#7422
Impact of Joint Laxity Before Total Knee Arthroplasty on Postoperative Ligament Balance
*
Yuji Arai - Kyoto Prefectural University of Medicine - Kyoto, Japan
Atsuo Inoue - Kyoto Prefectural University of Medicine - Kyoto, Japan
Manabu Hino - Kyoto Prefectural University of Medicine - Kyoto, Japan
Kenji Takahashi - Kyoto Prefectural University of Medicine - Kyoto, Japan
*Email: shushi@koto.kpu-m.ac.jp
Introduction: It is important to analyze the joint laxity preoperatively, to achieve good ligament balance post-total joint arthroplasty (TKA). Factors such as patient background, preoperative deformity, and surgical manipulation influence varus/valgus ligament balance after posterior stabilized (PS)-type TKA. In this study, we evaluated the medial/lateral joint stability before and after TKA and examined the characteristics of patients with soft-tissue imbalance.
Methods: In this retrospective study, 100 knees from 85 female patients who underwent PS-type TKA at our hospital were included. All patients had knee osteoarthritis with varus deformity, with the mean age at surgery being 75.4±6.1 years. Simple radiographs were taken preoperatively and 3 weeks postoperatively in both extension and flexion under varus and valgus stress (Figure 1). Patients were classified into two groups: one demonstrated good postoperative soft-tissue balance in both extension and flexion (well-balanced group, n=49), and the other demonstrated poor balance in at least one of the two positions (unbalanced group, n=51). Patient background, preoperative femoro-tibial angle (FTA), preoperative joint inclination angle, and intraoperative medial soft-tissue release were compared between the two groups.
Results: There were significant differences in employing intraoperative medial soft-tissue release (superficial medial collateral ligament), and in preoperative varus inclination angle in extension between the well-balanced and the unbalanced groups. Multivariate analysis showed a significant association of postoperative ligament balance with the preoperative angle of varus inclination in extension; according to the receiver operatorating characteristic (ROC) curve analysis, a joint inclination angle of 7° was found to be the cutoff for good ligament balance (Figure 2).
Conclusion: The normal knee has some degree of physiological lateral laxity, and mild lateral laxity is accepted after TKA. However, in patients with excessive preoperative lateral laxity, there is concern about the effect on postoperative ligament balance. In the present study, a poor postoperative ligament balance in patients was associated with a large varus inclination angle in extension. Therefore, patients with preoperative lateral laxity may have difficulty achieving a good ligament balance after TKA.
Figures
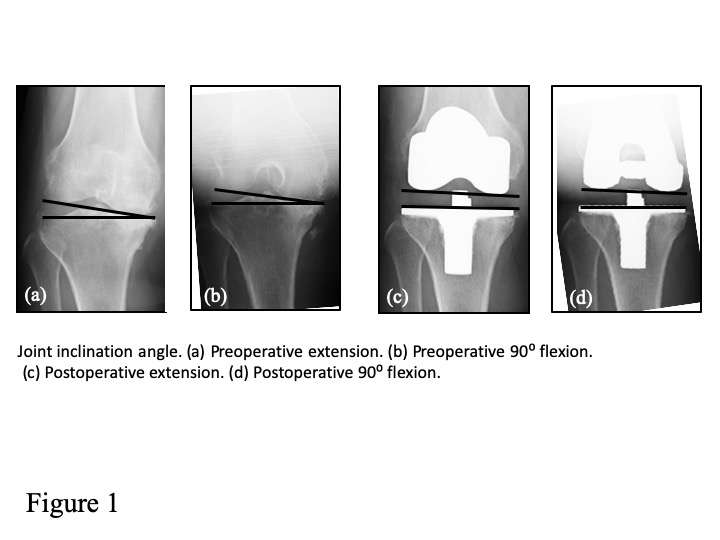
Figure 1
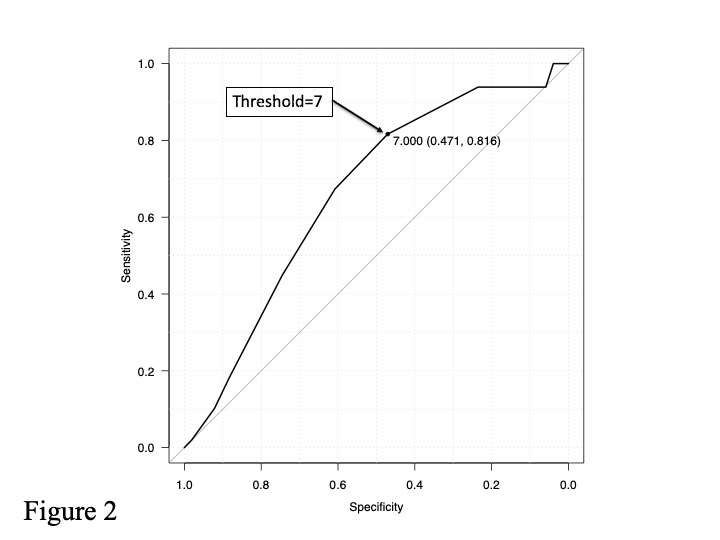
Figure 2#7572
Theoretically Finding Optimal Stem Positions That Minimize Cortical Bone Removal.
*
Michael LaCour - University of Tennessee - Knoxville, USA
Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Garett Dessinger - The University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: thangnguyen4796@gmail.com
Introduction: Preoperative templating serves as a valuable resource to help surgeons determine component sizes and plan positioning. However, preoperative templating is typically done in two dimensions (2D), and the stem version is often “driven” by the canal natural shape. Thus, surgeons may not have complete control over stem position, particularly neck version and anterior/posterior tilt, and may have to ream into the cortical bone to achieve desired positions. We developed an algorithm to model these situations theoretically by using the canal shape and the cancellous mantle bone thickness to determine the “Path of Least Resistance” (PLR) position of the stem. The objective of this study is demonstrate how such a tool can help orthopaedic companies design future stems and help surgeons plan more effectively.
Methods: The “PLR” algorithm uses Kane’s Dynamics to create a dynamic forward solution model. As the stem moves distally into the canal, we have implemented a contact detection algorithm to predict contact between the stem and the cortical or cancellous bone (Figure 1). Specifically, the stem is virtually pushed down the canal and a contact map between two meshes is calculated. If the stem penetrates/contacts the cortical bone, a counter-force will be applied to that area to reduce the penetration (Figure 2). The cancellous mantle thickness is also considered during force calculations. The stem is continually driven distally until it settles within the canal, fully seated with minimal penetration between the stem and cortical bone. The final result is the position of the stem that is “driven” by the shape of the canal.
Results: This model has been previously used to the predict stem position required to minimize the distance between the native and postoperative femoral head. Thus, the PLR algorithm is another surgical position that can be evaluated with the tool. In Figure 3, the amount of bone removal in PLR position is small compared to the Anatomical position, showing a difference of more than 0.8cm³ of cortical bone removal. Cortical bone that would need to be reamed away to achieve the desired positions are shown in red. While the PLR position visually and mathematically requires less to no bone removal, this does not come without consequence, as the distance between the preoperative femoral head center and the implanted head center is nearly 5mm larger in the PLR position than in the Anatomical position (Figure 3).
Conclusion: We developed an algorithm to model interoperative stem positioning within the canal by using forward solution dynamic modeling to broach or ream the femoral shaft and then driving the stem distally into the canal, attempting to yield a “natural” position of the stem with the least amount of cortical bone removal. It is evident from this pilot study that the PLR algorithm is indeed yielding less cortical bone removal. Often, desired interoperative fits may not be achievable without minor amounts of cortical bone removal. Therefore, developing a quantitative method to evaluate each different criteria would provide surgeons with additional data as they decide their personal, preferred stem fit.
Figures
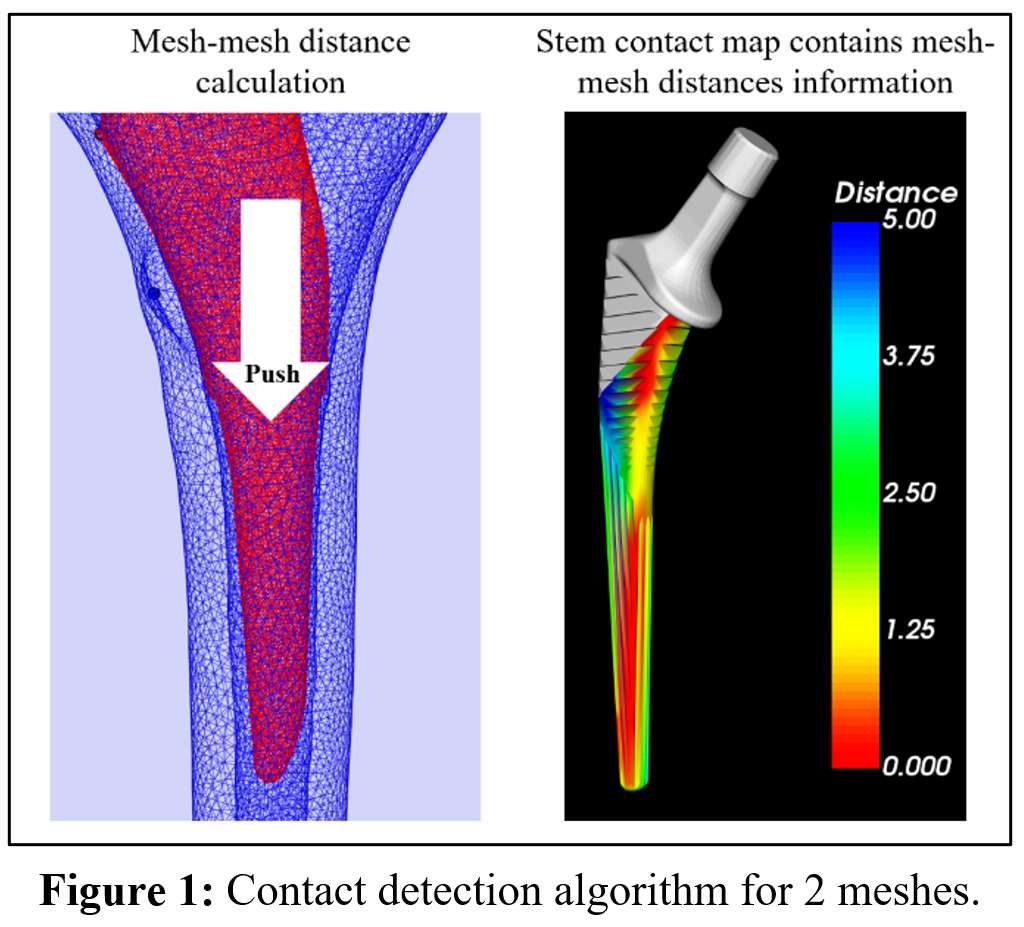
Figure 1
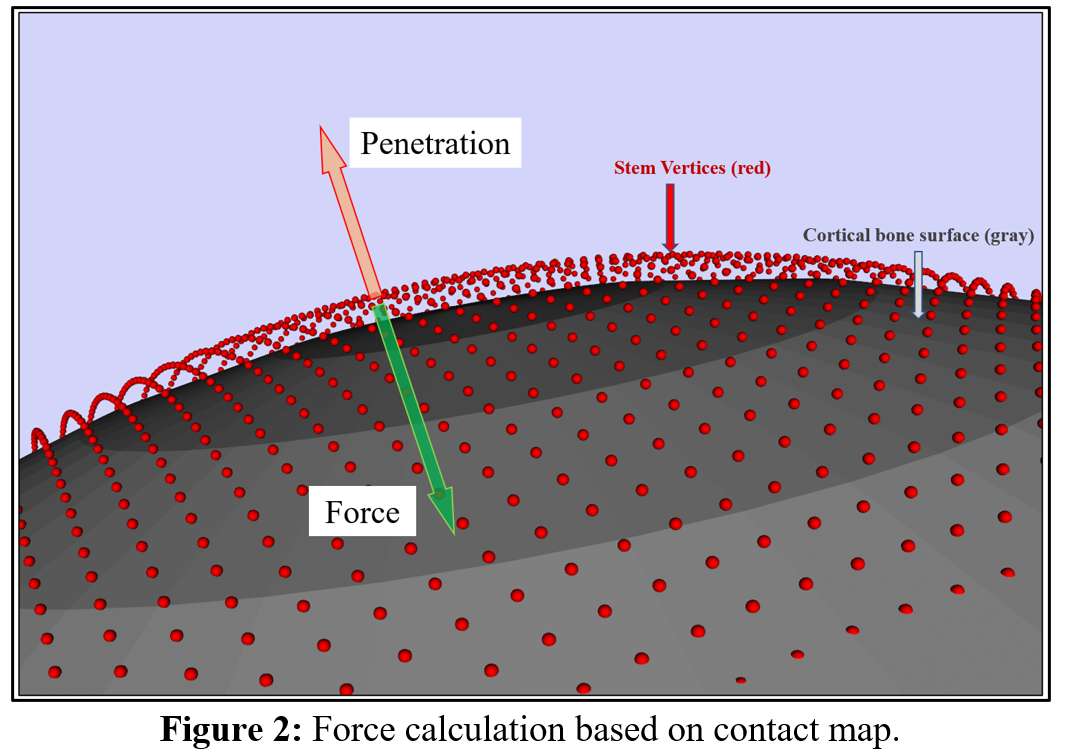
Figure 2
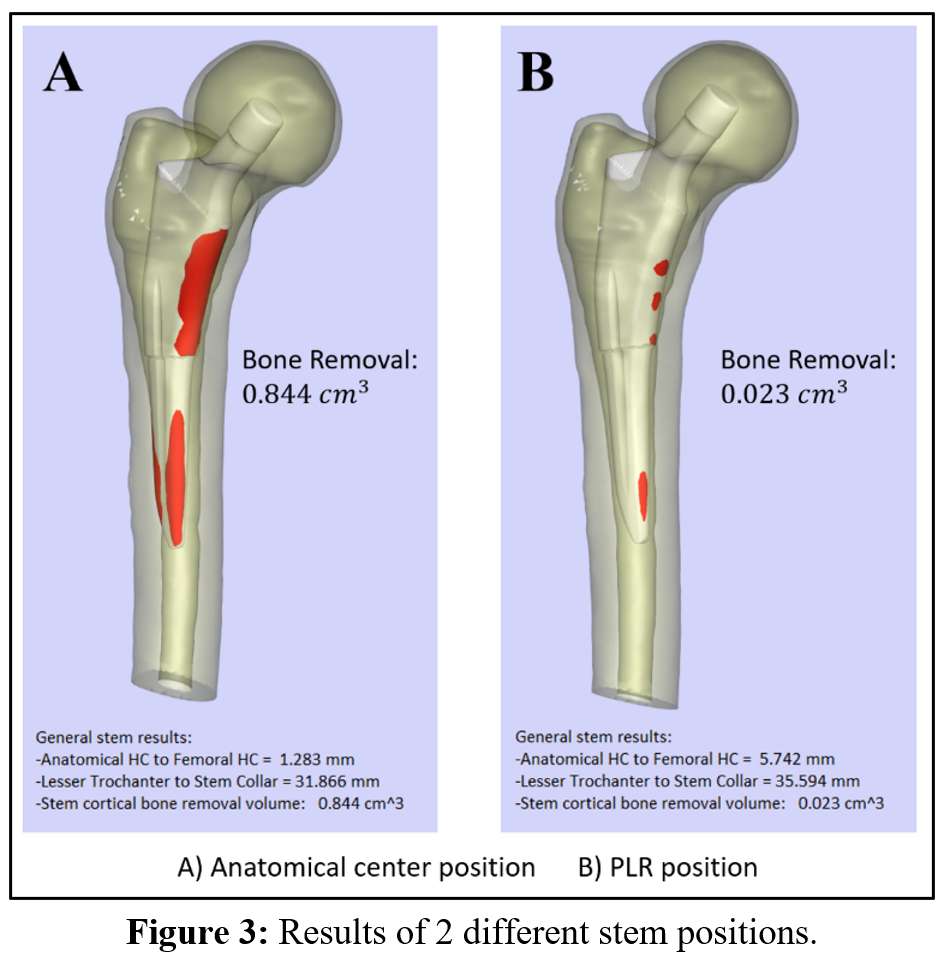
Figure 3#7569
Novel THA Component Positioning in Different Alignment Scenarios: Optimizing Performance Before Implantation
*
Michael LaCour - University of Tennessee - Knoxville, USA
Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Garett Dessinger - The University of Tennessee - Knoxville, USA
Manh Ta - Stryker Corporation - Fort Lauderdale, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
Andrew Jacobs - DePuy Synthes - Warsaw, USA
*Email: thangnguyen4796@gmail.com
Introduction:
In THA, each stem type has different broaching process in order to align the stem in the canal. In addition, once the canal is broached, the surgeon may at times need to further ream cortical bone to ensure proper stem fit. To address these issues, we have developed a validated pre-operative planning tool that assesses the shape of the canal and the fit and position of a femoral stem under different alignment conditions based on an in-depth computational understanding of the canal and femoral stem. By comparing different stem alignments, the objective of this study is to present quantitative evaluation tools to help orthopaedic surgeons find improved stem alignment options where the chosen stem position successfully assesses optimal femoral head position and stem version coupled with overall implant stability and a minimization of cortical bone removal.
Methods:
The preoperative planning tools used in this study is a continuation of previously published and validated virtual hip simulator and component alignment algorithms that automatically place a stem in a desired position and compare the resulting postoperative mechanics. In this study, a single stem system was compared under differing alignment conditions. The “Path of Least Resistance” (PLR) fit is where the stem is driven primarily by canal shape and cancellous mantle thickness, without considering preoperative femoral head position or femoral version. In contrast, the “Anatomical” fit assesses both the shape of the canal as well as preoperative femoral positioning and version. After stem alignment, a virtual dynamic hip simulator is used to analyze joint contact mechanics and kinematics during multiple post-operative activities.
Results:
In both alignment scenarios, contact between stem and cortical bone happens mostly on the medial face of stem, with more than 50% of the total contact area occurring on the medial side and shares a similar contact pattern with canal (Figure 1). The Anatomical fit successfully reduces the distance between anatomical femoral head center and stem head center by nearly 4 mm, from 4.146 mm to 0.357 mm, occurring predominantly in the anterior/posterior direction, and only requires an additional 0.067 cm3 of bone removal (Figure 2). When these positions are exported to the in vivo model, the maximum hip forces during stance phase for both alignment cases are similar, around 2.1 xBW each (Figure 3). Interestingly, while the separation and sliding magnitudes are similar, the model predicts that the PLR fit causes edge loading while Anatomical fit does not (Figure 3).
Conclusion:
The positioning planning tool has shown that having the stem head align closer to anatomical femoral head center could improve the contact mechanics (reduce edge loading) and kinetics (hip/ligaments/muscle forces), and this further highlights the need to consider patient-specific stem version angles intraoperatively. In this study, it was found that an “Anatomical” fit may not be fully achievable without minor amounts of cortical bone removal. Therefore, developing a quantitative method to evaluate each different criteria would provide surgeons with additional data as they decide on their own personal “optimal” stem fit.
Figures
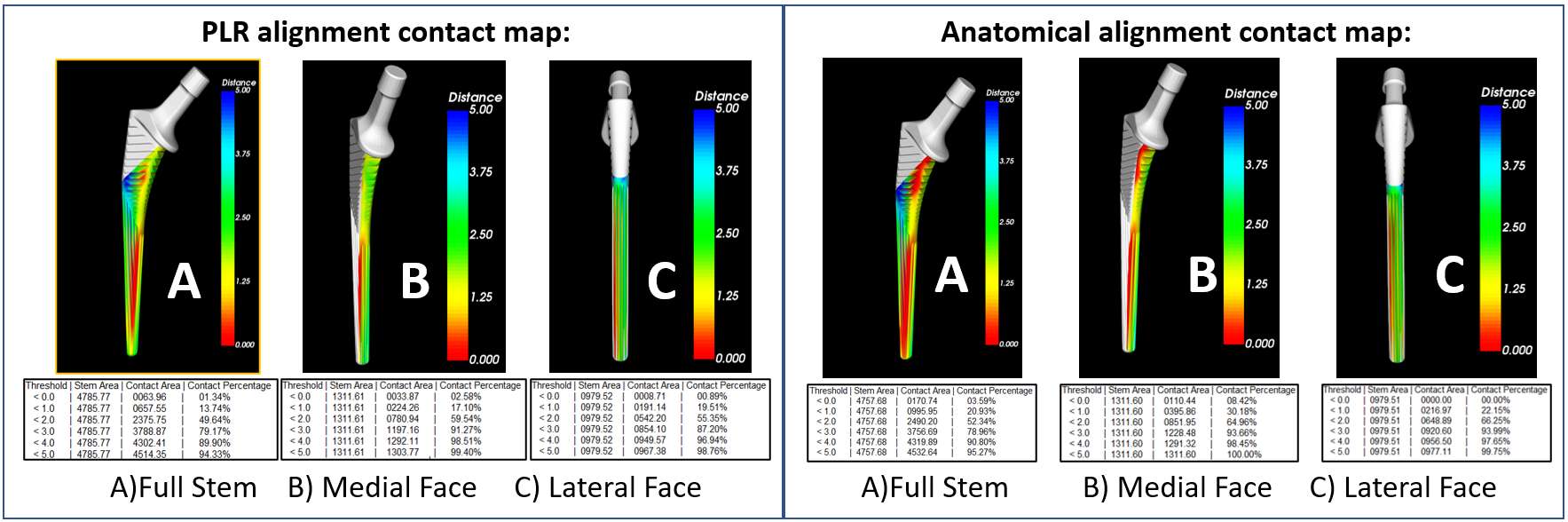
Figure 1
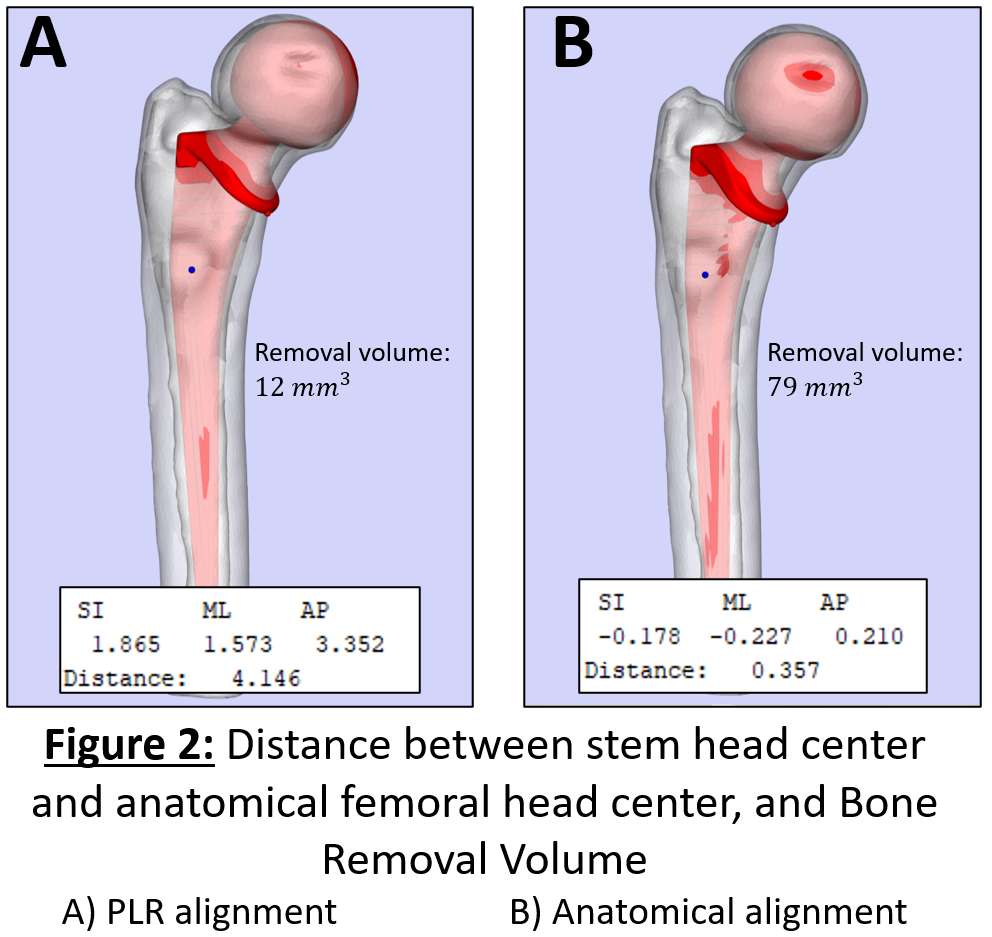
Figure 2
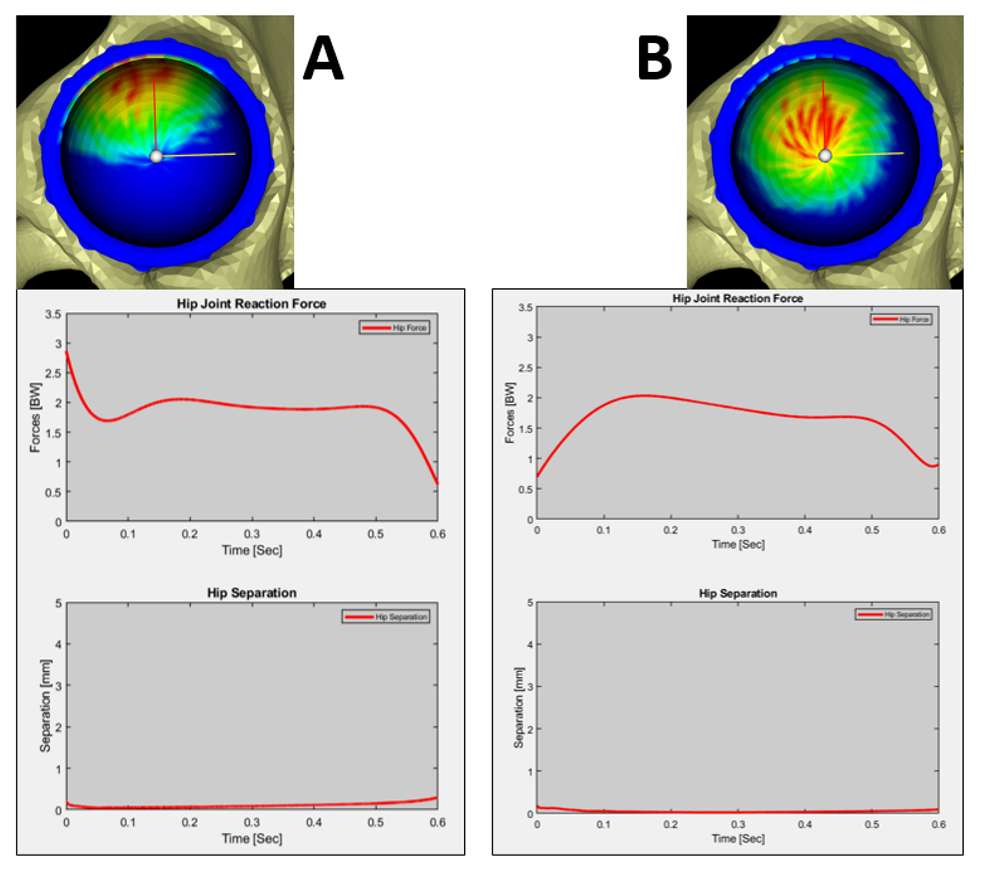
Figure 3#6908
Modified Gap Technique for Total Knee Arthroplasty (TKA) in Rheumatoid Arthritis
*Satomi Abe - Asahikawa Medical University - Asahikawa, Japan
Hitoshi Nochi - Asahikawa, Japan
Yusuke Sasaki - Asahikawa Medical University - Asahikawa, Japan
Go Sato - Asahikawa Medical University - Asahikawa, Japan
Hiroshi Ito - Asahikawa Medical College - Asahikawa, Japan
*Email: satomi@asahikawa-med.ac.jp
INTRODUCTION: It is reported that varus deformities were not medial side contractures and that the medial preserving gap technique improves the stability of mid-to-deep knee flexion in OA knees. Soft tissue balance is dependent on surgical techniques including soft tissue release skills and evaluation methods. Gap and balance of soft tissue during TKA varies by individual and measurement strength. Experientially the soft tissues look loose based on the pathologic condition in rheumatoid arthritis (RA), therefore we built up the gap and balance more tightly. However pathologic soft tissue loosening in RA were not reported. The purpose of this study is to understand of the characteristics of soft tissue balance in RA.
METHODS: We compared component gap OA 160 varus knees and RA 45 varus knees during TKA (NexGen LPS-Flex, fixed surface, or Persona, Zimmer) procedures, in which soft tissue releases were performed under Clayton Stage I medial release (capsule release and additional POL release). The average of DAS28 (CRP) scores, which indicates RA activity, is 2.51 and severely deformed knees were excluded. To assess the soft tissue balance, component gaps (CGs) were measured using an original two paddled tensor at 20lb, 30lb and 40lb, for each knee at a 0 degree extension and 90 degree flexion. To evaluate the characteristics of soft tissue rigidity of the medial side, we calculated the change of the distance of CGs 30-20lb, 40-30lbs and 40-20lbs, and the change of distance of CG flexion - CG extension. The statistical analysis software used was StatView and significant difference was defined as p<0.05.
RESULTS:(1) The medial side of CG (20/30/40lb) at extension were 9.7±1.9mm, 11.0±1.9mm and 12.2±2.3mm in OA, and 10.4±1.9mm, 11.6±2.2mm and 12.9±2.6mm in RA respectively. At flexion, they were 12.7±2.3mm, 15.0±2.8mm and 16.7±3.1mm in OA, and 13.4±3.0mm, 15.7±3.3mm and 17.2±2.3mm in RA, respectively. The joint gaps were bigger when the opening force increased. (Figure 1)
(2) The change of distance at extension 30-20/40-30/40-20lb were 1.3±1.2mm, 1.1±0.9mm and 2.5±1.6mm in OA, and 1.1±1.0mm and 1.3±1.0mm and 2.4±1.5mm in RA, respectively. At flexion, they were 2.2±1.2mm, 1.7±0.8 and 4.0±1.5mm in OA, and 2.3±0.7mm, 1.4±0.6mm and 3.7±0.9mm in RA respectively. There were not significant differences between OA and RA. (Figure 2)
(3) The changes in the medial distance of CG at flexion and extension (20/30/40lb) were 3.0±2.1mm, 3.9±2.6mm and 4.6±2.9mm in OA, and 3.0±2.3mm, 4.1±2.1mm and 4.2±2.5mm in RA. The change of distance of CGs were bigger when the opening force increased. There were not significant differences between OA and RA. (Figure 3)
DISCUSSION:We compared the soft tissue rigidity at the same rerelease without MCL release and we showed there were not significant differences between OA and RA. This means that we could use the same gap-control techniques in OA and RA knees, which are well controlled activities. In the future, we will evaluate the effect of the activity of RA and the difference in long term changes in OA and RA. This study’s limitations are the static evaluation, the value of opening force, and knee position.
#7904
Examination of Appropriate Gap Balance for Good Flexion Angle and Clinical Results in PS Type TKA
*Satomi Abe - Asahikawa Medical University - Asahikawa, Japan
Hitoshi Nochi - Asahikawa, Japan
Hiroshi Ito - Asahikawa Medical College - Asahikawa, Japan
*Email: satomi@asahikawa-med.ac.jp
INTRODUCTION:
The purpose of the study was to determine the individual soft-tissue characteristics depending on the opening force and gap balance for obtaining a good preoperative flexion and clinical results by cluster analysis.
METHODS: We examined 323 PS-type TKA (Zimmer LPS Flex, Gender, Persona) due to OA, age 67 ± 11 years. All cases were the medial parapatellar approach and modified gap-controlled techniques. The component gap (CG) of the medial and lateral side was measured after reducing the patella using a two-paddles tensioner at 20lbf, 30lbf, and 40lbf, for each knee at 0 degrees extension and 90 degrees of flexion. Cluster analysis was performed using the Ward method by the third party. The group-to-group comparison used a one-way analysis of variance and the Bonferroni method (P<0.01). Also, we analyzed the relationship between insert thickness and medial extension 30lfb CG.
RESULTS: (1) CG values could be divided into three groups by cluster analysis, group A (152 knees), B (77 knees), and C (94 knees). The ratio of the medial and lateral CG values could be divided into three groups, group I (202 knees), II (58 knees), and III (63 knees) by cluster analysis. (Figure 1) (2) There were no statistical differences in postoperative FTA, α, β, γ, and δ angle between groups A, B, and C, or I, group II and III. (3) There were no differences in the preoperative flexion or pre-and postoperative extension in groups A-C and group I-III. The postoperative flexion angles were 120± 11 degrees in group A, 121 ± 10 degrees in group B, 125 ± 9 degrees in group C, and group C showed a significant difference (P<0.05) only with group A. In addition, 121 ± 11 degrees in group I, 120 ± 7 degrees in group II, 125 ± 10 degrees in group III, and group III was significantly different from group I and II (P<0.05). (4) To find the soft tissue characteristics of each group A-C and I-III, we analyzed the trapezoid shape from 20 to 40lbf, and the relationship between the insert thickness and the medial CGs (figure 2). In Group A, a similar trapezoid shape was maintained from 20 to 40lbf and the thigh inserts (-0.31mm) compared to the medial extension CGs on 30lbfs. In Group B, the trapezoid shape became larger on both the medial side and lateral side from 20 to 40lbf, and their thin insert (+1.19mm). In Group C, the trapezoid shape on the lateral side became larger from 20 to 40lbf and the same thick inserts (+0.28mm) as the extension medial 30lbfs. Group I; The trapezoid shape with medial and lateral CG ratio 1.0 -1.1, Group II; The trapezoid shape with medial and lateral CG ratio 1.4, Group III; The trapezoid shape with medial and lateral CG ratio 1.2.
DISCUSSION:
These results suggested that the medial flexion CG was bigger than the extension CG and the medial and lateral balance ratio of about 1.2, gives a good postoperative flexion angle.
Figures
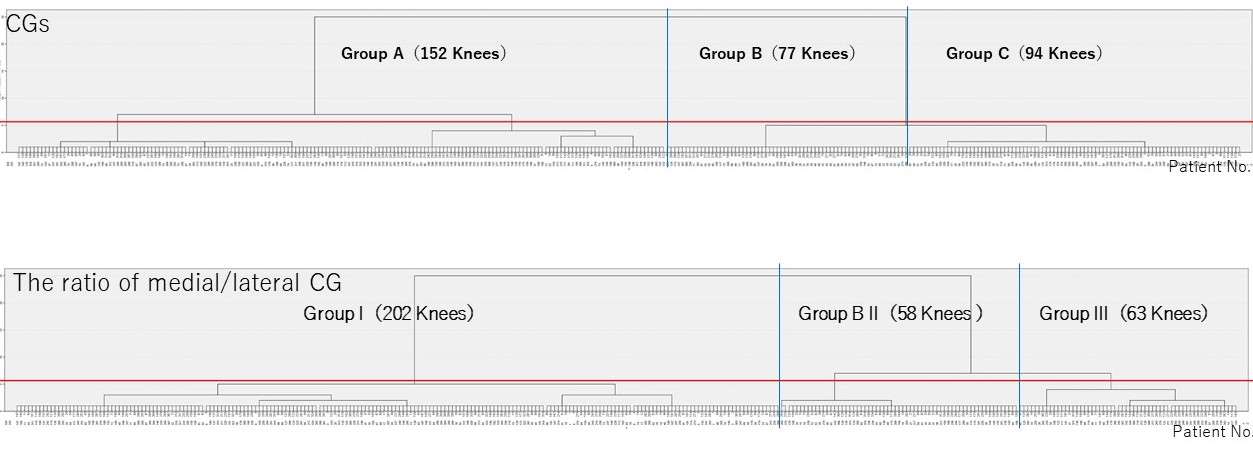
Figure 1
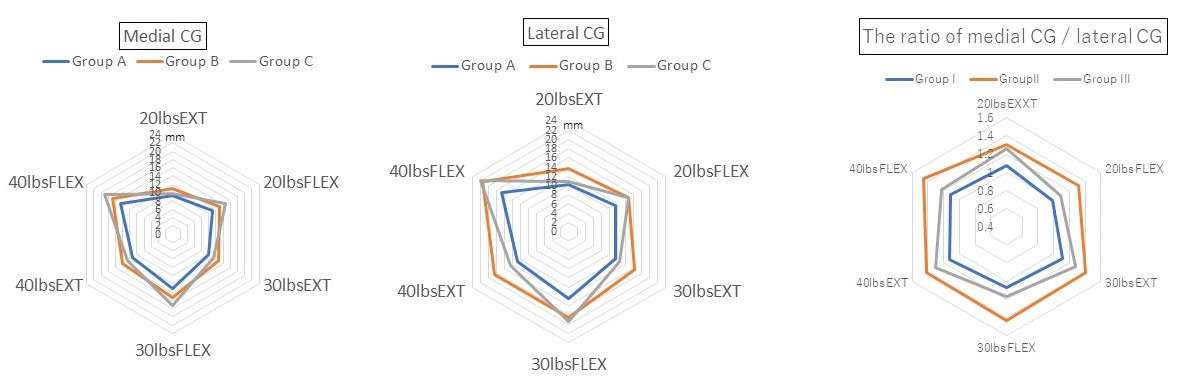
Figure 2#7839
In-Person Pre-Operative Patient Educational Classes May Not Be Necessary Prior to Elective Arthroplasty
Maveric Abella - University of Hawaii - Honolulu, United States of America
Krystin Wong - Straub Medical Center - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Scott Nishioka - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
*Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: onohunter@icloud.com
Introduction: In-person pre-operative patient education classes can prove to be an inconvenience to some patients in rural or low-income areas. Additionally, due to the COVID-19 pandemic and recommended social distancing per the Centers for Disease Control, these classes were prohibited from taking place to minimize in-person contact. This study examines the impact of replacing in-person pre-operative patient education classes with a pre-operative telephone call. While a pre-operative telephone call provided an easy and accessible way to prepare patients for surgery, it is unknown how this format impacts patient surgical outcomes. Furthermore, we assess the current and potential future implications of a telehealth pre-operative patient education class for elective arthroplasty surgery.
Methods: This retrospective review compared 232 patients (305 arthroplasties) who underwent in-person instruction and 155 patients (192 arthroplasties) that received telephone instruction, who underwent total hip arthroplasty (THA), total knee arthroplasty (TKA), or unicompartmental knee arthroplasty (UKA). Patients who underwent arthroplasty from May 2020 to October 2020 received pre-operative education via telephone. Primary outcomes included length of stay, clinic call burden and complications within 90-days, with parametric statistical analyses performed to compare groups.
Results: Patient demographics between groups were similar, except patients having undergone pre-operative education over telephone tended to be younger and have a lower body mass index. Compared to in-person classes, telephoned patients had significantly shorter length of stay for all unilateral telephoned groups (p<0.009), but the percentage of telephoned patients making at least one post-operative clinic call increased (22.8% to 40%; p<0.001). No differences were noted in post-operative complications, and emergency room visits significantly decreased for TKA telephoned patients (p=0.039).
Conclusion: Transition from in-person to telephone for pre-operative instruction resulted in similar post-operative complications, indicating that the condensed format sufficiently prepared patients for elective joint arthroplasty. However, pre-operative telephone instruction did increase the number of post-operative clinic calls related to wound care and symptom relief. With focused efforts to address these issues, pre-operative telephone instruction prior to joint arthroplasty may safely replace the more inconvenient, time consuming in-person instruction.
#7835
Fixed Distal Femoral Cut Consistently Achieves Neutral Alignment Across Races
Maveric Abella - University of Hawaii - Honolulu, United States of America
Vera Ong - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Tyler Thorne - University of Hawaiʻi at Mānoa - Mānoa, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
*Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: onohunter@icloud.com
Introduction: Mechanical axis (MA) alignment is used to evaluate lower extremity deformity and total knee arthroplasty (TKA) success. A neutral MA alignment is important to prevent implant failure and poor functional outcomes. It is widely known that pre-operative MA varies significantly across race and gender, but it is unknown if a fixed 6° distal femoral cut can attain the desired neutral alignment consistently across racial groups. Furthermore, MA alignment pre- and post- TKA has not been readily studied in Native Hawaiian and Pacific Islanders (NHPI), a demographic readily available at our hospital. Therefore, this study investigates MA alignment in Asians, Caucasians, and Native Hawaiian/Other Pacific Islanders before and after TKA.
Methods: In this retrospective study, pre- and post-TKA MA were measured from 835 Asian, 447 Caucasian, and 163 NHPI patient radiographs, in which a standard distal femoral cut of 6° valgus was performed. Data were evaluated as continuous variables and by groupings of varus (MA<-3°), valgus (MA>3°), and neutral (-3°<MA<3°) alignment.
Results: Pre-operative MA alignment ranged from 38° valgus to 29° varus. The proportion of Asian and NHPI with a varus MA was significantly greater than Caucasian patients in females (Asians: 66.1%; Caucasians: 45.7%; NHPI: 63.2%) and males (Asians: 80.6%; Caucasians: 67.0%; NHPI: 79.0%) [Figure 1]. Post-operatively, MA alignment ranged from 11° valgus to 8° varus. Achieving neutral MA was consistent across races for females (Asians: 75.2%; Caucasians: 76.8%; NHPI: 75.9%) and males (Asians: 77.3%; Caucasians: 79.4%; NHPI: 72.3%) [Figure 1].
Conclusion: As expected, MA prior to TKA was different between the evaluated race groups. In particular, greater varus alignment was presented in Asian and NHPI patients. However, the consistent distal femoral cut of 6° valgus successfully and consistently established neutral MA alignment across race and gender, necessary for ensuring good functional outcomes and minimizing implant failure. Although the majority of patients had a neutral MA post-surgery, methods such as computer-assisted navigation could be used to ensure neutral MA but may result in added costs and surgical time.
Figures
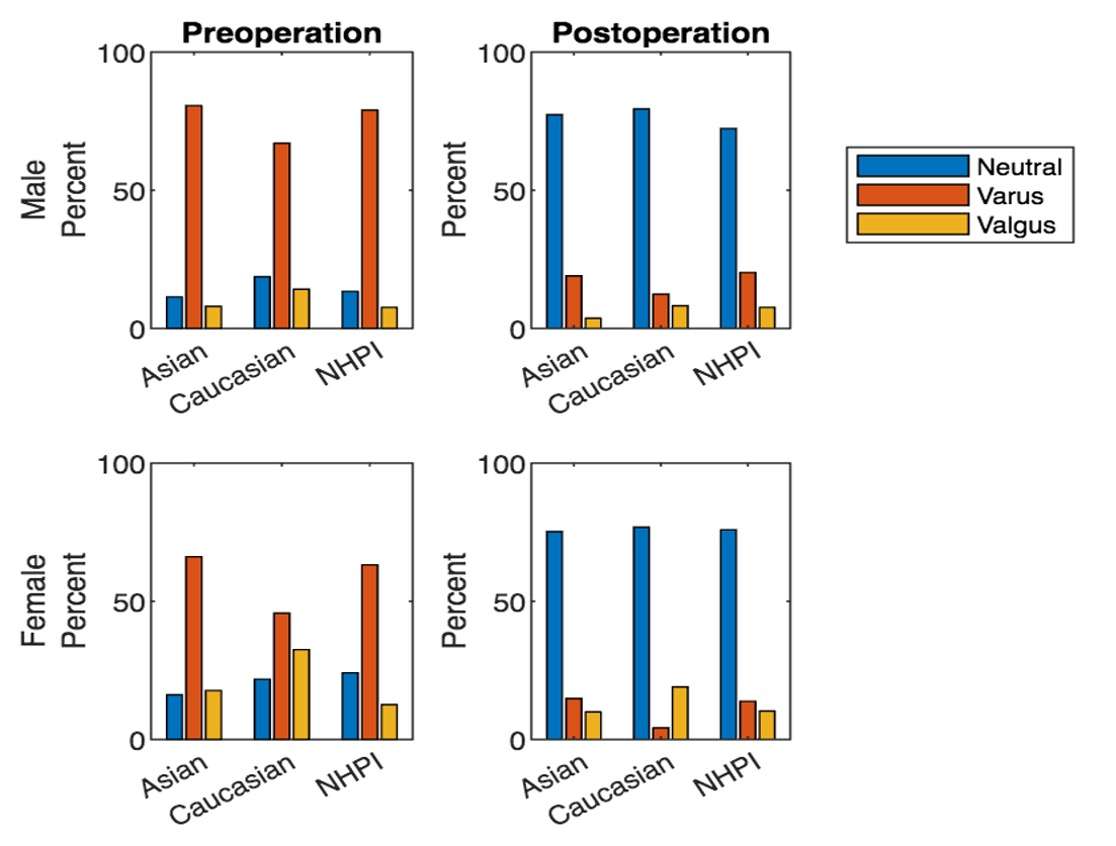
Figure 1#7565
Rotator Cuff Muscle Excursion During Abduction After Reverse Total Shoulder Arthroplasty (RTSA)
*Eric Hu - University of Illinois at Chicago College of Medicine - Chicago, United States of America
Martine Dolan - University of Illinois at Chicago - Chicago, USA
Farid Amirouche - University of Illinois at chicago - Highland park, United States of America
*Email: ehu9@uic.edu
Introduction: The rotator cuff (RC) is a group of four muscles that helps maintain dynamic stability of the glenohumeral joint and provides force rotation of the shoulder1. Out of the RC muscles, abduction of the shoulder is mediated primarily by the supraspinatus. External rotation is mediated by the teres minor and infraspinatus, while internal rotation is generated through the subscapularis. Rotator cuff tears, typically of the supraspinatus, are a common injury that may result in pain and limited joint stability1. Previous biomechanical studies have shown that complete rotator cuff tears decrease abduction force and glenohumeral joint stability2. Reverse total shoulder arthroplasty (rTSA) is a popular treatment option for complete RC tears that is indicated in patients with superior humeral head migration in the presence of osteoarthritis. This procedure has been shown to improve abduction strength and mobility3. It is important to assess various biomechanical properties of the RC after rTSA to explore potential measurable indicators of rehabilitation after surgery. The change in muscle length, or excursion, during joint rotation can be used to assess muscle function4. Therefore, the goal of this study is to determine excursion of the RC muscles during shoulder abduction after rTSA in order to show how each muscle contributes biomechanically during limb movement after surgery.
Methods: The experiment was performed using an apparatus (Figure 1) to abduct six cadaveric shoulders under two conditions: intact and rTSA. Within the apparatus, nylon strings connected the tendinous muscular insertion sites to suspended weights. Digital points were assigned and tracked at muscle origin and insertion to calculate muscle length during shoulder abduction. Muscles were divided into anterior/superior or posterior/inferior segments to determine nuances in recruitment within the same muscle. The excursion was calculated for each segment by subtracting muscle length at 0o of abduction from muscle length at 90o. ANOVA and post-hoc Tukey testing was done to compare the overall mean muscle length and excursion values of each muscle segment across the four conditions and identify any significant differences.
Results: Results showed that certain muscles after rTSA had significantly different excursion values when compared to the intact shoulder. (Figure 2, 3) Though the supraspinatus no longer contributes to abduction after rTSA, our results showed significantly greater values of theoretical excursion compared to the intact shoulder after rTSA (p<0.05). For infraspinatus, rTSA produced significantly smaller excursions (p<0.05). Teres minor showed no significant differences in excursion between conditions (p=0.54). Subscapularis also showed no significant differences (p=0.55).
Conclusion: Our findings suggest that rTSA may restore muscle excursions in the teres minor and subscapularis. In addition, rTSA seems to eliminate the excursion difference seen between superior and inferior segments of the infraspinatus (Figure 2B), potentially altering the muscle to be a more uniform stabilizer. Supraspinatus increased excursion could be due to the inferio-medial shift of the glenohumeral joint center of rotation present after rTSA. Subscapularis excursion seems to be restored, which supports previous studies showing that subscapularis biomechanics can be restored with rTSA following a complete RC tear5.
Figures
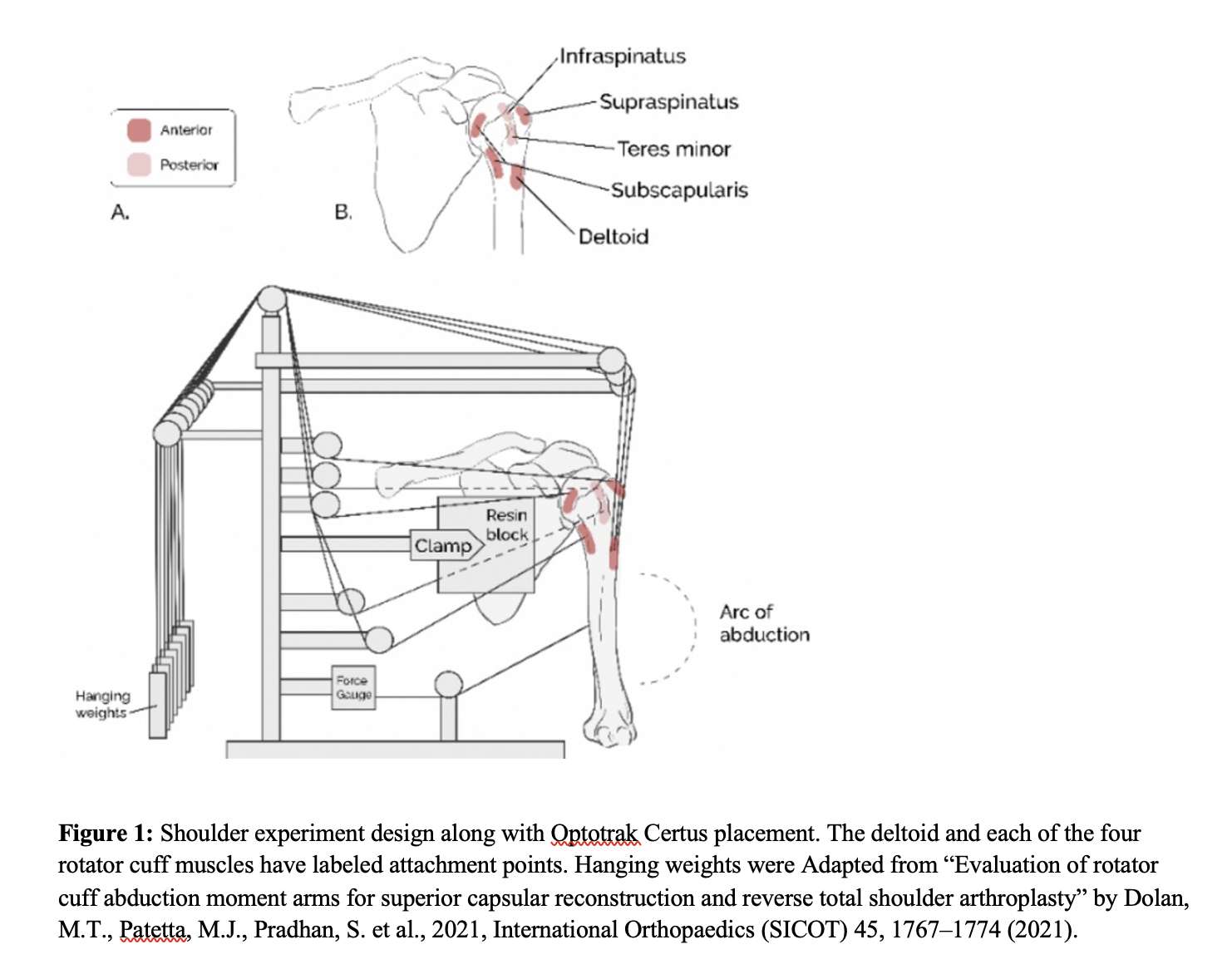
Figure 1
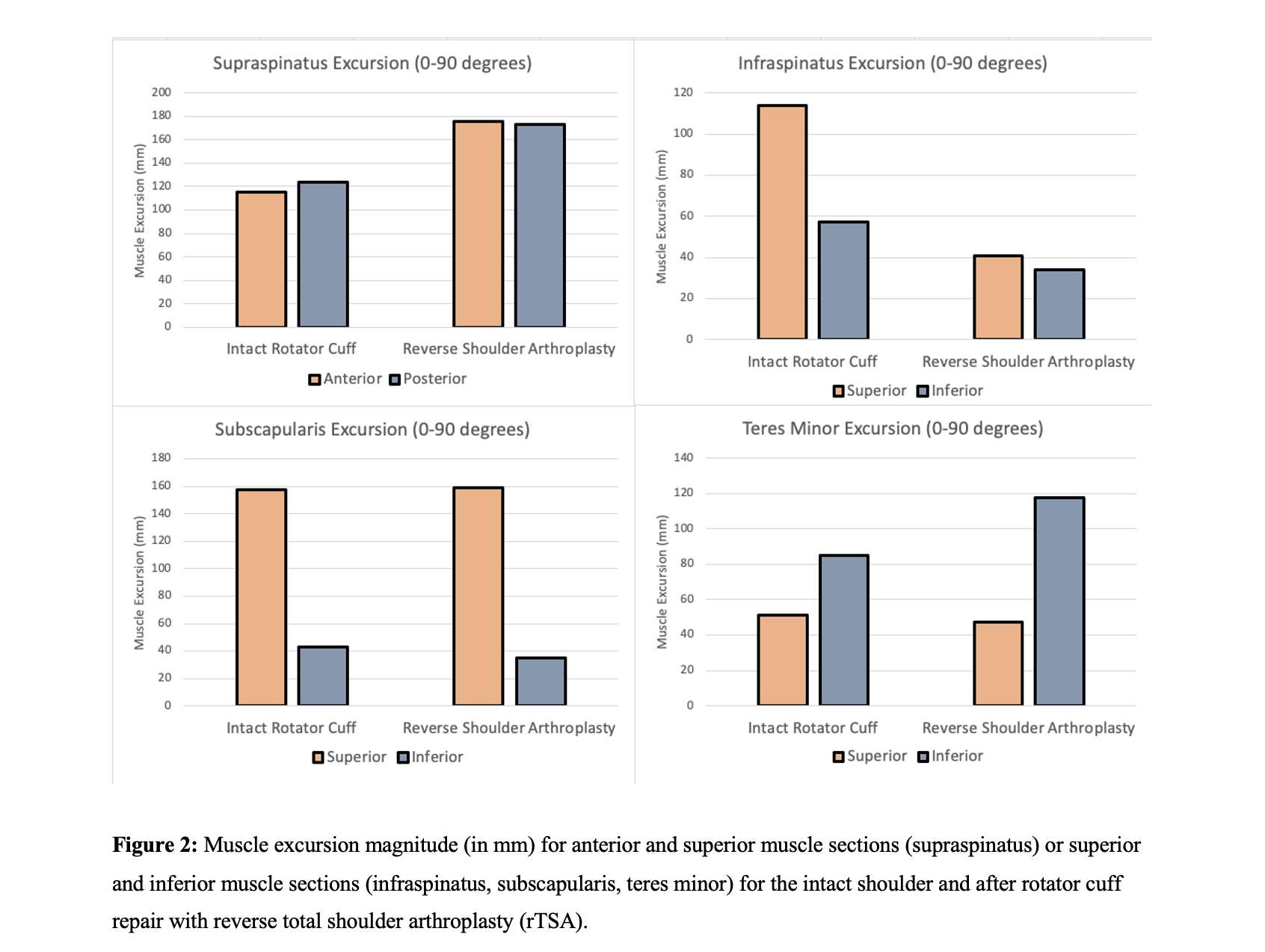
Figure 2
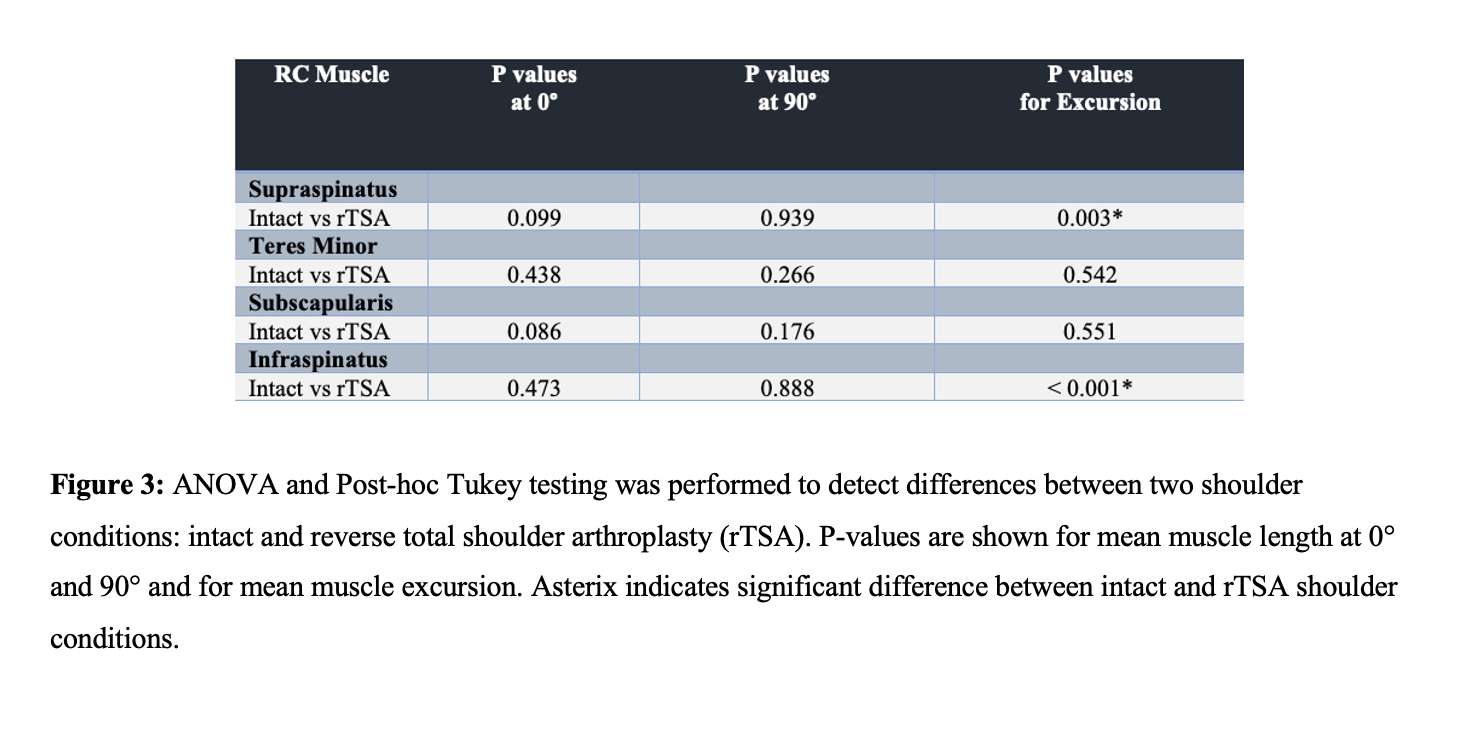
Figure 3#7731
Glenoid Implants Loosening in Shoulder Arthroplasty . Asymmetry and Conformity Versus Bounded and Frictionless Screw-Bone Interface.
Roberto Leonardo Diaz - University of Illinois at Chicago - Chicago, United States of America
*Farid Amirouche - University of Illinois at chicago - Highland park, United States of America
Lewis Shi - University of Chicago - Chicago, USA
Jason Koh - NorthShore University Health System - Evanston, USA
*Email: farid.amirouche@gmail.com
Introduction
Glenoid implant loosening is the most common complication of shoulder arthroplasty. Loosening the implant may cause pain, limit function, and lead to more complicated revision surgery. Causes of loosening include migration due to eccentric loading of the humeral head motion and poor bone quality. Two glenoid implants are designed based on the two common morphological erosion patterns: symmetric and asymmetric. The analysis of inlay and onlay resurfacing procedures during shoulder arthroplasty and their effect on the implant performance is necessary to highlight technical and clinical advantages. This study evaluates the biomechanical performance of glenoid implants asymmetry, threaded pegs bounded and not bounded to the bone in shoulder arthroplasty under compressive loading and resurfacing conditions that preserve the glenoid anatomical conformity using the finite element method.
Methods
Implant design: In the symmetric design, the thickness of the implant increases evenly from the centerline to both edges producing a uniform concavity and replicating the glenoid cavity curvature. In the asymmetric design, one of the borders is thicker with respect to the centerline to create a non-uniform concavity that may help correct the glenoid version angle in cases of eccentric reaming. The glenoid implant was modeled using HDPE material properties (E=900MPa, ν=0.3).
FEA: Finite element model of glenoid implants were built using ANSYS Workbench. The implant was fitted on a block simulating cortical bone (E=244.08 MPa, ν=0.3). A 500N load was applied at 5 points along the centerline of the implant using a ball simulating the humeral head. For the onlay case, the implant's base-paired the outer surface of the bone block, whereas, for the inlay case, bone was removed to fit the implant base 2mm depth inside the block. Frictional contact (Coefficient =0.2) was allowed between the surfaces in contact to simulate a cementless case. Micromotion and stress distribution was recorded to enable comparison between the two designs.
Results
Glenoid implants that simulate the onlay resurfacing technique showed higher motion values, on average 178.18μm for symmetric models and 174.54μm for asymmetric models [Fig. 1]. The asymmetric model showed 8% less displacement than the exact symmetric model location on the thicker side. The average maximum stress was 12 MPa in both symmetric and asymmetric implants.
Results for the inlay technique showed an average motion of 176.18μm for symmetric and 174.2μm for asymmetric models [Fig. 2]. The symmetric model showed larger displacement (10%) than the asymmetric models along the loading centerline. In this technique, maximum stress values were 12% higher in the asymmetric model (13.25 MPa) than in the symmetric model (11.67 MPa).
Conclusion
This study compared symmetric and asymmetric glenoid implant models simulating two shoulder arthroplasty resurfacing techniques. These simulations found that the asymmetric model has an advantage over the symmetric in preventing micromotion under similar loading conditions. The augmented thickness at one of the sides of the implant likely helps to decrease micromotion, which is important to avoid loosening and promote osseointegration. Results indicate similar micromotion values for the asymmetric models for onlay and inlay resurfacing techniques.
Figures
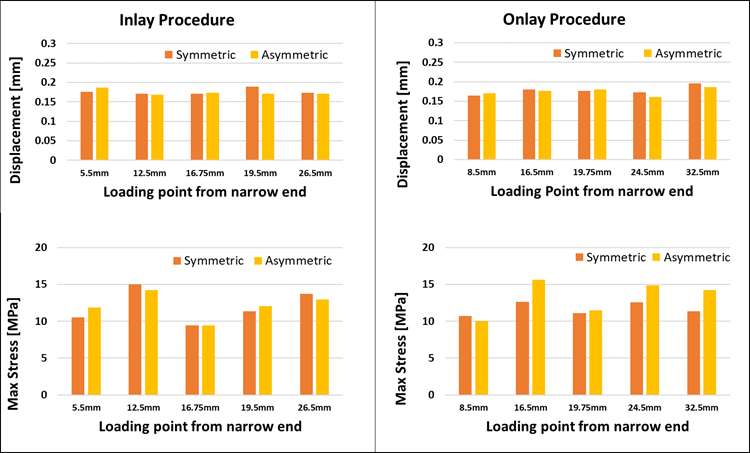
Figure 1
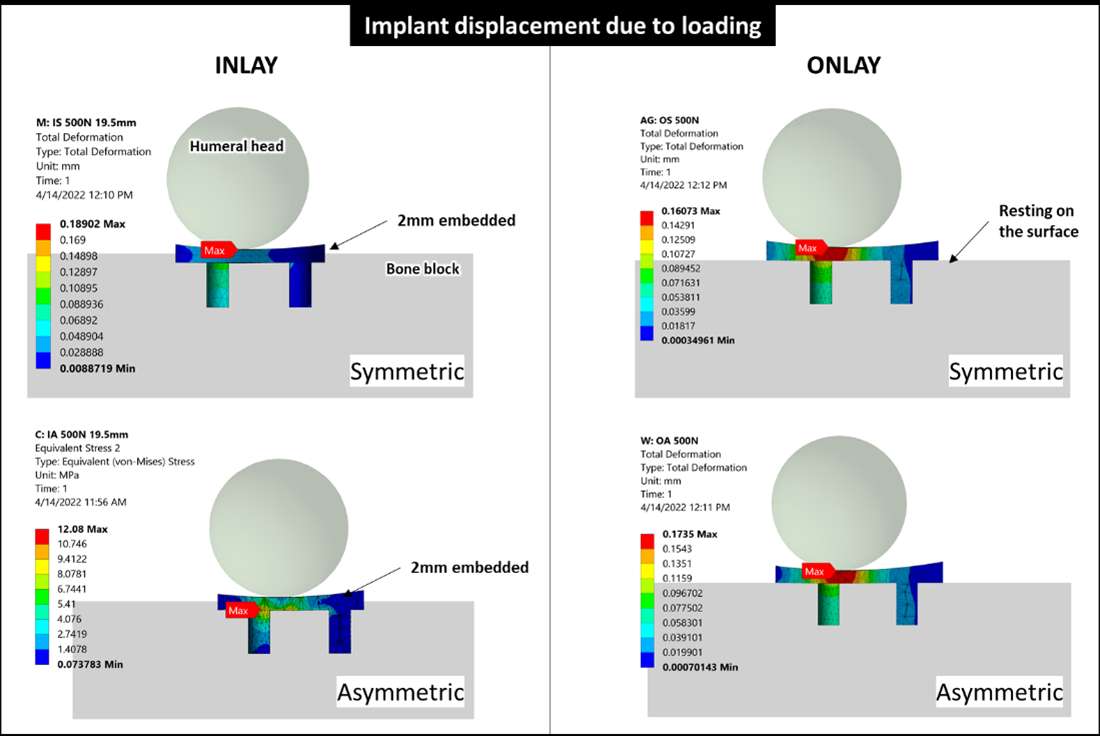
Figure 2#7921
Improved Mediolateral Gap Balance Achievement With Instrumented Navigated Total Knee Arthroplasty Compared to Conventional Instrumentation
*Laurent Angibaud - Exactech, Inc. - Gainesville, USA
Wen Fan - Exactech - Gainesville, USA
Florian Kerveillant - Blue-Ortho - Meylan, France
Philippe Dubard - Blue-Ortho - Meylan, France
Marine Torrollion - Blue-Ortho - Meylan, France
Matthew Rueff - Exactech - Gainesville, USA
Alexander Sah - Washington Hospital - Fremont, USA
James Huddleston
*Email: laurent.angibaud@exac.com
Introduction
Soft-tissue balance is assumed to be a crucial determinant in achieving a successful outcome in total knee arthroplasty (TKA). While soft-tissue balancing using conventional mechanical instrumentation was primarily based on subjective assessments at discrete flexion angles, recent technological advancements encompass the possibility of characterizing the soft-tissue envelope throughout the full arc of motion.
This study evaluated the ability to achieve targeted mediolateral (ML) gap balance throughout the arc of motion using conventional mechanical instrumentation versus a computer-assisted orthopedic surgery (CAOS) system featuring an intraarticular distractor according to two levels of user’s experience.
Methods
Four cadaveric specimens (8 knees) were assigned to four surgeons (2 seniors and 2 juniors) with the declared goal of achieving rectangular gaps in both extension and flexion.
For each specimen, conventional mechanical instrumentation was used for the right side TKA (conventional TKA), while an instrumented CAOS system was leveraged for the left side TKA (instrumented TKA) (Figure 1).
At the end of each procedure, a laxity test was conducted to assess the ML gap balance by placing the intraarticular distractor between the proximal tibial cut and the trial femoral component previously impacted onto the prepared distal femur. Then, the limb was manipulated from extension to full flexion and the spatial positions of the trial femoral component relative to the acquired proximal tibial cut were captured by the CAOS system.
For each degree of flexion from 5° to 90°, both the signed and the unsigned differences between the lateral and medial gaps were calculated and both the mean difference and the standard deviation through the range of motion were reported for each TKA among the four groups (i.e., 2 user experience levels and 2 types of instrumentation).
Results
Regardless of the experience level, the instrumented TKAs were associated with a significantly lower ML gap differential than the conventional TKAs (p<0.001). While the senior group achieved moderate gain regarding the ML gap differential between their conventional TKAs and their instrumented TKAs (p<0.001 for unsigned difference, p=0.220 for signed difference), the junior group achieved a significant reduction in the ML gap differential between their conventional TKAs and their instrumented TKAs (p<0.001 regardless of the signature) (Figure 2).
Discussion
Historically, soft tissue balancing during TKA has been reported as an art rather than a science. This statement is mostly due to the difficulty of objectively assessing the soft-tissue envelope leaving the surgeon with his/her subjective assessment. In this context, the surgeon’s experience is deemed crucial.
In this regard, the addition of a dedicated technology to characterize the soft-tissue envelope during TKA has the potential to provide an augmented perspective to the surgeon. As illustrated by the present study, this characterization may be particularly beneficial for junior surgeons.
Finally, in contrast with a similar recent cadaveric study comparing robot assisted TKA and conventional TKA where there were no significant intergroup differences for laxity, the present study established that the usage of instrumented CAOS led to significantly lower ML gap differences than conventional instrumentation.
Figures
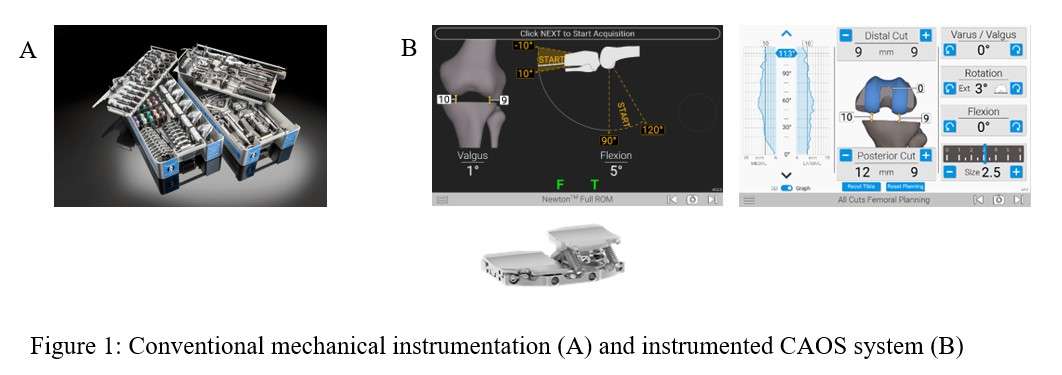
Figure 1
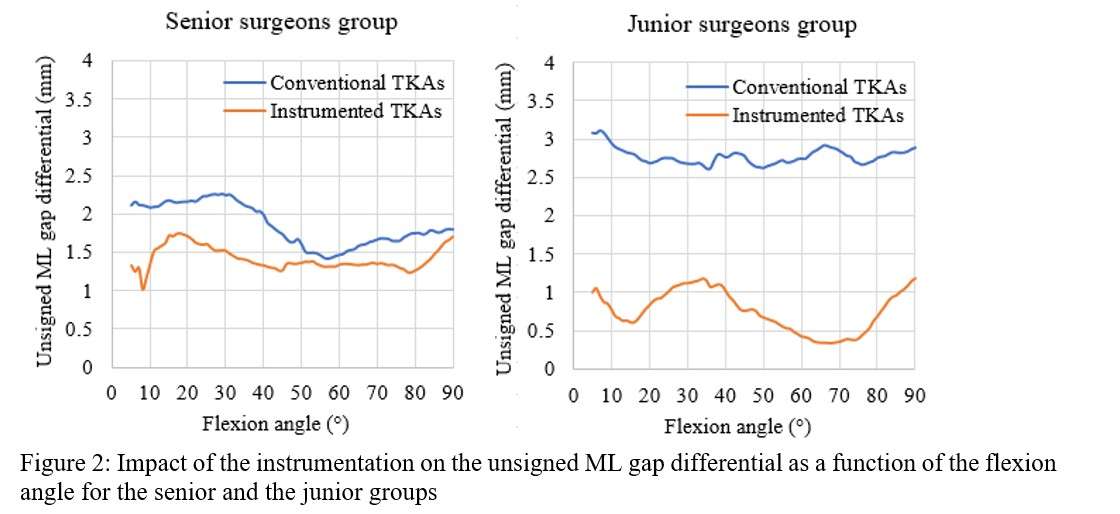
Figure 2#7939
Reliability of Laxity Acquisitions During Navigated Total Knee Arthroplasty - Comparison of Two Techniques
*Laurent Angibaud - Exactech, Inc. - Gainesville, USA
Wen Fan - Exactech - Gainesville, USA
Philippe Dubard - Blue-Ortho - Meylan, France
Matthew Rueff - Exactech - Gainesville, USA
Herman Prieto - University of Florida - Gainesville, USA
Hari Parvataneni - University of Florida - Gainesville, USA
*Email: laurent.angibaud@exac.com
Introduction
Total knee arthroplasty (TKA) continues to be one of the most successful surgical interventions in medicine. Most contemporary developments have been based on bony references to restore a neutral knee alignment. With an attempt to improve patient’s satisfaction, more recent developments have focused on the intra-operative management of soft-tissue balancing surrounding the knee joint throughout the full arc of motion when using a computer-assisted orthopedic surgery (CAOS) system. The aim of this study was to determine and compare the inter- and intraobserver reliabilities of acquiring knee joint laxities during navigated TKA using different techniques.
Methods
Bilateral TKAs using a CAOS system were performed on a fresh-frozen human cadaveric specimen. Prior to any bone cuts, joint laxities were acquired using conventional technique which applied a varus stress test to the knee joint while flexing the limb to acquire lateral laxities, followed by a valgus stress test to acquire medial laxities.
The proximal tibial cut was then performed neutrally to the mechanical axis and an intra-articular tibial distractor was introduced into the joint space. This distractor applied a quasi-constant distraction force regardless of the joint gap. The joint laxities were acquired by manually manipulating the limb through a full arc of motion with the knee joint stabilized by the distraction force.
For each technique, manipulations were performed by 4 surgeons (2 senior and 2 junior surgeons) on 6 occasions on both knees across medial and lateral compartments. The inter- and intraobserver reliabilities were assessed using intraclass correlation coefficients (ICCs) and 95% confidence intervals (CIs).
Results
A total of 96 laxity acquisitions were performed for each technique. Regardless of the compartment (i.e., medial or lateral), the instrumented technique was associated with a higher reliability than the conventional technique for the laxity acquisitions (p=0.017) (Figure 1). For the instrumented technique, the interobserver reliability ranged from moderate to good (Mean ICC=0.72), while for the conventional technique, it ranged from poor to moderate (Mean ICC=0.35) (table 1). Similarly, the intraobserver reliability was consistently higher for the instrumented technique (Mean ICC=0.66) than the conventional technique (Mean ICC=0.41) (table 1). Regardless of the technique, there was no significant difference in the reliability associated with the compartment (p=0.453). The experience level of the user had no statistically significant impact on the reliability of acquisitions (p>0.05).
Conclusion
This study established that the acquisition of knee joint laxities using an instrumented technique was associated with a significantly higher reliability than the conventional manual varus/valgus stress test technique. One aspect relates to the application of a distraction force to the knee joint, which greatly stabilizes the joint during the manipulation of the limb. Also, the manipulation of the limb in neutral alignment for the instrumented technique is easier to consistently apply compared to manual application of valgus or varus stress.
There are still discussions about the amount of distraction force to be applied to the knee joint during the acquisitions. Thus, future developments include fluctuating the input load according to patient-specific parameters.
Figures
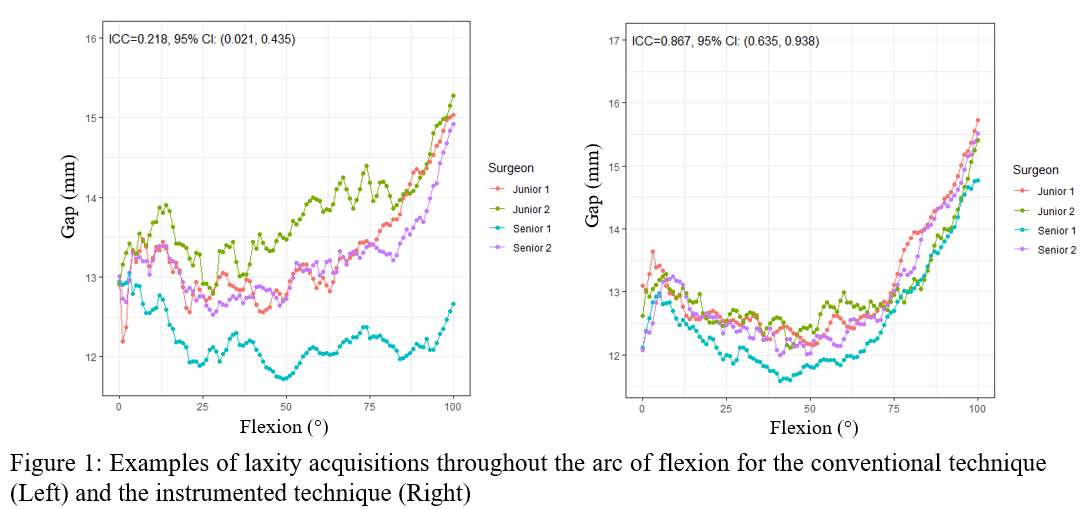
Figure 1
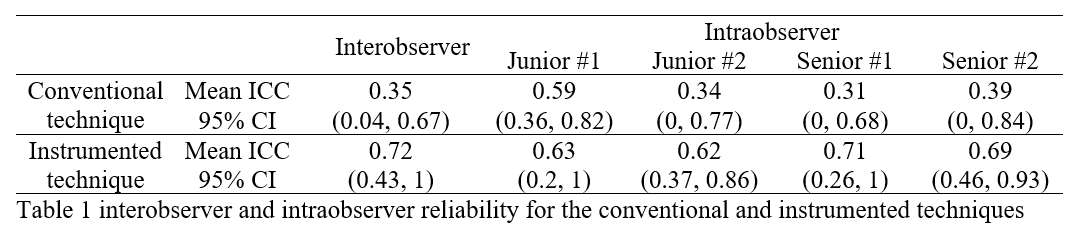
Figure 2#7586
Feeling Better After TKA: Reference Chart for Remotely Collected Pain Scores
*Ricardo Antunes - Stryker - Glasgow, GB
Paul Jacob - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Robert Marchand - Ortho Rhode Island - South County, USA
Andrew Meyer - Stryker - Mahwah, USA
Elaine Justice - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Emily Hampp - Stryker - Mahwah, USA
Matthias Verstraete - Stryker - Fort Lauderdale, USA
*Email: ricardo.antunes@stryker.com
Introduction:
Remote patient monitoring, using wearable devices and connected patient engagement platforms has the potential to improve timely clinical decisions. Patients can be monitored at a higher granularity than can be collected through in practice visits alone, allowing for early detection of complications such as infection. These platforms allow the collection of recovery data from multiple patients, often across multiple practices and spatial domains, that can be used to produce evidence-based reference to support clinical decisions at the level of the individual patient. While some normative references for functional measures (e.g. range of motion) have been published for total knee arthroplasty (TKA), these are still lacking for pain scores. This paper presents a normative recovery model for pain scores collected remotely from TKA patients using a remote data.
Methods:
The VAS pain scores on a 10-point Likert scale were analyzed for TKA patients enrolled in an observational study. Scores from 65 patients reporting at least five scores in the 90 days following surgery, were used to produce a normative recovery model. A nonlinear mixed effects model was fitted, whereby the response variable is assumed to be distributed following a beta-binomial distribution. This discrete value distribution allows to constrain model’s response variable to the non-negative integer domain values of the pain scores, by fixing its count parameter to 10. The mean population pain score was modelled using a smooth function, defined by a 12 hidden-layer neural networks taking the time of pain score collection (x days since surgery) as input. These functions allow to model non-linear relationships in both the expectation and dispersion of the pain scores. The model was fitted using a state-of-the-art Bayesian approach allowing for estimation of the fitted parameters’ uncertainty, including the neural network weights. Model fitting was carried out using Stochastic Variational Inference (maximizing the evidence lower bound, ELBO) with custom scripts in Python.
Results:
The population mean trend shows an increase in pain in the first few days following surgery, higher than the preoperative mean, with wide dispersion showing scores ranging throughout the 10-point scale (Figure 1). After the first week, the expected pain score steadily decreased, resulting in a score no higher than two in 65% of the population beyond 90 days after surgery. The fitted model allows referencing individual patient's pain scores at different stages of recovery, against the model’s predicted distribution. We present the case of a patient with pain scoring outside the model’s expectation coinciding with infection, as an illustration of the potential use of normative models to alert the occurrence of possible complications during recovery (Figure 2).
Conclusion:
We produced a useful reference curve for TKA patient pain scores collected remotely through engagement platforms. This can support early detection of patients that significantly deviate from the reference model and be a useful integration into clinical decision support software tools.
#7590
Evaluation of Range of Motion During Daily Activities Through Knee-Worn Wearable Sensor System After TKA Surgery
*Ricardo Antunes - Stryker - Glasgow, GB
Paul Jacob - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Robert Marchand - Ortho Rhode Island - South County, USA
Elaine Justice - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Andrew Meyer - Stryker - Mahwah, USA
Emily Hampp - Stryker - Mahwah, USA
Matthias Verstraete - Stryker - Fort Lauderdale, USA
*Email: ricardo.antunes@stryker.com
Introduction:
Remote patient monitoring through wearable devices and connected patient engagement platforms provide clinicians with additional visibility to patients’ recovery. These can also allow collection of patient recovery data at higher granularity than can be achieved by traditional outcomes measures, such as collected during practice visits. When these devices include sensors that measure knee angle metrics during activities of daily living, they can further be used for detecting post-operative stiffness and/or a lack of range of motion during the early post-operative period that might require manipulation under anaesthesia (MUAs). Here we present a comparison between range of motion measurements made using a novel knee-worn wearable system used for remotely monitoring patients’ recovery after surgery, and published reports.
Methods:
Following IRB approval and completing the consent process, 92 patients were enrolled in an observational study two to four weeks prior to undergoing unilateral total knee replacement surgery. Patients were instructed on the use a wearable sensor system during a single onboarding visit in clinic. The sensor system consists of two wireless inertial sensor nodes attached above and below the knee joint on the lateral aspect of the thigh and shank respectively. While worn, the sensors regularly measure the patient’s knee flexion angles, which are aggregated hourly into 5-degree bin histograms. These are used to calculate the maximum and minimum knee flexion and stored in a cloud-based platform. The hourly bins were further aggregated into daily knee flexion angle distributions for each patient and the study population. The observed measurements were assessed and compared with published TKA recovery progression studies (Kittelson et al 2020; Kornuijt et al 2019; Mutsuzaki et al 2017; Zhou et al 2015).
Results:
Sensor reported mean minimum and maximum knee flexion angles show a clear recovery trend following surgery (Figure 1). The wearable maximum flexion trend aligns very well with the Kittelson (2020) recovery model throughout the postoperative 90 days considered, and with both Zhou et al (2015) and Mutsuzaki et al (2017) at 30 days postoperative. The latter study reported ~20° less flexion than the wearable mean at day one after surgery. With respect to extension, mean wearable measurements tended to be below published reports, but showed a similar increase in extension range following surgery, particularly in the early post-operative period.
Conclusion:
We have shown that range of motion monitored remotely through a wearable sensor shows variation consistent with the expectation from recovery, and thus it is useful in supporting clinical decisions and facilitate the identification of patients with an abnormal recovery. While our trend was similar to some published reports, it differed from others, but the magnitude of these differences fall within the differences among the considered studies themselves.
#7296
In Vivo Bearing Movement During Non-Weight Bearing Knee Flexion in Mobile Bearing Unicompartmental Knee Arthroplasty
Takahiro Arakawa - University of Tokyo - Tokyo, Japan
*Kenichi Kono - The Scripps Research Institute - San Diego, USA
Tetsuya Tomita - Japan
Shuji Taketomi - Faculty of Medicine, The University of Tokyo - Bunkyo-ku, Japan
Ryota Yamagami - Tokyo University Hospital - Tokyo, Japan
Kohei Kawaguchi - Tokyo University Hospital - bunkyo, Japan
Tomofumi Kage - The University of Tokyo - Tokyo, Japan
Ryo Murakami - University of Tokyo - Tokyo, Japan
Hiroshi Inui - Faculty of Medicine, The University of Tokyo - Bunkyo-ku, Japan
Sakae Tanaka - The University of Tokyo - Tokyo, Japan
*Email: kkouno_tki@yahoo.co.jp
Introduction Mobile bearing unicompartmental knee arthroplasty (MB-UKA) is an effective treatment for patients with unicompartmental knee osteoarthritis or osteonecrosis. While appropriate surgery has been reported to result in high patient satisfaction and good functional recovery, bearing dislocation is a serious complication and its incidence is reported 0.7% among 1000 cases with a 15-year follow-up. Although postoperative bearing movement must be analyzed to determine the mechanism of dislocation, few studies have clarified it. In this study, we examined the inter-component antero-posterior (AP) translation during knee flexion using fluoroscopic kinematic analysis and estimated the AP movement of the bearing.
Method A total of 12 knees in 12 patients who underwent MB-UKA were investigated. Each patient performed knee flexion with their feet floating in a sitting position and the motion was recorded by a fluoroscope (a 17-inch flat panel detector system). A two-dimensional/three-dimensional (2D/3D) registration technique was used to obtain the spatial position and orientation of the implants. The lowest point of the femoral component relative to the tibial baseplate was projected onto it to evaluate the AP translation of the bearing. The AP midpoint of the tibial baseplate was defined zero position; positive and negative values were described as anterior and posterior, respectively. A paired t test was conducted for results. p values < 0.05 were considered statistically significant.
Results The center of the bearing was located -3.2 ± 3.1 mm at knee extension (defined as the initial position). It translated to -1.4 ± 3.6 mm (i.e., anteriorly) until 40° of flexion, then moved to -6.4 ± 5.3 mm (i.e., posteriorly) until 130° of flexion (defined as the final position). The amount of posterior translation from initial position to the final position was 2.7 mm on average, and 3.8 mm on median. Assuming a cutoff value of 3 mm posterior translation from the initial position, 6 cases moved more posterior than it (Group M) and 6 cases moved less than it (Group L). The final position was -9.8 ± 2.4 mm in Group M, whereas it was -2.4 ± 5.1 mm in Group L (p values < 0.05). Comparison of implant alignment, inter-component kinematics and inter-bone kinematics between the two groups showed significant differences in femoral component valgus angle (Group M, -1.3 ± 3.4°; Group L, 3.6 ± 1.0°), tibial component valgus angle (Group M, -1.6 ± 0.9°; Group L, -3.8 ± 1.0°) and external rotation of the femoral component relative to the tibial component at 130° of flexion (Group M, 6.7 ± 8.0°; Group L, 17.4 ± 6.4°). The bearing moved significantly posteriorly after 90° of flexion in group M.
Conclusion On average, during non-weight knee flexion, the center of the bearing was located -3.2 mm from zero position at knee extension, then translated 1.8 mm anterior by 40 degrees of flexion, and moved 5.0 mm posterior by 130 degrees of flexion. It was suggested that femoral component valgus angle, tibial component valgus angle and inter-component rotation at 130° of flexion may have affected the amount of AP translation.
#7720
The Impact of Implant Design and Surgical Alignment on Posterior Stabilized Knee Kinematics
*Luke Aram - DePuy Synthes Joint Reconstruction - Warsaw, USA
Amit Mane - DePuy Synthes - Warsaw, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: laram@its.jnj.com
Introduction: Studies have recognized the presence of patient-perceived noise generation after posterior stabilized (PS) knee replacement1. Such patients were more likely to report post-operative functional limitations and the presence of a limp, joint swelling and stiffness2. In another fluoroscopic study, researchers recorded vibrations (sound) during deep knee bend (DKB)fluoroscopy3 and found high vibrations correlated with impact spikes and an irregular transition during initial CAM-post engagement3. Comprehensive analysis of the T-F joint kinematics and CAM-post engagement mechanics may shed more light on such irregularities. Therefore, the objective of this study was to investigate the impact of implant design and surgical alignment on the T-F kinematics of two PS-knee solutions and observe mechanism of the impact spikes during CAM-post engagement.
Methods:
A half-factorial design of experiments (DOE) was constructed to evaluate the impact of tibial implant slope (0⁰ and 5⁰), femoral implant flexion (0⁰ and 5⁰), and collateral ligament stiffness (normal and 50% reduced) on the kinematics of two different PS TKA solutions. A DKB simulation, from 0⁰-120⁰, of all configurations was conducted using a previously validated4 Forward Dynamics Model (FDM)(See Figure 1).
Two PS TKA solutions included, the Attune® PS (DePuy-Synthes) and Sigma® PS (DePuy-Synthes) total knee arthroplasty (TKA). The Attune® femoral component includes the GRADIUS™ (gradually reducing sagittal radius) geometry while the Sigma® has a multi-radii J-curve. The medial and lateral Femoral Lowest Point (LP) motions for all runs were reported during simulated DKB. From LP motion, four output parameters were calculated: anterior medial slide in mid flexion, post engagement angle, internal-external rotation in flexion, and screw-home rotation in extension.
Results: The LP kinematic for both TKAs are shown in Fig.-2. Tibial implant slope influenced the Femoral anterior slide, showing increase in anterior slide with increasing posterior slope. Whereas CAM-post engagement occurred at later flexion angles with higher posterior slope. Additionally, with 5⁰-tibial slope, the LP motion curve observed an abrupt change in direction when the post engaged. Comparing the two implant designs, Sigma® experienced posterior slide in early flexion (≤20⁰ flexion), switched to anterior slide until CAM-post engagement, followed by abrupt reversal in motion to posterior until terminal flexion . In contrast, the Attune TKA demonstrates significantly less anterior translation and a smooth CAM-post engagement without abrupt changes in direction.
Conclusion: Previous clinical study found the incidence of hearing or feeling noise was less with the Attune1 (compared to Sigma, 17.7% vs 30.9%; P=0.02). The smooth CAM-post transition may have reduced the occurrence of noise. Additionally, the interactive DOE approach highlighted Tibial posterior slope as the most influencing factors, amongst studied variables, to affect the CAM-post mechanics and potentially leading to patient perceived noises. Therefore, in summary, the study indicated criticality of both implant design and surgical alignment impact PS TKA kinematics. Thus, surgeons should consider the CAM-post engagement and the potential for impact spikes and/or noise generation when selecting tibial slope.
References:
- Ranawat et.al-JOA 2016
- Nam et.al-CORR 2017
- Zingde PhD Dissertation 2015
- Khasian et.al. J. Arthroplasty 2020
- Fitzpatrick et al-JOR 2012
Figures
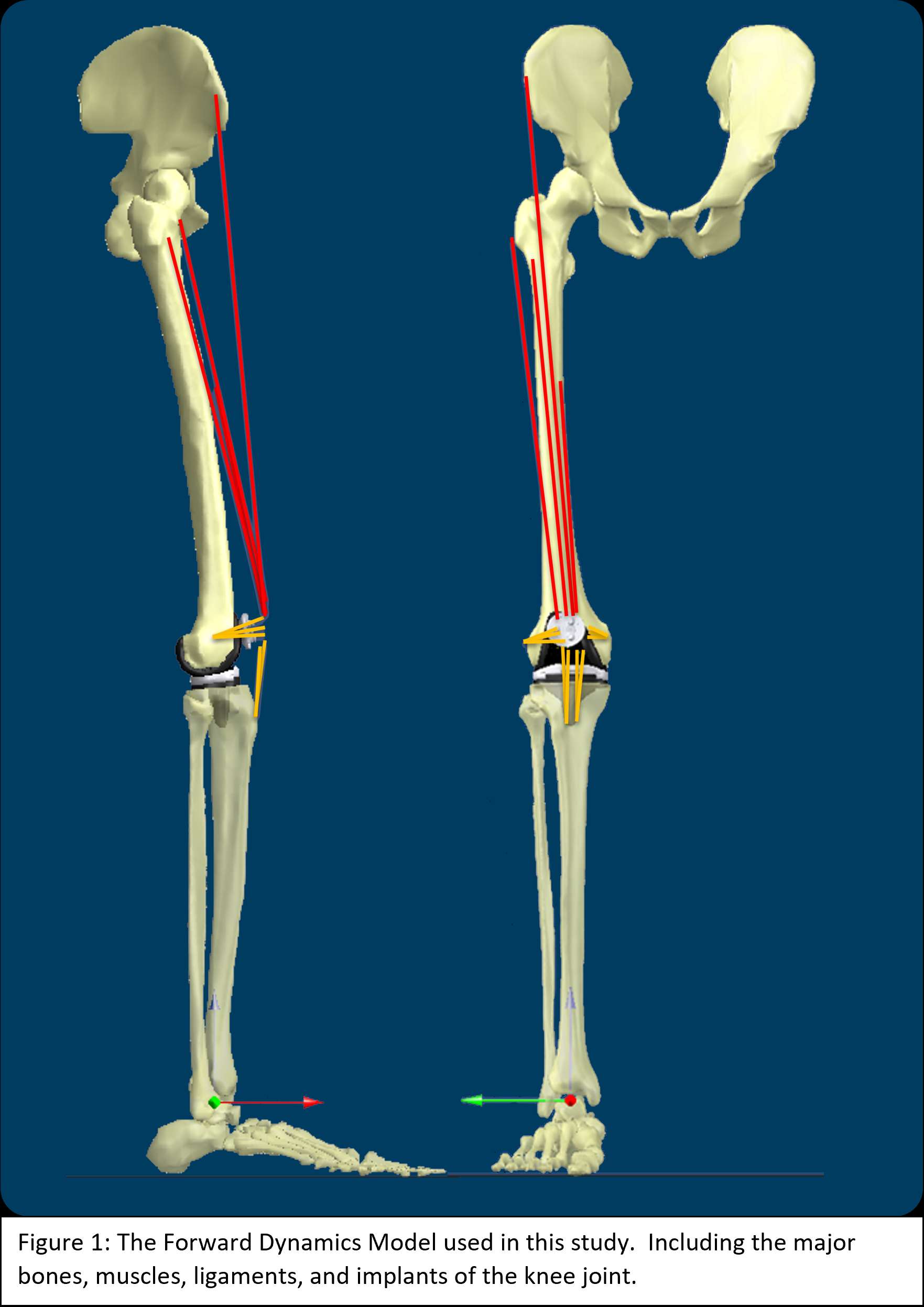
Figure 1
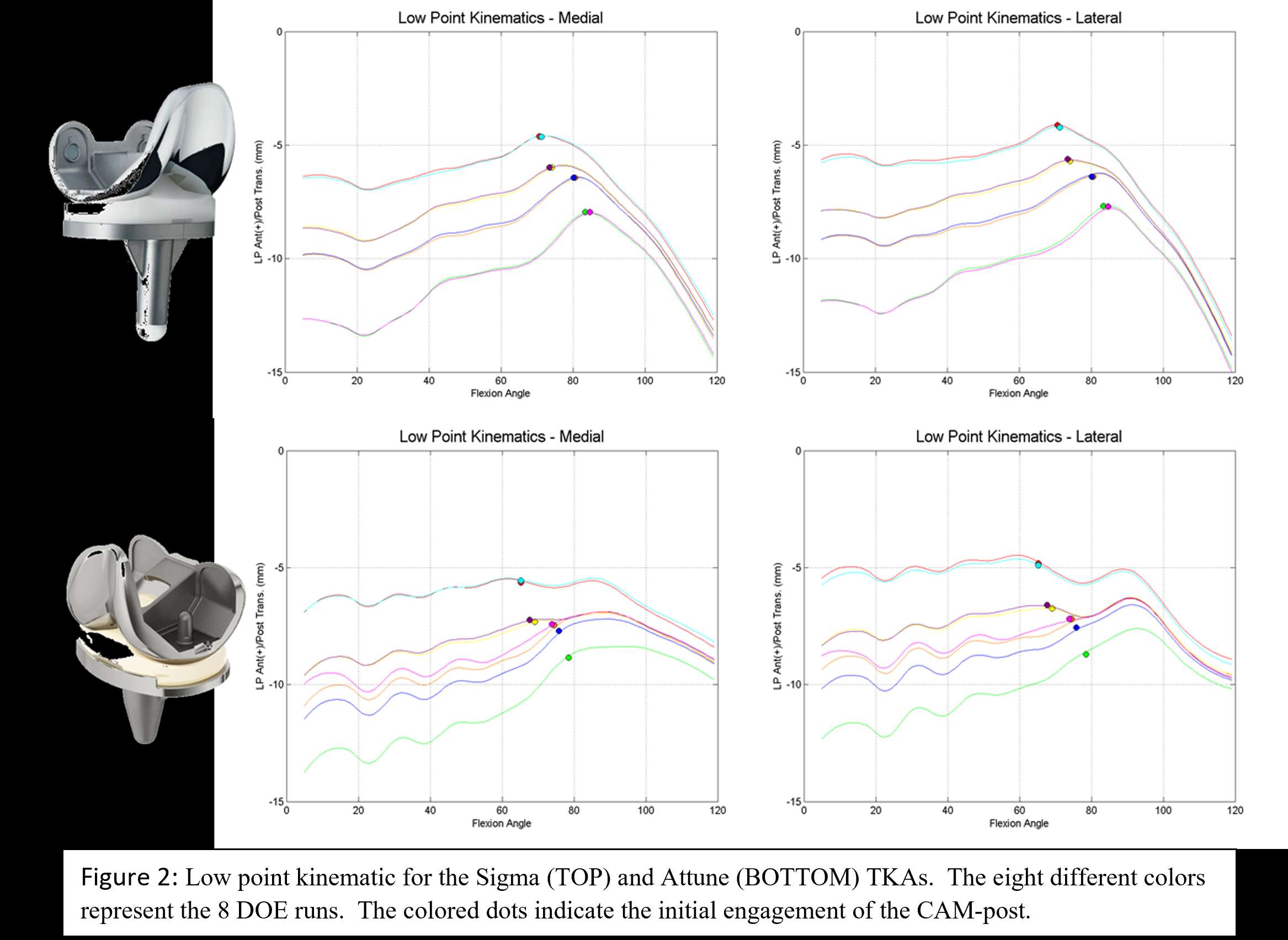
Figure 2#7740
The Impact of Patient Specific Alignment on Initial Fixation of Cementless Tibial Implants
*Luke Aram - DePuy Synthes Joint Reconstruction - Warsaw, USA
Eric Peckenpaugh - DePuy Synthes Joint Reconstruction - Warsaw, USA
Chase Maag - DePuy Synthes - Warsaw, USA
*Email: laram@its.jnj.com
Introduction: Design evolution of total knee arthroplasty (TKA) has improved implant durability and clinical outcomes. However, it has been reported that some patients have limited satisfaction with their operated knees1. To increase patient satisfaction, there has been growing interest in patient specific alignment in TKA2,3. The patient specific alignment (PSA) technique aims to replicate the natural joint line of the patient; typically, the tibial component is implanted in slight varus alignment while still maintaining the long leg (hip-knee-ankle) within ±3° from neutral alignment. However, there is limited data on how patient specific alignment impacts the fixation of cementless tibial implants.
The objective of this study is to investigate the initial fixation of the ATTUNE® cementless tibial implants in PSA by directly comparing it to Attune cementless tibial implants in mechanical alignment (MA). The micromotion between the implants and synthetic bone model will be directly measured while under loading from the AMTI VIVO test frame.
Methods: Alignment specific physiological loading was determined using telemetric tibial implant data from Orthoload4 and applying it to a validated finite element lower limb model developed by the University of Denver5. Three activities were selected for the loading section of this study: gait, stair descent, and deep knee bend. Using the lower limb model, hip and ankle external boundary conditions were applied to the ATTUNE® knee. The kinetics and kinematics for each activity were then extracted from the model for both MA and PSA.
Testing included impacting the tibial implants into the foam bone and securing the tibial construct to the AMTI VIVO joint simulator. Physiological loading conditions, including gait, stair-descent, and deep knee bend activities, were applied while images of the tibial construct were collected using a GROM DIC system to determine the micromotion of the tibial implant.
Point-to-point distance calculations were made for the tibial construct using the 4 reference point markers (Figure-1). The software tracked each point’s location through the images and could therefore track the distances through five captured cycles of each activity. The maximum distance increase within each cycle was calculated and the average of those values was calculated.
Results: A result summary is listed in Table-1. Testing included fixed bearing implant micromotion and rotating platform implant micromotion. A two-way ANOVA using a 0.95 confidence interval was conducted at each measurement location that examined the effect of physiological loading on initial fixation micromotion. For all three loading conditions evaluated (gait, stair descent, and deep knee bend), the average micromotion of the patient specific aligned Attune Cementless Tibial Base was not significantly different from the average micromotion of the Attune Cementless Tibial Bases in mechanical alignment.
Conclusion: This study indicated that patient specific alignment, as defined with the alignment limits of this study, does not adversely affect the initial fixation of ATTUNE® cementless tibial implants.
References:
- Bourne et.al CORR 2010
- Dossett et.al JBJSB 2014
- Hutt et.al Int-Orthop 2016
- Bergmann 2008. <http://Orthoload.com>
- Fitzpatrick et.al. Computer Methods in Biomechanics and Biomedical Engineering 2012
Figures
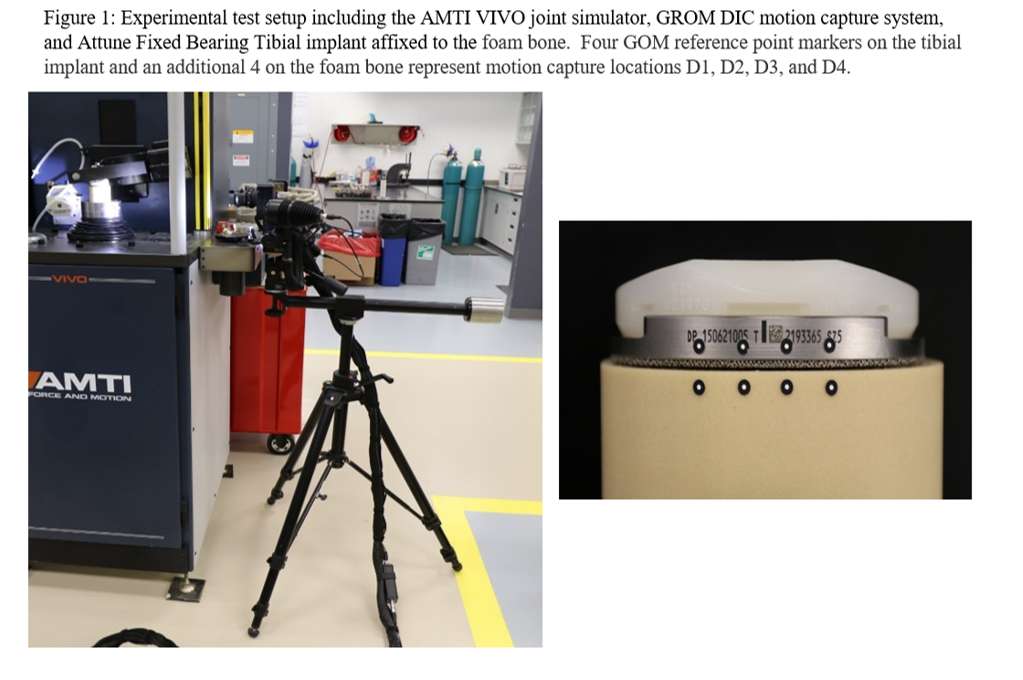
Figure 1
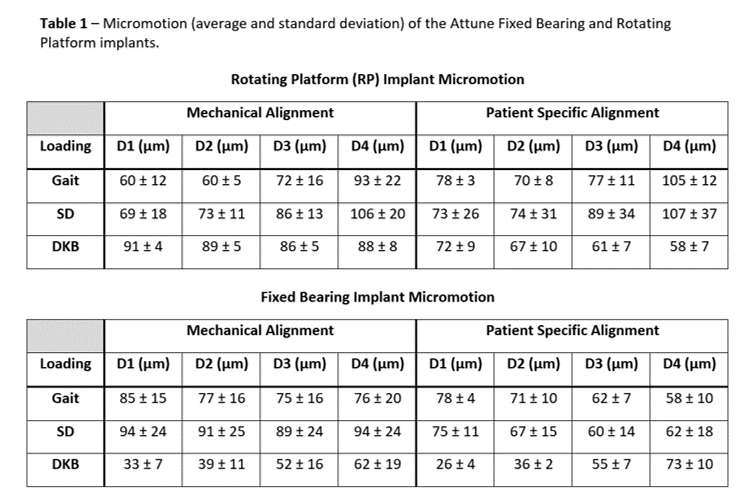
Figure 2#7495
Prediction of Soft Tissue Balancing in Total Knee Replacement
*Daniele Ascani - Medacta International SA - Chiasso, Switzerland
Massimiliano Bernardoni - Medacta International SA - Castel San Pietro, Switzerland
Claudia Mazza' - The University of Sheffield - Sheffield, United Kingdom
*Email: ascani@medacta.ch
Introduction
Inadequate soft tissue balancing is still one of the major unsolved problems in total knee replacement (TKR) [1], mostly caused by surgical techniques ineffectively addressing the balancing of the knee envelope [2]. Preoperative planning and advanced surgical execution tools such as patient-specific guides, or robotic/navigation, allow to accurately achieve what planned. However, the influence of the implants position on the soft tissue balancing is still ignored and left to the surgeon experience, intraoperatively.
The goal of this study was to develop a patient-specific knee model to account for the soft tissue balancing that can be integrated in the surgical workflow. This biomechanical model allows to predict intraoperatively the postoperative elongation of the knee ligaments allowing the surgeon to take data-driven decisions before performing the cuts.
Methods
The first part of the study was the design of an algorithm to accurately estimate the origins and insertions of the knee ligament from CT images, necessary for the creation of the biomechanical models [3] (Figure 1). Then, the study comprises the development of CT based static and quasi-static knee models able to estimate the postoperative length of the collateral lateral ligaments using a dataset of seven TKR patients; In addition, a subject-specific dynamic musculoskeletal model of the lower limb was created using in vivo knee contact forces to perform the same analysis during walking [4]. The three models of increased complexity were then compared in terms of outputs to understand if there was a significant correlation.
Results
The average difference of origins and insertions of the knee ligaments between the values predicted by the algorithm on CT images and those estimated on the MRI was 2.1mm (SD 1.2mm) for the femur and 2.7mm (SD 1.0mm) for the tibia, respectively. The results showed that the subject-specific static model was the best solution in terms of performance and results since there was a significant correlation between the three models. The possibility of using a static model which is computationally lighter, allowed the adoption of this prediction in a real time surgical workflow.
Conclusion
The procedure developed in this study allows to predict the postoperative length of the knee collateral lateral ligaments by using CT images of the patient. This algorithm, originally proposed in [3] has been implemented in the NextAR TKA system (Medacta International SA, Castel San Pietro, CH) which allows to intraoperatively measure in real time the length of the collateral lateral ligaments. The surgeon is finally able to see in real time how the angles and the heights of the bone cuts affects the soft tissue balancing before executing the planning. The final goal is to adjust intraoperatively the preoperative planning by using: real time data on the patient-specific soft tissue, and the prediction on how changing the planning would affect the ligaments postoperatively. Current studies are addressing the clinical benefit of including the prediction of the soft tissue balancing in the surgical workflow for TKR.
Figures
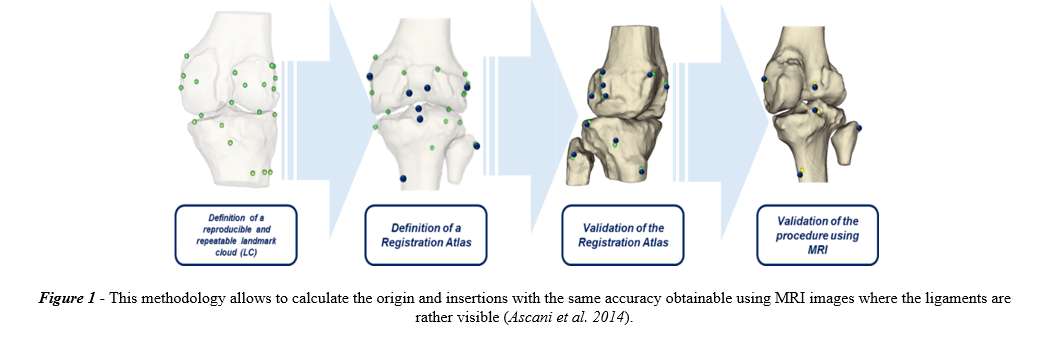
Figure 1#7498
Nextar Rsa: Augmented Reality Surgical Guidance for Accurate Glenoid Component Positioning in Reverse Shoulder Arthroplasty
*Daniele Ascani - Medacta International SA - Chiasso, Switzerland
Massimiliano Bernardoni - Medacta International SA - Castel San Pietro, Switzerland
*Email: ascani@medacta.ch
Introduction
Relevant literature[1], reported that glenoid components placed with conventional instrumentation had an average deviation from the preoperative planned position of 8° (SD 8.2°) in retroversion, 7° (SD 7.9°) in inclination and 3mm (SD 2mm) for the glenoid starting point (entry point of glenoid K-wire). The introduction of patient specific instrumentation (PSI) allowed to improve the accuracy, Hendel et al [2] compared the execution of a CT-based 3D preoperative planning by using PSI and conventional instrumentation in 31 patients undergoing to glenoid component positioning for total shoulder arthroplasty. The results showed that the combination of 3D preoperative planning with patient and implant specific instrumentation enhances the accuracy of the glenoid component compared to conventional instrumentation. The goal is to demonstrate that the NextAR RSA system, which is a novel augmented reality surgical guidance system, improves the accuracy of the glenoid component compared to the standard techniques.
Methods
The 3D models of 12 cadaveric shoulders were obtained from CT images, then 3 surgeons preoperatively planned the position of the glenosphere component virtually, simulating a reverse shoulder arthroplasty. The preoperative planning allowed to set the following parameters:
- Glenoid base plate insertion point
- Glenoid base plate retroversion
- Glenoid base plate inclination
- Glenoid base plate medio-lateral position
The cadaver specimens were operated using a delto-pectoral approach and the NextAR RSA system allowed to accurately place the glenoid components by guiding the surgeon, through the augmented reality glasses (Figure 2). The surgical parameter set during the preoperative planned were registered in real time during the surgery, the target was the accurate execution of the preoperative planning. Post-operative CT scans were performed to assess the glenoid component positioning: the accuracy is intended as the deviation between the preoperatively planned values compared with the postoperative CT images.
Results
The results showed a significant correlation between the planned and executed values, mean deviation for the angles was 1,5° (SD 0.8°), whilst for the distances 0,9 mm (SD 0.5mm), respectively. The comparison between the values measured during the cadaveric testing by the NextAR RSA system and the postoperative results obtained on the postoperative CT images showed an average accuracy of 0,6° (SD 0.4°) and 0,6 (SD 0.5mm).
Conclusion
The cadaveric study has been performed to demonstrate the accuracy of the NextAR RSA shoulder system in performing a complete total reverse shoulder arthroplasty surgery for glenoid preparation. The results have been calculated using as ground truth the 3D models created from postoperative CT images. In particular, the study investigated the deviation between the preoperative planning values and the postoperative analysis. The results confirmed the high accuracy of NextAR RSA system showing an average deviation of 1,5° for the angles and 0,9 mm for the distances. This study demonstrated that the augmented reality surgical guidance can largely improve the glenoid component positioning compared with the standard available techniques (PSI and conventional). In conclusion, the surgeons would benefit from the NextAR RSA augmented reality system to execute a preoperative plan to position the glenoid component accurately in the planned position.
Figures
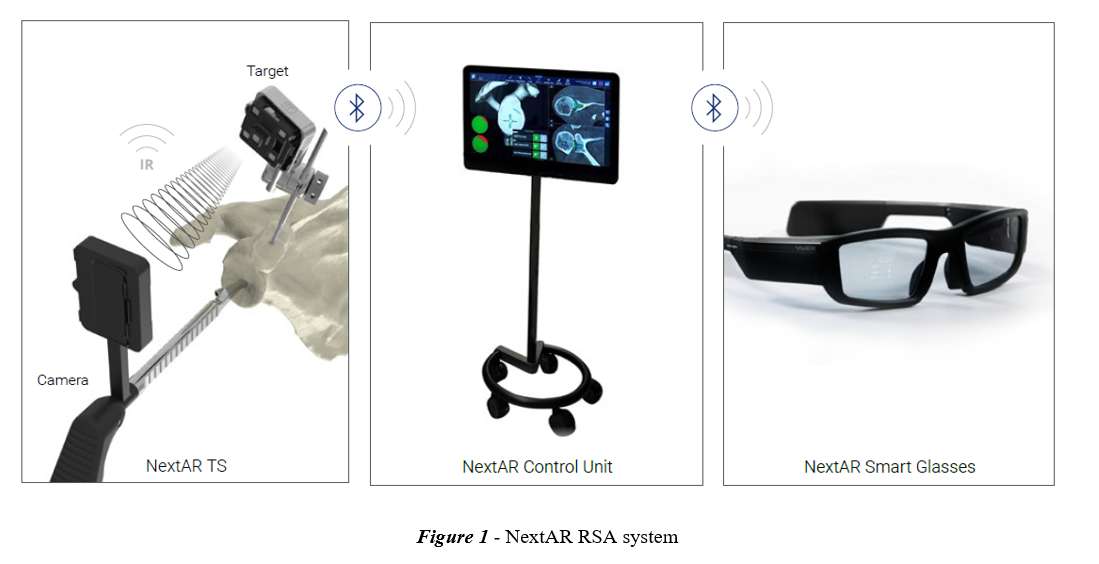
Figure 1#7502
Development of an Open-Loop Position Controller With Iterative Learning for Ex-Vivo Shoulder Motion Simulation
*David Axford - Western University - London, Canada
Robert Potra - Mathys Ltd Bettlach - London, Canada
Antonio Arenas-Miquelez - Hospital quironsalud San Jose - Madrid, Spain
Desmond Bokor - Macquarie University Hospital - Sydney, Australia
Richard Appleyard - Macquarie University - Sydney, Australia
Sumit Raniga - Roth|McFarlane Hand and Upper Limb Centre - London, Canada
Louis Ferreira - University of Western Ontario - London, Canada
*Email: david.t.axford@gmail.com
Introduction
Reverse total shoulder arthroplasty (RTSA) is growing in popularity and is an effective treatment for a variety of shoulder pathologies. RTSA can improve elevation range of motion by reversing the geometry of the joint and increasing deltoid efficiency. However, complication rates for RTSA remain higher than for a conventional prosthesis.
Ex-vivo shoulder motion simulators have been used to better understand RTSA biomechanics, but current simulators can only perform simple planar motions at quasi-static speeds. To better understand RTSA biomechanics in the context of activities of daily living, it is important to simulate movements associated with functional tasks.
The purpose of this study was to evaluate the use of open-loop position control with iterative learning to simulate faster and more complex motions than what has been previously reported.
Methods
A shoulder motion simulator was developed that uses an open-loop tendon position controller with iterative learning to control joint motion (Figure 1). This simulator controlled joint orientation by prescribing the excursions of eight linear actuators attached to shoulder muscle tendons. Prior to motion simulation, actuator excursions were mapped as a function of joint angle and these maps were used to determine initial actuator excursions. The initial excursions were played in an open-loop fashion and an iterative learning routine was used to reduce kinematic errors by adjusting the actuator excursions.
Using a single cadaveric specimen with an implanted RTSA prosthesis, a faceted circumduction motion was simulated to evaluate the simulators’ kinematic tracking accuracy while performing complex, multiplanar motion. Similarly, to evaluate the kinematic tracking accuracy for high simulation speeds, abduction/adduction was generated with a peak glenohumeral rotation speed of 25 degrees/second. The simulator’s kinematic tracking accuracy was assessed using maximum kinematic error and root mean square error (RMSE). The simulator’s repeatability was assessed by calculating the average standard deviation for three repeated trials of 25 degrees/second abduction/adduction.
Results
For faceted circumduction (Figure 2), RMSE was 0.2, 0.3, and 0.8 degrees for elevation, plane of elevation, and axial rotation, respectively. The maximum recorded error was less than 1.6 degrees for all three joint angles. For abduction/adduction (Figure 3), the RMSE was 0.3, 0.7, and 0.7 degrees for elevation, plane of elevation, and axial rotation, respectively. The maximum recorded error was less than 2.0 degrees for all three joint angles. The average standard deviation across three simulated abduction/adduction cycles was 0.2 degrees for all joint angles.
Conclusions
This study presents a preliminary evaluation of a shoulder motion simulator that uses a novel open-loop position control architecture. As demonstrated, the simulator has high accuracy and repeatability when simulating complex multiplanar and high-speed motions. With this functionality, the shoulder motion simulator can be used to simulate functional shoulder movements and can provide new insights into current understandings of RTSA biomechanics.
Figures
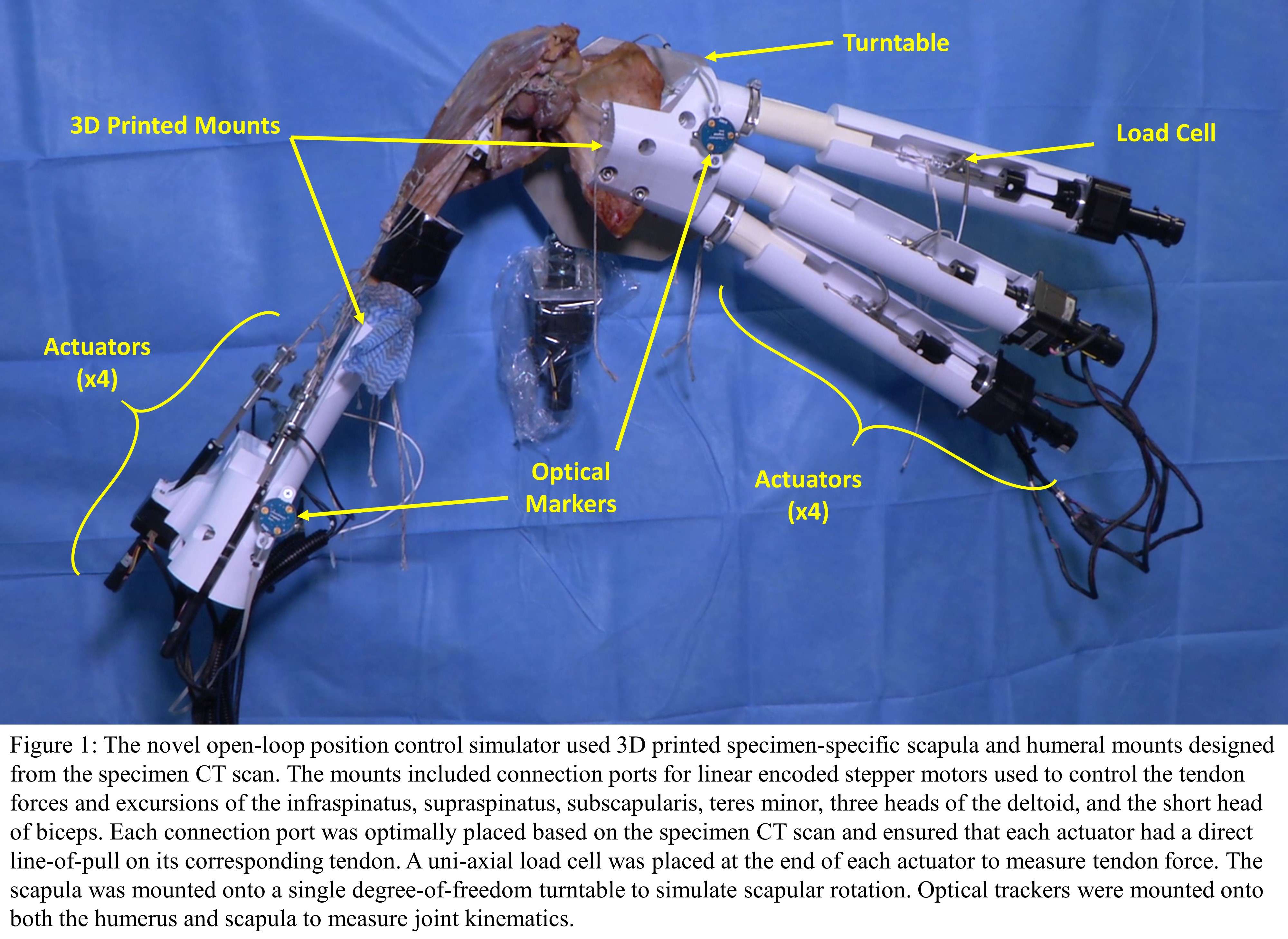
Figure 1
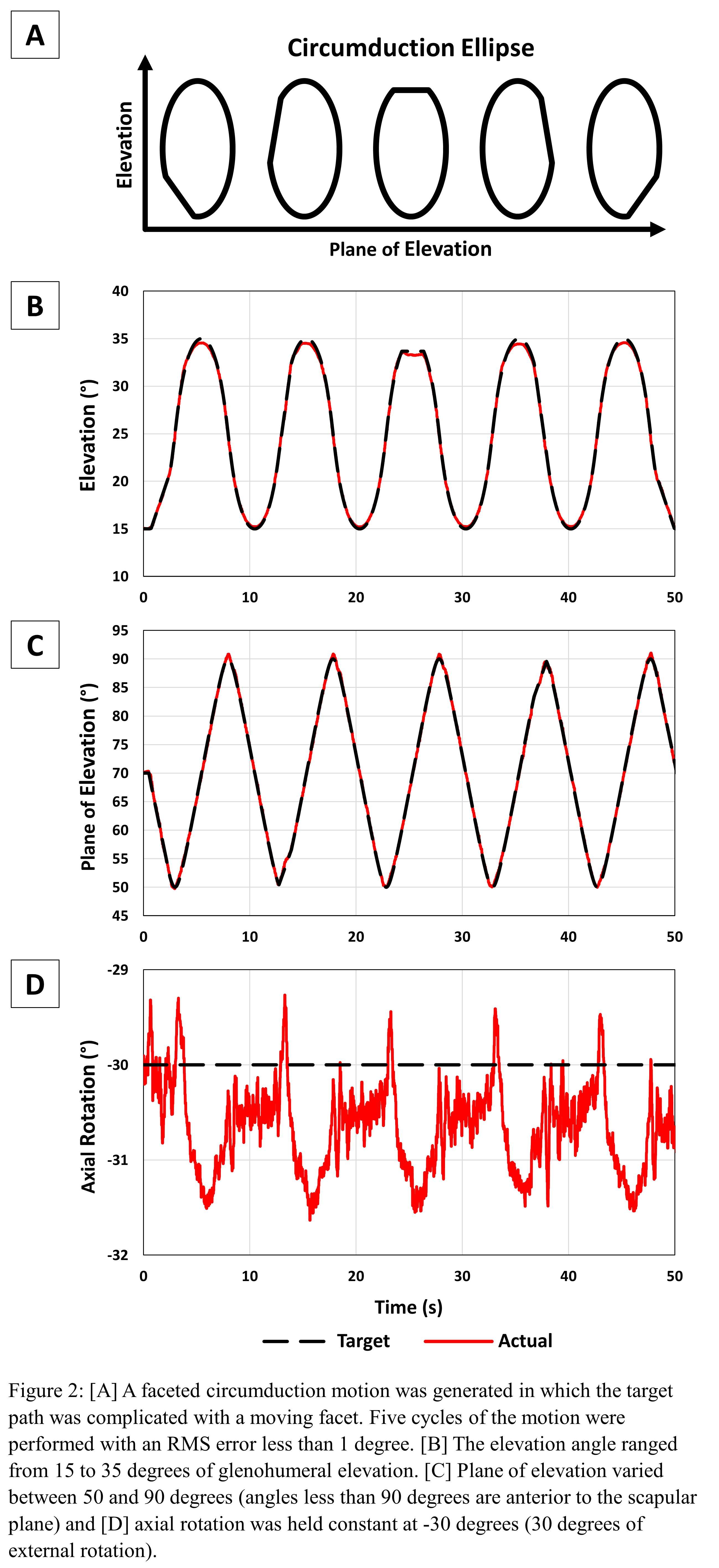
Figure 2
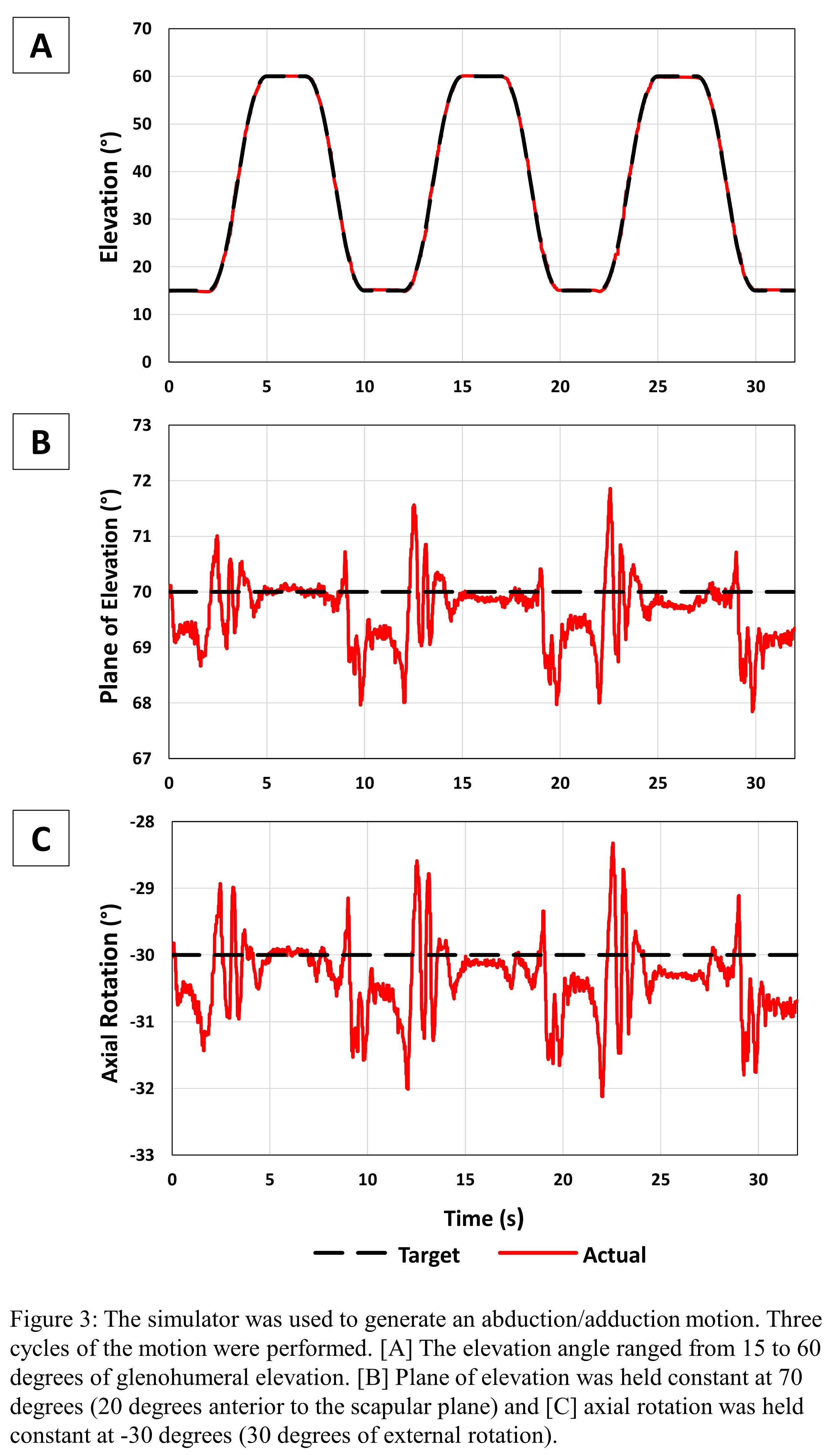
Figure 3#7504
The Effect of Repairing the Subscapularis Tendon Following Reverse Total Shoulder Arthroplasty: A Preliminary Ex-Vivo Study
*David Axford - Western University - London, Canada
Robert Potra - Mathys Ltd Bettlach - London, Canada
Antonio Arenas-Miquelez - Hospital quironsalud San Jose - Madrid, Spain
Desmond Bokor - Macquarie University Hospital - Sydney, Australia
Richard Appleyard - Macquarie University - Sydney, Australia
Sumit Raniga - Roth|McFarlane Hand and Upper Limb Centre - London, Canada
Louis Ferreira - University of Western Ontario - London, Canada
*Email: david.t.axford@gmail.com
Introduction
A topic often debated in reverse total shoulder arthroplasty (RTSA) is whether to repair the subscapularis tendon following RTSA implantation. Some suggest that there are no clinical benefits to repairing the tendon while others recommend repairing the subscapularis whenever possible.
Ex-vivo shoulder motion simulators are often used to study the effects of shoulder pathology and treatment on joint function. However, the controllers used by current simulators group muscles into antagonistic pairs based on their primary function and do not control each muscle individually. As a result, it is challenging to remove muscles such as the subscapularis from the controller without needing to alter the controller design.
The purpose of this study was to use an open-loop tendon excursion controller with individual muscle control to evaluate the effect of repairing the subscapularis tendon after RTSA in a cadaver biomechanical model.
Methods
A shoulder motion simulator that uses an open-loop tendon excursion controller was used to control joint motion (Figure 1). The controller specified muscle actuator excursions to produce a target motion. These excursions were determined using specimen-specific muscle actuator excursion maps. To reduce kinematic errors, an iterative learning routine was used to adjust each actuator excursion individually.
Using a single cadaveric specimen with an implanted RTSA prosthesis, abduction/adduction was generated. Initially, the motion was performed by actuating eight muscles including the subscapularis. Following this, the subscapularis actuator was deactivated, and the actuator excursions for the remaining seven actuators were replayed. To compensate for changes in joint kinematics due to the lack of the subscapularis, the remaining seven actuator excursions were adjusted using an iterative learning routine. For each motion, kinematic tracking accuracy was measured using maximum kinematic error and root mean square error (RMSE).
Results
The RMSE for abduction/adduction (Figure 2) with all eight muscles being simulated was 0.2, 0.3, and 0.3 degrees for elevation, plane of elevation, and axial rotation, respectively. The maximum recorded error was less than 1 degree for all joint angles. Repeating the same motion after deactivating the subscapularis muscle resulted in RMSE of 1.1, 0.4, and 13.8 degrees for elevation, plane of elevation, and axial rotation, respectively. The maximum errors for elevation and plane of elevation remained below 1.4 degrees but axial rotation error increased to 18.9 degrees. After compensating for the loss of the subscapularis, RMSE was 1.1, 6.2, and 12.4 degrees and the maximum recorded errors were 1.6, 12.9, and 22.6 degrees for elevation, plane of elevation, and axial rotation, respectively.
Conclusions
This controller allows muscles to be easily deactivated and a novel learning algorithm can adjust the remaining muscle excursions in an attempt to restore kinematics. This study showed that when the subscapularis was deactivated, there was a loss of internal rotation, and the remaining muscles were not able to compensate at low elevation angles, which is an observation often made clinically. This functionality will allow biomechanical investigation of arthroplasty components to be conducted while modeling clinically relevant losses of selected muscle/tendon functional units.
Figures
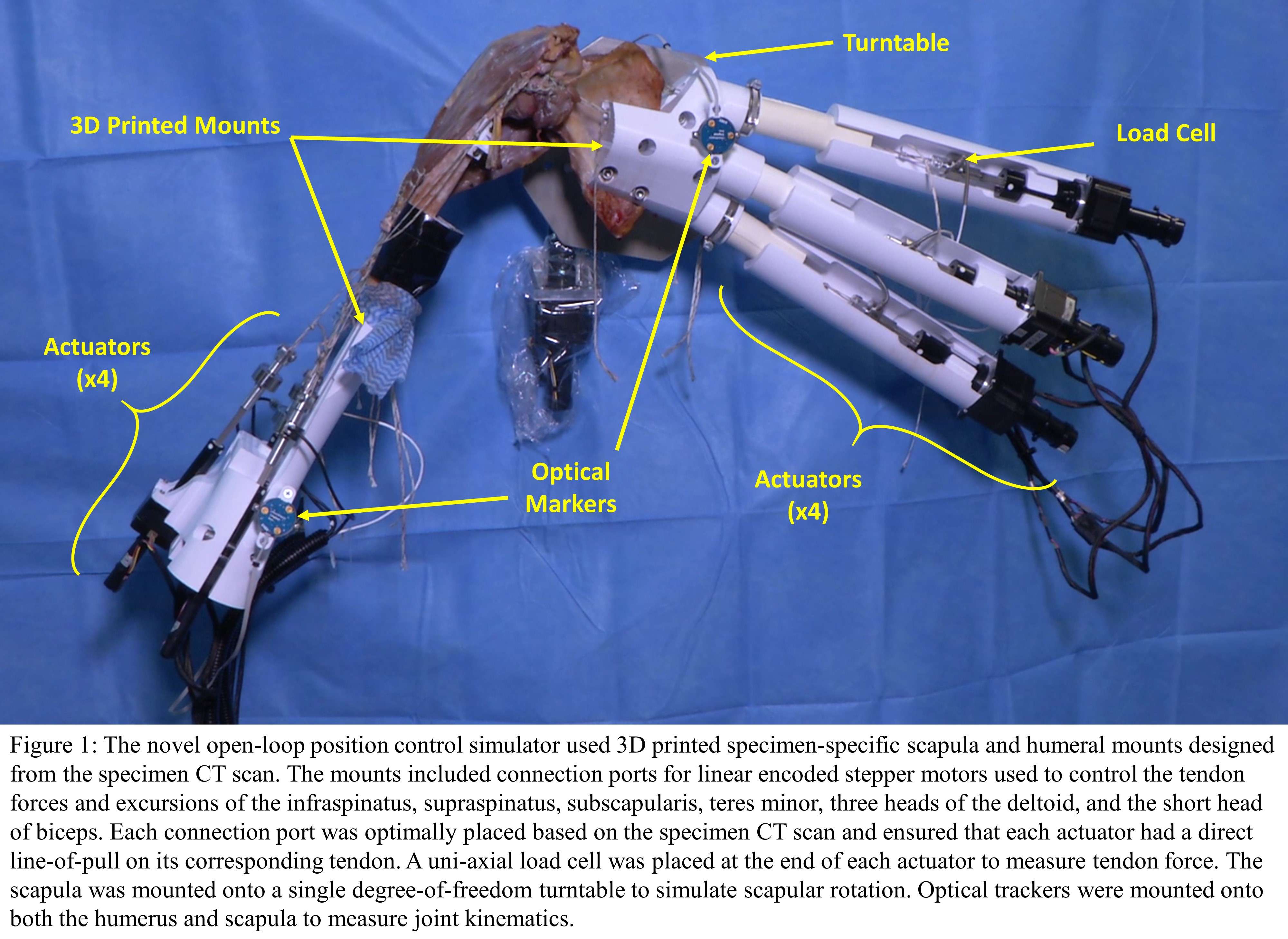
Figure 1
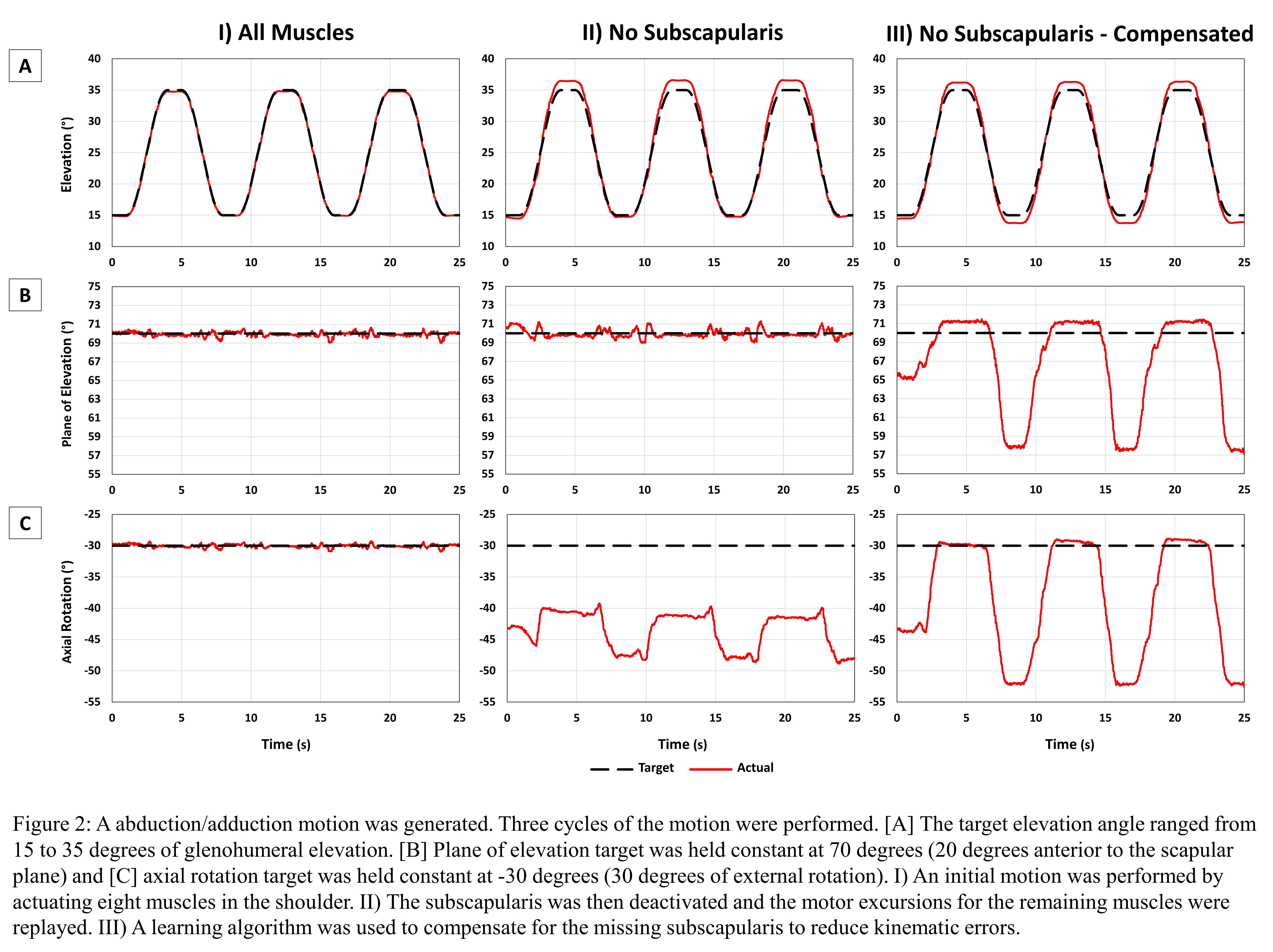
Figure 2#7314
Accuracy of Advanced Active Robot for Total Knee Arthroplasty: A Cadaveric Study
Yong-Beom Park - Chung-Ang University Hospital - Seoul, South Korea
*Han-Jun Lee - Chung-Ang University - Seoul, South Korea
Seong Hwan Kim - Hyundae general Hospital, Chung-Ang University - Namyangju-Si, South Korea
Seok-Ho Baek - Chung-Ang University Hospital - Seoul, South Korea
Kyu-Hwang Kim - Chung-Ang University Hospital - Seoul, South Korea
*Email: gustinoLHJ@nate.com
Purpose: Although the accuracy of other types of robotic systems for total knee arthroplasty (TKA) has been assessed in cadaveric studies, no investigations have been performed to evaluate this newly advanced active robotic system. Therefore, the authors aimed to analyze the accuracy of bone resection in terms of thickness and alignment in a cadaveric study.
Methods: Three cadaveric specimens (six knees) and an active robotic system (CUVIS Joint, CUREXO) were used in the study. Three surgeons with different experience of robotic TKAs performed this cadaveric study using the same robotic protocol with two different implant designs. The thickness and angle of bone resection planes obtained from the optical tracking system and the difference between resection planes and the planning data were assessed to determine accuracy (see Figure 1).
Results: With respect to the overall resection accuracy compared to the plan, the cutting depth accuracy was within 1.0 mm mean of root mean square (RMS), and the resection angle accuracy in terms of sagittal, coronal, and axial planes was within 1.0° mean RMS. In contrast, no significant differences were observed between the planned and measured values in terms of the resection angles and cutting thickness. The hip–knee–ankle angle at postoperative evaluation was 0.7° ± 0.7° (RMS 1.0°).
Conclusion: This in vivo study suggests that the use of this newly advanced active robotic system for TKA demonstrates a high degree of accuracy in terms of resection thickness and alignment. This finding supports the clinical application of this advanced robotic system.
Figures

Figure 1#7315
Advanced Active Robotic Total Knee Arthroplasty: A Learning Curve of Surgical Time and Alignment Accuracy
Yong-Beom Park - Chung-Ang University Hospital - Seoul, South Korea
*Han-Jun Lee - Chung-Ang University - Seoul, South Korea
Seong Hwan Kim - Hyundae general Hospital, Chung-Ang University - Namyangju-Si, South Korea
Seok-Ho Baek - Chung-Ang University Hospital - Seoul, South Korea
Kyu-Hwang Kim - Chung-Ang University Hospital - Seoul, South Korea
*Email: gustinoLHJ@nate.com
Background: Several robotics of total knee arthroplasty (TKA) has been introduced for improving outcomes. A newly advanced active robotic system with automated bony resections is recently applied in clinical practice (see Figure 1). As with all new technology, the new system is associated with a learning curve. Therefore, the aim of this study is to determine the learning curve necessary to minimize the operative time and to evaluate the alignment accuracy when using advanced active robotic (AR) TKA (AR TKA).
Methods:
In AR TKA, advanced active robotic technology refers to the use of a robot for planning and bone preparation by a milling tool under surgeon guidance and control. Operative times, implant and limb alignment were evaluated. Sixty patients were classified into 6 groups according to the day of surgery. The differences among 6 groups were analyzed to assess learning curves for operative time, implant alignment and lower leg alignment.
Results: AR TKA was associated with a learning curve of more than 40 cases for operative time (p<0.001). After 40 cases, the operative time was significantly decreased by approximately 15-20 minutes (see Figure 2). The precision of implant positioning and lower limb alignment showed no learning curve. An average deviation for the coronal planes of the femoral and tibial implants from the preoperative plan was observed less than 1.0°. Limb alignment showed a mean deviation of 1.6° towards varus postoperatively compared to the intraoperative plan.
Conclusion: Active Robotic total knee arthroplasty is associated with a learning curve of 40 cases for operative time. There was no learning curve-associated component position. This study demonstrated a high degree of accuracy with regard to implant position and lower limb alignment. Based on these findings, advanced active robotics represents a viable and safe technique for primary TKA.
Figures

Figure 1
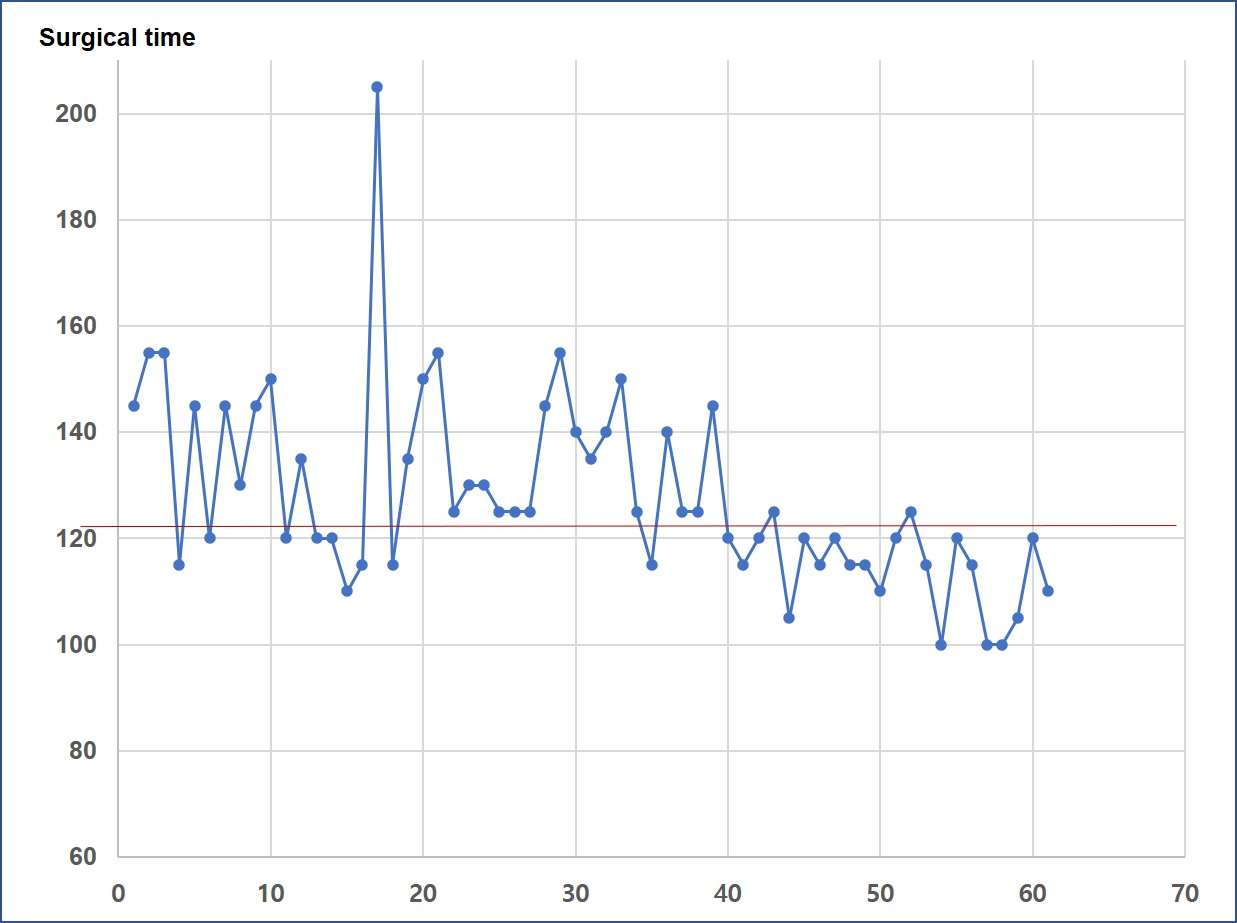
Figure 2#8029
Invited Talk: Machine learning enables clinically practical radiographic assessment of joint kinematics.
*Scott Banks - University of Florida - Gainesville, USA
*Email: banks@ufl.edu
#7344
A Postmortem Analysis of Polyethylene Damage in Rotating Platform and Fixed Tibial Inserts
*Elexis Baral - Hospital for Special Surgery - New York, USA
James B Chen - Hospital for Special Surgery - New York, USA
Robert Hopper - Anderson Orthopaedic Research Institute - Alexandria, USA
Hollis Potter
Thomas Bauer - The Cleveland Clinic Foundation - Cleveland, USA
C. Anderson Engh - Alexandria, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Douglas E Padgett - Hospital for Special Surgery - New York, USA
*Email: barale@hss.edu
Introduction: Rotating platform (RP) insert designs in total knee arthroplasty (TKA) are intended to reduce articular surface wear; however, mixed results have been reported from retrieval analyses. Postmortem implants provide the opportunity to assess polyethylene damage in successful implants rather than failed implants in retrieval studies. We compared the polyethylene damage patterns between RP and fixed bearing (FB) implants obtained from well-functioning, postmortem knee specimens and then compared these results to our prior findings from retrieval RP and FB implants. We also performed magnetic resonance imaging (MRI) and histological analyses of the periprosthetic tissues in the postmortem knees to determine if abnormal findings were detected by these methodologies.
Methods: 24 postmortem knees containing TKAs were separated into two groups: 11 RP (6 cruciate retaining [CR], 5 posterior stabilized [PS]) and 13 FB inserts (4 CR, 9 PS). Groups were matched for age and BMI. Specimens were thawed for multi-acquisition variable-resonance image combination (MAVRIC) sequence MRIs that were read by a trained radiologist. Pre-operative and post-operative radiographs were used for alignment measurements. Three standard tissue sections were collected for histologic assessment and, if detected on MAVRIC MRI review, a fourth, targeted specimen was obtained from a specific region of interest. Polyethylene inserts were removed in a standardized fashion and were then subjectively scored for surface damage (Fig. 1) by two independent graders, who assessed the articular, backside, and PS post surfaces.
Results: RP inserts had higher damage scores (53 ± 10 vs 34 ± 9; p<0.001) when compared to the FB inserts. The most common damage modes observed were burnishing, scratching, and pitting. The RP cohort had higher scratching (14 ± 7 vs 4 ± 4; p<0.001) and pitting (14 ± 5 vs 5 ± 3; p<0.001) scores than the FB cohort (Fig 2.). Post damage was comparable between the two cohorts (5 ± 3 vs 4 ± 3, RP vs Fixed; p=0.7). RP designs had more evidence of damage overall across the backside (medians: 12 vs 1, p<0.001) and the articular surface (37± 9 vs 30 ± 8, p=0.046) (Fig 2.). The ICC score of the two independent graders was found to be 0.908 corresponding to good to excellent agreement. Increased tibial slope was found to have a positive correlation with damage observed. MRI review found knees to be clinically benign in appearance. Histologic assessment of these samples showed both polyethylene and metallic debris in both cohorts, with corresponding scratches across the articular surface of the femoral component.
Conclusions: RP designs had more damage than FB designs, reflecting the increased macrophage response and particles in the tissues for the RP design. Second, though RP inserts were more damaged than FB, the damage overall was far less than seen in failed retrievals (Fig. 3), consistent with the fact that these PM knees had no failures. Finally, though the damage was less, the trends and damage modes were the same as seen in retrievals, thus confirming the usefulness of retrieval analysis in reflecting the performance of TKA tibial inserts.
Figures
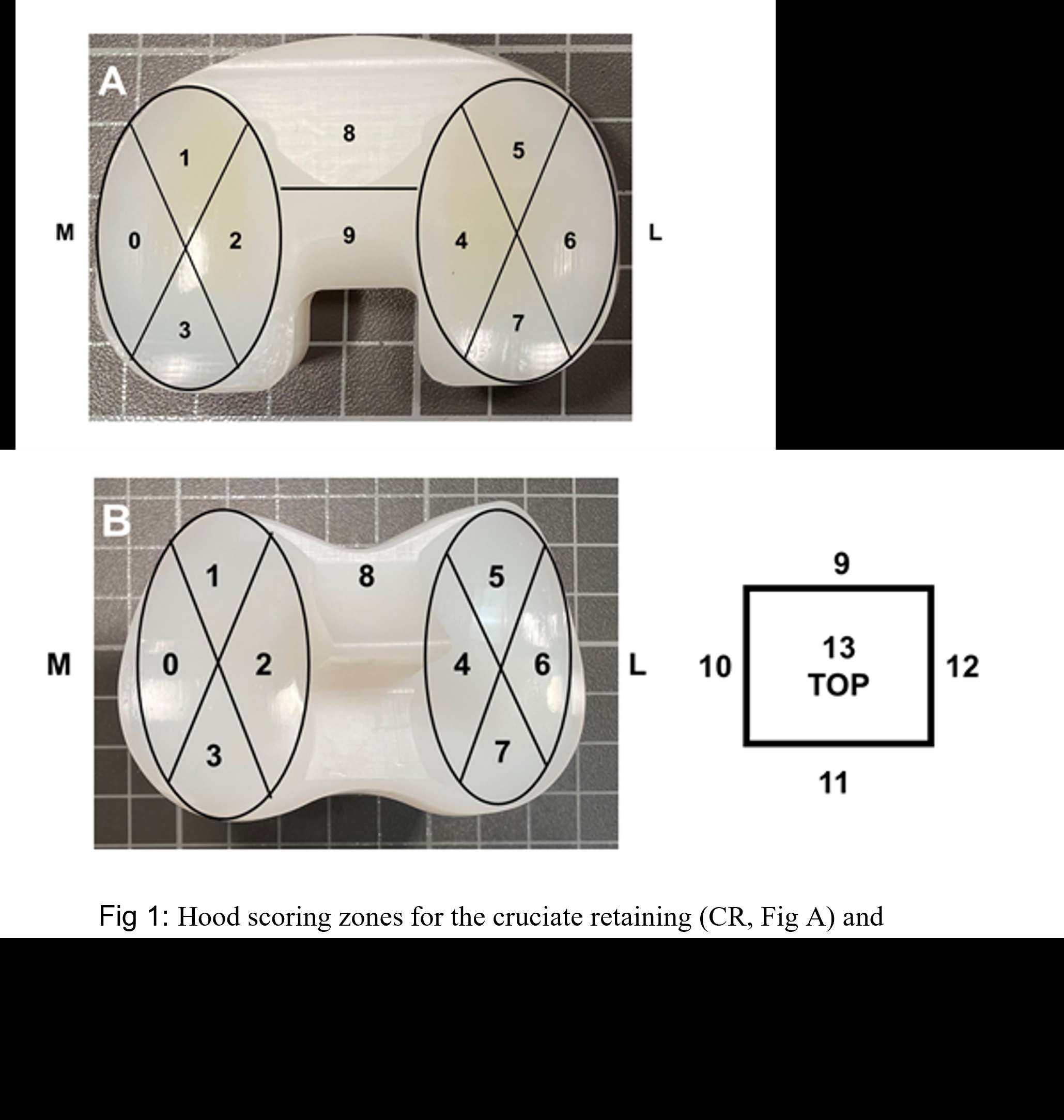
Figure 1

Figure 2
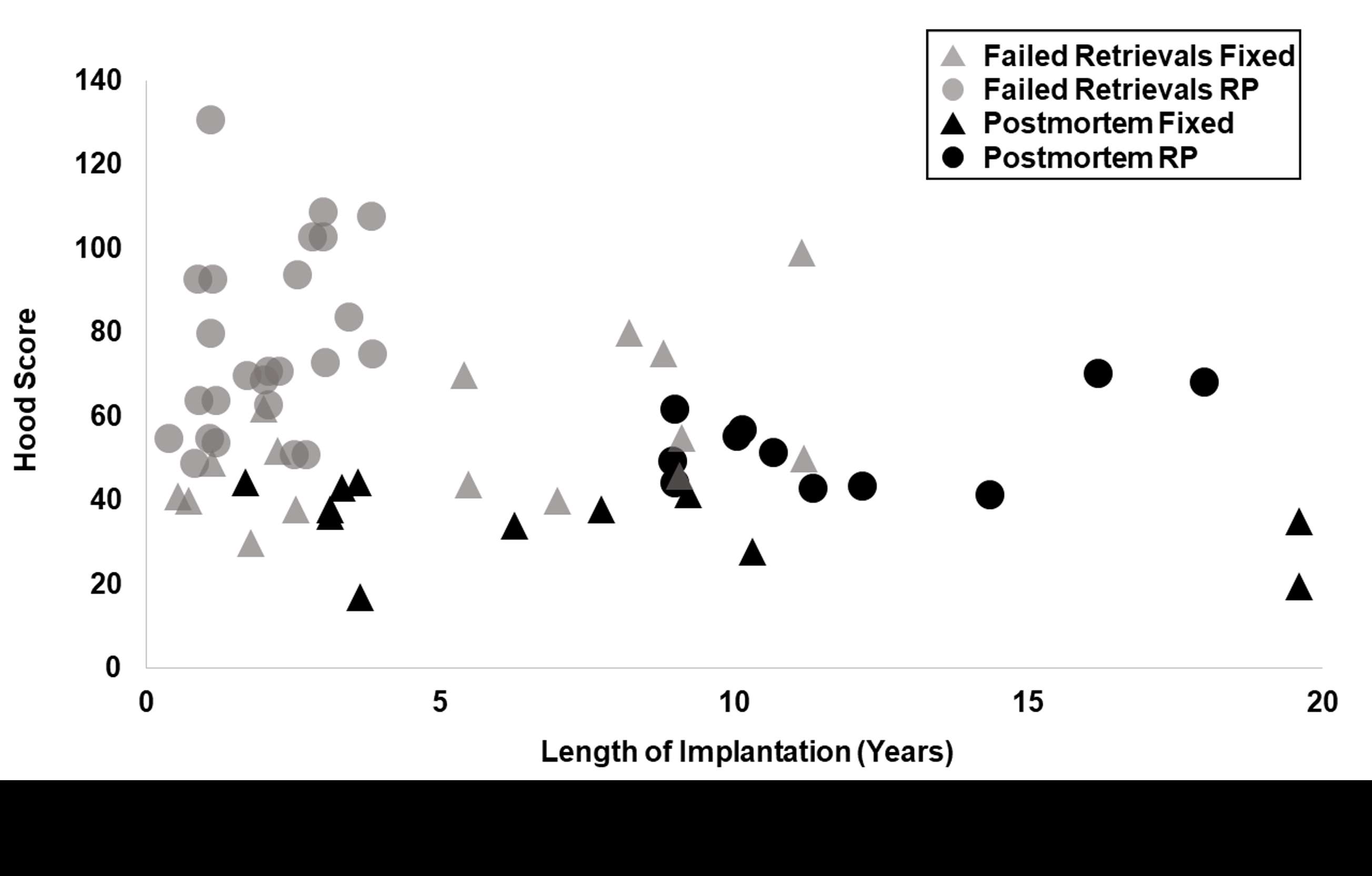
Figure 3#7996
Is Accuracy of Surgical Robotic Systems in Total Knee Arthroplasty (TKA) as Well Established as We Think? a Systematic Review
*Fatemeh Rasouli - Think Surgical Inc. - Fremont, United States of America
Valentina Campanelli - Think Surgical - Fremont, Italy
Jayson Zadzilka - JZ Biomedical LLC - Brunswick, USA
Joel Zuhars - Think Surgical Inc. - Fremont, USA
William Bargar - Sutter Joint Replacement Institute - Fair Oaks, USA
Bernard Stulberg - Saint Vincent Charity Medical Center - Cleveland, USA
*Email: frasouli@thinksurgical.com
Is accuracy of surgical robotic systems in total knee arthroplasty (TKA) as well established as we think? A Systematic Review
Abstract
Background: Robotic-Assisted Surgery (RAS) has pushed the limits of cutting accuracy in TKA. The consensus among the joint replacement community is RAS has significantly better accuracy than conventional TKA. This interpretation is derived by published studies in recent years reporting high RAS accuracy using a variety of measurement techniques. However, some techniques for measuring and reporting accuracy have limitations such as being dependent on the robotic system. As a result, it is unclear if accuracy results are reliable and comparable across studies and systems.
Methods: A systematic review of PubMed was conducted for robotic TKA accuracy. Included studies were assessed for appropriateness of the measurement and reporting technique. Data from qualified studies were evaluated for data gaps and missing accuracy reporting. Outcomes of inter-robot and intra-robot variability were compared.
Results: Twenty-six articles were identified during the systematic search. Each study was assessed for the appropriateness of measurement technique and reported descriptive statistics. Nineteen studies passed the quality assessment. Considering all reported descriptive statistics, qualified studies had significantly more component placement errors reported outside of (-1˚,1˚) range than not-qualified studies. The robotic systems indicated similar errors in coronal component placement, but more variability was seen in sagittal.
Conclusion: Optimal methods for measuring accuracy should be independent from the robotic system, include registration error, and report appropriate qualitative statistics. Otherwise, high reported accuracy in RAS may be unreliable or misleading. A standardized method for measuring and reporting accuracy of robotic systems is needed.
Keywords: Robotic Total Knee Arthroplasty, Accuracy, Measurement Technique
*This work has been registered at International prospective register of systematic reviews (PROSPERO) under ID number 292016.
Introduction
Robotic-Assisted Surgery (RAS) has pushed the limits of cutting accuracy in TKA and enabled knee arthroplasty surgeons to fine-tune their craft and more consistently achieve successful outcomes. Several robotic systems have been developed to help the surgeon execute a highly accurate surgical plan using tracking approaches, cutting strategies, level of automation, and imaging options. The consensus among the joint replacement community is RAS has significantly better cutting accuracy than conventional TKA [1], [2]. This interpretation is derived by published studies in recent years reporting high RAS accuracy using a variety of measurement techniques. However, some techniques for measuring and reporting accuracy have limitations such as being dependent on the robotic system, excluding registration errors, inadequate descriptive statistics, and/or missing proper accuracy reporting.
Measuring the cutting accuracy of a robotic technology requires developing a measurement technique that is, at a minimum, independent of the robotic device and inclusive of all sources of error. However, a variety of published studies have used the robotic system itself to measure cutting accuracy [3]–[8], resulting in a measurement dependent on RAS system that most often does not include registration errors (i.e., inaccuracies in estimating bone location during surgery). Additionally, some studies used as a gold standard measurement a navigation system that utilized the same registration process as RAS, thus being dependent on the robotic system [9], [10].
With each technique, the final cut or implant placement error is computed by measuring the intra- or postoperative cut or implant placement and comparing it with pre- or intraoperative planned values. Five different accuracy measurement techniques have been identified in the literature to compute robotic TKA (rTKA) accuracy in clinical or cadaveric settings:
- Robotic: Same robotic system (same software and digitizing device) that performed the TKA is used to collect points intraoperatively.
- Navigation: A separate navigation system measures final resection angles in the sagittal and coronal planes.
- Caliper: A caliper measures the bone resections to compute achieved resection thicknesses.
- Radiological: Implant placements are measured from postoperative radiographs or CT scans.
- Fiducial Cluster: Cut or implant placements are measured intraoperatively using a planar probe relative to fiducial markers installed in bones prior to preoperative CT scan.
The ‘Robotic’ and ‘Navigation’ techniques are providing an assessment that is dependent on the robot itself, while the ‘Radiological’ technique is an independent measurement that include all sources of error and thus the preferred technique for clinical studies. The ‘Fiducial Cluster’ technique would be considered a gold standard measurement for accuracy but is limited to cadaveric settings. For a given robotic system, it is unclear if the accuracy values obtained with these different techniques are comparable.
In addition to properly measuring accuracy, properly reporting on cutting accuracy is also important and ideally requires 1) quantifying both the bias and precision of the robotic system [11], 2) quantifying cut or implant placement errors for both the resection levels (translational) and resection angles (rotational) [12], 3) providing descriptive statistics that are appropriate for the statistical distribution of data (i.e., normality).
According to the ASTM definition [11], the accuracy of a computer-assisted surgical system involves a combination of a random error and a common systematic error called bias. A surgical system that has a low random error is defined as “precise” (i.e., cutting error is repeatable), while a system that has a low systematic error is defined as “unbiased” (i.e., mean error is close to zero). Therefore, it is important to report descriptive statistics that are representative of the overall accuracy, such as mean absolute errors or root mean square errors (RMSE). Additionally, when assessing the final implant placement, it is important to report not only the rotational but also the translational errors when possible, as they affect the joint line level restoration and Flexion/Extension (FE) gaps [13]–[16]. Lastly, cutting errors tend to not be normally distributed. Therefore, it is essential to check for normality and avoid using misleading statistics, or to use a large enough sample size (30 or higher) according to the central limit theorem [17].
As a result, it is unclear if accuracy results are reliable and comparable across studies and systems. Hence, the objective of this study is to 1) review appropriateness of measurement techniques and accuracy reporting in published literature, 2) identify RAS accuracy data gaps due to lack of reporting inclusive parameters 3) determine the intra- and inter-robot variabilities between component placement errors and malalignment rates reported by different studies for RAS systems.
Material and Methods
The study conducts a systematic review for publications in PubMed filtered between January of 2005 and 2022 using Medical Subject Headings (MeSH) as keywords in three different categories that cover concepts related to TKA, robotic, and accuracy (Appendix A). The MeSH keywords in each category were initially attached using the Boolean operator “OR”. Then, the outcomes in all categories were connected by the Boolean operator “AND”.
F.R and V.C. reviewed the abstracts for relevance to the research questions. F.R. initially screened the abstract and V.C. checked the decision. If a decision could not be made through abstract review, the full paper was screened. Papers were excluded if they were on unicompartmental knee arthroplasty, review papers, were not about accuracy, used only sawbones, only included conventional navigation systems, not written in English, were case studies, or studied robotic systems that are not currently commercially available in the US.
All included studies were rated for Level of Evidence based on Oxford Centre for Evidence-Based Medicine [18]. For the first objective, studies were critically assessed for the appropriateness of the measurement and reporting techniques used. Specifically, the quality assessment addressed three criteria: a) whether the measurement technique was independent of the robot, b) inclusive of all sources of error, and c) reported appropriate qualitative statistics.
To answer the second objective, extracted data from included studies were evaluated for data gaps and missing accuracy reporting. We also analyzed most and least reported cut or component placement errors across studies.
Final objective compares intra-robot variability between accuracy outcomes from different qualified studies reporting on the same RAS system as well as the inter-robot variability between different RAS systems. The only data that was not included in this analysis were resection thickness errors as those were not consistently reported and data on cutting accuracies when a study reported both cut and component placement error.
Results
The search initially found a total of 303 publications. After applying exclusion criteria, 26 studies [3], [4], [20]–[29], [5], [30]–[35], [7]–[10], [13], [14], [19] were included in the final literature review (Figure 1). Two studies, both RCTs, were rated as level I evidence, three were rated as level II, six level III, eight level IV, and seven cadaveric studies as level V (Appendix B).
Quality of reported outcomes was evaluated based on the three criteria (Table 1). Nineteen studies passed the quality assessment and seven failed one or more criteria. Reasons for failing the quality assessments were study used a technique dependent on RAS (4/7), was not inclusive of all sources of errors (6/7), or reported mean and standard deviation (SD) for errors without confirming the normality (3/7).
Reported statistics for Hip-Knee-Ankle (HKA) angle error, coronal femur, coronal tibia, and sagittal tibia component placement errors were compared between studies that passed or failed the quality assessment (Figure 2a). Considering all reported descriptive statistics (mean error, absolute mean error, SD, RMSE, median), qualified studies had significantly more component placement errors reported outside of (-1˚,1˚) range than not-qualified studies (p = 0.038 < 0.05). Four studies with four different RAS systems reported RMSE for component placement and the outcomes were compared between qualified and not-qualified studies (Figure 2b). Errors reported by studies that failed the quality assessment were consistently lower than studies that passed the three qualifying criteria.
Data gap assessment found 18/26 (69%) studies were missing reports on any translational errors for implant placement. For HKA angles, 15/26 (58%) studies did not report the outlier rate (outside ±3°) and 7/26 (27%) did not report any data on HKA accuracy. Number of studies that reported each rotational and translational component placement errors was counted (Figure 3). Tibial Anterior-Posterior (AP) translational error was missing in 25/26 (96%). Translational errors including Proximal-Distal (PD), and AP implant placement errors were consistently less reported than rotational errors for femur and tibia (coronal and sagittal).
For HKA angles and coronal component placement (Figure 4a), intra-robot variability across studies reporting on the same system was low and showed consistent reporting. Similarly inter-robot variability between mean errors of different RAS systems remained low. Mean reported errors ranged from 1˚ to 1.8˚ for HKA, -0.3˚ to 1.1˚ for coronal femur, and -0.7˚ to 1˚ for coronal tibia (Level of Evidence: I to V). However, standard deviations of HKA angles and coronal component placement in studies utilizing MAKO were approximately up to 1˚ (~1.5x times) higher than NAVIO.
For sagittal component placement (Figure 4b), intra-robot variability among studies reporting on the same system was considerably high. Furthermore, in sagittal direction, the inter-robot variability between different RAS systems as well as the overall error were higher than coronal direction. For NAVIO reported sagittal component placement, mean errors for tibia and femur were 9x to 10x times higher in one study (Level of Evidence: I) [13] than another (Level of Evidence: IV) [30]. On other hand for MAKO, standard deviation of sagittal tibia varied from 0.8˚ to 2.4˚ (Level of Evidence: III to IV). Overall sagittal component placement errors had the highest reported mean (+6.4˚ for NAVIO sagittal tibia) and standard deviation (2.9˚ for MAKO sagittal femur) compared to coronal component placement errors.
Comparing malalignment rates (outside ±3°) among qualified studies, MAKO reported results ranging from 0% to 22% (Level of Evidence: II and III), NAVIO ranged from 5% to 11% (Level of Evidence: I and III), ROSA reported 5% (III), and T-Solution One 9.4% (IV). Table 2 summarizes HKA malalignment rates. There are no reports for outliers on the Velys system.
Discussion
The objective of this study was to evaluate the current evidence on reliability and comparability of RAS accuracy results by performing a systematic review of the current literature on cutting accuracy for robotic TKA. The most important findings of the study are 1) some studies used inadequate measurement or reporting techniques (failing the 3-prong quality assessment) that minimized reported cutting errors, 2) gaps are present in the reported accuracy of RAS as the translational errors are not included most of the time, 3) comparisons were possible only in sagittal and coronal rotations as there is limited data in other directions. The robotic systems indicated similar errors in coronal component placement, but more variability was seen in sagittal. For a given system, some outcomes varied greatly such as malalignment rate in MAKO and tibial sagittal error in NAVIO.
The current study has limitations that require further investigations. Only the PubMed’s database was considered. Reviewers were not blinded to each other’s selection decisions. Also, addition of a meta-analysis could further synthesize the outcomes of the study.
While the rotational errors of the femoral and tibial component are well captured in literature, data on the translational accuracy is lacking. Klasan et al. [12] noted the implications of a wrong resection depth are similar if not worse than rotational errors, as they affect changes in joint line level and FE gaps. Some studies did not report translational errors such as AP error for the tibial component, and ML for femoral and tibial component as surgeons like to control those variables in the trialing process. However, there was no explanation for not measuring and reporting PD and AP error for the femoral component and PD error of the tibial.
For each system, mean errors for coronal femur, coronal tibia, and HKA angles were consistent between studies (within 1°), while the errors for sagittal femur and tibia had higher study-to-study variability (within 2.5°). The highest study-to-study variation was seen in the HKA outlier rate. The source of variability is unclear, but some explanations could be related to measurement technique or surgeon’s abilities to correctly collect points on the bone during the registration process. We noted that two qualified studies [4], [8] excluded cases during learning curve from the accuracy analysis. However, cutting accuracy should not be affected by the learning curve [14], [21].
Determining RAS cutting errors means being able to correctly identify errors around 1 mm/°. To achieve this resolution, measurement techniques need to have ideally (4-10) times less errors (0.25-0.1 mm/°) than what is measured [9]. Seven out 26 identified studies used measurement techniques that do not adequately capture the full system accuracy. Most of the studies used a technique that was not validated, or validation showed similar accuracies of the robotic system. The ASTM standard on “Measurement of Positional Accuracy of Computer-Assisted Surgical Systems” [11] was a first attempt to standardize the measurement of positional accuracy for Computer-Assisted Surgical (CAS) systems in 2010. The standard highlights new standards will be written to evaluate specific system types for specific imaging modalities. To the best of our knowledge, these additional standards have yet to be published after 12 years of the first version, and 4 years of the updated version. With lack of appropriate standards, five techniques have been used in literature to measure cutting accuracy. Below is a summary of the strengths and limitations of each one.
Robotic: Four articles [3], [5], [7], [28] quantified the accuracy of RAS using ‘Robotic’ technique. Main drawback of this technique is excluding registration errors if present. It relies on the registration process to measure cut surfaces and component placement. Thus, the difference between measured quantities in the robot space and true values in the real space remains unknown. Casper et. al. [3] indicated refinement and improvement in rTKA compared to manual TKA (Level of Evidence: V). However, the conclusion is derived by comparing the outcomes with previous literature [36]. This comparison raises another caveat: the referenced literature used the ‘Radiological’ technique. Different capabilities of these measurement techniques in reporting all or partial sources of inaccuracy in the final outcomes make them incomparable. Sires et al [28] assumed measurement errors related to the ‘Robotic’ technique is minimal. However, justifications for this assumption came from a different CAS system and does not provide sufficient information for the current ‘Robotic’ technique [7], [15].
Navigation: In ‘Navigation’, same rigid bodies as RAS system are used for tracking of the bone. Therefore, similar registration procedures are done consecutively for both RAS and ‘Navigation’ prior to the cutting, applying same level of uncertainty to ‘Navigation’ as RAS. Inaccuracies related to the placement of the rigid bodies (for optical tracking) as well as variation between the real-world coordinate and the software coordinate will remain unknown in this technique. Intraoperative measurements are useful only if they capture all sources of error [6]. At the very least, the uncertainty of the measuring tool should be computed to assess the confidence in the outcomes.
Radiological: ‘Radiological’ measurement is perhaps the most common method with 73% of the literature utilizing it (Table 1). In the ‘Radiological’ technique, preoperative plan and occasionally intraoperative adjustments are compared with the postoperative measurements from long-leg radiographs or CT scans. The complete independence of ‘Radiological’ measurement from the robotic device allows for better comparison between outcomes of different systems. One drawback is limitation to component placement measurements since bone cut accuracy cannot be computed due to the metal artifacts (implant). Additionally, radiographs and CT scans can introduce additional errors based on patient positioning, image resolution, inter- and intra-observer limitation, etc. [37], [38].
However, the advantages of ‘Radiological’ technique far outweigh these limitations. Previously discussed techniques highly depend on the accuracy of the systems to capture the true location of the bones and implant in the space and share similar sources of inaccuracy as the robotic device.
Few studies investigated the reliability of ‘Robotic’ or ‘Navigation’ techniques by comparing the results with ‘Radiological’ technique [6], [39]. One investigation found mean absolute differences between ‘Radiological’ and ‘Robotic’ measurements ranged from 1.09˚ to 1.97˚ with 8.97% of cases more than 3˚ different [6]. These differences highlight the importance of knowing the accuracy of the technique. For example, one identified study using ‘Robotic’ technique [28] reported absolute mean errors for cut and component placement to be less than 1˚ in all directions. If we look at the mean absolute difference between ‘Robotic’ and ‘Radiological’ techniques, our interpretation of the accuracy of the RAS system can change if a different measurement technique was used.
Caliper: Caliper is a validated measurement tool [15] but it could only be used for resection thickness.
Fiducial Cluster: This technique, used in one study [19], requires prior placement of fiducial clusters and therefore cannot be used in clinical studies. Pre- and postoperative CT scans with intraoperative registration capture all sources of measurement inaccuracy.
To summarize, each technique should clearly specify which sources of inaccuracy have been included or excluded in the reported outcomes as done by Hamp et al [19]. Furthermore, when reporting accuracy, the reliability and independence of the measurement tools need to be assessed. It is important to ask whether the method relies on the same process as the robotic device and whether the accuracy and precision of the measurement tool is known.
Finally, reporting all descriptive statistics (absolute or signed mean, SD, RMSE, and outliers) conveys a complete image on the accuracy of the robotic system. If only one could be reported, RMSE might be the best way to report RAS accuracy since it puts more weight on larger differences between planned and achieved values because these differences are squared. This is important in TKA because the clinical consequences of large errors are much greater than those of small errors.
Conclusion
Optimal methods for measuring accuracy should be independent from the robotic system, include registration error, and report appropriate qualitative statistics. Otherwise, high accuracy measurements reported in RAS may be unreliable or misleading. While the rotational errors of component placement were well captured, data on the translational accuracy and malalignment rate are lacking in many studies. Across all RAS systems, coronal component placements indicated similar errors, but more variability was seen in sagittal component placements. For a given system, some outcomes varied greatly such as malalignment rate in MAKO and tibial sagittal error in NAVIO. More studies with appropriate measurement and reporting techniques are needed to evaluate RAS system outcomes with higher certainty. A standardized method is needed to determine how accuracy should be measured and reported for RAS TKA.
Figure Legends
Figure 1. PRISMA Flow Diagram of the Systematic Search. Papers were excluded if they were unicompartmental knee arthroplasty (UKA), review papers, were not about accuracy, only included conventional navigation systems, not written in English, were case studies, or studied robotic systems that are not currently commercially available in the US (prototypes, robotic systems utilized only outside of US, etc.).
Figure 2. a) Total Reported Measurement Errors bigger than 1° or smaller than -1° compared among studies that meet and did not meet qualifying criteria. HKA: 86% (12/14 reported measurements) vs. 25% (2/8), Coronal Femur: 40% (10/25) vs. 0% (0/12), Coronal Tibia: 32% (8/25) vs. 8% (1/12), Sagittal Tibia: 61% (16/26) vs. 45% (5/12). b) RMSE reported Errors for HKA, Coronal Femur, Coronal Tibia, Sagittal Femur, and Sagittal Tibia
Figure 3. Number of studies that reported each rotational and translational component placement error.
Figure 4. a) Component placements mean and standard deviation errors for HKA, coronal femur, and coronal tibia. b) Component placements mean and standard deviation errors for sagittal femur, and sagittal tibia.
[1] J. B. Mason, T. K. Fehring, R. Estok, D. Banel, and K. Fahrbach, “Meta-Analysis of Alignment Outcomes in Computer-Assisted Total Knee Arthroplasty Surgery,” J. Arthroplasty, vol. 22, no. 8, pp. 1097–1106, Dec. 2007, doi: 10.1016/j.arth.2007.08.001.
[2] N. Agarwal, K. To, S. McDonnell, and W. Khan, “Clinical and Radiological Outcomes in Robotic-Assisted Total Knee Arthroplasty: A Systematic Review and Meta-Analysis,” J. Arthroplasty, vol. 35, no. 11, pp. 3393-3409.e2, 2020, doi: 10.1016/j.arth.2020.03.005.
[3] M. Casper et al., “Accuracy assessment of a novel image-free handheld robot for Total Knee Arthroplasty in a cadaveric study,” Comput. Assist. Surg., vol. 23, no. 1, pp. 14–20, 2018, doi: 10.1080/24699322.2018.1519038.
[4] S. Rossi, R. Sangaletti, L. Perticarini, F. Terragnoli, and F. Benazzo, “High accuracy of a new robotically assisted technique for total knee arthroplasty : an in vivo study,” Knee Surgery, Sport. Traumatol. Arthrosc., no. 0123456789, 2021, doi: 10.1007/s00167-021-06800-8.
[5] C. S. Sicat, J. C. Chow, B. Kaper, R. Mitra, J. Xie, and R. Schwarzkopf, “Component placement accuracy in two generations of handheld robotics ‑ assisted knee arthroplasty,” Arch. Orthop. Trauma Surg., no. 0123456789, 2021, doi: 10.1007/s00402-021-04040-6.
[6] J. D. Sires and C. J. Wilson, “CT Validation of Intraoperative Implant Position and Knee Alignment as Determined by the MAKO Total Knee Arthroplasty System,” J. Knee Surg., vol. 1, no. 212, 2020, doi: 10.1055/s-0040-1701447.
[7] N. Vaidya, T. N. Jaysingani, T. Panjwani, R. Patil, and A. Deshpande, “Assessment of accuracy of an imageless hand ‑ held robotic ‑ assisted system in component positioning in total knee replacement : a prospective study,” J. Robot. Surg., no. 0123456789, 2021, doi: 10.1007/s11701-021-01249-w.
[8] L. Vanlommel, E. Neven, M. B. Anderson, L. Bruckers, and J. Truijen, “The initial learning curve for the ROSA ® Knee System can be achieved in 6-11 cases for operative time and has similar 90-day complication rates with improved implant alignment compared to manual instrumentation in total knee arthroplasty ORIGINAL PAPER,” J. Exp. Orthop., 2021, doi: 10.1186/s40634-021-00438-8.
[9] S. Parratte, A. J. Price, L. M. Jeys, W. F. Jackson, and H. D. Clarke, “Accuracy of a New Robotically Assisted Technique for Total Knee Arthroplasty: A Cadaveric Study,” J. Arthroplasty, vol. 34, no. 11, pp. 2799–2803, Nov. 2019, doi: 10.1016/j.arth.2019.06.040.
[10] A. Seidenstein, M. Birmingham, J. Foran, and S. Ogden, “Better accuracy and reproducibility of a new robotically-assisted system for total knee arthroplasty compared to conventional instrumentation: a cadaveric study,” Knee Surgery, Sport. Traumatol. Arthrosc., vol. 29, no. 3, pp. 859–866, Mar. 2021, doi: 10.1007/s00167-020-06038-w.
[11] “Standard Practice for Measurement of Positional Accuracy of Computer Assisted Surgical Systems.” doi: 10.1520/F2554-18.
[12] A. Klasan, S. Edward, P. Samuel, G. Thomas, N. Myles, and R. Coolican, “Conventional instruments are more accurate for measuring the depth of the tibial cut than computer ‑ assisted surgery in total knee arthroplasty : a prospective study,” Arch. Orthop. Trauma Surg., no. 0123456789, pp. 3–8, 2020, doi: 10.1007/s00402-020-03403-9.
[13] N. V Vaidya, A. N. Deshpande, T. Panjwani, R. Patil, T. Jaysingani, and P. Patil, “Robotic ‑ assisted TKA leads to a better prosthesis alignment and a better joint line restoration as compared to conventional TKA : a prospective randomized controlled trial,” Knee Surgery, Sport. Traumatol. Arthrosc., no. 0123456789, 2020, doi: 10.1007/s00167-020-06353-2.
[14] B. Kayani, S. Konan, S. S. Huq, J. Tahmassebi, and F. S. Haddad, “Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning,” Knee Surgery, Sport. Traumatol. Arthrosc., vol. 27, no. 4, pp. 1132–1141, 2019, doi: 10.1007/s00167-018-5138-5.
[15] L. C. Biant, K. Yeoh, P. M. Walker, W. J. M. Bruce, and W. R. Walsh, “The accuracy of bone resections made during computer navigated total knee replacement. Do we resect what the computer plans we resect?,” Knee, vol. 15, no. 3, pp. 238–241, Jun. 2008, doi: 10.1016/j.knee.2008.01.012.
[16] E. Song and J. Seon, “Robotic-assisted TKA Reduces Postoperative Alignment Outliers and Improves Gap Balance Compared to Conventional TKA,” pp. 118–126, 2013, doi: 10.1007/s11999-012-2407-3.
[17] S. M. Ross, Introductory statistics. Academic Press, 2017.
[18] O. G. and M. H. Jeremy Howick, Iain Chalmers (James Lind Library), Paul Glasziou, Trish Greenhalgh, Carl Heneghan, Alessandro Liberati, Ivan Moschetti, Bob Phillips, Hazel Thornton, “The Oxford Levels of Evidence 2,” Oxford Centre for Evidence-Based Medicine. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
[19] E. Hampp et al., “Robotic-Arm Assisted Total Knee Arthroplasty Demonstrated Greater Accuracy and Precision to Plan Compared with Manual Techniques,” J. Knee Surg., vol. 32, no. 03, pp. 239–250, Mar. 2019, doi: 10.1055/s-0038-1641729.
[20] O. Mahoney et al., “Improved component placement accuracy with robotic-arm assisted total knee arthroplasty,” J. Knee Surg., vol. 10075, 2020, doi: 10.1055/s-0040-1715571.
[21] H. Vermue et al., “Robot-assisted total knee arthroplasty is associated with a learning curve for surgical time but not for component alignment, limb alignment and gap balancing,” Knee Surgery, Sport. Traumatol. Arthrosc., no. 0123456789, 2020, doi: 10.1007/s00167-020-06341-6.
[22] L. Y. Scholl et al., “How Does Robotic-Arm Assisted Technology Influence Total Knee Arthroplasty Implant Placement for Surgeons in Fellowship Training?,” J. Knee Surg., vol. 1, no. 212, 2020, doi: 10.1055/s-0040-1716983.
[23] B. T. Nickel et al., “The Accuracy and Clinical Success of Robotic-Assisted Total Knee Arthroplasty,” 2021, doi: 10.1177/15563316211026307.
[24] D. G. Deckey et al., “Robotic-assisted total knee arthroplasty improves accuracy and precision compared to conventional techniques,” Bone Jt. J., vol. 103-B, no. 7, pp. 74–80, 2021, doi: 10.1302/0301-620X.103B6.BJJ-2020-2003.R1.
[25] J. Thilak, B. C. Babu, M. Thadi, V. Mohan, T. A. Kumar, and P. P. Mane, “Accuracy in the Execution of Pre ‑ operative Plan for Limb Alignment and Implant Positioning in Robotic ‑ arm Assisted Total Knee Arthroplasty and Manual Total Knee Arthroplasty : A Prospective Observational Study,” Indian J. Orthop., vol. 55, no. 4, pp. 953–960, 2021, doi: 10.1007/s43465-020-00324-y.
[26] P. Bollars, A. Boeckxstaens, J. Mievis, S. Kalaai, M. G. M. Schotanus, and D. Janssen, “Preliminary experience with an image-free handheld robot for total knee arthroplasty: 77 cases compared with a matched control group,” Eur. J. Orthop. Surg. Traumatol., vol. 30, no. 4, pp. 723–729, 2020, doi: 10.1007/s00590-020-02624-3.
[27] K. Collins, P. A. Agius, A. Fraval, and J. Petterwood, “Initial experience with the navio robotic-assisted total knee replacement-coronal alignment accuracy and the learning curve,” J. Knee Surg., 2021, doi: 10.1055/s-0040-1722693.
[28] J. D. Sires, J. D. Craik, and C. J. Wilson, “Accuracy of Bone Resection in MAKO Total Knee Robotic-Assisted Surgery,” J. Knee Surg., Nov. 2019, doi: 10.1055/s-0039-1700570.
[29] T. Kaneko, T. Igarashi, K. Takada, S. Yoshizawa, and H. Ikegami, “Robotic-assisted total knee arthroplasty improves the outlier of rotational alignment of the tibial prosthesis using 3DCT measurements,” Knee, vol. 31, pp. 64–76, 2021, doi: 10.1016/j.knee.2021.05.009.
[30] M. Laddha and S. Gaurav, “Assessment of Limb Alignment and Component Placement After All Burr Robotic ‑ Assisted TKA,” Indian J. Orthop., vol. 55, no. s1, pp. 69–75, 2021, doi: 10.1007/s43465-020-00269-2.
[31] S. Thiengwittayaporn, P. Uthaitas, C. Senwiruch, and N. Hongku, “Imageless robotic ‑ assisted total knee arthroplasty accurately restores the radiological alignment with a short learning curve : a randomized controlled trial,” Int. Orthop., no. 0123456789, 2021, doi: 10.1007/s00264-021-05179-y.
[32] P. Savov, L. Rene, T. Henning, W. Jonathan, and E. Max, “Imageless robotic handpiece ‑ assisted total knee arthroplasty : a learning curve analysis of surgical time and alignment accuracy,” Arch. Orthop. Trauma Surg., vol. 141, no. 12, pp. 2119–2128, 2021, doi: 10.1007/s00402-021-04036-2.
[33] V. Singh, G. M. Teo, and W. J. Long, “Versatility and accuracy of a novel image ‑ free robotic ‑ assisted system for total knee arthroplasty,” Arch. Orthop. Trauma Surg., no. 0123456789, 2021, doi: 10.1007/s00402-021-04049-x.
[34] G. W. Doan, R. P. Courtis, J. G. Wyss, E. W. Green, and C. W. Clary, “Image-Free Robotic-Assisted Total Knee Arthroplasty Improves Implant Alignment Accuracy: A Cadaveric Study,” J. Arthroplasty, 2022, doi: 10.1016/j.arth.2021.12.035.
[35] B. N. Stulberg et al., “Safe and effective use of active robotics for TKA : Early results of a multicenter study,” J. Orthop., vol. 26, no. July, pp. 119–125, 2021, doi: 10.1016/j.jor.2021.07.001.
[36] C. Baier, C. Lu, F. Ko, F. Zeman, and J. Grifka, “Assessing patient-oriented results after revision total knee arthroplasty,” pp. 955–961, 2013, doi: 10.1007/s00776-013-0467-1.
[37] T. D. V Cooke and E. A. Sled, “Frontal Plane Knee Alignment : A Call for Standardized Measurement,” 2007.
[38] J. V. Johan Bellemans, William Colyn, Hilde Vandenneucker, “Is Neutral Mechanical Alignment Normal for All Patients? The Concept of Constitutional Varus,” Chitranjan Ranawat Award, pp. 45–53, 2012, doi: 10.1007/s11999-011-1936-5.
[39] S. Lustig, C. Fleury, D. Goy, P. Neyret, and S. T. Donell, “The accuracy of acquisition of an imageless computer-assisted system and its implication for knee arthroplasty,” Knee, vol. 18, no. 1, pp. 15–20, 2011, doi: 10.1016/j.knee.2009.12.010.
Figures
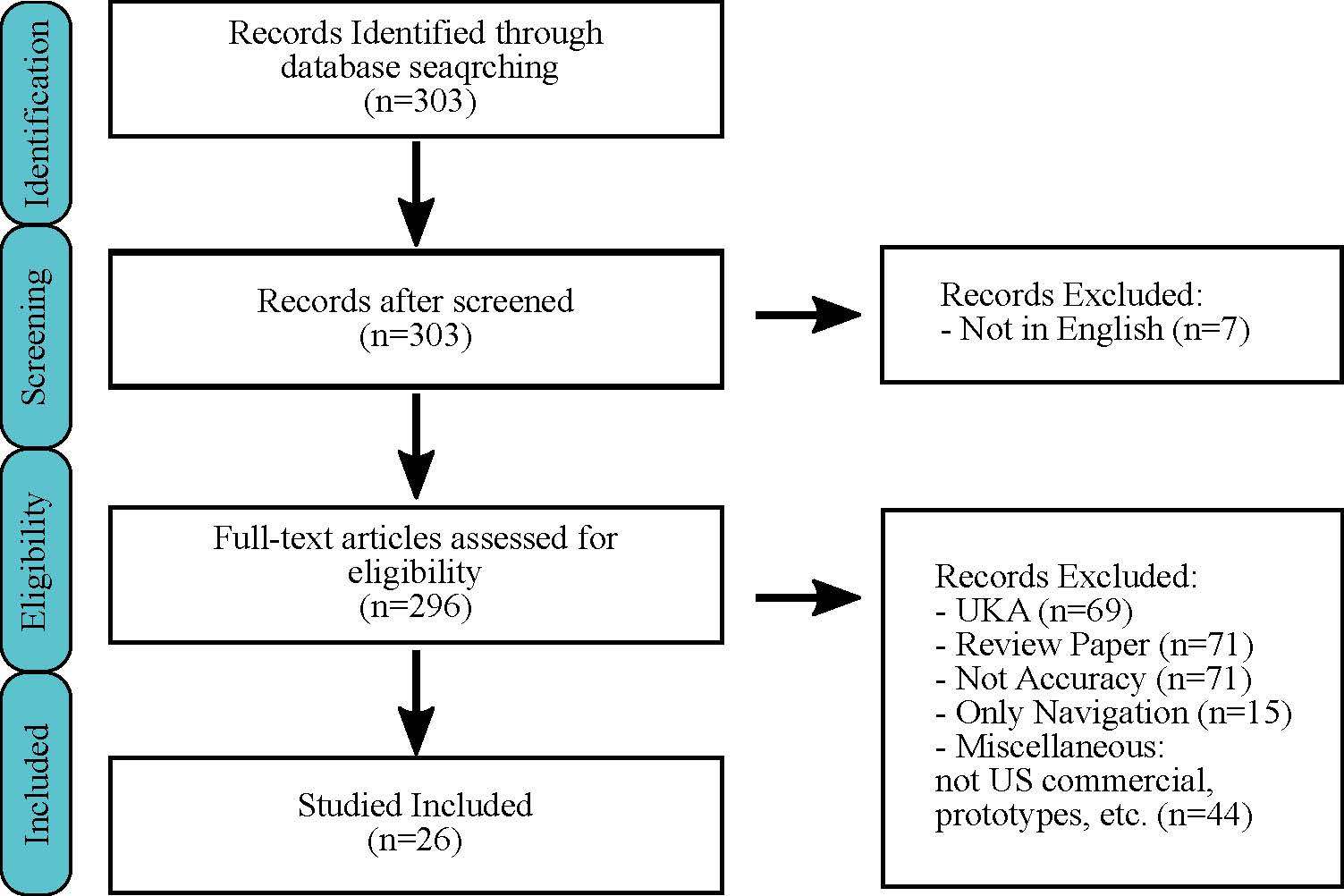
Figure 1
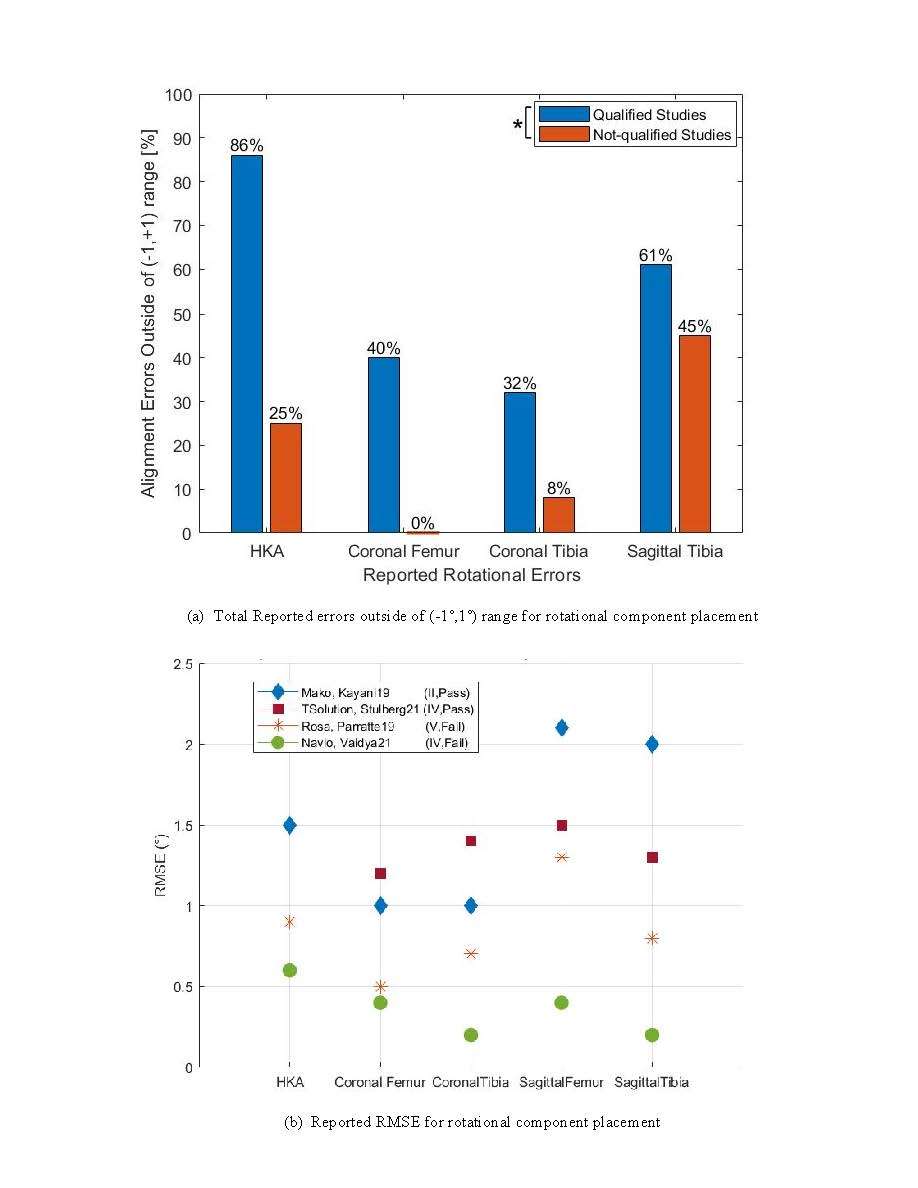
Figure 2
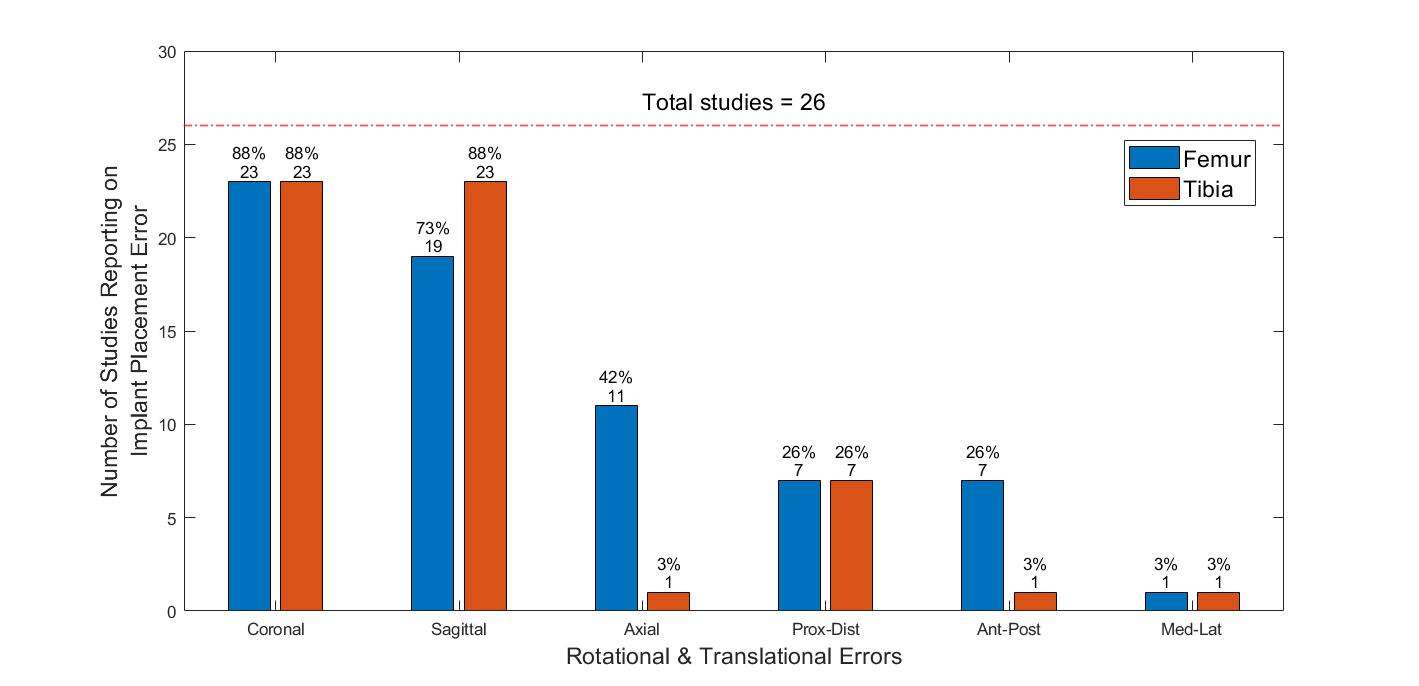
Figure 3
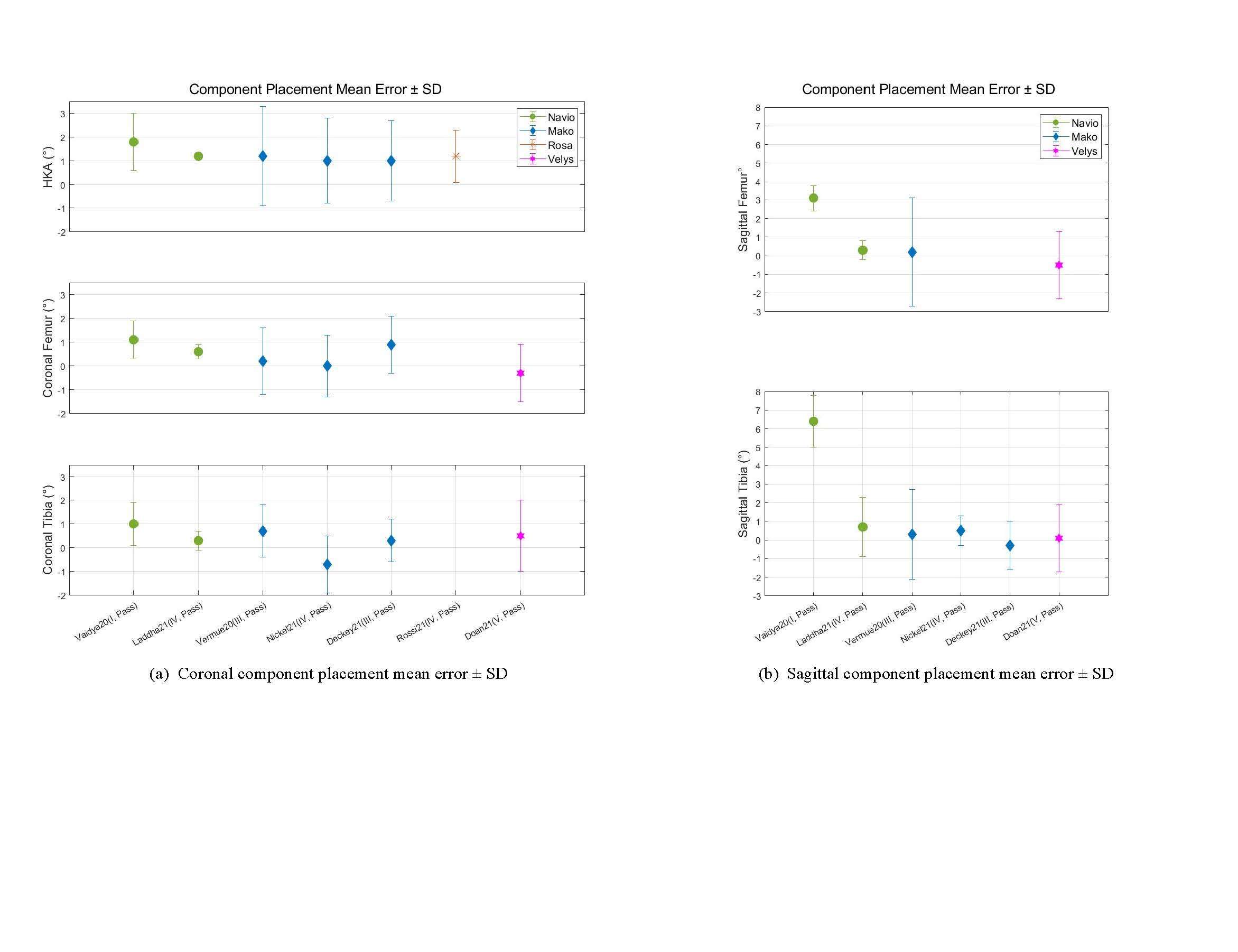
Figure 4

Figure 5
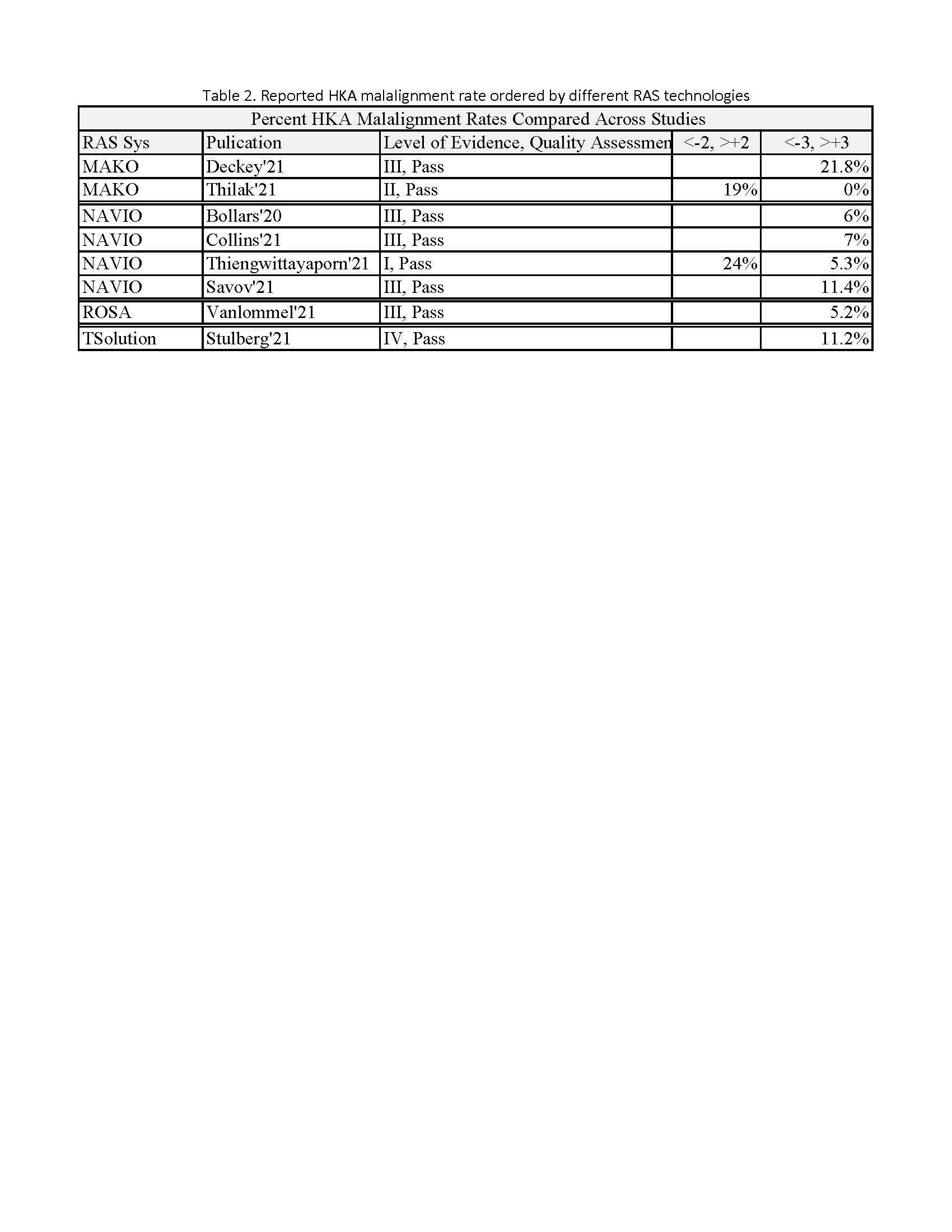
Figure 6

Figure 7
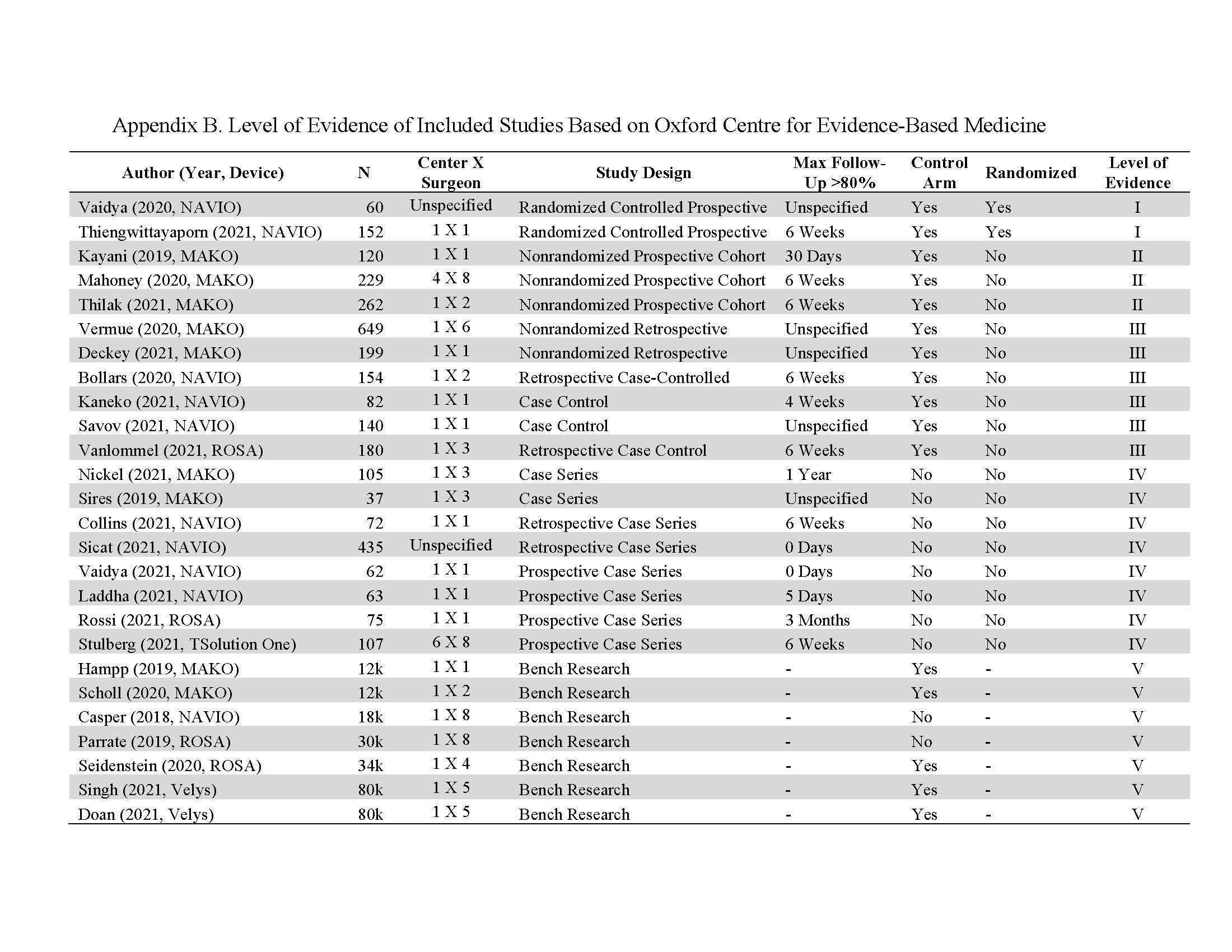
Figure 8

Figure 9#7603
Is Accuracy of Surgical Robotic Systems Used in Total Knee Arthroplasty (TKA) as Well Established as We Think?
*Fatemeh Rasouli - Think Surgical Inc. - Fremont, United States of America
Valentina Campanelli - Think Surgical - Fremont, Italy
Jayson Zadzilka - JZ Biomedical LLC - Brunswick, USA
William Bargar - Sutter Joint Replacement Institute - Fair Oaks, USA
Bernard Stulberg - Saint Vincent Charity Medical Center - Cleveland, USA
Joel Zuhars - Think Surgical Inc. - Fremont, USA
*Email: frasouli@thinksurgical.com
Introduction: Robotic-Assisted Surgery (RAS) has pushed the limits of cutting accuracy in TKA. The consensus among the joint replacement community is RAS has significantly better cutting accuracy than conventional TKA. This interpretation is supported by published studies in recent years reporting high RAS accuracy using a variety of measurement techniques. However, some techniques for measuring accuracy have limitations such as being dependent on the robotic system, excluding registration errors, inadequate descriptive statistics, and/or missing accuracy reporting. As a result, it is unclear if accuracy results are reliable and comparable across studies and systems. Hence, the purpose of this study is to 1) review appropriateness of measurement techniques and accuracy reporting in published literature, 2) identify RAS accuracy data gaps due to lack of reporting inclusive parameters 3) compare intra- and inter-variability of malalignment rates for RAS systems.
Method: A systematic review of the literature on RAS cutting accuracy was conducted for publications in PubMed between 2005-2022. Identified studies were screened for inclusion and exclusion (Figure 1). Next, included studies were critically assessed for appropriateness of the measurement and reporting technique. Specifically, the quality assessment addressed three criteria: whether the studies were independent of the robot, inclusive of all sources of error, and reported appropriate qualitative statics. Then, data from qualified studies were evaluated for data gaps and missing accuracy reporting. Finally, malalignment rates were compared across different RAS systems.
Results: Twenty-six studies were included (Figure 1). After quality assessment, 19/26(73%) of the studies met all three criteria and therefore were included in the follow-up analysis (Figure 2). The studies that did not use appropriate measurement and/or reporting techniques, consistently reported better accuracy and lower measurement errors within [-1,1] deg range (Figure 3a).
Data gap evaluation found 16/19(84%) of studies were missing reports on translational errors, 11/19(58%) of studies did not report malalignment rate for femoral and tibial alignments but only qualitative statistics. Reporting on the axial rotation for the femoral component was missing in 12/19(58%) of studies and no rotational error was reported in 2/19(10%) studies.
Comparing malalignment rates between qualified studies, MAKO reported results ranging from 0% to 22%, NAVIO ranged from 5% to 11%, ROSA reported 5%, and T-Solution One 9.4% (Figure 3b).
Conclusion: Optimal methods for measuring accuracy should be independent from the robotic system, include registration error, and report appropriate qualitative statistics. Otherwise, high accuracy measurements reported in RAS may be unreliable or misleading. While the rotational errors of component placement were well captured, data on the translational accuracy and malalignment rate are lacking in many studies. Across all RAS systems, malalignment rate ranged from 0%-22% with the highest inter-variability for MAKO and a moderate variation for NAVIO. ROSA and T-Solution One were each only reported in one study. More studies with appropriate measurement and reporting techniques are needed to evaluate RAS system outcomes with higher certainty. A standardized method is needed to determine how accuracy should be measured and reported for RAS TKA.
Figures
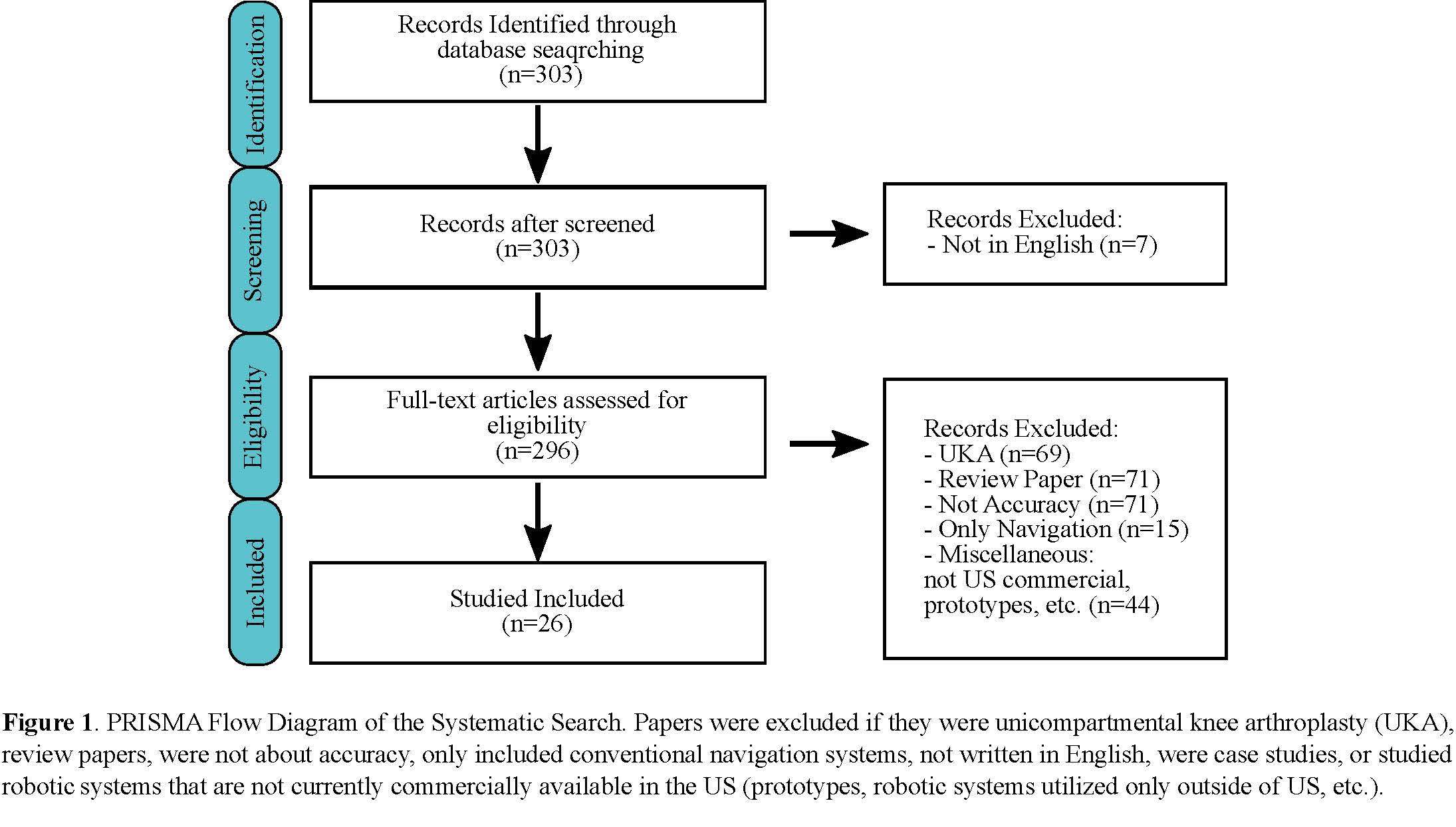
Figure 1
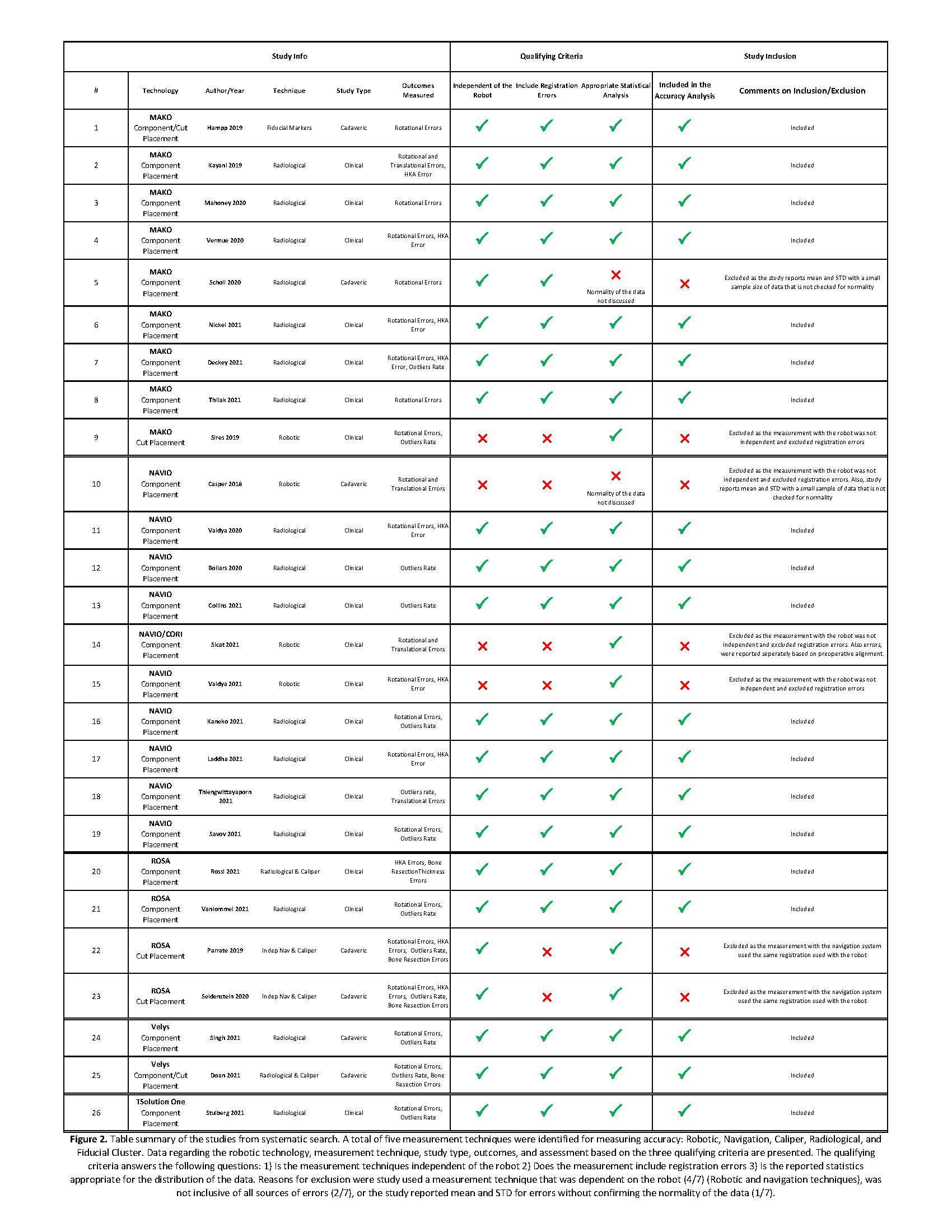
Figure 2
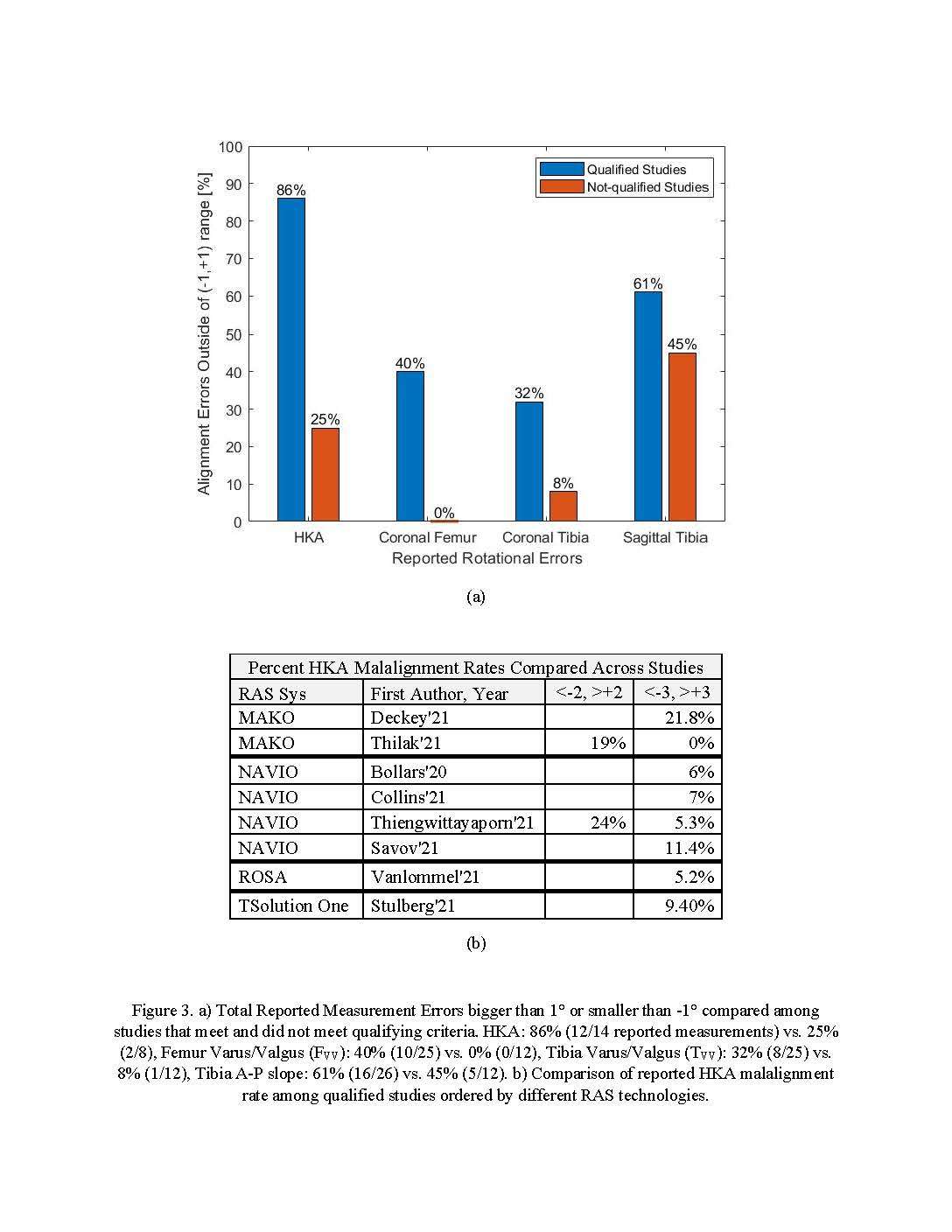
Figure 3#8032
Invited Talk: Intraoperative Imaging vs Robotics as the future for THA
*Robert Barrack - Washington University School of Medicine - Saint Louis, USA
*Email: barrackr@WUSTL.edu
Aims: The aims of this study were to examine the rate at which the positioning of the acetabular component, leg length discrepancy and femoral offset are outside an acceptable range in total hip arthroplasties (THAs) which either do or do not involve the use of intra-operative digital imaging.
Patients and methods: A retrospective case-control study was undertaken with 50 patients before and 50 patients after the integration of an intra-operative digital imaging system in THA. The demographics of the two groups were comparable for body mass index, age, laterality and the indication for surgery. The digital imaging group had more men than the group without. Surgical data and radiographic parameters, including the inclination and anteversion of the acetabular component, leg length discrepancy, and the difference in femoral offset compared with the contralateral hip were collected and compared, as well as the incidence of altering the position of a component based on the intra-operative image.
Results: Digital imaging took a mean of five minutes (2.3 to 14.6) to perform. Intra-operative changes with the use of digital imaging were made for 43 patients (86%), most commonly to adjust leg length and femoral offset. There was a decrease in the incidence of outliers when using intra-operative imaging compared with not using it in regard to leg length discrepancy (20% versus 52%, p = 0.001) and femoral offset inequality (18% versus 44%, p = 0.004). There was also a difference in the incidence of outliers in acetabular inclination (0% versus 7%, p = 0.023) and version (0% versus 4%, p = 0.114) compared with historical results of a high-volume surgeon at the same centre.
Conclusion: The use of intra-operative digital imaging in THA improves the accuracy of the positioning of the components at THA without adding a substantial amount of time to the operation. Other advanced technologies currently utilized at our center include imageless navigation (Intellijoint) and robotics (Mako). The upfront capital expense for Intraop imaging is about 10% of robotics and no pre-op CT is required (unless the new 3-D option is elected). Navigation and robotics also add additional cost per case of several hundred dollars for disposables while intra-op imaging does not. Differences in accuracy among the options appears negligible. While advanced technologies will likely become standard to more accurately position and customize THA component position, which platform will emerge as the leader is yet to be determined.
#7500
Early Outcomes of a Novel Cementless Unicompartmental Knee Arthroplasty System
*Tarik Bayoumi - Hospital for Special Surgery - New York, USA
Lindsey Ruderman - Hospital for Special Surgery - New York, USA
Joost Burger - Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Univ - Berlin, Germany
Edwin Su - Hospital for Special Surgery - New York, USA
Andrew Pearle - Hospital for Special Surgery - New York, USA
*Email: tbayoumi.md@gmail.com
INTRODUCTION: Unicompartmental knee arthroplasty is a well-established treatment for isolated medial osteoarthritis. Traditionally, UKA components are fixated using bone cement. However, cement-related issues such as third body debris, inappropriate cement penetration or incorrect implant positioning have led to a renewed interest in cementless fixation for UKA. Recent National joint registry studies have shown an increase in the use of cementless UKA over the last years and favorable long-term results are reported for these systems. However, concerns exist with regard to potential implant movement and its influence on early clinical outcomes. To facilitate a stable environment for osseointegration, provide a more durable fixation, and improve clinical outcomes, a cementless fixed-bearing UKA system with a blade-based bone anchor that locks into the tibial tray has recently been developed (Figure 1). This study reports the clinical and radiological outcomes of this system during the first postoperative year.
METHODS: Arthroplasty registries of two designer surgeons, consisting of prospectively collected data, were retrospectively screened for patients who had received a cementless UKA between July 2020 and March 2022. Patients were included if they had completed patient-reported outcome measures (PROMs) including the Oxford Knee Score (OKS), Visual Analogue Scale (VAS) for pain, and University of California, Los Angles (UCLA) Activity Score at one-year follow-up. Radiolucent lines (RLLs) were assessed on one-year postoperative radiographs. Descriptive statistics were used to describe PROMs. Association between demographics and PROMs were evaluated with use of Pearson’s correlation coefficient.
RESULTS: A total of 33 knees were included (29 patients, mean age 60.7 ±5.8 years, mean BMI 28.7 ±5.0 kg/m2, 76% male). Mean one-year OKS, VAS and UCLA scores were 41.5 ±5.8, 1.4 ±1.3, and 7.2 ±1.7, respectively. A total of 19 knees (58%) had excellent outcomes (OKS >41) at one-year follow-up. There was a strong negative association between BMI and one-year OKS scores (r = -0.64, [95% Confidence Interval (CI) -0.81– -0.3], p <0.001) (Figure 2). Physiological RLLs were present under the tibial tray in all 15 patients with one-year postoperative radiographs. No fractures or infections occurred in this series.
CONCLUSION: Early clinical results of the first series of patients treated with a novel cementless fixed-bearing UKA system demonstrate a promising trend and compare favorably to previously reported outcomes of cementless UKA designs. Higher BMI was associated with worse one-year OKS scores. RLLs were frequently present, however did not seem to influence PROMs at one-year follow-up given the favorable outcome scores.
Figures
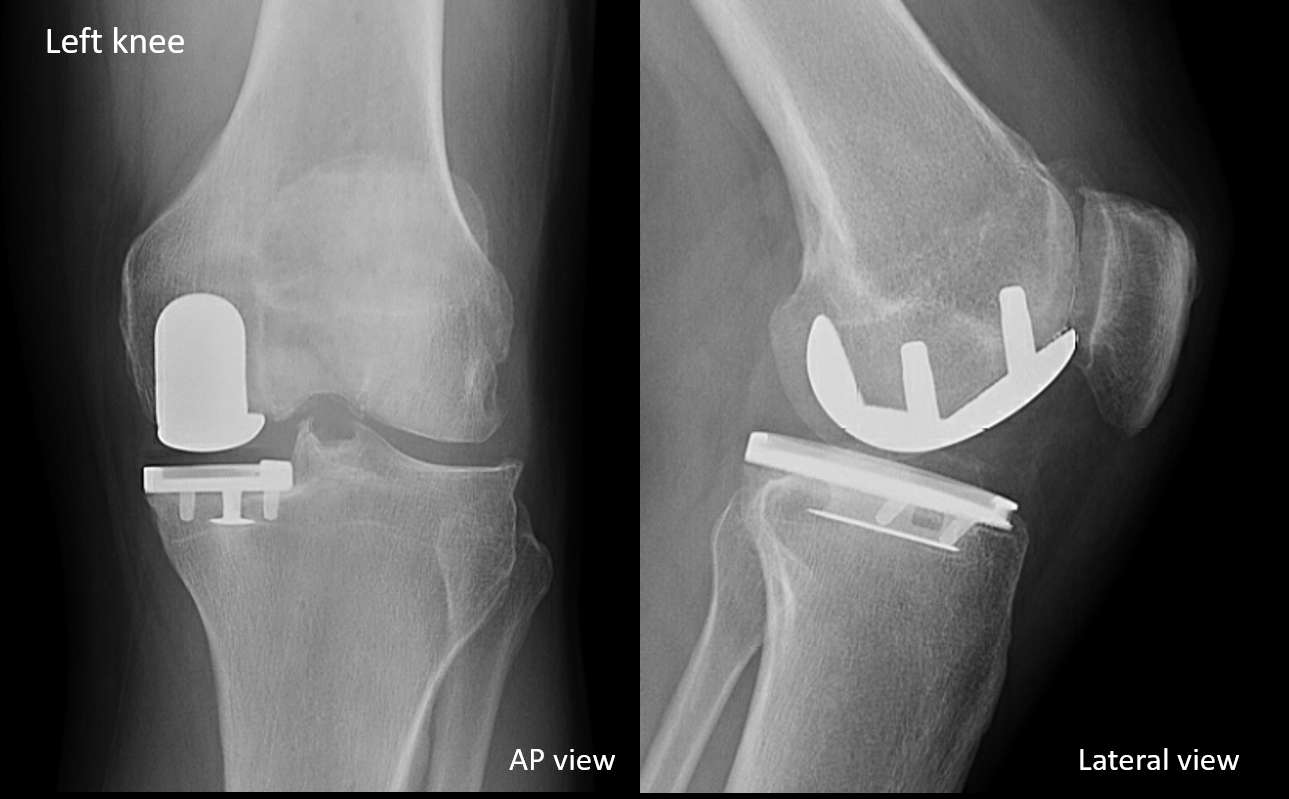
Figure 1
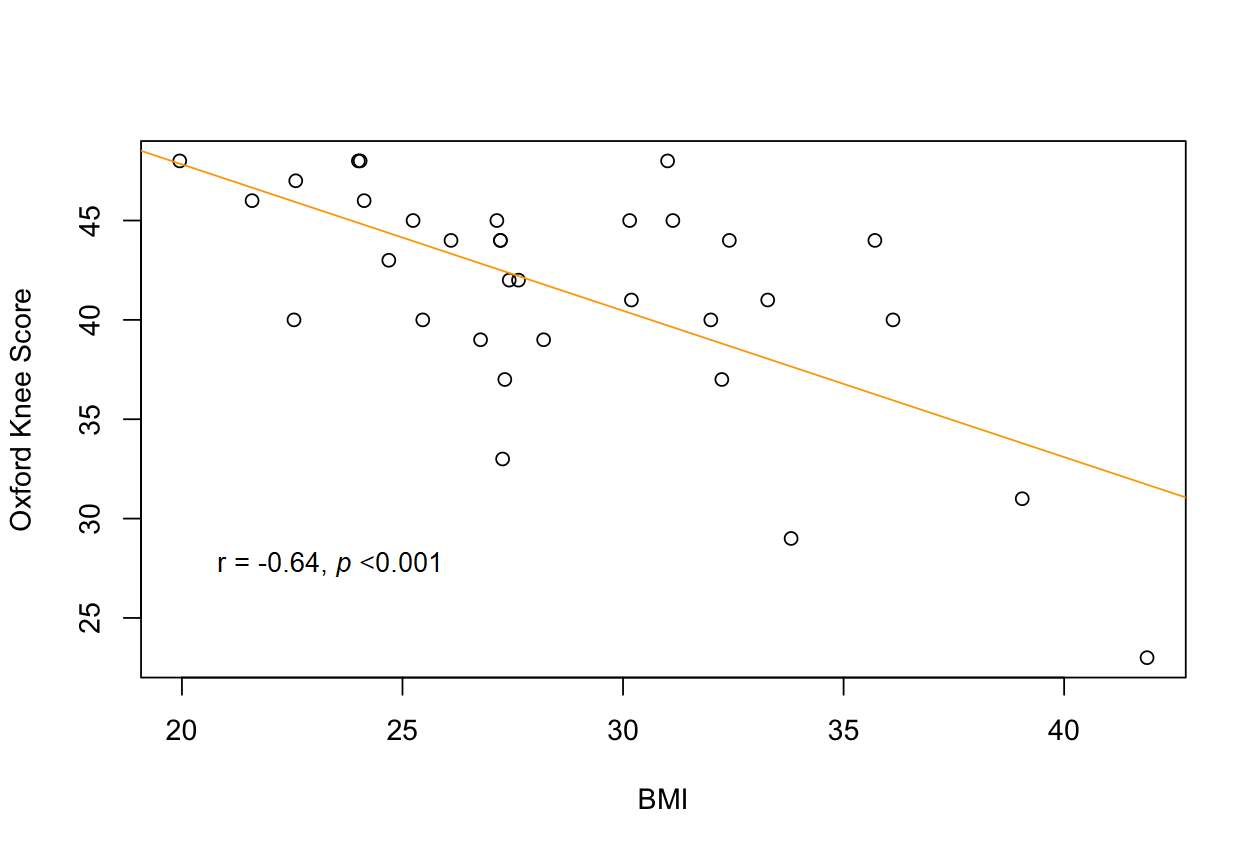
Figure 2#7453
Ten-Year Survivorship and Patient Satisfaction of Robotic-Arm Assisted Medial Unicompartmental Knee Arthroplasty: A Prospective Multicenter Study
*Tarik Bayoumi - Hospital for Special Surgery - New York, USA
Todd Borus - Rebound Orthopedics & Neurosurgery - Portland, USA
Thomas Coon - Coon Joint Replacement Institute - St. Helena, USA
Laura Jill Kleeblad - Northwest Clinics - Alkmaar, Netherlands
Jon Dounchis - Naples Community Hospital - Naples, USA
Joseph Nguyen - Hospital for Special Surgery - New York, USA
Andrew Pearle - Hospital for Special Surgery - New York, USA
*Email: tbayoumi.md@gmail.com
Introduction: Unicompartmental knee arthroplasty (UKA) has considerable benefits over total knee arthroplasty (TKA) in the treatment of isolated medial compartment osteoarthritis, but revision rates after UKA are generally found to be higher compared to TKA. Robotic-arm assisted systems for medial UKA have been introduced to provide improved surgical precision, soft tissue balancing, and component positioning in order to improve outcomes and implant survivorship. Previous studies have demonstrated high survivorship at short- to mid-term follow-up after robotic-arm assisted UKA. However, limited evidence is available on long-term outcomes following this procedure and it remains unclear whether the increased surgical precision translates into improved survivorship. The purpose of this prospective multicenter study was to determine long-term survivorship and patient satisfaction following robotic-arm assisted medial UKA.
Methods: A total of 287 consecutive patients (367 knees) underwent robotic-arm assisted medial UKA by three individual surgeons at separate institutions between 2009 and 2011. A fixed-bearing metal-backed onlay tibial component was used for all cases. Patients were contacted at 10-year follow-up to determine survivorship and their overall satisfaction using a five-series questionnaire. Implant survivorship was defined as the time from intial implantation to revision surgery. Revision to TKA was used as the primary endpoint, and revision for any reason was recorded as the secondary endpoint for survivorship. The Kaplan-Meier analysis was used to determine survivorship for each endpoint.
Results: Data was collected for 192 patients (250 knees) with an average follow-up of 10.3 ± 0.4 years. Two patients declined participation in the study, 62 were lost to follow-up and 31 patients deceased during the study period. Mean age at time of surgery was 64.3 ± 10.1 years, mean BMI was 29.9 ± 4.7 kg/m2, and 47% of patients were female. A total of 58 patients (30%) received bilateral UKA. At 10-year follow-up, 17 knees were reported as revised to TKA, resulting in a survivorship of 93.2% (95% Confidence Interval [CI] 90.0–96.3) (Figure 1). Additionally, two UKA components were revised, corresponding with an overall survivorship of 92.4% (95% CI 89.1–95.7) (Figure 2). Average time to revision was 5.6 ± 2.8 years. Of all patients without revision, 93% were either very satisfied or satisfied with the overall function of their operative knee.
Conclusions: In this prospective multicenter study, high 10-year survivorship and patient satisfaction were found following robotic-arm assisted medial UKA. Prospective comparative studies are warranted to assess differences in long-term survivorship and patient-reported outcomes between robotic-arm assisted UKA, conventional UKA and TKA.
Figures
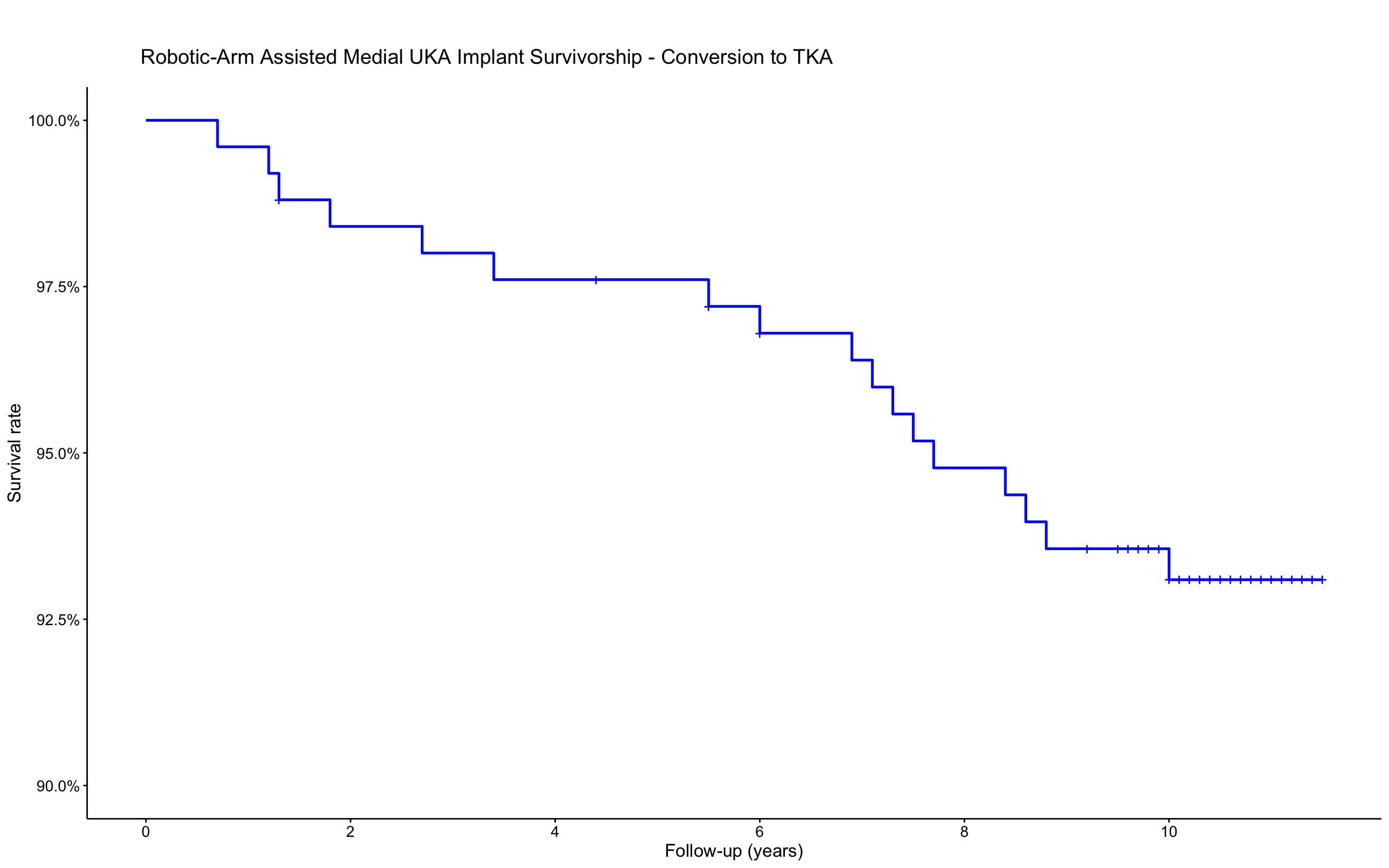
Figure 1
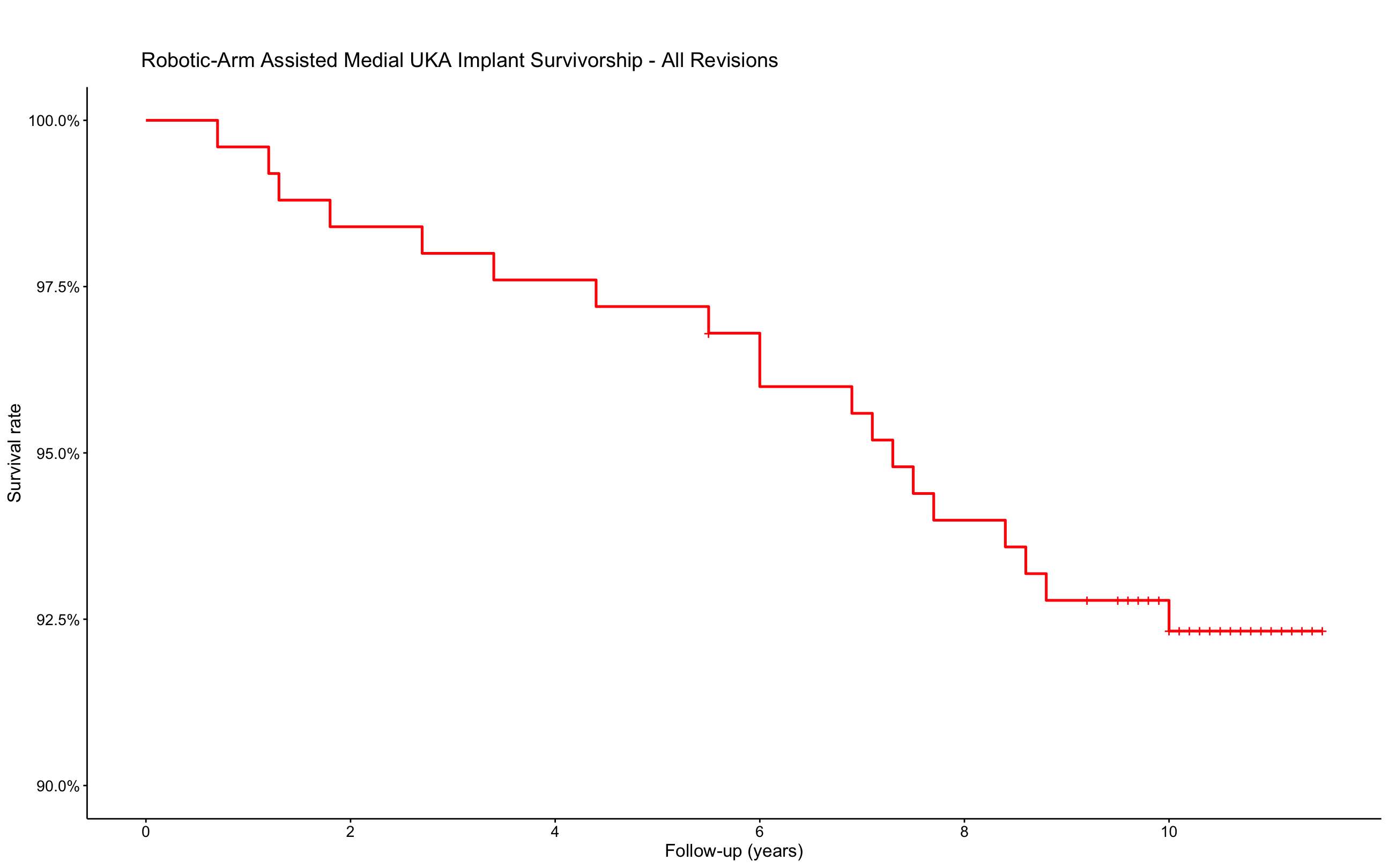
Figure 2#7414
Robotic-Assisted Medial Unicompartmental Knee Arthroplasty With a Ligament-Guided Technique Restores Pre-Arthritic Coronal Limb Alignment
*Tarik Bayoumi - Hospital for Special Surgery - New York, USA
Joost Burger - Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Univ - Berlin, Germany
Lindsey Ruderman - Hospital for Special Surgery - New York, USA
Joseph Nguyen - Hospital for Special Surgery - New York, USA
Hendrik Zuiderbaan - Medical Clinic Velsen - Velsen, Netherlands
Andrew Pearle - Hospital for Special Surgery - New York, USA
*Email: tbayoumi.md@gmail.com
INTRODUCTION: Robotic-assisted medial unicompartmental knee arthroplasty (UKA) with a ligament-guided technique is theorized to restore pre-arthritic coronal limb alignment in patients with medial compartment osteoarthritis and a correctable varus deformity. A ligament-guided technique differs from a “measured resection” or “alignment targeted” approach, as postoperative alignment results primarily from restoration of native medial collateral ligament (MCL) tension rather than pursuing a pre-determined alignment target. Intraoperative real-time feedback provided by the robotic system enables surgeons to restore ligament tension throughout the range of motion, thereby reconstructing normal knee kinematics and, theoretically, the patient’s pre-arthritic alignment This study aimed to assess whether postoperative alignment was equivalent to pre-arthritic alignment after robotic-assisted medial UKA, using the arithmetic hip-knee-ankle (aHKA) algorithm and contralateral unaffected knee to estimate pre-arthritic alignment.
METHODS: Patients with isolated medial osteoarthritis and a passively correctable varus deformity treated with robotic-assisted fixed-bearing medial UKA were retrospectively reviewed. Patients with an unaffected (Kellgren-Lawrence grade ≤2) contralateral knee and estimated pre-arthritic alignment of ≥0° of varus were included. Postoperative mechanical hip-knee-ankle (mHKA) angle of the operative knee was compared to aHKA of the operative knee and mHKA of the contralateral unaffected knee. Postoperative knee joint line obliquity (KJLO) was compared between the operative knee and contralateral unaffected knee. Equivalence between postoperative alignment and estimated alignment parameters was assessed through the two one-sided test (TOST) method with initial equivalence margins of ±2.0°.
RESULTS: A total of 102 patients were included (mean age 58.4 ±8.3, 75% male). Mean postoperative mHKA and aHKA were equivalent with a mean difference of -0.56° (1.68 SD, 01.7 SE, [90% CI -0.83 to -0.29], p <0.01) (Figure 1). Similarly, mean postoperative mHKA and KJLO of the operative knee were equivalent to the contralateral unaffected knee with mean differences of -0.61° (1.79 SD, 0.18 SE, [90% CI -0.90 to -0.31], p <0.01), and -0.40° (2.09 SD, 0.21 SE, [90% CI -0.74 to -0.06], p <0.01), respectively (Figure 1). Subsequent tests found that the TOST demonstrated equivalence for all alignment parameters with the margins further reduced to ±1.0° (Figure 2).
CONCLUSION: Mean postoperative alignment of the operative knees was equivalent within ±1.0° of mean estimated pre-arthritic alignment. These results imply that robotic-assisted medial UKA allows for successful restoration of pre-arthritic coronal limb alignment in patients with medial osteoarthritis and a correctable varus deformity, using re-tensioning of the MCL as primary guidance during balancing of the knee.
Figures
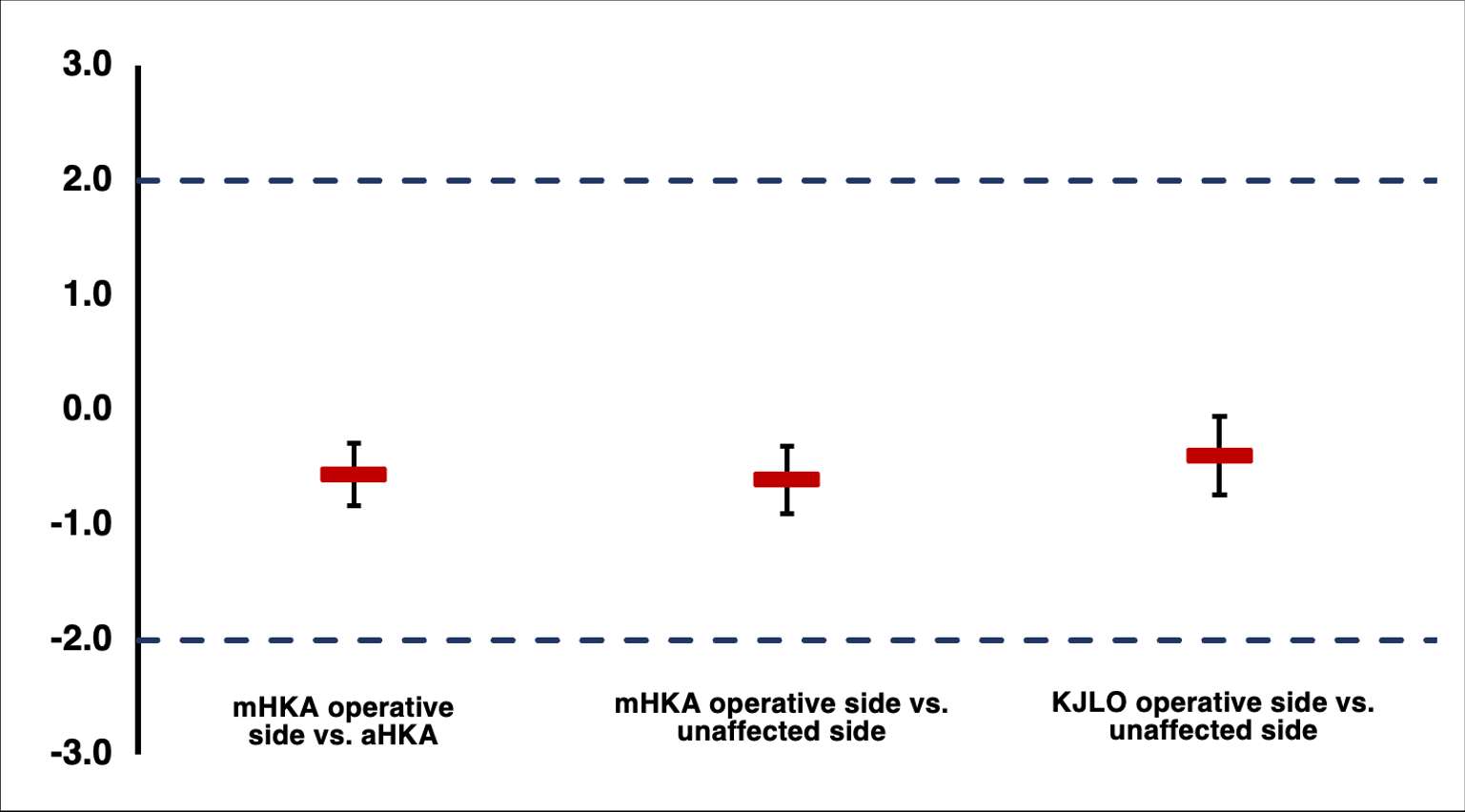
Figure 1
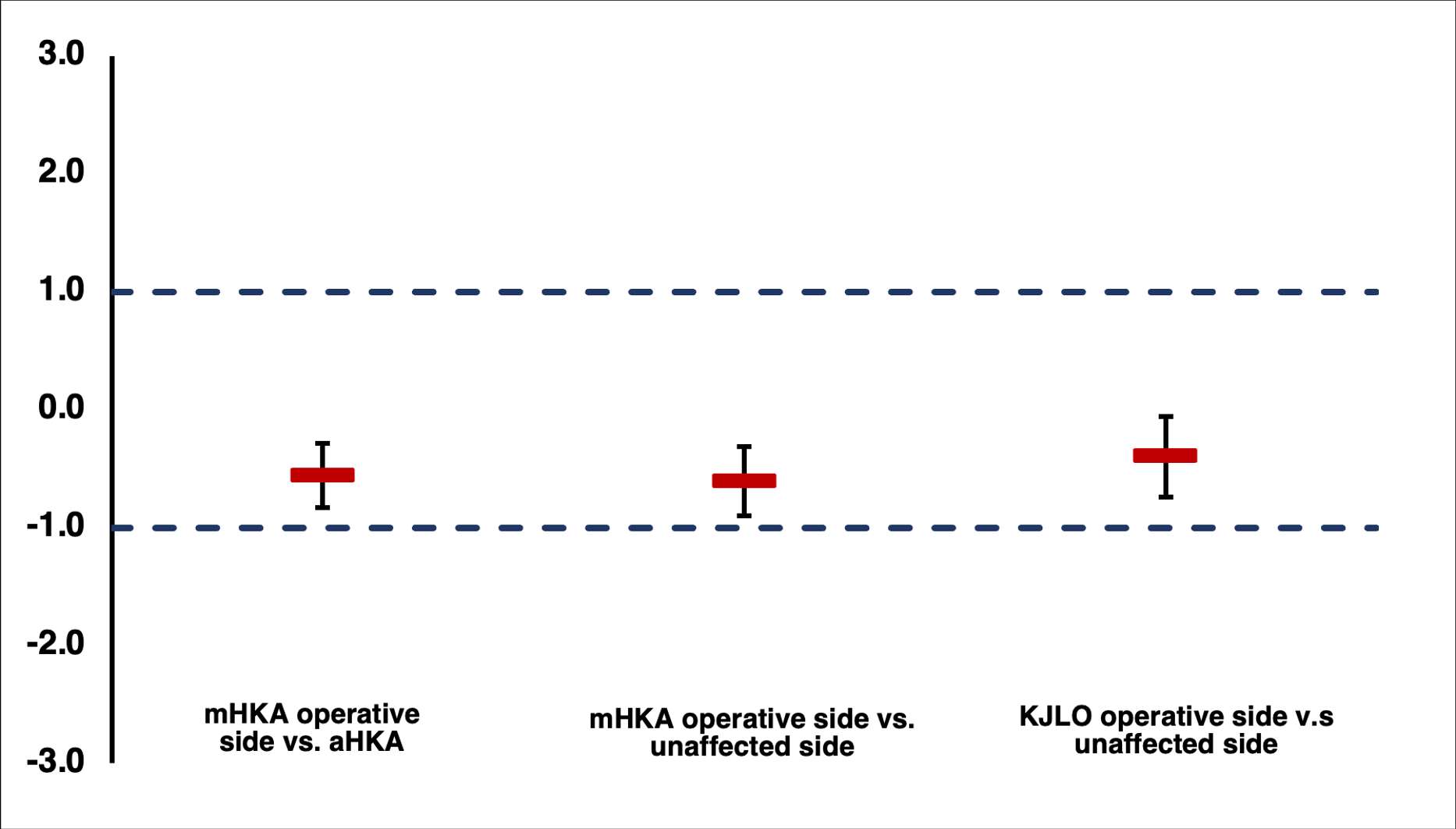
Figure 2#7897
Statistical Shape and Statistical Intensity Models of B2/B3 Eroded Scapulae With Reverse Shoulder Arthroplasty Research Applications
Claire Pearce - University of Victoria - Victoria, Canada
Aren Beagley - University of Victoria - Victoria, Canada
*Joshua Giles - University of Victoria - Victoria, Canada
*Email: jwgiles@uvic.ca
Introduction
Statistical Shape Models (SSMs) and Statistical Intensity Models (SIMs) describe bone variance in a population through Principal Component Analysis (PCA). SSM/SIMs can also be used to systematically generate scapulae with realistic shape and Hounsfield intensity, a surrogate for material properties. Our goal was to develop the first SSM/SIM based on patients with Walch-type B2/B3 eroded glenoids, which are challenging to treat with Reverse Shoulder Arthroplasty (RSA), and gain knowledge of this population’s full bone variation. We also investigated the significance of localized variation in the eroded glenoid.
Methods
SSM/SIM Development
Calibrated CTs from 39 patients with B2/B3 erosions were used. The SSM was constructed from corresponding surface meshes using an existing Non-Rigid Iterative Closest Point registration method and applying PCA. The SIM was constructed using PCA applied to corresponding volume meshes, created using Finite Element methods. Material properties were assigned using Mimics (Materialise).
Subset Determination
To understand how localized glenoid variation was explained by the SSM/SIM, eigenvectors from SSM/SIMs created for the full scapula were fitted to a glenoid-only data subset. The localized glenoid region was extracted using Python, while maintaining point/cell correspondence with the full model to allow for eigenvector fitting. The eigenvalues from the region-specific fitting were analyzed to determine the importance of each mode in glenoid variation.
Correlation
Generating scapulae with realistic shape and intensity requires both an SSM and SIM; however, if the modes of shape and intensity variation are strongly correlated, independently selecting weights for these models may not produce a realistic scapula when combined, in which case an all-in-one Statistical Shape & Intensity Model is required. To determine SSM-to-SIM correlation, the weights that reproduced each input patient model were determined for the 30 most important shape and intensity modes. All combinations (30x30=900) of SSM and SIM weights for each patient were correlated and ranked in descending order by R value.
Results
Figure 1 shows the difference in variance explained by each mode for the full scapula and glenoid-only subset. For the subset, Modes 3 and 1 explain 17.7% and 26.4% respectively, whereas for the full model they explain 12.3% and 50.4%. The top 30 correlations are only moderate and explain little variance within the full scapula analysis [Fig. 2]. The strongest correlation was between Shape Mode 30 and Intensity Mode 15 (R=0.563) [Fig. 3].
Conclusion
This analysis shows no strong/notable correlation between shape and intensity for B2/B3 eroded scapulae. A methodology for determining region-specific explanations of variance by modes of variation was developed. This methodology demonstrated that the relative importance of modes depends on the region considered; for instance, SSM Mode 1, which explains overall scaling, is less important to the glenoid while Mode 3 becomes more significant than Mode 2. Despite glenoid-specific differences in variance explained by each mode, no modes of variation were disproportionately important to the glenoid-only region compared to the full scapula. Therefore, SSM/SIM parameters can be varied independently to generate representative scapulae and be used in computational investigations of RSA (e.g. Finite Element modeling) that can yield more generalizable results.
Figures
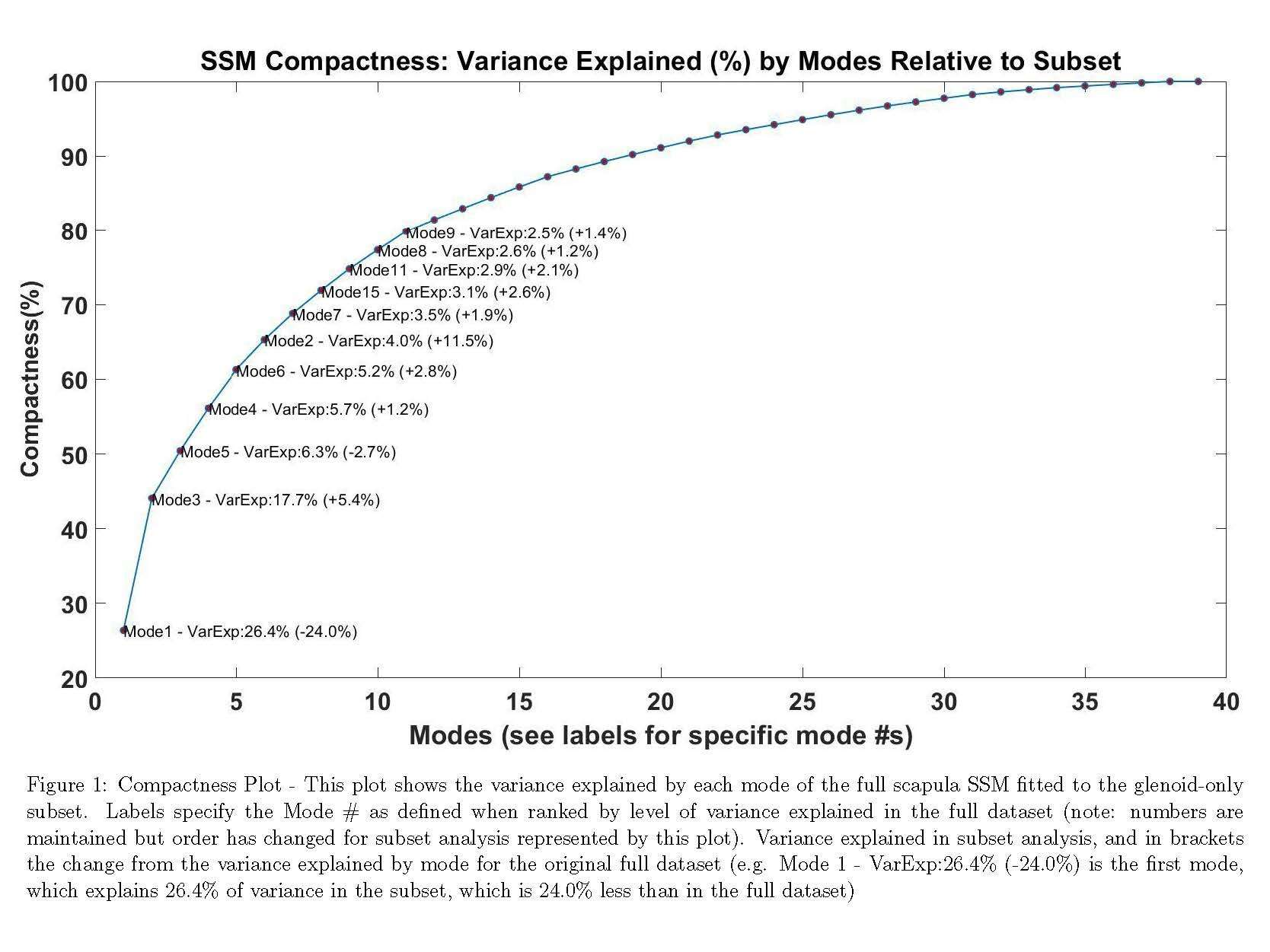
Figure 1
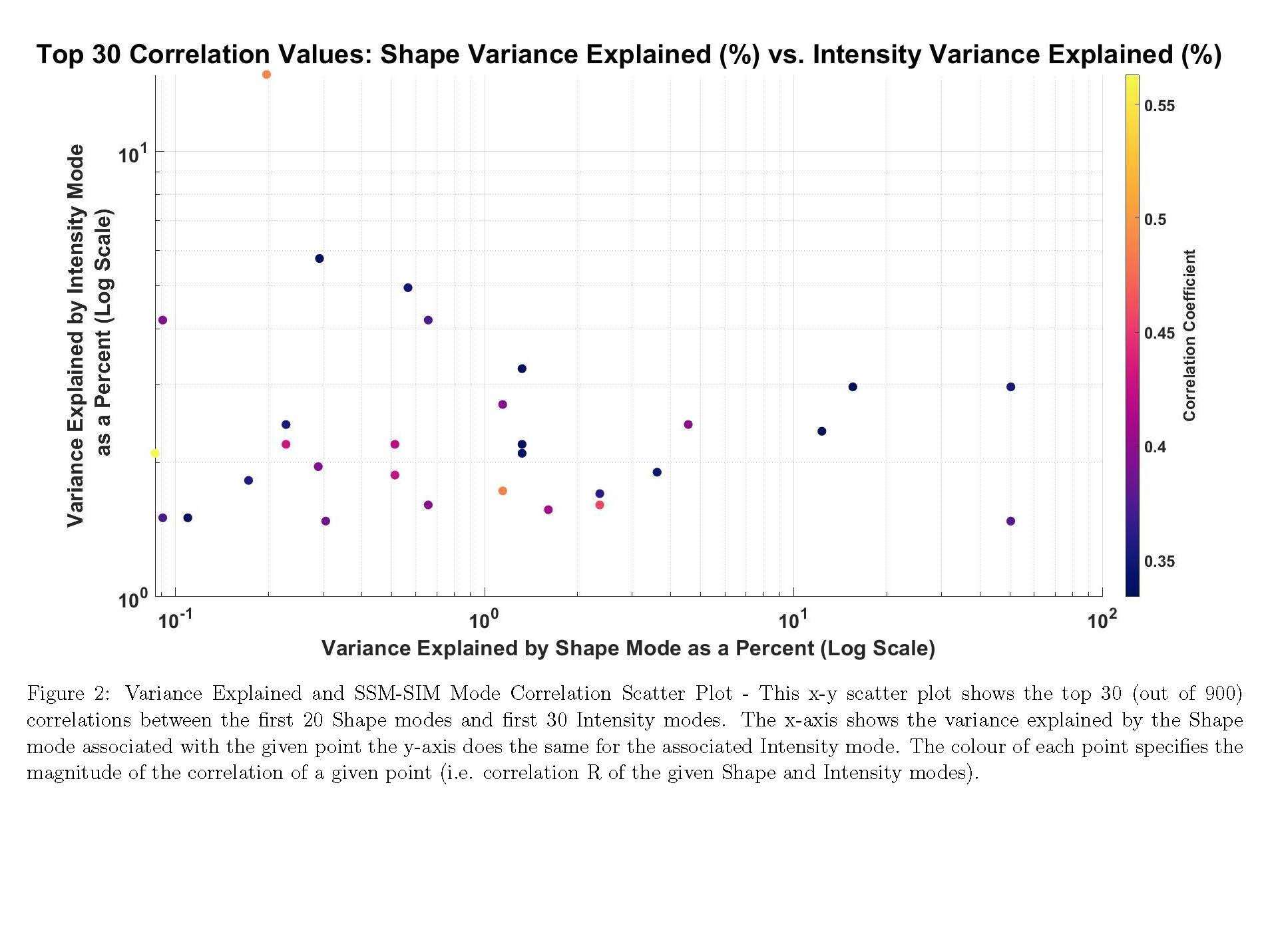
Figure 2
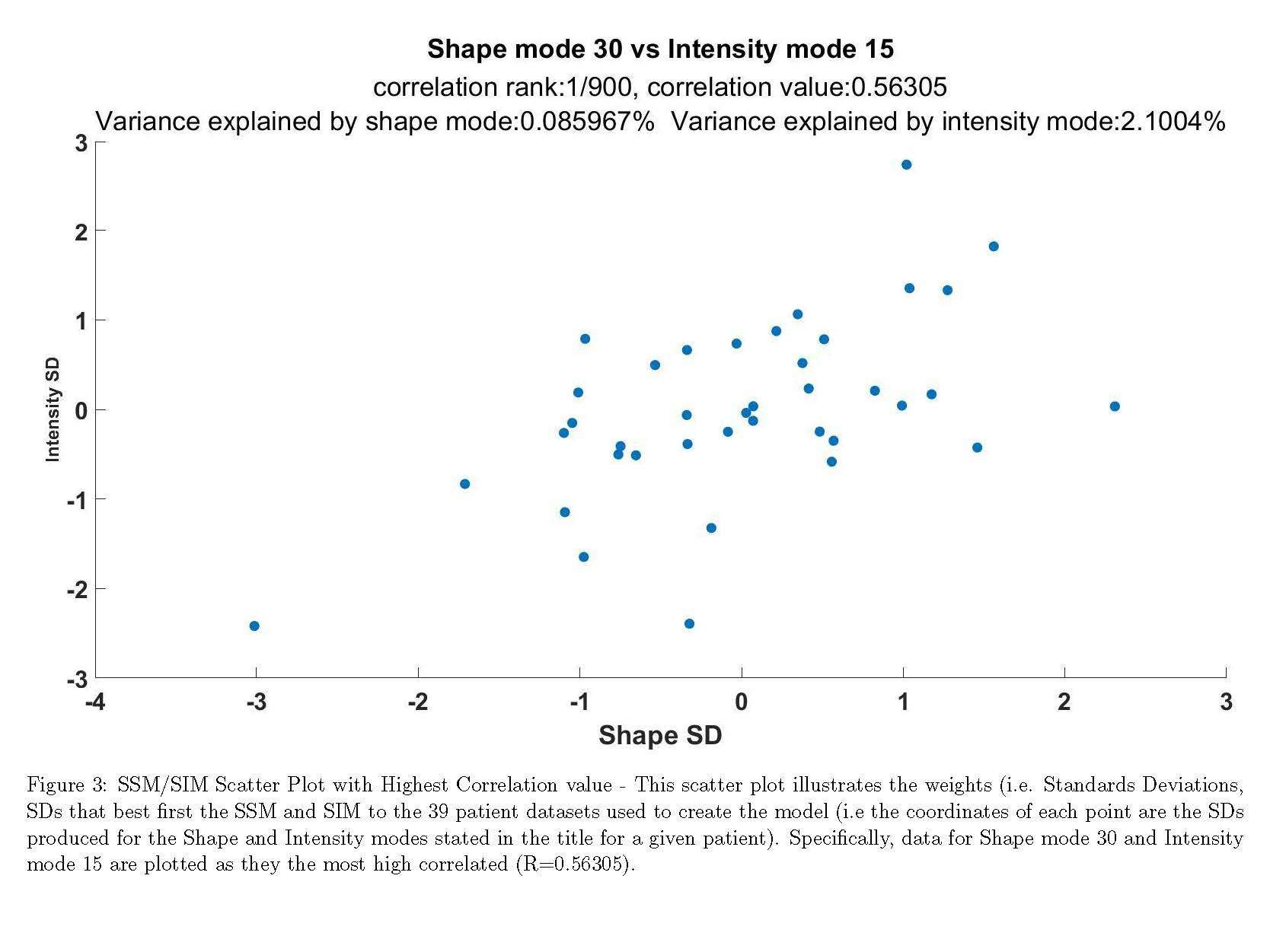
Figure 3#7819
Validation of a Method for Deriving Finite Element Simulations From a Statistical Bone Model
Aren Beagley - University of Victoria - Victoria, Canada
Asees Kaur - University of Victoria - Victoria, Canada
Claire Pearce - University of Victoria - Victoria, Canada
*Joshua Giles - University of Victoria - Victoria, Canada
*Email: jwgiles@uvic.ca
Introduction:
Integrating Statistical Shape & Intensity Models (SSIMs) with Finite Element (FE) simulations could generate simulations spanning the shape and material property variations in the population, thereby yielding more generalizable results and improving research efficacy. SSIM outputs, volumetric meshes with material properties, are difficult to integrate with existing FE workflows. Therefore, we developed a method to convert SSIM outputs into synthetic CT images compatible with virtual surgery and FE workflows. This work quantified conversion error under idealized conditions and estimated conversion accuracy relative to cubic-spline image reslicing under realistic conditions.
Methods:
Volumetric meshes of the scapula and humerus with realistic material properties comparable to SSIM outputs were created from 10 clinical CT scans, which served as ground truths. Material properties were in Hounsfield Units (HU). Meshes were converted into images using inverse distance weighted interpolation:
- u(x)=∑wi(x)·ui/∑wi(x), if d(x,xi)≠0
- u(x)=ui, if d(x,xi)=0
- where wi(x)=1/d(x,xi)8, r=2.1·(Voxel-Diagonal), and only points satisfying d(x,xi)≤r were considered.
Idealized Conditions: Synthetic images were generated by interpolating each mesh onto the voxel architecture of each source CT, thereby allowing direct comparison. Material property error was quantified as the absolute difference in HU at each voxel. Geometric error was quantified as the percentage of voxels added to and removed from the bone relative to the source CT.
Realistic Conditions: When converting an SSIM-derived mesh to a synthetic image, the original image properties are unknown, making one-to-one voxel correspondence unrealistic. Unaligned-synthetic image quality was compared against images created by reslicing each source CT onto each synthetic image using cubic-spline interpolation, which is a validated technique [Fig. 1]. The probability mass function (PMF) of HU, which gives the probability of a random voxel equaling a given HU value, was determined for the synthetic, cubic-resliced, and source images. Error was estimated as the mean absolute difference between the PMF of the source CT and the PMF of the derived images. An analysis of variance for a 22 factorial design with factors: bone type and image generation method, and paired t-tests (H0:μd=0, H1:μd≤0) comparing image generation methods for the scapula and humerus were performed.
Results:
Idealized Conditions: The aligned-synthetic images had a mean absolute HU error of 8.1 HU and standard deviation of 38.2 HU. The mean percentages of voxels added or removed were 0.059% and 0.103% respectively.
Realistic Conditions: See Figs. 2 & 3 for comparison of PMFs for the two techniques. There were significant effects for bone type (p<0.001), image generation method (p<0.001), and a significant interaction between these factors (p=0.001). The paired t-tests supported the synthetic images having less mean error than the cubic-resliced images for the scapula (p<0.001) and humerus (p=0.023).
Conclusion:
This study supports the validity of creating SSIM-derived synthetic CT images. The mean material property and geometric errors were low compared to CT scanner noise and inter-operator segmentation differences. Statistical analysis supports synthetic image generation being more accurate than cubic-spline reslicing and the synthetic images better preserved the bimodal distribution of HU compared to the cubic-resliced images. As such, this method may enable generation of FE simulations, derived from validated SSIMs, to accurately represent population-level variation.
Figures
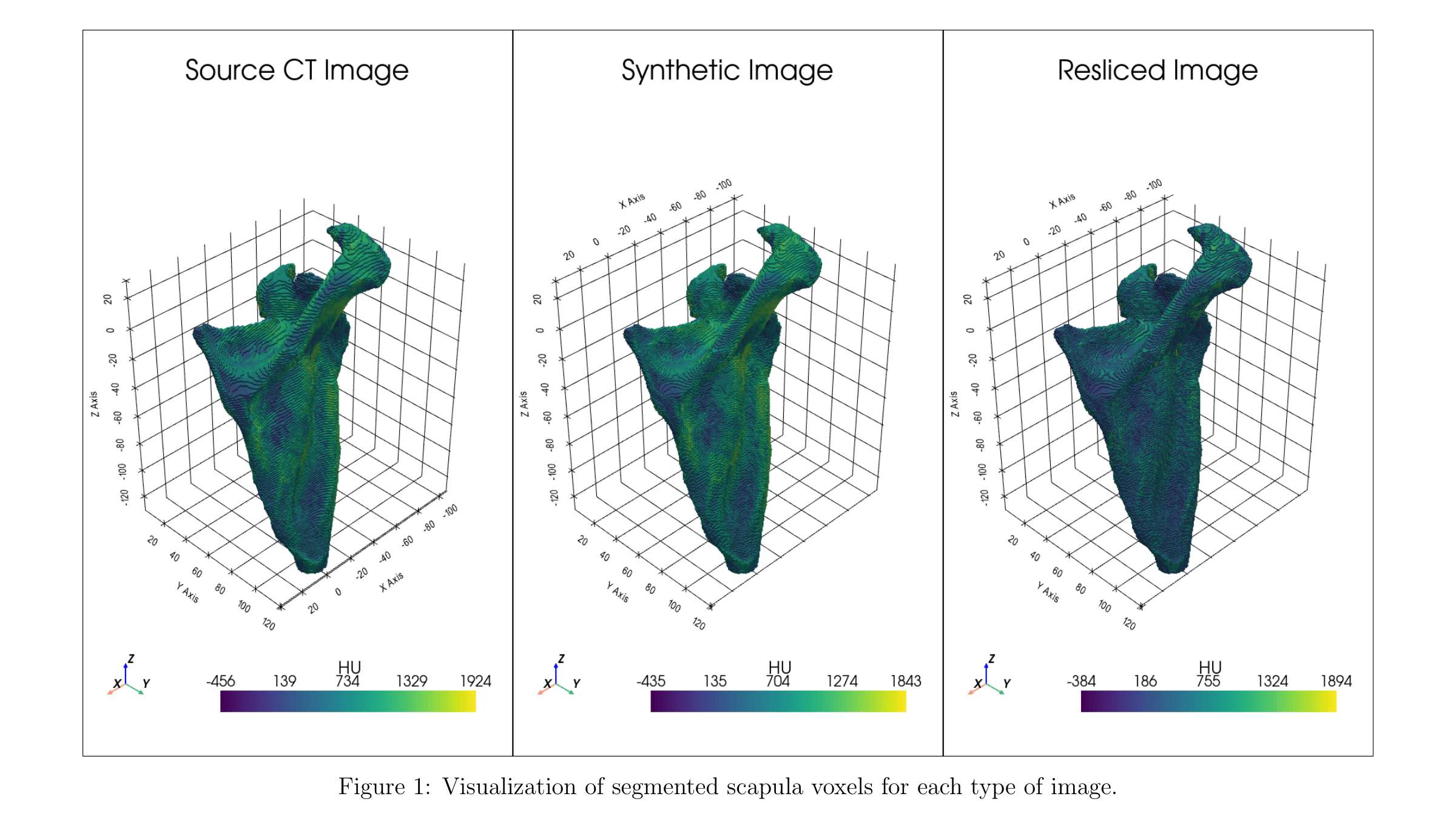
Figure 1
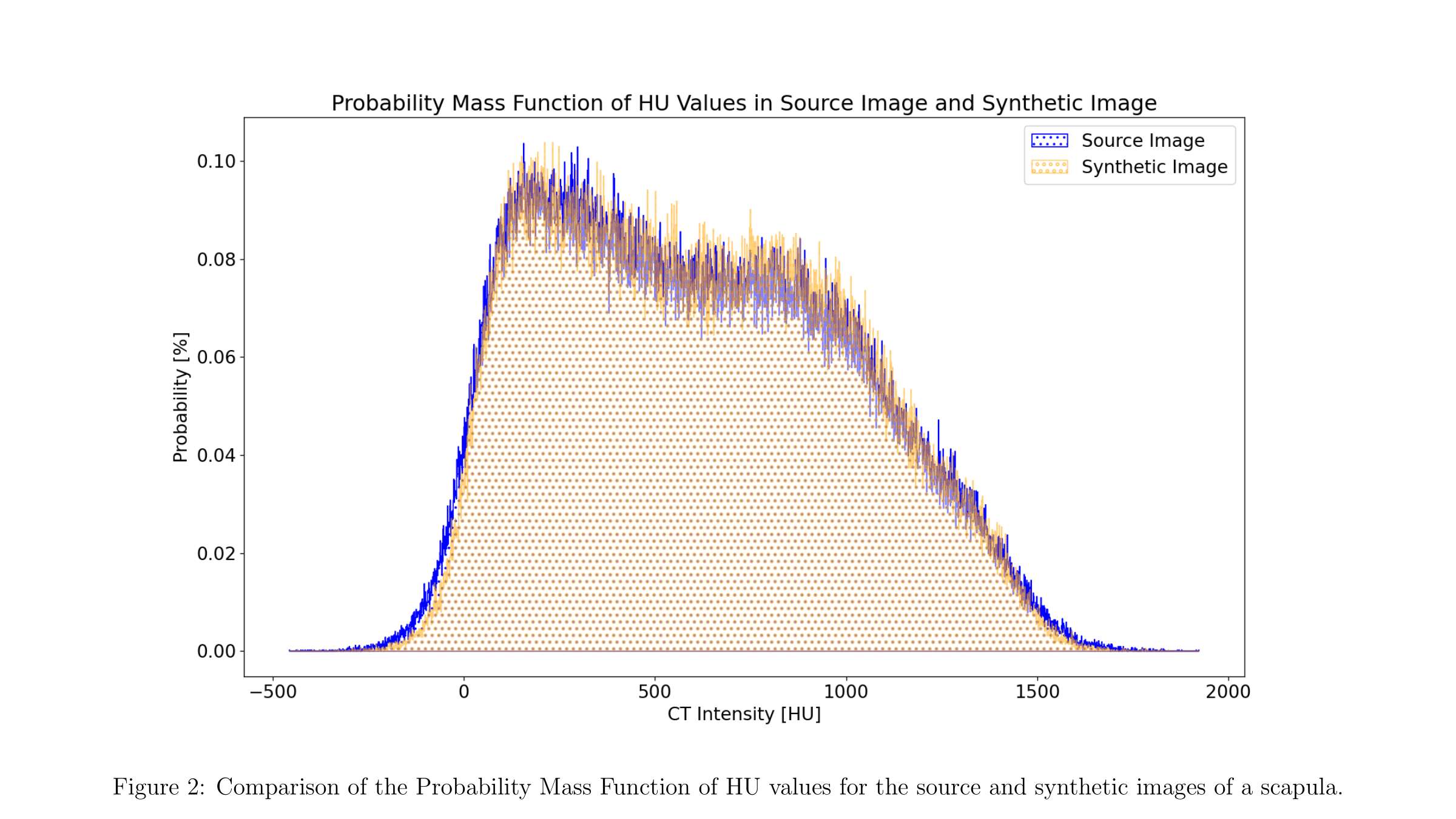
Figure 2
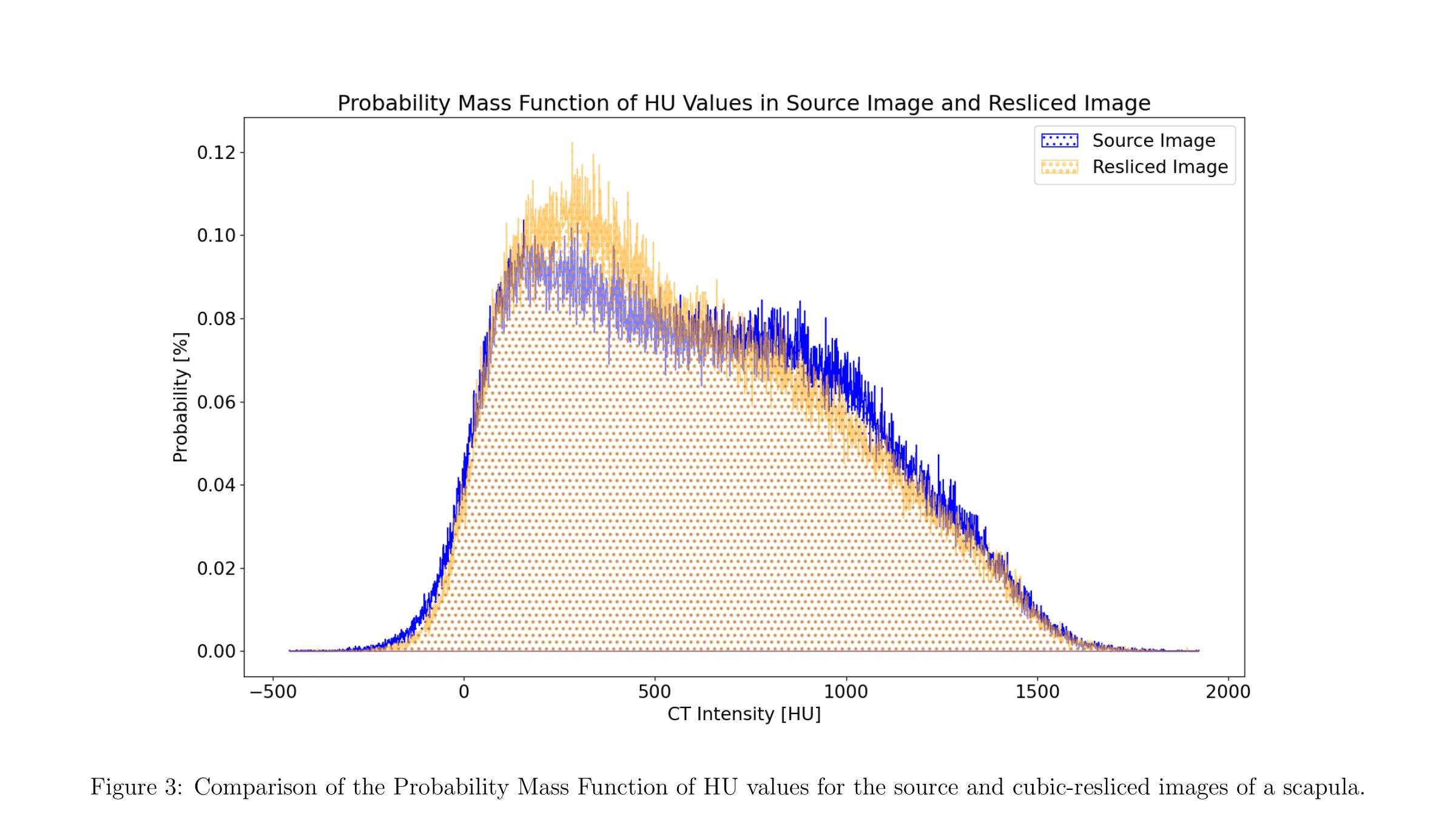
Figure 3#7901
Method to Preserve Thin Features of Bone During Synthetic CT Image Generation
Aren Beagley - University of Victoria - Victoria, Canada
Claire Pearce - University of Victoria - Victoria, Canada
*Joshua Giles - University of Victoria - Victoria, Canada
*Email: jwgiles@uvic.ca
Introduction:
Integration of Statistical Shape & Intensity Models (SSIMs) with Finite Element (FE) simulations can be achieved by converting SSIM volumetric mesh outputs into synthetic CT images compatible with existing virtual surgery and FE workflows. This could yield more generalizable results, thereby improving research efficacy. While there are existing methods for converting meshes into images, they require significant user input, introduce considerable noise, and are prone to thin feature loss. Therefore, we developed an algorithmic method to preserve thin features during mesh conversion. This work evaluated the effect of the thin feature preservation method when creating synthetic images of the scapula and humerus.
Methods:
Volumetric meshes of the scapula and humerus with realistic material properties comparable to SSIM outputs were created from 10 clinical CT scans, which served as ground truths. Material properties were in Hounsfield Units (HU). Meshes were converted into images using inverse distance weighted interpolation:
- u(x)=∑wi(x)·ui/∑wi(x), if d(x,xi)≠0
- u(x)=ui, if d(x,xi)=0
- where wi(x)=1/d(x,xi)8, r=2.1·(Voxel-Diagonal), and only points satisfying d(x,xi)≤r were considered.
When converting SSIM-derived volumetric meshes into synthetic CT images, voxel dimensions and axes must be set manually or algorithmically determined. For this work, axes were aligned with the global system and a voxel aspect ratio of 1:1:1 was chosen. Voxel dimensions were initially specified using the inverse of the ideal relationship between voxel and cell sizes established in previous work through a convergence analysis of mesh density’s effect on conversion error.
Thin features were identified by skeletonizing a high-resolution binary image created from the mesh and estimating thickness as twice the distance to the nearest mesh surface point for each skeletonized point [Fig. 1]. The minimum thickness was estimated as the mean of the thinnest 5% of points. To preserve thin features, if the estimated minimum thickness was less than the voxel dimensions calculated above, the voxel dimensions were set to equal the estimated minimum thickness. The origin was translated to create correspondence between a voxel in the synthetic image and the thinnest point.
Synthetic images were generated for all patient scapulae and humerii, with and without the thin feature preserving method. Synthetic image error was quantified as the mean absolute difference in Probability Mass Function of HU values, which gives the probability of a random voxel having a given HU value, between the synthetic and source images. Paired t-tests were performed to assess the effect of preserving thin features on the scapula (H0:μd=0, H1:μd≤0) and the humerus (H0:μd=0, H1:μd≠0).
Results:
The paired t-tests supported synthetic image error being reduced when using thin feature preservation for the scapula (p<0.001) but did not support a difference for the humerus (p=0.573).
Conclusion:
This study supports the validity of the developed thin feature preservation method as it demonstrates a reduction in conversion error for the scapula and produces similar error for the humerus. This matches expectations as the scapula may be a single voxel thick in some regions while the humerus has no thin features. As such, this method may be used with SSIMs of both flat and long bones to improve synthetic image quality.
Figures
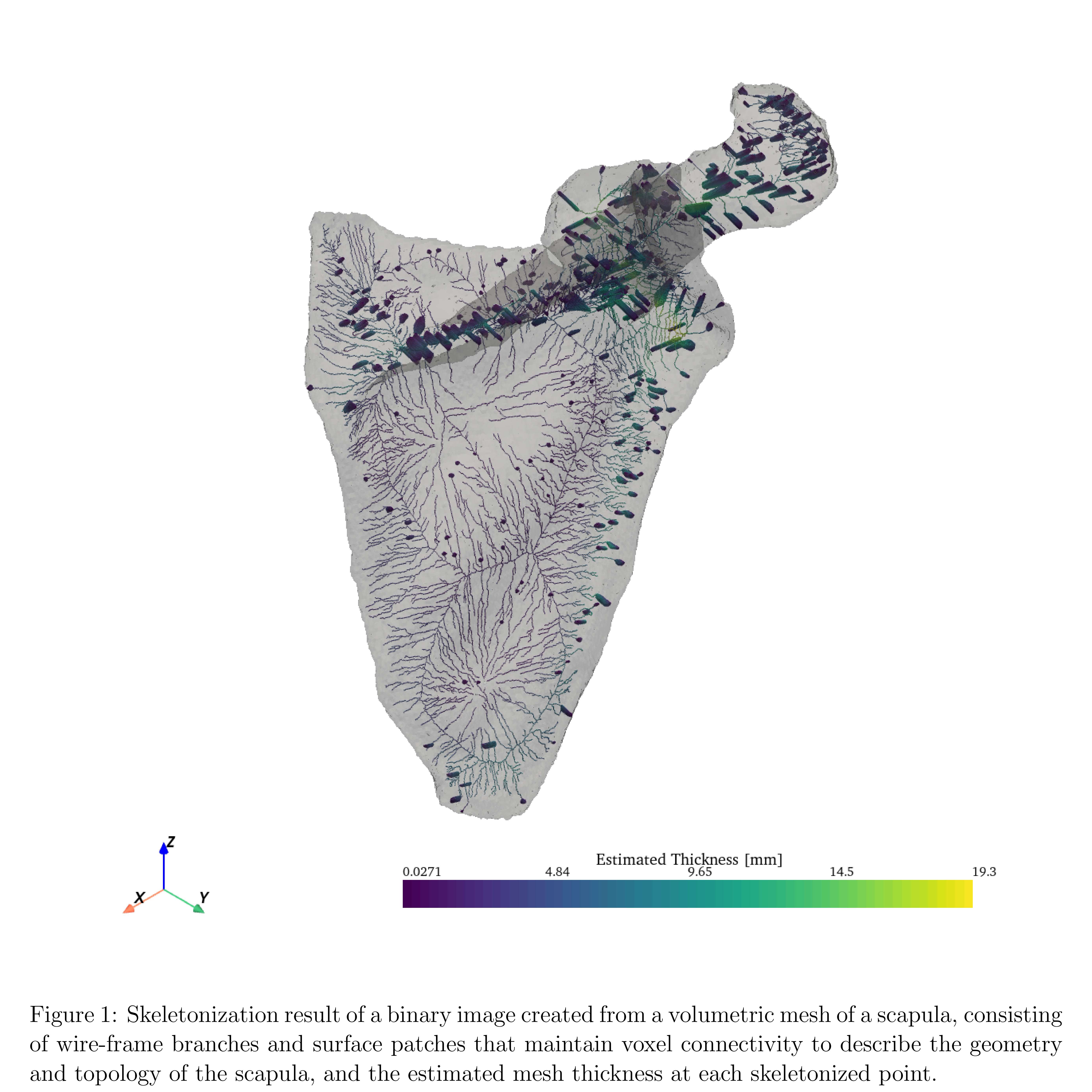
Figure 1#8018
Deep Learning-Based Automatic Segmentation of the Shoulder: Importance of Using Glenohumeral Joint Specific Metrics
*Joshua Giles - University of Victoria - Victoria, Canada
Erik Bedard - University of Victoria - Victoria, Canada
Alexandra Branzan Albu - University of Victoria - Victoria, Canada
*Email: jwgiles@uvic.ca
Introduction: Pre-operative planning for shoulder replacement relies on accurate CT scan segmentation, especially when these segmentations are used to design Patient Specific Guides (PSGs) because PSGs can become unstable intra-operatively if the actual bone geometry of the patient differs from the segmented 3D bone model. Therefore, inaccurate segmentation can lead to inaccurate surgeries and negatively impact clinical outcomes. Automatic deep learning-based medical segmentation methods have recently become popular, and have generally been shown to be effective, accurate, and reliable. However, there is currently a lack of published literature on accurate automatic segmentation of the shoulder for arthroplasty and existing evaluation methods do not explicitly consider glenoid segmentation accuracy, where segmentation is most challenging and accuracy is most important. Consequently, the aim of this paper is two-fold: (1) to develop state-of-the-art automatic deep learning segmentation models for shoulder arthroplasty, and (2) to develop methods to specifically evaluate glenoid segmentation accuracy.
Methods: A dataset of 58 clinically-relevant shoulder CT scans with varying arthritic changes were used. Manual ground-truth scapula and humerus segmentation labels were created with Mimics (Materialise) for network training and testing. For segmentation, the nnU-Net deep learning framework was used (Isensee et al., Nature Methods, 2021), which is a robust state-of-the-art method. The 3D patch-based full-resolution version of nnU-Net eas used to automatically segment the scapula and humerus. Network configuration, image pre-processing, data augmentation, network training, and post-processing were handled automatically by the framework. Five-fold validation was performed using 43 scans, and training took 27hrs for each fold using 16 CPU cores and a Tesla V100 GPU. The trained model then automatically segmented the scapula and humerus from unseen 15 test scans. To evaluate glenoid segmentation, the ground-truth glenoid geometry was automatically determined from the scapula labels using a mesh-growing algorithm (Ghafurian et al., JOR, 2016), which extracted a 10mm-thick section medial to the glenoid plane. The ground-truth geometry was then projected onto the nn-UNet scapula predictions to ensure the glenoid ground-truth and predictions had the same geometric constraints. The average surface distance (ASD), robust Hausdorff distance (HD), and volumetric dice (VD) evaluation metrics were computed for the full scapula and humerus, and the glenoid-only.
Results: Table 1 summarizes the segmentation prediction errors for the scapula, humerus, and glenoid, with the VD above 0.97 for all, ASD between 0.12-0.24mm, and HD under 1mm for all. The scapula and glenoid metrics were in good agreement on average across the 15 test scans, but one scan did exhibit HD errors in the glenoid double that of the scapula (0.98mm vs. 0.52mm; Fig.1).
Discussion: Based on the results, we have demonstrated the effectiveness of state-of-the-art deep learning methods for segmenting shoulder CT scans from patients undergoing arthroplasty. Although full scapula and glenoid-only segmentation metrics were similar on average, the 100% greater error in the worst test scan demonstrates the necessity of locally evaluating the glenoid segmentation due to its significant impact on surgical decisions and PSG design. Thus, glenoid-specific segmentation and evaluation methods should be integrated as a final step in segmentation pipelines.
Figures
Figure 1
Figure 2#7392
Vibratory Inserton of Orthopedic Implants
*Kambiz Behzadi - Behzadi Medical Device - Pleasanton, USA
*Email: kbehzadi@comcast.net
Vibratory Insertion of Orthopedic Implants
Total hip replacement is one of the most successful orthopedic operations, however it continues to be plagued with problems associated with poor alignment and poor fixation. Current technological advancements involve navigation and robotics which primarily focus on achieving desired alignment but ignore management of force for press fitting implants. Large robotic equipment in the OR space add to the workflow and complexity of the surgery, increasing cognitive load for the surgeon, arguably providing marginal improvements. We believe that in addition to cost, this issue is the primary reason that some of these technologies have not found universal adoption and acceptance within the general orthopedic community. We asked whether a simple handheld tool could provide better control over both the direction and magnitude of force, essentially making the operation easier rather than harder for the surgeon.
We theorized the vibratory insertion of the implants into bone involves a different physical phenomenon than what occurs with discrete impacts, as is done with a mallet or through commercially available automated percussive impacting devices. In contemplating the development of a vibratory insertion prototype we considered that if you are constrained by a constant level of energy (size of motor) and a given mass (the implant), frequency and amplitude/magnitude; or speed and torque are inversely related to each other. This is a limitation of classical mechanics. Figure 1.
Figure 1. Limitation of Classical Mechanics: Amplitude vs Frequency

We focused on emphasizing frequency and deemphasizing magnitude to produce a lightweight and less complicated handheld tool that is easy to use and allows the surgeon to maintain haptic connection with the patient. We developed several vibratory insertion tools with vibratory frequencies between 60Hz to 300Hz, all of which provided the ability to insert acetabular cups into bone proxies with between 300N to 800N of force, up to 90% lower than what was required with a mallet.
To monitor cup position and perform a controlled low force insertion of implants, we developed a mechatronic handle that uses existing IMU (Inertial Measuring Unit) technology to supplement the vibratory insertion tool. This tool allows the surgeon to place (not impact) the cup into the exact desired position and alignment, while monitoring the insertion process in a live fashion.
Investigations are continuing into additional dimensions of vibratory insertion. First, the prototypes we developed are only vibrating longitudinally in the Z axis. However, it is possible to include motion in one or more of six degrees of freedom. This would mean both longitudinal and rotational motion can be incorporated in any of the x, y, and z axes. Figure 2.
Figure 2. Oscillation Direction: In any one of six degrees of freedom.

Second, superimposition of ultrasonic vibrations on driven (sonic) vibrations, is thought to amplify the elastic response of bone, which could excite certain mode shapes and compression cycles that could be leveraged to decrease the hold of static friction. This could relieve interference fit and dramatically reduce the force required for insertion of implants.
#7560
Comparison of Numerical Methods for Modeling Trabecular Bone Indentation
Remy Benais - University of Waterloo - Waterloo, Canada
*Stewart McLachlin - University of Waterloo - Waterloo, Canada
Aleksander Rycman - University of Waterloo - Waterloo, Canada
*Email: stewart.mclachlin@uwaterloo.ca
Introduction: Computational modeling of trabecular bone indentation during implant subsidence has been extensively studied using the finite element (FE) method. Limitations of previous studies investigating implant subsidence have included simplified material properties, lacking consideration for continuum damage mechanics, and simplified bone-implant interface conditions that have prevented modeling of trabecular bone densification. As a result, studies have only inferred subsidence risk based on local stress and strain concentrations, lacking any inclusion of appropriate failure behaviour to accurately predict deformation with implant subsidence.
Recent work by Kulper et al. (2018) demonstrated a meshless smoothed particle hydrodynamics (SPH) based approach to model trabecular bone compaction upon implant insertion [1]. This novel FE approach yielded effective force-displacement results against experimental indentation test data, but there was no comparison performed by the authors to examine different numerical material models for trabecular bone behaviour.
The goal of this study was to implement a meshless SPH approach to compare different material models for the elastic-viscoplastic material behaviour of trabecular bone compaction.
Methods:The confined trabecular bone indentation test setup from the Kulper et al. [1] study was recreated in a commercial explicit solver (LS-Dyna, LST, Livermore, California).
Gathered literature data for time-dependent behaviour of bone tissues was used to identify appropriate constitutive material models for trabecular bone. Two numerical material models available within LS-Dyna were used as a starting point to represent the time-dependent bone behaviour: (1) a crushable foam material model (CF) [2], and (2) a plastic kinematic/isotropic material model (PKI) [3]. Both material models are compatible with SPH elements, which are effective in representing high strain, crushing, and localized densification and damage behaviours experienced during bone indentation.
Trabecular bone response for the two material models were compared based on the effective plastic strain fields at different indentation depths to examine the material model’s ability to accurately capture the crushing and densification phenomena.
Results: As shown in Figure 1, bone densification occurs predominantly below the indenter (punch) with the CF model. In comparison, trabecular densification for the PKI model is apparent all around the indenter. For this reason, CF’s behavior performs favorably to PKI in capturing the localized densification behavior in trabecular bone compaction. This is supported by previous evidence that showed trabecular bone exhibited whitening directly under the indenter during experimental indentation testing, as shown in Figure 2 [2].
Conclusion: The SPH method and its application in the modeling of trabecular bone has not been widely explored despite the promising applications for predicting trabecular bone damage. Additionally, CF models, thanks to their pressure-dependent yielding quality, have demonstrated improved post-yield response in comparison to PKI. The presented work shows the ability of the SPH method to qualitatively demonstrate trabecular bone crushing and densification behaviour, as well as the apparent benefit of pressure-dependent yielding in reproducing trabecular bone response.
References
[1] Kulper SA et al. J Orthop Res 2018.
[2] Kelly N et al. Biomech Model Mechanobiol 2013.
[3] Khor F UWSpace 2018.
Figures
Figure 1
Figure 2#7497
Nextar Tka: Augmented Reality Enhanced by Single Use Tracking System for Total Knee Replacement
*Daniele Ascani - Medacta International SA - Chiasso, Switzerland
Massimiliano Bernardoni - Medacta International SA - Castel San Pietro, Switzerland
*Email: ascani@medacta.ch
Introduction
The correct execution of a 3D-based preoperative planning in total knee replacement (TKR) is critical to reproduce the patient-specific alignment and to limit postoperative complications [1]. However, despite the availability of advanced tools, implant alignment due to the surgical execution is still a challenge [2].
Robotics, computer assisted surgical (CAS) systems, and lately augmented reality applications attempted to offer accurate surgical guidance to assist the surgeon in performing the surgical execution. Robotics and CAS applications have demonstrated to enhance the accuracy with respect to conventional instrumentation [3,4], at the cost of having bulky equipment in the surgical theater, and a significant increase of the costs [5]. Other augmented reality applications that embed passive QR images, to overcome bulky equipment and costs increase, seem to not have the required accuracy to reproduce a CT based preoperative planning [6].
The objective of the NextAR TKA system was to combine the augmented reality with a single use tracking system to execute a CT based preoperative planning for TKR.
Methods
The 3D models of 10 cadaveric knees were obtained from CT images, then 3 surgeons preoperatively planned the position of the femoral and tibial components virtually, simulating a total knee replacement. The execution of the preoperative planned was performed by using the NextAR TKA system which is composed by a single-use tracking system (small camera infrared and active tracker to be placed within the incision), augmented reality glasses, and a medical grade PC monitor (Figure 1).
Post-operative CT scans were performed to assess the implants positioning: the accuracy is intended as the deviation between the preoperatively planned values compared with the postoperative CT images.
Results
The results showed a significant correlation between the planned and executed values, mean deviation for the angles was 1,5° (SD 1°), whilst for the distances 1 mm (SD 0.6mm), respectively. The comparison between the values measured during the cadaveric testing by the NextAR TKA system and the postoperative results obtained on the postoperative CT images showed an average accuracy of 0,8° (SD 0.3°) and 0,7mm (SD 0.5mm).
The augmented reality was correctly used during the surgery (Figure 2) and the surgeons reported the following advantages:
- The data over imposed onto to the operative allowed to perform the surgical step with the sight always direct on the surgical area
- Light and wearable hardware worn under the surgical helmet
- Solution to the line-of-sight problem present in traditional navigation systems
Conclusion
The study successfully demonstrated the accuracy of the NextAR Knee system compared to published data on conventional instrumentation [3]. The combination of augmented reality and single use tracking system allows to accurately execute the positioning of the implants and the tracking of the bones through the range of motion. The novelty of the system lies on the use of an active tracking system which empowers the augmented reality hardware to ensure the high accuracy needed for surgical applications, compared to other surgical AR application which provides lower accuracy.
#7973
Assessment of 3D Positional Accuracy of a Surgical Tracker Based on the ASTM Standard: A Case Study
*Sylvain Bernhardt - Atracsys LLC - Lausanne, Switzerland
Alexander Eischeid - University of Nebraska Medical Center - USA
Hani Haider - UNMC - Omaha, USA
*Email: sylvain.bernhardt@smith-nephew.com
Navigation and robotics often rely on tracking to monitor the motion of surgical instruments and the patient’s anatomy. Objective assessment of a system’s tracking accuracy is necessary but is typically performed either in clinical trials or manufacturers’ laboratories without a standardized procedure of measuring and reporting. The authors helped draft and upgrade an international testing standard (1)for the objective assessment of the positional accuracy of such tracking systems. The standard describes a series of tests to be performed by means of a tracked pointer on a calibrated phantom. The aim is to assess the simplest of all functions; the accuracy of 3D tracking to locate a point in space. Such fundamental step governs the accuracy of all subsequent more advanced functions.
We performed the full standard procedure with an Atracsys optical tracking system used in clinical applications, to measure the accuracy at different locations in the measurable volume. Near the center where the phantom and the attached reference array were registered, the single point measurement accuracy was understandably best with a bias (mean error) of 0.06mm and precision (scatter) of 0.09mm across 20 separate measurements of a single point. That same operation, repeated at the furthest point in the measurable volume, yielded a bias of 0.22mm and precision of 0.39mm. Similarly, measuring 20 different points on the phantom yielded 190 measured distances which can be compared to the reference locations on the phantom as measured by CMM. In this distance test, the tracker scored 0.08mm and 0.30mm of mean error near the center and furthest location in the measurable volume, respectively.
The markers used in the tracked arrays were passive flat reflective disks, and therefore had restricted visibility under tilt with respect to the tracker compared to marker types. Nonetheless, our results showed that within [-50°, 50°] of pointer tilt (which was 10° beyond the nominal range), the precision (scatter) was 0.09mm near the center and 0.27mm at the furthest location of the measurable volume.
In this study, we provide further details and analysis regarding the variations of accuracy across the measurable volume, comparing other forms of optical tracking and flat markers. We offer our results publicly to start building a growing database for comparison between surgical tracking systems across labs and companies. More compared datasets are necessary to refine the methodology described in the international standard and to set more realistic and well-considered acceptance criteria to validate systems.
Nonetheless, other and more specific metrics should be used to better describe the overall performance of computer-aided orthopaedic systems (e.g., accuracy in orientation for cutting and drilling). The success in adopting this methodology will compel the production of other complementary standards. Enabling such standardized and objective performance comparisons between systems will help the regulatory bodies in their certification decision and hospitals in their purchase, ultimately improving the safety for the patient.
(1) ASTM F2554-18 Standard Practice for Measurement of Positional Accuracy of Computer Assisted Surgical Systems
Figures
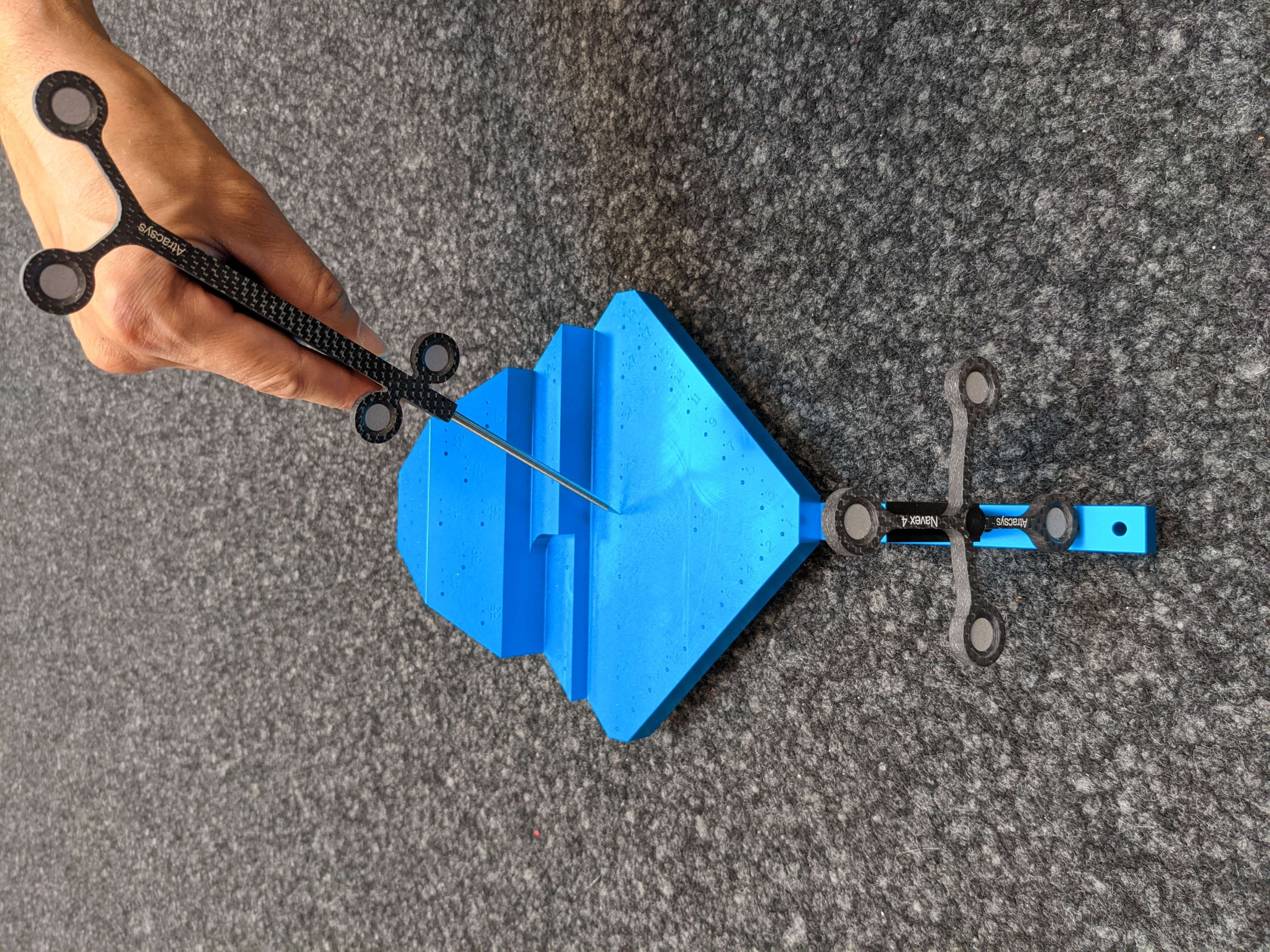
Figure 1
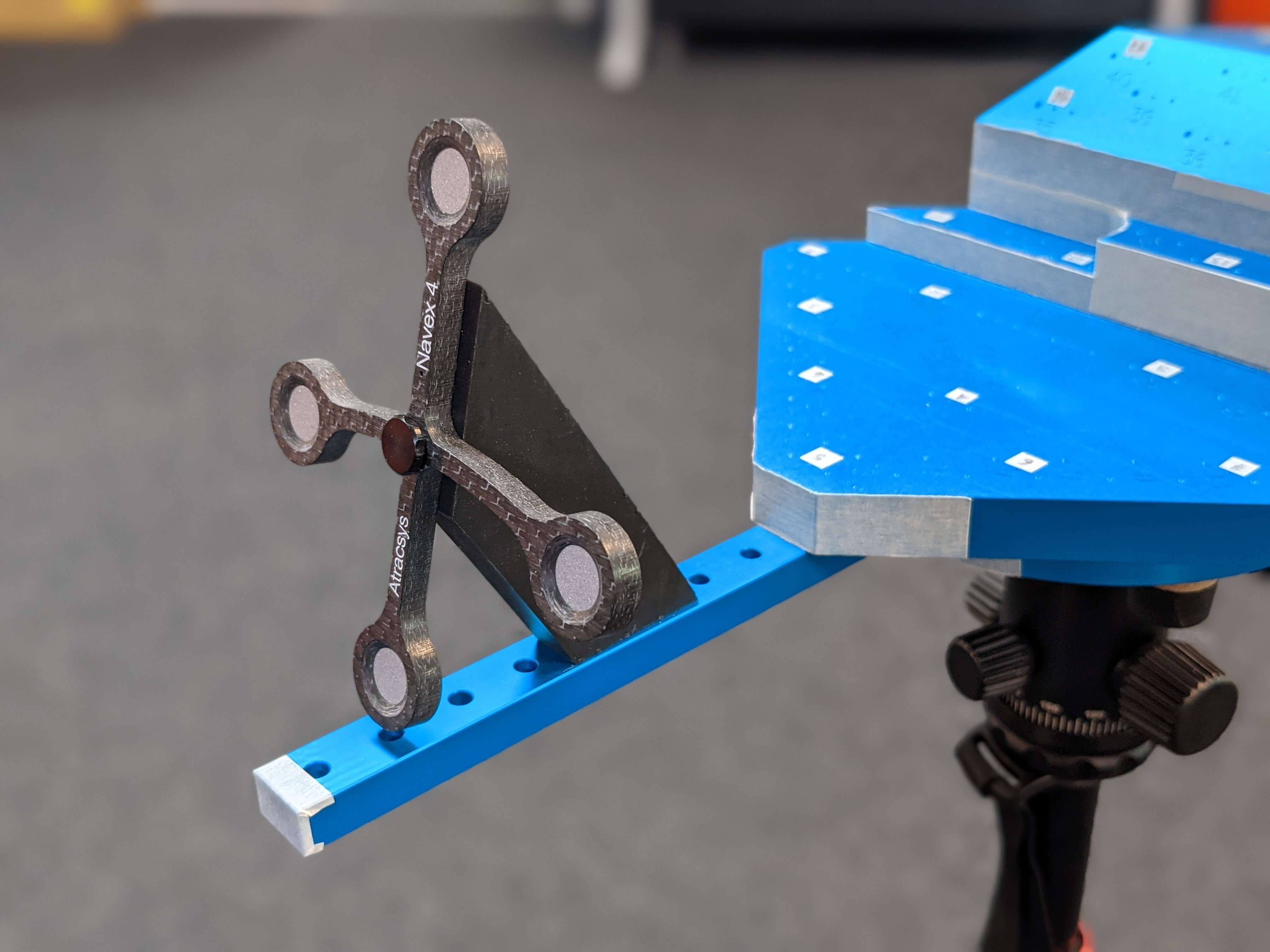
Figure 2#7793
Biomechanical Analysis of Posterior Stabilized Total Knee Arthroplasty Reveals Intraoperative Targets for Reducing Sagittal Plane Laxity in Midflexion
*Erin Berube - Hospital for Special Surgery - New York, United States of America
Cynthia Kahlenberg - Hospital for Special Surgery - New York City, USA
William Xiang - Hospital for Special Surgery - New York, USA
Joseph Manzi - Hospital for Special Surgery - New York, USA
Brian Chalmers - Hospital for Special Surgery - New York CIty, USA
David J. Mayman - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Michael B.Cross - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
Carl Imhauser - USA
*Email: berubee@hss.edu
INTRODUCTION: Knee instability in midflexion is a leading cause of patient dissatisfaction and revision surgery following total knee arthroplasty (TKA)1. Although surgeons assess coronal laxity intraoperatively, midflexion instability can involve abnormal motions and tissue loading outside of this plane2. Moreover, quantitative intraoperative targets for both coronal laxity and ligament tensioning to achieve clinically acceptable sagittal plane (i.e., anterior) laxity in midflexion remain ill-defined. Therefore, we posed the following research questions in posterior stabilized (PS) TKA. First, are laxities in the coronal and sagittal planes related? Second, are forces carried by the medial and lateral collateral ligaments (MCL/LCL) associated with sagittal plane laxity?
METHODS: Eight cadaveric knees (62.6 ±10.9 years; 5 male) underwent PS TKA (Zimmer, Persona) via measured resection by a board-certified orthopaedic surgeon. Each specimen was mounted to a robotic manipulator (ZX165U, Kawasaki) and then passively flexed from 0 to 90°. Coronal laxity was assessed by applying varus/valgus moments of ±6 Nm at 0 and 90° of flexion and measuring the resulting varus/valgus angulation. Anterior laxity in midflexion was quantified by applying an anterior load of 30 N at 30° of flexion. Forces carried by the collaterals were determined via serial ligament sectioning and the superposition principle. We related anterior laxity at 30° of flexion to coronal laxity and to MCL and LCL forces during passive flexion (i.e., pretension) via linear or nonlinear regressions to answer our first and second research questions, respectively. We reported regression coefficients (β or k), 95% confidence intervals, coefficients of determination (r2) and, for linear regression, the p-values (α=0.05).
RESULTS: Anterior laxity was positively associated with valgus and varus angulations at full extension (β = 5.0 mm/°, p = 0.001 and β = 4.5 mm/°, p = 0.03, respectively), but not at 90° of flexion (p≥0.2) (Fig. 1A) The median pretension in the MCL was 3.8 times greater than that of the LCL (MCL: 31 N, range: 1-161 N; LCL: 8 N, range: 0-45 N). Anterior laxity at 30° of flexion and pretension in the MCL were nonlinearly related (k= -0.02, r2 = 0.75) (Fig. 1B).
DISCUSSION: Anterior laxity at 30° of flexion was highly sensitive to valgus and varus angulations at full extension and to MCL pretension at 30° of flexion. Reducing anterior laxity in midflexion required MCL tensions that were greater than those of the native knee in this PS TKA design with relatively non-conforming bearing surfaces. Specifically, in the knees with AP translations ≤7.2 mm MCL pretensions averaged 79 ± 58 N, which exceeded that of the native MCL by more than three-fold3. Supraphysiological MCL tension may be related to clinical observations of post-operative increases in knee laxity over time. This cadaver model did not include muscle loading, but nonetheless revealed an important trade-off between MCL pretension and AP laxity. This trade-off could be an important consideration when selecting intraoperative targets for TKA ligament balancing.
ACKNOWLEDGEMENTS: Clark and Kirby Foundations
REFERENCES: [1] Paxton. JBJS 2010. [2] Abdel. BJJ 2014. [3] Kanamori. JOrthopSci 2000
KEYWORDS: Cruciate Resecting Fixed Bearing; Instability; Ligament Force
Figures
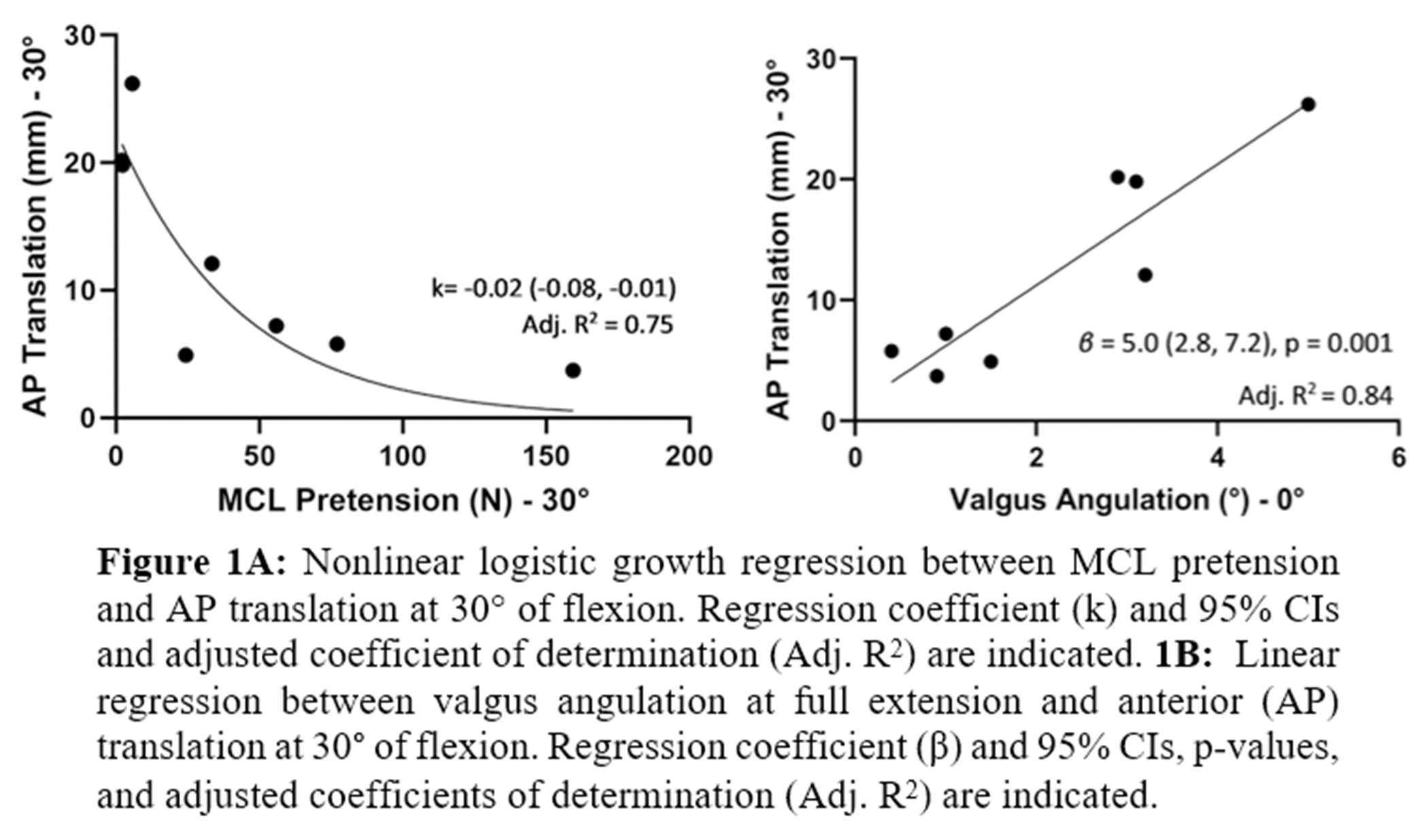
Figure 1#7830
Novel Arthrometer for Quantifying Knee Laxity in Three Planes: Safety and Reliability Assessment in Healthy Subjects
*Carl Imhauser - USA
Erin Berube - Hospital for Special Surgery - New York, United States of America
Thomas Fraychineaud - Hospital for Special Surgery - New York, USA
Zaid Zayyad - Hospital for Special Surgery - New York, USA
Jennifer Vazquez - Hospital for Special Surgery - New York, USA
Hamidreza Jahandar - Hospital for Special Surgery - New York, USA
Nicholas Sapountzis - Hospital for Special Surgery - New York, USA
Ethan Krell - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Andrew Pearle - Hospital for Special Surgery - New York, USA
Danyal H. Nawabi - Hospital for Special Surgery - New York, Select Country
Thomas Wickiewicz - Hospital for Special Surgery - New York, USA
Peter K. Sculco - Hospital for Special Surgery - NYC, USA
Brian Chalmers - Hospital for Special Surgery - New York CIty, USA
David J. Mayman - Hospital for Special Surgery - New York, USA
*Email: imhauserc@hss.edu
INTRODUCTION: Knee instability is a leading cause of patient dissatisfaction and revision surgery following total knee arthroplasty (TKA)1. Instability may involve abnormal knee laxity in multiple planes including varus-valgus (VV) angulation, anterior-posterior (AP) translation, and internal-external (IE) rotation 2. Unfortunately, few clinical measurement instruments quantitatively and objectively assess knee laxity in these three planes. Thus, the goals of this study were threefold: (1) to describe a custom-designed arthrometer that can quantify the VV, AP, and IE load-displacement responses (i.e., laxity) of the knee; (2) to assess its reliability; and (3) to determine its safety.
METHODS: The custom-designed arthrometer utilized an instrumented linkage with five degrees of freedom (DOF) (Fig. 1). Applied forces and moments were measured using a six DOF load cell (ATI, Inc), which was fixed to the arthrometer behind the subject’s proximal tibia. To conduct a test, the subject sat reclined in a chair, their leg was aligned in the arthrometer at 20° of flexion, the femur was fixed to the chair, and the tibia was fixed to the arthrometer with controlled forces ranging from 90 to 33 N via ratcheting mechanisms. The examiner manually applied AP forces (10 N posterior to 100 N anterior) and both VV (±4 Nm) and IE (±2.5 Nm) moments to the tibia and the corresponding translations and rotations were recorded (Fig. 1). With IRB approval, safety and reliability were quantified. For AP and IE testing, two examiners conducted two independent tests on the left knees of 34 healthy, uninjured volunteers (17 males, 17 females; mean age: 30 ± 7 years) with informed consent. The same protocol was followed for VV testing on the right knees of 10 more healthy, uninjured volunteers (5 males, 5 females; mean age: 24 ± 3 years). Reliability within a single test and within (intra) and across (inter) examiners was characterized via intra-class correlation coefficients (ICC) and 95% confidence intervals (CI). Pain was assessed on a visual analog scale from 0 (no pain) to 10 (excruciating pain).
RESULTS: Intra-trial reliability was excellent for all laxities (Table 1). For AP laxity, intra- and inter-examiner reliabilities were excellent. For IE rotation and VV laxities, intra- and inter-examiner reliabilities ranged from good to excellent. Pain across all tests averaged ≤0.7 ± 0.9. One volunteer discontinued testing due to skin irritation behind their calf.
CONCLUSION: We have developed a safe and reliable instrument to quantify knee laxity in three planes. AP translations had excellent ICC’s, potentially due to controlled fixation of the tibia and femur. IE rotations had acceptable but lower ICC’s, potentially due to inability to consistently control femoral rotation about its long axis. Safety and reliability assessments will next be conducted in the TKA population. Our arthrometer can provide data needed to link patient perceptions of instability with laxity in three planes towards improving implant design and surgical technique to address this common complication.
ACKNOWLEDGEMENTS: Clark and Kirby Foundations, Gosnell Family, Surgeon-in-Chief Fund
REFERENCES: [1] Paxton. JBJS 2010. [2] Abdel. BJJ 2014.
KEYWORDS: instability, arthrometer
Figures
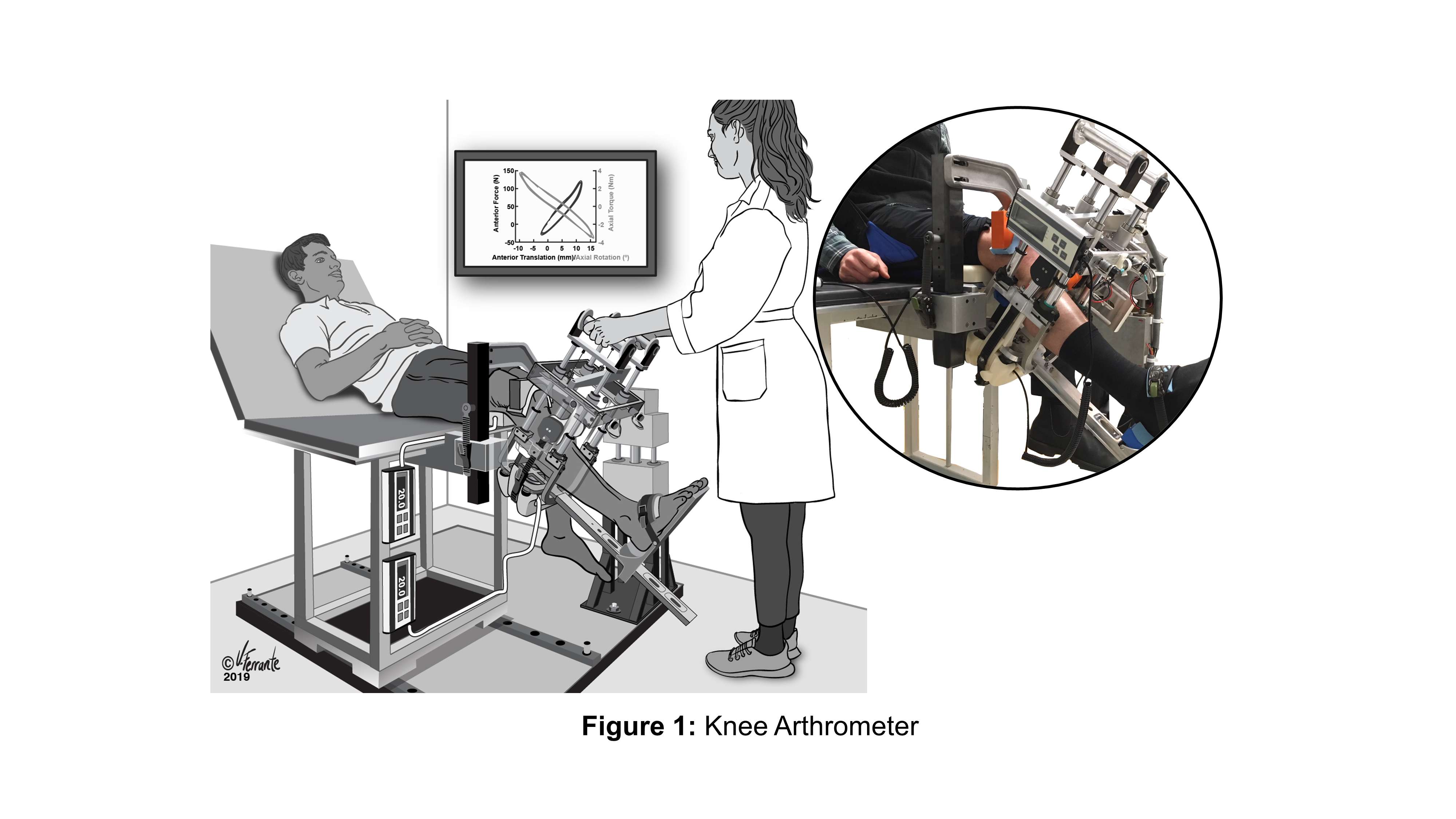
Figure 1
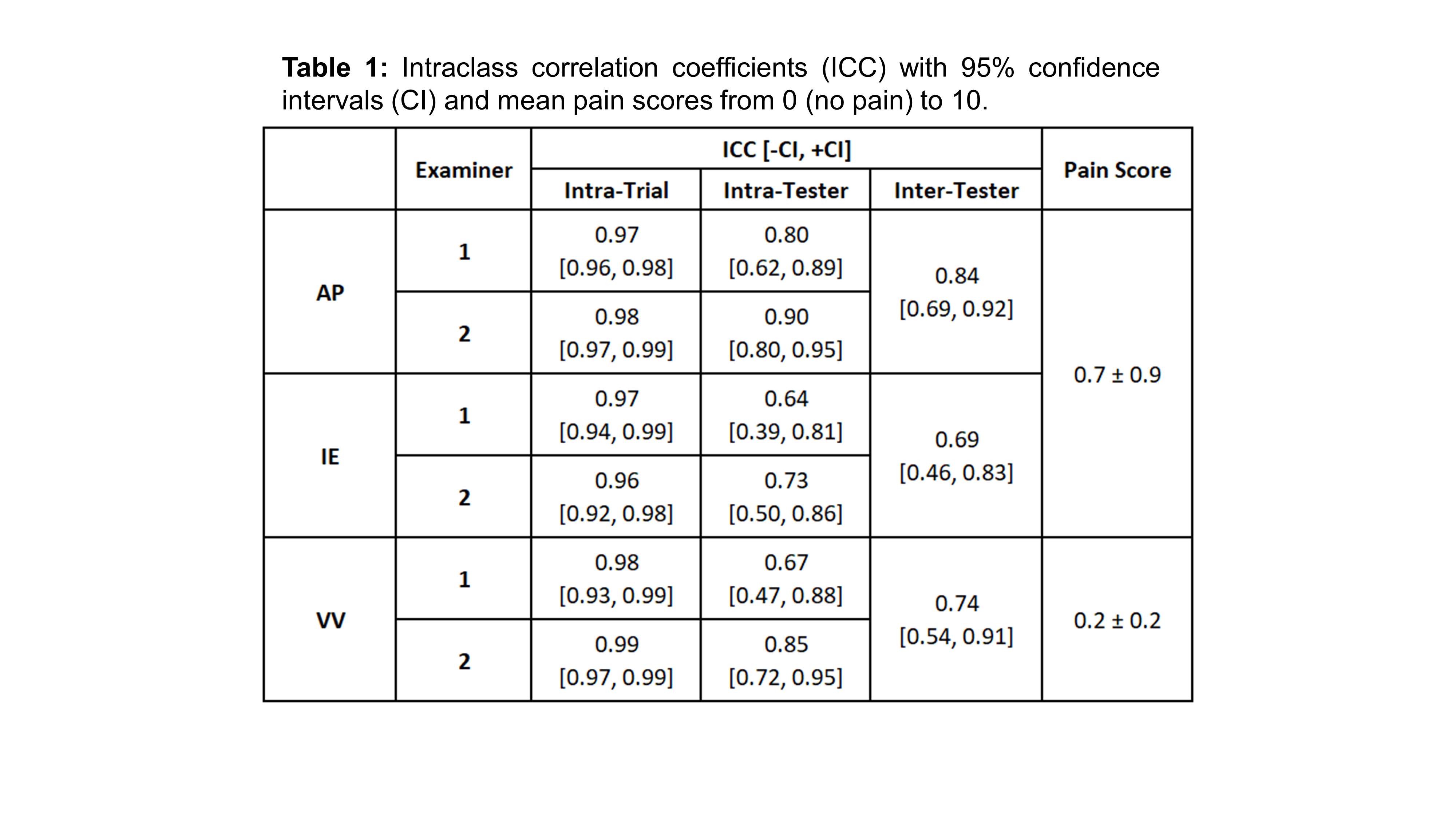
Figure 2#7602
Remote Evaluation of Post-Operative Outcomes Using Wearable Sensors Comparing Robotic-Assisted and Conventional Knee Arthroplasty
Faseeh Zaidi - University of Auckland - Auckland, New Zealand
Scott Bolam - University of Auckland - Auckland, New Zealand
Ted Yeung - University of Auckland - Auckland, New Zealand
Jacob T Munro - University of Auckland - Auckland, New Zealand
Michael M Hanlon - Auckland City Hospital - Auckland, New Zealand
Thor F Besier - University of Auckland - Auckland, New Zealand
*Andrew Paul Monk - University of Auckland - Auckland, New Zealand
*Email: apmonk@gmail.com
Introduction
Post-operative monitoring of patients following knee arthroplasty is essential to identify patients on a sub-optimal recovery course.Patient-reported outcome measures (PROMs) have a rapid ‘ceiling effect’ and fail to highlight differences in function or outcome when comparing knee replacement designs and implantation techniques. Ankle-worn inertial measurement units (IMUs) can be used to remotely measure and monitor the bi-lateral impact load of patients, augmenting traditional PROMs with objective data. The aim of this study was to compare IMU-based impact loads with PROMs in patients who had undergone conventional total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), and robotic-assisted TKA (RA-TKA).
Methods
57 patients undergoing primary knee arthroplasty (19 RA-TKA, 30 TKA, and 8 UKA) for osteoarthritis were prospectively enrolled. Remote patient monitoring was performed pre-operatively, then weekly from post-operative weeks two to six using bilateral ankle-worn IMUs and PROMs. IMU-based outcomes included: cumulative impact load, bone stimulus, and impact load asymmetry. PROMs scores included: Oxford Knee Score (OKS), EuroQol Five-dimension with EuroQol visual analogue scale, and the Forgotten Joint Score.
Results
Large variability in IMU-based outcomes were observed across the cohort, however, on average, patients improved impact load asymmetry by 67% (p=0.001), bone stimulus by 41% (p<0.001), and cumulative impact load by 121% (p=0.035) between post-operative week two and six (Figure 1). Differences in IMU-based outcomes were observed in the initial six weeks after surgery between surgical procedure (Figure 2). The mean change scores for OKS were 7.5 (RA-TKA), 11.4 (TKA), and 11.2 (UKA) over the early post-operative period (p=0.144). PROMs did not always reflect the same trend as IMU-based impact loads between the three surgical techniques. Improvements in OKS were consistent with IMU outcomes in the robot-assisted-TKA group, however, conventional TKA and UKA groups did not reflect the same trend in improvement as OKS, demonstrating a functional decline in the early post-operative period (Figure 3).
Conclusions
Ankle-worn IMUs provide objective measurement of bi-lateral impact loads, which can be used to augment PROMs to evaluate patient progress following knee arthroplasty. Our data illustrate that PROMs do not necessarily align with patient function, with some patients reporting good PROMs, yet show a decline in cumulative impact load or load asymmetry. These new IMU-based measures can supplement existing PROMs to provide a holistic overview of post-operative recovery and identify ‘at-risk’ outlier patients on a sub-optimal course.These data also provide evidence for a difference in the functional outcome of TKA and UKA patients that might be overlooked by using PROMs alone.
Acknowledgements
We would like to thank VICON-IMeasureU (Vicon, Oxford, UK) for providing the IMU sensors and database/cloud computing infrastructure for this study. This project was kindly funded by NZ Medical Technologies Centre of Research Excellence (MedTech CoRE, New Zealand). Thanks also to Megan Lovatt for her assistance with collecting the data.
Figures
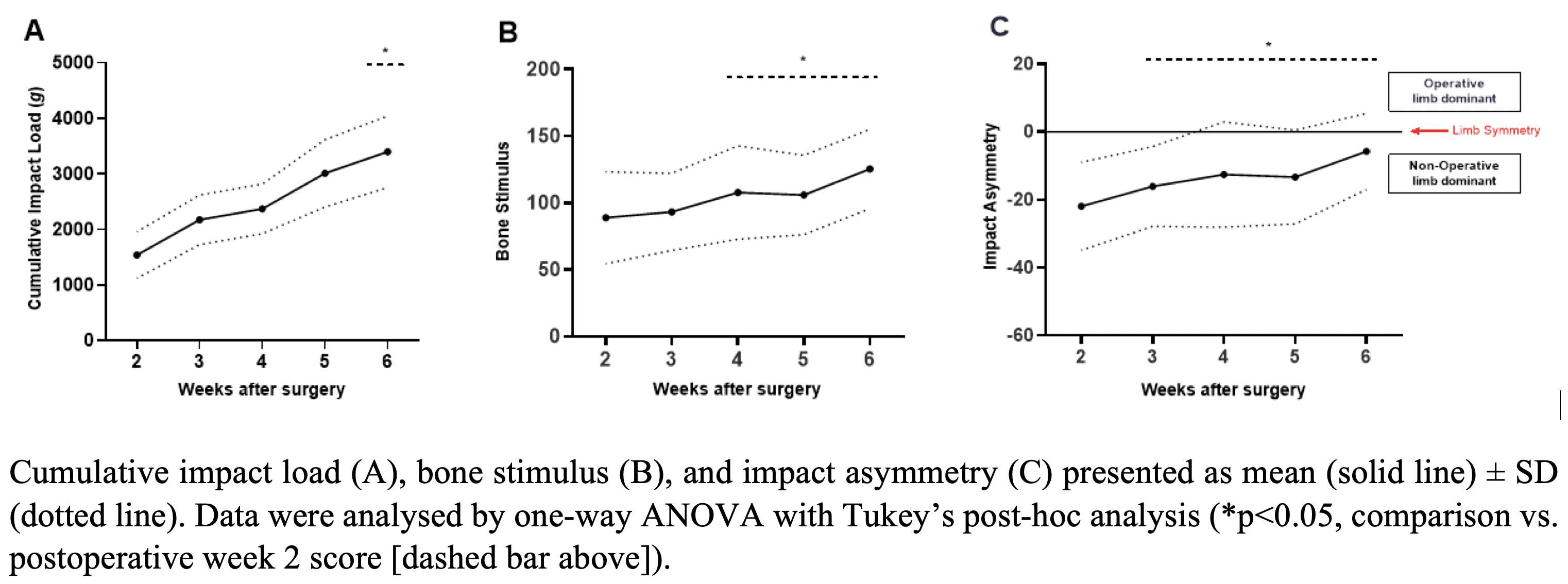
Figure 1
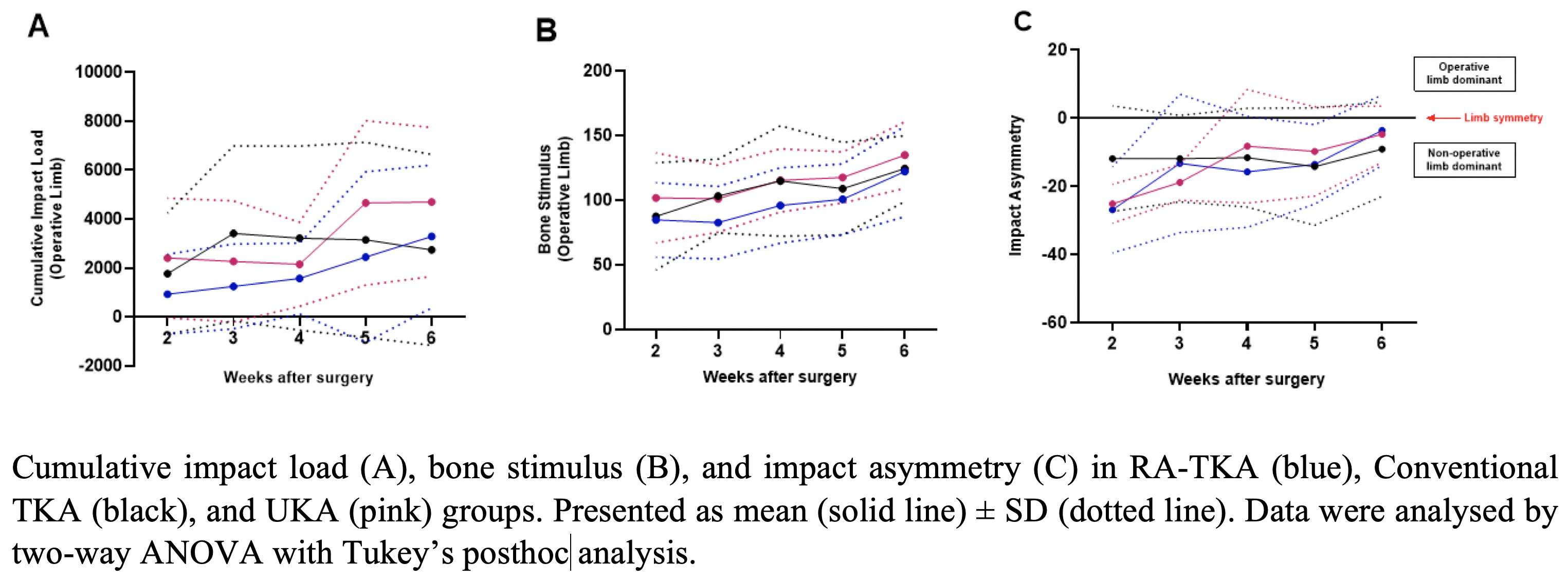
Figure 2
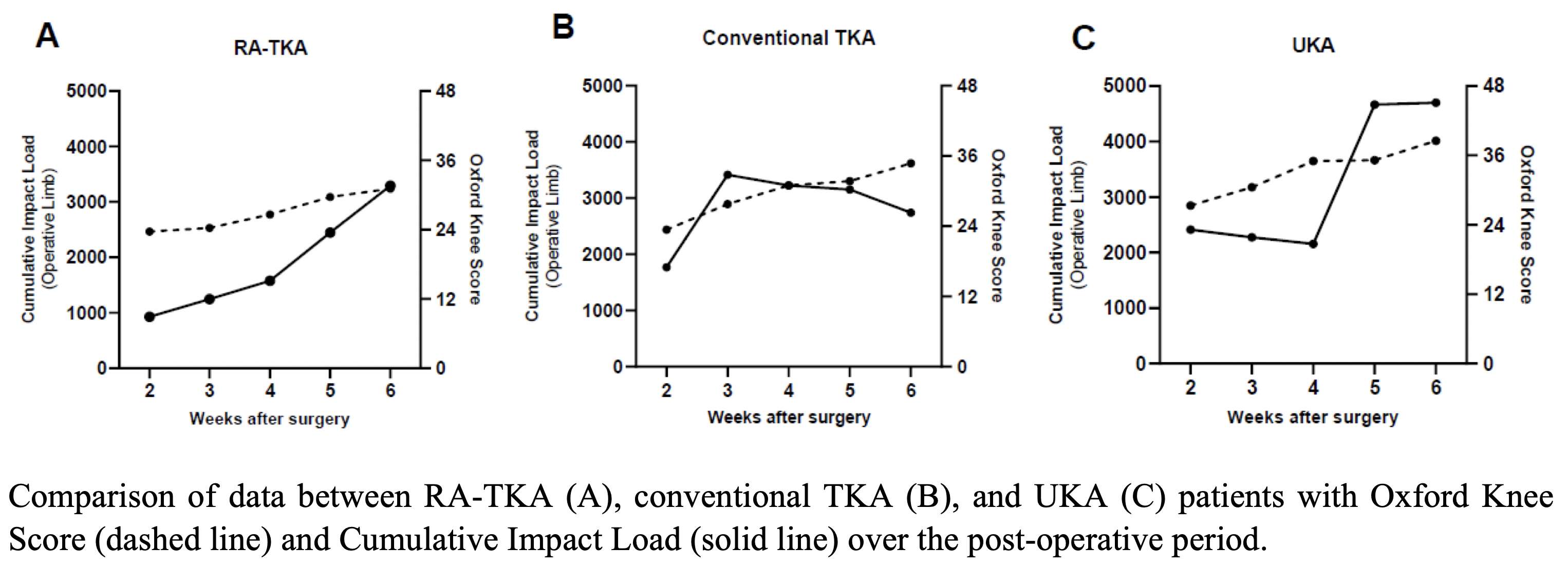
Figure 3#7468
Automated 3D Preoperative Planning Can Assist Surgeons in Restoring Native Hip Joint Biomechanics
Lilian Lim - FormusLabs - Auckland, New Zealand
Maximilian Pentecost - Zimmer Biomet - Belrose, Australia
Alex Carleton - FormusLabs - Auckland, New Zealand
Ju Zhang - Formus Labs - Auckland, New Zealand
David Liu - Gold Coast Centre for Bone and Joint Surgery - Tugun, Australia
Patrick Weinrauch - Brisbane Hip Clinic - Brisbane, Australia
*Thor F Besier - University of Auckland - Auckland, New Zealand
*Email: t.besier@auckland.ac.nz
Introduction
Although total hip arthroplasty (THA) is regarded as the “operation of the 20th century”, between 7% and 23% of patients experience unfavourable outcomes [1]. Restoring native hip kinematics, avoiding impingement, and maximizing range of motion can be challenging in THA, due to complex coupling between patient anatomy, kinematics, and implant design [2]. Pre-operative planning can assist surgeons to select and place implants, however, conventional templating from anterior-posterior (AP) radiographs cannot account for this complex coupling. CT scans provide accurate geometry for biomechanical simulation to optimize planning but have been limited to research use. The purpose of this study was to assess an automated CT-based pre-operative planner, comparing planned versus native 3D center of rotation (COR) and planned versus delivered cup size, position, and anteversion.
Methods
31 participants (8 males; 23 females, mean age 66.2 years) were included in this study and underwent routine surgery by two experienced surgeons. Patients were implanted with the Taperloc Complete Microplasty® and Reduced Distal stems (Zimmer Biomet, Warsaw, IN) using free-hand anterior and posterior approaches. Pre- and post-operative CT scans were taken within a month of surgery. Pre-op scans were input to an automated 3D planning software (FormusLabs, Auckland, NZ) that automatically segmented the pelvis to define the native acetabular COR and predict the cup size, position, and orientation using an optimization algorithm (Figure 1). The algorithm simulates contact with the acetabulum, whilst maximising coverage and range of motion with the fitted stem and minimising deviation from the native COR. Pre- and post-operative pelvis and cup models were co-registered to the pelvis to enable calculation of planned vs native COR and planned vs delivered COR.
Results
Planned COR was, on average, shifted 3.1 ± 2.9 mm more medially, 0.9 ± 1.8 mm posteriorly, and 0.1 ± 2.4 mm superiorly than the native COR. Good agreement was observed between planned and delivered COR, with mean differences <1 mm in all three planes (Figure 2, p > 0.1). A difference of 1.8° was observed between the planned cup anteversion (16.7 ± 5.1°) and delivered cup anteversion (18.5 ± 5.0°, p = 0.026). Predicted cup sizes were all within two sizes of delivered cup size, with 35% having an exact match, 52% within one size and 13% within two sizes.
Conclusion
Automated 3D functional planning from CT offers new opportunities to optimize implant selection and positioning for total hip arthroplasty, with advantages over 2D templating. The weighted-optimization criteria produced a plan with a COR that was close to the native COR, accounting for fixation, coverage and complex coupling of stem fit. CT scans provide an additional advantage over x-ray by enabling bone density information to inform the plan. The close match between the planned and delivered cup size and position provides confidence in the optimization approach. Finally, despite the lack of navigation, the 3D visualization assisted surgeons to execute the plan with reasonable accuracy.
References
- Beswick, A et al. 2012. BMJ Open, 2, e000435.
- Scott, C et al. 2022. The Bone & Joint Journal, 104, 189-192.
Figures
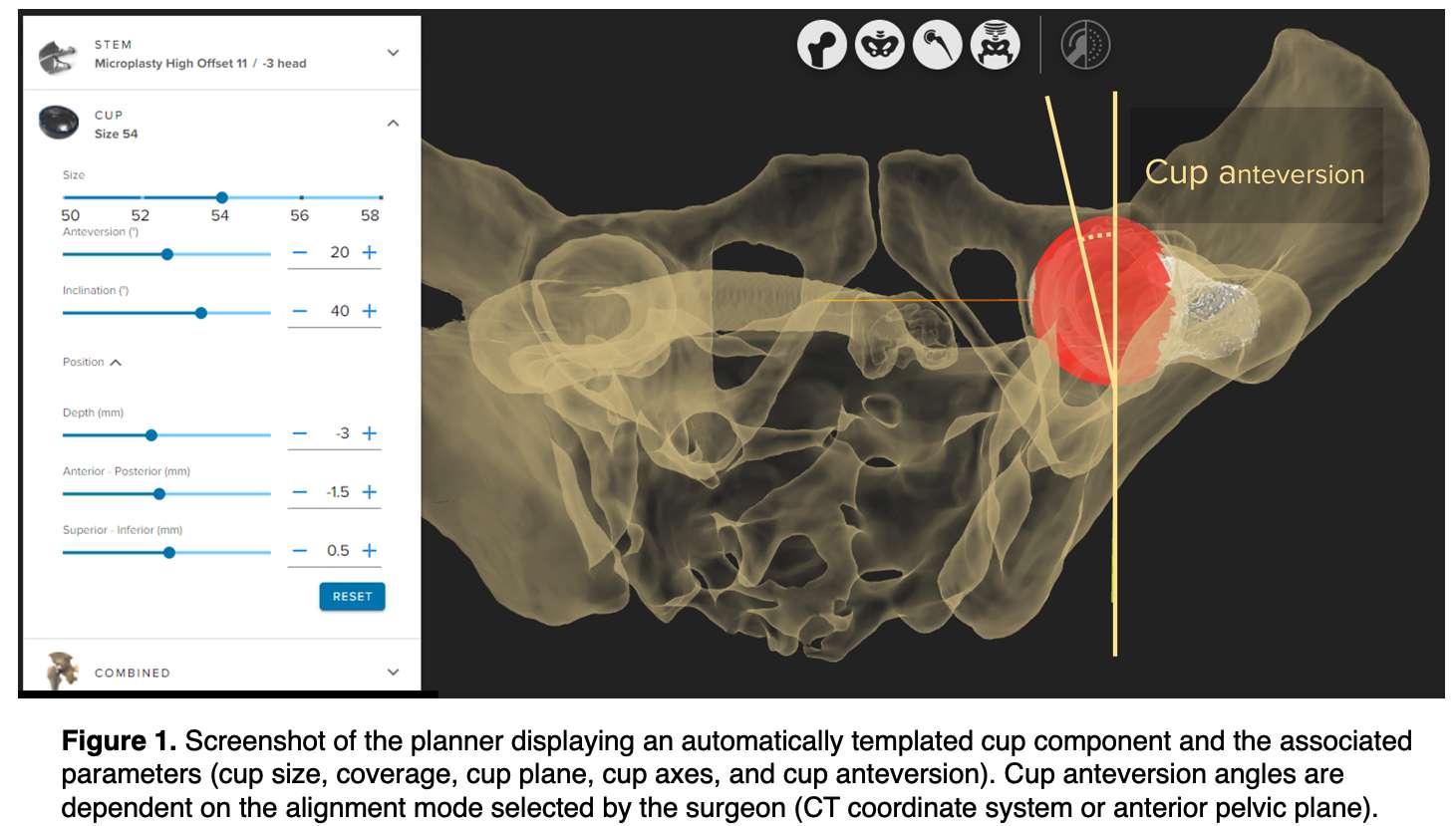
Figure 1
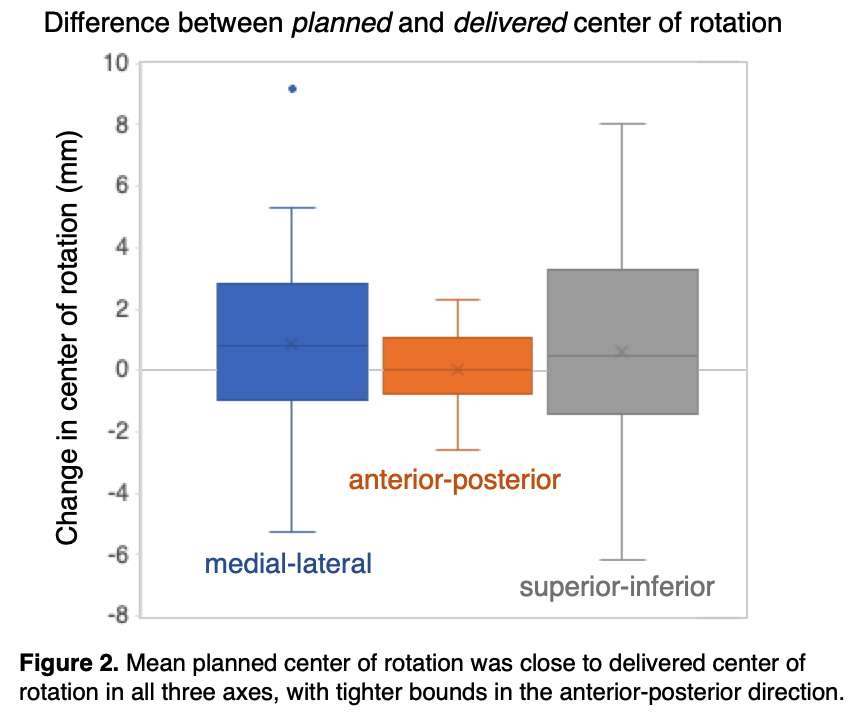
Figure 2#7547
Combining Genotyping and Machine Learning to Improve the Results of Arthroplasty
*David Langton - ExplantLab - Newcastle Upon Tyne, GB
Rohan Bhalekar - Newcastle University - Newcastle Upon Tyne, United Kingdom
Thomas Joyce - Newcastle University - Newcastle upon Tyne, United Kingdom
Matthew Nargol - ExplantLab - Newcastle Upon Tyne, United Kingdom
Nish Shyam - Explantlab - Newcastle, United Kingdom
Moreica Pabbruwe - CITRA - Perth, Australia
Edwin Su - Hospital for Special Surgery - New York, USA
Antoni Nargol - University Hospital of North Tees - Stockton, United Kingdom
*Email: davidl@explantlab.com
Background
Over five million joint replacements are performed across the world each year. Cobalt chrome (CoCr) components are used in most of these procedures. Some patients develop delayed type hypersensitivity (DTH) responses to CoCr implants, resulting in tissue damage and revision surgery. DTH is unpredictable and genetic links have yet to be definitively established.
Methods
At a single site, we carried out an initial investigation to identify HLA alleles associated with development of DTH following metal-on-metal hip arthroplasty. We then recruited patients from other centres to train and validate an algorithm incorporating patient age, gender, HLA genotype and blood metal concentrations to predict the development of DTH. Accuracy of the modelling was assessed using performance metrics including time dependent receiver operator curves.
Results
In total, 606 patients gave samples for next generation HLA sequencing. 176 of these patients experienced failure of their prostheses; the remaining 430 were asymptomatic at a mean follow up of twelve years. Development of DTH was associated with patient age, gender, the magnitude of metal exposure and the presence of certain HLA class II alleles. The predictive algorithm performed well, with weighted mean survival probability errors of 1.8% and 3.1% for pre-operative and post-operative models respectively.
Conclusion
The development of DTH following joint replacement appears to be determined by the interaction between implant wear and a patient’s genotype. Around 15% of patients of European descent have HLA genotypes which respond negatively to cobalt concentrations frequently seen in patients with commonly used arthroplasties, including TKRs. By identifying higher risk patients, the algorithm described in this paper may improve implant selection and help direct patient surveillance following surgery. On the basis of these results, we have developed "Orthotype", a product which is now available for commercial use in the United Kingdom.
#7918
Is Tibial Debonding Associated With Deformation of the Backsides of Polyethylene Tibial Inserts?
Rohan Bhalekar - Newcastle University - Newcastle Upon Tyne, United Kingdom
Matthew Nargol - ExplantLab - Newcastle Upon Tyne, United Kingdom
Nish Shyam - Explantlab - Newcastle, United Kingdom
Antoni Nargol - University Hospital of North Tees - Stockton, United Kingdom
*David Langton - ExplantLab - Newcastle Upon Tyne, United Kingdom
Stephen Wells - ExplantLab - Newcastle Upon Tyne, United Kingdom
*Email: djlangton22@yahoo.com
Introduction
Recently, there have been a number of reports of early failure of some contemporary total knee arthroplasties (TKA) secondary to tibial component loosening. Investigators have suggested this failure mechanism may be linked to surface roughness changes and the presence or absence of cement gutters on the tibial tray. For this study, we investigated whether geometrical changes of polyethylene (PE) tibial inserts may influence the amount of cement observed on the explanted tibial trays of commonly used knee arthroplasties.
Methods
We used validated techniques to analyse changes in tibial insert geometries using high accuracy coordinate measuring machines (Legex and Strato, Mitutoyo). These geometric changes are indicative of manufacturing imperfections, wear and/or deformation occurring in-vivo. Backside geometrical changes are reported as “planicity”, which refers to the difference between the maximum and minimum linear deviations (in the continuous data sections – i.e., those away from the damage which occurs during retrieval). During the geometrical analysis of the PE back surfaces, it became apparent that some inserts exhibited a characteristic pattern of deformation, with the outer edges of the polyethylene deviating inferiorly, leaving these areas as the primary contact area. We labelled this “batwinging” (Figure 1). Light microscopy was used for the non-quantitative analysis of specific features. We interrogated these data for this study, including all explanted fixed-bearing TKAs (n=113) of four widely used contemporary designs (Attune, NexGen, PFC, and Triathlon), revised for any reason. The amount of cement cover on the underside of explanted tibial trays is routinely quantified as a percentage of the total surface using Image J software. The trays were divided into two distinct groups to allow categorical statistical comparisons to be made, with ≤10% of cement cover labelled as “bare” and >10% as “cement”.
Results and Discussion
The Attune and NexGen (central-locking) trays were found to have significantly less cement cover than Triathlon and PFC trays (peripheral-locking) (p=0.012). The median planicity values of the PE inserts used with central-locking trays were significantly greater than of those with peripheral locking inserts (233 vs 93 microns; p < 0.001). All 4 of the Attune trays were bare of cement and the corresponding PE inserts exhibited batwing deformation (Figure 2a). There were 50 NexGen TKAs. 33 of the trays (66%) were bare of cement and 36 of these exhibited batwing deformations (Figure 2b). There were 39 design PFC TKAs, (25 CoCr, 14 Ti), 19 (49%) of which were bare of cement, none with batwinging (Figure 2c). There were 20 Triathlon TKAs, 3 (15%) of which were bare of cement, none exhibited batwinging (Figure 2d). Examination of the PE with light microscopy showed that of the deformed PE components, machining marks were lost (i.e., worn away) at the peripheral margins of the PE but retained at the central loading areas (Figure 3).
Conclusion
Explanted TKAs with central-locking mechanisms were significantly more likely to debond from the cement mantle. Batwinging deformation was associated with PE wear occurring at the outer edges of the articulation, potentially increasing the frictional torque generated at this interface.
Figures
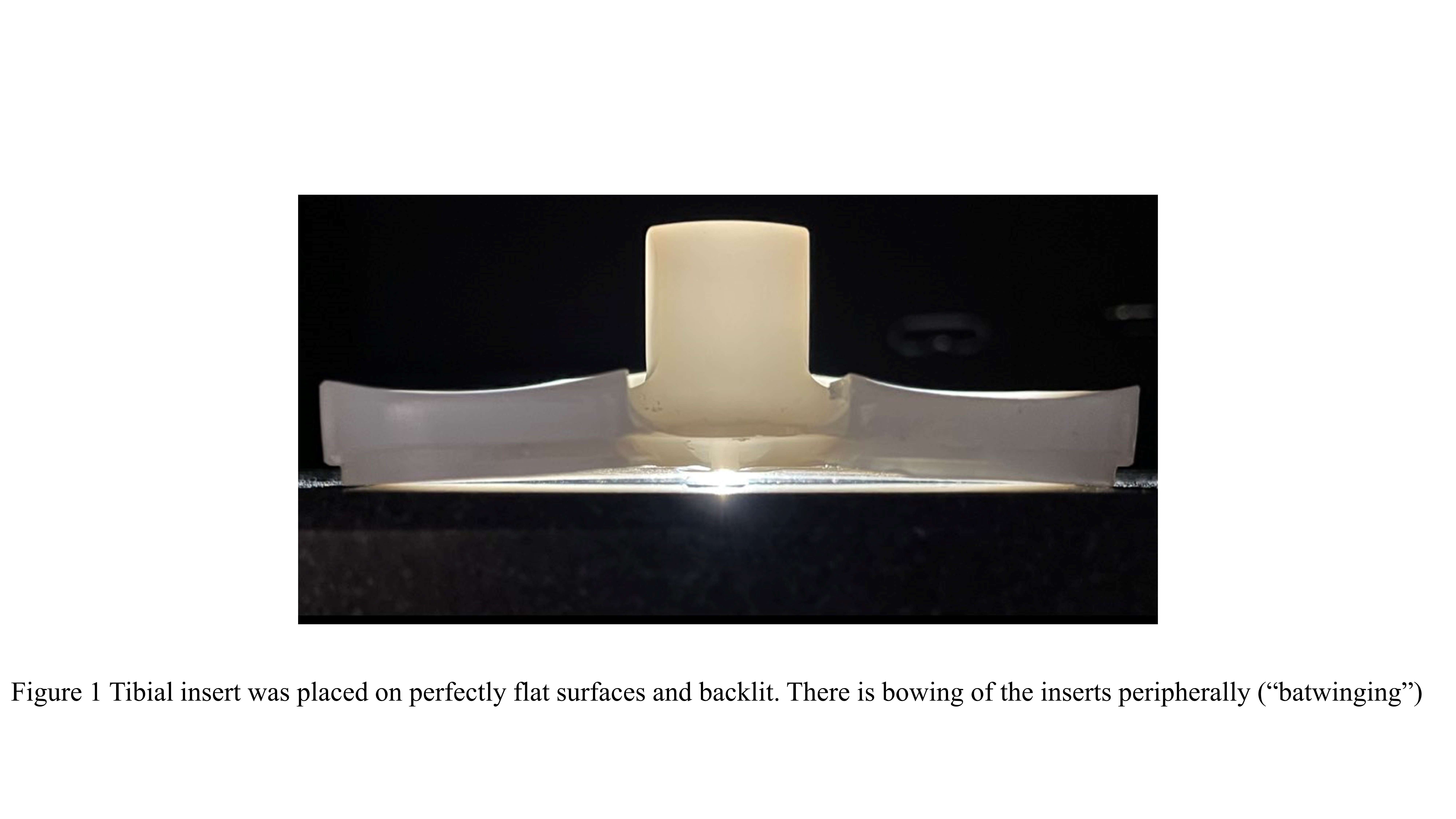
Figure 1
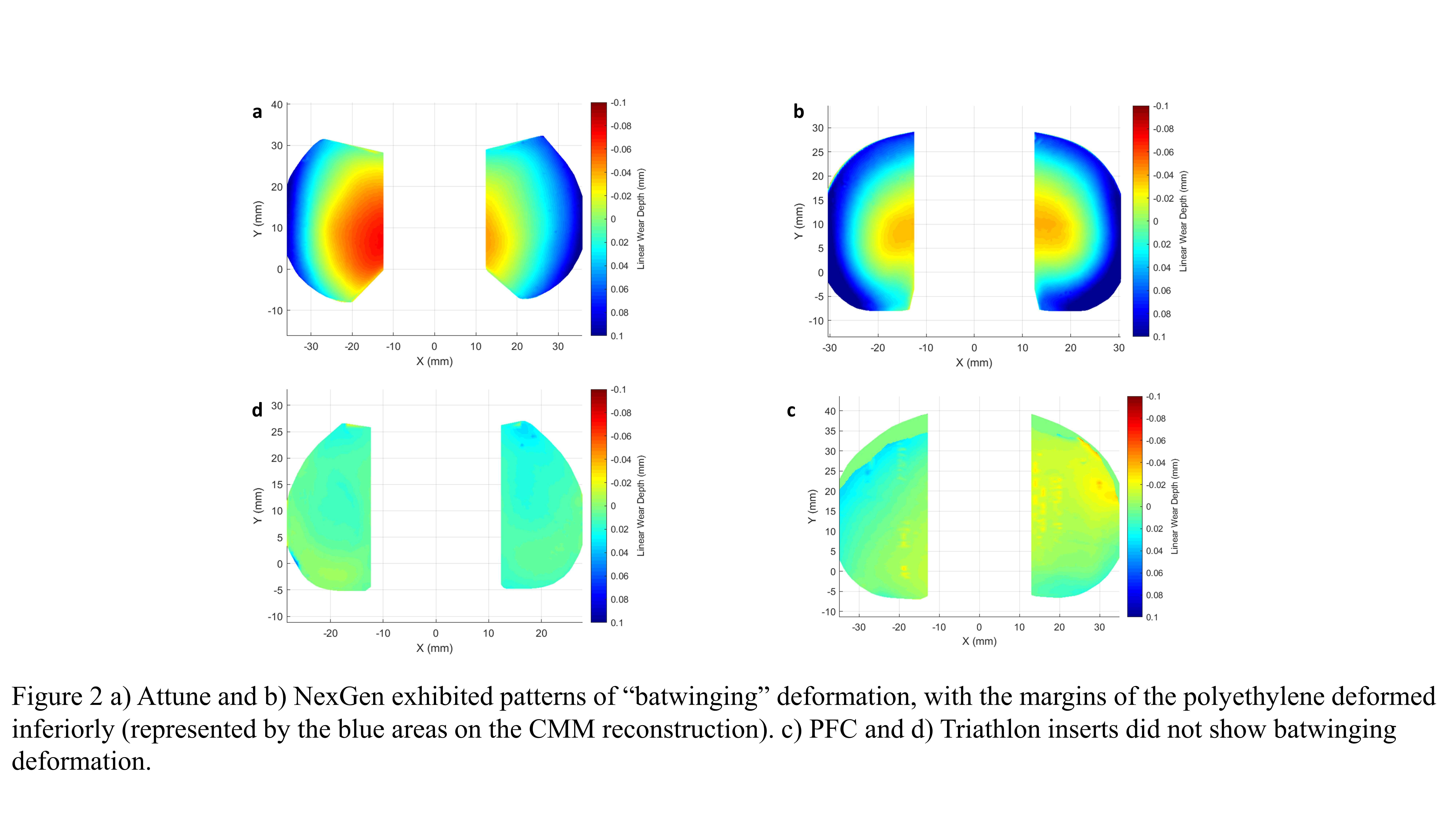
Figure 2
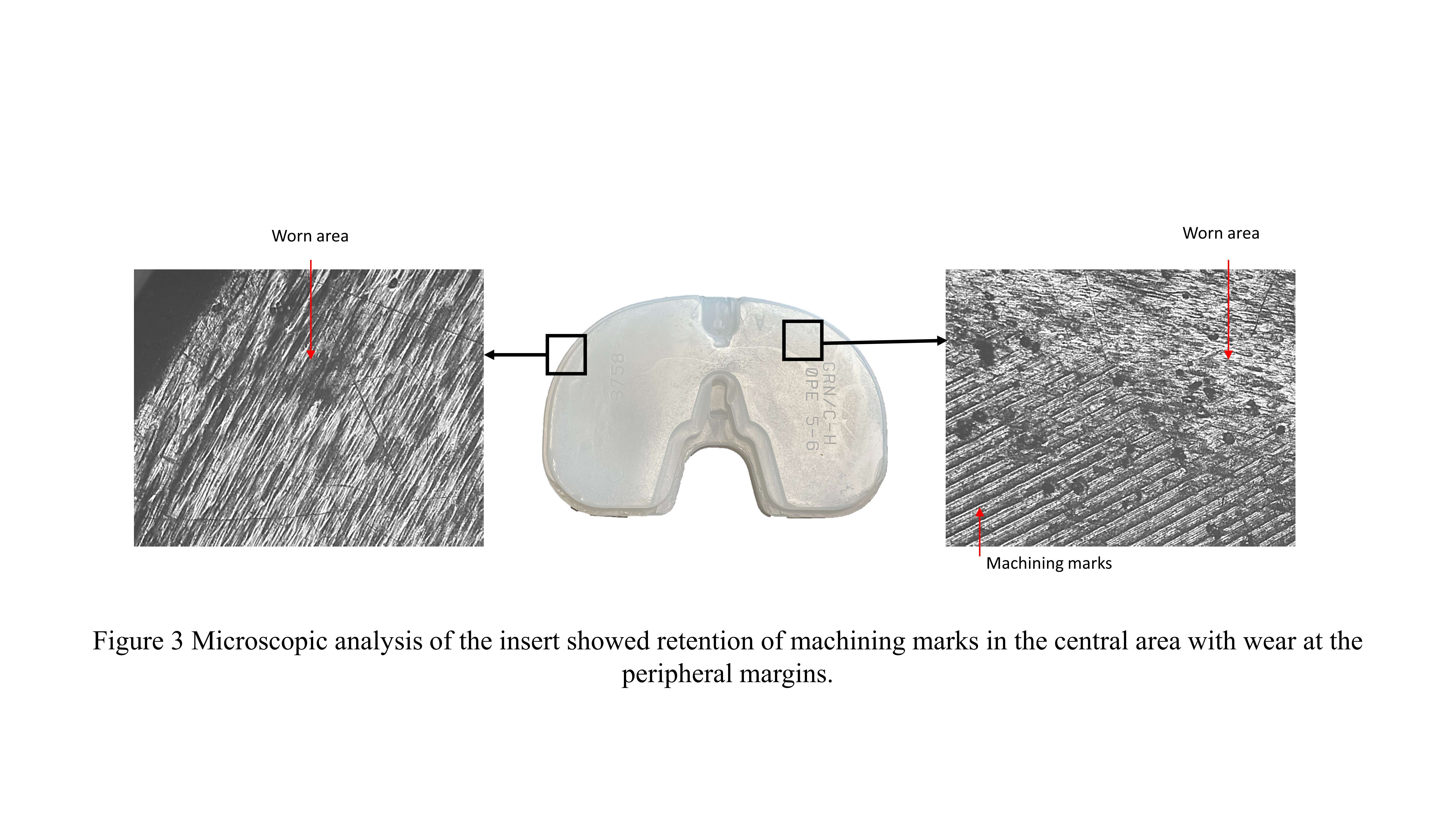
Figure 3#7936
Metal Debris Release in Total Knee Replacements: Explant Study
Rohan Bhalekar - Newcastle University - Newcastle Upon Tyne, United Kingdom
Shona Haston - Newcastle University - Newcastle upon Tyne, United Kingdom
Matthew Nargol - ExplantLab - Newcastle Upon Tyne, United Kingdom
Nish Shyam - Explantlab - Newcastle, United Kingdom
Antoni Nargol - University Hospital of North Tees - Stockton, United Kingdom
*David Langton - ExplantLab - Newcastle Upon Tyne, GB
*Email: davidl@explantlab.com
Introduction
In total knee replacements (TKRs) polyethylene (PE) inserts are present between metallic femoral and tibial tray components. Several studies have reported significant elevations of cobalt (Co) and chromium (Cr) in the blood of patients with TKRs (Lons et al. 2017,Reiner et al 2020). Moreover, Kurmis et al. 2019, observed a prevalence of pseudotumours or high-grade Aseptic lymphocyte-dominated vasculitis-associated lesion in >7% of their 321 patients with failed TKRs. Therefore, this explant study focused on investigating the source of metal debris release from TKRs.
Methods
We used peer-reviewed techniques to analyse changes in the wear and deformation of PE inserts using coordinate measuring machines (Legex and Strato, Mitutoyo). The study involved data from the explanted fixed-bearing components of five widely used contemporary designs of TKR (NexGen, Genesis II, Vanguard, Attune and PFC) revised for any indication, and we compared them with components that used the previous generation of PEs. Metal components were examined using visual and light microscopic analysis. Surface roughness analysis(Ra) was performed on the superior surface of Genesis II and Vanguard trays. These measurements were taken on two distinct areas based on microscopic analysis: worn (with pitting) and unworn (without pitting). A link between the rate of bearing wear/backside deformation or asymmetrical wear of the bearing was examined. Alloy compositions (CoCr or Ti) were assessed using x-ray fluorescence.
Results and Discussion
For the total (contemporary) PEs, the median (IQR) wear rate of the PE bearing surfaces was 10 mm3/year(6 to 17). The rates of wear of the older generation PEs were significantly higher at 31 mm3/year(7 to 78)(p = 0.034). The median PE backside planicity is shown in Figure 1. Microscopic analysis of 138 TKRs exhibited pitting or abrasive changes on the superior surface of 72 (52%) tibial trays(Figure 2). Pitting was observed on the superior surface of 14(74%) of Genesis II (n=19, Ti),10 (67%) of Vanguard (n=15, CoCr),3 (75%) of Attune (n=4, CoCr),8 (32%) of D∑GVF PFC (n=25, CoCr) and abrasive changes on 23 (50%) of NexGen (n=46, Ti alloy),3 (21%) of D∑GVF PFC(n=14, Ti) and 11(73%) of older generation PFC(n=15, Ti) trays. Surface roughness analysis of trays confirmed the presence of pitting. Ra [Median (IQR)] of tibial trays showed a statistically significant increase from 0.046(0.043to0.051) to 0.302(0.160to0.392) µm for Genesis II (p<0.001) and from 0.056(0.052to0.062) to 0.187(0.108to0.342) µm for Vanguard (p<0.001), on unworn and worn surfaces, respectively(Figure 3a). Visual inspection showed the presence of abrasive changes on the inferior surface of metal trays (Figure 3b). The bearing surfaces of Vanguard (n=15), and Genesis II (n=8) femoral components (CoCr), demonstrated abrasive changes, 67% and 50% respectively. Three TKRs (2 Genesis II and 1 D∑GVF PFC) exhibited direct femoral component and tibial tray contact due to the wear of the polyethylene insert.
Conclusion
Based on this explant analysis, the generation of metal particles was predominantly from the metal tray, which may explain elevated metal ions after TKRs, despite no direct metal-on-metal contact. We recommend the measurement of metal ion levels which may indicate tray wear or component instability.
Figures
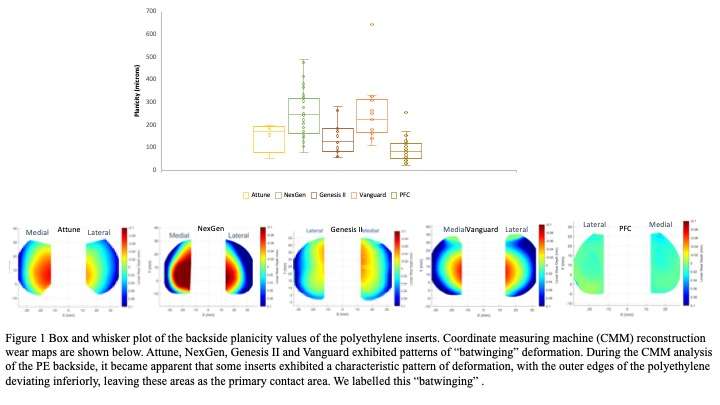
Figure 1
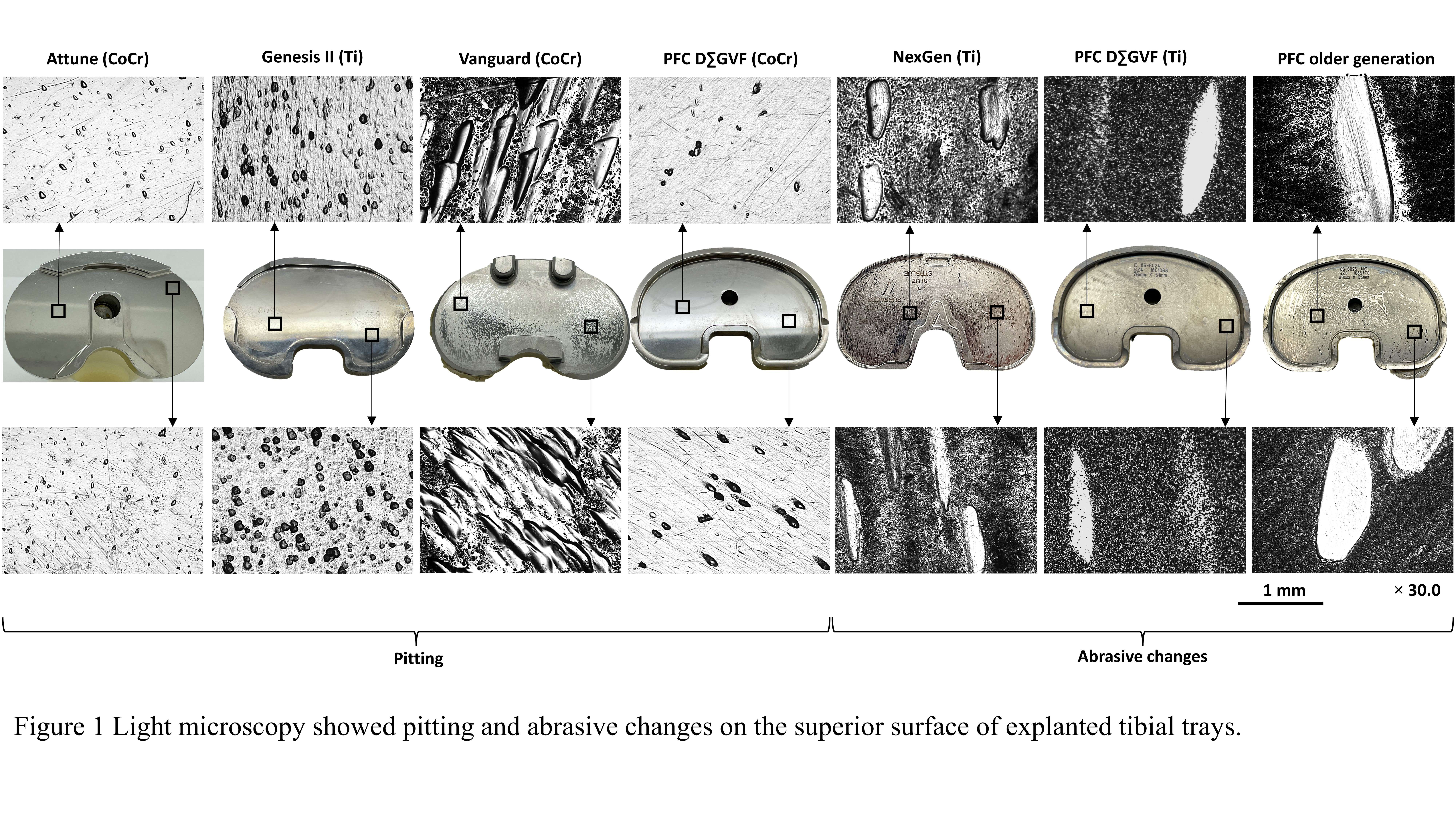
Figure 2
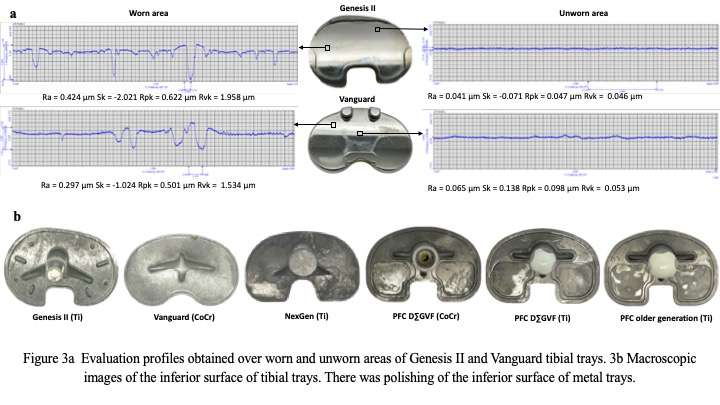
Figure 3#7336
Short-Term Functional Outcomes and Complications of Custom Patellofemoral Arthroplasty
*Joshua Rogers - University of Kansas - Wichita - Wichita, United States of America
Tarun Bhargava - The University of Kansas School of Medicine - Wichita - Wichita, USA
Brayden Strine - KU School of Medicine - Wichita - Wichita, USA
Jack Nolte - KU School of Medicine - Wichita - Wichita, USA
Rosey Zackula - KU School of Medicine - Wichita - Wichita, USA
*Email: jrogers14@kumc.edu
Background
One surgical option to address isolated patellofemoral arthritis resistant to conservative treatment is patellofemoral arthroplasty (PFA). PFA has shown promising results especially with the newer generation protheses; however, many disadvantages still exist with off-the-shelf prostheses. With newer technology and the concept of individualized medicine, custom patellofemoral protheses are designed to help improve complication rates seen with off-the-shelf prostheses. Custom-made patient-specific trochlear resurfacing implants replicate each patients’ unique trochlear anatomy theoretically improving patellofemoral tracking allowing patients to return to a high level of activity. The purpose of this study is to evaluate short-term functional outcomes and complications of the custom PFA in treatment of isolated patellofemoral arthritis.
Methods
A retrospective study was conducted to analyze patients who received a patellofemoral arthroplasty operation from a single surgeon. Inclusion criteria were surgical patients from 2012 to 2018 who underwent patellofemoral arthroplasty using a custom prosthesis implant. Minimum follow-up was two years. Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS, JR) and Lower Extremity Function Scale (LEFS) were collected both pre- and post-operative. Complications related to the index procedure were recorded.
Results
A total of 79 patients (94 knees) participated in the study; a majority, 55 (69.6%), were female. The mean age was 56.8 at the time of index arthroplasty; 15 patients (30 knees) were bilateral. Four patients were lost to follow-up and one patient was removed from the primary surgeon’s practice for illicit drug use for a 94% follow-up rate. 74 patients (89 knees) were included in the final analysis. Median follow up was 3.6 years (2 – 8.9). Overall pre- and post-functional scores differed significantly for both KOOS, JR and LEFS. Post operative scores increased for KOOS, JR by 27.5 points, and for LEFS they increased 26.0 points; p < 0.001 for both. This difference was greater for females in both scores. Complications in the 89 knees included six reoperations (6.7%) related to patellofemoral arthroplasty: four conversions (4.4%) to total knee arthroplasty at a mean of 2.3 (1.5-3) years after index procedure, one VMO advancement (1.1%) secondary to patellar maltracking, and one manipulation under anesthesia (1.1%).
Conclusions
The custom patellofemoral arthroplasty in patients with isolated patellofemoral arthritis showed good short-term functional outcomes and low revision rates with very few complications. We believe patients with isolated patellofemoral arthritis who have failed nonoperative management may benefit from custom PFA.
#7761
Total Knee Prosthesis With Potential for Full Motion
*J (John) Blaha - University of Michigan - ANN ARBOR, USA
*Email: jdblaha@med.umich.edu
Total Knee Prosthesis with potential for full motion
INTRODUCTION
Total knee arthroplasty components have been designed based on the premise that 1) the compartments of the knee are symmetric and 2) the motion of the knee is guided by the ligaments. The human knee is not symmetric and the ligaments are neither stiff enough or strong enough the guide the knee. Kinematic studies of the knee have shown that during the majority of flexion, the medial compartment of the knee moves largely as a simple ball-in-socket joint, whereas the lateral compartment moves such that the contact point changes from anterior to posterior in an arcuate path dependent largely on the longitudinal rotation of the tibia beneath the femur. The behavior of the knee in the terminal 20 degrees of extension and after 115 degrees of flexion differs from the motion in the mid-range of motion. In full extension, a cam-like effect of the distal medial articular surface moves the femur away from the tibial surface, tightens the medial and lateral collateral ligaments, and creates an external rotation of the tibia called "screw-home". Beyond 115 degrees of flexion the lateral tibial contacts the posterior lateral tibial surface in a rolling and sliding motion that moves the lateral femoral condyle off the back of the tibia ("roll off") and allows full flexion while decompressing the contents of the popliteal fossa. Thus the knee has three ranges of motion: full-extension, midrange flexion, and full-flexion.
A design concept for a total knee prosthesis that more closely mimics the motion of the normal knee has been patented the United States Europe, Japan, China and Hong Kong, This prothesis mimics the stiffness of the normal knee by 1) being stiff in terminal extension using a cam-like surface to move the femur away from the tibial surface and tighten ligaments; 2) being much less stiff in the midrange of flexion with a ball-in-socket articulation in the medial compartment and a less constrained articulation in the lateral compartment and 3) being stiff again in full flexion with a central articulation that lifts the condyle away from the tibial surface on the lateral side and mimics the “roll-off” of the lateral condyle.
CONCEPT TESTING
Using CAD models this design concept was tested by computational analysis. shows that flexion in excess of 140° is possible with the potential for “heel against buttock” flexion to accommodate full squatting. Insofar as possible based on confidentiality of data testing will be shared at presentation
SUMMARY
This patented implant for total knee arthroplasty relies on the conformation of interfacing surfaces during the full range of motion (i.e., all three ranges of motion full extension, mid-range flexion and full-flexion) to provide a large range of motion of the joint, and stability throughout flexion but not relying primarily on ligament tension to provide such. These features are provided through sets of cooperating convex and concave facet surfaces within the prosthesis joint compartment which cooperate in the ranges of motion.
#7815
Laser Embedding of Silicon Nitride Particles Into Bioinert Metallic Substrates to Impart Resistance to Bacterial Colonization
Jackson Hendry - SINTX Technologies - Salt Lake City, USA
Sean Ronayne - SINTX Technologies, Inc. - Salt Lake City, USA
Erin Jones - SINTX Technologies - Salt Lake City, USA
Douglas Hoxworth - SINTX Technologies - Salt Lake City, USA
Sonny Bal - Sintx - USA
*Ryan Bock - SINTX Technologies - Salt Lake City, USA
*Email: RBock@sintx.com
INTRODUCTION: Implant-associated infection remains a stubborn obstacle in orthopedics. Monolithic silicon nitride (Si3N4), a non-oxide ceramic commonly used in demanding industrial environments, has been successfully employed as a commercial spinal fusion device since 2008. To expand the applications where its beneficial biomedical properties[1] can be enjoyed, recent research has explored composite and coating applications. Previous work[2] demonstrated that a laser could be used to apply coarse Si3N4 particles as a relatively thick coating to a variety of substrates, including Ti6Al4V. Other efforts demonstrated that directed energy deposition could construct Si3N4-Ti-alloy composites. However, the resulting composites contained extraneous intermetallic phases and poorly controlled microstructures. In this work, attempts were made to embed individual non-contiguous Si3N4 particles on specimen surfaces while minimizing formation of extraneous phases by using much finer particles and reduced laser energy.
METHODS: Ti6Al4V-ELI (grade 23 titanium) discs (Ø 12.7mm x 1 mm thick) were coated by atomization and dip coating with slurries containing submicron β-Si3N4 particles suspended in isopropanol to obtain different surface coverage densities. Following drying to remove the isopropanol, a narrow range of laser parameters were employed to embed the Si3N4 particles into the Ti-alloy substrate surfaces under flood nitrogen conditions. Sample surface topographies and cross-sections were subjected to visible light microscopy (VLM), confocal laser scanning microscopy (CLSM), scanning electron microscopy (SEM) and energy dispersive spectroscopy (EDS) to assess surface coverage, depth of embedding, and chemical reactions between the particles and substrate. Resistance to bacterial colonization by a biofilm forming strain of S. epidermidis (ATCC®14990™) was assessed in vitro using a diluted human plasma-based inoculum at time points of 24- and 48-hours according to a previously published protocol[3]. PEEK was used as a positive control, and untreated Ti-alloy and monolithic Si3N4 were included in the biofilm assay for benchmarking.
RESULTS: Embedding of individual Si3N4 particles into the Ti-alloy surface, produced when the particle concentration on the surface prior to lasing was low, is apparent in Figure 1(a). Following lasing of a surface with a high concentration of Si3N4 particles, formation of a more complex and contiguous layer, rich in Si and N, occurs (Figure 1(c and d)). Figure 2 shows a detail of individual embedded particles imaged in back scatter (a) along with EDS maps for Si (b; purple) and Ti (c; teal). Limited local diffusion, on the order of 1-2 μm, of Si from the embedded particles into the Ti-alloy matrix is observed. Bacterial CFU counts are reduced significantly relative to the PEEK control and untreated Titanium benchmark samples. This reduction roughly correlates to embedded Si3N4 surface coverage.
CONCLUSION: These experiments show that embedding Si3N4 particles into a Ti-alloy surface without significant structural or chemical perturbation is possible. The resulting modified surface is imbued with the bioactivity of the Si3N4 particles, thus raising the possibility of retrofitting existing devices for improved resistance to biofilm formation and applying silicon nitride to device geometries otherwise unfavorable for construction from monolithic ceramics.
Figures
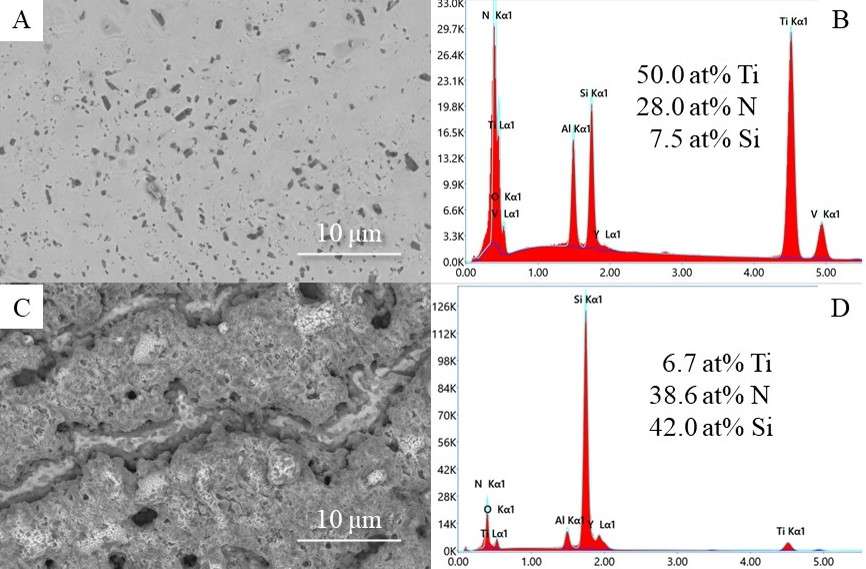
Figure 1
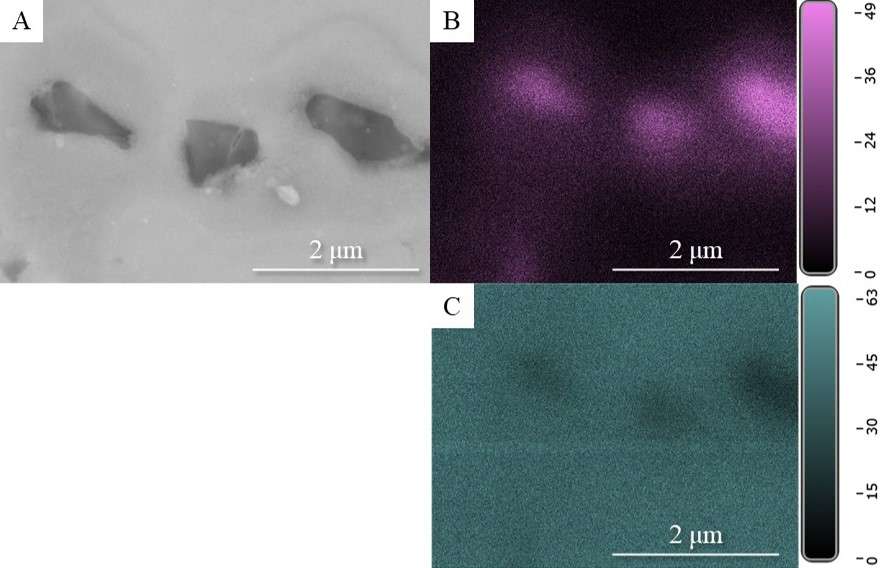
Figure 2#7482
Rotational Stability of Cementless Revision Hip Stems - a Study in Porcine Femurs
*Julius Boettcher - TUHH Hamburg University of Technology - Hamburg, Germany
Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
Kay Sellenschloh - TUHH Hamburg University of Technology - Hamburg, Germany
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: julius.boettcher@tuhh.de
INTRODUCTION
Implant loosening remains one of the major challenges in cementless revision total hip arthroplasty, leading to re-revisions [1]. Manufacturers try to increase primary stability after implantation by improving the force locking between stem and cortex. Tapered stems with longitudinal fixation fins that indent into the femoral cortex show promising results in achieving sufficient primary stability to enable bone ingrowth [2]. However, the influence of the shape (height, width) and the amount of these fins is unknown. The aim of this study was to investigate whether an implant with a second set of non-prominent, 0.3 mm shorter longitudinal fixation fins can achieve improved primary stability.
MATRIALS AND METHODS
Porcine femurs were either implanted with an established revision stem (Reclaim™ DePuy Synthes, n = 8) or with a prototype design (n = 8) with two different sets of longitudinal fixation fins (Figure 1).
Dynamic implantation was performed with a droptower (increasing energies; 2 J, 3 J, 4 J) and seating recorded by digital image correlation (Aramis 3D, MV 100, GOM, Germany). One femur of each group was sectioned after implantation and the cortex indentation analyzed with a 3D-laserscanning-microscope (Keyence VK-X100, Keyence Corporation, Osaka, Japan). All other femurs were torqued to failure under an axial preload (100 N) by increasing the torsion angle with 0.5 with a servo-hydraulic testing machine (MiniBionix II, MTS, Eden Prairie, MN, USA). Failure was defined as a sudden drop in torsional moment (> 3 Nm), indicating slip at the implant-bone interface. The torsional moment to failure as well as the torsion angle at failure were determined. The results were statistically analyzed using a Mann-Whitney U test.
RESULTS
Maximum torsional moments until failure were not significantly different (p = 0.71; Figure 2). The prototype design showed a larger spread but also the highest value (39.7 Nm). The maximum torsion angle showed values of approximately 1° for both groups (p = 0.62; Figure 2). The analysis of the cortex indentation showed similar values of about 0.4 mm for all prominent fins of both designs (Figure 3).
DISCUSSION & CONCLUSION
No difference in torsional moment to failure and torsion angle at failure may indicate a negligible effect of additional, non-prominent longitudinal fixation fins on the rotational stability of revision hip stems. This may be due to the limited ability to cut into the cortical bone of young, dense porcine femurs which might also explain why the additional less prominent fins did not show any permanent cortex indentation and no beneficial effect. This could be different for less dense bone in older patients.
Despite the dense porcine bone, the measured values for the maximum torsional moment are consistent with those reported in the literature for revision hip stems with distal fixation fins evaluated in human bone (25-35 Nm [3, 4]).
Support of DePuy Synthes by providing the prosthetic components and surgical instruments is kindly acknowledged.
REFERENCES
[1] AAOS, AJRR 2021
[2] Hancock et al., HIP INT 2019
[3] Kendrick et al., J ARTHROPLASTY 1995
[4] Meneghini et al., J ORTHOP SURG RES 2006
Figures
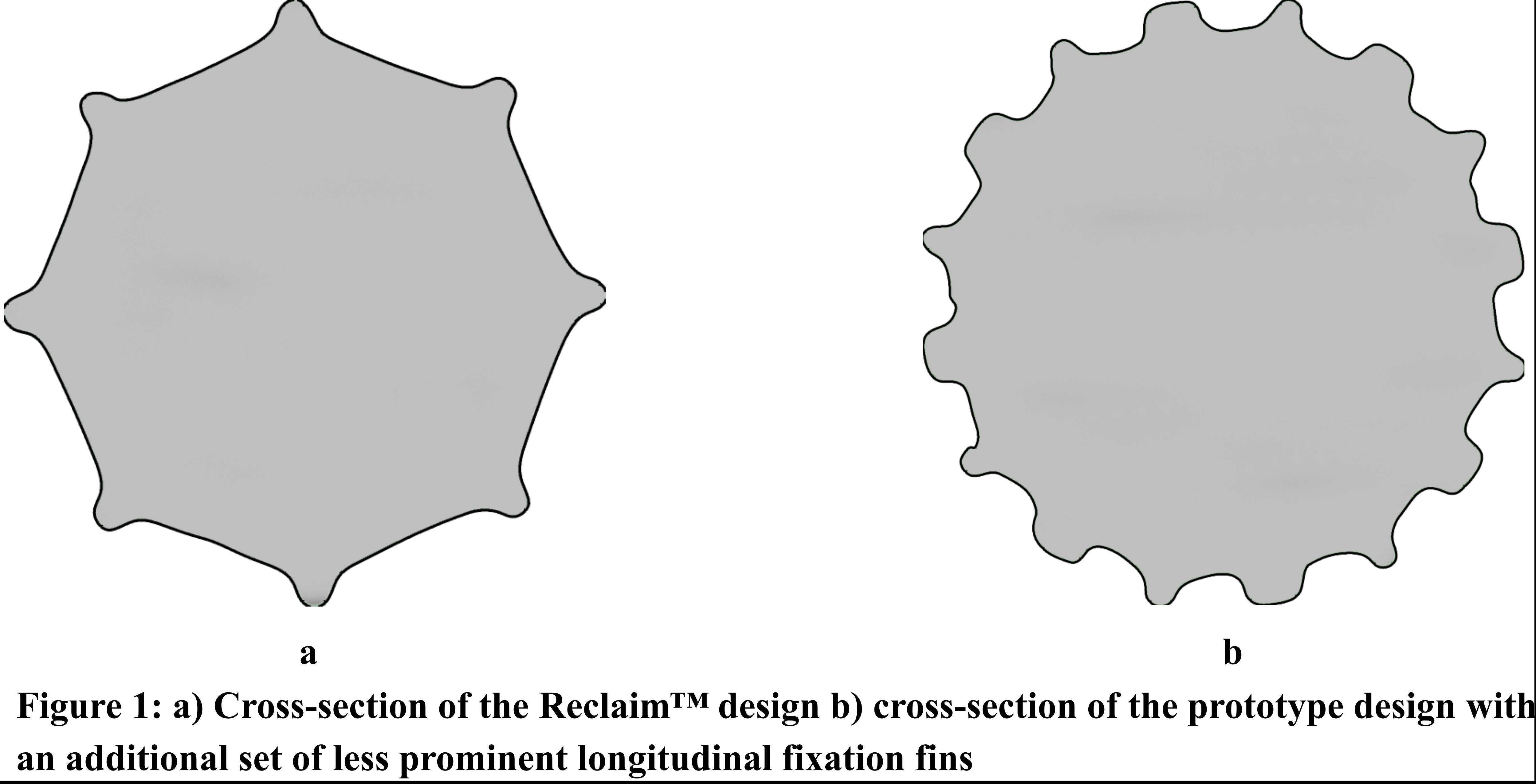
Figure 1
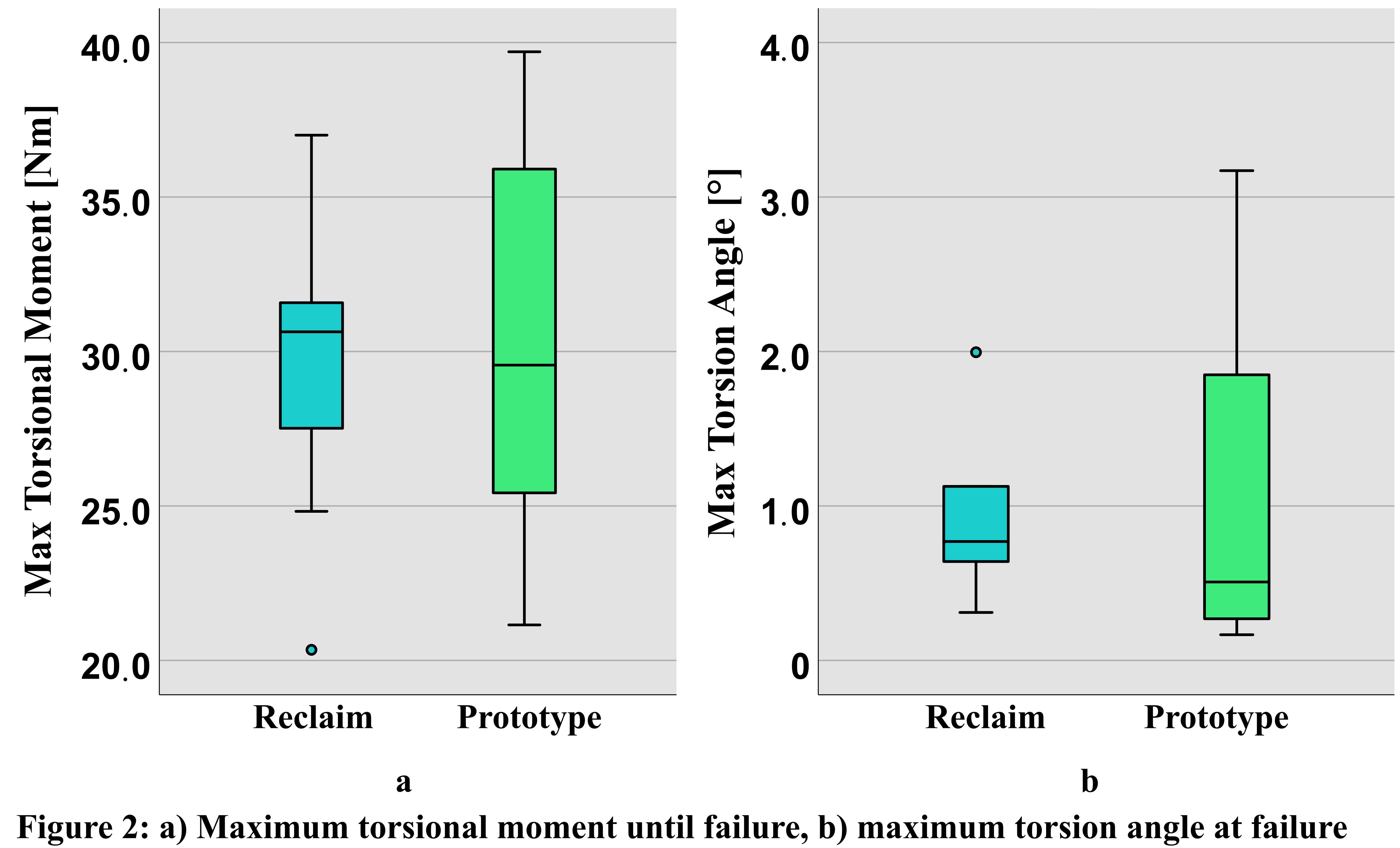
Figure 2
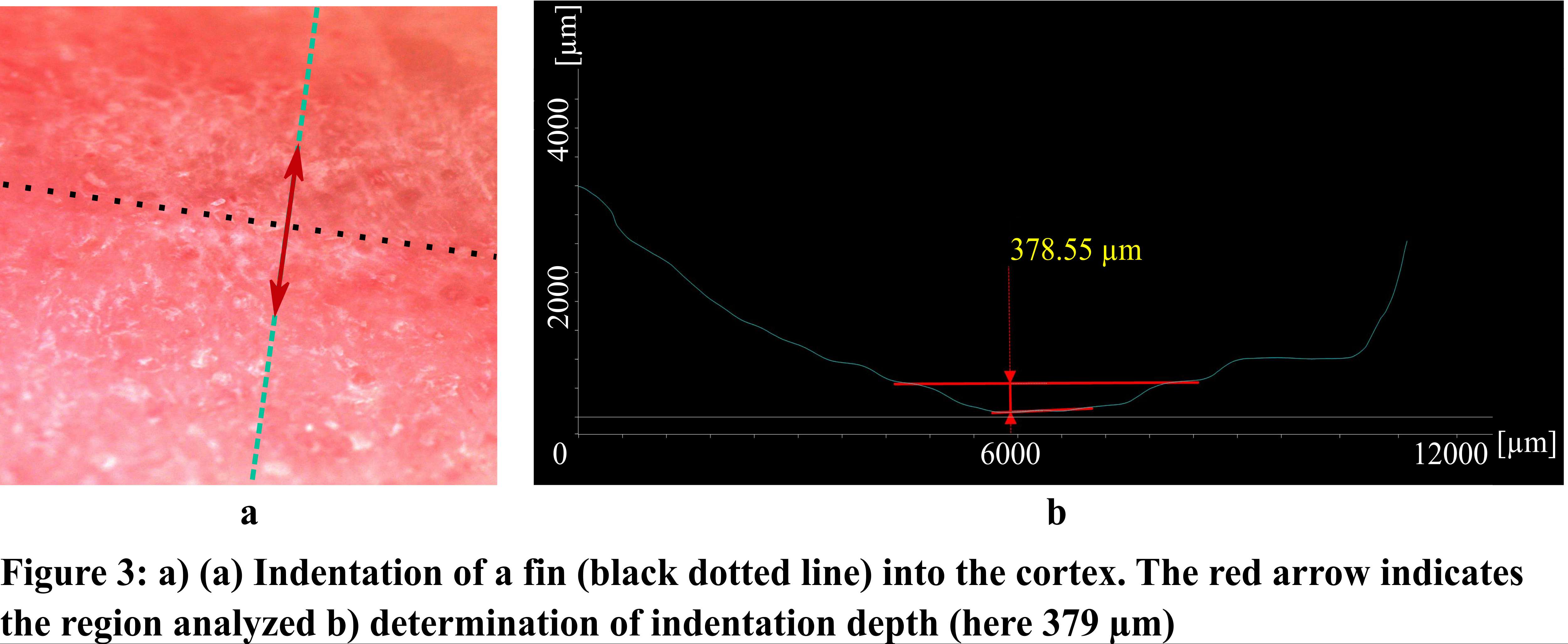
Figure 3#7409
An Introduction Into the Development of Wearable Technologies
*Richard Bolander - TracPatch - Orland Park, United States of America
*Email: rbolander@tracpatch.com
Recent advancements in sensing, data capture, communication, power optimization and access to data have increased the applicability of using wearable technologies to monitor musculoskeletal and physiological phenomena. These advancements have resulted in increased acceptance of these devices in clinical and remote settings. This trend has been accelerated due to the COVID-19 pandemic, which has changed the way in which traditional medicine has been conducted, including changes in billing codes, increasing cross border privileges, surges in telemedicine interactions and shifts in patient expectations.
As these trends continue, there will be an increase in people with diversified backgrounds who will be exposed to these technologies. A primary issue will be properly communicating and providing context about what these technologies can and cannot do in order establish reasonable expectations. The purpose of this presentation is to provide a high-level overview of the steps and resources required to develop a wearable technology. The primary audience will be academics, clinicians, and industry experts who are curious about how these technologies are developed. The presentation will provide a common frame of reference for each of these primary groups to better communicate about these topics.
The session will be divided into the following topics:
- Conduct market and technical analyses
- Provide a high-level overview of the primary components associated with a wearable device:
- Instrumentation used to measure the feature of interest
- Application or local interface used to receive data
- Remote or consolidated data infrastructure
- Discuss the required engineering specialties to build the system
- Mechanical: Device design and compatibility
- Electrical / Firmware: Electronic board design and programming
- Software: Application and website development
- Algorithm / Data Science: Content expert and analysis
- Provide an overview of the design and development process
- Basic research studies and proof of concept
- Analysis of biomechanical and physiological signals
- Development of metrics and algorithms
- Device design and development
- Software and application development
- System integration
- Discuss concepts of Verification and Validation of the technology
- Discuss concepts of intellectual property and FDA requirements, device classifications and data security
#7445
Daily Characterization of Leg Position and Step Count in TKA Patients During an Episode of Care Using Remote Monitoring Technology
*Richard Bolander - TracPatch - Orland Park, United States of America
S. David Stulberg - Northwestern Memorial Hospital - Chicago, USA
Ralph Mobbs - Prince of Wales Private Hospital - Sydney, Australia
Curt Wiedenhoefer - Consensus Orthopedics, Inc. - USA
*Email: rbolander@tracpatch.com
Introduction
The introduction of remote monitoring technology provides the ability to measure the musculoskeletal function of patients following medical intervention more frequently than reoccurring clinical visits. These data can be used to develop standardized recovery patterns and identify patients that fall outside of these norms for early intervention. In this study, we sought to characterize the position of the knee and general activity patterns of a cohort of patients following total knee arthroplasty (TKA) to understand daily behavior post intervention.
Methods
A retrospective analysis of TKA patient data collected using a remote wearable technology (TracPatch Duo, TracPatch, Sacramento, CA) to characterize the daily distribution of leg position. Tracpatch exports range of motion (ROM) data and step counts every minute. The position of the knee was classified into 7 categories, 6 corresponding to a range of static positions ranging from -2 to 150 degrees and 1 corresponding to walking movement during that minute. The distribution of each category was stratified by day from surgery, ranging from -5 to 69 days. Average step counts were stratified daily.
Results
Data were captured for 169 patients (62% Female) from 7 surgeons. Patient demographics included: age (yrs): M:71±8, F:65±18, height (in): M:70±2, F:65±7: Weight (lb): M:201±30, F:176±37. The total number of ROM samples was 1,844,689. The distribution of knee position and steps are shown in Figure 1 and Figure 2 respectively. The number of ROM samples and number of patients are provided in Figure 3.
The key findings include the following: There was an inverse non-linear relationship between knee position (preference towards extension) and active motion across the joint. A consistent trend was observed where the knee was statically in a degree of extension between 45 and 75 degrees throughout the day regardless of days post-surgery. Additionally, the classification of activity through ROM correlated with step count. Finally, the number of monitored patients decreased significantly beyond 40 days post episode of care, and the remaining data show that additional gains in increases in activity and less time being stationary can be achieved.
Conclusion
The results of this study provide the basis for a method to characterize activity and position of the knee following TKA. It was observed that the percent of time being active increases consistently following the intervention and that the longer that a patient continues to participate in monitoring, they will continue to increase their daily activity and reduce total static positioning time. Additionally, this preliminary data suggests that beyond 40 days of recovery may be required to achieve pre-surgical activity levels. Follow-on analyses will review larger data sets, create corridors for recovery and identify which factors best correlate to better or worse outcomes.
Figures
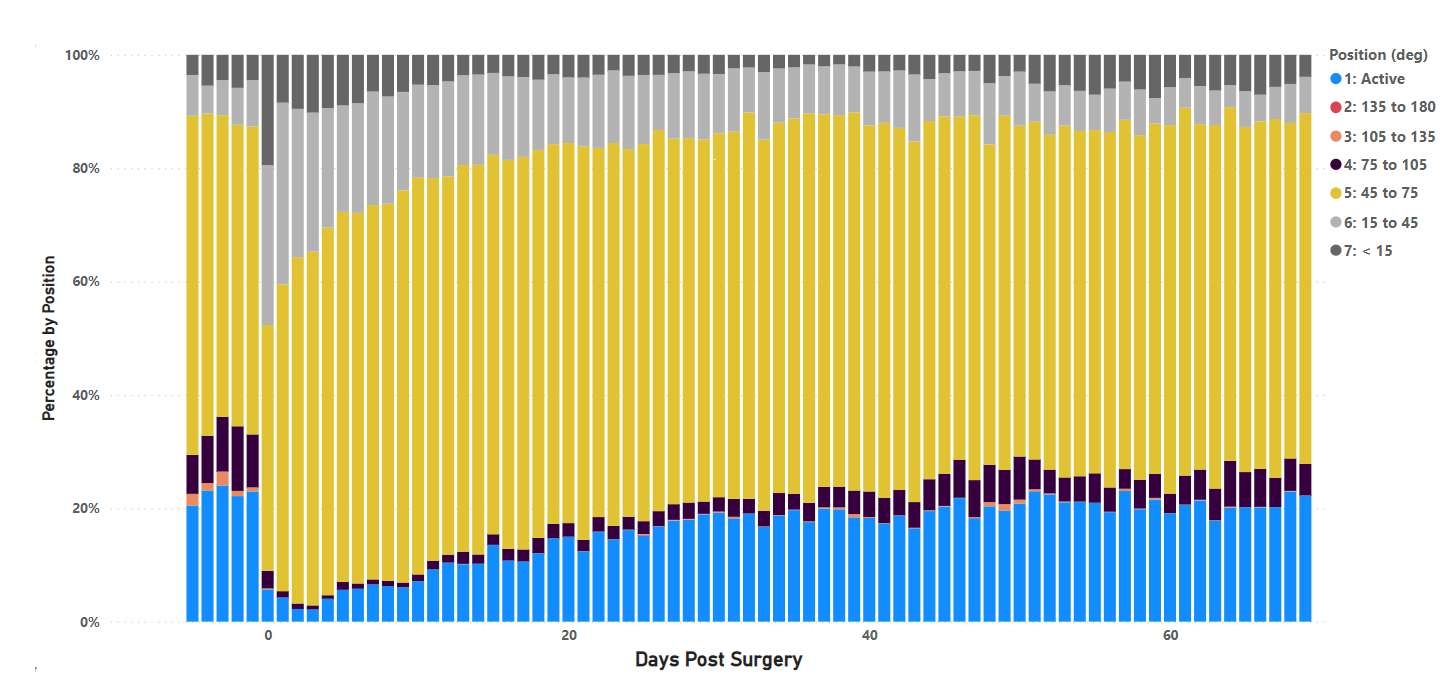
Figure 1
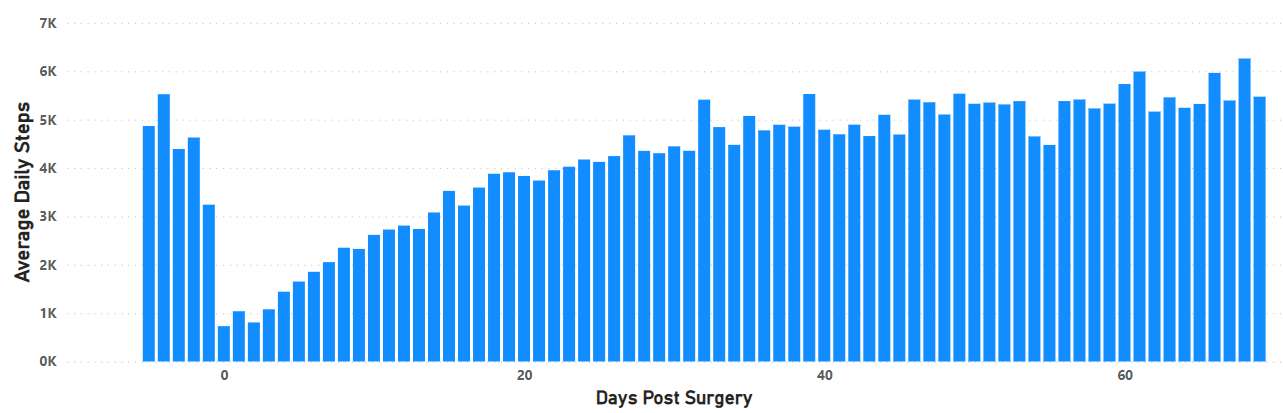
Figure 2
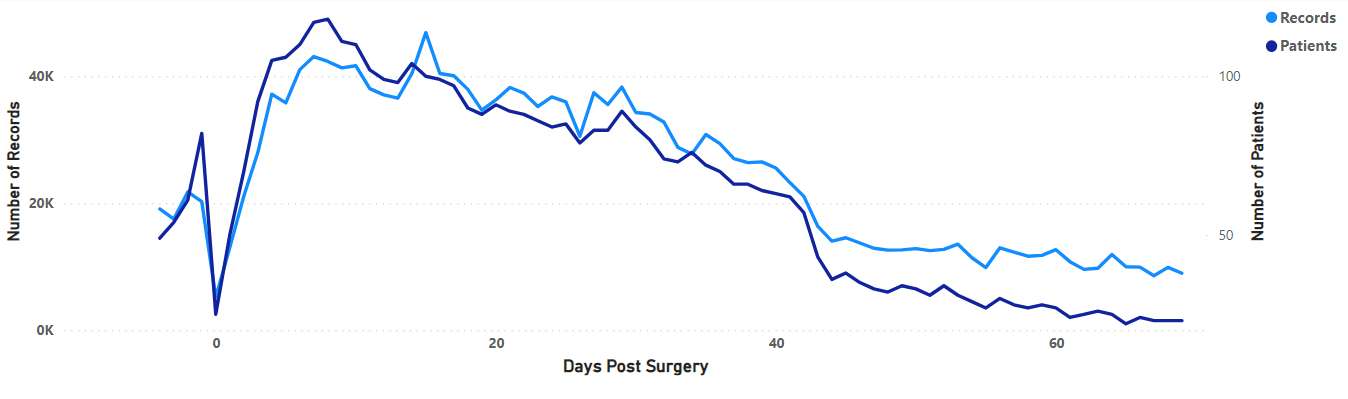
Figure 3#7474
Hip Cup Impaction Force. What Makes the Difference?
*Sebastian Jaeger - Heidelberg University Hospital - Heidelberg, Germany
Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Therese Bormann - University Hospital Heidelberg - Heidelberg, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: sebastian.jaeger@med.uni-heidelberg.de
Introduction:
Implantation of a cementless acetabular cup via impaction can be a challenging act. Press fit fixation must be obtained to ensure adequate ingrowth of the bone to the implant while avoiding fracture of the acetabulum. Therfore an appropriate impact technique may be the key to achieve adequate primary stability. Furthermore, the fixation depends on the force peaks that are reached during implantation. The impaction forces might be influenced by the instrumentation. Therefore, in this experimental in vitro study, we investigated the force peaks at the acetabular cup base using different instrumentations (intended and non-intended), cup sizes and implantation angles.
Methods:
Under standardized conditions, an acetabular cup system with two different implant sizes (MRS-TITAN, Size 60 and 68, Peter Brehm GmbH, Germany) was impacted with eight different instruments (group A-H) (Figure 1). Group A and G are intended to be used by the manufacturer.
Furthermore, the impaction angle orthogonal to the base of the cup at 0° and 28° was investigated. In order to exclude the influences of varying bone densities or the variations of the impaction force applied by the surgeon, a standardized test set-up was used (Figure 2). Hereby, the impaction force was normalized by a drop hammer. The resulting force peaks were recorded with a piezoelectric force probe below the cup. The identical set of instruments was used for group A and B (Figure 1). However, in group A the instrument was screwed to the cup as intended by the manufacturer whereas in group B it was not screwed. For each instrument set, five measurements were taken per cup size and angle setting.
Results:
The results are shown in Figure 3.
Impaction angle 0°:
For cup size 60, significant differences for group A-F were measured with values ranging from 1077.8 N ± 57.7 N to 3718.1 N ± 22.3 N (p<0.001). Size 68 also showed significant differences for group A-F with values ranging from 909.5 N ± 29.2 N to 2565.6 N ± 30.7 N (p<0.001).
Impaction angle 28°:
For cup size 60, significant differences for group C-H were measured with values ranging from 1097.3 N ± 106.5 N to 3610.8 N ± 66.6 N (p<0.001). Size 68 also showed significant differences for group C-H with values ranging from 1274.1 N ± 31.7 N to 3398.6 N ± 30.5 N (p<0.001).
The instruments of group A and G as intended to be used by the manufacturer showed significantly higher impaction forces compared to the non-intended.
Conclusion:
The results showed that the resulting peak force below the cup was significantly dependent on the design and the intended use of the instrumentation. This was also observed with different implant sizes and implantation angles. For clinical use, this could indicate for the surgeon that the use of different instruments could result in different primary stability and change the intraoperative fracture risk. However, this needs to be investigated in further studies.
Figures
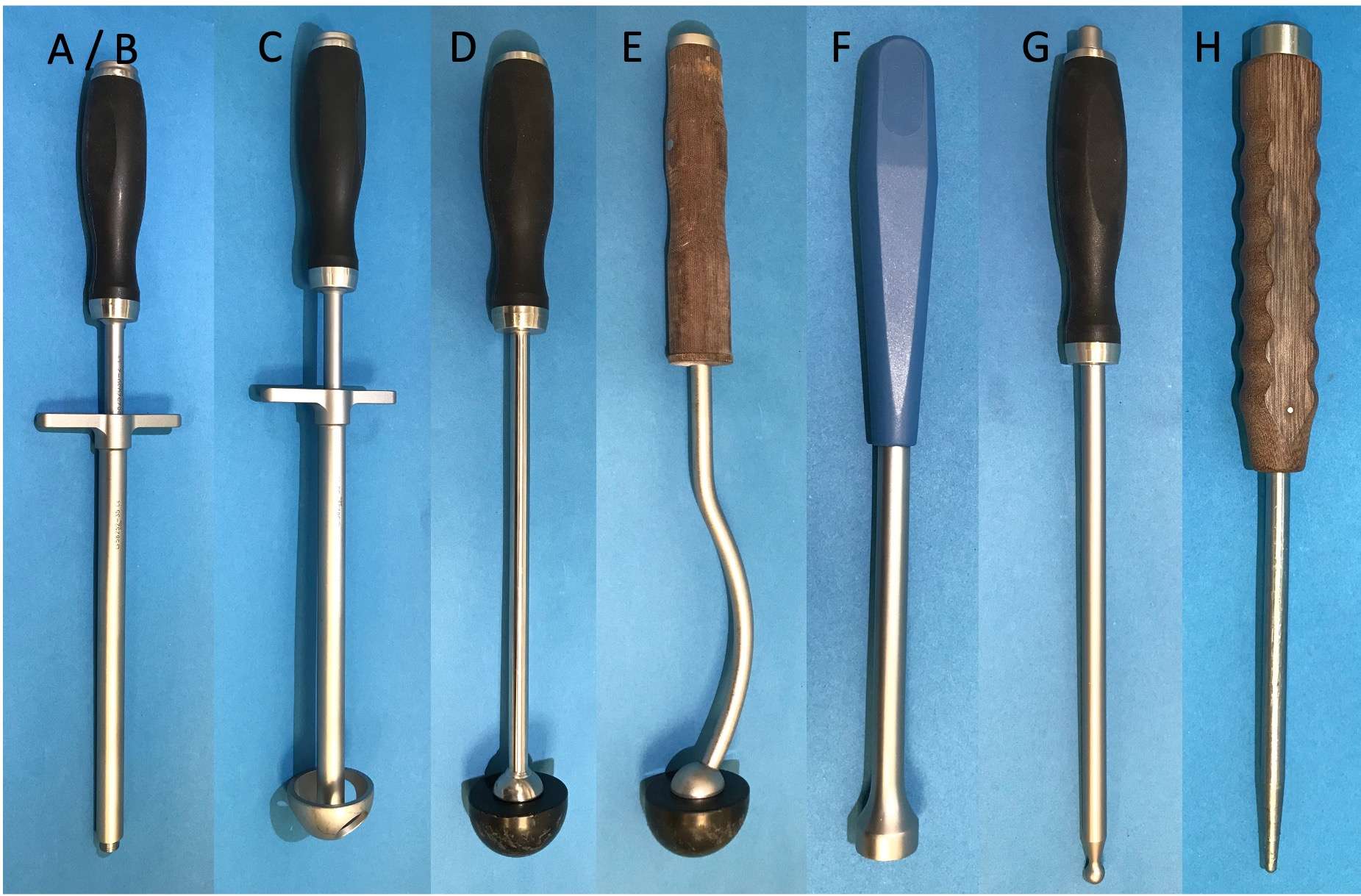
Figure 1
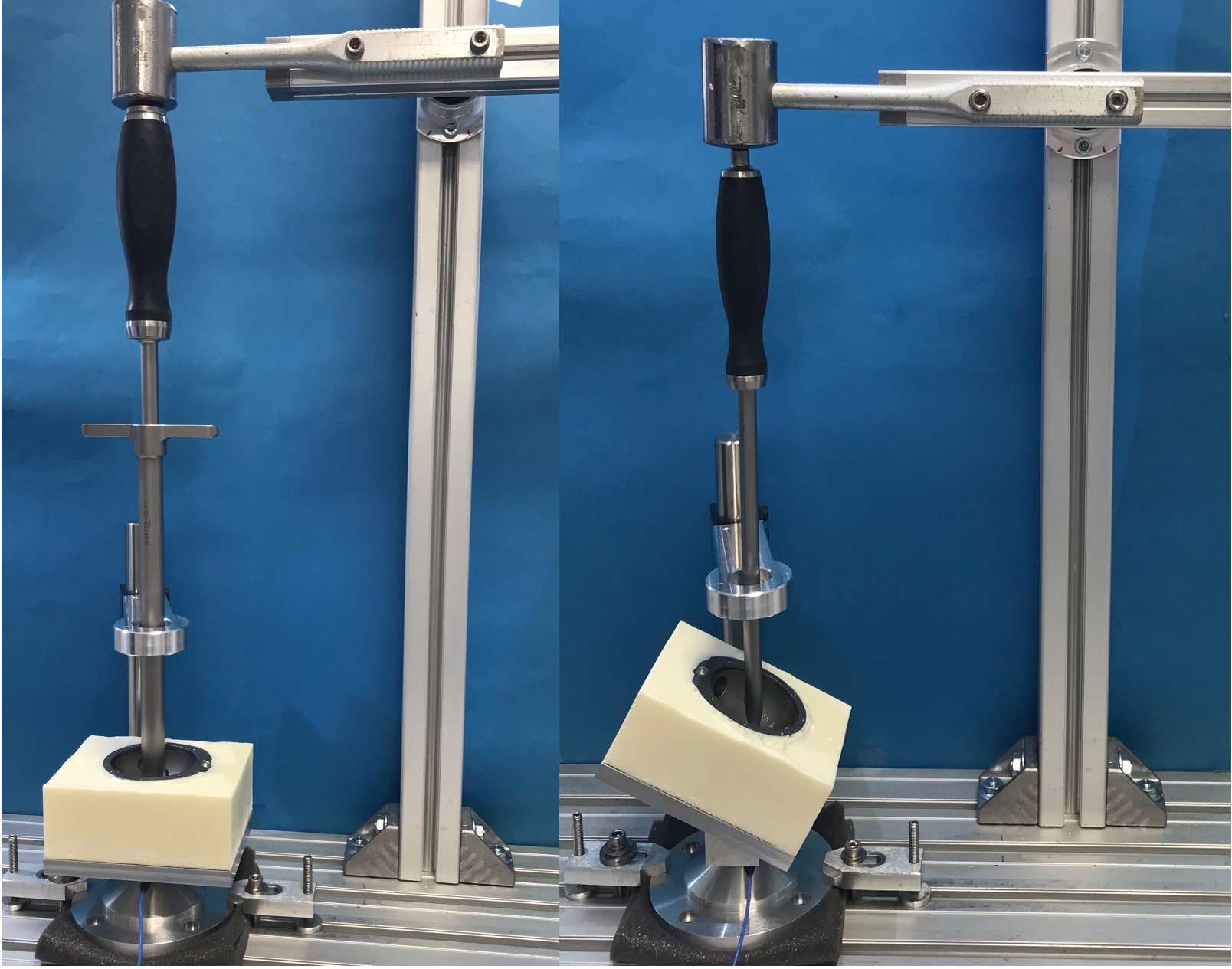
Figure 2
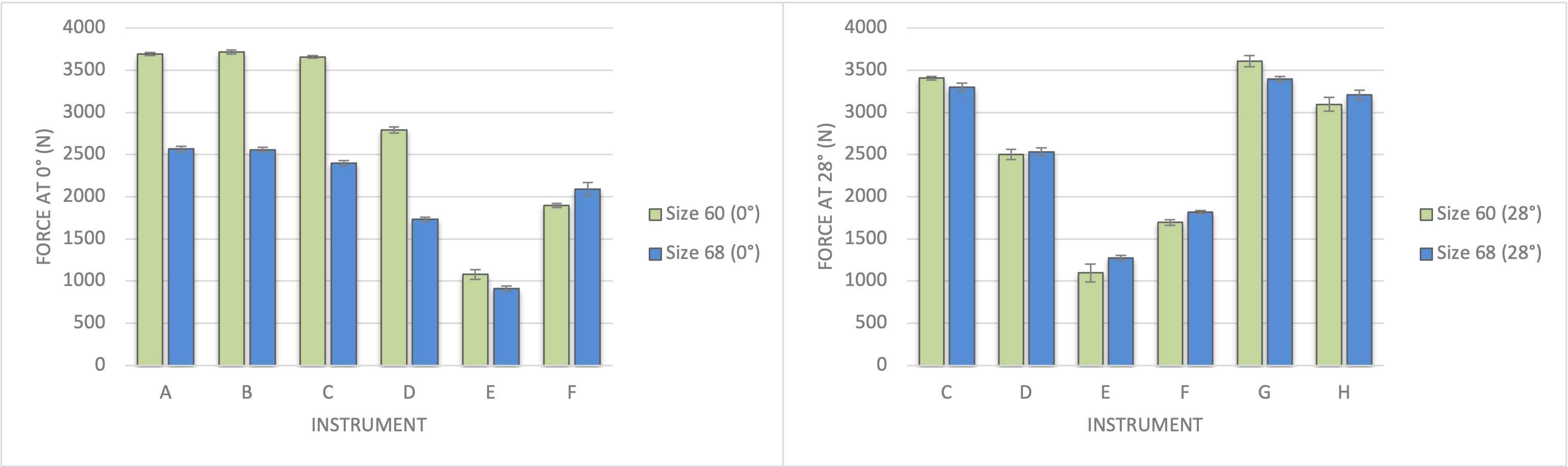
Figure 3#7535
Influence of FeCl3 and H2O2 in Corrosion Testing of Modular Taper Connections in Total Hip Arthroplasty: An in Vitro Study
*Therese Bormann - University Hospital Heidelberg - Heidelberg, Germany
Nebel, Laura - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Ulrike Mueller - University of Heidelberg - Heidelberg, Germany
Phuong Thao Mai - Karlsruhe Institute of Technology - Karlsruhe, Germany
Jens Gibmeier - Karlsruhe Institute of Technology - Karlsruhe, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: therese.bormann@med.uni-heidelberg.de
Corrosion at taper interfaces of orthopaedic implants can be a clinically relevant issue, because ions and debris generated during tribo-corrosive processes can induce adverse local tissue reactions. The latter can present itself as tissue necrosis, pseudotumor or osteolysis. For in vitro corrosion testing, saline solutions or bovine calf serum are frequently applied but this often does not introduce a clinically significant corrosive degradation of the tested interfaces. The addition of H2O2 and/or FeCl3 has been proposed to simulate inflammatory conditions in the joint1, which are thought to possibly aggravate corrosive processes at the taper connections. Also, it has been shown that H2O2 reduces the corrosion resistance of CoCrMo- and Titanium-alloys in corrosion and fretting tests1-3. These tests, however, do usually not comprise an actual taper design. Aim of the study was the investigation of the effect of H2O2 and FeCl3 on tribo-corrosion at realistic head-neck taper interfaces.
Corrosion testing was done at taper connections with a CoCrMo head taper and a Ti6Al4V neck taper, which comprised a realistic taper geometry and surface topography. As electrolytes, five different solutions were used: Pure ringer’s solution (RS), RS + 30mM H2O2, RS + 0.7 mM FeCl3, RS + 30 mM H2O2 + 0.7 mM FeCl3 and bovine calf serum (CS). The connections were dynamically loaded for five million load cycles. After completion of testing, the mass loss of the head and neck parts was determined gravimetrically as well as by ion analysis. The degradation mechanisms were investigated by light and electron microscopy.
Addition of FeCl3 led to an increase in mass loss at the head taper of about a factor of 2, while it increased the mass loss at the neck taper about a factor of 18 in comparison to pure RS, while the addition of H2O2 did not significantly increase the mass loss from head and neck tapers (Fig. 1). If H2O2 and FeCl3 were combined, an enhanced occurrence of microcracks at the neck taper surface was observed. Calf serum led to different material degradation mechanisms than the solutions based on RS, as it increased mass loss at the neck taper but decreased mass loss at the head taper in comparison to pure RS.
Adding FeCl3 increases mass loss from taper interfaces and is, therefore, suitable for the creation of a rather aggressive tribo-corrosion testing environment. The combination of FeCl3 and H2O2 increased the occurrence of microcracks at the Ti6Al4V neck taper surface and can be considered as a worst-case testing situation. The study further showed, that results from fretting test setups are not necessarily transferable to the tribo-corrosion behavior of tapers with a realistic geometry.
References
1 Liu et al., Wear 390-391 (2017) 302-311.
2 Prestat et al., Corros. Sci. 190 (2021) 109640.
3 Wimmer et al., Wear 477 (2021) 203813.
Figures
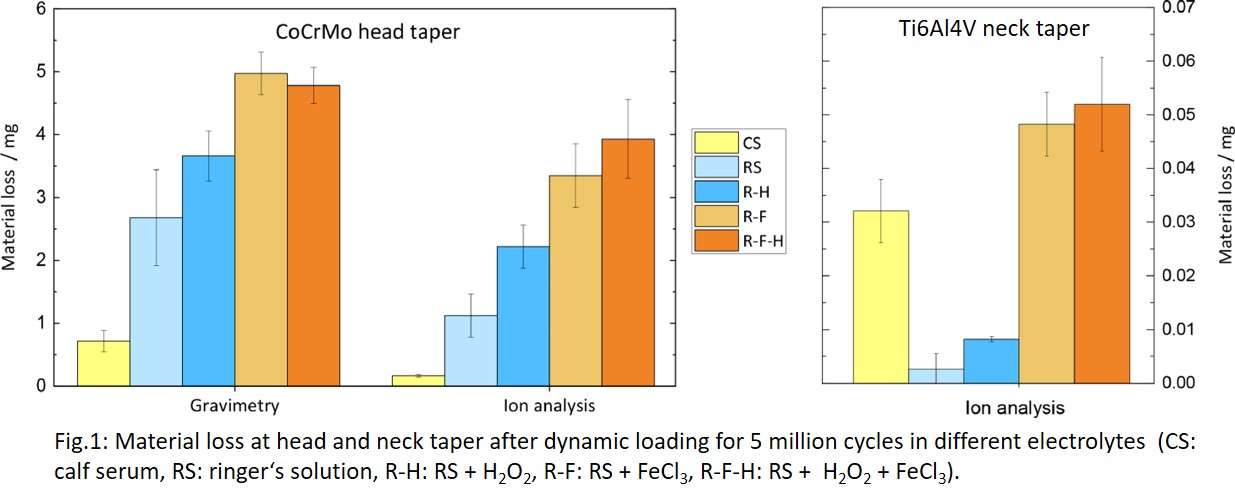
Figure 1#7480
Stability of Ceramic Coatings on Retrieved Knee Prosthesis
*Therese Bormann - University Hospital Heidelberg - Heidelberg, Germany
Simeon Kraenzler - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Daniel Kluess - University of Rostock - Rostock, Germany
Wolfram Mittelmeier - Universität Rostock - Rostock, Germany
Sebastian Jaeger - Heidelberg University Hospital - Heidelberg, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: therese.bormann@med.uni-heidelberg.de
Knee arthroplasty is a common and successful operation in the western world. The articulating femoral component is usually made of a cobalt-chromium-molybdenum-alloy because of its high wear resistance. The usage of such alloys can, however, be problematic for people with metal allergies. Also, ions that escape from the prosthesis may introduce adverse local tissue reactions. To avoid problems related to metal ions, femoral components with coated or ceramacised surfaces exist, which should shield the patient environment from the actual metal. Data on the in vivo behavior of prothesis with ceramic coatings are, however, rare. In this study, therefore, the stability of ceramic coatings is in investigated by means of retrieved femoral knee implants.
Thirty retrievals from our in-house retrieval registry with ceramic coatings were investigated, of which 25 comprised a monolayer and five a multilayer coating. Mean time in vivo of the collection was 4.4 ± 3.6 years. At all retrievals, the thickness of the coatings was measured in four different locations within the articulating area (Fig. 1) using a calotest system (Fig. 2). As original layer thickness, the coating thickness outside of the articulating area was measured. The reduction of the coating thickness was determined as the difference between the mean value from the articulation and the original layer thickness. In addition, the coatings at the retrievals were visually investigated with regard to signs of wear or damage like for example scratches or areas where the coating was completely worn away.
The mean original layer thickness of the collection was 3.7 ± 0.8 µm. In the articulating area the mean layer thickness was 3.1 ± 1.0 µm. The area medial 0° exhibited the lowest mean coating thickness of 2.9 ± 1.4 µm. There was no significant difference of the coating thickness between the individual areas within the articulation. The mean coating reduction of retrievals with a monolayer coating was 0.7 ± 0.9 µm while it was 0.3 ± 0.2 µm for the multilayer coating systems (p = 0.33). The coating reduction did neither correlate with the time in vivo (Pearson r = 0.32; p = 0.01) nor with the activity level of the patients (Spearman’s ρ = 0.32; p = 0.01). At 23 % (7 out of 30) of the retrievals, isolated areas with a completely worn away coating were found.
After revision surgery, the mean coating thickness referred to about 3 µm. This seems to be reasonable given that the mean original coating thickness was less than 4 µm. The mean time in vivo of the investigated retrievals was, however, less than 5 years, why no conclusions on the long-term behavior of ceramic coatings can be drawn from this study. The occurrence of isolated full coating abrasion at 23 % of the investigated retrievals shows that ceramic coatings should be optimized with respect to their stability.
Figures
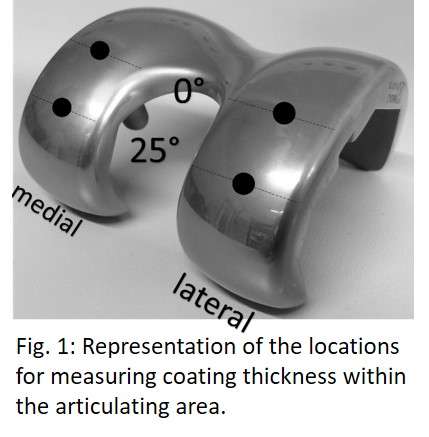
Figure 1
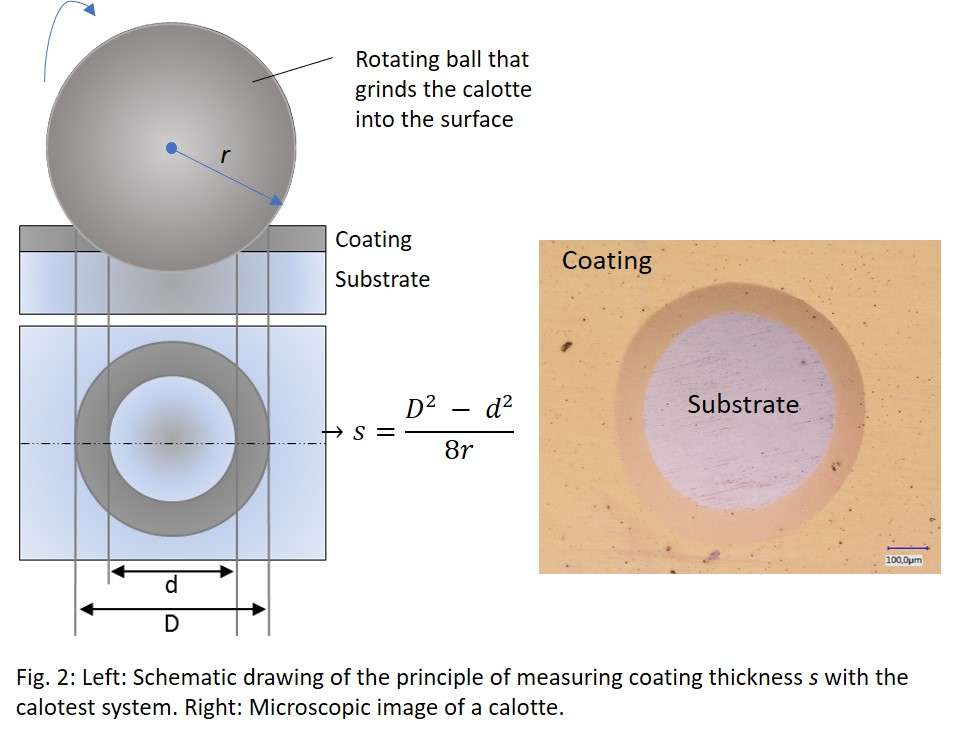
Figure 2#7708
How Does Number of Cerclage Cables Impact Titanium Tapered Stem Stability in Periprosthetic Femoral Fracture: A Biomechanical Cadaveric Study
*Troy Bornes - Hospital for Special Surgery - New York, USA
Haena-Young Lee - Hospital for Special Surgery - New York, USA
Mathais Bostrum - Hospital for Special Surgery - New York, USA
Christopher Anderson - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Jose Rodriguez - Lenox Hill Hospital - New York, USA
Friedrich Boettner - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
*Email: troy.bornes@gmail.com
Introduction: Periprosthetic femoral fractures around total hip arthroplasty stems are commonly treated with femoral component revision using a titanium tapered stem and cerclage fixation.1-3 Peri-isthmic periprosthetic fractures are particularly challenging to treat given that the fracture extends through the isthmus and compromises the zone of bone available for stem contact and stability. Limited biomechanical evidence exists to guide fixation strategies.4-5 We previously found that a 4-cm cortical contact length between intact bone and stem provided superior stability compared to shorter contact lengths.4 The objective of this study was to evaluate the difference in tapered stem stability when using 2 versus 3 cerclage cables in the treatment of simulated peri-isthmic fractures with a 4-cm contact length.
Methods: Fourteen fresh frozen cadaveric female femora (7 matched pairs) from donors with an age of 64.0±9.9 years were included. The femoral isthmus was identified using fluoroscopy and the bone proximal to the isthmus was resected. The femoral shaft was over-reamed in a retrograde fashion to create a consistent 4-cm contact length at the isthmus. A simulated oblique fracture was created using a 3D-printed cutting guide, reduced, and fixed using cerclage cables (Stryker Dall-Miles; 2 cables on one femur and 3 on the contralateral femur of each matched pair; Fig. 1A). The femur was prepared, and a 195-mm monobloc tapered stem (Exactech Alteon) was implanted. The distal end of each femoral specimen was loaded axially in a stepwise fashion to up 10000 N using a servohydraulic testing system (Fig. 1B). Stem subsidence and fracture displacement were determined at 2600 N (simulating load during gait).5-7 Load-to-failure was determined with failure defined as stem subsidence ≥10 mm, the initiations of a new fracture, and/or cable failure (Fig. 1C).
Results: At a 2600 N load, stem subsidence was significantly lower in specimens treated with 3 cables (3.0±1.9 mm) than 2 cables (5.7±2.0 mm; p=0.02; Table 1). Fracture displacement was <1.5 mm in all specimens at a 2600 N load (0.5±0.3 mm for 3 cables; 0.7±0.5 mm for 2 cables; p=0.03). During load-to-failure testing, all constructs failed. The load-to-failure was 3657±543 N in specimens treated with 3 cables and 3271±799 N in those with 2 cables (p=0.12). The initial failure mode was subsidence ≥10 mm in most specimens (6/7 of 3-cable specimens; 5/7 of 2-cable specimens). Forces at which stems subsided ≥10 mm were not significantly different between specimens with 2 and 3 cables (3829±545 N for 3 cables; 3464±729 N for 2 cables; p=0.16; Table 2). Force at which new fracture occurred was significantly higher in specimens treated with 3 cables (4971±1496 N) compared to those with 2 cables (3929±851 N; p=0.04).
Conclusions: In a peri-isthmic periprosthetic fracture model with a 4-cm cortical contact length, titanium tapered stems had improved initial axial stability and reduced stem subsidence in fractures treated with 3 cerclage cables compared to 2 cables. In load-to-failure testing, femora fixed with 3 cables demonstrated superior biomechanical properties to femora with 2 cables as higher loads were required for new fractures to develop.
Figures
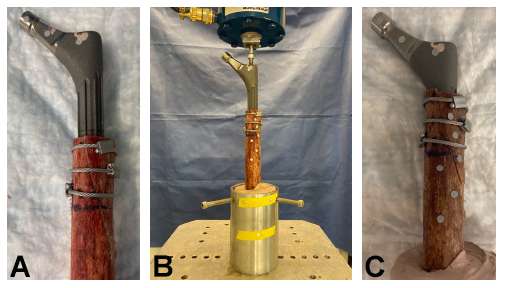
Figure 1
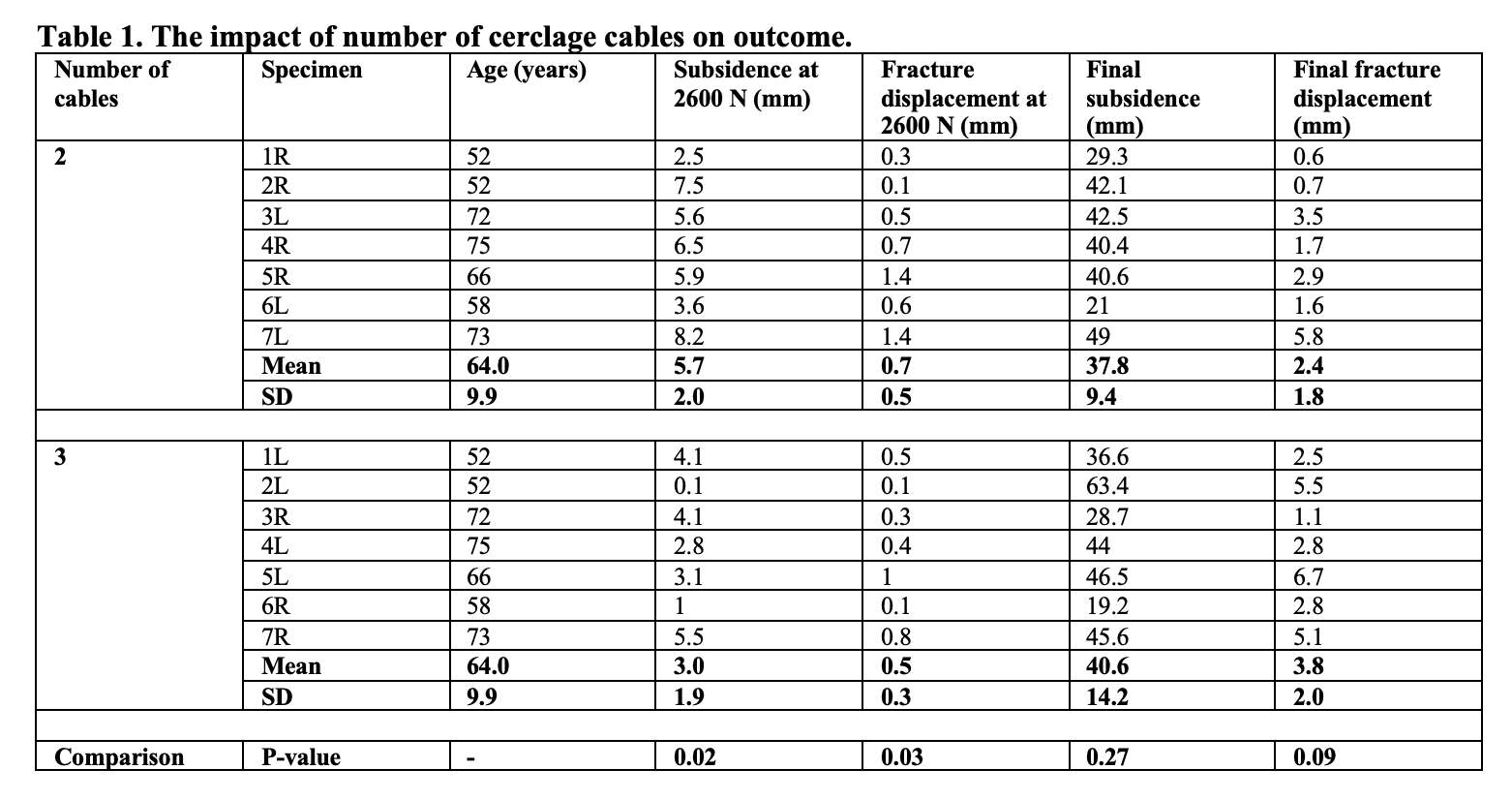
Figure 2
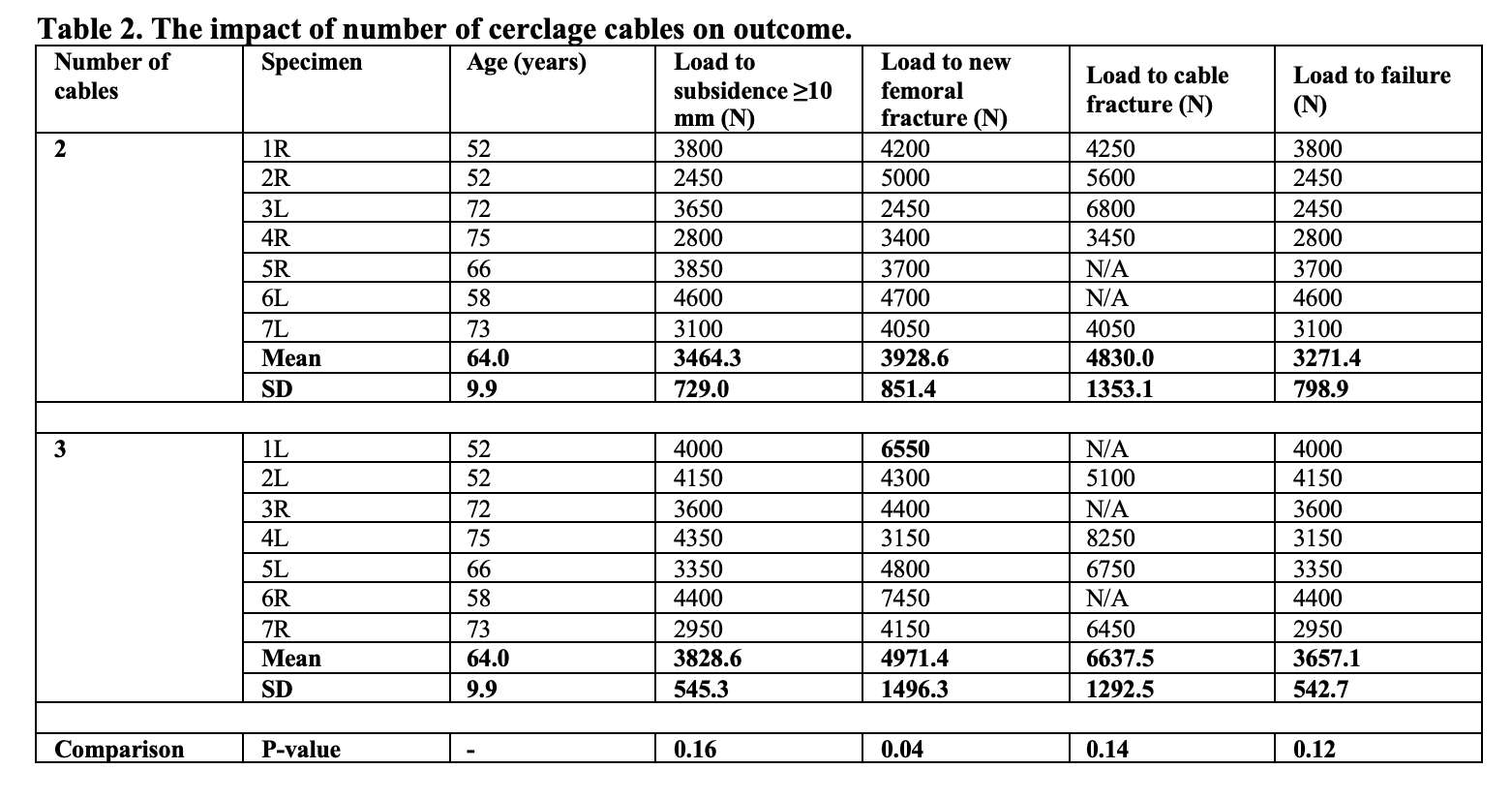
Figure 3#7816
Absolute Neutrophil Count: A Novel Marker for Diagnosing Chronic Periprosthetic Joint Infection Following Total Hip and Knee Arthroplasty
*Troy Bornes - Hospital for Special Surgery - New York, USA
Allina Nocon - Hospital for Special Surgery - New York, USA
Jonathan Yu - Cornell University - New York, USA
John Rezkalla - Hospital for Special Surgery - New York, USA
Mark Youssef - Hospital for Special Surgery - New York, USA
Alberto Carli - Hospital for Special Surgery - New York City, USA
David J. Mayman - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
*Email: troy.bornes@gmail.com
Introduction: Establishing the diagnosis of periprosthetic joint infection (PJI) is challenging. To date, no gold standard test exists.1-7 Criteria used to diagnose PJI include synovial white blood cell (WBC) count and polymorphonuclear neutrophil (PMN) percentage.3-5 Elevations in these markers suggest the presence of PJI. However, it is currently unclear whether PJI is present if levels are discordant with one marker elevated and the other within normal limits. Our objectives were to determine the performance of synovial absolute neutrophil count (ANC) in the diagnosis of chronic PJI and evaluate its accuracy in predicting PJI when discordance exists between WBC and PMN.
Methods: This retrospective study included 472 patients from a revision arthroplasty registry treated with revision total hip arthroplasty (THA) or revision total knee arthroplasty (TKA). All patients were evaluated with preoperative aspiration and 3 intraoperative cultures. Synovial fluid markers (WBC and PMN) and serum markers (CRP and ESR) were collected. ANC was calculated as the product of WBC count and PMN percentage. Chronic infection was defined using the definition from the 2013 International Consensus Meeting on PJI. ANC thresholds were generated using data-driven methods (upper quartile) and the literature-derived estimates. Patients with discordance were identified within the sample population. ANC was compared to other markers in the diagnosis of infection using area under the curve (AUC) analysis on receiver operating characteristic (ROC) curves, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
Results: Patient demographics are reported in Table 1 for 193 patients with chronic PJI and 279 patients with no infection. Levels of all infection markers including ANC were significantly higher in chronically infected patients compared with noninfected patients (p<0.0001; Table 1). Based on ROC curves generated from 472 patients, ANC (81.5%) and WBC (81.9%) performed significantly better in the diagnosis of chronic PJI compared to PMN, ESR, and CRP (Figure 1A). Discordance between WBC and PMN occurred in 38 patients within the study population (11.9%) including 14 patients in the chronic PJI group (8.4%) and 24 patients in the noninfected group (15.8%). In this subgroup of patients with discordance, an ANC threshold of 975 cells/mL had a sensitivity of 92.9% and NPV of 88.9%, while a threshold of 3819 cells/mL had a specificity of 87.5% and PPV of 66.7% (Table 2A). These values were superior to those found for other markers. In the study population of 472 patients, an ANC threshold of 2983 cells/mL yielded optimal balance between sensitivity, specificity, PPV, and NPV (Table 2B).
Discussion: ANC performed well in predicting chronic PJI in patients treated with revision THA and TKA. Discordance between WBC count and PMN percentage occurred in approximately 12% of patients. Based on the results, we propose a diagnostic algorithm for use in patients with discordance (Figure 1B). An ANC threshold of 2983 cells/mL was shown to effectively diagnose chronic PJI in the study population of 472 patients. Further investigation is required to validate the use of ANC in diagnostic algorithms.
Acknowledgements: Funding was provided by the Stavros Niarchos Foundation Complex Joint Reconstruction Center.
Figures
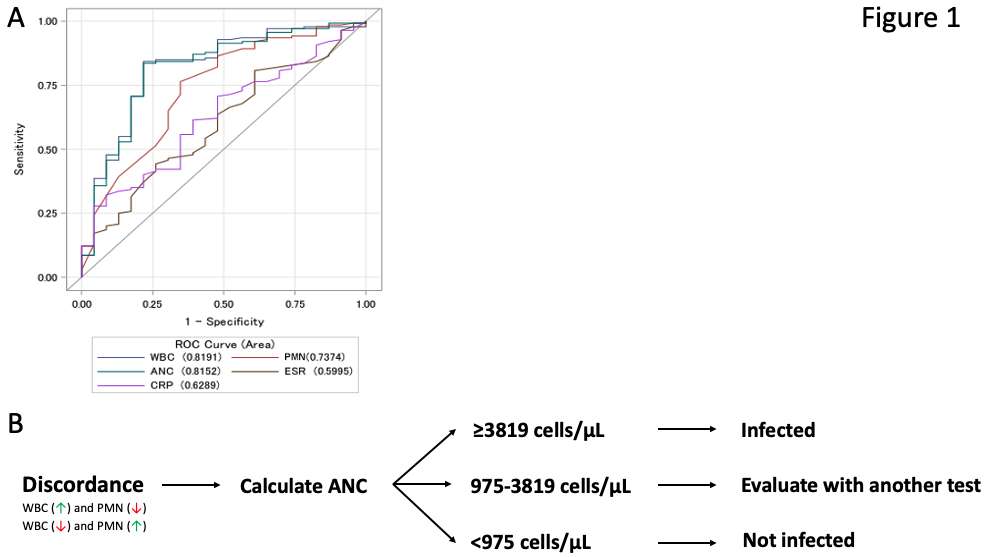
Figure 1
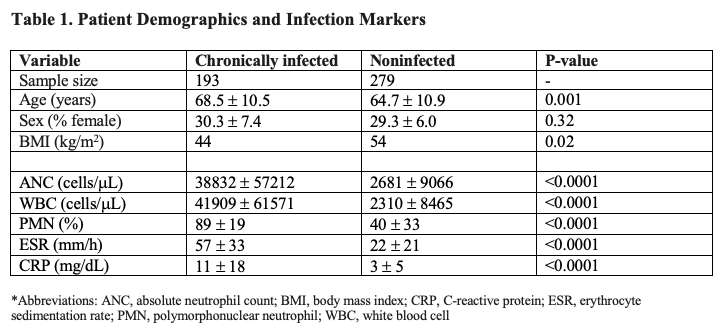
Figure 2
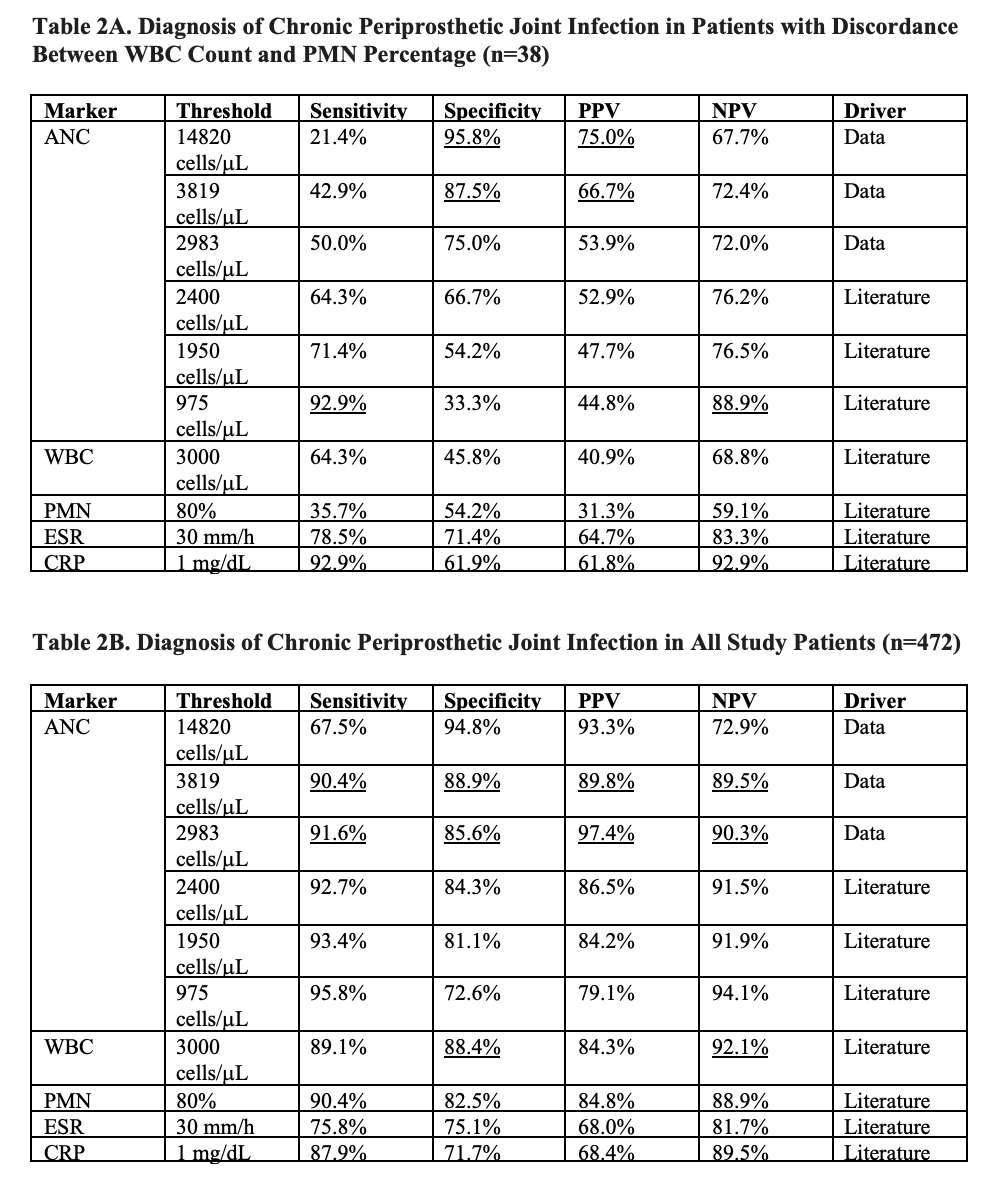
Figure 3#7745
Leg-Length Discrepancy in Revision Total Hip Arthroplasty: The Impact of Computer-Assisted Navigation
*Troy Bornes - Hospital for Special Surgery - New York, USA
Christopher Anderson - Hospital for Special Surgery - New York, USA
Gregory Schimizzi - Hospital for Special Surgery - New York, USA
Allina Nocon - Hospital for Special Surgery - New York, USA
Kathleen Tam - Hospital for Special Surgery - New York, USA
Jason Blevins - Hospital for Special Surgery - New York, USA
Alberto Carli - Hospital for Special Surgery - New York City, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
*Email: troy.bornes@gmail.com
Introduction
Leg-length discrepancy (LLD) following total hip arthroplasty (THA) is a source of patient dissatisfaction, morbidity, and litigation.1 Computer-assisted navigation can be used to monitor and optimize leg length during surgery. Several studies have reported improved leg-length correction during primary THA when navigation systems were employed.2-3 To date, there has been limited study of LLD following revision THA (rTHA).4 Furthermore, the impact of navigation during revision surgery on correction of LLD is currently unknown. The objectives of this study were to characterize LLD following rTHA and evaluate the difference in LLD in patients treated with navigated rTHA compared to non-navigated rTHA.
Methods
This retrospective cohort study included 202 patients from a single institution’s revision arthroplasty registry treated with rTHA during the period of 2017-2021. Demographic and surgical data and were collected. An a priori power analysis determined a sample size of 101 patients in each group was needed to determine a difference in LLD of 2 mm at 80% power at a significance level of 0.05. Patients treated with navigated rTHA and non-navigated (control) patients were randomly selected (Table 1). LLD was measured on pre-operative and post-operative X-rays (AP pelvis or full-length EOS) using consistent landmarks on the femur (lesser trochanter or greater trochanter) and pelvis (tear drop or obturator foramen). Outcomes of LLD (absolute value), re-revision rate, and patient-reported outcome measures were compared between groups using a Mann-Whitney U test. A sub-analysis was performed to compare post-operative LLD in patients who had a pre-operative LLD of <20 mm, <15 mm, <10 mm, and <5 mm.
Results
Patient demographics and pre-operative diagnoses are reported in Table 1. In navigated rTHA, post-operative LLD (3.69±4.73 mm) was significantly lower than pre-operative LLD (7.46±6.12 mm; p<0.001). In the non-navigated rTHA, post-operative LLD (4.88±4.34 mm) was significantly lower than pre-operative LLD (7.76±6.64 mm). Post-operative LLD was significantly lower in the navigated group compared to non-navigated group in all patients and in subgroups with pre-operative LLD <5 mm, <10 mm, <15 mm, and <20 mm (p<0.05; Table 2). Subsequent re-operation was required in 3 navigated rTHAs (2.97%) and 6 non-navigated rTHAs (5.94%; p=0.26). Change in patient-reported Hip Injury and Osteoarthritis Outcome Score Junior (HOOS Jr.) with surgery was 18.8±21.0 in navigated and 19.3±24.8 in non-navigated patients (p=0.86), change in Lower Extremity Activity Scale [LEAS] was 1.3±3.0 in navigated and 1.9±3.1 in non-navigated patients (p=0.28), and change in pain was -14.1±31.5 in navigated and -20.5±28.2 in non-navigated patients (p=0.48).
Conclusions
Post-operative LLD was improved relative to pre-operative LLD in rTHA with and without the use of computer-assisted navigation. Post-operative LLD was significantly lower in navigated rTHA than non-navigated rTHA. There was no difference in patient reported outcomes between groups. Based on these results, navigation appears to optimize leg-length correction and should be considered for use in revision arthroplasty surgery.
Acknowledgements
Funding was provided by the Stavros Niarchos Foundation Complex Joint Reconstruction Center.
Figures
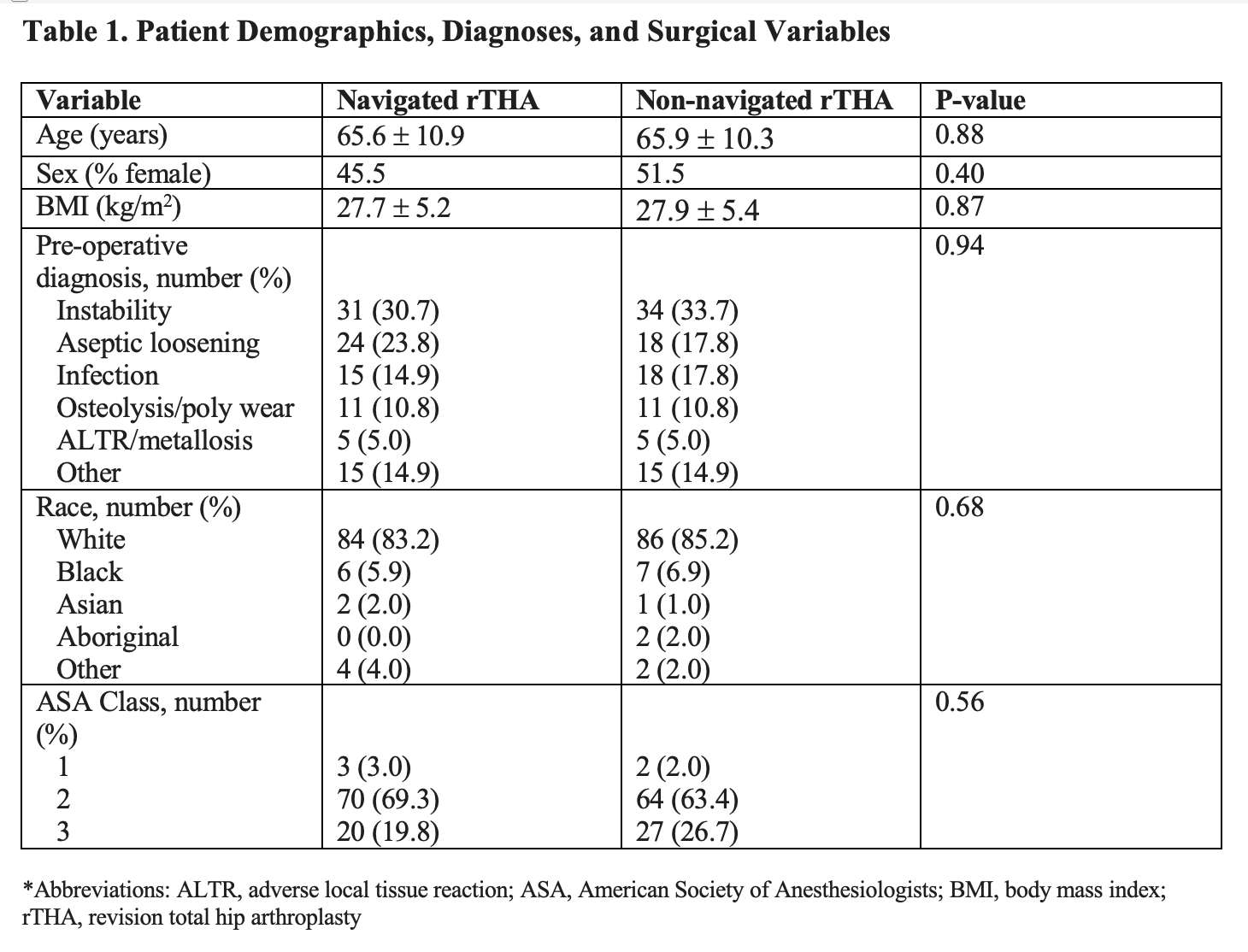
Figure 1
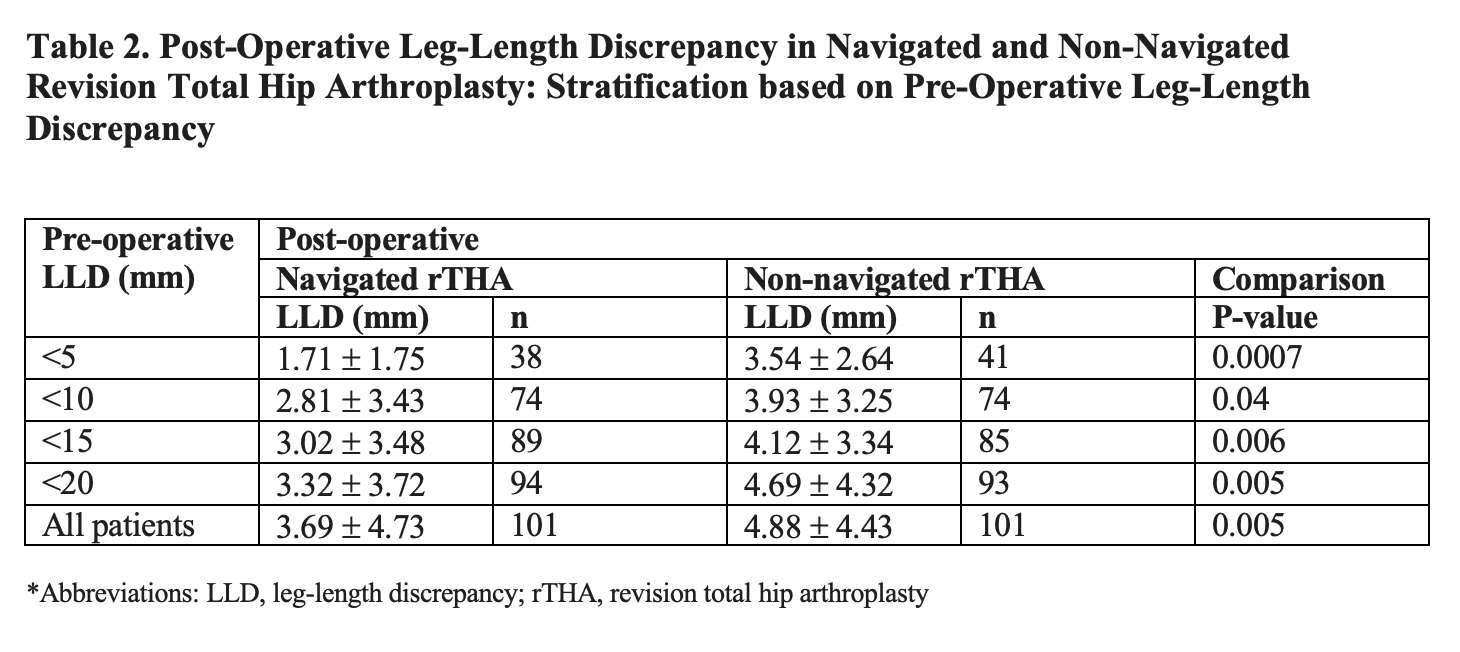
Figure 2#7619
The L1-Pelvic Angle: A Simplified Approach to Estimating the PI-LL Mismatch From Lateral Radiographs
*Yuan Chai - University of Sydney - Sydney, Australia
Mounir Boudali - University of Sydney - Sydney, Australia
John Farey - The Kolling Institute - Sydney, Australia
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: yuan.chai@sydney.edu.au
Introduction:
Pelvic Incidence-Lumbar Lordosis (PI-LL) mismatch is considered a measure of the spinopelvic alignment in the sagittal plane. This angle is obtained by measuring two separate angles (PI and LL) on lateral radiographs (Figure 1). Here we propose a simplified method of estimating the PI-LL mismatch through the measurement of the L1-Pelvis angle (L1P), reducing operator error linked to manual measurement and making the process more practicable for radiographic templating.
Methods:
A series of 126 consecutive standing lateral radiographs presenting for Total Hip Arthroplasty (THA) were examined. Landmark selection was completed by three operators and was repeated by one operator. In total, 6 landmarks were identified on digital radiographs as follows: 1 landmark at the midpoint of the center of the femoral heads, 2 landmarks at the anterior and posterior margins of the superior S1 endplate, 1 landmark at the midpoint of the superior S1 endplate, and 2 landmarks at the anterior and posterior margins of the superior L1 endplate. We compare the PI-LL mismatch obtained via the conventional method of measuring PI and LL, with our simplified method, where we estimate this mismatch by measuring an intermediary angle from the first lumbar vertebra to the pelvis (L1P) using the formula PI-LL = L1P - 90°. We also assess the reliability and repeatability of both methods using the intraclass correlation coefficient (ICC).
Results:
No difference (p > 0.05) was observed between the PI-LL mismatch from the conventional method (0.22° ± 13.6) and the simplified method (0.0° ± 13.1). The overall average normalized root mean square error for PI-LL mismatch across all three operators was 6.5% (-2.9° ± 4.9). This value increases slightly to 7.53% (-3.3° ± 6.0) for PI-LL measure using the conventional method, confirming that the simplified method of measuring PI-LL reliably reproduced similar measurements to the conventional method. The inter- and intra-operator reproducibility were excellent (all the ICCs > 0.9), where the new method had higher reliability (inter-operator ICC = 0.969 vs 0.951, intra-operator ICC = 0.981 vs 0.976). Furthermore, the NRMSE between the two sets of measurements was 9.96% for PI, 5.97% for LL, and 4.41% for L1P. The absolute error between the two sets of measurements shows the same trend.
Conclusion:
Results show that the simplified method produced similar measurements of PI-LL mismatch to the conventional method. Furthermore, reproducibility of the measurements and reliability between operators were improved compared to the conventional method. When considering the L1P angle, the classification of the sagittal spinal deformity – or flatback deformity – seen in [1] translates to the following: normal when L1P<100°, mild when 100°<L1P<110°, and severe when L1P>110°. Surgeons adopting our method should expect an improvement in the reliability and repeatability of the measurements and a significant improvement in assessing this mismatch through the visualization of the angle L1P.
References:
[1] Aoki Y, Nakajima A, Takahashi H et al. Influence of pelvic incidence-lumbar lordosis mismatch on surgical outcomes of short-segment transforaminal lumbar interbody fusion. BMC Musculoskelet Disord 16, 213 (2015). https://doi.org/10.1186/s12891-015-0676-1
Keywords:
L1-Pelvic angle; PI-LL mismatch; Lumbar lordosis;
Figures
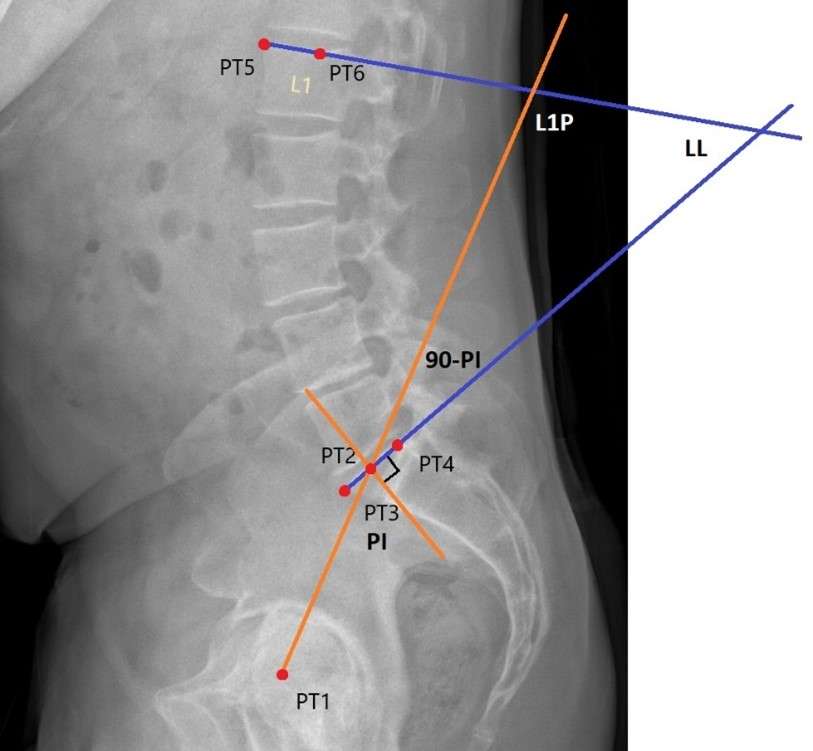
Figure 1#7610
Validation of a Machine Learning Technique for Single Plane Fluoroscopy
*Jordan Broberg - Western University - London, Canada
Andrew Jensen - University of Florida - Gainesville, USA
Scott Banks - University of Florida - Gainesville, USA
Matthew Teeter - Western University - London, Canada
*Email: jbroberg@uwo.ca
Introduction: Single plane fluoroscopy has been used to accurately track in vivo kinematics of total knee replacements (TKR). Modern single plane fluoroscopy obtains implant model poses with the use of optimization techniques to help automate the process, greatly reducing the amount of human error and time required to produce kinematic measurements. However, the process still requires a human operator to find the initial poses of the implant models in the first frame using an edge detection algorithm. A machine learning technique implementing two networks has been developed for use in a commonly used publicly available joint kinematic measurement software (JointTrack Auto). The first network segments each radiograph to identify the tibial or femoral component, and the second finds an initial pose that can be used as a starting point for the optimization algorithm. The goal of this study was to assess the accuracy of the machine learning technique in calculating the relative pose between the tibial and femoral components, using a biplanar radiostereometric analysis (RSA) technique as a gold standard.
Methods: Twenty-four patients were included in the present study, each with a cemented, single radius, posterior stabilized TKR design. Each patient underwent weightbearing, quasi-static RSA exams, where up to five radiographic image pairs at increasing angles of flexion were acquired for each patient to simulate a knee bend. A total of 113 image pairs were acquired. Model-based RSA (MBRSA) software used both the anterior-posterior (AP) and lateral radiographs to acquire the relative poses between the tibial and femoral implant components, which represented the gold standard kinematics. The same lateral radiographs implemented in the RSA measurements were used to simulate single plane fluoroscopy in a modified version of JointTrack Auto that could implement the machine learning technique. This was used to find the relative poses between the tibial and femoral components, which were then compared to the gold standard kinematics. Root-mean-square (RMS) error was calculated for all six translational and rotational axes, including (AP) translation, superior-inferior (SI) translation, medial-lateral (ML) translation, flexion-extension, abduction-adduction, and internal-external rotation. Bland-Altman plots were also generated with bias and 95% limits of agreement (LoA) reported. Correlations between the gold standard and machine learning techniques were also calculated.
Results: RMS error was 0.8mm for AP translation, 0.5mm for SI translation, 2.6mm for ML translation, 1.0° for flexion-extension, 1.2° for abduction-adduction, and 1.7° for internal-external rotation. Figure 1 contains the Bland-Altman plots for each of the three translational and rotational axes. There were significant correlations between the machine learning and gold standard techniques for AP translation (r=0.95, p<0.0001), SI translation (r=0.99, p<0.0001), flexion-extension (r=0.99, p<0.0001), and internal-external rotation (r=0.94, p<0.0001).
Conclusion: This study validates the use of the machine learning technique for obtaining TKR kinematics. RMS errors were on par with accuracies reported in literature for single plane fluoroscopy. Bland-Altman plots showed good agreement between techniques for the in-plane translational and rotational axes.
Figures
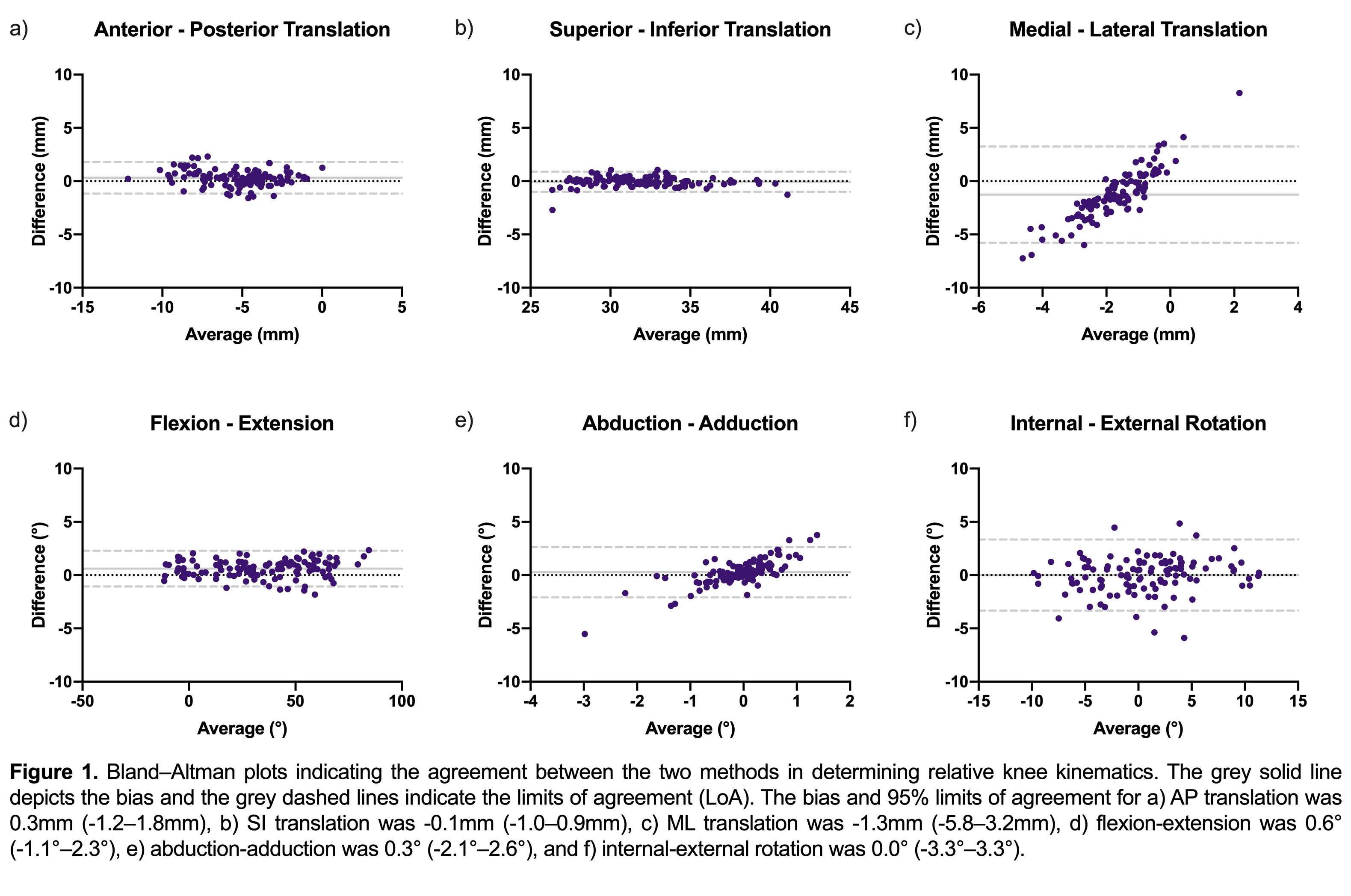
Figure 1#7612
Tibial Component Fixation of Cementless Total Knee Replacements Measured With RSA and MRI
*Jordan Broberg - Western University - London, Canada
James Howard - London Health Sciences Centre - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Hollis Potter
Matthew Teeter - Western University - London, Canada
*Email: jbroberg@uwo.ca
Introduction: Cementless total knee replacement (TKR) implants have porous metal surfaces that require bone ingrowth to create a biological fixation mechanism. Radiostereometric analysis (RSA) is the gold standard for investigating implant fixation but is limited to use on small groups of patients. Magnetic resonance imaging (MRI) is more available and can analyze the bone-implant interface for the presence of fibrous membrane formation and classify an implant as loose if there is diffusely poor bone integration. However, it is unknown how the status of implant fixation as measured by MRI relates to migration measured by RSA. The goal of this study is to investigate cementless TKR tibial component migration measured using RSA in comparison to evaluation of the corresponding bone-implant interfaces for bone ingrowth using MRI.
Methods: Ten patients (five male, five female) have been recruited. Supine RSA and 3 Tesla MRI (using metal artifact reduction sequences) were performed at a baseline of one day after TKR surgery and again at two-weeks, six-weeks, three-months, and six-months post-operation. Weight-bearing RSA exams were performed at all timepoints following the baseline exam. With RSA, maximum total point motion (MTPM) and migration in four distinct quadrants of the tibial baseplate (anterolateral, anteromedial, posterolateral, and posteromedial) were calculated. Longitudinal migration was determined between the supine baseline exam and each follow-up supine exam. Inducible displacement was determined between the supine and standing exams at each time point. With MRI, the bone-implant interface surrounding the tibial baseplate was assessed in the four quadrants and classified as normal, fibrous, fluid, or osteolytic and the percent contact of bone (<33%, 33%-66%, >66%). Implants were then scored as either loose or not loose.
Results: Figure 1 shows the longitudinal migration for each tibial baseplate quadrant as well as the MTPM. There were no differences (p=0.92) in longitudinal migration between the four quadrants. Figure 2 shows the inducible displacement for each tibial baseplate quadrant as well as the MTPM. There were no differences (p=0.85) in inducible displacement between the four quadrants. All patients had >66% integration of bone with the porous metal implant surface in all four quadrants at each timepoint, except for one patient who had 33-66% integration in the posteromedial region at six-months post-operation. Six patients had quadrants classified as fibrous, however all implants were scored not loose. Quadrants that had a fibrous membrane present within the first 6 weeks post-operation had significantly greater longitudinal migration at two-weeks (mean difference=0.22mm, p=0.002), six-weeks (mean difference=0.31mm, p=0.007), and three-months (mean difference=0.28mm, p=0.03) than quadrants that were classified as normal within the first six weeks (Figure 3).
Conclusion: This is the first study using RSA and MRI to examine implant fixation in the same cohort of patients. The significantly greater longitudinal migration in baseplate quadrants classified as fibrous within the first six weeks post-operation suggests a potential relationship may exist between RSA-measured migration and the MRI-evaluated integration of the bone-implant interface.
Figures
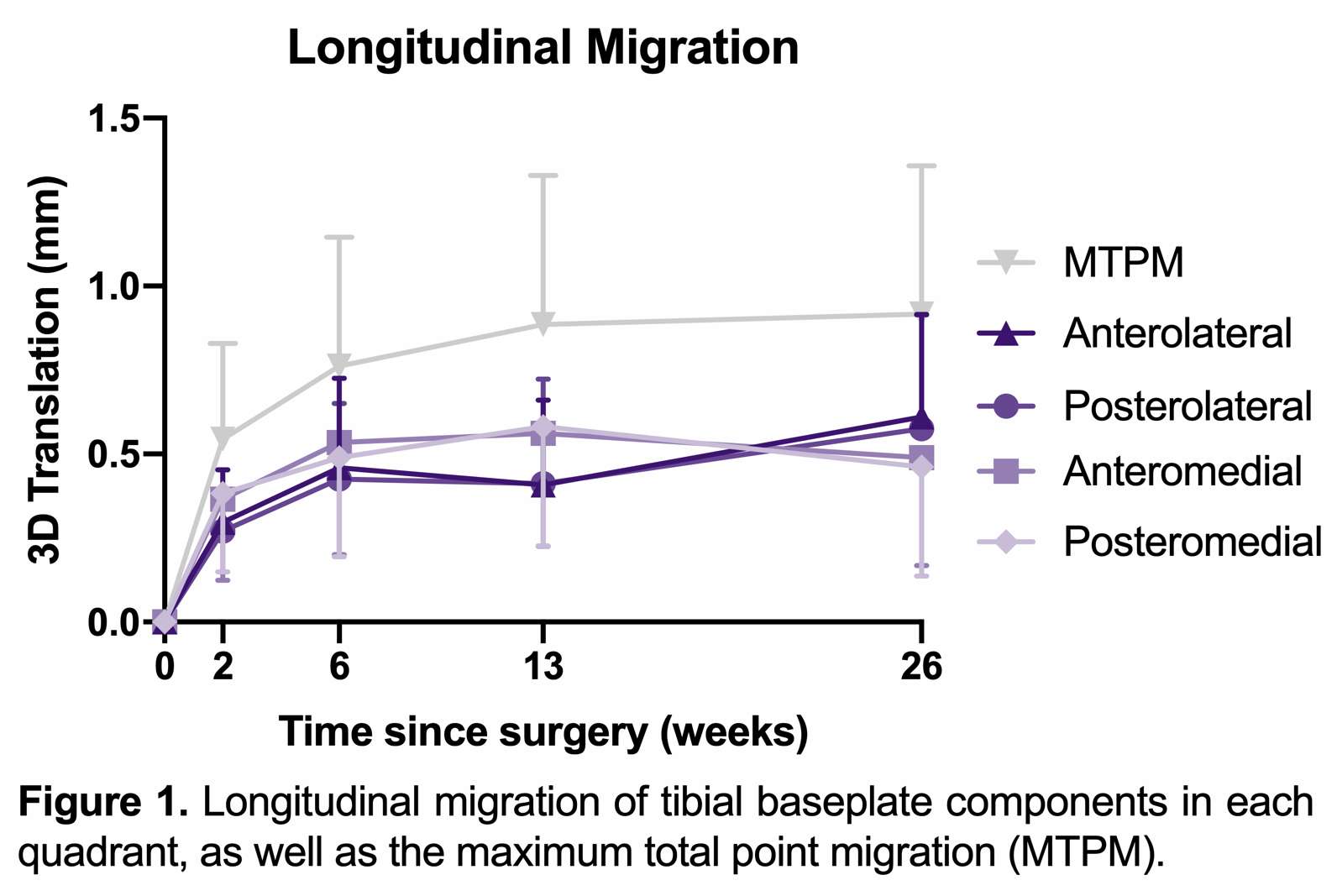
Figure 1
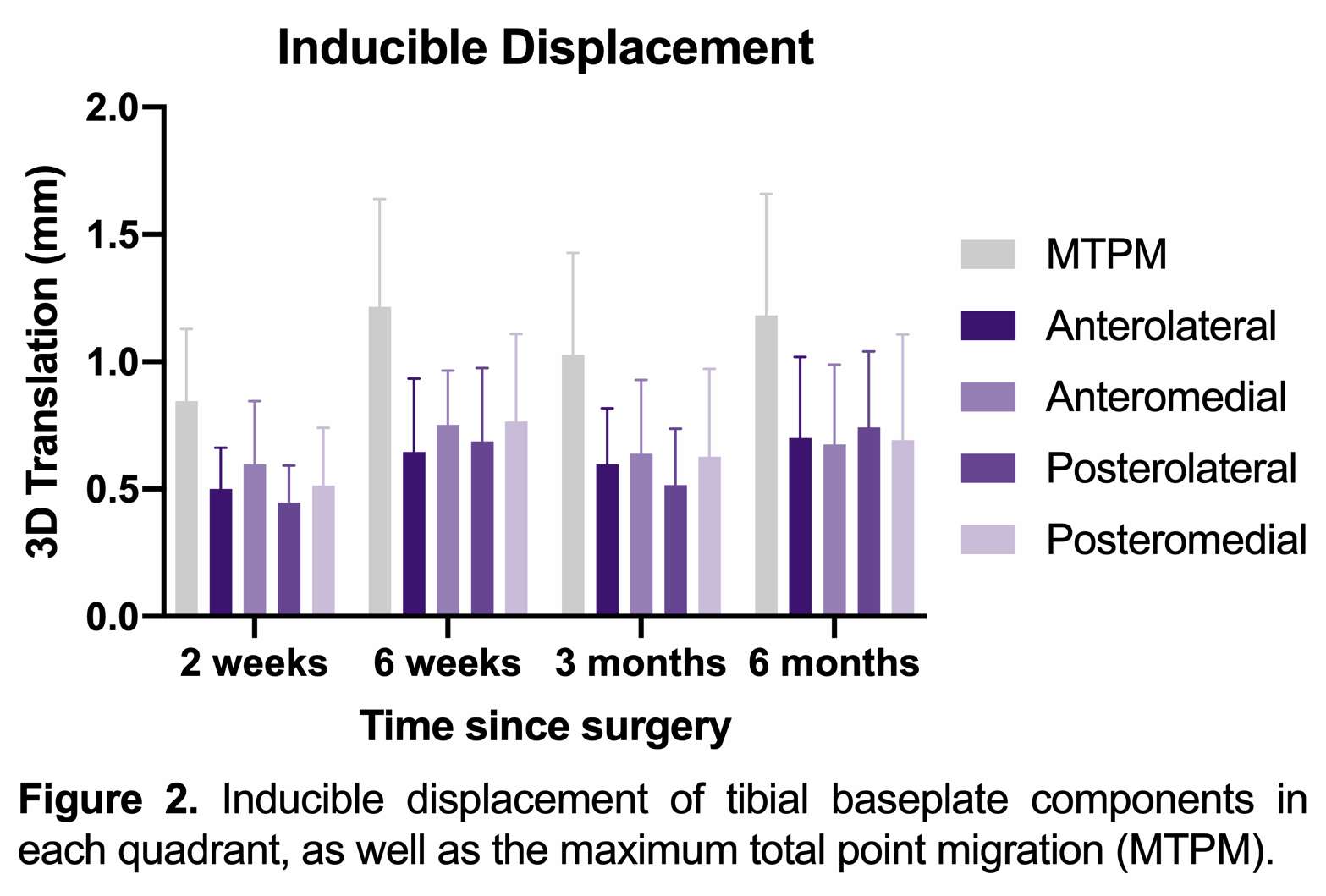
Figure 2
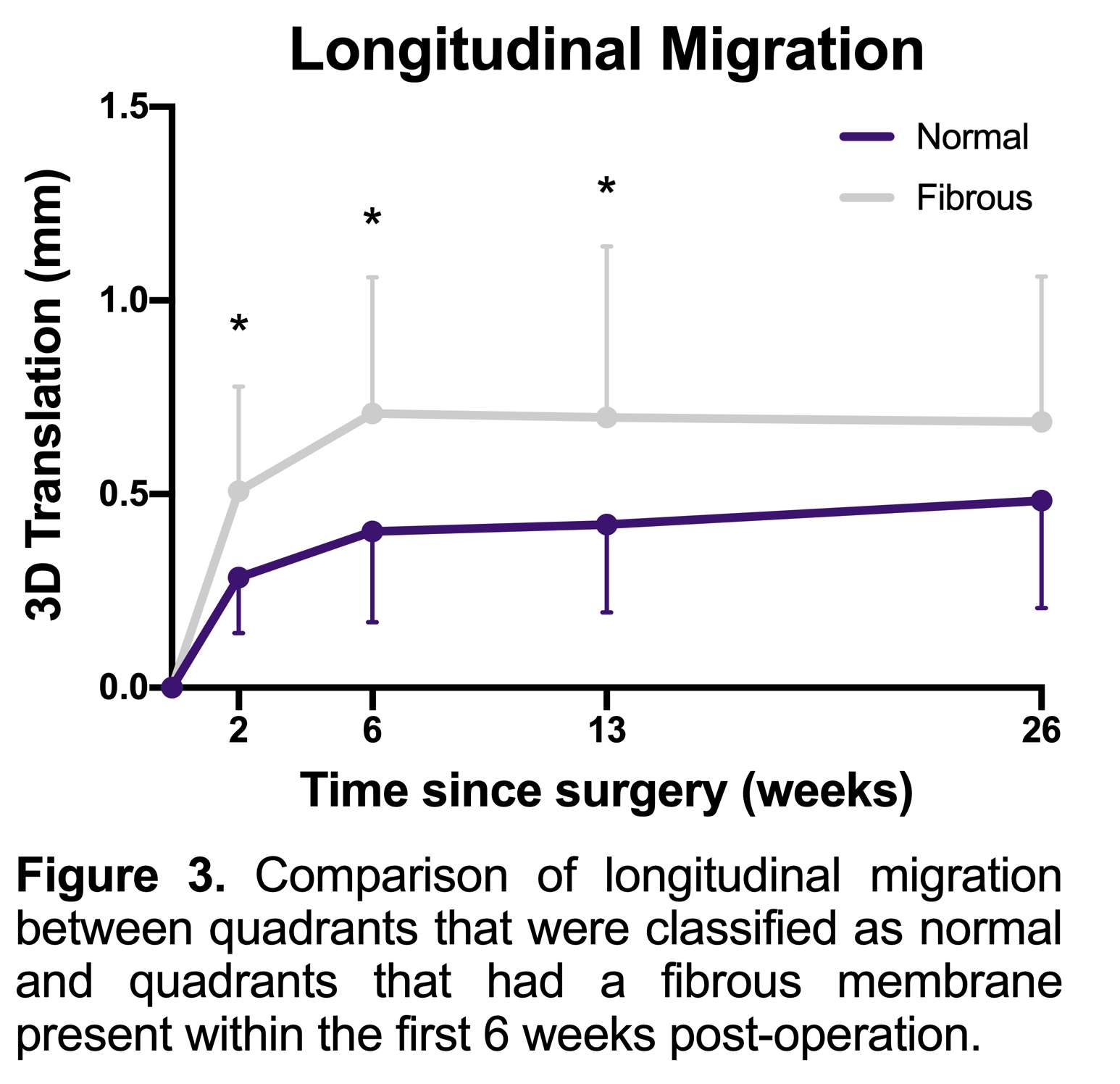
Figure 3#7620
Contact Kinematics Correlates to Tibial Component Migration Following Cemented Bi-Cruciate Stabilized Total Knee Replacement
*Jordan Broberg - Western University - London, Canada
Douglas Naudie
James Howard - London Health Sciences Centre - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Edward Vasarhelyi - Western University - London, Canada
Matthew Teeter - Western University - London, Canada
*Email: jbroberg@uwo.ca
Introduction: Total knee replacements (TKR) do not always restore the natural knee joint kinematics. Abnormal kinematics, such as paradoxical anterior motion, can occur in the newly replaced joint and may be a factor for the 20% dissatisfaction rate associated with TKR. Implant migration, measured with radiostereometric analysis (RSA), is a predictor of implant loosening, with greater implant migration suggesting an increased risk of implant loosening and early failure leading to revision. Contact kinematics between tibial and femoral implant components have been thought to influence implant migration. However, the relationship between implant migration and kinematics has been underexplored. A previous study concluded that kinematics can influence tibial component migration for a cemented, posterior stabilized TKR design, likely through alterations of force transmissions. The goal of the present study is to compare tibial component migration to contact kinematics for a cemented, bi-cruciate stabilized TKR design.
Methods: Fifty-four patients were included in this study, each with cemented, bi-cruciate stabilized TKR. Each patient underwent supine RSA at a baseline of 2 weeks, with follow-ups at 6 weeks, 3 months, 6 months, 1 year, and 2 years post-operation. Weightbearing, quasi-static RSA was done at 3 months and 1 year post-operation, where up to seven radiographic image pairs at increasing angles of flexion were acquired for each patient to simulate a deep knee bend. Model-based RSA (MBRSA) software was used to measure the longitudinal tibial component migration, defined as micromotions between the supine baseline examination and a follow-up supine examination. Migrations were reported as translations and rotations about the three orthogonal axes, and as 3D translations at seven points of interest on the tibial component known as fictive points (anterolateral, anteromedial, lateral, medial, posterolateral, posteromedial, and stem tip). MBRSA was also used to acquire the poses of the tibial and femoral components from the weightbearing RSA exams. These poses were used to obtain the most anterior and most posterior points of contact between tibial and femoral components for both the medial and lateral condyles. Correlations were then calculated between the tibial component migrations and the contact kinematics. Migrations at 6 weeks and 3 months post-operation were correlated with the 3 month post-operative kinematics, whereas migrations at 6 months, 1 year, and 2 years were correlated with the 1 year post-operative kinematics.
Results: Ten significant correlations were found. Figure 1 shows the significant correlations and linear regression analyses between tibial component orthogonal translations and rotations and contact kinematic measures. Figure 2 shows the correlations and linear regression analyses between fictive point 3D translations and contact kinematics measures. In general, more anteriorly positioned contact on the medial condyle resulted in more anterior translation, medial translation, and superior translation, but less anterolateral and lateral fictive point 3D translations. More anteriorly positioned contact on the lateral condyle resulted in greater posterolateral and stem tip fictive point 3D translations.
Conclusion: Contact kinematics driven by the bi-cruciate stabilized TKR design influenced the pattern of tibial component migration. Considering the previous report, these resultant migration patterns are a potentially important consideration in implant design.
Figures
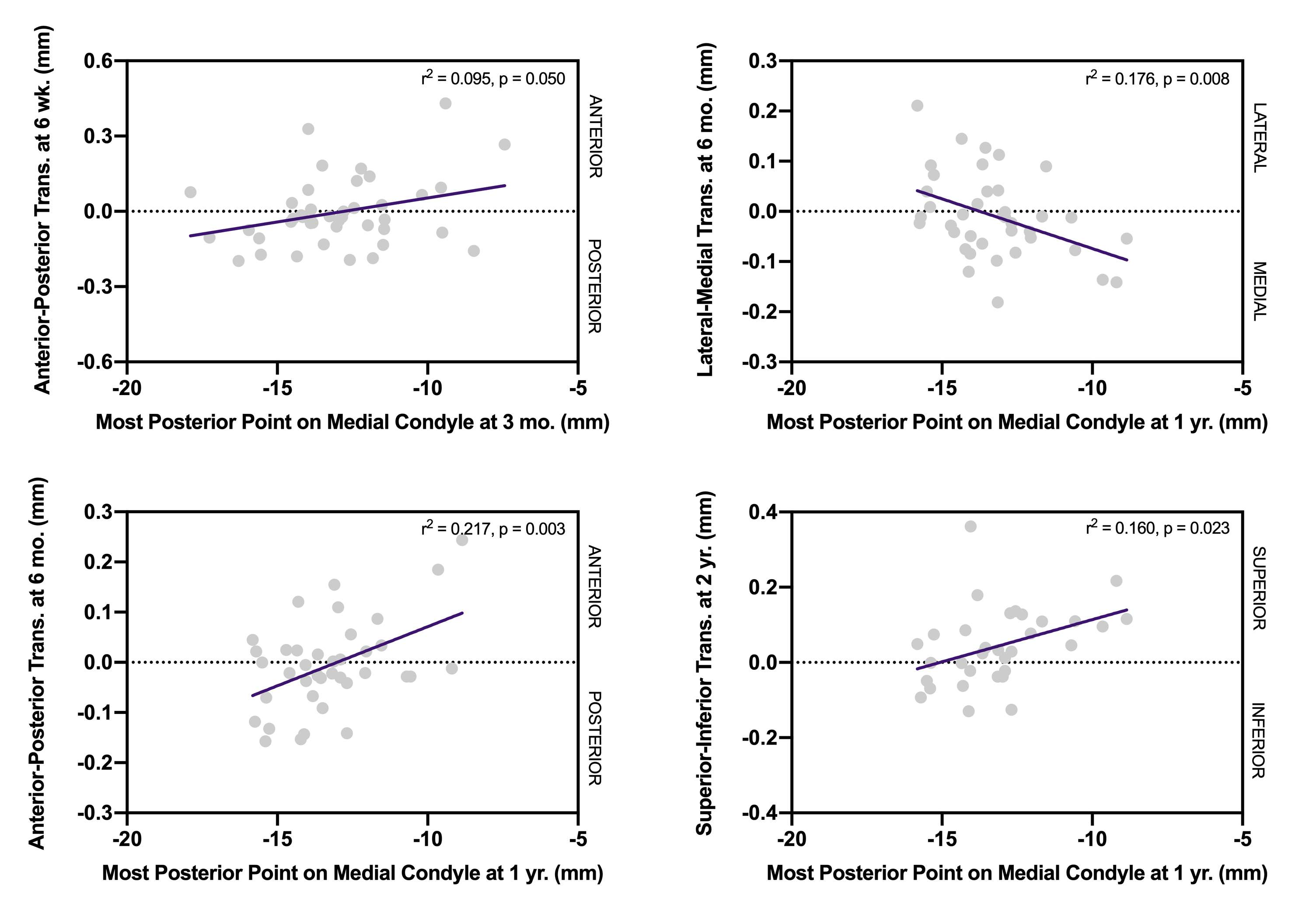
Figure 1
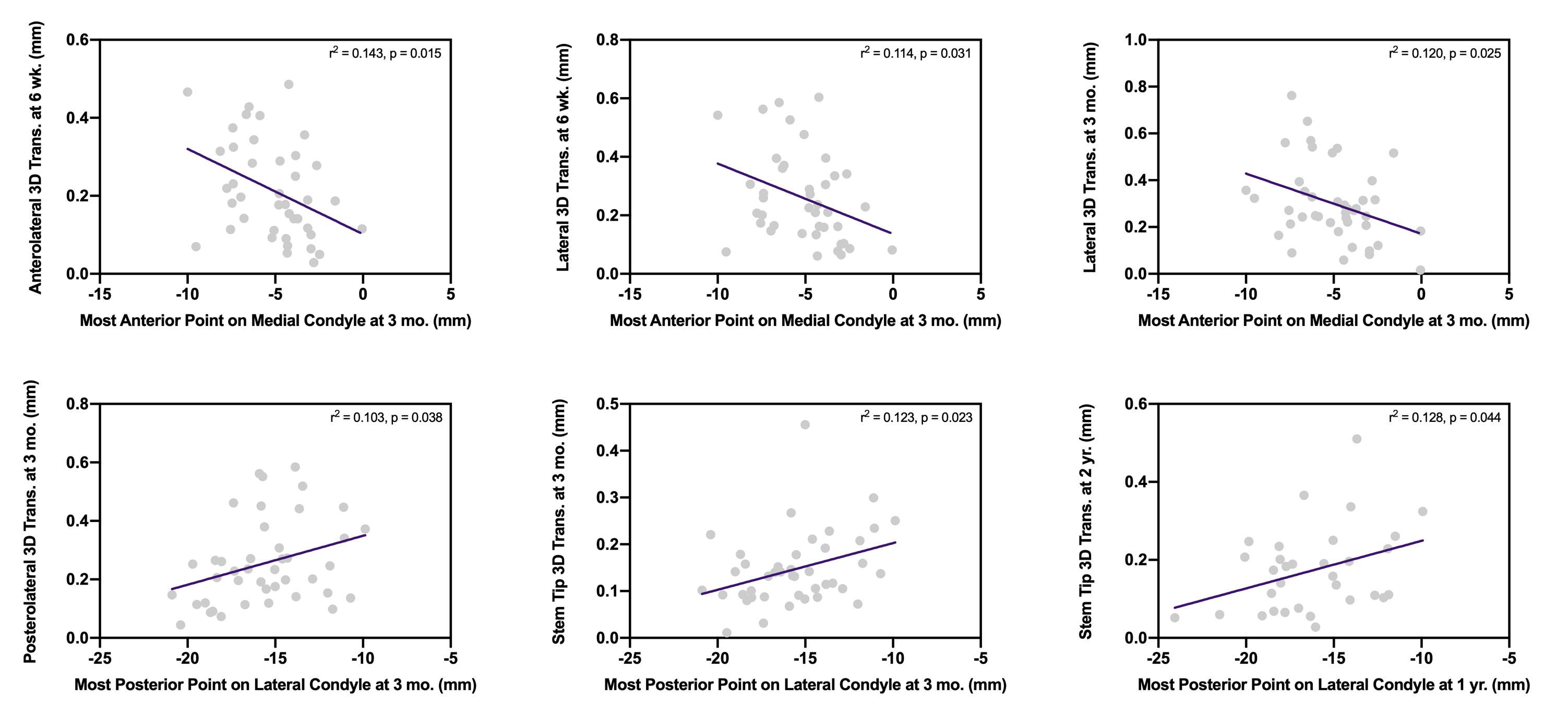
Figure 2#7457
Non-Metal Trauma Orthopedic Implants Using MP-1 Game Changing Material
*Alisa Buchman - MMATECH Ltd - Haifa, Israel
Simha Sibony - MMATECH - Haifa, Israel
Amir Oron - Kaplan Hospital - Rehovot, Israel
*Email: Alisa@mma-tech.com
Background: Orthopaedic fractures will increase in the coming years due to rise of the ageing population and sport activity. Bone fractures often require the surgical insertion of fixation implants such as nails or plates and screws to hold the bone pieces together during recovery. Conventionally made of metal or composite materials, they are subject to wear, resulting in inflammation, osteolysis and loosening of implants. Additional corrective revision surgeries are often necessary with obvious socioeconomic consequences, highlighting the need for wear-resistant biocompatible materials in orthopedic implants. EU funded MP-ORIF project for using a novel, biocompatible material that does not cause inflammation – polyimide MP-1. This biopolymer that MMATECH invented originated from the Aerospace industry and has many desirable features for orthopedic use such as toughness, wear resistance and self-lubrication. Easy to produce, MP-1 is friendly to the environment. It does not cause allergies like metals while its low thermal conductivity means that people will not suffer from weather changes. Importantly, it does not require implant removal after healing avoiding revision surgery.
Experimental: When first introduced, MP-1 obtained a CE mark for total hip liner implant replacing metal or ceramic or PE materials. Using compression molding, MP-ORIF partners successfully generated trauma implants such as nails, plates, screws and distal Radius implants. Testing included wear debris bio-compatibility, mechanical testing bending and fatigue, pull out test of screws and clinical testing in animal models and human corpses.
Results: showed excellent biocompatibility and mechanical results, very promising performance results in animals with cartilage and new bone formation indicative of fracture gap closing. The MP-1 material demonstrated excellent biocompatibility and short healing period. Orthopedic trauma surgeries involve long cuts, which leave ugly scars on the healed limb. The MP-ORIF solution enables the surgeon to execute minimally invasive surgeries with shorter surgery time. Concomitant hospitalization and recovery times are reduced, minimizing healthcare costs and improving patient quality of life.
Conclusion: MP-1 implants will be the game changing solution in trauma and other orthopedic devices.
Figures

Figure 1#7905
Novel Technique for the Identification of Hip Implants Using Artificial Intelligence
*Neil Antonson - University of Nebraska Medical Center - Omaha, United States of America
Brandt Buckner - University of Nebraska Medical Center - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Hani Haider - UNMC - Omaha, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
*Email: neil.antonson@gmail.com
Introduction:
The forecasted growth of total hip arthroplasty (THA) over the next decade will necessarily result in an increase in revision THA. A critical aspect of revision surgery is pre-operative planning, including identifying current implants to ensure implant-specific tooling for prosthesis extraction. Failing to plan properly may lead to difficulty with implant removal, which may result in increased operative time, blood loss, periprosthetic fracture, and/or other complications further exacerbated by prolonged time under anesthesia. Artificial intelligence (AI) has already shown promise in aiding clinical decision-making in medicine at-large, including studies demonstrating the ability to identify hip implants. Limitations of those studies include relatively small datasets, wildly variant stem designs, lack of path forward to scale solutions, and requirement of AI-expertise to design machine learning models. To address those limitations, we developed a novel technique to generate large datasets, tested against radiographically-similar stems, demonstrate ability to scale to any variety of implant, and utilized a no-code machine learning solution.
Methods:
We trained, validated, and tested an autoML-implemented convolutional neural network to classify 9 radiographically-similar femoral implants, all with a metaphyseal-fitting, wedge taper design. Our technique generated 27,020 images, split into training (22,957) and validation (4,063) sets. We obtained 786 test images from retrospectively-collected patient anterior-posterior (AP) plain radiographs (66.5%) at a single health system, AP radiographs from cadaver labs (28.2%), and journal articles (5.2%). Our novel technique utilizes CT-derived projections of a three-dimensional scanned model of an implant superimposed within a computed tomography (CT) pelvis. We used computer-aided design (CAD) modeling to place implants in proper position in 3D-space within the proximal femur of the CT pelvis volume [Fig. 1]. CAD models where then exported using a common coordinate system to maintain positioning relative to the CT imaging. We used MATLAB to superimpose the CAD model within the CT pelvis volume. The combined CT-implant volume was rotated to a varying degree randomly along the AP (±5 deg), medial-to-lateral (±25 deg), and longitudinal (±25 deg) axes; in addition, the Hounsfield-level corresponding to bone was randomly attenuated to create images of varying bone intensity. The resulting image projections were fed into our machine learning model. Performance of the model was evaluated by calculating the sensitivity, specificity, and accuracy.
Results:
Preliminary results of our machine learning model discriminated the 9 implant models with a mean accuracy of 97.4%, sensitivity of 88.4%, and specificity of 98.5% [Fig 2 & 3].
Conclusion:
Our novel technique to develop a hip implant detection model demonstrated the ability to accurately identify amongst 9 radiographically-similar implants. Furthermore, our technique is easily scalable with the ability to generate large datasets, as well as add historic and/or obscure implants that are not represented in current datasets. Lastly, the no-code machine learning model that we implemented demonstrated the feasibility of obtaining meaningful results without AI-modeling expertise, hopefully encouraging others to further build upon these results.
Figures
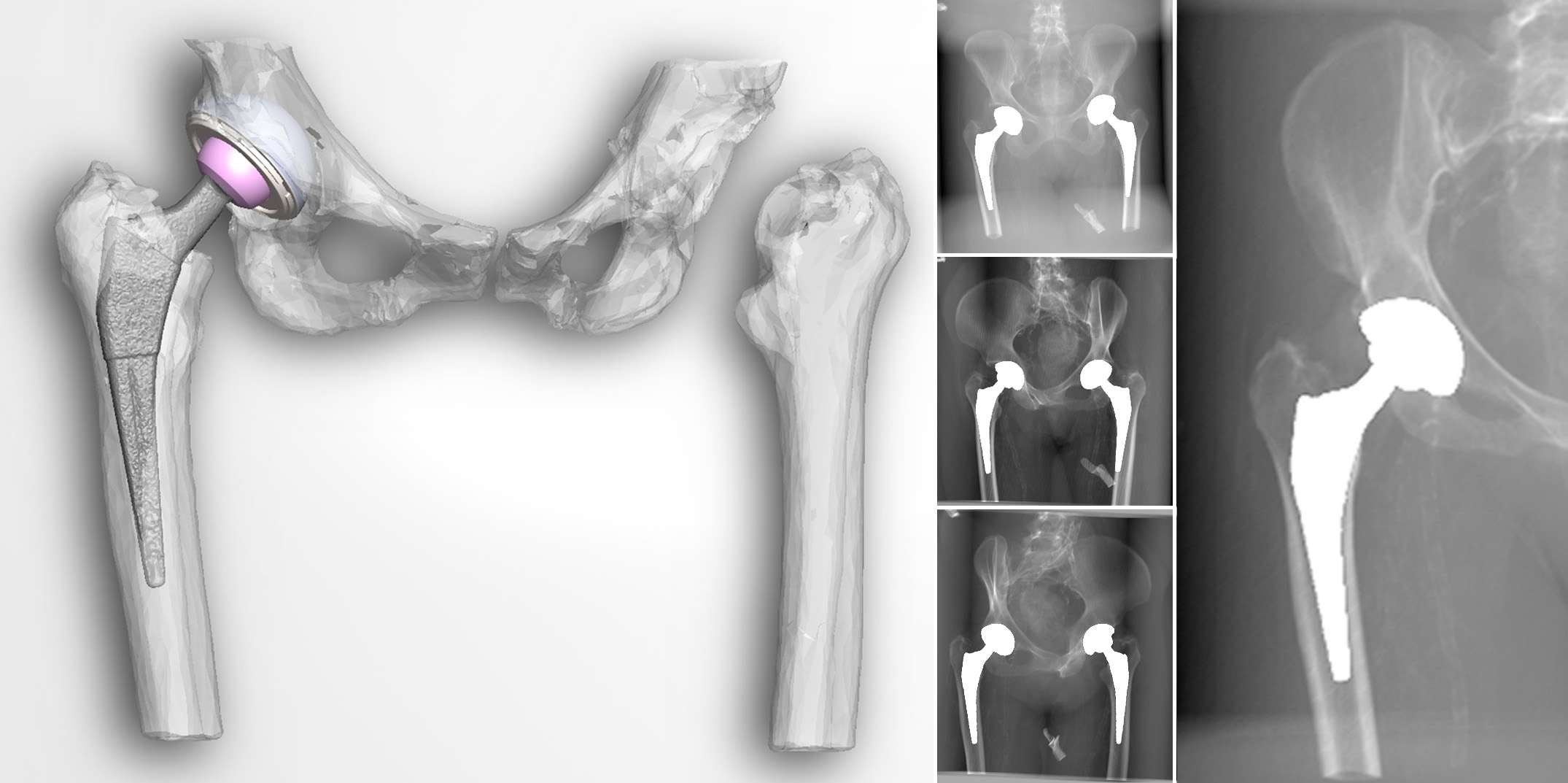
Figure 1
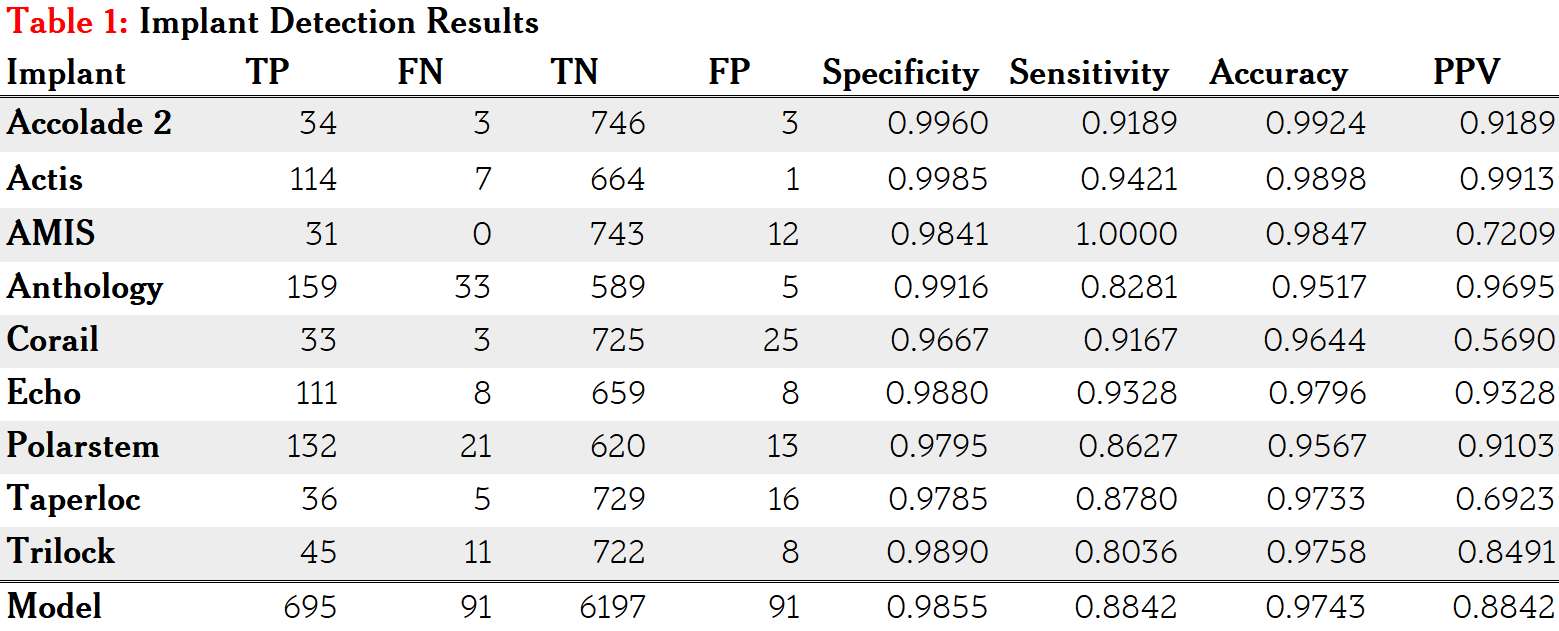
Figure 2
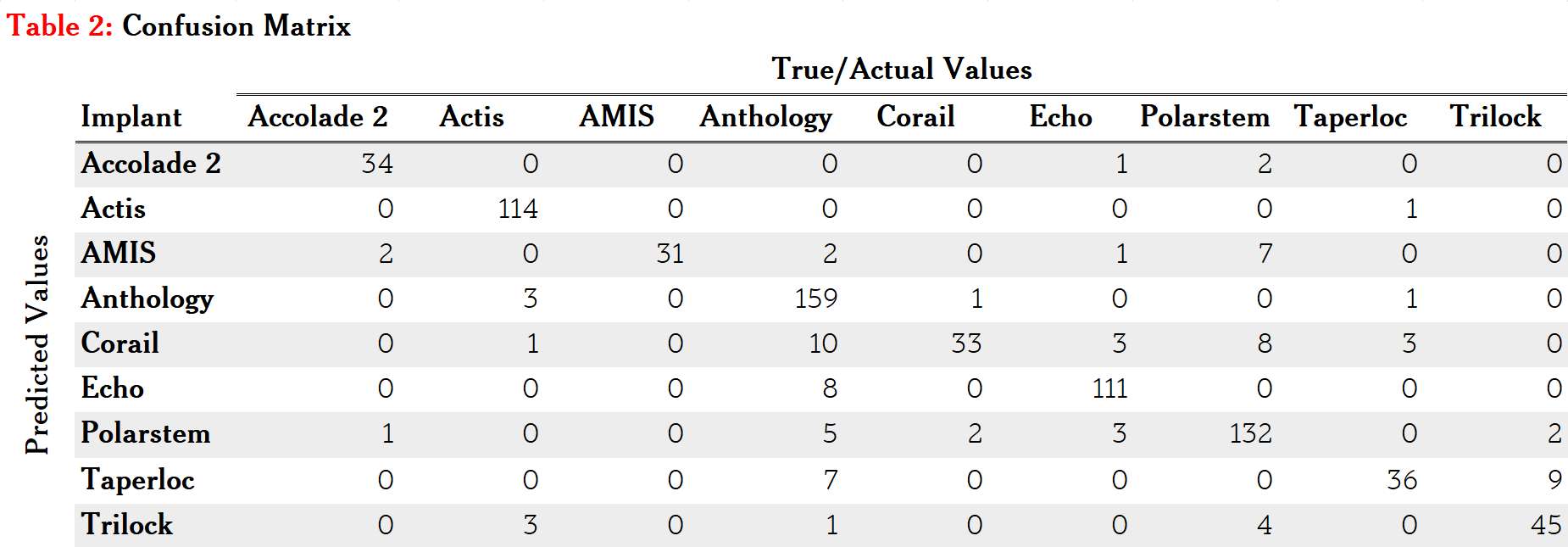
Figure 3#7530
Polyimide (MP-1) as a Bearing in Total Hip Arthroplasty (THR): First Ever Use and Clinical Study Results .
*James Burn - Canterbury District Health Board - Christchurch, New Zealand
*Email: pjamesburn@xtra.co.nz
Introduction
Polyimide ( MP-1, MMATech, Haifa, Israel), is a high performance aerospace thermoplastic used for its lubricity, stability, inertness and radiation resistance.
A wear resistant thin robust bearing is needed for arthroplasty.
After independent laboratory testing, in 2006 , the author used the material as a bearing in two Reflection (Smith and Nephew, USA) hip surgeries. The first, a revision for polyethylene wear, survives with no evidence of wear, noise , new osteolysis or complications related to the MP-1 bearing after 16 yrs. The second donated his asymptomatic MP-1 hip at 6.5yrs for post-mortem examination. The tissues were bland with no reaction.
Methods
In 2013 a clinical study with ethical committee approval was started using a Biolox Delta (Ceramtec, Germany) head against a polyimide liner in 97 patients. MMATech sold all liners, irradiated:steam 52:45. Sixteen were re-machined in New Zealand. Acetabular shells were Delta PF( LIMA, Italy). The liner locked by taper.
The cohort consisted of 46:51 M:F, and ages 43 to 85, mean 65. Ten received cemented stems. For contralateral surgery, a ceramic or polyethylene liner was used. Initial patients were lower demand, later, more active patients still running.
Results
All patients have on-going follow up , including MP-1 liner revision cases. There has been no measurable wear, or osteolysis around the acetabular components using weight-bearing radiographs. Squeaking within the first 6 weeks was noted in 39 number of cases and subtle increase in palpable friction, (passive rotation at 50 degrees flexion), but then disappeared. There were 6 revisions, four of which were related to cementless Stemsys implants ( Evolutis, Italy) fixed distally with proximal linear lucencies in Gruen zones 1 and 7, and 2 and 6. No shells were revised and MP-1 liners were routinely changed to ceramic or polyethylene. The liners showed no head contact at the apex, with highly polished contact areas.
No deep or superficial infections, but one traumatic anterior dislocation at 7 years associated with 5 mm subsidence of a non-collared stem.
Conclusion
The initial squeaking and increased friction was due to poor engineering of the liner / shell composite as implanted, not allowing adequate clearance for fluid film lubrication. The revised bearings were “equatorial” rather than polar, with lack of wear or creep this never fully resolved. Where the clearance was better, function was normal. The “slow” utilization was due to my ongoing concern with clearances not being correct. The revision of 4 Stemsys stems, tribology issues may have contributed, but non “MP-1” Stemsys combinations outside this study have shown the same response. A returned Stemsys stem showed the substrate Ra value under the hydroxyapatite was too low with possible “shedding”.
With correct engineering and clearances, a 3 mm thick MP-1 bearing, surface Ra<0.5 shows no appreciable wear or failure, and with confidence, can be used as a high performance THR bearing.
The author / surgeon has no financial interest in this material nor received financial support for this paper.
#7908
SmartSeg: Machine Learning Infrastructure Software for Automating Medical Image Analysis
*William Burton - Ortho Haus, LLC - Denver, USA
*Email: burtonw0814@gmail.com
Introduction
Medical image processing, and in particular segmentation, is a crucial process involved in multiple use cases spanning both academic and industry settings. The time-intensiveness of segmentation creates a bottleneck for relevant applications that rely on this procedure, as manual segmentation can necessitate multiple hours or days of human labor for a single scan. Machine learning is a powerful class of algorithms that can learn to make predictions based on annotated training data. These data-driven algorithms can augment conventional medical image processing by replacing cognitive labor with predictions from trained models. Unfortunately, model development comes with its own set of complications including specialized hardware requirements, complex data pipelines, and iterative design procedures. As a result, there is significant overhead involved when implementing custom machine learning infrastructure. The SmartSeg software solution is a cloud-based application that allows users to develop and employ custom machine learning models, in just a few clicks, for automating medical image segmentation. Use of automatic segmentation algorithms can reduce effort involved in multiple target use cases including 3D model generation, anatomical landmarking, development of anatomical statistical models, and generation of computational simulations. The current demonstration evaluates a custom-trained machine learning model developed in the software for the representative task of automatic segmentation of femoral cartilage from magnetic resonance imaging (MRI).
Methods
As a demonstration of the SmartSeg solution, a 2D convolutional neural network (CNN) [1] was developed in the software for automatic segmentation of femoral cartilage in the sagittal plane from MRI scans. The CNN was developed by initializing the model, using “data upload” functionality to associate 30 training scans with the model [2], and launching a training job in the software’s model management panel. Upon completion of the training job, the CNN was downloaded into the software from the cloud-based platform and applied to automatically segment 10 validation scans of healthy subjects held out from the training set (Fig. 1). Segmentation masks predicted by the CNN were compared to manually-annotated masks using Dice Similarity Coefficient (DSC) and Intersection-over-Union (IoU).
Results
The trained CNN accurately segmented femoral cartilage in the 10 validation scans (Fig 2.). Mean DSC over the validation set was 0.80 and mean IoU was 0.66 (Fig. 3). Application of the CNN to all slices in a volumetric scan required around 2 minutes of computation.
Conclusion
The current demonstration has presented a typical workflow in the SmartSeg software solution for developing custom machine learning models for automatic segmentation of medical images. Although the presented model was developed for automatic segmentation of femoral cartilage, the generality of the software allows users to employ the same workflow for automating a broad range of segmentation tasks, contingent on data availability. Future research will further investigate how custom-trained machine learning models can accelerate additional annotation tasks in the biomechanics and orthopaedics industries.
References
[1] Tan M, et al. (2019) Mnasnet: Platform-aware neural architecture search for mobile.
[2] Peterfy C, et al. (2008) The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee.
Figures
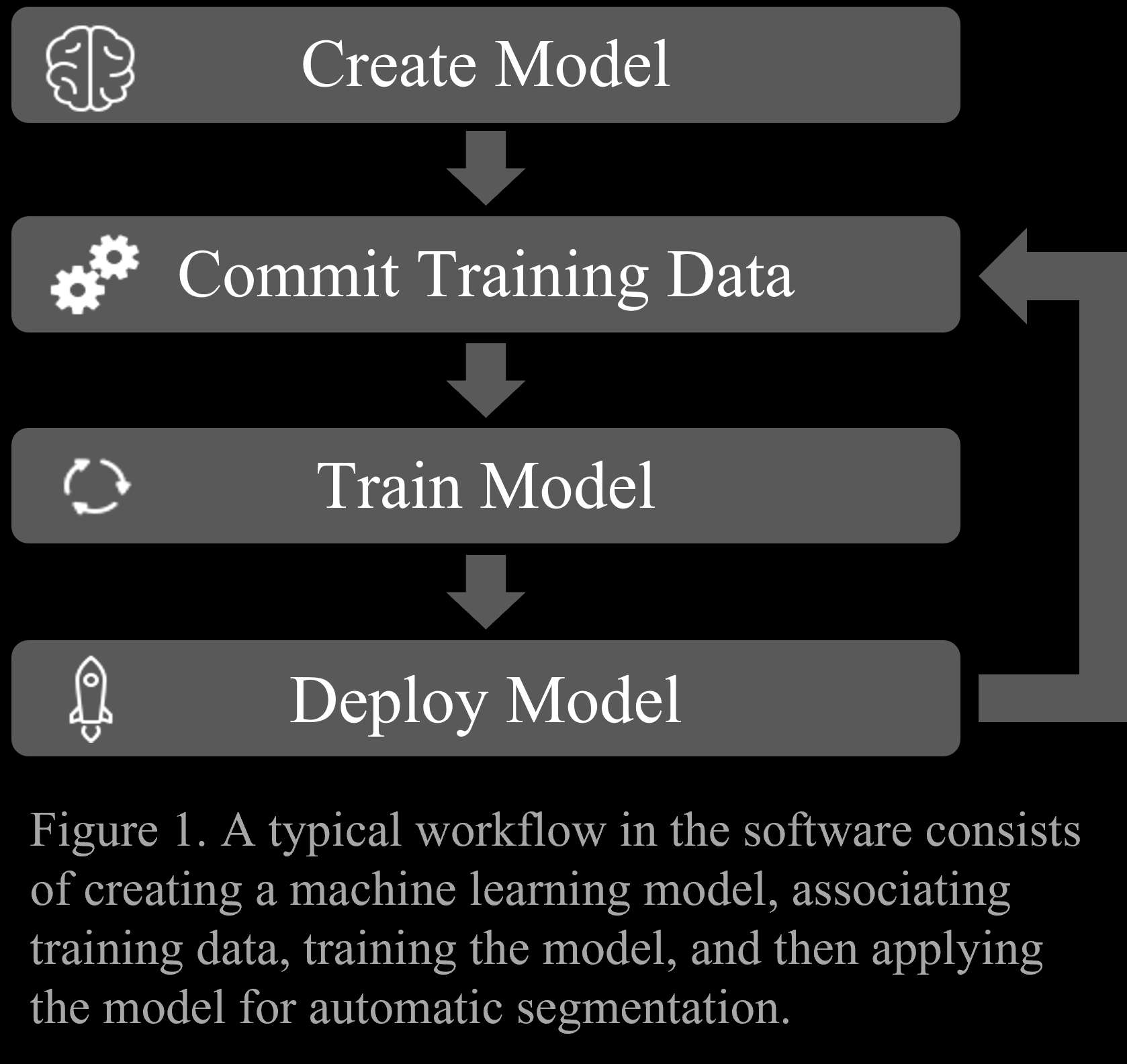
Figure 1
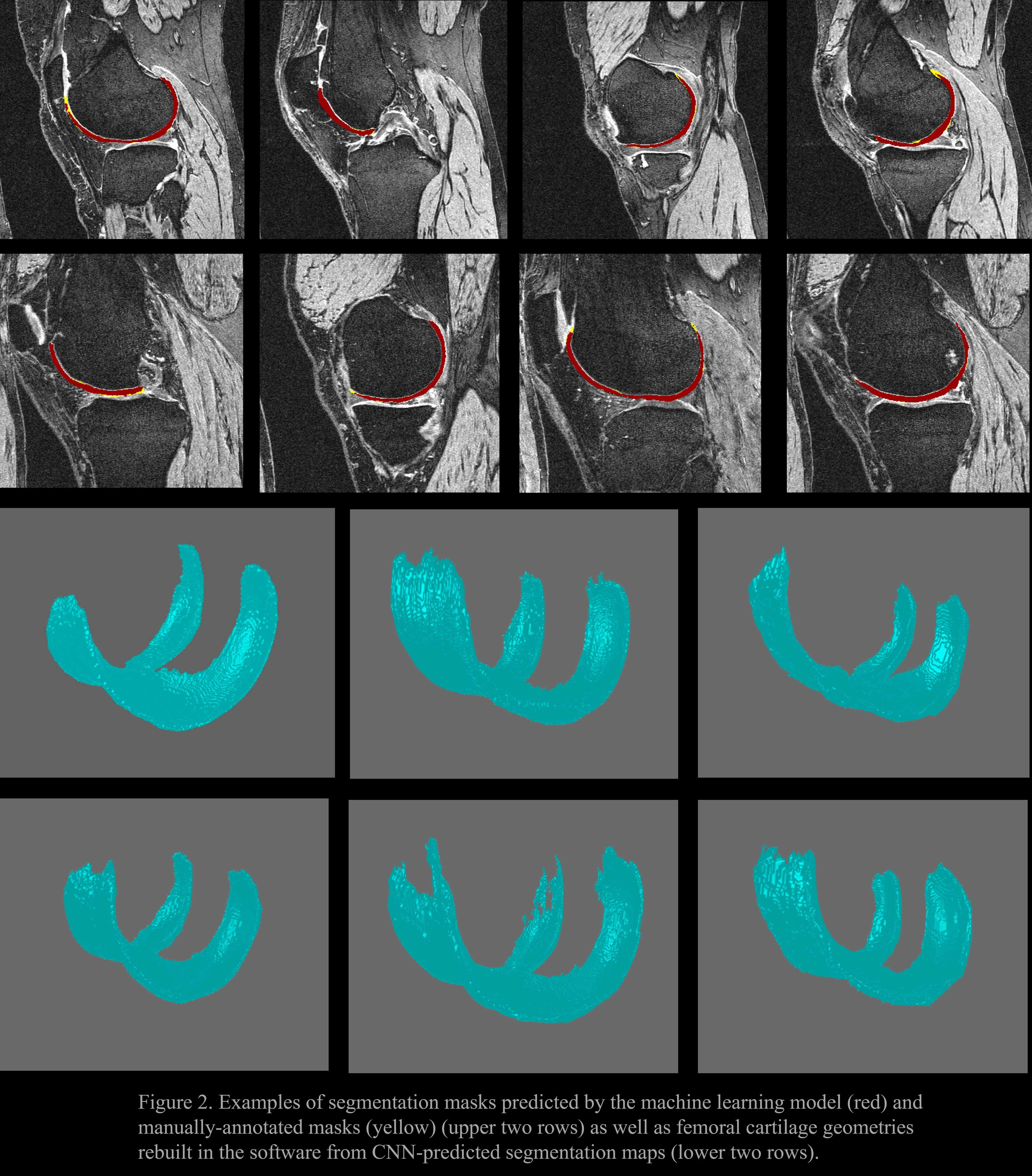
Figure 2
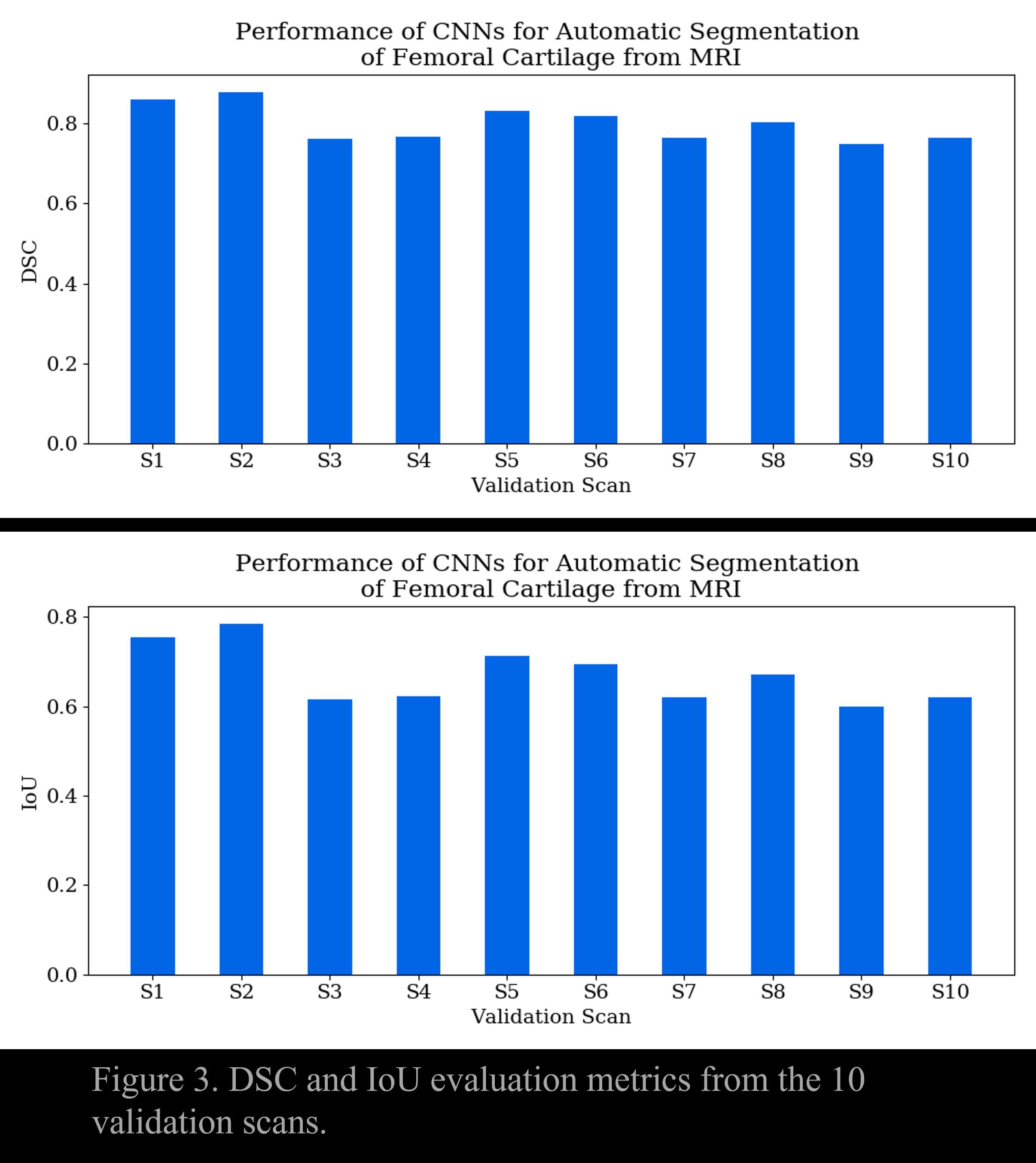
Figure 3#7775
Scan2Sim: Automatic Generation of Patient-Specific Finite Element Models From Computed Tomography With 3D Convolutional Neural Networks
William Burton - Ortho Haus, LLC - Denver, USA
Casey Myers - Ortho Haus - Denver, United States of America
Chadd Clary - Ortho Haus, LLC - Denver, USA
Clare Fitzpatrick - Ortho Haus, LLC - Boise, Select Country
*Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
*Email: prullkoe@theorthohaus.com
Introduction
Manual effort required for constructing geometric models of anatomical structures from medical images is a key hindrance that slows development of patient-specific finite element (FE) simulations. Over the past decade, advancements in computer vision technology have demonstrated that convolutional neural networks (CNNs) can accurately and automatically segment volumetric data from medical images. Application of these CNNs to computed tomography (CT) scans can enable automatic generation of FE models for evaluating patient-specific bony anatomy, bone quality, and mechanics under realistic loading conditions. The objective of the current study was to compare geometry and mechanics (displacement, stress, strain) values from patient-specific FE studies using anatomical structures obtained from both manually-annotated and CNN-predicted segmentation masks.
Methods
23 CT scans with manually-annotated segmentation masks were used to train a 3D CNN [1] for automatic segmentation of left and right healthy femurs. The trained CNN was applied to CT scans of 3 subjects to obtain predicted segmentation masks of both femurs. CNN-predicted segmentation masks were used to construct tetrahedral (tet) FE meshes by using alpha shapes [2] to first create triangular surface meshes from segmented voxels, and then applying a tet meshing algorithm [3] to fill surface meshes with volumetric elements (Fig. 1). Elements were assigned material properties by relating scan voxel intensities to Young’s moduli similar to previous work [4]. Additionally, FE models were obtained from the same 3 scans by constructing meshes from manually-annotated segmentation masks. The most inferior nodes of the meshes were encastered and a force was applied to the femoral head in the inferior direction. Static FE simulations were performed using FE models obtained from both CNN-predicted and manually-annotated segmentation masks. Geometric differences between surface meshes constructed from manual (ground truth) and predicted segmentation masks were computed by finding the closest point on a ground truth surface for all nodes in the corresponding predicted geometry, and then averaging. Additionally, FE studies that used ground truth and predicted geometries were compared by computing differences between the 5th and 95th percentile values of normal stresses and strains.
Results
The average geometric error between geometries obtained from manually-annotated and predicted segmentation masks was 0.48 mm (Fig. 2). Mean percent errors for 5th percentile values of medial-lateral (M-L), anterior-posterior (A-P), and superior-inferior (S-I) normal strains were 18%, 18%, and 36%, respectively (Fig. 3). Additionally, mean percent errors for 95th percentile values of M-L, A-P, and S-I normal strains were 34%, 33%, and 18%.
Discussion
The current work has demonstrated the viability of using CNN-predicted segmentation masks for automated analysis of patient-specific mechanics through the application of static stress analysis of the proximal femur. While manual segmentation of CT scans is associated with significant human effort, segmentation masks can be automatically generated in a matter of seconds with 3D CNNs. Note that small differences in resulting geometry alter predicted bone mechanics, further highlighting the need for automated processes.
Figures
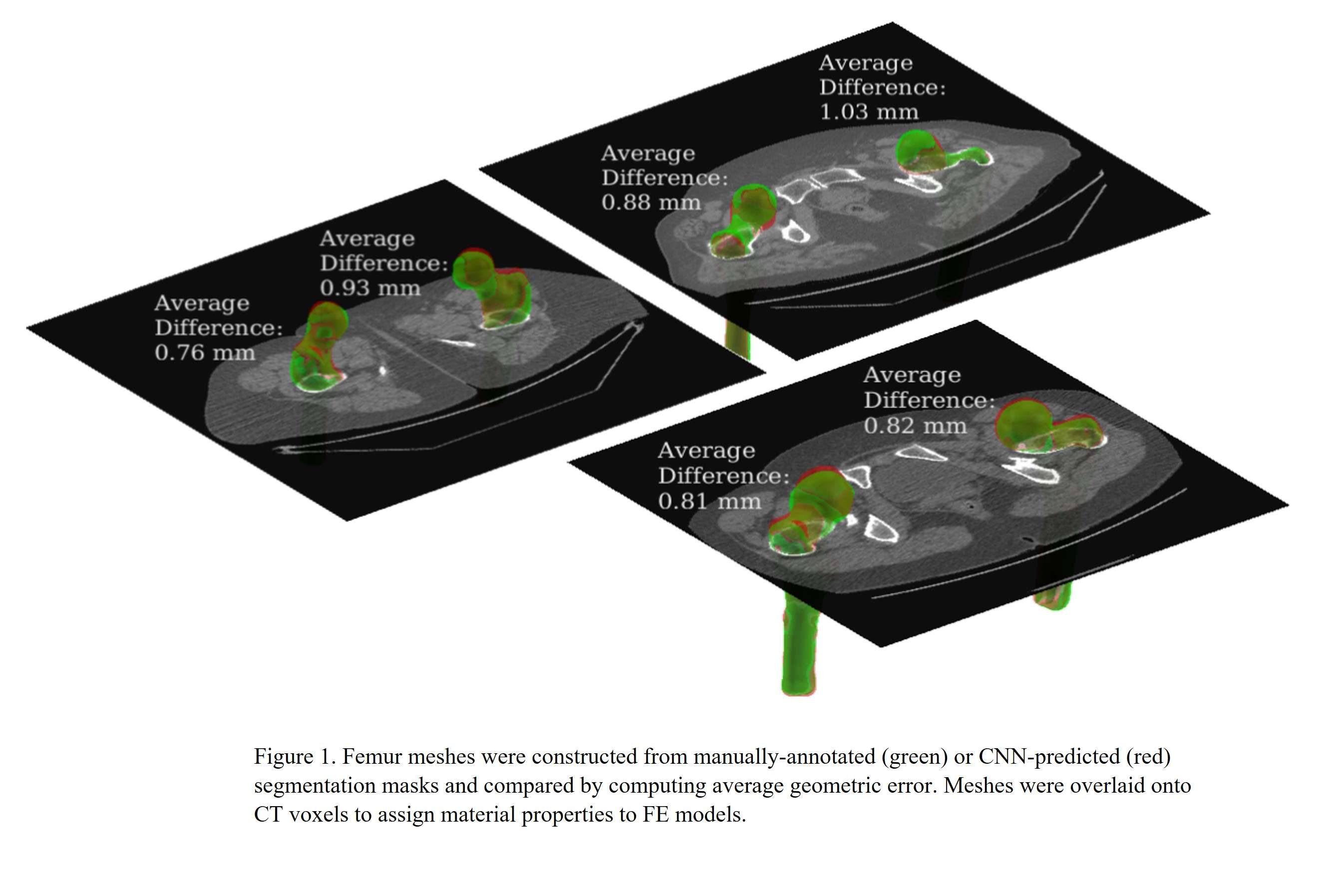
Figure 1
Figure 2
Figure 3#7600
After Betadine Irrigation, Novel Technology BioPrax Treats MRSA Infections Remaining on Implant and Bone Cement: An in Vitro Study
Jacob Opalinski - Garwood Medical Devices - Buffalo, USA
Bernadette Zumpano - Garwood Medical Devices - Buffalo, USA
Scott Nodzo - University at Buffalo - Buffalo, USA
*Mary Canty - Garwood Medical Devices - Buffalo, United States of America
*Email: mcanty@garwoodmedical.com
Introduction: Periprosthetic joint infection (PJI) is a devastating outcome of total joint arthroplasty. Debridement, antibiotic, and implant retention (DAIR) has been used clinically to treat patients; however, DAIR success varies widely (20-90%) [1-2]. Research indicates cathodic voltage-controlled electrical stimulation can reduce coupon-associated methicillin-resistant Staphylococcus aureus (MRSA) [3-6]. Garwood Medical Devices has developed BioPrax™, a novel application of this stimulation technology. This study evaluated MRSA viability after BioPrax and DAIR irrigation on cemented and uncemented patellofemoral implants.
Methods: MAKO Restoris® size 2 patellofemoral implants (Stryker) were sterilized prior to use. Experiments were conducted with orthopedic isolates of MRSA, strain CA-127. Fresh cultures were prepared in 5mL of TSB to an OD600 of 0.05, incubated overnight, then added to 500mL TSB media containing implants, with and without Simplex-P bone cement (Stryker). Implants incubated on a magnetic stir plate at 37°C and 130rpm for 24hrs, media was exchanged for fresh TSB, and incubated additional 24hrs. Implants were rinsed in PBS prior to use. BioPrax utilizes a three-electrode system with a working (MAKO implant), counter (platinum), and reference electrode (Ag/AgCl). Implants treated with BioPrax received a -1.9V vs. Ag/AgCl treatment for 24hrs. Custom agar flow chambers were fabricated (3.0% agar in sterile saline (0.9% NaCl)). After incubation, implants were rinsed in sterile PBS to remove loosely adherent cells. Implants that served as controls and wash alone (3min soak 10% Betadine wash) were harvested immediately after growth incubation. Remaining implants were placed into flow chambers supplying fresh TSB at 0.08mL/min, and treated with BioPrax alone, or 10% betadine+BioPrax. Implants were washed in sterile PBS+0.1% saponin, sonicated, and dilution plated for CFU. Three independent samples were evaluated in all conditions. A one-way ANOVA and Tukey post-hoc compared log-transformed CFU across conditions. If significant Levene’s test, a Welch’s test and Games-Howell post-hoc test were performed.
Results: Results are shown in Figure 1. Remarkably, 10% betadine+BioPrax showed a 7-log reduction in MRSA viability, to below detection, on uncemented implants. Cemented implants showed 97.6% more growth than uncemented (1.88x109 vs. 4.50x107 CFU/implant) Figure. As compared to controls, treatment with 10% betadine alone resulted in a 93.1% reduction in MRSA viability on uncemented implants (3.10x106 vs. 4.50x107 CFU/implant, p=0.001) and a 95.8% reduction on cemented implants (7.83x107 vs. 1.88x109 CFU/implant, p=0.002). BioPrax treatment was 99.9% effective at reducing MRSA bioburden from controls (Uncemented: 1.50x102 vs. 4.50x107 CFU/implant, p<0.001, Cemented: 6.17x104 vs. 1.88x109 CFU/implant, p<0.001). BioPrax combined with 10% betadine reduced MRSA to below detectable levels, a 99.9% increase in efficacy over 10% betadine irrigation alone across cemented and uncemented implants.
Conclusion: PJI is detrimental to the patient and early intervention often fails. This study shows BioPrax increases success of irrigation in DAIR by 99.9%, and reduces infection below detection in the absence of cement. This study also highlights the problematic nature of bone cement during infection and its recalcitrance to irrigation techniques. BioPrax is a promising technology to improve the outcomes of PJI.
References: [1]Urish et al. 2018 [2]Qasim et al. [3]Ehrensberger et al. 2015 [4]Nodzo et al. 2015 [5]Nodzo et al. 2016 [6]Canty et al. 2019
Figures
Figure 1#7655
Giving Your TKA a Voice- Early Experience With a Sensor-Enabled Implant
*Kaitlin Carroll - United States of America
Jeffrey Yergler - South Bend Orthopaedics - South Bend, USA
Derek Yocum - South Bend Orthopaedics - South Bend, USA
Barbara Elashoff - Canary Medical - Carlsbad, USA
Patrick Aubin - Canary Medical - Carlsbad, USA
William Hunter - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
BACKGROUND: Remote patient monitoring (RPM) continues to gain popularity as a tool to evaluate patients following total knee arthroplasty (TKA). The purpose of our study was to assess the ability of a novel, sensor-enabled tibial stem to remotely and objectively monitor a patient’s mobility following primary TKA.
METHODS: After receiving a waiver from the institutional review board, we retrospectively reviewed 27 consecutive patients, 28 knees, that underwent a primary TKA between October 4, 2021 and December 16, 2021 with a single anatomically designed knee system that was implanted in concert with a interconnected sensor-enable tibial stem extension. The extension containing a 3-D accelerometer, a 3-D gyroscope, a power source, and with telemetry transmission capability in 27 patients. This sensor enabled TKA has an IMU that allows step count and qualified gait movement data to be collected and sensor pairing accelerometers with gyroscopes to provide detailed analysis of limb movement and orientation within a spatial reference frame. This sensor enabled stem is intended to provide objective kinematic data is intended as an adjunct to other physiological parameter measurement tools applied or utilized by the physician during the course of patient monitoring and treatment post-surgery. The mean follow-up was 10  3.09 weeks (Range 6-13 weeks). Medium resolution data from ten-second bouts was collected three times per day, during three five-hour windows. The data was analyzed, and gait cycles were counted as “qualified gait cycles” (QGCs) if they met certain pre-specified criteria. The data were summarized using descriptive statistics.
RESULTS: There were a preponderance of female participants (67%, 18/27) and the average age was 61±7 years. The average body mass index (BMI) was 33.1 ± 8.5 kg/m2. The cumulative number of QGCs from all 28 knees was 16, 536. Data was reviewed in the dashboard for reliability for the first 6 weeks post-operatively with a mean step count transmission of 100% days 2-14, 98.9% days 15-28 and 99.2% days 29-42 (Table 1). There were no adverse events within the 6-week period. Overall kinematic data was recorded for all patients over the 6-week time period [Figure 2].
CONCLUSION: This novel sensor-enabled tibial stem reliably provided kinematic mobility data following primary TKA with greater than 98% collection during the study period. Furthur studies are needed to determine the clinical utility of these data to best support patient care where needed the most.
Figures
Figure 1
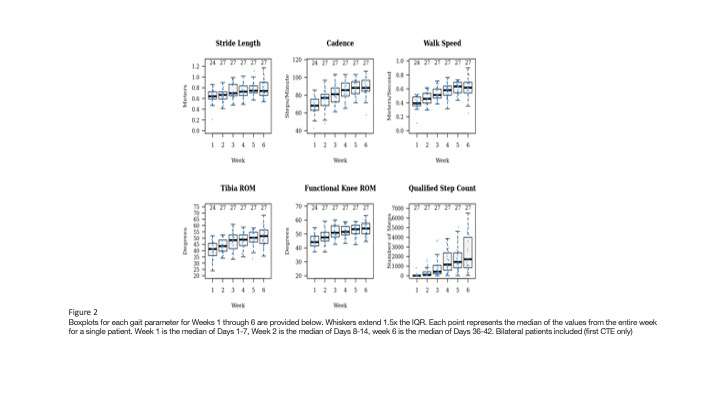
Figure 2
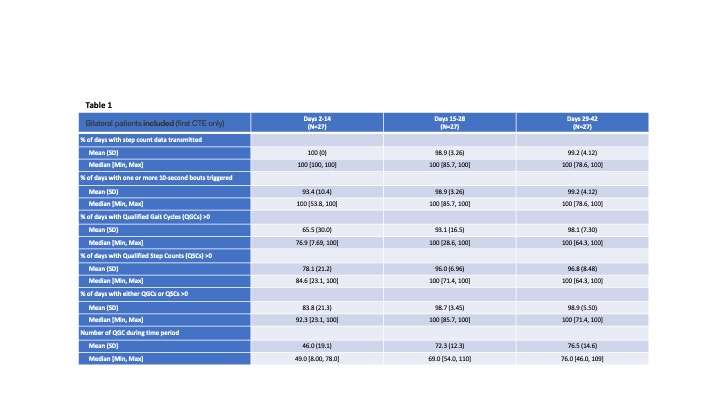
Figure 3#7890
A Pillar Based, Macro-Scale, Osseointegrative Interface With Variable Biomechanics Based on Material Composition and Pillar Geometry
*Greg Causey - Cortical Consulting, LLC - Erie, USA
Jamey Price - Applied Medical Technology, Inc - Brecksville, USA
George J Picha - Applied Medical Technology, Inc - Brecksville, USA
Matthew Pelletier - University of New South Wales - Sydney, Australia
Tian Wang - University of New South Wales - Randwick, Australia
William Walsh - University of New South Wales - Randwick, Australia
Elizabeth Mathey - University of Colorado Denver - Denver, USA
Dana Carpenter - University of Colorado Denver - Denver, USA
*Email: greg.causey@corticalconsulting.net
INTRO:
Our group has focused on a macro-scale in-growth surface with controllable biomechanics. While the shear strength of the interface between implant and bone is important, the compliance of the interface can enhance load-sharing and reduce stress-shielding. It is important to create an interface that is both adequately strong and appropriately compliant. Our discrete pillar geometry has been shown to allow for the design of a stiffness matched interface while also enabling a strong mechanical interlock.
METHODS:
Following ethical clearance, using a common ovine model, two studies were undertaken to examine in-growth and mechanical response of the pillar morphology. The first examined implants with different pillar morphologies or a grit-blast finish in titanium. The second study used a single pillar geometry with several implant materials (PEEK, PEEK-HA, Ti, UHMWPE). Pushout testing was conducted and shear strength and stiffness was calculated. Subsequently, a finite element model was created to further explore the effects of pillar variations and implant material on mechanical performance. A fixed strain was applied to the in-silico implant and shear strength and stiffness values calculated. Physical implants were made, over-molded with HDPE to simulate ingrowth, and pushout tested. Shear stress and stiffness were calculated and compared to the FEA output.
RESULTS:
Shear strength of the 12 week ovine samples demonstrated statistically similar results for all pillar configurations in titanium and PEEK while the grit-blast Ti and UHMWPE were notably different. In contrast, the interface stiffness between the titanium and PEEK implants were trending strongly different while the grit-blast Ti implant was similar to the PEEK group and the UHMWPE was more compliant. Animal to animal variability in the ovine model prevented discerning differences in pillar geometry within a single implant material group. Figure 1 summarizes results grouped by implant material. The max shear strength in UHMWPE was 3 times the smooth grit-blast Ti while both the PEEK and titanium groups were 5 times stronger. In contrast, the grit-blast Ti and PEEK were twice as compliant while the UHMWPE was 8 times as compliant as the titanium. Results of the initial FEA models with cortical bone ingrowth revealed titanium to be 4 times as stiff as PEEK (Figure 2). Greater load sharing was noted with the PEEK material. Comparison of the FEA models with the HDPE "in-growth" material and the benchtop testing (Figure 3) demonstrated agreement within 16%.
CONCLUSION:
Long-term effectiveness of an osseointegrative interface is dependent on its ability to effectively load-share with the in-growing bony tissue. We have demonstrated a novel, macro-scale, discrete surface morphology which can be biomechanically designed for both shear strength as well as stiffness. In-vivo evaluation of pillar morphologies is time consuming and costly as compared to in-silico. Developing an FEA model of the biomechanical response of various pillar configurations and implant materials will be critical to the rapid evaluation and optimization of the surface for a variety of clinical applicants. Early FEA work has demonstrated correlation with in-vivo results as well as good agreement with benchtop models.
Figures
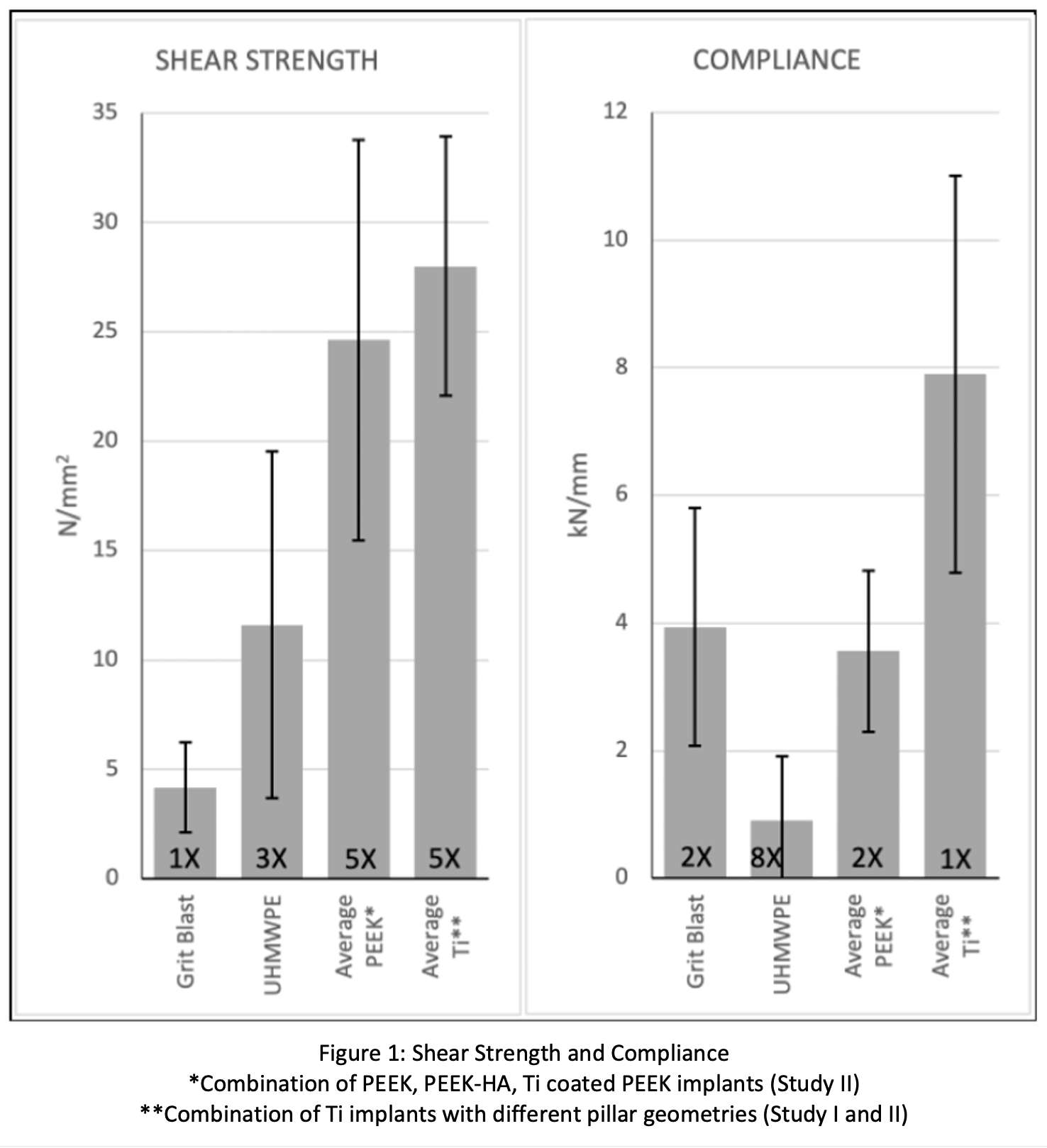
Figure 1
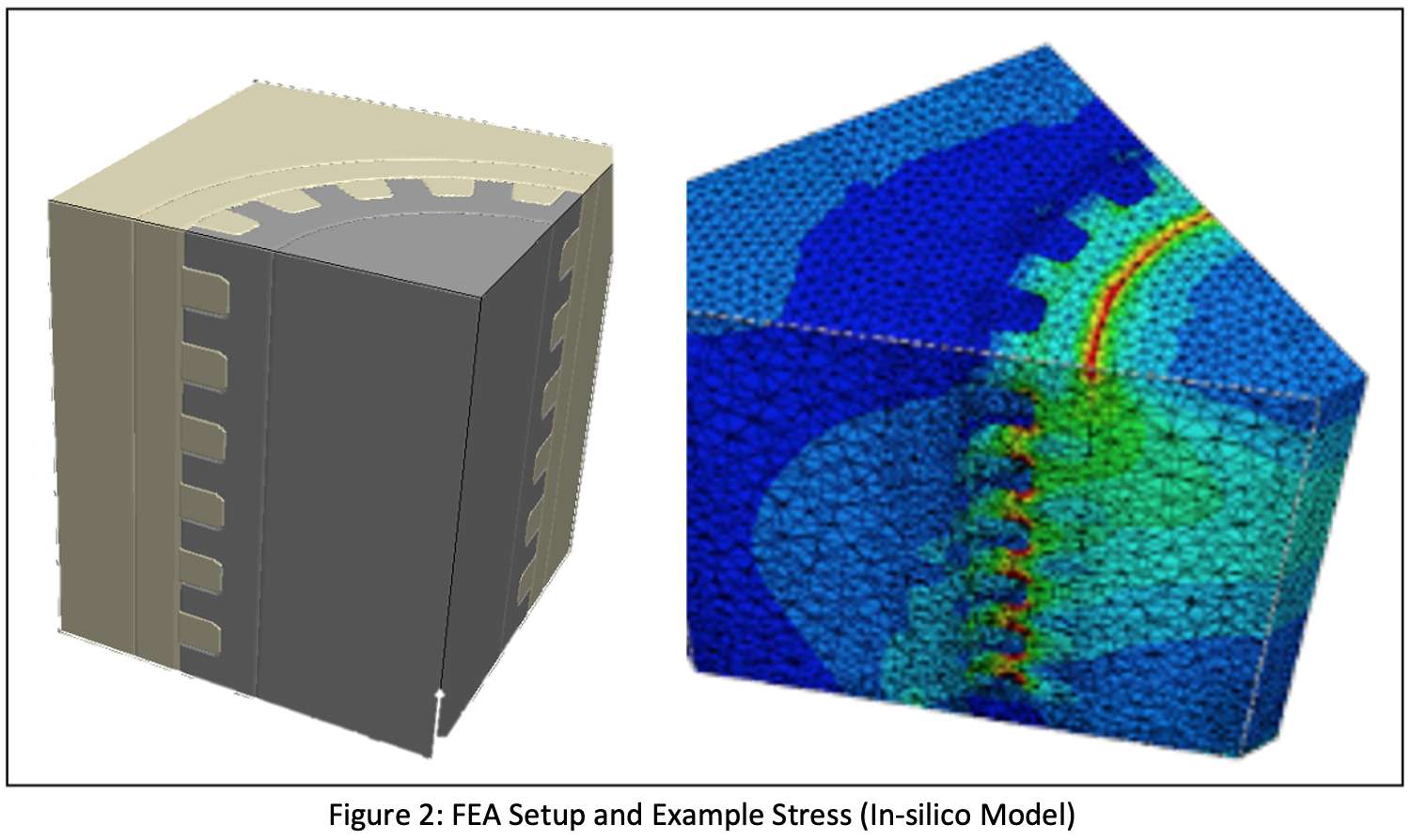
Figure 2
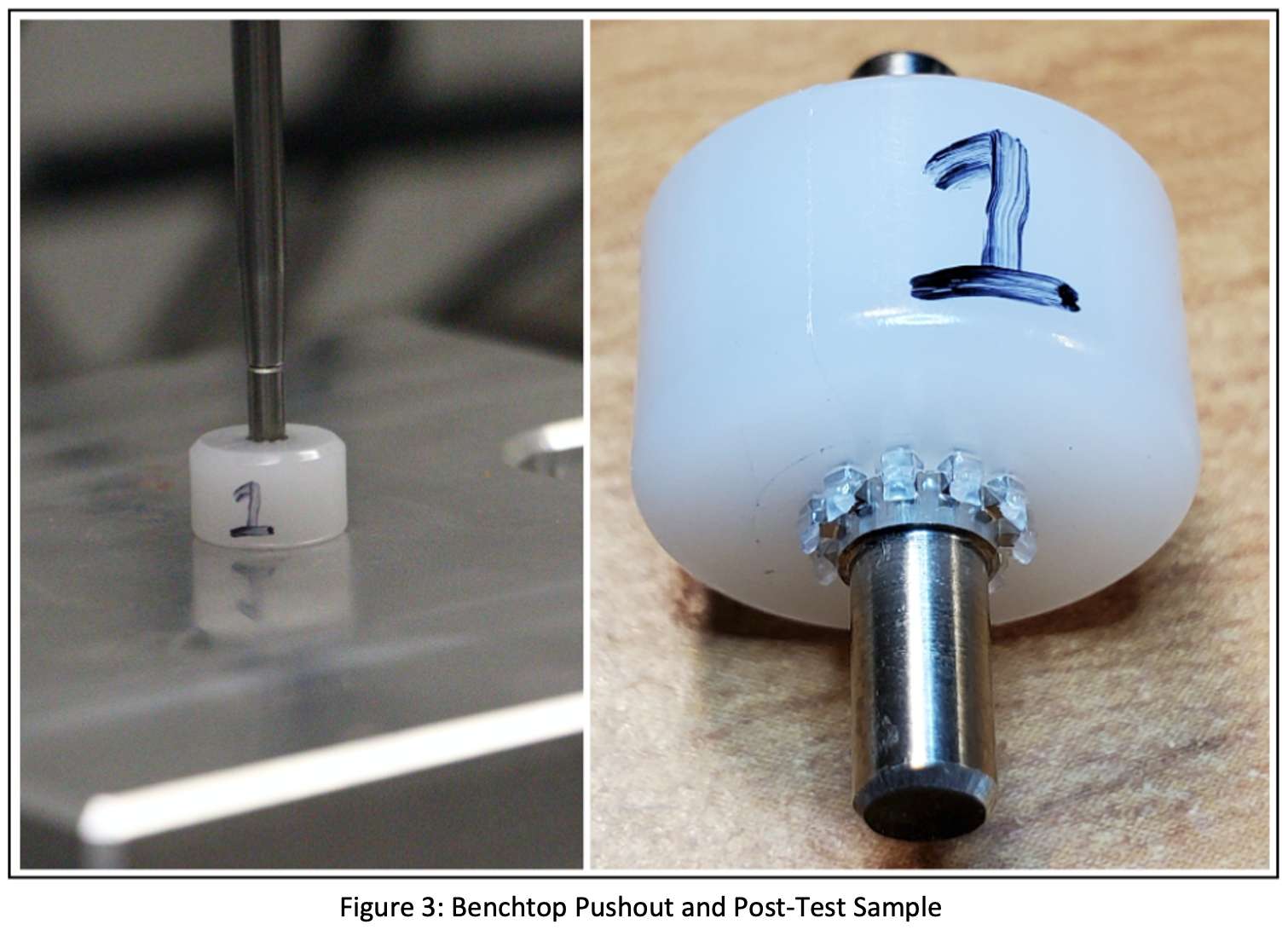
Figure 3#7900
System for High-Precision Biomechanical Testing of Motions of Multiple Small Bones in Close Anatomic Proximity
*Greg Causey - Cortical Consulting, LLC - Erie, USA
Callan Gillespie - Cleveland Clinic Biorobotics Lab - USA
Robb Colbrunn - Cleveland Clinic - Cleveland, USA
Tara F Nagle - Cleveland Clinic BioRobotics - CLEVELAND, USA
Jamey Price - Applied Medical Technology, Inc - Brecksville, USA
Kyle Grebb - University of Notre Dame - Notre Dame, USA
*Email: greg.causey@corticalconsulting.net
INTRO:
Development of new implant systems for in-vivo fixation of small bones often requires biomechanical evaluation of their effectiveness at reducing relative motions, especially when standard test methods are difficult or impossible to apply. Comparison with current treatments can assist development and support clinical claims. Many current motion tracking systems lack the accuracy needed for evaluation of arthrodesis conditions (50-150 microns) and are too bulky for fixation to multiple small bones in close proximity. We present a methodology and process to address this need. While the system was initially developed in support of a novel mid-foot fusion device, it can be widely applied to a variety of anatomic situations.
METHODS:
An industrial robotic system coupled with control software (simVITRO®) is used to simulate a gait cycle with a cadaveric foot (Fig1). Tendon actuation provided by linear actuators simulate muscle forces while a force plate under the stride surface provides ground reaction forces which are fed back into the overall gait control. Real forces from test subjects are used to ensure proper gait forces are achieved[1]. A low-profile, modular fiducial system is used to locate and track individual bone motions[2] (Fig2). CT scannable markers are attached to the anchors and the foot is scanned and segmented. The CT markers enable the locations of the fiducial anchors relative to the bones to be established. Vision tracking markers are attached to the anchors for subsequent motion tracking. The geometric relationship between CT markers and vision markers are used to establish the vision marker position relative to the bones (Fig1). A digital image correlation system (DIC)[3] is used to track motion of the vision markers with high precision. DIC software tools and custom data processing algorithms written in LabView are used to translate the motion of the vision markers to actual bone motion. Bone motion may be further analyzed using graphic or visual animation techniques.
RESULTS:
A matched pair of cadaveric feet were obtained and the modular anchors attached to the 3 cuneiforms and 1st-3rd metatarsals. CT markers were attached to the anchors and the feet scanned, segmented automatically using DISIOR and imported into SolidWorks. Each foot was attached to the simVITRO® system and driven thru gait cycles while a series of treatment options were performed (intact, staple fixation, plate fixation, mid-foot fusion device) with the DIC system collecting high precision motion data. Using predetermined vision marker to bone transforms, data was analyzed and relative bone motion determined. The system was able to resolve differences in intra-bone motion between treatment groups (Fig3).
CONCLUSION:
We have successfully demonstrated a high-resolution motion tracking system comprised of the combination of a robotic biomechanical simulator, a small modular fiducial system, a DIC system, and custom algorithms to track the individual motion of small bones in the mid-foot. The system can be applied to a variety of biomechanical test scenarios. Work continues on improved fiducials, streamlined data processing, and more robust visual analysis.
REF:
[1]Nagle, et.al., Paper 133, ORS2022
[2]Causey, et.al. Poster 1608, ORS2022
[3]Gillespie, et.al., Poster 1610, ORS2022
Figures
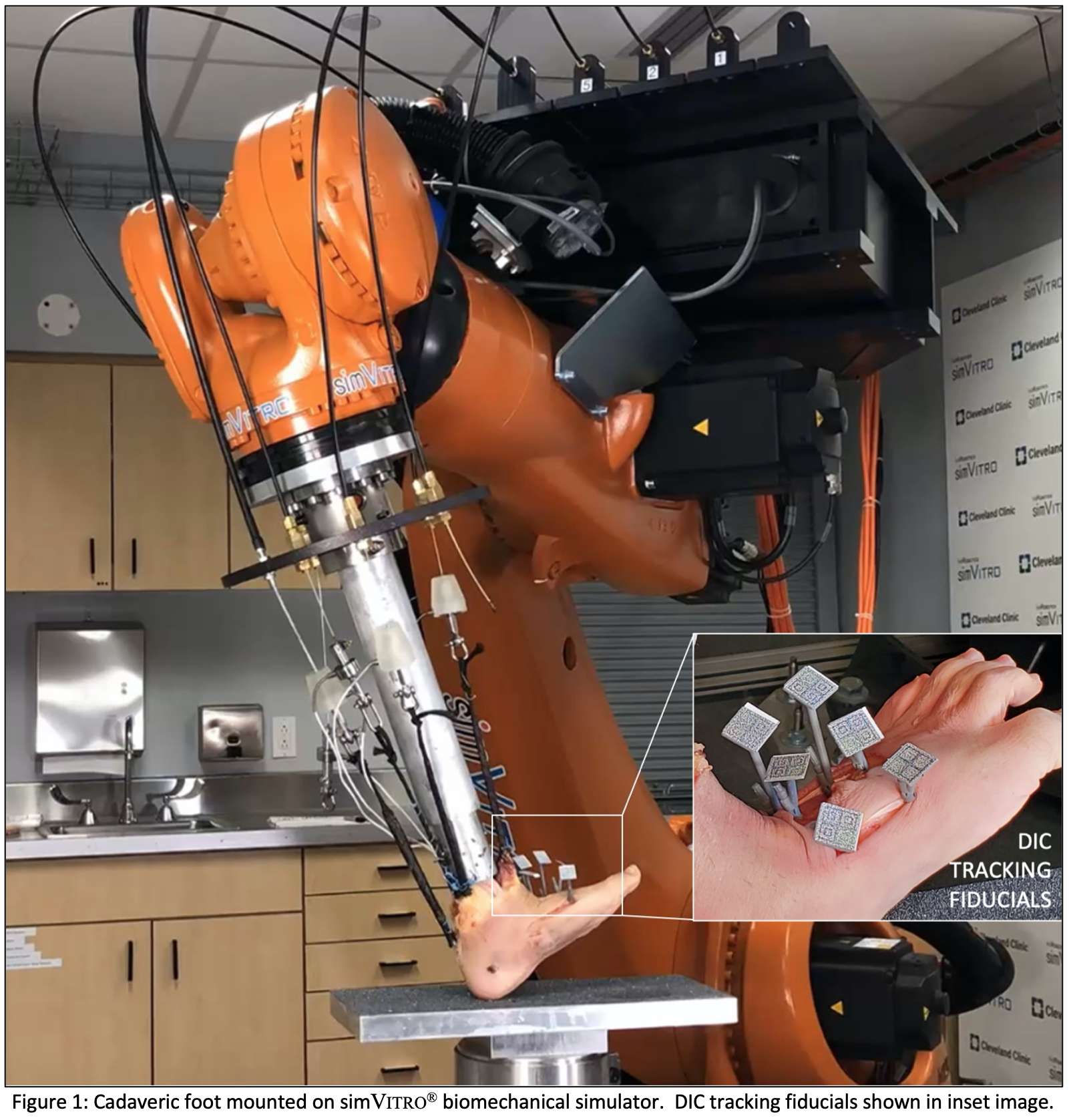
Figure 1
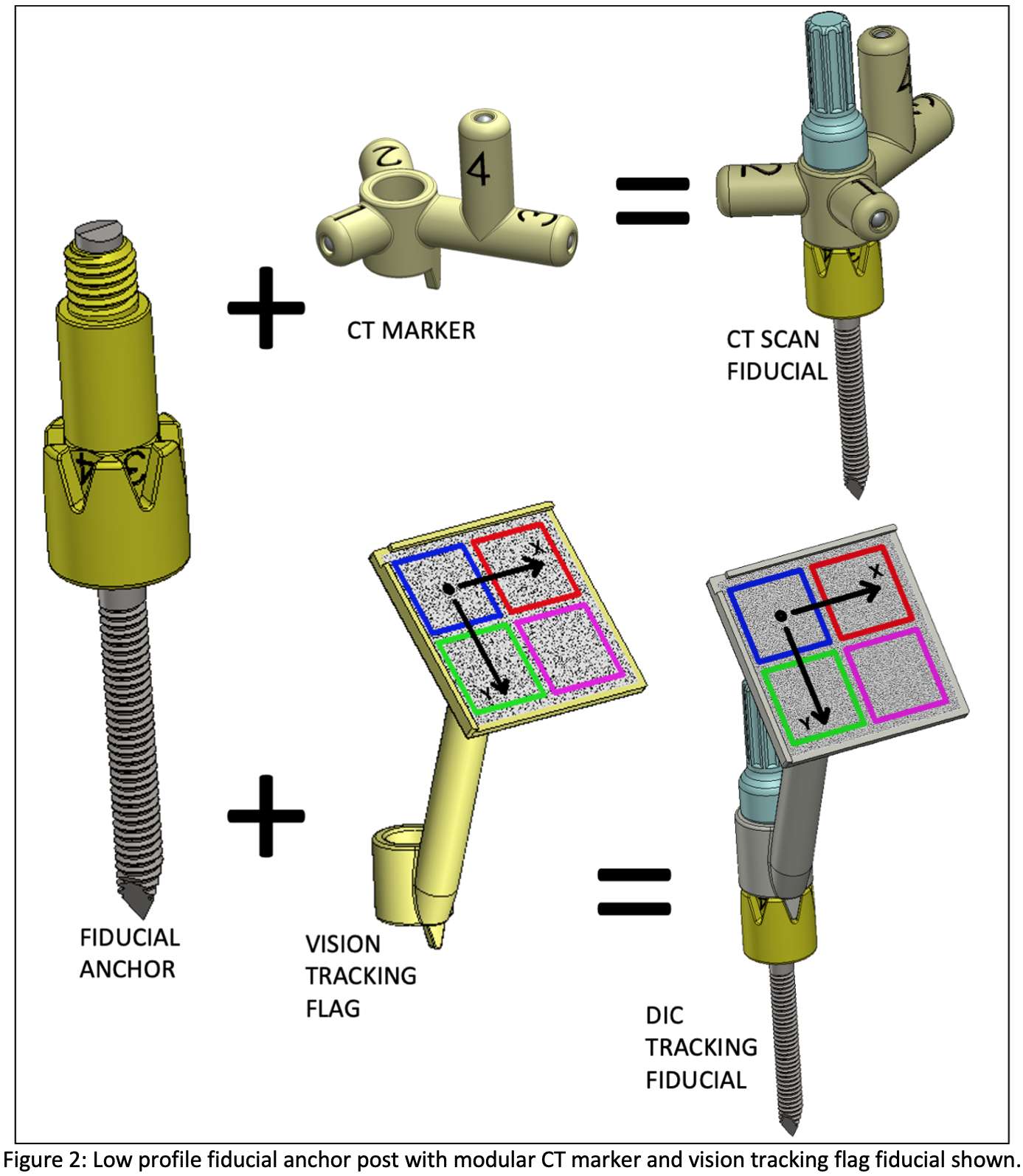
Figure 2
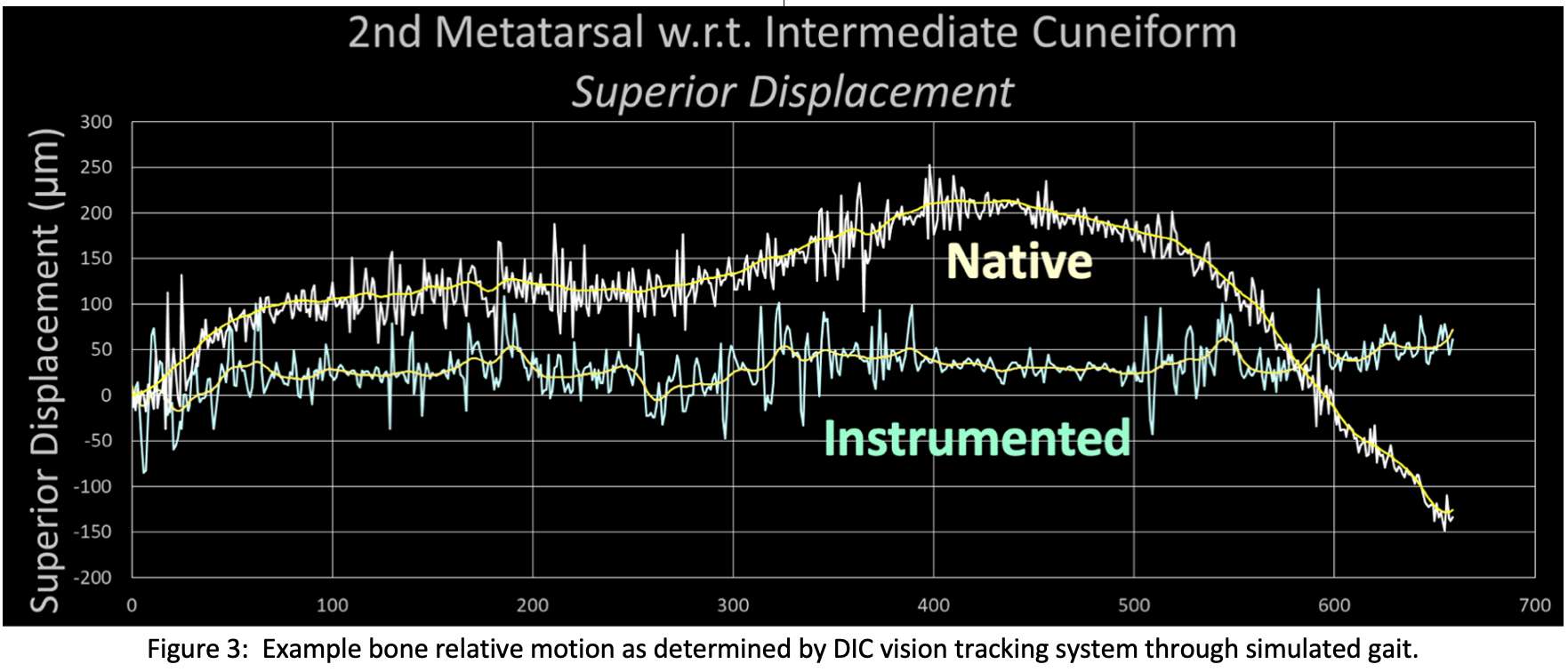
Figure 3#8001
Functional Outcomes of a Lima Modular Shoulder Replacement
*Elliot Cha - Guthrie Clinic - Sayre, USA
Nicholas Hager - Guthrie Clinic - Sayre, USA
Joseph Choi - Guthrie Clinic - Sayre, USA
*Email: deekaycha@gmail.com
Introduction: The use of a metal backed glenoid components over polyethylene for total shoulder arthroplasty (TSA) remains a point of contention. While their advantages are well documented, few, if any, studies exist demonstrating their efficacy in TSA and conversion rates to a total reverse shoulder arthroplasty (RSA). The current study evaluates acute post-operative complications, shoulder pain and functional outcomes, and conversion rates to RSA among patients undergoing a TSA using a modular metal backed glenoid component.
Methods: A retrospective review of adult patients undergoing a TSA using a metal backed glenoid component between 2014 and 2019 was performed. Exclusion criteria were set as patients undergoing surgery for infectious or revision etiologies. Patient baseline demographics and surgical characteristics such as operative duration and estimated blood loos (EBL) were collected. Surgical outcomes were defined as postoperative complications, rates of revision of the primary procedure to a reverse total shoulder arthroplasty (RSA), pain and physical function as evaluated using the Numerical Rating Scale (NRS) and American Shoulder Elbow Society score (ASES), respectively. NRS and ASES scores were collected preoperatively and at 1-year, 2-year and at final postoperative follow up. Rates of revision to a RSA were further evaluated for the indication. Summary statistics were performed for all included patients. Any significant differences between preoperative and postoperative NRS and ASES scores were evaluated using a two-tailed Student’s t-test.
Results: A total of 99 patients were identified as eligible for the study. After exclusion and inclusion criteria were applied the study’s final cohort was 91 patients. The mean age was 66.5 ± 8.1 years with an average body mass index of 32.8 ± 6.9 and 53.8% being male. Majority of patients underwent a TSA on the left side (53.8%), which corresponded to an average operative duration of 105 minutes and EBL of 148.8mL. A total of 13 patients (14.3%) went onto conversion to an RSA. Among these individuals, 4 suffered a traumatic a rotator cuff tear (RCT), 3 had evidence of excessive polyethylene wear, and 6 suffered a non-traumatic RCT. Overall mean time to revision was 27.7 ± 24.8 months,.17.5 ± 9.8 months for trauma patients, 51.0 ± 3.5 for excessive polyethylene wear, and 22.9 ± 31.3 months for non-trauma RCTs. Mean preoperative NRS was 6.8 ± 2.3 and ASES scores were 28.5 ± 15.6 and significantly improved by 1-year, 2-year, and final postoperative timepoints (p<0.001).
Conclusion: Patients undergoing a total shoulder arthroplasty using a metal backed glenoid component reported few if any acute postoperative complications. Additionally, patients demonstrated significant improvement in pain and shoulder function. A small proportion of patients were converted to a reverse total shoulder arthroplasty for signs of a rotator cuff tear and excessive component wear. This study may suggest that the metal backed glenoid design do not specifically place patients at an increased risk for postoperative complications and thereby be exposed to another subsequent revision procedure.
#7527
Evaluating Pelvic Tilt Using Measurements From Anteroposterior Pelvic Radiographs - a Meta-Analysis of Sacro-Femoral-Pubic (SFP) Method
*Yuan Chai - University of Sydney - Sydney, Australia
Sam Khadra - University of Sydney - Sydney, Australia
Mounir Boudali - University of Sydney - Sydney, Australia
Ibrahim Darwish - Royal North Shore Hospital - St. Leonards, Australia
William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
*Email: yuan.chai@sydney.edu.au
Introduction
Accurate measurement of pelvic tilt (PT) is critical in diagnosing hip and spine pathologies. PT is usually measured on a sagittal pelvic radiograph, yet the sagittal radiograph is sometimes not available or not measurable. Studies explored the correlation between the PT and different landmarks from an anteroposterior (AP) radiograph. The sacro-femoral-pubic (SFP) angle (Figure 1) is one of the most popular landmarks, which is defined as the angle between the midpoint of the upper sacral endplate, the centroid of the acetabulum, and the upper midpoint of the pubic symphysis. The SFP method has been posited as an accurate method to measure pelvic tilt from AP radiographic films, yet some other studies disagree with the claim. This study aims to perform a cohort-controlled meta-analysis to examine the correlation between the SFP angle and PT and proposes an application range of the method.
Methods
This study searched PubMed, Embase, Cochrane, and Web of Science databases for studies that evaluated the correlation between SFP angle and PT. The Pearson's correlation coefficient r from studies were tabulated and compared. Pooled correlation coefficients r for overall and gender/age (teenage or adult) controlled subgroup studies were reported with 95% confidence intervals (CI) using Fisher’s Z transformation with the random-effect model. Heterogeneity and publication bias were evaluated using Egger's regression test for the asymmetry of funnel plot of standard error by Fisher's Z.
Results
Eleven studies were recruited, with nine studies reporting the correlation coefficient between the SFP angle and the PT that was involved in the meta-analysis, totaling 1,247 patients (Figure 2). The overall pooled correlation coefficient was 0.61 (95% CI: 0.51 – 0.68) with high inter-study heterogeneity (I2 = 75.95%). Subgroup analysis showed that the adult group has a higher correlation coefficient than the teenage group (0.70 versus 0.56, p < 0.001), and the pooled correlations in the teenage group for males and females were 0.56 (95% CI: 0.45-0.66) and 0.62 (95% CI: 0.48-0.73), respectively. SFP angle performed statistically better correlation to PT in the female group than in the male group (p = 0.031), yet the confidence of the significance is low, and further subgroup analysis involving more data is suggested. Most of the analyses demonstrated high heterogeneities.
Conclusion
The SFP method must be used with caution and should not be used in the male teenage group. The current studies did not demonstrate a superior outcome of SFP over other AP landmarks. More predictability in the data would be required to evaluate the absolute error of this method. Identical heterogeneity was observed among studies, indicating that ethnicity-segregated subgroup studies might be necessary. Gender-specific studies with adult subjects would be highly recommended.
Acknowledgment
The authors acknowledge the technical assistance of Kathrin Schemann and Jim Matthews of the Sydney Informatics Hub, a Core Research Facility of the University of Sydney. We are also thankful to Dr. John Farey for the clinical consultations.
Keywords: Pelvic Tilt; Sacro-Femoral-Pubic Angle; Anteroposterior Radiograph; Coronal X-Ray; Pre-Operative Planning; Total Hip Arthroplasty
Figures
Figure 1
Figure 2#7526
The Correlations of Different Pelvic Tilt Definitions Interchangeable or Irrelevant?
*Yuan Chai - University of Sydney - Sydney, Australia
Mounir Boudali - University of Sydney - Sydney, Australia
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: yuan.chai@sydney.edu.au
Introduction
Pelvic tilt (PT) is an important parameter in hip and spine surgeries. Four different pelvic orientation definitions are used clinically for different purposes (Fig. 1). Anatomical pelvic tilt or anterior pelvic plane (PTa) is defined by the pubic tubercles and the anterosuperior iliac spines, which is mainly used to evaluate acetabular orientation and intra-operative navigation. Mechanical pelvic tilt (PTm) is defined by the femoral head centers and the midpoint of the sacral plate. In conjunction with sacral slope (SS), both landmarks are important in analyzing sagittal balance and spinal pathology. Hip pelvic tilt (PTh) is defined by the pubic symphysis and the sacral promontory (Fig. 1). PTh is popular in hip surgeries, such as evaluating femoroacetabular impingement. These landmarks quantify a similar concept about pelvic orientation, yet the understanding of their relationships was lacking. Some studies referred to the word "pelvic tilt" for horizontal comparisons. However, the PT landmarks might not be the same, and their anterior/posterior definitions might be opposite. This study aims at investigating the correlations of the four popular pelvic tilt definitions using the same radiographic dataset and proposing a better defined pelvic tilt.
Methods
This study recruited 105 sagittal pelvic radiographs from a single clinic awaiting their total hip replacement, in which 68 images were from male patients and 37 images from female patients. Four pelvic tilt definitions (PTm, PTa, PTh, SS) were examined in a gender-dependent manner by two observers and were repeated after six months. The linear regression model was applied to all the comparisons with a 95% significance interval. The intraclass correlation coefficient (ICC) was used to evaluate the measurement reproducibility.
Results
No gender difference was found in any measurement. The Pearson's correlation coefficient between PTa and PTm, PTa and PTh, PTa and SS, PTm and PTh, PTm and SS, PTh and SS was 0.59, 0.70, 0.29, 0.91, 0.16, -0.01, respectively (Fig. 2). All the inter- and intra- observer ICCs were above 0.90. Since the correlation coefficient between PTm and PTh was excellent, the linear regression model between them was established as PTm = 0.951 × PTh - 68.284.
Conclusion
The correlation between PTm and PTh is very strong. The two parameters are interchangeable under a simple linear regression model provided in the Results. Thus, one of the two definitions could be substituted. SS is a personalized spinal landmark that is independent of the pelvic anatomy. Patients with spinal pathology may have more static spinopelvic relationships following a certain pattern, yet more study is required. This study also proposes always defining the forward (anterior) pelvic tilt as a positive value, thus simplifying and optimizing the use of pelvic orientation for clinical purposes and study comparisons.
Acknowledgment
We thank Dr. John Farey from the Kolling Institute of Medical Research of the Royal North Shore Hospital for his professional consultation.
Keywords: Pelvic Tilt; Pelvic Orientation; Acetabular Coverage; Pelvic Navigation; Sagittal Balance; Total Hip Arthroplasty; Spinal Deformity
Figures
Figure 1
Figure 2#7623
A Novel Method of Evaluating the Accuracy of Radiographic Landmark Localization
*Yuan Chai - University of Sydney - Sydney, Australia
Mounir Boudali - University of Sydney - Sydney, Australia
John Farey - The Kolling Institute - Sydney, Australia
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: yuan.chai@sydney.edu.au
Introduction
Skeletal abnormalities are usually templated and diagnosed using radiographs. Manual landmark detection has been reported as a reliable data source for surgical decisions. However, human error always exists and is evaluated using statistical descriptions or coefficients. The technological advances popularized the "non-human" landmarking method. The errors are usually presented in a probability format that is not comparable to the manual method. The region-based landmark definition makes an arbitrary "ground truth" point impossible. The differences in patients' anatomies, radiograph qualities, and scales make the horizontal comparison difficult. Thus, the so-called "precise" AI landmarking algorithms that outperform human errors are not persuasive unless their errors can be compared. This study aims to explore manual landmark detection further and establish a probability-based landmarking analysis method to quantify human error.
Methods
This study recruited 115 sagittal pelvic radiographs from 93 adult patients. Three labeling procedures were designed. First, a senior surgeon labeled the images with severe pelvic axial rotations that would influence the estimation of landmarks. Second, four independent observers measured pelvic tilt (PT) on each image. Two PT definitions were used. Anatomical pelvic tilt (PTa) was defined by the pubic tubercles and the anterosuperior iliac spines. Mechanical pelvic tilt (PTm) was defined by the center of two femoral heads and the midpoint of sacral plate (Figure 1). PTm was both estimated and calculated by identifying the skeletal contours. Two observers repeated the process. Third, the angular errors with high standard deviations (SD > 3°) were isolated for further review by a senior surgeon to determine the wrong landmarks. The inter- and intra- observer reliabilities were evaluated using the intraclass correlation coefficients (ICC). This study scaled each image in accordance with the lengths of two PT lines and superimposed the label's centroid from different observers. The data distribution was projected to an average PT axis for a density vector to calculate the maximum possible error (Figure 2).
Results
All the measurements demonstrated excellent reliabilities (ICCs > 0.9). 53 PTs from 39 images exhibited high SDs among four observers, in which 84 measurements (6.09% of total labels) were qualified as wrong landmarks that failed to label the correct locations. All the highly rotated radiographs had at least one PT that exhibited high SDs. Cognitive differences were found in the landmarks from clearly identifiable skeletal edges (Figure 3). By removing wrong labels and rotated pelves, the error analysis found 6.77°-11.76° maximum PT disagreement with 95% data points.
Conclusion
This study proved that the landmarks with excellent reliability still have a chance (at least 6.09% in our case) of making wrong landmark decisions. Identifying skeletal contours resulted in higher accuracy (at least 24.64% more accurate) than estimating landmark locations. A very careful surgeon measures PT could reasonably result in a maximum 11.76° random difference in 95% cases. Although not necessarily influencing the length/angular outcome, the landmark at a clear skeletal contour is more likely to generate systematic errors due to cognitive differences. In this case, the data from a single observer could minimize the systematic error.
Figures
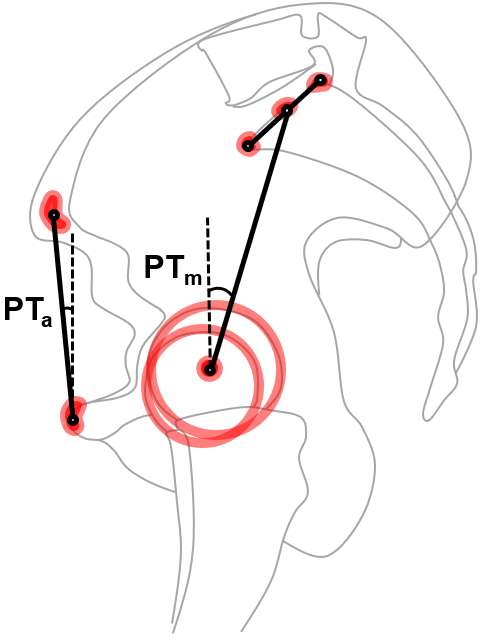
Figure 1
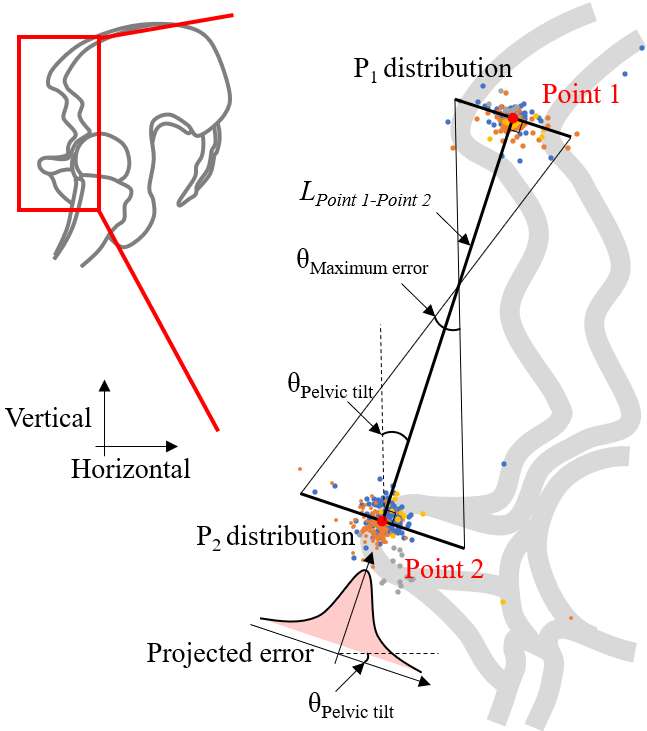
Figure 2
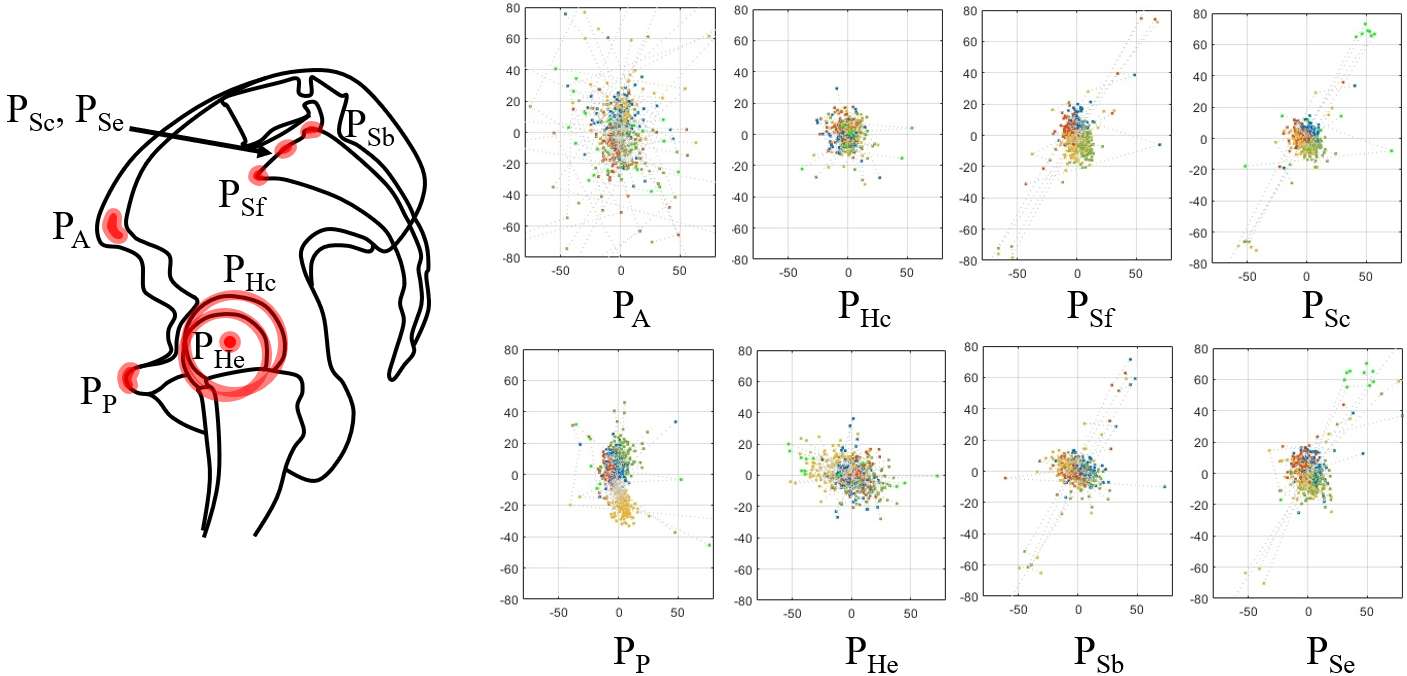
Figure 3#7972
Automated Assessment of Thigh Muscle Condition in Patients With Advanced Knee OA Using a Novel Deep Learning-Based Software: Correlation With Isokinetic Muscle Tests and Clinical Scores
Chong Bum Chang - Seoul National University College of Medicine - Seoul, South Korea
Chang-Jin Yon - Keimyung University - Daegu, South Korea
*Ja-Young Choi - Seoul National University Hospital - Seoul, South Korea
Seung-Baik Kang - Boramae Medical Center/ Seoul National University College of Medicine - Seoul, South Korea
*Email: drchoi01@gmail.com
Objective: This study aimed (1) to determine whether the isokinetic muscle strength test reflects the volume of the corresponding thigh muscle group, (2) to determine whether isokinetic muscle strength and muscle volumes are associated with the clinical scores, and (3) to examine the influence of the thigh muscle status and demographic data on the clinical scores in patients with advanced knee osteoarthritis (OA).
Design: The patients with advanced OA who underwent TKA were reviewed retrospectively. All the patients underwent measurement of isokinetic strength including knee extensor and flexor peak toque prior to TKA. The thigh muscle group volume was measured using a novel automated thigh segmentation software with axial CT images. KOOS and EQ-5D were assessed as preoperative clinical scores. The Pearson correlation coefficient was used to examine the correlation between the isokinetic muscle strength and thigh muscle volume. Linear regression analyses were used to examine the effect of the variables on the preoperative clinical scores.
Results: A moderate correlation was found between the muscle volume and the peak torque of the isokinetic strength test. In the multivariable linear regression analysis, the mean KOOS was significantly influenced by age, sex, and H/Q ratio, and the strongest factors correlating with the EQ-5D index score were age and flexor peak torque.
Conclusions: This study suggests that isokinetic muscle strength partially reflects thigh muscle volumes and could be an indicator of the degree of functional impairment. Furthermore, age and sex are predictors of clinical conditions in patients with advanced knee OA.
#7971
The Optimal Tibial Stem Position of Primary and Revision Total Knee Arthroplasty in Asian Knee: Three-Dimensional Analyses
Chong Bum Chang - Seoul National University College of Medicine - Seoul, South Korea
*Ja-Young Choi - Seoul National University Hospital - Seoul, South Korea
Jong Seop Kim - Seoul National University Bundang Hospital - Seoul, South Korea
Seung-Baik Kang - Boramae Medical Center/ Seoul National University College of Medicine - Seoul, South Korea
*Email: drchoi01@gmail.com
Background: The tibial stem position of the tibial component in total knee arthroplasty (TKA) is momentous for the longevity of the implant. The purpose of the present study was to investigate the optimal position of the tibial stem in primary and revision TKA using three-dimensional estimation.
Methods: 90 consecutive patients who had progressed knee osteoarthritis indicated for TKA were included. Radiographic parameters, including the medial proximal tibial angle (MPTA), tibia vara angle (TVA), medial and lateral distance from the tibial stem to the inner cortex at 4 cm below the resection surface, and the coronal offset measured by an extramedullary and an intramedullary guide at the resection surface were evaluated. The coordinates of the anatomic axis on the tibial plateau and the tibial stem tip were evaluated using 3D image processing software.
Results: Analysis of radiographs showed that the tibial stem tip position was centered in the intramedullary canal. The coronal offset of the anatomic axis to the intramedullary canal was 1.2±3.8 mm medial to the plateau center on the resection surface. The projected bisecting line on the section level of the tibial stem tip was medial to the center of the intramedullary canal, and the coronal offset was centered on the resection surface measured using 3D software.
Conclusions: The medialized tibial stem for primary TKA with an extramedullary guide could deviate medially in the intramedullary canal of the tibia, and the coronal offset for revision TKA or primary TKA with an intramedullary guide was centered in the Asian knee.
#8013
In Situ Relationship Between Load and Range of Motion in Reverse Total Shoulder Arthroplasty
*Alexander Greene - Exactech Inc. - Gainesville, USA
Prudhvi Tej Chinimilli - Exactech - Gainesville, USA
Josie Elwell - Binghamton University - Binghamton, USA
Christopher Roche - Exactech - Gainesville, USA
Ari Youderian - South County Orthopedic Specialists - Laguna Woods, USA
Moby Parsons - Wentworth Douglas Hospital - Portsmouth, USA
Richard Jones - Southeastern Sports Medicine - Asheville, USA
Allan Wang - St John of God Medical Centre - Murdoch, Australia
*Email: alex.greene@exac.com
INTRODUCTION:
In reverse total shoulder arthroplasty (RTSA), determining proper humeral and glenoid implant offset and the resulting impact on joint tension and range of motion (ROM) has traditionally been a subjective matter determined by the surgeon. This study aims to quantify the correlation between joint loads and ROM in RTSA using an intraoperative joint load sensor in a clinical setting.
METHODS:
14 RTSA procedures were performed by 5 different surgeons using a wireless load sensing humeral liner trial (VERASENSE for Equinoxe, OrthoSensor, Inc., Dania Beach, FL) during the ROM assessment portion of the procedure. Surgeons chose between 38mm and 42mm liner sizes based on patient sizing and individual preference. Each surgeon performed a consistent set of four maneuvers during the final implant reduction to simulate activities of daily living of the affected shoulder. These maneuvers consisted of a maximum internal/external rotation of the forearm at 0°, 45°, and 90° of humeral abduction, and a maximum flexion/extension motion. Each surgeon was instructed to start and end each motion at the same neutral rotation and abduction angles to generate as consistent data between cases as possible. Load values and total angular change of the liner were collected through three calibrated load sensors and a 6 degree of freedom inertial measurement unit within the liner trial at a 20 hertz sample frequency. Load vs. ROM was then plotted for each maneuver per case and the relationship between load magnitude and the change of load with respect to arm position was compared.
RESULTS:
6 38mm liner sizes and 8 42mm liner sizes were used by the surgeons. Maximum and minimum load values and the angles at which each value was achieved are presented in Figures 1 and 2 for 38mm and 42mm liner sizes, respectively. Visual plots of load vs. ROM for each maneuver are shown in Figure 3 for single representative cases of both 38mm and 42mm liner sizes. In every case observed, load magnitudes plotted a U-shaped curve when compared to ROM with the highest loads always occurring in end ROM, indicating that load is not a static measurement throughout ROM. In addition, the slope of the load curve tended to change more quickly as the arm approached end ROM.
CONCLUSION:
This is the first study to define the relationships between ROM and in situ load in RTSA in a clinical setting. The change in slope of the load curve at end ROM indicates that tissue elasticity may have a large impact on joint loads and potential achievable ROM and joint stability. Limitations of this study include interobserver variability, and collection of passive humeral-only (without scapula) ROM data in patients who are anesthetized and paralyzed with an open incision, which will be less relevant than values recorded in an awake patient with active muscle tension and full scapulohumeral motion in an enclosed joint. Clinical outcomes are being collected on a patient cohort to correlate load magnitude and ROM ranges to shoulder outcome scores and will be reported at a future date.
Figures
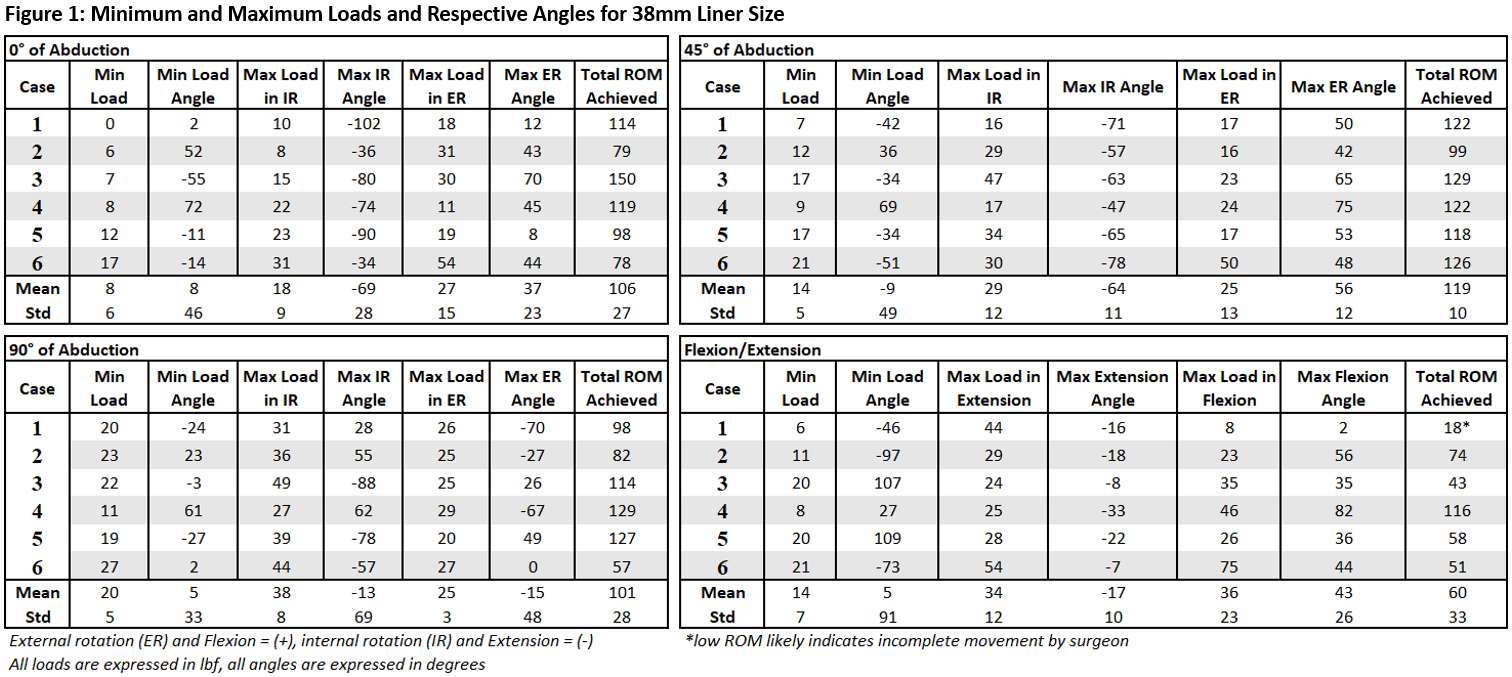
Figure 1
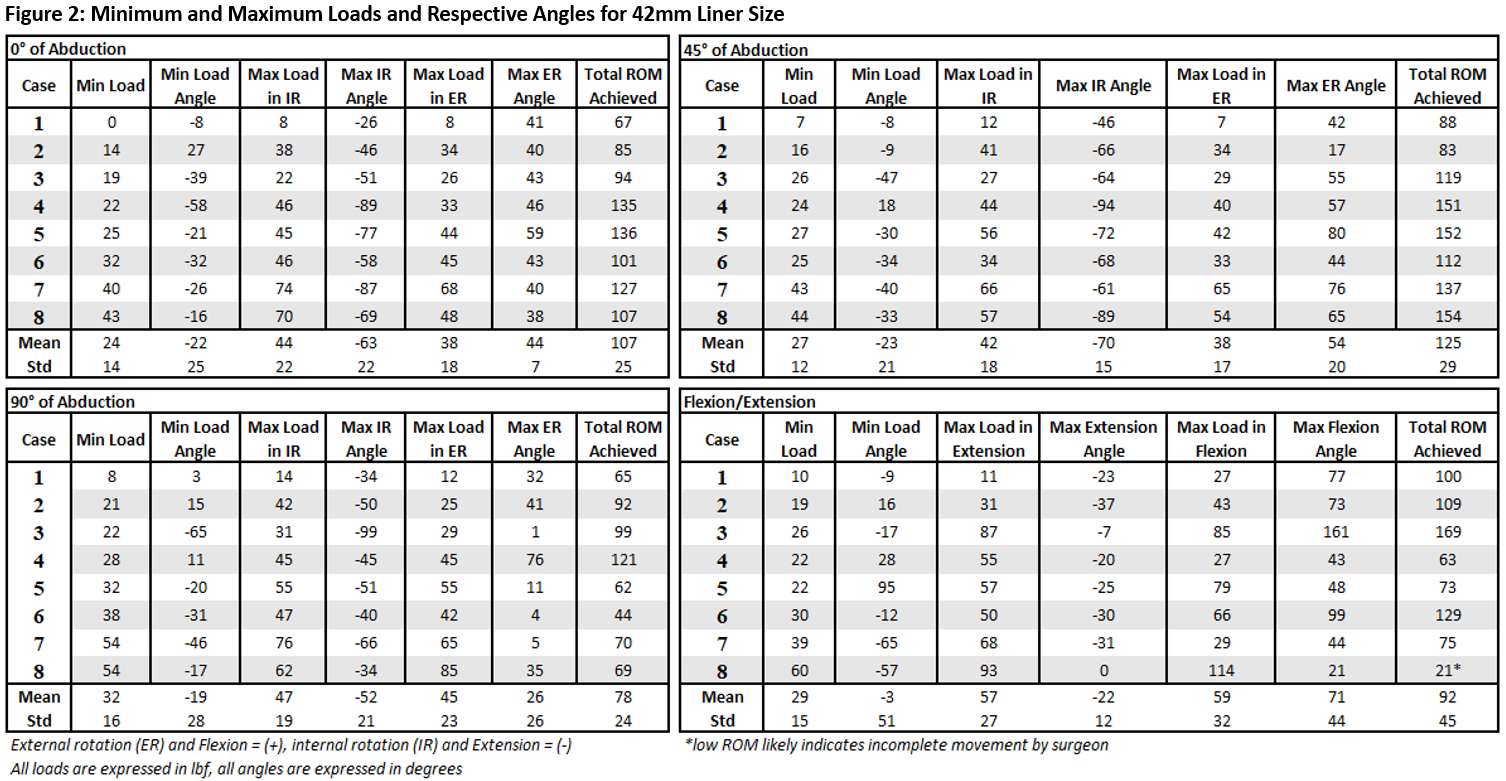
Figure 2
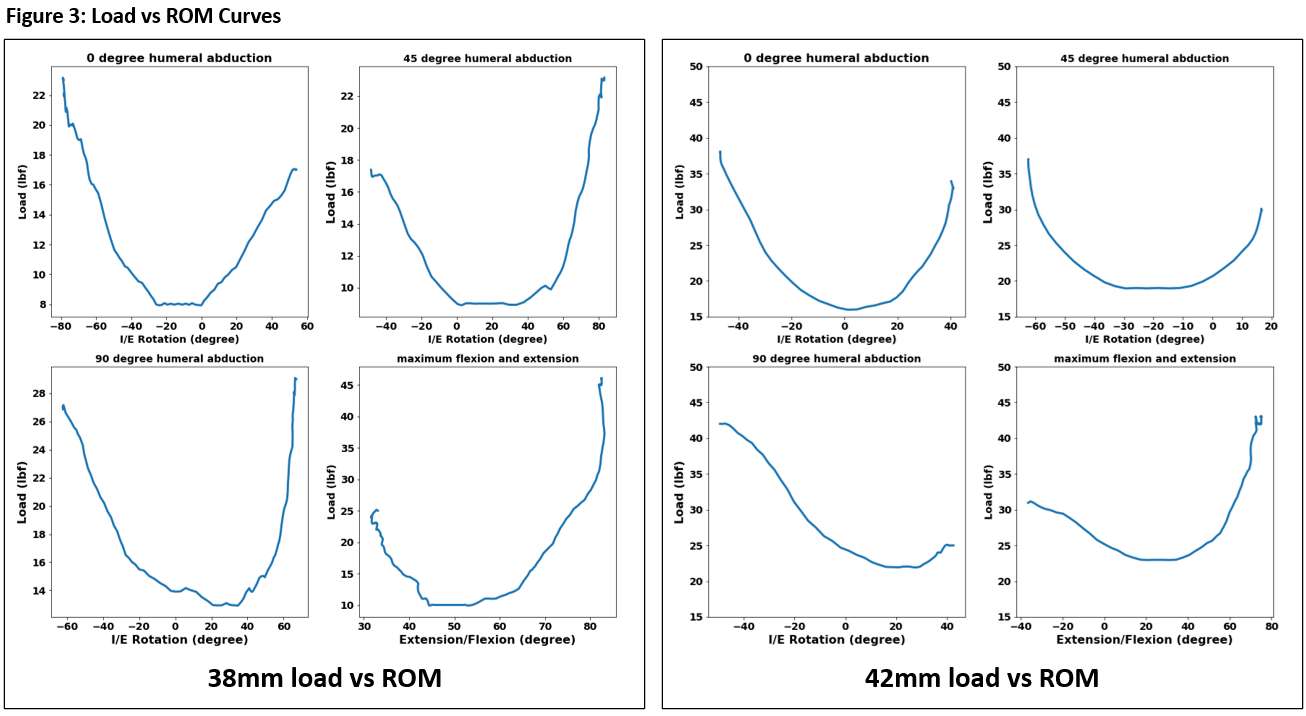
Figure 3#7922
New Cup Targeting Technology in Anterior Approach THA: Preliminary Results
*Ian Chun - John A. Burns School of Medicine at the University of Hawai'i - Honolulu, United States of America
Ashley Shirriff - John A. Burns School of Medicine at the University of Hawai'i - Honolulu, USA
James DeJesus IV - University of Hawaii - Honolulu, United States of America
Dylan Lawton - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: ikhchun@hawaii.edu
Introduction: The accuracy of acetabular cup placement during total hip arthroplasty (THA) has been shown to improve with intraoperative fluoroscopy (IF), however, only one previously evaluated system (System A) provided targeting for both abduction (ABD) and anteversion (ANT). This study compared previously reported cup positioning results using System A to results using a newly released IF supplementation software (System B) now with similar cup targeting capabilities.
Methods: Previously published (System A), cup positioning results from the current study site was compared to prospectively collected data from a consecutive cohort of patients utilizing System B. Both IF supplementations were used during unilateral or single staged bilateral THA, performed by a single surgeon using the anterior approach and a specialized fracture table. Radiographic evaluation was performed six-weeks post-THA, from which the acetabular cup ABD and ANT were measured. The target ABD was 42°±10° and 40°±10° for Systems A and B, respectively. Target ANT was 15°±10° for both systems. Fluoroscopy time was recorded directly from each system.
Results: System A included 178 patients (217 hips) and System B included 55 patients (72 hips). For System A and B, the average ABD was 41.8°±4.1° and 41.9°±4.0° and average ANT was 14.5°±4.3° and 18.3°±4.9°, respectively. For Systems A and B, target ABD was achieved in 98.2% and 98.6% and target ANT was achieved in 97.2% and 91.7%, respectively. Fluoroscopy time per hip for System A was 9.9±4.0 seconds compared to System B 13.9±5.3 seconds.
Discussion/Conclusion: Preliminary data suggests accuracy in acetabular cup positioning was similar between System A and B. Fluoroscopy time was slightly higher for System B, due to additional research related data collection requirements. Both systems resulted in excellent precision and accuracy regarding cup positioning for anterior approach THA.
#7754
Real-Time Prediction of THA Contact Mechanics for Hip Planning Applications
Casey Myers - Ortho Haus - Denver, United States of America
Clare Fitzpatrick - Ortho Haus, LLC - Boise, Select Country
Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
*Chadd Clary - Ortho Haus, LLC - Denver, USA
*Email: cclary@theorthohaus.com
Introduction: Edge loading in total hip arthroplasty (THA), when the femoral head contacts the periphery of the acetabular liner, has been associated with increased risks liner damage and dislocation. Cup placement to avoid edge loading may reduce the risk of adverse outcomes, but current methods for predicting contact mechanics (e.g., finite element analysis) are computationally intensive and not well suited for real-time surgical planning tools. The objective of this study was to develop and verify a computationally efficient algorithm to assess head-liner contact mechanics across multiple implant families and patient poses.
Methods: Contact patches for five different hip implant combinations, with both small and large diameter femoral heads in metal-on-poly, ceramic-on-poly, and ceramic-on-ceramic combinations, were experimentally measured in standing and seated poses with low (650 N) and high (1750 N) loads using an AMTI VIVO (Fig. 1A). Measurements were repeated 3 times for each configuration. Prior to loading, a fast-curing epoxy (Microset 101) was introduced to the articulation, allowed to cure under load, and then optically scanned (Space Spider, Artec) to identify the contact regions (i.e., regions where no epoxy was present, Fig. 1B). Contact areas, locations, and centroids of the contact regions were calculated using Matlab (Mathworks). Separately, Hertzian contact models were formulated for each implant configuration, pose, and loading condition. Contact stiffness was determined from the experimentally measured Young’s modulus of the materials, then calibrated within the uncertainty bounds to match the experimental contact area in one representative combination. The predicted contact area and centroid from the analytical models were compared to the experimental measurements (Fig. 1C). Finally, a linear response model (LRM) was trained using contact metrics from 10,000 randomly sampled unique contact configurations predicted by the analytical model, with cup inclination (range: 0°-70°), cup version (range: 0°-70°), liner/head diameters (range: 28mm-44mm), and implant materials (poly, CoCr, ceramic) as inputs and with contact centroid and radius as outputs. The accuracy of the LRM model was calculated across a test dataset of 3,600 unique implant configurations, sampled independently from the training set, as the root mean square (RMS) difference in contact centroid between the LRM and analytical models.
Results: The mean difference between experimental and model-predicted contact centroids was 1.5 mm with a maximum of 4 mm (Fig. 2). Differences were smallest for the small diameter metal/ceramic on poly articulations. The RMS difference between the contact LRM and analytical model over the entire test dataset was 0.22 mm and a maximum of 1.17 mm (Fig. 3).
Conclusions: The spherical contact conditions in THA enables the Hertzian contact model to accurately predict contact centroids and areas. Although considered gold-standard, uncertainty in the experimental set-up (e.g., small variations in implant alignment or uncertainty in contact boundaries identification) potentially contribute more error than the analytical prediction. Hertzian contact is particularly well suited for approximation using LRMs. This overall approach to predict hip contact mechanics resulted in sub-millimeter accuracy with minimal computational cost, making it particularly applicable for real-time surgical planning applications to reduce the occurrence of edge loading in THA.
Figures
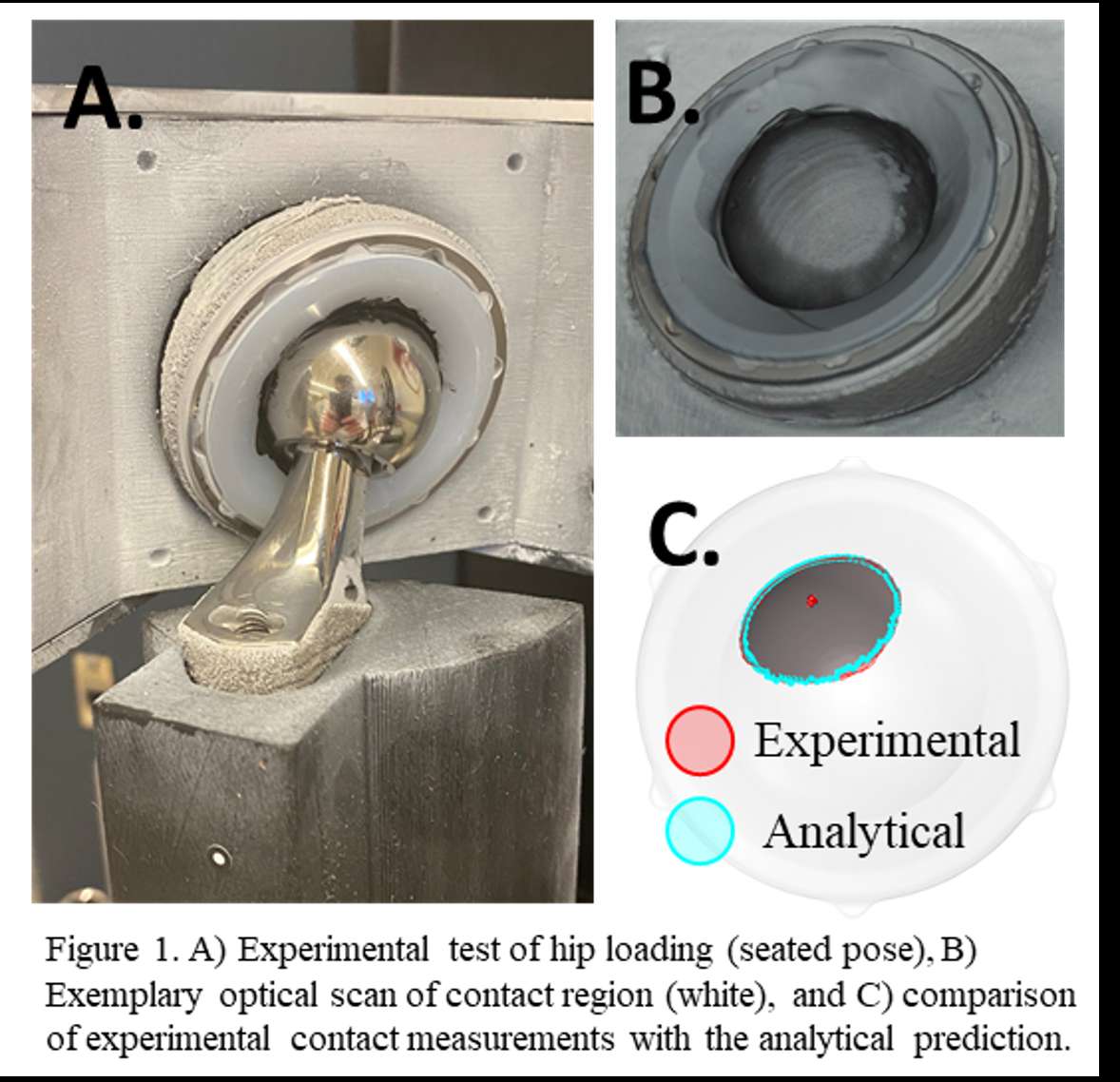
Figure 1
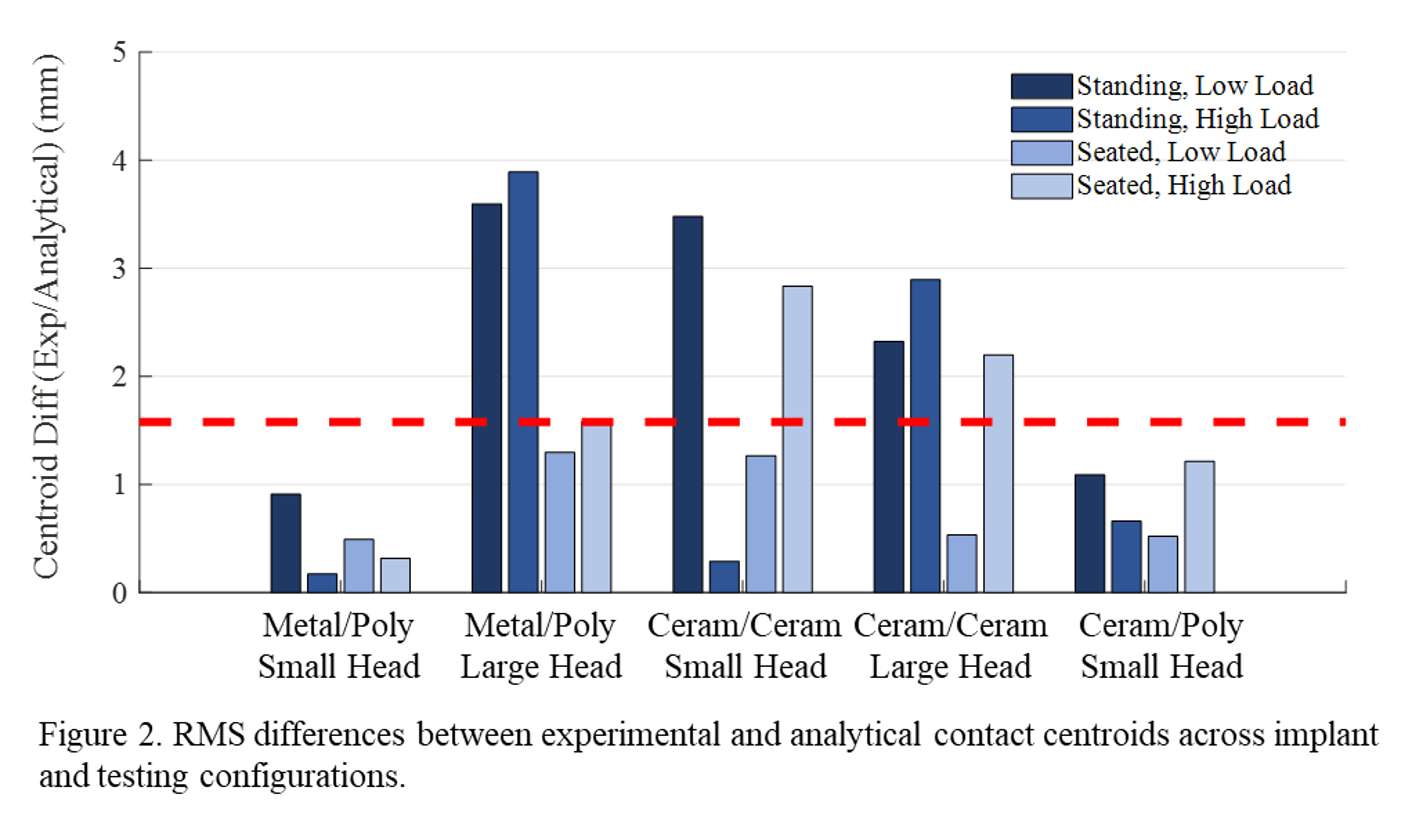
Figure 2
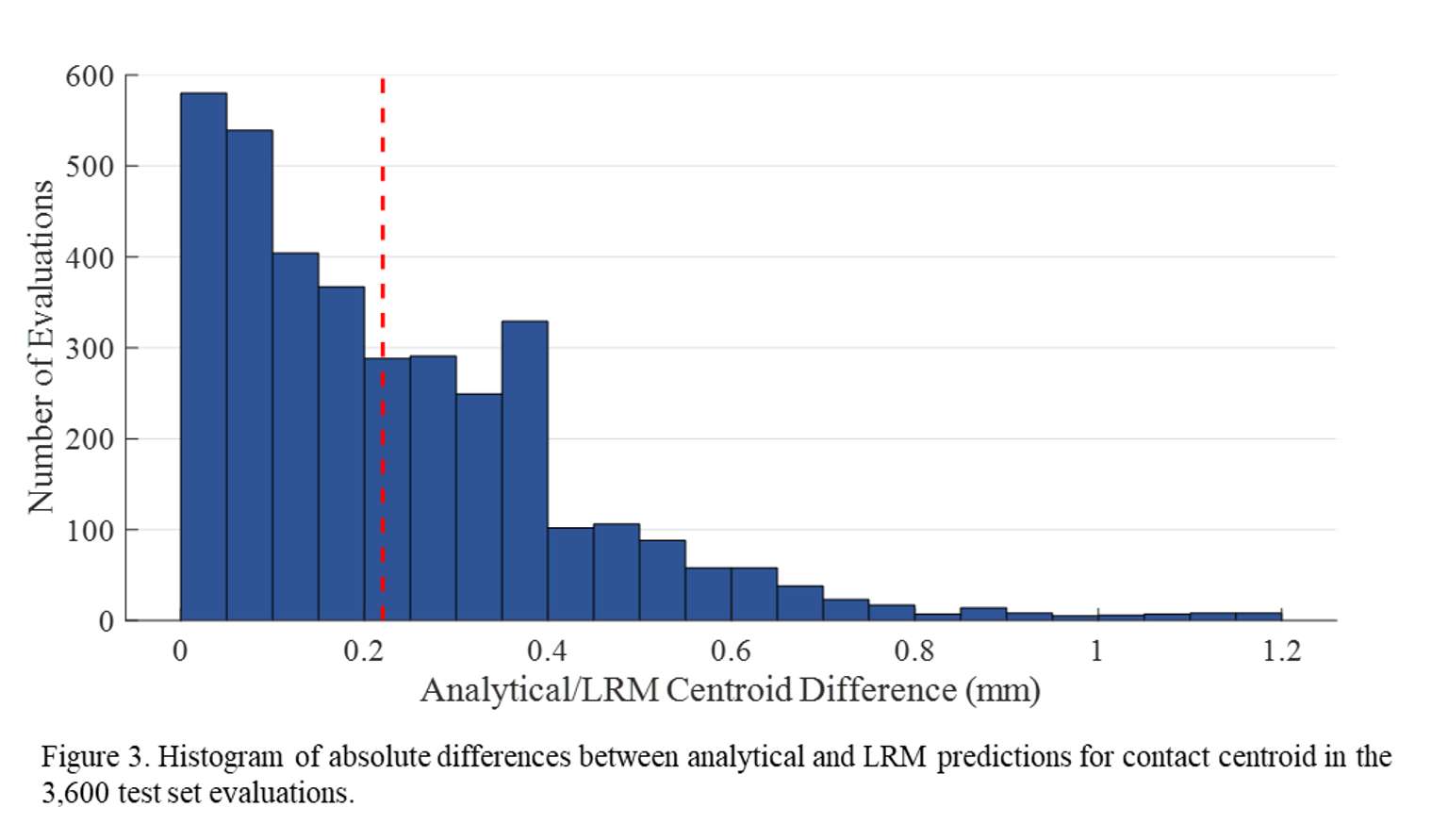
Figure 3#7773
Automated Tool for Real-Time Cup Alignment to Avoid Edge Loading and Implant Impingement in THA
Casey Myers - Ortho Haus - Denver, United States of America
Clare Fitzpatrick - Ortho Haus, LLC - Boise, Select Country
Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
Chris Hunt - DePuy Synthes Joint reconstruction - Leeds, United Kingdom
Brittany Marshall - Depuy Synthes - Warsaw, USA
*Chadd Clary - Ortho Haus, LLC - Denver, USA
*Email: cclary@theorthohaus.com
Introduction: Pre-operative total hip arthroplasty (THA) planning tools have recently been developed to avoid edge loading, minimizing potential polyethylene damage and propensity for dislocation. Current tools commonly require CT scans and manual processing that significantly increases the time required for plan generation. The focus of the current study was to develop an automated, real-time algorithm to calculate bounds for acceptable cup alignment based on patient-specific pelvic mobility, accounting for both edge loading and implant impingement.
Methods: The planning algorithm calculates patient-specific cup anteversion and inclination alignments that prevent 1) edge loading and 2) implant impingement. Algorithm inputs are pelvic tilt angles from the standing and seated flexed positions, commonly determined from functional x-ray images, and the implant type. Pelvic tilt angles, defined by the orientation of the anterior pelvic plane, are used to query a verified linear response model (LRM) which reports contact areas and centroids between the head and liner in the standing and seated positions for a range of cup alignments (Fig. 1a). The set of cup alignments which do not result in edge loading (i.e., contact centroids within 2-mm of the liner periphery) in both functional poses are identified (Fig. 2a). A second verified LRM is subsequently used to evaluate the external rotation of the femoral implant to impingement in the patient’s standing pose and the corresponding internal femoral rotation to impingement in the patient’s seated pose for each cup alignment in the set (Fig. 1b). The set of cup alignments is then truncated to those which maximize femoral rotation to impingement in both functional poses (Fig. 2b). Two theoretical subjects representing low pelvic mobility (-14° standing tilt, -5° seated tilt, Fig. 2) and high pelvic mobility (0° standing tilt, 40° seated tilt, Fig. 3) were evaluated by the algorithm, formulating the edge loading free cup orientations and the associated rotations to impingement.
Results: The range of cup positions which prevent edge loading is heavily influenced by the magnitude of the change in pelvic tilt from the standing to seated poses. Low-mobility patients (e.g., Subject 1) have a large range of cup alignments that effectively avoid edge loading (Fig. 2). Conversely, high-mobility patients (e.g., Subject 2) have a narrower range of acceptable cup alignments (Fig. 3) and may require lipped liners to provide sufficient coverage. Variation in the seated pose affects the minimum version for the cup, while the standing pose affects the maximum allowable version. Excluding cup positions that have the highest likelihood of impingement further limits the acceptable cup alignments, particularly cup inclination. The run time of the algorithm to establish the acceptable cup alignments for a patient was 2.8 seconds.
Conclusions: Consideration of both edge loading and impingement demonstrates that impingement is an important factor in acceptable cup alignments compared to contact alone. Leveraging computationally efficient analytical tools to assess how patients’ pelvic mobility affects functional cup alignment and the associated impacts on edge loading and impingement will help surgeons address the range of pelvic tilt behavior seen in the THA.
Figures
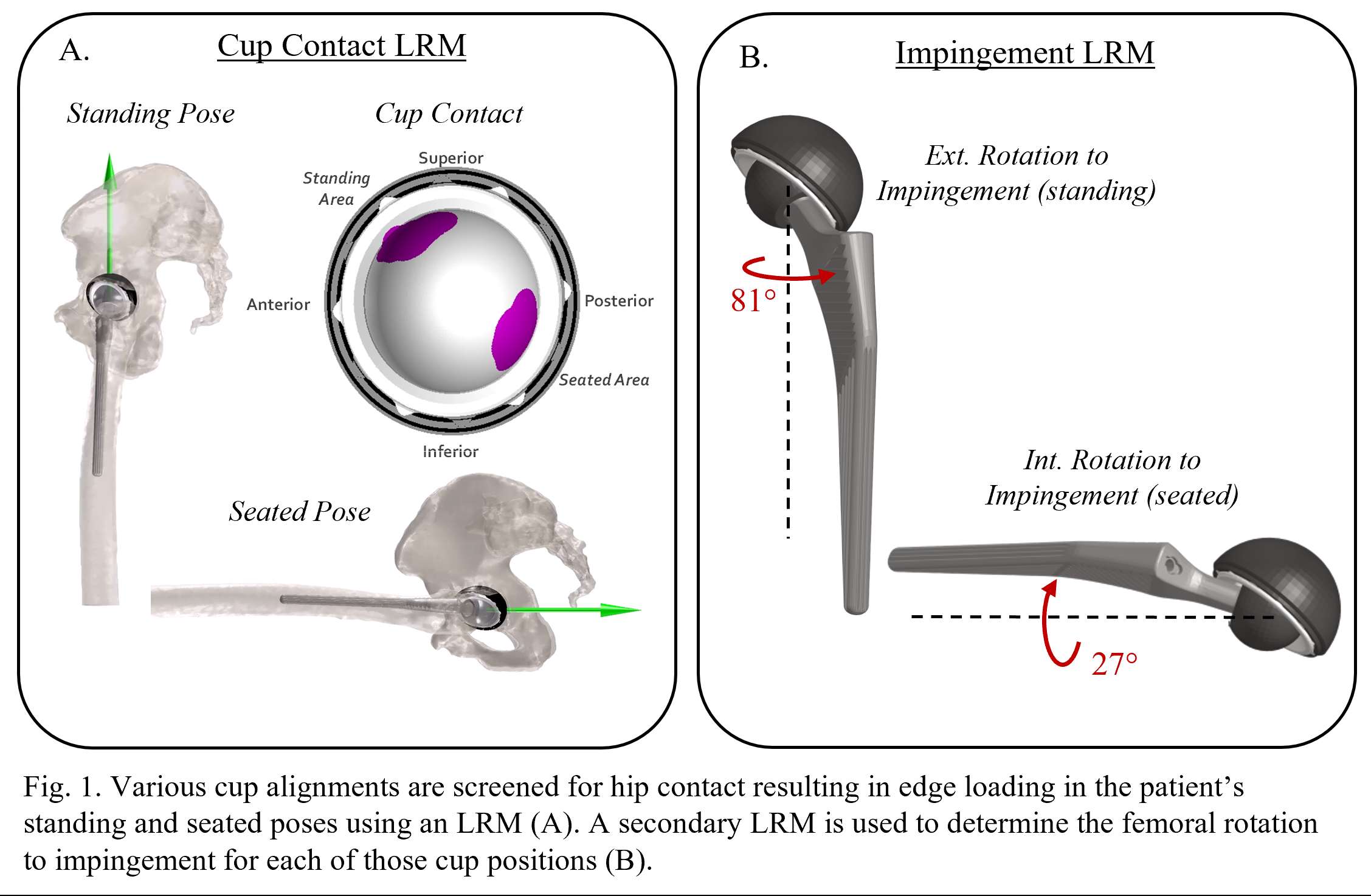
Figure 1
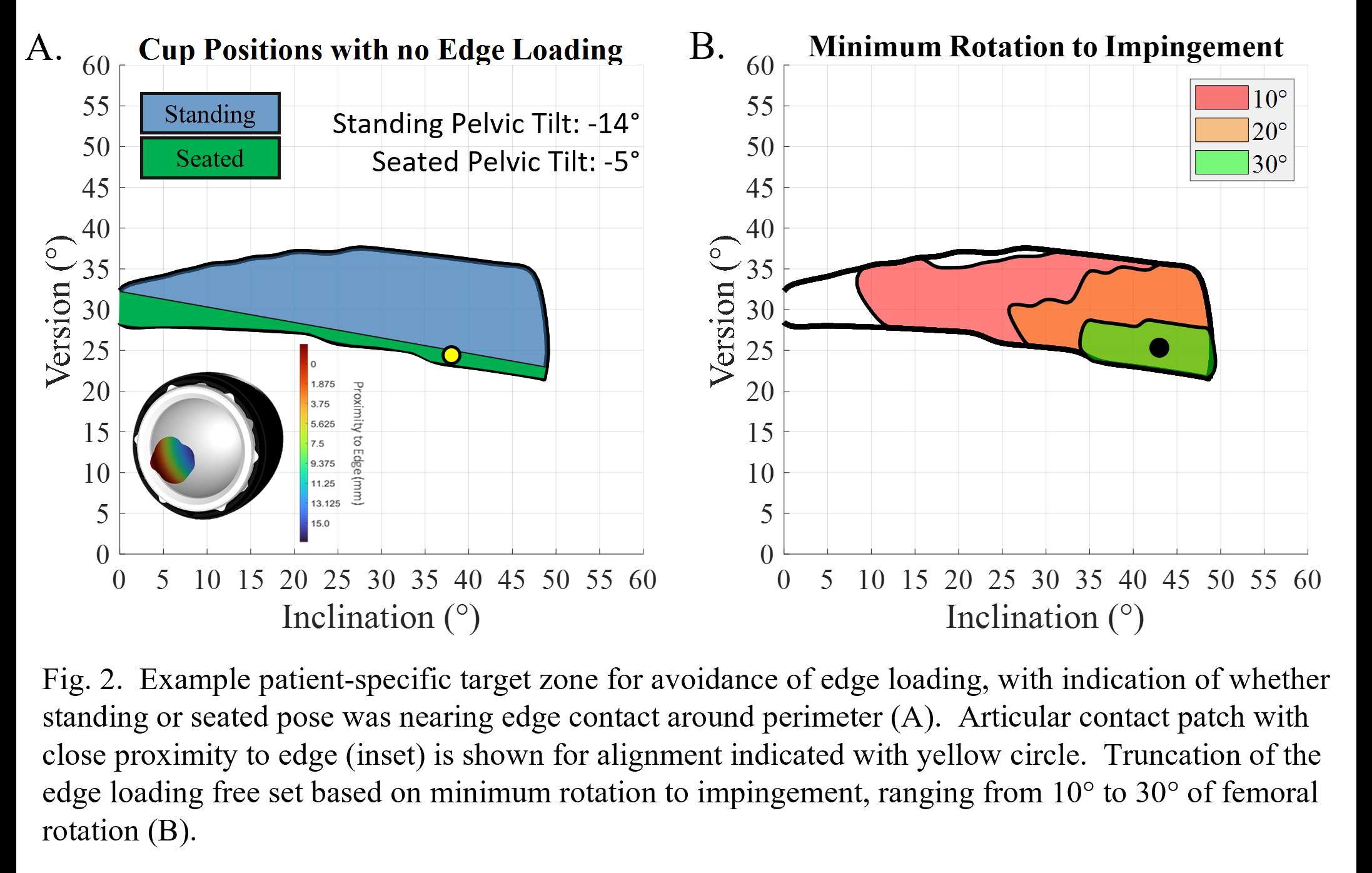
Figure 2
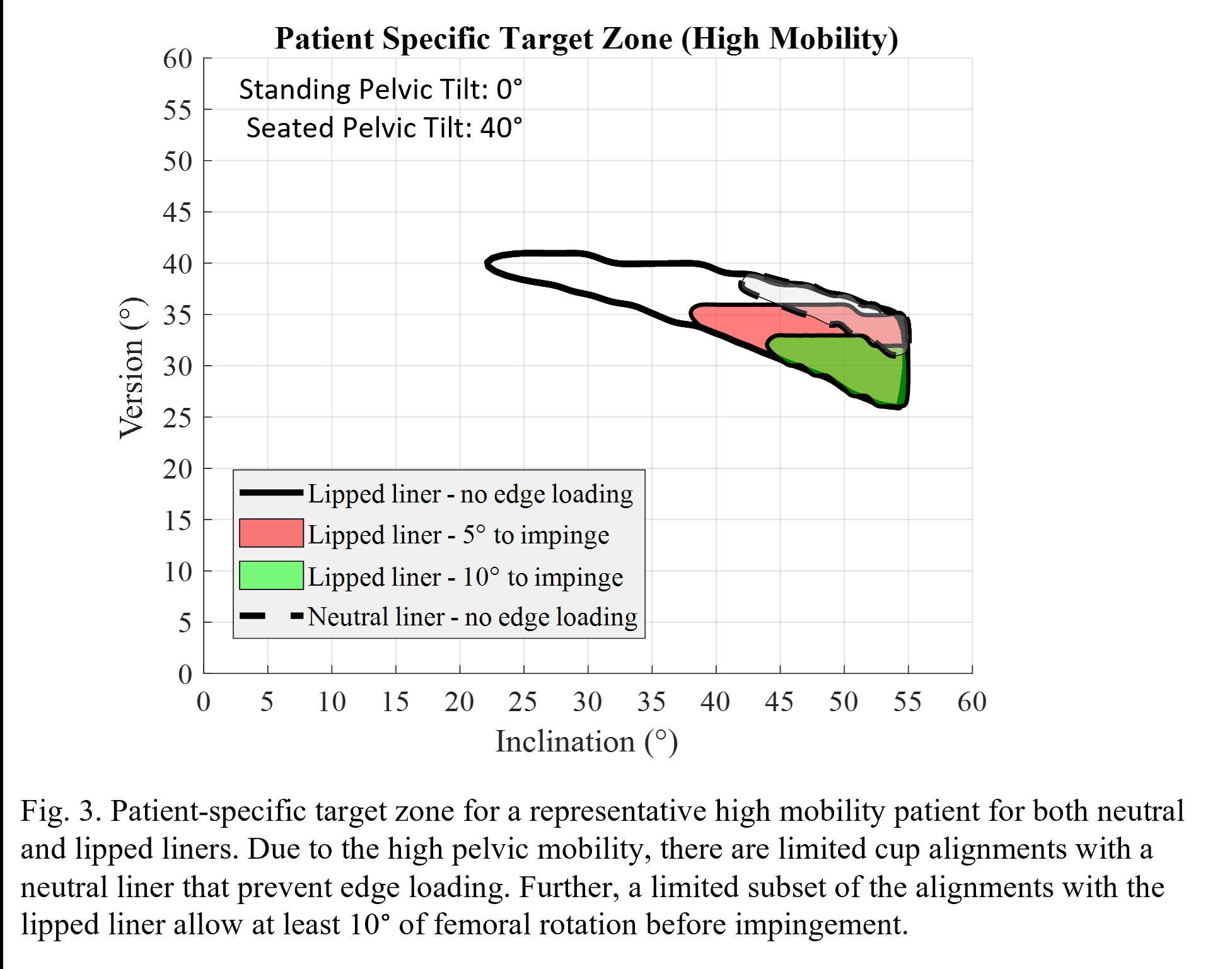
Figure 3#7864
Dislocation After Total Hip Arthroplasty for Acute Hip Fracture. the Effect of Approach, Headsize or Dual-Mobility?
*Peter Cnudde - HDUHB - Llanelli, GB
Cecilia Rogmark - LUND UNIVERSITY - LUND, Sweden
Jonatan Natman - SWEDISH ARTHROPLASTY REGISTER - GOTHENBURG, Sweden
Nils Hailer - UPPSALA UNIVERSITY - UPPSALA, Sweden
Ammar Jobory - Lund university - Lund, Sweden
*Email: peter.cnudde@icloud.com
INTRODUCTION:
Due to the potentially increased risk of dislocation of the hip in patients, treated with a total hip arthroplasty (THA) for acute femoral neck fractures(FNF), it is unclear whether they should receive a conventional (cTHA) or dual-mobility total hip arthroplasty (DMC-THA) and whether lateral approach and increased head size confer a reduced dislocation risk.
METHODS:
We designed a longitudinal cohort study linking a national joint register with the National Patient Register, including patients presenting with an acute FNF and treated with a THA from 2005 to 2014. The total dislocation rate at 1-year, and 3-year revision, reoperation and mortality rates were recorded. Cox multivariable regression models were fitted to calculate adjusted hazard ratios (HR) stratified by approach (lateral versus posterior) and implant type/head size. Adjustments were made for age, sex, Charlson comorbidity index, premorbid neurological disease, year of surgery, implant type and approach respectively.
RESULTS:
11,289 patients received a unilateral arthroplasty for acute FNF in the study period. After exclusions for uncemented stems, bilateral procedures and missing data 8,031 patients were included in the study group and followed up until reoperation, revision, death or end of study period. When stratified for approach the 1-year total dislocation rate was 8.33% for the posterior approach versus 2.73% for the lateral approach (p<0.001) (Fig 1). When stratified for implant type/head size the 1-year total dislocation rate was 0.8% after DMC-THA, 6.4% after conventional THA with head size smaller than 32 mm (cTHA<32), 3.8% after conventional THA with head size of 32 mm (cTHA=32) and 4.6% after conventional THA with head size bigger than 32 mm (cTHA>-32) (p<0.001) (Fig 2). In the posterior approach group a lower risk of dislocation was associated with DMC-THA compared to cTHA=32 (HR=0.21, CI 0.07-0.68, p=0.009). When stratified by implant type/head size the posterior approach was associated with higher incidence of dislocations (HR=3.48, CI 2.85-4.24, p<0.001) (Fig 2). No differences in reoperation-free survival were identified between the head sizes and approach. However, at 3 years there were more revisions in the posterior approach group (p=0.016) (Fig 3). No difference in revision rate could be identified at any time interval between the implant types.
DISCUSSION AND CONCLUSION:
Although there is a tendency towards a lower rate of dislocation with the use of DMC-THA, our study suggests that when using a lateral approach, type of implant and head size is not associated with different dislocation rates. However, when using a posterior approach, DMC-THA is associated with a lower dislocation rate and cTHA<32 with a higher dislocation rate. On the basis of our findings, we would suggest avoiding the posterior approach altogether but if posterior approach is used a DMC-THA might be the better choice.
Figures
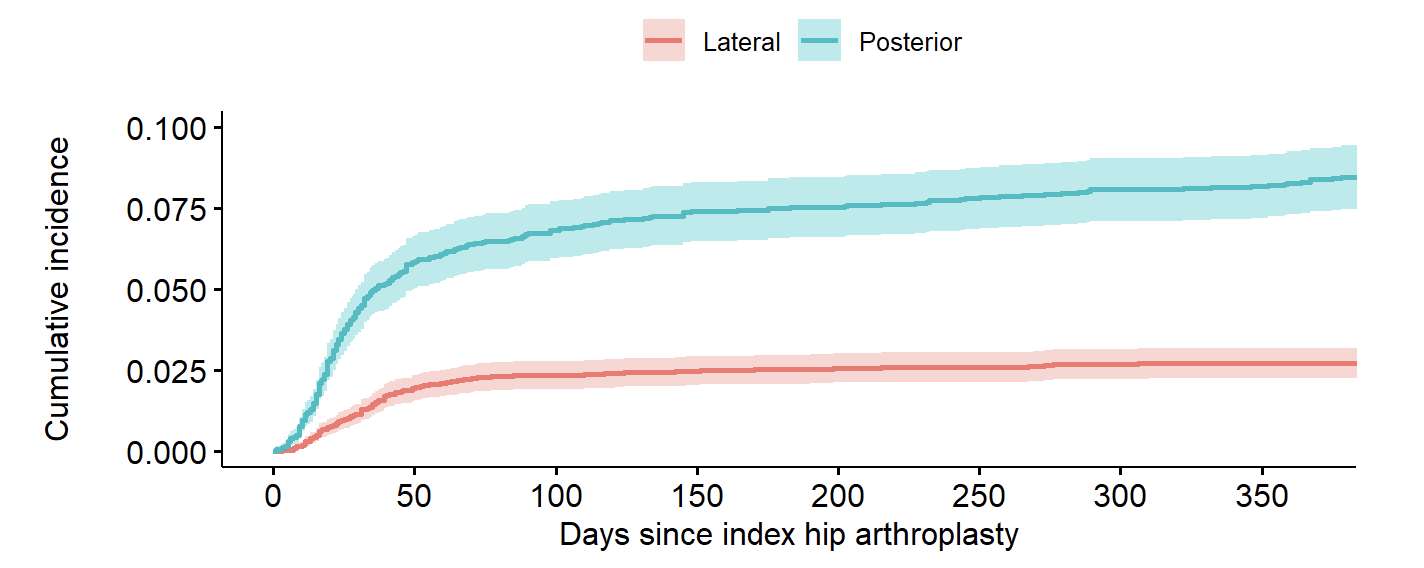
Figure 1
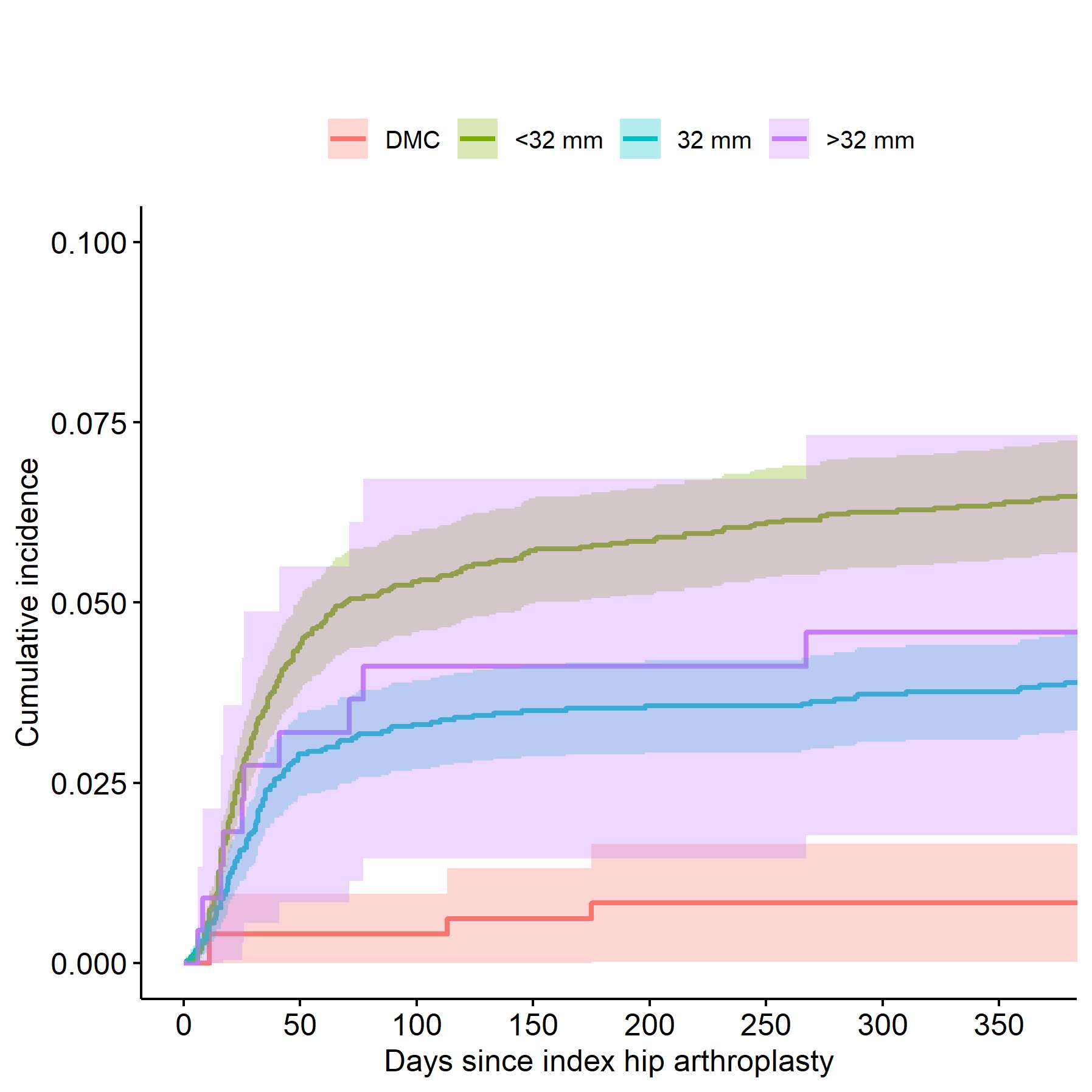
Figure 2
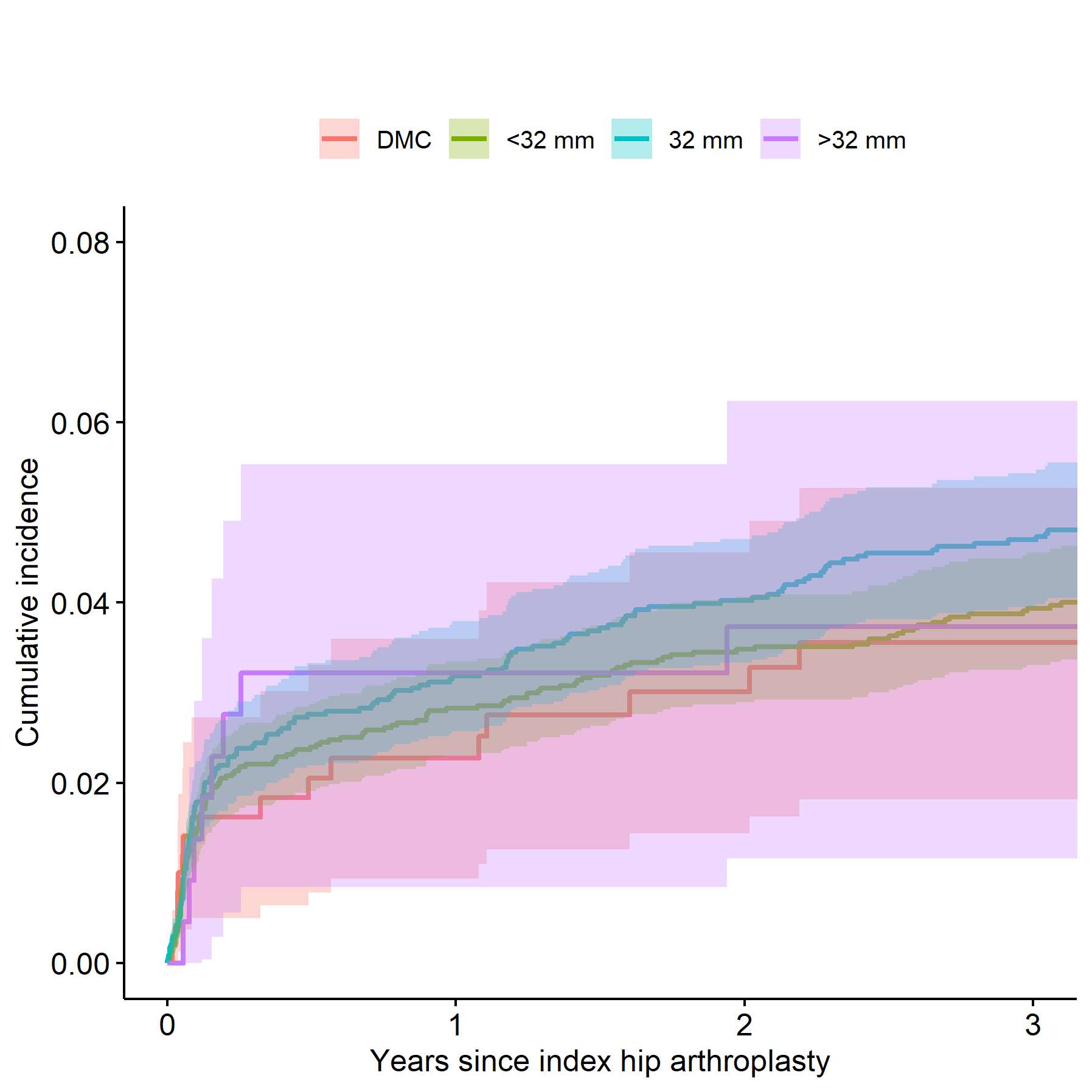
Figure 3#7713
Using Digital Image Correlation to Track Joint Fusion Micromotion in 6 Degrees of Freedom
*Callan Gillespie - Cleveland Clinic Biorobotics Lab - USA
Greg Causey - Cortical Consulting, LLC - Erie, USA
Jamey Price - Applied Medical Technology, Inc - Brecksville, USA
Robb Colbrunn - Cleveland Clinic - Cleveland, USA
Kyle Grebb - University of Notre Dame - Notre Dame, USA
*Email: gillesc2@ccf.org
Introduction: Fixation of implants to bone is essential for boney ingrowth and fusion of the bone to the implant. In bone – implant fusions motion of greater than 150 µm is associated with formation of fibrous tissue at the interface rather than bone tissue ingrowth. Conversely, bone tissue in-growth occurs at values lower than 40-70 µm. [1] As a result, it’s imperative to track these micromotions to evaluate fixation. Unfortunately, many infrared motion capture systems have noise greater than 50 µm when tracking static motions, with dynamic motion and rigid body transformations further increasing noise. [2]The aim of this study was to use a digital image capture (DIC) system to track 6-DOF kinematics of metatarsal and cuneiform bones in a cadaveric foot during a gait cycle before and after implantation of clinically relevant options indicated for mid foot fusion.
Methods: First, static data was obtained from a speckle pattern and the noise was recorded via a VIC3D DIC system (Correlated Systems) (Figure 1). Second, VIC3D output was compared to Optotrak Certus (Northern Digital, Inc.) kinematic data and VIC3D was found to be similar, but with less noise. Third, a custom, modular fiducial system incorporating 3D printed posts with 16mm x 16mm square speckle patterns [4] were screwed into the cuneiform and metatarsal bones in a cadaveric foot and tracked throughout time (Figure 2). The cadaveric foot was attached to a simVITRO® robotic testing system (Cleveland Clinic), put through a gait cycle, and DIC data was obtained. DIC kinematic data was then transformed to the bone’s local coordinate system.
Results: The second metatarsal’s superior displacement from initial position were plotted with respect to the intermediate cuneiform’s anatomical coordinate frame (Figure 3). Transformed relative motion between the bones decreased after implantation, with noise on 1 DOF approximately 50-100 µm. Further, zero phase low pass filtering was able to reduce noise to 10-20 µm.
Conclusion: DIC decreased kinematic noise and uncertainty compared to an Optotrak Certus motion capture system. This reduction was vital because noise and uncertainty are amplified when transforming kinematic data from different reference frames and comparing sensor data. DIC speckle patterns also enabled tracking within the small spaces above mid foot bones that traditional motion capture markers would not have. Physical limitations with using a VIC3D DIC system were that the systems are sensitive to lighting, reflections, the angle of the speckle pattern relative to the cameras, occlusion, and calibration errors. Some of these limitations are present in some motion capture systems. Further, DIC is often intended for strain field mapping rather than 6-DOF rigid body motion tracking. It was therefore necessary to develop custom post processing software to obtain 6-DOF rigid body motions in an anatomical coordinate system.
References: 1. Gao X et al. (2019) J. R. Soc. Interface. 16:20190259 2. Eichelberger P et al. (2016) J. Biomech. 49(2016) p2085-88 3. Windolf M et al. (2008) J. Biomech 41(2008) p2776-80 4. Causey et al. (2022) ORS Annual Meeting, Poster #1608
Acknowledgements: Applied Medical Technology
Keywords: implant instability, navigation
Figures
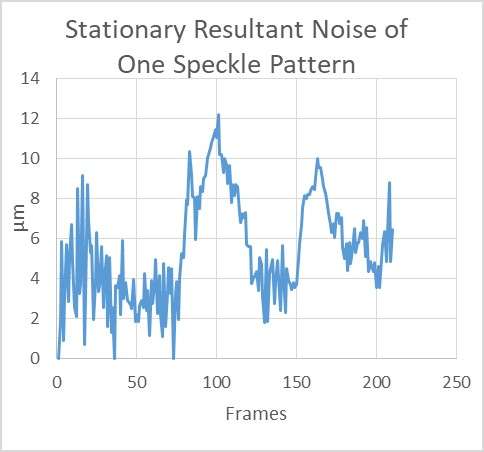
Figure 1

Figure 2
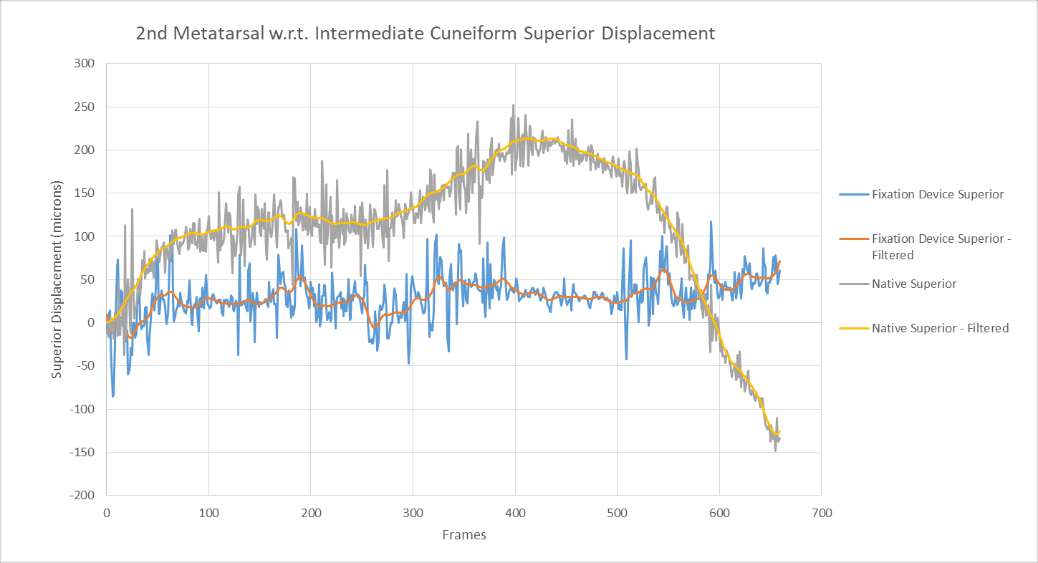
Figure 3#7719
Improving Accuracy of Multi-Axial Simulators and Testing of Orthopaedic Implants Using Sensor Fusion
*Callan Gillespie - Cleveland Clinic Biorobotics Lab - USA
Tara F Nagle - Cleveland Clinic BioRobotics - CLEVELAND, USA
Robb Colbrunn - Cleveland Clinic - Cleveland, USA
*Email: gillesc2@ccf.org
Introduction: Understanding in vivo kinematics of orthopaedic implants is an important part in evaluating performance. Simulation is often done via multi-axial mechanical simulators. As with any mechanical testing apparatus, compliance of the machine and associated fixtures are sources of uncertainty in acquiring kinematic data. Kinematic data from motion capture eliminates the influence of machine compliance, but is less reliable due to noise and visibility concerns. The aim of this study was to improve simulator kinematic accuracy by understanding and leveraging the individual benefits of machine and motion capture kinematic data in a sensor fusion algorithm.
Methods: A knee implant was tested using a robotic simulator that consisted of a pedestal base, 6-axis ATI Omega 85 load cell, and a Kuka KR300 robot. Active motion capture sensors were mounted to the femur and tibia implants and motion was measured with a NDI Optotrak Certus stereoscopic motion capture camera (Figure 1). The relative relationship of the femur and tibia coordinate systems was calculated using the Grood and Suntay knee joint coordinate system (JCS). The implant was tested using simVITRO® software by applying motions and loads specified by a standard gait profile (ISO 14243-1) and constraint test (ASTM F1223). Two versions of JCS kinematic data, measured by 1) motion capture sensors and 2) robot position, were collected throughout the tests. System compliance was calculated for each degree of freedom, as the difference in the two kinematic measurements, divided by the applied load.
Results: Differences between JCS kinematics from motion capture and robot data were identified. The measurement noise range was more favorable using robot data (5-40 µm) vs motion tracking data (60-800µm). Because robot data accuracy decreased with increasing forces, errors were therefore due to system compliance (Figure 2). Compliance was identified in several degrees of freedom, with the greatest difference between the motion capture and robot data in the inferior-superior direction and likely due to large applied compression forces. The system stiffness was calculated as 877 N/mm in the inferior-superior direction. Due to system compliance, at high loads (~2500 N) seen in the ISO standard gait profile, robot data incorrectly suggested ~3 mm of reported penetration of the femur into the tibia (Figure 3).
Conclusion: While the robot kinematic data was more precise than motion capture, it suffered from compliance induced accuracy problems. Figure 3 shows the overlap contact relationship between implant components. While motion capture based kinematic data was more accurate than robot data, it had more stochastic noise and visibility constraints. Occlusion of one or more markers on an Optotrak rigid body can shift its reported position or occlude the rigid body entirely. After completing this study, a real-time sensor fusion algorithm was implemented in the Cleveland Clinic BioRobotics lab that fuses the accuracy of motion capture with the precision of robot data. Future studies will examine the effect of this algorithm on compliance induced kinematic errors in wear testing, superposition testing, and mathematical modeling.
Acknowledgements: 360 Knee Systems
Keywords: robotics, navigation, multi-axial simulators, implant
Figures

Figure 1
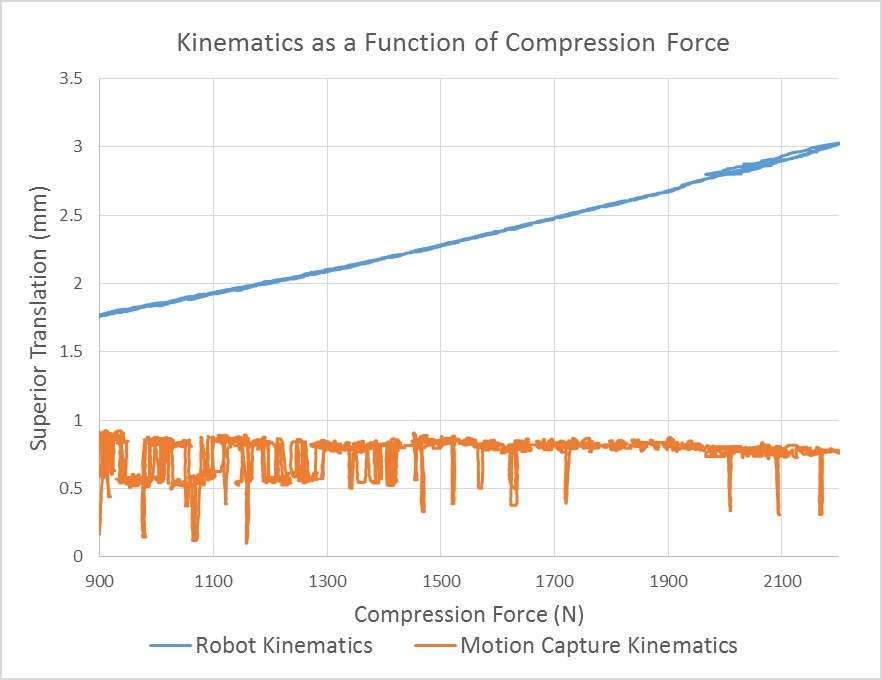
Figure 2
Figure 3#7381
Are We Able to Define the Pre-Diseased Coronal Constitutional Alignment?
*William Colyn - AZ Turnhout - Turnhout, Belgium
Axel Cleymans - UZ Leuven - Leuven, Belgium
Bruckers Liesbeth - UHasselt - Diepenbeek, Belgium
Jan Truijen
Kristof Smeets - AZ Vesalius - Tongeren, Belgium
Johan Bellemans - ZOL Genk - Genk, Belgium
*Email: william_colyn@hotmail.com
Introduction
It was thought for many years that young healthy adults had neutrally aligned knees. However, by introducing the concept of constitutional varus, this dogma was nullified. Therefore, a patient specific target must be pursued. Previous attempts to use the contralateral limb for predicting the constitutional alignment have shown us that it cannot be used effectively. The purpose of this study is to outline how to predict the original pre-diseased coronal alignment, the so-called predicted Hip Knee Ankle-angle (HKAPRED). A mathematical formula, based on independent cohorts of different arthritic stages, could in theory serve this purpose. Using such formula, it was our hypothesis that the distribution of the predicted HKA’s (HKAPRED’s) is equal to the distribution of HKAYHA’s of our young healthy adult cohort.
Methods
A radiological analysis of three cohorts was used: (1) arthritic patients with consecutive X-rays (138knees) (2) young healthy adults (355 knees) and (3) an arthritic population scheduled for primary total knee arthroplasty (99 knees). Only varus knees were included. Five alignment parameters were determined using the full-length X-rays: HKA-angle, mechanical lateral distal femoral angle (mLDFA), medial proximal tibial angle (MPTA), joint line convergence angle (JLCA) and the tibial joint line angle (TJLA). Inter-observer reliability was determined. To calculate the patient’s change in HKA-angle (∆ HKA) the mathematical formula was used: ∆ HKA = 0.61195 + ∆MLDFA*0.4065 – ∆MPTA*0.717 – ∆TJLA*0.135 + ∆JLCA*0.5378. All knees were subdivided according their CPAK-phenotype and Kellgren-Lawrence scale (KL-scale). The former formula was specified for each CPAK-phenotype. Correction-factors were calculated to integrate the degree of arthrosis (KL-scale).
Result
All measurements demonstrated a very good accuracy with an intra-class correlation coefficient for inter-observer reliability within a range of 0.877 and 0,97. The HKA-angle will increase by KL-grade (p< 0.001) from -2,47° to -10,46°. (fig. 1). There is a positive correlation between the HKA and the Delta HKA (fig. 2) (R = 0,87. R2 = 0,76). The mean HKA-angle of the YHA-adults (HKAYHA) subdivided in CPAK 1(130 knees, 37%) was 4° varus (SD,1.42°) and 1.34° varus in CPAK 2 (142 knees, 40%). In the arthritic cohort, subdivided according CPAK 1 and 2, mean HKAPRED were respectively 3,86° (SD,1,3°) and 1.68°(SD, 1,9°). The distribution of the HKAPRED’s is equal to the distribution of HKAYHA’s. Also, the 25th,50th and 75th percentiles of the HKApred and the HKAYHA are equal (table 1).
Conclusion
The most important finding from this study was that the pre-diseased coronal alignment can be predicted with an accuracy of £ 0.5°. Therefore, the KL-grade, CPAK-phenotype and four radiographic parameters should be measured on a full-length X-ray. The HKAPRED can be very useful in current clinical practice especially as the prevalance of robotic surgery in total knee surgery is on the rise. Robotic-assisted surgery could enhance surgical precision; however, this will only result in better outcomes if the correct goal is pursued. Restoring the constitutional alignment needs a tool to predict the original pre-diseased alignment. Based on these results, the specific coronal alignment target in TKA can now be calculated in 80 percent of the varus knees.
Figures
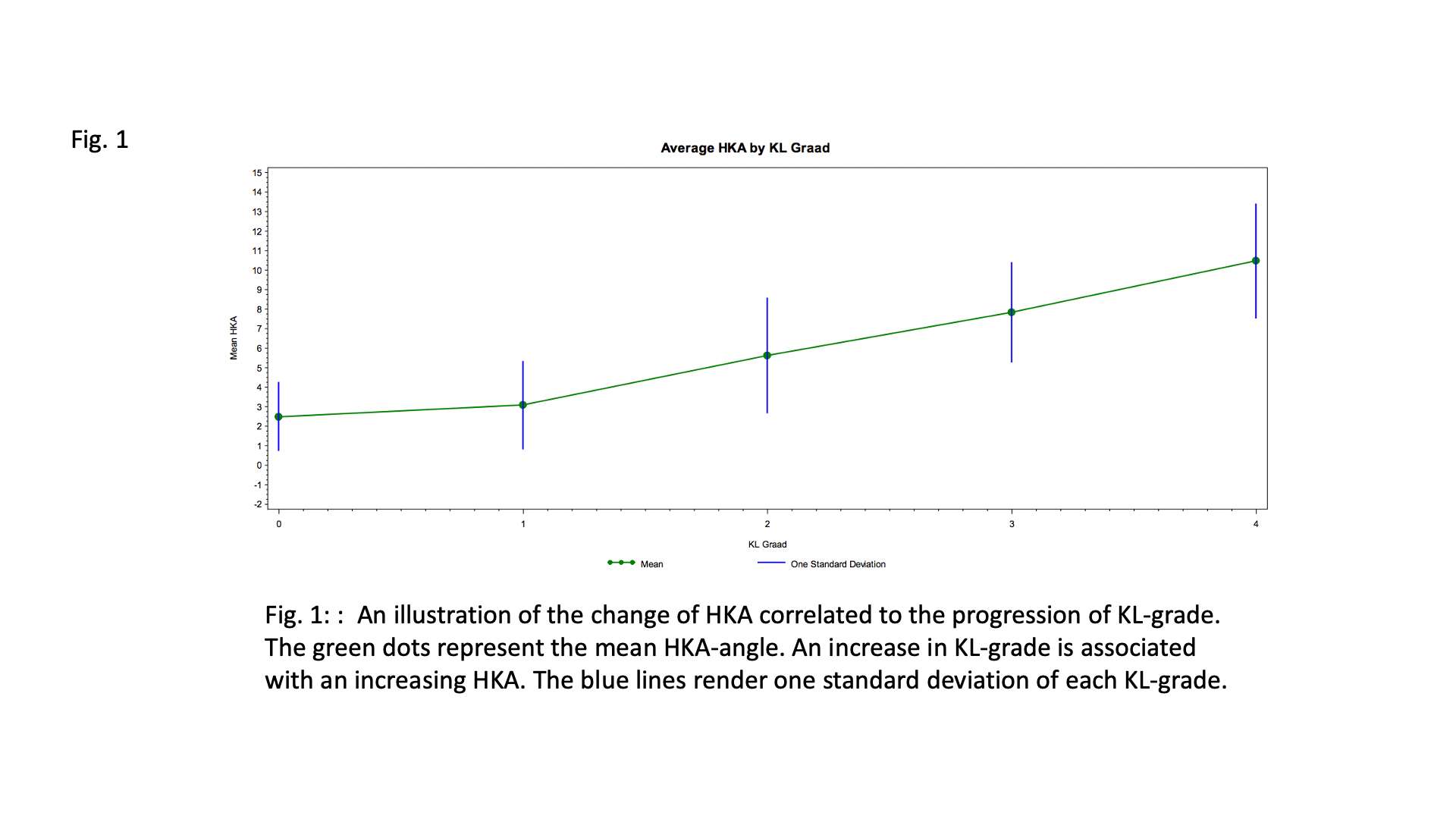
Figure 1
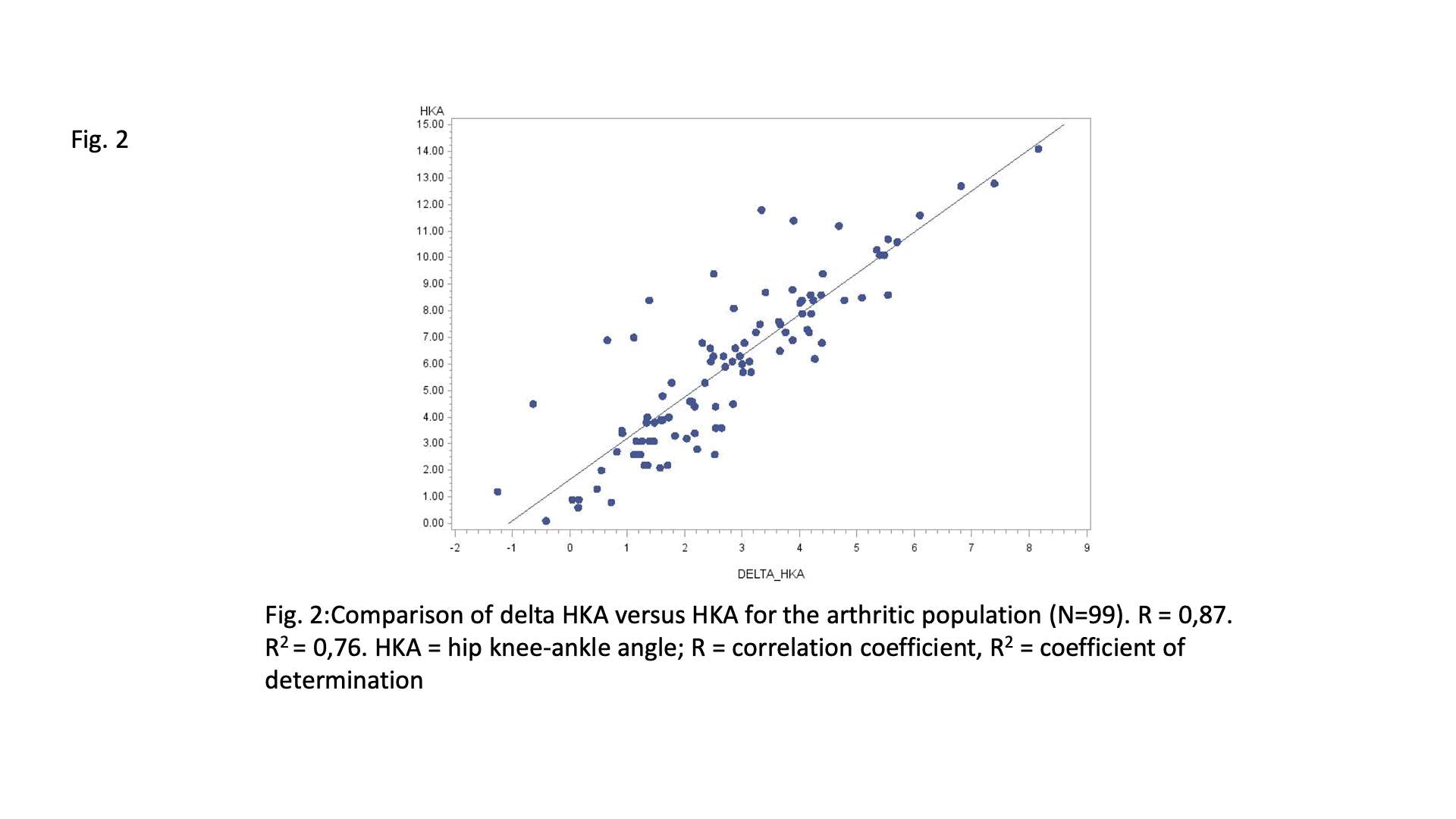
Figure 2
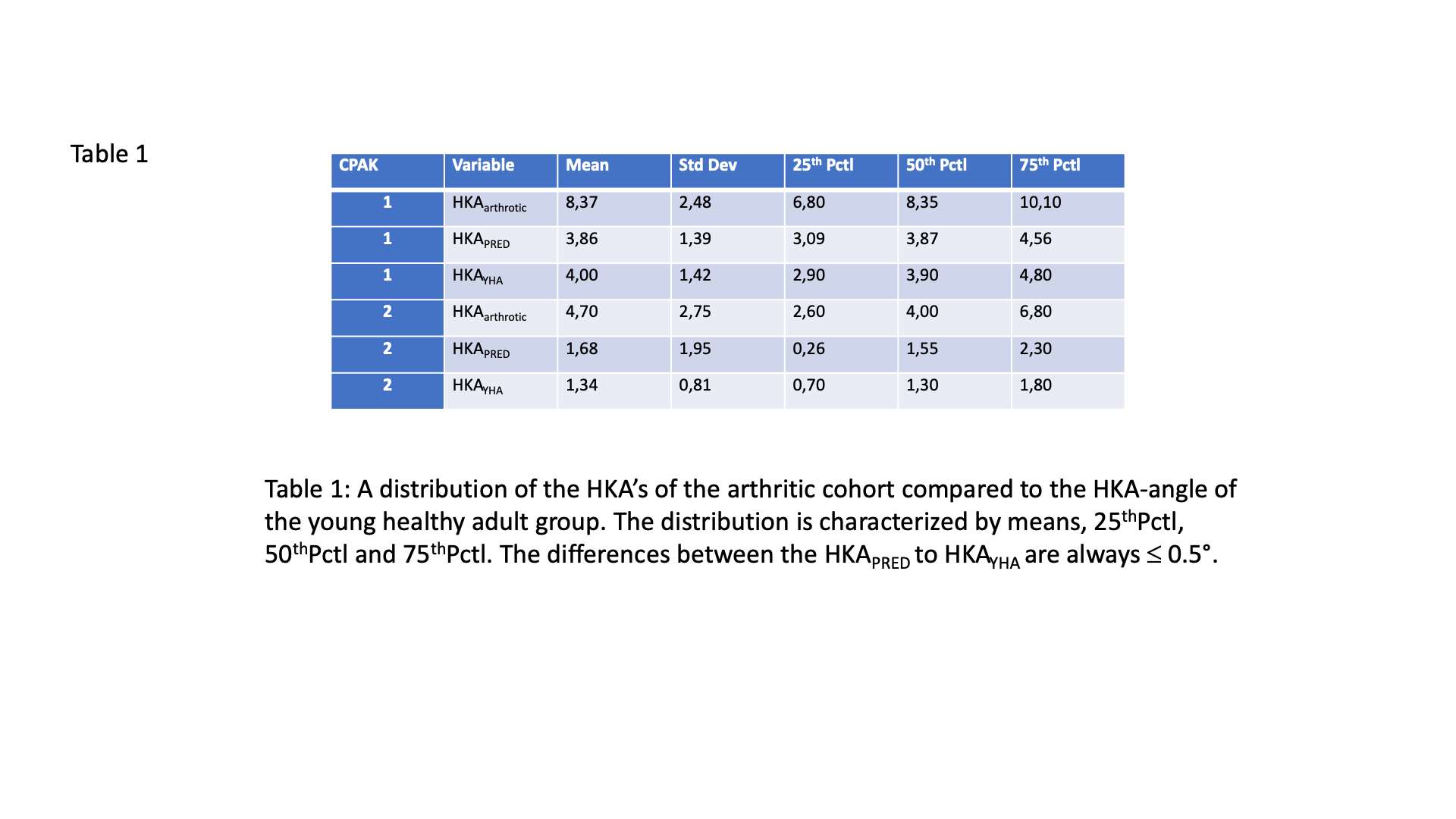
Figure 3#7683
How Does Cam/Post Geometry in TKAs Affect Contact Stress?
*Seth Coomer - University of Tennessee in Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
Bradley Meccia - University of Tennessee Knoxville - Knoxville, USA
*Email: scoomer2@utk.edu
INTRODUCTION: Minimizing contact stresses in Total Knee Arthroplasty (TKA) has been the driving force behind many TKA design changes in the past. Lower contact stress leads to lower component wear and higher implant longevity. However, it can be difficult to determine how proposed new design changes affect contact stresses in vivo. One area where orthopedic companies have made changes is the shape of the cam/post mechanism. Rounding the edges of the posterior stabilized (PS) cam/post mechanism has been done to reduce edge loading and provide lower contact stresses.
METHODS: A contact mapping algorithm has been developed to assess in vivo contact areas and stresses for two fixed bearing PS TKA systems. To assess cam-post contact, this algorithm utilizes a point cloud to represent the femoral cam geometry, while a polynomial surface is matched to the polyethylene post’s surface. The faces of the polynomial surface that the point cloud penetrates make up the contact area. A validated mathematical model is used in conjunction with this contact mapping algorithm to provide in vivo kinematics and kinetics. Using these contact forces and contact areas, contact stresses can then be calculated. To assess the effect of changing post shape a PS TKA with a flat post and PS TKA with a rounded post were virtually implanted in a subject in the mathematical model and underwent a DKB activity to 120⁰ flexion (Figure 1).
RESULTS: The shape of this post has significant effects on the contact areas and contact stresses. In early cam/post engagement the flat post TKA shows higher contact areas with an area of 85.56 mm2 at 85⁰ flexion. However, edge loading occurs as the axial rotation of the femur increases leading to a decrease in contact area with a contact area of 28.22 mm2 at 120⁰ flexion. The rounded post TKA shows a contact area of 32.54 mm2 at 85⁰ flexion, but shows an increased contact area as flexion increases, with a contact area of 52.25 mm2 at 120⁰ flexion (Figure 2). The flat post TKA shows a maximum contact stress of 38.51 MPa, while the rounded post TKA shows a maximum contact stress of 19.25 MPa (Figure 3).
CONCLUSIONS: The rounded post provided a significant decrease in peak contact stress. Although a flatter post may provide larger contact areas in earlier flexion, as axial rotation increases, the medial compartment of the post experiences edge loading, resulting in lower contact areas and higher contact stresses. These findings are consistent with other investigations into this topic [1] and supports many recent design changes which have moved to rounded posts.
REFERENCES:
[1] Toshifumi Watanabe, Hideyuki Koga, Masafumi Horie, Hiroki Katagiri, Ichiro Sekiya, Takeshi Muneta. Post-Cam Design and Contact Stress on Tibial Posts in Posterior-Stabilized Total Knee Prostheses: Comparison Between a Rounded and a Squared Design. The Journal of Arthroplasty. Volume 32, Issue 12,2017. https://doi.org/10.1016/j.arth.2017.07.010.
Figures

Figure 1
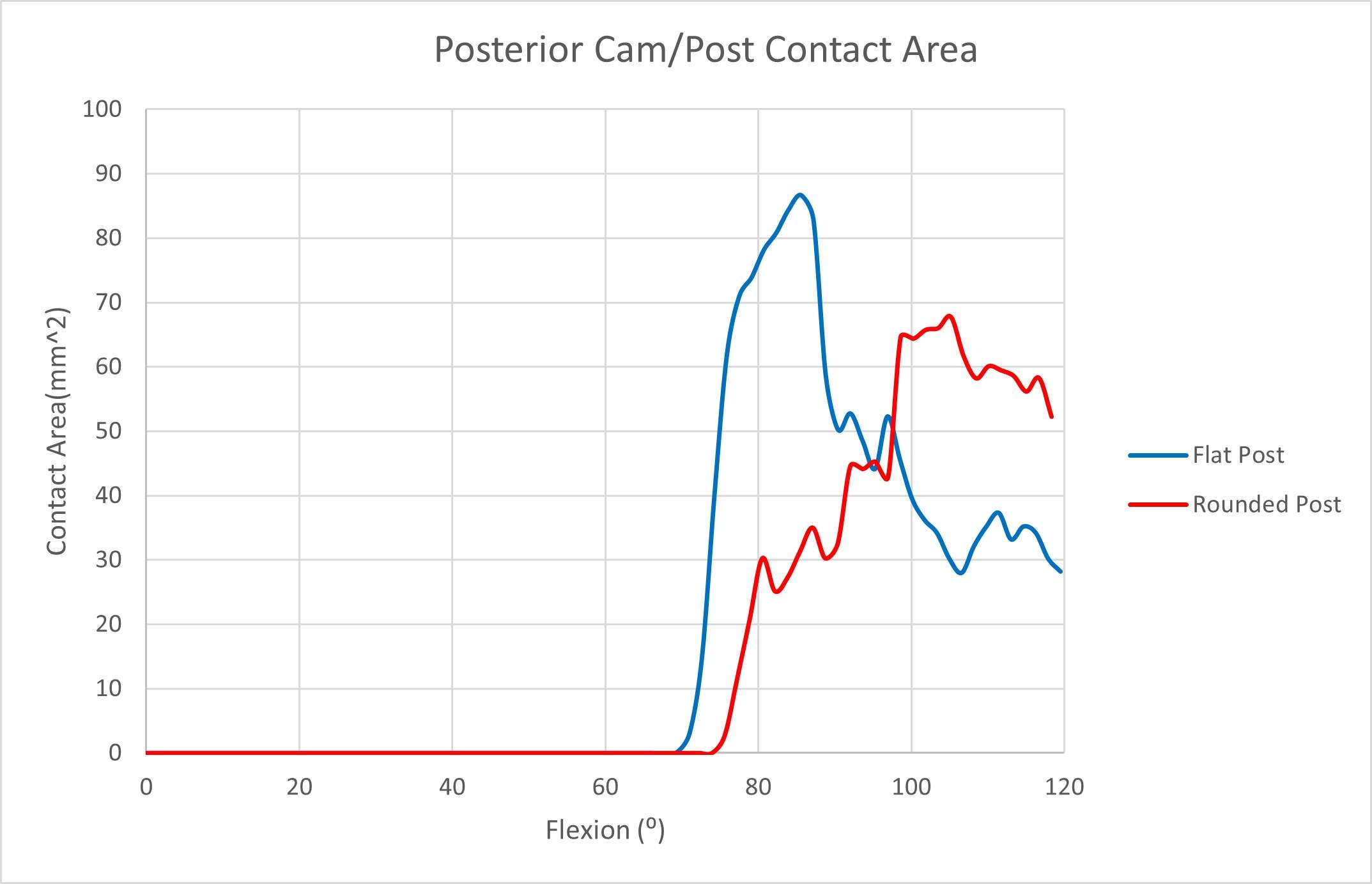
Figure 2
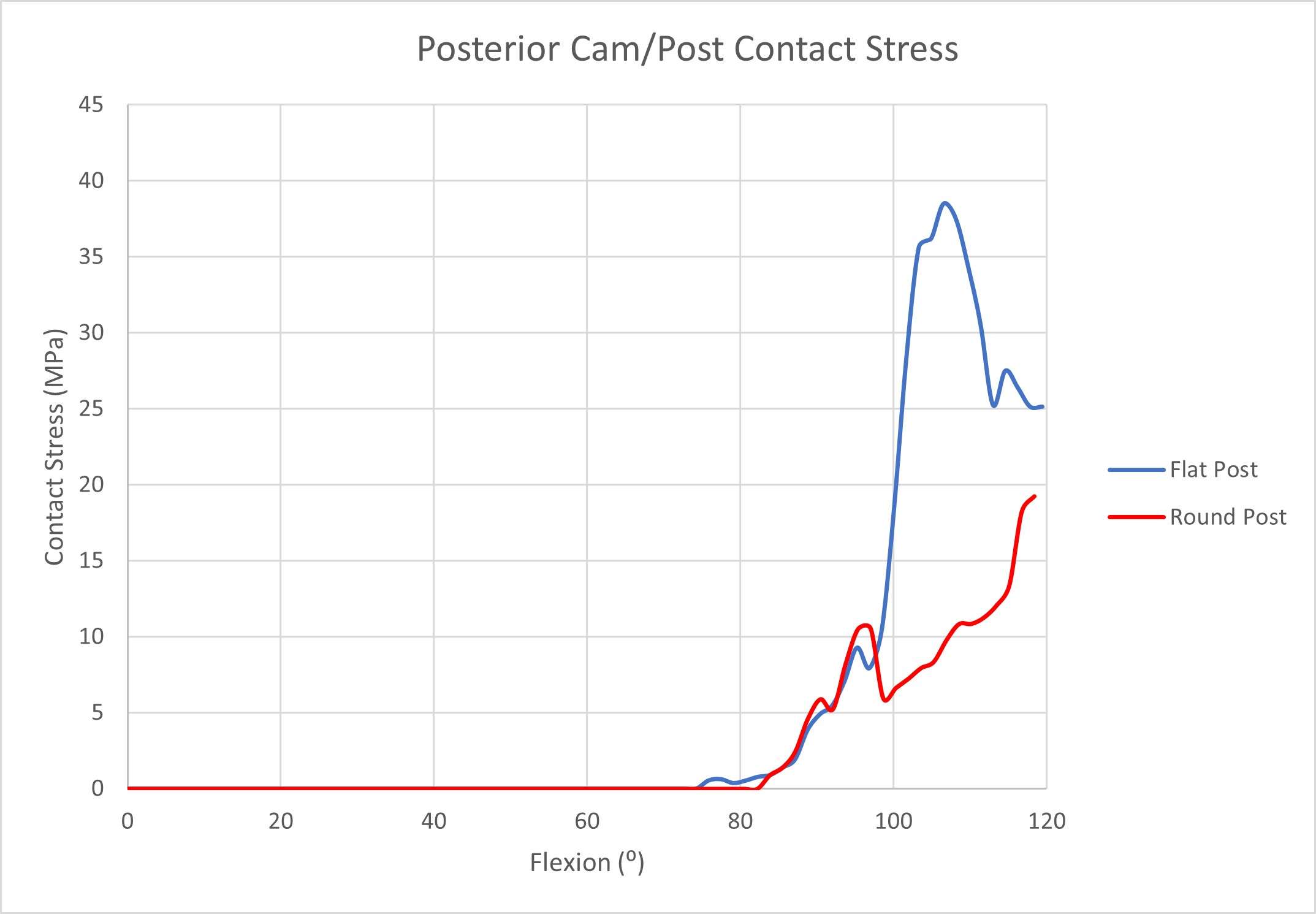
Figure 3#7688
Predicting Patient-Specific in Vivo Tibiofemoral Contact Stresses in TKAs
*Seth Coomer - University of Tennessee in Knoxville - Knoxville, USA
Bradley Meccia - University of Tennessee Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: scoomer2@utk.edu
INTRODUCTION: Component wear has long been a major factor in total knee arthroplasty (TKA) longevity and performance. However, predicting subject-specific contact stresses in vivo has proved to be a challenge. While current methods of wear testing provide valuable information, they often do not utilize accurate force profiles for in vivo activities, which can significantly vary from subject to subject. Mathematical modeling has shown great promise as a tool to predict knee kinematics and kinetics. Utilizing the kinematics and kinetics from a validated mathematical model could allow for more accurate contact area and contact stress predictions. This will allow for orthopedic companies to accurately evaluate design changes and their potential effects on component wear.
METHODS: Using a validated forward mathematical model, 10 subjects underwent a deep knee bend activity (DKB) to 120° flexion. Kinematics and kinetics were calculated for each subject. A contact mapping algorithm has been developed to predict in vivo contact areas and contact stresses. This algorithm utilizes a point cloud to represent the femoral component’s geometry, while a polynomial surface is matched to the bearing’s surface. The faces of the bearing which are in contact with the femoral point cloud create the contact area (Figure 1). The calculated contact areas, combined with the calculated tibiofemoral contact forces, can predict contact stress.
RESULTS: The average medial contact area was 201.22 mm2 at 0° flexion and steadily decreased to 104.22 mm2 at 120° flexion. The average lateral contact area was 247.54 mm2 at 0° flexion and steadily decreased to 103.28 mm2 at 120° flexion (Figure 2). Other literature has shown this decrease in tibiofemoral contact areas, with one study showing total tibiofemoral contact areas beginning at 368.22 mm2 at 0⁰ flexion and decreasing to 129.54 mm2 at 120⁰ flexion [1]. The average medial contact stress was 1.3 MPa at 0° flexion and increases to 12.1 MPa at 120° flexion. The average lateral contact stress was 1.7 MPa at 0° flexion and increases to 9.0 MPa at 120° flexion (Figure 3). Medial contact stresses were higher than lateral contact stresses, which is consistent with other literature which has shown peak medial contact forces of 22 MPa and peak lateral contact forces of 13 MPa in other implants [2].
CONLCUSIONS: Utilizing this contact algorithm in conjunction with a validated forward mathematical model has been shown to produce realistic tibiofemoral contact area and contact stress values for a deep knee bend activity in ten different subjects. Accurate contact stress calculations are vital for developing a better understanding of possible wear patterns or component life predictions, and these findings offer a faster alternative to FEA simulations and can be utilized with subject specific boundary conditions and in vivo forces.
REFERENCES:
[1] Kittipong Kitisak, et al. " Finite Element Analysis in Posterior Stabilized Total Knee Arthroplasty on Kneeling," International Journal of Pharma Medicine and Biological Sciences, 2016. doi: 10.18178/ijpmbs.5.1.67-70
[2] Sharma A, et al. High-flexion TKA designs: what are their in vivo contact mechanics? Clin Orthop Relat Res. 2007 Nov;464:117-26. doi: 10.1097/BLO.0b013e318157e478. PMID: 17975375.
Figures
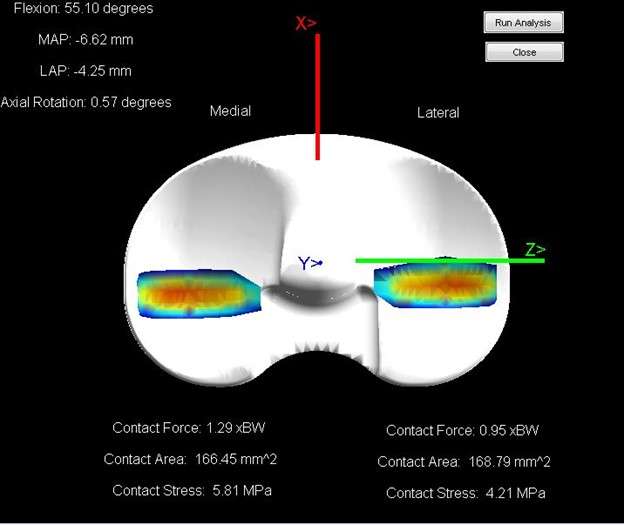
Figure 1
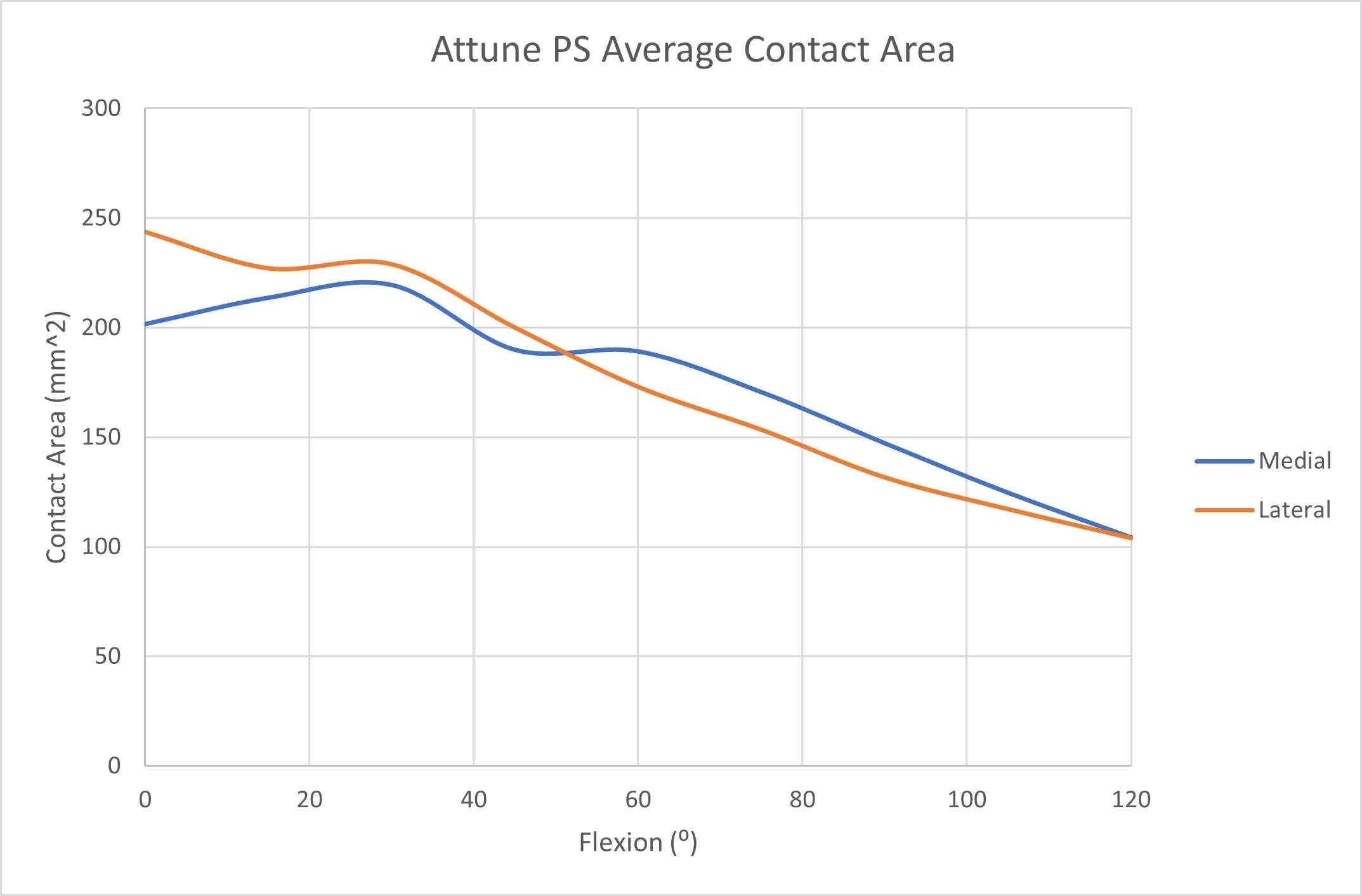
Figure 2
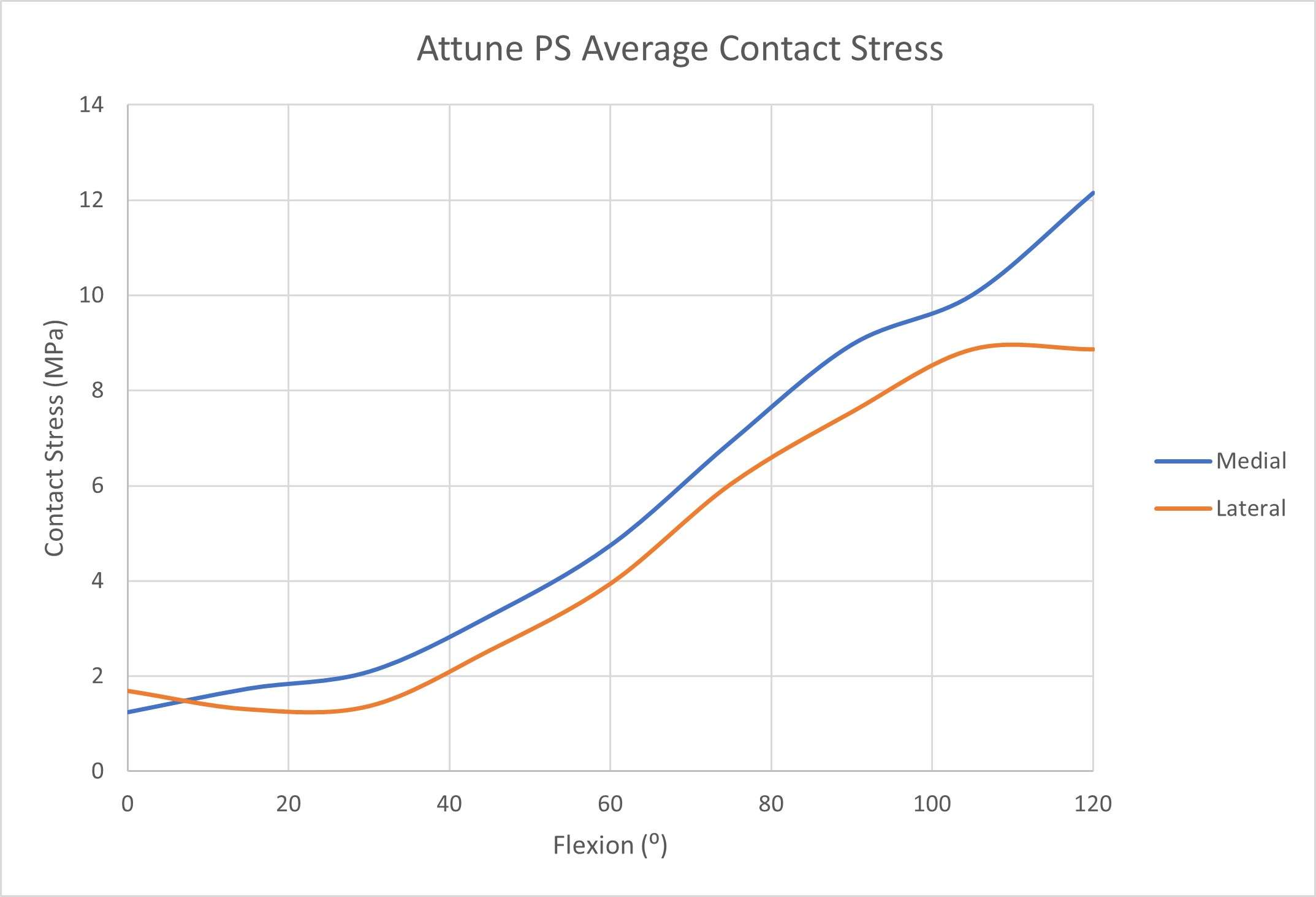
Figure 3#7357
Assessing the Wear and Kinematics of Two Medial Ball-and-Socket Total Knee Replacements, MRK and SAIPH
*Raelene Cowie - University of Leeds - Leeds, United Kingdom
Jo Cullum - MatOrtho Ltd. - Leatherhead, United Kingdom
Simon Collins - MatOrtho Limited - Leatherhead, United Kingdom
Louise M. Jennings - University of Leeds - Leeds, United Kingdom
*Email: r.cowie@leeds.ac.uk
Medial ball-and-socket total knee replacements aim to provide a more natural feeling knee with increased stability through flexion. The aim of this study was to compare the wear and kinematics of two different medial ball-and-socket total knee replacements. The MRK is an early medial ball-in-socket knee with >20 years clinical success, the SAIPH being an evolution of the original design.
Three size 8 SAIPH implants and three size 5 MRK implants (MatOrtho, UK) were investigated; these are the largest implants in the respective ranges. Prior to the start of the study the implants were set up on custom fixtures; the conventional polyethylene was aged as per ASTM F2003. The study was carried out on a ProSim electromechanical knee simulator with input kinematic and environmental conditions consistent with ISO 14243-1. The axial force (max 2800N), anterior-posterior (AP) force and tibial rotation (TR) torque was delivered through the tibial component via load control with soft tissue constraints simulated with virtual springs. The flexion/extension was position controlled. The lubricant used was 20 g/l bovine serum supplemented with 0.03% sodium azide, the temperature of which was elevated to 37 ± 2°. 6 million cycles (MC) of wear simulation was carried out with the wear of the UHMWPE tibial components assessed gravimetrically every 1MC and a loaded soak control used for compensation of moisture uptake by the polyethylene. The resulting AP translation and TR position was measured throughout the study. The mean wear rate was calculated with 95% confidence limits and statistical analysis was carried out to compare the implant designs using ANOVA with significance taken at p<0.05.
Over the duration of the 6 MC wear test the mean wear rate was 0.57 ± 0.71 and 1.24 ± 2.0 mm3/MC for the SAIPH and MRK implants respectively (Figure 1). There was no significant difference in the wear of the two implant types (p=0.24). Analysis of the output kinematics (Figure 2 and 3) shows a larger range of anterior-posterior motion for the SAIPH implant which was offset anteriorly compared to the MRK. The magnitude of the tibial rotation was low for both implants with internal rotation of the tibia with increasing flexion for the SAIPH implants.
Wear rates of both implants were very low particularly as the conventional polyethylene (non-cross-linked) was used. The magnitude of both the AP and TR motion was relatively small for both implants demonstrating the inherent stability of this design of implant particularly through flexion. The magnitude and the shape of the output kinematics was similar to investigations of the kinematics of the natural knee1. Less conforming implants investigated under similar conditions have been shown to have much larger magnitudes of motion2.
-
Andriacchi, T P., et al. "A point cluster method for in vivo motion analysis: applied to a study of knee kinematics." J biomedl eng 120.6 (1998): 743-749.
-
Johnston, H., et al. (2018). Representing the effect of variation in soft tissue constraints in experimental simulation of total knee replacements. JMBBM, 87, 87-94.
Figures
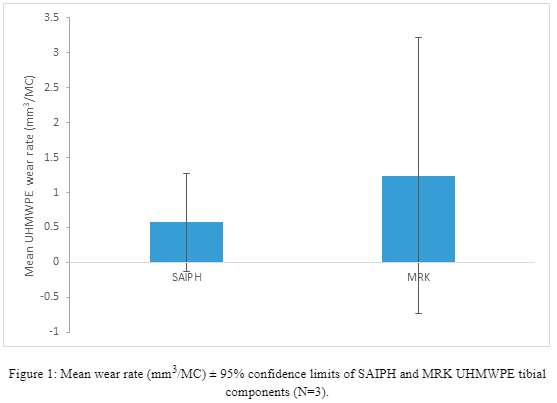
Figure 1
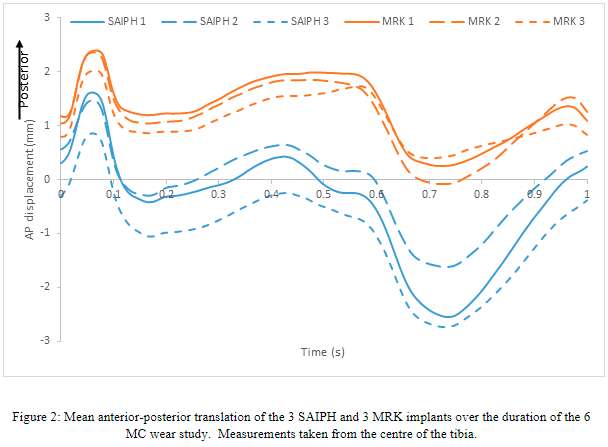
Figure 2
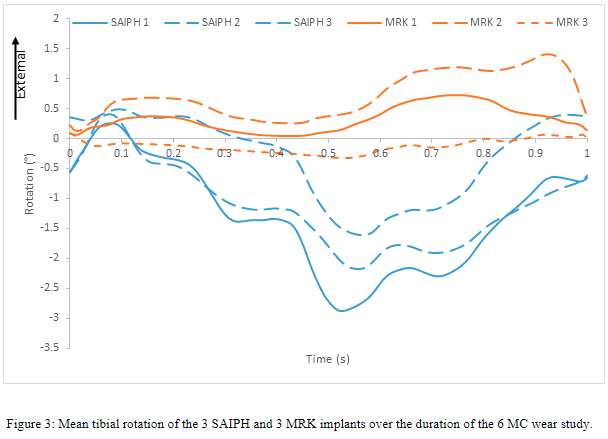
Figure 3#7577
Third Body Wear of an All-Polymer Knee
*Raelene Cowie - University of Leeds - Leeds, United Kingdom
Jens Schwiesau - Aesculap AG - Tuttlingen, Germany
Adam Briscoe - Invibio Ltd - Lytham St. Annes, United Kingdom
Louise M. Jennings - University of Leeds - Leeds, United Kingdom
*Email: r.cowie@leeds.ac.uk
Introduction
Experimental wear simulation of a PEEK-OPTIMA™ polymer-on-UHMWPE total knee replacement has shown an equivalent rate of UHMWPE wear to conventional implant materials (CoCr-on-UHMWPE).1 To date, wear simulation of this implant has been carried out in a clean environment. The aim of this study was to investigate the influence of third body particles from bone and PMMA cement on UHMWPE wear and surface topography of this all-polymer knee.
Methods
Three PEEK-OPTIMA™ polymer and three CoCr femoral components of similar initial surface topography and geometry were set up against all-polyethylene (GUR1020, conventional, EO sterile) tibial components in a 6-station ProSim electromechanical knee simulator. Initially, 1 million cycles (MC) wear simulation was carried out in clean lubricant (25% bovine serum ± 0.03% sodium azide) under displacement controlled, Leeds high kinematic conditions1 followed by 2 subsequent MC with the lubricant contaminated first with porcine bone particles, then PMMA (Palacos R&G) particles. The particles were sieved within a size range of 500-1000µm and 5mg/ml2 was added to the test cell with particles replaced at each measurement point. The loss in mass of the tibial components was determined gravimetrically every 0.3MC and converted to a wear rate using the UHMWPE density. All data is presented as mean ± 95% confidence limits, statistical analysis was carried out using one-way ANOVA to compare PEEK to CoCr with significance taken at p<0.05.
Results
The wear of the UHMWPE tibial components is shown in Figure 1 and images of the surface topography in Figures 2 and 3. In clean lubricant, there was no significant difference (p>0.05) in the wear of UHMWPE against the different femoral component materials. Scratching was visible on the PEEK implants and burnishing of the tibial components. With bone particles in the serum, there was no significant difference in wear of UHMWPE against the different femoral component materials and the wear rates were similar to those in clean lubricant. There was a high density of scratching on the PEEK implants, similar findings were not seen on CoCr. With PMMA particles, there was a dramatic increase in polyethylene wear for both implants but there was no significant difference in wear rate of UHMWPE against different femoral component materials. Scratching was visible on both femoral components and roughening of the tibial components. In the metal-on-polyethylene study, the lubricant was discoloured. There was no evidence of particles becoming embedded in the PEEK.
Conclusion
PEEK implants were more easily scratched than CoCr but under the conditions investigated, there was no significant difference in the mean wear rate of the UHMWPE components. Wear of both implants was higher with PMMA than bone particles showing that harder particles are more likely to accelerate wear. Discolouration of the lubricant in the CoCr-on-UHMWPE investigation suggests release of metal ions into the lubricant, it is not known whether PEEK particles were also removed from the implant surface.
- Cowie RM, et al. 2016, JEIM, 230(11):1008-1015.
- Schroeder C, et al. 2013, J Mater Sci: Mater in Med 24(5):1319-1325.
Acknowledgements: Implants provided by Maxx Orthopedics Inc
Figures
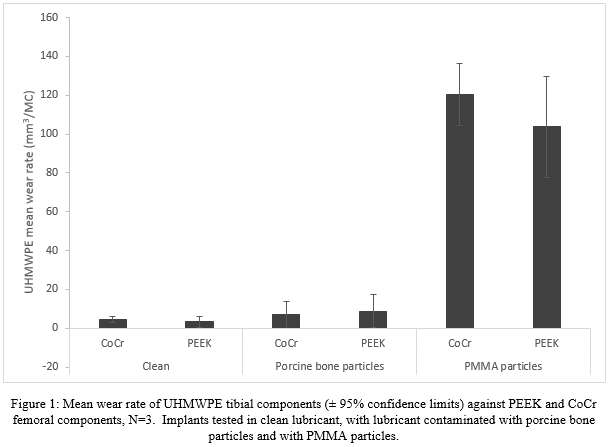
Figure 1
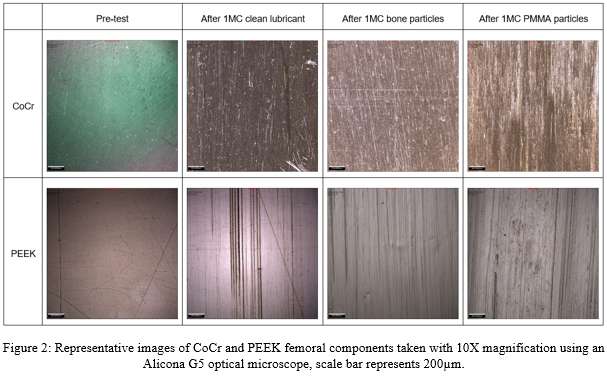
Figure 2
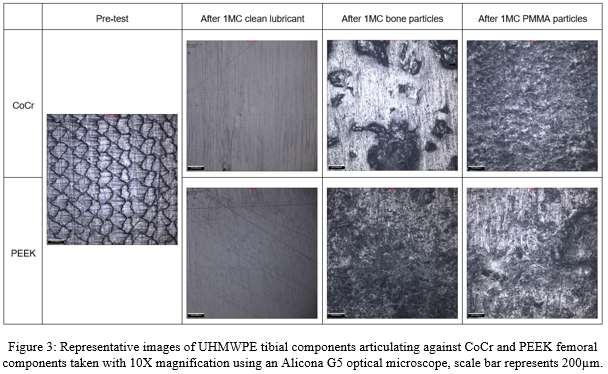
Figure 3#7709
In Vivo Arthrokinematics and the Potential Role of Implant Alignment in Total Wrist Arthroplasty
Bardiya Akhbari - Harvard Univ - Boston, USA
Amy Morton - Brown University - Providence, USA
Douglas Moore - Brown University - Providence, USA
Kalpit Shah - Brown University - Providence, USA
Janine Molino - Brown University - Providence, USA
Arnold-Peter Weiss - Brown University - Providence, USA
Scott Wolfe - HSS - New York, USA
*J.J. Trey Crisco - Brown University - Providence, USA
*Email: joseph_crisco@brown.edu
Introduction: Total wrist arthroplasty (TWA) is a treatment of unrealized potential. Because of unacceptably high failure rates, TWA has been viewed as an alternative to arthrodesis only for low-demand patients. In contrast, hip and knee arthroplasty, which utilize the same metal-on-polyethylene bearing surfaces, are extremely successful and implemented widely. A key difference is that hip and knee replacements have been refined by decades of testing and evaluation, while there are no comparable datasets on wrist arthroplasty. Thus, the aim was to determine the in vivo arthrokinematics and the role of implant alignment of TWA during activities of daily living that we hope will provide new insight and eventually assist with future designs and pre-clinical testing.
Methods: Six patients (74.7 ± 5.6 yrs) with size 2 Freedom® TWA implants (Integra LifeSciences) provided informed written consent after IRB approval. Radiographic images of the wrists and clinical outcomes were recorded. A computed-tomography (CT) scan of each wrist was acquired. Biplane videoradiography (BVR) captured dynamic implant motion at 200 Hz. Each participant performed 5 tasks: flexion-extension, radial-ulnar deviation, circumduction, simulated hammering, and simulated pitcher pouring. Outcome measures included 1) center of contact (CoC) between components, 2) component alignment using radiographs and CT, and 3) TWA ROM. Radiographic measurements were validated using Bland–Altman analysis. Linear regression assessed the associations between alignment and wrist ROM.
Results: CoC at neutral posture was not at the geometric centers but was located 3.5 mm radially on the carpal component and 1.2 mm ulnarly on the radial component. From extension to flexion, the CoC moved 10.8 mm from dorsal to volar side on the carpal component and 7.2 mm from volar to dorsal on the radial component. From radial to ulnar deviation, the CoC moved 12.4 mm from radial to ulnar on the carpal component, and 5.6 mm from ulnar to radial on the radial component. Radiographic measures of alignment had a 95% limit-of-agreement of 3 degrees and 3mm with CT values. Wrist flexion–extension and radial–ulnar deviation were highly correlated with volar–dorsal tilt and volar–dorsal offset of the radial component and demonstrated a ROM increase of 3.7 and 1.6 degrees per degree increase in volar tilt, and 10.8 and 4.2 degrees per millimeter increase in volar offset. The carpal component’s higher volar tilt was also associated with improvements in patient-reported pain.
Conclusions: We found that articular contact patterns of TWA were a function of the direction of wrist motion. Although we hypothesized that the CoC moves along the principal arcs of curvature, our assessment showed that the CoC are primarily restricted to the radial side of the convex surface of the carpal component and the ulnar side of the concave surface of the radial component. We also found the volar tilt and volar offset of the radial component strongly influenced wrist ROM. Future studies must evaluate these finding in a larger cohort and in a longitudinal study design to determine the impact of these factors on the survival success of TWA.
Acknowledgements: AFSH and NIH-P30GM122732
#7998
Evaluating the Effect of Anatomical Loading Scenarios on the Fixation Evaluation of Anatomical Shoulder Glenoid Implants
*David Cunningham - University of Western Ontario - London, Canada
Cole Fleet - Western University - London, Canada
Devin Ferguson - St. Joseph’s Hospital/HULC - London, Canada
George Athwal - University of Western Ontario - London, Canada
James Johnson - SJHC - London, Canada
*Email: dcunni9@uwo.ca
Introduction:
Fixation is an important outcome measure in the evaluation of shoulder implants. The ASTM F2028 standard for the dynamic evaluation of glenoid loosening and disassociation outlines criteria for the quantification of the initial fixation of glenoid implants. To date, studies evaluating bone-implant fixation have employed loading protocols mostly isolated to simulating forces in the local coronal plane as a proxy to evaluate bone-implant relative motion when the maximum shear load in a normal shoulder is naturally sustained. This experimental study was conducted to determine if additional loading protocols are also warranted during the evaluation of glenoid baseplate primary stability. The objective of this study was to evaluate the effects of loading magnitude and load direction that not only characterize the objective ASTM-suggested inferior-superior shear load (0.42*BW in shear, 0.51*BW in compression), but also those that represent a clinically relevant range of activities of daily living.
Methods:
Five human cadaveric scapulae (male, 83±11 years) were implanted with keeled polyethylene glenoid baseplates (Olympia™ Total Shoulder System, Wright Medical Group) using bone cement. An optical machine vision USB3 camera (acA4096-30uc, Basler AG, Ahrensburg, SH, Germany) outfitted with a c-mount premium lens (FL-BC3518-9M, Ricoh Canada, ON, Canada) was used in conjunction with ProAnalyst ® to measure relative bone-implant motion at the inferior edge of the glenoid component. Five separate loading scenarios were employed. These included 4 loading conditions intended to approximate those experienced during daily living, as well as the ASTM-suggested standard loading protocols for the S-I direction. A custom designed synchronously loaded 3-dimensional loading apparatus was employed.
Results:
The mean relative bone-implant displacements ranged from [0.113 mm – 0.031 mm] (Figure 1) over all loading cases, indicating a limited variability in the response to loading states developed at the glenoid. It was noted that the no-weight forward-flexion motion caused similar bone-implant displacements to the ASTM inferior-superior profile. An ANOVA test resulted in only slight statistically significant differences in bone-implant relative motion at the glenoid baseplate-bone interface (p = 0.049), but no relative bone-implant displacements were larger than those experienced by the ASTM-suggested worst-case scenario values. These results suggest that the existing method of evaluating fixation of polyethylene glenoid baseplate designs is ultimately sufficient, but may benefit from replicating anatomically relevant loading scenarios, as the varied loading magnitudes and directions ultimately result in slightly different levels of liftoff at the inferior edge of the glenoid baseplate; dependent on the load profiles utilized.
Conclusion:
The precedent methods of evaluating the efficacy of (polyethylene) glenoid components are sufficient in representing the worst-case scenarios in an adequately wide range of activities that might be experienced by a patient post-surgery. The results of this investigation validate the existing suggested loading protocols in the evaluation of the fixation of polyethylene glenoid baseplates. Further work is needed to determine if the testing of implants with metal baseplates and reversed shoulder arthroplasty components follow similar patterns.
Figures
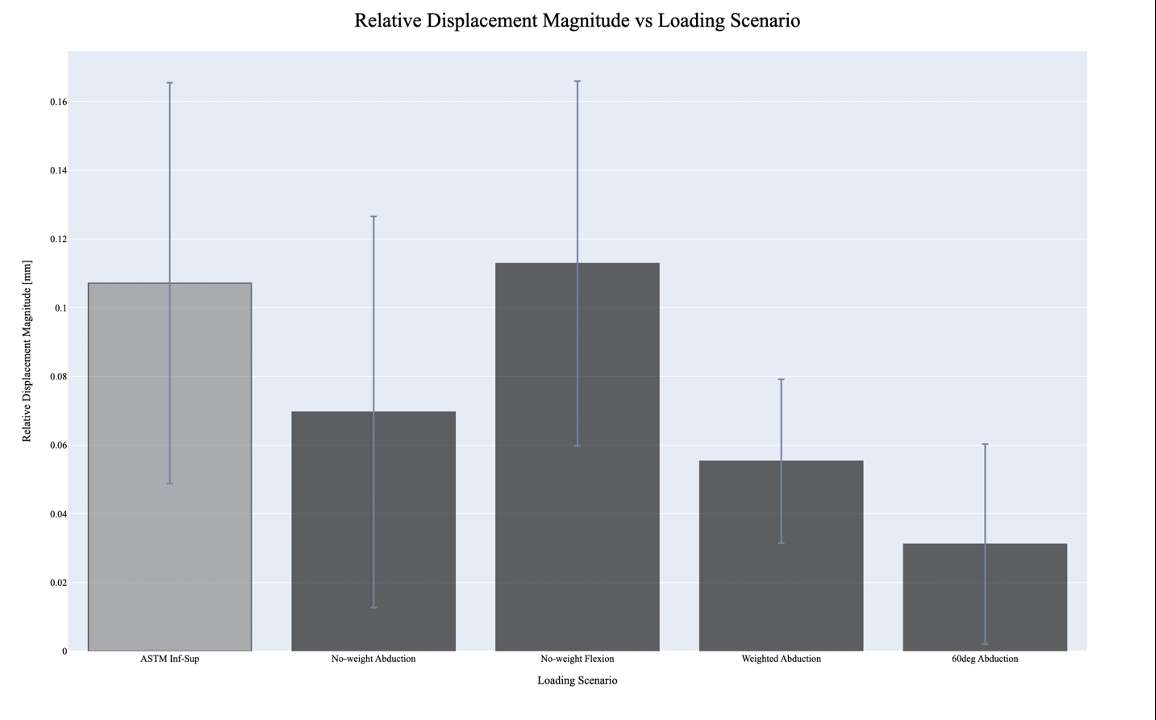
Figure 1#7930
Fracture and Fatigue in Highly Cross-Linked UHMWPE
*Barbara Currier - Dartmouth College - Hanover, USA
Kori Jevsevar - Dartmouth College - Hanover, USA
Rebecca Thomson - Dartmouth College - Hanover, United States of America
Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: barbara.h.currier@dartmouth.edu
Introduction
Early time rim fracture of highly cross-linked (HXL) acetabular liners was shown to result from overly vertical cup placement combined with local stress-concentrators. Analysis of retrieved HXL liners and inserts over time has shown fracture and fatigue occurring in both acetabular liners and tibial inserts. Historically, oxidation was shown to correlate with decreased mechanical properties in shelf-aged, never-implanted and retrieved gamma-air sterilized UHMWPE, explaining fatigue and fracture seen in those retrievals. The questions explored in this study are:
- Does increasing oxidation in HXL retrievals from time in vivo effect UHMWPE mechanical properties?
- What factors contribute to fracture/fatigue damage in HXL liners and inserts?
Methods:
An IRB-approved retrieval database identified HXL acetabular and tibial inserts (n=354), received at retrieval from 2016 to the present. The 229 remelted and 125 annealed retrievals with in vivo time of 0-19.3 years were rated for clinical damage as received, and analyzed for oxidation within 3 months of retrieval using a Thermo-Scientific iN10-FTIR microscope. Oxidation was reported as maximum ketone oxidation index (KOI). Tibial insert retrievals of sufficient size and thickness (n=13) were evaluated for mechanical properties by uniaxial tensile testing of 200-micron thin sections (n=10-15, dependent on initial thickness of the insert), cut parallel to the insert non-articular surface with a microtome and stamped into ASTM Type V samples. Testing was performed on an Instron 5544 load frame equipped with a 2-kN load cell, pneumatic sample grips, and video extensometer. Statistical analyses used SPSS, with p-value <0.05 considered statistically significant.
Results:
Thirty-one HXL liners and inserts in this cohort either exhibited cracking and/or delamination fatigue at retrieval or fractured in vivo (Fig.1). Fracture and fatigue occurred in both remelted and annealed retrievals (Fig.2). Occurrence of fatigue/fracture correlated with maximum KOI (Spearman rho=0.323, p<0.001), time in vivo (Spearman rho=0.288, p<0.001) and patient BMI (Spearman rho=0.111, p=0.042). Mean time in vivo for the occurrence of fatigue/fracture was 8.9±3.2 years. Oxidation increased with time in vivo (Spearman rho=0.506, p<0.001), with knees oxidizing more rapidly than hips (knees=0.162/year, hip=0.082/year, p<0.001, Fig.3). Ultimate tensile strength (UTS) and/or elongation at break (EaB) in both remelted and annealed HXL UHMWPE decreased with increasing oxidation.
Discussion:
Consistent with earlier studies, these HXL implants oxidized over time in vivo. Oxidation has been shown to adversely affect mechanical properties in historical gamma-air sterilized UHMWPE, where critical oxidation (KOI=1.2) led to loss of UHMWPE strength and ductility. Oxidation appears to have similar effects on HXL UHMWPE, answering the first question explored in this study. However, more retrievals with a larger range of oxidation are needed to firmly establish trends of mechanical properties by material.
Knees in this cohort oxidized more rapidly than hips, and fatigue/fracture occurred more frequently in knees (11%) than hips (6%), suggesting that stress may be a contributing factor to both oxidation and fatigue/fracture. As HXL materials have longer time in vivo, the potential for bearing fatigue/fracture increases with increasing oxidation and cycles of use. Additionally, device design, patient factors, and implant placement/alignment all have potential to affect the performance of implants.
Figures
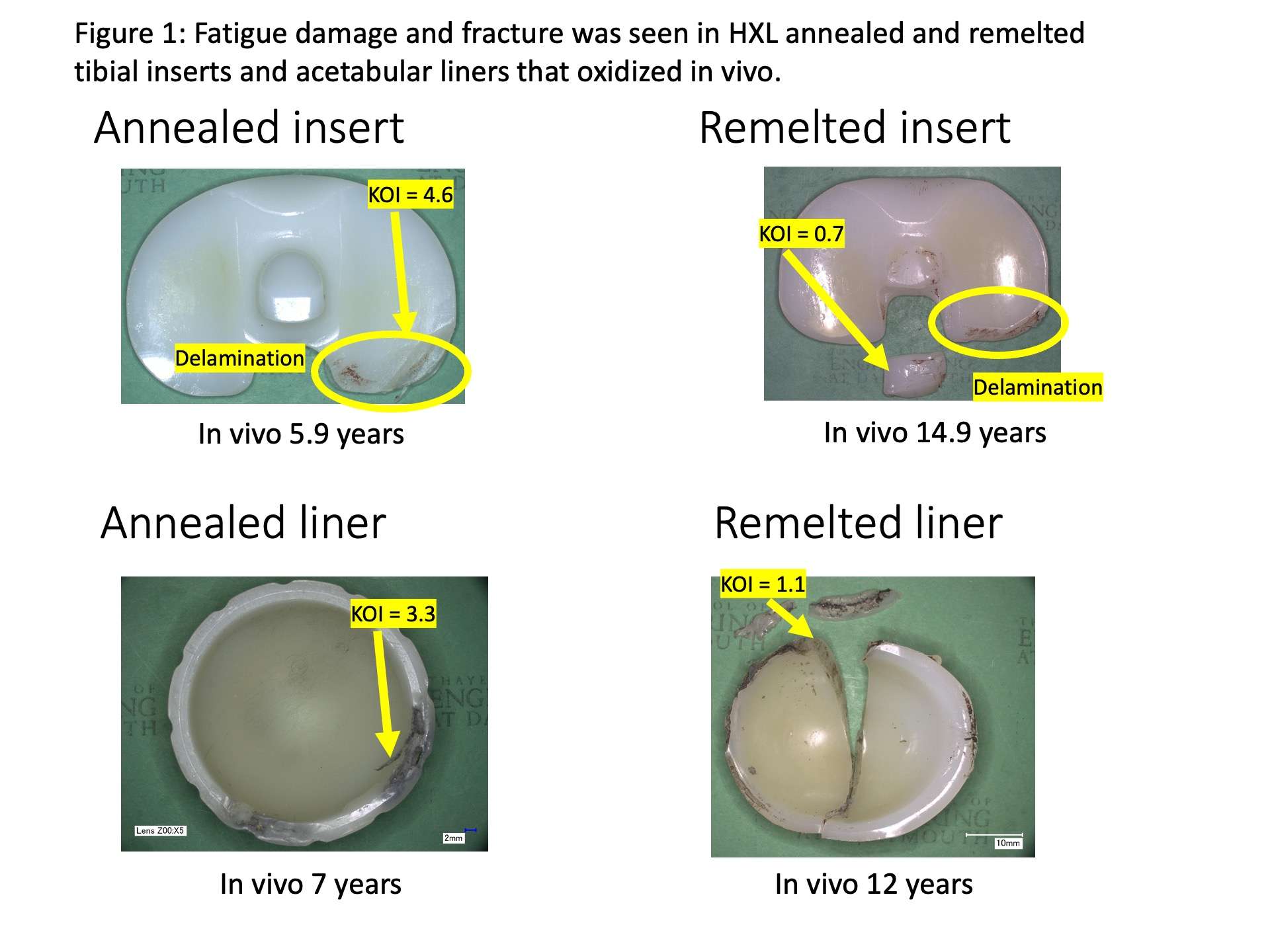
Figure 1
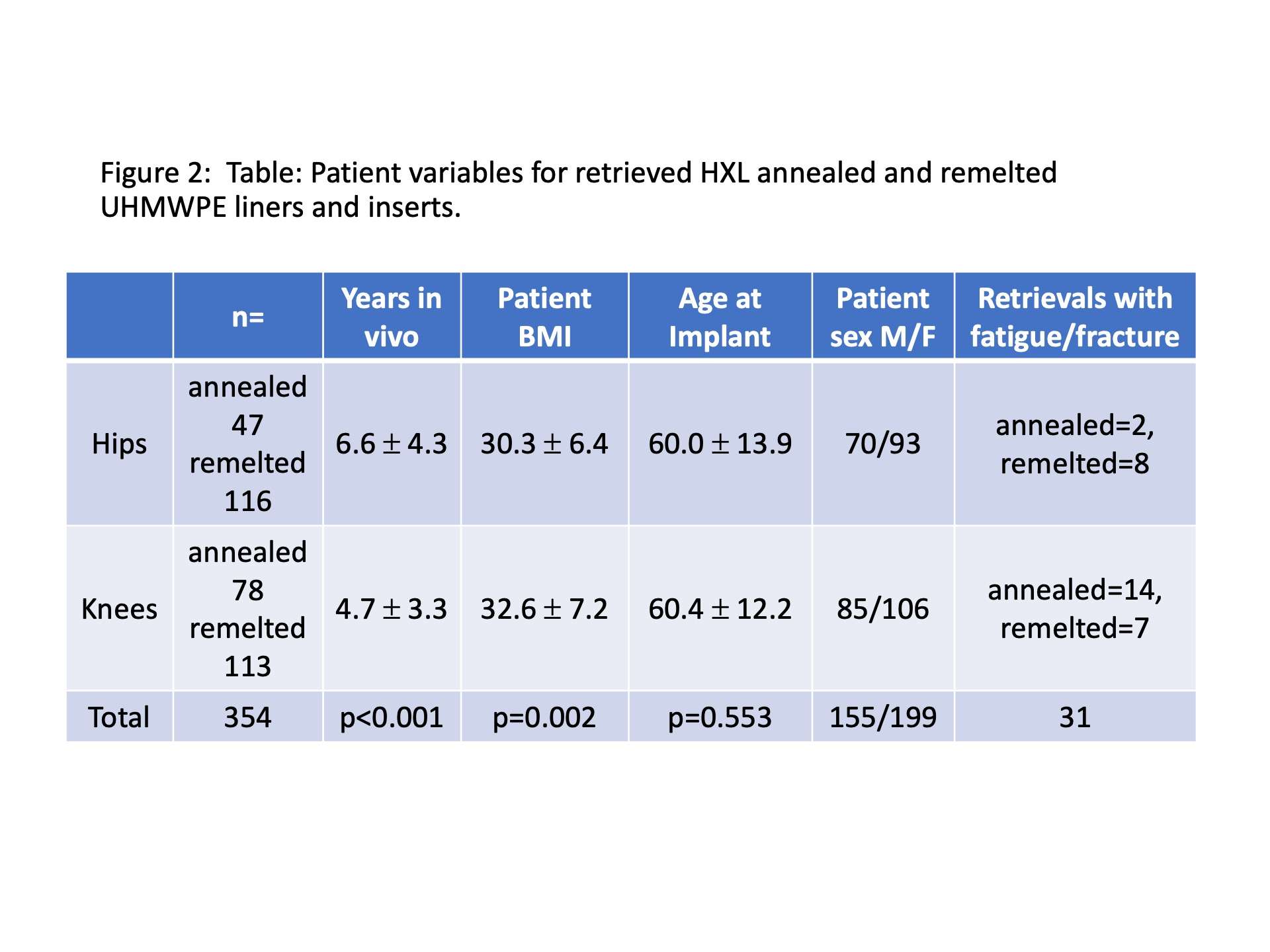
Figure 2
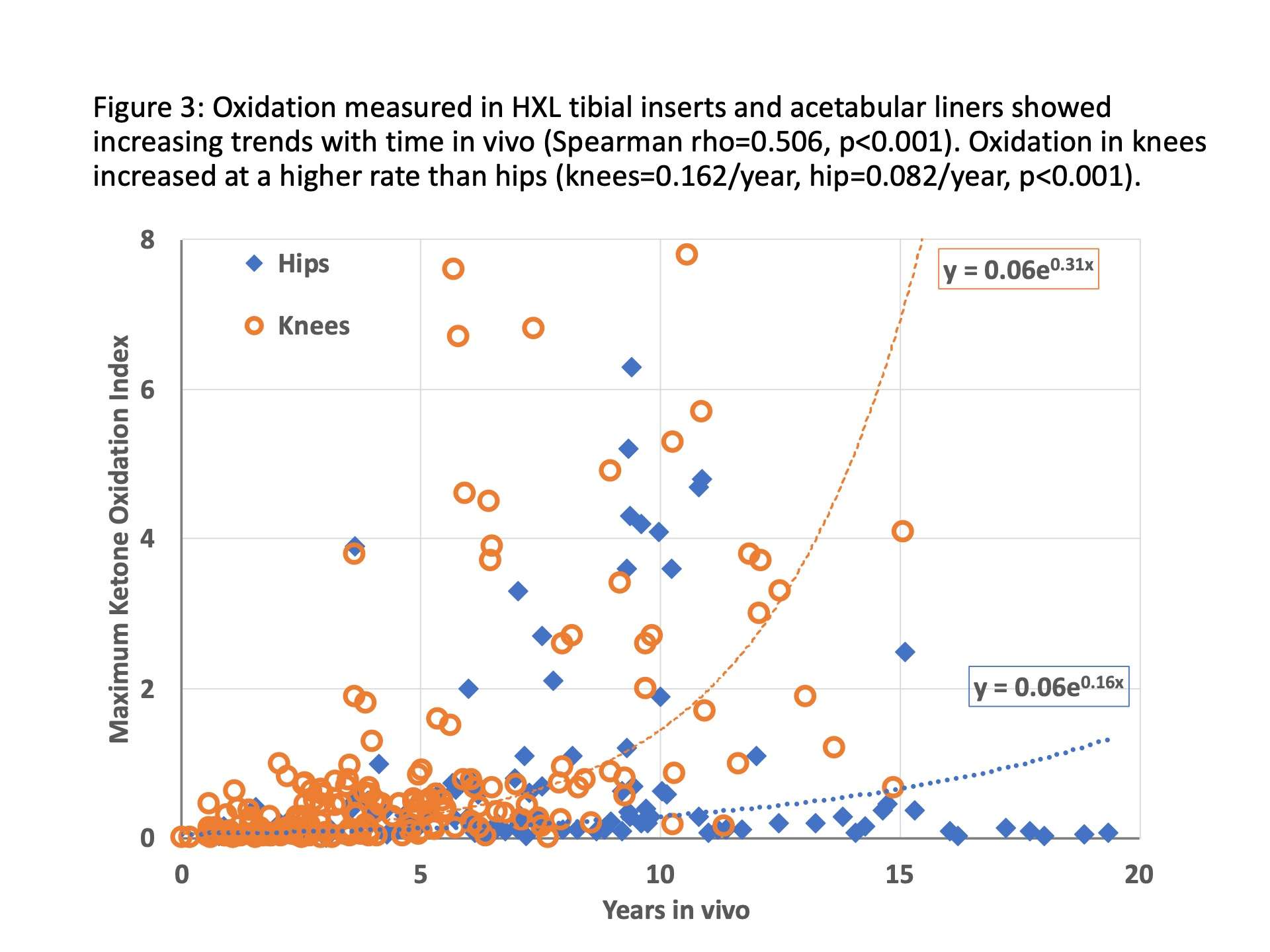
Figure 3#7650
Activity Recognition in Remote Patient Monitoring for Total Knee Arthroplasty
*Kaitlin Carroll - United States of America
Felix Chan - Canary Medical - Carlsbad, USA
David Lee - Canary Medical - Carlsbad, USA
Esther Hsu - Canary Medical - Carlsbad, USA
Barbara Elashoff - Canary Medical - Carlsbad, USA
Patrick Aubin - Canary Medical - Carlsbad, USA
John Savage - Canary Medical - Carlsbad, USA
William Hunter - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
Introduction: The COVID-19 pandemic has triggered a marked rise in the use of telemedicine to evaluate patients following total knee arthroplasty (TKA). The purpose of our study was to identify and quantify patient activities using a novel stem with an embedded sensor that can remotely and objectively monitor a patient’s mobility following TKA.
Methods: An analysis was performed on the data (consisting of 3-axis acceleration and 3-axis angular velocity) coming from 71 knees (68 patients) who underwent a primary TKA with a smart tibial extension (STE) implant. Principal component analysis (PCA) was done to align the axis of the sensors with the tibia [Figure 1]. A sensor fusion technique transformed measurements observed in the sensor’s frame of reference to measurements as observed on earth. As a result, 3D angular movement of the tibia could be visualized and quantified [Figure 2 and Figure 3]. Activities were then identified based on orientation of the device with respect to earth’s gravity and the angular range spanned by the activity.
Results: Five activities were identified based on their differences in the tibia’s orientation and range of motion including: level walking, turning, leg raising, knee extension, and heel sliding. For example, the angle relative to gravity typically ranges from -40 to 40 degrees for level walking, 80 to 160 degrees for leg raising, -10 to 80 degrees for knee extension, and 20 to 80 degrees for heel sliding. Relevant metrics such as functional range of motion, cadence, and turning speed were also determined. For example, cadence for leg raising activity is typically 4-5 repetitions over 10 seconds.
Conclusion: These results confirm signals generated from embedded sensors, analyzed appropriately, can provide insights into patients’ activities post TKA. Such insights could be valuable to doctors to remotely monitor their patients’ recovery.
Figures
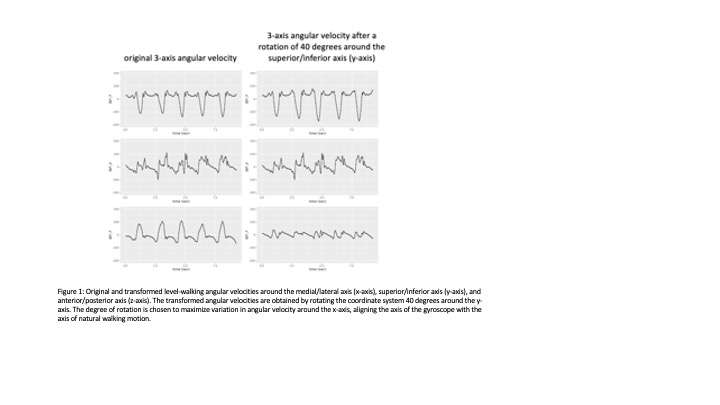
Figure 1
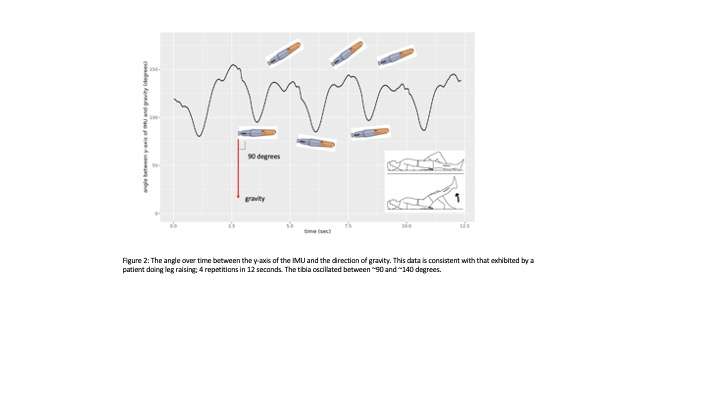
Figure 2#7659
Bone Loss Following Revision of Cemented Stems- Dependent on Technique ?
*Kaitlin Carroll - United States of America
Jeffrey Yergler - South Bend Orthopaedics - South Bend, USA
James C Ballard - Regnerative Orthopedic Center - Portland, USA
Kevin Gemmell - Canary Medical - Carlsbad, USA
Peter Schiller - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
Introduction: While standard cement techniques are most commonly used during total knee arthroplasty (TKA), often times surgeons will elect to use a full cemented stem in high risk populations. The primary objective of this study was to evaluate the degree of tibial bone loss at the time of revision surgery between a standard component with a short (30 mm) stem versus a longer sensor enabled tibial stem extension (seTE) (58mm).
Methods: Six cadaveric specimens (12 knees) were used a primary TKA performed by two surgeons. The specimens were considered to be high risk for bone fracture both by DEXA T-Score and clinical assessment. Four posterior stabilized (PS) TKA designs with + 30 mm stem tibial constructs with standard cementation, four PS TKA with seTE implant constructs with standard cementation, and four PS TKA with seTE with full cementation implant constructs were used. Primary total knee arthroplasties (tibia only) were performed and the specimens set for 30 minutes to allow cement to cure. Following the 30-minute cure time, the tibial construct of each specimen was removed. After removal, each surgeon visually assessed bone loss and each specimen underwent fluoroscopic imaging. All fluoroscopic images were reviewed for bone loss by an independent radiologist. Comparisons of the pre TKA and post implant removal images were assessed in anteroposterior and lateral views using standard grading criteria (Table 1).
Results: All specimens were documented to have poor bone quality, but the use of the seTE was proven to be clinically-acceptable without increased bone loss or risk of an unsuccessful revision. While the seTE construct is 28mm longer, there was no significant bone loss upon removal with either cement technique as noted by the radiologic and visual assessment of bone loss (Table 2). The use of full cement did not increase the risk of bone loss during removal compared to the standard technique as noted in the radiologic comparison. There were no differences between the two techniques with either construct. There was no cortical bone perforations on any specimen post-removal. All revision TKAs were performed successfully for both constructs and cement techniques (Table 3).
Discussion: Our findings demonstrate that the use of a longer tibial stem with a seTE construct did not increase bone loss upon removal, and a successful revision can be performed in a population at high-risk for fracture and bone loss. Successfully completing this study with osteoporotic specimens further suggests that the use of the seTE does not increase the bone loss or fracture risks during removal in the range of normal to high-risk populations compared to a shorter tibial stem.
Figures
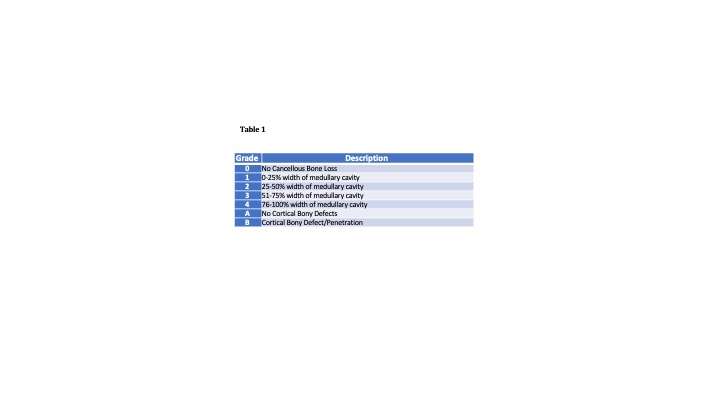
Figure 1

Figure 2
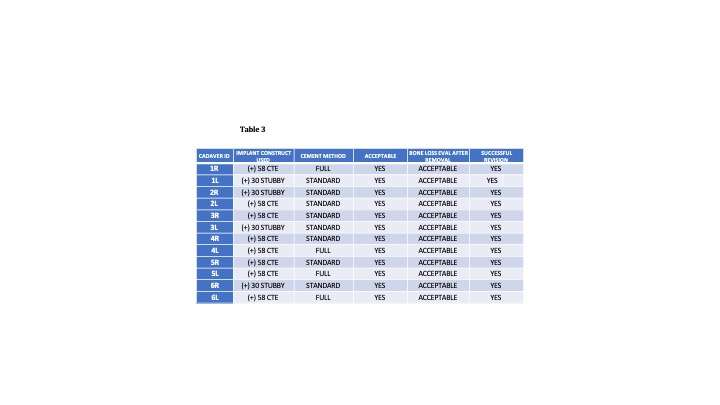
Figure 3#7652
Smart Knee Prosthesis Enables Remote Patient Monitoring of Walking Speed Following Total Knee Arthroplasty: The Digital Health Revolution
*Kaitlin Carroll - United States of America
Jeffrey Yergler - South Bend Orthopaedics - South Bend, USA
Derek Yocum - South Bend Orthopaedics - South Bend, USA
Barbara Elashoff - Canary Medical - Carlsbad, USA
Patrick Aubin - Canary Medical - Carlsbad, USA
Peter Schiller - Canary Medical - Carlsbad, USA
Jeffrey Gross - Canary Medical - Carlsbad, USA
William Hunter - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
Introduction: Primary total knee arthroplasties (TKA) in the United States are projected to grow by 673% to 3.48 million procedures by 2030[1] [2].In the traditional health care setting, the ability to continuously monitor rehabilitation progress is limited. Validated functional evaluations to assess post-operative progress, such as the 6-minute walk test, stair climb test, Time Up and Go test, among others, are typically administered by a health care professional in a clinical setting during an in-person visit. Rehabilitation monitoring and performance evaluations is conducted infrequently because of the barriers and costs associated with administering them. Consequentially, there is a sparsity of quantitative data regarding the time course of rehabilitation progress following TKA.
Methods: In our study, 50 patients received a PS TKA with a sensor enabled smart total knee implant [Figure 1]. This enabled stem is a smart implant with embedded sensors that enable the health care team and patients to monitor step count, walking speed, cadence, functional knee range of motion, tibia range of motion, and walking speed for up to 10 years following TKA. In this cohort, we monitored daily self-selected walking speed, at home and in the community, for 8 weeks following TKA. From the aggregate data, we calculated seven percentile bands (5th, 10th, 25th,50th, 75th, 90th, and 95th percentile) for daily walking speed following TKA. We introduce the novel concept of a recovery walking speed curve to understand the natural time course of walking speed recovery following TKA to enable the patient and health care team a novel way to monitor rehabilitation progress compared to similar demographic groups (e.g. females aged 65 and above).
Results: The cohort had a mean age of 62 years and mean BMI of 33 kg/m2, 33 patients were female, and 14 were 65 years and older. We recorded 7,879 bouts of motion from 52 knees (two patients were biliteral) that were transmitted to the a HIPPA compliant cloud database for processing. There were 23,624 qualified gait cycles that were parsed from the inertial data resulting in an average of 472.5 qualified gait cycles per patient. The walking speed recovery curves (Figures 2 and 3) demonstrate that for TKA patients mean walking speed recovers quickly for the first seven weeks following surgery, then asymptotes beyond seven weeks towards 0.7 m/s, which has been reported as mean walking speed prior to surgery [3]. The older patients had a faster cadence (steps/min) at all time points as compared to younger patients, perhaps due to differences in BMI (34.9 kg/m2 (<65) versus 28.6 kg/m2 (≥65). The ability to walk ≥100 steps/min has been shown to predict a reduction in mortality among community-dwelling older adults [4].
Conclusion: This represents one of the largest and richest kinematic datasets of patient during normal daily living following TKA. High fidelity, dense (daily), monitoring of all-activity ambulation will provide the research and healthcare community with the quantitative data necessary to improve outcomes by comparing the efficacy of different models of rehabilitation following TKA.
Figures

Figure 1
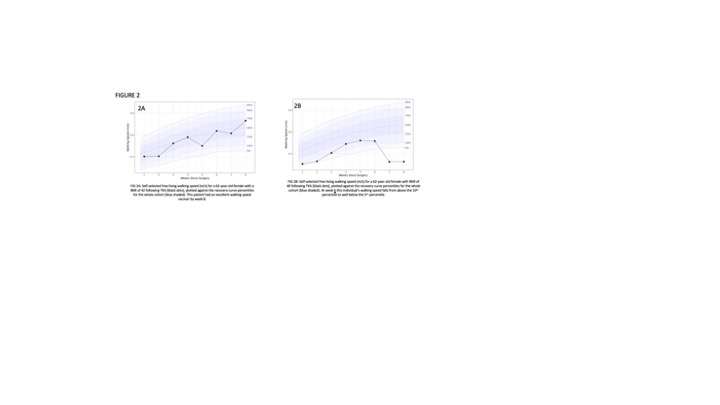
Figure 2
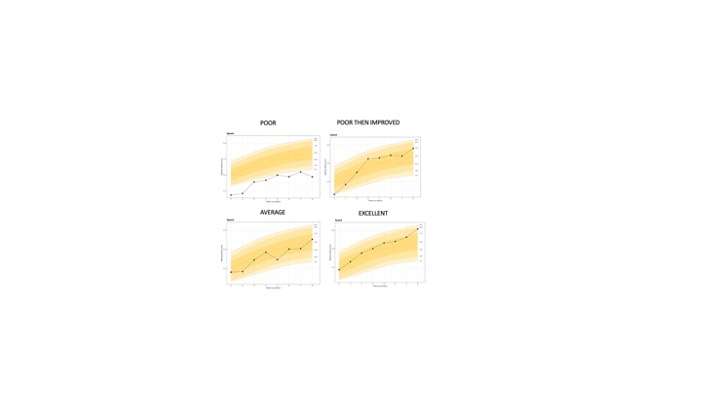
Figure 3#8022
Do Obese Patients Benefit From a Kinematic Appropriate Knee?
*Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: fcushner@canarymedical.com
Introduction: Modern total knee arthroplasty (TKA) using the Journey 2 implant utilizes a bicruciate stabilized technique. However, whether bicruciate stabilized TKA is equally effective across weight classes is unknown.
Methods: We identified patients who underwent primary bicruciate stabilized TKA during 2016 and 2017, at a single institution. All included patients had, at minimum, 2-year follow-up. Patients were categorized into body-mass index (BMI) groups as follows: underweight, normal, or overweight (<30 kg/m2), obese (³30 to <35 kg/m2), and severely obese (³35 kg/m2). Patient reported outcome measures (PROMs) were measured at baseline. Both KSS and KOOS JR, along with the Visual Analogue Scale (VAS), were also recorded at follow-up. Pre-operative, post-operative, and pre- to post-operative changes in PROMs were analyzed using analysis of variance (ANOVA) and linear regression.
Results: The 292 patients had a mean age of 64.8 years and mean BMI of 32.3 kg/m2. There were 116 (39.7%) patients in the underweight, normal, or overweight group, 88 (30.1%) in the obese category, and 88 (30.1%) in the severely obese group. There were no differences between PROMs at baseline or at follow-up (p > 0.10 for all comparisons). There were also no differences in the improvement from pre- to post-operative KSS (p = 0.21) and KOOS JR (p = 0.62).
Conclusions: Bicruciate stabilized TKA has similar effects on PROMs across BMI groups. These results suggest that bicruciate stabilized TKA is a viable treatment option both for low-weight and high-weight patients.
Key words: Arthroplasty; total knee arthroplasty; body mass index
#8033
Invited Talk: Look Who�s Talking - My Implant !
*Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: fcushner@canarymedical.com
#7950
Is a Nickel Allergy Related to Poor Outcomes in Total Knee Arthroplasty
Bhumit Desai - Ochsner Medical Center - New Orleans, United States of America
Jimmy Daher - Ochsner Medical Center - New Orleans, USA
Cruz Velasco-Gonzalez - Ochsner Medical Center - New Orleans, USA
*George Chimento - Ochsner Health System - New Orleans, USA
*Email: chimento2@cox.net
Introduction
Reasons for failure requiring revision following total knee arthroplasty (TKA) are commonly related to infection, instability, or malalignment. Revisions due to Metal allergy (MA) have become more common in the last decade. 10-48% have been reported to be sensitive to metal, with Nickel being the most common offender. A controversy surrounds the validity of whether MA leads to sub-optimal outcomes requiring revision arthroplasty. Two studies showed that symptoms were resolved following revision surgery with hypoallergenic material, however, evidence has been lacking to support the hypothesis of whether these outcomes are directly related to the MA. The only consensus between studies is that MA is considered a diagnosis of exclusion. The study goal is to show that metal allergy is not detrimental to outcomes post TKA by evaluating asymptomatic post-operative TKA patients with well-functioning implants through quantitative MA testing.
Methods
With approval from the institutional review board (IRB), we performed a prospective cohort study that included a total of 41 patients (26 females, 15 males, mean age 70.9 ± 6.67, average BMI 34.3 ± 7.65) who underwent primary TKAs (L: 17 R: 24) between 2010 and 2020. Inclusion criteria included a primary TKA and a well-functioning implant with minimum 12-month post-operative follow up. Patients with an Oxford Knee Score (OKS) less than 40 and those with a TKA implant that did not contain cobalt chromium and nickel were excluded from the study. An informed consent was signed by all patients. A commercially available Lymphocyte Transformation Test (LTT) measures the amount of a Delayed Type Hypersensitivity lymphocyte immune response after exposure to a particular antigen. The level of immune reactivity to each metal is measured as a Stimulation Index (SI) with a score over 2 indicating a positive reaction to an allergen. MA results were divided into non-reactive, mildly reactive(2-4), reactive(4-8), and highly reactive(>8). T-test and Wilcoxon-Mann-Whitney test were performed to compare individual metal reactivity. Proportional odds ordinal logistic regression and exact chi-square test was used for testing homogeneity of metal reactivity.
Results
41 knees were included for analysis with mean follow up 73.7 months. Nickel had the highest incidence when compared to cobalt and chromium and is the only metal to show reactive (n=7) and highly reactive (n=10) scores based on the SI (Table 1; p-value <0.01). There was no correlation between metal reactivity and OKS score by metal (Table 2; Nickel rho = -0.082; Cobalt rho = 0.014; Chromium rho = -0.166).
Conclusions
To our knowledge, this is the first study looking at metal allergy in well-functioning TKAs. There is no correlation between clinical outcomes and the presence or absence of Nickel allergy. Based on the results of this study, surgeons should not base their decision to revise a painful or poorly functioning total knee solely based on a “positive” Nickel allergy test. Further studies are ongoing to see if sensitivity to other metals may be associated with poorer outcomes following TKA.
Figures

Figure 1
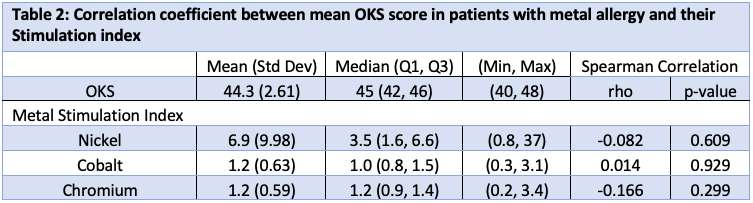
Figure 2#7962
Long-Term Follow-Up on Revisions of a Recalled Large-Head Metal-on-Metal Hip Prosthesis
Bhumit Desai - Ochsner Medical Center - New Orleans, United States of America
Jimmy Daher - Ochsner Medical Center - New Orleans, USA
Michael Warren - Ochsner Clinic Foundation - New Orleans, USA
Michael Nammour - Ochsner Medical Center - New Orleans, USA
*George Chimento - Ochsner Health System - New Orleans, USA
*Email: chimento2@cox.net
Introduction
Total hip arthroplasty (THA) remains one of the safest and most successful procedures in orthopedics. In the early 2000’s, metal on metal (MoM) THA gained popularity, increasing from 11.9% of primary THA in 2003 to a peak of 22.3% in 2008. Advantages include smaller wear particle size compared to metal on polyethylene (MoP) hip prosthesis and larger head size thus increasing stability. In 2010 a recall was issued for monoblock large head MoM prosthesis citing metallosis, pseudotumor, and aseptic lymphocytic vasculitis-associated lesions which lead to an unacceptably high revision rate of 12-13%. There are no known studies with long-term follow-up for revisions of this recalled system reported in the literature. Our purpose is to report long term outcomes and trend metal ion levels of revised monoblock large head MoM hip prosthesis
Methods
A retrospective chart review was performed on all patients that underwent revision of large MoM hip replacements between 2010-2015. This was a single site, single surgeon study. Patients that were deceased, paralyzed due to stroke, or lost to follow up were excluded from the study. Pre- and post-revision Harris hip score (HHS), cup abduction angles, anteversion angles, combined angles and cup sizes were compared. HHS was the primary outcome measured; serum cobalt and chromium levels were the secondary outcome and were followed throughout the study period for each patient. Multivariate linear regression was used to examine the correlation between pre-revision serum metal ion levels and pre-revision HHS. ​
Results
A total of 21 patients with 24 hips (mean age= 67.2 ± 11.0; 11 Males, 13 females; Mean BMI = 30.29 ± 5.8) met inclusion criteria. Revision surgeries were for pain, high metal ions, infection, aseptic loosening, failure of ingrowth, leg length discrepancy and/or pseudotumor. Mean time to revision was 4.12 years ± 1.1. Mean cup anteversion pre-revision was 24 degrees, most frequent cup and stem size were 50 and 4 respectively. Long term follow up was obtained on all patients with a mean follow up of 10 years. Mean HHS increased significantly after revision from 48.5 to 89.5 (p < 0.001) and were 84.8 at most recent follow up. Higher pre-revision cobalt levels were correlated with lower pre-revision HHS (cobalt R = 0.25; chromium R = 0.3160). There was no correlation for cobalt (p = 0.2671) or chromium (p = 0.3160) with pre-revision HHS. Most recent metal ion testing revealed a significant decrease in both cobalt (40.9 to 2.5 μg/L; p = 0.0084) and chromium (15.6 to 6.3 μg/L; p = 0.0115). Revision survival rate is 100% at time of submission with no prosthetic joint infections to date. ​
Conclusion
Our study showed significant improvements in HHS and significant decreases in Cobalt and Chromium levels after revision surgery for recalled monoblock large head MoM prosthesis. There were no early, midterm or long-term failures requiring revision in this series.
#7637
Anatomical Patellar Resurfacing in Patellofemoral Arthroplasty
Oliver Dandridge - Imperial College London - London, United Kingdom
Amy Garner - Imperial College London - London, United Kingdom
Andrew Amis - Imperial College of London - London, UK
Justin Cobb - Imperial College - London, United Kingdom
*Richard van Arkel - Imperial College London - London, United Kingdom
*Email: r.vanarkel@imperial.ac.uk
One in five of people with knee osteoarthritis have disease isolated to the patellofemoral compartment, yet Patellofemoral Arthroplasty (PFA) is used for <1% of patients. This may be in part due to poorer outcomes compared to total knee arthroplasty. Most innovations to date in PFA have focused on the femoral component and hence this study sought to establish biomechanical effects of patellar component design in PFA, comparing an anatomical component to a standard patellar button.
Nine cadaveric knees were tested in a knee extension rig using a validated repeated-measures protocol. Physiologically directed muscle loads totalling 205 N were applied, whilst extension moment, Medial Patellofemoral Ligament (MPFL) length-change, and tibiofemoral and patellofemoral kinematic trajectories were measured. Knees were tested in four states: 1) intact; 2) anatomical patellar resurfacing with trochlea intact; 3) anatomical patella with standard trochlear replacement; 4) standard patella button with replaced trochlea. All arthroplasties were planned from CT images in a virtual environment and implemented using bespoke, patient-specific cutting guides to ensure implant position. Patellar cartilaginous geometry was obtained by separating the patella and trochlear prior to scanning using a radiolucent joint separator. The anatomical patella was shape matched to the native patellar geometry of each specimen, thus restoring the articular geometry. A transpatellar approach was used to access the joint, avoiding variable soft tissue tensions between tests. One-dimensional statistical parametric mapping with Bonferroni-Holm corrected provided statistical comparison between the states.
Introducing the anatomical patella component alone did not affect knee biomechanics, indicating that the anatomical resurfacing well replicated the native patellofemoral joint and that the patient specific instrumentation was able to implant the component in the desired position. However, when combined with a femoral component in PFA, knee extensor moment was altered (p<0.001) (Fig.1). PFA with the conventional button was different from both the native knee, and PFA with the anatomical button (p<0.001). Patellar tilt was affected by introducing the femoral component (p<0.001) (Fig.2) but no other patellofemoral kinematic differences were apparent. No differences in tibiofemoral kinematics or MPFL length change were observed between any implant states.
Patellar component design influences PFA biomechanics. An anatomical patellar component could enhance biomechanics after PFA, but there would be little benefit to using one with a conventional femoral component in their current state. The patellar and femoral components would need to be designed as a mating pair to realise the full benefit.
Figures
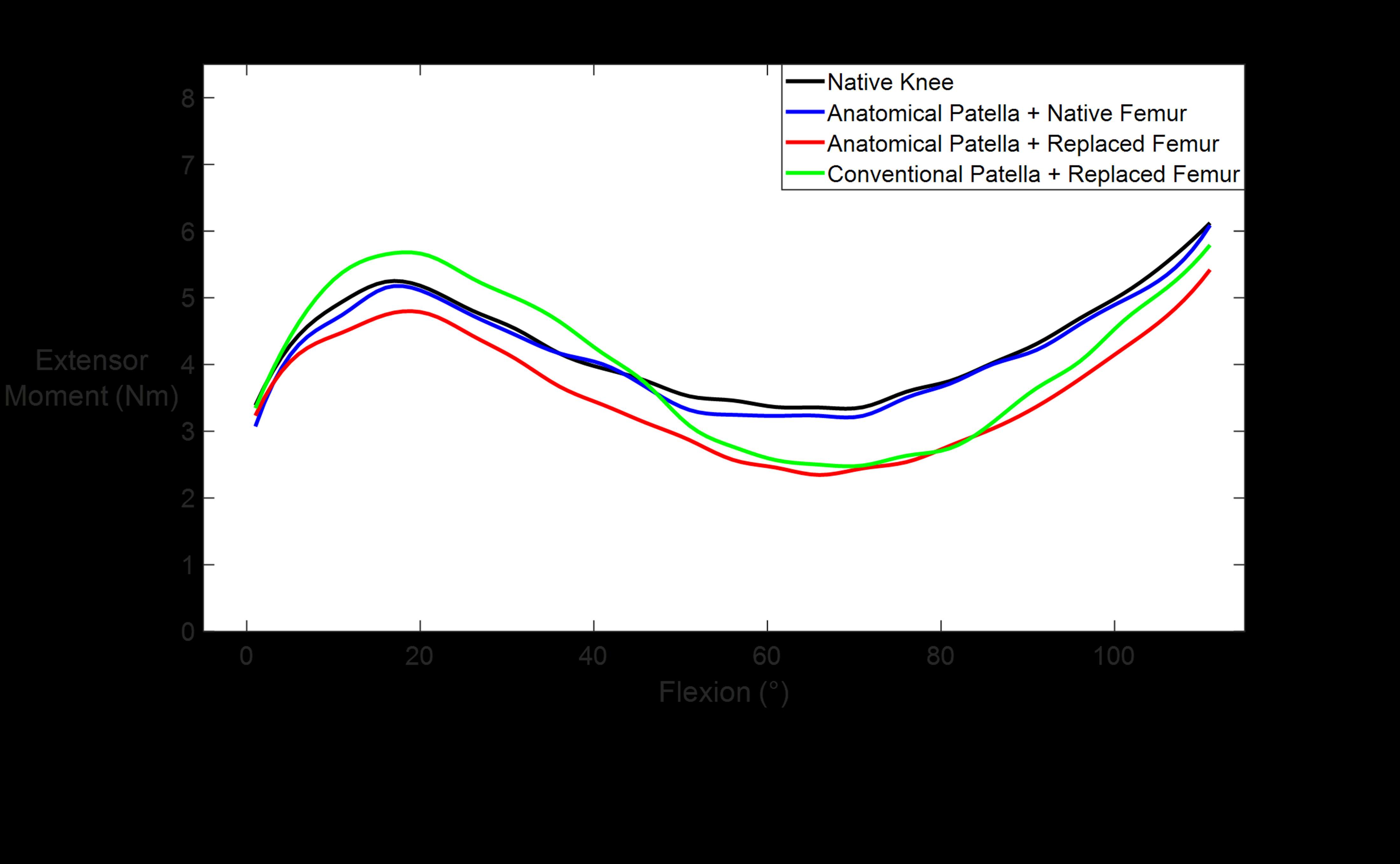
Figure 1
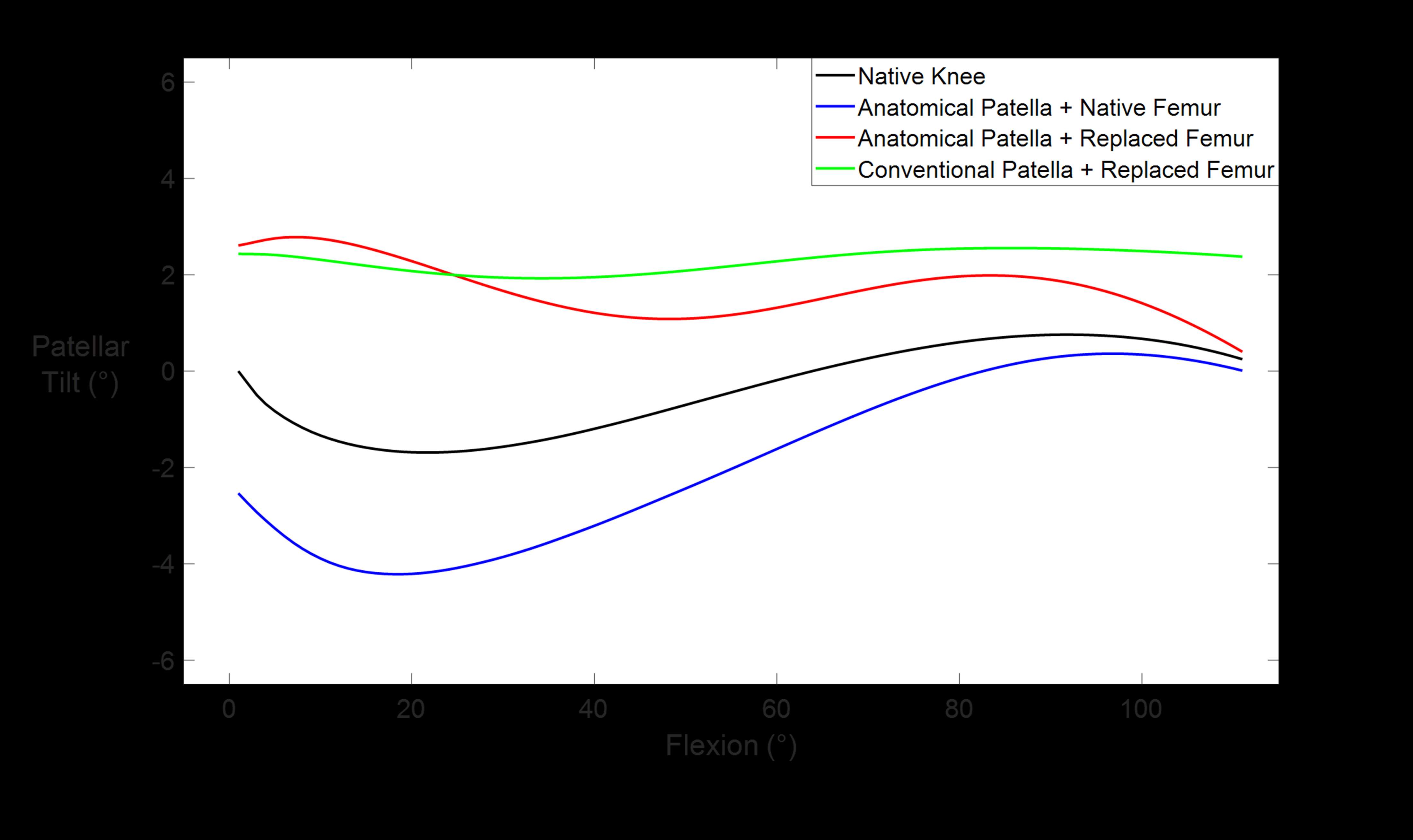
Figure 2#7636
Biomechanical Effects of Implant Position in Patellofemoral Arthroplasty
Oliver Dandridge - Imperial College London - London, United Kingdom
Amy Garner - Imperial College London - London, United Kingdom
Andrew Amis - Imperial College of London - London, UK
Justin Cobb - Imperial College - London, United Kingdom
*Richard van Arkel - Imperial College London - London, United Kingdom
*Email: r.vanarkel@imperial.ac.uk
The rise in assistive technologies, such as virtual planning, surgical robotics, and patient specific instrumentation, has led to renewed interest in a compartmental approach to knee arthroplasty – treating diseased compartments of the knee with one or combined partial knee arthroplasty implants. These technologies allow greater control and accuracy of implant positioning but for Patellofemoral Arthroplasty (PFA), little is known about how implant position affects knee biomechanics. This is especially true regarding patellar resurfacing, where surgical techniques and implant designs remain comparatively rudimentary. This study, therefore, aimed to elucidate how femoral and patellar component positioning influences knee kinematics and kinetics, hypothesising that femoral implant positioning is more important.
Nine cadaveric knees were studied using a validated repeated-measures protocol, varying both femoral and patellar implant positions between tests. Knees were tested intact, then after PFA in different positions: neutral (as-planned), patellar over-/understuffing (±2mm), patellar tilt, patellar flexion, femoral rotation, and femoral tilt (all ±6° from neutral). Tibio- and patellofemoral cartilaginous and bony geometries were obtained from CT scans, using a novel joint spacing technique to allow trochlear and patellar articular surface separation. Arthroplasties were planned virtually, then implemented with bespoke, patient-specific instrumentation, minimising inter-test variation. Extension moment, MPFL length-change, and tibio-/patellofemoral kinematic trajectories were measured under physiologically directed muscle loads totalling 205 N. One-dimensional statistical parametric mapping provided statistical inference with Bonferroni-Holm correction for multiple comparisons.
PFA changed knee function, altering extension moments (p<0.001) (Fig.1) and patellofemoral kinematics (p<0.05), but not tibiofemoral kinematics. Patellar component positioning affected patellofemoral kinematics: over/understuffing influenced patellar anterior translation (Fig.2) and the patellar tendon moment arm (p<0.001). Medially tilted patellar cuts produced lateral patellar tilt (p<0.001) and vice versa (Fig.3). A similar inverse effect occurred with extended/flexed patellar cuts, causing patellar flexion and extension (p<0.001), respectively (Fig.3). Of all variants, only extending the patellar cut produced near-native extension moments throughout (Fig.1). Conversely, the only femoral position difference was MPFL length change between medially/laterally rotated components.
PFA is capable of restoring native knee biomechanics. Provided anterior femoral cuts are controlled and smooth condyle-to-component transition is ensured, careful patellar management may provide more benefit than currently thought and warrants further research attention.
Figures
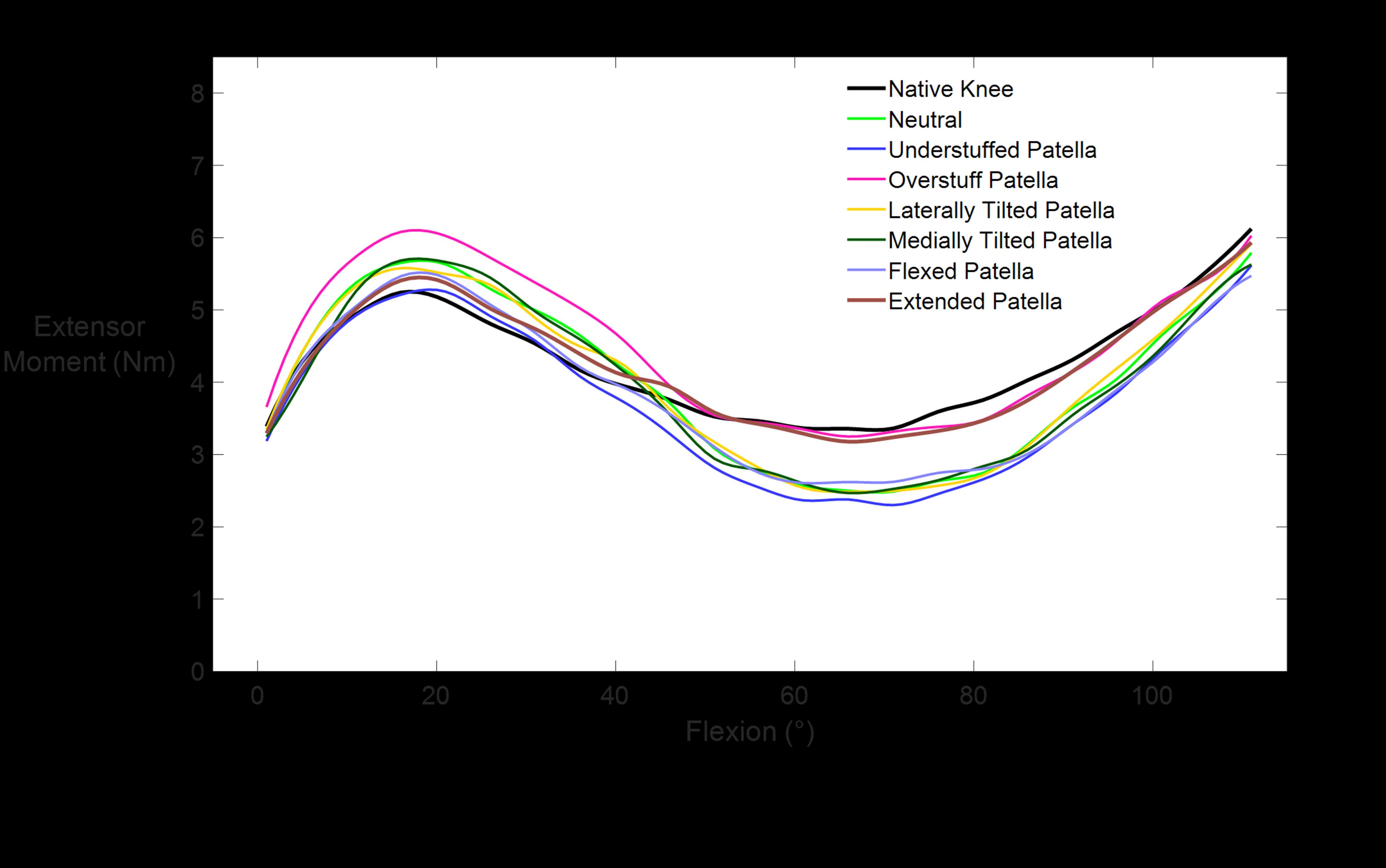
Figure 1
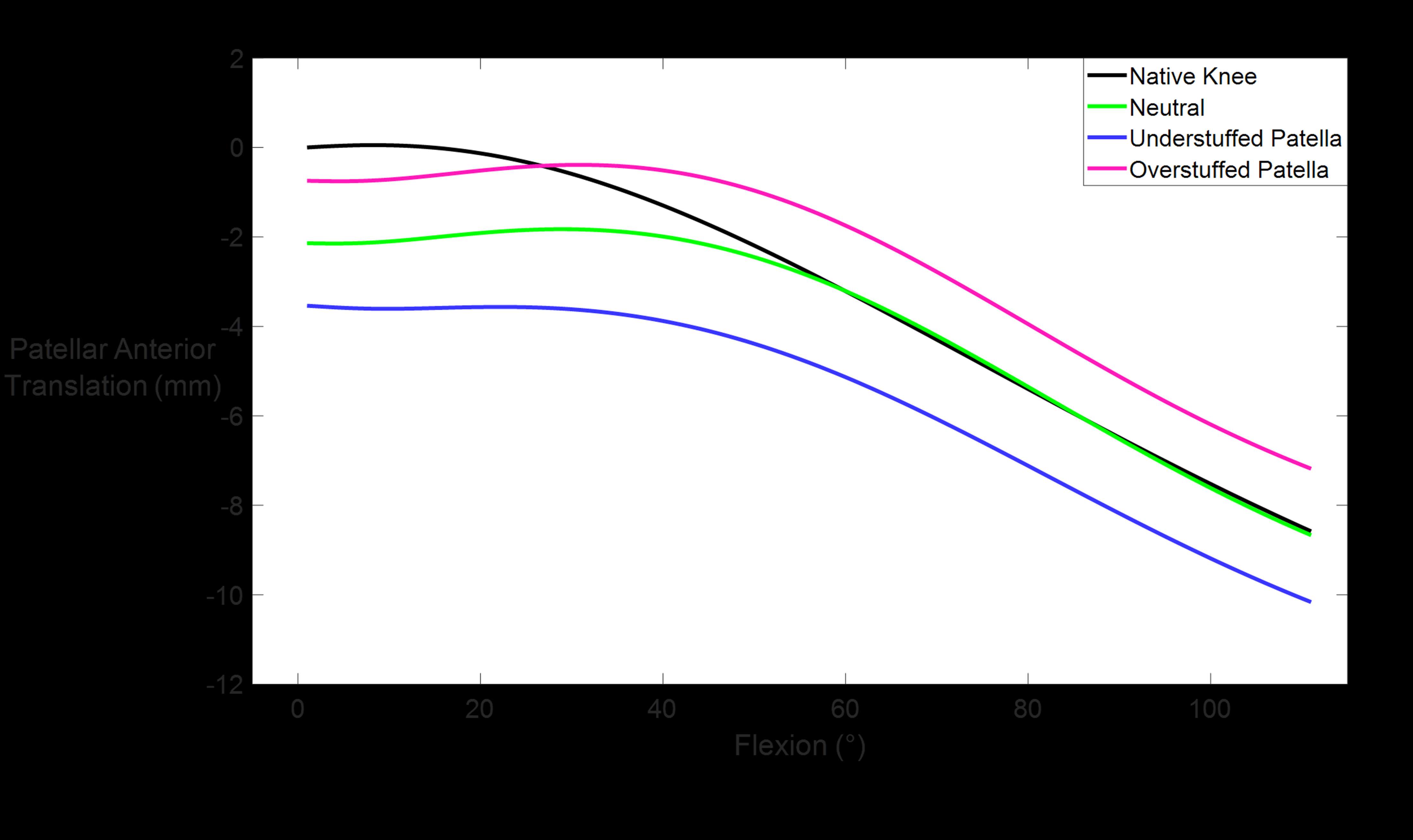
Figure 2
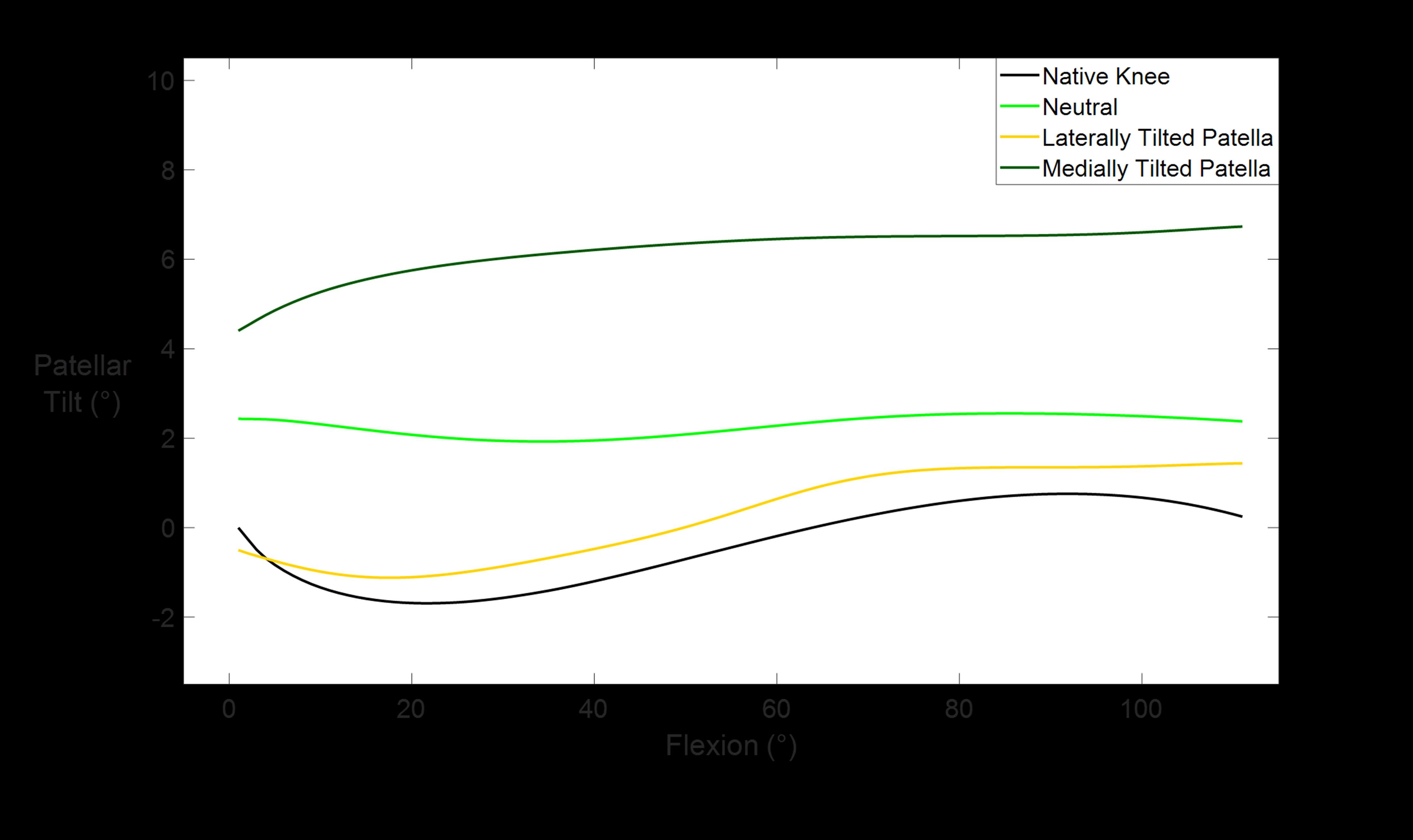
Figure 3#7828
A Subhemispheric Acetabular Component Increases Dislocation Risk
*Brian Darrith - Henry Ford Hospital - Detroit, USA
Tahsin Rahman - Henry Ford Health System - Detroit, USA
Lindsay Miller - Henry Ford Health - Detroit, USA
Robb Weir - Henry Ford Health - Detroit, USA
*Email: bdarrit1@hfhs.org
Introduction
Instability after primary total hip arthroplasty (THA) remains a leading cause for revision. Multiple patient, surgical and implant factors contribute to dislocation. The purpose of the current study is to identify patient and component related risk factors for dislocation, with particular interest in the type of acetabular component utilized.
Methods
A consecutive series of 1,724 primary THAs performed at a single community teaching hospital by three different fellowship trained arthroplasty surgeons were retrospectively compared. Only manual THAs were included in the study. Acetabular components from three different manufacturers were used during the 6-year time period. The primary outcome of dislocation was tracked via review of electronic medical records and postoperative radiographs. Univariate and multivariate logistic regression was used to identify risk factors for dislocation.
Results
Of the 1724 primary THAs, 2.6% (n=45) dislocated postoperatively. Half of these dislocations occurred with Zimmer Continuum acetabular components (Warsaw, IN), which demonstrated a 7.3% rate of dislocation compared to a 1.6% dislocation rate for non-Continuum cups (p<0.001). Primary THAs utilizing a continuum cup were at 5 times higher odds of dislocation in both univariate and multivariate analyses (p<0.001). Of the 22 dislocations from the Continuum cup cohort, 21 used a standard polyethylene liner. Increased patient age (p=0.02) and prior lumbar fusion (p=0.004) were also associated with dislocation.
Discussion
The current study suggests that increased age, prior lumbar fusion, and use of the Zimmer Continuum cup (Warsaw, IN) are associated with increased dislocation risk. Specifically, use of Continuum cup with a standard liner is associated with increased dislocation rate. The subhemispheric design of the Continuum standard liner (Figures 1 &2) leads to the center of rotation of the femoral head lying outside the plane of the cup opening, which decreases the jump distance necessary for dislocation. For a 36 mm head, the diameter of the liner in the plane of its opening is only 35 mm, leading to an approximate 0.5 mm decrease in jump distance. Surgeons should be aware of the impact of subhemispherical acetabular component design on jump distance and dislocation risk. The use of elevated “high-wall” liners may minimize the dislocation risk by increasing jump distance, and these liners should especially be considered for patients at increased odds of dislocation due to risk factors such as prior lumbar fusion.
Figure Legend: Figure 1 depicts 36 mm head with a continuum neutral 36 mm liner. The line drawn on the head demonstrates the border of the neutral liner for the hemispherical G7 cup, as shown in Figure 2 (Zimmer-Biomet, Warsaw IN).
#7284
Survivorship Analysis of Cementless Total Knee Arthroplasty With and Without Patellar Resurfacing at Midterm Follow-Up
Brian Darrith - Henry Ford Hospital - Detroit, USA
*Tahsin Rahman - Henry Ford Health System - Detroit, USA
Logan Hansen - Henry Ford Health - Detroit, USA
Kevin Lindsay-Rivera - Henry Ford Health - Detroit, USA
Hailey Heil - Henry Ford Health System - Detroit, USA
Mary Hennekes - Henry Ford Health - Detroit, USA
Madison Mervis - Wayne State University School of Medicine - Detroit, USA
Craig Silverton - Henry Ford Hospital - Detroit, USA
*Email: trahman1@hfhs.org
Background:
Cementless total knee arthroplasty has become more prevalent in the past several years due to improvements in new generation systems. Follow up data of newer designs is limited in literature. Likewise, the outcomes of cemented patellar resurfacing with cementless tibial and femoral components deserves further attention. The purpose of our study was to evaluate reoperations and complications at midterm follow up from cementless total knee arthroplasty with and without patellar resurfacing.
Methods:
A retrospective review was completed on 216 consecutive cementless total knee arthroplasties (Zimmer Natural Knee Flex, Warsaw, IN) conducted by a single fellowship trained surgeon at an urban, academic hospital. Initially the surgeon routinely resurfaced the patella, then selectively, and then routinely did not resurface the patella. If resurfaced, the same symmetric all-polyethylene cemented patellar button was used. Patient demographics, medical history, component details, and surgical data were collected through electronic medical record review. Surgical and medical complications as well as all cause reoperation and revision were collected. Student’s t-test, Pearson’s chi-square test, multivariate logistical regression, and Kaplan-Meier survivorship analyses were completed.
Results:
There was an average of 4.8 years of follow-up prior to retrospective review. 60 of the 216 patients underwent patellar resurfacing during the index surgery. Follow-up for the patellar resurfacing cohort was significantly longer (6.3 vs 4.0 years, p<0.001). No differences were found between the two groups with regards to demographics, operative time, or all-cause reoperation (Tables 1 & 2). Reoperation-free survivorship was similar between groups (Figure 1). One of the 60 resurfaced pateints underwent subsequent medial capsular imbrication for recurrent patellar dislocation. Only one patient from the unresurfaced cohort underwent subsequent isolated patellar resurfacing, but another two patients were revised for instabiliy and tibial loosening and during these procedures the patella was resurfaced.
Conclusions:
Assuming appropriate component positioning, cementless total knee arthroplasty showed all-cause revision rates comparable to published rates of midterm revision rates in cemented total knee arthroplasty. Despite the theoretical risk of developing symptomatic patellofemoral osteoarthritis in patients who do not undergo patellar resurfacing, our cohorts did not show any differences in patellar reoperations or all-cause reoperation at midterm follow-up. Further long term follow up may support the elimination of routine patellar resurfacing in the context of cementless knee arthroplasty.
Figures
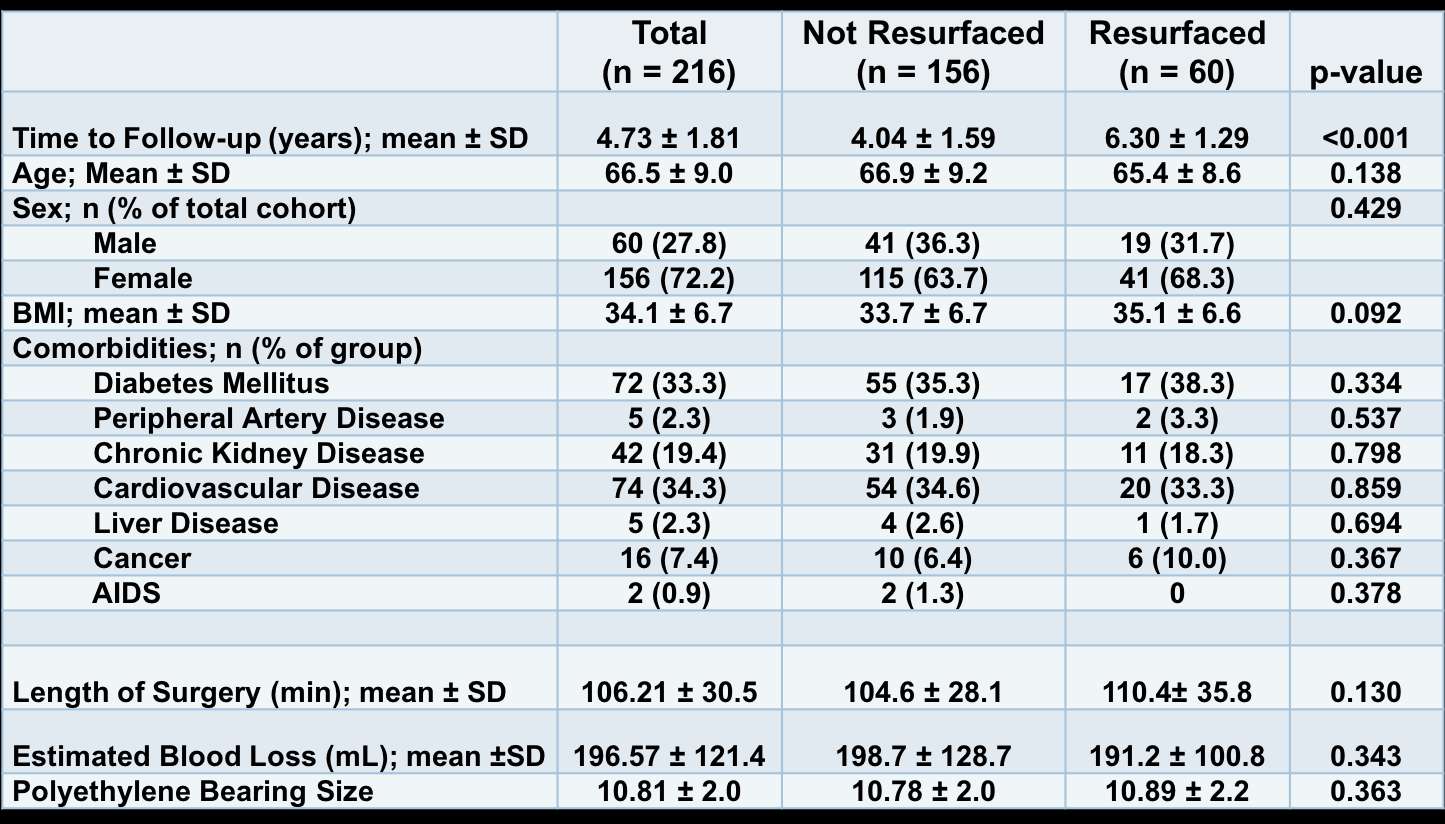
Figure 1
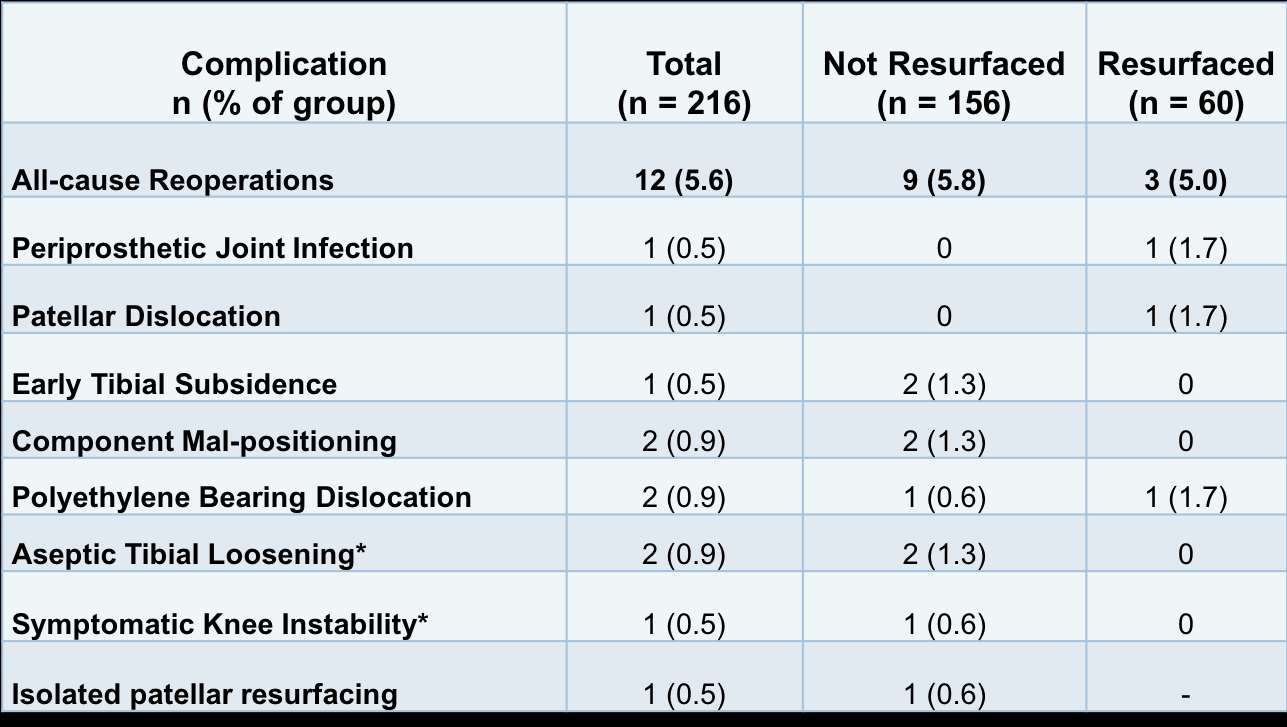
Figure 2
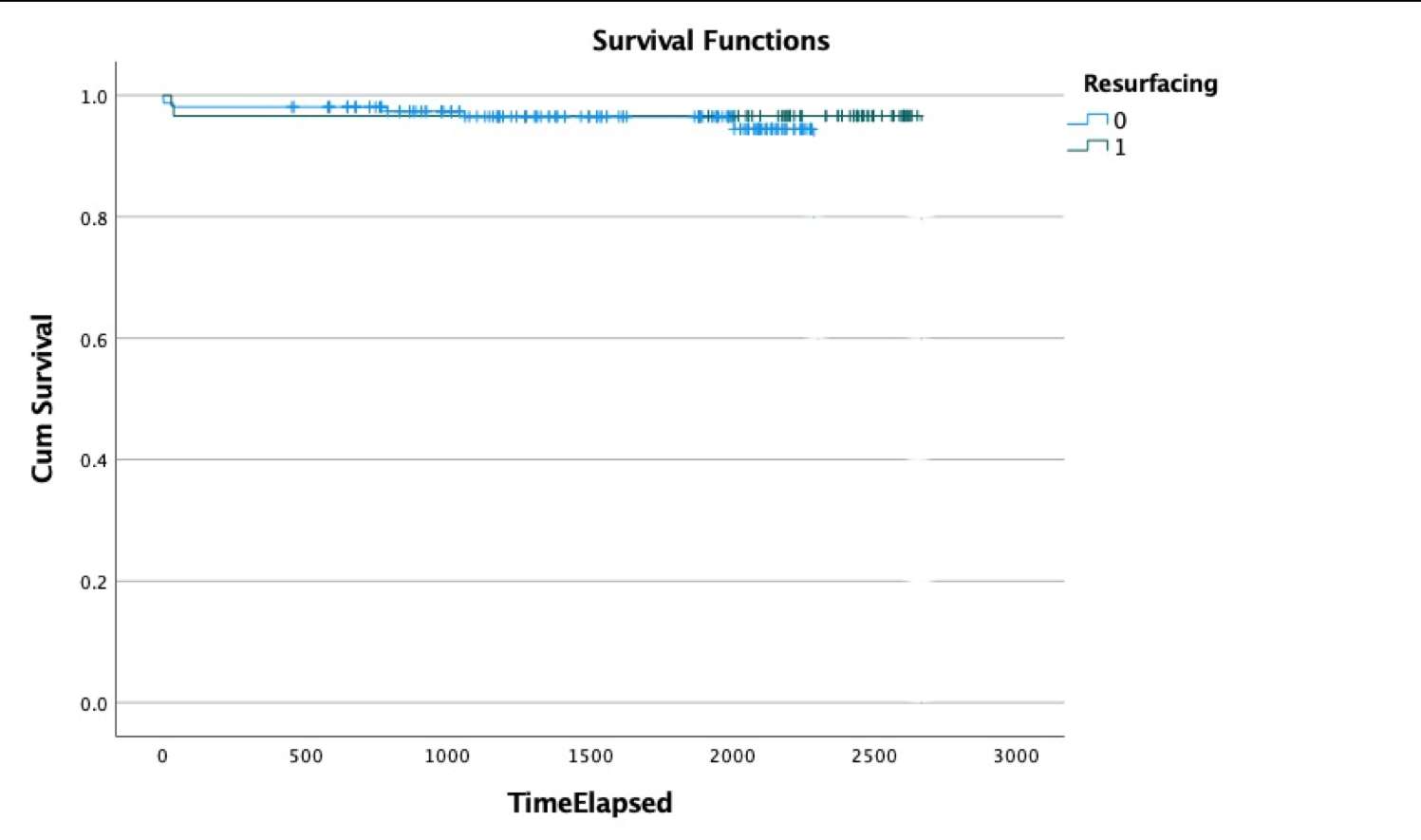
Figure 3#7328
The Impact of Free Radical Stabilization Techniques on in-Vivo Subsurface Mechanical Properties in Highly Cross-Linked Polyethylene Acetabular Liners
*Jordan Kump - University of New Mexoco - Albuquerque, United States of America
Mathew G Teeter - Schulich School of Medicine and Dentistry, Western University and London Health Sciences Centre - London, Canada
Robert Klassen - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Michael Decker - University of New Mexico School of Medicine - Albuquerque, USA
*Email: jorkump@salud.unm.edu
Introduction:
The overwhelming success of total hip arthroplasty in improving the quality of life for patients with end-stage degenerative hip disease relies significantly on clinical implant performance and longevity, which are influenced heavily by the mechanical properties of the modular components. Polyethylene component wear has been associated with instability, osteolysis, aseptic implant loosening, adverse local tissue reaction, and need for revision surgery; this has been shown to be particularly significant with the use of conventional ultra-high molecular weight polyethylene (UHMWPE). 1–3 Highly cross-linked polyethylene (HXLPE) for total hip arthroplasty was developed to improve wear resistance in-vivo and associated complications in comparison to UHMWPE. 4–10 The purpose of this study was to determine if there is evidence of subsurface microhardness changes in retrieved HXLPE liners at the rim and articular subsurface after extended in-vivo time that could be associated with oxidation and evaluate the possible effects on mechanical properties and implant integrity.
Materials and Methods:
Prior work by Decker et al. tested vertical cross-sections prepared of 16 retrieved and 5 control liner rims and then assessed for oxidation using a Bruker Hyperion 2000 Fourier transform infrared (FTIR) microscope (Bruker Daltonics Inc, Billerica, MA) attached to a Tensor II spectrometer.34 Eight liners that exhibited the highest subsurface Oxidation Indices based on FTIR testing were selected for analysis at the articular subsurface. These included 2 remelted, 3 single annealed, and 3 sequentially annealed liners. Each was mechanically tested for subsurface microhardness at both the rim and articular subsurface using a validated microindentation technique according to ASTM E384, using a Micromet II Vickers microhardness tester (Buehler Ltd, Lake Bluff, IL). The Vickers hardness (HV) for each sample was calculated using the following equation: HV=1.8544xF/d2.
Results:
Rim testing demonstrated a decrease in mechanical integrity that corresponded to higher subsurface oxidation values regardless of the free-radical stabilization technique. At the articular subsurface, a decrease in mechanical integrity was observed near the surface corresponding to peak oxidation and Vicker’s hardness, which decreased and normalized with increasing depths. This was found in all liners, with the exception of the single-annealed liners, which demonstrated decreased mechanical integrity trends at greater depths beyond peak oxidation, between 1.0 – 2.0mm. Interestingly, the single-annealed liners had a mean in-vivo time of 13.17 years, compared to a mean of 8.25 years for remelted and 7.29 years for sequentially-annealed liners.
Conclusion:
Our results suggest that subsurface mechanical properties do change in-vivo for certain implants. Though it is likely that the mechanical failures are multifactorial, we have shown that mechanical property degradation of HXLPE liners does occur with long-term in-vivo exposure and should be considered a possible risk factor. It is hypothesized that oxidation at the implant rim and articular surface may lead to an altered biomechanical environment and ultimately lead to mechanical property changes of the polyethylene liners as a whole, predisposing them to implant complications and failure. It is important to further delineate this relationship as a possible means to identify at-risk liners in order to improve long-term mechanical properties and implant longevity.
#7633
Reverse Shoulder Arthroplasty: An in Vitro Comparative Evaluation of the Tightening Torques and the Compressive Forces on the Glenoid Component Using Different Designs of Central Compressive Screw
*Nicola Del Negro - LimaCorporate Spa - Villanova di San Daniele del Friuli, Italy
Thomas Ferro - Limacorporate - Villanova di San Daniele del Friuli, Italy
Andrea Fattori - Lima Corporate - Villanova Di San Daniele del Friuli, Italy
Michele Pressacco - LimaCorporate Spa - Villanova di San Daniele del Friuli, Italy
*Email: Nicola.DelNegro@limacorporate.com
Introduction. One of the most common complications in RSA is glenoid baseplate loosening. To guarantee bone ingrowth and avoid aseptic loosening, a stable bone to implant interface during the first few months after surgery is key. Multiple options have been developed to increase primary stability of glenoid components by reducing micromotions, such as the use of central compressive screw fixation. With this aim, an appropriate compressive force should be applied while trying to minimize the amount of torsional load transmitted to the bone and the implant to not compromise the primary stability. The relationship between tightening torque and baseplate compression have been evaluated, even considering different baseplate designs but without consider the influence of different central screws. The aim of this study was to evaluate the compression strength and the related torque applied using central screws with different designs.
Methods. Different screw designs and assemblies were included in this study (fig.1): a Ø25mm baseplate (Stryker) coupled with its Ø6.5mm central compressive screw; a Ø25mm baseplate simulacrum coupled with a commercial Ø6.5mm screw (Limacorporate) and other three screw prototypes. Each screw was implanted in three different bone surrogate densities (PCF 20/30/40, three repetitions each) prepared with the appropriate pilot hole. A dedicated metal spacer was used to reach 15mm grip depth length for each screw to allow a homogeneous comparison. An annular load-cell was placed between the PCF and the baseplates to measure the maximum compressive force (fig.2) and the correspondent maximum allowed torque (until stripping of the screw occurred) was measured with a torsiometer (fig.1). An additional test was performed to compare the untightening torque of the Ø5mm cancellous double lead and single lead screws after a non-stripping 2.5Nm tightening torque on PCF30 (fig.3).
Results. Compared to other study parameters, the change of bone density highlighted the highest effect on the maximum compressive force reached. In fact, overall, the external screw diameter, the thread geometry and the number of threads starts didn’t affect much the maximum compressive force. The only exception was the Ø5mm double lead screw showing -15.5% compressive force compared to the correspondent design with single lead in the PCF 40 specimen. In contrast, all the parameters seemed to affect more the maximum torque: the diameter increase led to noticeably higher torques to reach the maximum force (fig.2), especially in higher density specimens (up to 9.5Nm). Finally, the torque needed to untighten the double lead screw in a defined insertion condition is significantly lower (-19,7%) than the same screw with a single lead thread (fig.3).
Discussion and Conclusions. When using large diameters screws in high density bones there is the risk to apply high value torques to maximize the compressive forces; this might be difficult to transmit through a screwdriver and might be dangerous for bone-implant interface. On the other hand, lower diameters central screws are able to give comparable compressive forces with lower tightening torques required. The tested double lead thread design has less compressive forces and lower residual torque if compared with a single lead screw.
Figures
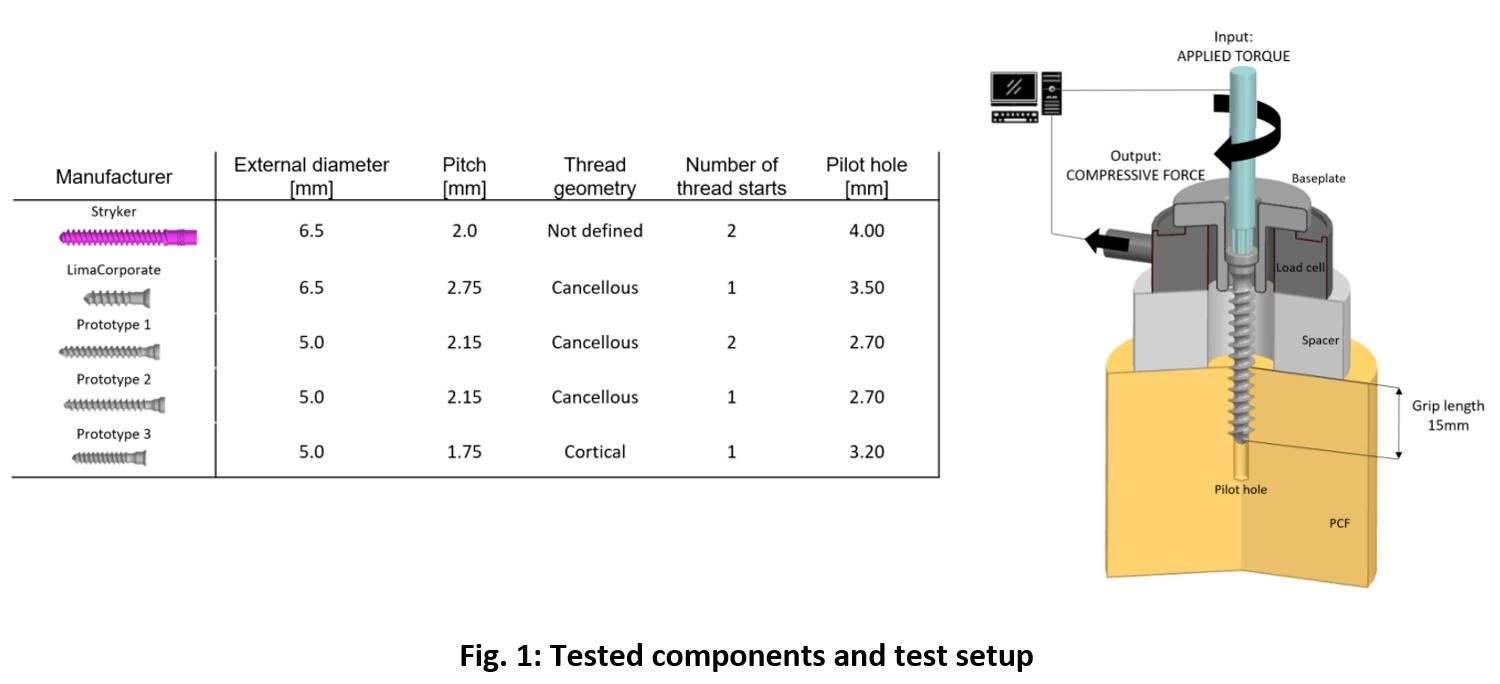
Figure 1
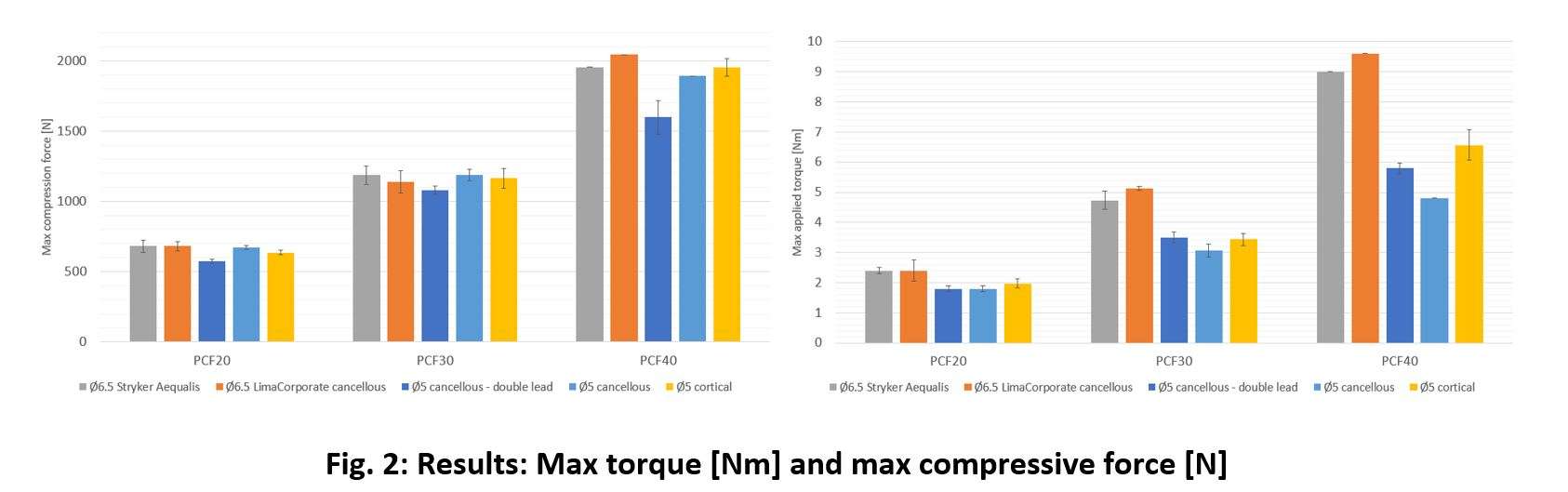
Figure 2
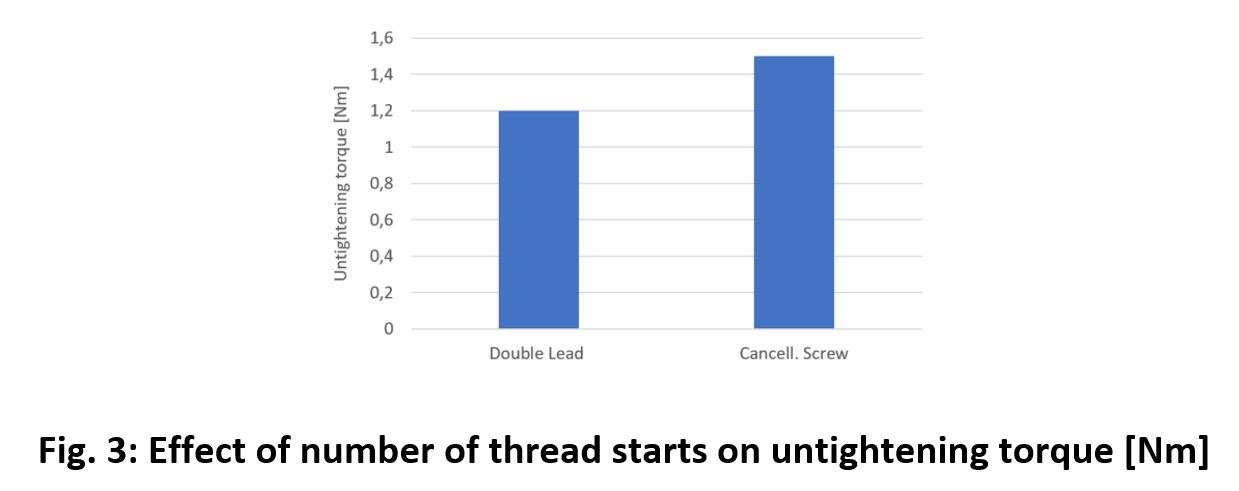
Figure 3#7455
Electrophoretic Deposition of Gentamicin and Chitosan Into Titanium Nanotubes to Prevent Periprosthetic Joint Infection
Greta Della Fara - Rush University Medical Center - Chicago, United States of America
*Markus Wimmer - Rush University - Chicago, USA
John Hamilton - Rush University Medical Center - Chicago, USA
Adrienn Markovics - Rush University Medical Center - Chicago, USA
*Email: markus_a_wimmer@rush.edu
Background
Periprosthetic joint infection (PJI) occurs in around 1-2% of primary total hip and knee arthroplasties, but rates of PJI can be greater than 20% in certain patient risk groups. Development of PJI can lead to devastating complications including requirement of multiple operations, poor outcomes and morbidity, and mortality. Systemic antimicrobials are routinely utilized as a preventative measure and treatment for PJI. However, systemic drug treatments can provide low bioavailability of antimicrobial drugs around the implant and can fail to prevent or eradicate the infection. Therefore, the development of localized drug delivery systems is of great clinical significance. Titanium (Ti) is known to form a nanotubular oxide layer under appropriate electrochemical conditions; this layer can be used to load antibacterial drug. Here we describe the use of electrophoretic deposition (EPD) as drug loading and coating of nanotubes (NTs) on a mouse femoral nail to establish a local application of antibiotic capable of prolonged antimicrobial drug delivery.
Methods
A two-step anodization process was performed to create NTs on 0.6 mm diameter and 3 cm length Ti-6Al-4V wire. For gentamicin deposition, EPD with different voltages and durations was tested and compared to air-dry method (ADM). To establish a prolonged drug release, simultaneous gentamicin deposition and crosslinked chitosan coating were carried out by a two-step EPD. Gentamicin release was determined by fractional volume sampling and quantified by UV-Vis spectrophotometry using the ninhydrin reaction. The antibacterial effect of the gentamicin-loaded wires was tested against Staphylococcus aureus (S. aureus) in vitro by agar diffusion and liquid culture growth methods. Eventually, a toxicity analysis in osteoblast cultures was performed.
Results
The NTs created on Ti wire with two-step anodization process (70V 1h + 15 min sonication + 70V 30 min) are characterized by a 100 nm diameter and 7 µm depth. This process allowed a highly ordered nanotube morphology maintaining a high diameter but with lower variability with respect to the other methods tested [Figure 1]. EPD resulted in a higher amount of gentamicin deposited with all parameters tested as compared to the air-dry method, up to 10x higher values were obtained. The amount of antibiotic with EPD was controllable by adjusting the two parameters of the deposition, increasing voltage and duration led to more drug loaded [Figure 2A]. The application of a crosslinked chitosan layer allowed logarithmic release kinetics for up to 3 days [Figure 2B]. Gentamicin-loaded Ti wires significantly inhibited S. aureus growth in liquid culture (p<0.0001) and resulted in a larger elliptical inhibition zone (4.5 cm x 3.5 cm) compared to anodized but unloaded wires. Toxicity analysis resulted in non-significant difference in viability within samples (LW, NLW, cells only) [Figure 3].
Conclusion
EPD proved to be an effective method for gentamicin loading and coating of Ti NTs. Crosslinked chitosan coating was also successfully applied by EPD and resulted in prolonged drug delivery. Antibiotic loaded Ti NTs created on Ti-alloy surface, may represent a powerful technology in the fight against PJI; we plan to test it in a murine PJI model next.
Figures
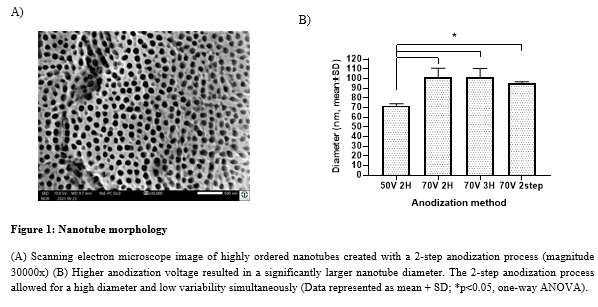
Figure 1
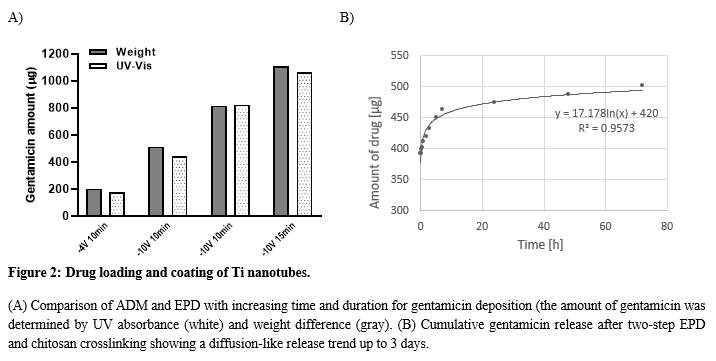
Figure 2
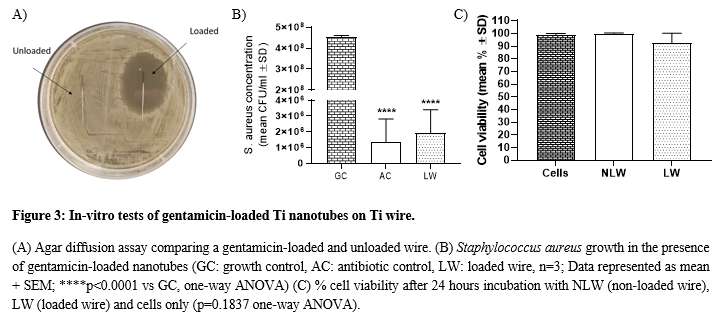
Figure 3#7814
Retrieval Analysis of Vitamin E Doped Total Knee Arthroplasty Inserts and Comparison Between Incorporation by Blending Versus Diffusion
*Hannah Spece - Drexel Implant Research Center - Philadelphia, USA
Tabitha Derr - Drexel University - Philadelphia, USA
Daniel MacDonald - Drexel University - Philadelphia, USA
Greg Klein - Hartzband Center for Hip and Knee Replacement - Hackensack, USA
Michael Mont - Northwell Hospital - New York, USA
Arthur Malkani - Jewish Hospital - Louisville, USA
Steven Kurtz - Drexel University - Philadelphia, USA
*Email: hannahspece@gmail.com
Introduction
Vitamin E doping is a popular strategy for reducing free radicals and improving the oxidation resistance of highly crosslinked polyethylene (HXLPE) for orthopaedic devices. The antioxidant can be incorporated either by blending, in which vitamin E is mixed with polyethylene resin powder prior to compression molding, or by diffusing vitamin E into the polyethylene following crosslinking.
The purpose of this study was to provide an update to a previously published retrieval analysis of vitamin E polyethylene (VEPE) inserts for total knee arthroplasty (TKA). A secondary goal was to compare the in vivo performance of VEPE components created by diffusion versus blending.
Methods
148 TKA inserts were retrieved during revision surgery as part of a multi-institutional implant retrieval program. The cohort represented VEPE formulations from 4 manufacturers with n = 121 manufactured via diffusion and n = 27 via blending. The inserts were evaluated for 7 surface damage mechanisms according to the semiquantitative Hood scoring method. Sample slices approximately 200 µm in thickness were then created using a microtome, and the samples were boiled in heptane for 6 hours and sonicated in water to remove lipids that may have diffused into the material in vivo. The samples were then analyzed for oxidation using Fourier-transform infrared spectroscopy. To compare vitamin E incorporation methods, blended and diffused components were matched on the basis of implantation time, BMI, and age at insertion, resulting in 27 matched pairs for statistical analysis.
Results
The cohort had an average implantation time of 1.1 ± 1.3y and average patient of BMI 32.6 ± 6.5 kg/m2. The components were revised most often for infection (n = 33/148), instability (n = 32/148), and loosening (n = 17/148). Across the entire cohort, at least minimal pitting was observed on 99% (n = 146/148) of inserts, at least minor scratching was observed on 97% (n = 143/148), and at least minor burnishing was observed on 95% (n = 140/148). We found no correlation between total surface damage and implantation time or BMI. Measured oxidation for the cohort was low, with an average oxidation index (OI) of 0.09 ± 0.05 for the articulating surface, 0.09 ± 0.21 for the backside, 0.13 ± 0.29 for the anterior/posterior surfaces, and 0.08 ± 0.05 for the stabilizing post. We found a weak correlation between maximum oxidation index and implantation time (Spearman’s rho = 0.25, p < 0.05).
Comparison between matched blended and diffused components showed no significant difference in maximum oxidation index (p > 0.05 for articulating surface OI, backside surface OI, and overall maximum OI) or total surface damage. The frequency of revision reasons between the groups also did not differ.
Conclusion
In this study we examined the in vivo damage and oxidation for retrieved vitamin E-doped TKA inserts, and found that while certain damage mechanisms (i.e., scratching, pitting, and burnishing) were highly prevalent, oxidation was minimal. We did not find differences for the in vivo oxidation or surface damage when comparing VEPE created via diffusion versus blending.
Figures
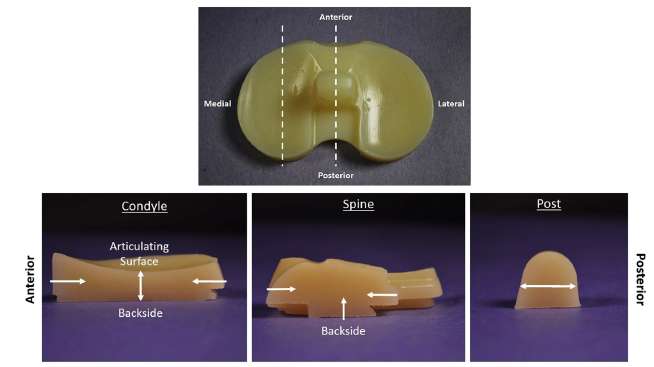
Figure 1#7706
iTemplating: The Future of Templating for Hip and Knee Arthroplasty
*Parth Desai - Ochsner Clinic Foundation - New Orleans, USA
*Email: parthdesai1234@yahoo.com
Problem: Templating is an important component of pre-operative planning for hip and knee arthroplasty. On the implant manufacturers side, companies rely on templating for supply-chain management and to provide value to their surgeons. Digital templating has become the predominant method of templating world-wide, however these solutions can be costly, time-consuming and require significant on-boarding. Accessibility is often limited to orthopaedic surgeons within the confines of hospital and PACS networks. With the growing number of total joint arthroplasty cases completed worldwide, there is a need for newer smartphone-based modalities of digital templating.
Solution: Augmented-reality (AR) based digital templating represents an innovative solution for fast and accurate templating from virtually any location where a templating x-ray is available. The application allows for a more kinesthetic templating experience using the touch screen on a smartphone, rather than a computer mouse. This simplification of templating can transform the tedious task of templating before every case into a more enjoyable activity. Furthermore, the accuracy of this modality is comparable to the established modalities of acetate and digital templating.
Market: The digital templating market is dominated by 2 key players that control over 80% of the market share. These companies offer end-to-end digital templating for a variety of use-cases, however subscription costs can be over $2,000.00 annually per user. Lowering the price-point for digital templating will improve access to templating for surgeons, while also increasing the size of the overall templating market.
Product: iTemplating is an AR-based mobile application which allows for simple and efficient templating for hip and knee arthroplasty. The application covers every major implant and includes a wide variety of calibration options. The current version of the application has shown over 90% prediction accuracy within 1 implant size in retrospective trials and over 80% accuracy within 1 size in prospective trials. The speed and simplicity of the application is its core advantage over other digital solutions. The application is designed to be accessible to surgeons, as well as implant representatives and physician-extenders. The goal of the product is to eventually use the templates created within the application to develop a machine learning model which can instantly generate an accurate template using only a templating radiograph.
Timescales: The application is in a closed beta period which began in Q3 2021. It is currently available on iOS by invitation only. The first consumer version of the application will be available by subscription in early 2023, with plans for AI automation to be added thereafter.
Funding: The research and development of iTemplating was funded by a single angel investor.
Figures
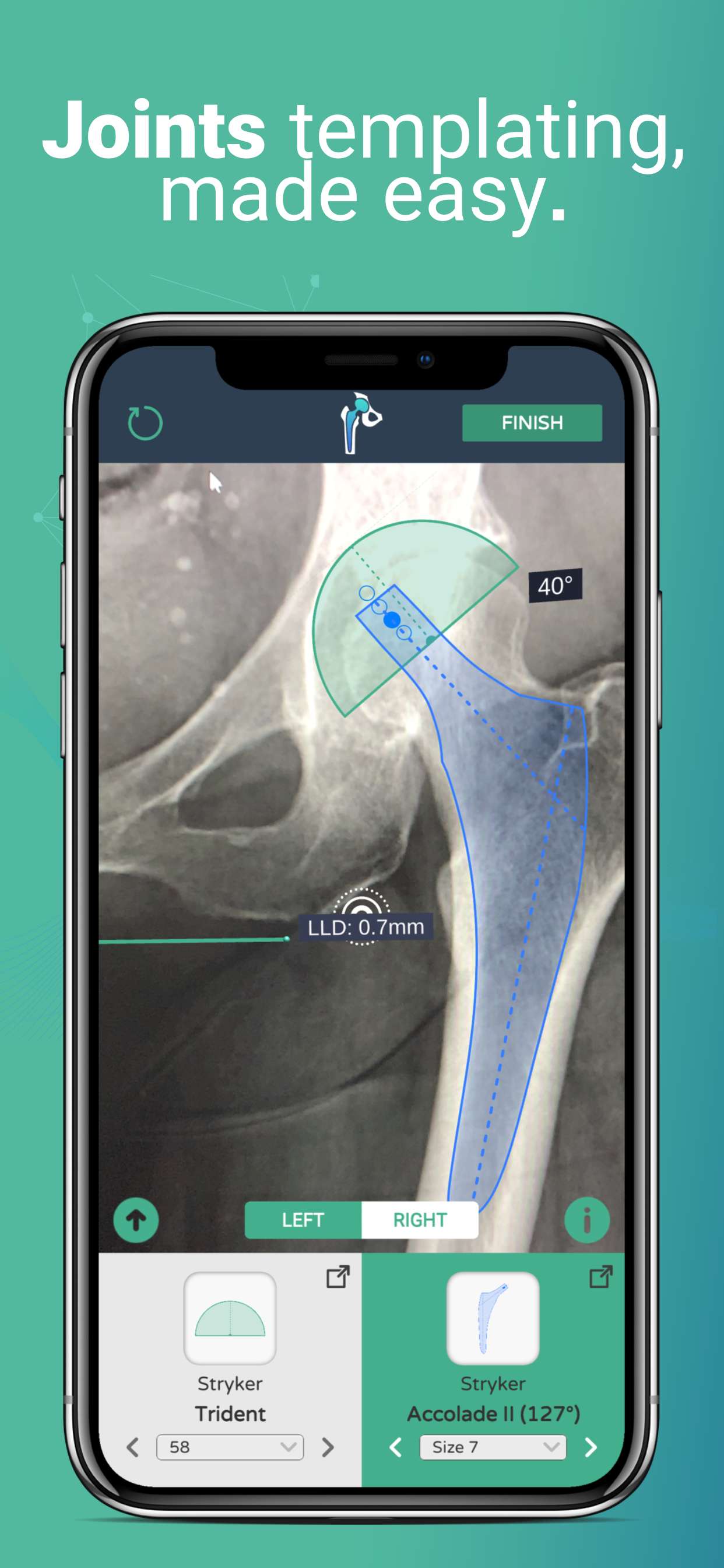
Figure 1
Figure 2
Figure 3#7718
Novel Augmented-Reality Templating Application for Total Hip Arthroplasty: A Retrospective Analysis
*Parth Desai - Ochsner Clinic Foundation - New Orleans, USA
Michael Stallard - Ochsner Medical Center - New Orleans, USA
Hunter Starring - Ochsner Medical Center - New Orleans, USA
George Chimento - Ochsner Health System - New Orleans, USA
Connor Soles - University of Queensland- Ochsner Clinic Foundation - New Orleans, USA
*Email: parthdesai1234@yahoo.com
Introduction: Templating is an important component of pre-operative planning for total hip arthroplasty (THA). The current modalities of acetate and digital templating allow for accurate determination of implant size and position, however have limitations in accessibility. With the advent of augmented-reality capable mobile devices, new technological solutions leveraging these frameworks have been proposed. The purpose of this pilot study was to evaluate the accuracy of a novel augmented-reality (AR) based mobile application at predicting implant size for primary total hip arthroplasty.
Methods: Templating analysis using the AR-based templating application was conducted retrospectively on 20 randomized pre-operative radiographs of THA patients completed by 1 orthopaedic surgeon over a 6 month period. The acetabular cup size and femoral stem size were predicted by one trained user of the templating application were compared to the actual implant sizes utilized.
Results: The exact acetabular cup size was predicted in 40% of patients (8/20) while 85% (17/20) of patients were predicted within one cup size of the eventual implant used. The exact femoral stem size was predicted in 25% (5/20) of cases while 75% (15/20) of cases were predicted within 1 stem size. For both acetabular cup and femoral stem, 100% (20/20) cases were predicted within two implant sizes.
Conclusions: Based on the limited results of this pilot study, AR-based templating appears to be a viable option for predicting within 1 implant size for both acetabular cup and femoral stem. These results indicate the need for future, high-powered prospective studies to validate the accuracy of AR-based templating.
#7725
The Use of Machine Learning to Develop an Automated Orthopaedic Implant Identification Tool
*Parth Desai - Ochsner Clinic Foundation - New Orleans, USA
Michael Stallard - Ochsner Medical Center - New Orleans, USA
Hunter Starring - Ochsner Medical Center - New Orleans, USA
Connor Soles - University of Queensland- Ochsner Clinic Foundation - New Orleans, USA
George Chimento - Ochsner Health System - New Orleans, USA
*Email: parthdesai1234@yahoo.com
Introduction: The identification of unknown joint implants is a major problem faced by orthopaedic surgeons during the preoperative planning of revision joint arthroplasty. Due to the large number of implants on the market, as well as the paucity of available resources, identification can be a time and resource-consuming task. To solve this problem, we propose a machine learning based image classification method, deployed as a mobile application.
Methods: The proposed solution first requires creation of a robust implant x-ray library consisting of every commonly used implant model. This is followed by development of a rudimentary machine learning algorithm to stratify implant x-rays into groups based on similar morphologic features. Next, surgeons must manually confirm the precise identity of the implant to allow for a larger training database to train a more complex machine learning algorithm capable of precisely identifying any individual implant.
Results: The proposed solution has been developed and tested with success for all major hip, shoulder, wrist, and ankle implants. Based on these positive preliminary results, the solution should be released to orthopaedic surgeons worldwide to develop a further, more complex machine learning algorithm.
Conclusion: The problem of implant identification is one that will continue to increase as the number of revision joint arthroplasties continues to rise. Using the frameworks delineated in this paper, a clear path has been conceived to solve this problem. A tool based on machine-learning and an app-based image storage protocol appears to be the first step towards faster and more efficient implant identification.
Figures

Figure 1

Figure 2
Figure 3#7690
3D-Printed Silicon Nitride-PEEK Composite Promotes Osteogenic Activity in Vitro
*Paul DeSantis - Drexel University - Philadelphia, United States of America
Ryan Bock - SINTX Technologies - Salt Lake City, USA
Sean Ronayne - SINTX Technologies, Inc. - Salt Lake City, USA
Bryan McEntire - SINTX Technologies, Inc. - Salt Lake City, USA
Noreen Hickok
Steven M. Kurtz - Drexel - Philadelphia, USA
*Email: pmd67@drexel.edu
INTRODUCTION: Aseptic loosening and infection are prevalent reasons for revision in total knee and total hip arthroplasty [1,2]. A proposed material for implants is silicon nitride (Si3N4), which is a synthetic non-oxide ceramic with many industrial applications. An in vivo experiment where rats were induced with Staphylococcus epidermidis found after 3 months that Si3N4 implants had strong antibacterial and osseointegrative properties when compared to titanium and PEEK [3]. Due to its ceramic nature, Si3N4 can be susceptible to brittle fracture [4], however it is proposed that a composite material made from both Si3N4 and polyetheretherketone (PEEK) could have the potential to combine the favorable bioactive properties of Si3N4, with the biomechanical properties of PEEK. PEEK is a semi-crystalline thermoplastic that can be 3D printed into various geometries and has a similar elastic modulus to bone, making it useful in many arthroplasty procedures.
METHODS: Samples with dimensions of 10x10x1 mm were printed using SiN-PEEK composite containing 30% Si3N4 (Apium P220). Samples were imaged using scanning electron microscopy (SEM) in order to verify the presence of Si3N4 on their surface. MC3T3E1 pre-osteoblast cells (ATCC) were cultured and seeded on sterilized SiN-PEEK composite, Ti6Al4V, pure Si3N4, and pure PEEK surfaces (n=6). MTT and ALP assays at Days 7, 14, and 21 acted as markers for cell proliferation and osteogenic activity, respectively. Normalized ALP was calculated to measure osteogenic activity relative to cell number. An alizarin red assay was used on Day 21 to determine the amount of cumulative mineralization. ANOVA with multiple comparisons was used to determine statistical significance.
RESULTS: SEM images of 3D-printed composite SiN-PEEK samples show characteristic Si3N4 structures, indicating that cells would be able to interact with surface Si3N4 (Figure 1). Figure 2 shows the normalized ALP activity for each of the four materials tested, and cells grown on tissue-culture-plastic (TCP). The SiN-PEEK composite showed the highest activity at Days 7 and 14, but was only significantly greater than the Ti6Al4V and positive control groups at Day 14. At Day 21, the SiN-PEEK group was not significantly different from the positive control and was significantly less than the Ti6Al4V, PEEK, and pure Si3N4 groups. This could indicate that the composite surface better supports osteogenic differentiation as opposed to cellular proliferation in the short term. Figure 3 show that the the SiN-PEEK composite had the highest amount of alizarin red stain with 0.0982±0.0171 mM, and the pure SiN sample had the lowest amount of stain at 0.0595±0.00699 mM.
CONCLUSION:. These experiments establish the feasibility of using 3D printing for the creation of a sample that contains both PEEK and Si3N4. This combined SiN-PEEK supports cell adhesion, proliferation, and mineralization as indicated by normalized ALP and alizarin red results. We suggest that a SiN-PEEK composite could be used in custom implants produced using fused filament fabrication to utilize the osteoconductive properties of Si3N4 and the biomechanical properties of PEEK.
Figures
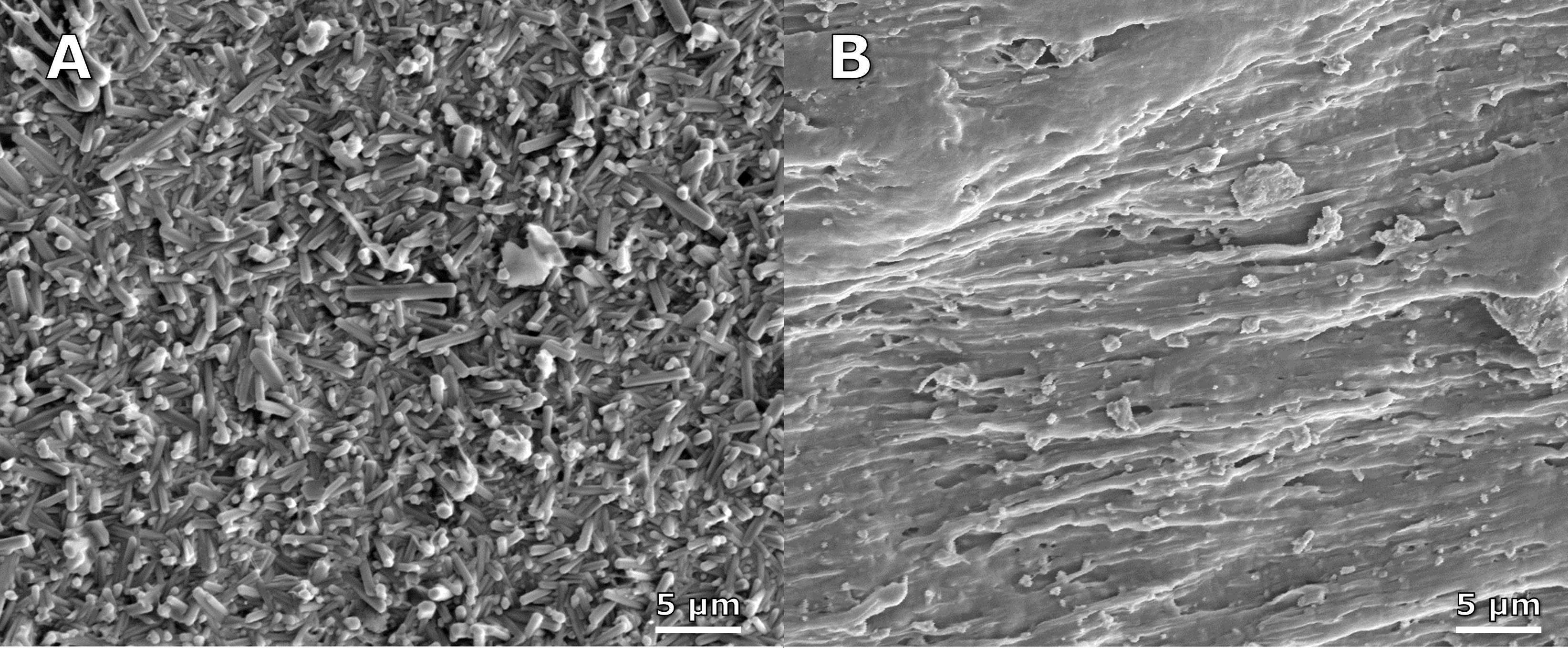
Figure 1
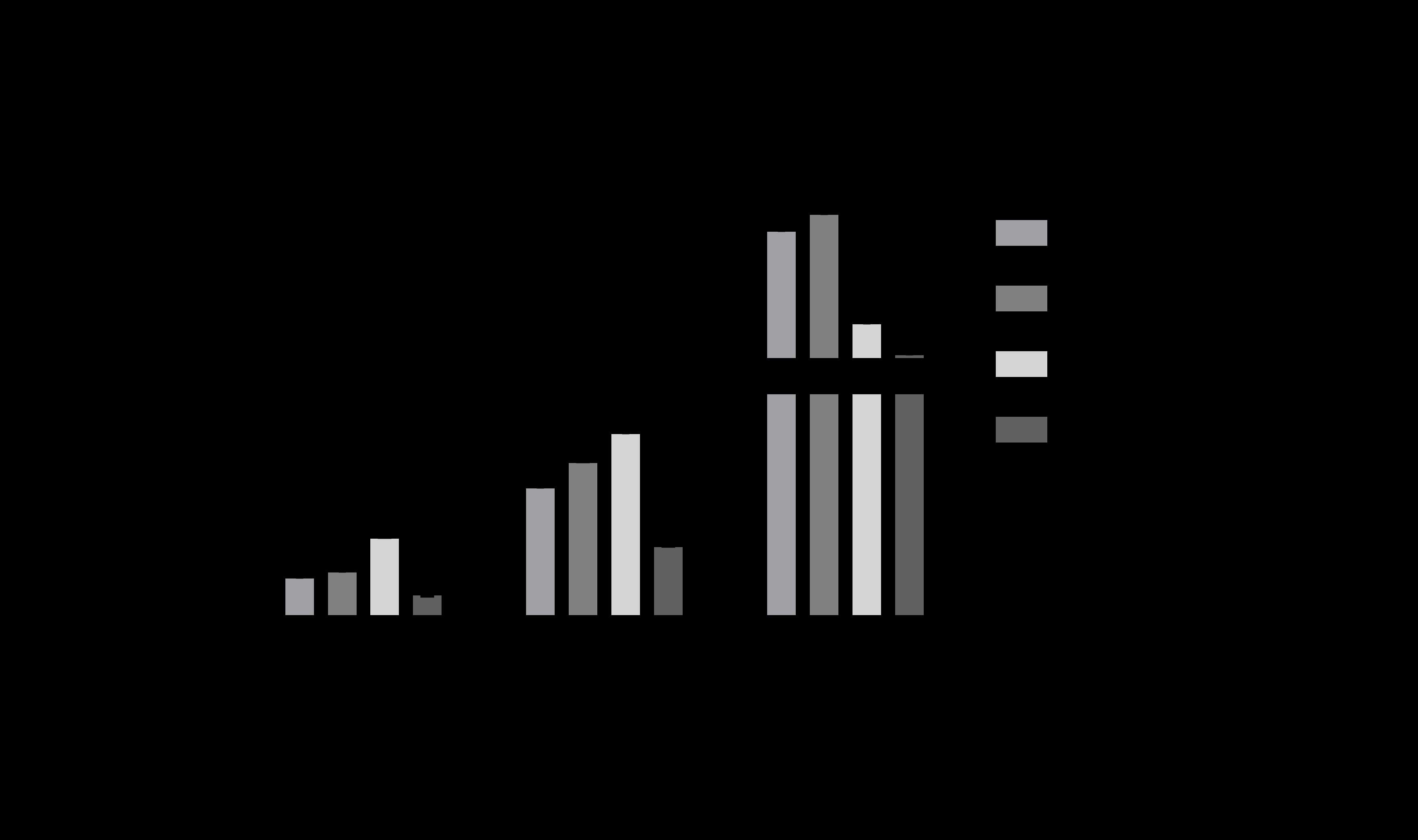
Figure 2
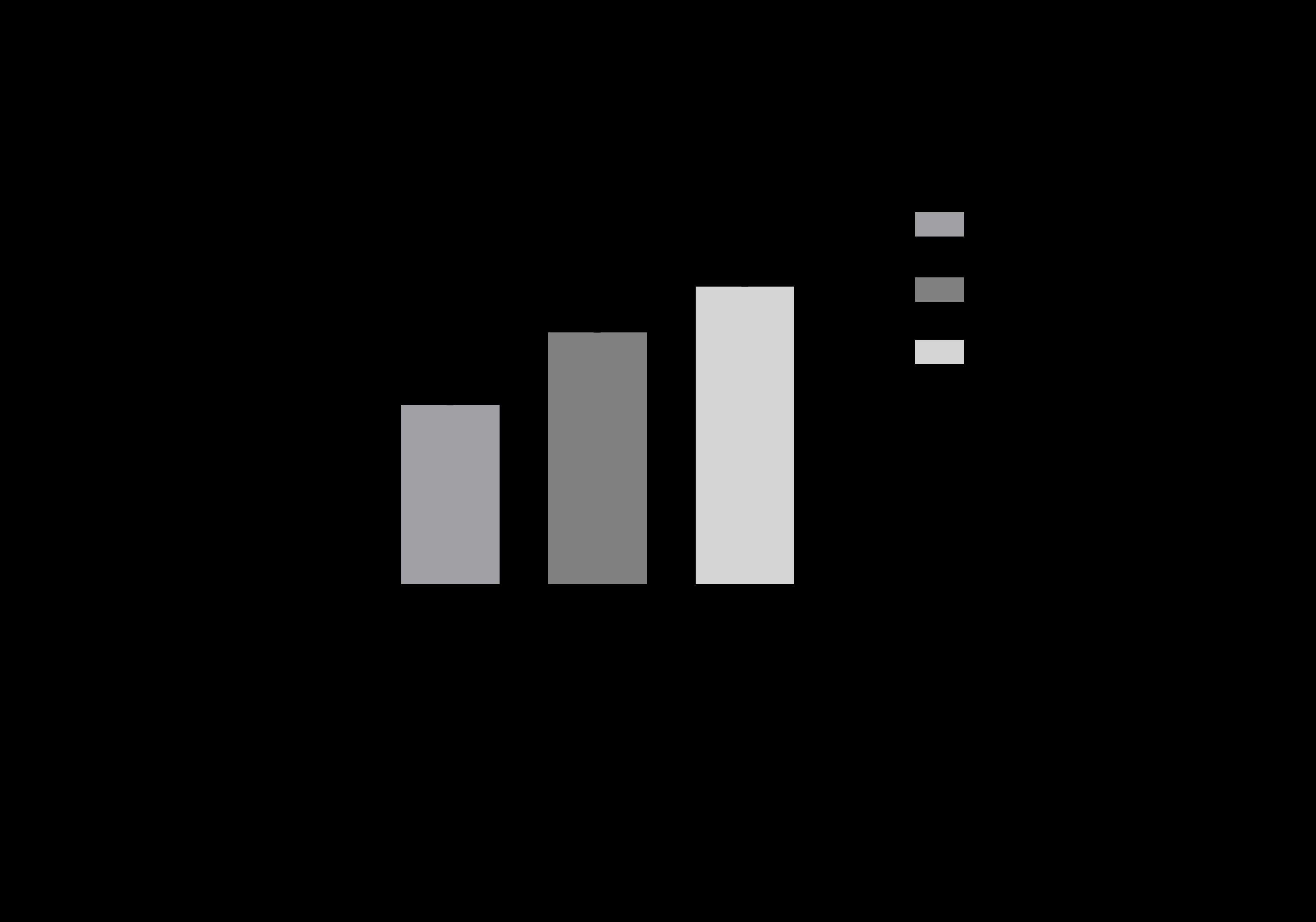
Figure 3#7963
Automating Pre-Operative Joint Kinematics: Segmenting Native Bones With Deep Learning for Improved TKA Diagnostics
*Sasank Desaraju - University of Florida - Gainesville, United States of America
Andrew Jensen - University of Florida - Gainesville, USA
Selena Tinga - Cornell University - Ithaca, USA
Stephen Jones - University of Florida - Gainesville, USA
Scott Banks - University of Florida - Gainesville, USA
*Email: sasank.desaraju@ufl.edu
Introduction and Aims: Pre-operative measurement of knee bone kinematics does not have a mature solution despite the clinical advantages it offers such as quantification of disease state before intervention and range-of-motion comparison with post-surgical outcomes. This study seeks to lay the foundation for a native bone kinematics pipeline by creating a neural network model for bone segmentation from x-ray images. The study has three aims. The first aim (1) is to determine the general performance of a convolutional neural network (CNN) at segmenting bones from fluoroscopy images. Next (2), we determine the effect of TPLO (Tibial Plateau Leveling Osteotomy) implants on performance. This small tibial implant may suggest how other implants impact segmentation. Finally (3), we evaluate the ability of a CNN to guess bone anatomy that extends beyond the x-ray.
Materials and Methods: A canine model was used for simple data acquisition and similarity to human anatomy. 2,079 total images from 10 patients were used, with patients having gait cycle trials from the surgical leg pre-op, the surgical leg post-op, and the contralateral leg post-op. The data was split into groups with implants (n=1180) and without implants (n=899). Different CNN models were trained based on the bone (femoral or tibial) and presence of implant (clean, implanted, or mixed). Finally, a new model was trained with the portion of the image label that extends off screen removed (see Figure 2). All models had a training/validation split of 80/20 using the same sets of randomly selected images. During all image loading of all models (save one pair for demonstration), the x-ray images were all cropped to a small region around the mask label in an effort to eliminate the second, irrelevant leg from the image (Figure 1). In all models, the training images were augmented using the Albumentations package for increased robustness.
Results and Discussion: The CNN models performed strongly, with IOU values of over 0.98 for both bones when using all data (Figure 3). The differences between the models with different implant presence was minimal. The slightly increased IOU of the mixed models of both bones are likely due to the larger sample size when using all images. This means that training the data on heterogeneously implanted data will likely result in a network that can segment both clean and implanted bones, at least for small implants like TPLO. The paltry increase in IOU in the “bordered” trial (Figure 3) yields the surprising result that the CNN models can “guess” where the femur and tibia ends are when they go off screen.
Conclusion: We present a model for segmenting native bones from single-plane x-ray images that is highly accurate, is proofed against the presence of TPLO implants, and can even segment off-screen segments of bone based on the bone sections that are visible. This is a promising step towards development of a pipeline that automatically extracts 3D joint kinematics from x-ray images, enabling novel clinical diagnostic tools as well as pre-operative measurements of mobility to compare with post-op evaluations.
#7553
Worldwide in-Vivo Weight-Bearing Kinematics for Three BCS TKA Cohorts Compared to the Normal Knee
*Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: gdessing@vols.utk.edu
Introduction:
The bi-cruciate stabilized (BCS) total knee arthroplasty (TKA) features a dual cam-post mechanism meant to substitute for both the anterior and posterior cruciate ligaments (ACL, PCL), as proper substitution of both cruciate ligaments may result in more normal-like kinematics throughout a larger flexion range compared to designs that only account for the PCL through substitution or retention. The objective of this research study was to compare the kinematics of three independent cohorts around the world using the same BCS-TKA design to normal knee kinematics under in vivo, weight-bearing conditions.
Methods:
In vivo kinematics were assessed for 70 subjects – 60 BCS-TKA (20 from the US, 20 from Portugal, and 20 from Belgium) and 10 healthy, normal knees from the US – using a C-ARM fluoroscopic system for data acquisition and then evaluated using a 3D-to-2D registration technique. Each location offered subjects from a single surgeon that met recruitment criteria while normal knees were chosen through volunteers that met separate participation conditions. All subjects performed a deep knee bend (DKB) activity while under fluoroscopy, flexing from extension (0°) to a maximum (MAX) weight-bearing flexion. The kinematic parameters that were assessed for each subject were lateral and medial anterior/posterior (LAP, MAP) position and axial orientation.
Results:
All three cohorts experienced excellent weight-bearing flexion and condylar rollback patterns. The BCS1 cohort had an average flexion of 131.8° and experienced continuous lateral rollback (Figure 1). The BCS1 cohort also exhibited greater magnitudes of medial rollback (Figure 2) compared to the other cohorts, leading to less axial rotation (Figure 3). The BCS2 cohort had an average flexion of 108.6° and experienced LAP trends similar to that of the normal knee (Figure 1). The BCS3 cohort had an average flexion of 114.9° and also saw very similar LAP trends to that of the normal knee (Figure 1). Both BCS2 and BCS3 displayed minor anterior motion through mid-flexion (30°-90°) (Figure 2), which resulted less than normal-like axial orientation (Figure 3). The normal knee cohort averaged 139.0° of flexion, the LAP displayed continuous rollback through flexion, with larger magnitudes in both early- (0°-30°) and deep-flexion (90°-MAX) (Figure 1). The MAP position of the normal cohort had less rollback (Figure 2), which contributed to a greater internal orientation in early-flexion carrying to a greater external orientation in deep-flexion (Figure 3).
Discussion:
The BCS cohorts exhibit kinematics that compared well to those of the normal knee during certain ranges of motion of DKB with more variability in mid- and deep-flexion. The similarities that exist in early-flexion suggest that the anterior cam-post is indeed capable of holding the role held by the ACL in the normal knee. It can also be seen that the posterior cam-post facilitates PCL function by assisting with rollback from mid- into deep-flexion to achieve more normal-like kinematic trends. However, in mid-flexion, when neither the anterior nor posterior cam-post are engaged, anterior motion can still be seen among the BCS cohorts that differ from normal knee kinematics.
Keywords: BCS, TKA, Normal, Knee, Fluoroscopy, Kinematics
Figures
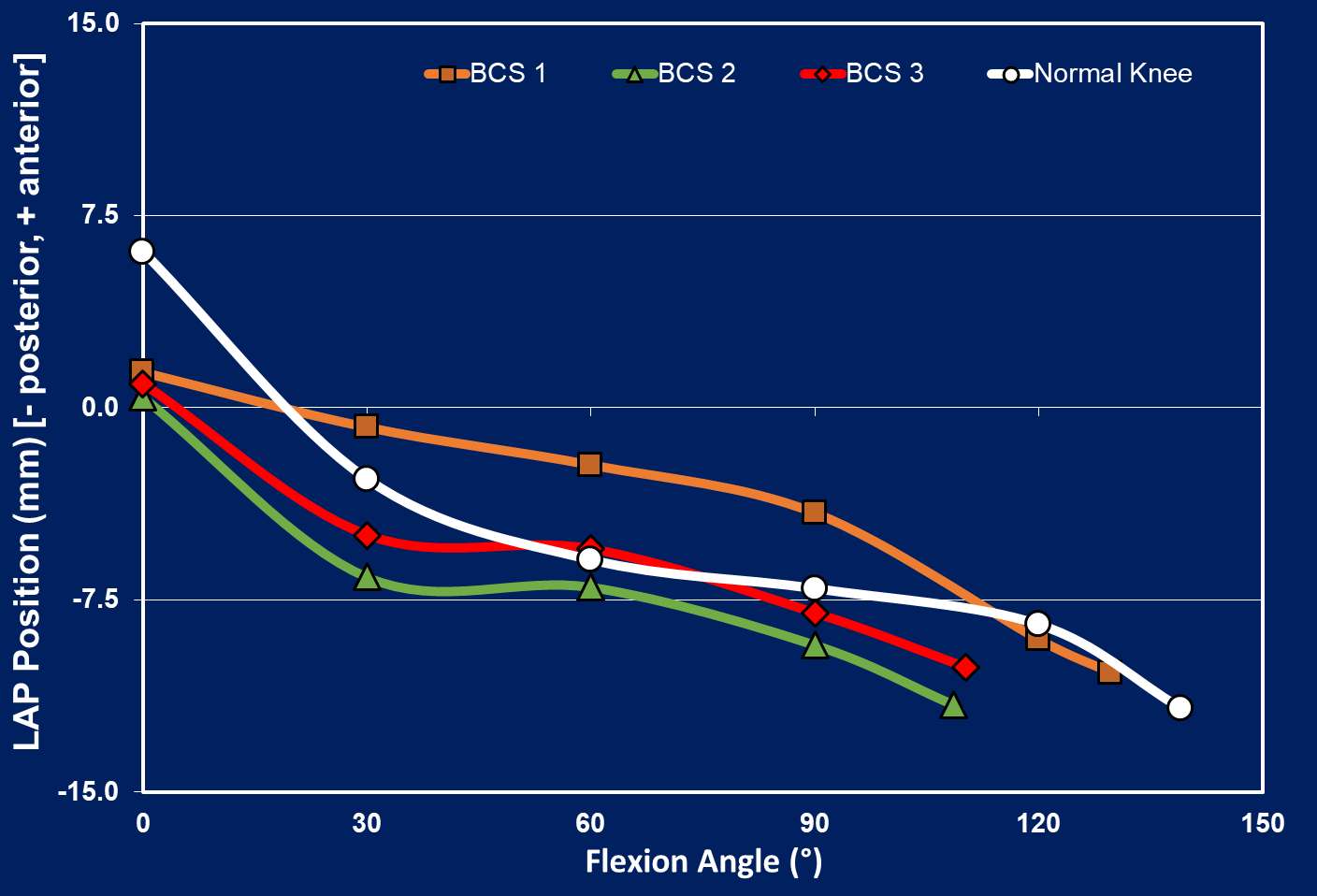
Figure 1
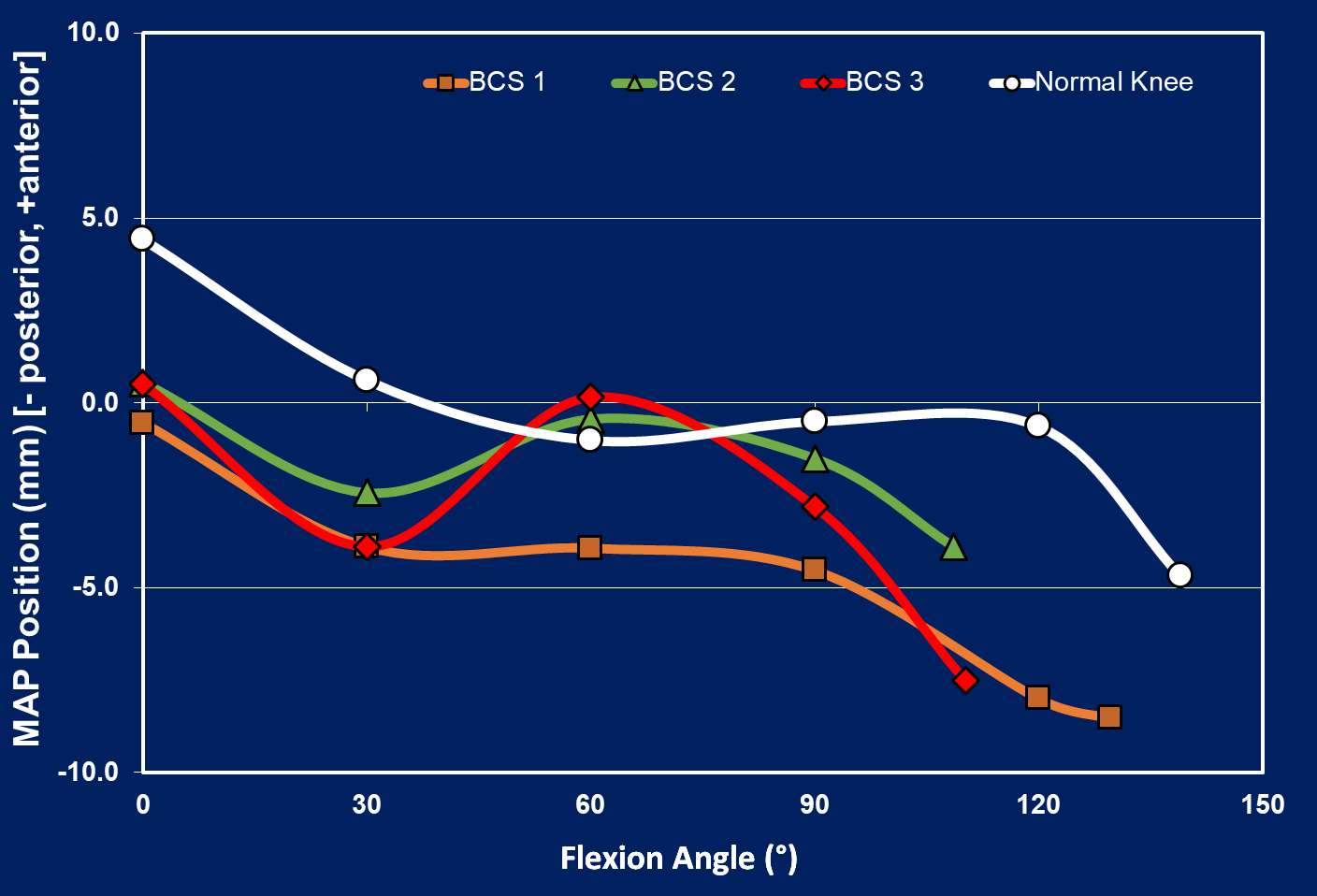
Figure 2
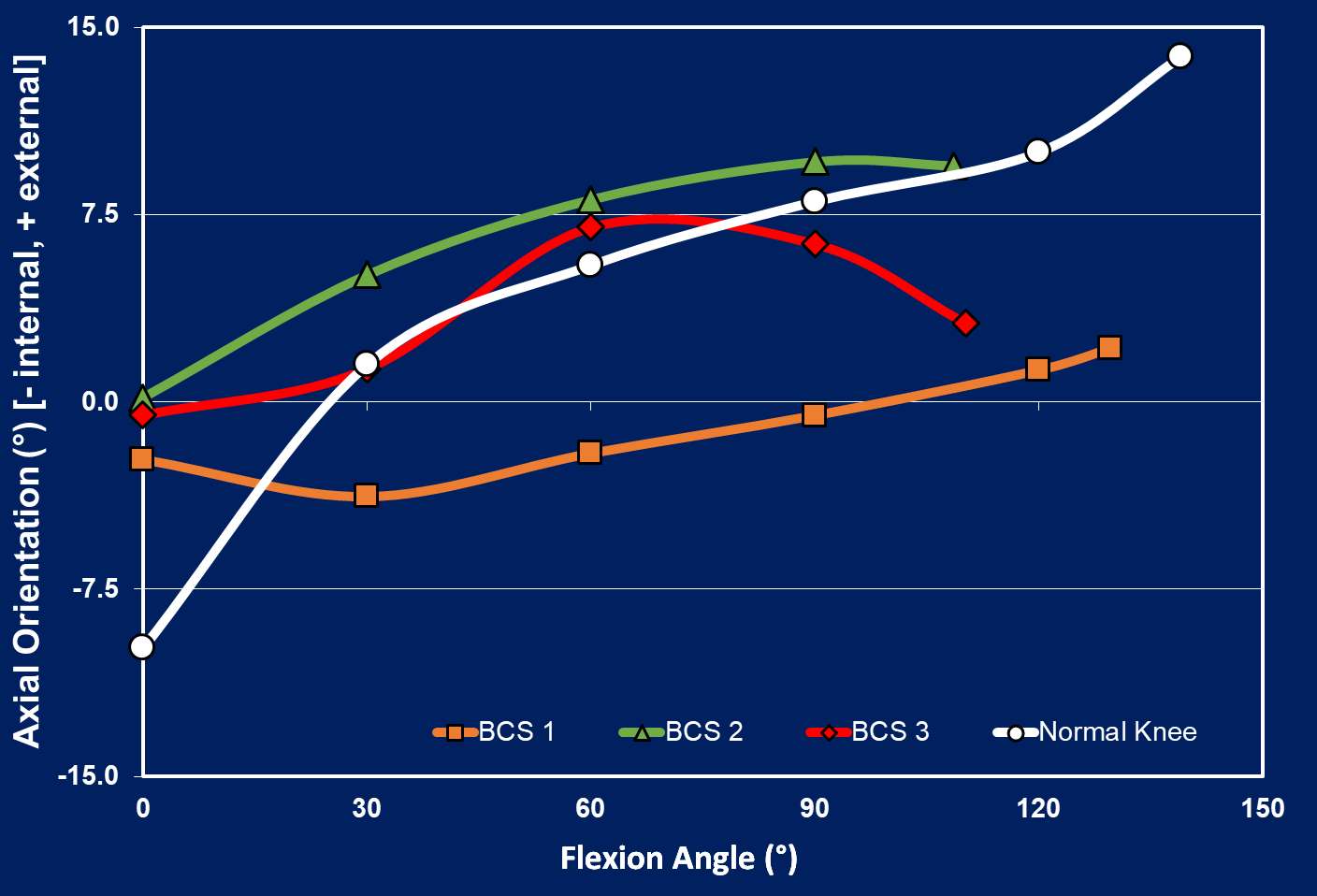
Figure 3#7554
In-Vivo Kinematics of Over 1300 Total Subjects, Including Four Implant Types and Normal Knee Comparisons
*Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: gdessing@vols.utk.edu
Introduction:
Through the history of total knee arthroplasty (TKA), it has often been discussed which cruciate ligaments of the knee joint should be retained, substituted, or removed entirely. Similar discussions regarding how the postoperative mechanics of TKAs should compare to normal knees have also been entertained. Should the “success” of a TKA design be awarded purely by subjective patient-reported outcome scores, the ability to replicate the normal knee kinematics, or something else? The objective of this analysis is to evaluate the different trends within implant types that exist as compared to normal knee kinematics using data collected over the last decade.
Methods:
In vivo kinematics were assessed for 1228 TKA subjects – 61 bi-cruciate retaining (BCR), 196 bi-cruciate stabilized (BCS), 503 posterior cruciate retaining (PCR), 468 posterior stabilized (PS) – and 114 normal knees. In vivo kinematics were obtained using fluoroscopic 3D-to-2D registration techniques. All data in this analysis was collected through various studies that have been conducted over several years. All subjects performed a weight-bearing, deep knee bend (DKB) activity while under fluoroscopy and this analysis focused on the kinematics between full-extension (0°) and deep-flexion (120°). The kinematic parameters that were assessed for each subject were lateral and medial anterior/posterior (LAP, MAP) condylar position and axial orientation.
Results:
During DKB, the average lateral rollback for the BCS cohort was 16.4mm posterior while the average medial rollback was 10.4mm posterior. The BCS cohort also exhibited an average axial rotation of 7.3° of external rotation. The BCR average lateral rollback was 9.3mm posterior, the average medial rollback was 2.9mm posterior, and the average axial rotation was 8.5° external. The PS cohort had an average lateral rollback of 7.8mm posterior and an average medial rollback of 3.8mm posterior, with an average axial rotation of 4.4° external. The PCR average lateral rollback was 3.4mm posterior, the average medial rollforward was 1.4mm anterior, and the average axial rotation was 5.8° external. Lastly, the normal knee cohort had an average lateral rollback of 17.5mm posterior, an average medial rollback of 7.4mm posterior, and 21.7° of external axial rotation. Detailed kinematics can be found in Figures 1-3.
Discussion:
Comparing the TKA cohorts to the normal knee averages, it can be interpreted that the BCS TKA, with its dual cam-post mechanism design, is able to most closely replicate normal knee position in early flexion compared to the other design averages. The BCR TKA also appears to maintain a similar trend throughout flexion, indicating that the retention of both cruciate ligaments helps guide posterior movement on the lateral side with less on the medial side, leading to axial rotation patterns similar to the normal knee. By not accounting for the functionality of the ACL, the PS and PCR designs both show general posteriorized positions of both condyles on average compared to the normal knee.
Keywords: BCS, BCR, PS, PCR, Normal, Knee, Fluoroscopy, Kinematics
Figures
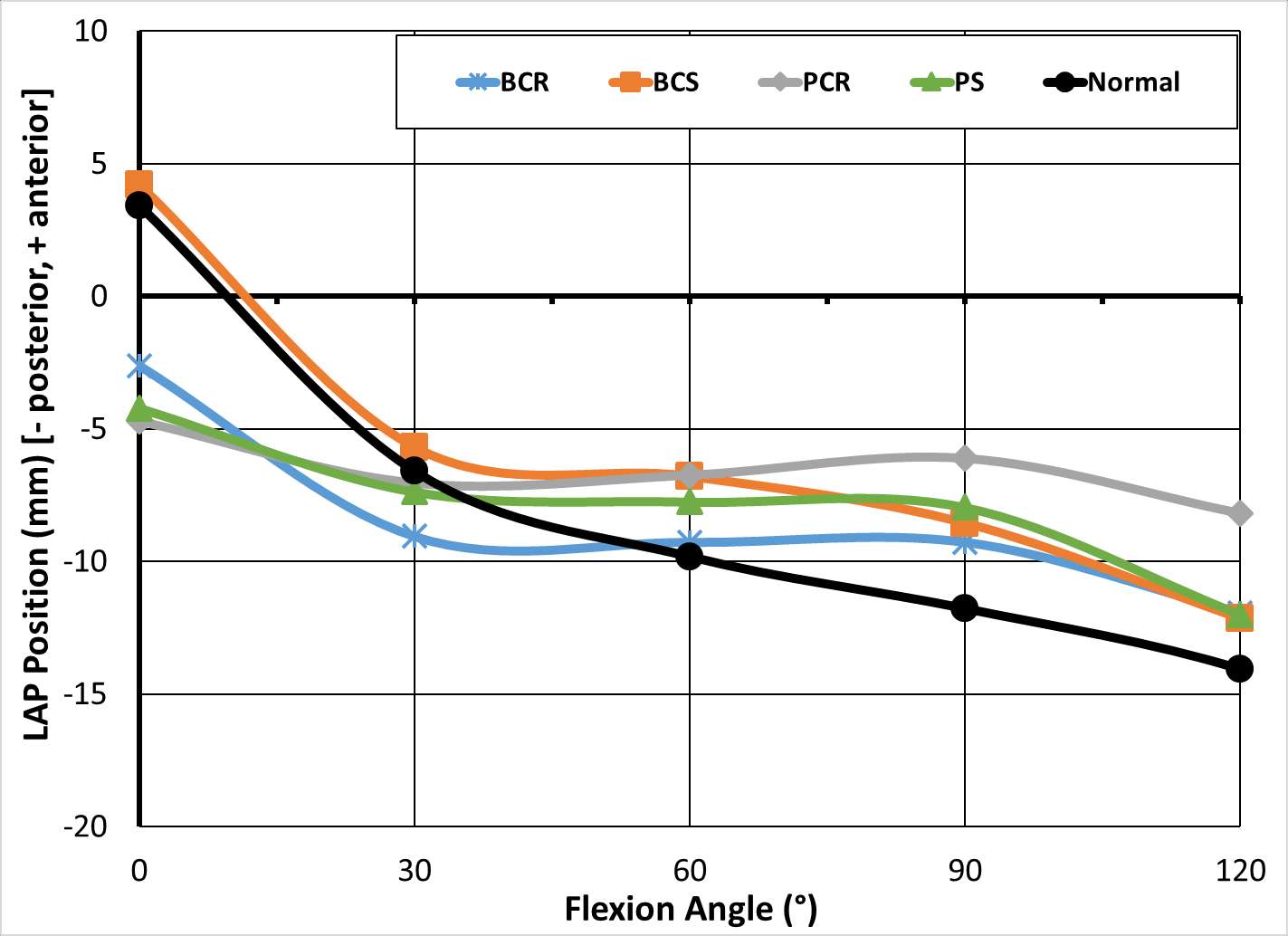
Figure 1
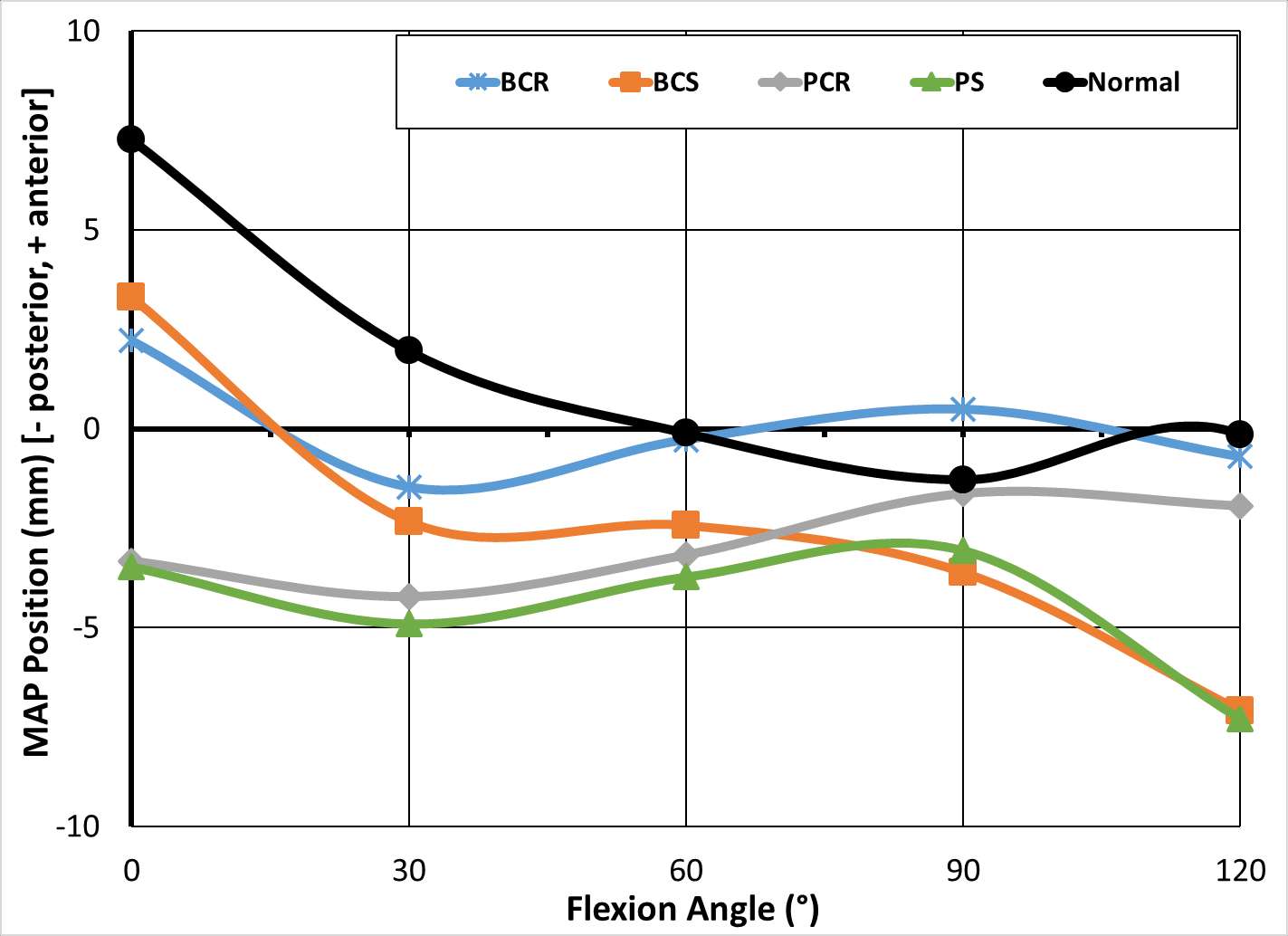
Figure 2
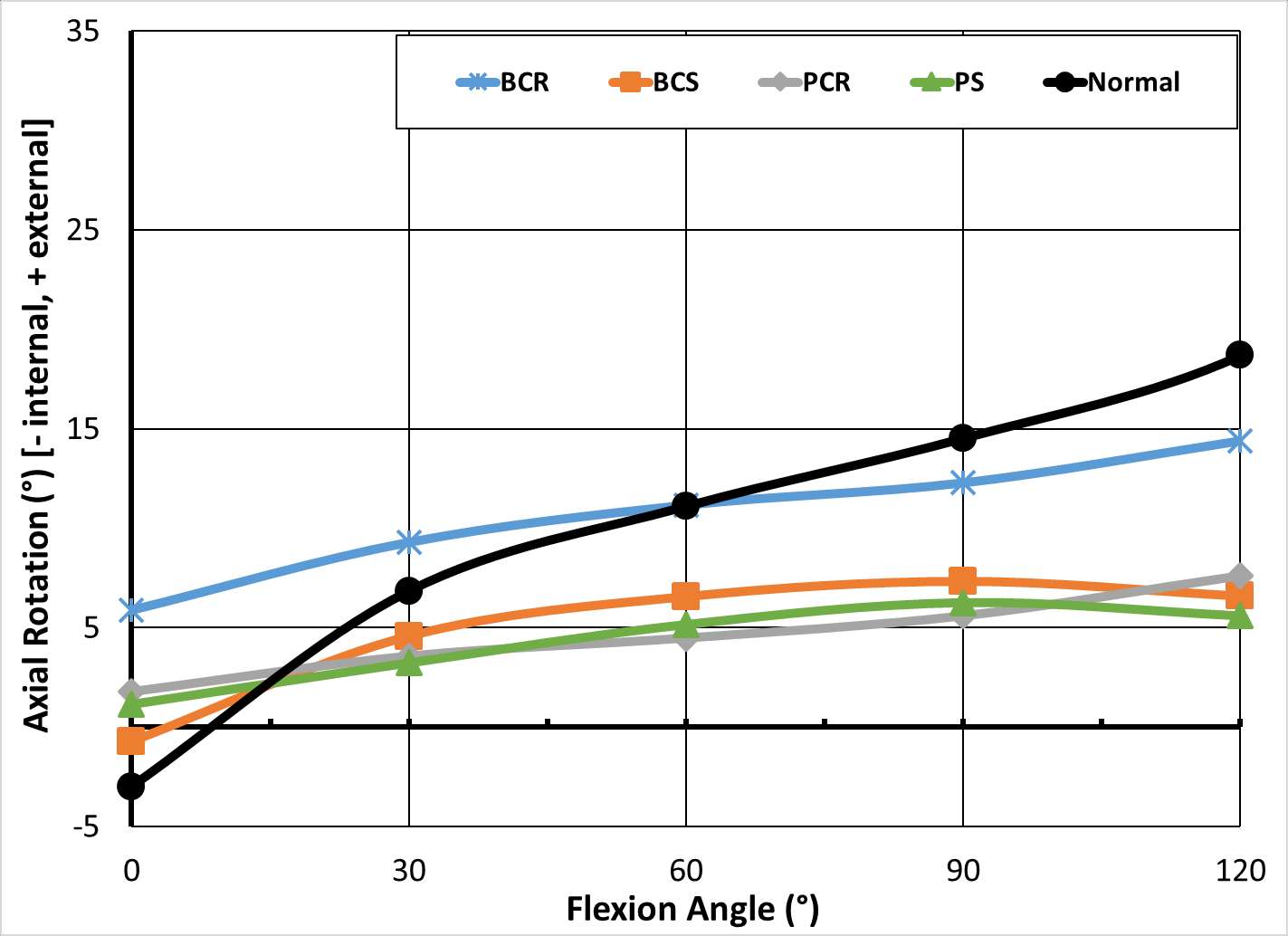
Figure 3#7521
Spanish Translation of the HOOS, JR. for Primary Total Hip Arthroplasty
*Stephen Lyman - Hospital for Special Surgery - Fukuoka, Japan
Amethia Joseph - Hospital for Special Surgery - New York, USA
Allison Diaz - Hospital for Special Surgery - New York, USA
Alejandro Gonzalez Della Valle - Hospital for Special Surgery - New York, USA
Jose Rodriguez - Lenox Hill Hospital - New York, USA
Bella Elogoodin - Hospital for Special Surgery - New York, USA
*Email: lymans@hss.edu
Introduction
The HOOS, JR. was endorsed as an acceptable patient reported outcomes measure (PROM) by the Centers for Medicare and Medicaid Services (CMS) in 2015 as part of their Comprehensive Joint Replacement (CJR) bundled payment program. Since that time hospitals and ambulatory surgery centers have been incentivized to collect the HOOS, JR. on all Medicare eligible patients undergoing primary total hip arthroplasty (THA). However, approximately 13% of the American public speaks Spanish at home and to date, the HOOS, JR. has only been available in English. We, therefore, endeavored to translate and cross culturally adapt the HOOS, JR. into Spanish.
Methods
Following the best practices for cross cultural adaptation of health surveys, we performed two simultaneous forward translations of the HOOS, JR. into Spanish using two native Spanish speakers (one hip surgery expert and one non-expert). These simultaneous translations were then harmonized through a discussion between the translators until consensus was reached. Back translation then proceeded with two native English speakers fluent in Spanish. These were also harmonized until consensus. The Spanish and back-translated English HOOS, JR. surveys were then evaluated by our expert panel (4 translators, 2 Spanish speaking orthopedic surgeons, one linguist, and one research methodologist). This panel came to a consensus on a pre-final translation of the HOOS, JR.
This pre-final translation was then administered to 22 Spanish speaking patients undergoing THA with a board-certified orthopedic surgeon at our hospital. These patients were invited to provide feedback on their understanding of the items (questions) and response options for each item. All interviews were audio recorded for reference and any challenging language revealed by these interviews was modified through a consensus process within the expert panel.
Results
Eleven discrete phrasing discrepancies in the instructions (5 discrepancies), items (6 discrepancies), or responses (none) were identified and resolved through the translation, back-translation, and consensus process. Recruited patients were 68% female, with a median age of 63 years (45-74), 41% had acquired less than a college degree while 50% were from the Caribbean, 41% from South America, and 9% from Central America. The introductory instructions and all items were scored as “no difficulty” or “low difficulty by more than 90% of patients (Figure 1). Two sub-section instructions (stiffness and function/daily living) were scored as moderately difficult or worse by 12-14% of patients.
Discussion
We were able to successfully translate the HOOS, JR. into Spanish using best practices for the cross cultural adaptation of health surveys. Our translation is well understood by native Spanish-speaking patients residing in the United States. Our next step will be confirm that this Spanish HOOS, JR. demonstrates similar psychometric properties to the original English HOOS, JR.
Figures
Figure 1#7697
Influence of the Deep and Superficial Medial Collateral Ligament on Knee Stability During Simulated Clinical Laxity Tests
*Callahan Doughty - Western University - London, Canada
Ryan Willing - Western University - London, Canada
Alan Getgood - Fowler Kennedy spirt medicine Clinic - London, Canada
Thiago Vivacqua - Fowler Kennedy Sport Medicine Clinic. - Lonndon, Canada
Tina Khazaee - Fowler Kennedy Sport Medicine Clinic. - London, Canada
Samira Vakili - Western University - London, Canada
*Email: cdought@uwo.ca
Purpose: Injuries to medial ligamentous structures of the knee are common among athletes. Previous cadaver studies have measured knee stability (or laxity) in vitro, through the application of forces and torques across the joint. Loads applied using a 6 degree of freedom robot [1,2,4,5] mimic those applied during clinical laxity tests, and resulting kinematics are measured after simulated ligament injuries are compared with intact knee kinematics. Previous studies examined the roles of the superficial medial collateral ligament (sMCL) and deep MCL (dMCL) in maintaining knee stability [2-4], with conflicting findings. Thus, the objective of this study is to evaluate changes in knee kinematics and in situ ligament forces during simulated laxity tests following complete sMCL and complete dMCL injuries.
Methods: Sixteen cadaver knees were potted and mounted onto 6 degrees of freedom force- and displacement-controlled joint motion simulator (AMTI VIVO). During laxity testing, the joint motion simulator applied loads including an 8 Nm valgus moment, a 4 Nm external rotatory torque, a 4 Nm internal rotatory torque, and loads for testing anteromedial rotatory laxity (89 N anterior tibial force plus a 4 Nm external rotatory torque) at the flexion angles of 0°, 30°, 60° and 90°. Intact joint behavior was recorded, followed by one of three different injury sequences: Sequence 1 (n = 8) comprised cutting the ACL, dMCL, and then sMCL; Sequence 2 (n=4) comprised cutting the ACL, dMCL, and then sMCL; and Sequence 3 (n=4) comprising cutting the dMCL, sMCL and then ACL.
Results: With the ACL deficient, a significant increase (p<0.01) in valgus laxity was observed across flexion upon sectioning of the dMCL and sMCL. Although, with the ACL intact, under the same conditions, laxity increased, however, it was not significant (p>0.05). In ACL deficient specimens, the sMCL restrained 63% of the load, with the dMCL only restaining 16%. While in extension in ACL deficient knees the dMCL restrained 22% of the ER load, and the sMCL restrained 20%, however, throughout flexion the sMCL restrained 32% and the dMCL restrained 20% of the ER load.
Conclusion: The sMCL is the main restraining ligament to valgus forces and utilizes the dMCL and co-stabilizing ligaments to restrain joint laxity. Additionally, the sMCL is the major contributor to knee stability in the case of ER loading. Differing from previous literature [1], the sMCL’s role in IR restraint was found to be insignificant. Furthermore, it was determined that kinematics and force contribution are not entirely correlated, small laxity increases can cause large load transfer to co-stabilizers, an undetectable observation by physical assessment.
References: [1] S. Ball et al. Knee Surgery, Sports Traumatology, Arthroscopy, 2020. [2] LaPrade et al. Am J of S medicine, 2009. [3]Robinson et al. Am J of S medicine, 2006. [4] LaPrade et al. Am J of S medicine, 2009. [5] Weirer et al. Knee Surgery, Sports Traumatology, Arthroscopy, 2021.
Figures
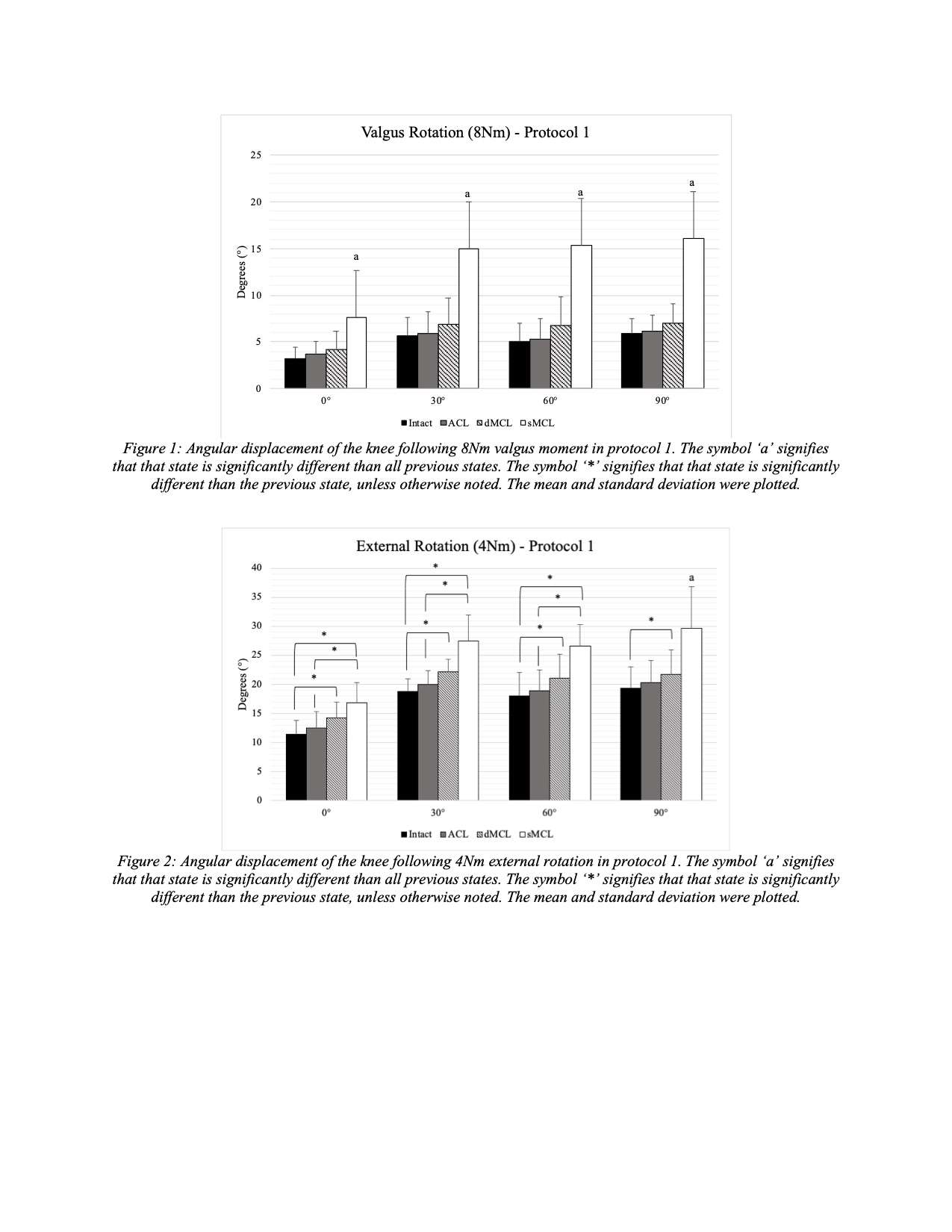
Figure 1
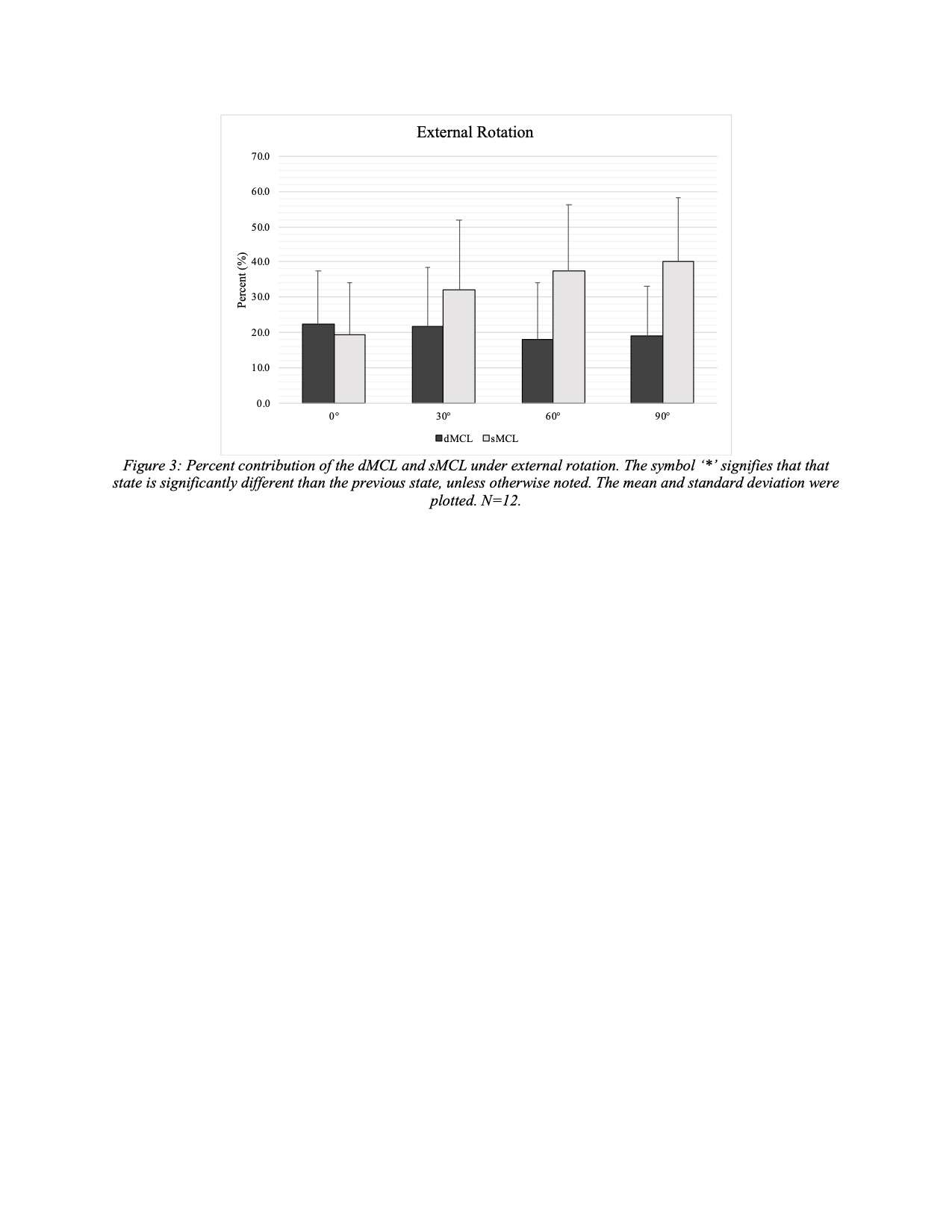
Figure 2#7407
Disruption of Arthroplasty Rehabilitation Episode of Care
*Charles Fisher - Hospital for Special Surgery - New York, USA
Danielle Edwards - Hospital for Special Surgery - Manhattan, United States of America
*Email: fisherc@hss.edu
Introduction:
As arthroplasty numbers in the world continue to increase along with a push for more value-based care, there is need to rethink how arthroplasty rehabilitation is performed. Historically, acute care rehabilitation has focused on providing care only to patients admitted to the hospital. Impactful rehabilitative pre-operative care wasn’t typically performed, while post-acute care was provided by either outpatient, subacute/acute or home physical therapists. Disciplines such as social work and physical therapy requested similar information from patients to assist in discharge planning. This results in many layers of providers, duplication, inefficiencies, waste along with increased utilization and cost.
Our innovative expansion of a traditional acute care rehabilitation role to a peri-operative model includes pre-operative, acute and post-acute phases of care with the goals of providing consistent, cost-effective care and communication to streamline the patient experience.
We leveraged technology to facilitate this expansion allowing for necessary communication, workflows and clinician information to flow amongst patients and our interdisciplinary team of healthcare providers.
Methods
We leveraged technology to create a collaborative perioperative rehabilitation program. We combined the role of a PT and a social worker and use logic-based rules within the electronic medical record to send clinical intake to patients pre-operatively to collect valuable pre-op information that is shared across the episode of care to multiple departments. Patient responses received within the patient portal triggered appropriate discharge planning responsibilities to either the PT or social worker to match patient need to provider type. A virtual decision tree allowed for patient choice for treatment location and type of pre-operative rehabilitation visit: virtual vs in-person.
Our post-acute program utilizes EMR integrated and synchronous telehealth to provide virtual PT visits to patients after hospital discharge. Clinical information from the pre-op and acute phases is shared to provide most accurate care to patient. All is done through one application for ease of use. Specialized work queues were created for patient scheduling which allowed the administrative team to use information gathered at pre-op visit to help schedule post-op visits.
Results
Pre-op PT with discharge planning has become standard of care. 52% of patients did not need social work (figure 1). PTs were just as accurate in determining discharge disposition as social workers for appropriate patients (figure 2). Our post-acute telehealth program continues to be successful with high levels of patient satisfaction and outcomes at lower utilization levels to transitional home PT (figure 3).
Conclusions
Patient care workflows and outcomes can be greatly enhanced by utilizing technology to connect patients and patient information to providers. This expansion is not a destination but a step in our journey of utilizing technology to reduce utilization cost while improving outcomes.
References
LeBrun, D.G., Martino, B., Biehl, E. et al. Telerehabilitation has similar clinical and patient-reported outcomes compared to traditional rehabilitation following total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc (2022). https://doi.org/10.1007/s00167-022-06931-6
Fisher C, Biehl E, Titmuss MP, Schwartz R, Gantha CS (2019) HSS@Home, physical therapist-led telehealth care navigation for arthroplasty patients: a retrospective case series. HSS J 15:226–23
Figures
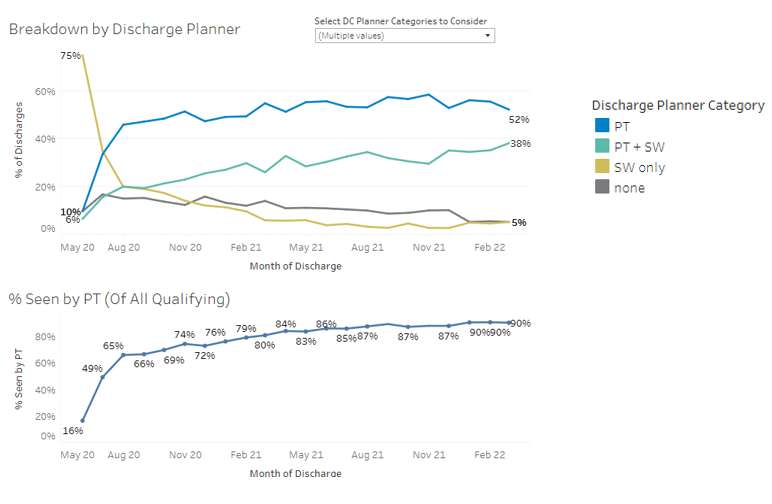
Figure 1
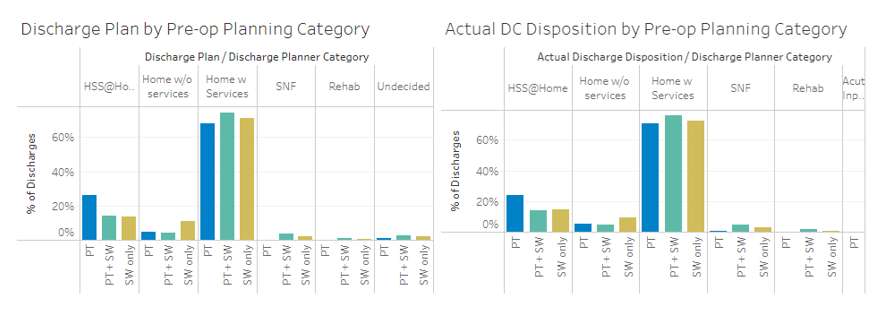
Figure 2
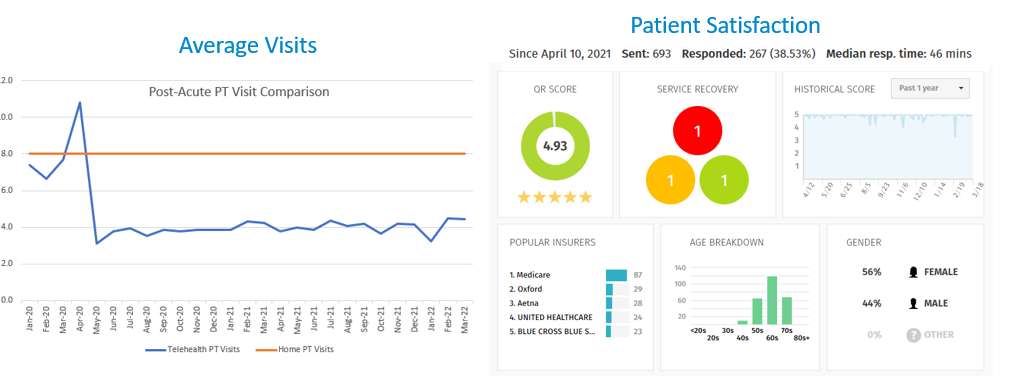
Figure 3#7850
An Automated, Web-Based Triage Tool May Optimise Referral Pathways in Elective Orthopaedic Surgery: A Proof of Concept Study
*Alexandra Stanley - Imperial College London - London, GB
Gareth Jones - Imperial College - London, United Kingdom
Thomas Edwards - Imperial College London - London, United Kingdom
Johnathan Lex - University of Toronto - Toronto, Canada
Martin Jaere - Imperial College London - London, United Kingdom
*Email: astanley1298@gmail.com
Introduction: Knee pain is common, representing a significant socioeconomic burden. Caused by a variety of pathologies, its evaluation in primary-care is challenging. Subsequently, an over-reliance on magnetic resonance imaging (MRI) exists. Prior to orthopaedic surgeon referral, many patients receive no, or incorrect, imaging. Electronic-triage (e-triage) tools represent an innovative solution to address this problem. The primary aim of this study was to ascertain whether an e-triage tool is capable of outperforming existing clinical pathways to determine the correct pre-hospital imaging based on knee pain diagnosis.
Methods: Patients ≥18 years with a new presentation of knee pain were retrospectively identified. The timing and appropriateness of imaging was assessed.A symptom-based e-triage tool was developed, using the Amazon LEXbot platform, and piloted to predict five common knee pathologies and suggest appropriate imaging.
Results: 1462 patients were identified. 17% of arthroplasty patients received an ‘unnecessary MRI’, whilst 28% of arthroscopy patients did not have a ‘necessary MRI’, thus requiring a follow-up appointment, with a mean delay of three months (SD 2.6, range 0.2-20.2) (Fig. 1). Using National Health Service (NHS) tariffs, a wasted cost through unnecessary/necessary MRIs and subsequent follow-up appointments was estimated at £45,816. The e-triage pilot was trialled with 41 patients (mean age:58.4 years, 58.5% female). Preliminary diagnoses were available for 34 patients. Using the highest proportion of reported symptoms in the corresponding group, the e-triage tool correctly identified three of the four knee pathologies (Fig. 2). The e-triage tool did not correctly identify anterior cruciate ligament injuries (n=3). User feedback was promising with 79.2% of participants stating they would use the tool again.
Conclusion: A significant number of knee pathology patients received incorrect imaging prior to their initial hospital appointment, incurring delays and unnecessary costs. A symptom-based e-triage tool was developed, with promising pilot data and user feedback. With refinement and use of larger datasets and robust machine learning algorithms, this tool has the potential to improve wait-times and referral quality, whilst reducing costs.
Figures
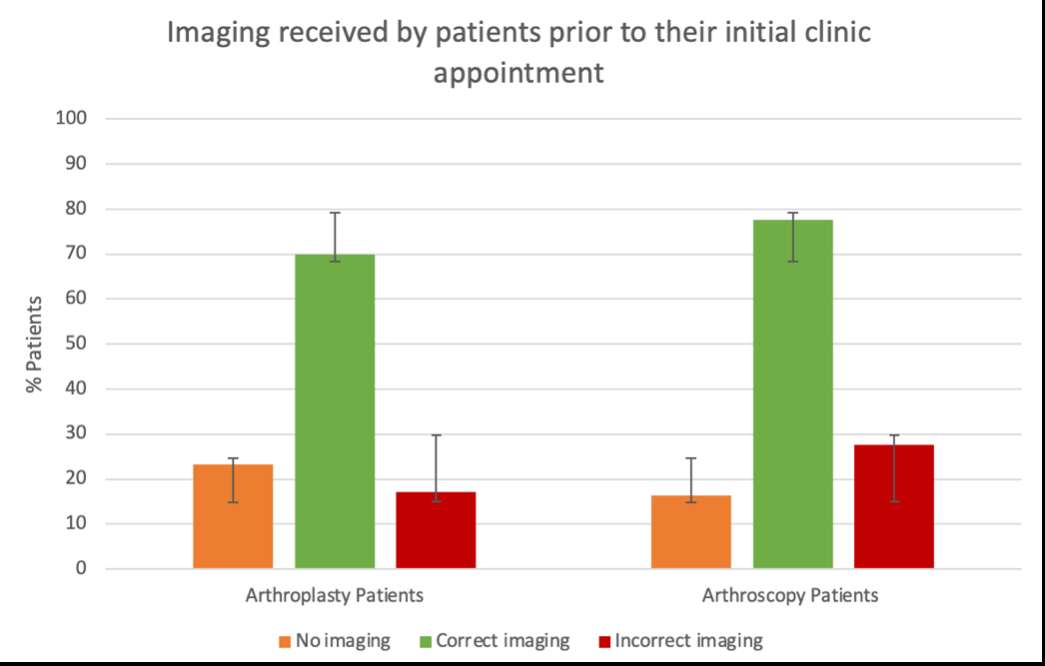
Figure 1
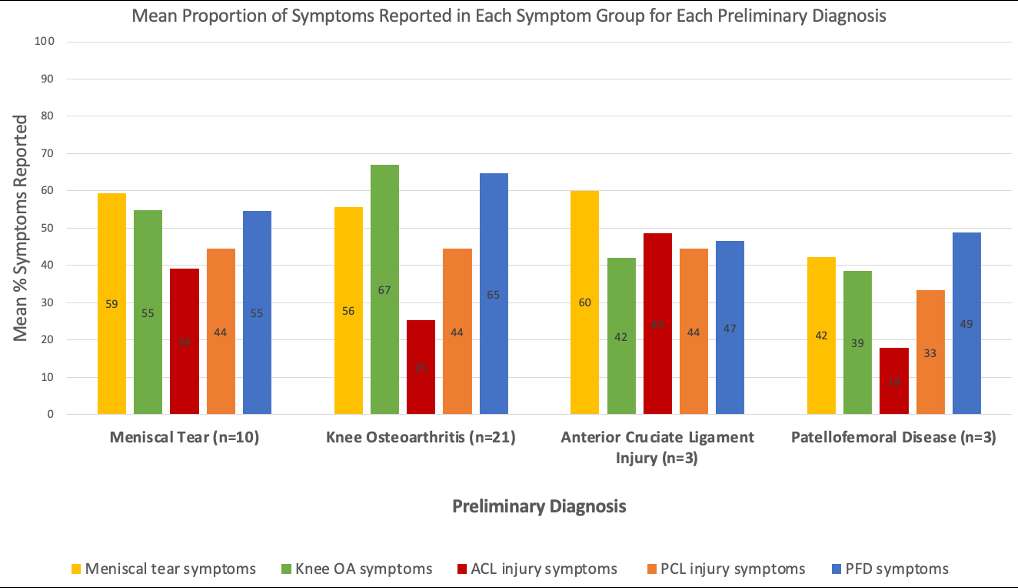
Figure 2#8017
Collaborative Team Training in Virtual Reality Is Superior to Individual Learning for Performing Anterior Approach Total Hip Arthroplasty: A Randomised Controlled Trial
*Thomas Edwards - Imperial College London - London, United Kingdom
Shubham Gupta - Imperial College London - London, United Kingdom
Daniella Soussi - Imperial College London - London, United Kingdom
Arjun Patel - Imperial College London - London, United Kingdom
Amogh Patil - Imperial College London - London, United Kingdom
Sikandar Khan - Imperial College London - London, United Kingdom
Alexander Liddle - Imperial College - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
Kartik Logishetty - Imperial College - London, United Kingdom
*Email: thomas.edwards@imperial.ac.uk
Introduction: Current evidence suggests that superior surgical team performance is linked to fewer intraoperative errors, reductions in mortality and even improved patient outcomes [1, 2]. Virtual reality has demonstrated excellent efficacy in training surgeons and scrub nurses individually, however its impact on training teams together is currently unknown [3, 4]. The anterior approach total hip arthroplasty is known to be a difficult operation to learn with a well established, strenuous early learning curve [5]. This study aimed to assess if training together (scrub nurse and surgeon) in an innovative multiplayer virtual reality program was superior to single player training for novices learning the difficult anterior approach total hip arthroplasty (AA-THA).
Methods: 40 participants (20 novice surgeons (PGY 1 to 3) and 20 novice scrub nurses) were enrolled in this study and randomised to individual or team virtual reality training. Individually-trained participants played with virtual avatar counterparts, whilst teams trained live in pairs (surgeon and scrub nurse) (Figure 1). Both groups underwent 5 VR training sessions over 6 weeks. Subsequently, they underwent a real-life assessment in which they performed AA-THA on a high-fidelity model with real equipment in a simulated operating theatre (Figure 2). Teams performed together and individually-trained participants were randomly paired up with a solo player of the opposite role. Videos of the assessment were marked by two blinded expert assessors. The primary outcome was team performance as graded by the validated NOTECHs II score. Secondary outcomes were procedure time and number of technical errors from an expert pre-defined protocol.
Results: Teams outperformed individually-trained participants for non-technical skills in the real-world assessment (NOTECHS-II score 50.3 ± 6.04 vs 43.90 ± 5.90, p=0.0275). They completed the assessment 28.1% faster (31.22 minutes ±2.02 vs 43.43 ±2.71, p=0.01), and made close to half the number of technical errors when compared to the individual group (12.9 ± 8.3 vs 25.6 ± 6.1, p=0.001).
Conclusions: Multiplayer, team training appears to lead to faster surgery with fewer technical errors and the development of superior non-technical skills in performing the difficult anterior approach total hip arthroplasty.
References
1. Fecso AB, Kuzulugil SS, Babaoglu C, Bener AB, Grantcharov TP. Relationship between intraoperative non-technical performance and technical events in bariatric surgery. Br J Surg 105(8): 1044, 2018
2. Mazzocco K, Petitti DB, Fong KT, Bonacum D, Brookey J, Graham S, Lasky RE, Sexton JB, Thomas EJ. Surgical team behaviors and patient outcomes. Am J Surg 197(5): 678, 2009
3. Logishetty K, Rudran B, Cobb JP. Virtual reality training improves trainee performance in total hip arthroplasty: a randomized controlled trial. Bone & Joint Journal 101B(12): 1585, 2019
4. Edwards TC, Patel A, Szyszka B, Coombs AW, Liddle AD, Kucheria R, Cobb JP, Logishetty K. Immersive virtual reality enables technical skill acquisition for scrub nurses in complex revision total knee arthroplasty. Archives of Orthopaedic and Trauma Surgery: 1, 2021
5. Hartford JM, Bellino MJ. The learning curve for the direct anterior approach for total hip arthroplasty: a single surgeon's first 500 cases. Hip Int 27(5): 483, 2017
Figures

Figure 1
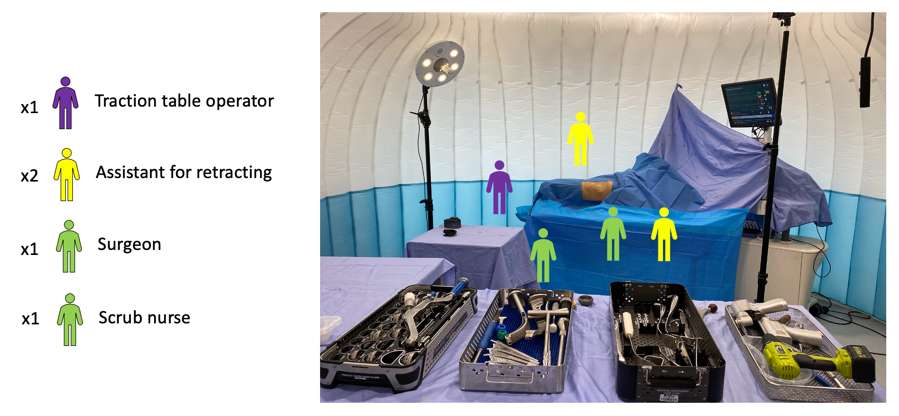
Figure 2#7597
Computational Modeling of Cathodic Voltage-Controlled Electrical Stimulation Applied to Total Knee Replacements
Priyanshu Vishnoi - University at Buffalo - Buffalo, USA
Elise Martin - University at Buffalo - Buffalo, USA
Mary Canty - Garwood Medical Devices - Buffalo, United States of America
Jackson Hobble - Garwood Medical Devices - Buffalo, USA
Tim Kopera - Garwood Medical Devices - Buffalo, USA
*Mark Ehrensberger - University of Buffalo - USA
*Email: mte@buffalo.edu
Introduction: Previous studies have shown that cathodic voltage-controlled electrical stimulation (CVCES) of titanium (Ti) implants is an effective and broad-spectrum antimicrobial treatment for implant-associated infections[1,2]. We have recently developed and validated a computational model of the electrochemical modifications that occur in the microenvironment adjacent to cathodically polarized, planar coupons of Ti [3]. The purpose of this study was to develop a computational model to generate temporal and spatial mapping of the electrochemical changes in the microenvironment adjacent to cathodically polarized total knee arthroplasty implants composed of cobalt-chromium-molybdenum (CoCrMo) in the presence and absence of bone cement coverage.
Methods: Human-sized, CoCrMo, femoral and tibial components of a total knee replacement system were subjected to potentiodynamic polarization tests within a custom test chamber filled with saline. An Ag/AgCl reference electrode was used and a custom flexible counter electrode was wrapped around the perimeter of the electrochemical cell. Curve-fitting was done on the polarization scan data using Matlab to evaluate the charge transfer coefficients and exchange current densities for the two dominant reduction reactions taking place on the implant’s surface, namely oxygen reduction reaction and hydrogen evolution reaction. Charge transfer coefficients and exchange current density serve as the input parameters for the Butler-Volmer equation. Computational models are developed using COMSOL Multiphysics (v 5.6). CAD models of human-sized knee implant structures the presence and absence of bone cement coverage (Fig 1) were imported into COMSOL. Cement coverage was modeled with a simple block or cone of inert material merged along the bone facing implant surface. Mathematical models are developed with Tertiary Current Distribution, Nernst-Planck physics interface of the Electrochemistry module in COMSOL. The model simulates the electrode surface reactions using Butler-Volmer kinetics. The Nernst-Planck equation and the condition of electroneutrality govern the mass transport of species through the electrolyte. The 3D computational simulations were performed with a saline electrolyte (0.154 M) and CVCES magnitudes of -1.9 V and -2.2V (vs Ag/AgCl) applied to all implant constructs for a period of 10 mins. The reportable outcomes included the spatial and temporal distributions of current density and pH.
Results: Fig. 2 displays the spatial distribution of the current density and pH values along the surface of the femoral and tibial components (with and without cement coverage) after 10 mins of CVCES at -1.9V has been applied. Fig.3 displays plots of the surface averaged current density and surface averaged pH values.
Conclusion: A novel computational model has been developed to simulate the electrochemical modifications associated with CVCES applied to human-sized, CoCrMo total knee replacement components in the presence and absence of bone cement coverage. This model will be used to optimize parameters for clinical translation of CVCES therapy to prevent/ eradicate implant infections.
References: 1.Ehrensberger,M et al. Biomaterials,2015.41(0)97-105. 2.Nodzo,S et al. Clin ortho rel res, 2016. 474(7): 1668-75 3.Clark,C et al. Electrochimica Acta, 2021 393:138853
Figures
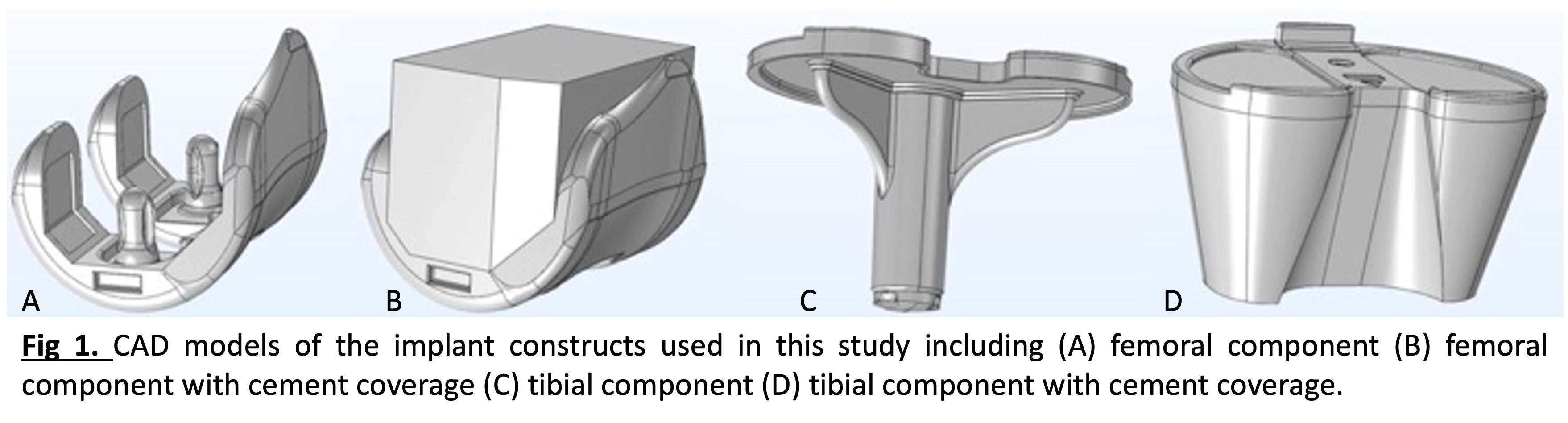
Figure 1
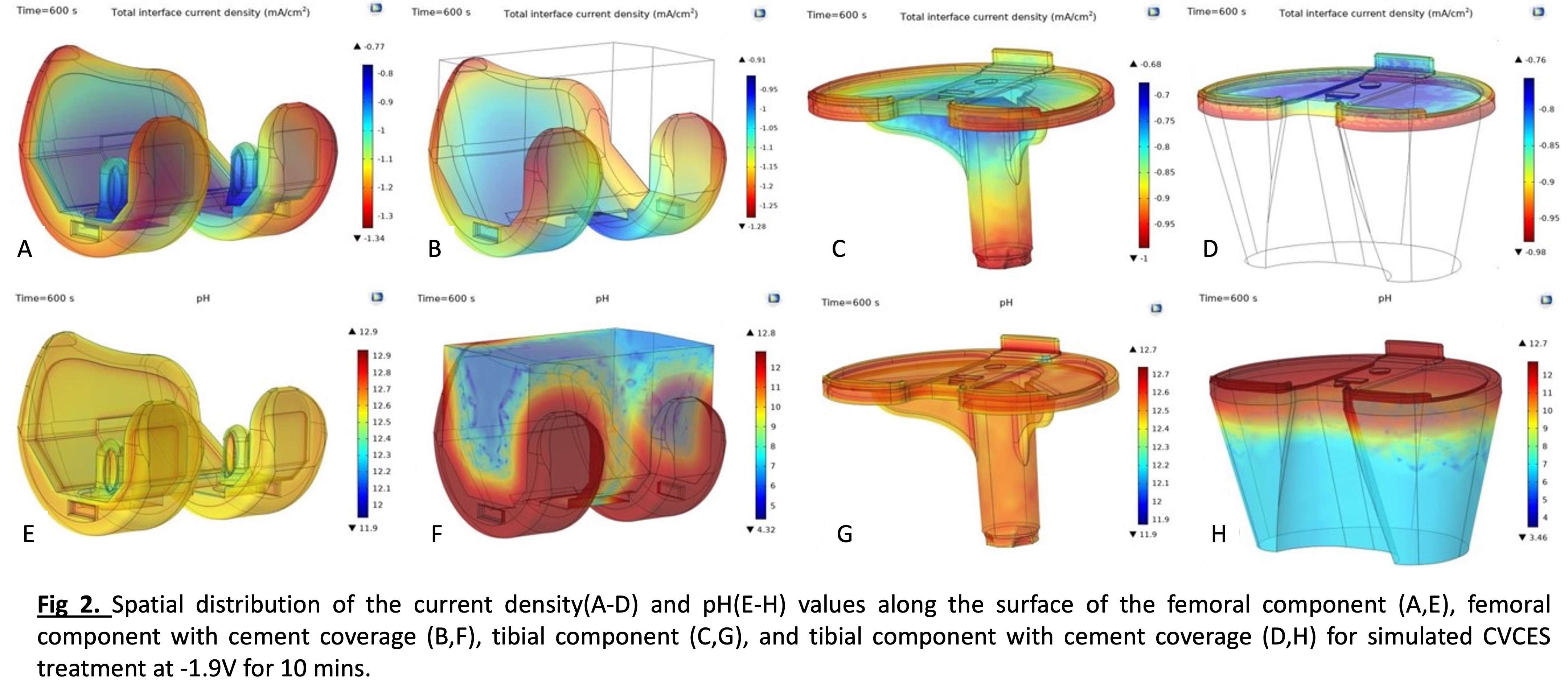
Figure 2
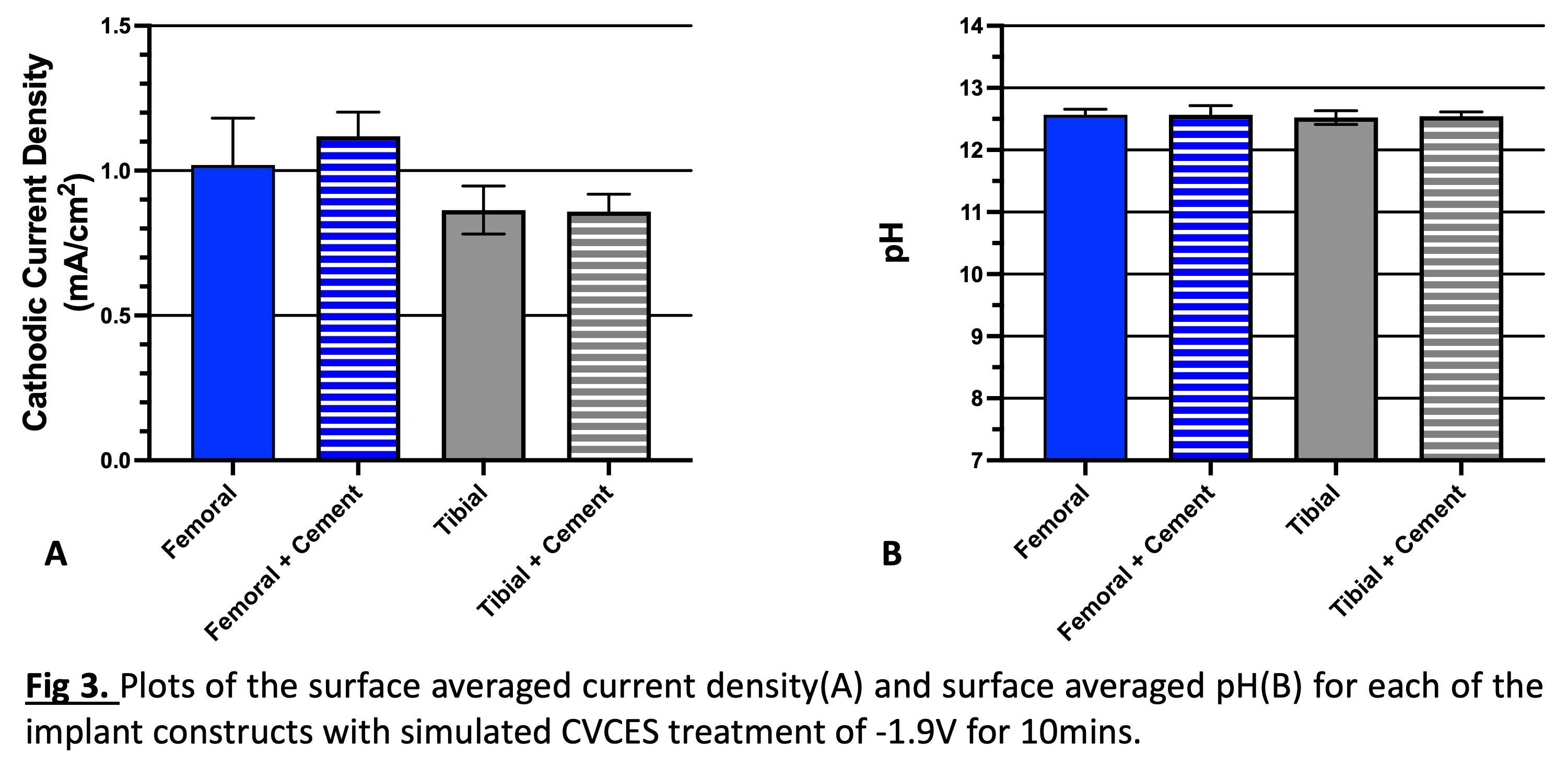
Figure 3#7437
New BCR Knee Arthroplasty Design
*Mohamed Elfekky - Dubai Health Authority - Dubai, United Arab Emirates
Samih Tarabichi - BURJEEL HOSPITAL FOR ADVANCED SURGERY - Dubai, United Arab Emirates
Diego Zamagni - ETH Zurich - Zurich, Switzerland
*Email: mohamelfekky2@yahoo.com
New BCR knee arthroplasty design
Dr Samih Tarabichi
Dr Mohamed Elfekky (presenter)
Introduction
Total knee arthroplasty are now needed in younger generation with higher needs. One of the solutions for this change in age limit was thought to be the BCR knee.
Since the first design of BCR knee arthroplasty and until now it didn’t meet inventors expectations either due to early failures or difficult insertion.
A new BCR implant design and a new surgical approach was suggested to change this case scenario.
Materials and methods
Systematic review of causes of failure of BCR knees were studied and design solution was proposed and tested through FEA.
Results
The new design showed high resistance to failure compared to other BCR knees, and new surgical approach showed to be more convenient in insertion
Discussion
The current design should go through further testing for clinical trials and FDA approvals
Conclusion
A new BCR knee design with modified surgical approach is presented with expectations for better performance
#7462
New Device to Detect Ligament Best Kinematic Position
*Mohamed Elfekky - Dubai Health Authority - Dubai, United Arab Emirates
Peter Theobald - Cardiff university - Cardiff, United Kingdom
Samih Tarabichi - Dubai, UAE
*Email: mohamelfekky2@yahoo.com
Introduction
Bicruciate retaining knee replacement was tho to be of better outcome and with better postoperative patient function and
Consequently better patient satisfaction
There was problem of possible attenuated ACL or possible other ligaments laxity with need for augmentation or reconstruction of ligaments.
The same case scenario can happen in other designs of knee arthroplasty
A new device was invented to detect the best kinematic position for reconstruction or augmentation of lax ligaments
Methods
Designing of a device that detects the best kinematic position of ligament
Testing of the device through bone models and cadavers was done
Results
The device detect the best near isometric point of ligaments to be tested
Discussion
This device is under development to be surgeon friendly and to get more applications
Conclusion
An invented device that detects the best isometric ligament position is discussed
#7977
Role of Midlevel Constraint in Reducing Midflexion Laxity After Additional Distal Femoral Resection in Posterior Stabilized TKA
*Shady Elmasry - Hospital for Special Surgery - New York City, USA
Brian Chalmers - Hospital for Special Surgery - New York CIty, USA
Cynthia Kahlenberg - Hospital for Special Surgery - New York City, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
David J. Mayman - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Michael Cross - Hospital for Special Surgery - New York City, USA
Carl Imhauser - USA
*Email: shady.elmasry.cu@gmail.com
INTRODUCTION: Surgeons commonly resect additional distal femur during primary posterior-stabilized (PS) total knee arthroplasty (TKA) to correct for flexion contracture. However, this procedure elevated the joint line, which is linked to increased midflexion laxity and may contribute to knee instability; a common cause of patient dissatisfaction [1]. A mid-level constrained (MLC) insert has been introduced to reduce knee laxity; however, the effect of MLC on tibiofemoral kinematics following this procedure is not well understood [2]. The goal of this study was to determine whether an MLC insert reduces mid-flexion laxity after joint line elevation in TKA.
METHODS: Six computational knee models with standardized capsular and collateral ligament properties specific to TKA were developed using measured resection principles (Fig. 1.a) [3]. PS and MLC inserts were utilized on each model (Fig. 1.b). A 10° flexion contracture was modeled by reducing the slack in the spring elements representing the medial and lateral posterior capsule while simulating a standard clinical exam of knee extension [4]. Distal femoral resections of 2 mm and 4 mm were simulated with both the PS and MLC models (Fig. 1.c). Subsequently, varus and valgus (VV) moments of ±10 Nm under 50 N of compression were applied to the tibia at 30°, 45°, and 60° of flexion for the baseline (i.e., no additional resection) and after additional distal resections of 2 mm and 4 mm. The coronal laxity, defined as the sum of VV angulations in response to the VV moments, and coupled axial rotation, defined as the sum of coupled internal and external rotation in response to the VV moments, were measured at the three flexion angles and compared between PS and MLC using RM-ANOVA with alpha set to 0.05.
RESULTS: At 30° of flexion, the coronal laxities with the PS insert at the +2 mm and +4 mm resections averaged 7.9 ±0.6° and 11.3 ±0.6°, respectively. With the MLC insert, coronal laxity did not achieve statistical significance decreasing by 0.8° (p= 0.06) and 1.0° (p= 0.07) with the +2 mm and +4 mm resections, respectively (Fig. 2). With the PS insert, coupled axial rotation at the +2 mm and +4 mm resections averaged 11.1 ±3.9° and 12.5 ±4.6°, respectively, and decreased by 5.6° (P= 0.01) and 7.1° (P=0 .02), respectively, with the MLC insert (Fig. 3). Similar patterns were observed at 45° and 60° of flexion.
DISCUSSION: With additional resections of the distal femur in primary TKA, the MLC insert slightly reduced coronal laxity compared to the PS insert, but more substantially reduced coupled axial rotation at midflexion. Midflexion instability could be attributed not only to increased primary motions, like coronal laxity, but also coupled rotations of the knee at midflexion [1]. Therefore, our findings might suggest that MLC insert could contribute to reducing the incidence of midflexion instability. However, the increased constraint in MLC may increase the mechanical burden on the bone-implant interface. Therefore, understanding the trade-offs between constraint, stability, and bone-implant loading are critical considerations. These findings are specific to the simulated implant system.
Figures
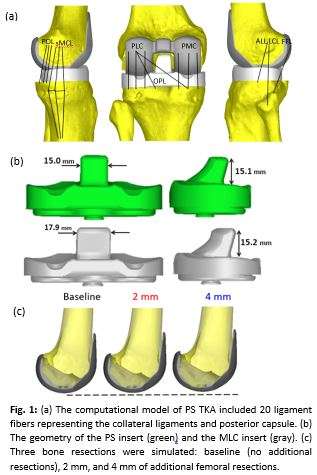
Figure 1
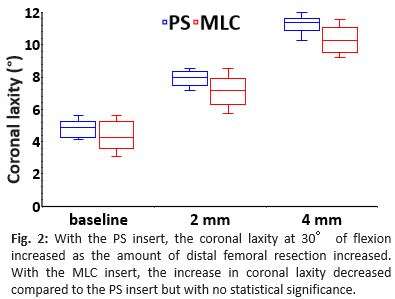
Figure 2
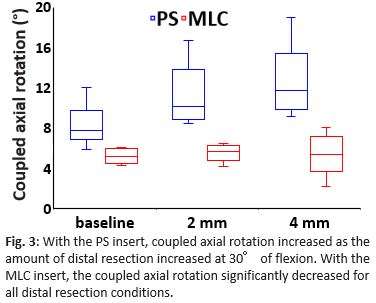
Figure 3#7300
Novel Well-Fixed Cemented Cup Removing Technique While Performing Revision Total Hip Arthroplasty With Dedicated Original Device
Hirosuke Endo - Japan - krashiki, Japan
*Toyohiro Kawamoto - Kawasaki Medical School - Kurashiki city, Japan
Kazuki Yamada - Okayama medical center - Okayama, Japan
Tomonori Tetsunaga - Okayama Medical Center - Okayama City, Japan
Yoshifumi Namba - Kurasiki-city, Japan
Shigeru Mitani - Kawasaki Medical School - Kurashiki-city, Japan
*Email: kawaben@med.kawasaki-m.ac.jp
There have been excellent long-term results reported regarding the improved cemented cup technique in primary total hip arthroplasty. When cup revision surgery was performed, the cemented cup, which was grossly loosened at the bone-cement interface, was easily removed. However, in a well-fixed bone-cement interface, it remains difficult to remove the cemented cup for a revision in the event of a recurring dislocation. In addition, the protrusion of the cement (cement anchors) cause unpredictable bone defects. Thus, a new removal device was created that was used successfully to remove even a well-fixed cemented cup safely and efficiently. This report introduces both the device and the technique usedin cemented cup removal.
Figures
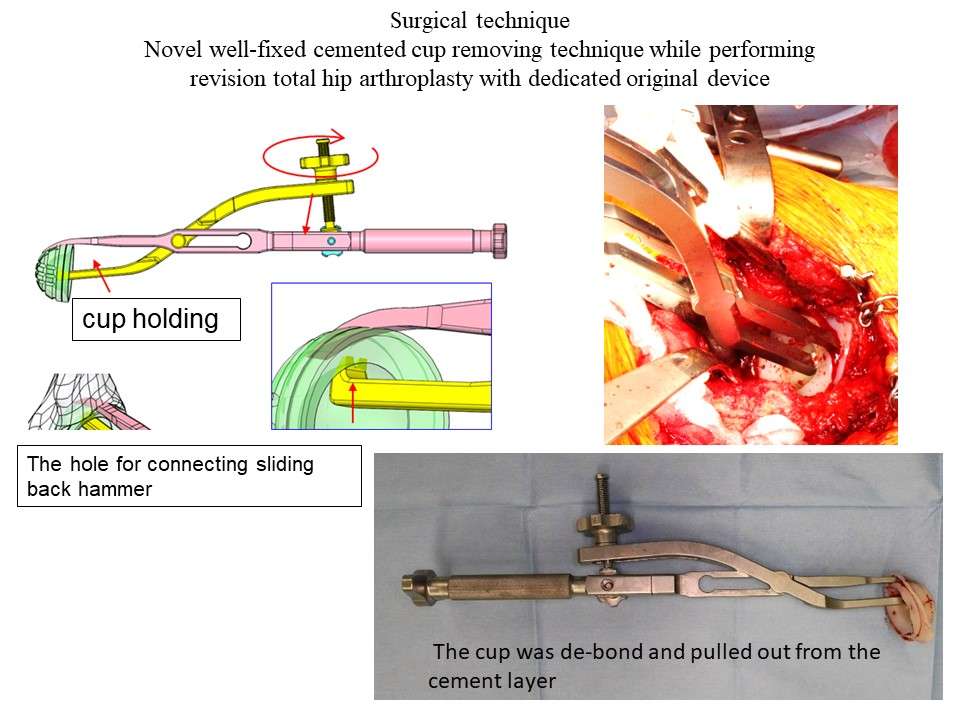
Figure 1#7666
Assessment of Cup Orientation During Gait: Implications for Preclinical Hip Replacement Testing
*Lee Etchels - University of Leeds - Leeds, United Kingdom
Ksenija Vasiljeva - Institute of Medical and Biological Engineering, University of Leeds - Leeds, United Kingdom
Swati Chopra - University of Leeds - Leeds, United Kingdom
Sarah Kingsbury - University of Leeds - Leeds, United Kingdom
Philip Conaghan - University of Leeds - Leeds, United Kingdom
Lin Wang - DePuy Synthes Joint Reconstruction - Leeds, United Kingdom
Jonathan Thompson - DePuy Synthes Joint Reconstruction - Leeds, United Kingdom
Graham Isaac - University of Leeds - Leeds, United Kingdom
Sophie Williams - University of Leeds - Leeds, United Kingdom
Ruth Wilcox - University of Leeds - Leeds, United Kingdom
Alison Jones - University of Leeds - Leeds, United Kingdom
*Email: l.w.etchels@leeds.ac.uk
Introduction: Hip replacements are tested under standard and also separation conditions in pre-clinical hip simulation. In separation conditions, typically occurring during the swing phase of gait, the head-liner contact location is forced onto the liner rim rather than the bearing surface. The orientation recommended by ISO14242-4 (Figure 1) is a static 55° inclination and 0° version. The aim of this study was to determine whether this configuration represents clinically relevant separation directions and contact conditions, particularly when taking into account pelvic motions during gait.
Methods: Thirty participants (15 male, 15 female) with symptomatic hip pain were analysed from a larger cohort (BLINDED). The native acetabular inclination and version angles for each subject were extracted from 3D Magnetic Resonance (MR) images and used to define a hypothetical patient-specific acetabular cup orientation. Three-dimensional pelvic movement was derived from marker-camera data captured for walking over force plates at a self-selected speed. The native orientation occurred when pelvic tilt = obliquity = internal-external rotation = 0°, with pelvic rotations then leading to a change in the acetabular orientation relative to the lab coordinate system. The measured pelvic rotations were applied to generate a subject-specific predicted acetabular cup orientation for two points in the gait cycle: toe-off and heel-strike, marking the start and end of swing phase. The analysis was repeated with all patients having the same initial cup orientation (45° radiographic inclination (angle between acetabular axis projected onto frontal plane and transverse plane), 18° anatomic version (angle between acetabular axis projected onto transverse plane and frontal plane)), representing a consistent surgical plan, to separate differences caused by patient specific anatomy and patient specific motions.
Results: The mean native inclination and version angles were 51° (range 39 to 64°) and 18° (5 to 34°), respectively, and the version angles reached a maximum of 40° at heel-strike (Figure 2). Inclination and version changes from toe-off to heel-strike peak were 0.5° (-4 to 4°) and 5.6° (-4 to 11°). An increase in angle was seen in 17/30 (inclination) and 29/30 (version) patients during swing phase.
Conclusion: The mean inclination angle is well represented by the 55/0° ISO test setting, but the mean version is less well represented. There was relatively little inclination variation between patients when using a fixed initial acetabular orientation (Figure 3), suggesting that most of the variation was anatomical. There was more variation in version angles however, likely due to differing patterns of pelvic tilt and internal-external rotation. The limited inclination changes between toe-off and heel-strike, and relatively even split between patients with increasing and decreasing inclinations, suggest that a static inclination for separation testing may be a reasonable representation of the cohort. The increasing version during swing phase was much more consistent amongst the patient group and larger in magnitude. Further work is needed to assess the implications for test severity and device damage mechanisms, however.
In summary, these results show acetabular cup version varies during gait and this may need to be considered in the application of preclinical testing standards.
Figures
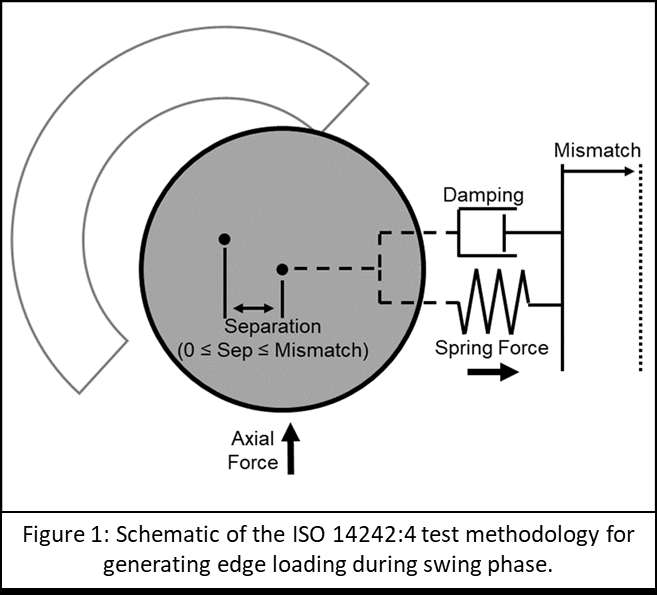
Figure 1
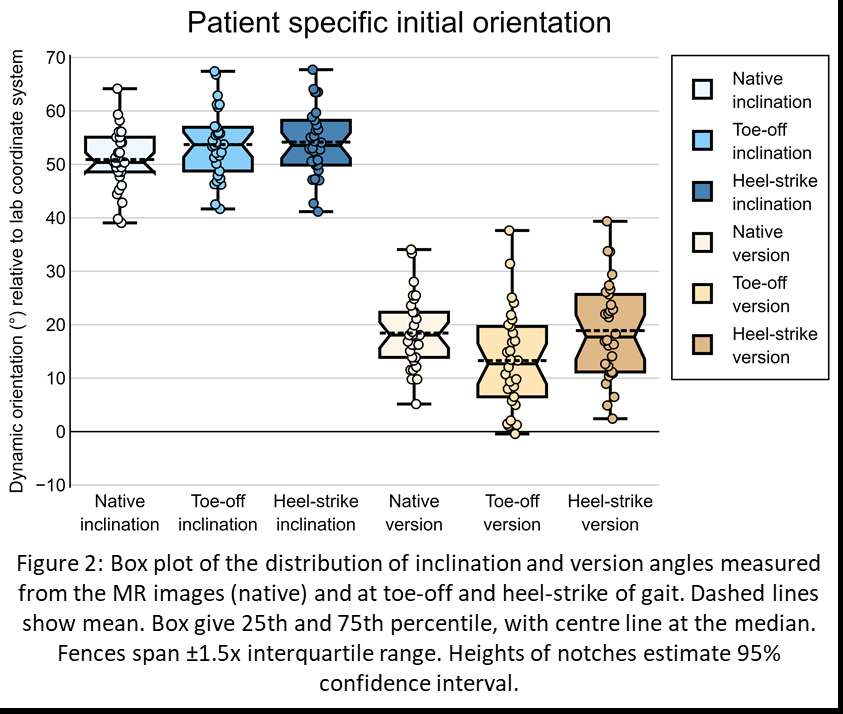
Figure 2
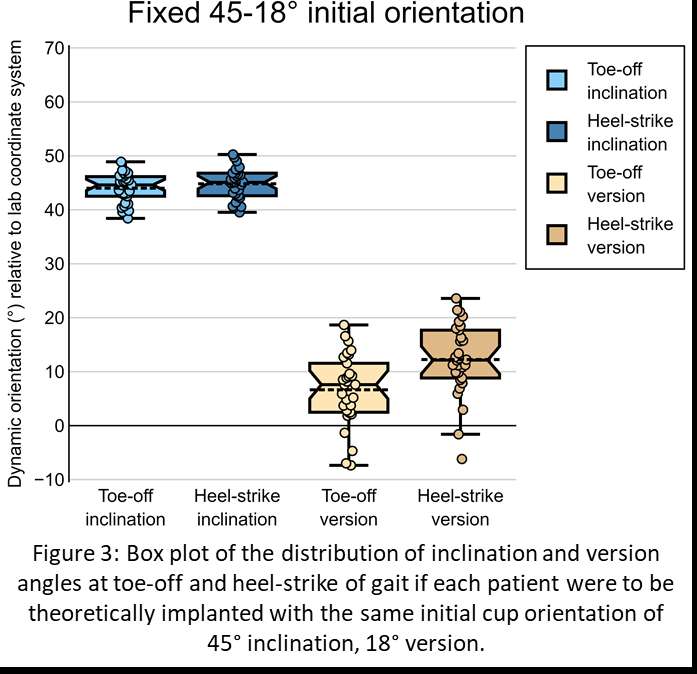
Figure 3#8004
Public Perception of Robotic Assisted Total Hip Replacement Surgery
*James Feng - Beaumont Health - Royal Oak, United States of America
Marvee Espiritu - Oakland University William Beaumont - Rochester, USA
Phillip Vartanyan - Beaumont Health - Royal Oak, USA
Drew Moore - Beaumont Health System - Royal Oak, USA
Robert Runner - Beaumont Health System - Royal Oak, USA
Mark Karadsheh - Beaumont Health - Royal Oak, USA
*Email: jef351@gmail.com
Purpose: Computer-assisted and robotic (CA/R) total hip arthroplasty (THA) has gained considerable attention due to its superior accuracy and precision. However, few studies have evaluated the public’s understanding and appraisal of this technology. Here, we evaluate the public’s initial perception of technology-assisted compared to traditional THA, and if interactive education may alter an individual’s preferences.
Materials and Methods: A prospective cohort study was developed utilizing a 48-question, paid survey distributed via a clinically validated, public, online marketplace in April 2022. After collecting baseline demographics and knowledge regarding THA, participants were queried whether they would prefer a CA/R THA or traditional THA without additional information. Participants were then separated into “Tech” and “Traditional” THA cohorts. Respondents then completed an educational questionnaire which gathered respondent preferences while presenting evidence-based information regarding the surgical modalities. Upon completion of the educational questionnaire, cohorts were asked again which THA modality they would prefer. Statistical analyses were performed with Student’s t-tests and χ2 tests.
Results: 507 surveys were completed with 311 (61.34%) Tech and 196 (38.66%) traditional THA respondents. Tech respondents took fewer daily prescription medications (1.07±1.83 vs 1.48±2.41, p<.05; Table 1). These respondents were also more likely to have heard of CA/R THA (45.02% vs 28.57%; p<.001), but less likely to have any previous orthopaedic surgery (12.22% vs 22.45%, p<.05). All other demographics were similar between the cohorts (Table 1).
After completing the educational questionnaire, 95 (48.47%) of traditional and 267 (85.85%) of Tech THA respondents (total 71.40%) would choose CA/R THA if they needed a hip replacement now. Among this subset of individuals, 73.20% would switch surgeons for CA/R THA. With regards to cost, 88.27% traditional and 94.53% Tech respondents believed health insurance should cover the costs of CA/R THA (p<.05). However, the percentage of individuals willing to supplement their insurance costs was lower (40.51% Tech vs 27.04% traditional, p<.01).
Although significantly different, both groups in general indicated current surgeons should be trained for CA/R THA in its current state (aggregate 69.63%). Similarly, semi-active robotic THA would be preferable to fully-active robotic and computer-assisted THA.
Conclusion: Computer-assisted and robotic THA appears well regarded and valued by the public, with a sizable proportion willing to change surgeons in favor of those trained in this technology. Given this bias, it is recommended younger surgeons be familiar with this technology to accommodate the growing demand.
Figures
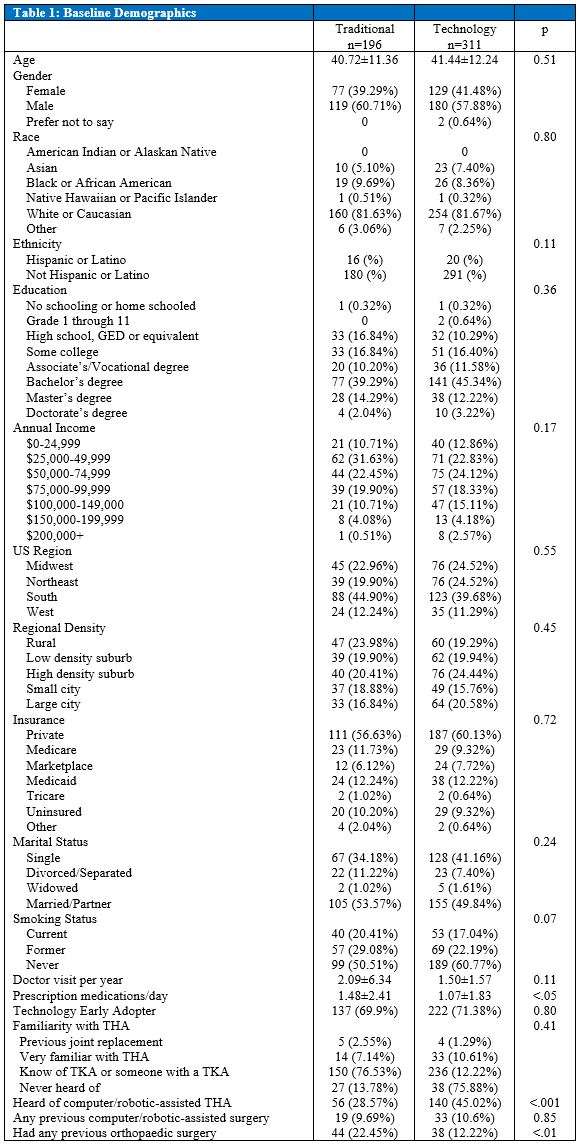
Figure 1
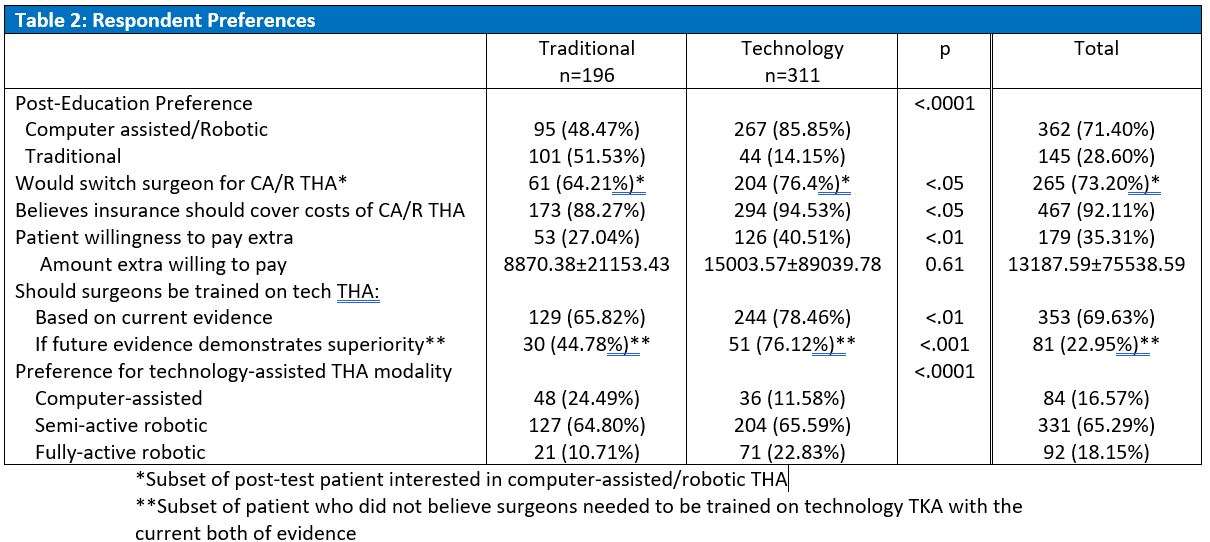
Figure 2
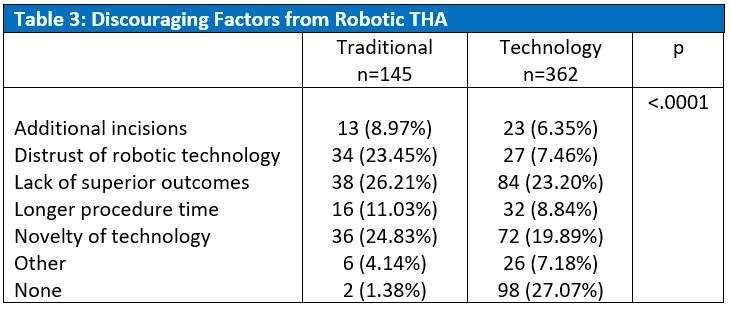
Figure 3#7968
Assessing Patient Preferences for Technology-Assisted Versus Traditional Total Knee Arthroplasty Using a Validated Online Survey Marketplace: Before and After Patient Education
*Tanner Hafen - Oakland University William Beaumont School of Medicine - Auburn Hills, Select Country
James Feng - Beaumont Health - Royal Oak, United States of America
Phillip Vartanyan - Beaumont - Royal Oak, USA
Drew Moore - Beaumont Health System - Royal Oak, USA
Robert Runner - Beaumont Health System - Royal Oak, USA
Mark Karadsheh - Beaumont Health - Royal Oak, USA
*Email: tannerhafen15@gmail.com
Introduction: Although technology-assisted total knee arthroplasty (TKA) is becoming increasingly prevalent, insight into its reception and value by the public is limited. Here we evaluate the general population’s perception of technology-assisted TKA compared to traditional TKA, and how patient education may alter an individual’s preferences.
Methods: A prospective cohort study was performed utilizing a 35-question, paid, survey distributed via a clinically, validated, public, online marketplace in March 2022. After collecting baseline demographics, participants were queried whether they would prefer a computer-/robotic-assisted (technology) TKA or traditional TKA without additional information. Participants were then separated into “Tech TKA” and “Traditional TKA” cohorts based on their responses. All respondents then sequentially completed a pre-test, an evidence-based education table (Figure 1), and a post-test survey focused on the differences between technology versus traditional TKA. Upon completion, cohorts were again asked which TKA modality they would prefer. Statistical analyses were performed with Student’s t-tests and χ2 tests.
Results: In total, 500 surveys were completed with 402 (80.4%) respondents in the tech TKA and 98 (19.6%) in the traditional TKA cohort. Tech TKA respondents were more educated (Bachelor’s degree: 46.88% vs 31.63%, p<.01), had higher annual incomes (>$75,000: 35.6% vs 18.4%), took more daily prescription medications (1.32±1.8 vs 0.92±1.4; <.05) and more familiar with TKA (know of, very familiar, or underwent TKA: 93.2% vs 82.65%; p<.01; Table 1). Age, gender, race, ethnicity, and annual doctor visits were similar.
After reviewing the educational table, 33 (33.67%) of the traditional TKA respondents switched their preferences to technology TKA. Conversely, 95 (23.63%) Tech TKA switched to traditional TKA (Table 2). Among post-test respondents interested in technology-assisted TKA, 75.00% were willing to switch their surgeons and 35.29% would pay an additional sum of moneys if not covered by insurance (35.29%). This was valued by respondents at $3157.35±4498.61 USD. The most important information from the table for technology-assisted TKA respondents was length of stay, while traditional TKA was “who does the surgery”.
Conclusion: Technology-assisted TKA appears to be well-regarded and valued amongst the public. Educational material does not appear to dramatically change preferences, while a sizable proportion of the public are even willing to change surgeons for this technology. Given this bias, it is recommended younger surgeons be familiar with this technology to accommodate the growing demand.
Figures
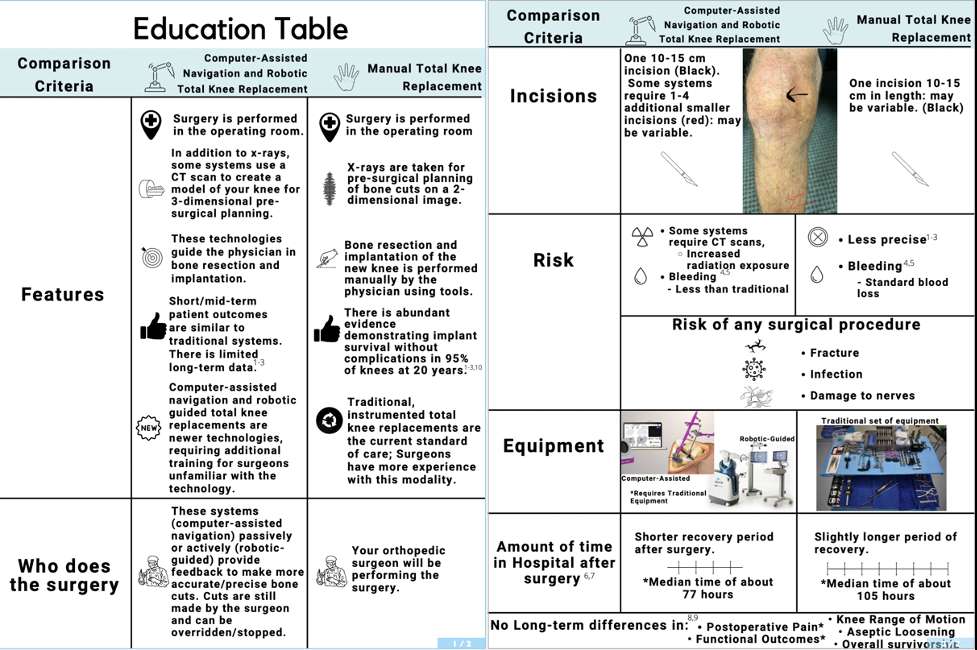
Figure 1
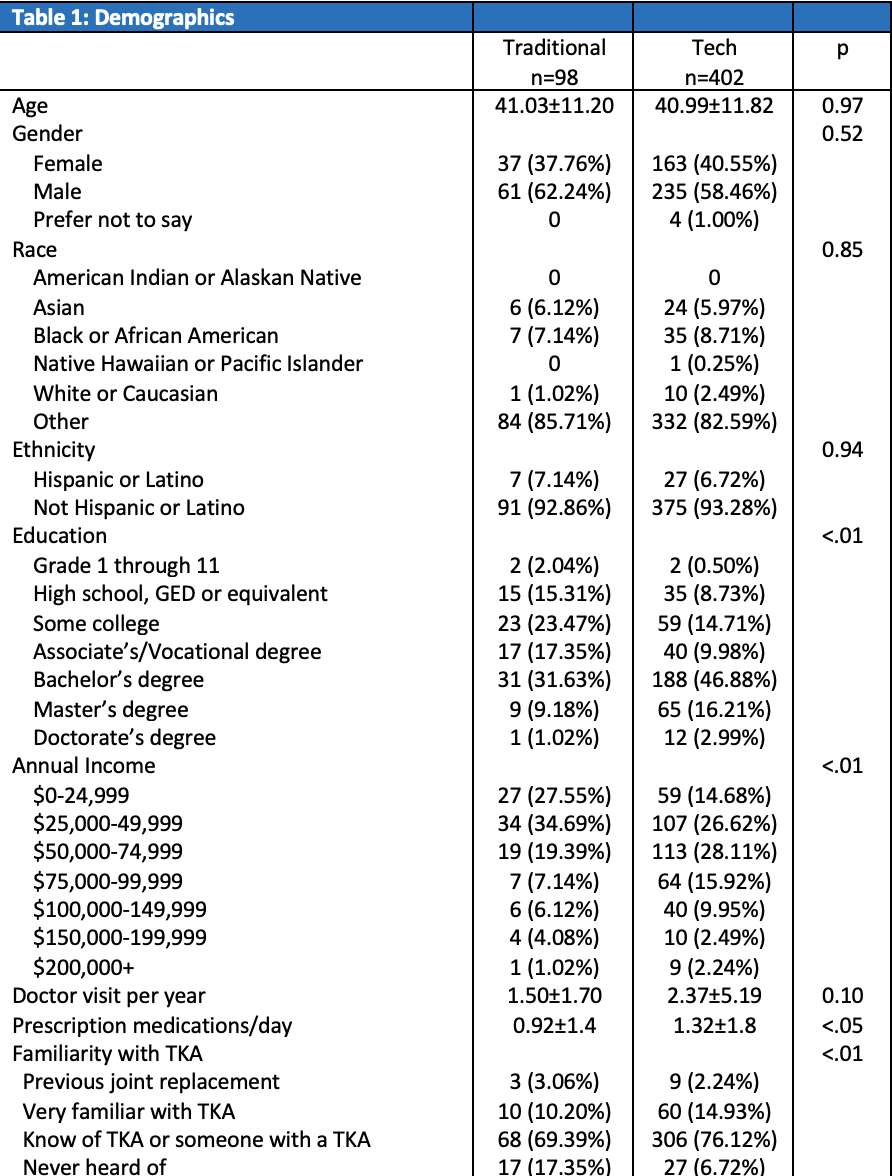
Figure 2
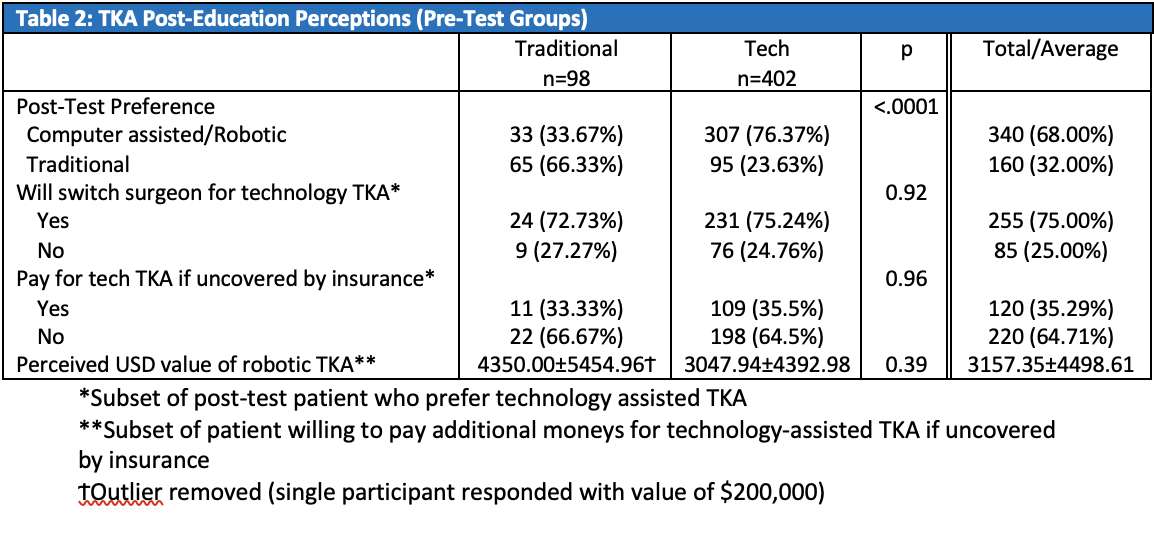
Figure 3#7585
Performance of QCT-Derived Scapula Finite Element Models in Predicting Local Displacements Using Digital Volume Correlation
*Louis Ferreira - University of Western Ontario - London, Canada
Jonathan Kusins - Western University - London, Canada
Nikolas Knowles - University of Calgary - Calgary, Canada
Enrico Dall'Ara - University of Sheffield - Sheffield, United Kingdom
Melissa Ryan - University of Sheffield - Sheffield, United Kingdom
*Email: Lferreir@uwo.ca
Introduction
Subject-specific finite element models (FEMs) of the shoulder complex are commonly used to predict differences in internal load distribution due to injury, treatment or disease. However, the accuracy of these models is to some extent unknown. Currently, experimental validation of shoulder QCT-based FEMs is limited to the cortical shell, while the accuracy of internal predictions within trabecular bone has yet to be explored. The goal of the current study was to quantify the accuracy of local displacements predicted by subject-specific QCT-based FEMs of the scapula, compared to experimental measurements obtained by combining digital volume correlation (DVC) and mechanical loading of cadaveric scapulae within a microCT scanner.
Methods
A custom-designed six degree-of-freedom hexapod robot was fabricated with carbon fiber struts for compatibility with a cone beam microCT scanner (Nikon XT H 225ST) (Figure 1). MicroCT scans (33.5 µm resolution) were acquired of four cadaveric scapulae in a pre- and post-loaded state (500 N compressive applied load, settling time of 20 minutes). BoneDVC was used to derive full-field experimental displacement measures (sub-volume size of ≈ 1 mm). QCT-FEMs were generated for each specimen. Three separate boundary conditions (BCs) were modelled. Experimentally-idealized BCs were simulated by rigidly fixing the medial border of the scapulae and applying either a force (idealized-force BC) or displacement (idealized-displacement BC) to a virtual loading platen. Also, a DVC-derived BC was modelled by directly imposing the local displacements quantified by the DVC algorithm to the top and bottom face of the QCT-FEMs (Figure 2).
Linear regression analysis between local displacements along the x, y, and z directions predicted by the QCT-FEMs and experimental DVC results was performed.
Results and Discussion
DVC-derived BCs resulted in the closest match to the experimental results (best agreement (range of m = 0.93-1.05) and highest correlation (range of r2 = 0.83-1.00)) compared to the idealized-displacement and idealized-force BCs (Table 1, Figure 3). In addition, a two order of magnitude decrease was observed in RMSE, with the lowest errors found using DVC-derived BCs (average RMSE = 4.7±1.3 µm, N=4) compared to the idealized-displacement (average RMSE = 538±239 µm, N=4) and idealized-force (average RMSE = 749±379 µm, N=4) BCs.
Conclusions
The results of this study show that errors in local displacements predicted by QCT-based FEMs of the shoulder can be minimized using DVC-derived BCs. This has the potential to significantly improve the accuracy of QCT-based FEMs, which could be used to preoperatively optimize patient outcomes associated with a variety of surgical interventions.
Figures
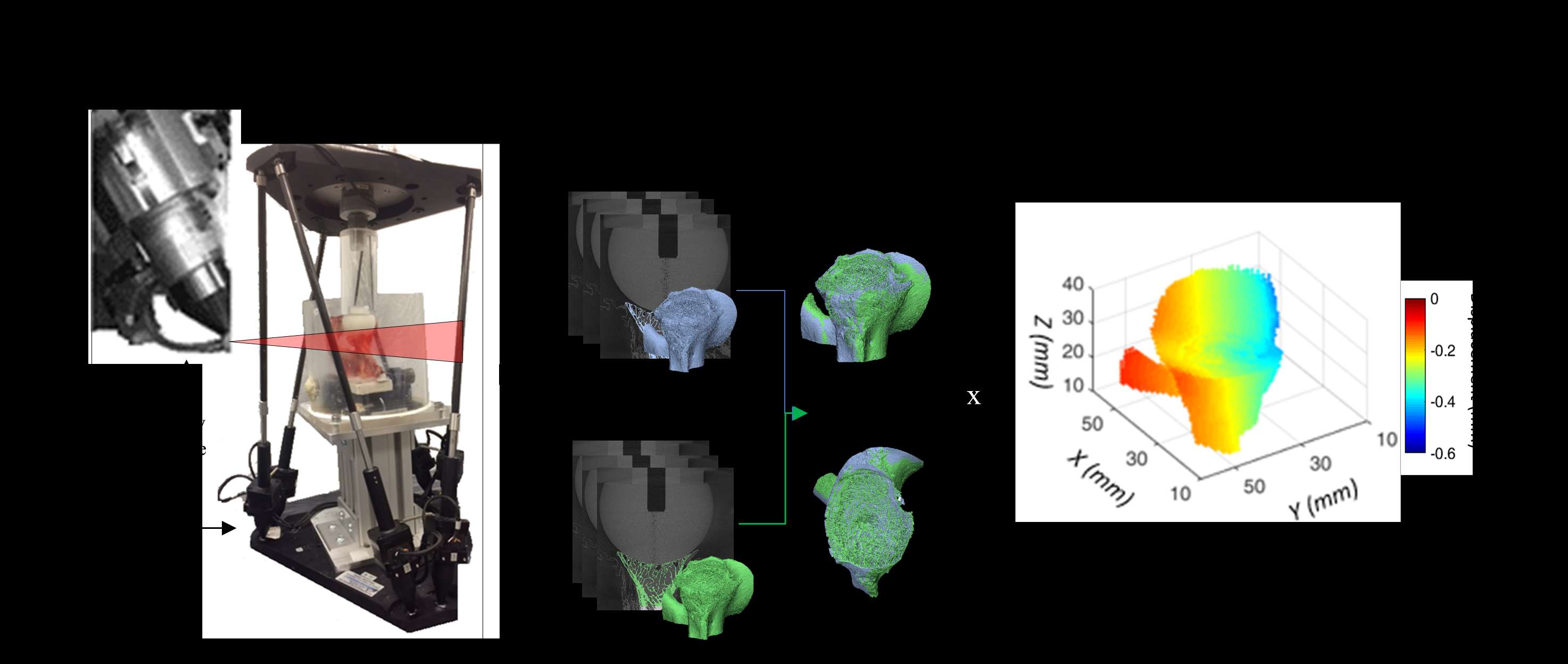
Figure 1
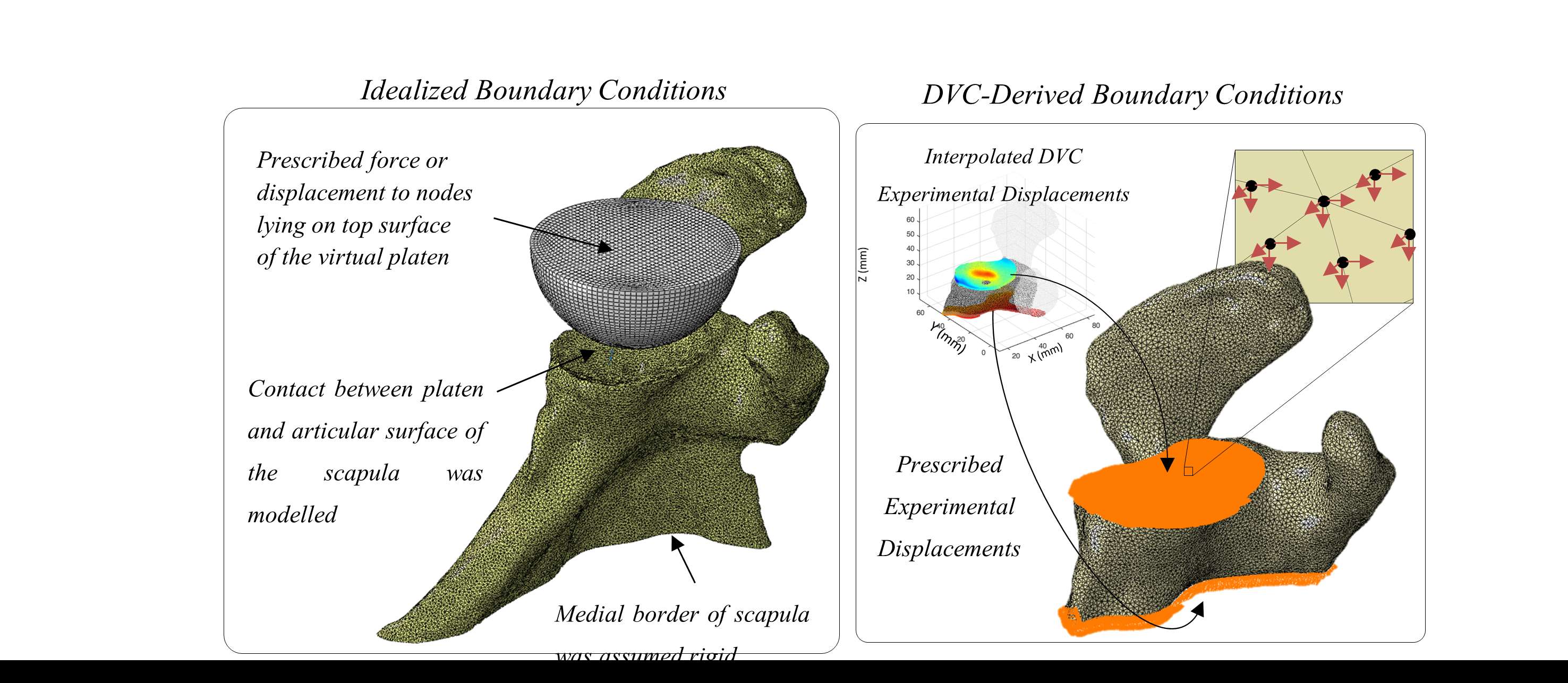
Figure 2
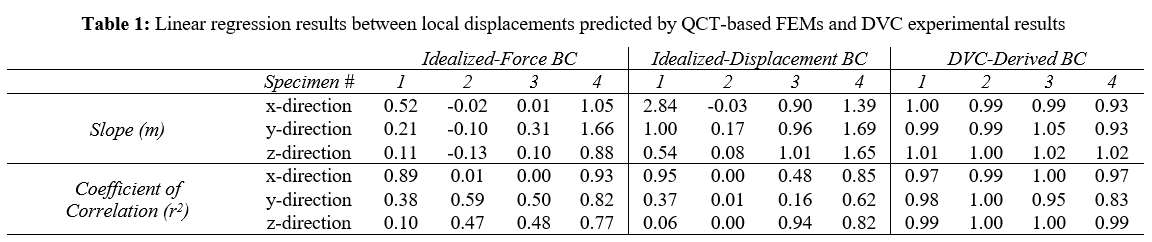
Figure 3#7591
Assessment of Local Displacement Predictions Generated by MicroFEMs of Trabecular Bone Cores Retrieved From the Shoulder
*Louis Ferreira - University of Western Ontario - London, Canada
Jonathan Kusins - Western University - London, Canada
Nikolas Knowles - University of Calgary - Calgary, Canada
Melanie Columbus - The University of Western Ontario - London, Canada
George Athwal - University of Western Ontario - London, Canada
*Email: Lferreir@uwo.ca
Introduction: Micro finite element models (µFEM) of the shoulder can be used to evaluate joint replacement designs preclinically [1]. However, the predictive outcomes generated by µFEMs are influenced by underlying assumptions. Therefore, experimental validation is necessary to ensure accurate clinical conclusions are achieved [2]. The aim of the current study was to assess local displacements predicted by shoulder trabecular bone core µFEMs compared to full-field experimental displacements quantified using digital volume correlation (DVC) techniques.
Methods: Six humeral osteotomies were collected from patients that had undergone total shoulder arthroplasty due to end-stage osteoarthritis. Cubic trabecular bone cores (edge length of 5.5 mm) were excised from the center of the resection surface of the humeral osteotomies. Experimental stepwise compressive loading was performed within a microCT scanner (image resolution = 4.75 µm) and volumetric images were captured at varying loading steps (Figure 1). DaVis DVC was used to quantify full-field experimental local displacements throughout the trabecular structure.
MicroFEMs with voxel sizes of 20 and 40 µm were generated for each trabecular bone core using the pre-loaded microCT image. Homogeneous and heterogeneous material properties were assigned. Local DVC displacements were prescribed to the medial and lateral surfaces [3]. Linear regression was performed on the pooled results to quantify the agreement between the µFEMs’ predicted local displacements in the main loading direction compared to the experimental results.
Results: The µFEMs were able to replicate the experimental local displacements with high accuracy (slope ≥ 0.85, R2 ≥ 0.88) regardless of the material property or voxel size used as indicated by the pooled linear regression results (Table 1, Figure 2). At a voxel size of 20 µm, higher errors in axial force were predicted for all six µFEMs using homogenous material properties (225% error [range: 85-385%]) compared to heterogenous material properties (85% error [range: 4-235%]). Similar trends were observed for µFEMs generated with a voxel size of 40 µm.
Discussion: The results of this study indicate that accurate local displacement predictions can be obtained with shoulder µFEMs generated using either homogeneous or heterogenous material properties and with varying voxel sizes (20 or 40 µm). These findings may be useful to reduce the computational resources associated with the µFEM approach, but other outcome measures (e.g., yield strength, trabecular strains) should also be evaluated in this context. The accuracy of predicted axial force was improved with the use of heterogenous material properties, but the relative error was still high (85% error). Future work should investigate varying methodologies associated with heterogeneous material mapping at the tissue level. Nevertheless, continual development of shoulder µFEMs combined with full-field DVC validation techniques can improve the predictive capabilities to efficiently screen joint replacement designs prior to clinical adoption.
References: [1] Chevalier et al. J Biomech 2016. [2] ASME Verification & Validation 40 - 2018 [3] Chen et al. J Mech Behav Biomed Mater 2017
Figures
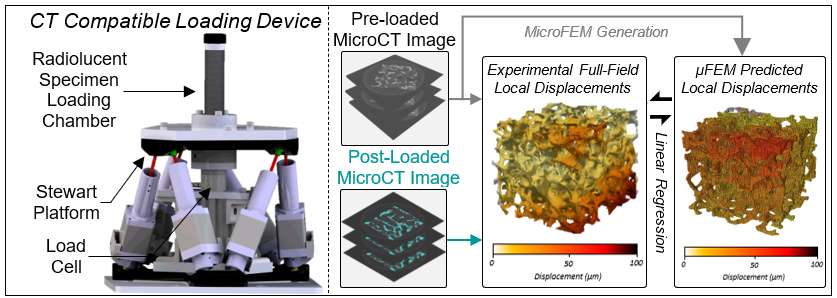
Figure 1
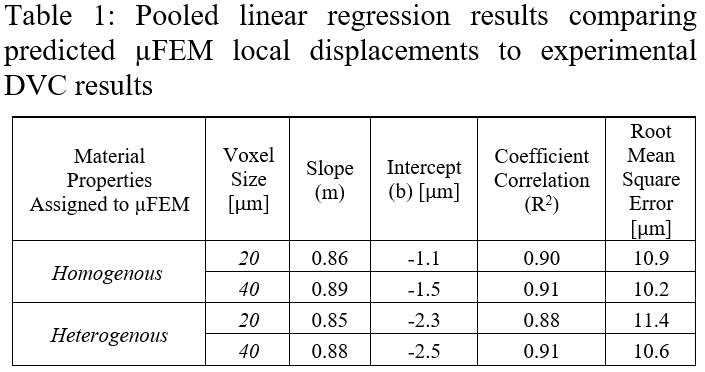
Figure 2#7592
Accuracy of Local Strains Predicted by QCT-Based Finite Element Models Within Osteoarthritic Humeral Heads
*Louis Ferreira - University of Western Ontario - London, Canada
Jonathan Kusins - Western University - London, Canada
Nikolas Knowles - University of Calgary - Calgary, Canada
Melanie Columbus - The University of Western Ontario - London, Canada
Enrico Dall'Ara - University of Sheffield - Sheffield, United Kingdom
George Athwal - University of Western Ontario - London, Canada
*Email: Lferreir@uwo.ca
Introduction: Continuum-level finite element models (FEMs) are gradually becoming common practice to evaluate and predict failure associated with joint replacements. However, the accuracy of internal strain predictions generated by quantitative CT (QCT) FEMs is currently unknown. This study aimed to evaluate the accuracy of local full-field strains predicted by QCT-FEMs compared to experimental digital volume correlation (DVC) measurements.
Methods: Two osteoarthritic humeral osteotomies were harvested from patients being treated with total shoulder joint replacement surgery. A 500N load was applied within a microCT using a custom-designed CT-compatible loading device (Figure 1). BoneDVC (≈1mm voxel resolution) was used to quantify experimental full-field displacements and strains. Corresponding continuum-level FEMs were generated from clinical QCT scans. Mechanical properties were assigned using three separate density-modulus relationships. Two boundary conditions (BCs) were applied: force-controlled and DVC-driven. Local 3rd principal strains were probed within seven cylindrical volumes of interest (7mm diameter x 7 mm length) located 0.5 mm underneath the loading platen. Linear correlation was performed to compare QCT-FEM predictions and experimental DVC results.
Results: Accuracy of QCT-FEM predictions was found to be sensitive to the boundary condition applied (Figure 2). High variations of error due to the density-modulus relationship used were observed when using force-controlled BCs (RMSE ranging from 2385-6381 µstrain); however, this effect was reduced with DVC-driven BCs (RMSE ranging from 1314-1768 µstrain) (Table 1, Figure 3). When using DVC-driven BCs, RMSE% less than 10% was achieved for both specimens.
Conclusion: This study compared local strains from QCT-FEMs to experimental DVC measurements within bone from patients that have undergone total shoulder joint replacement. Fair agreement between models was achieved when using DVC-driven BCs. Continual development of these methods will improve our ability to predict the success rate of joint replacement procedures preoperatively.
Figures

Figure 1
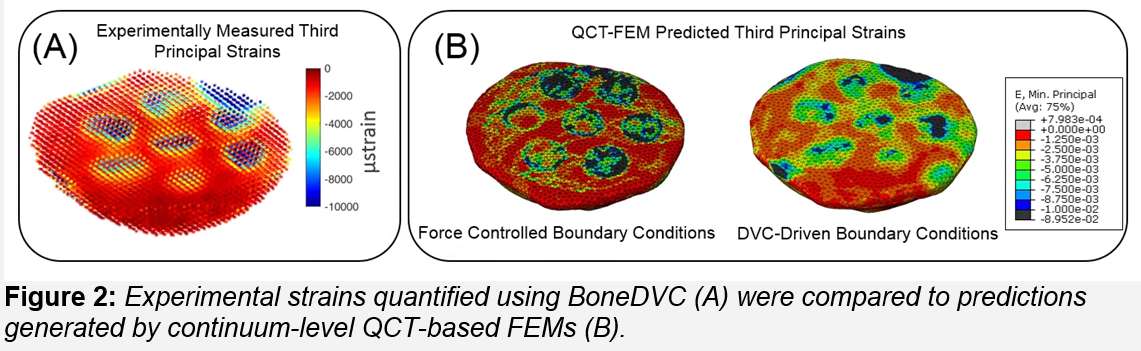
Figure 2
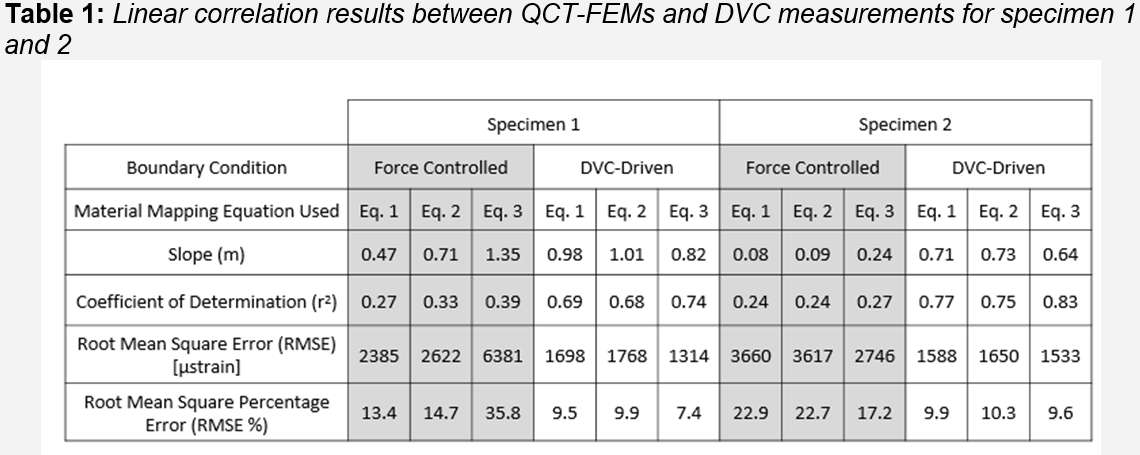
Figure 3#7501
Assessing Knee Mechanics of Revision TKA Solutions and Continuum of Care
*Lauren Ferris - DePuy Synthes - Warsaw, United States of America
Amit Mane - DePuy Synthes - Warsaw, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
Paul Sade - DePuy Synthes - Warsaw, USA
*Email: lferris3@its.jnj.com
Introduction: More than 700,000 Primary Total Knee Arthroplasty (TKA) are performed annually in the US; 12% of these TKA require revisions (rTKA)1. TKA failures leading to debilitating conditions are loosening, infection, and instability, resulting in decreased function. TKA revision surgery initially require a surgeon to determine, based on many options, which rTKA system provides the patient the best outcomes with respect to bony fixation, stability, and range of motion. Furthermore, implant continuity between TKA and rTKA solutions must be considered. If a legacy design philosophy of a Primary solution is carried over to rTKA, patients can benefit from the Continuum of Care. Therefore, the first objective was to evaluate performance of one rTKA solution compared to the corresponding Primary solution, and second, to further extend rTKA comparisons with two additional commercially available rTKA solutions.
Methods: Three Fixed Bearing (FB) rTKA systems and one FB PS TKA were assessed using a previously validated Forward Dynamics Model (FDM) (Fig.1)2. rTKA solutions analyzed were Construct-ATR, Construct-ST and Construct-NXG (Fig.2). The FB PS offering of Construct-ATR was referred to as Construct-AT. For each construct, a Deep Knee Bend (DKB) from 5⁰ to 120⁰ flexion with neutral tibial rotational alignment was simulated. Analyses were focused on kinematic measures included AP translation of the femoral medial and lateral condylar lowest points (LP), and force measures of Quadriceps, Patella-Femoral (PF) Contact, and Patellar Tendon (PT).
Results: The AP motion of the medial and lateral condyles of Construct-ATR were within 0.5mm of Construct-AT (Fig.3). Construct-AT and Construct-ATR experienced anterior medial translation of 0.9mm and 1.25mm respectively, until cam-post engagement at 72⁰ and 73⁰ of flexion, while Construct-ST and Construct-NXG translated anteriorly 2.4mm and 3.8mm respectively, until cam-post engagement at 83⁰ and 82⁰, respectively. Peak Quadricep, PF, and PT forces for Construct-AT and Construct-ATR were within 150N (Fig.3). Construct-ST and Construct-NXG experienced peak forces higher than those of Construct-ATR and Construct-AT.
Discussion: Construct-AT LP motion characteristics observed are similar to those reported by Khasian2 with twenty patients performing DKB. Observed similarities of LP results with in vivo patients demonstrates the predictive capabilities of the FDM. Construct-ATR and Construct-AT are designed with identical sagittal plane Femoral J-Curve-GRADIUS™, PF mechanism-GLIDERIGHT™ and cam-post engagement-SOFCAM™. The observed similarities in Tibio-Femoral AP motions and PF mechanics between Construct-AT and Construct-ATR demonstrates continuation of the design philosophies from Primary and Revision solutions. J-Curve of Construct-ST and Construct-NXG contains distinctive multiple radii potentially influencing observed larger anterior translation until cam-post engagement, which was concurrent with the increased Quad, PF and PT forces. Fitzpatrick et al. correlated post-cam engagement velocity and abrupt changes in LP kinematics in PS TKA solutions3. Construct-AT and Construct-ATR utilizes ‘S’ shape design of the post, promoting smooth transition from condylar control to cam-spine control, unlike Construct-ST and Construct-NXG. In summary, as the design of rTKA evolves, implementation of primary design philosophies, kinematics, and force measurements can aid in determining the optimal design parameters for rTKA patients.
References:
1. Hamilton et al 2015, 2. Khasian et al 2020, 3. Fitzpatrick et al 2013
Figures
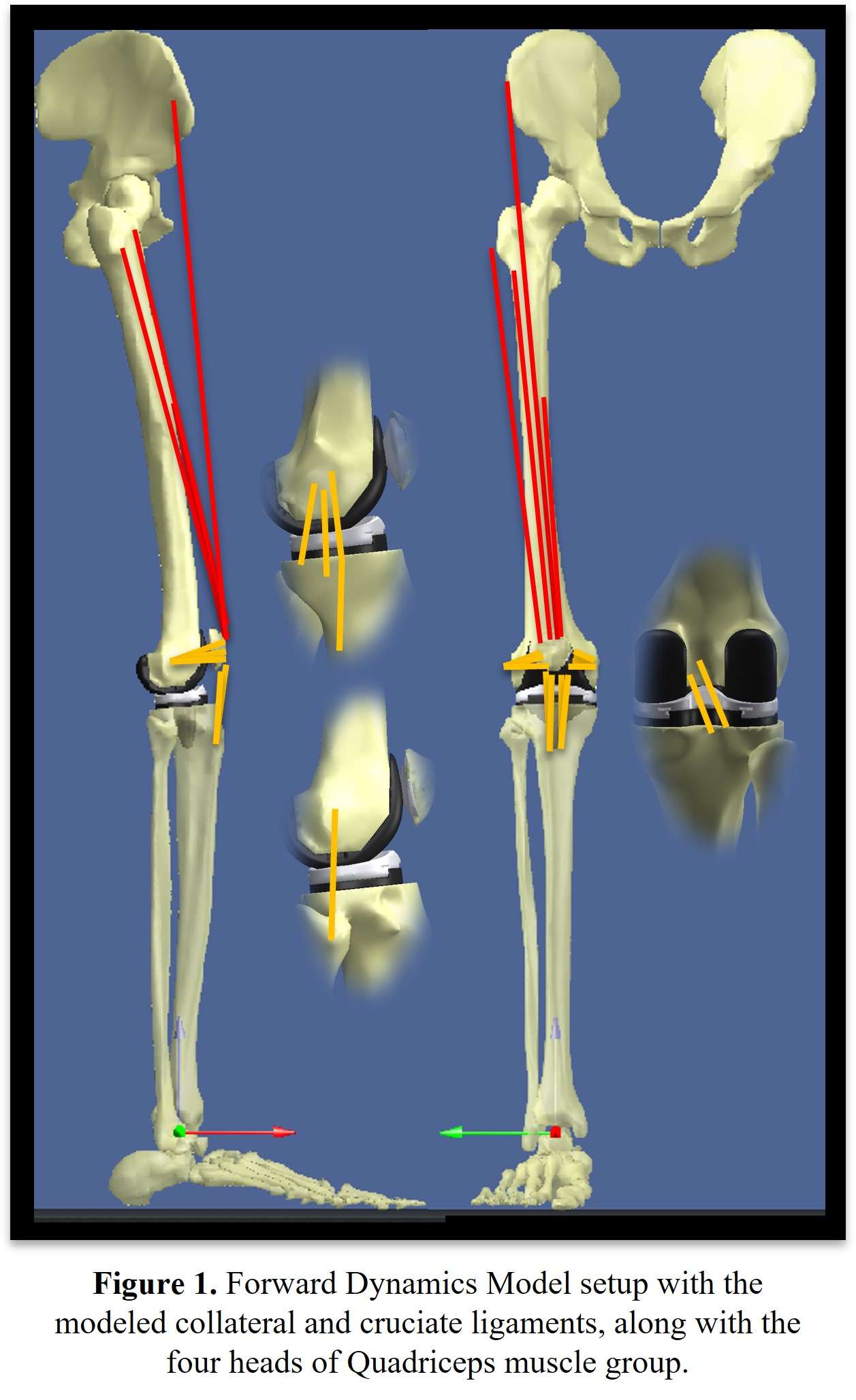
Figure 1
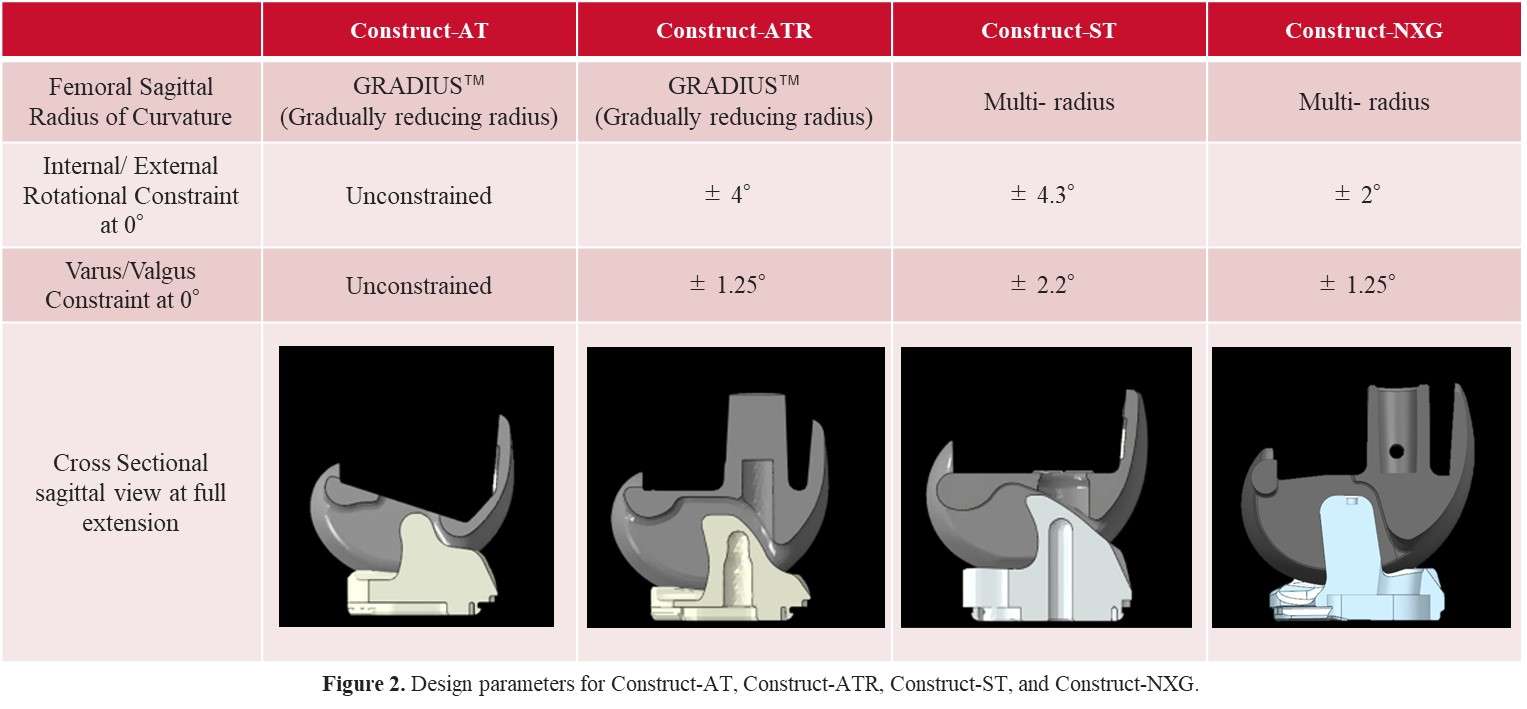
Figure 2
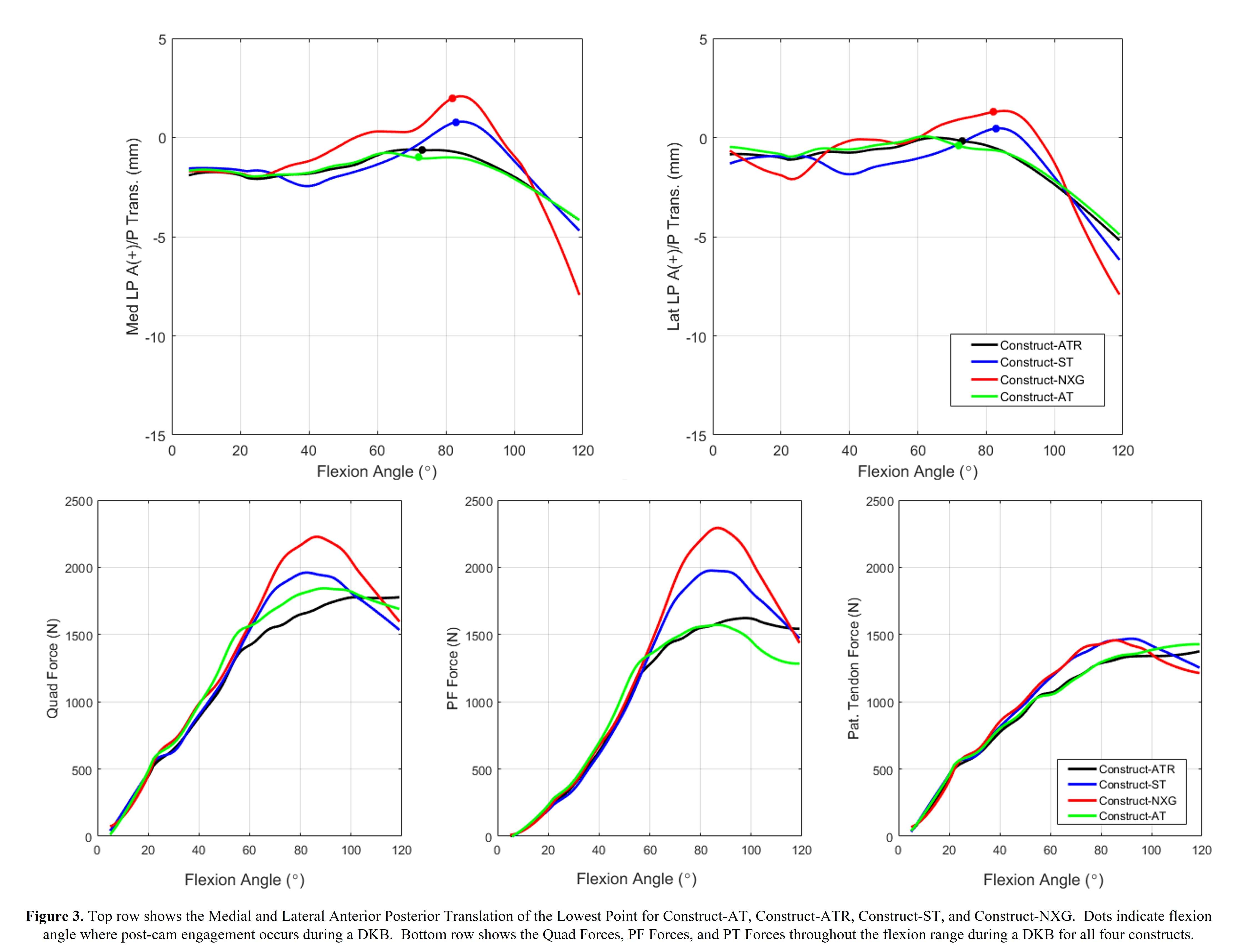
Figure 3#7757
Real-Time Prediction of THA Implant Impingement in Standing and Seated Positions for Multiple Implant Configurations
*Clare Fitzpatrick - Ortho Haus, LLC - Boise, Select Country
Casey Myers - Ortho Haus - Denver, United States of America
Chadd Clary - Ortho Haus, LLC - Denver, USA
Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
*Email: cfitzpat@theorthohaus.com
Introduction: Implant-implant impingement is a risk factor for dislocation and implant wear after total hip arthroplasty (THA) [1]. Cup placement is a major contributor to whether implant-implant impingement will occur [2]. However, the wide variety of THA implant sizes and designs, in addition to variability in patient-specific mobility, make it difficult to determine implant-implant impingement pre- or intra-operatively. The objective of this study was to develop an algorithm to predict THA implant-implant impingement across a selection of implant configurations.
Methods: An implant library was assembled for several families of primary THA implants. The library included full size ranges for 3 stem designs with both collared and collarless variants, 1 shell design (sizes 38-72mm) with 3 liner options (neutral, lipped, face changing) and head sizes from 22.225-44mm. Standing (femur in full extension) and seated (femur flexed to 90°) finite element simulations were developed for the library of THA implant configurations (Fig. 1). Internal and external rotations of the femur were applied until contact with the shell or liner occurred (Figs. 1, 2). Rotation to impingement, cup inclination and anteversion pose, and key implant metrics (including liner/shell sizes, stem length and neck shaft angle) were recorded. These simulations were repeated for 1,800 unique implant configurations with 60 cup poses per configuration. These data were used to train a linear response model (LRM) [3] where cup pose, and implant design metrics were used as inputs and femoral rotation to impingement was predicted. Accuracy of the LRM was assessed using a test dataset of 120 unique implant configurations at 30 cup poses per configuration. All test configurations were independent from training configurations. LRM predictions were compared to predictions from the finite element simulations for these same implant/pose conditions (Fig. 3).
Results: The root-mean-square error for the impingement LRM across the entire test dataset was 2.3°. The average rotations to impingement from a neutrally aligned femur were 46.0° and 25.9° in standing and seated poses, respectively. The majority (97.4%) of conditions evaluated had maximum errors in rotation to impingement predictions of less than 5°. However, LRM accuracy decreased in three regions of cup placement; in the standing pose: high inclination (>55°) with high version (>35°); inclination <35° with mid-range version; and in the seated pose: low version (<8°). Higher errors were associated either with (1) implant combinations that resulted in unusual contact conditions (e.g., collar/shoulder contact); or (2) conditions where the cup was almost flat with respect to femoral rotation, such that impingement was particularly sensitive to cup placement.
Conclusions: It is not feasible to use numerical or CAD simulations to evaluate impingement for every possible implant/pose combination. Our LRM approach provides a computationally efficient path to predict implant-implant impingement in real-time at any cup pose for any implant configuration in our library. This algorithm may enhance the capability of software tools to assist the surgeon in selecting cup placements and/or implant configurations which maximize rotation to impingement.
References: [1] Palit et al., ABME, 2019. [2] Widmer, CORR, 2020. [3] Gibbons et al., JBiomech, 2019.
Figures
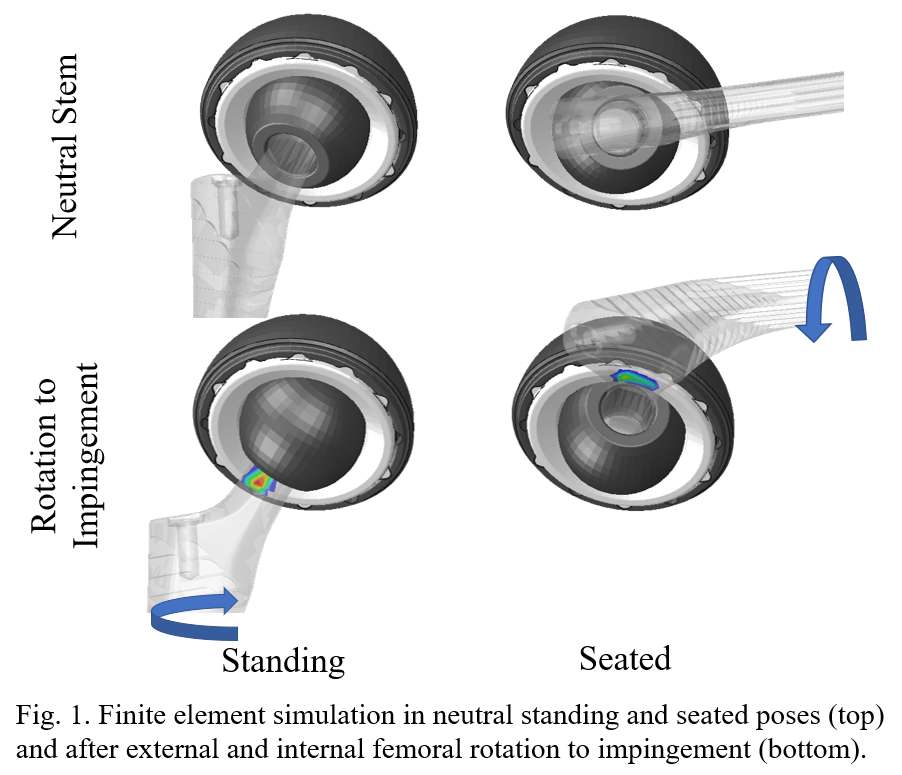
Figure 1
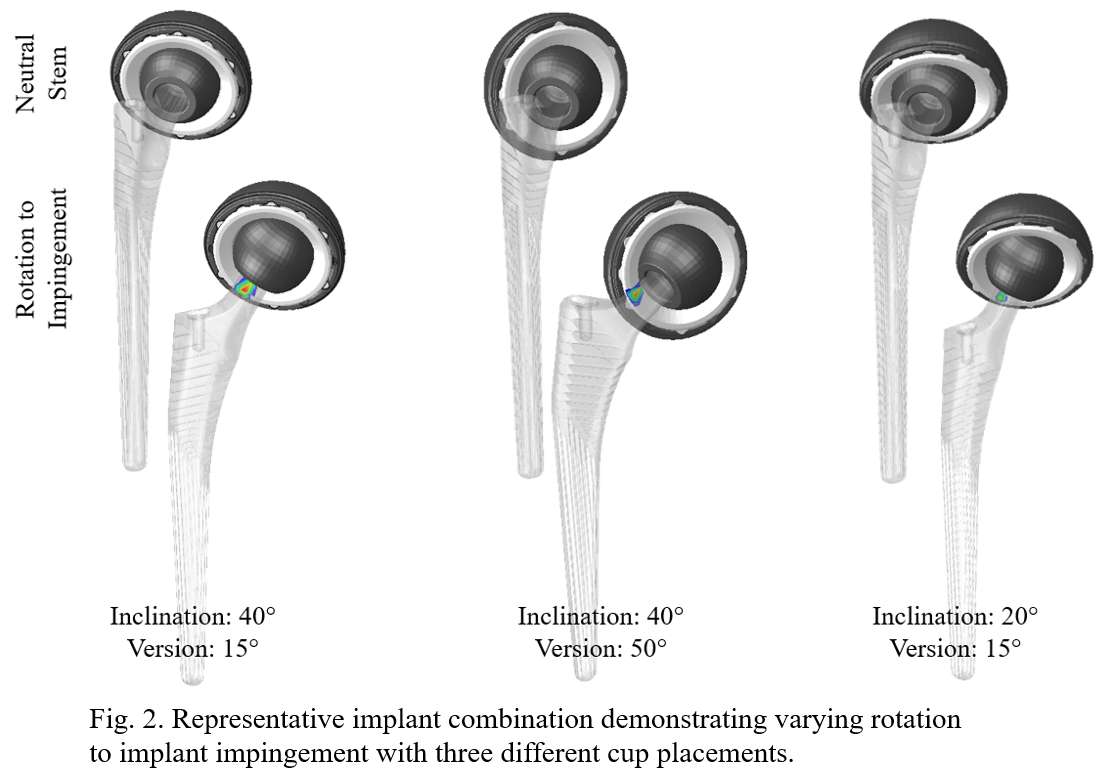
Figure 2
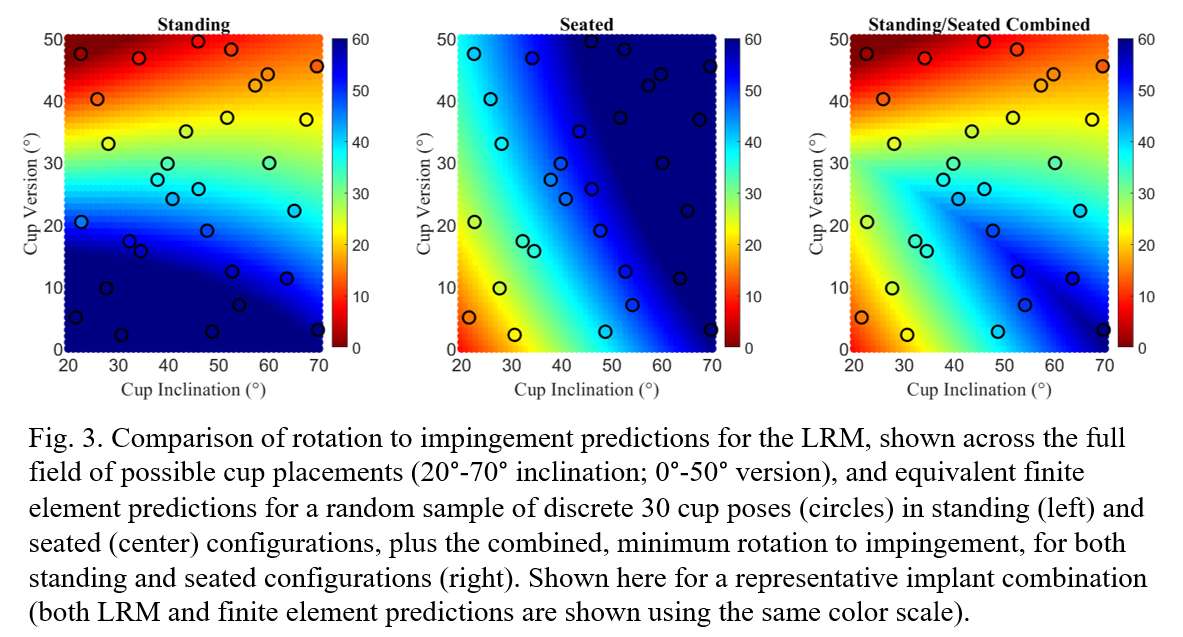
Figure 3#7686
A Subacromial Implant to Restore Shoulder Stability in the Setting of Massive Irreparable Rotator Cuff Tears
Cole Fleet - Western University - London, Canada
Daniel McNeil - Roth McFarlane Hand and Upper Limb Clinic, St. Joseph's Hospital - London, Canada
James Johnson - SJHC - London, Canada
*George Athwal - University of Western Ontario - London, Canada
Andrew Trenholm - Dalhousie University - Halifax, Canada
*Email: gsathwal@hotmail.com
Background
Massive irreparable rotator cuff tears often lead to superior migration of the humeral head, which can markedly impair glenohumeral kinematics and function. Several treatments for this pathology currently exist, however, the literature has not demonstrated a clearly superior choice of treatment. Therefore, a subacromial implant was designed and tested to assess its ability in restoring normal glenohumeral stability. It was hypothesized that (1) the implant would restore near normal humeral head position and (2) the implant shape could be optimized to improve restoration of the normal humeral head position.
Methods
A subacromial implant was designed based on average acromial morphology from a series of upper extremity computer tomography (CT) scans. The final implant design was modular and consisted of four design variables that varied in both implant thickness (5mm and 8mm) and curvature of the humeral articulating surface (high constraint and low constraint) (Fig. 1). To assess these different designs, the implants were 3D printed using medical grade titanium and assessed in a cadaver-based biomechanical testing protocol. Eight cadaver specimens (64 ± 13 years old) were loaded at 0, 30, and 60 degrees of glenohumeral abduction using a previously developed shoulder simulator. An 80N load was equally distributed across all three deltoid heads while 10N tone loads were applied to all rotator cuff muscles. Testing states included a fully intact rotator cuff state, a posterosuperior massive rotator cuff tear state (cuff deficient state), and the four implant designs. An optical tracking system (Northern Digital, Ontario, Canada) was used to record the translation of the humeral head relative to the glenoid. All results for the cuff deficient and implant test states were compared relative to the position of the humeral head in the intact cuff state.
Results
Superior-Inferior (SI) Translation
The creation of a posterosuperior massive rotator cuff tear resulted in significant superior translation of the humeral head relative to the intact cuff state (P=0.016). No significant differences were observed between each implant design and the intact cuff state as all implants reduced the superior migration of the humeral head that was observed in the cuff deficient state (Fig. 2). The 5mm low and high constraint implant models were most effective at restoring SI humeral head position (-1.3 ± 2.0mm, P=0.223; and -1.5 ± 2.3mm, P=0.928 respectively).
Anterior-Posterior (AP) Translation
No significant differences were observed across all test states for AP translation of the humeral head (Fig. 3). The implant designs most effective at restoring humeral head position were found to be both 5mm and 8mm thickness high constraint implant models (5mm high constraint: 2.0 ± 4.7mm, P=1.000; 8mm high constraint: 1.6 ± 4.9mm, P=1.000).
Conclusion
The 5mm high constraint implant was most effective in restoring normal humeral head position. The results from this study suggest this subacromial implant may be an effective treatment for restoring normal glenohumeral kinematics and function in patients with massive irreparable rotator cuff tears. Future studies are needed to access the implant’s effect on mechanical efficiency during arm abduction.
Figures
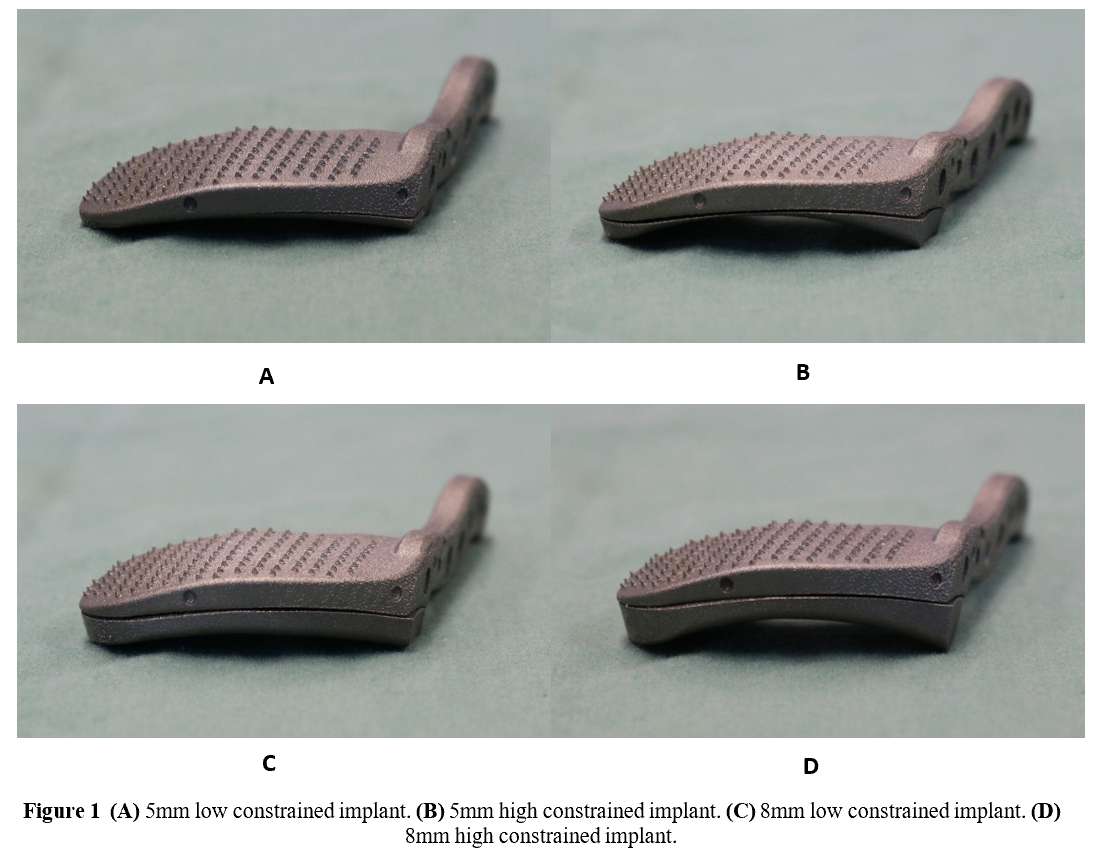
Figure 1
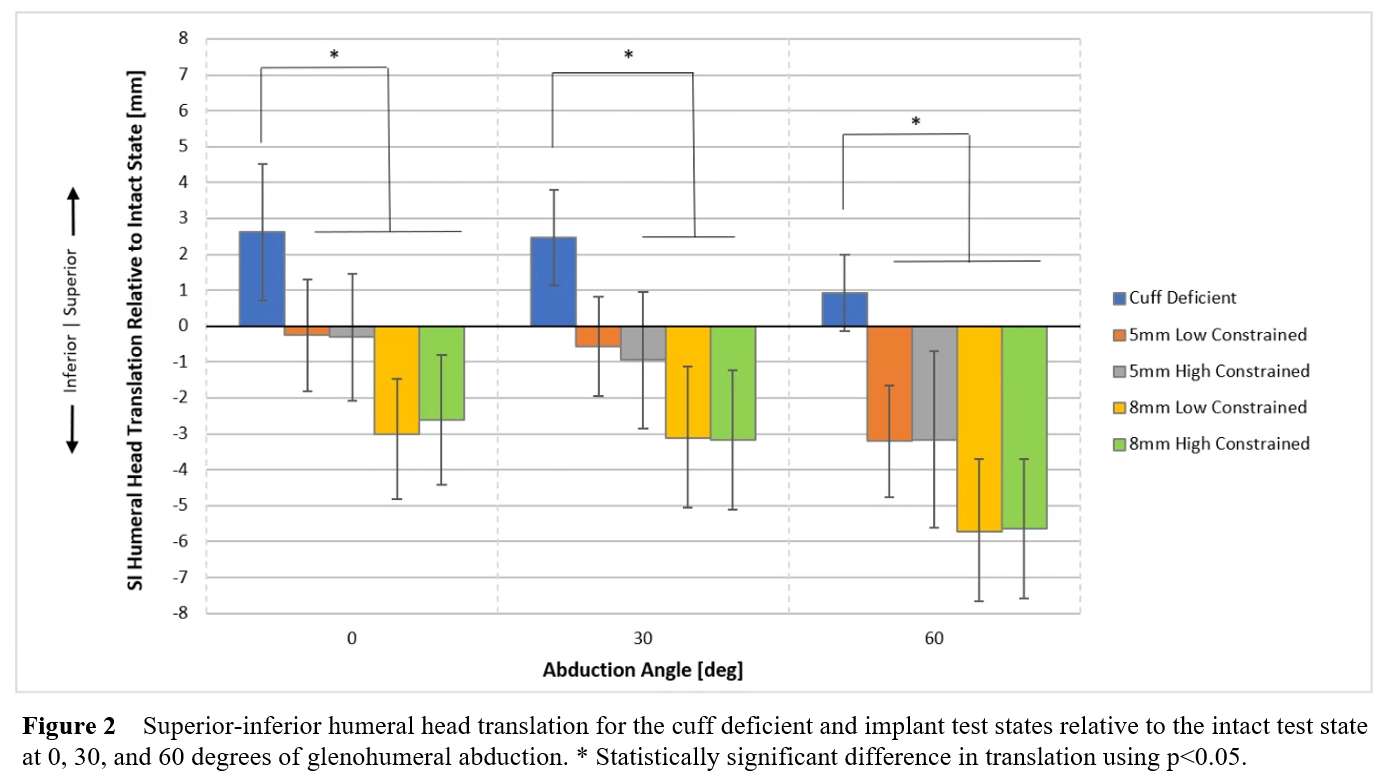
Figure 2
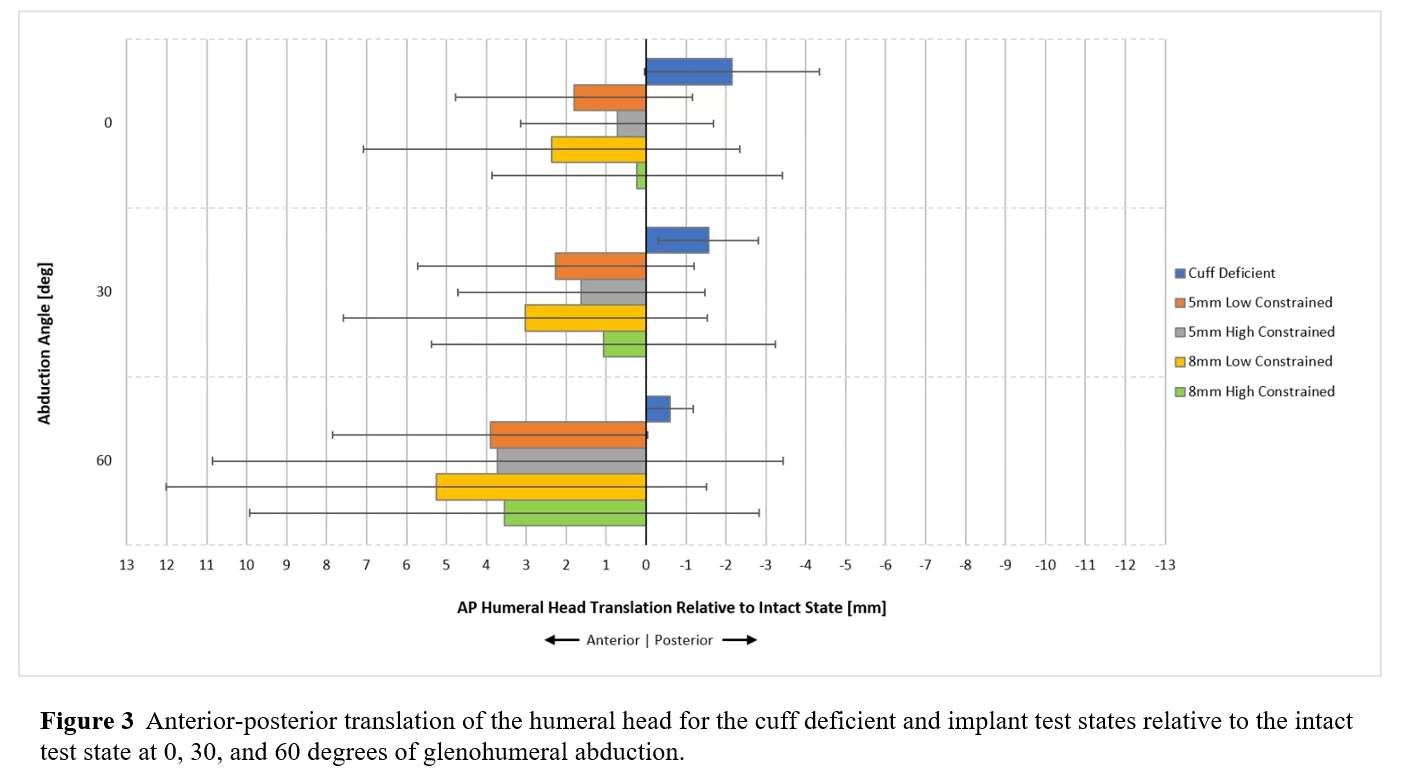
Figure 3#7648
Oxidised Zirconium Versus Cobalt-Chrome Femoral Heads in Total Hip Arthroplasty: a Multicentre Prospective Randomised Controlled Trial With 10 Years Follow-Up
*Babar Kayani - University College Hospital London - London, United Kingdom
Joanna Baawa - University College London Hospital - London, United Kingdom
Andreas Fontalis - University College London Hospitals - London, United Kingdom
Jenni Tahmassebi - UCLH - London, UK
Nic Wardle - UCLH - London, UK
Robert Middleton - Royal Bournemouth Hospital - Bournemouth, UK
Arthur Stephen - Royal Derby Hospital - Derby, United Kingdom
James Hutchinson - Royal Derby Hospital
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: babar.kayani@gmail.com
Introduction:
This study reports the ten-year polyethylene liner wear rates, incidence of osteolysis, clinical outcomes and complications ofa multicentre randomised controlled trial comparing Oxidised Zirconium (OxZr)versus Cobalt-Chrome (CoCr) femoral heads with ultra-high molecular weight polyethylene (UHMWPE) and highly cross-linked polyethylene (XLPE)liners in total hip arthroplasty (THA).
Methods:
Patients undergoing primary THA were recruited from four institutions and prospectively allocated to the following treatment groups: Group A - CoCr femoral head with XLPE liner; Group B - OxZr femoral head with XLPE liner; and Group C - OxZr femoral head with UHMWPE liner. All study patients and assessors recording outcomes wereblinded to the treatment groups. The outcomes of 262 study patients were analysed at ten years follow-up (figure 1).
Results:
Patients in group C were associated with increased liner wear rates compared to patients in group A (0.133 ± 0.21 mm/yr vs 0.031 ± 0.07 mm/yr respectively, p<0.001) and group B (0.133 ± 0.21 mm/yr vs 0.022 ± 0.05 mm/yr respectively, p<0.001) at ten years follow-up (figure 2). Patients in group C were also associated with increased risk of osteolysis and aseptic loosening requiring revision surgery compared with patients in group A (7/133 vs 0/133 respectively, p=0.007) and group B (7/133 vs 0/135 respectively, p=0.007). There was a non-statistically significant trend towards increased liner wear rates in group A compared with group B (0.031 ± 0.07 mm/yr vs 0.022 ± 0.05 mm/yr respectively, p=0.128) (figure 3). All three groups were statistically comparable preoperatively and at ten years follow-up when measuring normalised Western Ontario and McMaster Universities Osteoarthritis Index(p=0.410), short-form-36 (p = 0.465 mental, p = 0.713 physical), and pain scale scores (p=0.451).
Conclusion:
The use of UHMWPE was associated with progressively increased annual liner wear rates after THA. At ten years follow-up, this translated to UHMWPE leading to an increased incidence of osteolysis and aseptic loosening requiring revision surgery compared to XLPE. Femoral heads composed of OxZr were associated with trend towards reduced wear rates compared to CoCr, but this did not reach statistical significance and did not translate to any differences in osteolysis, functional outcomes, or revision surgery between the two femoral head components.
Key words:
Bearing surface
Cobalt–chrome
Highly-crosslinked polyethylene
Oxidised zirconium
Ultra-high molecular weight polyethylene
Legends:
Figure 1:CONSORT flow diagram demonstrating passage of patients through the randomised controlledtrial, with details on enrolment, intervention allocation, follow-up and analysis at ten years follow-up. UHMWPE, ultra-highmolecular weight polyethylene; CoCr, cobalt–chrome; OXZr, oxidised zirconium; XLPE,highly cross-linked polyethylene.
Figure 2: Graph showing mean linear wear rates (with 95% confidence intervals) in all treatment groups at ten years follow-up
Figure 3: Line graph demonstrating mean ten year linear wear of acetabular liner for groups of Cobalt-chrome (CoCr)/cross-linked polyethylene (XLPE), Oxidised zirconium (OxZr)/XLPE and OxZr/ultra-high molecular weight polyethylene (UHMWPE) (standard deviation in error bars)
Figures
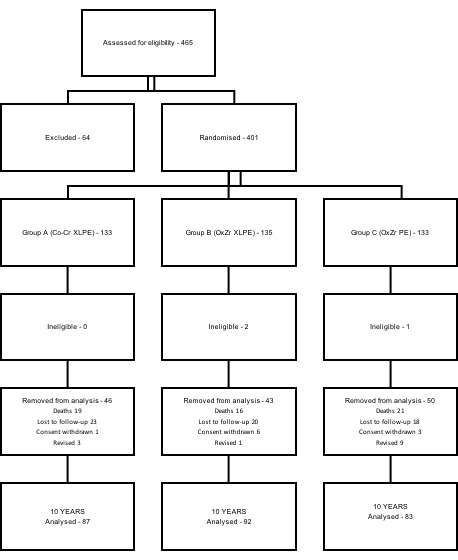
Figure 1
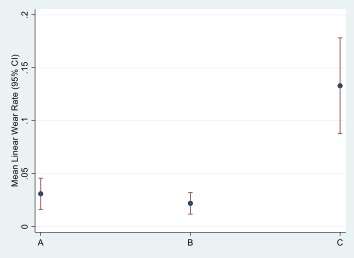
Figure 2
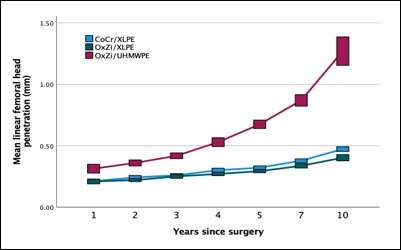
Figure 3#7669
Spinopelvic Mobility and Functional Component Positioning in Total Hip Arthroplasty Patients With Spinal Pathology and the Role of Robotic-Arm Assistance: A Prospective Cohort Study.
*Andreas Fontalis - University College London Hospitals - London, United Kingdom
Fabrice Glod - Hôpitaux Robert Schuman-Fondation Hôpitaux Robert Schuman - Luxembourg-City, Luxembourg
Babar Kayani - University College Hospital London - London, United Kingdom
Pierre Putzeys - Hôpitaux Robert Schuman-Fondation Hôpitaux Robert Schuman - Luxembourg-City, Luxembourg
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: andreasfontalis@gmail.com
Introduction
The complex relationship between spinopelvic mobility and component positioning in Total Hip Arthroplasty (THA), presents a challenge in achieving functional implant positioning. It has been reported that more than half of patients suffering a dislocation post-operatively had their acetabular component positioned withing the Lewinnek "safe zone" and there is mounting evidence highlighting the importance of functional component positioning. Patients with spinal pathology, especially those with stiff spines who have little change in sacral slope are in high risk of instability. The objective of this study was to investigate the effect of spinopelvic parameters on patient-specific component positioning, impingement and elucidate the role of robotic arm-assistance.
Methods
This prospective cohort study included 109 patients with previous spinal pathology undergoing robotic arm-assisted primary THA; incorporating spino-pelvic motion into planning and allowing dynamic evaluation of range-of-motion (ROM). Study participants were allocated in three groups based on their spinopelvic movement as measured by the difference in sacral slope between sitting and standing (Delta SS); <10, stiff spine; <10<Delta SS<30, normal movement; <30, hypermobile. The ROM where impingement occurred, utilising the virtual ROM tool (vROM) of the robotic software, was documented. In addition, the inclination and anteversion of the cup, spinopelvic parameters, combined offset and leg length were collected.
Results
Pre-operative ROM was comparable among the groups (N=10 stiff spine, N=69 normal mobility, N=31 hypermobile, one-way ANOVA p>0.05). Delta SS was 8.2 (3.5), 18.8 (10.9) and 36 (6) respectively. Based on the pre-operative plan, impingement with the vROM tool was evident in 100% patients with stiff spines, 69.6% in patients with normal spinopelvic motion and 45.2% in the hypermobile group, p=0.003. Intra-operative measurements revealed a significant difference in final component positioning between the groups; cup inclination was 43.2 (3.32) vs. 40.46 (2.9) vs. 39.8 (2.02), p=0.003[Fig.1], one-way ANOVA; anteversion was 22.5 (2.4) vs. 21.42 (2.45) vs. 20.55 (1.85), p=0.049[Fig.2]. No significant difference was identified in relation to combined anteversion p>0.66. Patients with stiff spines had their offset increased by 3.33mm (6.9)[Fig.3], compared to -1.3 (5.2) and 0.3 (6.03) in the other groups, p=0.046. With regards to the precision of achieving the planned component positioning utilising robotic arm-assistance; the median precision for achieving the desired anteversion and inclination was 0mm (IQR, 1); for achieving the desired offset 1mm (IQR, 5). Additionally, the median precision for achieving the desired leg length was 1mm (IQR, 2). There were no dislocations post-operatively.
Conclusion
In our study, patient specific component positioning was significantly affected by the individual spinopelvic motion. We found that in the challenging subgroup of patients with spinal pathology, robotic-arm assistance demonstrated high accuracy in achieving the planned component positioning and enabled the execution of a patient specific plan, avoiding impingement and maximising ROM; especially utilising the latest platform that encompasses a vROM tool to dynamically assess impingement. This could conceptually translate to lower risk of dislocation, less pain and better implant survivorship; however, this needs to be corroborated by long term studies.
Keywords
spinopelvic mobility, functional component positioning, total hip arthroplasty, robotic arm-assistance, virtual range of motion
Figures
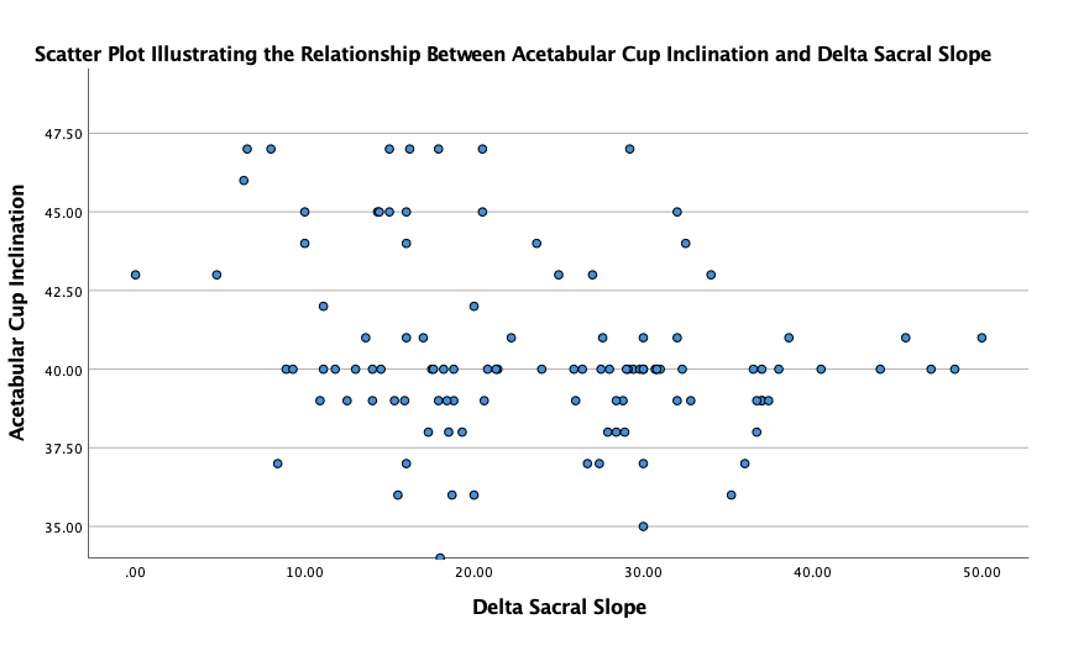
Figure 1
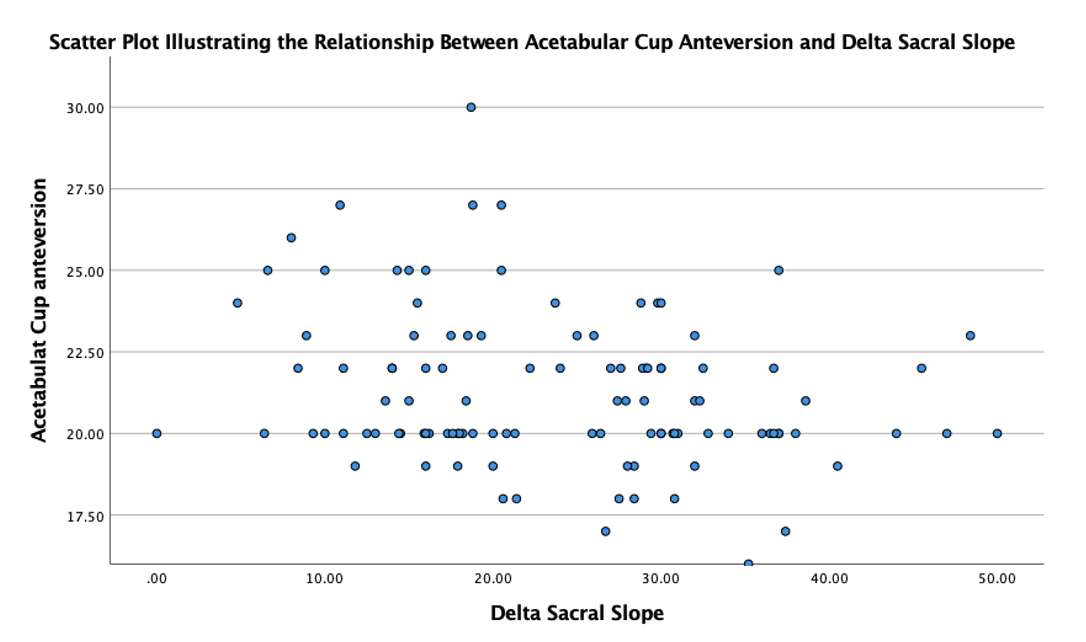
Figure 2
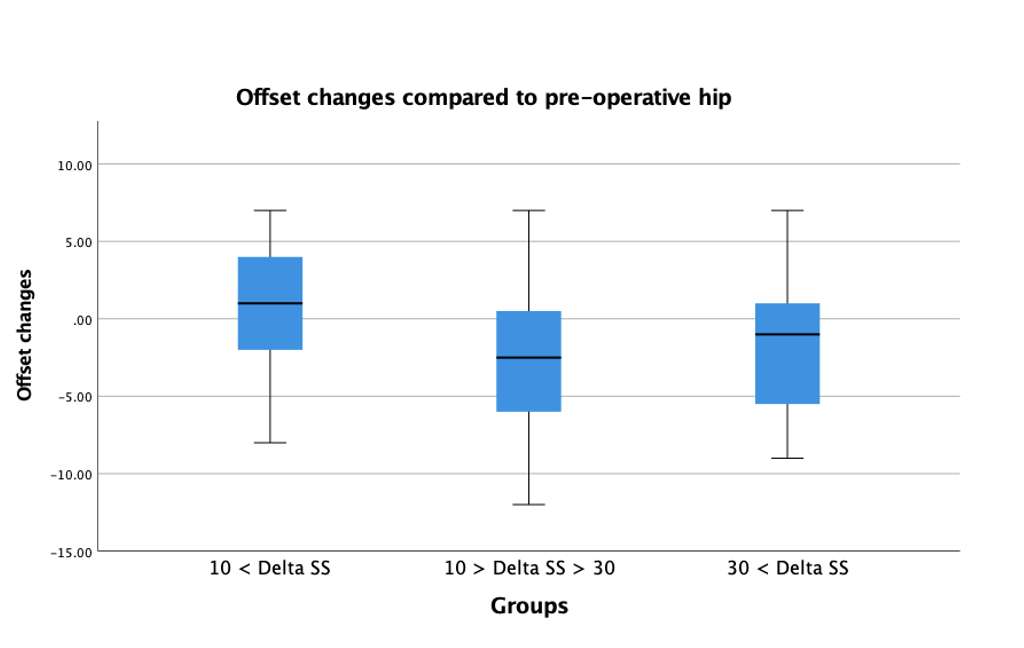
Figure 3#7853
Inflammatory Response in Robotic Total Knee Arthroplasty Versus Conventional Jig-Based and the Correlation With Functional Outcomes and Patient Reported Outcome Measures: A Randomized Controlled Trial
*Andreas Fontalis - University College London Hospitals - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Ajay Asokan - University College London Hospital - London, United Kingdom
Isabella Catrina Haddad - University College London Hospital - London, United Kingdom
Jenni Tahmassebi - UCL Hospitals NS Foundation Trust - London, United Kingdom
Sujith Konan - University College Hospital London - London, United Kingdom
Sam Oussedik - Sydney Orthopaedic Research Institute - Chatswood, Australia
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: andreasfontalis@gmail.com
Abstract
Background
Robotic Total Knee Arthroplasty (TKA) has been shown to result in reduced bone and soft tissue trauma. The objective of this study was to compare the inflammatory response in conventional jig-based TKA versus robotic-arm assisted TKA and examine the relationship with early functional outcomes and Patient Reported Outcome Measures (PROMs).
Methods
This prospective randomised controlled trial included 30 patients with symptomatic knee osteoarthritis undergoing conventional TKA versus robotic-arm assisted TKA. The local inflammatory response was assessed by analysing samples from the intraarticular drain fluid at 6 and 24 hours. Markers of serum inflammation were measured in blood samples collected for up to 28 days post-operatively.
Results
Patients in the robotic group demonstrated reduced drain fluid levels of IL-6 at 6- hours [798.54 vs. 5699.2, p=0.026] and 24- hours and IL-8 at 6 hours. Robotic TKA was associated with lower pain scores. PROM scores were comparable between the two groups at 2 years. A significant correlation was observed between self-reported pain and serum markers on the 7th postoperative day; between drain IL-8 levels and pain on postoperative day 1 (r= 0.458), 2 and 7; between knee flexion and extension and drain IL-6, IL-8 and TNF-a levels (6-hours).
Conclusion
Robotic-arm assisted TKA was associated with a reduction in the early postoperative local inflammatory response. We also found a moderate relationship with self-reported pain, knee flexion and extension. Further validation of these findings on a larger scale and looking at longer-term data, will be key to developing the optimal TKA procedure.
Keywords: Total Knee Arthroplasty; Robotic arm-assistance; Inflammatory Response;
Interleukin; Patient Reported Outcome Measures; Functional Outcomes
Introduction
There is still a high incidence of patient dissatisfaction in patients undergoing Total Knee arthroplasty (TKA)1,2, despite the good clinical outcomes reported by mid- to long term follow up studies3,4. Several causes and predictors have been suggested, including worse baseline Patient Reported Outcome Measures (PROMs), decreased Range of Motion (ROM), depression, unmet patient expectations and socioeconomic status1,2. With the advent of surgical technologies, such as navigation and robotic arm assistance5, attention has also been drawn to alignment philosophies and their implication on patient satisfaction6. Another potentially modifiable factor is the trauma of surgery which may lead to localized and systemic inflammatory responses that impair postoperative clinical recovery and in turn influence long-term functional outcomes1,7.
The evolution of surgical technology has led to the development of robotic-arm assisted TKA (RO TKA), where the haptically bounded saw blade and stereotactic boundaries could help minimise bone and peri-articular soft tissue trauma8–10. Cadaveric studies in conventional, jig-based TKA (CO TKA) have demonstrated that even in the hands of experienced surgeons, the oscillating saw significantly surpasses the bone edge when performing the tibial cut; resulting in direct injury to the capsule and stabilising structures11–13.
The optimal method for quantifying the surgical insult and invasiveness of a procedure is contentious. Several cytokines have been put forward as a surrogate measure, however the synthesis of interleukin-6 (IL-6) by monocytes, macrophages and other cells is instantly mediated by surgery14. Attempts to evaluate the magnitude of surgical insult in TKA have focused predominantly on quantifying serum inflammatory markers15,16 and these have been shown to correlate with post-operative recovery pain and functional outcomes14,17. Notwithstanding this, it has been postulated that the local inflammatory response is more important in determining postoperative recovery18.
We recently conducted a Randomised Controlled Trial (RCT) studying the levels of serum inflammatory markers at distinct post-operative timepoints between robotic-arm assisted and conventional TKA19. Robotic TKA was associated with a transient reduction of the systemic inflammatory response on the 7th post-operative day; this reduction attenuated and reached non-statistical levels in the late post-operative period (28th day). We also noted that participants in the robotic group sustained decreased iatrogenic soft tissue injury and less bone trauma8. Conceptually, we hypothesised that robotic-arm assisted TKA could be associated with a reduction in local inflammation.
As there are no published studies in relation to the local inflammatory response between conventional and robotic-arm assisted TKA; in this subsequent analysis of the RCT, we aimed to produce pilot data by measuring the levels of inflammatory markers obtained from the intra-articular drain fluid. Moreover, we aimed to study functional outcomes and Patient Reported Outcome Measures (PROMs) at 2-years following surgery; and explore whether there was any correlation with local and systemic inflammation. To our knowledge, this is the first RCT comparing the local post-operative response between Conventional and Robotic TKA.
Materials and Methods
Study design and objectives:
This is a prospective randomised controlled study investigating the local inflammation and patient reported outcomes in robotic-arm assisted versus conventional TKA.
This study was conducted in a single unit and encompassed 30 adult patients aged between 18 and 80 years, with symptomatic knee osteoarthritis, undergoing primary TKA (Figure 1). Participants undergoing revision surgery or with concomitant cancer, autoimmune or neurological diseases were excluded to limit any confounding effect. Other exclusion criteria comprised the presence of bone loss requiring augmentation and symptomatic arthritis of the contralateral knee. The study was reviewed by the institutional Joint Research Office and the local Research Ethics Committee and a favourable opinion was given (Ref: 18/LO/0926). Written consent was obtained from all research participants and the study was also registered with clinical.trials.gov(NCT04192006)20.
Patients with symptomatic knee osteoarthritis requiring TKA were screened and provided with a Research Ethics Committee approved information leaflet, during their visit to the outpatient clinic. Patients agreeing to participate, were randomly allocated to undergo robotic-arm assisted or conventional TKA. Sequence generation was achieved with the assistance of an online random number generator and participants were allocated with equal probabilities to the interventions.
The objectives of this study were to compare the local inflammatory response, Patient Reported Outcome Measures and functional outcomes in Robotic versus Conventional TKA. Moreover, we aimed to explore whether there was any correlation between the inflammatory responses, PROMS and functional outcomes.
Surgical technique and post-operative care:
All procedures were performed under general anaesthetic and a medial parapatellar approach was utilised. A tourniquet was applied, but not inflated to minimise bias on measurements owing to reperfusion or muscle ischaemia. The Mako Robotic Arm Interactive Orthopaedic System (Stryker Limited, Kalamazoo, Michigan) was used to perform the bone preparation and guide implant positioning according to the pre-operative plan.
The cemented Stryker Triathlon (Stryker Navigation, Kalamazoo, Michigan), cruciate retaining knee system was utilised in both groups. Tibial and femoral bone resections were performed to achieve neutral mechanical alignment. Patellar resurfacing was performed in both groups. An intraarticular vacuum drain was inserted, which was removed 24 hours post-operatively. All study participants followed standardised rehabilitation with full weight-bearing and active range of movement (ROM) exercises.
Pre-defined local inflammatory markers: Interleukin-6 (IL-6), Interleukin-8 (IL-8), Tumour necrosis Factor alpha (TNFa) were measured from the drain fluid at 6- and 24 hours following surgery. Pain, opiate requirements, knee joint ROM, time to discharge and number of physiotherapy sessions were additionally collected. The Oxford Knee Score (OKS), Knee Injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster University Osteoarthritis Index (WOMAC), 12-Item Short Form Health Survey (SF-12) and the EuroQol- 5 Dimension (EQ-5D) were collected pre-operatively and at 2 years.
Sample size calculation:
As previously described, the sample size calculation for this RCT was performed utilising the systemic levels of CRP at 48 hours post-operatively as the primary outcome19. In this subsequent analysis, we utilised pilot data to investigate the local inflammatory response between RO TKA and CO TKA. Several papers have been published in relation to identifying an appropriate sample in pilot studies; Connelly21 advocated a pilot study sample should be 10% of the sample projected for the larger parent study; Isaac and Michael 22 suggested 10 – 30 participants; Hill 23 recommended 10 to 30 participants for pilots in survey research; van Belle 24 suggested 12 and Treece and Treece 25 10% of the project sample size. In line with the current literature26,27, our study encompasses 15 participants in each group.
Statistical analysis:
Continuous variables are presented as mean (standard deviation) or median (Interquartile range). Differences in continuous outcomes were assessed with the independent samples Mann-Whitney U Test or two-samples t-test. The Spearman and Pearson coefficients were employed to determine if a correlation was evident between the cytokines measured from the drain fluid and PROMs.
Results
The mean age of patients undergoing robotic TKA was 67.9 (SD 8.6) and conventional TKA 68.7 (SD 8.6, p = 0.81). Upon comparison of the groups’ baseline characteristics (gender, BMI, ASA score, side of intervention)19, no significant differences were noted. No serious adverse events occurred in any participant.
Local Inflammatory Response
Patients in the robotic group demonstrated reduced levels of IL-6 in the drain fluid at 6- hours [798.54 (3954) vs. 5699.2 (6550), p=0.026] and 24- hours [1474 (64678) vs. 147400 (55079), p=0.002] and reduced levels of IL-8 at 6-hours following surgery [401.3 (1176.44) vs. 1986 (2797.5), p=0.001]. Levels of TNFa were comparable between groups at each time point (Table 1 and Figures 2-4).
Pain, opiates consumption and early functional outcomes
Patients in the robotic TKA group demonstrated a significantly lower pain score on post-operative day 1, 2 and 7, measured on a numerical scale ranging from 0-10 (Table 2). Opiates consumption, length of stay, number of physiotherapy sessions and early functional outcomes were comparable between the two study arms (Tables 2 and 3).
Patient Reported Outcome Measures (PROMs)
No significant differences were evident upon comparison of the baseline PROMs and quality of life between the two groups (Table 4). At two-years of follow up, PROM scores were also comparable between the two treatment groups (Table 5).
Correlational analyses
Self-reported pain and inflammatory markers
Upon studying the correlation between self-reported pain measured on a numerical scale on the seventh postoperative day and serum markers; a positive correlation was noted for all markers except IL-1b (Table 6 and Figure 5). Spearman rank correlation coefficient for IL-6 was 0.536 (p=0.002), TNF-a 0.402 (p=0.028), ESR 0.409 (p=0.025), CRP 0.512 (p=0.004), CK 0.443 (p=0.014).
With respect to the correlation with drain inflammatory markers, a significant relationship was manifested between the drain IL-8 levels at 6-hours and pain on postoperative day 1 (r= 0.458, p=0.011), day 2 (r=0.404, p=0.027) and day 7 (r=0.449, 0=0.013). A moderate positive relationship was also evident between the drain IL-6 levels at 24-hours and pain on day 1, 2 and 7 (Tables 7 and 8).
Early functional outcomes and opiate consumption
Knee flexion and extension were significantly correlated with drain IL-6 levels at 6- hours, drain IL-8 and TNF-a levels at 6- hours (Figure 6) and the serum ESR levels on the seventh postoperative day (r=0.470, P=0.009) (Tables 6 - 8).
No significant relationship was shown between inflammatory markers and the number of physiotherapy sessions, time to discharge and opiate consumption (Tables 6 - 8).
Changes in PROMs and quality of life
In an exploratory analysis we evaluated the correlation among changes in PROMs and the systemic and local inflammatory response utilising the Pearson Correlation Coefficient. Higher levels of cortisol at 28 days were moderately associated with larger gains in WOMAC scale (r= 0.380, p= 0.042). Gains in KOOS were inversely correlated with Cortisol levels at 48 hours (r= -0.477, p=0.008), IL-1β levels at 28 days (r= -0.400, p=0.028) and CRP levels at 28 days (r= -0.452, p=0.012). Improvement in OKS was inversely correlated with IL-1β levels at 28 days (r= -0.422, p=0.20), while improvement in quality of life showed a weak positive correlation with WCC levels at 48 hours (r=0.566, p=0.001) and weak negative correlation with Neutrophil levels at 7 days (r= -0.374, p=0.42). In relation to SF-12; MCS-12 gains were negatively correlated with local IL-6 levels at 24 hours (r= -0.421, p=0.21), LDH levels at 6 hours (r= -0.421, p=0.21), CRP levels at 6 hours (r= -0.458, p=0.11) and positively correlated with WCC levels at 28 days (r=0.367, p=0.046). Improvements in PCS-12 scores were positively correlated with ALP at 6 hours (r=0.412, p=0.024), ALP at 28 days (r=0.535, p=0.002) and negatively correlated with Neutrophils at 7 days (r= -0.459, p=0.011).
Discussion
Serum inflammatory markers could represent an objective way of ascertaining the invasiveness of a surgical procedure and this approach has been employed in the context of TKA15,28,29. Preserving the periarticular soft tissue envelope in TKA and minimising the surgical insult is key and has been shown to affect rehabilitation and clinical outcomes30. Trials have suggested robotic TKA is associated with a reduction in bone trauma, soft tissue injury and early systemic inflammatory response8,19,31. However, there is no published evidence of clinical correlation with pain, recovery and early functional outcomes.
This is the first RCT studying the local post-operative inflammation between conventional and robotic TKA and assessing the correlation with early functional outcomes and PROMs at 2 years.
In our study, robotic TKA was associated with reduced postoperative levels of IL-6 and IL-8 measured in the drain fluid at 6 hours and IL-6 at 24 hours. Differences were particularly pronounced with respect to IL-6 levels. This could reflect the reduced bone and soft tissue injury with robotic technology, owing to averting multiple cuts and more precisely executing the pre-operative plan. Several parameters that could have influenced the measurements including operative time and length of incision, were previously reported to be comparable between the groups19.
Furthermore, research performed in animals has shown that the use of conventional cutting blocks and saw blades is associated with the production of significant metal debris; only particles released from the saw blades were estimated at 500,00032. These may enter the joint and be responsible for a more pronounced inflammatory response owing to macrophage activation32. An alternative interpretation could embrace the use of intramedullary femoral referencing in conventional TKA that has been suggested to trigger an inflammatory reaction33. Another parameter that should be appreciated is the inflammatory response that may have been induced by the introduction of the femoral and tibial registration pins in robotic TKA. Conceivably, they are perhaps less likely to induce substantial inflammation, due to their topographic placement in relation to the joint and smaller diameter. Finally, we found levels of local TNF-a were comparable between groups at each time point. This could reflect the inherent difficulty in reliably measuring TNF-a levels, owing to its very short half-life (15 to 30 minutes34).
Ugras et al 7 reported postoperative intraarticular IL-6 was correlated to KSS and WOMAC scores. Notwithstanding, no correlation was shown with serum IL-6 and CRP levels, hence authors suggested that local inflammatory response is more important.
In our study we found that both local and systemic response were correlated with pain. A moderate positive correlation was evident between self-reported pain and drain IL-6 (24 hours) and IL-8 (6 hours). Furthermore, a moderate to strong correlation was found between serum markers on the seventh postoperative day and pain.
In our trial we found no significant correlation between either local or systemic markers and the number of physiotherapy sessions, in-hospital stay, and opiate consumption. Notwithstanding this, we need to consider potential confounding factors such as standardized protocols for discharge and rehabilitation when interpreting the findings in the setting of the National Health System (NHS). Enhanced recovery pathways and day-case TKA have been introduced in the NHS, however there is careful patient selection and an inherent bias owing to the qualifying inclusion criteria35.
Our findings are to a certain extent in concordance with previous studies; Poehling-Monaghan et al36 studied the correlation of serum markers in 100 patients undergoing conventional THA and reported no predictive value with respect to functional outcomes and time to discontinuing narcotics. Similarly, Lanklide et al37 reported that only IL-10 levels were associated with long term rehabilitation following TKA and functional performance. Notwithstanding, in our study a weak to moderate relationship was evident between drain inflammatory markers at 6-hours postoperatively and knee flexion and extension.
PROM scores and quality of life were comparable between the two groups at 2 years. However, as our primary objective was to ascertain the inflammatory response, our pilot study encompassed a relatively small sample size. Hence, unmasking any statistically significant difference would be rather improbable, considering the large effect size of TKA. Upon evaluating the correlation among changes in PROMs and the systemic and local inflammatory response, a moderate relationship with several systemic and local inflammatory markers was unveiled that can fuel further research and targets in the future.
Finally, pain scores in the robotic group were significantly lower and this was found to be correlated predominantly with systemic inflammatory markers. This could represent a signal that robotic TKA potentially results in faster recovery and shorter length of stay. This has been reported in bigger datasets38–40, nevertheless owing to our relatively small sample size we were unable to substantiate it.
However, our study has several limitations that should be considered when interpreting the results. First, owing to the pilot character of our trial, it encompasses a limited sample. Second, owing to the nature of the fluid sample (intra-articular fluid), it would be unethical to obtain a baseline sample; hence baseline differences in the magnitude of the inflammation between individuals could have impacted final results. Third, a potential source of bias could be the trauma caused by the intramedullary femoral referencing in conventional jig-based TKA and the tibial and femoral registration pins in robotic TKA, which is impossible to quantify.
Conclusions
Results of the RCT, showed that robotic TKA was associated with a reduction in the postoperative drain fluid levels of IL-6 and IL-8 at 6 hours and IL-6 at 24 hours.
Furthermore, correlational analyses unveiled that both the local and systemic responses were correlated with pain, and pain scores in the robotic group were significantly lower. However, no significant correlation was unveiled with length of stay, number of physiotherapy sessions or opiate consumption. PROM scores and quality of life at two years were comparable between the two study cohorts.
Further validation of the findings and signals that emerged on a larger scale, as well as scrutinising longer-term data, will be key to developing the optimal TKA procedure that confers better functional and patient reported outcomes, in addition to reducing soft tissue and bone injury.
Source of funding
Funding for this study was received from Stryker Limited, Kalamazoo, Michigan, USA. The funding source did not play a role in the investigation or interpretation of the results. The study was sponsored by University College London, Bloomsbury, London, UK.
Figure Legends:
Figure 1. Flow diagram depicting the progress of the two groups through the phases the randomised controlled trial.
Figure 2. Boxplot depicting the levels of Interleukin 6 between the two groups, 6- and 24 hours post-operatively.
Figure 3. Boxplot depicting the levels of Interleukin 8 between the two groups, 6- and 24 hours post-operatively.
Figure 4. Boxplot depicting the levels of Tumour Necrosis Alpha factor between the two groups, 6- and 24 hours post-operatively.
Figure 5. Scatterplot matrix demonstrating the correlation between self-reported pain and serum inflammatory markers on the 7th postoperative day.
Figure 6. Scatterplot matrix illustrating the correlation between knee flexion and extension and drain inflammatory markers 6 hours post-operatively.
References
1. Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJK, Robertson BW. Patient Dissatisfaction Following Total Knee Arthroplasty: A Systematic Review of the Literature. J Arthroplasty. 2017;32(12):3854-3860. doi:10.1016/J.ARTH.2017.07.021
2. Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ. Three groups of dissatisfied patients exist after total knee arthroplasty: early, persistent, and late. Bone Joint J. 2018;100-B(2):161-169. doi:10.1302/0301-620X.100B2.BJJ-2017-1016.R1
3. Hampton M, Mansoor J, Getty J, Sutton PM. Uncemented tantalum metal components versus cemented tibial components in total knee arthroplasty: 11- to 15-year outcomes of a single-blinded randomized controlled trial. https://doi.org/101302/0301-620X102B8BJJ-2019-1448R1. 2020;102(8):1025-1032. doi:10.1302/0301-620X.102B8.BJJ-2019-1448.R1
4. Haddad FS, Plastow R. Is it time to revisit cementless total knee arthroplasty? Bone Joint J. 2020;102-B(8):965-966. doi:10.1302/0301-620X.102B8.BJJ-2020-0962
5. Fontalis A, Epinette JA, Thaler M, Zagra L, Khanduja V, Haddad FS. Advances and innovations in total hip arthroplasty. SICOT-J. 2021;7. doi:10.1051/SICOTJ/2021025
6. Oussedik S, Abdel MP, Victor J, Pagnano MW, Haddad FS. Alignment in total knee arthroplasty. https://doi.org/101302/0301-620X102B3BJJ-2019-1729. 2020;102 B(3):276-279. doi:10.1302/0301-620X.102B3.BJJ-2019-1729
7. Ugraş AA, Kural C, Kural A, Demirez F, Koldaş M, Çetinus E. Which is more important after total knee arthroplasty: Local inflammatory response or systemic inflammatory response? Knee. 2011;18(2):113-116. doi:10.1016/J.KNEE.2010.03.004
8. Kayani B, Konan S, Pietrzak JRT, Haddad FS. Iatrogenic Bone and Soft Tissue Trauma in Robotic-Arm Assisted Total Knee Arthroplasty Compared With Conventional Jig-Based Total Knee Arthroplasty: A Prospective Cohort Study and Validation of a New Classification System. J Arthroplasty. 2018;33(8):2496-2501. doi:10.1016/J.ARTH.2018.03.042
9. Hampp EL, Sodhi N, Scholl L, et al. Less iatrogenic soft-tissue damage utilizing robotic-assisted total knee arthroplasty when compared with a manual approach: A blinded assessment. Bone Jt Res. 2019;8(10):495-501. doi:10.1302/2046-3758.810.BJR-2019-0129.R1/ASSET/IMAGES/LARGE/2046-3758.810.BJR-2019-0129.R1-FIG3.JPEG
10. Plaskos C, Wakelin E, Shalhoub S, et al. SOFT-TISSUE RELEASE RATES IN ROBOTIC-ASSISTED GAP-BALANCING AND MEASURED-RESECTION TOTAL KNEE ARTHROPLASTY | Orthopaedic Proceedings. Orthop Proc. 2019;102-B(No.SUPP_2). https://online.boneandjoint.org.uk/doi/abs/10.1302/1358-992X.2020.2.001. Accessed December 10, 2021.
11. Leopold MSS, McStay C, Klafeta K, Jacobs JJ, Berger RA, Rosenberg AG. Primary repair of intraoperative disruption of the medical collateral ligament during total knee arthroplasty. J Bone Joint Surg Am. 2001;83(1):86-91. doi:10.2106/00004623-200101000-00012
12. Wijdicks CA, Griffith CJ, Johansen S, Engebretsen L, LaPrade RF. Injuries to the medial collateral ligament and associated medial structures of the knee. J Bone Joint Surg Am. 2010;92(5):1266-1280. doi:10.2106/JBJS.I.01229
13. Herregodts S, Verhaeghe M, Paridaens R, et al. Soft-tissue penetration of the oscillating saw during tibial resection in total knee arthroplasty. https://doi.org/101302/0301-620X102B10BJJ-2019-1602R2. 2020;102(10):1324-1330. doi:10.1302/0301-620X.102B10.BJJ-2019-1602.R2
14. Honsawek S, Deepaisarnsakul B, Tanavalee A, et al. Relationship of serum IL-6, C-reactive protein, erythrocyte sedimentation rate, and knee skin temperature after total knee arthroplasty: a prospective study. Int Orthop. 2011;35(1):31. doi:10.1007/S00264-010-0973-0
15. Niki Y, Mochizuki T, Momohara S, Saito S, Toyama Y, Matsumoto H. Is minimally invasive surgery in total knee arthroplasty really minimally invasive surgery? J Arthroplasty. 2009;24(4):499-504. doi:10.1016/J.ARTH.2008.04.002
16. Tsunoda K, Sonohata M, Kugisaki H, et al. The Effect of Air Tourniquet on Interleukin-6 Levels in Total Knee Arthroplasty. Open Orthop J. 2017;11(1):20. doi:10.2174/1874325001711010020
17. Si HB, Yang TM, Zeng Y, et al. Correlations between inflammatory cytokines, muscle damage markers and acute postoperative pain following primary total knee arthroplasty. BMC Musculoskelet Disord. 2017;18(1). doi:10.1186/S12891-017-1597-Y
18. Ugraş AA, Kural C, Kural A, Demirez F, Koldaş M, Çetinus E. Which is more important after total knee arthroplasty: Local inflammatory response or systemic inflammatory response? Knee. 2011;18(2):113-116. doi:10.1016/J.KNEE.2010.03.004
19. Kayani B, Tahmassebi J, Ayuob A, Konan S, Oussedik S, Haddad FS. A prospective randomized controlled trial comparing the systemic inflammatory response in conventional jig-based total knee arthroplasty versus robotic-arm assisted total knee arthroplasty. Bone Joint J. 2021;103-B(1):113-122. doi:10.1302/0301-620X.103B1.BJJ-2020-0602.R2
20. Inflammatory Response Conventional Total Knee Replacement Versus Mako Total Knee Replacement - Full Text View - ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT04192006. Accessed December 12, 2021.
21. Connelly LM. Pilot studies. Medsurg Nurs. 2008;17(6):411-412. http://www.ncbi.nlm.nih.gov/pubmed/19248407. Accessed February 26, 2019.
22. Isaac S, Michael W. Handbook in Research and Evaluation 3 Rd Ed San Diego. San Diego, CA : Educational and Industrial Testing Services.; 1995. https://www.coursehero.com/file/p5bi092/Isaac-S-Michael-W-B-1995-Handbook-in-research-and-evaluation-3-rd-ed-San-Diego/. Accessed February 26, 2019.
23. Hill R, Hamilton WP. WHAT SAMPLE SIZE is “ENOUGH” in INTERNET SURVEY RESEARCH? | Semantic Scholar. Psychology. 1998. https://www.semanticscholar.org/paper/WHAT-SAMPLE-SIZE-is-%22ENOUGH%22-in-INTERNET-SURVEY-Hill-Hamilton/88134689f8eb30296cd67bf8f11c0a0856927ee6. Accessed May 11, 2021.
24. van Belle G. Statistical Rules of Thumb. New York: John Wiley; 2002.
25. Treece EW, Treece JW. ELEMENTS OF RESEARCH IN NURSING : Nursing Research. Nurs Res. 1977;26(3):239-239. https://journals.lww.com/nursingresearchonline/Citation/1977/05000/Elements_of_Research_in_Nursing.32.aspx. Accessed May 11, 2021.
26. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057-1073. doi:10.1177/0962280215588241
27. Bell ML, Whitehead AL, Julious SA. Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin Epidemiol. 2018;10:153. doi:10.2147/CLEP.S146397
28. Tanavalee A, Honsawek S, Rojpornpradit T, Sakdinakiattikoon M, Ngarmukos S. Inflammation related to synovectomy during total knee replacement in patients with primary osteoarthritis. J Bone Joint Surg Br. 2011;93-B(8):1065-1070. doi:10.1302/0301-620x.93b8.26719
29. Mayer C, Franz A, Harmsen JF, et al. Soft-tissue damage during total knee arthroplasty: Focus on tourniquet-induced metabolic and ionic muscle impairment. J Orthop. 2017;14(3):347-353. doi:10.1016/j.jor.2017.06.015
30. Peters CL, Jimenez C, Erickson J, Anderson MB, Pelt CE. Lessons learned from selective soft-tissue release for gap balancing in primary total knee arthroplasty: An analysis of 1216 consecutive total knee arthroplasties :AAOS Exhibit Selection. J Bone Jt Surg - Ser A. 2013;95(20). doi:10.2106/JBJS.L.01686
31. Khlopas A, Chughtai M, Hampp EL, et al. Robotic-Arm Assisted Total Knee Arthroplasty Demonstrated Soft Tissue Protection. Surg Technol Int. 2017;30:441-446. doi:10.29007/8bxp
32. Gotterson PR, Nusem I, Pearcy MJ, Crawford RW. Metal debris from bony resection in knee arthroplasty--is it an issue? Acta Orthop. 2005;76(4):475-480. doi:10.1080/17453670510041448
33. Albert V, Subramanian A, Trikha V, Veerappan SK, Jothi A. Acute coagulofibrinolytic and inflammatory changes in response to intramedullary nailing and its impact on outcome. J Clin Orthop Trauma. 2018;9(Suppl 1):S67-S73. doi:10.1016/j.jcot.2018.01.003
34. Ma Y, Zhao S, Shen S, et al. A novel recombinant slow-release TNF α-derived peptide effectively inhibits tumor growth and angiogensis. Sci Reports 2015 51. 2015;5(1):1-17. doi:10.1038/srep13595
35. Thompson JW, Wignadasan W, Ibrahim M, Plastow R, Beasley L, Haddad FS. The introduction of day-case total knee arthroplasty in a national healthcare system: A review of the literature and development of a hospital pathway. Surgeon. 2021. doi:10.1016/J.SURGE.2021.01.017
36. Poehling-Monaghan KL, Taunton MJ, Kamath AF, Trousdale RT, Sierra RJ, Pagnano MW. No Correlation Between Serum Markers and Early Functional Outcome After Contemporary THA. Clin Orthop Relat Res. 2017;475(2):452-462. doi:10.1007/s11999-016-4904-2
37. Langkilde A, Jakobsen TL, Bandholm TQ, et al. Inflammation and post-operative recovery in patients undergoing total knee arthroplasty-secondary analysis of a randomized controlled trial. Osteoarthr Cartil. 2017;25(8):1265-1273. doi:10.1016/j.joca.2017.03.008
38. Archer A, Salem HS, Coppolecchia A, Mont MA. Lengths of Stay and Discharge Dispositions after Total Knee Arthroplasty: A Comparison of Robotic-Assisted and Manual Techniques. J Knee Surg. 2021. doi:10.1055/S-0041-1735280
39. Kayani B, Konan S, Pietrzak JRT, Tahmassebi J, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty. Bone Jt J. 2018;100B(7):930-937. doi:10.1302/0301-620X.100B7.BJJ-2017-1449.R1/ASSET/IMAGES/LARGE/BJJ-2017-1449.R1-GALLEYFIG6.JPEG
40. Mitchell J, Wang J, Bukowski B, et al. Relative Clinical Outcomes Comparing Manual and Robotic-Assisted Total Knee Arthroplasty at Minimum 1-Year Follow-up: https://doi.org/101177/15563316211028568. 2021;17(3):267-273. doi:10.1177/15563316211028568
Appendix
Tables
|
Table 1. Levels of drain inflammatory markers between the two groups
|
|
|
6 hours
|
24 hours
|
|
Variables
|
Robotic TKA
|
Conventional TKA
|
P Value
|
Robotic TKA
|
Conventional TKA
|
P Value
|
|
Interleukin-6
|
798.54 (3954)
|
5699.2 (6550)
|
0.026*
|
1474 (64678)
|
147400 (55079)
|
0.002*
|
|
Interleukin-8
|
401.31 (1176.44)
|
1986 (2797.50)
|
0.001*
|
9834 (21959)
|
12512 (11473)
|
0.202*
|
|
Tumour Necrosis Factor - a
|
10.61 (12.07)
|
12
(48.21)
|
0.345*
|
8.78
(8.91)
|
12
(12)
|
0.267*
|
|
Data presented as median (Interquartile range), *Independent samples Mann-Whitney U Test
|
|
Table 2. Pain and opiates consumption between the robotic and conventional TKA groups.
|
|
Variables
|
Robotic TKA
|
Conventional TKA
|
P Value
|
|
Pain (numerical scale 1-10)
Post-operative day 1
Post-operative day 2
Post-operative day 3
Post-operative day 7
|
3 (1)
3 (2)
3 (2)
3 (1)
|
5 (2)
6 (1)
4 (1)
6 (2
|
<0.001*
<0.001*
0.285*
<0.001*
|
|
Opiates consumption (mg)
Post-operative day 1
Post-operative day 2
Post-operative day 3
|
28 (15)
5 (10)
0 (5)
|
20 (20)
5 (10)
0 (5)
|
0.870*
0.683*
0.902*
|
|
Data presented as median (Interquartile range), Independent samples Mann-Whitney U Test
|
|
Table 3. Length of stay, number of physiotherapy sessions and early functional outcomes between the two groups.
|
|
Variables
|
Robotic TKA
|
Conventional TKA
|
P Value
|
|
Number of physiotherapy sessions
|
6.93 ± 1.43
|
7.26 ± 1.53
|
0.544$
|
|
Time to discharge (Hrs)
|
76.4 ± 15.38
|
78.6 ± 14.85
|
0.693$
|
|
Knee extension
|
0 (0)
|
0 (0)
|
0.858*
|
|
Knee flexion
|
90 (5)
|
95 (10)
|
0.452*
|
|
Data presented as mean ± standard deviation or median (Interquartile range) based on whether normality was observed, *Independent samples Mann-Whitney U Test, $Independent samples t-test
|
|
Table 4. Baseline Patient Reported Outcome Measures and Quality of Life between the two groups.
|
|
Variables
|
Robotic TKA
|
Conventional TKA
|
P Value
|
|
WOMAC
|
68.66 (13.40)
|
67.60 (12.61)
|
0.824
|
|
KOOS
|
29.20 (6.51)
|
28.73 (5.43)
|
0.833
|
|
OKS
|
18.13 (7.18)
|
18.20 (4.73)
|
0.976
|
|
EQ-5D
|
0.629 (0.076)
|
0.620 (0.077)
|
0.740
|
|
EQ-5D VAS
|
60.33 (13.57)
|
59.60 (15.05)
|
0.890
|
|
12-item Short Form Survey (SF-12)
Mental Component Score (MCS-12)
Physical Component Score (PCS-12)
|
40.77 (11.14)
28.34 (4.68)
|
42.69 (7.58)
27.57 (6.10)
|
0.586
0.668
|
|
Data presented as Mean (Standard Deviation)
All comparisons made using the Independent samples T-Test
WOMAC: Western Ontario and McMaster University Osteoarthritis Index, KOOS: Knee injury and Osteoarthritis Outcome Score, OKS: Oxford Knee Score, EQ-5D: EuroQol-5D
|
|
Table 5. Patient Reported Outcome Measures and Quality of Life at 2-years follow up between the robotic and conventional groups and differences compared to the baseline scores.
|
|
Variables
|
Robotic TKA
|
Conventional TKA
|
P Value
|
|
WOMAC
Delta-WOMAC
|
4.86 (5.81)
63.80 (12.85)
|
6.13 (5.12)
61.46 (11.71)
|
0.532+
0.607+
|
|
KOOS*
Delta-KOOS
|
97 (14)
61.33 (13.91)
|
94 (7)
61.53 (12.17)
|
0.308$
0.967+
|
|
OKS
Delta-OKS
|
44.93 (2.78)
26.80 (7.97)
|
45.20 (2.75)
27 (4.84)
|
0.794+
0.934+
|
|
EQ-5D
Delta EQ-5D
|
0.881 (0.092)
0.252 (0.108)
|
0.838 (0.094)
0.217 (0.134)
|
0.211+
0.448+
|
|
EQ-5D VAS*
Delta EQ-5D VAS
|
75 (20)
8.33 (25.22)
|
75 (8)
8.73 (23.70)
|
0.983$
0.965+
|
|
12-item Short Form Survey (SF-12)
Delta SF-12
Mental Component Score (MCS-12)
Delta MCS-12
Physical Component Score (PCS-12)
Delta PCS-12
|
50.70 (13.04)
9.92 (14.04)
43.20 (11.54)
13.49 (12.84)
|
53.54 (9.54)
10.84 (8.78)
36.67 (9.33)
9.09 (10.79)
|
0.503+
0.832+
0.099+
0.319+
|
|
Data presented as Mean (Standard Deviation)
*Median (Interquartile range), +Independent samples T-Test, $Independent samples Mann-Whitney U Test
WOMAC: Western Ontario and McMaster University Osteoarthritis Index, KOOS: Knee injury and Osteoarthritis Outcome Score, OKS: Oxford Knee Score, EQ-5D: EuroQol-5D
|
|
Table 6. Correlation matrix displaying serum inflammatory markers 7 days post-operatively and pain, early functional outcomes.
|
|
|
IL-1B
|
IL-6
|
ESR
|
TNF-a
|
CRP
|
CK
|
|
Pain (numerical scale 1-10)
Post-operative day 7
|
0.314
(P=0.91)
|
0.536
(P=0.002)
|
0.409
(P=0.025)
|
0.402
(P = 0.028)
|
0.512
(P=0.004)
|
0.443
(P=0.014)
|
|
Number of physiotherapy sessions
|
-0.200
(P=0.289)
|
0.097
(P=0.611)
|
0.252
(P=0.179)
|
-0.057
(P=0.764)
|
0.038
(P=0.842)
|
0.162
(P=0.392)
|
|
Time to discharge
|
-0.038
(P=0.842)
|
0.166
(P=0.382)
|
0.213
(P=0.259)
|
0.069
(P=0.717)
|
-0.038
(P=0.842)
|
0.233
(P=0.216)
|
|
Knee extension
|
-0.290
(P=0.121)
|
-0.074
(P=0.697)
|
-0.136
(P=0.473)
|
0.023
(P=0.903)
|
-0.176
(P=0.353)
|
0.139
(P=0.463)
|
|
Knee flexion
|
0.041
(P=0.831)
|
0.265
(P=0.157)
|
0.470
(P=0.009)
|
0.176
(P=0.353)
|
0.180
(P=0.341)
|
-0.069
(P=0.719)
|
|
Results are presented as Correlation Coefficient (Spearman’s rank test), statistical significance (p-value).
ESR: Erythrocyte Sedimentation Rate, CK: Creatine Kinase, CRP: C-Reactive Protein, IL: Interleukin, TNF-a: Tumour Necrosis Factor-alpha.
|
|
Table 7. Correlation matrix displaying drain inflammatory markers 6 hours post-operatively and pain, opiate consumption.
|
|
|
IL-6 (6 hours)
|
IL-8 (6 hours)
|
TNF-a (6 hours)
|
|
Pain (numerical scale 1-10)
Post-operative day 1
Post-operative day 2
Post-operative day 3
Post-operative day 7
|
0.233 (P = 0.215)
0.077 (P = 0.685)
0.182 (P = 0.337)
0.321 (P = 0.083)
|
0.458 (P = 0.011)
0.404 (P = 0.027)
0.191 (P = 0.312)
0.449 (P = 0.013)
|
0.068 (P = 0.722)
0.143 (P = 0.451)
0.166 (P = 0.380)
0.022 (P = 0.908)
|
|
Opiate consumption (mg)
Post-operative day 1
Post-operative day 2
Post-operative day 3
|
0.197 (P = 0.297)
0.207 (P = 0.272)
0.111 (P = 0.561)
|
-0.073 (P = 0.703)
0.077 (P = 0.685)
-0.039 (P = 0.839)
|
0.114 (P = 0.549)
- 0.153 (P = 0.42)
0.157 (P = 0.406)
|
|
Number of physiotherapy sessions
|
0.220 (P=0.244)
|
0.123 (P = 0.517)
|
0.164 (P=0.387)
|
|
Time to discharge
|
-0.071 (P=0.710)
|
0.002 (P = 0.993)
|
0.43 (P = 0.822)
|
|
Knee extension
|
-0.432 (P = 0.017)
|
-0.287 (P = 0.125)
|
-0.416 (P = 0.022)
|
|
Knee flexion
|
0.376 (P = 0.041)
|
0.452 (P = 0.012)
|
0.164 (P =0.387)
|
|
Results are presented as Correlation Coefficient (Spearman’s rank test), statistical significance (p-value). IL: Interleukin, TNF-a: Tumour Necrosis Factor-alpha.
|
|
Table 8. Correlation matrix displaying drain inflammatory markers 24 hours post-operatively and pain, opiate consumption.
|
|
|
IL-6 (6 hours)
|
IL-8 (6 hours)
|
TNF-a (6 hours)
|
|
Pain (numerical scale 1-10)
Post-operative day 1
Post-operative day 2
Post-operative day 3
Post-operative day 7
|
0.433 (P = 0.017)
0.388 (P = 0.034)
-0.202 (P = 0.285)
0.623 (P < 0.001)
|
0.041 (P = 0.828)
-0.021 (P = 0.914)
-0.176 (P = 0.352)
0.250 (P = 0.182)
|
0.198 (P = 0.294)
0.110 (P = 0.564)
0.093 (P = 0.626)
0.150 (P = 0.430)
|
|
Opiate consumption (mg)
Post-operative day 1
Post-operative day 2
Post-operative day 3
|
- 0.051 (P = 0.790)
0.274 (P = 0.143)
- 0.150 (P = 0.430)
|
0.021 (P = 0.912)
0.270 (P = 0.149)
-0.268 (P = 0.152)
|
-0.138 (P = 0.468)
0.415 (P = 0.022)
0.013 (P = 0.946)
|
|
Number of physiotherapy sessions
|
0.153 (0.420)
|
0.043 (P = 0.820)
|
- 0.220 (0.244)
|
|
Time to discharge
|
0.177 (0.349)
|
0.076 (P = 0.690)
|
-0.265 (P = 0.157)
|
|
Knee extension
|
0.135 (P = 0.475)
|
-0.024 (P = 0.899)
|
-0.210 (P = 0.265)
|
|
Knee flexion
|
0.152 (P = 0.423)
|
-0.077 (P = 0.687)
|
0.036 (P = 0.849)
|
|
Results are presented as Correlation Coefficient (Spearman’s rank test), statistical significance (p-value). IL: Interleukin, TNF-a: Tumour Necrosis Factor-alpha.
|
Figures
Figure 1
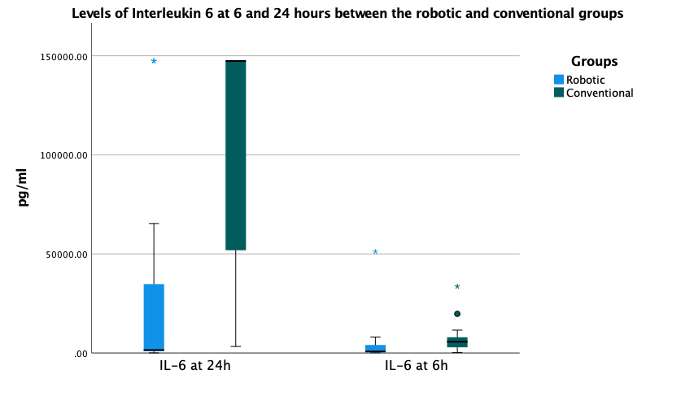
Figure 2
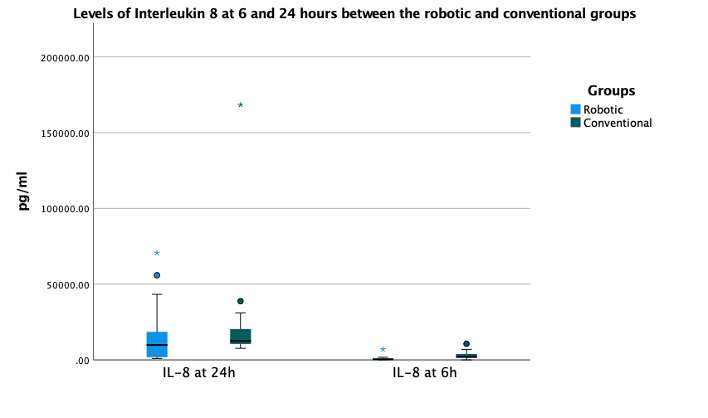
Figure 3
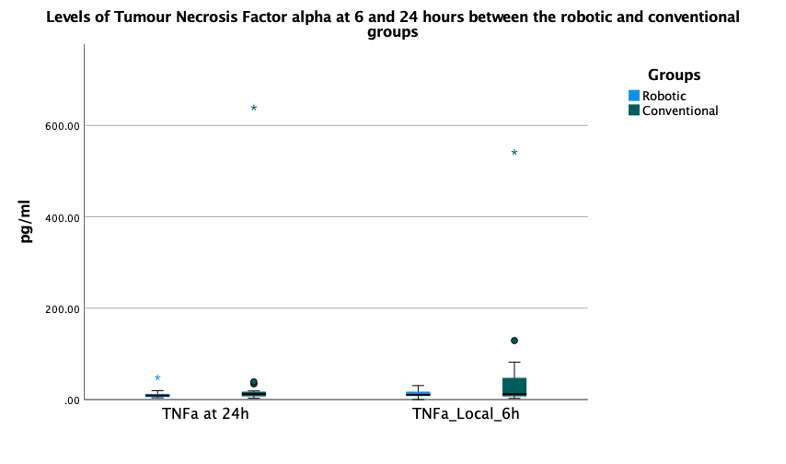
Figure 4
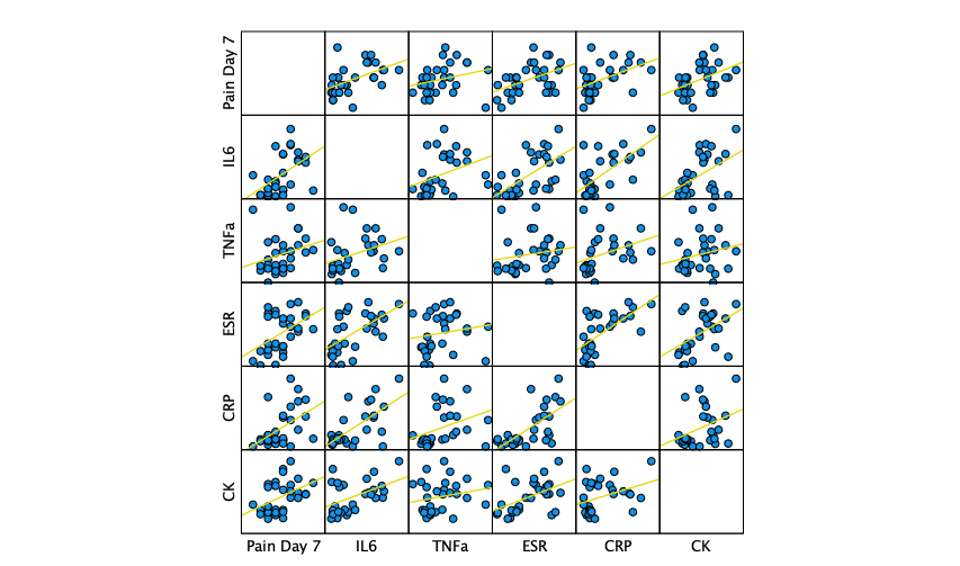
Figure 5
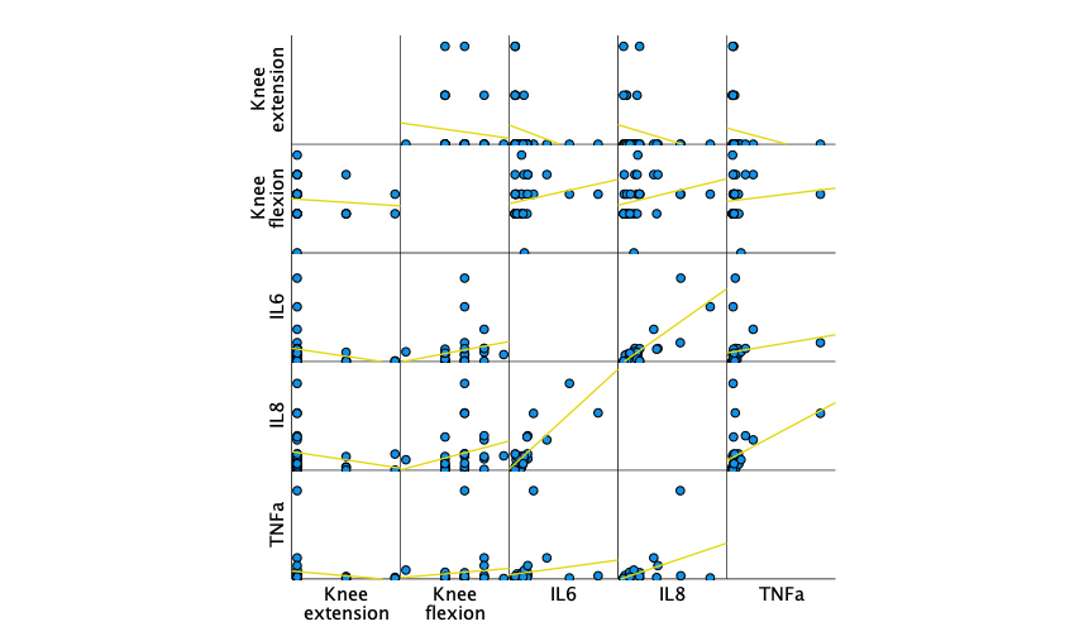
Figure 6#7714
2-Year Radiostereometric Analysis Evaluation of a Short, Triple-Taper, Proximally Coated Femoral Stem Versus a Self-Locking Stem With Reinforced Proximal Body: A Randomized Controlled Trial.
*Andreas Fontalis - University College London Hospitals - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Ivor Vanhegan - University College London - Stanmore,, United Kingdom
Jenni Tahmassebi - UCL Hospitals NS Foundation Trust - London, United Kingdom
Isabella Catrina Haddad - University College London Hospital - London, United Kingdom
Dia Giebaly - University College London Hospital - London, United Kingdom
Vishal Rajput - University College London Hospital - London, United Kingdom
Shanil Hansjee - University College London Hospital - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: andreasfontalis@gmail.com
Introduction
Cementless stem designs in total hip arthroplasty differ in relation to geometry and area of fixation. A well-documented method for gauging implant success and longevity is through the measurement of its stability. Radiostereometric analysis (RSA) is considered the gold standard to quantifying motion and several studies have reported that early migration over the first 2-years after surgery is predictive of late aseptic failure. The purpose of this prospective, randomised controlled trial (RCT) was to evaluate the 2-year migration and clinical outcomes of two cementless femoral stems.
Methods
60 participants undergoing primary total hip replacement for any cause were recruited in this RCT. Patients were randomly allocated to receiving either a novel, proximally coated, short blade stem, with a reduced lateral shoulder and narrow triple taper geometry or a triple-taper, self-locking design stem, with reinforced proximal body and proximal grooves perpendicular to load transmission. RSA radiographs were performed post-operatively and at 6 weeks, 6 months, 1- and 2 years. The Harris Hip Score (HHS), Oxford Hip Score (OHS) and EQ-5D were also collected.
Results
At two years the median subsidence of the novel, short-blade stem was 0.097 (IQR, 0.76), the median medial translation 0.023 (IQR, 0.20) and the median anterior translation 0.035 (IQR, 0.57)[Fig.1]; the respective subsidence in the comparator group was 0.086 (IQR, 0.29, p=0.683); medial translation 0.029 (IQR, 0.18, p=0.907); posterior translation 0.07 (IQR, 0.21, p=0.268)[Fig.2]. The median total migration of the short blade, triple-taper stem at different timepoints was 0.29 (IQR, 0.65) versus 0.29 (IQR, 0,28, p=0.567) at 6 weeks; 0.57 (IQR, 0.80) versus 0.21 (IQR, 0.20, p=0.005) at 6 months; 0.61 (IQR, 0.78) versus 0.25 (IQR, 0.27, p=0.010) at 1 year; 0.52 (IQR, 1.08) versus 0.26 (IQR, 0.32) at 2 years. Baseline PROM scores improved significantly at 2-years from pre-operatively and were comparable among groups. At 2 years HHS was 92 (IQR, 19) versus 91 (IQR, 19.75, p=0.692), OHS 42 (IQR, 4.25) versus 42 (IQR, 5, p =0.832), EQ5D 0.94 (IQR, 0.17) versus 0.837 (IQR, 0.19, p=0.489). There were no stem revisions and one patient randomised to the larger, triple-taper self-locking stem had evidence of heterotopic ossification.
Conclusion
2-year migration results utilising RSA, showed that both cementless stems exhibited a predictable migration pattern and achieved initial stability. The larger, triple-taper, self-locking stem with reinforced proximal body demonstrated less total migration that reached statistical significance at 6 months, 1- and 2-years. Participants in both groups demonstrated excellent clinical, and patient reported outcomes after 2 years of follow up. The biological fixation of both implants as evidenced by the RSA analysis is likely to translate to good mid and long-term stability and outcomes, which need to be corroborated by longer-term outcome studies.
Keywords
Total Hip Arthroplasty, Radiostereometric Analysis, Cementless implants, Proximally coated stem, Migration, Triple-taper, Patient Reported Outcome Measures
Figures
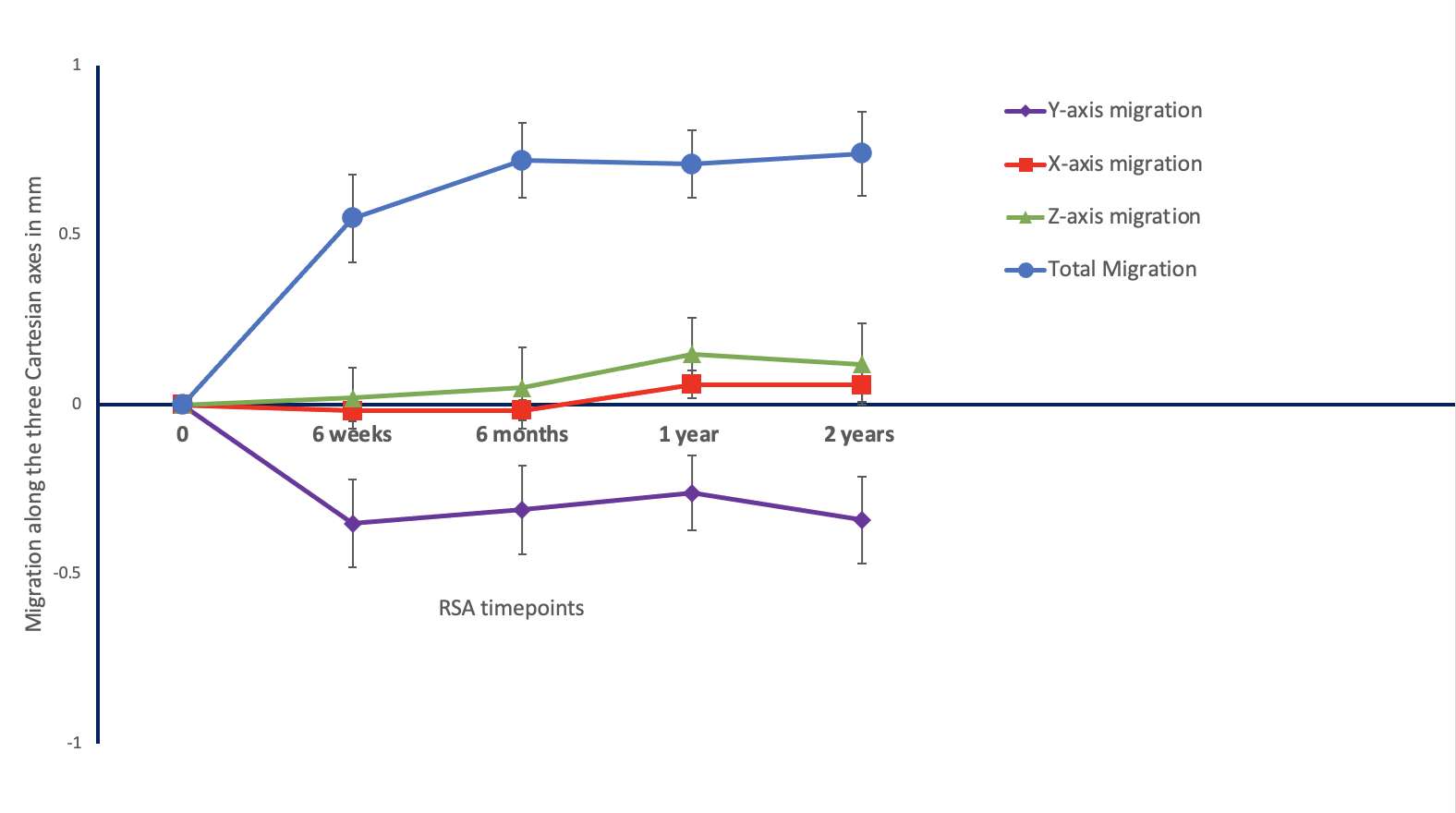
Figure 1
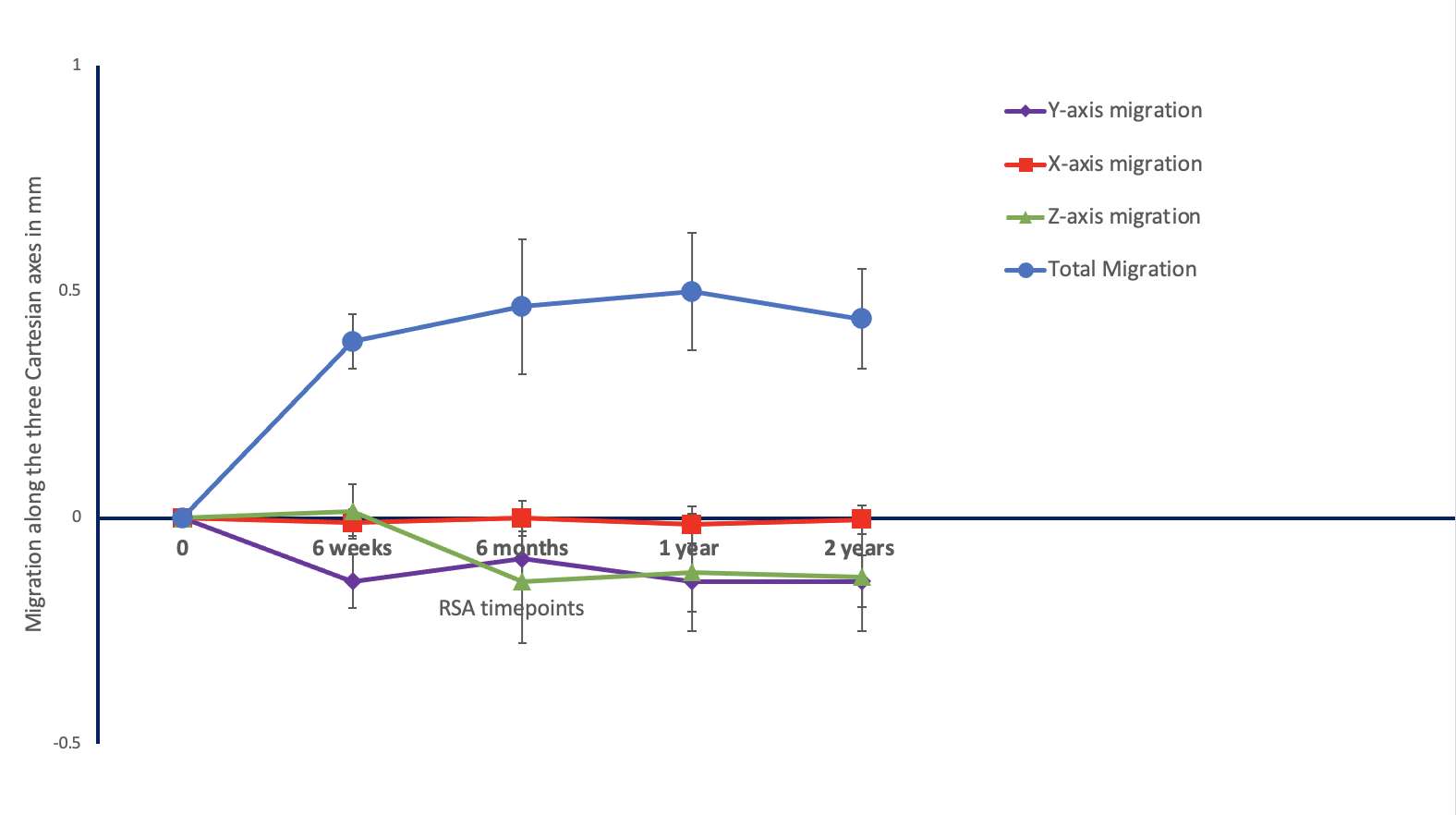
Figure 2#7532
Kinematic Biomechanical Markers After Total Knee Arthroplasty Are Associated With Patient Outcome Measures and Satisfaction Levels
*Alex Fuentes - Emovi - Montreal, Canada
Gabriel Larose
Nicola Hagemeister - Ecole de technologie superieure - Montreal, Canada
Ilona Turnes - Ecole Technologie Superieure - Montreal, Canada
Pierre Ranger - Hopital Jean-Talon - Montreal, Canada
*Email: afuentes@emovi.ca
Introduction: It is well documented that knee kinematics are not fully restored after total knee arthroplasty (TKA) and that up to 20% of patients remain unsatisfied postoperatively. Studies have shown associations between dynamic biomechanical markers and patient-reported outcome measures (PROMs) in knee osteoarthritis (OA) patients; however, such associations are not well understood after TKA. Therefore, this study explored the associations between biomechanical markers and PROMs post-TKA.
Methods: A retrospective study was conducted on 43 knees from 37 patients who underwent TKA. Surgeries were performed by one of three experienced orthopaedic surgeons. All knees had patella resurfacing and used a similar implant (Genesis II or Legion, posterior stabilizing, Smith and Nephew, Auckland, New Zealand). Eleven biomechanical markers previously described in OA literature were quantified during gait between 12- and 36-months post-surgery with a dynamic knee kinesiography exam with the KneeKG® system (Emovi Inc., Montreal, Canada). This procedure, done in a clinical context, identifies and analyzes biomechanical markers in flexion-extension, varus-valgus, and external-internal rotation (Figure-1). Patients completed a Knee Injury and Osteoarthritis Outcome Score (KOOS) and a 4-point Likert scale regarding their satisfaction level related to the improvements in performing activities of daily living (ADL) arising from the surgery. Bivariate Pearson correlations were assessed between biomechanical markers and the five KOOS subscales. ANOVA was performed to assess biomechanical markers differences between satisfaction levels. Considering the exploratory nature of this study, significance thresholds were set at p<0.1.
Results: There was 51.4% of women, the mean age at the time of the assessment was 66.7 years (95%CI: 63.8;69.5), and the mean BMI was 29.7 kg/m2 (28.2;31.3). Mean KOOS scores and values for the eleven assessed biomechanical markers, as well as their significant associations are presented in Table-1. Four biomechanical markers showed statistically significant associations with at least one KOOS subscales (all 0.001<p<0.06, see Table 1). Globally, greater flexion amplitudes during loading and stance phases of the gait, as well as greater varus at heel strike and during stance were associated with better KOOS scores (all 0.29<r<0.43). Pain and Abilities during recreative/sport activities subscales were both associated with three or these four dynamic biomechanical markers, while Function during ADL subscale was associated with two markers. Moreover, there were significant differences between satisfaction levels in three of these biomechanical markers: very unsatisfied patients presented with dynamic valgus alignment (-2.1° at heel strike -3.6° and during stance) and limited flexion during stance (8.8°) compared to more satisfied ones (all p<0.1; see Table-2).
Conclusion: Dynamic biomechanical markers measured by a knee kinesiography exam are associated with pain, function, and satisfaction after TKA. Interestingly, markers identified in this study were the same reported in the literature to be associated with pain and function in knee OA patients. While results suggest that such markers may not be fully addressed by the surgery, they are known to be modifiable through targeted conservative care. This supports the need to document pre- and post-TKA biomechanical markers to better understand residual dysfunctions and design targeted care plans post-TKA to achieve better outcomes.
Figures

Figure 1
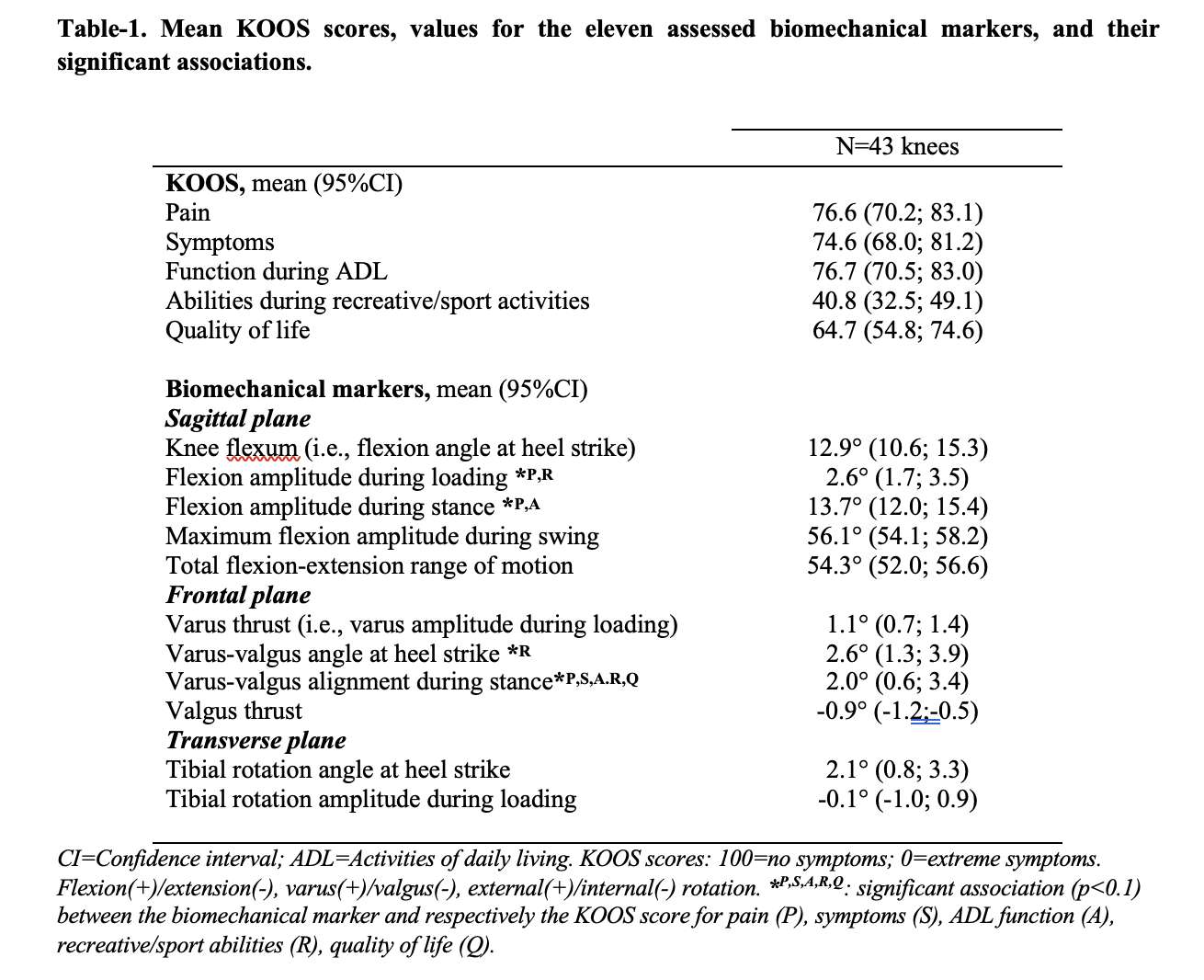
Figure 2
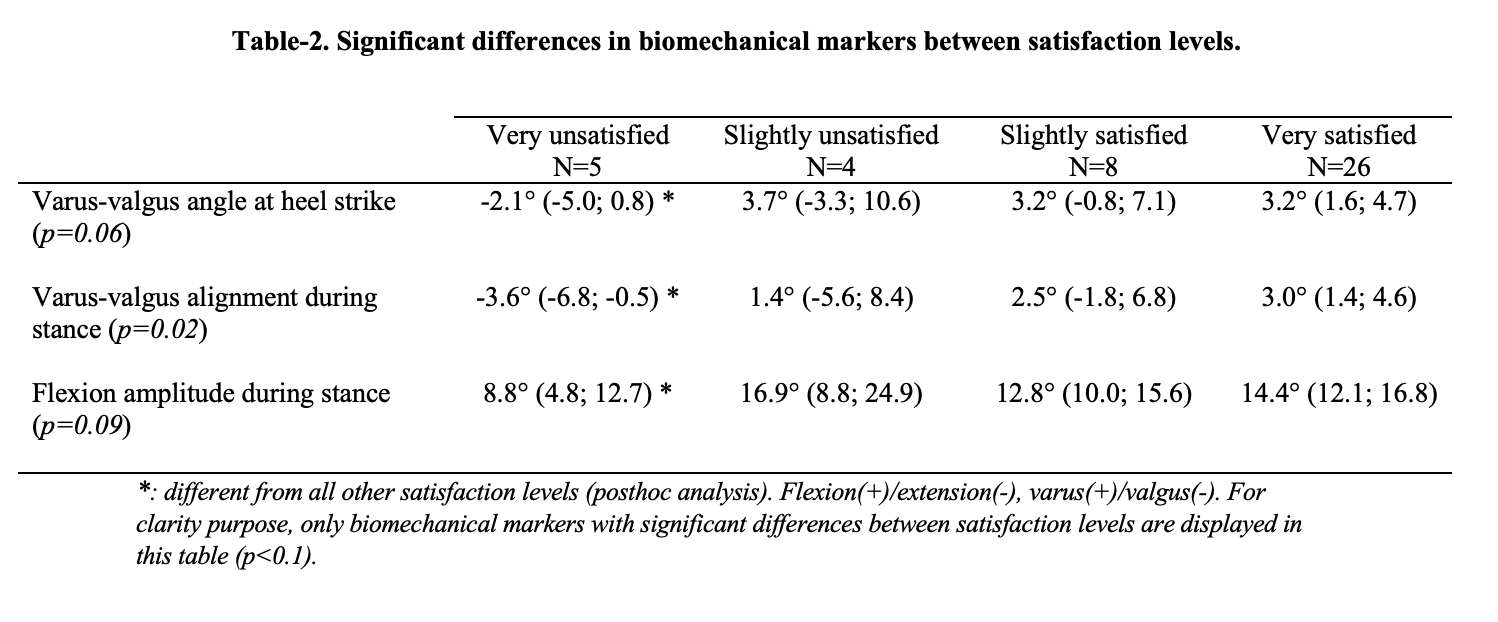
Figure 3#7567
Biomechanical Markers of the Knee Kinesiography Exam: Literature Review on Their Interest in the Management of Knee Osteoarthritis From Its Onset to Its Post-Surgical Management
*Alex Fuentes - Emovi - Montreal, Canada
Laurene Lenoir - Emovi Inc. - Montreal, Canada
Alix Cagnin - Emovi Inc - Montreal, Canada
Pierre Ranger - Hopital Jean-Talon - Montreal, Canada
Patrick Lavigne - Hopital Maisonneuve Rosemont - Montreal, Canada
David Baillargeon - Hopital Cite de la Sante - Laval, Canada
Guy Grimard - Hopital Sainte-Justine - Montreal, Canada
Neila Mezghani - TELUQ University - Montreal, Canada
Nicola Hagemeister - Ecole de technologie superieure - Montreal, Canada
*Email: afuentes@emovi.ca
Introduction: There is a well-documented discordance between radiographic findings and both symptoms and dynamic lower-limb alignment in knee osteoarthritis (OA) patients. Contrastingly, literature supports how dynamic biomechanical markers provide valuable functional information linked to OA progression and symptoms. In the age of personalized medicine, objective functional data can help develop effective targeted care plans and aid in clinical decision-making; however, this type of data is not easily accessible in clinic. Knee kinesiography exams, which assess and quantify 3D knee biomechanical markers during gait in a clinical setting (Figure-1), can fill this gap.
Methods: A comprehensive review on the use of the knee kinesiography exam (KneeKG®, Emovi Inc.) was conducted within MEDLINE and RESEARCHGATE databases to update a technical literature review from 20121 (Figure-2 for references).
Results: Besides validation studies presented in the technical review, a recent study demonstrated the association between lower-limb alignment measured from a surgical robotic system and knee kinesiography exam2. Several studies further confirm that compared to OA radiographic severity, biomechanical markers are significantly better associated with both patient-reported outcome measures (i.e., KOOS, OKS, etc.) and objective physical function (i.e., Timed-up and go test, strength, etc.)3,4.
A recent randomized controlled trial investigated and demonstrated how addressing biomechanical markers through targeted conservative OA management allows significant improvements in clinical outcomes and correction of identified markers compared to standard of care (i.e., control)5,6. In addition, this approach, when used as an integral part of patient education, had a positive impact on the patient's adherence to treatment. Results also showed that patients in control group were 2.5 times more likely to deteriorate their biomechanical markers compared to intervention group7.
Knee kinesiography exams allow the assessment of biomechanical markers such as varus thrust, hyperextension and flexion contracture, providing valuable information for orthopedists regarding total knee arthroplasty (TKA) surgical planning. Studies using artificial intelligence (AI) models including markers showed the data to be sensitive enough to differentiate diverse biomechanical profiles (phenotypes) in both OA and healthy participants, an important step toward personalized medicine8. Other AI models reported the value of biomechanical markers to document and support appropriateness to TKA, which in turn could be beneficial for third party payors9. In the past years, multiple clinical trials used the KneeKG® as a functional outcome measuring tool. These studies either assessed the impact of implant designs10,11,12, surgical approaches13, or alignment techniques14. A study using knee kinesiography helped to gain new insight on mechanical causes of symptoms post-TKA15. Results showed the painful TKA group presented with dynamic valgus alignment and stiffer gait compared to asymptomatic TKA and healthy participants. Notably, these markers have been shown to be modifiable in knee OA patients through conservative management6,7.
Conclusion: This review illustrates how a knee kinesiography exam provides actionable functional data throughout the knee OA continuum of care. Studies confirm that this exam can help document biomechanical markers to support medical decision-making for providers as well as arthroplasty decision-making and post-operative management for surgeons. Studies illustrate the high potential of 3D biomechanical markers to help towards personalizing arthroplasty.
Figures

Figure 1
Figure 2#7852
Dual Mobility Hips Have Advantages...Is Reduced Wear One of Them?
Joel Weisenburger - The University of Nebraska Medical Center - Omaha, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
*Hani Haider - UNMC - Omaha, USA
*Email: hhaider@unmc.edu
Dual Mobility (DM) Total Hip Replacements (THR) are showing promising results with improved range of motion with less dislocation risk, viable in both primary and revision surgeries. A DM THR typically consists of a small femoral head captive within a mobile ultra-high molecular weight polyethylene (UHMWPE) bearing liner which articulates against a hard, fixed acetabular liner. This in vitro hip simulator study investigated the wear rates of UHMWPE bearing components from DM and standard fixed-bearing (FB) THRs that have been highly crosslinked (HXL) and stabilized with vitamin E to preserve mechanical properties. We introduced novel methods in testing to simulate/isolate and measure the wear from the outer articulation of a DM and compared the full DM and isolated outer DM wear rates to those of two types of fixed bearing controls.
Twelve THRs were tested, in four different groups (n=3 each), 2 FB and 2 DM groups. The DM groups were either full dual mobility articulations, or with the outer articulation surfaces allowed only. Both DM groups had inner 28mm CoCr femoral heads, and an outer UHMWPE bearing diameter of 59.1mm (Fig.1). The FBs groups had either 36mm CoCr or 40mm Biolox Delta ceramic heads (Fig.2). All UHMWPE material in all four groups was identical GUR1020E 100KGy stabilized with vitamin E.
Tests were conducted on a 12-station hip simulator (AMTI, Boston). The specimens were mounted in a physiologically correct manner, lubricated with bovine serum (30g/L protein, 37°C) and subjected to the walking cycle specified in ISO-14242-1 at 1Hz up to 5million cycles (Mc). The bearings were carefully cleaned and gravimetrically weighed at standard intervals, and the wear was corrected with the weight gain of active load soak controls.
The isolated outer articulation group showed the highest UHMWPE wear (37.4±8.02mg/Mc, Fig.3) with clear elliptical scratches appearing on the CoCr acetabular liners. The wear of this group was significantly higher than the other three groups. The 36mm MOP FB group was the next highest wearing (14.4±1.07mg/Mc) which differed significantly from the other groups. The full DM design group and the 40mm COP FB group showed almost identical wear rates of 11.0±0.865mg/Mc and 10.3±0.486mg/Mc, respectively (not significantly different, p=0.308).
The results show that fully DM THR systems do not show higher UHMWPE wear rates than FB THR systems with large femoral heads, despite the DM designs having a large outer UHMWPE surface on which to articulate against the acetabular liner. The isolated outer articulation DM group showed much higher wear than the fully DM group. In the full DM group, it is likely that little motion was taking place between the DM UHMWPE bearing and CoCr acetabular liner making the 28mm CoCr head/UHMWPE bearing the main articulating interface, while the isolated outer articulation group functioned essentially as a FB THR with a very large UHMWPE femoral head. With modern, mechanically stable UHMWPE, wear due to increased contact area tends to dominate that caused by higher stress, and therefore smaller modern THRs tend to wear less than larger THRs which supports these findings.
Figures
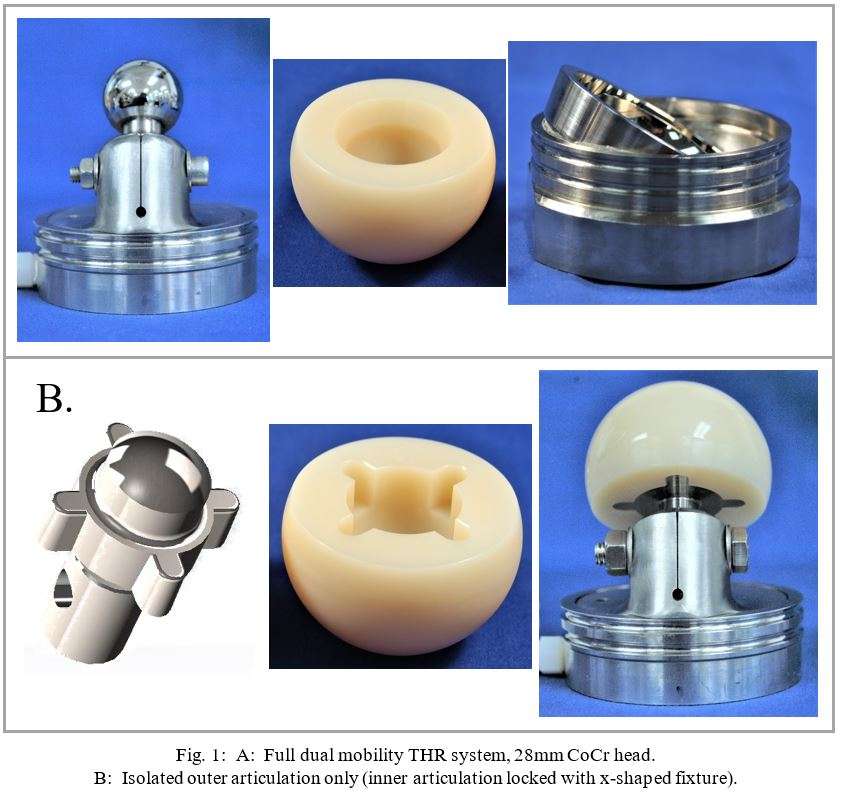
Figure 1
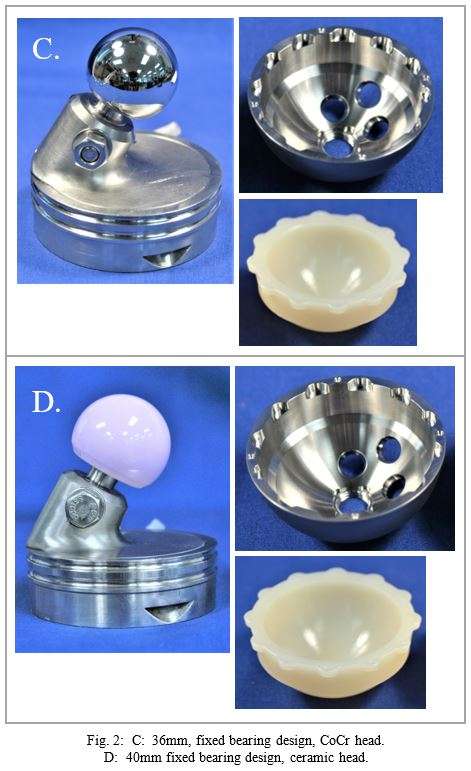
Figure 2
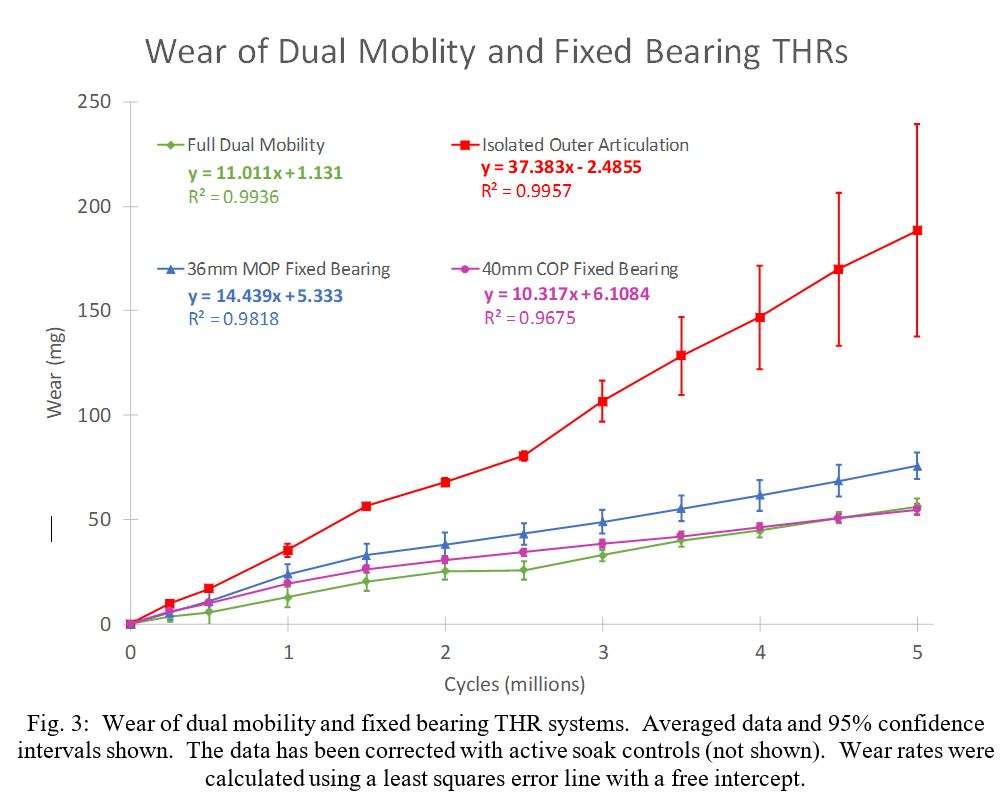
Figure 3#7966
3D Printed Clinical Techniques for Repair of Tibial Segmental Defects
*Jay Garza - McGovern Medical School - Houston, USA
Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Savannah Baimbridge - McGovern Medical School - Houston, USA
David McClendon - McGovern Medical School - Houston, USA
Jacob Su - McGovern Medical School - Houston, USA
*Email: jay.e.garza@uth.tmc.edu
Introduction: Large segmental defects remain a challenging problem within orthopedic surgery. A segmental bone defect (SBD) is a bone void that will not fill without intervention. This diagnosis is typically subjective, but generally if the defect has >50% circumferential loss or >2cm length then intervention is required. These injuries are often riddled with complications such as nonunion and infection deeming non-operative approaches illogical. These defects can result from trauma, infection, or removal of malignancy. Whatever the method of injury, the tibial SBD remains a particularly difficult injury to treat. There are multiple established treatment strategies for these defects including Vascularized fibular graft, Ilizarov technique, and the Masquelet technique, but each comes with its own set of disadvantages. With the advent of 3D titanium printing clinicians and researchers now have a material strong enough for load-bearing while also having a customizable fabrication method for each patient fracture presentation.
Methods: Our systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology (Figure 1). Our search strategy encompassed four databases in total. We began with a basic search strategy through Embase, Pubmed, and Cochrane libraries with our keyword search dating from January 10th 2010 to January 2nd 2021. The gathered articles were then sent through Web of Science for associated relevant articles. The final articles were then thoroughly reviewed by each member of the team, and the data points extracted from each were the mean length, length of follow-up time, union percentage for each bone affected, and complication percentage.
Results: The main outcome of our study was that 3D printing as an adjunct or an alternative to tibial SBDs is still unknown. This paper seeks to guide further investigation in clinical efficacy of 3D printing as well as provide an anchor for future studies. While 3D printing is an exciting and promising alternative for tibial segmental bone defect repair, the outcomes are still unknown because of the limited number of studies that have included 3D printing. Additionally, our study showed the comparability between the 3 gold standards for tibial defect repair Ilizarov limb lengthening and Masquelet technique (Figure 2 & 3).
Conclusion: Our study illustrates the advantages and disadvantages of the three first line treatment options for segmental bone defects in the tibia along with the newer application of 3D printing techniques. The results provide some evidence that 3D printing could be a viable alternative therapy for this pathology. Reports on its clinical usage are limited however and demand further trials analyzing its efficacy and cost-benefit before a concrete recommendation can be made for or against its implementation.
Figures
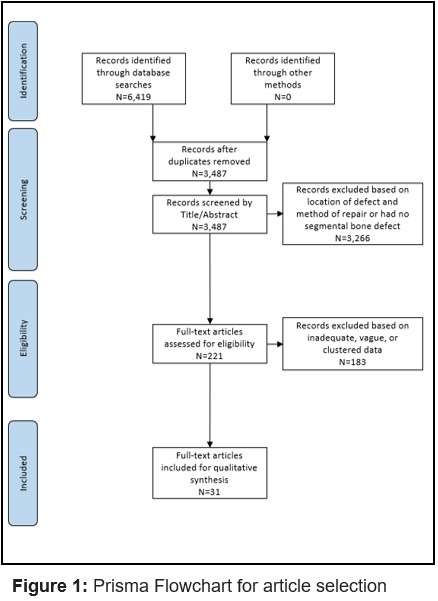
Figure 1
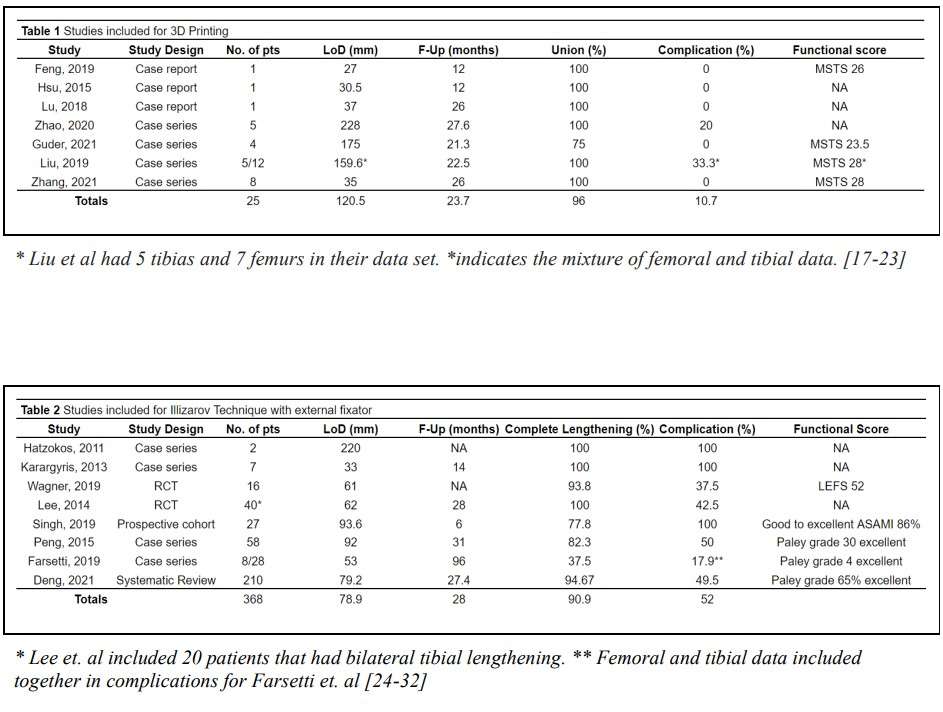
Figure 2
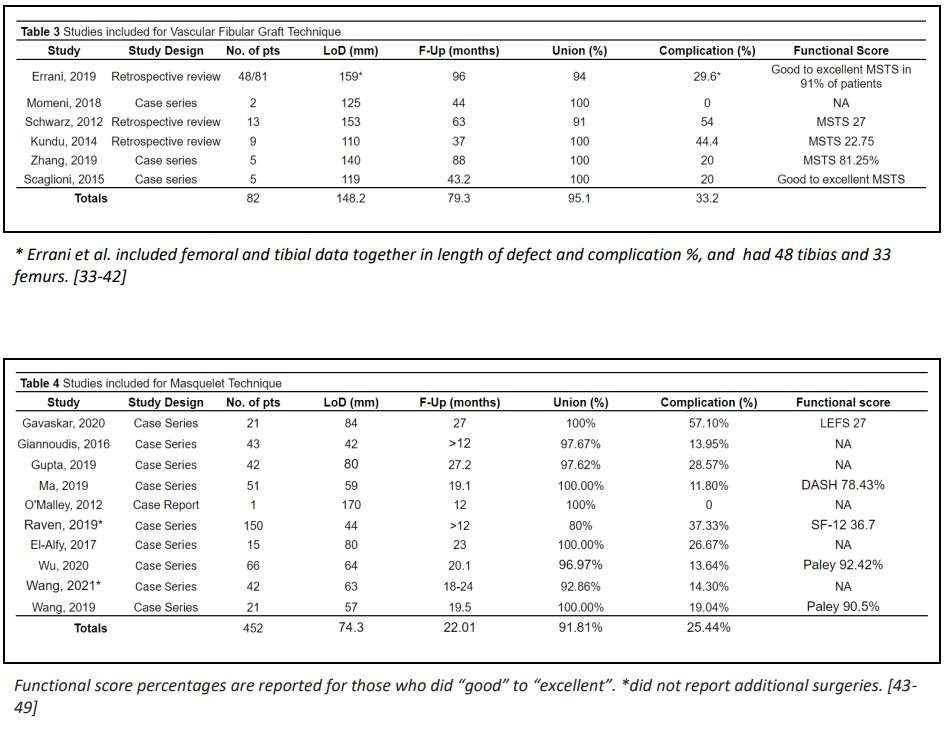
Figure 3#7660
The Sensor Enabled TKA: More Tech in the OR, No Disruption to Procedure
*Kaitlin Carroll - United States of America
Kevin Gemmell - Canary Medical - Carlsbad, USA
Peter Schiller - Canary Medical - Carlsbad, USA
Jeffrey Gross - Canary Medical - Carlsbad, USA
William Hunter - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
Introduction:
The introduction and advancement of technologies like robotics and smart devices in hospitals, operating rooms (OR), and clinics presents the need to assess human factors and usability (HFU) to ensure the design, training, and other mitigations keep health care professionals (HCP) and their patients safe while using these technologies. As patient care continues to evolve, and moreover when responsibility is given to the patient to use devices in private homes, HCPs and less skilled patients and caregivers must be able to safely use these complex devices. The objective of this study was to evaluate HFU of the novel canturio™te system to ensure the system is able to be used as intended and is not vulnerable to use errors that could cause harm.
Materials and Method:
Fifteen OR nurse users were asked to perform the tasks required using all canturio™te system components and answer critical knowledge questions. A predefined acceptance criteria was established prior to testing, such that each task or critical knowledge question had a defined expected result. All user errors or difficulties were also recorded to identify any root causes within the system design. Seven surgeon users performed a total of 16 implantations on cadaveric specimens using the canturio™te system following the prescribed surgical technique. A pass/fail acceptance test was used to ensure the canturio™te system can be used to perform clinically acceptable total knee arthroplasties (TKAs). Fifteen lay users representing TKA patients, were asked to imagine specific use-scenarios and perform the tasks required using all canturio™te system components and answer critical knowledge questions. A predefined acceptance criteria was established prior to testing, such that each task or critical knowledge question had a defined expected result.
Results:
Participants were able to complete all the tasks associated with canturio™te system within the OR environment. A total of 150 critical tasks were attempted with an overall 99.33% success rate (1 observed use error as a result of a study artifact). There were no significant patterns of difficulties or use errors. All surgeons performed each task successfully without use error or difficulty. Each canturio™te implant was communicated to evaluate the implant functionality after implantation. 100% of 98 attempts succeeded in connecting to the implant. 97.98% of attempts were under 60 seconds to connect to the implant. Participants were able to complete all the tasks associated with canturio™te system within the home environment and found the system easy to use and intuitive. The findings from the study demonstrate that the majority of simulated-use tasks were completed without use error or difficulty, however, small changes to the interface could improve the overall user experience. The canturio™te system was determined safe and effective for the intended patient users, uses, and within the private home environment and the OR.
Conclusion:
The canturio™te system was assessed for use problems associated with potential for serious harm that were evaluated during simulated-use tests. After completing the HFU evaluations, the canturio™te system has been found to be safe and effective for the intended users, uses, and use environments.
#7667
Determining Stress Relaxation of Trabecular Bone to Simulate Realistic Press-Fit Conditions of Cementless Implants
*Thomas Gersie - RadboudUMC - Nijmegen, Netherlands
Thom Bitter - Raboud University Nijmegen Medical Centre - Nijmegen, Netherlands
David Wolfson - DePuy International Ltd - Leeds, United Kingdom
Robert Freeman - DePuy International Ltd. - Leeds, United Kingdom
Nico Verdonschot - Radboudumc - Nijmegen, Netherlands
Dennis Janssen - Radboud University Nijmegen Medical Centre - Nijmegen, Netherlands
*Email: thomas.gersie@radboudumc.nl
Introduction
Accurate modeling of bone-implant interfaces and the primary stability of implants depend on accurate material properties. The trabecular bone is generally modelled as a linear elastic material, with the Young’s modulus being related to the density of the bone. However, in reality the mechanical response of trabecular bone is time-dependent, displaying a distinct stress-relaxation response. Therefore, bone should be modelled as a viscoelastic material, with a response that varies with the strain level. To our knowledge, nonlinear stress relaxation of trabecular bone has not yet been quantified in relation to bone mineral density, which may influence the primary fixation of orthopaedic implants. In this abstract we present the preliminary results of stress relaxation experiments on bovine femoral bone.
Methods
Eight trabecular bone cylinders were harvested from distal bovine femora under 30 months of age. Before mechanical testing, computed tomography (CT) scans were made to determine the bone mineral density. Mechanical experiments were performed with a servo-hydraulic MTS. The samples were pre-conditioned at 0.1% strain for ten cycles, and were then allowed to recover for 30 minutes. Stress relaxation experiments were then conducted by applying a uniaxial compressive strain ranging from 0.2% to 0.8% for 24 hours. A water basin filled with physiological saline at 37°C was used to keep the specimens hydrated during the mechanical testing.
Results
After 24 hours, stress relaxation ranging from 43.3 to 66.5% was observed which can be seen in Figure 1. Large proportions of stress relaxation occurred in the first 10 minutes in which the maximal peak force decreased by 25.6 to 48.3% (Figure 2).
Conclusion
The initial results show that stress relaxation up to almost 50% already occurs after 10 minutes, which in clinical practice is still during surgery. This viscoelastic behavior can have implications for the primary fixation of press-fit implants, and the magnitude of the micromotions occurring at the implant-bone interface. We previously found that the initial mechanical conditions at the interface have a significant effect on interface micromotions. For instance, computational models using linear elastic bone material properties typically predict interface micromotions that are much smaller relative to experimental findings. Adding plasticity to the material model increases the micromotions, but still leads to an underestimation of the micromotions [1]. The addition of viscoelastic bone material response to the models may contribute to achieving a more realistic prediction and simulation of the primary fixation of press-fit implants.
We here present preliminary experimental results. Further testing will illuminate the relation between bone mineral density and viscoelastic response. The next step is to incorporate the viscoelastic behavior in finite element simulations of primary fixation of femoral and tibial total knee arthroplasty components to demonstrate the influence of bone relaxation on primary fixation, which may further optimize the implant design process.
References
[1]: S. Berahmani et al. J. Biomech. (2017), http://dx.doi.org/10.1016/j.jbiomech.2017.07.023
Acknowledgements
The collaboration project is co-funded by the PPP Allowance made available by Health~Holland, Top Sector Life Sciences & Health, to stimulate public-private partnerships, and DePuy Synthes Knee Research and Development (Leeds, UK).
Figures
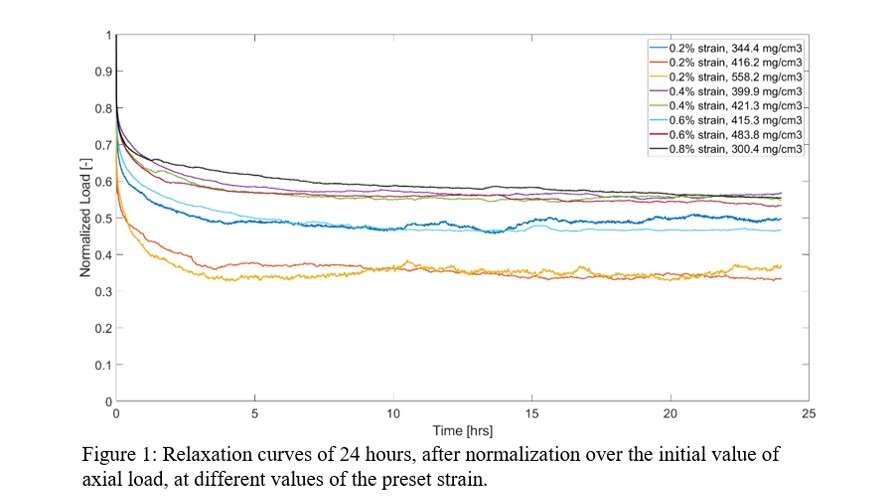
Figure 1
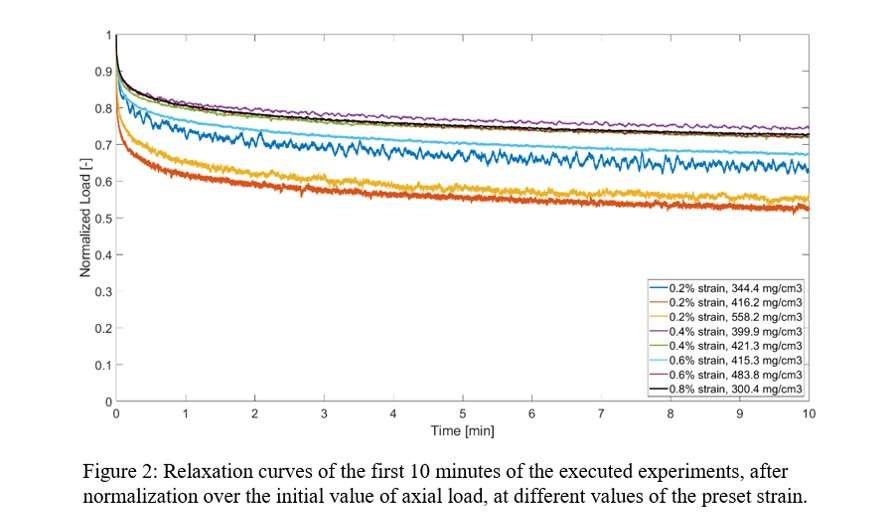
Figure 2#7987
Investigating the Capability of Machine Learning on Detecting and Classifying Failure in Piezoresistive Bone Cement Using Impedance Measurements
*Hamid Ghaednia - Massachusetts General Hospital - Boston, USA
Lily Keiderling - Massachusetts General Hospital - Boston, USA
Jessica Rosendorf - Massachusetts general Hospital - Boston, USA
Crystal E. Owens - Massachusetts Institute of Technology - Cambridge, USA
A. John Hart - Massachusetts Institute of Technology - Cambridge, USA
Joseph Schwab - Massachusetts General Hospital/Harvard Medical School - Boston, USA
Tyler N Tallman - Purdue University - West Lafayette, USA
*Email: hghaednia@mgh.harvard.edu
Introduction: Joint replacement is one of the most common orthopedic procedures, with over 2 million surgeries performed at a cost of $8 billion annually in the United States. Loss of implant fixation, or aseptic loosening, is the leading cause of revision following primary joint replacement accounting for ~25% of all revision cases. However, diagnosing aseptic loosening remains a challenge due to the minuscule scale in which cracks form, and the low sensitivity of plain radiographs at that scale. To address this, we propose a novel approach that utilizes self-sensing bone cement, electrical impedance tomography (EIT), and machine learning. This work explores the efficacy of these three methods in cement condition characterization.
Methods: Experiments were designed to assess whether EIT combined with piezoresistive cement and machine learning algorithms can be used to detect the location and type of cracks in simulated joint replacement interfaces. The EIT setup consists of a circular water tank with 16 electrodes equally spaced around the region, Fig 1. The simulated interfaces included a male and female conical component, with a metallic coating in the middle. Known failure conditions were induced in the samples: healthy, loose, cracked vertically and cracked horizontally. EIT signals were collected with the samples in various radial and angular locations throughout the tank. In total, over 1000 experiments were performed. We then applied machine learning using the MATLAB toolbox on both the raw data signals and the data after being processed with principal component analysis (PCA). The algorithms were intended to calculate the radial and angular location of the sample in the tank, the crack orientation (horizontal vs vertical), and the failure type.
Results: Table 1 shows a summary of the machine learning results for each category of analysis. Overall, we found that certain machine learning algorithms were able to identify the locations and failure types of the samples more accurately. For radial location tracking, the raw data returned higher accuracy than the PCA data. We found the Linear Discriminant, Cubic SVM, and Subspace Discriminant had 100% accuracy in classifying the angular location during testing. Similarly, the raw data returned higher accuracy for the angular coordinate of the sample. Matern 5/2 GPR, Exponential GPR, and Rational Quadratic GPR models had a root mean square errors ranging from 5.808 to 6.980 degrees. In predicting the crack orientation, the Medium Tree, Boosted Trees, and Rational Quadratic GPR models had the lowest root mean squared error, ranging from 4.454 to 6.637 degrees. Lastly, for the failure classification, multiple algorithms had 100% accuracy, including Fine KNN, Subspace Discriminant, and Narrow Neural Network.
Conclusion: The results validate our hypothesis that machine learning will be able to identify various crack parameters, even when reconstructed conductivity maps have no clear pattern to the naked eye. The next steps include validating this theory via surrogate and cadaver testing. If validated, this method could be implemented to provide earlier detection of aseptic loosening, leading to a decreased need for revision operations.
Figures
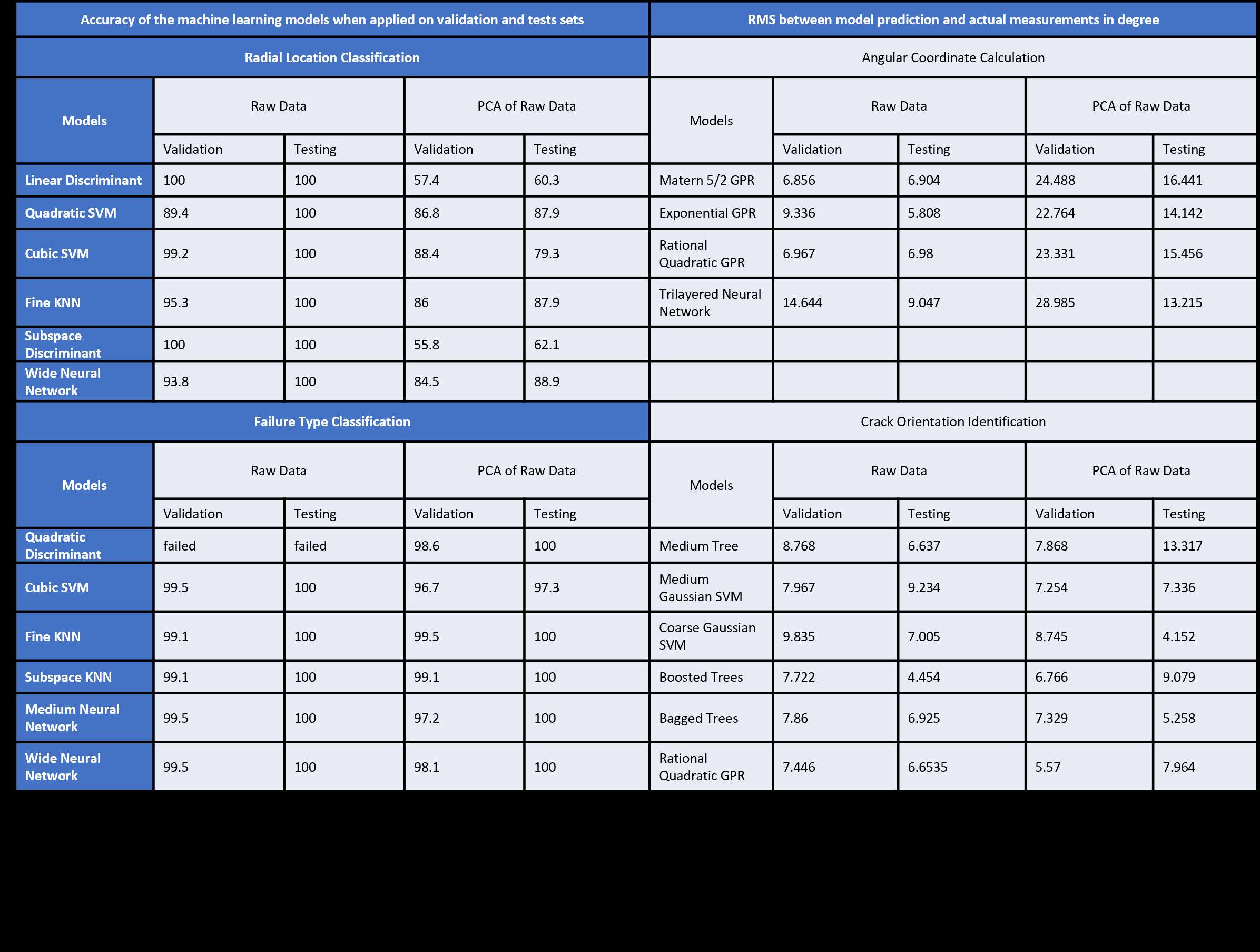
Figure 1#7760
A Modified Technique for Two Stage Revision in Periprosthetic Joint Infections Treatment
raffaele iorio - la sapienza roma - roma, Italy
*veronica giuliani - sant'andrea la sapienza roma - roma, Italy
Ferdinando Iannotti - Sapienza - Roma, Italy
Edoardo Viglietta - la sapienza - roma, Italy
Leonardo Previ - La Sapienza - roma, Italy
Giulia Rescigno - la sapienza - rome, Italy
Carlo Massafra - University of Rome La Sapienza - Rome, Italy
Andrea Ferretti - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
*Email: giuliani.veronica1@gmail.com
Background
Periprosthetic joint infection (PJI) represent one of the most important complcation after joint replacement surgery, the incidence varies between 0.5 and 2.2%. The “debridement, antibiotic pearls and retention of the Implant" (DAPRI) protocol represents a surgical technique for the treatment of PJI that allows to save the implant. It consists of aggressive soft-tissue debridement, including culture sampling, extensive pulse lavage, inserts replacement, and the use of local calcium sulfate antibiotic beads plus systemic antibiotic therapy. When it is not possible to save the implant, one or two stage revision is used. Two stage revision can be implemented using antibiotic calcium sulfate beads and tumor like debridement guided by methylene blue. The aim of the study is to compare the implemented two-stage revision technique with the standard technique in order to assess its effectiveness.
Material and Methods
Twenty patients with PJI of the hip or knee were prospectively enrolled from June 2019 to December 2022. The patients were randomly divided in two groups; group 1 was composed by 10 patients treated with implemented two-stage revision technique; group 2 included 10 patients underwent the standard two-stage revision technique. Each patient underwent routine laboratory tests including inflammatory markers (CRP, ESR and procalcitonin), clinical evaluation and radiographic control with a mean follow-up of 16 months ( range 8-24 months). Parameters evaluated were time of the reimplantation and duration of antibiotic therapy.
Results
No patients were lost at follow up. There was no statistically significant difference between the two groups with regard to demographic parameters, host immunity status according to McPherson and the type of microorganisms responsible. In both groups, 6 revisions of TKA and 4 revisions of THA were performed. In group A and in group B inflammatory markers normalised in 7.2 ± 2.3 weeks and 15.5 ± 4.6 weeks respectively (p<0.05); the difference of the duration of antibiotic therapy and of the time reimplantation were statistically significant between group A and group B (p<0.05).
Reinfection occurred in only one case in group B.
Discussion and Conclusion
The implemented two-stage revision technique demonstrated a faster normalization of inflammatory markers, as well as a decrease in reimplantation time and duration of antibiotic therapy, compared to the traditional technique.
The use of calcium sulphate antibiotic beads and tumor-like debridment seems to improve the results and to reduce the time of healing. This leads to a more rapid and less stressful course for the patient, as well as a reduction in health care costs.
#7763
Accuracy and Cost-Effectivenss of a Novel Method for Alpha-Defensins Measurement in the Diagnosis of Peri-Prosthetic Joint Infections
Edoardo Viglietta - la sapienza - roma, Italy
*veronica giuliani - sant'andrea la sapienza roma - roma, Italy
Giulia Rescigno - la sapienza - rome, Italy
Leonardo Previ - La Sapienza - roma, Italy
Fabio Conteduca - Rome University - Rome, Italy
Mazza Daniele - la sapienza - rome, Italy
raffaele iorio - la sapienza roma - roma, Italy
Andrea Ferretti - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
*Email: giuliani.veronica1@gmail.com
Background: Two methods for detecting synovial fluids alpha-defensins are available: the enzyme-linked immunosorbent assay and the lateral flow test. For both the proper role and accuracy remain uncertain. The purpose of this study was to assess the accuracy of the matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) for alpha-defensins detection in synovial fluids of patients with total knee/hip arthroplasty (TKA/THA) failures. The hypothesis was that the MALDI-TOF MS detects alpha-defensins with high diagnostic accuracy.
Methods: The study included 138 patients. The 2018 MSIS criteria were used to diagnose PJIs. Synovial fluids were assessed for routinely synovial fluid tests and alpha-defensins measurement through MALDI-TOF MS. A thorough description of the novel diagnostic test was reported. Sensitivity, specificity, overall diagnostic accuracy, positive and negative predictive values (PPV and NPV), receiver operator curves (ROCs) and area under the curve (AUC) were calculated.
Results: According to the 2018 MSIS criteria 59 PJIs (43%) and 79 aseptic failures (57%) were diagnosed. The MALDI-TOF MS assay showed an overall accuracy of 94.9%. The sensitivity was 93%, the specificity was 96%, the PPV was 95% and the NPV was 95%. ROC analysis demonstrates an AUC of 0.95 (p < 0.001).
Conclusion: The MALDI-TOF MS assay showed high sensitivity and specificity for alpha-defensins detection in case of TKA/THA failures. The advantages of the technology, such as the few milliliters of sample needed, the rapidity of obtaining results and the cost-effectiveness of the procedure could make the MALDI-TOF MS alpha-defensins assay a useful and widespread test in clinical practice.
#7765
Single-Use Reamer Technique Can Influence the Hip Center of Rotation? a CT Study
raffaele iorio - la sapienza roma - roma, Italy
*veronica giuliani - sant'andrea la sapienza roma - roma, Italy
Attilio Speranza - Sapienza University of Rome/Sant' Andrea Hospital - Rome, Italy
Carlo Massafra - University of Rome La Sapienza - Rome, Italy
Leonardo Previ - La Sapienza - roma, Italy
Giulia Rescigno - la sapienza - rome, Italy
Edoardo Viglietta - la sapienza - roma, Italy
Andrea Ferretti - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
*Email: giuliani.veronica1@gmail.com
Background
The positioning of the acetabular component in total hip arthroplasty (THA) has a crucial role in establishing the center of rotation (COR). The goal of successful acetabular preparation are: re-establish joint kinematics closer to native condition; ensure permanent fixation; reduce complications as dislocation, wear, and impingement. Two acetabular reaming techniques have been described: anatomical or peripheral reaming and conventional or progressive reaming. The peripheral reaming technique allows easier restoration of native condition while respecting the quadrilateral lamina and avoiding over reaming and over sizing, improving hip ROM and decreasing risk of bone impingement. Conventional acetabular preparation consists of reaming down to the true floor, which medialises the centre of rotation of the hip (COR) and reduces the acetabular offset.
Objectives
The aim of the study is to evaluate the modification of the Acetabular Off-Set (AO) and Acetabular Floor distance (AF), in two groups of patients treated by uncemented total hip arthroplasty (THA) using Single use Reamer (peripheral technique) and conventional technique. Our hypothesis was that “anatomical” technique achieves better restoration of hip centre of rotation.
Materials & Methods
Thirty-nine patients were enrolled prospectively; they were randomly divided into two groups. In the Group A (20 patients, 20 THA ) the acetabulum was reamed by sequentially larger reamers (conventional technique). In the Group B (19 patients, 20 THA) the acetabulum was reamed peripherally, using a single reamer 2 mm larger than native femoral head. All patients underwent a CT scan pre and post-operatively. The parameters evaluated were AO and AF. In addition, surgical time were evaluated.
Results
Preoperatively, there is no statistically significant difference between the two groups in terms of: age, sex, BMI, femoral head size, mean AO and AF values. In group A, the pre-operative mean AO was 3.31 mm and post operative was 2.38 mm, with a difference of 0.93 mm (p< 0.05); pre operative mean AF was 0.91 mm and post operative was 0.25 mm, with a difference of 0.66 mm (p< 0.05). In group B the pre operative mean AO was 2.89 mm and post operative was 2.47 mm, showing a difference of 0.41mm (p>0.05); pre operative mean AF was 0.67 mm and post operative 0.31 mm, with a difference of 0.36 mm (p>0.05). The variation of AO and AF between the two groups was statistically significant. No statistical difference was found about surgical time.
Conclusions
The use of single-use reamer with peripheral reaming technique allows to restore native COR, preserving bone stock, guaranteeing good reaming quality and reducing surgical time-associated risks.
#7770
Patient Specific Instrumentation in Laser Guide Navigated THA: Experience in the First 100 Cases, a CT Study
Andrea Ferretti - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
*veronica giuliani - sant'andrea la sapienza roma - roma, Italy
Carlo Massafra - University of Rome La Sapienza - Rome, Italy
Leonardo Previ - La Sapienza - roma, Italy
Attilio Speranza - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
Giulia Rescigno - la sapienza - rome, Italy
Edoardo Viglietta - la sapienza - roma, Italy
raffaele iorio - la sapienza roma - roma, Italy
*Email: giuliani.veronica1@gmail.com
Background
Functional positioning of components in total hip arthroplasty (THA) and its relationship with individual spino-pelvic kinematics and patient’s anatomy are being extensively studied with the purpose to optimise the functional orientation of the implant during patient’s daily life activities, thus avoiding potential impingement and instability. Patient specific dinamic planning could be a game-changer, however, it should be accurately delivered intraoperatively. The main purpose of this study was to verify the reliability and accuracy of a patient-specific instrumentation (PSI) and laser-guided technique to replicate the preoperative dynamic planning in the first consecutive 100 cases.
Materials and methods
One hundred consecutive patients were prospectively enrolled and received a dynamic hip preoperative planning based on three functional lateral spinopelvic X-rays and a low dose CT scan. 3D printed PSI (including femoral and acetabular guides) and laser guided instrumentation were used intraoperatively. The accuracy of the system was measured using post-operative CT, as approved by the ethics committee, performed in 60 cases. Components size and orientation, osteotomy level, and change in hip-length and offset were measured and compared with the planned pre-operative values.
Results
The mean absolute deviation from the planned inclination and anteversion was 4.3° and 5.4° respectively. In 93% of cases, both inclination and anteversion were within +/- 10° of the planned values . Regarding osteotomy level, offset change, and limb length change, the mean deviation was respectively 1,2 mm, 2,3 mm, and 1,9 mm. No statistically significant difference was detected comparing the planned and the achieved values. One case of anterior dislocation was reported in the 100 patients treated, due to inaccurate positioning of the acetabular guide intraoperatively (anteverted 38°).
Conclusions
Patient-specific and laser-guided instrumentation is safe and accurately reproduce the dynamic planning in terms of components orientation, osteotomy level, leg length and offset.
#7959
A Comparison Between Robotic-Assisted Surgery and Laser Guide Navigation With PSI in THA: Preliminary Results
*veronica giuliani - sant'andrea la sapienza roma - roma, Italy
Raffaele Iorio
Giulia Rescigno - la sapienza - rome, Italy
Leonardo Previ - La Sapienza - roma, Italy
Attilio Speranza - Sapienza University of Rome/Sant' Andrea Hospital - Rome, Italy
Edoardo Viglietta - la sapienza - roma, Italy
Carlo Massafra - University of Rome La Sapienza - Rome, Italy
Andrea Ferretti - Sant'Andrea Hospital II University of Rome "La Sapienza" - rome, Italy
*Email: giuliani.veronica1@gmail.com
Introduction: Accurate components positioning in Total Hip Artrhtroplasty (THA) is a key to optimize functional outcomes and to reduce rates of dislocation, impingement, aseptic loosening and other wear-related complications. Robot-assisted total hip arthroplasty (RA-THA) is a recent technology that should provide optimal positioning of implants. Intraoperative Laser guided navigation is a new technology that provides patient-specific component alignment as a result of pre-operative dynamic analysis and patient-specific instrumentation (PSI). The aim of this study is to compare the accuracy, in terms of component positioning, of RA-THA with Laser-guided navigated THA, as evaluated by a post-operative CT scan.
Methods: Forty patients were enrolled and randomly divided in two groups. Group A was composed by 20 patients treated with RA-THA, group B by 20 patients operated with laser-guide navigation THA. Both technologies required a pre-operative CT scan. All patients underwent a post-operatively X-Ray and CT scan. Parameters measured and compared with the planned pre-operative values were: component sizes (cup and femoral stem), cup abduction, cup anteversion, osteotomy level, hip-length and femoral off-set.
Results: The suggested cup abduction was 40.5° (range 40°- 45°) in group A and 39,5° (range 34°-45°) in group B; the anteversion was 20° in all cases in group A e 20.26° in group B (range 12°-25°). The mean deviation from the planned cup abduction and anteversion were 1.9° and 7.1° in group A and 3.9° and 4.2° in group B respectively No statistically significant difference was detected comparing planned and the achieved values, in both groups or in the registered deviation from the planning between the two groups. Regarding osteotomy level, off-set and limb length, the mean post-operative mismatch was 3.2 mm, 4.5 mm and 6 mm in Group A 1.6 mm, 2.6 mm and 2 mm in Group B respectively. Intraoperatively, planned cup and femoral stem size corresponded to the actual implant in 35% and 70% of cases and in Group B in 85% and 90% in Group B respectively. A statistically significant difference in surgical times was found: in group A mean surgery time was 72 minutes while in group B was 54 minutes (p<0.05). No early dislocation were detected in both groups. One case of early periprosthetic infection in group A was successfully treated by DAPRI.
Conclusion: To our knowledge, this is the first study comparing these two advanced technologies. While the RA-THA seems to be more accurate in respecting pre operative cup abduction; laser guided navigated THA seems to be more accurate in anteversion, osteotomy level, femoral off-set and sizing. However all this differences don’t reach statistical significance. Quite surprising in most cases of RA-THA, pre-operative planning suggested an abduction of 40° and an anteversion of 20, while Laser-guided THA system showed a much greater variability. This mismatch could be explained by the functional planning provided by laser-guide navigated THA, which also evaluates functional spino-pelvic parameters. Despite several limitations, on the basis of this preliminary results, the Laser guided intraoperative use of PSI seems not inferior to RA-THA.
#7658
Tibial Baseplate Motion Relates to Tibiofemoral Kinematics During Gait: A Holistic Evaluation of TKA Biomechanics Using a Patient-Specific Computational Workflow
*Jonathan Glenday - Hospital for Special Surgery - New York, USA
Peter K. Sculco - Hospital for Special Surgery - NYC, USA
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
Joseph Lipman - Hospital for Special Surgery - New York, USA
Cynthia Kahlenberg - Hospital for Special Surgery - New York City, USA
David J. Mayman - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Fernando Quevedo Gonzalez - Hospital for Special Surgery - New York, USA
*Email: glendayj@hss.edu
Introduction: Approximately two thirds of total knee arthroplasty (TKA) failures are related to either joint mechanics (e.g., instability) or fixation mechanics (e.g., aseptic loosening) [1]. While joint and fixation mechanics are interrelated [2], biomechanical studies often treat them separately, which hampers our understanding of how joint kinematics and forces combine to influence component fixation. Therefore, we developed a computational workflow to holistically assess TKA biomechanics and asked: is the tibial baseplate motion after cemented TKA correlated with anterior-posterior (AP) tibiofemoral translation during gait?
Methods: Our computational workflow integrates a multibody musculoskeletal model to evaluate joint mechanics with a finite element (FE) model to evaluate fixation mechanics (Fig.1). We used data from the fourth Grand Challenge Competition to Predict In Vivo Knee Loads [3], which included preoperative and postoperative CT-scans and motion analysis data of five gait trials from a 68-year-old male with an instrumented TKA. We adapted a generic lower extremity musculoskeletal model [4] to include the patient-specific anatomy and TKA implantation. We utilized an enhanced static optimization algorithm (https://simtk.org/projects/opensim-jam) to determine the tibiofemoral joint forces and kinematics throughout the stance phase of gait, which we directly transferred to the corresponding patient-specific FE model to evaluate the bone-cement-implant interaction. The tibia was fixed 150 mm distal to the resection. The tibia was modeled with a Poisson’s ratio (υ) of 0.3 and a non-homogenous elastic modulus (E) determined from the preoperative CT-scan, using density-modulus relationships specific to the proximal tibia [5,6]. The tibial component, insert, and cement were modeled as a titanium alloy (E=114 GPa, υ=0.33), ultra-high molecular weight polyethylene (E=463 MPa, υ=0.46), and polymethylmethacrylate (E=2.2 GPa, υ=0.33), respectively. We tied the bone-cement interface and considered cohesive contact between implant and cement [7]. We computed the rigid body motion of the baseplate relative to the bone, similar to CT-based radiostereometric analysis [8]. We quantified the correlation between the peak tibial baseplate motion and the AP position of the medial and lateral tibiofemoral contact points.
Results: The medial and lateral compartments translated 5.8–7.8 mm and 11.3–15.4 mm, respectively (Figs. 2 and 3). The baseplate translations and rotations were less than 0.036 mm and 0.08°, respectively. The maximum total point motion of the baseplate was less than 0.07 mm. The lateral translation of the implant was correlated with the AP position of the lateral compartment (R2=0.82, p=0.03). The valgus tilt and external rotation of the implant were correlated to the AP position of the medial compartment (R2=0.85, p=0.03 and R2=0.91, p=0.01, respectively).
Conclusion: The relationships between tibial baseplate motion and AP tibiofemoral kinematics during level walking, identified from our holistic workflow, underscore the interdependence between joint and fixation mechanics.
References: [1] AJRR Annual Report 2020. [2] Teeter et al., J Arthroplasty 2017. [3] Fregly et al., J Orthop Res 2011. [4] Arnold et al., Ann Biomed Eng 2010. [5] Morgan et al., J Biomech 2003. [6] Snyder & Schneider. J Orthop Res 1991. [7] de Ruiter et al., J Exp Orthopaed 2017. [8] Brodén et al., Acta Orthop 2021
Figures
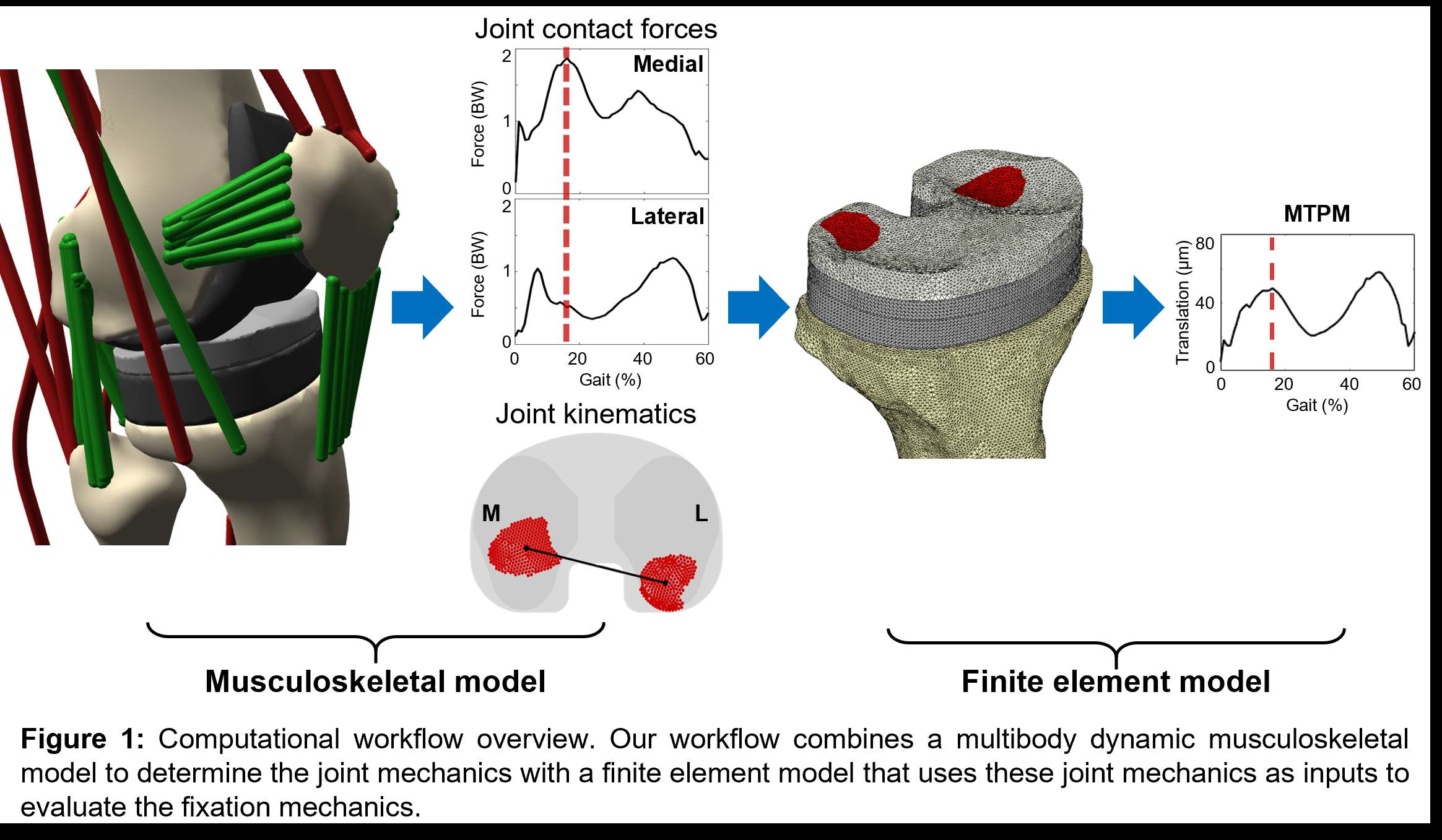
Figure 1
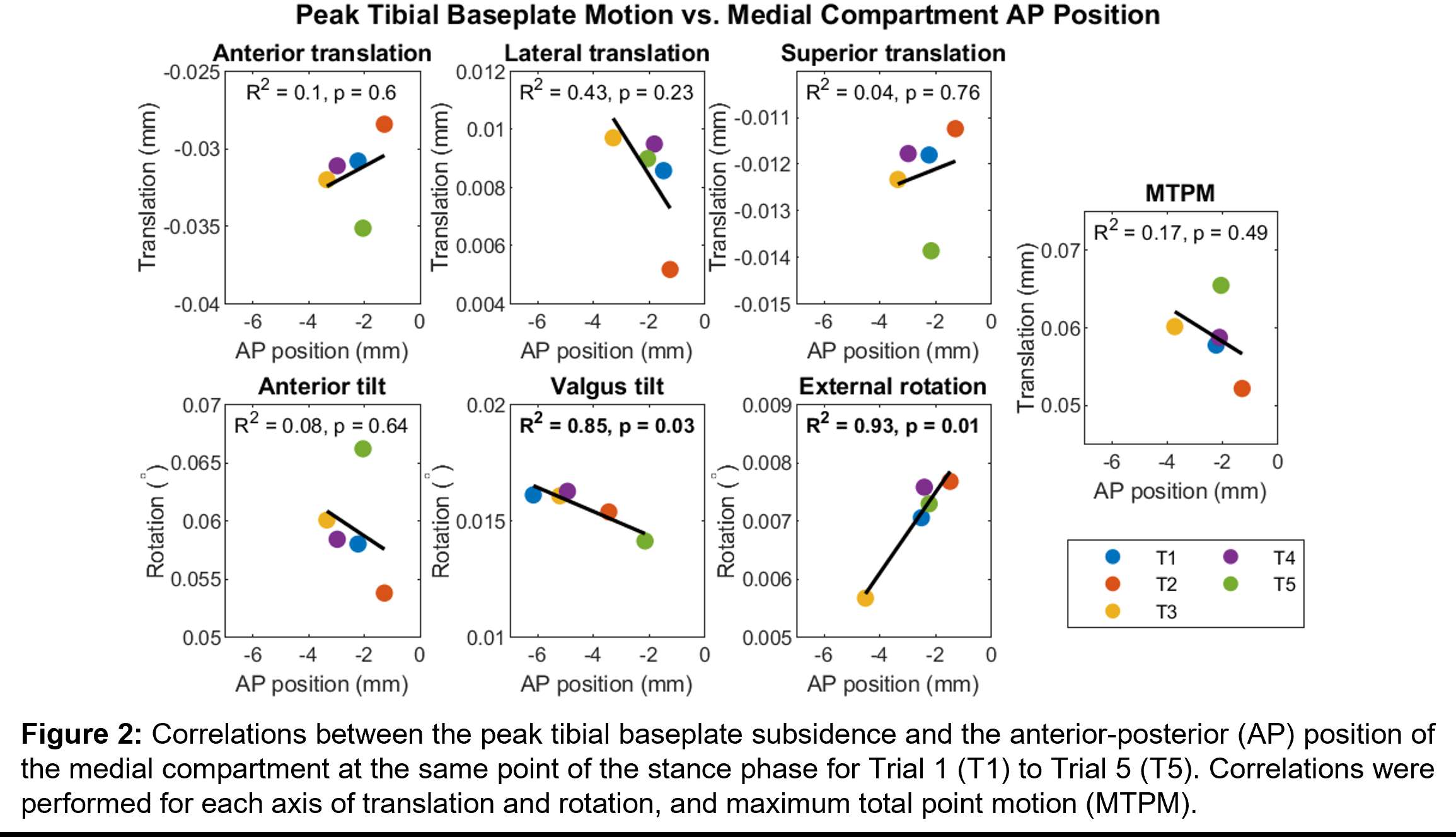
Figure 2
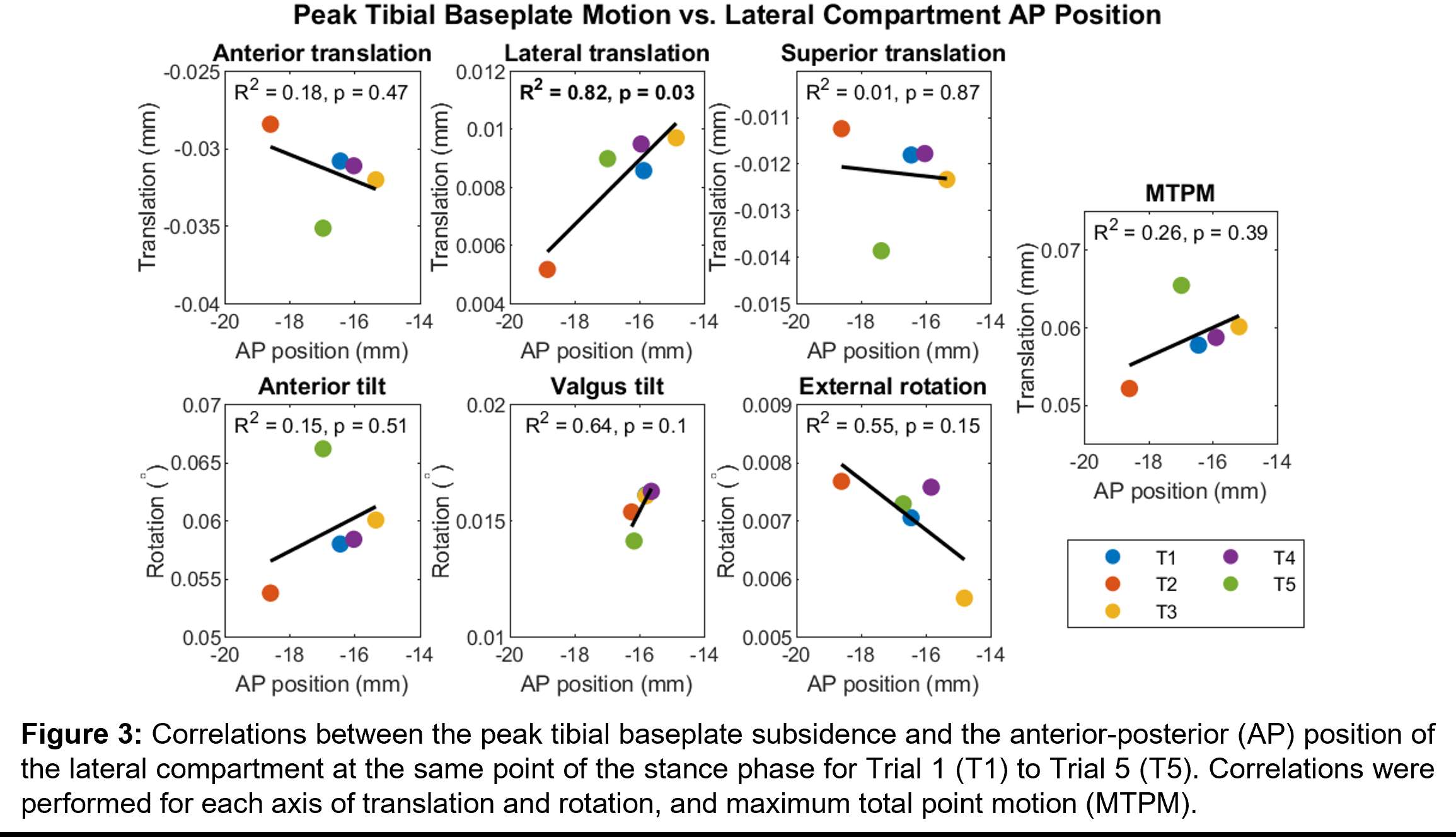
Figure 3#7490
Measurement of the Impaction Force and Broach Acceleration During Femur Preparation in Hip Arthroplasty
*Katja Glismann - TUHH Hamburg University of Technology - Hamburg, Germany
Tobias Konow - TUHH Hamburg University of Technology - Hamburg, Germany
Marius Vorbeck - University of Technology - Hamburg, Germany
Frank Lampe - Hamburg University of Applied Science
Matthias Vollmer - TUHH Hamburg University of Technology - Hamburg, Germany
Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: katja.glismann@tuhh.de
INTRODUCTION
Periprosthetic femoral fractures (PPF) are one of the main reasons for revisions in total hip arthroplasty [1]. One of the reasons for a PPF may be excessive impaction energy (IE) during broaching and the implantation process [2].
IE is typically determined using instrumented mallets and high-speed camera systems [3]. In such an approach energy loss e.g. by the mass of the instruments are not considered. In order to include them, the additional measurement of acceleration is required. The aim of this study was to investigate a measuring system which combines force and acceleration measurements in the direction of impaction for the calculation of the IE.
MATRIALS AND METHODS
Cementless femoral stems (Corail, DePuy Synthes, US) were implanted in six cadaveric femur pairs (71 ± 13 years) divided into two groups. Six experienced surgeons templated implant sizes. The results were averaged for each femur to obtain a templated reference stem size. Two consecutive implantations were performed: Femur group 1: implantation of an undersized stem followed by the implantation of the reference size; group 2: reference size first followed by an oversized stem.
During broaching, forces and accelerations were recorded continuously (800 kHz) using an impactor instrumented with the sensors (Figure 1). The absolute maxima of each stroke were evaluated (Figure 2). Calculation of the IE was performed by integration of the acceleration signal (velocity of the broach) and the force (impulse) [2], such including the effect of the involved masses. The final 8 strokes for every broach were statistically analyzed by Kruskal-Wallis tests.
RESULTS
Impaction forces (2421.8 ± 844.8 N), accelerations (-10131.36 ± 5459.3 m/s^2), and the calculated energies (‑0.09 ± 0.11 J) during broaching were similar regardless of the used stem size (p = 0.17, p = 0.22, p = 0.85). Forces and accelerations were significantly higher for the broaching of oversized stems (p < 0.001, p = 0.003, Figure 3a); the IE showed a similar trend (p = 0.06; Figure 3b). Smaller forces and accelerations for undersized stems compared to the reference stems were not seen (p = 0.44, p = 0.981).
DISCUSSION & CONCLUSION
The instrumented impaction tool permits direct measurement of force and acceleration, enabling the calculation of IE for every single stroke. The mean energy in this study was smaller than literature values (0.45 ± 0.18 J [3]). This could be due to the careful implantations by the surgeon, trying to prevent PPFs. It is, however, hypothesized that the difference is mainly due to differences in the sensor positions (broach vs mallet [3]), since measurement at the impaction mallet does not guarantee measurements in the direction of the force flow during impaction. The high sampling rate of the accelerometer enables a more accurate investigation of broach progression during the implantation process compared to measurements with high-speed cameras [3]. The setup will be used to determine PFF risk dependent on stem size and impaction method.
Financial support by DePuy Synthes and the templating done by the surgeons is kindly acknowledged.
REFERENCES
[1] AAOS, AJRR: 44, 2021
[2] Doyle et al., Biomechanics 82: 2019
[3] Scholl et al., ORS: 2012
Figures
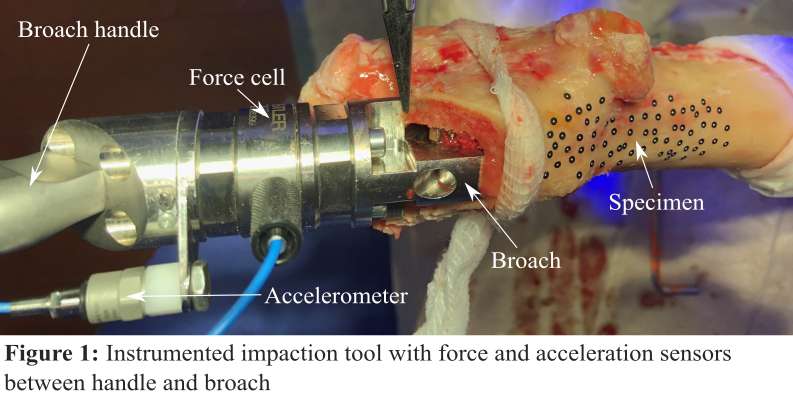
Figure 1
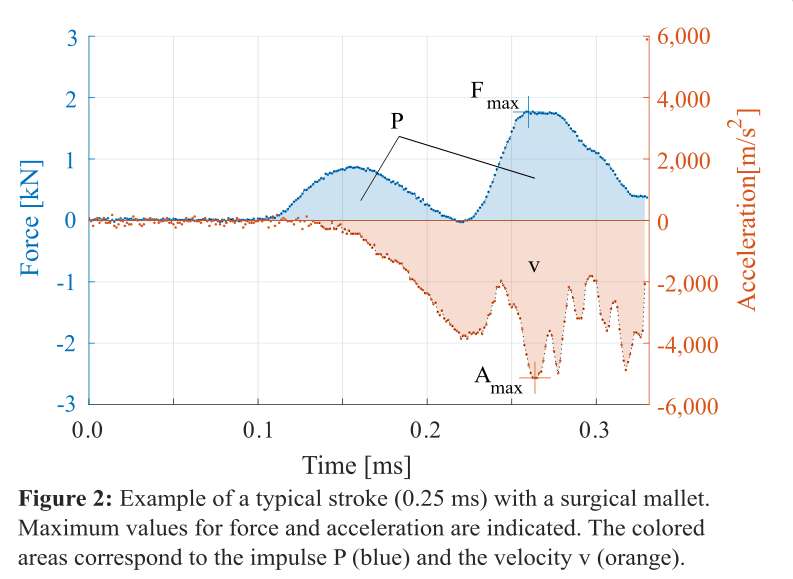
Figure 2
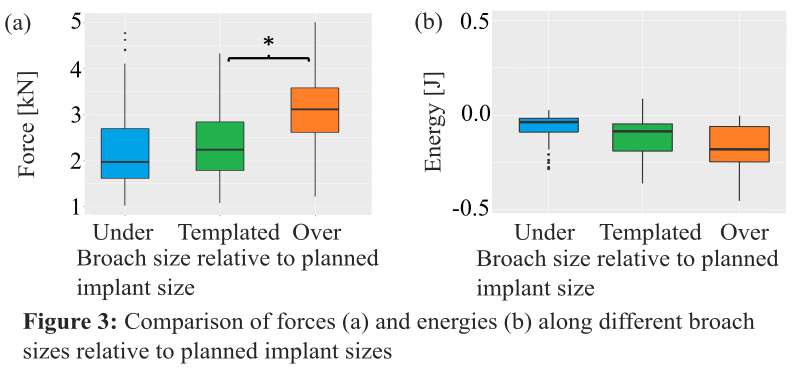
Figure 3#7767
Characterization of Waviness and Effect on Total Hip Replacement Stem Taper Contact Mechanics
*Michael Godoy - Rush University Medical Center - Chicago, USA
Jonathan Gustafson - Rush University Medical Center - Chicago, USA
Steven Mell - Rush University Medical Center - Chicago, USA
Alfons Fischer - University of Duisburg-Essen - Duisburg, Germany
Brett Levine - Rush University Medical Center - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
Hannah Lundberg - Rush University Medical Center - Chicago, USA
*Email: michael_godoy@rush.edu
INTRODUCTION: Head-neck modularity, a standard for total hip replacements (THRs), has been linked to reports of failure, which may require revisions, causing detrimental effects on patients. Our previous work has shown that damage at the junction starts mechanically, influenced by surface topography, and progresses to different modes of fretting-corrosion. Surface topography on machined surfaces, like micro-grooved tapers, is split into two groups: roughness and waviness. Previous studies have not characterized waviness and the potential influence on modular taper assembly. Our head-stem modular taper assembly experiments have shown inconsistent contact distributed across the entire length of tapers. We noted the presence of waviness in the stem tapers and postulated that this variability on the surface might contribute to contact inconsistencies. This study aims to characterize waviness across a group of well-functioning stem tapers and use a validated finite element analysis (FEA) model to determine the effect of waviness on contact mechanics under multiple surgeon-applied implant assembly loads.
METHODS: Thirty postmortem retrieved hip stems were chosen from an IRB-approved repository to characterize the taper waviness of well-functioning THRs. Three-dimensional models of the surfaces of each stem taper were generated using an optical coordinate measuring machine (CMM). The measured profile was filtered (Gaussian filter, 0.8mm cut-off frequency), and the mean amplitude and period of the resulting waviness profile were quantified (Fig. 1). A validated FEA model was used to investigate the effect of surface waviness on stem taper contact mechanics during implant assembly. Stepwise-multiple linear regression was performed at a load of 6kN to understand the effect of waviness (height and spacing) on four model outputs (displacement, contact area, contact pressure, and peak plastic strain).
RESULTS: The median value of waviness height was 0.8 (range 0.50 – 1.23) µm. FEA found that for the case of no surface waviness, full contact is present throughout the length of the stem taper. In contrast, models with waviness exhibited less total contact for surgeon-applied assembly loads less than 6kN. At 6kN, stepwise-multiple linear regression (Fig. 2) found waviness height to be a significant predictor on displacement (p<<0.001) and strain (p<<0.001), and found waviness spacing to be a significant predictor on contact area (p<<0.001), strain (p=0.004), and pressure (p<<0.004).
CONCLUSION: This study aimed to quantify waviness (height and period) on postmortem stem tapers. Additionally, we investigated how waviness, in the presence of microgrooves, affects the contact mechanics at the head-stem interface. We expected variability in both waviness height and period across the postmortem group. Although the heights of waviness were low compared to microgrooves, they have a large predicted effect on contact mechanics. In terms of THR procedures, our results suggest surgeons must apply forces at or over 6kN to obtain maximum microgroove peak contact at the modular junction. This study mapped out a broad range of waviness values from our cohort of postmortem stem tapers, however, we need to further understand waviness in context with angular mismatch, out-of-roundness, and microgroove geometry on both head and stem tapers.
Figures
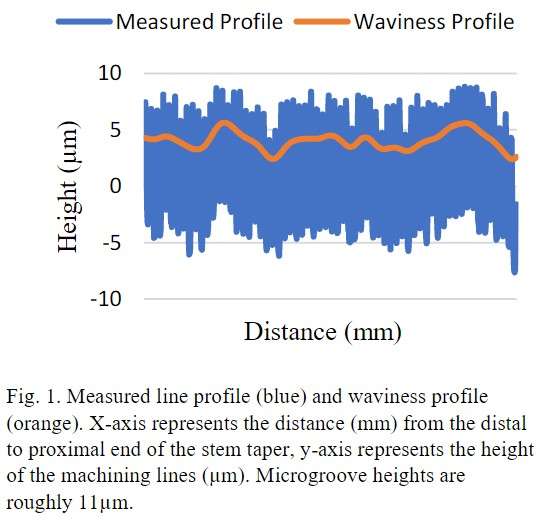
Figure 1
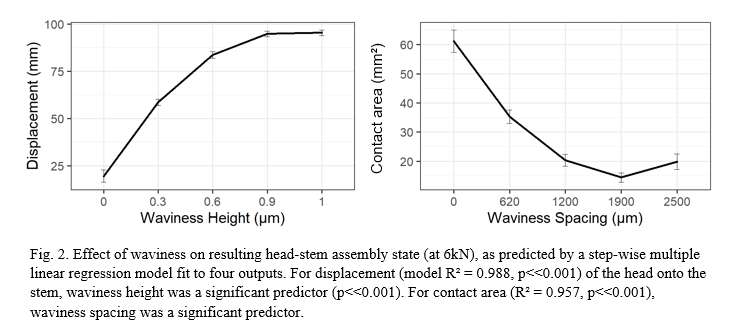
Figure 2#7769
Out-of-Roundness on Postmortem-Retrieved Head-Stem Taper Couples
*Michael Godoy - Rush University Medical Center - Chicago, USA
Jonathan Gustafson - Rush University Medical Center - Chicago, USA
Brett Levine - Rush University Medical Center - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
Hannah Lundberg - Rush University Medical Center - Chicago, USA
*Email: michael_godoy@rush.edu
INTRODUCTION: Modularity of total hip replacements (THRs) has been associated with fretting-corrosion that, in some cases, can lead to implant failure. Previous studies have assessed different design variations of the head and stem tapers, such as angular mismatch, to determine their potential influence on fretting-corrosion. Although angular mismatch is critical in identifying potential causes of fretting-corrosion within the modular junction, most in silico studies assume a perfect cone for both the head and stem taper. Out-of-roundness (OOR), or ovality, of head and stem tapers, is a measurement of deviation from circularity or roundness, which is not well understood in the literature. Engagement or contact area is specific to a particular head-stem couple subject to differences in geometrical form. Recent studies have shown inconsistent contact distributed across the entire length of tapers when performing THA head-stem taper assembly experimentally. Our objective is to determine OOR from postmortem retrieved head and stem taper couples in this study and investigate the implications of OOR on contact mechanics during femoral head assembly with finite element analysis (FEA).
METHODS: Thirty postmortem retrieved head-stem taper couples were chosen from an IRB-approved repository to determine the OOR of well-functioning THRs. Three-dimensional models of each head and stem taper surface were generated using an optical coordinate measuring machine (Redlux, Romsey, UK). Inner head taper surfaces were obtained from high-precision molds (Microset Blue, Microset). Each model was fitted to a cone using the CMM software (RedLux Studio) (Fig. 1). Next, circumferential profiles of the deviation from the fitted cone were extracted at four locations on the head and stem taper proximal to distal (Fig. 2). Median and range values are reported for total deviation from the ideal surface, the sum of the maximum (peak) and minimum (valley) deviations of the circumferential profiles. A three-dimensional FEA model was used to investigate the effect of OOR on contact mechanics during femoral head assembly by modeling the cone cross-section as a 2nd order harmonic with minor and major axis.
RESULTS: The median total deviation of postmortem retrieved heads from perfectly round was 6.21µm (range: 3.79 – 16.39µm). Seven heads displayed 2nd order harmonic profiles, while eight heads displayed 3rd order harmonic profiles. In terms of stem tapers, OOR was seen in four of 30 cases (median: 7.88µm, range: 7.14-7.96µm). All four stem tapers with OOR displayed 2nd-order harmonic profiles. FEA showed that contact distribution changed with increasing OOR (Fig. 3). At the largest OOR deviation, 16µm, contact was only present on 11% of the stem taper length at the minor radius of OOR.
CONCLUSION: OOR was found in 50% of head tapers and 14% of stem tapers, with deviations as large as 16µm. Head taper OOR led to inconsistent contact between the stem and head taper during femoral head assembly. Future studies aim to incorporate a broader range of head-stem taper couples to obtain a larger dataset of OOR values and to investigate the interaction between taper contact mechanics, OOR, and other implant design variables.
Figures
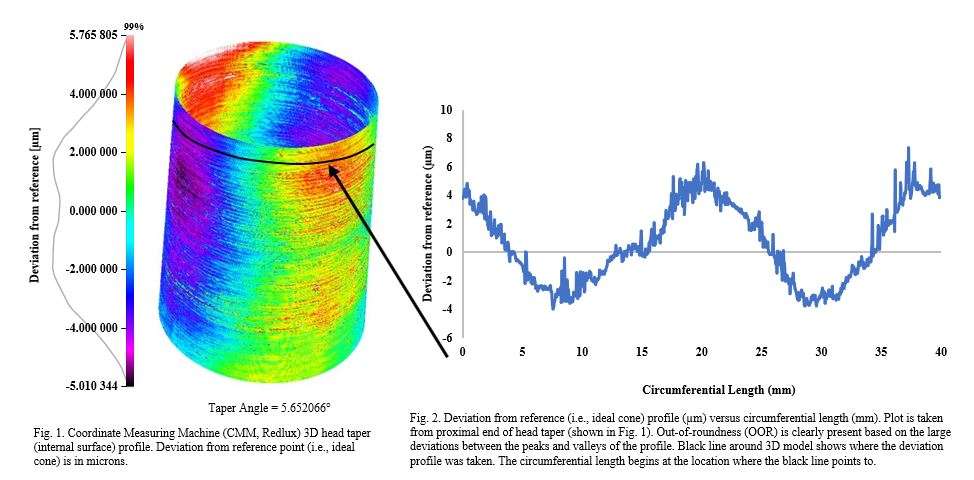
Figure 1
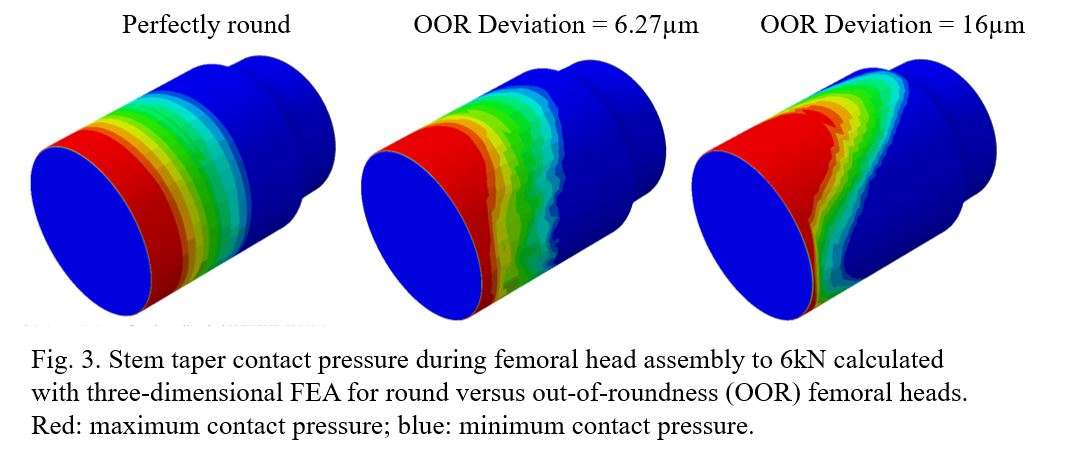
Figure 2#7933
Simultaneous Bilateral Versus Unilateral Total Joint Arthroplasty Outcomes in Octogenarians
*Thomas Kane - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Paige Casil - Straub Medical Center, Bone and Joint Center - Honolulu, USA
Anna Gragas - John A. Burns School of Medicine at University of Hawaii - Honolulu, United States of America
*Email: kane25@hawaii.edu
Introduction:
As advances in medicine have increased life expectancy, more octogenarians are undergoing total hip and knee arthroplasty than ever before. Elderly patients with bilateral end-stage hip or knee arthritis want to know if it is safe to have bilateral surgery under a single anesthetic, to restore their quality of life as quickly as possible. Yet, simultaneous bilateral total joint arthroplasty (SBTJA) in octogenarians remains controversial.
The purpose of this study was to compare 90-day outcomes of simultaneous bilateral total joint arthroplasty versus unilateral total joint arthroplasty in patients ≥ 80 years old.
Methods:
We conducted a descriptive, observational cohort study that included all patients ≥ 80 years old who underwent elective primary TJA performed by a single surgeon in a high-volume arthroplasty center between February 2014 and July 2021 as simultaneous or unilateral procedures. Patients were excluded if the procedure was performed for any reason other than degenerative joint disease or if hardware was removed at the time of surgery.
Outcome variables assessed in this study were hospital length of stay (LOS), blood transfusion rate, discharge disposition, and 90-day adverse events (i.e., emergency department visits, unplanned readmissions, complications, and mortality). Any patients who had an ER visit or readmission in the first 90 days after surgery were identified, and a detailed chart review was performed. Descriptive statistics were performed for all patients, and then separated by unilateral/bilateral procedures.
Results:
Of the 241 patients included in this study, 101 underwent unilateral TKA, 92 underwent unilateral THA, 40 underwent simultaneous bilateral TKA, and 8 underwent simultaneous bilateral THA. Overall, the patients included in this study had an average age of 83.4 years old, a BMI of 26.1, ASA of 3, and 66.5% were female. There were no significant differences in age, gender, ASA, and BMI among unilateral TJA and simultaneous BTJA groups. The simultaneous bilateral TJA cohort had a higher rate of postoperative blood transfusions (20.8% versus 3.6%) and a greater proportion of patients discharged to a rehabilitation facility rather than home (95.8% versus 39.9%). There was no major difference in 90-day ED visit rates between simultaneous bilateral TJA (2/48, 4.2%) and unilateral TJA (5/193, 2.6%) cohorts. In addition, 90-day hospital readmission rates were similar between simultaneous bilateral and unilateral TJA cohorts (4.2% versus 3.6%). No patients died within 90 days postoperatively.
Conclusion:
Although octogenarians who underwent simultaneous bilateral TJA were more likely to be discharged to a rehabilitation facility and required significantly more perioperative transfusions compared to those undergoing unilateral TJA, the odds of a 90-day major complication and readmission were similar between groups.
Simultaneous bilateral total hip and knee arthroplasty can be a safe and effective option for octogenarians. Complications and mortality are not higher for SBTJA compared to UTJA in this population.
#7297
Use of a Novel Imageless Navigation System Reduced Fluoroscopy Exposure and Improved Acetabular Positioning in Anterior Approach Total Hip Arthroplasty. a Case-Control Study.
*Christian Ong - Hospital for Special Surgery - New York, United States of America
Yu-Fen Chiu - Hospital for Special Surgery - New York, USA
Alejandro Gonzalez Della Valle - Hospital for Special Surgery - New York, USA
Ajay Premkumar - Hospital for Special Surgery - New York, USA
Jacqueline Grubel - USA
*Email: ongc@hss.edu
Introduction: Direct anterior approach (DAA) total hip arthroplasty (THA) has become increasingly popular. DAA cases frequently utilize fluoroscopic radiation for intraoperative imaging, which is known to carry several health risks for patients and providers. In June of 2020, a new, miniature imageless hip navigation system received FDA approval for use in total hip arthroplasty (THA). As a novel product, the purpose of this study is to assess the impact of using a novel imageless THA navigation system on fluoroscopic radiation exposure. Secondary objectives are to assess impacts of using the device on operative duration and acetabular cup placement quality.
Methods: This was a retrospective, single-surgeon cohort study of a consecutive group of patients who underwent primary anterior approach THA for a diagnosis of osteoarthritis between October 2017 – January 2022 in a single specialty hospital. A novel imageless navigation system that required temporary fixation of an optical pelvic tracker (Naviswiss, Switzerland) was used to determine intraoperative acetabular inclination and anteversion angles referenced off of a generic coronal and sagittal plane. Seventy-one navigated cases (study group) were compared 1:1 with 71 manual cases for fluoroscopy exposure, operative duration and acetabular placement variation. Cohorts were similar in their distributions of sex, race, ethnicity and body mass index. Comparisons between groups were investigated using independent samples t-tests. Statistical significance was defined as p<0.05.
Results: On average, Naviswiss patients experienced significantly less fluoroscopy exposure time (3.59 [±1.95] vs. 9.15 [±5.98] seconds; p<0.001) and dosage (0.30 [±0.23] vs. 0.78 [±0.63] mGy; p<0.001). Use of the system did not increase operative duration (82.69 [±11.70] vs. 89.54 [±14.60] minutes; p=0.09). The study group had a significantly lower placement variation for inclination and anteversion, based on mean proximity to the centroid of each cohort (3.55 [±1.88] vs. 5.39 [±3.51]; p<0.001) and also a greater proportion of cases that fell within 1 SD of the mean cohort inclination and anteversion (40.8% vs. 21.1%; p=0.009) (Figure 1, Table 1).
Conclusion: Use of a novel imageless navigation system for DAA THA significantly reduced fluoroscopic radiation exposure duration and dosage. The system also improved acetabular cup positioning consistency without resultant increases in operative duration.
Keywords: Navigation; Anterior; Fluoroscopy; Hip; Arthroplasty
Figures
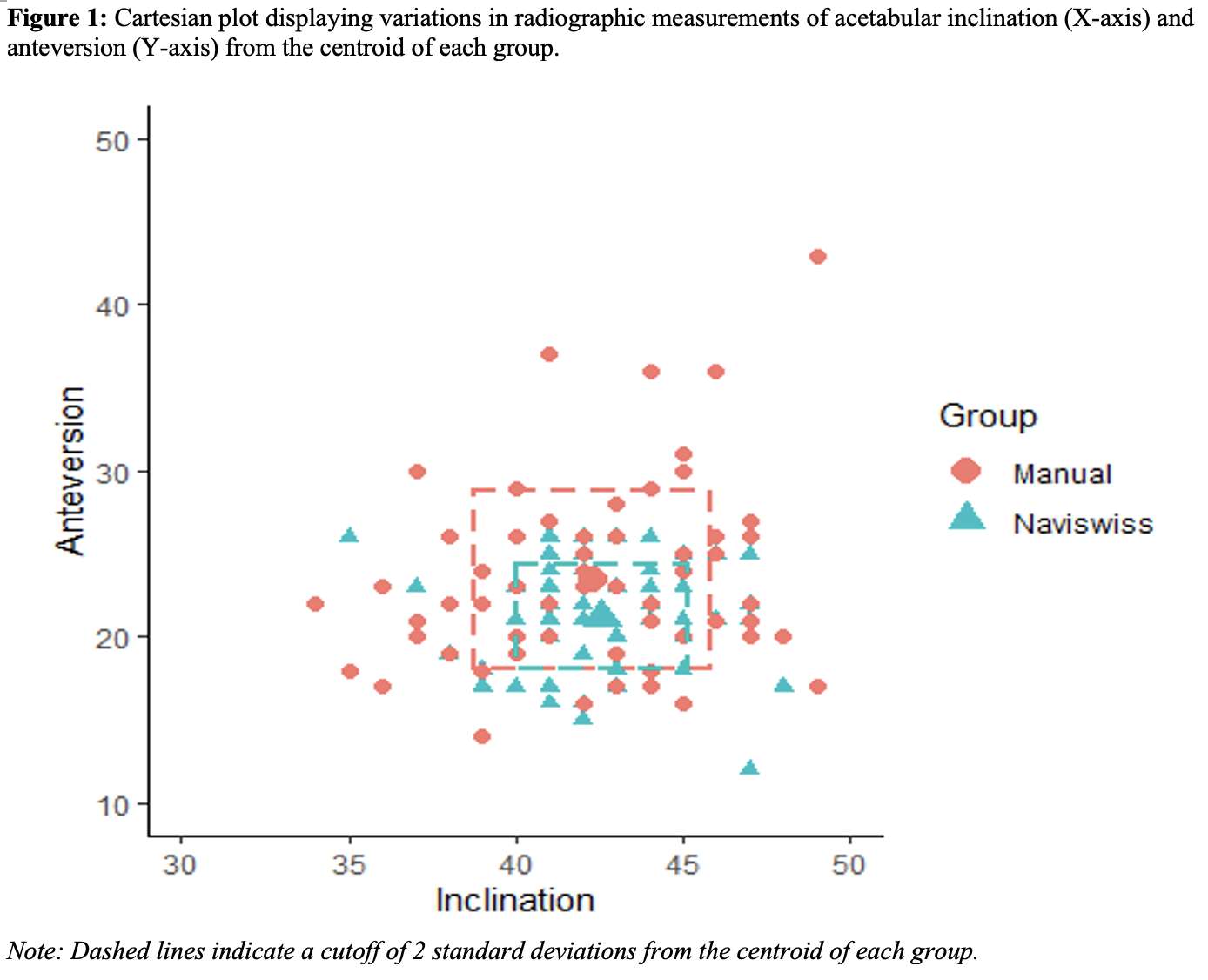
Figure 1
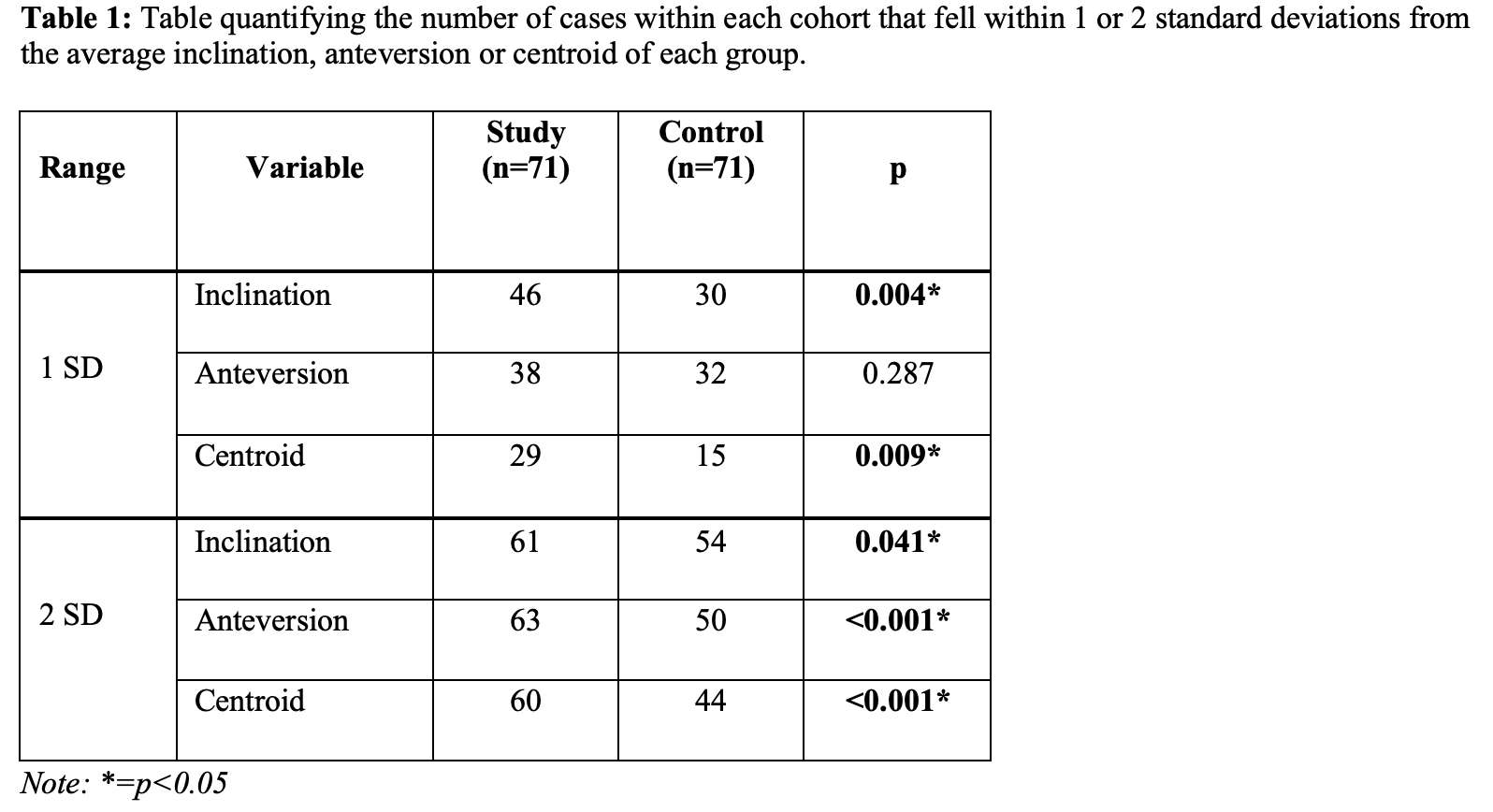
Figure 2#7298
The Learning Curve of Adopting an Optical, Miniature Imageless Navigation System for Total Hip Arthroplasty (THA)
*Christian Ong - Hospital for Special Surgery - New York, United States of America
Alejandro Gonzalez Della Valle - Hospital for Special Surgery - New York, USA
Ajay Premkumar - Hospital for Special Surgery - New York, USA
Yu-Fen Chiu - Hospital for Special Surgery - New York, USA
Jacqueline Grubel - USA
*Email: ongc@hss.edu
Introduction: The adoption of new surgical technologies is often associated with an initial learning period, which may be reflected by increased operative times and/or inconsistent outcomes. In June of 2020, a new, miniature imageless hip navigation system received FDA approval for use in total hip arthroplasty (THA). As a novel product, the purpose of this study was to assess the duration of the learning curve from the perspectives of surgical time and accuracy of acetabular positioning. A secondary objective was to investigate patient characteristics which influenced accuracy.
Methods: This was a prospective, single-surgeon observational study of a consecutive group of patients who underwent primary total hip arthroplasty (THA) for a diagnosis of osteoarthritis between September 2020 – May 2021 in a single specialty hospital. All procedures were performed through a posterior approach with the aid of an imageless navigation platform that required temporary fixation of an optical pelvic tracker (Naviswiss, Denver, CO). The platform was used to determine intra-operative acetabular inclination and anteversion angles referenced off of a generic coronal and sagittal plane. Acetabular accuracy was determined by assessing differences between intraoperative inclination and anteversion values and those obtained from measuring standardized 6-week follow-up radiographs. Operative time and acetabular accuracy were visualized by plotting simple moving averages (SMA) of 5, 7, 10 and 20 consecutive cases. The conclusion of the learning period was defined as no statistically significant difference between three consecutive SMA using Analysis of Variance (ANOVA). Acetabular accuracy by patient race, ethnicity, sex, and procedure laterality was reported in frequencies and percentages and compared using t-tests. The association between acetabular accuracy and age, BMI, and operative duration was assessed using Pearson correlation. Statistical significance was defined as p<0.05.
Results: A total of 74 patients were included in this analysis. No formal learning period was detected for operative duration and/or acetabular accuracy (Figure 1). Patient sex had a significant impact on acetabular inclination accuracy (male -1.4 vs. female 1.2, p=0.001) (Table 1). Pearson’s correlation coefficients indicated a weak relationship between acetabular accuracy and patient age, BMI and surgical time (all absolute γ < 0.2) (Table 2).
Conclusion: Adoption of a new imageless hip guidance system did not display an observable learning curve traditionally associated with utilizing novel technologies. Patient sex was the only significant predictor of acetabular positioning accuracy. Further research amongst a larger, more longitudinal cohort incorporating outcomes data is needed to validate these findings.
Keywords: Hip, Arthroplasty, Navigation, Learning, Acetabulum
Figures
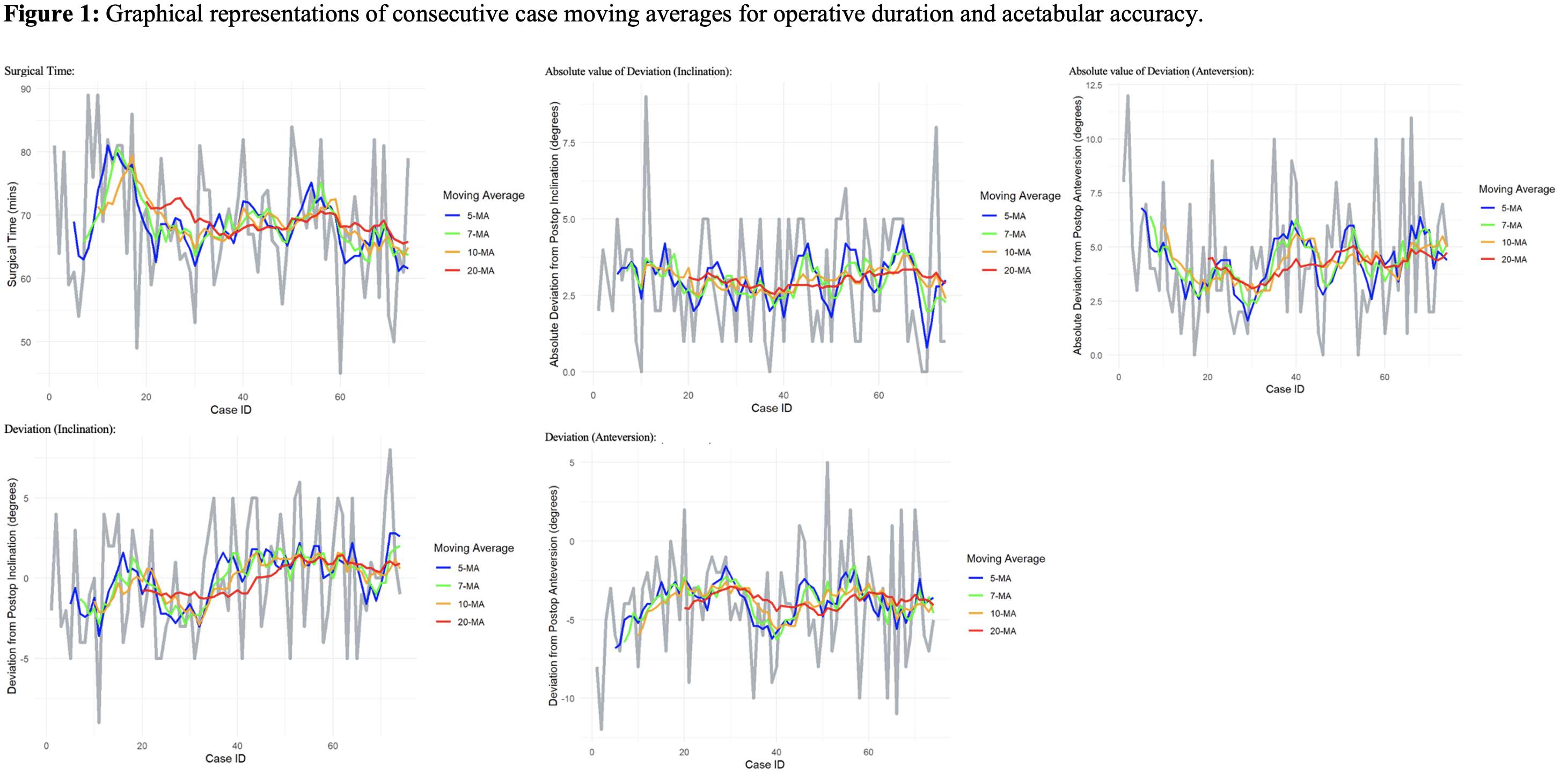
Figure 1
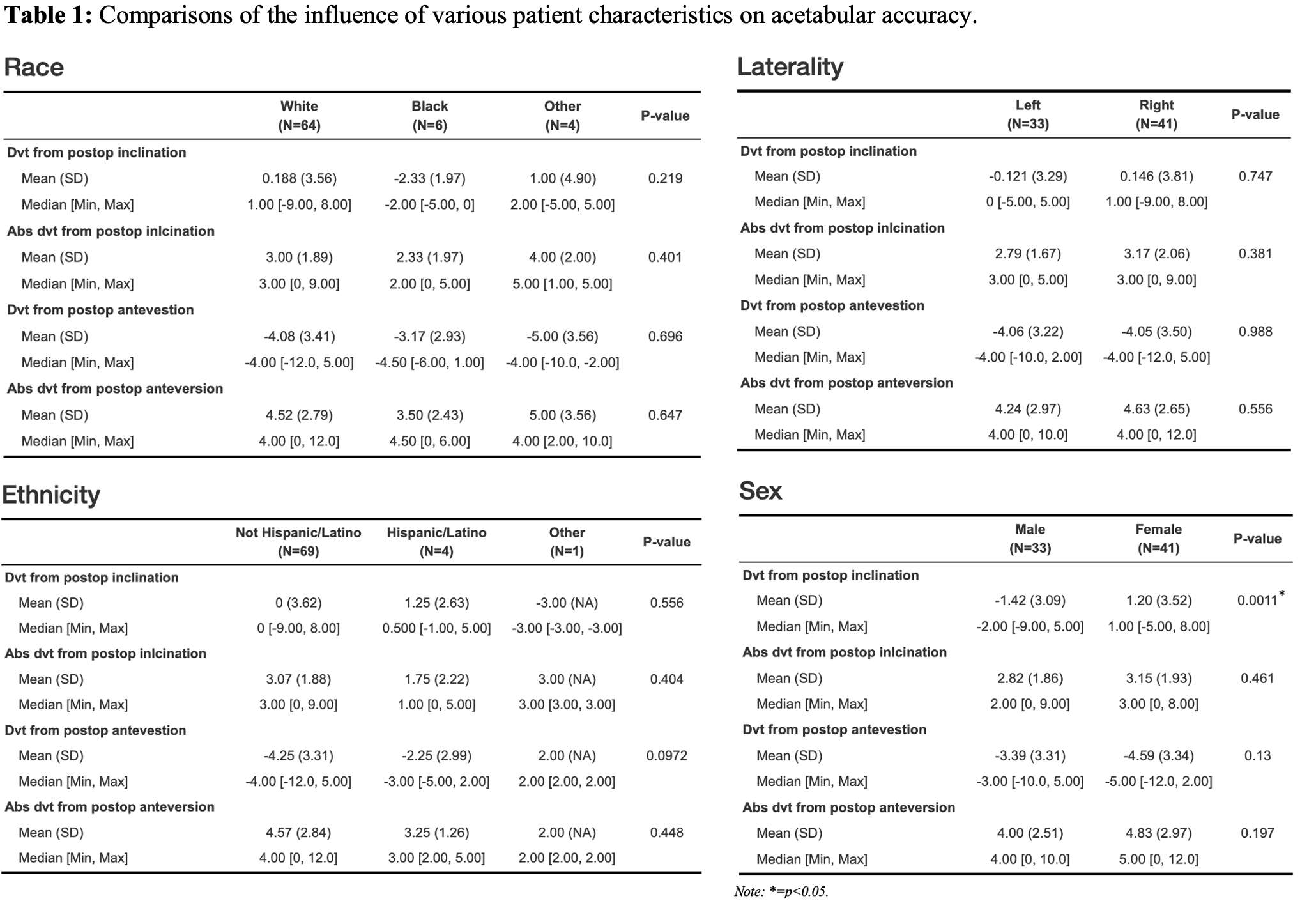
Figure 2
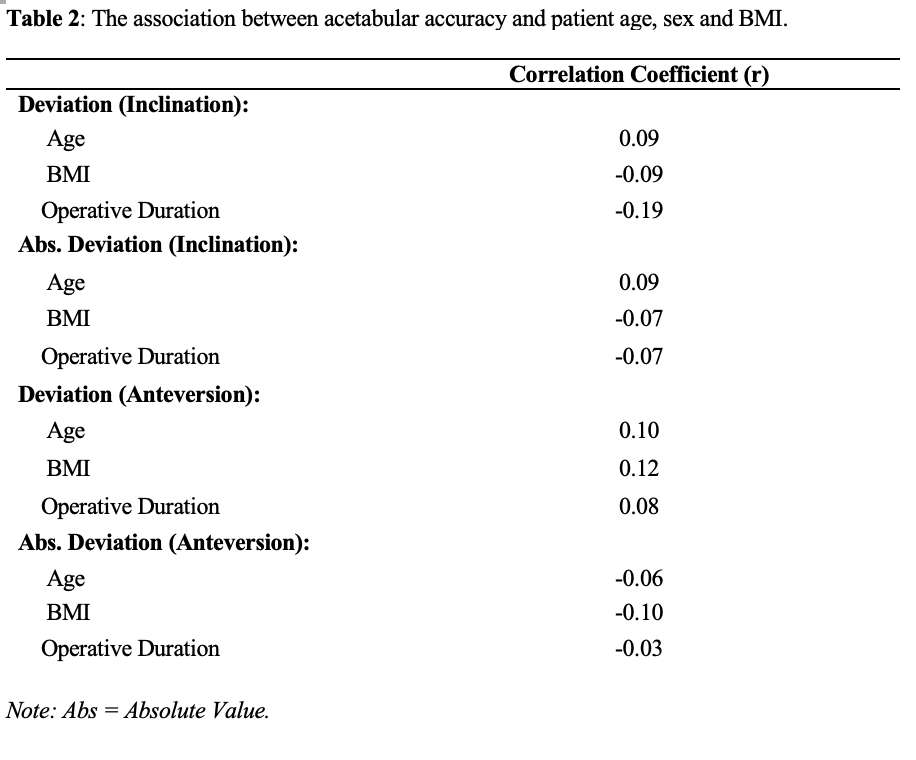
Figure 3#8052
Invited Talk: Can Bi-cruciate substituting TKA function similar to a normal knee?
*steven haas - Hospital for Special Surgery - New York, United States of America
*Email: haass@hss.edu
#7747
Patient Specific Mega Spacers for Severe Bone Loss in Cases of Periprosthetic Joint Infection (PJI)
*Mahmoud Hafez - October 6 University - October 6 City, Egypt
*Email: mhafez@msn.com
Patient Specific Mega Spacers for Severe Bone Loss in cases of Periprosthetic Joint Infection (PJI)
Mahmoud A Hafez, FRCS Ed, MD1; Ahmed Abdel Moghny1; Abdelrahman M Makram1; Omar Mohamed Makram, MBBCh1,2;
1The Orthopaedic Department, Faculty of Medicine, October 6 University, Giza, Egypt.
2Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom.
MAH: mhafez@msn.com (ORCID: 0000-0002-6285-5720)
AAM: amughny@gmail.com (ORCID: 0000-0001-9171-7127)
AMM: abd-makram@hotmail.com (ORCID: 0000-0003-2011-8092)
OMM: omarmakram95@gmail.com (ORCID: 0000-0001-8361-9068)
Corresponding author
Mahmoud A Hafez
Institutional address: 1/1 Main Axis, 12566, 6th of October City, Giza, Egypt
Phone: +20 1007 566 299
Email: mhafez@msn.com
Website: www.egyorth.org
Authors’ contribution
MAH developed the idea.
Acknowledgments
The authors acknowledge the work of engineer Ahmed Abdel Moghny Salem, who helped in the development of the patents.
Conflict of interest
This paper is part of two self-funded patents submitted by MAH.
Source of funding
No funding was received for this study.
ABSTRACT
Introduction
In cases with PJI and tumors, amputation is the last resort to prevent further local spread. Limb salvage techniques have evolved to overcome this problem. One of the ways is to insert a permanent bone spacer that fits the size of the individual’s contralateral bone.
Materials and Methods
The templating of each PSS is done using a CT scan, some calculations of the bone anatomy based on the contralateral side, and a 3D printer. We used our templates to treat two cases of PJI and tumors: one at the proximal part of the humerus and one at the distal part of the femur. In one setting, extraction of the affected bone and soft tissue and surgical debridement was done, and the spacer was then implanted. In another setting, the spacer was removed to be replaced with a permanent implant.
Results
The two cases recovered completely from the two operative stages with no side effects or complications related to the spacer itself.
Conclusion
The PSS provides size matching implants for patients. Because it is based on printing 3D models, this technique can be used to treat cases of bone infections and traumatic bone loss.
Keywords
Cancer; PJI and tumor; Spacer; Patient-specific; Treatment; 3D-Printing; Pediatrics
INTRODUCTION
Neoplastic growth within the skeletal system may be of primary origin, whether benign or malignant, or secondary origin (metastatic bone disease). Most tumorous tissues of the bone will need to be curetted or resected and replaced with a graft [1]. Although PJI and tumors are not common, metastatic spread to bones is the third most common site of the solid cancerous (e.g., breast, lung, prostate) [2]. However, metastasis is commonly observed in the vertebrae, ribs, pelvis, and ends of long bones because it is hypothesized that bones with trabecular organization, red marrow, higher blood supply, and pacier tissue turnover are better in harboring tumor cell seeding [2-4].
Different modalities have been suggested in treating bone metastasis. Bone-targeting agents (BTAs) have been proposed to limit metastatic growth within bones by a multitude of actions. The most used class of BTAs is the osteoclast inhibitor denosumab that depends on hindering osteolysis by preventing osteoclastic differentiation, through targeting the RANKL, which ultimately leads to bone destruction and altered remodeling [5-7]. Bisphosphonates are a less potent choice that can also help in impeding osteoclastic bone resorption. Both drugs can also be used for preventing bone resorption associated with cancer treatment [8]. Moreover, BTAs have been and are being studied for their possible efficacy in preventing bone metastasis in breast [9-11] and prostate [12, 13] cancers.
Surgical interventions such as bone curettage can leave the remaining bone prone to fractures [2]. Other modalities can also be done after complete bone resection, such as insertion of an intramedullary rod/nail or spacer implantation. In cases where there is extensive local infiltration, amputation is the last resort to control the disease [14]. In PJI and tumors, external fixation can be used to reduce the incidence of pathological fractures, correct limb length discrepancy, and improve bone deformity [1]. The Masquelet (aka induced membrane) technique, which is a two-step procedure to treat bone defects, has proven itself to be a good approach in dealing with such cases, no matter what the original pathology is. The first step involves tissue debridement till the healthy tissue bleeds, while the second step involves the placement of a polymethyl methacrylate cement spacer in the defect area. The role of the spacer is to provide stability, counteract against fibrosis, and form a pseudo-synovial membrane that is used to implant cancellous bone in a third reconstructive operation [15-17]. A similar technique is used in the mandibular reconstruction, where a three-dimensional model is printed to provide the functions of the spacer till bone implantation is done [18-20].
In this paper, we present two cases of PJI and tumors managed by uniquely designed patient-specific spacers (PSS) using CT imaging.
METHODS AND RESULTS
This manuscript is based on three patents (PCT/EG2013/000014), (PCT/EG2018/000021), (WO/2019/076421) published in 2013, 2018, and 2019, respectively, by the first author (MAH). The first patent discusses the invention of a patient-specific spacer (PSS) that fits into a debrided joint in the case of prosthetic joint infection [21]. The second one is aimed at 3D-printing a template that can replace the bone removed due to tumorous growth [22].
Designing (imaging and templating)
As it is a type of computer-assisted surgery, the intended spacer is designed using the patient’s preoperative CT scan which is used to determine the sizes and dimensions of the spacer based on the anatomic configuration of the patients’ joint and the cavities of the bones forming the target joint. These CT images are converted into a 3D model using specialized software and printed using FDA-approved implantable medical materials (e.g., Nylon). This process ensures the best fit of the spacer inside the patient’s body as it is unique for each induvial as well as being disposable, so it prevents contamination and infection.
Spacer components
The spacer is patient specific as it provides exact sizing compatible with both the acetabulum and proximal femoral canal of the patient as well as delivering the specific antibiotics selected based on culture and sensitivity tests.
The patient specific spacer PSS consists of three main parts: stem, head, and a nerve that connects the head with the stem (Figure 1). First, the stem has a conical shape in the case of ball and socket joint (e.g., hip, shoulder) replacement, where the larger diameter forms the upper part and the smaller one forms the lower part to facilitate its insertion and fixation into the cavity of the socket. Second, the head of the spacer has a spherical shape with the lower third being cut to ensure the free mobility of the implant (e.g., the head of the femur inside the acetabulum) as well as facilitating the connection with the nerve connected to the stem. Third, the nerve has a square shape where it connects the conical shape of the stem and the spherical shape of the head. This square shape of the nerve helps with the support of the body and balancing its mass, as well as withstanding the loads resulting from the patient’s weight, and both fixed and motor daily activities.
There are two mechanisms for antibiotic release directly to the infected site: first one, from a feeder reservoir in the head and neck of the spacer that connects to internal canals that open into six holes spread all around the spacer. Antibiotics should be injected in liquid format through the opening in the centre of the head that is sealed with a plug afterwards. The seconded one, from a paste composed of at least two sensitive antibiotics (one in powder and another in liquid format, e.g., Vancomycin and Gentamycin). The paste should be applied to the stem surface to fill in the gaps between the beads.
Internal paths are also present in both the stem and the head to allow installing surgical metal wires to maintain the stability and rigidness of the spacer and increase its ability to withstand the patient’s weight and daily activities such as walking, standing up, sitting down, and other simple motor skills. These internal paths extend longitudinally across the stem and transversely across the head. Finally, these paths have one open end and one closed end which also contributes to the prevention of infections and the overall spacer stability. These paths could be loaded with different quantities of antibiotics according to the patient’s needs and the surgeon’s decision. For better fixation in PJI and tumor patients, the head and stem may be printed with holes that can help in fixating the spacer (Figure 2).
The exact sizing of the spacer is based on preoperative imaging using X-ray, CT or MRI. However, ready-made, off-the-shelf spacers are available for those cases where the sizing
Materials used
This PSS is made of nylon, which has both the physical and mechanical properties that enable it to withstand shear, vertical forces, and horizontal loads resulting from the activities of daily life. Nylon, which is an FDA-approved material, is known to be safely used in implantations inside loving tissues without any medical complications. Nylon can last for about 6 months inside the body, which gives enough time for infection resolution and the temporary spacer to be replaced with the permanent one. The external surface of the spacer is also rough enough to enable the surgeon to coat it with medical cement to ensure its fixation in the proper position inside the cavity. In the case of infection, the surgeon has the option to coat the spacer with antibiotics, too.
3D-Printing process
There are two methods of 3D printing technology that may be used to produce the spacer: (1) the fused deposition modeling (FDM) where plastic wires made of nylon are used in the printing process; (2) selective laser sintering (SLS) where a laser is used for sintering the nylon powder to produce the required profile of the PSS.
Patients included
We prospectively included patients with surgically indicated tumorous bone growth. The final included number of patients was two (Table 1): one with proximal humerus tumor and the other with distal femur PJI (Figure 3). All surgeries were performed by MAH. The intervention was done in two operations: 1) bone debridement and spacer implantation; 2) spacer removal after six-to-eight weeks and insertion of a permanent implant (e.g., total knee arthroplasty).Outcomes were assessed based on achieving the main objectives of the PSS, which are control tumorous growth, maintenance of stability, and preservation of the space. The two patients recovered completely from the two operations and had no complications related to the operations or the spacers implanted. Further follow-up is pending.
DISCUSSION
The authors in this paper present a new model in dealing with pediatric bone tumors. We present two cases of planned bone resection because of tumorous growth. Normally, a spacer resembling the bone tissue loss should be placed to allow tissue regeneration and membrane formation [23]. This is due to the poor outcomes when the length of the removed bone part exceeds five centimeters [24-26], which is the case in most malignant swellings that require resection with a safety margin [27]. Although there is a scantiness of information on the outcomes of this new treatment prototype, we believe that a size-matching PSS can help regeneration and bone growth, in children, along the normal body planes that correspond to the contralateral side. This is because our technique allows the surgeon to provide a perfect match to the bone tissue lost. Moreover, the 3D printing technology implemented can be used to treat traumatic or infectious bone loss.
According to the market prices, this technology of 3D printing (the SLS) would be 12 times less expensive compared to the conventional spacers. This would reduce the burden on both individual patients and governments and allow the use of safer complication-free technology which consequently helps with reducing the number of patients on the surgical waitlists.
This study has some limitations as well. This technique is very novel in managing PJI and tumors, so it is unlikely to know its efficacy in the meantime. The surgeries were performed in the near past, hindering the ability to have a longer follow-up. We only tried this technique in three patients, two of which are presented in this paper. The third patient had a sacrococcygeal tumor that was resected, and the spacer was implanted; however, the second operation is not done yet. There are potential complications of this spacer as well. One of the main ones is the possible loosening. The spacer may also break as it is made of polymers that can’t withstand intense exercise, for instance.
CONCLUSION
In this study, we introduced a new technique for making and inserting a bone spacer in patients using three published patents by MAH. The technique used depended on 3D-printing a patient-specific spacer (PSS) that needed preoperative CT scanning and an experienced engineer to measure the contralateral bone and template an inverted duplicate. The templates were used to treat one proximal humerus tumor and one distal femur PJI through bone debridement and spacer placement. In the next setting, the spacer was removed to be replaced with a permanent implant. The two operative stages of the two included participants were uncomplicated.
CLINICAL CORREALTION
The 3D-printed PSS provides size matching implants for patients. This technique can be used in other patients with traumatic or infectious bone loss.
REFERENCES
1. Matsubara H, Tsuchiya H. Treatment of bone tumor using external fixator. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2019;24(1):1-8. doi: 10.1016/j.jos.2018.06.022.
2. Fornetti J, Welm AL, Stewart SA. Understanding the Bone in Cancer Metastasis. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2018;33(12):2099-113. doi: 10.1002/jbmr.3618.
3. Kakhki VR, Anvari K, Sadeghi R, Mahmoudian AS, Torabian-Kakhki M. Pattern and distribution of bone metastases in common malignant tumors. Nuclear medicine review Central & Eastern Europe. 2013;16(2):66-9. doi: 10.5603/nmr.2013.0037.
4. Krishnamurthy GT, Tubis M, Hiss J, Blahd WH. Distribution pattern of metastatic bone disease. A need for total body skeletal image. Jama. 1977;237(23):2504-6.
5. Dionísio MR, Mansinho A, Abreu C, Cavaco-Silva J, Casimiro S, Costa L. Clinical and translational pharmacology of drugs for the prevention and treatment of bone metastases and cancer-induced bone loss. Br J Clin Pharmacol. 2019;85(6):1114-24. doi: 10.1111/bcp.13852.
6. Mundy GR. Mechanisms of bone metastasis. Cancer. 1997;80(8 Suppl):1546-56. doi: 10.1002/(sici)1097-0142(19971015)80:8+<1546::aid-cncr4>3.3.co;2-r.
7. Weilbaecher KN, Guise TA, McCauley LK. Cancer to bone: a fatal attraction. Nature reviews Cancer. 2011;11(6):411-25. doi: 10.1038/nrc3055.
8. Murad MH, Drake MT, Mullan RJ, Mauck KF, Stuart LM, Lane MA, et al. Clinical review. Comparative effectiveness of drug treatments to prevent fragility fractures: a systematic review and network meta-analysis. The Journal of clinical endocrinology and metabolism. 2012;97(6):1871-80. doi: 10.1210/jc.2011-3060.
9. Gnant M, Pfeiler G, Dubsky PC, Hubalek M, Greil R, Jakesz R, et al. Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2015;386(9992):433-43. doi: 10.1016/s0140-6736(15)60995-3.
10. Coleman RE, Finkelstein D, Barrios CH, Martin M, Iwata H, Glaspy JA, et al. Adjuvant denosumab in early breast cancer: First results from the international multicenter randomized phase III placebo controlled D-CARE study. Journal of Clinical Oncology. 2018;36(15_suppl):501-. doi: 10.1200/JCO.2018.36.15_suppl.501.
11. Gnant M, Pfeiler G, Steger GG, Egle D, Greil R, Fitzal F, et al. Adjuvant denosumab in early breast cancer: Disease-free survival analysis of 3,425 postmenopausal patients in the ABCSG-18 trial. Journal of Clinical Oncology. 2018;36(15_suppl):500-. doi: 10.1200/JCO.2018.36.15_suppl.500.
12. Denham JW, Joseph D, Lamb DS, Spry NA, Duchesne G, Matthews J, et al. Short-term androgen suppression and radiotherapy versus intermediate-term androgen suppression and radiotherapy, with or without zoledronic acid, in men with locally advanced prostate cancer (TROG 03.04 RADAR): an open-label, randomised, phase 3 factorial trial. The Lancet Oncology. 2014;15(10):1076-89. doi: 10.1016/s1470-2045(14)70328-6.
13. Wirth M, Tammela T, Cicalese V, Gomez Veiga F, Delaere K, Miller K, et al. Prevention of bone metastases in patients with high-risk nonmetastatic prostate cancer treated with zoledronic acid: efficacy and safety results of the Zometa European Study (ZEUS). European urology. 2015;67(3):482-91. doi: 10.1016/j.eururo.2014.02.014.
14. Clara-Altamirano MA, Garcia-Ortega DY, Martinez-Said H, Caro-Sánchez CHS, Herrera-Gomez A, Cuellar-Hubbe M. Surgical treatment in bone metastases in the appendicular skeleton. Revista espanola de cirugia ortopedica y traumatologia. 2018;62(3):185-9. doi: 10.1016/j.recot.2017.12.001.
15. Morelli I, Drago L, George DA, Gallazzi E, Scarponi S, Romanò CL. Masquelet technique: myth or reality? A systematic review and meta-analysis. Injury. 2016;47 Suppl 6:S68-s76. doi: 10.1016/s0020-1383(16)30842-7.
16. Karger C, Kishi T, Schneider L, Fitoussi F, Masquelet AC. Treatment of posttraumatic bone defects by the induced membrane technique. Orthopaedics & traumatology, surgery & research : OTSR. 2012;98(1):97-102. doi: 10.1016/j.otsr.2011.11.001.
17. Masquelet AC, Fitoussi F, Begue T, Muller GP. [Reconstruction of the long bones by the induced membrane and spongy autograft]. Annales de chirurgie plastique et esthetique. 2000;45(3):346-53.
18. Bender-Heine A, Petrisor D, Wax MK. Advances in Oromandibular Reconstruction with Three-Dimensional Printing. Facial plastic surgery : FPS. 2020;36(6):703-10. doi: 10.1055/s-0040-1721110.
19. Bender-Heine A, Wax MK. Reconstruction of the Midface and Palate. Seminars in plastic surgery. 2020;34(2):77-85. doi: 10.1055/s-0040-1709470.
20. Cohen A, Laviv A, Berman P, Nashef R, Abu-Tair J. Mandibular reconstruction using stereolithographic 3-dimensional printing modeling technology. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics. 2009;108(5):661-6. doi: 10.1016/j.tripleo.2009.05.023.
21. Hafez MA. A PATIENT-SPECIFIC SPACER. In: Bureau WIPOI, editor. A61F 2/36 (2006.01) ed. Egypt 2019.
22. Hafez MA. A METHOD FOR TREATING AND REPAIRING KNEE FRACTURES RESULTING FROM BENIGN TUMORS USING PATIENT - SPECIFIC ELECTRONIC TEMPLATES. In: Office USPaT, editor. A61B 34/10 (2006.01); A61B 17/17 (2006.01) ed. Egypt 2020.
23. Walker M, Sharareh B, Mitchell SA. Masquelet Reconstruction for Posttraumatic Segmental Bone Defects in the Forearm. The Journal of hand surgery. 2019;44(4):342.e1-.e8. doi: 10.1016/j.jhsa.2018.07.003.
24. Regan DK, Crespo AM, Konda SR, Egol KA. Functional Outcomes of Compression Plating and Bone Grafting for Operative Treatment of Nonunions About the Forearm. The Journal of hand surgery. 2018;43(6):564.e1-.e9. doi: 10.1016/j.jhsa.2017.10.039.
25. Ring D, Allende C, Jafarnia K, Allende BT, Jupiter JB. Ununited Diaphyseal Forearm Fractures with Segmental Defects: Plate Fixation and Autogenous Cancellous Bone-Grafting. JBJS. 2004;86(11).
26. Weiland AJ, Phillips TW, Randolph MA. Bone Grafts: A Radiologic, Histologic, and Biomechanical Model Comparing Autografts, Allografts, and Free Vascularized Bone Grafts. Plastic and Reconstructive Surgery. 1984;74(3).
27. Ritter J, Bielack SS. Osteosarcoma. Annals of oncology : official journal of the European Society for Medical Oncology. 2010;21 Suppl 7:vii320-5. doi: 10.1093/annonc/mdq276.
FIGURES AND TABLES CAPTIONS
Table 1. Basic characteristics of the patients undergone spacer implantation.
Figure 1. The diagram shows the different views of the patient-specific spacer (PSS). (A) Two-dimensional front elevation for PSS; (B) two-dimensional elevation view for PSS; (C) three-dimensional view for PSS; (D) two-dimensional internal sector for PSS. (1) head; (2) stem; (3) nerve; (4) the opening of the longitudinal internal path passing across the stem; (5) the longitudinal path; (6) the transverse path.
Figure 2. Two photos of the fixation holes in a template of the distal femur (left) and the proximal humerus (right).
Figure 3. The resection bone of the patient with tumor at the distal femur (left) and the 3D-printed PSS (right). Note the similarities in the morphology and the size.
Table 1. Basic characteristics of the patients undergone PSS implantation.
|
Patient Number
|
Sex
|
Age
|
Weight in Kg
|
Replacement
|
Stem Length in mm
|
Stem Diameter in mm
|
Indication
|
|
1
|
F
|
16
|
42
|
Proximal Humerus Spacer
|
122
|
16
|
Tumor
|
|
2
|
M
|
13
|
40
|
Distal Femur Spacer
|
170
|
22
|
Tumor
|
Figure 1. The diagram shows the different views of the patient-specific spacer (PSS). (A) Two-dimensional front elevation for PSS; (B) two-dimensional elevation view for PSS; (C) three-dimensional view for PSS; (D) two-dimensional internal sector for PSS. (1) head; (2) stem; (3) nerve; (4) the opening of the longitudinal internal path passing across the stem; (5) the longitudinal path; (6) the transverse path.
Figure 2. Two photos of the fixation holes in a template of the distal femur (left) and the proximal humerus (right).
Figure 3. The resection bone of the patient with tumor at the distal femur (left) and the 3D-printed PSS (right). Note the similarities in the morphology and the size.
Figures
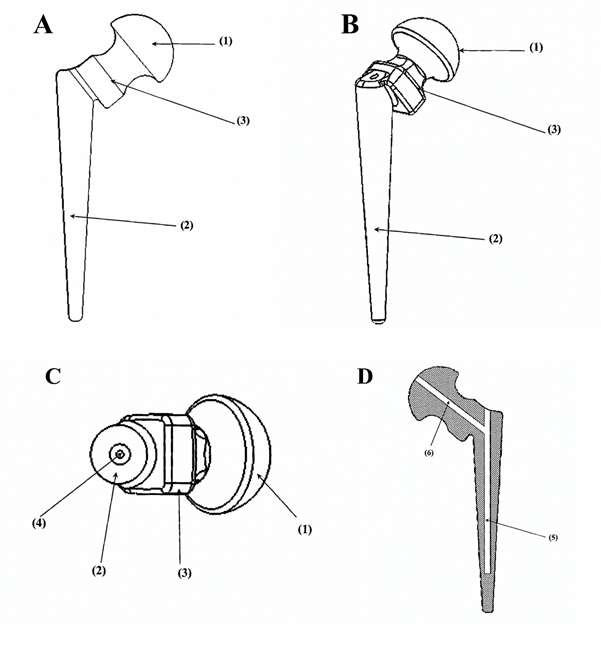
Figure 1

Figure 2

Figure 3#7887
Egyptian Community Arthroplasty Register
*Mahmoud Hafez - October 6 University - October 6 City, Egypt
*Email: mhafez@msn.com
Introduction:
Currently, there is neither a record in literature nor official documentations of arthroplasty procedures in the Arab countries. The indications for arthroplasty, types of implants, ratio between total hip and knee arthroplasty (THA & TKA) or the outcome are not known.
Materials and methods:
This community Register is an individual initiative to prospectively document arthroplasty procedures performed from 2007 to date in Cairo, Egypt. The registry sheet is available in printed format and online www.knee-hip.com/arthroplastyRegister.aspx The register started by one surgeon (MAH). We present the initial analysis of 1190 cases of TKA and THA with a ratio: 1.24 to 1.0.
Results:
For THA: Mean age was 51 years (19-86), Female to male ratio was 1.15:1. Indications were paeds hip diseases, failed ORIF of # NoF, AVN, posttraumatic and OA. Uncemented THA was 85%, Cemented 10% and hybrid 5%. Primary THA was 49%, complex primary 30%, while revision 21%.
For TKA: A female to male ratio was 3.14:1. The Indication was OA in 73%. 47% had severe varus and 15 17% had significant bone defect. Both THA and TKA had a revision rate of 2% and their implants were made by 8 companies.
Conclusion:
This study has limitations as the initial analysis was predominantly related to cases done by one surgeon (MAH), which may not be representative of the region. However, the registry revealed unexpected results that are not surgeon dependent such as; young age and indications for THA other than OA, the high % of complex THA & TKA due to late presentations and complex pathology. Establishing a register in this region is very difficult due to lack of funding, low interest in research and dominance of private practice.
#7886
10 Years Outcome of Bilateral Simultaneous Total Knee Arthroplasty in Patients With Deformities and Comorbidities: Comparison Between Bilateral PSI, Unilateral PSI, and Unilateral Conventional Techni
*Mahmoud Hafez - October 6 University - October 6 City, Egypt
Ahmed Abdel Moghny - October 6 University - Giza, Egypt
Emad Samuel Saweeres - El Sahel Teaching Hospital - Cairo, Egypt
Omar Makram - Faculty of Medicine, October 6 University, Giza, Egypt - Giza, Egypt
*Email: mhafez@msn.com
Background: In low-income settings, patients with knee osteoarthritis usually present late, when bilateral deformities become well established. These patients are in a deadlock and are usually deprived of the privilege of TKA because of the expected poor results of having one TKA, while the other arthritic side is still deformed. Most of these patients do not fit the criteria for bilateral simultaneous TKA due to the associated comorbidities and age.
Methods: The aim of this work is to compare the outcome of bilateral simultaneous TKA using the patient specific template (PST) versus unilateral PST and conventional TKA in patients with deformities and comorbidities. 739 consecutive TKA procedures were included in this study (bilateral simultaneous 428, unilateral 165, conventional unilateral 146). All patients had more than 10O of varus, valgus, or flexion deformities and one comorbidity. Survival of patients and the implants, function (knee society score & ROM) and complications were reported.
Results: More than 53% of the patients showed more than 15O up to 40O of varus deformity. 4% of the patients had valgus deformity between 15 O and 40 O degrees; 31% of the patients had fixed flexion deformity more than 20O up to 60O. The severe deformities such as varus deformity >15O (265 bilateral PST, 90 Unilateral PST and 83 conventional) and flexion deformity >20 degrees (163 bilateral PST, 75 Unilateral PST and 63 conventional) have undergone PST intervention more than the conventional technique. Hospital stay was significantly lower in both group of bilateral PSI and unilateral PSI when compared to the conventional technique (4.24±0.90, 4.35±0.57 and 6.95±2.92 respectively). KSS has significantly improved in the group <60 years when simultaneous bilateral PST or unilateral PSI is performed compared to the conventional technique (67.0, 68.2 and 60.3 respectively).
33 knees face complications after the surgery, (31 bilateral PST, 1 Unilateral PST and 1 Conventional.
Conclusion: Hospital and KSS improver in bilateral PST and unilateral PST in compare with conventional technique.
Keywords: total knee arthroplasty; bilateral simultaneous; PST; survival; mortality; morbidity; function; conventional.
#7986
Apparatus and System for Acquiring Data From Bones and Joints, Plan Surgery and Manufacturing Instruments or Implants (US10966787B2)
*Mahmoud Hafez - October 6 University - October 6 City, Egypt
*Email: mhafez@msn.com
This invention relates to Patient-Specific Templates (PST) which have already been used by implant manufacturers and clinically applied by orthopedic surgeons. This work presents an apparatus comprised of a unit acquiring data from the surface of bones and joints, a computerized unit for surgical planning and a desktop 3D printer for manufacturing PST, which are functionally, physically and electrically connected. The apparatus is compact, portable and suitable for hospital-based or clinic-based service. The data-collection unit has electro-magnetic (EM) device, diagnostic ultrasound machine, laser scanner and a receiver for acquisition of external data. It integrates the data from multiple sources and has sensor fusion ability. The surgical planning unit has specific software program capable of merging the collected data through mathematical model of specific parts of bones, joints and a library of implants and prostheses.
Figures
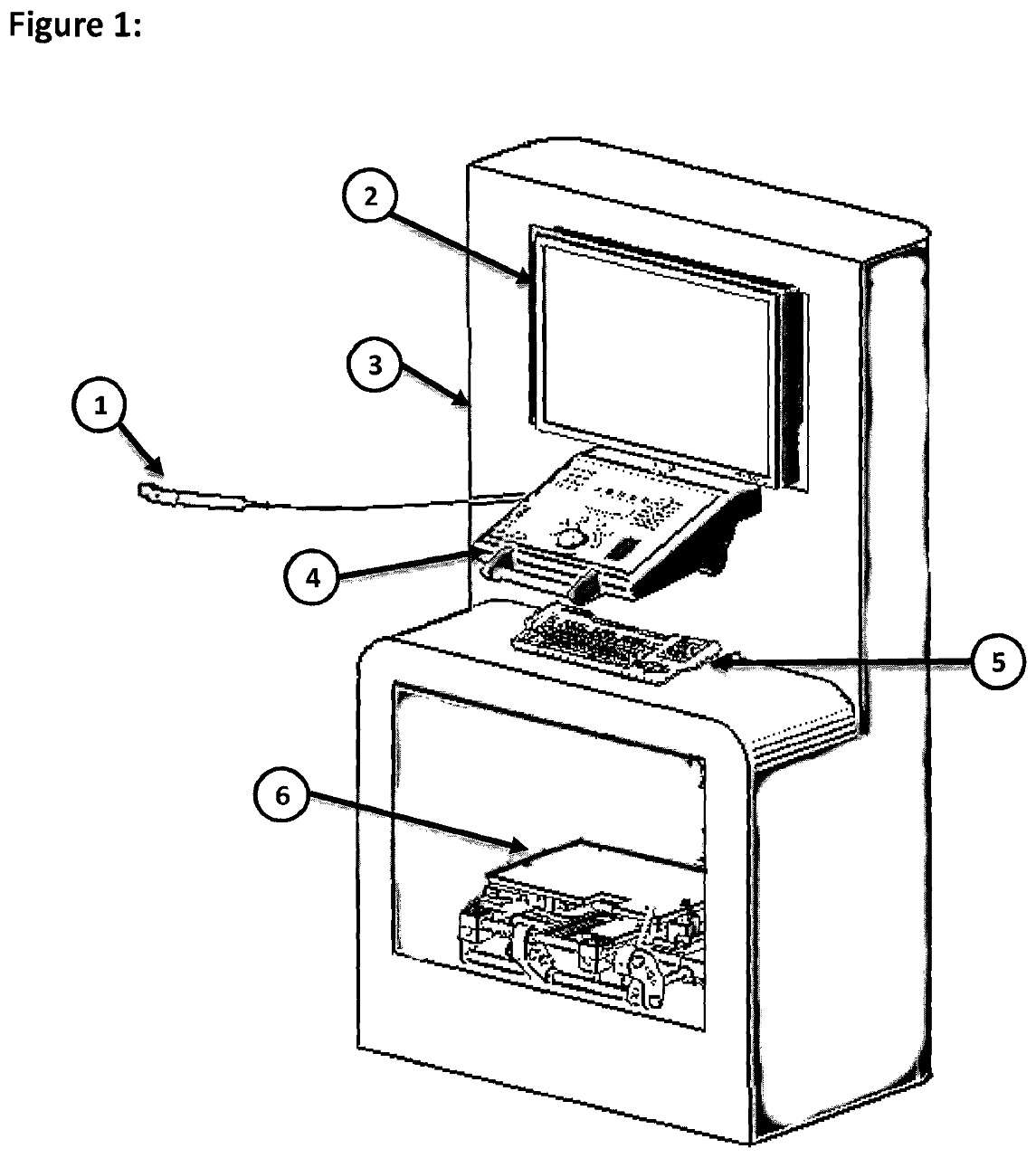
Figure 1
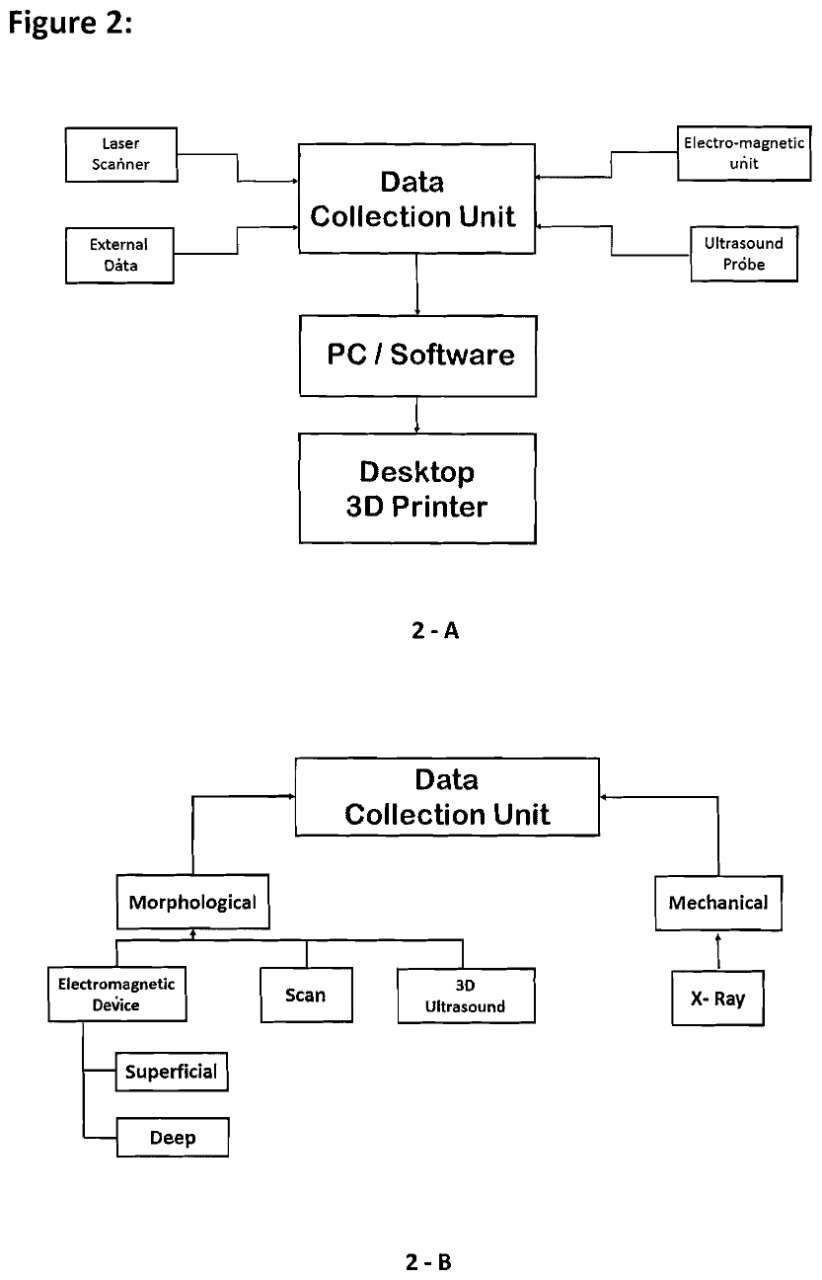
Figure 2#8035
Invited Talk: History and current practice of Patient Specific Instruments and arthroplasty
*Mahmoud Hafez - October 6 University - October 6 City, Egypt
*Email: mhafez@msn.com
#7777
Where Does the Wear of a Dual Mobility Hip Come From, Outer or Inner Articulation?
*Hani Haider - UNMC - Omaha, USA
Joel Weisenburger - The University of Nebraska Medical Center - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
Ryan Siskey - Exponent - Philadelphia, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
*Email: hhaider@unmc.edu
Dual Mobility (DM) Total Hip Replacements (THR) have emerged as a viable option in primaries and when revision surgery is necessary for improved range of motion with less dislocation risk. A DM THR consists of a small femoral head captive within a mobile ultra-high molecular weight polyethylene (UHMWPE) liner which articulates against a hard, fixed acetabular liner. This in vitro hip simulator study investigated the wear rates of UHMWPE bearing components from DM and fixed-bearing (FB) THRs that have been highly crosslinked (HXL) and stabilized with vitamin E to preserve mechanical properties. We introduced novel methods to simulate/isolate and measure the wear from the inner and outer articulations of a DM. Finally, the DM wear rates are compared to those of fixed bearing controls.
12 hips were tested, in four different groups (n=3 each), 1 FB and 3 DM groups. The DM groups were as follows: fully dual mobility articulations, outer articulation surfaces allowed only, and inner articulation only (Fig.1). All DM groups had inner 28mm CoCr femoral heads, while the FB had 44mm dia. heads. The UHMWPE components in all groups were made from GUR1020E 150KGy UHMWPE (very high HXL). The DM and outer articulation UHMWPE bearings had identical 58mm outer dia.
Testing was conducted on a 12-station hip simulator (AMTI, Boston). The specimens were mounted in a physiologically correct manner, lubricated with bovine serum (30g/L protein, 37°C) and subjected to the walking cycle specified in ISO-14242-1 at 1Hz up to 10million cycles (Mc). The UHMWPE bearings were carefully cleaned and weighed at standard intervals and corrected with the weight gain of active soak control bearings.
The bearings showed extremely low wear in general compared to other in-house tests. The isolated outer articulation group showed the highest wear (7.49±0.431mg/Mc, Fig.2) with clear elliptical scratches appearing on the CoCr acetabular liners. The wear of this group was significantly higher than the other three groups. The FB group was the next highest wearing (5.32±0.391mg/Mc) which differed significantly from the other groups. The inner articulation group was the next highest wearing (1.04±0.060mg/Mc) followed by the full DM design showing the lowest wear of all designs tested (0.362±0.602mg/Mc) but not significantly lower than the isolated inner design (p=0.190).
The custom fixtures successfully isolated the inner and outer articulations, allowing full wear characterization of the DM design. The low wearing DM group was surprising, as it had an additional large outer articulating surface on which to wear. Since the DM and isolated inner groups showed wear that was nearly identical, it is likely that most of the DM wear originated from the inner articulation, rather than outer. We speculate that the DM mobile liners predominately moved together with the CoCr acetabular liner, so little/no outer articulation was taking place. Additionally, the full DM possibly allowed for some decoupling of the rotations which resulted in less cross-shear. This likely is why the DM group showed (insignificantly) less wear than the isolated inner group. Perhaps concerns with DM hips having large outer articulating surfaces are unfounded.
Figures
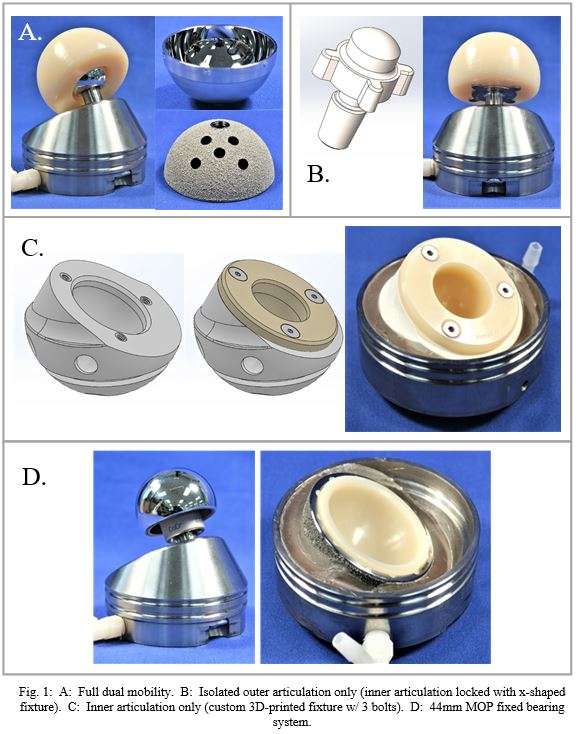
Figure 1
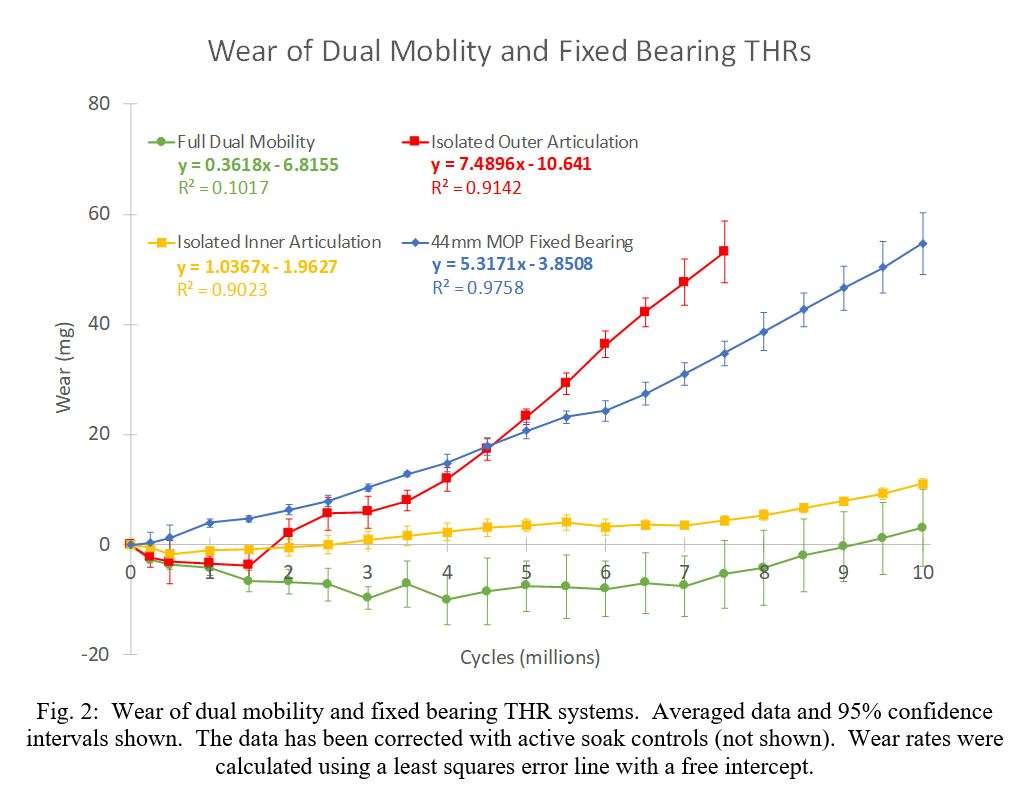
Figure 2#7985
Assessing Contact Stresses in TKR With Pressure Sensitive Film: Is It Reliable?
*Hani Haider - UNMC - Omaha, USA
Max Twedt - UNMC - Omaha, USA
Joel Weisenburger - The University of Nebraska Medical Center - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
*Email: hhaider@unmc.edu
Understanding how stresses are distributed across the ultra-high molecular weight polyethylene (UHMWPE) tibial bearing surfaces of a total knee replacement (TKR) is vital prior to clinical use. If stresses are excessively high or the contact area is too large, high UHMWPE wear can occur leading to implant failure. A method to determine contact area/stress uses thin, pressure-sensitive film placed between the femoral and tibial components and then engaging the components under known loads. The film has a layer of small color-forming capsules which break open under mechanical stress, releasing a chemical that reacts with an adjacent developer layer which chemically reacts and changes color. The intensity of color corresponds directly to the pressure applied. This reacted area is then digitized/scanned alongside a calibration sheet to determine color density, which is then converted to pressure. This study investigates sources of error and tests methods of correction to improve accuracy in TKR contact stress tests.
Three flat ½ in diameter highly-polished CoCr discs were used to apply load to the films. Ten loads were selected along the range of “medium” range film (10-50 MPa range) and were applied for 5 seconds through a single-axis MTS Mini Bionix test frame. The reacted film was scanned alongside the provided calibration sheet using an Epson V600 scanner. Scans were completed with various DPI and color correction settings and analyzed using our newly developed image analysis software. Scans were completed with no image processing by the scanning software and then analyzed with MATLAB (Fig. 1). Calibration stamps that did not saturate the film were selected to realign results by a scalar factor to account for uncontrolled differences in the scanner or the film. Reference standards defined by the international commission of illumination that are compared in this study are the CIELAB and the CIELUV color spaces, as well as the HSV and RGB color models. The percent of the film that reacted and percent error in forces were used in a regression analysis to determine the best color compression model.
The regression analysis results are shown in Table 1 including data from 30 samples. Color compression methods produced repeatable results, regardless of scanner settings and image encoding methods. Methods that showed high degrees of accuracy were CIELUV Luminance, CIELAB Luminance, CIELAB red/green channel, and HSV Saturation. RGB Red channel did not perform well due to its high speckle patterns leading to a large error in measured contact area. Representative data is included to show percentage errors in calculated force greater than 75% of the film reacted.
Our results align with the theoretical basis for the color spaces where CIELAB is designed for perceived color, CIELUV is used for produced colorations, and HSV is useful for relative differences in color. This study indicates that using the CIELAB red/green channel produces that highest accuracy when measuring forces. Future work may involve combining color spaces to produce greater resolution between applied forces as well as quantifying or modeling forces outside of the prescribed range of the actively used film.
Figures
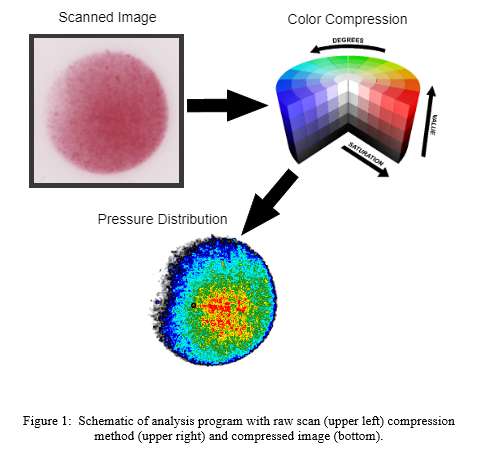
Figure 1
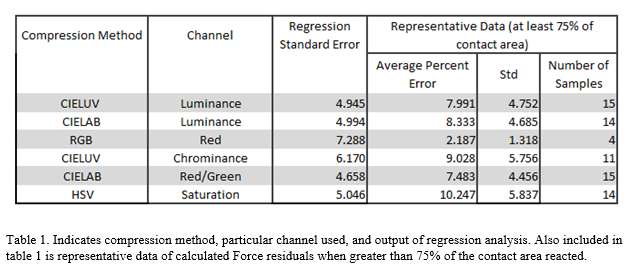
Figure 2#7593
MOP Patients With High ALVAL Tissue Scores Had CoCrMo Femoral Heads Exhibiting a Chemical Attack of Preferential Corrosion Sites
*Deborah Hall - Rush University Medical Center - Chicago, USA
Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Jennifer Wright - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: deborah_hall@rush.edu
Introduction: Fretting-corrosion at modular THA taper junctions can manifest in the form of different damage modes and subsequent cellular responses to corrosion products that vary greatly among patients. Cellular responses can range from an innate macrophage response to lymphocyte-dominated adverse local tissue reactions (ALTRs). Among the most severe damage modes occurring in corroded head tapers are imprinting (mechanically-driven) and column damage (chemically-driven). Column damage is dictated by molybdenum-poor segregation bands within the alloy that can preferentially corrode with greater volume loss compared to heads with only mechanically-dominated fretting damage. The purpose of this study was to evaluate joint capsule specimens from patients with MoP THA for cellular response and degree of ALTR, and determine their association with the occurrence of imprinting and column damage modes within the tapers of corresponding CoCrMo femoral heads.
Methods: The study entailed retrieved joint pseudocapsule and wrought CoCrMo femoral heads from 70 patients with MOP THA (36 collected at revision surgery and 34 postmortem). H&E sections of pseudocapsule were evaluated for the extent and type cellular response and scored for the overall number of macrophages, giant cells, lymphocytes, plasmacytes, eosinophils, and neutrophils. The tissues were also given an ALVAL score. CoCrMo head tapers were visually scored using a modified Goldberg score (1=minimal to 4=severe). Tapers demonstrating more than minimal damage were sectioned and global damage patterns were characterized using SEM. Patients were divided into 3 head taper damage groups: 1) Column Damage, 2) Imprinting, 3) None (Figure 1). Comparisons were made using Kruskal-Wallis and Mann-Whitney tests.
Results: A dominant macrophage response was observed in 39% of the 70 joint capsule specimens, 36% had a lymphocyte-dominated response and 26% had a mild cellular response. Thirty-nine percent of the modular heads received a damage score 4 and 37% received a damage score of 1. Overall, 40% of heads exhibited imprinting of stem taper topography into the head taper surface, 26% showed column damage and 34% had no damage. Head tapers with column damage had significantly higher ALVAL scores and perivascular lymphocyte scores compared to imprinted tapers or heads with no damage (p≤0.003) (Figure 2). Heads with imprinting also had significantly higher ALVAL and perivascular lymphocyte scores compared to heads with no damage (p≤0.019). Particle-laden macrophage scores were similar between the damage groups.
Conclusion: Lymphocyte-dominated ALTRs were associated with a chemical attack of preferential corrosion sites (i.e. column damage) within CoCrMo head tapers in MoP THA. This finding may be explained with the higher material loss observed in column damage cases compared to those with no damage or fretting-corrosion only. However, even the reported median material loss of 1.2 mm3 in cases with column damage is small compared to wear volumes of up to 250 mm3 in MoM THA. Yet, MoP and MoM can exhibit lymphocyte-dominated ALTRs, raising the question if the nature of the generated corrosion products under chemically vs. mechanically-dominated damage modes dictates the nature and severity of the tissue response, rather than the quantity of material loss generated from the CoCrMo head taper.
Figures
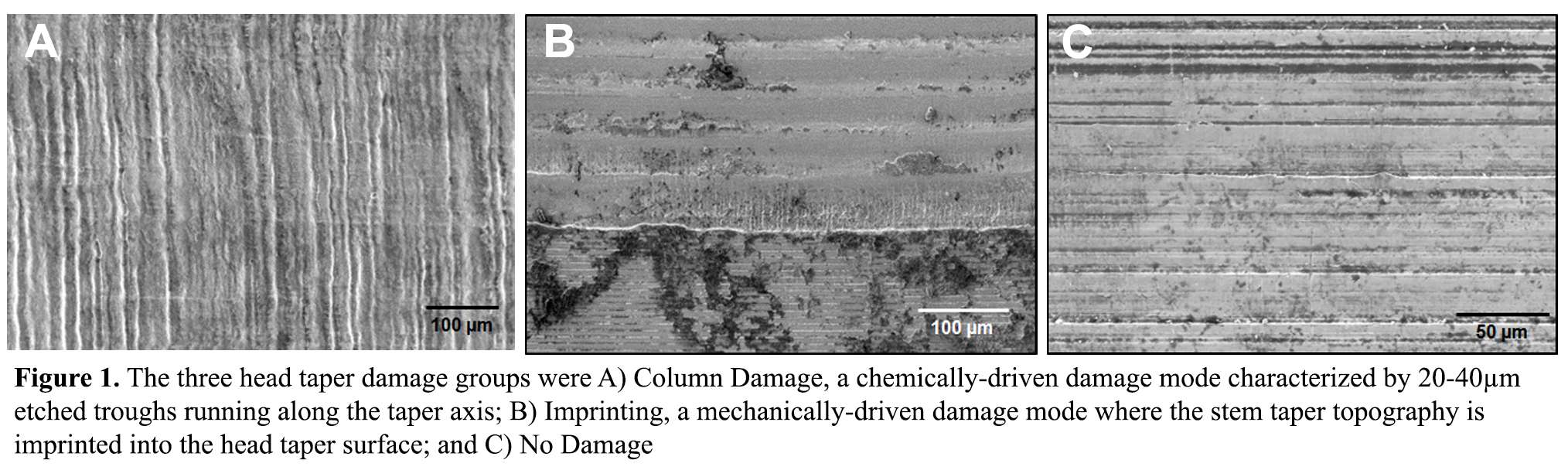
Figure 1
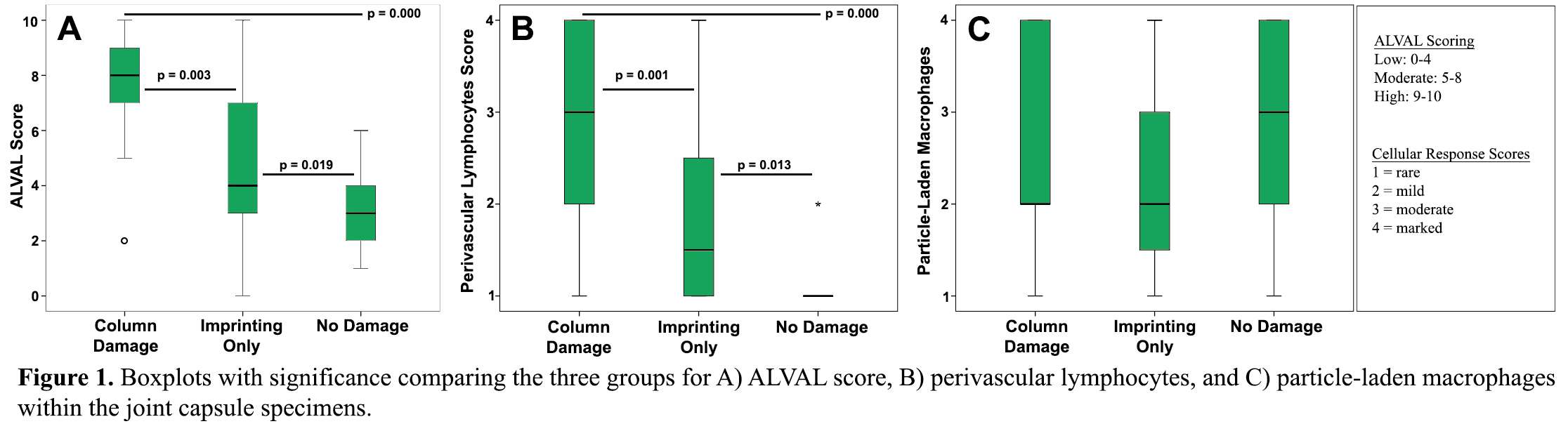
Figure 2#7702
Preclinical Evaluation of an Active Osseointegrative Implant in a Bioreactor
*Thomas Hall - Imperial College London - London, United Kingdom
Konstantinos Theodoridis - Imperial College London - London, United Kingdom
Nupur Kohli - Khalifa University - Abu Dhabi, United Arab Emirates
Benjamin Lovat - Imperial College London - London, United Kingdom
Frederic Cegla - Imperial College London - London, United Kingdom
Richard van Arkel - Imperial College London - London, United Kingdom
*Email: thomas.hall14@imperial.ac.uk
INTRODUCTION: Cementless fixation, also referred to as osseointegration, harnesses the innate regenerative properties of bone to establish a direct structural and functional connection between the implant and the host bone1. In passive implants, this process is dependent on the implant surface chemistry, topography, and loading environment, which modulate the host inflammatory response and promote bone remodeling2,3. Recently, there has been interest in active osseointegrative implants, which use controllable biophysical stimuli to enhance and accelerate bone formation in periprosthetic tissue4–6. This study uses an ex vivo bioreactor model to investigate the effects of an active osseointegrative implant under regulated conditions whilst preserving the natural cellular diversity and extracellular structure.
METHODS: Fresh cancellous bone cylinders (n = 24; Ø10 mm x 5 mm) were extracted from distal porcine femora. The specimens were held in contact with additive-manufactured, surface-roughened titanium discs (cp-Ti; Ra = 75 µm; Ø10 mm x 3 mm) under light static load, submerged in cell culture medium (DMEM + 10% FBS + 1% P/S) and incubated within five hours of euthanization. Specimens were rested for 24 hours before undergoing 21 days of active (n = 12) or passive (n = 12) culture in the bioreactor. Calcium-binding fluorophores (Calcein/Alizarin Red S) were administered to the specimens via the media (50 µg/ml) on the seventh and fourteenth days of culture, and removed after 24 hours. At termination, specimens were separated at the implant-bone interface. Ongrowth onto the titanium implants was visualized using fluorescent widefield microscopy and scanning electron microscopy (SEM). The effects of active stimulation on the bone were evaluated by monitoring calcium levels in the media and conducting histology (H&E; Masson-Goldner Trichrome; Movat Pentachrome; Picrosirius Red).
RESULTS: Cell viability was maintained throughout the 21-day culture period in all specimens. Superior ongrowth of tissue onto the titanium discs during culture was observed in the actively stimulated specimens (Fig. 1), which was further supported by evidence of fibrous extracellular matrix deposition and mineralization from the endpoint SEM imaging. Moreover, histological analyses revealed increased bone remodeling at the implant-bone interface in the actively stimulated specimens compared to the passive controls.
CONCLUSION: Enhanced osseointegrative properties were observed at tissue level when an actively stimulated implant was evaluated in a bioreactor. The ex vivo model provided supportive evidence to osteogenic effects that had previously been observed in simple cell cultures4–6, thereby advancing the clinical readiness of this technology.
ACKNOWLEDGEMENTS: This research was supported by the Engineering and Physical Sciences Research Council (EPSRC) through a Doctoral Training Account award and Grant EP/S022546/1.
REFERENCES:
1. Shah et al. Acta Biomater. 2019;84:1–15.
2. Albrektsson and Wennerberg. Clin Implant Dent Relat Re. 2019;21(S1):4–7.
3. Kohli et al. Sci Rep. 2021;11(1):1–11.
4. Dos Santos et al. Sci Rep. 2016;6(1):1–15.
5. Gittens et al. Bioelectromagnetics. 2013;34(8):599–612.
6. Pettersen et al. Sci Rep. 2021;11(1):1–8.
Figures
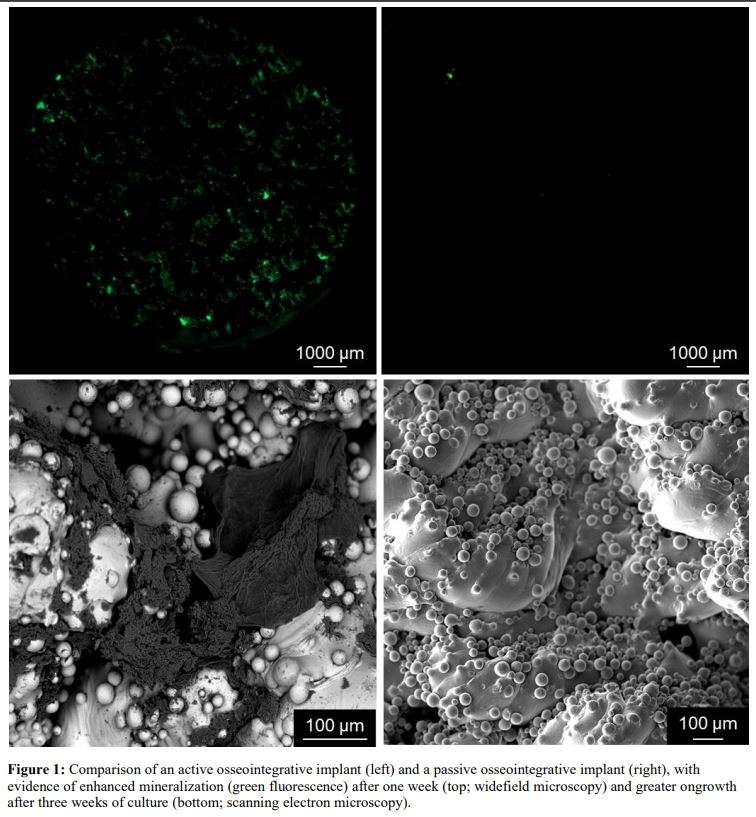
Figure 1#7705
Wireless, Battery-Free Smart Implants for on-Demand Implant Fixation Monitoring
*Thomas Hall - Imperial College London - London, United Kingdom
Frederic Cegla - Imperial College London - London, United Kingdom
Richard van Arkel - Imperial College London - London, United Kingdom
*Email: thomas.hall14@imperial.ac.uk
INTRODUCTION: The field of orthopaedics has been using sensor-embedded implants for several decades to generate valuable information for orthopaedic research1–3, whilst clearance for a mass-market instrumented implant was only granted by the FDA for the first time in 20214. One of the challenges faced by designers has been minimizing the overall size and cost of the onboard circuitry used for power, communication, sensing, and processing, with inflated architectures having been associated with increased bone loss5. Batteries, in particular, have limited power reserves and increase device size, but can be offloaded when using passive interrogation techniques. This study investigated the consistency of battery-free, on-demand measurements from a commercial unicondylar knee replacement, which can be used to detect implant-cement debonding.
METHODS: The tibial component of a commercial unicondylar knee replacement was instrumented with a single-element sensor (volume: <5 mm3) and an inductive coil, establishing a communications link to an external reader. The instrumented implant was used to measure implant fixation in four conditions: well-fixed, partially debonded, fully debonded in situ, and fully debonded with migration. Sensitivity to reader alignment was quantified with respect to translation (posteroanterior, mediolateral, and caudocranial directions; range: −10 to +10 mm) and rotation (coronal and sagittal planes; range: −10 to +10 °), whilst sensitivity to femoral component positioning and musculoskeletal tissue (porcine) were also quantified.
RESULTS: The implant fixation measurement (acquisition rime: 1 s) rose with respect to the well-fixed measurement when partially debonded (+7.1%), fully debonded in situ (+6.3%), and fully debonded with migration (+6.4%) (Fig. 1); the maximum deviation in all of the reader positions was +0.7% (Fig. 2). Mean deviations caused by the femoral component position and musculoskeletal tissue were <0.5%. The maximum drops in signal-to-noise ratio due to reader position (−4.1 dB), component position (−1.6 dB) and anatomy (+0.5 dB) were small and could be counteracted by extended measurement intervals (~20 dB per decade increase in acquisition time).
CONCLUSION: This study has demonstrated that is possible to robustly detect implant-cement debonding on a commercial implant with only two embedded components: a sensor and a coil. Moreover, the wireless, battery-free architecture has a small onboard footprint and concomitant cost; it is therefore applicable as a platform technology to multiple implant designs.
ACKNOWLEDGEMENTS: This research was supported by the Engineering and Physical Sciences Research Council (EPSRC) through a Doctoral Training Account award. Implants used in this research were provided by Zimmer Biomet.
REFERENCES:
1. Rydell. Acta Orthop Scand. 1966;37(Suppl. 88):1–132.
2. Waugh. Acta Orthop Scand. 196637(Suppl. 93):1–87
3. Graichen and Bergmann. J Biomed Eng. 1991;13(5):370–4.
4. Food and Drug Administration. DEN200064 Aug 27, 2021.
5. Martin et al. J Arthroplasty. 2017;32(1):79–82.
Figures
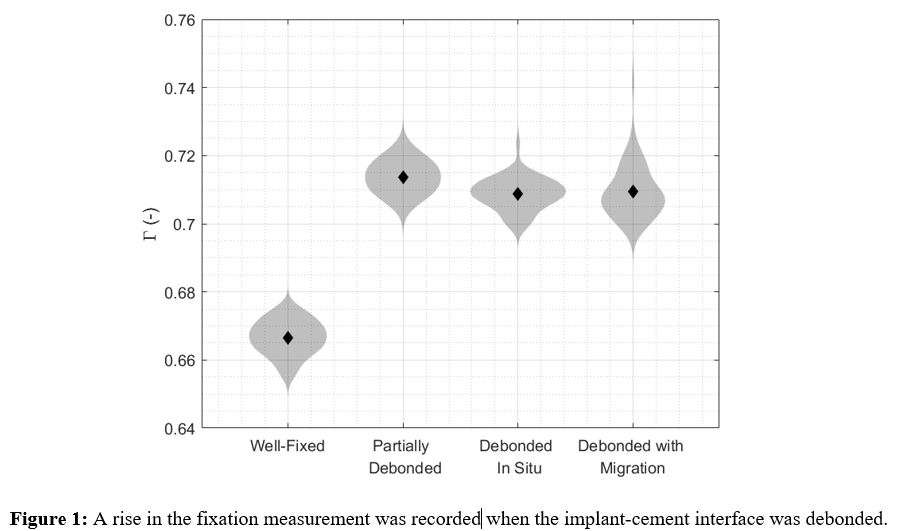
Figure 1
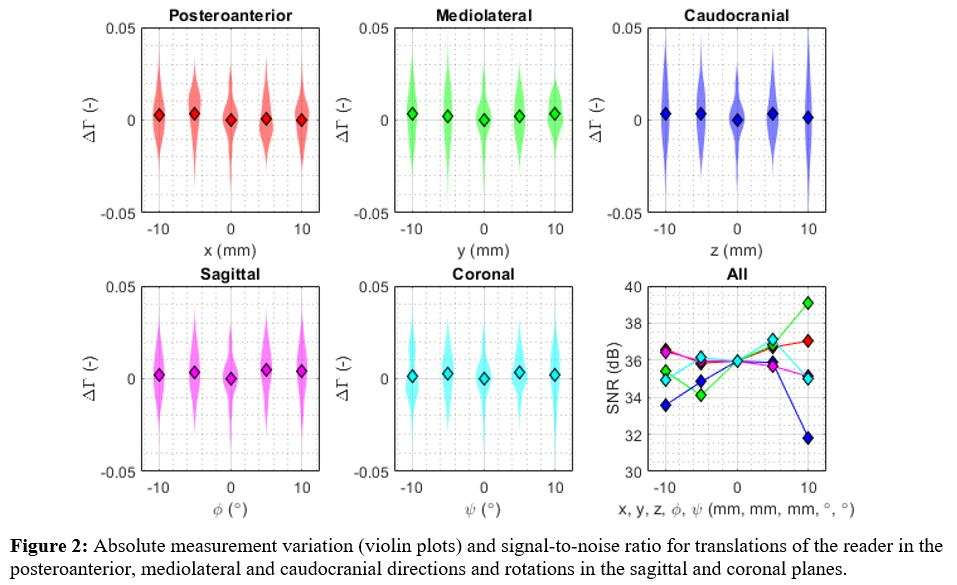
Figure 2#7771
Successful Long-Term Bone Ingrowth and Minimal Polyethylene Wear of Bilateral MOP THA in a Lowland Gorilla Compared to Human Postmortem Retrievals
*Deborah Hall - Rush University Medical Center - Chicago, USA
Thomas M. Turner - Rush University Medical Center - Chicago, USA
Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Jennifer Wright - Rush University Medical Center - Chicago, USA
Robert Urban - Rush Medical Center - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: deborah_hall@rush.edu
Introduction: In 1986, a lowland gorilla living in an accredited zoological park received bilateral MOP THA for severe osteoarthritis by board-certified orthopedic surgeons. Implanted into both hips were a cemented CoCrMo femoral stem with CoCrMo modular head and a c.p. titanium porous coated acetabular component with conventional UHMWPE liner. The gorilla did well with her hips for 22 years until death at age 47 in 2008 due to respiratory and cardiac arrest following anesthesia for uterine surgery. The purpose of this study was to investigate the long-term performance of these bilateral implants with regard to implant fixation and PE wear and to compare these values to 3 bilateral human postmortem cases.
Methods: The proximal femurs and acetabular bone with in situ implants were harvested postmortem and contact radiographs were made. The overall extent of tissues within the porous coating and at the implant-bone interface was quantified by pointcounting of plastic embedded, undecalcified, stained sections using light microscopy. PE bearing surface wear was quantified with an optical coordinate-measuring-machine (OrthoLux, RedLux). Three bilateral postmortem patients hosting identical components were selected for comparison. The mean time in situ for the human subjects was 5 years, with implantation between 1984 and 1987. Data was collected using the same methods as the gorilla.
Results: There was excellent bone ingrowth into the porous coating (L:70%, R:51%) and at the interface (L:71%, R:57%) for both acetabular components (Figure 1). Fibrous tissue was greater on the right side. Particle-induced macrophage responses within the coating/at the interface were minimal (≤ 2%). For the bilateral human cohort, mean extent of bone was 27% in the coating and 36% at the interface. On contact radiographs, the femoral components appeared well fixed with no radiolucencies or osteolysis apparent. Both PE liners exhibited symmetric wear scars that did not have the same characteristic “kidney bean” shape known from surgically retrieved PE liners of that generation (Figure 2). The left and right PE liners had a wear volume of 152.33 and 124.82 mm3, respectively. The corresponding wear rates were 6.92 and 5.67 mm3/year compared to 28.39±15.6 mm3 and 30.49±25.24 mm3 in the bilateral patient cohort with the same implant type (Figure 3).
Conclusion: The gorilla tolerated the implant well with excellent osseointegration and low PE wear. Although differences between human and great ape bone metabolism are not fully understood, the gorilla had considerably more bone ingrowth than the human cohort, or previously published postmortem porous acetabular data (mean 33%)(Figure 1). The difference in wear scar between the gorilla and the patient cohort can likely be explain by differences in motion and loading patterns associated with gait. The lower PE wear rate can be explained by low activity in a caged environment, and the fact that gorillas use their arms during gait for most activities. Nonetheless, the PE debris burden did not cause any local tissue reactions. The bilateral THA surgery enabled the gorilla to live a life free of osteoarthritis pain for 22 years and can therefore be considered a great success.
Figures
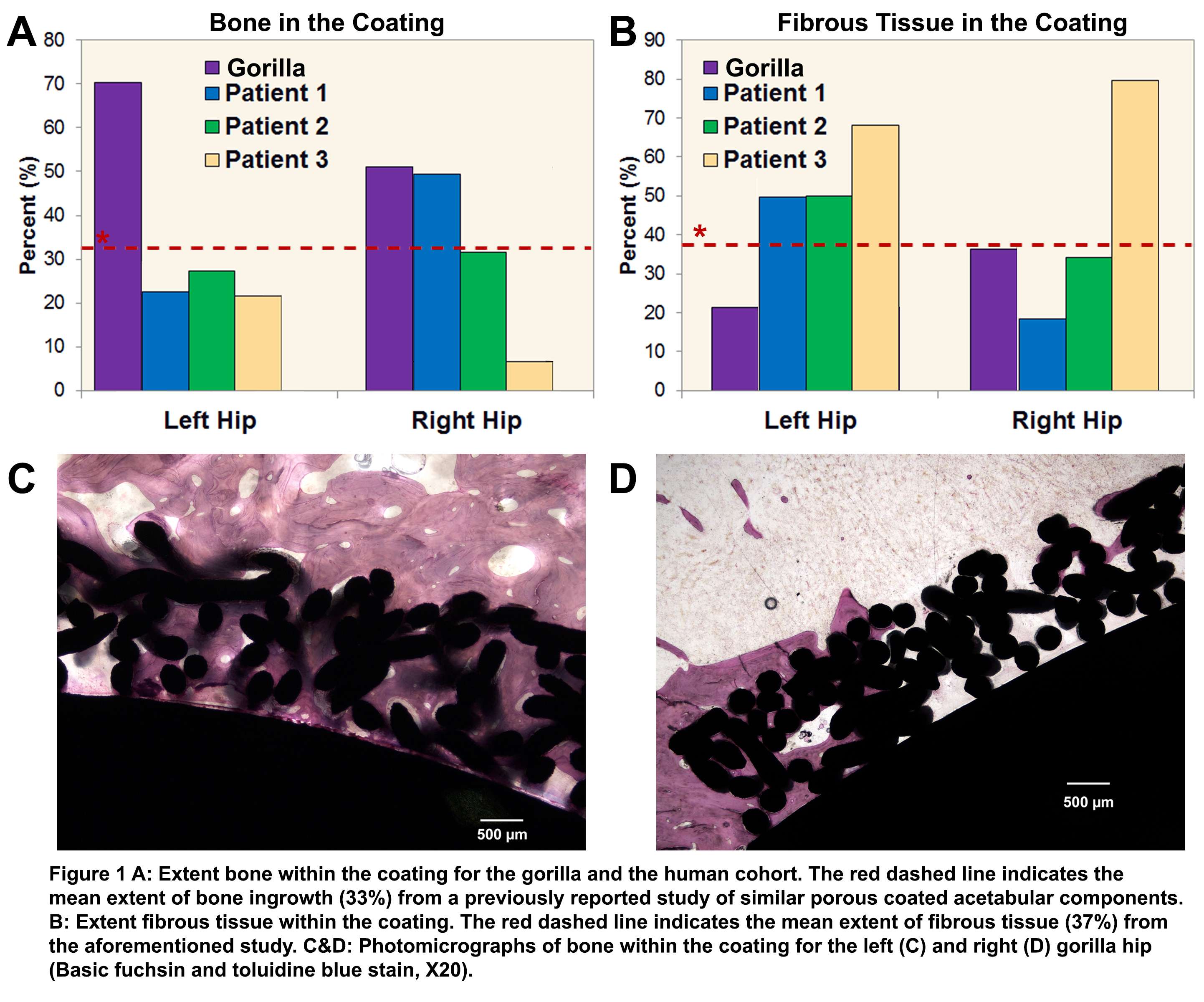
Figure 1
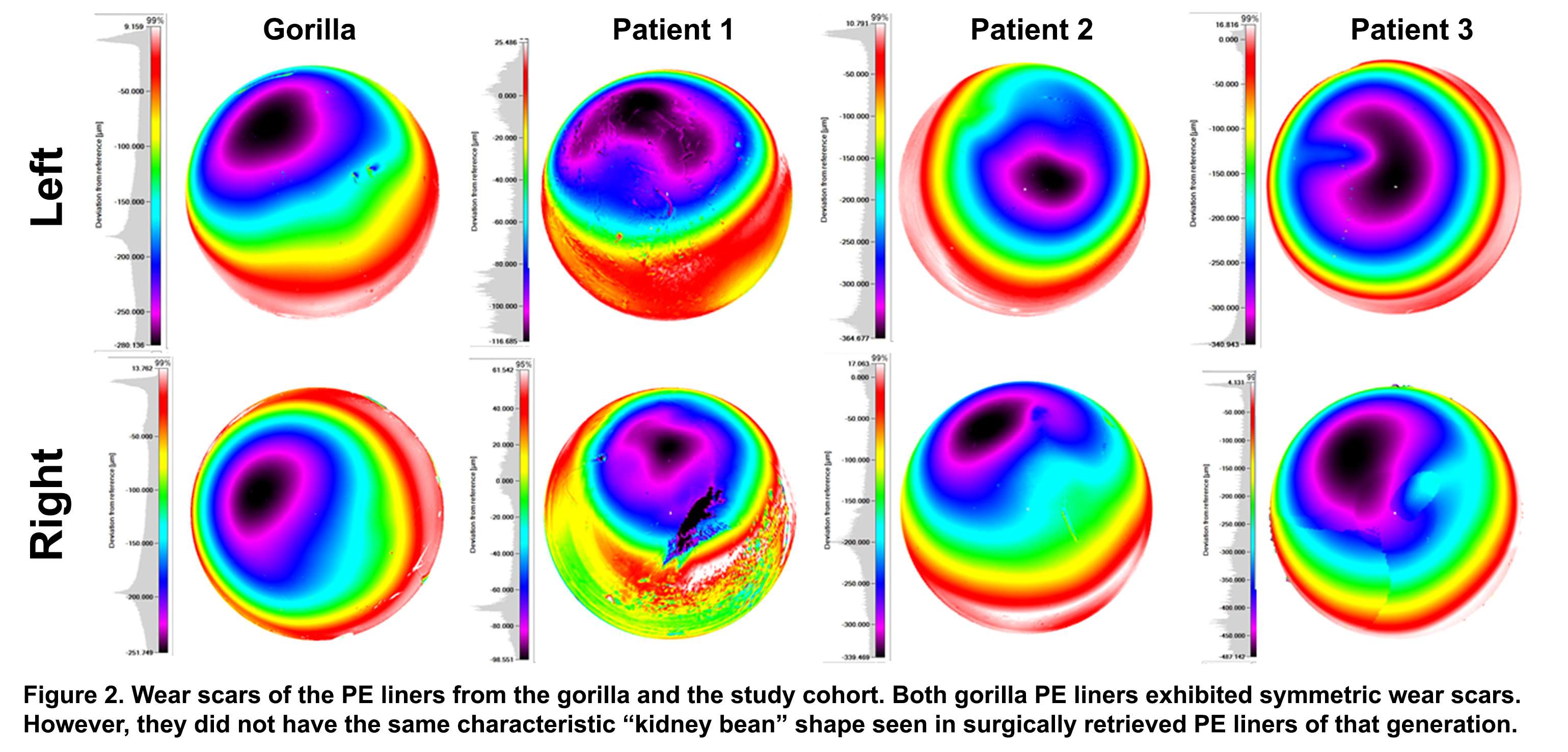
Figure 2
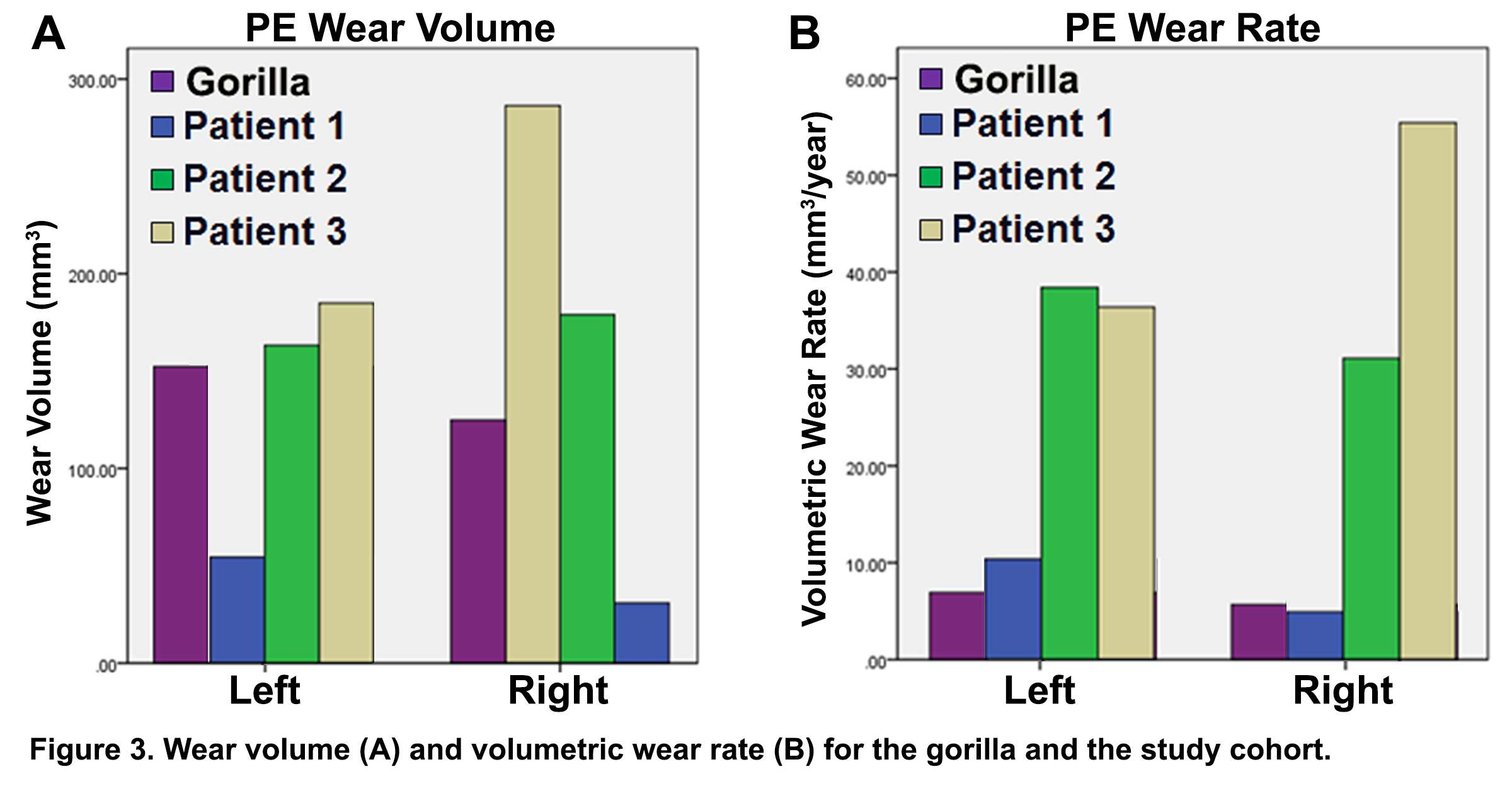
Figure 3#7452
Kinematic Comparison of Medial Pivot Total Knee Arthroplasty and Non-Symptomatic Controls
*Landon Hamilton - University of Denver - Denver, United States of America
Kevin Shelburne - University of Denver - Denver, USA
Paul J. Rullkoetter - University of Denver - Denver, USA
C. Lowry Barnes - HipKnee Arkansas Foundation - Little Rock, United States
Erin M. Mannen - Boise State University - Boise, USA
*Email: landon.hamilton@du.edu
Introduction
Total-knee arthroplasty (TKA) is a surgical intervention that can relieve pain and restore function in severely disabled knee joints. The medial-pivot implant design is intended to limit anterior-posterior (AP) translation in the medial compartment while allowing translation in the lateral compartment1, approximating the motion of the native knee. Prior investigators have measured medial-pivot kinematics; each design is unique and kinematic validation is required for each implant. The purpose of our study was to compare in-vivo knee-joint kinematics using high-speed stereo radiography (HSSR) in patients who have undergone cruciate sacrificing medial-pivot TKA (Medtronic, Responsive Orthopedics) with native knee non-symptomatic, age-matched controls.
Methods
Seven TKA patients (4 female, 69.6 ± 4.4 yrs) and 8 non-symptomatic controls (4 female, 64.4 ± 8.2 yrs) performed 6 functional tasks in HSSR: deep-knee lunge, chair rise, step down, gait, gait with 90° turn, and seated knee extension. Patient-reported outcome (KOOS) was obtained pre- and post-TKA; post-TKA knee-extensor and flexor strength was measured at 70° knee flexion.
Patient-specific femoral component and tibial-tray geometries were oriented in accordance with Grood and Suntay decomposition2 while control geometries were assigned with the tibia coincident to the femur (Figure 1A). Geometries were tracked in both HSSR planes to recreate subject-specific movement in 3D space for each task (Autoscoper, Brown University; Figure 1B). Medial and lateral low points of the femoral component were identified as the lowest point relative to the transverse plane of the tibial plateau and were used to calculate medial- and lateral-compartment AP translations across the full range of motion3 (Figure 1C).
Results
Kinematic assessment occurred 17.5 ± 7.6 months post-TKA for the surgical group with patients reporting greater knee function post-surgery (KOOS: pre = 62.2 ± 7.4 [47.5, 67.2]; post = 90.2 ± 9.8 [77.8, 96.9]). Knee torque was similar between the operated and non-operated limb in knee extension (difference = -0.053 ± 0.095 Nm/kg [-0.278, 0.112]; Figure 2A) and flexion (-0.088 ± 0.071 Nm/kg [-0.233, 0.043]; Figure 2B) indicating measurable post-surgery recovery.
The emerging trend among the TKA cohort was greater AP translation for the lateral low point, relative to the medial low point, during weightbearing activities and greater medial compartment translation during non-weightbearing knee extension (Figure 3A). Despite similar trends in chair rise and lunge, the controls demonstrated greater posterior translation of the medial (-5.8 mm [-6.6, -4.9]) and lateral low point (-10 mm [-12, -9]) across 100° flexion during chair rise. Greater anterior translation of the medial compartment across 100° flexion was only observed for controls during lunge (7.2 mm [5.9, 8.4]; Figure 3B). Uniquely during knee extension, the surgical group displayed anterior translation of the medial low point (2.6 mm [1.9, 3.2]) while the controls exhibited posterior translation of the lateral low point (8.1 mm [7.2, 9.2]) for 100° flexion.
Conclusion
Our results highlight the limited medial and lateral compartment AP translation during weightbearing activities for patients who have undergone medial-pivot TKA. The trends toward lateral compartment translation exceeding medial compartment translation in weightbearing activities are consistent for the surgical group but intermittent for the non-symptomatic controls.
Figures
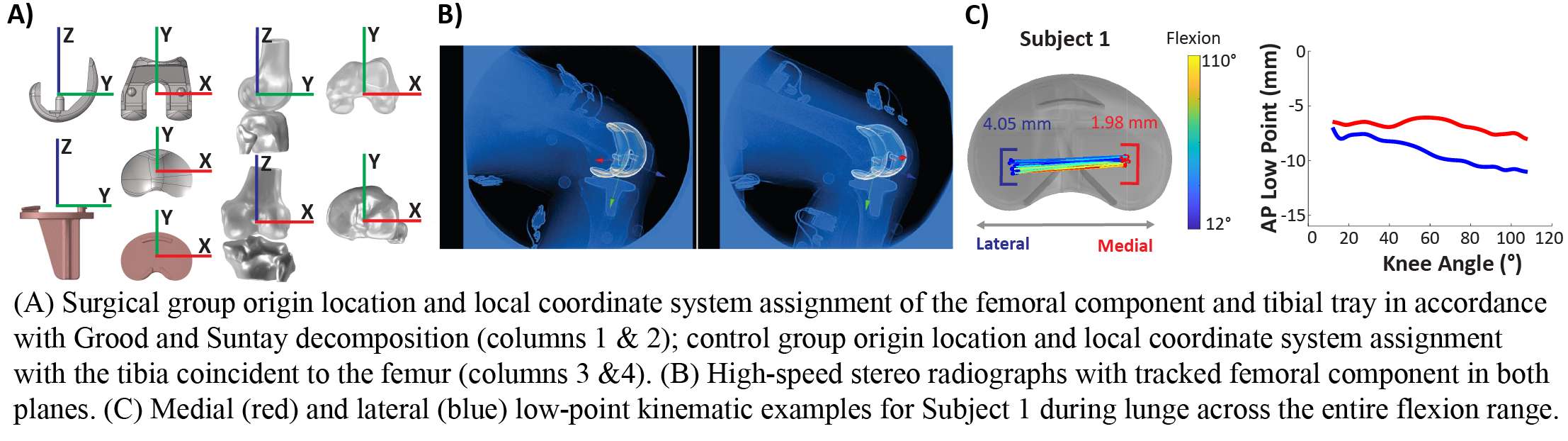
Figure 1
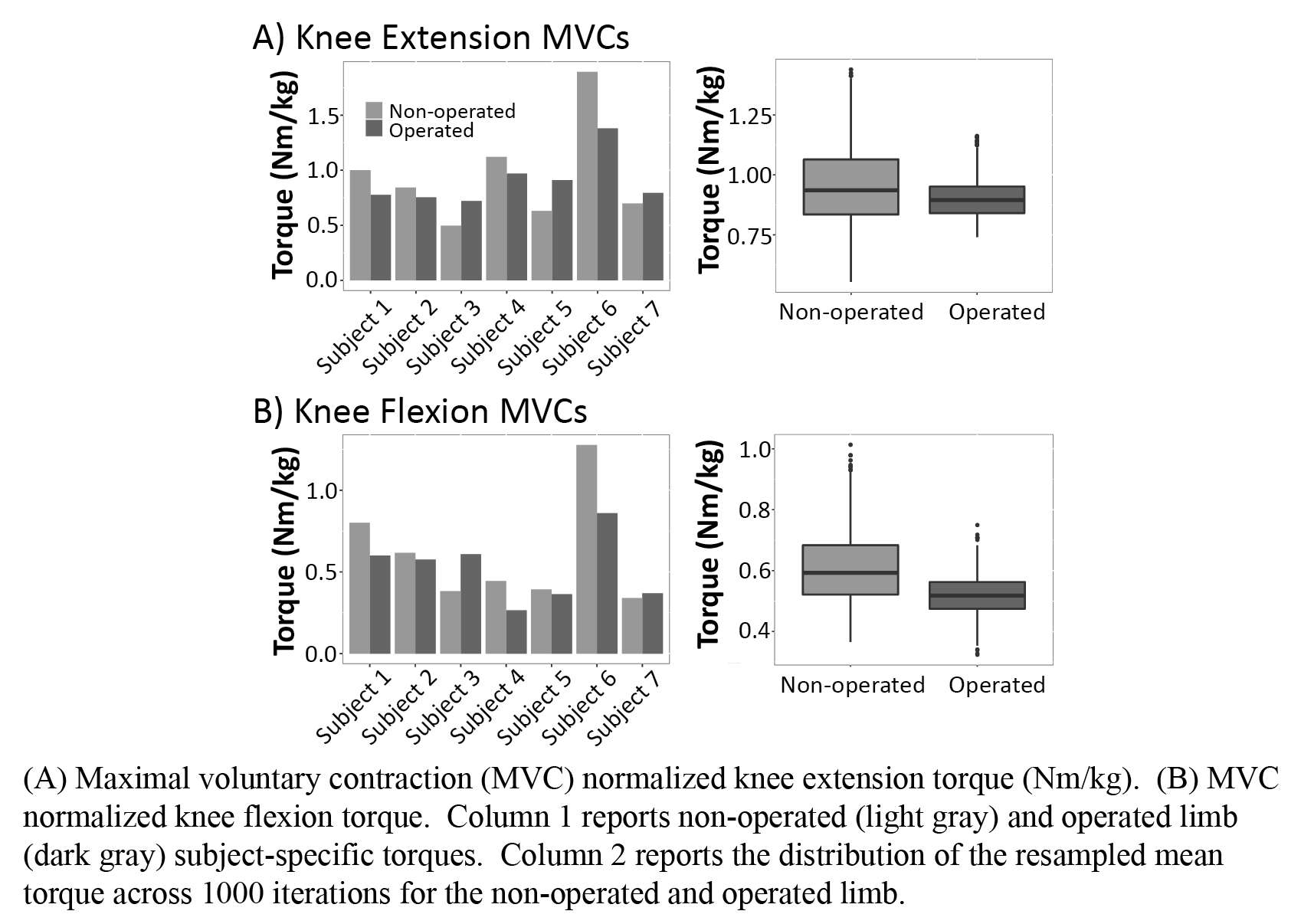
Figure 2
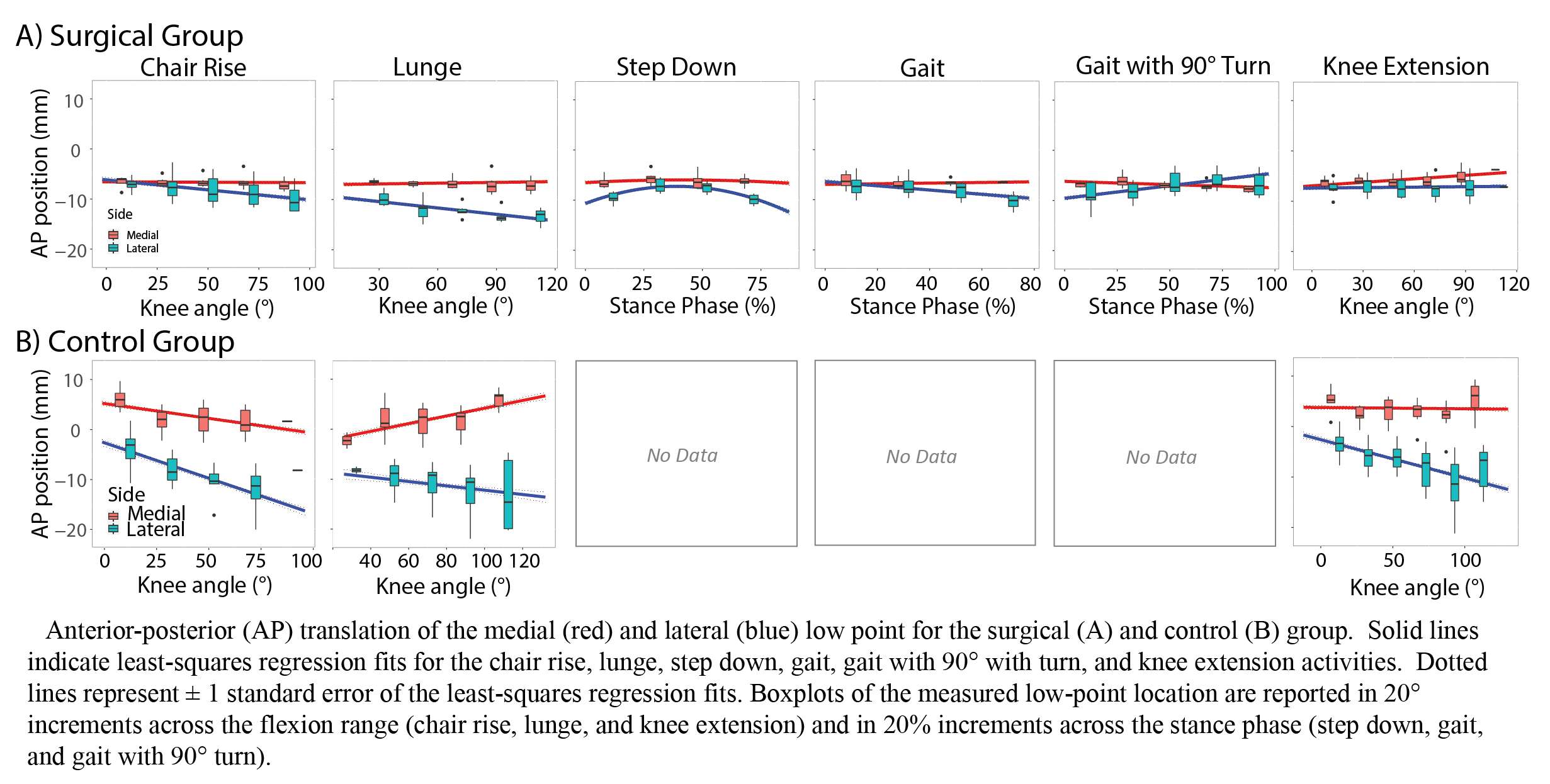
Figure 3#7948
Use of Electrophoretic Deposition in the Hospital Setting to Coat Medical Implants With Therapeutic Agents to Prevent or Treat Biomaterial Associated Infection
*John Hamilton - Rush University Medical Center - Chicago, USA
Adrienn Markovics - Rush University Medical Center - Chicago, USA
Greta Della Fara - Rush University Medical Center - Chicago, United States of America
AMANDINE IMPERGRE - Rush University Medical Center - Chicago, USA
Markus Wimmer - Rush University - Chicago, USA
*Email: john_l_hamilton@rush.edu
Introduction: Despite use of systemic antibiotic prophylaxis, biomaterial associated infections from joint replacement, spine surgery, or fracture fixation range from 0.5%–50% of cases depending on patient and surgical risk factors. Once bacterial adhesion occurs on the implant surface, bacterial biofilm formation occurs, making these bacteria resistant to the host immune response or antimicrobials. Biomaterial infections can lead to requirement of implant removal and replacement, long courses of medical treatment, as well as poor surgical outcomes and mortality. Total hospital costs for infection associated with joint replacement can often exceed $100,000. We developed a method of coating biomaterials with therapeutic agents, such as antibiotics, with electrophoretic deposition (EPD) for use in the operating room or clinical office to prevent or treat biomaterial infection.
Methods: We recently used EPD to coat medical grade titanium (Ti-6Al-4V ELI) wire. In this EPD application, we coated Ti with gentamicin antibiotic alone as well as in combination with controlled-release drug carrier chitosan. We were able to create a negative charge on the Ti surface by applying -5 V potential difference; this allowed the attraction and deposition of gentamicin and chitosan on the Ti surface due to their positive charge in solution over 5 minutes. We assessed the efficacy of EPD coating through i) assessment of amount gentamicin loaded on Ti; ii) ability to neutralize Staphylococcus aureus (S. aureus) infection in vitro; as well as iii) toxicity in osteoblast culture.
Results: Using EPD, we were able to generate more than 10x the amount of gentamicin at the Ti surface as compared to the method of air-drying a gentamicin solution over the wire. Dual coating of Ti wires with gentamicin and chitosan killed and neutralized bacterial infection with S. aureus and resulted in non-toxicity in osteoblast culture in vitro. Furthermore, dual coating with gentamicin and chitosan provided a sustained delivery of gentamicin from the Ti surface over 3 days.
Conclusion: Use of EPD led to the accumulation of gentamicin at the Ti surface within minutes, which neutralized S. aureus in vitro and was non-toxic in osteoblast culture. We believe EPD could be used for but not limited to prevention and eradication of biomaterial associated infection. While implant associated biofilms are resistant to antibiotics, recent evidence demonstrates biofilms can be eradicated if the localized concentration of antibiotic is high enough. EPD could be set up in the operating room with sterile and disposable components for coating of implant material to prevent or treat biomaterial associated infection [Figure 1 and Figure 2]. EPD could also be designed to eradicate implant associated biofilm in the clinical office setting [Figure 3]. We filed a provisional patent for use of EPD with therapeutic agents in the hospital setting. Sterilization of orthopedic implants through methods such as autoclave, which are often repeated in the hospital, would destroy most therapeutic coatings. Therefore, we believe EPD coating would often be most suitable in the hospital setting after sterilization. We are actively working on in vivo animal models of biomaterial associated infection using EPD.
Figures
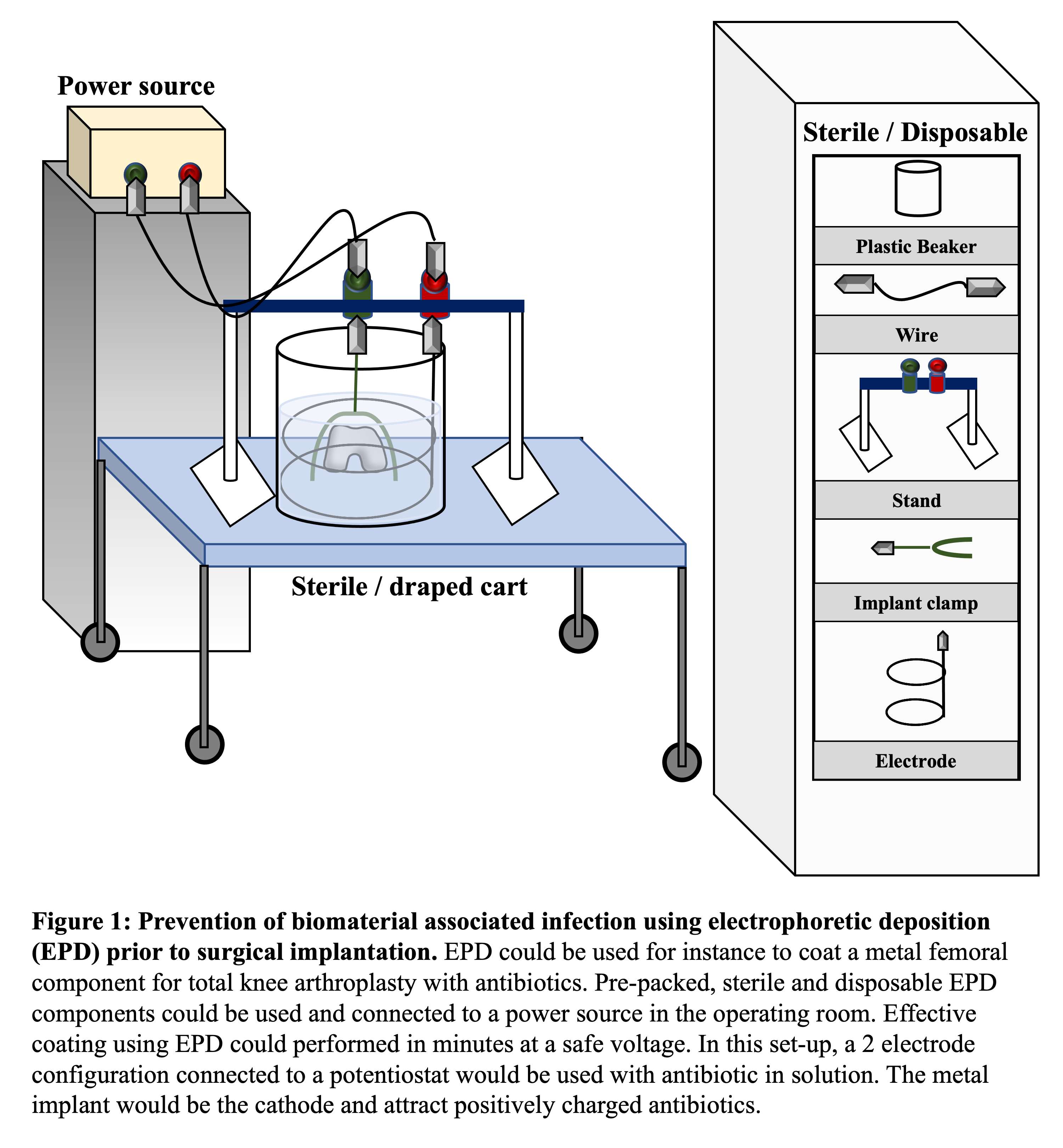
Figure 1
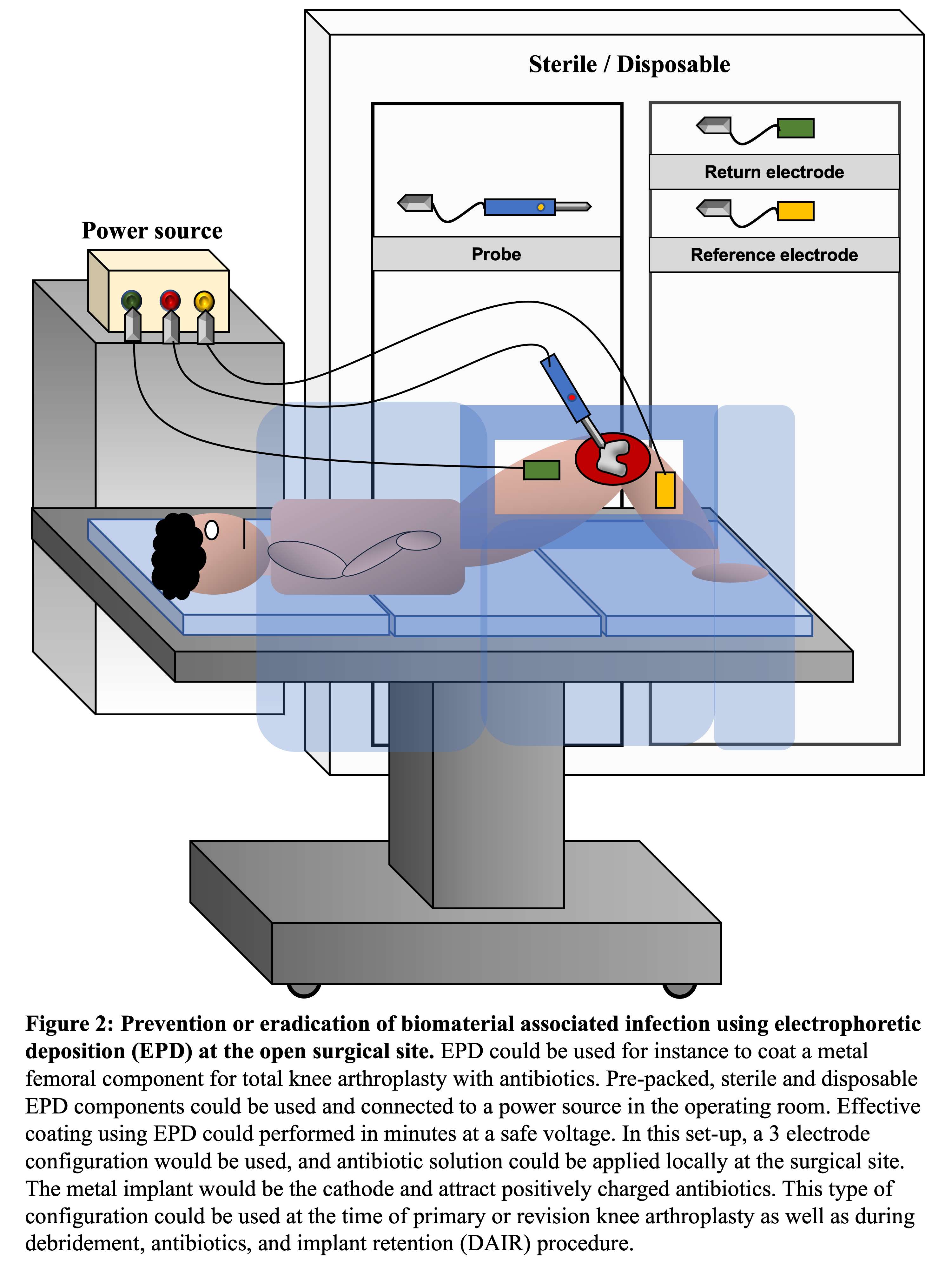
Figure 2
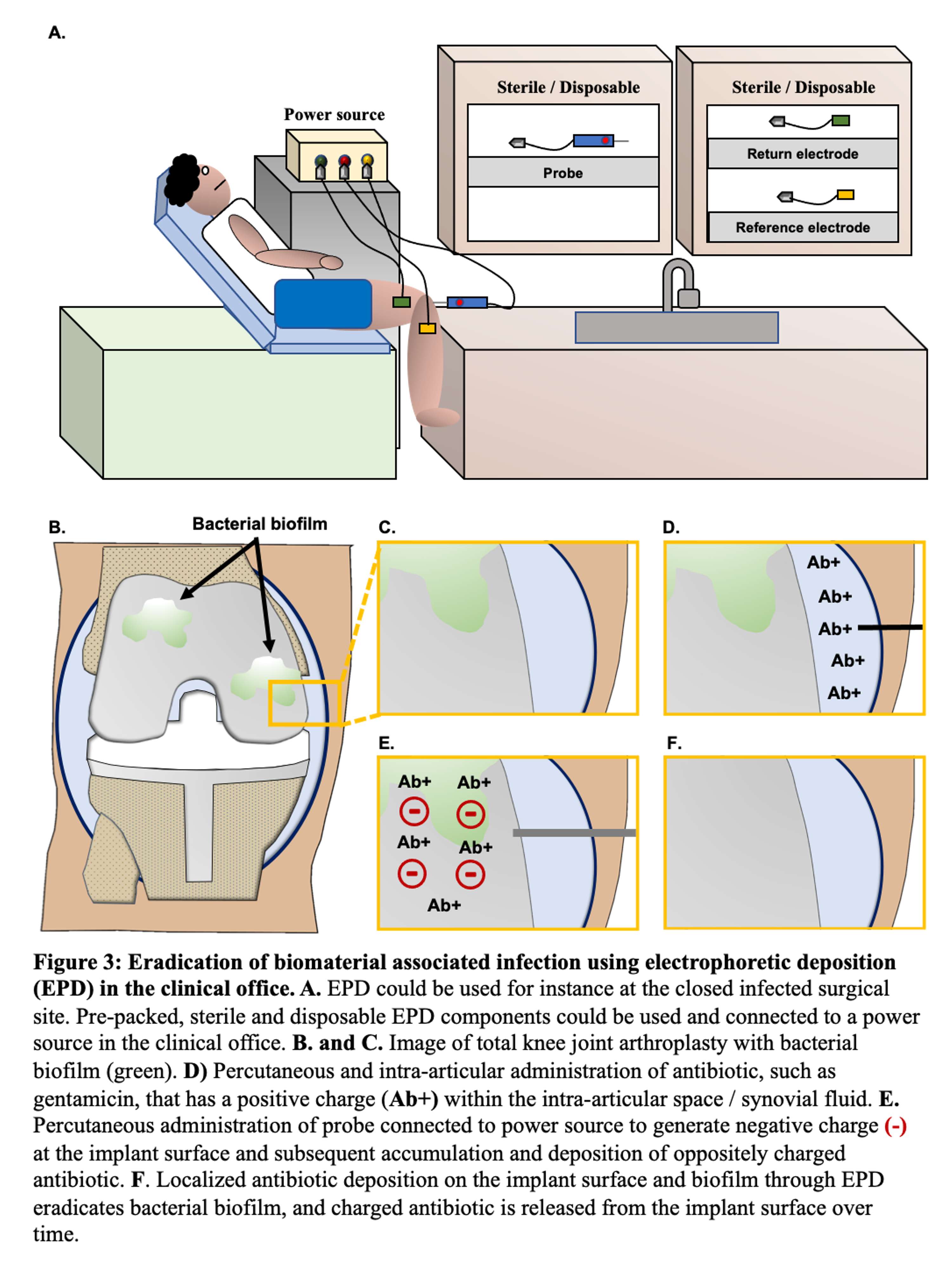
Figure 3#7878
A Sterile Barrier Reduces the Risk of Contamination of the Instrument Table During Orthopaedic Procedures
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Robert Frangie - University of Texas - Houston, United Kingdom
Hugh Jones - UT Health Science Center at Houston - Houston, USA
Jasmine Gonzalez - The Institute of Orthopedic Research and Education - Houston, USA
Shuyang Han - University of Texas Health Science Center at Houston - Houston, USA
*Email: philipnoble66@gmail.com
Introduction
Infection remains a major cause of failure of orthopedic surgeries. Within the operating room, a major threat to sterility of the surgical site is the close proximity of the sterile periphery to the sterile instrument table and surgical instruments. We performed an experimental study to determine: (i) the influence of separation of the operative staff from the instrument table on the rate of contamination, and (ii) the efficacy of a sterile transparent bonnet in mitigating contamination in the presence of activity within the operating room.
Methods
A sterile table was placed in the center of an isolated, simulated operating room. Three sets of agar plates, each having one Sabouraud (fungi) and one tryptone (bacteria), were positioned at different sites on the table. An active particle counter (AeroTrak, TSI Inc) was mounted at the center of the table and programmed to capture 2.8L/min of air (Figure 1). To simulate OR traffic, a staff member in laundered surgical scrubs walked around 3 sides of the table (3-foot separation) for 1min every 5 mins for a total of 1hr. To simulate the location of a surgical technician, the 4th edge was kept free of any traffic. The particle counter was programmed to collect 13 air samples/hr during the presence of the staff member within the test facility. The experimental procedure was repeated with: (i) the same staff member walking along a path 1-foot from the instrument table and (ii) exposure of the agar plates for one-hour in a closed room without traffic (control exposure). The procedures performed with a 1- and 3-foot separation were repeated with the addition of a bonnet-type barrier to the instrument table. The barrier consisted of a sterile transparent drape mounted on an aluminum frame shielding the instruments from three sides and above. One side was left open to allow the surgical technician to access the instruments. Contamination rates and particle counts were compared using Student’s t-test (p< 0.05).
Results
Compared to the control (52±16 CFUs/m2/hr), traffic within 3-feet of the edge of the instrument table increased the average rate of contamination by approximately 2.5-fold (125±26 CFUs/m2/hr; p=0.002) compared to approximately 5-fold (255±46 CFUs/m2/hr; p< 0.001) at 1 foot. The presence of the bonnet was associated with a 40% reduction (151±27 vs 255±46 CFUs/m2/hr; p=0.014) with one foot proximity traffic. There was no difference with and without the bonnet when traffic was restricted to 3 feet (Figure 2).
Conclusions
● There was a clear relationship between the proximity of traffic to the edge of the instrument table and the rate of contamination of sites on the table. Keeping a clear 3-foot perimeter from the table reduces the contamination rate by half compared to 1-foot.
● When this is not feasible due to the size of the operating room or the need for essential personnel to get closer, addition of a transparent sterile cover will reduce the contamination by approximately 40%.
Figures
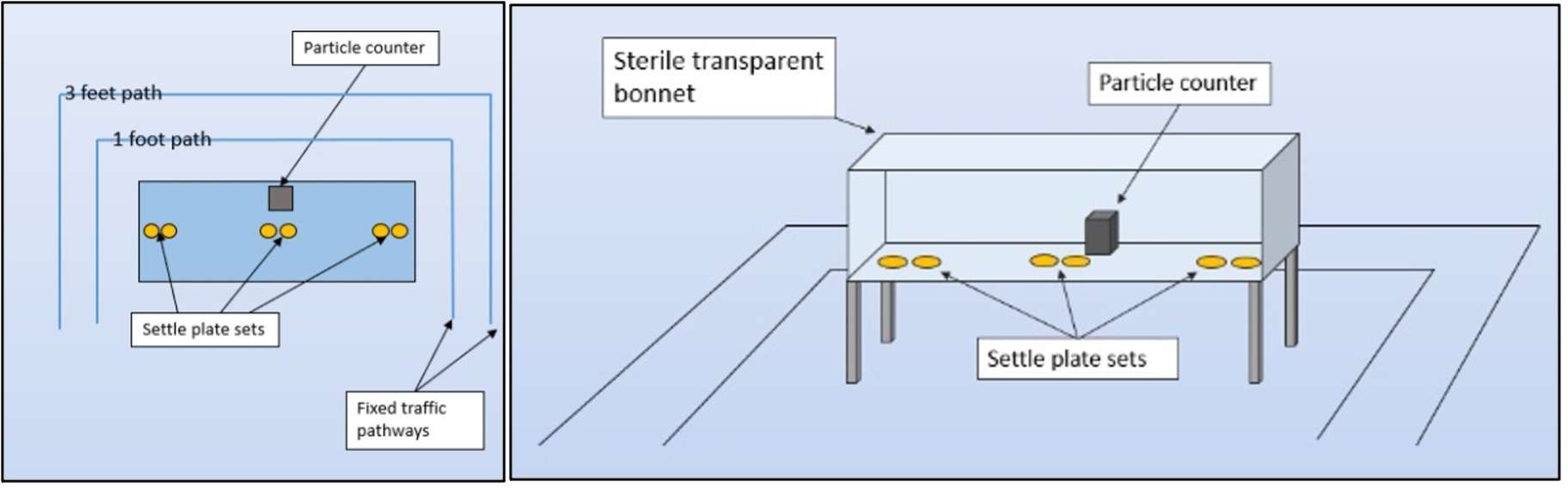
Figure 1
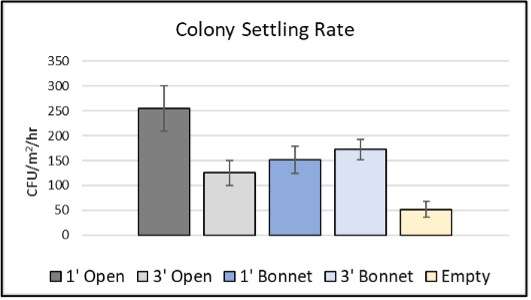
Figure 2#7876
Prophylactic Cerclage as an Adjunct to Fixation of Periprosthetic Fractures: The Effect of Cable Location
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Analisa Narro - McGovern Medical School at UT Health Houston - Houston, USA
Carson Viglione - University of Texas Health Science Center - Houston, USA
Hugh Jones - UT Health Science Center at Houston - Houston, USA
Shuyang Han - University of Texas Health Science Center at Houston - Houston, USA
Jonathan Gold - Institute of Orthopedic Research and Education - Houston, USA
David Rodriguez - University of Texas - Houston, USA
*Email: philipnoble66@gmail.com
Background: During internal fixation of proximal femoral periprosthetic fractures (PPF) cerclage cables are often placed below the most distal fracture to prevent propagation of cortical cracks during subsequent loading. However, definitive biomechanical data guiding the location of cerclage cables is lacking, with different publications recommending placement at levels ranging from 0-20mm below the fracture. In this study we examine the research questions:
(i) Does a cerclage cable increase the resistance of the construct to crack propagation?
(ii) If so, what is the effect of the location of the cerclage cable with respect to the tip of the cortical fracture?
Methods: A preliminary study examined fracture initiation and propagation in tubular composite materials compared to cortical bone. Based on the results, 25 fiber-reinforced polyester test specimens (ID: 3/4”; length: 6”, wall thickness: 1/8”) were prepared. A longitudinal crack (length: 8.0+0.5mm) was created in each specimen and stained with ink to facilitate visualization. A stainless-steel tapered rod (4°) was inserted under axial load at 10mm/min until 15mm displacement or a 10% drop in insertion resistance. The insertion force, displacement of the rod, and the tension within the cerclage cable were continuously monitored. In 4 sets of 5 specimens, a circumferential multi-filament CoCr cerclage cable (diameter: 1.8mm) was placed at 5 mm, 10 mm, 15 mm, and 20 mm from the distal end of the longitudinal fracture prior to loading. Each cable was tightened to the same nominal load, as indicated by the manufacturer’s tensioning instrument. An additional group of 5 specimens was tested without cerclage to act as a control. Differences between groups were evaluated with ANOVA and post hoc analysis using Fisher’s PLSD test.
Results: For the control group, the fracture propagated 32.4+1.6mm under an ultimate load of 883+71N. In comparison, placement of the cerclage cable at 5mm, 10mm, and 15mm below the fracture increased the peak resistance to fracture propagation by 75% (p<0.0001), 38% (p=0.0008), and 34% (p=0.002). Conversely, the length of propagation of the fracture decreased by 48% (p=0.0005), 44% (p=0.001) and 38% (p=0.023), respectively. Placement of the cable 20mm below the fracture did not increase the resistance to fracture propagation (p=0.602) or the growth of the fracture during loading (p=0.072). The average force required to initiate growth of the fracture was not significantly affected by cerclage location (p=0.925). The average force applied during tensioning the cerclage cable was 290+10N and was maintained during fracture initiation and the initial phase of propagation (Figure 2).
Conclusion: Our results demonstrate that placement of prophylactic cerclage cables with respect to the initial fracture does matter. A CoCr cable placed at 5mm proved to provide the best support when looking at total propagation distance and ultimate force. Cable placement at 10mm and 15mm also provided improvements with regard to these same measurements. Whereas placing a cerclage cable 20mm from the most distal end of a fracture provided no significant difference for all measurements assessed.
Figures

Figure 1
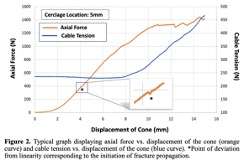
Figure 2

Figure 3#7937
Bone Morphological Risk Factors for Extraarticular Bony Impingement in Total Hip Arthroplasty
*Xuzheng Han - University of Denver - Centennial, USA
Casey Myers - University of Denver - Denver, USA
Chadd Clary - University of Denver - Denver, USA
*Email: xuzheng.han@du.edu
Introduction
Hip dislocation secondary to impingement is a common complication after total hip arthroplasty (THA). Recent studies into pelvic mobility and functional acetabular cup positioning may reduce the occurrence of implant-implant impingement. However, extraarticular bony impingement, like ischiofemoral impingement, requires balancing patient morphology with implant positioning to maximize impingement free range of motion (RoM). Preoperative imaging can be used to reconstruct the hip anatomy and evaluate the impingement risk but is not standard of care and is time consuming. The purpose of the current study was to investigate relationships between natural variation in bony anatomy and the impact on impingement free RoM with the goal of identifying simple radiographic measurements that indicate high risk patients.
Methods
Bone-on-bone impingement free RoM was analyzed in a database of 91 reconstructed CT scans (182 femurs, 39% Female, Age:73±10, Height: 67±3in., Weight:146±37lbs.). Anatomic coordinate systems were assigned to the bones and several anatomic measurements were extracted (Fig. 1), including the A-P width of the femur at the intertrochanteric crest, distances from the center of the femoral head to the lesser trochanter, most posterior, lateral, and distal points on the ischium, the anterior inferior iliac spine, and version and inclination angles of the femur and acetabulum. With the hip fully extended, the femur was rotated externally about the femoral head until impingement between the femoral shaft and pelvis. Likewise, with the hip flexed to 90°, the femur was rotated internally until impingement between the femoral shaft and the anterior inferior iliac spine (AIIS). Contact between the femoral neck and acetabular rim were excluded due to their resection during THA. A statistical shape and function model (SSFM) was constructed, including the hip anatomy and impingement free RoM, to identify anatomic relationships causing early impingement.
Results
On average, patients accommodated 46°±16° of external femoral rotation in extension and 34°±15° of internal rotation in flexion prior to bony impingement (Fig. 2). Impingement in extension occurred between the posterior intertrochanteric crest (57%) or lesser trochanter (33%) and the posterior horn of the ischium. Earlier extension impingement was primarily a function of Mode 4 of the anatomic variation, which correlated with increased femur version, a more lateral posterior horn of the Ischium, and a wider intertrochanteric crest (Fig. 3). Patients with early impingement had a significantly higher PC4 score (175) versus patients with larger RoM (115). Impingement in flexion primarily occurred between the intertrochanteric crest (80%) and the AIIS. Earlier impingement in flexion was strongly correlated with a lateral AIIS and reduced femoral version (r2 = 0.57 and 0.50) and was a function of Mode 2 of the anatomic variation, which influenced the AIIS location. Patients with early impingement had a significantly higher PC2 score (450) versus patients with larger RoM (195).
Conclusion
Extraarticular bony impingement was strongly correlated with anatomic features that are easy to measure from anteroposterior and lateral radiographs, including femoral version, AIIS location, and width of the ischium. The SSFM from this analysis can be used to predict early impingement risk based on these measurements.
Figures
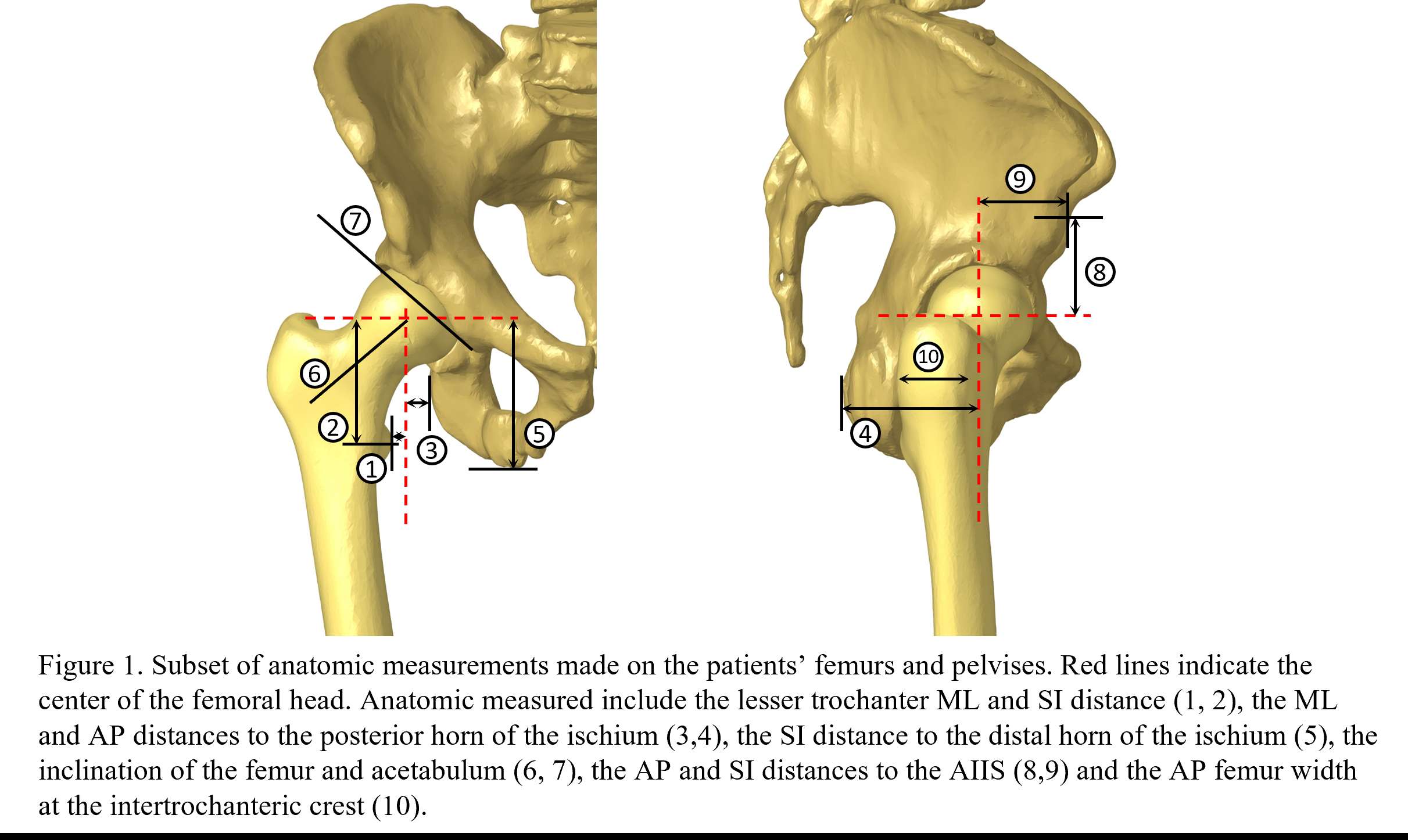
Figure 1
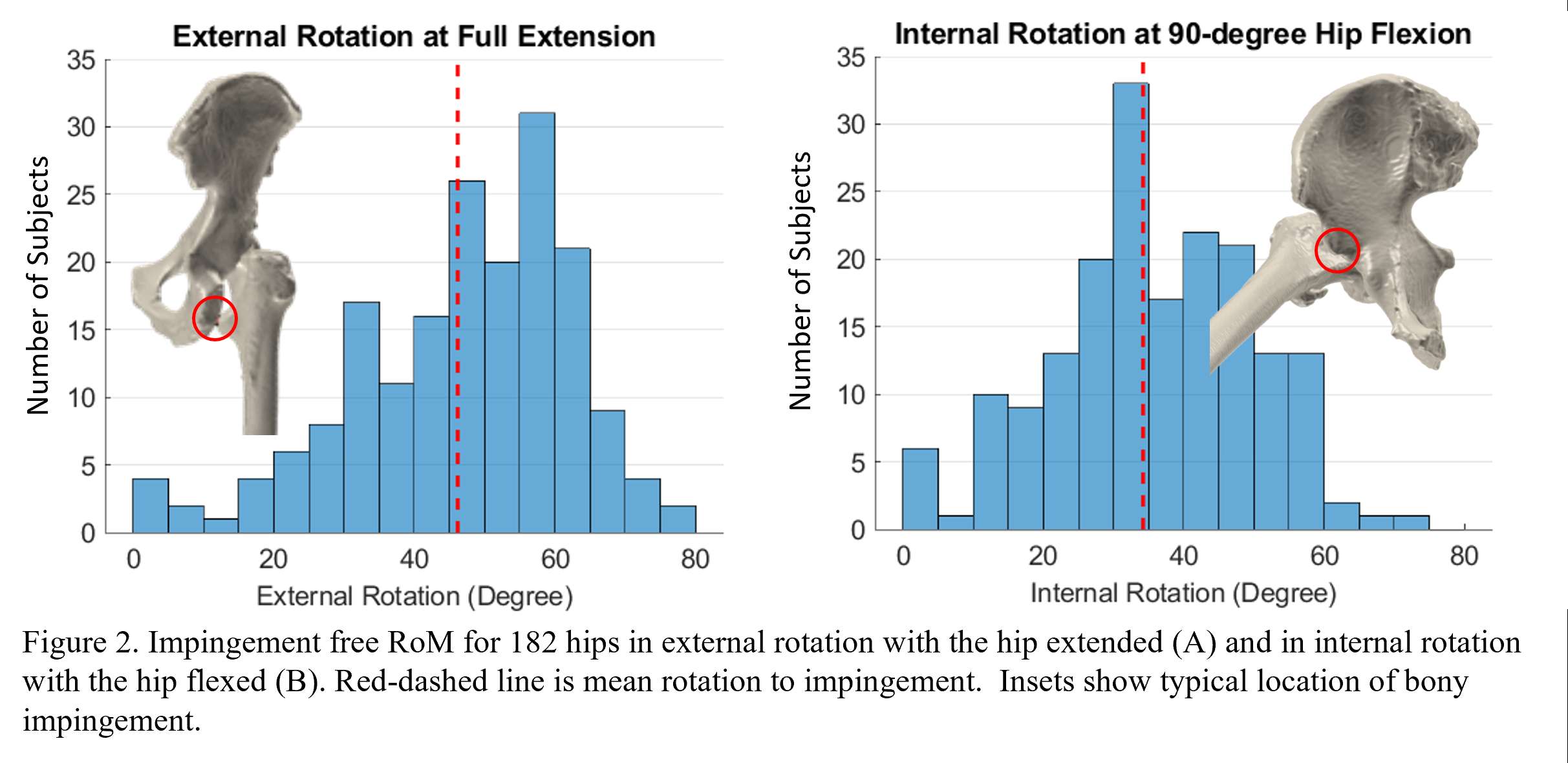
Figure 2
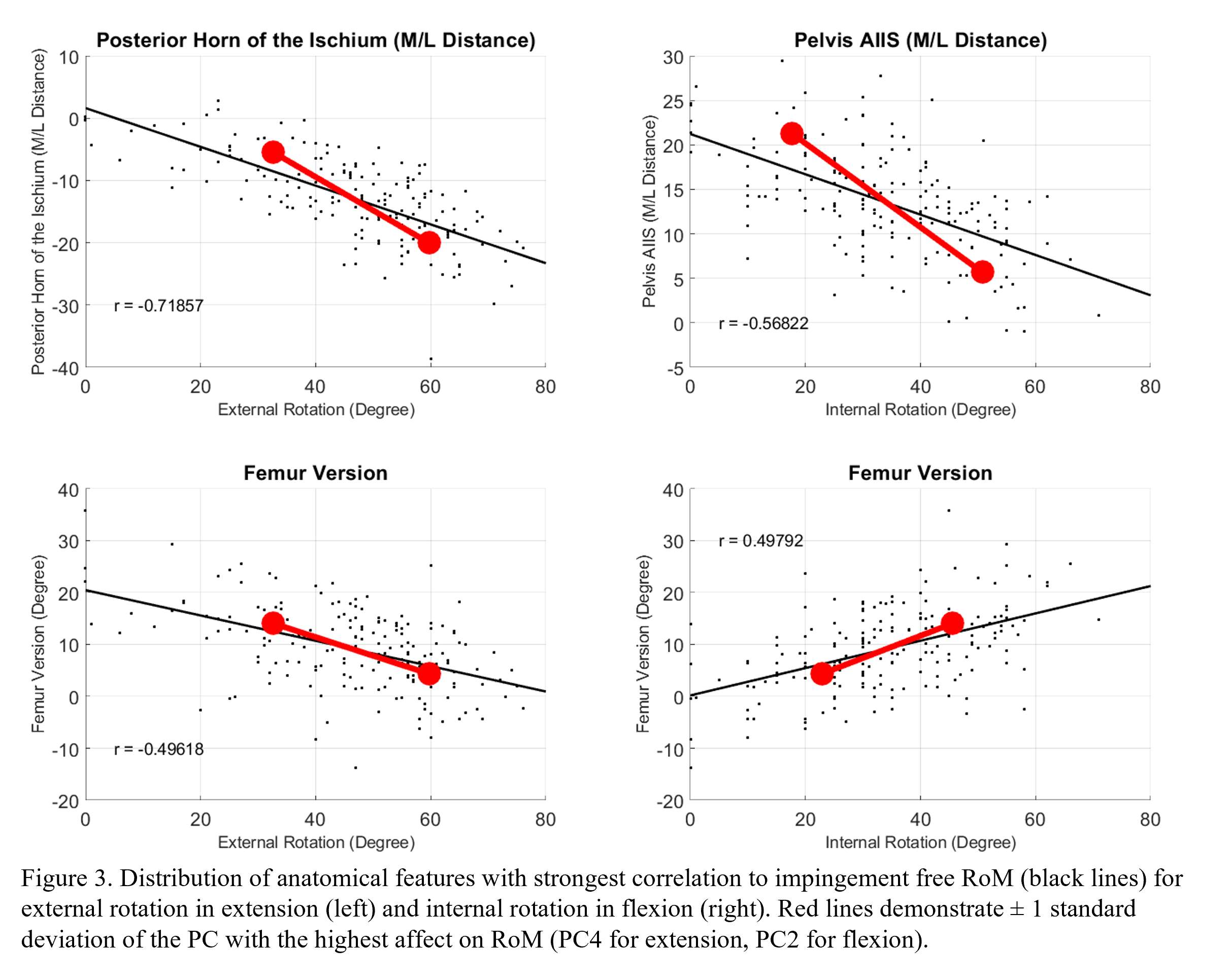
Figure 3#7461
Evaluating the Initial Stability in Cementless Patellar Implant During a Single-Leg Lunge
*Xuzheng Han - University of Denver - Centennial, USA
Huizhou Yang - University of Denver - Denver, USA
Alessandro Navacchia - University of Denver - Denver, USA
Paul J. Rullkoetter - University of Denver - Denver, USA
Chadd Clary - University of Denver - Denver, USA
*Email: xuzheng.han@du.edu
Introduction
Initial stability of cementless implants after total knee arthroplasty is crucial to establish bony ingrowth into the porous interface surface and maintain long-term fixation [1]. Previous studies mainly focused on quantifying tibial micromotion via experimental or computational models [2,3]. However, few have investigated patellar implant micromotion. The goal of this study was to investigate cementless patellar implant micromotion under implant-specific loading conditions and assess the initial fixation stability for different patellar implant designs.
Methods
Ten different cementless patellar prostheses with variations in articulating surfaces and sizes were implanted onto synthetic bones machined from sheets of 12.5 lb/ft3 closed-cell polyurethane foam (Sawbones, Pacific Research Lab) (Fig. 1). All implants had three cylindrical pegs coated with porous titanium for fixation to the host bone. The experimental simulation included seven variations of a single-leg lunge activity. In the experimental simulations, the anterior-posterior and medial-lateral axis were force controlled and displacement controlled in other degrees of freedom [4]. Bone-implant micromotion was measured using digital image correlation with marker pairs on either side of the bone-implant interface. Finite element (FE) models of the constructs were created, verified against the experimental measurements, and subsequently evaluated in a design-of-experiment fashion to quantify the influence of implant shape, patellar size, and patella contact mechanics on implant interface micromotion. Micromotion on the implant-bone interface surfaces was computed based on changes in distance between each node on the implant fixation surface and the closest node on the corresponding bone mesh over the cycle for each model configuration.
Results
Positive correlations between FE surface marker displacements and interface micromotions were observed, ranging from r2 = 0.25 to 0.95. These correlations were strongest for the smallest patella sizes (Fig. 2). Peak interface micromotions consistently occurred on the pegs and not on the plateau of the implant-bone interface. For six of the seven loading conditions, the largest compressive interface micromotions were observed on the 31-mm symmetric patella which had the smallest size among the implants studied, ranging from 100~174µm (Fig. 3). The predicted peak compressive interface micromotions for implants with different articulating surfaces were on average 95.5µm (medialized dome), 96.8µm (anatomic), 126.0µm (symmetric dome), and 73.0µm (asymmetric dome).
Conclusion
The peak interface micromotions were primarily influenced by implant size, possibly due to smaller contact areas and corresponding deformation of the underlying foam bone in smaller implants. The impact of variation in the articulating surfaces was less significant but should still be considered in pre-clinical evaluations. The relative displacements measured between marker pairs across the exposed bone-implant interface were correlated with the actual micromotions on the interfacing surfaces, but were larger in magnitude, indicating the necessity for computational modeling to evaluate cementless patellar implant fixation. All patella evaluated in this study exhibited interface micromotions within the threshold necessary for osteointegration.
Acknowledgements
Supported by DePuy Synthes Products, Inc.
References
- Pillar, et al., Clinical Orthopaedics and Related Research. 1986
- Crook, et al., J Arthroplasty. 2017
- Fitzpatrick, et al., J Biomechanics. 2016
- Navacchia, et al., J Mech Behav Biomed Mat. 2018
Figures
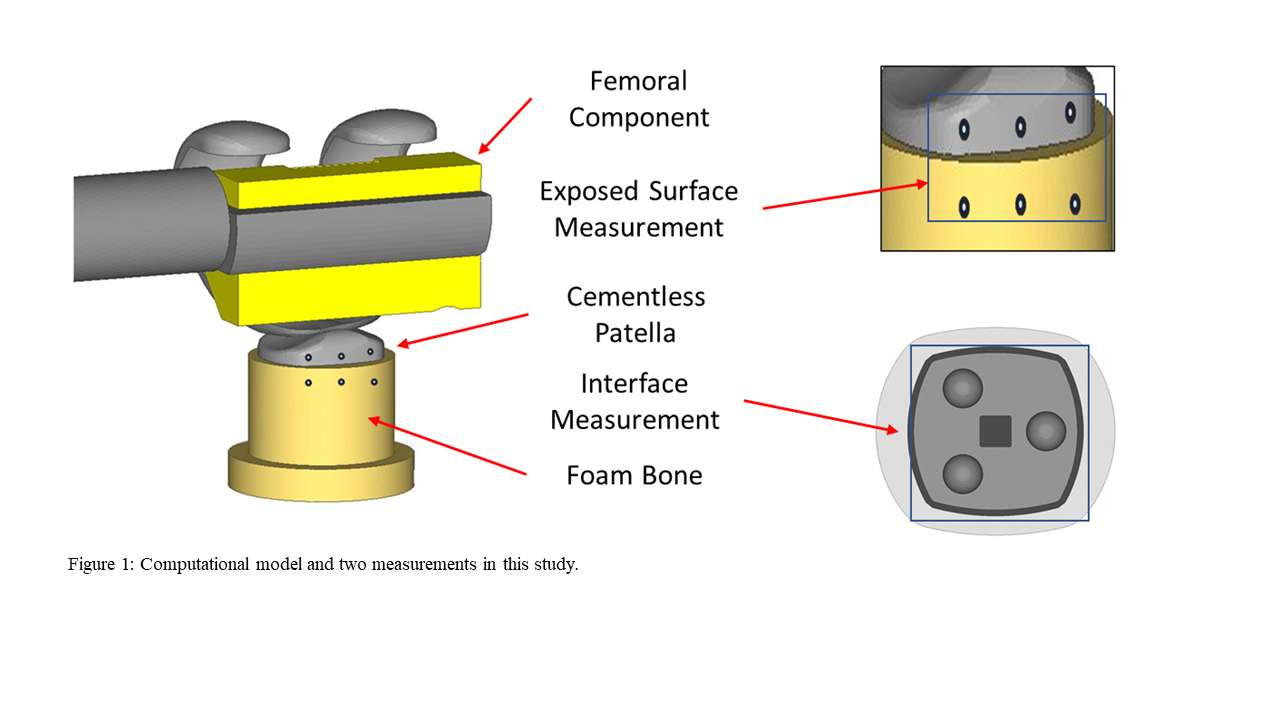
Figure 1
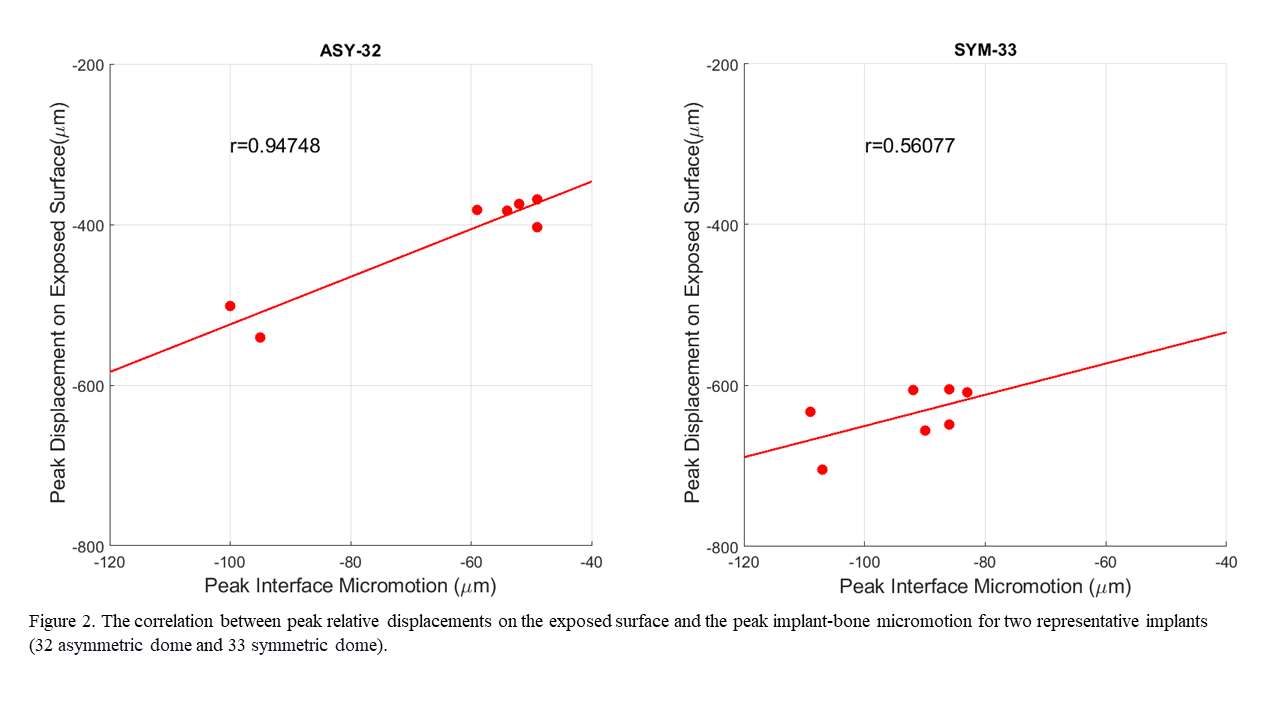
Figure 2
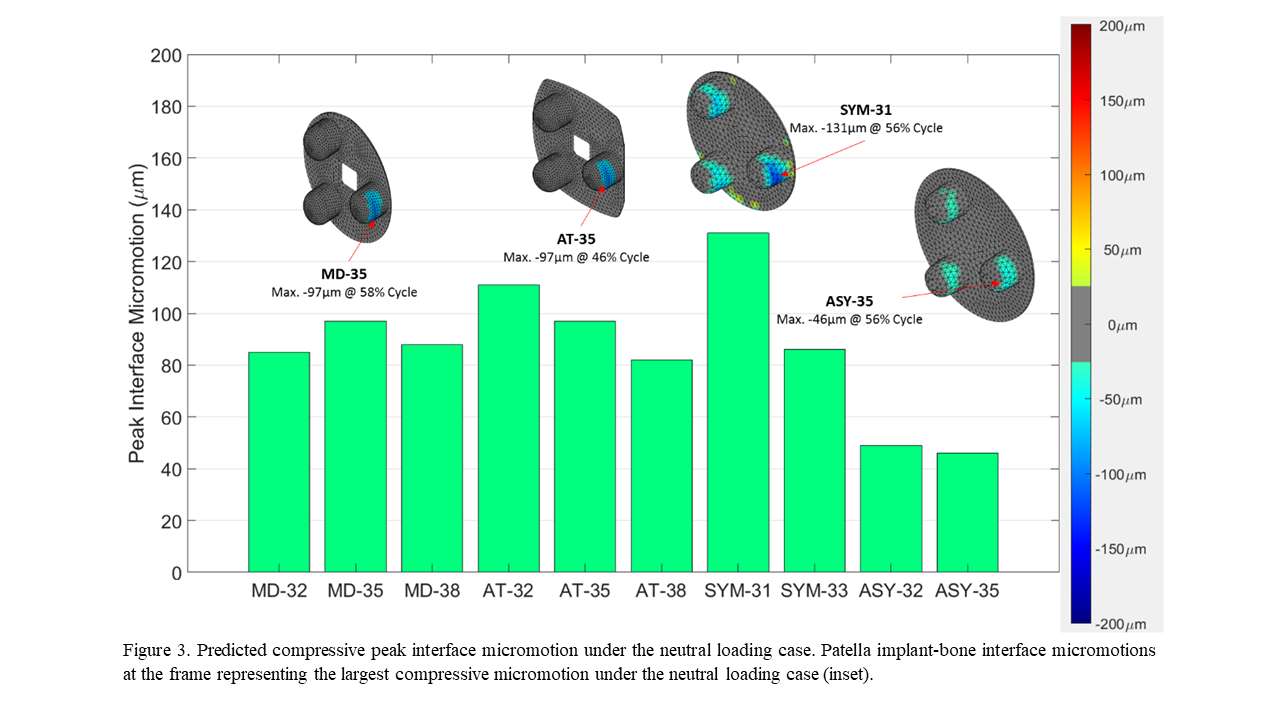
Figure 3#7305
Meta-Analysis and Systematic Review of Revision Rates for Patients With ACL Deficiency and ACL Intact After Unicompartmental Knee Arthroplasty (UKA)
*Maya Hara - Higashitotsuka Memorial Hospital - Tokyo, Japan
Tokito Tatsuo - Showa University Fujigaoka - Yokohama, Japan
Tomoyuki Matsuoka - Higashitotsuka Memorial Hospital - Yokohama, Japan
Kyosuke Shiohara - Higashitotsuka Memorial Hospital - Yokohama, Japan
Ken Yamazaki - Higashitotsuka Memorial Hospital - Yokohama, Japan
*Email: maya.hara85@gmail.com
Introduction
It has been reported that unicompartmental knee arthroplasty (UKA) is less invasive than total knee arthroplasty (TKA) and has a lower risk of intraoperative bleeding, postoperative infection, and postoperative pain. In addition, unlike TKA, UKA can be done without damaging the lateral compartment and can preserve soft tissue. However, due to the high revision probability, it is currently applicable only to anterior cruciate ligament (ACL) intact cases.
In recent years, studies suggest a good prognosis for patients who underwent UKA even if ACL was not intact. If UKA is indicated in a wider range of cases including ACL deficiency, it will be an option for more patients. We aim to compare the revision rate of patients who had UKA with ACL intact and ACL deficient patients.
Methods
We performed a meta-analysis based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) instruction. The authors carried out systematic research of Cochrane Library, PubMed, and Google scholar. A meta-analysis of revision rate in patients with ACL deficiency and ACL intact was conducted using Review Manager 5.4 software. The inclusion criteria were as follows: studies which were performed on humans, written in English. Studies included RCTs, cohort studies, and case control studies. We excluded review papers, case reports, studies performed on cadavers, in vivo and vitro, and those conducted on unrelated topics.
Results
The initial search identified 2812 articles. Of these, 2701 were excluded on the basis of the title, because they were a review paper, or because they covered an unrelated topic. The abstracts of the remaining 111 articles were examined further. That review resulted in a sample of 8 articles. The total number of the sample was 2128. We performed a meta-analysis with a random effects model using Review Manager 5.4 software. The result of the meta-analysis was Odds ratio 1.54(Confidence interval 0.91-2.63)(fig1). Therefore, the result does not indicate an increased revision rate with ACL deficient patients. Consequently, there are possibilities to consider that would extend the indication of UKA for ACL deficient patients. Funnel plot shows no obvious publication bias (fig2).
Conclusion
We performed a meta-analysis of revision rates for patients who underwent UKA with or without ACL in existing articles. Results showed that there was no statistically significant difference of revision rate with or without ACL. Therefore, it may be possible to increase the indication of UKA for ACL deficient patients. However, the number of articles included in this study was still small and there was no RCTs. Consequently, further research is needed to address the issue. In addition, results reported this study reflect the pooled data without period stratification, since the measurement time points varied among included studies.
Figures
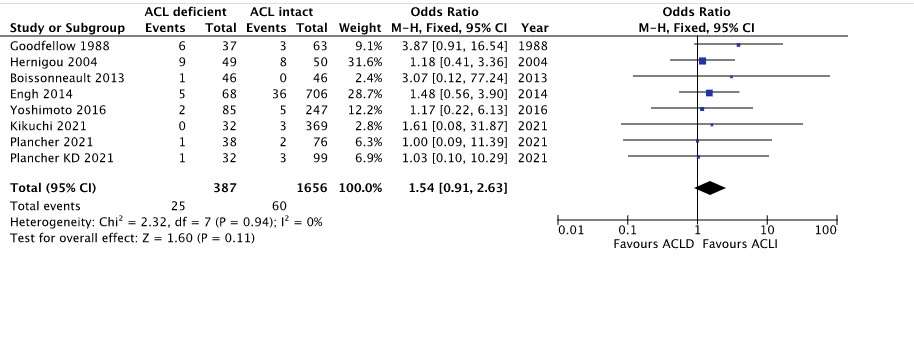
Figure 1
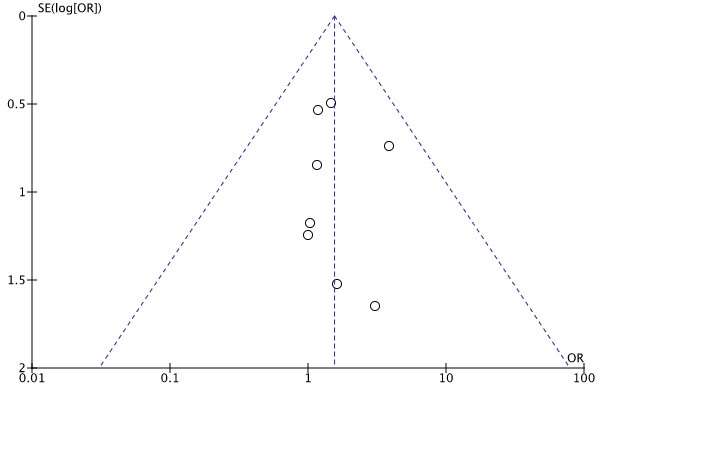
Figure 2#7874
Multi-Center Study to Assess Influence of Surgical Approach on Hip Functional Implant Placement
*Bob Marchand - ortho rhode island south county - Wakefield, United States of America
Ajay Lall - American Hip Institute - Chicago, USA
Seth A. Jerabek - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Benjamin Domb - American Hip Institute - Des Plaines, USA
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
Benjamin Harder - Stryker - Nashville, TN, United States of America
*Email: marchand33@cox.net
INTRODUCTION: Surgical approach during total hip arthroplasty (THA) continues to be debated between surgeons with each approach having its own benefits and drawbacks. When performing direct anterior (DA) approach, the anterior capsule is released, and even when repaired there can be increased concern for anterior dislocation. For posterior approach, the posterior capsule and other structures are released, and even if repaired there is increased concern for posterior dislocation, particularly while these repairs heal. These differences may influence a surgeon’s decision making on where to place THA implants. A study on THA dislocations showed that greater anteversion increased the likelihood of anterior dislocation whereas reduced anteversion was associated with increased risk of posterior dislocation. In addition, increased inclination was associated with risk of anterior dislocation and decreased inclination was associated with risk of posterior dislocation. The purpose of this study was to understand how surgical approach may influence functional implant placement when performing robotic-assisted THA (RA-THA).
METHODS: A multi-center, prospective study was performed on a cohort of 73 consented patients who received RA-THA with integration of software to assess patient’s pelvic tilt (PT) and virtual range-of-motion (VROM) to impingement. Preoperative CT scans were obtained in addition to standing and sitting lateral radiographs which were used to plan femoral and acetabular component as well as evaluate patient’s VROM to impingement, PT, and cup position in supine, standing and sitting poses. If impingement was identified using VROM tool, the surgeon was able to adjust implant positioning to try to avoid impingement. Intraoperatively, either DA or posterior approach was used based on surgeon preference performing the case. Data on final acetabular cup planned position were collected intraoperatively. A two-way ANOVA and Tukey post hoc test at a 95% confidence level were used to evaluate difference in implant placement plan between DA and posterior approach.
RESULTS: Cases were separated into groups based on pre-operative spinopelvic mobility moving from standing to seated. 74% of cases were considered normal (change ≥10°) and 26% of cases stiff (change <10°). Planned acetabular cup inclination and version for these patient groups are provided in Table 1. There was a significant difference in implant placement between the two surgical approaches. DA approach used statistically significant less inclination and anteversion for cup placement for both patient groups when compared to the posterior approach group.
DISCUSSION: Differences in THA surgical approach influences how a surgeon considers implant placement, where DA is associated with greater concern for posterior impingement and therefore anterior dislocation, and posterior approach is associated with greater concern for anterior impingement and therefore posterior dislocation. Functional implant placement plans in the current study reflected these considerations where the posterior approach was associated with statistically significant more inclination and anteversion when compared to DA plans. These results convey that surgical approach may influence a surgeon’s functional implant placement. Follow-up will be needed on these patients to report on their clinical outcomes; however, literature has reported no difference in clinical outcomes for patients who received the DA versus posterior approach using robotic-assisted THA.
Figures
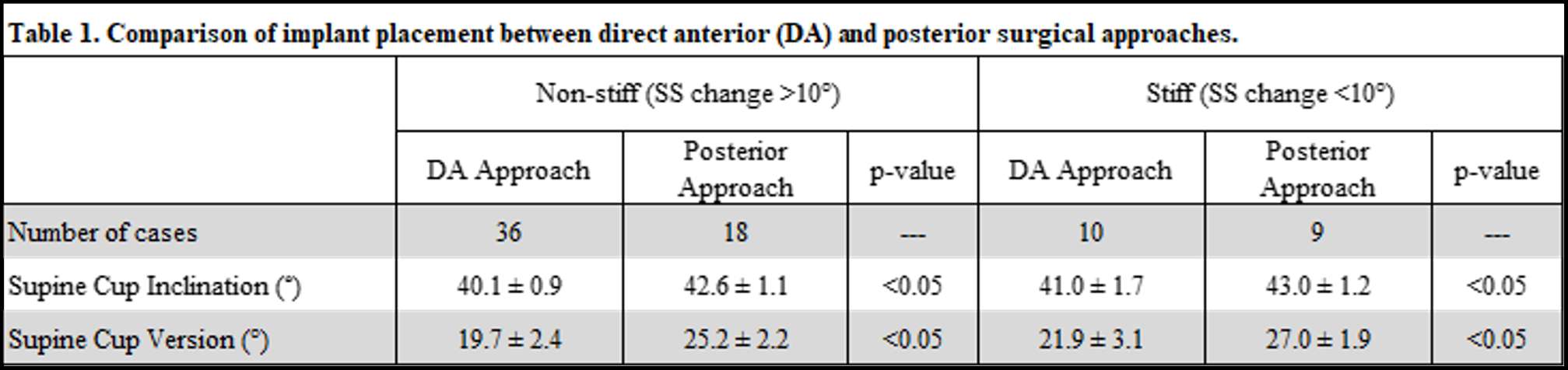
Figure 1#7746
Assessment of Robotic Assisted Total Hip Arthroplasty With Functional Hip Positioning: 1-Year Outcomes
*Laura Yanoso-Scholl - Stryker Orthopaedics - USA
Kevin Marchand - Ortho Rhode Island - South County, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Daniel Erwin - Ortho Rhode Island - Wakefield, USA
Robert Marchand - Ortho Rhode Island - South County, USA
Benjamin Harder - Stryker - Nashville, TN, United States of America
*Email: Laura.Scholl@stryker.com
INTRODUCTION: Robotic assisted total hip arthroplasty (RA-THA) has shown to provide accurate implant positioning and enhanced patient outcomes.1 With previous software versions, RA-THA has not considered a patient’s functional hip positioning. The purpose of this study was to report on patient outcomes for an initial cohort receiving RA-THA with new software that incorporates functional hip positioning.
METHODS: A single-center, retrospective review was performed on a consecutive cohort of 100 patients who received an anterior approach RA-THA with integration of software to assess patient’s standing and sitting pelvic tilt and virtual range-of-motion (VROM) to impingement. If impingement was identified using the VROM tool, the surgeon was able to adjust implant positioning to avoid impingement. HOOS-JR scores were collected preoperatively and at 6-weeks, 3-months, 6-months and 1-year postoperatively. A one-way ANOVA and a Tukey post hoc test at a 95% confidence level were used to evaluate difference in HOOS JR scores over time.
RESULTS: Between preoperative to 6 weeks postoperative, the RA- THA cohort achieved a statistically significant improvement (p<0.05) in their HOOS Jr score where this delta was also considered to be a substantial clinical benefit.2 At 3-month, 6-month and 1-year follow-up, patients continued to have statistically significant improvement in HOOS Jr which represented a minimal clinically important difference.2
CONCLUSION: It is critical to understand spinopelvic mobility prior to performing a THA.3,4 We now have technology that can allow the surgeon to perform intraoperative VROM to assess impingement and optimize implant position. Patients reported substantial clinical benefit when receiving RA-THA that included assessment of functional hip positioning. Further research is needed to continue to evaluate this patient cohort and compare to a manual THA cohort.
REFERENCES: [1] Domb et al. J Am Acad Orthop Surg. 2020 Oct 15;28(20):847-856. [2] Lyman et al. Clin Orthop Relat Res (2018) 476:2432-2441. [3] Buckland et al. Bone Joint Journal. 2017 Nov;99-B,5. [4] McCarthy et al. J Arthroplasty. 2016 Sep;31(9 Suppl):264-8.
#8006
Patient Outcomes in Total Knee Arthroplasty With Internal Rotation of the Femoral Component
*Bob Marchand - ortho rhode island south county - Wakefield, United States of America
Kevin Marchand - Ortho Rhode Island - South County, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Daniel Erwin - Ortho Rhode Island - Wakefield, USA
Benjamin Harder - Stryker - Nashville, TN, United States of America
*Email: marchand33@cox.net
Introduction: Total knee arthroplasty (TKA) is often described as a soft tissue procedure aimed at achieving a well-balanced knee. Often with traditional TKA instruments, the femoral component is neutrally or externally rotated relative to the transepicondylar axis. Robotic technologies allow a surgeon to intraoperatively adjust component position, like femoral rotation, to achieve a more balanced knee prior to making bone resections. Due to differences in patient anatomy, the rotation of the femoral component may vary to achieve desired knee balance. The purpose of this study was to perform a longitudinal, observational, single-surgeon, cohort study of robotic-arm assisted TKA cases to assess whether internal femoral rotation adversely affected patient outcomes and the ability to achieve a minimally clinical important difference (MCID) at six months for a large patient cohort who underwent a robotic TKA (RTKA) procedure.
Methods: 876 knees were reviewed for final femoral internal and external rotation relative to the transepicondylar axis. Femoral rotation was used to categoried patients into <0° to 6° internal, and 0° to 6° external. Intraoperative medial and lateral gaps in flexion and extension were collected as well as r-WOMAC surveys preoperatively and at 6-month follow-up. MCID achievement was determined by taking one-half of the standard deviation of preoperative scores and compared between patient groups.
Results: The internal group included 466 patients with an average femoral angle of -2.8° ± 1.5°. The external group included 388 patients with an average femoral angle of 1.9° ± 1.8°. r-WOMAC and MCID results are shown in Table 1. There was no significant difference in preoperative, postoperative, and MCID improvement for the reduced WOMAC when comparing patients with an internally or externally rotated femoral component.
Discussion: Very few studies investigate patient outcomes as related to internal or external rotation of the femoral component and for a large patient cohort. This study demonstrated patient outcomes were not affected by femoral component internal or external rotation. This study has some limitations in that it was a single-surgeon study and dynamic kinematics were not evaluated in these patients to determine the effect of femoral rotation. In conclusion, variability in femoral component rotation may help achieve a more functional component position and was demonstrated to have no effect on patient outcome.
Figures
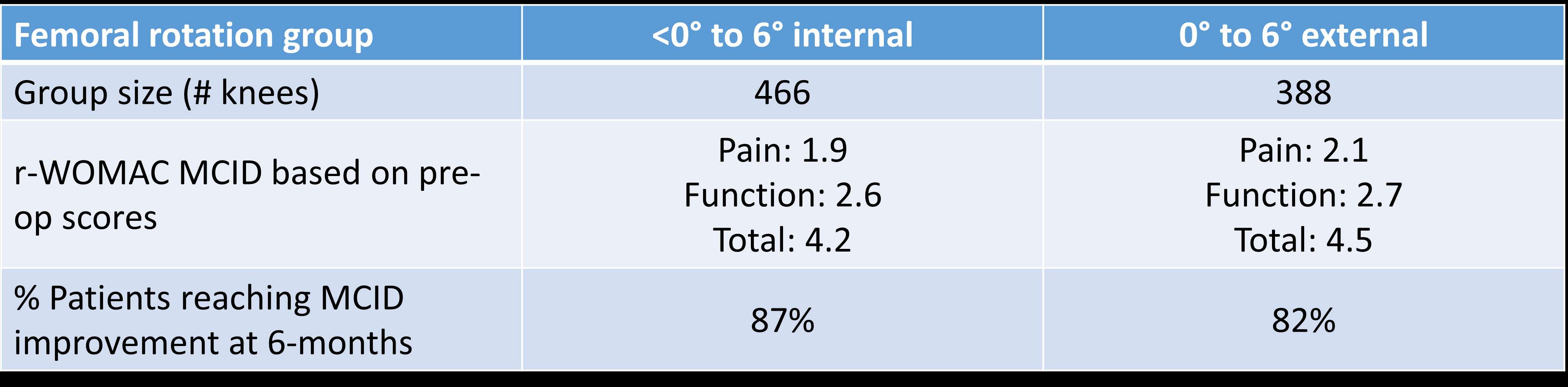
Figure 1#7926
Patient Compliance With Remote Monitoring: Findings From a Multi-Center Study
*Emily Hampp - Stryker - Mahwah, USA
Ricardo Antunes - Stryker - Glasgow, GB
Robert Marchand - Ortho Rhode Island - South County, USA
Paul Jacob - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Andrew Meyer - Stryker - Mahwah, USA
Elaine Justice - Oklahoma Joint Reconstruction Institute - Oklahoma City, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Kelly Luttazi - Ortho Rhode Island - Wakefield, USA
Matthias Verstraete - Stryker - Fort Lauderdale, USA
Benjamin Harder - Stryker - Nashville, TN, United States of America
*Email: emily.hampp@stryker.com
Introduction:
There has been an increase in the use of technology to remotely administer rehabilitation and monitor recovery after total knee arthroplasty (TKA). However, the implementation and adoption of these devices is not well-characterized. The purpose of this study is to review the preliminary findings related to patient compliance from a multi-center study for a newer generation wearable device after TKA.
Methods:
A total of 101 patients (mean age of 65 y/o, range 50 to 79 y/o) were enrolled at two centers. Device worn time compliance was characterized by the mean percent of expected worn days, per each 30-day period pre- and post-surgery, which was defined as the total number of worn days in each period (pre-operative period, 1-30 days post-operative, 31-60 days post-operative, and 61-90 days post-operative) over the total expected worn days in that period to normalize for any dropped patients. The mean hours per day the wearable sensors were worn by the patient were also characterized for each of these 30-day periods and throughout the recovery journey.
Results:
On average, patients wore the device for 80%, 70%, 70% and 40% of the expected days for the pre-operative period, 1-30 days post-operative, 31-60 days post-operative, and 61-90 days post-operative, respectively. When the device was worn, the mean worn time for the pre-operative period, 1-30 days post-operative, 31-60 days post-operative, and 61-90 days post-operative, was 9.8, 9.8, 9.8, and 10.3 hours per day, respectively.
Conclusion:
The average device worn time demonstrated high compliance in terms of the percent of expected days that the device was worn (pre-operatively and up to 60 days post-operatively), and the number of hours the device was worn per day throughout recovery. A limitation in the expected worn time is the assumption that the mean percent is constant within the 30-day period if a patient drops out of the study. These preliminary findings demonstrate the potential for remote therapeutic monitoring reimbursement, while also giving an objective view on the patient’s functional recovery after surgery.
#7472
Functional Femoral Anteversion: Axial Rotation of the Femur and Its Implications for Stem Version Targets in THA
*Max Hardwick-Morris - 360 Med Care - Sydney, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
Kunaal Kacker - Alfred Health - Melbourne, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Jitendra Balakumar - Melbourne Orthopaedic Group - Melbourne, Australia
*Email: max@360med.care
INTRODUCTION: It is well known that the pelvis undergoes sagittal rotation during Activities of Daily Living (ADLs), altering the functional position of an implanted cup in THA. Less well known is that the femur undergoes functional femoral rotation (FFR) with a similar impact on femoral version. Prior studies have investigated anatomic femoral anteversion (AFA) but have failed to consider the impact of rotation in functional positions. This study aimed to profile the variability of an under-studied measurement – Functional Femoral Anteversion (FFA) (Figure 1) – in a large sample of patients undergoing total hip arthroplasty (THA), assess its implications for femoral stem version targets, and investigate the number of individuals whose femoral rotation may place them at-risk of malorientation. Further, we measured FFR using a novel and reproducible x-ray protocol.
METHODS: 1008 consecutive patients who underwent THA surgery were assessed for preoperative FFA as part of a preoperative Range of Motion planning protocol. Each patient had a long limb CT scan as well as a standing lateral X-ray capture of the hip and distal femur. From this data, supine and standing FFR (the Posterior Condylar Line (PCL) to the coronal plane angle) as well as AFA (neck angle to the PCA) were assessed. Adding the standing or supine FFR and the AFA gives FFA for that position. Positive FFR values and positive changes in FFR from supine-to-standing were external femoral rotation. Pearson’s correlations were used to assess the linear relationship between continuous variables.
RESULTS SECTION: The mean AFA was 15.6° ± 9.8°. The mean standing FFR was -2.7° ± 13.1°. The mean standing FFA was 13.2° ± 12.2°. The mean change in FFR from supine to standing was -2.2° ± 11.8°. The mean absolute change in FFR from supine to standing was 8.7° ± 7.2°. 16% patients had standing FFA version of greater than 25°. 46% patients had standing FFR (internal or external) of greater than 10°. 12% patients exhibited an increase in external rotation from supine to standing of greater than 10°. 33% patients exhibited an absolute change in FFR (internal or external rotation) of greater than 10° (Figure 2). A moderate, negative linear relationship was also observed between AFA and standing external femoral rotation (p << 0.001, R = -0.46).
DISCUSSION: Functional alignment of the femur in patients requiring THA is under-studied. We have shown that the femur can rotate significantly between functional positions, altering its functional alignment. Given the degree of rotation variability observed in our study, combined anteversion targets may need to consider FFA and surgeons may consider the use of lateral knee x-rays to incorporate femoral rotation into their planning. Further, the moderate correlation between decreasing AFA and increasing external FFR in standing indicated the possibility of a compensatory mechanism occurring around the joint where the functional positioning of the femur corrects for anatomical variation, which could be occurring to maintain tension in the capsule. Further investigation is required, but this compensatory mechanism may have implications for both stem and acetabular alignment.
Figures
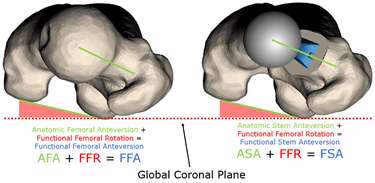
Figure 1
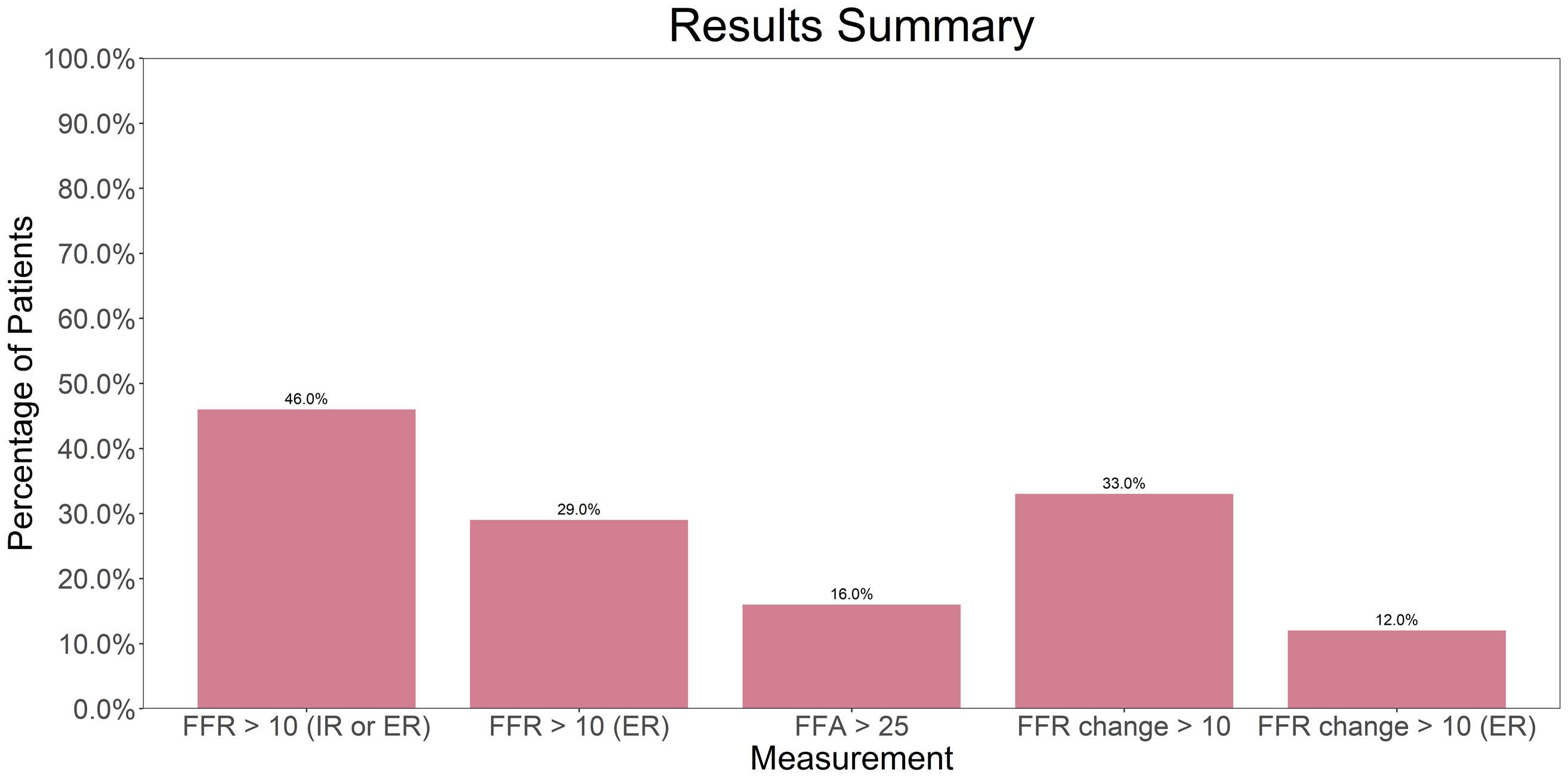
Figure 2#7470
Leg Length Discrepancy Assessment in Total Hip Arthroplasty: Time to Get It Right
Joshua Twiggs - University of Sydney - Sydney, Australia
*Max Hardwick-Morris - 360 Med Care - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Christopher Jones - Fiona Stanley Hospital Group - East Fremantle, Australia
Piers Yates - University of Western Australia - Perth, Australia
*Email: max@360med.care
INTRODUCTION: Leg length discrepancy (LLD) is a common pre- and postoperative issue in total hip arthroplasty (THA) patients. Consequences of LLD include patient dissatisfaction, dislocation, abnormal gait, and pain. The ‘Gold Standard’ for measuring LLD has historically been on a weightbearing AP pelvic radiograph (inter-teardrop measurement). However, this does not capture many potential sources of LLD (Figure 1). Clinical LLD can be broadly broken down into two sources: ‘True’ LLD and ‘Apparent’ LLD. Apparent LLD is more strongly perceived by patients – a postoperatively equal apparent LLD is the target. Therefore, the aim of this study was to determine if Long Leg (EOS) radiology can provide a more reproducible & holistic measurement of LLD.
METHODS: 93 patients from two experienced surgeons who underwent a THA received a standardized preoperative EOS scan, AP Radiograph, and clinical LLD assessment by the surgeons. 7 of the 93 patients were bilateral, giving 100 joints analysed. 16 measurements were taken, including the inter-teardrop line on the short AP Radiograph as a reference standard. Other measurements included pelvic obliquity and measurements of the femur, tibia, head-centre-to-ankle/floor, and anterior superior iliac spine (ASIS)-to-ankle/floor along both anatomic and functional (weightbearing line) axes. Measurements were taken on the operative and contralateral side. Each measurement was measured twice by an Orthopaedic Fellow and twice by a Surgical Planning Engineer with repeat measurements taken at least 2 weeks apart to calculate intra-operator reproducibility and correlations between measurements compared.
RESULTS SECTION: Strong correlations were observed for all EOS measurements (r > 0.9). The strongest correlation with AP x-ray (inter-teardrop line) was observed for functional-ASIS-to-floor (functional) (r = 0.57), much weaker than the correlations between EOS measurements. Mean AP LLD was 1.7mm (± 5.6), and 4.2% patients had an absolute LLD of greater than 10mm. ASIS-to-ankle (anatomic) exhibited a high ( r > 0.8) correlation to other linear measurements, the highest ICC (r = 0.97), and had a mean LLD of 3.1mm with 32.6% of patients having an absolute LLD of greater than 10mm. This percentage was statistically different from the AP inter-teardrop LLD measurement (p < 0.005). Most measurements had an Intra-Class Correlation Coefficient of > 0.9.
DISCUSSION: We found that the ‘Gold Standard’ measurement of LLD does not correlate well with other, long leg measurements and may not provide a holistic understanding of LLD. With its high repeatability (ICC > 0.9) and strong correlations with pelvic obliquity & X-ray measurements, the ASIS-to-ankle measurement demonstrated greater detection of potential clinical LLD than other measurements. Therefore, where available, there is a strong case for use of this measurement on EOS scans to determine LLD. However, it should be noted that there is a potential oversensitivity of the ASIS-to-ankle measurement to sources of LLD that naturally correct postoperatively (e.g., a hip contracture). Therefore, clinical correlation should be sought (blocks, gait observation) as usual. When confirmed, EOS measurements may provide a better quantitative target than conventional methods (AP x-ray). Further research will involve postoperative, 12-month follow-up with patients to correlate achieved LLD recreation with outcomes.
Figures
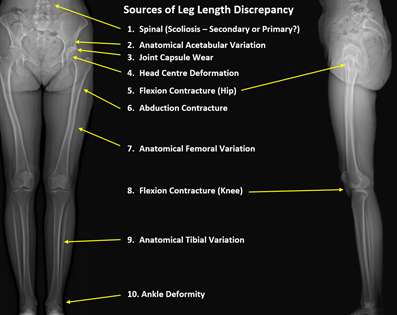
Figure 1
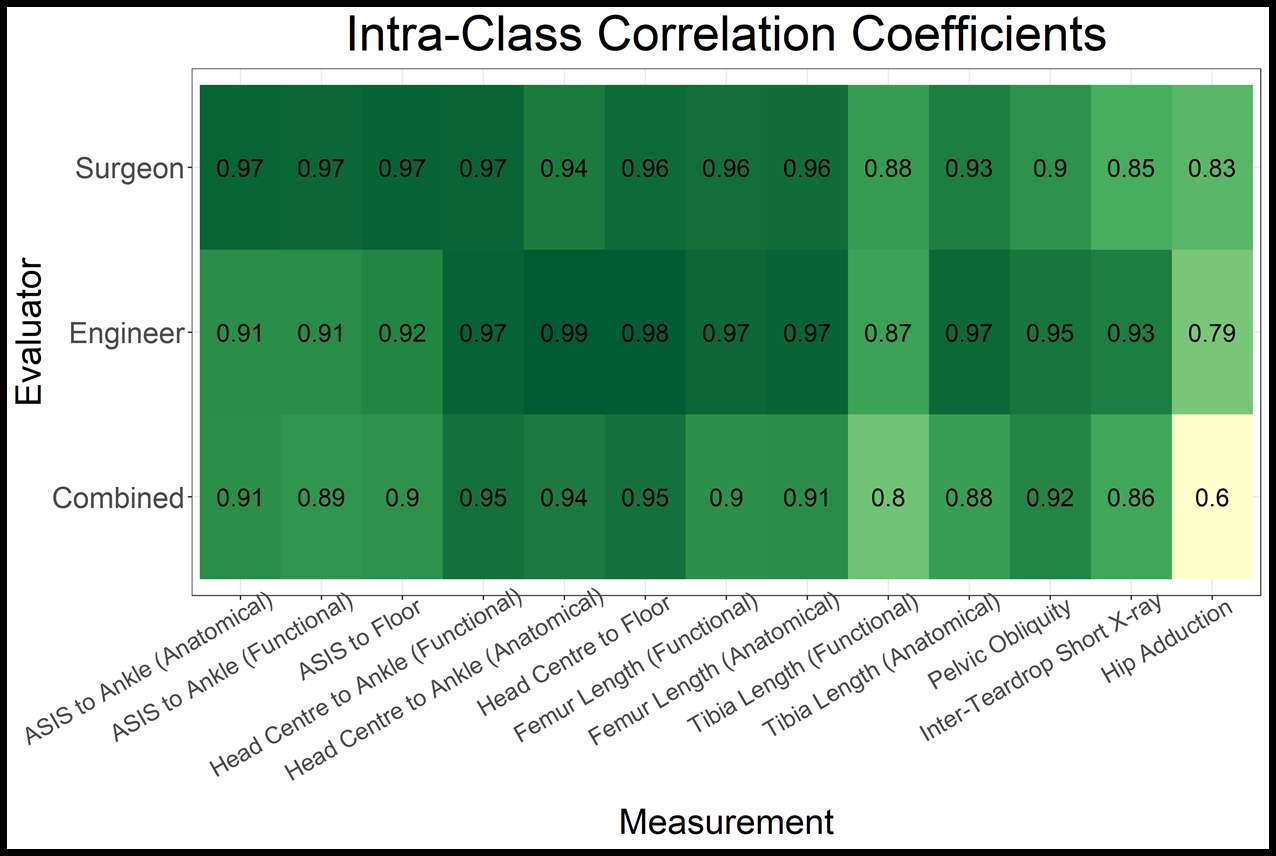
Figure 2#7522
Validation of a Novel Computational Iliopsoas Impingement Detection Simulation for Surgical Planning
*Max Hardwick-Morris - 360 Med Care - Sydney, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Yuan Chai - University of Sydney - Sydney, Australia
Jitendra Balakumar - Melbourne Orthopaedic Group - Melbourne, Australia
Rami Al-Dirini - Flinders University - Adelaide, Australia
Mark Taylor - Flinders University - Adelaide, Australia
William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
*Email: max@360med.care
INTRODUCTION: There are several reasons a patient may experience pain after total hip arthroplasty (THA) including infection, incorrect indication, instability, or soft tissue complications, such as iliopsoas tendonitis. Despite a relatively high incidence, occurring in 4-30% of patients after undergoing hip arthroplasty, there are few attempts at modelling the impingement between the iliopsoas and acetabular cup, and no attempts at modelling this in a representative cohort of subjects. The purpose of this study was to develop a novel computational model for quantifying the impingement between the iliopsoas and acetabular cup and validate its utility in a case-controlled investigation.
METHODS: We conducted a retrospective search for THA patients with psoas tendonitis and control patients without psoas tendonitis. Inclusion criteria included a postoperative CT scan, standing x-ray, and patient having exceeded 6 months from surgery. Exclusion criteria included resurfacings, metal-on-metal implants, and dual mobility cups. This resulted in two cohorts of 25 patients. Using the CT scans, 3D models of the femur, pelvis, femoral stem, and a registered hemispherical acetabular component were generated and landmarked. These 3D models were used to simulate the psoas impingement in R Studio (Figure1) in supine and standing pelvic tilt positions. Three discrete impingement values were recorded, and the mean and maximum of these values were reported. Cup prominence was measured using a novel, nearest-neighbour algorithm.
RESULTS SECTION: The average standing mean impingement for the symptomatic cohort was 0.4mm and 0.02mm for the asymptomatic cohort (p < 0.001). The average standing maximum impingement for the symptomatic cohort was 0.8mm and 0.1mm for the asymptomatic cohort. The difference was statistically significant (p < 0.001) (Figure2). The mean cup prominence for the symptomatic cohort was 8.3mm and 5.0mm for the asymptomatic cohort (p < 0.001) (Figure2). Pearson’s correlations found statistically significant linear relationships between cup prominence & standing mean impingement (R = 0.78, p < 0.001) and cup prominence & cup anteversion (R=-0.36, p = 0.02). Impingement significantly predicted the probability of pain in logistic regression models and the simulation had a sensitivity of 80%, specificity of 80%, and an AUC of 0.83.
DISCUSSION: Using one of the largest samples of patients who have been diagnosed with iliopsoas tendonitis after THA, we demonstrated that our novel simulation could detect impingement between the iliopsoas and cup through a retrospective, case-controlled investigation. This was demonstrated with the symptomatic patients exhibiting significantly greater levels of impingement than the asymptomatic patients. Other noteworthy findings included: (1) 5 symptomatic patients had little-to-no impingement, indicating the multicausal nature of iliopsoas tendonitis; (2) no impingement was observed in some asymptomatic patients who also had high cup prominence values, indicating the simulation can differentiate between cup prominence that results in impingement and cup prominence that does not; (3) minor impingement was detected in some asymptomatic patients, which may indicate a threshold for irritation/pain. In conclusion, this tool has the potential to be used preoperatively, to guide decisions about optimal cup placement, and postoperatively, to assist in the diagnosis of iliopsoas tendonitis and determine an appropriate treatment pathway.
Figures
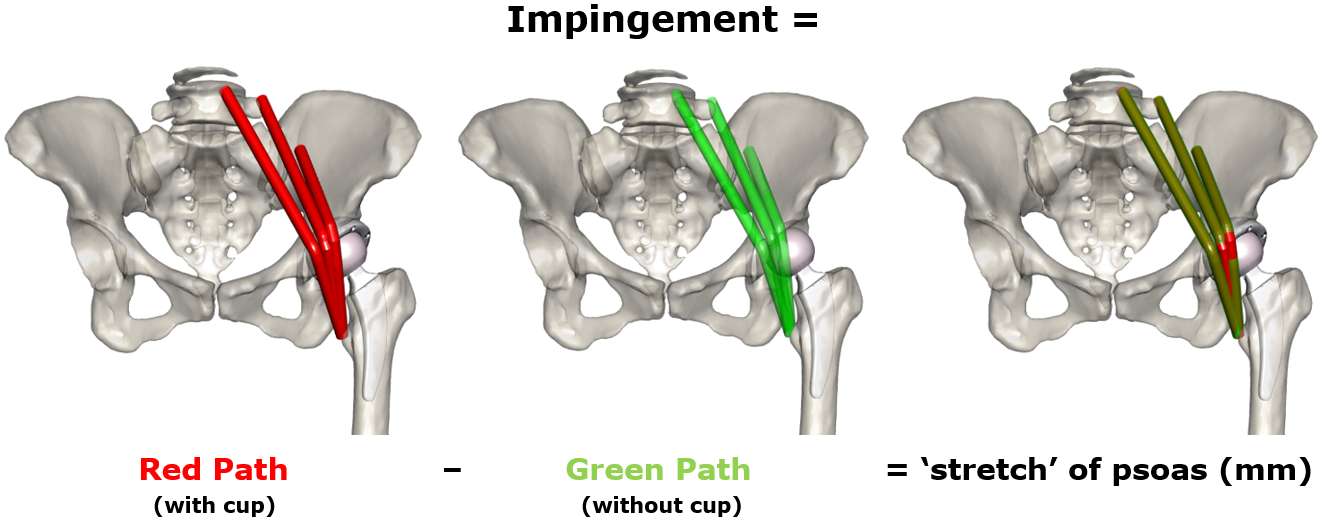
Figure 1
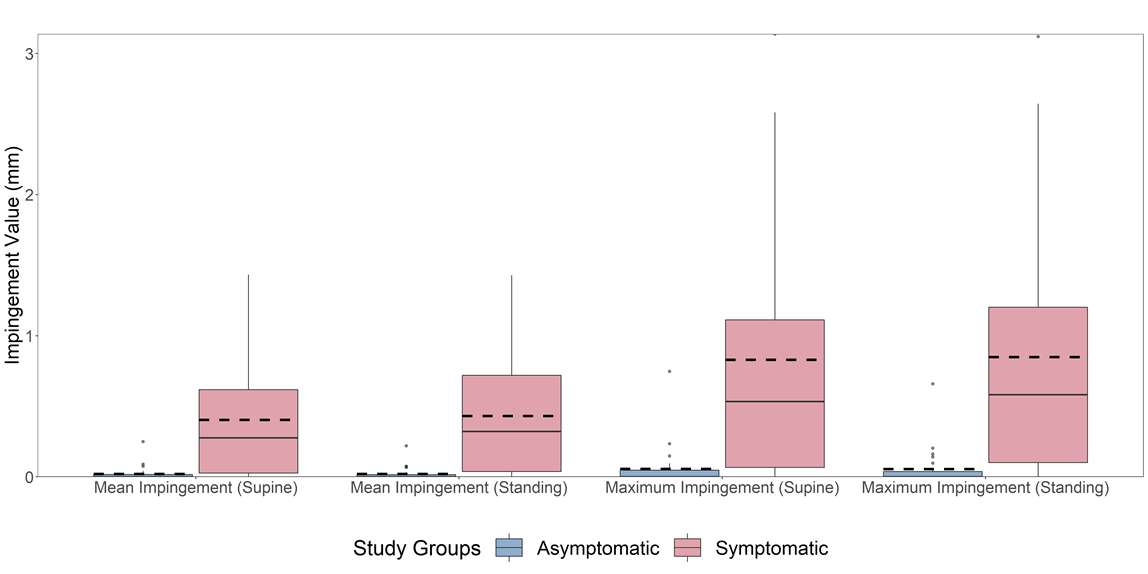
Figure 2
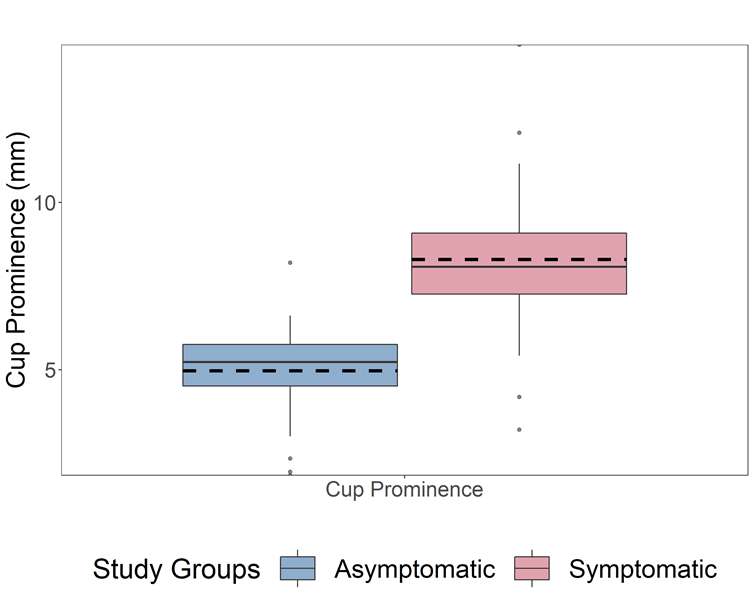
Figure 3#7696
An Eighty Patient Clinical Demonstration of a Settle Plate Method to Assess Intraoperative Airborne Microbial Contamination During Orthopedic Total Joint Replacement
*John Harp - ORAQ Labs, LLC - Fort Smith, USA
*Email: jhharp@hotmail.com
Introduction
Periprosthetic joint infection (PJI) is a dreaded complication of total joint replacement. A risk factor for PJI is sterile wound contamination[1] by airborne microbe-carrying particles (MCPs). Measurement of intraoperative MCP levels would allow quantification of this risk factor and such data could be used in OR quality programs and PJI risk factor research projects.
A straightforward settle plate technique to quantify MCP intraoperative bioburden loads has been described[2] recently. This investigation concerns the clinical application of this system in a series of eighty lower extremity total joint replacement cases at a single hospital.
Methods
Cases were monitored in a prospective observational study approved by the institutional review board. Eighty TKA and THA cases ( 4 surgeons, 20 cases per surgeon ) were monitored over 16 months. Surgeons used surgical helmet systems and strict protocols. Only intravenous antibiotic prophylaxis was used.
Two ORs with ANSI/ASHRAE/ASHE Standard 170 – 2021[3] ventilation systems were used for all cases. These systems provide a HEPA filtered air supply through a dispersed array of “non-aspirating” ceiling diffusers. Air return is via near floor exhausts grills. This system does not appear to produce traditional unidirectional airflow[4,5].
The technique captures sedimenting MCPs on commercially available terminally sterilized Petri dishes. Two zones were monitored: the backtable zone; and the wound zone around the patient’s operative extremity. Plates were opened from time of sterile field creation until fascia closure. Plates were incubated for 48 h at 35°C, then colony counts were performed. The bioburden for each zone, reported as Microbial Deposition Total (MDT, colonies/m2) were calculated. Benchmark MDT values of 100 and 450, corresponding to the historic orthopedic ultraclean air (UCA) limits of 1 colony/m3 and 10 colonies/m3, were applied to the results. Statistical analysis of zone UCA compliance was performed using Fisher’s exact t-test. Patient follow-up was performed for PJI events.
Results
Average MDT levels were 205 (+/- 166) MDT and 461 (+/- 331) MDT respectively for the wound and backtable zones. 75/80 (93.8%) of cases had wound zone MDT levels under 450. The five wound zone outliers had explainable causes due to cases length or complexity. 53/80 (66.3%) of cases had backtable zone MDT levels under 450. (See Figure 1) There was a statistically significant difference in UCA compliance between the wound and backtable zones (p<0.001). No PJIs were detected at average 2.15 years follow-up (range, 1.56−3.76).
Conclusion
This intraoperative clinical study found the settle plate technique to be compatible with usual TJR OR practices without additional personnel and at low cost. Almost all cases complied with the historic UCA standard in ORs without using a high ACH unidirectional airflow system. Outlier cases had explainable variations suggesting MDT data may be used as a simple quality indicator.
This settle plate system produced low-cost quantitative data suitable for larger studies investigating intraoperative airborne microbial contamination abatement measures or PJI risk.
Figures
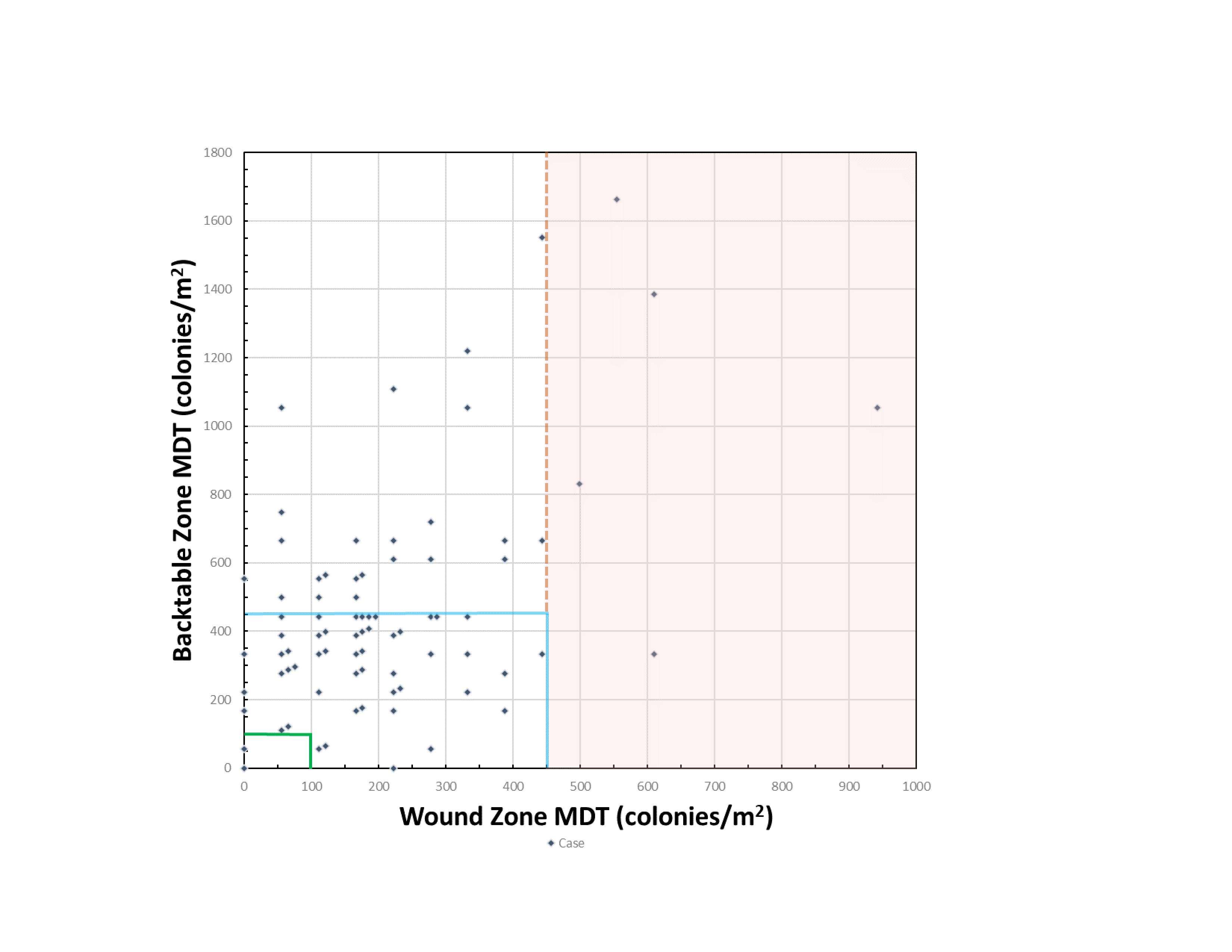
Figure 1#7687
Can Spino-Pelvic Alignment Be Improved After Hip Arthroplasty? : Focus on the Value of PI-LL
*Shigeki Hayashi - Zenshukai Hospital - Maebashi, Japan
Takahisa Sato - Public Tomioka General Hospital - Tomioka, Japan
Masashi Kimura - Zenshukai Hospital - Maebashi, Japan
Kenji Takahashi - Kyoto Prefectural University of Medicine - Kyoto, Japan
*Email: shige-h8@koto.kpu-m.ac.jp
Introduction:
The Schwab classification is very famous to examine relationship between spinal and pelvic alignment for the adult patient with spinal deformity. Many spine-surgeon try to correct lumbar lordosis (LL) according to pelvic incidence (PI). The goal of spinal corrective surgery (SCS) is to achieve a |PI-LL| value of less than 10. Recently there are some reports about dislocation of total hip arthroplasty (THA) after SCS. Especially dislocation of THA due to anterior impingement at seated position after SCS. To prevent such dislocation, it remains controversial which surgery should be done firstly. The purpose of this study is to evaluate spino-pelvic alignment after THA especially focusing on the value of standing and seated PI-LL values.
Methods:
This study included 69 patients (mean age 62.0 years, male 14) who were treated by THA at our hospital between January and July 2019. Thirty-seven patients received unilateral THA and 32 received bilateral THA. |PI-LL| was calculated and the patients were divided into two groups, group A with a |PI-LL| value of less than 10 and group B with a |PI-LL| of 10 or greater. T5-12 angle, LL, PT, Sacral slope (SS), PI, Sagittal Vertical Axis (SVA), L1 slope, LL at seated position, PT at seated position, SS at seated position, and PI at seated position were measured at standing and seated position respectively according to Schwab classification on pre-THA and 1 year follow-up radiographs. These parameters were analyzed using t-test among group A and group B, and using paired t-test among pre- and post-THA. P<0.05 was considered to be statistically significant.
Results:
There were 38 cases in group A and 31 cases in group B. There was significant difference in LL, PT, SVA, and L1 slope between group A and B before and after surgery. In group A, T5-12 angle, PT, PI, SVA and L1 slope were lesser and LL, SS, and L1 slope were greater on pre- and post-operatively (Table1,2). At standing position, post-operative LL and L1 slope were greater than pre-operative. On the other hand, there were no significant differences in the measured items in group B. At seated position, only PT were statistically decreased after surgery in group A, but in group B all of the measured items at seated position were significantly difference after surgery (Table3).
Conclusion:
In group B, there were no significant differences in the measured items between pre- and post THA. This indicated compensatory mechanisms of spino-pelvic alignment were failed in the group B. There were pre- and post-operative spino-pelvic sagittal malalignment in the group B. If the patient had good pre-oprative spino-pelvic alignment, post-operative alignment might be improved. Overmore, in group B all of the measured items at seated position were significantly difference after surgery. This indicated if the patient had pre-operative spino-pelvic sagittal malalignment it was difficult to predict the spino-pelvic alignment at seated position after THA. This result will be helpful to decide which surgery should be done for the hip spine syndrome.
Figures
Figure 1
Figure 2
Figure 3#7910
Association of Ethnicity and Patient Satisfaction Following Total Knee Arthroplasty
Jeffrey Hayashi - John A. Burns School of Medicine - Honolulu, United States of America
Kyung Moo Kim - John A. Burns School of Medicine - Honolulu, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
Tyler Thorne - University of Hawaiʻi at Mānoa - Mānoa, USA
Samantha Andrews - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
*Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: onohunter@icloud.com
Introduction: Nearly 20% of patients are not satisfied following total knee arthroplasty (TKA) and, despite previous research, no clear reason for dissatisfaction has been identified. Additionally, satisfaction data for certain minority groups following TKA are sparse. Therefore, the purpose of this study was to evaluate the influence of ethnicity and patient demographics on patient reported outcomes and satisfaction following TKA amongst a diverse population of patients in Hawaii.
Methods: Data were prospectively collected from April 2019 to April 2021 and included unilateral and bilateral procedures. Patients were grouped based on self-reported identities Asian, White or Native Hawaiian/Pacific Islander (NHPI). Patient demographics, Charlson Comorbidity Index (CCI) and six-month clinical and patient reported outcomes were collected. Analyses of variance and Chi-squared tests were performed for continuous and categorical variables, respectively. Logistic regression was performed to evaluate variables influencing satisfaction.
Results: Overall, 212 patients were included (White=123, Asian=68, and NHPI=21). Compared to Asian and White patients, NHPI had a higher body mass index (34.4±5.2kg/m2), higher CCI (2.9±2.5) and lower functional scores (42.9±18.0) before surgery. Despite NHPI having significantly lower max flexion angles (109.6Ëš±12.1Ëš) six months following TKA, there was no difference in functional scores (70.5±23.0) amongst all three racial groups. Additionally, there was no significant difference in top-box patient satisfaction scores between groups both 6-weeks and 6-months following TKA. Neither ethnicity nor patient demographics contributed to satisfaction; however, logistic regression revealed six-month functional patient-reported outcomes were the most significant contributors to satisfaction (Odds Ratio: 1.072; 95% Confidence Interval: 1.040-1.104)
Conclusion: Patient satisfaction did not appear to be affected by either racial or demographic differences. Higher perceived functional recovery, however, appeared to be associated with increased patient satisfaction. While NHPI patients had poorer self-reported functional scores prior to surgery, there was no difference six months following surgery. Racial disparities regarding function or satisfaction following TKA were not present for the minority groups studied here.
Acknowledgements: Straub Bone and Joint Center
#7654
Flexible Versus Standard Intramedullary Rod in Primary Total Knee Arthroplasty: RCT of Effects on Sagittal Contour of the Distal Femur, Implant Positioning, Functional Outcome and Sizing
*Petra Heesterbeek - Sint Maartenskliniek - Nijmegen, Netherlands
Ate Wymenga - Sint Maartenskliniek - Nijmegen, Netherlands
Menno Benard - Sint Maartenskliniek - Ubbergen, Netherlands
Thomas Bolhuis - Sint Maartenskliniek - Nijmegen, Netherlands
*Email: p.heesterbeek@maartenskliniek.nl
Introduction: In total knee arthroplasty (TKA) a flexible intramedullary rod can be used to accommodate the sagittal bowing of the distal femur. Whether a more flexed orientation of the femoral component will result in better functional outcome remains to be investigated. The goal of this RCT was to compare the flexible rod to the standard intramedullary rod in primary TKA in terms of fit of the TKA, functional outcome and component sizing.
Methods: A single-blind randomized controlled trial with two groups (flexible vs standard rod, Figure 1) in 60 patients (30/30 male/female, mean age 65.9 (SD 7.1 yrs)) with posterior-stabilized TKA (Triathlon, Stryker) was performed. Patients were evaluated up and until two years postoperative with fluoroscopic images, functional tests and patient-reported outcomes. The 3D volume images from fluoroscopy were used to determine the flexion angle of the TKA in the sagittal plane, and the sagittal profile (medial, lateral and trochlea) of the distal femur (pre and postoperative). Knee function was assessed with functional tests and patient-reported outcomes.
Results: Flexion angle of the femoral component in the sagittal plane was 2.9 degrees higher (i.e. more flexed) with the flexible rod (9.8 degrees (95% CI 8.6-11.0) vs 7.0 degrees (95% CI 6.1-7.8), p=0.0001). However, this difference in flexion did not result in any measurable differences in the other parameters: There were no differences in the sagittal profile of the distal femur (Figure 2), component sizing, nor knee function. The number of knees showing over- or understuffing was comparable between the groups.
Conclusion: Although use of a flexible intramedullary rod led to a more flexed orientation of the femoral component in the sagittal plane compared to a standard intramedullary rod, this did not result in different component fit or better functional outcome.
Figures
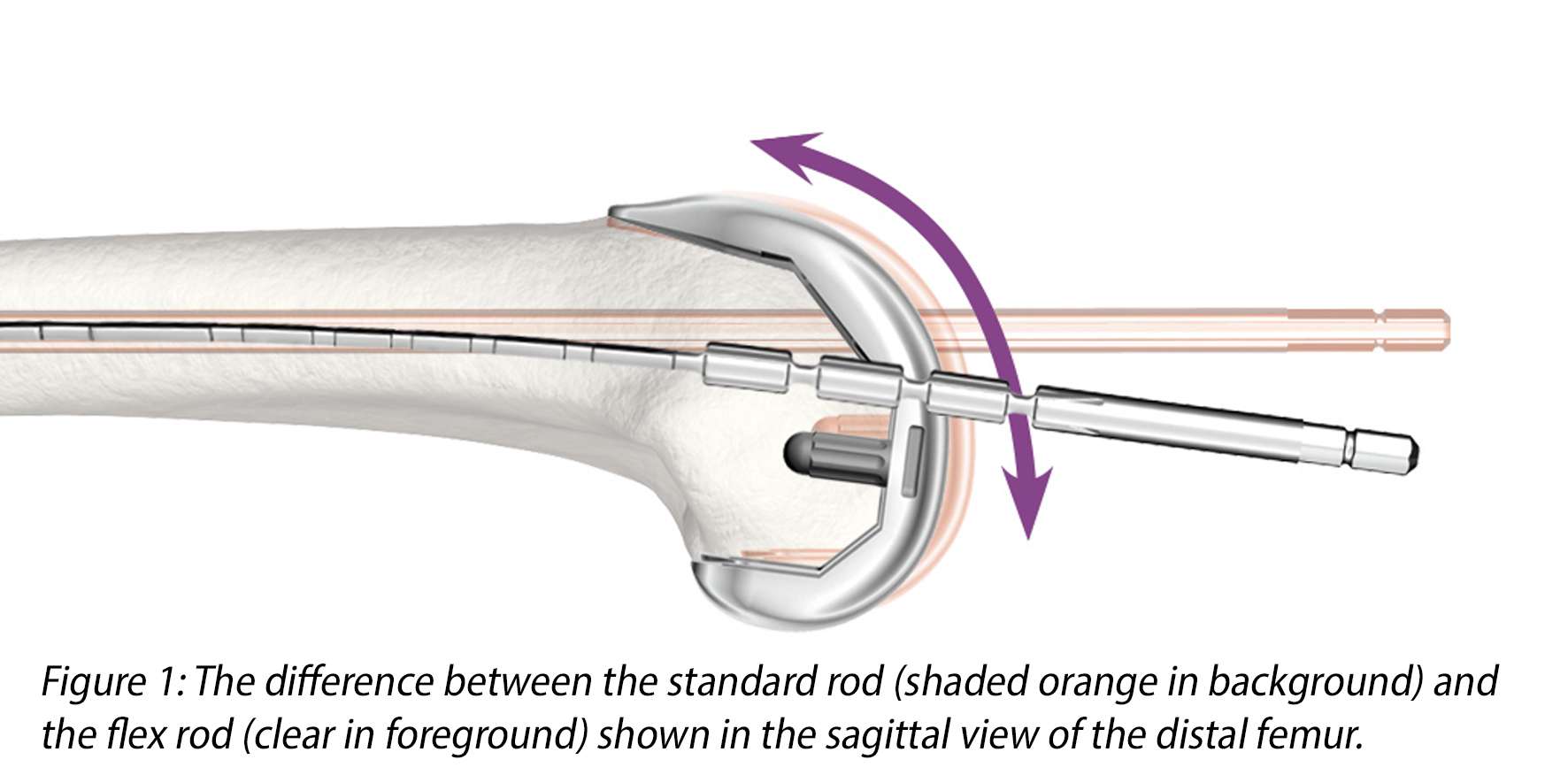
Figure 1
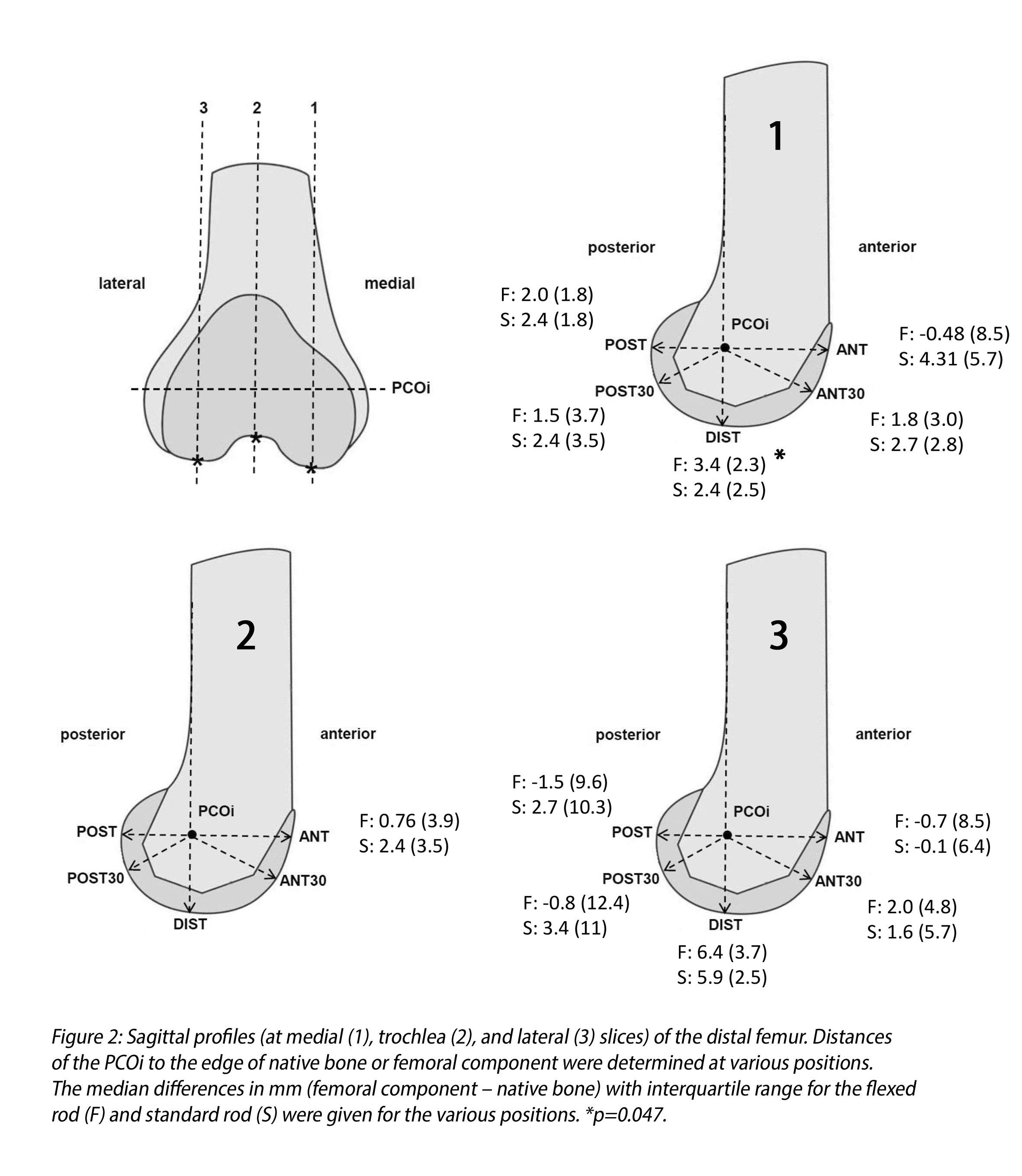
Figure 2#7893
Invited Talk: Construct Stability of Revision Total Knee Arthroplasty With Tibial Cones: Preliminary Results of a Radiostereometric Analysis (RSA)
*Petra Heesterbeek - Sint Maartenskliniek - Nijmegen, Netherlands
Gijs Van Hellemondt - Ubbergen (Near Nijmegen), Belgium
Maartje Belt - Sint Maartenskliniek - Ubbergen, Netherlands
*Email: p.heesterbeek@maartenskliniek.nl
Introduction: In (re-)revision total knee arthroplasty (TKA), cones can be used to ensure sufficient fixation of the revision construct in the bone in cases with suboptimal metaphyseal bone stock (Fig. 1). Together with press-fit placed stems of sufficient length, cones can reduce interface stresses of damaged bone in the distal femur or proximal tibia and provide additional prosthetic surface for implant fixation. Whether this construct in revision cases results in adequate stable and safe fixation of the implant in the bone, remains to be investigated. With radiostereometric analysis (RSA) it is possible to investigate the stability of the construct in a precise way. We aim to investigate the stability of the fixation in the bone of the Legion revision TKA with cones until 5 years postoperatively.
Methods: Patients who underwent a revision TKA with a tibial cone (Smith+Nephew, Memphis (TN), USA) were included in this prospective study. Patients were not eligible for the study when they were older than 78 years, had ASA>2, were planned for a hinged-type revision system, had an active local or systemic infection, or had a immunosuppressive disorder. During surgery, tantalum markers were inserted in the tibial bone to enable stability assessment using RSA analysis. RSA analysis combines two simultaneous radiographs to construct a 3D model (Fig. 2). Bone markers were used as a model representation for the bone, and 3D models of the tibia components (based on CAD models of the implants) were fitted onto the radiographs for a representation of the prosthesis. RSA radiographs were made post-operative (baseline measurement), after 6 weeks, 3 months, 6 months, 1 year, 2 years, and 5 years. Migration of the tibial component was assessed using model-based RSA software (RSAcore, Leiden, the Netherlands) by calculating the migration of the prothesis with respect to the bone over time. Migration was measured as total translation (TT) and total rotation (TR) in the x,y,z-direction. Clinical results were evaluated using the Oxford Knee Score, KOOS-PS, Knee Society Score, VAS pain and VAS satisfaction.
Results: Currently, 20 patients were included and of those, 14 patients completed the 6 months follow-up, and 13 the 1-year follow-up. The mean age at the time of surgery was 65 years (SD 6.5 years), and mean BMI was 30.7 (SD 4.7). The reason for revision was loosening (12/14), instability (1/14) and malalignment (1/14). One of the patients was lost to follow after 1 year due to a repeat revision TKA for loosening.
Discussion: So far, one patient had a repeat revision TKA for loosening, not evidently related to migration as measured with RSA. At the time of the conference, we expect to share the 1-year migration results of 16 out of 20 patients.
Figures

Figure 1
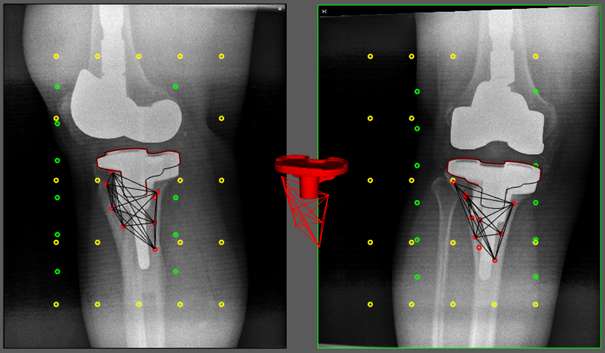
Figure 2#7974
Bonding of Silicon Nitride Particles to Ti-6Al-4V via Aqueous PEKK Solutions to Improve Biological Response
*Jackson Hendry - SINTX Technologies - Salt Lake City, USA
Tony Decarmine - Oxford Performance Materials - South Windsor, USA
Erin Jones - SINTX Technologies - Salt Lake City, USA
Douglas Hoxworth - SINTX Technologies - Salt Lake City, USA
James Porteus - Oxford Performance Materials - South Windsor, USA
Bryan McEntire - SINTX Technologies, Inc. - Salt Lake City, USA
Sonny Bal - Sintx - USA
Ryan Bock - SINTX Technologies - Salt Lake City, USA
*Email: jhendry@sintx.com
INTRODUCTION: While advances in 3D printing technology have enabled advances in implant design, infection is still a major concern [1]. Current spinal implant designs commonly leverage titanium alloy’s (Ti-alloy) mechanical properties to include intricate porous structures that facilitate bone ingrowth, but the associated increased surface area also increases risk of infection. Alternatively, silicon nitride (Si3N4) is a ceramic material that exhibits inhibition of biofilm formation and improved osteogenic properties relative to those of Ti-alloy [2]. Monolithic Si3N4 has been commercialized as a spinal fusion device material. However, Si3N4’s inherent properties present challenges for production of complex geometries and in applications where the device will undergo significant tensile loading. Using a high strength polyetherketoneketone (PEKK) matrix to bond Si3N4 particles to a Ti-alloy implant surface couples the cost and mechanical properties of titanium with the antibacterial and osteogenic properties of Si3N4.Aqueous PEKK solution (OXPEKK-SC, OPM) functions as a suspension medium allowing dispersed ß-Si3N4 particles to infiltrate and cover the surface of intricate implant geometries. Ultra-thin, composite PEKK-Si3N4 films on titanium implants could provide improved functionality to titanium implants by reducing the incidence of post-operative implant infections and enhancing osseointegration.
METHODS: Si3N4-PEKK composite coatings were adhered to Ti6Al4V ELI (Grade 23 ASTM F136) discs (Ø 12.7mm x 1mm thick) by dip coating into various concentrations of submicron ß-Si3N4 particles suspended in an aqueous PEKK solution (OXPEKK®-SC, Oxford Performance Materials). Acid functional groups were thermally driven from the dried composite coatings and subsequently heated to peri-melting temperatures to form a fully contiguous composite film. Coupons treated with the composite coating were characterized by visible light microscopy (VLM), scanning electron microscopy (SEM), confocal laser scanning microscopy (CLSM), and progressive load scratch testing to quantify mechanical properties of the coating. Resistance to bacterial colonization by a biofilm-forming strain of S. epidermidis (ATCC®14990™) was assessed in vitro using a diluted human plasma-based inoculum at time points of 24 and 48 hours according to a previously published protocol [2].
RESULTS: Modulation of Si3N4 surface coverage density was achieved by varying the quantities of dispersed Si3N4 and dissolved PEKK in the aqueous solution. Relatively low volume fractions of Si3N4 in the casting slurry resulted in dense areal coverage of uniformly dispersed Si3N4 particles on the composite surface. Figure 1 shows SEM imagery used to correlate the areal loading of Si3N4 in the final composite film with the dip coating slurry composition. Figure 2 shows that a roughly 12% increase in area occupied by Si3N4 is achieved with every 1% increase of ceramic volume in the slurry. Thicknesses of the composite coatings ranged from 0.25µm to ~3µm as a function of slurry composition. Coatings reproduced surface topography with high resolution. PEKK-Si3N4 coatings readily wet titanium surfaces which would allow its infiltration into scaffold or cage design implants. Bacterial CFU counts are reduced relative to the PEKK control and untreated titanium benchmark samples. This reduction roughly correlates to the Si3N4 surface coverage.
Figures
Figure 1
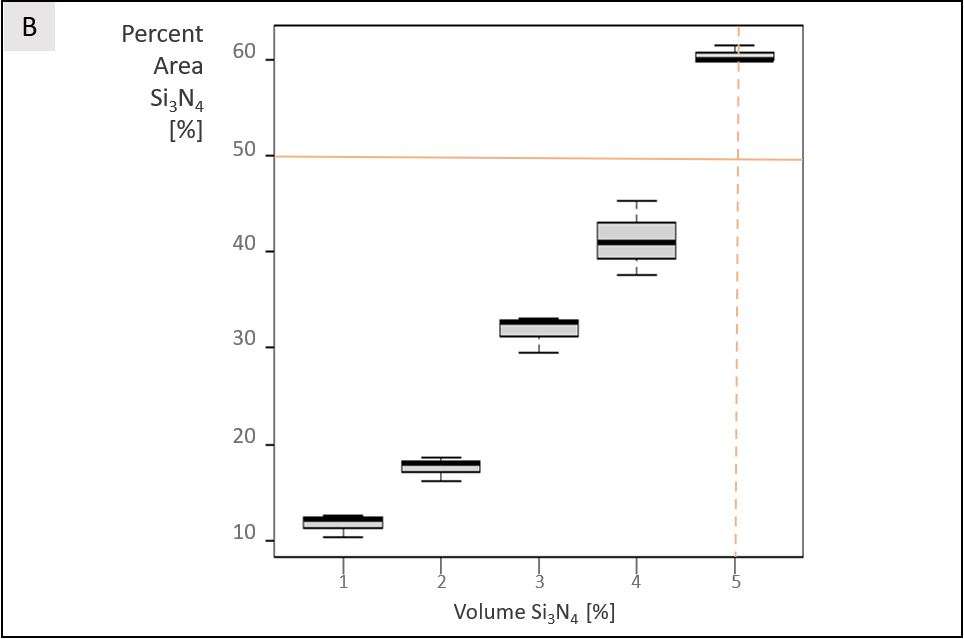
Figure 2#7420
Restrictions, Compensations, and Anatomic Biases in Reverse Total Shoulder Arthroplasty
Hema Sulkar - University of Utah - Salt Lake City, USA
Klevis Aliaj - University of Utah - Salt Lake City, USA
K. Bo Foreman - University of Utah - Salt Lake City, USA
Peter Chalmers - University of Utah - Salt Lake City, USA
Robert Tashjian - University of Utah - Salt Lake City, USA
*Heath Henninger - University of Utah - Salt Lake City, USA
*Email: heath.henninger@utah.edu
Introduction
Scapulothoracic and glenohumeral motion are altered after reverse total shoulder arthroplasty (rTSA), with greater scapulothoracic contributions [1, 2]. While prior motion analysis studies generally focused on average rTSA patients, examining deficient populations with highly accurate 3D biplane fluoroscopy provides insight into the origins of functional limitations. This technique also avoids skin artefact that corrupts interpretation of underlying motion. The objective of this study was twofold: 1) quantify 3D rTSA shoulder kinematics without and with a handheld weight, and 2) quantify 3D shoulder orientations of rTSA patients who can and cannot perform internal rotation in adduction.
Methods
Subjects >1-year post-operative to rTSA provided informed consent at enrollment. A total of N=10 subjects performed scapular plane elevation without and with a 2.2 kg handheld weight. A total of N=15 subjects performed internal rotation in adduction, where static resting neutral and maximum achievable internal rotation poses were collected. The biplane fluoroscopy system was spatially and temporally synchronized to an optical motion analysis system, which quantified the torso relative to scapulothoracic and glenohumeral orientations. Model-based markerless tracking aligned 3D models of the bones generated from subject-specific CT scans to calculate joint angles. Paired statistics compared (un)weighted scaption activities within subjects, whereas independent group statistics compared individuals who could and could not achieve internal rotation. Data from healthy individuals [3] provided context for relative restrictions, compensations, and biases in rTSA subjects.
Results
When performing scapular plane abduction with a handheld weight, 4 of 10 rTSA subjects could not achieve 90° humerothoracic elevation (-25±29°, Fig. 1). In these individuals, over 90% of arm elevation originated from scapulothoracic lateral rotation with virtually no glenohumeral elevation. Restricted elevation was thus limited by achievable scapulothoracic rotation. In resting neutral poses, individuals with high internal rotation capabilities demonstrated more scapular lateral rotation and anterior tilt (Fig. 2), and less glenohumeral elevation. At maximum internal rotation these differences were not present. Counterintuitively, individuals with high internal rotation had more pose differences versus healthy controls than those with low internal rotation, most notably with 10° more scapulothoracic retraction. Anatomic biases in humeral internal rotation (torsion) may also influence the ability to perform internal rotation in adduction (Fig. 3).
Conclusions
Individuals with functional limitations after rTSA provide important data for consideration in surgery, implant design/selection, and rehabilitation. For example, the inability of 40% of individuals to perform arm elevation with modest loading was previously observed in the laboratory but omitted from analysis [4], and is not considered in clinical assessments [5]. The present data precisely quantify the large kinematic changes within these individuals. Only recently have the 3D relationships of the scapula, humerus, and torso been considered with respect to functional capabilities after rTSA using 3D models [6]. The present data systematically quantify how the 3D relationships of the shoulder and torso relate to functional limitations in living individuals. More research is required to determine how these identified factors are affected by surgical technique and implant design, and determine predictive measures to identify patients at risk of functional deficit.
Figures
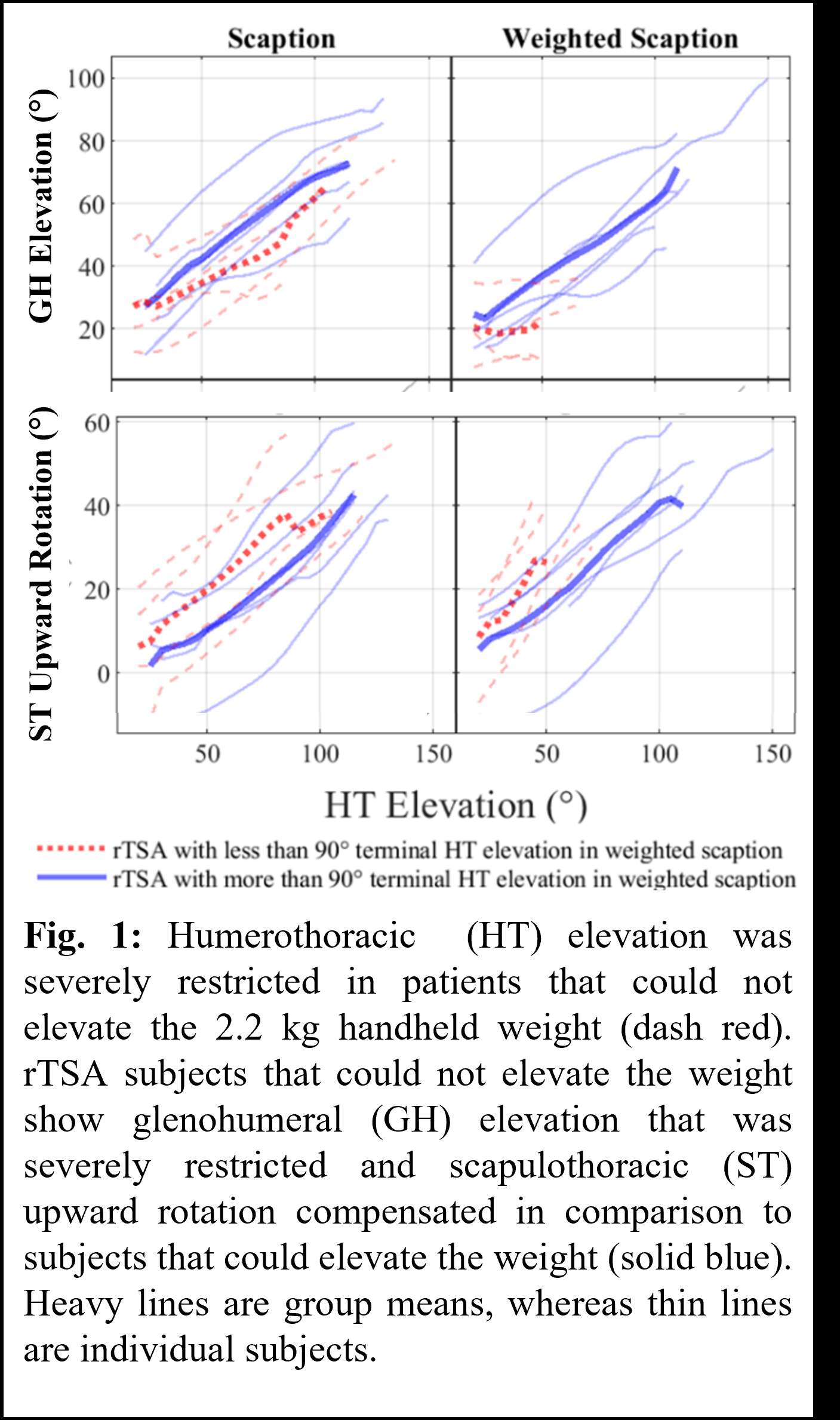
Figure 1
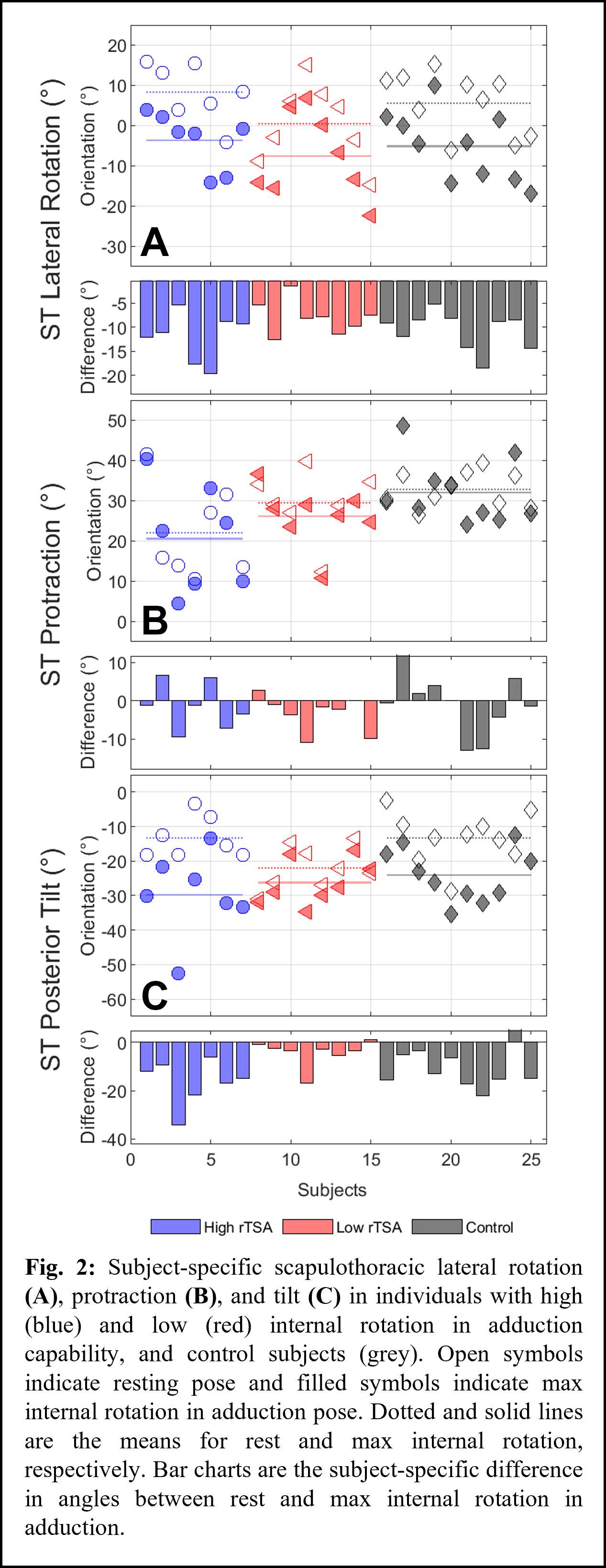
Figure 2
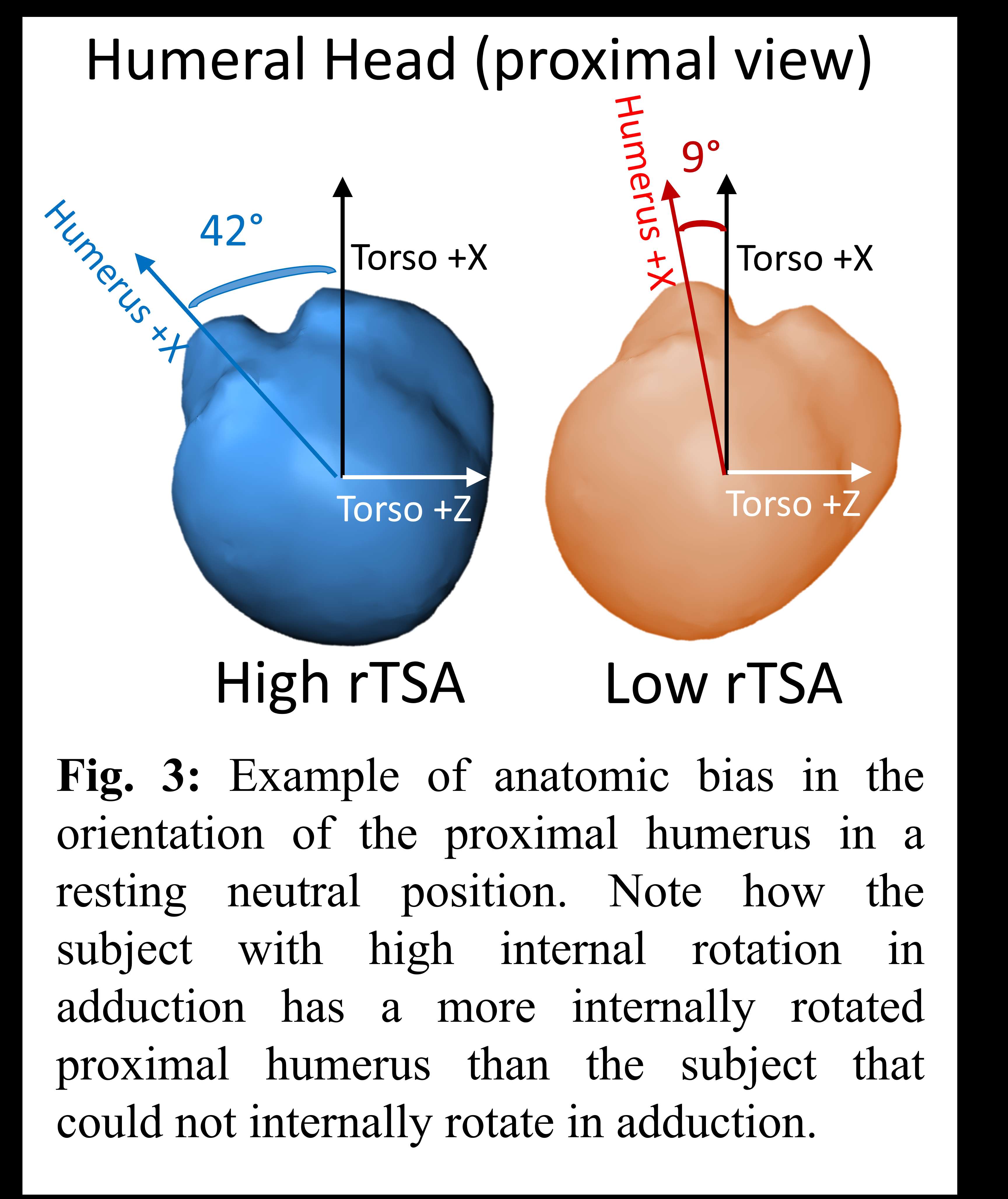
Figure 3#7459
An Efficient Experimental Design for Determining Functional Relationships Between Surgeon-Controlled Variables and Risk of Revision
*Matthew Hickey - The University of British Columbia - Vancouver, Canada
Carolyn Anglin - University of Calgary - Calgary, Canada
Bassam Masri - University of British Columbia / Department of Orthopaedics - Vancouver, Canada
Antony J Hodgson - The University of British Columbia - Vancouver, Canada
*Email: matthew.hickey@hiphealth.ca
Introduction: Innovations in surgical robotics and navigation have significantly improved implant placement accuracy in total knee arthroplasty (TKA), however, they have not substantially reduced revision rates (Kim 2020, Ollivier 2018). This disconnect between improved surgical accuracy and limited changes in clinical outcomes reflects a deficiency in the fundamental understanding of the causal factors affecting implant failure. We conducted a simulation study to investigate if a match-controlled study design would be an efficient analysis strategy to determine functional relationships between surgical variables and risk of revision.
Methods: To determine the feasibility of this approach, we generated large populations of simulated TKA patients and assigned individual estimated risks of revision based on patient-specific factors (age at index, BMI, gender) and two surgeon-controlled variables (overall coronal alignment and tibial slope) using a previously developed method in which the effects of these variables are presumed to be known (Hickey 2021). We randomly sampled patients presently experiencing implant failure in our simulation. For each revision candidate, a simulated functioning patient was randomly matched based on patient-specific factors and length of implant survival. Simulations were conducted with various group sizes (N=50–200) in each of the experimental and control arms. For each study size, 10 Naïve Bayes classifiers representing individual mock studies were trained based on different samplings of the patient population. Within each mock study, the optimal overall coronal alignment and tibial slope was calculated in addition to the predicted functional relationships between orientation and implant life factor (k, a normalized measure of the impact of changes in surgical variables on revision risk (Hickey 2021)).
Results: Across different study sizes, our classifier predicted the functional relationships between k and two surgeon-controlled variables (overall coronal alignment and tibial slope, Fig.1), with average errors of less than 5% and 3% (Fig.2) and predicted optimums within 1.5⁰ and 0.1⁰ (Fig.3), respectively, with as few as 100 patients in each study arm.
Discussion: The results of this simulation show that a match-controlled methodology may be an efficient approach to determine the impact of surgeon-controlled variables on revision risk in TKA. Unexpectedly, the classifier consistently predicted a more valgus knee to be optimal compared to neutral, likely due to the varus/valgus asymmetry in the assumed function for k, though this only represents a change of ~2% in the estimated k between the assumed and predicted optimum. In future iterations, we will explore alternative machine learning techniques that might better capture this asymmetry while also handling additional surgeon-controlled variables. In practice we imagine this type of analysis would be used retrospectively, with patient implant positions either measured directly at the time of revision or using intraoperative measurements obtained from navigated/robotic devices at the time of index surgery. In the former case, there is a risk that implants may have moved compared to the index surgery, so pre-revision implant position estimates may need to be corrected by cross-reference to radiographs obtained at the time of index surgery. Accurate functional relationships generated from this type of study design could improve future surgical planning processes.
Figures
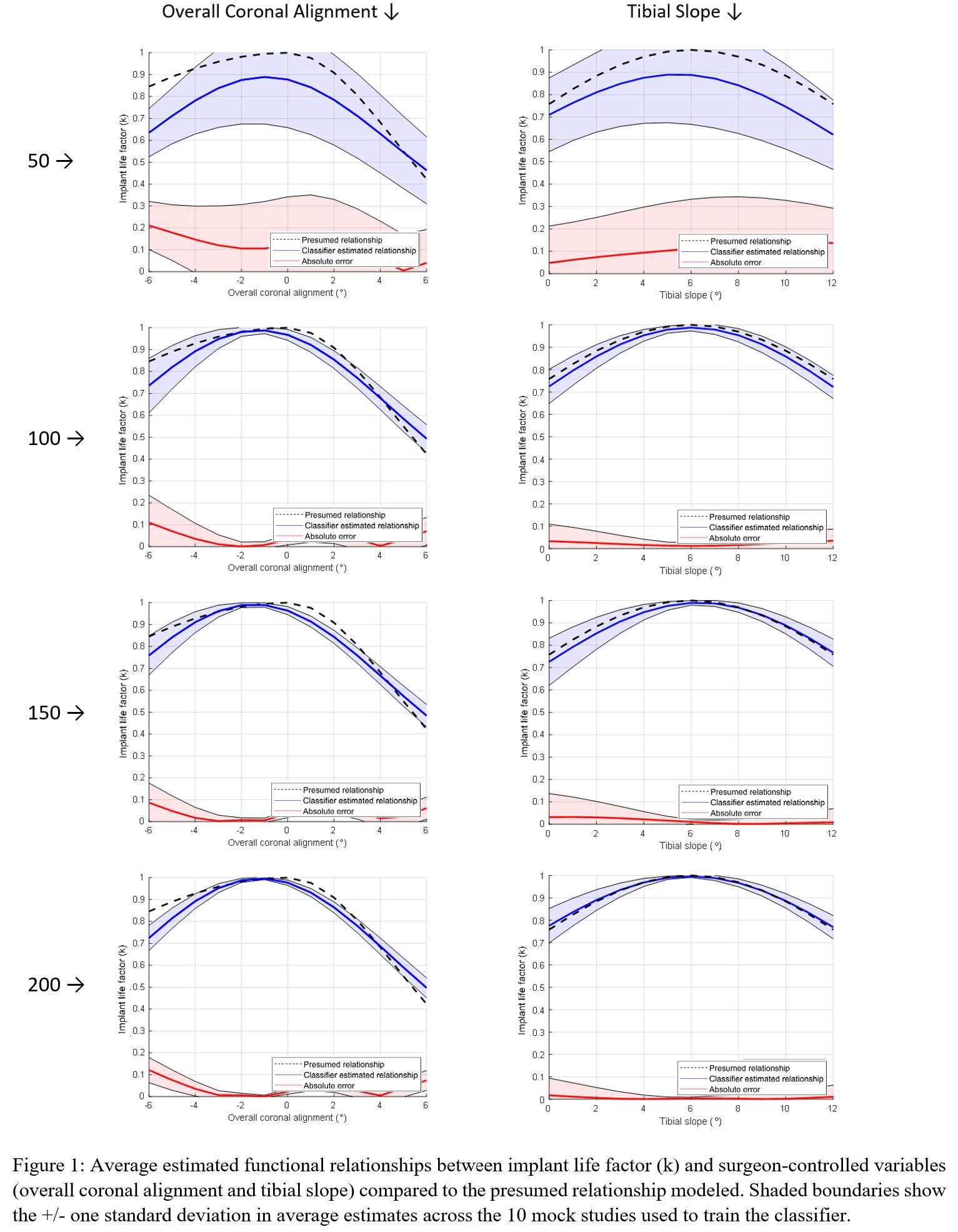
Figure 1
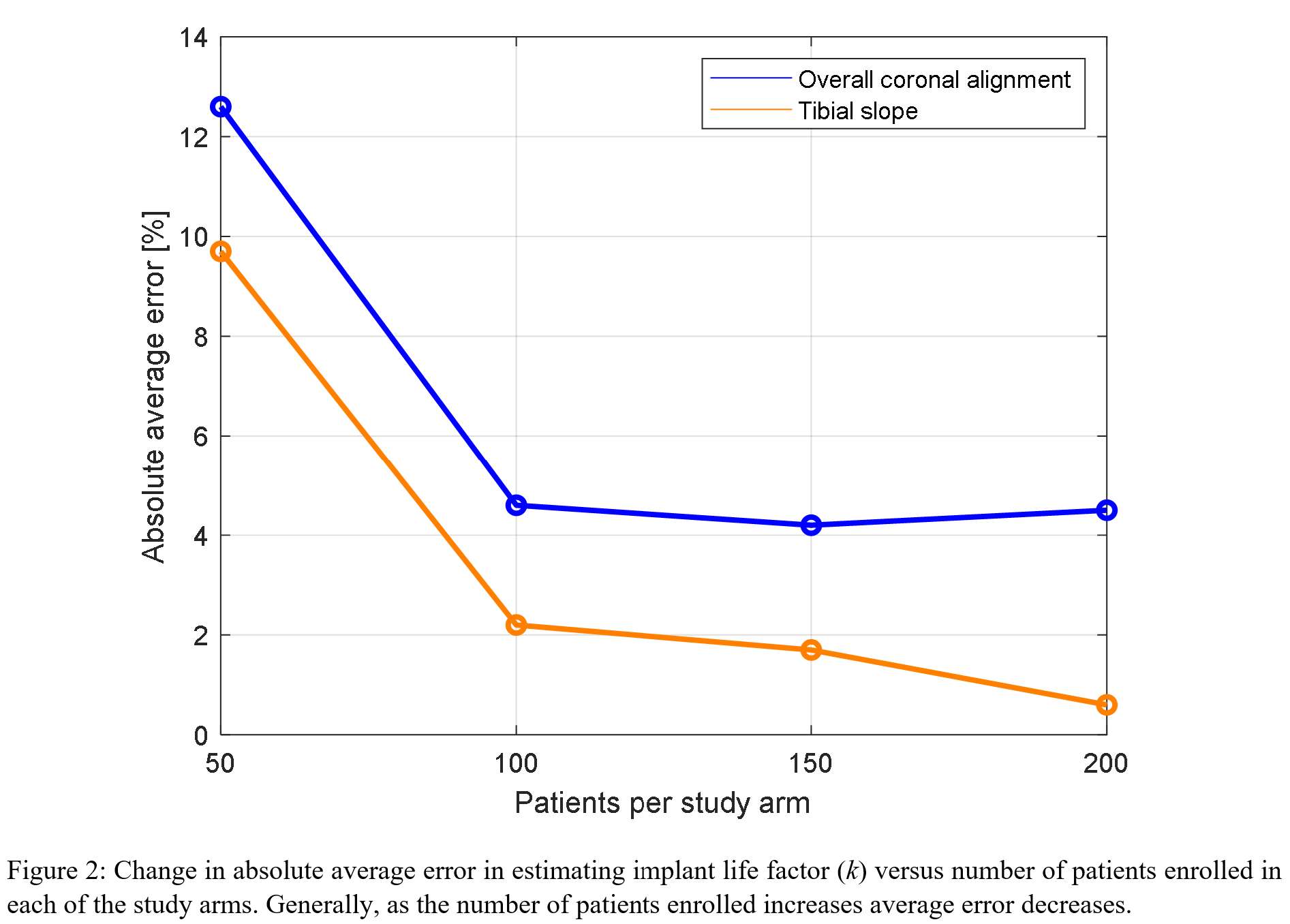
Figure 2
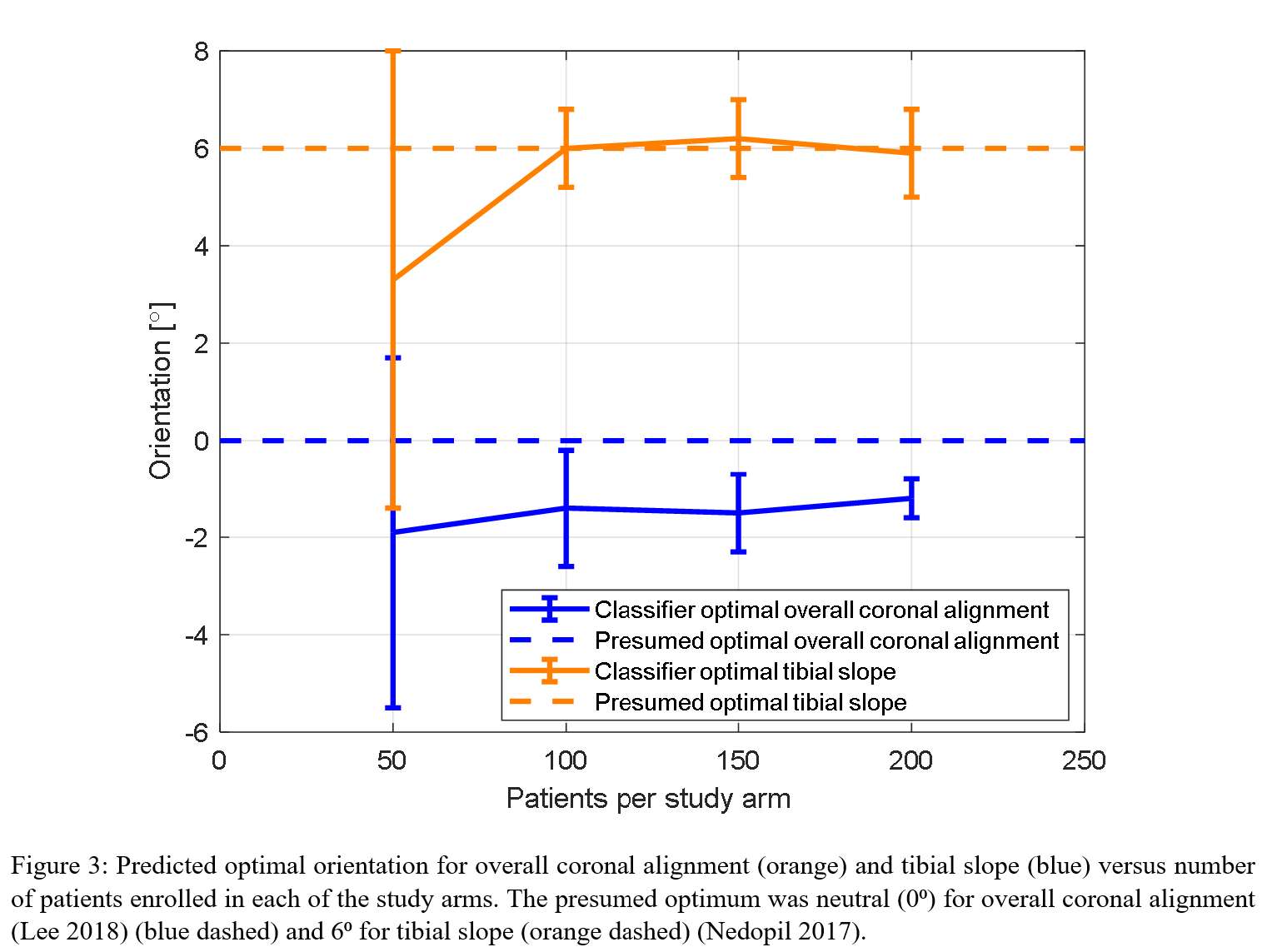
Figure 3#7578
Impact of Porous Shoulder Implant Stems in Various Humeri Densities
*Sydney Hitchon - University of Western Ontario - London, Canada
Jaques S. Milner - University of Western Ontario - London, Canada
David Holdsworth - Western University - London, Canada
Ryan Willing - Western University - London, Canada
*Email: shitcho2@uwo.ca
Introduction: Two-staged revision surgeries for orthopaedic device-related infection (ODRI) are strenuous on patients and healthcare systems. A permanent porous implant, loaded with antibiotics, could allow for a single-stage revision surgery following ODRI. Gyroids are porous structures with reduced stress concentrations compared to other periodic porous structures whose porosities can be altered to manipulate their stiffness [1]. The purpose of this research is to evaluate porous humeral stem components for their mechanical strength and their resulting effects on load transfer through proximal humeri of different bone densities, using finite element models (FEM).
Methods: Porous humeral stems were constructed in gyroid structures at porosities of 60%, 70%, and 80% using computer-aided design (CAD) software and assumed to be made of titanium (Ti6Al4V). These CAD models were analyzed using FEM (Abaqus) to look at the stress distributions throughout the stem components and resulting stress and strain distributions within the proximal humeri. An average bone shape was created using a statistical shape and density model (SSDM) based on 75 cadaveric shoulders (57 males and 18 females, 73 +/- 12 years) [2]. The Young’s moduli (E) of the cortical and trabecular bones were defined on an element-by-element basis, with a minimum allowable E of 15 MPa. Three bone densities, representing a healthy, osteopenic, and osteoporotic humerus were analyzed. Boundary and loading conditions were applied to the humeri to represent the arm being actively held in four positions: 45° and 75° of abduction and 90° and 120° of flexion. The strain energy densities within the humeri were compared with corresponding intact bone to calculate the volume fraction of resorption/formation of each bone density.
Results: The volume fraction of resorption/formation of each bone density were averaged over all loading scenarios for each stem porosity and compared to a solid stem (Figure 1). The porous stems do not cause further bone resorption than the solid stem and show a reduction in bone resorption as stem porosity increases in the osteoporotic bone. With the exception of a few mesh dependent singularities, all three porous stems show stress distributions below the yield strength of Ti-6Al-4V (880 MPa) for each loading and bone density scenario (Figure 2) [3].
Conclusion: This study indicates that these gyroid stems have adequate strength for implantation and do not negatively influence bone mechanobiology within the proximal humerus and may provide mechanobiological benefits when employed in the osteoporotic bone. Although a fatigue analysis has not been performed, the stress distributions do not predict catastrophic failure under physiologically-relevant loads. Future work should explore the employment of these porous stems across different bone geometries and a formal prediction of their fatigue lives. These results show that use of porous gyroid stems is mechanically viable, and so could play a role in drug delivery for single-stage revision surgery.
References: [1] Kelly et al. Acta Biomaterialia 2019; 94: 610-626. [2] Soltanmohammadi et al. Journal of Biomechanical Engineering 2020; 142 [3] Boyer et al. Materials Properties Handbook: Titanium Alloys 1994
Figures
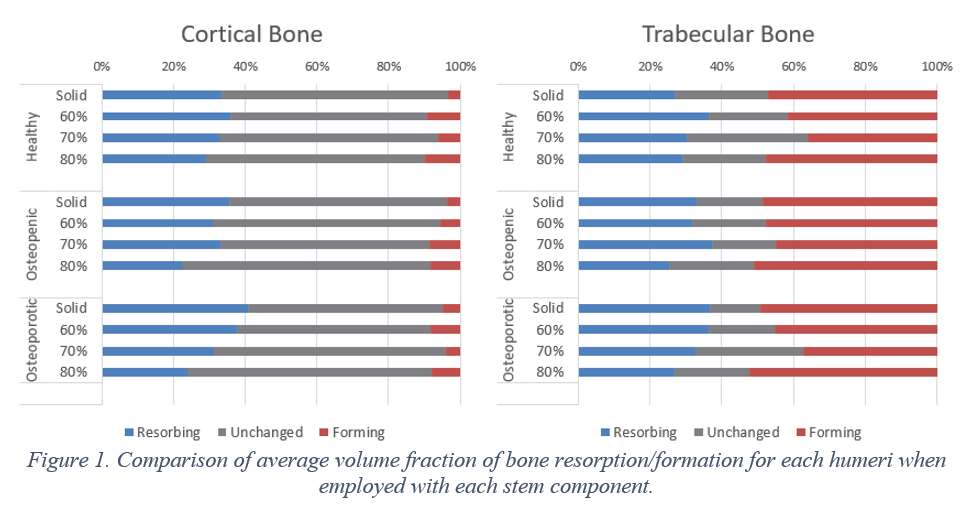
Figure 1
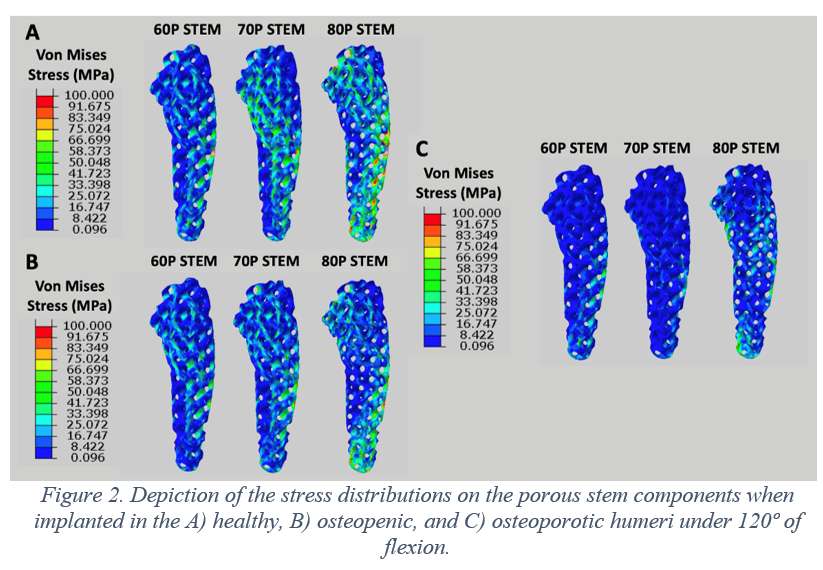
Figure 2#7842
Outcomes of Cementless Short-Stem Total Hip Arthroplasty in Elderly Patients
*Nathaniel Villanueva - University of Hawaii John A. Burns School of Medicine - Honolulu, United States of America
Richard Ho - John A. Burns School of Medicine, University of Hawaii at Manoa - Honolulu, United States of America
Thomas Kane - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: nvillanu@hawaii.edu
INTRODUCTION
Cementless short-stemmed femoral components for total hip arthroplasty (THA) have conventionally been avoided in older patients due to poorer bone quality. However, cementless implants eliminate the risk of cement-related systemic adverse events, save time, and facilitate less invasive surgical approaches. The purpose of this study was to examine fracture rates and patient-reported outcomes in elderly patients receiving a cementless, taper-wedged short-stem THA.
METHODS
This was a prospective evaluation of 158 osteoarthritic patients (185 hips) aged ≥ 70 years undergoing elective unilateral or bilateral THA. All patients received the same cementless short stem and the same orthopedic surgeon performed all surgeries. Pre-operative Hip Disability and Osteoarthritis Outcome Score for Joint Replacement (HOOS JR), intra-/post-operative fractures and 90-day complications were reported for all patients. Improvements in patient-reported outcomes for patients with a minimum six-month follow-up (131 patients; 152 hips) were calculated.
RESULTS
Demographics for unilateral and bilateral patients included: age (75.4±5.0; 74.4±3.8 years), males (47.3%; 25.9%), body mass index (27.0±5.1; 26.1±4.3kg/m2) and Charlson Comorbidity Index (2.5±2.0; 2.3±1.6). Two (1.1%) intraoperative calcar fractures occurred and two (1.1%) post-operative fractures were incidentally noticed on six-week radiographs but did not require treatment. For unilateral and bilateral patients with a minimum six-month follow-up, improvements in HOOS JR were present (38.4±18.6; 33.4±21.5) and 94.5% and 95.1% of patients were “very satisfied” or “satisfied” at their last visit, respectively.
CONCLUSION
The results of the current study suggest a cementless short stem can be used during THA in the elderly patient population for the treatment of osteoarthritis. The low fracture rate and good patient reported outcomes demonstrate the safety and effectiveness of this traditionally avoided approach in the elderly.
#7954
Is the ASTM Standard Sufficient to Test Total Knee Arthroplasty Anterior-Posterior Constraint?
*Sander Holthof - Imperial College London - London, GB
Richard van Arkel - Imperial College London - London, United Kingdom
Andrew Amis - Imperial College of London - London, UK
Michael Rock - DePuy Synthes Joint Reconstruction - Leeds, United Kingdom
*Email: sholthof@ic.ac.uk
Introduction: Instability following knee arthroplasty leads to poor outcomes, affects up to 20% of patients and remains a leading cause of revision and hence is an area of active research interest. Cadaveric, computational and fluoroscopic studies have observed paradoxical anterior translation of the femur (i.e. posterior tibial translation) in patients (Clary et al., 2013; Khasian et al.,2020; Pfiztner et al., 2018) and it has been hypothesised that this is caused by multi-radius knee designs, with the instability triggered by the change in radius. However, current stability tests (ASTM-F1223) focus on analysing implant constraint at discrete angles of knee flexion and hence may be unable to detect any instability arising from the change in radius if it occurs between the discrete positions analysed. This study aimed to analyse total knee arthroplasty anterior-posterior constraint during flexion/extension movements to examine how changing implant radius affects constraint.
Methods: Two implants were tested: 1) a traditional implant with a multi-radius femoral component and 2) a modern implant with gradually reducing radius. An industrial robotic arm (KR160-R1570-nano, Kuka, Germany) (figure 1), with 160 kg payload and simVITRO control software (simVITRO, USA), was used to analyse implant anterior-posterior constraint under static and dynamic loading. First, it was measured in accordance with ASTM-F1223 at discrete angles of knee flexion (0,15,30,60,90). Then, the implants were re-analysed throughout a continuous flexion-extension arc between 0-90° under fixed anterior tibial translation loading (-100 N, 0 N and 100 N). For all tests, 710 N compression was applied and the implant was lubricated using de-ionised water, in line with ASTM-F1223. Tibial anterior translation was measured in relation to the midpoint of a femoral transcondylar axis derived kinematically, in accordance with a built-in simVITRO optimisation algorithm (Nagle et al, 2021).
Results: Static testing revealed little difference in constraint between the implants, however, dynamic testing revealed kinematic differences between the implants. Under anterior tibial drawer, paradoxical anterior femoral translation of up to 2 mm was observed in the multi-radius design in low flexion, with posterior femoral rollback in higher flexion (figure 2). The angle at which the paradoxical anterior translation transitioned to femoral rollback correlated with load-bearing contact at the change in radius of the knee implant design. Conversely, the implant with gradually reducing radius exhibited a smoother translation pattern throughout flexion, with anterior tibial translation under anterior tibial force at all angles of knee flexion (figure 2). The gradually reducing radius design was more stable overall (ranging from 0.3 to 4.9 mm) compared to the traditional multi-radius design (ranging from -1.8 to 5.6 mm).
Conclusion: Testing implant constraint at discrete flexion angles misses important effects of implant design that are detected when testing across a complete flexion-extension arc. The gradually reducing radius design did not lead to the paradoxical anterior femoral translation apparent for the multi-radius design, and exhibited greater overall anterior-posterior constraint during flexion/extension movements.
References:
Clary, C. W. et al. (2013). J.Biomech, 46(7), 1351-1357.
Khasian, M. et al.(2020). J.Athroplasty, 35(4), 1101-1108.d
Pfitzner, T. et al. (2018). KSSTA, 26(6), 1645-1655.
Nagle, T. et al. (2021). J.Biomech 127 : 110664.
Figures

Figure 1
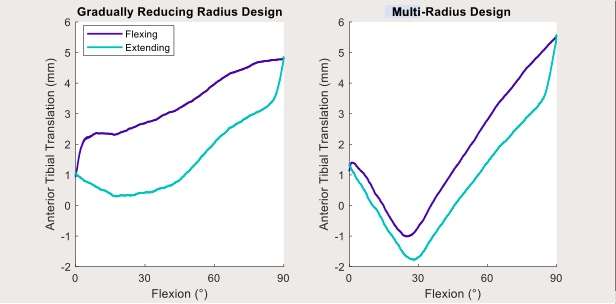
Figure 2#7576
Can Models Help to Identify Modular Revision Stems at Risk for Failure?
*Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
Klaus-Peter Günther
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: g.huber@tuhh.de
INTRODUCTION
Failure of uncemented modular revision stems is a rare but serious event. It mainly occurs at the taper junction and has been reported independent of manufacturer or design. Based on numerical estimations of taper loading, implant configurations that are mechanically less prone to failure have been identified [1]. The question remains, whether the mechanical analysis of implant configuration is sufficient to explain clinical failures. The aim of the study was to determine individual implant loading of clinically fractured revision stems using a mechanical model.
MATRIALS AND METHODS
Anthropometric and implant data of 6 patients with failed modular revision stems were available (Revitan, Zimmer Biomet, Warsaw, Indiana). The modular titanium (Ti) alloy stem is assembled with a Protasul®-21 taper to the Ti alloy neckpiece. A estimate of the finite life fatigue strength for the taper material of 800 MPa is assumed [2].
A parametrical analytical 3-D model was adapted based on the individual clinical data (patient weight, neck segment length and offset), but the proximal bone support was neglected. The anteversion angle was unknown and set to 12.5° [3]. Loading at the taper junction between neck segment and stem was determined for different common activities [3].
RESULTS
Mean patient age was 71.7 ± 7.8 years, implant offset 51.1 ± 5.7 mm, neck segment length 67.8 ± 4.8 mm, time in-situ 5.1 ± 1.6 years, and body weight 91.2 ± 16.3 kg (missing weight of one patient was replaced by mean value).
Stresses at the taper junction varied greatly between patients and activities (Figure 1) and amounted to more than 500 MPa even for low load activities such as walking (505 ± 76 MPa; Figure 2). For higher load activities such as stair climbing (606 ± 91 MPa), the finite life fatigue strength is nearly reached in 1 patient (patient 118, Figure 1). Jogging would risk plastic deformations in 6 of the 7 patients (939 ± 140; Figure 2). No correlation between taper stress during any activity and time to failure was observed.
DISCUSSION & CONCLUSION
Optimum neck segment length with minimum taper stress at the taper junction depends on patient and activity due to the differences in loading magnitude and direction.
It is unknown how active the aged patients will be after surgery, but taking the high loading during jogging, a slightly longer neck segment could have caused a minor reduction of stresses at the taper junction for all patients - just for this this specific activity (Figure 1).
High differences in stress magnitude at the taper junction were observed, even though only implants with fractured tapers were simulated. It is probable that the highly loaded taper junctions are always at risk, but that implant geometry is only one factor influencing the risk for failure. Other factors like taper assembly, specific activity or proximal bone support might play a similarly important role.
REFERENCES
[1] Huber et al., Clin Biomech, 2021
[2] Streicher et al., Proc Inst Mech Eng H, 210(3), 1996
[3] Bergmann et al., PLoS One 11 (5), 2016
Figures
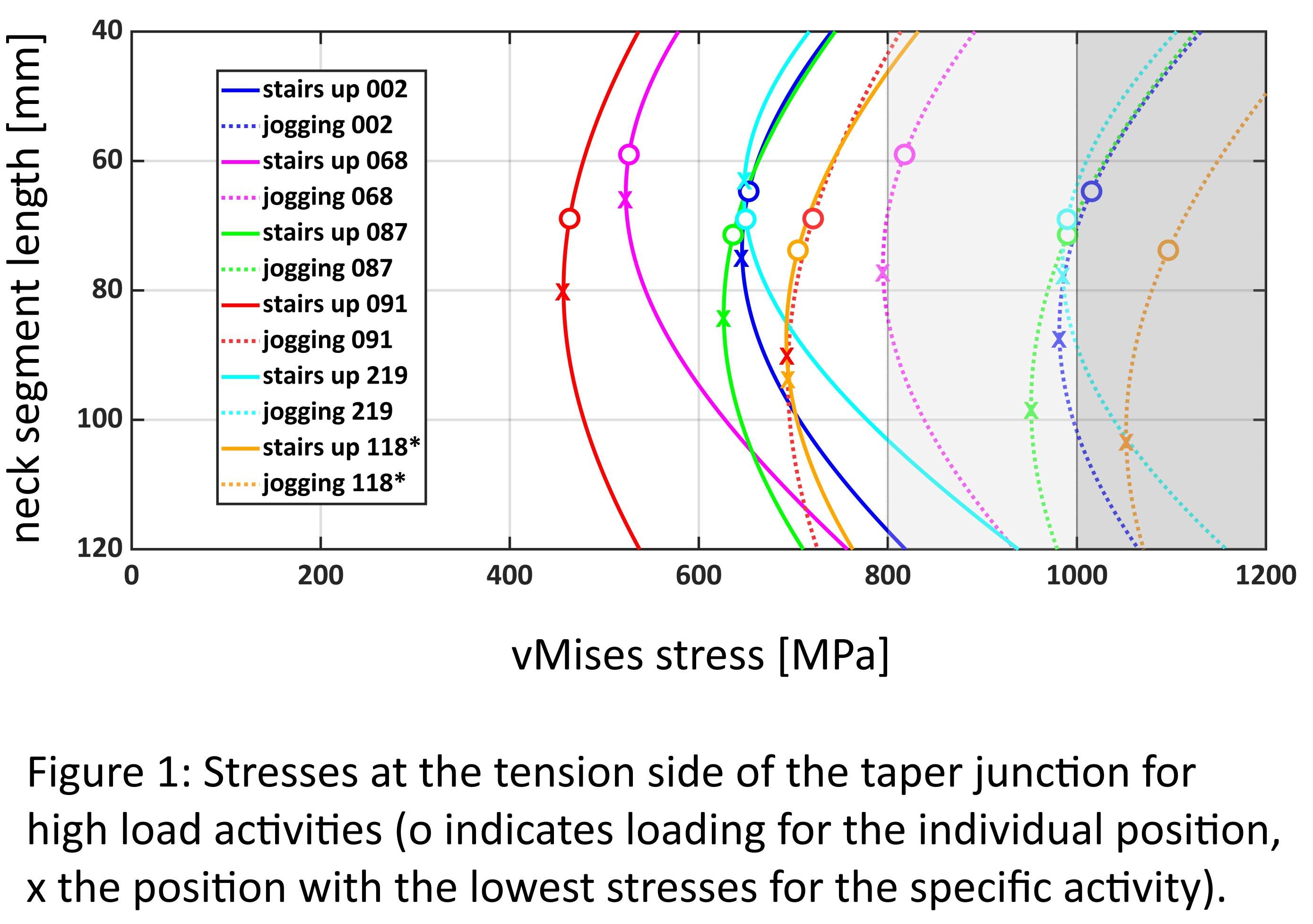
Figure 1
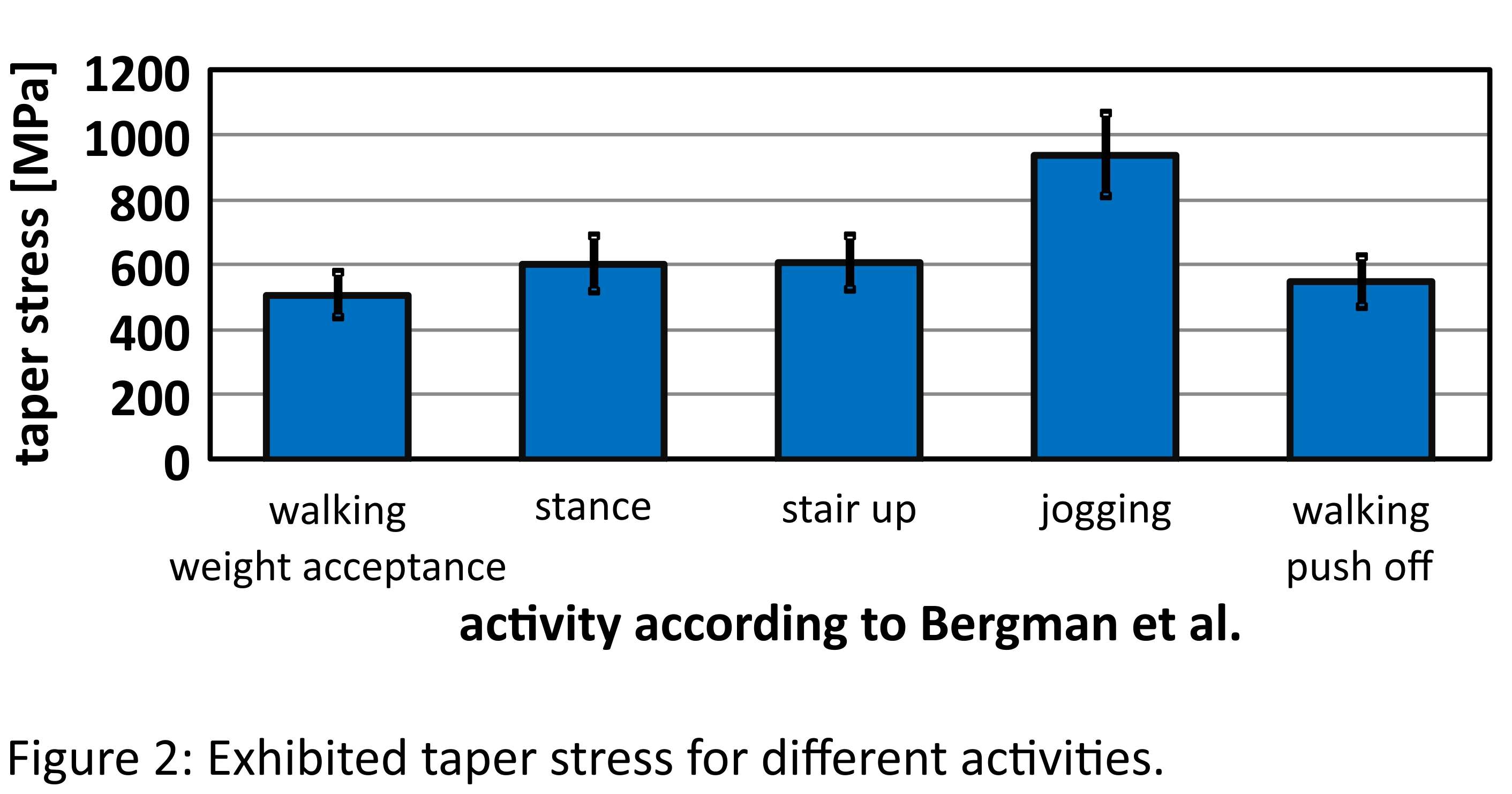
Figure 2#7978
Ability to Achieve Mediolateral Gap Balance With Instrumented Navigated Total Knee Arthroplasty - a Review of the First 273 Cases
*James Huddleston - Stanford University - Woodside, United States of America
Laurent Angibaud - Exactech, Inc. - Gainesville, USA
Amaury Jung - Blue Ortho - La Tronche, France
Cyril Hamad - Blue Ortho - La Tronche, France
Wen Fan - Exactech - Gainesville, USA
Mark Davis - Davis Orthopaedics - Prescott Valley, USA
Brian Zirgibel - Tallahassee Orthopedic Clinic - Tallahassee, USA
Jake Deister - Stormont Vail Hospital - Topeka, USA
*Email: jamesh3@stanford.edu
1 Introduction
Appropriate management of soft tissue envelope at the time of the surgery is critical to the long-term success of total knee arthroplasty (TKA) [1]. Recent computer-assisted orthopedic surgery (CAOS) systems encompass the possibility of characterizing the soft-tissue envelope throughout the full arc of motion so the planning for bone cut parameters can be based on thorough soft-tissue information [2], as well as performing a final check of the achieved ligament balance of the knee joint. However, only few studies have detailed the ability to achieve targeted mediolateral (ML) gap balance [3].This study assessed this ability by comparing the final ML laxity measured during the trial reduction with the planned ML laxity defined prior to any bone resections.
2 Methods
A retrospective review was performed on a proprietary, cloud-based web database that archived technical logs of cases performed using an instrumented CAOS system (Newton, Exactech, Gainesville, FL & ExactechGPS, Blue-Ortho, Meylan, FR). The study cohort included the first 273 cases associated with a tibia first technique performed by 24 different surgeons.
All cases followed a similar surgical workflow which measured both planned and checked lateral and medial gaps (Figure 1). The ability to achieve the plan in terms of ML laxity was defined as:
- Signed ML laxity = Checked (Gaplateral-Gapmedial) – Planned (Gaplateral-Gapmedial)
- Unsigned ML laxity = | Signed ML laxity| (absolute value)
The overall difference of ML laxities was tested by ANOVA test. To examine heterogeneity of distributions of signed ML laxity on a surgeon basis (with > 30 cases), a pairwise two-sided Kolmogorov-Smirnov test was performed. Significance was defined as p ≤ 0.05.
3 Results
The average signed ML laxity was well-aligned with a neutral differential throughout the full arc of motion, ranging from -0.04mm (15° flexion) and 0.27mm (95° flexion) (Figure 2A); the range of average unsigned ML laxity was 1.04mm (0° flexion) to 1.30mm (120° flexion) (Figure 2C). There was no statistical difference between signed/unsigned ML laxities acquired at 15°, 45°, 75°, and 105° (p=0.06). The signature of the signed ML laxity was found to be surgeon specific among 4 surgeons associated with more than 30 cases. Each two of surgeons had a significantly different ML laxity distribution (p<0.05) (Figure 2B).
4 Conclusion
This study investigated the ability to achieve ML gap balance during tibia-first TKA using a force-controlled intraarticular distractor integrated with a CAOS system to optimize the soft-tissue balance. The proposed technique achieved final ML laxity that was similar to the planned ML laxity throughout the full arc of motion, which demonstrated its ability to successfully execute the expected plan. Such ability is aligned with the outcomes from a previous study using a robotic tensioning device integrated with a CAOS system [3]. However, in this study, data from all users (not only surgeons-designers) involved with this pilot release were considered and the learning curve cases were not excluded.
5 References
[1] Gustke KA et al. Bone Joint J. 2014;96-b:1333–1338
[2] Shalhoub S et al. J Arthroplasty. 2018;33(9):3043–3048
[3] Shalhoub S et al. Arthroplast Today. 2019;5(3):334-340
Figures
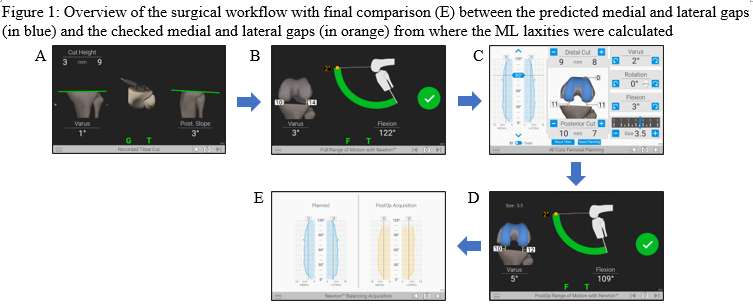
Figure 1
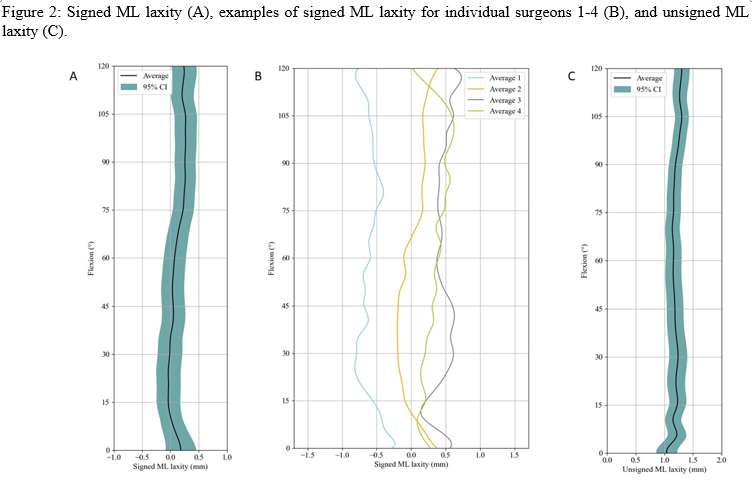
Figure 2#7980
High Prevalence of Spinopelvic Risk Factors in Patients With Post-Operative Hip Dislocations
*James Huddleston - Stanford University - Woodside, United States of America
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
Chameka Madurawe - Corin - Pymble, Australia
Christopher Plaskos - Corin - Raynham, USA
Jim Pierrepont - Corin - Cirencester, United Kingdom
*Email: jamesh3@stanford.edu
Introduction: Excessive standing posterior pelvic tilt (PT), lumbar spine stiffness, low pelvic incidence (PI), and severe sagittal spinal deformity (SSD) have been linked to increased dislocation rates. We aimed to determine the prevalence of these 4 parameters in a cohort of unstable THA patients and compare these to a large representative control population of primary THA patients.
Methods: Forty-eight patients with instability following primary THA were compared to a control cohort of 9414 THA patients. Lateral X-rays in standing and flexed-seated positions were used to assess PT and lumbar lordosis (LL). CT scans were used to measure PI and acetabular cup orientation. Thresholds for “at risk” spinopelvic parameters were standing posterior PT ≤ -15°, lumbar flexion (LLstand – LLseated) ≤ 20°, PI ≤ 41°, PI ≥ 70°, and SSD (PI – LLstandmismatch ≥ 20°).
Results: There were significant differences in mean spinopelvic parameters between the dislocating and control cohorts (p < 0.001) (Figure 1). There were no differences in mean PI (58° v 56° respectively, p = 0.29) or prevalence of high and low PI between groups. 67% of the dislocating patients had one or more significant risk factors, compared to only 11% of the control (Figure 2). 71% of the dislocating patients had cup orientations within the traditional safe zone (Figure 3).
Conclusion: Excessive standing posterior PT, low lumbar flexion and a severe SSD are more prevalent in unstable THAs. Pre-op screening for these parameters combined with appropriate planning and implant selection may help identify at risk patients and reduce the prevalence of dislocation.
Figures
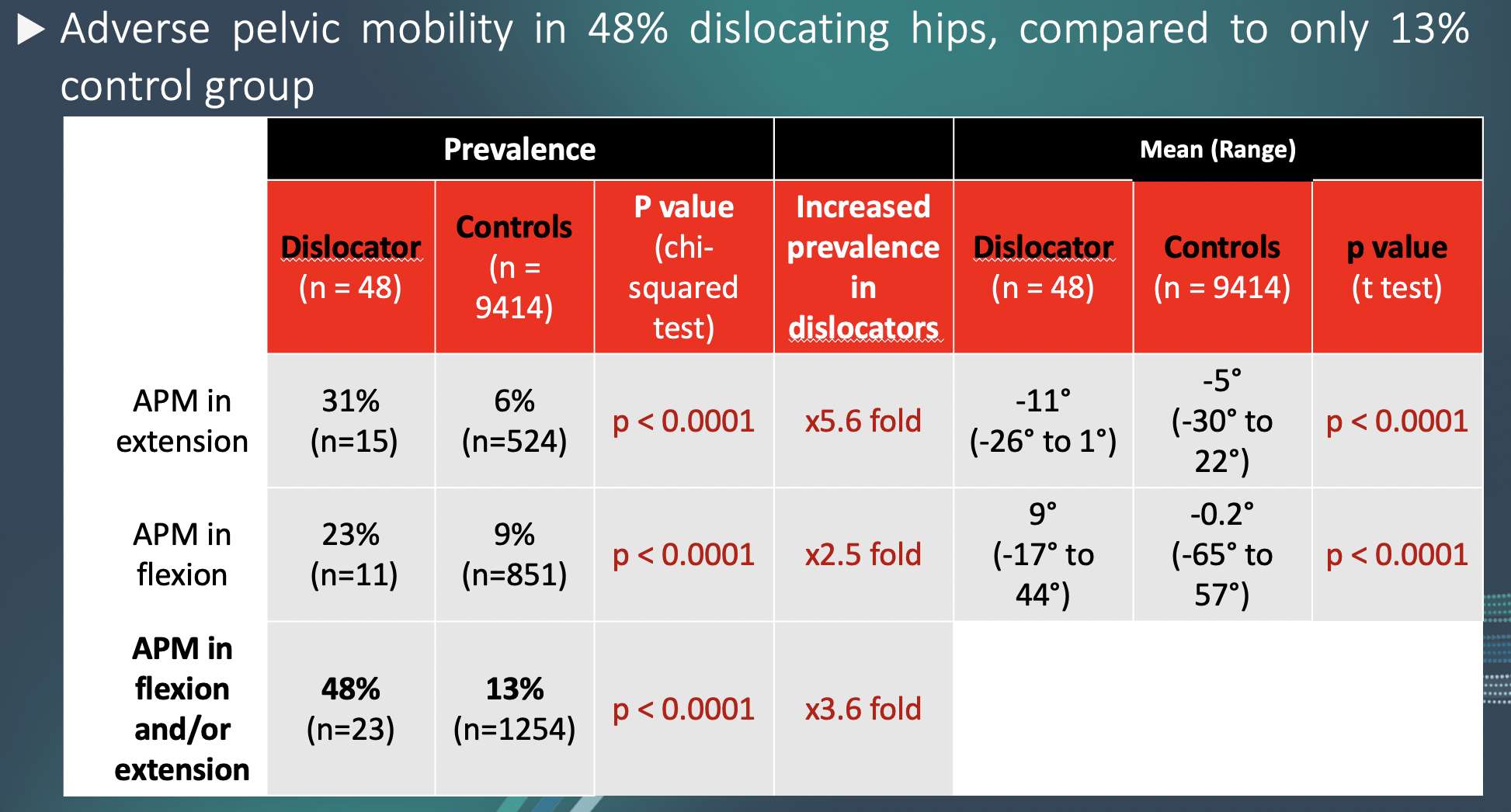
Figure 1
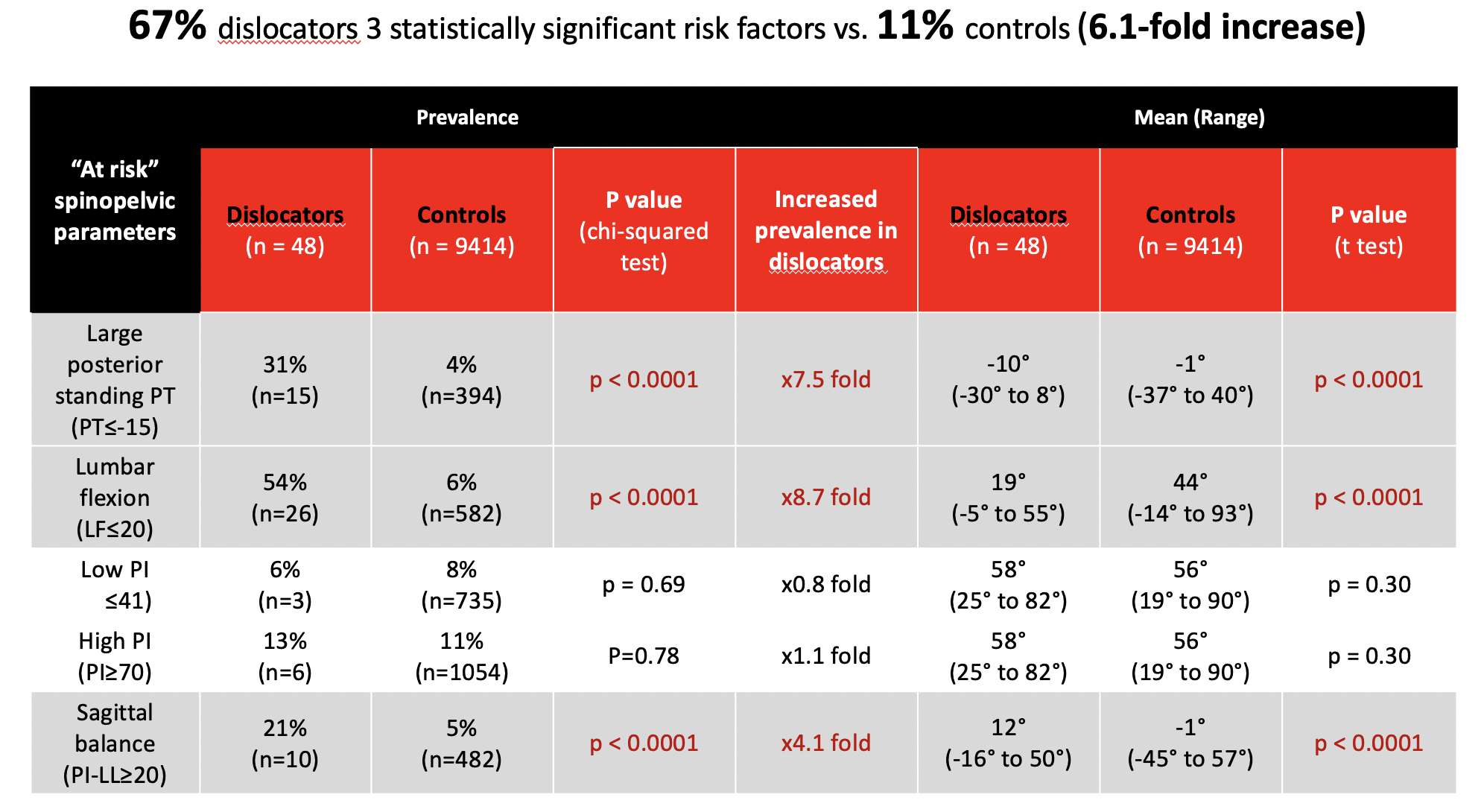
Figure 2
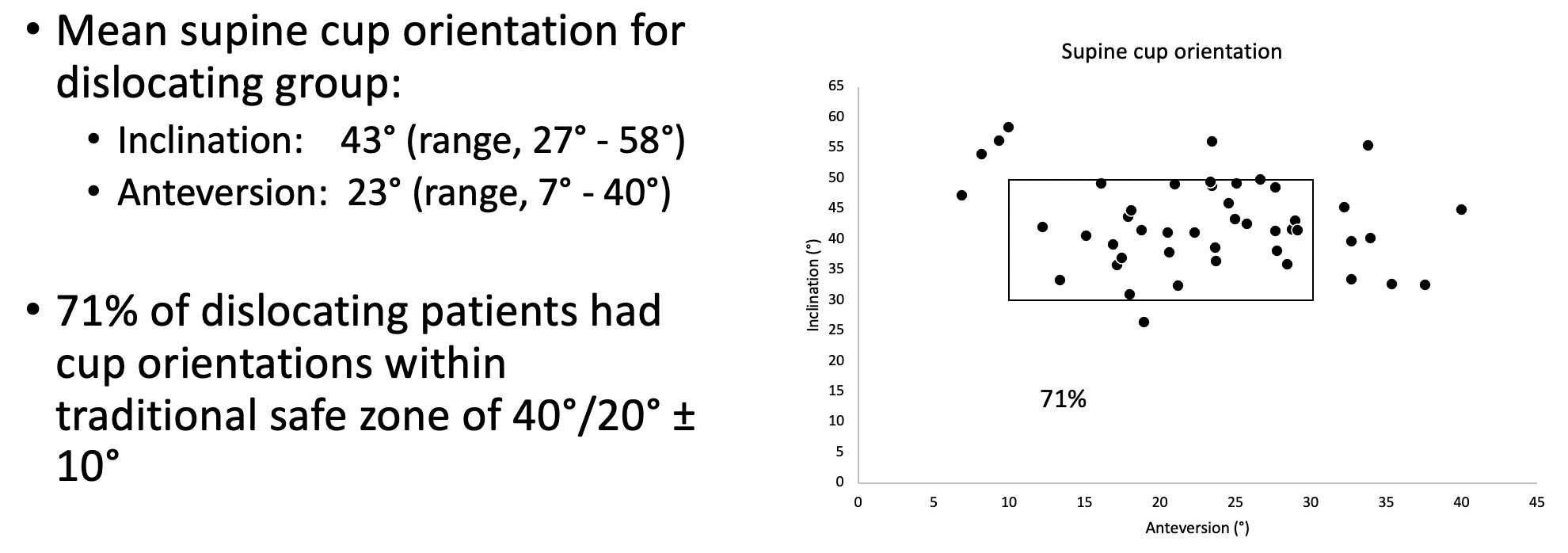
Figure 3#7983
Endoscopic Iliopsoas Lengthening for Treatment of Recalcitrant Iliopsoas Tendinitis After Total Hip Arthroplasty
*James Huddleston - Stanford University - Woodside, United States of America
John Bonano - Stanford University - Stanford, USA
Marc Safran - Stanford University - Stanford, United States of America
Chris Jamero - Stanford University - Stanford, USA
Nicole Segovia - Stanford University - Stanford, USA
*Email: jamesh3@stanford.edu
Introduction: Iliopsoas (IP) tendinitis from impingement upon the acetabular component after total hip arthroplasty (THA) has been treated with open and endoscopic IP tenotomy or acetabular component revision. This study describes the results of a consecutive series of patients treated with endoscopic IP tenotomy as a less invasive alternative.
Methods: Twenty-eight patients with IP impingement after THA underwent endoscopic IP lengthening from 2012 to 2021 at a single-center academic institution. Follow up of 24 of these patients was achieved with a mean follow up of 7.6 months (range 1 – 28). Outcomes included Modified Harris Hip Score (mHHS), visual analog pain scale (VAS), satisfaction, component positioning, and complications.
Results: Seventy one percent of patients were satisfied or very satisfied after their operation (Table 1). The median mHHS preoperatively was 57 (IQR 43 – 60) and postoperatively was 75 (IQR 66 – 92, p<0.001) (Table 2). Clinically meaningful improvements in mHHS were seen in patients with VAS pain scores <5, cup prominence >8mm, BMI >30, and less than 2 years from their index THA (Table 3). Two patients developed a deep infection 7 and 10 months postoperatively (neither related to the release) and one patient underwent open psoas release for persistent impingement.
Conclusion: Endoscopic IP tenotomy is a safe and effective treatment for impingement after THA. Patients with cup prominence >8mm, BMI >30, and less than 2 years from their index THA may have more clinically meaningful improvements in pain and function.
Figures
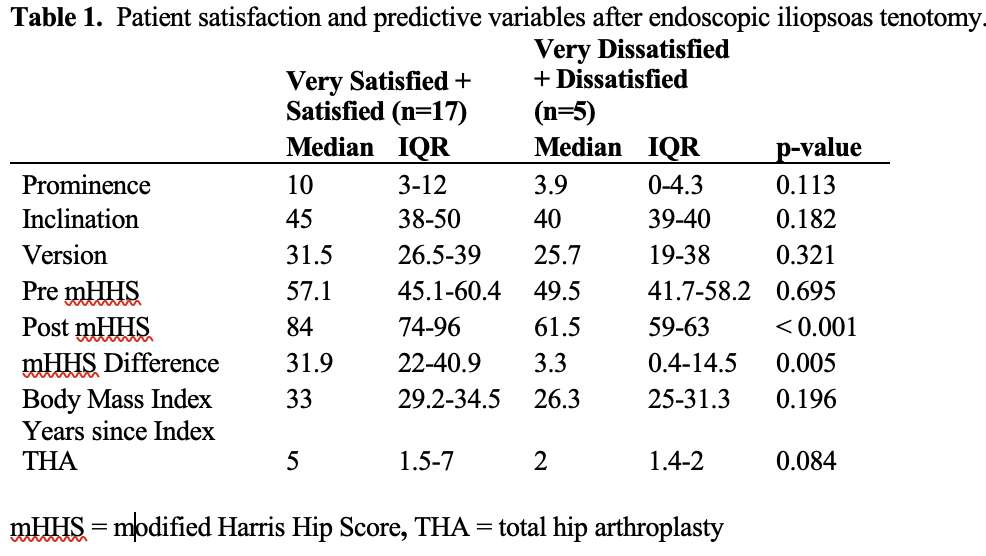
Figure 1
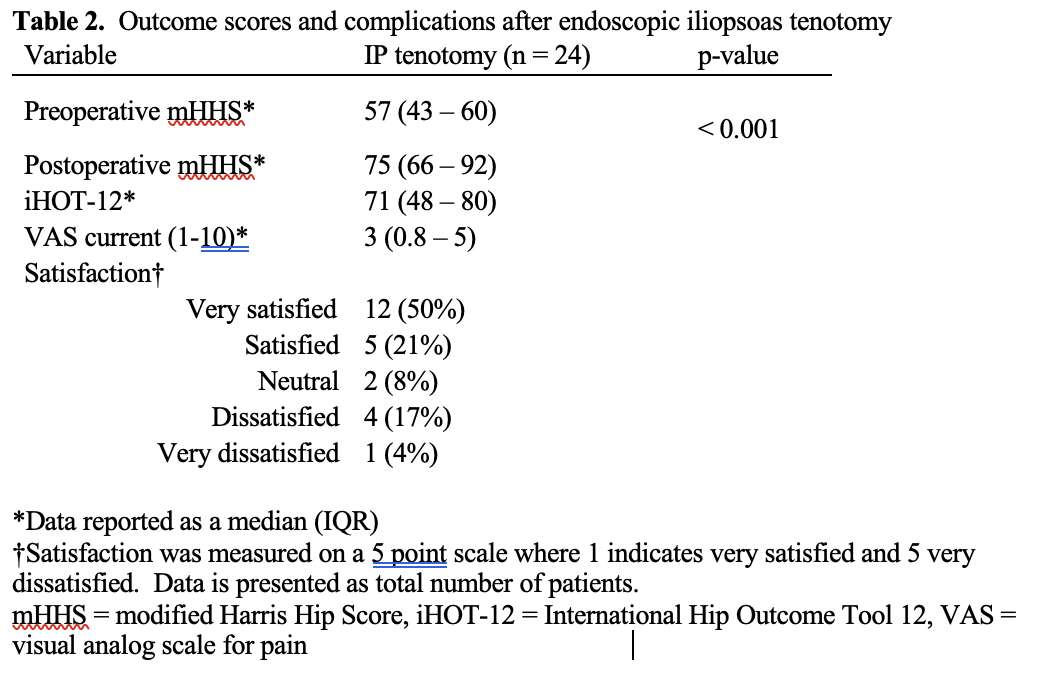
Figure 2
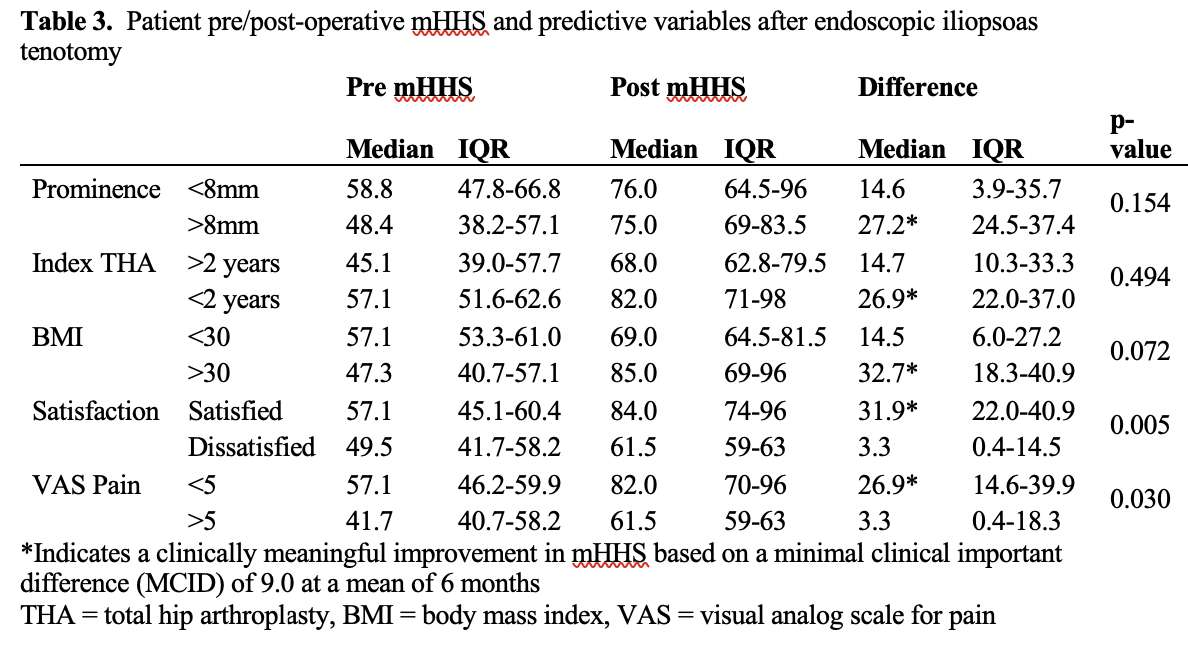
Figure 3#7710
The Effect of Changes in Coronal TKA Alignment on Loading of Adjacent Joints
*Daniel Huff - DePuy Synthes Joint Reconstruction - Warsaw, USA
Chase Maag - DePuy Synthes - Warsaw, USA
*Email: dhuff4@its.jnj.com
Introduction: Changes in knee alignment can affect the hip and ankle joints, as these three joints operate as a kinetic/kinematic chain during gait. The present study investigates the effect of Patient Specific (anatomic) and mechanical alignment of TKA on the loading conditions of adjacent joints. Drongelen et al. showed that changes in lower limb alignment associated with THA can increase knee adduction moment and the risk for osteoarthritis of the knee medial compartment [1]. Similarly, Lewinson et al. showed that shod gait with the introduction of lateral wedge insoles changes the location of peak contact load in cartilage of the knee [2]. Further, much research has been done to understand deleterious effects that changing joint kinematics can have on healthy cartilage. Paschos et al. theorized a chronic derangement of local joint loading patterns causes irreversible changes to cartilage homeostasis [3]. Chaudhari et al describes the mechanism by which these kinematics shifts cause degenerative metabolic changes in regions of cartilage where the tissue cannot adapt to the new loading pattern [4].
Methods: Using a validated lower extremity model (Fitzpatrick et. al.), external boundary conditions of step down, gait and deep knee bend were created using Orthoload telemetric tibial loads [5,6]. Using these external boundary conditions, an Cruciate Retaining Fixed Bearing implant was placed into 50 discrete alignments chosen by latin hypercube sampling with Joint Line (JL) angles between 0° and 7° and HKA varus angles between 0° and 5°, in all instances. Each alignment was run through Step Down, Gait and Deep Knee Bend (DKB), recording the 6-degree of freedom loads seen at the Hip, Knee, and Ankle. Changes in hip and ankle loads across the sampled design space was calculated across all activities.
Results: In moving from natural anatomic alignment to neutral mechanical alignment (0HKA, 0JL) M/L forces of the hip and ankle changed, at most in the design space, >100% in each of the three activities tested. A/P and compressive forces of both hip and ankle were largely unaffected by changes in knee coronal plane alignment. All moments about the hip in all activities were affected by >100%. In each of these instances except for flexion moment, these sensitivities resulted in marked absolute changes in load or moment (fig 2). Contributions of changes in HKA angle and JL Angle independently may be seen in Figure 3.
Conclusion: Prior work has described the pathway by which changes in joint loading can lead to osteoarthritis. With a prevalence of a little over 2% of the US population in 2010, an estimated 7.2million people in the US were living with TKA or THA prostheses [7]. Even without a further rise in incidence, simply the aging of the population would result in an estimated 11 million individuals with total hip or knee replacement (4 million total hip and 7.4 million total knee) in 2030 [7]. Understanding the impact of these changes in load on the cartilage in the adjacent joints is necessary to further plan on the patients’ long-term health.
Figures
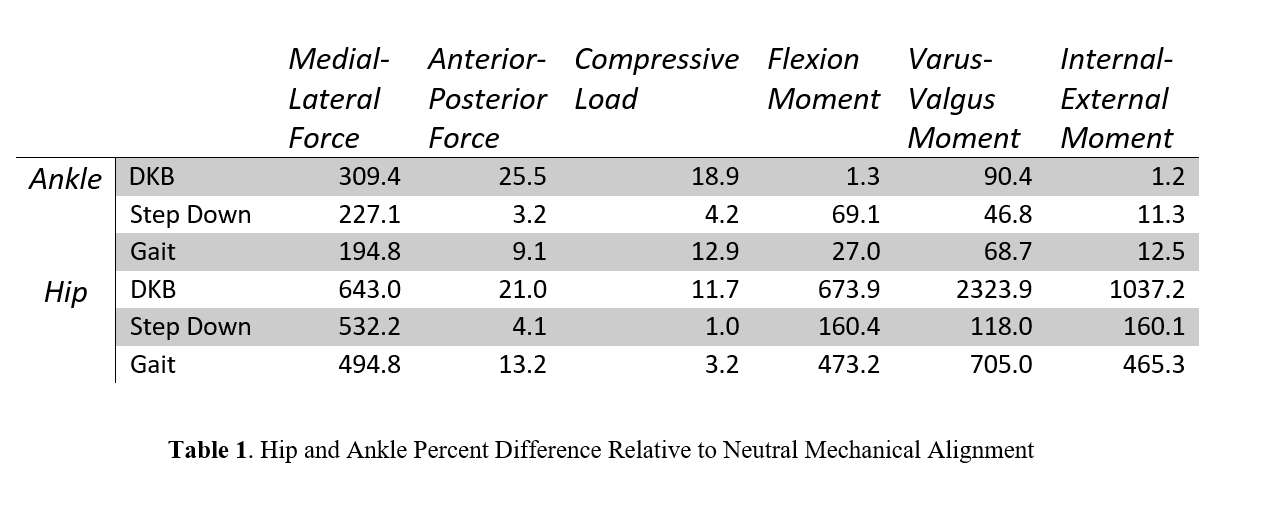
Figure 1
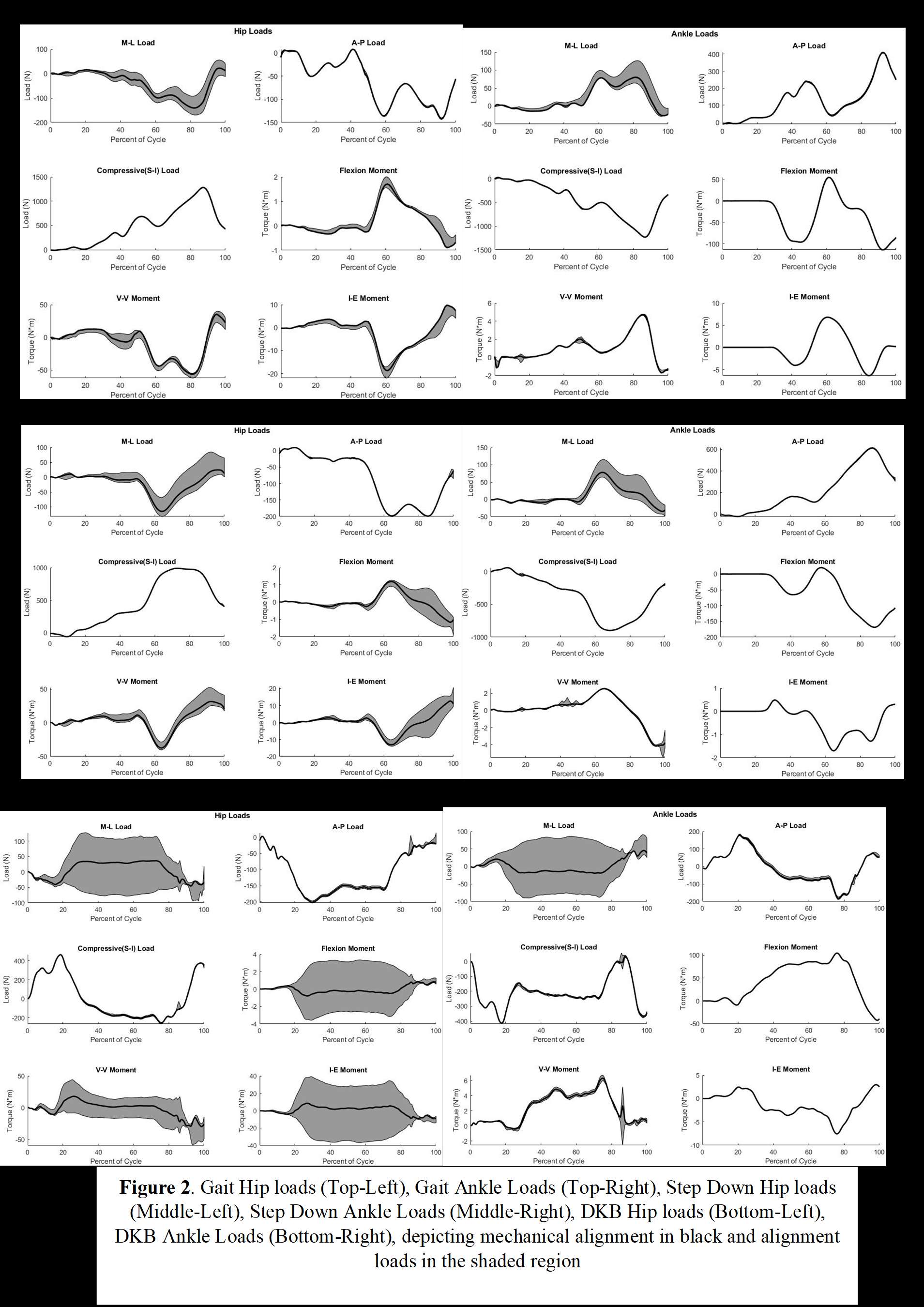
Figure 2
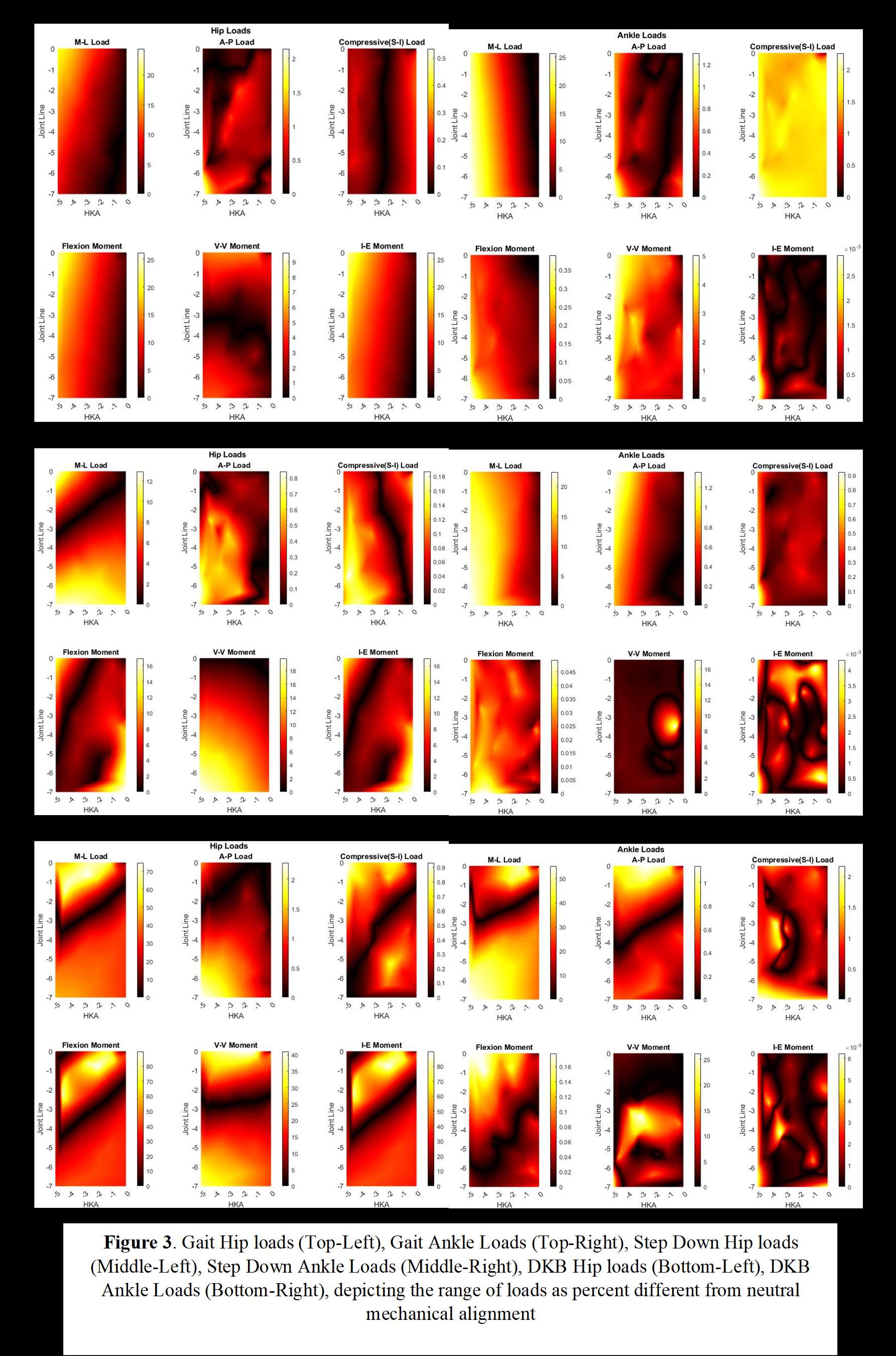
Figure 3#7310
Flexion Facet Centers Should Not Be Used to Determine Tibiofemoral Kinematics Following Total Knee Arthroplasty
*Maury Hull - University of California Davis - Sacramento, USA
*Email: mlhull@ucdavis.edu
Introduction: A common approach to determine planar 2D tibiofemoral kinematics is based on analysis of fluoroscopic images recorded as patients perform activities of daily living. Following 3D model-to-2D image registration, images are processed to determine the anterior-posterior (AP) position of each femoral condyle in relation to the tibia. By tracking movement of AP positions during flexion, tibiofemoral kinematics can be determined. One common method to determine AP positions is the flexion facet center (FFC) method (Figure 1). The primary objective was to determine whether fixed FFCs based on circle fits accurately indicate AP positions of variable radius femoral components, which are the most common designs.
Methods: Using two multi-radius femoral component designs, instant radii of curvature and instant centers of curvature (termed variable FFCs) were determined for each femoral condyle as the radii and centers, respectively, of best-fit circles to 20º segments of the sagittal profile from 0º to 120º of flexion in 15° increments (Figure 2). The fixed FFC of each condyle was the center of the best-fit circle from 0º to 120º. Errors in AP positions were differences between AP positions of fixed FFCs and variable FFCs.
Results: Sagittal profiles and errors in AP positions of the two designs differed. One was a 3-radius design with a relatively early decrease in radius of curvature at 60° and the other was a 2-radius design with a late decrease in radius of curvature at 120°. For the 2-radius design, absolute errors in the AP positions for fixed FFCs were limited to 0.2 mm at all flexion angles except 120° where the error increased to 2.0 mm and root mean squared errors (RMSEs) were limited to 0.7 mm for both condyles. In contrast, for the 3-radius design, errors in the AP positions for fixed FFCs were greatest at 0º approaching 7 mm and RMSEs were 2.8 mm for both femoral condyles.
Discussion: Errors in AP positions of fixed FFCs were greatly increased for the 3-radius design with an early decrease in radius of curvature. Because the best-fit circle over 0°– 120° better represented the sagittal profile for the 2-radius design with the late decrease in radius of curvature, errors in AP positions were smaller except at the flexion angle after the decrease. Hence, fixed FFCs should not be used to indicate AP positions particularly of multi-radius designs with an early decrease in radius of curvature. Although fixed FFCs might be used to indicate AP positions with lower error for designs with a late decrease in radius of curvature in activities where knee flexion is limited to 90°, a better method is the lowest point method. This is because AP positions of lowest points are identical to those of variable FFCs in which case the lowest point method can be used generally for any multi-radius femoral component design.
Conclusions: Condylar AP positions indicated by fixed FFCs for multi-radius designs are subject to large error and should not be used in determining tibiofemoral kinematics. AP positions of lowest points should be used instead.
Figures
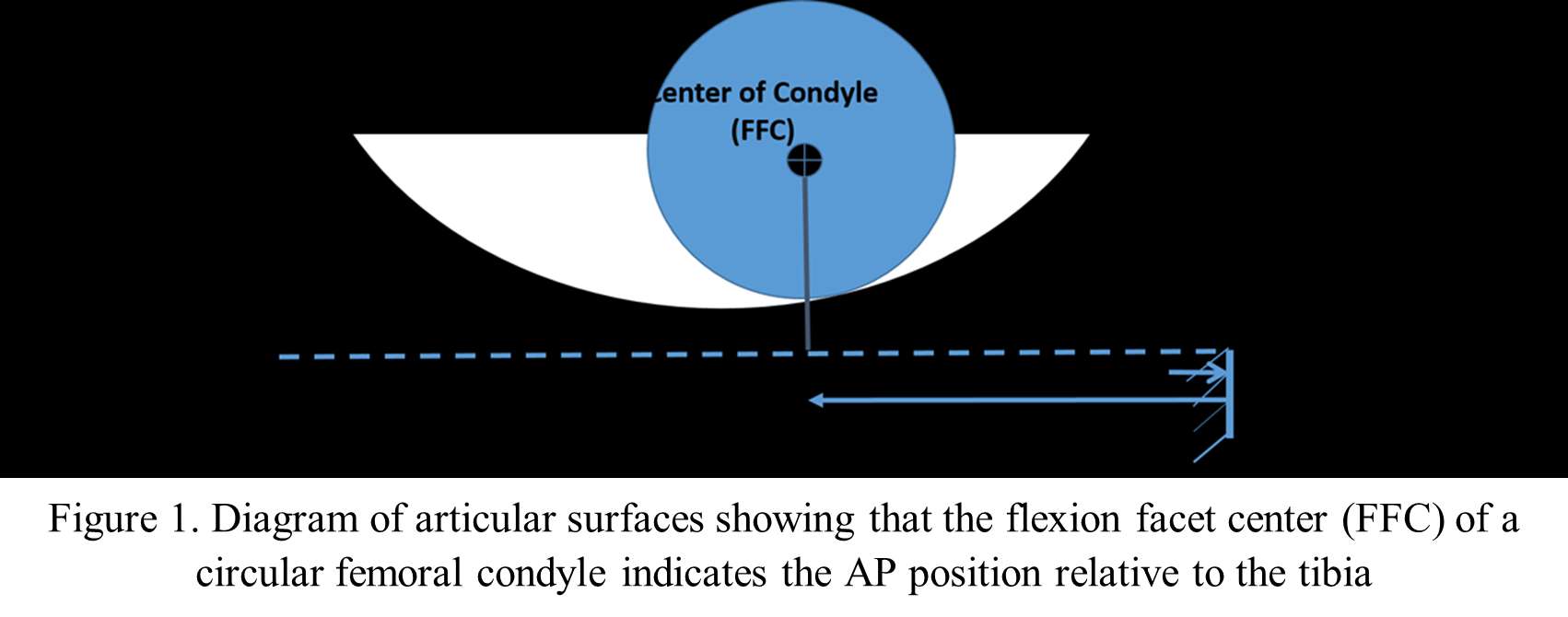
Figure 1
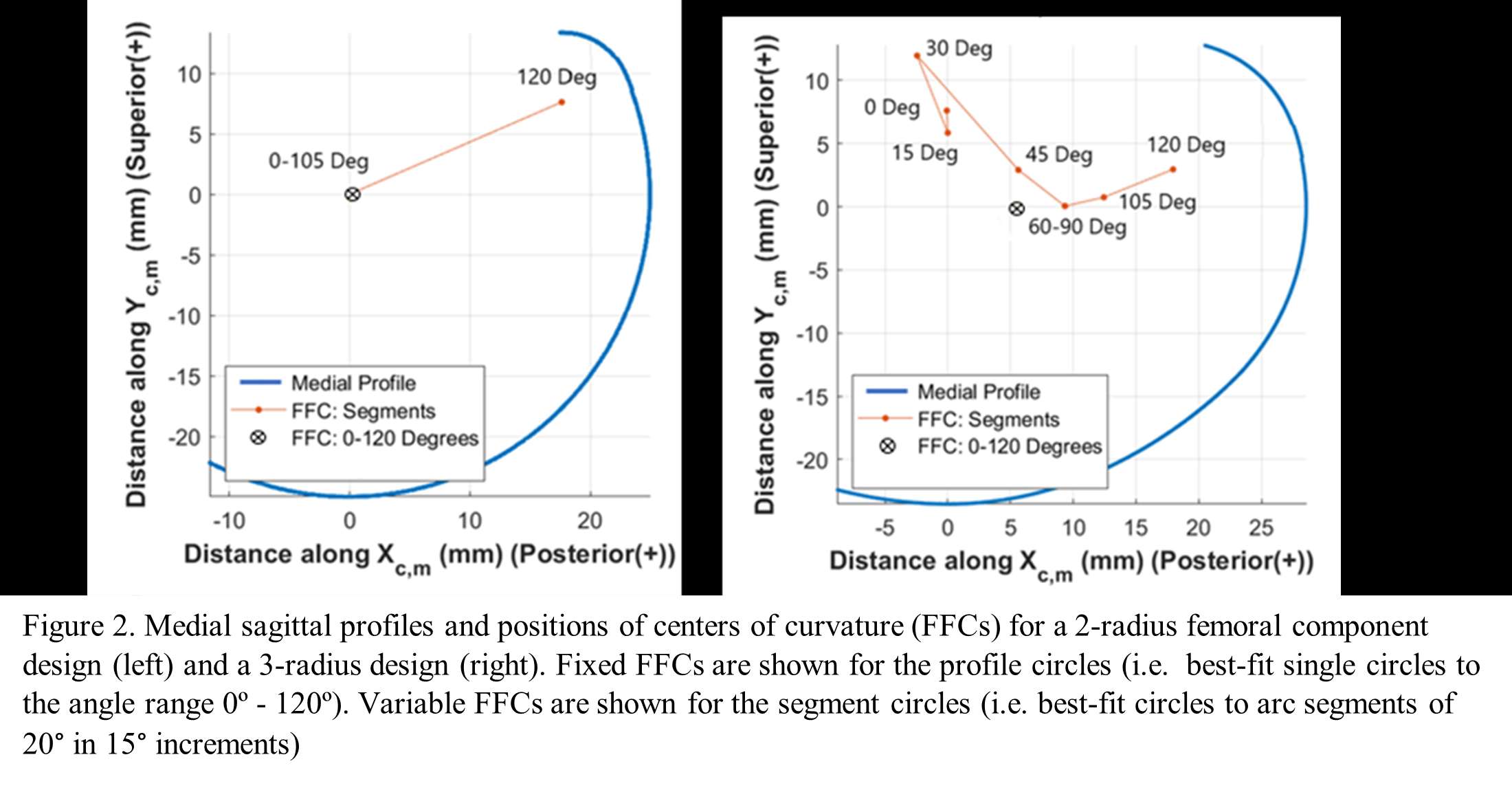
Figure 2#7387
A Surgeon With No Experience in Performing Kinematic Alignment With Manual Instruments Has a Short Learning Curve and Comparable Accuracy and Results to Those of an Experienced Surgeon
*Alexander Nedopil - University of Wuerzburg - Wuerzburg, Germany
Anand Dhaliwal - California Northstate University - Elk Grove, USA
Stephen Howell
Maury Hull - University of California Davis - Sacramento, USA
*Email: nedopil@me.com
Purpose: The study determined a surgeon's learning curve, who has no experience in performing kinematic alignment (KA) TKA using manual instruments (=inexperienced (IE)), by assessing the deviation of the femoral resections from the KA target and operative time. A secondary objective was to test the hypotheses that the femoral resection accuracy, operative time, and postoperative patient-reported outcome measures (PROMs), implant positioning, and limb alignment were not different from an experienced (E) surgeon.
Methods: This prospective cohort study included the first 30 TKAs performed by an IE surgeon in private practice after an arthroplasty fellowship and 30 consecutive TKAs performed by an E surgeon (> 4000 KA TKAs). Independent observers recorded thickness of the distal medial (DM), distal lateral (DL), posterior medial (PM), and posterior lateral (PL) femoral resections and their deviation from target (Figure 1). The 30 TKAs performed by the IE surgeon were divided into three groups by chronological order and the bias (mean deviation) and precision (standard deviation of deviation) of the femoral resections were compared between the groups. To assess the effect of surgeon experience, these same deviation quantities were computed for the E surgeon. The cumulative summation (CUSUM) analysis assessed the learning curve for operative time. In addition, operative time, PROMs and alignment variables including the distal lateral femoral angle (DLFA), proximal medial tibial angle (PMTA), posterior slope, internal-external rotation deviation from target, and hip-knee-ankle angle (HKAA) were measured for both the IE and E surgeons. Statistical analyses were performed to compare resection thickness deviations from target, PROMs, and mean and variance of the alignment variables between the two surgeons.
Results: The IE surgeon's deviation of the distal and posterior medial and lateral femoral resection was within the caliper resolution of ± 0.5 mm or did not significantly change between three groups of ten consecutive patients, which indicated no learning curve. The learning curve for the operative time was 20 cases (p = 0.01) (Figure 2). Between the IE and E surgeon, only the accuracy of the posterolateral femoral resection was different (p < 0.000). There was no difference in the patient's Forgotten Joint, Oxford Knee, and KOOS scores, and coronal and sagittal alignment of the components and limb at a mean follow-up of 9 and 17 months, respectively (p ≥ 0.1287). The IE surgeon's operative time was 39 minutes longer (p < 0.000).
Discussion: Surgeons transitioning to KA TKA might be interested to know there is no learning curve for setting the femoral component with manual instruments and that the resection accuracy, postoperative PROMs, and alignment is comparable to an E surgeon, although the operative time is longer.
Figures
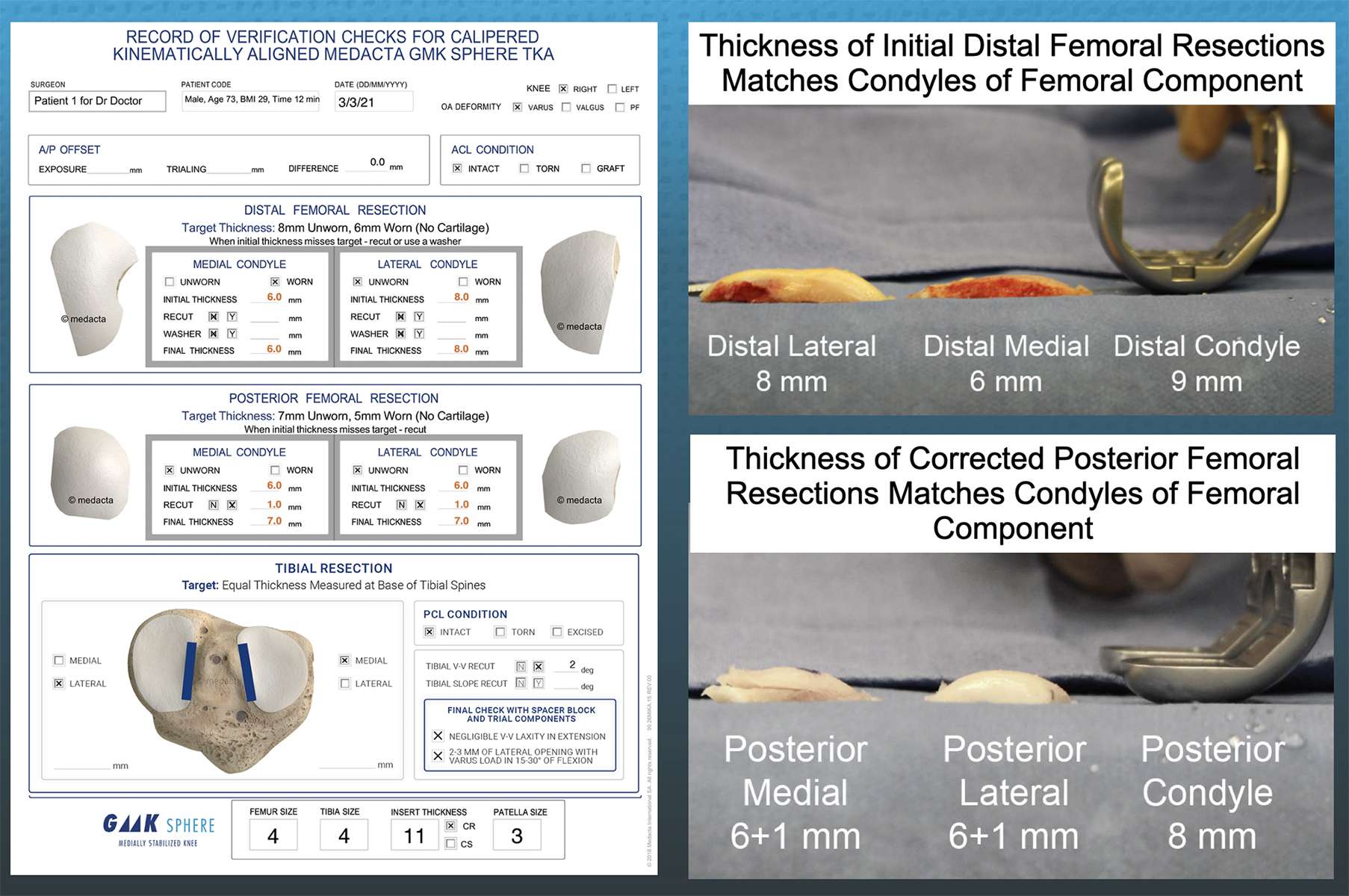
Figure 1
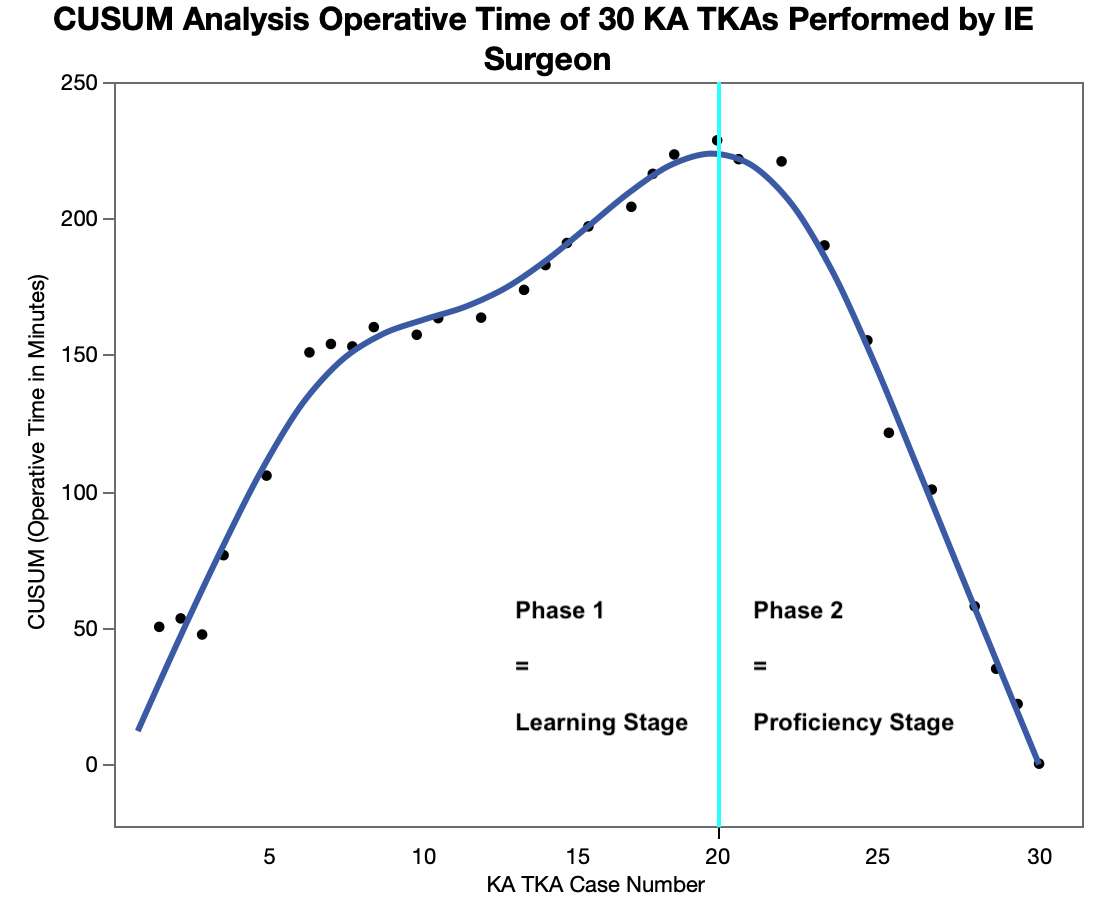
Figure 2#7311
Pitfalls to Avoid in Using the Joint Coordinate System of Grood & Suntay to Quantify Knee Kinematics
*Maury Hull - University of California Davis - Sacramento, USA
*Email: mlhull@ucdavis.edu
Introduction: In analysis of 3D tibiofemoral kinematics, the joint coordinate system (JCS) of Grood and Suntay is often used. For this JCS to yield clinically meaningful motions however, pitfalls which introduce kinematic crosstalk errors must be avoided. One objective was to describe requirements to avoid kinematic crosstalk errors and another objective was to illustrate the consequences of failing to meet these requirements using results from a JCS based on the International Society of Biomechanics (ISB) recommendation.
Methods: The kinematic model which forms the basis of the Grood and Suntay JCS is a chain of three cylindric joints (Figure 1). Movements in this JCS occur along and about each axis. Flexion-extension (F-E) rotation occurs about a femoral body-fixed axis and internal-external (I-E) axial rotation occurs about a tibial body-fixed. Varus-valgus (V-V) rotation occurs about the ‘floating’ axis which is mutually perpendicular to the body-fixed axes. Translations are determined by projecting the vector connecting femoral and tibial Cartesian coordinate system origins onto the JCS axes. To avoid the pitfall of kinematic crosstalk errors in rotations, body-fixed axes must coincide with functional axes [1]. To avoid the pitfall of kinematic crosstalk errors in translations, origins of femoral and tibial Cartesian coordinate systems must lie on the body-fixed functional axes [2]. A JCS based on the ISB recommendation [3] was formed where the body-fixed FE axis passed through the most distal point of the trochlear groove and the body fixed I-E axis was parallel to the tibial mechanical axis. The origins of the femoral and tibial Cartesian coordinate systems coincided. Fluoroscopic images of 13 patients with healthy knees performing a dynamic, weight bearing deep knee bend were processed to determine 3D relative motions between femur and tibia using the ISB JCS.
Results: Greatest absolute mean V-V rotation occurred at 90º flexion and was 12° valgus. Greatest absolute mean translations occurred at 120º flexion and were 13 mm posterior for A-P, 28 mm distraction for C-D, and 4.5 mm medial for M-L.
Discussion: The ISB JCS produced non-physiological motions. The mean valgus rotation of 12° manifests as a medial flexion gap of nearly 12 mm. With a strain at yield below 20% and a length of 50 mm, this gap would create a strain of 24% in the medial collateral ligament which is sufficient to cause acute damage. Likewise, the 12.5 mm posterior tibial translation is non-physiologic since A-P translation is minimal due to the constraint in the medial compartment to medial femoral condyle linear displacement. Lastly the near 30 mm distraction arguably would disrupt every major ligament in the tibiofemoral joint. These non-physiological motions are evidence of significant kinematic crosstalk errors in the ISB JCS.
Conclusions: To avoid significant kinematic crosstalk errors rendering results of little clinical relevance, a JCS which adheres to specific requirements must be strictly followed.
References: 1) Piazza, S. & Cavanagh, P. (2000) J. Biomech, 33: pp. 1029-1034; 2) Hull, M. L. (2020) J. Biomech, 109: 109928; 3) Wu et al, (1995) J. Biomech, 28: 1257-1261.
Figures
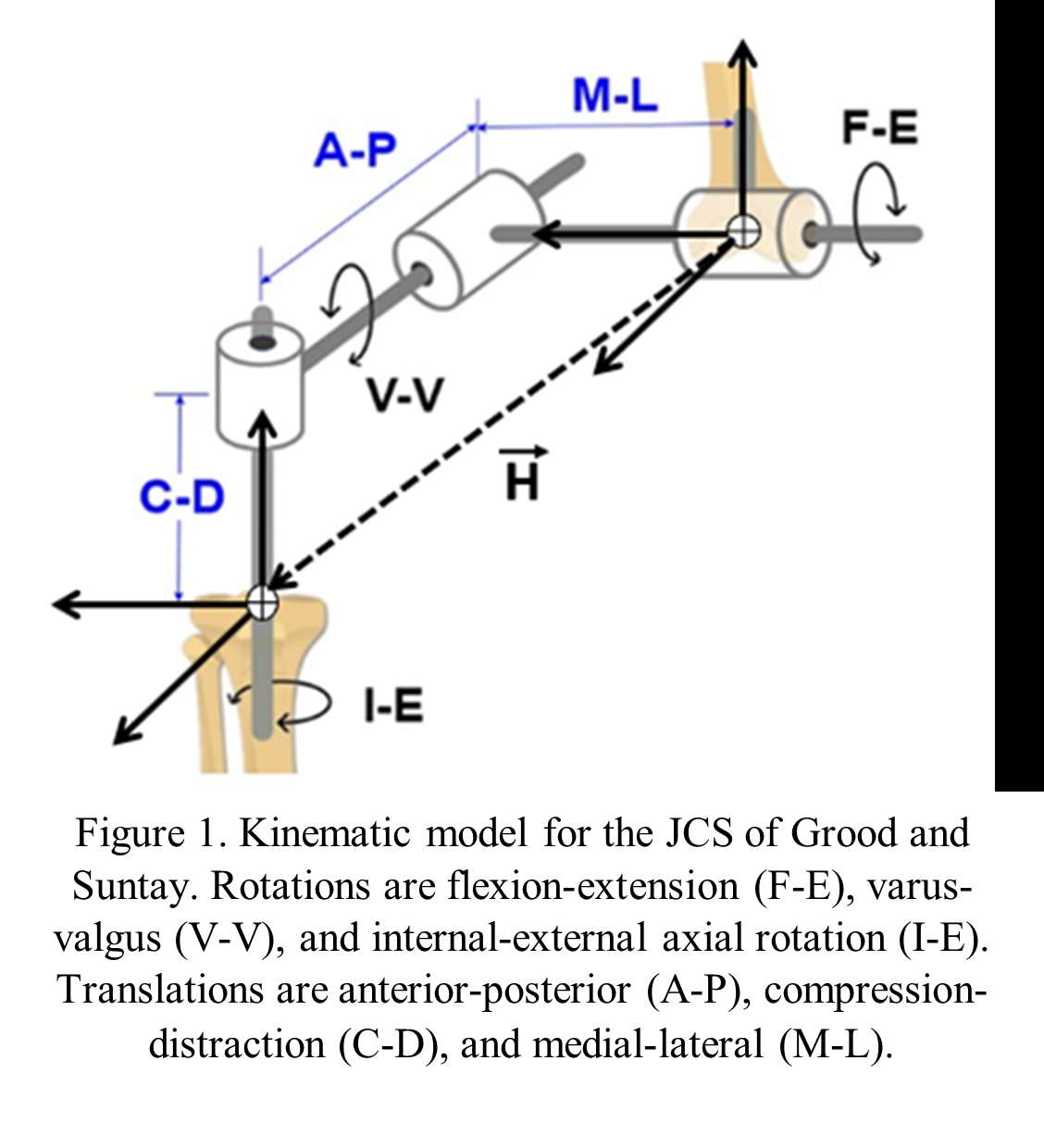
Figure 1
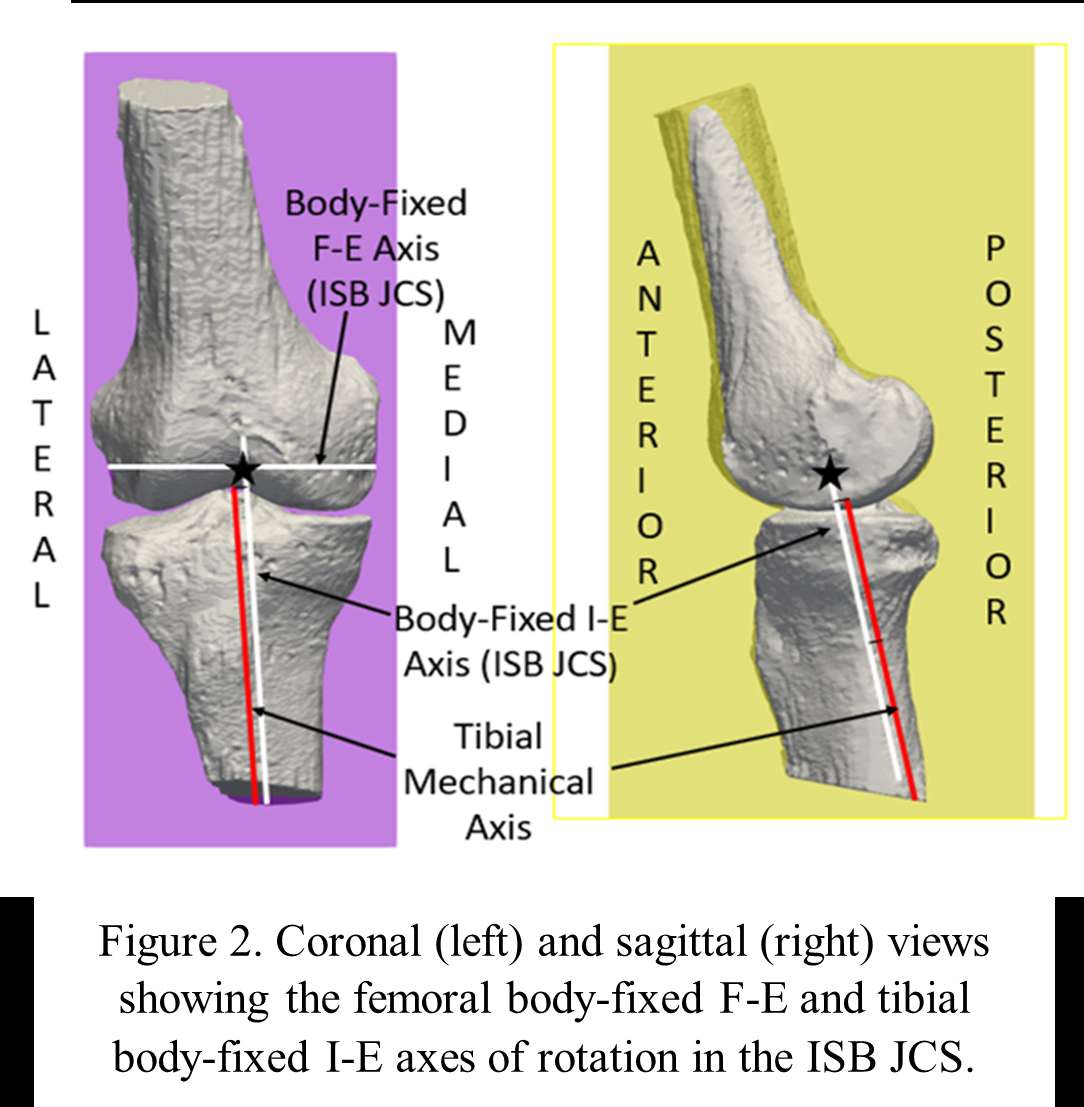
Figure 2#7628
Utility of the Femoral Elevator System for Direct Anterior Approach in Total Hip Arthroplasty
Takahiro Igei - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
*Satoshi Nakasone - Graduate School of Medicine, University of the Ryukyus - Nishihara, Japan
Masamichi Onaga - Graduate school of medicine, university of the Ryukyus - Nishihara Nakagami-gun, Japan
Fumiyuki Washizaki - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
Masato Ishihara - Graduate School of Medicine, University of the Ryukyus - Nishihara, Japan
Kotaro Nishida - Graduate school of medicine, University of the Ryukykus - Nishihara Nakagamigun, Japan
*Email: satoshi_nakasone@hotmail.com
Introduction:Total hip arthroplasty (THA) through direct anterior approach (DAA) has become widely known as muscle tendon-sparing technique, using an inter-muscular and inter-neural tissue approach. Advantage of the DAA-THA include less soft tissue trauma, earlier post-operative recovery and lower dislocation rate. In the usual DAA-THA, preparation of the femur requires extending the operating table and elevating the femur with a trochanteric retractor. Failure to obtain proper femoral elevation may result in stem malalignment or femoral perforation. In addition, excessive extension of the hip is a risk for femoral nerve palsy, and excessive retraction forces are a risk for greater trochanteric fractures. Therefore, we performed femoral preparation by directly elevating the femur using the femoral elevator system. In this study, we investigated the results of DAA-THA using the femoral elevator system and examined its usefulness.
Methods:Retrospectively, 124 patients (46males, 78 females, mean age was 61.4 years old), including 137 hips undergoing DAA-THA (by three surgeons) between January 2017 and December 2020 were included in this study. The mean follow-up period was 36 months. The femoral elevator system (Tedan Inc, USA) was used in all cases. Three-dimensional computed tomography (3DCT) data was obtained before and after THA. The stem placement angles (stem anteversion, varus-valgus, flexion-extension) and cup placement angles (RI: radiographic inclination, RA: radiographic anteversion) were measured using 3D template software. In surgery, after the cup placement, the femoral exposure was performed. The femoral hook was placed around proximal femur along vastus lateralis and lifted the femur (Fig.1). The trochanteric retractor put into the posterior of great trochanter for skin protection. Finally, femoral preparation and stem insertion were performed without operation table extension (Fig.2-3). The stem and cup alignment after THA, Japanese orthopedic association (JOA) hip score before and after THA, Postoperative complication were assessed.
Results:The mean JOA hip score before THA was 49.4 (10-88), that after THA was 92.5 (67-100). DAA-THA improved JOA hip score (p<0.05). There were no cases of nerve injury, dislocation, infection and femoral perforation. Two cases (1.5%) including after femoral osteotomy and dialysis patient for 20 years had a complication of grater trochanteric fracture after surgery.The mean stem anteversion, varus-valgus, and flexion-extension after THA was respectively 26.2 (-7.9-56.5)˚, varus 0.5 (valgus 4.7-varus 5.1)˚, and flexion 2.0 (extension 4.4-flexion 7.3)˚. The cases with varus stem alignment were 9 cases (6.6%), with flexion stem alignment in flexion were 53 cases (38.7%). The mean cup-alignment (RI, RA) was 40.0 (32.5-52.3)˚, 16.4 (6.6-35.5)˚. Compared to preoperative plan, the mean absolute value of difference in the angles (RI, RA), was 2.4 (0.0-12.3)˚, 2.8 (0.0-20.5)˚.
Conclusion:This study has several limitations including retrospective, single approach and no comparison with other systems. Postoperative femoral stem alignment was good with the femoral elevator hook system Using the femoral elevator system provided good alignment of the stem, and no postoperative nerve palsy was observed though two complicated cases had identified trochanteric fractures. The femoral elevator hook system is safely and useful for the femoral preparation and stem insertion in DAA-THA.
Figures
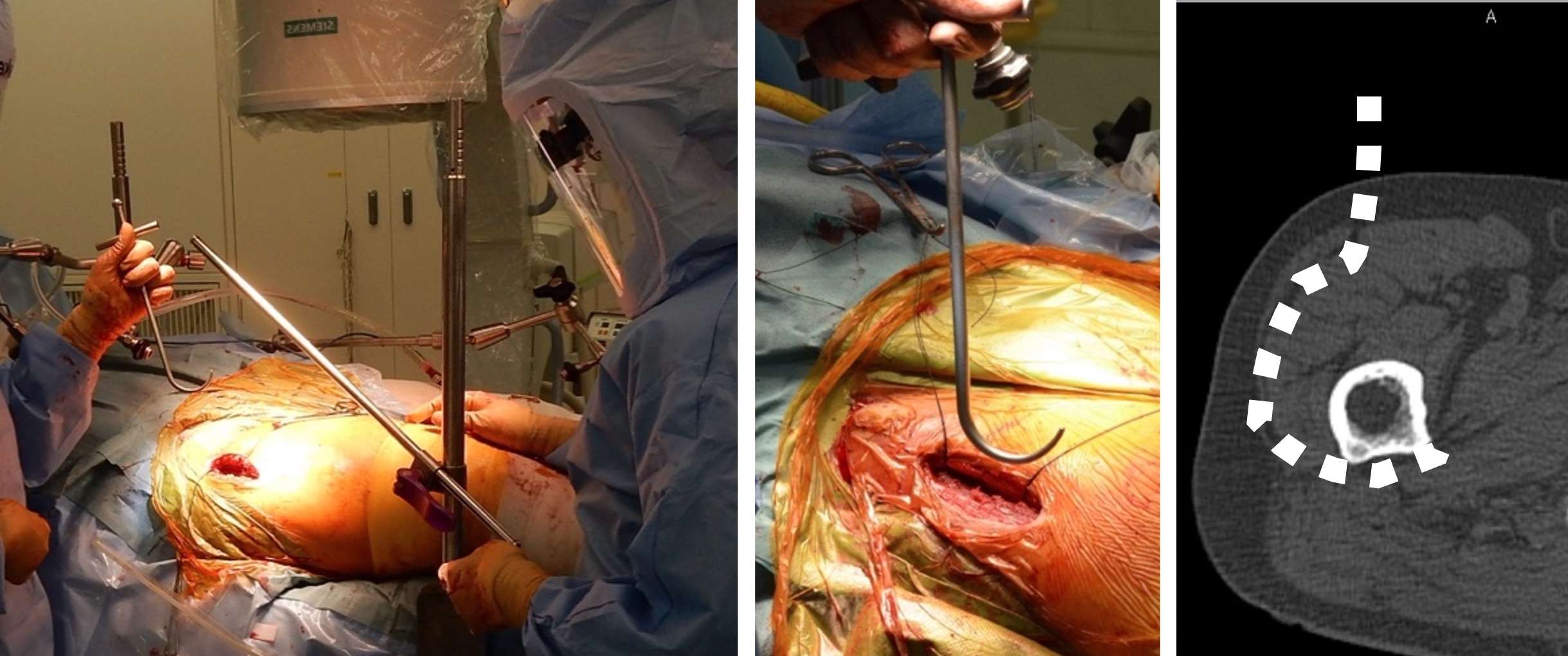
Figure 1
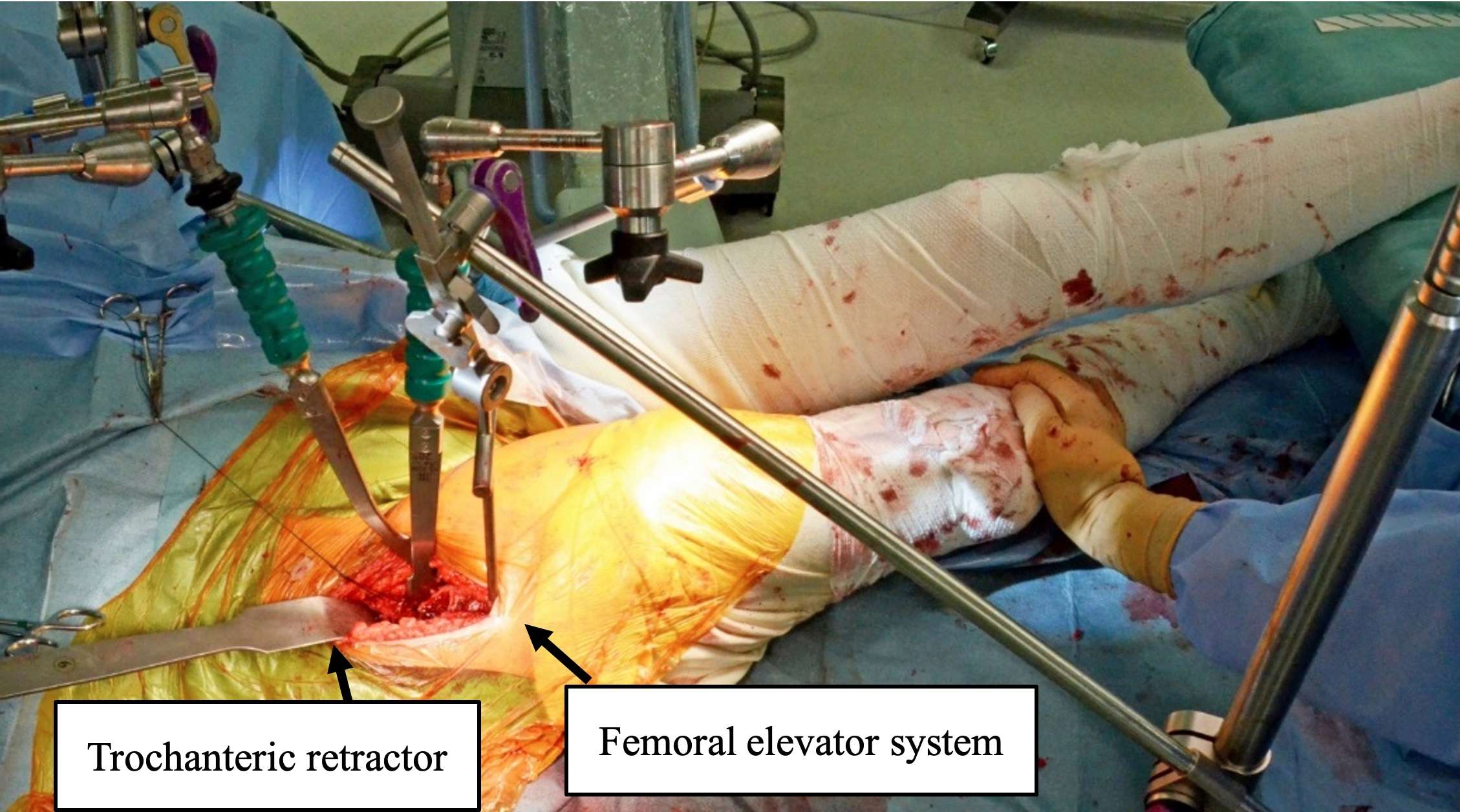
Figure 2
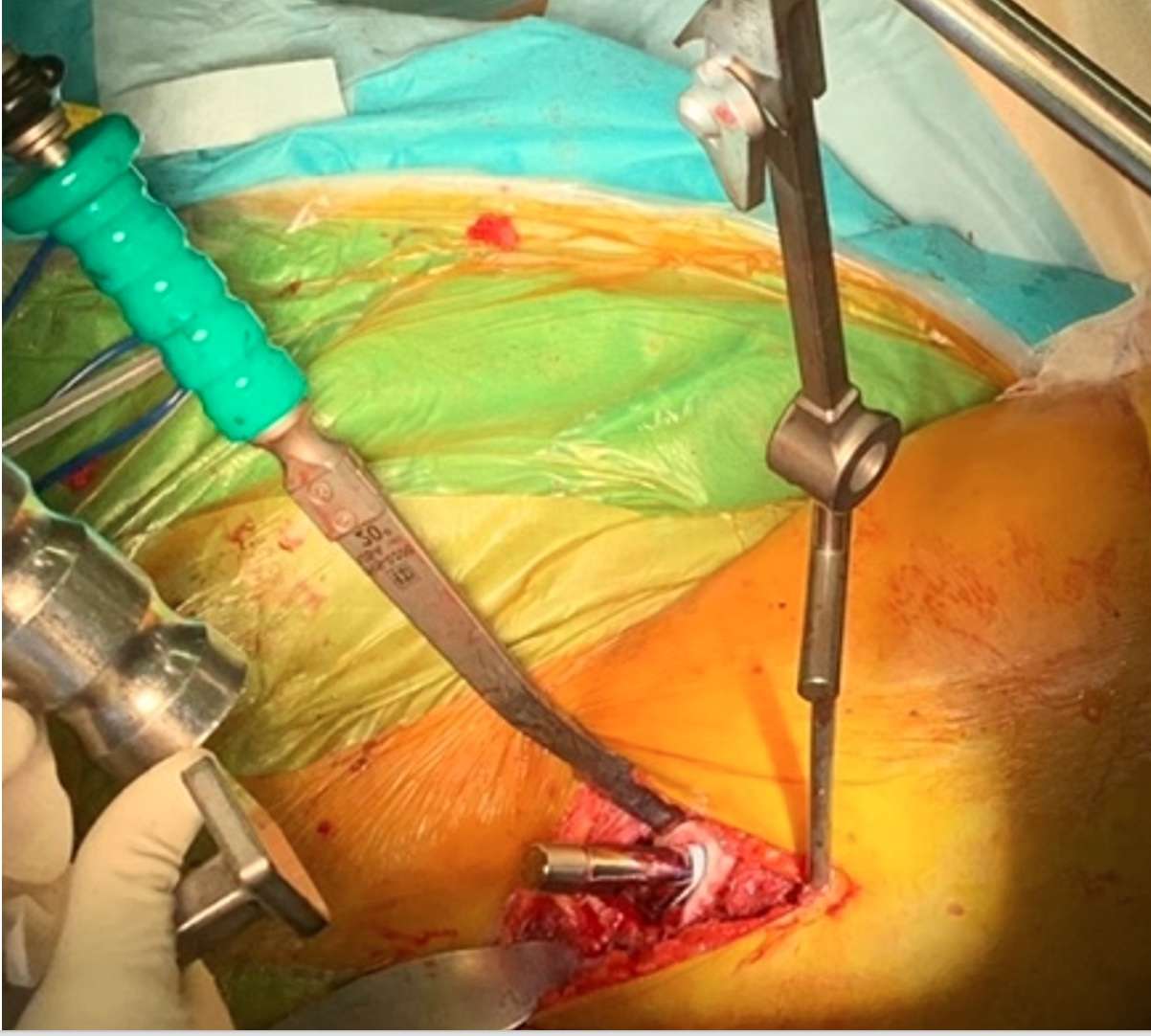
Figure 3#7508
Tribological Evaluation of a Pyrolytic Carbon Interposition Implant Against Live Cartilage in Comparison With Alumina Ceramic and CoCrMo-Alloy
*AMANDINE IMPERGRE - Rush University Medical Center - Chicago, USA
Markus Wimmer - Rush University Med Ctr - Chicago, USA
Ana-Maria Sfarghiu - Laboratoire de Mécanique des Contacts et des Structures - Villeurbanne, France
Nathalie Bernoud-Hubac - Laboratoire de Mécanique des Contacts et des Structures (LaMCoS) INSA de Lyon - CNRS UMR5259 - Villeurbanne, France
*Email: Amandine_Impergre@rush.edu
INTRODUCTION: Degenerative shoulder diseases associated with a functional rotator cuff are currently treated by hemi-arthroplasty or total prosthesis replacement. However, patients may suffer from post-operative pain due to glenoid erosion associated with metal compounds. The Pyrolytic carbon (PyC) spherical interposition implant is a new type of shoulder hemi-arthroplasty device. It consists of a freely moving ball, which is inserted between the glenoid cavity and the shaped humeral head. PyC has been successfully used for cardiac valve replacement thanks to its excellent fatigue and wear resistance properties, as well as its excellent biocompatibility. In addition, a low elastic modulus supports the use of PyC in orthopedics to counter stress shielding and improve the transmission of mechanical stresses to bone. Few studies, however, have investigated if PyC will preserve articular cartilage during articular motion. The aim of this research was to elucidate lubrication mechanisms and investigate cartilage changes after in vitro tribological testing against PyC, and traditional biomaterials: zirconium toughened alumina (ZTA) and cobalt-chromium alloy (CoCrMo).
METHODS: Live bovine articular cartilage explants were subjected to tribological testing using a dual-axis joint simulator housed in an incubator against PyC, CoCrMo or ZTA balls (diam. 32 mm). A compressive load of 40N was maintained for 3 hours per day for 5 days. Free swelling cartilage (FSC) samples served as control. A synthetic biomimetic synovial fluid, based on DMEM/F12 and hyaluronic acid (HA)-phospholipid vesicles (PLs), was used as lubricant. Biological tissue response was assessed by 1) metabolic activity of chondrocytes (PrestoBlueTM), 2) histological analysis using haematoxylin-eosin saffron and Safranin-O staining, 3) measurement of sulfated glycosaminoglycans (sGAG). Vesicles of HA-PLs adsorbed on the biomaterials were quantified by HPLC. Statistical differences between biomaterials and FSC were performed using a nonparametric Kruskal-Wallis test.
RESULTS: CoCrMo significantly reduced the number of metabolically active chondrocytes (55±4%), but similar numbers for FSC, PyC and ZTA (72-76±9% N=9, p=0.84) were maintained. sGAG quantification and histological analysis pointed in the same direction, showing a more advanced state of degradation of the cartilage matrix and a more damaged and thinner articular superficial zone after tribological testing against CoCrMo than for other biomaterials [Fig 1 and 2]. Although not significant, PyC showed the highest amount of PLs adsorbed after rubbing (ZTA=1.56±0.32; CoCrMo=1.92±0.48; PyC=2.79±0.94 with p=0.037 between ZTA vs PyC) [Fig 3]. The adsorbed PLs likely protect the cartilage surface from shear damage.
CONCLUSION: While most hemi-arthroplasty implants are made of CoCrMo alloy, this study reveals that among the three biomaterials tested, it induces the most severe cartilage degradation. ZTA and PyC performed similarly, while PyC adsorbed more phospholipid vesicles than ZTA, which may improve its frictional properties. Future studies should investigate the frictional evolution and correlate it with the findings of this study.
Figures
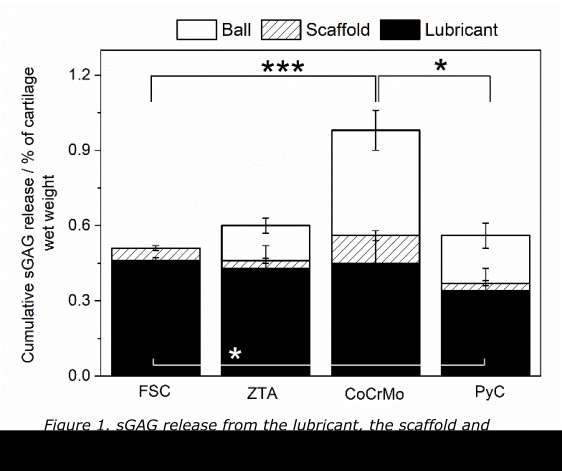
Figure 1
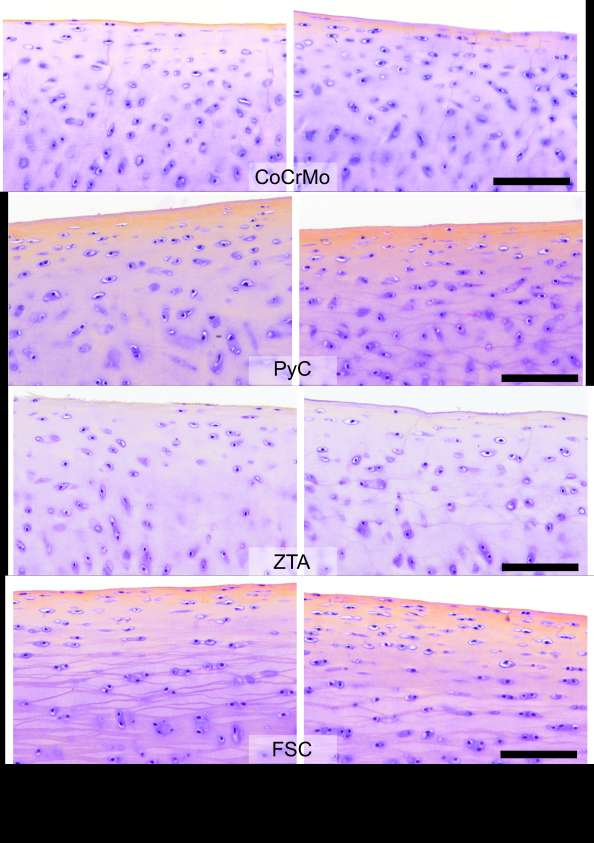
Figure 2
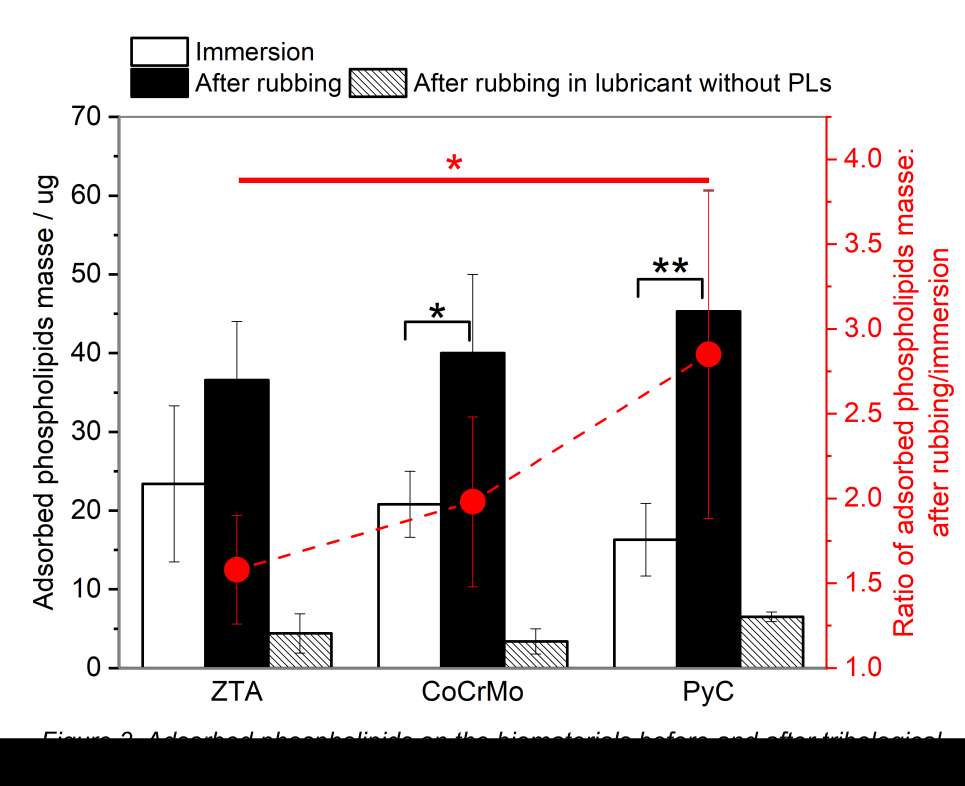
Figure 3#7454
Unicompartimental to Total Knee Arthroplasty Revision Using Intraoperative Sensing Technology: A New Surgical Technique.
*Pier Indelli
Karlos Zepeda MD - Touro College of Osteopathic Medicine - New York, USA
Stefano Ghirardelli - Mount Sinai Hospital - Toronto, Canada
*Email: pindelli@stanford.edu
Unicompartmental Knee Arthroplasty (UKA) is an effective option for managing unicompartmental knee osteoarthritis. Despite evolution in surgical technique and implant design, long-term survivorship of UKA have been lower than Total Knee Arthroplasty (TKA). Historically, UKA revisions have presented technical challenges mainly related to managing residual bone defects and ligament insufficiency ultimately leading to knee instability: the fear of instability has often pushed surgeons to lower the threshold for an increase of the intra-articular level of constraint. Unfortunately, the use of more constrained implants requires sacrificing bone stock and has been related to higher rates of re-revision secondary to recurrence of aseptic loosening.
Methods: The authors developed a surgical technique that combines balancing the knee during revision surgery with the use of the less constrained polyethylene option. We started utilizing, in a revision setting, a device (VERASENSE, Orthosensor, FL) designed to support soft tissue balancing during primary TKA. This intraoperative sensing technology dynamically quantifies intra-articular loads during TKA trial with the goal of correcting any residual imbalance in real time. This technique allows the use of a primary TKA design characterized by a lower level of constraint, instead of a constrained or hinged revision knee system, during UKA revision.
After components removal, the level of constraint (primary PS or semi-constrained) was determined. The general rule followed was that if the distal femoral and proximal tibial bone loss was <15 mm on each side, a primary PS design was chosen, making the final decision on the stability of the implant and the integrity of the collateral ligaments at the time of sensor-guided trial testing.
After all bone cuts have been completed, the femoral and tibial component trials were inserted and the Postero-Stabilized Verasense tibial sensor was inserted, the knee was brought to extension and load measurements are then documented at 10°, 45°, and 90° of flexion.
At this point, the distribution of compartment forces during intraoperative ROM drives the selection of the liner and, accordingly, the level of constraint. The authors considered stable knees those showing a pressure of <50 lbs on the medial compartment, <35 lbs on the lateral compartment, and a mediolateral intercompartmental difference within 15 lbs. The mean intercompartmental force differences during trial ultimately drived our surgical technique
and 15 lbs is usually considered as the parameter to differentiate “balanced” from “unbalanced” knees. To obtain the desired values, the authors performed soft tissue releases [“pie-crusting” of the lateral compartment or superficial MCL release] or bone re-cuts after removal of the trial components. Once these “fine tunings” have been performed, a new sensor trial was performed to confirm stability. Once the final implants have been chosen and cemented, a standard closure of the soft tissues was performed.
Conclusion: The clear advantage of using this sensor- guided technology in UKA revision is to allow an intraoperative evaluation of the medial and lateral compartmental load pressures, tracking soft-tissue balance throughout the entire range of motion arc with trial implants in place, and accordingly, modify any residual imbalance.
#7366
Postoperative Callus Around Tapered Wedge Short Stem: Undiagnosed Fracture After Total Hip Arthroplasty.
*Seiya Ishii - Juntedndo University School of Medicine - Tokyo, Japan
Yuichi Shirogane - Juntendo University - Tokyo, Japan
Koju Hayashi - Juntendo university - Tokyo, Japan
Taiji Watari - Juntendo University - Tokyo, Japan
Yasuhiro Homma - Juntendo University - Tokyo, Japan
Tomonori Baba - Juntendo University - Tokyo, Japan
Kazuo Kaneko - Juntendo University - Tokyo, Japan
Muneaki Ishijima - Juntendo University - Tokyo, Japan
*Email: seiya.isii@gmail.com
Background: Although total hip arthroplasty(THA) using a short tapered wedge stem is popular for its advantage of realizing minimally invasive surgery concept, high risk of periprosthetic fracture and potential postoperative stress fracture has become a clinical concern. Tamaki et al reported that 57 % of postoperative early fracture is caused nontraumatically, and Harper et al observed postoperative callus(PC) after THA and consecutive displaced periprosthetic fracture at the location of that PC has observed. PC might be a reactive phenomenon of undiagnosed periprosthetic fracture after THA. The aim of this study is to investigate the PC after THA with a short tapered wedge short stem.
Methods: We retrospectively assessed the medical records of all patients who received primary THA at our university hospital from 2017 to 2021. 127 THAs in 120 patients using Taperloc Complete Microplasty stem were included in this analysis. Dual mobility system (DM) was used in 92cases (inner head; 22.2-mm in 32 cases, 28mm in 60 cases), and conventional 32-mm femoral head was used in 35 cases. The distance from the lateral corner of the stem to the most medial point of lesser trochanter along to body axis was measured as stem depth (SD). We defined characteristic X-ray finding of lateral border of the femoral cortex at the height of distal margin of porous coating is doubly observed as PC. Radiograph at preoperative and immediate postoperative and at 1, 3, 6 months after the surgery was used to assess femoral morphology (morphologic cortical index, canal-calcar ratio, and canal flare index), canal fill ratio, stem alignment, and SD, and PC. Univariate and multivariate logistic regression analysis was performed to identify the independent predictors of PC.
Results: PC was observed in 40% of the all patients (mean 3.1 ± 1.4months). PC were not associated with weight (p = 0.254), and subsidence (p = 0.74). The multivariate logistic regression analysis with dependent variables of PC revealed that SD (odds ratio; 1.178 , 95% confidence interval; 1.086–1.278, P = 0.000) and the diameter of femoral head (odds ratio; 0.243 , 95% confidence interval; 0.077–0.765, P = 0.015) were significant and independent risk factors for PC.
Conclusion: High incidence of PC after THA using a short tapered wedge stem was presented in this study. This might be a sign of stress fracture around the stem, and a potential risk of consecutive complete fracture. Initial callus after fracture is radiographically evident in an average of 21 days, PC might not be a reactive phenomenon of intraoperative fracture caused by stem insertion. Stress concentration on the lateral side of the femur caused by deep insertion of the stem, and high frictional torque of large femoral head transmitted to the stem may have led to stress fracture with PC during postoperative rehabilitation. Our results showed that deep insertion of tapered wedge short stem and use of a large femoral head are the major risks of PC and potential periprosthetic fracture, this combination should be avoided in case of short tapered wedge stem.
Figures
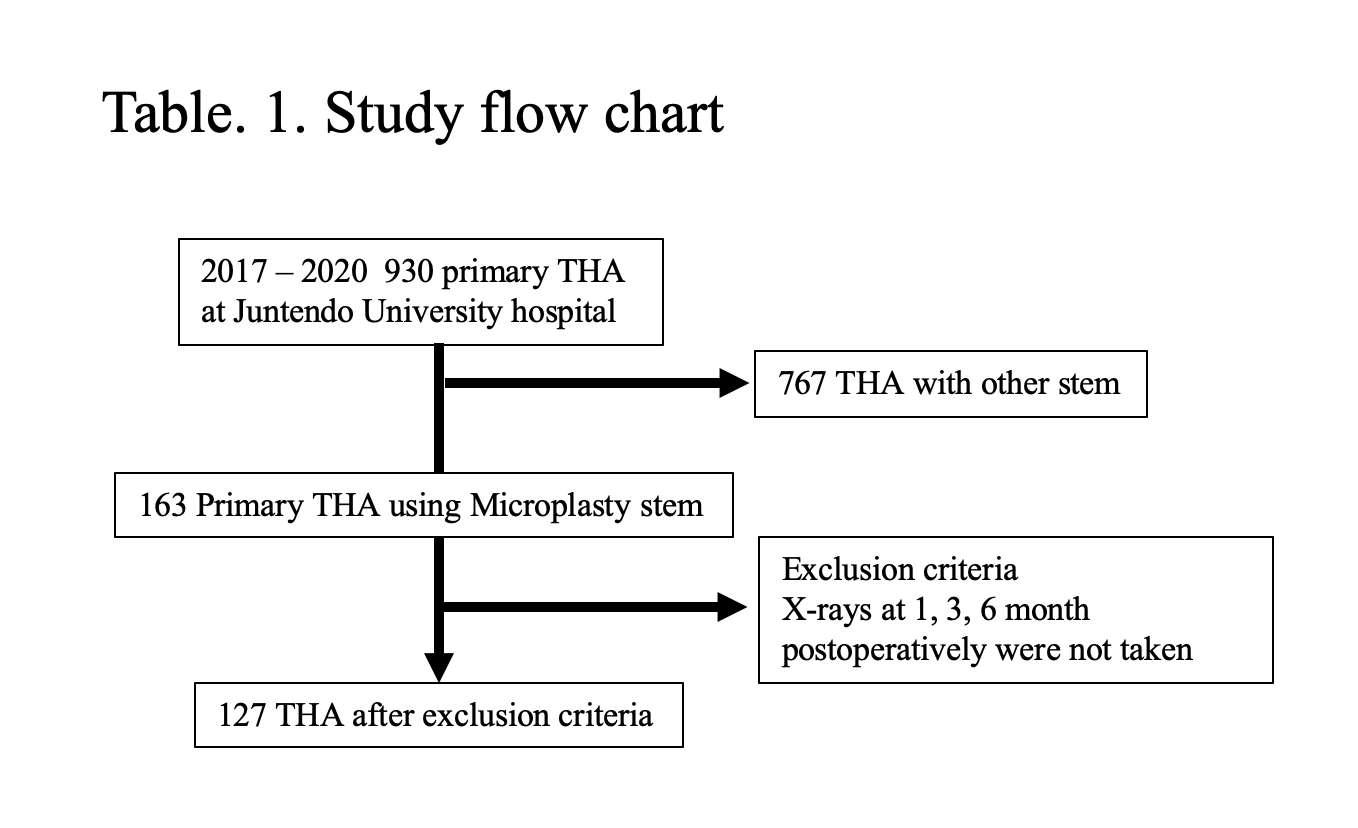
Figure 1
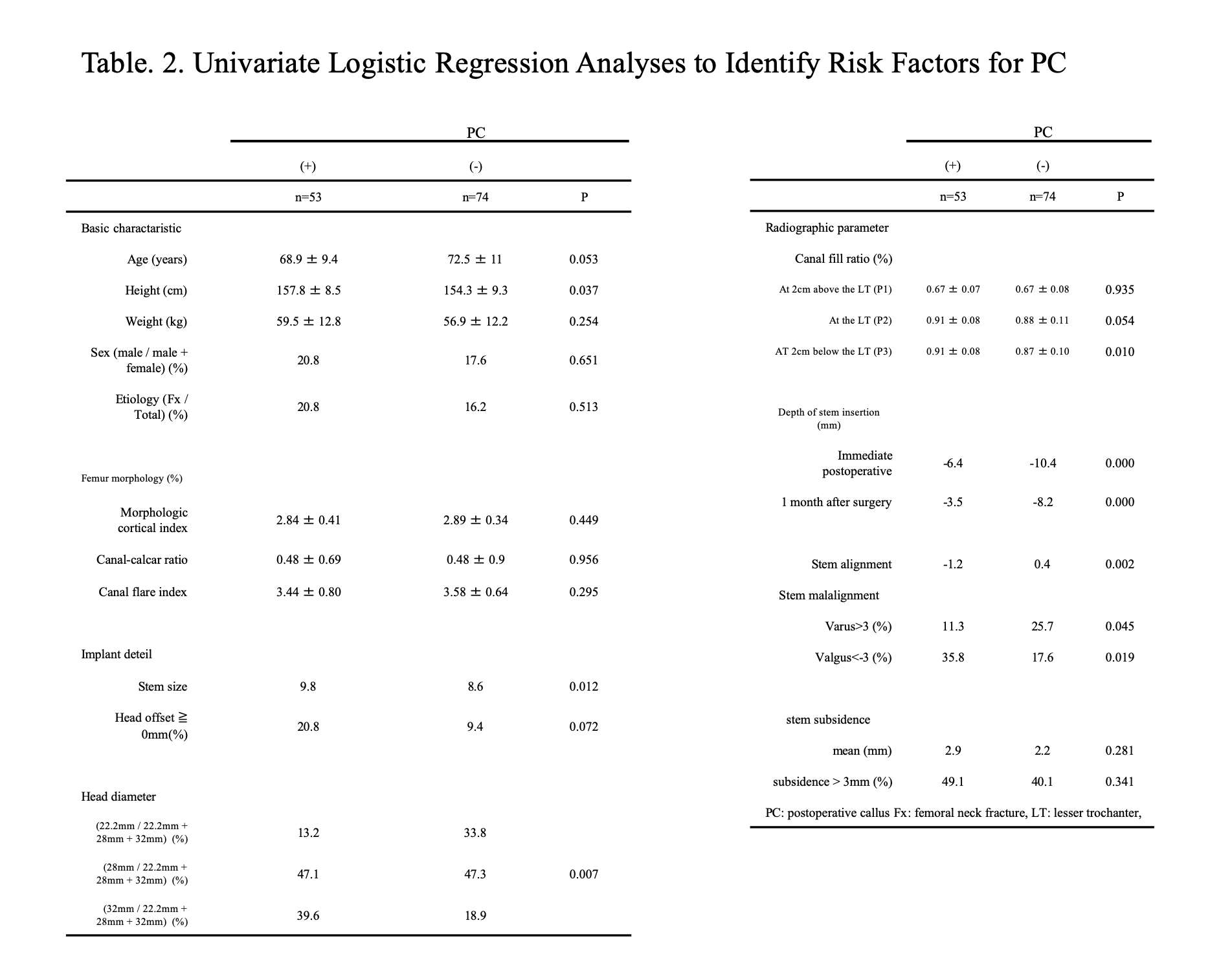
Figure 2
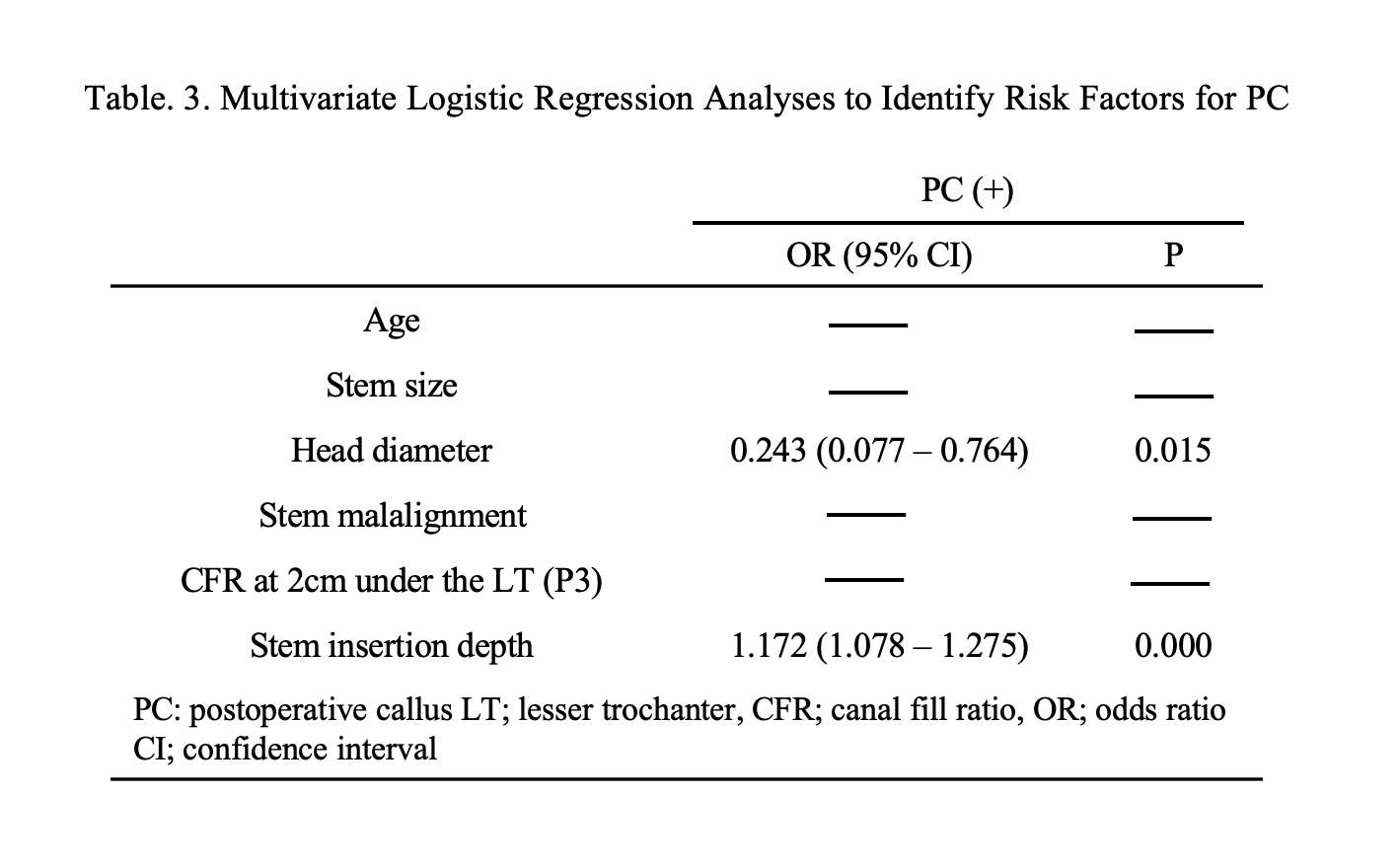
Figure 3#7524
Postoperative Callus Around Tapered Wedge Short Stem: Undiagnosed Fracture After Total Hip Arthroplasty
*Seiya Ishii - Juntedndo University School of Medicine - Tokyo, Japan
Yasuhiro Homma - Juntendo University - Tokyo, Japan
Tomonori Baba - Juntendo University - Tokyo, Japan
Yuichi Shirogane - Juntendo University - Tokyo, Japan
Koju Hayashi - Juntendo university - Tokyo, Japan
Kazuo Kaneko - Juntendo University - Tokyo, Japan
Muneaki Ishijima - Juntendo University - Tokyo, Japan
Taiji Watari - Juntendo University - Tokyo, Japan
*Email: seiya.isii@gmail.com
Abstract
Background: Although total hip arthroplasty(THA) using short tapered wedge stem is popular for its advantage of realizing minimally invasive surgery concept, high risk of periprosthetic fracture and potential postoperative stress fracture has become a clinical concern. Tamaki et al reported that 57 % of postoperative early fracture is caused nontraumatically, and Harper et al observed postoperative callus(PC) after THA and consecutive displaced periprosthetic fracture at the location of that PC has observed. PC might be a reactive phenomenon of undiagnosed periprosthetic fracture after THA. The aim of this study is to investigate the PC after THA with a short tapered wedge short stem.
Methods: We retrospectively assessed the medical records of all patients who received primary THA at our university hospital from 2017 to 2021. 127 THAs in 120 patients using Taperloc Complete Microplasty stem were included in this analysis. Dual mobility system (DM) was used in 92cases (inner head; 22.2-mm in 32 cases, 28mm in 60 cases), and conventional 32-mm femoral head was used in 35 cases. The distance from the lateral corner of the stem to the most medial point of lesser trochanter along to body axis was measured as depth of the stem(DS). We defined characteristic X-ray finding of lateral border of the femoral cortex at the height of distal margin of porous coating is doubly observed as PC. Radiograph at preoperative and immediate postoperative and at 1, 3, 6 months after the surgery was used to assess PC, DS, femoral morphology (morphologic cortical index, canal-calcar ratio, and canal flare index), canal fill ratio, and stem alignment. Univariate and multivariate logistic regression analysis was performed to identify the independent predictors of PC.
Results: PC was observed in 53/127 cases (41.7%, mean 3.1 ± 1.4 months after THA). PC were not associated with weight (p = 0.254), and subsidence (p = 0.74). The multivariate logistic regression analysis with dependent variables of PC revealed that DS (odds ratio; 1.178 , 95% confidence interval; 1.086–1.278, P = 0.000) and the diameter of femoral head (odds ratio; 0.243 , 95% confidence interval; 0.077–0.765, P = 0.015) were significant and independent risk factors for PC.
Conclusion: High incidence of PC after THA using short tapered wedge stem was presented in this study. This might be a sign of stress fracture around the stem, and potential risk of consecutive complete fracture. Initial callus after fracture is radiographically evident in an average of 21 days, PC might not be a reactive phenomenon of intraoperative fracture caused by stem insertion. Stress concentration on the lateral side of the femur caused by deep insertion of the stem, and high frictional torque of large femoral head transmitted to the stem may have led to stress fracture with PC during postoperative rehabilitation. Our results showed that deep insertion of tapered wedge short stem and use of a large femoral head are the major risks of PC and potential periprosthetic fracture, this combination should be avoided in case of short tapered wedge stem.
Introduction
Total hip arthroplasty(THA) is the only solution for end-stage osteoarthritis and enables to excellent pain relief and functional improvement. Although THA has developed for elder people for concerning poor results with THA in active young patients due to their high activity [1], the England registry reported the acceptable implant longevity that 15-year implant survival rates of cementless stem THA aged at <55 years old is 9.71% compared with 7.89% of all surgery [2]. It is projected that 52% of the patients receiving THA will be younger than 65 years old by 2030 [3], surgical planning and implant selection considered revision surgery are getting demanded at the time of initial THA. THA using short stem has become increasingly popular in recent years for its advantage for maintaining proximal femur bone and minimally invasion of soft tissue. Insertion of short stems enables to preserve of proximal femur bone mass compared with conventional stem[4], the overall decrease in BMD value was less when using the short stem compared to the cementless standard femoral stem [5]. Additionally, short stems realize the minimally invasive surgery concept as it enables muscle and soft tissue preservation compared to insertion of conventional stems which needs highly detachment of soft tissue. We started to use colorless tapered wedge short stems in 2017 for these reasons.
In recent years, high risk of periprosthetic fracture has become a recent clinical concern after THA with tapered wedge short stem. Keith et al. reported a 1.9 times higher periprosthetic fracture rate of a short tapered wedge stem than a standard tapered wedge stem. A finite element analysis study also showed high fracture risk and femoral strain of short tapered wedge stem during implant insertion and single-leg stance compared with another stem[6]. Moreover, several researchers indicate the risk of potential postoperative stress fracture after THA with tapered wedge short stem. Tamaki et al reported that 57 % of postoperative early fracture is caused nontraumatically[7], and Harper et al observed postoperative callus(PC) after THA and consecutive nontraumatic displaced periprosthetic fracture at the location of that PC has observed[8].
These might indicate potential postoperative microfracture with PC and consecutive displaced fracture induced by postoperative loading stress. However, the incidence of PC and factors that influence emerging PC are unclear.
The aim of this study is to investigate the PC after THA with a tapered wedge short stem.
Material and method
After obtaining institutional review board approval, we retrospectively reviewed the medical records of all patients who had undergone THA at our university hospital from January 2017 to November 2021. In total, 930 THA procedures were performed during that period. Taperloc Complete Microplasty stem (Zimmer Biomet, Warsaw, IN, USA) was used in 163 THAs in 152 patients. The exclusion criteria were (1) previous hip surgery, (2) early revision surgery, (3) ankylosing spondylitis, (4) cases who could not complete a total of 3 times of radiographic follow-ups at 1, 3, and 6 months after the surgery. After the exclusion criteria, 127 THAs in 120 patients were included in this analysis. The implanted acetabular component was a G7 Acetabular System (Zimmer Biomet, Warsaw, Indiana). Dual mobility system (DM) with E1 Active Articulation all-polyethylene outer shell was used in 92 cases, of which the 22.2 mm femoral heads were used for 32 cases (Cobalt Chromium head; 1 case, ceramic head; 31cases), and the 28 mm ceramic femoral heads were used for 60 cases. Exception for the DM cases, the bearing surface was highly cross-linked polyethylene (E1 Antioxidant Infused Technology; Zimmer Biomet, Warsaw, IN, USA) and all of the femoral head was the 32 mm ceramic head (Table. 1).
Operative procedure
All surgery was performed by a group of eight orthopaedists specializing in hip joint arthroplasty. Direct anterior approach was used in all cases.
Radiographic evaluation
Radiographic evaluation was performed using an anteroposterior radiograph in the supine position with both legs internally rotated 10°. Emerging PC was assessed using an immediate postoperative radiograph and a radiograph at 1 month ± 1 week, 3 months ± 2 weeks, and 6 months ± 2 weeks after the surgery.
PC group was defined as cases with blurred or doubled lateral border of the femoral cortex at the distal end of stem porous coating at 1, 3, or 6 months after THA compared with immediate postoperative X-ray. (Fig. 1). The distance from the lateral corner of the stem to the most medial point of the lesser trochanter along to body axis was measured as depth off the stem (DS) (Fig. 2).
Pre-operative radiographs were used to analyze the proximal femoral geometry using previously described radiographic parameters, including the morphologic cortical index, canal-calcar ratio, and CFI using the method described by Yeung et al [9]. Immediate postoperative radiographs were used to assess stem alignment, acetabular offset, femoral offset, and the canal fill ratio of the stem (CFR). The CFR was defined as the width of the stem divided by the width of the canal at four points: at the lesser trochanter and 2 cm above, 2 cm below, and 7 cm below the lesser trochanter. All measurements were conducted using a computerized picture archiving and communication system (SYNAPSE; Fujifilm, Tokyo, Japan).
Statistical analysis
The patients’ baseline characteristics are expressed as mean ± standard deviation. The independent-sample Student’s t-test or the Mann–Whitney test was used for continuous variables, and the chi-squared test was used for dichotomous variables. Data were statistically analyzed using IBM SPSS Statistics for Macintosh, Version 22.0 (IBM Corp., Armonk, NY, USA).
Univariate and multivariate logistic regression analyses were performed to identify the risk factors for CH. Before conducting the multivariate analysis, we assessed the relationships between the variables by Spearman’s rank correlation coefficient to prevent the effects of confounders. A P value of < 0.05 was considered statistically significant, and all tests were two-sided.
Result
The background of each group of femoral heads was different because we use DM only patients aged over 70 years old (Table. 2).
PC was observed in 53/127 cases (41.7%, mean 3.1 ± 1.4 months after THA), and the incidence of PC was different between the femoral head (Incidence of EC ; DM (22.2 mm); 17.6%, DM (28 mm); 42.9%, 32 mm; 75%, p=0.007).
The univariate logistic regression analysis indicated that height (p = 0.037), stem size (p = 0.012), head diameter (p = 0.007), canal fill ratio at P3 (p = 0.010), DS (immediate postoperative; p=0.000, 1 month after surgery; 0.000), stem alignment (p = 0.002) were significantly associated with PC. PC were not associated with weight (p = 0.254), and subsidence (p = 0.74) (Table. 3).
The multivariate logistic regression analysis with dependent variables of PC revealed that DS (odds ratio; 1.178 , 95% confidence interval; 1.086–1.278, P = 0.000) and the diameter of femoral head (odds ratio; 0.243 , 95% confidence interval; 0.077–0.765, P = 0.015) were significant and independent risk factors for PC (Table. 4).
Discussion
A high incidence of PC after THA using tapered wedge short stem has been revealed in our study. This is the first report to reveal factors of PC that relative contact positioning between stem and femur, and the difference in the diameter of the femoral head. PC might be a sign of stress fracture around the stem, and potential risk of consecutive complete fracture. The risk factors of PC can be divided as 1. Relative contact positioning between stem and femur (SD at immediate and 1 month after the surgery; p = 0.000, canal fill ratio at 2cm below the LT; p = 0.010, Stem alignment; p = 0.002) and 2. Diameter of the femoral head (p = 0.007).
1, Relative contact positioning between stem and femur
A high incidence of emerging PC was observed in cases where the stem was inserted deeply and valgus alignment. Stress concentration on the lateral side of the stem might be caused by this positioning of the stem against the femur, which may have led to stress fracture with PC. Three-point fixation of tapered wedge stem in the coronal plane is obtained (1) medially at the neck cut, (2) laterally at the margin of the stem shoulder, and (3) medially at the distal aspect of the stem. [11]. Valgus and deep position of the stem will increase stress concentration for lateral edge of the stem, especially at the distal end of the porous coating where the coefficient of friction changes compared with further distal area. Moreover, changes in the postoperative load transfer environment would influence this stress distribution. The mean time until the EC observe for the first time is 3.0± months. Initial callus after fracture is radiographically evident in an average of 21 days for patients over 44 years old[12], EC is unlikely to be the result of a fracture caused by stem insertion during surgery If EC was a sign reflecting fracture healing. We assumed microfracture around the femur was induced by postoperative weight loading after the surgery. Walking can be considered as supporting the entire body weight in single-leg, and force of 2.4 times the body weight in the standing position by single leg[13], 7.2〜7.4 times the body weight in stair crimb[14] are exerted on the femoral head in a direction outward relative to the femur axis. As rehabilitation progresses and the angle of load stress gradually increases relative to the femoral axis, the vertical femoral axis component of the force increases. This point of force and distal medial thick cortex as a point of fulcrum would induce higher stress on the lateral cortex as a point of load. This high stress to the lateral cortex of the femur caused by this leverage is greater with the short stem than with the conventional stem because the shorter stem length reduces the ratio of the distance between the fulcrum-action point distance divided distance between the fulcrum-force point distance. Stress distribution in specific implant position and change of stress direction in daily activity a few month after the surgery could be the reasons for emerging callus in patients after THA with a short stem, and of the period that callus occurs about 3 months after the surgery. When preoperative planning for THA using a short stem, we should not hesitate to change the selection of the stem if an implant position with a high risk of callus, which is a potential fracture risk, is anticipated.
2. Diameter of the femoral head.
The diameter of the femoral head has influenced the development of EC. The high frictional torque of the large femoral head(citation needed) might be transmitted distally to the stem and contributed to stress fracture. Although THA with a large femoral head has low dislocation rate because a large femoral head has high jumping distance[15] and oscillation angle [16], negative aspects of a large femoral head are not well understood. A registry from Netherlands showed that the use of a large head decreased the revision rate due to dislocation but increased the revision rate for other reasons [17]. This high revision risk other than dislocation is mainly thought to be due to its high frictional torque. Scholl et al. reported that study reported that the frictional torque was 1.5 times higher for a 44mm head compared to a 22mm head[18]. We also demonstrated high frictional torque of large femoral head in vivo study, cases after THA using 36mm head has a higher risk of cortical hypertrophy than that of 32mm head(36mm; 51.6%, 32mm; 17.7%) [19]. This high frictional torque characteristic of a large femoral head cause trunnion failure, and cup loosening[20][21]. 90 % of cases for revision surgery after trunnion failure has been used 36mm femoral head[20]. Investigation using Nordic registry revealed a higher rate of cup loosening associated with 36 mm heads than with 32 mm (hazard ratio, 2.29; 95% confidence interval, 1.79-2.92; P < .001) [21]. The use of large femoral heads is a trade-off relationship between improved dislocation risk and decreased long survivorship. Our study suggests insufficiency fracture might be induced by the high frictional torque of the large femoral head. A combination of a large femoral head and implants with high fracture risk such as a short tapered wedge stem should be carefully selected after evaluation of bone quality.
Limitation
This investigation has several limitations. First, we can’t determine whether the callus that we observe in this study is the same as the callus after a fracture. We experienced similar cases after THA using tapered wedge short stem without pain at the time of discharge from hospital and admitted with severe hip pain outpatient clinic at 1 month after the surgery, and the pain disappeared at 3 or 6 months after the surgery. Although postoperative stress fracture might cause this pain and consecutive emerging PC as fracture healing, we have not been able to demonstrate an association between pain scores and PC in the present study because of incomplete pain score collection. We believe that further studies showing an association with pain scores will clarify the relationship between callus and fractures. Second, we have also used this stem in cases with bone fragility. However, we strictly limited the use in our institution for the fracture risk after this study. Inappropriate contact between this stem against the femur should be avoided in cases of strong bone fragility, and the choice of a large head diameter should be carefully selected.
Conclusion
We observed postoperative callus around the femur after total hip arthroplasty using tapered wedge short stem. Stem insertion position and diameter of the femoral head were the factors in the development of the callus. The use of tapered wedge short stem should be carefully selected after evaluating the risk of potential fracture.
1. Charnley J. Arthroplasty of the hip. A new operation. Lancet 1(7187): 1129, 1961
2. National Joint Registry. National joint registry for England, Wales, Northern Ireland and the Isle of Man: 18th annual report 2021, http://www.njrcentre.org.uk (2021, accessed 11 November 2021).
3. Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Future young patient demand for primary and revision joint replacement: national projections from 2010 to 2030. Clin Orthop Relat Res 467(10): 2606, 2009
4. Yan SG, Woiczinski M, Schmidutz TF, Weber P, Paulus AC, Steinbrück A, Jansson V, Schmidutz F. Can the metaphyseal anchored Metha short stem safely be revised with a standard CLS stem? A biomechanical analysis. Int Orthop 41(12): 2471, 2017
5. Samy AM, El-Tantawy A. Stem length in primary cementless total hip arthroplasty: Does it make a difference in bone remodeling? Eur J Orthop Surg Traumatol 29(6): 1235, 2019
6. Nandi S, Shah A, Joukar A, Becker K, Crutchfield C, Goel V. Short single-wedge stems have higher risk of periprosthetic fracture than other cementless stem designs in Dorr type A femurs: a finite element analysis. Hip Int: 1120700020949185, 2020
7. Tamaki T, Jonishi K, Miura Y, Oinuma K, Shiratsuchi H. Cementless Tapered-Wedge Stem Length Affects the Risk of Periprosthetic Femoral Fractures in Direct Anterior Total Hip Arthroplasty. J Arthroplasty 33(3): 805, 2018
8. Harper KD, Incavo SJ, Clyburn TA. Short-Stem Prostheses in Total Hip Arthroplasty: An Unexpected Short-Term Complication: A Report of 2 Cases. JBJS Case Connect 10(1): e0159, 2020
9. Yeung Y, Chiu KY, Yau WP, Tang WM, Cheung WY, Ng TP. Assessment of the proximal femoral morphology using plain radiograph-can it predict the bone quality? J Arthroplasty 21(4): 508, 2006
10. Hallgren KA. Computing Inter-Rater Reliability for Observational Data: An Overview and Tutorial. Tutor Quant Methods Psychol 8(1): 23, 2012
11. Warth LC, Grant TW, Naveen NB, Deckard ER, Ziemba-Davis M, Meneghini RM. Inadequate Metadiaphyseal Fill of a Modern Taper-Wedge Stem Increases Subsidence and Risk of Aseptic Loosening: Technique and Distal Canal Fill Matter! J Arthroplasty 35(7): 1868, 2020
12. Hufnagl K. An Investigation of Time Since Injury: A Radiographic Study of Fracture Healing. 2005
13. Kamel HM. MODELING AND SIMULATION OF A HIP PROSTHESIS IMPLANTATION. The International Conference on Applied Mechanics and Mechanical Engineering 18(18th International Conference on Applied Mechanics and Mechanical Engineering.): 1, 2018
14. Nordin M. Basic biomechanics of the musculoskeletal system. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2012
15. Sariali E, Lazennec JY, Khiami F, Catonné Y. Mathematical evaluation of jumping distance in total hip arthroplasty: influence of abduction angle, femoral head offset, and head diameter. Acta Orthop 80(3): 277, 2009
16. Malik A, Maheshwari A, Dorr LD. Impingement with total hip replacement. J Bone Joint Surg Am 89(8): 1832, 2007
17. Zijlstra WP, De Hartog B, Van Steenbergen LN, Scheurs BW, Nelissen R. Effect of femoral head size and surgical approach on risk of revision for dislocation after total hip arthroplasty. Acta Orthop 88(4): 395, 2017
18. Scholl L, Longaray J, Raja L, Lee R, Faizan A, Herrera L, Thakore M, Nevelos J. Friction in modern total hip arthroplasty bearings: Effect of material, design, and test methodology. Proc Inst Mech Eng H 230(1): 50, 2016
19. Ishii S, Homma Y, Baba T, Shirogane Y, Kaneko K, Ishijima M. Does increased diameter of metal femoral head associated with highly cross-linked polyethylene augment stress on the femoral stem and cortical hypertrophy? Int Orthop 45(5): 1169, 2021
20. Bansal T, Aggarwal S, Dhillon MS, Patel S. Gross trunnion failure in metal on polyethylene total hip arthroplasty-a systematic review of literature. Int Orthop 44(4): 609, 2020
21. Tsikandylakis G, Kärrholm J, Hailer NP, Eskelinen A, Mäkelä KT, Hallan G, Furnes ON, Pedersen AB, Overgaard S, Mohaddes M. No Increase in Survival for 36-mm versus 32-mm Femoral Heads in Metal-on-polyethylene THA: A Registry Study. Clin Orthop Relat Res 476(12): 2367, 2018
Figures
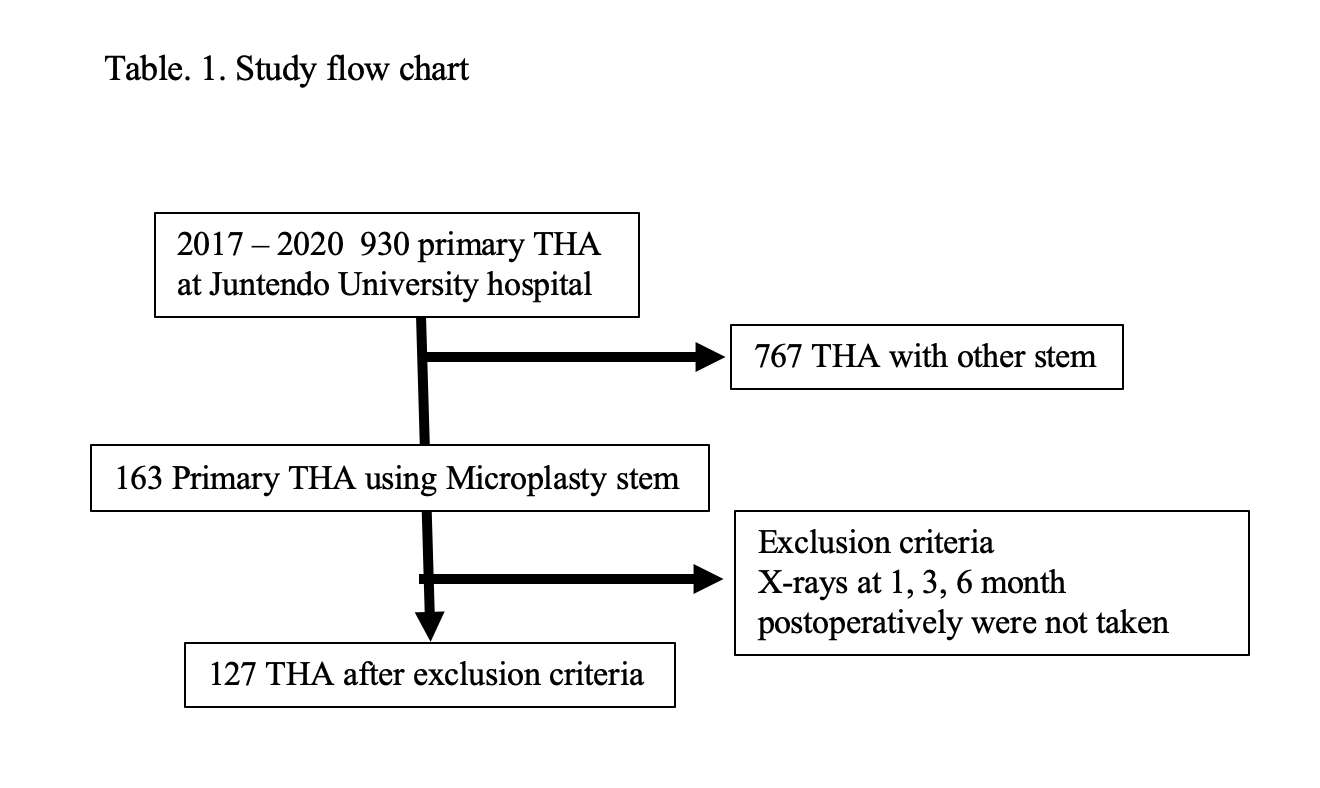
Figure 1
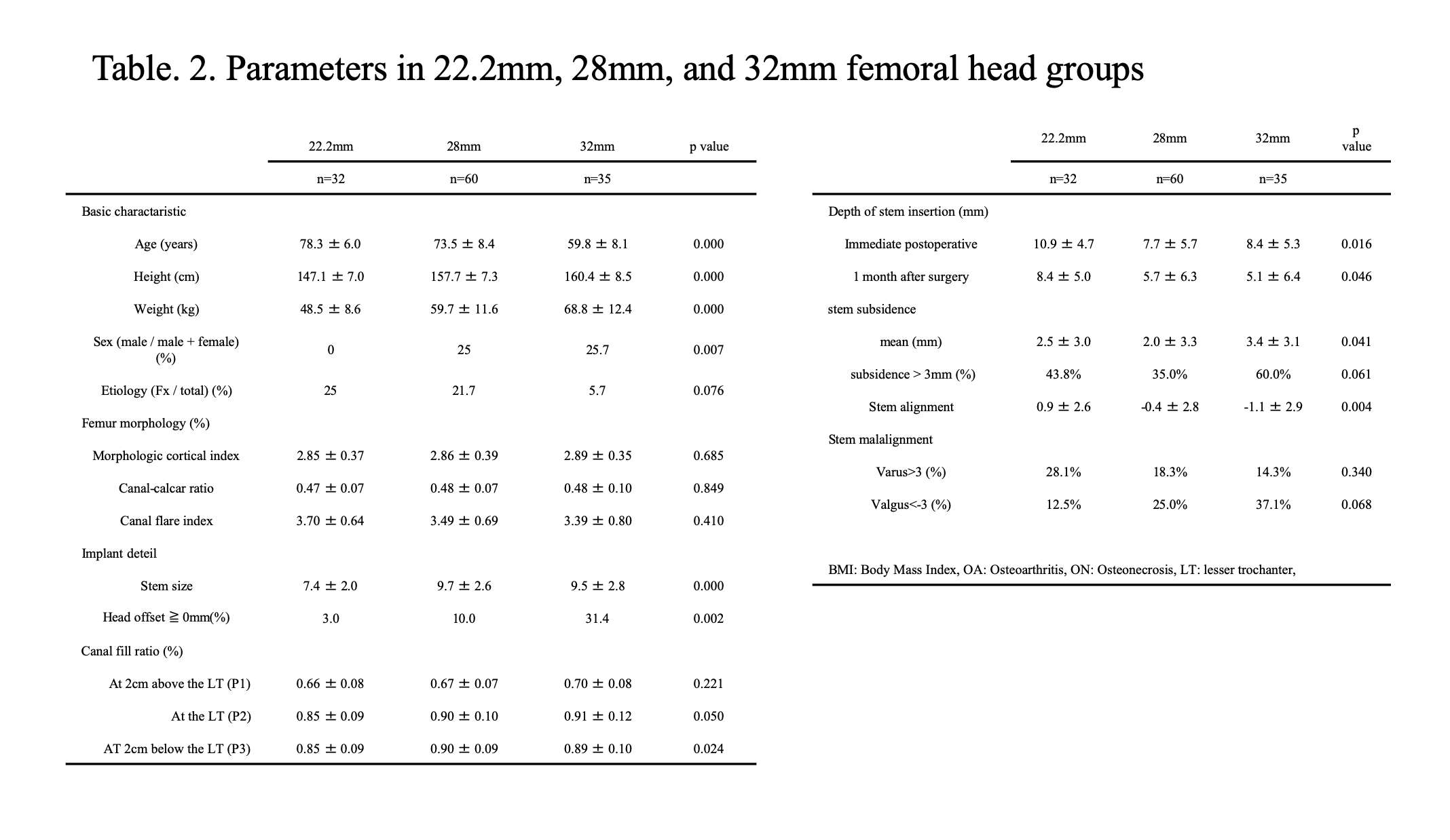
Figure 2
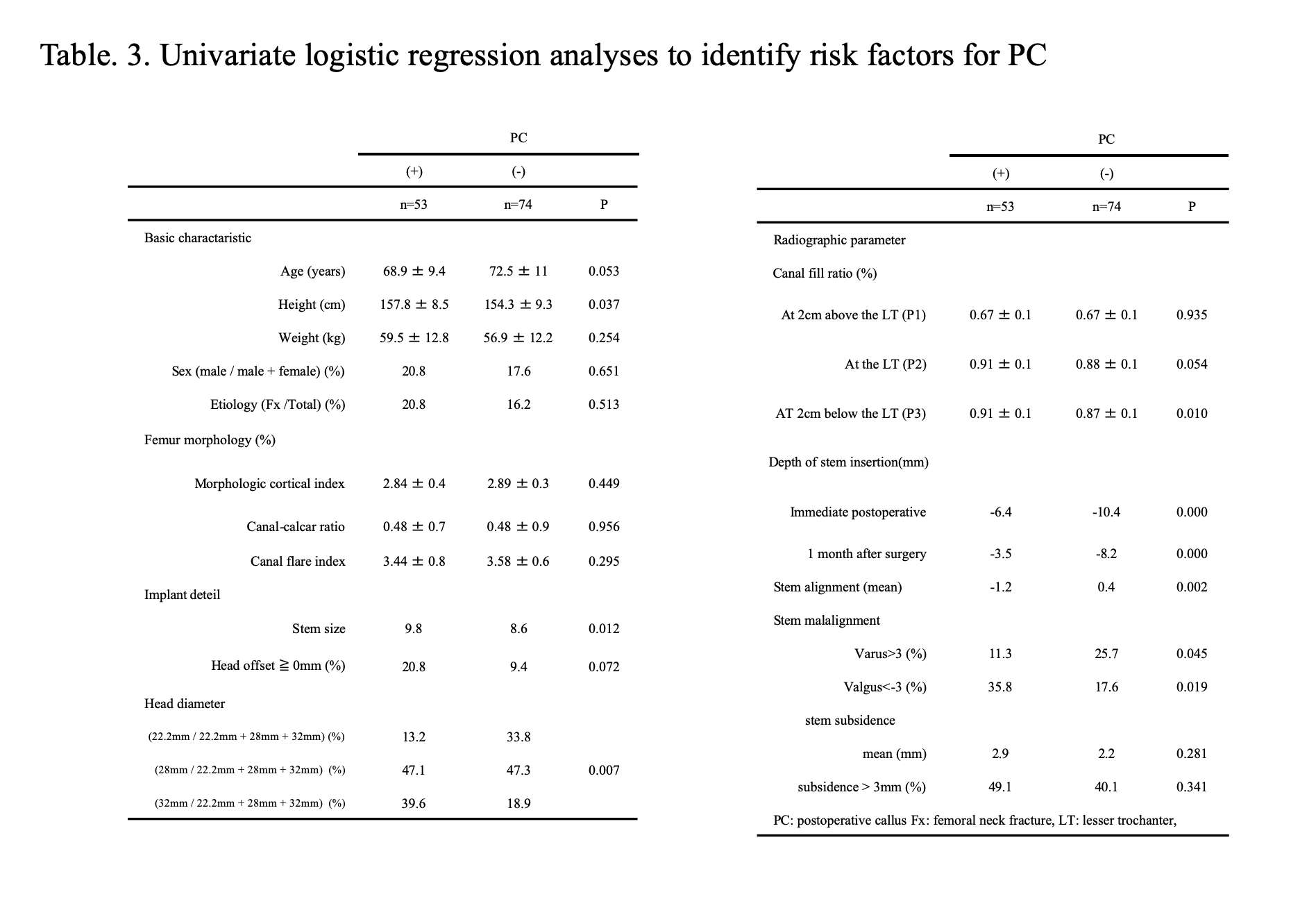
Figure 3
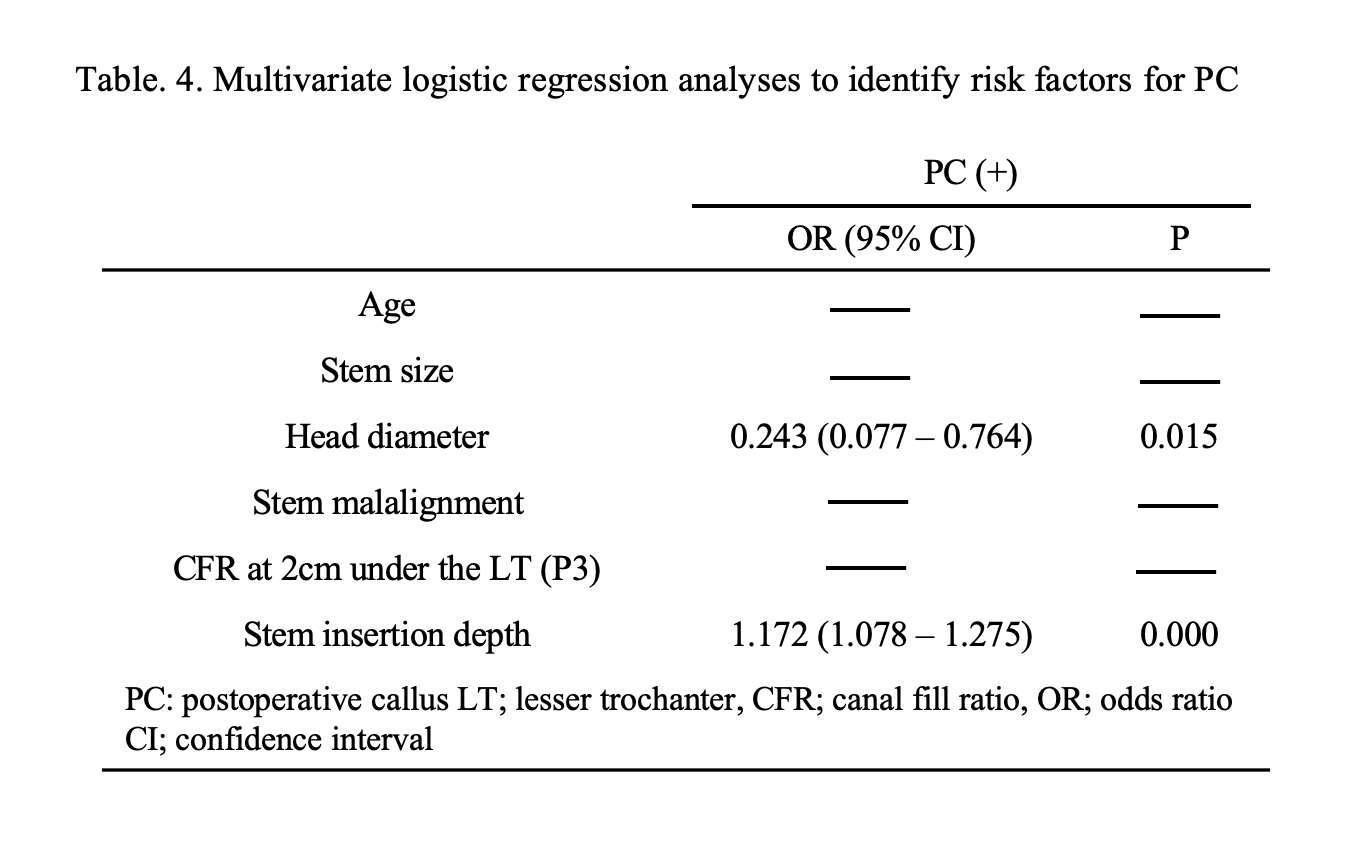
Figure 4
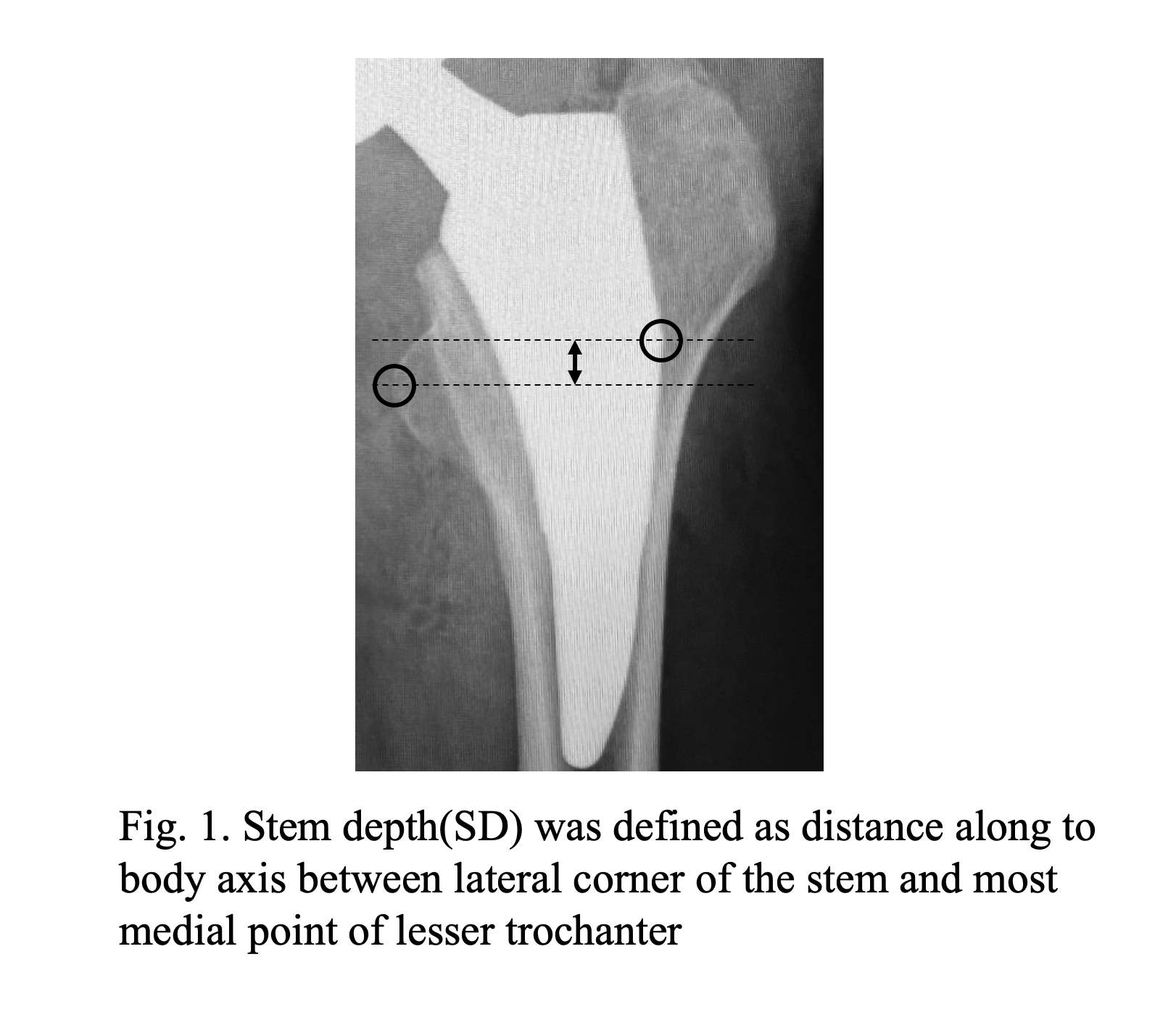
Figure 5
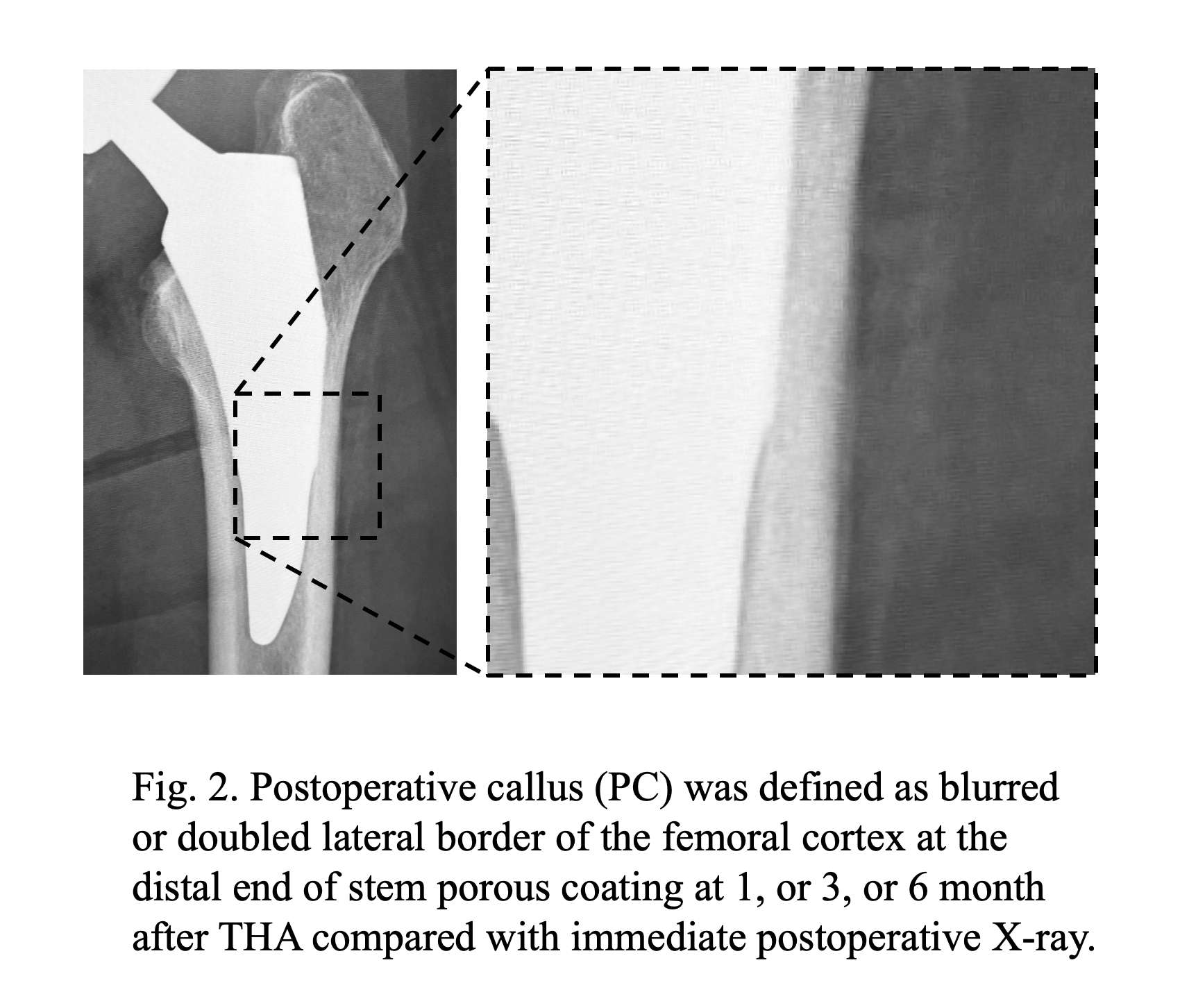
Figure 6#7877
The Glove-Gown Interface: Methods to Inhibit a Potential Source of Surgical Contamination
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Lee Swiderek - Advanced Ortho and Spine - Bellaire, USA
Jasmine Gonzalez - The Institute of Orthopedic Research and Education - Houston, USA
Hugh Jones - UT Health Science Center at Houston - Houston, USA
Kenneth Mathis - The Methodist Hospital - Houston, USA
Sabir Ismaily - Institute of Orthopedic Research and Education - Houston, USA
*Email: philipnoble66@gmail.com
Introduction
The junction between a surgical glove and the sleeve of a surgical gown is recognized as a potential source of contamination during joint replacement procedures. Moreover, when the air between the gown and the skin is positively pressurised, as in the “space suits”, the possibility of contaminants escaping into the operative field increases. Multiple studies have demonstrated that the glove/gown junction can become contaminated during the donning procedure; however, no studies have demonstrated that this pathway leads to contamination of the perioperative environment. This study was undertaken to determine:
1) Does air escape via the glove-gown interface during operative procedures?
2) Does this deliver viable contaminants into the surrounding environment?
3) If so, can alternative gloving techniques inhibit particle transport?
Methods
1. Schlieren imaging was used to visualise air flow from the surgical gown to the surrounding air.
2. A surgeon performed 7 mock TKR procedures under sterile conditions. After each procedure, he blotted his palm and forearm circumferentially on an agar tray in a laminar flow biosafety cabinet (Fig 2). The trays were then incubated and checked for bacterial growth after 24 and 48 hours.
3. To evaluate alternative gloving techniques, the surgeon performed 24 simulated surgeries after bilateral application of 2gm of fluorescent powder (5µm) up to the elbow to serve as a surrogate for skin flakes. On one hand, the surgeon donned two pairs of sterile Ortho gloves overlapping the cuff in a typical manner. The other hand was donned using one of 3 alternative dressing techniques (8 each; Fig 3):
1. Inner glove and gown circumferentially taped.
2. Gown cuff positioned in-between the inner and outer gloves.
3. An expanded pad was worn at the wrist to fill the internal gown space.
Results
Glove/gown interface
Schlieren imaging demonstrated that manual compression of the gloved palmar surface caused air to escape from the interior of the sleeve (Fig 1).
Sterile Surgeries
2/7 sterile mock surgeries were found to be contaminated proximal to the glove-gown interface.
Aseptic training powder surgeries
Standard gloving was breached during 18 of the 24 (75%) surgeries. In comparison, the contamination rate using the alternative dressing techniques was 25% for the taped group (p=0.015 vs. controls), 38% for the over-&-under technique was (p=0.333), and 25% with the wrist pad (p=0.053) (Fig 3). For all groups combined, 68% of contaminants were dorsal vs. 40% volar (p=0.006). 36% of the contaminants were found on the left hand and 64% on the right (p=0.006). When separating the groups, 78% of the contaminants were found dorsally for standard gloving and 28% were found volar (p=0.001). The number of contaminations using alternative gloving was low and no dorsal/volar or left/right pattern emerged.
Conclusions
â—� Air escaping via the glove-gown interface carries viable contaminants from within the gown itself.
â—� Gloving techniques that create an airtight barrier and reduce at the glove/gown interface can reduce breaching of particles. However, a large number of trials would be needed to determine if alternate gloving techniques inhibit contamination in surgical practice.
Figures
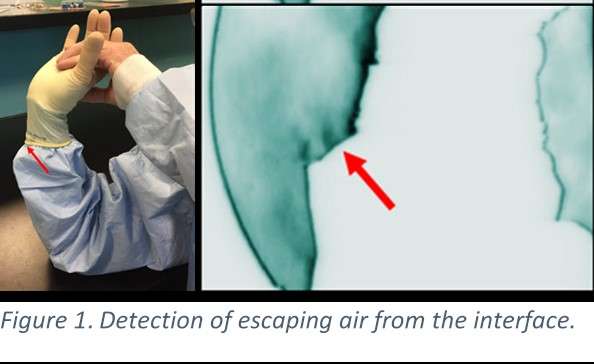
Figure 1

Figure 2
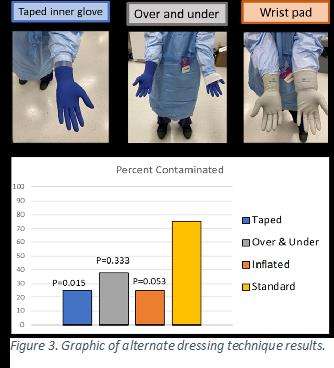
Figure 3#7891
Balancing the Knee Through Robotic Arm Assisted Component Positioning Avoids Soft Tissue Releases in Total Knee Arthroplasty for Varus Pattern Osteoarthritis
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Jonathan Peterson - University of Texas Health Science Ctr - Houston, USA
Lauren Pupa - Baylor College of Medicine - Houston, USA
Sabir Ismaily - Institute of Orthopedic Research and Education - Houston, USA
Kevin Tran - University of Texas Health Science Ctr - Houston, USA
Adam Freedhand - The University of Texas Health Science Center at Houston - Houston, USA
*Email: philipnoble66@gmail.com
Introduction
Component positioning methodologies in TKA range from Mechanical Alignment (MA) which restores a neutral hip-ankle axis and achieves ligamentous balance through soft tissue releases to Kinematic Alignment (KA) which aims to restore the pre-arthritic knee alignment and thereby minimize the need for soft tissue adjustments. The purpose of this study was to quantify the changes made in a hybrid technique of TKA balancing through changes in component positioning using a robotic assisted arm platform.
Methods
56 knees with a varus deformity of at least 3° due to osteoarthritis were templated for a standard MA TKA through measured resection (Standard Plan). A Robot Assisted surgical platform (MAKO, Stryker, Mawah NJ) was used intra-operatively to quantify the angular deformity and stiffness of the knee and the gap in mm between the planned bone resections on the femur and tibia in full extension and at 90° of flexion. Tibia and femur component position adjustments were made in the coronal, sagittal, and axial planes to achieve a gap of 18mm +/-1mm. Maximum coronal angulation of the components was limited to 2° varus/valgus or less. Changes in the final plan were recorded for all knees and compared to the initial parameters. Clinically significant changes in the final vs standard plans were chosen based on standard deviation and surgeon preference.
Results
Average initial alignment was 8.6° varus with gaps between the planned bone resections of 13.5mm medially and 19.6mm laterally in extension and 12.8mm medially and 17.4mm laterally in flexion on the standard plan. The most commonly changed parameters that were clinically significant are shown in Table 1 and include medial posterior condyle resection (3mm more resection in 75% of knees), tibial component rotation, femoral component rotation, femoral component flexion, distal femur resection, and tibial component varus/valgus. All knees required changes in at least 1 component position. 9 knees (16%) which had significantly worse initial average varus deformity of 11.2° required soft tissue releases in addition to component position changes including medial reduction osteotomy, posterior medial corner, or semimembranosus release. The maximum width of osteophytes in the coronal plane did not correlate significantly with coronal deformity. Final gaps with trials in place were well balanced within 1mm medially and laterally in flexion and extension.
Conclusion
Despite pre-operative planning based on CT scans, all patients in a group of standard varus pattern knee OA required intra-operative adjustments to component positioning to achieve balance while avoiding additional soft tissue releases. Even while restricting coronal alignment changes to 2° or less, 84% of varus knees were able to be balanced with component positioning alone. The most common changes were additional posterior condyle resection, external rotation of the femoral component and tibial component, tibial component varus, and decreasing distal femur resection.
#7561
The Effects of Femoral Stem Misalignment and How Next Generation Implant Systems Can Help Improve Postoperative Outcomes
*Michael LaCour - University of Tennessee - Knoxville, USA
Andrew Jacobs - DePuy Synthes - Warsaw, USA
Thang Nguyen - University of Tennessee - Knoxville, USA
Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: mlacour@utk.edu
Introduction
Total hip arthroplasty (THA) is a very successful procedure, but many patients still remain unsatisfied with their implant, often related to function and appearance. One such complication, less visible in clinical settings but easily confirmed online, is changes in foot angle after surgery. Commonly referenced as “pigeon-toe” and “duck-toe” throughout online public communities, one user posted online that “I had both hips replaced. Now when I walk, I noticed that my legs get achy and sore, and today I noticed that my toes are pointing in (pigeon-toe) and they never did that before.” Similar concerns are common and easy to locate. Thus, it becomes essential to continue to strive for both precision and accuracy, and the goal of this study is to utilize a validated theoretical hip model to predict causes and effects of toe angle changes and to demonstrate how next-generation THA systems can help alleviate patient concerns.
Methods
A previously published three-dimensional hip model was developed to assess component fit and outcome mechanics based on subject-specific anatomy. The preoperative planning tool searches a database and chooses components for patients that result in optimal positioning while minimizing bone loss. This study evaluates 62 statistical shape model bones and evaluates 3 stems-of-interest: a newly-designed stem (NDS) and two currently marketed hip systems (HS1 and HS2). From here, differences between the implanted head center and the preoperative femoral head center were compared as well as effects of version angle changes.
Results
Using the algorithm’s chosen position, the NDS was able to position the implanted femoral head an average of 1.2 mm ± 0.6 mm away from the preoperative head center, with 29/62 (47%) of the subjects achieving less than 1.0 mm difference. HS1 was able to position the implanted head within 1.6 mm ± 0.7 mm, with 9/62 (15%) achieving less than 1.0 mm difference, and HS2 was able to position the implanted head within 2.2 mm ± 0.8 mm, with only 1/62 (2%) subject achieving less than 1.0 mm difference. All three of these averages were statistically different between cohorts (p < 0.002). A sample datapoint can be seen in Figure 1.
Interestingly, misalignment occurrences in stem version angle produced changes in postoperative foot angle as well as instances of edge-loading. Specifically, 10° of excess anteversion of the stem yielded 10° of “pigeon-toeing” (Figure 2a) and 10° of excess retroversion yielded 10° of “duck-toeing” (Figure 2b). Excess anteversion scenarios also produced edge-loading conditions on the anterior aspect of the liner, where the predicted contact area decreased from approximately 400mm2 to 250 mm2 at toe off (Figure 3).
Conclusion
The results presented here directly corresponds to the concerns discovered online. Malalignment of the components can lead to undesirable postoperative mechanics, including changes in foot angle and edge-loading, which can further lead to patient dissatisfaction, premature component wear, and increased opportunity for dislocation. Fortunately, as new hip systems are released and orthopaedic technology continues to improve, accurate component alignment becomes continually more achievable and postoperative outcomes will continue to improve.
Figures
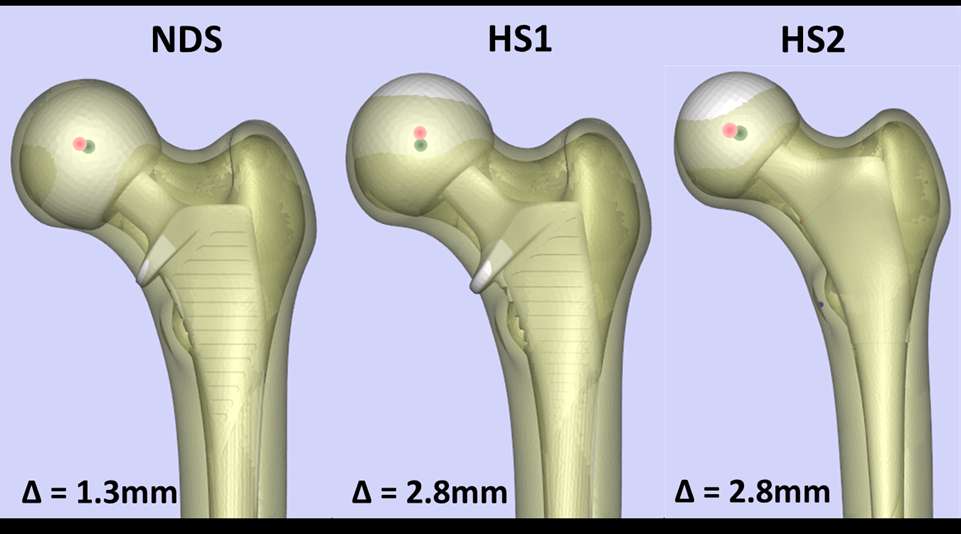
Figure 1
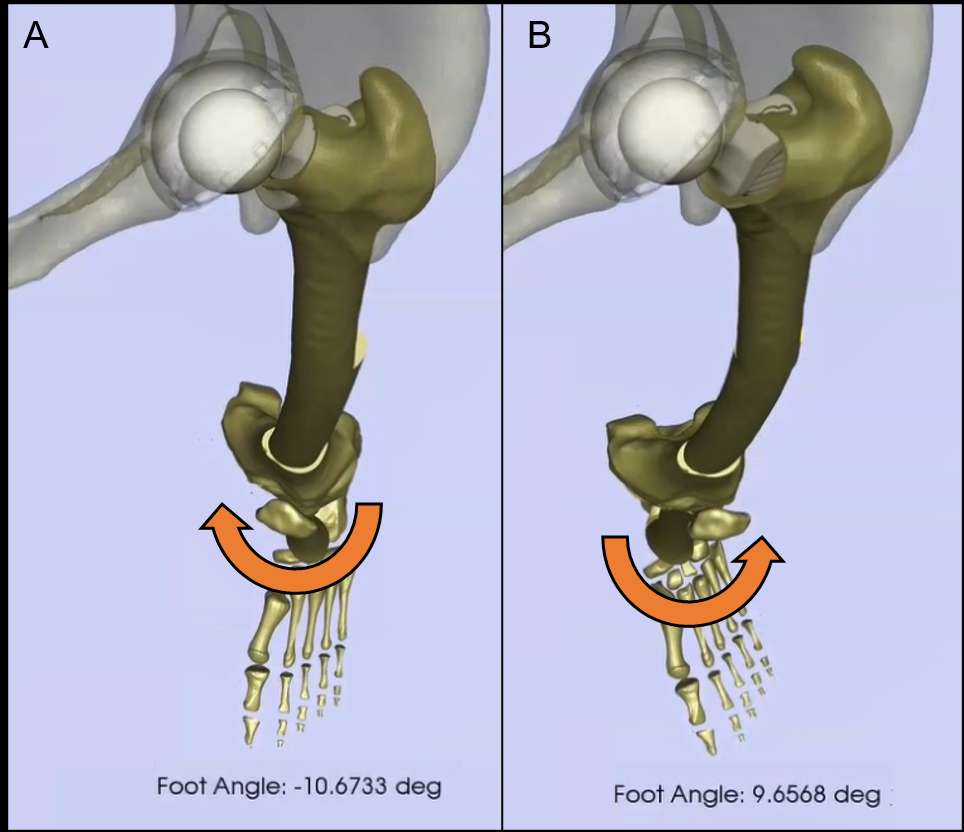
Figure 2
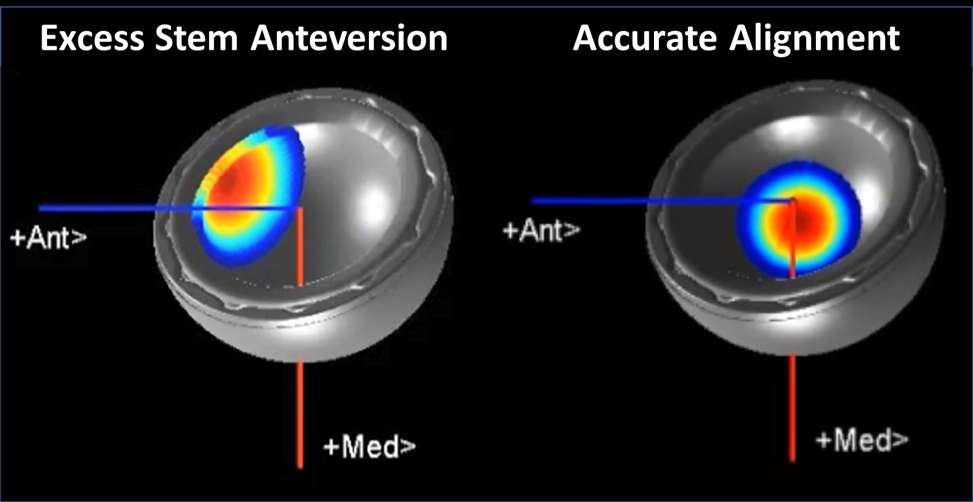
Figure 3#7347
Antibacterial Infection and Immune-Evasive Coating for Orthopedic Implants
*Woo-Young Jang - Korea University - Seoul, South Korea
Seung-Beom Han - Korea University Medical center - Seoul, South Korea
Jun-gu Park - Korea university - SEOUL, Select Country
JI HYE Choi - Korea University Anam Hospital - Seoul, South Korea
Gi Won Choi - Korea University Ansan Hospital - Ansan, South Korea
Taeyeong Kim - Anam hospital,Korea university - Seoul, Korea (Republic of)
Joonsuk Lee - Korea University Anam Hospital - Seoul, Korea (Republic of)
SungJin Ahn - Korea University - Seoul, Korea (Republic of)
*Email: opmanse@gmail.com
Bacterial infection and infection-induced immune response have been a life-threatening risk for patients having orthopedic implant surgeries. Conventional biomaterials are vulnerable to biocontamination, which causes bacterial invasion in wounded areas, leading to postoperative infection. Therefore, development of anti-infection and immune-evasive coating for orthopedic implants is urgently needed. Here, we developed an advanced surface modification technique for orthopedic implants termed lubricated orthopedic implant surface (LOIS), which was inspired by slippery surface of Nepenthes pitcher plant. LOIS presents a long-lasting, extreme liquid repellency against diverse liquids and biosubstances including cells, proteins, calcium, and bacteria. In addition, we confirmed mechanical durability against scratches and fixation force by simulating inevitable damages during surgical procedure ex vivo. The antibiofouling and anti-infection capability of LOIS were thoroughly investigated using an osteomyelitis femoral fracture model of rabbits. We envision that the LOIS with antibiofouling properties and mechanical durability is a step forward in infection-free orthopedic surgeries.
Figures
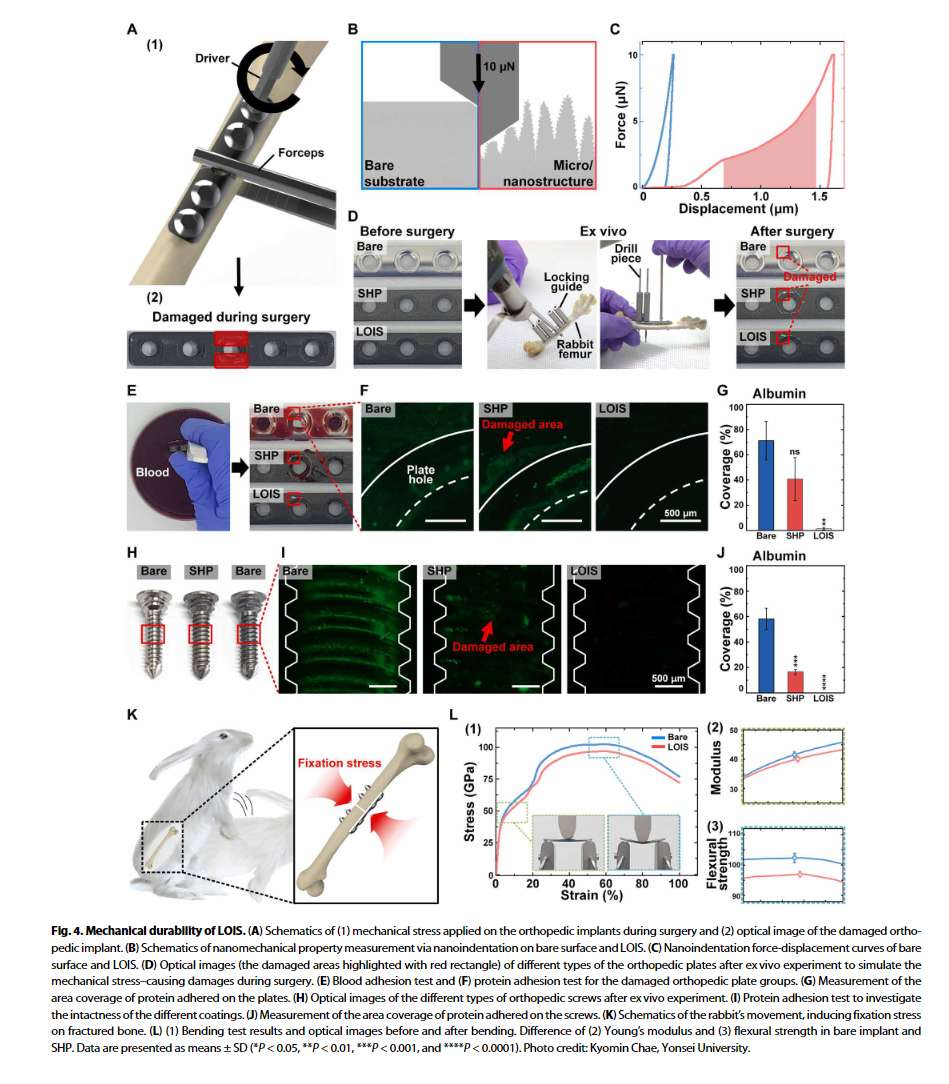
Figure 1
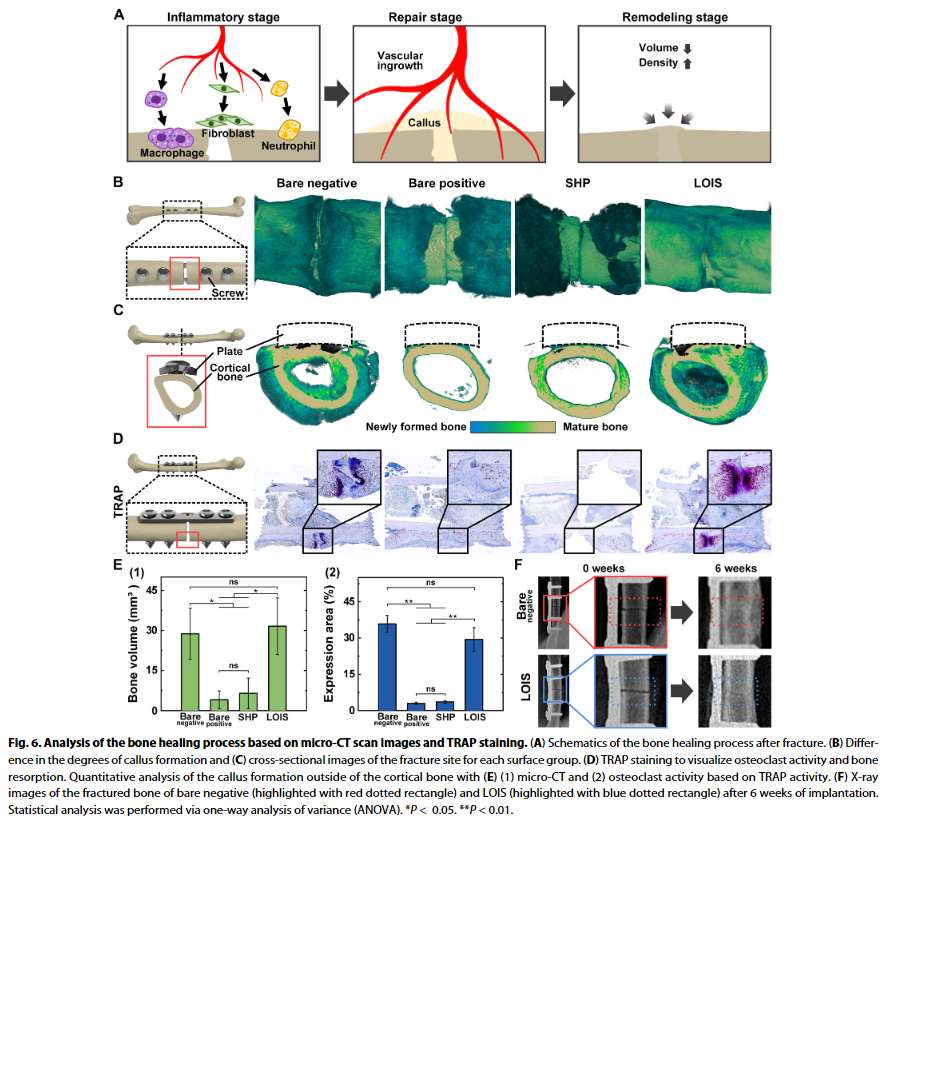
Figure 2#7349
Monitoring Wound Healing With Topically Applied Optical NanoFlare mRNA Nanosensors
*Woo-Young Jang - Korea University - Seoul, South Korea
Seung-Beom Han - Korea University Medical center - Seoul, South Korea
Gi Won Choi - Korea University Ansan Hospital - Ansan, South Korea
Jun-gu Park - Korea university - SEOUL, Select Country
Taeyeong Kim - Anam hospital,Korea university - Seoul, Korea (Republic of)
Joonsuk Lee - Korea University Anam Hospital - Seoul, Korea (Republic of)
SungJin Ahn - Korea University - Seoul, Korea (Republic of)
*Email: opmanse@gmail.com
An effective wound management strategy needs accurate assessment of wound status throughout the whole healing process. This can be achieved by examining molecular biomarkers including proteins, DNAs and RNAs. However, existing methods for quantifying these biomarkers such as immunohistochemistry and quantitative polymerase chain reaction are usually laborious, resource-intensive, and disruptive. This article reports the development and utilization of mRNA nanosensors (i.e. NanoFlare) that are topically applied on cutaneous wounds to reveal the healing status through targeted and semi-quantitative examination of the mRNA biomarkers in skin cells. In 2D and 3D in vitro models, the efficacy and efficiency of these nanosensors are demonstrated in revealing the dynamic changes of mRNA biomarkers for different stages of wound development. In mouse models, this platform permits the tracking and identification of wound healing stages and normal and diabetic wound healing process by wound healing index in real time.
Keywords: mRNA nanosensor; spherical nucleic acids; NanoFlare; wound healing; diabetic wound
Figures
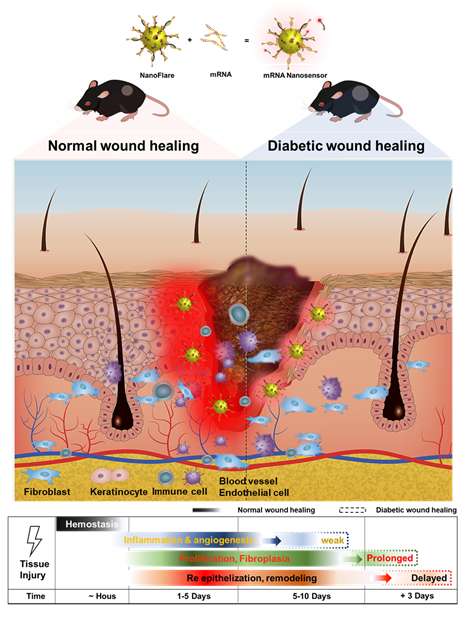
Figure 1#7478
The HINTEGRA Total Ankle Arthroplasty
Won-young Jang - Chonnam national university hospital - Gwangju, South Korea
*Keun-Bae Lee
Gun-Woo Kim - Chonnam national university hwasun hospital - Hwasun, South Korea
Hong-Yeol Yang - Chonnam national univertisy bitgoeul hospital - Gwangju, South Korea
*Email: kbleeos@chonnam.ac.kr
Introduction
The purpose of this study was to determine the functional outcome and implant survivorship of mobile-bearing total ankle arthroplasty (TAA) performed by a single surgeon.
Patients and Methods
We reviewed 205 consecutive patients (210 ankles) who had undergone mobile-bearing TAA (205 patients) for osteoarthritis of the ankle between January 2005 and December 2015. Their mean follow-up was 6.4 years (2.0 to 13.4). Functional outcome was assessed using the Ankle Osteoarthritis Scale, American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score, 36-Item Short-Form Health Survey (SF-36) score, visual analogue scale, and range of movement. Implant survivorship and complications were also evaluated.
Results
There were significant improvements in all functional outcome categories between the preoperative and final follow-up assessments (p < 0.001). Patients showed marked improvement in clinical outcomes in terms of pain, function, and quality of life. The overall implant survivorship was 91.7% at a mean follow-up of 6.4 years. In all, 33 major complications were identified with a 15.7% rate, resulting in 12 prosthesis failures (5.7%). Periprosthetic osteolysis (19 cases; 9.0%) was the most frequent complication.
Conclusion
Mobile-bearing TAA resulted in improved functional outcomes, a low major complication rate, and excellent implant survivorship at a mean follow-up of 6.4 years.
#7484
Comparison of Intermediate to Long-Term Outcomes of Total Ankle Arthroplasty in Ankles With Preoperative Varus, Valgus, and Neutral Alignment
Won-young Jang - Chonnam national university hospital - Gwangju, South Korea
Gun-Woo Kim - Chonnam national university hwasun hospital - Hwasun, South Korea
*Keun-Bae Lee
*Email: kbleeos@chonnam.ac.kr
Background
Preoperative ankle coronal malalignment has been considered as a risk factor for poor outcomes and failure after total ankle arthroplasty. The present study evaluated whether intermediate to long-term outcomes of total ankle arthroplasty in ankles with preoperative varus and valgus malalignment (5° to 20°) are comparable with those with neutral alignment (<5°).
Methods
We enrolled 144 consecutive ankles that underwent primary total ankle arthroplasty (140 patients) using a mobile bearing HINTEGRA prosthesis with a minimum follow-up of 4 years; the mean overall follow-up duration was 89 months (51 to 145months). We divided all patients into 3 groups according to the preoperative coronal plane tibiotalar angle: the varus group (59 ankles, 5° to 20° of varus), the valgus group (34 ankles, 5° to 20° of valgus), and the neutral group (51 ankles, <5°). Patients in each group showed similar characteristics in mean age, sex, body mass index, and follow-up period.
Results
The mean Ankle Osteoarthritis Scale pain and disability score, American Orthopaedic Foot & Ankle Society ankle-hindfoot score, Short Form-36 Physical Component Summary score, visual analog scale pain score, and ankle range of motion did not differ meaningfully among the 3 groups at the final follow-up. The final tibiotalar angle showed that the degree of coronal alignment of the varus group was significantly less corrected compared with the neutral group (p = 0.010). The varus group had significantly more concomitant procedures (42 procedures [71.2%]) compared with the neutral group (p = 0.003). The prevalence of major complications did not differ among the 3 groups (p = 0.124). The overall probability of implant survivorship was 91.1% (97.7% in the varus group, 81.1% in the valgus group, and 90.9% in the neutral group) at a mean follow-up of 7.3 years.
Conclusions
In the intermediate to long-term follow-up, mobile-bearing total ankle arthroplasty showed similarly good outcomes in patients with varus and valgus malalignment up to 20° compared with the neutral alignment group when neutrally aligned ankles were achieved postoperatively.
#7536
Development of Patient-Specific Metaphyseal Stabilized Augment and Design Automation System
YoungWoong Jang - Corentec Co Ltd - Seoul, South Korea
Junkyu Park - Corentec Co. Ltd. - Seoul, South Korea
Jong-Min Kim - University of Ulsan College of Medicine Asan Medical Center - Seoul, Korea (South)
Yong In - Seoul St. Mary's Hospital, The Catholic University of Korea - Seoul, South Korea
Jae Ang Sim - Gil Hospital, Gachon University - Incheon, South Korea
SeongJin Kim - Corentec Co. Ltd. - Seoul, South Korea
AhReum Han - Corentec Co. Ltd. - Seoul, South Korea
*JungSung Kim - Corentec Co., Ltd - Seoul, South Korea
*Email: jskim@corentec.com
Introduction
Revision TKA was reported to have a lower survival rate compared to Primary TKA. Its main cause is the instability and aseptic loosening in interface bone and TKA. The block, cone augments and sleeves are developed for stability to replace more various bone defect areas. However, most of these augments are applied with the anthropometry data of Caucasian. Therefore, the use of the products is limited for Asians with small overall size of the bone. In addition, it is difficult to use for patients who need to use an offset device due to lack of space in the metaphysis with augment block near the articular surface.
In this study, a metaphyseal stabilized augment (MSA) that can be used with an offset device was developed to improve the problems. And based on the patient's individual medical image, we developed an API-based automation design system that can be provided to all rTKA patients with Asians.
Materials and Method
A general augment block can be used in Type1-2A in The AORI classification. We developed MSA to be used with augment blocks. The combination was designed to be usable even in Type2B. The knee joint was divided into three-fixation zones. The TKA implant and stem extension are inserted to improve the stability of the knee joint in zone 1 and zone 3, respectively. The developed MSA was inserted in zone 2 for strengthen around the offset device and stem extension. Finally, a porous structure was applied on the outside surface in contact with the bone. The porous structure can increase the bone contact surface to increase the bone regeneration. Also it was produced a geometric shape similar to cancellous bone structure of the human body. MSA was designed using Solidworks (Dassault Systèmes, USA) which provides API (application programming interface). It enables iterative model design according to design parameters input from the external environment.
Results
MSA consists of two type products that can be used for the femur and tibia, respectively (Figure 1.). The shape of the central hole can be adjusted depending on whether an offset device is used. The product was printed using Ti in biocompatible materials. Most of the body was designed to be porous structure for bone regeneration and lightweight.
The design automation system was developed to enable automation design using medical image data and parameter set in the pre-operative plan in a GUI environment (Figure 2.). In addition, it applies an algorithm that can limit the design of shapes that cannot be manufactured or are not guaranteed for product safety. Finally, we were able to get MSA's 3D modeling and surgical tool drawings through of the program.
Conclusion
In this study, we completed the development of an MSA implants that can be applied to all patients in need of rTKA and a program for its patient-specific rapid production. Currently, we are in the process of obtaining domestic approval for MSA, and we will update the clinical results of the product.
Figures
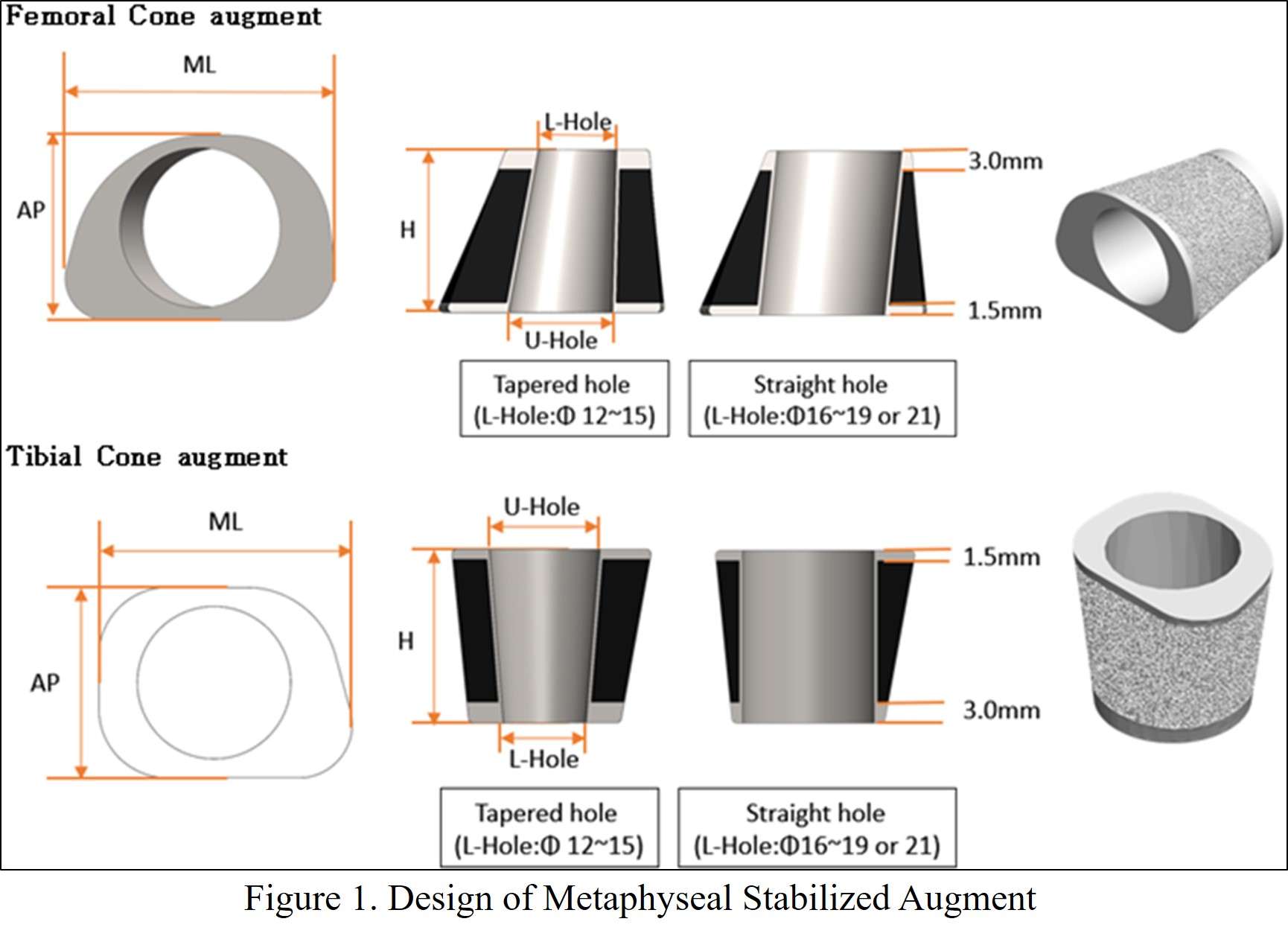
Figure 1
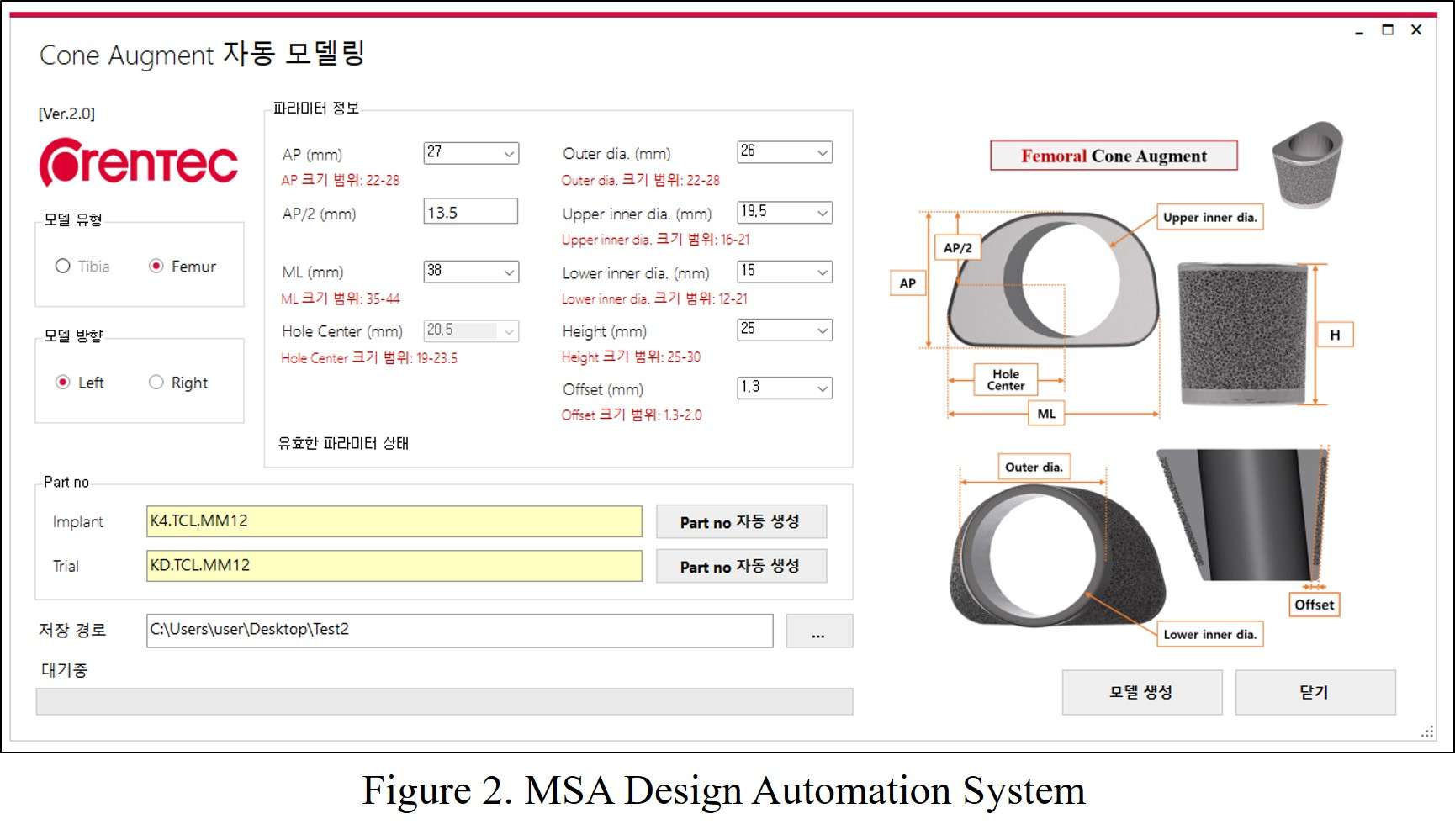
Figure 2#7641
The Effect of Periprosthetic Bone Loss on the Failure Risk of Tibial Total Knee Arthroplasty
*Navid Soltanihafshejani - Radboud University Medical Center - Nijmegen, Netherlands
Thom Bitter - Raboud University Nijmegen Medical Centre - Nijmegen, Netherlands
Nico Verdonschot - Twente - Nijmegen, Netherlands
Dennis Janssen - Radboud University Nijmegen Medical Centre - Nijmegen, Netherlands
*Email: navid.soltanihafshejani@radboudumc.nl
Introduction: Subsidence of the tibial implant after TKA is influenced by periprosthetic bone loss. Bone adapts to the changes in the load distribution in the tibia following TKA, which leads to bone remodeling which affects the bone strength. While the TKA reconstruction is able to withstand the loads occurring during activities of daily living, excessive physiological loads as occurring during events such as stumbling may cause permanent damage to the tibial bone, and may even lead to collapse of the proximal tibia and gross failure of the tibial reconstruction. Considering the bone damage, it is crucial to capture the plastic behavior in a proper material model in finite element analysis (FEA). The objective of the current study was therefore to investigate the effect of periprosthetic bone loss on tibial TKA failure in FEA simulations incorporating a crushable foam bone material model.
Methods: Subject-specific models of two proximal tibiae (male of 65 yrs, 85 kg, and a female of 90 yrs, 65 kg) were constructed based on QCT images as a representation of good and poor primary bone quality . The models were implanted with a simplified CAD model based on an optical scan of a cemented Triathlon tibial component (Stryker Orthopaedics) [Fig 1-a]. Clinically reported bone loss occurring over a 7-year follow-up period [1] were used to simulate post-operative bone loss in both FEA models. The models were loaded with a gait load for 150 cycles [2], followed by a stumbling load. As a measure of tibial collapse, the angular deviation of the tibial tray was calculated, and a threshold of 10° was considered as gross failure due to tibial collapse [Fig 1-b].
Results: At baseline bone densities (directly post-operatively), no significant permanent deformation was observed for level walking, neither in strong or the weak tibia. Applying the stumble load led to some permanent bone damage in the weaker bone. Incorporating the bone loss occurring 7 years after surgery led to a significant increase in bone damage, particularly in the poor quality tibia. While the angular deviation in the weak bone was 3.7° directly post-operatively, it increased to 16.5° after 7 years. For the strong bone the angular deviation remained smaller than 1° [Fig 2].
Conclusion: This study shows the feasibility of simulating the long-term collapse of the tibial reconstruction in TKA. As expected, gait loading did not lead to noticeable bone damage for both tibiae, but a stumbling load triggered the failure process of the reconstruction. Bone resorption significantly increased the risk of failure after TKA, particularly in case of a poor initial bone quality.
Keywords: Total Knee Arthroplasty, Bone resorption, Bone Mineral Density, Finite Element Analysis, Medial Tibial Collapse
Figures
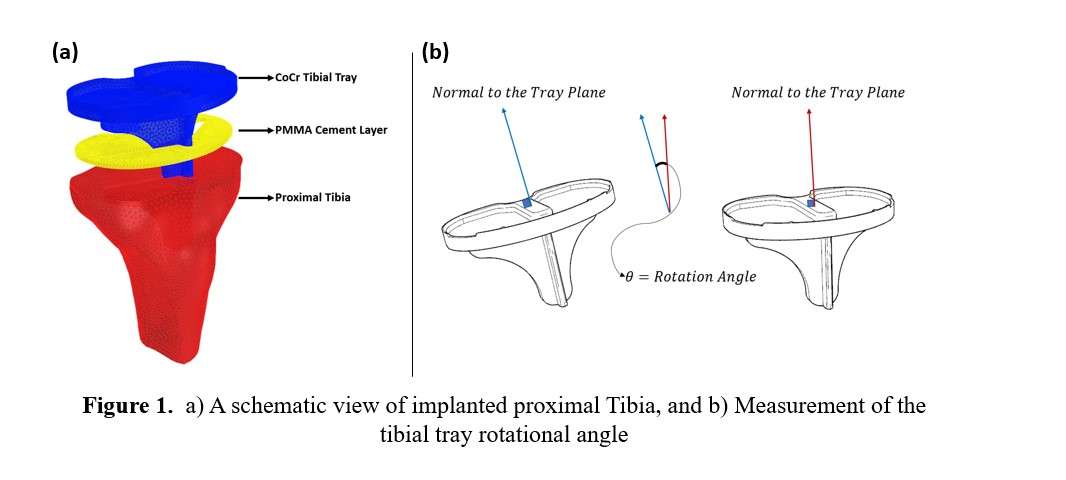
Figure 1
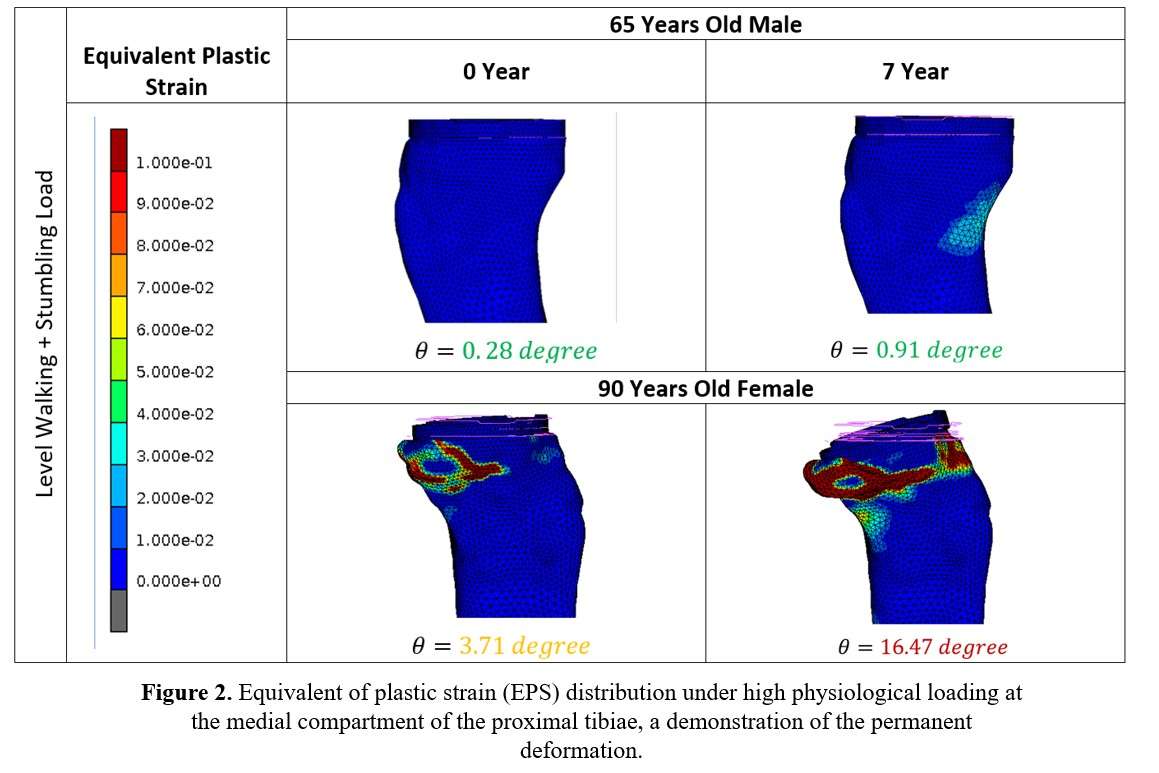
Figure 2#7642
The Influence of Plasticity Models on the Micromotion Predictions in Total Knee Arthroplasty
*Navid Soltanihafshejani - Radboud University Medical Center - Nijmegen, Netherlands
Thom Bitter - Raboud University Nijmegen Medical Centre - Nijmegen, Netherlands
Dennis Janssen - Radboud University Nijmegen Medical Centre - Nijmegen, Netherlands
Nico Verdonschot - Twente - Nijmegen, Netherlands
*Email: navid.soltanihafshejani@radboudumc.nl
Introduction: The primary fixation of cementless total knee arthroplasty (TKA) implants depends on the press-fit conditions between the implant and the bone. The press-fit fixation is a result of the interference fit that is achieved during surgery, when the implants are impacted onto the bone. During impaction the bone is deformed permanently, leading to plastic deformations which affect the primary fixation. To capture this non-linear bone behavior in finite element analysis (FEA) adequate material models are required. In the current study we incorporated a crushable foam model (CFM) for femoral bone in an FEA model of a femoral TKA reconstruction to investigate its effect on the prediction of implant-bone interface micromotions. The same model was also analyzed using a softening Von Mises (sVM) model which served as a comparator.
Methods: The CFM models was previously developed based on experiments with 64 femoral bone samples. At the first phase, to demonstrate the effect of cyclic loading on permanent deformation and hysteresis, three cylindrical samples (70 yrs. male donor) were subjected to cyclic displacement-controlled loading [Fig 1-a]. Subsequently, QCT-based specimen-specific FEA models were generated and loaded according to the experimental loading configuration using the two different material models (CFM and sVM).
In the second phase, the two material models were applied to FEA models of three femoral TKA reconstructions (male 57, 73 and 90 yrs.). The models were cyclically loaded with a gait load for 100 cycles. Micromotions were computed at 7 ROIs [Fig 1-b], and the average micromotions values were reported at each cycle.
Results: The force-displacement results of the experimentsdemonstrated a series of hysteresis loops, with a dissipation energy that gradually decreased with each loading cycle [Fig 2-left]. The simulations with the CFM representing the bone behavior displayed a similar trend of decreasing dissipation energy [Fig 2-middle], while in the models with the sVM all energy was dissipated after the first loading cycle [Fig 2-right].
The simulations of the femoral reconstruction models also indicated a time-dependent effect of the CFM models, with average micromotions that deviate over time [Fig 3]. The absolute values differed between the three models, with the largest micromotions seen in the model of the 90-year old male. The simulations incorporating the sVM for the femoral bone led to micromotion predictions that were almost two times lower than the CFM models. No gradual increase in micromotions was seen in the 73 and 90-year old models.
Conclusion: Replicating the non-linear mechanical processes occurring with press-fit fixation of cementless TKA components is challenging. However, previous studies have shown that using linear elastic bone properties may lead to an excessive bone strains (beyond the yield threshold) and an underestimation of micromotions when compared to experimental findings. Our results demonstrate the effect of the material model that is chosen to represent the periprosthetic bone, and illustrate the significance for simulations of primary fixation and interface micromotions. Further comparison against experimental results is required to demonstrate the validity of the CFM material model.
Keywords: TKA, Primary Stability, Micromotion, FEA, Bone Material Model.
Figures
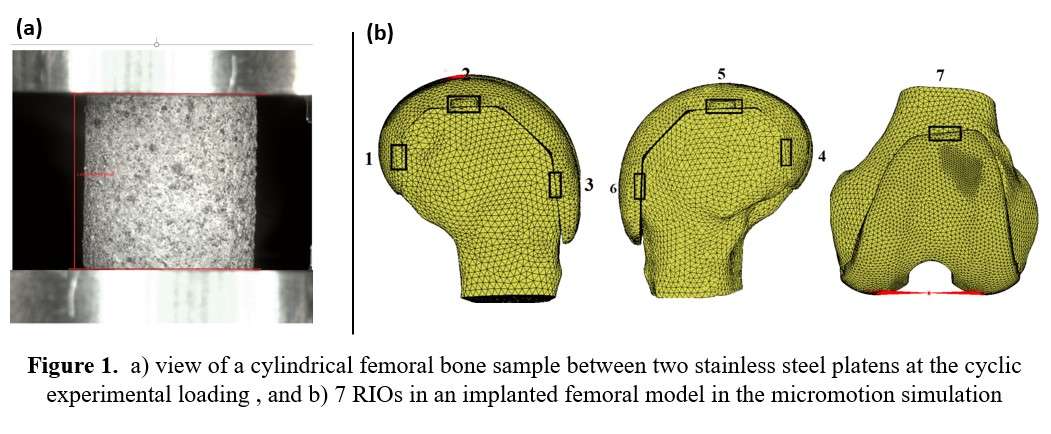
Figure 1
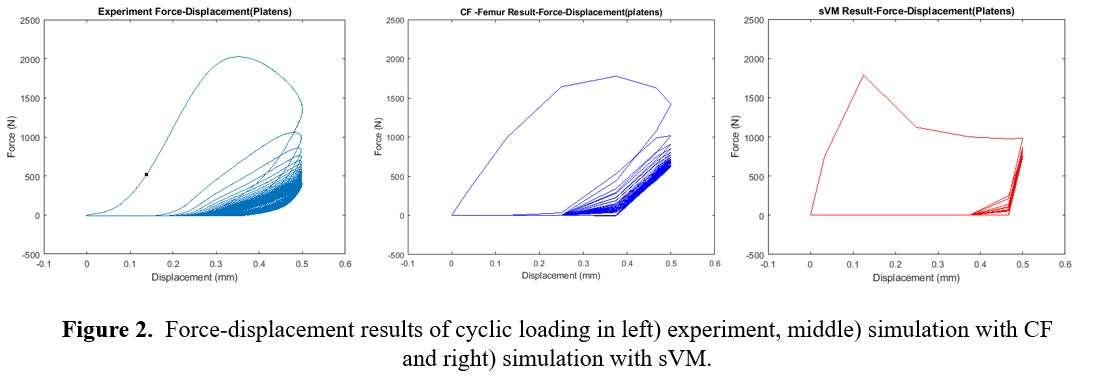
Figure 2
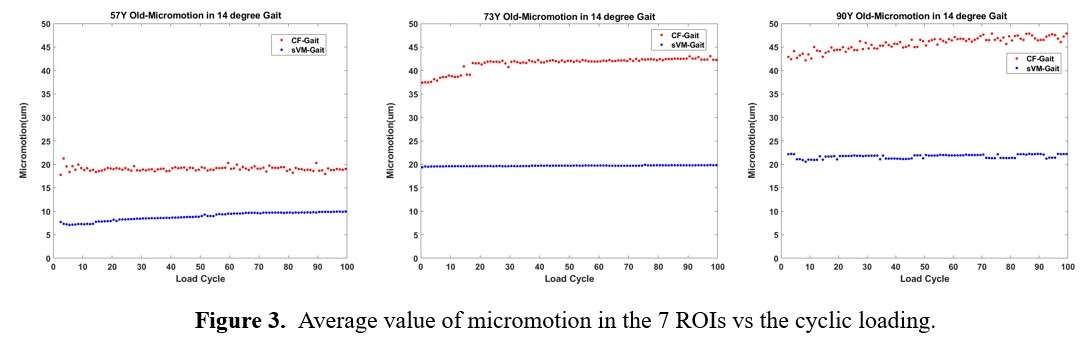
Figure 3#7491
Invited Talk: Influence of Positioning on the Biomechanics of Metal-on-Polyethylene Hip Replacements
*Louise M. Jennings - University of Leeds - Leeds, United Kingdom
Raelene Cowie - University of Leeds - Leeds, United Kingdom
Susan Partridge - University of Leeds - Leeds, United Kingdom
John Fisher - University of Leeds - Leeds, United Kingdom
Mazen Al-Hajjar - University of Leeds - Leeds, United Kingdom
*Email: l.m.jennings@leeds.ac.uk
Introduction
Surgical positioning influences the biomechanics and wear of metal-on-polyethylene hip implants. Introducing a medial-lateral translational offset (mismatch) with high cup inclination angle has been shown to result in edge loading and accelerate in vitro wear.1 The aim of this study was to further investigate the influence of translational and rotational positioning by expanding the envelope of conditions. The influence of two translational offsets (medial-lateral (ML) and anterior-posterior (AP)) coupled with two rotational offsets (inclination angle and version angle) on the biomechanics of the hip were investigated through a series of short-term studies.
Methods
Three 36mm diameter metal-on-polyethylene implants (Pinnacle®, Marathon®, DePuy Synthes Joint Reconstruction, UK) were studied in a ProSim electromechanical hip simulator, EM16 (Simulation Solutions, UK). Studies were carried out in 25% bovine serum with input kinematics taken from ISO 14242-1 with a 70N swing phase load as per ISO 14242-4.2,3 All offsets were applied to the cup (Figure 1). The rotational offsets investigated were inclination angle (35 and 55° simulator angle equivalent to 45 and 65° in vivo) and version angle (0, 10, 20, 40 and 60°); translational offsets were introduced in the medial-lateral and anterior-posterior directions (0, 2 and 4mm). Springs (100 N/mm) were positioned horizontally in the medial-lateral and anterior-posterior directions to hold the cup at the specified translational offset. Under high vertical load, the springs were compressed, and the components became concentric; as the load was released, the cup translated. Each condition was run for 150 cycles, the resulting medial-lateral and anterior-posterior dynamic separation were measured. The mean of the maximum medial-lateral and anterior-posterior dynamic separations were measured and the total dynamic separation = √ (AP2 +ML2) was calculated.
Results
A summary of the maximum displacement of the cup from its concentric position for all the conditions investigated is shown in Figure 2. Higher cup inclination angle coupled with either an anterior-posterior or medial-lateral offset led to higher separation. Introducing medial-lateral offsets had a greater influence on separation than introducing the same magnitude anterior-posterior offset. With increasing version angle, a larger magnitude of separation was measured.
Conclusion
Introducing rotational and translational offsets to the cup influenced the magnitude of dynamic separation with a trend of increasing separation with larger offsets for all the parameters investigated. Increasing separation is likely to reduce joint stability and increase edge loading, the findings from this study will inform future investigations to understand how the different rotational and translational offsets influence implant wear.
- Ali, M., et al.(2017). Wear and deformation of metal-on-polyethylene hip replacements under edge loading conditions due to variations in surgical positioning. Orthopaedic Proceedings (Vol.99, No. SUPP_3, pp.12-12).
- ISO 14242-1:2014/Amd:2018
- ISO 14242-4:2018
Figures
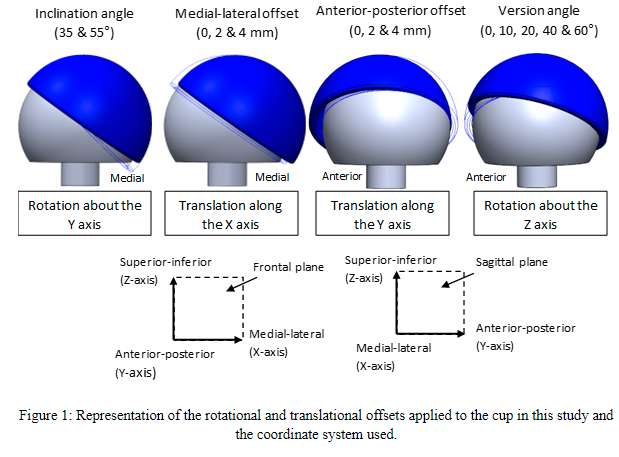
Figure 1
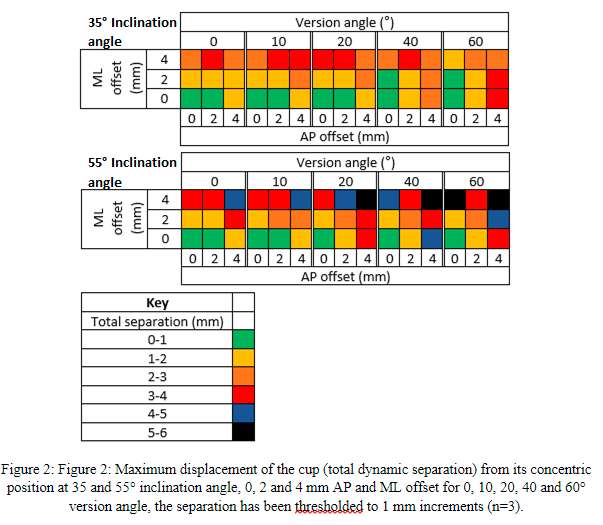
Figure 2#7558
Development of a Computational Model to Predict Kinematics, Contact Mechanics and Wear of a Total Knee Replacement
*Bethany Lowe - University of Leeds - Leeds, GB
Abdellatif Abdelgaied - University of Leeds - Leeds, United Kingdom
Louise M. Jennings - University of Leeds - Leeds, United Kingdom
David Wolfson - DePuy International Ltd - Leeds, United Kingdom
*Email: brlowe1@outlook.com
Introduction
Pre-clinical evaluation methods of total knee replacements have traditionally involved experimental simulation to determine the biomechanical and tribological performance of the bearing. However, these methods are both resource and time intensive and not practical for investigating a wide range of variables. Relatively recent developments in computational modelling provides an opportunity to utilise finite element models as a fast and low-cost tool to aid in pre-clinical assessment. The aim of this study was to use a combined experimental and computational approach to develop a finite element model of a fixed bearing cruciate retaining total knee replacement to predict walking kinematics, contact mechanics and wear outputs.
Methods
A 3-million cycle standard walking gait study using force control inputs (ISO 14243-1:2009) was completed on a knee simulator using cobalt chrome ATTUNETM femoral components and ultra-high-molecular-weight polyethylene AOXTM tibial total knee replacement bearings (n=6). The experimental outputs included tibial anterior-posterior displacement and internal-external rotation calculated as a 100-cycle average and an average volumetric wear rate at intervals of 1 million cycles with 95% confidence intervals. A finite element model controlled using loads and spring constraints was developed to simulate the experimental methods. An experimental study to investigate contact pressures from 0%-100% gait cycle at 10% intervals was completed using Tekscan sensors, the methods were also repeated in the computational model at all 11 gait cycle intervals. Output kinematic motions and contact pressure results from the computational simulation were used to calculate a wear prediction for the model using a previously developed wear framework [1]. R-squared values for the tibial component kinematic outputs were determined to quantify the correlation between an experimental 100-cycle average and the computational prediction.
Results
The R-squared value over the gait cycle for anterior-posterior translation was 0.76 (Fig. 1) and for internal-external rotation was 0.83 (Fig. 2). The model contact pressure predictions at the 11 points along the gait cycle were in good agreement with the experimentally measured average contact pressure values (n=5) using the Tekscan (Fig. 3). During high-loaded periods of the gait cycle the predicted values fell within the 95% confidence interval of the experimentally measured values, during the swing phase (low-load) the model predicted more anterior values than the experimental outputs, possibly due to internal friction of the simulator. The experimental average volumetric wear rate of Attune AOX total knee replacement bearings after 3 million cycles was 2.7mm3/MC (± 1.08 mm3/MC CI) in agreement with historical wear data (3.6 mm3/MC) [2]. The computational wear prediction (3.0mm3/MC) was within the experimental wear confidence interval.
Conclusion
A newly developed finite element model of an Attune AOX total knee replacement predicted kinematics, contact mechanics and wear values in good agreement with experimentally determined values under the same conditions. This provides confidence in the computational models ability to predict pre-clinical wear and, with additional experimental studies, can be adapted to simulate other total knee replacement variables of interest.
References:
[1] Abdelgaied et al.2018. J. Mech. Behav. Biomed. Mater., 78(2018):282-291
[2] Dressler et al. 2012. Trans. Ortho Res. Soc. Poster 959.
Figures
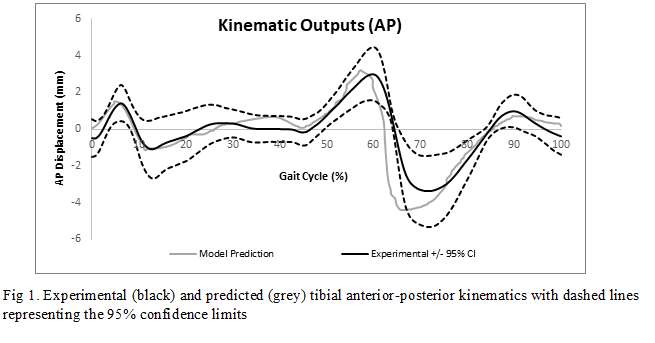
Figure 1
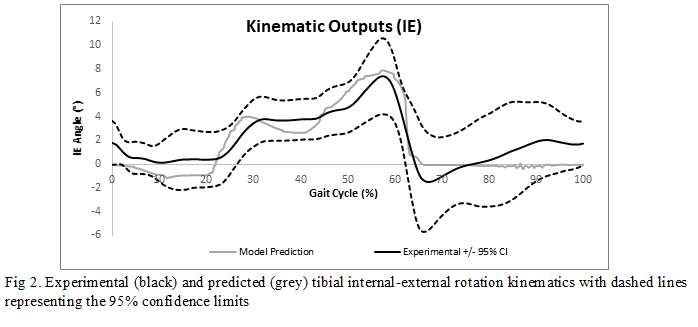
Figure 2
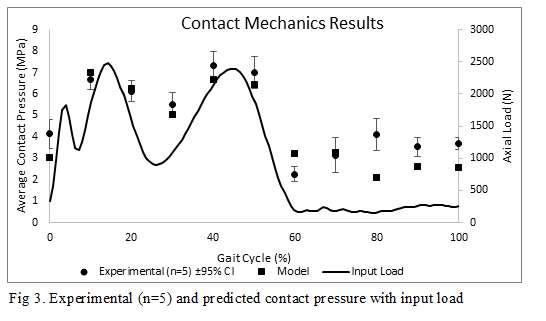
Figure 3#7317
Cement Loaded With High-Dose Gentamicin and Clindamycin Reduces the Risk of Subsequent Infection After One-Stage Hip or Knee Arthroplasty Exchange for Peri-Prosthetic Infection: A Preliminary Study
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
Introduction
The aim of the study was to quantify the prophylactic and therapeutic effect of a combination of high-dose gentamicin with clindamycin (GCC) for one-stage hip and knee revision arthroplasty (RA) for chronic periprosthetic joint infection. We hypothesized that the raw surgical site infection (SSI) rate after implant fixation with GCC cement is lower than when cement loaded with standard-dose gentamicin (GC) is used during one-stage hip and knee revision arthroplasty for chronic periprosthetic joint infection.
Methods
All patients who were operated for hip or knee RA due to a chronic periprosthetic joint infection between February 2017 and January 2019 were eligible. The patients were divided into two consecutive cohorts based on the type of cement used: GC in the first cohort (control group), GCC in the second cohort (study group). All patients were followed for a minimum of 24 months. A SSI was defined as the presence of a fistula or a positive deep surgical site sample on microbiological analysis. The occurrence of a SSI was recorded, and the survival curve after the occurrence of a SSI was established. The bacteria found in the SSI was noted. The SSI were differentiated between recurrence or persistence of the initial infection (same germ found a second time) and a new infection (germ identified is different from initial one). The outcomes of the infection at 2 years were defined according to the four-tier classification proposed at the International Consensus Meeting on periprosthetic joint infections in August 2018.
Results
171 patients were included: 96 men (56%) and 75 women (44%) with a mean age of 69 ± 12 years and a mean BMI of 31.3 ± 8 kg/m². The hip was operated in 97 patients (57%) and the knee in 74 patients (43%). There were 86 patients in the study group (50%) and 85 patients in the control group (50%). There was no significant difference in the preoperative parameters between the two groups.
Thirty-three patients suffered a SSI (19%) in the overall cohort: 11 in the study group (13%) and 22 (26%) in the control group (p=0.03). Recurrence of the index infection was observed in 1 case in the study group (1%) and 4 cases in the control group (5%) (NS). A new infection was observed in 8 cases in the study group (9%) and 17 cases in the control group (20%) (p=0.05). Two SSIs in the study group and one in the control groups could not be classified (fistula with no germ found).
The SSIs were treated mainly by debridement, antibiotics and implant retention in both groups. The percentage of patients who were still alive, infection-free and had their implants in place at 2 years was significantly higher in the study group (98%) than in the control group (91%) (p=0.01). The results according to the four-tier classification proposed at the International Consensus Meeting on periprosthetic joint infections are reported in figure 1.
Conclusion
Routine use of this newer cement can be recommended for one-stage hip and knee revision arthroplasty for infection.
Figures
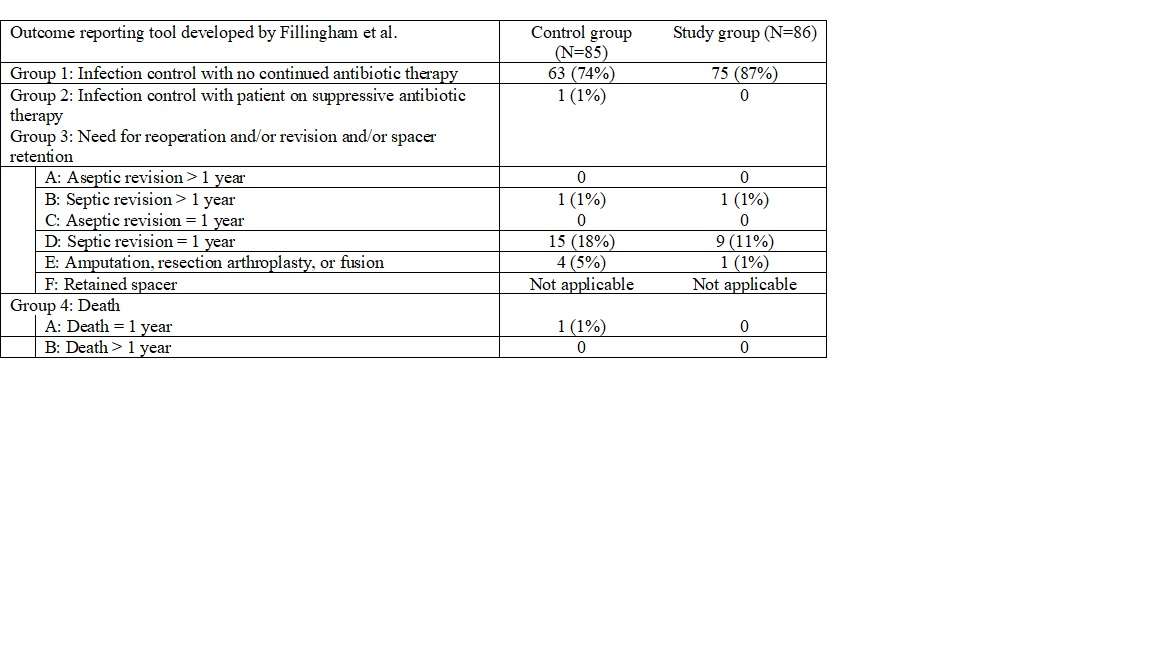
Figure 1#7320
Patient-Specific Prescription of Aspirin as Thromboprophylaxis After Total Hip or Total Knee Arthroplasty: Case-Control Study With Propensity Score Matching
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
Introduction
The aim of this study was to validate the most recent recommendations of the European Society of Anaesthesiology (ESA)by comparing the thromboembolic and haemorrhagic risk in a population of unselected patients undergoing unilateral total hip (THA) or knee (TKA) arthroplasty who followed a fast-track procedure (FTP), according to the thromboprophylactic medication given: either systematic low molecular weight heparin (LMWH - control group), or aspirin or LMWH depending on the patients’ risk factors (study group). The primary hypothesis was that the risk of postoperative TEE would be greater after the patient-specific administration of aspirin or LMWH than after systematic administration of LMWH.
Methods
All patients who underwent unilateral THA or TKA between January 2018 and December 2020, and who were operated on by the principal investigator, were eligible for inclusion in the study group. The control group was extracted from a historic series of 1949 patients who were operated on between October 2016 and October 2017. The patients were matched in the two groups by propensity score matching using logistic regression, including age, sex, body mass index (BMI), ASA classification, personal history of a TEE, previous use of anticoagulant medication and the intervention performed.
All patients followed a FTP. In the control group, patients received treatment with LMWH. In the study group, aspirin was administered if the patient was not morbidly obese and had no previous history of a serious TEE, or LMWH was administered for other patients according to the same protocol as the control group.
The primary evaluation criterion was the rate of TEEs in the 90 days after the intervention. The secondary criterion was the rate of haemorrhagic complications in the 90 days after the intervention.
Results
203 consecutive patients were included into the study group: 81 males (43%) and 122 females (57%), with a mean (SD) age of 68 ± 13 years and a mean (SD) BMI of 30.2 ± 5.8 kg/m². The matched control group, extracted from the historic series, consisted of 79 males (39%) and 124 females (61%), with a mean (SD) age of 67 ± 12 years and a mean (SD) BMI of 29.8 ± 5.7 kg/m². There were no significant differences in preoperative criteria between the control and study groups except for the prophylactic treatment administered.
Results are summarized in table 1. Two TEEs occurred in the control group (1%) and three in the study group (1%) (P=0.65): 2/51 patients treated with LMWH and 1/152 patients treated with aspirin (P=0.09). Five haemorrhagic complications occurred in the control group (2%) and four in the study group (2%): 2/51 patients treated with LMWH and 2/152 patients treated with aspirin (P=0.77).
Conclusion
The selective use of aspirin as thromboprophylaxis in patients considered at low risk of TEEs appears acceptable after unilateral THA or TKA following a FTP. The recommendations of the ESAcan therefore be considered valid.
Figures
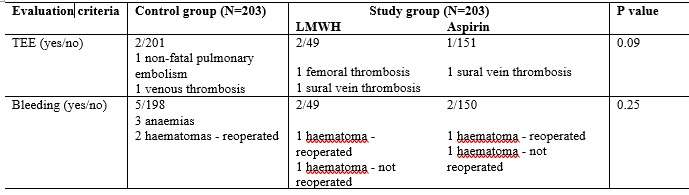
Figure 1#7321
Functional Knee Phenotypes of OA Patients Undergoing Total Knee Arthroplasty Are Significantly More Varus or Valgus Than in a Non-OA Control Group
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
Florent Baldairon - University Hospital Strasbourg - Strasbourg, France
Michael Hirschmann - Kantonsspital Baselland - Basel, Switzerland
*Email: Jean-yves.jenny@chru-strasbourg.fr
Introduction
The aim of this study was to analyze the coronal alignment of a population of patients undergoing TKA using a modern classification of the different phenotypes found in a population of non-OA patients. The hypothesis of this study was that the distribution of coronal alignment of the operated patients was significantly different from that of the reference non-OA patients.
Methods
All patients were operated on using an image-free navigation system allowing the anatomical parameters of the subject to be measured during the operation before implantation. Five hundred and twenty cases were randomly selected among the files with a complete anatomical analysis. The following data were specifically analyzed for this study: the femorotibial mechanical angle (FTMA), the native femoral angle (NFA) (defined as the femoral mechanical angle increased by 2° for varus deformities or decreased by 2° for valgus deformities to compensate for degenerative femoral cartilage wear, the native tibial angle (NTA) (calculated as the FTMA decreased by the NFA and increased by 2° for varus deformities or decreased by 3° for valgus deformities to account for normal medial or lateral laxity in extension).
Numerical data were transformed into categorical data according to Hirschmann's classification into 3° classes and compared with those published by Hirschmann et al. in a non-OA population, considered as a control group. The main criterion was the percentage of subjects with normal overall coronal alignment, defined by the association of a normal NFA and a normal NTA. The most frequent phenotypes in the study group were identified and compared to the most frequent phenotypes in the control group.
Results
The study group included 171 men (32.9%) and 349 women (67.1%). The gender distribution was significantly different from the control group (p<0.001). Normal overall coronal alignment was found in 66 patients in the study group (12.7%) and 76 patients in the control group (24.7%) (p<0.001). The distribution of the FTMA was significantly different, with fewer normal cases in the study group than in the control group. The distribution of the NTA was significantly different, with fewer normal cases in the study group than in the control group (p=0.001).
Thirty-eight different phenotypes were present in the study group out of a possible 81, compared to 18 in the control population (p=0.002). The most frequent phenotype was the association of neutral NFA and neutral NTA in both groups, but the percentage was smaller in the study group (15.0%) than in the control group (24.7%) (p<0.001).
Conclusion
This study, with a normal anatomy rate of 17% for the mechanical femorotibial angle, 37% for the MDNFA (or LPNFA) and 37% for the NTA in OA patients, suggests that the role of bony architectural abnormalities is predominant in the occurrence of knee OA, compared to cartilage factors. No particular morphotype favoring the occurrence of knee OA was detected. It is only the deviation of the phenotype with respect to the average that seems to favor the occurrence of knee OA by increasing the mechanical loading.
#7322
Same Complication Rate After Day-Case Procedure or Fast-Track Procedure After Total Hip and Knee Arthroplasty. a Prospective, Propensity Score-Matched Case-Control Study
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
Vincent Gisonni - University Hospital Strasbourg - Strasbourg, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
Introduction
The optimal course of postoperative rehabilitation after total hip (THA) or knee (TKA) arthroplasty is still debated.
The current surgeon’s resistance to use day-case procedures (DCPs) concerns the potential delay in the management of these complications and the potentially higher risk of complications related to the very short stay. The objective of this study was to compare the respective risks of complications, readmission and reintervention after the DCP or fast-track procedure (FTP)
Methods
All patients operated on by two experienced joint reconstruction surgeons for unilateral primary THA or TKA between July 2016 and December 2019 were eligible. 265 cases were included.
The anesthetic, operative and post-operative procedures were standardized. The selection of FTP or DCP was done according to surgeon’s and patient’s choice. All patients were contacted after 3 months. Complications, readmissions and reinterventions were recorded.
The primary endpoint was the occurrence of a complication within 90 days after the arthroplasty. The secondary criteria were the severity of complications assessed according to the Clavien-Dindo classification, and the need for readmission and reintervention within three months after the arthroplasty.
Patients were matched in both groups with a ratio of 1:1 by a propensity score calculation using logistic regression including five factors: age, gender, body mass index (BMI), ASA score, procedure performed. The data collected were compared in the two groups by a Chi² test or Fisher's exact test and by calculation of the Odd-Ratio (OR) for qualitative data, and by a Student's t test or a Mann-Whitney test for quantitative data. All tests were performed at the 5% threshold.
Results
91 FTPs (control group) and 91 DCPs (study group) were paired. There were 72 man and 110 women, with a mean age of 67 ± 8 years, and a mean BMI of 30 ± 5 kg/m². There was no significant difference between the two groups for preoperative data. There were no lost to follow-up or missing data. The mean length of stay in the control group was 3 ± 2 days.
The complication rate was not significantly higher in the study group (15% versus 11%) (p=0.38), with an OR of 1.47 (95% confidence interval: 0.62 - 3.51). The other criteria were not significantly worse in the study group (table 1). Only the TKA procedure increased the risk of complication (p=0.018), readmission (p=0.001) and reintervention (p=0.001).
Conclusion
The hypothesis was not confirmed. The complication rate within the first 3 months was not significantly higher after DCP than after FTP in matched populations. Similarly, complication severity, readmission rates and reintervention rates within the first 3 months were not significantly higher after DCP. Concern about the safety of DCPs for THA and TKA appear to be unfounded.
#7323
Avoiding Stem Extension During Revision Total Knee Arthroplasty
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
Objectives
Revision implants with stem extensions are routinely implanted in revision TKAs, but they involve bone loss. The present study was designed to evaluate the possibility of implanting routinely primary instead of revision implants during revision TKAs.
The hypothesis of this study will be that the 5 survival rate of primary TKAs implanted for revision cases will not be negatively impacted in comparison to revision implants.
Methods
All patients undergoing TKA exchange between January 2013 and December 2017 were included. All patients were operated on by two senior surgeons experienced with revision TKA. The target for reimplantation was: neutral mechanical alignment, orthogonal position of both implants in anteroposterior and lateral planes, restoration of the joint line within 2 mm of the native one, medial and lateral gaps in flexion and in extension less than 5 mm. All these parameters were controlled by a navigation system. Bone loss was filled by bone allografting and/or metal augments without increasing bone defects by additional resection. The smallest implant was chosen, which allowed primary fixation of both implants and graft/augment.
Information about follow-up was collected from the individual patient files. All patients were recalled for clinical and radiological examination. The survival curve was plotted.
Results
158 patients were included: 96 women and 62 men, with a mean age at surgery of 71 ± 10 years. The mean body mass index was 31.6 ± 6.7 kg/m². Reasons for revision were infection (65%), aseptic loosening (13%), implant malposition (10%), and instability (6%).
11 cases were reimplanted with a smaller implant than the implant removed (Group A). 37 cases were reimplanted with the same size of implant than the implant removed (Group B). 31 cases were reimplanted with a longer implant than the implant removed for only one tibial or femoral component (Group C), and 79 cases were reimplanted with a longer implant than the implant removed for both components (Group D). There was no significant difference between all groups for demographic data: age, gender, body mass index, ASA score. Bone defects were significantly larger in group D than in all other groups.
The survival rate at 5years was 100% in group A, 96% in group B, 94% in group C and 92% in group D. The differences were not statistically significant.
Conclusions
Reimplantation of a TKA smaller or with the same size than the removed implant was possible in 30% of the cases, without a negative impact on the survival rate after 5 years. Both tibial and femoral extension stems were necessary only in 48% of the cases. Navigation offers the possibility to decrease significantly the size of the implants during TKA revision. This might allow preserving bone stock for a possible repeat revision, especially in cases of infected TKA where the failure rate is significantly higher.
#7324
Diagnosis of Peri-Prosthetic Knee Infection: What Do the New Msis Definition Criteria Bring?
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
Nicolas Giordano-Orsini - University Hospital - Strasbourg, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
OBJECTIVES
Accurate diagnosis of peri-prosthetic joint infection is critical to allow adequate treatment. Currently, the criteria of the Musculo-Skeletal Infection Society (MSIS) serve as a validated reference tool. More recently, these criteria have been modified for better accuracy. The goal of this study was to compare retrospectively the diagnostic accuracy of these two different tools in cases of known peri-prosthetic total knee arthroplasty (TKA) infection or in aseptic cases and to analyze one additional criterion: presence of an early loosening (prior to 2 years after implantation).
Methods
All cases of knee prosthesis exchange operated on at our department during the year 2017 have been selected. There were 130 cases in 127 patients: 67 men and 60 women, with a mean age of 69 years. 74 cases were septic and 53 cases were aseptic.
All criteria included in both classifications were collected: presence of a fistula, results of bacteriological samples, ESR and CRP levels, analysis of the joint fluid, histological analysis. Additionally, the presence of an early loosening was recorded.
The diagnosis accuracy of the classical MSIS classification and of the 2018 modification were assessed and compared with a Chi-square test at a 0.05 level of significance.
Results
The conventional MSIS classification correctly discriminated between infected and non-infected cases in 128/130 cases (98%). There were two failures by infected cases: one case was considered infected with no major criteria and only three minor criteria; one case was considered infected with no major criteria and only two minor criteria. There was no failure by non-infected cases.
The new MSIS classification correctly discriminated between infected and non-infected cases in 129/130 cases (99%). There was one single failure by infected cases: one case was considered infected despite a score of 4 points.
There was no significant difference between the diagnostic accuracy of both classifications.
The presence of an early loosening had a high specificity (85%) but a low sensitivity (22%).
CONCLUSIONS
The conventional MSIS classification had a high diagnostic accuracy. The new MSIS classification offered only minor, non significant increase of this accuracy. As the new classification involves several additional biological assays, these results might question the cost-effectiveness of the new classification. The presence of an early loosening might be an interesting additional criterion at no additional cost.
#7325
Deviation From Native Knee Anatomy After Total Knee Arthroplasty Depends on the Technique of Coronal Alignment Used. Analysis by a Navigation System.
*Jean-Yves Jenny - University Hospital Strasbourg - Illkirch, France
Florent Baldairon - University Hospital Strasbourg - Strasbourg, France
*Email: Jean-yves.jenny@chru-strasbourg.fr
Introduction
The implantation of a TKA can significantly alter the native anatomy of the operated patient. To date, there are several philosophies regarding the anatomical goals of TKA implantation in the coronal plane. The classic goal of systematically restoring a neutral mechanical axis of the lower limb is currently being challenged by proponents of kinematic alignment, which is believed to individually restore the native alignment of the surgical patient; The aim of the present study was to analyze the modification of the native coronal alignment of a population of TKA patients according to different alignment goals.
Methods
Five hundred and twenty TKAs were analyzed. The following angles were measured using an image-free navigation system prior to prosthetic implantation: medial femorotibial mechanical angle without constraint and with maximum manual constraint to reduce deformity, medial distal femoral mechanical angle, medial proximal tibial mechanical angle. The native angles were derived from the osteoarthritic knee angles using a validated correction technique. Femoral and tibial angular data before TKA were pooled for the same patient and transformed into categorical data according to the frontal alignment phenotype.
Data after TKA implantation were calculated by simulating five different coronal alignment techniques: mechanical alignment, restricted mechanical alignment, anatomical alignment, kinematic alignment and restricted kinematic alignment. Femoral and tibial angular data after TKA were pooled for the same patient and transformed into categorical data according to the frontal alignment phenotype as before. The overall phenotype, combining both femoral and tibial phenotypes, as well as the femoral and tibial phenotypes individually were compared before and after TKA. The primary endpoint was the binary endpoint of whether or not TKA restored the natural global phenotype. Secondary endpoints were the binary criterion of whether or not the natural femoral phenotype and the natural tibial phenotype were restored by TKA.
Results
The global phenotype was restored significantly differently by the five alignment techniques (figure 1), and there was a significant difference between each of the pairs of techniques, except for the pair mechanical alignment - restricted mechanical alignment. The femoral (figure 2) and tibial (figure 3) phenotypes were restored significantly differently by the five alignment techniques, and there was a significant difference between each pair of techniques for both phenotypes.
Conclusion
Apart from the kinematic alignment technique, the different alignment techniques induce significant changes in the pre-arthrosis anatomy of the TKA patient. The surgeon must be aware of these modifications. The clinical relevance of this alteration remains to be defined.
Figures
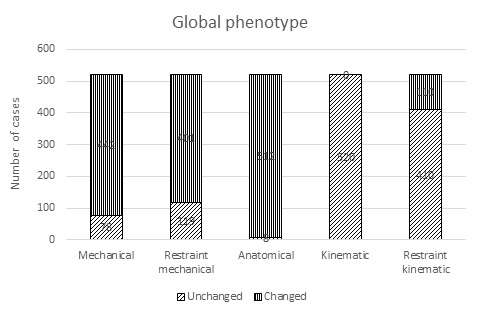
Figure 1
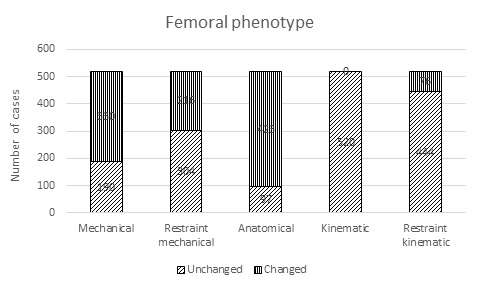
Figure 2
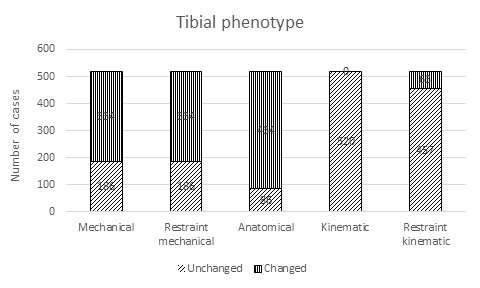
Figure 3#7925
Joint Track Machine Learning: An Autonomous Method for Measuring 6DOF TKA Kinematics From Single-Plane X-Ray Images
*Andrew Jensen - University of Florida - Gainesville, USA
Paris Flood - University of Cambridge - Cambridge, United Kingdom
Lindsey Palm - University of Florida - Gainesville, USA
Will Burton - University of Denver - Denver, USA
Paul Rullkoetter - University of Denver - Denver, USA
Scott Banks - University of Florida - Gainesville, USA
*Email: ajensen123@ufl.edu
Abstract
Dynamic radiographic measurement of 3D TKA kinematics has provided important information for implant design and surgical technique for over 30 years. However, current methods of measuring TKA kinematics are too cumbersome or time-consuming for practical clinical application. Even state-of-the-art techniques require human-supervised initialization or human supervision throughout the entire optimization process. Elimination of human supervision could potentially bring this technology into clinical practicality. Therefore, we propose a fully autonomous pipeline for quantifying TKA kinematics from single-plane imaging. First, a convolutional neural network segments the femoral and tibial implants from the image. Second, segmented images are compared to Normalized Fourier Descriptor shape libraries for initial pose estimates. Lastly, a Lipschitzian optimization routine minimizes the difference between the segmented image and the projected implant. This technique reliably reproduces human-supervised kinematics measurements from internal datasets and external validation studies, with RMS differences of less than 0.7mm and 4° for internal studies and 0.8mm and 1.7° for external validation studies. This performance indicates that it will soon be practical to perform these measurements in a clinical setting.
Joint Track Machine Learning is available for download at https://github.com/BRIO-lab/Joint-Track-Machine-Learning
Introduction
Total Knee Arthroplasty (TKA) is a standard procedure for alleviating symptoms related to osteoarthritis in the knee. In 2018, orthopaedic surgeons performed more than 715,000 TKA operations in the United States [1]. This number is projected to increase to 3.48 million by 2030 [2]. While TKA largely relieves symptomatic osteoarthritis, roughly 20% of TKA patients express postoperative dissatisfaction, citing mechanical limitations, pain, and instability as the leading causes [3]–[5]. Standard methods of musculoskeletal diagnosis cannot quantify the dynamic state of the joint, either pre- or post-operatively; clinicians must rely on static imaging (radiography, MRI, CT) or qualitative mechanical tests to determine the condition of the affected joint, and these tests cannot easily be performed during weight-bearing or dynamic movement when most pain symptoms occur. Unfortunately, most of the tools used to quantify 3D dynamic motion are substantially affected by soft-tissue artifacts [6]–[8], are prohibitively time-consuming or expensive [9], or cannot be performed with equipment available at most hospitals.
Model-image registration is a process where a 3D model is aligned to match an object’s projection in an image [10]. Researchers have performed model-image registration using single-plane fluoroscopic or flat-panel imaging since the 1990s. Early methods used pre-computed distance maps [11], [12], or shape libraries [13]–[15] to match the projection of a 3D implant model to its projection in a radiographic image. With increasing computational capabilities, methods that iteratively compared implant projections to images were possible [16]–[18]. Most model-image registration methods provide sufficient accuracy for clinical joint assessment applications, including natural and replaced knees [19]–[22], natural and replaced shoulders [23]–[26], and extremities [27]–[29]. One of the main benefits of this single-plane approach is that suitable images can be acquired with equipment found in most hospitals. The main impediment to implementing this approach into a standard clinical workflow is the time and expense of human operators to supervise the model-image registration process. These methods require either (1) an initial pose estimate [17], [18], (2) a pre-segmented contour of the implant in the image [10], [11], or (3) a human operator to assist the optimization routine out of local minima [16]. Each of these requirements makes model-image registration methods impractical for clinical use. Even state-of-the-art model-image registration techniques [17] require human initialization or segmentation to perform adequately.
Machine learning algorithms automate the process of analytical model building, utilizing specific algorithms to fit a series of inputs to their respective outputs. Neural networks are a subset of machine learning algorithms that utilize artificial neurons inspired by the human brain’s connections [30]. These networks are successful in many computer vision tasks, such as segmentation [31]–[33], pose estimation [34], [35], and classification [36]–[38]. These capabilities might remove the need for human supervision from TKA model-image registration. Therefore, we propose a three-stage data analysis pipeline (Fig. 1) where a convolutional neural network (CNN) is used to segment, or identify, the pixels belonging to either a femoral or tibial component. Then, an initial pose estimate is generated comparing the segmented implant contour to a pre-computed shape library. Lastly, the initial pose estimate serves as the starting point for a Lipschitzian optimizer that aligns the contours of a 3D implant model to the contour of the CNN-segmented image.
This paper seeks to answer the following three questions: (1) How well does a convolutional neural network segment the femoral and tibial implants from fluoroscopic and flat-panel images? (2) Can a Fourier descriptor-based pose estimation method produce useful initial guesses of 3D implant pose from the CNN-segmented images? (3) Can the Lipschitzian optimizer, given reasonable initial guesses, replicate human-supervised TKA kinematic measurements?
Methods
Data from seven previously reported TKA kinematics studies were used for this study [39]–[45]. These studies utilized single-plane fluoroscopy or flat-panel imaging to measure tibiofemoral implant kinematics during lunge, squat, kneel, and stair climbing movements from 8248 images in 71 patients with implants from 7 manufacturers, including 36 distinct implants. From each of these studies, the following information was collected: (1) deidentified radiographic images, (2) x-ray calibration files, (3) manufacturer-supplied tibial and femoral implant surface geometry files (STL format), and (4) human supervised kinematics for the tibial and femoral components in each of the images. CNNs were trained with images from six of the studies using a transfer-learning paradigm with an open-source network [32]. CNN performance was tested using two image collections: a standard test set including images from the six studies used for training and a wholly naïve test set using images from the seventh study, where the imaging equipment and implants were different from anything used in training (Fig. 2). We used both test image sets to compare human-supervised kinematics with autonomously measured kinematics. Separately, two independent groups utilized our software to assess the accuracy of TKA kinematics measurements compared to their previously reported reference standard systems using RSA [46] or motion capture [9].
Image Segmentation
Images were resized and padded to 1024x1024 pixels. Images containing bilateral implants had the contralateral knee cropped from the image. Segmentation labels were created by taking the human-supervised kinematics for each implant and generating a flat-shaded ground-truth projection image (Fig. 3). Two neural networks [32] were trained to segment the tibial and femoral implants, respectively, from the x-ray images. Each network was trained using a random 6284/1572 (80/20) training/validation split. Augmentations were introduced in the training pipeline to improve the network's generalization to new implants and implant types [47]. Each neural network was trained on an NVIDIA A100 GPU for 30 epochs. The performance of the segmentation networks was measured using the Jaccard Index [48]. This calculates the intersection between the estimated and ground-truth pixels over the union of both sets of pixels. The ideal Jaccard index is 1.
Initial Pose Estimate
Initial pose estimates were generated from bounding contours of the CNN-segmented implant regions using Normalized Fourier Descriptor (NFD) shape libraries [13]–[15]. Shape libraries were created by projecting 3D implant models using the corresponding x-ray calibration parameters with ±30° ranges for the out-of-plane rotations at 3° increments (Fig. 4). Pose estimates were determined as previously described [13]. NFD-derived femoral and tibial implant poses were transformed to anatomic joint angles and translations [49] and compared to the human-supervised kinematics for the same images using RMS differences for each joint pose parameter. The performance of this method was also assessed using flat-shaded projection images with perfect segmentation as a ground-truth reference standard.
Pose Refinement
A modified Dividing Rectangles (DIRECT) algorithm called DIRECT-JTA [17] generated the final pose estimates. This method of Lipschitzian optimization divides the search into three stages, the “trunk,” “branch,” and “leaf.” Each of the three stages was assigned distinct cost function parameters and search regions. The cost function used a computationally efficient L1-norm between the dilated contour from the segmentation label and the projected implant. Successively decreasing the dilation coefficient allowed the optimization routine to escape local minima, and the leaf branch served to find the optimal out-of-plane translation. Transversely symmetric tibial implants posed problems during registration because two distinct poses produced roughly identical projections [50]. Because of this pose ambiguity, the tibial implant was always optimized after the non-symmetric femoral implant. In addition to the dilation metric, the tibial mediolateral translation and varus/valgus rotations relative to the femur were penalized. Final implant poses were transformed into knee joint rotations and translations [49] and compared to the human-supervised kinematics for the same images using RMS differences for each joint pose parameter. Squared differences between data sets were compared using one-way MANOVA with post-hoc multiple pair-wise comparisons using the Games-Howell test (R v4.2.0 using R Studio, rstatix, and stats).
Pose Ambiguities and Registration Blunders
A blunder was defined as an image frame with the squared sum of rotation differences greater than 5° between autonomous and human-supervised measures. These blunder frames contain errors considerably larger than would be clinically acceptable and warrant further exploration. Blunders were analyzed with respect to the tibial implant’s apparent varus/valgus rotation relative to the viewing ray (Fig. 5). A probability density function and cumulative density function were calculated for the blunder likelihood. Due to the high likelihood of blunders in this region, an ambiguous zone was defined for all apparent tibial varus/valgus-rotation less than 3.6 degrees, which is the mean + 1std of the blunder distribution (Fig. 5). Squared measurement differences between images inside and outside the ambiguous zone were also compared using one-way MANOVA with post-hoc multiple pair-wise comparisons using the Games-Howell test.
Results
CNN segmentation of standard test set images produced Jaccard indices of 0.936 for the femoral and 0.883 for the tibial components. CNN segmentation performance on the completely naïve test set was lower, 0.715 and 0.753, respectively.
The initial pose estimates were within the range of convergence for the DIRECT-JTA optimizer and offered a robust initialization for optimization (Table 1). The RMS differences for initial pose estimates on ground-truth images were smaller (better) than for CNN-segmented images, but the differences were mostly within a few millimeters or degrees. Due to poor sensitivity for measuring out-of-plane translation with monocular vision, the mediolateral translation had the largest RMS differences for both image types.
RMS differences between DIRECT-JTA optimized kinematics and human-supervised kinematics were sub-millimeters for all in-plane translations (Table II). Mediolateral translations and out-of-plane rotation differences were smaller when the pose of the tibia was outside the ambiguous zone. The RMS differences for the completely naïve test set were within 0.5 mm or 0.5 deg compared to the standard test set, indicating similar performance on the entirely novel dataset.
There was one femoral blunder and 43 tibial blunders out of 392 test images. Using the definition of the ambiguous zone as apparent tibial varus/valgus rotation less than 3.6 deg, 11% of images have a tibial blunder within this zone, compared to 3.2% outside. Sixty-six percent of tibial blunders were due to symmetry ambiguities (Fig 6).
One-hundred thirteen image pairs from an RSA study of TKA were used to independently assess the accuracy of the autonomous kinematics measurement for single-plane lateral TKA images. RMS errors were 0.8mm for AP translation, 0.5mm for SI translation, 2.6mm for ML translation, 1.0° for flexion-extension, 1.2° for abduction-adduction, and 1.7° for internal-external rotation. At a different institution, 45 single-plane radiographic images were acquired with an instrumented sawbones phantom that was independently tracked using motion capture. Comparing the motion capture and autonomously measured radiographic kinematics, the RMS errors were 0.72mm for AP translation, 0.31mm for SI translation, 1.82mm for ML translation, 0.56° for flexion-extension, 0.63° for abduction-adduction, and 0.84° for internal-external rotation.
Discussion
Dynamic radiographic measurement of 3D TKA kinematics has provided important information for implant design and surgical technique for over 30 years. Many surgeons have expressed an interest in utilizing this type of measurement in their clinical practices; however, current methods are impractical. We developed a completely autonomous TKA kinematics measurement pipeline that can potentially provide a practical method for clinical implementation. This study sought to answer three questions, (1) How well does a neural network segment TKA implants from fluoroscopic and flat-panel images? (2) How well can an NFD shape library estimate the pose of a TKA implant given a CNN-segmented image? And (3) How well does a Lipschitzian optimization routine replicate human-supervised kinematics for TKA implants given an approximate initial guess?
CNN image segmentation of TKA implants worked well, with Jaccard indices greater than 0.88 for the standard test set, and greater than 0.71 for the naïve test set. Segmentation performance for the standard test set outperformed published examples by 0.05-0.1 Jaccard points [51], [52], with the naïve test set on par with other segmentation examples. The most notable decrease in segmentation performance occurred along the perimeter of the segmented pixel region, especially in areas where implant projections occluded each other. These imperfectly segmented perimeter regions likely affect the initial pose estimate and the DIRECT-JTA optimization solution since both methods rely heavily on the segmented implant boundary. Further improvements can be made for the perimeter segmentation results by introducing intelligent augmentations during training using generative models [53] and performing neural network bolstered contour improvement strategies [54].
Our initial pose estimates were satisfactory as an initialization for the DIRECT-JTA optimization, falling within the convergence region of ±30° [17]. However, the performance for the ground-truth projections was not as good as the cited method [13], which achieved errors of less than 1mm for in-plane translation and 2° for rotation. The cited method utilized an additional refinement step for the NFD estimation, interpolating the apparent out-of-plane angles between nearest shapes in the library. This extra step was not done because only approximate initial pose estimates were needed. In addition, the current study incorporated a vastly larger set of implant shapes (36 vs. 2) and image quality and calibration variations. Distinct implant shapes manifest unique normalization maps, where there can be discontinuities or jumps in normalization angles which affect the best-fitting library entry (Fig. 3) [14], [15]. These details are easily upgraded with additional code using previously reported methods but were not pursued because the initial pose results were well within the DIRECT-JTA convergence region. The initial pose estimates for the CNN-segmented images were not as good as for the ground-truth projections. This follows directly from the fact that the perimeter of the segmented implants was not as accurately rendered, leading to poorer results with the edge-based NFD method. Finally, the out-of-plane translation estimates were relatively poor for both ground-truth projects and CNN-segmented images. This translation estimate is extremely sensitive to model projection and edge detection details and can be adjusted for better results if required.
RMS differences between human-supervised and DIRECT-JTA optimized kinematics demonstrate the two methods provide similar results. In-plane translation differences of less than 0.8mm and out-of-plane less than 1.8 mm, indicate good consistency in determining the relative locations of TKA implants. Rotation differences of 4° or less for frames within the ambiguous zone, and less than 1.7° for frames outside the ambiguous zone, indicate joint rotation measures with sufficient resolution to be clinically useful. We observed two important characteristics in the measurement comparisons that will affect future implementations and use. First, we identified an ambiguous zone of apparent tibial rotations wherein there is a higher incidence of registration errors. These errors resulted in significant differences in measurement performance for the out-of-plane translations and rotations. This phenomenon, resulting from the nearly symmetric nature of most tibial implants [11]–[13], [16], [17] prompts either practical modification to imaging protocols to bias the tibial view outside the ambiguous zone or modifications of the model-image registration code to enforce smooth kinematic continuity across image frames and/or to impose joint penetration/separation penalties [55]. Second, we observed similar measurement performance for the standard and naïve test sets, which differed only in the superior/inferior joint translation. This suggests that the autonomous kinematic processing pipeline can provide reliable measures for implants and imaging systems that were not part of the training set, which will be important for application in novel clinical environments.
Two independent research teams utilized our software to evaluate the accuracy of our autonomous measurement pipeline compared to their reference standard methods using implants and image detectors that were not part of our training sets. In both cases, the accuracy results were comparable to results reported for contemporary human-supervised single-plane model-image registration methods for TKA kinematics [13], [17], [19]–[21]. Interestingly, the independent accuracy results appeared superior to our assessment of differences between autonomous and human-supervised measures of TKA kinematics. In both cases, the independent centers used high-resolution flat-panel detectors that provided better spatial resolution and grayscale contrast than most of the imaging systems included in our datasets. With images of similar quality, it is reasonable to expect similar measurement accuracy.
This work has several limitations. First, the image data sets resulted from previous studies in our labs, so there was no prospective design of which implant systems and image detectors should be included for a pipeline that generalizes well to other implants and detectors. Nevertheless, the naïve data set and the independent assessments, all involving implants and detectors not used for training, performed well and suggest that the method can usefully generalize to measurements of traditionally configured TKA implants. Future work is required to evaluate measurement performance with partial knee arthroplasty or revision implants. Second, many methodologic and configuration options and alternatives remain to be explored, and the current pipeline implementation should not be considered optimal. How best to disambiguate tibial poses and determine the most effective and robust optimization cost functions are areas of current effort.
We present an autonomous pipeline for measuring 3D TKA kinematics from single-plane radiographic images. Measurement reproducibility and accuracy are comparable to contemporary human-supervised methods. We believe capabilities like this will soon make it practical to perform dynamic TKA kinematic analysis in a clinical workflow, where these measures can help surgeons objectively determine the best course of treatment for their patients.
Conflicts of Interest
None
Acknowledgments
This work was supported by a grant from the McJunkin Family Charitable Foundation.
References
[1] Agency for Healthcare Research and Quality, “HCUP Fast Stats,” Healthcare Cost and Utilization Project. https://hcup-us.ahrq.gov/faststats/NationalProcedures (accessed Apr. 26, 2022).
[2] S. Kurtz, K. Ong, E. Lau, F. Mowat, and M. Halpern, “Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030:,” J. Bone Jt. Surg., vol. 89, no. 4, pp. 780–785, Apr. 2007, doi: 10.2106/JBJS.F.00222.
[3] P. N. Baker, J. H. van der Meulen, J. Lewsey, and P. J. Gregg, “The Role of Pain and Function in Determining Patient Satisfaction After Total Knee Replacement: Data From the National Joint Registry for England and Wales,” J. Bone Joint Surg. Br., vol. 89-B, no. 7, pp. 893–900, Jul. 2007, doi: 10.1302/0301-620X.89B7.19091.
[4] R. B. Bourne, B. M. Chesworth, A. M. Davis, N. N. Mahomed, and K. D. J. Charron, “Patient Satisfaction after Total Knee Arthroplasty: Who is Satisfied and Who is Not?,” Clin. Orthop., vol. 468, no. 1, pp. 57–63, Jan. 2010, doi: 10.1007/s11999-009-1119-9.
[5] C. E. H. Scott, C. R. Howie, D. MacDonald, and L. C. Biant, “Predicting Dissatisfaction Following Total Knee Replacement: A Prospective Study of 1217 Patients,” J. Bone Joint Surg. Br., vol. 92-B, no. 9, pp. 1253–1258, Sep. 2010, doi: 10.1302/0301-620X.92B9.24394.
[6] B. Gao and N. (Nigel) Zheng, “Investigation of soft tissue movement during level walking: Translations and rotations of skin markers,” J. Biomech., vol. 41, no. 15, pp. 3189–3195, Nov. 2008, doi: 10.1016/j.jbiomech.2008.08.028.
[7] R. Stagni, S. Fantozzi, A. Cappello, and A. Leardini, “Quantification of soft tissue artefact in motion analysis by combining 3D fluoroscopy and stereophotogrammetry: a study on two subjects,” Clin. Biomech., vol. 20, no. 3, pp. 320–329, Mar. 2005, doi: 10.1016/j.clinbiomech.2004.11.012.
[8] C.-C. Lin, T.-W. Lu, H.-L. Lu, M.-Y. Kuo, and H.-C. Hsu, “Effects of soft tissue artifacts on differentiating kinematic differences between natural and replaced knee joints during functional activity,” Gait Posture, vol. 46, pp. 154–160, May 2016, doi: 10.1016/j.gaitpost.2016.03.006.
[9] R. Daems, J. Victor, P. De Baets, S. Van Onsem, and M. Verstraete, “Validation of three-dimensional total knee replacement kinematics measurement using single-plane fluoroscopy,” Int. J. Sustain. Constr. Des., vol. 7, no. 1, p. 14, Oct. 2016, doi: 10.21825/scad.v7i1.3634.
[10] L. G. Brown, “A survey of image registration techniques,” ACM Comput. Surv., vol. 24, no. 4, pp. 325–376, Dec. 1992, doi: 10.1145/146370.146374.
[11] S. Lavallee and R. Szeliski, “Recovering the position and orientation of free-form objects from image contours using 3D distance maps,” IEEE Trans. Pattern Anal. Mach. Intell., vol. 17, no. 4, pp. 378–390, Apr. 1995, doi: 10.1109/34.385980.
[12] S. Zuffi, A. Leardini, F. Catani, S. Fantozzi, and A. Cappello, “A model-based method for the reconstruction of total knee replacement kinematics,” IEEE Trans. Med. Imaging, vol. 18, no. 10, pp. 981–991, Oct. 1999, doi: 10.1109/42.811310.
[13] S. A. Banks and W. A. Hodge, “Accurate measurement of three-dimensional knee replacement kinematics using single-plane fluoroscopy,” IEEE Trans. Biomed. Eng., vol. 43, no. 6, pp. 638–649, Jun. 1996, doi: 10.1109/10.495283.
[14] T. P. Wallace and O. R. Mitchell, “Analysis of three-dimensional movement using Fourier descriptors,” IEEE Trans. Pattern Anal. Mach. Intell., vol. PAMI-2, no. 6, pp. 583–588, 1980, doi: 10.1109/TPAMI.1980.6447707.
[15] T. P. Wallace and P. A. Wintz, “An efficient three-dimensional aircraft recognition algorithm using normalized fourier descriptors,” Comput. Graph. Image Process., vol. 13, no. 2, pp. 99–126, Jan. 1980, doi: 10.1016/S0146-664X(80)80035-9.
[16] M. R. Mahfouz, W. A. Hoff, R. D. Komistek, and D. A. Dennis, “A robust method for registration of three-dimensional knee implant models to two-dimensional fluoroscopy images,” IEEE Trans. Med. Imaging, vol. 22, no. 12, pp. 1561–1574, Dec. 2003, doi: 10.1109/TMI.2003.820027.
[17] P. D. L. Flood and S. A. Banks, “Automated registration of 3-D knee implant models to fluoroscopic images using lipschitzian optimization,” IEEE Trans. Med. Imaging, vol. 37, no. 1, pp. 326–335, 2018, doi: 10.1109/tmi.2017.2773398.
[18] D. G. Lowe, “Fitting parameterized three-dimensional models to images,” IEEE Trans. Pattern Anal. Mach. Intell., 1991, doi: 10.1109/34.134043.
[19] S. A. Banks, G. D. Markovich, and W. A. Hodge, “In vivo kinematics of cruciate-retaining and -substituting knee arthroplasties,” J. Arthroplasty, vol. 12, no. 3, pp. 297–304, Apr. 1997, doi: 10.1016/S0883-5403(97)90026-7.
[20] S. A. Banks and W. A. Hodge, “2003 Hap Paul Award paper of the International Society for Technology in Arthroplasty,” J. Arthroplasty, vol. 19, no. 7, pp. 809–816, Oct. 2004, doi: 10.1016/j.arth.2004.04.011.
[21] R. D. Komistek, D. A. Dennis, and M. Mahfouz, “In Vivo Fluoroscopic Analysis of the Normal Human Knee,” Clin. Orthop., vol. 410, pp. 69–81, May 2003, doi: 10.1097/01.blo.0000062384.79828.3b.
[22] W. Burton et al., “Automatic tracking of healthy joint kinematics from stereo-radiography sequences.,” Comput. Biol. Med., 2021, doi: 10.1016/j.compbiomed.2021.104945.
[23] T. Kijima et al., “In vivo 3-dimensional analysis of scapular and glenohumeral kinematics: comparison of symptomatic or asymptomatic shoulders with rotator cuff tears and healthy shoulders,” J. Shoulder Elbow Surg., vol. 24, no. 11, pp. 1817–1826, Nov. 2015, doi: 10.1016/j.jse.2015.06.003.
[24] M. Mahfouz, G. Nicholson, R. Komistek, D. Hovis, and M. Kubo, “In Vivo Determination of the Dynamics of Normal, Rotator Cuff-Deficient, Total, and Reverse Replacement Shoulders,” VO LU M E, p. 8.
[25] K. Matsuki et al., “In vivo 3-dimensional analysis of scapular kinematics: comparison of dominant and nondominant shoulders,” J. Shoulder Elbow Surg., vol. 20, no. 4, pp. 659–665, Jun. 2011, doi: 10.1016/j.jse.2010.09.012.
[26] A. Sugi et al., “Comparing in vivo three-dimensional shoulder elevation kinematics between standing and supine postures,” JSES Int., vol. 5, no. 6, pp. 1001–1007, Nov. 2021, doi: 10.1016/j.jseint.2021.07.005.
[27] F. Cenni et al., “Kinematics of the Three Components of a Total Ankle Replacement: In Vivo Fluoroscopic Analysis,” Foot Ankle Int., vol. 33, no. 4, pp. 290–300, Apr. 2012, doi: 10.3113/FAI.2012.0290.
[28] F. Cenni et al., “Functional performance of a total ankle replacement: thorough assessment by combining gait and fluoroscopic analyses,” Clin. Biomech., vol. 28, no. 1, pp. 79–87, Jan. 2013, doi: 10.1016/j.clinbiomech.2012.10.008.
[29] R. J. de Asla, L. Wan, H. E. Rubash, and G. Li, “Six DOF in vivo kinematics of the ankle joint complex: Application of a combined dual-orthogonal fluoroscopic and magnetic resonance imaging technique,” J. Orthop. Res., vol. 24, no. 5, pp. 1019–1027, Apr. 2006, doi: 10.1002/jor.20142.
[30] D. Marr, “Early processing of visual information,” 1976.
[31] L. Chan, M. Hosseini, C. Rowsell, K. Plataniotis, and S. Damaskinos, “HistoSegNet: Semantic Segmentation of Histological Tissue Type in Whole Slide Images,” in 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Korea (South), Oct. 2019, pp. 10661–10670. doi: 10.1109/ICCV.2019.01076.
[32] Jingdong Wang et al., “Deep High-Resolution Representation Learning for Visual Recognition.,” IEEE Trans. Pattern Anal. Mach. Intell., 2020, doi: 10.1109/tpami.2020.2983686.
[33] O. Ronneberger, Philipp Fischer, and Thomas Brox, “U-Net: Convolutional Networks for Biomedical Image Segmentation,” 2015, doi: 10.1007/978-3-319-24574-4_28.
[34] A. Wu et al., “Deep Graph Pose: a semi-supervised deep graphical model for improved animal pose tracking,” Animal Behavior and Cognition, preprint, Aug. 2020. doi: 10.1101/2020.08.20.259705.
[35] A. Kendall and R. Cipolla, “Geometric Loss Functions for Camera Pose Regression with Deep Learning,” in 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, Jul. 2017, pp. 6555–6564. doi: 10.1109/CVPR.2017.694.
[36] A. Krizhevsky, I. Sutskever, and G. E. Hinton, “ImageNet Classification with Deep Convolutional Neural Networks,” Commun. ACM, vol. 60, no. 6, pp. 84–90, 2017, doi: 10.1145/3065386.
[37] C. R. Qi, H. Su, K. Mo, and L. J. Guibas, “PointNet: Deep Learning on Point Sets for 3D Classification and Segmentation,” ArXiv161200593 Cs, Apr. 2017, Accessed: Jan. 13, 2022. [Online]. Available: http://arxiv.org/abs/1612.00593
[38] C. R. Qi, Li Yi, Hao Su, and Leonidas J. Guibas, “PointNet++: Deep Hierarchical Feature Learning on Point Sets in a Metric Space,” 2017.
[39] V. Kefala et al., “Assessment of Knee Kinematics in Older Adults Using High-Speed Stereo Radiography,” Med. Sci. Sports Exerc., vol. 49, no. 11, pp. 2260–2267, Nov. 2017, doi: 10.1249/MSS.0000000000001350.
[40] L. Palm-Vlasak, R. Leitz, H. Parvateneni, L. Pulido, M. B. Horodyski, and S. Banks, “Minimal Variation in Top Level and Decline Walking Speeds Between Pivoting TKA Subjects and Healthy Controls,” presented at the Orthopaedic Research Society Annual Meeting, Tampa, FL, 2022.
[41] N. Okamoto, L. Breslauer, A. K. Hedley, H. Mizuta, and S. A. Banks, “In Vivo Knee Kinematics in Patients With Bilateral Total Knee Arthroplasty of 2 Designs,” J. Arthroplasty, vol. 26, no. 6, pp. 914–918, Sep. 2011, doi: 10.1016/j.arth.2010.07.018.
[42] T. Watanabe, M. Ishizuki, T. Muneta, and S. A. Banks, “Knee Kinematics in Anterior Cruciate Ligament-Substituting Arthroplasty With or Without the Posterior Cruciate Ligament,” J. Arthroplasty, vol. 28, no. 4, pp. 548–552, Apr. 2013, doi: 10.1016/j.arth.2012.06.030.
[43] J.-Y. Jenny, S. Banks, and F. Baldairon, “Registration of Knee Kinematics With a Navigation System: A Validation Study,” presented at the International Society for Technology in Arthroplasty, Emerging Technologies in Arthroplasty, Online, 2015. [Online]. Available: https://online.boneandjoint.org.uk/doi/abs/10.1302/1358-992X.2021.9.004
[44] T. Watanabe et al., “In-vivo kinematics of high-flex posterior-stabilized total knee prosthesis designed for Asian populations,” Int. Orthop., vol. 40, no. 11, pp. 2295–2302, Nov. 2016, doi: 10.1007/s00264-016-3176-5.
[45] G. Scott et al., “Can a total knee arthroplasty be both rotationally unconstrained and anteroposteriorly stabilised?: A pulsed fluoroscopic investigation,” Bone Jt. Res., vol. 5, no. 3, pp. 80–86, Mar. 2016, doi: 10.1302/2046-3758.53.2000621.
[46] M. G. Teeter et al., “Quantification of in vivo implant wear in total knee replacement from dynamic single plane radiography,” Phys. Med. Biol., vol. 58, no. 9, pp. 2751–2767, May 2013, doi: 10.1088/0031-9155/58/9/2751.
[47] A. Buslaev, V. I. Iglovikov, E. Khvedchenya, A. Parinov, M. Druzhinin, and A. A. Kalinin, “Albumentations: Fast and Flexible Image Augmentations,” Information, vol. 11, no. 2, p. 125, Feb. 2020, doi: 10.3390/info11020125.
[48] P. Jaccard, “The Distribution of the Flora in the Alpine Zone,” New Phytol., vol. 11, no. 2, pp. 37–50, Feb. 1912, doi: 10.1111/j.1469-8137.1912.tb05611.x.
[49] E. S. Grood and W. J. Suntay, “A Joint Coordinate System for the Clinical Description of Three-Dimensional Motions: Application to the Knee,” J. Biomech. Eng.-Trans. Asme, 1983, doi: 10.1115/1.3138397.
[50] D. G. Kendall, “Shape Manifolds, Procrustean Metrics, and Complex Projective Spaces,” Bull. Lond. Math. Soc., vol. 16, no. 2, pp. 81–121, Mar. 1984, doi: 10.1112/blms/16.2.81.
[51] Z. Zhou, M. M. Rahman Siddiquee, N. Tajbakhsh, and J. Liang, “UNet++: A Nested U-Net Architecture for Medical Image Segmentation,” in Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support, vol. 11045, D. Stoyanov, Z. Taylor, G. Carneiro, T. Syeda-Mahmood, A. Martel, L. Maier-Hein, J. M. R. S. Tavares, A. Bradley, J. P. Papa, V. Belagiannis, J. C. Nascimento, Z. Lu, S. Conjeti, M. Moradi, H. Greenspan, and A. Madabhushi, Eds. Cham: Springer International Publishing, 2018, pp. 3–11. doi: 10.1007/978-3-030-00889-5_1.
[52] P. Rodrigues, M. Antunes, C. Raposo, P. Marques, F. Fonseca, and J. P. Barreto, “Deep segmentation leverages geometric pose estimation in computer‐aided total knee arthroplasty,” Healthc. Technol. Lett., vol. 6, no. 6, pp. 226–230, Dec. 2019, doi: 10.1049/htl.2019.0078.
[53] R. Hataya, J. Zdenek, K. Yoshizoe, and H. Nakayama, “Faster AutoAugment: Learning Augmentation Strategies using Backpropagation,” ArXiv191106987 Cs, Nov. 2019, Accessed: Mar. 22, 2022. [Online]. Available: http://arxiv.org/abs/1911.06987
[54] Y. Yuan, J. Xie, X. Chen, and J. Wang, “SegFix: Model-Agnostic Boundary Refinement for Segmentation,” in Computer Vision – ECCV 2020, vol. 12357, A. Vedaldi, H. Bischof, T. Brox, and J.-M. Frahm, Eds. Cham: Springer International Publishing, 2020, pp. 489–506. doi: 10.1007/978-3-030-58610-2_29.
[55] S. Mu, “JointTrack: An Open-Source, Easily Expandable Program for Skeletal Kinematic Measurement Using Model-Image Registration,” p. 27, 2007.
Figures
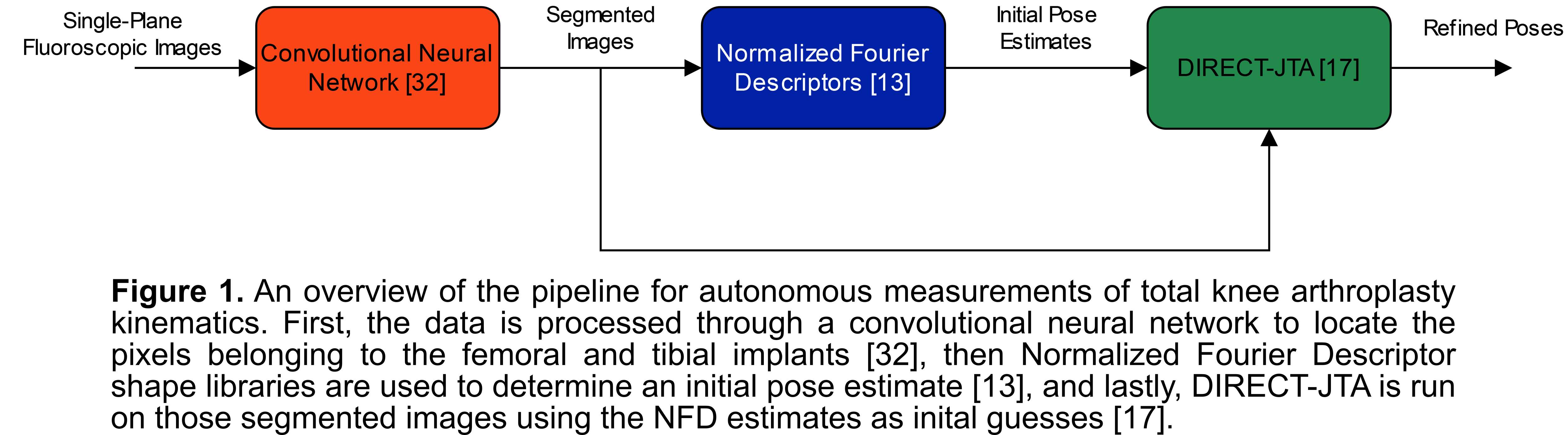
Figure 1
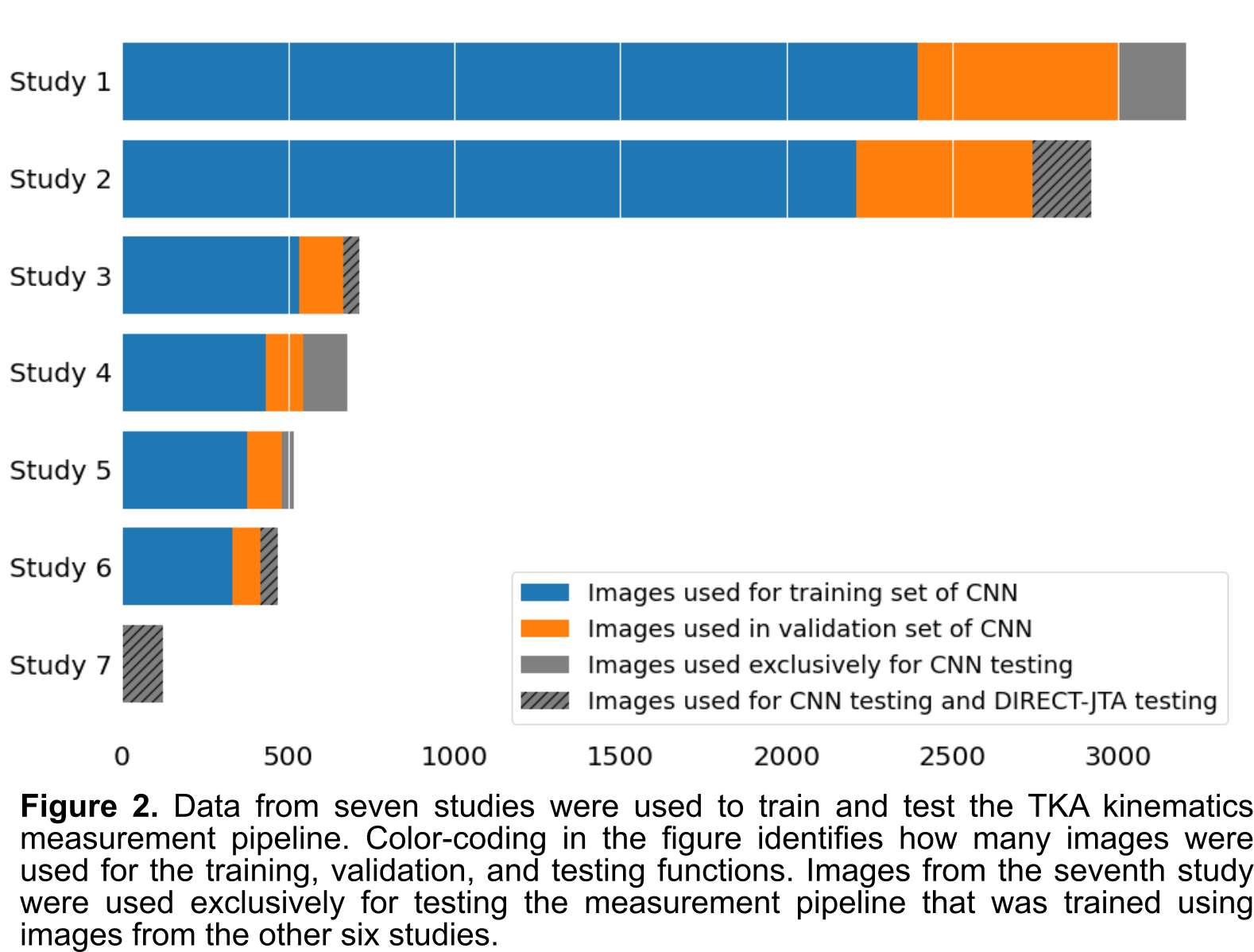
Figure 2
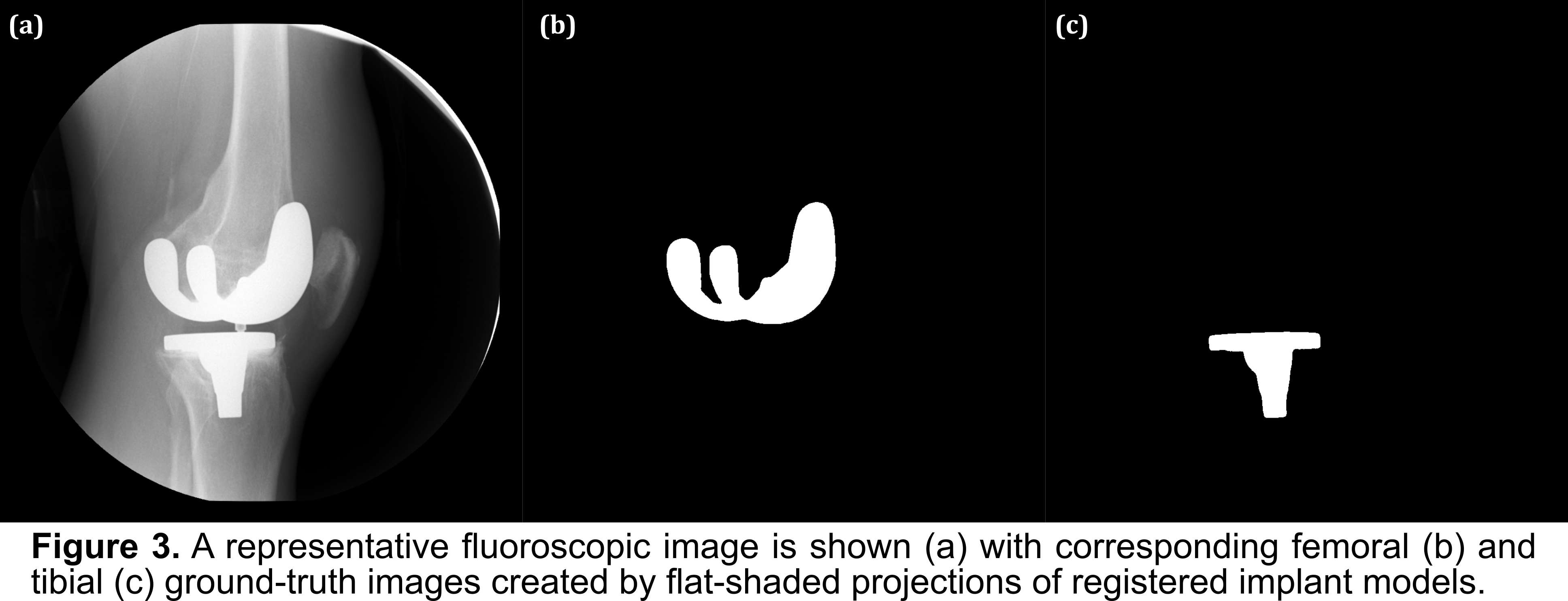
Figure 3
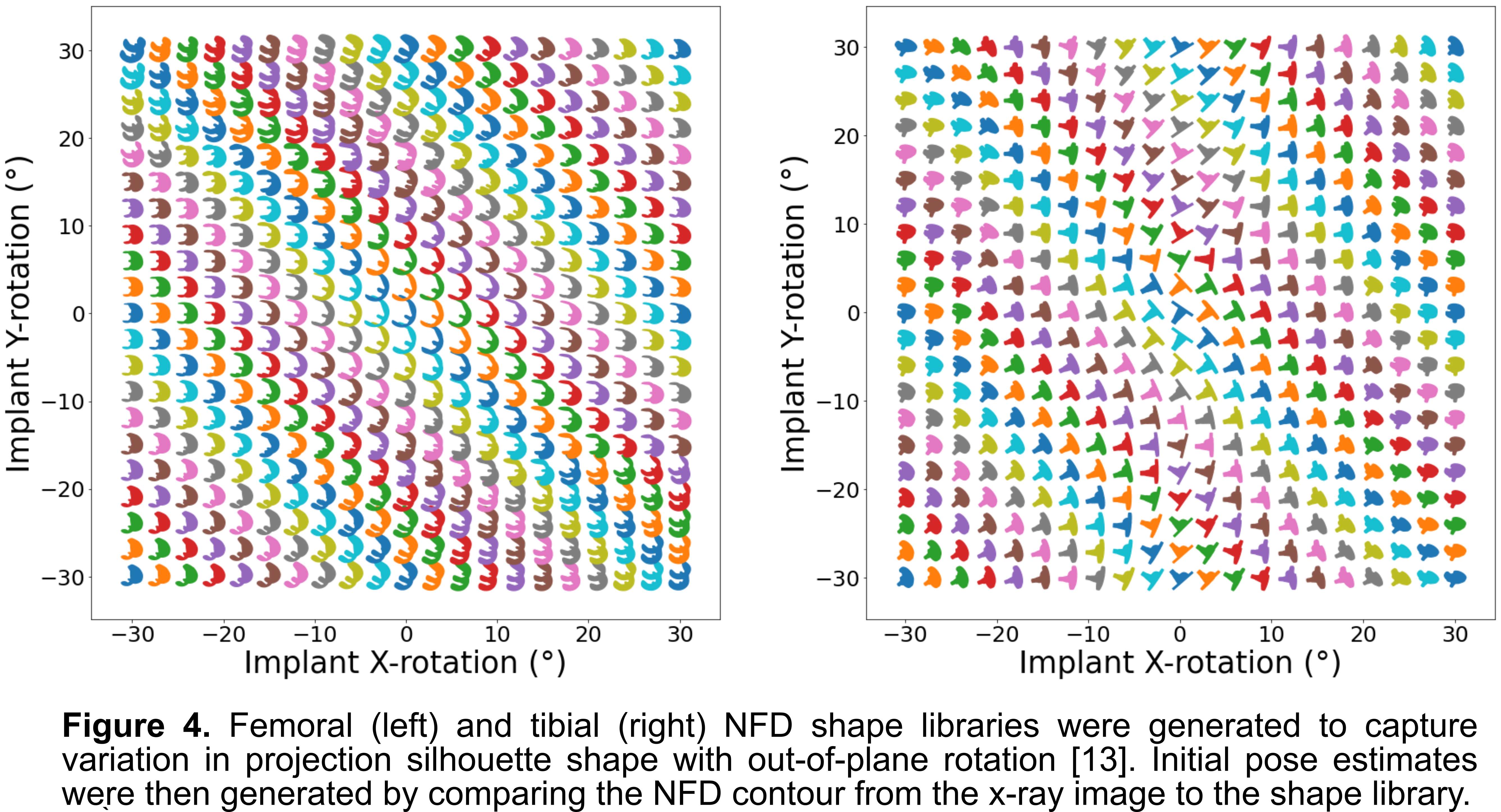
Figure 4
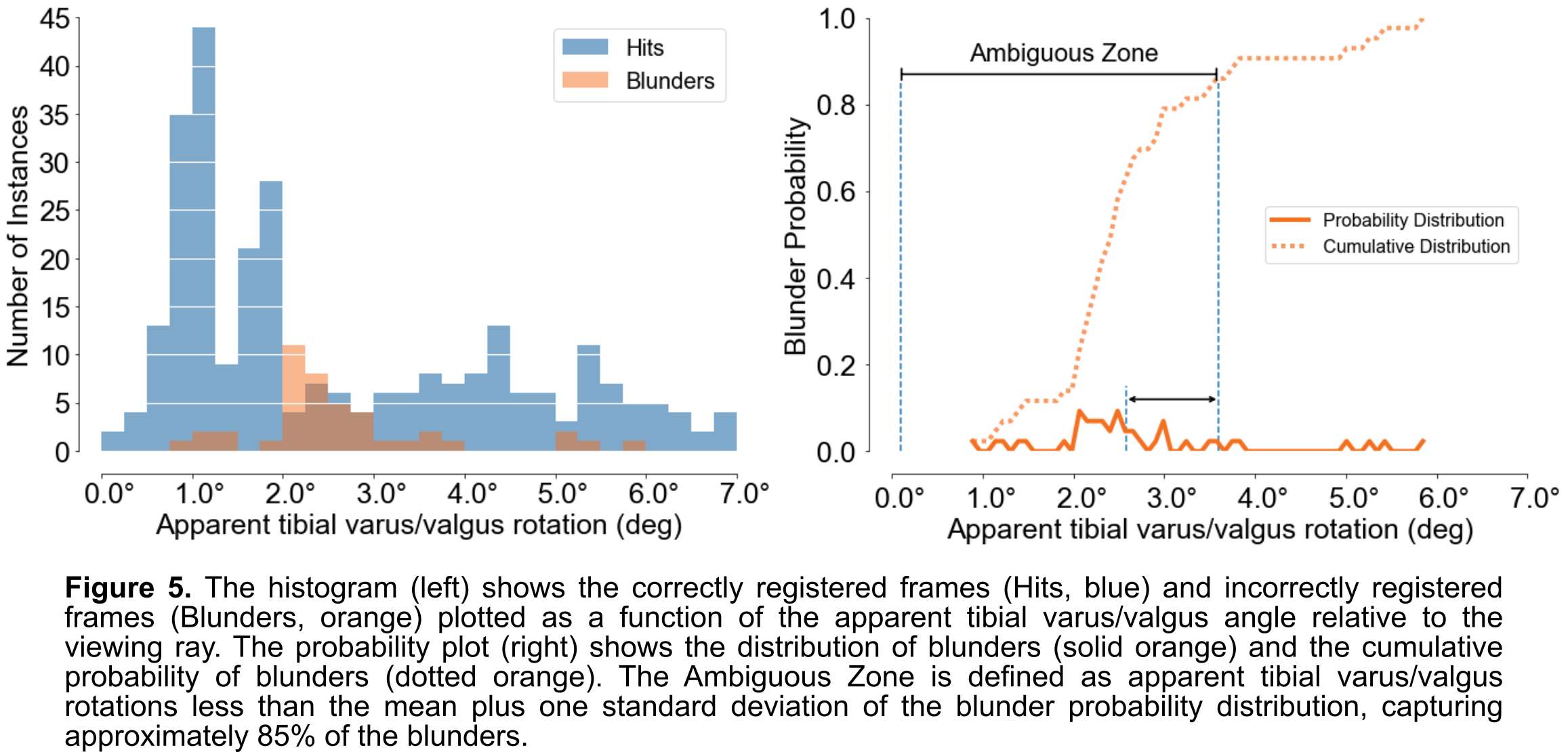
Figure 5
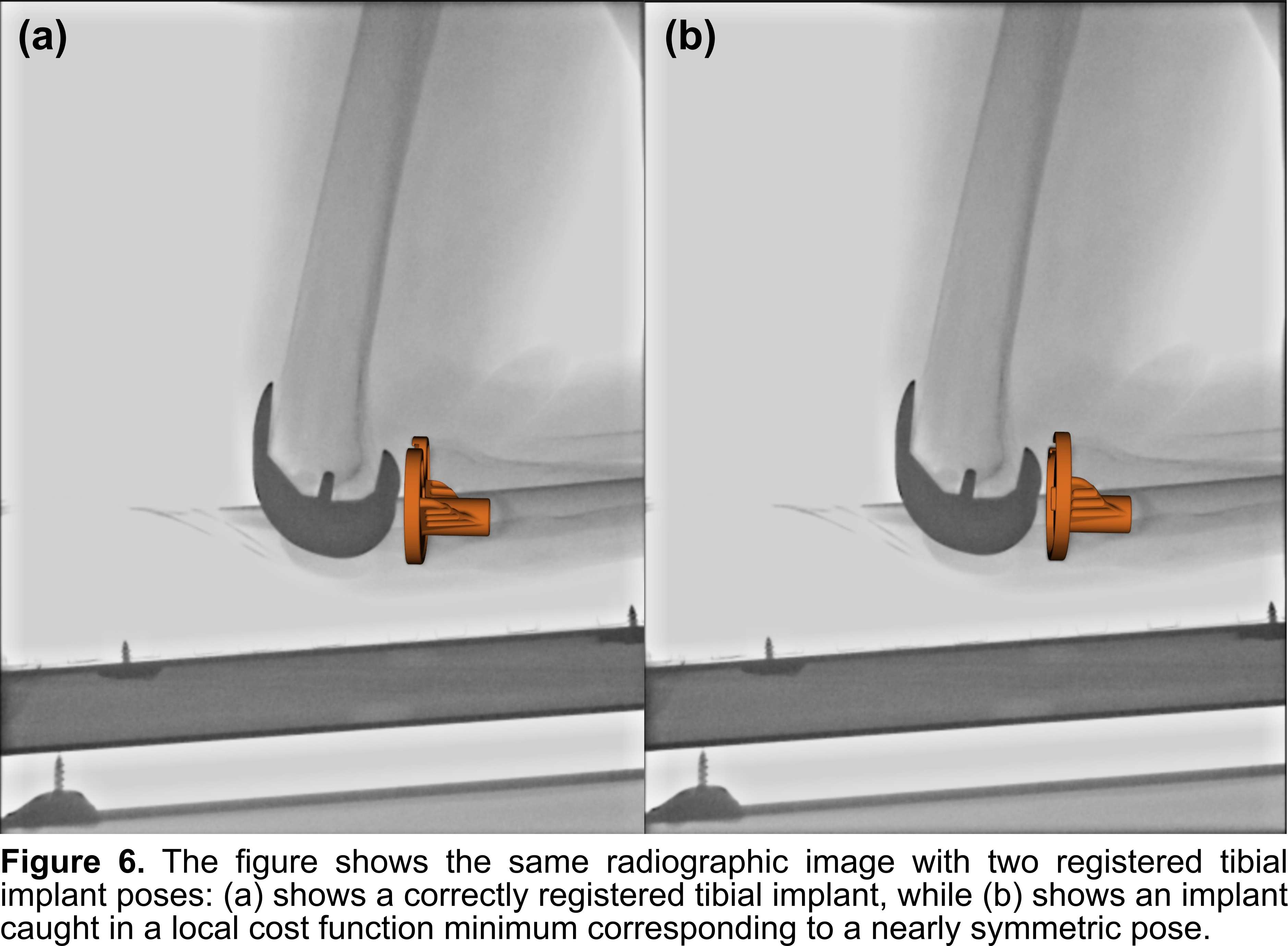
Figure 6
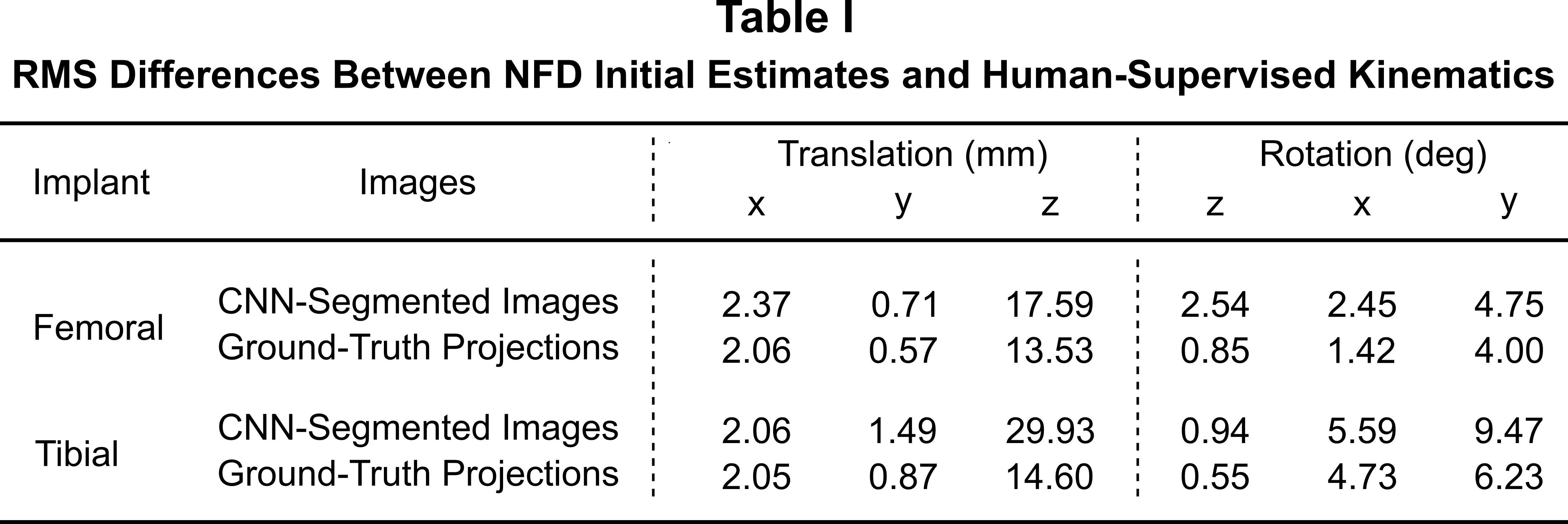
Figure 7
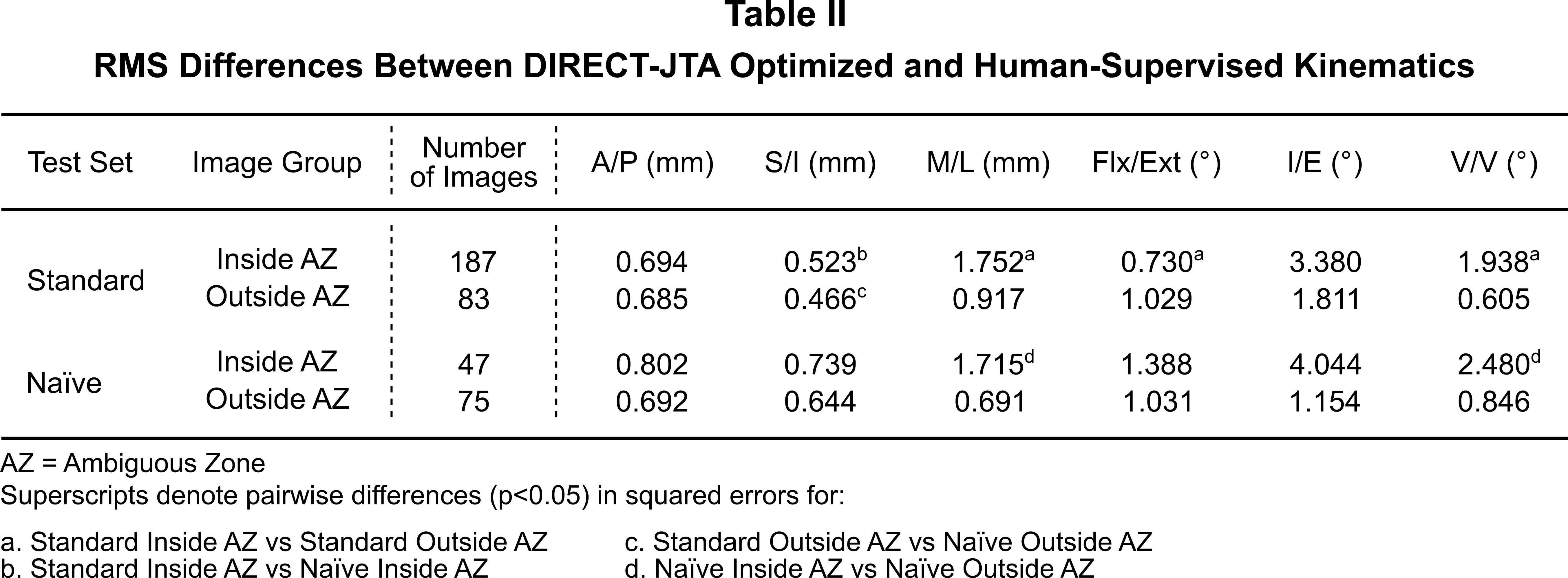
Figure 8#7319
Safety and Efficacy of Uninterrupted Warfarin Anticoagulation With Supplemental Tranexamic Acid in Total Joint Arthroplasty Patients
*Michael Johnston - Washington State University, Elson S. Floyd College of Medicine - Spokane, USA
Matt Porter - Washington State University, Elson S. Floyd College of Medicine - Spokane, USA
Kade Eppich - Washington State University, Elson S. Floyd College of Medicine - Spokane, USA
David Scott - Spokane Joint Replacement Center - Spokane, USA
Celeste Gray - Orthopaedic Specialty Clinic - Spokane, USA
Jason Kowitz - Massachusetts General Hospital - Boston, USA
*Email: michael.g.johnston@wsu.edu
Purpose: The continuation of chronic Warfarin therapy is gaining acceptance in minor surgeries but maintaining patients at therapeutic INR values during major orthopaedic procedures raises concern for excessive blood loss. While bridging therapy with low molecular weight heparin is currently recommended for anticoagulated patients, few studies have evaluated the safety of continuing patients on warfarin during total joint arthroplasty – making concerns about increased perioperative bleeding largely theoretical and based on minimal empirical data. Our study evaluates the safety and efficacy of continuous warfarin anticoagulation in conjunction with primary hip and knee replacement with and without the use of prophylactic tranexamic acid (TXA).
Methods: We conducted a retrospective, matched-pair analysis of two experimental groups of patients who underwent primary THA or TKA performed by a single surgeon. Our first experimental group, Warfarin + TXA Group, consisted of 21 patients who underwent arthroplasty while therapeutically anticoagulated with warfarin (INR 2.0-3.0) and who received prophylactic TXA. Our TXA group was then matched with a control group, consisting of 21 non-anticoagulated controls. Additionally, our second experimental arm, Warfarin without TXA Group, consisted of 40 patients who underwent arthroplasty while therapeutically anticoagulated with warfarin (INR 2.0-3.0) without prophylactic TXA. Both experimental groups utilized matched pairs based on age, sex, BMI, date of surgery, type of surgery, and pre-operative hemoglobin value.
Results: In our first experimental group, Warfarin + TXA, the Warfarin and control groups were similar for age (p=0.46), sex (p=1.0), BMI (p=0.61), and pre-operative hemoglobin value (p=.58). 19% of matched pairs underwent THA (4 patients), while 81% underwent TKA (17 patients). The percentage change in hemoglobin value post-surgery was not greater in the warfarin group than in controls (p=0.30). Additionally, units RBCs transfused (p=0.33), surgical site infection rates (p=0.31), bleeding complication rates (p=0.31), and thrombotic complication rates (p=n/a) were similar between groups. In our second experimental group, Warfarin without TXA, the Warfarin and control groups were similar for age (p=0.58), sex (p=1.0), BMI (p=0.05), and pre-operative hemoglobin value (p=.75). 37.5% of matched pairs underwent THA (15 patients), while 62.5% underwent TKA (25 patients). The percentage change in hemoglobin value post-surgery was not greater in the warfarin group than in controls (p=0.40). Additionally, units RBCs transfused (p=0.16), surgical site infection rates (p=0.15), bleeding complication rates (p=0.31), and thrombotic complication rates (p=0.31) were similar between groups. Additionally, between our patients who underwent prophylactic TXA vs those who did not, we saw a statistical decrease in average RBC transfused (p=0.0003) and estimated blood loss (p=0.023). We also saw no difference in thrombotic complications (p=0.47), bleeding complications (p=1.0), or surgical site infections (p=0.97) in patients who received prophylactic TXA compared to those who did not.
Conclusion: Many considerations must be made when choosing perioperative thromboembolic prophylaxis for arthroplasty candidates with medical comorbidities requiring chronic anticoagulation. While current guidelines suggest that patients on chronic warfarin anticoagulation should discontinue warfarin and undergo bridging therapy, our data suggests that it is safe to continue therapeutic warfarin administration along with adding prophylactic TXA prior to and during hip and knee arthroplasty.
Figures
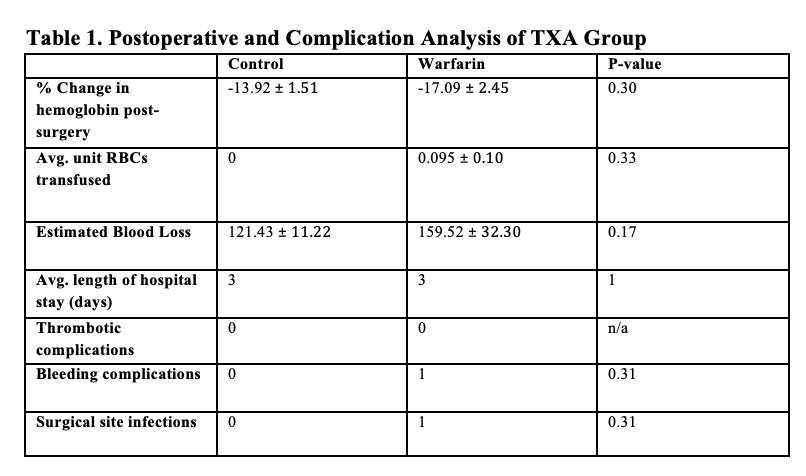
Figure 1
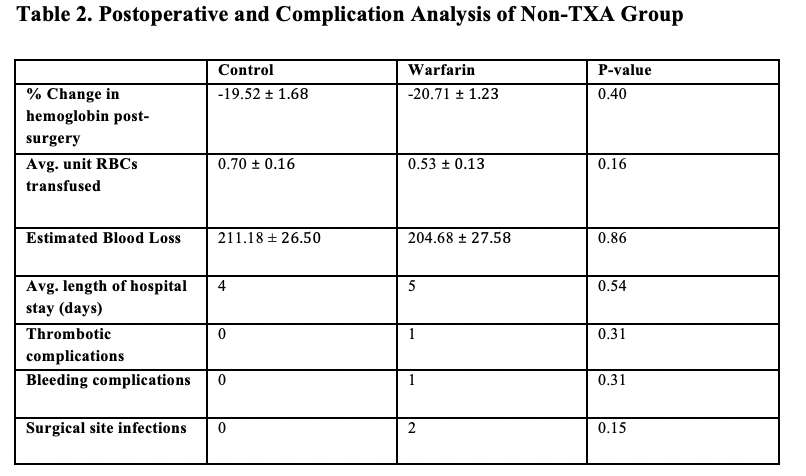
Figure 2
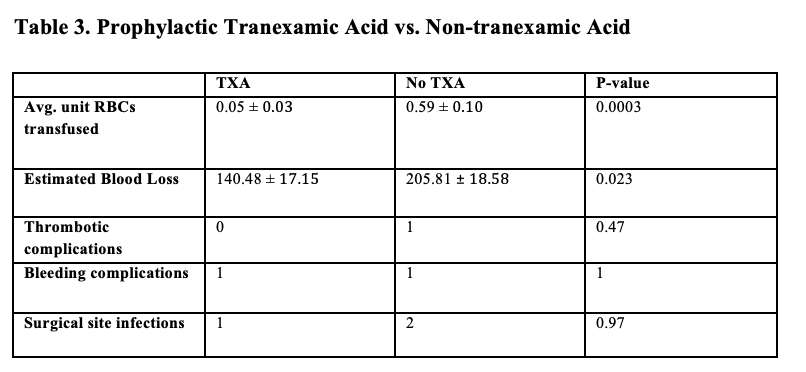
Figure 3#7703
Does Preoperative Vastus Medialis Volume and Quality Affect Functional Outcomes After TKA?
Hojung Jung - Hallym Univ. - Seoul, Korea (Republic of)
*Joong Il Kim - Hallym Univ. - Seoul, South Korea
JongHwa Lee - Hallym Univ. - Seoul, South Korea
*Email: oskji@hallym.or.kr
Background: Vastus medialis (VM) function has been implicated in the development and progression of knee osteoarthritis, however, studies evaluating the influence of preoperative VM volume and quality on functional outcomes following total knee arthroplasty (TKA) are limited. The purpose of this study is to determine the association between VM volume and quality and clinical outcome after TKA.
Methods: Among the patients who underwent unilateral TKA between July 2019 to February 2021, 92 patients (mean age, 71.2 ± 6.3 years) who had magnetic resonance imaging (MRI) images before TKA were included. The preoperative VM volume and quality were assessed by maximal cross-sectional area (mCSA) on axial and fatty infiltration ratio on axial MRI images respectively. The clinical outcomes were evaluated using the Knee Society (KS) pain and function scores at 1 years after TKA. The relationship between preoperative VM mCSA and fatty infiltration ratio and KS pain and function scores were analyzed with univariate and multivariate linear regression analysis.
Results: In univariate linear regression analysis, preoperative VM mCSA and fatty infiltration ratio were not associated with postoperative KSKS. Although preoperative VM mCSA was not associated with postoperative KSFS, preoperative VM fatty infiltration ratio was significantly associated with postoperative KSFS (β = -2.046; p < 0.001). In multivariate linear regression analysis, age (β = -0.533; p = 0.020) and VM fatty infiltration ratio (β = -1.7444; p < 0.001) were significantly associated with postoperative KSFS.
Conclusion: Increased VM fatty infiltration was associated with worse functional outcomes after TKA. Preservation of VM quality may have the potential to improve functional outcomes after TKA and orthopedic surgeons should encourage patients to performed quadriceps strengthening exercise before TKA for maintenance of VM quality.
Figures
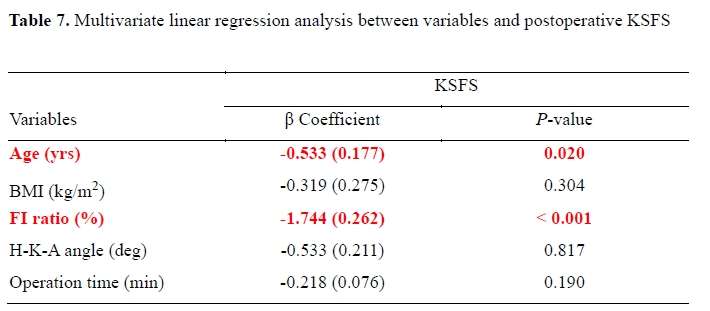
Figure 1
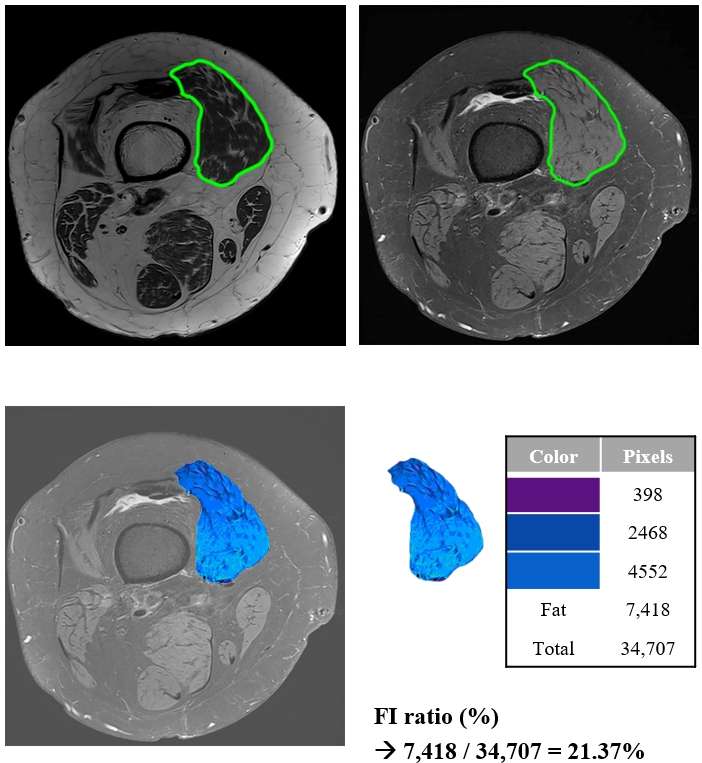
Figure 2#7331
Biomechanical Performance of Improved Designs of Tibial Component for Mobility Total Ankle Replacement
*Rajesh Ghosh - Indian Institute of Technology Mandi - Mandi, India
Jyoti Jyoti - IIT Mandi - Mandi, India
*Email: rajesh@iitmandi.ac.in
Introduction:
Mobility is one of the popular implants for total ankle replacement (TAR); however, its failure by aseptic loosening of the tibial component is a major cause of concern. Its tibial component design utilizes only one single stem to achieve fixation but the addition of pegs can improve its performance. The aim of the present study is to investigate the biomechanical performance of two improved designs of tibial component for Mobility TAR considering the implant-bone micromotion and tibial bone stresses (von Mises).
Methods:
The geometry of the bone was extracted from the CT data. The cortical bone was taken as homogeneous and the cancellous bone was given location-dependent heterogeneous material properties 1. The tibial and polythene components were modelled as linear elastic 2. Four finite element (FE) models were developed, one for the natural bone, one for the standard/ existing Mobility design with a single stem and two for the modified/improved designs i.e., Mobility with two pegs in the Anterior-Posterior (AP) direction and Mobility with two pegs in the Medial-Lateral (ML) direction to the main stem (Figure 1). The load 937.5 N was applied to the polythene component to represent the neutral loading condition. The implant-bone interface coefficient of friction was taken as 0.5. The proximal part of the tibia was fully constrained.
Results: The micromotions for the Mobility with a single stem design were maximum in the posterior portion of the stem; these values decreased with the addition of pegs (Figure 2). Also, for the tibial tray maximum micromotions were seen in the anterior portion for the single stem design, they became lesser and more uniform in the designs with pegs. The peak and mean values of micromotion were least for Mobility with two pegs AP design. The tibial bone stresses present in the natural model in the distal part of the tibia and medial malleolus were shielded by the implant in the model with a single stem by taking the bulk of the load (Figure 3). When compared to Mobility with a single stem the stress shielding was only affected slightly with the addition of pegs.
Conclusion: This study establishes that the addition of pegs to the tibial component improves the performance of Mobility TAR by reducing the peak micromotion and mean micromotion. The additional pegs do not affect the tibial stresses and stress shielding substantially. The Mobility with two pegs AP design is somewhat better than the Mobility with two pegs ML design when neutral loading is considered due to lesser micromotion.
References:
1. Mondal, S. & Ghosh, R. The Effects of Implant Orientations and Implant–Bone Interfacial Conditions on Potential Causes of Failure of Tibial Component Due to Total Ankle Replacement. J. Med. Biol. Eng. 39, 541–551 (2019).
2. Terrier, A., Fernandes, C. S., Guillemin, M. & Crevoisier, X. Fixed and mobile-bearing total ankle prostheses: Effect on tibial bone strain. Clin. Biomech. 48, 57–62 (2017).
Figures
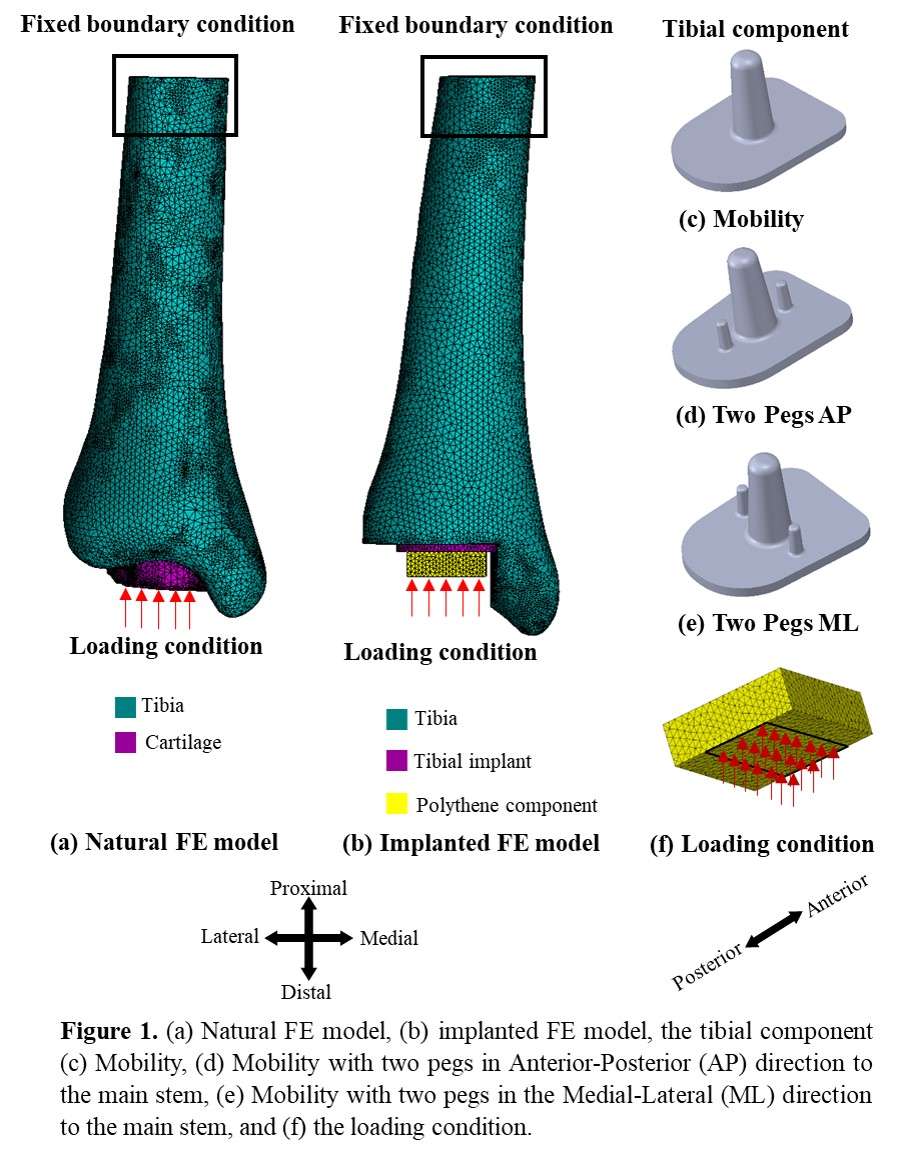
Figure 1

Figure 2
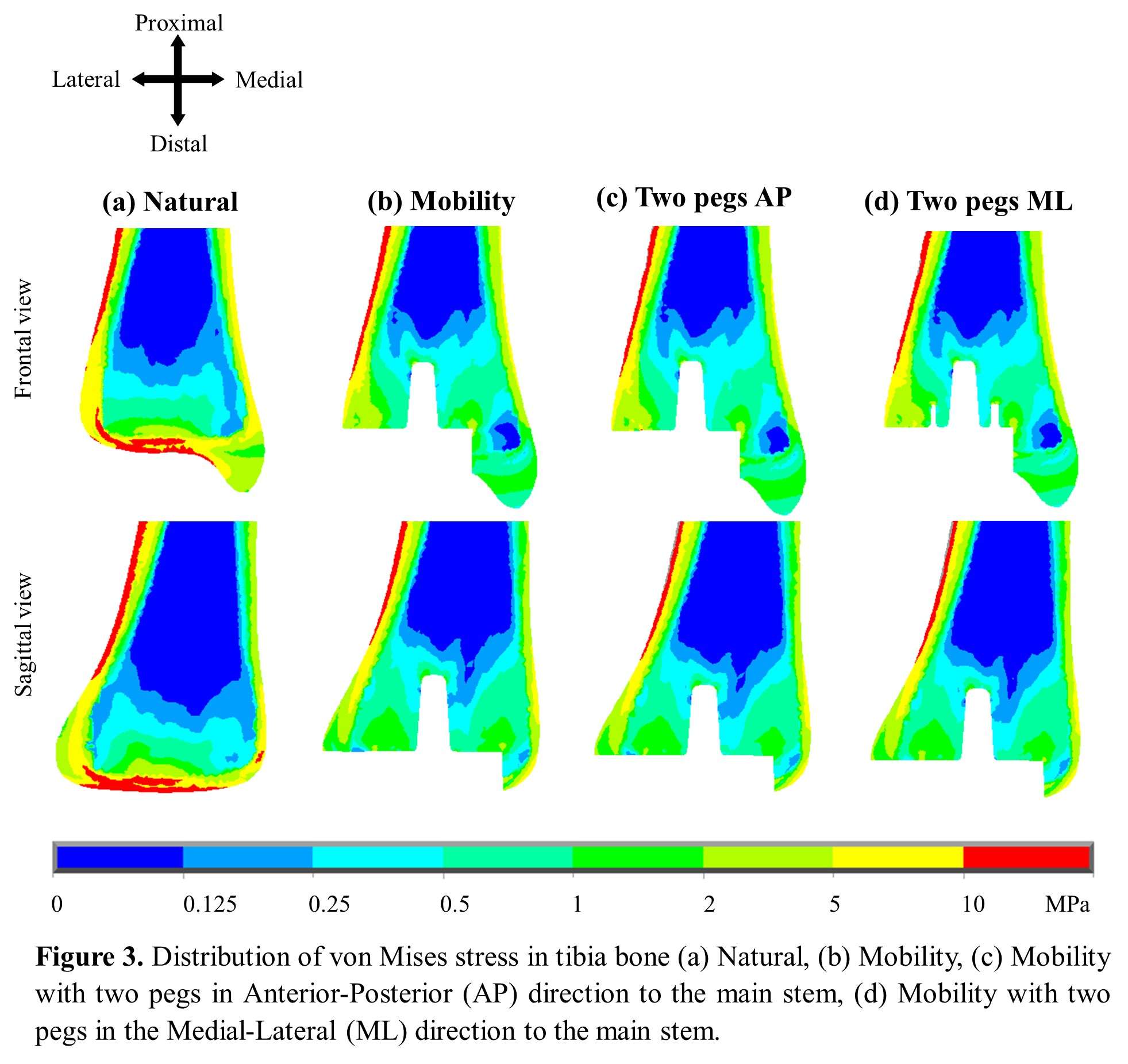
Figure 3#8020
Immersive Virtual Reality for Novice Scrub Nurses Improves Efficiency, Confidence and Knowledge in Learning Skills for Anterior Approach Total Hip Arthroplasty: A Randomised Controlled Trial
Thomas Edwards - Imperial College London - London, United Kingdom
*Jonathan Edwards - Imperial College - London, GB
Isabelle Poole - Imperial College - London, United Kingdom
Francesca Kablean-Howard - Imperial College London - London, United Kingdom
Kathryn King - King's College London - London, United Kingdom
Monil Karia - Imperial College London - London, United Kingdom
Julie Bliss - King's College London - London, United Kingdom
Alexander Liddle - Imperial College - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
Kartik Logishetty - Imperial College - London, United Kingdom
*Email: jonathanwedwards@me.com
Introduction: Superior team performance in surgery leads to fewer technical errors, reduced mortality and improved patient outcomes. Scrub nurses are a pivotal part of this team, yet they have very little structured training. This lack of training leads to high levels of stress, low confidence and concerns that their poor knowledge may cause patient harm. Furthermore, efficiency is paramount in arthroplasty surgery, with prolonged operations leading to a substantial increase in the risk of a serious complication. Immersive virtual reality (iVR) simulation is a low cost, easily accessible technology which allows novice scrub nurses to enter a virtual operating theatre and repetitively practise these skills in a risk-free environment. It has demonstrated excellent efficacy in training surgeons, however there is a paucity of literature investigating its role in training scrub nurses. This study examines the impact of iVR on acquisition of skill, knowledge and confidence for novice scrub nurses.
Materials and Methods: 60 undergraduate nursing students were included in this study and randomised in a 1:1 ratio to learning the scrub nurse role for an AA-THA using either conventional training or iVR. Participants were excluded if they had previously scrubbed for >5 AA-THA operations or had prior iVR surgical simulation experience. The conventional training was derived through expert consensus, consisting of a 1-hour seminar with a Q&A and 2 hours of e-learning in which participants were taught the equipment and sequence of steps. The iVR training consisted of 3 separate hour-long sessions where participants performed the scrub nurse role with an avatar surgeon in a virtual operation. The iVR outcomes were time taken to complete the virtual operation and dominant hand motion across the 3 training sessions. Real world transfer was assessed through improvement from baseline on an expert-derived theoretical knowledge test and self-perceived levels of confidence/ability as measured using a validated 5 point Likert scale.
Results: 53 participants successfully completed the study (26 iVR, 27 conventional) with a mean age of 31 ± 9 years. There were no significant differences in baseline characteristics or baseline knowledge test scores between the two groups (p>0.05). Procedure time decreased across the 3 sessions by 30.2%, dominant hand motion decreased by 7.7%. The iVR group demonstrated superior improvement in knowledge (84.2% vs 47.2%, p<0.0001) and significant improvements in confidence identifying, understanding and assembling equipment for the operation beyond that of the conventionally-trained group.
Conclusion: Immersive virtual reality training improves efficiency, knowledge and confidence for novice scrub nurses learning AA-THA. This easily accessible, low cost training modality could be integrated into scrub nursing curricula to address the current shortfall in training.
#8015
Immersive Virtual Reality Is Superior to Conventional Training for Novice Scrub Nurses Learning Anterior Approach Total Hip Arthroplasty: A Randomised Controlled Trial
*Thomas Edwards - Imperial College London - London, United Kingdom
Francesca Kablean-Howard - Imperial College London - London, United Kingdom
Jonathan Edwards - Imperial College - London, GB
Isabelle Poole - Imperial College - London, United Kingdom
Monil Karia - Imperial College London - London, United Kingdom
Kathryn King - King's College London - London, United Kingdom
Julie Bliss - King's College London - London, United Kingdom
Alexander Liddle - Imperial College - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
Kartik Logishetty - Imperial College - London, United Kingdom
*Email: thomas.edwards@imperial.ac.uk
Introduction: Superior team performance in surgery leads to fewer technical errors, reduced mortality and improved patient outcomes. Scrub nurses are a pivotal part of this team, however they have very little structured training. This lack of training leads to high levels of stress, low confidence and concerns that their poor knowledge may cause patient harm. Immersive virtual reality (iVR) simulation is a low cost, easily accessible technology which allows novice scrub nurses to enter a virtual operating theatre and repetitively practice these skills in a risk-free environment. It has demonstrated excellent efficacy in training surgeons, however there is a paucity of literature investigating its role in training scrub nurses. This randomised study therefore investigates the impact of an iVR curriculum on training prospective scrub nurses in performing their role in an anterior approach total hip arthroplasty (AA-THA).
Methods: 60 undergraduate nursing students were included in this study and randomised in a 1:1 ratio to learning the scrub nurse role for an AA-THA using either conventional training or iVR. Participants were excluded if they had previously scrubbed for >5 AA-THA operations or had prior iVR surgical simulation experience. The conventional training was derived through expert consensus, consisting of a 1-hour seminar and 2 hours of e-learning where participants were taught the equipment and sequence of steps. The iVR training involved 3 separate hour-long sessions where participants performed the scrub nurse role with an avatar surgeon in a virtual operation. The primary outcome was their performance in a physical world practical assessment with real equipment, where participants were asked a series of questions designed to reflect the knowledge and skills needed to perform their role in the operation. This assessment was developed and validated using a modified Delphi process with a panel of experts consisting expert scrub nurses, surgeons and industry representatives.
Results: 53 participants successfully completed the study (26 iVR, 27 conventional) with a mean age of 31 ± 9 years. There were no significant differences in baseline characteristics or baseline knowledge test scores between the two groups (p>0.05). The iVR group significantly outperformed the conventionally trained group in the real-world assessment, scoring 66.9 ± 17.9% vs 41.3 ± 16.7%, p<0.0001.
Conclusion: Immersive virtual reality training was superior to conventional training in teaching novice scrub nurses to perform their role in AA-THA surgery. This easily accessible, low cost training modality could be integrated into scrub nursing curricula to address the current shortfall in training.
#7529
National Trend of Total Hip Arthroplasty in Japan From the Database on Hospital Charge
*Masaru Kadowaki - Shimane University - Izumo, Japan
Yuji Uchio - Department of Orthopaedic Surgery Shimane University
*Email: masaru11@med.shimane-u.ac.jp
Introduction: A new calculation method of hospital charges, based on the combination of diagnostic procedures, was introduced in Japanese hospitals this decade. Each hospital reports items about patients' characteristics and information on hospital charges to the National Institute of Health and Labor. This database is open to the public and available for analysis. The study aimed at revealing the national trend of total hip arthroplasty (THA) in Japan.
Method: Data from the national database, on patients who underwent primary THA from 2006 to 2017, were extracted and analyzed. Number of surgeries, ratio of males to females, age at surgery, condition requiring surgery, and duration of hospital stay were investigated.
Results: As the number of hospitals that used this method increased, the number of THA surgery entries also increased from 4,227 surgeries in 2006 to 15,039 in 2012 and 37,421 in 2017[Fig.1]. The male (18%) to female (82%) ratio was almost always constant. The proportion of patients aged above 80 years at surgery increased from 7.6% in 2006 to 10.1% in 2012 and 13.7% in 2017, whereas that of patients aged 41-60 years at surgery gradually decreased from 34.7% in 2006 to 25% in 2017 [Fig.2]. About the condition that necessitated surgery, primary osteoarthritis was the most frequent at 38~40%, followed by secondary osteoarthritis, including hip dysplasia, at 32~34%, and osteonecrosis at 10% during the period [Fig.3]. Mean hospital stay gradually decreased annually from 34.9 days in 2006 to 23.3 days in 2017.
Conclusion: The age of the population undergoing THA increased with the aging of society. Minimally invasive techniques have become popular and may allow early discharge.
Figures
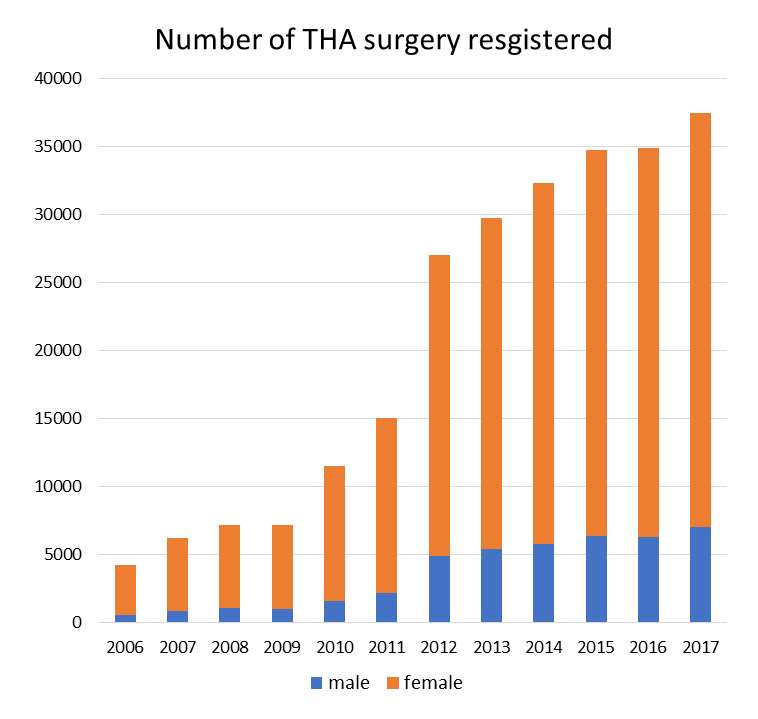
Figure 1
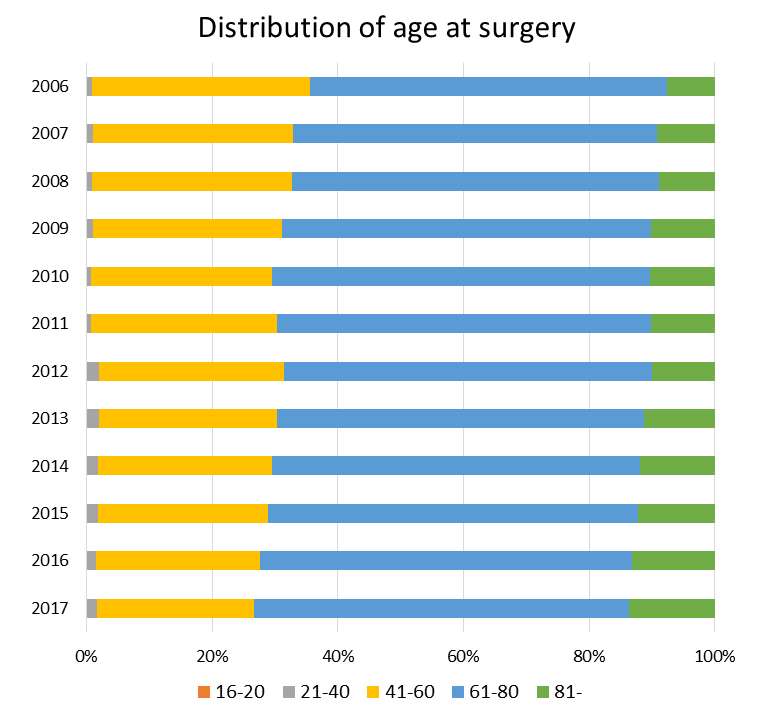
Figure 2
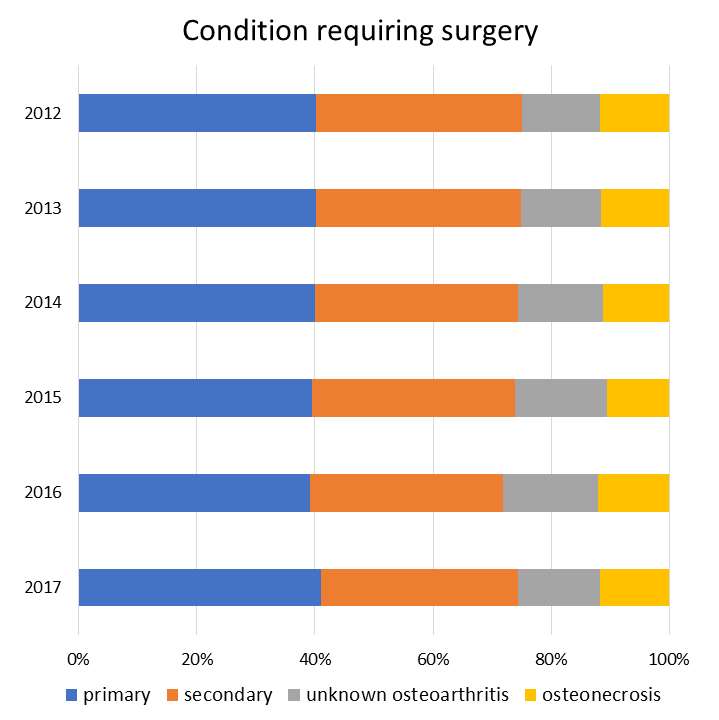
Figure 3#7292
Comparative Biotribological Analysis of Explanted NuNec, Mobi-C and Discocerv Cervical Discs
*Göksu Kandemir - Newcastle University - Newcastle Upon Tyne, United Kingdom
Thomas Joyce - Newcastle University - Newcastle upon Tyne, United Kingdom
*Email: goksu.kandemir@newcastle.ac.uk
Introduction: Cervical total disc replacement (TDR) is an alternative to the gold-standard anterior cervical discectomy and fusion which aims to relieve pain and restore the natural motion of the cervical spine [1]. However, the biotribological performance of cervical TDRs is not well known. Therefore, explant analyses are essential to provide such understanding.
Materials and methods: The analysis was conducted at the nano and macroscales using three different contemporary cervical discs, namely, the NuNec (self-mating, all-polyether ether ketone (PEEK), semi-constrained, 2 years in-vivo), Mobi-C (metal-on-polymer (cobalt chromium-on-ultra high molecular weight polyethylene (UHMWPE)), non-constrained, 6 years in-vivo) and Discocerv (ceramic-on-ceramic (alumina-on-zirconia), semi-constrained, 1-year in-vivo) cervical discs (figure 1). The surface topographies of the articulating surfaces of the explants were analysed using a Zygo NewView 5000 non-contacting profilometer. The roughness measurements were compared with the data reported for unworn surfaces that were made from the same materials and had the same geometry as the articulating surfaces of the explants. Dimensional measurements were taken using a Mitutoyo non-contacting vision measuring machine. For the semi-constrained discs, the predominant lubrication regime was estimated using the theoretical elastohydrodynamic lubrication theory.
Results and discussion: The average roughness of the explanted NuNec inferior cup and the superior head was 0.067 ± 0.056 µm and 0.037 ± 0.023 µm, respectively. The inferior and superior endplates of the explanted Mobi-C disc had an average roughness of 0.055 ± 0.020 µm and 0.016 ± 0.006 µm, the inferior and superior surfaces of the explanted Mobi-C insert had an average roughness of 0.446 ± 0.083 µm and 1.210 ± 0.154 µm, respectively. The inferior cup and the superior head of the explanted Discocerv disc had an average roughness of 0.015 ± 0.002 µm and 0.016 ± 0.003 µm, respectively. Boundary lubrication regime was found to be the predominant regime for the semi-constrained discs.
Compared to unworn surfaces (figure 2), PEEK, CoCr and ceramics surfaces roughened in vivo, whereas both surfaces of the UHMWPE surfaces became smoother.
This was the first study that investigated the biotribological performance of the NuNec, Mobi-C, and Discocerv cervical discs. The articulating surfaces of the semi-constrained discs showed less damage than the non-constrained disc, although the ceramic surfaces showed dark grey wear marks, similar to the ones observed on explanted ceramic hips [2]. In addition, traces of impingement were observed at the metallic rims of the articulating surfaces of the ceramic-on-ceramic Discocerv disc. The surfaces of the metal-on-polymer Mobi-C disc showed significant damage; the inferior endplate lost its shiny appearance. The insert was significantly damaged (figure 1) due to excessive migration. Traces of impingement was observed on the endplates.
Conclusions: The non-constrained Mobi-C disc showed significantly more damage than the explanted NuNec and the Discocerv discs, mainly due to excessive migration of the polymeric insert which took place in vivo.
References
[1] T. M. Grupp et al., “Alternative bearing materials for intervertebral disc arthroplasty”, Biomaterials, 2010; 31(3):523-531
[2] A. Ruggiero et al., “Metal transfer and surface roughness in ceramic femoral heads: recent investigations and future research trends”, Conference ECOTRIB, 2017.
Figures
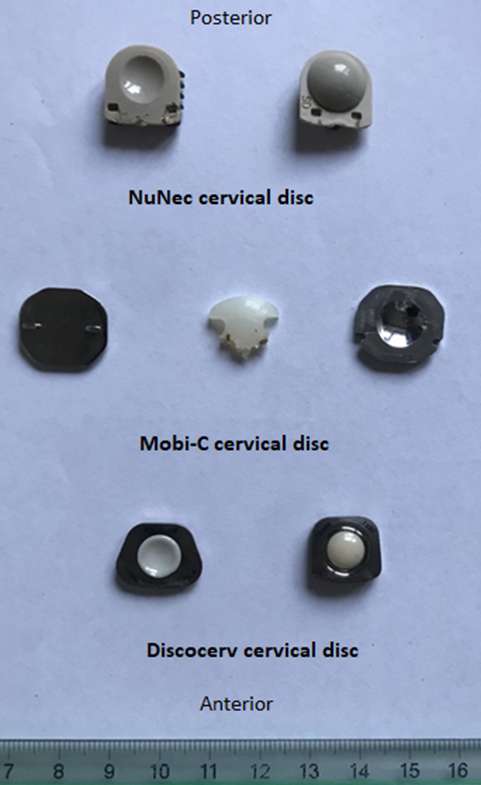
Figure 1
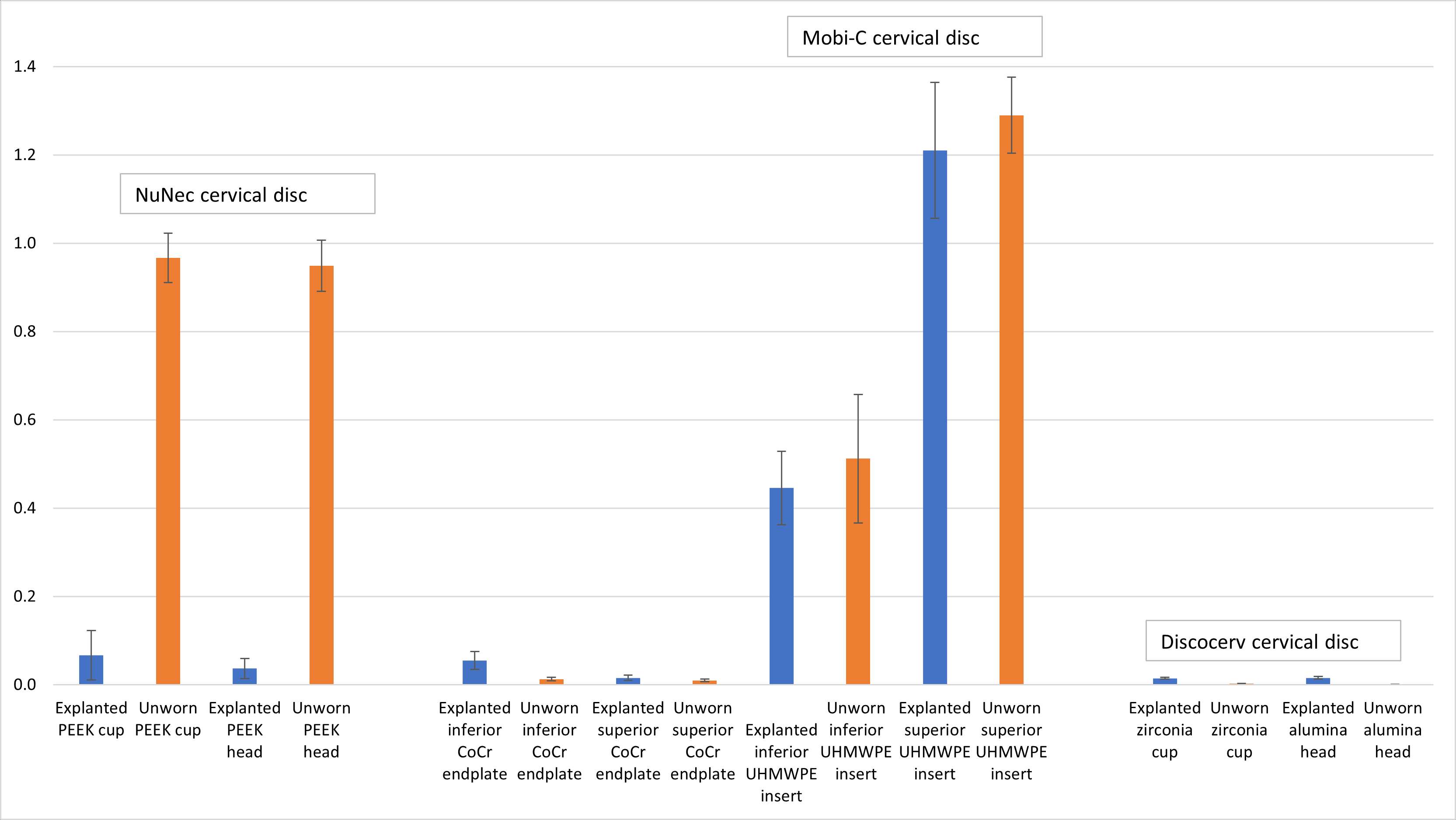
Figure 2#8016
Component Positioning and Limb Alignment Restoration Using an Imageless, Robotic-Assisted Total Knee Arthroplasty Technique
*Bertrand Kaper - Orthopaedic Specialists of Scottsdale - Scottsdale, USA
Marco Kaper - USA
*Email: bonebroke@yahoo.com
Introduction: Robotic-assisted (RA) surgical techniques have been introduced to improve the surgical performance of and the outcomes in total knee arthroplasty (TKA). The ability of this RA technology to achieve desired component position and limb alignment restoration needs to be thoroughly understood. The objective of this study was to evaluate the effectiveness of an imageless, handheld RA-TKA technique to achieve accurate and precise post-operative component positioning and limb alignment.
Methods: This study was designed as a retrospective analysis of a non-randomized, single-blinded study. One-hundred and ninety-four patients who underwent primary TKA were studied. Pre-operative alignment, intra-operative, and post-operative component orientation and alignment were documented. Average and absolute deviations between the intra-operative and post-operative component position, as well as the planned and achieved alignment were analyzed. Data cohort subsets were analyzed for potential confounding factors.
Results: The absolute angular deviation from the specified target component orientation, a measure of technique accuracy, was demonstrated to be less than 1° for all parameters assessed: 0.8° for DFA, 0.9° for FF, 0.6° for PTA, and 0.8° for TS. The mean angular deviation from final intra-operative measurements for the entire study cohort, as a measure of reproducibility, was also noted to be less than 1° for all parameters assessed: 0.3° for DFA, 0.7° for FF, 0.0° for PTA, and 0.9° for TS. The average angular deviation from the planned alignment was 0.1°. The absolute deviation was on average 1°, with 98.5% of all cases demonstrating <3° deviation from planned alignment. In cases with known pre-operative risk factors such as obesity and substantial pre-operative limb malalignment (>7° of varus or valgus), surgical plan was not compromised.
Conclusions: Imageless robotic-assisted TKA produces highly accurate and reproducible post-operative outcomes about both component orientation and restoration of planned limb alignment.
Figures
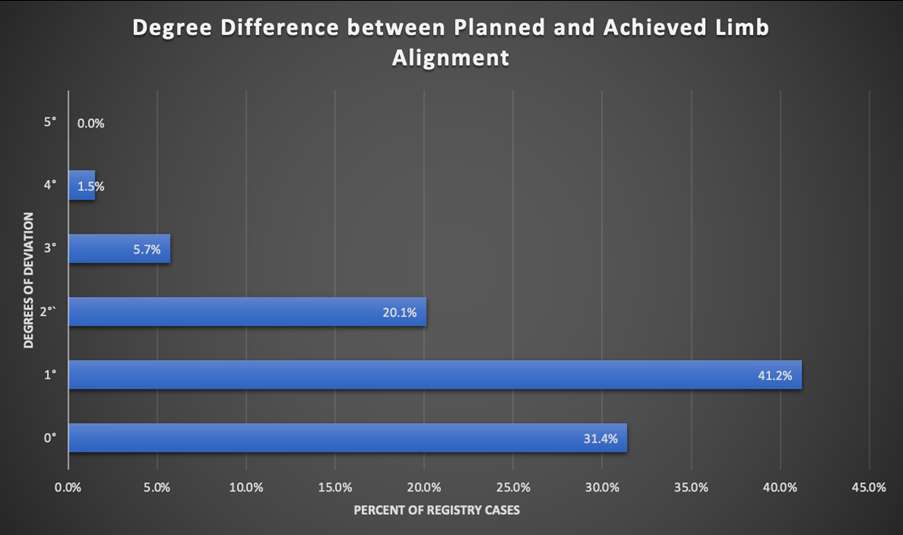
Figure 1#7550
A Case of THA Revision Due to Trunniosis: a Case Report
Toyohiro Kawamoto - Kawasaki Medical School - Kurashiki city, Japan
Yoshifumi Namba - Kurasiki-city, Japan
Shigeru Mitani - Kawasaki Medical School - Kurashiki-city, Japan
*Hirosuke Endo - Japan - krashiki, Japan
*Email: hirosukeendol@yahoo.co.jp
A 35-year-old male (height 174 cm, weight 65.6 kg, BMI 21.7), working in manufacturing, suffered a left femoral neck fracture due to traffic trauma at the age of 16. Seven years later, he developed pain due to traumatic osteonecrosis and underwent THA with a Stryker ADEPT®️ cup and CentPillar ®︎ stem via a posterior approach with a metal-on-metal, 46 mm head. He was pushing a 400 kg cart every day at work. 12 years after THA, he felt discomfort in his left hip joint, then abnormal sound and pain appeared when he walked, and he visited his local doctor. The patient was referred to our clinic with suspicion of fracture at the neck area on radiograph. Allogeneic bone grafting was performed from a bone bank.
The cause of trunnionosis is thought to be the high torque and high workload of the large-diameter head, which resulted in a defect at the neck.
#7967
Does Previous Hip Osteotomy Affect Cementless Conversion Total Hip Arthroplasty?
*Tsutomu Kawano - Kyushu Rosai Hospital - Kitakyushu City, Japan
Kyohei Shiomoto - Kyushu Rosai Hospital - Kitakyushu, Japan
Satoshi Shin - Kyushu Rosai Hospital - Kitakyushu, Japan
*Email: tsutomu417@gmail.com
Background
As the previous hip osteotomies may alter the anatomies, and the deformities following the progression of the hip arthritis would be severe compared to the common hip arthritis, therefore, performing the hip arthroplasty (THA) after the hip osteotomy is considered to be technically challenging. Furthermore, because of the effect of previous operation on both bone and soft tissues, outcomes of the THA after the hip osteotomy remain controversial, compared to the routine THA.
Objectives
The clinicoradiologic outcomes of the THA after the hip osteotomy were reviewed retrospectively. We focused on these questions regarding the THA after the hip osteotomy as follow: How cementless THA can be performed? Are the clinical outcomes equivalent to the routine THA?
Study Design & Methods
Between 2009 and 2017, 54 hips in 52 patients underwent cementless THA following hip osteotomy at our institution. Previous osteotomy at the pelvic side and the femoral side had been performed for 23 hips and 34 hips, respectively. The interval between osteotomy and conversion THA was averaged 23.4 years. The mean follow-up period for this series was 4.5 years. A radiographic examination was performed at three months after THA and a clinical assessment was performed at the final follow-up using Japanese Orthopaedic Association (JOA) hip score.
Results
Compared with the mean operative time in the routine THAs (103min), there was significant difference was observed in the THAs after the hip osteotomy (133min), and the mean operative blood loss was 400ml. All the THAs after the hip osteotomy underwent using the hemispherical cementless cups and the monoblock cenentless stems, and no bulkbone augmentation to the acetabular defect was performed. Radiographic examination showed the high hip centre with the distance from the head centre to the interteardrop line > 30 mm in 6 hips (11.8 %), and excessive stem anteversion measured by computer tomography > 50 degrees was observed in 1 hip.
THA provided significant relief of pain and improvement in function for all patients, and the mean JOA hip score in the THAs after the hip osteotomy was similar to the routine THAs. However, there were nine patients in this series who were taken the routine THA in the contralateral side, and four of them showed slight lower score in the THA after the hip osteotomy than in the contralateral routine THA.
Conclusions
Our data revealed the acceptable hip centre height and appropriate stem alignment in most of the conversion cementless THAs without bulkbone graft. Furthermore, the favorable clinical outcomes were also achieved in the THA after the hip osteotomy. On the other hand, inferior outcome of the THA after the hip osteotomy may be concerned if compared with the contralateral routine THA.
#7503
Miniaturised Instrumentation for the Detection of Impingement Events in Total Hip Replacements
*Matthew Shuttleworth - University of Leeds - Leeds, Select Country
Oliver Vickers - University of Leeds - LEEDS, GB
Tim Board - Wrightington, Wigan & Leigh NHS Foundation Trust - Wigan, United Kingdom
Graham Isaac - University of Leeds - Leeds, United Kingdom
Peter Culmer - University of Leeds - Leeds, United Kingdom
Sophie Williams - University of Leeds - Leeds, United Kingdom
Robert Kay - University of Leeds - Leeds, GB
*Email: m.p.shuttleworth@leeds.ac.uk
Introduction
Impingement in total hip replacements (THR) can lead to issues including accelerated implant wear, joint instability and pain. Whilst the effects of impingement have been reported, to-date methods of recording the occurrence, location or severity of impingement under typical real-world motions have not been reported.
Advances in microelectromechanical systems (MEMS) have allowed miniaturised sensory devices, such as inertial measurement units (IMUs) to become increasingly accurate while reducing their physical size. This study details the initial development and validation of an inertial-tracking method, using an IMU, for inferring the occurrence, location and duration of impingements events in conventional THR’s, without line of sight.
Methods
Impingement events were recreated using a robot arm (UR3, Universal Robots, Denmark) by articulating a 3D printed polymer (PETG) femoral stem and cobalt chrome head, in a horizontally mounted acetabular shell and polyethylene liner. The inertial impingement inference device was mounted to the stem and starting from a vertical inclination was pivoted downwards using the robot arm until impingement occurred; upon which, it partially retracted and at a new polar location repeated the process. This was performed at 32 unique locations around the circumference of the liner and the experiment was repeated 5 times. To signal the robot to retract, self-adhesive copper tape (PRO 25mm Copper Tape, RS Components, UK) was moulded around the stem and the rim of the implant that would contact during impingement, forming electrical continuity. These were connected to inputs on the control box of the robot arm using wires soldered to the tape. The setup is illustrated in Figure 1.
Robot and tracker data was recorded synchronously during the experiments and at points when impingement occurred a marker was added to the data. For the trackers impingement was inferred whenever the measured inclination was greater than a threshold angle calculated from 3D models of the components. For the robot this was whenever there was electrical continuity.
Results
Upon comparison with the inclination from the robot arm, the tracker measurement error was found to be on average 0.01°±0.26° (mean±SD), and was consistent in location around the liner between tests. In total 160 impingements events were recorded, with the tracker detecting 93.8% of these to within 1.0° of the true value. Observing the pattern of peak inclination (Figure 2) shows repeated over- and under-shooting on opposing sides of the liner by equal amounts. This indicated a small degree of angular misalignment of the liner to the robot arm.
Conclusion
This work has documented for the first-time a non-contact method for the detection of impingement in THR’s during dynamic testing. The measurement accuracy of the device consistently matched the outputs of the test equipment, with a 93.8% success rate for detection. The introduction of a second tracker to measure relative liner inclination could be used to further enhance the system by accounting for relative positioning of the stem to the liner.
Acknowledgements
This work was funded by the UK Engineering and Physical Sciences Research Council (EP/R003971/1)
Keywords
Total Hip Replacement, Impingement, Sensor, Tracking
Figures
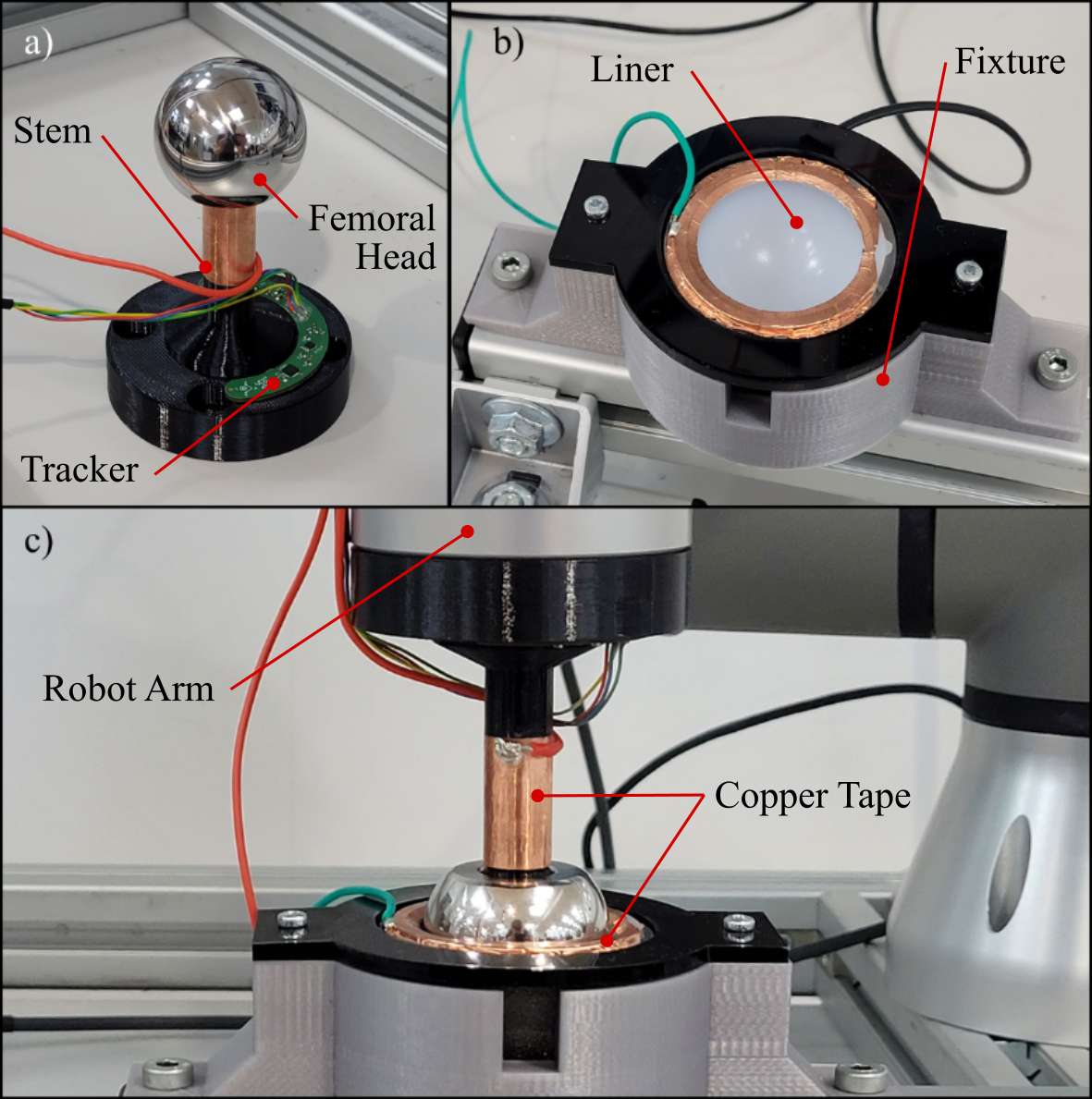
Figure 1
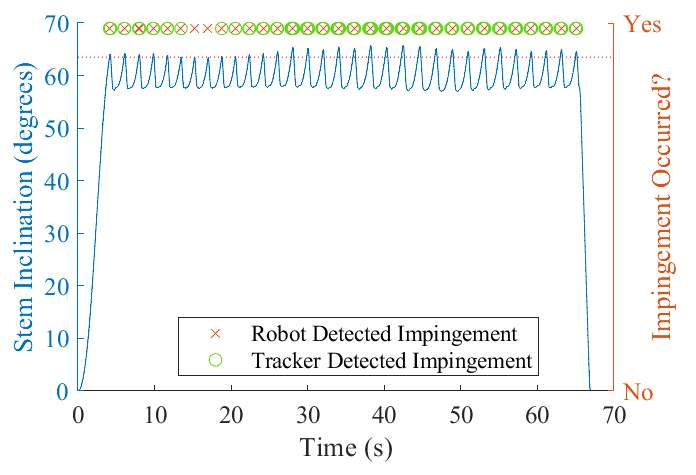
Figure 2#7356
Increasing Nodal Connectivity Increases the Fatigue Strength of Lattice Structures
*Stylianos Kechagias - Imperial College London - London, United Kingdom
Reece Oosterbeek - Imperial College London - London, United Kingdom
Maxwell Munford - Imperial College London - London, United Kingdom
Shaaz Ghouse - Imperial College London - London, United Kingdom
Jonathan Jeffers - Imperial College London - London, United Kingdom
*Email: s.kechagias20@imperial.ac.uk
Introduction
Lattice structures are widely used in orthopaedic implants owing to their ability to promote osseointegration and eliminate stress shielding. High open porosity, typically more than 70%, is essential to provide space for bone in-growth and to lower the stiffness of a lattice. Although built by materials which are many times stiffer than bone when in solid form, additively manufactured lattices can be designed with controllable micro-architecture and tailored mechanical properties which match the ones of bone and maintain its physiology upon implantation. However, high porosities lead to significant reduction in fatigue strength of lattices which hinders their use in load-bearing implants which are subject to cyclic loading.
Early studies on cellular materials, like foams and lattices, have shown that their structural material, porosity and topology can regulate their yield strength and stiffness. This study aims to investigate how topology (specifically nodal connectivity) of lattices can further affect their fatigue performance.
Methods
Stochastic lattices were designed by filling a design volume with randomly distributed points which were connected to each other with struts based on a desired connectivity and number of struts (strut density). Cylindrical specimens were designed using constant strut density of 5 struts per mm3 and four levels of nodal connectivity Z (4, 8, 12, 14). Lattices were then fabricated via Selective Laser Melting using pure titanium powder and two nominal strut thicknesses t (230 and 300 μm).
Quasi-static compression tests were carried out to calculate the elastic modulus E and the yield strength Sy (n=5 per design). Subsequently, compression-compression fatigue tests were performed at 15 Hz with R=0.1. Five stress levels (80%, 65%, 50%, 35%, and 25% of Sy) were tested to produce S-N curves (n≥2 per stress level per design), while the staircase method was used to estimate the fatigue strength at 1mllion cycles (n=6 per design).
Results
Results validated that increasing connectivity and strut thickness – over constant strut density – decrease porosity which results in an increase in stiffness, yield, and fatigue strength (see Figure 1). Regarding static properties, lattices designed with different values of connectivity and strut thickness exhibited a wide range of stiffness values (0.3-2.5 GPa) similar to the stiffness range of cancellous bone while maintaining high porosity (>79%). From fatigue data, S-N curves (see Figure 2) further demonstrated that increasing connectivity improves the fatigue life of structures since high connectivity lattices could bear higher stress levels for the same number of cycles. When comparing lattices of constant porosity (79%), lattices with Z=14 and t=230μm demonstrated 62% higher fatigue strength (at 1million cycles) compared to lattices with Z=4 and t=300μm.
Conclusion
Increasing nodal connectivity increases stiffness and fatigue life of lattice structures over constant strut thickness or porosity. This means that lattice-based implants can be designed with different connectivity levels to meet different static and fatigue requirements without being dependent solely on controlling strut thickness which is the current golden standard.
Figures
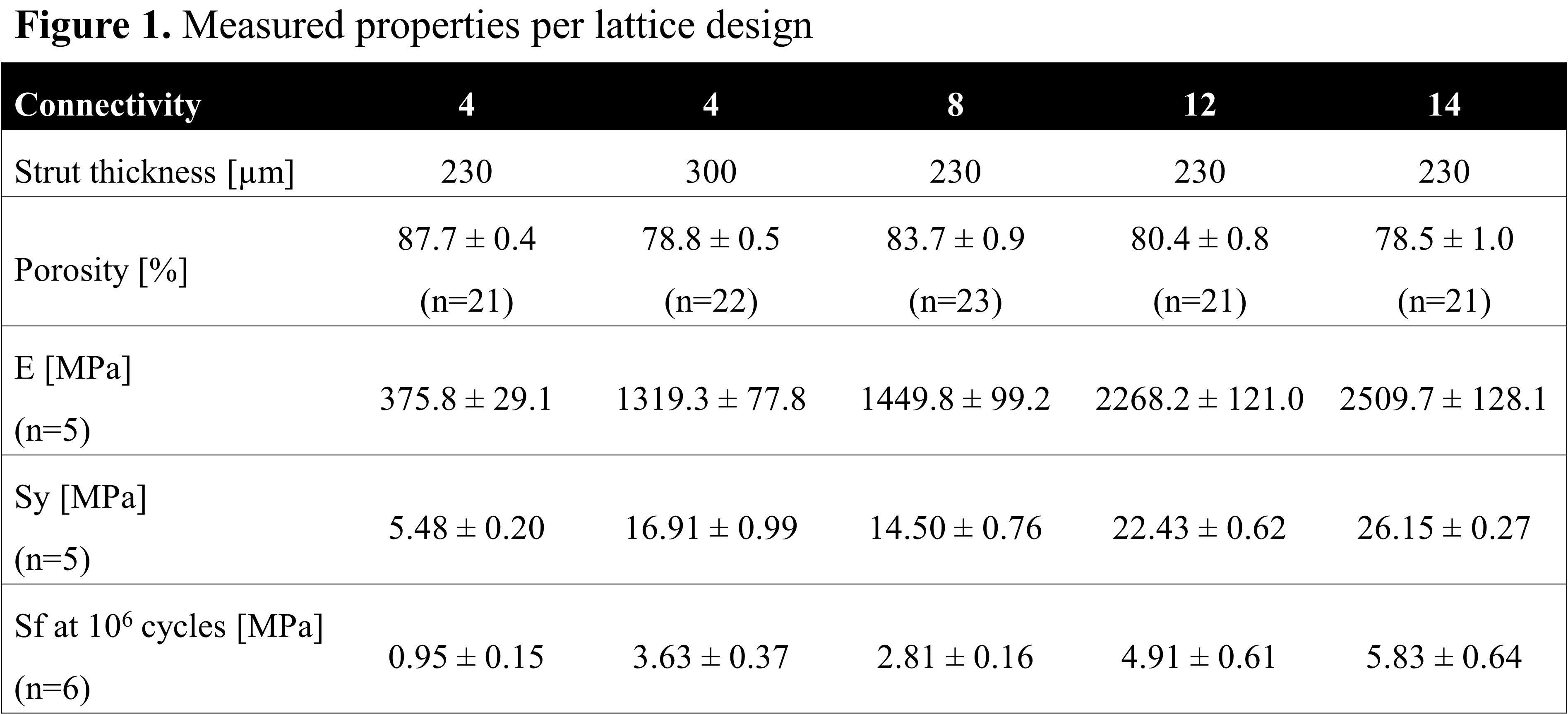
Figure 1
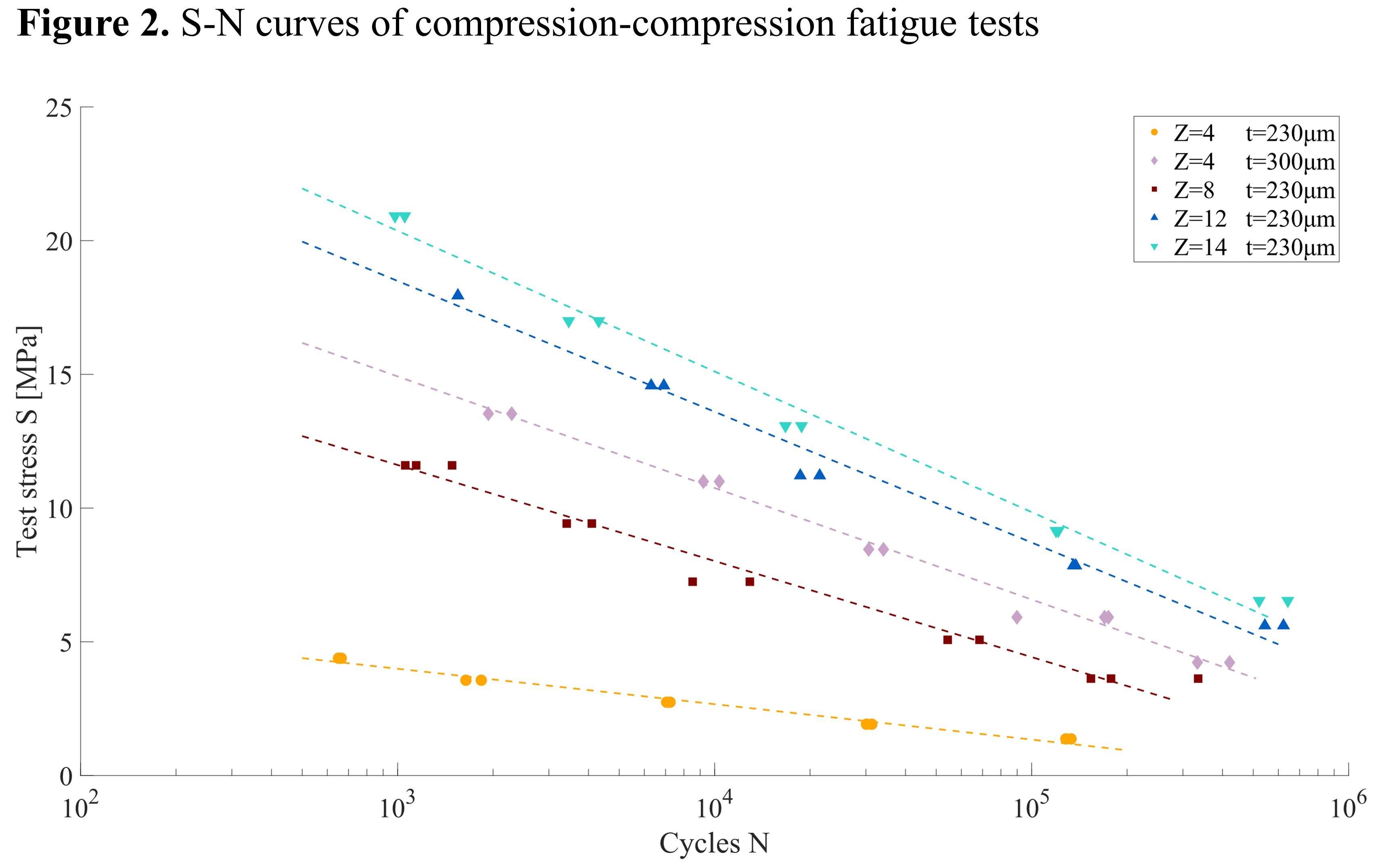
Figure 2#7494
Optimised Subtrochanteric Canal Fill Ratio Prevents Subsidence of Cementless Stem in Femoral Neck Fracture in Elderly
*Yuttana Nilanont - Phyathai2 International Hospital - Bangkok, Thailand
Saradej Khuangsirikul - Phramongkutklao Hospital - bangkok, Thailand
Danai Heebthamai - Phramongkutklao Hospital - Bangkok, Thailand
Thanainit Chotanaphuti - Phramongkutklao Hospital - Bangkok, Thailand
*Email: chengo071@hotmail.com
Introduction: Femoral neck fracture is a common orthopedic challenge in aging population because of high failure and mortality rate. Hip arthroplasty shows an excellent outcomes and reduces the risk of revision surgery for the displaced femoral neck fracture. Nowadays, the cementless stem has good survivorship, no risk of cement implantation syndrome, and less operative time comparing to cemented stem. Several factors, such as femoral canal morphology, prosthetic design, and surface coating, are studied to predict the outcome of the cementless stem. This study aims to analyse (1)relationship between subsidence of cementless stem and canal fill ratio at 4 locations (2)relationship between subsidence and Dorr type in femoral neck fracture, and (3)relationship between femoral neck fracture and femoral morphology according to Dorr type.
Methods: The digital radiographs of femoral neck fracture in Thai population who undergone hip arthroplasty with collarless, fully HA-coated, single wedge taper stem from 2011 to 2019 were reviewed. Age, gender, Dorr type, subsidence of stem[Fig.1] and canal fill ratio were measured at 4 locations[Fig.2]; 2 cm above lessor trochanter (LT), at level of LT, 2 cm below LT, and 7 cm below LT. Stem subsidence were recorded postoperatively at 6 weeks, 3 months, 6 months, 1 year, and then annually. The threshold of subsidence > 3 mm was considered as significant migration.
Results: A multivariate regression analysis was done in 207 hips (49 males, 158 females) with average age of 74.2 (range, 52-98 years)[Fig.3]. 22 hips(10.6%) of Dorr A, 97 hips(46.9%) of Dorr B, and 88 hips(42.5%) of Dorr C were analysed[Fig.4]. 48 hips(23.2%) were subsidence > 3 mm and subgroup analysed to Dorr type A 3 hips(6%), Dorr type B 20 hips(42%), and Dorr type C 25 hips(52%)[Fig.5]. Dorr type B group had statistically significant relationship between subsidence of stem and canal fill ratio at level of LT (P<0.016) and 2 cm below LT (P<0.030). The greater canal fill ratio of more than 70% at LT level and more than 73% at 2 cm below LT could prevent stem subsidence[Fig.6]. There was no significant relationship between canal fill ratio and subsidence of stem in Dorr type A(P<0.41) and Dorr type C(P< 0.28)[Fig.3]. Although many cases showed stem subsidence more than 3mm, but there was no clinical symptom or revision after 2-year follow-up.
Conclusion: This study showed stem subsidence in all Dorr types. The Dorr type A group had least subsidence. Optimised subtrochanteric canal fill ratio could be a good predictor for stem stability in Dorr type B. However, there was no association in Dorr type C group. We recommend the stem sitting proud technique, collared stem, or cemented stem in Dorr C femoral canal.
Keyword:Fracture neck of femur, Subsidence of cementless stem, Subtrochanteric canal fill ratio, Dorr type
Figures
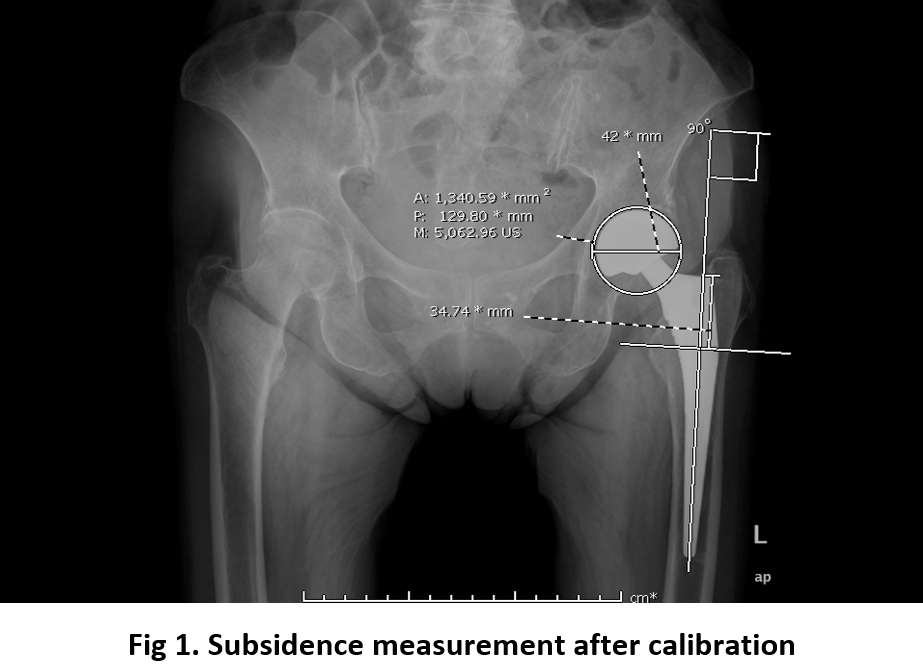
Figure 1
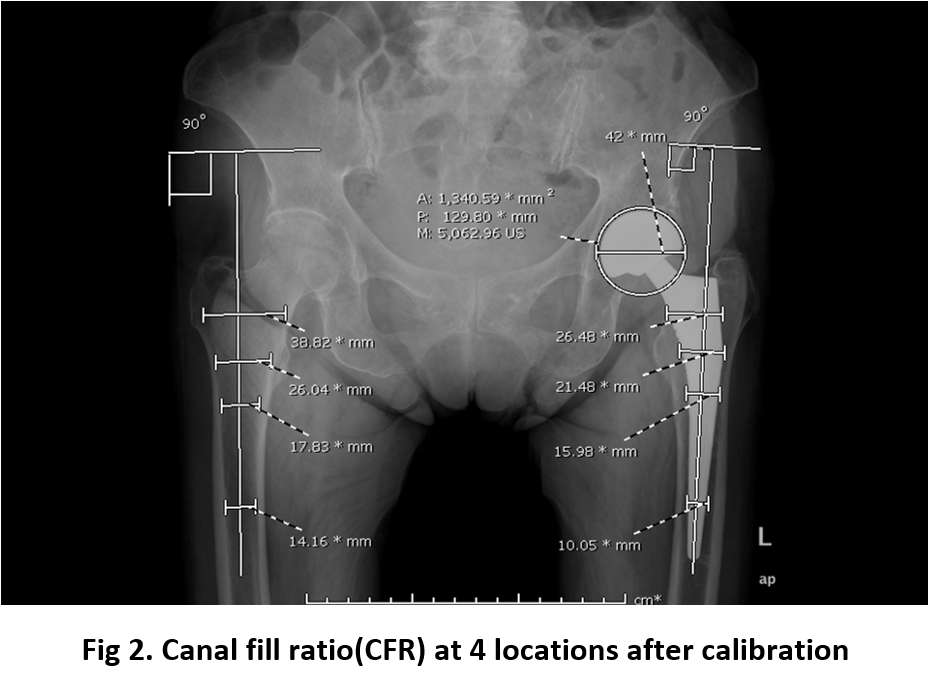
Figure 2
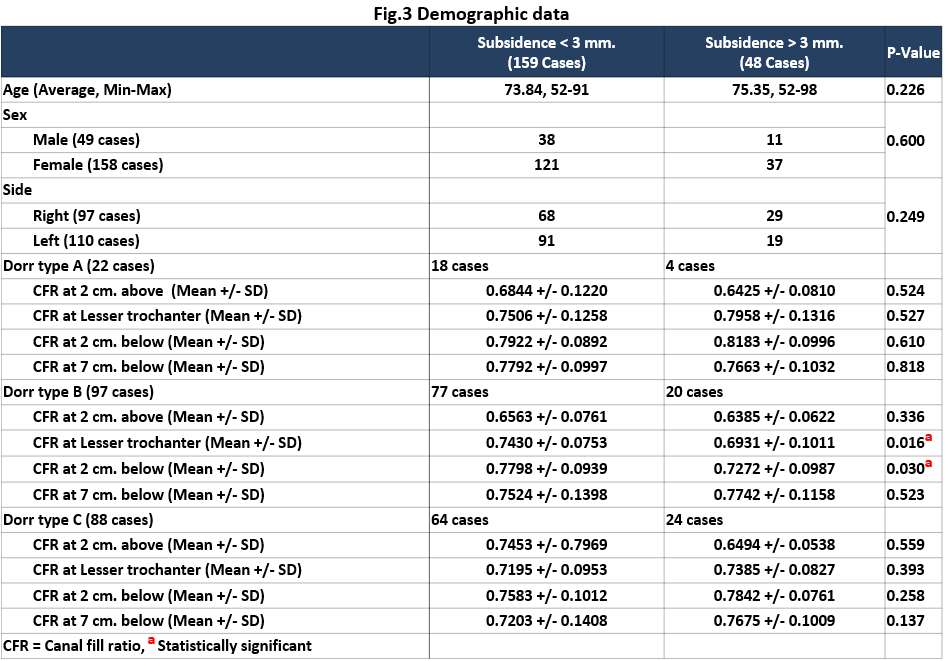
Figure 3
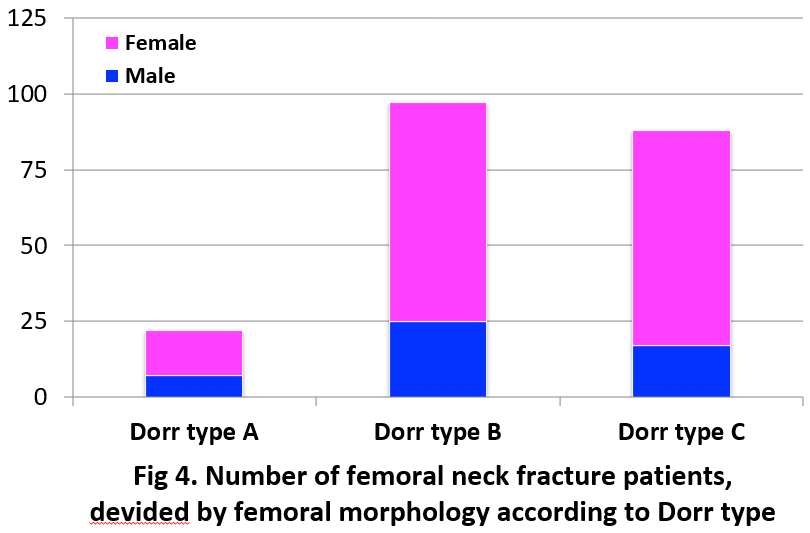
Figure 4
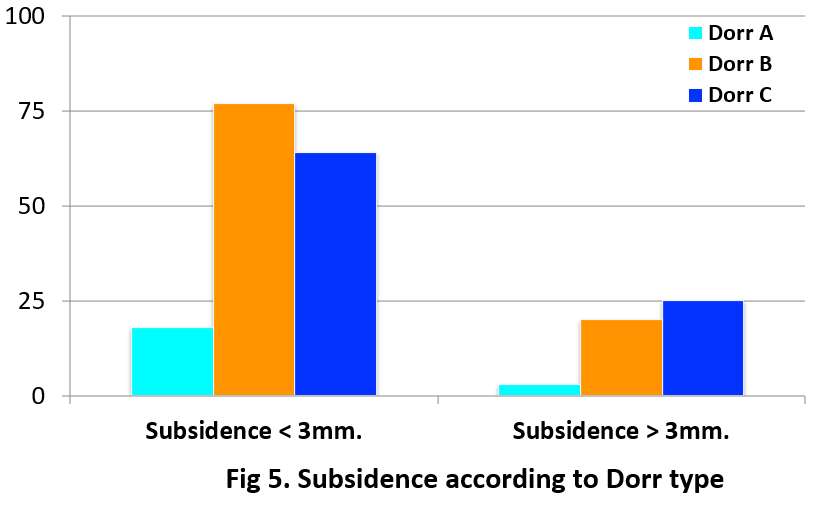
Figure 5
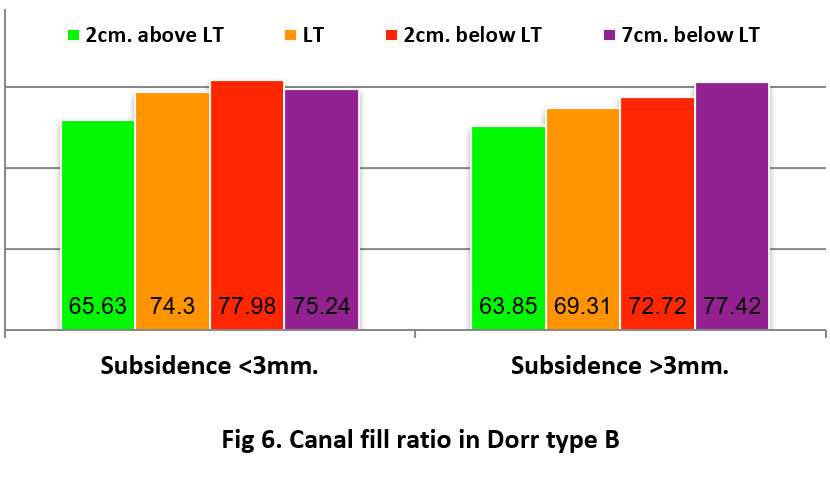
Figure 6#7580
Levels of Constraint Affect Functional Outcome of Femoral Sleeve in Revision Total Knee Arthroplasty
*Phatrapol Sthavorn - Phramongkutklao Hospital - Bangkok, Thailand
Saradej Khuangsirikul - Phramongkutklao Hospital - bangkok, Thailand
Thanainit Chotanaphuti - Phramongkutklao Hospital - Bangkok, Thailand
Danai Heebthamai - Phramongkutklao Hospital - Bangkok, Thailand
*Email: p.sthavorn@gmail.com
Revision total knee arthroplasty is a challenging procedure,resulting in a gradual increase in its necessity.Some main obstacles that we encountered are bone loss and quality of soft tissue.Usually, a metaphyseal sleeve is used in metaphyseal bone loss. However, different constrains utilizes the same metaphyseal sleeves. Factors which determine constrain type includes collateral ligament insufficiency, severity of varus or valgus deformity, gross flexion, extension gap imbalance, and hyper-laxity. These problems can be fixed with constraint prosthesis such as varus-valgus constrain and rotational hinge knee. Our study was designed to demonstrate the level of constrain that affects functional outcome of femoral sleeve in various types of revision total knee arthroplasty. We measure KOOS score, canal filled ratio and survival rate in different level of constrains to find correlation among these types of prosthesis.
From September 2012 to December 2020, we retrospectively analyzed all revision total knee arthroplasty in our institute. This retrospective study involved moderate to severe bone loss as classified by the AORI; 100 cases were included into the study. Mean postoperative KOOS score was lowest in rotational hinge knee prosthetic especially those caused by hyper-laxity. Most failure cases in all groups were peri prosthetic infection resulting from 4 out of 5 cases. A satisfactory canal filled ratio of 0.77 was achieved in the metaphyseal areas of all the groups, without any significant differences between them. Semi constrain TKA, varus-valgus constrain TKA and a rotational hinge knee with metal sleeve have no different functional outcome and radiographic outcome at minimal one year follow up.
#7371
Minimal Pre-Operative Leg Length Discrepancy as a Risk Factor of Post-Operative Leg Length Discrepancy After Total Hip Arthroplasty in Patients With Non-Traumatic Osteonecrosis of the Femoral Head
HONG SEOK Kim - Seoul National University Hospital - Seoul, South Korea
Han Jin Lee - Seoul National University Hospital - Seoul, South Korea
*Jeong Joon Yoo - Seoul National University College of Medicine - SEOUL, South Korea
*Email: jjyos@snu.ac.kr
Background: Leg length discrepancy (LLD) is one of the troublesome complications of total hip arthroplasty (THA). It may cause low back pain, change the patient’s gait and lead to disability to the patient. Previously, several risk factors were suggested, but they were subjected to their inherent limitations. By controlling several confounding variables, this study aimed to analyze the independent risk factors of LLD after primary THA in patients with non-traumatic osteonecrosis of the femoral head.
Methods: We retrospectively reviewed 186 patients with non-traumatic ONFH who underwent unilateral THA between 2014 and 2021 to treat symptomatic hips. All patients were operated by one senior surgeon using a single implant. The demographic data of the patients (age, sex, and body mass index), surgery (femoral stem size, acetabular cup size, head size, and neck length), and radiological findings (pre-operative LLD, Dorr classification, and femoral neck resection) were analyzed to identify the risk factors of ≥5 mm post-operative LLD based on the radiological measurement and to calculate odds ratios by logistic regression analysis.
Results: Of the 186 patients, 96 were female (52%) and the mean age of all patients was 58.8 years at the time of initial THA. The average post-operative LLD were 1.2±2.9mm in the control group and 9.7±3.2mm in the LLD group, respectively. The LLD group tended to have minimal pre-operative LLD than the control group (-3.2±5.1mm vs. -7.9±5.8mm p <0.001). No significant difference was found between groups in age, gender, body mass index, femoral cortical index, and implant size.
Conclusion: Mild pre-operative LLD is associated with an increased risk of a post-operative LLD after primary THA in ONFH patients. Thus, surgeons should recognize the pre-operative LLD to achieve an optimal outcome. Moreover, surgeons must inform patients about the risk of developing LLD pre-operatively.
Keywords: Pre-operative leg length discrepancy, proximal femoral shape, Osteonecrosis of the femoral head, unilateral total hip arthroplasty
Figures
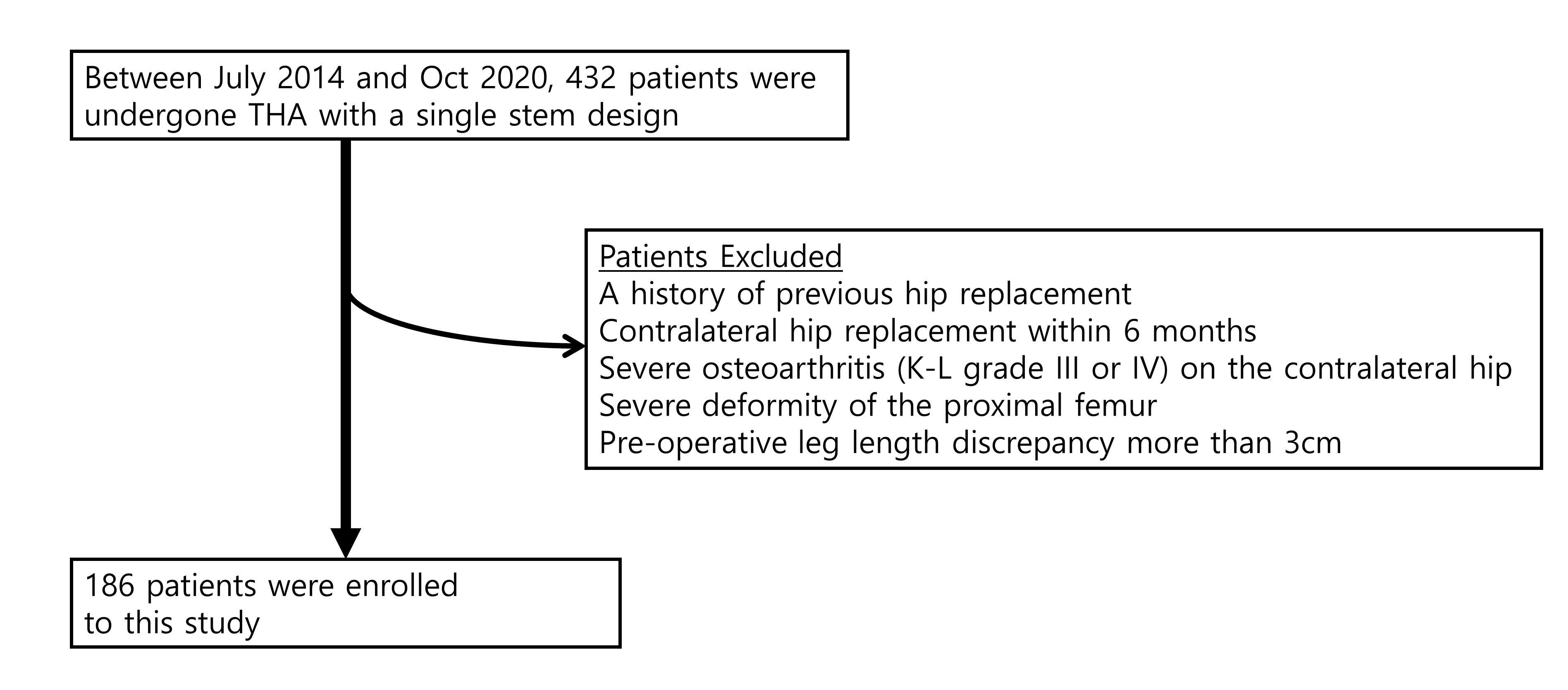
Figure 1
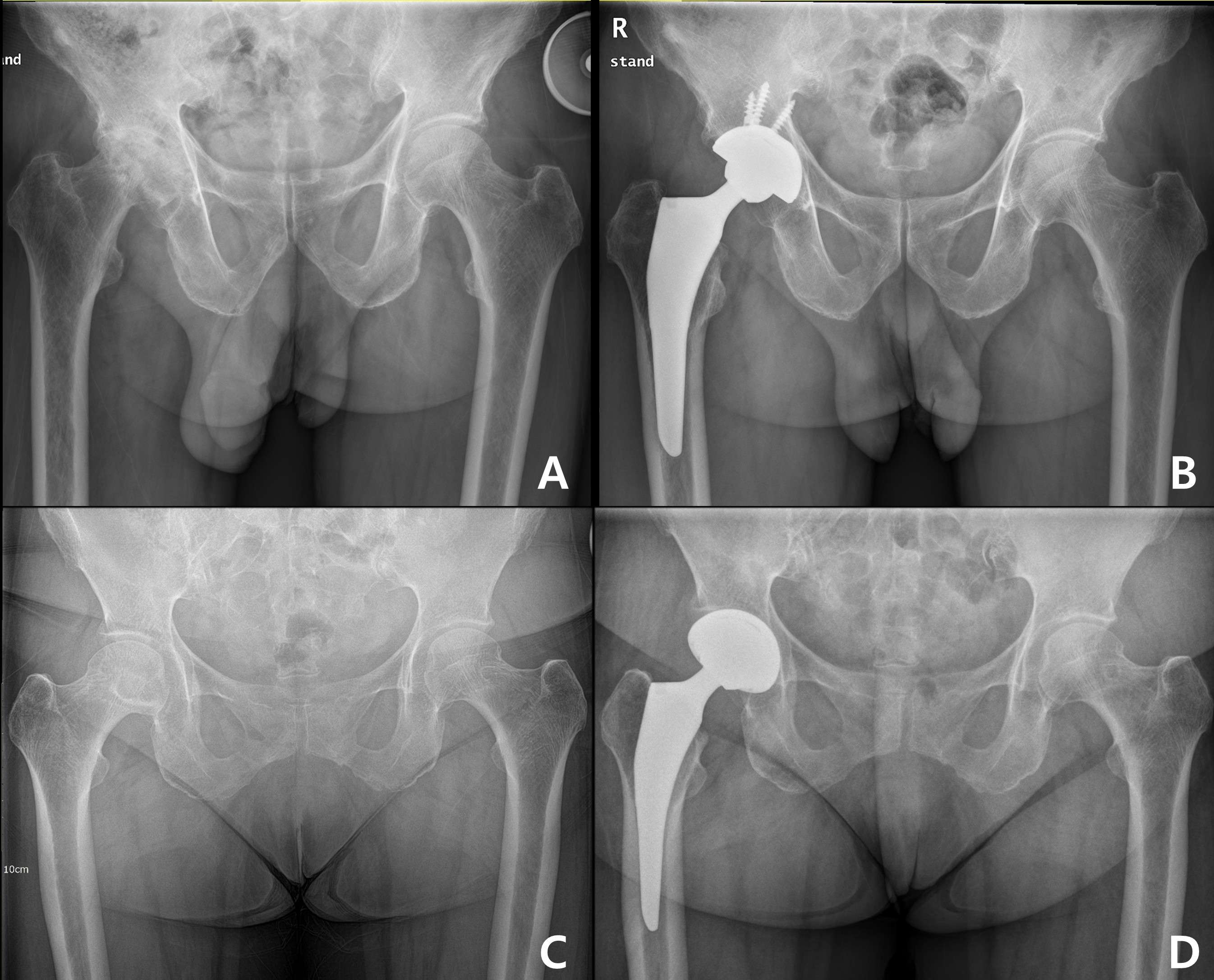
Figure 2#7372
The Mid-Term Outcome of a Novel Cementless Modular Femoral Stem in East Asian Patients
HONG SEOK Kim - Seoul National University Hospital - Seoul, South Korea
Han Jin Lee - Seoul National University Hospital - Seoul, South Korea
*Jeong Joon Yoo - Seoul National University College of Medicine - SEOUL, South Korea
*Email: jjyos@snu.ac.kr
Background: Early firm fixation of the femoral implant is crucial in total hip arthroplasty (THA) with unstable metaphysis or a large degree of femoral bone loss. This study aims to evaluate the mid-term results of the novel cementless modular fluted tapered stem in such cases.
Methods: From 2015 to 2020 at two tertiary hospitals, 105 hips (101 patients) had surgery by two surgeons with a cementless modular, fluted, tapered stem due to peri-prosthetic fracture, massive bone loss, prosthetic joint infection sequelae, or tumorous condition. Clinical outcomes, radiographic results, and survivorship of the implant were evaluated.
Results: The average follow-up period was 2.8 years (range, 1-6.2 years). The Koval grade was 2.7±1.7 preoperatively and maintained at 1.2±0.8 at the latest follow-up. The plain radiograph showed bone ingrowth fixation in 89 hips (84.8%). The average stem subsidence at postoperative one year was 1.6±3.2 mm (range, 0 to 11.0 mm). Five (4.8%) re-operations were needed, including one for occult intra-operative peri-prosthetic fracture; one for recurrent dislocation; and three for chronic peri-prosthetic joint infection. Kaplan-Meier survivorship with re-operation for any reason as the end-point was 94.6%.
Conclusions: The mid-term results of hip arthroplasty with the novel cementless modular, fluted, tapered THA stem system are satisfactory clinically and radiologically. Although the shortcomings inherent to its modularity did still exist, this modular femoral system may provide adequate fixation and be a practical option in the setting of complicated THA.
Keywords: revision total hip arthroplasty, femoral revisions, tapered modular stem
Figures
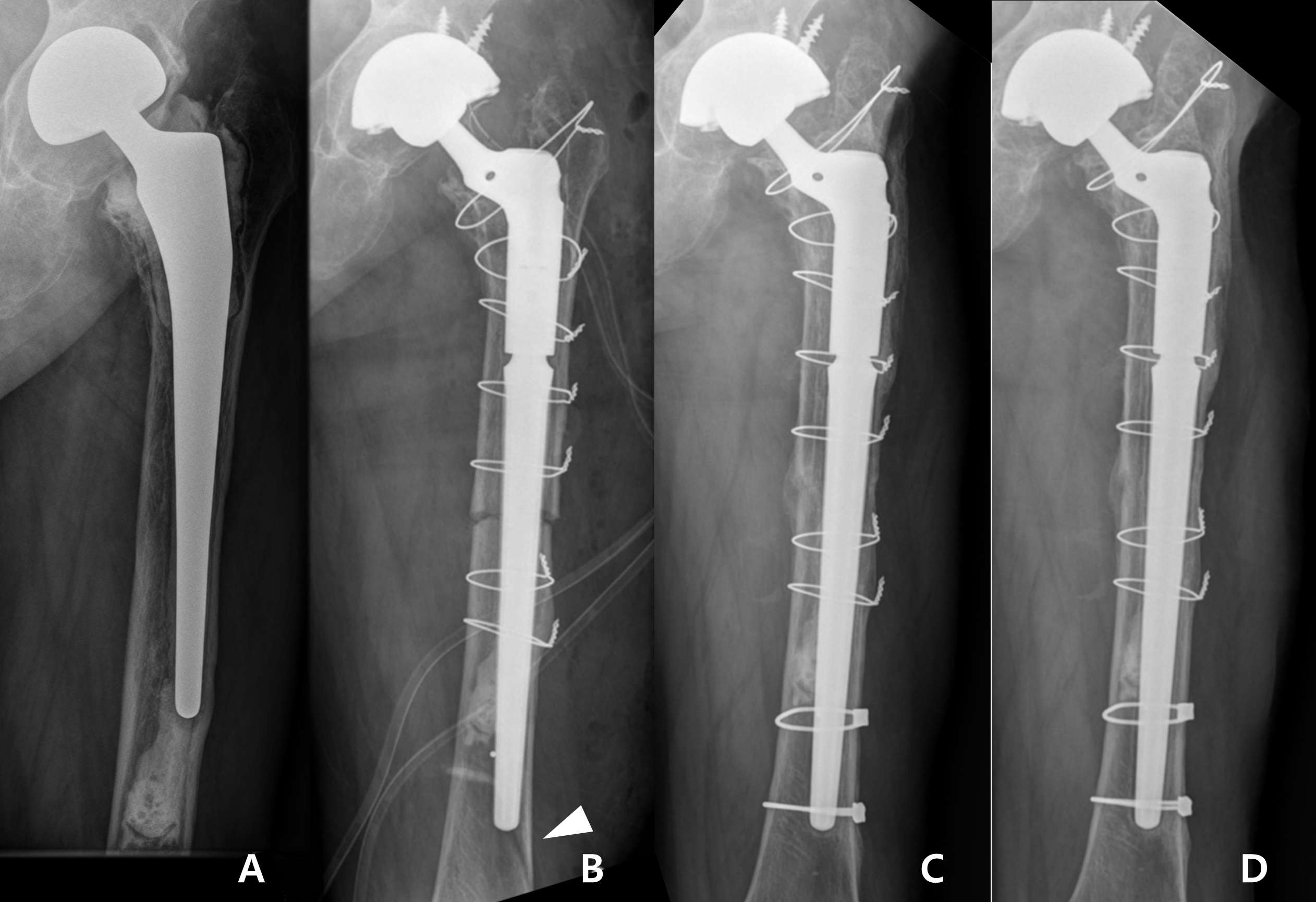
Figure 1
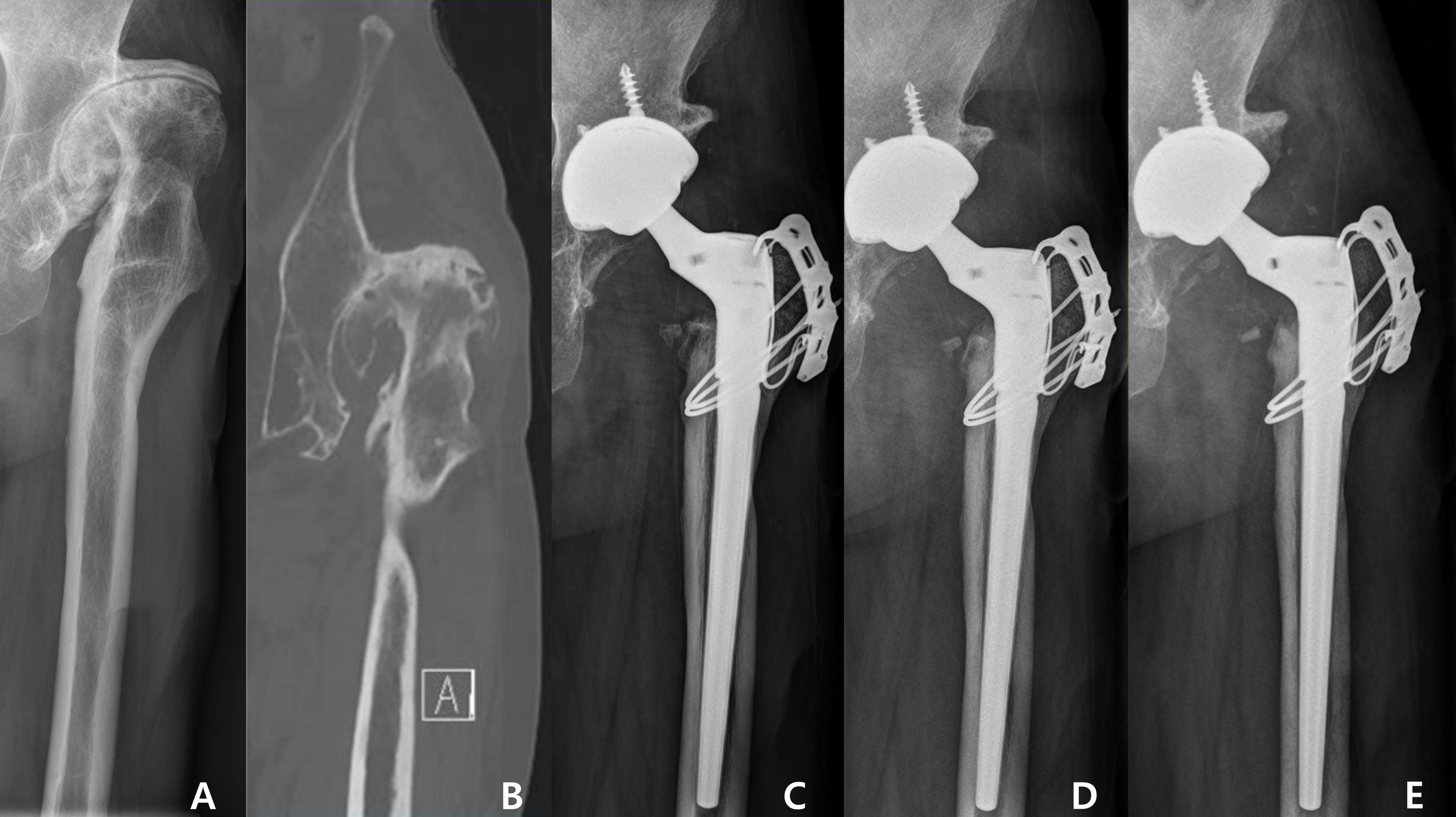
Figure 2
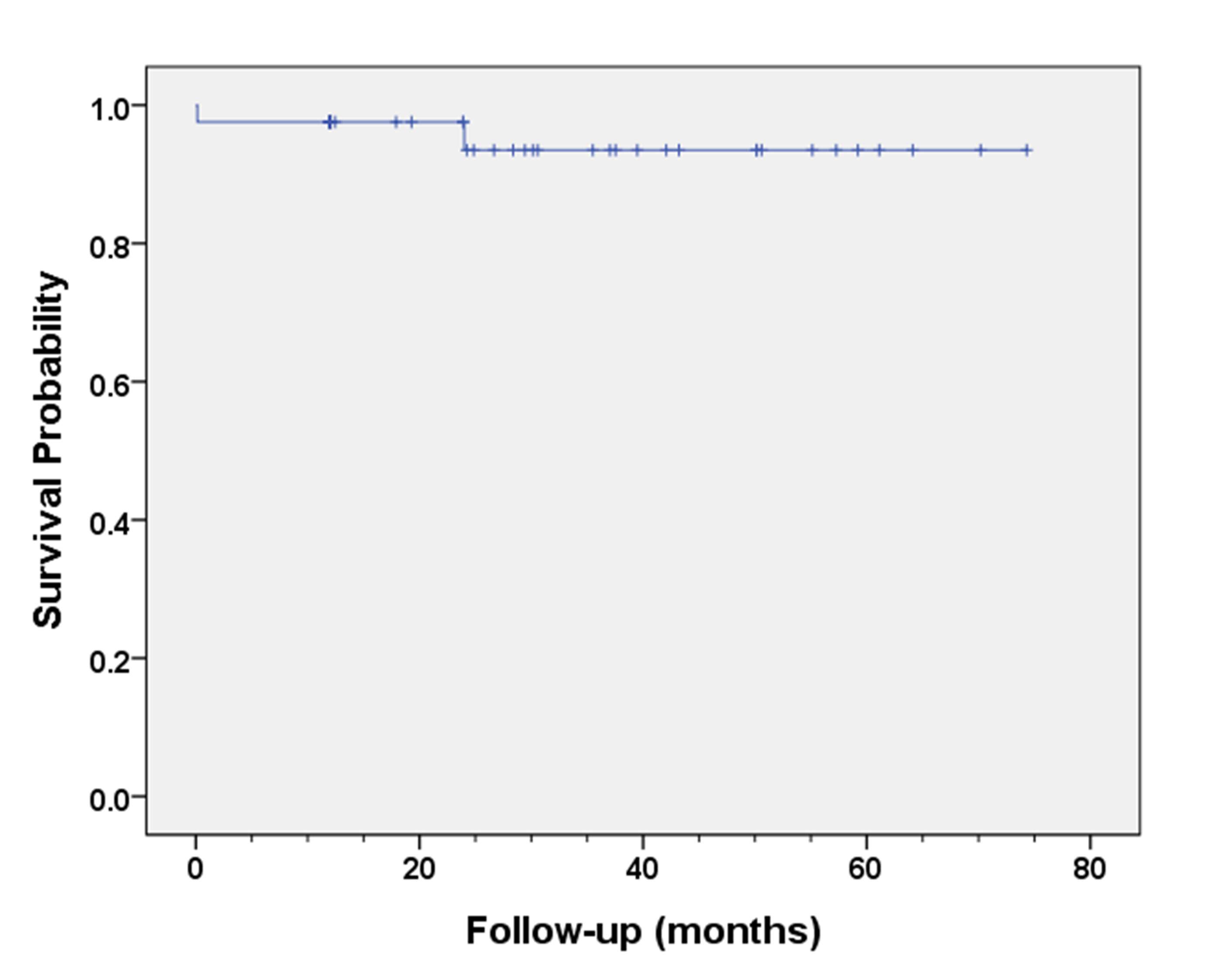
Figure 3#7418
Development of the Novel Patellar Reamer During Total Knee Arthroplasty
Hee-June Kim - Kyungpook National University Hospital - Daegu, South Korea
*Hee-Soo Kyung - Kyungpook National University Hospital - Daegu, South Korea
Ji-Yeon Shin - Department of Preventive Medicine, School of Medicine, Kyungpook National University - Daegu, Korea (Republic of)
Jae Hwi Han - Daegu Fatima Hospital - Daegu, South Korea
Kyeong-Hyeon Park - Kyungpook National University - Daegu, South Korea
*Email: hskyung@knu.ac.kr
Introduction
Patellar resurfacing can help prevention of the anterior knee pain following total knee arthroplasty (TKA). However, because the difficulty to perform accurate resection can result in complications, such as a fracture, a new patellar resection device was required to ensure accurate resection.
Methods
We used a method of resection to the desired thickness by vertically reaming from the center of the target point, rather than the conventional method of horizontal patellar resection from medial to lateral. The resection was implemented using a total of 36 femur heads. Two surgeons performed the reaming using each 14 and 22 femur heads. After reaming, the thickness of the remaining portion was measured to calculate the actual thickness and determine whether it had the appropriate thickness. In addition, each 7 actual patellae were resected duting TKA to check that they were resected to the exact thickness. The difference of thickness between two surgeons was also evaluated.
Results
The mean resection thickness of the 14 femoral heads was 9.07 mm and of 22 femoral heads was 8.85 mm, respectively. There was no statistical difference from the actual 9 mm target (p = 0.79 and p= 0.15, respectively). Between two surgeons, there was also no statistical difference in the average thickness (p=0.463). As a result of the 7 patients of TKA, the average thickness of the patella before surgery was 21.93 mm, and the total thickness measured after insertion of the patella replacement after resection was 22.29 mm on average. There was also no statistical difference in the average thickness before and after surgery (p=0.22).
Conclusion
A patella resection can be easily and accurately performed using the new patellar resection device. It is expected to be used in the actual TKA to perform simple and accurate techniques.
#7539
Rapid Prototyping Pelvic Model in Total Hip Arthroplasty: Mid-Term Follow-Up
*Sang-Min Kim - Korea University College of Medicine, Guro Hospital - Seoul, South Korea
*Email: heavystone75@gmail.com
Introduction
Total hip arthroplasty (THA) is challenging in cases of acetabular deficiency or implant loosening after primary THA, and osteoarthritis secondary to hip dysplasia. Three-dimensional (3D) prototyping models manufactured from computed tomography scans enhance surgeon's understanding of patient-specific patho-anatomy and provides precise preoperative planning. The purpose of this study was to determine the effectiveness of rapid prototyping pelvic model in total hip arthroplasty.
Methods
This was a retrospective study of 20 hips within 18 patients [8 men, 10 women; mean age 60.9 years, 2 patients with bilateral side] with acetabular deficiency in primary and revision THA situation. In accordance with Paprosky classification, we involved one hip with 2B type, eleven hips with 2C type, and five hips with 3A type. Additionally, two exceptive patients (3 hips) with pseudo-acetabular formation after developmental dysplasia of the hip and acetabular bone defect due to cancer metastasis were included. Data obtained by CT-scan were transferred to the planning workstation using a DICOM interface and were 3D reconstructed. Fused deposition model (FDM) module 3D printer was applied for actual printing of prototypes using polylactic acid (PLA) filament. Preoperatively, simulated acetabular reaming and positioning of cup or cage, sometimes with metal augment were conducted on the reconstruction of proportional pelvis model. Radiographic assessments including acetabular cup position including inclination and anterversion, osteolysis and prosthesis loosening were investigated. Postoperative surgical complications such as dislocation, periprosthetic infection, and periprosthetic fracture were also analyzed.
Results
Acetabular cup inclination and anteversion was mean 49.1˚ [43.5-54.7] and 15.0˚ [2.0-28.0], respectively. Radiologic measurements did not show implant loosening or progression of osteolysis in any case. There were no surgical complications after surgery at the mean 15.5 months follow-up. In order to plug the bony defect, trabecular metal augment was applied for seven cases, and acetabular cage was utilized for two cases. Additional stability was obtained using bone screws penetrating holes of acetabular cups in most cases except two patients.
Conclusion
Favorable outcomes were achieved in patient with preoperative planning assisted by 3D reconstructed model. Despite the efficacy of rapid prototyping pelvic model in THA, furthermore clinical studies with long-term follow-up should be required.
#7606
Effect of Severity and Cause of Preoperative Anemia on the Transfusion Rate After Total Knee Arthroplasty
Tae Woo Kim - Seoul National University College of Medicine, SMG-SNU Boramae Medical Center - Seoul, South Korea
*Seung-Baik Kang - Boramae Medical Center/ Seoul National University College of Medicine - Seoul, South Korea
*Email: ossbkang@gmail.com
Introduction: This study aimed to (1) evaluate the preoperative Hb cut-off value for transfusion after unilateral and bilateral staged (1week apart) TKAs, respectively, and (2) determine whether cause of preoperative anemia can affect transfusion rate after TKA.
Methods: A total of 951 patients who underwent TKA (unilateral: 605, bilateral staged: 346) from 2016 to 2019 were reviewed retrospectively. Patient demographics, comorbidities, preoperative Hb level, surgery types, and cause of anemia were evaluated as possible risk factors. The cut-off values for preoperative Hb level to reduce transfusion after TKA were evaluated in each surgery type.
Results: Preoperative Hb level, surgery type, and cardiac disease were identified as the risk factors for transfusion after TKA, and preoperative Hb levels of 11.8 (AUC=0.88) and 12.8 (AUC=0.76) were the cut-off values for transfusion after unilateral and staged bilateral TKAs, respectively. Although transfusion rate was higher in anemia with iron deficiency (ID) group than anemia without ID group, preoperative Hb level was also lower in anemia with ID group than anemia without ID group.
Conclusion: Single use of preoperative Hb level with different cut-offs depending on the surgery types can be useful indicator for preoperative optimization regardless of cause of anemia.
#7618
Incidence and Outcomes of Intraoperative Periprosthetic Acetabular Fractures in Cementless Total Hip Arthroplasty: A Prospective Three-Dimensional CT-Based Study.
Seung-Chan Kim - Eunpyeong St. Mary's Hospital, The Catholic University of Korea, Seoul, South Korea - Seoul, South Korea
Young Wook Lim - Seoul St. Mary's Hospital - Seoul, Korea
Woo Lam Jo - Catholic University of Korea - Seoul, South Korea
Soon Yong Kwon - St. Mary's Hospital - Seoul, Korea
*Hwanhee Lee - Daejeon St. Mary's Hospital / College of Medicine / the Catholic University of Korea - Daejeon, South Korea
*Email: hwanhee337@naver.com
Introduction: Unlike periprosthetic femoral fractures, periprosthetic fractures of the acetabulum in total hip arthroplasty (THA) have not been fully understood. Furthermore, published studies have been conducted in a nonprospective fashion with highly selected patient groups, and it is unclear if outcomes vary with location and type of the fractures. We aimed to prospectively identify the incidence, patterns, and clinical outcomes of intraoperative periprosthetic acetabular fractures with the use of pre- and postoperative CT scans, as well as risk factors for these fractures.
Methods: From January 2016 to January 2018, 234 consecutive patients (250 hips) who underwent THA with hemispheric acetabular components and who routinely underwent three-dimensional CT before and after surgery within a week were eligible for this prospective study. We assessed the incidence and pattern of fractures, outcomes for each fracture pattern, and reoperation and revision rates. A Harris hip score and a visual analog scale (VAS) pain score were also evaluated. Multivariate regression models were used to identify risk factors for periprosthetic acetabular fractures while adjusting for age, sex, body mass index (BMI), preoperative diagnosis, surgeon, size and orientation (inclination and anteversion) of the cup, and fixation of dome screws. There were 94 men and 140 women with a mean age of 58.5 ± 15.4 years (range, 20-92 years). The minimum followup was 2 years (mean, 2.8 years; range, 2-4.1 years).
Results: There were 18 periprosthetic femoral fractures (7.2%) and 41 periprosthetic acetabular fractures (16.4%) identified on CT scan; among those, 3 periprosthetic acetabular fractures (1.2%) were visible on plain radiographs. Fractures occurred most frequently at the posterior column (16 hips), followed by anterosuperior wall (11 hips), superolateral wall (8 hips), posterior wall (2 hips), combined location (2 hips), medial wall (1 hip), and anterior column (1 hip). Early cup migration occurred in 3 hips (2 displaced posterior column fractures, 1 medial wall fracture), with stabilization prior to 1-year followup in all hips. At the last followup, no radiographic evidence of component loosening or nonunion was observed and no patients underwent revision surgery for acetabular loosening. On regression modeling, patients with rheumatoid arthritis (odds ratio [OR], 7.00 compared to primary osteoarthritis; 95% confidence interval [CI], 1.37 to 35.68; p = 0.019) and osteonecrosis of the femoral head (OR, 3.64; 95% CI, 1.19 to 11.14; p = 0.024) were found to be significant predictors for periprosthetic acetabular fracture.
Conclusion: Periprosthetic fractures of the acetabulum during cementless THA are not infrequent and are more common in patients whose diagnosis is rheumatoid arthritis or osteonecrosis. Although no revisions were required due to these surgical complications in outcome analyses, surgeons need to closely follow patients when the fractures are detected on plain radiograghs with a displacement postoperatively. These findings may help understand unexplained pain after THA surgery.
#7646
Different Trochlear Groove Length Between Natural and Arthroplasty Knees Can Change Patellofemoral Contact Kinematics Related With Crepitus
Tae Woo Kim - Seoul National University College of Medicine, SMG-SNU Boramae Medical Center - Seoul, South Korea
*Seung-Baik Kang - Boramae Medical Center/ Seoul National University College of Medicine - Seoul, South Korea
*Email: ossbkang@gmail.com
Introduction : Although trochlear groove length (TGL) change after total knee arthroplasty (TKA) can affect patello-femoral(PF) contact kinematics and related symptoms, TGL of TKA implants have rarely investigated yet. This study aimed to (1) compare the TGL between natural and arthroplasty knees, and (2) determine whether TGL change after TKA can alter PF contact kinematics related with crepitus.
Materials and Methods : On the lateral plain radiography of 300 knees (female :150, male :150, age 62-75 ), the noble trochlear groove length index (TGLI) that was defined as the ratio between TGL/anterior-posterior dimension of distal femur were measured (Figure 1-A). After 3D modeling of 5 TKA implants using 3D scanner ( MDS 500, Maestro 3D, Italia ), the TGLI of implants were measured using Mimics 21.0 software (Materialise, Leuven, Belgium), and compared with native knee (Figure 1-B). Then, whether patellar superior pole pass through trochlear edge was compared between preoperative and postoperative lateral knee radiograph at 120 ° flexion. Finally, in 100 TKA patients, the incidence of PF crepitus generated during deep knee flexion (90~120 °) were investigated at postoperative 1 year.
Results: The TGLI of native knee was 0.49±0.03 (0.42-0.54) in female, and 0.48±0.02 (0.44-0.53) in male(Figure 2-A). The TGLI of TKA implants were 45.44±6.16 (35.8-50.4) in cruciate-retaining (CR) TKAs, and 35.9±3.03 (30.1-39.0) in posterior-stabilized (PS) TKAs (Figure 2-B). In lateral knee radiograph at 120 ° flexion, patellar superior pole did not pass trochlear groove edge preoperatively, but passed through trochlear groove edge postoperatively in all 50 cases (Figure 3). At postoperative 1year after patellar-preserving PS TKAs, 32 of 100 patients showed PF crepitus, and 23 of 32 PF crepitus were generated during deep knee flexion.
Conclusion : Current TKA implants could not reproduce TGL of natural knee, especially in PS TKAs. Reduced TGL after TKA led to the unnatural contact kinematics of patellar superior pole that passed through the trochlear groove edge during deep flexion. This findings can be related with post-TKA PF crepitus generated during deep knee flexion.
Figures

Figure 1
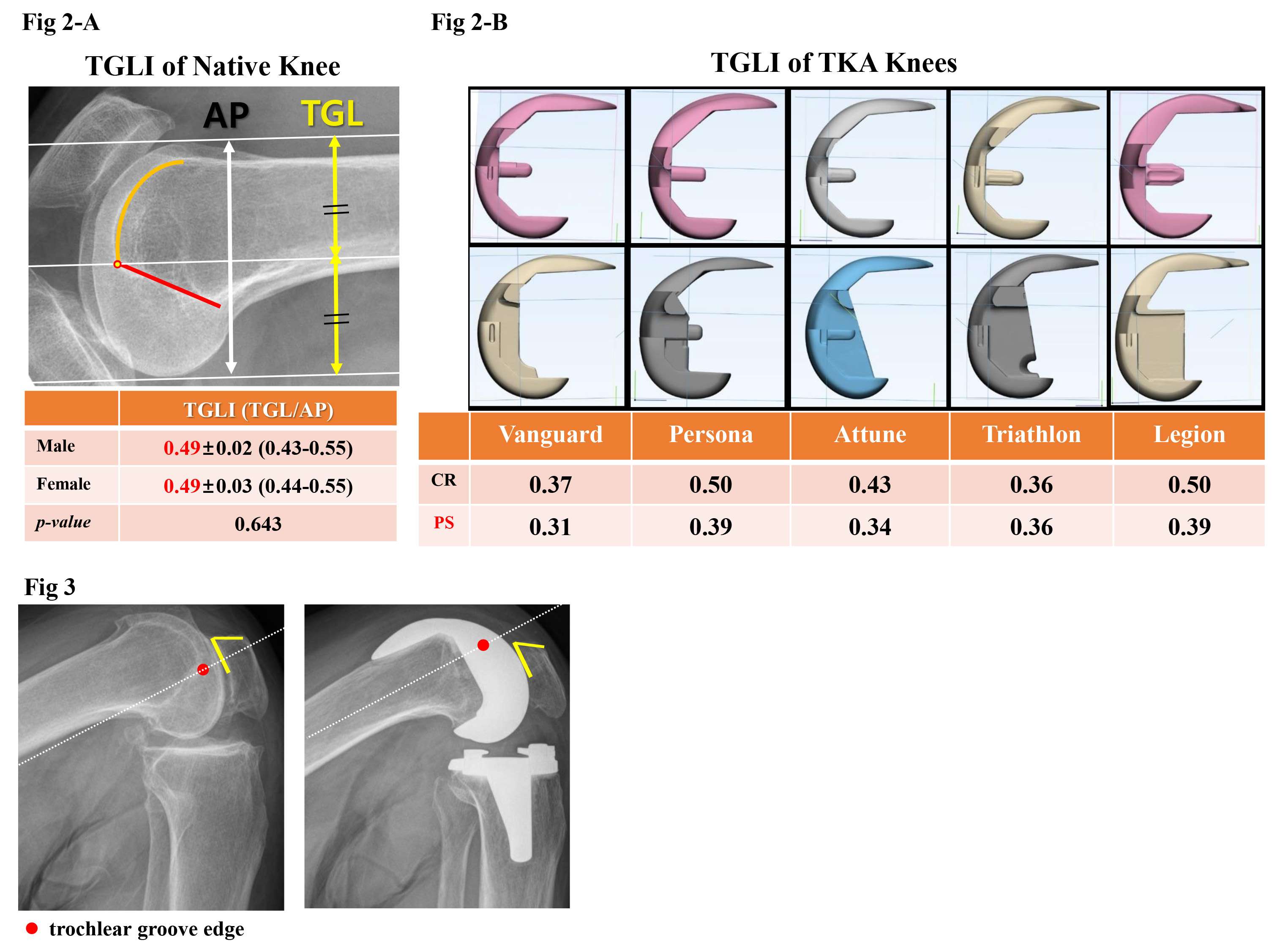
Figure 2#7678
Comparison Between Simultaneous Bilateral Total Hip Arthroplasty With and Without Drainage; a Retrospective Cohort Study.
MIN GWANG KIM - CHONNAM NATIONAL UNIVERSITY HOSPITAL - Gwangju, South Korea
Chae Jin Lim - Chonnam national university - Hwa sun, South Korea
Yoon Taek Rim - Chonnam National University - Hwasun-Gun, Korea
Joon Kyoo Kang - Chonnam national university - Gwangju, South Korea
*Kyung-Soon Park - Center for Joint Disease,Chonnam National University Hwasun Hospital - Hwasun-gun, South Korea
*Email: chiasma@hanmail.net
Introduction
Simultaneous bilateral Total hip arthroplasty (SBTHA) is an effective procedure for patients with disease bilaterally. But there is concern about increased blood loss and complications of SBTHA. This study aimed to evaluate the differences in the clinical outcomes and complication rate of SBTHA with drainage and without drainage for reducing the concerns.
Methods
Between October 2015 and April 2019, a retrospective cohort study was conducted with modified minimally invasive two-incision method and a consecutive series of 41 SBTHA performed with drainage (Group I) were compared to 37 SBTHA performed without drainage (Group II). It was assessed clinically and radiographically for a mean of 2.1 ± 0.8 years (range, 1.0-4.8 years). Postoperative hematologic values (Hgb drop, Hct drop, total blood loss, transfusion rate), pain susceptibility, functional outcome, and complication were compared in the drained group and the non-drained group.
Results
Mean postoperative Hgb drop (I: 5.1 ± 1.3 g/dL, II: 3.9 ± 1.0 g/dL; p < 0.001) & Hct drop (I: 15.3 ± 4.2 %, II: 11.6 ± 3.0 %; p < 0.001), mean total blood loss (I: 1684.4 ± 512.3 ml, II: 732.4 ± 243.8 ml; p < 0.001) and mean transfusion unit (I: 0.7 ± 1.0 IU, II: 0.1± 0.3 IU; p < 0.001) were significantly lower in the SBTHA without drainage than in the SBTHA with drainage group. But the mean dose of morphine equivalent (I: 132.7 ± 314.1 mg, II: 732.2 ± 591.5 mg; p < 0.001) was significantly larger in SBTHA without drainage.
Conclusion
SBTHA without drainage can reduce postoperative blood loss and the requirement for transfusion without increasing other complication. But SBTHA without drainage is more painful method than SBTHA with drainage. Therefore, SBTHA without drainage will be a good option to reduce the burden on the patient by reducing postoperative bleeding if it can control pain well after surgery.
Keywords: bilateral simultaneous, total hip arthroplasty, drainage, blood loss, pain.
Figures
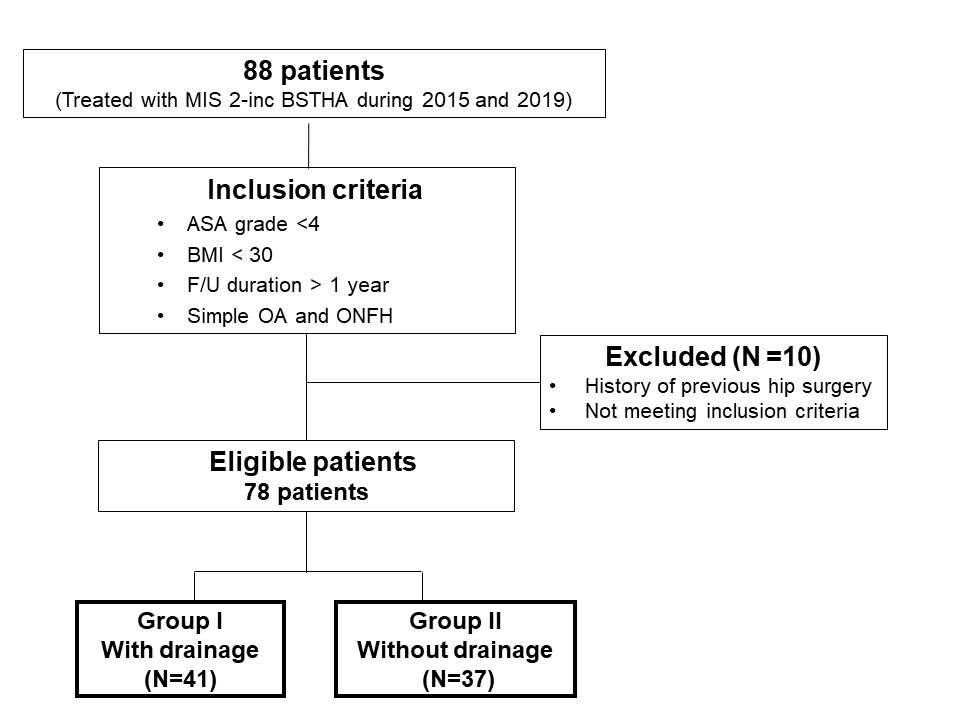
Figure 1
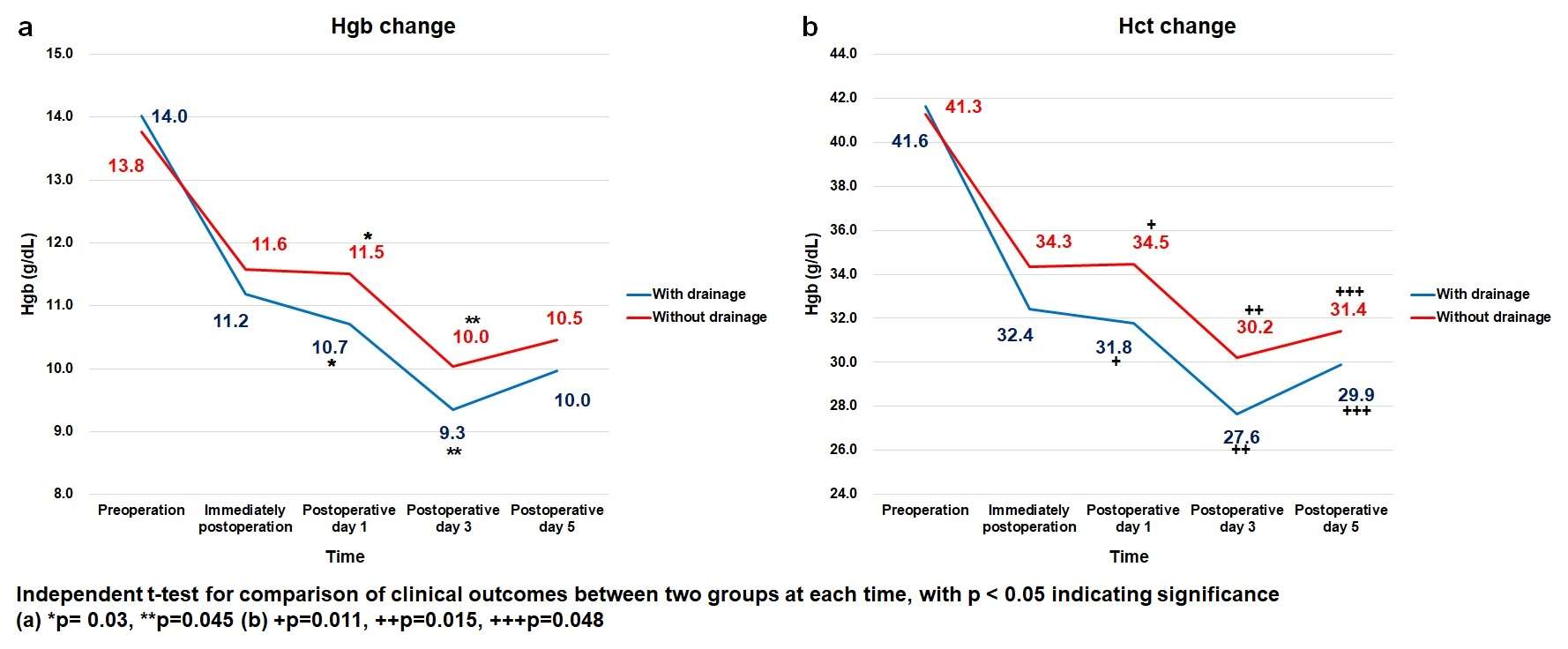
Figure 2
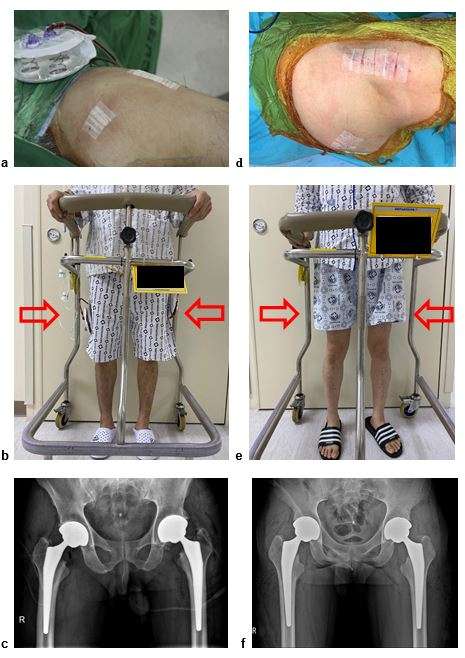
Figure 3#7282
Changes of Acetabular Anteversion According to Pelvic Tilt on Sagittal Plane Under Various Acetabular Inclinations
*Suk Kyoon Song - Daegu Catholic University Medical Center - Daegu, South Korea
Myung-Rae Cho - South Korea
Cheol-Hwan Ryu - Daegu Catholic University Medical Center - Daegu, South Korea
Hee-Chan Kim - Daegu Catholic University Medical Center - Daegu, South Korea
*Email: ryansong10@naver.com
Introduction:Improper functional orientation of the acetabular cup can result in improper posi�tions when dynamic pelvic positions are not considered. The purpose of this study was to evaluate changes on acetabular anteversion according to pelvic tilt under various acetabular inclinations.
Methods: Two artificial pelvic models were selected for this study. Acetabular inclinations on the coronal plane were 25°, 32°, 50°, and 60°. Acetabular anteversion of all components were 15°. Changes of anteversion according to pelvic tilt were measured at angles of 0°, 10°, 20°, 30°, and 40°. Computer Navigation, PolyWare 3D pro, CT, and plain radiography were used to measure each angle.
Results: The anatomical anteversions against pelvic tilt were calculated using the following formulae: anatomical anteversion (°) = −14.48Χ + 90.18 (in�clination angle 25°); anatomical anteversion (°) = −12.26Χ + 80.10 (inclination angle 32°); anatomical anteversion (°) = −7.468Χ + 61.13 (inclination angle 50°); and ana�tomical anteversion (°) = −5.328Χ + 44.84 (inclination angle 60°) (Χ: pelvic tilt angle). Radiographic anteversion against pelvic tilt were calculated using the following formulae: radiographic anteversion (°) = −9.50Χ + 57.09 (inclination angle 25°); radiographic anteversion (°) = −8.577Χ + 50.89 (inclination angle 32°); radiographic anteversion (°) = −6.794Χ + 45.73 (inclination angle 50°); radiographic anteversion (°) = −5.226Χ + 33.08 (inclination angle 60°).
Conclusion: Changes in anteversion according to pelvic tilt were lesser at higher degrees of acetabular inclination.
Keywords: acetabular anteversion, acetabular inclination, pelvic tilt
#7857
Learning Curve of Robot Assisted Total Knee Arthroplasty and Its Effects on Implant Position and Limb Alignment
Hojung Jung - Hallym Univ. - Seoul, Korea (Republic of)
*Joong Il Kim - Seoul National University Hospital - Seoul, South Korea
JongHwa Lee - Hallym Univ. - Seoul, South Korea
*Email: jungil@hanmail.net
Background: Recent studies have shown that robot‑assisted total knee arthroplasty (rTKA) achieve a more accurate implant position and limb alignment, compared to conventional TKA (cTKA) leading to an increase in the popularity of rTKA. The purpose of this study is 1) to determine the learning curve for rTKA and 2) to compare implant position and limb alignment between rTKA and cTKA according to the learning curve of rTKA.
Methods: This prospective study included 30 consecutive cTKAs (C group) followed by 30 consecutive rTKAs using MAKO robotic system (Stryker, USA) performed by a single surgeon. Cumulative summation (CUSUM) analyses were used to assess learning curve for operative time in rTKAs. Based on CUSUM analysis, rTKA cases were divided into initial cases (I group) and proficiency cases (P group). Femoral and tibial component position in coronal, sagittal, axial plane and limb alignment were compared between three groups.
Results: rTKA was associated with a learning curve of 15 cases for operative times (p < 0.05). Operative time was significantly shorter in C and P groups compared to I group and it was not different between C and P groups (92.57 ± 12.69 min in C group vs. 116.47 ± 10.24 min in I group vs. 97.4 ± 7.18 min in P group, p < 0.05). I and P groups showed less deviation from planned femoral component axial position (1.60 ± 1.38° in C group vs. 0.37 ± 1.27° in I group vs. 0.47 ± 1.0° in P group, p < 0.05) and tibial composition sagittal position (3.13 ± 2.86° in C group vs. -0.27 ± 0.73° in I group vs. 0.27 ± 1.11° in P group, p < 0.05) compared to C group and it was not different between I and P groups.
Conclusion: Although, rTKA has learning curve of 15 cases, operative time was not different between rTKA and cTKA after the learning curve. Moreover, surgeon could expect more accurate and reproducible implant position compared to cTKA, regardless of the learning curve.
Figures
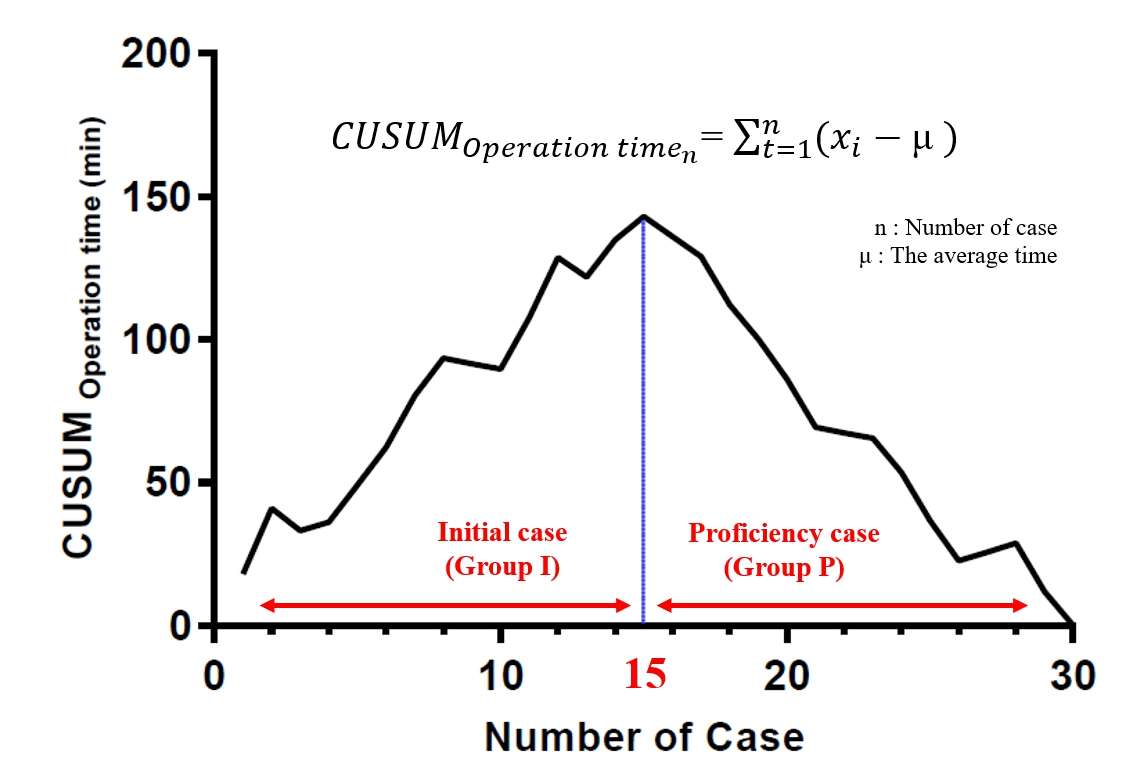
Figure 1
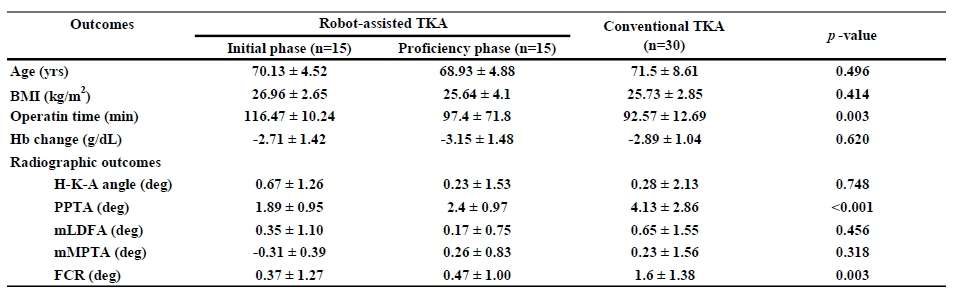
Figure 2#7858
The Incidence of Focal Osteonecrosis of the Femoral Head and Its Impact on Conversion Hip Arthroplasty After Screw Fixation of Femoral Neck Fractures: A Multicenter Study Based on Postoperative MRI
Eungsic Kim - Daejeon St. Mary’s Hospital, The Catholic University of Korea, - Daejeon, Select Country
*Seung-Chan Kim - Eunpyeong St. Mary's Hospital, The Catholic University of Korea, Seoul, South Korea - Seoul, South Korea
*Email: kschb129@naver.com
Purpose Osteonecrosis of the femoral head (ONFH) and subsequent head collapse is a major concern after internal fixation of femoral neck fracture (FNF). Previous studies focused on ONFH incidence using plain radiography; postoperative magnetic resonance imaging (MRI) was rarely performed. We performed a multicenter study to investigate the incidence of ONFH and the need for conversion hip arthroplasty after FNF screw fixation.
Methods We reviewed 195 patients who underwent screw fixation during closed FNF reduction between 2012 and 2017 at three institutions. Except for patients who did not consent to MRI, all patients underwent postoperative MRI either 1 to 3 years after screw fixation. The occurrence of ONFH was investigated through plain radiography and MRI.
Results 30 patients were diagnosed with ONFH through plain radiography, and an additional 33 patients were diagnosed with MRI, resulting in a total of 63 patients (32.3%) were diagnosed with ONFH. The mean time to ONFH diagnosis was 18.9 months and the conversion rate to hip arthroplasty was 10.2%. Of the 33 patients who were normal on hip radiography but exhibited ONFH on MRI, all had small focal lesions not associated with head collapse at the last follow-up[Fig.1]. The ONFH group diagnosed through plain radiography had more unstable FNFs than the group diagnosed through MRI.
Conclusion Although postoperative MRI revealed a higher incidence of ONFH after FNF screw fixation than reported previously, the small focal MRI lesions were not associated with increased risks of femoral head collapse or conversion to arthroplasty.
Keywords Osteonecrosis of the femoral head · femoral neck fracture · magnetic resonance imaging · conversion hip arthroplasty
Figures

Figure 1#7871
Robot-Assisted Total Knee Arthroplasty in Patients With Hemophilic Arthropathy
*Kang-Il Kim - Kyung Hee University Hospital at Gangdong - Seoul, South Korea
Jung-Kwon Bae - Kyung Hee Univ - Seoul, South Korea
*Email: kangilkm@gmail.com
Background – Robot-assisted total knee arthroplsty (TKA) are used to improve the accuracy of component positioning and radiographic alignment, with the goal of improving patient satisfaction and implant survivorship. In the treatment of hemophilic arthritis there have also been efforts to improve outcomes in TKA. Furthermore, there is no literature regarding long-term results of robot-assisted TKA in patients with hemophilia. Therefore, the purpose of this study was to evaluate long-term outcomes of robot-assisted TKA in hemophilic arthropathy.
Materials and Methods – Current study retrospectively assessed the long-term clinical and radiological outcomes of 38 knees that had undergone robot-assisted in hemophilic arthropathy with a minimum 10 years follow-up. Clinical outcomes were evaluated using American Knee Society (AKS) knee score, Short Form-36 (SF-36) and complications. Radiologic outcomes were evaluated mechanical axis (MA) angle, outliers (>±3°) for coronal plane and long-term survivorship of robot- assisted TKA were assessed.
Results – The mean follow-up period was 11.4 years (range 9.7-13.5). The mean AKS score and SF-36 score increased significantly during follow up (P<0.001). Postoperative complications appeared in 6 knees (15.8%). Revision TKA was performed in three knees for periprosthetic joint infection (n=2 knees) and tibial component loosening (n=1 knee). The outlier for the MA within a range of 0 ± 3° was in 6 knees (11.5%) and the Kaplan-Meier 10 year prosthesis survival rates were 94.6%.
Conclusion –The current study suggests that the long-term results of robot-assisted TKA in patients with hemophilic arthropathy are favorable for all outcome measures at a minimum of 10 years of follow up. Moreover, it showed satisfactory with successful long-term prosthesis survival which seems comparable with outcomes of TKA in patients with primary osteoarthritis.
Keywords: hemophilia, robot assisted, total knee arthroplasty, long-term, outcome, complication, survival
#7906
The Morphology of TKA Implant Does Not Influence Periprosthetic Bone Resorption, Remodeling and Clinical Outcome
Eungsic Kim - Daejeon St. Mary’s Hospital, The Catholic University of Korea, - Daejeon, Select Country
*Dong Whan Suh - SMG-SNU Boramae Medical Center - Seoul, South Korea
*Email: eastlight83@gmail.com
Purpose
Concern over periprosthetic bone resorption due to the possibility of stress shielding in TKA exist. Such problem may limit the life expectancy of the implant. The morphology of implant and its position on bone could influence bone resorption and remodeling. The hypothesis of this study was to find whether 1) asymmetric morphology of tibial component (ATC) is more fit to the designated position than symmetric design, 2) symmetric morphology of tibial component (STC) would show greater degree of bone resorption and remodeling in tibia due to the less fit conformation and 3) such influence of implant morphology on bone physiology would translate into clinical outcome.
Method
The retrospective case control study was done. 120 patients who underwent TKA (60 ATC, 60 STC) in our institution between 2018 to 2020 were the subject of this study. All TKA was performed by two surgeons (DWS, JHJ) and the 2 types of implants; STC & ATC were used. To assess whether morphology of implant influence bone resorption and hence the clinical outcome, we measured periprosthetic radiolucent line (RLL) & bone mineral density at femoral and tibial condyle (BMD) and position of component on CT scan. Propensity score matching for age and sex was done.
Result
#1 Assessment of tibial component fit was ; underhang (3 cases), overhang (6 cases) and cortical fit (111 cases).
#2 Mean BMD among STC (ROI 1,2,3,4) was 0.857 (g/cm2) and ATC (ROI 1,2,3,4) 0.862 (g/cm2)
#3 Overall incidence of RLL of 3mm or more in length was 6 cases in STC and 8 cases in ATC, at POD 1Y
#4 Incidence of complete RLL along the medial side of tibial implant was not different between Attune (CoCr_STC) and Persona (Ti_ATC) (3 cases vs. 4 cases)
Conclusion
In terms of complete RLL(+) & BMD change, position and morphology of implants did not influence medial periprosthetic bone resorption. Degree of periprosthetic bone resorption was not associated with clinical outcome (ROM and WOMAC)
#7956
Changes in the Ratio of Patients Who Underwent Total Hip Arthroplasty for Osteonecrosis of Femoral Head After Bone Marrow Transplantation
GEON-U Kim - cartholic university - Seoul, Korea (Republic of)
Ji Hoon Bahk - Seoul St. Mary's Hospital - Seoul, Korea (Republic of)
Yoon Vin Kim - The Catholic University of Korea Bucheon St. Marys Hospital - Bucheon-Si, South Korea
Woo Lam Jo - Catholic University of Korea - Seoul, South Korea
Kee-Haeng Lee - Catholic University of Korea - South Korea
*Young Wook Lim - Catholic university of Korea - Seoul, South Korea
*Email: cmcoslpart2@gmail.com
Introduction
Bone marrow transplantation (BMT) is one of the essential treatment option in treating hematologic diseases. However, high doses of immuno-suppressants and steroids have to be used for successful bone marrow transplantation. Therefore, after bone marrow transplantation, many patients develop osteonecrosis of femoral head (ONFH) and undergo total hip arthroplasty (THA). In this study, we investigate the rate of patients who have undergone bone marrow transplantation using clinical data warehouse (CDW) of our institute.
Material and Methods
We retrospectively reviewed patients who underwent BMT for hematologic disorders between January 2009 and May 2018. Among them, we searched for patients who underwent THA in our institute using the CDW. The total count and ratio of hematologic disorders causing BMT was reviewed and rate of THA as a treatment of ONFH after BMT in each disease were analyzed respectively.
Results
3351 patients underwent BMT in our institute and 93 THAs for 64 patients were performed. It took average of 28.4 ± 22.1 months after BMT to THA. The total occurrence rate of THA after BMT was 2.78%, which exhibited a gradually decreasing trend from 2009 to 2018 (Table 1, Fig.1). Of all patients who underwent BMT of all hematologic disorders, myelodysplastic syndrome (MDS) showed highest risk in occurrence of THA (MDS; 3.6 %, aplastic anemia (AA); 2.7 %, acute lymphocytic leukemia (ALL); 2.3 %, acute myeloid leukemia (AML); 1.5 %, multiple myeloma (MM); 1.3 %, Lymphoma; 0.7 %, chronic myeloid leukemia (CML); 0 %) (Table 2). In terms of type of BMT, allogenic transplantation showed higher rate of THA than autogenic transplantation, but no statistical difference was found (allogenic; 2.2 %, autogenic; 1.1 %, p = 0.056). Patient underwent BMT at 40.32 ± 17.63 of age and patients between 20 to 29 showed highest rate of THA (20 to 29; 4.0%, 30 to 39; 2.6%, 60 to 69; 2.3 %, 40 to 49; 4.6 %, 10 to 19; 1.5 %, 50 to 59; 1.4%, less than 10; 0 %, over 70; 0 %) (Fig.2). By logistic regression analysis, age at BMT (p=0.308), sex (p=0.119), body mass index (p=0.230), pre-BMT diagnosis (p=0.240), and methods of BMT (p=0.231) showed no statistical difference (Table 3, 4).
Discussion
The use of corticosteroids has decreased due to the development of immuno-suppressants. Furthermore, with great advancement in post-BMT care, incidence of allogenic BMT has been increasing and the number of HLA types which needs to be matched have decreased. But on the other hand, incidence of graft-versus-host disease (GVHD) could rise and total corticosteroid used could also increase in this view.
The percentage of patients who underwent THA after BMT was 2.78% and in annual comparison, it showed declining trend which might have been owing to decreased total corticosteroid use. However, it showed no statistical difference between the methods of BMT or types of diseases which required BMT, for the rate of THA.
For clarifying relationship between ONFH and corticosteroid use in BMT, further study is required.
Figures
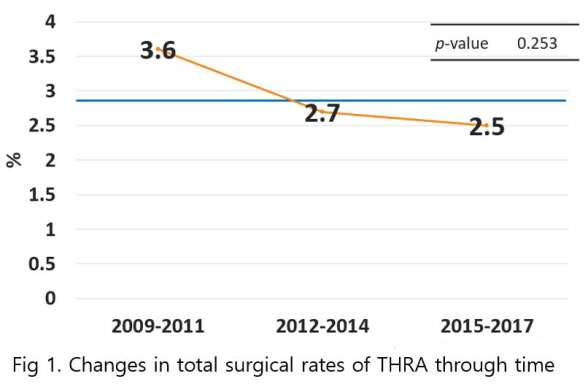
Figure 1
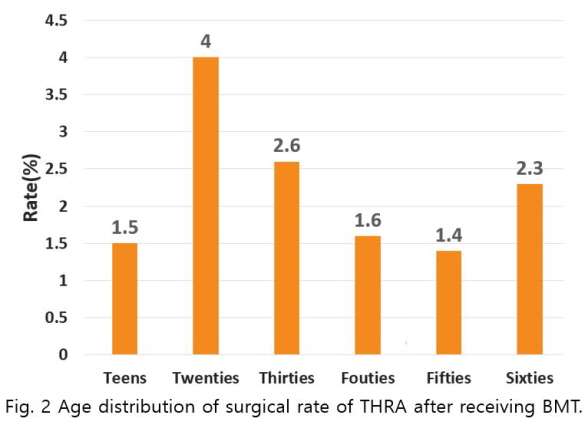
Figure 2#7981
Contralateral Knee Osteoarthritis: Does It Influence Satisfaction After Total Knee Arthroplasty
Nathan Kim - John A. Burns School of Medicine - Mililani, United States of America
Kylie Popovich - John A. Burns School of Medicine - Honolulu, USA
Andrew Takata - University of Hawaii at Manoa - Honolulu, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
*Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Samantha Andrews - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
*Email: onohunter@icloud.com
Introduction:
Approximately 15-25% of patients remain dissatisfied following total knee arthroplasty (TKA), often citing post-operative pain, limited function, and limited range of motion as the reason for dissatisfaction. Although not yet evaluated, nearly 90% of patients present with contralateral osteoarthritis (OA) which could result in compensatory motion and increased pain, thereby decreasing satisfaction. Therefore, the purpose of this study was to compare function and satisfaction between patients with or without contralateral knee OA.
Methods:
This prospective study included a consecutive cohort of 96 patients having undergone elective unilateral TKA between April 2019 and June 2021 and had a six-month follow-up visit. Prior to surgery, each patient received bilateral, weight-bearing radiographs and completed the Knee Disability and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), Patient-Reported Outcomes Measurement Information System Global Physical Health (GPH), and Global Mental Health (GMH) scores. A Kellgren-Lawrence (KL) score was assigned for each knee by the senior surgeon, with patients presenting with contralateral OA further categorized by KL score ≤2 and ≥3. Statistical analyses included only patients with contralateral OA and included independent t-test and Chi-squared tests to compare differences in KL≤2 and KL≥3 groups.
Results:
Overall, 88 (91.7%) of patients presented with contralateral OA, with 18 (20.5%) with KL≤2 and 70 (79.5%) with KL≥3. Compared to KL≤2, body mass index was higher in patients with KL≥3 (27.1±3.5 vs 30.6±6.3; p=0.030), yet no other differences were noted in patient demographics or pre-operative patient reported outcomes. Post-operatively, there were no differences in patient reported outcomes at six weeks or six months between KL≤2 and KL≥3 patients. Additionally, patient satisfaction ≥4 was also similar at six weeks (KL≤2: 64.7% and KL≥3: 79.7% p=0.169) and six months (KL≤2: 82.4% and KL≥3: 86.6% p=0.455).
Conclusion:
Similar to previous literature, over 90% of the patients in the current study presented with contralateral OA. However, post-operative patient satisfaction and outcomes were similar between the OA severity groups. Although not significant, patients with KL≤2 generally had lower patient satisfaction, which could indicate a mismatching of expectations in patients with less severe knee OA.
#7475
The Progression of Varus Deformity in Osteoarthritis Induces Anterior Paradoxical Motion of Femur Relative to Tibia in Early Flexion
*Tomofumi Kinoshita - Ehime University - Toon City, Japan
Kazunori Hino - Ehime University - Toon, Japan
Tatsuhiko Kutsuna - Ehime University Graduate School of Medicine - Toon-city, Japan
Kunihiko Watamori - Ehime University Graduate School of Medicine - Toon-city, Japan
Takashi Tsuda - Ehime University Graduate School of Medicine - Toon, Japan
Hiromasa Miura - Kyushu Rosai Hospital - Kitakyushu, Japan
Masaki Takao - Ehime University - Toon City, Japan
*Email: de29d8bed7upj@gmail.com
Introduction
Recently, due to the technical improvement of evaluation instruments, we are able to comprehend knee kinematics in detail. However, little study has been done about the changes in knee kinematics caused by a progression of knee deformity. In this study, we aimed to evaluate the position of femur relative to tibia throughout range of motion in osteoarthritis knee, and to assess the relationship between the degree of varus deformity and knee kinematics.
Methods
We evaluated 116 preoperative knees with varus deformity using a navigation system. Internal-external (IE), anteroposterior (AP) and medio-lateral (ML) position of femur relative to tibia was measured at maximum extension angle, 15°, 30°, 45°, 60°, 90°, 105°, 120° and maximum flexion angle using a navigation system. From these parameters, two-dimensional translation of the surgical epicondylar axis was projected to the tibial axial plane and evaluated femoral movement relative to tibia. In addition, we retrospectively classified 116 preoperative knees into 3 groups according to degree of preoperative hip-knee-ankle (HKA) angle: mild varus group (<10°), moderate varus group (10°-20°), and severe varus group (>20°). Then, we investigated the difference of each parameter among these groups.
Results
The mean AP translation of femur relative to tibia throughout range of motion (ROM) was 34.0, 30.0, 25.9mm in mild, moderate and severe group, respectively. The mean AP translation in mild group showed significantly high compared with moderate and severe groups (p=0.02, 0.01). On the other hand, the mean IE rotation and ML movement throughout ROM was not differed among 3 groups. AP translation throughout ROM correlated with AP position of femur relative to tibia at maximum extension (ρ=0.61, p<.0001). Regarding knee kinematics, anterior paradoxical motion of femur relative to tibia during early knee flexion was observed 54.4%, 65.3% and 90% in mild, moderate and severe group, respectively.
Conclusion
Progression of varus deformity in osteoarthritis knee influences AP position of femur relative to tibia, especially during knee extension to early flexion. The posterior deviation of femur at knee extension to early flexion changes AP movement of femur relative to tibia. Surgeon should notice that severe osteoarthritis induces abnormal knee kinematics such as anterior paradoxical motion.
Figures
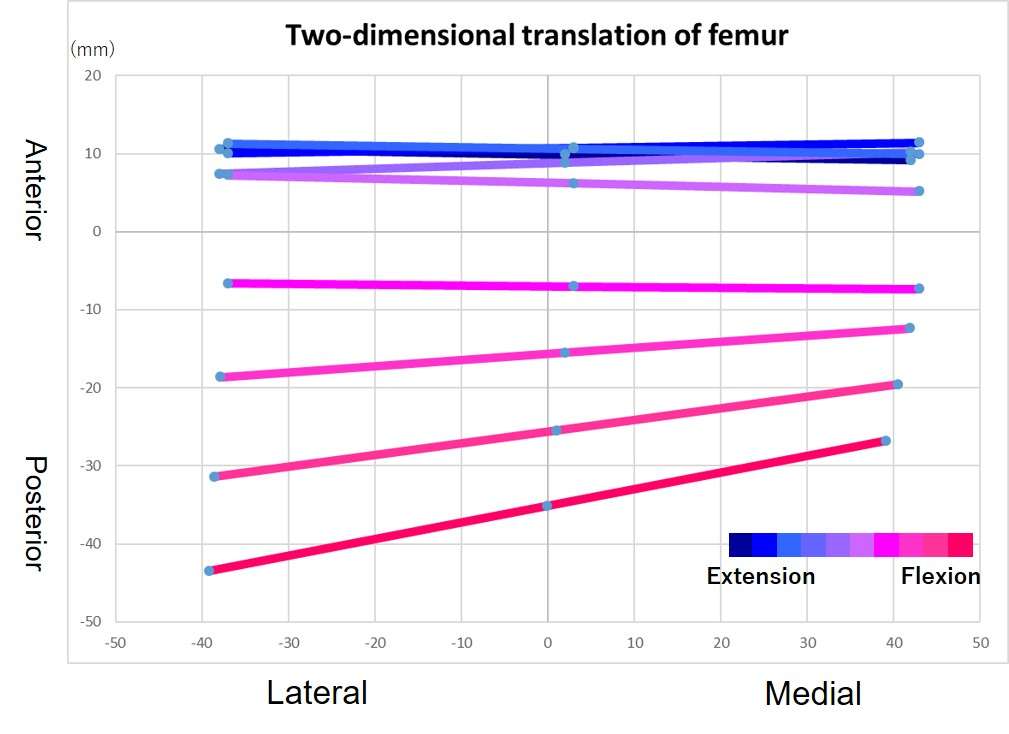
Figure 1
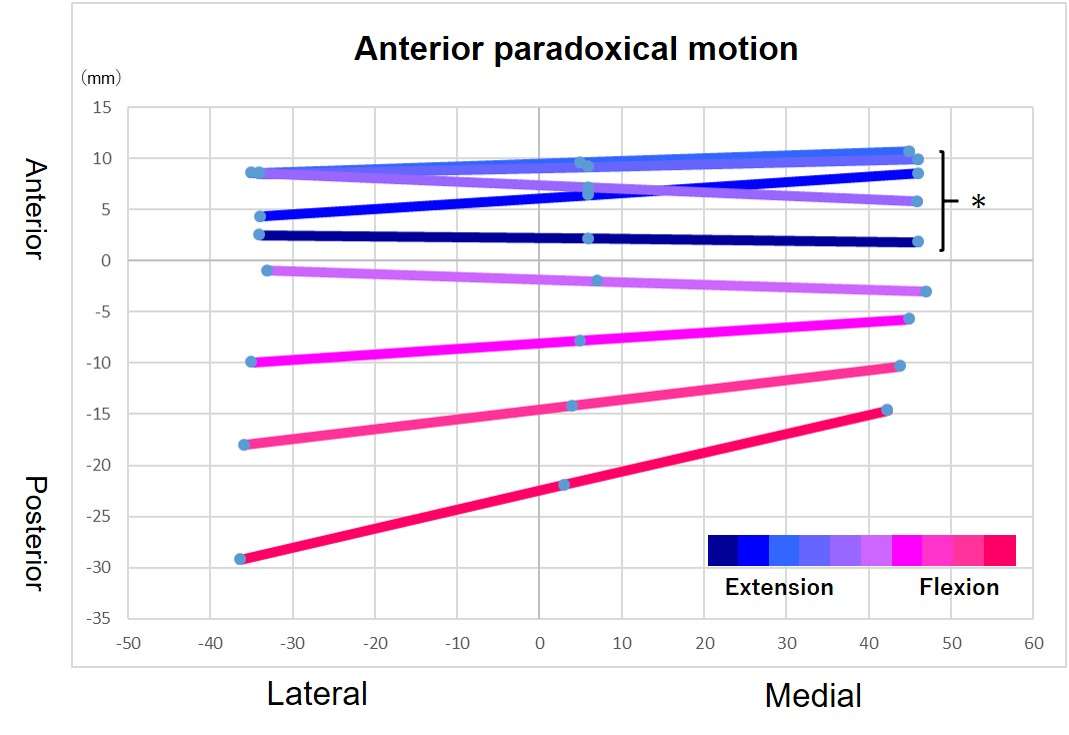
Figure 2#7573
AI Produced Hip Stem Design Improves Predicted Performance
*Bryan Kirking - Enovis - Austin, USA
*Email: bryan.kirking@enovis.com
INTRODUCTION
Artificial intelligence (AI) and machining learning (ML) algorithms have gained popularity as they demonstrate their usefulness in addressing complex problems. Generative adversarial networks (GANs) are particularly exciting for their ability to allow computers to generate unique content and recent works have investigated the benefits of integrating GANs with topology optimization. A GAN structured AI that produces viable implant designs could be used to address unique patient specific requirements and could serve as a valuable tool in improving the performance of population specific implants. This study presents the results of a first generation GAN developed to design implants with optimized fixation.
METHODS
The GAN consisted of a generator component and discriminator component. The network requires 3D shapes that approximate implant shapes for training, boney anatomy, bone density, specified activities of daily living, specified bench test requirements, and relevant design objectives such as minimizing bone removal. For this study, the anatomy was taken from a cadaver CT scan with density phantom. A gait cycle was used to evaluate implant performance during ADL, fatigue resistance was evaluated similar to ISO 7206-04, and an additional objective to minimize implant volume was included.
Generated designs from the network consisted of the 3D shape, material, and locations of surface coatings for bone ingrowth. The network evaluates coatings as fully osseointegrated.
Implant performance was evaluated using the predicted head displacement during gait, the implant’s fatigue resistance, and implant volume. For comparison, DJO’s Linear Hip Stem, which been in use for over 17 years, was separately evaluated by the discriminator component of the GAN.
RESULTS
The GAN produced a large variation of implant shapes as shown in Figure 1. As training progressed, shapes approached the bone anatomy, but lacked some features seen in the commercial design such as cement grooves. The DJO Linear and AI design 2 are shown overlaid with the femur geometry in Figure 2. The values predicted by the discriminator for the two best performing AI generated designs relative to the benchmark design are presented in the table.
DISCUSSION
Using a GAN structure, the AI was able to produce hip stem designs with predicted fixation performance that was a good as the DJO Linear Hip stem. The AI generated designs demonstrated less motion and better fatigue resistance than the benchmark design. While the AI volumes were larger, that was likely due to lateral-superior aspect where the commercial design was reduced for easier insertion.
Training the generator with appropriate shapes was a key component to producing viable designs in an efficient manner using the GAN. Once trained, the network was able to tune to the design conditions and produced designs that matched the fixation performance of the benchmark design. Improvements to the AI performance could be realized with increased training and more robust design constraints.
Figures
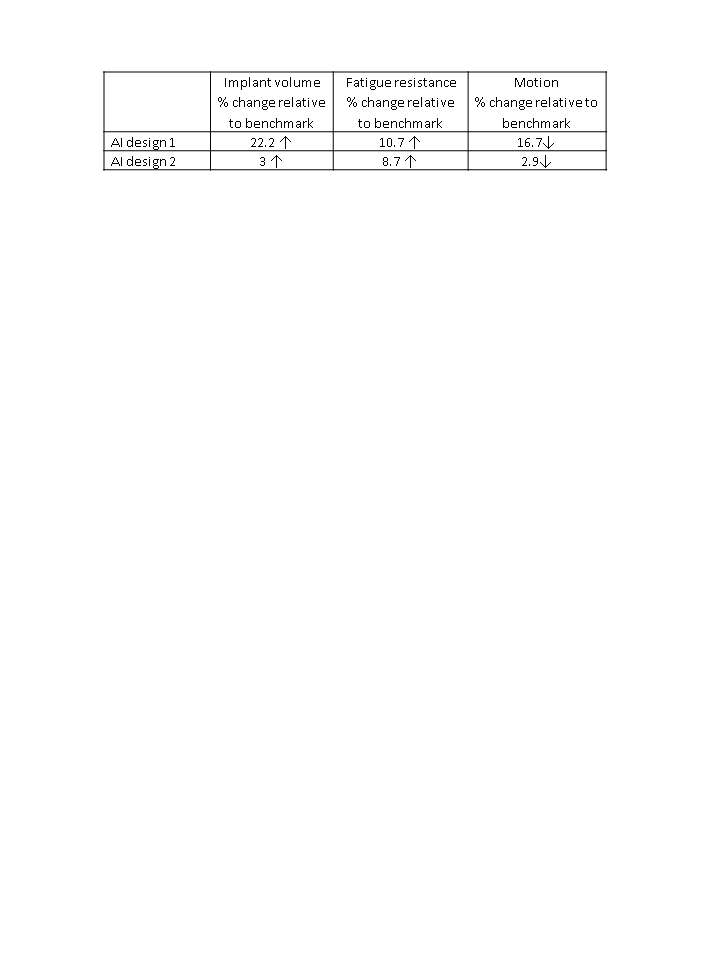
Figure 1

Figure 2
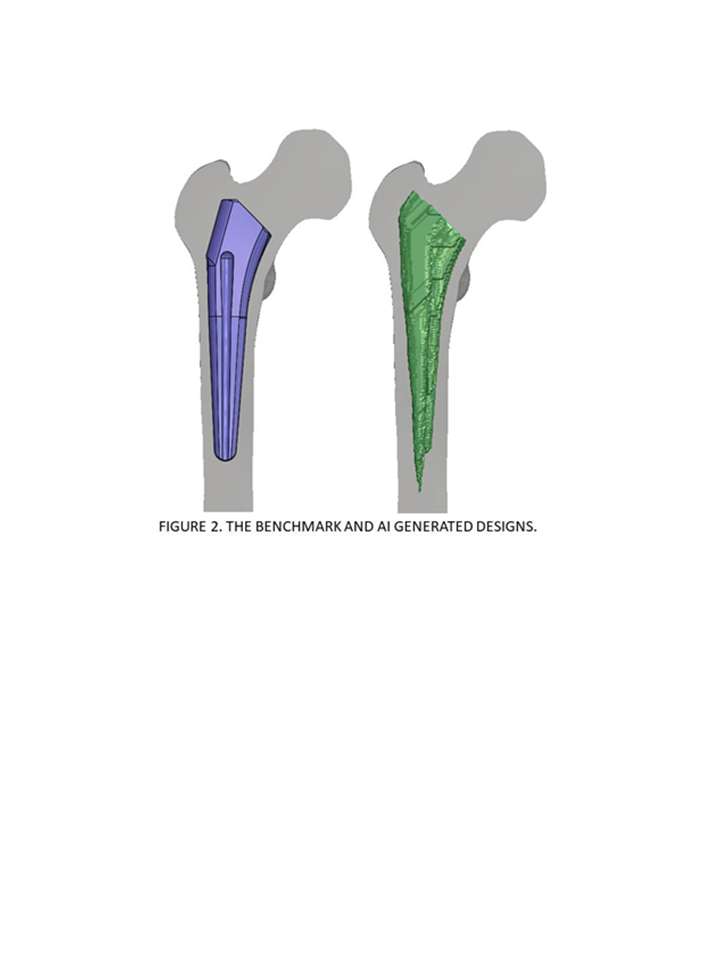
Figure 3#7564
A Machine Learning Assessment of the Predictive Power of FEA-Based Metrics for Estimating Bone Remodeling in a Novel Osseointegrated Device
*Bryan Kirking - Enovis - Austin, USA
Nathaniel Pyle - DJO Surgical - Austin, USA
*Email: bryan.kirking@enovis.com
Introduction
Long term stability of a press-fit implant depends on maintaining sufficient bone density to support the loads at the device/bone interface. The principle of Wolff’s law governs bone remodeling, but its’ use is most often qualitative. Validated, quantitative models that predict bone remodeling could improve orthopedic device design by enhancing implant long-term stability.
Patients with transfemoral amputations received the POP (Percutaneous Osseointegrated Prosthesis) under an FDA Early Feasibility Study (Figure 1). Each patient had CT scans and gait analysis performed preoperatively and 12-months post-implantation, providing a data set well suited to building models that relate bone remodeling and FEA output.
Methods
Each femur was reconstructed at both time points into a tetrahedral mesh from the CT scan (Mimics/3-matic). Bone density of each element was calculated using qCT and then isotropic bone modulus was estimated from bone density. At the post-op timepoint, the implant’s porous coated region was modeled using contact with a surface offset to achieve press-fit with cortical bone. Knee loadings from the gait analysis were applied over 20 steps through a rigid element onto either the implant or intact femur at the corresponding implant location.
For each element, the initial and remodeled bone densities and associated stresses, strains, and strain energy densities were extracted at each loading step and the average and maximum of these parameters over all 20 steps were calculated for each element. Random Forest machine learning regressions (MLR) were performed using Python’s SciKit-Learn to build explanatory models relating the FEA to bone density changes. It is important to note that these FEA were conducted with the true bone densities and would not be available when predicting bone remodeling with only the initial state.
Results
The table summarizes the linear correlation and MLR scores for both training and testing data sets.
Discussion
The change in von Mises Stress (ΔVMS) had the best linear correlation to change in bone density (0.2809). The magnitude of the correlation coefficients was similar for ΔVMS, remodeled von Mises Stress (VMS_f), and the initial bone density (P_init). The relative strain energy density (rSED) which is sometimes used as an indicator for bone remodeling, did not score well either with linear correlation or as a single input in the MLR.
Combining ΔVMS, VMS_f, rSED, and P_init in a MLR to predict change in bone density produced scores > 0.9 for both training and test sets. In Figure 2, a reconstructed femur is shown with the elements color coded to density for one subject. There was excellent agreement between the predicted FEA/MLR densities (left image) and for the qCT densities (right image).
Conclusion
The FEA\ML model predictions of bone density from the multi-variate model using stress and strain energy density showed excellent agreement with the qCT determined bone densities. Relative strain energy density alone was not a good predictor of bone density change, even when calculated using the known final density.
Figures
Figure 1
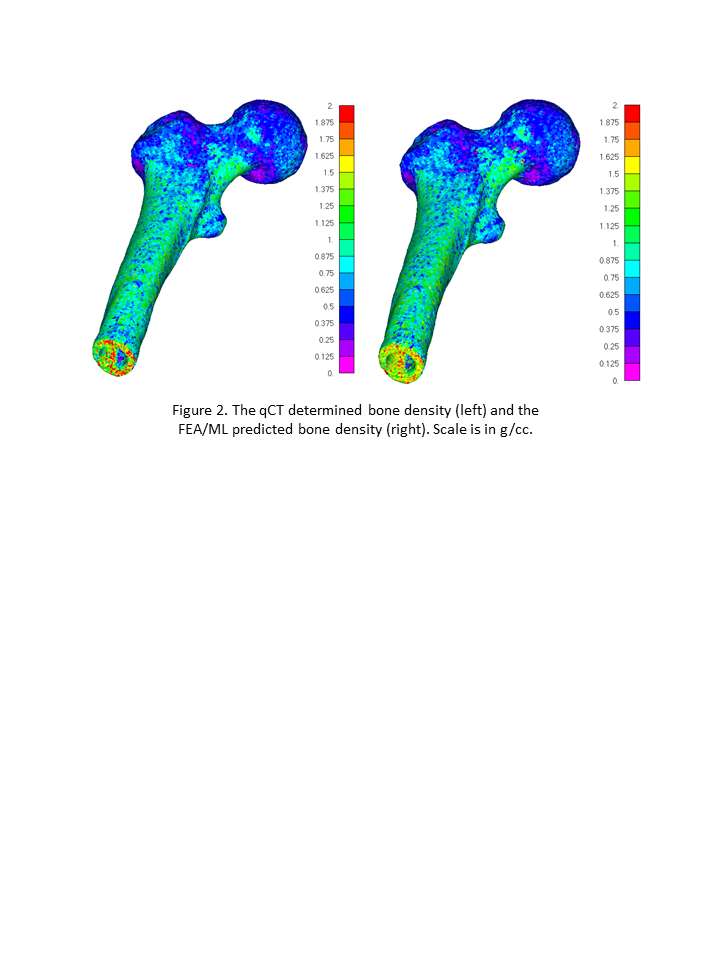
Figure 2
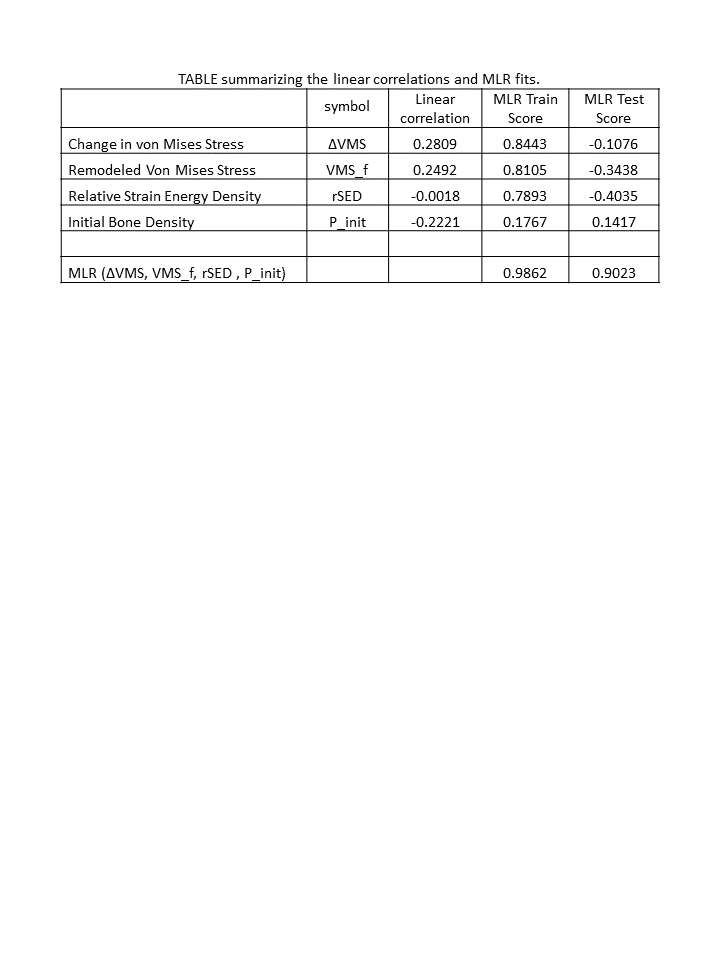
Figure 3#6893
Characterizing Comorbidities in Total Joint Arthroplasty Patients in a Safety-Net Hospital Using the Age-Adjusted Charlson Comorbidity Index
*Ira Kirschenbaum - Bronx-Lebanon Hospital - Bronx, USA
Noshin Nuzhat - Brown University - Providence, USA
Melanie Anaya - Brown University - Providence, USA
Gabriela De Queiroz Campos - Brown University - Providence, USA
Ariel R.C. Silverman - BronxCare Orthopaedics - Bronx, USA
Ronald Huang - BronxCare Orthopaedics - Bronx, USA
Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
*Email: IKIRSCH@bronxleb.org
Introduction
The presence of multiple comorbid diseases has been shown to increase patient’s length of stay and lead to greater utilization of resources after a total knee arthroplasty [3]. It may also delay diagnosis, alter treatment, lead to complications, influence survival, and confound analysis of outcomes [4]. The goal of the present study is to analyze the distribution of comorbid diseases in patients who have undergone total joint arthroplasty at BronxCare Health System, which serves the poorest congressional district in the United States.
Methods
A retrospective analysis was conducted reviewing consecutive total joint arthroplasty patients at BronxCare Hospital System receiving surgery between 2008 and 2018 (N=1836). All procedures were performed by two fellowship-trained joint replacement surgeons. The total number of conditions per person was determined using the department’s own formula which takes into account additional comorbidities and risk factors common in our particular patient population proven to increase risk of complications. Additionally, the relevant comorbidities were used to calculate the Age-Adjusted Charlson Comorbidity Index (ACCI), which is includes fewer comorbidities, but weights them based on severity. From this, we determined the score distribution of both the hospital score and of the ACCI of the population. The most frequent conditions present were also identified. Descriptive statistical analysis was performed to find central tendency and variance.
Results
Within the patient population, 5% had no comorbidities, 36.7% had between 1 and 4, 41.6% had
between 5 and 9, and 16.8% had over 10 comorbid conditions (mean: 6; sd: 3.66; mode: 4) [Graph 1].
Regarding AACI scores, 5.5% of the patient population scored 0, 48% scored between 1 and 4, 43% scored
between 5 and 9, and 4% scored above 10 (mean: 4.4; sd: 2.6; mode: 4) [Graph 2]. Out of the total patient population, 26% presented with one or more psychiatric issues. The most frequently occurring comorbid conditions according to the hospital criteria in this population were hypertension (N=1228), obesity (N=755), diabetes (N=583), anemia (N=533), and valve disorder (N=522).
Conclusion/Discussion
Using the described methodology, our analysis uncovered the presence of a high incidence of comorbidities in the BronxCare Orthopedics total joint replacement patient population which represents a closed urban population.
Gaining a better understanding of the severity of pooled comorbidities within a hospital’s respective patient population can lead to a more accurate assessment in developing efficacious payment systems adopted for the procedure [6]. [7]. In our opinion it is critical that payors include these risk adjustments for pooled comorbidities so that hospitals with medically complex patients, such as BronxCare and other safety net hospitals, are not penalized or disadvantaged [8].
Therefore, rather than stratifying individuals for individual payment, pooled comorbidity information can be used to better inform bundled payments for joint replacements based on severity of comorbidities of the population served by the center.
#6894
Time-Driven Activity-Based Costing to Determine Personnel Expenses in Total Joint Replacement Surgery in a Closed Urban Setting
*Ira Kirschenbaum - Bronx-Lebanon Hospital - Bronx, USA
Eva Kitlen - Brown University - Bronx, USA
Melanie Anaya - Brown University - Providence, USA
Gabriela Batista - Brown Universiy - Providence, USA
Gabriela De Queiroz Campos - Brown University - Providence, USA
Noshin Nuzhat - Brown University - Providence, USA
Natasha Richmond - Brown University - Providence, USA
Lindsey Ruda - Brown University - Providence, USA
Lisa Schulmeyer - Brown University - Providence, USA
Ariel R.C. Silverman - BronxCare Orthopaedics - Bronx, USA
Ronald Huang - BronxCare Orthopaedics - Bronx, USA
*Email: IKIRSCH@bronxleb.org
Introduction
There are many ways to calculate costs in the OR, including time-driven activity-based costing (TDABC) in the perioperative area. The aims of the present study include calculating personnel costs for TKA and THA, identifying inefficiencies in the surgical process, and identifying major cost drivers with the goal of streamlining the process to reduce costs.
Methods
Data Collection: Personnel observation during four TKAs and two THAs led to the development of process maps for each surgery, including all patient interactions, all operating room use, and administrative activity. For each event, we recorded the time that relevant personnel were involved and used it in conjunction with internal salary data to calculate personnel expenses.
Results
Costs: TKA personnel costs fall between $2201 and $3720, with a mean cost of $3171. THA personnel costs fall between $2040 and $2378, with a mean of $2209.
Efficiency: Figures 1-4 are Gantt charts representing process maps of TJAs. Figure 1 illustrates the turnover time between a THA and a TKA. There is significant overlap between the final events in the first case (THA) and the initial events the second case (TKA). There is significant overlap and continuity between events within each case. Figure 4 depicts the turnover time between a TKA and an inpatient THA. Unlike Figure 1, however, it shows a short period of unoccupied time between the two cases. Figures 2 and 3 both illustrate single TKAs. Similarly to Figure 1, there is minimal lag time between events in each of these cases.
Consistency: Table 1 shows the %RSD by event numerically. Consistency was only assessed for TKA because there were only 2 THA cases, which is too small a sample size to give significant data regarding consistency in the process.
Cost Drivers: Figure 6 shows the relative contribution of each event to TKA personnel costs. The procedure is the only major cost driver at $2046. Figure 7 illustrates the cost contributions of different groups of personnel. The anesthesia team is the primary cost driver at $1216, followed by the surgeon at $921.
Conclusions
Costs: Personnel costs are a significant and highly variable cost in TJA
Efficiency: Examination of the Gantt charts suggests that there are minimal inefficiencies in the surgical process, as many events overlap or immediately follow each other. Inefficiencies were due to delays in pre-operative medication administration
Consistency: Based on the %RSD of each relevant event in TKA, events throughout the entire surgical process are highly variable. The CRNA’s involvement in anesthesia induction had 160.2% RSD and every segment of the draping and sterile preparation process had RSD>50%.
Cost Drivers: Personnel-based analysis indicates that the anesthesia team and the surgeon are both major cost drivers.
Significance: The present study finds that TKA involves, on average, $3171 of personnel costs while THA personnel costs are $2209 on average. We believe it would be useful to follow up this analysis with further studies taking into account the cost of material goods as a factor, including devices.
Figures
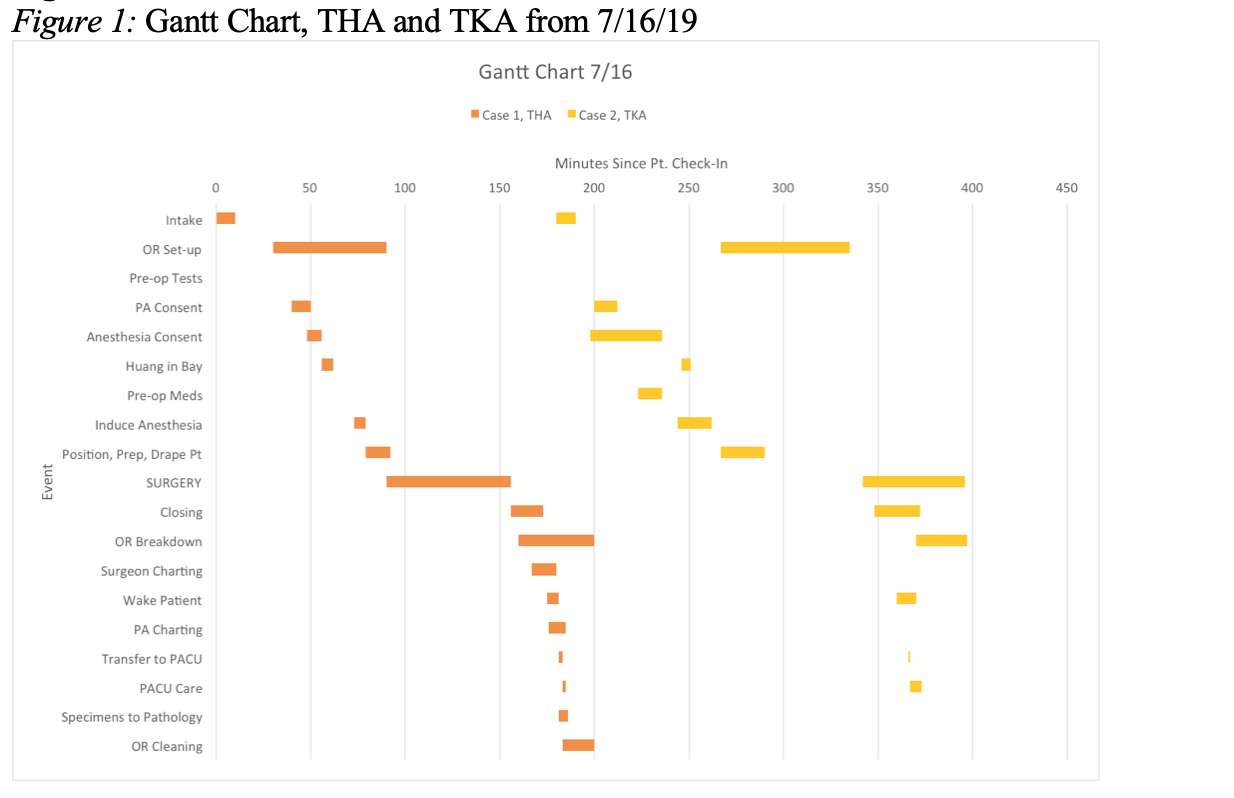
Figure 1
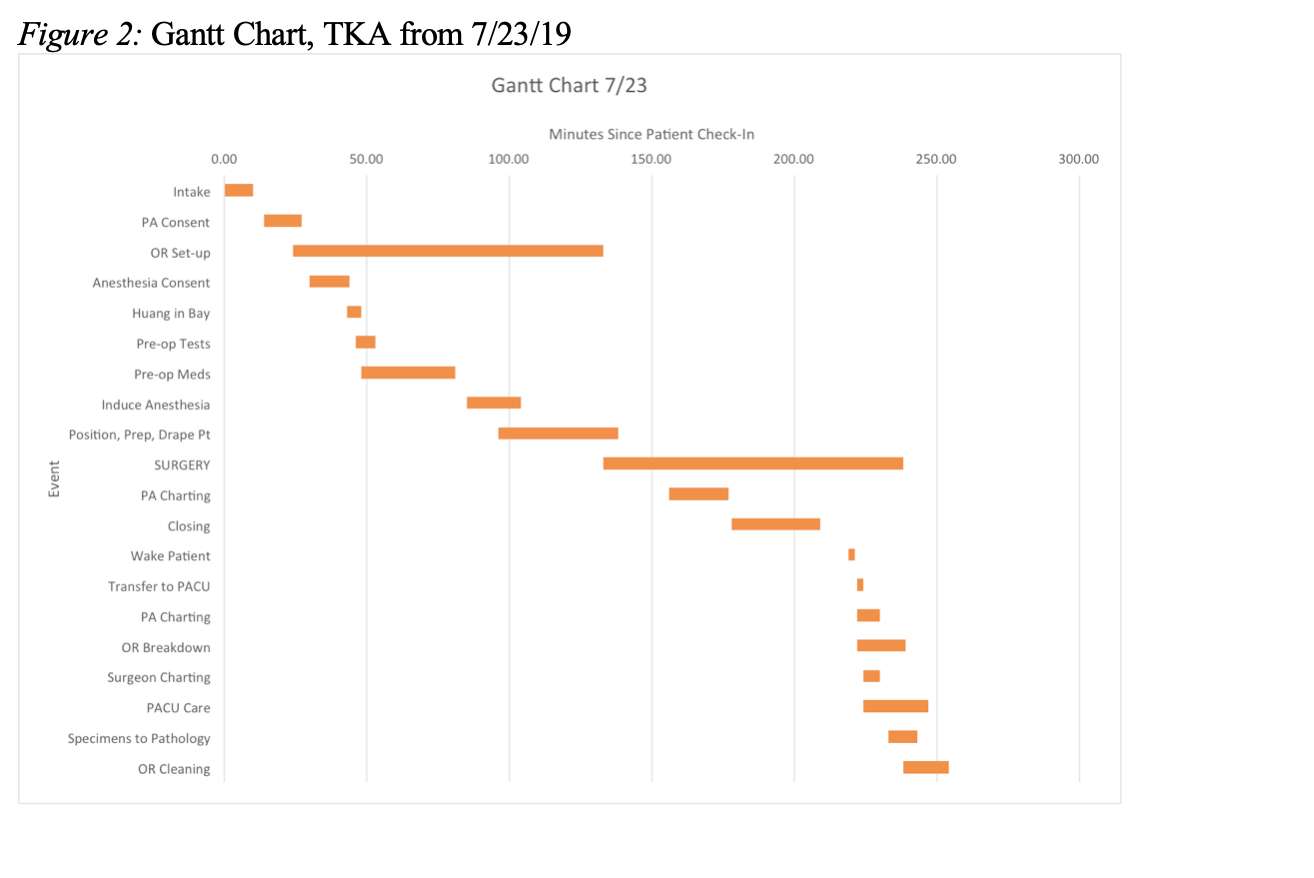
Figure 2
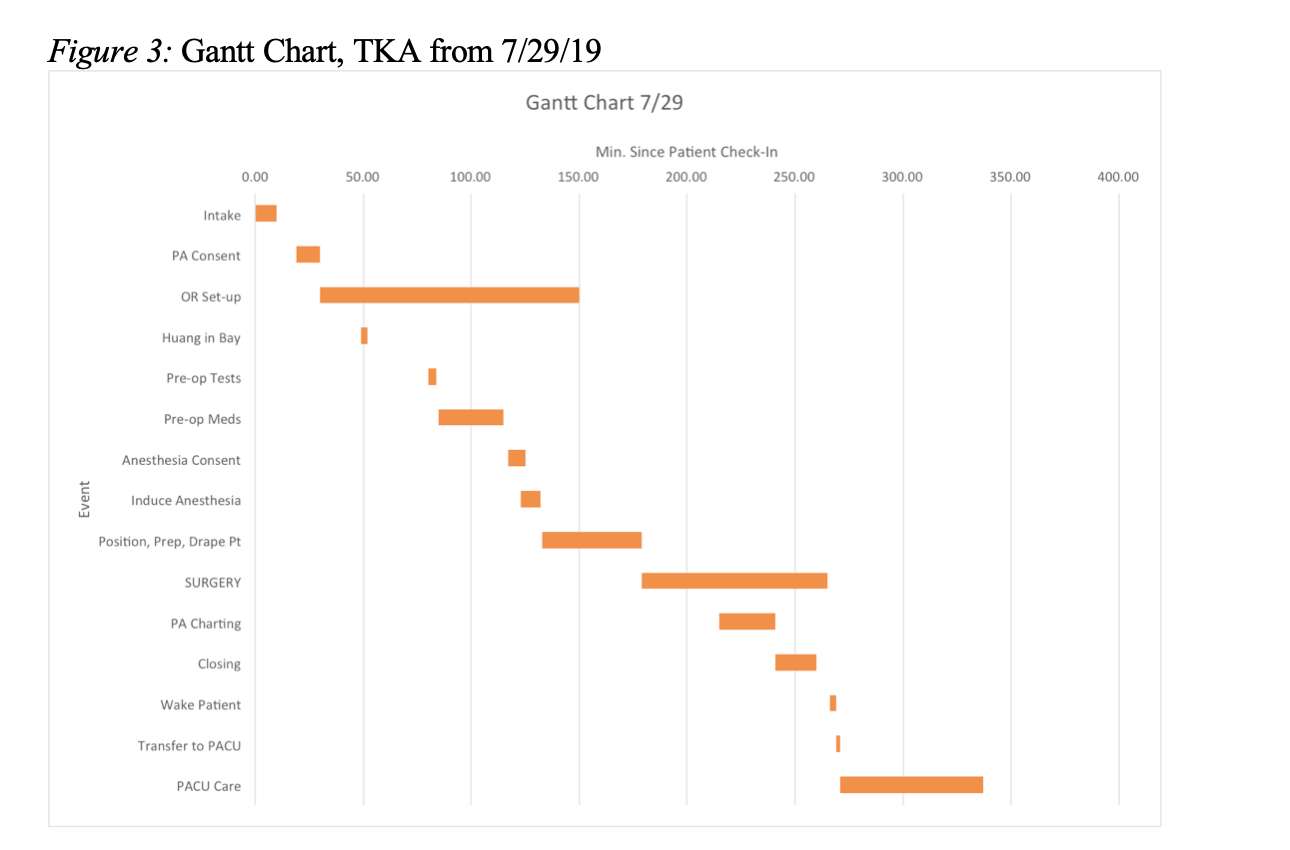
Figure 3
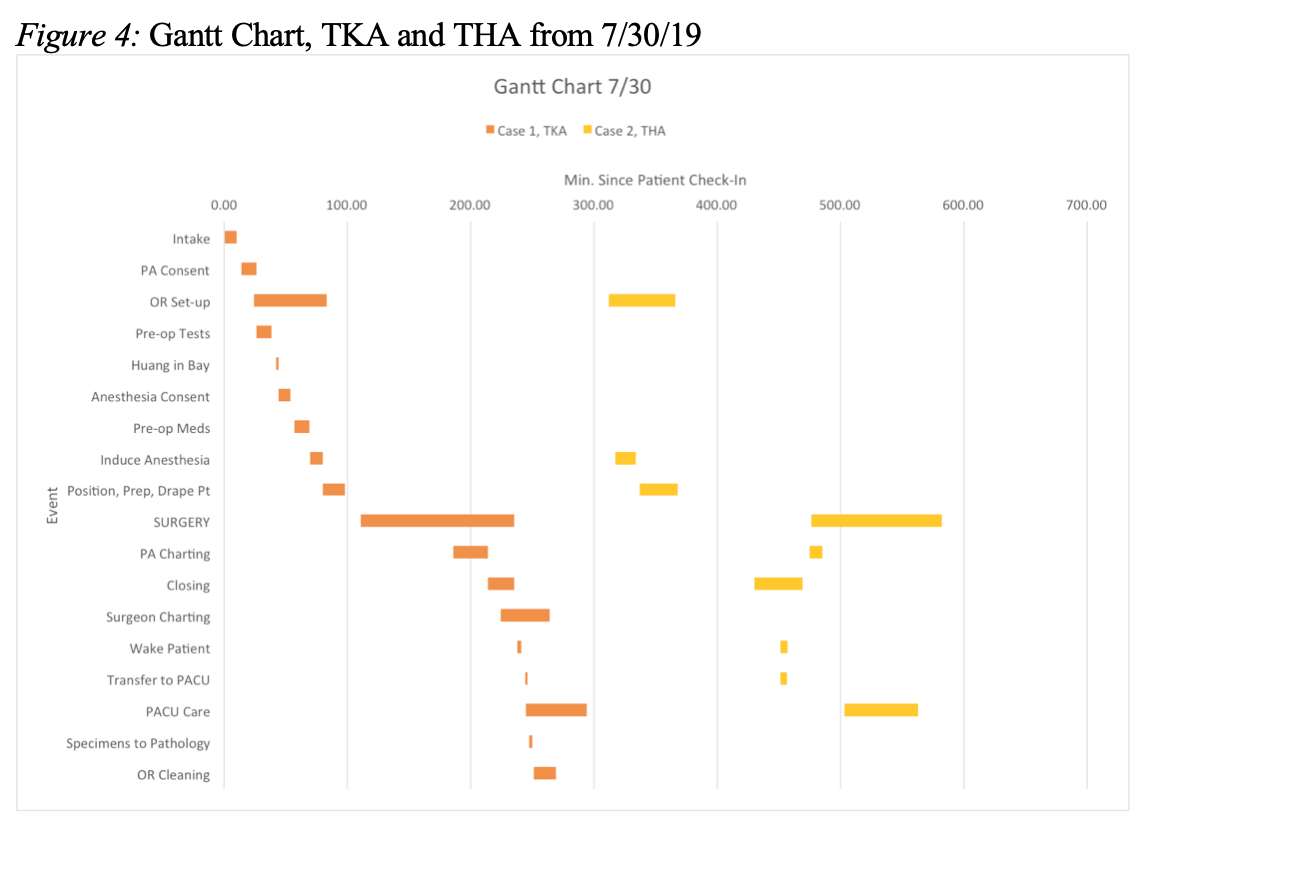
Figure 4
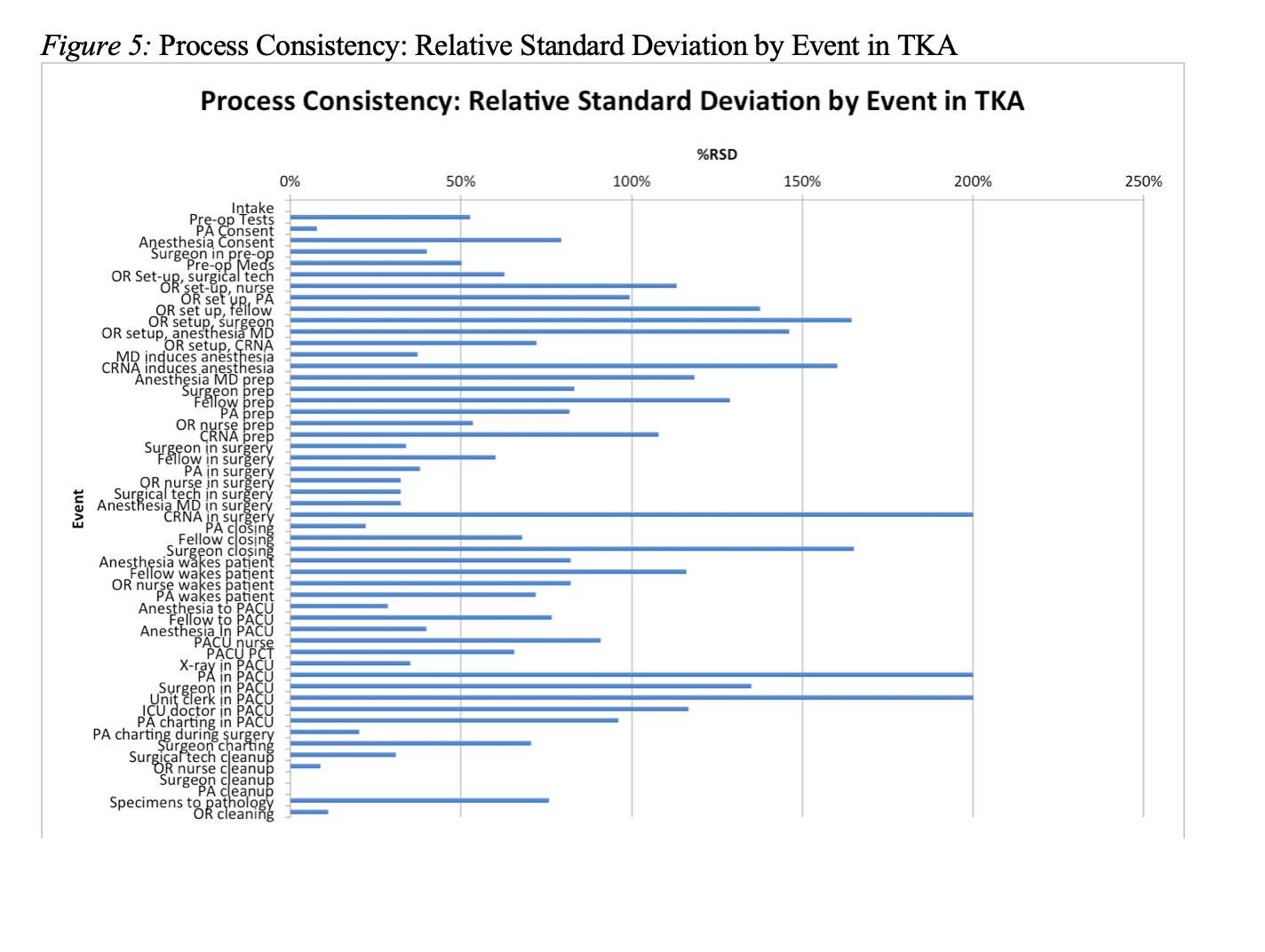
Figure 5
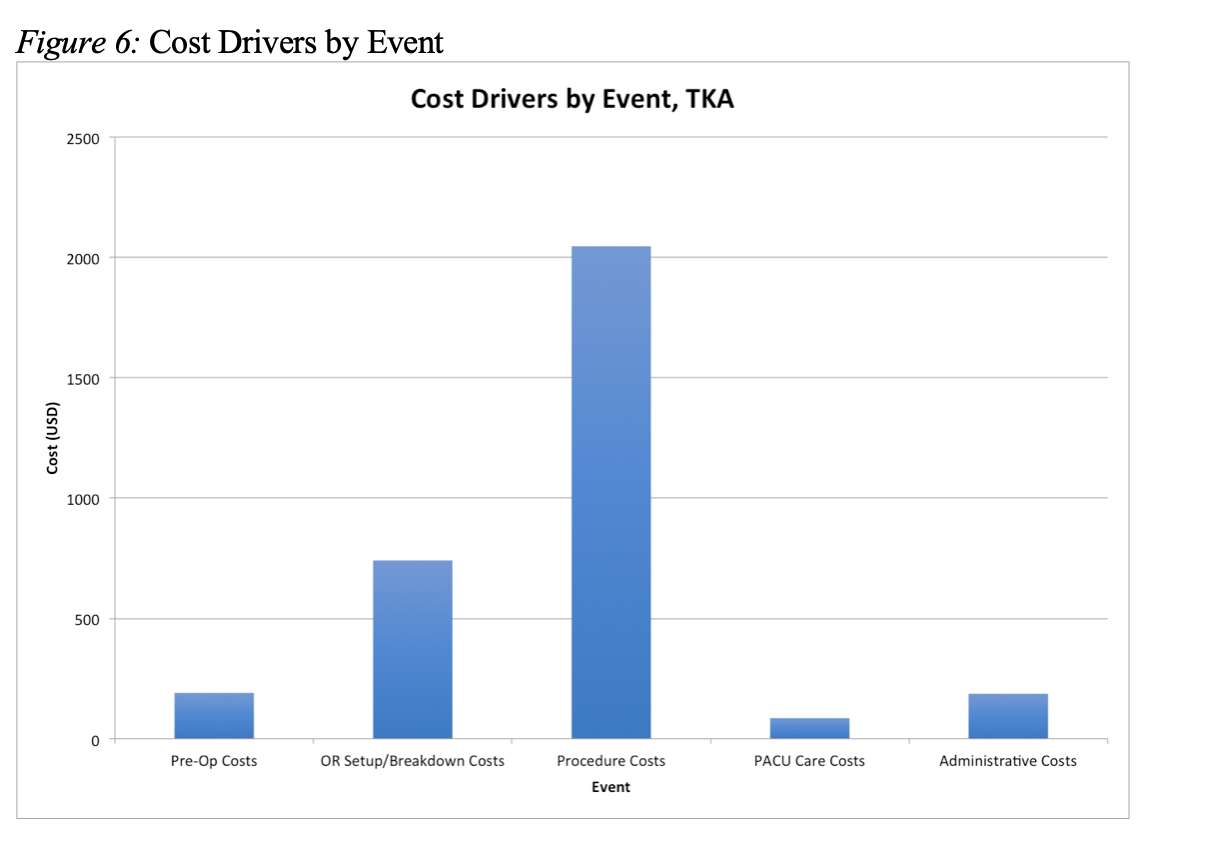
Figure 6
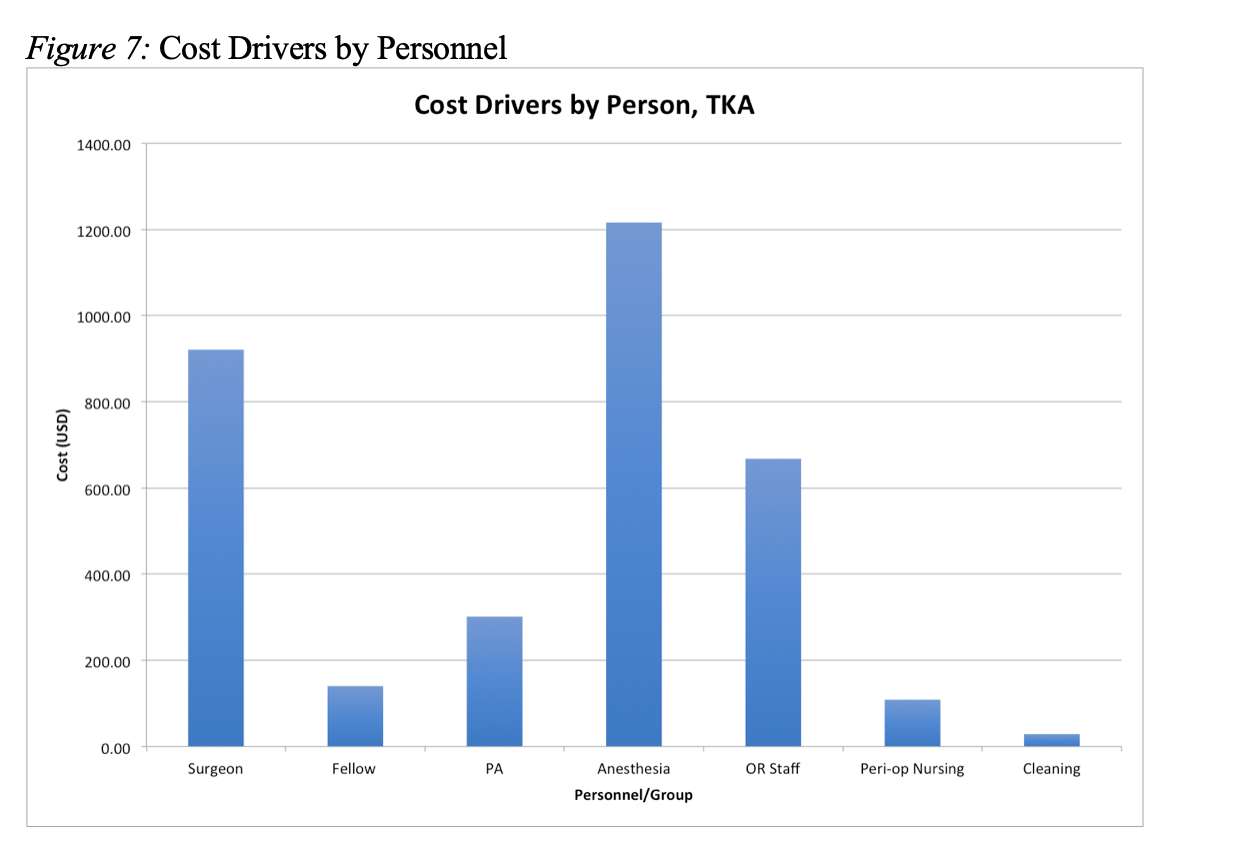
Figure 7
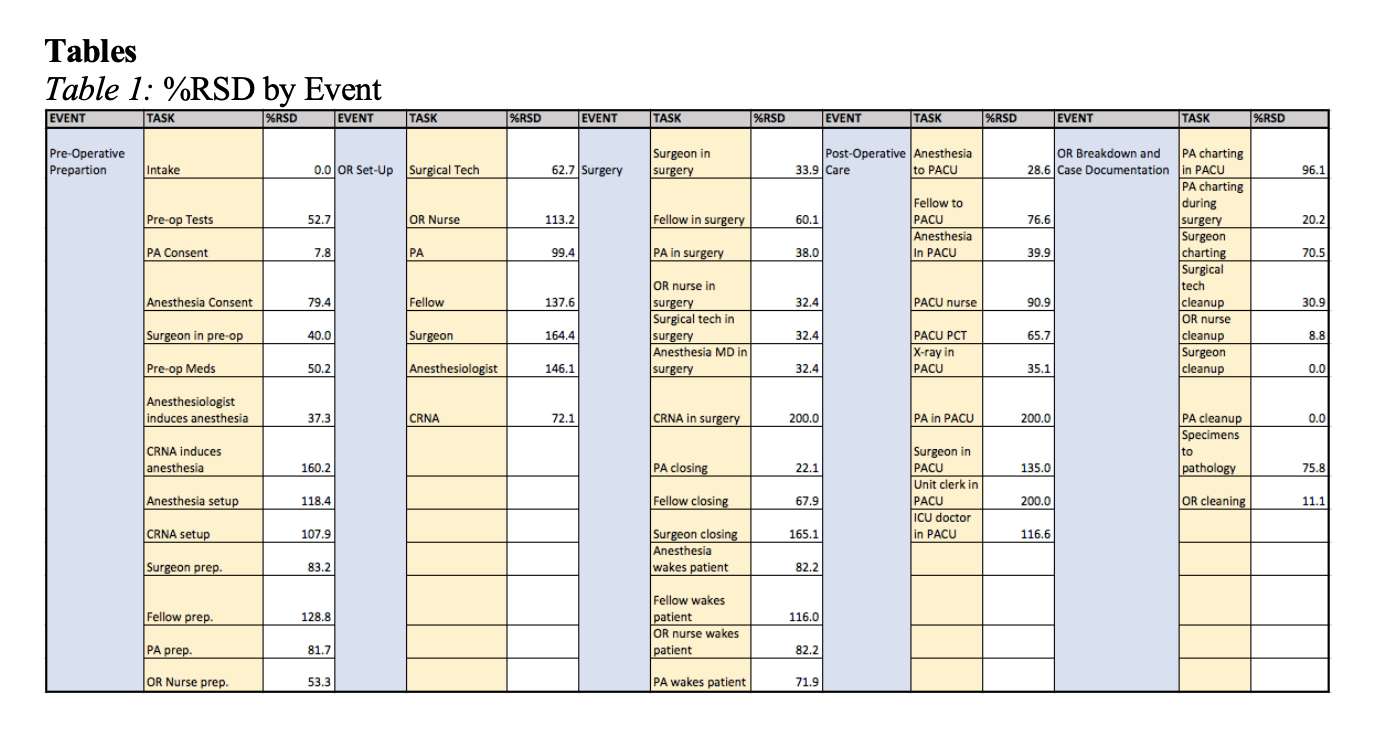
Figure 8#6895
Health Literacy in English vs. Spanish-Speaking Orthopaedic Chronic Pain Patients in a Closed Urban Setting
*Ira Kirschenbaum - Bronx-Lebanon Hospital - Bronx, USA
Gabriela Batista - Brown Universiy - Providence, USA
Eva Kitlen - Brown University - Bronx, USA
Natasha Richmond - Brown University - Providence, USA
Lindsey Ruda - Brown University - Providence, USA
Ariel R.C. Silverman - BronxCare Orthopaedics - Bronx, USA
*Email: IKIRSCH@bronxleb.org
Introduction
Health literacy is an essential element of doctor-patient communication. Inadequate literacy was also a risk factor for hospital admission among elderly Medicare patients. Additionally, patients with low levels of literacy have been shown to hold a deep sense of shame, which is often exacerbated when hospital staff express frustration when interacting with such patients.
We developed and administered a novel survey that investigates the following main questions:
- How well do patients comprehend their medical conditions?
- What is the nature of the patient’s social connectivity to others as it relates to their health?
- How do patients perceive both their doctor’s and their ownability to influence their health outcomes?
Methods
Chronic Pain Patients (CPPs) presenting for treatment (either general or specialized) at BronxCare’s orthopaedic clinic were randomly selected and asked to complete a 5-minute survey prior to their appointments. The survey assessed English speaking and comprehension abilities, current pain level and chief complaint, persistence of condition, comprehension of condition, whether the patient had discussed the condition with others, whether the patient was accompanied to appointments, confidence in the physician, and confidence in self. The inclusion criterion for analysis was self-reported pain for greater than 3 months in orthopaedic patients over the age of 18.
Results
44% of patients chose to complete the survey in Spanish and 56% did so in English. Over 60% of patients reported their English speaking and comprehension abilities to be either good, very good, or excellent. CPPs reported an average pain score of 6.25/10 for conditions mostly related to the hip, leg, or knee. 42% of all CPPs could both name and describe their condition (n=24). Most CPPs came unaccompanied to their appointments (n=36, 65%), but over 85% reported previously discussing their conditions with members of their community (n=47). Of all CPPs, 75% reported confidence in their physician (n=42) and 59% reported self-confidence in improving their health outcomes (n=33).
Regressors Influencing Condition Comprehension:
Condition comprehension was significantly positively correlated with both English Speaking and English Comprehension abilities (p<0.02). There were no other factors significantly correlated with condition comprehension.
English vs. Spanish-Speaking Comparisons:
Survey responses for English- and Spanish-speaking cohorts were further compared for significant differences. Non-English-comprehending and speaking patients reported significantly lower confidence in their physicians to improve their health outcomes (X2=6.705, p=0.009). The two cohorts were comparable for all other responses.
Conclusions
The present study aimed to examine health literacy in a closed, urban community with a high proportion of Spanish-speaking patients. Despite the extensive interpretation services available at our hospital, patients with poor English capabilities still showed significant decreases in their condition comprehension and overall confidence in their physician.
Language differences can interrupt the flow of health information from practitioner to patient, leaving the patient less informed regarding their health. The Spanish-speaking cohort also showed significantly lower levels of confidence in their physicians. The results beg further investigation into a detailed analysis of this issue.
#6896
Retrospective Comparative Analysis of Opioid Issuance Trends for Total Joint Arthroplasty in 2014 and 2017
*Ira Kirschenbaum - Bronx-Lebanon Hospital - Bronx, USA
Chloe Zana - Brown University - Providence, USA
Lauren McAllister - BronxCare Orthopaedics - Bronx, USA
Kylen Soriano - University of California at San Francisco - San Francisco, USA
Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
*Email: IKIRSCH@bronxleb.org
Objective
The increasing number of overdoses and deaths caused by opioids spotlights a complex public health crisis faced by the American society. Hence, concerns surrounding the dependence and abuse of narcotics have led to new laws and regulations of opioid prescriptions. In 2017, New York state implemented a Mandatory Prescriber Education for prescribers licensed to issue controlled substances, including opioids. This study tracked opioid prescriptions of orthopedic surgeons following total joint arthroplasty in both 2014 and 2017 to evaluate trends in opioid prescriptions following changes in legislation and an increased public awareness of the opioid crisis.
Methods
Retrospective analysis was conducted on 35 randomized patients from 2014 and 35 randomized patients from 2017 who underwent total joint arthroplasty (TJA) at BronxCare Health System. The data collected included the total number of opioid prescriptions and the total morphine equivalent for each patient. These variables were evaluated for both six months prior to and six months post-surgery. Opioid prescription information was derived from computerized pharmacy records, pre-operative risk assessments, and operative reports.
Results
Between 2014 and 2017, a significant decrease in the total morphine equivalent dosage (MED) prescribed was observed (p = 0.009, N = 70), going from 3437.57 to 960.07 morphine equivalents. A significant decrease in the number of months a TJA patient stays on opioids post-op was also observed (p = 0.015), from 1.89 months in 2014 to 0.93 months in 2017.
Pre-op opioid users were suggestively prescribed more opioids (p = 0.008) for longer (p = 0.001), with a mean MED of 5665 compared to a mean of 999 for non-pre-op opioid users, and a mean period of 2.96 months compared to 0.87 months for non-pre-op opioid users. This study had 18 such patients with additional conditions that were treated by prescription opioids within 6 months prior to surgery.
Among the variables analyzed, prior substance abuse (PSA) was a significant indicator: patients with PSA were prescribed more opioids (p = 0.027) for longer (p = 0.026), with a total MED of 7662 compared to 1288 for patients without substance abuse history, and a mean period of 3.04 months compared to 1.13 months. Among the 70 patients, 10 reported polysubstance abuse prior to their TJA.
Obesity, hypertension, and gender all proved to be insignificant determinants of opioid prescription amount (p = 0.0155, 0.487, 0.408) or length of usage (p = 0.480, 0.408, 0.320).
Conclusion
This study revealed a decrease in orthopedic surgeon issuance of opioids for patients who underwent total joint arthroplasty in 2017, as compared to patients who underwent the same procedure in 2014. As the patient population of BronxCare Health System exists within the urban setting of the South Bronx, New York is at a greater risk of developing opioid dependence, this study provides data to support the positive effects of increased public awareness, as well as increased legislature and regulations, on decreasing opioid dependence and abuse.
#6897
The Impact of a Comprehensive Orthopaedic Delivery System on Referral Patterns of Knee Pain in a Closed Urban Environment
*Ira Kirschenbaum - Bronx-Lebanon Hospital - Bronx, USA
Lindsey Ruda - Brown University - Providence, USA
Eva Kitlen - Brown University - Bronx, USA
Ariel R.C. Silverman - BronxCare Orthopaedics - Bronx, USA
Chrissy Manning - BronxCare Orthopaedics - Bronx, USA
*Email: IKIRSCH@bronxleb.org
Background
Historically, non-governmental safety net hospitals (SNH) treating patients of low socioeconomic status (SES) have had difficulty providing specialty care, leaving it to public hospital systems. In 2008, BCHS underwent significant administrative and structural changes in its orthopaedic delivery system by increasing services and quality. We hypothesize that safety net hospitals should invest in comprehensive orthopedic departments, as this hospital did for issues related to access and quality. We believe that the growth of this orthopaedic delivery system was accompanied by a concomitant rise in musculoskeletal visits in the treat-and-release divisions of BCHS, showing a pull-through effect that quality can have across a health system.
Methods
Using hospital-based, administrative claims data, we analyzed the growth of orthopaedic outpatient clinic volume from 2009 to 2018 in all musculoskeletal visits. Additionally, surgical volume was analyzed with an internal departmental surgical tracking database (TrackVia, Inc.). Separately, emergency department treat-and-release data for knee-related complaints for all Bronx residents was obtained with IBM Market Expert® in order to compare referral volume and patterns for BCHS compared to other regional hospitals in 2009 versus 2018.
Results
Orthopaedic Department: BCHS had over a ten-fold increase in the number of clinic visits from 3,500 to 36,000 per year and a corresponding increase in surgical volume, while the population of the Bronx only grew between 3-4%.
Treat and Release Patterns and Data: Referral volume for BronxCare showed a 44.4% increase in knee pain treat and release over this time period with no significant increase (3.9%) in general ER volume. Of the five other major hospitals in the Bronx region, one saw a 25% increase, one saw a 4% increase, and the three others saw losses of 5.6%, 33.9% and 62.5% respectively.
Conclusions
Specialty care matters in health systems. Using knee pain as a proxy, the market-based analysis illustrates a general increase in treat-and-release musculoskeletal visits across BCHS that we believe can be attributed to the development of a comprehensive, high-quality orthopaedic delivery system. The findings demonstrate a positive disruption in the marketplace based on improved specialty care delivery system.
Public or private health systems that are in underserved areas should not ignore the value of high-quality specialty care, not only to meet community needs, but also due to its necessity in constructing a complete healthcare and business mission of the healthcare delivery system.
#7398
Increased Early Mortality After Total Knee Arthroplasty Using Conventional Instrumentation, Compared to Technology-Assisted Surgery: An Analysis of Linked National Registry Data
*David Kirwan - Insight Private Hospital - ALBURY, Australia
Ian Harris
*Email: kirwan@hotkey.net.au
Abstract
Introduction: Recent studies have demonstrated improving mortality rates over time, in both hip and knee arthroplasty. Navigation has been shown to reduce complication rates, including bleeding, but not VTE. These outcomes are not routinely collected by arthroplasty registries.
All TKA operations are associated with some fat emboli. At body temperature, bone marrow fat exists as liquid, as a low viscosity oil, which can be instilled with ease into venous sinusoids in bone, when surgical trauma is combined with hydrostatic pressure. The insertion of intra-medullary rods (which is necessary with conventional instrumentation) may increase the risk of complications, including death.
We hypothesised that technology assistance (navigation, PSI and robotics), which avoids intra-medullary instrumentation, would be associated with a lower rate of early postoperative death, compared with the use of conventional instrumentation.
Methods: Using data from a large national arthroplasty registry we compared available 7-day, 30-day and 90-day rates of mortality, following bilateral simultaneous (BSTKA) and unilateral TKA, when performed with conventional versus technology-assisted instrumentation. Logistic regression and Cox proportional models were used, adjusted for known potential confounders.
Results: A total of 34,908 BSTKAs and 581,818 unilateral TKA procedures were identified. The proportion of cases utilising technology-assisted instrumentation increased over the study period (2003 - 2019 incl).
For the BSTKA patients, the odds ratio of mortality at 30-days and 90-days was approximately 4 times higher with conventional instrumentation, compared to technology-assisted.
For the unilateral TKA patients, the odds ratio of 7-day, 30-day and 90-day mortality rates were, 2.3, 1.7 and 1.4 respectively, in the conventional instrumented group, compared to the technology-assisted group.
In both groups, results were adjusted for age, gender, ASA grade, BMI and year of procedure.
Discussion:Fat Embolism Syndrome (FES) has been in existence since fractures of bone first occurred. FES was described in Roman times. The Gurd and Wilson classification of FES was described in 1970. A contemporary understanding of fat embolism following orthopaedic surgery is provided, including clinical and pathological manifestations and, the reduction in FES associated with the use technology in knee arthroplasty surgery. Implications for the design and use of instrumentation are considered.
Conclusions: Technology-assisted BSTKA and TKA were both associated with significantly lower early mortality, compared with the use of conventional instrumentation. This difference may be explained primarily by the reduced quantum of fat emboli associated with technology-assisted BSTKA. These differences are likely to be clinically important, on a population scale.
Level of evidence: Therapeutic Level III.
#7611
THR: Presentation of Novel Femoral Components, Designed to Mitigate Impingement, Instability, Peri-Prosthetic Fracture & Revision.
*David Kirwan - Insight Private Hospital - ALBURY, Australia
*Email: kirwan@hotkey.net.au
Abstract:
An analysis of common non-infective mechanisms of wear, failure, fracture and revision is presented, with novel femoral components, intended to mitigate these problems. Successful early bench studies and computational studies are presented. This new design is tendered for the ISTA membership to consider, before wider publication.
Background:
THR revision presents a significant cost and morbidity. Non-infective indications include impingement, wear, instability and peri-prosthetic fracture.
Technologies, including Leewinek charts, combined version, pelvic inclination and tilt, sacral angles, OPS, navigation and robotics, have improved component placement, to optimise outcomes and reduce these risks.
The high success rate of THR has encouraged many authors to assert that component design is now optimal, such that further improvements are unlikely to occur.
We hypothesised that a modified femoral stem component, could reduce the incidence and severity of both posterior prosthetic impingement (PPI) and anterior bony impingement (ABI) and by inference, reduce rates of impingement, instability, wear and revision.
Methods:
We compared our novel stem with a generic (Corail style) stem, to determine the range of motion (ROM), using anterior bony impingement (ABI) and posterior prosthetic impingement (PPI), as the respective end points of flexion and extension.
Planning was performed by experienced planning engineers, using “Lexi” software, to determine ideal component placement for both stems.
Terminal flexion was measured at zero degrees of abduction and rotation. Terminal extension was performed at 60 degrees of hip ER and zero degrees of abduction.
All hips were modelled and tested with a standardised acetabular component, at 40/20.
Results:
Compared to the generic stem, terminal flexion and extension angles were increased using the novel stem, in all hips modelled. In both groups, flexion was limited by ABI and extension by PPI. There were no cases of anterior prosthetic impingement. Further results are pending and will be released at ISTA, Maui.
Discussion:
Without soft tissue constraints, hip components have a finite ROM (FROM) in each plane, before impingement occurs. Soft tissues often prevent these limits being reached.
Logically, edge loading and impingement are far more common than failure or revision for these problems. And, contemporary efforts have been directed at idealising acetabular component placement, to mitigate these same problems. However, THR failures still occur.
Initial results show that our novel stem design allows an increased ROM before the two most common examples of impingement occurs (ABI and PPI). Positive inferences may be drawn from these increases, in relation to wear, stability and revision rates. Peri-prosthetic fracture rates may also be improved. Further work is required, including clinical trials.
Conclusions:
Contemporary technologies have improved component placement and outcomes. However, a substantial improvement in component design is presented for consideration. The novel stem appears to improve ROM before impingement can occur. This difference is likely to be clinically important, on a population scale.
#8023
Extracorporeal Shockwave Technology (ESWT) for Orthopaedic Treatment
*Jih-Yang Ko - Kaohsiung Chang Gung Memorial Hospital - Kaohsiung, Taiwan
Ching-Jen Wang - Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan - Kaohsiung, Taiwan
*Email: kojy@adm.cgmh.org.tw
Extracorporeal shockwave therapy (ESWT) has developed over the past 40 years. This treatment was originally designed for disintegration of kidney stones and has remained the gold standard for the treatment of urolithiasis because of its clinical success. An incidental observation of osteoblast responses in bone after ESWT triggered the clinical use of this practice for musculoskeletal disorders. This paradigm shift resulted in expanding ESWT from a destructive force for stone disintegration into a regenerative treatment modality.
Nowadays, ESWT had emerged as the leading choice in the treatment of some orthopedic disorders including plantar fasciitis of the heel, lateral epicondylitis of the elbow, calcific tendinitis of the shoulder and non-union of long bone fracture.
In biological tissues, ESWT reportedly modulates angiogenesis (vWF, VEGF, eNOS, and PCNA), bone healing (BMP2, osteocalcin, alkaline, phosphatase, DKK1 and IGF-1), anti-inflammatory (si-CAM and sVCAM) and wound healing (Wnt3 and B-catenin).
These advancements in research and technology further widened the indications of ESWT from musculoskeletal disorders to non-skeletal diseases such as ischemic heart disease, Peyronie's disease, erectile dysfunction, diabetic foot ulcers, acute or chronic wounds and burn lesion.
The future application of ESWT may be combined with advances and innovative technology including stem cell therapy, miRNA analysis, gene sequencing, and genomic medicine. In the orthopaedic field, combined ESWT with other treatment modalities has been performed increasingly for osteoarthritis of the knee, avascular necrosis of the femoral head, non-calcific rotator cuff tendinopathy, and anti-biofilm effect in peri-prosthesis joint infection (PJI). As such, ESWT has evolved into a multidisciplinary and multifunctional medical subspecialty to promote the health and wellbeing of humans.
#8024
Invited Talk: Avoidance of Intramedullary Violation in Computer-Assisted TKA Lowers the Incidence of Periprosthetic Joint Infection Compared With Conventional TKA
*Jih-Yang Ko - Kaohsiung Chang Gung Memorial Hospital - Kaohsiung, Taiwan
Cheng-Fong Chen - Taipei Veterans General Hospital - Taipei, Taiwan
Jeng-Wei Chen - Kaohsiung Chang Gung Memorial Hospital - Kaohsiung, Taiwan
Feng-Chih Kuo - Kaohsiung Chang Gung Memorial Hospital - Kaohsiung, Taiwan
Shu-Jui Kuo - China Medical University Hospital, - Taichung,, Taiwan
Ka-Kit Siu - Park One International Hospital - Kaohsiung, Taiwan
*Email: kojy@adm.cgmh.org.tw
Background: Conventional total knee arthroplasty (CONV-TKA) inevitably perturbs femoral medullary canal, disturbs medullary micro-architecture and increases blood loss and inflammatory responses. We hypothesized that avoidance of intramedullary violation in computer-assisted total knee arthroplasty (CAS-TKA) may lower the incidence of periprosthetic joint infection (PJI), as compared with CONV-TKA.
Methods: A propensity score matchings tudy of 5342 patients who underwent CAS-TKA (n = 1085) or CONV-TKA (n = 4257) for primary osteoarthritis of the knee from 2007 to 2015 in our institute was performed. Patients who underwent CAS-TKA were matched to those who received CONV-TKA at a 1:2 ratio according to age, gender, BMI, CCI, year of surgery, surgical duration, preoperative anemia, blood transfusion, and usage of antibiotics-impregnated cement. PJI was defined according to the Musculoskeletal Infection Society diagnostic criteria from the 2013 International Consensus Meeting.
Results:According to the data of Taiwan national health service and Taiwan joint reconstruction society, we have 371 joint reconstruction surgeons. The annual amount of THA, TKA, revision THR, and revision TKA were 8977, 24120, 1287, 1149, and 8399, 22636, 1191 and 1176 in 2020 and 2021 respectively. The overall PJI rate was 1.29% (69/5342) after a mean follow-up duration of 8.3years in our institute.After controlling potential risk factors, the use of CAS-TKA resulted in a lower incidence of PJI as compared with CONV-TKA [adjusted hazard ratio (HR), 0.42; 95% confidence interval (CI), 0.18-0.99]. The same trend in PJI reduction was observed with the usage of CAS-TKA under sensitivity testing [HR, 0.33; 95% CI, 0.12-0.95]. The cumulative incidence of PJI was lower in the CAS-TKA group than the CONV-TKA group (log-rank test, p = 0.013).
Conclusion: Through avoidance of intramedullary violation during TKA, the use of CAS-TKA can reduce the incidence of PJI, with a better survival rate in terms of being free of PJI, as compared with CONV-TKA.
#7947
Patient Specific Instrument in Resurfacing Hip Arthroplasty.
*Daisuke Koga - Orthopaedic Surgery Saitama Red Cross Hospital - Saitama, Japan
*Email: koga.orth@tmd.ac.jp
Background: The use of resurfacing hip arthroplasty (RHA) for idiopathic osteonecrosis of the femoral head and other conditions has decreased since the report of adverse reaction to metal debris (ARMD). However, if the application is considered appropriately, it can provide advantages such as physiological loading. In RHA, the insertion angle of the guidewire determines the insertion alignment of the implant, and it is necessary to rely on the surgeon's experience and intraoperative radiography.
Objectives: In the present study, we developed a patient-specific instrument (PSI) as a tool to assist in the insertion of guide pins, and we report on its usefulness.
Study Design & Methods: The subjects were three patients with four joints who underwent RHA in 2021. Preoperative planning was performed based on 3D-CT data, and PSI was created using AUTODESK FUSION360 CAD software and an optical 3D printer. We evaluated implant alignment using postoperative CT.
Results: The intraoperative fitting of the PSI to the femur was good, and the implant could be inserted with the planned alignment in all the cases.
Discussion: The PSI can be used as a support tool for accurate implant insertion by bridging the gap in skill between surgeons. In addition, the 3D preoperative planning has a secondary effect of allowing the surgeon to have a clear image of the operation preoperatively.
#7543
Comparison of Robotic-Assisted TKA and Patient Specific Instrumentation TKA
*Takeshi Kojima - Tachibana Hospital - Miyazaki, Japan
*Email: t-koji-1173@kaz.bbiq.jp
[Introduction]We installed surgery assist robot, Mako (Stryker Triathlon CS) , in November 2021. We compared and examined the component installation accuracy of MakoTKA and PSITKA (Medacta GMK Sphere CS).
[Subjects] From April 2016 to December 2021, 68 cases of PSITKA and 11 cases of MakoTKA were performed by the same surgeon, and the average age at the time of surgery was 79.6 years (66-90 years).
[Methods]:At Patient’s first postoperative clinic visit, standing AP hip-to-ankle radiographs were obtained. And Hip-Knee-Ankle angle (HKA), Femoral component angle (FCA), and Tibial component angle (TCA) were measured. An error of 3 ° or more from the planned installation angle was defined as the outlier.
[Results] The outlier rate of HKA of PSITKA was 35% (25/68 cases), and that of MakoTKA was 9% (1/11cases). The FCA was 25% (17/68 cases) and 9% (1/11cases), and the TCA was 31% (21/68 cases) and 0%.
[Conclusion] Compared with PSITKA, MakoTKA was able to install components more accurately. MakoTKA also has a leaning curve, and the outlier in one case was due to the antenna being displaced in the third case of introduction. We would like to continue to examine the installation accuracy by repeating cases.
#8038
Invited Talk: The Role of the ACL for knee function
*Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: rkomistek@aol.com
#7481
Influence of Stem Size and Position on Periprosthetic Fracture Risk and Primary Stability in Total Hip Arthroplasty
*Tobias Konow - TUHH Hamburg University of Technology - Hamburg, Germany
Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
Frank Lampe - Hamburg University of Applied Science
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: tobias.konow@tuhh.de
INTRODUCTION: Implant loosening and periprosthetic fracturs (PPF) are major complications in uncemented Total Hip Arthroplasty (THA). Complications decrease with increasing surgical experience and volume [1]. Even between highly experienced surgeons, variations with regard to the implanted stem size and position have been observed [2]. These may be related to different surgical philosophies (e.g. cortical/ trabecular bone fixation) during preoperative planning. The influence of small stem size variations (±1 size) around a reference size combined with variations in stem positioning on PPF risk and primary stability is unclear. The aim of this study therefore was to evaluate the PPF risk during broaching and stem implantation for a variation of the stem sizes and stem position and to assess the initial implant stability.
METHODS: The reference stem size for each femur was determined as the mean templated stem size (TSZ) by six experienced surgeons (Corail, Depuy Synthes, US). Two concessive implantations were performed in 6 femur pairs. On one side of each pair, first an undersized stem was implanted followed by a second implantation of the reference size stem. On the contralateral sides, first the reference size was implanted followed by an oversized stem. In the remaining 9 femur pairs reference size stems were implanted in 3 different alignments (6 varus, 6 neutral, 6 valgus). Cortex strains as an indicator for PPF were measured during broaching and stem implantation using digital image correlation. Laser scans were conducted to determine the stem position in the femur. All specimens were exposed to dynamic physiological loading (800 N, 600 cycles, 1 Hz). Primary stability was estimated from micromotion measurements and pull-out force.
RESULTS: The TSZ varied between the six surgeons (size 13 ± 1; p = 0.005). Higher stem subsidence was found for undersized stems compared to normal- or oversized stems (p < 0.001; Figure 1a). Oversized stems had higher pull-out forces compared to normal- and undersized stems (p = 0.008, p = 0.001, Figure 1b). Higher cortex strains were observed for varus-tilted stems compared to neutral- or valgus-tilted stems (Figure 2). High stem subsidence and low pull-out forces were found for valgus-tilted stems in comparison to neutral and varus (both: p = 0.043; Figure 3a,b). Lowest stem subsidence was observed for varus-tilted stems (p = 0.100, Figure 3a), yet micromotion was higher (17 ± 11 µm, neutral/valgus: 8 ± 2 µm, p = 0.043).
CONCLUSION: The differences in templating philosophies explain the variations in chosen stem sizes [2]. Undersizing is associated with reduced primary stability possibly causing implant loosening or increased PPF risk due to excessive stem subsidence [3]. If lateralized positioning (eg. slight valgus-tilt) is achieved, oversizing may improve primary stability without observing an increased PPF risk. Varus-tilt of the stem is associated with higher cortex strains increasing PPF risk and increased micromotions due to higher lever arms and bending moments.
REFERENCES:
[1] Konow et al., Bone Joint J 2021
[2] Konow et al., ARTD 2022
[3] Korsnes et al., HIP Int. 2020
ACKNOWLEDGEMENTS: The study has been financially supported by DePuy Synthes.
Figures
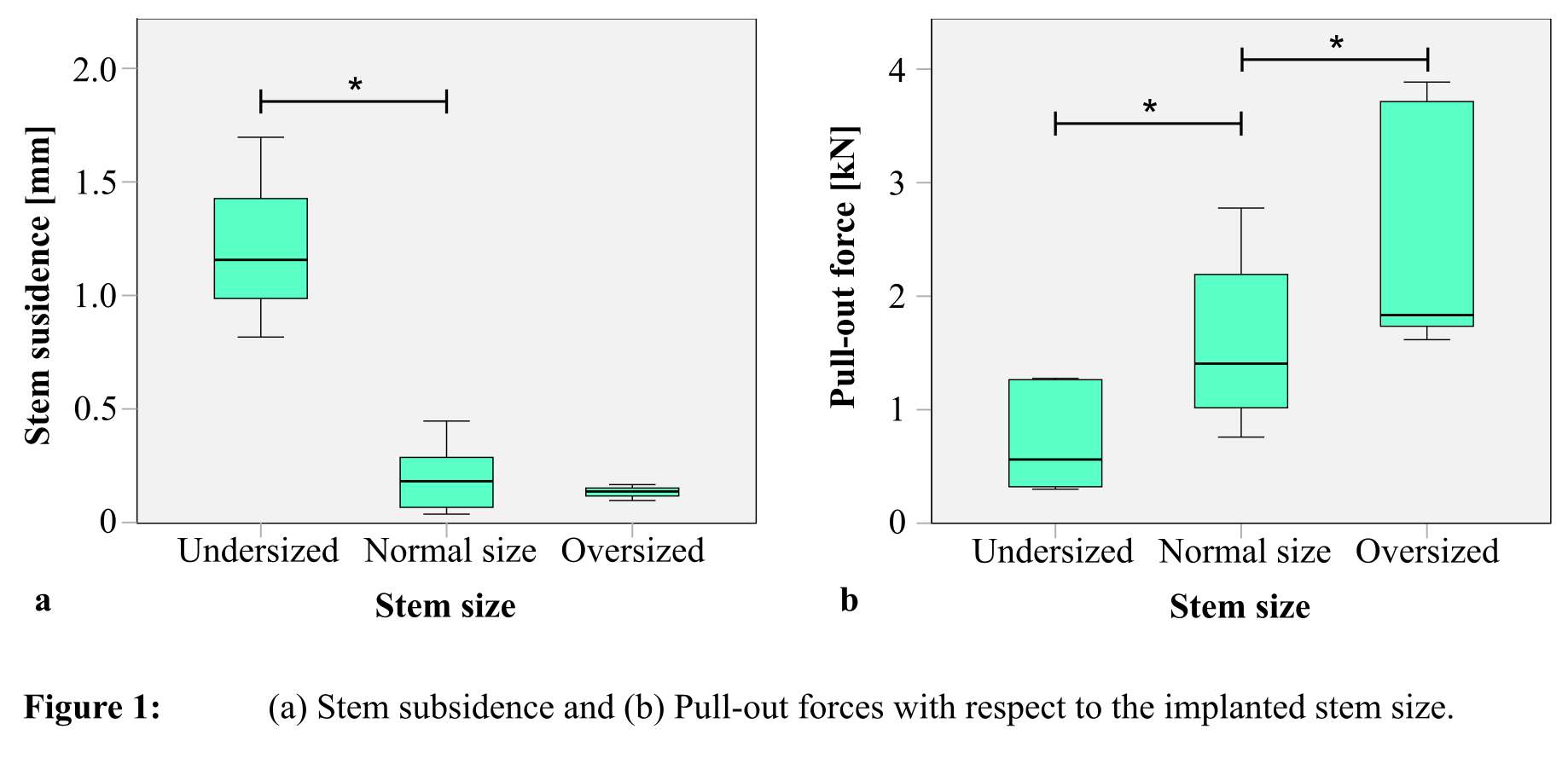
Figure 1
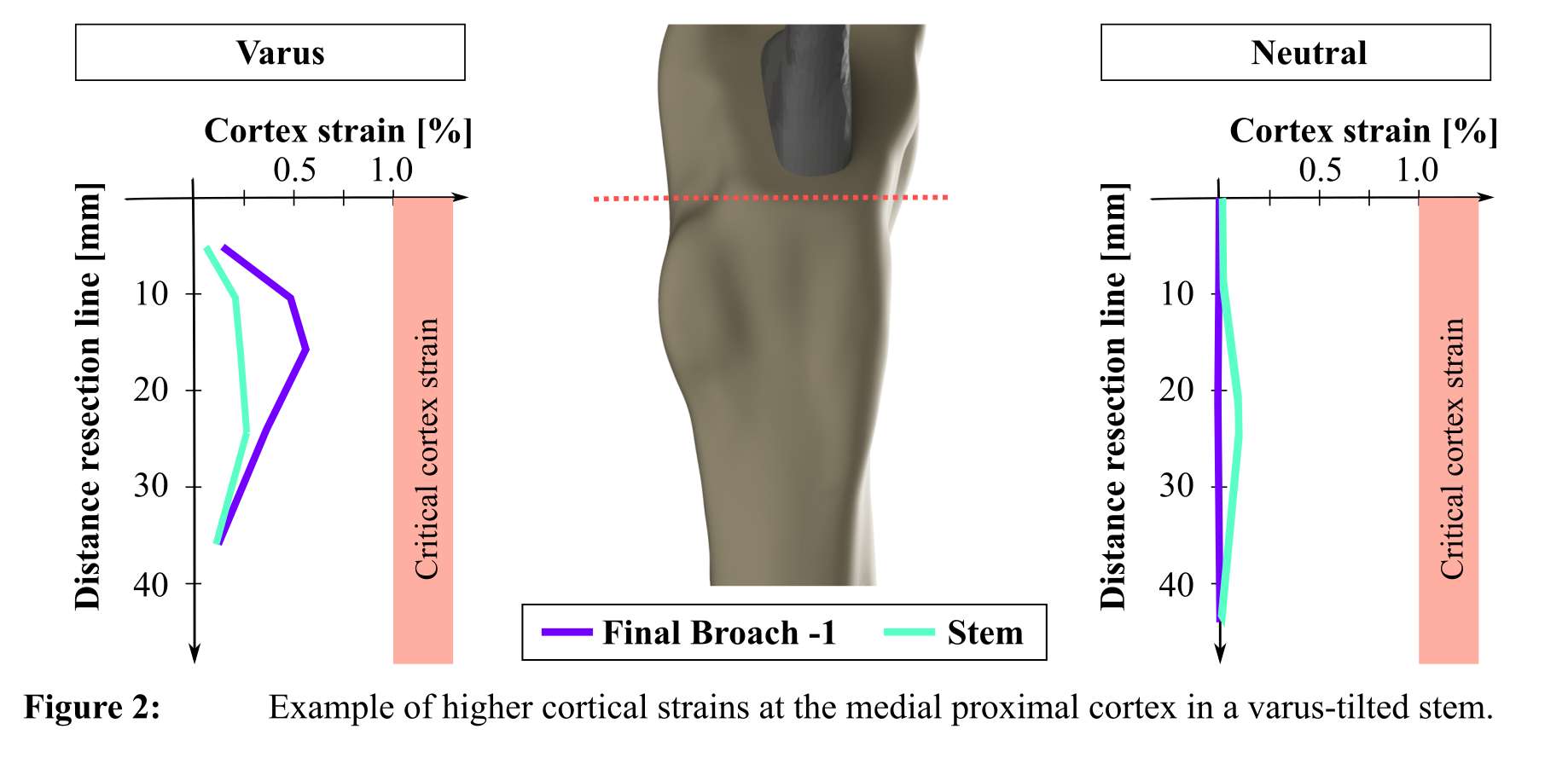
Figure 2
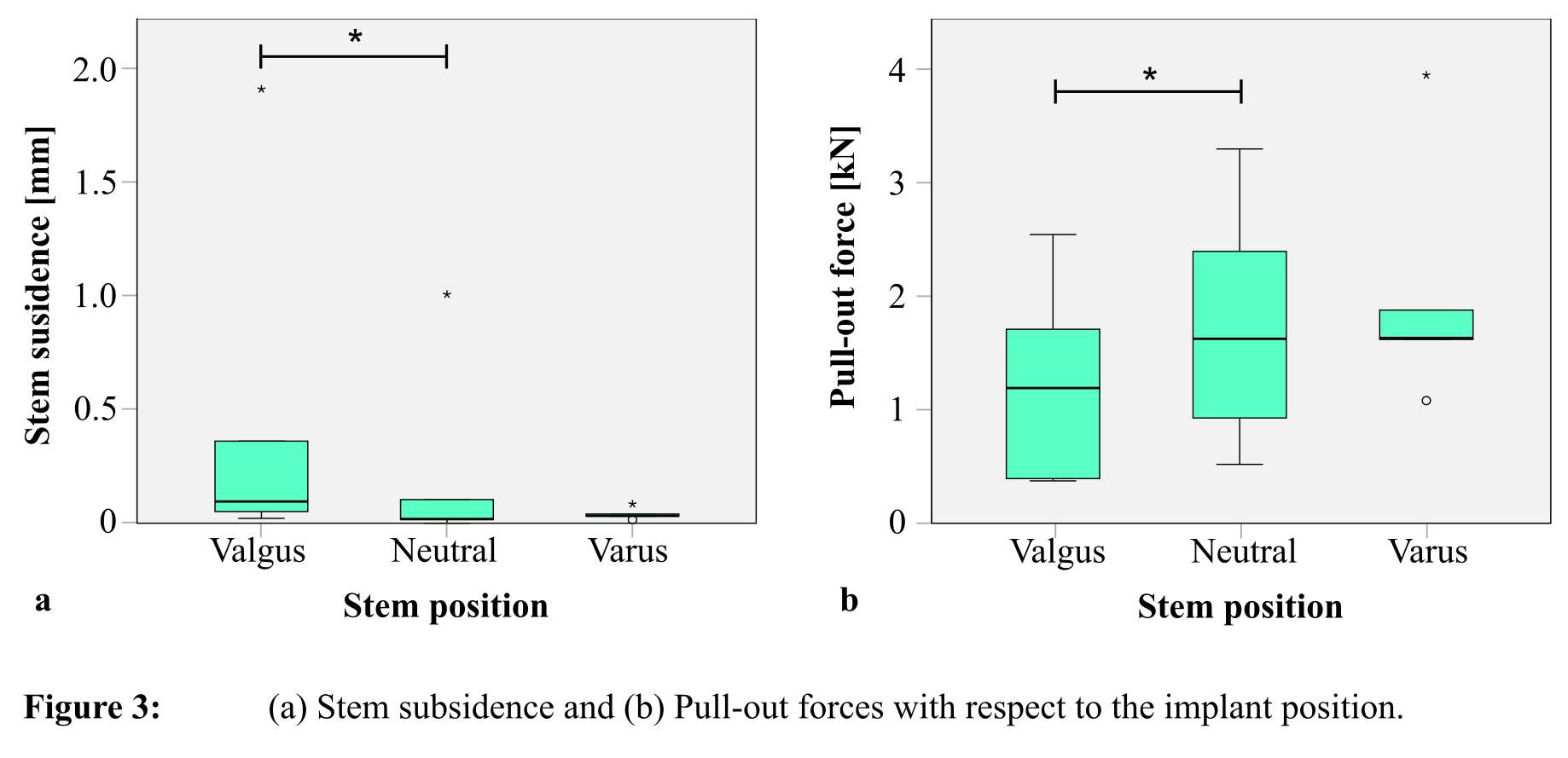
Figure 3#7849
Influence of Bone Morphology and Femur Preparation Method on the Primary Stability of Hip Revision Stems
*Tobias Konow - TUHH Hamburg University of Technology - Hamburg, Germany
Peter Schlieker - TUHH Hamburg University of Technology - Hamburg, Germany
Frank Lampe - Hamburg University of Applied Science
Benjamin Ondruschka - Medical Center Hamburg-Eppendorf (UKE) - Hamburg, Germany
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: tobias.konow@tuhh.de
Abstract
Background: Aseptic loosening is one of the major reasons for re-revisions of cementless revision stems. Insufficient primary stability is associated with bone characteristics and the surgical process. This study aimed to investigate how femur morphology and preparation methods influence the primary stability of revision stems.
Methods: Femur morphology was described by the proximal femur curvature (UFC) and an individualized Dorr type classification based on the ratio between the canal-to-calcar ratio (CCR*) and the cortical index (CI*). Manual and powered reaming in combination with helical and straight reamers were used to prepare the bone cavity of 10 cadaveric human femur pairs. Forces during stem impaction were recorded (Reclaim, Depuy Synthes, Leeds, UK). Micromotion at the bone-implant interface during cyclic axial loading and torsional load to failure was determined.
Results: CCR*/CI* ratio and impaction forces (R² = 0.817, p < 0.001) or torsional strength (R² = 0.577, p < 0.001) are reciprocal. CCR*/CI* did not affect micromotion during axial loading (R² = 0.001, p > 0.999), but proximal femoral curvature did (R² = 0.462, p = 0.015). Powered reaming and straight reamers led to an improved torsional strength (both: p = 0.043).
Conclusion: Individualized Dorr classification CCR*/CI* and UFC allows a good estimation of the primary stability of revision stems. For severely curved Dorr type-C femurs, an alternative anchorage method should be considered clinically.
Keywords
Revision THA, primary stability, bone morphology, Dorr type, femur curvature, canal reaming
Introduction
Primary total hip arthroplasty (THA) exhibits success rates above 96 % within the first 5 years [1–3]. Changing demographics come along with increasing physical activities among older patients and increased expectations for life quality. Hence, the worldwide number of primary THA and revision procedures is also increasing [4], especially in the elderly [2]. With ageing and consecutive interventions, the bone quality and the remaining bone stock decline [5–9], and surgeons cannot rely on the proximal trabecular bone structure [10]. Tapered revision stems, anchoring distally in the diaphysis, become the preferred choice of the surgeon [11–13]. The majority of re-revisions are caused by aseptic loosening - potentially introduced by excessive micromotion between stem and bone [14–17]. In particular, stem subsidence occurs frequently with cementless revision stems [18,19]. Postoperative stem subsidence less than 2 mm [20] and micromotions of less than 30 µm are considered harmless [21,22], while over 150 µm is regarded as crucial [23].
Patient-related factors such as femur shape or bone quality but also upper femoral curvature (UFC) may have an impact on the primary stability of cementless revision stems. Bone quality and decreased femoral strength are often age-related [24] and associated with comorbidities [25]. Macroscopically, the femoral morphology is usually described by the Dorr type [26]. Femurs of young, active patients often have a funnel-shaped medullary cavity with a thick cortex categorized as Dorr type A. Femurs with a stove-piped shaped canal and a thin cortex - common in the elderly [27] - are assigned to Dorr type C . Since revision stems are anchored in the diaphysis, the cortical morphology of the femur influences the stability. Dorr type C bones with reduced bone strength often require stems with larger diameters [27]. Preoperative determining of the bone morphology according to the Dorr type is important for planning but usually is only performed qualitatively. Dorr’s classification either refers to the canal-to-calcar ratio (CCR) or the cortical index (CI), determined at fixed positions without considering body-specific factors such as patient height [26,28], and an ideal AP or ML view orientation cannot be guaranteed. Furthermore, using the CCR or the CI does not necessarily yield the same Dorr type for a specific femur, which makes a unique classification impossible in some cases. Combined, this can lead to ambiguous results even for the most experienced surgeons [29,30]. A unique classification to evaluate the morphology of the proximal femur based on the original work of Dorr is desirable to support surgeons’ implant choices and to elucidate differences in clinical outcomes.
In addition to proximal femur morphology, especially important for elderly [2], the cavity preparation method bears the potential to influence the outcome of the procedure. Likewise, in primary THA, where preparation affects stem seating for low bone mineral density (BMD) [31], broach design influenced the shape of the cavity [31], this could also apply to the reamer design in revision THA. Furthermore, manual reaming could cause more variable cavities compared to powered reaming. However, the effect of these factors on primary stability of revision stems has not been fully investigated.
This study aimed to investigate how femur morphology and preparation methods influence the primary stability of revision stems.
Methods
10 femur pairs from human donors (7 female, 3 male, 74.8 ± 6.1 years, range 65 to 84 years) were excised post mortem and stored below -20 °C [32]. The Ethics Commission of the Medical Association Hamburg (WF-067/18) approved this study.
Femur analysis
CT scans (Brilliance 16, Philips, Amsterdam, Netherlands) with a calibration phantom (QSA, QRM, Möhrendorf, Germany) were taken (voxel size: 0.5 x 0.5 x 0.5 mm³) and Hounsfield units were converted to BMD in terms of Calcium-Hydroxyapatite per milliliter (Structural Insight 3, University Medical Center Schleswig-Holstein, Kiel, Germany [33]). The BMD of the cortical bone was determined at a 10 mm wide ring of the femur shaft, 100 mm below the trochanter minor (threshold: [500, 1500 mgHA/cm³]; AVIZOLite 9.7.0, Thermo Fisher Scientific, Waltham, MA, USA). The cortical bone and medullary canals were segmented based on thresholds (cortical bone: 500 to 1500 mgHA/cm³; medullary canal: -250 to 500 mgHA/cm³, [31]). CT-data were pre-aligned based on the homogeneously distributed point cloud of the cortical shell using its three main principal components (Matlab 2020b, The MathWorks, Natick, MA, USA).
Percentages of donors’ body height (BH) were used as body-specific measures for femur classification. The anatomical femur axis was defined by a best-fit line through the diaphysis between 2 % BH (z2%) and 8 % BH (z8%) distally to the trochanter minor (TM). This femur section was further divided into two equal sub-sections (z2% to z5% and z5% to z8%) and used to determine the UFC (β) as the angle between the respective canal axes of the sub-sections (Figure 1A).
Individual body-height-specific femur types CCR* and CI* on the bases of Dorr et al. [23] were determined, by replacing the fixed positions of 30 mm (z30mm) and 100 mm (z100mm) below the TM with body-specific measures of 1.7 % BH (z1.7%) and 5.8 % BH (z5.8%). Positions are the same for an average German body height of 172 cm [34] (Figure 1B). AP and ML (Lauenstein) radiographs were replaced by cross-sectional areas of the cortical shell (Acort) and the intramedullary canal (Aim) determined from CT-data (Eq. 1). Hence, the individualized CI* was determined from the medullary cross-sectional area Aim,5.8% and the cortical cross-sectional area Acort,5.8% (Figure 1B; Eq. 2).
To describe the cone shape of the intramedullary canal, the canal diameter originally determined 30 mm (Dim,30mm) and 100 mm below the TM (Dim,100mm) were replaced by cross-sectional areas (Eq. 3). In line with the former, the individual CCR* was expressed as percentage of the body height (Figure 1B, Eq. 4). The ratio between CI* and CCR* is further used to evaluate the in vitro experiments.
In-vitro experiment
Revision stems (Reclaim Revision Hip System, stem-length: 140 mm; Depuy Synthes, Leeds, UK; Figure 2) were implanted by one experienced surgeon using different cavity preparation methods. First, the drive method for reaming was varied, with manual reaming on one femur (n = 5) and powered reaming on the contralateral femur (n = 5) using helical reamers. Second, standard helical reamers (n = 5) were used on one and straight reamers (n = 5) on the contralateral femur both with powered mode. During cavity preparation, reamer diameters were stepwise increased (1 mm) until the surgeon perceived sufficient stability. The final depth and position of the reamer were measured with respect to the greater trochanter by a digitalized caliper.
Afterwards, specimens were embedded (Technovit 4004, Kulzer GmbH, Wehrheim, Germany) aligned with the reamer axis. Stems were implanted using a drop tower with subsequently stepwise increasing energy (10 impactions at 3 J and 5 impactions at 4, 5, 6 and 7 J each) until the desired stem position (as reamed) was reached (Figure 3A). In case the intended stem position could not be achieved after this protocol, implantation was discontinued. Impaction forces (Kistler 9333A, Winterthur, Switzerland) and the implantation depth per impact were recorded.
Specimens were mounted with the implant axis aligned from joint center to joint center of two cardan joints (Figure 3B). Primary stability was determined during force-controlled cyclic sinusoidal axial compression load (1 Hz, 200 N – 2000 N, 30 min; Bionix II, MTS, Eden Prairie, USA). Micromotions between the stem and the bone were measured contactless by digital image correlation (DIC, ARAMIS 3D Camera, GOM, Braunschweig, Germany) at seven definite time points (10 cycles at the beginning and 10 cycles every 300 cycles, 25 fps, measuring volume: 100 x 80 x 50 mm³, 2752 x 2200 pixels, marker diameter 0.4 mm, 5 µm measurement noise). The distal stems were modified for the torque-to-failure test to enable high torsional load transfer. Ultimate torque to failure (angular velocity: 0.5 °/s) was determined in combination with a static axial preload (500 N).
Statistical analysis
Statistics were performed with a type I error level of 0.05 (SPSS 24.0, SPSS Inc., Chicago, USA). Multiple Pearson correlations were used to identify relations between the parameters. Wilcoxon sign-rank analysis was performed to determine effects within paired femurs.
Results
The cortical BMD (1012.4 ± 67.3 mgHA/cm³) was the same within femur pairs (p = 0.970) and in both study groups (p = 0.462). A high level of symmetry between femur sides was found regarding the UFC (p = 0.389) and the CCR*/CI* (p = 0.954). UFC and CCR*/CI* were also similar for specimens of both study groups (4.2° ± 1.3°, p = 0.526; 1.14 ± 0.18, p = 0.668). Femur length increased with increasing body height (R² = 0.83, p < 0.001).
Body-specific CCR* yielded results similar to standard Dorr CCR (p = 0.349). Differences were seen with regard to CI* for small patients (< 165 cm; p = 0.043) and larger patients (> 175 cm; p = 0.028). In 90 % of the observed specimens, the CCR* and the CI* classification led to different Dorr types - alike CCR and CI. A negative correlation between CCR* and CI* (R² = 0.399, p = 0.003; Figure 4) was found. To differentiate between Dorr types A*, B*, and C* Dorr’s cut-off limits for the CCR and the CI were applied to the ratio CCR/CI and CCR*/CI* respectively (Table 1 [26]). A linear function from the origin through those herby generated points represents the new cut-off limits (Figure 4). The majority of femurs were assigned to the Dorr type A* (A* = 12, B* = 4, C* = 4). Patient’s height did not correlate with CCR*/CI* ratio (p = 0.588).
13 implants (65 %) were impacted to the desired position while 7 implants (35 %) showed an elevated position (Mean elevation: 6.0 ± 3.0 mm). Maximum impaction forces and energies were similar independent of the reaming method (Forces: 6.5 ± 1.9 kN, p = 0.946; Energy: 90.6 ± 50.4 J, p = 0.830). A paired analysis of the isolated subgroups neither revealed differences. UFC neither affected impaction forces (R² = 0.006, p = 0.743) nor the required impaction energy (R² = 0.003, p = 0.805). Impaction forces increased with decreasing CCR*/CI* ratio (R² = 0.806, p < 0.001; Figure 5). Higher demand of impaction energy was associated with decreasing CCR*/CI* ratio (R² = 0.721, p < 0.001).
7 specimens (35 %) exhibited small cyclic micromotions of less than 5 μm (0.5 ± 2.4 μm; 5 fully seated, 2 not fully seated), which is within the noise of the DIC system. 13 specimens exhibited reasonable micromotions of 32.7 ± 30.9 μm. Micromotions did neither depend on reaming method (p = 0.405) nor on cortical BMD (R² = 0.096, p = 0.183) nor on the CCR*/CI* ratio (R² = 0.019, p = 0.552). For specimens exhibiting micromotions above 5 µm, a positive correlation was found with increasing UFC (R² = 0.453, p = 0.015; Figure 6). Moreover, micromotions came along with increased stem subsidence (R² = 0.317, p = 0.010), but stem subsidence was found to be small (-10.5 ± 22.7 μm). Bone morphology did not affect stem subsidence (CCR*/CI*: R² = 0.004, p = 0.778; UFC: R² = 0.025, p = 0.509).
Powered reaming resulted in 21 % increased torsional strength compared to manual reaming (p = 0.043, Figure 7B). Straight reamers appeared to be 11 % superior compared to helical reamers in terms of torsional strength (p = 0.043, Figure 7B). With a decreasing CCR*/CI* quotient higher torsional strength was observed (R² = 0.579, p < 0.001, Figure 7A).
Discussion
Specimens of the given cohort had a superior bone quality compared to the clinical situation. No degenerated bone structures were found with the majority having a CCR*/CI* below 1.3 (Dorr type A* or B*). Whether the results would be different if more Dorr type C* samples with poor bone quality were included remained unclear. The homogeneity of paired specimens between study groups concerning BMD and CCR*/CI* indicates that the evaluation of the different preparation methods was not recently influenced by donor-specific anthropometric characteristics. The contact area between bone and implant, which was found to influence the torsional strength [35], was similar for the whole study, since the same stem-length was used in all specimens and fortunately, the variations in stem diameter were small (size 15 ± 1). The observed torsional strength within the bone-implant-interface was slightly above the loads projected for high load activities like jogging [36].
The use of body-height-specific measures to determine CCR* and CI* is justified by the correlation of BH and femur length found in this study alike to previous ones [37,38]. The body-specific normalization solely results in minor changes for most femurs, but larger or small patients might benefit from this approach. Percentages of donors’ body heights with decimal places were used to reflect the constant positions suggested by Dorr and the average BH of the donors’ population. However, simplified percentages e.g. 2 % and 6 % should work similarly. Threshold-based CT detection of cortical and trabecular bone is advantageous compared to 2D projections due to its reproducible results without positioning errors during image acquisitions but requires quantitative CT scans. Since CT scans are recommended before revisions, the patient would not be exhibited to additional radiation [39]. The semi-automatic, numerical determination of femoral morphology, additionally improves the inter- and intra-observer reliability deplored in literature [29,30] and could be implemented fully automatically in modern preoperative planning software. The negative correlation between CCR and CI was already mentioned by Dorr et al. but not pursued further [26]. Thus, the Dorr type is often determined by just one parameter, either by CCR or CI with potentially contradictory results, limiting the comparability of different studies. The newly introduced CCR*/CI* ratio not only describes the correlation between CCR* and CI*, but also serves as a unique measure to quantify femoral morphology, which may positively influence preoperative planning through correct implant selection and might prevent complications during or after revision surgery.
Standard powered reaming appears to be superior compared to the manual approach since it is time-efficient, involves less physical work and yields to higher torsional strength, presumably due to a more uniform cavity. It is uncertain whether straight reamers further improve the junction due to their changed geometry or merely due to the sharper cutting edges caused by less previous operating time of the reamer.
One third (35 %) of stems exhibited micromotions of less than 5 μm, in the range of the signal noise, and therefore, no correlations between micromotion and CCR*/CI* ratio or BMD were observed. The lower performance observed in curved femurs in terms of increase in micromotion may be related to a smaller contact area within the less congruent interface, which is known to reduce primary stability [35]. Mechanically, a low CCR*/CI* with a high BMD (R² = 0.47, p = 0.002), as found in Dorr type A bones, increases system stiffness leading to higher impaction forces and energies which improves primary stability. In contrast, the thin cortex of Dorr type C bones with low BMD, often found in elderly patients most commonly affected by revision THA [2,27], does not provide comparable radial pressures at the implant-bone interface to achieve similar torsional strength. For these specimens in particular, the maximum torsional moments are close to loads projected for activities like jogging [36].
Overall, femur morphology appears worthwhile to be considered during cementless revision THA, because of the exhibited correlation between impaction force, impaction energy and bone-related parameters (BMD, CCR*/CI*, UFC) with primary stability.
Conclusion
With the CCR*/CI* ratio a unique Dorr type* can be determined for any femur. Including body-height-specific measures and a semi-automatic computation of the CCR* and the CI* from 3-dimensional CT-data improves the reproducibility and reduces inter-/ intra-observer variations. CCR*/CI*appears to represent the achievable mechanical situation and might foster adequate prosthesis selection. Apart from the clinical situation, this allows objective body-specific femoral morphological parameters to be used for in-vitro analysis. Since micromotion is affected by UFC and torsional stability by CCR*/CI*, it may be worthwhile to consider both parameters in combination. In contrast to bone morphology, the preparation method plays a minor role for primary stability. Slight advantages of powered compared to manual reaming and the reamer geometry will most likely not decide the revision’s success. A combination of several adverse factors may lead to early implant failure and re-revision. In severely curved type C* femurs that have been manually prepared, primary stability could be critically compromised, so an alternative anchorage method may be beneficial for these patients.
Conflict of interest statement
Financial support by Depuy Synthes to carry out this study is kindly acknowledged.
Literature
1. No Authors Listed. Hip, Knee & Shoulder Arthroplasty: Annual Report 2019. AOANJRR. 2019;
2. Grimberg A, Jansson V, Lützner J, Melsheimer O, Morlock M, Steinbrück A. Jahresbericht 2021. EPRD Deutsche Endoprothesenregister; 2021.
3. No Authors Listed. Hip, Knee & Shoulder Arthroplasty: Annual Report 2020. AOANJRR. 2020;
4. Kurtz SM, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of Primary and Revision Total Hip and Knee Arthroplasty in the United States From 1990 Through 2002. J Bone Jt Surgery-American Vol. 2005;87:1487–97.
5. Venesmaa PK, Kröger HPJ, Jurvelin JS, Miettinen HJA, Suomalainen OT, Alhava EM. Periprosthetic bone loss after cemented total hip arthroplasty: A prospective 5-year dual energy radiographic absorptiometry study of 15 patients. Acta Orthop Scand. 2003;74:31–6.
6. Harris WH, Schiller AL, Scholler JM, Freiberg RA, Scott R. Extensive localized bone resorption in the femur following total hip replacement. JBJS. 1976;58:612–8.
7. Dan D, Germann D, Burki H, Hausner P, Kappeler U, Meyer RP, et al. Bone loss after total hip arthroplasty. Rheumatol Int. 2006;26:792–8.
8. Harris WH. Wear and periprosthetic osteolysis the problem. Clin Orthop Relat Res. 2001;66–70.
9. Kang MN, Huddleston JI, Hwang K, Imrie S, Goodman SB. Early Outcome of a Modular Femoral Component in Revision Total Hip Arthroplasty. J Arthroplasty. 2008;23:220–5.
10. Amanatullah DF, Howard JL, Siman H, Trousdale RT, Mabry TM, Berry DJ. Revision total hip arthroplasty in patients with extensive proximal femoral bone loss using a fluted tapered modular femoral component. Bone Jt J. 2015;97-B:312–7.
11. Böhm P, Bischel O. The Use of Tapered Stems for Femoral Revision Surgery. Clin Orthop Relat Res. 2004;148–59.
12. Skyttä ET, Eskelinen A, Remes V. Successful femoral reconstruction with a fluted and tapered modular distal fixation stem in revision total hip arthroplasty. Scand J Surg. 2012;101:222–6.
13. Nadaud MC, Griffin WL, Fehring TK, Mason JB, Tabor OB, Odum S, et al. Cementless revision total hip arthroplasty without allograft in severe proximal femoral defects. J Arthroplasty. 2005;20:738–44.
14. No Authors Listed. National Joint Registry - 17th Annual Report 2020. Natl Jt Regist. 2020;
15. Streit MR, Haeussler D, Bruckner T, Proctor T, Innmann MM, Merle C, et al. Early Migration Predicts Aseptic Loosening of Cementless Femoral Stems: A Long-term Study. Clin Orthop Relat Res. 2016;474:1697–706.
16. Kassi JP, Heller MO, Stoeckle U, Perka C, Duda GN. Stair climbing is more critical than walking in pre-clinical assessment of primary stability in cementless THA in vitro. J Biomech. 2005;38:1143–54.
17. Sundfeldt M, Carlsson L V., Johansson CB, Thomsen P, Gretzer C. Aseptic loosening, not only a question of wear: A review of different theories. Acta Orthop. 2006;77:177–97.
18. Moreland JR, Bernstein ML. Femoral revision hip arthroplasty with uncemented, porous-coated stems. Clin Orthop Relat Res. 1995;141–50.
19. Hancock DS, Sharplin PK, Larsen PD, Phillips FTS. Early radiological and functional outcomes for a cementless press-fit design modular femoral stem revision system. HIP Int. 2019;29:35–40.
20. Walker PS, Mai SF, Cobb AG, Bentley G, Hua J. Prediction of clinical outcome of THR from migration measurements on standard radiographs: A study of cemented Charnley and Stanmore femoral stems. J Bone Jt Surg - Ser B. 1995;77:705–14.
21. Bragdon CR, Burke D, Lowenstein JD, Connor DOO, Ramamurti B, Jasty M, et al. Differences in Stiffness Between a Cementless and Cancellous Bone into Varying Amounts of of the Interface Porous Implant vivo in Dogs Due Implant Motion. Clin Orthop. 1996;11:945–51.
22. Kawahara H, Kawahara D, Hayakawa M, Tamai Y, Kuremoto T, Matsuda S. Osseointegration under immediate loading: Biomechanical stress-strain and bone formation-resorption. Implant Dent. 2003;12:61–8.
23. Pilliar RM, Lee JM, Maniatopoulos C. Observations on the effect of movement on bone ingrowth into porous-surfaced implants. Clin Orthop Relat Res. 1986;108–13.
24. Keaveny TM, Kopperdahl DL, Melton LJ, Hoffmann PF, Amin S, Riggs BL, et al. Age-dependence of femoral strength in white women and men. J Bone Miner Res. 2010;25:994–1001.
25. Grynpas M. Age and disease-related changes in the mineral of bone. Calcif Tissue Int. 1993;53.
26. Dorr LD, Faugere M-C, Mackel AM, Gruen TA, Bognar B, Malluche HH. Structural and cellular assessment of bone quality of proximal femur. Bone. 1993;14:231–42.
27. Toro G, Bothorel H, Saffarini M, Jacquot L, Chouteau J, Rollier JC. Uncemented total hip arthroplasty in octogenarian and nonagenarian patients. Eur J Orthop Surg Traumatol. 2019;29:103–10.
28. Karayiannis PN, Cassidy RS, Hill JC, Dorr LD, Beverland DE. The Relationship Between Canal Diameter and the Dorr Classification. J Arthroplasty. 2020;35:3204–7.
29. Nakaya R, Takao M, Hamada H, Sakai T, Sugano N. Reproducibility of the Dorr classification and its quantitative indices on plain radiographs. Orthop Traumatol Surg Res. 2019;105:17–21.
30. Najd Mazhar F, Jafari D, Nojoomi M, Mirzaei A, Tayebi H. Inter and Intra-Observer Reliability of Dorr Classification in Proximal Femur Morphology. Shafa Orthop J. 2018;5.
31. Bätz J, Messer-Hannemann P, Lampe F, Klein A, Püschel K, Morlock MM, et al. Effect of cavity preparation and bone mineral density on bone-interface densification and bone-implant contact during press-fit implantation of hip stems. J Orthop Res. 2019;37:1580–9.
32. Püschel K, Heinemann A, Dietz E, Hellwinkel O, Henners D, Fitzek A. New developments and possibilities in the field of post-mortem medicine mortui vivos docent. Rechtsmedizin. 2020;30:425–9.
33. Graeff C, Timm W, Nickelsen TN, Farrerons J, Marín F, Barker C, et al. Monitoring teriparatide-associated changes in vertebral microstructure by high-resolution CT in vivo: Results from the EUROFORS study. J Bone Miner Res. 2007;22:1426–33.
34. Statistisches Bundesamt. Mikrozensus - Fragen zur Gesundheit - Körpermaße der Bevölkerung, 2017. 2018;49:1–17.
35. Michael Meneghini R, Hallab NJ, Berger RA, Jacobs JJ, Paprosky WG, Rosenberg AG. Stem diameter and rotational stability in revision total hip arthroplasty: A biomechanical analysis. J Orthop Surg Res. 2006;1:1–7.
36. Huber G, Morlock MM. Which length should the neck segment of modular revision stems have? Clin Biomech. 2021 Feb;105286.
37. Mahakkanukrauh P, Khanpetch P, Prasitwattanseree S, Vichairat K, Troy Case D. Stature estimation from long bone lengths in a Thai population. Forensic Sci Int. 2011;210:279.e1-279.e7.
38. Baba M, Hyodoh H, Okazaki S, Shimizu J, Mizuo K, Rokukawa M, et al. Stature estimation from anatomical landmarks in femur using postmortem CT. J Forensic Radiol Imaging. 2016;7:28–32.
39. Kuroda K, Kabata T, Maeda T, Kajino Y, Watanabe S, Iwai S, et al. The value of computed tomography based navigation in revision total hip arthroplasty. Int Orthop. 2014;38:711–6.
Figures
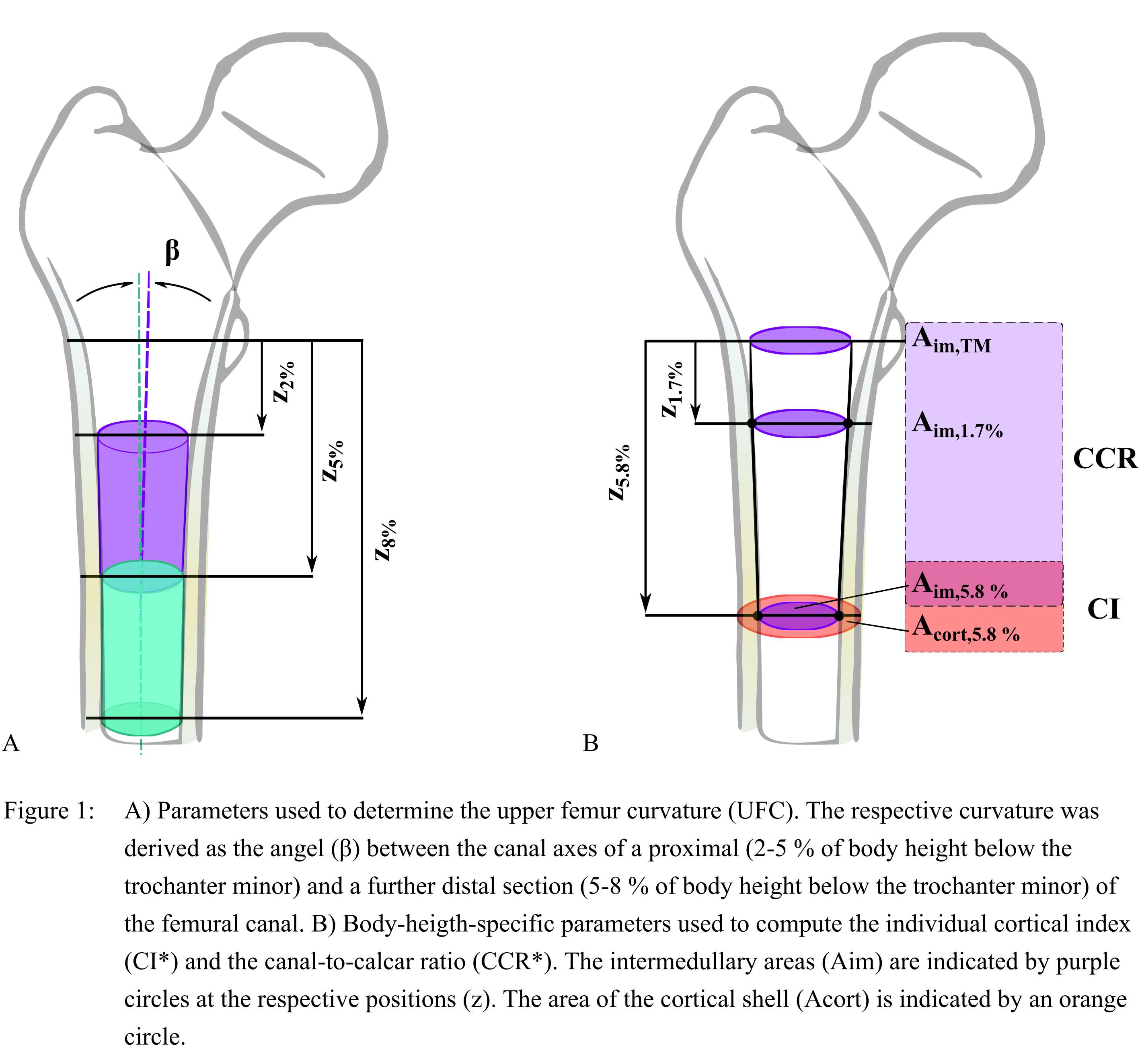
Figure 1
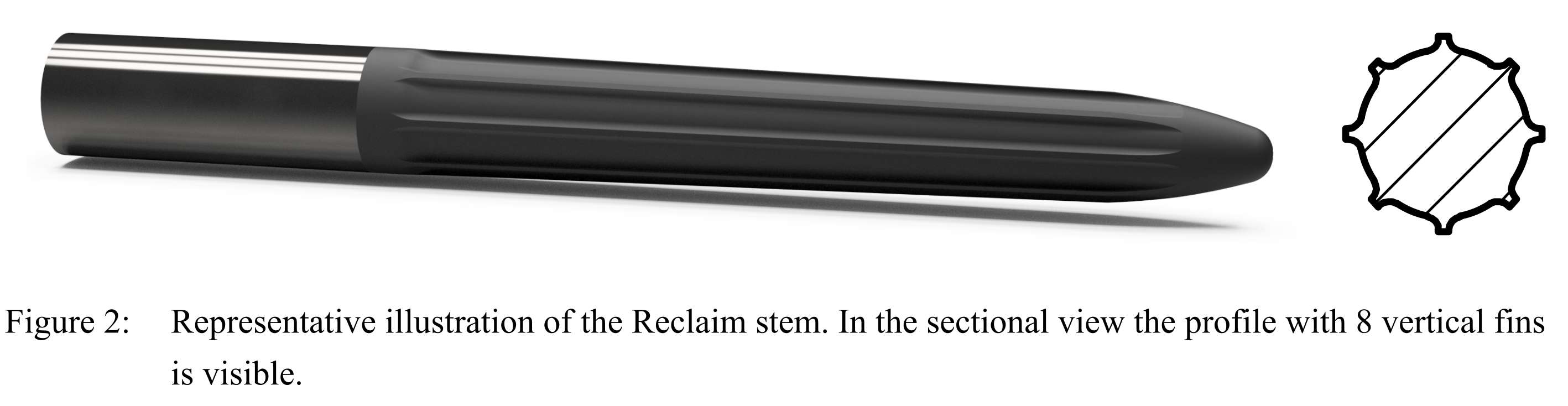
Figure 2
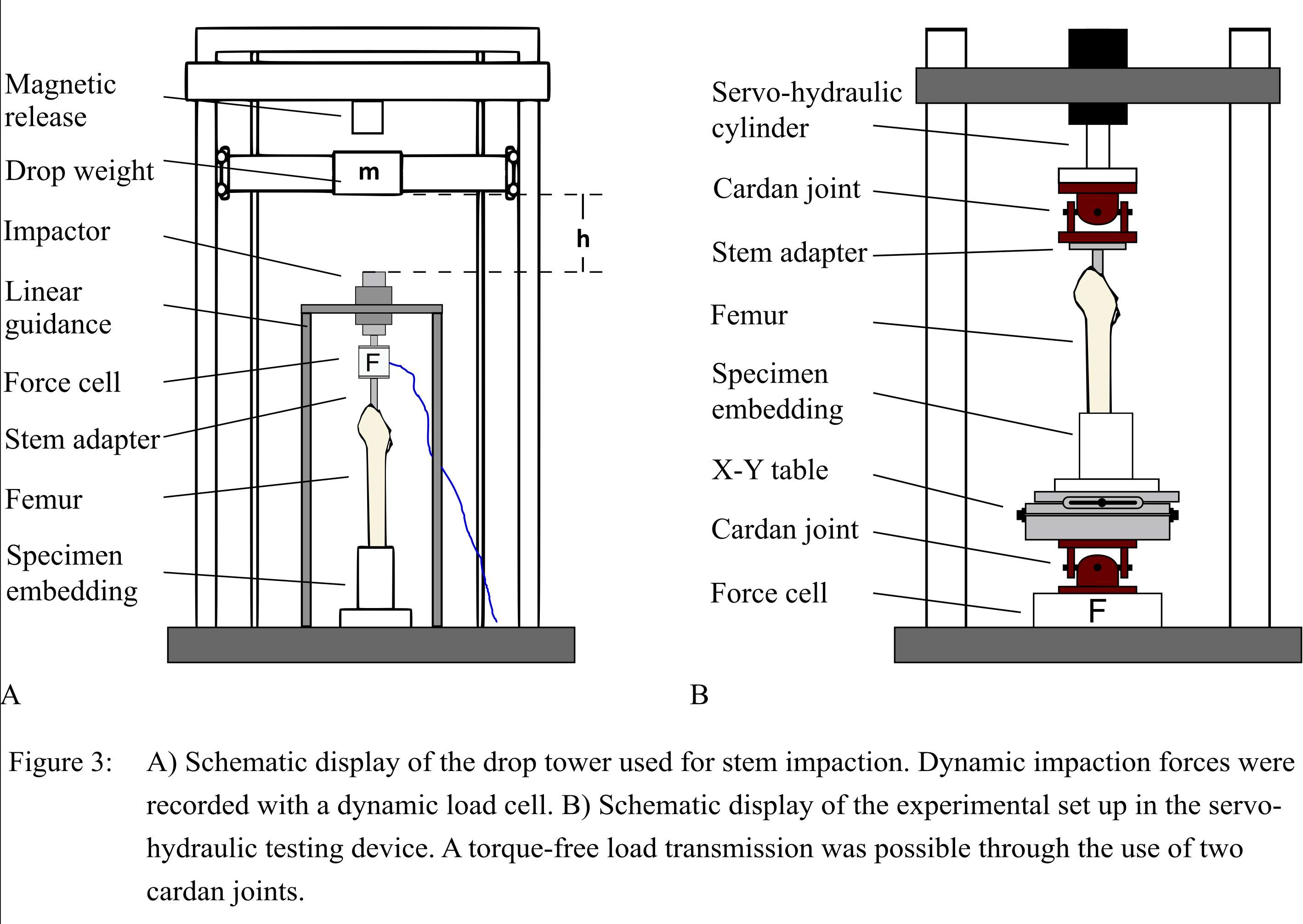
Figure 3
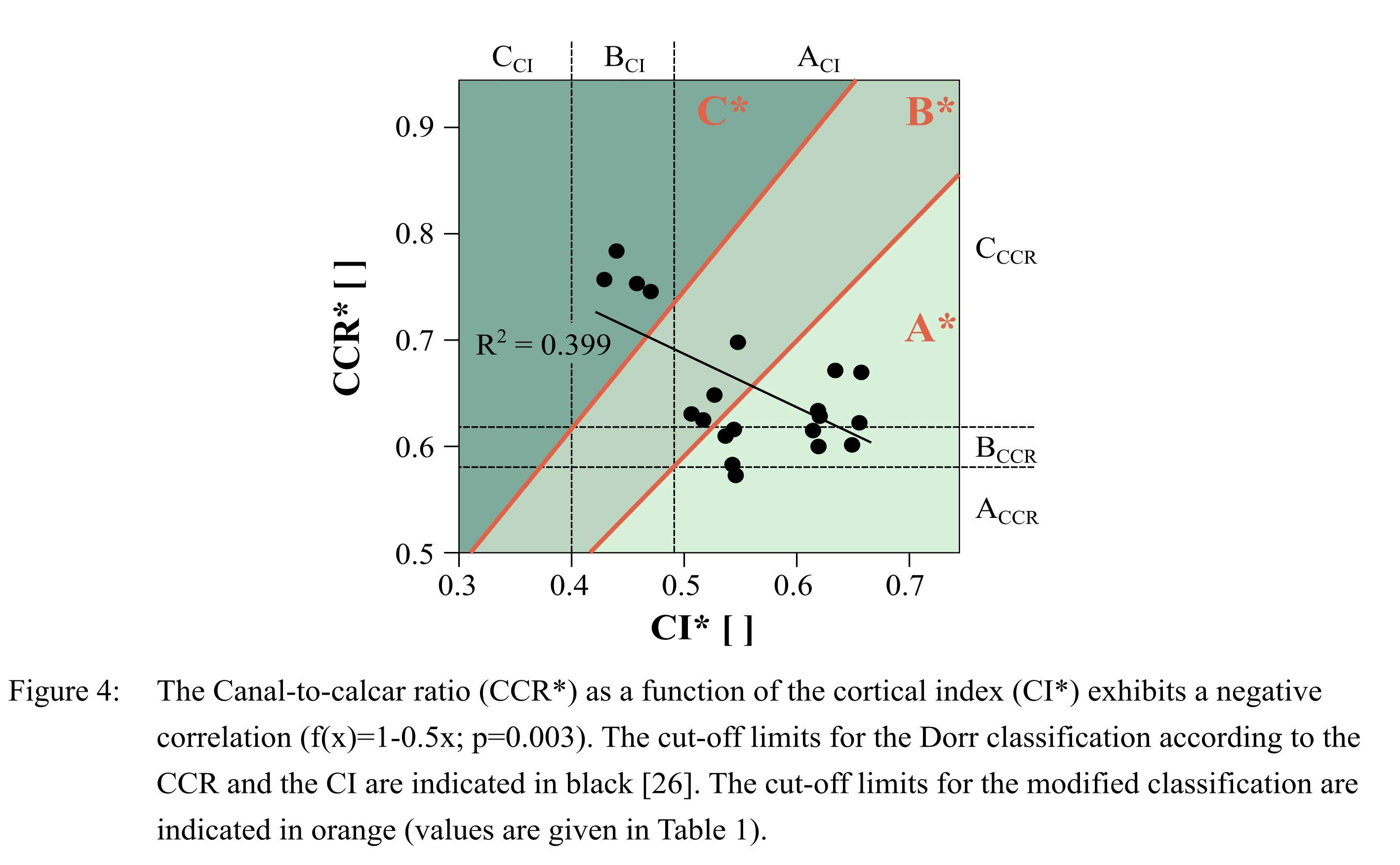
Figure 4
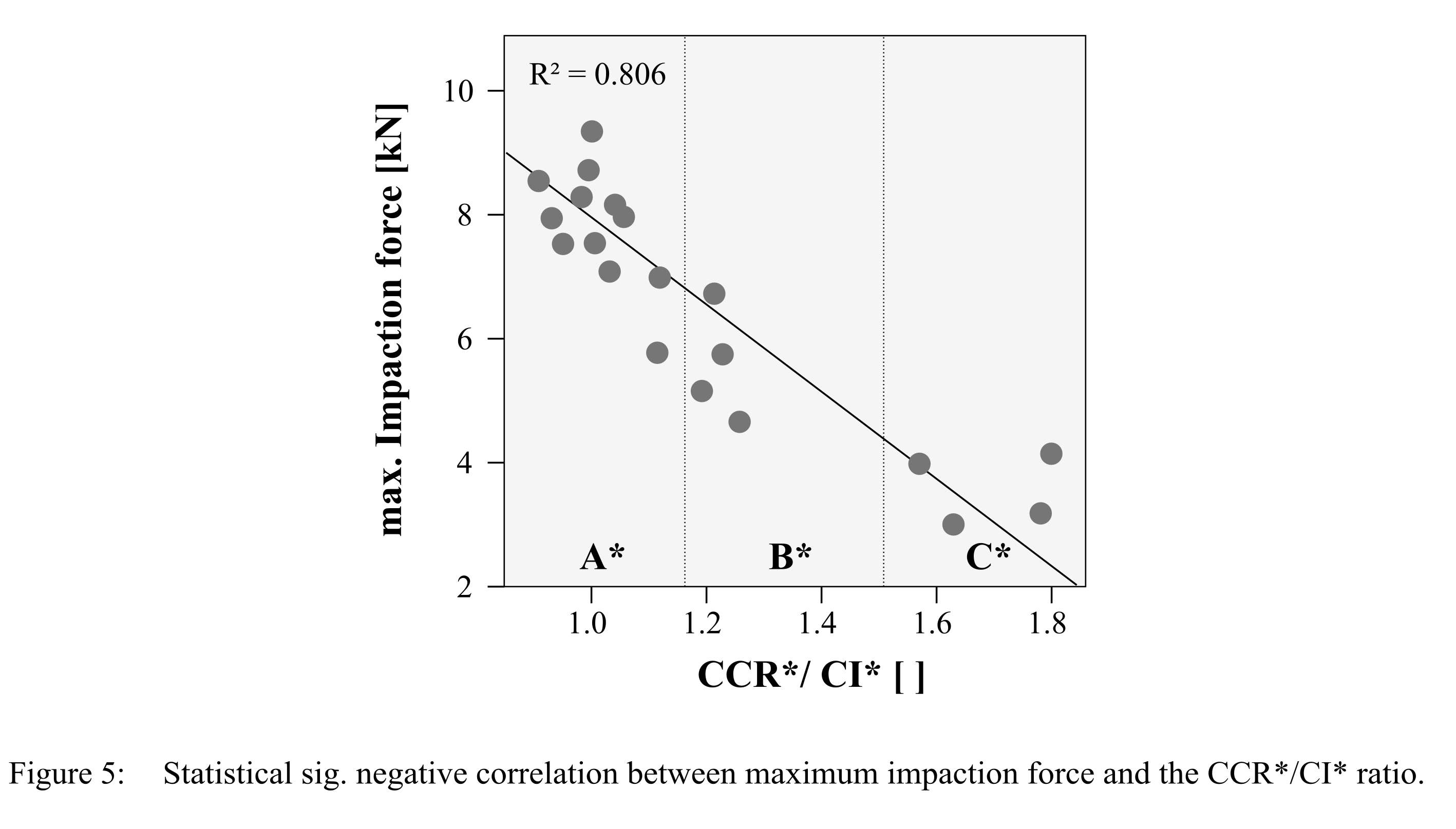
Figure 5
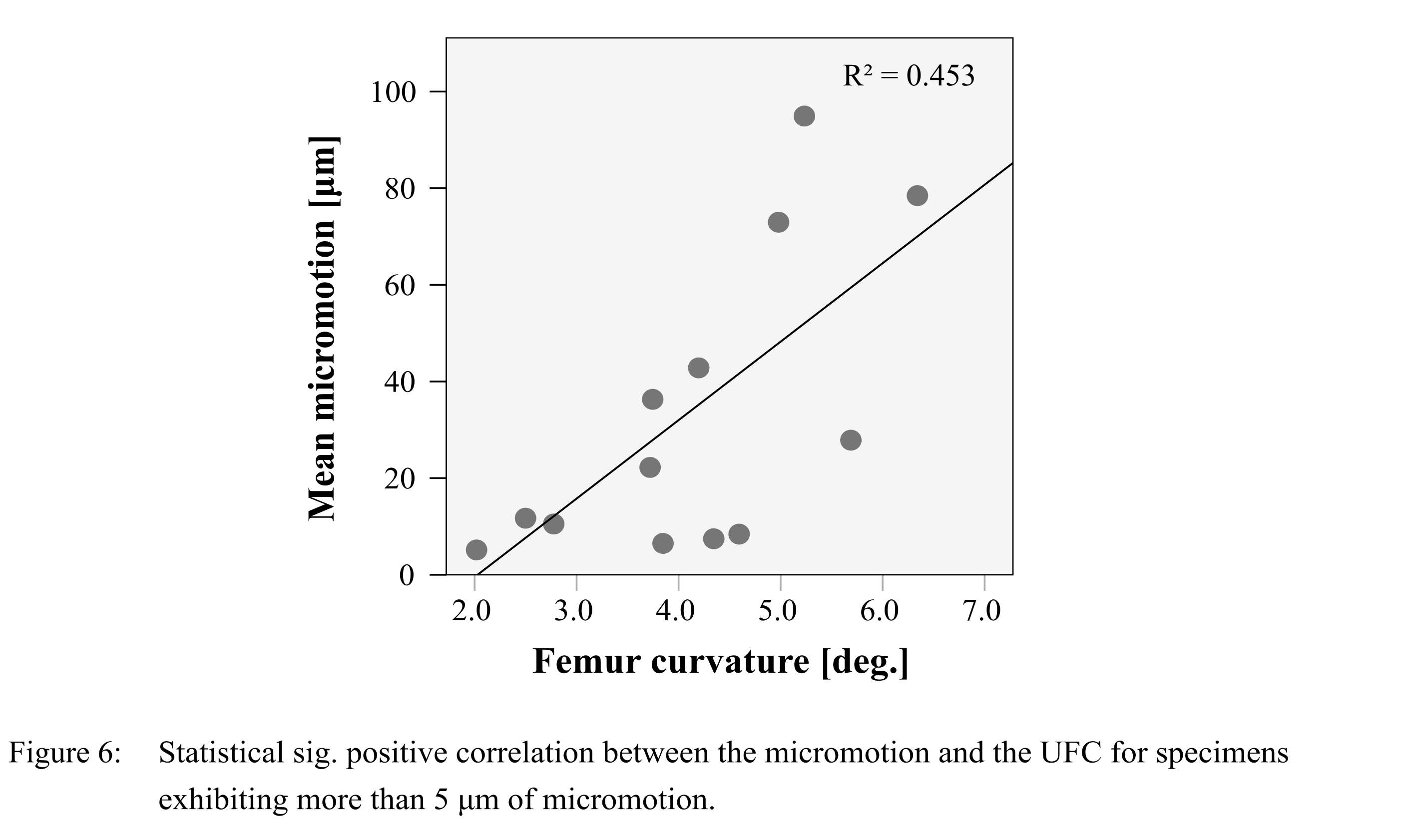
Figure 6
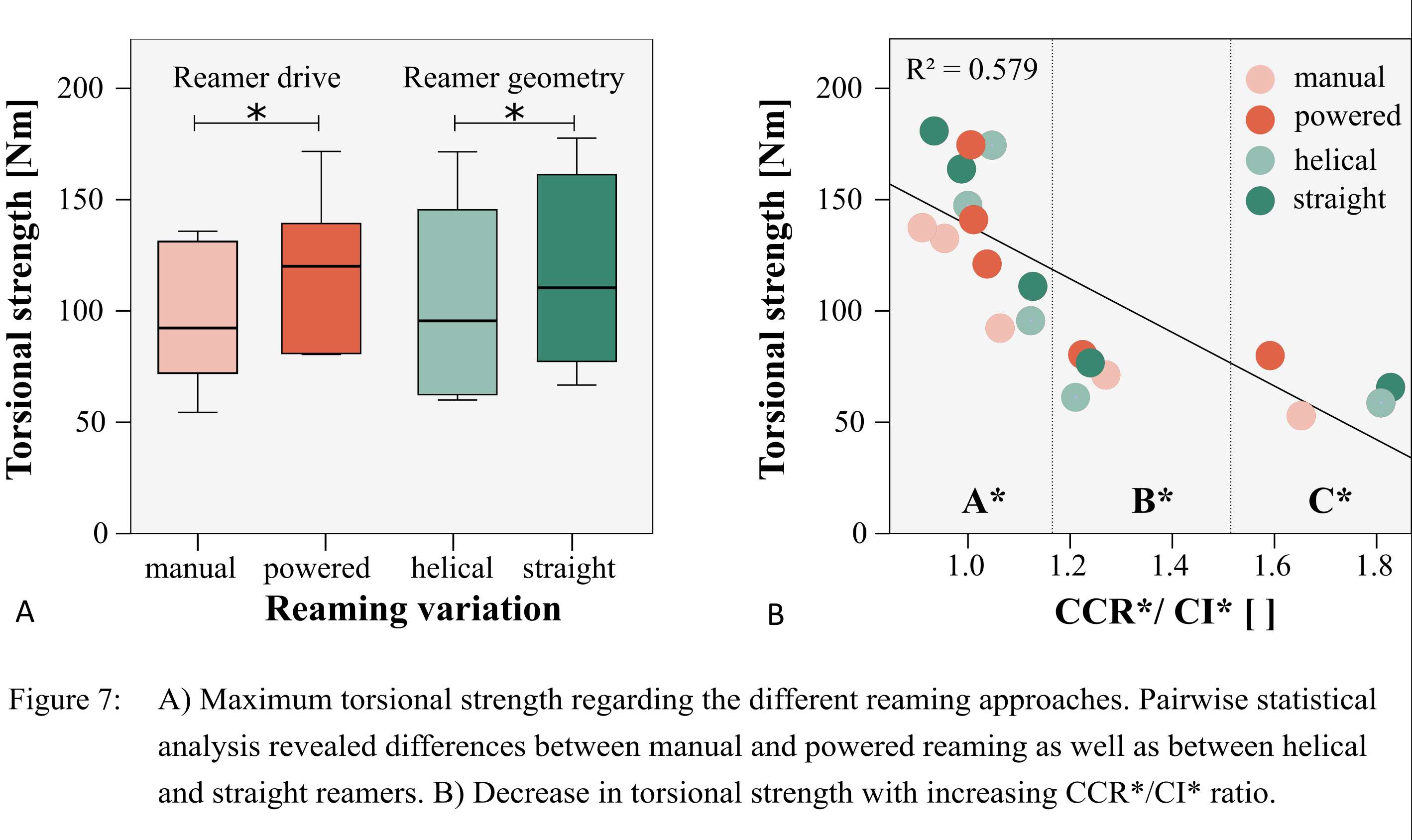
Figure 7
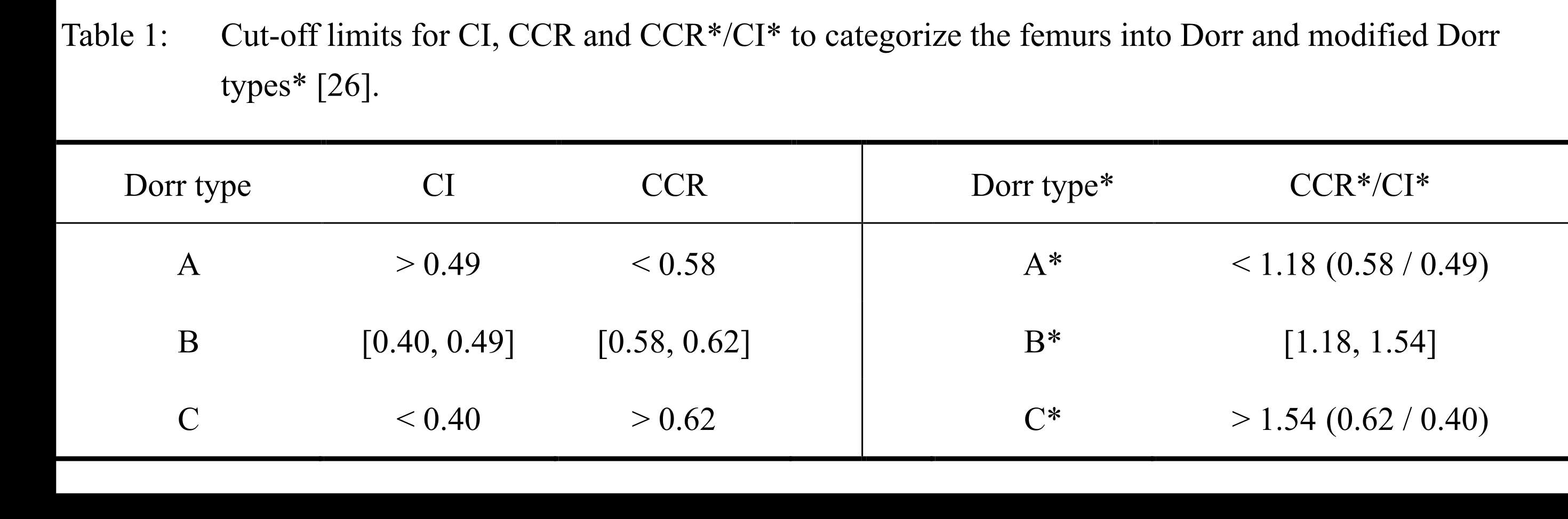
Figure 8
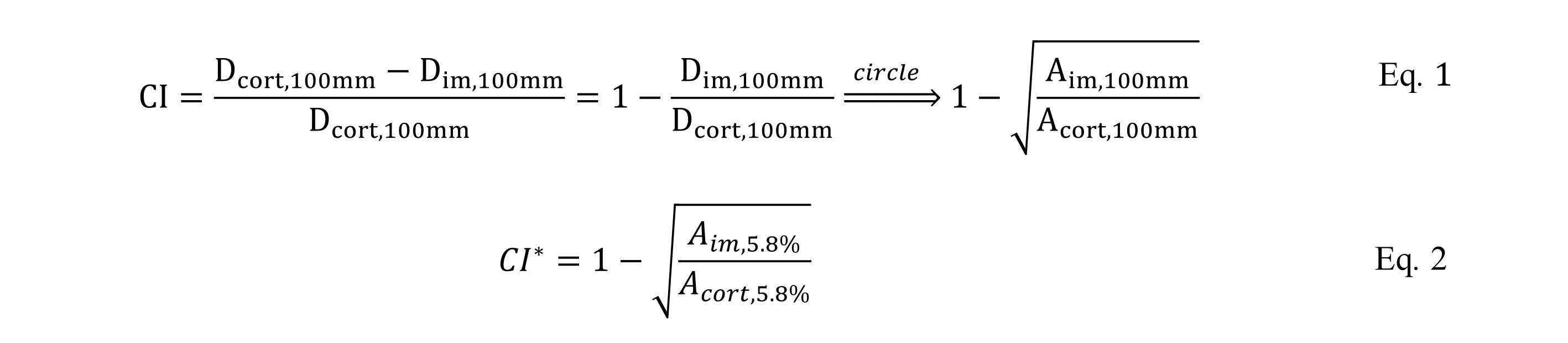
Figure 9
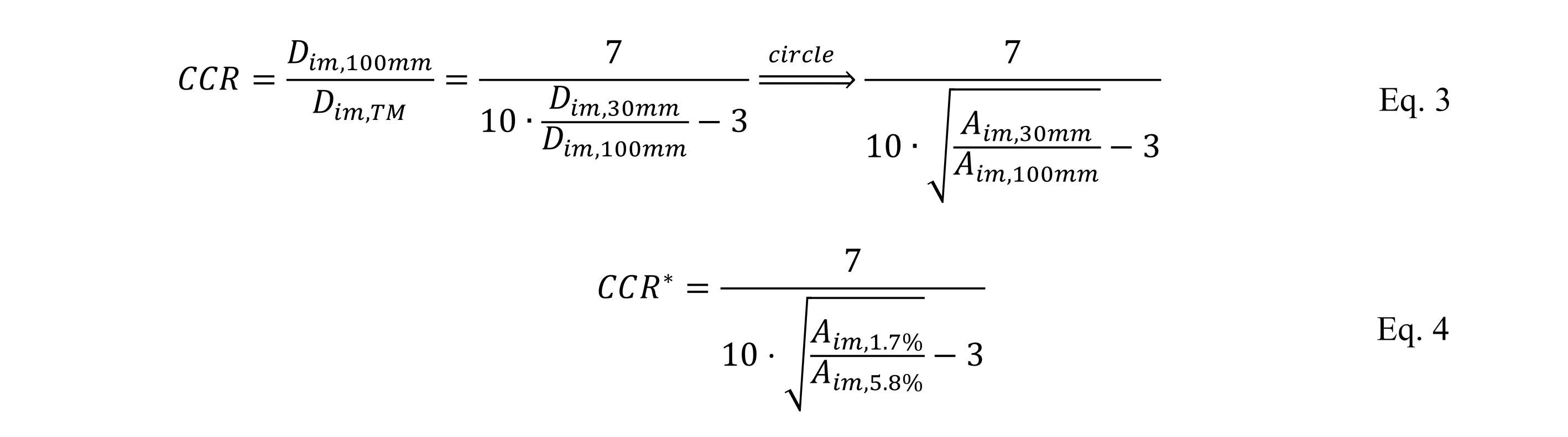
Figure 10#7965
Biomechanical Comparison of Medial Pivot and Posterior Stabilized Implants During Ramp and Stair Descent Following Total Knee Arthroplasty
Erik Kowalski - University of Ottawa - Ottawa, Canada
Danilo Catelli - University of Ottawa - Ottawa, Canada
Geoffrey F Dervin - Ottawa, Ontario, CAN
*Mario Lamontagne - University of Ottawa - Ottawa, Canada
*Email: mlamon@uottawa.ca
Abstract
Background
The purpose of this study was to evaluate knee biomechanics during a ramp and stair descent task before and twelve months after total knee arthroplasty(TKA), and to compare biomechanical outcomes between the TKA groups and a control group.
Methods
Twenty-eight participants who underwent TKA with either a medial pivot(MP) or posterior stabilized(PS) implant and fourteen healthy control subjects participated in three-dimensional motion analysis.
Results
Pre-operatively, no differences in age, body mass index, or knee biomechanics for either task existed between the MP and PS group, suggesting both groups were similar and had comparable movement patterns pre-operatively. Post-operatively the MP group had greater knee range of motion during both tasks, and the MP group achieved greater knee flexion during the ramp descent task compared to the PS group.
Conclusion
Knee excursion was indistinguishable between the MP and control group for both tasks, whereas the PS group had less knee flexion during both ramp and stair descent tasks. Neither implant group improved with their knee moments or powers, with both groups displaying differences when compared to the control group in knee extension moments during the ramp descent task, and in knee powers during the stair descent task. During the stair descent task, the PS group walked with less knee excursion and knee extension moment during the load response phase, indicating a stiff knee gait pattern to reduce joint loading.
Keywords: kinematics, kinetics, statistical parametric mapping
Introduction
Patients with end stage knee osteoarthritis(OA) often undergo total knee arthroplasty(TKA) to alleviate pain, improve their quality of life and allow them to perform most activities of daily living[1]. Previous research has shown that TKA is successful at reducing pain and that the majority of patients are satisfied with their operation[2]. However, ~20% of patients remain dissatisfied[3], and have persistent pain or have limitations in performing functional daily activities following surgery[3, 4]. TKA should restore normal joint function during walking, and during more demanding activities of daily living.
Descending a ramp or staircase are more demanding on the knee joint than level walking [5, 6]. Within patient reported outcome measures (PROMs), patients often report [7]feeling uncomfortable to perform these tasks[7]. However, PROMs cannot capture the objective functional deficits that may remain following TKA[8], therefore, a biomechanical analysis is imperative to understand the deficiencies that may persist following surgery[9].
Several studies have identified altered biomechanics in patients after TKA while descending a staircase[10-14] or ramp[15-17]. Additionally, only a few studies had the purpose of comparing different implant designs during these tasks. Considering that implant designs can influence knee joint function following TKA[18], studies should report which implants were used in their studies and not pool different implant designs together for analysis.
While different knee implant designs exist[19], the debate is still ongoing on if one implant design provides better functional outcomes with fewer complications[20, 21]. Three primary designs exist within fixed-bearing designs and include posterior stabilized (PS), cruciate-retaining(CR), and medial pivot(MP) implants[22]. MP implants, with their highly congruent medial compartment and less conforming lateral compartment, were designed to reduce the anterior sliding of the femoral component on the tibial plateau that is experienced in with CR or PS implants[23]. To our knowledge, no other study has compared MP and PS implants during a ramp or stair descent task. However, during level walking, findings were inconsistent with either PS[24] or MP[25] implants having similar knee kinematics to healthy controls.
Previous gait studies comparing TKA implants examined discrete biomechanical outcome measures, such as peak knee extension moment or sagittal knee range of motion (RoM). However, gait is a continuous process, therefore, methods that examine the entire movement cycle may uncover additional information which may have been missed with discrete analyses. Statistical parametric mapping(SPM) analyses the entire gait cycle by providing a point-by-point comparison[26]. This provides additional temporal information on where statistical differences occur [26].
To our knowledge, no study exists in the TKA literature which compared knee biomechanics throughout the entire movement cycle during ramp and stair descent. Therefore, the aim of this study was to evaluate knee biomechanics throughout the entire movement cycle during a ramp and stair descent task in patients before and after a TKA with either a MP or PS implant and compare them to a group of similarly aged healthy controls. It is hypothesized that the MP group will have closer knee biomechanics to the control group than the PS group.
Material and methods
Subjects
This was a prospective case-control study which included subjects with end-stage knee OA who were scheduled to undergo TKA by a senior orthopedic surgeon(GD). Prior to enrollment, subjects were screened for eligibility by research staff (Table 1). Three-dimensional motion analysis was completed within one month prior to TKA and 12±1 months after TKA.
All surgical procedures were performed with a midline incision and subvastus approach at a tertiary hospital by a single senior arthroplasty surgeon(GD). The protocol required for resurfacing of all patellae. All components were cemented, and tourniquet use was restricted to the time of cementation and then deflated prior to closure[27]. Patients were randomly assigned to receive a MP (MicroPort EVOLUTION® MP System with Cruciate Sacrificing tibial inserts) or PS (Zimmer® NexGen® PS TKA system with PS inserts) implants.
A sample of similarly aged healthy participants were recruited from the community to form a control group(CTRL). Inclusion and exclusion criteria for the CTRL group is described in Table 1. The CTRL group completed a single motion analysis visit.
This study was approved by the university and hospital review boards and was conducted following approval by the U.S. Food and Drug Administration. The trial was registered in the ClinicalTrials.gov database (NCT02589197) in October 2015. All participants provided informed consent prior to participation.
Anthropometric Measurements
Age, height, weight, and sex were recorded, and BMI was calculated for participants in the TKA and CTRL groups (Table 2).
Motion Analysis
Motion analysis was completed using a three-dimensional 10-camera motion capture system (200Hz, VICON, Oxford Metrics, Oxford, England) synchronized with four force platforms (1000Hz, Bertec Corp., Worthington, OH, USA and Kistler, Winterhur, Switzerland). A three-step staircase had force platforms on the first and second steps, and two force platforms were embedded in the ground at the bottom of the staircase. An instrumented ramp was inclined to 9° and had two force platforms embedded in the middle of the ramp to record a step from each foot as participants walked down the ramp. Forty-five spherical passive-reflective markers were placed bilaterally on all participants[28]. Participants completed a static trial and completed five trials at their preferred pace for both the ramp descent(RD) and stair descent(SD) tasks.
Motion capture data were processed using Vicon Nexus 2.9.2 software (Oxford Metrics, Oxford, England). Trajectories were filtered using a Woltring filter with a mean standard error of 15mm and force platform data were filtered using a 4th order (zero lag) Butterworth filter with a cut-off frequency of 10Hz. Gait event detection was done with the assistance of the ground reaction forces, and the trials were modeled[28] to compute the variables of interest. A custom-written Matlab script (2019b, MathWorks, Natick, USA) was used to extract relevant data.
Outcome Variables
Comparisons were made on the affected side undergoing TKA for the MP and PS groups, and the dominant limb in the CTRL group[29], which was defined as the limb they would use to kick a ball[30]. The variables of interest were knee flexion/extension and abduction/adduction angles and moments, as well as joint powers. Knee moments were expressed as external moments normalized to body mass (Nm/kg) and knee power was normalized to body mass (W/kg). Knee biomechanical variables were normalized to 100% gait cycle (GC). Knee moments and powers were analyzed during the stance phase which was represented as 0 to 62% GC[31].
Several temporospatial variables were extracted. Since stature of participants can affect these parameters, i.e., taller individuals tend to walk with longer steps, several temporospatial variables were normalized to leg length and included: walking speed, stride length, step length, and step width[32].
Data Analysis
All discrete statistical analyses were done using SPSS v.27 software (IBM Corporation, Armonk, USA). A paired t-test (P<.05) was used to assess changes between pre-operative and post-operative time points. A One-Way ANOVA with a Bonferroni post hoc correction to measure differences between the groups.
Point-by-point analysis of knee biomechanics along the entire movement cycle were completed using statistical parametric mapping (SPM)[26]. To assess differences between pre-operative and post-operative time points, a paired SPM (P<.05) was used, whereas between-group comparisons were completed using analysis of variance SPM (P<.05).
Several biomechanical outcomes may be influenced by walking speed[33], therefore, if walking speed was identified to be significantly different, it would be used as a covariate.
Results
Comparison of pre- and post-operative time points for the knee biomechanics during RD and SD tasks are displayed in Figure 1. MP and PS groups demonstrated to be equivalent pre-operatively, as no differences existed between the groups for any variable during either the RD or SD tasks. The MP group had a significant increase in knee flexion prior to toe-off in the RD(44-65%GC) and throughout stance (0-7%; 22-56%GC) and swing phases (60-78%GC) during the SD. Post-operatively, the MP group achieved more knee flexion during swing phase (69-83%GC) compared to the PS group during the RD.
Comparison of post-operative knee biomechanics after TKA with healthy CTRL group during RD and SD tasks are displayed in Figure 2. The PS group had less knee flexion than the CTRL group during stance (2-30%GC) and swing (67-90%GC) of the RD, and during stance phase (6-25%GC) of the SD. During the RD task, both the MP (53-58%GC) and PS (35-46%; 57-59%GC) groups had different knee extension moments compared to the CTRL group. Peak knee extension moment was significantly lower in the PS group compared to the CTRL group during the SD (13-18%GC). Knee power generation during midstance was significantly lower in both the MP (22-25%GC) and PS (18-24%GC) compared to the CTRL group during the SD.
Temporospatial outcomes during the RD and SD tasks are displayed in Figure 3. Pre-operatively, walking speed was significantly (p=.009) lower in the PS (1.06±0.23) group compared to the MP (1.36±0.28) during the RD -.308(95%CI, -.56 to -.05), and between pre- and post-operative visits for the PS group during the SD, t(12)=-2.819, p=.018, d=.85. Therefore, walking speed was used as a covariate when comparing the MP and PS group pre-operatively during the RD, and when comparing the PS group pre- and post-operatively during the SD.
PS group walked post-surgery with a significantly longer step length during the RD, t(12)=-2.507, p=.028, d=.70, and with a significantly faster stride, t(12)=2.908, p=.014, d=.84, and step time, t(12)=2.202, p=.050, d=.64, during the SD. No differences in temporospatial outcomes existed post-operatively between the MP and CTRL groups(P>.05). Post-operatively, the PS group (.74±.08) walked with a wider step width compared to the CTRL (.76±.09) group,(.052, 95%CI( .017 to .087)), during the RD, which was significantly different (p<.001).
BMI was significantly different between the groups, F(4,65)=5.647, p<.001, Table 2. Bonferroni post hoc analysis revealed differences between the PS pre-op (29.8 ± 3.4kg/m2) and CTRL (24.9±2.1kg/m2) group (4.87,95% CI(1.16 to 8.59), p=.003), and between the PS post-op (30.3±3.9kg/m2) and CTRL group, (5.42, 95% CI(1.70 to 9.14), p<.001).
Discussion
This study compared knee biomechanics across the entire gait cycle during RD and SD tasks in patients pre- and post unilateral TKA to that of a healthy CTRL group. No pre-operative differences in age or BMI existed between the MP and PS groups. Although the PS group walked slower prior to TKA compared to the MP group during the RD, walking speed was used as a covariate to compare both groups during the RD. No differences in biomechanics existed for either task existed between the two groups, suggesting that both groups were similar and had comparable movement patterns pre-operatively. Therefore, observed post-operative differences in knee biomechanics are likely attributed to the implant they received.
Twelve months post-surgery, the MP implant group showed larger knee flexion compared to their pre-surgery visit during both tasks. The PS group had the same knee flexion angle pre- and post-surgery during both tasks, and had significantly less knee flexion during the swing phase of the RD task compared to the MP group(Figure 1). Compared to the healthy controls, knee flexion angle for the MP group was statistically indistinguishable, while the PS group had significantly less knee flexion compared to the CTRL group during both tasks(Figure 2).
Knee joint loading was not improved after TKA, as both PS and MP groups did not have any measurable differences in knee joint moments during either task. Some differences in knee joint power were observed during terminal stance of the RD task, however, this difference may not have clinical relevance, as the mean values were around 0W/kg, and these differences did not occur during the transition from single- to double-limb support(Figure 1).
The increased demands of walking down a ramp was evident, as both groups displayed different joint loading patterns compared to the CTRL group(Figure 2). During the RD task, the second peak knee extension moment occurred earlier in the stance phase in the MP and PS groups compared to the CTRL group. This was identified as a significant difference between the groups, which may not have been identified if discrete statistics using peak moments were used. Although the unaffected limb was not analyzed, it is suspected that the TKA groups adapted a shorter swing phase for the unaffected limb during the RD condition. This would shorten the duration the TKA group spent in single-limb support on their affected limb, allowing them to return to double-limb support earlier in the gait cycle. This would have the second peak knee extension moment occurring earlier than in the CTRL group. Previous research identified that individuals with knee OA walked with a significantly shorter total swing time, spent less time in single-limb support, and spent more time in double-limb support than similarly aged healthy controls during SD tasks[34]. Therefore, it is possible that this phenomenon existed with the present cohort and existed during the RD condition as well.
During SD, the PS group had lower knee extension moment during midstance (13-18%GC) compared to the CTRL group. During this period, the body is transitioning from double-limb support to single-limb support on the affected limb. The PS group may have been adapting a strategy to minimize knee joint loading by reducing knee excursion and lowering knee extension moments[35].
Examining knee joint powers provides further insight into how the joint generates and absorbs energy, which is represented by positive and negative values, respectively. Following load response, there is a transition from negative to positive work while the limb is loaded and transitions from double-limb to single-limb support[36]. Both MP and PS groups displayed an inability to generate sufficient knee power during this period while descending the staircase. Descending a staircase produces the highest axial knee forces of 3.52 body weight(BW), greater than level walking (2.76BW) or ascending a staircase (3.06BW)[37].
Taken together, the reduced knee excursion, lower extension moment, and limited power generation at load response indicated the PS group adopted a strategy to minimize joint loading which could indicate a pain avoidance strategy while descending the staircase[35]. This gait pattern was present prior to TKA (Figure 1), so the surgery did not improve gait biomechanics for the PS group.
Although the MP group did not have a post-operative improvement in knee moments or powers, they did improve with knee excursion for both the RD and SD task (Figure 1). This would indicate that they are walking with a less stiff knee gait pattern, as dynamic knee joint stiffness is a function of knee excursion and knee extension moment[38]. The MP group also walked with a more similar gait pattern to the CTRL than the PS group, as the MP group did not have any differences in knee power during the RD task, or in knee moments during the SD task. When differences occurred compared to the CTRL group, the period within the gait cycle was less for the MP group than the PS group. These smaller periods existed with knee extension moment during RD (MP:Δ5%GC, PS:Δ13%GC) and knee power during SD (MP:Δ3%GC, PS:Δ8%GC)(Figure 2). Our hypothesis was partially correct, as the MP group did have similar knee joint angles as the control group, but some differences did exist for knee extension moment during RD and knee power during SD.
This study was not without limitations. It compared patients at 12±1 months after surgery, so perhaps patients were still recovering, as studies which evaluated MP and PS groups at 24 months post-TKA found fewer differences between groups[24, 39]. This study excluded obese (BMI>35kg/m2) individuals as excessive adiposity can affect the accuracy for the placement of the reflective markers for gait analysis and cause changes in gait biomechanics[40]. It also excluded individuals with a previous lower limb joint replacements, therefore, findings from this study would not be applicable to those cohorts. Finally, this study did not control for the post-operative rehabilitation. In Ontario (Canada), where this study was conducted, TKA patients are provided with eight publicly funded physiotherapy sessions. Some patients may have continued beyond these sessions and that information was not recorded.
Conclusions
This study used SPM to compare knee biomechanics across the entire movement cycle in patients before and 12 months after TKA with either a MP or PS implant during a RD and SD task. TKA with a MP implant improved knee RoM and had similar knee joint angle patterns as healthy controls. The PS group did not improve in knee RoM and had more differences compared to the control group for knee extension moments and joint powers during the RD and SD tasks. The PS group walked with a stiff knee gait pattern which was characterized by less knee excursion and more knee extension moment, which was likely done to reduce loading on their operated knee[38]. The MP group walked with a less stiff knee pattern, indicating they were better able to load their knee during the more demanding tasks of walking down a ramp and staircase.
Acknowledgements
Institutional support for this research was provided by MicroPort Orthopedics.
References
1. Roos EM, Toksvig-Larsen S. Knee injury and Osteoarthritis Outcome Score (KOOS) - validation and comparison to the WOMAC in total knee replacement. Health and quality of life outcomes 1: 17, 2003
2. Choi Y-J, Ra HJ. Patient Satisfaction after Total Knee Arthroplasty. Knee surgery & related research 28(1): 1, 2016
3. Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJK, Robertson BW. Patient Dissatisfaction Following Total Knee Arthroplasty: A Systematic Review of the Literature. The Journal of Arthroplasty 32(12): 3854, 2017
4. Noble PC, Conditt MA, Cook KF, Mathis KB. The John Insall Award - Patient expectations affect satisfaction with total knee arthroplasty. Clinical orthopaedics and related research (452): 35, 2006
5. Pickle NT, Grabowski AM, Auyang AG, Silverman AK. The functional roles of muscles during sloped walking. Journal of biomechanics 49(14): 3244, 2016
6. Nadeau S, McFadyen BJ, Malouin F. Frontal and sagittal plane analyses of the stair climbing task in healthy adults aged over 40 years: what are the challenges compared to level walking? Clin Biomech (Bristol, Avon) 18(10): 950, 2003
7. Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis care & research 63 Suppl 11(0 11): S208, 2011
8. Stevens-Lapsley JE, Schenkman ML, Dayton MR. Comparison of Self-Reported Knee Injury and Osteoarthritis Outcome Score to Performance Measures in Patients After Total Knee Arthroplasty. PM&R 3(6): 541, 2011
9. Lamontagne M, Beaulieu ML, Varin D, Beaule PE. Gait and Motion Analysis of the Lower Extremity After Total Hip Arthroplasty: What the Orthopedic Surgeon Should Know. Orthopedic Clinics of North America 40(3): 397, 2009
10. Komaris DS, Tedesco S, O'Flynn B, Govind C, Clarke J, Riches P. Dynamic stability during stair negotiation after total knee arthroplasty. Clin Biomech (Bristol, Avon) 87: 105410, 2021
11. McClelland JA, Feller JA, Menz HB, Webster KE. Patterns in the knee flexion-extension moment profile during stair ascent and descent in patients with total knee arthroplasty. Journal of Biomechanics 47(8): 1816, 2014
12. Standifird TW, Cates HE, Zhang S. Stair ambulation biomechanics following total knee arthroplasty: a systematic review. J Arthroplasty 29(9): 1857, 2014
13. Sumner B, McCamley J, Jacofsky DJ, Jacofsky MC. Comparison of Knee Kinematics and Kinetics during Stair Descent in Single- and Multi-Radius Total Knee Arthroplasty. J Knee Surg 33(10): 1020, 2020
14. Valenzuela KA, Zhang S, Schroeder LE, Weinhandl JT, Cates HE. Increased knee loading in stair ambulation in patients dissatisfied with their total knee replacement. Clinical Biomechanics 67: 38, 2019
15. Simon JC, Della Valle CJ, Wimmer MA. Level and Downhill Walking to Assess Implant Functionality in Bicruciate- and Posterior Cruciate–Retaining Total Knee Arthroplasty. The Journal of Arthroplasty 33(9): 2884, 2018
16. Wen C, Cates HE, Weinhandl JT, Crouter SE, Zhang S. Knee biomechanics of patients with total knee replacement during downhill walking on different slopes. J Sport Health Sci 11(1): 50, 2022
17. Wiik AV, Aqil A, Tankard S, Amis AA, Cobb JP. Downhill walking gait pattern discriminates between types of knee arthroplasty: improved physiological knee functionality in UKA versus TKA. Knee Surg Sports Traumatol Arthrosc 23(6): 1748, 2015
18. Andriacchi TP, Yoder D, Conley A, Rosenberg A, Sum J, Galante JO. Patellofemoral design influences function following total knee arthroplasty. J Arthroplasty 12(3): 243, 1997
19. Dall'Oca C, Ricci M, Vecchini E, Giannini N, Lamberti D, Tromponi C, Magnan B. Evolution of TKA design. Acta Biomed 88(2S): 17, 2017
20. Kahlenberg CA, Lyman S, Joseph AD, Chiu YF, Padgett DE. Comparison of patient-reported outcomes based on implant brand in total knee arthroplasty: a prospective cohort study. The bone & joint journal 101-b(7_Supple_C): 48, 2019
21. Wright G, Chitnavis J. Which design of TKR–does it matter. J Bone Joint Surg Br: 1, 2011
22. Sabatini L, Risitano S, Parisi G, Tosto F, Indelli PF, Atzori F, Massè A. Medial Pivot in Total Knee Arthroplasty: Literature Review and Our First Experience. Clinical medicine insights Arthritis and musculoskeletal disorders 11: 1179544117751431, 2018
23. Atzori F, Salama W, Sabatini L, Mousa S, Khalefa A. Medial pivot knee in primary total knee arthroplasty. Ann Transl Med 4(1): 6, 2016
24. Kulshrestha V, Sood M, Kanade S, Kumar S, Datta B, Mittal G. Early Outcomes of Medial Pivot Total Knee Arthroplasty Compared to Posterior-Stabilized Design: A Randomized Controlled Trial. Clin Orthop Surg 12(2): 178, 2020
25. Gray HA, Guan S, Young TJ, Dowsey MM, Choong PF, Pandy MG. Comparison of posterior‐stabilized, cruciate‐retaining, and medial‐stabilized knee implant motion during gait. Journal of Orthopaedic Research 38(8): 1753, 2020
26. Pataky TC, Robinson MA, Vanrenterghem J. Region-of-interest analyses of one-dimensional biomechanical trajectories: bridging 0D and 1D theory, augmenting statistical power. PeerJ 4: e2652, 2016
27. Hofmann AA, Plaster RL, Murdock LE. Subvastus (Southern) approach for primary total knee arthroplasty. Clinical orthopaedics and related research (269): 70, 1991
28. Mantovani G, Lamontagne M. How Different Marker Sets Affect Joint Angles in Inverse Kinematics Framework. Journal of biomechanical engineering 139(4), 2017
29. Kowalski E, Catelli DS, Lamontagne M. Side does not matter in healthy young and older individuals – Examining the importance of how we match limbs during gait studies. Gait & Posture 67: 133, 2019
30. Chapman JP, Chapman LJ, Allen JJ. The measurement of foot preference. Neuropsychologia 25(3): 579, 1987
31. Winter DA. Kinematic and kinetic patterns in human gait: Variability and compensating effects. Human Movement Science 3(1): 51, 1984
32. Hof AL. Scaling gait data to body size. Gait & Posture 4(3): 222, 1996
33. Fukuchi CA, Fukuchi RK, Duarte M. Effects of walking speed on gait biomechanics in healthy participants: a systematic review and meta-analysis. Systematic reviews 8(1): 153, 2019
34. Hicks-Little CA, Peindl RD, Fehring TK, Odum SM, Hubbard TJ, Cordova ML. Temporal-spatial gait adaptations during stair ascent and descent in patients with knee osteoarthritis. J Arthroplasty 27(6): 1183, 2012
35. Briem K, Snyder-Mackler L. Proximal gait adaptations in medial knee OA. Journal of Orthopaedic Research 27(1): 78, 2009
36. Winter DA, Robertson DG. Joint torque and energy patterns in normal gait. Biological cybernetics 29(3): 137, 1978
37. Heinlein B, Kutzner I, Graichen F, Bender A, Rohlmann A, Halder AM, Beier A, Bergmann G. ESB Clinical Biomechanics Award 2008: Complete data of total knee replacement loading for level walking and stair climbing measured in vivo with a follow-up of 6-10 months. Clinical biomechanics (Bristol, Avon) 24(4): 315, 2009
38. McGinnis K, Snyder-Mackler L, Flowers P, Zeni J. Dynamic joint stiffness and co-contraction in subjects after total knee arthroplasty. Clinical biomechanics (Bristol, Avon) 28(2): 205, 2013
39. Stolarczyk A, Maciąg BM, Mostowy M, Maciąg GJ, Stępiński P, Szymczak J, Żarnovsky K, Świercz M, Oleksy Ł, Stolarczyk M. Comparison of Biomechanical Gait Parameters and Patient-Reported Outcome in Patients After Total Knee Arthroplasty With the Use of Fixed-Bearing Medial Pivot and Multi-radius Design Implants—Retrospective Matched-Cohort Study. Arthroplasty Today 14: 29, 2022
40. da Silva-Hamu TCD, Formiga CKMR, Gervásio FM, Ribeiro DM, Christofoletti G, de França Barros J. The impact of obesity in the kinematic parameters of gait in young women. Int J Gen Med 6: 507, 2013
Figures
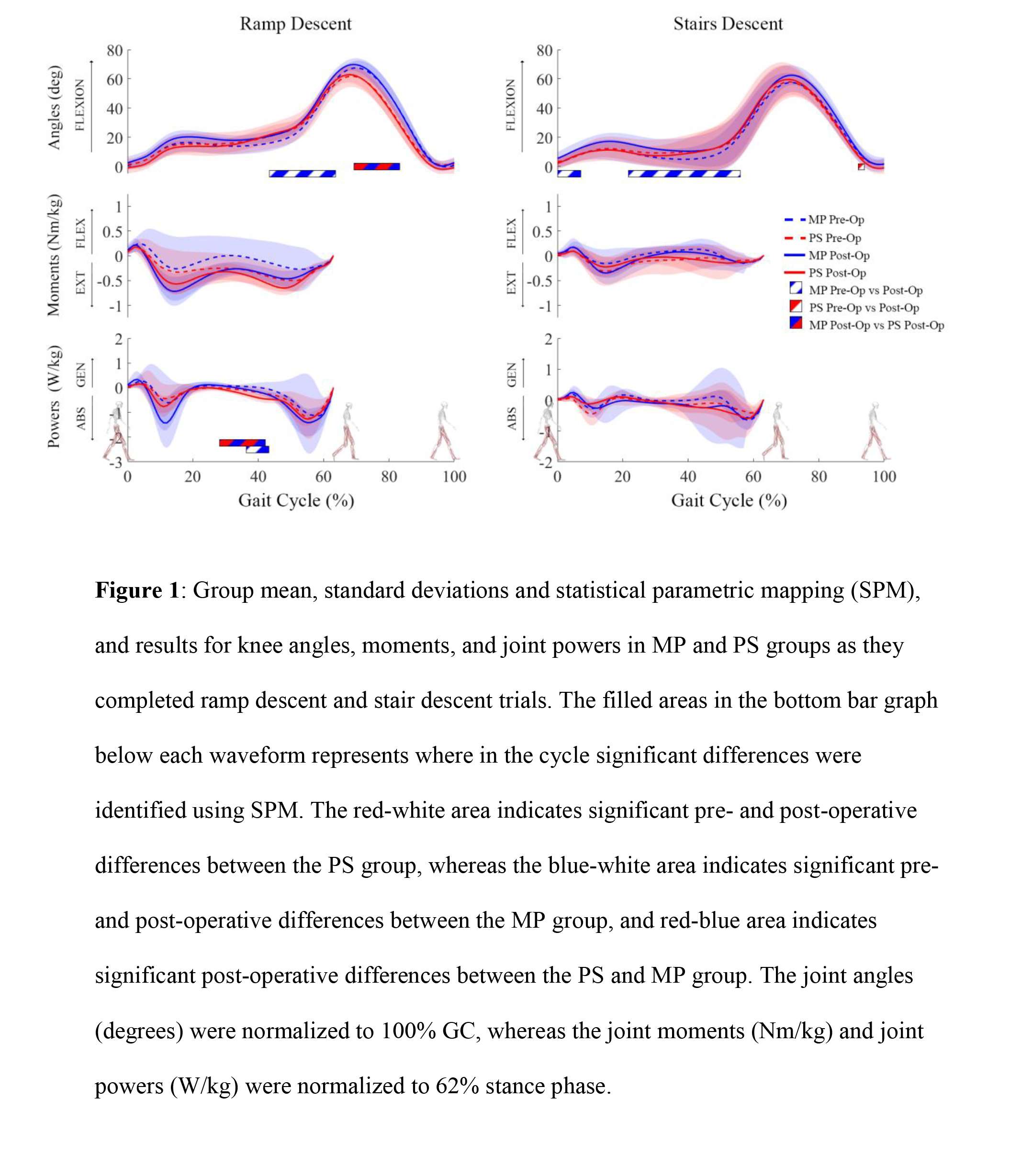
Figure 1
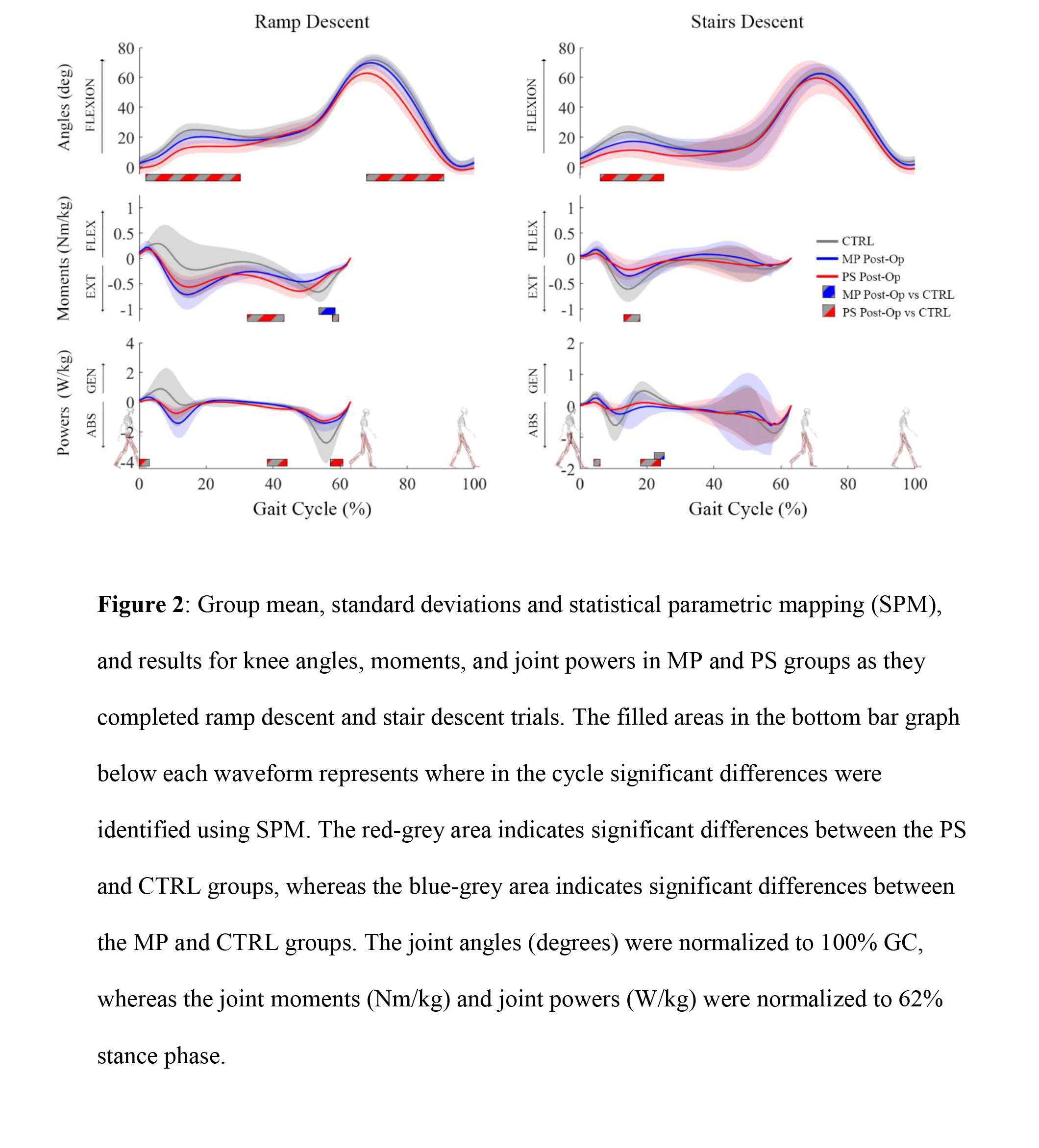
Figure 2
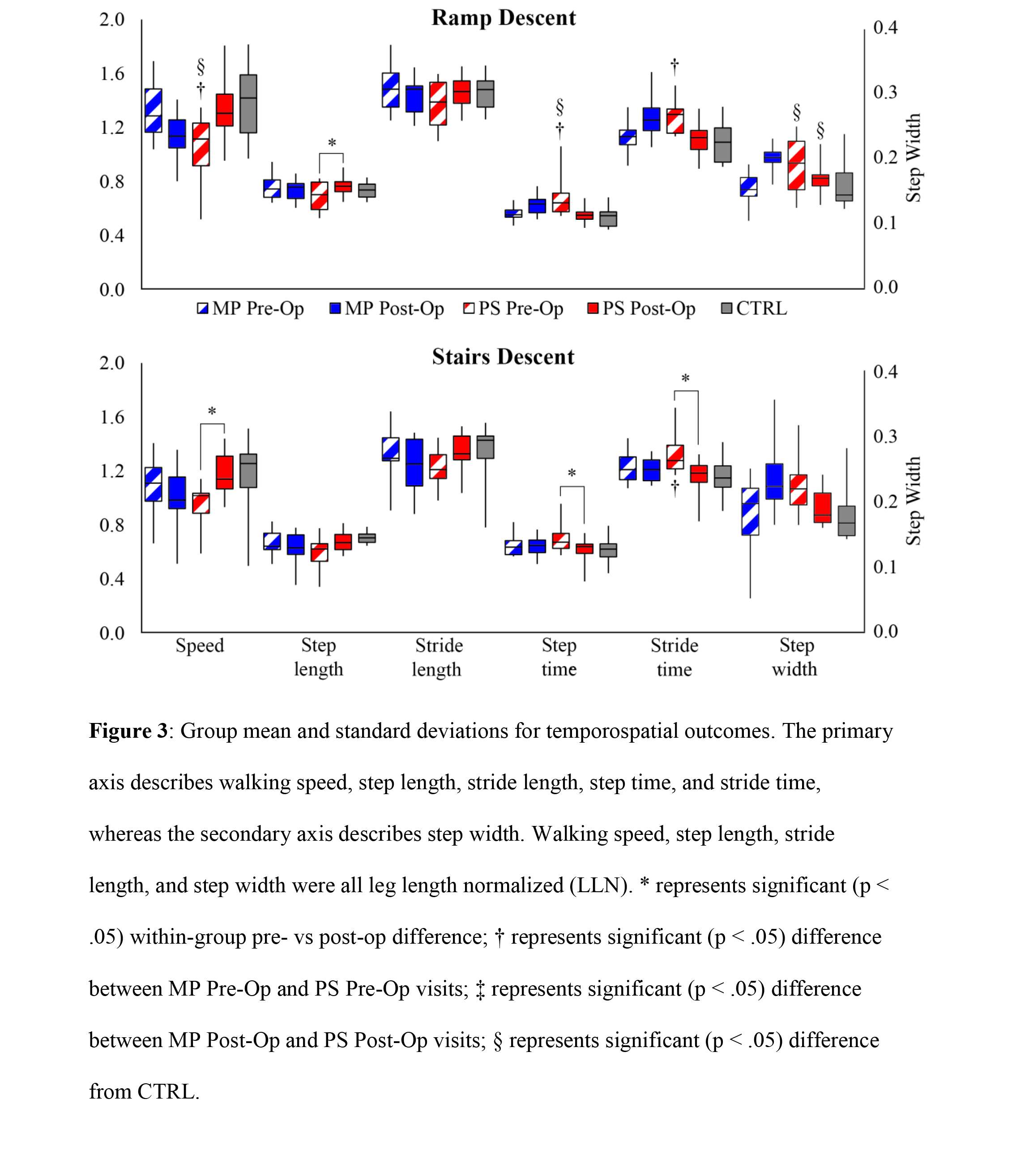
Figure 3
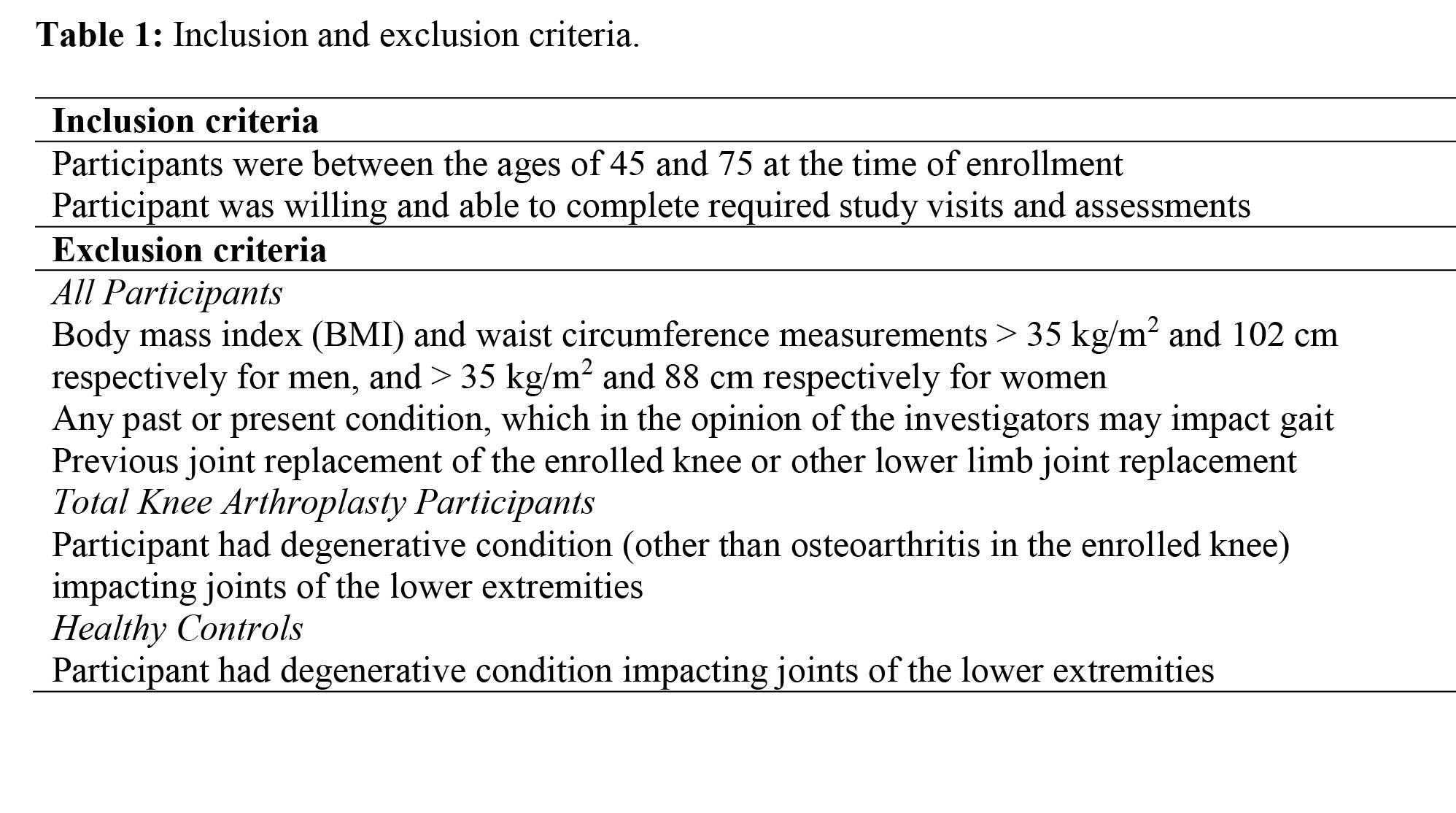
Figure 4
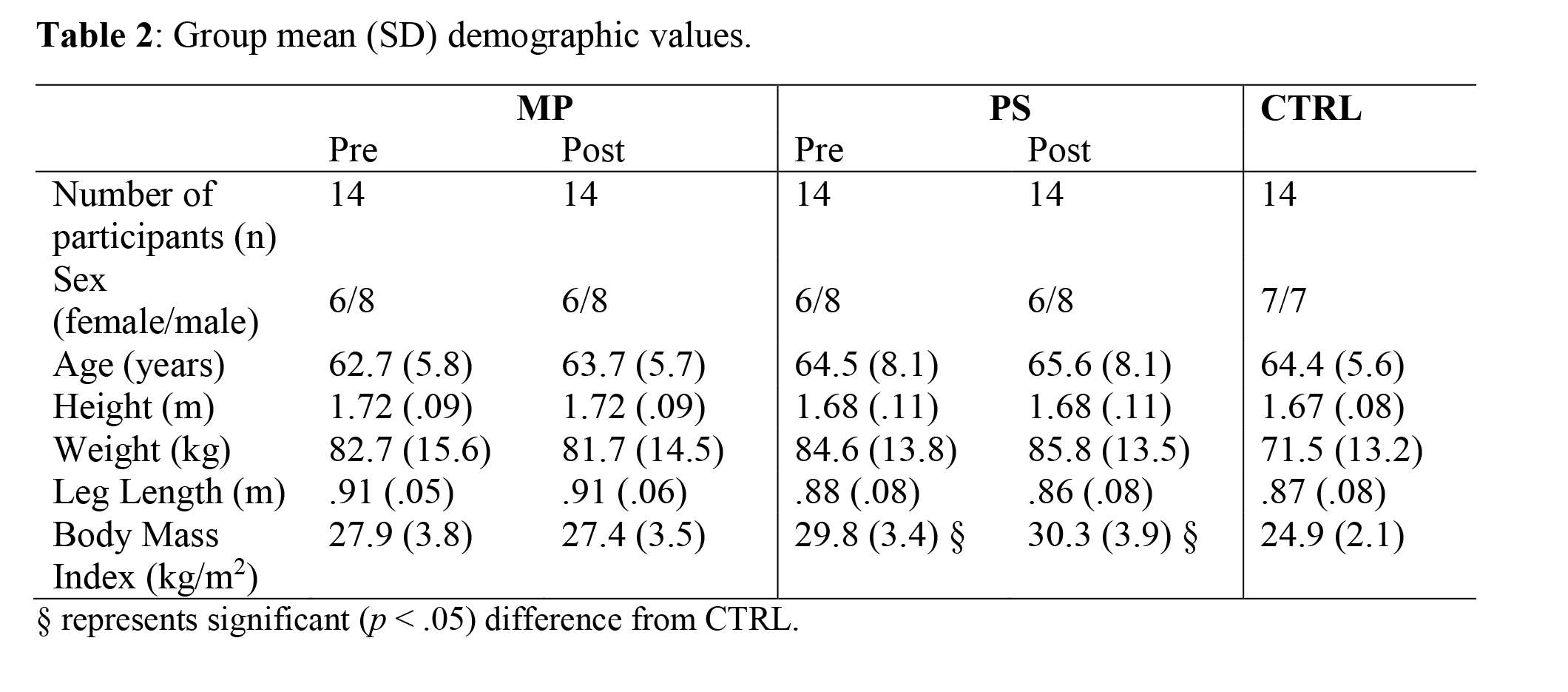
Figure 5#7375
Development of a New Impaction Device to Securely Connect Stem and Head Tapers.
*J. Philippe Kretzer - University of Heidelberg - Heidelberg, Germany
Ulrike Mueller - University of Heidelberg - Heidelberg, Germany
*Email: philippe.kretzer@med.uni-heidelberg.de
In total hip joint replacements taper associated complications like wear and corrosion have been frequently reported in the past years. Several causes for taper corrosion have been considered and the connection strength is one of them. Insufficient taper fixation may accelerate micro motions at the connection leading to fretting and corrosion. In common practice the head of the hip joint replacement is connected to the stem by the surgeon using a mallet blow. However, a mallet blow is highly individual and of limited reproducibility. In some cases the applied forces are even too low to ensure a tight fixation.
Therefore, the aim of this project was do develop and validate a new surgical instrument that ensures a sufficient and reproducible impaction force to assembly the head on the stem properly. For the validation, it was intended to study the reproducibility based on different applicants as well as the influence of different tissue damping properties.
Different technical concepts were considered based on a morphological analysis and the optimum solution was designed and manufactured as a prototype. To assess the functionality as well as the reproducibility, the impaction force was measured under laboratory conditions considering different applicants and long term tests were performed, too. Additionally, in vitro tests were done to analyze to what extend different tissue damping properties influence the taper connection strength. Furthermore, handling tests of the prototype have been performed on cadavers.
An impaction force of 4kN was predefined. As a technical solution the instrument (Fig. 1) contains a pretensioned mass which is released with a high velocity to an integrated tappet. The mechanism is triggered by the contact of the tappet to the implant’s head and a predefined contact force. Therefore, it is ensured that the impulse is completely transferred from the instrument to the implant components.
Evaluating three different users revealed no significant differences (p=0.212) of the impaction force (3.96 to 4.03kN (Min-Max) and thus a good reproducibility could be confirmed. Furthermore, the impaction force remained stable over 1000 applications without any significant variations (initial: 3.99±0.03kN and finally 3.98±0.01kN) (p=0.759). The torque off taper connection strength resulted in 15.34±0.54Nm if stiff implant bedding was simulated. Simulating soft-elastic bedding resulted in a torque off taper connection strength of 17.12±0.63Nm and in 16.31±0.68Nm if the bedding was simulated by muscle tissue. There was no significant reduction in taper connection strength considering muscle tissue in comparison to a soft-elastic bedding (p=0.181) or stiff implant bedding (p=0.087). The cadaver tests revealed optimal functionality and effective handling of the instrument (Fig. 2).
A new instrument to securely connect stem and head tapers was developed and validated. It was shown that the impaction force is independent from the applicant and highly reproducible over multiple applications even if different tissue damping properties are considered. Currently, the new instrument is under clinical evaluation and will be available soon for broad application.
Figures

Figure 1

Figure 2#7953
Accuracy of a Handheld CT-Based Navigation System
*Stefan Kreuzer - INOV8 Orthopedics - Houston, USA
*Email: skreuzer@inov8hc.com
Keywords: Hip, Arthroplasty, Navigation, Computed Tomography
ABSTRACT
Introduction: Pre-operative computed tomography (CT) and 3-dimensional pre-operative planning has become increasingly popular in total hip arthroplasty (THA) because it allows for precise planning of components and assessment of simulated range of motion. There are several tools available to intra-operatively execute what has been planned, including robotics, navigation and patient specific guides. The present study involves a novel handheld navigation system (Naviswiss, Switzerland) which offers both, image-free and CT-based navigation modalities. The purpose of this study was to evaluate the accuracy of acetabular cup placement using a CT-based workflow.
Methods: This was a retrospective, single-surgeon cohort study of a group who underwent primary THA using the direct anterior approach (DAA) for a diagnosis of osteoarthritis between December 2021 and February 2022 in an ambulatory surgery center. Pre-operative CT and 3-dimensional functional planning was performed using the OPS system (Corin, UK). The Naviplan (Naviswiss, Switzerland) software was used to auto-segment and prepare the case for the navigation system. Intra-operatively, a novel image-based navigation system (Naviswiss, Switzerland) was used to guide acetabular inclination and anteversion angles referenced according to the pre-operative plan. The acetabular cup inclination and anteversion accuracy was analyzed using commercially available software (Mimics 2D/3D - Materialize, Belgium).
Results: On average, the cup placement was accurate within 0.69° [SD ±1.98°] of the plan for inclination and 0.29° [±2.22°] for anteversion. The maximum difference between plan and execution ranged from -2.94° to 3.81° for inclination and -3.36° to 3.08° for anteversion.
Conclusion: Use of a novel handheld CT-based navigation system for DAA THA provides accurate and consistent execution of 3-dimensional preoperative planning. Future studies involving a larger patient population will be needed.
Figure 1: Cartesian plot displaying the difference between planned and executed cup alignment in acetabular anteversion (X-axis) and inclination (Y-axis).
Figures
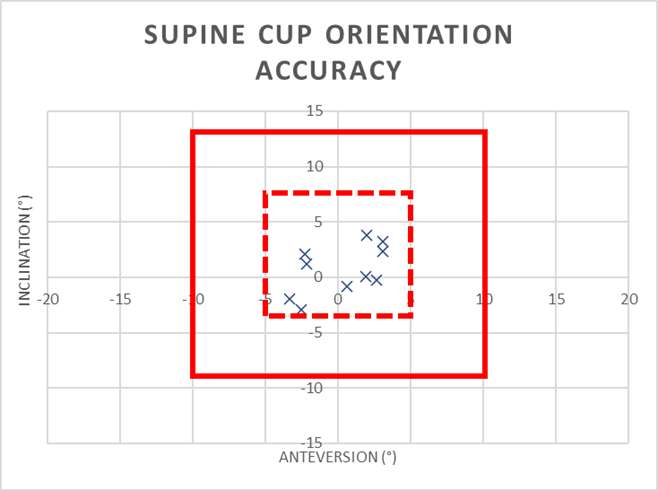
Figure 1#8039
Invited Talk: Robotics in Orthopedics: Why it is the future?
*Stefan Kreuzer - INOV8 Orthopedics - Houston, USA
*Email: skreuzer@inov8hc.com
#7584
Ultrasonic Measurement of MCL Strain During Knee Flexion-Extension
*Isabelle Kuder - Imperial College London - London, Select Country
Joe Lawton - DePuy Synthes - Leeds, United Kingdom
Richard van Arkel - Imperial College London - London, United Kingdom
*Email: ik1616@ic.ac.uk
Introduction & Aims
Assistive technologies have enabled repeatable collateral ligament balancing during total knee arthroplasty (TKA). However, it is not known how their function changes postoperatively – can a balanced knee become unbalanced, or vice versa, and if so, which patients are affected and why? Ultrasound technology could provide a means to non-invasively assess collateral ligament function pre, intra and postoperatively by measuring ligament strain during knee extension-flexion cycles. However, due to the small and complex anatomy of the ligaments, existing ultrasonic strain measurement technology is unable to reliably track the MCL over large ranges of knee flexion. The aim of this research is to optimise ultrasonic strain measurement algorithms to facilitate research into collateral ligament function post-TKA.
Method
First, n=2 porcine knees were dissected free of all soft-tissue except for the MCL. The femur and tibia were potted to enable controlled loading of the MCL in a material-testing machine. The MCL was loaded to 3% tensile strain and then relaxed back to zero. Strain was measured with optical camera digital image correlation (DIC) and with ultrasound. The ultrasound strain algorithm was then optimised based on repeatability, accuracy at peak strain compared to the DIC measurements, and accuracy for calculating zero strain at the end of the test. 2160 variations of the strain measurement algorithm were analysed. Second ultrasound measurements were then taken of the MCL for an undissected cadaveric human knee, with it extended/flexed between 0° and 90° in a knee extension rig over 5 seconds. 20 measurements were recorded and analysed using the optimum protocol measured with the porcine study. The knee was then dissected free of soft-tissue and strain in the MCL was re-calculated optically.
Results
The strain algorithm was successfully optimised to match the DIC measurements in the porcine knees (Figure 1). For the human knee, the MCL was tracked for two-thirds (n=14) of the measurements, leading to reliable measurements of increasing strain from 0° to 90° of flexion (Figure 2), agreeing with previous ligament length change values reported in the literature for the intermediate bundle of the MCL (Figure 3). Measurements where the MCL was poorly tracked (n=6) by the ultrasound were easy to identify and rule out as invalid measurements as the strain variation within the ligament was greater than 15%.
Conclusions
Ultrasound strain algorithms have been optimised to enable non-invasive measurement of collateral ligament strain throughout knee extension-flexion cycles. The optimised algorithm was insensitive to anatomical variation, working for both porcine and human MCLs. This advance will facilitate research into changes in collateral ligament function post-TKA.
Figures
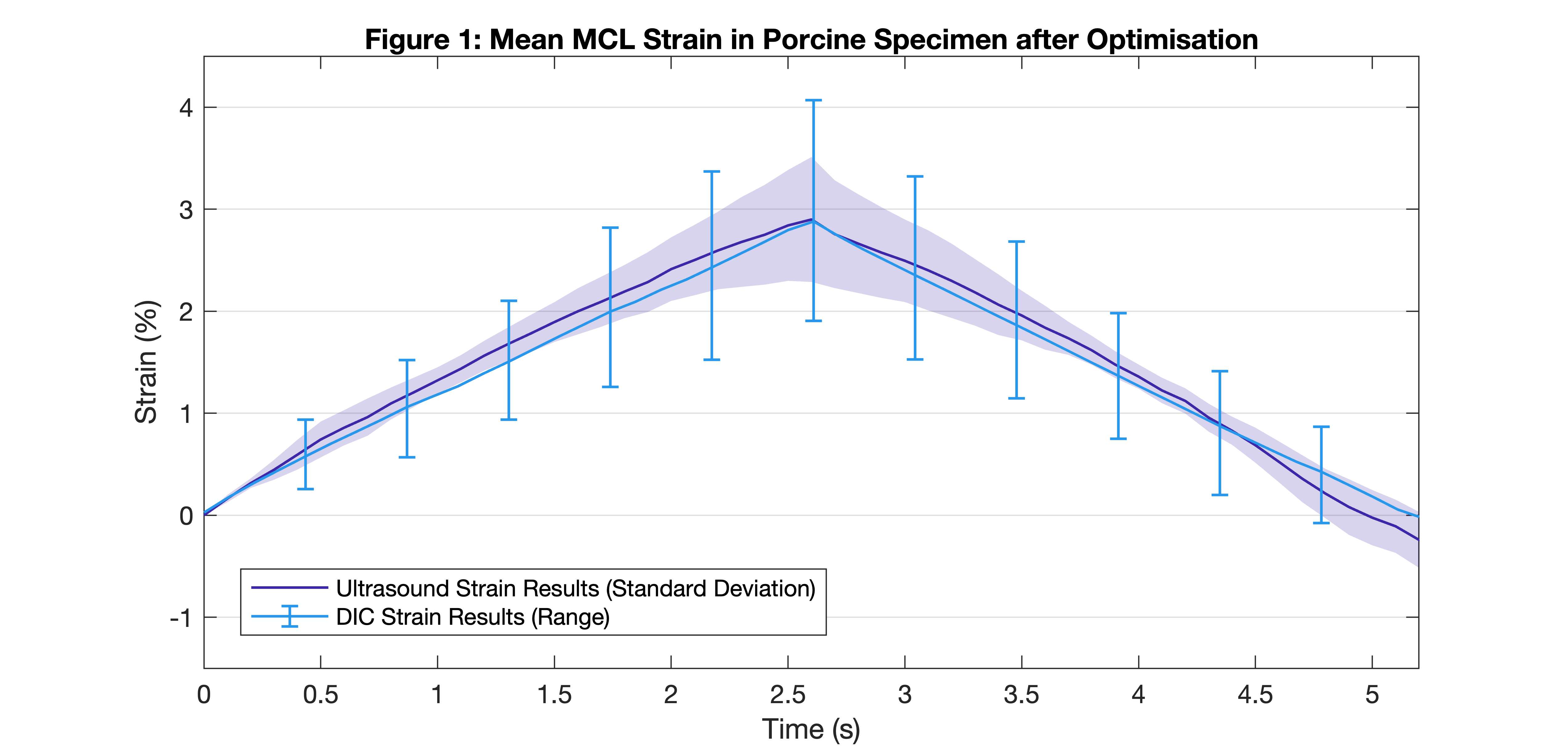
Figure 1
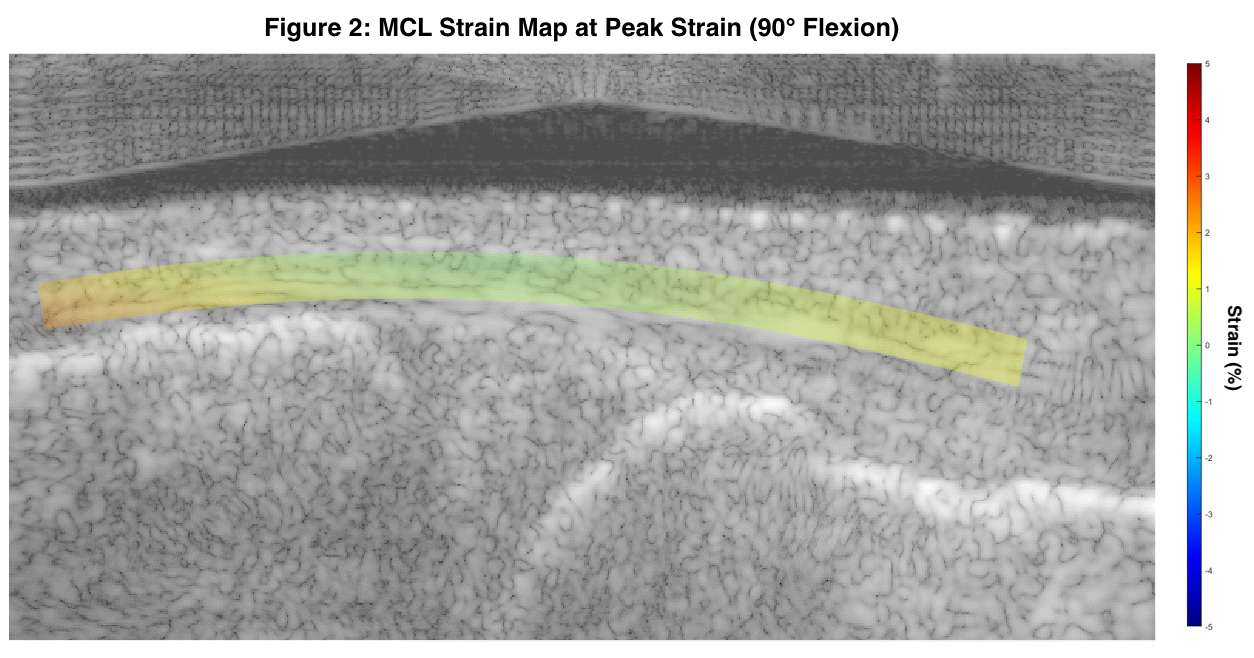
Figure 2
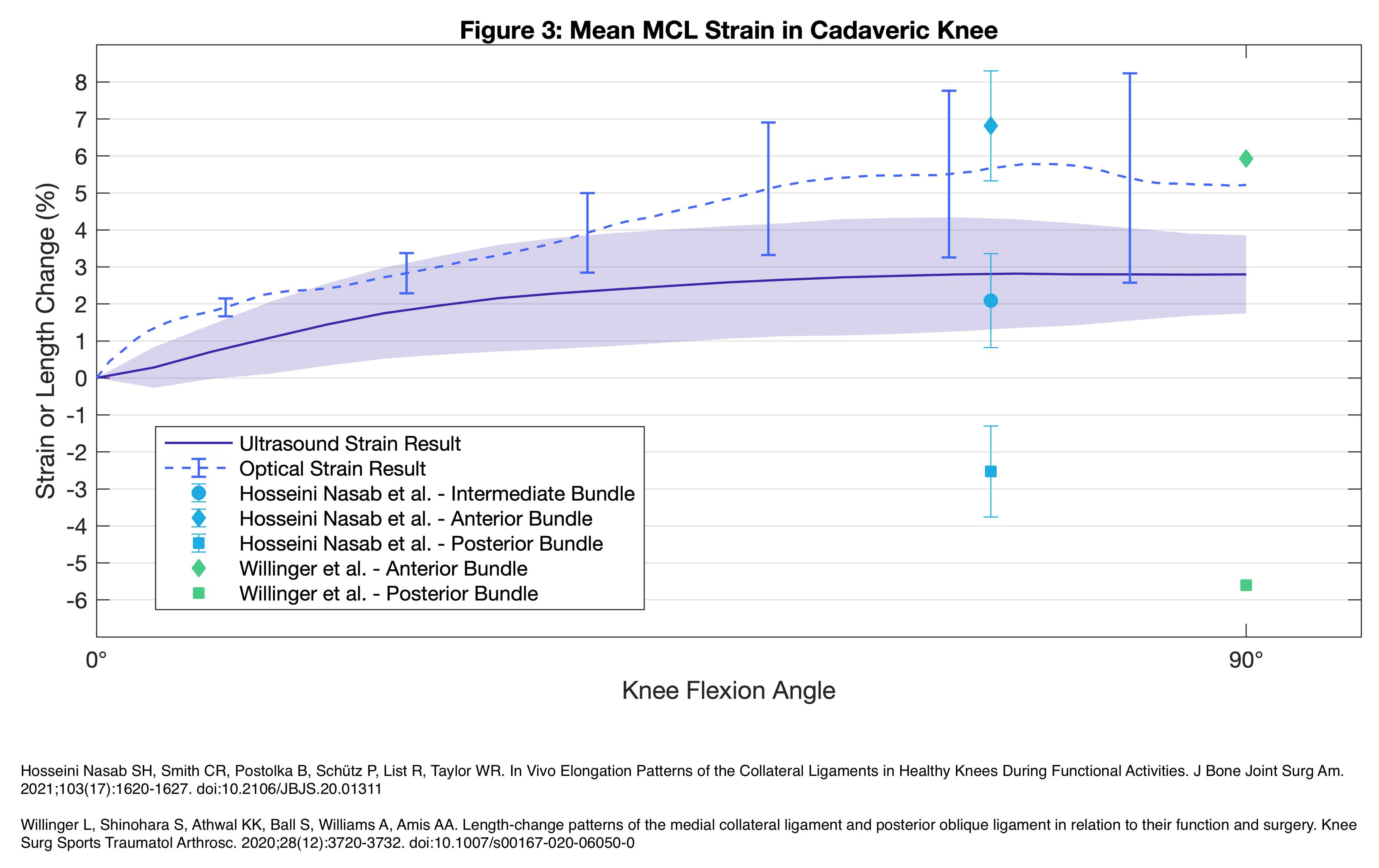
Figure 3#7823
A Novel Mesh-Free Method for Accurately Simulating the Crushing and Cracking Behavior of Trabecular Bone Tissue With a Wide Range of Clinically Relevant Bone Mineral Density Values
Sloan Kulper - Lifespans - Wong Chuk Hang, Hong Kong
*Ren Xiaodan - Tongji University - Shanghai, China
Tsui Hin Lin - Lifespans, Ltd. - Hong Kong, Hong Kong
Dana Coombs - Depuy Synthes - Westchester, USA
Michael Bushelow - DepuySynthes Trauma - West Chester, USA
Evan Fang - The University of Hong Kong - Hong Kong, Hong Kong
Ahmed Abbas Alvi - Lifespans, Ltd. - Wong Chuk Hang, Hong Kong
Erica Ueda - Lifespans, Ltd. - Wong Chuk Hang, Hong Kong
Christian Xinshuo Fang - The University of Hong Kong - Pok Fu Lam, Hong Kong
Teng Zhang - The University of Hong Kong - Pok Fu Lam, Hong Kong
*Email: rxdtj@tongji.edu.cn
Conflict of Interest and Sources of Funding: Kulper, Ueda, and C. Fang are co-founders of Lifespans Limited, and Lin, Alvi, and Zhang are paid staff and/or consultants of Lifespans Limited. Coombs and Bushelow are paid staff of DePuy Synthes. Research reported in this manuscript was supported by the Hong Kong Innovation and Technology Fund (ITF) under grant award number ITS-470-16. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Hong Kong Innovation and Technology Commission.
Objectives: Accurate simulation of trabecular bone biomechanics is critical to the development of orthopedic implants resistant to post-surgical migration, particularly for patients with osteoporosis. Conventional meshed-based simulation techniques such as finite element analysis (FEA) are limited in their ability to model the crushing, cracking, fragmentation, and compaction phenomena that occur during implant migration. Recent studies have shown that newer mesh-free simulation techniques – such as smoothed-particle hydrodynamics (SPH) – can overcome many such limitations, though validation was only completed for a narrow range of bone densities and morphologies. In the present study, an improved mesh-free simulation method was developed capable of accurately simulating the cracking, fragmentation, and compaction of trabecular bone specimens with a wide range of bone densities and morphologies. Results were validated by examining the concordance between physical and simulated results when crushing human cadaveric trabecular tissue.
Methods: Cylindrical trabecular bone specimens (n=22) with height of 12 mm and radius of 3.7 mm were extracted from the proximal heads of nine fresh-frozen human cadaveric humeri (seven female, two male donors; mean age 73.7 years, range 45–86). MicroCT scans of these specimens (15 μm/pixel) were used to measure volumetric bone mineral density (vBMD; range 0.040–0.214 gHA/cm3) and to construct mesh-free models for simulation. Physical and simulated specimens were compressed under axial loading to 20-30% of their original height while recording force-displacement data. To improve concordance with the physical data, simulation parameters were systematically iterated to develop an equation (power law) that adjusted the Young’s modulus for each specimen according its vBMD score.
Results: Across all vBMD values (0.040–0.214 gHA/cm3), the concordance correlation coefficient (CCC) between physical and simulated force-displacement data was 0.762, with a 95% CI of 0.746–0.777, a Pearson ρ (precision) value of 0.911, and a bias correction factor Cb (accuracy) value of 0.837. For the 15 least-dense specimens (vBMD values of 0.040–0.150 gHA/cm3), the CCC was 0.8792 (95% CI 0.866–0.891, ρ = 0.936, Cb = 0.940). From the literature, this range of density (0.040–0.150 gHA/cm3) accounts for between 80–99.9%, 91%, and 87% of the trabecular bone tissue present in the proximal humeri, proximal femora, and lumbar vertebrae of postmenopausal women, respectively.
Conclusion: The improved mesh-free model presented here accurately simulated the behavior of trabecular bone specimens with a range of densities representing the majority of trabecular bone present in the humeri, femora, and lumbar vertebrae of post-menopausal women. Further research is necessary to improve accuracy for denser tissue. This is the first such model of which the authors are presently aware.
Figures
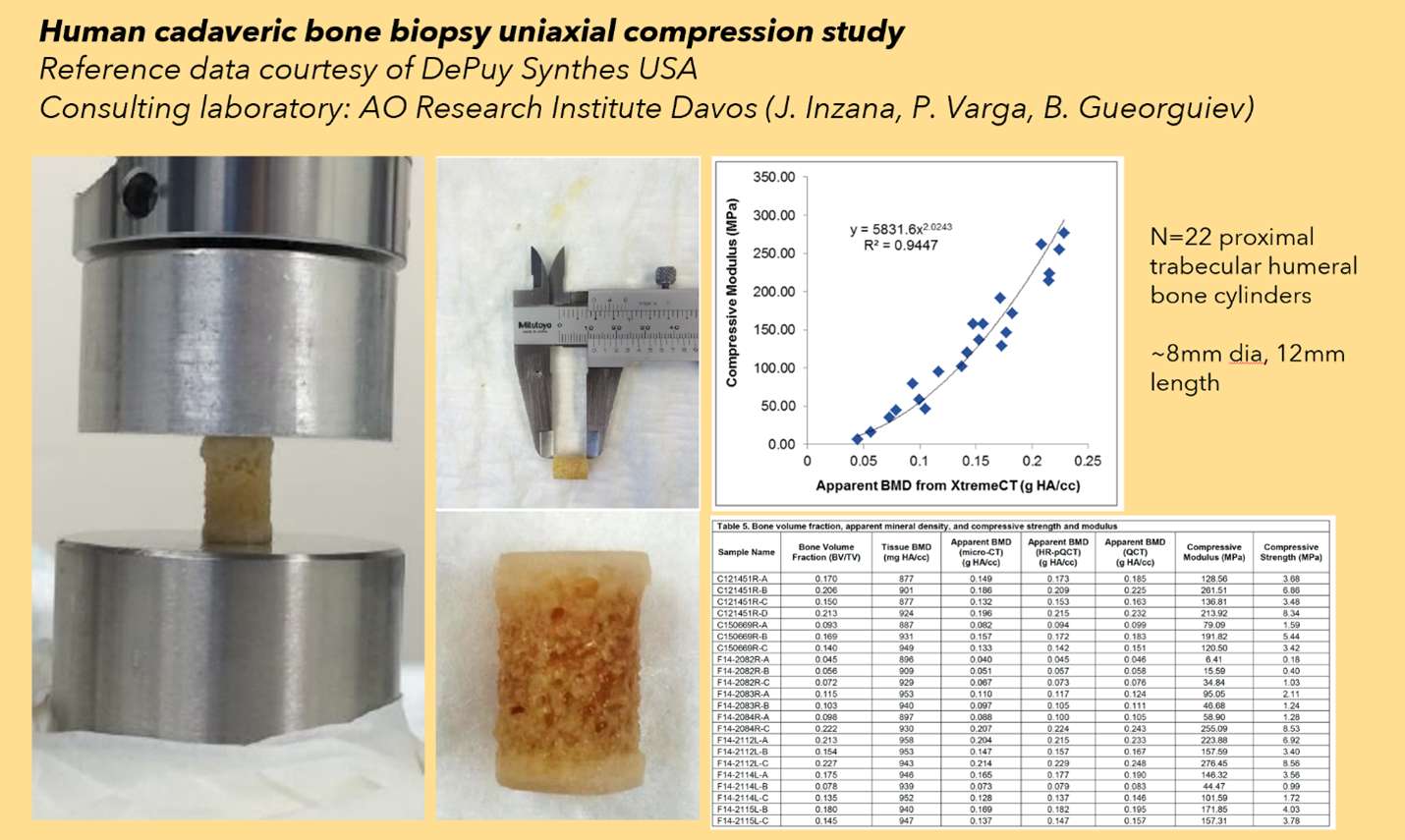
Figure 1
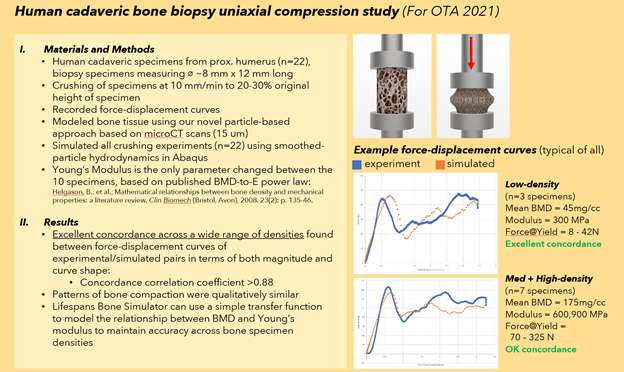
Figure 2
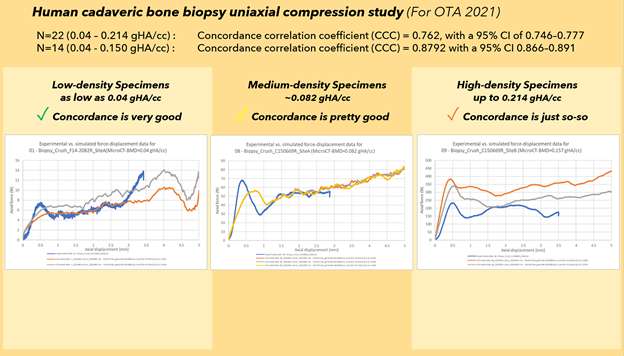
Figure 3
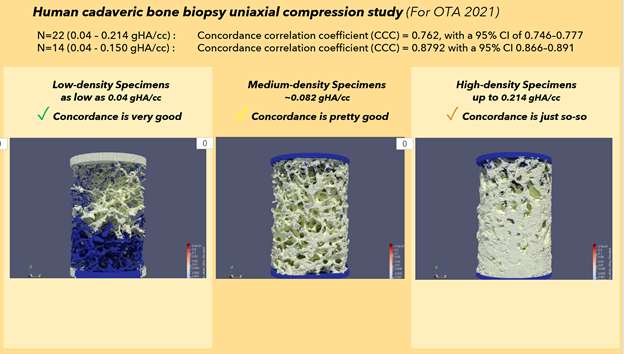
Figure 4
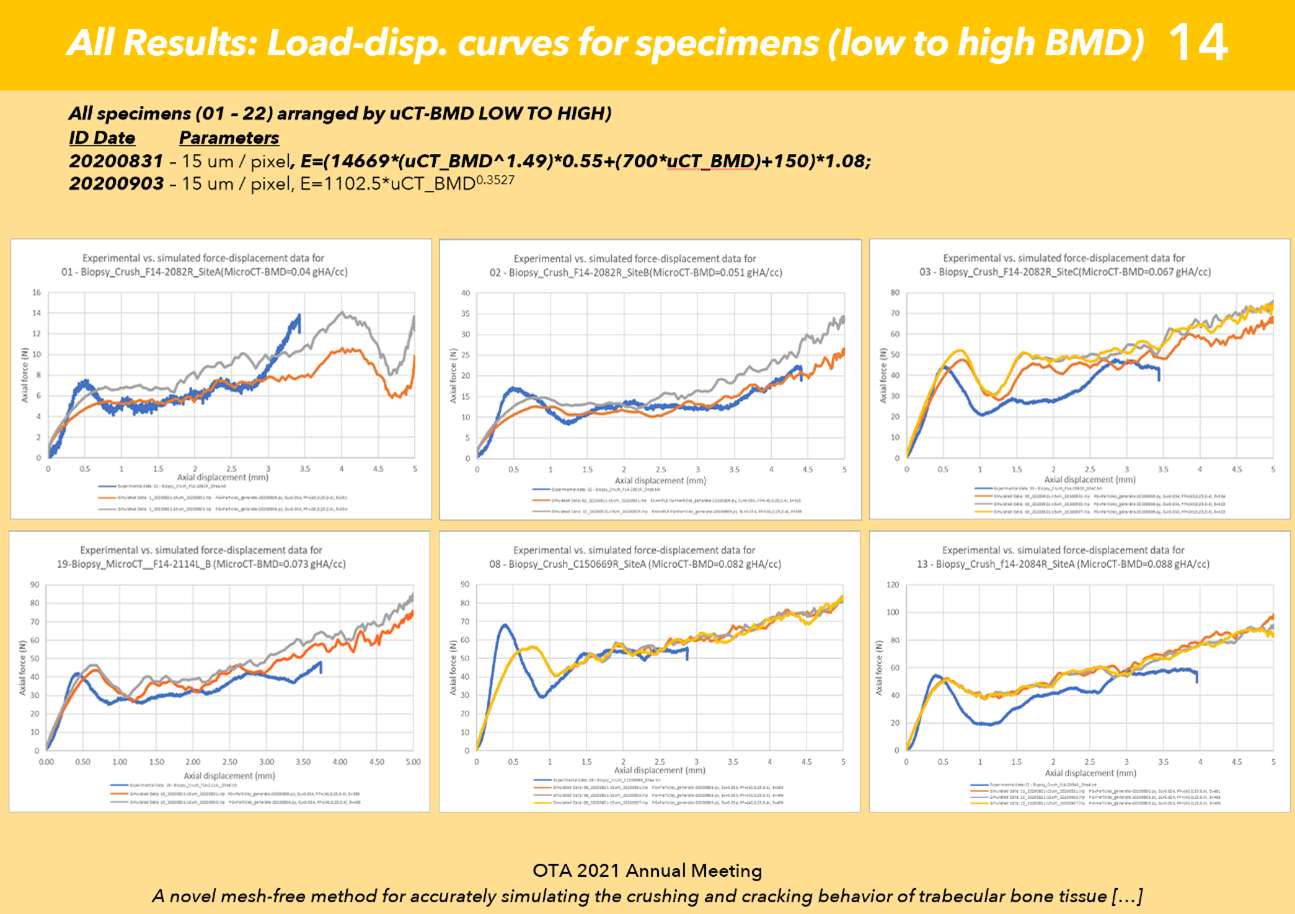
Figure 5
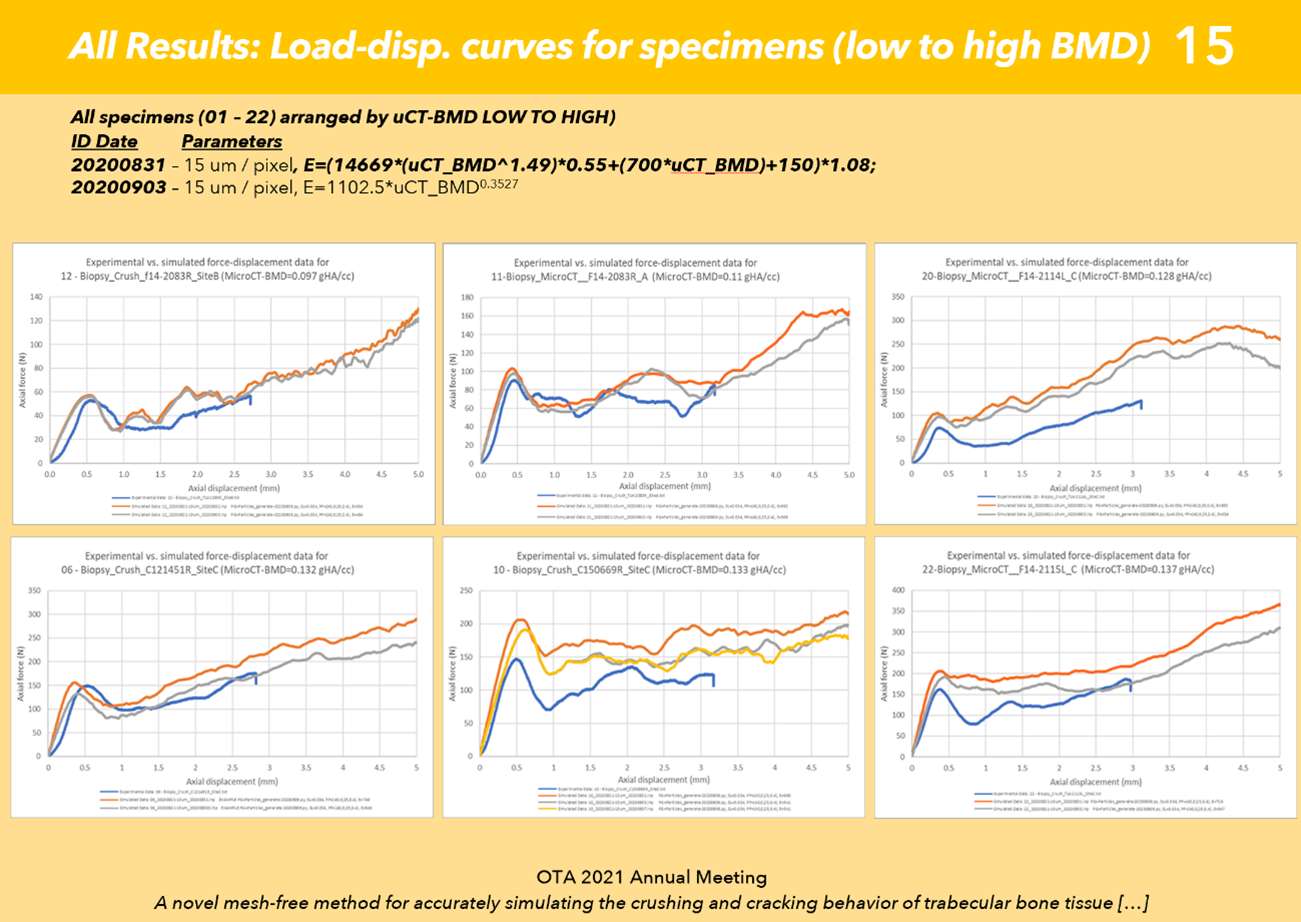
Figure 6
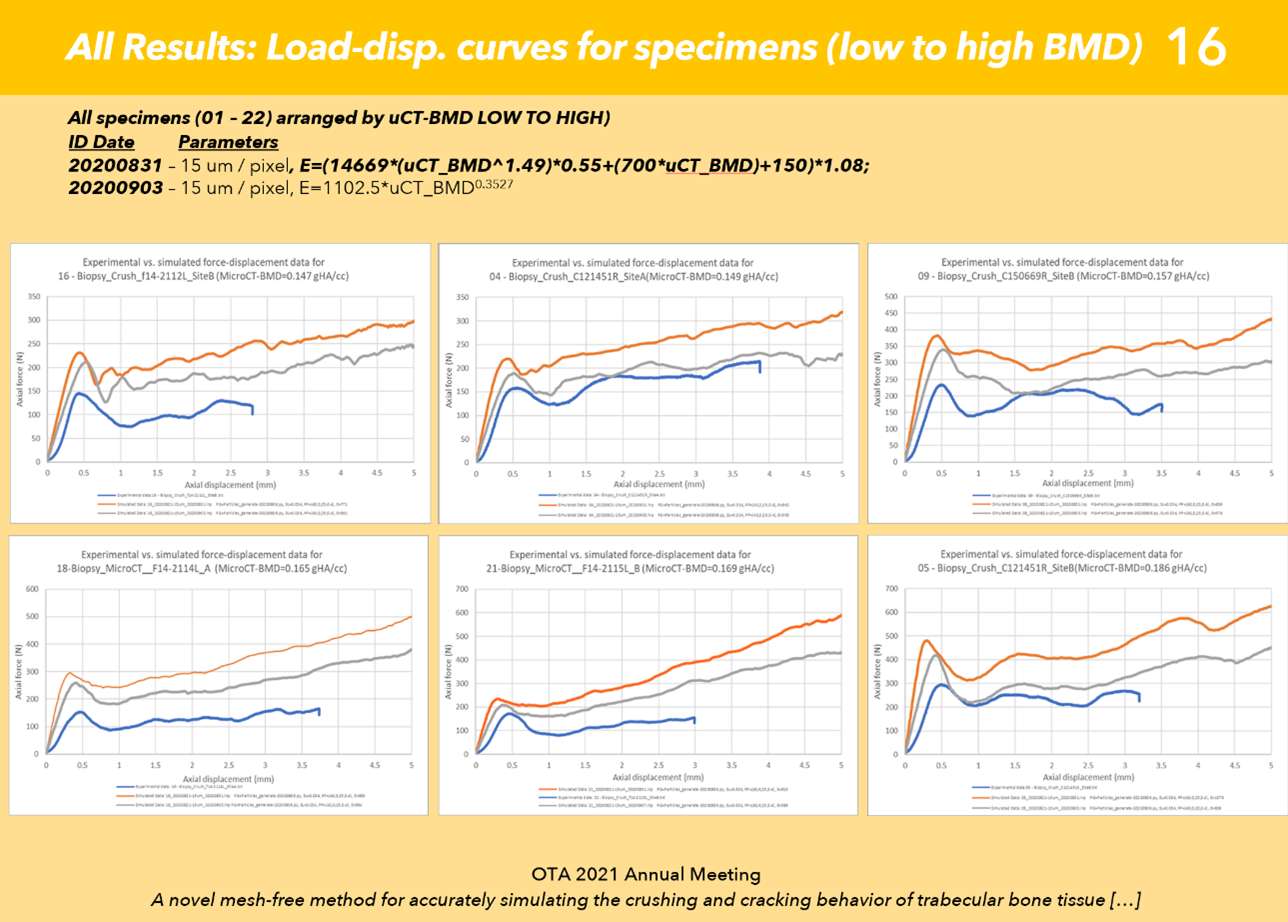
Figure 7
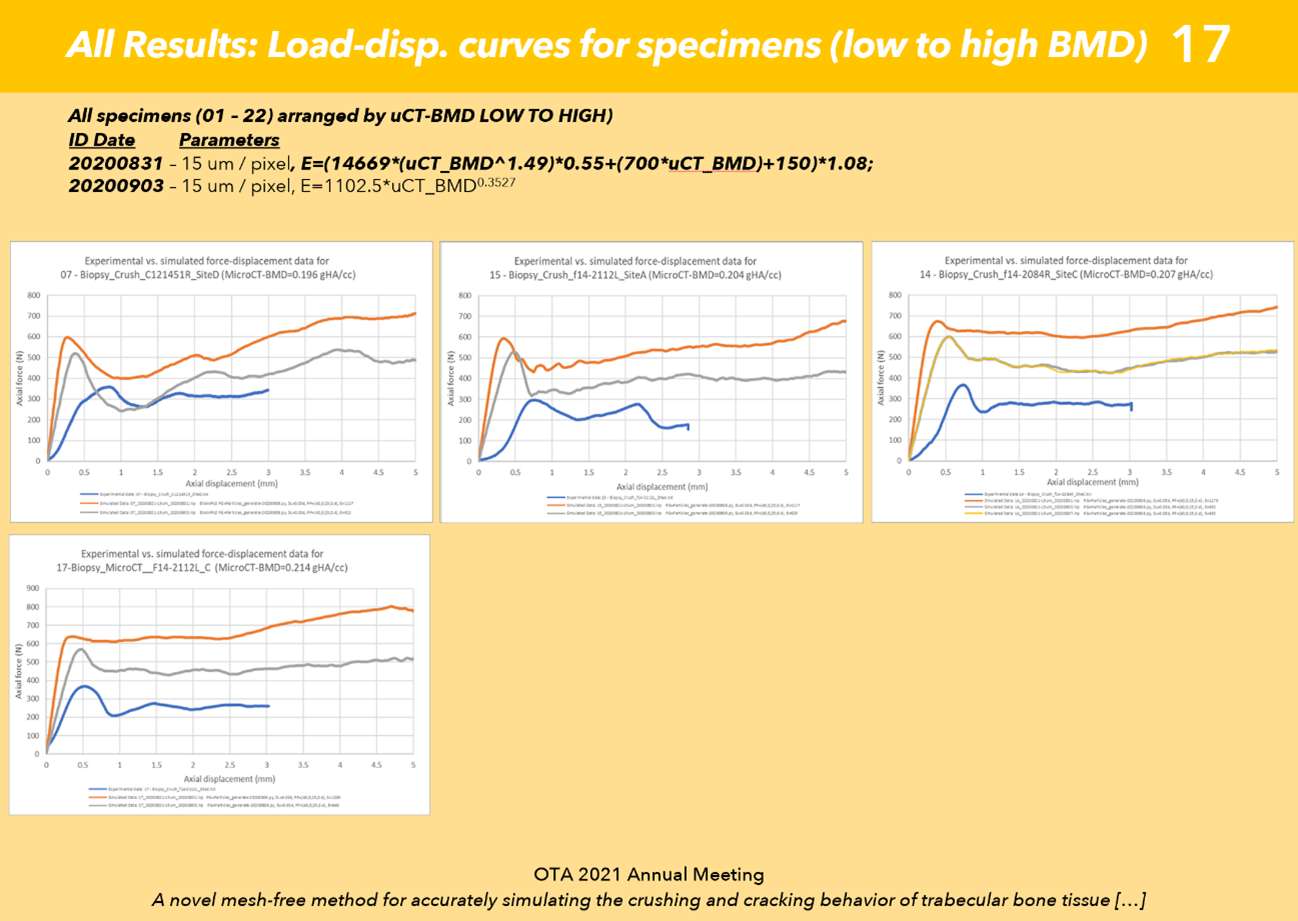
Figure 8#7701
Corrosion of Additively Manufactured Titanium Alloys in Simulated Inflammatory Solution: Ti-29Nb-21Zr Shows Improved Corrosion Resistance
Michael Kurtz - Clemson University - Charleston, USA
*Jeremy Gilbert - Clemson University - Charleston, USA
Audrey Wessinger - Clemson University - Charleston, USA
Aldo Moreno-Reyes - Clemson University - Charleston, USA
*Email: jlgilbe@clemson.edu
Introduction: Additively manufactured (AM) titanium alloy implants are increasingly implanted in vivo. Despite a clinical need for AM implants, their long-term in vivo behavior remains poorly understood. Until recently, AM biomaterial selection has mostly been limited to legacy alloys. However, laser-powder bed fusion opens possibilities for development of alloy admixtures, where distinct metal particle compositions are combined by rapid melting and solidification. In vivo, conventionally manufactured (CM) Ti-6Al-4V implants can severely corrode, damage that has been reproduced in vitro from the combination of inflammatory species and cathodic activation1. We investigated the effects of inflammatory species (H2O2) on AM titanium alloys and admixtures compared to CM Ti-6Al-4V. We hypothesized that AM titanium biomaterials will be less susceptible to corrosion in inflammatory species than CM titanium alloys.
Methods: Samples, provided by Z3DLAB, were printed on an SLM 125HL machine using these alloy and admixture powders: Ti-6Al-4V, Ti-6Al-4V with 1% added yttria stabilized zirconia powder (nYSZ), and Ti-29Nb-21Zr. Samples were stress relieved at 600 oC for three hours followed by air cooling. Scanning electron microscopy (SEM) was used to image polished samples and powders. Experiments (n=3) were conducted in both phosphate buffered saline (PBS) and 0.1M H2O2/PBS solutions. Following one hour at open circuit potential (OCP), electrochemical impedance spectra (EIS) were captured from 104 to 10-2 Hz. Next, samples were anodically polarized from -0.2 V below OCP to +1 V vs Ag/AgCl. Randles circuit elements from EIS were fit using phase angle symmetry2. CM Ti-6Al-4V (ELI) was used as a control. Repeated measures ANOVA was used to assess the effect of solution on passivation resistance (Rp) and a one-way ANOVA was used to determine Rp differences between groups in 0.1M H2O2.
Results: SEM micrographs of AM Ti-6Al-4V and Ti-6Al-4V 1% nYSZ powder (Fig. 1 A-B) show pre-alloyed powder beads. Ti-29Nb-21Zr admixture powder (Fig. 1 C) beads are comparatively smaller. Both AM Ti-6Al-4V and Ti-6Al-4V 1% nYSZ have martensitic microstructures with elongated needle-like alpha grains (Fig. 1 D-E). Ti-29Nb-21Zr microstructure (Fig. 1F) shows distinct boundaries where various Ti, Nb, and Zr powder beads melted and resolidified. In 0.1M H2O2, both AM Ti-6Al-4V and Ti-29Nb-21Zr OCPincreased by 0.2 V (Fig. 2 A-B). The passive current density for AM Ti-6Al-4V also increased by a factor of 10 (Fig. 2 A). Rp (Fig. 3) significantly decreased in 0.1M H2O2/PBS solution (p = 0.000). Ti-29Nb-21Zr Rp (1.24E+06 Ωcm2) was higher by a factor of 10 compared to other titanium alloys in 0.1M H2O2, a significant increase(p = 0.004).
Conclusion: Introducing H2O2 significantly decreased Rp for all alloys. Ti-29Nb-21Zr’s Rp in 0.1M H2O2 was significantly higher when compared to the other alloys, supporting our hypothesis. In vivo, inflammatory species and cathodic activation may contribute to severe corrosion of orthopedic devices. Improved resistance to inflammatory species may make Ti-29Nb-21Zr more suitable for in vivo use.
References: 1. Kurtz et al, ORS 2022, 2. Gilbert et al, J Electrochem. Soc, 2020.
Acknowledgements: Z3DLAB sas, Amine Hattal Ph.D, Jeff Holliday, William Nelson, Partially supported by the Wyss Endowment.
Figures
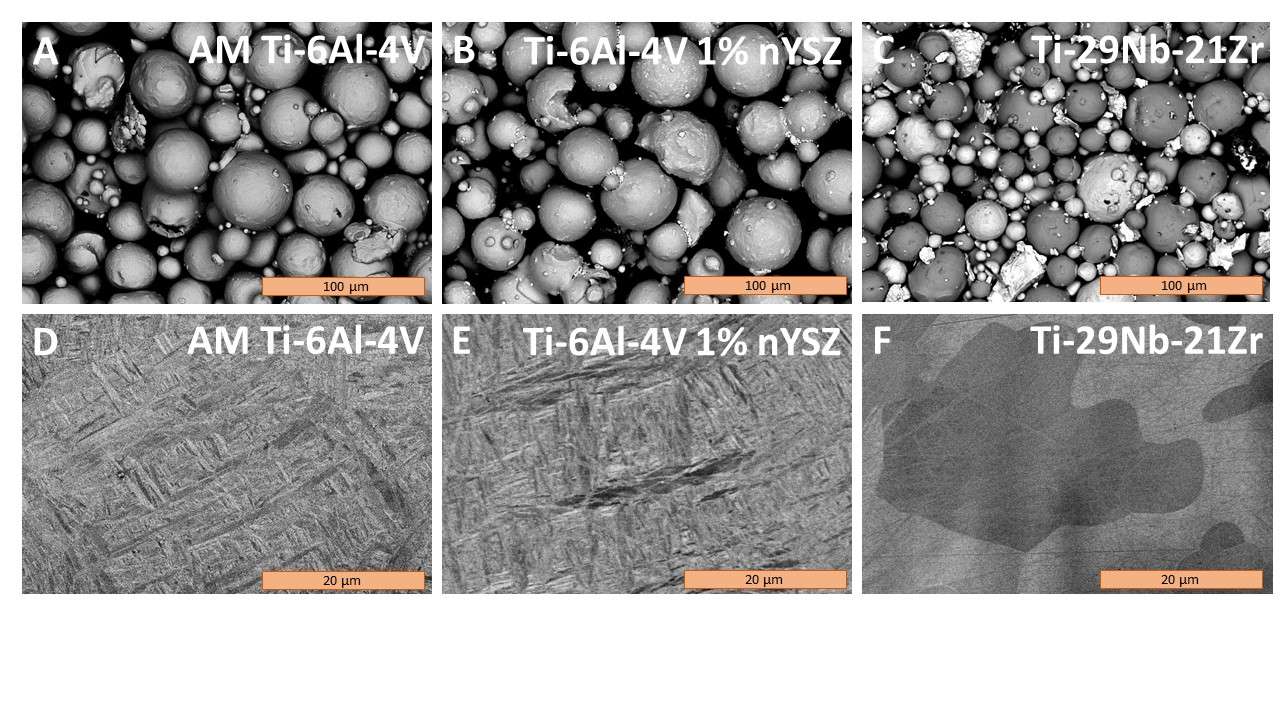
Figure 1
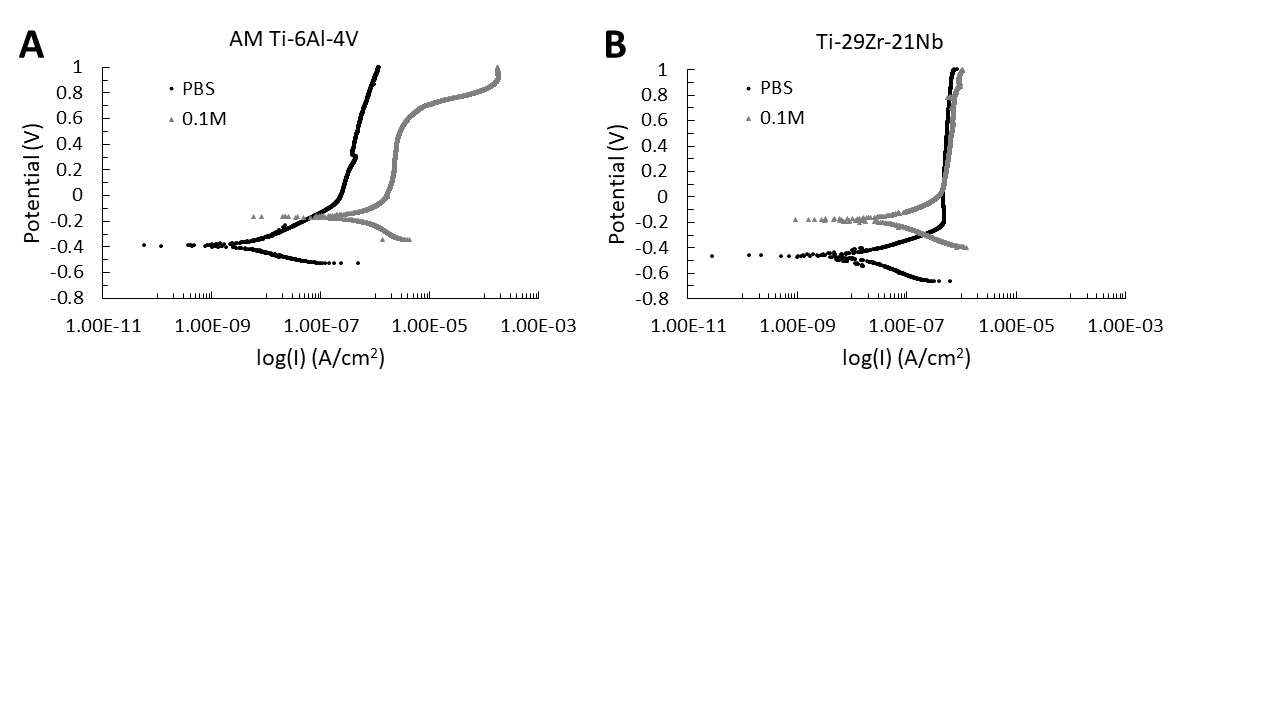
Figure 2
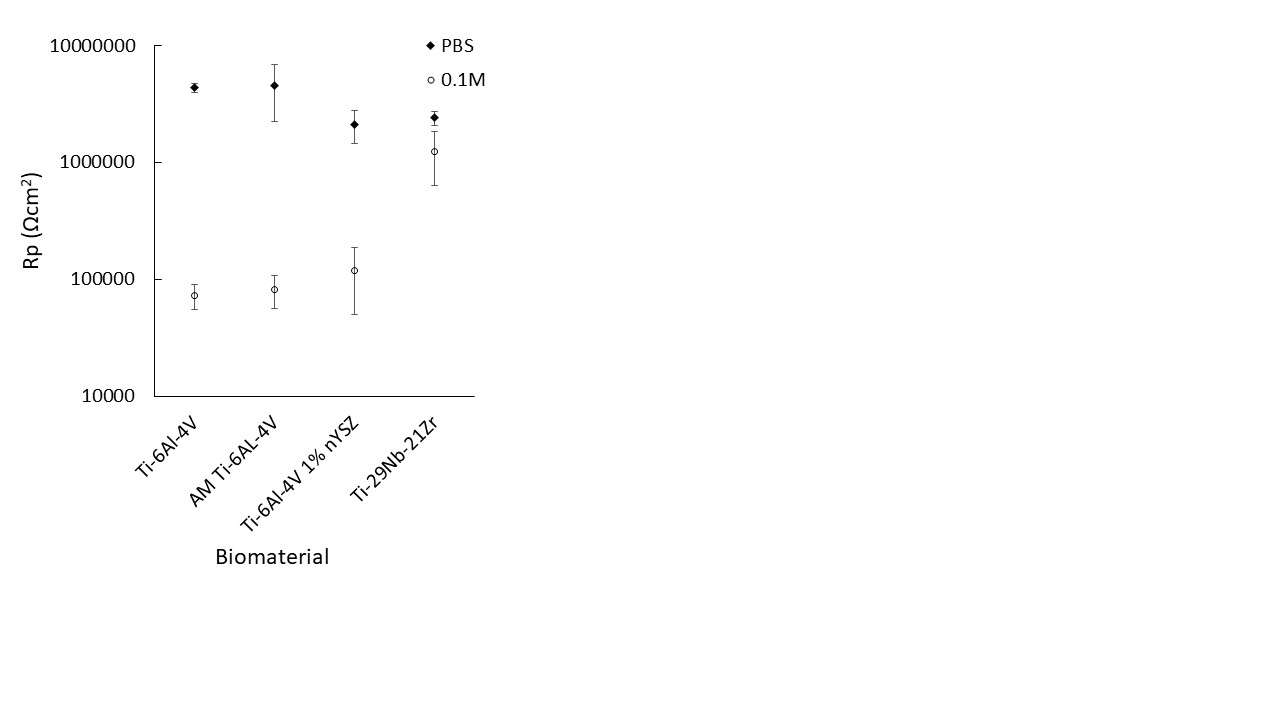
Figure 3#7419
Total Knee Arthroplasty With Patella Retention in Rheumatoid Arthritis
Hee-June Kim - Kyungpook National University Hospital - Daegu, South Korea
*Hee-Soo Kyung - Kyungpook National University Hospital - Daegu, South Korea
Ji-Yeon Shin - Department of Preventive Medicine, School of Medicine, Kyungpook National University - Daegu, Korea (Republic of)
Jae Hwi Han - Daegu Fatima Hospital - Daegu, South Korea
Kyeong-Hyeon Park - Kyungpook National University - Daegu, South Korea
*Email: hskyung@knu.ac.kr
Introduction
We evaluated functional and radiographic results of the TKA with resurfaced and non-resurfaced patella in patients with rheumatoid arthritis.
Methods
We retrospectively followed up 68 patients (94 knees) with rheumatoid arthritis who had total knee arthroplasties(TKA) from 1994 to 2020. The mean age was 61.5 years(range, 32-82). 25 knees underwent TKA with patella resurfacing and 69 knees underwent TKA without patella resurfacing. Mean follow-up period was 70 months (range, 24 – 180). Clinical results were compared, including Hospital for special Surgery (HSS) score, Knee Society Knee Score (KS) , Function Score (FS) and modified patellar score. anterior knee pain and complications were also evaluated. Radiographs were used for final evaluation. Patello-femoral tracking was classified into type I(normal), type II(shift), type III(tilt) and type IV(tilt & shift) by patellar skyline view.
Results
In patients with patellar resurfacing, ROM improved from 109 to 119 degrees. HSS improved from 57.7 to 82.4, KS improved from 54.3 to 90.4, FS improved from 49.2 to 69.8. and modified patella score improved from 14.8 to 22.4. In patients without patellar resurfacing, ROM improved from 99 to 116 degrees. HSS improved from 55.67 to 83.6, KS improved from 50.5 to 90.2, FS improved from 46.1 to 68.7 and modified patella score improved from 15.7 to 22.0. In both group, the all clinical scores improved significantly, and between two groups, there are no significant difference in all clinical scores. In both group, the anterior knee pain was all improved significantly, and there were no patella complications postoperatively. Postoperative patellar tracking was not different between two groups.
Conclusion
By retaining the native patella we were still able to obtain satisfactory results in terms of pain relief and function. We consider that TKA without patellar resurfacing is suitable for rheumatoid arthritis group with small patella and bony deficiency.
#7507
Assessing Correlations Between Patient-Reported Outcomes and Knee Kinematics Following TKA Procedure
*Michael LaCour - University of Tennessee - Knoxville, USA
Milad Khasian - University of Tennessee - Knoxville, USA
Douglas Dennis - Colorado Joint Replacement - Denver, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: mlacour@utk.edu
Introduction
Quantitative, non-subjective means to evaluate the “success” of Total Knee Arthroplasty (TKA) can be quite difficult to determine. Clinically, outcome scores such as Knee Society Scores (KSS) or Knee Injury and Osteoarthritis Outcome Score (KOOS) are often considered a gold standard, and many groups further consider intraoperative or postoperative passive flexion to be a good indicator of postoperative success. From a more mechanical perspective, in vivo weight-bearing kinematics such as weight-bearing flexion or condylar rollback are also believed to be indicators of postoperative success, as previous fluoroscopy studies have demonstrated that there are many parameters that affect weight-bearing range-of-motion. The objective of this study to investigate the correlations between patient-reported outcomes, passive flexion, and weight-bearing knee kinematics.
Methods
The femorotibial kinematics, passive and weight-bearing range-of-motion, and KOOS and KSS for 291 TKA subjects were collected in a retrospective study. The average age, BMI, and post-op time was 69.2±7.2 years, 29.3±4.6, and 22.4±16.3 months, respectively. Pearson correlation analysis was used to find the statistical correlations between the various parameters, and two-tailed t-tests were carried out to find statistical differences.
Results
Increased weight-bearing flexion was statistically correlated with both higher KOOS (r=0.20, p=0.0145) and KSS (r=0.27, p<.0001). Conversely, there was no correlation between passive flexion and KOOS (r=0.10, p=0.24), and correlations between KSS and passive flexion were not analyzed.
Furthermore, subjects with paradoxical anterior sliding of either condyle had significantly lower KSS scores than those without anterior sliding (81.1±11.9 versus 84.4±12.4 for lateral, p=0.03, and 82.2±12.1 versus 85.1±12.5 for medial, p=0.03). Similarly, subjects with anterior sliding of the medial condyle had significantly lower KOOS scores than those without (82.6±13.6 versus 86.8±11.6 for medial, p=0.03). The lateral condyle showed similar trends for KOOS but lacked statistical correlation (83.4±10.3 versus 85.2±13.0 for lateral, p=0.24).
Finally, subjects who experienced reverse axial rotation had significantly lower KOOS scores than those without (79.7±11.8 versus 85.8±12.6, p=0.02). Similar trends between KSS and reverse axial rotation were present but were not statistically significant (82.0±11.9 versus 84.1±12.4, p=0.13). Summary data can be found in Figure 1.
Conclusion
Unfortunately, subject-reported outcome measures will always be subjective, and weight-bearing kinematics are difficult to determine in vivo. Nonetheless, the results of this study revealed that weight-bearing kinematics, and not passive flexion, appear to be better predictors of TKA outcomes. Subjects having greater weight-bearing flexion demonstrated higher KOOS and KSS scores. Also, subjects that experienced a paradoxical femorotibial kinematics had a statistically lower clinical scores than those subjects that experienced “normal-like” kinematics. Therefore, it may be important for the orthopaedic community to begin evaluating weight-bearing kinematics instead of non-weight-bearing kinematics as a measure of postoperative success.
Figures
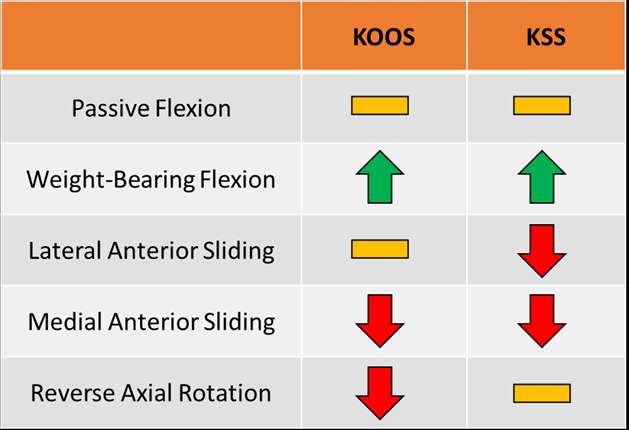
Figure 1#7866
Optimizing Femoral Head Positioning and Stem Alignment Within the Canal for Total Hip Arthroplasty: Can Both Be Accomplished Simultaneously?
*Michael LaCour - University of Tennessee - Knoxville, USA
Manh Ta - Stryker Corporation - Fort Lauderdale, USA
Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Thang Nguyen - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: mlacour@utk.edu
ABSTRACT
The orthopaedic industry is constantly pursuing advancements in supportive technology to improve postoperative implant outcomes and patient satisfaction. Accordingly, it has been shown that theoretical tools such as mathematical modeling can be a fast and inexpensive design evaluation tool focused on improving interoperative precision and accuracy. The objective of this study is to build from a previously published and validated mathematical model to further enhance a theoretical evaluation tool used for implanting Total Hip Arthroplasty (THA) components into subject-specific bones to evaluate their fit, performance, and ability to restore anatomical conditions.
The proposed algorithm automatically computes the morphology of femoral bones and suggests a specific implant size and placement to match the subject-specific bone. The program allows for detailed evaluations including component head positioning and canal fit. This study specifically focuses on stem fit evaluation for three total hip replacement stems.
The automatic femoral stem selection algorithm accurately selected the same stem as the surgeon for all assessed subjects, and according to the algorithm, the novel Emphasys™ Stem was able to more closely recreate the anatomical femoral head center compared to existing Corail® and Tri-Lock® BPS stems. The theoretical design evaluation tool proved to be highly consistent and reliable and can therefore be a powerful tool for future implant design and evaluation as well as clinical preoperative applications, thereby improving surgical outcomes and accelerating the implant development process.
INTRODUCTION
Total hip arthroplasty (THA) has consistently been considered one of the most successful orthopaedic procedures in the modern era. With recent advancements in technology, the frequency of these procedures will undoubtedly increase in the upcoming decade [1]. Although THA is very successful, the industry continues to strive for improvements related to longevity and function. Implants do not reproduce kinematics and mechanics associated with native joints and a subset of patients remain unsatisfied with their implant function [2] [3] [4] [5] [6] [7]. Fortunately, as technology continues to improve and additional tools are provided to surgeons and design engineers, the importance of intraoperative positioning of THA components is constantly being investigated. Tools such as robotic-assisted surgery [8] [9], patient-specific jigs and implants [10], surgical planning software [11], and theoretical modeling [12] [13] [14] [15] [16] have all provided valuable insight into the importance of accurate component positioning.
It has been suggested that preoperative surgical planning has become one of the most important steps towards successful THA [17], as effective preoperative planning enables surgeons to select and orient femoral and acetabular components for individual patients [18] [19]. Combined with research that focuses on additional aspects of component alignment such as cup orientation [20] [21] [22], component offset [23] [24], femoral head size [25], and component fixation [26] [27], it is undeniable that successful postoperative mechanics is a complicated and multi-faceted challenge. Previous research has suggested generalized guidelines and “safe zones” for various component positions [21], but more recent investigations have indicated that component positioning should be patient-specific to ensure ideal outcomes [20] [28] [29].
An important but often under-reported consideration is translational mismatch between the native femoral head center and the implanted head center. While it has been previously documented that improper component placement, mismatched offsets, and leg length discrepancy can cause poor muscle function, increased wear, and implant loosening [23] [24] [30], more recent studies have begun to demonstrate that joint center mismatches can also generate hip instability in the form of sliding, separation, pistoning, and edge-loading [4] [6] [12] [31]. Consequently, as tools that help surgeons more precisely place components become more readily available, it becomes even more imperative that the orthopaedic community focuses on developing implants and surgical techniques that can recreate native anatomy as closely as possible, ultimately pushing for improved postoperative outcomes, patient satisfaction, and a more detailed understanding of the effects of component malpositioning.
The objective of this study is to use the stem fit module of a previously validated mathematical model of the hip joint [12] [13] to predict and compare the femoral stem component fits between three implant designs, evaluating the 3-dimensional proximity (Anterior/Posterior, Superior/Inferior, and Medial/Lateral) that each stem system can place the implanted femoral head center with respect to the anatomical femoral head center.
METHODS
A validated and previously published three-dimensional (3D) mathematical model of the hip joint was developed to assess component fit and outcome mechanics based on subject-specific kinematics and anatomy [12] [13]. This model can be used to virtually place a hip implant component into a subject-specific bone model, observe the quality of the component fits, run comparisons between different surgical conditions (including implant sizing choices, placement, designs, surgical approaches, and soft tissue modifications), and analyze resultant biomechanics. This software package allows for visualization of fit throughout the canal and the location and amount of bone removal that is required for a specific stem placement (Figure 1).
The stem fit module for this study evaluates the proximal portion of a subject-specific femoral bone model, automatically generating subject-specific femoral bone morphology parameters such as the anatomical femoral head center (defined as the center of a best-fit sphere in 3D), the neck shaft axis and angle, a 3D proximal femoral canal description, the proximal femoral canal axis, and various anatomical landmarks [13]. Similarly, all stem and femoral head components in the database are automatically assigned morphological parameters, including the component head center, neck axis, and shaft axis. A detailed visualization of the mathematical parameters for both the bones and the implant components is shown in Figure 2. Using these parameters, the software automatically suggests component sizes based on the subject-specific bone models and will automatically place these components in the algorithm’s “ideal” orientation, including suggested canal position and component version.
Determination of the ideal stem for each subject is conducted by evaluating each stem in the database iteratively compared to the selected femoral bone model, focusing on the shape of the canal and the location of the femoral head. For each stem, the software determines how far distally the femoral stem fits within the canal before “collision” is detected between the stem and the cortical bone. This collision threshold can be manually adjusted to allow for broaching or reaming directly to the cortex or to account for a cancellous mantle. Next, the femoral component version is adjusted about the shaft axis to minimize the relative distance from the anatomical femoral head center to the component head center, and the optimal femoral stem fit is established when the distance between head centers is the smallest. Since the model is based on mathematics, the component placements are highly precise and repeatable [13]. In all cases, component fit can also be modified manually based on surgical expertise, if desired. This way, specific clinical concerns can be alleviated by using a different size stem or by adjusting component offsets or positions accordingly.
Two separate evaluations were done for this study: 1) a retrospective evaluation of seven subjects receiving a Corail THA from a previous fluoroscopy study [4] was conducted, comparing the algorithm-predicted stem size and position versus the actual size that the surgeon chose during surgery. Stem positioning with respect to the bone and the canal was determined in vivo using single plane fluoroscopic image registration and 3D model-fitting [32]; and 2) an investigation using 63 proximal statistical shape model (SSM) femoral bone models to compare fits between different commercially available stem systems. The SSM bone models were derived from a database of 320 subject-specific CT scans, designed to robustly account for morphological variations found in the global population based on gender, age, and country-of-origin [33]. Six sample bones demonstrate the variability from subject to subject in Figure 3.
In both cases, each bone model under investigation was evaluated using the automated algorithm’s chosen stem. The stem component database consists of all standard and high-offset implant CAD models as well as all head length options. This study compared three hip systems, the newly designed Emphasys™ Stem, the Corail® stem, and the Tri-Lock® BPS stem (DePuy Synthes, Warsaw, IN). For this study, the primary parameters of interest are the distances between the anatomical and component head centers in the anterior/posterior (A/P), medial/lateral (M/L), and superior/inferior (S/I) directions (with respect to the femur) for each subject. Mismatches between the two joint centers were established based on how far a stem head center differentiated from the anatomical head center. The mismatch between the anatomic femoral head (shown as the green dot) and the component femoral head (shown as the red dot) is easily seen during an analysis (Figure 4), where superior, lateral, and anterior mismatches are designated as positive values. The investigation included examining overall placement distances for each implant independently as well as reviewing the direct same-subject comparisons between femoral stems, generating comparison differences.
Statistical analyses were conducted using the JMP statistical analysis suite (SAS Institute, Cary, NC). All analyses were carried out at a 95% confidence level. In all cases, the data was first checked for normality. If the data was normally distributed, means and groups were analyzed using t-testing. If the data was not normally distributed, means were analyzed using Wilcoxon Signed Rank testing and group means were compared using the Wilcoxon/Mann-Whitney test with two-sided exact p-values.
RESULTS
Retrospective Evaluation
Using data from a previously published fluoroscopy study, the automatic femoral stem selection algorithm accurately suggested the same stem as the surgeon for all seven subjects during the in vivo comparison (100% - Table 1). The algorithm revealed high consistency with the surgeon, even in difficult coxa vara and abnormal femoral neck geometry cases. For example, Subject 1 was implanted with the high offset coxa-vara (HO - KLA) stem, and Subject 6 had abnormal femoral neck geometry resulting in small femoral offset. A sample comparison of the femoral stem suggested by the proposed algorithms and the surgeon’s selection for Subject 3 can be seen in Figure 5.
After automatic stem fit and positioning, three analysis tools can be used to further examine the fit. Specifically, the cross-sectional analysis tool (Figure 6-A) allows the user to visualize the fit anywhere along the femoral canal, allowing for visualizations of fit within the canal or of concerning aspects at the stem-canal interface that may lead to loosing or possible future locations of radiolucent lines. The user can also utilize the bone removal analysis (Figure 6-B) and contact map analysis (Figure 6-C) features to identify potential stem penetration into or gaps between the femoral canal, which again could be an area for potential radiolucent lines to appear after surgery.
Stem Fit Assessment
For the SSM stem fit assessment, the Emphasys™ Stem consistently yielded the closest placements of the implanted femoral head system, followed by the Corail® and then the Tri-Lock® BPS stems, respectively. Among all models, the Emphasys™ Stem head center mismatched the femoral head center by an average resultant value of 1.2mm (σ = 0.6mm, 0.2mm – 3.2mm), the Corail® stem head center mismatched the anatomical femoral head center by an average resultant value of 1.6mm (σ = 0.7mm, 0.5mm – 4.7mm), while the Tri-Lock® BPS stem mismatched by an average resultant value of 2.2mm (σ = 0.8mm, 0.7mm – 5.9mm). While the differences between all groups (p < 0.002) is clinically small, they do represent the “best case” scenario that can be achieved intraoperatively, and additional surgical variability may exacerbate these differences.
Additionally, the Emphasys™ Stem was able to place the implanted head within 1mm of the anatomic femoral head for 29/63 (46%) of the models, while Corail® did so for 9/63 (14%) of the models and Tri-Lock® BPS did so for only 1/63 (1.6%). Similarly, the Emphasys™ Stem was able to place the implanted head within 2mm of the anatomic femoral head for 59/63 (94%) of the models, while Corail® did so for 47/63 (75%) of the models and Tri-Lock® BPS did so for 29/63 (46%). Among all models, the Emphasys™ design maintained the anatomic femoral head center closest for 57/63 bones (90.5%) while the Corail® stem was closer for the remaining six (9.5%). Interestingly, Tri-Lock® BPS stem was never able to outperform both Emphasys™ and Corail® for a single bone.
Further investigation into the directional placements of the stem systems reveals that the Tri-Lock® BPS stem tends to place the femoral head more superiorly than both other systems (1.6mm vs 0.2mm/0.6mm, p < 0.0001) as well as more laterally (0.3mm lateral vs 0.5mm medial, p < 0.0001) than the Corail® system. Detailed data for all 63 femurs can be found in Table 2, and a sample comparison for a single subject can be found in Figure 7. Interestingly, very few trends exist when comparing the ability to recreate the head center of these stem systems at different sizes.
A unique advantage of this model is the ability to assess outcomes using the post-operative analysis. Once the components are chosen and positioned in the bones, the algorithm can predict virtual mechanics during weight-bearing activities to assess kinematics, stability, and contact mechanics. Resultant hip joint forces for Patient 1 can be found in the bottom right graph within Figure 1.
DISCUSSION
Common in vivo complications after total hip arthroplasty include edge loading, joint instability, leg length discrepancy, hip pain, dislocation, infection, and more. Determining solutions to these issues is complicated and multi-faceted, and theories generally include developing progressive new implant designs, establishing the least destructive surgical methods, and determining and executing ideal intraoperative component alignments. This study focuses on overcoming these issues from a component alignment and implant design perspective. The theoretical simulations and modern computational tools used in this study can help successfully develop and verify THA components that were designed with the intention of more accurately recreating the original location of the anatomical femoral head.
The intraoperative positioning of hip components is an important area of THA research. While most current research studies focus primarily on the angular orientation of the acetabular cup, fewer analyses investigate the effects of translational shifts of the cup or head joint center. The topic of component shifting remains controversial, and it is beyond the scope of this paper to suggest that certain positions are “better” than others. Regardless of preference, surgical accuracy and precision are certainly of importance, as minor inaccuracies in component positioning can quickly compound. Additionally, it is important to remember that the theoretical model presented in this study is mathematically repeatable and therefore will “perfectly” place the components in ideal position and orientation based on a set of pre-defined surgical target inputs for the scenario being analyzed. Intraoperatively, since there are multiple surgical technique variations, including exposure angles, incision size, joint clarity, and other factors, there is often large variability in intended component positioning versus actual component positioning, both rotationally and translationally [34] [35] [36] [37]. Low repeatability rates for freehand accuracy are evident after total hip arthroplasty, with cup inclination ranges as high as 48° [34], cup anteversion ranges as high as 82° [34], joint offset ranges as high as 47mm [35], and successful placement rates within desired safe zones as low as only 26% [34]. Proper alignment is essential for successful postoperative biomechanics, and errors this large are of significant concern to the orthopaedic community.
Fortunately, given the wide array of component positioning theories and methodologies, there are a plethora of tools and techniques that have been developed to assist surgeons, ensuring maximum intraoperative precision. For example, a substantial amount of research has been conducted regarding the precision of navigation tools or specialized jigs, and the results overwhelmingly show that some form of navigation yields highly precise component placements [9] [36] [37] [38] [39] [40]. The results from this study attempt to define the “accuracy” aspect of component placement as a supplement to “precision.”
Additional research, such as the study presented herein, demonstrates the robustness and versatility of computational modeling and modern component designs. The Corail® stem analyzed in this study is one of the most popular hip stems available to surgeons [41], but non-ideal positioning during surgery remains quite possible. In general, designing implant systems with fixed sizes and shapes that can be used to successfully treat millions of different patients with a wide array of bone morphologies is undeniably a difficult task. Nonetheless, the results presented in this paper demonstrate that it is still possible to make design improvements. In this study, the proposed algorithms can be extended as design evaluation tools, allowing the user to gain valuable and instant feedback for a new design. Unlike long-term follow-up studies, which often take 5-10 years before a new design can be evaluated for success [42] [43] [44], this mathematical model allows the user to quickly assess new component designs for multiple subjects with components being placed using various surgical techniques and locations. Accordingly, the proposed algorithms can provide instant feedback on how well the stem will fit within many types of canals, and it can then be used in conjunction with other theoretical tools to predict post-implantation mechanics and the restoration of the anatomic femoral head center.
This study does have its limitations. First, because the computational model is based on a repeatable mathematical algorithm, component placements are highly precise and repeatable. Thus, the magnitude of the results from this study are clinically small and may appear negligible to some. However, this analysis does not account for additional surgical technique, approach, and philosophy variability that may be unexpected or may exacerbate the presented differences. Next, while the computational model has been tested using multiple different bone models, the accuracy of the predictions can be limited by the CT-scan quality, and scans with larger slices or metal artifacts may limit accuracy. Similarly, if the anatomical landmarks are predicted incorrectly, then the fit and size will be suggested incorrectly. Thirdly, the bone models used are statistical shape models, indicating that they have been mathematically created as an attempt to represent specific populations. Future analyses will analyze actual bone models derived from CT scans. Similarly, the retrospective evaluation only considered a single surgeon with a single implant type. A more rigorous validation across a wider range of surgeons and implant types is planned as future work and will further improve the strength of the model. Finally, the stem fit algorithm does not consider bone quality and instead only considers geometrical and morphological information of the bone. In fact, the size of the stem can vary slightly from the results of this study if the bone quality is a considerable factor.
CONCLUSIONS
The stem fit module of a previously validated mathematical model of the hip joint successfully predicted and compared the femoral stem component fits between three implant systems, Emphasys™, Corail®, and Tri-Lock® BPS, with respect to the anatomical femoral head center. The results suggested that, for mathematically precise placements, the novel Emphasys™ design generated closer potential placements of the implanted femoral head center compared to both the Corail® and Tri-Lock® BPS stems.
ACKNOWLEDGEMENTS
This study was funded through a research grant from DePuy Synthes.
CAPTIONS
Figure 1: Visualization of the software GUI to analyze patient-specific bone models.
Figure 2: Visualization of the mathematical parameters use to define the bones and the stem components.
Figure 3: Visualization of six SSMs of the femur, demonstrating variability in bone morphology and size.
Figure 4: Depiction of mismatch coordinate system. If the component head center (shown in red) is placed superiorly, laterally, and anteriorly with respect to the anatomical head center (shown in green), these are indicated by positive values, respectively.
Figure 5: Comparison of the surgeon’s selection (left images) and the femoral stem predicted by the proposed algorithm (right images) for Subject 3.
Figure 6: (A) Cross-sectional analysis, (B) bone removal analysis, and (C) contact map analysis of Subject 1 where the algorithm and the surgeon picked the same stem (KLA high offset stem size 12).
Figure 7: Data showing fits for all three stem systems under investigation for a single, sample subject.
Table 1: Comparison of the femoral stem size predicted by the proposed algorithm and the surgeon’s selection.
Table 2: Summary data for all 63 subjects. Positive values indicate superior, lateral, and anterior component head placement with respect to the anatomical femoral head.
Bibliography
[1] Singh JA, Yu S, Chen L, and Cleveland JD, "Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample," The Journal of Rheumatology, 2019.
[2] Thoms RJ and Marwin SE, "A Unique Failure Mechanism of a Constrained Total Hip Arthroplasty. A Brief Review of the Literature," The Journal of Arthroplasty, vol. 23, no. 2, pp. 293-298, 2008.
[3] Nevelos J, et. al., "Microseparation of the Centers of Alumina-Alumina Artificial Hip Joints during Simulation Testing Produces Clinically Relevant Wear Rates and Patterns," The Journal of Arthroplasty, vol. 15, no. 6, pp. 793-795, 2000.
[4] DeCook CA, et al., "In Vivo Determination and Comparison of Total Hip Arthroplasty Kinematics for Normal, Preoperative Degenerative, and Postoperative Implanted Hips," The Journal of Arthroplasty, vol. 35, no. 2, pp. 588-596, 2020.
[5] Lombardi AV, et al., "An In Vivo Determination of Total Hip Arthroplasty Pistoning During Activity," The Journal of Arthroplasty, vol. 15, no. 6, pp. 702-709, 2000.
[6] Liu F and Fisher J, "Effect of an edge at cup rim on contact stress during microseparation in ceramic-on-ceramic hip joints," Tribology International, vol. 113, pp. 323-329, 2017.
[7] Hua X et al., "The contact mechanics and occurrence of edge loading in modular metal-on-polyethylene total hip replacement during daily activities," Medical Engineering & Physics, vol. 38, no. 6, pp. 518-525, 2016.
[8] Kayani B, et al., "The current role of robotics in total hip arthroplasty," EFORT Open Rev, vol. 4, no. 11, pp. 618-625, 2019.
[9] Redmond JM, et al, "Accuracy of Component Placement in Robotic-Assisted Total Hip Arthroplasty," Orthopedics, vol. 39, no. 3, pp. 193-199, 2016.
[10] Reimann P, et al, "Patient satisfaction - A comparison between patient-specific implants and conventional total knee arthroplasty," Journal of Orthopaedics, vol. 16, no. 3, pp. 273-277, 2019.
[11] Knafo Y, et al, "Value of 3D Preoperative Planning for Primary Total Hip Arthroplasty Based on Biplanar Weightbearing Radiographs," Biomed Res Int, 2019.
[12] LaCour MT, Ta MD, Komistek RD, "Development of a hip joint mathematical model to assess implanted and non-implanted hips under various conditions," Journal of Biomechanics, vol. 112, 2020.
[13] Ta MD, "Development and Implementation of a Computational Surgical Planning Model for Pre-Operative Planning and Post-Operative Assessment and Analysis of Total Hip Arthroplasty," Doctoral Dissertation, University of Tennessee, 2019.
[14] Delp SL, et al., "OpenSim: Open-Source Software to Creat and Analyze Dynamic," IEEE Transations on Biomedical Engineering, vol. 54, no. 11, pp. 1940 - 1950, 2007.
[15] Damsgaard M, et al, "Analysis of musculoskeletal systems in the AnyBody," Simulation Modelling Practice and Theory, pp. 1100 - 1111, 2006.
[16] Halloran JP, Petrella AJ, Rullkoetter PJ, "Explicit finite element modeling of total knee replacement mechanics," J Biomech, vol. 38, no. 2, pp. 323-331, 2005.
[17] Eggli S, Pisan M, and Müller ME, "The value of preoperative planning for total hip arthroplasty," The Journal of bone and joint surgery. British volume, vol. 80, no. 2, pp. 382-390, 1998.
[18] Miashiro EH, et al., "Preoperative planning of primary total hip arthroplasty using conventional radiographs," Revista Brasileira de Ortopedia (English Edition), vol. 49, no. 2, pp. 140-148, 2014.
[19] Stiehl JB, et al, Navigation and MIS in orthopedic surgery, 2007.
[20] Abdel MP, et al., "What safe zone? The vast majority of dislocated THAs are within the Lewinnek safe zone for acetabular component position," Clinical Orthopaedics and Related Research, vol. 474, no. 2, pp. 386-391, 2016.
[21] Lewinnek GE, et al., "Dislocations after total hip-replacement arthroplasties," The Journal of bone and joint surgery. American volume, vol. 60, no. 2, pp. 217-220, 1978.
[22] Dorr LD and Callaghan JJ, "Death of the Lewinnek “Safe Zone”," The Journal of arthroplasty, vol. 34, no. 1, pp. 1-2, 2019.
[23] Terrier A, Florencio FL, and Rüdiger HA, "Benefit of cup medialization in total hip arthroplasty is associated with femoral anatomy," Clin Orthop Relat Res, vol. 472, no. 10, pp. 3159 - 3165, 2014.
[24] Bonnin MP, et al, "Do we medialise the hip centre of rotation in total hip arthroplasty? Influence of acetabular offset and surgical technique," Hip Int., vol. 22, no. 4, pp. 371-378, 2012.
[25] Tsikandylakis G, et al, "Head size in primary total hip arthroplasty," EFORT Open Reviews, vol. 3, no. 5, 2018.
[26] Karuppal R, "Biological fixation of total hip arthroplasty: Facts and factors," J Orthop, vol. 13, no. 3, pp. 190 - 192, 2016.
[27] Sumner DR, "Long-term implant fixation and stress-shielding in total hip replacement," Journal of Biomechanics, vol. 48, no. 5, pp. 797-800, 2015.
[28] McLawhorn A, et al, "Targeting a New Safe Zone: A Step in the Development of Patient-Specific Component Positioning for Total hip Arthorplasty," Am J Orthop, vol. 44, no. 6, pp. 270-276, 2016.
[29] Pierrepoint J, et al, "Variation in functional pelvic tilt in patients undergoing total hip arthroplasty," Bone Joint J, Vols. 99-B, no. 2, pp. 184-191, 2017.
[30] Scheerlinck T, "Cup positioning in total hip arthroplasty," Acta Orthop Belg, vol. 80, no. 3, pp. 336-347, 2014.
[31] Pierrepont J, et al., "Integration of Functional Pelvic Orientation into Patient-Specific Computational Modeling for Acetabular Cup Positioning," in Poster presented at ORS, 2013.
[32] Mahfouz MR, Hoff WA, Komistek RD, Dennis DD, "A Robust Method for Registration of Three-Dimensional Knee Implant Models to Two-Dimensional Fluoroscopy Images," IEEE Transactions on Medical Imaging, vol. 22, no. 12, pp. 1561-74, 2004.
[33] Roose J, "Correlation of Femoral Head Center Variation With Intraosseous Femoral Anatomy," in ICJR 3rd Annual Pan Pacific Orthopaedic Congress, Kona, Hawaii, 2016.
[34] Saxler G, et al., "The accuracy of free-hand cup positioning - a CT based measurement of cup placement in 105 total hip arthroplasties," International Orthopaedics, vol. 28, pp. 198-201, 2004.
[35] Bjarnason JA and Reikeras O, "Changes of center of rotation and femoral offset in total hip arthroplasty," Ann Transl Med, vol. 3, no. 22, pp. 1-7, 2015.
[36] Nishihara S, et al., "Comparison between hand rasping and robotic milling for stem implantation in cementless total hip arthroplasty," The Journal of Arthroplasty, vol. 21, no. 7, pp. 957-966, 2006.
[37] Nakamura N, et al., "A Comparison between Robotic-assisted and Manual Implantation of Cementless Total Hip Arthroplasty," Clin Orthop Relat Res, vol. 468, pp. 1072-1081, 2010.
[38] Ryan JA, Jamali AA, and Bargar WL, "Accuracy of Computer Navigation for Acetabular Component Placement in THA," Clin Orthop Relat Res, vol. 468, pp. 169-177, 2010.
[39] Gupta A, et al., "Does Robotic-Assisted Computer Navigation Affect Acetabular Cup Positioning in Total Hip Arthroplasty in the Obese Patient? A Comparison Study," The Journal of Arthroplasty, vol. 30, pp. 2204-2207, 2015.
[40] Chang JD, et al., "The Evolution of Computer-Assisted Total Hip Arthroplasty and Relevant Applications," Hip Pelvis, vol. 29, no. 1, pp. 1-14, 2017.
[41] Vidalain JP, "Twenty-year results of the cementless Corail stem," Int Orthop, vol. 35, no. 2, pp. 189-194, 2011.
[42] Buechel Sr FF, "Long-term followup after mobile-bearing total knee replacement," Clinical Orthopaedics and Related Research, vol. 404, pp. 40-50, 2002.
[43] Callaghan JJ, et al, "Charnley total hip arthroplasty with cement: minimum twenty-five-year follow-up," Jbjs, vol. 82, p. 487, 2000.
[44] LaCour MT et al, "Confirmation of Long-term In Vivo Bearing Mobility in Eight Rotating-platform TKAs," Clinical Orthopaedics and Related Research, vol. 472, pp. 2766-2773, 2014.
Figures
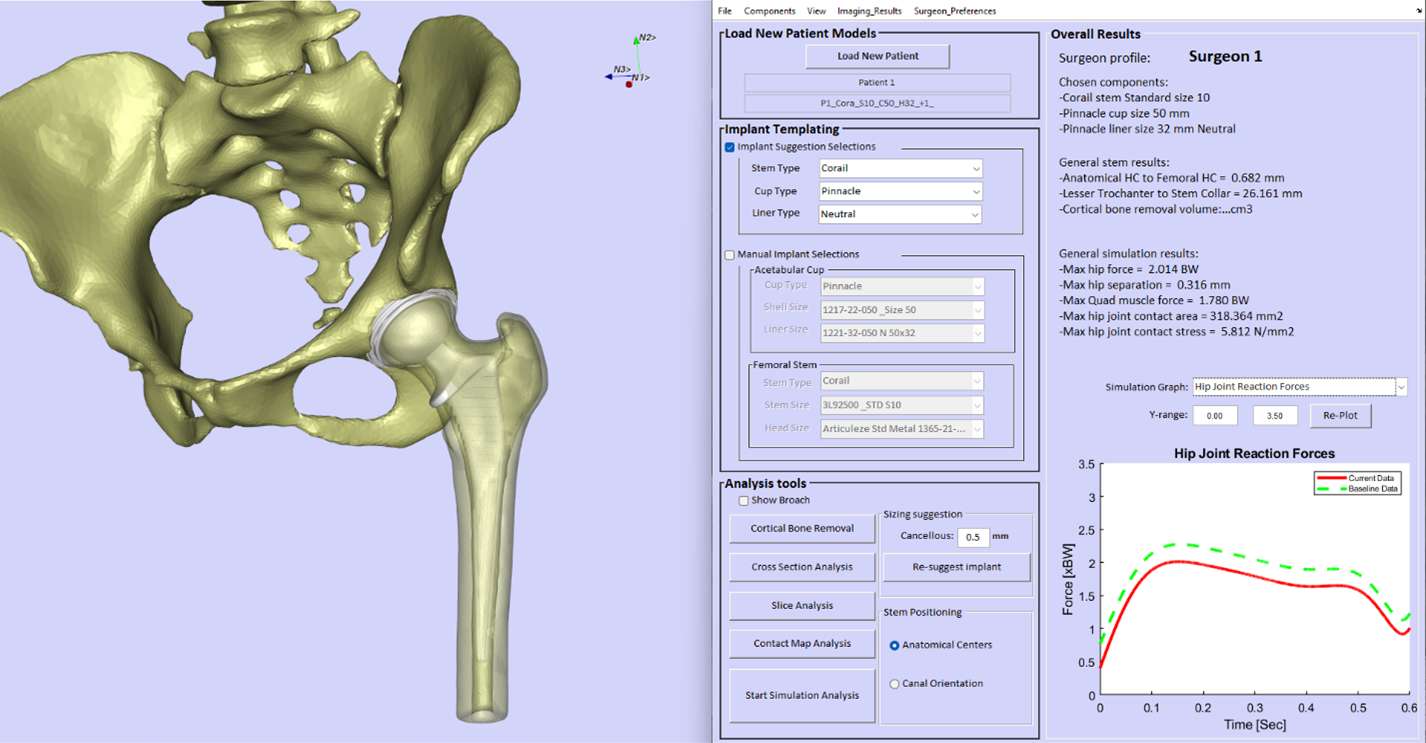
Figure 1
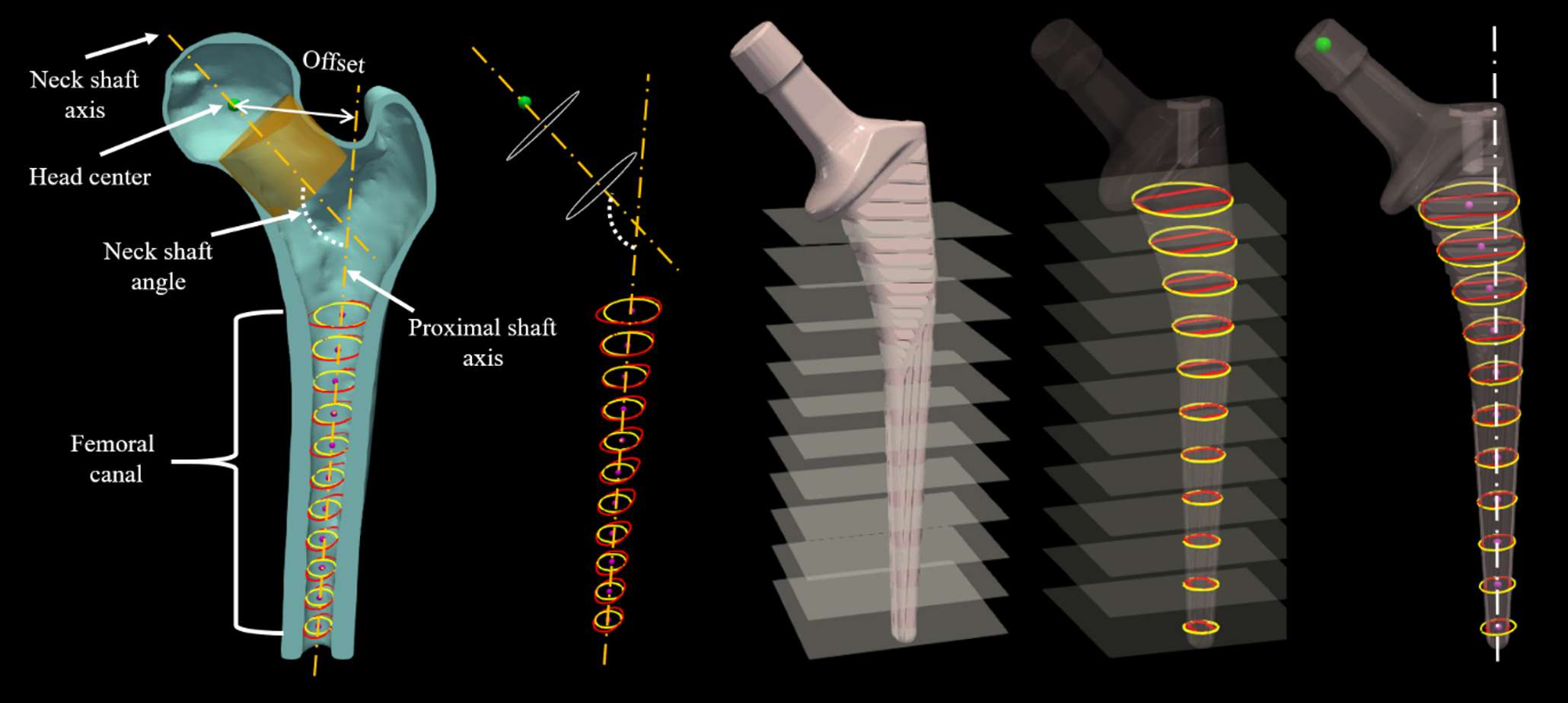
Figure 2
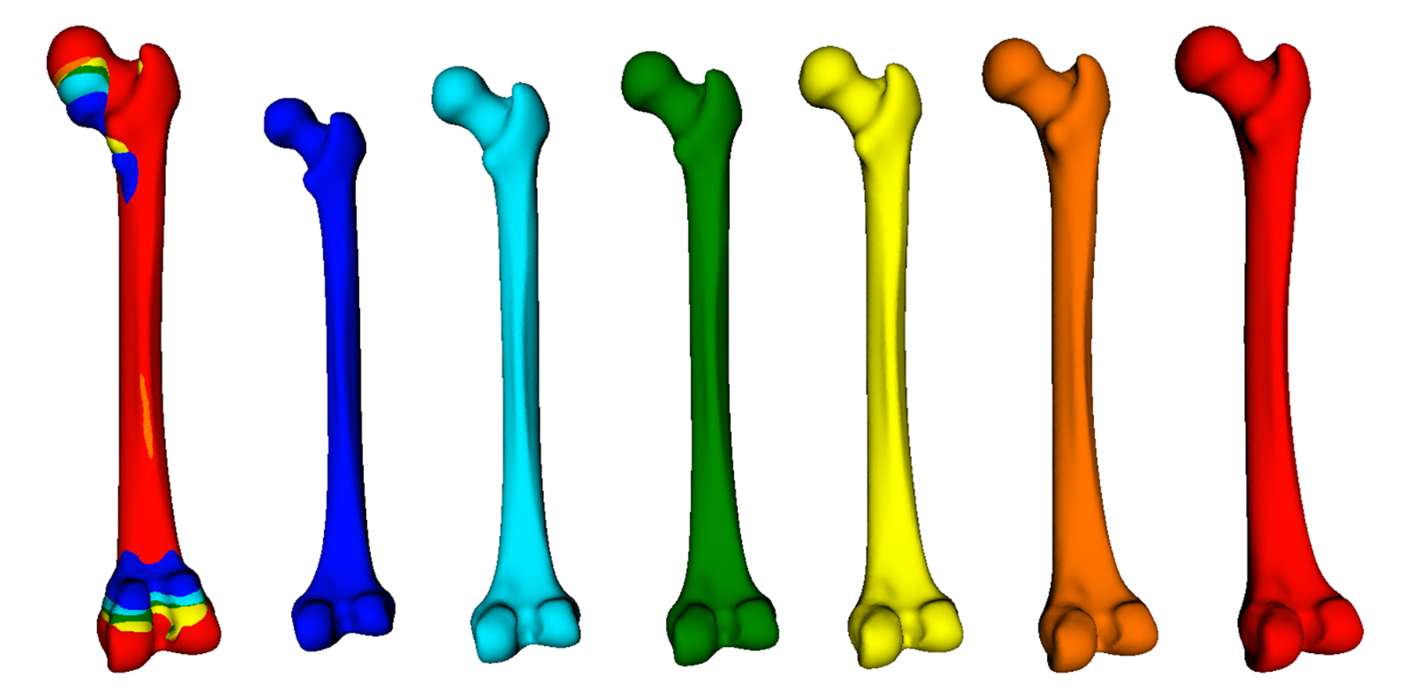
Figure 3
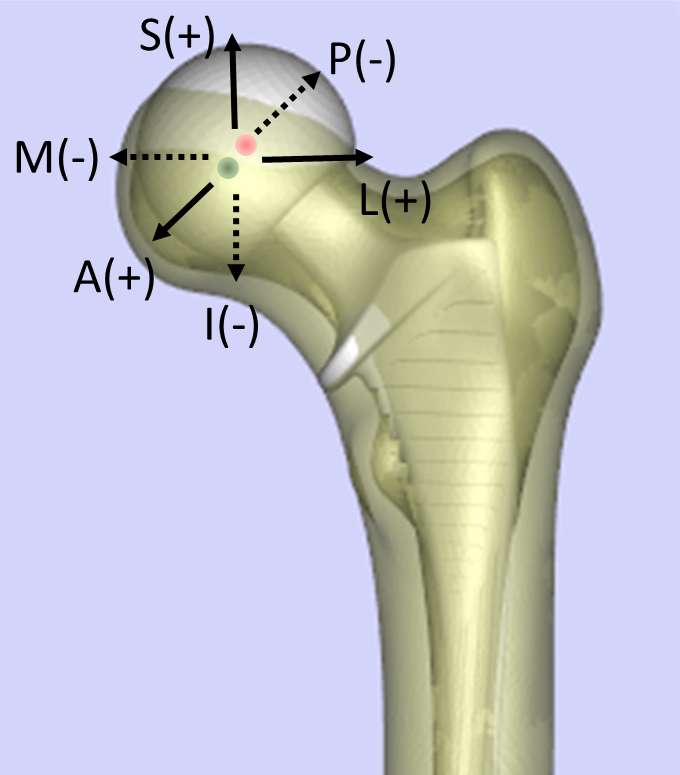
Figure 4
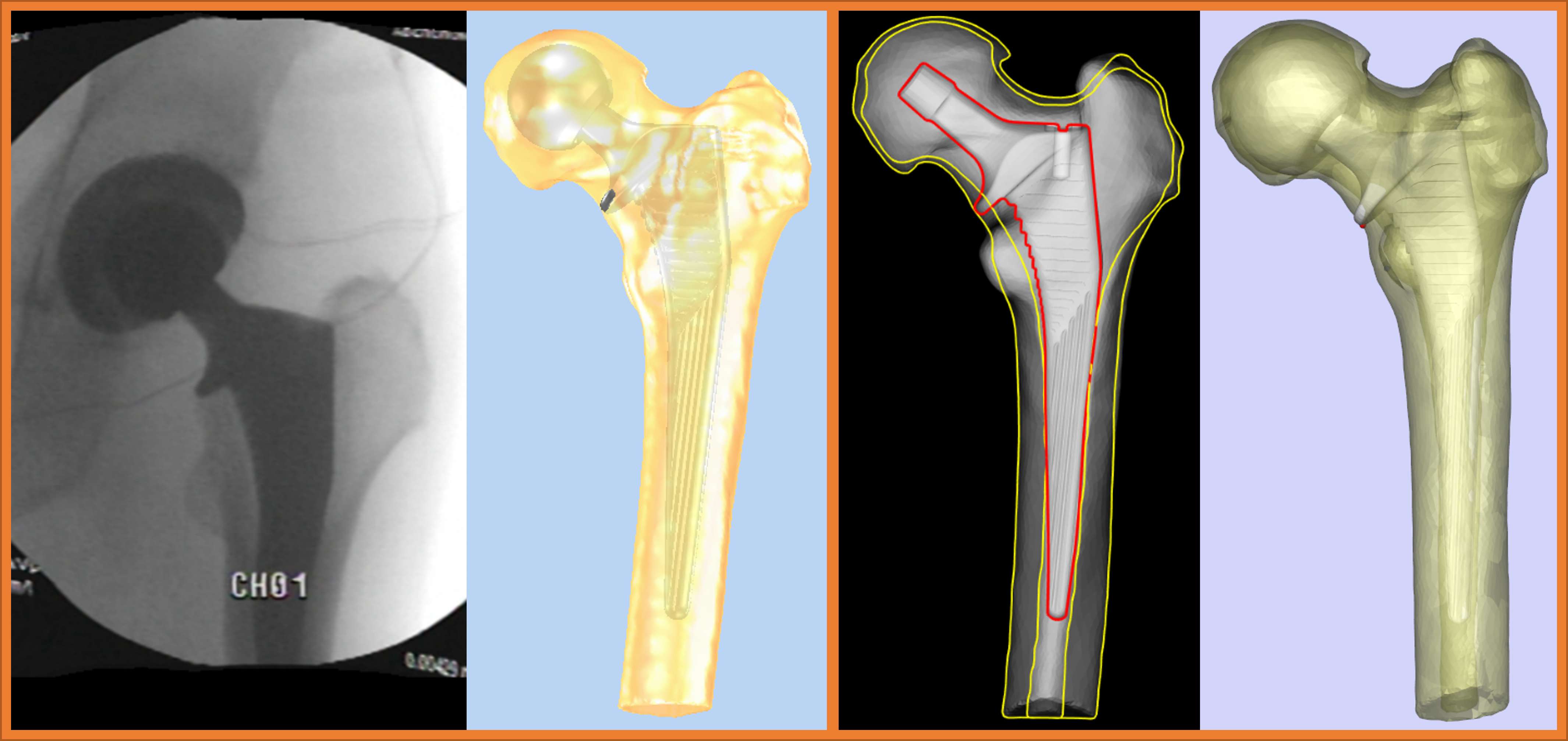
Figure 5
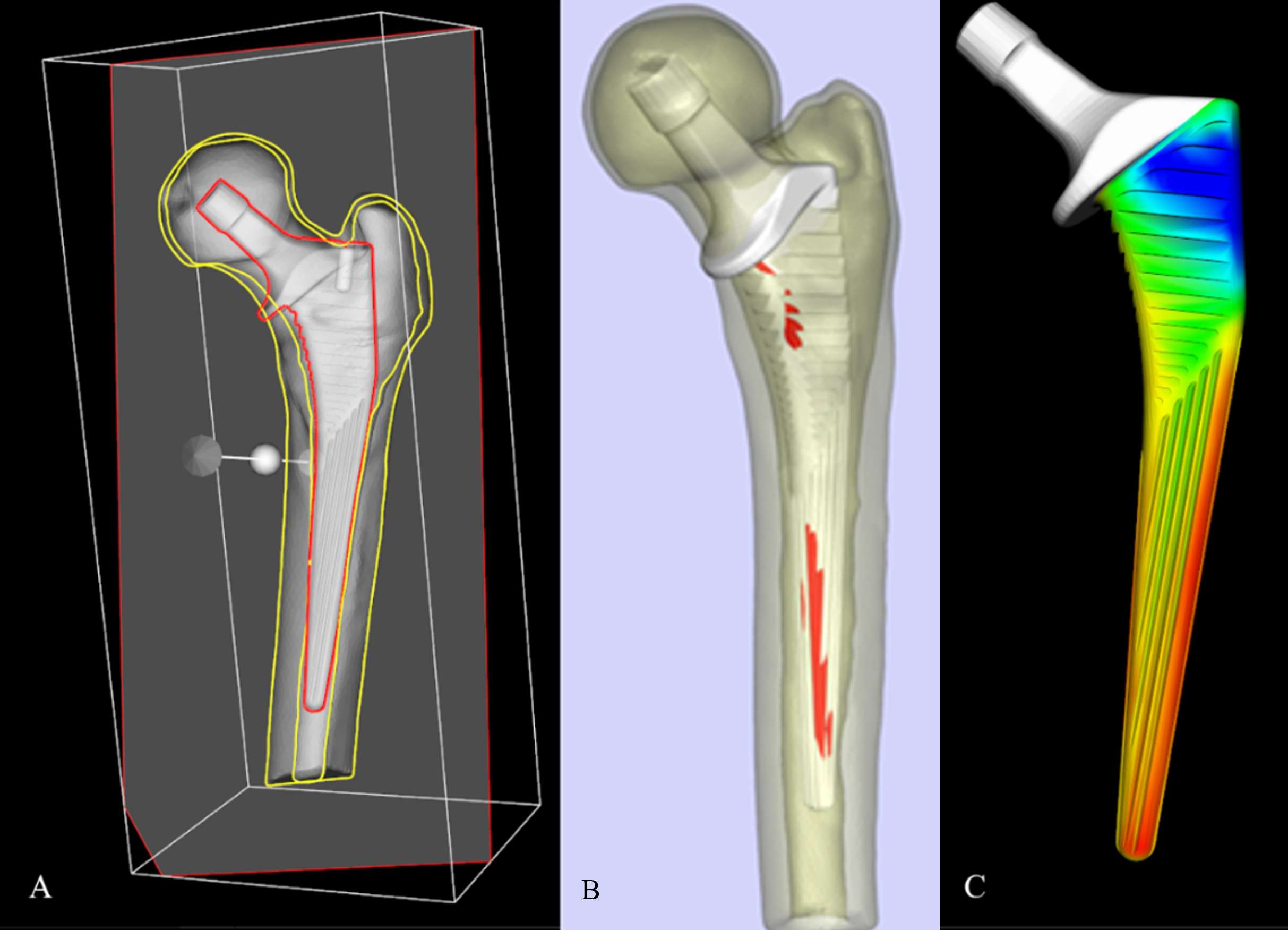
Figure 6
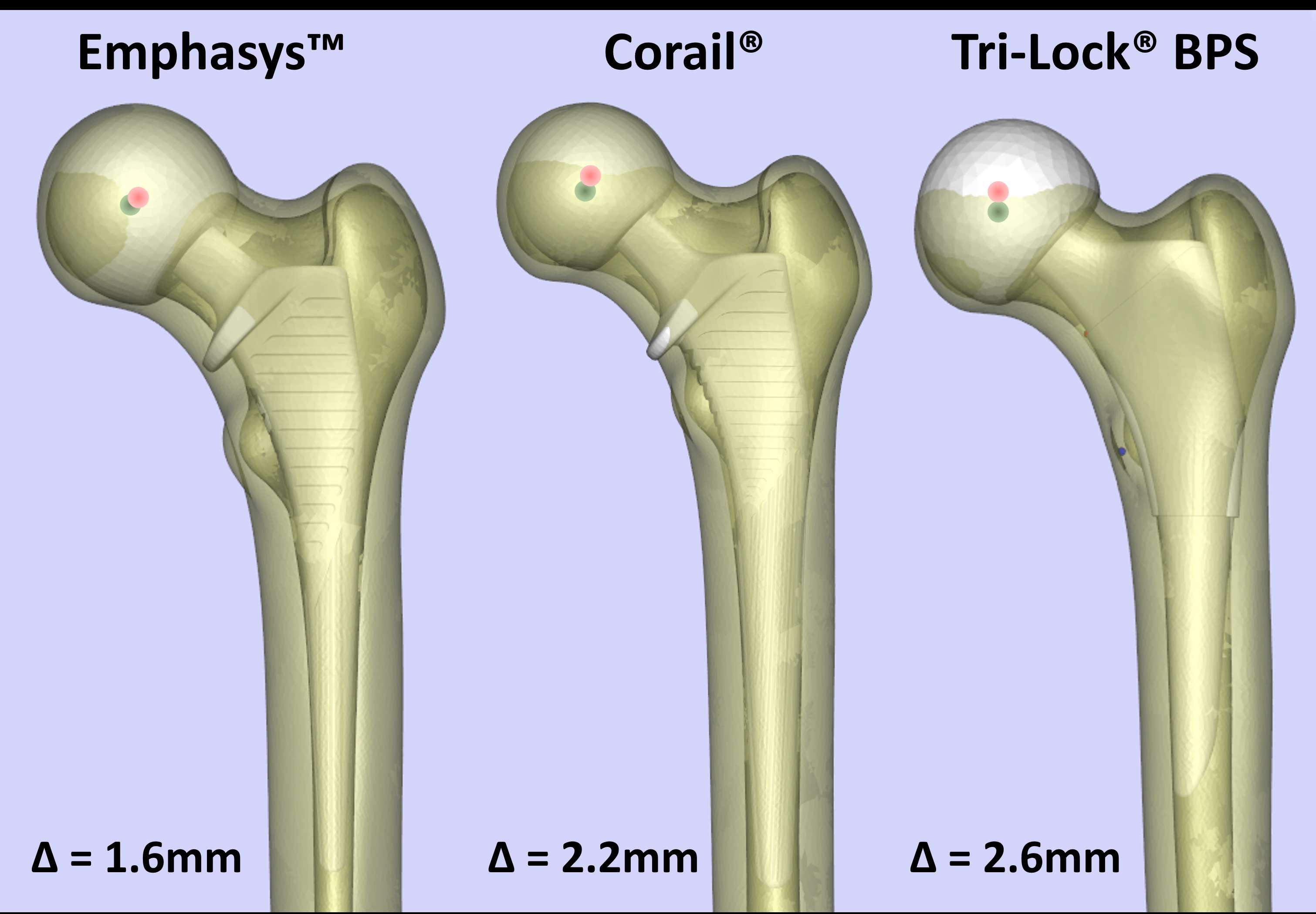
Figure 7
Figure 8
Figure 9#7722
An Original Technique Which Guarantees Excellent Femoral Component Positioning in Hip Resurfacing
*Gustavo Lage - Clinica Lage - S�o Paulo, Brazil
Lafayette Lage - Clinica Lage - sao paulo, Brazil
*Email: gustavo.lage622@gmail.com
Introduction: The good positioning of the femoral component in hip resurfacing is a crucial element for the outcome and longevity of the procedure. A varus positioning can be related with femoral neck fracture and femoral component loosening. A valgus positioning combined with femoral superior neck notching can also be related with femoral neck fracture. Valgus positioning induces a more physiological strain pattern and reduces the risk of femoral neck fracture when notching does not occur. On profile view it is interesting to get an anterior offset specially in athletes who need hip hiperflexion like ballet dancer, hockey goalkeeper, martial arts, soccer, beach tennis, volleyball and any other sports or activities who hiperflexion the hip including gardening.
Methods: We devised a new very simple technique which guarantees the desired femoral component positioning and also the acetabular component positioning. An ideal inclination of the acetabular component is achievable through this method, but it's ideal anteversion still remains as an unsolved problem until now. So we are reporting this technique as ideal for femoral component positioning! The femoral guide pin is passed through the femoral head and neck using the prosthesis guide. Each Resurfacing prosthesis has its own specialized instrumentation which aims to place the pin in the center of the femoral neck, but it's precision is variable. In special patients who need hiperflexion it is nice to place the femoral component a little bit anterior on profile view allowing an increased range of flexion of the hip improving the anterior offset. Our method allows a very precise femoral pin positioning since we cut the femoral guide just 2 to 3 mm above the femoral head and reduce the femoral head back to its place and take AP and Profile views intraoperatively using the image intensifier. If the position of the Kirschner wire is not desirable, we dislocate the hip and pass another pin again, and again if necessary, until we achieve the ideal desirable surgeon's position by rechecking its positioning on image intensifiers. Once we achieved the desired position we took off the kirschner a few centimeters and continued the surgery as usual.
Results: We started using this technique after the implantation of two initial unfortunate cases in 2003. We adapted this method using the femoral intensifier as if we perform a hip arthroscopy in lateral positioning. Since then we had never had a bad femoral component positioning.
Conclusions: For better positioning of the femoral component we do recommend the use of image intensifiers in all hip resurfacings which improves the surgical time less than 5 minutes and is affordable to any patient in any hospital, so it’s possible to avoid complications related with femoral component mal positioning . Acetabular ideal anteversion still remains a problem which might be solved with navigation, robotic, sterile 3D preop models or special surgical glasses with virtual 3D augmented reality.
Key words: -Hip -Surgical technique -Resurfacing -Surface -Replacement -Arthroplasty -Metal-on-metal
#7766
Mobility Outcomes Testing Following TKA: Improving on Subjective Outcomes Reporting
*Bradley Lambert - Houston Methodist Hospital - Houston, USA
Jordan Ankersen - Texas A&M University - College Station, USA
Thomas Sullivan - Houston Methodist Hospital - Houston, USA
Terry Clyburn - Houston Methodist Hospital - Houston, USA
Kwan Park - Houston Methodist Hospital - Houston, USA
Caleb Shin - Texas A&M University - College Station, USA
Stephen Incavo - The Methodist Hospital - Houston, USA
*Email: bslambert@houstonmethodist.org
INTRODUCTION: Tracking of patient reported outcome measures (PROMs) is common following total joint replacement via various self-reported survey formats. However, such measures are highly subjective and limited. The purpose of this study was to (1) develop a simple mobility outcomes testing battery (MOTB) incorporating movements of daily living as well as real-time pain assessment in patients following primary total knee arthroplasty (TKA); (2) evaluate MOTB performance in conjunction with classical outcome surveys before surgery (pre-op) and at 3- and 6-months post-surgery.
METHODS: Thirty-six patients (M=14, F=22; 667yr) undergoing primary TKA at a single institution underwent measurements of body composition and bone density (DEXA) in addition to mobility testing prior to surgery (pre) as well as 3 and 6 months post-TKA (3m, 6m). During testing, patients performed the following: walking (3 meters), sit-to-stand, ambulation up and down 4 stairs (hands on 2 rails, a single rail, and no rail assistance), and a body weight squat. Patients were scored on the following scale: 0=could not complete/attempt movement, 1=partial completion, 2=completion of movement. For each trial, patients rated their pain (VAS, 0-10). MOTB scoring incorporated both function and pain scores as follows for each movement: Function Score(0-2) x [(10 – VAS)/10]. A composite score for the entire MOTB was calculated as the sum of movement-specific scores divided by 18. At each timepoint, patients also completed the KOOS Jr, Pain Catastrophizing Scale (PCS), and the TSK-11 kinesiophobia survey as traditional PROMs. A generalized mixed model ANOVA was used to compare outcome measures over time. Correlation analysis was used to determine the degree to which MOTB scores correlated with the traditional PROM surveys and to determine which patient demographic measures were correlated with MOTB performance. Type-I error, =0.05.
RESULTS: Pain measures significantly decreased at the 3m timepoint (P<0.001) relative to pre-op and continued to improve out to 6m for stair decent while holding both (P=0.012) or a single rail (P=0.019)(Fig.1). Stair and squat movements were observed to have the highest VAS pain ratings on average (Fig.1). MOTB scores increased at the 3m timepoint for walking, sit-to-stand, stair movements utilizing both rails, and the squat (P<0.01) with stair movements (ascending and descending) without the use of handrails peaking at 6m post-op (Fig 1). Composite scores for the MOTB and other PROMs are shown in Figure 2. All metrics showed similar improvements by 3m (P<0.001) with continued improvement in the MOTB score which was sentitive enough to detect additional improvements at 6m (P<0.001). Significant correlations were observed between MOTB and all survey measures (KOOS Jr, r=0.715| PCS, r=-0.445| TSK-11, r=-0.359, P<0.05). Lastly, BMI (r=-0.451), %Body Fat (r=-0.474), and fat mass index (r= -0.561) were observed to be negatively correlated with MOTB performance.
CONCLUSIONS: The testing battery developed here significantly correlates with traditional survey-based PROMs while reducing subjectivity in patient reporting through a combination of objective in-clinic measures paired with real-time patient feedback. Such metrics may also be incorporated into clinical tracking software. These findings also highlight the impact of obesity on outcome measures following TKA.
Figures
Figure 1
Figure 2#8026
Accuracy of Acetabular Cup Positioning Using Patient-Specific Augmented Reality Guidance
Dan Sun - Tufts University - Boston, USA
*William Murphy - Harvard Medical School - Boston, USA
Patrick Lane - Surgical Planning Associates - USA
Stephen Murphy - New England Baptist Hospital - Boston, USA
*Email: wmurphy13@gmail.com
Introduction:
Malposition of the acetabular cup has been shown to contribute to postoperative complications following Total Hip Arthroplasty, including dislocations and revisions [1]. Surgeons have used many methods to achieve optimal placement of the acetabular cup, including preoperative planning, traditional navigation, robotics, and intraoperative radiography. More recently, an augmented reality guidance solution has been developed for implant positioning intraoperatively, allowing the surgeon to see 3D models including of the patient’s pelvis and planned cup and cup handle orientation through AR glasses in and around the patient in real-time during surgery. The purpose of this study was to evaluate the accuracy of cup placement relative to the goal for surgeries performed using the augmented reality guidance platform.
Methods:
Twenty four patients underwent CT based preoperative planning for use of the augmented reality guidance system. This includes 3D models of the patient’s pelvis and femur and planned placement of the components. 3D holograms were created for display during surgery. At the time of the procedure, a smart mechanical navigation tool was docked to the patient with a tracking image located outside of the body in a predicted position. The holograms were then displayed in surgery on a headmounted device (Microsoft HoloLens 2) by anchoring and tracking the image. The surgeon then aligned the real cup handle as closely as possible to the projection of the cup handle. All cases were performed by the senior author.
After surgery, all patients underwent standing EOS biplanar imaging at their postoperative appointment [2]. These two images were used to calculate the achieved cup orientation. This was compared to the planned cup orientation.
Results:
The mean error in achieved vs planned operative anteversion of the acetabular cup was -1.6° (SD: 2.2°, Min -6.0°, Max 2.0°), the mean error in operative inclination was -1.7° (SD: 2.6°, Min -6.0°, Max 5.0°). The average absolute error was 2.1° for operative anteversion, and 2.4° for operative inclination. Demographic information for patients is summarized in table 1.
Conclusion:
The augmented reality guided acetabular components were well placed with low mean error, and all cases within +/- 6 degrees in both planes. Further studies may provide additional data on the accuracy of augmented reality guidance for accurate acetabular component placement in total hip arthroplasty.
References:
[1] Techniques for Optimizing Acetabular Component Positioning in Total Hip Arthroplasty: Defining a Patient-Specific Functional Safe Zone. JE Feng, AA Anoushiravani, N Eftekhary, D Wiznia, R Schwarzkopf, JM Vigdorchik; JBJS Reviews. 2019 Feb;7(2):e5. doi: 10.2106/JBJS.RVW.18.00049
[2] Geometry of the EOS® Radiographic Scanner, B. N. Groisser, Department of Mechanical Engineering Technion-Israel Institute of Technology Haifa, Israel, arXiv:1904.06711
Figures
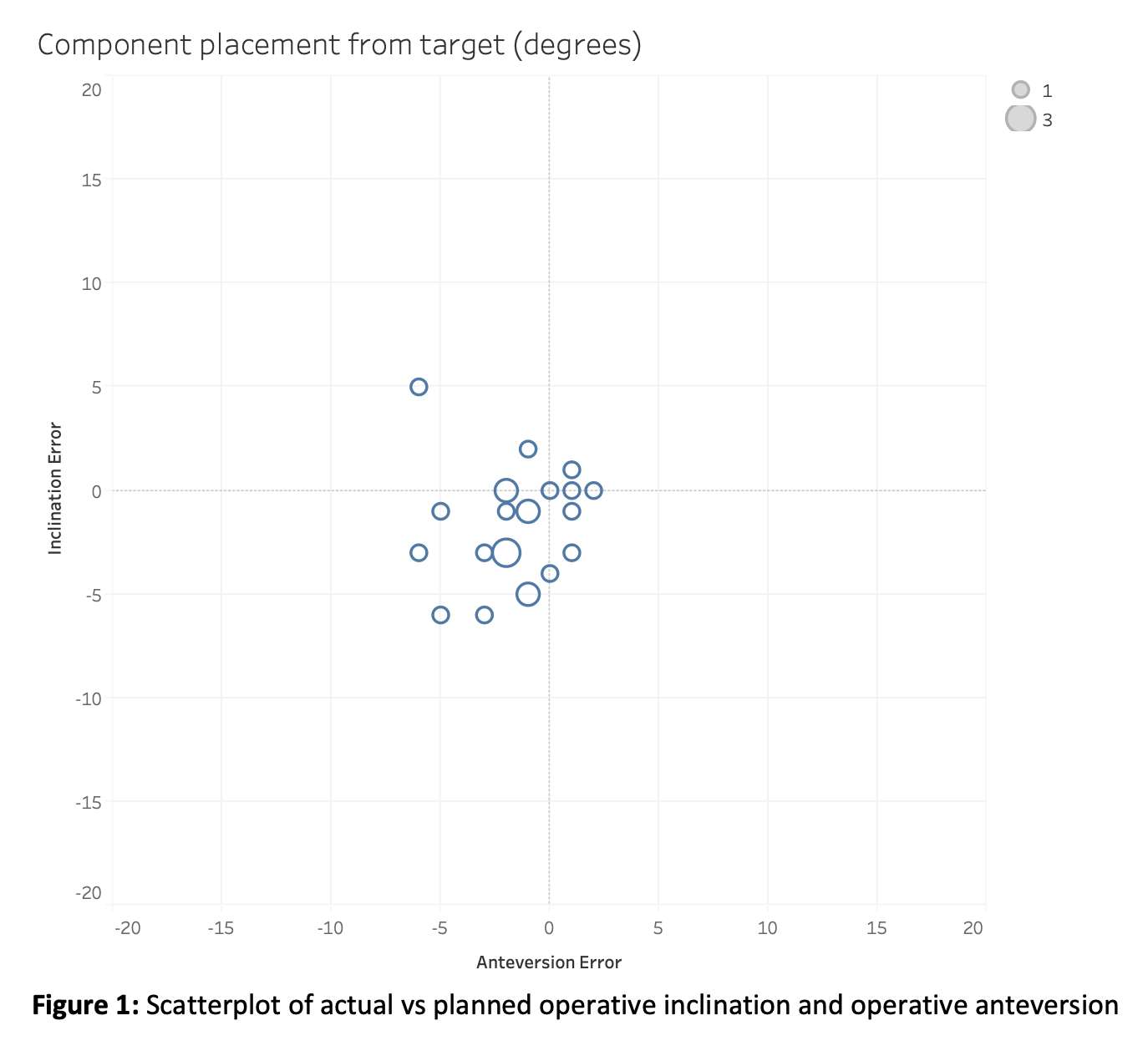
Figure 1
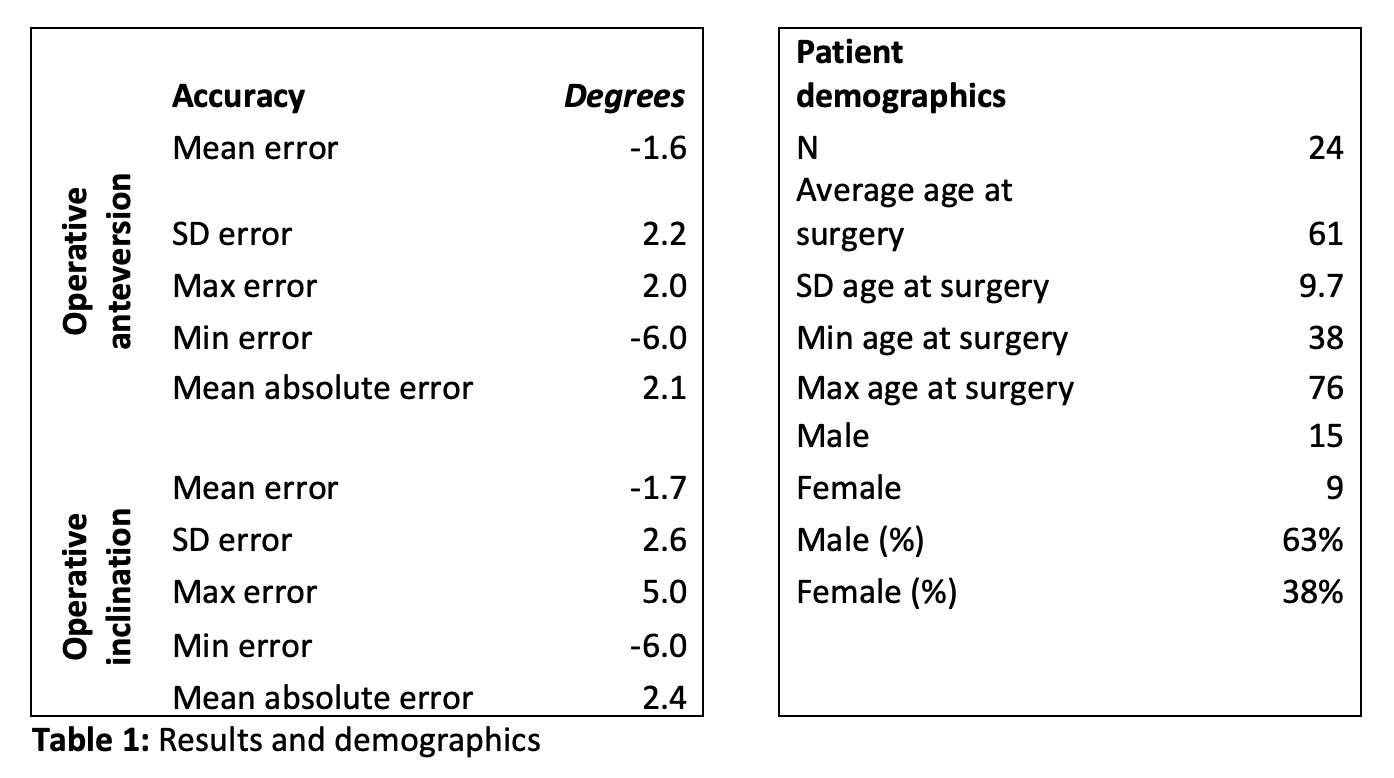
Figure 2#7492
A Pilot Study on Preferences From Surgeon to Deal With an Innovative Personalized and Connected Knee Prosthesis
*Mathieu Le Stum - Inserm - Brest, France
Myriam Le Goff Pronost - Institut Mines Telecom Atlantique - BREST, France
Eric Stindel - Latim, University Hospital of Brest - Brest, France
*Email: mathieu.le-stum@inserm.fr
Introduction
Knee arthroplasty (TKA) is one of the most predominant orthopedic intervention worldwide with respectively 720,000 in 2019 and more than 700,000 interventions in Europe (Eurostat) and USA (Sloan, 2018). This number is continuously increasing from several decades and is expected to exploded in the next years (+147% by 2030 in the USA [Sloan, 2018]). This is the results of the population ageing, a strong demand from young (<65 years), often overweight, and more active people. Implanted for 20 years in active subjects, these prostheses are more frequently revised, leading to expensive and less effective procedures.
To face this major public health problem, the project FollowKnee (www.followknee.com) is providing an innovative response by proposing a new care chain. With an efficient AI based software, surgeons automatically customize the design of the prosthesis that are then 3D printed. To allow a precise and optimal implantation, augmented reality tools, easy to use in the operating room, are developed. And to better drive patients’ care and rehabilitation, an integrated set of sensors will transmit data to monitor the mechanical behavior of the prosthesis and detect early infections. Patient recovery and optimized follow up will be eased.
This personalized and connected prosthesis, bringing together several technologies, would represent a breakthrough and would lead to an adaptation and changes in practices for surgeons. We aimed to assess how surgeons’ preferences will affect acceptability to use this new prosthesis and associated technologies.
Method
We assessed surgeons’ preferences using a discrete choice experiment questionnaire (De Bekker-2012, Lancsar-2008, McFadden-1973) with 16 choice set scenarios with an status quo option. Surgeons were asked to select the one they would prefer. Based on literature review, experts’ consultation and pre-testing questionnaire, we characterize four attributes (table 1): customized prosthesis, integrated sensors, augmented reality tools and extra cost. A status quo option (ie “no change with my usual practice”) is include. Conditional logit model was used to estimate surgeons’ preferences. The questionnaire was distributed in France via the French national association of orthopaedic surgeons.
Results
The questionnaire was return by 56 surgeons, that were all males. 46.4% have 10 and less years of experience whereas 53.6% have more. 48.3% work in public hospital and 51.7% in a private structure.
The random parameters are presented in table 2. Non-significant status quo’s coefficient indicates no influence of this alternative on surgeons’ preferences. All preference for FollowKnee’s technologies were important for surgeons and were in the expected direction. Overall, the conditional relative most important attribute on surgeons’ choice is “customized prosthesis” (0.62), followed by “Augmented Reality” (0.47), Extra Costs (0.41) and “Integrated sensors” (0.34).
Conclusion
This study demonstrate that surgeons want to used a customized prosthesis implemented by augmented reality for a measured extra cost. Although interesting, embedded sensors technology seems to be too early for them.
Aknowledgement
This work benefited from State aid managed by the French National Research Agency under the Future Investment Program bearing the reference ANR-17-RHUS-0005 (Project FollowKnee).
Figures
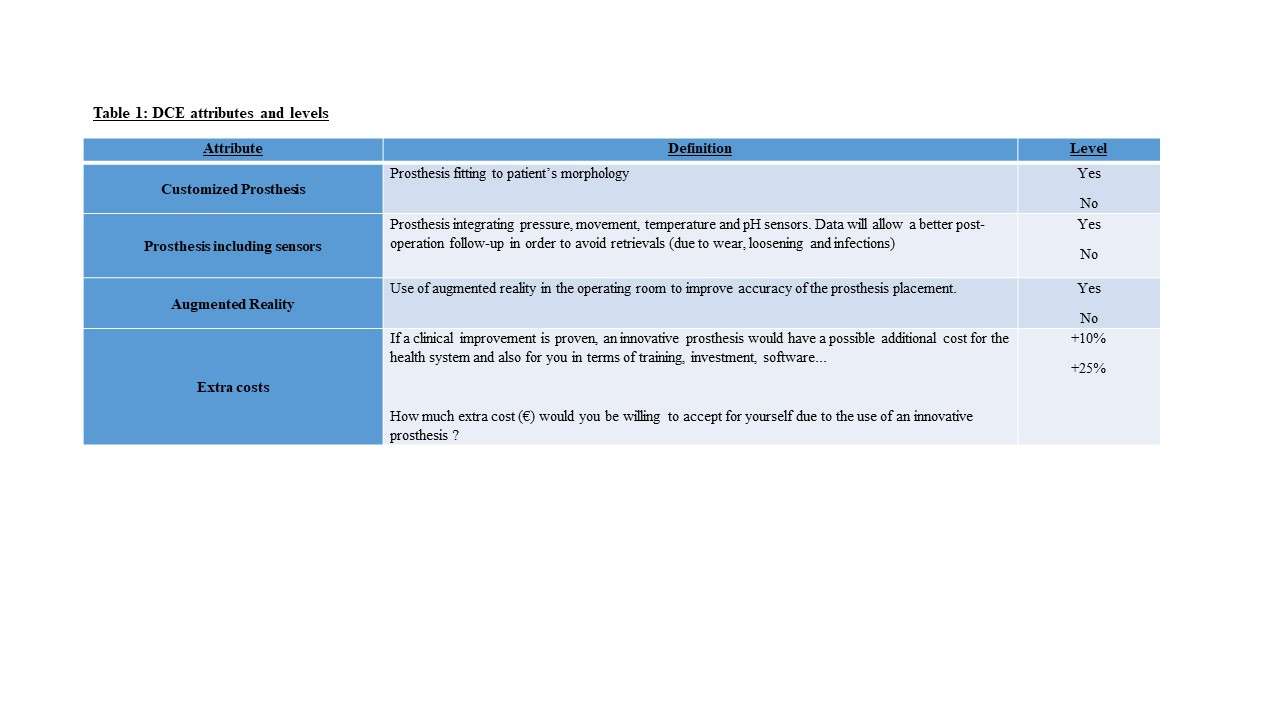
Figure 1
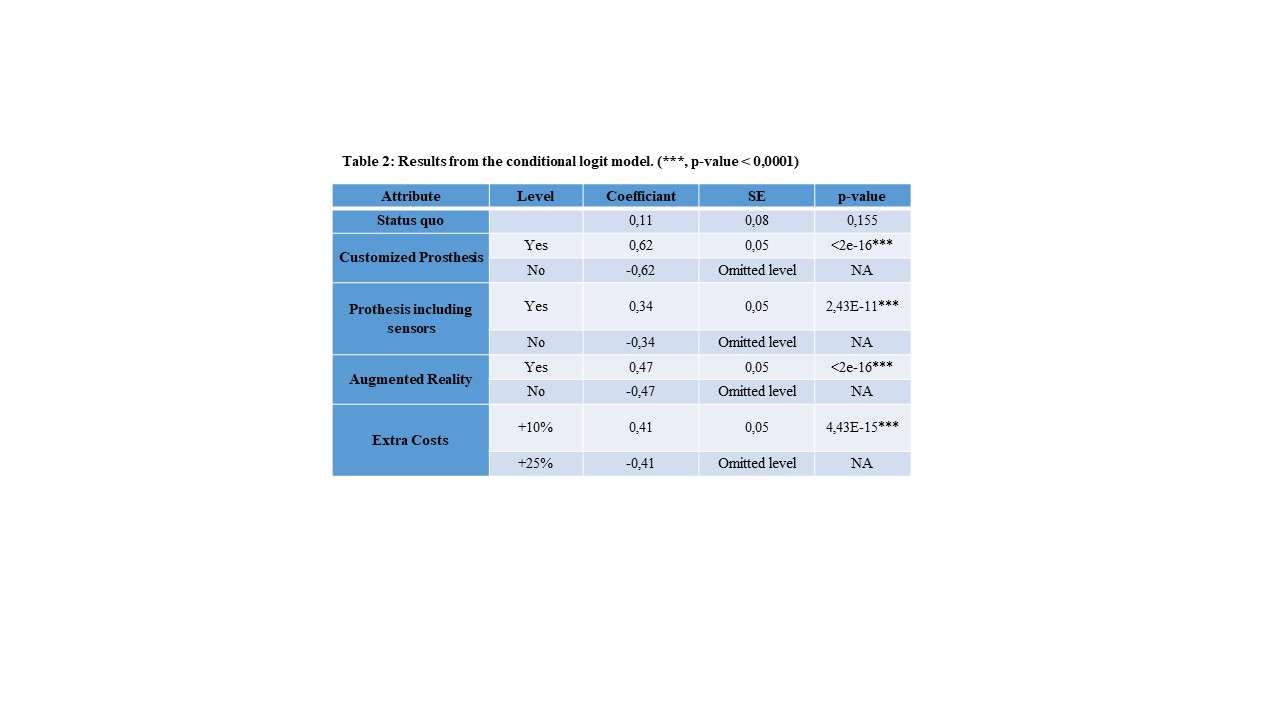
Figure 2#7440
Quantifying the Pelvic Mobility Impact on the Functional Cup Orientation for THA
*Aziliz Guezou-Philippe - LaTIM, University of Western Brittany - Brest, France
Arnaud Clave - Saint-George Private Hospital - Nice, France
Mathieu Le Stum - Inserm - Brest, France
Wistan Marchadour - LaTIM, University of Western Brittany - Brest, France
Eric Stindel - Latim, University Hospital of Brest - Brest, France
Christian Lefevre - LaTIM, University hospital of Brest - Brest, France
Dardenne Guillaume - University Hospital of Brest - Brest, France
*Email: aziliz.guezouphilippe@univ-brest.fr
How to optimize the cup orientation in total hip arthroplasty (THA) has been an ongoing question for years. Since Lewinnek suggested a safe zone around 40° inclination and 15° anteversion, various other safe orientations have been proposed in the literature. More recently, the spino-pelvic mobility has been shown to impact the stability of the total hip prosthesis (THP) and should therefore be considered when orienting the cup. Thus we propose a functional safe zone (FSZ) to determine the cup orientations suited to the patient pelvic mobility, evaluated by the pelvic tilts (PTs) in sitting, standing and supine positions. Based on Hsu method*, this FSZ combines the safe zones computed for the three positions. Our goals were (1) to validate the proposed FSZ and (2) to quantify the PTs’ impact on the FSZ mean orientation.
A FSZ was computed for 30 patients whose PTs were acquired in sitting, standing and supine positions as part of a clinical study (NCT03555812 in the clinicaltrials.gov database). The FSZ was validated for 10 patients randomly chosen, by comparing the computed FSZ to the “true” FSZ obtained by simulating the motions of a THP 3D model. Both computed and true FSZ were compared in terms of difference of mean anteversion, mean inclination and edges. The correlations between the FSZ mean orientation and the PTs were identified by computing the Pearson correlation coefficients rp and quantified using linear regressions. Correlations were strong if ±rp>0.8, high if ±rp>0.6, moderate if ±rp>0.4 and poor otherwise.
The true and computed FSZs differed by -0.2±0.3° (range: -0.6° to 0.4°) for mean anteversion, 0.0±0.1° (range: -0.1° to 0.2°) for mean inclination and 0.2±0.2° (range: 0.0° to 1.0°) for edges. The correlation coefficients and linear regressions between the FSZ mean orientation and the PTs are presented in Figures 1 and 2.
To adapt the cup orientation in THA to the patient mobility, we proposed a FSZ computed from the patient PTs in three positions. The FSZ was validated through a simulation study, with mean errors <0.5°. The FSZ mean anteversion was found modified by 0.3° and 0.5° per degree of PT in standing and supine position respectively, and the mean inclination by 0.2° per degree of supine PT. Thus, the more anteverted the pelvis is in these positions, the higher the cup anteversion and inclination should be, and conversely, the more retroverted the pelvis, the lower the anteversion and inclination. While those effects are statistically significant and coherent with the literature, the FSZ mean orientation stays in the Lewinnek safe zone boundaries. However, the size and shape of the FSZ differ from Lewinnek safe zone, thus reducing the margin of error around the optimal orientation (Figure 3). Such observations confirm the need to consider the PTs in different positions before implanting a THP and the usefulness of a FSZ to estimate the optimal cup orientation and its margin of error.
* Hsu et al., Calculation of impingement-free combined cup and stem alignments based on the patient-specific pelvic tilt, J. Biomech., 2019
Figures

Figure 1
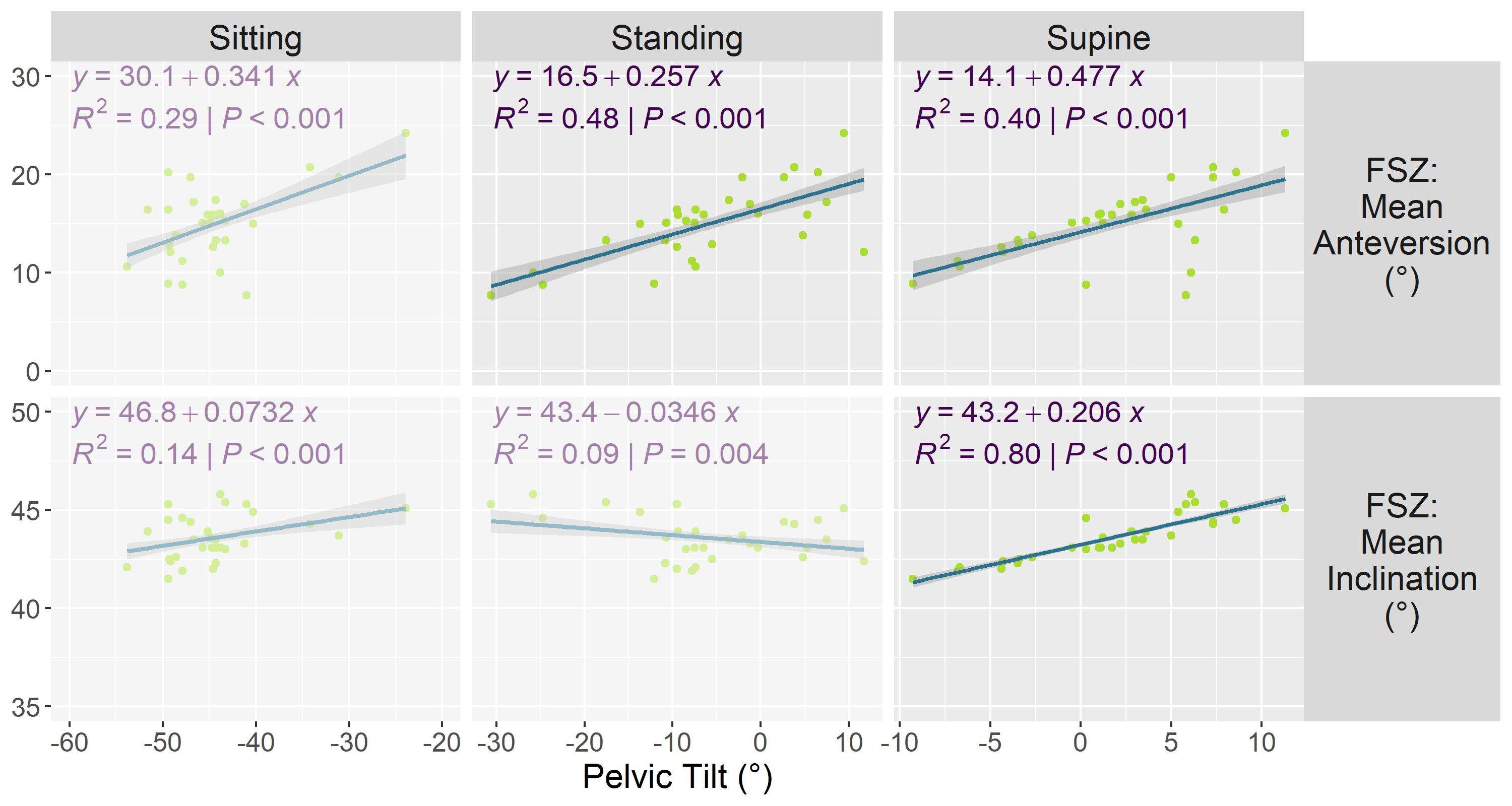
Figure 2
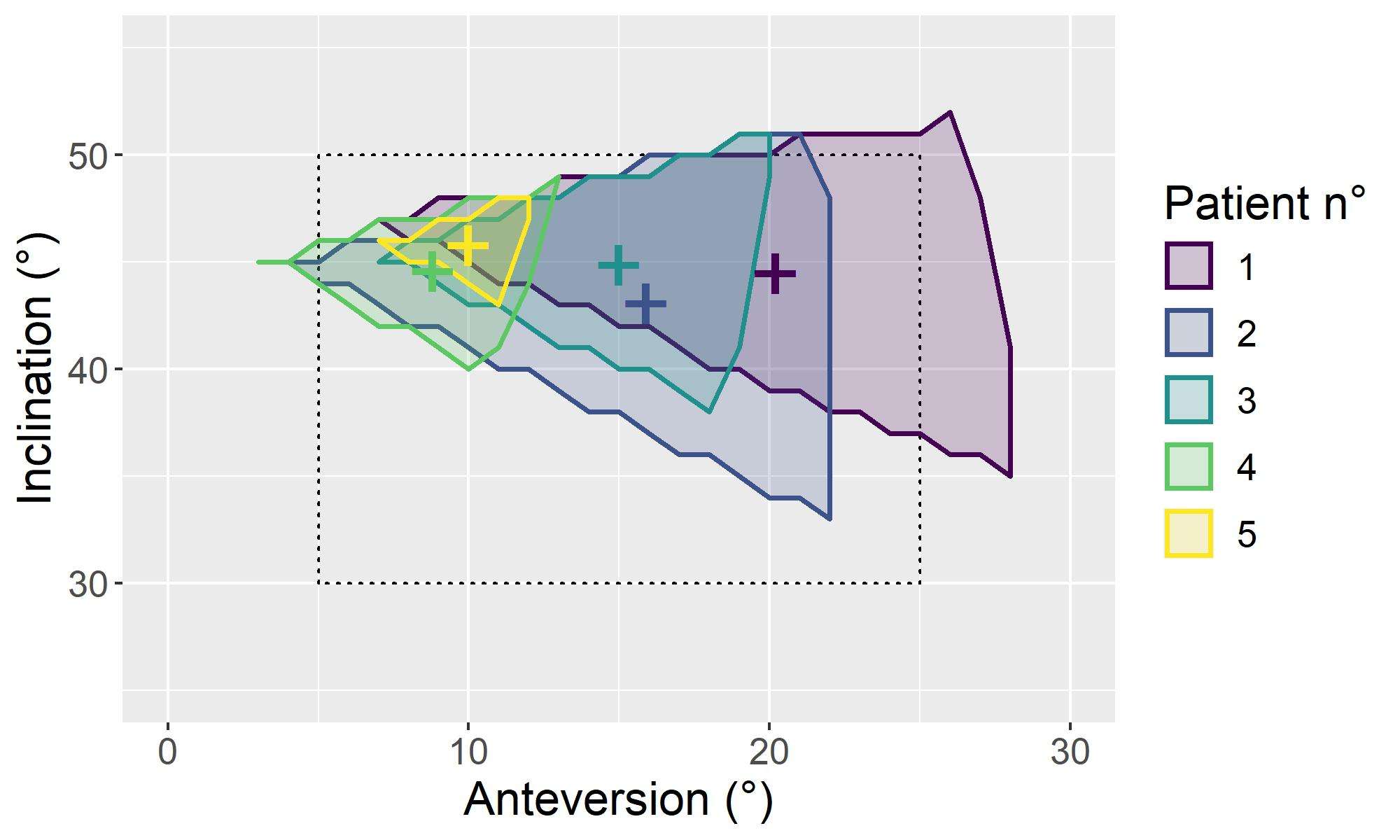
Figure 3#7499
Clinical and Radiological Mid-Term Results of Stemless Shoulder Arthroplasty
*Myung-Sun Kim - Chonnam National University Hospital - Gwangju, South Korea
Sun-Ho Lee - Chonnam National University Hospital - Gwangju, South Korea
Woo-Jong Kim - Chonnam National University Hospital - Gwangju, South Korea
Jun-Hyeok Lim - Chonnam National University Hospital - Gwangju, South Korea
*Email: rhamses@chol.com
Abstract
Introduction: Through an iteration of various advancements, stemless options for humeral fixation have been proposed and have shown numerous theoretical advantages, including preserved bone stock, reduced rate of intraoperative humerus fracture, and flexibility of anatomic reconstruction. Therefore, The purpose of this study was to evaluate the clinical and radiological results of shoulder arthroplasty using a single type of stemless humeral component with a minimum follow-up of 4 years.
Methods: A retrospective review was conducted of primary shoulder arthroplasties performed with stemless humeral component since 2014. Shoulder arthroplasty using Comprehensive Nano stemless shoulder system (Biomet ®, Warsaw, IN, USA) was performed in 16 shoulders; 7 underwent hemiarthroplasty (HA), 7 underwent totoal shoulder arthroplasty (TSA), and 2 underwent reverse total shoulder arthroplasty (RTSA). 15 patients (16 shoulders) who were aged 56.8 years were available for clinically and radiologically at a mean follow-up of 63.2 months.Clinical evaluations were documented using Constant-Murley Score (CMS); American Shoulder and Elbow Society (ASES) score; Korean Shoulder Scoring (KSS) System. Radiological evaluations was based on geometrical joint parameters and the occurrence of radiolucent lines around implants.
Results: Overall survival rate at 4.6 years was 94%. 1 patient who underwent RTSA had revision to cement stem due to immediate operative humeral component displacement. Clinically, CMS improved from 43.9 to 85.3 and ASES score improved from 44.8 to 86.2 and KSS improved from 54.5 to 82.6 (P=0.001). Active range of motion improved significantly for flexion (from 116.5° to 163.5°), abduction (from 95.0° to 158.2°; P=0.001), and external rotation (from 38.5° to 59.6°; P=0.001). Radiologically, most of center of rotation showed superomedial deviation and lateral glenohumeral offset increased significantly after total shoulder arthroplasty. Also radiolucent lines could be detected around humeral component, but none of them have had clinical relevance yet.
Conclusion: The functional and radiologic results of the Comprehensive Nano stemless shoulder system are promising in mid-term follow-up. However, synthetical preoperative evaluation is essential in performing the stemless RTSA. Long-term study including a large number of patients are needed to support this mid-term results.
Key words: Stemless shoulder arthroplasty; hemiarthroplasty; total shoulder arthroplasty; reverse total shoulder arthroplasty
#7656
Concurrent Repair of Medial Meniscus Posterior Root Tear Provides Additional Benefits Toward Restoring Tibiofemoral Contact Biomechanics Conferred by Opening-Wedge High Tibial Osteotomy: A Cadaveric B
Hyung Jun Park - Seoul National University College of Medicine, SMG-SNU Boramae Medical Center - Seoul, South Korea
*Seung-Baik Kang - Boramae Medical Center/ Seoul National University College of Medicine - Seoul, South Korea
Chong Bum Chang - Seoul National University Boramae Hospital - Seoul, South Korea
Moon Jong Chang - SMG-SNU Boramae Medical Center - seoul, South Korea
Tae Woo Kim - Seoul National University College of Medicine, SMG-SNU Boramae Medical Center - Seoul, South Korea
Tae Soo Bae - Jungwon University - Chungbuk, South Korea
Dai-Soon Kwak - The Catholic University of Korea - Seoul, South Korea
Eunah Hong - 6. Department of Biomedicine & Health Science, College of Medicine, The Catholic University of Korea - Seoul, South Korea
Kyung-Hwi Kim - Department of Orthopedic Surgery, Seoul National University College of Medicine, SMG-SNU Boramae - Seoul, South Korea
Siyung Lee - Seoul National University College of Medicine, SMG-SNU Boramae - Seoul, South Korea
Tae Seon Kim - Seoul National University College of Medicine, SMG-SNU Boramae - Seoul, South Korea
*Email: ossbkang@gmail.com
Background
Repair of the medial meniscus posterior root (MMPR) and opening-wedge high tibial osteotomy (OWHTO) are both reportedly effective in reducing the load on the medial compartment of the knee, respectively. However, the effectiveness of concurrent repair of the MMPR tear during OWHTO is controversial.
Purpose
This study aimed to determine whether the degree of improvement in the tibiofemoral contact biomechanics after OWHTO differed according the state of the MMPR (intact, torn, and repaired). We also aimed to determine whether the degree of restoration of tibiofemoral contact biomechanics after MMPR repair differed according to the degree of correction during OWHTO.
Study Design
Controlled laboratory study
Methods
Nine fresh-frozen human cadaveric knee specimens were included in this study. Each specimen was tested under nine conditions comprising 3 different degrees of correction during OWHTO (neutral, 5°, and 10°) and 3 different types of MMPR conditions (intact, torn, and repaired, Figure 1). The contact pressure (CP) and contact area (CA) generated by a tibiofemoral axial load of 650 N was recorded using the Tekscan sensor’s pressure mapping software.
Results
The pattern of tibiofemoral contact biomechanics worsened after MMPR tear, but improved after repair compared to the intact MMPR. These results were consistent, irrespective of whether OWHTO was performed. The absolute amount of biomechanical restoration after MMPR repair decreased depending on the degree of correction (Figure 2,3). However, based on the tibiofemoral contact biomechanics in the torn MMPR state, the rate of restoration of tibiofemoral contact biomechanics after MMPR repair was constant, irrespective of the degree of correction during OWHTO.
Conclusion
The protective effect of MMPR repair on the medial compartment of the knee persisted even after OWHTO was performed, irrespective of the degree of the correction, including the valgus overcorrection status. Therefore, concurrent repair of the MMPR during OWHTO can be useful to further improve tibiofemoral contact biomechanics. The findings of our cadaveric biomechanical study should be confirmed using clinical studies.
Figures
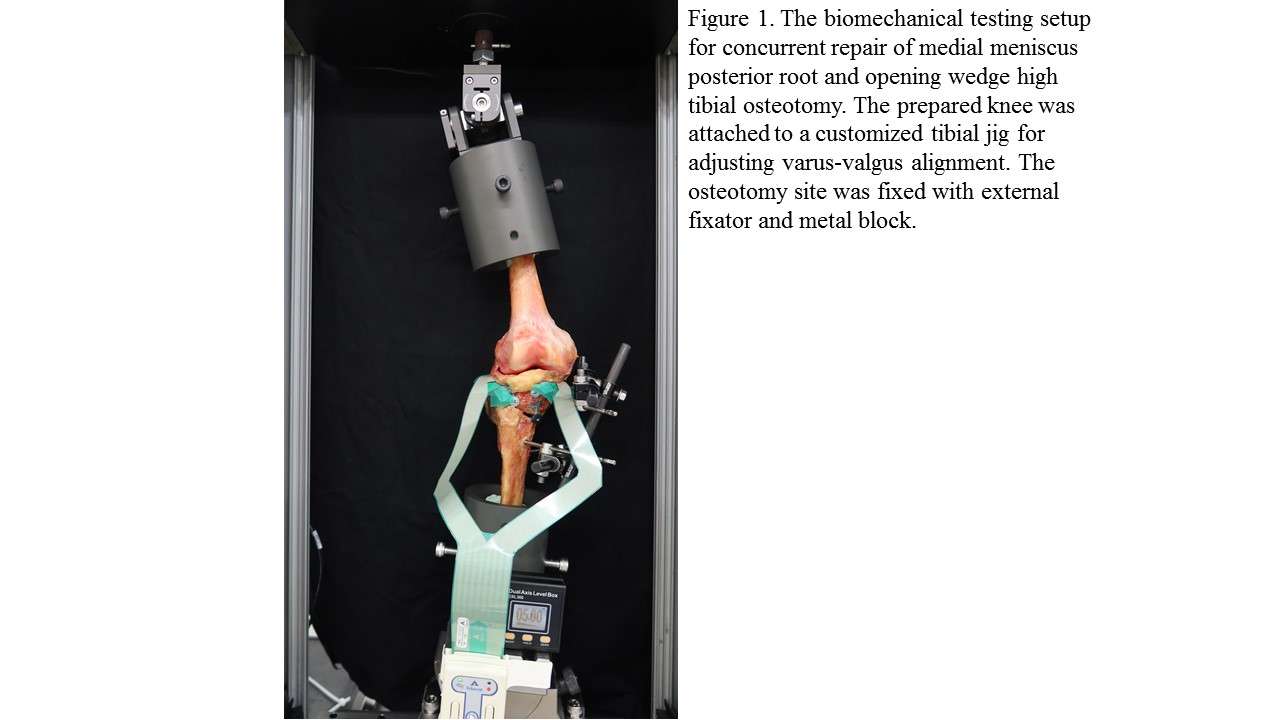
Figure 1
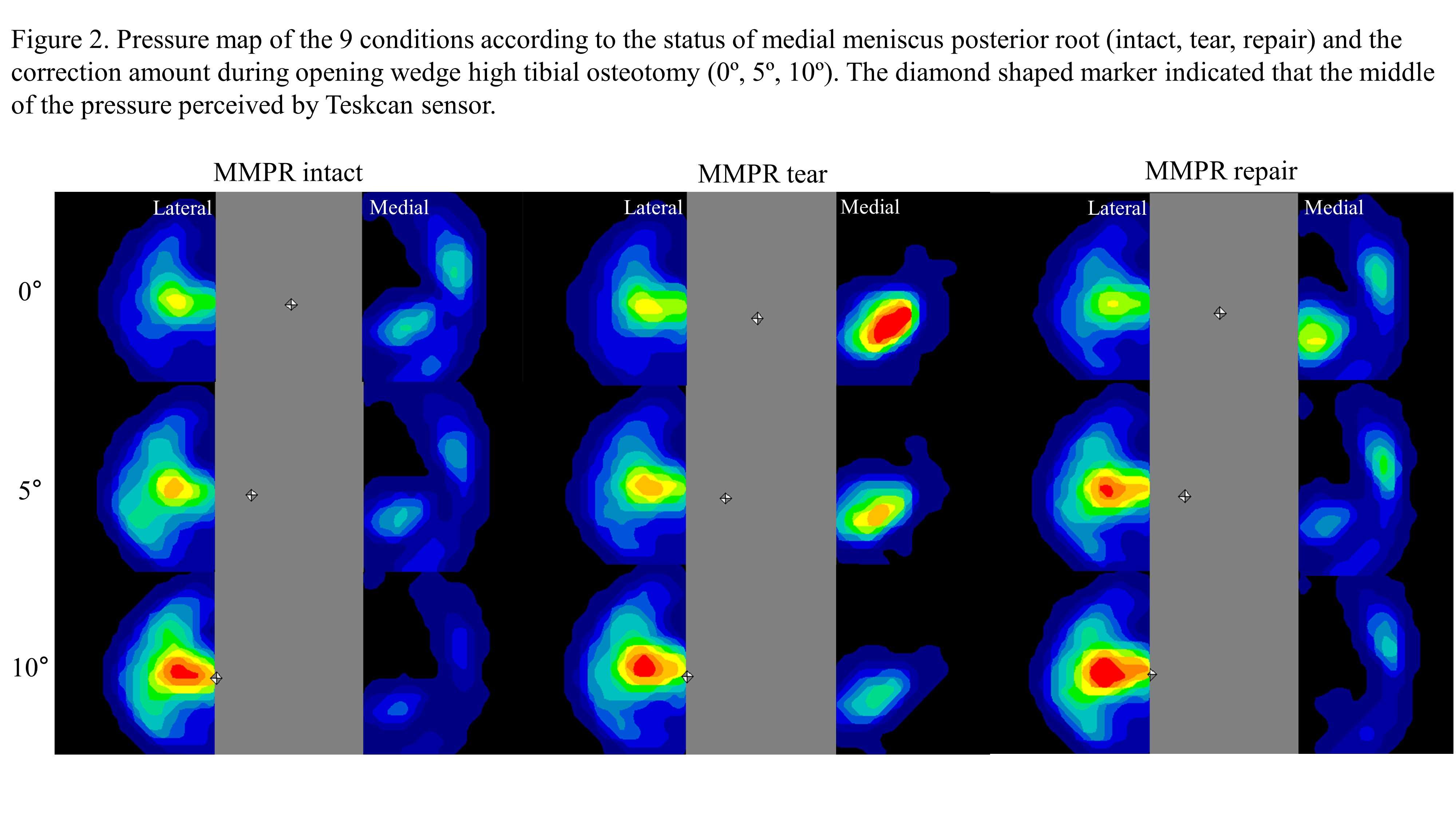
Figure 2
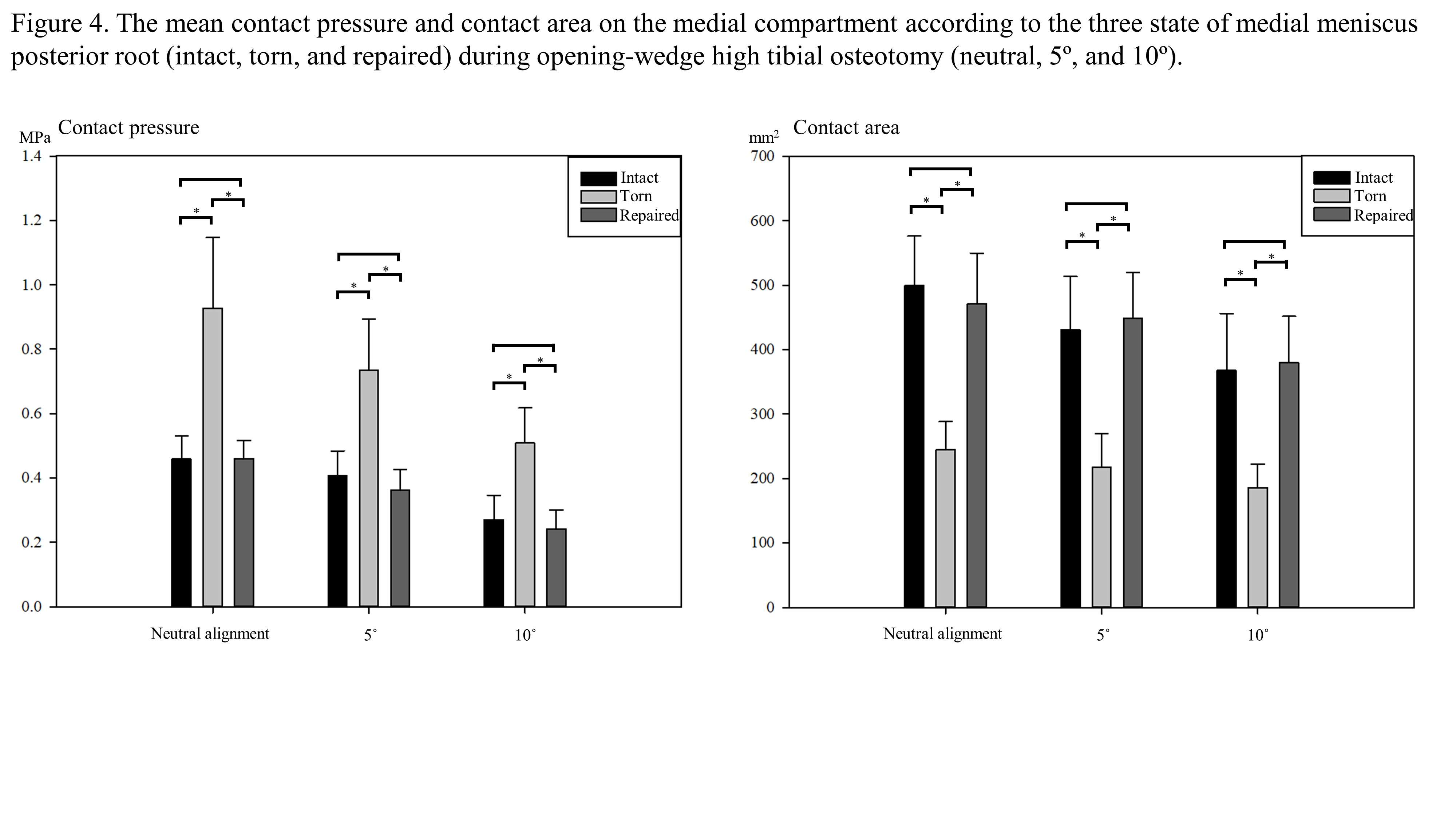
Figure 3#7632
The Newly Developed Robot Arthroplasty System -Dr. LCT-
*SungHwan Yoon - LeeChunTek Orthopaedic Specialty Hospital - Suwon City, South Korea
Soo-hyun Lee - LeeChun Tek Otehopaedic Specialty Hospital - Suwon city, Select Country
OhMyoung Kwon - LeeChunTek Orthopaedic Specialty Hospital - Suwon, Korea (Republic of)
HangJae Lee - LeeChunTek Orthopaedic Specialty Hospital - Suwon, Korea
Richard Yuseok Bang - LCT Medical Research Center - Suwon-si, South Korea
Yoo Wang Choi - Gangbuk Yonsei Hospital - Seoul, South Korea
*Email: osman1973@hanmail.net
Introduction: In order to improve post-operative outcomes of total knee arthroplasty, several robot-aid systems have been used over the past few decades. ROBODOC (robot-assisted surgery ISS inc., CA USA) & ORTHODOC (planning system, ISS inc., CA USA) was one of the first methods to be invented and has long shown good results. Since 2002, we have successfully performed more than 15,000 surgeries using ROBODOC and ORTHODOC. However, as time went by, it became difficult to improve and make further progress. So we developed new robot–assisted total knee system (named Dr.LCT) based on our experience. We would like to introduce our newly developed system.
Material and Methods: Dr. LCT is CT based full active, 7 axis arm robotic system, (Figure 1.) This is prospective randomized controlled study. From June 2021 to September 2021, 50 osteoarthritis patients (average age: 69.7, male:7, female :43 ) was preformed bilateral TKA with mechanically alignment. The operations were performed by one author (Dr, Yoon), one Knee with ROBODOC and the other knee with Dr LCT, same times or in a week. Postoperative results were analyzed by other authors without knowing which side was operated by Dr LCT. The radiological evaluations included mechanical axis, implant position (α,β,γ,δ angle ) according to the system of American Knee Society. Clinical outcomes and motion were measured preoperatively, 6 weeks, 3 months, and 6 months postoperatively.
Results: There was no difference in the postoperative α, β, γ angle and mechanical axis between two groups (p<0.05). In group ROBODOC, mechanical axis angle changed from preoperative varus 8.5±6.4° to postoperative varus 0.3±1.2° with 1 outlier. In group Dr. LCT, mechanical axis angle changed from varus 7.8±6.3° to varus 0.2±1.2° with 1 outlier. In group ROBODOC, the mean α, β, γ, δ angle were 96.2°, 1.5°, 89.9°, 84.3° and 96.2°, 1.4°, 90.2°, 83.4° in group B. There was no difference of clinical results between two groups. Mean knee society score was improved in both group (pain score; from 46.3 ±11.7(preoperative) to 83.4±4.7(postoperative) in ROBODOC, from 50.3±9.2 to 85.0±6.0 in Dr. LCT, function score: from 43.2±14.4 to 86.7±4.7 in ROBODOC, from 39.1± 12.5 to 86.7± 4.7 in Dr. LCT). WOMAC score showed similar results; 68.1±4.5 to 15.6 in ROBODOC, 69.6±6.0 to 15.74.0 in Dr. LCT). There was significant difference in surgery times between two groups (Match time(minutes): 7.9±2.0 in ROBODOC, 2.8±1.0 in Dr. LCT, Cut time: 23.5±4.2 in ROBODOC, 8.2 ±1.2 in Dr. LCT)
Conclusion: In our extremely short experience, both Dr.LCT and ROBODOC showed good radiological & clinical results without difference, whereas operative time and cutting time were founded to be much less with Dr. LCT which can hardly be compared. We think that Dr. LCT system has clinically safety and effectiveness not only to patient also to surgeon with improvement. However, additional follow up and evaluation will be needed.
Figures

Figure 1#7534
Quadriceps Muscle Volume Has No Effect on Patellofemoral Cartilage Lesions in Patients With End-Stage Knee Osteoarthritis
Jung-Ro Yoon - Veterans Health Service Medical Center - Seoul, South Korea
Kyu Bok Kang - VHS medical center - Seoul, South Korea
*Seung Hoon Lee - VHS medical center - Seoul, South Korea
Jung Taek Im - VHS medical center - Seoul, Korea (Republic of)
Phil-Sun Park - VHS medical center - Seoul, South Korea
*Email: lsh5931k@hanmail.net
Purpose: The quadriceps muscle has a positive effect on anterior knee pain. However, its effect on the patellofemoral (PF) cartilage in patients with end-stage knee osteoarthritis is unknown. The present study aimed to evaluate whether the quadriceps muscle area had a positive effect on the PF cartilage and whether this muscle had a positive effect on the clinical scores.
Materials and methods: Patients with confirmed cartilage status and clinical scores who underwent total knee arthroplasty (TKA) were included. The PF cartilage status was evaluated during TKA. The thickness and the area of the quadriceps muscle were measured using a knee computed tomography scan obtained before the surgery. The Q-angle, hip-knee-ankle angle, alignment, and Insall-Salvati ratio were measured by radiography.
Results: Altogether, 204 patients were included in the study. Logistic regression was performed including factors associated with PF cartilage lesions. The regression model was found to be statistically significant (Hosmer-Lemeshow test, χ2 = 0.493). A smaller hip-knee-ankle (HKA) angle was associated with a higher incidence of PF cartilage lesions (p = 0.033) and only the alignment had an effect on the PF cartilage lesions. PF cartilage lesions did not correlate with the clinical scores. A thicker medial portion of the quadriceps muscle was associated with a significantly higher Knee Society Knee Score (KSKS) (p = 0.028).
Conclusions: Quadriceps muscle thickness and area, Q-angle, and patellar height were not associated with PF cartilage lesions, while a smaller HKA angle was associated with PF cartilage lesions. The presence of PF cartilage lesions did not affect the clinical symptoms. However, a thicker medial portion of the quadriceps muscle was associated with a higher KSKS.
#7533
Biomechanical Efficacy of Hyperlordotic Cage According to Lordotic Angle in Posterior Lumbar Interbody Fusion(PLIF) in the Lower Lumbar: A Finite Element Study
Ye-Ji Lee - Inje university - Gimhae, Select Country
Sung-Jae Lee - Inje Univ. - Gimhae, South Korea
*Sung-Woo Choi - Soonchunhyang Medical College, Seoul Hospital - Seoul, South Korea
Ji-Eun Jang - GS medical - Cheongju, South Korea
Jae-Won Lee - GS medical - Cheongju, South Korea
*Email: osfx1209@naver.com
Introduction: Although posterior lumbar interbody fusion(PLIF) with cage is frequently used to restore lumbar lordosis in degenerative spinal disease, recent studies have shown its clinical effectiveness decreases at the lower lumbar spine(L4-L5-S1), where lordotic curve(Lordosis 26-40º) is more pronounced. The increases in cage subsidence and motion at the adjacent segments have been attributed to the sagittal imbalance arising from the lack of a sufficient lordotic angle provided by the conventional cage. This imbalance can cause chronic back pain by making the uneven load distribution of the spine. Therefore, the recovery of the lordotic angle is important. Recently, hyperlordotic cages with enlarged lordosis angles similar to those of the lower lumbar segments have been introduced, but biomechanical studies supporting their efficacy are lacking. In this study, the subsidence risk and degeneration of the adjacent segments of hyperlordotic cages were investigated using a finite element(FE) analysis.
Methods: A previously validated intact lumbar(L1-S1) FE model was used to construct three surgical models with PLIF cages(Lordotic PEEK cage, GS Medical Co. Ltd, Korea) for different lordotic angles(Type A:low hyperlordotic angle, 12º;Type B:middle hyperlordotic angle, 18º;Type C:extreme hyperlordotic angle, 21º) with pedicle screws(Scoli Poly Screw(self)TM, GS Medical Co. Ltd, Korea)[Fig. 1]. Partial removal of the annulus, ligament, and facets was simulated to accommodate the PLIF cage insertion(L5-S1). Follower load of 400N and pure moment of 10Nm were applied in flexion/extension, lateral bending and axial rotation with the inferior S1 fixed in all directions. The motion in each direction was noted and the other constructed models were loaded by increasing the moment until the primary L1-S1 motion matched the intact(healthy) L1-S1 motion. Compared to the yield strength(16MPa) of the vertebrae, the peak von Mises stress(PVMS) at the lower vertebral body was predicted to investigate the risk of cage subsidence. Degeneration of the adjacent segments was investigated by comparing the ROM of superiorly adjacent segments of intact and surgical models.
Results: Overall, a low subsidence risk and degeneration of adjacent segments were confirmed to have the highest hyperlordotic cage(Type C). Especially in flexion, Type C showed the lowest PVMS(3.7MPa), followed by Type B(5.5MP) and Type A(5.8MPa). The higher the hyperlordotic angle, the lower the PVMS, and the possibility of subsidence of the vertebral body due to load concentration was lowest(Type A: 35%, Type B: 33%, Type C: 22%). Thus the subsidence risk was increased by decreasing cage lordosis, which is similar to the ROM tendency[Fig. 2]. The ROM at the adjacent segments was highest in Type A(4.4º, 118%). This was approximately 11% higher than Type C(4.0º, 107%) with a higher lordosis cage in lateral bending. This is expected to reduce the possibility of degeneration by preventing the excessive movement of the adjacent segments. These results suggest that Type C is the least likely to degenerate at adjacent segments compared to the other types[Fig. 3].
Conclusions: This study demonstrates that a hyperlordotic cage with a high lordosis angle at lumbar fusion(L5-S1) reduces the risk of subsidence and secures surgical stability by minimizing the movement of adjacent segments.
Figures
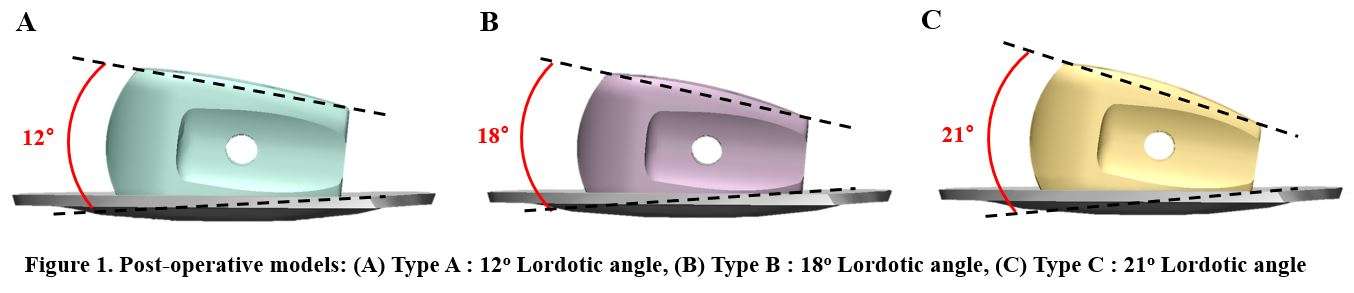
Figure 1
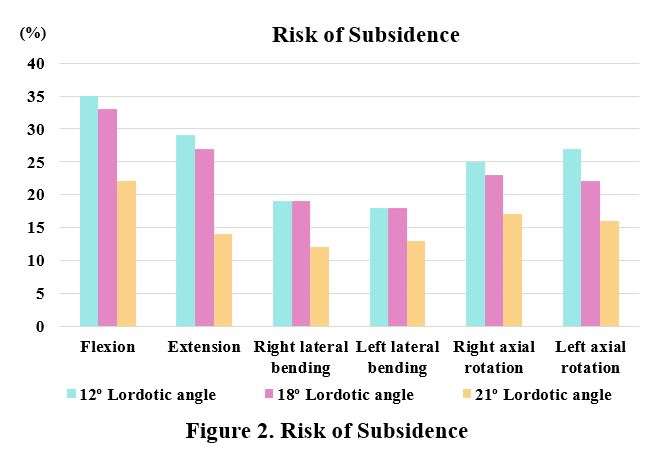
Figure 2
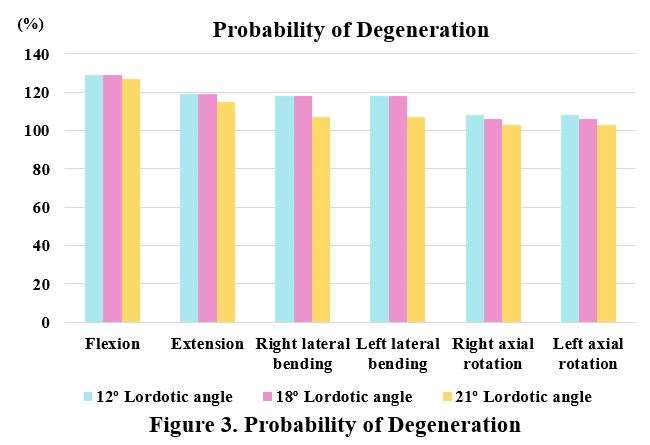
Figure 3#7779
Finite Element Model of Custom Flange Acetabular Components Provides Biomechanical Insight Into the Risks of Hip Joint Center Lateralization
*Haena-Young Lee - Hospital for Special Surgery - New York, USA
Friedrich Boettner - Hospital for Special Surgery - New York, USA
Jason Blevins - Hospital for Special Surgery - New York, USA
Jose Rodriguez - Hospital for Special Surgery - New York City, USA
Joseph Lipman - Hospital for Special Surgery - New York, USA
Fernando Quevedo Gonzalez - Hospital for Special Surgery - New York, USA
Mathais Bostrum - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
*Email: leeha@hss.edu
Introduction: Custom flange acetabular components (CFAC) are increasingly utilized to treat failed total hip arthroplasties (THA) with large acetabular defects. A design-related factor associated with clinical CFAC survivorship is the post-implantation position of the hip joint center; more lateralized centers correlate to higher aseptic loosening risk [1,2]. Our goal was to develop a computational finite element (FE) model to quantify how hip center location affects the strain distributions in the implant and surrounding pelvic bone and the micromotions between implant and bone.
Methods: We created a FE model using the preoperative CT scan of a 54-year-old female with standard pelvic bone geometry [2]. We modeled a defect type that commonly requires CFAC reconstruction – a superior-medial bone defect with bone loss in the anterior wall and acetabular rim. We then designed a patient-specific CFAC that lateralized the hip center 9.7 mm from the native acetabular center (Fig. 1). The CFAC was modeled as Ti6Al4V alloy with an elastic modulus (E) of 114 GPa and Poisson’s ratio of 0.33. We derived the non-homogeneous E of the bone from the Hounsfield units in the preoperative CT scan. We assumed line-to-line contact between CFAC and bone, with a friction coefficient of 0.6, and modeled the screws as perfect fixation without motion with the implant and bone. Based on a prior study, we applied the maximum hip contact force during gait at the center of the cup and the corresponding abductor muscle force along the superior region of the ilium [3]. We compared the bone strains against the fatigue strength of the bone (0.3% strain) [4] and the bone-implant micromotion against the threshold for a stable interface (20 µm) [5] under two configurations: the as-designed CFAC and the CFAC with an additional 10 mm of hip center lateralization.
Results: For both configurations, the area of bone with strains above the fatigue strength was concentrated at the proximal end of the ilial flange and around the iliac screws (Fig. 2). Lateralization of the hip center increased the areas of bone at risk of failure around the ilial flange by 50% (from 16% to 23%). For both configurations, the micromotion at the bone-implant interface was below the threshold for a stable interface.
Conclusion: Lateralization of the hip center from 9.7 mm to 19.7 mm increased regions of bone at risk of failure, in agreement with our previous clinical study, which reported higher survivorship of CFACs lateralized by ~10 mm compared to those lateralized by ~20 mm [2]. Future studies will investigate other important design variables (e.g., ischial flange length, bone-implant contact conditions, and screw geometries and contacts). This first FE study of CFAC implants establishes the utility of our modeling approach, an approach that we plan to use in developing a robust biomechanically-based classification system to guide treatment of acetabular bone defects.
References: [1] Barlow et al., J Arthroplasty 2016; [2] Jones et al., Bone Joint J 2019; [3] Bergmann et al., OrthoLoad.com, [4] Dendorfer et al., J Biomech 2008, [5] Jasty et al., JBJS 1997
Figures
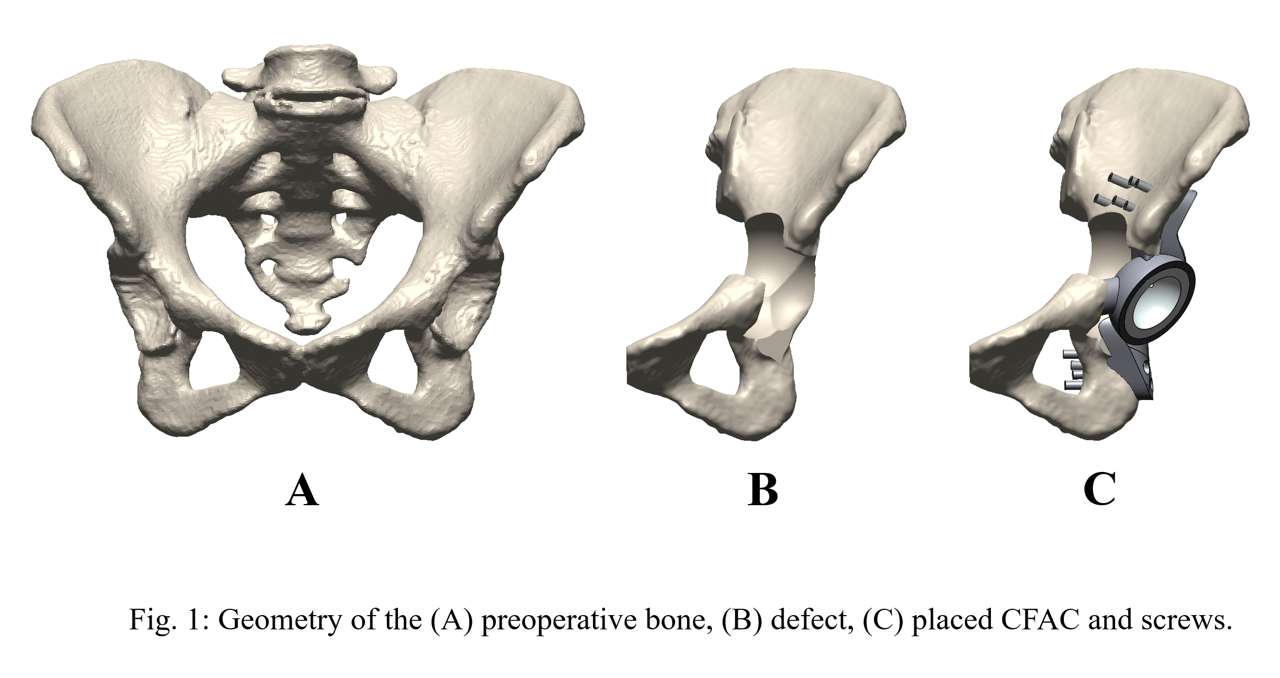
Figure 1
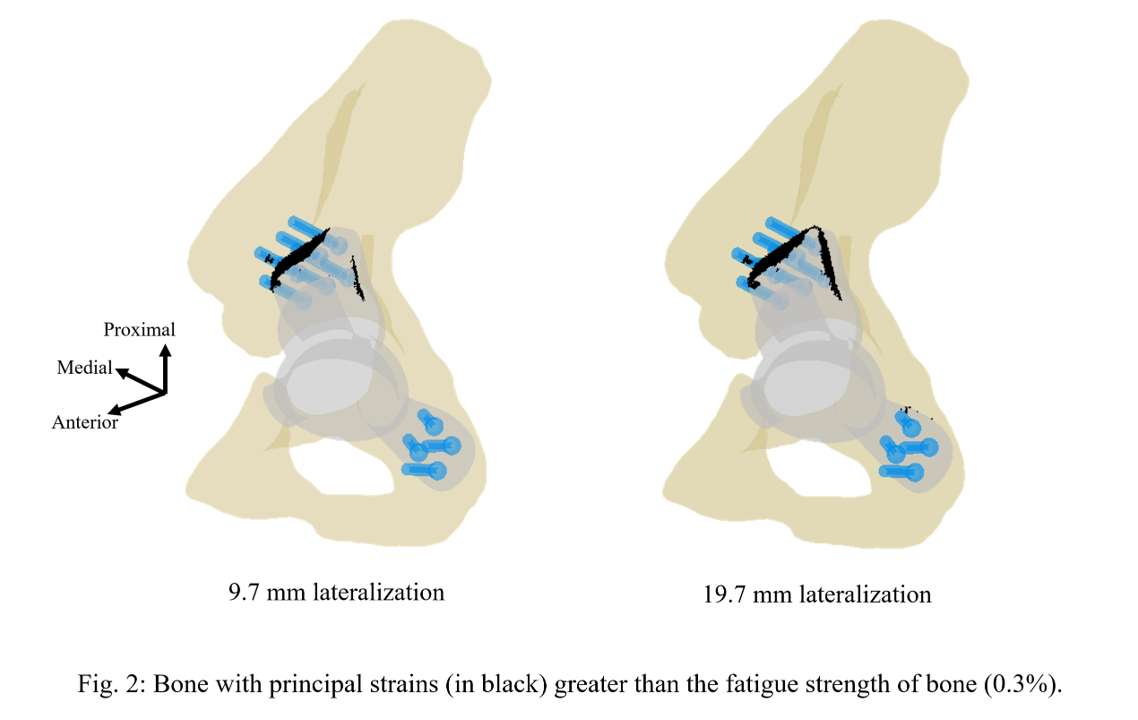
Figure 2
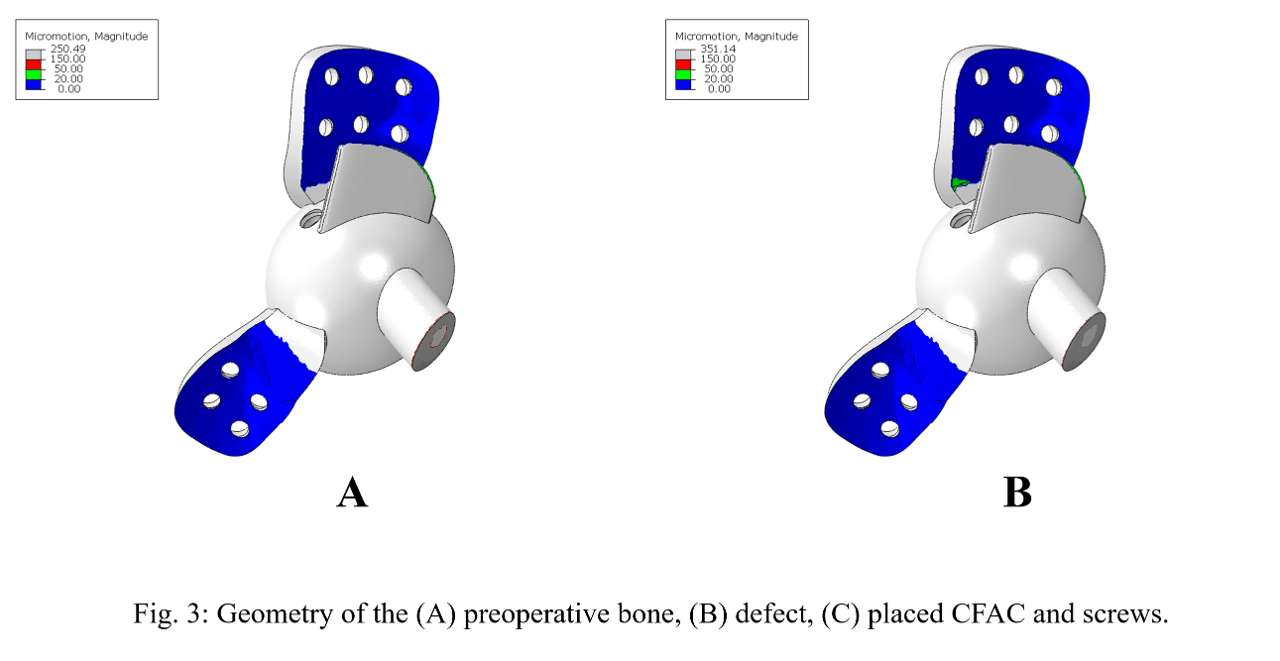
Figure 3#7903
A Finite Element Analysis of the Foot and Ankle to Predict Contact Pressure Changes at the Medial Ankle Joint After Supramalleolar Osteotomy With or Without Fibula Osteotomy
Jung-Min Lee - Inje University - Gimhae-si, South Korea
*Chul-Hyun Park - Yeungnam University Medical Center - Daegu, South Korea
Sung-Jae Lee - Inje Univ. - Gimhae, South Korea
Jeong-Jin Park - Yeungnam University Medical Center - Daegu, South Korea
*Email: chpark77@naver.com
Introduction
Supramalleolar osteotomy(SMO) is regarded as a representative surgical treatment for different medial ankle arthritis(MAA) types. However, controversies remain for the treatment effect, whether additional fibula osteotomy(FO) brings more effect on contact pressure reduction at the medial ankle joint. Thus, in this study, a finite element(FE) analysis was performed by constructing 3D FE models including MAA with or without varus tilting model and SMO with or without FO procedure model to predict contact pressure changes at the medial ankle cartilage.
Methods
The normal model was modified from the previous validated model by reconstructing the ankle cartilages including the talar dome and tibia plafond in 1mm thickness.
The normal model was consisted of bony, cartilages, and soft-tissue part those were meshed in 2mm. In addition, the passive soft-tissue for foot structure stabilization was constructed of the plantar fascia and ligaments applying ‘3D trust element(T3D2)’ with ‘non-compressive’ condition.
The pathological MAA models were determined by following the classification of MAA stage, MAA with medial translation for stage-3a, MAA with varus tilting(7.5°) for stage-3b. Based on the normal model, MAA with medial translation model was constructed by obliterating inter-surface of the medial talar and tibial cartilage without varus tilting. MAA with varus tilting was additionally applied by 7.5° varus tilting.
The post-operative models(isolated SMO and SMO combined with FO) were constructed by corresponding to each MAA model. In both procedures, the tibial osteotomy was performed 10mm opening tibial wedge and the bone allograft was inserted at corresponding osteotomized space. The graft was produced as 10mm wedge and applied bone material property. The interface of the osteotomized tibia and wedge was considered as bone union applying the ‘tie contact’ condition.
The FE analysis conditions were commonly applied. The boundary condition of ankle joint was defined as ‘sliding condition’ and applied 0.002 friction coefficient to realize lubricative property. Loading condition was assumed as a two-leg standing position and half of the subject body-weight(325N) was loaded on center of ground to vertical direction.
Contact pressure changes were predicted at the medial talar cartilage.
All of the 3D foot and ankle FE analysis was performed in Abaqus(v2021, Dassault System, France).
Results
Comparing between pathological and post-operated models, in MAA with medial translation, isolated SMO reduced pressure by 58.4% at the medial talar dome. However, SMO combined with FO showed pressure reduction over 20% at the medial talar dome. Moreover, in MAA with varus tiling, isolated SMO decreased pressure at the medial talar dome by 4.1%. SMO with combined FO indicated pressure reduction at the medial dome over 11%.
Discussion/Conclusion
In MAA with medial translation, isolated SMO could provide sufficient pressure reduction at the medial talar dome. However, in MAA with varus tilting, SMO combined with FO could appropriately relieve concentrated pressure at the medial talar dome.
Keywords
Supramalleolar osteotomy, Fibular osteotomy, Varus tilting arthritis, Medial translation arthritis, Finite element analysis
Figures
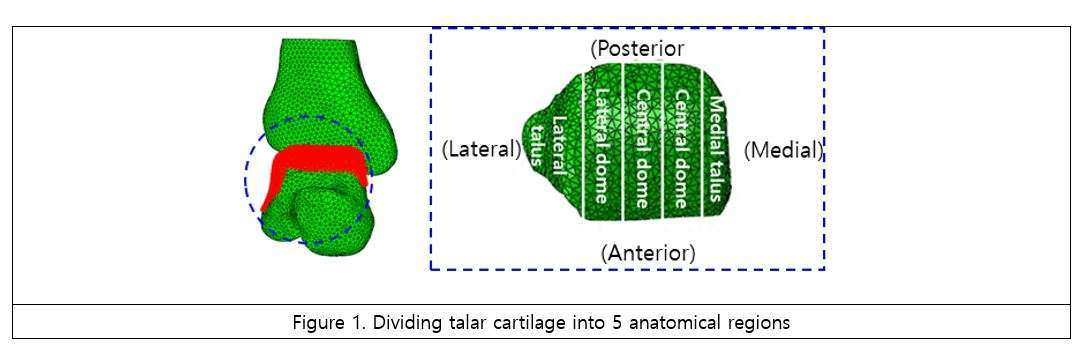
Figure 1
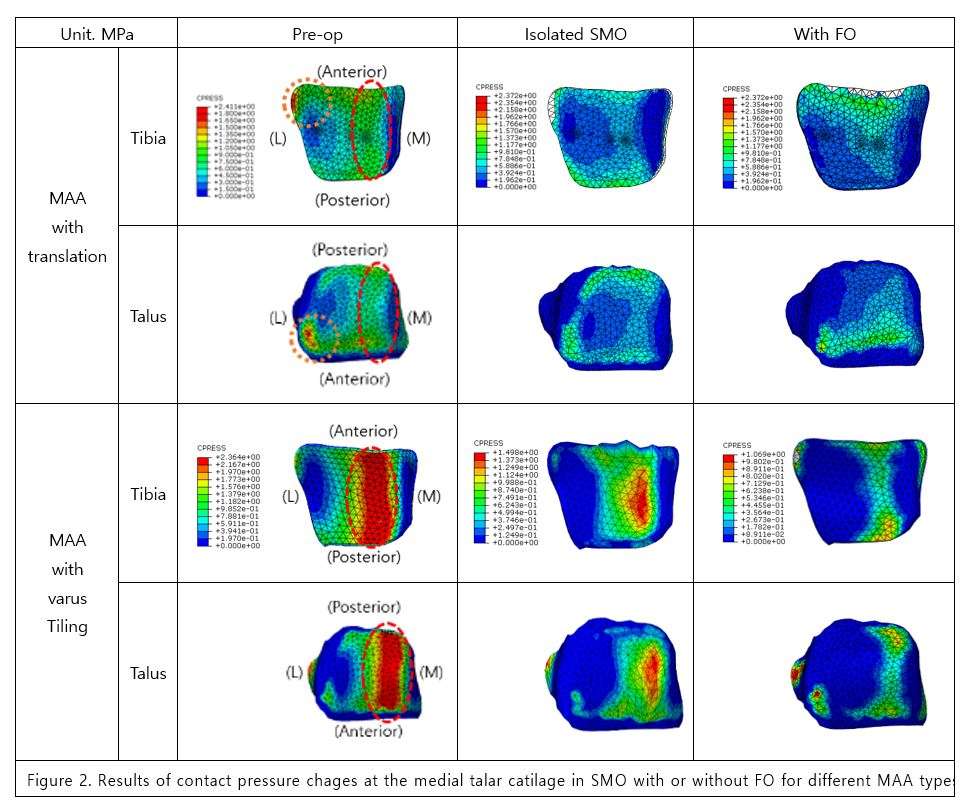
Figure 2
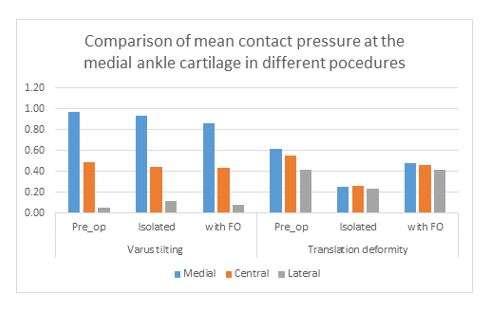
Figure 3#8009
Comparison of Survival Rates Between Total Knee Arthroplasty After a Previous Anterior Cruciate Ligament Reconstruction and Primary Total Knee Arthroplasty via Propensity Score Matching
Sun-Ho Lee - Chonnam National University Hospital - Gwangju, South Korea
*Jong-Keun Seon - Chonnam National University - Hwasun Gun, South Korea
*Email: seonbell@jnu.ac.kr
Abstract
Purpose: Although the survival rate of total knee arthroplasty (TKA) in patients treated with anterior
cruciate ligament reconstruction (ACLR) is not as favorable as that in patients treated with primary
TKA without ligament reconstruction, the exact survival rates and complications associated with these
procedures are still controversial. Therefore, the purpose of the current study was to compare the
revision rates of TKA in patients with knee osteoarthritis (OA) with a previous ACLR and those of
patients with primary TKA with no history of knee surgery by using propensity score matching analysis.
Methods: A list of patients who underwent TKA from January 1, 2008 to May 31, 2019 was obtained
from the Korean National Health Insurance database. Among these, 460 patients underwent TKA in a
knee with a previous ACLR and 569,766 patients who underwent primary TKA due to degenerative
OA. We performed propensity scoring matching to compare the revision rates including septic revision
due to prosthetic joint infection after TKA and perioperative complication rates within 90 days after
revision TKA between the two groups.
Results: Matched patients were assigned to one of the two groups (group A: 2,201 patients who
underwent TKA due to primary OA, group B: 448 patients who underwent TKA in a knee with a
previous ACLR) based on the propensity score. The total number of revisions per 1000 person-years
was significantly higher in group B than in group A (10.16 vs 4.66, respectively). Group B showed a
higher risk of revision than group A at 10 years post-TKA (hazard ratio: 2.49, 95% confidence interval:
1.30-4.77). However, group B showed a similar risk of septic revision as group A (p=0.44).
Perioperative complications within 90 days after TKA showed no significant differences between the
groups.
Conclusions: Surgeons should be aware of the relatively higher revision rate of TKA in patients who
had previously undergone an ACLR compared to that in patients who underwent primary TKA.
Level of Evidence: III (Retrospective cohort study)
#7337
Patellar Fracture After Total Knee Arthroplasty With Retention: A Retrospective Analysis of 2954 Consecutive Cases
Jongjin Lee - Asan Medical Center - Seoul, South Korea
Bum-Sik Lee - Asan Medical Center - Songpa-Gu, Korea (Republic of)
*Seong-Il Bin - Asan Medical Center, Ulsan University School of Medicine - seoul, South Korea
Jung-Su Choe - Cheju Halla General Hospital - Jeju, South Korea
Jong-Min Kim - University of Ulsan College of Medicine Asan Medical Center - Seoul, Korea (South)
*Email: sibin@amc.seoul.kr
BACKGROUND: To the best of our knowledge, there have been no large case studies on patellar fracture after total knee arthroplasty (TKA) with patella retention.
METHODS: From 2005 to 2019, 2954 consecutive TKAs with patella retention were retrospectively reviewed. The incidence of patellar fracture was confirmed. Perioperative demographic factors associated with patellar fracture were compared between the nonpatellar fracture control (randomly selected after age and sex matching) and patellar fracture patient groups. To confirm the prognosis of identified patellar fractures, Hospital for Special Surgery knee score, union rates, and complications after treatment were evaluated. Treatment outcomes were compared as per the treatment method, and fracture type was classified by shape(Fig 1).
RESULTS: For primary TKAs with patella retention, patellar fracture occurred in 32 of 2883 cases (incidence 1.11%). When c
omparing the preoperative demographic factors between the patellar fracture and control groups, there was a significant difference in knee flexion of the affected limb. Twenty-three cases were treated nonoperatively, and nine cases were treated operatively. Of the 32 patellar fractures, 28 had confirmed union, and the HSS score at the latest follow-up increased significantly from the preoperative score. The only complication noted after treatment was nonunion in three cases. We found no significant differences in treatment results as per the treatment method and fracture type.
CONCLUSION: Patellar fracture after TKA with retained patella is infrequent, with relatively improved clinicoradiological results over those of patellar fracture after TKA with resurfaced patella reported in the literature. The improved results did not differ as per the treatment method and fracture type.


#7339
Long-Term Survivorship of Contemporary Posterior-Stabilized Total Knee Prostheses in Asian Patients: A 20-Year Single-Surgeon Single-Implant Cohort Study
Jongjin Lee - Asan Medical Center - Seoul, South Korea
Bum-Sik Lee - Asan Medical Center - Songpa-Gu, Korea (Republic of)
*Seong-Il Bin - Asan Medical Center, Ulsan University School of Medicine - seoul, South Korea
Jong-Min Kim - University of Ulsan College of Medicine Asan Medical Center - Seoul, Korea (South)
Jung-Su Choe - Cheju Halla General Hospital - Jeju, South Korea
*Email: sibin@amc.seoul.kr
Purpose: (1) to assess the proportion of potential revision candidates who remained living at more than 20 years after primary TKAs; (2) to evaluate the implant longevity regarding mechanical failures such as aseptic loosening and polyethylene (PE) wear; and (3) to determine the risk factors for revision surgery in Asian populations.
Methods: We conducted this age-stratified survival analysis in a consecutive series of 368 NexGen Legacy Posterior Stabilized (LPS) TKAs performed by a single surgeon. These cases were divided into four age groups (<60 years, early 60s, late 60s, and ≥70 years). The patients’ survival in each age group and the implant longevity against aseptic mechanical failures was calculated using the Kaplan-Meier method. The revision surgery risk was evaluated using postoperative factors including a deep flexion capability(> 135°), and postoperative mechanical alignments.
Results: Death rates without implant revision were higher in the older group (6%, 27%, 50%, and 59% in each age group). The cumulative 20-year implant longevity was more than 95% in the two oldest groups, but less than 60% in the youngest group. Aseptic loosening was observed with an earlier onset (3.1 to 18.9 years) trend than PE wear (9.8 ~ 17.9 years), with most cases arising in the youngest groups. Flexion limitation and varus alignment were significant risks to aseptic loosening and PE wear.
Conclusion: A younger age (<60 years), inability of postoperative deep flexion, and varus alignment were significant risk factors for aseptic loosening and PE wear after modern PS design in this Asian cohort.
Table 1. Revision surgeries for the indicated reasons in each age group during the study period
|
|
No. of Knees
|
Revision for each reason(n)
|
|
Prosthetic joint infection
|
Aseptic Loosening
|
Polyethylene wear
|
Traumatic
|
|
Age Group
|
< 60y
|
52
|
0
|
9
|
6
|
2
|
|
early 60s
|
102
|
1
|
6
|
1
|
1
|
|
late 60s
|
110
|
1
|
0
|
0
|
2
|
|
≥70y
|
104
|
0
|
3
|
0
|
1
|
|
Total
|
|
368
|
2
|
18
|
7
|
6
|
Table2. Revision surgeries due to the indicated mechanical issues stratified by the postoperative flexion arc and alignment.
|
|
No. of Knees
|
Revision for each reason(n)
|
|
Prosthetic joint infection
|
Aseptic Loosening
|
Polyethylene wear
|
Trauma
|
|
Flexion arc
|
< 135°
|
214
|
2
|
16
|
6
|
5
|
|
≥ 135°
|
154
|
0
|
2
|
1
|
1
|
|
Postoperative Alignment
|
Valgus (< -3)
|
22
|
0
|
0
|
0
|
0
|
|
Neutral (-3~3)
|
233
|
1
|
6
|
2
|
3
|
|
Varus (> 3)
|
113
|
1
|
12
|
5
|
3
|
|
Total
|
|
368
|
2
|
18
|
7
|
6
|
Figures
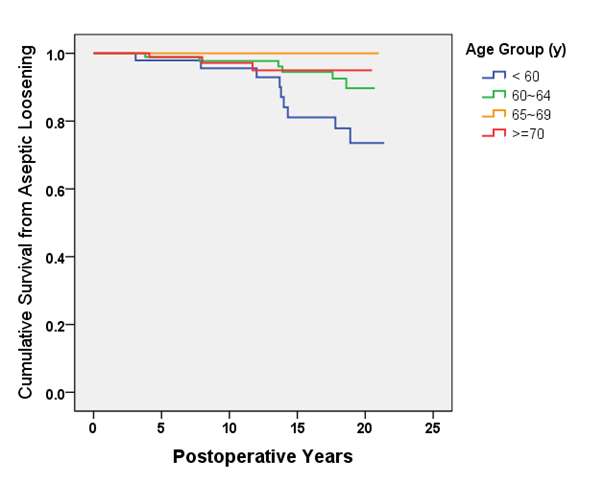
Figure 1
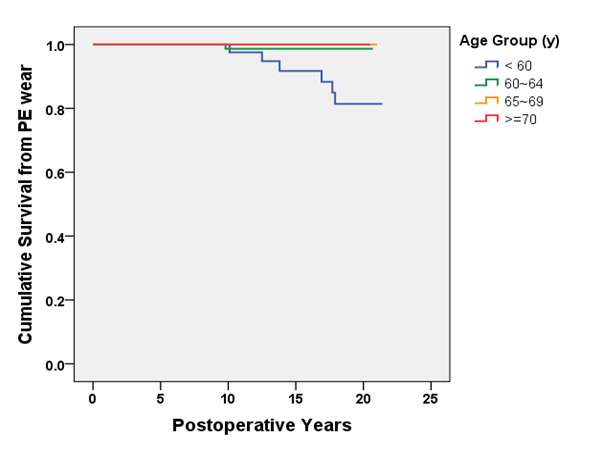
Figure 2
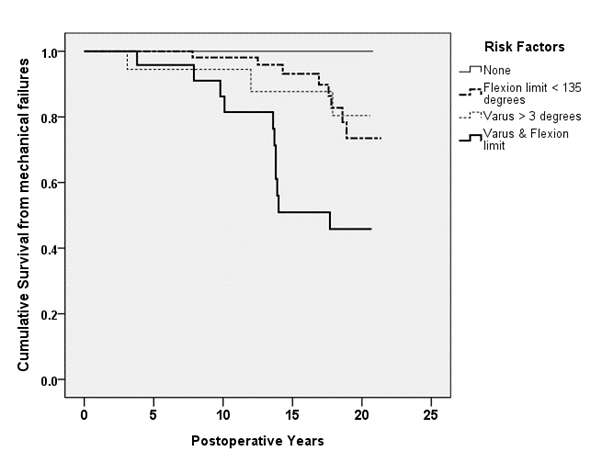
Figure 3#7281
Impact of Chronic Obstructive Pulmonary Disease on Outcomes After Total Joint Arthroplasty: A Meta-Analysis and Systematic Review
*Kyun-Ho Shin - Nanoori Hospital Incheon - Incheon, South Korea
Seung-Beom Han - Korea University Medical center - Seoul, South Korea
Joonsuk Lee - Korea University Anam Hospital - Seoul, Korea (Republic of)
*Email: kyunho.shin@gmail.com
Background
Comorbid chronic obstructive pulmonary disease (COPD) is increasingly common and may have an adverse impact on outcomes in patients undergoing total joint arthroplasty (TJA) of lower extremity. The purpose of this meta-analysis is to compare the postoperative complications between COPD and non-COPD patients undergoing primary TJA including total hip and knee arthroplasty.
Methods
PubMed, Embase, and Cochrane Library were systematically searched for relevant studies published before December 2021. Postoperative outcomes were compared between patients with COPD versus those without COPD as controls. The outcomes were mortality, re-admission, pulmonary, cardiac, renal, thromboembolic complications, surgical site infection (SSI), periprosthetic joint infection (PJI), and sepsis.
Results
Figure 1 summarizes the details of the study identification and selection process. The quality assessment results for the included studies are shown in Fig 2. All the included studies were considered low-risk in terms of overall risk of bias. A total of 1,002,779 patients from nine studies were finally included in this meta-analysis. Patients with COPD had an increased risk of mortality (OR [odds ratio] = 1.69, 95% confidence interval [CI] 1.42–2.02), re-admission (OR = 1.54, 95% CI 1.38–1.71), pulmonary complications (OR = 2.13, 95% CI 1.75–2.59), cardiac complications (OR = 1.40, 95% CI 1.15–1.69), thromboembolic complications (OR = 1.19, 95% CI 1.03–1.37), renal complications (OR = 1.41, 95% CI 1.04–1.90), SSI (OR = 1.23, 95% CI 1.18–1.30), PJI (OR = 1.26, 95% CI 1.15–1.38), and sepsis (OR = 1.36, 95% CI 1.22–1.52).
Conclusion
Patients with comorbid COPD showed an increased risk of mortality and postoperative complications following TJA compared with patients without COPD. Therefore, orthopedic surgeons can use the study to adequately educate these potential complications when obtaining informed consent. Furthermore, preoperative evaluation and medical optimization are crucial to minimizing postoperative complications from arising in this difficult-to-treat population.
Figures
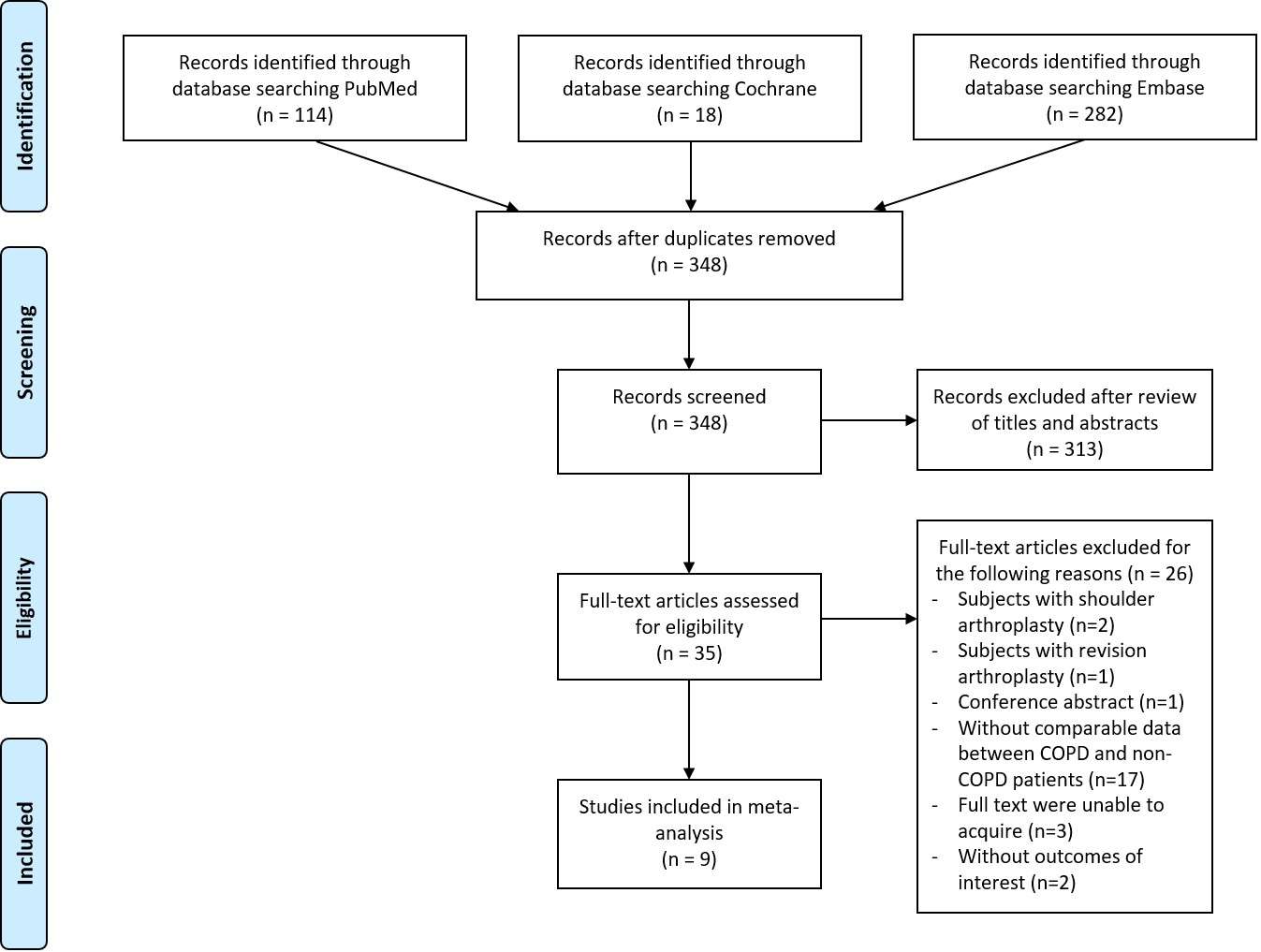
Figure 1
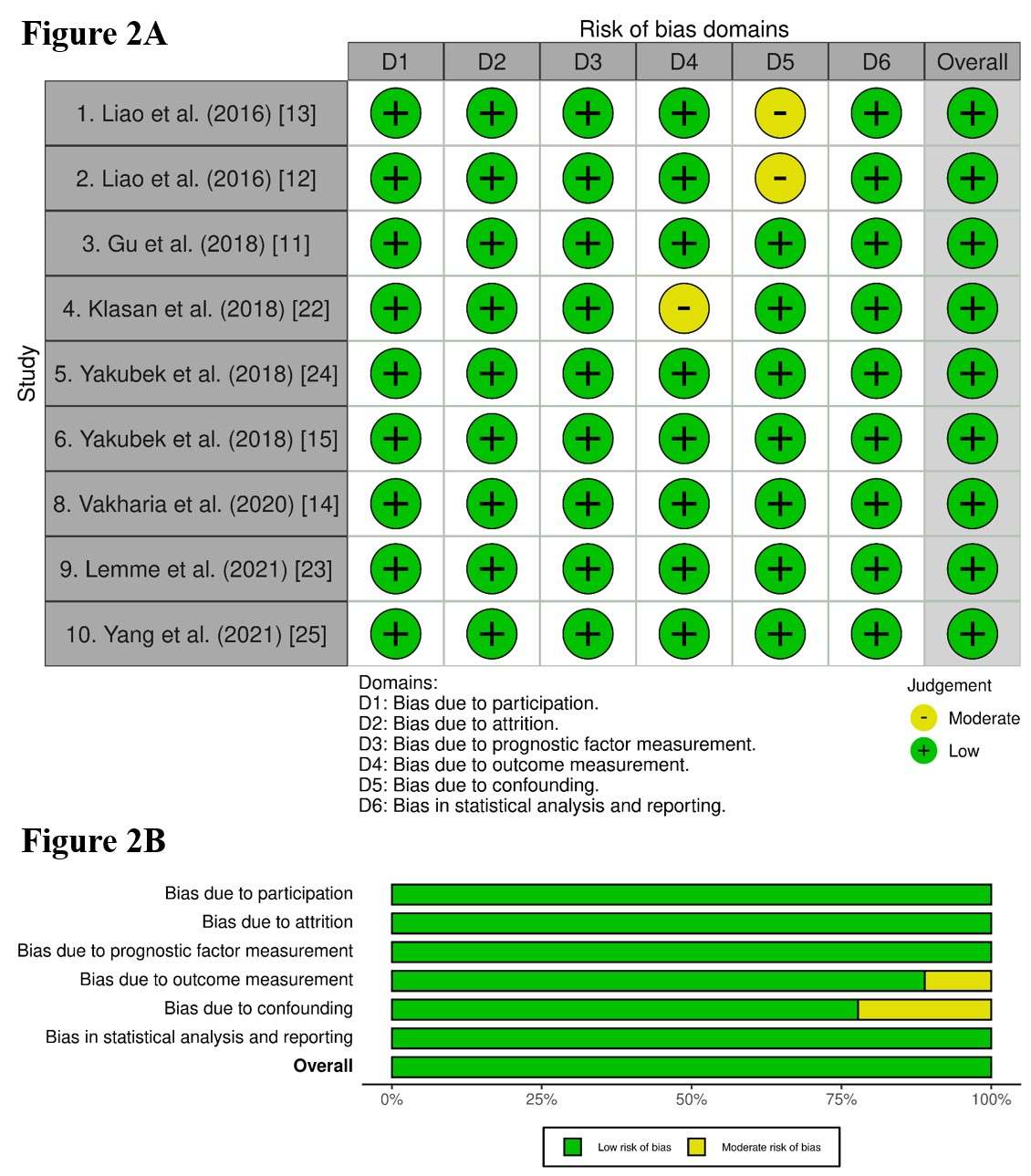
Figure 2#7711
TKA Implant Placement Affects Quadriceps Mechanism Efficiency
*Nathan Lenz - Smith & Nephew - Memphis, USA
Brian Chalmers - Hospital for Special Surgery - New York CIty, USA
Paola Jimenez - Smith & Nephew Inc. - Memphis, United States of America
steven haas - Hospital for Special Surgery - New York, United States of America
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: nathan.lenz@smith-nephew.com
Introduction:
Anterior knee pain is one common complication following total knee arthroplasty (TKA). Increased quadriceps force after TKA is a potential cause of anterior knee pain as surgical techniques attempt to restore or improve the pre-operative muscle function through varying the implant positions and thicknesses. One thought is quadriceps muscle function can be improved by increasing the moment arm of the quadriceps tendon through increasing the distance between the knee flexion axis and the quadriceps through implant positioning or design. This study investigates the relationship between the effective quadriceps mechanism moment arm and relevant femur, tibia, and patella positioning variables.
Methods:
A computational analysis was performed simulating knee flexion 0-120° of a PS TKA using previously validated software (LifeMOD/KneeSIM; LifeModeler Inc.) that includes MCL, LCL, popliteal-fibular ligament, iliotibial band, iliopatellar band, and medial retinaculum. A five-factor, ½ fraction central composite response surface DOE was performed (Design-Expert 13, Stat-Ease Inc.) varying implant positions from restoring native thicknesses: femur anterior-posterior (AP) 0±2mm, femur superior-inferior (SI) 0±2mm, femur flexion 2°±2°, tibia superior-inferior (SI) 0±2mm, and patella thickness 0±2mm. The quadriceps mechanism moment arm was calculated as the weighted average knee extension moment arm of the forces of the quadriceps muscle, quadriceps tendon wrapping contact, patellofemoral contact, patellar tendon wrapping contact, and patellar tendon force (Figure 1). Linear regression coefficients for implant position variables were calculated for every 10° knee flexion with the DOE software.
Results:
The quadriceps muscle and patellar tendon forces generate extension moments while the quadriceps tendon, patellofemoral, and patellar tendon contact forces generate flexion moments (Figure 1). The quadriceps mechanism moment arm generally decreases with knee flexion and is more affected by implant placement for <90° knee flexion (Figure 2). Positioning the femur more posterior and superior, the tibia more inferior, and decreasing patella thickness increased the quadriceps mechanism moment arm while femur flexion had little effect (Figure 3). The effect of femur AP position decreases with flexion while effect of femur SI, tibia SI, and patella thickness peaks around 20° flexion. Positioning the femur more superior and decreasing patella thickness decreased the quadriceps muscle moment arm, but they also decreased the patella contact force, which reduced the flexion moment effect of the patella contact resulting in an overall increase in quadriceps mechanism efficiency.
Conclusion:
Implant positioning that increases the moment arm of the quadriceps muscle force results in a reduction of overall quadriceps efficiency because it increases patellofemoral contact force and the resulting knee flexion moment due to increased tension on the retinaculum. This contradicts traditional thinking that increasing patella offset from the femur results in improved quadriceps muscle function.
Figures
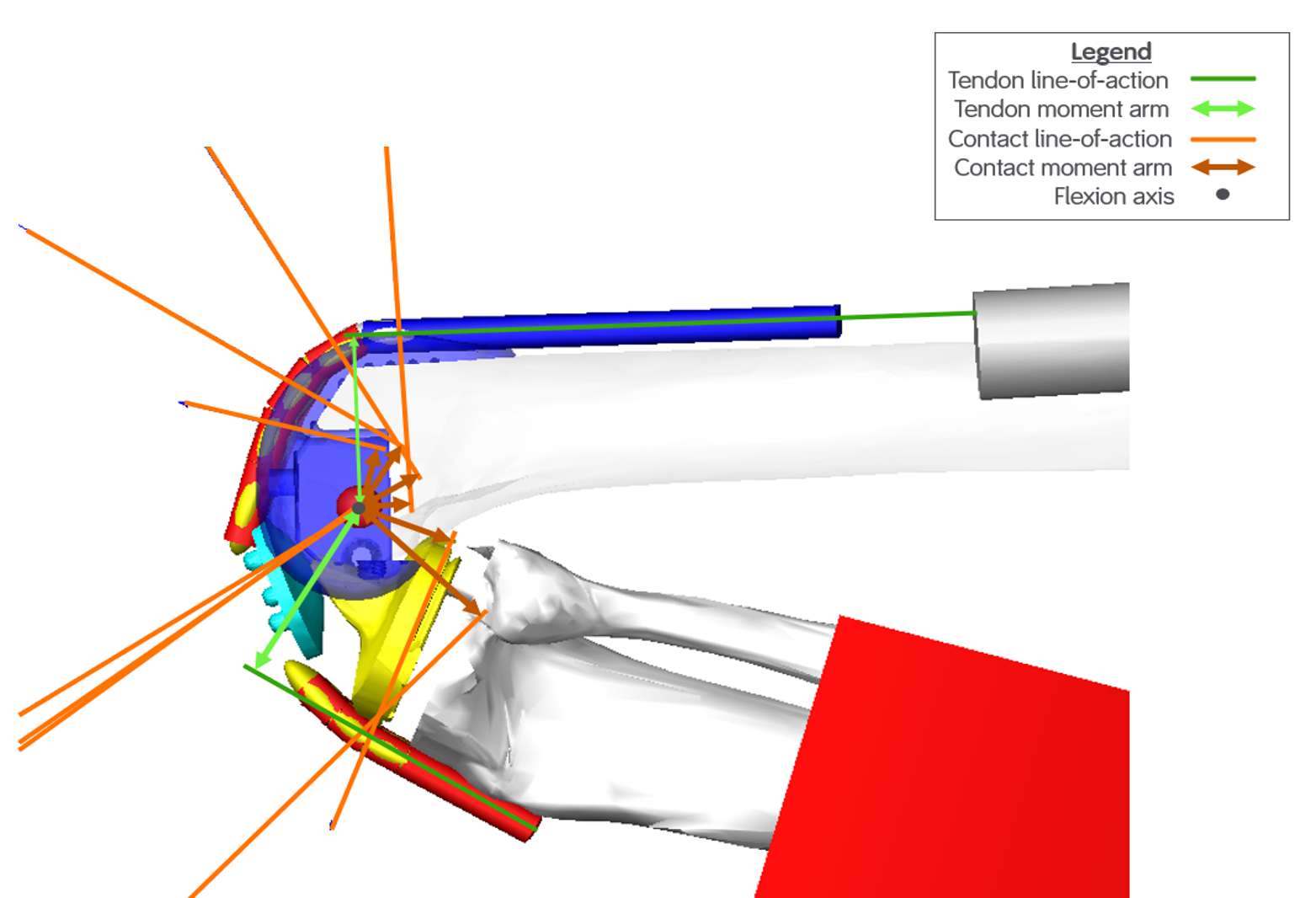
Figure 1
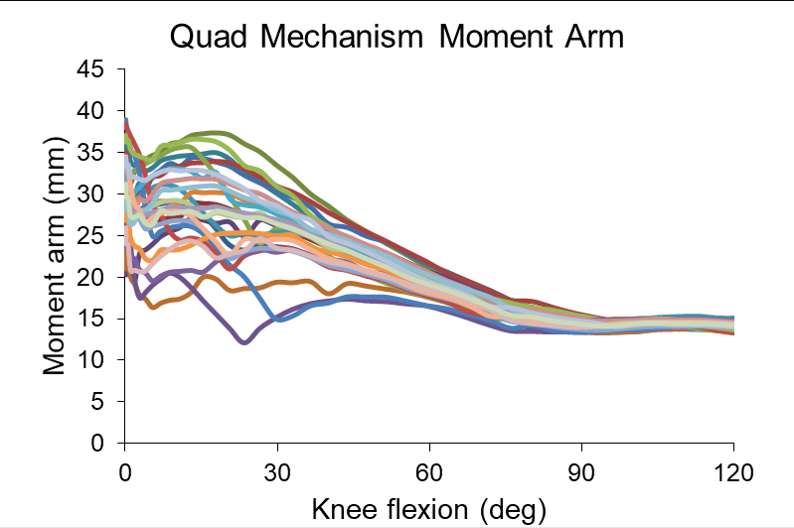
Figure 2
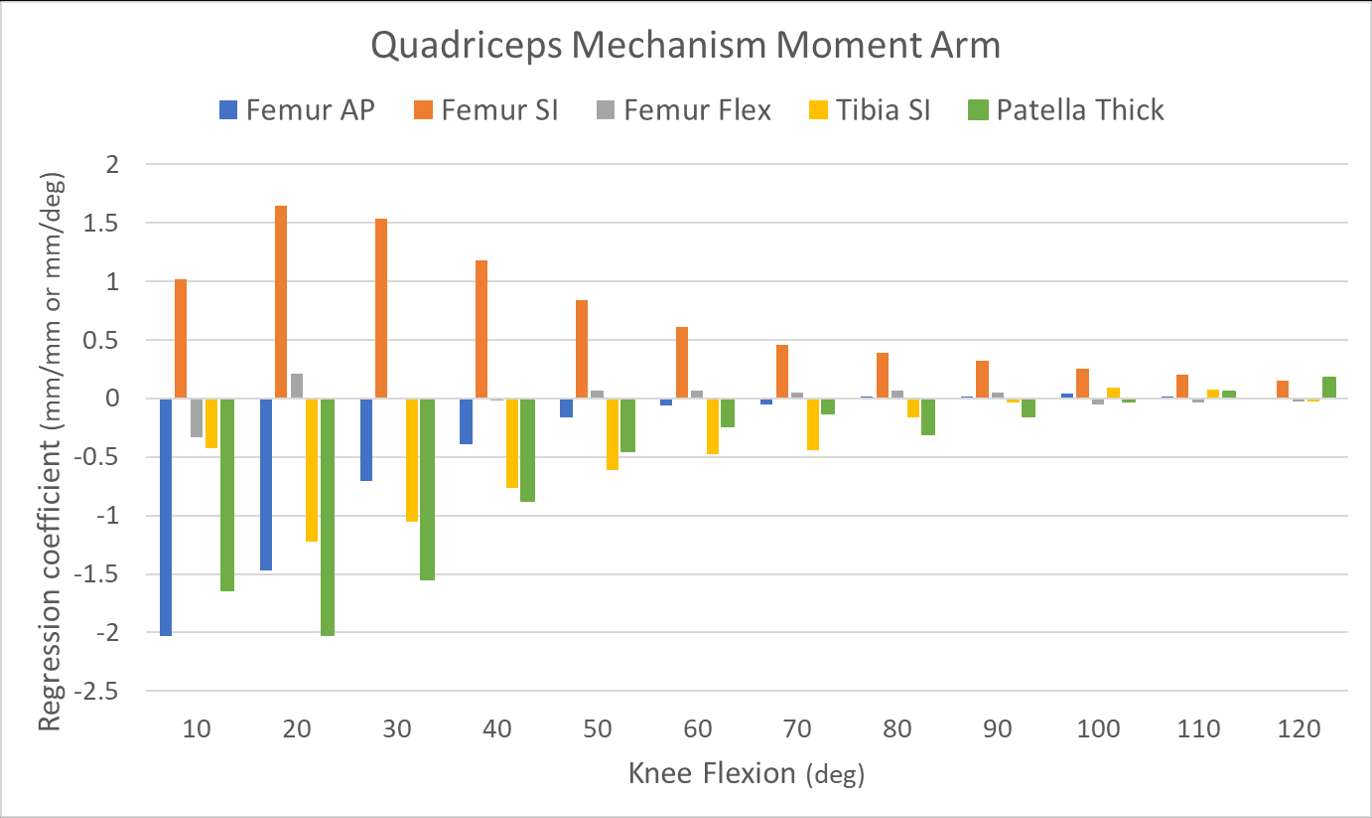
Figure 3#7818
TKA Implantation Effects on Quadriceps Length
*Nathan Lenz - Smith & Nephew - Memphis, USA
Richard D. Komitek - University of Tennessee - Knoxville, USA
Brian McKinnon - Smith & Nephew - Cordova, USA
*Email: nathan.lenz@smith-nephew.com
Introduction:
It has been reported that active weight bearing flexion is less than and better correlates to functional outcomes after total knee arthroplasty (TKA) than passive flexion1. It’s unknown what limits active flexion in TKA patients. One potential cause is the quadriceps muscle is lengthened to its maximum physiological limit and therefore is unable to generate the necessary force to continue active flexion due to implant positioning or design. Sagittal plane TKA implant malpositioning that changes femur anterior-posterior (AP), femur superior-inferior (SI), femur flexion, and tibia SI positions or changes patella thickness have the potential to influence quadriceps length. The effects of these variables on quadriceps length were studied in a computer simulated knee rig, which provides a controlled environment to isolate the effects of these factors.
Methods:
A computational model simulating a knee test rig (LifeMOD/KneeSIM; LifeModeler Inc.) analyzed a PS TKA flexing 0-120°. A five-factor, ½ fraction central composite response surface DOE was performed (Design-Expert 13, Stat-Ease Inc.) varying implant positions from restoring native thicknesses: femur anterior-posterior (AP) 0±2mm, femur superior-inferior (SI) 0±2mm, femur flexion 2°±2°, tibia superior-inferior (SI) 0±2mm, and patella thickness 0±2mm. The quadriceps length throughout flexion was recorded. Linear regression coefficients for implant position variables were calculated for quadriceps length for every 10° knee flexion with the DOE software.
Results:
Quadriceps length increased with progressive knee flexion and had a consistent range between the simulations of the DOE across the flexion range (Figure 1). The quadriceps was lengthened by positioning the femur inferior, the tibia superior, and increasing the patella thickness while femur AP position and femur flexion had little effect on quadriceps length (Figure 2). The effect of femur SI is relatively consistent at 1mm of femur inferior shift correlating to a 1mm increase in quadriceps length throughout flexion, the effect of tibia SI decreases from greater than 1mm increase in quadriceps length per 1mm superior shift to as low as 0.5mm, and the effect of patella thickness increases from less than 0.4mm increase in quadriceps length per 1mm thickness increase to 0.8-1mm in beyond 70° flexion. In lower flexion angles femur SI and tibia SI have nearly equal and opposite effects. In higher flexion angles where active knee flexion may be limited patella thickness, femur SI has a larger effect than tibia SI while patella thickness has also become a significant effect.
Conclusion:
Given the relative effects of femur SI and tibia SI, quadriceps length isn’t affected by tibiofemoral joint line changes at low flexion angles as long as the joint space is not changed. As flexion increases lowering the joint line increases quadriceps length due to femur SI having a larger effect than tibia SI. Any change that tightens the extension gap lengthens the quadriceps throughout flexion. Similarly, increasing patella thickness has a strong correlation to lengthening the quadriceps in mid-to-high knee flexion.
References:
- Song YD, et al. Active Flexion in Weight Bearing Better Correlates with Functional Outcomes of Total Knee Arthroplasty than Passive Flexion. Knee Surg Relat Res. 2016 Jun;28(2):118-29.
Figures
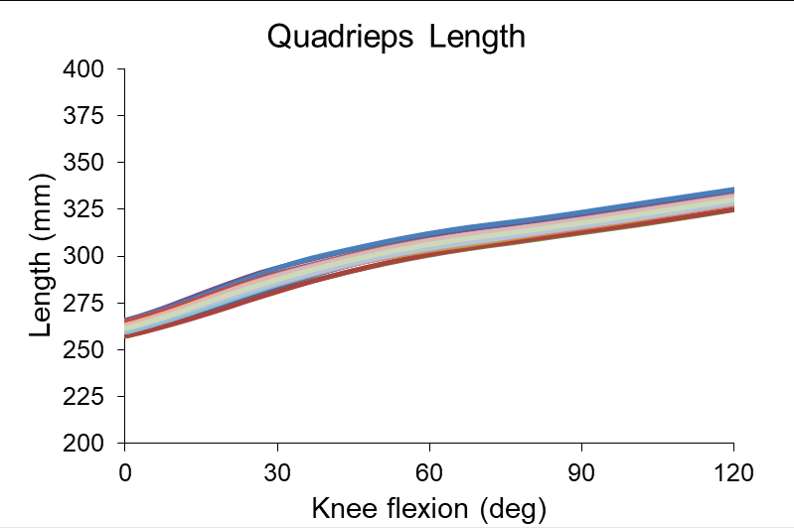
Figure 1
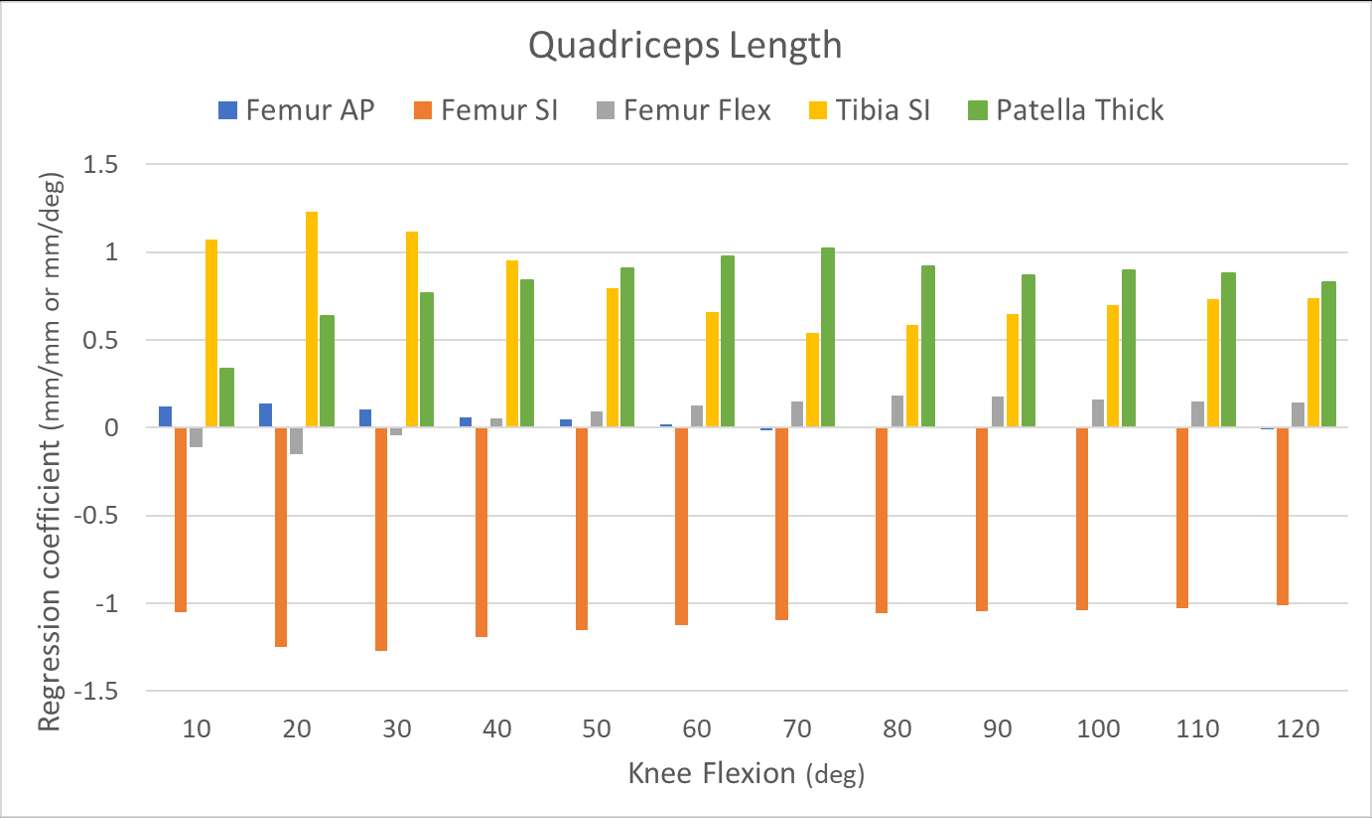
Figure 2#7691
Utilization and Outcomes of Total Hip and Knee Arthroplasty in the Canadian Immigrant Population
Johnathan Lex - University of Toronto - Toronto, Canada
Daniel Pincus - University of Toronto - Toronto, Canada
Michael Paterson - Institute for Clinical Evaluative Sciences - Toronto, Canada
Harman Chaudhry - University of Toronto - Toronto, Canada
Rob Fowler - University of Toronto - Toronto, Canada
Gillian Hawker - University of Toronto - Toronto, Canada
*Bheeshma Ravi - University of Toronto - Toronto, Canada
*Email: bheeshma.ravi@utoronto.ca
Background:
Immigrated Canadians make up approximately 20% of the total population in Canada, and 30% of the population in Ontario. Despite universal health coverage and an equal prevalence of severe arthritis in immigrants relative to non-immigrants, the former may be underrepresented amongst arthroplasty recipients secondary to challenges navigating the healthcare system. The primary aim of this study was to determine if utilization of arthroplasty differs between immigrant populations and persons born in Canada. The secondary aim was to determine differences in outcomes following total hip and knee arthroplasty (THA and TKA, respectively).
Methods:
This is a retrospective population-based cohort study using health administrative databases. All patients aged ≥18 in Ontario who underwent their first primary elective THA or TKA between 2002 and 2016 were identified. Immigration status for each patient was identified via linkage to the ‘Immigration, Refugee and Citizenship Canada’ database. Outcomes included all-cause and septic revision surgery within 12-months, dislocation (for THA) and total post-operative case cost and were compared between groups. Cochrane-Armitage Test for Trend was utilized to determine if the uptake of arthroplasty by immigrants changed over time.
Results:
There was a total of 186,528 TKA recipients and 116,472 THA recipients identified over the study period. Of these, 10,193 (5.5%) and 3,165 (2.7%) were immigrants, respectively. The largest proportion of immigrants were from the Asia and Pacific region for those undergoing TKA (54.0%) and Europe for THA recipients (53.4%). There was no difference in the rate of all-cause revision or septic revision at 12 months between groups undergoing TKA (p=0.864, p=0.585) or THA (p=0.527, p=0.397), respectively. There was also no difference in the rate of dislocations between immigrants and people born in Canada (p=0.765, respectively).
Conclusion:
Despite having similar complication rates and costs, immigrants represent a significantly smaller proportion of joint replacement recipients than they represent in the general population in Ontario. These results suggest significant underutilization of surgical management for arthritis among Canada’s immigrant populations. Initiatives to improve access to total joint arthroplasty are warranted.
#7695
MRI Use Leading Up to Total Knee Arthroplasty: A Retrospective Cohort Study
Johnathan Lex - University of Toronto - Toronto, Canada
*Tiffany Lung - University of Toronto - Toronto, Canada
Daniel Pincus - University of Toronto - Toronto, Canada
Suriya Aktar - Institute for Clinical Evaluative Sciences - Toronto, Canada
David Wasserstein - University of Toronto - Toronto, Canada
Michael Paterson - Institute for Clinical Evaluative Sciences - Toronto, Canada
Bheeshma Ravi - University of Toronto - Toronto, Canada
*Email: t.lung@mail.utoronto.ca
Introduction:
Demand for total knee arthroplasty (TKA) is increasing as it remains the gold-standard treatment for end-stage osteoarthritis (OA) of the knee. While magnetic-resonance imaging (MRI) scans of the knee are not indicated for diagnosing knee OA, they are commonly ordered prior to the referral to an orthopaedic surgeon. The purpose of this study was to determine the proportion of patients who underwent an MRI in the two years prior to their primary TKA for OA. Secondary outcomes included determining patient and physician associations with increased MRI usage.
Method:
This is a population-based cohort study using billing codes in Ontario, Canada. All patients over 40 years-old who underwent a primary TKA between April 1, 2008 and March 31, 2017 were included. Statistical analyses were performed using SAS and included the Cochran-Armitage test for trend of MRI prior to surgery, and predictive multivariable regression model. Significance was set to p<0.05.
Results:
There were 172,689 eligible first-time TKA recipients, of which 34,140 (19.8%) received an MRI in the two years prior to their surgery. The majority of these (70.8%) were ordered by primary care physicians, followed by orthopaedic surgeons (22.5%). Patients who received an MRI were younger and had fewer comorbidities than patients who did not (p<0.001). MRI use prior to TKA increased from 15.9% in 2008 to 20.1% in 2017 (p<0.0001). Reduction of unnecessary MRIs prior to patients undergoing TKA in Ontario by 33.3% or 66.7% (overall 13% or 6.5% of patients receiving an MRI prior to TKA, respectively) would represent a yearly savings of CA$946,121 to CA$1,895,084 per year.
Conclusion:
Despite MRIs rarely being indicated for the work-up of knee OA, nearly one in five patients have an MRI in the two years prior to their TKA. Reducing the use of this prior to TKA may help reduce wait-times for surgery.
#7727
Machine Learning Prediction and Optimization Improves Elective Orthopaedic Surgery Scheduling
*Johnathan Lex - University of Toronto - Toronto, Canada
Jacob Mosseri - University of Toronto - Toronto, Canada
Aazad Abbas - University of Toronto - Toronto, Canada
Jay Toor - University of Toronto - Toronto, Canada
Cari Whyne - University of Toronto - Toronto, Canada
Elias Khalil - University of Toronto - Toronto, Canada
Bheeshma Ravi - University of Toronto - Toronto, Canada
*Email: johnathanlex@gmail.com
Introduction:
Total knee and hip arthroplasty (TKA and THA) are the most commonly performed surgical procedures, the costs of which constitute a significant healthcare burden. Improving access to care for THA/TKA requires better efficiency. It is hypothesized that this may be possible through a two-stage approach that utilizes prediction of surgical time to enable optimization of operating room (OR) schedules.
Methods:
Data from 499,432 elective unilateral arthroplasty procedures, including 302,490 TKAs, and 196,942 THAs, performed from 2014-2019 was extracted from the American College of Surgeons (ACS) National Surgical and Quality Improvement (NSQIP) database. A deep multilayer perceptron model was trained to predict duration of surgery (DOS) based on pre-operative clinical and biochemical patient factors. A two-stage approach, utilizing predicted DOS from a held out “test” dataset, was utilized to inform the daily OR schedule. The objective function of the optimization was the total OR utilization, with a penalty for overtime. The scheduling problem and constraints were simulated based on a high-volume elective arthroplasty centre in Canada. This approach was compared to current patient scheduling based on mean procedure DOS. Approaches were compared by performing 1000 simulated OR schedules.
Results:
The predict then optimize approach achieved a 3% increase in OR utilization over the mean regressor, which equates to a reduction in 403 minutes of OR underutilization over five days across five ORs. The two-stage approach reduced overtime by 21-minutes per OR day, however it created a 5-minute increase in underutilization. Better objective value was seen in 93.4% of the simulations.
Conclusions:
With deep learning prediction and mathematical optimization of patient scheduling it is possible to improve overall OR utilization compared to typical scheduling practices. Maximizing utilization of existing healthcare resources can, in limited resource environments, improve patient’s access to arthritis care by increasing patient throughput, reducing surgical wait times and in the immediate future, help clear the backlog associated with the COVID-19 pandemic.
#7456
Physiological Axial Tibial Rotation of the Knee During a Weightbearing Flexion
*Guoan Li - Orthopaedic Bioengineering Research Center, Newton-Wellesley Hospital - Newton, USA
*Email: GLI1@partners.org.edu
Introduction
Axial tibial rotation is recognized as a characteristic motion of the knee, but, it is controversial on how it occurs with knee flexion. We investigated the mechanisms of axial tibial rotations of human knees during a weightbearing flexion using a previously validated dual fluoroscopic imaging system.
Methods
Twenty normal human knees were investigated using a combined MRI and dual fluoroscopic imaging system. Each subject performed a weightbearing single legged lunge. Tibiofemoral articular contact motions were analyzed at flexion intervals of 15° from 0° to 120°. Articular contact distances on femoral condyles and tibial surfaces and the axial tibial rotations due to both articulations were compared.
Results
The data showed that articular contact distances were longer on femoral condyles than on tibial surfaces at all flexion intervals (p<0.05). The internal tibial rotation was 6.8±4.5° at the flexion interval of 0°-15°, where 6.1±2.6° was due to articulations on femoral condyles and 0.7±5.1° due to tibial surface articulations (p<0.05). The axial tibial rotations due to articulations on femoral condyles are significantly larger than those on tibial surfaces until 60° of flexion (p<0.05). Minimal additional axial tibial rotations were observed beyond 60° of flexion.
Conclusion
The data indicated that axial tibial rotations of the knee were mainly attributed to articulations on femoral condyles than on tibial surfaces. The fact that the articular distance on medial femoral condyle is longer than on lateral condyle indicated that the axial tibial rotation is with respect to a rotation center at the lateral side of the knee. These data can provide new insights into the understanding of mechanisms of axial tibial rotation of the knee.
Keywords: Knee kinematics, Axial knee rotation, Internal tibial rotation, Medial pivoting,Lateral pivoting,Articular contact motion
#7545
One and Two Year Results of a Novel Ceramic on Ceramic Hip Resurfacing Implant in Australia
*David Lin - Sydney Orthopaedic Group - North Sydney, Australia
Joshua Xu - Royal North Shore Hospital - St Leonards, Australia
Patrick Weinrauch - Brisbane Hip Clinic - Brisbane, Australia
Piers Yates - University of Western Australia - Perth, Australia
David Young - Melbourne Orthopaedic Group - Melbourne, Australia
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: david.lin1@nhs.net
Introduction:
Hip Resurfacing Arthroplasty (HRA) is a bone conserving option to Total Hip Arthroplasty (THA) suitable for young patients with intrinsically higher physical and athletic demands. [1] Certain poorly designed , poorly implanted Metal on Metal HRA suffered early failures and unacceptably high revision rates. Ceramic on Ceramic (CoC) bearings have performed well in THA over a 20 year period [2] but have not previously been used extensively in HRA. We present the early 1 and 2 year clinical and radiographical follow-up of a novel CoC HRA (ReCerf, MatOrtho Surrey, UK) in a multi-centric Australian cohort.
Methods:
All Australian patients undergoing ReCerf HRA between the September 2018 and April 2021 were included in this prospective cohort. Patient-reported outcome measures (PROMS) in the form of the Forgotten Joint Score (FJS), HOOS Jr, WOMAC
(Pain, Stiffness and Physical Function), Oxford Hip Score (OHS) and UCLA Activity Score were collected preoperatively and at 1- and 2-years post-operation. Serial radiographs were assessed for migration, component alignment and evidence of osteolysis/ loosening. All complications over the follow up period were reported.
Results:
There were 209 patients identified of which 106 reached 2-year follow-up. Of these, 187 completed PROMS at 1 year and 90 at 2 years. There was significant improvement in HOOS Jr (49.6 v 91.0 v 91.5, p< 0.001) and OHS (22.0 v 44.8 v 44.9, p< 0.001) between the pre-operative, 1 year and 2 years outcomes. Patients also reported improved pain (9.6 v 1.0 v 1.0, p<0.001 ), function (33.2 v 4.2 v 4.0, p<0.001) and reduced stiffness (4.8 v 1.0 v 0.9, p<0.001) as measured by the WOMAC score. Patients had improved UCLA Activity Scores (4.9 v 7.7 v 8.0, P<0.001) with 53% reporting return to impact activity at 2 years . FJS at 1 and 2 years were not significantly different (80.1 v 82.7, p =0.38). There was no migration, osteolysis or loosening of any of the implants. The mean cup inclination angle was 41.3 degrees and the femoral component shaft angle was 137 degrees.
There was 1 early femoral neck fracture requiring conversion to THA, 1 sciatic nerve palsy and 1 deep infection that resolved on washout and antibiotics.
Conclusions:
The results of CoC resurfacing at 2 years post-operation are promising with satisfactory outcomes in all recorded PROMS. Early return to impact activities was noted in more than half our patients at 2 years. No clinical or radiological complications related to the implant were noted. Longer term follow up with increased patient numbers are required to restore surgeon confidence in HRA and expand the use of this novel product.
References
1. Girard J Hip Resurfacing: International Perspectives. HSS J 2017 Feb;13(1):7-11
2. Vendittoli, P.A., et al., Ceramic-on-ceramic total hip arthroplasty is superior to metal-on-conventional polyethylene at 20-year follow-up: A randomised clinical trial. Orthop Traumatol Surg Res, 2021. 107(1): p. 102744.
Figures

Figure 1

Figure 2#7772
Correlation of the Chemical Signature of Periprosthetic Macrophages With the CoCrMo Head Wear Rate in Total Hip Replacements and Resurfacings
*Songyun Liu - University of Illinois at Chicago - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: Songyun_Liu@rush.edu
INTRODUCTION: The release of CoCrMo wear debris and in some cases corrosion products remains a major concern in total hip replacement (THR) and hip resurfacing (HR) due to adverse local tissue reactions (ALTR) characterized by a strong macrophage and lymphocyte presence. Specifically, particles engulfed and phagocytosed by macrophages help to explain the acting processes leading to ALTR. It was our goal to utilized infrared spectroscopy (IR) to characterize the chemical nature of macrophages associated within periprosthetic tissues from patients with different types of hip replacements and degrees of CoCrMo wear.
METHODS: Joint pseudo-capsule tissues retrieved from 13 MoM-HR and 8 MoM-THA patients were analyzed. The average time in situ was 5 and 6.73 years, respectively. Wear of the corresponding metal head bearing and taper surfaces was assessed using a coordinate-measuring-machine. H&E histological evaluation and IR spectroscopy were performed on sequential thin sections. The calculated wear volume and rate were incorporated to the spectral datasets to perform Principal Component Analysis (PCA) and further data visualization using Python-based custom-made programs. A control group of postmortem retrieved metal-on-polyethylene (MoP) THRs (N=12) with negligible wear and taper corrosion was analyzed previously for comparison.
RESULTS: The mean wear volume and wear rate of the femoral heads were 17.73 mm3 (0.16, 77.97) and 4.76 mm3/year (0.06, 24.64) in the MoM-HR group, and 34.67 mm3 (1.53, 152.53) and 6.0 mm3/year (0.03, 22.32) in MoM-THR group. THRs had material loss from taper surfaces of 2.08 mm3 (0, 13.97) and 6.0 mm3/year (0, 2.68). The marked presence of debris-laden macrophages throughout the tissue was commonly observed within samples corresponding to higher wear rates. The corresponding score plot clearly isolates IR signatures of collagenous tissue from those of macrophages from different groups (Fig. 1). Cases with higher CoCrMo wear rates and/or higher total volumetric loss tended to have higher PC1 scores. Plotting PC1 against the phosphate peak integral centered near 1062cm-1 resulted in a linear correlation (r2=0.96) (Fig. 2).
DISCUSSION: We found that the chemical signature of periprosthetic macrophages associated with MoM hips correlated with the wear rate of the CoCrMo. Particle-laden macrophages exhibited a strong absorbance in the phosphate region and exhibited similar spectral features as CrPO4. Under well-functioning conditions MoM bearings predominately produce small amounts of Cr2O3 nanoparticles. Such cases overlap well with the MoP controls (Fig. 1). High wear cases usually result from edge loading under which abrasion dominates and larger CoCrMo particles (100nm to µm-range) are generated. Thus, it seems likely that higher wearing hips are also associated with the formation of CrPO4 within macrophages, which is likely the result of phagocytosis of large cobalt-containing particles as evidenced by large dome shaped ν(PO43-) peaks (Fig. 2A). There were several cases in the MoM-THA group that overlapped with neither of the other groups (Fig. 1), among those extracellular chromium phosphate flakes were identified, indicating that cases with corrosion products from the taper surface may emit different types of debris resulting in a different macrophage chemistry.
Figures
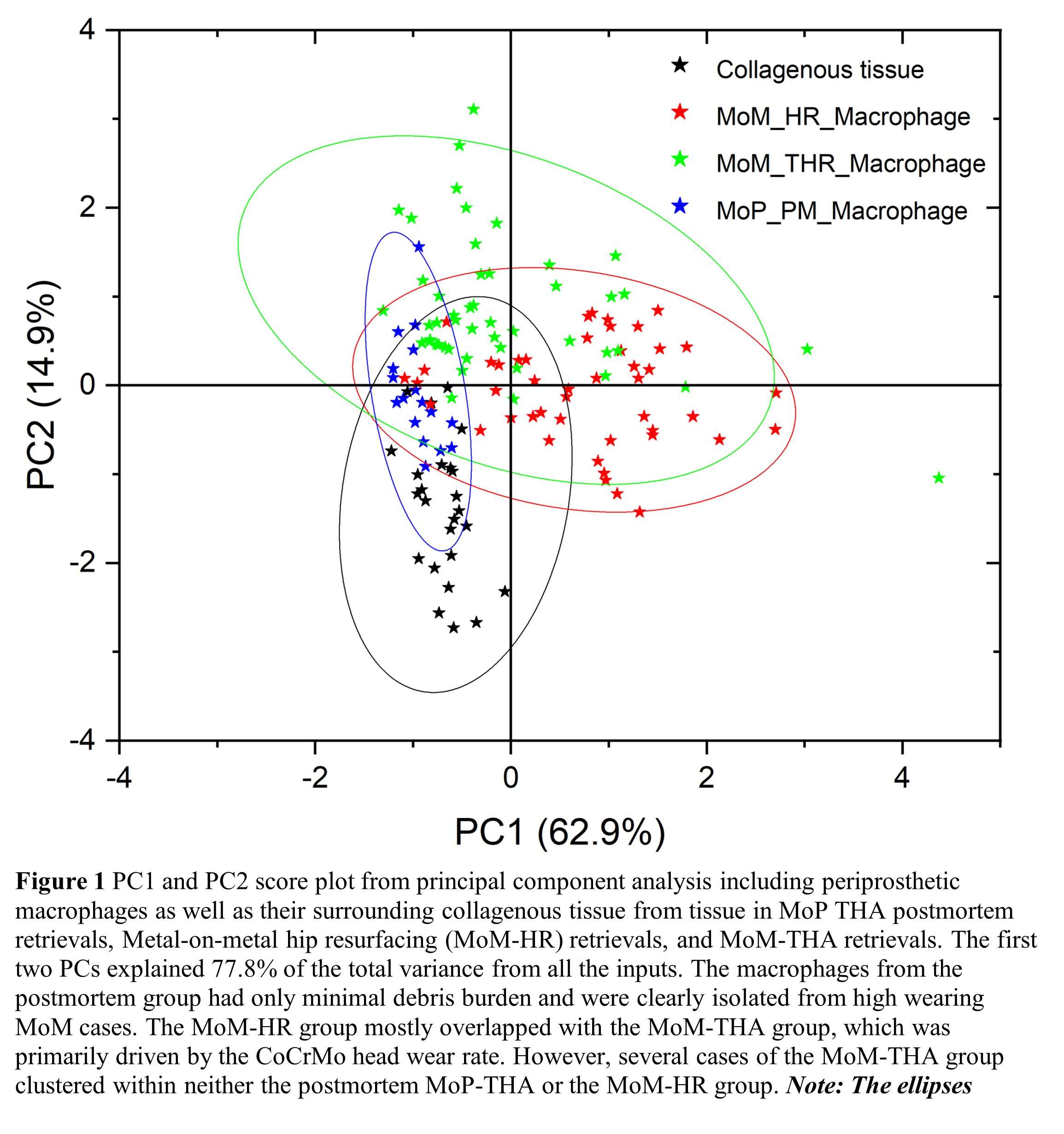
Figure 1
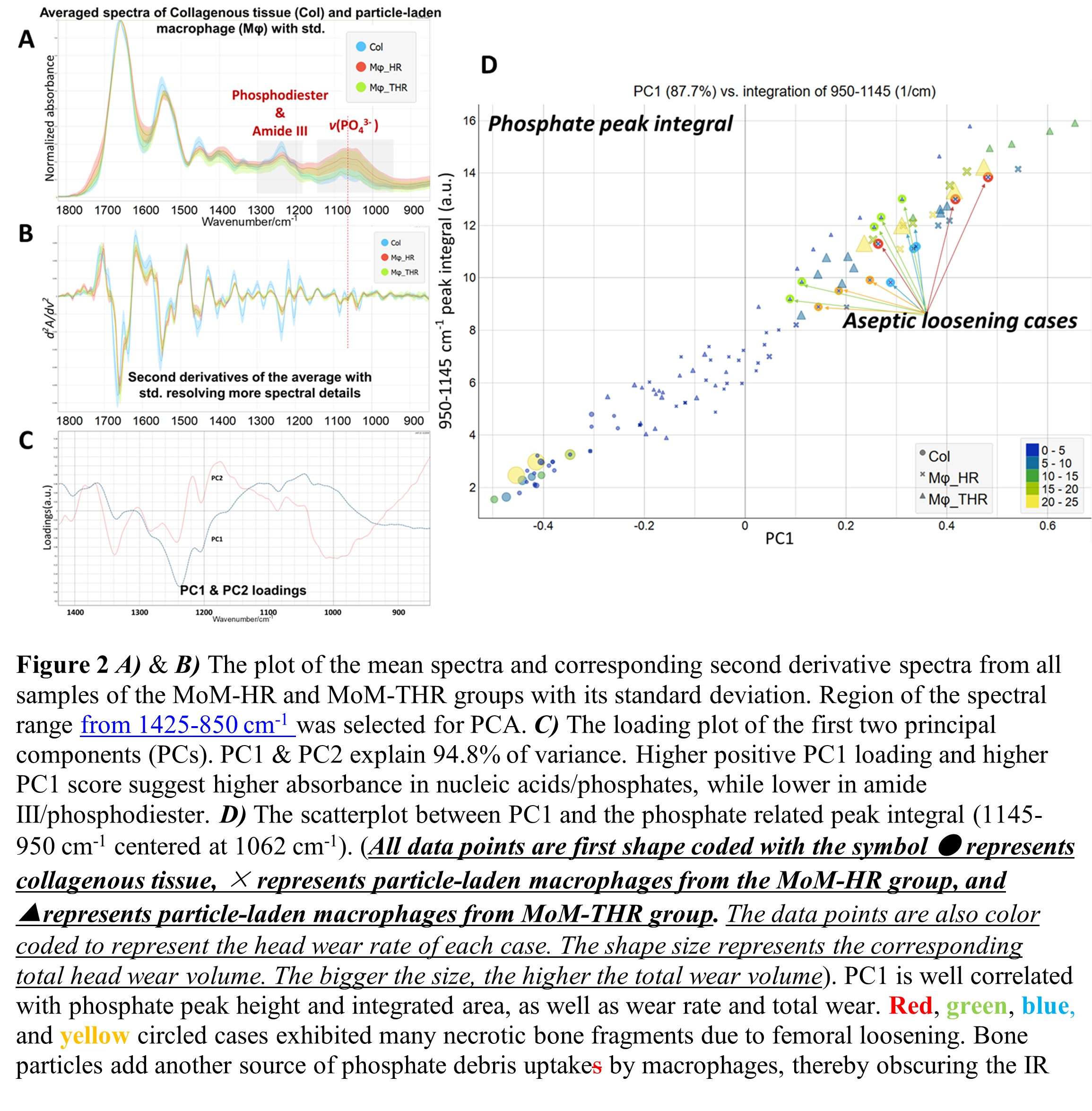
Figure 2#7809
Chemical Characterization of Corrosion Products From Ti6Al4V Stems Coupled With CoCrMo Heads
Songyun Liu - University of Illinois at Chicago - Chicago, USA
Mozart Neto - Rush Medical Center - Chicago, USA
Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Bianca Romay - Rush University Medical Center - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Hannah Lundberg - Rush University Medical Center - Chicago, USA
*Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: robin_pourzal@rush.edu
Introduction: Much emphasis has been given to the characterization of damage modes on total hip arthroplasty (THA) components made from CoCrMo suffering in vivo corrosion. Yet less has been done on the Ti6Al4V counterpart.Therefore, this study aimed to determine what damage modes occur on the Ti6Al4V stem taper surfaces paired with corroding CoCrMo heads from a group of retrieved contemporary THA.
Materials and Methods: 17 retrieved stems were analysed. Taper damage on the Goldberg scale were minimal (5), mild (1), moderate (1) and severe (10). All implants were analysed in a scanning electron microscope (SEM) (Jeol) with an energy dispersive X-ray spectroscopy (EDS) detector to confirm damage modes. The material loss from the head taper and stem taper were assessed by an optical coordinate measuring machine (CMM). The degradation products on Ti6Al4V stem taper surfaces were measured by Raman micro-spectroscopy (Horiba) using a 100x objective and 532nm laser in concert with EDS.
Results: CMM data revealed thatmost tapers exhibited shape deviations such as out-of-roundness and waviness. Damage modes ranged from plastic deformation and localized fretting (N=9) to severe fretting along machining lines (N=4), and in some cases pitting like corrosion along deformed machining lines (N=4) (Fig. 1). Eight stems were suffering from imprinting of which 3 also underwent chemically induced column damage as well. The average time in situ was 47.3 months (6.4, 155.4). The average material loss was 0.355 mm3 (0, 2.319) for the head taper and 0.294 mm3 (0, 2.61) for the stem taper. Typically, the undamaged/non-contact area on the stem taper showed Ti2O3 signals, and no Al or V associated oxides were detected. Within the damage scars, amorphous TiO2, Ti2O3, Cr2O3, CrO(OH), AlO(OH), MoO3 were identified, as well as some residual organic constituents, e.g., Phenylalanine, Tyrosine, and Tryptophan. Additionally, round features with cell-like morphology were identified as cells within the machining line valleys in two cases (Fig. 2). Among those tapers with damage score 4, black, flaky degradation products were seen stuffed in between deformed machining lines. They were identified mainly as amorphous and hydrated CrO(OH), Cr2O3 ,Ti2O3, CrO42-/CrO3, and in some cases, CoMoO4. In the contact area with pitting corrosion, weak TiO2 in rutile phase was observed as well as AlO(OH). In cases with column damage, the Ti2O3, amorphous TiO2, and CrO(OH) were always present.
Conclusion: This preliminary study showcases the different oxides, organic deposits and metallo-organic complexes formed on Ti6AL4V stem tapers in vivo under different fretting and corrosion processes against CoCrMo. Knowledge of these species may help to better understand adverse reactions to corrosion products within periprosthetic tissue. Specific concern lies in the occurrence of Cr(VI), although such complexes are likely short lived in vivo. Another highlight is the identification of cells which would support recent reports of cell-accelerated-corrosion within modular junctions. Also, shape deviations and machining lines provide reservoirs for corrosion product accumulation and potentially alteration. More work is being conducted to link specific corrosion products to material loss rate from both surfaces and the specific damage processes identified by SEM.
Figures
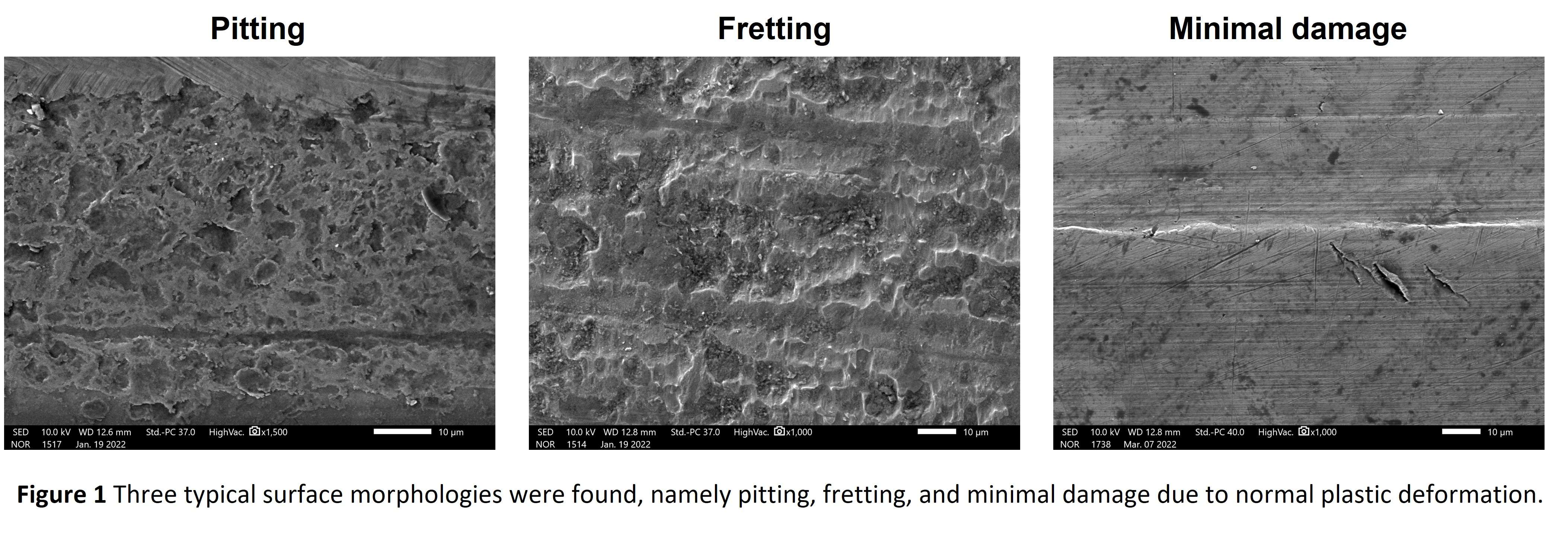
Figure 1
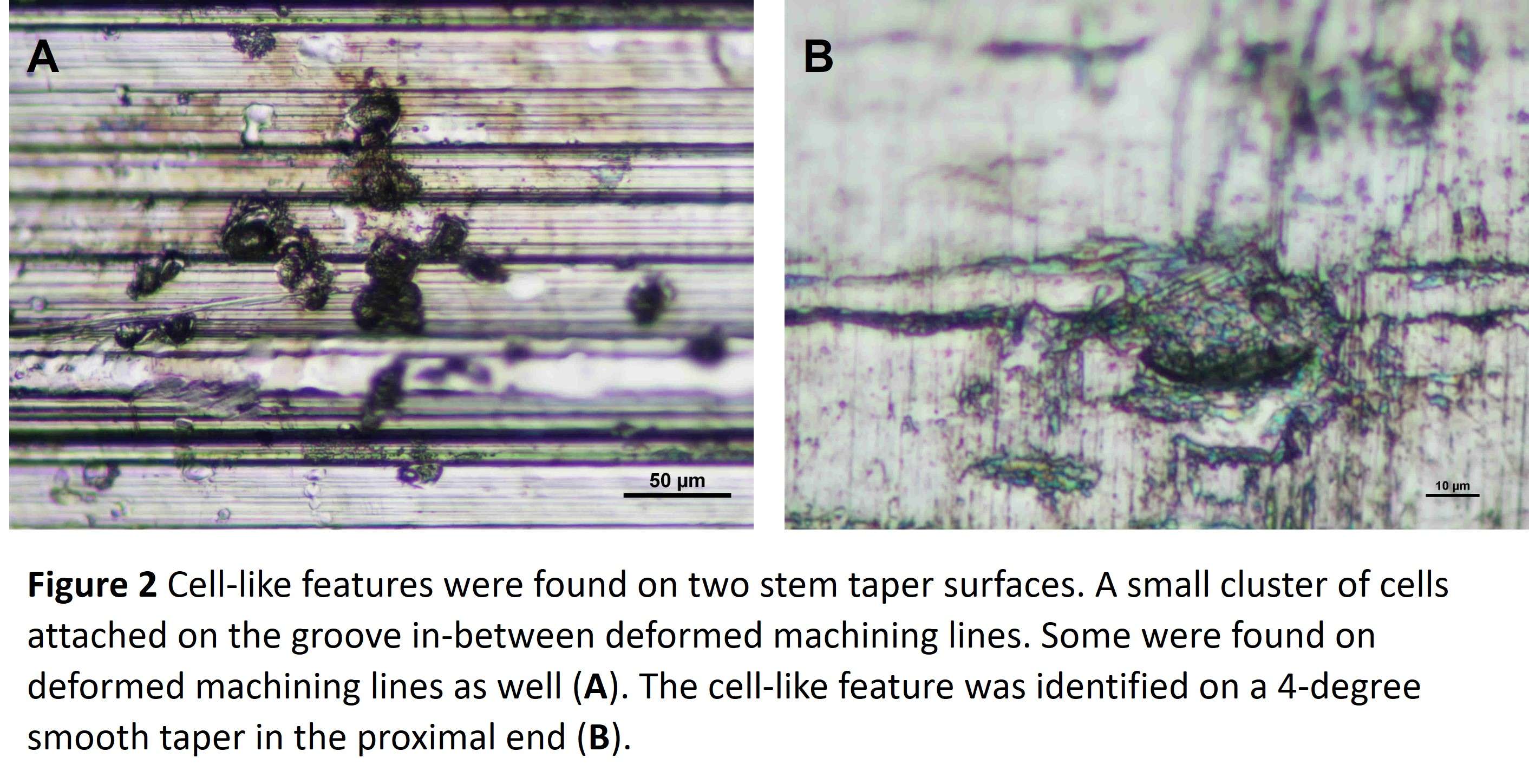
Figure 2#7970
Efficacy of the Pre-Operative Three Dimensional (3D) Templating in a Robot Assisted TKA in Predicting the Correct Implant Sizes and Alignment.
*Sanjay Londhe - India
Ravi Shah - Sujay Hospital (Juhu) BSES - Mumbai, India
Santosh Shetty - Criticare Asia Hospital - Mumbai, India
Rakesh Nair - Criticare Asia Hospital - Mumbai, India
Vijay Shetty - Criticare Asia Hospital - Mumbai, India
Ashit Shah - BSES MG Hospital - Mumbai, India
Niraj Vora - India
*Email: sanlondhe@yahoo.com
Background: Although Total knee Arthroplasty has a successful outcome in majority of the patients, roughly 20 % of TKA patients remain dissatisfied. Patient dissatisfaction after TKA is a major concern in 21 st century arthroplasty practice. Accurate femoral and tibial implant sizing is shown to improve the implant survival, knee balance and patient reported outcome measures. The purpose of the current study is to assess the efficacy of pre-operative three dimensional (3D) templating in a robot assisted TKA in predicting the correct implant sizes and alignment.
Materials and methods: Prospectively collected data in a single RA-TKA center from 30 RA-TKAs was assessed to determine its efficacy in correctly predicting the implant size and positioning. An inclusion criterion was patients with end stage (grade 4) bone on bone arthritis undergoing primary TKA. Patients undergoing revision TKA and patients not willing to participate in the study were excluded. Preliminary study of 10 patients had indicated almost 100% accuracy in determining the implant size and position. Sample size was estimated to be 28 for 90% reduction in implant size and position error with α error of 0.05 and beta error of 0.20 with power of study being 80 %. Post-operative radiographs were assessed by an independent observer with respect to implant size and position. The independent observer was not part of the RA-TKA operative team.
Statistical analysis: The accuracy of femoral component and tibial component sizing proportions in the study were compared with the historic control proportions with Chi-squared test. The p value < 0.05 was considered to be significant.
Results: The pre-operative CT scan 3D templating accuracy was 100 % (30 out of 30 knees) for femoral component and 96.67% (29 out of 30 knees) for tibial component. The implant position and limb alignment was accurate in 100 % of patients. The accuracy of femoral component and tibial component sizing is statistically significant (Chi-squared test, p value 0.0105 and 0.0461 respectively).
Conclusion: The results of our study show the effectiveness of pre-operative CT scan 3D planning in predicting the implant sizes and implant positioning. This will help in improving the implant longevity, clinical outcomes and patient satisfaction.
Key words: Robotic assisted Total Knee Replacement, Dissatisfied patient, Femoral component sizing, Tibial component sizing.
#7750
The Influence of Assembly Load and Angular Mismatch on THR Head-Neck Modular Junction Contact Mechanics in Ceramic Head Tapers: A Computational Analysis
*Hannah Lundberg - Rush University Medical Center - Chicago, USA
Steven Mell - Rush University Medical Center - Chicago, USA
Denis Ovoshchnikov - Rush University Medical Center - Chicago, USA
Brett Levine - Rush University Medical Center - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
Jonathan Gustafson - Rush University Medical Center - Chicago, USA
*Email: hannah_lundberg@rush.edu
INTRODUCTION: To combat the potential for corrosion between metallic modular components in total hip replacement (THR), the use of ceramic femoral heads has significantly increased [1]. Prior work has shown that both conical mismatch angle and machining lines on the metallic stem and head tapers can influence modular junction stability during assembly, but there is a paucity of evidence in understanding the mechanics of ceramic head tapers during THR assembly. The purpose of this study was to compare the effect of femoral head material on modular junction contact mechanics during assembly using a computational model in the context of three variables: assembly load, conical mismatch angle, and machining lines of the stem taper.
METHODS: Previously developed 2D axisymmetric finite element analysis (FEA) models [2,3] were used to investigate the effect of femoral head material on contact mechanics during dynamic femoral head assembly. The models consisted of a half cross-section of a 32mm femoral head (CoCrMo or ceramic) and stem taper (Ti6Al4V) with a nominal 12/14 taper design. Circumferential machining lines were modeled on both the stem and head taper surfaces. Assembly loads (2 – 12 kN) were applied dynamically to the femoral head and contact was modeled between the stem and head taper surfaces with a 0.2 coefficient of friction. A total of 32 simulations were performed. To understand the effect of material and its potential interactions with load and mismatch angle on final assembly state, stepwise-multiple linear regression (MLR) was performed up to second order terms and including interactions for four model outputs (displacement, contact area, peak contact pressure, and peak plastic strain).
RESULTS: Stepwise-MLR found that femoral head material had a large influence on contact mechanics (Figure 1). Material was a significant contributor to displacement (p<<0.001), with ceramic heads displacing less than CoCrMo heads. Contact area between the head and stem, was significantly less for ceramic heads (p<0.001) and there was an interaction between material and load (p=0.0119) for this output. Average plastic deformation across the stem was significantly higher in ceramic heads (p<0.01). Material was not a significant predictor of contact pressure and was dropped from the final model by the stepwise algorithm. Angular mismatch was a significant quadratic predictor (p<0.05) of displacement, strain, and contact pressure, consistent with previous studies. Assembly load was a significant predictor (p<0.001) of displacement and contact area, but not of strain (p=0.015) or contact pressure (p=0.09).
CONCLUSION: CoCrMo heads displaced further with higher contact areas than their ceramic counterparts. This is an important finding because it indicates that ceramic heads may be less stable than CoCrMo heads under lower assembly loads. For the output factors we investigated, load and angular mismatch angle had a larger effect on contact mechanics than material, suggesting that surgeons may need to hit ceramic heads harder to achieve similar assembly conditions.
REFERENCES: [1] AAOS AJRR Annual Report 2020. [2] Bechstedt et al. J Biomech 2020, 103:109689. [3] Gustafson et al. Bone Joint J 2020, 102:33-40.
ACKNOWLEDGEMENTS: This study was supported by NIH/NIAMS R01 AR07181.
Figures
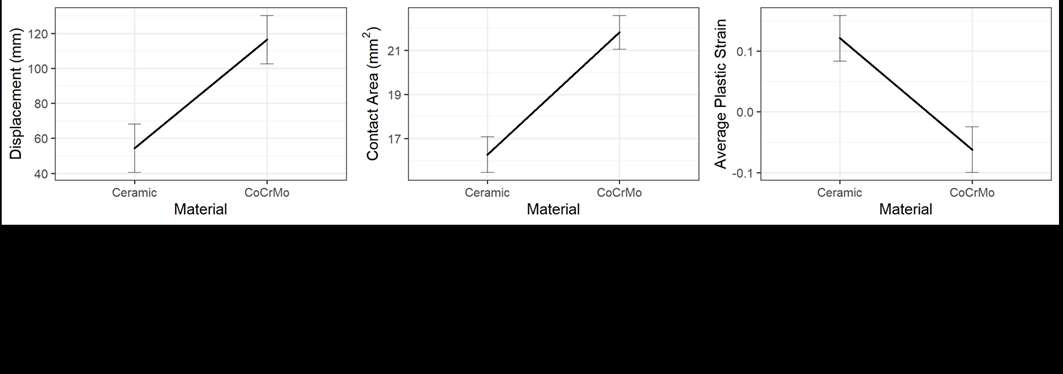
Figure 1#7912
Influence of Obesity and Intra-Operative Image Guidance Technology on Acetabular Cup Positioning in Total Hip Arthroplasty
*Kayti Luu - JABSOM - Honolulu, United States of America
Scott Nishioka - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Emily Unebasami - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: kaytiluu@hawaii.edu
Background: Accuracy of acetabular cup positioning during total hip arthroplasty (THA) can be improved with intraoperative imaging but may be influenced by body mass index (BMI). This study assessed the influence of BMI on cup accuracy when using intraoperative fluoroscopy (IF) alone or supplemented with a commercial product.
Methods: This retrospective review included four consecutive cohorts of patients having undergone anterior approach THA with IF alone (2011 to 2015), IF and Overlay (2015 to 2016) (Radlink Inc., Los Angeles, CA), IF and Grid (2017 to 2018) (HipGrid Drone™, OrthoGrid Systems Inc., Salt Lake City, UT) and IF and Digital (2018 to 2020) (OrthoGrid Phantom®, OrthoGrid Systems, Inc., Salt Lake City, UT). Component placement accuracy was measured on six-week postoperative weight bearing radiographs and compared between BMI≤25, 25<BMI≥30, BMI 30<BMI≥35, and BMI>35 patients. Total fluoroscopy times were also obtained from the c-arm machine.
Results: Abduction angle significantly increased as BMI increased (p=0.003) with IF alone but no difference was present in groups with guidance technology. Anteversion was significantly different between BMI groups for IF alone (p=0.028) and Grid (p=0.027) but was not different in Overlay (p=0.107) or Digital (p=0.210). Fluoroscopy time was significantly different between BMI categories for IF alone (p=0.005) and Grid (p=0.018) but was not different in Overlay (p=0.444) or Digital (p=0.170).
Conclusion:Morbid obesity (BMI>35) increases risk for malpositioning of acetabular cups and increases surgical time with IF alone or the Grid. Additional IF guidance technology (Overlay or Digital) increased cup positioning accuracy without decreasing surgical efficiency.
#7519
How Does Obesity Influence Patient Outcomes After Primary TKA?
*Stephen Lyman - Hospital for Special Surgery - Fukuoka, Japan
Fred Cushner - Hospital for Special Surgery - New York, USA
Michael Parks - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Amethia Joseph - Hospital for Special Surgery - New York, USA
Ilan Fleisher - Hospital for Special Surgery - New York, USA
Gina Mosich - Hospital for Special Surgery - New York, USA
Yu-Fen Chiu - Hospital for Special Surgery - New York, USA
*Email: lymans@hss.edu
Background: Obesity in the United States is reaching epidemic proportions. Given the potential for functional limitations in the obese population, the purpose of this study was to evaluate the Knee Osteoarthritis Score for Joint Replacement (KOOS-JR) within the World Health Organization (WHO) defined by body mass index (BMI) classifications.
Methods: Using our institutional joint replacement registry, 3,961 primary TKAs for osteoarthritis were identified (2016-2019). BMI was classified according to WHO: normal-weight (<25kg/m2), overweight (25<30kg/m2), Obese-I (30<35kg/m2), Obese-II (35<40kg/m2), Obese-III (>40kg/m2). Patient demographics, Charlson Comorbidity Index, length of stay, operative time, and preoperative and 1-year KOOS-JR-scores were analyzed.
Results: Of the 3961 patients, only 613 (16%) were normal-weight, with 1253 (31.5%) overweight, 1104 (27.8%) Obese-I, 595 (15.0%) Obese-II, and 396 (10%) Obese-III. Higher BMI patients had TKA at a younger age and had longer operative times and longer hospital length of stay. Higher obesity class patients were also less likely to be discharged home with 23% of Obesity-III patients discharged to a skilled nursing facility (p=0.005). Overweight and obese patients had worse preoperative KOOS-JR-scores (p<0.0001), but larger improvement/delta KOOS-JR-scores at 1-year (p<0.0001) compared to normal-weight patients. Even with the larger increase in KOOS-JR scores, higher BMI patients had slightly lower 1-year scores when compared to non-obese patients (Figure 1, p<0.0001).
Conclusions: Patients undergoing primary TKA in higher BMI categories require more resources during the perioperative (operative time) and early post-opeartive (LOS, need for in-patient rehabilitation) than lower BMI patients. These patients start with lower KOOS-JR scores preoperatively but achieved larger improvements in their scores one year postoperatively. This information should be considered by providers when counseling patients on the outcomes of TKA.
Figures
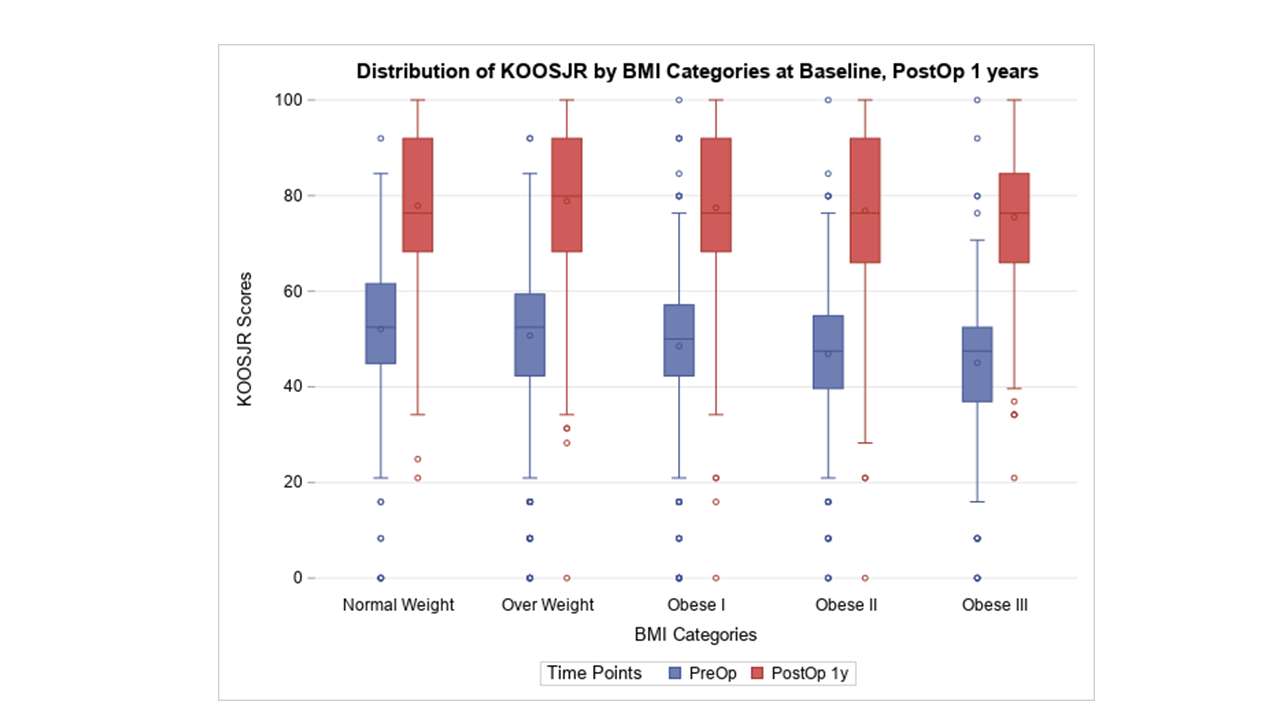
Figure 1#7621
Validation and Utility of the Japanese JKOOS+: A Culturally Relevant Knee Outcome Measure
*Stephen Lyman - Hospital for Special Surgery - Fukuoka, Japan
Go Omori - Niigata University of Health and Welfare - Niigata, Japan
Takahisa Sasho - Chiba University - Chiba, Japan
Tomoyuki Saito - Yokohama City University - Yokohama, Japan
Matsutaka Deie - Aichi Medical University - Nagakute, Japan
Norimasa Nakamura - Osaka Health Science University - Osaka, Japan
Wataru Ando - Osaka University Graduate School of Medicine - Suita, Japan
Hiroshi Ikeda - Juntendo University - Tokyo, Japan
Naoshi Fukui - Univesrity of Tokyo - Tokyo, Japan
*Email: lymans@hss.edu
INTRODUCTION: Existing knee related patient reported outcome measurements (PROMs) have overwhelmingly been developed and validated in western countries, suggesting a potential for a western bias in PROMs evaluation of patients with knee conditions. One of the most frequently used knee PROMs, the Knee Injury and Osteoarthritis Outcomes Survey (KOOS), has been translated into more than 50 languages worldwide. These translations have largely adhered to standarts for cross cultural adaptation of health surveys. However, after release of the Japanese KOOS (JKOOS) we discovered the JKOOS was not fully culturally relevant to Japanese patients. We, therefore, undertook the cultural adaptation of the Japanese version of the knee injury and osteoarthritis outcome survey (JKOOS) and evaluated the responsiveness of our novel JKOOS+ PROM.
METHODS: We completed this project in 3 phases across 10 hospital outpatient knee clinics in Japan. In Phase 1, 187 surgically naïve patients with knee pain were asked about activities limited by their pain. An expert panel reconciled these activities against existing KOOS items to identify potential novel items. In Phase 2, 241 surgically naïve patients with knee pain were administered the Japanese Oxford Knee Survey (OKS), JKOOS, and these novel items. An Rasch analysis was used to test item fit for each novel item within the KOOS Activities of Daily Living (ADL). Unidimensionality was assessed using principle component analysis. Internal consistency (Cronbach's alpha) and external validity (Spearman's Correlations) were assessed for Japanese ADL (J-ADL). In phase 3, we enrolled 114 patients scheduled for total knee arthroplasty (TKA) across 8 knee clinics across Japan. Patients completed the Oxford Knee Score (OKS) and JKOOS+ both at the time of enrollment and again 1 year post-TKA. Responsiveness was evaluated using effect size and standardized response mean (SRM). An effect size or SRM >0.8 is considered adequately responsive. We further tested the difference in responsiveness between the original JKOOS activities of daily living (ADL) domain and the novel Japanese ADL (JADL) domain using the modified Jacknife test.
RESULTS: Phase 1 identified 4 activities relevant to Japanese knee patients: sitting seiza, using a Japanese toilet, climbing hills, and getting on/off a bus/train. In Phase 2, climbing hills and bus/train were well fit in JADL. JADL was deemed to be unidimensional with high internal consistency (Cronbach's alpha 0.96) and external validity (Spearman Correlations 0.723-0.893). The JADL domain outperformed the ADL domain in both effect size (Figure 1, 1.51 v. 1.45) and SRM (Figure 2, 1.67 v. 1.57) (p<0.001).
CONCLUSIONS: We were able to successfully culturally adapt and validate the JKOOS+ to create a knee PROM more culturally relevant to Japanese sufferingfrom knee pain. The JKOOS+ JADL domain is significantly more responsive than the Europe-developed ADL domain to TKA in Japanese knee patients suffering from knee osteoarthritis (OA).
Figures
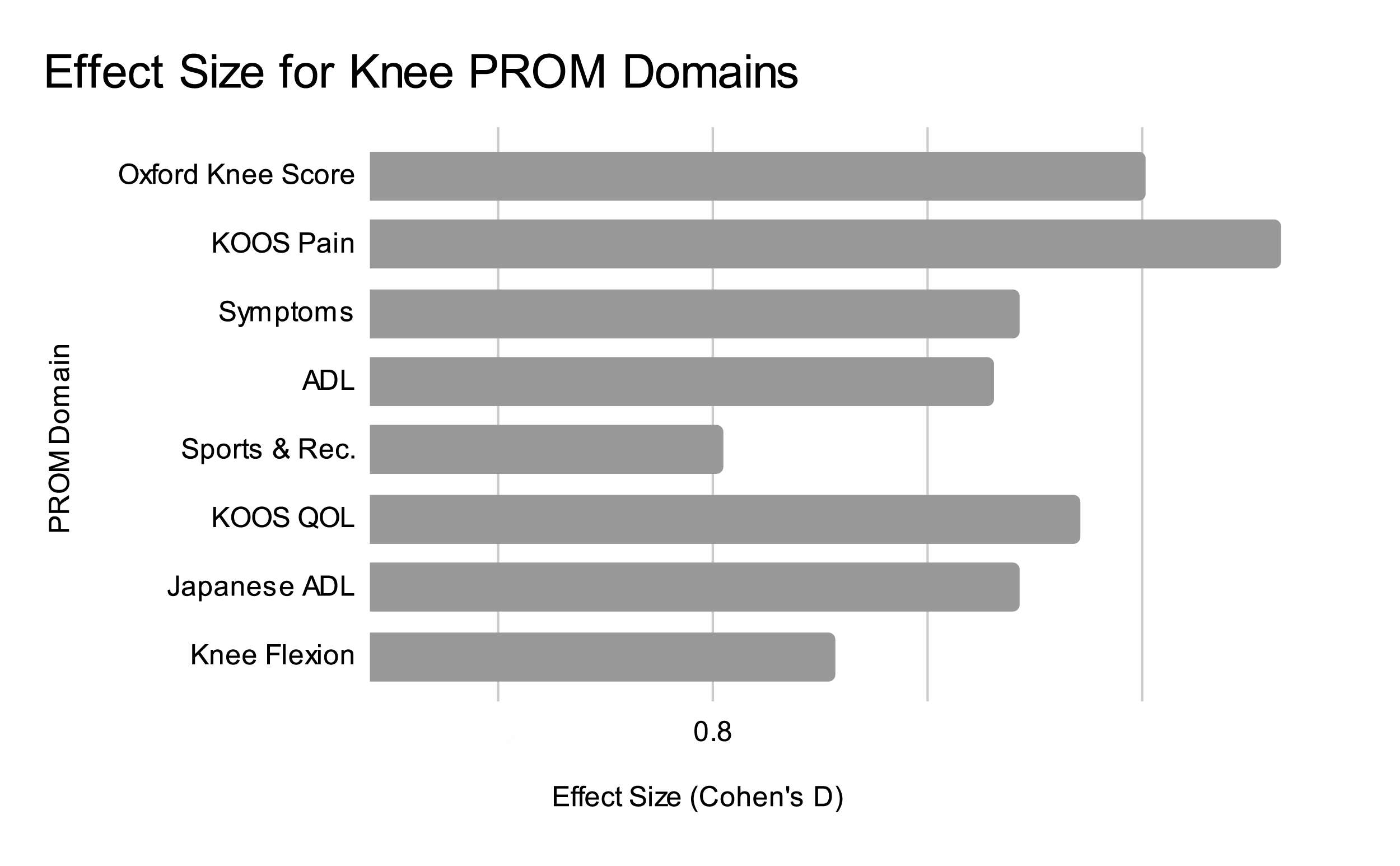
Figure 1
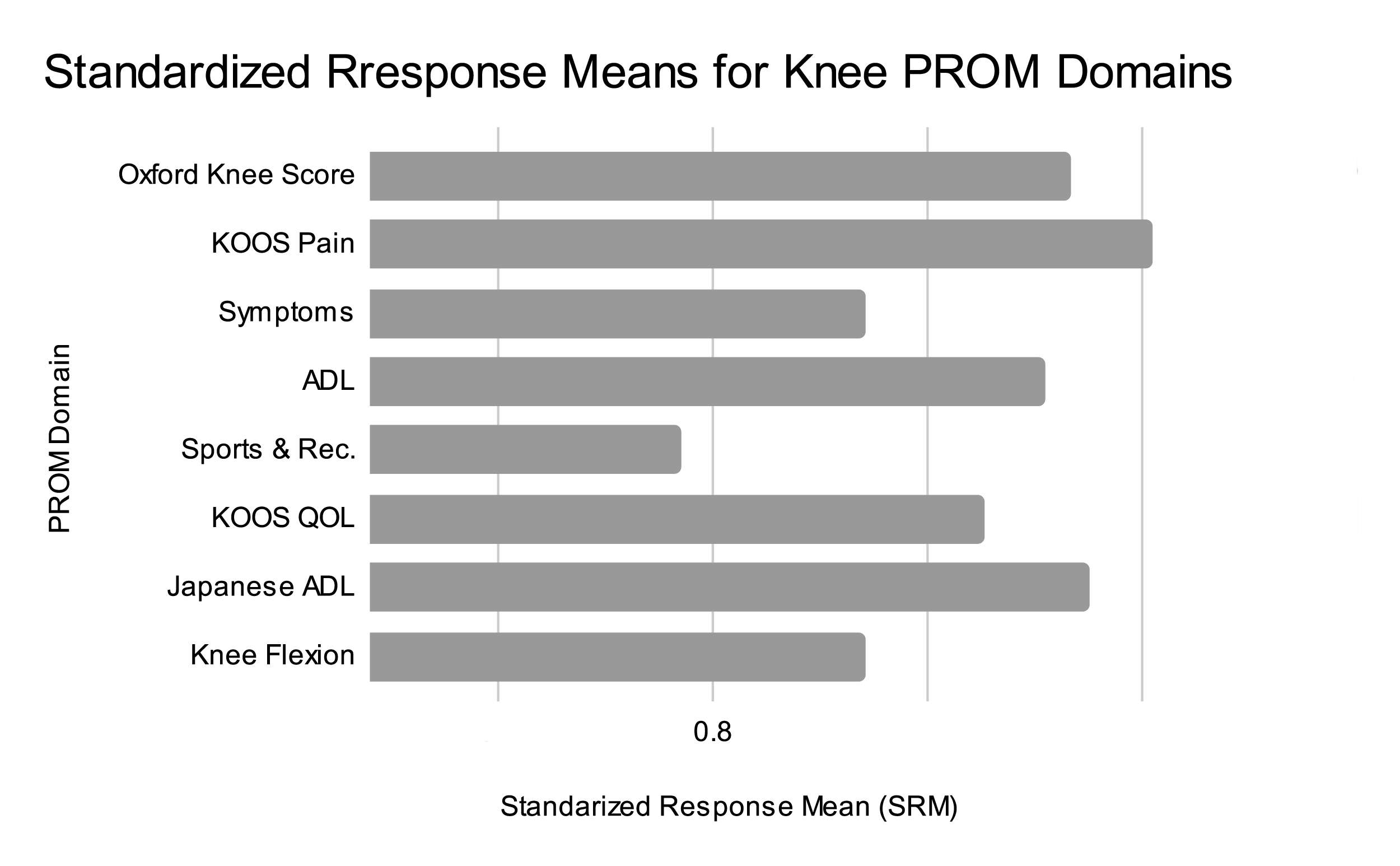
Figure 2#7989
Nickel Allergies Associated With Titanium-6 Augments in Total Knee Replacement
*Gerhard Maale - Medical Center Plano - Plano, USA
Arianna Mixon - Dallas Ft. Worth Sarcoma Group - Plano, USA
*Email: gerhardmaale53@gmail.com
INTRODUCTION: Total knee arthroplasty (TKA) is the most commonly performed orthopedic surgical procedure in the United States. Current literature reports multidirectional instability (MDI) and arthrofibrosis secondary to metal allergies, specifically nickel, have been associated in 1.5% of all primary knees. Increased awareness of metal hypersensitivity in total knee prostheses are driving the effort to develop devices that are ‘hypoallergenic’. The Porex Hinge system, which has a Niobium Nitride and pure Titanium coating, is used at the time of revision for patients with known nickel allergies. Titanium-6 augments used in this system contained very little nickel (<0.05%), and were completely encased in cement. Although the augments were not exposed to the joint or the patient, some patients still demonstrated signs of chronic inflammation, arthrofibrosis and perivascular cuffing with lymphocytes after revision with these hypoallergenic prosthetic devices. The purpose of this study is to show that Titanium-6 augments used at the time of revision, showed all the features that the patients had prior with MDI associated with the nickel allergies.
METHODS: This study retrospectively reviewed 18 patients that had a total knee replacement with a pure Titanium- Niobium Nitride coating and Titanium-6 augments. All patients underwent the Metal-Lymphocyte Transformation Test (metal-LTT) to confirm nickel allergy diagnosis. Additionally, all patients had routine labs (CBC, CRP, and ESR) and were staged with x-rays, WBC scan, CT scan and tri-phase bone scan. Patients were followed for a minimum of two-years.
RESULTS: Of the 18 patients in our cohort, 4 were male and 14 were female. The average age was 63 years with a range from 41-78. All patients demonstrated a recurrence of inflammatory capsular pain on an average of 8.2 months after revision with a Porex hinge, with the onset of symptoms ranging from 3 to 19 months. 9 out of 18 (50%) patients required a revision to exchange the Titanium- 6 augment to polyethylene components.
CONCLUSION: Titanium-6 alloy contains very little nickel (0.05%), yet patients had inflammatory response, arthrofibrosis, and perivascular lymphocytic infiltration of the capsule following total knee replacements with a Porex hinge. Even when the augments were covered in cement, patients still demonstrated signs of pain, chronic inflammation, and arthrofibrosis. It is possible the porus composition of the cement allows nickel particles to pass through to the joint space causing the recurrence of the inflammatory response. Revision of the Titanium-6 augments to polyethylene augments was a suitable treatment option for recurrence of inflammatory capsular pain with most patients noting a relief of pain.
#7515
Evaluation of Vascular Proximity to the Acetabulum in Severely Dysplastic Hips to Assess the Risk of Vascular Injury in Total Hip Arthroplasty
*Yuki Maeda - Osaka University Graduate School of Medicine - Suita, Japan
Wataru Ando - Osaka University Graduate School of Medicine - Suita, Japan
Hidetoshi Hamada - Osaka University - Suita, Japan
Keisuke Uemura - Osaka University - Suita, Japan
Nobuhiko Sugano - Osaka University Graduate School of Medicine - Suita, Japan
Kazuma Takashima - Osaka University Graduate School of Medicine - Suita, Japan
*Email: yktmaeda@nike.eonet.ne.jp
Introduction: The purpose of this study was to evaluate the vascular proximity to the acetabulum that is associated with the risk of vascular injury when exposing the acetabulum in total hip arthroplasty (THA) for osteoarthritis (OA) in patients with severe hip dysplasia.
Materials & Methods: The study participants were 15 patients with unilateral Crowe type IV OA who underwent THA using CT-based navigation. Three-dimensional planning software was used to place a cup in the affected acetabulum and the contralateral normal acetabulum. The femoral artery/vein and iliopsoas muscle were identified on CT images. A circle that matched the outer contour of the cup was drawn on cross-sectional images every 5 mm from 10–25 mm proximal to the pelvic teardrop (Figure 1). The shortest distances from the intersection between the anterior wall and each circle to the femoral artery and vein were measured (Figure 2). The site at which the iliopsoas muscle passed the acetabulum was compared between the affected and unaffected sides (Figure 3).
Results: Mean minimum distances from the anterior wall–circle intersection to the femoral artery/vein on the affected side/unaffected side were 13.9/20.2 mm for the artery and 10.0/16.5 mm for the vein at 10 mm; 13.6/17.6 mm for the artery and 9.0/15.2 mm for the vein at 15 mm; 13.8/16.4 mm for the artery and 10.0/15.8 mm for the vein at 20 mm; and 16.0/18.2 mm for the artery and 13.5/19.2 mm for the vein at 25 mm. The femoral artery at 10–20 mm proximal to the pelvic teardrop and the femoral vein at the 10–25 mm level were significantly closer to the anterior wall on the affected side than the unaffected side. On the unaffected side, the iliopsoas muscle passed between the anterior pelvic wall and femoral artery/vein in all cases. However, on the affected side at the 10–15 mm level, the iliopsoas muscle passed lateral to the acetabulum without passing between the anterior pelvic wall and femoral artery/vein.
Discussion: Cup placement in the original acetabulum in Crowe type IV OA provides stable fixation but requires removal of the elongated capsule to expose the hypoplastic acetabulum, which increases the risk of vascular injury. The femoral artery/vein are close to the intersection between the anterior wall and the outer contour of the cup. The iliopsoas muscle protects the femoral artery and vein during exposure of the anterior acetabulum in normal hips, but not in hips with Crowe type IV OA.
Conclusions: When placing an acetabular component in THA in patients with severe hip dysplasia, particular care is needed when performing surgical procedures at around 10–15 mm proximal to the pelvic teardrop.
Figures
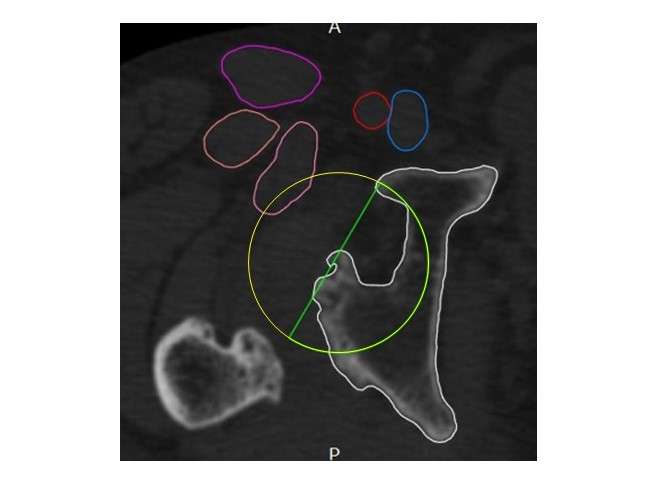
Figure 1
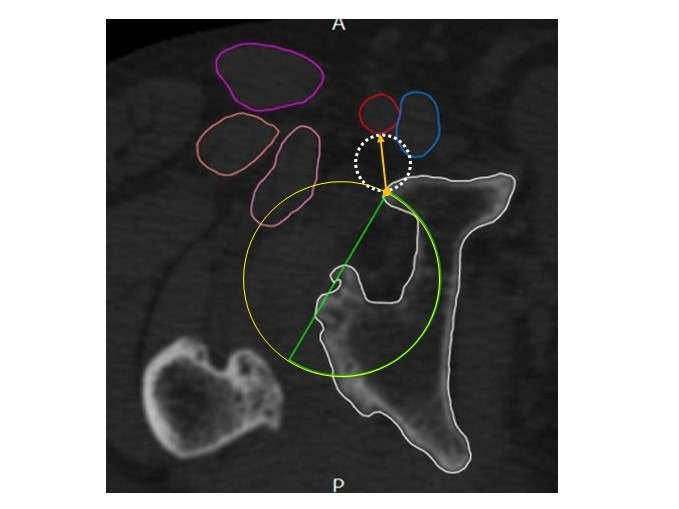
Figure 2
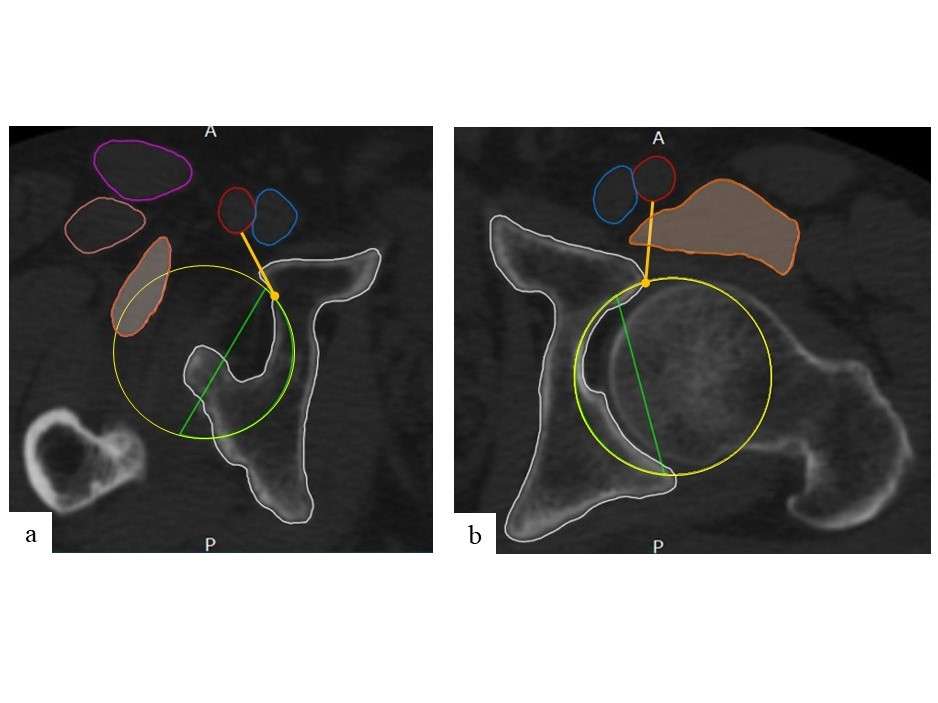
Figure 3#7995
The Change in Fixed Flexion Deformity During Robotic-Arm Assisted Unicompartmental Knee Arthroplasty
*ahmed magan - University College London Hospital - London, GB
Alastair Chambers - UCLH - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Vishal Rajput - University College London Hospital - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
Dia Giebaly - University College London Hospital - London, United Kingdom
*Email: ahmedmagan@gmail.com
Introduction
Unicompartmental knee arthroplasty (UKA) is an effective surgical treatment for patients with unicompartmental knee arthritis. Residual fixed flexion deformity (FFD) may lead to worse functional outcomes, but the change in FFD with UKA remains unknown. The objective of this study was to assess the change in FFD in patients undergoing medial UKA.
Methods
This prospective cohort study included 63 patients with medial compartment arthritis undergoing robotic-arm assisted UKA at a single tertiary centre between 2018 and 2022. This study included 30 males and 33 females with a mean age of 62 ± 5.7 years. Patients were divided into four study groups based on the degree of preoperative FFD: < 3 degrees, 3 – 6 degrees, 6-9 degrees, and >9 degrees. Intraoperative optical motion capture technology was used to assess pre- and postoperative FFD. The Oxford Knee Score (OKS) was assessed in all patients before surgery and at one-year follow-up.
Results
This study found statistically significant increase in mean preoperative to mean postoperative FFD for each of the four treatment groups: : < 3 degrees (pre op FFD = 1.53, post op FFD = 0.61 degrees, P = 0.004), 3 - 6 degrees (pre op FFD = 4.94 degrees, post op FFD = 3.71, P = 0.015), 6 – 9 degrees (pre op FFD = 7.96 degrees, post op FFD = 3.63, P < 0.001), >9 degrees(pre op FFD = 11.63 degrees, post op FFD = 7.18, P value < 0.001). All treatment groups showed a statistically significant improvements from preoperative to postoperative OKS (p<0.001) at one year follow-up. There were no significant differences in OKS between the four treatment groups at one-year follow-up.
Conclusion
This is the first study to use optical motion capture technology to quantify the change in FFD during robotic-arm assisted UKA. The FFD was reduced by approximately half in all four treatment groups with no difference in functional outcomes based on the degree of preoperative FFD. These findings may help to modify existing clinical criteria for medial UKA.
#7997
Time for Return to Sport Following Total Knee Arthroplasty: A Meta-Analysis
*ahmed magan - University College London Hospital - London, GB
Babar Kayani - University College Hospital London - London, United Kingdom
Ganan Radhakrishnan - Univeristy College London - London, United Kingdom
Flaminia Ronca - University College London - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: ahmedmagan@gmail.com
Introduction
The frequency of total knee arthroplasty (TKA) is increasing, particularly in younger and more active patients. There may be greater functional demands in these patients, with an expectation to return to sporting activities (RTS) following TKA. There is a paucity of data on time to RTS following TKA and this meta-analysis aims to determine the time to RTS following TKA.
Methods
Using the PRISMA guidelines, an electronic search of PUBMED, MEDLINE, EMBASE, and the Cochrane Library for trails was performed on TKA and RTS in the English language, published from the database's inception to 31st October 2020. Data evaluating the time to RTS and functional outcomes were recorded by two authors independently in the analysis. Pooled analysis using the random-effect model on overall proportions at the different time intervals and the end of the follow-up was carried out for all studies.
Results
In total, 1,611 studies were retrieved from the literature search. Of these, nine studies met the inclusion criteria with 1,307 patients. Two studies with 148 patients demonstrated an overall pooled proportion of 18.7% (95% CI: 8.2% - 32.3%) of patients RTS at 3 months post-TKA; Three studies reported RTS rate at 6 months 70.% (95% CI: 48-88.4).Two studies with 123 patients demonstrated an overall pooled proportion of 84.0% (95% CI: 77.1% – 89.9%) patients RTS at 12 months. 986 patients returned to sport from a total of 1,307, with an overall adjusted proportion return to sport of 87.9 (95% CI: 80.5-93.8% ) at the end of follow-up; mean 14 months (range 3 – 36 months).
Conclusion
Patients undergoing TKA were found to successfully RTS; pooled proportion analysis showed an increasing rate of RTS with time, at a mean of 14 months following TKA, where 87.9% of patients had returned to sports. The findings of this study will enable more informed discussions and rehabilitation planning between patients and clinicians on RTS following TKA.
#7999
Time for Return to Sport Following Hip Resurfacing: A Meta-Analysis
*ahmed magan - University College London Hospital - London, GB
Babar Kayani - University College Hospital London - London, United Kingdom
Ganan Radhakrishnan - Univeristy College London - London, United Kingdom
Flaminia Ronca - University College London - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
Warran Wignadasan - University College London Hospital - London, United Kingdom
*Email: ahmedmagan@gmail.com
Introduction
The aim of this study was to establish the time for a return to sport (RTS) following hip resurfacing arthroplasty (HRA) from studies published in the literature.
Methods
A literature search was performed on PUBMED, MEDLINE, EMBASE, and the Cochrane Library for trials on HRA and RTS, in the English language and published from the inception of the database to October 2020. A further manual search was performed in appropriate sports medicine and orthopaedic journals—all relevant studies reported on time to RTS after HRA were included. The PRISMA guidelines for reporting meta-analyses were used to undertake this study.
Results
A total of 1568 studies were identified. After scanning for duplicates, the remaining articles were screened before 37 full articles were selected for a full-text review. 11 studies involving 659 patients matched our inclusion criteria. Two studies involving 94 patients demonstrated that a pooled proportion of 91.8% (95% CI 71.8-100) of patients were able to RTS post-HRA by three months post-operatively. Four studies involving a total of 265 patients determined a pooled proportion of 96.8% (95% CI 91.0-99.7) of patients were able to RTS by the 6-month post-operative stage. Pooled proportion analysis from all 11 studies comprising 659 patients showed that 90.9% (95% CI 82.2-96.9) of patients were able to RTS by a final follow-up of 3 years. There is a trend toward patients partaking in low-contact sports post-operatively.
Conclusion
There are marked inter-and intra-study variations in the time that patients were able to RTS after HRA. Pooled analysis shows that greater than 80% of patients were able to RTS at six to 12 months postoperatively. The findings of our meta-analysis allow for more informed discussions between surgeons and patients about the time to RTS post-HRA.
#8000
Tourniquet Use in Total Knee Arthroplasty and the Risk of Infection: A Meta-Analysis of RCTs
*ahmed magan - University College London Hospital - London, GB
Olivia Dunseath - University College London Hospital - London, United Kingdom
Panagiotis Armonis - University College London Hospital - London, United Kingdom
Andreas Fontalis - University College London Hospital - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: ahmedmagan@gmail.com
Introduction
Background: The intra-operative use of tourniquets during Total Knee Arthroplasty (TKA) is common practice. The advantages of tourniquet use include decreased operating time and the creation of a bloodless visualisation field. However, tourniquet use has recently been linked with increased postoperative pain, reduced range of motion, and slower functional recovery. Importantly, there is limited evidence of the effect of tourniquet use on infection risk. This systematic review and meta-analysis aim to fill this gap in the literature by synthesising data pertaining to the association between tourniquet use and infection risk in TKA.
Methods: A systematic literature search was performed on Pubmed, Embase, Cochrane and clinicaltrials.gov until May 2021. Randomised control trials (RCTs) were included, comparing TKA outcomes with and without tourniquet use. The primary outcome was the overall infection rate. Secondary outcomes included superficial and deep infection, skin necrosis, skin blistering, DVT rate, and transfusion rate.
Results: 14 RCTs with 1,329 patients were included. The pooled incidence of infection in the tourniquet group (4.0%, 95% CI=2.7-5.4) was significantly higher compared to the non-tourniquet group (2.0%, 95% CI=1.1-3.1) with an OR of 1.9 (95% CI=1.1–3.76, p=0.03). The length of hospital stay, haemoglobin drop (0.33 95% CI =0.12 – 0.54), P=0.002) and transfusion rates (OR of 2.7, 95%CI = 1.4 - 5.3, P=<0.01) were higher in the tourniquet group than the non-tourniquet group. The difference in the length of in-hospital stay was 0.24 days favouring the non-tourniquet group (95% CI = 0.10 – 0.38, P=<0.01). The incidence of skin blistering (OR 2.6, 95% CI=0.7-9.9, p=0.17), skin necrosis (OR 3.0, 95% CI=0.50-19.3, p=0.25), and DVT rates (OR 1.5, 95% CI=0.60- 3.60, p=0.36) did not differ between the two groups.
Conclusion: Quantitative data synthesis showed that tourniquet use was associated with an increased overall risk of infection, intraoperative blood loss, need for blood transfusion, and longer hospital stay. Tourniquet use did not increase the risk of skin blistering or DVT. Arthroplasty surgeons should be considerate of these additional risks and complications associated with tourniquet use in TKA. This systematic review and meta-analysis do not support the routine use of tourniquets in TKA.
#8008
Return to Sports and Physical Activity After Unicompartmental Knee Arthroplasty: A Systematic Review and Meta-Analysis
*ahmed magan - University College London Hospital - London, GB
Ganan Radhakrishnan - Univeristy College London - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Flaminia Ronca - University College London - London, United Kingdom
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: ahmedmagan@gmail.com
Introduction
With OA affecting a younger population keen to maintain an active lifestyle, patients often question the time taken to RTS. Unicompartmental knee arthroplasty (UKA) is particularly used in patients who suffer from isolated medial or lateral OA. This is the first systematic review and meta-analysis that attempts to guide both surgeons and patients.
Objective
The primary objective was to carry out a systematic review and meta-analysis of published literature on UKA and the time to RTS following surgery.
Methods
The PRISMA guidelines were followed to undertake this meta-analysis. A search was performed on MEDLINE, EMBASE and the Cochrane Library with the keywords “arthroplasty” and “return to sports” from inception to August 2020. The quality of the articles was graded according to the Methodological Index for Nonrandomised Studies checklist. The primary outcome assessed was the time taken for RTS. The secondary outcomes were the percentage of RTS patients and validated patient recorded outcome scores.
Results
A total of 10 studies were reviewed with a patient population of 730. The time taken to RTS was between 1 month and 24 months, 53.28% RTS within 3 months, and 76.68% RTS within 6 months. Walking had the quickest return to sports with an average 7.87 weeks (SD: 8.4), whilst tennis had an average RTS of 10.1 weeks (SD: 2.5). Robotic UKA had a significantly quicker RTS of 4.2 months compared to the conventional jig based approach of 10.5 months (p<0.001)
Conclusion
Using the random effect model, the overall pooled data highlighted that 91.70% of the total number of patients RTS between 1 and 24 months after surgery, 76.68% of patients returned within 6 months of surgery. Low-intensity sports such as walking had the highest number of patients returning to sports, whilst robotic surgery had the best outcomes for patients. This systematic review and meta-analysis serve as useful guidance for clinicians and patients to predict the time patients are likely to RTS after UKA.
#8012
Gait Studies of Robotic Total Knee Arthroplasty Versus Conventional Jig-Based Outcomes: Results of a Prospective Randomised Controlled Trial
*Dia Giebaly - University College London Hospital - London, United Kingdom
Shanil Hansjee - University College London Hospital - London, United Kingdom
ahmed magan - University College London Hospital - London, GB
Vishal Rajput - University College London Hospital - London, United Kingdom
Andreas Fontalis - University College London Hospital - London, United Kingdom
Babar Kayani - University College Hospital London - London, United Kingdom
Jenni Tahmassebi - UCLH - London, UK
Fares Haddad - University College London Hospital - London, United Kingdom
*Email: dia.giebaly@doctors.org.uk
Background
The exact aetiology of patient dissatisfaction (up to 20%) in Total Knee Arthroplasty (TKA) is unclear. There is growing literature showing that robotic-arm assisted knee arthroplasty is associated with improved accuracy of implant positioning, better short- to mid-term functional scores and reduced revision rates compared with conventional jig based TKA. Altered tibial rotation and intercomponent rotation in TKA have been shown to link to increased knee pain, and patellofemoral complications. The recent evolution in intraoperative surgical aids, such as computer navigation and robotic technology, have offered the opportunity to assess patient-specific knee kinematics intraoperatively and obtain more physiological limb alignment targets and potentially better markers of gait function post operatively.
Objectives
The aim of this study is to detect differences in gait between robotic assisted and conventional knee arthroplasty. We hypothesized that patients after robotic TKA would reach higher walking speeds and inclines compared with conventional TKA and would enable a more natural gait.
Study Design & Methods
This prospective randomised controlled trial included 30 patients with symptomatic knee osteoarthritis undergoing conventional TKA versus robotic TKA. This study included 13 male patients and 17 female patients. All patients had primary TKA by two surgeons under the direct supervision of the senior author at UCLH.
Gait analysis was performed with an instrumented dual-belt treadmill, with force plates underneath both belts to record the kinetics of each step, left and right, independently at increasing speed and inclination (maximum 10 degrees).
Results
There were no differences in baseline demographics or preoperative radiological deformity between the two groups. Mean age 68.7 in the conventional TKA group and 67.9 in the robotic TKA group. Mean BMI was 27.5 in the conventional TKA group and 27.0 in the robotic TKA group. Mean pre-operative limb alignment was 3.4 degrees in the conventional TKA group and 3.1 degrees in the robotic TKA group.
Gait studies were performed at mean follow up at 27.8 months. No difference was found in the two groups at low walking speed. With increasing walking speed, the robotic TKA group reached a higher speed compared with conventional TKA. Gait analysis revealed significantly better cadence, walking speed, stride length and stance time in the robotic TKA group.
Robotic TKA patients tolerated more weight on the operated side at high walking speed. Fixed walking speed and an increasing incline showed no statistically significant differences were seen between robotic TKA and conventional TKA patients.
Conclusions
Robotic assisted surgery in total knee arthroplasty improves outcomes of gait performed under increased physical demand. robotic assisted TKA patients reached a higher walking speed and preserved a more normal weight acceptance compared with conventional TKA patients.
#7787
General Versus Regional Anesthesia in Shoulder Arthroplasty: A NSQIP Analysis Between 2008 and 2016
*David Mai - SUNY Downstate Health Sciences University - New York, United States of America
Thy Vo - SUNY Downstate Health Sciences University - Brooklyn, USA
Elver Ho - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Nayeem Uddin - SUNY Downstate Medical Center - BROOKLYN, United States of America
Ryan Kong - SUNY Downstate - Brooklyn, United States of America
Shreya Jain - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Benjamin Sanits - SUNY Downstate Health Sciences University - Staten Island, United States of America
Adam Wolfert - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Faisal Elali - SUNY Downstate Health Sciences University - Brooklyn, Select Country
Benjamin Krasnyanskiy - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Danielle Casagrande - SUNY Downstate Health Sciences University - Brooklyn, USA
*Email: david.mai@uwalumni.com
Shoulder arthroplasty is a commonly performed procedure. It is used to relieve pain and restore functions in degenerative and traumatic conditions affecting the glenohumeral joints. This study compared 30-day postoperative morbidity and mortality in patients who were given either general anesthesia or regional anesthesia for shoulder arthroplasty.
The ACS NSQIP database was queried via CPT codes between 2008 and 2016 for total, revision, and hemi-shoulder arthroplasty procedures (23472, 23470, 23473, and 23474). These procedures were then categorized into general or regional anesthesia. One-to-one propensity score matched controlling for estimated probability of morbidity, age, and gender were performed. Patient demographics, comorbidities, and 30-day post-operative outcomes were collected. Univariate analysis and multivariate logistic regression models controlling for the above covariates were used to identify general or regional anesthesia as risk factors for postoperative outcomes.
From 2008 to 2016, 17891 patients underwent shoulder arthroplasty procedures. 341 patients were given general anesthesia and 11900 patients were given regional anesthesia. Using 1:1 propensity score matching, 338 patients having undergone general or regional anesthesia were isolated. For the propensity matched cohort, the mean age was 69.29, 230 (48.7%) were male, 242 (51.3%) were female, and 393 (83.3%) were white. 75 (15.9%) of patients had diabetes, 297 (62.9%) had hypertension requiring medication, 47 (10%) were smokers, 42 (8.9%) had chronic obstructive pulmonary disease (COPD), 102 (21.6%) had anemia, 22 (4.7%) had steroid usage, and 10 (2.1%) had bleeding disorder. 226 (47.9%) patients were ASA class 2 and 221 (46.8%) were ASA class 3. Patients with ASA class 3 or 4 were more likely to be given general anesthesia (177, 54.0%) compared to regional anesthesia (151, 46.0%) (p=0.045). Patients with COPD were more likely to undergo general anesthesia than regional anesthesia (15, 4.5% vs 28, 8.6%, p = 0.029). Anesthetic type was not associated with increased rates of postoperative complications, adverse events, readmission, reoperation, or mortality (all, p ≥0.373). Anesthetic type was not found to be an independent predictor for postop complications, readmission, reoperation, or mortality between the two groups (all, p ≥0.210).
In the setting of total, revision, or hemi-arthroplasty procedures, general anesthesia was associated with higher rates of DVT/Thrombophlebitis compared to regional anesthesia. Neither regional nor general anesthesia was an independent predictor for post-op morbidities, readmission, reoperation, or mortality. Previous studies have shown that regional anesthesia was associated with greater rates of discharge, lower hospital complications, and reduced rates of hospital readmission compared to general anesthesia with and without regional blockade in the setting of total shoulder arthroplasty. Our study provides additional evidence for potential benefits of regional anesthesia in patients undergoing shoulder arthroplasty.
#7789
Effects of Having Acquired Immunodeficiency Syndrome on Postoperative Outcomes of Primary Shoulder Arthroplasty Patients
*David Mai - SUNY Downstate Health Sciences University - New York, United States of America
Elver Ho - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Ryan Kong - SUNY Downstate - Brooklyn, United States of America
Jigar Govind - SUNY Downstate Health Sciences University - Brooklyn, USA
Benjamin Krasnyanskiy - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Faisal Elali - SUNY Downstate Health Sciences University - Brooklyn, Select Country
Adam Wolfert - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Danielle Casagrande - SUNY Downstate Health Sciences University - Brooklyn, USA
*Email: david.mai@uwalumni.com
Acquired Immunodeficiency Syndrome (AIDS) is a chronic, potentially life-threatening condition caused by the HIV virus that results in severe immune dysfunction. The impact of having AIDS on postoperative outcomes of patients undergoing Primary Shoulder Arthroplasty (PSA) is poorly understood.
The National Inpatient Sample was queried to identify patients who underwent PSA surgery (ICD9: 8180, 8181, 8188) from the years 2005 – 2012. Patient demographics and incidence rates of patients that had been diagnosed with AIDS were reported from the years 2005 – 2012. 1:1 propensity score match controlling for age, sex and obesity was performed. Univariate analysis was used to compare differences in postoperative complications, revision of shoulder arthroplasty (ICD9: 8197) and in-hospital mortality in the AIDS cohort. Multivariate logistic regression analysis controlling for age, sex and obesity was done to determine AIDS status as an independent risk factor for postoperative complications between the two cohorts.
A cohort of 53 AIDS patients and 53 non-AIDS patients were identified. Both cohorts had similar sex (5.7% vs 11.3% female), age (54.11 vs 51.17 years) and obesity (1.9% vs 1.9%) distributions. The average incidence rate of patients who had AIDS from 2005 – 2012 was 0.22 (95%CI: 0.18 – 0.27) per 1,000,000 person years [Figure 1]. Incidence rates of AIDS patients increased by 2.43% from the years 2005 – 2012 [Figure 1]. AIDS patients who underwent a PSA did not experience higher rates of postoperative surgical or medical complications (all, p>0.05) [Table 1]. Moreover, AIDS patients who underwent PSA surgery were not at increased risk for postoperative surgical or medical complications (all, p>0.05) [Table 2].
AIDS patients who underwent PSA did not experience higher rates of postoperative surgical complications or medical complications. These findings should be taken into consideration for these patients prior to PSA surgery.
Key Words: Acquired Immunodeficiency Syndrome; Primary Shoulder Arthroplasty; Postoperative Complications
Figures
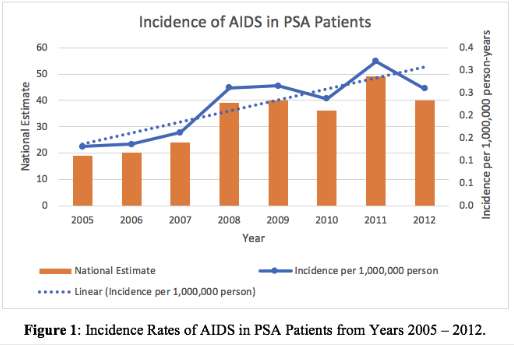
Figure 1
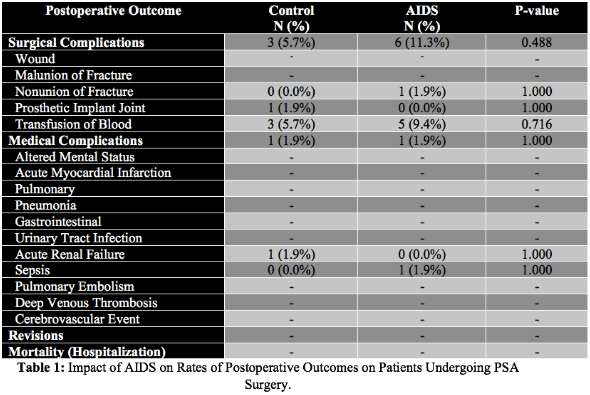
Figure 2
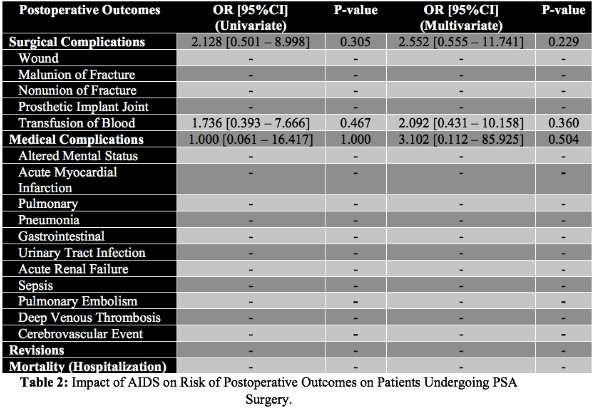
Figure 3#7791
Effect of Congestive Heart Failure on Postoperative Outcomes of Primary Shoulder Arthroplasty Patients
*David Mai - SUNY Downstate Health Sciences University - New York, United States of America
Elver Ho - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Ryan Kong - SUNY Downstate - Brooklyn, United States of America
Alex Jung - SUNY Downstate Health Sciences University - Staten Island, USA
Kurt Moskovitz - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Faisal Elali - SUNY Downstate Health Sciences University - Brooklyn, Select Country
Benjamin Krasnyanskiy - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Adam Wolfert - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Danielle Casagrande - SUNY Downstate Health Sciences University - Brooklyn, USA
*Email: david.mai@uwalumni.com
Congestive Heart Failure (CHF) is a condition in which the heart cannot pump sufficient blood to meet metabolic demand. The weakened heart may cause fluid to accumulate in other body tissues such as the lungs and lower limbs and can potentially be life-threatening. The impact of having CHF on postoperative outcomes of patients undergoing Primary Shoulder Arthroplasty (PSA) surgery is poorly understood.
The National Inpatient Sample was queried to identify patients who underwent PSA surgery (ICD9: 8180, 8181, 8188) from the years 2005 – 2012. Patient demographics and incidence rates of patients that had been diagnosed with CHF were reported from the years 2005 – 2012. 1:1 propensity score match controlling for age, sex, race, and obesity status was performed. Univariate analysis was used to compare differences in postoperative complications, revision of shoulder arthroplasty (ICD9: 8197) and in-hospital mortality in the CHF cohort. Multivariate logistic regression analysis controlling for age, sex and obesity status was performed to determine CHF status as an independent risk factor for postoperative outcomes between the two cohorts.
A cohort of 2,677 CHF patients and 2,677 non-CHF patients were identified. Both cohorts had similar sex (63.2% vs 64.8% female), age (74.5 vs 74.6 years) and obesity (17.6% vs 18.7%) distributions. The average incidence rate of patients who had CHF from 2005 – 2012 was 13.6 (95%CI: 11.8 – 15.4) per 1,000,000 person years [Figure 1]. Incidence rates of CHF patients increased by 107.4% from the years 2005 – 2012. (Figure 1). CHF patients who underwent a PSA procedure experienced higher rates of surgical complications, wound complications, non-union of fracture, prosthetic implant joint complications, transfusions, acute myocardial infarctions, pulmonary complications, pneumonia, urinary tract infections, acute renal failure, sepsis, pulmonary embolisms, cerebrovascular events, and in-hospital mortality (all, p<0.05) [Table 1]. Patients with prior CHF diagnosis who underwent PSA were at increased risk for postoperative surgical complications (OR=2.5), wound complications (OR=2.3), non-union of fracture (OR=2.6), prosthetic implant joint complications (OR=2.1), transfusions (OR=2.6), medical complications (OR=3.5), acute myocardial infarction (OR=4.8), pulmonary complications (OR=3.7), pneumonia (OR=4.2), urinary tract infection (OR=2.1), acute renal failure (OR=5.0), sepsis (OR=9.4), pulmonary embolism (OR=2.7), cerebrovascular event (OR=2.0) and in-hospital mortality (OR=10.8) [Table 2].
CHF patients who undergo PSA experienced higher rates of postoperative surgical, medical complications and in-hospital mortality. These findings should be taken into consideration in CHF patients to optimize them prior to PSA surgery and to prepare providers for such potential complications in the postoperative period.
Key Words: Congestive Heart Failure; Primary Shoulder Arthroplasty; postoperative Complications
Figures
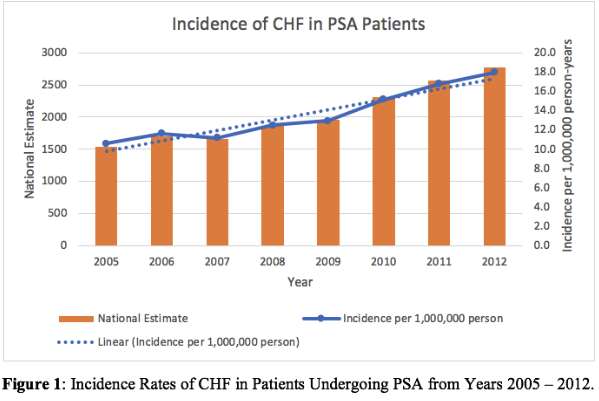
Figure 1
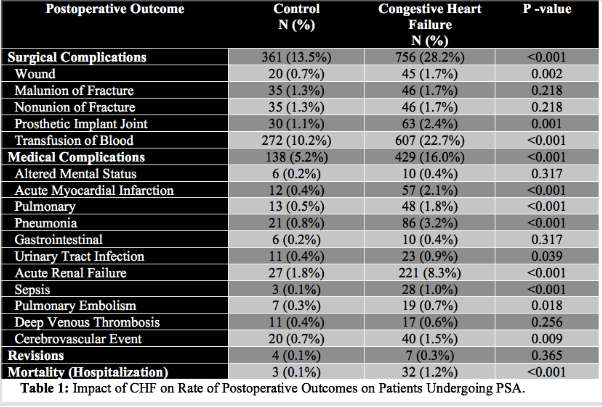
Figure 2
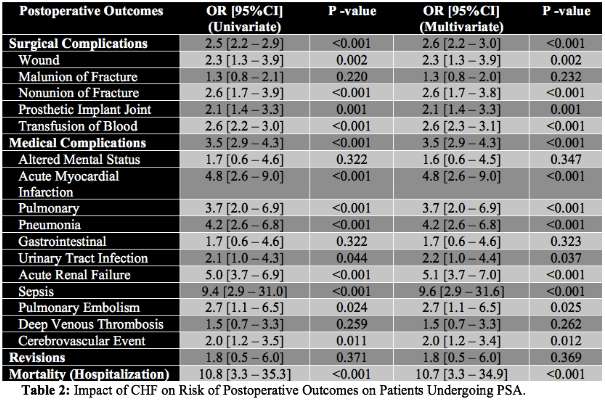
Figure 3#7792
Effect of Sickle Cell Anemia on Postoperative Outcomes of Primary Shoulder Arthroplasty Patients
*David Mai - SUNY Downstate Health Sciences University - New York, United States of America
Elver Ho - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Ryan Kong - SUNY Downstate - Brooklyn, United States of America
Naomi Newen - SUNY Downstate Health Sciences University - Stony Brook, United States of America
Faisal Elali - SUNY Downstate Health Sciences University - Brooklyn, Select Country
Adam Wolfert - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Benjamin Krasnyanskiy - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Danielle Casagrande - SUNY Downstate Health Sciences University - Brooklyn, USA
*Email: david.mai@uwalumni.com
Sickle cell anemia (SCA) is an inherited blood disorder caused by abnormal hemoglobin causing red blood cells to take an abnormal shape. This decreases the lifespan of red blood cells and can potentially cause blockage that stymies the flow of blood. The impact of SCA on patients undergoing primary shoulder arthroplasty (PSA) surgery is poorly characterized.
The National Inpatient Sample was queried to identify patients who underwent PSA surgery (ICD9: 8180, 8181, 8188) from the years 2005 – 2012. Patient demographics and incidence rates of patients that had been diagnosed with SCA were reported from the years 2005 – 2012. 1:1 propensity score match controlling for age, sex, race, and obesity status was performed. Univariate analysis was used to compare differences in postoperative complications, revision of shoulder arthroplasty (ICD9: 8197) and in-hospital mortality in the SCA cohort. Multivariate logistic regression analysis controlling for age, sex and obesity status was performed to determine SCA status as an independent risk factor for postoperative outcomes between the two cohorts.
A cohort of 141 SCA patients and 141 non-SCA patients were identified. Both cohorts had similar sex (61.0% vs 63.1% female) and obesity (10.6% vs 10.6%) distributions. The average incidence rate of patients who had an SCA from 2005 – 2012 was 0.66 (95%CI: 0.48 – 0.84) per 1,000,000 person years (Figure 1). Incidence rates of SCA patients increased by 10.25% from the years 2005 – 2012. (Figure 1). SCA patients who underwent a PSA procedure experienced higher rates of surgical complications and transfusions (all, p<0.05) (Table 1). Moreover, patients with prior SCA diagnosis who underwent PSA were at increased risk for surgical complications [OR=2.880, 95%CI=1.495 – 5.548, p=0.002) and transfusions (OR=3.550, 95%CI=1.755 – 7.178, p<0.001) (Table 2).
SCA patients who undergo PSA experienced higher rates of post-operative surgical complications and transfusions. These findings should be taken into consideration in SCA patients prior to PSA surgery.
Figures
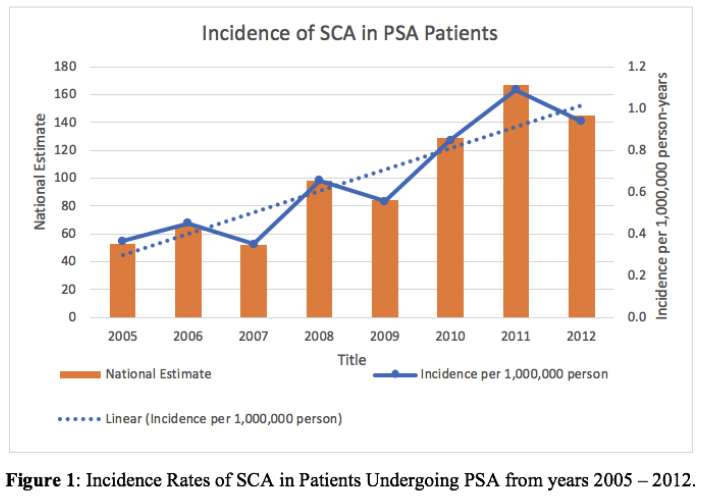
Figure 1
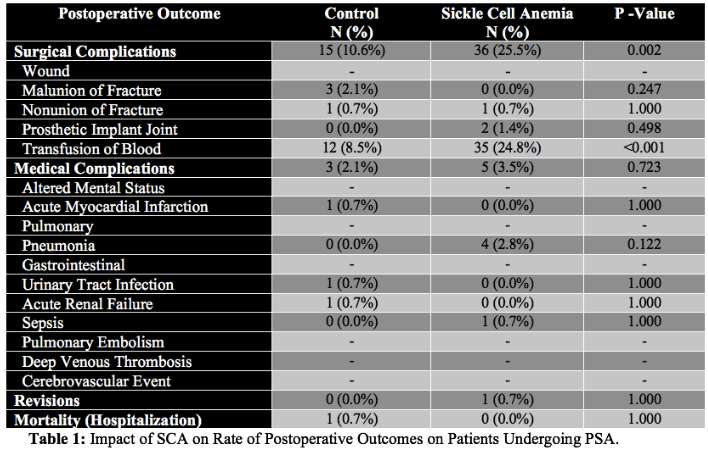
Figure 2
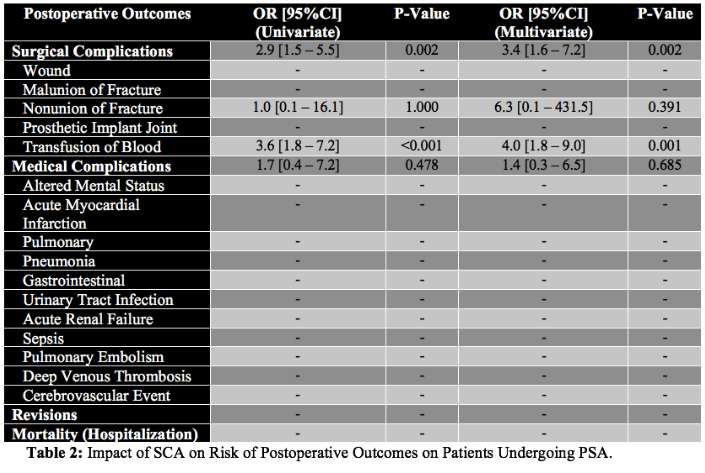
Figure 3#7790
Effect of Atrial Septal Defect on Postoperative Outcomes of Primary Shoulder Arthroplasty Patients
*David Mai - SUNY Downstate Health Sciences University - New York, United States of America
Elver Ho - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Ryan Kong - SUNY Downstate - Brooklyn, United States of America
Alexandra Nerantzinis - SUNY Downstate Health Sciences University - Brooklyn, United States of America
David Kim - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Adam Wolfert - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Benjamin Krasnyanskiy - SUNY Downstate Health Sciences University - Brooklyn, United States of America
Faisal Elali - SUNY Downstate Health Sciences University - Brooklyn, Select Country
Danielle Casagrande - SUNY Downstate Health Sciences University - Brooklyn, USA
*Email: david.mai@uwalumni.com
An Atrial Septal Defect (ASD) is a congenital heart defect in which there is a channel between the atria. This channel can vary in size and may lead to potentially life-threatening complications such as arrhythmias and/or heart failure. The impact of having an ASD on postoperative outcomes of patients undergoing Primary Shoulder Arthroplasty (PSA) is poorly understood.
The National Inpatient Sample was queried to identify patients who underwent PSA surgery (ICD9: 8180, 8181, 8188) from the years 2005 – 2012. Patient demographics and incidence rates of patients that had been diagnosed with an ASD were reported from the years 2005 – 2012. 1:1 propensity score match controlling for age, sex and obesity status was performed. Univariate analysis was used to compare differences in postoperative complications, revision of shoulder arthroplasty (ICD9: 8197) and in-hospital mortality in the ASD cohort. Multivariate logistic regression analysis controlling for age, sex and obesity status was performed to determine ASD status as an independent risk factor for postoperative outcomes between the two cohorts.
A cohort of 72 ASD patients and 72 non-ASD patients were identified. Both cohorts had similar sex (66.4% vs 66.2% female), age (73.08 vs 71.97 years) and obesity (18.2% vs 19.5%) distributions. The average incidence rate of patients who had an ASD from 2005 – 2012 was 0.30 (95%CI: 0.19 – 0.41) per 1,000,000 person years [Figure 1]. Incidence rates of ASD patients increased by 4.96% from the years 2005 – 2012 [Figure 1]. ASD patients who underwent a PSA procedure did not experience different rates of postoperative complications (all, p>0.05) [Table 1]. Patients with prior ASD diagnosis who underwent PSA were not at increased risk for postoperative complications (all, p>0.05) [Table 2].
ASD patients who underwent PSA did not experience higher rates of post-operative surgical or medical complications. These findings should be taken into consideration in ASD patients prior to PSA surgery.
Key Words: Atrial Septal Defect; Primary Shoulder Arthroplasty; Postoperative Complications
Figures
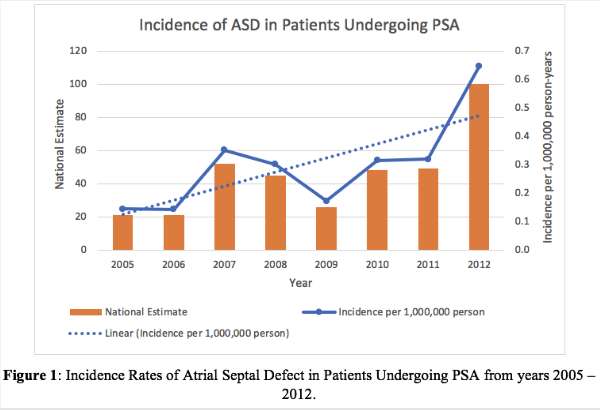
Figure 1
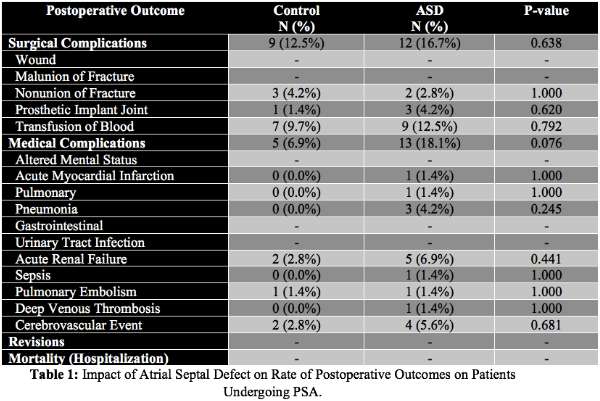
Figure 2
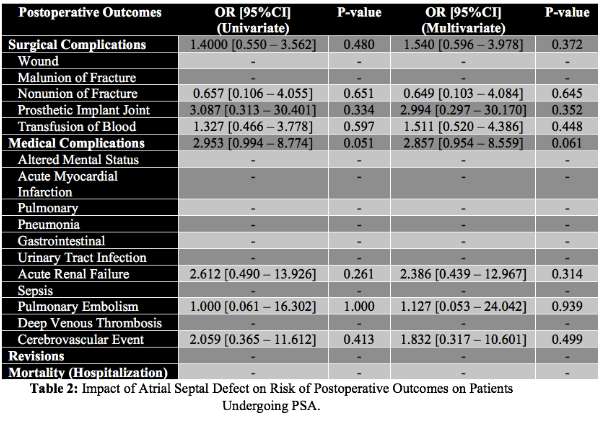
Figure 3#8040
Invited Talk: The uncemented paradox - current evidence for THA fixation
*Henrik Malchau - Massachusetts General Hospital - USA
*Email: hmalchau@partners.org
#8041
Invited Talk: Hip Replacement Bearings: Problem Solved
*William Maloney
*Email: wmaloney@stanford.edu
#7380
Perioperative Sleep Quality After Total Knee Arthroplasty.
*Takeo Mammoto - Mito, Japan
*Email: mammototakeo@mitokyodo-hp.jp
Introduction
Sleep is a vital and restorative human function. However, it has been reported that up to 50% of postoperative patients experience sleep disturbance during hospitalization. Sleep disruption could lead to intensified pain and even poor recovery. Orhtopaedic surgery, including total knee arthroplasty (TKA), could induce moderate to severe postoperative pain. Patients tend to suffer from postoperative pain, leading to sleep problems.
The purpose of this study was to evaluate postoperative sleep quality in patients undergoing TKA. It was hypothesized that postoperative patients would be very painful and that their sleep would be disturbed.
Methods
This was a single-center, prospective observational study approved by the IRB authority, and informed consent was obtained from the patients before their participation.
Thirty-three patients were included. Postoperative pain and sleep scores were evaluated by the visual analogue scale (VAS). Sleep status was evaluated from the day of admission through 7 days after surgery, by a mattress-type actigraphy without any direct sensor including bioelectrodes on the human body. Sleep status included that time of sleep, sleep cycle, hours of nocturnal awakening, latency of sleep onset, sleep stage (awaking - rapid eye movement (REM) sleep – non REM sleep), frequency of body motion, and sleep efficacy. Sleep efficacy was defined as the rate of actual sleeping time over total bedtime hours.
Results
Postoperative VAS pain scores were highest and sleep score was lowest at day 1. After then, pain score gradually decreased, and sleep score improved accordingly by day 7. Time of sleep was constant throughout the survey period. Sleep cycle and nocturnal awakening hours were shorter at the day of surgery. Latency of sleep onset was shorter at the day of surgery. The ratio of deep sleep stage (stage 3 to 4 of non-REM) was large and that of light sleep was low at the day of admission. After surgery, the ratio of deep sleep decreased, and the ratio of light sleep increased. Frequency of body motion was fewer at day of surgery. Sleep efficacy was superior at the day of surgery.
Conclusions
After surgery, VAS pain and sleep score showed a bi-directional relationship. Postoperative pain could lead to poor sleep quality. Poor sleep quality aggravates pain sensations. This results in a vicious circle of poor sleep quality, leading to intensified pain and even poorer sleep quality. Sleep disturbance could contribute to postoperative pain, which causes the inability to participate in postoperative rehabilitation, leading to delayed recovery and hospital discharge. The interaction between postoperative pain and sleep quality should be considered for postoperative care for patients.
ACKNOWLEDGEMENTS:
Japan Society for the Promotion of Science (JSPS) KAKENHI (19K18486).
#7505
Effect of Femur-Insert Size Mismatch on Tibiofemoral Joint Motions and Soft Tissue Structures
*Amit Mane - DePuy Synthes - Warsaw, USA
Michael Rock - DePuy Synthes Joint Reconstruction - Leeds, United Kingdom
Luke Aram - DePuy Synthes Joint Reconstruction - Warsaw, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
Stephen White - DePuy Synthes - Warsaw, USA
*Email: amane5@its.jnj.com
Introduction: Success of TKA surgery could be influenced by appropriate Implant sizing1 and its effect on optimal soft tissue balance2. The TKA solutions with matching Insert-Tray size typically allows mating multiple femoral components to one polyethylene-Insert, leading to size mismatched Femur-Insert (F-I) construct. Contrary, TKA solutions with matching F-I sizes offer mating of multiple Tray components to desired F-I construct. The F-I mismatch could alter T-F motions and its harmony with surrounding soft tissue. Therefore, primary objective of this research was to assess effect of size mismatched F-I construct on T-F motions and soft tissue behavior of three TKA solutions; and later compare their performances with size matched F-I TKA solution.
Methods: Previously validated Forward dynamics model (FDM, Fig.1)3 simulated deep knee bend (DKB) activity from 5⁰-100⁰ flexion in CR configuration. Study included one matched F-I construct, Concept-AMS, and three mismatched F-I constructs: Concept-PMC, Concept-PCR and Concept TCS (Fig.1). In Concept-PMC and Concept-PCR, two consecutive femoral sizes articulated with one Insert, and in Concept-TCS, one Femur mated with three compatible Insert sizes (Fig.1). In Concept-AMS, two consecutive matched sizes were simulated (Fig.1). Femoral lowest point (LP) motions, and Collaterals and PCL forces were reported.
Results: Concept-AMS experienced medial A-P translation of 1.1mm and continuous lateral roll-back of 6.3mm (Fig.2); furthermore, A-P motions were similar (≤ 0.4mm) for both matched F-I constructs. Concept-PMC and Concept-PCR demonstrated reversal of A-P motions in both mismatched F-I constructs. The A-P motions occurred within 2mm of each other on same Insert. In Concept-TCS medial condyle A-P translations were within 8.0-9.2mm for all F-I constructs; while A-P motions occurred within 6.0mm of each other. Concept-AMS experienced least changes in ligament forces, which increased gradually with flexion (Fig.3). Ligament forces variedwithin ±0.3BW for Concept-PMC and Concept-PCR, and within ±0.25BWfor Concept-TCS.
Conclusion: Intra-operatively, surgeons select Femur size using its A-P width4, and Tray size to achieve better tibial coverage5. When Insert-Tray are size-matched, smaller or larger Femur size can result in F-I mismatch. This mismatch is addressed at F-I articular interface by modifying Insert conformity, to allow mating with multiple Femoral sizes. Results demonstrated effect of compromised conformity when multiple Femurs mate with one Insert. The Femoral A-P translation varied within 2.0mm-6.0mm for Concept-PMC, Concept-PCR, and Concept-TCS (Fig.2). Although small, these magnitudes can significantly alter moments at knee during weight-bearing activities; especially, at tibial bone-Tray interface, while altering ligament contribution within ±0.3BW. Concept-AMS utilizes a LOGICLOCK™ locking mechanism, which allows mating of ±2 Insert sizes to a Tray, ensuring size matched F-I configuration by decoupling interface at Insert and Tray junction. Results highlighted benefits, similar T-F A-P motions and corresponding soft tissue recruitments, in Concept-AMS, which have been previously shown in harmony with each other6. In summary, F-I mismatch may introduce variation in the T-F A-P motions, potentially influencing the moments experienced at a knee joint, while introducing suboptimal soft tissue interaction.
References:
1. Dantany et al.-2016, 2. Wyss et al.-2006, 3. Khasian et al.-2020, 4. Yan et al.-2013, 5. Clary et al-2014, 6. Mane et al.-ORS-2022
Figures
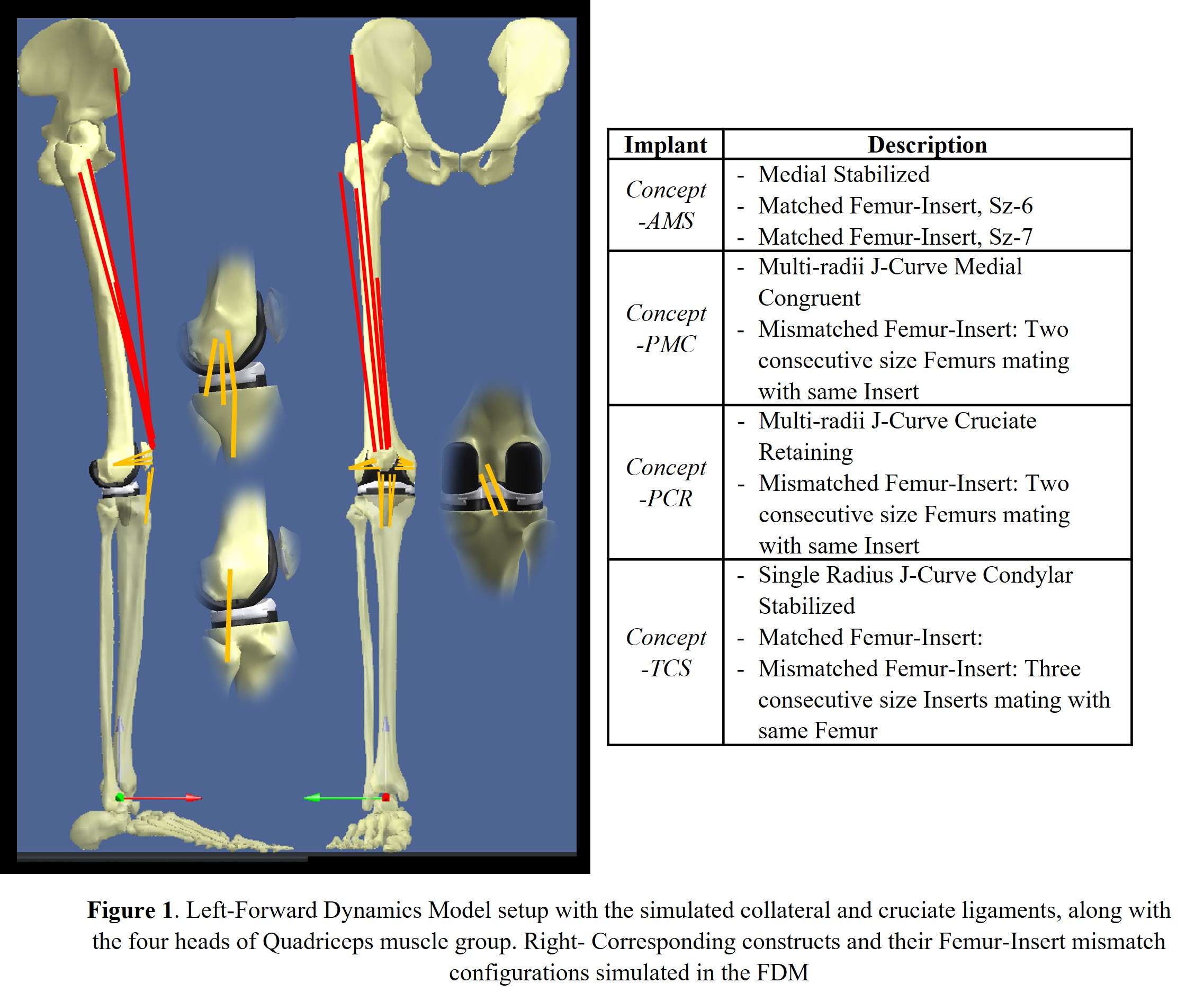
Figure 1
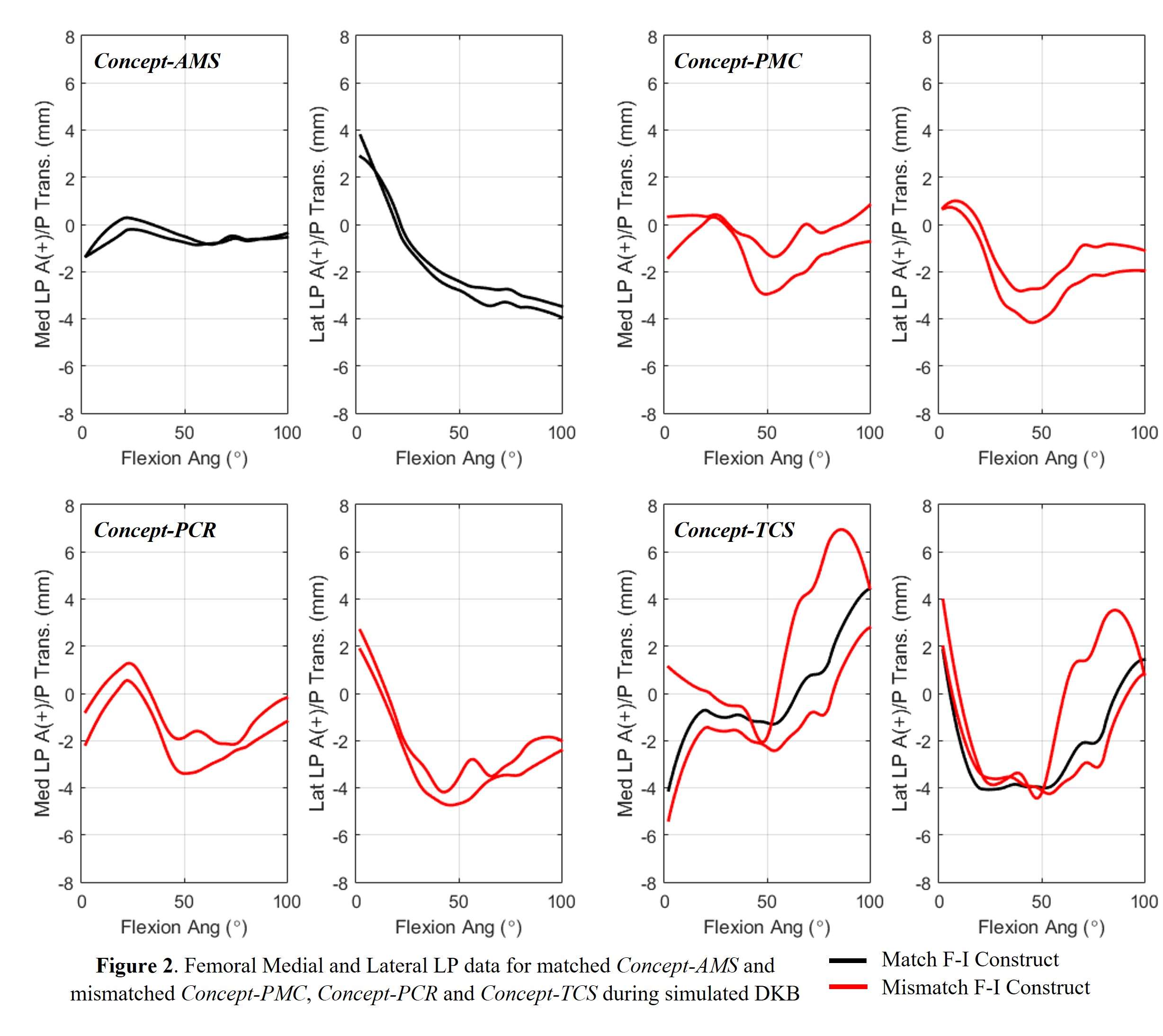
Figure 2
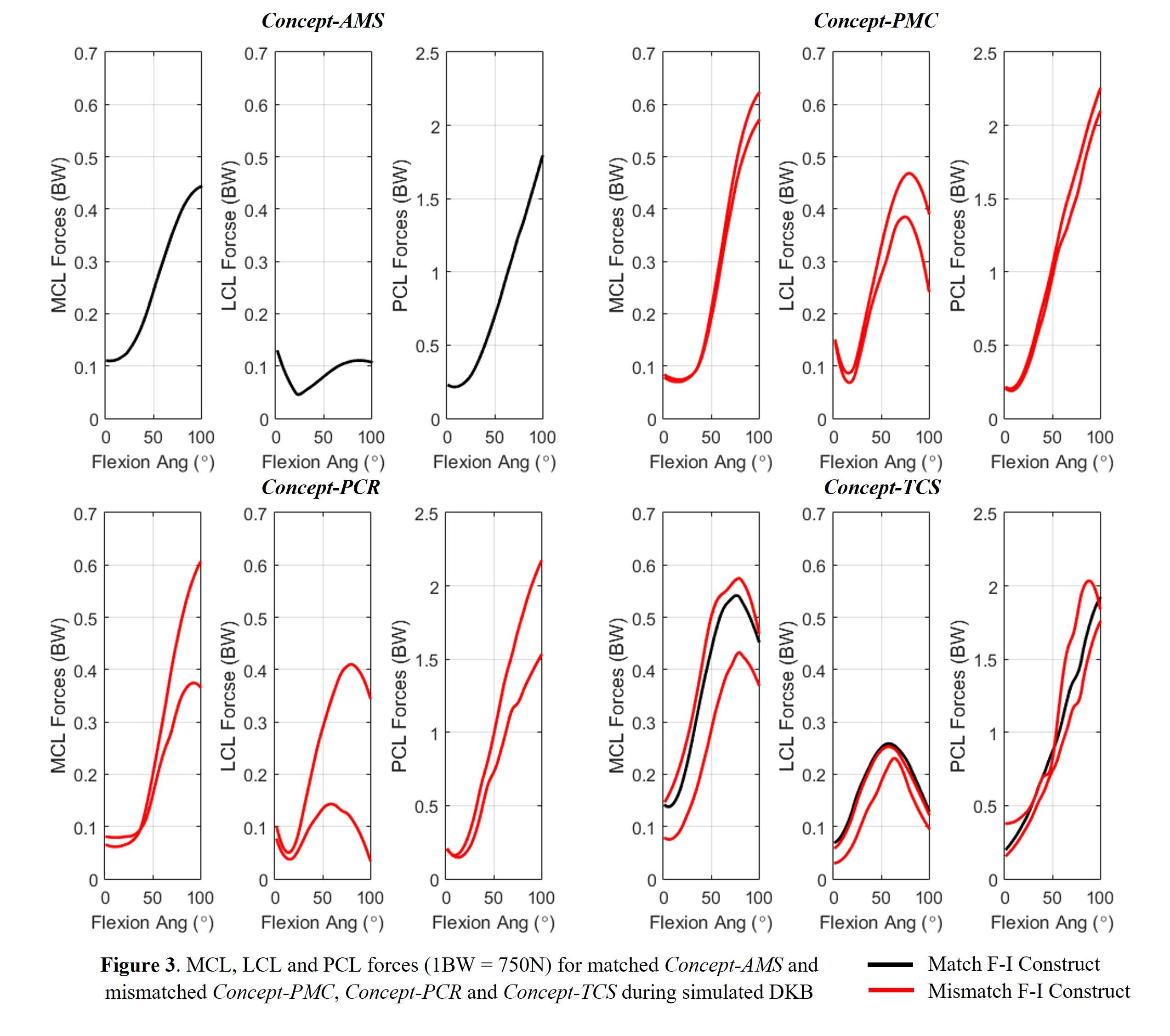
Figure 3#7506
Harmony Between Tibiofemoral Motions and Soft Tissue Structures of Two Unique Femoral J-Curves
*Amit Mane - DePuy Synthes - Warsaw, USA
Michael Rock - DePuy Synthes Joint Reconstruction - Leeds, United Kingdom
Luke Aram - DePuy Synthes Joint Reconstruction - Warsaw, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
Stephen White - DePuy Synthes - Warsaw, USA
*Email: amane5@its.jnj.com
Introduction: The medial pivot ball-and-socket knee has spherical medial tibiofemoral (T-F) articulation1. Their J-Curves utilizes a spherical radius (SR) section, followed by closing radius. These constructs have demonstrated minimal medial A-P translations during ADL1,2; however, motions occurring outside SR section of the J-Curves have not been studied thoroughly. Therefore, the objectives of this work were: First, to assess the interaction of SR designs with T-F A-P motion and soft tissues; especially, motions occurring after SR section of a J-Curve, and second, compare joint mechanics to that of non-SR medial stabilized design.
Methods: Previously validated Forward dynamics model (FDM) simulated deep knee bend (DKB) activity (Fig.1)3. The SR design, Concept-eMP, and medial stabilized design, Concept-AMS, were modeled in CR configuration, and DKB activity (5⁰-120⁰) was simulated in six subjects. The medial-lateral femoral lowest point (LP) motions, MCL and PCL forces, and deep and oblique MCL strains were reported in absolute magnitudes and normalized (to full-extension) magnitudes. The t-tests were performed to detect significant differences (p ≤ 0.05).
Results: The Concept-eMP revealed mean A-P translation of 2.4mm; with medial condyle translating posteriorly in early flexion, then anteriorly after 70⁰ flexion, followed by posterior and anterior translation at 90⁰ and 105⁰ respectively (Fig.2). The medial condyle of Concept-AMS remained stable and experienced mean A-P translation of 1.6mm. The absolute mean MCL and PCL forces were higher for Concept-eMP than those of Concept-AMS (Fig. 3), with significant differences in MCL forces during entire flexion, and during early flexion for PCL forces. Deep and oblique MCL strains were higher for Concept-eMP (Fig.3), with significant difference in oblique MCL strain. Normalized data demonstrated similar results, additionally highlighting significant increase in deep MCL strain in Concept-eMP.
Conclusion: Low-point motion patterns experienced by Concept-AMS demonstrated smaller medial A-P translation; similar to that of native patients4. The SR femur may force knee flexion-extension (F-E) axis to Implant derived F-E axis, irrespective of surrounding soft tissue and their preferences. Contrary, Concept-AMS uses CR femoral component, characterized with GRADIUS™ J-Curve, which has demonstrated harmony between T-F motions and soft tissue structures5,6. Observed higher absolute MCL and PCL forces, and increased absolute MCL Strains in Concept-eMP may indicate conflict between T-F motions and surrounding soft tissues. Intra-operatively, surgeon may detect and address increased ligament forces at full extension, by using thinner Insert or ligament release philosophies. However, normalized ligament data still demonstrated increased MCL force and strain for Concept-eMP. After 100⁰ flexion, i.e. beyond 0⁰-100⁰ of SR flexion arc, Concept-eMP experienced significantly larger medial anterior translation (Fig.2). At deeper flexion, both condyle of native knee translates posteriorly7. Despite smaller closing femoral radius, increased sagittal posterior-medial conformity of SR Insert may not allow femoral posterior translation with flexion, consequently keeping it more anterior. In summary, SR ball-on-socket may influence T-F A-P motions and its harmony with the surrounding soft tissue.
References:
1. List et. al. -2019, 2. Banks et al.-2016, 3. Khasian et al. -2020, 4. Johal et al.-2004, 5. Mane et al.- ORS-2021, 6. Mane et al.- ORS-2022, 7. Johal et al-2005
Figures
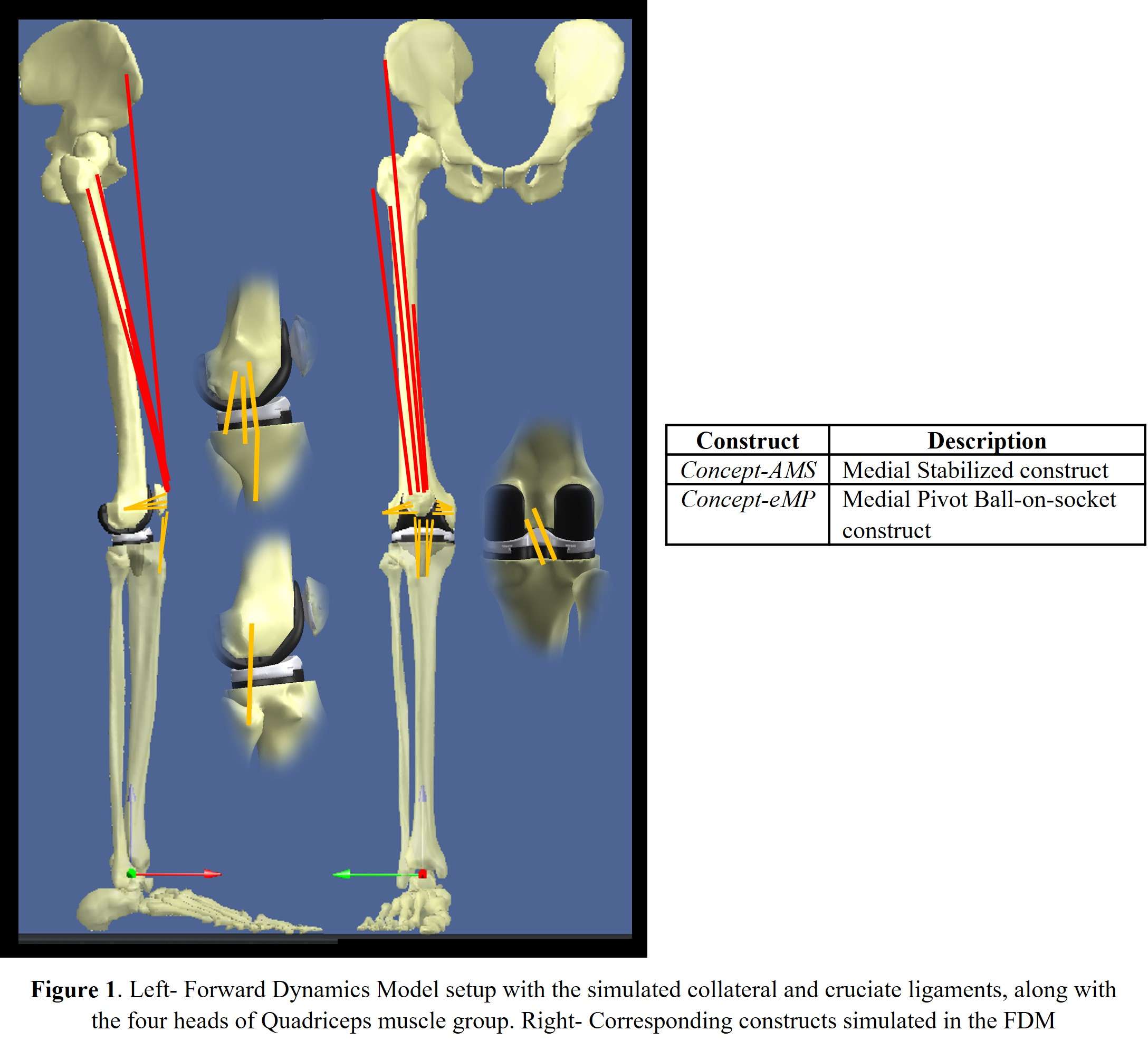
Figure 1
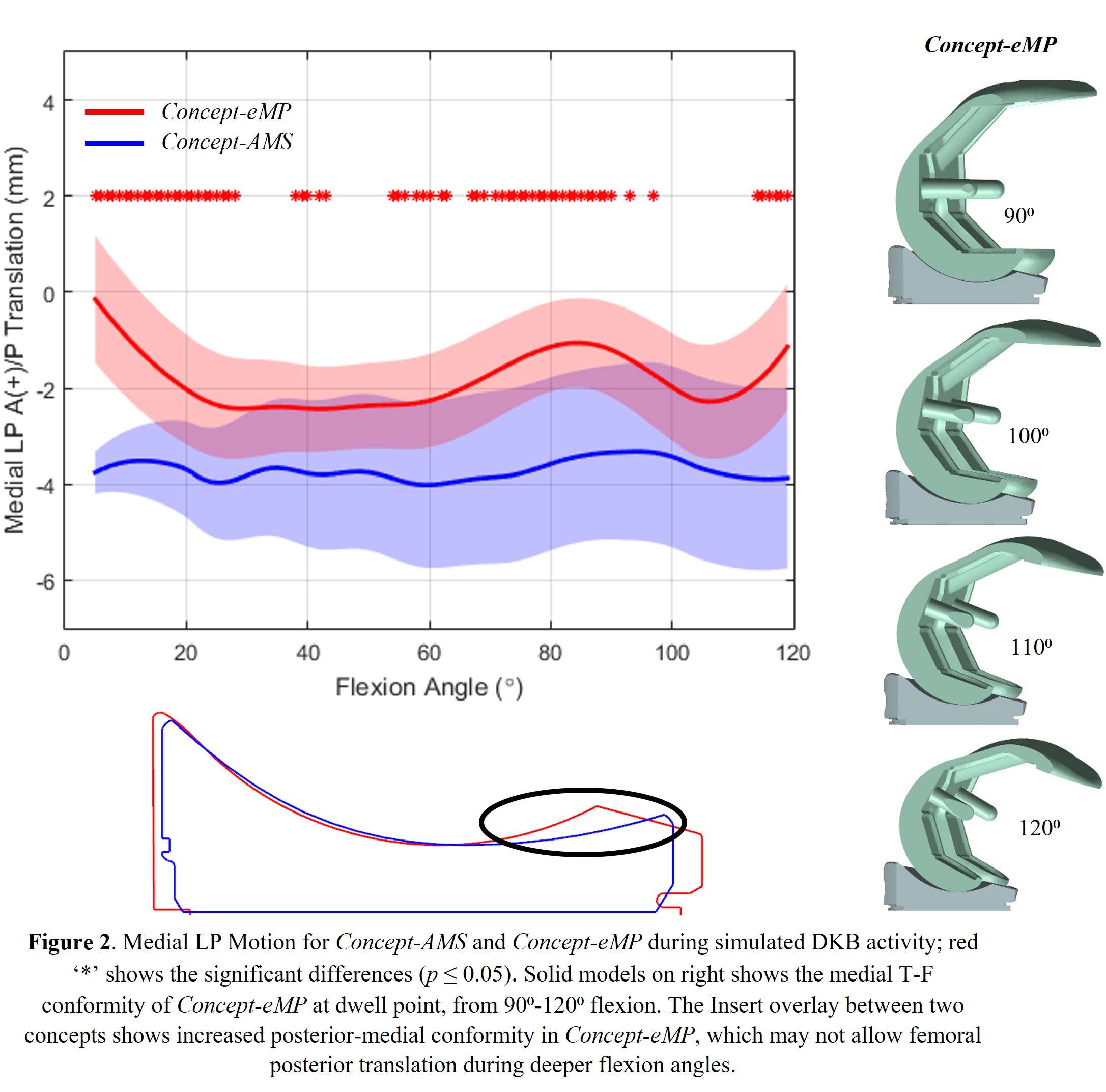
Figure 2
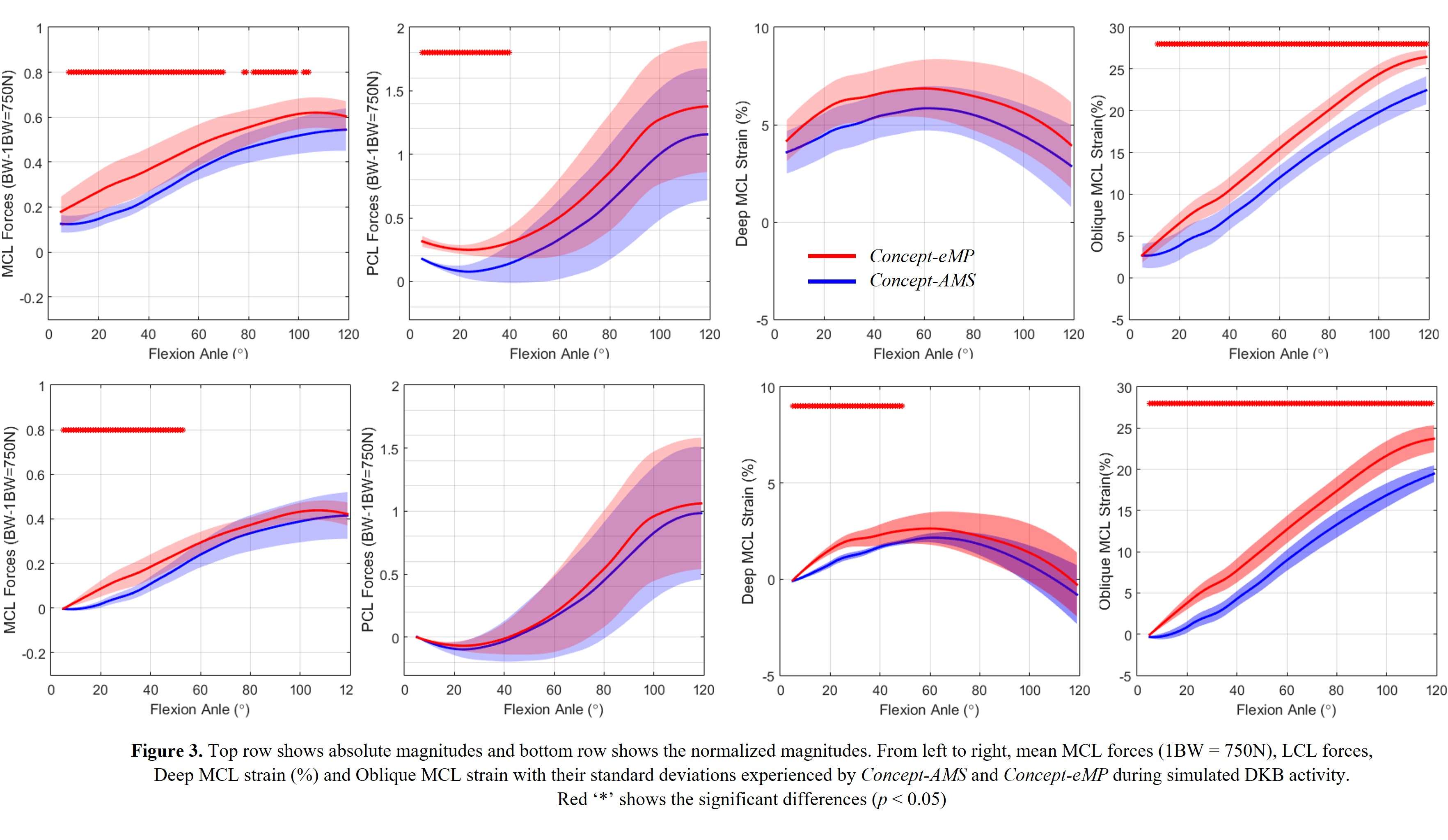
Figure 3#7730
Evaluating Primary Axial Stability of Cementless Humeral Stems
*Saandeep Mani - Zimmer Biomet - Warsaw, USA
Steven Meulink - Zimmer Biomet - Warsaw, USA
*Email: saandeep.mani@zimmerbiomet.com
Introduction: The ability to achieve and maintain biological fixation in shoulder arthroplasty relates in part to the ability to achieve good primary stability. Poor primary stability, defined in this case to be excessive bone-implant micro-motion under physiological loading prior to any bone ingrowth/ongrowth, may result in the generation of fibrous tissue rather than bone at the implant interface leading to a higher potential for eventual loosening of the implant. Therefore, the risk of loosening of cementless stems in shoulder arthroplasty under dynamic loading needs to be understood and shown to be sufficient. The objective of this study was to develop a test method to investigate stem loosening and evaluate the primary stability of cementless stem designs.
Methods: Based on the orientation and magnitude of glenohumeral forces (GHF), a load of 870N was determined to be appropriate in anatomic configuration. The orientation range for the physiological load vector is between 20°-40° with respect to the stem axis; the axial component of the worst-case orientation of the load was calculated as F = 870 X cos (20°), or F = 818N, and this load was applied along the stem axis as that is the worst-case configuration for this loading scenario. The summary of test parameters is given in Table 1 (Figure3). Displacement micro-motion measurements were collected via small mechanical linear displacement transducers (DVRTs) anchored to the foam block. Micro-motion was defined as the relative displacement between the stem and the foam block occurring between maximal and minimal load levels and this was considered to be representative of the interface micromotion between the stem and the foam block.
This test was performed in machined blocks of polyurethane foam (20pcf) conforming to the specifications of ASTM F1839 standard representing average proximal humeral bone properties. Six cementless humeral stems with porous coating on the proximal region intended to achieve a press-fit condition were tested. Before the stem was inserted into the foam block, the foam block was manually rasped using an appropriate size rasp. The stem was mated with the test fixture (Figure 1) and then inserted axially into the foam block until the desired insertion level was reached. The foam block was clamped at its base and the test was performed according to the general configuration illustrated in Figure 1 and details outlined in Table 1.
Results: The average micromotion of the stems were observed to be 52.12 ± 4.26 µm and a representative image of micromotion is shown in Figure 2.
Conclusion: Interface micro-motion in excess of 150µm has been associated with the formation of fibrous tissue and this 150µm value has been used as a threshold level by many investigators to determine whether a specific implant may be expected to provide sufficient primary stability to provide for bone on-growth. From the results, it is observed that the average micromotion values are considerably lower than 150µm. Future studies could compare the initial stability of different stem designs under different loading scenarios and investigate how that translates to clinical performance.
Keywords: stem loosening, shoulder, micromotion
Figures
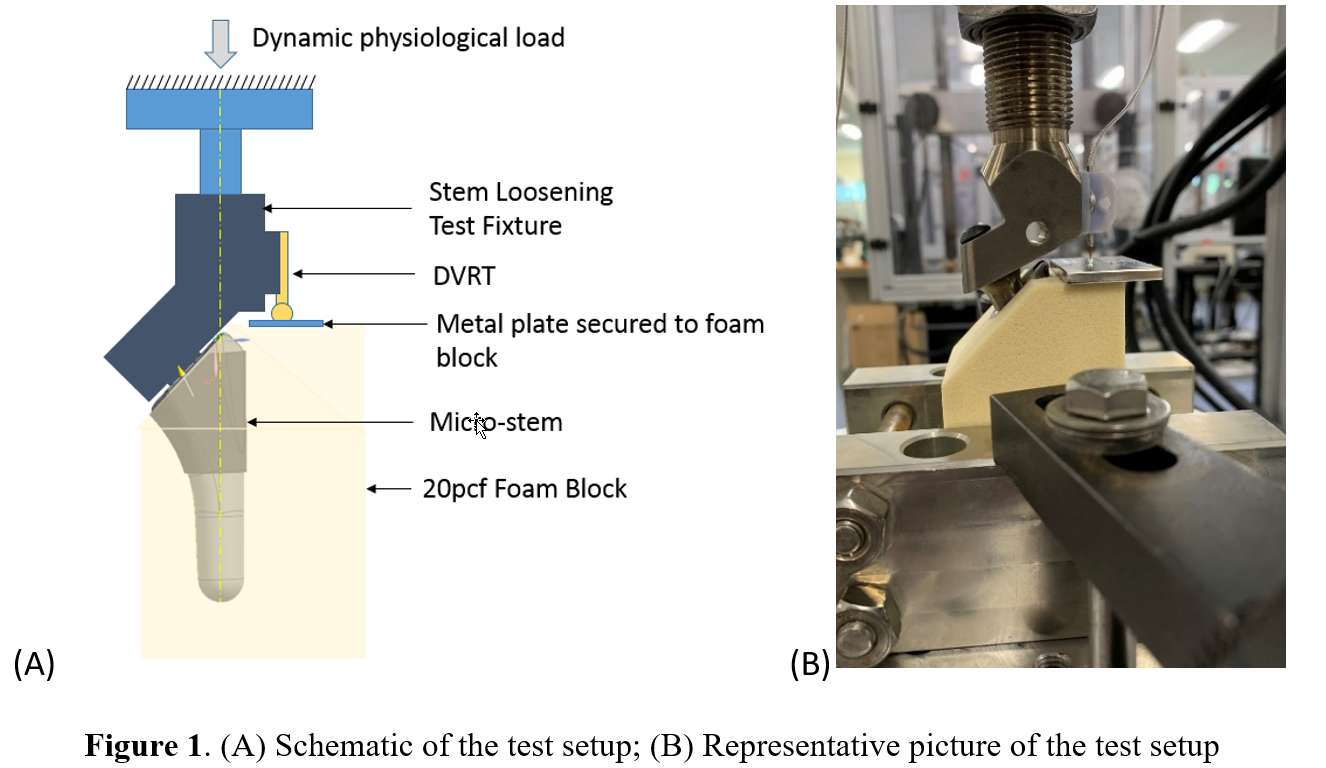
Figure 1
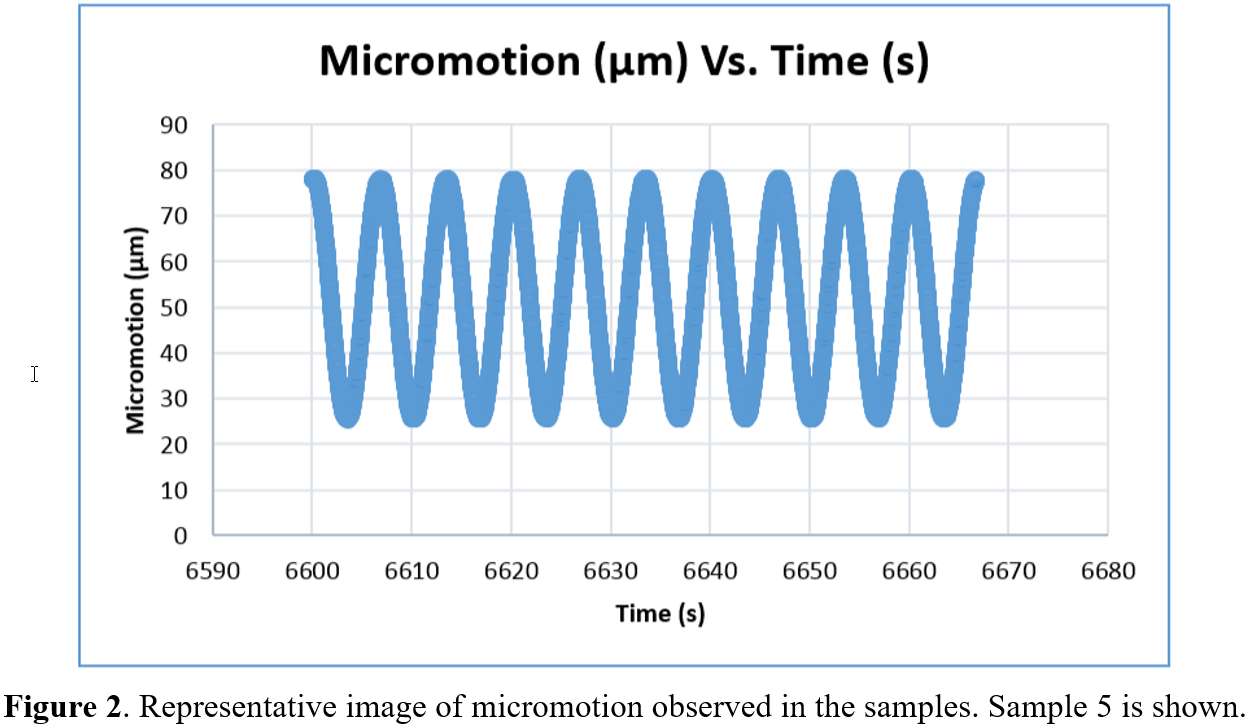
Figure 2
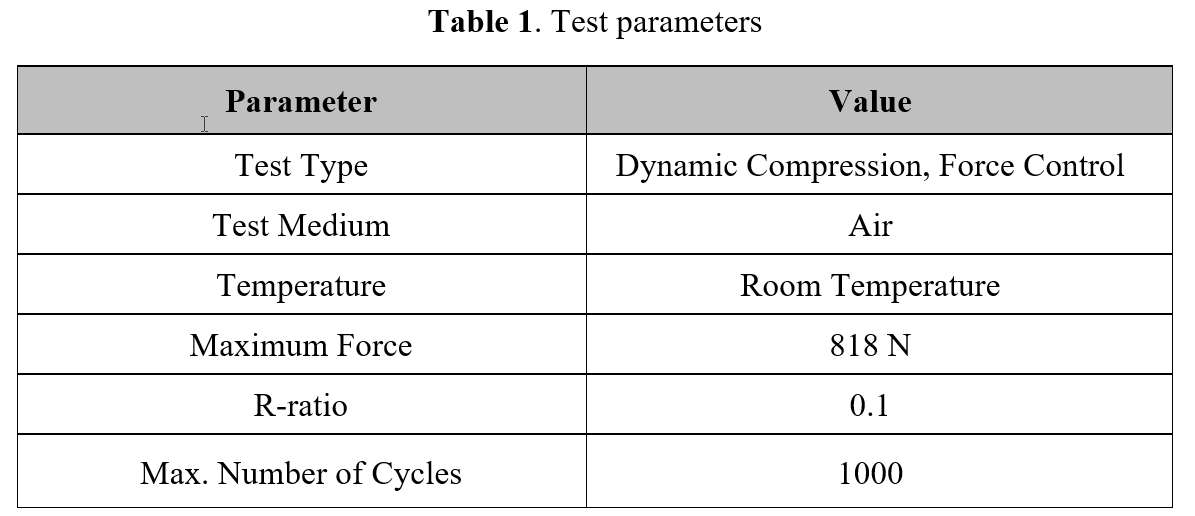
Figure 3#7824
Addressing Valgus Knees Using Robotic Assisted Total Knee Arthroplasty Methods
*Laura Yanoso-Scholl - Stryker Orthopaedics - USA
Kevin Marchand - Ortho Rhode Island - South County, USA
Kelly Taylor - Ortho Rhode Island - South County, USA
Daniel Erwin - Ortho Rhode Island - Wakefield, USA
Manoshi Bhowmik-Stoker - Stryker Orthopaedics - Mahway, USA
Robert Marchand - Ortho Rhode Island - South County, USA
*Email: Laura.Scholl@stryker.com
Introduction: Valgus deformity in an osteoarthritic knee can be difficult to correct with no clear consensus on case management. It has been reported that the surgeon must have detailed understanding of location, orientation and physical characteristics of soft tissues providing medial and lateral stability to address coronal and joint line restoration. To reduce inadvertent soft tissue damage in a valgus case, it has been suggested that precise bone resections could be applied while maintaining integrity of the soft tissue envelope. Robotic assisted (RA) technology has been shown to have 3D cut accuracy which could assist with addressing complex cases. The purpose of this work was to determine the number of soft tissue releases and component orientation of valgus cases performed with RA total knee arthroplasty (TKA).
Methods: This study was a retrospective chart review of cases performed by a single surgeon from July 2016 to December 2017. The surgeon performed 565 RA TKA of which 72 were defined as having valgus deformity pre-operatively. Initial and final 3D component alignment, knee balancing gaps, and component size were collected intraoperatively (Figure 1). Full or partial releases were documented intraoperatively. Post-operatively, radiographs, adverse events, and reduced WOMAC pain and KOOS Jr scores were collected at 6 months post-operatively.
Results: Pre-operatively, knee deformities ranged from reducible knees with less than 5mm of medial laxity to up to 12° with fixed flexion contracture. All knees were corrected within 2.5° (Figure 2) of mechanical neutral. All cases were adjusted intraoperatively prior to bony resection. In the final plan, average component position of the femur was 0.26o valgus, 4.07o flexion, 2.20o internal rotation. Where 68% of the femur were placed in internal rotation. Average component position of the tibia was 0.37o valgus, 2.96o slope, and 0.01o internal rotation. Where all tibial components were either placed with a neutral or valgus orientation. Medial and lateral gaps were balanced in extension 100% of cases and flexion 93% of cases. For component size prediction, the surgeon achieved their planned within one size on the femur 93.8% and tibia 100% of the time. The surgeon upsized the femur in 6.2% of cases. No soft tissue releases were reported in this study.
At latest follow-up, radiographic evidence suggested well seated and well-fixed components. Radiographs also indicated patella components were tracking well within the trochlear groove. Patient reported outcomes measures collected at 6-month follow up indicated an improvement in WOMAC pain score from 9.6 to 3.2 and improvement in KOOS JR from 44.7 to 74.4 points.
Discussion: In this retrospective case review, soft tissue releases were not needed to address valgus knees ranging from 1-12° of deformity. The surgeon was able to balance the knee with bone resections and avoid disturbing the soft tissue envelope. To achieve this balance, it was noticed for many of the valgus knees, the femoral component was oriented with internal and valgus rotations while the tibial component was oriented with valgus rotations. This allowed the surgeon to close the lateral gap and balance it with the medial gap.
Figures
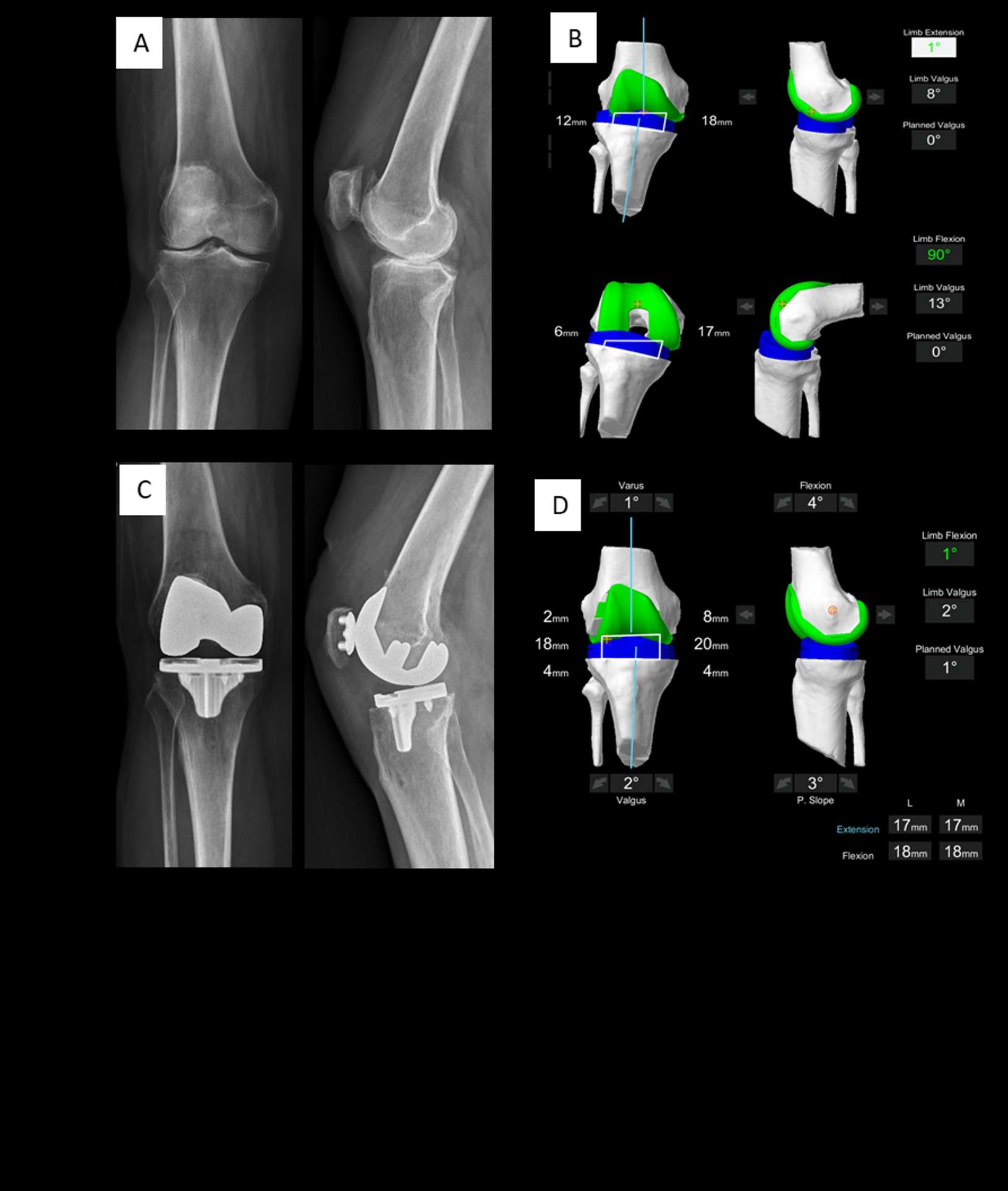
Figure 1
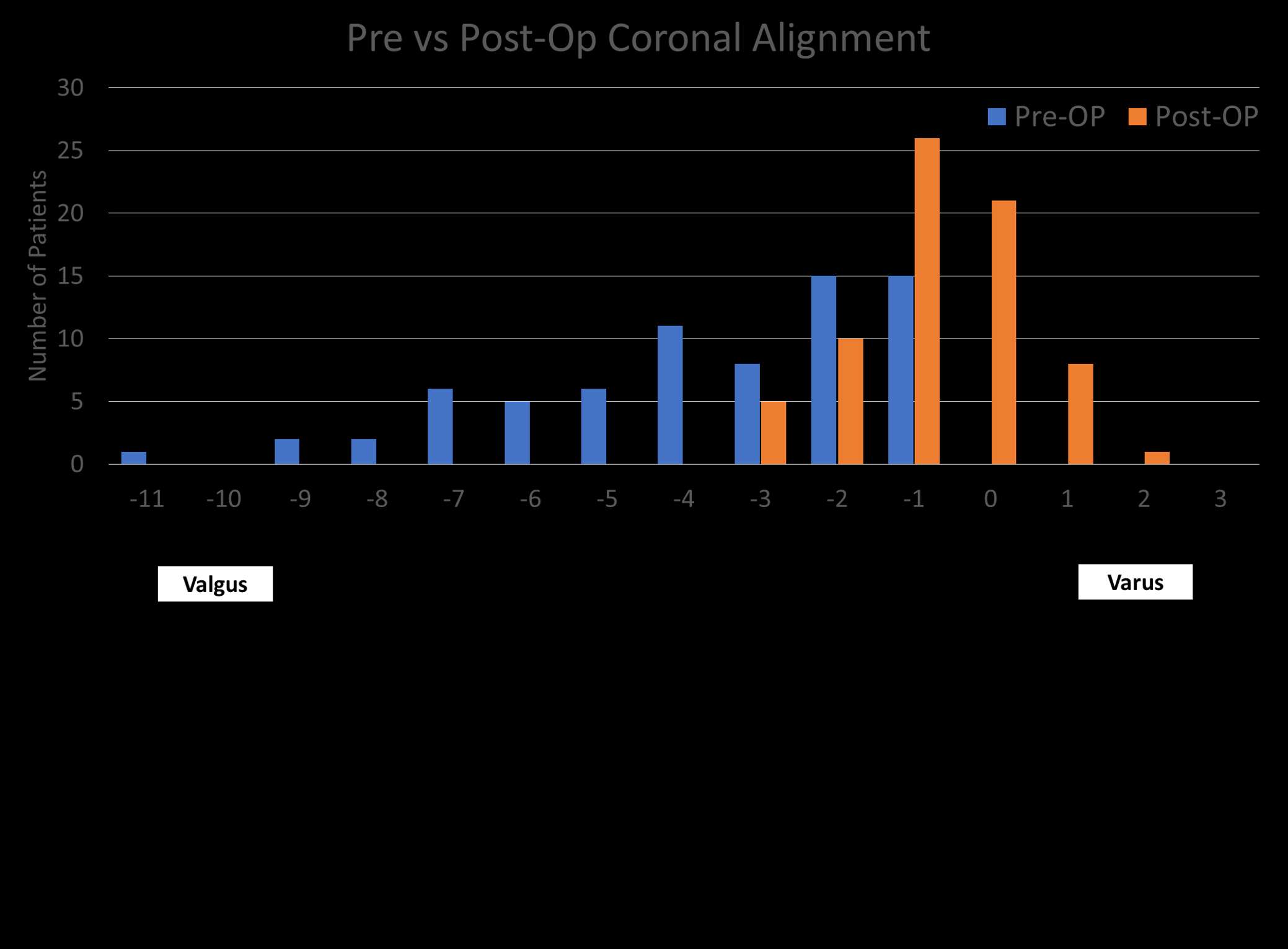
Figure 2#7875
Does Implant Positioning Change When Considering Functional Positioning? a Multi-Center Analysis
*Robert Marchand - Ortho Rhode Island - South County, USA
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
Ajay Lall - American Hip Institute - Chicago, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
Benjamin Domb - American Hip Institute - Des Plaines, USA
Seth A. Jerabek - Hospital for Special Surgery - New York, USA
*Email: bmarchand@orthopedicsri.com
INTRODUCTION: A common target for acetabular cup position during total hip arthroplasty (THA) is 40° inclination and 20° anteversion. However, optimal acetabular cup position can vary widely based on consideration of patient anatomy and pelvic position. Literature highlights influence of spinopelvic mobility where the type of spinal imbalance will cause surgeons to change acetabular cup position. The purpose of this study was to quantify percentage of cases where surgical plan deviates from a 40° inclination and 20° anteversion target based on spinopelvic mobility when considering functional implant planning.
METHODS: A multi-center, prospective study was performed on a cohort of 192 consented patients who received robotic-assisted THA with integration of software to incorporate patient’s pelvic tilt and virtual range-of-motion (VROM) to impingement. Preoperative CT scans were obtained in addition to standing and sitting lateral radiographs which were used to plan the femoral and acetabular component position as well as evaluate the patient’s range-of-motion to impingement, pelvic tilt, and cup position in the supine, stand and sit poses. If impingement was identified using the VROM tool, the surgeon was able to preoperatively adjust the planned implant positions to try to avoid impingement. Intraoperatively, either the direct anterior (DA) or posterior approach was used based on surgeon preference. Data on implant position were collected intraoperatively. A student’s t-test with a 95% confidence level was used to evaluate difference in implant position based on functional pelvic tilt. A Chi square test with 95% confidence level was used to compare percentage of cases outside of a 40° inclination and 20° version preoperative target.
RESULTS: Cases were separated into groups based on their pre-operative spinopelvic mobility moving from standing to sitting. 79.2% of cases were considered normal (change ≥10°) and 20.8% of cases were considered stiff (change <10°). The stiff cohort had a statistically significant larger planned supine cup version compared to the normal cohort (p=0.0001, 2.2° difference) while there was no difference in planned supine cup inclination (p=0.6882). Both cohorts had a majority of cases deviating from the 40° inclination and 20° version target (Table 1).
DISCUSSION: When considering a patient’s functional hip position, acetabular cup placement may deviate from the traditional target of 40° inclination and 20° version implant placement plan. This study evaluated the functional implant plan for a cohort of patients with either a stiff or normal preoperative spinopelvic mobility. For both groups, the average cup placed had greater inclination and version when compared to the 40°/20° target. It was also noticed that patients with stiff spinopelvic mobility had higher average anteversion which would reduce the risk of anterior impingement which is a concern for stiff patients when sitting. Based on these findings, considering factors such as pelvic tilt and VROM may influence a surgeon’s implant plan and obtaining additional preoperative imaging appears warranted. As such, this methodology allows a more personalized surgical plan that incorporates spinopelvic mobility rather than using the traditional generic target. Further studies are needed to report on the clinical success of patients with a functional hip plan.
Figures
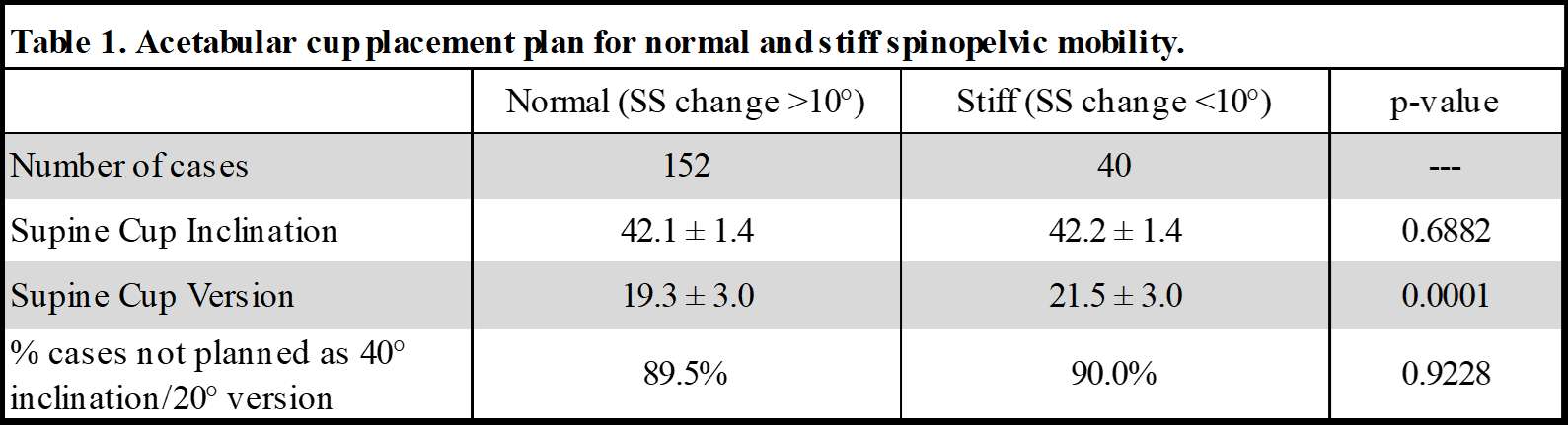
Figure 1#7883
Computed Tomography (CT) Required to Perform Robotic-Assisted Total Hip Arthroplasty (RaTHA) Can Reliably Measure Femoral Bone Mineral Density and Identify Previously Undiagnosed Femoral Osteoporosis
Brett Bukowski - University of Wisconsin - Madison, United States of America
Kevin Sandhu - University of Wisconsin - Madison, USA
James Bernatz - University of Wisconsin - Madison, USA
Neil Binkley - University of Wisconsin - Madison, USA
Perry Pickhardt - University of Wisconsin - Madison, USA
Paul Anderson - University of Wisconsin - Madison, USA
Robert Marchand - Ortho Rhode Island - South County, USA
*Richard Illgen - University of Wisconsin Hospital - Madison, USA
*Email: Illgen@ortho.wisc.edu
Title.
Computed Tomography (CT) Required to Perform Robotic-assisted Total Hip Arthroplasty (raTHA) Can Reliably Measure Femoral Bone Mineral Density and Identify Previously Undiagnosed Femoral Osteoporosis
Author names and affiliations.
Brett R. Bukowski BS, Kevin P. Sandhu MD, James T. Bernatz MD, Neil Binkley MD, Perry J. Pickhardt MD, Paul A. Anderson MD, and Richard L. Illgen II MD. University of Wisconsin School of Medicine and Public Health, Madison, WI.
Corresponding author.
Richard Illgen II, MD.
illgen@ortho.wisc.edu
Present/permanent address.
East Madison Hospital
4602 Eastpark Blvd
Madison, WI 53718
Background
Osteoporosis is underdiagnosed prior to total hip arthroplasty (THA). The purposes of this study were to: 1) utilize hip computed tomography (CT) to measure femoral bone mineral density (BMD) using CT X-ray absorptiometry (CTXA), 2) determine if routine CTXA analysis would improve identification of low BMD compared with dual energy X-ray absorptiometry (DXA), and 3) determine if improved recognition of decreased BMD would the affect the rate of cement fixation.
Methods
Retrospective chart review identified 78 patients with CTXA performed prior to robotic-assisted THA (raTHA) (Group 1). Group 1 was age- and sex-matched to 78 raTHAs that had a pre-operative hip CT, but did not have CTXA analysis (Group 2). Clinical demographics, femoral fixation method, CTXA, and DXA data were recorded.
Results
No significant demographic differences were noted comparing Groups 1 and 2. Pre-operative femoral BMD was available for 100% of Group 1 patients (CTXA) and 43.6% of Group 2 patients (DXA). CTXA analysis for all Group 1 patients pre-operatively identified 13 osteopenic and 8 osteoporotic patients that were not identified by the available pre-operative DXA data. Cemented fixation was used with higher frequency in Group 1 vs. Group 2 (28.2% vs 14.3%, respectively. P=0.03)
Conclusion
Valuable information can be obtained regarding proximal femoral BMD from pre-operative hip CT scans routinely obtained prior to raTHA. Systematic pre-operative evaluation with CTXA identified double the number of patients with femoral osteopenia, five-times the number with osteoporosis, and doubled the rate of cemented femoral fixation compared with the group with DXA alone.
Keywords:
total hip arthroplasty (THA); osteoporosis; osteopenia; pre-operative CT scan; robotics, fracture risk
Support was provided by an internal award from the University of Wisconsin School of Medicine and Public Health and the Herman and Gwendolyn Shapiro Foundation for one author (B.B.).
Introduction
Total hip arthroplasty (THA) has demonstrated excellent implant survivorship at long term follow-up intervals and has been termed by some as the “operation of the century” [1,2]. Outstanding clinical and radiographic results can be expected if complications can be avoided. Certain subgroups are at increased risk for complications related to periprosthetic fracture including elderly females with osteoporosis when cementless femoral fixation is utilized [3].
In the United States, cementless femoral fixation was used in 94% of all elective primary THA cases reported to the American Joint Replacement Registry (AJRR) in 2021, including 85% of patients age 80-89 and 66% of patients age >90 [4]. Remarkably, cementless femoral fixation still predominates when THA or hemiarthroplasty (HA) are performed to treat patients with femoral neck fractures (FNF) [4]. This high utilization of cementless femoral fixation in elderly osteoporotic patients in spite of evidence that cemented fixation results in reduced risk of fracture and revision has been termed the “uncemented paradox” [5]. This pattern has been noted in the United Kingdom with a documented correlation between the increased use of cementless femoral fixation and an increased prevalence of femoral periprosthetic fracture [6]. Such femoral periprosthetic fractures are associated with significant morbidity, mortality, and cost [7–10]. Systematically identifying patients at increased risk for periprosthetic fracture due to femoral osteoporosis would be clinically valuable and could represent an opportunity for bone health optimization and help guide the choice of femoral fixation.
Computed tomography (CT) performed for other indications can be utilized to diagnose osteoporosis, a method generally known as opportunistic screening [11,12]. This technique has been validated and has excellent correlation with dual-energy X-ray absorptiometry (DXA) scans [13]. One commercially available software for CT-based osteoporosis screening has been referred to as CT X-ray absorptiometry (CTXA) [13,14]. To our knowledge, utilizing opportunistic CT to identify osteoporosis prior to THA has not been studied to date. Hip CT scans are routinely performed prior to robotic-assisted THA (raTHA) with one robotic platform. The purposes of our study were to: 1) use the hip CT performed prior to raTHA to measure proximal femoral bone mineral density (BMD) and generate T-scores, 2) determine if systematic evaluation of pre-operative femoral BMD with CTXA would improve identification of osteopenia and osteoporosis compared with available standard pre-operative DXA analysis, and 3) determine if improved recognition of reduced proximal femoral BMD would affect the rate of cemented femoral fixation.
Materials and Methods
Institutional Review Board approval was obtained for this study. All raTHAs performed by a single surgeon at one institution between January 2018 and February 2021 were identified using a departmental database. Inclusion criteria were age ≥ 30 years undergoing primary raTHA during this time period. Exclusion criteria included cases of trauma and tumor. Retrospective chart review identified 78 patients (Group 1) that had pre-operative CTXA. CTXA analysis utilizes a validated software (Mindways Software, Inc., Austin, TX) and a phantom to calibrate the CT scanner. This process allows for accurate conversion of CT Hounsfield units (HU) generated with custom regions of interest in the proximal femur and total hip to calculate areal BMD (g/cm2) and DXA-equivalent T-scores (Figure 1) [13,15]. This methodology has been well-described in previous reports and there has been high correlation noted between CTXA and DXA [13,15]. Group 1 was age- and sex-matched to a group of 78 patients who had a pre-operative hip CT performed according to the standard protocol required for use of the raTHA platform (Stryker Mako, Kalamazoo, MI), but did not have pre-operative CTXA analysis available (Group 2).
Clinical and radiographic records were retrospectively reviewed. Demographics, medical co-morbidities, medications, prior DXA testing, and femoral fixation methods were recorded (Tables 1-2). The CTXA generated BMD and T-scores for the femoral neck, greater trochanter, intertrochanteric region, and total hip were recorded (Figure 1). The lowest T-score from either the femoral neck or the total hip was used to categorize patients as normal, osteopenic, or osteoporotic consistent with WHO guidelines [16].
Subgroup analysis was performed to evaluate females <65, females ≥ 65, and males ≥ 70 years old in Groups 1 and 2. The femoral BMD and T-scores were recorded based on available DXA and CTXA data for each group. Chi-square tests were used to compare categorical values, while continuous variables were evaluated with 2-sample t-tests assuming unequal variance.
Results:
Demographics
A total of 156 patients were included in the study with 78 patients in the Group 1 and 78 patients in Group 2. No significant differences were noted comparing patient demographics (Table 1).
Radiographic analysis
DXA
DXA data was available for 38.5% of Group 1 cases and 43.6% of Group 2 cases with 60% and 47.1% occurring within 2 years of raTHA in Groups 1 and 2 respectively. Bone health based on available DXA was categorized as 36.7% normal, 56.7% osteopenic, and 6.7% osteoporotic for Group 1 and as 29.4% normal, 61.8% osteopenic, and 8.8% osteoporotic in Group 2 (Table 2). No significant differences were noted comparing rates of normal, osteopenic, or osteoporotic patients for Group 1 vs. Group 2 based on available pre-operative DXA analysis (Table 2).
CTXA
CTXA identified 30 osteopenic patients in Group 1 including an additional 13 cases that were previously not recognized by available pre-operative DXA analysis (Tables 2 and 3). Similarly, CTXA identified 10 osteoporotic patients in Group 1 including an additional 8 cases of osteoporosis not identified on DXA analysis (Tables 2-3). CTXA identified 5-times the number of osteoporotic patients compared with DXA analysis alone (2 cases of femoral osteoporosis identified with DXA compared with 10 cases of femoral osteoporosis identified with CTXA). The percentage of normal, osteopenic, and osteoporotic cases were similar in Group 1 and 2 (Table 2), but less than half of Groups 1 and 2 had available pre-operative DXA data available.
Subgroup analysis of women ≥ 65 years of age and men ≥ 70 years of age
DXA was available within 2 years in less than 50% of females ≥ 65 and 0% of men ≥ 70 in both groups (Table 4). Systematically applying CTXA to Group 1 patients provided femoral BMD for all women ≥ 65 and men ≥ 70 for Group 1 (Table 5). In women ≥ 65, CTXA evaluation of Group 1 patients revealed an additional 6 patients with osteopenia and 7 patients with osteoporosis compared to DXA alone (Table 4-5). In men ≥ 70, CTXA identified 2 cases of osteopenia and zero cases of osteoporosis (Table 4-5).
Subgroup analysis of women ≥ 65 years of age and men ≥ 70 years of age
DXA was available within 2 years in less than 50% of females ≥ 65 and 0% of men ≥ 70 in both groups (Table 4). Systematically applying CTXA to Group 1 patients provided femoral BMD for all women ≥ 65 and men ≥ 70 for Group 1 (Table 5). In women ≥ 65, CTXA evaluation of Group 1 patients revealed an additional 6 patients with osteopenia and 7 patients with osteoporosis compared to DXA alone (Table 4-5). In men ≥ 70, CTXA identified 2 cases of osteopenia and zero cases of osteoporosis (Table 4-5).
Subgroup analysis of Women < 65 years of age
DXA was available within two years for two women age <65 (18.2%) with one identified as normal and one as osteopenic. CTXA revealed low BMD in the majority of women age <65 with six cases of osteopenia and one case of osteoporosis. (Table 6).
Impact of preoperative identification of femoral osteoporosis on cemented femoral fixation
It should be noted that the pre-operative femoral BMD status was available in less than half of Group 2 (DXA) and 100% of Group 1 (CTXA). When the status of femoral BMD was known, rates of cemented femoral fixation were similar for osteopenic and osteoporotic patients in Group 1 and Group 2 (Table 7). Applying CTXA systematically to all 78 patients in Group 1 substantially improved the number of identified cases of osteopenia and osteoporosis compared with available pre-operative DXA data. This improved recognition of pre-operative femoral BMD substantially increased the number of overall cases of cemented femoral fixation in Group 1 compared with Group 2 (Table 7). In Group 2, over half (N=44) of the patients did not have known BMD based on DXA within 2 years. The vast majority (95.5%) of raTHA cases utilized cementless femoral fixation when BMD status was unknown. There were no periprosthetic fractures in either group.
Discussion
Valuable information can be obtained regarding proximal femoral BMD from pre-operative CT scans routinely obtained prior to raTHA. Our study supported the previously reported findings that osteoporosis is underdiagnosed prior to primary THA [17]. Despite National Osteoporosis Foundation (NOF) guidelines recommending routine DXA screening for women age ≥ 65 and men age ≥ 70 [18], DXA was performed within 2 years prior to raTHA in less than half of women age ≥ 65 and in 0% of men age ≥ 70 in both of our study groups. Systematic evaluation of femoral BMD with CTXA substantially improved the number of cases identified with low femoral BMD with twice the number of patients identified with osteopenia and five-times the number identified with osteoporosis compared with DXA alone. Additional long-term benefits for these patients include identifying previously undiagnosed osteoporosis. Patients with newly identified osteoporosis were counseled post-operatively and referred for long-term bone health optimization either by their primary care physician or our institutional osteoporosis management consult service. Such efforts to diagnose and treat previously unrecognized patients with osteoporosis may help reduce their long-term risk for osteoporotic related fractures and represents a significant health benefit.
In our study, sub-group analysis revealed that 83.3% of women age ≥ 65 had low femoral BMD based on CTXA (30% osteoporosis, 53.3% osteopenia). Women age < 65 would not normally qualify for routine BMD screening with DXA based on age alone according to NOF guidelines. Surprisingly, in our study the majority of women age < 65 had low femoral BMD based on CTXA analysis (54.4% osteopenia, 9.1% osteoporosis). These findings suggest that further study in a larger patient cohort is warranted to determine if all women might benefit from pre-operative assessment with CTXA prior to raTHA. The value of routine CTXA analysis in men age ≥ 70 is less clear. International guidelines regarding BMD screening in men is controversial [18]. The NOF recommends obtaining a baseline screening in all men age ≥ 70 [18]. In our study, no men age ≥ 70 had DXA within 2 years of surgery and CTXA analysis of all men age ≥ 70 in Group 1 revealed that the majority had normal BMD (85.7%) with zero cases of osteoporosis. Further study in larger patient cohorts is required to determine appropriate indications for CTXA screening in men.
Choice of femoral fixation was consistent when the pre-operative femoral BMD was known in our single surgeon study (Table 7). The small differences in the rate of cement fixation for osteopenic and normal bone groups comparing the DXA and CTXA groups were not statistically significant, but may be related to the immediate availability of CTXA prior to raTHA. The CTXA analysis was performed in conjunction with the CT required for use of raTHA, the femoral BMD and T-scores were routinely included in the radiology CT report, and CTXA data was routinely reviewed prior to surgery. DXA data was available in the medical record, but may have been less consistently reviewed pre-operatively compared with CTXA. It should be noted that even when osteoporosis was diagnosed with DXA, it was inconsistently noted in the patient problem list and frequently was not treated. This pattern of under-diagnosis and under-treatment of osteoporosis for prior to THA noted in our study is consistent with previous reports [17]. Applying CTXA systematically to all Group 1 patients substantially improved the number of identified cases of osteopenia and osteoporosis compared with available pre-operative DXA data. This improved recognition of pre-operative femoral BMD was reflected by more than doubling the number of overall cases of cemented femoral fixation in Group 1 compared with Group 2 (Table 7).
Our study has several limitations. CTXA analysis requires the use of a phantom to calibrate the CT scanner in order to accurately convert HU measurements to femoral BMD and requires the use of a proprietary software. Although this opportunistic CT approach is well described and validated [12–15,19,20], software availability and phantom calibration represents potential barriers for the widespread adoption of this technique. Additionally, the majority of primary THAs worldwide are not performed with CT-based robotic assisted technique. Multiple alternative methods also exist based on plain radiographs that quantify proximal femoral bone geometry and have been validated to identify patients at risk for femoral periprosthetic fracture when cementless femoral fixation is utilized [21,22]. Patients that lack pre-operative hip CT data would benefit if the alternative methods were used to assess proximal femoral bone quality and influenced surgeons to choose cemented femoral fixation in properly selected patients to reduce the risk or early periprosthetic fracture. Both the Dorr Classification of proximal femur geometry and the Cortical Index have moderate correlation to BMD and were recommended by the International Society for Clinical Densitometry to identify those patients at risk for osteoporosis [22]. Surveys of surgeons have shown that pre-operative knowledge of osteoporosis would affect surgical technique and pre-operative planning, however less than 10% of surgeons obtain DXA scans preoperatively [23,24]. It is possible that lack of familiarity with plain radiographic techniques to identify patients at risk for periprosthetic fracture and inadequate surgical experience with cemented femoral fixation techniques contributes to the under-utilization of cement in properly selected patients in the United States. These data suggest that additional educational efforts are needed to improve surgeon recognition of femoral osteoporosis prior to primary THA and to increase surgeon comfort level with cemented femoral fixation. The art of cemented femoral technique in primary THA is potentially being lost and effort is required to address this issue.
Additional limitations include our study design. This is a single surgeon series at one academic institution. The fellowship-trained surgeon in our study has substantial previous experience with cemented femoral fixation that may have affected decisions to proceed with cemented fixation in appropriate cases. The retrospective nature of the study limits the findings and prospective randomized clinical trials would be advised to better define these relationships. Our study was also underpowered to evaluate the impact of femoral fixation on the incidence of periprosthetic fractures in these groups. Further study in larger patient cohorts is warranted.
In summary, our study demonstrates a simple, effective, and reliable method to evaluate proximal femoral BMD using a validated software to analyze hip CTs routinely obtained prior to primary raTHA using one robotic platform. This CTXA technique pre-operatively identified twice the number of osteopenic and 5-times the number of osteoporotic patients compared with DXA analysis alone. Improved recognition of femoral osteoporosis with CTXA more than doubled the percentage of cases with cemented femoral fixation compared with a group with DXA alone. Patients with newly diagnosed osteoporosis were referred for bone health optimization and this represents another significant health benefit for these patients to reduce their long-term risk of osteoporotic-related fractures. Additional prospective studies in larger patient cohorts are required to determine if improved recognition of femoral osteoporosis and appropriate use of cemented femoral fixation will result in reduced risk of periprosthetic fracture. Future educational efforts to improve surgeon recognition of femoral osteoporosis prior to primary THA and to increase surgeon comfort level with cemented femoral fixation are warranted in the United States.
Acknowledgement
We would like to thank Dr. William H. Harris for his inspirational leadership throughout his lengthy and distinguished career. The senior author (Richard Illgen II, MD) served as his fellow (1999-2000) and Dr. Harris has provided tremendous mentorship and guidance over the last 25 years. He has set the standard of excellence for others to follow as clinician scientists.
References
[1] Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. The Lancet 2007;370:1508–19. https://doi.org/10.1016/S0140-6736(07)60457-7.
[2] Gwam CU, Mistry JB, Mohamed NS, Thomas M, Bigart KC, Mont MA, et al. Current Epidemiology of Revision Total Hip Arthroplasty in the United States: National Inpatient Sample 2009 to 2013. J Arthroplasty 2017;32:2088–92. https://doi.org/10.1016/J.ARTH.2017.02.046.
[3] Abdel MP, Watts CD, Houdek MT, Lewallen DG, Berry DJ. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hip arthroplasties: A 40-year experience. Bone and Joint Journal 2016. https://doi.org/10.1302/0301-620X.98B4.37201.
[4] American Joint Replacement Registry (AJRR): 2021 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2021
[5] Bunyoz KI, Malchau E, Malchau H, Troelsen A. Has the Use of Fixation Techniques in THA Changed in This Decade? The Uncemented Paradox Revisited. Clin Orthop Relat Res 2020;478:697–704. https://doi.org/10.1097/CORR.0000000000001117.
[6] Thien TM, Chatziagorou G, Garellick G, Furnes O, Havelin LI, Mäkelä K, et al. Periprosthetic femoral fracture within two years after total hip replacement: analysis of 437,629 operations in the nordic arthroplasty register association database. J Bone Joint Surg Am 2014;96:e167. https://doi.org/10.2106/JBJS.M.00643.
[7] Smolle MA, Hörlesberger N, Maurer-Ertl W, Puchwein P, Seibert FJ, Leithner A. Periprosthetic fractures of hip and knee-A morbidity and mortality analysis. Injury 2021;52:3483–8. https://doi.org/10.1016/J.INJURY.2021.01.015.
[8] Chitnis AS, Mantel J, Vanderkarr M, Putnam M, Ruppenkamp J, Holy CE, et al. Medical resource utilization and costs for intraoperative and early postoperative periprosthetic hip fractures following total hip arthroplasty in the medicare population: A retrospective cohort study. Medicine 2019;98:e15986. https://doi.org/10.1097/MD.0000000000015986.
[9] Jennison T, Yarlagadda R. Mortality in patients sustaining a periprosthetic fracture following a hemiarthroplasty. Journal of Orthopaedics 2018;15:798–801. https://doi.org/10.1016/j.jor.2018.05.031.
[10] Reeves RA, Schairer WW, Jevsevar DS. The national burden of periprosthetic hip fractures in the US: costs and risk factors for hospital readmission. HIP International 2019;29:550–7. https://doi.org/10.1177/1120700018803933.
[11] Pickhardt PJ, Graffy PM, Perez AA, Lubner MG, Elton DC, Summers RM. Opportunistic screening at abdominal CT: Use of automated body composition biomarkers for added cardiometabolic value. Radiographics 2021;41:524–42. https://doi.org/10.1148/RG.2021200056/ASSET/IMAGES/LARGE/RG.2021200056.FIG21.JPEG.
[12] Pickhardt PJ. Value-added Opportunistic CT Screening: State of the Art. Radiology 2022. https://doi.org/10.1148/RADIOL.211561.
[13] Ziemlewicz TJ, Maciejewski A, Binkley N, Brett AD, Brown JK, Pickhardt PJ. Opportunistic Quantitative CT Bone Mineral Density Measurement at the Proximal Femur Using Routine Contrast-Enhanced Scans: Direct Comparison With DXA in 355 Adults. J Bone Miner Res 2016;31:1835–40. https://doi.org/10.1002/JBMR.2856.
[14] Lee SJ, Anderson PA, Pickhardt PJ. Predicting Future Hip Fractures on Routine Abdominal CT Using Opportunistic Osteoporosis Screening Measures: A Matched Case-Control Study. AJR Am J Roentgenol 2017;209:395–402. https://doi.org/10.2214/AJR.17.17820.
[15] Brown JK, Timm W, Bodeen G, Chason A, Perry M, Vernacchia F, et al. Asynchronously Calibrated Quantitative Bone Densitometry. J Clin Densitom 2017;20:216–25. https://doi.org/10.1016/J.JOCD.2015.11.001.
[16] Kanis JA, Melton LJ, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res 1994;9:1137–41. https://doi.org/10.1002/JBMR.5650090802.
[17] Bernatz JT, Brooks AE, Squire MW, Illgen RI, Binkley NC, Anderson PA. Osteoporosis Is Common and Undertreated Prior to Total Joint Arthroplasty. Journal of Arthroplasty 2019;34:1347–53. https://doi.org/10.1016/j.arth.2019.03.044.
[18] Viswanathan M, Reddy S, Berkman N, Cullen K, Middleton JC, Nicholson WK, et al. Screening to Prevent Osteoporotic Fractures: An Evidence Review for the U.S. Preventive Services Task Force 2018.
[19] Jang S, Graffy PM, Ziemlewicz TJ, Lee SJ, Summers RM, Pickhardt PJ. Opportunistic Osteoporosis Screening at Routine Abdominal and Thoracic CT: Normative L1 Trabecular Attenuation Values in More than 20 000 Adults. Radiology 2019;291:360–7. https://doi.org/10.1148/RADIOL.2019181648.
[20] Pickhardt PJ, Pooler BD, Lauder T, del Rio AM, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Annals of Internal Medicine 2013;158:588–95. https://doi.org/10.7326/0003-4819-158-8-201304160-00003.
[21] Bigart KC, Nahhas CR, Ruzich GP, Culvern CN, Salzano MB, della Valle CJ, et al. Does Femoral Morphology Predict the Risk of Periprosthetic Fracture After Cementless Total Hip Arthroplasty? J Arthroplasty 2020;35:S359–63. https://doi.org/10.1016/J.ARTH.2020.02.048.
[22] Anderson PA, Morgan SL, Krueger D, Zapalowski C, Tanner B, Jeray KJ, et al. Use of Bone Health Evaluation in Orthopedic Surgery: 2019 ISCD Official Position. J Clin Densitom 2019;22:517–43. https://doi.org/10.1016/J.JOCD.2019.07.013.
[23] Kadri A, Binkley N, Hare KJ, Anderson PA. Bone Health Optimization in Orthopaedic Surgery. J Bone Joint Surg Am 2020;102:574–81. https://doi.org/10.2106/JBJS.19.00999.
[24] Maier GS, Kolbow K, Lazovic D, Maus U. The Importance of Bone Mineral Density in Hip Arthroplasty: Results of a Survey Asking Orthopaedic Surgeons about Their Opinions and Attitudes Concerning Osteoporosis and Hip Arthroplasty. Adv Orthop 2016;2016. https://doi.org/10.1155/2016/8079354.
Figures
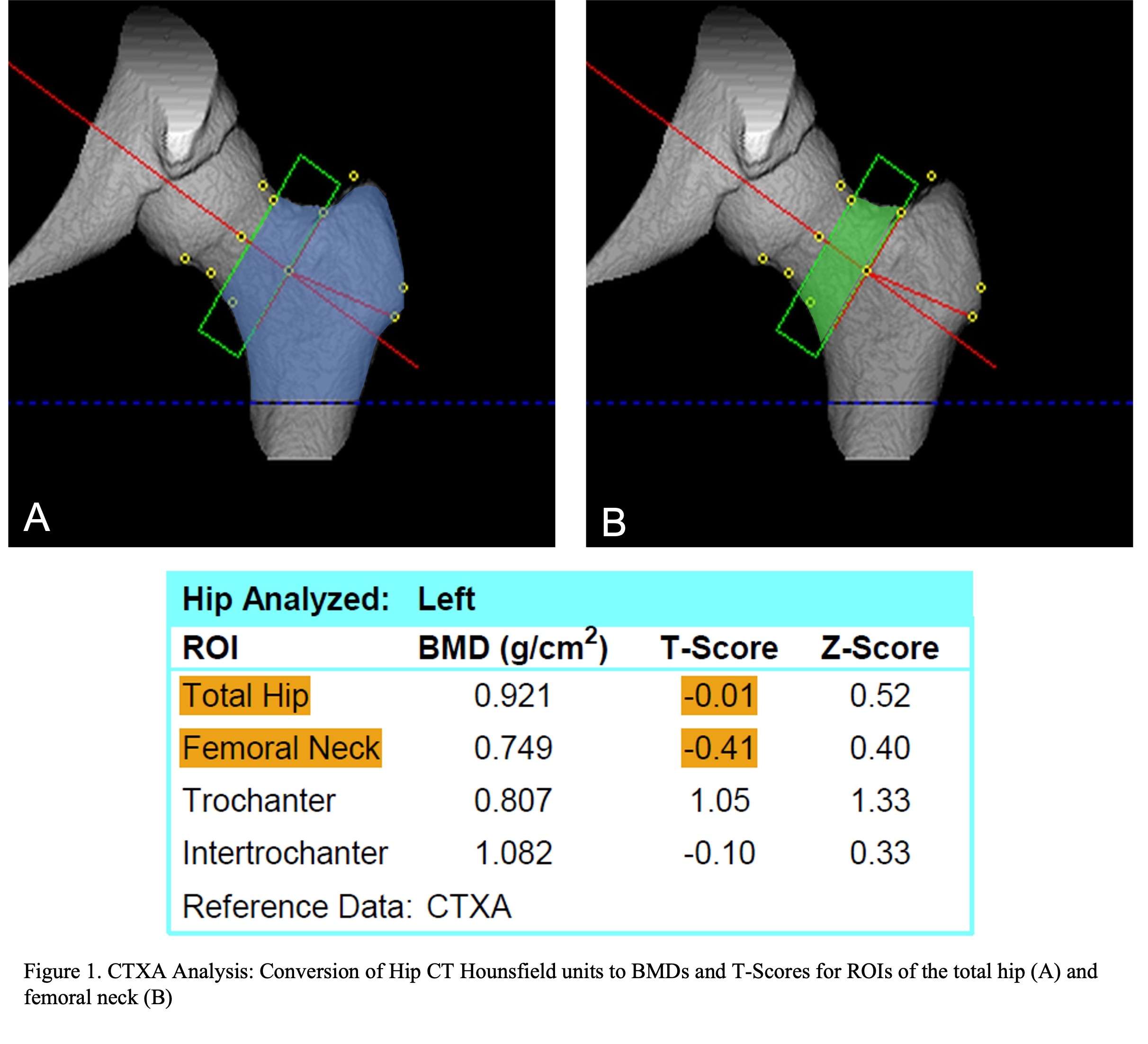
Figure 1
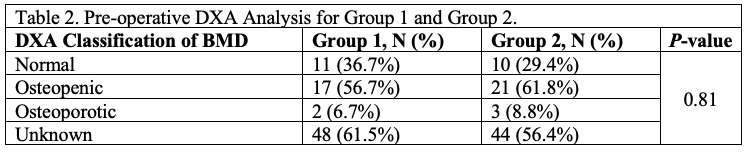
Figure 2
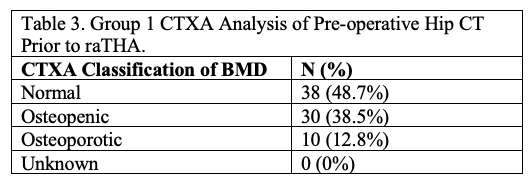
Figure 3
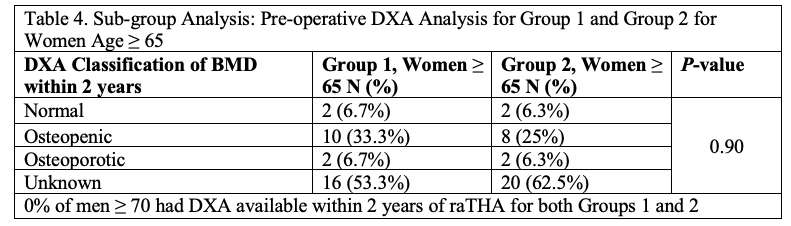
Figure 4
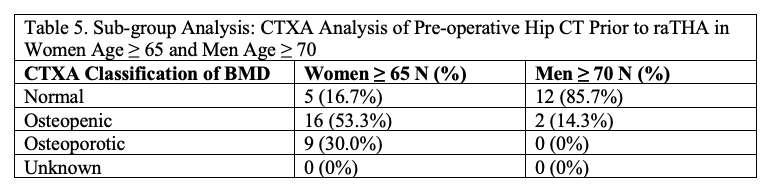
Figure 5
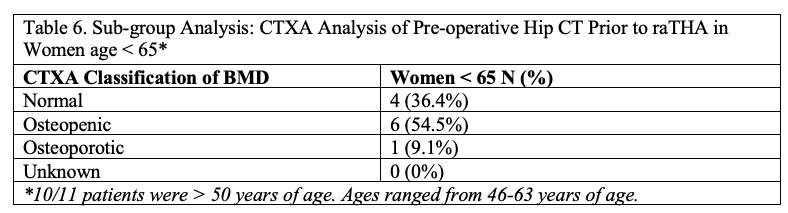
Figure 6
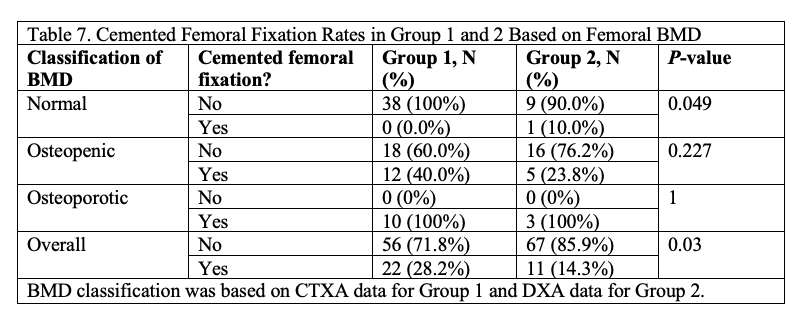
Figure 7
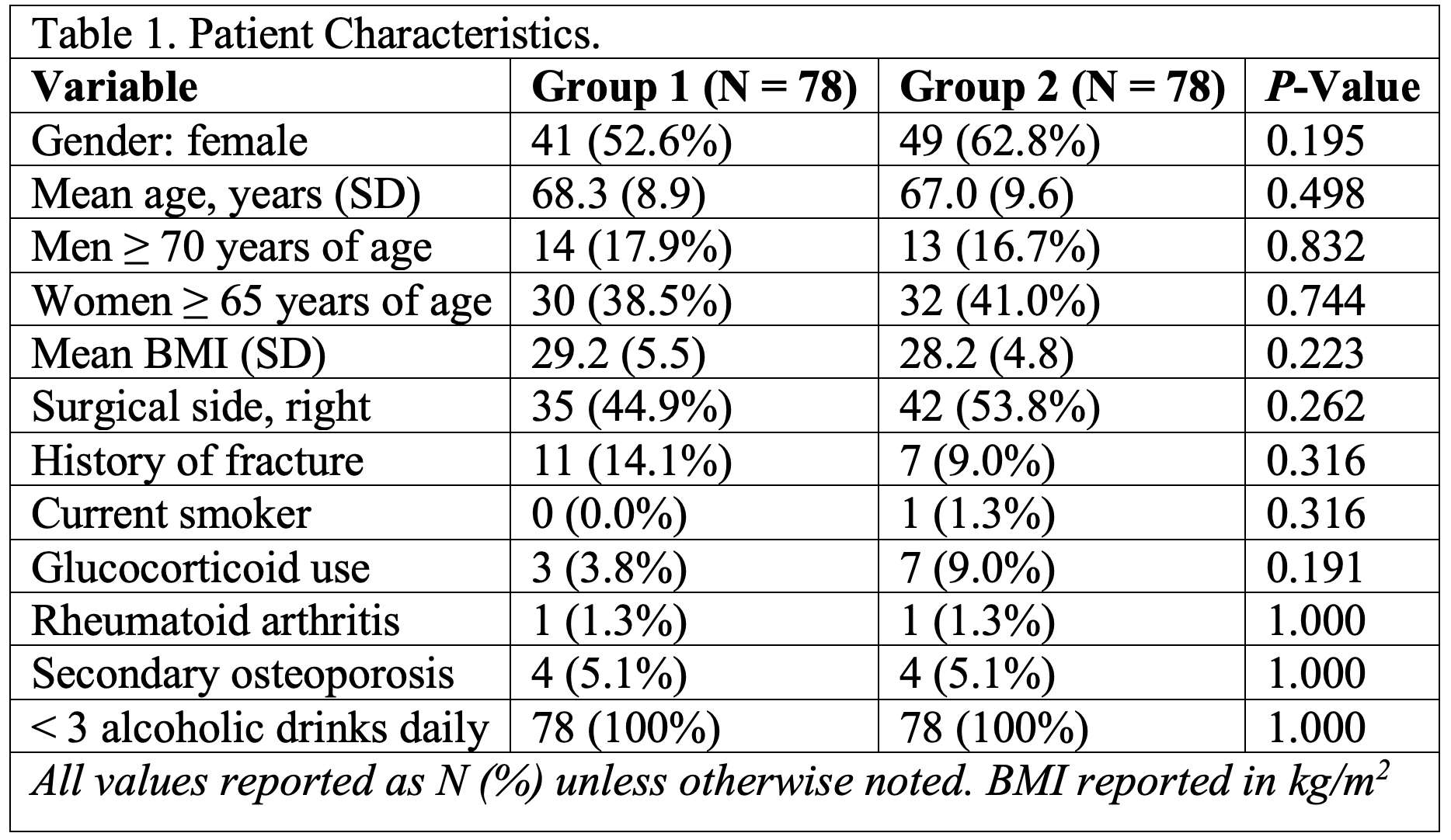
Figure 8#7616
Body Composition Changes Following Total Joint Arthroplasty as Determined by Bioimpedance Analysis
*Michael Marinier - University of Iowa
Jacob Elkins - University of Iowa - Iowa City, USA
David DeMik - University of Iowa - Iowa City, USA
*Email: michael-marinier@uiowa.edu
Introduction: Bioimpedance Analysis (BIA) is an emerging tool for identifying body composition including body fat, body water, and skeletal muscle mass (SMM). While BIA has been introduced in other specialties, its role has yet to be established in orthopaedic surgery. Given the association between malnutrition and obesity with increased risks for perioperative complications, BIA has potential to provide greater insight into segmental body composition and nutritional status than more commonly used measures, such as body mass index (BMI). This study aimed to identify changes in SMM in patients following total joint arthroplasty (TJA). It was hypothesized that patients with increased BMI will experience greater loss of SMM following TJA, with obesity class III patients (BMI ≥ 40 kg/m2) experiencing the greatest reduction in SMM.
Methods: Patients undergoing elective total hip or knee arthroplasty (THA, TKA respectively) were prospectively enrolled. Multi-frequency segmental BIA (InBody 770; InBody USA; Cerritos, CA USA) scanning was performed at the pre-operative work-up visit and post-operatively at 3 and 6 weeks (± 1 week) following TJA. Patients’ maximal hand grip strength (HGS) was also recorded during each visit using a hydraulic dynamometer (Jamar Hydraulic Hand Dynamometer; Sammons-Preston-Rolyan; Bolingbrook, IL USA). Patients were stratified into obesity cohorts: non-obese (< 30 kg/m2), class I (30 to < 35 kg/m2), class II (35 to < 40 kg/m2), and class III (> 40 kg/m2). The primary outcome was change in SMM. Analysis of descriptive statistics, comparison of means and Pearson’s correlations between pre-operatively measured variables was conducted.
Results: 87 patients scheduled for elective TJA were enrolled. Mean age was 63.1 years, 50.6% were female, and 48.3% underwent THA. Of those undergoing THA, 33 were performed via posterior approach and 9 were via direct anterior approach. 26 patients were designated as non-obese, 24 as obesity class I, 13 as obesity class II, and 22 as obesity class III at enrollment. Relationships between changes in SMM and several preoperative measurements are shown in Figure 1. Changes in SMM stratified by obesity class and surgical procedure are illustrated in Figures 2-3.
Conclusion: BIA allows for rapid, non-invasive, longitudinal assessments of body composition. While it was initially hypothesized that increased BMI would result in increased losses of SMM, this was not observed. Better predictors of SMM loss were pre-operative measures of lean tissue and strength. This may indicate that patients who are more habitually active prior to surgery experience larger decrement of muscle mass during the intensive post-operative recovery period. In addition, using a direct anterior approach rather than a posterior approach for THA allowed patients to reclaim more of their initial SMM loss by week 6, which corroborates claims that the direct anterior approach is muscle sparing. Further studies are needed to further elucidate these associations, as well as the role of body composition as a risk factor for post-operative complications. This pilot study demonstrates promise as regards moving away from BMI-based surgical indication and risk-stratification in a specialty naïve to this emerging technology. This is an inviting arena of ongoing and future research.
Figures
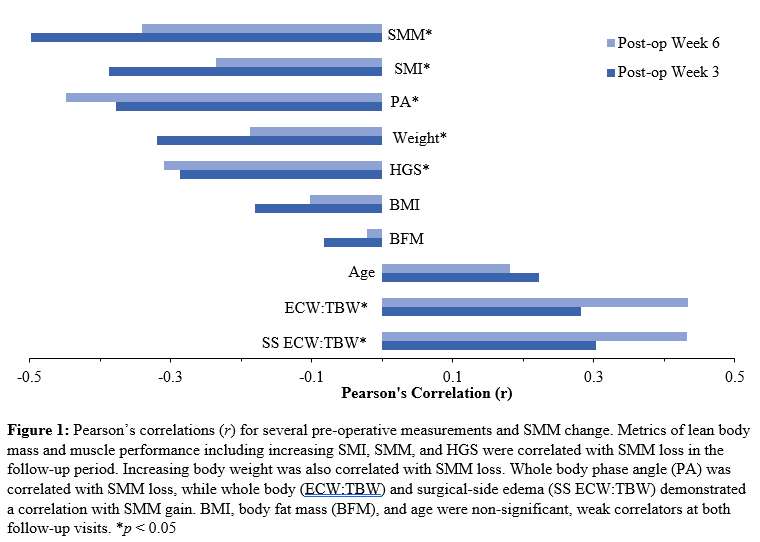
Figure 1
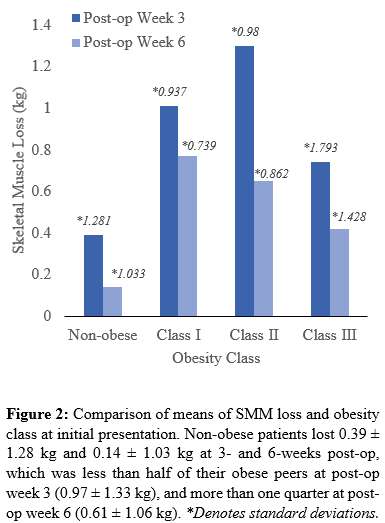
Figure 2
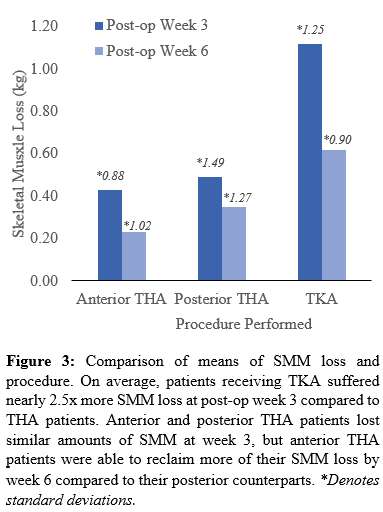
Figure 3#7728
Body Composition Changes in the Immediate Peri-Operative Period Following Total Joint Arthroplasty
*Michael Marinier - University of Iowa
Jacob Elkins - University of Iowa - Iowa City, USA
Ayobami Ogunsola - University of Iowa - Iowa City, USA
*Email: michael-marinier@uiowa.edu
Background: Bioimpedance analysis (BIA) is a readily available tool to assess body composition in a clinical setting. Relative to other specialties, BIA is under-utilized in orthopaedics, especially regarding joint arthroplasty. Previous reports have demonstrated that metallic orthopaedic implants, in the setting of fracture fixation, cause an increase in post-operative fat-free mass, which is equivalent to lean body mass (LBM). However, there are no similar studies examining these changes in an arthroplasty population. This investigation aims to quantify changes in body composition, namely dry lean mass (DLM) and LBM, in the immediate peri-operative period following total hip (THA) and total knee arthroplasty (TKA).
Methods: Following IRB approval, adults scheduled for elective total joint arthroplasty were recruited to participate. Patients underwent three portable, research-grade, multi-frequency BIA scans (InBody S10; InBody USA; Cerritos, CA USA) in the immediate peri-operative period: pre-operative on their day of surgery (DOS), post-operative day 0 (POD0), and post-operative day 1 (POD1). Peri-operative fluid balance, as documented by the anesthesia team, was recorded. Patients were positioned supine unless they were required to be seated due to room availability. The primary outcome for this was DLM changes. Secondary outcomes include LBM changes. Statistical analysis was completed using SAS (SAS Institute; Cary, NC USA) and Microsoft Excel (Microsoft Corporation; Redmond, WA USA).
Results: 67 patients were enrolled to undergo BIA. Mean age was 62.64 ± 10.28 years old, 49.2% were females, and 49.2% underwent THA. Patients received 1.16 ± 0.58 kg of fluid mass peri-operatively, on average. 48 of the enrolled patients underwent exclusively supine scans. The all-supine cohort exhibited a 0.36 ± 0.61 kg increase in DLM (p < 0.001) and 1.30 ± 2.14 kg increase in LBM on post-operative day 0 (p < 0.001). Table I summarizes these findings. On POD0, patients undergoing THA exhibited an increase of 0.22 ± 0.62 kg in DLM, while those undergoing TKA experienced a DLM increase of 0.68 ± 0.65 kg. An independent t-test demonstrated a statistically significant (p = 0.0043) difference between the procedures’ mean DLM changes (Figure 1).
Conclusion: BIA is a rapid, portable tool that allows for body composition analysis of an inpatient surgical population. The results identified a statistically significant gain in DLM following their procedure, but there was not a statistically significant difference in the two post-operative scans. These findings may indicate that changes in DLM are at least partially explained by the prosthesis mass. In addition to DLM changes, there was a statistically significant gain in LBM from the pre- to post-operative scans, and there was not a statistically significant difference identified between the two post-operative scans. As LBM is simply DLM without water mass, the difference in these body composition markers is presumably the patients’ net fluid balance. These findings will assist surgeons in interpreting peri-operative body composition changes.
Figures
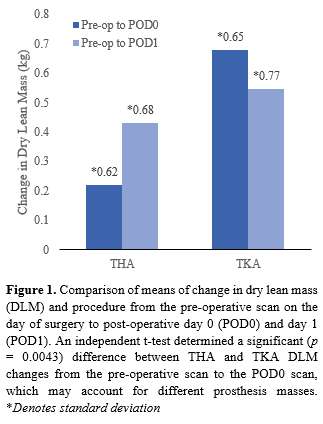
Figure 1
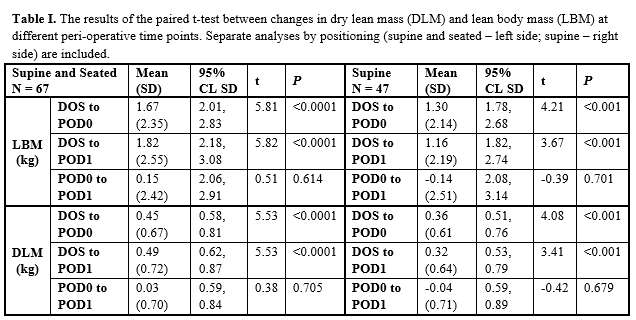
Figure 2#7945
Exploring the Utility of Bioimpedance Analysis in Total Joint Arthroplasty
*Michael Marinier - University of Iowa
Jacob Elkins - University of Iowa - Iowa City, USA
Ayobami Ogunsola - University of Iowa - Iowa City, USA
David DeMik - University of Iowa - Iowa City, USA
*Email: michael-marinier@uiowa.edu
Abstract
Introduction: Bioimpedance analysis (BIA) is a readily available tool to assess body composition in a clinical setting, which may have substantial implications regarding pre-operative risk-assessment. However, BIA has received little attention in orthopedics, much less in joint arthroplasty. This study aims to compare pre-operative markers to BIA-specific values and quantify changes in body composition following total joint arthroplasty (TJA).
Methods: Adults scheduled for primary total hip (THA) or total knee arthroplasty (TKA) were prospectively enrolled to undergo three outpatient and three inpatient BIA scans. Patients underwent hand-grip strength (HGS) testing as outpatients. Parameters including skeletal muscle mass (SMM), fat, and edema were compared across the study period.
Results: 87 patients were enrolled. Mean age was 63.1±9.6 years, 44 (50.6%) were female, and 42 patients (48.3%) underwent THA. On average, patients experienced a loss in overall body weight, SMM, and fat mass. Greater baseline skeletal muscle index, body weight, HGS, and whole-body phase angle correlated with loss of SMM at post-operative week-three and six (p<0.05), while increased pre-operative edema correlated with SMM gain (p<0.05). Patients undergoing TKA demonstrated more SMM loss than THA. Post-operative muscle loss was independent of body mass index. Patients experienced an immediate gain in dry lean mass on post-operative day zero (p<0.001).
Conclusion: Markers of physical fitness are risk factors for muscle loss. There was large heterogeneity among the various body-type phenotypes regarding post-operative muscle loss, the identification of which permits patient-specific intervention and preventative therapies. This study introduces the utilization of an emerging technology to TJA and demonstrates promising potential.
Key Words: Obesity; Total Joint Arthroplasty; Post-operative Complications
Introduction
Obesity is a well-established epidemic in the US which despite decades of attempted intervention and mitigation continues to rise unabatedly with a current prevalence at 40% in the United States. [1] It is typically defined and stratified by body mass index (BMI, in kg/m2), which is limited to describing body size rather than body type or composition.
Body composition including body fat mass (BFM) and skeletal muscle mass (SMM) plays an important role in a myriad of disease processes. [2-5] While obesity is characterized by excessive body mass, sarcopenia is defined as the generalized decline in SMM and function, and it has been associated with increased complications following arthroplasty procedures. [6-16] Specific to orthopaedics, patients on the obesity and/or sarcopenia spectrum experience increasing rates of post-surgical complications such as perioperative infections, falls, length of stay, mortality, edema, and inferior patient-reported outcomes. [3, 17-24] When there exists the concomitant presence of both obesity and sarcopenia, so-called sarcopenic-obesity (SO), there is markedly elevated rates of overall morbidity and mortality. [6, 25]
With conventional anthropomorphic body composition analyses such as the skinfold tests or hydrodensitometry becoming less common due to inherent inaccuracies, modalities including dual x-ray absorptiometry (DEXA), CT scan, air displacement plethysmography, and full-body MRI have emerged to assess body composition. [26] While these methods are regarded as accurate and reliable, there is limited applicability to the clinical setting due to cost, labor, and ionizing radiation exposure. In contrast, bioimpedance analysis (BIA) has emerged as a non-invasive, cost-effective, and efficient tool that allows for precise quantification of body composition in a clinic setting. [26, 27] BIA determines body composition by measuring resistance and reactance of tissues and has been extensively validated for clinical use. [27-29]
Additionally, BIA can quantify cellular health and permeability via the measurement of the whole-body phase angle (φ). This marker has been utilized in various medical and surgical specialties including critical care and surgical oncology, where decreased φ has been shown to independently predict mortality and decreased survivorship of severe illness. [8, 30] However, few studies have examined the utility of φ as a surrogative measure of health and function within the fields of orthopaedic surgery and musculoskeletal health. [31, 32] Furthermore, in addition to φ, BIA can directly quantify extremity lymphedema, which is an emerging risk marker for TJA complications. [33, 34]
Given the associations between malnutrition and obesity with increased risks for peri-operative complications, BIA has potential to provide greater insight into body composition and nutritional status than conventional measures such as body weight, BMI, or serum nutritional markers. Post-operative muscle dysfunction has been well-described in multiple surgical fields including general surgery, surgical oncology, vascular surgery, and transplant surgery, however there are scarce investigations specific to orthopaedics with even fewer in the realm of arthroplasty. [4, 35, 36] In orthopaedics, BIA has been primarily investigated in the setting of native hip fractures with individual factors of bioimpedance (reactance and resistance) and lean body mass predicting future falls, incident disability, bone loss, and death. [5, 11, 37-40] In arthroplasty, BIA has been used only for quantification of BFM, which was correlated with post-operative complications. [39-42] Thus, with only limited research available, this powerful and emerging technology has been under-utilized in joint arthroplasty specifically – and within the field of orthopaedics in general – compared to other surgical specialties. [39, 40, 43-46]
In addition to the applications of BIA in an outpatient setting, portable bioimpedance analyzers that can be transported readily to an inpatient unit are available for patients that require bed rest. Furthermore, there exists a gap in knowledge regarding the immediate perioperative body composition changes that patients experience. In a recent case report, Wagner has found that metallic implants (titanium alloy nails) increase the fat-free mass, which is equivalent to lean body mass (LBM) as determined by BIA. [47] To the study team’s knowledge, there have been no similar studies examining these changes in an arthroplasty population.
The purpose of this study was to identify the peri- and post-operative body composition changes in patients following TJA. In addition, this study aimed to identify sub-populations at risk of SMM loss following TJA. Through outpatient and inpatient BIA measurements, this study also aimed to ascertain the utility of this technology and assess its performance in orthopaedic practice. Hypotheses include (1) patients with greater baseline BMI, and namely those with class III obesity, will experience greater SMM losses secondary to sedentary lifestyles; and (2) patients will show an immediate gain in LBM following their procedure.
Methods
Study Population
This study was received Institutional Review Board approval. Eligible patients (³18 years of age) presenting for their pre-operative visit for elective primary total hip or knee arthroplasty (THA, TKA) with one of four fellowship-trained arthroplasty surgeons were identified. Consenting patients were prospectively enrolled to undergo six multi-frequency, segmental BIA scans: three as outpatients and three as inpatients. Patients were excluded if they were unable to stand for approximately 60-seconds to complete BIA testing, perform maximal effort hand-grip strength (HGS) testing, or if there was a medical contraindication to BIA testing, such as presence of an implanted electronic cardiac device.
Patient demographical information, medical history, pre-operative lab testing, and pre-operative patient-reported outcomes (PROs) were recorded at the time of enrollment. The enrollment occurred over a 10-week period between 6/1/2020 and 8/7/2020.
Outpatient Testing
Patients underwent three outpatient, stationary BIA scans (InBody 770; InBody USA; Cerritos, CA USA). BIA occurred at their pre-operative work-up visit, 3-weeks (±1 week) post-operatively, and 6-weeks (±1 week) post-operatively. Height was obtained using a calibrated, wall-mounted stadiometer. Patients were stratified into obesity cohorts based on their baseline BMI: non-obese (<30 kg/m2), class I (30 to <35 kg/m2), class II (35 to <40 kg/m2), and class III (>40 kg/m2).
Additionally, patients were subjected to three HGS measurements per hand using a calibrated hydraulic dynamometer (Jamar Hydraulic Hand Dynamometer; Sammons-Preston-Rolyan; Bolingbrook, IL USA). Maximal HGS was assessed using the Southampton Protocol which had modification that the mean of the top three of six trials was recorded. [48]
Inpatient Testing
In addition, patients underwent three inpatient, portable BIA scans (InBody S10; InBody USA; Cerritos, CA USA). Two scans were conducted on the day of surgery: one pre-operative (DOS) and one post-operative (POD0). The third inpatient scan was conducted on post-operative day 1 (POD1). Height and body weight measurements from the first outpatient visit were utilized throughout the inpatient cohort. To complete these BIA, scans were conducted in a seated or supine position based on the available pre- and post-operative facilities.
The patients’ peri-operative net volume change was also recorded to account for perceived peri-operative changes. Net volume change was defined as the change in volume (e.g. fluid replacement, blood loss, urine output) that patients experienced in the immediate peri-operative period. No additional HGS measurements were collected alongside the inpatient BIA scans.
Statistical Analysis
Baseline φ was compared to patient demographics, baseline body composition measurements, HGS, and routine pre-operative metrics including laboratory specimen values and patient-reported outcomes (PROs). The primary outcome for the outpatient testing was SMM changes. The primary outcome for the inpatient testing was dry lean mass (DLM) changes. The secondary outcome for the inpatient testing was lean body mass (LBM) changes. Statistical analysis was completed using SAS (SAS Institute; Cary, NC USA) and Microsoft Excel (Microsoft Corporation; Redmond, WA USA).
Results
Study Population
87 patients scheduled for elective TJA were enrolled in the study. Mean age was 63.1 ± 9.6 years, 44 (50.6%) were female, and 42 patients (48.3%) underwent THA. Of those undergoing THA, 33 were performed using a posterior approach and 9 were performed via the direct anterior approach. Demographics and select baseline measurements are summarized in Table I. Patient follow-up is shown in Table II.
Outpatient Testing
85 (97.7%) completed all procedures of the enrollment visit and were included in pre-operative data analysis. Pearson’s correlations for baseline φ and several pre-operative measurements are summarized in Fig 1. Figs 2-3 illustrate the relationships between φ and maximal HGS and skeletal muscle mass (SMM) by sex, respectively.
On average, participants experienced a decrement in overall body weight (Δ3w= -1.01 ± 2.70 kg, Δ6w= -0.76 ± 2.67 kg) and SMM (Δ3w= -0.80 ± 1.34 kg, Δ6w= -0.48 ± 1.07 kg) at both follow-up visits. Among the baseline body composition measurements, increasing aSMI, SMM, φ, body weight, and HGS were significantly correlated with SMM loss in the follow-up period (p<0.05). Whole body edema and surgical side edema demonstrated a significant correlation with SMM gain (p<0.05). Age, BMI, and BFM did not correlate with SMM change. Figure 4 summarizes these relationships between changes in SMM and several pre-operative measurements.
Among the obesity cohorts, obesity class II patients experienced the highest SMM loss at week-3 (1.30 ± 0.98 kg), while obesity class I patients saw the greatest SMM loss at week-6 (0.77 ± 0.74 kg). Non-obese patients experienced less SMM loss (week-3: 0.39 ± 1.28 kg; week-6: 0.12 ± 1.06 kg) than obese patients (week-3: 0.97 ± 1.33 kg; week-6: 0.74 ± 0.91 kg). There was no statistically significant difference in SMM among the obesity classes. The relationship between obesity classes and SMM loss are characterized in Figure 5.
Patients undergoing TKA experienced more SMM loss at each time point (week-3: 1.12 ± 1.25 kg; week-6: 0.62 ± 0.90 kg) compared with all THA procedures (week-3: 0.47 ± 1.36 kg; week-6: 0.32 ± 1.21 kg). Patients undergoing direct anterior THA experienced the least SMM loss at week-3 (0.43 ± 0.88 kg) and week-6 (0.23 ± 1.02 kg) compared to those undergoing a posterior THA (0.49 ± 1.49 kg and 0.35 ± 1.02 kg at 3- and 6-weeks, respectively). There was no statistically significant difference in SMM among the procedures. Figure 6 illustrates the mean SMM loss by procedure.
Inpatient Testing
Overall, patients gained 0.45 ± 0.67 kg of DLM and 1.67 ± 2.35 kg of LBM on POD0, which was, on average, 0.46% and 1.70% of their baseline body mass, respectively. Patients experienced 1158.85 ± 577.10 mL of net volume change in the peri-operative period (DOS to POD0), which is equivalent to 1.16 ± 0.58 kg of fluid mass. Following the procedure (POD0), patients undergoing THA exhibited an increase of 0.22 ± 0.62 kg in DLM, while those undergoing TKA experienced 0.68 ± 0.65 kg DLM change. Changes in DLM by procedure are shown in Figure 7.
Forty-eight of the enrolled patients underwent exclusively supine scans. The all-supine cohort exhibited a 0.36 ± 0.61 kg change in DLM and 1.30 ± 2.14 kg change in LBM on post-operative day 0. Their changes in DLM and LBM on POD1 were 0.32 ± 0.64 kg and 1.16 ± 2.19 kg, respectively. In the entire sample, the difference between DLM and LBM, which estimates water mass change, was 1.22 kg from DOS to POD0.
The changes in LBM and DLM demonstrated significant (p<0.001) differences between pre-operative (DOS) and post-operative (POD0 and POD1) in both the supine and supine+seated cohorts. There was no significant difference between the two post-operative measurements (POD0 to POD1) for both DLM and LBM and in both positioning cohorts. Table III summarizes these results. Furthermore, comparison of DLM and LBM between the supine+seated and supine showed that there is no significant difference between these means regardless of the positioning.
Discussion
Outpatient Testing
In this study, patients undergoing TJA experienced a decrement in multiple body composition metrics including body weight, SMM, and BFM at 3- and 6-weeks post-operatively. In addition, specific subpopulations such as patients with higher baseline muscle mass and lower baseline extracellular edema and those undergoing TKA were observed to have greater loss of SMM, on average.
While it was initially hypothesized that BMI would correlate with SMM loss and that patients classified as obesity class III would experience the most SMM loss assuming that more obese individuals would not have the conditioning capacity to maintain SMM following surgery, this was not observed. . Instead, better predictors of SMM loss were found to be pre-operative measures of lean tissue and strength, which may indicate that patients who are more habitually active prior to surgery experience larger loss of muscle mass during the intensive post-operative recovery period. Furthermore, body water metrics indicative of poor cellular health including decreasing φ and increasing extracellular edema were seen as protective against reduction in SMM. This may further indicate that patients with baseline deconditioning are more habituated to the expected inactivity in the initial post-operative period.
Surgery and surgical approach were also investigated as factors affecting post-operative SMM change: losses following TKA more than doubled those following THA. This can possibly be attributed to THA patients experiencing less pain and post-operative disability, and thus returning to ambulatory tasks more rapidly while undergoing faster recovery following their procedure. [17, 49] Surgical approach for THA also demonstrated variable SMM changes, as those undergoing the direct anterior approach recovered more of their initial SMM loss by 6-weeks compared to posterior THA. As the direct anterior approach is often regarded as a muscle sparing procedure with a more rapid recovery compared to other approaches, the inter-muscular planes utilized in this approach may explain these preliminary results on muscle loss following hip replacement. [50-53] However, subjects undergoing direct anterior THA are often less obese, and despite our general finding that patients with increased pre-operative muscle mass demonstrated greater SMM loss, those undergoing direct anterior THA demonstrated the least SMM loss after surgery compared with any other procedure. Further investigation specifically related to body composition changes following THA with varied surgical approaches is currently underway.
Inpatient Testing
In addition to the outpatient BIA testing, this study quantified body composition changes in the immediate perioperative period following total joint arthroplasty. A 2014 report has shown that knee prostheses have an average mass of approximately 0.47 kg. [54] This value is roughly 30% less than this study’s average DLM changes which likely indicates that changes in DLM are at least partially explained by the prosthesis mass. This increase in DLM was found to be a statistically significant change between DOS and POD0-1. There was not a statistically significant difference between POD0 and POD1, which further corroborates that the entirety of the calculated changes occurs during the procedure.
These results build on the limited previous studies that demonstrate metallic implants lead to increased fat-free mass. [47] They also may guide surgeons utilizing BIA in their practice as the post-operative changes in body composition likely do not account for the mass of the metallic components. Thus, a gain in DLM secondary to metallic components may lead to unaccounted for losses in important tissue mass during follow-up. Like the identified increases in DLM, there was a significant gain in LBM from the DOS to POD0, and there was not a difference identified between POD0-1. As LBM is simply DLM without water mass factored in, the difference in these body composition markers is likely the patients’ net fluid balance. In this study population, the mass of the net volume change was just 0.06 kg lower than the calculated water mass differential over the same period.
As for patient positioning with the portable bioimpedance analyzer, there was not a significant difference between the supine and supine+seated cohorts. This result implies that positioning during testing does not affect the outcome of the analysis, which may allow flexibility in testing practices. As both cohorts produced significant differences in DLM and LBM, this result signifies that varying patient positioning may not sacrifice the utility of the results; however, following uniform study and practice protocols is favored.
Applications of BIA in Arthroplasty
This study demonstrated a wide heterogeneity in body composition among the various obesity cohorts investigated. Here, BIA proved to be a valuable tool to identify and quantify additional variables in this population, some of which are thought to be protective against adverse outcomes (such as total SMM), as well as those that are strongly intuited to predispose to complications (such as increased lower extremity edema, decreased φ, increased BFM). In an age of bundled payments and increased scrutiny on surgical outcomes and value, it has become routine practice to deny elective surgery to those patients with a BMI greater than 40 kg/m2, which may lead to denial of care and loss to follow-up. [55] However, BIA offers the unique ability to quantify both body composition and cellular health in a non-invasive, rapid, and cost-effective procedure conducive to the office immediately challenges this BMI-threshold practice.
Limitations
This study is not without limitations. First, this study was performed at a single center with limited patient sample size and follow-up. Secondly, there may have been selection bias in patients undergoing direct anterior compared to posterior THA, although three of the surgeons at our institution perform exclusively posterior THA. Finally, patients body composition was not analyzed in a uniform position during the inpatient testing, and, due to the limitations of the portable BIA device, the body weight used during this testing arm was from patients’ enrollment office-based visit. Therefore, changes in body weight from their last clinic visit to their surgical date are unaccounted for. However, these pilot data demonstrate promising results for the incorporation of BIA in orthopaedic practice, as well as improving upon current BMI-based surgical guidelines and surgical thresholds.
Future Directions and Conclusions
BIA offers many attractive avenues for further investigation, including: the impact of nutritional supplementation on post-operative muscle wasting and recovery, correlation with body and water composition parameters with TJA complications, and assessment of body composition changes in revision scenarios due to various diagnoses.
In conclusion, patients, on average, experienced greater body mass and SMM losses if they underwent TKA or had higher baseline SMM and HGS. BIA is a powerful tool that allows for low-cost, rapid, non-invasive and longitudinal assessments of body composition. Despite its wide potential in identification of patient-specific risk factors for increased morbidity after musculoskeletal injury or surgery, BIA has not been well-investigated in orthopaedics. This study describes the use of BIA in the arthroplasty population, demonstrating clear promise for future investigations. φ holds great potential as a new marker for potential adverse outcomes and risk stratification following total joint arthroplasty. In addition, measures of physical fitness (LBM, SMM, HGS, etc.) identify those most at-risk for muscle wasting following elective surgery, indicating an opportunity for education and prevention. This study illustrates promising pilot data in a specialty largely naïve to this emerging technology, and this is an exciting avenue of ongoing and future research.
References
1. Hales, C.M., et al., Prevalence of Obesity Among Adults and Youth: United States, 2015-2016. NCHS data brief, 2017(288): p. 1-8.
2. Obesity and total joint arthroplasty: a literature based review, in J Arthroplasty. 2013, 2013 Elsevier Inc: United States. p. 714-21.
3. Oosting, E., et al., The Influence of Muscle Weakness on the Association Between Obesity and Inpatient Recovery From Total Hip Arthroplasty. The Journal of arthroplasty, 2017. 32(6): p. 1918-1922.
4. Huang, D.-D., et al., Effect of surgery-induced acute muscle wasting on postoperative outcomes and quality of life. The Journal of surgical research, 2017. 218: p. 58-66.
5. González-Montalvo, J.I., et al., Prevalence of sarcopenia in acute hip fracture patients and its influence on short-term clinical outcome. Geriatr Gerontol Int, 2016. 16(9): p. 1021-7.
6. Santilli, V., et al., Clinical definition of sarcopenia. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases, 2014. 11(3): p. 177-180.
7. Sousa-Santos, A.R. and T.F. Amaral, Differences in handgrip strength protocols to identify sarcopenia and frailty - a systematic review. BMC geriatrics, 2017. 17(1): p. 238-238.
8. Tanaka, S., et al., Low Bioelectrical Impedance Phase Angle Is a Significant Risk Factor for Frailty. Biomed Res Int, 2019. 2019: p. 6283153.
9. Genton, L., et al., Association of mortality and phase angle measured by different bioelectrical impedance analysis (BIA) devices. Clin Nutr, 2018. 37(3): p. 1066-1069.
10. Genton, L., et al., Bioimpedance-Derived Phase Angle and Mortality Among Older People. Rejuvenation Res, 2017. 20(2): p. 118-124.
11. Sánchez-Castellano, C., et al., [Prevalence of sarcopenia and characteristics of sarcopenic subjects in patients over 80 years with hip fracture]. Nutr Hosp, 2019. 36(4): p. 813-818.
12. Cruz-Jentoft, A.J., et al., Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing, 2019. 48(4): p. 601.
13. Hirase, T., et al., Sarcopenia predicts perioperative adverse events following complex revision surgery for the thoracolumbar spine. Spine J, 2021. 21(6): p. 1001-1009.
14. Wang, H., et al., Sarcopenia as a predictor of postoperative risk of complications, mortality and length of stay following gastrointestinal oncological surgery. Ann R Coll Surg Engl, 2021. 103(9): p. 630-637.
15. Hendrickson, N.R., et al., Sarcopenia is associated with increased mortality but not complications following resection and reconstruction of sarcoma of the extremities. J Surg Oncol, 2020. 121(8): p. 1241-1248.
16. Ho, K.K., et al., End-stage knee osteoarthritis with and without sarcopenia and the effect of knee arthroplasty - a prospective cohort study. BMC Geriatr, 2021. 21(1): p. 2.
17. DeMik, D.E., et al., Complications and Obesity in Arthroplasty-A Hip is Not a Knee. The Journal of arthroplasty, 2018. 33(10): p. 3281-3287.
18. Friedman, R.J., et al., Complication rates after hip or knee arthroplasty in morbidly obese patients. Clinical orthopaedics and related research, 2013. 471(10): p. 3358-3366.
19. Halawi, M.J., et al., Effect of morbid obesity on patient-reported outcomes in total joint arthroplasty: a minimum of 1-year follow-up. Arthroplasty today, 2019. 5(4): p. 493-496.
20. Hanly, R.J., et al., Morbid Obesity in Total Knee Arthroplasty: Joint-Specific Variance in Outcomes for Operative Time, Length of Stay, and Readmission. The Journal of arthroplasty, 2017. 32(9): p. 2712-2716.
21. Ji, H.-M., et al., Sarcopenia and Sarcopenic Obesity in Patients Undergoing Orthopedic Surgery. Clinics in orthopedic surgery, 2016. 8(2): p. 194-202.
22. Martin, J.R., J.M. Jennings, and D.A. Dennis, Morbid Obesity and Total Knee Arthroplasty: A Growing Problem. The Journal of the American Academy of Orthopaedic Surgeons, 2017. 25(3): p. 188-194.
23. Tohidi, M., et al., Ten-Year Mortality and Revision After Total Knee Arthroplasty in Morbidly Obese Patients. The Journal of arthroplasty, 2018. 33(8): p. 2518-2523.
24. Babu, J.M., et al., Sarcopenia as a Risk Factor for Prosthetic Infection After Total Hip or Knee Arthroplasty. The Journal of arthroplasty, 2019. 34(1): p. 116-122.
25. Roubenoff, R., Sarcopenic obesity: the confluence of two epidemics. Obes Res, 2004. 12(6): p. 887-8.
26. Wells, J.C. and M.S. Fewtrell, Measuring body composition. Arch Dis Child, 2006. 91(7): p. 612-7.
27. Kyle, U.G., et al., Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr, 2004. 23(5): p. 1226-43.
28. Ward, L.C., et al., Validation of a three-frequency bioimpedance spectroscopic method for body composition analysis. Nutrition, 2007. 23(9): p. 657-64.
29. Gutiérrez-Marín, D., et al., Validation of bioelectrical impedance analysis for body composition assessment in children with obesity aged 8-14y. Clin Nutr, 2021. 40(6): p. 4132-4139.
30. Uemura, K., et al., Predictivity of bioimpedance phase angle for incident disability in older adults. J Cachexia Sarcopenia Muscle, 2020. 11(1): p. 46-54.
31. Wada, O., et al., Implications of evaluating leg muscle mass and fat mass separately for quadriceps strength in knee osteoarthritis: the SPSS-OK study. Clin Rheumatol, 2020. 39(5): p. 1655-1661.
32. Wada, O., et al., Structural severity, phase angle, and quadriceps strength among patients with knee osteoarthritis: the SPSS-OK study. Clin Rheumatol, 2020. 39(10): p. 3049-3056.
33. Qin, E.S., et al., Multi-segment bioimpedance can assess patients with bilateral lymphedema. J Plast Reconstr Aesthet Surg, 2020. 73(2): p. 328-336.
34. Kolz, J.M., et al., Lymphedema: A Significant Risk Factor for Infection and Implant Failure After Total Knee Arthroplasty. J Am Acad Orthop Surg, 2020. 28(23): p. 996-1002.
35. Crisp, A.H., et al., Changes in Physical Activities and Body Composition after Roux-Y Gastric Bypass Surgery. Obes Surg, 2018. 28(6): p. 1665-1671.
36. Sandini, M., et al., Perioperative Interstitial Fluid Expansion Predicts Major Morbidity Following Pancreatic Surgery: Appraisal by Bioimpedance Vector Analysis. Ann Surg, 2019. 270(5): p. 923-929.
37. Suominen, T.H., et al., Physical function and lean body mass as predictors of bone loss after hip fracture: a prospective follow-up study. BMC Musculoskelet Disord, 2020. 21(1): p. 367.
38. Pichonnaz, C., et al., Effect of Manual Lymphatic Drainage After Total Knee Arthroplasty: A Randomized Controlled Trial. Archives of physical medicine and rehabilitation, 2016. 97(5): p. 674-682.
39. Pichonnaz, C., et al., Bioimpedance for oedema evaluation after total knee arthroplasty. Physiother Res Int, 2013. 18(3): p. 140-7.
40. Pichonnaz, C., et al., Bioimpedance spectroscopy for swelling evaluation following total knee arthroplasty: a validation study. BMC Musculoskelet Disord, 2015. 16: p. 100.
41. Ledford, C.K., et al., Percent Body Fat Is More Predictive of Function After Total Joint Arthroplasty Than Body Mass Index. J Bone Joint Surg Am, 2016. 98(10): p. 849-57.
42. Ledford, C.K., et al., Percent body fat more associated with perioperative risks after total joint arthroplasty than body mass index. J Arthroplasty, 2014. 29(9 Suppl): p. 150-4.
43. Wada, O., et al., Influence of the severity of knee osteoarthritis on the association between leg muscle mass and quadriceps strength: the SPSS-OK study. Clin Rheumatol, 2019. 38(3): p. 719-725.
44. Hidding, J.T., et al., Measurement Properties of Instruments for Measuring of Lymphedema: Systematic Review. Phys Ther, 2016. 96(12): p. 1965-1981.
45. Kim, S.M., et al., The effect of mechanical massage on early outcome after total knee arthroplasty: a pilot study. J Phys Ther Sci, 2015. 27(11): p. 3413-6.
46. Beswick, A.D., et al., What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open, 2012. 2(1): p. e000435.
47. Wagner, D.R., Case study: Effect of surgical metal implant on single frequency bioelectrical impedance measures of an athlete, in Physiol Rep. 2020, © 2020 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society. p. e14464.
48. Roberts, H.C., et al., A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing, 2011. 40(4): p. 423-9.
49. Meermans, G., et al., The direct anterior approach in total hip arthroplasty: a systematic review of the literature. Bone Joint J, 2017. 99-b(6): p. 732-740.
50. Matta, J.M., C. Shahrdar, and T. Ferguson, Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res, 2005. 441: p. 115-24.
51. Barrett, W.P., S.E. Turner, and J.P. Leopold, Prospective Randomized Study of Direct Anterior vs Postero-Lateral Approach for Total Hip Arthroplasty. 2013. 28(9): p. 1634-1638.
52. Lovell, T.P., Single-Incision Direct Anterior Approach for Total Hip Arthroplasty Using a Standard Operating Table. Advances in Surgical Technology, 2008. 23(7, Supplement): p. 64-68.
53. Antoniadis, A., et al., Is Direct Anterior Approach a Credible Option for Severely Obese Patients Undergoing Total Hip Arthroplasty? A Matched-Control, Retrospective, Clinical Study. 2018. 33(8): p. 2535-2540.
54. Gibon, E., et al., Doctor, what does my knee arthroplasty weigh? J Arthroplasty, 2014. 29(11): p. 2091-4.
55. Foreman, C.W., et al., Total Joint Arthroplasty in the Morbidly Obese: How Body Mass Index ≥40 Influences Patient Retention, Treatment Decisions, and Treatment Outcomes. J Arthroplasty, 2020. 35(1): p. 39-44.
Figures
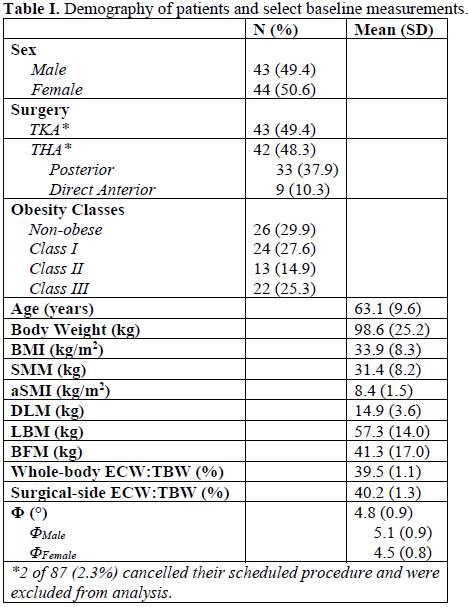
Figure 1
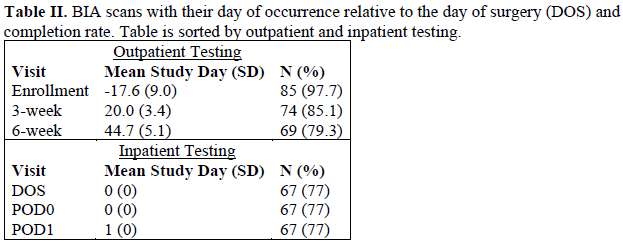
Figure 2
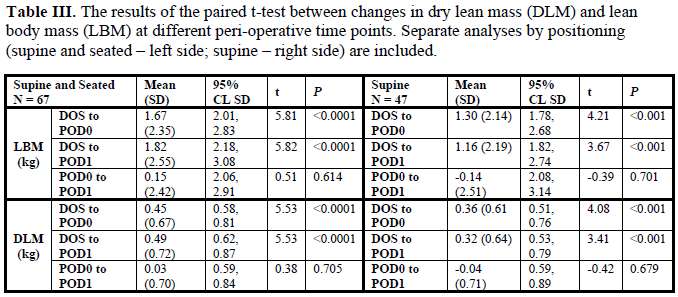
Figure 3
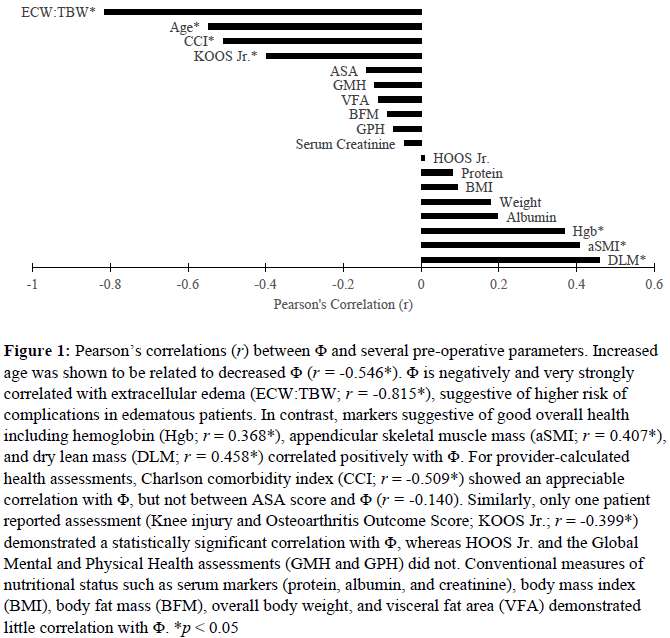
Figure 4
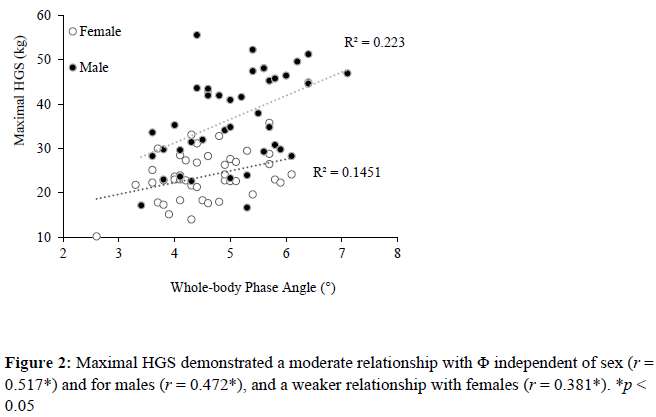
Figure 5
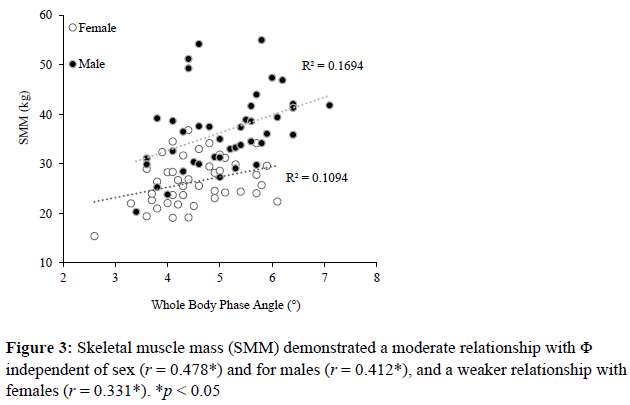
Figure 6
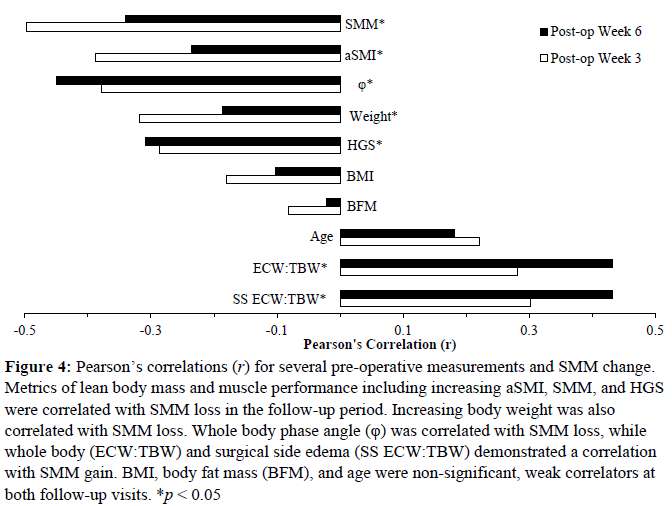
Figure 7
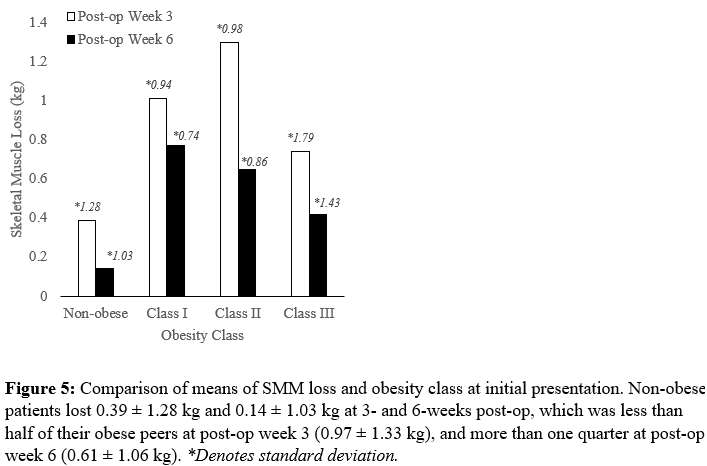
Figure 8
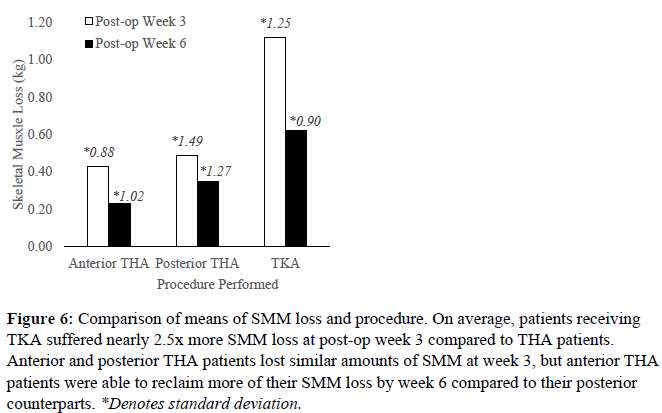
Figure 9
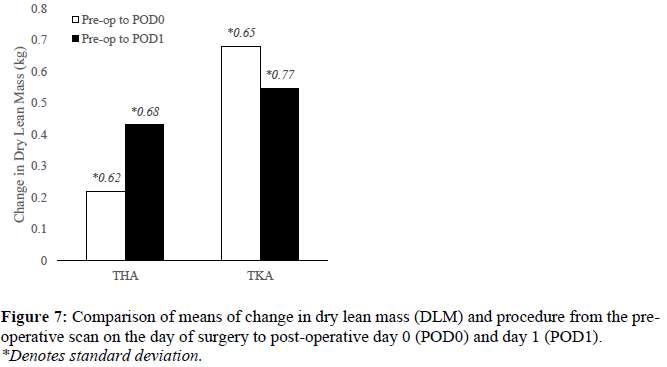
Figure 10
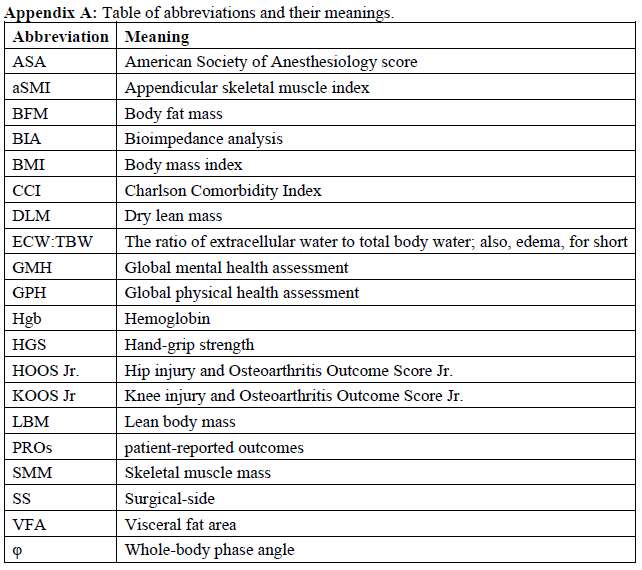
Figure 11#6898
Modified Supercapsular Percutaneous Assisted Approach for Japanese Dysplastic Hip Cases.
*Shogo Maruyama - Hamamatsu south Hospital - Hamamatsu, Japan
*Email: shoyumomo@gmail.com
Introduction
Supercapsular percutaneous assisted hip approach is a minimally invasive approach and very useful for preventing postoperative dislocation, but frequently difficult for dysplastic hip cases. I modified and adjusted this approach for my patients.
I will explain the modified this approach and clinical results for Japanese patients.
Methods
This approach is carried out in the lateral and hip flexion(about 70 to 80 degrees), complete the operation without taking the apparent dislocation position in all the steps, almost completely preserving the joint capsule and the conjoint tendon. Although there is an advantage that postsurgical dislocation is less likely to occur. The original method which performs rasping before cutting the femoral neck has particularly narrow working space for the dysplastic hip, so in our hospital we changed to the first cervical double cutting and taking out the femoral head (Fig 1), and sometimes the patient needs detaching the capsule from grater trochanter. And sometimes, highly dysplastic cases(F need first step reaming from main incision toward inside direction and secondary step reaming through the second incision (through the Cannula. Fig 2). By these procedure, all cases by Super Path® were able to preserve the joint capsule totally, and postoperative X-ray show good reposition of hip center, and leg length (Fig 3). And all cases had no postoperative prohibited limb position.
Results
Since July 2016 we performed this operation for 79 cases (97.4%) during consecutive 81THAs, remaining two cases were one ankylosis hip and one congenital dislocation hip (Crowe type4). These patient’s diagnosis are 44(55.7%) Dysplastic Hips (36cases as Crowe1 and 8 cases as Crowe 2),14(17%) Primary OAs, 12(15%) Necrosis Hips, 5 Fractures, 3 RDCs(rapidly destructive coxopathy), and one RA hip. There was no postsurgical dislocation in these cases. Especially, the THA female case for RDC (Rapidly Destructive Coxarthropathy) became delirium and japanese sitting at one day after surgery but she didn’t dislocate. In addition, out of the recent 40 cases in this case group, 38 cases (95%) are capable of elevation of lower limb extensions immediately after surgery (arousal of anesthesia) and are a measure of early recovery. And they were able to walk without cane within 5.0(1-10) days.
Discussion
However, there are many precautions in this procedure and we think that careful advance training is necessary before introduction this approach. In the lecture, I will introduce many pitfalls and useful tools for dysplastic Hips.
Figures
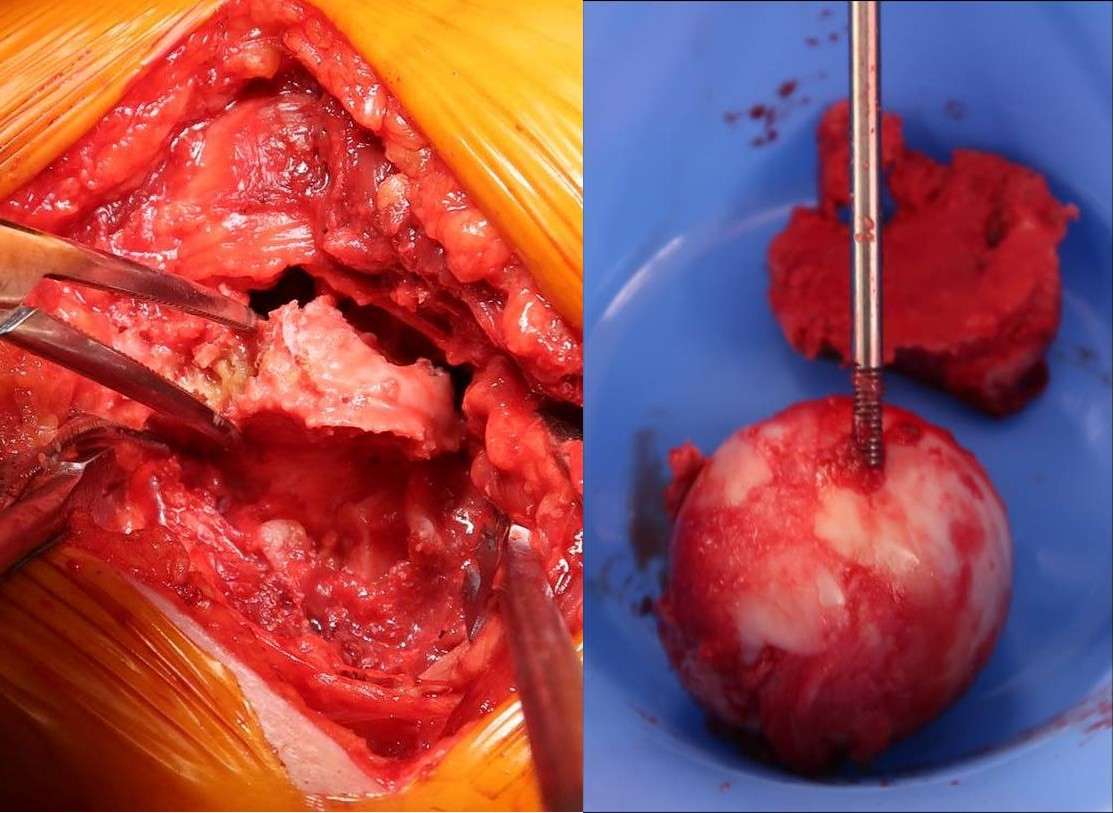
Figure 1

Figure 2

Figure 3#7436
Electronic Force Sensor Is Sensitive for Detecting Tight but Not Loose Soft Tissue in Total Knee Arthroplasty
*Shuichi Matsuda - Kyoto University - Kyoto city, Japan
Shinichi Kuriyama - kyoto university - kyoto, Japan
*Email: smat522@kuhp.kyoto-u.ac.jp
Introduction: Postoperative knee instability is a leading cause of revision total knee arthroplasty (TKA). An electronic force sensor was developed to detect increased joint load for adjusting ligament balance during primary TKA. However, it is unclear whether the sensor is reliable for detecting loose soft tissue.
Methods: Changes in medial and lateral tibiofemoral joint loads during knee flexion were evaluated with insert-shaped sensors with thickness ranging from 10 to 16 mm in six medial collateral ligament (MCL)-intact and MCL-deficient knees. Values from the sensor were compared with those from a conventional tension device. Correlations between joint loads and maximum knee extension angle were also evaluated.
Results:
Measurements with the Tension Device
In MCL-intact knees, mean lateral and medial joint gaps between the femoral component and the tibial cut surface were 11.7 ± 2.4 mm and 10.3 ± 2.2 mm in knee extension, respectively. In MCL-deficient knees, joint gaps were significant wider than in MCL-intact knees in knee extension and 45°, 90°, and 120° of knee flexion (all P < .05) (Fig. 1).
Measurement with the Electronic Force Sensor
For MCL-intact knees in extension, mean lateral and medial TF contact loads with sensor thickness of 10 mm were 10.2 ± 10.9 lb and 25.5 ± 29.7 lb, respectively (Fig. 2). As sensors thickness increased up to 16 mm, lateral and medial loads increased linearly in knee extension. In MCL-deficient knees, the medial load was difficult to detect at 45°, 90°, and 120° of knee flexion. Even when as insert thickness increased from 10 to 16 mm, corresponding to a theoretical joint gap reduction of up to 6 mm, lateral and medial loads remained almost unchanged (Fig. 3).
Correlation between TF Contact Load and Knee Extension Angle
As force sensor thickness increased, maximum knee extension angle remained limited up to -20° in MCL-intact knees. Extension angles were significantly smaller as total TF contact load increased (ρ = -0.35, P = 0.04). Knees with extension restriction less than 5° had a mean total TF contact load of 42.4 ± 18.3 lb.
Discussion and Conclusion: This study found that an electronic force sensor is highly sensitive for detecting a tight TF joint gap during PS-TKA and could predict knee flexion contractures. Excessively loose TF joint gaps were clearly detected by the tension device, but the force sensor had lower accuracy for detecting loose joint gaps. When the sensor shows a low load, this value should be carefully interpreted along with measurements based on other methods, such as the tension device.
Figures
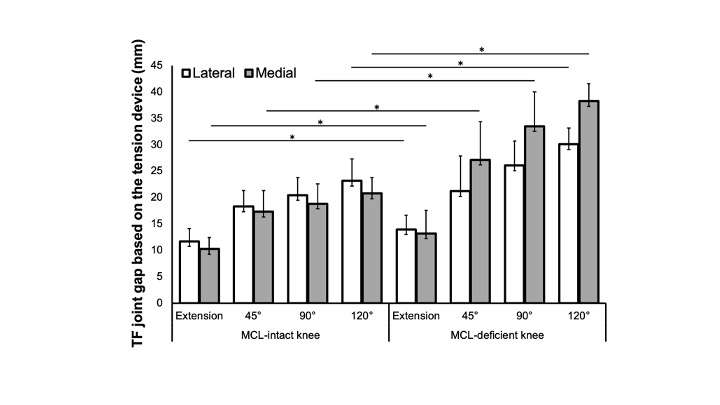
Figure 1
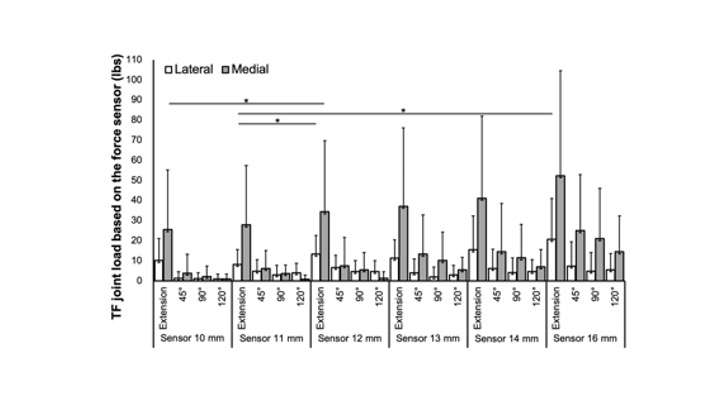
Figure 2
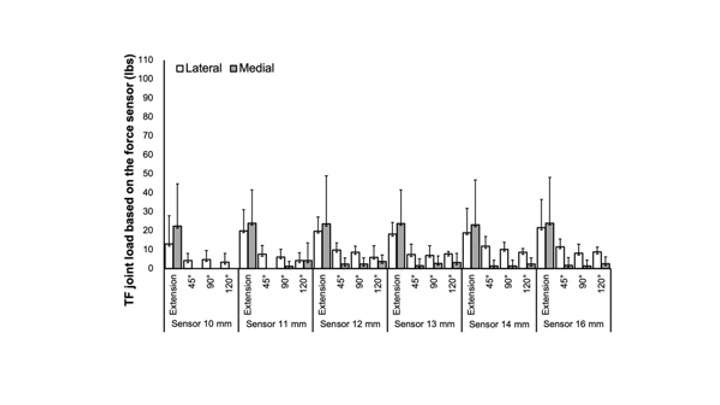
Figure 3#7914
A Comparison of Early Failures and Patient Reported Outcomes Between Press-Fit and Cemented TKA
*Makoa Mau - University of Hawaii, John A. Burns School of Medicine - Honolulu, United States of America
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Kyle Obana - University of Hawai'i John A. Burns School of Medicine - Honolulu, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
Charissa Tan - University of Hawaii, John A. Burns School of Medicine - Honolulu, USA
*Email: mkktmau@hawaii.edu
INTRODUCTION: Although cemented implants have been the gold standard in total knee arthroplasty (TKA) for the past three decades, shifts in younger patients requiring TKA have raised concerns for decreased integrity at the cement-bone interface. Press-fit implants have been introduced to minimize the cement-associated risk for loosening. However, press-fit implants have not demonstrated lower rates of early failures. The purpose of this study was to evaluate patient reported outcomes and rates of early failure (<1 year) between press-fit and cemented TKA.
METHODS: A consecutive cohort of 129 cemented and 95 press-fit TKA patients were prospectively evaluated. Pre-operative patient demographics were collected [Table 1]. Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR), Patient-Reported Outcomes Measurement Information System (PROMIS) Global Physical Health (GPH) and Global Mental Health (GMH) and satisfaction (very satisfied, satisfied, unsatisfied) were collected pre-operatively and post-TKA at six weeks, six months, and one-year. Revisions, manipulation under anesthesia (MUA), and other complications were evaluated with a minimum one-year follow-up.
RESULTS: There were no differences between groups regarding KOOS JR, PROMIS GPH, PROMIS GMH, or satisfaction throughout the year following surgery [Table 2]. At one-year, 80.6% and 70.9% of patients reported “very satisfied” and 12.9% and 12.6% reported “satisfied” in the cemented and press-fit groups, respectively. There were no revisions. The rate of MUA was similar for cemented (6.7%) and press-fit (10.4%) groups. There were no differences in complications [Table 3]. There were four deep vein thromboses (2.2%), one infection (0.6%) and one pulmonary embolism (0.8%) in the cemented group, and one fracture (0.7%) in the press-fit group.
CONCLUSION: Without differences in clinical or patient reported outcomes between cemented and press-fit implants, these results would suggest both implant designs are sufficient for TKA. Furthermore, similarities in complications between cemented and press-fit groups support previous research on the latest generation of press-fit prosthesis.
Figures
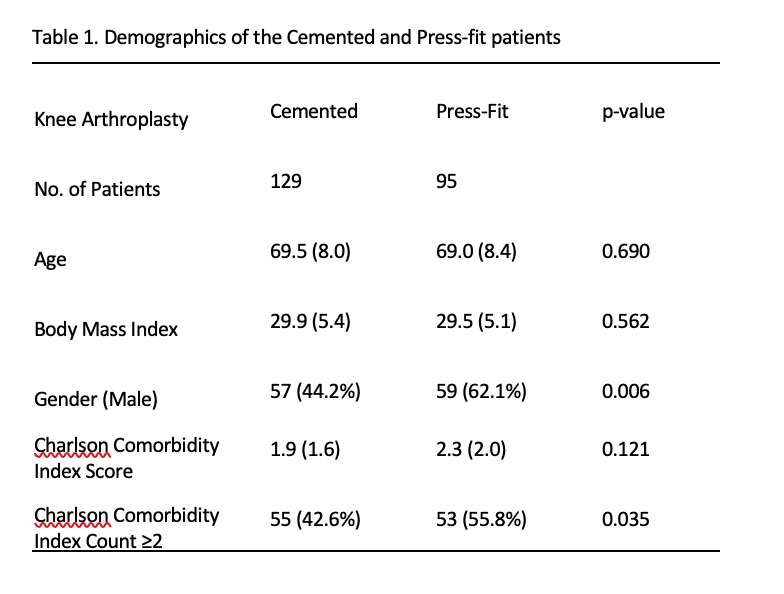
Figure 1
Figure 2
Figure 3#7293
Comparison of Early Outcomes Comparing Two Total Knee Implant Designs
*Julian Rimm - Straub Bone & Joint Center - Honolulu, United States of America
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Makoa Mau - University of Hawaii, John A. Burns School of Medicine - Honolulu, United States of America
*Email: jrimm@hawaii.edu
Introduction: Numerous total knee arthroplasty (TKA) implants are currently available, incorporating variations in tibial base symmetry and radius of curvature of the femoral component. Traditional implants have symmetric tibial base plates and multi-radius femoral components (SYM-MR), while newer TKA systems incorporate asymmetric tibial baseplates and single-radius femoral components (ASY-SR). However, literature comparing outcomes between these implant designs are conflicting. This study analyzed short-term patient-reported and radiographic outcomes between a SYM-MR and an ASY-SR TKA system.
Methods: This prospective study evaluated a consecutive cohort of unilateral and bilateral TKA patients receiving the SYM-MR or ASY-SR TKA system between 2019 and 2021. Improvements in the Knee Society Function Score, maximum knee flexion and Knee Injury Osteoarthritis Outcome Survey, Joint Replacement (KOOS JR) were calculated from pre-operative to six-months post-operatively. Mechanical axis was measured at six-weeks post-TKA from standing hip-to-ankle radiographs, with neutral defined as 0°±3°and negative values indicating varus alignment.
Results: Overall, 71 patients (96 knees) and 54 patients (79 knees) were included in the ASY-SR and SYM-MR groups, respectively. Six-month and overall improvements in clinical and patient reported outcomes were similar between groups. Post-operative MA was also similar between groups, with 79.2% and 82.3% of SYM-MR and ASY-SR patients having neutral post-TKA MA.
Discussion/Conclusion: The results of the current study demonstrated similar post-operative outcomes between a more traditionally designed SYM-MR and more novel ASY-SR. This suggests early outcomes are not affected by implant design and surgeons should not be overly concerned that one type of design offers clear advantages or disadvantages.
#7759
Has Wrought CoCrMo Alloy Changed for the Worse Over Time?
*Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Steven Mell - Rush University Medical Center - Chicago, USA
Brett Levine - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: stephanie_mccarthy@rush.edu
Introduction: Modular taper corrosion in total hip arthroplasty (THA) has been a clinical problem for over 30 years. THA failure due to adverse local tissue reactions (ALTR) to corrosion products has also seemingly increased over time. Recent studies have focused on comparing THAs with mechanical and/or chemical damage processes, specifically column damage. Chemically induced column damage is enabled by alloy segregation bands caused during thermomechanical processing of bar stock material. It is unclear if alloy banding is a recent phenomenon. The purpose of this study was to examine THAs implanted in the 1990s, 2000s, and 2010s to determine damage score distribution, occurrence of column damage, and prevalence of alloy banding over time.
Methods: 522 modular heads from 12 different manufacturers were analyzed. Implant damage was assessed using a modified Goldberg damage scoring system (1 minimal damage, 2 mild, 3 moderate, 4 severe damage). Implant characteristics and patient demographics were recorded. A subset of heads (n=122) was processed for metallographic analysis to visualize CoCrMo alloy banding. All head tapers from the subset group were measured with an optical coordinate measuring machine to determine column damage presence (Fig.1). Heads were grouped based on decade of implantation (1990s, 2000s, 2010s), serving as a proxy measure of manufacturing time, and chi-square tests were performed to compare differences between groups.
Results: Damage score distribution was consistent over the time periods (Fig.2). 28mm heads were the predominate size in the 1990s. In the 2000s, 28, 32 and 36mm heads were used, with the majority being 32mm. The most used head sizes of the 2010s were 32 and 36mm. Incidence of column damage significantly increased between the 1990s (n=24) and 2000s (n=68), from 21% to 55% (p=0.04), but decreased to 33% in the 2010s (n=28). Microstructural banding increased significantly from the 1990s (52%) to the 2000s (97%) (p<0.001) and 2010s (79%) (p=0.06) (Fig.3). Comparisons between banding in specific head sizes revealed a 76% increase in banding between the 1990s to 2000s in 28mm heads, but no change in 32mm heads from the 2000s to 2010s (92% and 100% banded, respectively). Interestingly, banding in 36mm and larger heads decreased from the 2000s and 2010s by 28%, suggesting a slight recovery in homogenous microstructure in larger heads.
Conclusion: Microstructural banding, which provides preferential corrosion sites enabling column damage, has increased over the last three decades. This increase can be partially explained by growing heads sizes, although the decrease in banding in 36mm heads warrants additional analysis to solidify this finding. Larger diameter bar stock material undergoes less deformation and is subject to lower degrees of microstructural homogenization. However, the increase in banding in 28mm heads from the 1990s to 2000s suggests changes in thermomechanical processing may also have occurred. Of note, no difference between manufacturers was seen, which could be explained by shared suppliers of bar stock material. These findings are significant because alloy banding can be avoidable, reducing the risk of column damage which is associated with more severe ALTRs than other fretting corrosion processes.
Figures
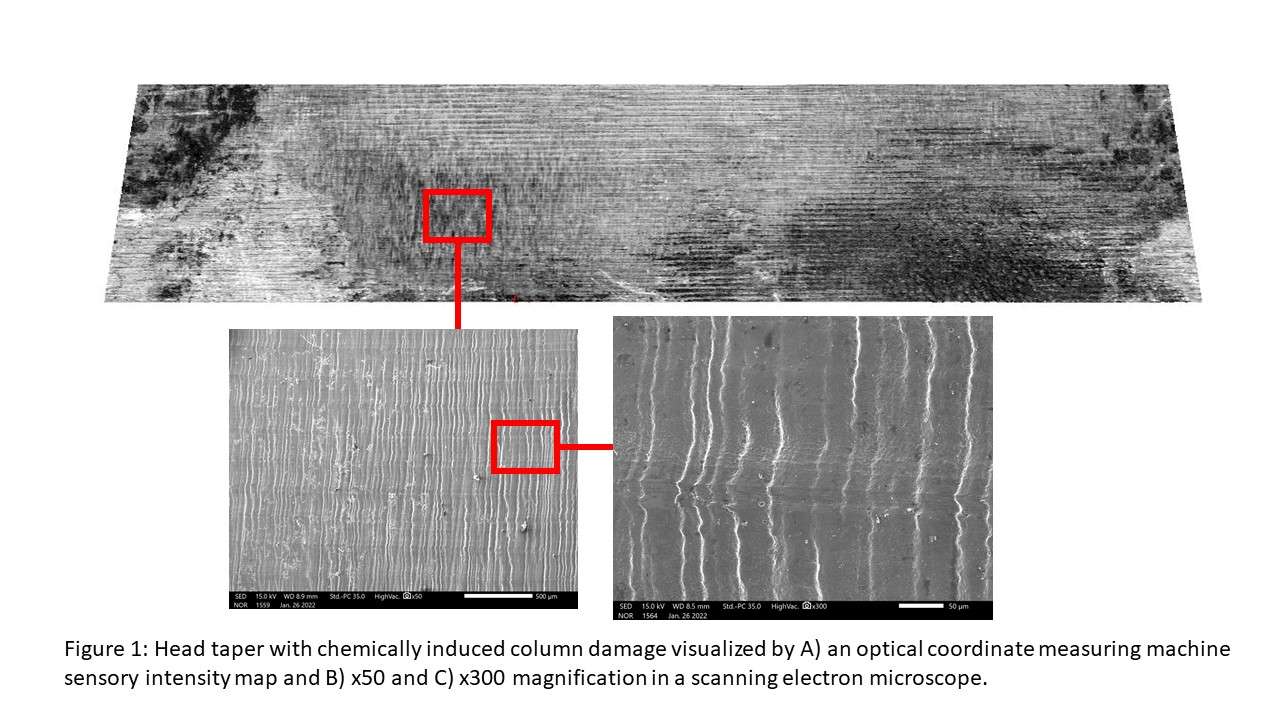
Figure 1
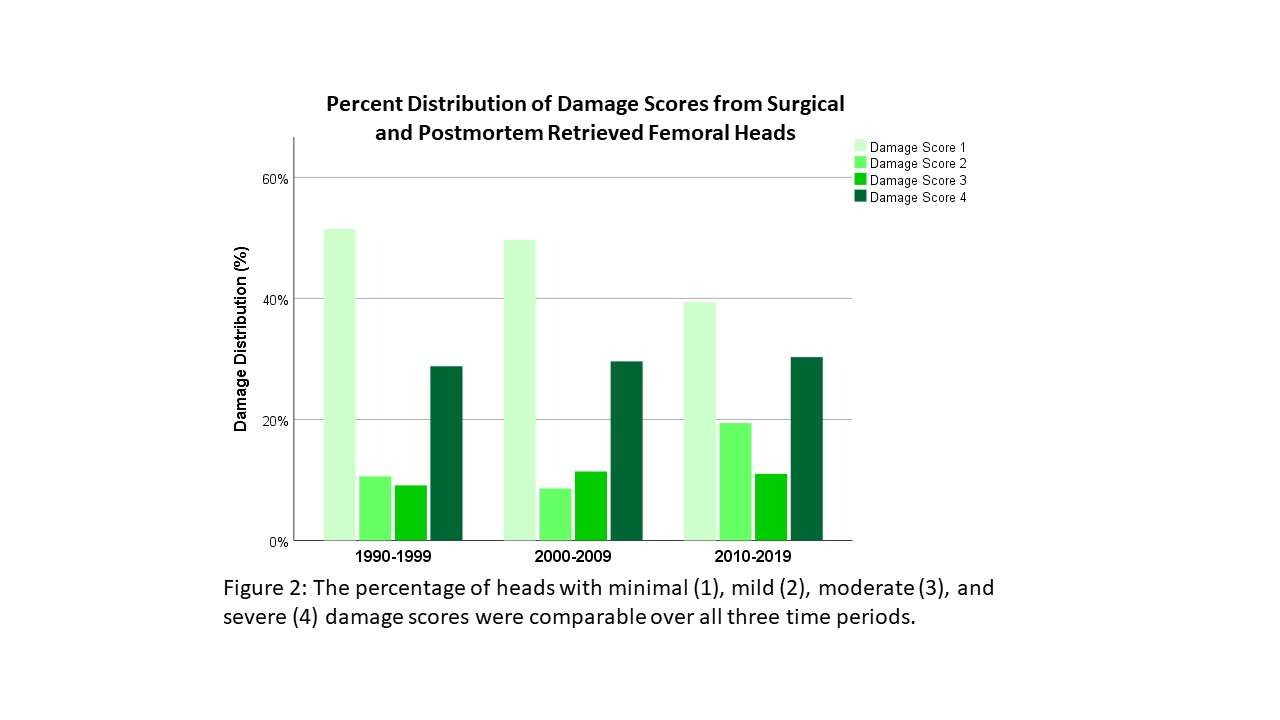
Figure 2
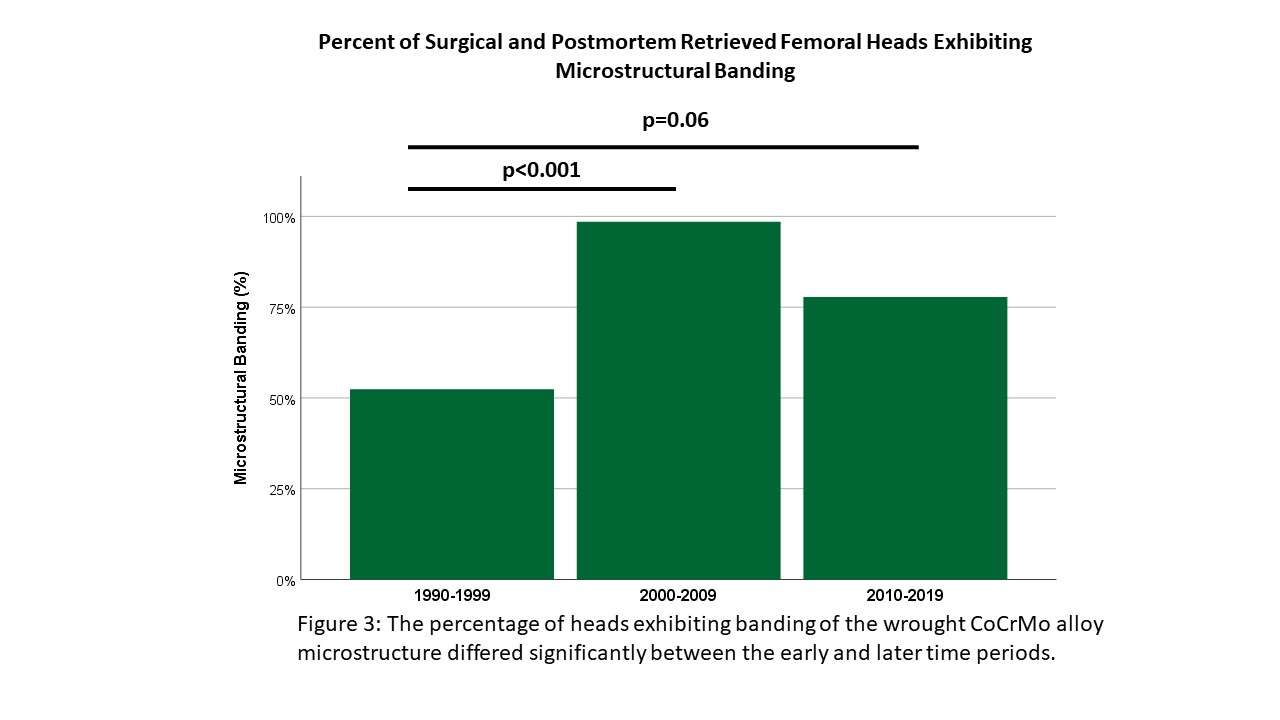
Figure 3#7806
Chemically Dominated Corrosion Modes in CoCrMo and Ti-Alloy Femoral Stem Tapers
*Stephanie McCarthy - Rush University Medical Center - Chicago, USA
Mozart Neto - Rush Medical Center - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: stephanie_mccarthy@rush.edu
Introduction: Total hip arthroplasty (THA) modular junctions can undergo micromotion induced fretting-corrosion and subsequent implant failure. Besides fretting, other chemically dominated corrosion modes can occur, leading to elevated material loss and higher risk of adverse tissue responses. In wrought CoCrMo femoral heads, the most severe chemical damage mode is column damage driven by a chemical attack on segregation bands, or preferential corrosion sites, within the alloy. Column damage of femoral stems has not been reported, although a harsh chemical environment within the modular junction should affect both taper surfaces. Therefore, the purpose of this study was to examine stem tapers corresponding to femoral heads exhibiting chemically induced column damage to document the resulting damage modes.
Methods: 753 contemporary modular stem and head taper pairings were evaluated for this study. Implant damage was assessed using a modified Goldberg damage score (1 minimal damage, 2 mild, 3 moderate, 4 severe). All heads exhibiting column damage with a paired stem taper available were selected for further analysis (n=29). Head and stem tapers were measured with an optical coordinate measuring machine to identify damage modes and calculate volumetric material loss (Fig.1). CoCrMo and Ti-alloy stem tapers were visualized in a scanning electron microscope for further distinction of chemical and mechanical damage modes (Fig.2). Implant characteristics and patient demographics were recorded. Comparisons between stem taper alloys were made using Chi-square tests and one-way ANOVA.
Results: 27 CoCrMo modular heads from 6 different manufacturers and 2 CoCrMo adaptor sleeves in ceramic heads had severe (score 4) taper damage. Average implant time in situ was 74.02 ±58 months. 62% of the paired stem tapers were made of CoCrMo alloy, with 16 exhibiting severe damage and 2 exhibiting moderate damage. 38% of stem tapers were Ti-alloy, with 5 severe, 4 moderate, 1 mild, and 1 minimal damage scores. Of the CoCrMo alloy stem tapers, 89% exhibited chemical damage of the stem taper. Ti-alloy stems exhibited chemical damage in 27% of cases, significantly less than the CoCrMo group (p=0.001). Average volumetric material loss also differed between stem alloys, with 0.6mm3 (95%CI [.26,.93]) and 0.07mm3 (95%CI [.01,.14]) (p=0.011).
Conclusion: We found the majority of CoCrMo stem tapers paired with CoCrMo alloy heads with column damage also suffered chemically dominated corrosion in addition to fretting damage. Unlike the head, stem corrosion damage manifested as intergranular corrosion, pitting, phase boundary corrosion and local etching. Like femoral heads, stem corrosion was driven by preferential corrosion sites such as grain boundaries, hard phases, and other alloy inhomogeneities. Titanium alloys were less likely to exhibit chemically induced damage due to its superior corrosion properties, yet a quarter of cases exhibited pitting corrosion along deformed machining lines. This study confirms that severe cases of THA modular junction corrosion experience a chemical change within the crevice that targets preferential corrosion sites on both taper surfaces. Why certain cases experience a change of the chemical environment needs to be further studied, but preferential corrosion sites can be eliminated from these alloys to improve implant performance.
Figures
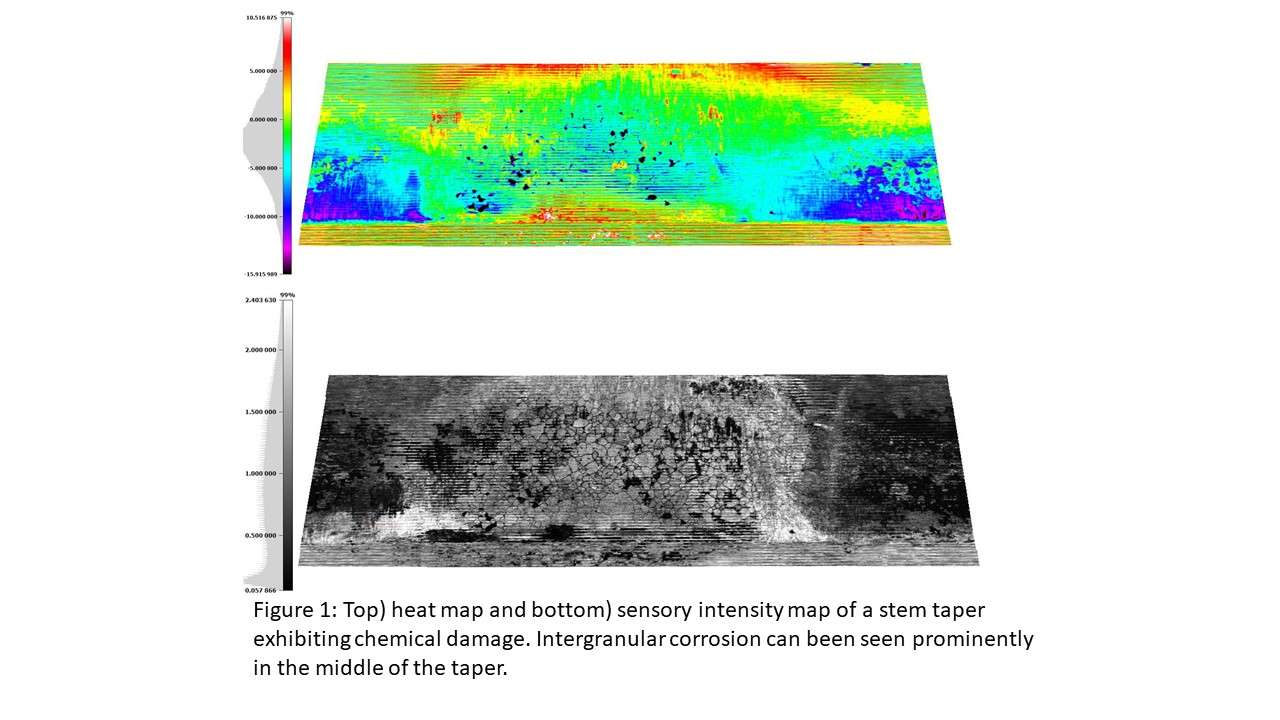
Figure 1
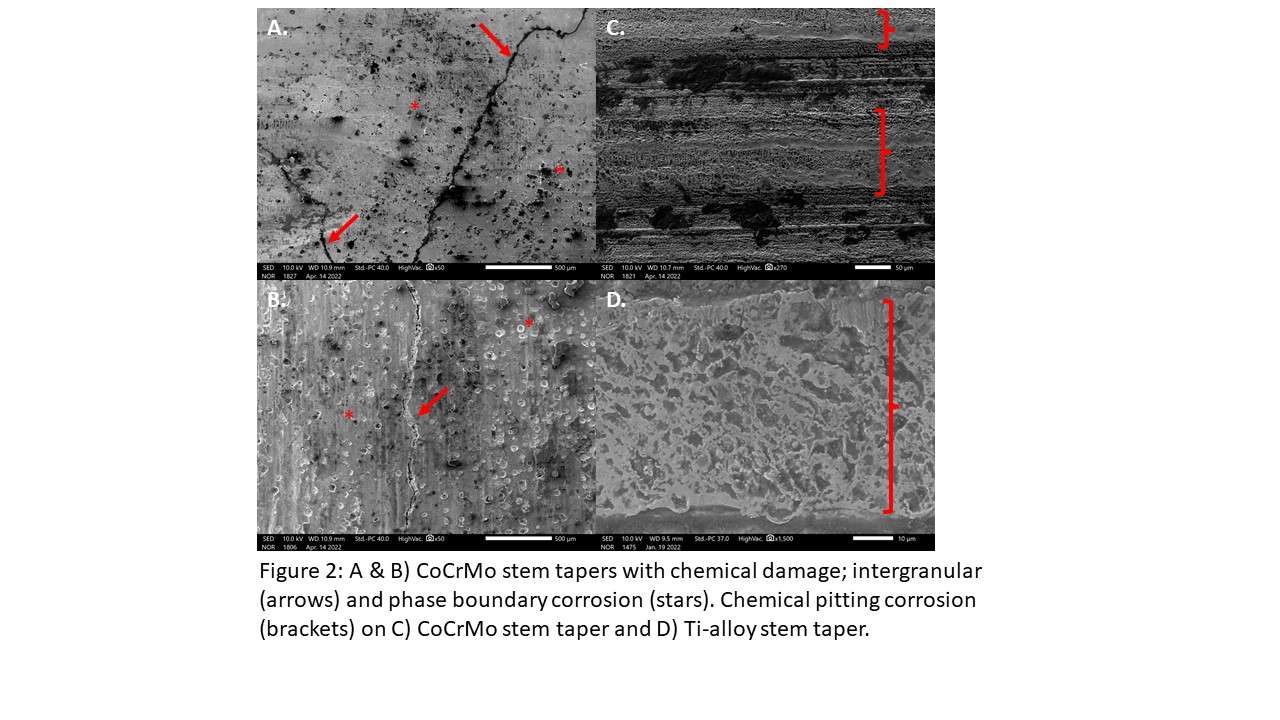
Figure 2#7601
Printability of Porous Lattice Architectures Using Metal Additive Manufacturing
Martine McGregor - University of Waterloo - Waterloo, Canada
Sagar Patel - University of Waterloo - Waterloo, Canada
Kevin Zhang - University of Waterloo - Waterloo, Canada
Mihaela Vlasea - University of Waterloo - Waterloo, Canada
*Stewart McLachlin - University of Waterloo - Waterloo, Canada
*Email: stewart.mclachlin@uwaterloo.ca
Introduction: Metal additive manufacturing (AM) has created opportunities to tailor orthopaedic implant designs with porous lattice architectures for osseointegration, functional topology optimization, stiffness reduction and light-weighting. Surface lattice structures, like triply periodic minimal surfaces (TPMS) and spinodoids, have established advantages over strut lattices for osseointegration; however, surface lattices are less compliant than strut lattices, such as the face centred cubic (FCC), body centred cubic (BCC), graphical diamond, octet, and Voronoi. Despite advantages of AM, these lattice geometries can be challenging to print using technologies such as laser powder bed fusion (LPBF) due to unsupported and downward facing surfaces (<45° to horizontal) that can induce part defects (porous regions, reduced dimensional fidelity, uneven rough surfaces), warping, and even build part failure in objects. The printability of different lattice types and variations is not well understood when tailoring orthopaedic implant designs for manufacturability using metal AM. The purpose of this study was to examine the printability of common lattice structures using LPBF based on geometric and defect analysis.
Methods: Nine unique homogenous lattice structures were designed as triangular meshes using nTopology software and MATLAB: FCC, BCC, graphical diamond, octet, Voronoi, TPMS gyroid, TPMS schwarz, TPMS diamond, and spinodoid (Figure 1). The lattices geometries filled 20 x 20 x 20 mm cubes with a lattice unit cell of 10 mm and a feature thickness of 1 mm. Lattice structures were manufactured in maraging steel using metal AM via LPBF (M290, EOS, Germany) and subjected to X-ray computed tomography (XCT) images for non-destructive evaluation of manufacturing outcomes. The important core process parameters used for manufacturing the lattice structures included a laser power of 370 W, 90 μm beam spot diameter, beam velocity of 0.92 m/s, a powder layer thickness value of 40 μm, and a hatching distance of 100 μm. Maraging steel was used due to material availability; however, print parameters and printability outcomes are expected to be similar to biocompatible metals such as Ti6Al4V. Lattice structures were geometrically analyzed using a custom Python script. Downward facing surfaces at 15° increments to horizonal (0-15° to 75-90°) were quantified based on a percentage of total lattice surface area. Volumetric part quality was quantified through an automated layer-by layer comparison of the lattice design mesh and XCT data from the printed lattice structures (Figure 2).
Results: Geometric deviations between the designed lattice mesh and XCT data were the highest in the lattice designs with more proportional downskin area (Figure 3). Surface lattices were successfully printed with fewer porous defects and excellent geometric fidelity between mesh and XCT data. Strut lattices had variable printability, being more susceptible to build orientation due to the greater interconnectivity of downward facing surfaces (Figure 3).
Conclusions: Printability of lattices is an important consideration for effective use of metal AM for tailoring orthopaedic implant designs. As metal additive manufacturing technology matures, it is imperative that the orthopaedic community benefits from its advances while ensuring patient safety through best manufacturing practices.
Figures
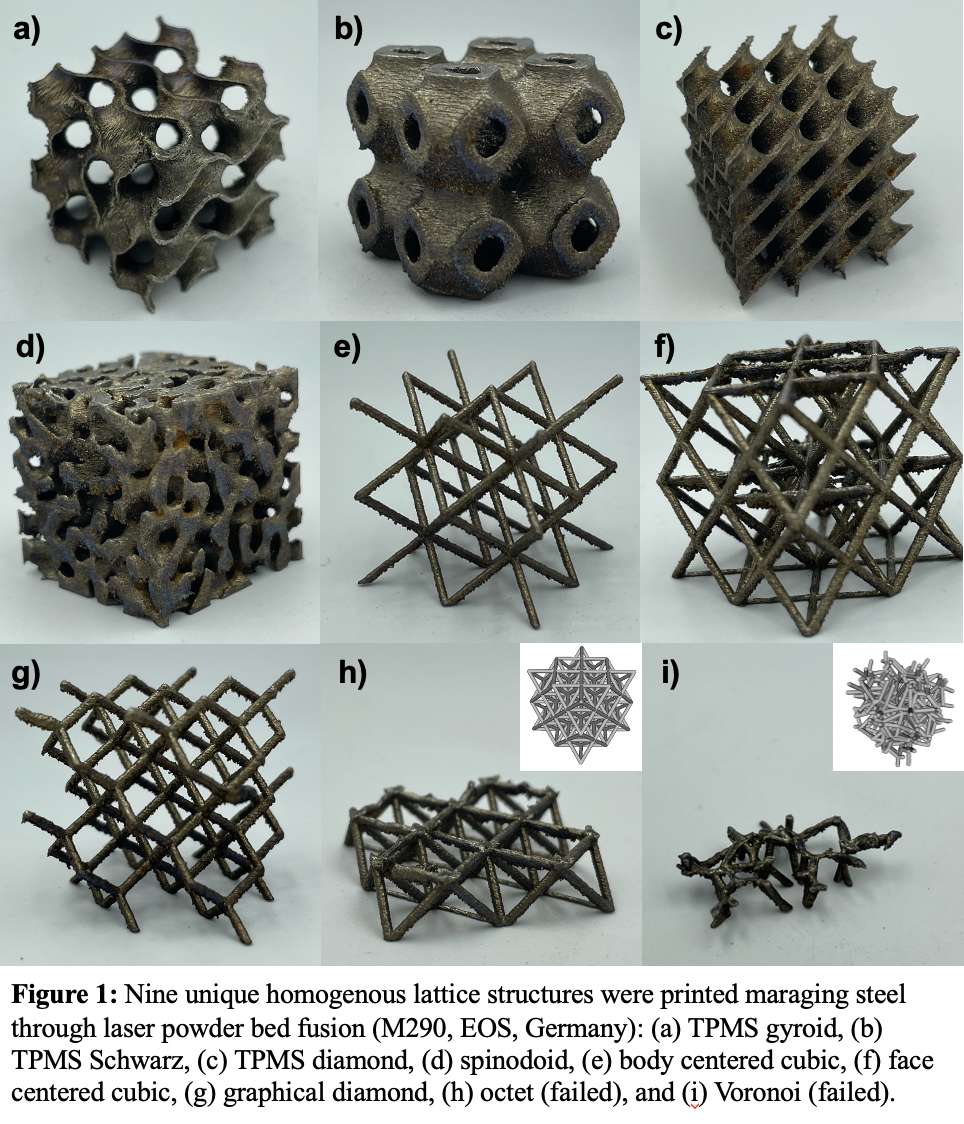
Figure 1
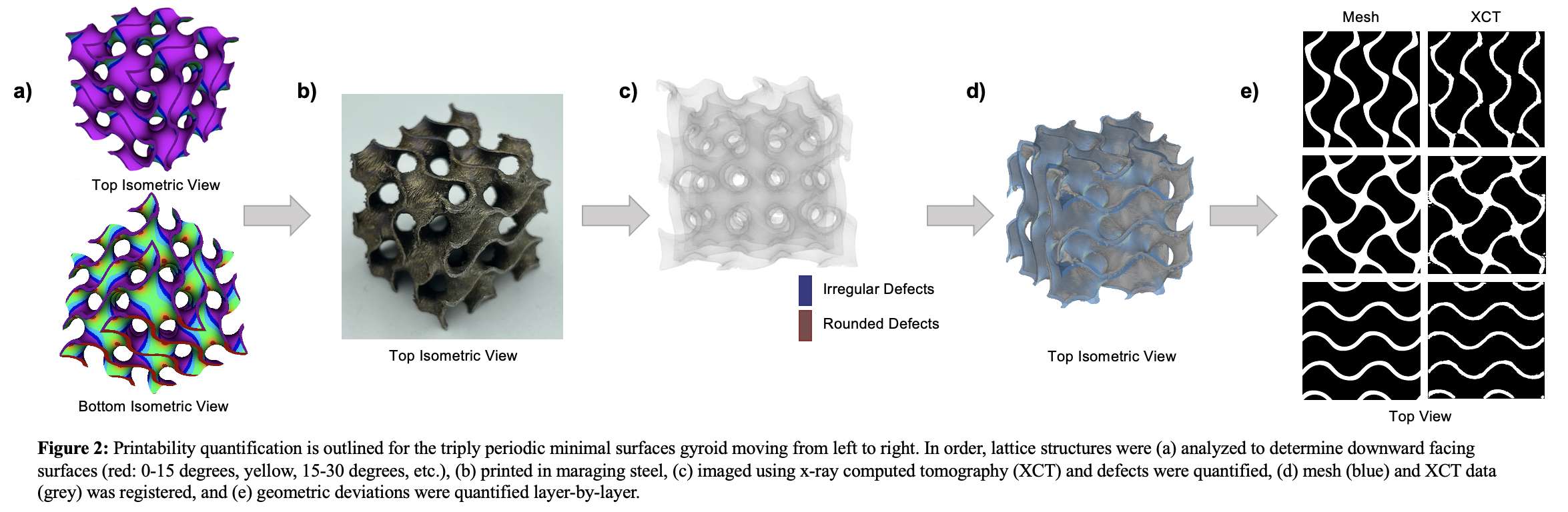
Figure 2
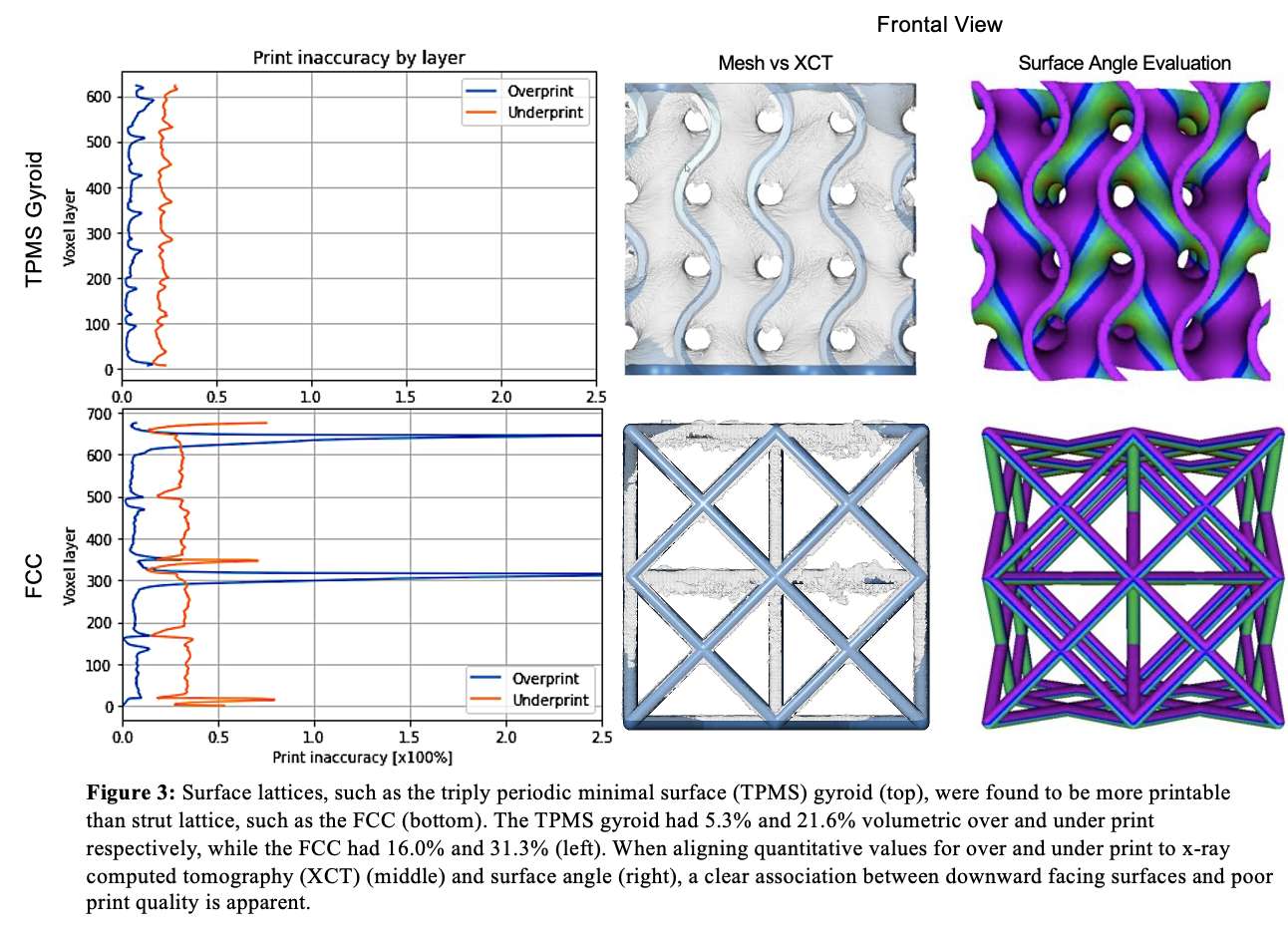
Figure 3#7931
Evaluating Spinal Implant Fixation Under Physiologically Derived Multi-Axial Loading Waveforms Using an AMTI VIVO Joint Motion Simulator
Martine McGregor - University of Waterloo - Waterloo, Canada
*Stewart McLachlin - University of Waterloo - Waterloo, Canada
*Email: stewart.mclachlin@uwaterloo.ca
Background: Implant loosening remains a clinically relevant complication associated with instrumented spinal fusion surgeries. Upwards of 15% of patients with healthy bone and 60% of patients with osteoporotic bone will experience pedicle screw loosening following posterior instrumented lumbar fusion surgery. Spinal implant fixation has typically been quantified biomechanically through either pullout strength or cyclic toggle testing. However, these in vitro testing methods occur in a single axis or plane and do not reflect the physiologic multiaxial loading that is applied to spinal implants in the lumbar and lumbosacral spine, as shown by the Orthoload group in Germany. Yet, in vitro application of multiaxial physiologic loading to spinal implants remains challenging due to the complex mechanical and control systems required to replicate in vivo spinal loading waveforms. Therefore, the goal of this work was to develop a novel approach to evaluate spinal implant fixation under physiologically derived multiaxial loading of the lumbar spine by adapting the six degree of freedom (6DOF) loading capabilities of the AMTI VIVO™ joint motion simulator.
Methods: In vivo 6DOF load data for common activities of daily living from telemeterized internal spinal fixator implants were collected from 5 patients in the Orthoload online repository (www.orthoload.com). A custom MATLAB script was used to convert the raw in vivo 6DOF data to multiaxial waveforms compatible with the AMTI VIVOTM (Figure 1). The created multiaxial loading waveforms were resolved to use the built-in Grood-Suntay coordinate system to enable 6DOF force control around the anatomical reference axis of the vertebra. To maintain this common anatomical reference position, custom fixtures were developed to position and hold lumbar vertebrae so that the long axis of the pedicle screw was in-line with the system’s superior-inferior axis (e.g. vertebra rotated to have screw positioned vertically) (Figure 2). In this orientation, the system’s actuators used to produce knee flexion/extension, abduction/adduction, and internal/external rotation were adapted to produce loads associated with spinal axial rotation, flexion/extension, and lateral bending respectively (Figure 3). Sixteen human lumbar vertebrae (L2-L5) will be tested to compare posterior spinal implant loosening under applied multiaxial loading and uniaxial toggle testing.
Results: The testing setup demonstrates how the AMTI VIVO™ can be adapted to simulate multiaxial spinal implant loading, using a combination of the large actuator range of motion, loading capacity and 6DOF force control around an anatomical vertebral reference axis. On-going testing efforts are expected to further reveal how multiaxial loading associated with activities of daily living contributes to spinal implant loosening.
Conclusion: This study presents a novel approach to improve biomechanical evaluation of spinal implant performance under multiaxial loading.To the best of our knowledge, this is the first report of the AMTI VIVO™ joint motion simulator being used to produce anatomical multiaxial loading for the purpose of testing spinal implants. As implant technologies advance, so must our testing approach to investigate potential causes and solutions to implant loosening.
Acknowledgements: Thank you to Dr. Ryan Willing for providing the custom MATLAB script required to convert raw Orthoload data files to AMTI VIVOTM compatible waveforms.
Figures
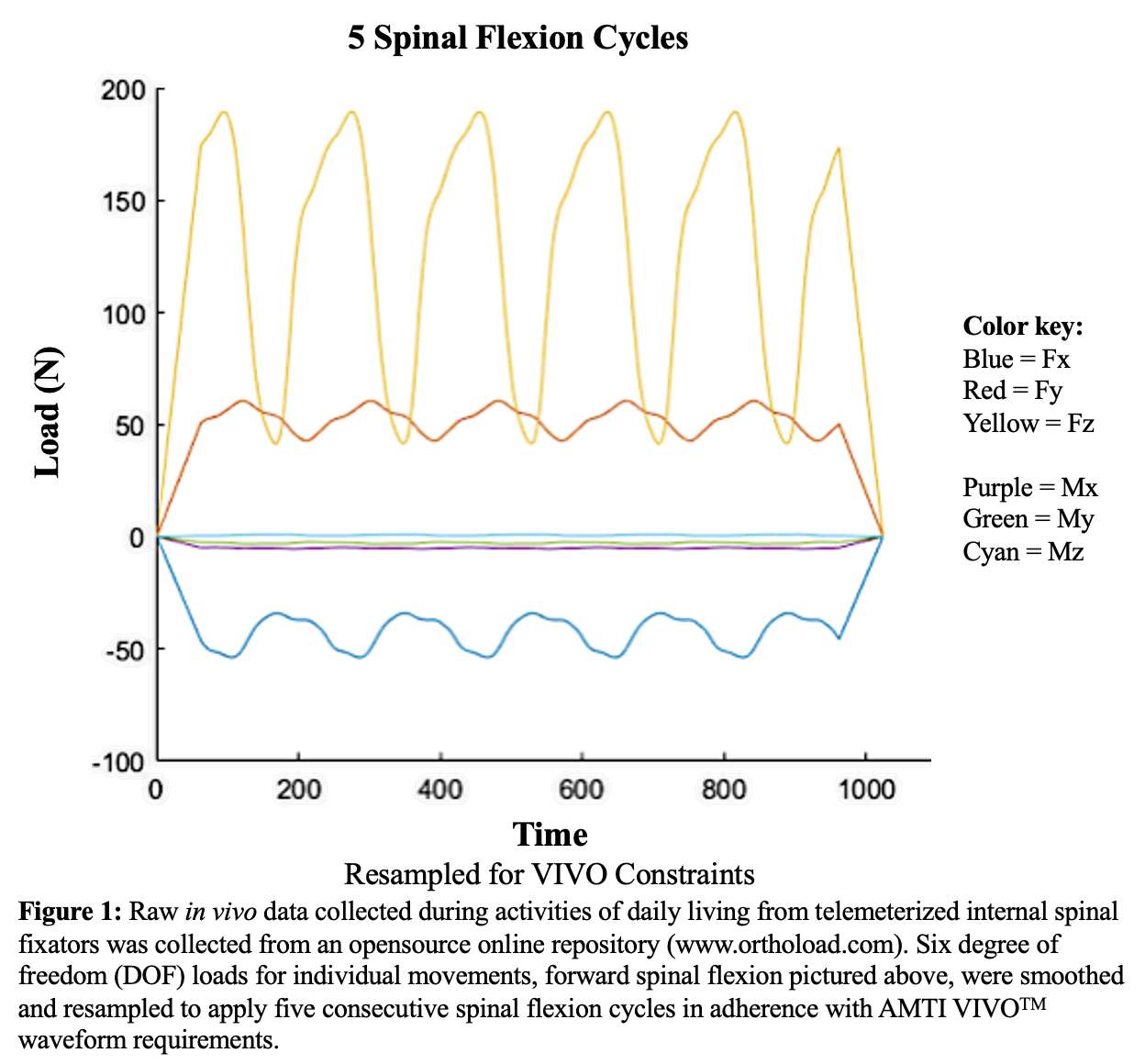
Figure 1
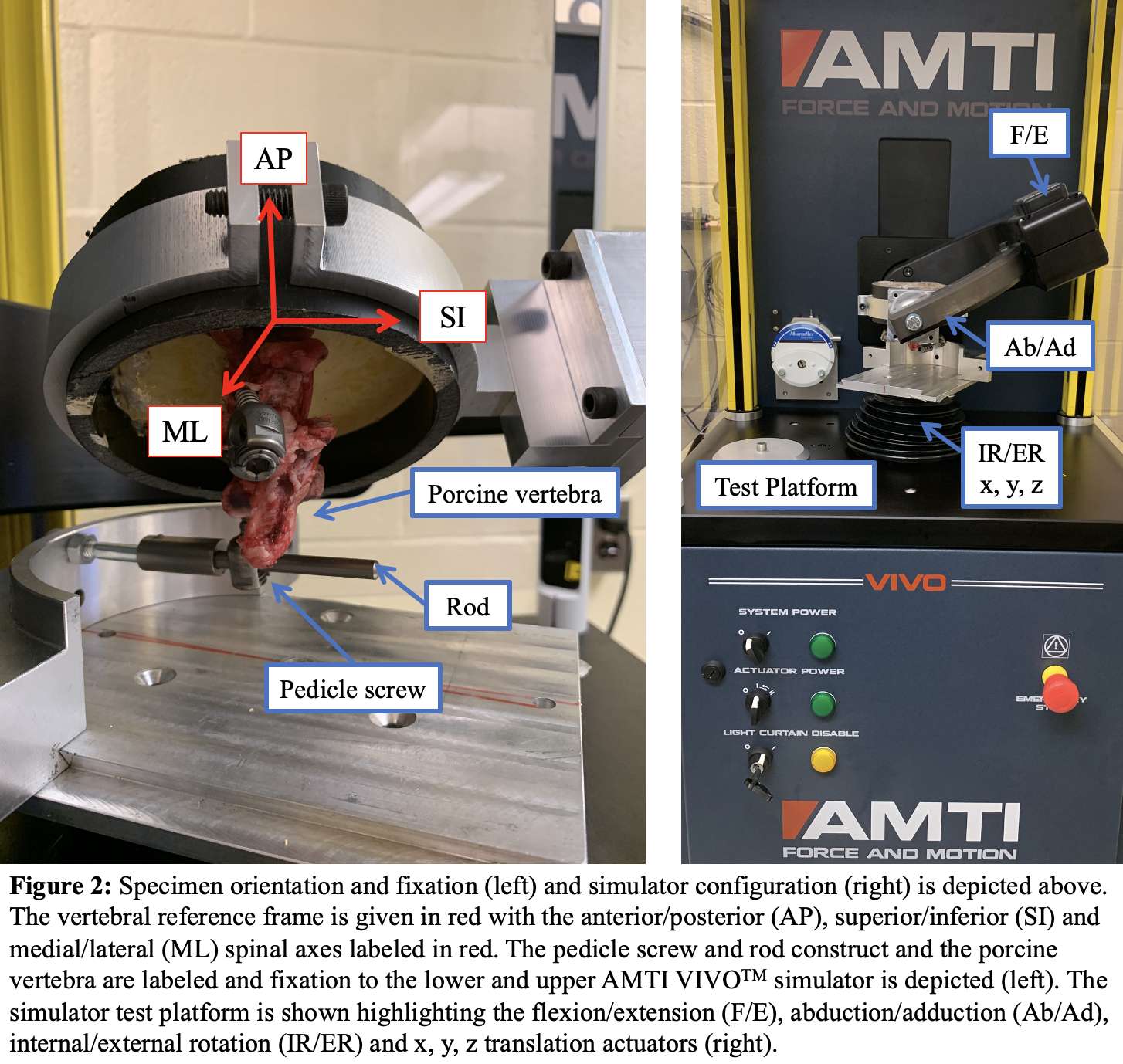
Figure 2
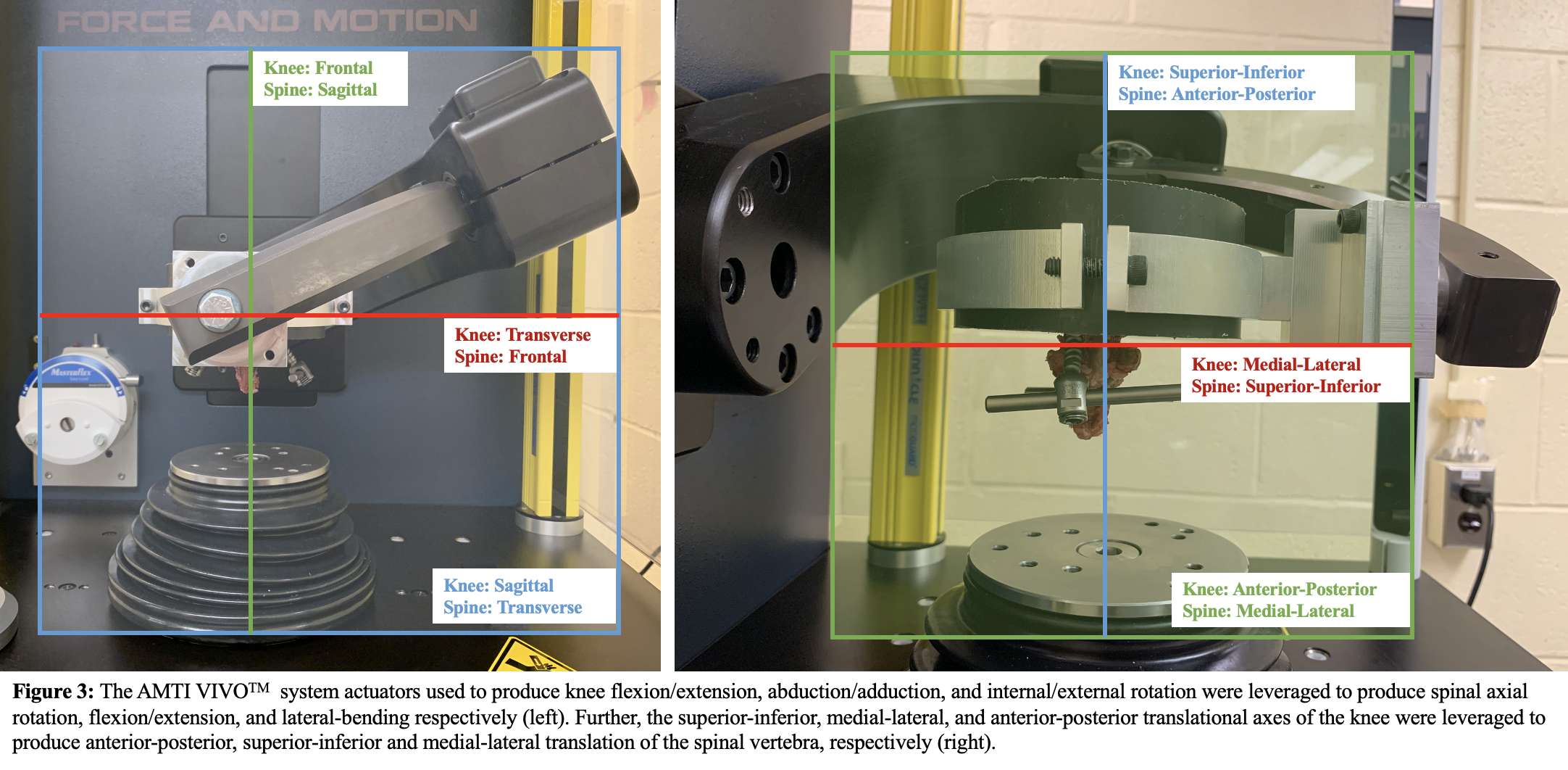
Figure 3#7752
Constrained Insert Design Provides Consistent V/V Constraint After Fatigue Loading With a Modern, Universal Primary Femur
Anna Sullivan - Total Joint Orthopedics - Salt Lake City, USA
Chris Weaber - TJO Inc. - Salt Lake City, USA
*Andi Cragen - Total Joint Orthopedics, Inc. - Austin, United States of America
Paul Postak
Dermott McHugh - Total Joint Orthopedics - Salt Lake City, USA
*Email: acragen@tjoinc.com
Introduction: Constrained tibial insert designs provide increased joint constraint in varus/valgus (V/V) and internal/external (I/E) rotation by way of interaction between an enlarged tibial post and the intercondylar box of the femur implant. The objective of this study is to evaluate the I/E and V/V constraint of the PS-Max tibial insert design with a modern, universal primary femur, and evaluate constraint after repeated physiological loading. Testing was performed to measure initial contact constraint values, apply physiologic cyclic loading, and measure constraint values after fatigue loading for comparison.
Methods: Size 1PS-Max tibial inserts were paired with Size 1 Klassic PS-Post femurs. The use of the smallest size implants maximizes loading under I/E and V/V controlled torque.
Initial contact constraint per ASTM F1223 was performed to establish the initial I/E and V/V tibial post and intercondylar box contact angle, using 710N and 45N joint loads, respectively, at flexion angles of 0°, 90° and 135°. Five samples were tested for each flexion angle in both I/E and V/V.
I/E fatigue of One TKR construct was tested in coronal plane rotation under severe internal rotation loading2. An I/E rotational moment of ±10.5 Nm (R=-1) was applied for 10,000 cycles. Under this severe loading, the I/E rotation constraint was provided by the articular interface only, and no post and intercondylar box contact was noted. The maximum I/E angle during cycling was recorded.
V/V fatigue of three total knee replacement (TKR) constructs were tested to simulate activities of daily living at 0° flexion with repeated frontal plane rotation (V/V) under severe varus loading1. Maximum varus moments of 54.5 Nm, 57 Nm, and 57 Nm (R=0.1) were applied for 1MM cycles, and the maximum varus angle was recorded.
A compressive joint load of 2250N was applied for all I/E and V/V fatigue testing.
Results: I/E testing per ASTM F1223 determined initial tibial post and intercondylar box contact to be ±6.9° and ±6.5°, at femur flexion angles of 0° and 90°, respectively (Figure 1).
V/V testing per ASTM F1223 determined initial tibial post and intercondylar box contact to be between ±1.64° and ±°2.65 (Figure 2). After Fatigue testing, none of the three samples experienced failure of the post or the locking mechanism and maximum varus angles observed were 6.1°, 6.45°, and 5.78°
Conclusion: This testing demonstrates that the subject PS-Max tibial insert design with a modern, universal primary femur provides a high level of V/V constraint and a moderate amount of I/E constraint under static testing.
Fatigue testing in I/E rotation shows that the articular surface of the tibial insert provides sufficient constraint to withstand repeated physiological loading, per reported in-vivo moments2, without loading the post.
In V/V rotation, fatigue testing results indicate that the post withstands repeated loading higher than reported in vivo moments2 and continues to provide constraint after 1MM cycles. These values compare favorably to currently marketed revision systems, which have reported similar amounts of constraint after fatigue testing under similar parameters1.
References:
1LiArno,S.,Gopalakrishnan,A.,Schmidig,G.,Schmidt,W.,Racanelli,J.,StrykerOrthopedics(2016)FrontalPlaneRotationofaTotalStabilizedTotalKneeReplacementunderSevereVarusLoading.Orlando,FL:ORS2016AnnualMeetingPosterNo.1002
2BergmannG,BenderA,GraichenF,DymkeJ,RohlmannA,etal.(2014)StandardizedLoadsActinginKneeImplants.PLoSONE9(1):e86035.doi:10.1371/journal.pone.0086035
Figures
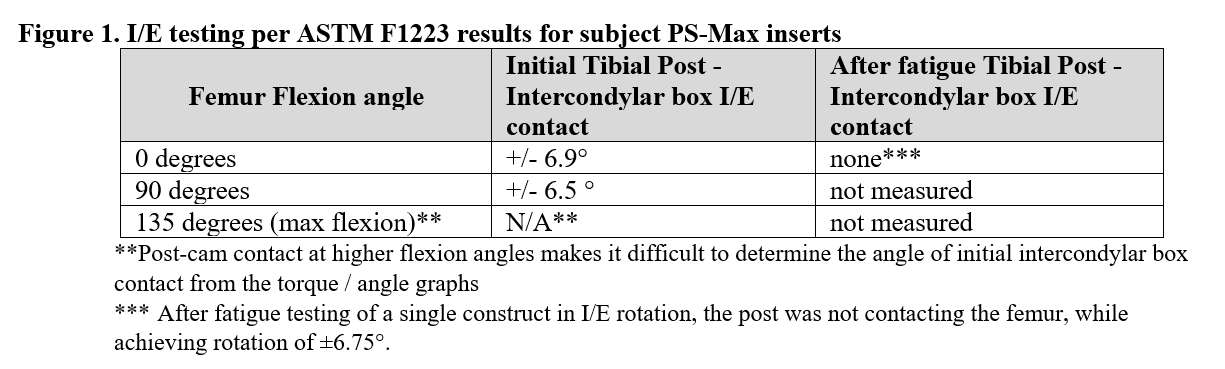
Figure 1
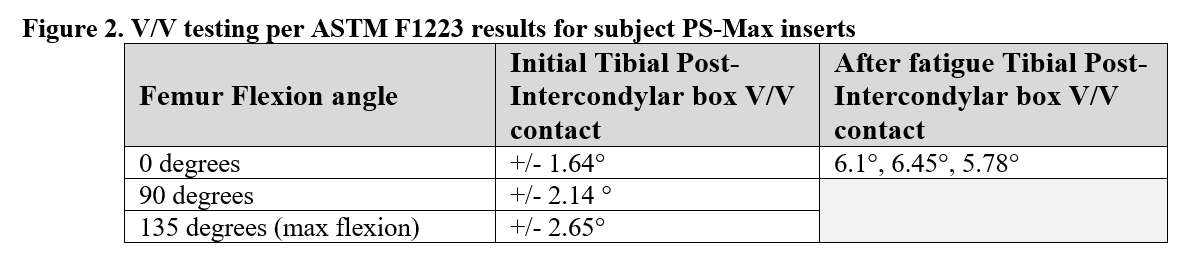
Figure 2#7594
Validation and Reliability of the Hip-Spine Assessment Feature of a Novel Surgical Planning Tool
*Emily McIntosh - Intellijoint Surgical - Kitchener, Canada
Nana Sarpong - Columbia University Medical Center - New York, USA
John Steele - Hospital for Special Surgery - New York, USA
ELIZABETH DAVIS - Hospital for Special Surgery - NEW YORK, USA
Jeff Muir - Intellijoint Surgical - Waterloo, Canada
Haley Canoles - Hospital for Special Surgery - New York, USA
Jonathan Vigdorchik - Hospital for Special Surgery - New York, USA
*Email: e.mcintosh@intellijointsurgical.com
Introduction
Dislocations remain a common cause of revision surgery following total hip arthroplasty (THA). The incidence of dislocations in a population with spinal pathologies has been reported to be up to 8%. As the frequency of spinal fusion procedures increases, and with an additional 17.6% of THA patients without lumbar fusion presenting with spinopelvic mobility issues, there is a growing consensus that functional cup placement should be considered. A novel surgical planning software offers a solution to allow surgeons to easily perform hip-spine assessments and functional cup planning. The purpose of this study was to determine the reliability and validity of this software.
Methods
Pre-operative stereoradiographic images (EOS Imaging, Paris, France) were obtained for 40 patients who underwent primary THA from October 2019-2021. Imaging included: standing anteroposterior pelvic (AP) view as well as standing and seated lateral views. To determine the reliability and validity of the new surgical planning software (Intellijoint VIEWTM, Intellijoint Surgical, Kitchener, ON), spinopelvic parameters for each case were measured retrospectively. The resulting cup targets were compared to the recommended clinical targets from a 5-year follow-up study in a large cohort with a 0.8% dislocation rate1. To evaluate user reliability, each image was read by three arthroplasty fellows and two researchers.
Relevant spinopelvic parameters required to complete the assessment included pelvic obliquity on the AP view, anterior pelvic plane tilt on the standing lateral view, and sacral slope on both lateral views. In addition to these necessary inputs, the reviewers also measured the pelvic incidence (PI) and lumbar lordosis (LL) angles on the standing lateral image.
Intraclass correlation coefficients (ICC) were performed on the delta sacral slope (dSS) and the PI-LL mismatch values. Sacral slope was selected since it has the largest impact on the calculated cup targets. PI-LL mismatch was chosen since it was used, along with dSS, to classify patients according to the reference study1. These classifications provided clinically relevant cup target values to compare to the functional cup targets provided by the program. Agreement was defined as a cup position within the range or within 3° of a specific target (e.g., 40° Inclination) when no range was provided.
Results
There was excellent reliability amongst reviewers. The intraclass correlation coefficient among fellows was 0.89 and 0.88 for all reviewers when comparing dSS measurements. PI-LL mismatch showed similar reliability (0.91 for fellows, 0.92 for all reviewers).
Targets generated through the program were in agreement with the current literature in 100% of cases for inclination targets, and in 80% of cases for anteversion targets. In the cases that exceeded the agreement criteria, 50% were within 1˚, and there were no cases that exceeded the criteria by >3˚.
Conclusion
The novel surgical planning software yielded consistent results with excellent reliability when used by five different reviewers. The resultant target values were clinically meaningful and agree with current clinical recommendations, with differences in anteversion targets likely a product of the patient-specific nature of the software, in contrast to the use of broad categories.
Reference
1-BoneJointJ 2021;103-B(7 Supple B):17–24
Figures
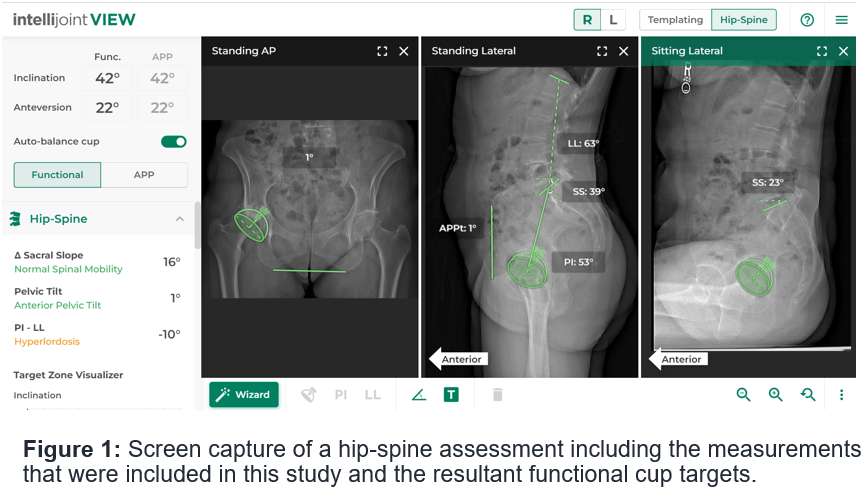
Figure 1#7941
Novel Total Hip Arthroplasty Surgical Planning Tool Provides Target Values Within the Sagittal Functional Safe Zone
*Emily McIntosh - Intellijoint Surgical - Kitchener, Canada
Jeff Muir - Intellijoint Surgical - Waterloo, Canada
Jennifer Wang - Keck School of Medicine of USC - Los Angeles, USA
Nathanael Heckmann - Keck School of Medicine of USC - Los Angeles, USA
*Email: e.mcintosh@intellijointsurgical.com
Introduction
Despite the success of modern total hip arthroplasty (THA), dislocations remain a common cause of revision surgery. The increased frequency of dislocations that occur in patients with spinal pathology has led to the belief that consideration of hip-spine mechanics is important when planning these surgeries. The combined sagittal index (CSI) was established to predict impingement and dislocation risk by considering the sagittal angle of the cup position in relation to the active movement of the femur from standing to sitting1. A sagittal functional safe zone has been reported (CSIsitting > 151, CSIstanding < 243)2 based on data obtained from late dislocations. The objective of this study was to determine if the acetabular component target from a novel surgical planning tool would fall within the sagittal functional safe zone.
Methods
Pre-operative x-rays were obtained for 30 patients who underwent primary THA at the research hospital. Each set of images contained a standing anteroposterior view as well as lateral sitting and standing x-rays. A novel THA planning software, Intellijoint VIEWTM (Intellijoint Surgical, Kitchener, ON), was used by two researchers to perform hip-spine assessments and plan functional cup targets. These analyses were performed retrospectively to determine whether the target values would correspond to the sagittal functional safe zone.
The following parameters were measured to obtain a functional cup target from the program: pelvic obliquity on the anteroposterior view, anterior pelvic plane tilt on the standing lateral view, and sacral slope on both lateral views. CSI was then calculated as the sum of pelvic femoral angle (PFA) and anteinclination (AI) angles measured on the sitting and standing lateral x-rays1 (refer to Figure 1). AI was measured from the target cup position, with the assumption that this would be the orientation in which the cup would be placed during surgery, and not the native acetabulum. An intraclass correlation coefficient (ICC) was performed using the grouped sitting and standing PFA measurements to determine the reliability between the two researchers.
Results
The target cup positions that were suggested by the novel surgical planning tool resulted in CSI sitting and standing values that fell within the sagittal functional safe zone in 90% (27/30) of cases. The ICC for the PFA values was 0.976.
Conclusion
This novel surgical planning tool produced acetabular component targets within the sagittal functional safe zone in 90% of the THA patients with excellent reliability between users. The three patients who fell outside of the functional safe zone all had lower than average pelvic incidences, posterior pelvic tilt, and stiff spines. These characteristics have been previously described as the ‘terrible triad’ in terms of dislocation risk and it has been suggested that patients who exhibit these do not have a functional safe zone3.
References
1Heckmann et al., J Bone Joint Surg Am. 2018
2Tezuka T et al., J Arthroplasty. 2019
3Ike H et al., J Bone Joint Surg Am. 2020
Figures
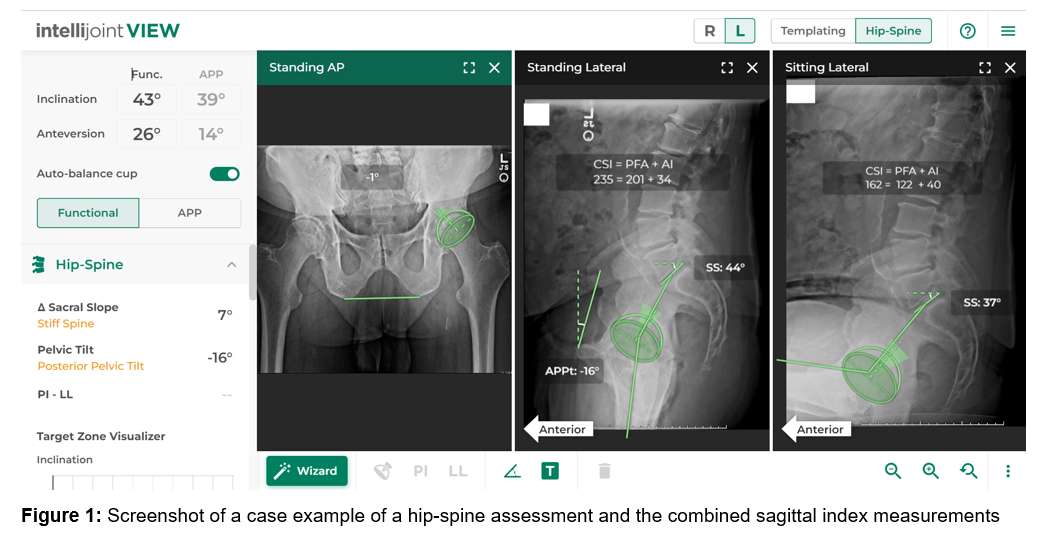
Figure 1#7563
Pelvic Rotation Correction on Anteroposterior Pelvic Radiographs
Jeff Muir - Intellijoint Surgical - Waterloo, Canada
John Vincent - McMaster University School of Medicine - Hamilton, Canada
Joseph Schipper - Intellijoint Surgical - Waterloo, Canada
*Emily McIntosh - Intellijoint Surgical - Kitchener, Canada
*Email: e.mcintosh@intellijointsurgical.com
Introduction
Anteroposterior (AP) pelvic radiographs remain the standard imaging modality for pre-operative planning and post-operative evaluation during total hip arthroplasty (THA); however, their accuracy can be limited by patient positioning errors and image distortion. While pelvic obliquity is easily corrected for using horizontal reference lines, errors in the sagittal plane (i.e., pelvic tilt) and the transverse plane (i.e., pelvic rotation) present greater challenges. We have previously developed a validated method for pelvic tilt correction and have previously discussed early findings evaluating a method for correction of pelvic rotation. The purpose of the current study was to complete our work on pelvic rotation correction and present our final results.
Methods
Computed tomography (CT) scans from 10 male cadavers and 10 female THA patients were segmented using 3D Slicer and used to create 3D renderings for each pelvis. Synthetic radiographs for each pelvis were then created using XRaySim software. XRaySim allows for the manipulation of the orientation of each synthetic image while retaining its 3-dimensional features and scaling. We used this feature to create individual images for each pelvis representing rotation (about a central axis) from between 30° of left rotation to 30° of right rotation in 5° increments (13 total images per pelvis). On each image, 4 unique parameters were measured: i) the horizontal distance from the midline of the pubic symphysis to the sacroiliac joint midline (PSSI), ii) the ratio of the horizontal distances from the midline of the pubic symphysis to the outer lateral border of both obturator foramina (PSOF), iii) the width ratio of the obturator foramina (OFW) and iv) the ratio of the horizontal distance from each anterior superior iliac spine to the sacroiliac joint midline (ASIS-SI) (Figure 1). Rotation correction equations resulting from measurements of each parameter were used to calculate pelvic rotation and the results compared with the known magnitude and direction of rotation in each image to determine the measurements that most accurately estimated pelvic rotation. For the parameter deemed most accurate, nomograms for both male and female pelvises were created. Nomograms were validated using 50 synthetic images set at random rotation magnitudes unknown to the reviewers.
Results
The ASIS-SI parameter was found to be the most accurate and reliable (r=0.98 (male) and 0.99 (female)) and was used to create sex-specific nomograms (Figure 2). Using these nomograms, the mean rotation as calculated (male: -0.5°±13.5°, female: 1.1°±9.3°) did not differ significantly from the known rotation values (male: -0.5°±12.6°, p=0.95; female: 1.2°±10.1°, p=0.96). The mean absolute difference between known and calculated rotation magnitude was 0.02°±1.8° for males and -0.01°±1.5° for females.
Conclusion
Our data indicate that the ratio of the lateral distance between the ASIS and the sacral midline provides a reliable and accurate method for calculating the magnitude and direction of pelvic rotation on AP pelvic radiographs. Our nomograms provide a simple and reliable method for calculating this pelvic rotation. These findings should prove valuable during planning and post-operative assessment in THA.
Figures
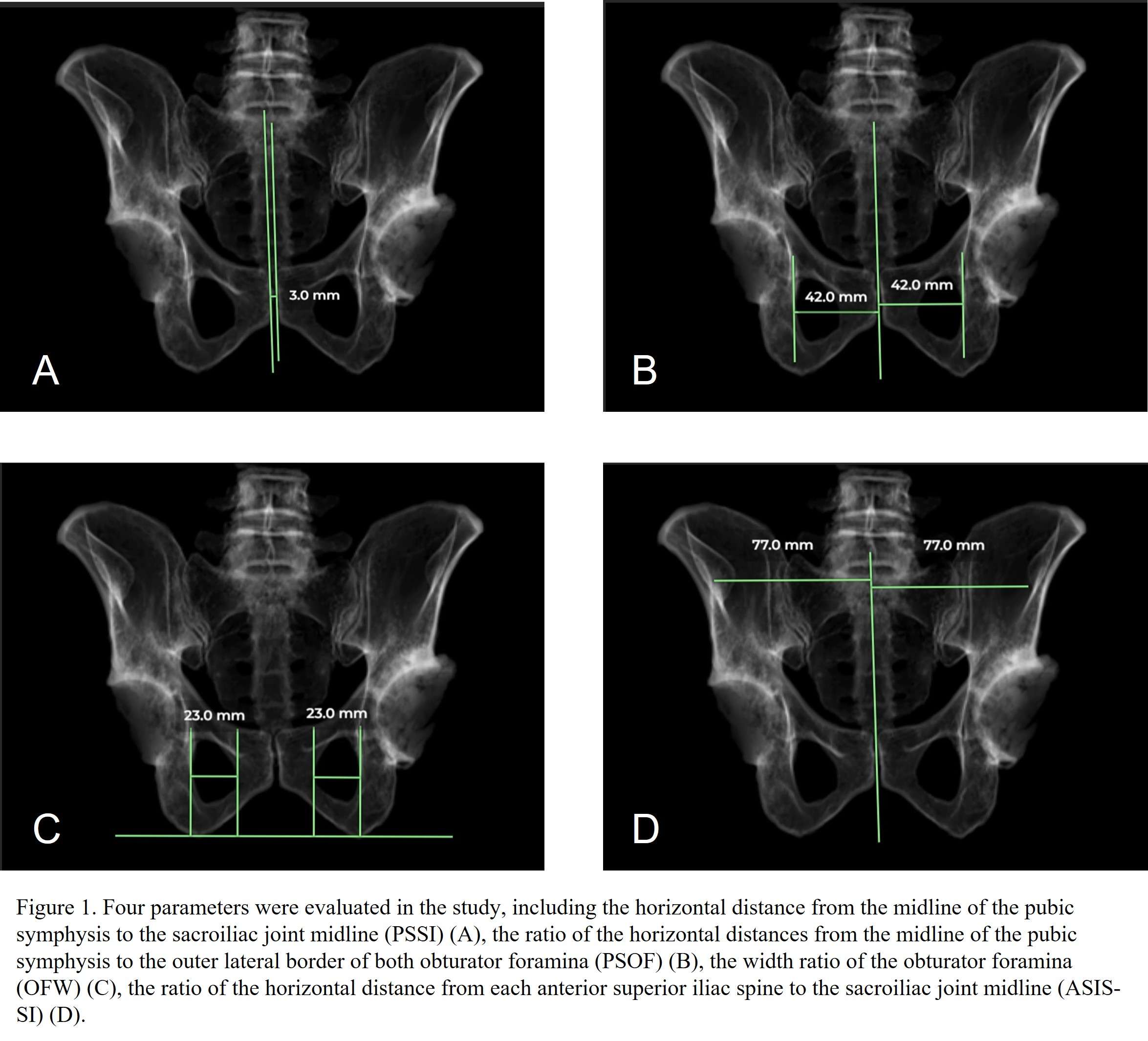
Figure 1
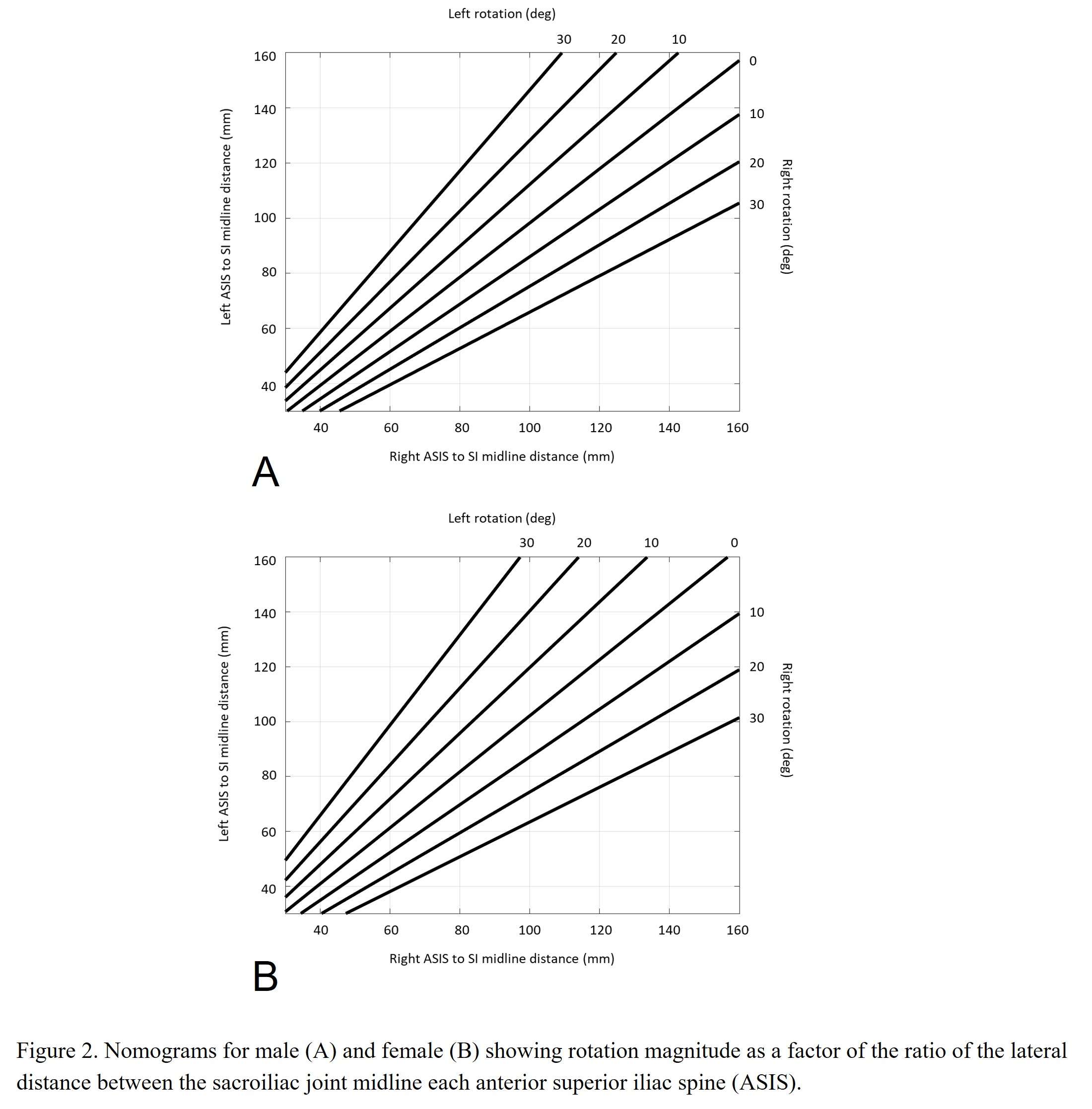
Figure 2#7598
Multivariate Time Series Clustering for Visualization of Telemeterized Implant Datasets
Martine McGregor - University of Waterloo - Waterloo, Canada
Adam Yu - University of Waterloo - Waterloo, Canada
Trevor Yu - University of Waterloo - Waterloo, Canada
*Stewart McLachlin - University of Waterloo - Waterloo, Canada
*Email: stewart.mclachlin@uwaterloo.ca
Introduction: Human joint motion and stability involves temporal coordination of six degree-of-freedom (6DOF) joint forces and moments. As a multivariate time-series (MTS), 6DOF joint forces and moments across different subjects and activities can be challenging to interpret due to their complex nature. Previously, maxima, minima, or waveform features were used to simplify MTS datasets for comparison. Newer machine learning techniques, like MTS t-Distributed Stochastic Neighbour Encoding (mTSNE) and Uniform Manifold Approximation and Projection (UMAP), allow for more comprehensive comparisons of MTS datasets by retaining and analysing more information for visualization purposes. The objective of this project was to develop a mTSNE framework [1] to examine in vivo 6DOF MTS data recorded from telemeterized internal spinal fixators at the lumbar spine and compare outputs to common dimensionality reduction methods such as principal component analysis (PCA).
Methods: An open-source MTS dataset reporting 6DOF in vivo loading from telemeterized internal spinal fixators located in the posterior column of the lumbar spine (L1 & L3) was obtained from [2] (Figure 1). The MTS dataset included 10 subjects, five postures (standing, sitting, walking supine, prone), and five movements (no movement, flexion, extension, torsion, and lateral bending). MTS data, recorded at 130 Hz, included three forces along the superior-inferior, anterior-posterior, and mediolateral axes and three moments in the frontal, sagittal and transverse planes of the implant. A total of 215 files were obtained for the 10 subjects (S1(90), S2(10), S3(13), S4 (9), S5(41), S6(18), S7(8), S8(5), S9(16), S10(5)). The original mTSNE framework proposed by Nguyen et al. [1] was implemented and modified to accommodate the format of the in vivo Orthoload data [2]. The developed mTSNE framework was initially applied on in vivo MTS dataset for the internal spinal fixator to visually identify if MTS data clustering was driven primarily by movement, posture, or another factor. PCA was applied on the same datasets as a comparison.
Results: Use of mTSNE for MTS clustering demonstrated that the in vivo spinal implant data appeared more visually separated (e.g. distinct) when analyzed based on subject (Figure 2). Both the PCA and mTSNE frameworks revealed loose clustering of the spinal fixator data based on posture (Figure 3) and movement.
Conclusion: Visualization and characterization of MTS data from human movement and activities is an important part evaluating orthopaedic implants, interventions, and rehabilitation. Visual demonstration of this MTS dimension reduction technique may indicate greater intersubject variability in 6DOF force and motion data from spinal implants compared to analysis of spinal loading in the same subject for different postures and activities, though further investigation is still needed.
[1] M. Nguyen, S. Purushotham, H. To, and C. Shahabi, “m-TSNE: A Framework for Visualizing High-Dimensional Multivariate Time Series” in Workshop on Visual Analytics in Healthcare, VAHC2016 in conjunction with AMIA 2016, Chicago, IL, USA, November 12 - 16, 2016.
[2] OrthoLoad, orthoload.com.
Figures
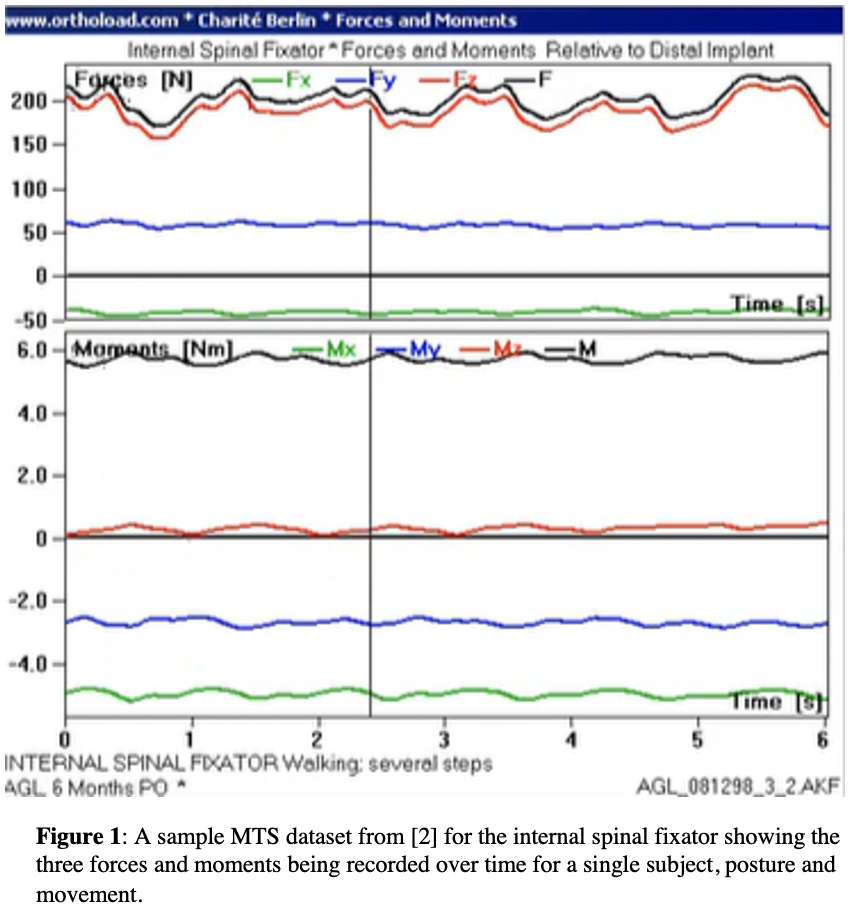
Figure 1
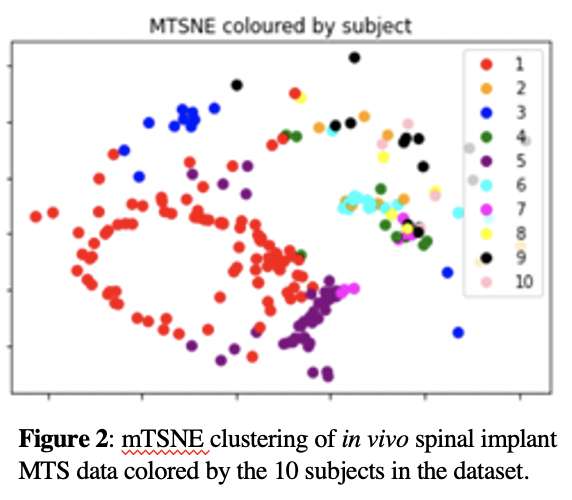
Figure 2
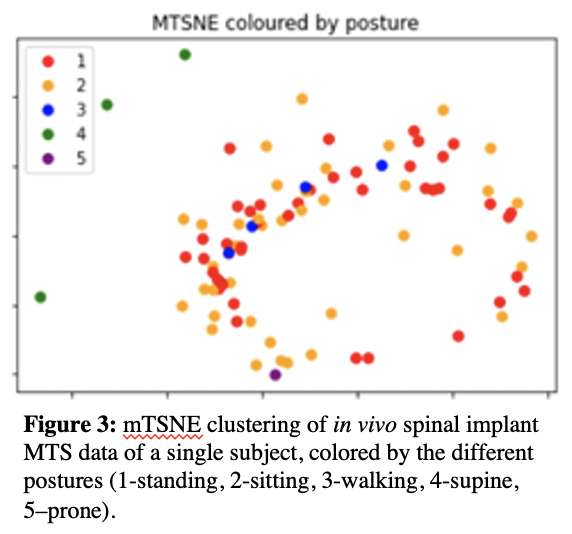
Figure 3#7813
Analyzing the Effect of Posterior Tibial Tilt in Medial UKA on Kinematics and Kinetics Using Mathematical Modeling
*Bradley Meccia - University of Tennessee Knoxville - Knoxville, USA
Seth Coomer - University of Tennessee in Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: allenbrad3@gmail.com
Introduction: When performing unilateral knee arthroplasty (UKA), the posterior tilt of the tibial component is commonly matched to the anatomical slope of the medial plateau, creating a postoperative geometry comparable to the native geometry. This is believed to produce native-like kinematics. Therefore, this study will analyze the effect of posterior tibial tilt (PTT) of the medial tibial component in UKA using mathematical modeling.
Methods: A previously developed and validated mathematical model of the human knee was expanded from only including total knee arthroplasty (TKA) to include UKA. In the mathematical model, a subject underwent virtual UKA reproducing this subject’s native PTT of 8°. The virtual surgery was redone with PTT values ranging from 0° to 14° in 2° increments (reported PTTs ranges from 0° to 15°). For each alignment, a simulated deep knee bend was analyzed.
Results: Changing the PTT had minimal effect on the resulting kinematics. The medial condyle anteroposterior (MAP) position started at approximately -5 mm (negative numbers denote posterior positioning) and translated posteriorly to approximately -15 mm for all simulations (Figure 1). The lateral condyle anteroposterior (LAP) position started at approximately -7 mm and rolled posteriorly to -15 mm at maximum flexion. The LAP and MAP had approximately 2 mm of variation for the different PTT with more tilt resulting in more posterior positioning. The external rotation angles at full extension ranged from 0.1° to -3.3° with more PTT having more external rotation and were 7.0° at maximum flexion for all PTT. Peak quadriceps and patella ligament forces were similar for all simulations with maximum forces of approximately 3.7 times body weight (xBW) and 2.0 xBW, respectively (Figure 2). The peak tibiofemoral forces ranged from 3.5 xBW to 4.0 xBW with more PTT resulting in less force. Lateral collateral ligament forces peaked at 0.45 xBW for all simulations. Peak medial collateral ligament forces ranged from 0.30 xBW to 0.55 xBW with more PTT resulting in lower forces (Figure 3). Peak ACL and PCL forces ranged from 0.40 to 0.60 xBW and 0.70 to 1.20 xBW, respectively. More PTT resulted in less PCL force and more ACL force.
Discussion: Based on these results, PTT has minimal effect of the kinematics with almost no effect on LAP or MAP and only a small effect on the initial axial rotation. However, ligament forces are heavily affected by the PTT with the MCL and PCL increasing by almost 100% when comparing the 0° PTT simulation to the 14° simulation. This increase in forces was partially offset by a decrease in ACL forces. Overall, this resulted in slightly higher tibiofemoral forces for the 0° PTT simulation. In conclusion, selecting the correct PTT is an exercise in ligament balancing which may not affect kinematics but could still affect patient satisfaction. Care must be taken not to cause any ligaments to be excessively tight in mid or late flexion. Continued research may lead to the ability to customize PTT based on preoperative templating and patient specific geometries to achieve a desired ligament force profile.
Figures
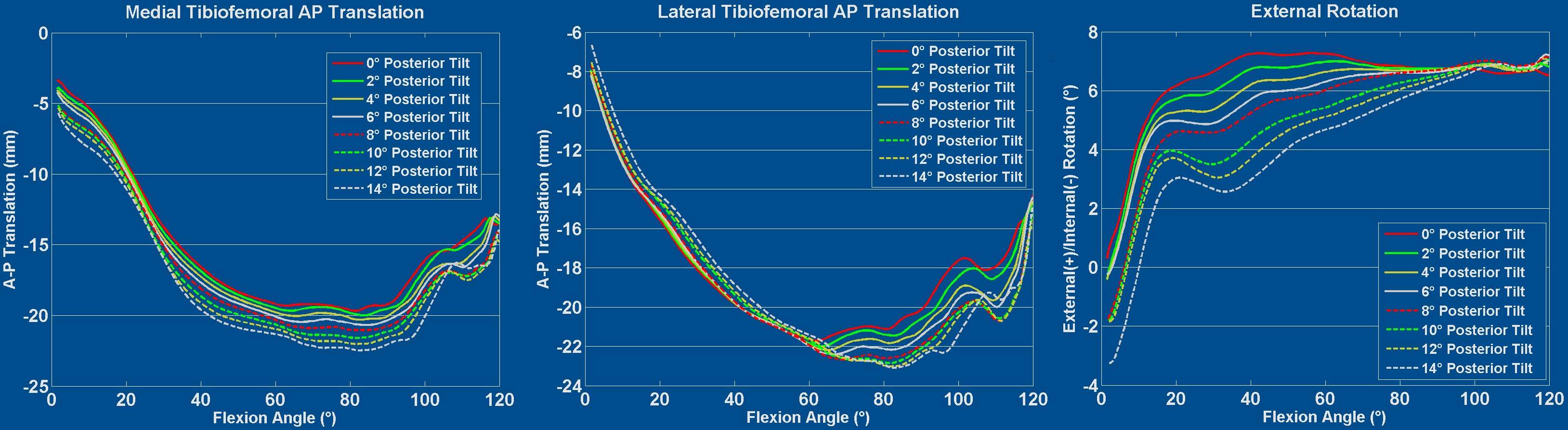
Figure 1
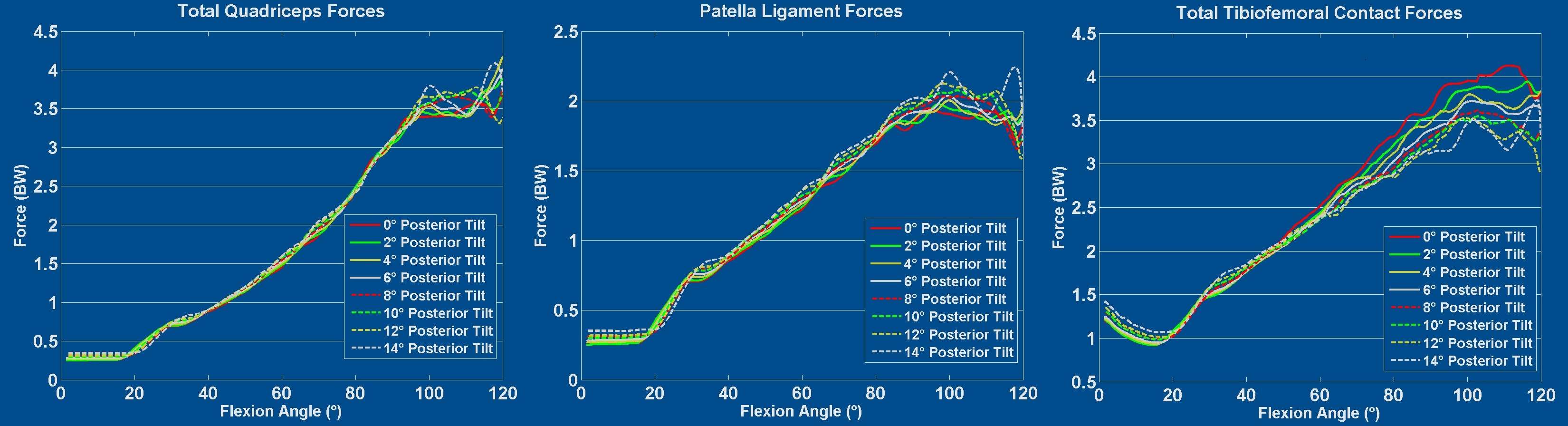
Figure 2
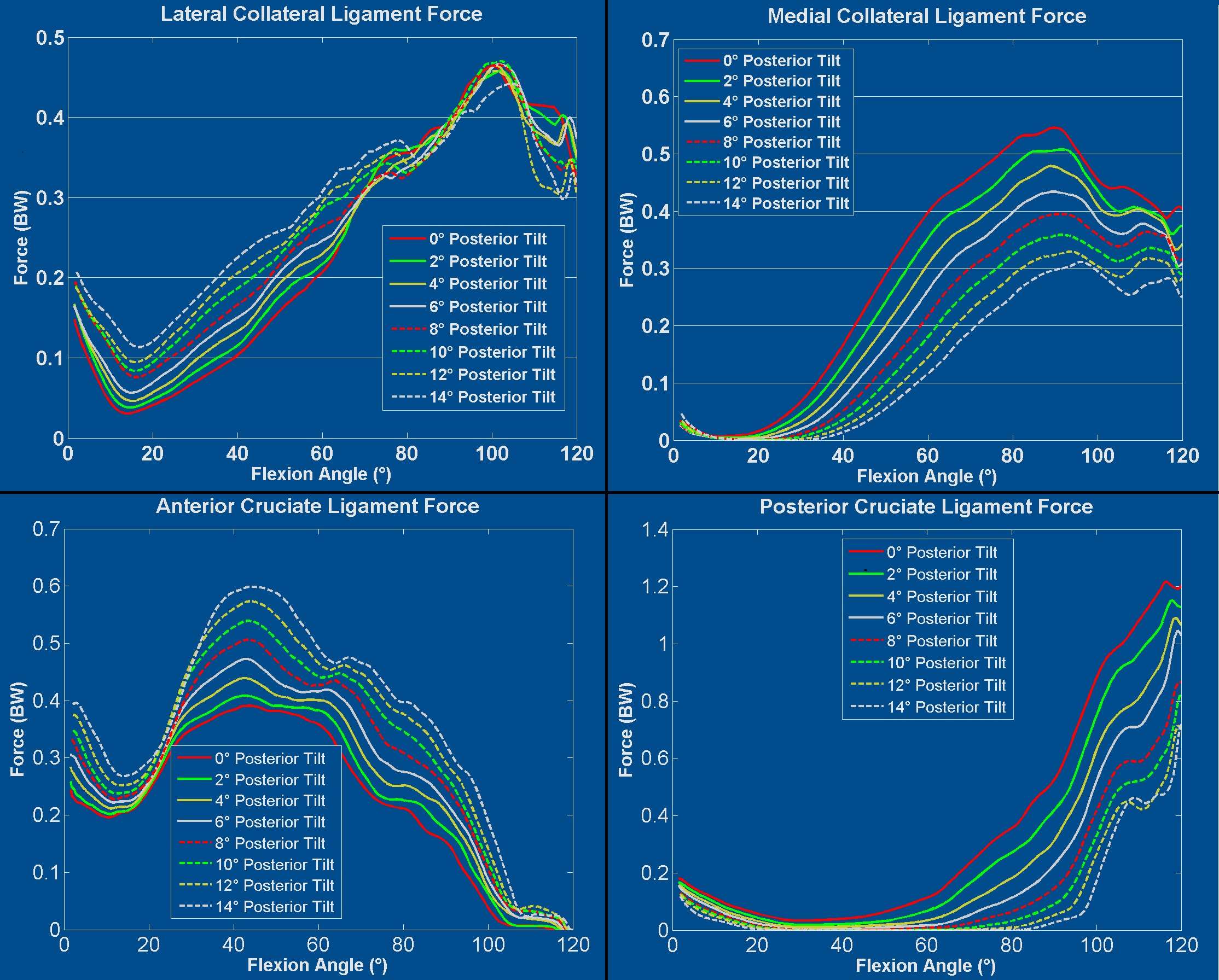
Figure 3#7663
Resection Magnitudes and Angles in Total Knee Arthroplasty: Insights From Robotic-Assisted Ligament Balancing
Michael Sybert - NYU Langone Health - New York, USA
*Christian Oakley - NYU Langone Health - New York, USA
Thomas Christensen - NYU Langone Health - New York, USA
Thomas Bieganowski - NYU Langone Health - New York, USA
Jerry Arraut - NYU Langone Health - New York, Select Country
Ittai Shichman - NYU Langone Health - New York, USA
Matthew Hepinstall - Lenox Hill Hospital - New York, USA
Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
*Email: Christiantoakley@gmail.com
Introduction
Various technologies seek to optimize the alignment and magnitude of bone resections in total knee arthroplasty (TKA). However, target resections that generate acceptable alignment and reliably enable ligament balance have been enigmatic. We utilized robotically balanced TKA to explore how target resections may vary by implant design and preoperative limb alignment.
Materials and Methods
Intraoperative bony resection metrics were collected from navigation software during 201 primary, unilateral TKAs with a single robotic platform. Preoperative coronal alignment was measured on standing full-length films. Resection metrics were compared between cruciate-retaining (CR) and posterior-stabilized (PS) implants and knees with preoperative varus (>3°), neutral (0±3°), or valgus (>3°) alignment. Metric variability was characterized as low (standard deviation [SD] <1 millimeter [mm] or degree), average (SD 1-2 mm or degrees), moderate (2-3 mm or degrees), or high (>3 mm or degrees). P-values <0.05 were considered significant.
Results
There were 147 CR (73%) and 54 PS (27%) TKAs. Overall, CR and PS resections differed only in mean posterior slope (2.8 vs 2.4 degrees). There were no significant resection differences between CR and PS when varus, neutral, or valgus knees were analyzed separately.
Preoperative alignment was varus in 116 (58%), neutral in 45 (22%), and valgus in 40 (20%) knees. There were small but significant differences between varus, neutral, and valgus knees in overall planned coronal alignment (1.4±2.2 vs 0.6±1.0 vs 0.0±1.2 degrees), distal femur angle (0.1±0.5 vs 0.0±0.6 vs -0.2±0.7 degrees), proximal tibial angle (1.2±2.2 vs 0.5±0.8 vs 0.2±0.7 degrees), femoral flexion angle (3.3±1.5 vs 3.8±1.4 vs 4.2±1.2 degrees), posterior tibial slope (2.8±0.8 vs 2.6±0.6 vs 2.3±0.7 degrees), lateral distal femur resection (5.7±1.8 vs 4.9±1.6 vs 3.5±1.8 mm), medial distal femur resection (7.7±1.3 vs 7.8±1.1 vs 8.3±0.8 mm), medial posterior femur resection (9.9±1.3 vs 9.2±1.2 vs 9.0±1.2 mm), lateral tibial resection (6.7±1.7 vs 6.0±1.5 vs 5.1±2.6 mm), the sum of lateral (12.4±2.2 vs 10.8±1.7 vs 8.6±3.5 mm) and medial (11.6±2.0 vs 11.9±2.1 vs 12.5±1.5 mm) extension resections, and medial flexion resection sum (13.8±1.7 vs 13.5±1.5 vs 13.2±1.6 mm).
For varus knees, low variability was found for distal femur angle and posterior tibial slope; moderate variability was found for overall coronal alignment, proximal tibial angle, and the sum of lateral and medial extension resections. For neutral knees, low variability was observed for distal femur angle, proximal tibial angle, and posterior tibial slope; moderate variability was found for the sum of medial extension and lateral flexion resections. For valgus knees, low variability was observed in distal femur and proximal tibial angles, posterior tibial slope, and medial distal femur resections; moderate variability was found for lateral tibial resection; high variability was observed for the sum of lateral extension and flexion resections.
Conclusion
Specific resection parameters were relatively conserved between knees of each alignment category, whereas other parameters varied. Valgus knees had more low- and high-variability metrics compared to neutral and varus knees. Understanding similar implant-specific data could improve preoperative planning of resection alignments and magnitudes, simplifying technology-assisted TKA procedures.
Figures
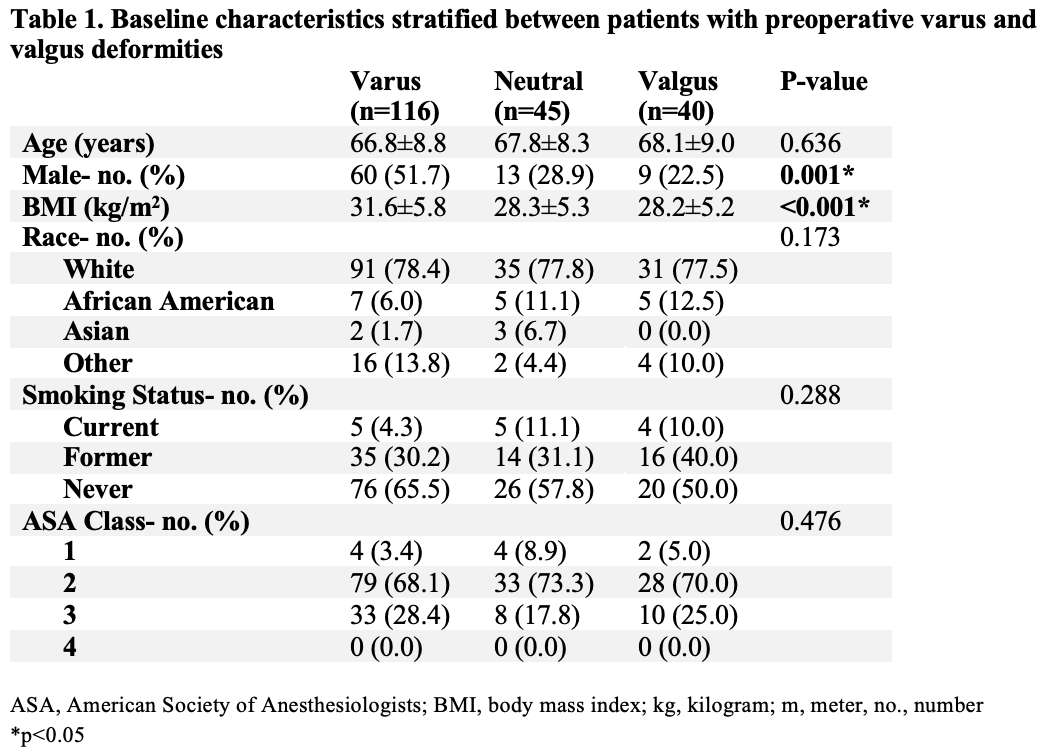
Figure 1
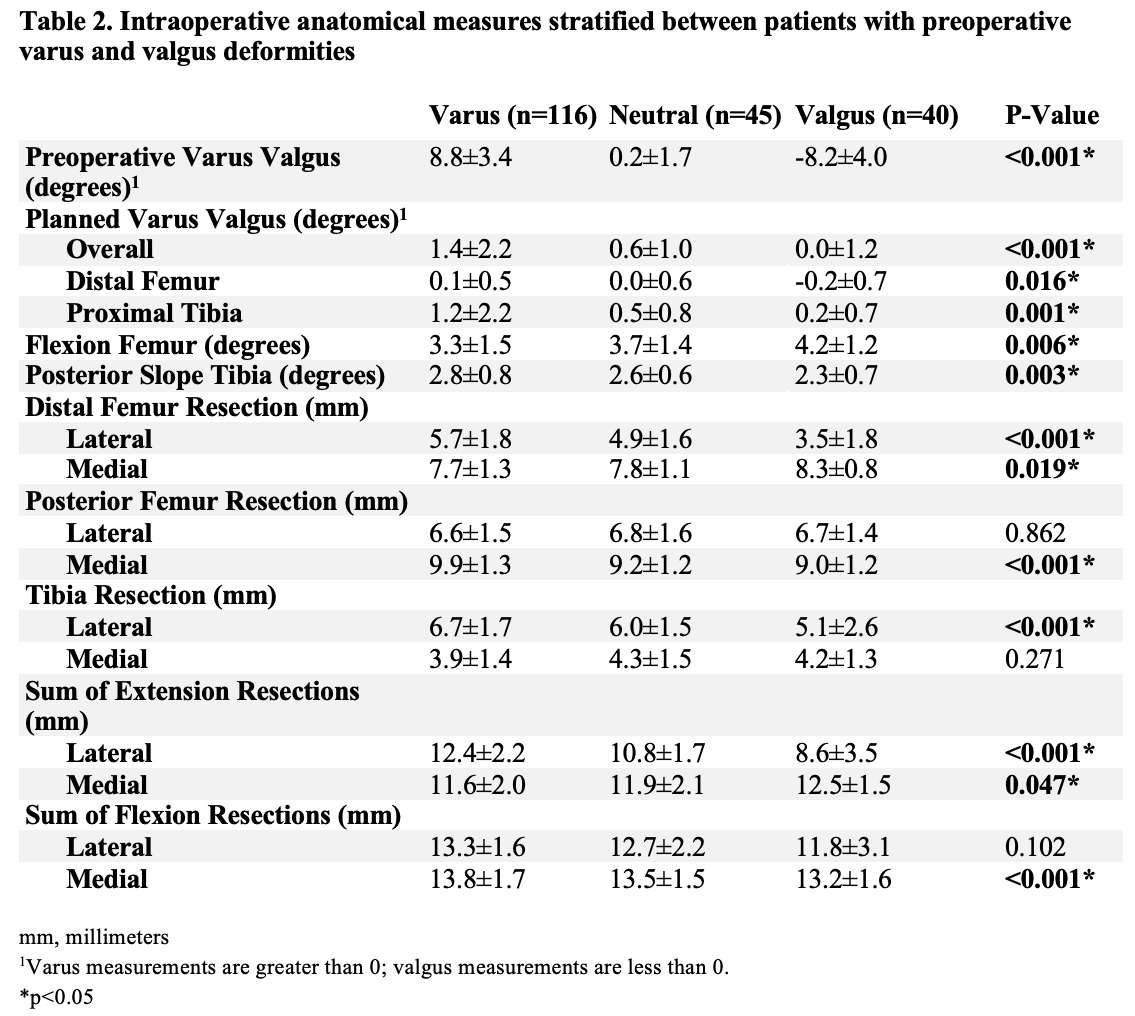
Figure 2#7776
Unable to Fully Sit or Stand, Some Hip Arthritis Patients Are Stuck in the Middle
*Christopher Scanlon - New York University Langone Medicine - New York, United States of America
Thomas Christensen - NYU Langone Health - New York, USA
Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
Matthew Hepinstall - Lenox Hill Hospital - New York, USA
Thomas Bieganowski - NYU Langone Health - New York, USA
*Email: christopher.scanlon@nyulangone.org
Introduction
Spinopelvic mobility drives functional acetabular position in sitting and standing, influencing dislocation risk after total hip arthroplasty (THA). Thought leaders have sought to simplify this complex topic, introducing the term “stuck sitting” to describe a pelvis that does not tilt anteriorly when standing and “stuck standing” to describe a pelvis that does not tilt posteriorly when sitting. We hypothesized that some patients are “stuck in between,” meaning their pelvic tilt changes very little from sitting to standing and does not reach the normal range in either position – placing these patients at risk of dislocation in both positions.
Methods
We reviewed our institution’s THA database, identifying 195 patients with standing and upright sitting whole body radiographs before and after THA as part of a standard perioperative imaging protocol. Patients were not selected for spinal pathology. Standing anterior pelvic plane tilt (APPT) and standing and sitting sacral slope (SS) were measured on preoperative images. Sitting APPT (which is difficult to measure radiographically) was calculated based on the standing APTT and the change in SS from standing to sitting. Based on prior work, normal standing APPT was defined as <2 degrees of posterior pelvic tilt and normal sitting APPT was defined as >12 degrees of posterior pelvic tilt. Patients were thus defined as able to fully stand if their APPT was <2 degrees of posterior pelvic tilt while standing and as able to fully sit if their APTT was >12 degrees of posterior pelvic tilt while sitting. Pelvic mobility was then categorized as (A) able to fully sit and stand, (B) able to fully sit but unable to fully stand, (C) able to fully stand but unable to fully sit, (D) unable to sit or stand fully. (Table 1)
Results
According to our proposed definitions, 52 patients were able to sit and stand normally (A), whereas 60 patients were able to sit fully but unable to stand fully (B), 72 patients were able to stand fully but unable to sit fully (C), and 11 patients were unable to sit or stand fully (D). (Table 2)
Discussion
We identified a subset of patients, representing 5.6% of our elective THA population, with abnormal pelvic mobility resulting in abnormal pelvic position in both sitting and standing. This included a substantial 15.5% of the patients who did not achieve normal standing pelvic position. The term “stiff and balanced” may not communicate the high-risk nature of these patients, who may be at risk of both anterior and posterior THA dislocations. Assessing pelvic mobility on standing (but not sitting) radiographs could lead these cases to be erroneously categorized as “stuck sitting.” Placing acetabular implants in less than anatomic anteversion in these patients – to reduce anterior dislocation risk – may increase the risk of posterior dislocation. This phenomenon should be considered before altering anatomic anteversion based on incomplete (or incompletely understood) functional imaging such as an isolated standing radiograph of the pelvis.
#7808
Pre-Operative Patient-Specific Risk Stratification Using Machine Learning
*Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
Ebrahim Mortaz - NYU Langone - New York, USA
Sam Barzideh - NYU Langone - New York, USA
*Email: morteza.meftah@nyulangone.org
Background: Preoperative risk stratification is essential to optimization and reduce peri-operative complications after elective orthopedic procedures. Such unfavorable outcomes include 30- and 90-day readmissions, long hospital stays (>2 nights) and the need for discharge to skilled nursing facilities. The goal of this study was to develop a machine learning based platform for accurate risk profile prediction in total joint arthroplasty patients.
Methods: This is a retrospective study analyzing patients’ data from 2015-2021 that underwent joint arthroplasty at a tertiary urban hospital center. Patient demographics, prior medical, surgical, and social history were assessed from Epic electronic health records. Multiple classes of machine learning models including linear models, ensembles such as boosted trees and random forests, and neural nets were trained and tested to perform the prediction task.
27,000 patients were included in the study, with over 1000 attributes for each patient to be analyzed. To compare machine learning models multiple accuracy metrics including overall accuracy, AUROC, and AUPRC were used. The gradient boosted trees provided the highest accuracy compared to all the models and was used to determine the most important features impacting the risk.
Results: The obtained accuracy, AUROC, and AUPRC were 75%, 69% and 62% respectively. We also trained a logistic regression model to be able to explain the impact of the important features obtained from the boosted trees on the risk of unfavorable outcomes. Using the logistic regression reduces the accuracy values but allows the surgical team to measure the impact of risky factors. Gender, age, BMI, congestive heart failure, diabetes, pulmonary circulation, fluid electrolyte disorders and some selected list of historical surgeries and medical conditions and medications were among the risk factors that have impact on the risk and are obtained through conditional independence test.
Conclusions. Machine learning models showed promising results for prediction of unfavorable outcomes in total joint arthroplasty patients. These algorithms can be integrated into clinically useful decision support systems to help the surgical teams decrease such risks and improve the quality care for patients.
#7810
Pre-Operative Patient-Specific Risk Stratification Using Machine Learning
*Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
*Email: morteza.meftah@nyulangone.org
Background: Preoperative risk stratification is essential to optimization and reduce peri-operative complications after elective orthopedic procedures. Such unfavorable outcomes include 30- and 90-day readmissions, long hospital stays (>2 nights) and the need for discharge to skilled nursing facilities. The goal of this study was to develop a machine learning based platform for accurate risk profile prediction in total joint arthroplasty patients.
Methods: This is a retrospective study analyzing patients’ data from 2015-2021 that underwent joint arthroplasty at a tertiary urban hospital center. Patient demographics, prior medical, surgical, and social history were assessed from Epic electronic health records. Multiple classes of machine learning models including linear models, ensembles such as boosted trees and random forests, and neural nets were trained and tested to perform the prediction task.
27,000 patients were included in the study, with over 1000 attributes for each patient to be analyzed. To compare machine learning models multiple accuracy metrics including overall accuracy, AUROC, and AUPRC were used. The gradient boosted trees provided the highest accuracy compared to all the models and was used to determine the most important features impacting the risk.
Results: The obtained accuracy, AUROC, and AUPRC were 75%, 69% and 62% respectively. We also trained a logistic regression model to be able to explain the impact of the important features obtained from the boosted trees on the risk of unfavorable outcomes. Using the logistic regression reduces the accuracy values but allows the surgical team to measure the impact of risky factors. Gender, age, BMI, congestive heart failure, diabetes, pulmonary circulation, fluid electrolyte disorders and some selected list of historical surgeries and medical conditions and medications were among the risk factors that have impact on the risk and are obtained through conditional independence test.
Conclusions. Machine learning models showed promising results for prediction of unfavorable outcomes in total joint arthroplasty patients. These algorithms can be integrated into clinically useful decision support systems to help the surgical teams decrease such risks and improve the quality care for patients.
#7841
Does Total Hip Arthroplasty Lead to Changes in Anterior Pelvic Plane Tilt?
*Thomas Christensen - NYU Langone Health - New York, USA
Thomas Bieganowski - NYU Langone Health - New York, USA
Shankar Narayanan - NYU - New York, United States of America
Ran Schwarzkopf - NYU Langone Medical Center Hospital for Joint Diseases - New York, USA
Morteza Meftah - NYU Hospital for Joint Diseases - New York, USA
Matthew Hepinstall - NYU Langone Health - New York, USA
*Email: tchristensen28@gmail.com
Introduction
Anterior pelvic plane tilt (APPT) is one of several parameters used by surgeons for preoperative planning and assessment of hip-spine deformity prior to total hip arthroplasty (THA). This study sought to examine if THA leads to a change in pelvic tilt in patients with preoperative anterior, neutral, or posterior pelvic tilt.
Methods
A retrospective review was conducted identifying patients with standing lateral full-body EOS images before and after their index THA. APPT was measured from lateral radiographs preoperatively and postoperatively, with a negative value indicating anterior tilt. Patients were stratified into three groups: anterior tilt (>5 degrees anterior pelvic tilt preoperatively), posterior tilt (>5 degrees posterior pelvic tilt preoperatively), and neutral tilt (<5 degrees in either direction preoperatively). Acetabular cup anteversion and inclination were measured from postoperative AP radiographs using a templating software (TraumaCad). Patient baseline demographics as well as THA bearing type were collected. Data was analyzed using basic statistical analysis.
Results
193 patients were identified in our cohort with 27 (14.0%) having greater than 5 degrees APPT preoperatively, 50 (25.9%) having greater than 5 degrees posterior pelvic tilt, and 116 (60.1%) with less than 5 degrees tilt in either direction. In the full cohort, there was a significant change in pelvic tilt posteriorly of 1.51±6.86 degrees after THA (p=0.002), from a preoperative mean of 0.38±7.86 to 1.90±9.05 postoperatively. The anterior tilt cohort experienced a significant change in pelvic tilt with a posterior change of 2.42±5.40 after THA (p=0.028) from a preoperative mean of -9.85±3.95 to a postoperative mean of -7.43±5.89. The neutral tilt cohort exhibited a posterior tilt change of 2.02±6.73 degrees (p=0.002), from a preoperative mean of -1.41±4.91 to 0.61±7.26 degrees postoperatively. There was no significant change in pelvic tilt for the posterior tilt cohort. Acetabular cup anteversion varied significantly between groups (p=0.049), with the greatest mean anteversion in the posterior tilt group, followed by the neutral tilt group and then the anterior tilt group (23.49 vs. 21.15 vs. 19.93). There was no significant difference between groups in cup inclination or THA bearing type.
Conclusion
Posterior pelvic tilt after THA was noted in patients who had preoperative anterior or neutral tilt, though no change was noted in the preoperative posterior tilt cohort. This suggests that APPT is corrected toward neutral in patients with anterior pelvic tilt preoperatively while there is no such change in patients with preoperative posterior tilt.
Figures
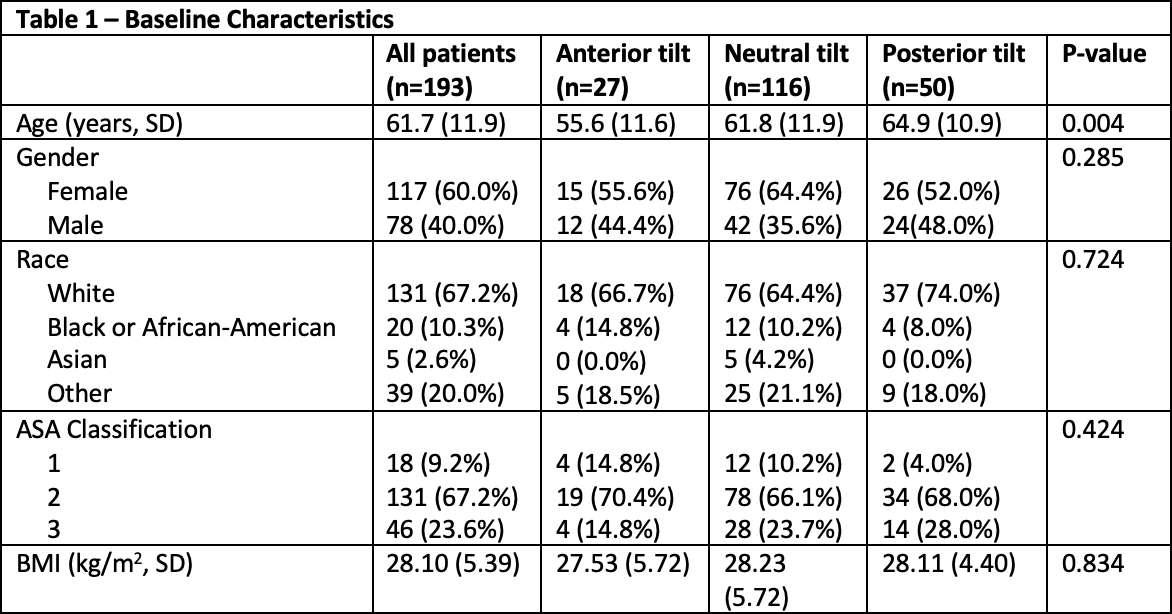
Figure 1
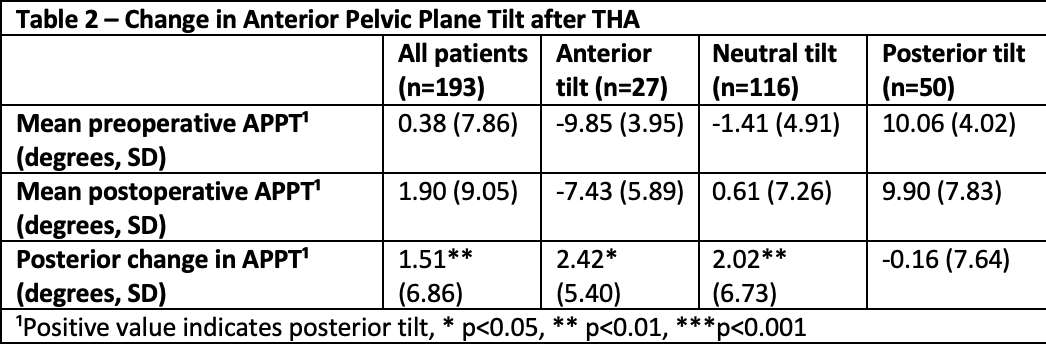
Figure 2
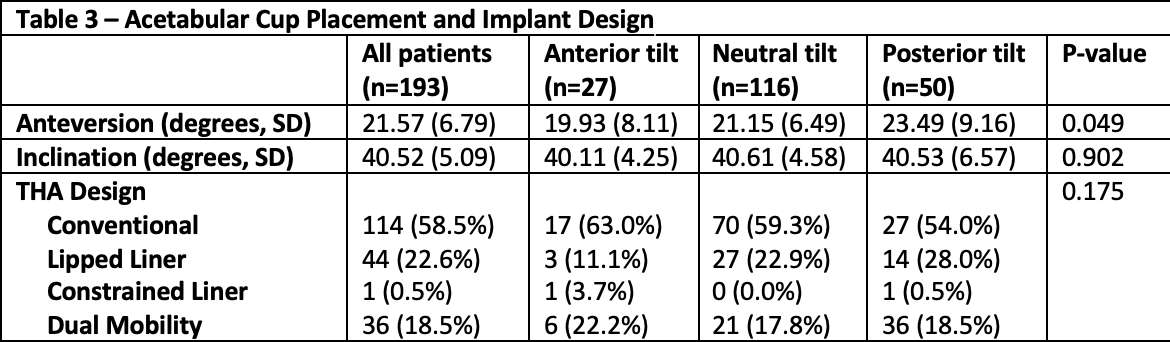
Figure 3#7308
US Versus European Experience With a Short Femoral Neck Retaining Stem for Primary THA
*William Mihalko - University of Tennessee - Memphis, USA
rick Gehlert - ortho surgery - SANDIA PARK, USA
Nathan Jove - Atlanta Knee and Sports Medicine - Decatur, USA
Nathan Jove - Atlanta Knee and Sports Medicine - Decatur, USA
*Email: wmihalko@campbellclinic.com
Introduction:
Efforts have been made at utilizing bone sparing implants for primary THA. These efforts have included shorter femoral components, hip resurfacing and femoral neck retaining implants. In Europe since 1998 a femoral neck retaining stem (Metha, Aesculap, Tuttlingen, Germany) has been reported with excellent midterm survivorship. No reports in the US however have surfaced on whether these results have been realized. We utilized a systemic review approach to compare the survivorship of the Metha in Europe to a series in the US.
Methods:
A systematic review was performed on PubMed with search terms: Hip, replacement, arthroplasty, and Metha. Four publications met the criteria of reporting survivorship and reasons for revision surgery. The results from these four articles combined reported on a total of 4179 total hip replacements with the Metha stem.[1-4] Three orthopaedic groups in the US were then used to combine their experience over the 11 years with the Metha for primary total hip replacement. A review from manufacturer distributor records and office records showed that 824 surgeries had been performed 2008-2019. We then reported on revisions for aseptic loosening, infection and modular neck failures for comparison to the European survivorship analysis from the literature.
Results:
In the reports from PubMed there were 4179 procedures. There were 26 titanium modular neck failures, with 4.8% revisions reported over the 5-10 years. If Ti neck failures are removed the survivorship for any reason was 96.3%. In the past 11 years from 1/2008 to 8/2019 there were 824 Metha THAs performed by four US surgeons. In this group there were 41 that had a modular neck and the remaining were monoblock. There have been no reported modular neck fractures; 3 revisions for septic loosening; 4 periprosthetic fractures; 2 for other reasons. If stem revisions for any reason are taken into account the Kaplan-Meier Survivorship at 5 year is 94.0%, and 87.1% at 10 years (Figure 1). If aseptic loosening is considered reason for revision this improves to 99.1% at 5 years and 98.4% at 11 years. (Figure 2)
Conclusion:
Bone sparing implants for primary THA have seen the popularization of midstems in the US but femoral neck retaining stems have not seen significant popularity. This report has excellent survivorshipp for this series in the US at 11 years of 98.4% which matches many reports of mid length or standard length primary THA stems in registry databases.
References
[1]. von Lewinski G, Floerkemeier T. 10-year experience with short stem total hip arthroplasty. Orthopedics. 2015 Mar;38(3 Suppl):S51-6. [2]. Schnurr C1,et al Low Short-Stem Revision Rates: 1-11 Year Results From 1888 Total Hip Arthroplasties. J Arthroplasty. 2017 Feb;32(2):487-493. [3]. Epinette JA1, et al. A predictive radiological analysis of short stems versus both shortened and long stems in primary hip replacement: A case-control study of 100 cases of Metha versus ABG II and Omnifit HA at 2-8years' follow-up. Orthop Traumatol Surg Res. 2017 Nov;103(7):981-986.[4]. Wittenberg RH1, et al. Five-year results of a cementless short-hip-stem prosthesis. Orthop Rev (Pavia). 2013 Mar 19;5(1):e4.
Figures
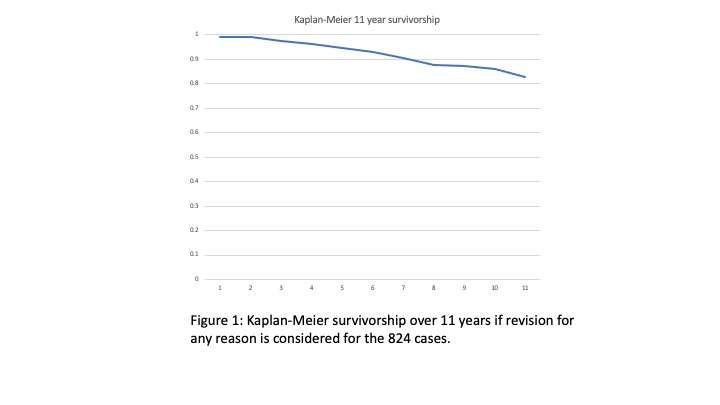
Figure 1
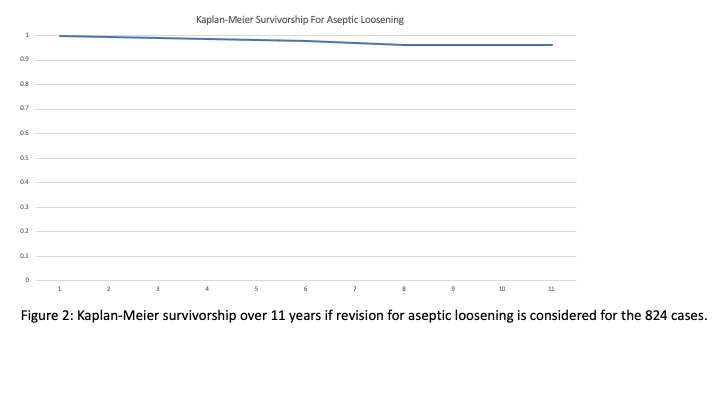
Figure 2#7316
Is There an Influence of Dilute Povidone-Iodine (Betadine) Lavage on the Interface Fixation of Tibial Baseplates Under Clinical Relevant Conditions?
*William Mihalko - University of Tennessee - Memphis, USA
Thomas M. Grupp - Aesculap AG - Tuttlingen, Germany
Ana Laura Puente Reyna - Ludwig Maximilians University Munich - Munich, Germany
Christoph Schilling - Aesculap - Tuttlingen, Germany
Byron Masi - Aesculap USA - Center Valley, USA
Bernhard Fritz - Aesculap AG - Tuttlingen, Germany
Charles Taunt - Michigan Orthopedic Center - Lansing, USA
*Email: wmihalko@campbellclinic.com
Introduction
In total knee arthroplasty (TKA), aseptic tibial component loosening remains a major cause of TKA failure, beneath infection, instability and malalignment [1]. This emphasizes the need for a stable primary and long-term fixation of tibial baseplates [2-5].
To reduce the risk of acute post-operative peri-prosthetic joint infection (PJI) dilute betadine lavage has been established in primary and aseptic revision TKA [6]. Thereby TKA patients receive a 3-minute dilute betadine lavage (0.35 %) before surgical wound closure instead of normal saline lavage [6].
The objective of our study was to setup a suitable test method to evaluate the influence of dilute betadine lavage on the implant-cement-bone fixation strength for tibial baseplates under clinical relevant time points of dilute betadine application.
Materials & Methods
Using Palacos® R HV bone cement, AS VEGA System® tibial baseplates (size T0) with a ZrN-multilayer coating were implanted in Sawbones® PU blocks (20 pfc). After implantation, the tibial baseplates were soaked in either saline solution (0.9% NaCl) or betadine solution (0.35%). A total of five testing groups, with six components each, were defined: Control (no use of saline nor betadine solution), early use of saline solution (during bone cement application time), early use of betadine solution (during bone cement application time), late use of saline solution (after bone cement hardening), and late use of betadine solution (after bone cement hardening). The timelines for the cementation and use of each solution were based on the working times for vacuum mixing of the Palacos® R HV bone cement. After the cementation procedure, the tibial baseplates were stored upside-down in saline solution at 37 °C for 48 hours.
Finally, each tibial baseplate was mounted into a testing frame and the maximum push-out strength was determined based on an established method [3].
Results
From the final push-out testing no statistical differences between the groups could be seen. (See Figure 1)
Discussion
The newly setup method allows to mimic clinically relevant conditions to evaluate the influence of dilute betadine lavage. In implant-cement-bone tibia fixation strength no significant differences were seen between dilute betadine lavage and normal saline lavage applied during the application phase or after curing of the bone cement. For dilute betadine lavage with a concentration of 0.35 % our results are in accordance with basic compression testing of Bingham et al. [7] on PMMA test cylinders.
References
- Dyrhovden et al., Clin Orth Rel Res, 475:1874-87,2017
- Cawley et al., Clin Biomech, 27:390-7, 2012
- Grupp et al., J Arthroplasty, 35(2):579-87,2020
- Gebert deUhlenbrock et al., Clin Biomech 27:929-35,2012
- Grupp et al., J Biomech, 59:9-22,2017
- Calkins et al., J Arthroplasty, 35:538-43,2020
- Bingham et al., Poster No. 913, ORS 2014
Figures
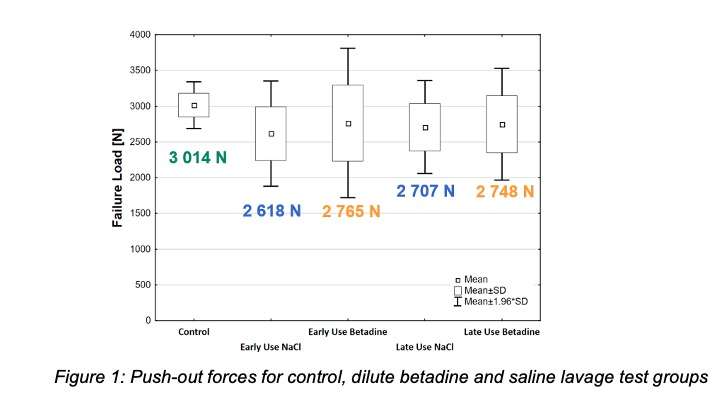
Figure 1#7406
The Association of Total Knee Arthroplasty on Weight Loss in the Look AHEAD (Action for Health in Diabetes) Clinical Trial
*William Mihalko - University of Tennessee - Memphis, USA
Karen Johnson - University of Tennessee Health Science Center - Memphis, USA
Phyllis Richey - University of Tennessee Health Science Center - Memphis, USA
Kunal Singhal - UTHSC - Memphis, USA
Rebecca Neiberg - Wake Forest University School of Medicine - Winston Salem, USA
Judy Bahnson - Wake Forest University - Winston Salem, USA
LookAHEAD Research Study Group - Wake Forest University - Winston Salem, USA
*Email: wmihalko@campbellclinic.com
Introduction: Patients who undergo a (Total Knee Arthroplasty) TKA and are obese seldom lose weight. The Look AHEAD trial randomized persons with type 2 diabetes who were overweight or obese to either an intensive lifestyle intervention (ILI) or to diabetes support and education (DSE).
Methods: A total of 5,145 participants were enrolled with a median 14 years of follow-up. ILI aimed at achieving and maintaining at least a 7% weight loss by focusing on reduced caloric intake and increased physical activity. The purpose of this analysis was to examine the impact of TKA during the trial on intervention effects of weight change and physical health related quality of life(HRQL) as determined by the SF-36. To determine this we first compared intervention response in participants with and without TKA using a time-varying TKA status model with annual visits categorized as ‘before’ or ‘after’ in participants with TKA and ‘no TKA ever’ for participants with no TKA. We excluded those that had partials, revisions, and bilateral TKA during the trial.
Results: There were a total of 872 TKAs during a median of 14 years of follow-up with 408 meeting our inclusion criteria (201 in DSE and 207 in ILI), with 22% occurring within the intensive intervention phase (years 1-4), 46% during extended follow-up(years 4+ to 9), and 32% occurring in the post-intervention phase. Both analyses suggest the ILI group remained effective in participants’ ability to maintain or lose weight after TKA. In the time-varying analysis, ILI lost significantly more weight than DSE in all three time categories (ILI-DSE before TKA mean[95%CI]: -3.6[-5.0, -2.3], after TKA: -3.7[-4.1, -3.3] and in no TKA group -3.6 [-4.9,-2.2]; all p<.0001). When we compare the weight loss before and after TKA only in the ILI group, we see no significant difference. (ILI: -0.36±0.3, p=0.21) A similar finding before and after TKA in the DSE group was seen (DSE: -0.41±0.29, p=0.16). For participants with no TKA, ILI had significantly better physical HRQOL scores (ILI-DSE mean[95%CI]: 1.2 [0.8,1.6], p<.0001). However, there was no difference between randomization groups in physical HRQL before or after TKA (ILI-DSE before: 1.0 [-0.5,2.4]; after: 0.4 [-1.1,1.9]). Both ILI and DSE improved their physical HRQL after TKA compared to before (both p<.001).
Conclusions: Intensive Lifestyle Intervention participants who underwent a TKA during the trial did not have diminished ability to maintain or obtain further weight loss. TKA improved HRQL in both the ILI and DSE groups.
#7408
Electrochemical Properties of Human Synovial Fluid and the Relationship to Patient Reported Outcomes
*William Mihalko - University of Tennessee - Memphis, USA
Nico Mascia - University of Tennessee Health Science Center - Memphis, USA
Kirsten Miller - University of Tennessee Health Science Center - Memphis, USA
Lisa Phan - University of Tennessee Health Science Center - Memphis, USA
Marc Mihalko - Campbell Clinic Orthopaedics - Germantown, USA
Marcus Ford - Campbell Clinic Orthopaedics - Germantown, USA
James Guyton - Campbell Clinic Orthopaedics - Germantown, USA
John Crockarell - Campbell Clinic Orthopaedics - Germantown, USA
James Harkess - Campbell Clinic - Collierville, USA
*Email: wmihalko@campbellclinic.com
Introduction
Total knee arthroplasties (TKA) are one of the most common and cost-effective elective surgeries worldwide. Cobalt Chromium-Molybdenum (CoCrMo) and Titanium (TiAlV) metal alloys are typically chosen for their durability, strength, and biocompatibility. As high as 20% of surgery recipients report dissatisfaction after their TKA, and synovial fluid electrochemical properties are potentially a factor. The objective of this study was to investigate the variation in the electrochemical properties of primary TKA patients’ synovial fluid when introduced to CoCrMo and TiAlV orthopedic alloys and identify any correlations between corrosion rate and patient-reported outcomes. We hypothesized that corrosion rates would be higher for those with low KOOSJR scores.
Methods
IRB approval was obtained for our study and patient consent was obtained prior to surgery. Fifty-seven human synovial fluid samples were collected in the operating room at the time of TKA and transferred to a three-electrode low volume electrochemical cell (Bioanalytical Systems, Inc.) within 30 minutes of collection. Each sample was divided to be tested with two separate alloys (ASTM F1537 CoCrMo and ASTM F136 TiAlV). Using a potentiostat (PalmSens4), three electrochemical tests were performed on each metal alloy: open circuit potential (OCP); electrochemical impedance spectroscopy (EIS); and linear polarization (LP). Individual corrosion rates were then calculated using the properties of each sample and compared to calculate statistical outliers. A statistical outlier was classified as being two standard deviations above the mean. The patient’s stiffness, pain, and daily function were self-reported using a Knee injury and Osteoarthritis Outcome Score, Joint Replacement (KOOSJR) survey after 3 or more months post-op. A t-test was performed on the corrosion rates using outliers and non-outliers as variables for each alloy. Another t-test was performed on the KOOSJR scores using outliers and non-outliers as variables for each alloy.
Results
The average corrosion rates of CoCrMo and TiAlV metal alloys were 3.35 and 0.01 mm/yr respectively. Of the 57 CoCrMo corrosions rates calculated, 2 were outliers with values of 59.62 and 107.7 mm/yr. Of the 40 TiAlV corrosion rates calculated, 2 were outliers with a value of 0.051 and 0.039 mm/yr. Forty KOOSJR scores have been collected with an average of 76.42. Non-paired t-test comparing outliers to nonoutliers resulted in: CoCrMo KOOSJR (n = 40, p = 0.012), TiAlV KOOSJR (n = 24, p = 0.023). (Figure 1)
Conclusion
Approximately 20% of patients report a poor outcome from their TKA. CoCrMo shows a relationship with high corrosion rates and statistically lower KOOSJR scores. Two of the 40 KOOSJR scores recorded for the CoCrMo reveal a significantly higher corrosion rate accompanied by a markedly decreased KOOSJR score. Unexpectedly, two of the 24 KOOSJR scores recorded for the TiAlV reveal a significantly lower corrosion rate accompanied by a markedly decreased KOOSJR score. We continue to enroll patients into our study and follow patients up to a year after surgery to look for stronger or continued correlations to poor reported KOOSJR scores.
Figures
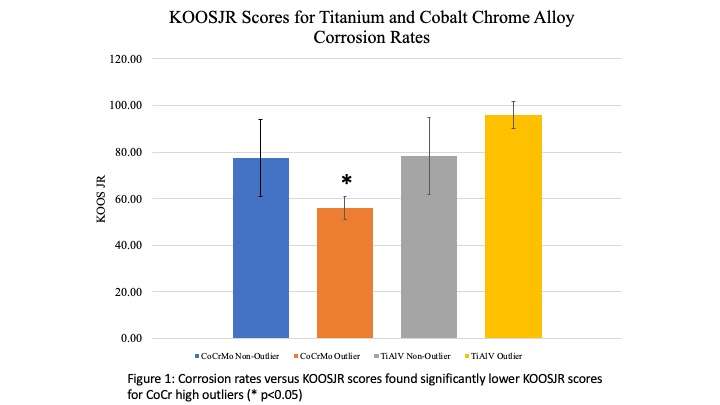
Figure 1#7410
In Vitro Effects of Macrophages on CoCr Alloy With and Without Electrocautery Damage
*William Mihalko - University of Tennessee - Memphis, USA
Kirsten Miller - University of Tennessee Health Science Center - Memphis, USA
Richard Smith - Univerisity of Tennessee Health Science Center - Memphis, USA
Matthew Holloway - University of Tennessee Health Science Center - Memphis, USA
*Email: wmihalko@campbellclinic.com
INTRODUCTION: Cobalt-Chromium (CoCrMo) alloy is one of the most commonly used materials in total joint arthroplasties due to its high strength, high resistance to corrosion, and biocompatibility. However, release of metal ions from these implants remains a topic of interest to researchers due to reports showing evidence of metal release in joint replacement patients experiencing adverse effects in the local tissue surrounding the implants. Many of these patients present with local tissue reactions, pain, and potentially revision of the implant. Two of the more recently investigated processes leading to the corrosion of metal implants include Electrocautery-Induced Corrosion (ECIC) and Inflammatory Cell-Induced Corrosion (ICIC). The objective of this study is to examine if macrophages are ingesting CoCr particles from the surface of the alloy, and how EC damage performed at the time of surgery influences the concentration of CoCr inside the macrophages.
METHODS: IC-21 ATCC peritoneal macrophages were cultured with growth medium of RPMI 1640 with 10%FBS, L-glutamine, and gentamicin. IFNy and Lipopolysaccharide (LPS) were used to induce activation of macrophages. CoCr disks were cut, polished, and placed into a 96 well plate. CoCr disks were damaged with an Electrocautery device using a 3 second hover method at 45W. CoCr testing included 8 groups: Undamaged disks + standard medium, EC disks + standard medium, Undamaged disks + 20,000 cells, Undamaged disks + 20,000 activated cells, EC disks + 20,000 activated cells, no disks + standard medium, no disks + 20,000 cells, no disks + 20,000 activated cells. After cells were attached to the surface of the CoCr disks, culture media was replaced every 12 hours and collected every 4 days starting on the second day. At the end of 30 days cells were taken from the CoCr disk surfaces and digested. ICP-MS, conducted at Brooks Applied Labs (Bothwell, WA), was used to determine metal concentrations found in the supernatant and digested cells. A Welch’s t-test was used to compare the metal release of each group with that of the group containing media with no cells and disks.
RESULTS: The supernatant Co for the undamaged disks with activated cells and Electrocautery disks with activated cells were both shown to have a statistically significant increase in metal ion release (p<0.01. ICP-MS analysis of the digested cells showed that the Co concentration in EC disks w/ Medium + LPS/IFNy was substantially higher at 0.742 ug/L while remaining groups had a Co concentration of 0.174(±0.52) ug/L. (Figures 1 and 2)
CONCLUSION: This experiment was able to test for the release of metal particles and their ingestion by macrophages. Specifically, lysed cells from groups with CoCrMo disks had higher concentrations of metal ions than lysed cell groups without CoCr disks. This suggests that various cell types may effectively change metal ion release profiles in different ways. Evidence of Inflammatory Cell-Induced Corrosion was seen on CoCr disks as well. This points to the need for future studies being aimed at possibly mitigating damage due to cellular corrosion and released metal ions about total knee replacement implants.
Figures
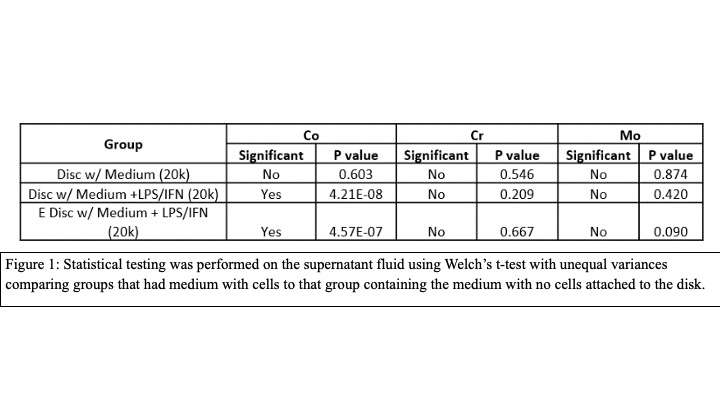
Figure 1
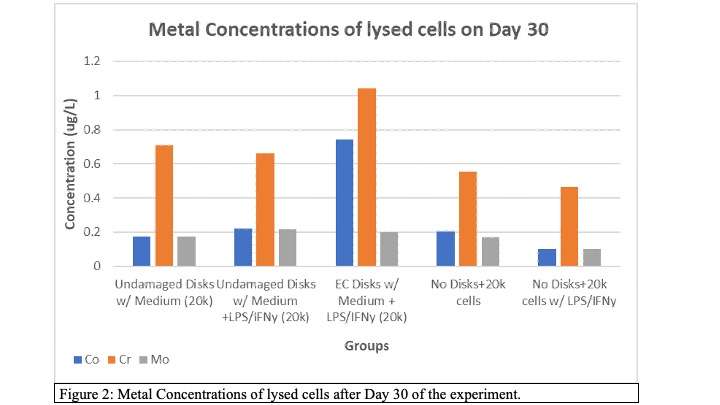
Figure 2#7880
Changes in Neuraxial Anesthesia Protocols Lead to Improved Efficiency of Same Day Discharge Total Knee Arthroplasty in an Ambulatory Surgery Center
*Tyler Calkins - University of Tennesse Health Science Center - Campbell Clinic Orthopaedics - Memphis, United States of America
Clayton Wing - University of Tennessee Health Science Center - Campbell Clinic Orthopaedics - Memphis, USA
Zachary Diltz - University of Tennessee Health Science Center - Campbell Clinic Orthopaedics - Memphis, USA
William Mihalko - University of Tennessee - Memphis, USA
Patrick Toy
*Email: tcalkins@uthsc.edu
Introduction: With the exponential rise in outpatient total joint arthroplasty, improving rapid recovery protocols for same-day discharge (SDD) total knee arthroplasty (TKA) may help to increase patient satisfaction and provide substantial economic benefit. This study evaluates how bupivacaine versus mepivacaine spinal anesthesia and preoperative adductor canal blocks (ACB) influence outcomes in SDD TKA at a free-standing ambulatory surgery center (ASC).
Methods: Ninety consecutive primary TKA patients with planned SDD in a free-standing ASC from March 2018 to September 2019 were retrospectively reviewed from a single-surgeon's practice and grouped by neuraxial anesthetic regimen: bupivacaine with ACB (n=50), bupivacaine without ACB (n=20), and mepivacaine without ACB (n=20). Preoperative ACBs stopped in December 2018 and mepivacaine spinals began in March 2019. All patients received a local peri-articular injection consisting of 10 mL of 0.25% bupivacaine and 20 mL of 1.3% liposomal bupivacaine at time of closure. There were no other changes in perioperative protocols during the study period. Time to discharge from post-anesthesia care unit (PACU), controlled void, and ambulation as well as postoperative pain, morphine equivalents, transient neurologic symptoms and rate of SDD were compared among mepivacaine and bupivacaine patients without ACB and separately among bupivacaine patients ± ACB with Student’s t-test and Fisher’s exact test. VAS pain and KOOS Jr. scores at 2-weeks, 6-weeks and 90-days were similarly compared between cohorts. Post-hoc power analyses found 20 patients in each mepivacaine versus bupivacaine without ACB cohorts could detect a 70-minute difference in time to discharge and bupivacaine with (n=50) and without (n=20) ACB cohorts could detect a 1.5-point difference in pain at discharge with 80% power.
Results: All patients underwent successful SDD. Mepivacaine spinals decreased time to PACU discharge (231±64 vs 324±95 minutes, p<0.001), controlled urinary voiding (164±75 vs 279±103 minutes, p<0.001), successful ambulation (183±62 vs 243±84 minutes, p=0.024), and total facility time (428±117 vs 537±100, p=0.003), but increased morphine equivalent consumption (13.1±8.6 vs 7.3±9.3 mg, p=0.049) despite similar pain at discharge (2.3±2.6 vs 2.4±2.8, p=0.908) compared to bupivacaine. Patients receiving bupivacaine with and without ACB, respectively, had statistically similar pain at discharge (1.3±2.1 vs 2.4±2.8, p=0.100), morphine equivalent usage (4.5±8.2 vs. 7.3±9.3 mg, p=0.214), minutes to ambulation (237±80 vs 243±84, p=0.793) and PACU discharge time (302±94 vs 324±95 minutes, p=0.372). There were no transient neurologic symptoms. There were no differences in VAS-pain or KOOS Jr. scores at any time point between cohorts, with the exception of lower VAS pain in the bupivacaine without ACB cohort compared to those with an ACB at 2-weeks (3.5±2.0 vs. 4.5±1.9, p=0.029). Patient demographics were statistically similar between cohorts (Table 1 & 2) and no patients were on preoperative opioids.
Conclusion: Mepivacaine spinals for TKA facilitated quicker SDD via decreased times to void and ambulation with a small increase in morphine equivalent requirement. Discontinuing preoperative ACBs had minimal effect on PACU outcomes.
Figures
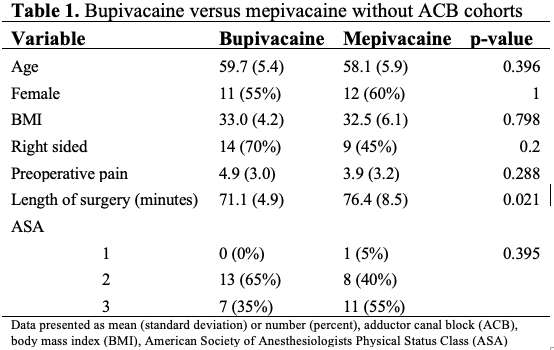
Figure 1
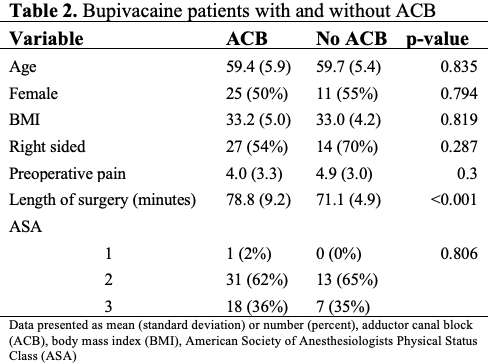
Figure 2#7881
Hip Arthroplasty Femoral Stem Design and Their Association With Early Postoperative Periprosthetic Femur Fractures
*Tyler Calkins - University of Tennesse Health Science Center - Campbell Clinic Orthopaedics - Memphis, United States of America
Devon D Goetz - West Des Moines, USA
Jacob Zalewski - University of Tennessee Health Science Center - Campbell Clinic Orthopaedics - Memphis, USA
Caleb Jones - University of Tennessee Health Science Center - Campbell Clinic Orthopaedics - memphis, USA
Peyton Gaumer - Des Moines University School of Medicine - Des Moines, USA
Marcus Ford - Campbell Clinic Orthopaedics - Germantown, USA
Patrick Toy
John Crockarell - Campbell Clinic Orthopaedics - Germantown, USA
James Harkess - Campbell Clinic - Collierville, USA
William Mihalko - University of Tennessee - Memphis, USA
James Guyton - Campbell Clinic Orthopaedics - Germantown, USA
*Email: tcalkins@uthsc.edu
Introduction
Periprosthetic femur fractures (PFF) in total hip arthroplasty (THA), especially those in contact with the diaphyseal stem, carry high morbidity and mortality burden. This study evaluates how stem design influences risk of Vancouver B and any PFF requiring operative intervention following THA.
Methods
A multi-center retrospective cohort study of 3,433 primary cementless THAs from 2014 to 2021 was performed including 2,302 single-taper [micro M-L (n=1169); M-L (n=1133)] and 1,131 double-taper [fit and fill (n=420); compaction collared (n=711)] stems with mean 2.2 year follow up. Primary outcomes were Vancouver B and surgically treated postoperative PFF risk among the 4 femoral stem groups compared with cox regression hazard ratios (HR) to control for confounding variables and any between group demographic differences. Secondarily, rates of intraoperative and postoperative Vancouver A and C PFFs as well as patient demographics differences among those who sustained PFF and those who did not were compared using two-tailed t-tests and Fisher’s exact test.
Results
Forty-five postoperative PFFs (1.3%) occurred within a median of 8.8 weeks. There were 25 Vancouver B (0.7%) and 20 surgically-treated postoperative PFFs (0.6%) with no statistical differences in rates between the four stem groups (Table 1). Compaction collared stems had decreased risk of Vancouver B (HR 0.18, 95% CI: 0.03 - 0.97 p=0.044) and surgically treated PFF (HR 0.10, 95% CI: 0.01 - 0.95; p = 0.037) with no other surgical or patient variables found to have significant associations in regression analyses. Intraoperative PFFs were most common with fit and fill stems (3.6%, p<0.001) and Vancouver A most common with compaction collared stems (1.8%, p<0.001) (Table 1). There were no Vancouver C PFFs in any cohort. Two postoperative Vancouver A (10%) and 18 postoperative Vancouver B PFFs (72%) required operative management, and only two intraoperative PFFs (5%) led to later postoperative PFFs that required operative management. There were more females, higher Charlson comorbidity index, more Dorr A or C femurs and posterior or lateral surgical approaches in the cohort that sustained PFFs compared to those without (p ≤0.014; Table 2).
Conclusion
Compaction broach collared double-taper stems led to a 5.6-fold reduced risk of Vancouver B PFFs and 10-fold reduced risk of postoperative PFFs that require surgical management after controlling for confounding variables. The authors recommend considering this implant in patients thought to be at higher risk for these clinically significant PFFs following cementless primary THA. However, the risk of intraoperative and early postoperative proximal metaphyseal PFFs may be higher with fit and fill and compaction collared stems, but the majority can successfully be treated nonoperatively.
Figures
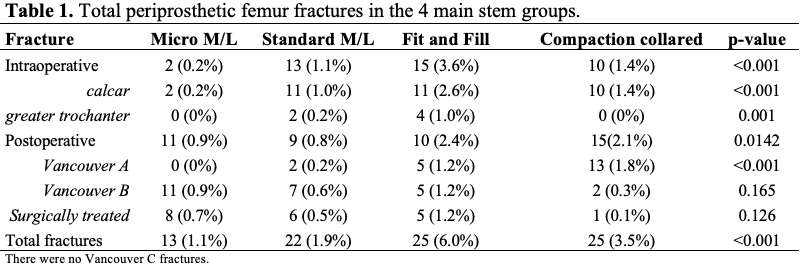
Figure 1
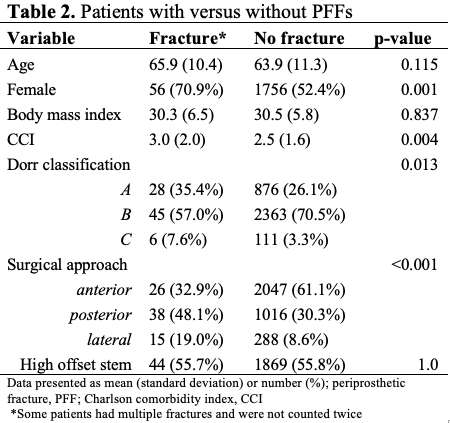
Figure 2#7848
Prescription Drug Monitoring Reveals Varied Sources of Opioid Prescriptions Following TKA
*William Mihalko - University of Tennessee - Memphis, USA
Karen Johnson - University of Tennessee Health Science Center - Memphis, USA
Karen Derefinko - University of Tennessee Health Science Center - Memphis, USA
Sarah Hand - University of Tennessee Health Science Center - Memphis, USA
Zoran Bursac - Florida International University - Miami, USA
*Email: wmihalko@campbellclinic.com
Introduction: Chronic opioid use following total knee arthroplasty (TKA) continues to be reported in a large number of patients. Due to this issue orthopaedic surgeons often follow strict guidelines of prescribing to minimize risk. However, it is possible that patients could turn to other physicians to obtain opioid prescriptions after their orthopaedic surgeon stops prescribing. The current study explored this possibility in a large sample of TKA patients from a single large multispecialty group. We hypothesized that of all controlled substances provided to patients following TKA, a significant number of these prescriptions would be provided by outside providers within the first year after their TKA surgery.
Methods: This study was a review of TKA patient’s records from the Prescription Drug Monitoring Database in the state of Tennessee. After IRB approval, identifiers from a subsample of patients who underwent a primary TKA during the calendar year 2018 in a large private clinic were included for a statewide scheduled pharmaceutical database search. Only patients who resided in the state of Tennessee were included in the study. Controlled substance prescriptions for the 12 months after surgery were coded as 1) from the TKA clinic, or 2) from an outside provider. Results were also categorized as type of medication (non-opioid, oxycodone, hydrocodone, other opioid, or Tramadol).
Results: Prescription drug monitoring incidents of TKR patients (N=453) indicated that in the year following surgery, these patients received 2,514 opioid prescriptions, an average of 5.55 opioid prescriptions per patient. Importantly, 992 (38.4%) of these opioid prescriptions were written by physicians outside of the orthopaedic clinic. Prescriptions from outside providers accounted for a significant proportion of controlled substances (χ2 = 11389.60, DF = 4, p<.001). Outside providers prescribed more hydrocodone than TKA surgeons (284 vs. 129 prescriptions, respectively), as well as opioids other than oxycodone and tramadol (i.e., codeine, morphine; 84 vs. 19 prescriptions, respectively).
Conclusions: Our statewide database search of scheduled prescriptions in TKA patients over their first postoperative year indicates that opioid prescribing goes beyond the surgeon, and should be monitored to assure outside providers are not providing prolonged access to opioid pain medication. This long-term prescribing of opioids could lead to chronic, recurrent use, which does little to address the underlying pain and has the negative added issue of fostering addiction. Communication with primary care physicians about this issue may aide in keeping patients off narcotics long term after TKA surgery.
#7898
Same Day Discharge From an Ambulatory Surgery Center After Total Joint Arthroplasty in Patients With Obesity Is Safe
*Zachary Diltz - University of Tennessee Health Science Center - Campbell Clinic Orthopaedics - Memphis, USA
Marcus Ford - Campbell Clinic Orthopaedics - Germantown, USA
William Mihalko - University of Tennessee - Memphis, USA
Zachary Mosher - University of Tennessee-Campbell Clinic - Memphis, USA
Andrew Gailey - Univ of Tennessee-Campbell Clinic - Memphis, USA
*Email: zdiltz@uthsc.edu
Introduction: Total joint arthroplasty (TJA) is increasingly performed in the outpatient setting, with equivalent safety and satisfaction when compared to inpatient procedures. However, careful patient selection is used to avoid potential complications in those with co-morbidities. Obesity is a major risk factor for osteoarthritis, and obese patients have also been shown to have increased complication rates in TJA. At the same time, TJA utilization by obese patients has increased substantially. There is a paucity of data regarding the safety and outcomes of TJA performed in the ambulatory setting on obese patients. Our study aimed to evaluate the safety of TJA performed at an ambulatory surgery center (ASC) with planned same day discharge (SDD) in patients with a body mass index (BMI) ≥35.
Methods: This study is a retrospective review of all patients with a BMI ≥35 who underwent total hip arthroplasty (THA) or total knee arthroplasty (TKA) at 2 free-standing ASCs from June 2013 through December 2020. The medical records were queried to collect demographic variables and pre-operative co-morbidities, as well as day of surgery data and post-operative complications. The primary outcome was successful SDD. Secondary outcomes included 90-day unplanned emergency department (ED) visits, readmissions, and re-operations.
Results: A total of 645 patients were included, 443 underwent TKA and 202 underwent THA. The average age and BMI for the included patients were 57.5 years and 38.7. 327 patients (50.7%) were female and 318 (49.3%) were male. 14 patients (2.2%) were ASA class I, 372 (57.7%) were ASA class II, and 259 (40.2%) were ASA class III. The most common medical co-morbidities were hypertension (HTN; 68.4%), obstructive sleep apnea (OSA; 27.0%), and diabetes mellitus (DM; 21.7%). Only 2 patients (0.3%) were kept overnight the day of surgery for a next day discharge (NDD), one for urinary retention requiring indwelling foley catheter and the other due to provider preference. All others underwent SDD. There were 9 total unplanned ED visits (1 THA and 8 TKA), 14 hospital readmissions (3 THA and 11 TKA), 25 re-operations (4 THA and 21 TKA), and 43 total post-operative complications (5 THA and 38 TKA).
Conclusion: Carefully selected patients with a BMI ≥35 may undergo TJA in an ASC with reliable SDD and similar or lower re-admission, surgical site infection, and overall complication rates compared to inpatient TJA.
#8042
Invited Talk: Cobalt Chromium and biologic Corrosion in TKA
*William Mihalko - University of Tennessee - Memphis, USA
*Email: wmihalko@campbellclinic.com
#7541
Over 50% of Patients at Risk of Impingement After THA Surgery Are Not Captured With Neutral Bony Alignment
Joshua Twiggs - University of Sydney - Sydney, Australia
*Max Hardwick-Morris - 360 Med Care - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Estelle Liu - 360 Med Care - Sydney, Australia
*Email: max@360med.care
INTRODUCTION:
Dislocation is one of the common complications in total hip arthroplasty (THA) and is primarily driven by bony or prosthetic impingement. Modelling impingement can therefore assist in optimizing component alignment at a patient-specific level. The aim of this study was two-fold. First, to develop a simulation that incorporates the functional position of the femur and pelvis and instantaneously determines range of motion (ROM) limits. Second, to assess the number of patients who would fall outside previously established ROM requirements with a standardised and conventional cup orientation. Third, to assess the number of patients for whom their functional bony alignment escalates impingement risk.
METHODS:
468 patients underwent a preoperative THA planning protocol that included functional x-rays and a lower limb CT scan. The CT scan was segmented and landmarked in ScanIP, and the x-rays were measured for pelvic tilt, femoral rotation, and preoperative leg length discrepancy (LLD). All patients received 3D templating with the same implant combination (Depuy; Corail/Pinnacle). Implants were positioned according to the following criteria: 40°/20° standing cup orientation, hip lengthening to restore any LLD, recreation of native femoral anteversion, and recreation of native centre of rotation.
Each patient was simulated in a novel ROM simulation that instantaneously calculates bony and prosthetic impingement limits in functional movements. The simulation was performed by converting the individual nodes of the bone and components bodies into a polar coordinate system reflecting the angle of motion. Proximity on the angular axis was then used to instantly detect portions of the bodies likely to impact. Simulated motions included flexion and standing-external rotation (ER). Each patient’s ROM was simulated with their bones oriented in both functional and neutral (0° pelvic tilt, 0° femoral rotation) positions. ROM limits were compared against previously established references for pure joint motion at the hip in flexion (120°), extension (30°), and external rotation (45°).
RESULTS:
For functional extension-ER, 121 (26%) of patients suffered a ROM impingement. For neutral extension-ER, 110 (24%) of patients suffered a ROM impingement. 63 (13%) patients suffered a ROM impingement for functional but not neutral extension-ER. As a result, 58 (48%) patients who failed the functional-ER simulation would not be detected without consideration of the functional bony alignment. For functional flexion, 211 (45%) of patients suffered a ROM impingement. For neutral extension-ER, 221 (47%) of patients suffered a ROM impingement. 73 (16%) patients suffered a ROM impingement for functional but not neutral extension-ER. As a result, 138 (65%) patients who failed the functional-ER simulation would not be detected without consideration of the functional bony alignment.
DISCUSSION:
We have developed a ROM simulation for use with THA surgery that can solve bony and prosthetic impingement limits instantaneously, which has the potential to be used in planning patient-specific component alignment for THA surgery. The advantage of our ROM simulation over previous simulations is instantaneous impingement detection, not requiring implant geometries to be analysed prior to use, and addressing the functional position of both the femur and pelvis.
Figures
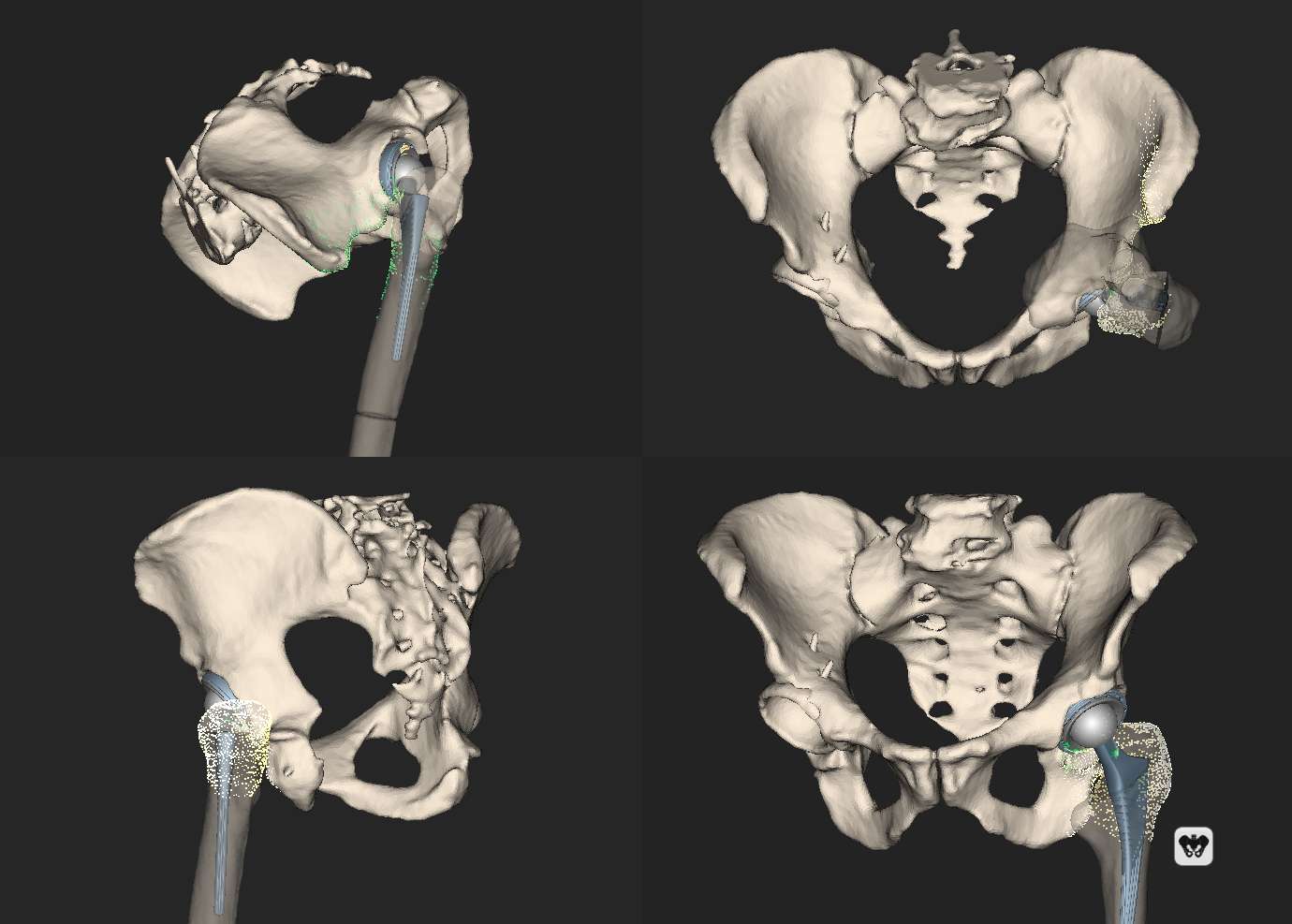
Figure 1#7867
Validation of a Novel Computational Iliopsoas Impingement Detection Simulation for Surgical Planning
*Max Hardwick-Morris - 360 Med Care - Sydney, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
Yuan Chai - University of Sydney - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Jitendra Balakumar - Melbourne Orthopaedic Group - Melbourne, Australia
Rami Al-Dirini - Flinders University - Adelaide, Australia
Mark Taylor - Flinders University - Adelaide, Australia
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: max@360med.care
Abstract:
Introduction: Iliopsoas impingement occurs in 4-30% of patients after undergoing hip arthroplasty. Despite a relatively high incidence, there are few attempts at modelling the impingement between the iliopsoas and acetabular cup, and no attempts at modelling this in a representative cohort of subjects. The purpose of this study was to develop a novel computational model for quantifying the impingement between the iliopsoas and acetabular cup and validate its utility in a case-controlled investigation.
Methods: This was a retrospective cohort study that included 25 symptomatic patients diagnosed with iliopsoas tendonitis and 25 patients not diagnosed with iliopsoas tendonitis. 3D models of each patient’s pelvis, operative femur, femoral stem, and acetabular cup were generated, and landmarked. These 3D models were simulated in a novel iliopsoas impingement detection model in both supine and standing pelvic positions. Impingement was quantified as ‘stretch’ of the iliopsoas by the acetabular cup, measured in millimeters. Logistic regression models were implemented to determine if the probability of pain could be significantly predicted. Receiver operating characteristic (ROC) curves were generated to determine the model’s sensitivity, specificity, and area under the curve (AUC).
Results: Statistically significant differences between the symptomatic and asymptomatic cohorts were observed for cup prominence and iliopsoas impingement in both supine and standing pelvic orientations. Logistic regression models determined that the impingement values significantly predicted the probability of groin pain. The simulation had a sensitivity of 80%, specificity of 80%, and an AUC of 0.83.
Conclusions: We developed a computational model that can quantify iliopsoas impingement and verified its accuracy in a case-controlled investigation. This tool has the potential to be used preoperatively, to guide decisions about optimal cup placement, and postoperatively, to assist in the diagnosis of iliopsoas tendonitis and determine an appropriate treatment pathway.
Introduction
With its low revision rates, Total Hip Arthroplasty (THA) is broadly viewed as a highlysuccessful operation for relieving pain and restoring mobility after osteoarthritis (OA) of the hip[1]. However, revision rates do not provide a holistic understanding of patient outcomes as they do not capture postoperative pain or dissatisfaction rates[2,3], whichmay persist for several reasons[4].These include infection, incorrect indication, instability, or soft tissue complications[4], such as greater trochanteric pain syndrome and iliopsoas tendonitis[5]. Iliopsoas tendonitis can occur due to protruding screws or cement[4,6] excessive increases in offset or leg lengthening[7], an overhanging femoral collar[8], or large diameter femoral heads[9–13]. However, it is most frequently attributed to an anteriorly exposed acetabular cup resulting from retroversion, lateralization, or oversizing of the component[14–16].
The incidence of iliopsoas tendonitis and postoperative groin pain is reported to be up to 29% of patients after THA[4,7,9,14,17–19] and up to 32% of patients after Hip Resurfacing Arthroplasty (HRA)[9,11,19]. It should be noted that several of the most frequently cited papers investigating the incidence of iliopsoas impingement after THA have found the incidence to be below 5%[7,14,17]. However, these studies were limited by small samples of symptomatic patients[7,14,17], were retrospective[7,14,17], and are now two decades old[7,14]. Large variability in rates of reported incidence may be explained by the heterogeneity in regards to the duration of follow-up and varying criteria of pain for inclusion[20]. Therefore, it may be that the true and current incidence of iliopsoas impingement is unknown, particularly given the widespread adoption of larger diameter femoral heads and different surgical approaches in recent years[10,13,21,22].
Despite its relatively high incidence, iliopsoas tendonitis is difficult to diagnose with certainty, can require multiple iterations of treatment, and is lacking in attempts to computationally model. As far as the authors are aware, only one previous study has attempted to quantify impingement between the iliopsoas and cup[23]. This in-vitro cadaveric study concluded that impingement increased as cup anteversion decreased and offset head centre cups with anterior recess reduced iliopsoas impingement[23]. However, being a cadaveric study, it had several limitations. First, the authors could not determine whether the impingement between the iliopsoas and acetabular cup would result in irritation and groin pain. Second, the iliopsoas was simplified as a single wire and wire clearance was used as a proxy for impingement. Finally, the study did not assess if and by how much the impingement altered in functional positions.
We sought to develop an in-silico model that could quantify impingement between the acetabular cup and iliopsoas and then validate its utility by simulating impingement in a case-controlled investigation of symptomatic and asymptomatic patients. The secondary aim was to identify anatomical and surgical parameters that correlate with impingement. Our primary hypothesis was that the simulation, using anatomic and kinematic information about the pelvis, femur, and acetabular cup, would detect a significantly greater level of iliopsoas impingement in the symptomatic cohort. Secondary hypotheses included that the impingement would be strongly correlated with anterior cup prominence, negatively correlated with cup anteversion, and would increase with posterior pelvic rotation.
Methods
This was a retrospective cohort study comparing iliopsoas impingement between a group of symptomatic patients who were diagnosed with iliopsoas tendonitis after THA surgery and a group of asymptomatic patients who were not diagnosed with iliopsoas tendonitis. The primary outcome was a difference in detected impingement values. Secondary outcomes were differences in cup prominence, cup size, pelvic tilt, and cup orientation, where cup orientation was measured relative to the anterior pelvic plane (APP). This retrospective study was approved by the Bellberry Human Research Ethics Committee (study number 201203710).
Patient Population
A retrospective search for THA patients in an experienced surgeon’s database who were diagnosed with postoperative iliopsoas tendonitis was conducted, returning 28 patients. Years searched included 1994-2020. Inclusion criteria was for patients to have minimum 6 months’ follow-up, a postoperative computed tomography (CT) scan, and a standing radiograph. Exclusion criteria included hip resurfacing implants, metal-on-metal (MoM) implants, and dual mobility cups. After this eligibility assessment, the cohort was reduced to 12 patients. A power calculation determined sample sizes of 12 with an alpha value of 0.05 only had a power of 65% to detect a difference in mean impingement of 0.4mm. To expand the sample size, additional patients who were referred to 360 Med Care for postoperative analysis for iliopsoas-related groin pain and who met the above inclusion criteria were included. This increased the sample size to 25 patients.
The asymptomatic cohort similarly consisted of 25 patients. 12 of these patients were randomly selected from the same experienced surgeon’s database of patients after ensuring that they were not diagnosed with postoperative iliopsoas tendonitis. The remaining 13 patients were randomly selected from a database of patients referred to 360 Med Care for postoperative THA analysis for non-groin pain related causes. The same inclusion criteria that were applied to symptomatic cohort were applied to the asymptomatic cohort. A flow chart of the retrospective cohort selection process can be found in Figure 1.
Generation and Landmarking of 3D models of the Bony Anatomy and Prostheses
All CT scans had a Z-direction pixel thickness of 1.25-1.5mm and in-plane resolution of 0.8-1mm x 0.8-1mm. Segmenting and landmarking was performed in ScanIP R-2020.09 (Synopsys, California, USA) to generate 3D models of the patients’ bony anatomy and prostheses with quality checks of the segmentation and landmarks by qualified surgical planning engineers to ensure accuracy. Segmentation was performed semi-automatically using in-built functions augmented with manual segmentation to finalise the models. The 3D models included the pelvis, operative femur, acetabular cup, and femoral stem. A hemispherical cup was registered to all acetabular cups to reduce inaccuracies associated with flare in the CT distorting the segmented model of the acetabular cup. Registration of the femoral head and stem was not required as we were not quantifying changes in the iliopsoas length due to the femoral components so it would not impact the simulation.
Landmarks (Figure 2) were taken manually of the patient’s left and right anterior superior iliac spine (ASIS) points, left and right pubic symphysis (PS) points, the femoral head centre, three superior iliopsoas attachment sites, and one inferior iliopsoas attachment site. The ASIS and PS points were taken to determine the patient’s APP which was used to measure their supine pelvic tilt and reference the cup orientation to. The iliopsoas insertion sites included one point on the lateral superior plateau of the patient’s L5 vertebrae, the lateral-most point on the patient’s L5 transverse process, a point approximately 3-5mm’s lateral of the patient’s sacroiliac joint, and the medial-most point of the patient’s lesser trochanter (LT). These points were chosen as they provided a reproducible and accurate representation of the width of the iliopsoas and the location it passes over the acetabular margin[24].
Simulating Iliopsoas Impingement
The simulation, which was developed in R Studio v1.3.1903 (Boston, MA, USA), began by importing the bony and prosthetic 3D models in their supine (CT) positions. A representation of the iliopsoas was generated with a novel algorithm by tracing a path from each superior attachment site around the acetabular margin of the pelvis to the inferior attachment site. Within each segment was a green path and a red path. The green path did not include the acetabular cup and the red path did. The impingement, which could be intuitively thought of as the ‘stretch’ of the iliopsoas due to the acetabular cup, was calculated as the difference in these path lengths (Figure 3). Therefore, in cases with no iliopsoas impingement, the path lengths were equal length. In cases with impingement, the red path was lengthened relative to the green path.
Three separate impingement values were calculated in supine (one for each segment) and reported as the mean and maximum of these values; supine mean impingement and supine maximum impingement. The pelvis was then rotated into its standing pelvic orientation using measurements of the supine and standing pelvic tilts and the same impingement detection algorithm was applied by tracing the representative segments of the iliopsoas and measuring the difference in path lengths. These standing pelvic tilt values were reported as standing mean impingement and standing maximum impingement.
Calculating Cup Prominence
Due to the highly variable quantification of acetabular prominence in previous literature [6,25,26], we developed a novel approach to measuring cup prominence. This approach reduced the STL files of the pelvis and registered acetabular cup to point clouds and applied a nearest neighbour algorithm to determine the greatest 3D distance between the cup and pelvis (Figure 4).
Statistical Analysis and Power Calculation
Statistical analysis was performed in R Studio. An alpha value of 0.05 was used to determine clinical significance. Two-way Student’s T-Tests were used to determine significant difference for continuous variables and Chi-Squared tests for categorical variables. Pearson’s correlations were used to assess the linear relationship between continuous variables. Logistic regression models were used to test if the standing mean impingement and standing maximum impingement values predicted the probability of groin pain. Receiver operator characteristic (ROC) curves were generated to determine the simulation’s area under the curve (AUC) and optimal predictive threshold for sensitivity and specificity. A post hoc power calculation with an alpha of 0.05 determined that samples of 23 patients in each cohort had a power of 95% to detect a difference in mean impingement of 0.45mm. The final sample sizes were therefore deemed sufficient.
Results:
No statistically significant difference between symptomatic and asymptomatic cohorts was found for cup anteversion, cup inclination, cup size, femoral head size, supine pelvic tilt, or standing pelvic tilt (Table 1). The mean cup prominence for the symptomatic cohort was 8.3mm and 5.0mm for the asymptomatic cohort. The difference was statistically significant (p < 0.001) (Figure 5). The average supine mean impingement for the symptomatic cohort was 0.4mm (±0.4mm) and 0.02mm (±0.1mm) for the asymptomatic cohort. The difference was statistically significant (p < 0.001). The average standing mean impingement for the symptomatic cohort was 0.4mm (±0.4mm) and 0.02mm (±0.04mm) for the asymptomatic cohort. The difference was statistically significant (p < 0.001). The average supine maximum impingement for the symptomatic cohort was 0.8mm (±0.9mm) and 0.1mm (±0.2mm) for the asymptomatic cohort. The difference was statistically significant (p < 0.001). The average standing maximum impingement for the symptomatic cohort was 0.8mm (±0.9mm) and 0.1mm (±0.1mm) for the asymptomatic cohort. The difference was statistically significant (p < 0.001) (Figure 6).
Pearson’s correlations found statistically significant linear relationships between cup prominence and standing mean impingement (R = 0.78, p < 0.001) & cup prominence and cup anteversion (R=-0.36, p = 0.02) (Table 2). Similarly significant relationships were also observed with other impingement measures (standing maximum impingement, supine mean impingement, and supine maximum impingement).
Standing mean impingement and standing maximum impingement significantly predicted the probability of pain in the logistic regression models (Figure 7, Table 3, and Table 4). The optimal cut-off point for mean impingement as a predictor of groin pain was 0.016mm (Figure 8). Using this cut-off point, the logistic regression model showed a sensitivity of 80%, specificity of 76%, and an AUC of 0.83. The optimal cut-off point for maximum impingement as a predictor of groin pain was 0.036mm (Figure 8). Using this cut-off point, the logistic regression model showed a sensitivity of 80%, specificity of 80%, and an AUC of 0.83.
Discussion:
Iliopsoas impingement is a relatively common cause of postoperative pain and dissatisfaction after THA surgery. Previous studies have noted its incidence within populations of THA patients[7,9,11,12,14,17,19], outlined successful treatment protocols[5,6,17,20,21,27,28], and assessed methods of measuring cup prominence[6,25,26], but only one previous study has attempted to quantify impingement between the acetabular cup and iliopsoas[23].
We demonstrated that our novel simulation could detect symptomatic groin pain via modelling the iliopsoas and cup through a retrospective, case-controlled investigation with the symptomatic patients exhibiting significantly greater levels of simulated impingement. Impingement was also observed to be correlated with cup prominence, calculated using our novel approach. However, contrary to our other hypotheses, the impingement did not increase significantly with posterior pelvic rotation and, unlike the study by Ries et al.[23], was not correlated with anteversion. The authors believe this to be related to sample size limitations, and, in a larger sample of patients, the symptomatic patients would likely have a significantly lower mean anteversion value.
Impingement demonstrated a strong correlation (R = 0.78, p < 0.001) with our novel approach to measuring cup prominence, which produced similar levels of prominence to the investigation by Dora et al.[6]. An explanation for our higher mean and range of prominence values is that the approach taken by Dora et al. used a horizontal measurement in CT scans at the level of the femoral head centre whereas our approach measured the largest nearest-neighbour distance between the cup and pelvis. This means our approach which will traverse across multiple CT slices and may be at a different level to the femoral head centre. In the same vein, a limitation of our method is that it does not address cups that are completely buried by bone (negative values). Therefore, several low prominence values relate to cups that are completely covered by bone, but the algorithm is measuring the slice thickness of the CT scan and differences in rendering of the 3D meshes. This impacted the results mostly by artificially increasing the mean cup prominence values of the asymptomatic cohort, yet a statistical difference between the cohorts was still observed.
Interestingly, six symptomatic patients had little-to-no impingement (standing maximum impingement < 0.05mm) detected by the simulation, yet also had relatively high cup prominence values. However, five of these patients had very large diameter femoral heads (>40mm) with monoblock cups. We believe that, in these cases, the femoral head may be preventing the iliopsoas and cup from interacting by ‘lifting it off’ the exposed cup. Despite no impingement between the iliopsoas and cup, these patients were still diagnosed with iliopsoas tendonitis and there may be multiple other reasons for their diagnosis. First, large diameter femoral heads may irritate the iliopsoas by ‘stretching’ it[9,10,13]. Second, a high combined functional anteversion may lead the iliopsoas to function more as an ‘anterior stabiliser’ to the prosthetic joint, causing irritation[4,29,30], or leading to posterior prosthetic impingement that irritates the iliopsoas through repeated anterior micro-instability. Third, there may have been excessive lengthening or offset changes made intraoperatively[7]. The existence of these patients led to the baseline risk of approximately 22% chance of groin pain after THA, despite zero impingement. This reflects the multi-causal nature of postoperative groin pain, which may be caused by a multitude of reasons other than impingement with the cup[4,6–13].
It was noteworthy that, despite several patients in the asymptomatic cohort having relatively high cup prominence values, no impingement was observed between the iliopsoas and cup in these patients. This indicated that the simulation could differentiate between cup prominence that results in impingement and cup prominence that does not. These results are likely a function of the patients’ anteriorly rotated pelvis combined with external rotation of their femur. The combined effect of these two motions prevents the iliopsoas from interacting with the acetabular cup, and this interaction might shed light on the kinematic relevance of spinopelvic and pelvic-femoral motion to the iliopsoas. Further, the minor impingement detected in 10 asymptomatic patients may reflect a threshold level of impingement for irritation or the error margin of the model. This warrants further investigation.
Our study had several limitations. First, the retrospective nature of the study meant that not all patients had the requisite imaging, necessitating exclusion from the study. Second, sample size-related limitations are likely the reason for not observing a difference in cup anteversion or cup size, as these have been shown to be a risk factor for iliopsoas impingement[21]. Third, we did not report on the treatment outcomes for the symptomatic patients and relate this to their level of impingement. Approaches to treating iliopsoas tendonitis are well documented in previous literature and this was not an objective of the study. However, further study may correlate different treatment options with the level of impingement to determine if the treatment path can be optimized.
Further research will involve investigating the impingement values in cohorts of symptomatic and asymptomatic patients with hip resurfacing arthroplasties. This may provide insight into differing mechanisms of groin pain as these two operations have been reported to have significantly different incidences of groin pain[7,9,11,12,14,17]. However, ultimately, the ambition for this simulation is to assist with preoperative planning for THAs by guiding decisions about optimal cup placement in concert with other tools, such as prosthetic and bony impingement simulations.
In conclusion, we have developed a computational model that can quantify impingement and verified its accuracy in a case-controlled investigation by simulating impingement in symptomatic and asymptomatic patients. This tool has the potential to be used preoperatively, to guide decisions about optimal cup placement, and postoperatively, to aid in the diagnosis of iliopsoas tendonitis and determine an appropriate treatment pathway.
Figure Captions
Figure 1 Flow chart of the patient selection process for the symptomatic cohort, which includes patients who were diagnosed with iliopsoas tendonitis, and asymptomatic cohort, which includes patients that were not diagnosed with iliopsoas tendonitis.
Figure 2 Illustration of the landmarks taken for the simulation. The ASIS points and pubic symphysis form the anterior pelvic plane (APP) and allow calculation of the supine pelvic tilt. Psoas Superior 1-3 and Psoas Inferior represent the ‘attachment sites’ of the iliopsoas. The Femoral Head Centre was used as the point at which the pelvis rotates around.
Figure 3 Schematic of the iliopsoas impingement simulation in a patient's standing pelvic position. Three segments approximate the width of the iliopsoas and the location it passes over the acetabular margin. These segments are comprised of two paths; a green and a red path. The green path does not include the cup and the red path does. The difference between these paths is equal to the impingement, and could be considered the ‘stretch’ of the iliopsoas due to the cup.
Figure 4 Our approach to calculating cup prominence values included reducing the pelvis and cup meshes to point clouds and implementing a nearest neighbour algorithm to determine the greatest distance between the point clouds. In this example, the cup prominence would be the straight-line distance between the two enlarged black spheres; one from the cup, one from the pelvis.
Figure 5 Cup prominence results for the symptomatic and asymptomatic cohorts. The symptomatic cohort had significantly greater cup prominence values. The edges of the box represent the 25th and 75th percentiles, the solid line within the box represents the median, the dashed line represents the mean, the lines represent the ranges, and the dots represent the outliers.
Figure 6 Mean and maximum impingement results for the symptomatic and asymptomatic cohorts. The symptomatic cohort had significantly greater mean and maximum impingement values in both standing and supine.
Figure 7 Logistic regression models for standing mean and maximum impingement to predict groin pain.
Figure 8 Receiver operating characteristic (ROC) curves for the standing mean impingement and standing maximum impingement logistic regression models.
Tables
Table 1 Implant, patient, cup prominence, and iliopsoas impingement-related information for both cohorts of patients.
|
Table 1
|
Cohort
|
Mean
|
Range
|
Standard Deviation
|
p-Value
|
|
APP Inclination
|
Symptomatic
|
43.1
|
29.9 – 59.5
|
7.8
|
n.s†
|
|
Asymptomatic
|
42.2
|
33.6 – 55.2
|
5.1
|
|
APP Anteversion
|
Symptomatic
|
18.3
|
-16.4 – 35.5
|
10.5
|
n.s†
|
|
Asymptomatic
|
19.8
|
1.4 – 36.3
|
8.6
|
|
Supine Pelvic Tilt
|
Symptomatic
|
1.3
|
-15.1 – 15.5
|
6.1
|
n.s†
|
|
Asymptomatic
|
2.9
|
-6.0 – 9.4
|
4.0
|
|
Standing Pelvic Tilt
|
Symptomatic
|
-4.2
|
-19.8 – 13.3
|
7.9
|
n.s†
|
|
Asymptomatic
|
-3.7
|
-14.8 – 6.2
|
5.3
|
|
Head Size
|
Symptomatic
|
35.8
|
28 – 48
|
6.2
|
n.s‡
|
|
Asymptomatic
|
33.7
|
22 – 36
|
3.4
|
|
Cup Size
|
Symptomatic
|
53.4
|
48 – 62
|
4.4
|
n.s‡
|
|
Asymptomatic
|
52.0
|
48 – 60
|
3.2
|
|
Cup Prominence
|
Symptomatic
|
8.3
|
3.2 – 14.7
|
2.5
|
< 0.001†
|
|
Asymptomatic
|
5.0
|
1.8 – 8.2
|
1.5
|
|
Supine Mean Impingement
|
Symptomatic
|
0.4
|
0.0 – 1.4
|
0.4
|
< 0.001†
|
|
Asymptomatic
|
0.02
|
0.0 – 0.3
|
0.1
|
|
Standing Mean Impingement
|
Symptomatic
|
0.4
|
0.0 – 1.4
|
0.4
|
< 0.001†
|
|
Asymptomatic
|
0.02
|
0.0 – 0.2
|
0.04
|
|
Supine Maximum Impingement
|
Symptomatic
|
0.8
|
0.0 – 3.1
|
0.9
|
< 0.001†
|
|
Asymptomatic
|
0.1
|
0.0 – 0.7
|
0.2
|
|
Standing Maximum Impingement
|
Symptomatic
|
0.8
|
0.0 – 3.1
|
0.9
|
< 0.001†
|
|
Asymptomatic
|
0.1
|
0.0 – 0.7
|
0.1
|
|
n.s = not significant
† = Student’s T-Test
‡ = Chi-Squared Test
|
Table 2 Pearson's correlations to determine linear relationships between variables. Similarly significant relationships with standing maximum impingement, supine mean impingement, and supine maximum impingement were observed, but not not reported.
Table 2
|
Correlator 1
|
Correlator 2
|
Correlation Coefficient
|
p-Value
|
|
Cup Prominence
|
Standing Mean Impingement
|
0.78
|
p < 0.001
|
|
Cup Prominence
|
Cup Anteversion
|
-0.36
|
p = 0.02
|
|
Standing Mean Impingement
|
Cup Anteversion
|
-0.08
|
n.s
|
|
Standing Mean Impingement
|
Cup Size
|
0.15
|
n.s
|
|
Change in Pelvic Tilt
|
Change in Impingement
|
-0.09
|
n.s
|
Table 3 Logistic regression model for predicting the probability of pain with standing mean impingement.
|
Table 3
|
Parameter
|
Standard Error
|
Coefficient
|
p-value
|
|
(intercept)
|
0.4438
|
-1.2930
|
< 0.01
|
|
Standing Mean Impingement
|
4.9725
|
12.9460
|
< 0.01
|
Table 4 Logistic regression model for predicting the probability of pain with standing maximum impingement.
|
Table 4
|
Parameter
|
Standard Error
|
Coefficient
|
p-value
|
|
(intercept)
|
0.4419
|
-1.2825
|
< 0.01
|
|
Standing Max Impingement
|
1.8294
|
5.4996
|
< 0.01
|
References
[1] Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. The Lancet 2007;370:1508–19. https://doi.org/10.1016/S0140-6736(07)60457-7.
[2] Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012;2:e000435. https://doi.org/10.1136/bmjopen-2011-000435.
[3] Scott CEH, Bugler KE, Clement ND, MacDonald D, Howie CR, Biant LC. Patient expectations of arthroplasty of the hip and knee. J Bone Joint Surg Br 2012;94-B:974–81. https://doi.org/10.1302/0301-620X.94B7.28219.
[4] Zhu J, Li Y, Chen K, Xiao F, Shen C, Peng J, et al. Iliopsoas tendonitis following total hip replacement in highly dysplastic hips: A retrospective study. J Orthop Surg 2019;14:1–8. https://doi.org/10.1186/s13018-019-1176-z.
[5] Capogna BM, Shenoy K, Youm T, Stuchin SA. Tendon Disorders After Total Hip Arthroplasty: Evaluation and Management. J Arthroplasty 2017;32:3249–55. https://doi.org/10.1016/j.arth.2017.04.015.
[6] Dora C, Houweling M, Koch P, Sierra RJ. Iliopsoas impingement after total hip replacement: the results of non-operative management, tenotomy or acetabular revision. J Bone Joint Surg Br 2007;89-B:1031–5. https://doi.org/10.1302/0301-620X.89B8.19208.
[7] Ala Eddine T, Remy F, Chantelot C, Giraud F, Migaud H, Duquennoy A. Anterior iliopsoas impingement after total hip arthroplasty: Diagnosis and conservative treatment in 9 cases. Rev Chir Orthopédique Réparatrice Appar Mot 2002;87:815–9.
[8] Brew CJ, Stockley I, Grainger AJ, Stone MH. Iliopsoas Tendonitis Caused by Overhang of a Collared Femoral Prosthesis. J Arthroplasty 2011;26:504.e17-504.e19. https://doi.org/10.1016/j.arth.2009.12.020.
[9] Bartelt RB, Yuan BJ, Trousdale RT, Sierra RJ. The Prevalence of Groin Pain After Metal-on-Metal Total Hip Arthroplasty and Total Hip Resurfacing. Clin Orthop 2010;468:2346–56. https://doi.org/10.1007/s11999-010-1356-y.
[10] Cobb JP, Davda K, Ahmad A, Harris SJ, Masjedi M, Hart AJ. Why large-head metal-on-metal hip replacements are painful: The anatomic basis of psoas impingement on the femoral head-neck junction. J Bone Joint Surg Br 2011;93-B:881–5. https://doi.org/10.1302/0301-620X.93B7.26054.
[11] Bin Nasser A, Beaulé PE, O’Neill M, Kim PR, Fazekas A. Incidence of groin pain after metal-on-metal hip resurfacing. Clin Orthop 2010;468:392–9. https://doi.org/10.1007/s11999-009-1133-y.
[12] Lavigne M, Laffosse JM, Ganapathi M, Girard J, Vendittoli P. Residual groin pain at a minimum of two years after metal-on-metal THA with a twenty-eight-millimeter femoral head, THA with a large-diameter femoral head, and hip resurfacing. J Bone Jt Surg - Ser A 2011;93:93–8. https://doi.org/10.2106/JBJS.J.01711.
[13] Browne JA, Polga DJ, Sierra RJ, Trousdale RT, Cabanela ME. Failure of larger-diameter metal-on-metal total hip arthroplasty resulting from anterior iliopsoas impingement. J Arthroplasty 2011;26:978 e5-8. https://doi.org/10.1016/j.arth.2010.10.002.
[14] Bricteux S, Beguin L, Fessy MH. Iliopsoas impingement in 12 patients with a total hip arthroplasty. Rev Chir Orthop Reparatrice Appar Mot 2001;87:820–5.
[15] Trousdale RT, Cabanela ME, Berry DJ. Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty 1995;10:546–9.
[16] Odri GA, Padiolleau GB, Gouin FT. Oversized Cups as a Major Risk Factor of Postoperative Pain After Total Hip Arthroplasty. J Arthroplasty 2014;29:753–6. https://doi.org/10.1016/j.arth.2013.07.001.
[17] O’Sullivan M, Tai CC, Richards S, Skyrme AD, Walter WL, Walter WK. Iliopsoas Tendonitis. A Complication After Total Hip Arthroplasty. J Arthroplasty 2007;22:166–70. https://doi.org/10.1016/j.arth.2006.05.034.
[18] Buller LT. Iliopsoas Impingement After Direct Anterior Approach Total Hip Arthroplasty: Epidemiology, Risk Factors, and Treatment Options. J Arthroplasty 2021:7.
[19] Nam D, Nunley RM, Sauber TJ, Johnson SR, Brooks PJ, Barrack RL. Incidence and Location of Pain in Young, Active Patients Following Hip Arthroplasty. J Arthroplasty 2015;30:1971–5. https://doi.org/10.1016/j.arth.2015.05.030.
[20] Henderson RA, Lachiewicz PF. Groin pain after replacement of the hip: Aetiology, evaluation and treatment. J Bone Jt Surg - Ser B 2012;94 B:145–51. https://doi.org/10.1302/0301-620X.94B2.27736.
[21] Buller LT, Menken LG, Hawkins EJ, Bas MA, Roc GC, Cooper HJ, et al. Iliopsoas Impingement After Direct Anterior Approach Total Hip Arthroplasty: Epidemiology, Risk Factors, and Treatment Options. J Arthroplasty 2021;36:1772–8. https://doi.org/10.1016/j.arth.2020.12.012.
[22] Meermans G, Konan S, Das R, Volpin A, Haddad FS. The direct anterior approach in total hip arthroplasty: a systematic review of the literature. Bone Jt J 2017;99-B:732–40. https://doi.org/10.1302/0301-620X.99B6.38053.
[23] Ries M, Faizan A, Zhang J, Scholl L. Effects of Acetabular Cup Orientation and Implant Design on Psoas Impingement in Total Hip Arthroplasty. Reconstr Rev 2019;9. https://doi.org/10.15438/rr.9.1.220.
[24] Nakano N, Yip G, Khanduja V. Current concepts in the diagnosis and management of extra-articular hip impingement syndromes. Int Orthop 2017;41:1321–8. https://doi.org/10.1007/s00264-017-3431-4.
[25] Brownlie CA, Evans R, Morrison D, Hayes A, Song S, Kuster MS. Improved accuracy of CT based measurements for anterior prominence of acetabular prosthesis using a novel protocol based on anatomical landmarks. Orthop Traumatol Surg Res 2020;106:563–8. https://doi.org/10.1016/j.otsr.2019.10.019.
[26] Cyteval C, Sarrabère MP, Cottin A, Assi C, Morcos L, Maury P, et al. Iliopsoas impingement on the acetabular component: Radiologic and computed tomography findings of a rare hip prosthesis complication in eight cases. J Comput Assist Tomogr 2003;27:183–8. https://doi.org/10.1097/00004728-200303000-00014.
[27] Chalmers BP, Sculco PK, Sierra RJ, Trousdale RT, Berry DJ. Iliopsoas Impingement After Primary Total Hip Arthroplasty: Operative and Nonoperative Treatment Outcomes. J Bone Joint Surg Am 2017;99:557–64. https://doi.org/10.2106/JBJS.16.00244.
[28] Fish DE, Chang WS. Treatment of iliopsoas tendinitis after a left total hip arthroplasty with botulinum toxin type A. Pain Physician 2007;10:565–71.
[29] Fabricant PD, Bedi A, De La Torre K, Kelly BT. Clinical Outcomes After Arthroscopic Psoas Lengthening: The Effect of Femoral Version. Arthrosc J Arthrosc Relat Surg 2012;28:965–71. https://doi.org/10.1016/j.arthro.2011.11.028.
[30] Jacobsen JS, Hölmich P, Thorborg K, Bolvig L, Jakobsen SS, Søballe K, et al. Muscle-tendon-related pain in 100 patients with hip dysplasia: prevalence and associations with self-reported hip disability and muscle strength. J Hip Preserv Surg 2018;5:39–46. https://doi.org/10.1093/jhps/hnx041.
Figures
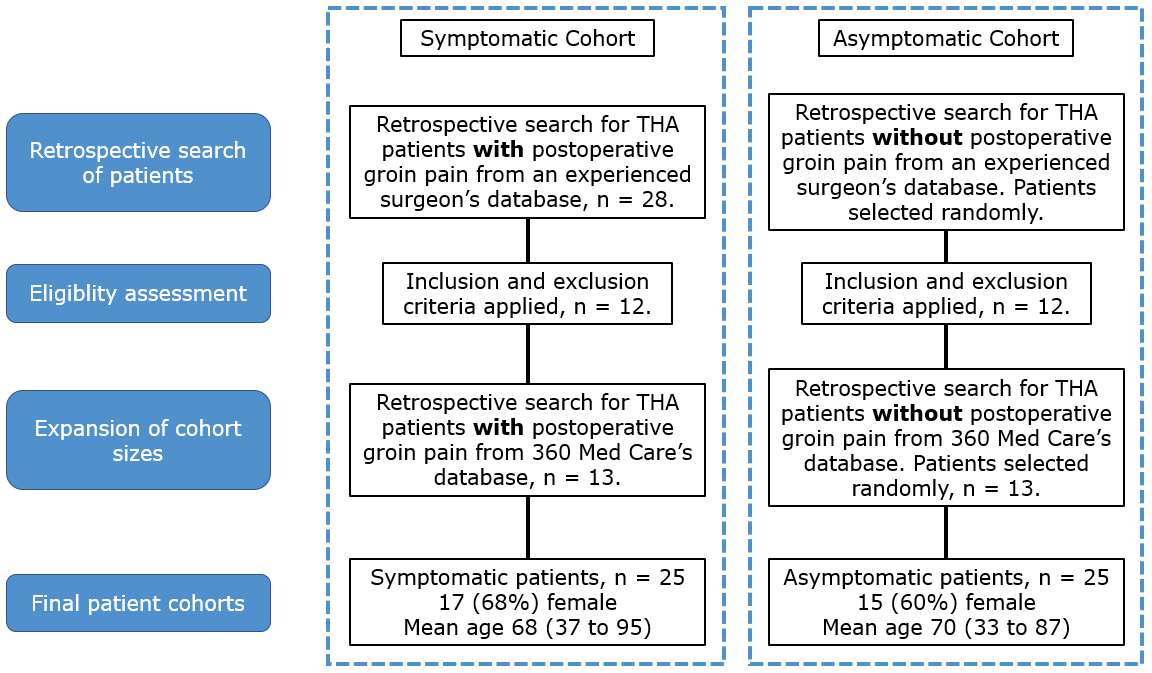
Figure 1
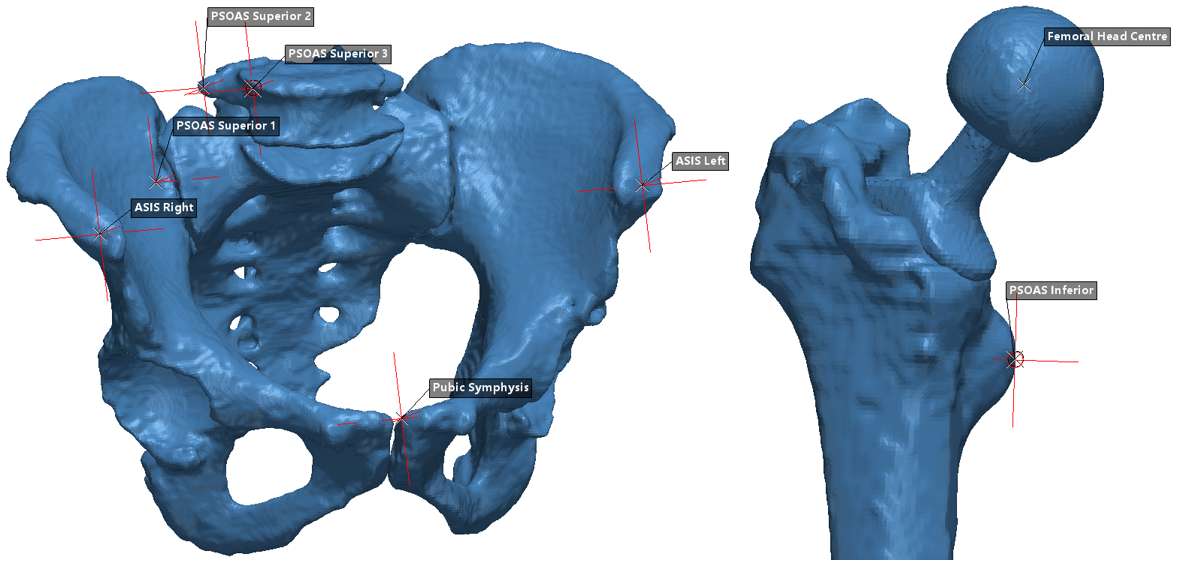
Figure 2
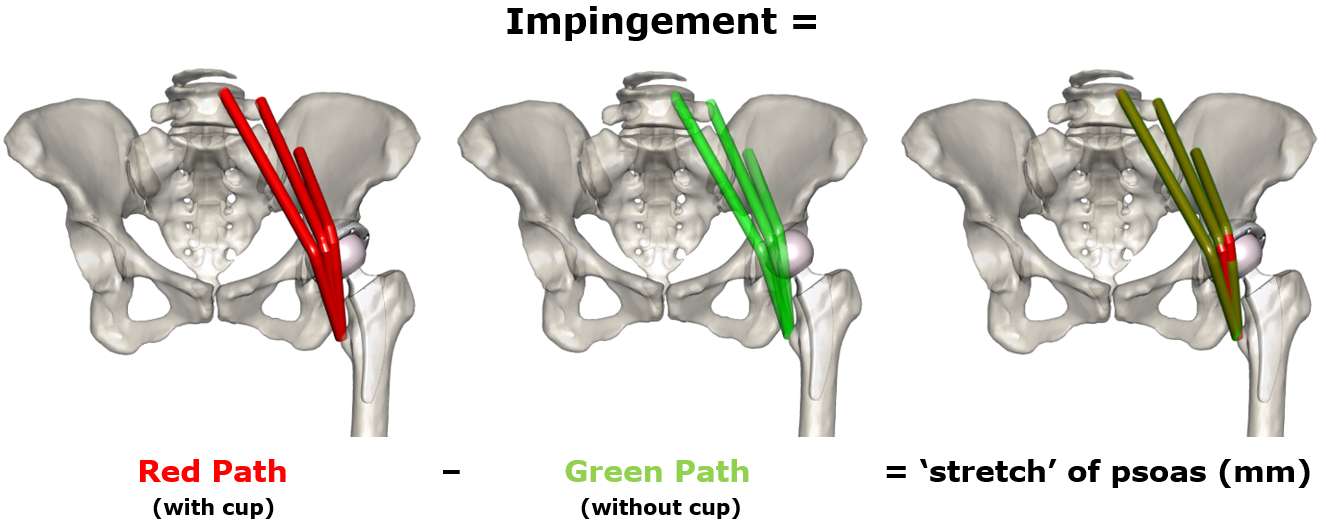
Figure 3
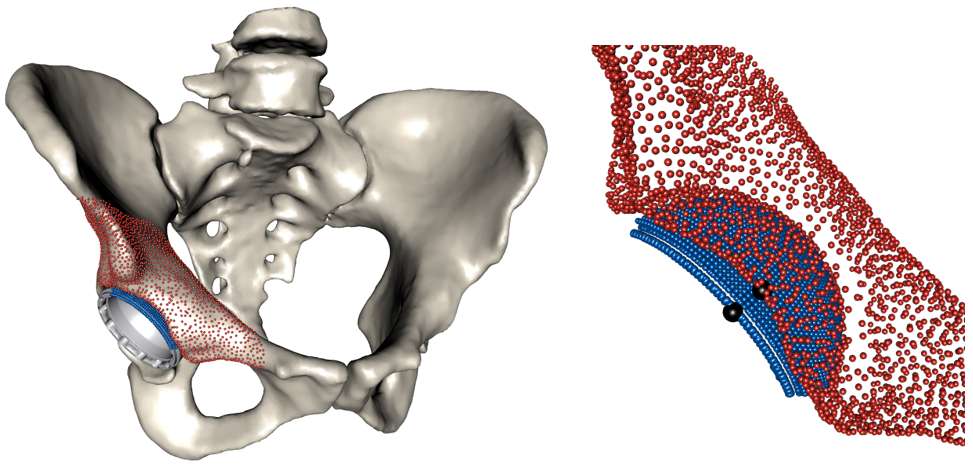
Figure 4
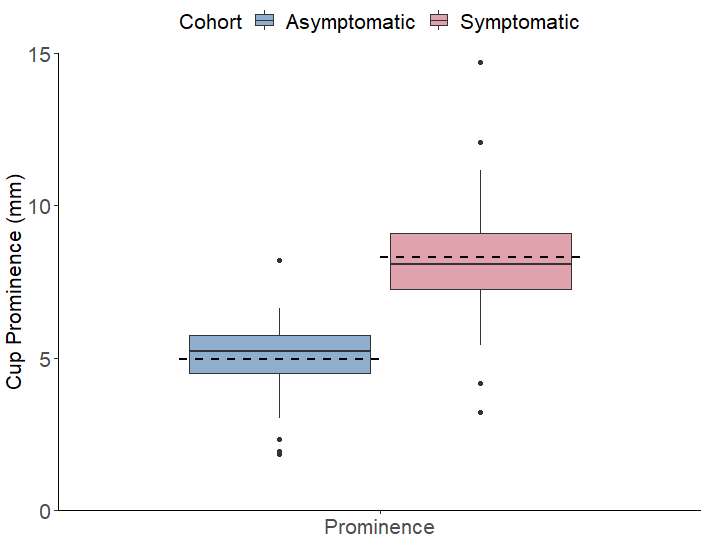
Figure 5
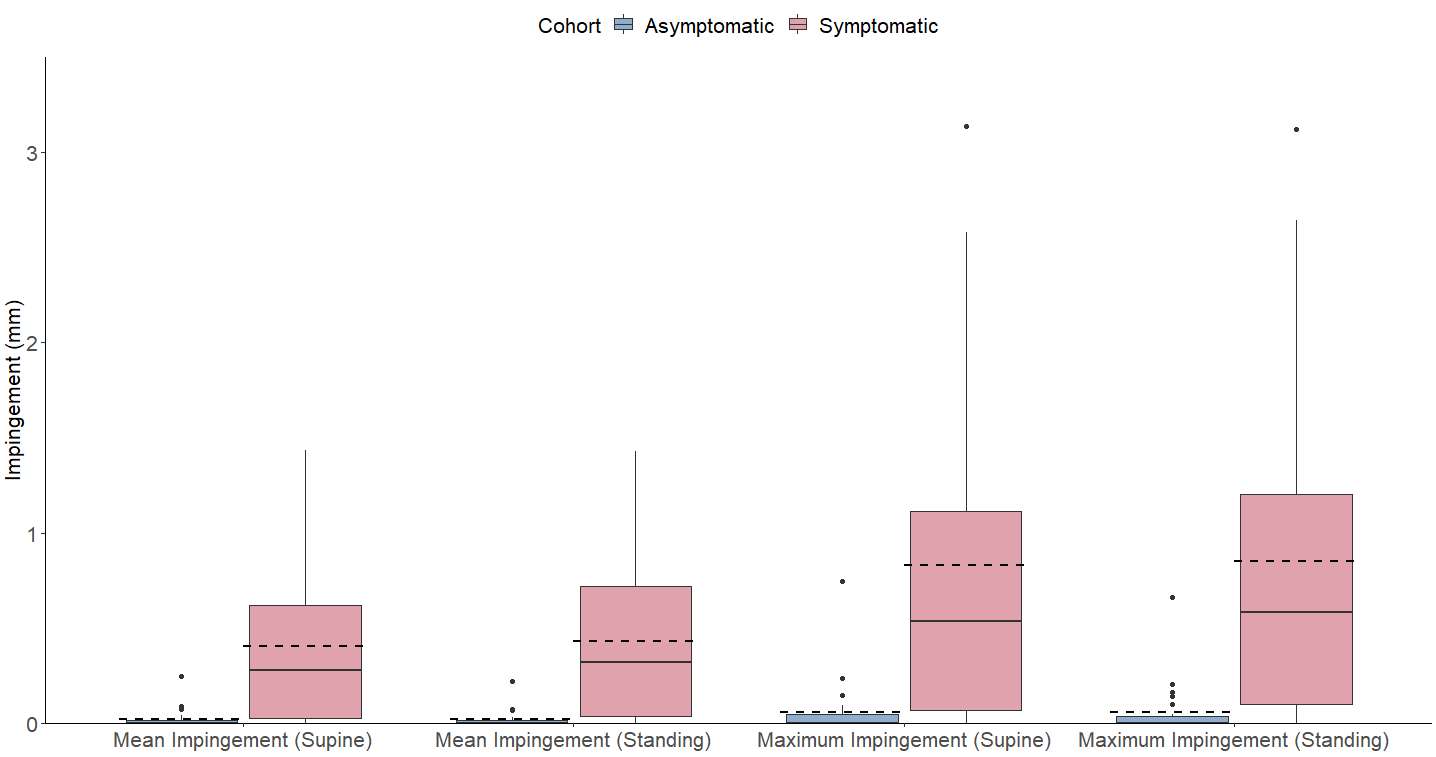
Figure 6
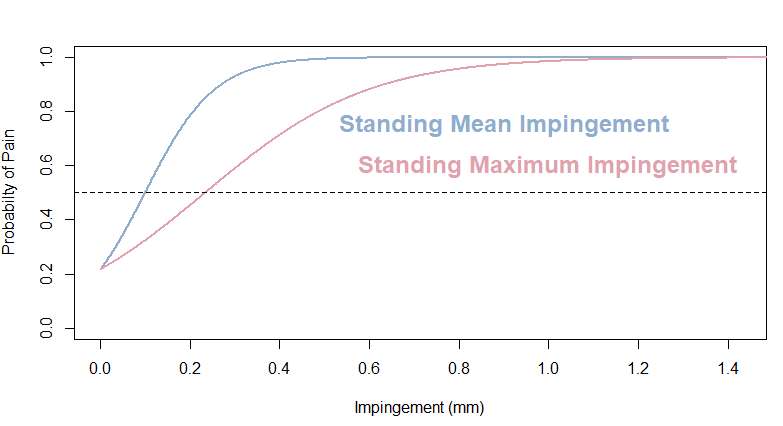
Figure 7
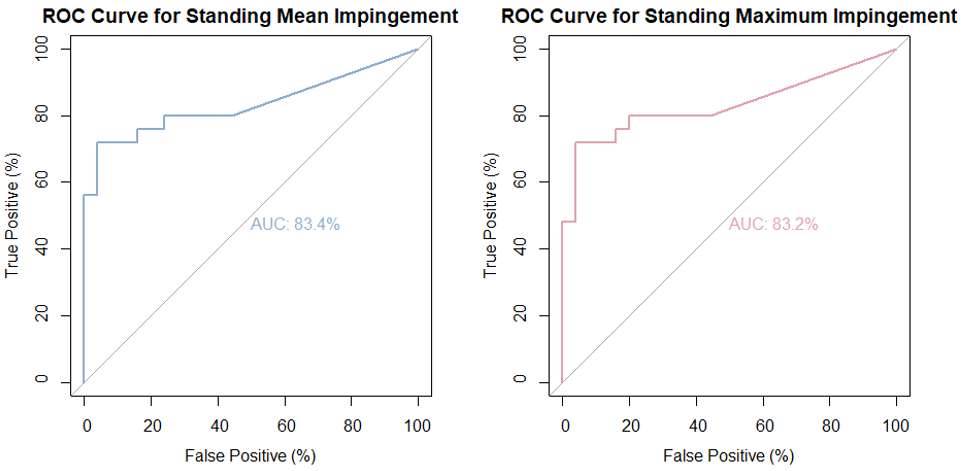
Figure 8#7583
Mid-Term Performance of a Bicruciate-Retaining TKA, a Radiostereometric Analysis
*Kelly Mills - Sint Maartenskliniek - Nijmegen, Netherlands
K.C. Defoort - Sint Maartenskliniek - Ubbergen (near Nijmegen), The Netherlands
Gijs Van Hellemondt - Ubbergen (Near Nijmegen), Belgium
Petra Heesterbeek - Sint Maartenskliniek - Nijmegen, Netherlands
*Email: k.mills@maartenskliniek.nl
Introduction: With a bicruciate-retaining (BCR) total knee arthroplasty (TKA), due to the preservation of both cruciate ligaments, the horse shoe-shaped implant design is different compared to a TKA where one or both cruciate ligaments are removed. Thereby, the preservation of both cruciate ligaments creates a different balance of forces. Both causes can affect the fixation of the implant in the bone. Our previous study using radiostereometric analysis (RSA) showed higher micromotion of a BCR-TKA until two years postoperatively compared to cruciate-retaining TKA. Therefore, we decided to further investigate this micromotion of the BCR-TKA group at five years postoperatively to see the development of the migration patterns over time.
Methods: All available patients from the original BCR-TKA group, who completed two years follow-up, were invited back to the clinic at five years postoperatively. An RSA x-ray was made and all patients filled out questionnaires: the Forgotten Joint Score (FJS), the OXFORD Knee Score + APQ supplement (OKS-APQ), the Knee injury and Osteoarthritis Outcome Score - Physical Function Short Form (KOOS PS) and VAS pain and satisfaction, also Range Of Motion (ROM) was determined. From the RSA x-rays the micromotion of both components was determined and expressed as Total Translation (TT) and Total Rotation (TR) and the change in Maximum Total Point Motion from two to five years postoperatively (ΔMTPM2-5yr).
Results: Of the 16 patients who completed two years follow-up one patient died, one had a major revision (total system revision due to instability) and one declined participation for further follow-up. Given this is preliminary data, we are still awaiting data for two patients. For the remaining 11 patients the median TT of the femoral component at five year postoperatively was 0.47 mm (0.28 to 0.57) and femoral TR was 0.52° (0.19 to 0.62) (Figure 1). For the tibia component the median TT was 0.24 mm (0.16 to 0.76) and TR was 0.60° (0.52 to 1.35) (Figure 2). The median ΔMTPM2-5yr was -0.029 mm (-0.11 to -0.032) for the femoral component and 0.022 mm (-0.048 to -0.15) for the tibial component. The median scores for all clinical outcomes were: 77.1 (49.0 to 83.7) for the FJS, 44 (43 to 46.5) and 84.4 (70.3 to 98.4) for the OKS and OKS-APQ respectively, 29.7 (14.6 to 31.7) for the KOOS-PS, 1 (0.95 to 1) and 80 (77.5 to 87.5) for the EQ-5D and VAS component respectively, 1 (0 to 16.5) and 100 (85 to 100) for VAS pain and satisfaction respectively and 130° (122.5 to 132.5) maximum knee flexion.
Conclusion: The BCR-TKA shows stabilization of the micromotion pattern from two to five years follow-up, with the exception of a couple outliers. However, the patients who show relatively higher migration patterns did show good scores on the clinical outcomes. In general the FJS was high and all clinical outcomes from two to five years follow-up remained constant, with only one revision. Based on these results the BCR-TKA seems to form a stable construct in the bone and satisfied patients.
Figures
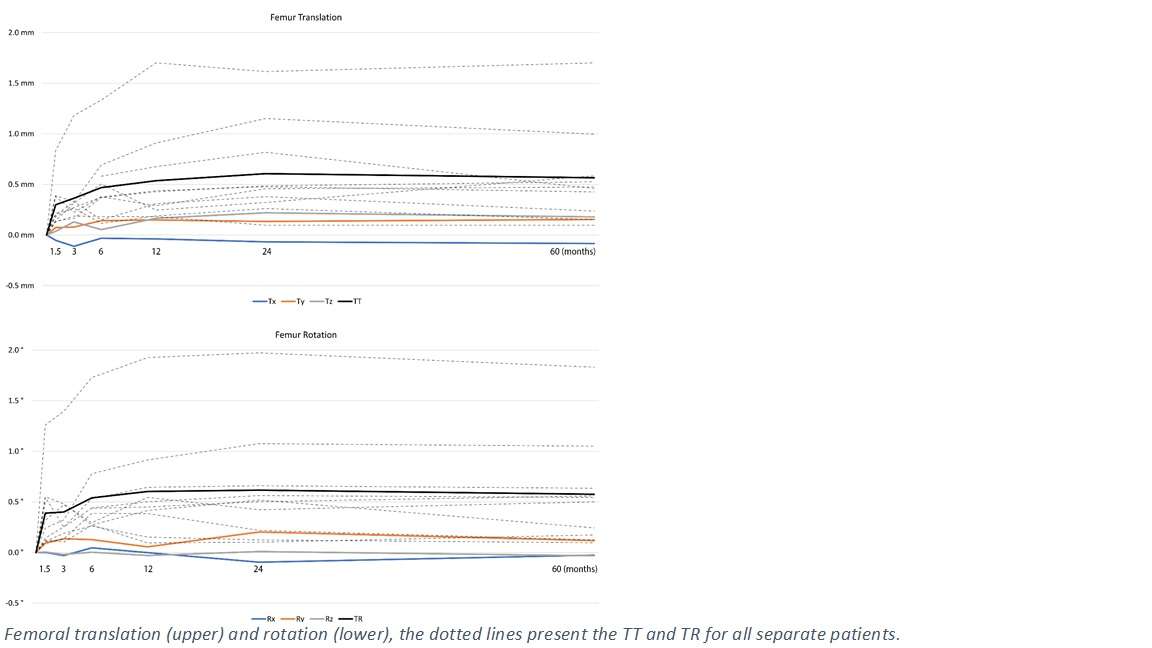
Figure 1
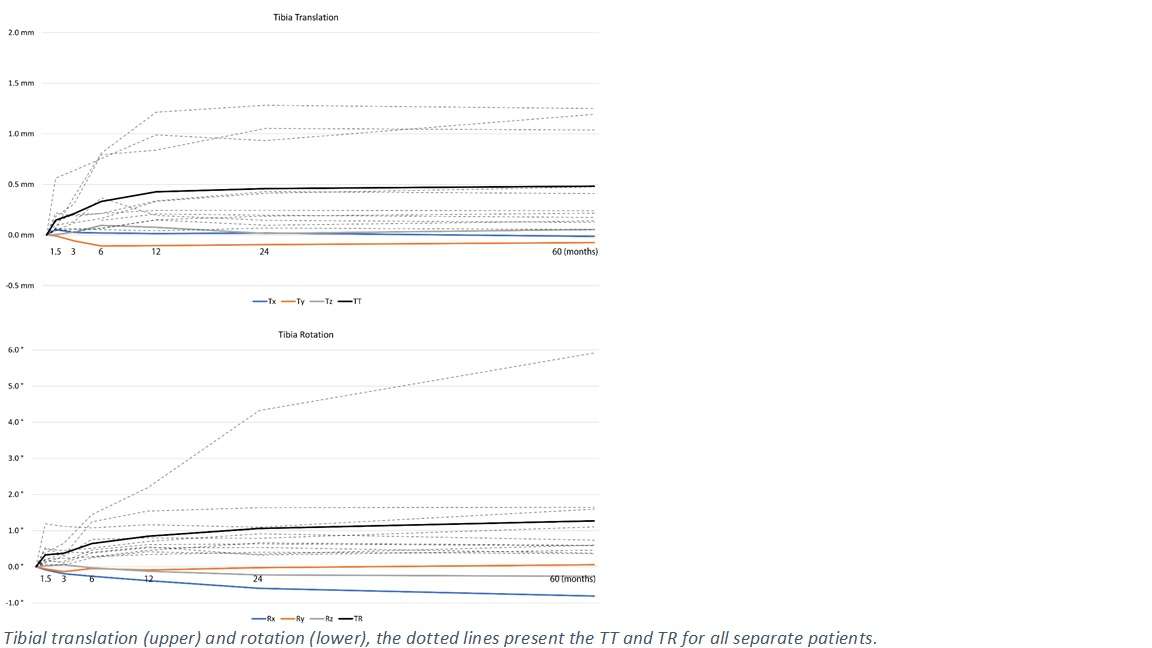
Figure 2#7587
Fluoroscopic and Radiostereometric Analysis of a Bicruciate-Retaining Versus a Posterior Cruciate-Retaining TKA: A Randomized Controlled Trial
*Kelly Mills - Sint Maartenskliniek - Nijmegen, Netherlands
Menno Benard - Sint Maartenskliniek - Ubbergen, Netherlands
Ate Wymenga - St. Maartenskliniek, University Medical Centre Nijmegen
Bart Kaptein - LUMC - Leiden, Select Country
K.C. Defoort - Sint Maartenskliniek - Ubbergen (near Nijmegen), The Netherlands
Gijs Van Hellemondt - Ubbergen (Near Nijmegen), Belgium
Petra Heesterbeek - Sint Maartenskliniek - Nijmegen, Netherlands
*Email: k.mills@maartenskliniek.nl
Introduction: A bicruciate-retaining (BCR) total knee arthroplasty (TKA) is thought to lead to more natural knee movement compared to a posterior cruciate-retaining (CR) TKA. The idea is that preserving the anterior cruciate ligament (ACL) facilitates proprioception and balance in the knee, leading to more natural knee kinematics. However, surgery is more challenging and the stemless design of tibial BCR-TKA may lead to differences in fixation of the components in the bone. The aim of the present study was to compare a BCR- and CR-TKA in terms of in vivo kinematics during functional tests and to compare micromotion measured using radiostereometric analysis (RSA).
Methods: A total of 40 patients with end-stage osteoarthritis were included into this randomized controlled trial. All patients performed a step-up and lunge task in front of a monoplane fluoroscope one year postoperatively. Femorotibial contact point (CP) locations were determined at every flexion angle and compared between the groups. Secondary, RSA images were taken at baseline, six weeks, three, six, 12 and 24 months postoperatively to determine implant micromotion of both components with respect to the bone. Clinical and functional outcome scores were compared up until two years postoperatively.
Results: Figure 1 presents the mean anterior-posterior (AP) CP ratios during both tasks, for both groups separately. Figure 2 shows the differences (BCR minus CR) in CP ratios and the 95% CI of this difference. In the step-up task, laterally, the BCR CP is more posterior from 20° to 0° flexion. In the lunge task the medial CP of the BCR group was more anterior in the early flexion phase compared to the CR group, while laterally the CP was more posterior during the entire movement cycle. Both groups showed paradoxical anterior translation of the CP and the BCR-TKA CP showed a wide within-group variation (Figure 1). Figure 3 presents micromotion (translation and rotation) of both components over time. Multilevel regression analyses showed statistically significantly more micromotion of the tibial component for the BCR-TKA compared to the CR-TKA. No significant differences between both groups were found for the clinical or functional outcome scores, but there were two insert exchanges and one total system revision in the BCR group (no minor/major revisions in CR group).
Conclusion: The BCR-TKA demonstrated a kinematic pattern comparable to the natural knee’s screw home mechanism and more natural rollback during the early flexion phase compared to the CR group. The difference between both implants is especially visible in the flexion phase in which the ACL is effective. However, both designs seem to fail to fully replicate the natural knee’s motion. In addition, the tibial component of the BCR-TKA showed more micromotion compared to the CR-TKA within the first two years after surgery. The femoral components were equally stable. At this stage we found no clinical differences between both implants, but the combination of higher tibial migration and overall higher complication rate does not support the routine use of this implant at this stage.
Figures
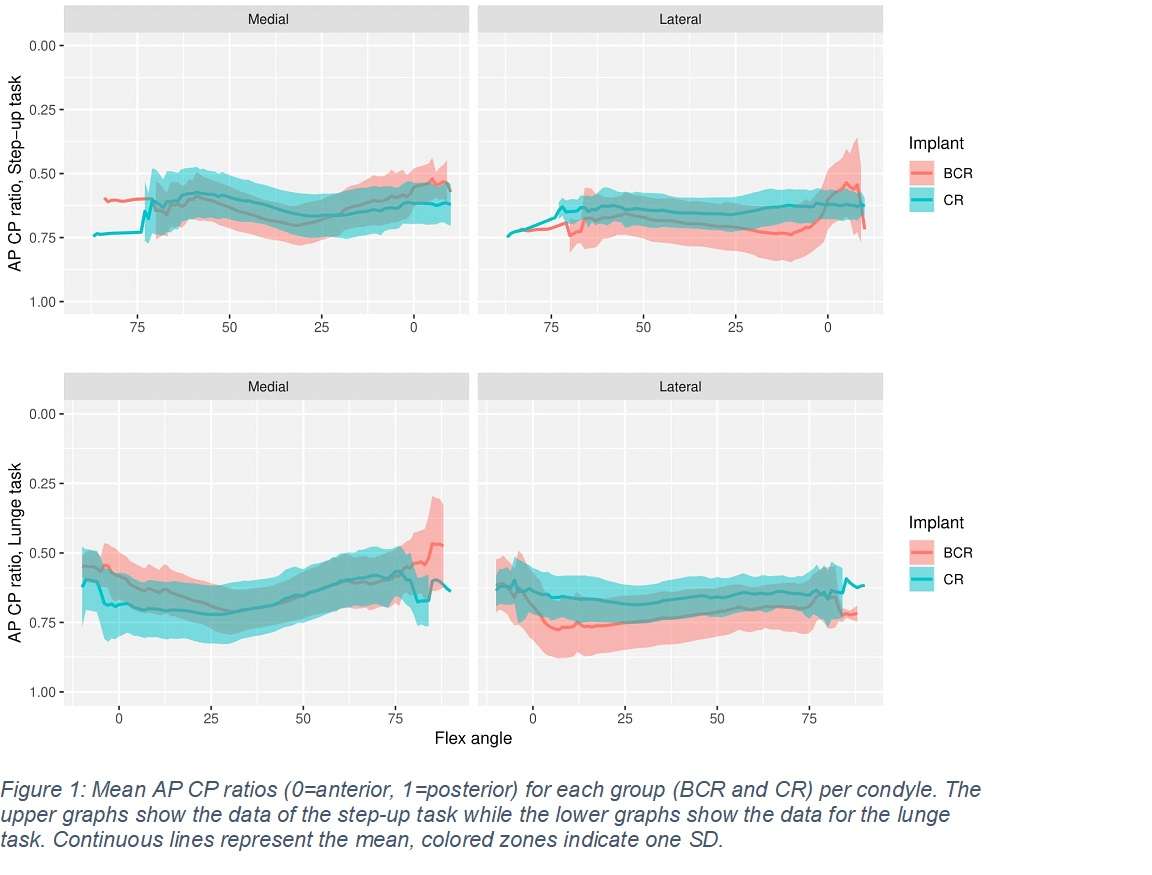
Figure 1
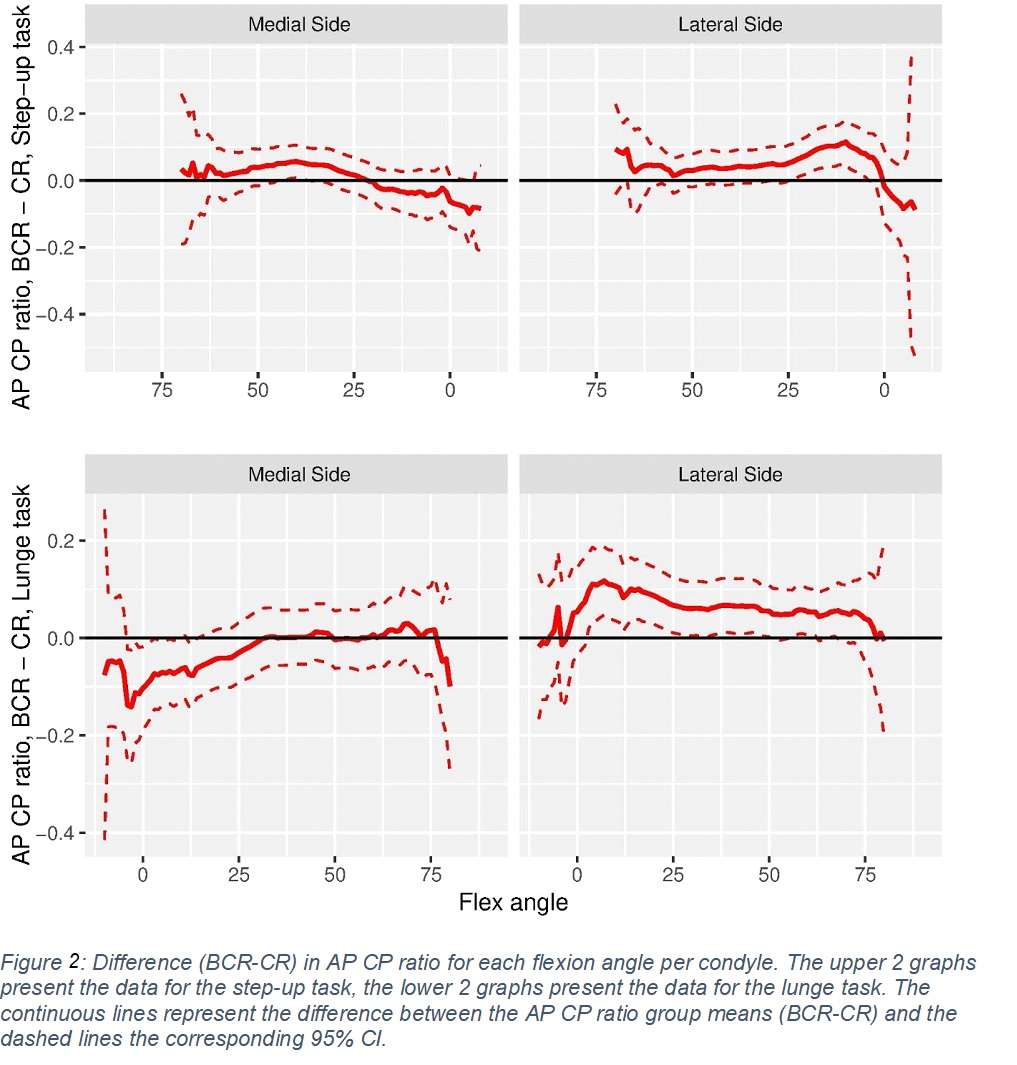
Figure 2
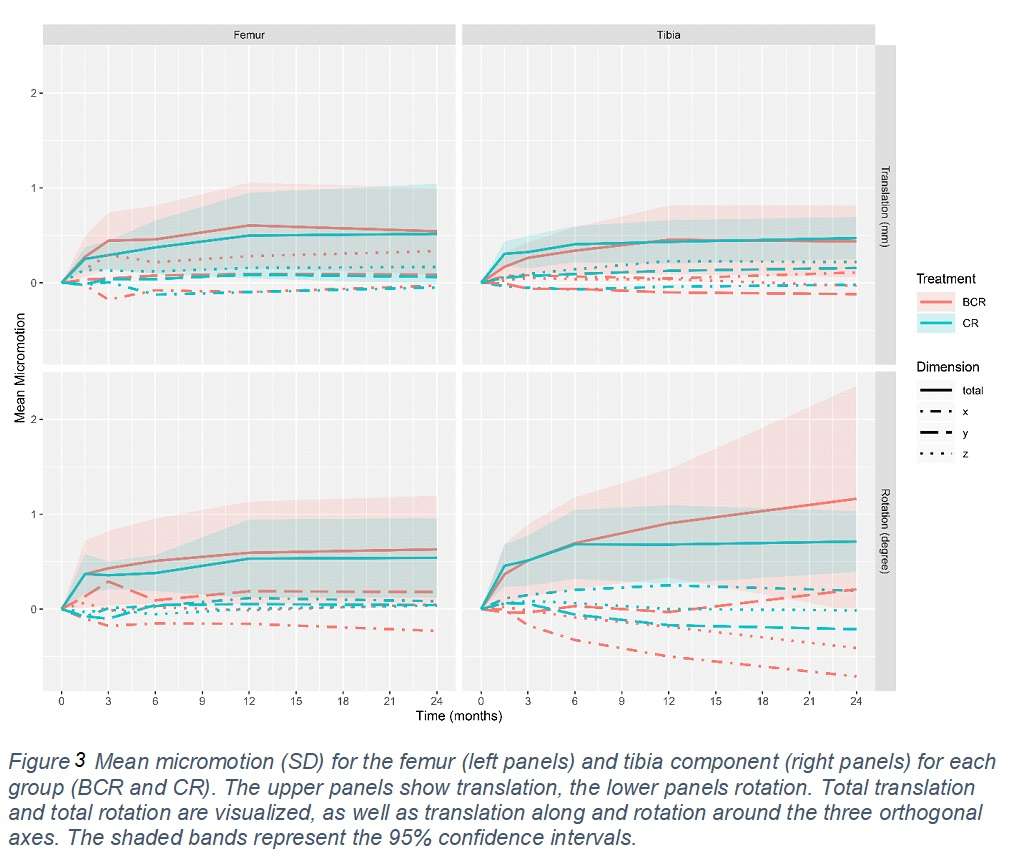
Figure 3#7279
Evaluations of MIS-TKA Without Femoral Intramedullary Reaming Using CT-Free Compact Navigation System.
*Genya Mitani - Department of Orthopaedic Surgery, Surgical Science, Tokai University School of Medicine - Isehara, Japan
Tomonori Takagaki - Tokai University School of Medicine - Kanagawa, Japan
Kosuke Hamahashi - Tokai University School of Medicine - Kanagawa, Japan
Daichi Takizawa - Tokai University School of Medicine - Kanagawa, Japan
Takehisa Suzuki - Tokai University School of Medicine - Kanagawa, Japan
Masahiko Watanabe - Tokai University School of Medicine - Kanagawa, Japan
*Email: genya@syd.odn.ne.jp
Purpose: The purpose of this study is to evaluate the radiographic alignment, perioperative items and DVT onset in minimally invasive surgery (MIS) total knee arthroplasty (TKA) without femoral intramedullary reamingusing CT-free compact navigation system comparison with conventional MIS TKA. Methods: 12 cases who underwent MIS TKA using CT-free compact navigation system (N group) and 28 cases underwent conventional MIS TKA (C group) were enrolled. Coronal femoral angle (CFA), coronal tibial angle (CTA), hip-knee-ankle angle (HKA), sagittal femoral angle (SFA), sagittal tibial angle (STA), surgical duration, blood loss, incision length, onset rate of DVTPE, D-dimer and Soluble Fibrin Monomer Complex(SFMC) at POD#1,3,5,7,10,14 were evaluated. Results and discussions: DVT onset, SFMC @POD#1 and dispersion of SFA, STA in N group were significantly lower than in C group. (N/C DVT onset: 0% / 35.7%,SFMC@POD#1:4±0.7/13.8±15.0, SFA:90.3±1.0°/88.3±3.2°, STA: 89.2±1.2°/89.4±4.5°) Surgical duration in N group was significantly longer than in C group. (134.2min. /120.5min.) Dispersion of CFA, CTA, HKA, incision length, blood loss, D-dimer, and SFMC except POD#1 have no significant difference in two groups. (CFA:88.9±1.0°/89.6±1.3°, CTA:90.6±1.3°/90.9±1.3°, HKA:180.7±1.6°/181.2±1.7°, incision length: 9.3cm/9.2cm, blood loss:703.3ml/710.0ml) Use of CT free compact navigation in MIS-TKA allowed reducing DVT onset and accurate implantation without increasing incision length and blood loss.
#7988
Arthroplasty at Very High Altitude With Restricted Resources: Our Experience and Review of Literature
*Samarth Mittal - All India Institute of Medical Sciences (AIIMS) - New Delhi, India
Chandra Shekhar Yadav - All India Institute of Medical Sciences - Delhi, India
*Email: samarthmittal@gmail.com
BACKGROUND : Patients living in high altitudes are often deprived of Total Knee Arthroplasty (TKA) due to logistic reasons and other challenges in performing surgical procedures for management of knee pain. TKA in high altitude dwellers has associated risk of deep venous thrombosis/ pulmonary embolism (DVT/PE) and if conducted at lower altitudes, return to high altitudes can cause high altitude pulmonary oedema.
METHODS : A retrospective study of patients undergoing Total Knee Arthroplasty at a camp set up at 11,000 feet above sea level between 2014 to 2020 was undertaken. At every follow-up, patients were assessed clinically for KSS and complications like DVT, infection, residual deformity etc. and patients were also evaluated radiologically to look for evidence of implant loosening.
RESULTS : 132 patients (202 knee joints in 50 male and 82 female patients) underwent TKA during annual camps. The average follow-up of patients was 60 months. There was no evidence of DVT or superficial or deep infection in any patient in the post-operative period. Mean pre-operative KSS was 38, which was increased to 83 at 1 year follow-up post-surgery.
CONCLUSION : With this study, we can safely conclude that Total knee arthroplasty can be safely performed at high altitudes and remote areas with limited health facilities and is a safer and more convenient prospect for the residents of high-altitude regions.
#7460
Combined Subjective & Objective Health Related Quality of Life (SO.QOL) Score, and Usefulness in a Musculoskeletal Population for Pre and Post Intervention Assessment
*Ralph Mobbs - Prince of Wales Private Hospital - Sydney, Australia
*Email: ralphmobbs@hotmail.com
Background:
Quality of Life (QOL) is an individual's perception of their situation in life in the context of culture and community. Health related QOL (HRQOL) is an evaluation of QOL and its relationship with physical and mental health. Objective measures such as reduced walking speed and activity (1,3) (daily step count) is a sign of advancing age, multiple disease states, cognitive impairment, and early mortality. Subjective validated questionnaires that assist in the measurement of health can help in measuring QOL. The authors present a novel tool for HRQOL evaluation that is easy to measure based on a simplified app questionnaire (subjective), and mobility metrics as recorded on a patient’s smartphone (objective).
Methods:
SO.QOLTM is a health measure with a range of 0 (poor health) to 100 (excellent health). The objective component is based on the SMoS algorithm(2), including daily step count and walking speed (measured as a weekly average). The subjective component is based on 5 health measures: i. Patient perception of their overall health status, ii. Personal care, iii. Day-to-Day activities, iv. Pain levels and v. Anxiety/Depression status. The score is delivered via a phone App to simplify data entry and extraction.
Results:
Validation of SO.QOLTM for the spine, hip and knee population includes normative datasets compared to pathology groups including hip osteoarthritis (HO), knee osteoarthritis (KO) and spinal stenosis (SS). From a cohort of 659 patients presenting to spine, hip and knee clinics over a 2-year period, the HO group was the most disabled based off SO.QOLTM scores, then followed by SS, and finally KO. All groups scored significantly lower than aged matched normative cohorts.
Conclusions:
SO.QOLTM is a simple and effective health scoring tool which is demonstrably altered in musculoskeletal pathologies of the hip, knee and spine, and serves as a rapid, App based tool for general health assessment in large populations. The SO.QOLTM has potential to be used as a screening tool in primary and specialised care settings, in addition to assessment of post intervention disability and recovery.
References
1. Mobbs RJ, Mobbs RR, Choy WJ. Proposed objective scoring algorithm for assessment and intervention recovery following surgery for lumbar spinal stenosis based on relevant gait metrics from wearable devices: the Gait Posture index (GPi). J Spine Surg. 2019 Sep;5(3):300-309. doi: 10.21037/jss.2019.09.06. PMID: 31663040; PMCID: PMC6787370.
2. Betteridge C, Mobbs RJ, Ho D. Proposed objective scoring algorithm for walking performance, based on relevant gait metrics: the Simplified Mobility Score (SMoS™)-observational study. J Orthop Surg Res. 2021 Jul 1;16(1):419. doi: 10.1186/s13018-021-02546-8. PMID: 34210345; PMCID: PMC8247222.
3. Mobbs RJ. Gait velocity (walking speed) is an indicator of spine health, and objective measure of pre and post intervention recovery for spine care providers. J Spine Surg. 2020 Jun;6(2):353-355. doi: 10.21037/jss-20-602. PMID: 32656370; PMCID: PMC7340824.
#7844
Objective Walking Metrics of Patients With Hip, Knee and Spine Pathology.
*Ralph Mobbs - Prince of Wales Private Hospital - Sydney, Australia
*Email: ralphmobbs@hotmail.com
Introduction
The clinical assessment of knee, hip, and spine disease severity has been traditionally performed using patient-reported ratings of symptoms and function and the visual assessment of gait by the treating physician. However, these assessments are limited by their subjective nature. We objectively constructed gait profiles of patients with spine, hip, and knee disease using gait metrics derived from a small and lightweight chest-based inertial measurement units (IMU / wearable device).
Methods
We performed a cross-sectional observational study of preoperative patients including 30 patients with lumbar spinal stenosis (Laminectomy), 30 with knee osteoarthritis (TKA), 30 with hip osteoarthritis (THA), and 30 healthy controls in a similar age bracket. Each participant walked along a straight unobstructed pathway at a self-selected pace for a self-selected distance (maximum 120 m). Gait metrics (spatiotemporal, asymmetry, and variability) were measured using the MetaMotionC (9-axis IMU) single-point wearable sensor placed at the sternal angle. Gait metrics were compared between patients and healthy controls.
Results
Compared to healthy controls, all pathological groups demonstrated significantly (p<0.04) reduced gait velocity (13.8-22.2%) and step length (8.32-10.7%), and significantly (p<0.03) increased step time (7.05-15.7%), double limb support time (7.30-13.4%), single limb support time (7.92-18.2%), stance time (7.02-14.4%), and swing time (6.92-16.8%). Patients with hip and knee disease had significant (p<0.02) marked alterations in asymmetry, particularly step time asymmetry (84.0-90.0%) and step length asymmetry (109-123%).
Conclusions
We objectively demonstrated alterations in gait metrics in patients with spine, hip, and knee disease compared to controls using a small and lightweight single-point inertial measurement unit. We also found unique gait patterns between pathological subgroups, and future studies may examine possibilities of disease diagnosis and quantification of disability using gait analysis. This technology may allow clinicians of the future to determine pre-intervention disability, track progress post-intervention, and to assist with post-operative rehabilitation.
#7979
Comparison of in Vivo Kinematic and Radiological Parameters of Three Cervical Disc Prostheses
*Ralph Mobbs - Prince of Wales Private Hospital - Sydney, Australia
*Email: ralphmobbs@hotmail.com
Introduction:
Cervical total disc replacement (CTDR) is an alternative to anterior cervical discectomy and fusion for select patients that may preserve range of motion and reduce adjacent segment disease. Various CTDR prostheses are available; however, comparative data are limited. This study aimed to compare the short‑term kinematic and radiological parameters of the M6‑C, Mobi‑C, and the CP‑ESP prostheses.
Methods:
This retrospective cohort study included patients treated with CTDR between March 2005 and October 2020 at a single institution. Patients were included if their follow‑up assessment included lateral erect and flexion/extension radiographs. The primary outcome assessed at 3‑months postoperatively was range of motion, measured by the difference in functional spinal unit angle between flexion and extension.
Results:
A total of 131 CTDR levels (120 patients, 46.2 ± 10.1 years, 57% male) were included. Prostheses implanted included the
M6‑C (n = 52), Mobi‑C (n = 54), and CP‑ESP (n = 25). Range of motion varied significantly (8.2° ± 4.4° vs. 10.9° ± 4.7° vs. 6.1° ± 2.7°, P < 0.001). On post hoc analysis, the Mobi‑C prosthesis demonstrated a significantly greater range of motion than either the M6‑C prosthesis (P = 0.003) or CP‑ESP (P < 0.001).
Conclusion:
Although the optimal range of motion for CTDR has not been established, short‑term differences in the range of motion may
guide the selection of CTDR prosthesis. Further studies with longer follow‑up and consideration of clinical outcome measures are necessary.
Keywords: Cervical total disc replacement, CP‑ESP, disc arthroplasty, M6‑C, Mobi‑C, total disc replacement
#7544
Vancomycin Resistance Enterococcus and Implications to Trauma and Orthopaedic Care
*Ali Mofidi - Morriston hospital - Swansea, United Kingdom
Medhi Tofighi - Morriston hospital - Swansea, United Kingdom
Owain Davies - Morriston Hospital - Swansea, United Kingdom
Karunakar Veravalli - ABM university trust - Swansea, UK
Parag Panwalkar - Morriston hospital - Swansea, United Kingdom
Phillip Butterick - HARP - Cardiff, United Kingdom
Brendan Healy - Public health wales - Cardiff, United Kingdom
*Email: mofidi71@hotmail.com
Vancomycin Resistance Enterococcus is a devastating nosocomial infection. We studied VRE outbreak in orthopaedic unit in Morriston hospital.
Twenty-four cases of VRE infection and 34 cases of VRE colonisations were identified in patients who were treated for orthopaedic care in a 15-month period. Cases were reviewed to identify predisposing-factors specifically looking at patient characteristics, risk-factors, VRE risk and clearance (PREVENT) scores, and impact on outcome and institution. The presenting condition, treatment, presence of postoperative infection, VRE-scores, was compared between colonised and the infected cohort.
Predominant VRE type was Van A, Enterococcus Faecium. Diabetes, advancing age, high ASA score, and peri-femoral surgery was associated with VRE infestation. All of the VRE infected patients had an infected complication of their fracture fixation or arthroplasty requiring reoperation and prolonged antibiotics therapy. The infected group had an average VRE risk score of 8.5 versus of 2 in the colonised group (p<0.001). PREVENT-score was 7 in the infected group and 2 in the colonised group (p<0.001).
Time to positivity was 36+/-33 days for the colonised group and 44+/-26 days for the infected group. Hospital stay was 71.6+/-34 days for the colonised group and 71.5+/-26 days for infected group. Mortality was significantly higher for VRE infected cases (p<0.05).
We advise surveillance, prompt therapy and discharge of patients undergoing peri-femoral surgery especially infected metalwork, avoidance of infective complications, antibiotic stewardship and radical surgery and beyond infective precautions. PREVENT-score shows that the infected group are unlikely to clear their VRE in the future but not the colonised group.
#7639
Assessing the Biomechanical Effect of Femoral Component Malrotation Following TKA Using a Novel Computational Model Including Ligament Wrapping
*Liam Montgomery - Western University - Whitby, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Ryan Willing - Western University - London, Canada
*Email: lmontgo7@uwo.ca
INTRODUCTION: Total knee arthroplasty (TKA) dissatisfaction and revision rates remain too high, in many cases as a result of instability which may be attributed to prosthesis malalignment. At the development stage of prosthesis components, or during surgical planning it would be beneficial to characterize how changes in prosthesis component alignment will influence stability. While the technology has been embedded into some robotic TKA systems, to some extent, these models do not incorporate contributions from individual ligament bundles, nor do they account for potential ligament wrapping. The objective of this study is to use a digital twin of a six degrees of freedom (6-dof) joint motion simulator, capable of including multiple ligaments and ligament wrapping, to examine the effects of femoral component rotational malalignment on joint kinematics/stability and ligament.
METHODS: A TKA was performed on a healthy knee model within the digital twin – VIVO Sim Visualization Software – with three conditions of malrotation: Baseline had a femoral component external rotation of 3° relative to the femur, External was over-rotated to 4.5°, Internal was under-rotated to only 1.5°. The standard rotation of 3.0±1.2° has been shown to reduce the need for retinacular release. Our TKA used single radius of curvature femoral components articulated against a cruciate-retaining UHMWPE insert appropriately sized for the modelled knee. The virtual twin is also capable of simulating multi-bundle virtual ligaments that exhibit non-linear elastic behaviour. Our knee model represented the superficial medial collateral ligament (sMCL) and the lateral collateral ligament (LCL) with five bundles each and the posterior cruciate ligament (PCL) with three bundle. Additionally, wrapping of the sMCL was simulated about the proximal medial edged of the tibia. Knee models underwent discrete motions within the digital twin including neutral flexion, posterior laxity, varus-valgus laxity, and internal-external laxity. Kinematics and ligament tensions were recorded for all motions. Laxity was calculated as the absolute difference between the position during neutral flexion and the position during the laxity test at a given flexion angle.
RESULTS: Average laxities are shown in Figure 1. Though the absolute position varies with femoral component rotation, overall laxity remains similar for all degrees of freedom measured. Figure 2 describes collateral ligament engagement patterns during neutral flexion which shows increased sMCL engagement as the knee is flexed for the Internal model, and decreased sMCL engagement for the External model. The opposite pattern is observed for the LCL. Figure 3 compares ligament tensions with and without simulated ligament wrapping. Simulating wrapping lead to increased sMCL and LCL engagement in late flexion.
CONCLUSION: This study examined the effects of femoral implant malrotation following TKA. Over-rotating the femoral implant lead to a more varus knee complete with increased LCL engagement as exemplified by the External model. Under-rotating had a more valgus knee with increased sMCL tension. Though laxity was not noticeably affected by component malrotation, malalignment of the femoral component clearly leads to different ligament engagement patterns during flexion. Furthermore, neglecting ligament wrapping will artificially reduce sMCL and LCL contributions by allowing more medial-lateral movement.
Figures

Figure 1
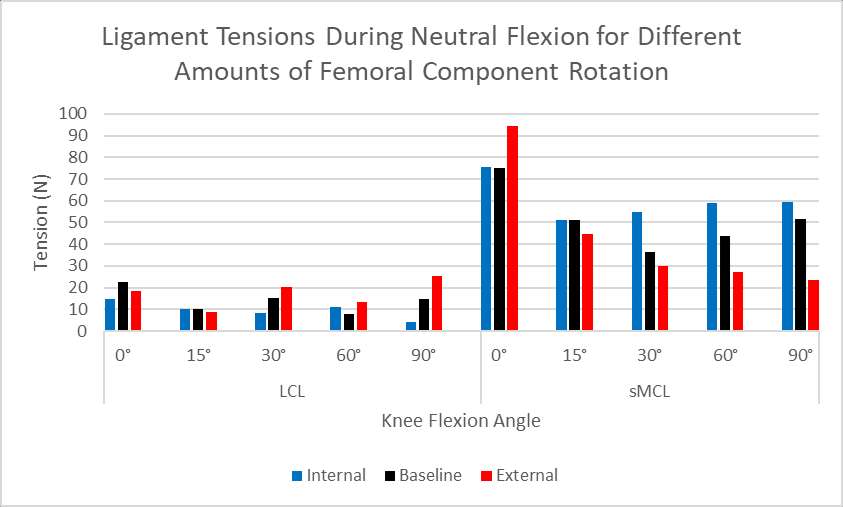
Figure 2
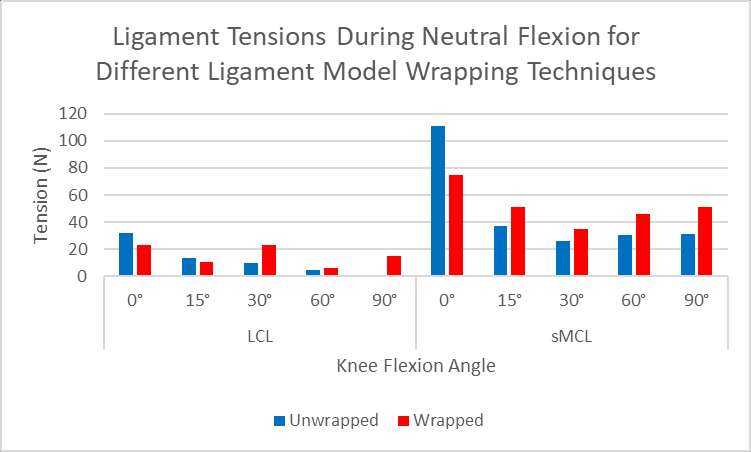
Figure 3#6899
Similar Radiological Results With Accelerometer-Based Navigation Versus Conventional Technique in Total Knee Arthroplasty
*Ing How Moo - Changi General Hospital - Singapore, Singapore
Raghuraman Raghavan - Changi General Hospital - Singapore
*Email: zell53@hotmail.com
Background: Proper alignment of the prosthesis in total knee arthroplasty is critical in maximizing implant survival and ensure optimal functional outcome. Malalignment of the prosthesis has been reported to lead to abnormal tibial–femoral and patellar tracking, asymmetric distribution of stresses at the weight-bearing surfaces, accelerated polyethylene wear, aseptic loosening and poor functional outcome. Navigation systems using accelerometer-based device are a relatively new concept with a limited number of systems available and there is a paucity of literature evaluating its intraoperative accuracy and clinical effectiveness in TKA. The authors hypothesize that accelerometer navigation will improve coronal and sagittal alignments when compared to conventional techniques in TKA, without a significant increase in the duration of surgery.
Methods: A single surgeon randomly assigned patients who underwent TKA to either accelerometer-based navigation or conventional method. Two groups of 30 patients each with primary osteoarthritis underwent TKA using either conventional method or accelerometer-based navigation in a single institution was retrospectively studied. Patients were matched according to body mass index (BMI), gender and age. A senior arthroplasty surgeon performed all the operation using the same surgical approach. Perioperative and post-operative regimens were the same. The primary outcome of this study was post-operative radiographic assessment of lower limb alignment and components placement, while the secondary outcomes include the duration of surgery, perioperative drop in serum haemoglobin (Hb) level and blood transfusion incidence. Complications of TKA were also recorded.
Results: There was no difference between the two groups for age, BMI, gender, side of operated knee and preoperative mechanical axis (p > 0.05). There was no difference in the proportion of outliers for mechanical axis (p= 0.38), coronal femoral angle (p= 0.50), coronal tibia angle (p= 0.11), sagittal femoral angle (p=0.28) and sagittal tibia angle (p= 0.33). The duration of surgery, post-operative drop in haemoglobin level and transfusion incidence did not show statistically significant differences between the two groups (p > 0.05).
Conclusions: Our article showed that accelerometer-based navigation was safe and remains a useful tool to restore mechanical axis. It did not increase the duration of the operation. However, our data demonstrated no difference in lower limb alignment and component placement between the TKA that used accelerometer-based system and those that underwent conventional method.
#7942
Safety of Bilateral Total Hip Arthroplasty in Patients Age >70
*Landon Morikawa - University of Hawaii - John A. Burns School of Medicine - Honolulu, Select Country
Scott Nishioka - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: landonmo@hawaii.edu
INTRODUCTION: Despite the efficiency and financial benefits of bilateral total hip arthroplasty (BTHA), it remains unclear if the procedure is safe to perform in the elderly population. The purpose of this study was to compare early post-operative complications between unilateral THA and BTHA performed in patients younger and older than 70.
METHODS: Prospective data was collected for 315 patients who had undergone THA (≤70, N=143; >70: N= 103) or single-stage BTHA (≤70: N=46; >70: N=23) between April 2019 and January 2021 by a single, fellowship trained arthroplasty. Variables of interest included Charlson Comorbidity Index (CCI), transfusion rate, length of stay, pre- and six-week post-THA Hip Disability and Osteoarthritis Outcome Score (HOOS JR), and 90-day complications and readmissions.
RESULTS: Compared to THA>70 patients, BTHA>70 patients remained at the hospital longer (0.9 days vs 2.2 days, respectively) and were less likely to be discharged directly home (85% vs 74%, respectively). Transfusion requirement was not significantly different between BTHA>70 (13%) and BTHA≤70 (4.3%). The complication rate in BTHA>70 (4.3%) was similar to that of THA>70 (4.9%) and BTHA≤70 (2.2%). The lone readmission in the BTHA>70 group was due to a component dislocation requiring revision but no cases of pulmonary embolism or deep vein thrombosis were reported. There were no differences in pre- or post-THA satisfaction or HOOS JR scores.
DISCUSSION/CONCLUSION: Although BTHA>70 patients were most likely to require transfusion, this cohort demonstrated comparable complication rates and patient reported outcomes as THA>70 and BTHA≤70 patients. These data suggest BTHA may be a reasonably safe treatment option for patients >70 with symptomatic bilateral hip osteoarthritis.
#7943
Posterior-Stabilizing Versus Ultracongruent Inserts in Total Knee Arthroplasty With Patellar Resurfacing
*Landon Morikawa - University of Hawaii - John A. Burns School of Medicine - Honolulu, Select Country
Maya Matsumoto - University of Hawaii - John A Burns School of Medicine - Honolulu, USA
Kyle Obana - University of Hawai'i John A. Burns School of Medicine - Honolulu, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: landonmo@hawaii.edu
INTRODUCTION: Patellar resurfacing in total knee arthroplasty (TKA) has demonstrated improved postoperative range-of-motion, however it is unclear if this benefit is influenced by the type of tibial insert used. Therefore, this study aimed to compare six-month outcomes of TKA with resurfacing between posterior-stabilizing (PS) and fixed-bearing ultracongruent (UC) inserts.
METHODS: Patients were selected from a prospective, on-site joint registry if the patient (1) underwent unilateral or bilateral TKA with patella resurfacing, (2) received either a PS or UC tibial insert and (3) had a minimum six-month clinical follow-up. The same orthopedic surgeon performed all procedures, in which the posterior cruciate ligament was sacrificed in both groups. Knee flexion, Knee Society Function Scores, and Knee Injury and Osteoarthritis Outcome Scores (KOOS, JR.) were evaluated at minimum 6-month follow-up. Independent t-tests and Chi-squared tests were performed to compare implant groups.
RESULTS: Overall, 53 UC and 33 PS patients were included in data analysis. The average post-cut patella thickness was similar between PS (21.8mm) and UC knees (21.2mm). Average post-operative knee flexion was comparable between PS (115.9 ̊±8.5 ̊) and UC knees (116.3 ̊±9.4 ̊). There were no group differences between PS and UC inserts in post-operative function (66.0 vs. 68.4, respectively) or KOOS, JR. scores (69.3 vs. 70.5, respectively).
DISCUSSION/CONCLUSION: PS and UC patients demonstrated similar post-operative knee flexion, functional scores, and patient-reported outcomes. These findings suggest that PS and UC inserts are acceptable when the patella is resurfaced and are equally successful approaches to TKA.
#7907
Impact of Over- or Under-Correction of Patella Thickness in Total Knee Arthroplasty
*Sean Chan - University of Hawai'i John A. Burns School of Medicine - Honolulu, United States of America
Kyle Obana - University of Hawai'i John A. Burns School of Medicine - Honolulu, USA
Brent Shimoda - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Landon Morikawa - University of Hawaii - John A. Burns School of Medicine - Honolulu, Select Country
*Email: chansean@hawaii.edu
INTRODUCTION: Restoration of native patellar thickness has always been a primary goal in performing total knee arthroplasty (TKA). No consensus has been reached regarding whether to resurface or not, but potential benefits of patellar resurfacing during TKA include a lower risk of patellar reoperation and better functional outcomes. Females have a higher incidence of patellar over-resection and experience poorer functional scores following TKA. However, the effect of over- or under-correction of native patellar thickness on postoperative range of motion (ROM) in both males and females remains unclear. Therefore, the purpose of this study was to report the incidence of patellar under- or over-correction and compare early range of motion (ROM) recovery between genders following TKA with patellar resurfacing.
METHODS: A retrospective chart review of 101 patients undergoing posterior-stabilized TKA with patellar resurfacing was conducted. Pre- and 6-week postoperative ROM, Knee Society function, KOOS Jr., and intraoperative patellar thickness measurements before and after resurfacing were collected. Multiple independent t-tests and Chi-squared tests were performed for continuous and categorical variables, respectively.
RESULTS: The average change in patellar thickness following resurfacing was -0.7±(1.6) and -0.6±(1.3) mm for males and females, respectively. Overall, postoperative patella thickness was equal to native thickness in 64.5% of males and 70.7% of females, with a decrease in patella thickness in 27.4% and 22.4% of males and females, respectively. Compared to preoperative, females and males had a comparable loss in knee flexion; however, females had lower function and patient reported outcome scores. At 6-weeks postoperatively, patients with a decrease in patella thickness had a greater loss of knee flexion (14.5°±21.7°) compared to patients with the same thickness (1.8°±16.5°).
CONCLUSION: Despite high success of restoring native patella thickness, a decrease in patella thickness results in a greater loss of knee flexion. Nevertheless, the change in patella thickness did not alone result in difference for knee function or patient reported outcomes; therefore, postoperative outcomes are likely more influenced by patient demographics and preoperative functional status.
Figures
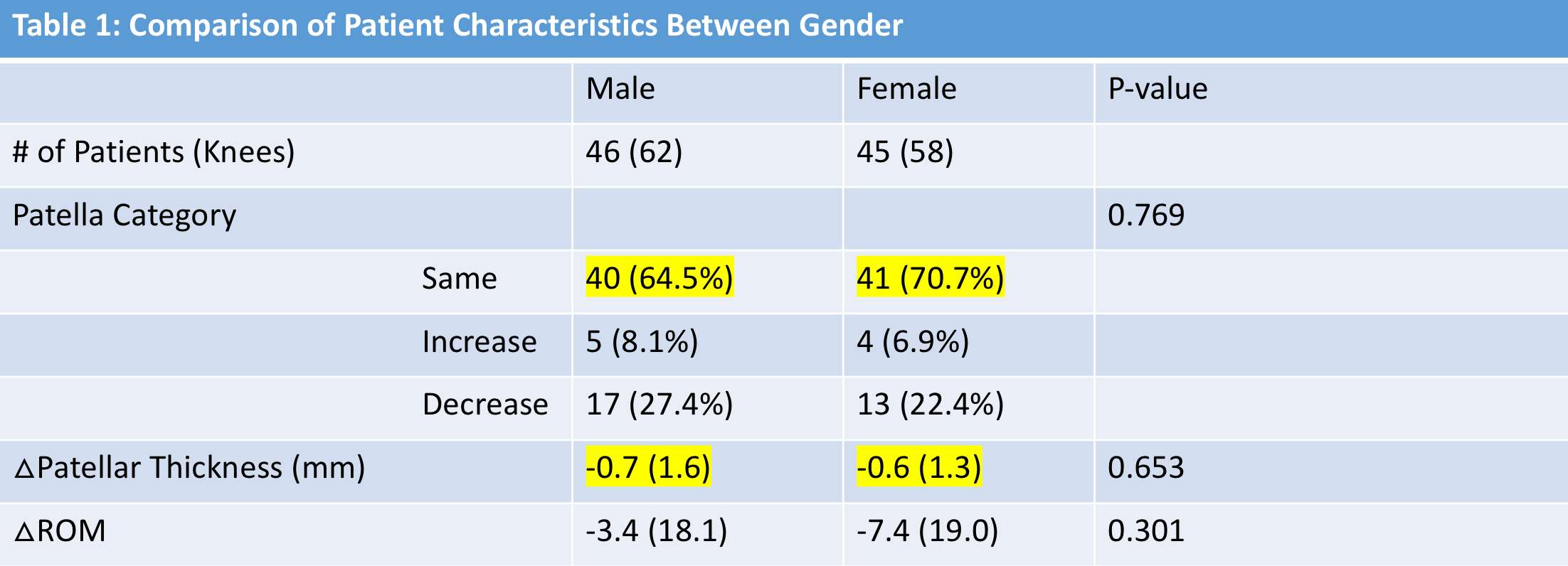
Figure 1
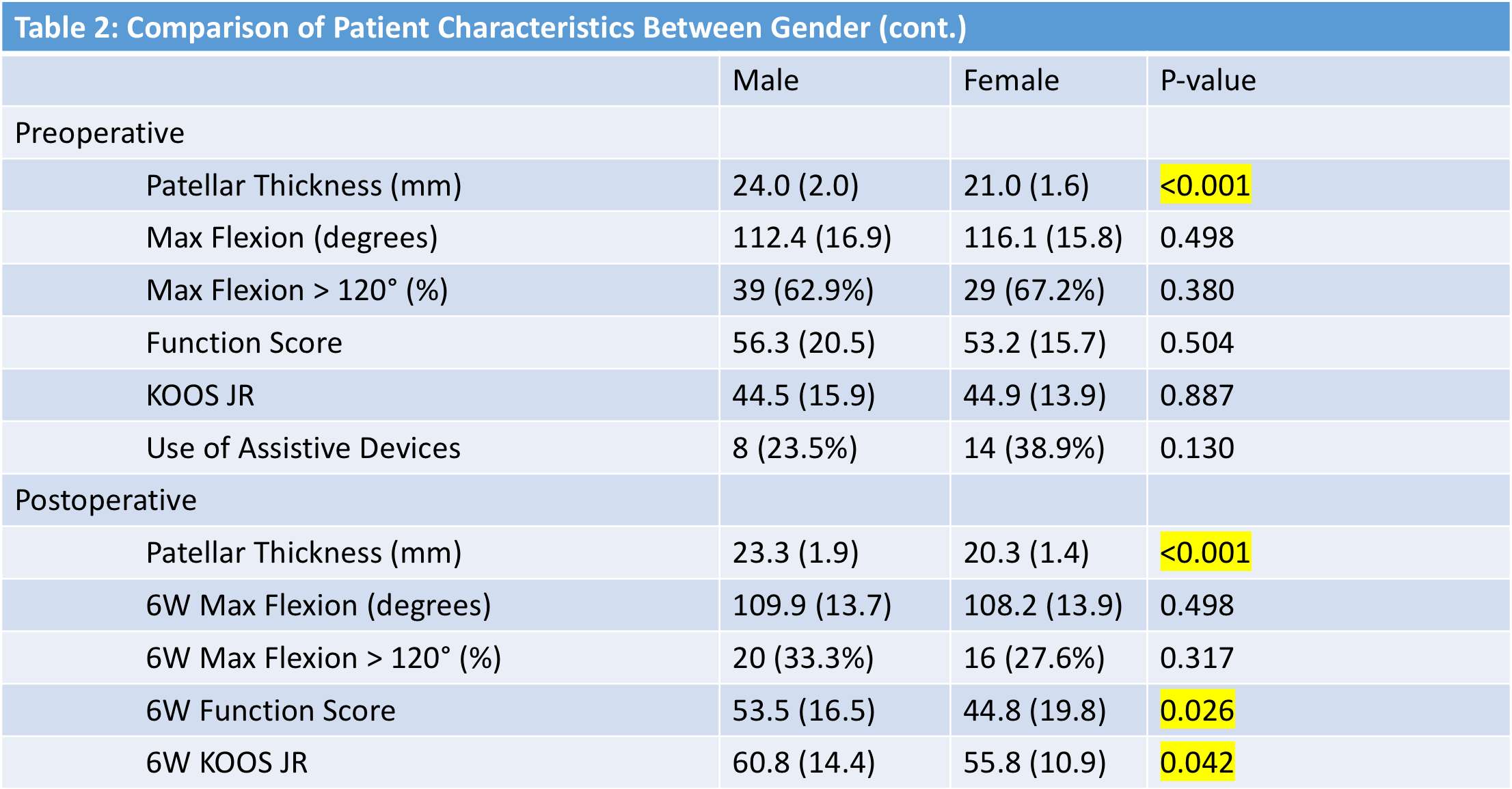
Figure 2

Figure 3#7385
Explant Analysis for Implants Suspected to Cause Revision Surgery
*Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
D.C. Wirtz - University Hospital Bonn - Bonn, Germany
Enrique Gomez-Barrena - Hospital La Paz - Madrid, Spain
Alister Hart - Imperial College - London, UK
Rainer Bader - University of Rostock - Rostock, Germany
Matthias Woiczinski - University Hospital of Munich (LMU) - Munich, Germany
Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: morlock@tuhh.de
Arthroplasty registries are very effective to document the long-term clinical performance of implants. Implant failures comprise today only 2-3% of the reasons for revision surgeries, which is a result of the material and design improvements in combination with the standardization of pre-clinical testing and post market surveillance. The reason for these implant failures, however, are not sufficiently identified and analysed. Explant analysis including patient, clinical and imaging documentation is crucial to identify failure mechanisms to prevent future failures, even if they occur only in small numbers, especially for implants, which are less frequently used. In the past, timely reaction to explant analysis results did not always happen, since detailed explant analysis studies are time consuming and frequently performed after the discontinuation of a product or perceived as singular cases. In order to improve patient safety, a system that screens all explants from revisions attributed to implant failure is mandatory to achieve transparency of the clinical reality and to improve the risk assessment for regulatory processes.
In Germany explants from revision cases directly related to mechanical failure or wear of the implant have to be reported to the BfArM (Federal Institute for Drugs and Medical Devices) and the manufacturer, who is legally mandated to analyze the failed implants. Long response times and inconclusive reports from the manufacturers have resulted in little interest by the surgeons to report cases and provide explants. The desire for a system providing an independent analysis has grown bigger and bigger.
The German Orthopedic Society DGOOC in cooperation with the EFORT Implant and Patients Safety Initiative IPSI has started a pilot study to establish such a system for the collection and analysis of explants. It is hypothesized that most failures are due to already known failure modes, which can be identified with sufficient probability without very detailed analysis by experienced researchers. Fifteen hospitals with high volumes of revision surgeries participate in the study and provide hip and knee explants of cases reported to the BfArM. The required documentation is kept small to reduce the burden for the submitting surgeon. Each explant is screened free of charge by one of the 4 University laboratories strongly experienced in explant analysis (Hamburg, Heidelberg, Munich, Rostock). Simple analysis methods combined with literature and registry results are used to decide whether the reason for failure can be sufficiently assessed or if a detailed explant analysis is indicated. The submitting hospital receives a short report of the result within 4 weeks. The 4 labs share their reports and meet regularly to discuss the process. In the first 3 month of the study, 8 explants of which 7 were fractured revision implants were received, no explant required detailed analysis (Figure 1).
A quickly responding collection and analysis system, which is accepted by the surgeons, will allow to identify implant related problems early and implant categories at higher risk, improving the risk assessment. The study is interposed into the standard process guided by the BfArM and such does not interfere with the legal requirements.
#7447
MyPROM - a New Smartphone App Utilizing Gamification to Acquire PROMs and Patient Activity
*Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
Carlos Marques - Schoen Clinic Hamburg - Hamburg, Germany
Arne Klingenberg - Patient Zero Games - Hamburg, Germany
Fabian Jaeger - Patient Zero Games - Hamburg, Germany
Franziska Fiedler - Schön Klinik Eilbek - Hamburg, Germany
Frank Lampe - Hamburg University of Applied Science
Gerd Huber - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: morlock@tuhh.de
Introduction The importance of Patient-Reported Outcome Measurements (PROMs) as a measure of success after joint replacement, in addition to the revision rate, is continuously increasing. Multiple questionnaires are used (paper&pencil or digital). However, no one solution exists for successful PROM acquisition in total hip (THR) or knee replacement (TKR) [1]. Remote collection of patients activity after surgery would be a meaningful supplement to PROMs [2]. Patients engagement is the crucial basis for both approaches. The aim was to investigate whether patients can be motivated to stay engaged with PROM and physical activity data acquisition with the use of gamification.
Methods In a prospective cohort studythe new Smartphone-App MyProm was tested. The App consists of three parts: (1) monitoring of patient activity, (2) the WOMAC and EQ5D questionnaires and (3) a game section (Figure 1). Patients could answer the questionnaires as often as they wanted, but they were reminded to answer the 2 questionnaires 4 weeks after surgery and then every 3 month by push messages. Activity data were transferred from the Smartphone of the patient to a safe server hosted by TUHH each time a patient completed a questionnaire (Figure 1b). Completing a questionnaire was rewarded by coins, which could be used for the games (Figure 1c). Patients can compete against each other in the games using a pseudonym, assigned to them during their registration in the App (Figure 1a: “Ärger”). The approval for a pilot study (12 month, 100 TKA, 100 THA patients) was obtained from the ethics commission (PV7363). Patient consent was obtained at the first consultation prior to THA or TKA. Due to the rigorous data security laws in Germany, the whole data collection had to be anonymized; age, sex, height, weight and joint treated were the only available patient data.
Results Unexpected problems such as old operating systems proved initially to be a major issue since the patients could not be contacted directly due to the pandemic situation and the German data security issues. Presently 93 THR and 84 TKR patients (mean age THR 64.4 +/-11.0 years, TKA 64.8 +/-9.0 years) are providing data in the study with slightly more females (95 vs 82 males). Patients filled out the questionnaires frequently (THR male 1.2 +/- 1.9 times per week, female 1.1 +/- 2.5; TKR male 2.1 +/- 3.3, female 1.1 +/- 1.0). Activity varied between the patients in both groups (Figure 2). Pain level decreased in both patient cohorts with time after surgery (Figure 3).
Discussion The gamification approach seems to work very well in keeping the patients committed to providing their PROMS and activity data. The study has several limitations such as the activity monitoring through their Smartphone, which is not carried throughout by the participants. The gamification approach should be further investigated.
Acknowledgements: The study has been financially supported by the Health Authority of the State of Hamburg.
[1] Franklin P JBJS 2021; 103(24)
[2] Ramkumar P., JoA 2019; 34(10)
Figures
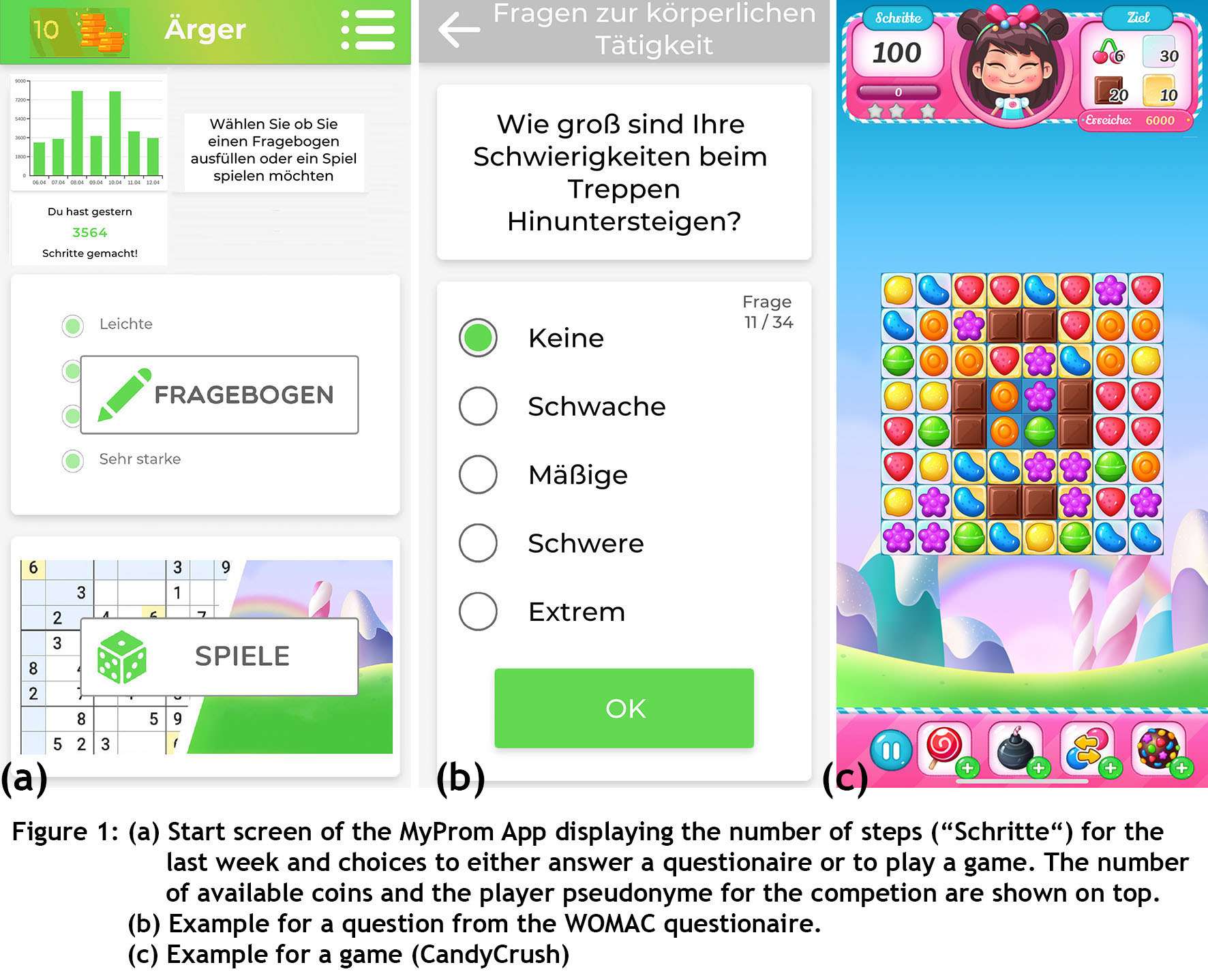
Figure 1
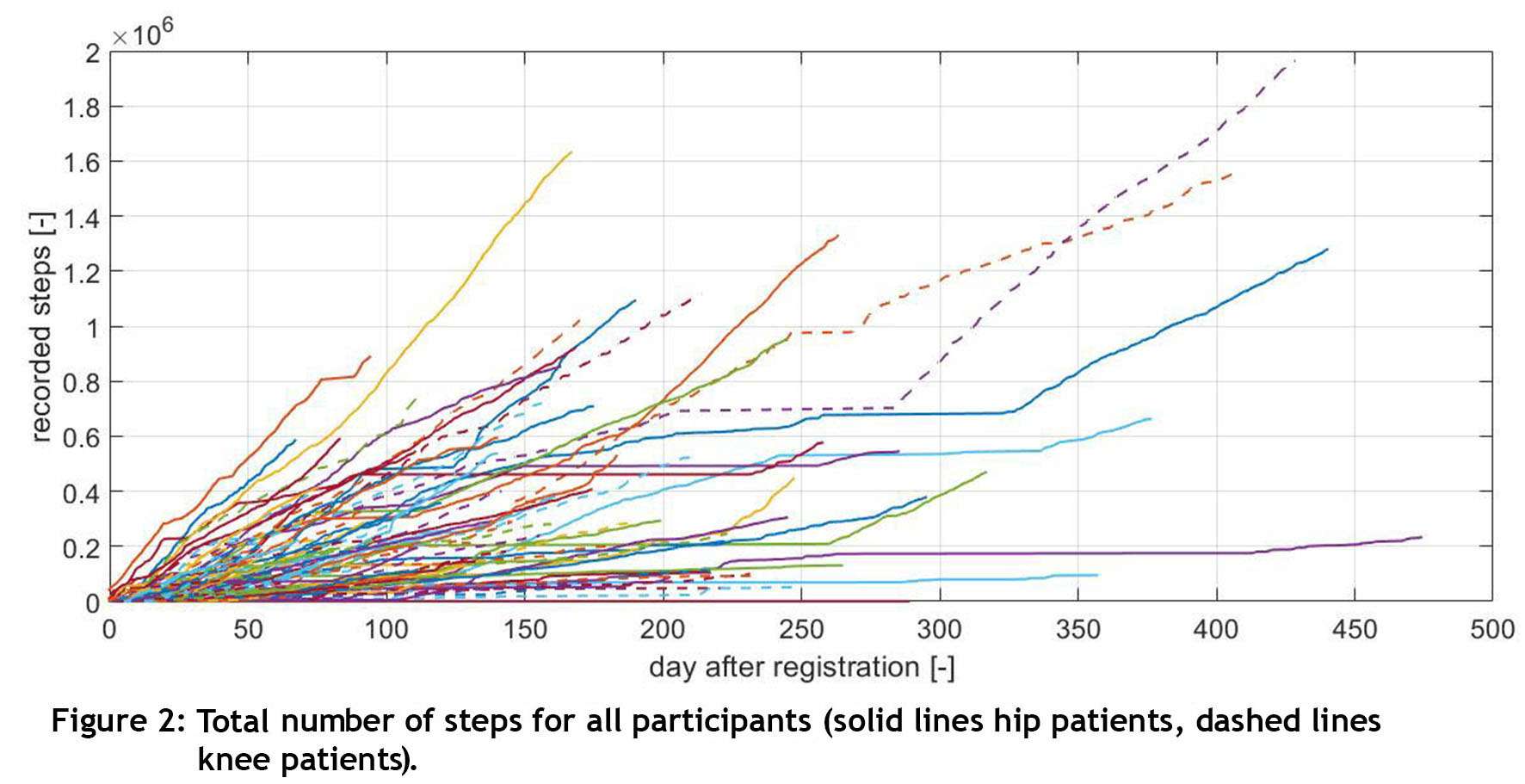
Figure 2
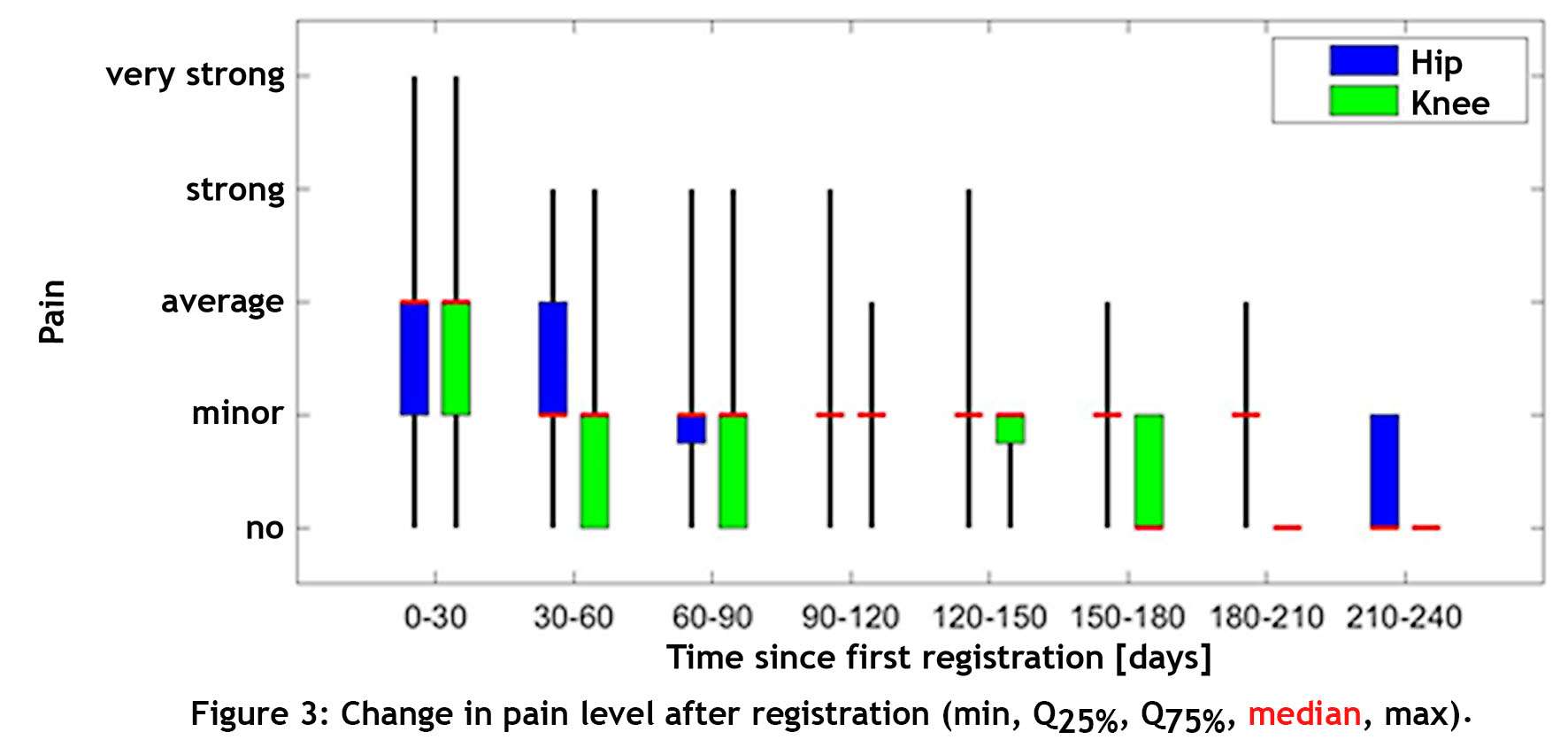
Figure 3#7549
Assessing Concordance in Post-Op Knee Implant Position Analysis Between Automated Image Analysis Algorithm and Human Radiologists
*Arman Motesharei - Stryker - Glasgow, United Kingdom
Kevin de Souza - Stryker - Manchester, United Kingdom
Benjamin Harder - Stryker - Nashville, TN, United States of America
Alexandre Moreau-Gaudry - Centre Hospitalier Universitaire Grenoble Alpes - Grenoble, France
Regis Pailhe - Centre Hospitalier Universitaire Grenoble Alpes - Grenoble, France
*Email: arman.motesharei@stryker.com
Introduction:
Identifying post-op implant position is essential for the analysis of orthopedic implants in knee
replacement surgery. Annotating these landmarks is time-consuming and requires trained medical
specialists. Stryker have developed a methodology for locating implants in post-op CT images where all stages of
the process are automated, thus eliminating human error and variability. Initial results have proven promising and
will be subject to statistical analysis to validate the algorithm's effectiveness.
Methods:
Data:
We analyzed the difference between our image analysis algorithm vs. manual radiologist-defined implant
orientation (Figure 1). Implant orientation is expressed as rotational angles about the X, Y and Z axes
(flexion/extension, varus/valgus and internal/external respectively) for 192 observations – 48 unique patients for
the tibia and femur. Two radiologists participated in this study.
Our analysis aims to determine if concordance exists between two radiologists and the automated
algorithm. The dependent variable is the difference between the algorithm and the radiologist. For example, a
value of zero would mean that the annotation performed by the radiologist is indistinguishable from the algorithm.
For true concordance it is critical that each radiologist agrees with each other in addition to the algorithm.
Therefore, the model will evaluate corroboration between both the radiologists and the algorithm. This analysis
seeks not to reject but accept the null hypothesis. Since frequentist statistical approaches do not offer a way to
accomplish this easily, Bayesian methods were used because they provide greater flexibility and interpretability.
Model specification:
We developed a novel statistical model using proven Bayesian methods to determine the difference
between the accuracy of the algorithm and both radiologists. In addition, given the innovative nature of this
research, we selected broad priors to represent the uncertainty in the data, minimizing their influence on the model.
Lastly, the femur and tibia were modeled independently, given fundamental differences in the underlying anatomy
of each bone.
The model assumed a varying intercept by patient but a fixed slope. This approach reduced model
complexity but introduced the assumption that their difference would be consistent while radiologists might
vary. For this study, we propose a Region of Practical Equivalence (ROPE) to +/- 0.5 degrees of accuracy along
with the following decision rules. If the posterior density falls within the ROPE, there is concordance between the
radiologists and the algorithm; alternatively if 95% of the posterior highest density interval (HDI) excludes the
ROPE, there is no concordance. Lastly, if part of the HDI excludes the ROPE, a decision will be withheld.
Results:
We found concordance for both varus/valgus and internal/external rotation angles for the femur, while
flexion/extension was inconclusive. The same results were observed for the tibia. For femoral flexion/extension
angle, both radiologists disagreed with the algorithm and each other. In contrast for tibial flexion/extension the
annotations of neither radiologist corroborated with the algorithm (Figure 2).
Conclusion:
Based on the model results, we conclude that algorithmically generated landmarks are indistinguishable
from human-generated for both varus/valgus and internal/external rotation angles for both the tibia and femur.
However, there is not enough data to conclude that the same is true for the flexion/extension angle; meaning this
is a difficult parameter to measure. Future research with multiple radiologists will be required to continue
monitoring the algorithm's performance.
Figures
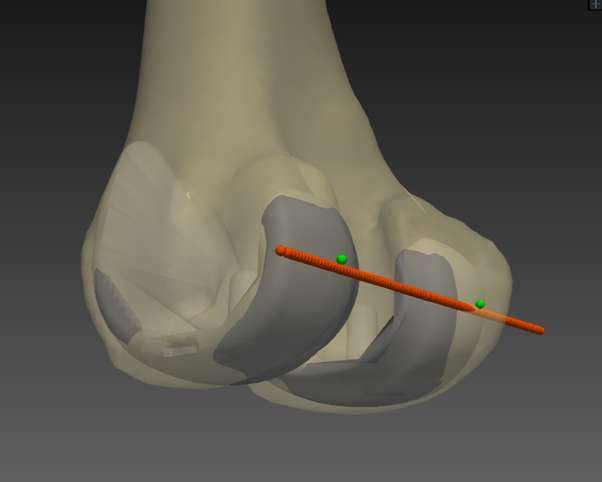
Figure 1
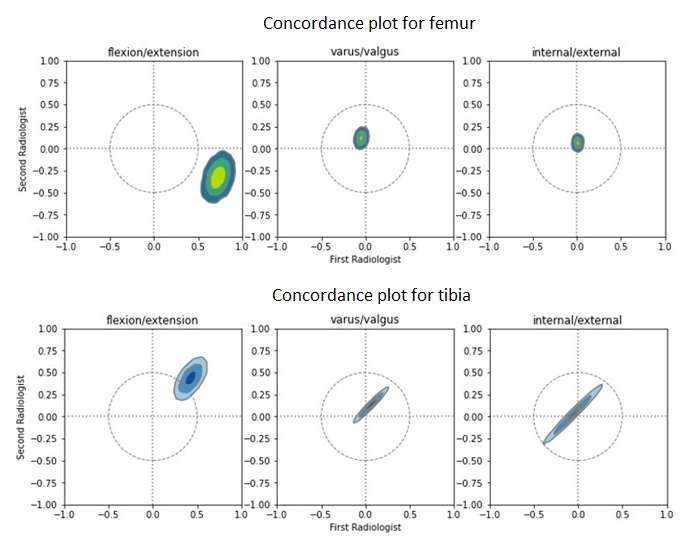
Figure 2
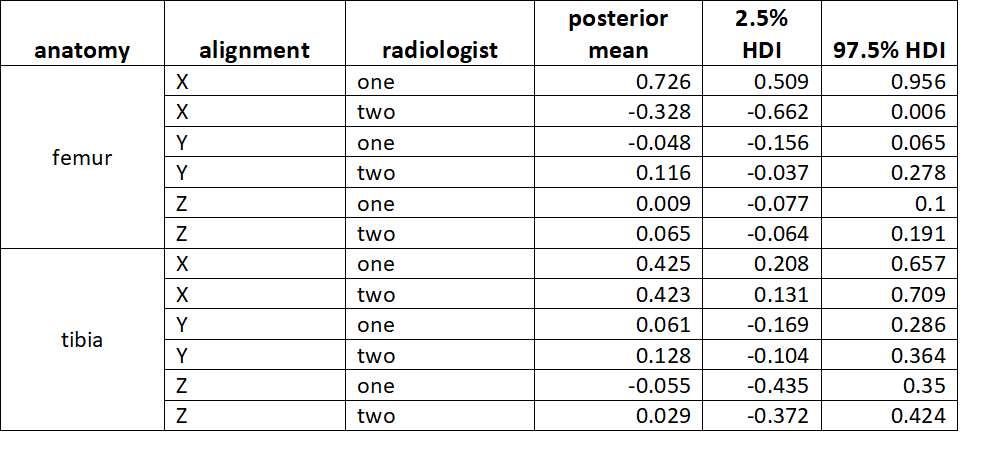
Figure 3#7332
Total and Partial Knee Replacement Implants That Maintain Native Load Transfer in the Tibia
*Maxwell Munford - Imperial College London - London, United Kingdom
Jonathan Jeffers - Imperial College London - London, United Kingdom
Jennifer Stoddart - Imperial College London - London, United Kingdom
Alexander Liddle - Imperial College - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
*Email: mjm214@ic.ac.uk
Introduction
Unicompartmental and total knee arthroplasty (UKA and TKA) are successful treatments for osteoarthritis, but monolithic solid metal implants disrupt the natural homeostasis of bone which leads to bone loss over time. This can cause problems with long-term fixation and loss of bone density which is a significant issue if the implant needs to be revised.
This study aimed to demonstrate that tibial implants made from titanium lattice could replace the tibial condyle surface while minimising disruption of the bone’s natural mechanical loading environment. A secondary aim was to determine whether implants perform better if they replicate more closely bone’s mechanical modulus, anisotropy and spatial heterogeneity. This study was conducted in a human cadaveric model.
Methods
In a cadaveric model, UKA and TKA procedures were performed on 8 fresh-frozen knee specimens by a board-certified consultant orthopaedic surgeon, using tibial implants made from (a) conventional monolithic solid metal and (b) titanium lattice structures. 4 titanium lattice implant variants were manufactured by powder bed fusion with varying degrees of matching between implant modulus and the surrounding bone. Implant variants mechanical properties were: 113GPa (solid metal), 0.6GPa (matching average tibial bone modulus), 0.6GPa (matching average tibial bone modulus and anisotropy), 3.3GPa (compromise between modulus matching and implant strength) and 0.4-0.7GPa (graded modulus precisely matching bone).
Stress at the bone-implant interface was measured with pressure film and compared to the native knee. Comparisons between all implant cases and the native knee were made for maximum stress, area underloaded and the similarity of the stress distribution (Jaccard similarity).
Results
All titanium lattice implants were able to restore the mechanical environment seen in the native tibia for both UKA and TKA (Figures 1 and 2). Maximum stress at the bone-implant interface ranged from 1.2-3.3MPa for titanium lattice implants compared to 1.3-2.7MPa for the native tibia (Table 1). In contrast, conventional UKA and TKA implants both reduced the maximum stress in the bone by a factor of 10.
Titanium lattice UKA and TKA implants caused negligible underloading of bone surface area compared to the native tibia. For titanium lattice UKA and TKA implants the stress distribution at the bone-implant interface was at least 71.2% and 67.8% similar to the native case, whereas in conventional UKA and TKA the stress distribution was only 19.8% and 20.5% similar to the native case respectively (Table 1). The conventional UKA and TKA implants underloaded 71%-77% of the bone surface.
Conclusions
Titanium lattice implants can maintain the natural mechanical loading in the proximal tibia after UKA and TKA. They maintain maximum stress and a stress distribution which closely matches the native tibia and underload only a very small area of bone-implant interface. No differences were determined between the 4 titanium lattice variants.
Implants like these may help maintain normal bone homeostasis throughout the life of the implant using manufacturing methods already in widespread use, possibly leading to improved biologic fixation and long-term bone density maintenance. This would maintain bone quality throughout the life of the implant and alleviate complications at revision surgery.
Figures
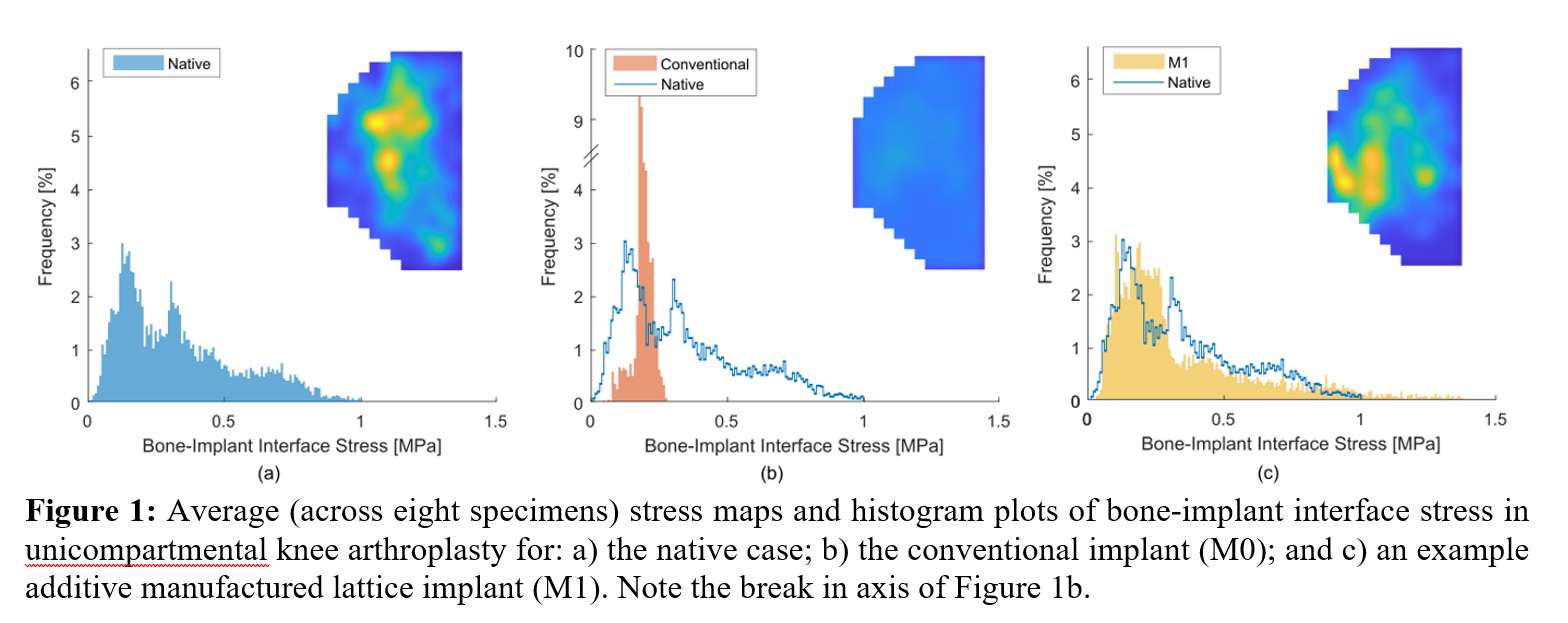
Figure 1
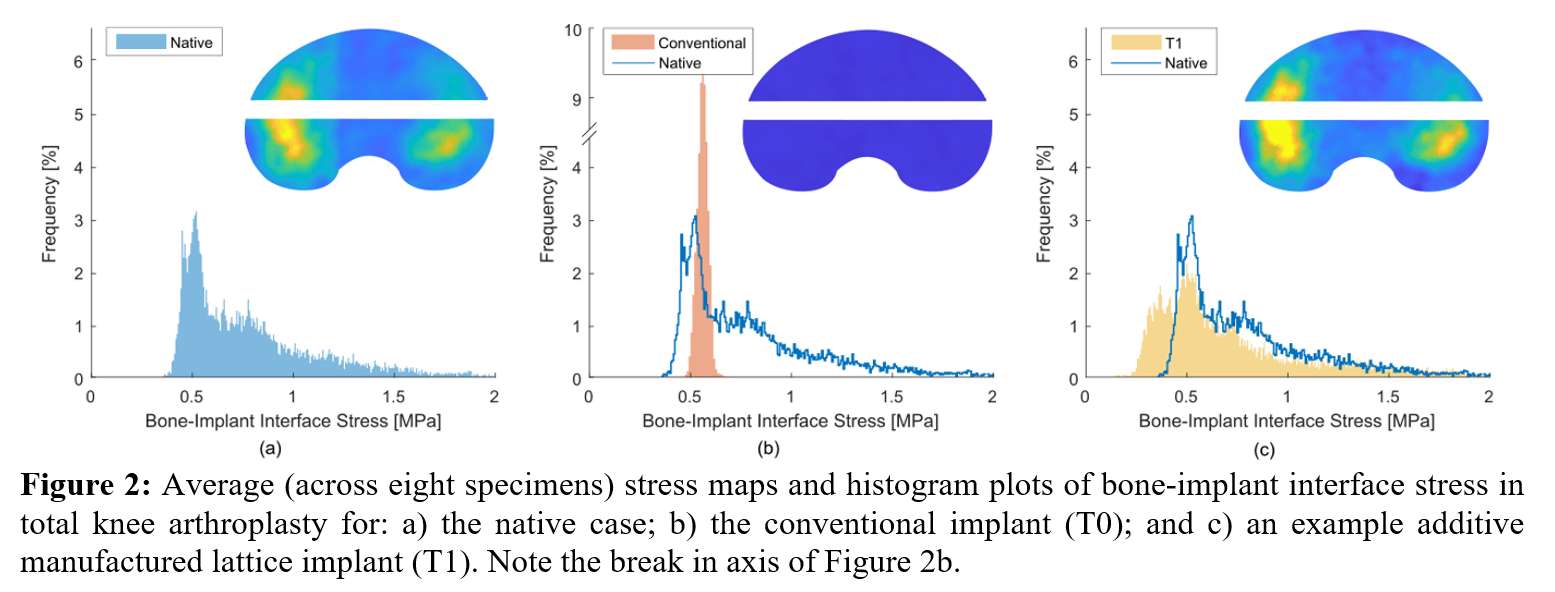
Figure 2
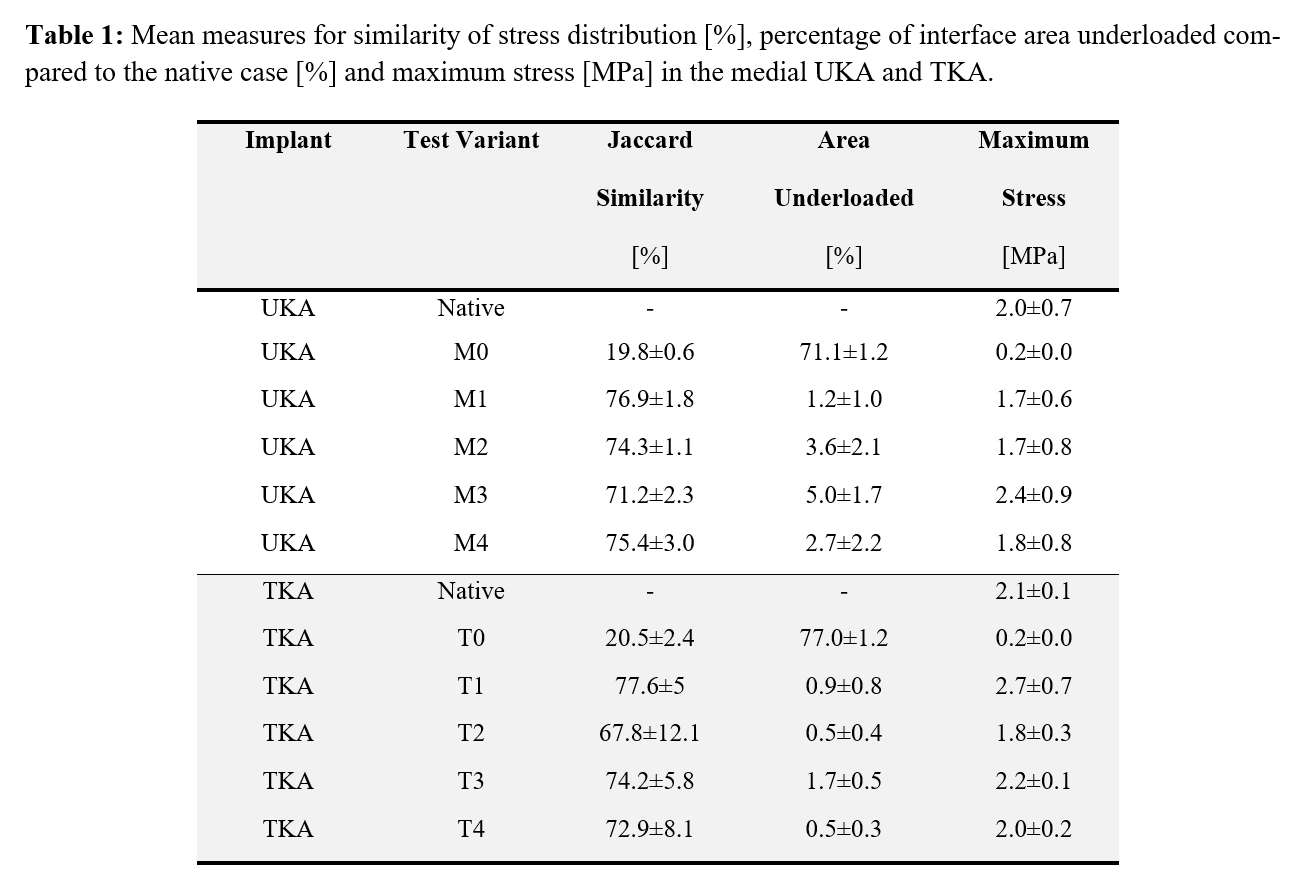
Figure 3#7753
Knee Simulator Wear Performance of CoCr and IBED TiN-Coated Femoral Components Against UHMWPE
Brad Micheli - Massachusetts General Hospital - Boston, USA
Keith Wannomae - Massachusetts General Hospital - Boston, USA
Chris Weaber - TJO Inc. - Salt Lake City, USA
Anna Sullivan - Total Joint Orthopedics - Salt Lake City, USA
*Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
*Email: omuratoglu@partners.org
INTRODUCTION
Cobalt chrome femoral components have been used successfully in knee replacements for decades. The rising incidence of metal sensitivity makes finding an alternate material important. Aurum® femoral components utilize a novel Ion Beam Enhanced Deposition titanium nitride coating applied to a Ti6Al4V femoral component. Aurum femoral components could provide an improved articulating surface but must be shown to not adversely affect the wear rate of UHMWPE and to resist scratching from third body particles which could lead to increased long-term wear of UHMWPE.
METHODS
Ultra-PS® GUR 1050 UHMWPE inserts were accelerated aged per ASTM F2003 [1] and then subjected to simulated gait at 1.0 Hz for wear testing against CoCr and Aurum femoral components. Wear testing was carried out using ISO 14243-3 kinematic waveforms with an increased peak axial load of 3200 N in 37°C bovine serum prepared per ISO 14243-3 [2]. Testing was interrupted every 0.5 million cycles (MC) where tibial bearings were washed, weighed, and photographed. Constructs were tested to a total of 5MC of gait, at which time femoral components were articulated against 400 grit sandpaper (Fig 1), and then the same constructs were tested for a further 3.5MC of gait. Wear rates of the tibial bearings were calculated by correcting for fluid absorption with matched load-soak components and then applying a linear regression on weight measurements excluding the first 0.5MC of testing in each phase. Wear particles were isolated from used serum during both phases of testing and analyzed via scanning electron microscopy. Groups were compared with a Student’s t-test, with a p<0.05 indicating a significant difference.
RESULTS
The calculated linear wear rate of bearings articulating against CoCr femoral components was 52.5 milligrams per million cycles (mg/MC) ± 4.1, which increased (p=0.01) to 71.6 mg/MC ± 0.9 after the femoral components were scratched with sandpaper (Fig 2). The calculated linear wear rate of bearings articulating against Aurum femoral components was 47.4 mg/MC ± 1.7 and held steady (p=0.14) at 43.1 mg/MC ± 2.7 after the Aurum femoral components were scratched. The distribution of wear particle size or shape was equivalent between all scratched and unscratched samples.
CONCLUSION
Aurum femoral components provide a durable articular surface for knee replacements and are a viable alternative to traditional CoCr femoral components. UHMWPE bearings articulating against pristine Aurum femurs had a similar wear rate to bearings articulating against CoCr femoral components. Furthermore, the Aurum femoral components resisted scratching, showing a 40% lower UHWMPE wear rate as compared to scratched CoCr femoral components (p=0.002). Therefore, third body particles should not adversely affect the long-term wear of the UHMWPE bearing when coupled with Aurum femoral components.
REFERENCES
[1] ASTM Standard F2003, 2015, "Standard Practice for Accelerated Aging of Ultra-High Molecular Weight Polyethylene after Gamma Irradiation in Air," ASTM International, West Conshohocken, PA, 2015.
[2] International Organization for Standardization. (2014). Implants for surgery – Wear of total knee-joint prostheses – Part 3: Loading and displacement parameters for wear-testing machines with displacement control and corresponding environmental conditions for test (ISO Standard No. 14243-3:2014).
Figures
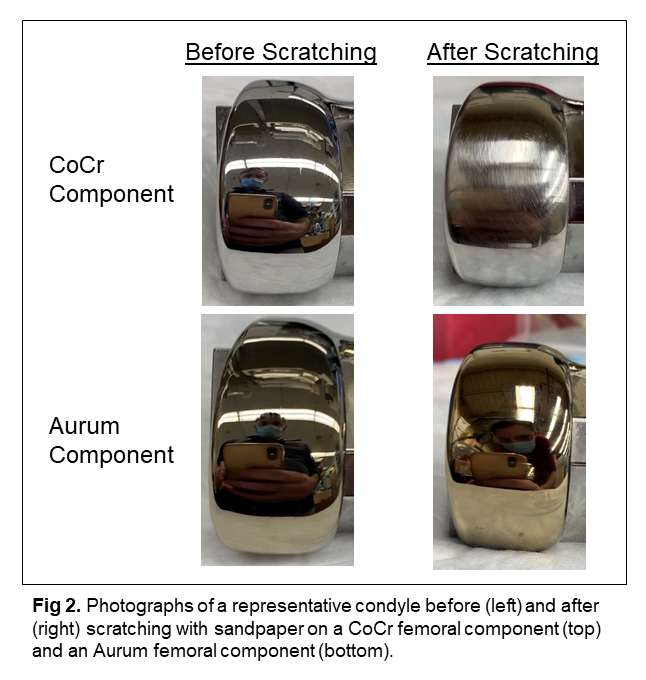
Figure 1
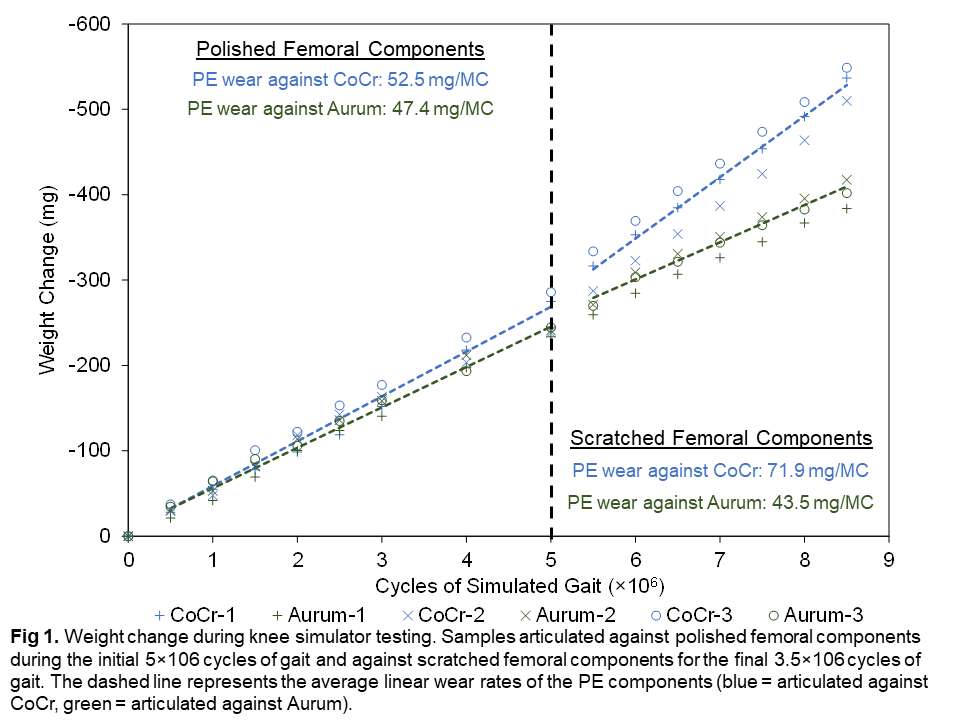
Figure 2#7804
Oxidative Changes in Irradiated and Melted Polyethylene Tibial Inserts During Second Decade of in Vivo Service
Keith Wannomae - Massachusetts General Hospital - Boston, USA
David Chan - Massachusetts General Hospital/Harris Orthopaedic Lab - Boston, USA
Jacquelyn Dunahoe - Massachusetts General Hospital - Boston, USA
Andrew Freiberg - Massachusetts General Hospital - Boston, USA
*Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
*Email: omuratoglu@partners.org
INTRODUCTION
Highly crosslinked irradiated and melted polyethylene (HXLPE) was developed to minimize wear particle induced osteolysis and was thought to have long term oxidative stability due to the absence of residual free radicals. We have since learned that the absorption of reactive species from the synovial fluid along with cyclic loading could alter the stability of UHMWPE [1,2]. Here we present the analysis of two long-term implanted HXLPE knee components.
METHODS
Both explanted bearings were fabricated from Prolong HXLPE, which, according to the manufacturer, is GUR1050 that was warm e-beam irradiated to 65 kGy and subsequently melted. Component HK-21-011 was explanted after 156 months in vivo, and component HK-21-033 was explanted after 187 months in vivo. Thin films were cut from the cross-section of the condyle, and additional blocks were cut from the cross-section of the component and quartered (Fig 2). The films were boiled in hexanes for 16 hours, dried, and analyzed via Fourier transform infrared spectroscopy (FTIR) per ASTM F2102 [3], and the blocks were analyzed to determine crosslink density [1].
RESULTS
Both bearings exhibited yellowing, indicating absorbed species from long-term in vivo use, and both had patches of embrittlement and possible oxidative damage on the articular surface (Fig 2).
Component HK-21-011: A large subsurface oxidation peak (OI = 4.0 ± 0.2) was observed approximately 0.8 – 0.9 mm below the articular surface. A smaller oxidation peak (OI = 0.13 ± 0.07) was seen on the backside, with OI levels essentially at 0 in bulk. The crosslink density measured at the articular surface (Q1) was 0.071 mol/dm3 ± 0.033, a sharp decrease from the bulk material’s crosslink density of 0.225 mol/dm3 ± 0.001 and 0.224 mol/dm3 ± 0.014 for Q2 and Q3, respectively. The component backside (Q4) also showed much lower crosslink density (0.073 mol/dm3 ± 0.035), even though it did not show the same level of oxidation.
Component HK-21-033: A subsurface oxidation peak (OI = 1.2 ± 0.2) was also observed approximately 1.7 – 2.0 mm below the articular surface, though no oxidation was seen on the backside or bulk. The crosslink density measured at the articular surface was 0.078 mol/dm3 ± 0.009, a decrease from the bulk material’s crosslink density of 0.232 mol/dm3 ± 0.021, 0.240 mol/dm3 ± 0.012, and 0.242 mol/dm3 ± 0.005 for Q2-Q4, respectively.
CONCLUSION
Neither component was revised due to polyethylene-related complications. While the data here supports previous findings showing that the in vivo environment can affect some materials, the induced oxidative changes did not yet appear to affect the material’s performance.
REFERENCES
[1] Muratoglu OK, et al. J Bone Joint Surg Am. 2010 Dec; 92(17): pp 2809-16.
[2] Oral E, et al. J Biomed Mater Res B Appl Biomater. 2012 Apr; 100(3): pp. 742-51.
[3] ASTM Standard F2102, 2017. ASTM International, West Conshohocken, PA, 2017.
Figures
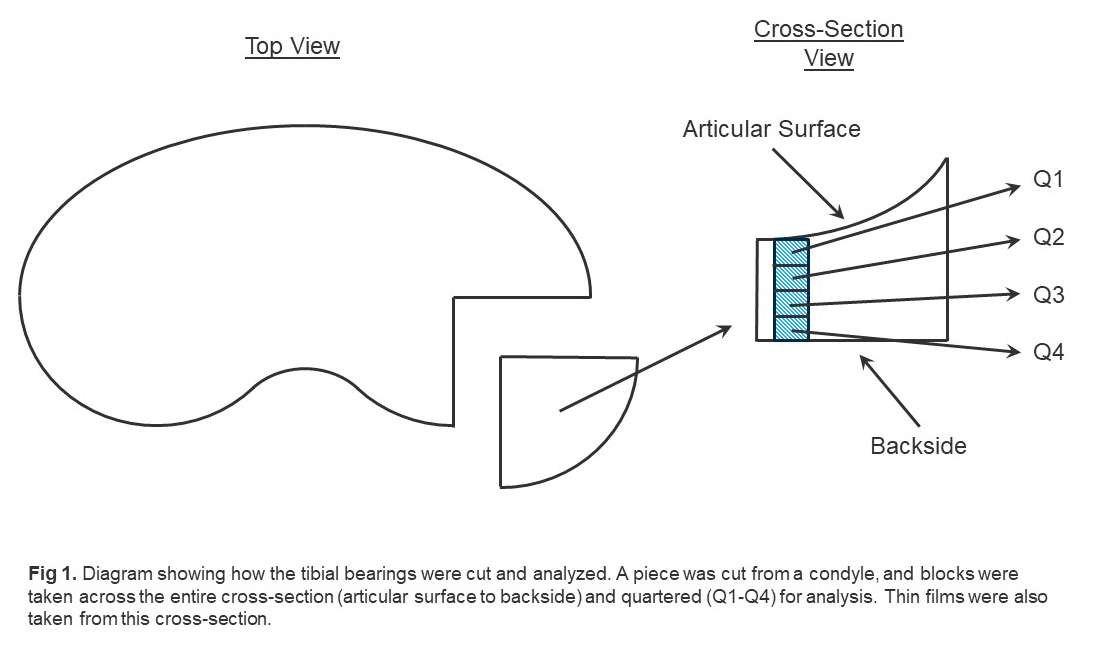
Figure 1
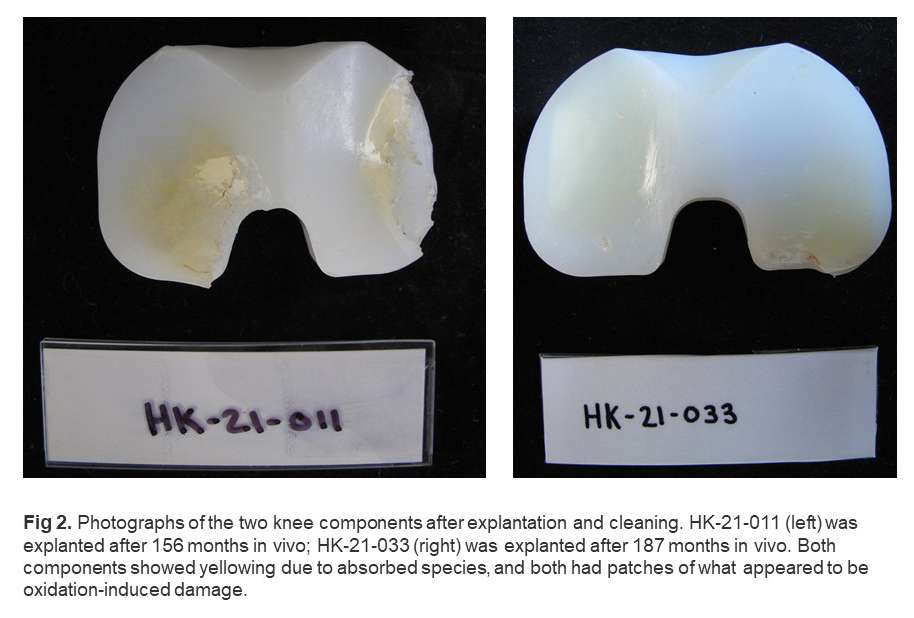
Figure 2#7716
The GPE Spacer: An Antibiotic-Loaded Total Knee Prosthesis Made From Ultra-High Molecular Weight Polyethylene (UHMWPE)
Cecilia M. Nepple - Massachusetts General Hospital - Boston, USA
Meghna Krishnagiri Tupal - Massachusetts General Hospital - Boston, USA
Keith Wannomae - Massachusetts General Hospital - Boston, USA
Brad Micheli - Massachusetts General Hospital - Boston, USA
Rachel Connolly - Massachusetts General Hospital - Boston, USA
Ali Atici - Massachusetts General Hospital - Boston, USA
Alireza Borjali - Harvard Medical School/ Massachusetts General Hospital - Boston, USA
Ebru Oral - Massachusetts General Hospital - Boston, USA
*Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
*Email: omuratoglu@partners.org
Introduction: Currently, periprosthetic joint infection (PJI) is the leading cause of arthroplasty failure. While only prevalent in 1-2% of surgeries, PJI has a mortality rate that rivals some forms of cancer.1 The primary treatment is two-stage revision arthroplasty where a temporary spacer is implanted, typically composed of antibiotic-loaded bone cement. However, these spacers suffer from poor material strength.2 This property limits both the dose of antibiotic and the mechanical function of the knee. In this study, we elaborate on our previous work developing the GPE spacer for the treatment of PJI.3
Methods: Gentamicin sulfate was incorporated into UHMWPE (9wt% GPE) by compression molding (Figure 1). The tibial component molded GPE atop a highly crosslinked UHMWPE base. Machining exposed the crosslinked UHMWPE on the load-bearing surfaces. The femoral component was uniformly fabricated with GPE. Mechanical testing included tensile, IZOD, pin-on-disc (POD), and AMTI knee simulation. For elution, full devices were fixed with bone cement and eluted into 100-300mL of PBS (volume depending on size) at 37°C and 100rpm. The eluent was characterized using o-phthaldialdehyde tagging.4 Intraarticular drug concentration was estimated by a single-component pharmacokinetic model. The synovial half-life was assumed to be 7 hours and 3 hours (worst-case scenario).5,6
Results: Mechanical testing showed insignificant change in elongation at break, IZOD impact strength, and POD wear in GPE concentrations up to 10wt%, suggesting dose-independent material strength (Figure 2A). While bone cement had higher ultimate tensile strength, GPE was more ductile, decreasing the relative risk of device fracture. Additionally, GPE exhibited a reduction in gravimetric wear, likely due to drug elution over the first one million cycle of simulation (Figure 2B). Its wear was 356mg/MC. In contrast, bone cement wear was reported as 1003mg/MC.7
The pharmacokinetic model suggested that the GPE spacer could maintain antibiotic concentrations above minimum inhibitory concentration (MIC) for S. Aureus (4µg/mL) for more than 180 days using the worst-case scenario (Figure 3). Bone cement’s drug concentration dropped below MIC after Day 50. Despite bone cement’s large initial burst, the GPE spacer outpaced the bone cement elution rate within 4 to 6 hours. The reduced burst could be attributed to manufacturing. GPE was pre-formed and washed. Washing eliminated drug at the surface, which was present in the intraoperatively molded bone cement.
Conclusion: There is no in vitro data dictating the duration and required levels of locally delivered antibiotics for PJI treatment.2 However, the GPE spacer offers major advancements in the availability of drug at steady state and accordingly, more antimicrobial activity relative to bone cement devices. Our novel device not only outperforms bone cement in all relevant elution parameters, but it ultimately offers markedly improved wear, material strength, and standardized drug formulation. The results support the possible use of GPE as a more effective spacer for two-stage revision arthroplasty.
[1] Rezapoor et-al. J.Arthroplasty (2015); [2] McLaren et-al. PJI of the Hip and Knee (2014); [3] Gil et-al. BoneJt.J (2020); [4] Gubernator et-al. IntJ.Pharm (2006); [5] Grigoletto et-al. Cienc.Rural (2020); [6] Pezzanite et-al. FrontVet.Sci (2021). [7] Villa et-al. Knee (2007).
Figures
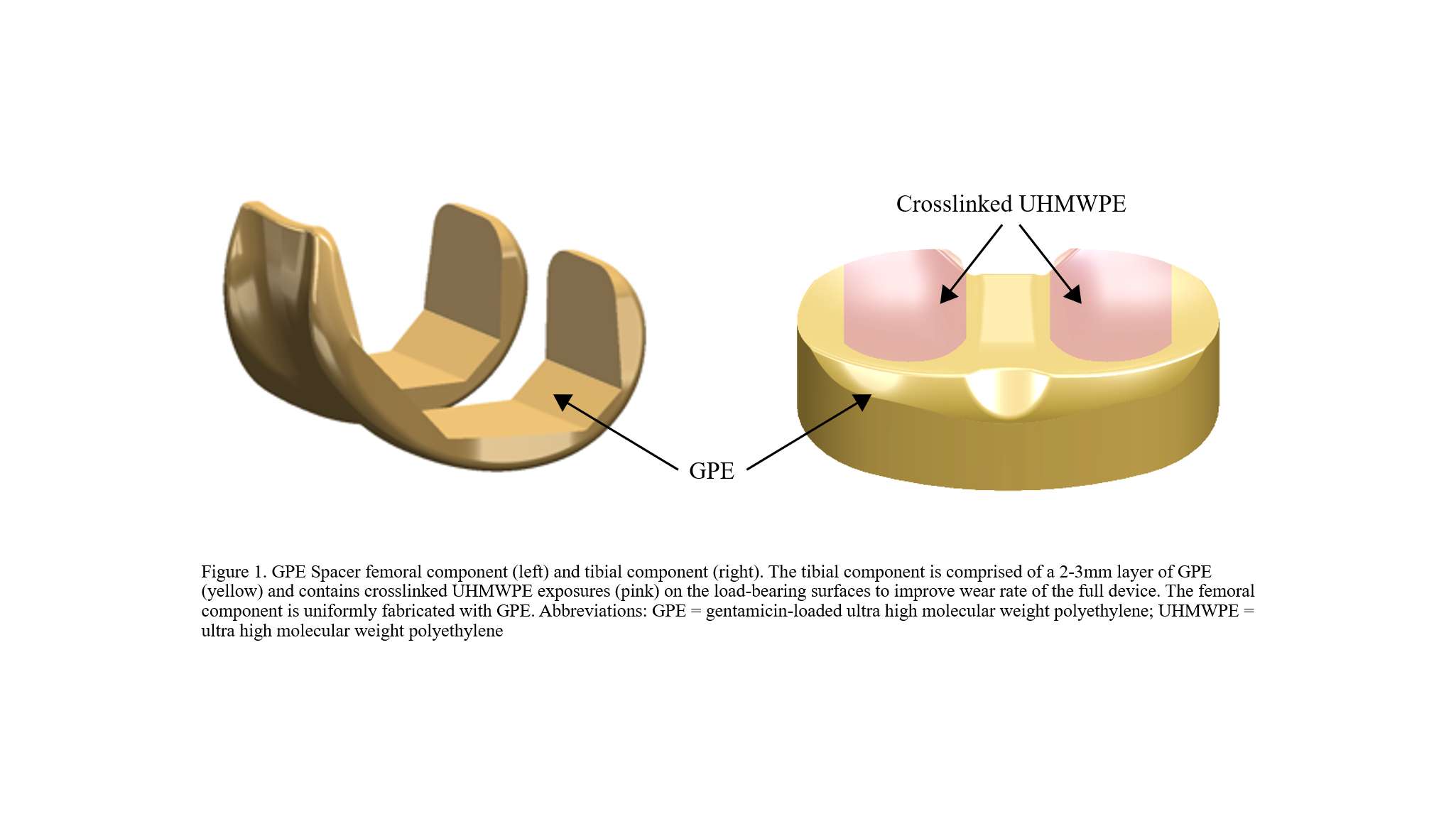
Figure 1
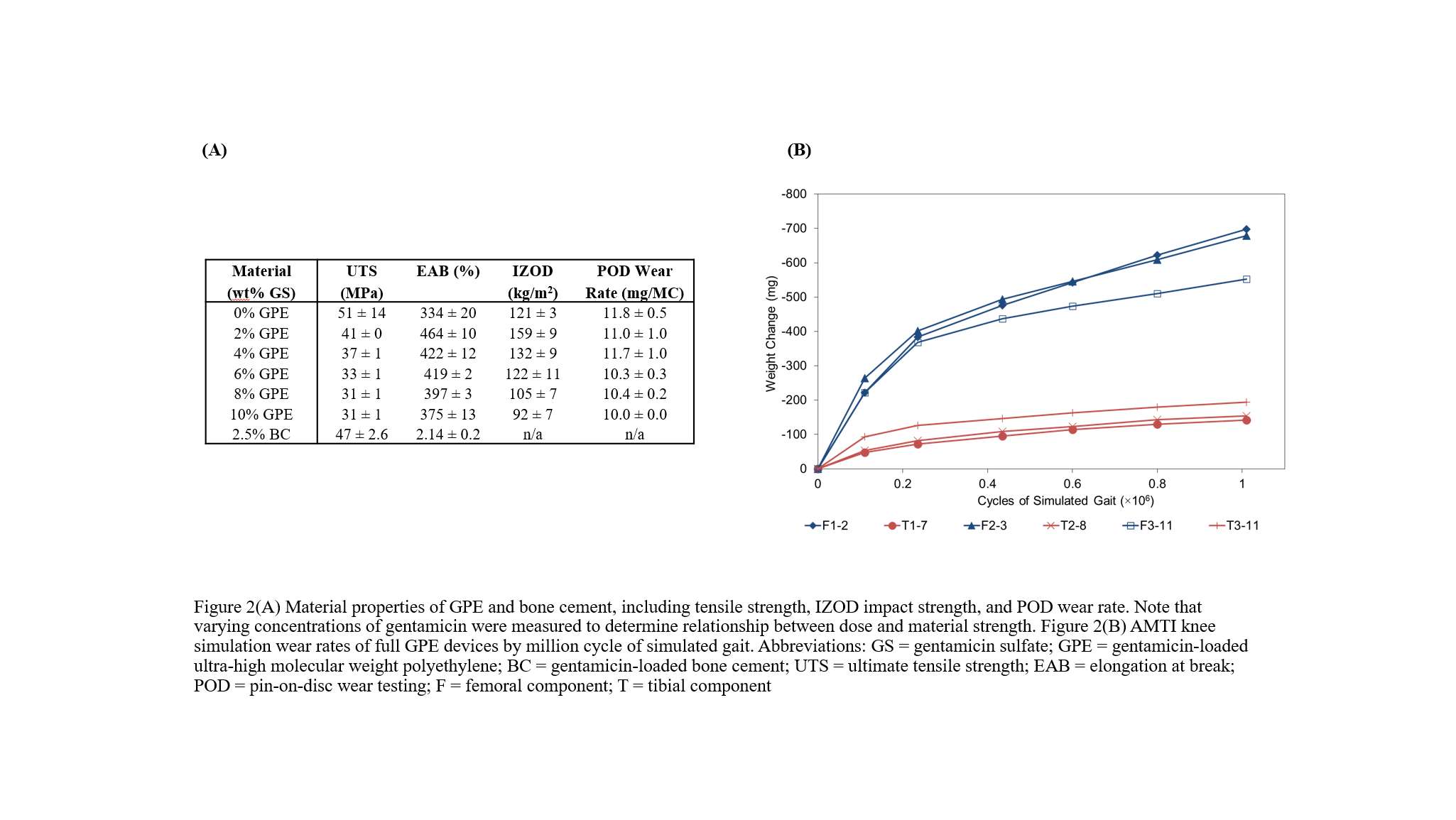
Figure 2
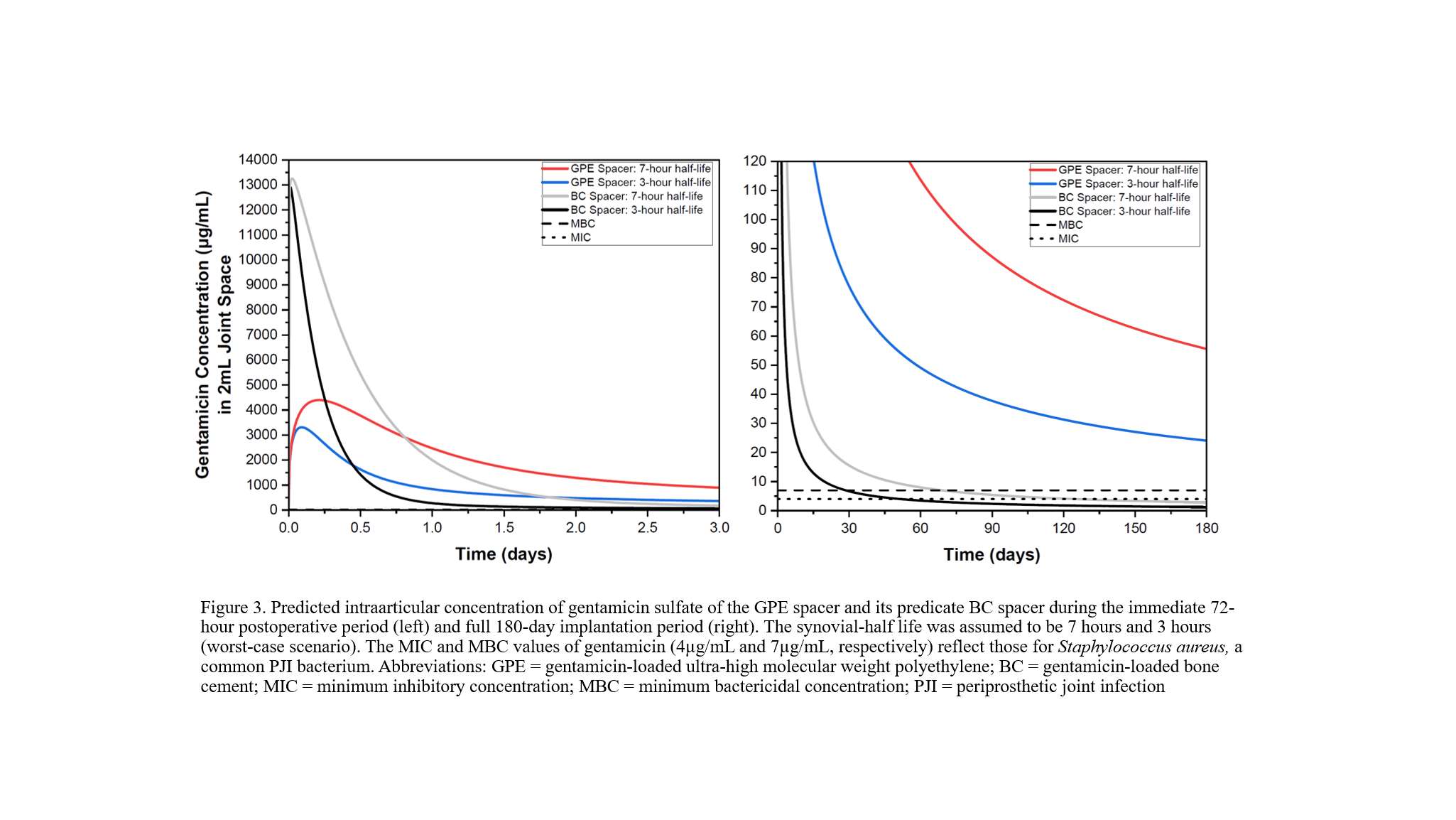
Figure 3#8043
Invited Talk : Clinical Introduction of a Chemically Crosslinked UHMWPE
*Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
Ebru Oral - Massachusetts General Hospital - Newtonville, USA
Brinda Badwe - Stryker - USA
Rachel Connolly - Massachusetts General Hospital - Boston, USA
Keith Wannomae - Massachusetts General Hospital - Boston, USA
Mehmet Asik - USA
Cecilia M. Nepple - Massachusetts General Hospital - Boston, USA
*Email: omuratoglu@partners.org
Ultra-high molecular weight polyethylene (UHMWPE) has undergone many iterations over the past two decades. In 1990s, UHMWPE particulate induced periprosthetic osteolysis and oxidation induced damage in UHMWPE implants were the dominant causes of revision in total joint patients. We addressed these by first eliminating air from packaging in gamma sterilized implants, followed by the clinical introduction of radiation crosslinked and thermally stabilized polyethylenes. More recently, added antioxidants further improved the oxidative stabilization of UHMWPE implants. These advances, particularly high levels of crosslinking, resulted in excellent clinical outcomes in total hips, knees, and shoulders. While all highly crosslinked UHMWPEs in clinical use are treated with ionizing radiation, chemical crosslinking with peroxides is also an option. We demonstrated that peroxide crosslinking (PRX) of UHMWPE is a viable technique and requires antioxidant stabilization. The technique comprises blending di-cumyl peroxide (DCP), vitamin-E and polyethylene followed by consolidation, during which UHMPE crosslinks. DCP undergoes thermal dissociation into peroxy free radicals that abstract protons from UHMWPE and lead to its crosslinking. The residual by-products of DCP are small molecules that are then removed by high temperature melting (HTM) of the consolidated blend. We optimized the formulation and the HTM cycle to reduce the concentration of the by-products to well below those that could raise toxicological concerns. The optimized formulation can be gamma sterilized without any stability concerns. Wear resistance is comparable to those of other clinically successful formulations. In addition, the PRX-HTM polyethylene has higher strength, ductility, and toughness than other crosslinked polyethylenes – these are properties that could improve long-term performance in high-demand patients. The FDA cleared the use of this technology in tibial knee inserts and patellae components in a specific total knee replacement implant system. As gamma radiation availability is becoming more scarce, peroxide crosslinked and high temperature melted UHMWPE will be a feasible option for continued clinical success of highly crosslinked UHMWPE implants.
#8005
Accurate Xray Measurement of Acetabular Cup Positioning Using Biplanar Xrays: A CT Validation of EOS Measurements
William Murphy - Harvard Medical School - Boston, USA
*Stephen Murphy - New England Baptist Hospital - Boston, USA
Dan Sun - Tufts University - Boston, USA
Patrick Lane - Surgical Planning Associates - USA
Jens Kowal - USA
*Email: stephenbmurphymd@gmail.com
Introduction:
Accurate acetabular component positioning is paramount to the success of total hip arthroplasty. The utility of the historic Lewinnek “safe zone” has recently been called into question and has been replaced by the concept of “functional safe zones”. These zones vary based upon individual patient spinopelvic pathology and achieving these goals requires precise methods of component placement. Intraoperative 2D imaging alone remains a popular tool for implant position assessment despite its known limitations[1]. Therefore, the purpose of this study was to evaluate the accuracy of a novel method for assessing acetabular component position based upon EOS biplanar Xray images.
Methods:
Thirty consecutive patients who underwent preoperative evaluation for THA with CT imaging and biplanar Xray imaging with the EOS system and also had a pre-existing implant were selected for this study. The operative inclination and operative anteversion of the acetabular cup were measured directly on CT as the ground truth, and then again measured using an EOS biplanar Xray reconstruction as described below. The EOS measurements were compared to the CT measurements to determine accuracy. All cases were measured by the senior author.
The EOS biplanar measurement methodology was created as follows: Standard Standing AP and lateral EOS images were taken. According to Groisser et al [2] the images were positioned in the iso center of the EOS coordinate system. An AP-Plane was constructed for each patient by digitizing and back-projecting ASIS- and Symphysis-points in both the ap- and lateral-EOS images. Subsequently, an initial 3d cup center was defined using the same projection mechanism, and 3D surface models of the acetabular components were created and positioned in the 3D reconstruction (Figure 1).
Using the fan-beam projection model from the EOS images, all vertices defining the cup model were projected on the EOS images as semi-transparent dots. Finally the operative anteversion and inclination (as defined by Murray [3]) and cup center position of the 3D cup model were aligned to maximize the fit between cup shadow shown in both EOS image and the projected overlays from the 3D cup model (Figure 2), and the operative inclination and anteversion were calculated.
Results:
The mean error in operative anteversion measurement of the acetabular cup between EOS at CT imaging was 0.4° (SD: 1.7°, Min -4.0°, Max 4.0°), the mean error in operative inclination was 0.2° (SD: 1.5°, Min 3.0°, Max 4.0°). The average absolute error was 1.1° for operative anteversion, and 1.1° for operative inclination. Demographic information for patients is summarized in table 1.
Conclusion:
The method utilized in this study was accurate for determination of acetabular component positioning when comparing biplanar Xray to CT measurements, well within traditional “safe zone” definitions. Limitations include the small sample size and single measurer. Further studies may provide additional data on the accuracy of this technique, or additional intraoperative tools to assist in precise component placement in total hip arthroplasty.
Figures
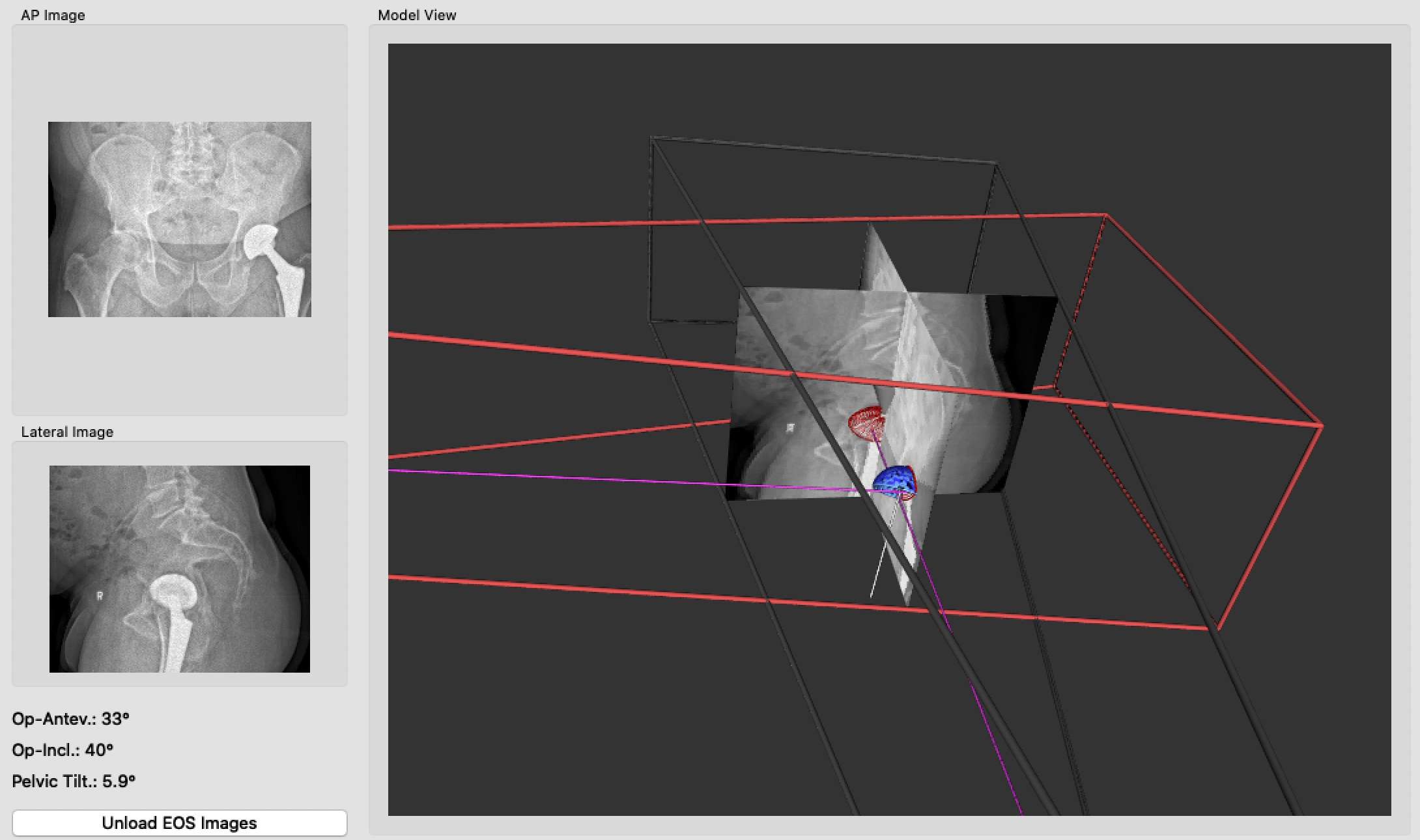
Figure 1
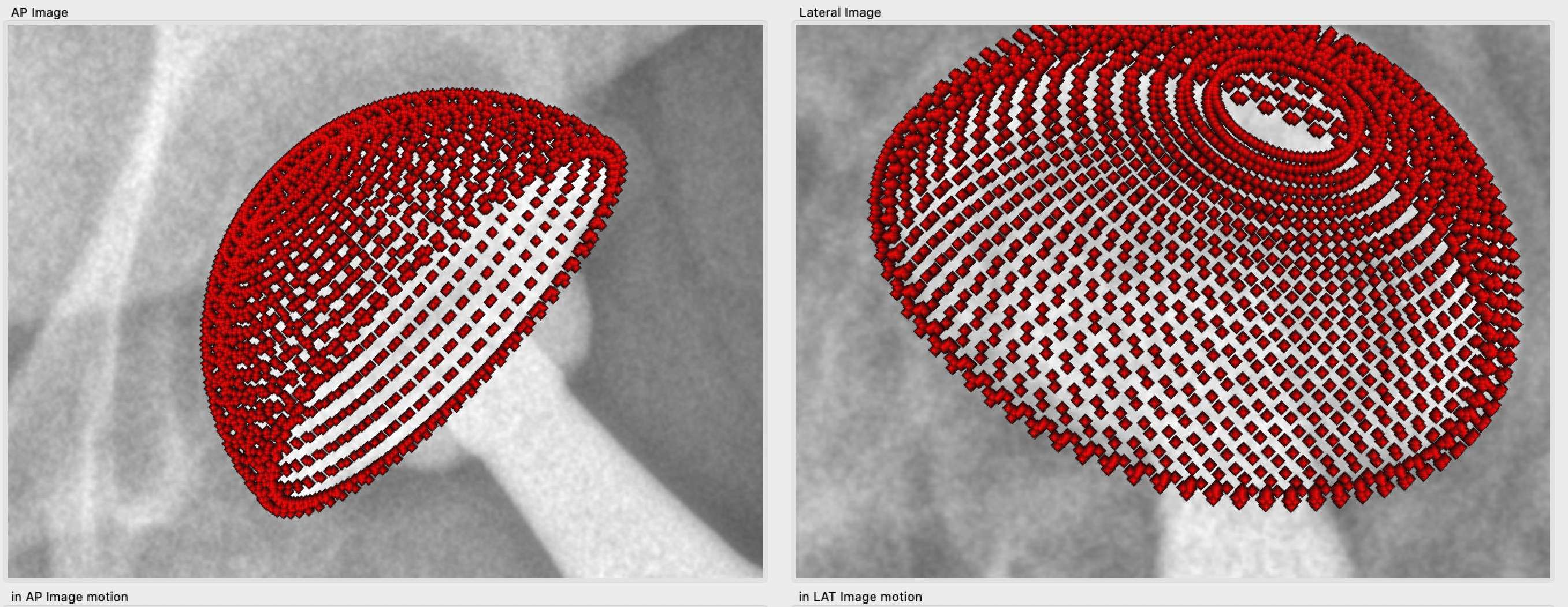
Figure 2
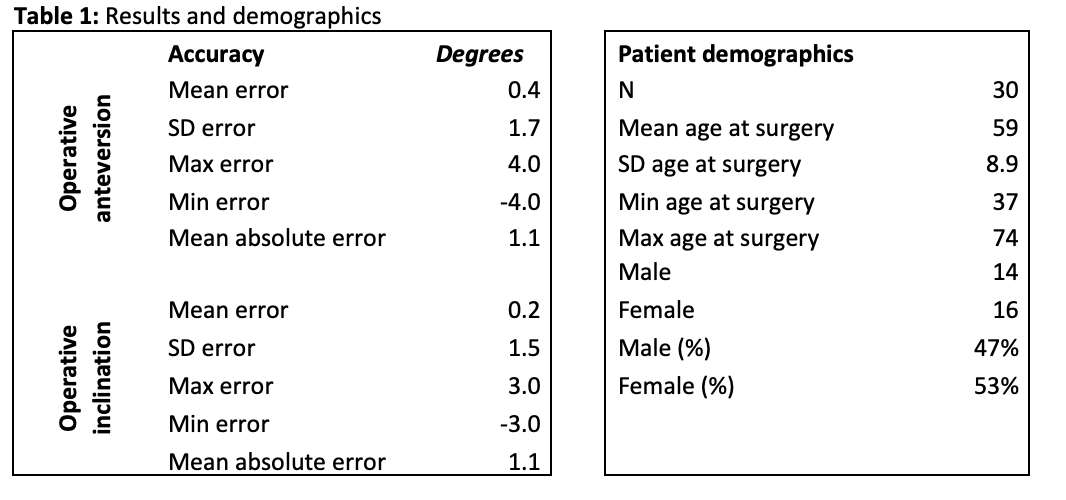
Figure 3
Figure 4#8044
Invited Talk: Augmented Reality in Hip Replacement
*Stephen Murphy - New England Baptist Hospital - Boston, USA
*Email: stephenbmurphymd@gmail.com
#7758
The Range of Spinopelvic Mobility in Lumbar Fusion Patients
Kathryn Colone - University of Denver - Denver, USA
Sam Mattei - University of Denver - Denver, USA
*Casey Myers - Ortho Haus - Denver, United States of America
Kevin Shelburne - University of Denver - Denver, USA
Chadd Clary - Ortho Haus, LLC - Denver, USA
Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
*Email: cmyers@theorthohaus.com
INTRODUCTION: Preoperative spinopelvic alignment and mobility has been identified as a risk factor for THA dislocation and has recently become an area of investigation [1]. Radiographic assessment of functional positions has shown pelvic orientation can be highly patient-specific and vary significantly across the population [2]. Certain pelvic positions in patients with spinal fusioncan lead to increased dislocation risk compared to individuals without spinal fusion [3,4]. Therefore, understanding spinopelvic mobility in individuals with spinal pathology may be valuable in making surgical decisions from radiographic images. The objective of this study was to compare spinopelvic mobility of patients with lumbar fusion to healthy controls using stereo radiography over a range of common functional positions.
METHODS: Twenty patients were enrolled in two cohorts (age-matched healthy controls, n=10; spinal fusion, n=10) and provided informed consent as part of a larger IRB-approved study. Data was collected using stereo radiography to capture 3D pelvis positions for five static activities including 1) neutral seated 2) flexed seated 3) neutral standing 4) slouch standing and 5) standing with thigh raised at 90° (Fig. 1). Patient-specific pelvic anatomy was reconstructed from CT images in ScanIP (Simpleware, Inc.) and used to track bone motion with DSX (C-Motion, Inc.) for 2D/3D image registration (Fig. 1). The anterior pelvic plane angle (APPA) was defined as the angle between the anterior pelvic plane and a global vertical reference frame, where negative values indicate posterior pelvic tilt. Spinopelvic mobility was determined for each patient as the greatest anterior pelvic tilt minus the greatest posterior pelvic tilt.
RESULTS: Overall spinopelvic mobility for the healthy and spinal fusion cohorts was 35.3 ± 12.2° and 33.9 ± 9.1°, respectively, exhibiting similar overall range of motion across activities. Both groups exhibited similar posterior pelvic tilt from the neutral standing to neutral seated poses (healthy, 10.0 ± 5.0°; spinal fusion, 9.8 ± 9.0°, Fig. 2) and anterior pelvic tilt from the neutral seated to flexed seated poses (healthy, 26.6 ± 8.9°; spinal fusion, 26.0 ± 6.77°). Due to the healthy cohort exhibiting more posterior pelvic tilt during slouch standing (Fig. 3), they also showed greater anterior tilt from the slouch standing to flex seated positions (healthy, 34.5 ± 13.0°; spinal fusion, 29.8 ± 11.0°) (Fig. 2).
CONCLUSION: Despite clinical reports that spinal fusion patients have higher risks of dislocation, both cohorts demonstrated similar ranges of overall spinopelvic mobility. On average, spinal fusion patients had more anterior tilt than healthy controls in the flexed seated and slouch standing positions (Fig. 3), which would result in decreased functional inclination and anteversion of the cup [5]. Both cohorts exhibited significant variability in pelvic mobility within their groups, with both low mobility subjects (healthy, 17.4°; spinal fusion, 18.2°) and high mobility subjects (healthy, 54.5°; spinal fusion, 46.8°). This demonstrates the value of patient-specific functional tilt measurements, regardless of previous spinal surgery, to determine effective placement of THA components to reduce the likelihood of dislocation.
REFERENCES: 1.Lum. J Arthroplasty (2018). 2.Pierrepont. Bone Joint J (2017). 3.Lazennec. J Arthroplasty (2017). 4.Sultan. J Arthroplasty (2018).
Figures
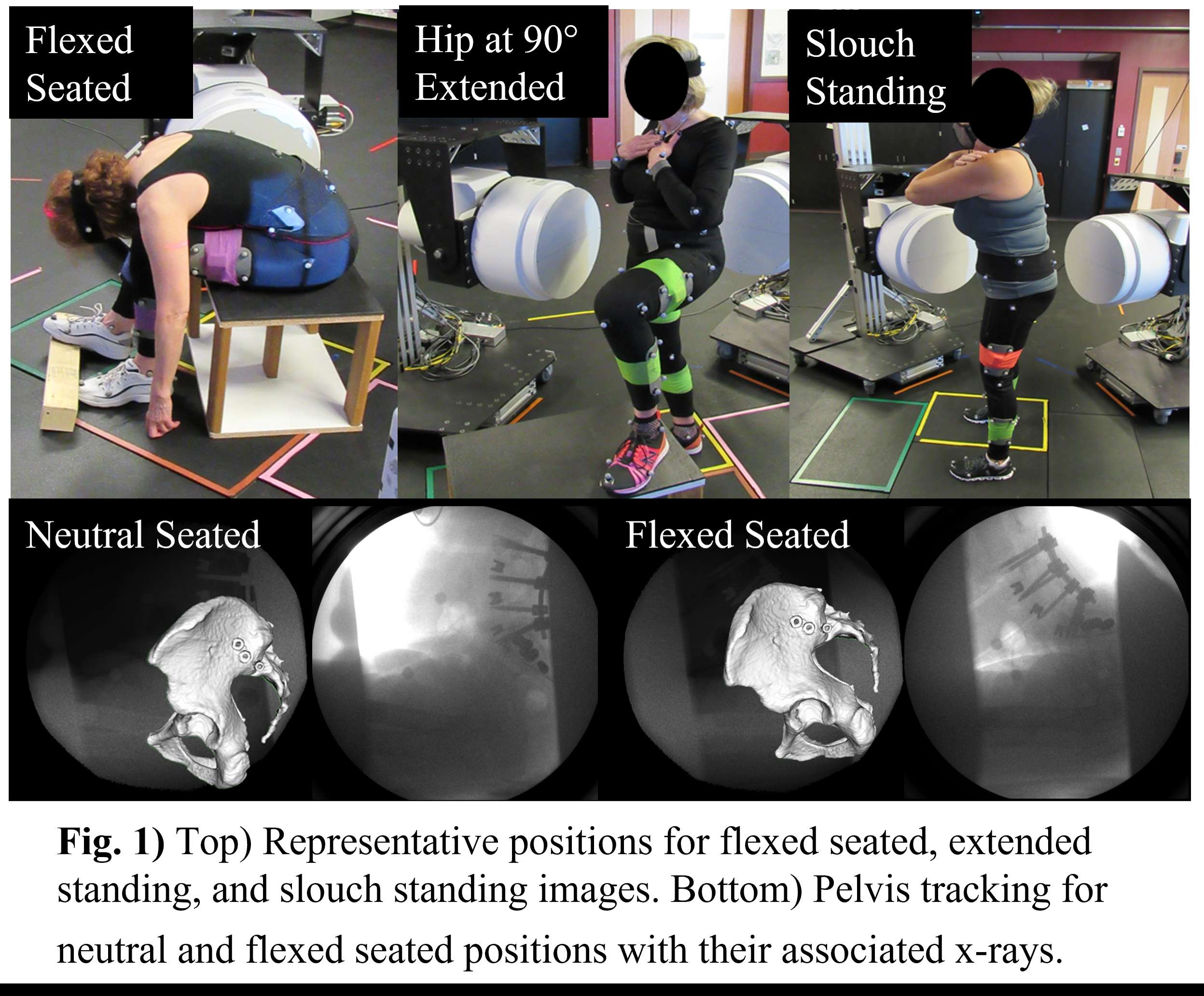
Figure 1
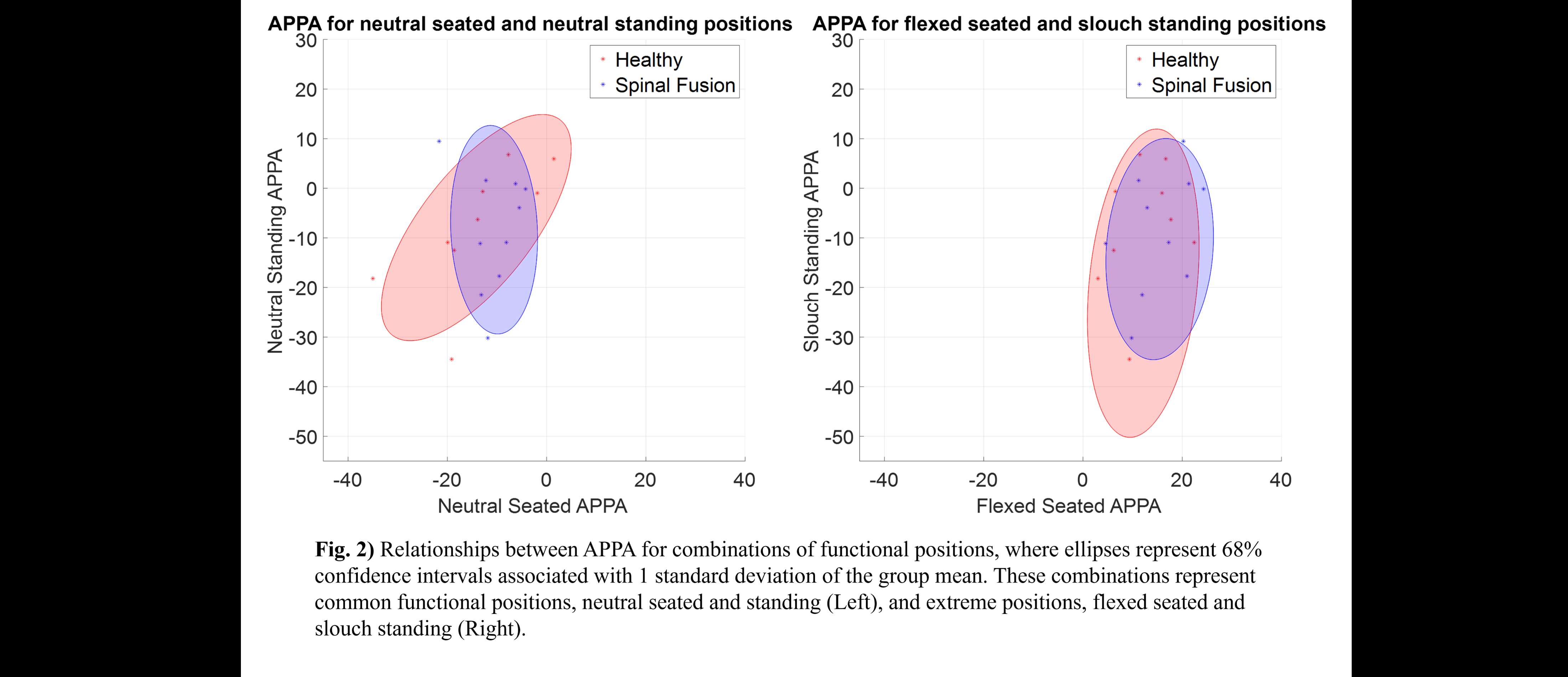
Figure 2
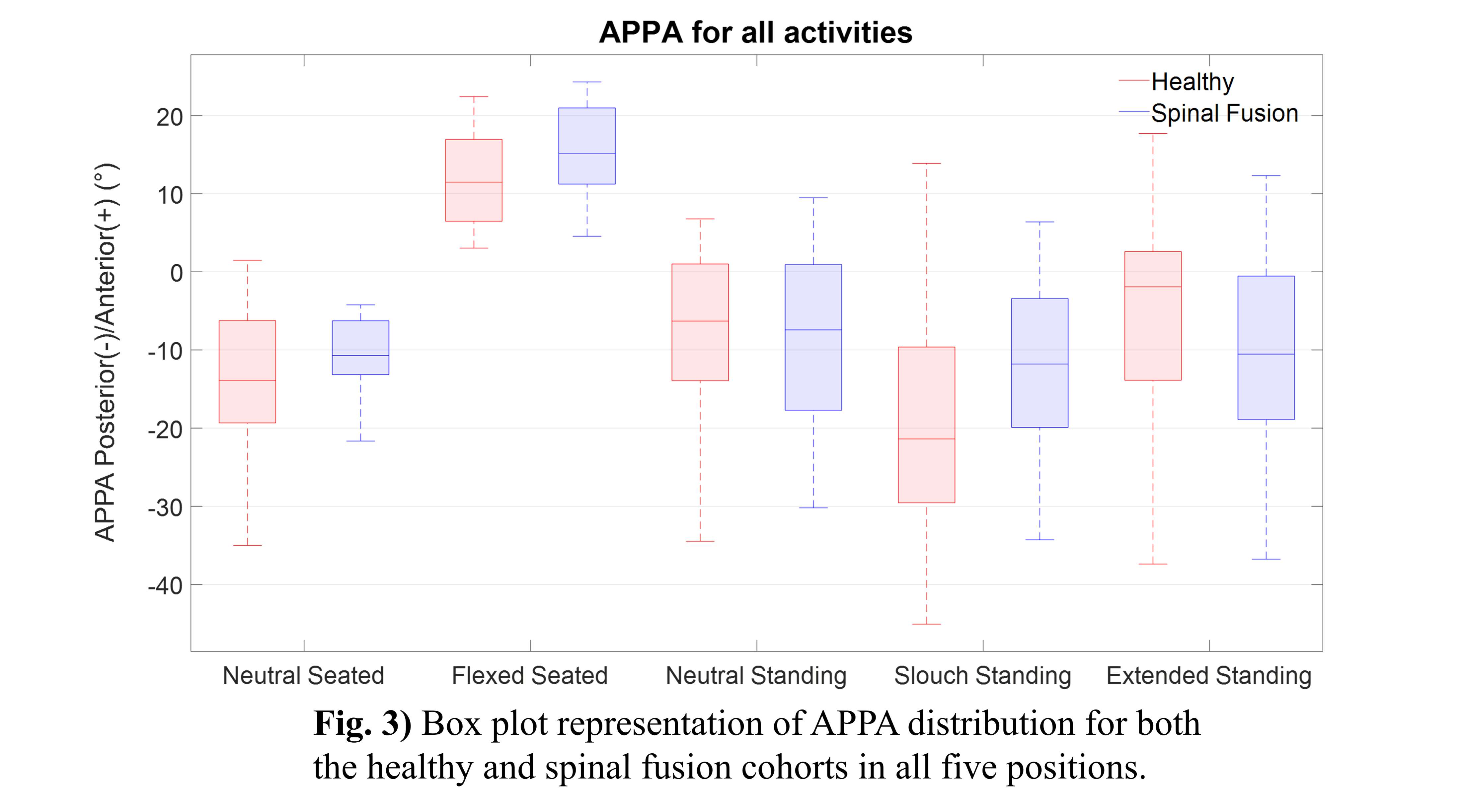
Figure 3#7768
Software-Driven Cup Alignment Recommendations for THA Patients With Varying Degrees of Spinopelvic Mobility
*Casey Myers - Ortho Haus - Denver, United States of America
Clare Fitzpatrick - Ortho Haus, LLC - Boise, Select Country
Chadd Clary - Ortho Haus, LLC - Denver, USA
Chris Hunt - DePuy Synthes Joint reconstruction - Leeds, United Kingdom
Matthew Dressler - DePuy Synthes Joint Reconstruction - Warsaw, USA
Paul Rullkoetter - Ortho Haus, LLC - Lyons, United States of America
*Email: cmyers@theorthohaus.com
INTRODUCTION: Pelvic tilt impacts the functional position of the cup following total hip arthroplasty (THA) and has been increasingly considered for determining component placement. There is significant variation in the direction and magnitude of pelvic tilt in patients that are due to receive THA [1,2]. One definition of adverse spinopelvic mobility is an anterior pelvic tilt change of greater than 20° when transitioning from standing to a flexed-seated position [3]. Patient-specific spinopelvic mobility can help explain why a large percentage of THA dislocations are in the Lewinnek “Safe Zone” for component position, which does not consider the functional orientations achievable for a given patient [4]. The objective of this study was to demonstrate the utility of a decision support tool for THA by determining the patient-specific cup target zones based on different levels of pelvic mobility. We hypothesized that both the level of mobility and magnitude of pelvic orientation would determine the target zone for the cup.
METHODS: The tool assesses cup inclination and anteversion using a previously developed algorithm that uniquely incorporates patient-specific spinopelvic mobility and accounts for edge loading and implant-implant impingement in real time. Inputs to the algorithm include the anterior pelvic plane angle measured during lateral functional x-rays captured in the standing and seated-flexed position as well as the selected implant size/type. Patient-specific outputs include the range of inclination and anteversion angles that make up a recommended target zone. Virtual patients (n=441) were created and evaluated in combinations of standing and seated-flexed pelvic tilt at 5° increments from ±50° [1]. Virtual patients were categorized by pelvic mobility into high and low mobility categories based on previously defined risk factors [3,4] (Figure 1). In-vivo pelvic tilt data of 28 real patients were available from a previous study that evaluated different patient cohorts [2]. Three representative real patients were selected from the study who were in the high and low mobility categories (Figure 1) to compare acceptable cup placement ranges.
RESULTS: Patients 1 and 2 were both categorized as low mobility; however, their patient-specific target zones were substantially different in anteversion targets. The anterior emphasis of the pelvic tilt in both functional positions for patient 1 resulted in a target position with higher anteversion than patient 2 (24° vs 17°) and smaller target zone ranges (patient 1 inclination:[34°-49°] version:[21°-28°] ; patient 2: inclination:[34°-52°], version:[10°-25°]). Patient 3 was high mobility and anteriorly oriented and characterized by acceptable cup positions that require anteversion angles of 35° or higher (Figure 2).
CONCLUSIONS: We have illustrated the performance of a real-time automated surgical decision support tool for THA. The algorithm offers increased resolution in assessing the potential impact of patient-specific spinopelvic mobility on cup orientation. The overall range of pelvic mobility and the directional magnitude of pelvic orientation proved to be important factors in determining patient-specific cup target zones. Furthermore, the fast-solving algorithm facilitates real-time decision making during preoperative and intraoperative planning.
References: 1.Pierrepont. Bone Joint J (2017). 2.Myers. Annual ORS Proceedings (2022). 3.Vigdorchik. J. Arthroplasty (2021). 4.Abdel. Clin Orthop Relat Res (2016).
Figures
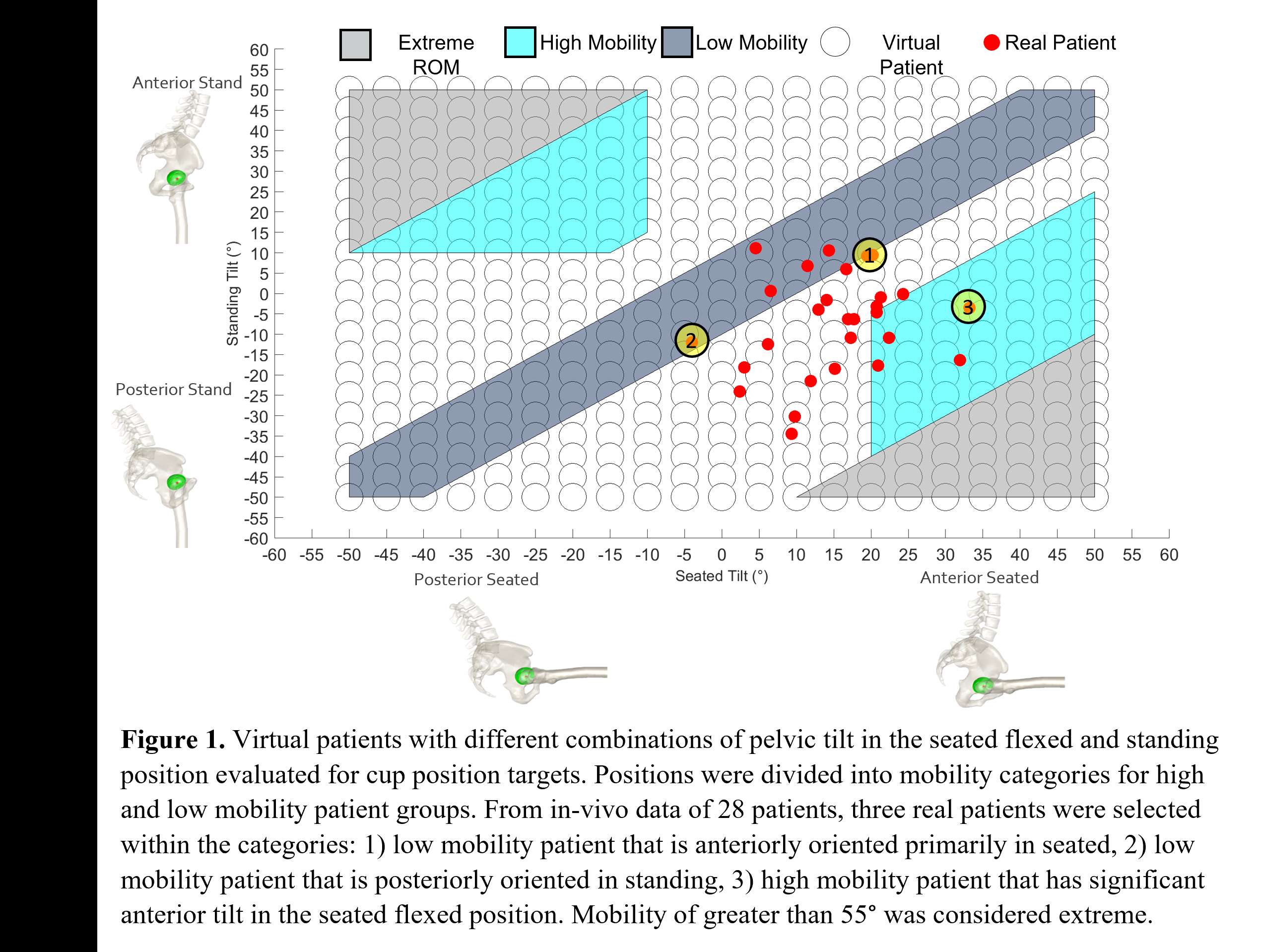
Figure 1
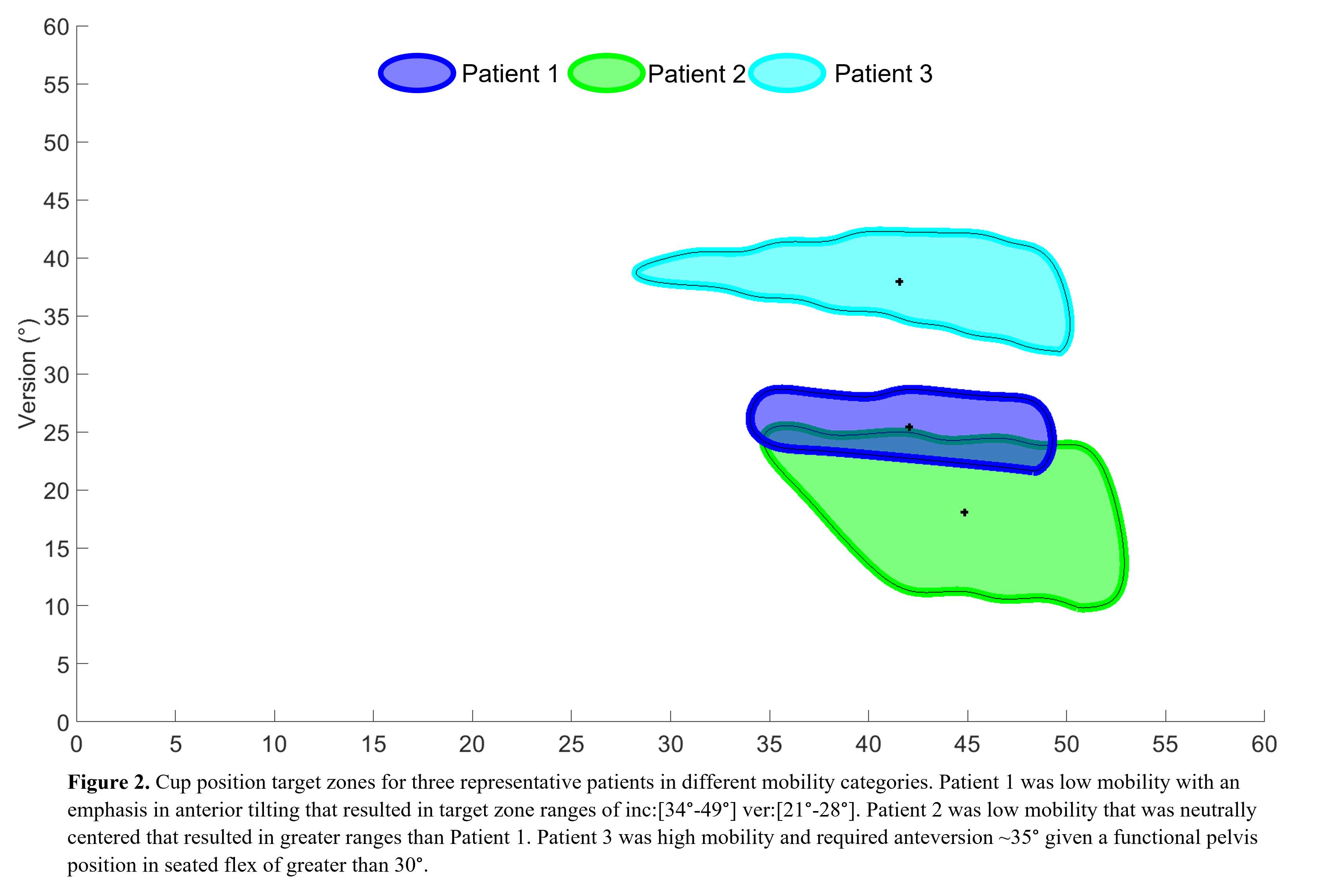
Figure 2#7450
Evaluation and Comparison of THA Component Fits Across Different Dorr Canal Types
*Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Thang Nguyen - University of Tennessee - Knoxville, USA
Andrew Jacobs - DePuy Synthes - Warsaw, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: jnachtra@vols.utk.edu
INTRODUCTION:
Total hip arthroplasty (THA) has been considered one of the most successful orthopaedic procedures in the modern era, but in the past most THA stems have struggled to maintain a good fit across all Dorr Types. As preoperative planning technology continues to improve, the accuracy of intraoperative positioning of THA components will improve too. The objective of this study is to determine and compare the femoral stem component fit between three different implants for all Dorr canal types.
METHODS:
A total of 60 proximal femurs from segmentation of CT scans (20 Dorr Type A, 20 Dorr Type B, and 20 Dorr Type C) were evaluated in this study. A previously validated pre-operative planning tool was used to evaluate the proximal portion of each subject-specific femoral bone model. The three stem systems used in this study, Hip Implant I (HI1), Hip Implant 2 (HI2), and a newly designed stem (NDS), are shown in Figure 1. Three parameters were evaluated for this study: the distance from the implanted head center to the anatomical head center (IHC-AHC); the volume of bone removal needed for each stem, calculated volume of the stem that overlapped with the cortical bone; and the contact percentage of each stem within the canal, calculated area of the stem in contact with the cortical wall as a percentage of the total contact area of the stem.
RESULTS:
Dorr Type A:
For ICH-ACH distances, NDS’s average was 0.4mm±0.3mm (0.2mm–1.0mm), HI2’s average was 0.6mm±0.4mm (0.3mm–1.6mm), and HI1’s average was 0.5mm±0.2mm (0.3mm–0.9mm). Both NDS and HI2 had 0.0cm3 of bone removal on average, whereas HI1 had 0.2cm3 on average. Similarly, the NDS yielded low overall contact percentage (0.2%) leading to bone removal when compared to HI1 (7.0%) and HI2 (1.4%).
Dorr Type B:
For ICH-ACH distances, NDS’s average was 0.6mm±0.6mm (0.2mm–2.0mm), HI2’s average was 0.8mm±0.7mm (0.3mm–2.4mm), and HI1’s average was 0.6mm±0.1mm (0.4mm–0.8mm). Both NDS and HI2 had 0.0cm3 of bone removal on average, whereas HI1 had 0.6cm3 on average. NDS yielded low overall contact percentage (0.7%) leading to bone removal when compared to HI1 (17.0%) and HI2 (2.1%).
Dorr Type C:
For ICH-ACH distances, NDS’s average was 0.3mm±0.2mm (0.2mm–0.5mm), HI2’s average was 0.4mm±0.2mm (0.2mm–0.6mm), and HI1’s average was 0.6mm±0.2mm (0.4mm–0.8mm). Both NDS and HI2 had 0.0cm3 of bone removal on average, whereas HI1 had 0.7cm3 on average. NDS yielded no overall contact percentage leading to bone removal when compared to HI1 (15.9%) and HI2 (0.4%).
CONCLUSION:
This study demonstrates how theoretical modeling can be used as a powerful tool to provide surgeons and engineers alike feedback on component designs and placement options. The tool was used to demonstrate that NDS had a more consistent fit across all Dorr Types. Both NDS and HI2 required less reaming of the cortical bone when compared to HI1, but NDS’s design also led to a minimized IHC-AHC distance compared to HI2. Clinically, small mismatches in stem orientation may sound negligible, but these misalignments can compound leading to undesirable postoperative mechanics.
Figures
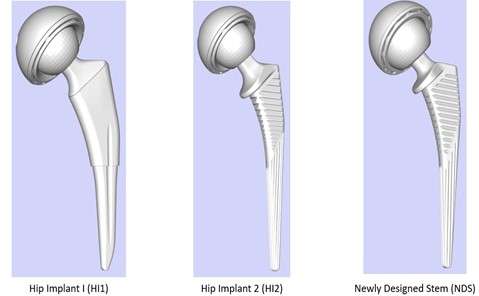
Figure 1
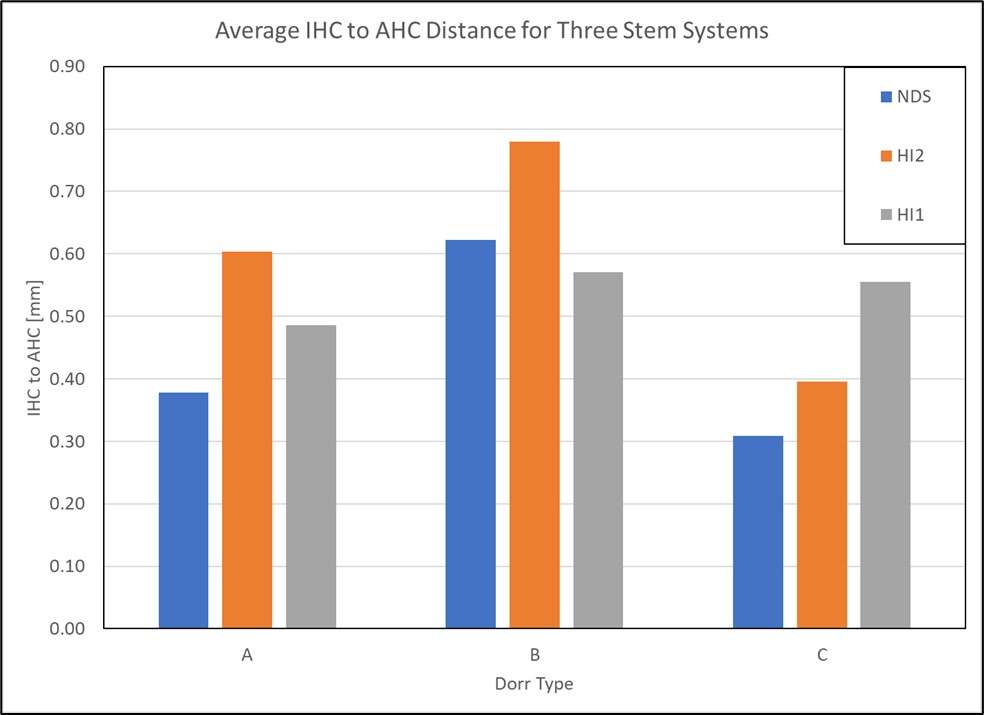
Figure 2
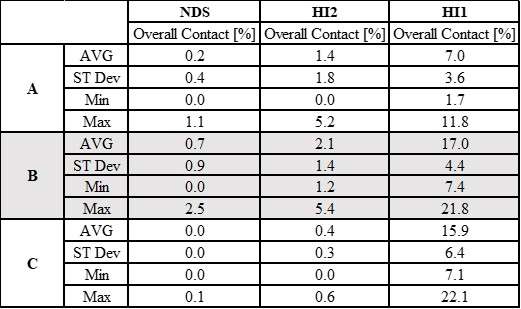
Figure 3#7451
Are Total Hip Bone Sparing Stems Truly Bone Sparing?
*Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Thang Nguyen - University of Tennessee - Knoxville, USA
Andrew Jacobs - DePuy Synthes - Warsaw, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: jnachtra@vols.utk.edu
INTRODUCTION:
Some stem systems are being marketed as bone sparing, but does that mean they require less overall bone removal? Many groups only look at the Lesser Trochanter to Lowest Calcar Point Distance (LT-LCP) when this claim is made. This means any extra reaming of the canal that a surgeon may have to perform to achieve the stem orientation and canal fit that they want is not considered. The objective of this study is to determine and compare three stem systems for the main bone sparing parameter as well as a volumetric analysis within the canal to get a better idea of overall bone removal for a given stem system.
METHODS:
A total of 60 proximal femurs from segmented CT scans were evaluated in this study. A previously validated pre-operative planning tool was used to evaluate the proximal portion of each subject-specific femoral bone model. The three stem systems used in this study, Hip Implant I (HI1), Hip Implant 2 (HI2), and a newly designed stem (NDS) are shown in Figure 1. Of these three, HI1 has been marketed as bone sparing. The main bone sparing parameter used is the LT-LCP. For this study, this distance was found and broken into all anatomical directions. Additionally, the volume of bone removal needed for each stem was calculated by finding the volume of the stem that overlapped with the cortical bone surrounding the canal.
RESULTS:
When comparing the overall LT-LCP, HI1 had an average of 36.91mm±4.36mm (29.65mm–48.15mm), HI2 had an average of 31.31mm±3.29mm (27.56mm–39.96mm), and NDS had an average of 32.81mm±3.60mm (26.33mm–41.76mm). Because this includes the Anterior/Posterior (AP) and Medial/Lateral (ML) directions, we decided to look at only the Superior/Inferior (SI) distances to get a better idea of bone removal when removing the femoral head. In this case, the LT-LCPs in the SI direction were as follows: HI1 had an average of 32.40mm±5.53mm (21.89mm–45.38mm), HI2 had an average of 24.44mm±5.15mm (13.62mm–35.27mm), and NDS had an average of 26.45mm±5.50mm (18.58mm–37.63mm). The rest of the LT-LCP data can be found in Table 1. Additionally, the required volume of bone removal by reaming the canal was found for each stem system: HI1 required 0.497cm3±0.309cm3 (0.018cm3–1.143cm3) on average, HI2 required 0.026cm3±0.050cm3 (0.000cm3–0.222cm3) on average, and NDS required 0.002cm3±0.006cm3 (0.000cm3–0.028cm3) on average.
CONCLUSION:
The results of this study do show that HI1 is the most bone sparing of the three according to the LT-LCP that is commonly used to signify a bone sparing stem system. However, HI1 appeared to require the most bone removal through reaming of the canal to achieve these fits, as the other two stem systems had nearly negligible amounts of bone removal required within the canal. Conversely, the NDS required the least amount of cortical reaming while maintaining a comparable LT-LCP. These results make us reconsider whether bone sparing stems truly are bone sparing, as excess or improper reaming within the canal has been shown to lead to many complications including bone fracture in extreme cases.
Figures
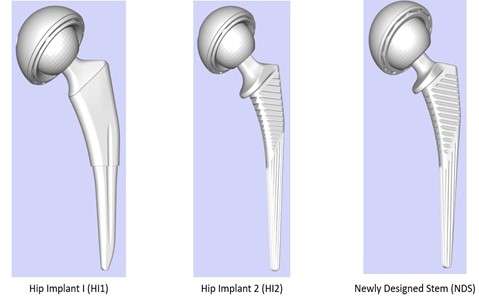
Figure 1
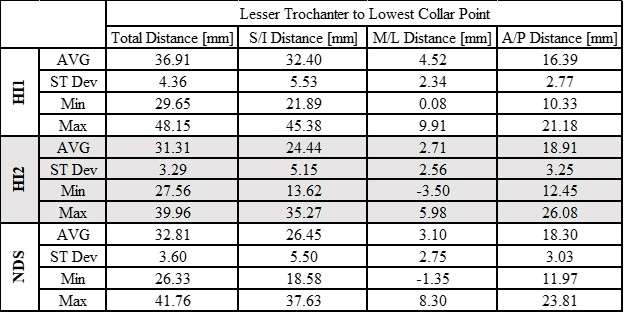
Figure 2#7379
Effects of Body Mass Index on Cup Placement Accuracy During Total Hip Arthroplasty in Supine Position Using a Pelvic Rotation Correction Device
*Satoshi Nakasone - Graduate School of Medicine, University of the Ryukyus - Nishihara, Japan
Masamichi Onaga - Graduate school of medicine, university of the Ryukyus - Nishihara Nakagami-gun, Japan
Takahiro Igei - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
Fumiyuki Washizaki - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
Kotaro Nishida - Graduate school of medicine, University of the Ryukykus - Nishihara Nakagamigun, Japan
Mika Takaesu - Chubu Tokushukai Hospital - Kitanakagusuku, Japan
Yoshihide Miyata - Chubu Tokushukai Hospital - Kitanakagusuku, Japan
*Email: satoshi_nakasone@hotmail.com
Introduction:
Accurate cup placement during total hip arthroplasty (THA) is very important. A simple device was developed for assisting in cup placement intra-operatively, the HipPointer, that can be to correct pelvic rotation intraoperatively using the functional pelvic plane (FPP) as a reference. HipPointer consists of a long and narrow base frame, and two hollow arms that can be adjusted to match the width between the left and right ASISs (Fig. 1). The level holder attached parallel to the base frame is used to ensure that the pelvic rotation is parallel to the horizontal plane, while the other level holder attached orthogonally to the device is used to ensure the base frame is parallel to the operating table (Fig. 2). In surgery, the parallel guide is attached to the cup impactor handle, and the cup was fixed in place so that the parallel guide is parallel to the alignment rod (Fig. 3). It has been reported that pelvic position change intra-operatively was reported a significant negative correlation between change in absolute axial rotation and BMI. This was caused excessive anteversion of the cup in supine THA. The purposes of this study were to investigate the effect of body mass index on accuracy of cup placement using pelvic rotation correction device.
Patients and methods:
This study examined 353 hips in 308 patients (93 male) who underwent cup placement using the HipPointer in THA through direct anterior approach with supine position. Their mean age at the time of surgery was 63.9 (17-90) years, and their mean BMI was 24.9 (16.6-42.0) kg/m2. The mean observation period was 40.2 (12-73) months. Preoperative 3-D CT imaging was performed, followed by 3-D preoperative planning using 3-D preoperative software. Surgery was performed using the HipPointer for cup placement. To investigate of the accuracy of HipPointer, the preoperative planning and postoperative cup placement angles relative to the FPP were examined, and their absolute value errors were measured, and the correlation between error and patient demographics especially body mass index was investigated.
Results:
The mean radiographic inclination (RI) of the cup was 40.2±3.0° (SD), and the mean radiographic anteversion (RA) was 15.8 ± 3.6°. The absolute error for cup placement was 2.2 ± 2.0° for RI and 2.7 ± 2.3° for RA. The ratio of the cup placement angle for which both RI and RA are ≤10° in the target zone was 99% (350/353 hips), and the ratio of the absolute errors for which both RI and RA are ≤5° was 80.4% (284/353 hips). There was no correlation between each error of RI or RA with BMI (Spearman correlation, RI: -0.01. RA: -0.08).
Conclusion:
In this study, pelvic rotation was observed with HipPointer following acetabular exposure using retractors. However, the HipPointer provided good cup placement accuracy regardless of body mass index values. The HipPointer is a cup placement assistance device that corrects the pelvic rotation and creates FFP intra-operatively has a simple structure, fast to mount, and is easy to use, and is useful for DAA-THA with supine position.
Figures
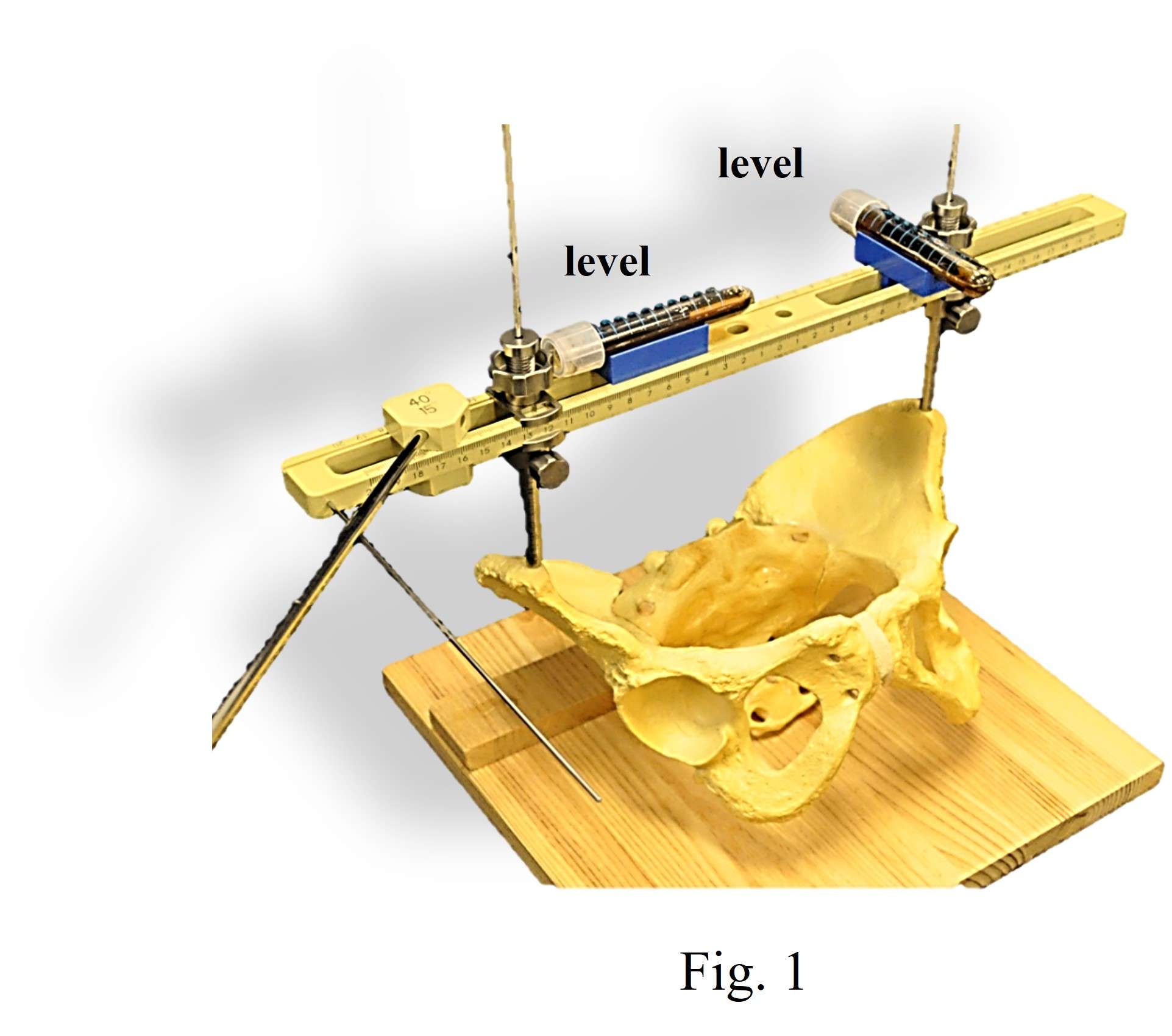
Figure 1
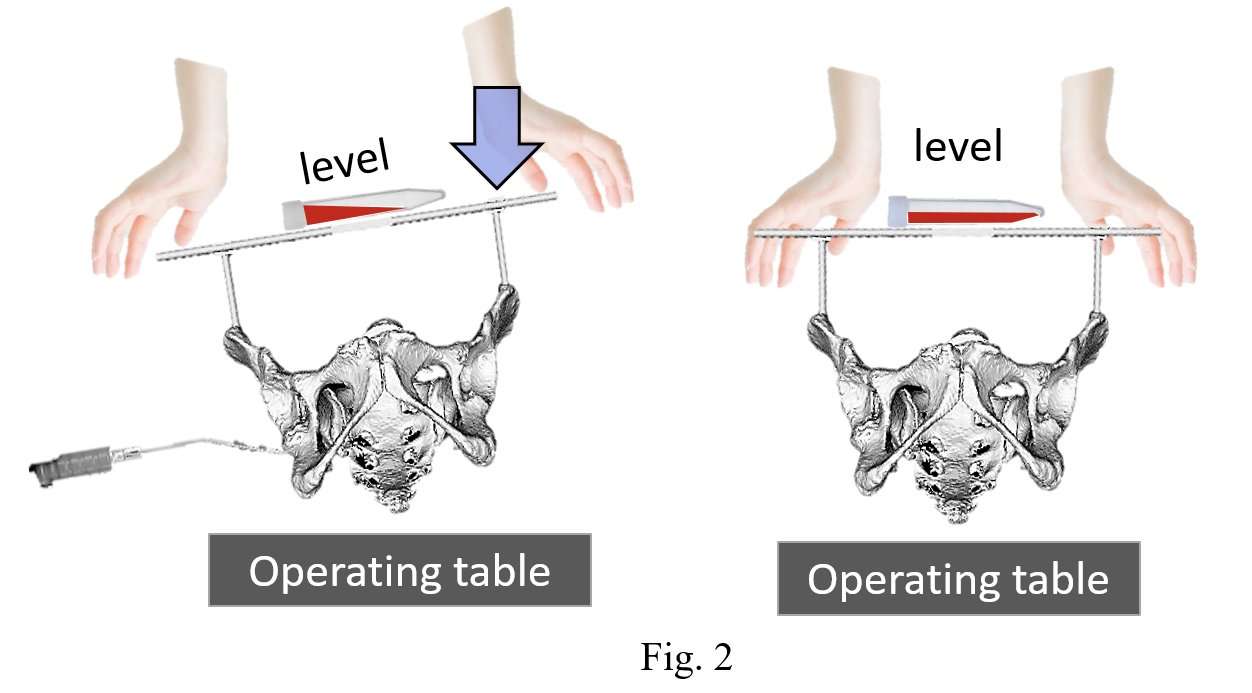
Figure 2
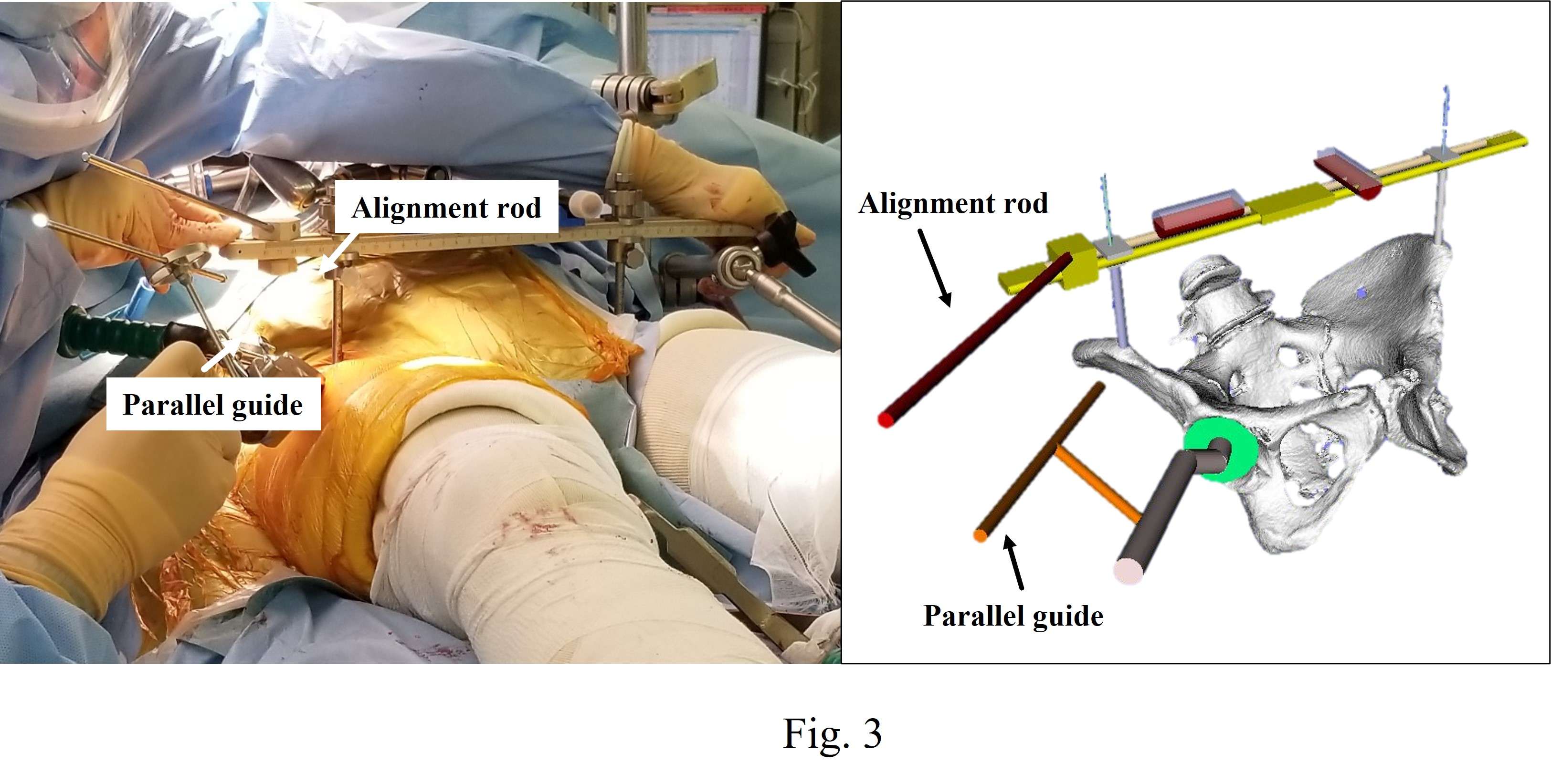
Figure 3#7469
Effect of Positive and Negative Body Taper Junction on Corrosion of Modular Revision Stem: Biomechanical Study
Byungwook Nam - corentec - seoul, South Korea
*JungSung Kim - Corentec Co., Ltd - Seoul, South Korea
TaeJin Shin - Corentec - Cheonan-Si, South Korea
Choongsoo Shin - Sogang University - Seoul, South Korea
Sang-Min Kim - Korea University College of Medicine, Guro Hospital - Seoul, South Korea
Seung-Chan Kim - Eunpyeong St. Mary's Hospital, The Catholic University of Korea, Seoul, South Korea - Seoul, South Korea
*Email: jskim@corentec.com
Keywords: Revision Hip Arthroplasty; Modular Revision Hip Stem; Positive and Negative Angular Mismatch; Fretting Corrosion
Introduction: In revision hip arthroplasty, the modular femoral stem is more widely used than the monobloc stem because of the advantage of being able to easily adjust the leg length and anteversion [Fig.1a]. Although fracture due to fretting corrosion on the taper interface has been reported occasionally, the effect on fretting corrosion due to positive and negative angular mismatches on the taper junction of modular stem has not been analyzed [Fig.1b]. In this study, we compared the effect of positive and negative angular mismatches on the taper interface of a modular stem through the biomechanical analyses.
Materials and Methods: Firstly, finite element analysis for positive and negative angular mismatch models was performed by using ANSYS workbench. The FE models consist of proximal body and distal stem made of Ti6Al4V ELI and have angular interference of -6 to +6 minutes for the male taper [Fig.1b]. A friction coefficient of 0.3 was applied at the taper junction and normal stiffness is appropriately controlled by software. Initial axial load of 2kN along the taper junction axis was applied on the proximal body to assemble with the distal stem. Sequentially, a functional load of 3,300N was applied on the trunnion of the proximal body according to ASTM F1875-98 [Fig.1c].
Secondly, electrochemical evaluation for two angular mismatch specimens was performed to assess the effect on the corrosion by measuring the static/dynamic currents following to the ASTM F1875-98 [Fig.3a].
Results: FE results showed that the lateral displacement of proximal body in positive mismatch was 18μm, which is 38% lower than 26μm in negative mismatch [Fig.2a]. It resulted from the bending moment by the functional loading on the trunnion of the proximal body. Additionally, the maximum stresses of positive and negative were 122Mpa and 92.2Mpa in different area, respectively [Fig.2b]. The most important factor in fretting corrosion is micromotion at the taper interface, and the lower the lateral displacement value means the lower the risk of corrosion.
Experimental results showed that mean static current of positive and negative mismatch was 2.23μA and 8.60μA and mean dynamic current of 3.76μA and 4.06μA were measured after 3,600 load cycles with electrochemical evaluation [Fig.3b]. The lower the current value means oxide film on the surface is better maintained, and lower risk of corrosion.
Conclusion: It is suggested that positive mismatch can reduce micromotion and lower the risk of corrosion, providing lower fatigue damage. This study is expected to help surgeons choose a better modular stem in revision hip arthroplasty.
Acknowledgement: This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, Republic of Korea, the Ministry of Food and Drug Safety) (Project Number:2014X49)
Figures
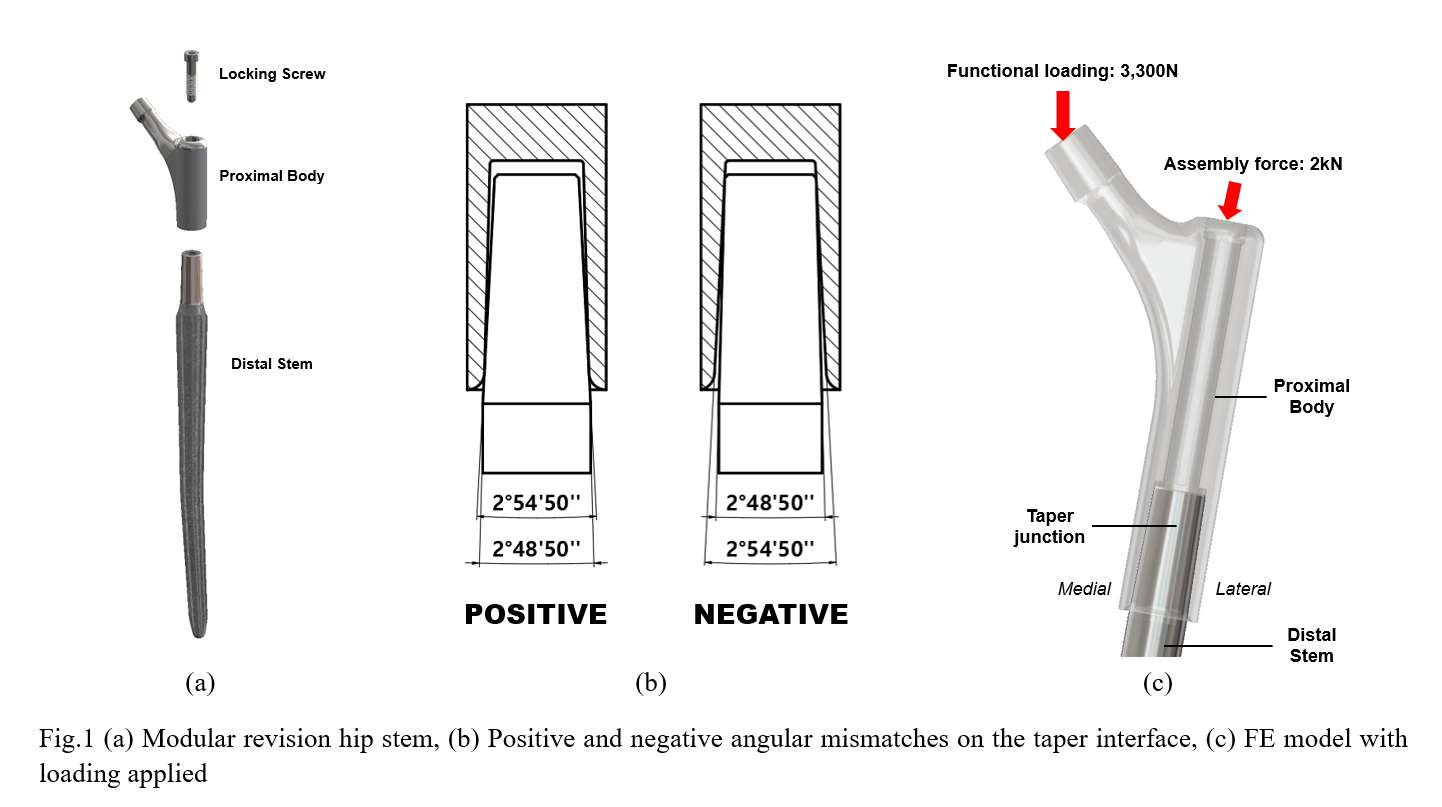
Figure 1
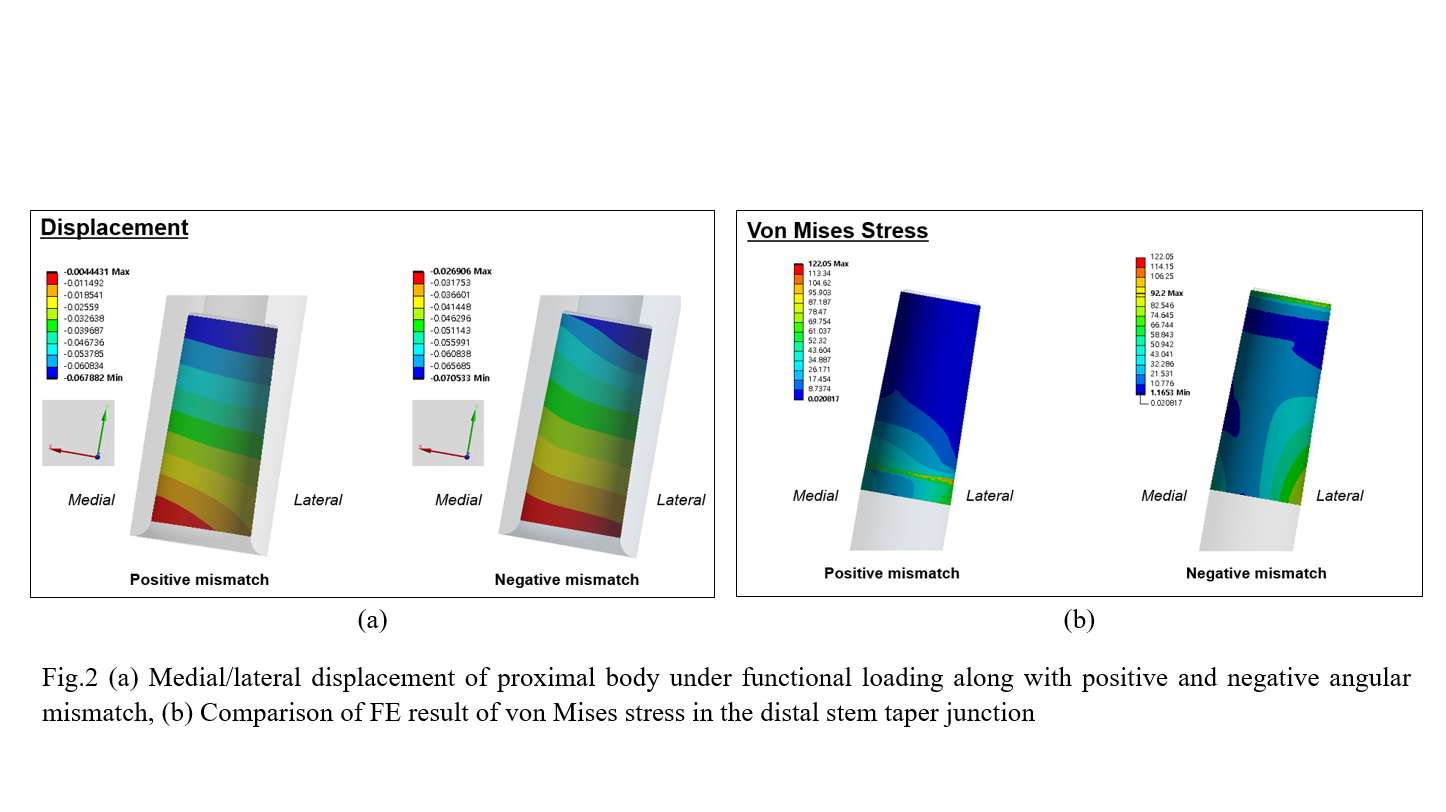
Figure 2
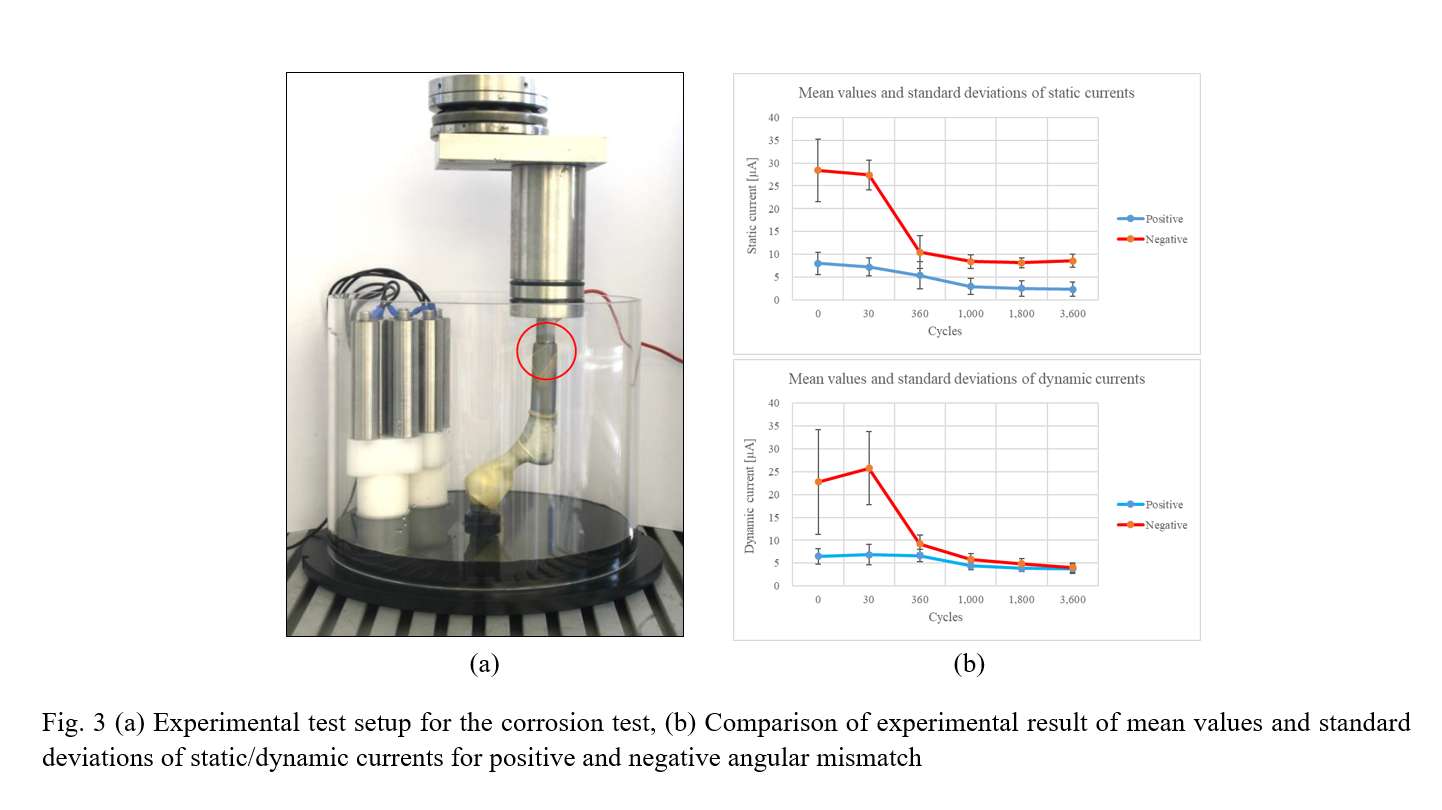
Figure 3#7895
What Lipped Liner Orientation Maximizes Jump Distance During Physiologically Relevant Hip Motions?
*Alessandro Navacchia - Smith & Nephew - Broomfield, USA
Edward Davis - The Dudley Group NHS Foundation Trust - Dudley, United Kingdom
*Email: alessandro.navacchia@smith-nephew.com
Introduction
Total hip arthroplasty (THA) elevated rim or lipped liners increase the travel distance of the femoral head before dislocation and demonstrated increased survivorship compared to flat liners, especially with posterior approach1. However, there remains controversy on the lip position, since a trade-off between range of motion (RoM) and jump distance is inevitable. This study compared the effect of three lip positions on joint RoM and jump distance at impingement with different cup alignments to identify the lip position that provides the best trade-off.
Methods
The computer model of an implanted hip was developed in LifeMOD© and included an R3◊ acetabular cup (48-mm outer diameter), a 20° lipped liner, a 32-mm femoral head with a +4 offset, and a POLARSTEM◊ Standard stem size 3 (Smith+Nephew). Three lip orientations were evaluated: posterior-inferior (8 o’clock for a right hip), posterior (9 o’clock), and posterior-superior (10 o’clock) (Fig. 1).
Implant RoM was calculated using the impingement diagram of the THA planning software RI.HIP MODELER (Smith+Nephew) (Fig. 2a). Only implant-to-implant impingement was considered.
Nine implant placements were evaluated, combining the following parameters:
- Cup inclination (CI) = 30°, 40°, 50°.
- Cup anteversion (CA) = 5°, 15°, 25°.
- Stem anteversion = 15°.
Impingement was assessed for three hip motions associated with dislocation risk2: flexion to 90° followed by internal rotation until impingement (FLEX+IR), external rotation until impingement (ER), and extension until impingement (EXT) (Fig. 2a). For each motion, stem position at impingement was recorded, together with the jump distance required to dislocate the head from the impingement position (Fig. 2b).
Results
RoM for the FLEX+IR motion changed with cup angles, ranging from 112° (90° of flexion + 22° of rotation) with lower cup angles (CI=30° and CA=5°) to 152° with larger cup angles (CI=50° and CA=25°). However, minimal differences (≤1°) were observed when changing lip orientation (Fig. 3a-b). RoM for ER and EXT presented an opposite trend, decreasing with larger cup angles.
Jump distance at impingement for FLEX+IR was consistently larger for the posterior-inferior lip orientation, with increases of 1 mm (10%) and 4 mm (67%) with respect to the posterior and posterior-superior orientations, respectively (Fig. 3c). For both the ER and EXT motions, jump distances ranged from 8 mm to 11 mm. In ER, no consistent trend was observed across cup placements, whereas in EXT posterior-inferior and posterior orientations presented the largest jump distance in 5 and 4 cases, respectively.
Conclusions
This study demonstrated that a posterior-inferior lip orientation provides equivalent RoM and increased jump distance in FLEX+IR when compared to posterior and posterior-superior orientations. Flexion to 90° and internal rotation until impingement is a test often performed intra-operatively to simulate physiologically relevant anterior impingement. Stability when impinging in flexion is particularly relevant for posterior approach surgeries in which risk of posterior dislocation is higher due to resection of the posterior capsule. Therefore, the posterior-inferior lip orientation might be the most appropriate choice in posterior approach surgeries, regardless of cup angles.
References
1. Wyatt, Clin Orthop Relat Res, 2020
2. Klemt, J Orthop Res, 2020
Figures
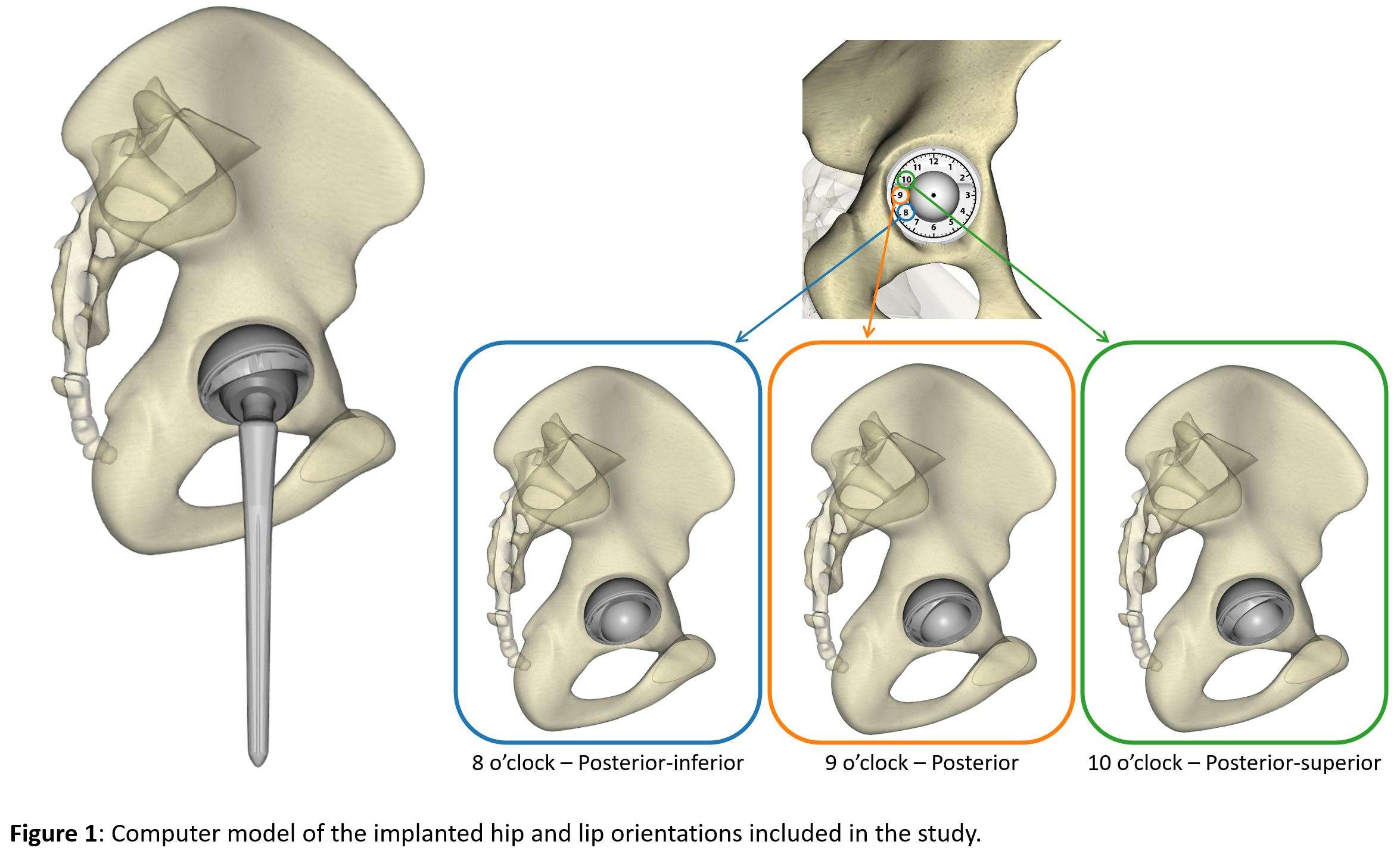
Figure 1
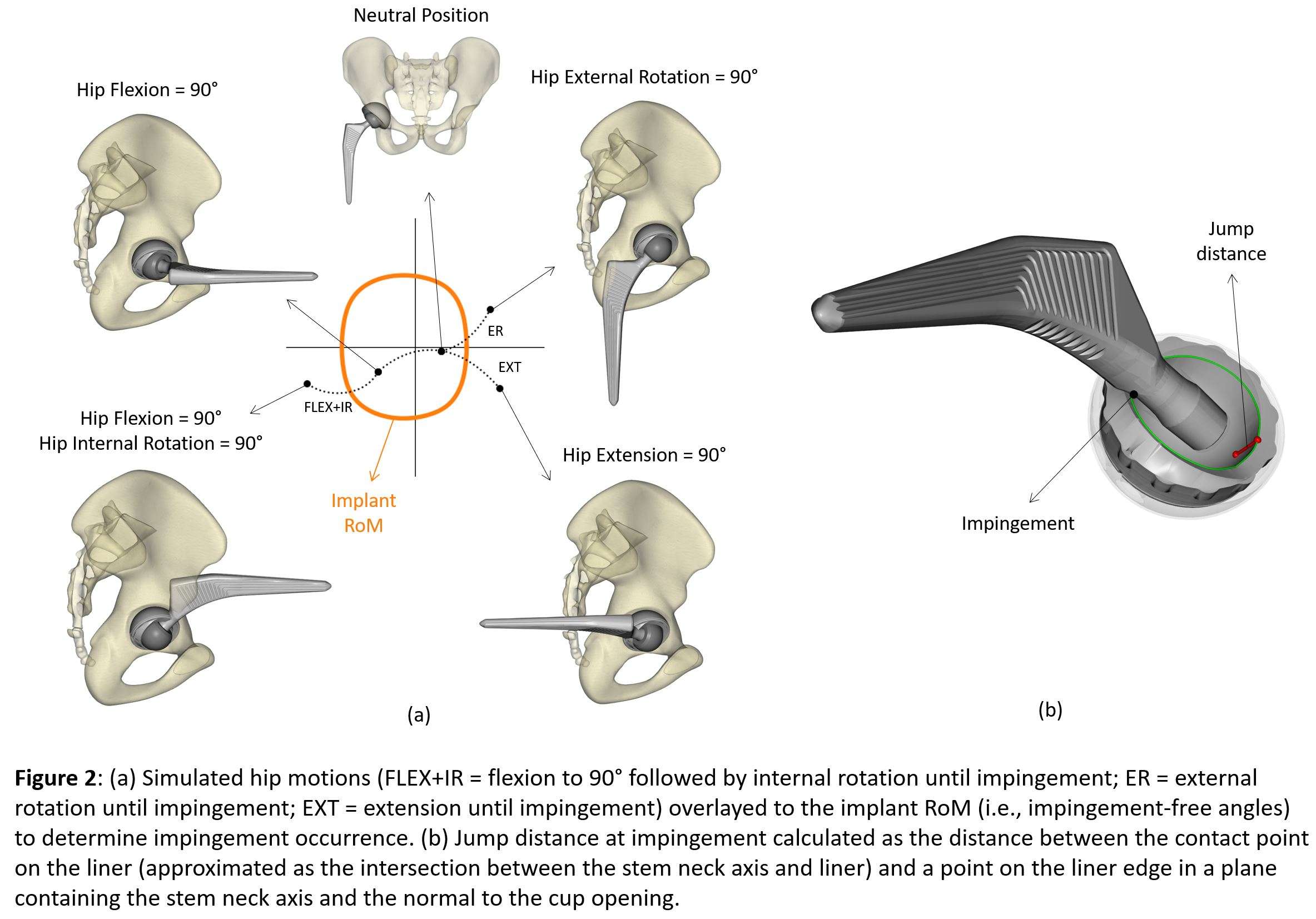
Figure 2
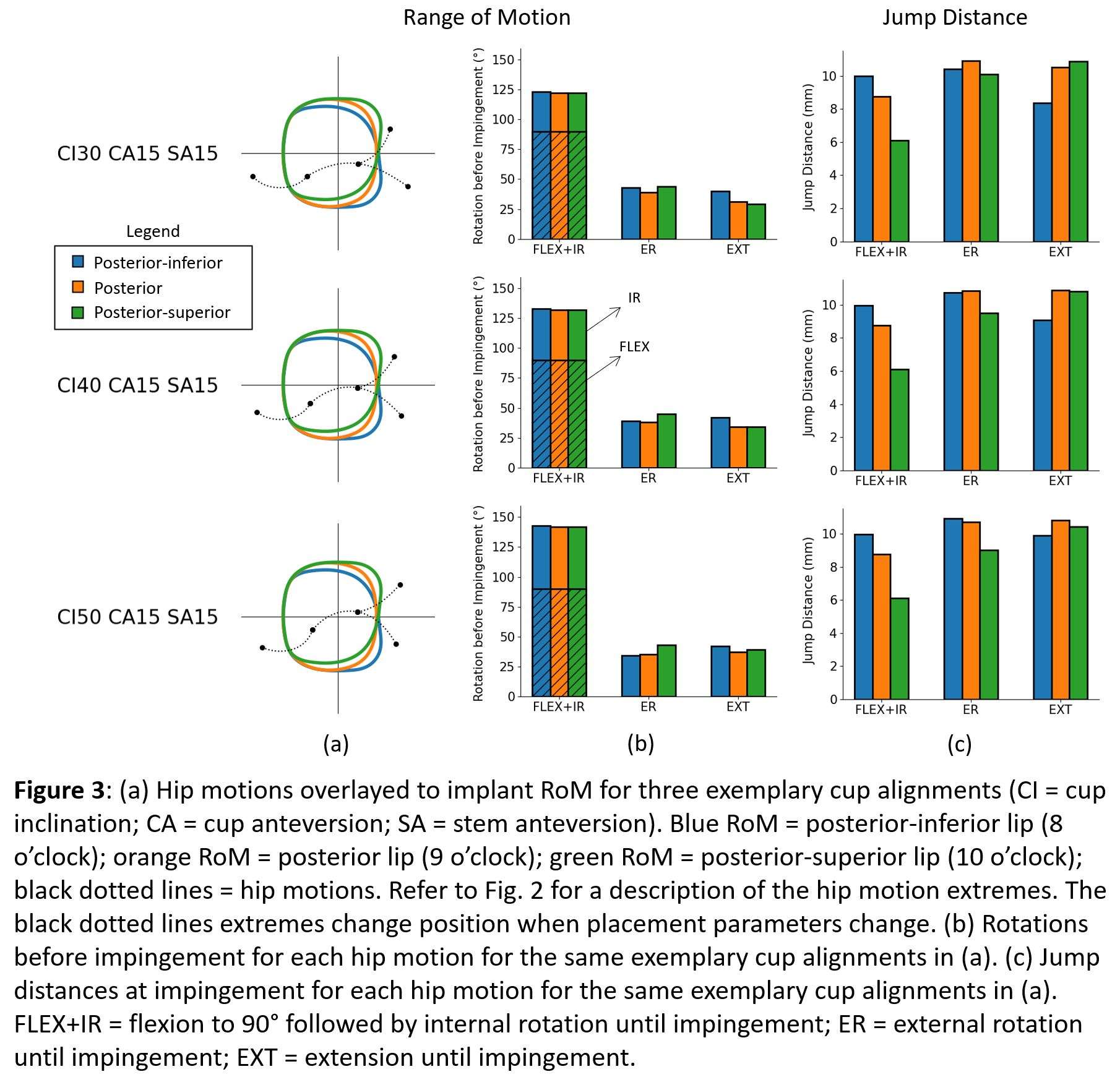
Figure 3#7894
Can Lipped Liners Be Oriented to Maximize Hip Range of Motion Before Impingement?
*Alessandro Navacchia - Smith & Nephew - Broomfield, USA
Edward Davis - The Dudley Group NHS Foundation Trust - Dudley, United Kingdom
*Email: alessandro.navacchia@smith-nephew.com
Introduction
Total hip arthroplasty (THA) elevated rim or lipped liners increase the travel distance of the femoral head before dislocation and demonstrated increased survivorship compared to flat liners, especially with posterior approach1. However, there remains controversy on the position of the lip, which can have a marked effect on range of motion (RoM) prior to impingement2. The purpose of this study was to compare the effect of three lip positions on joint RoM with different cup and stem placement combinations and identify the lip position that least constrained physiological RoM for each combination.
Methods
The computer model of an implanted hip was developed in LifeMOD© and included an R3◊ acetabular cup (48-mm outer diameter), a 20° lipped liner, a 32-mm femoral head with a +4 offset, and a POLARSTEM◊ Standard stem size 3 (Smith+Nephew). Three lip orientations were evaluated: posterior-inferior (8 o’clock for a right hip), posterior (9 o’clock), and posterior-superior (10 o’clock) (Fig. 1).
Implant RoM was calculated for each liner orientation using the impingement diagram of the THA planning software RI.HIP MODELER (Smith+Nephew) (Fig. 2). Only implant-to-implant impingement was considered.
Impingement occurrence was assessed for the following hip physiological motions3: 40° of extension to 130° of flexion, 40° of external rotation to 80° of internal rotation, and 50° of adduction to 50° of abduction (Fig. 2). For impinging motions, the rotation prevented by impingement was quantified.
Twenty-seven implant placements were evaluated, combining the following parameters:
- Cup inclination = 30°, 40°, 50°.
- Cup anteversion = 5°, 15°, 25°.
- Stem anteversion = 0°, 15°, 30°.
Lip orientations that prevented hip rotation by more than 10° for at least one hip motion were considered not acceptable. Within the acceptable cases, best lip orientation was determined based on two criteria:
- Lower number of impinging motions.
- Lower prevented rotation when the same number of impinging motions was observed.
Results
Compared to a posterior lip orientation, the posterior-inferior lip increased RoM in the top-right quadrant of the impingement diagram (adduction and external rotation) and decreased RoM in the bottom-right quadrant (abduction and extension). On the contrary, the posterior-superior lip increased RoM in abduction and extension and decreased RoM in adduction and external rotation (Fig. 3b).
A total of 13 acceptable cases (prevented hip rotation lower than 10°) were observed within the 27 placement combinations (Fig. 3a). Posterior-inferior, posterior, and posterior-superior lip orientations were the best orientation in 7 cases (mostly with 30-40° of cup inclination), 5 cases (mostly with 40° of cup inclination), and 5 cases (only with 50° of cup inclination), respectively (Fig. 3a).
Conclusions
This study identified the lip orientations that decrease risk of impingement during physiological hip motions for a set of implant placements. The posterior-inferior orientation presented lower impingement for the largest number of combinations, compared to the other two orientations, and might be the most appropriate choice when cup and stem alignments are not navigated intra-operatively.
References
1. Wyatt, Clin Orthop Relat Res, 2020
2. Insull, Bone Joint J, 2014
3. Widmer and Zurfluh, J Orthop Res, 2004
Figures
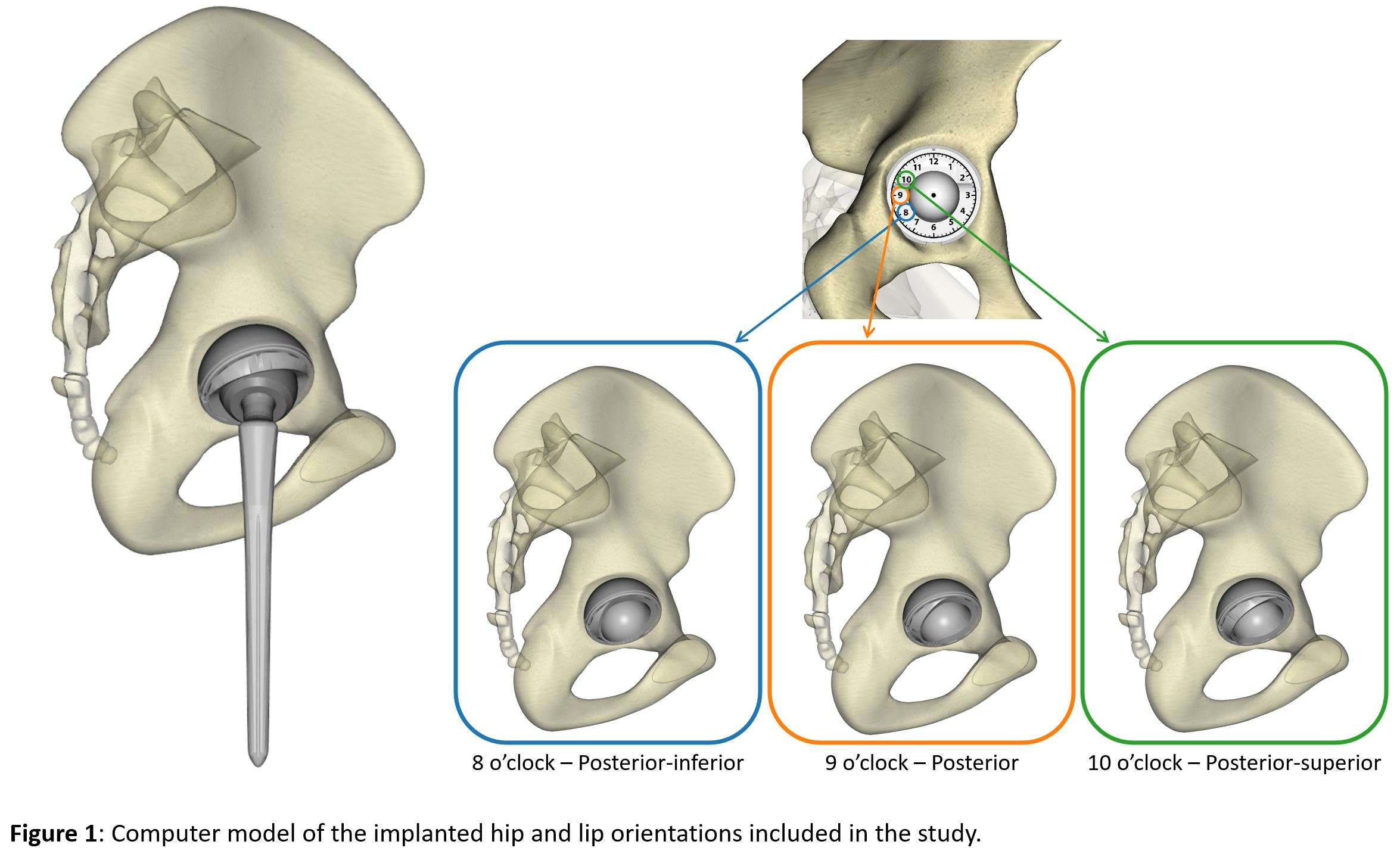
Figure 1
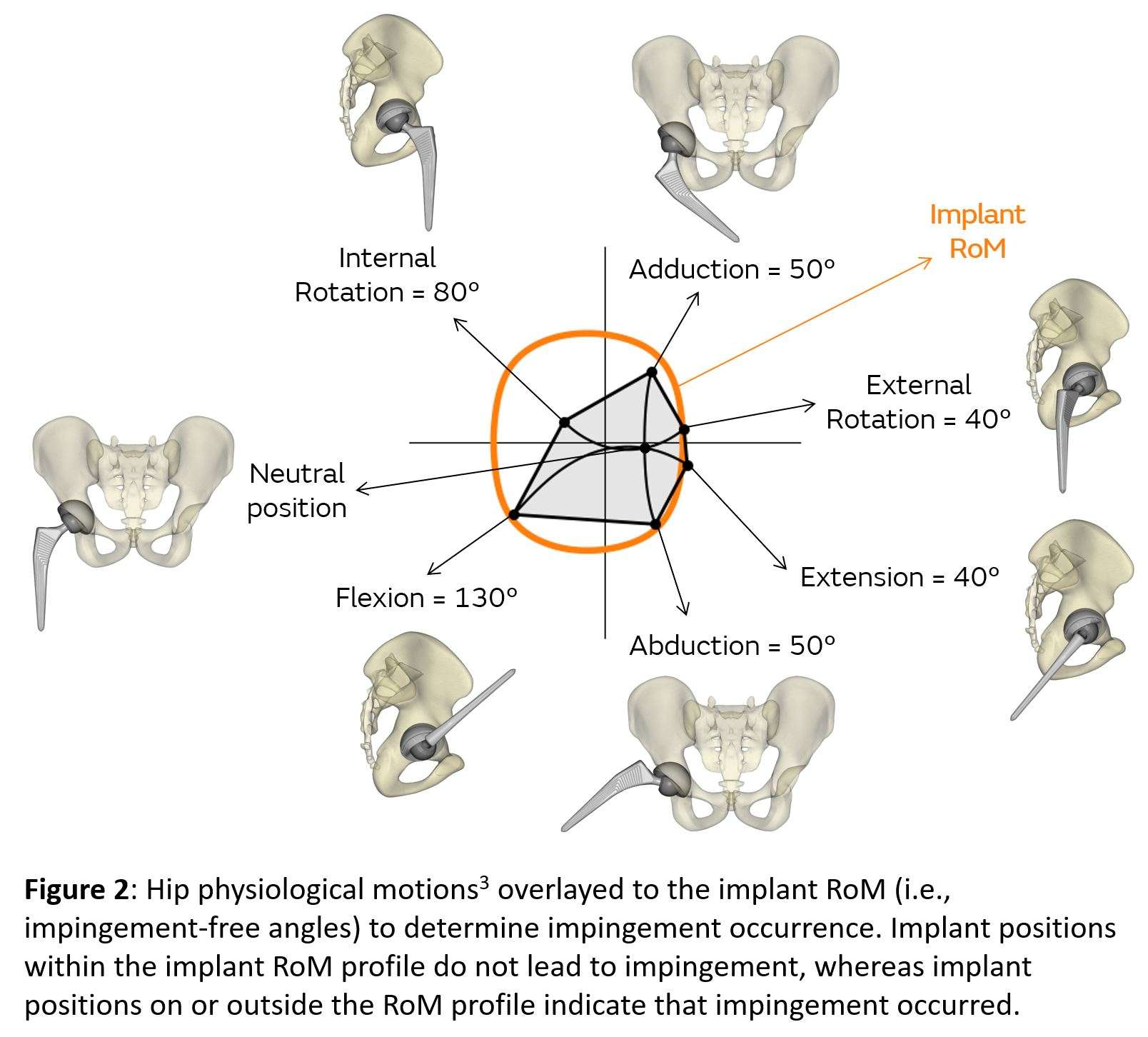
Figure 2
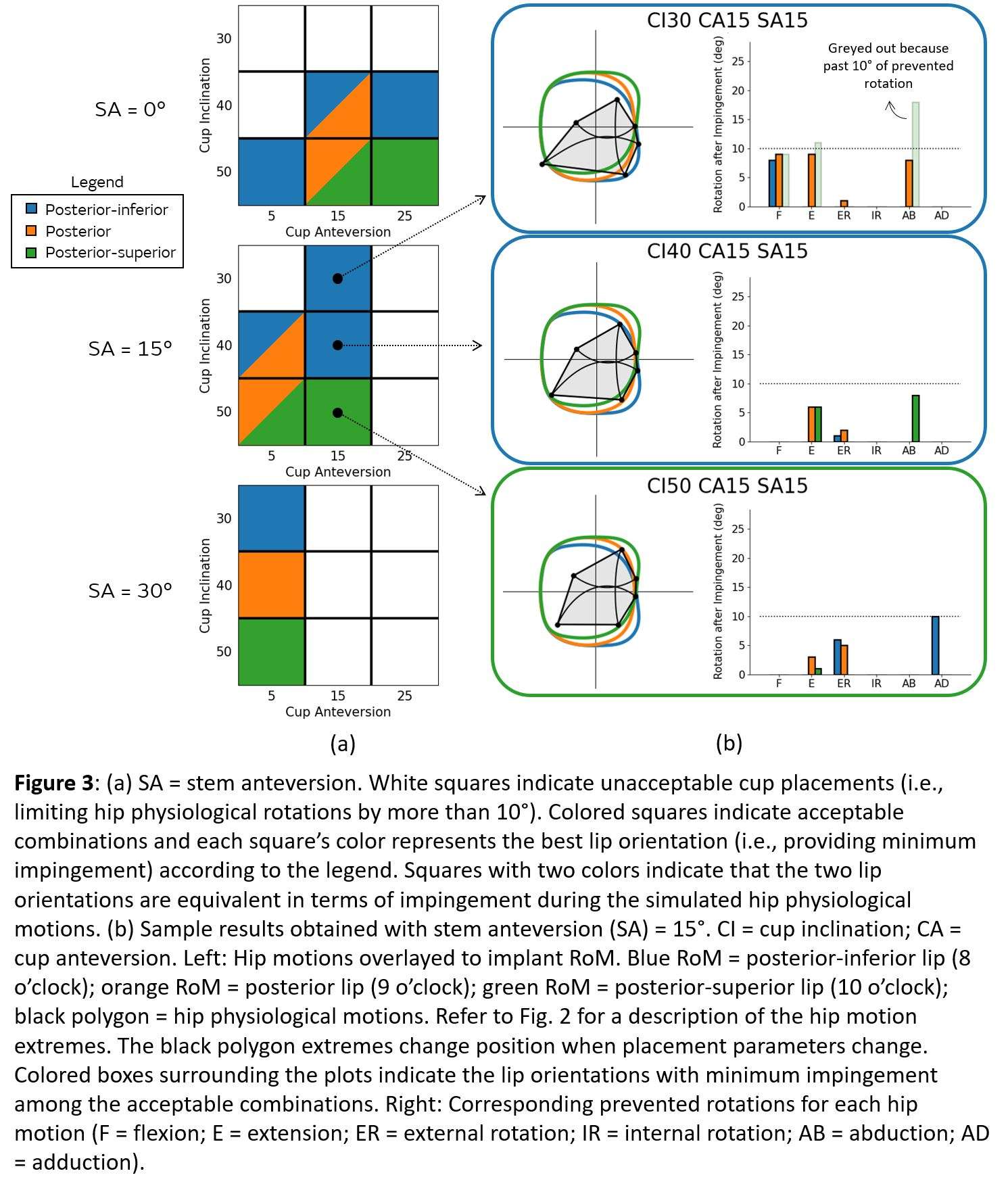
Figure 3#7309
Muscle Activation Patterns and Torque Output During Internal and External Rotation After a Reverse Total Shoulder Arthroplasty
*Alexis Nelson - UTHSC - Memphis, Select Country
William Mihalko - University of Tennessee - Memphis, USA
Thomas Throckmorton - Campbell Clinic - Germantown, USA
Tyler Brolin - Campbell Clinic - Memphis, USA
Blake Hajek - UTHSC - Memphis, USA
Willie Polio - Campbell Clinic - Memphis, USA
Kunal Singhal - UTHSC - Memphis, USA
Shannon Hughes - UTHSC - Memphis, USA
Tristan Hayes - UTHSC - Memphis, USA
Chi-Yang Chiu - UTHSC - Memphis, USA
David Bernholt - Campbell Clinic - Memphis, USA
Frederick Azar - Campbell Clinic - Memphis, USA
*Email: anelso70@uthsc.edu
Introduction: Reverse total shoulder arthroplasty (RTSA) is a reliable treatment for restoring shoulder function. RTSA patient outcomes to return to functional external rotation (ER) is less predictable and needed for activities of daily living. ER muscle activation patterns with RTSA are not well understood. Therefore, the purpose of this study was to examine the timing of upper extremity muscle activation patterns and torque output during shoulder ER and internal rotation (IR) in patients who have a well-functioning RTSA.
Methods: Sixteen patients who had a well-functioning RTSA were recruited to participate. Biomechanical analysis of their post-operative shoulder during ER and IR were performed in two movements: moderate neutral (MN) and abduction (AB). MN and AB are described as follows: MN position; arm at side with 90 degrees of elbow flexion and AB; abduction of shoulder to 90 degrees with 90 degrees of elbow flexion. At the respected positions the patients were informed to rotate as far as they could without pain. Seven surface EMGs and 3 needle EMGs were placed prior to participation. Dynamometer recorded torque and position at (100 Hz) mathematically pattern matched to electromyography (2000 Hz; EMG). Patients performed AB and MN during dynamometer session for 5 trails in each condition. Visual 3D was used to identify external rotation time series during kinematic data collection. Custom software (MATLAB, 2021a) was utilized to perform Teager-Kaiser energy operator on EMG signals to determine EMG onset and offset from which integrated RMS EMG was calculated.
Results: In the AB position, the sequence of iEMG (microvolts*msec) muscle activation timing from maximal IR to maximal ER began with the scapular stabilizers (upper trapezius (48.8, SD 46.1), middle trapezius (56.4 SD 59.4), and latissimus dorsi (11.3, SD 9.8)) followed to external rotation the anterior deltoid activated until neutral (52, SD 33.8), past neutral: teres major (9.6, SD 9.2), teres minor (14.1, SD 18.2) and posterior deltoid (11.1, SD 9.3) (Figure 2). In MN muscle activation patterns were similar compared to AB (Figure 3). Torque was found to be greater in the abduction condition compared to the moderate neutral (Figure 1, p < 0.01).
Conclusion: After RTSA, individually mapped muscle activation patterns were similar in AB compared MN. The upper trapezius timing of activation altered in AB to MN due to the muscle’s role to elevate and upwardly rotate the scapula to aid in abduction. Torque was greater in AB compared to MN potentially due to the AB movement’s need to overcome gravity. Our findings show the import role of the anterior deltoid (AD) to perform external rotation for this transition in AB to overcome gravity, AD aids external rotators to perform external rotation to neutral, past neutral teres major, teres minor, and posterior deltoid perform ER. This study elaborates the complexity of the upper extremity for rehabilitation post RTSA operations where rehabilitation should include the altered anatomy muscle activations of the RTSA shoulder to recover ER fully. Future studies should analyze the EMG intensity in addition to activation timings.
Figures
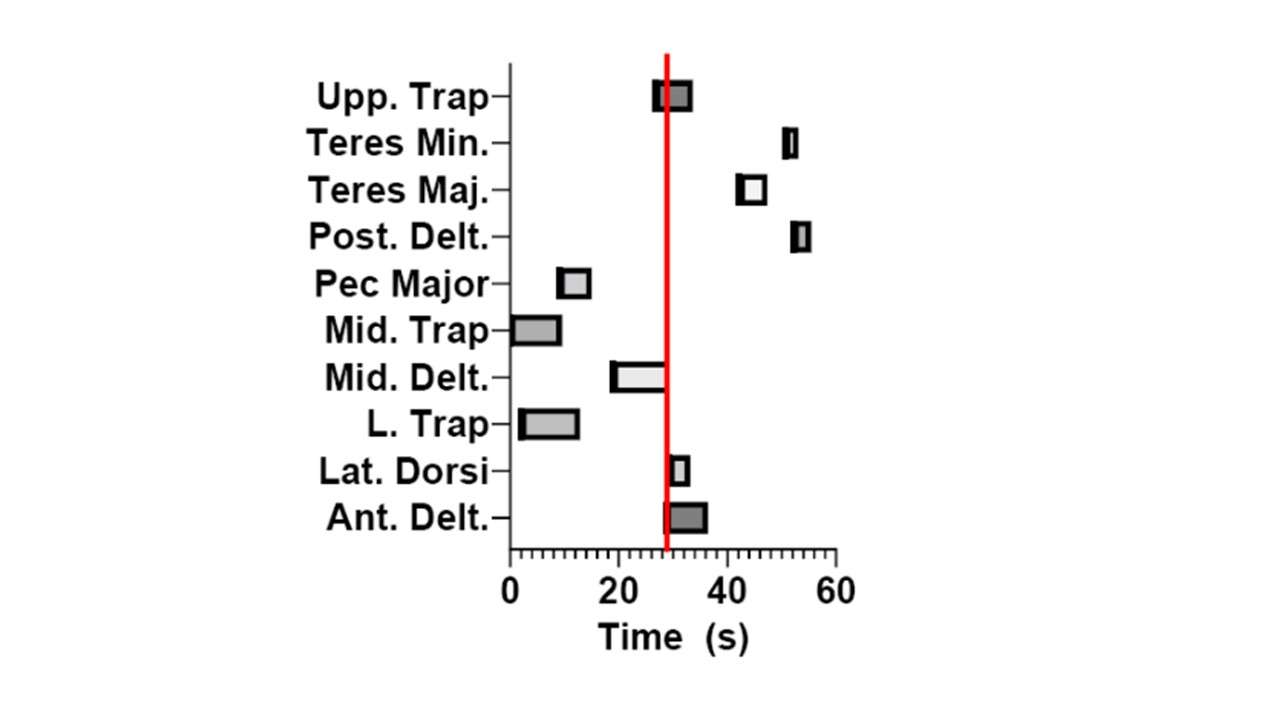
Figure 1
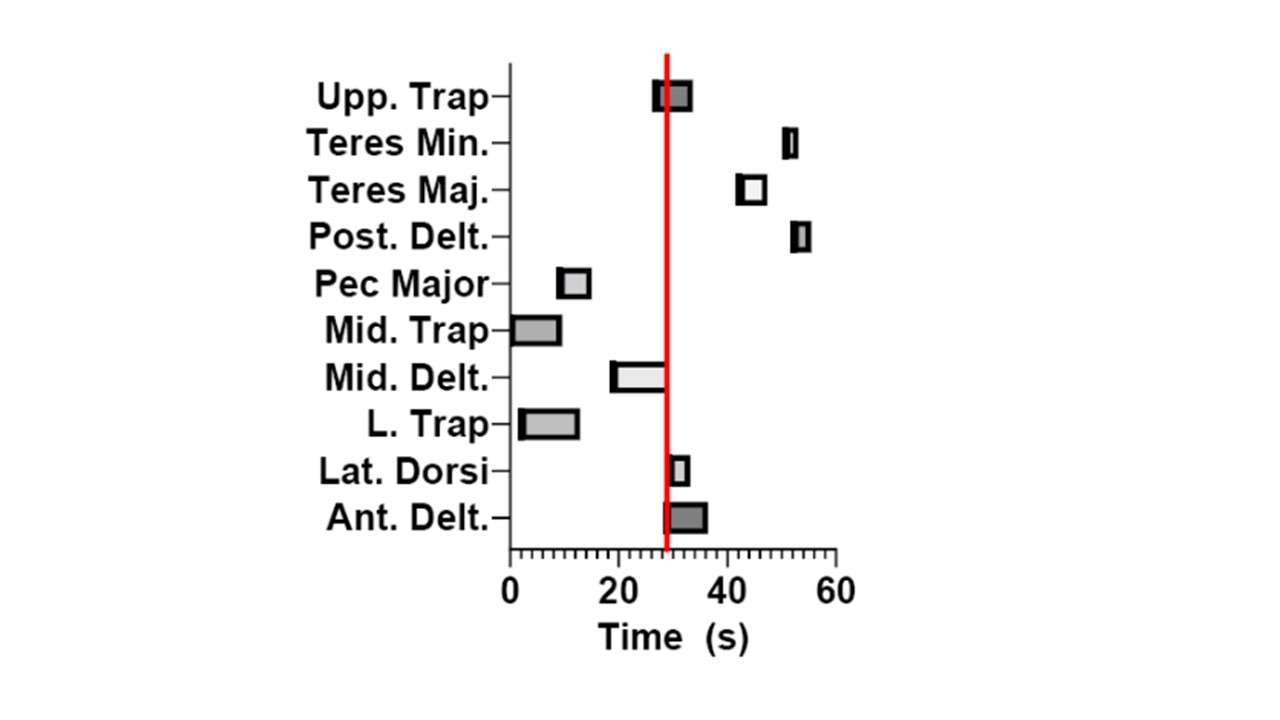
Figure 2
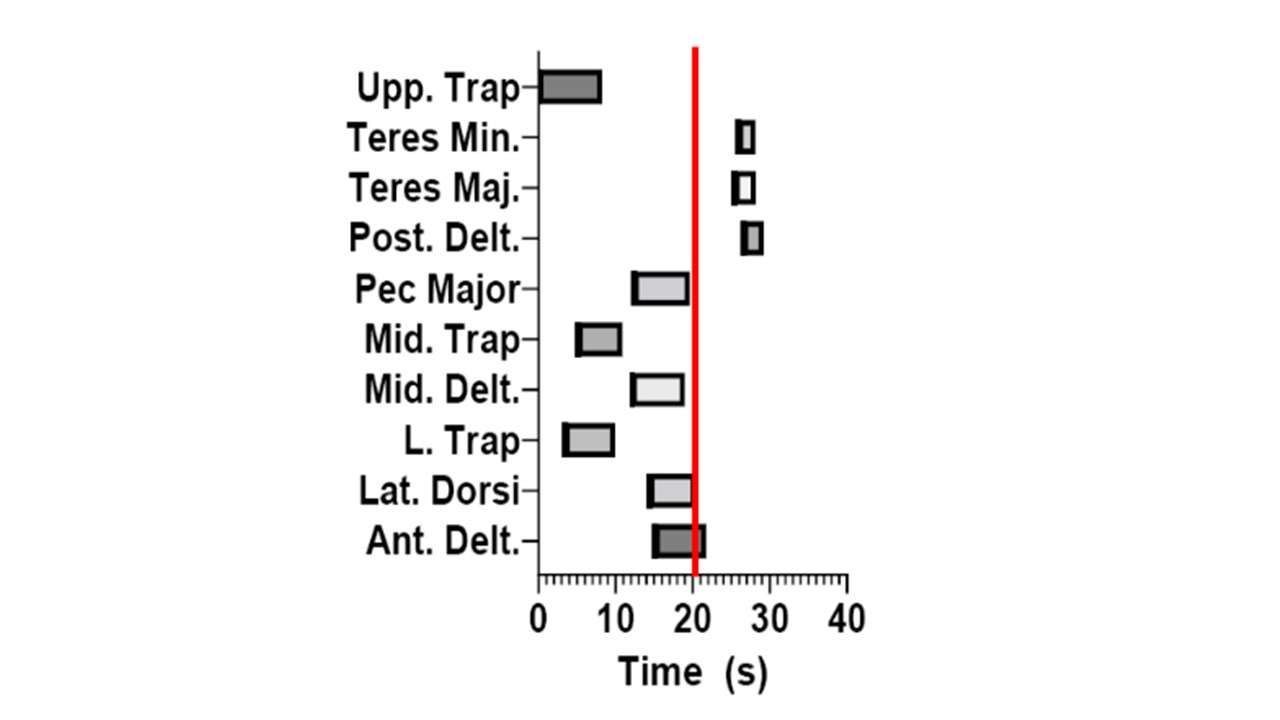
Figure 3#7742
Does TMZF Alloy Microstructure Play a Role in Corrosion Behavior and the Occurrence of Gross Trunnion Failure?
*Mozart Neto - Rush Medical Center - Chicago, USA
Jennifer Wright - Rush University Medical Center - Chicago, USA
Bianca Romay - Rush University Medical Center - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
W Mark Rainforth - University of Sheffield - Sheffield, United Kingdom
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: mozart_q_neto@rush.edu
Introduction: Titanium-molybdenum-zirconium-iron (TMZF) alloy has been introduced as an alternative femoral stem material due to its relatively low elastic modulus providing lower stress shielding. However, TMZF femoral stems failed in vivo at elevated rates due to catastrophic Gross Trunnion Failure (GTF) and were discontinued. The overall magnitude of the problem is uncertain and may be multifactorial. Specifically, the role of alloy microstructure is rarely discussed. Therefore, this study aims to characterize retrieved TMZF tapers and to identify if microstructure may have an impact on the TMZF electrochemical behaviour and the occurrence of GTF, and to determine the fretting-corrosion performance of non-GTF cases.
Materials and Methods: 23 retrieved TMZF femoral stems from a single manufacturer were available. Four cases exhibited GTF. TMZF stem and CoCrMo head tapers were first measured with an optical coordinate-measuring-machine (Redlux) to determine material loss due to fretting-corrosion. Stems were sectioned for microstructural analysis via electron backscatter diffraction (EBSD) in a scanning electron microscope (SEM). A custom made TMZF alloy was made for reference. Alloy samples were categorized as: a) No GTF-stems, b) GTF-stems and c) Custom-made. Three implants from groups a) and b) were selected for corrosion tests. Two electrochemical tests were performed in sequence: 1) Electrochemical impedance spectroscopy (EIS), and 2) potentiodynamic polarization. Both were performed in a three-electrode cell within simulated joint fluid (30 g/L protein, pH 7.4, 37°C). We assessed polarization resistance (Rp), capacitance (Q), corrosion potential (Ecorr) and corrosion current density (icorr). Samples were tested 5 times. Group differences were determined by Kruskal-Wallis and Mann-Whitney-U tests.
Results: EBSD showed that all groups had a homogenous microstructure characterized by equiaxed β phase grains ranging in size from: a) 52±6μm, b) 45±6μm and c) 24±7μm (Kruskal-Wallis, p<0.01) (Figure 1). The “GTF” group had an inferior corrosion behavior with respect to Ecorr, icorr, and Rp and intermediate values of Q. Although the “No GTF” group had the noblest Ecorr and highest values for Rp, the “Custom-made” group had the lowest icorr and Q (Figure 2). The mean in vivo material loss of Non-GTF stems and heads were 0.034±0.07mm3and 0.68±1.54mm3, respectively. GTF stems were worn off entirely, and corresponding heads had prominent fretting-corrosion with 10.9±1.3mm3 material loss.
Conclusion: TheGTF group exhibited the worst TMZF alloy corrosion behavior while also having a finer grain size than “No GTF” cases. Custom-made TMZF exhibited the lowest corrosion rate as measured by icorr. Despite differences, corrosion behavior did not correlate with grain size. Also, GTF occurred despite finer grain size which should provide higher strength. However, the custom-made alloy appeared to have an overall superior corrosion behavior compared to either alloy, while also providing higher strength due to the much finer grain size. Interestingly, in vivo material loss of non-GTF TMZF stems and the corresponding CoCrMo damage are negligible, while GTF CoCrMo heads exhibit severe corrosion loss in addition to TMZF wear. High resolution microstructural analysis is needed to better understand differences in the cases with/without GTF, and to determine if TMZF can be optimized to prevent GTF.
Figures

Figure 1
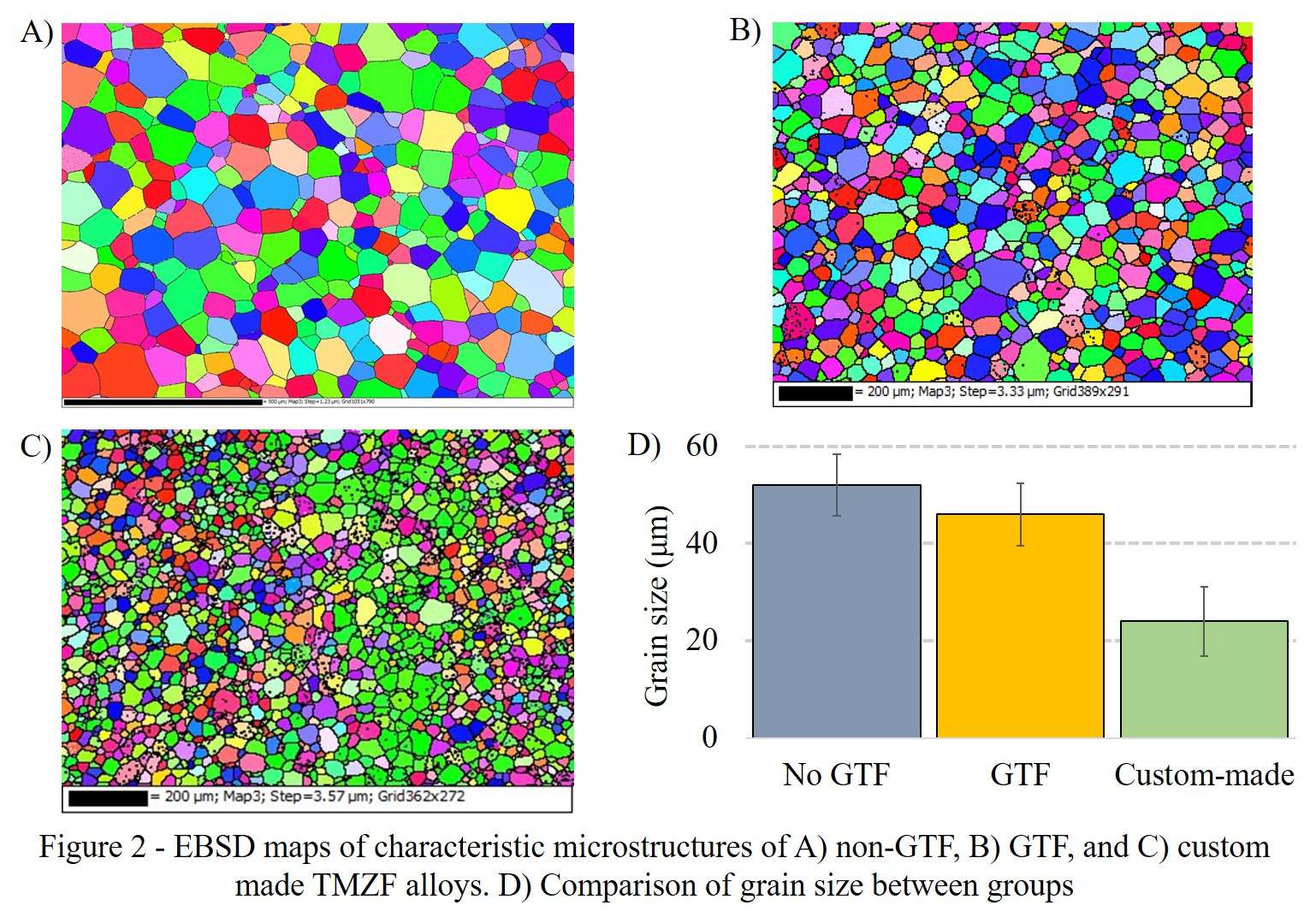
Figure 2
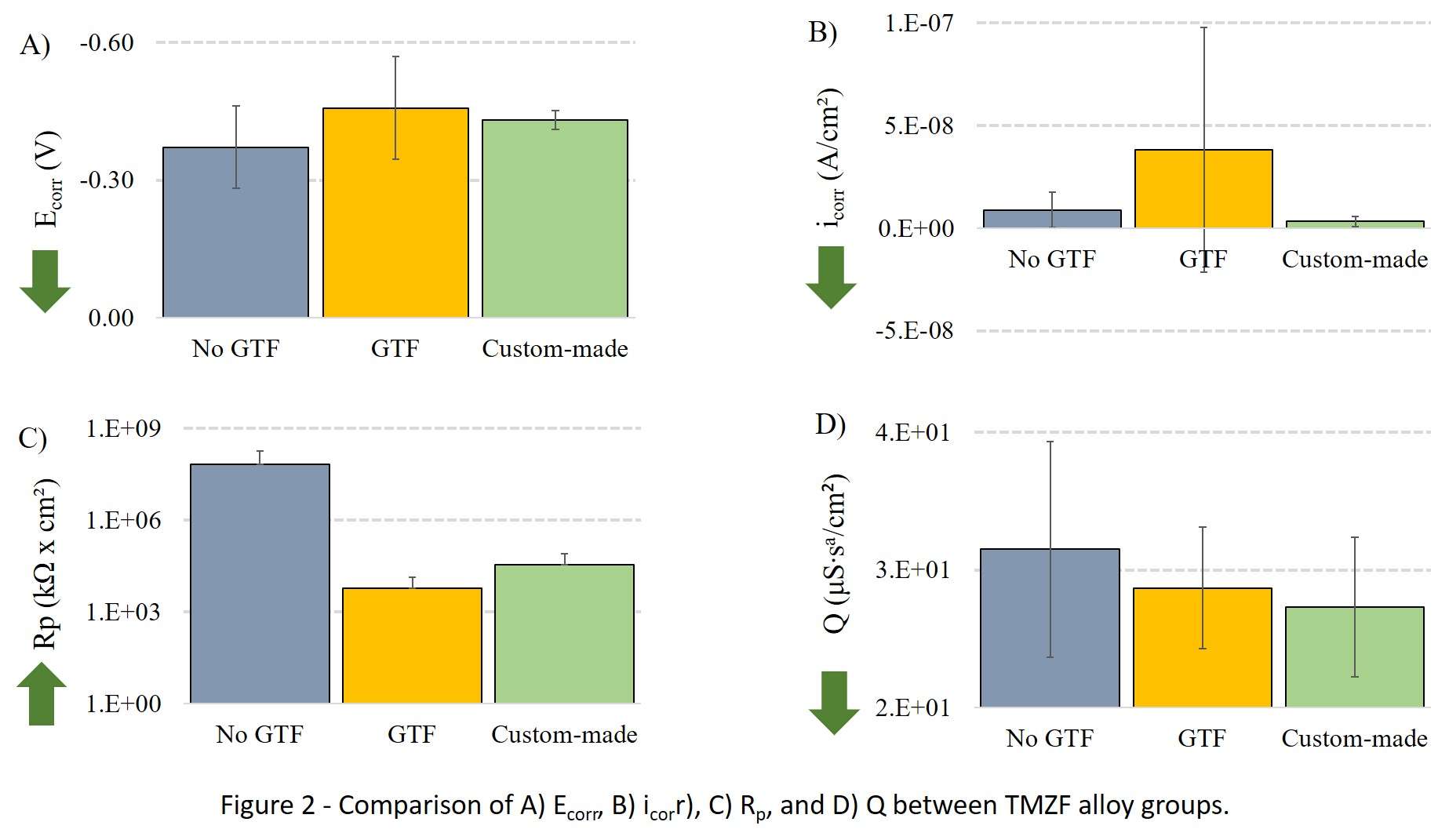
Figure 3#7741
Intra-Manufacturer Microstructural Variations of Additively Manufactured Implants and Its Implications on Corrosion Behavior
*Mozart Neto - Rush Medical Center - Chicago, USA
Nicholas Frisch - Henry Ford Hospital - Detroit, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Brett R. Levine - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: mozart_q_neto@rush.edu
Introduction: Additively manufactured (AM) implants made from Ti6Al4V are increasingly used for orthopedic implants. Our previous work has shown that AM implants have a variable microstructure that is distinctly different from wrought and cast alloys with implications on the corrosion behavior. However, intra-manufacturer variability of AM components is not yet well reported. Our hypothesis was that despite identical chemical composition and design, AM implants have intra-manufacturer microstructural variations that can lead to dissimilar corrosion behaviour.
Materials and Methods: We analysed five acetabular cups from the same manufacturer and design. Implants were either surgically retrieved or in a new state. The microstructural analysis was conducted in a scanning electron microscope (SEM) with electron backscatter diffraction (EBSD) and energy dispersive X-ray spectroscopy (EDS) detectors. We measured grain shape and size, phase content and distribution, alloying elements distribution (homogenization) and presence of defects. Potentiodynamic-polarization tests were conducted on 2 acetabular cups with the biggest difference in microstructure (N=5). Two electrochemical tests were performed in sequence: 1) Electrochemical impedance spectroscopy (EIS), and 2) potentio-dynamic polarization. Both were performed in a three-electrode cell within simulated joint fluid (30 g/L protein, pH 7.4, 37°C). We assessed polarization resistance (Rp), capacitance (Q), corrosion potential (Ecorr) and corrosion current density (icorr). Samples were tested 5 times. Group differences were determined by Kruskal-Wallis Mann-Whitney-U tests.
Results: Our results showed that the AM implants had a wide variation in microstructure from coarse lath-type to fine needle-like grains. Variations also included grain size, β phase content and alloying element distribution. For the components with coarse grains, the β phase was located along the α-boundaries in a network-like fashion, matching the vanadium distribution. The difference in vanadium content varied across phases up to ΔV=10.2%. The fine-grained alloys exhibited nearly no β phase. We observed differences in corrosion behaviour such as Ecorr, Icorr, Rp, and Q, where the fine-grained microstructure consistently exhibited an inferior corrosion resistance.
Conclusion: This study showed that intra-manufacturer microstructural variations can occur in AM implants. These variations can result from process parameters such as printing speed, strategy, powder quality, laser power and final heat treatment. The coarse microstructure is a typical microstructure that was heat treated, normally by hot isostatic pressing (HIP) and the fine microstructure is a non-heat-treated structure, also known as martensite. The coarse microstructure may have implications on the fatigue behaviour due to large elongated grains, network-like β distribution, and residual grain boundaries. The martensitic structure had the worst corrosion behaviour attributed to the metastable nature α’ (martensite) and the presence of built defects (local crevice corrosion). However, the large ΔV observed in the coarsest alloy was also recently linked to inferior corrosion behaviour and is likely the result from excessively long HIPing and slow cooling. Overall, it was surprising to find a range from non-heat treated to extensively heat treated Ti6Al4V microstructures within the same AM implant type. Intra-manufacturer alloy variations in AM implants and its implications on performance need to be further investigated.
Figures
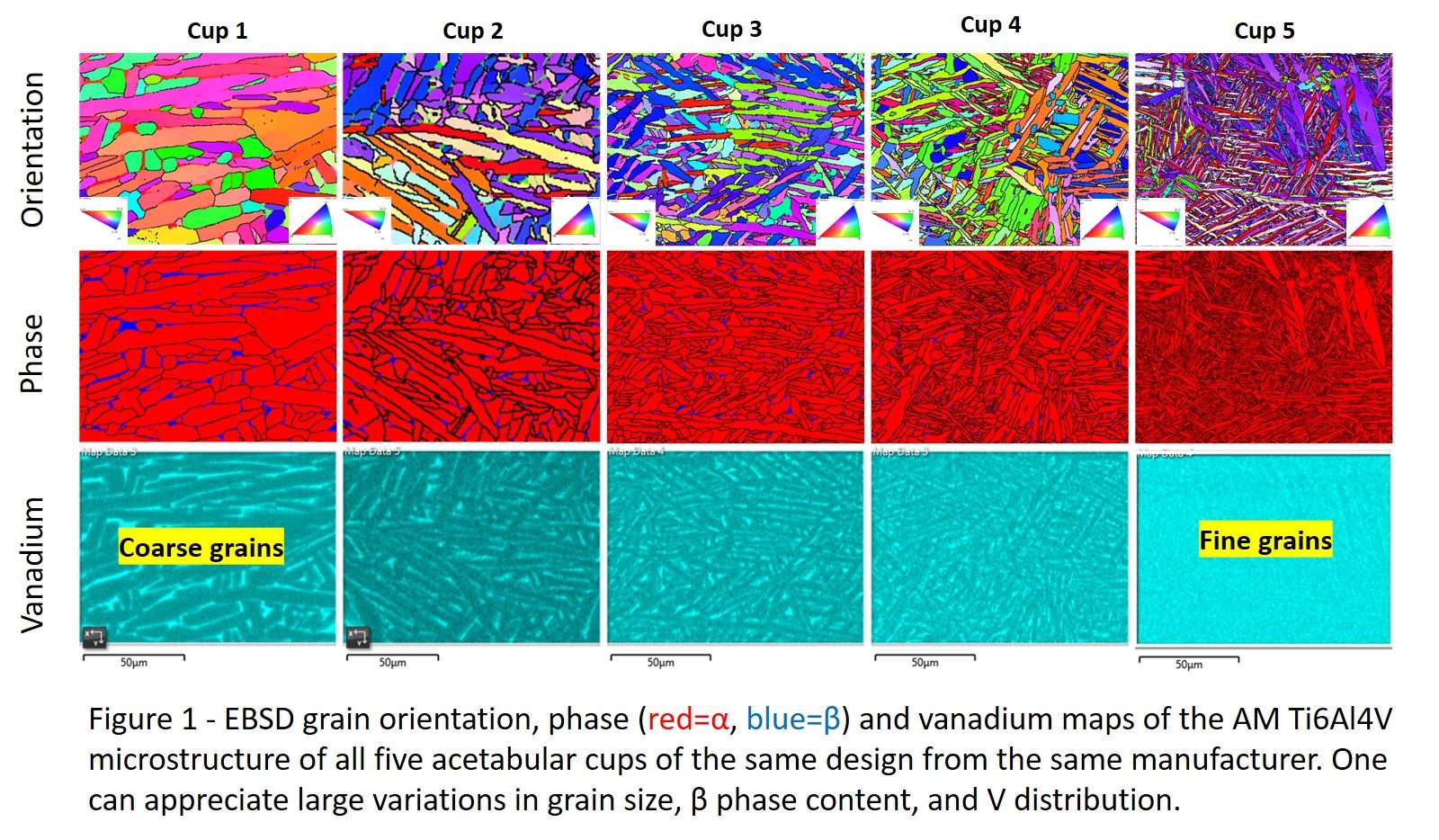
Figure 1
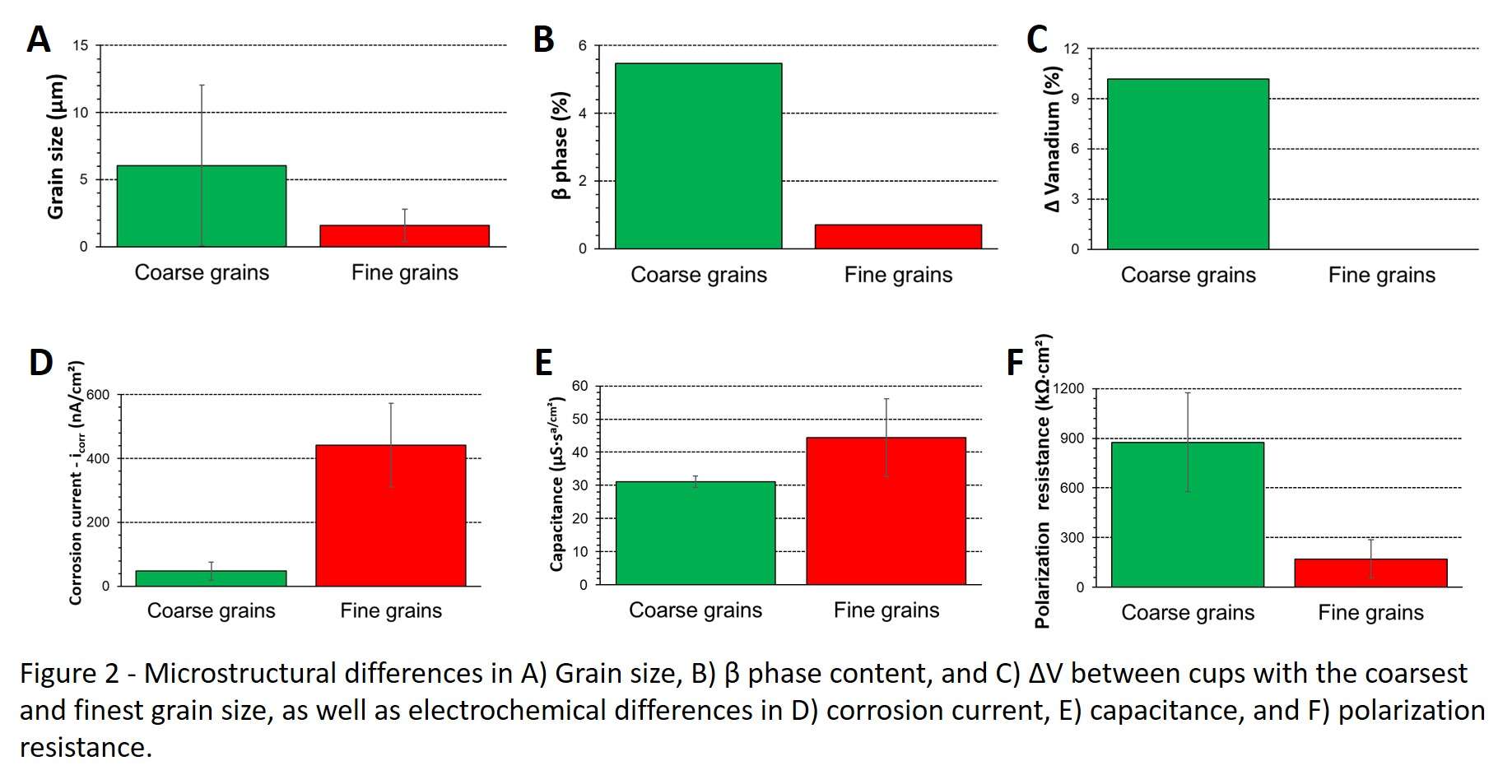
Figure 2#7423
Risk Stratification for Same Day Discharge: An Evaluation of Three Comorbidity Indices
*Ryan Nguyen - JABSOM - - Honolulu, HI - Honolulu, United States of America
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Brian Buchner - Hawaii Pacific Health Medical Group - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
*Email: nguyenry@hawaii.edu
Background:
Same day (SD) discharge following unicompartmental knee arthroplasty may be difficult from a community hospital due to treatment of unselected patients with various comorbidities commonly present. Therefore, this study evaluated the efficacy of three comorbidity indices in predicting successful SD discharge from a community hospital.
Methods:
Data for 97 UKA patients were retrospectively collected to determine the American Society of Anesthesiology (ASA) comorbidity classification, Charlson Comorbidity Index (CCI) and Outpatient Arthroplasty Risk Assessment (OARA). Multivariable logistic regression were performed to evaluate the influence of independent variables.
Results:
Overall, 77 (79.4%) patients achieved SD discharge, with SD discharge failure best predicted by gender (Odds Ratio (OR) 4.45, 95% Confident Interval (CI) 1.307-15.147) and pre operative use of an assisted walking device (OR: 3.633, CI: 1.218-10.832). The ASA, CCI, and OARA demonstrated similar positive predictive values but were not significant indicators of SD discharge success. While race was not different between SD and next day discharge groups, racial differences were present with OARA score >79 and >110 with White patients having a greater proportion in these classifications than Asian and Native Hawaiian/Pacific Island patients (p=0.046 and p=0.010, respectively).
Conclusion:
While no evaluated comorbidity index well predicted the failure of SD discharge, the OARA score was the only measure different between races. Future research should evaluate comorbidities and risk stratification in more ethnically diverse patient populations.
#7630
Comparing Patella Function Between Non-Implanted Knees, Posterior Cruciate Retaining TKAs, and Bi-Cruciate Stabilized TKAs
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Seth Coomer - University of Tennessee in Knoxville - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction
Total knee arthroplasty (TKA) has shown impressive progress over the last five decades, thanks to countless studies dedicated to improving in vivo mechanics. However, the current TKA revision rate is still a concern, at approximately 6% after five years and 12% after ten years. One necessary condition of normal motions includes proper patellar tracking and normal patella kinematics throughout flexion. Unfortunately, the influence of the patellar kinematics on TKA outcomes is generally understudied. Therefore, the objective of this study is to analyze the patella kinematics throughout flexion to determine influencing factors that may lead to patient dissatisfaction.
Methods
Ninety subjects were evaluated in this study, 40 having a Posterior Cruciate Retaining (CR) TKA, 40 having a Bi-Cruciate Stabilized (BCS) TKA, and 10 having healthy non-implanted knees. Similar demographics were controlled for each group. Each subject performed a deep knee bend. Knee kinematics were evaluated using a validated 3D-to-2D fluoroscopic technique while patella kinematics were calculated by using computer graphics measurements. Multiple angles were measured between various bones and components, but one particular angle of interest was the angle between the tibia axis and patella ligament, called the patella ligament angle and labeled as θ1 in Figure 1.
Results
The patella ligament angles throughout flexion for BCS, CR, and normal cohorts are shown in Figure 2, and the corresponding condylar kinematics throughout flexion is shown in Figure 3. At the full extension, Figure 3 clearly demonstrates that the normal knees sit more anteriorly than both TKAs, and with CR TKAs starting more posteriorly than BCS TKAs. Similarly, Figure 2 demonstrates that normal knees start with the greatest patellar ligament angle (19°) and CR TKAs start with the lowest (5°). In this case, larger patellar ligament angles correspond to a more anterior patella, which logically corresponds to a more anterior femur with respect to the tibia, which directly correlates with the AP positioning from Figure 3.
On the same note, according to Figure 3, all 3 cohort knees move posteriorly with increasing flexion, with the normal knee cohort demonstrating the most rollback (18 mm in LAP and 9 mm in MAP) and the CR cohort demonstrating the least (3 mm in LAP and 0 mm in MAP). This again appears to correspond to patellar ligament angle changes seen in Figure 2, with the CR cohort only showing a 5° change in patellar ligament angle throughout flexion and the normal cohort showing 33°. Similarly, BCS cohort magnitudes fall in between the two aforementioned cohorts.
Conclusion
Unfortunately, the patella seems to be considered an afterthought by much of the orthopedic community, and these results indicate that this needs to change. While the data presented here may only serve as an initial study, this analysis provides an approach to studying the influence of the patella on TKA patients’ motion in comparison with the non-implanted knees. This further supports the notion that the entire patellar extensor mechanism is correlated with condylar positioning and therefore overall TKA outcome success.
Figures
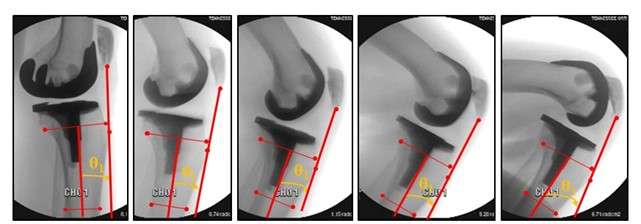
Figure 1
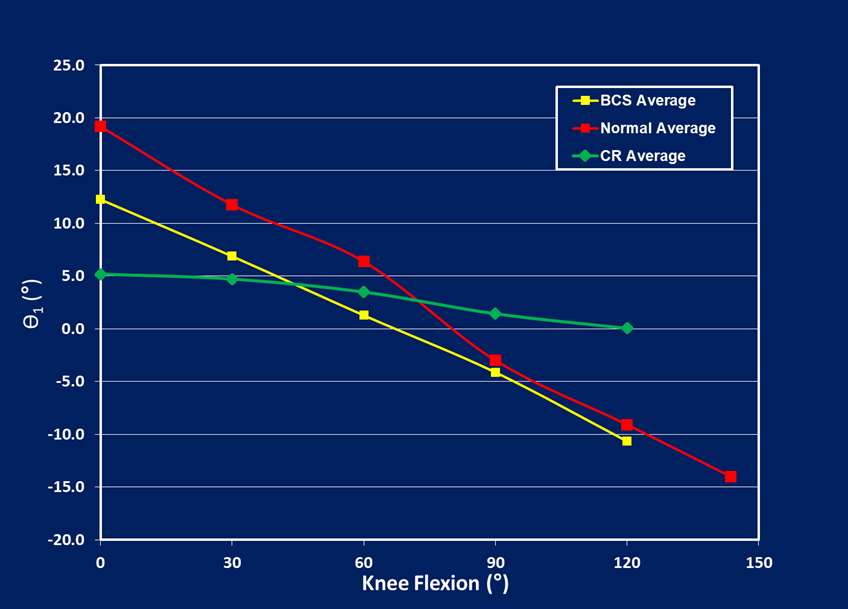
Figure 2
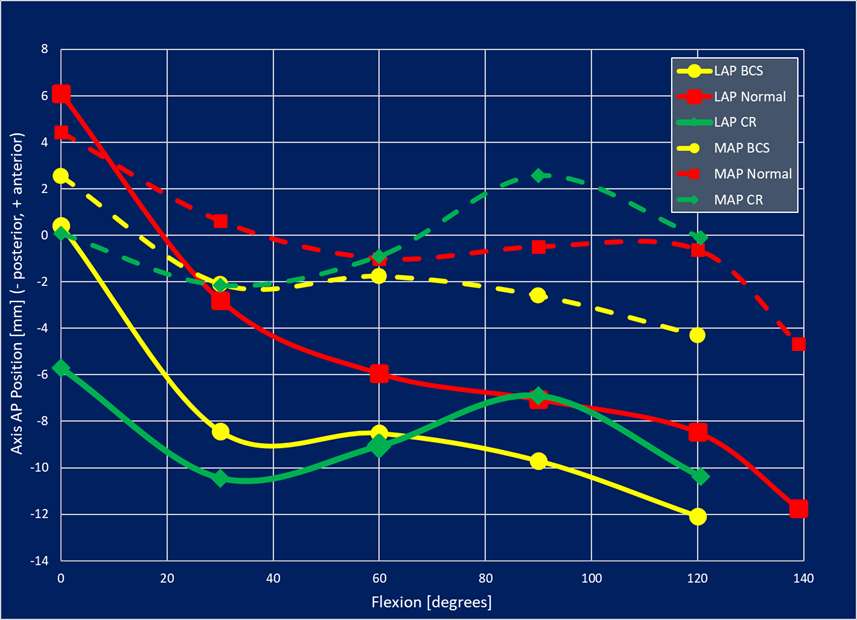
Figure 3#7704
Kinematics Comparisons of the Patella Alta With the Normal Patella After Total Knee Arthroplasty
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction: Patella complications are one of the most common reasons for total knee arthroplasty (TKA) revision. Several studies have shown that patellar height affects the range of motion (ROM) and causes anterior knee pain after TKA. While patella height relates to pseudo patella alta directly, the evidence on the effects of patella atla is still limited. Thus, evaluating correlations between pseudo-patella alta and postoperative TKA mechanics will provide a more in-depth understanding of patellar compilations after TKA.
Methods: The Insall-Salvati Ratio is typically used for classifying the patella height. However, when using fluoroscopic videos, classification based on a single image can introduce bias. We propose an enhanced Insall-Salvati Ratio (eISR) to classify patellar height from fluoroscopic video based on the average ISR from five still images, shown in Figure 1 [Fig. 1], to improve the accuracy of the classification step. In this case, the patella alta is detected for TKA patients with eISR>1.2 (patella baja has eISR<0.8; normal patella has 0.8≤eISR≤1.2). This study was conducted on 40 subjects implanted with a Bi-Cruciate Stabilized (BCS) TKA, 40 subjects implanted with a Posterior Cruciate Retaining (PCR) TKA, and 10 normal, non-implanted knees. No instances of patella baja occurred in our dataset. Kinematic and kinetic data of those 90 subjects were collected using validated 3D-to-2D fluoroscopic registration techniques. Specific parameters of interest were anterior/posterior motion of either condyle (LAP/MAP), femorotibial axial rotation, and weight-bearing range-of-motion (ROM).
Results: The patella height classification results are shown in Table 1 [Fig. 2]. While around 20% of non-implanted subjects have patella alta, the percentage for both implanted cohorts is around 40%. In other words, this indicates that TKA subjects are more likely to have patella alta than non-implanted subjects. There were no significant differences between the normal patella and patella alta groups for lateral antero-posterior (LAP), medial antero-posterior (MAP), and axial rotation (AR) for both BCS and PCR implants, as shown in Table 2 [Fig. 3]. Interestingly, however, there was a significant statistical difference in ROM for both the BCS cohort (P=0.016) and PCR cohort (P=0.04), with normal patellar groups having significantly higher weight-bearing range of motion than patella alta groups. The non-implanted group shows no significant differences for all the kinematics indexes.
Conclusion: Two significant findings were discovered in this study. First, TKA subjects appear to have higher occurrences of patella alta compared to non-implanted subjects, and second, there was a significant difference in weight-bearing ROM between the normal patella and patella alta groups for TKA patients. This is likely because quadricep wrapping happens earlier for the patella alta group, leading to a tighter extensor mechanism and a limited range-of-motion. This phenomenon did not happen with the non-implanted cohort, which is particularly interesting and may indicate that patella alta might reduce ROM after TKA. Thus, it’s important to maintain the natural position of the patellar joint line for TKA patients by choosing the correct implant sizes and polyethylene thickness.
Figures
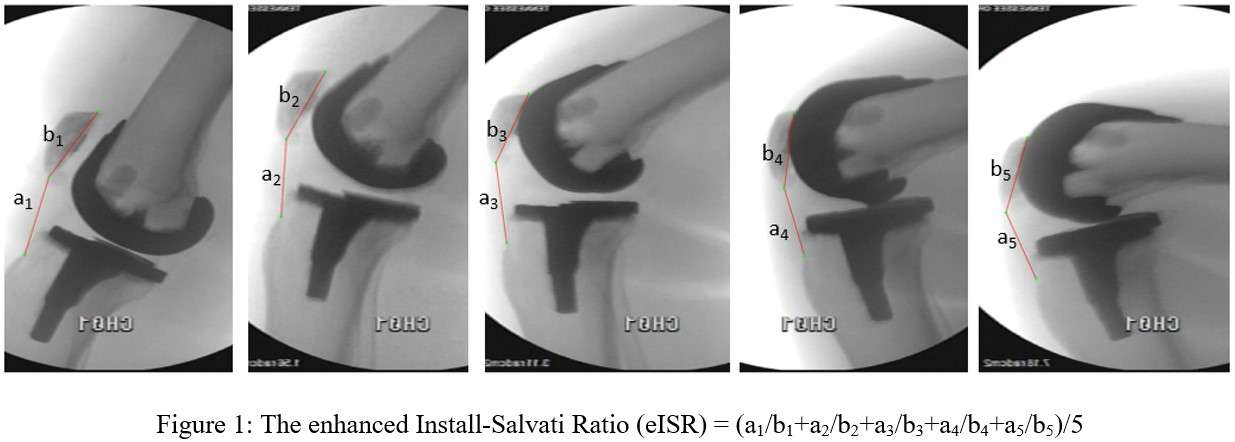
Figure 1

Figure 2
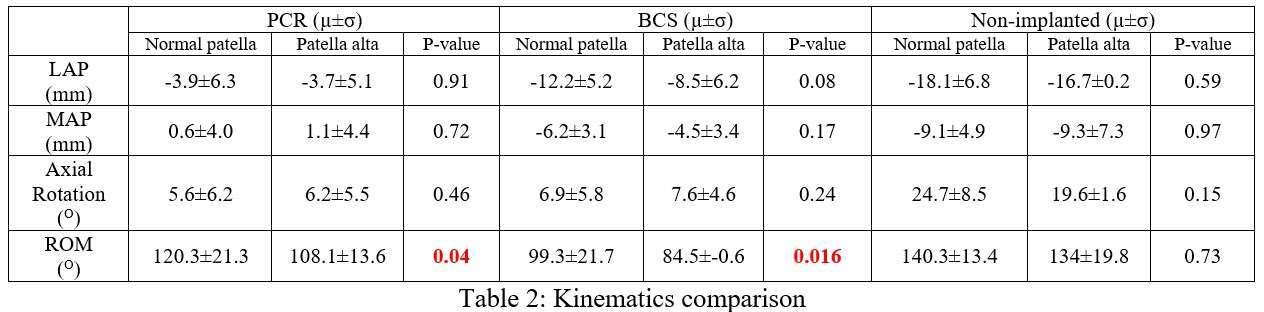
Figure 3#7827
Optimal Methodology for Creating 3D Implant CAD Models Using a Morphing Algorithm That Utilizes Either X-Ray or Fluoroscopic Images
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Jarrod Nachtrab - University of Thennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction: 3D reconstruction is not only an attractive problem for many researchers but also a challenging goal, especially for the anatomy of Total-Knee-Arthroplasty (TKA). While three-dimensional (3D) Computer-Aided-Design (CAD) is necessary for the TKA kinematics and kinetics analyses as well as design improvements, those CAD models are not always available. 3D models are usually reconstructed by the Computed-Tomography (CT) scan that contains a high radiation exposure and cost consumption. Reconstructing a 3D component from a limited number of X-ray images eliminates the need for a CT scan but is a challenging task. Thus, we propose a new approach to designing an unavailable CAD model using only one template model and a few X-ray or fluoroscopic images.
Methods: The first step involves multiple overlays of the initial CAD model with respect to the X-ray images, but those overlays might not be fitted due to the incorrect CAD model shape. This CAD model is processed by finding the initial bound in 3D, called X. The X-ray image is processed to find the two-dimensional (2D) bound. An optimization problem is solved to find the optimized target bound in 3D, called Y. The proposed morphing algorithm is an enhancement of Coherent-Point-Drift (CPD) to morph the required CAD model from a set of vertices. This is done so that bound X of this set fits with bound Y without changing the structure of the designing model since all vertices are transformed coherently (Figure 1). In this study, the algorithm was used to morph a TKA template component model and compare it to an available known model. We also utilized a scenario where we did not have the “correct” models and thus the morphed results are compared to the X-ray silhouette.
Results: In general, the morphed model showed excellent results when compared to a known model. By using a single CAD model and 4 fluoroscopy images (Medial/Lateral, Anterior/Posterior, and ±45-degree rotations of the knee implant about the Superior/Inferior axis), a comparison of the resulting morphed model to the known target CAD model can be found in Figure 2. The RMS error was 0.37 mm, and the absolute largest source of error was 1.08 mm and occurred on the internal surface, which is not a concern for fluoroscopic studies. Those errors could be reduced if additional X-ray images are provided for the input of the morphing algorithm. Additionally, the morphing results revealed that the overlay of the new morphed model fits almost exactly like the silhouette of the corresponding X-ray images (Figure 3).
Conclusion: A novel methodology was introduced to overcome common 3D-to-2D registration limitations by recreating entire families of 3D CAD models from a limited number of X-ray images. Our algorithm has demonstrated high levels of accuracy with multiple potential extended applications. While this evaluation focused only on the femoral component model, our algorithm is robust enough to be extended to additional components or joints, and the algorithm can also be extended to bones, which may help eliminate the need for CT scans and segmentation.
Figures
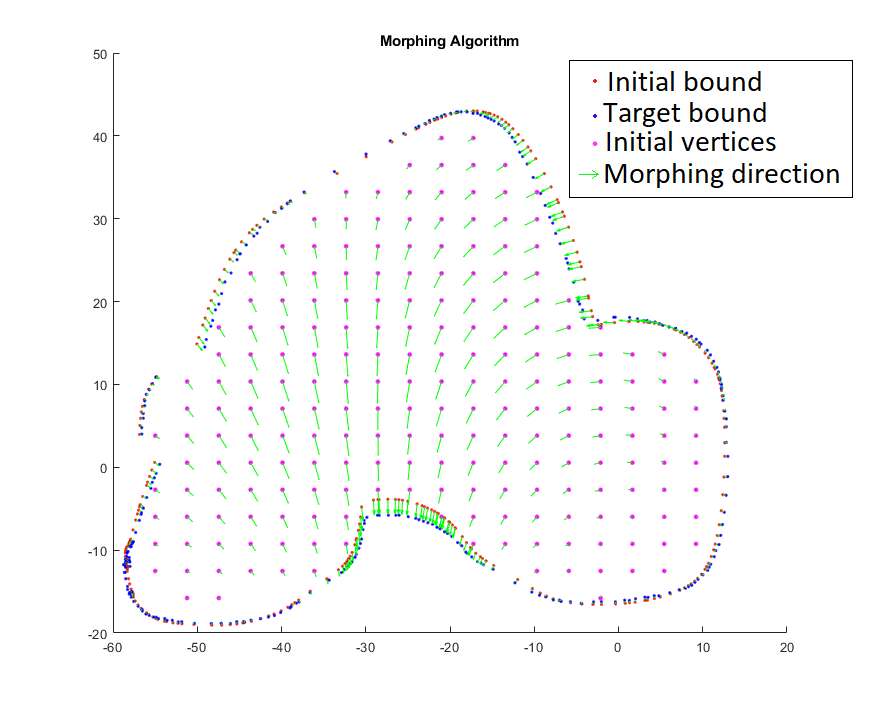
Figure 1
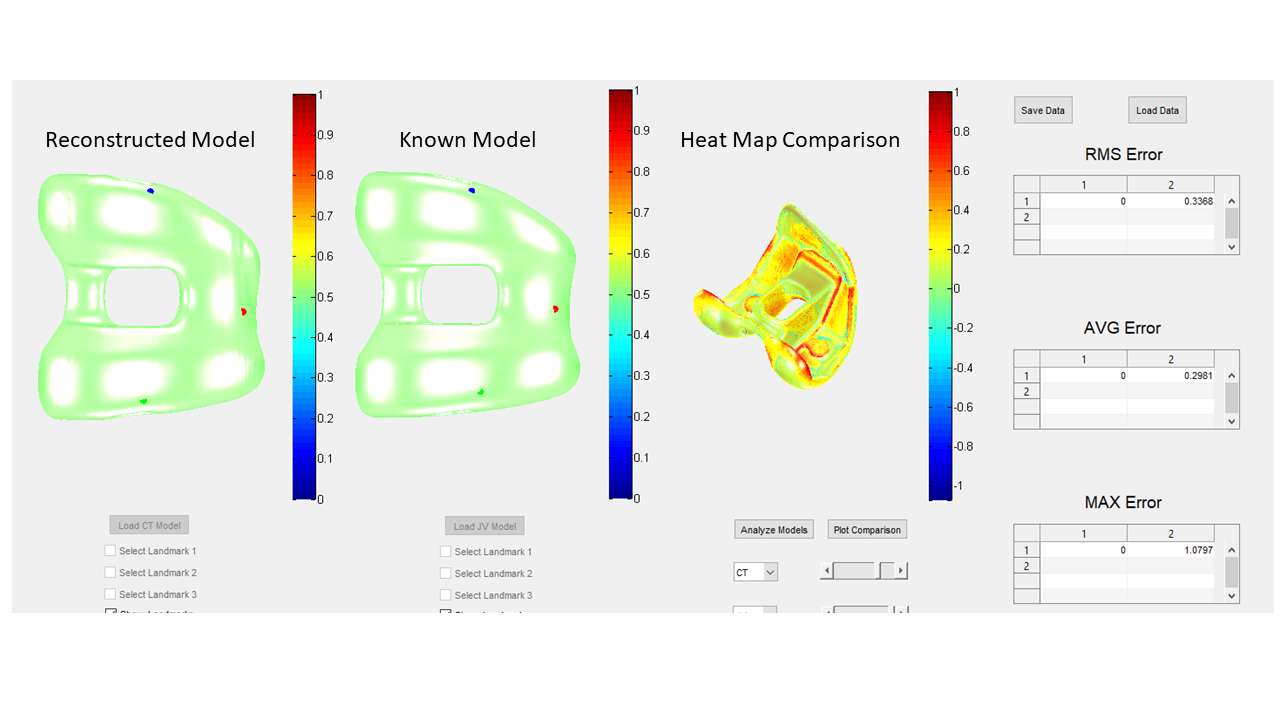
Figure 2
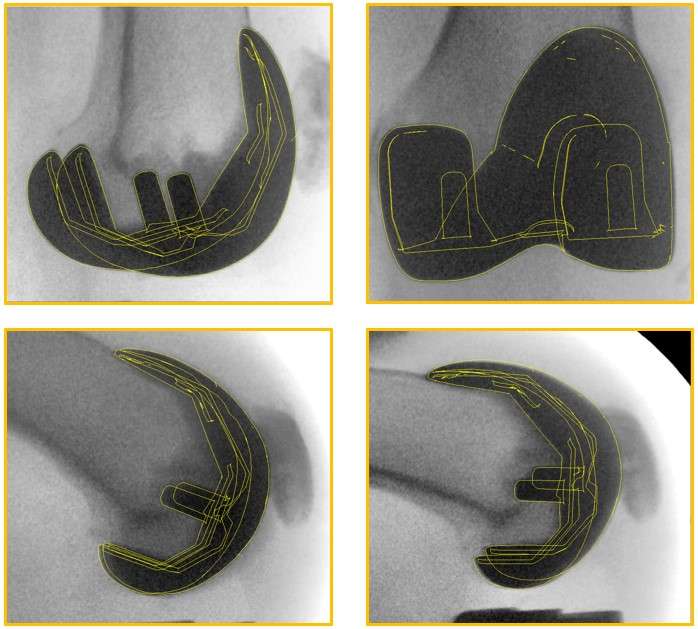
Figure 3#7832
A Comprehensive Comparison of Automatic 3D-to-2D Registration Techniques for Total Knee Arthroplasty by Non-Learning Optimization Methods
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction: The 3D-to-2D technique is an important step in analyzing the TKA kinetics and kinematics. Many studies have tried to implement optimization techniques in the past, but typically the results from these algorithms can be unstable and usually require human intervention or confirmation. Thus, the 3D-to-2D registration often requires manual work. With the development of computer technology, many powerful tools have been invented to find the solutions to the 3D-to-2D registration problem. While machine learning is a useful tool to solve this problem, it relies on a large dataset and is not always available. This study compares the performance of existing non-learning methods for the 3D-to-2D TKA registration problem to see which is the best.
Methods: We compared 7 different optimization methods, 4 for edge-based (including interior point, Quasi-Newton, sequential quadratic programming, and Powell-Brent) and 3 for region-based (particle swarm optimization, simulated annealing, and genetic algorithm), as summarized in Table 1 [Figure 1]. The edge-based method aims to fit the boundary of the knee implant onto the contour of its silhouette, while the region-based method overlays the projection of the knee implant onto the region of its silhouette. Those methods are evaluated by registering a 3D model on 20 fluoroscopy frames representing a weight-bearing high flexion activity. Convergence frequency, speed, and accuracy were used to evaluate the results.
Results: For the edge-based model of TKA, the Powell-Brent method shows excellent registration result (red contour) for TKA as shown in Figure 2 if the initial pose (green contour) is “close” enough to the correct pose. The Powell-Brent and interior-point methods converge to the minimum point of searching for the solution for the 3D-to-2D registration problem, while the quasi-newton and sequential quadratic programming methods failed to converge to the minimum point. The Powell-Brent method provides the highest accuracy and shortest run time to search for the registration result. For the region-base model of TKA, the success rate of the particle swarm optimization, as shown in Figure 3, is 100% of registering, while those numbers of the simulated annealing and genetic algorithms are 93% of the frames and 40% of the frames, respectively.
Conclusion: This study provides a comprehensive review of the existing methods and non-learning optimization tools for 3D-to-2D registration and its application in TKA. Both Powell-Brent edge-based and particle swarm optimization methods show excellent results for the 3D-to-2D TKA registration problem. However, Powell-Brent edge-based requires a “good” initial pose, while particle swarm optimization takes a longer running time to search for the result. Because each research lab uses a different protocol for 3D-to-2D registration on different joints, understanding the advantages and disadvantages of each method is important to find an appropriate method to analyze the dynamics of the corresponding joint for the highest accuracy.
Figures
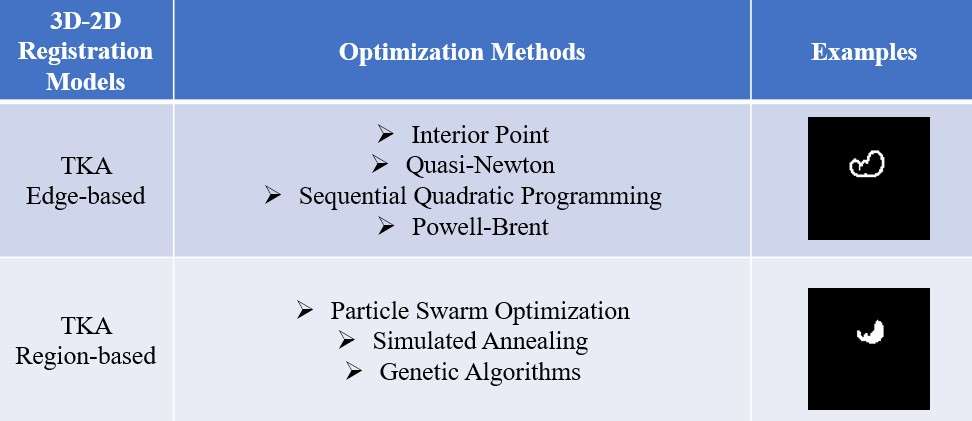
Figure 1
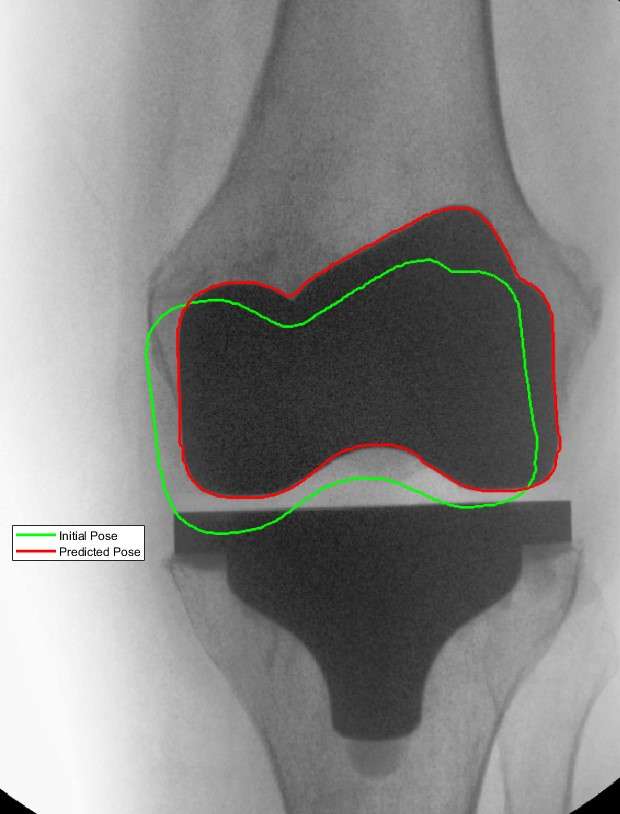
Figure 2
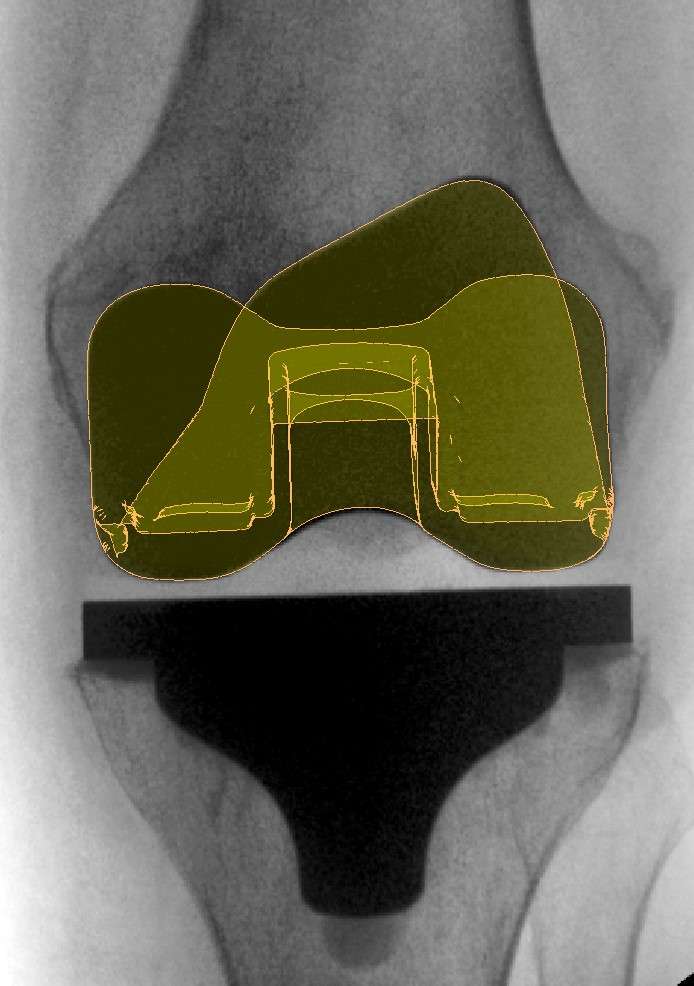
Figure 3#7820
Recreating 3D Femoral Component Catalogs Using Novel Non-Rigid Registration Morphing Algorithms
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction: 3D-to-2D registration methodologies have been around for nearly 30 years, involving both single-plane and bi-planar fluoroscopic registration. While the fluoroscopic videos are readily available through data collection, three-dimensional (3D) Computer-Aided-Design (CAD) models of the associated components are not always readily available. Unfortunately, these CAD models are necessary for accurate postoperative kinematic evaluations. Without such models, 3D-to-2D kinematic evaluations become nearly impossible. Reconstructing a 3D component from a limited number of X-ray images is a challenging task, yet current approaches involve using statistical shape methods and modern machine learning algorithms to achieve success. Thus, we propose a new approach to design a complete component sizing range using a single template CAD model using a limited number of static X-ray images and a template model.
Methods: The proposed non-rigid morphing algorithm, based on the coherent point drift (CPD) algorithm, scales and transforms the shape of the template model to fit with the silhouette of the corresponding X-ray images without changing the structure of the knee implant. While a greater number of X-ray images can lead to higher accuracy, our study utilizes only 4 images (Medial/Lateral, Anterior/Posterior, and ±45-degree rotations of the knee implant about the Superior/Inferior axis) as illustrated in Figure 1. This allows for good reconstruction results while also reducing the radiation exposure for all personnel. In this study, we use the proposed approach to reconstruct 2 catalogs (16 knee models) of cruciate-retaining (CR) and posterior-stabilized (PS) which include 8 sizes for each implant. Those reconstructed models are compared with the known models to analyze the algorithm performance.
Results: In general, the morphed model showed excellent results when compared to known models. By using the proposed morphing algorithm on reconstructing 16 testing models, we achieved an average root mean square (RMS) error of 0.41±0.08 mm. The average absolute largest source (MAX) of error was 1.55±0.48 mm, but these larger sources of error typically occur on the internal surfaces of the component, which are less important in fluoroscopic studies. A sample comparison of the resulting morphed model to the known target CAD model can be found in Figure 2 (RMS error = 0.46 mm, AVG error = 0.37 mm, MAX error = 1.8 mm). Those errors could be reduced if additional X-ray images are provided as input to the morphing algorithm. The entire morphed catalog, showing the original template model and all other morphed models, is shown in Figure 3.
Conclusion: A novel methodology was introduced to overcome common 3D-to-2D registration limitations by recreating entire families of 3D CAD models from a limited number of X-ray images for both CR and PS TKA implants. Our algorithm has demonstrated high levels of accuracy with multiple potential extended applications. While this evaluation focused only on the femoral component model, our algorithm is robust enough to be extended to additional components or joints, and the algorithm can also be extended to bones, which may help eliminate the need for CT scans and segmentation.
Figures
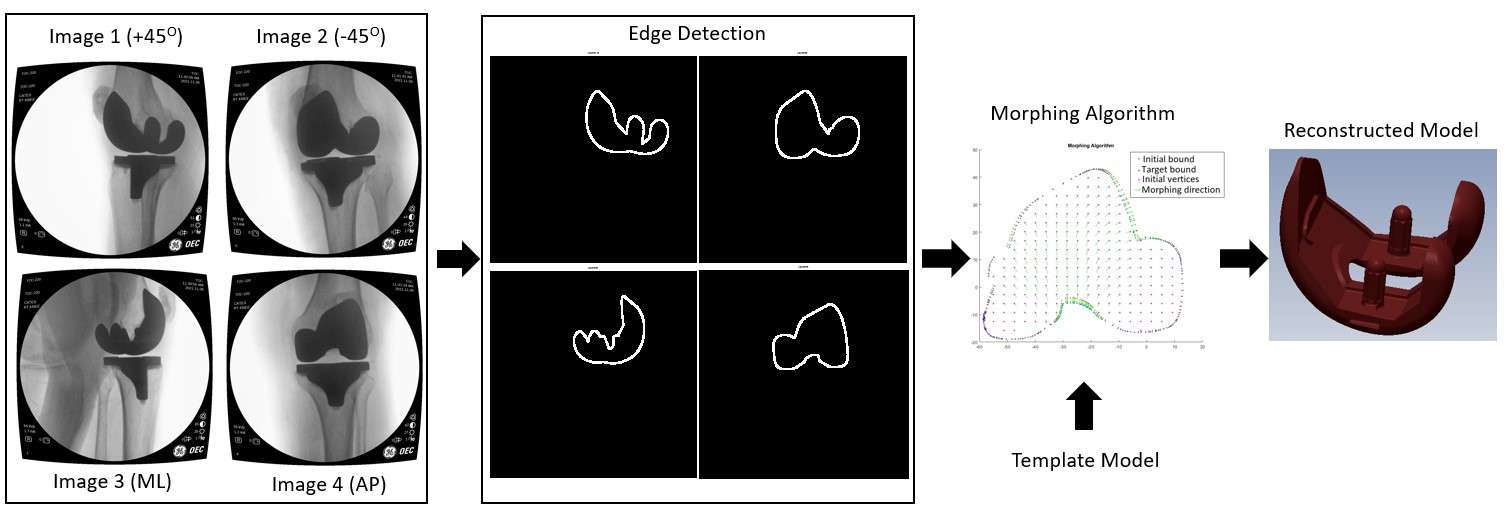
Figure 1
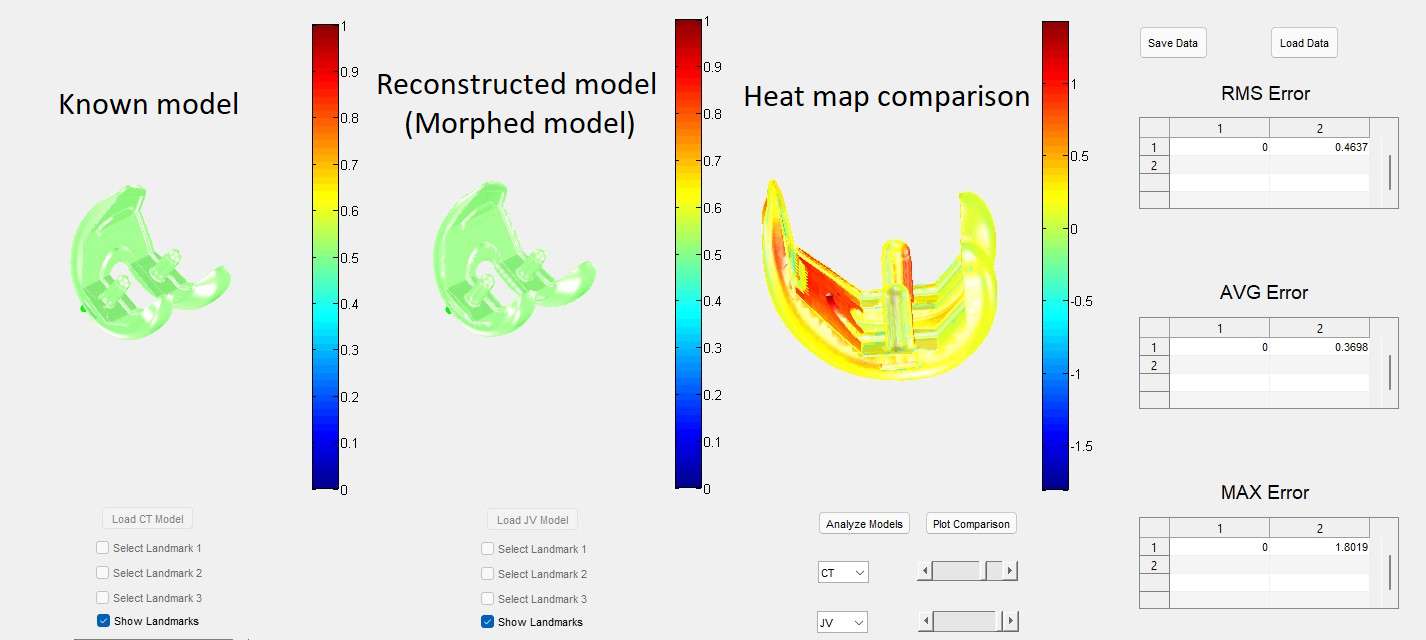
Figure 2
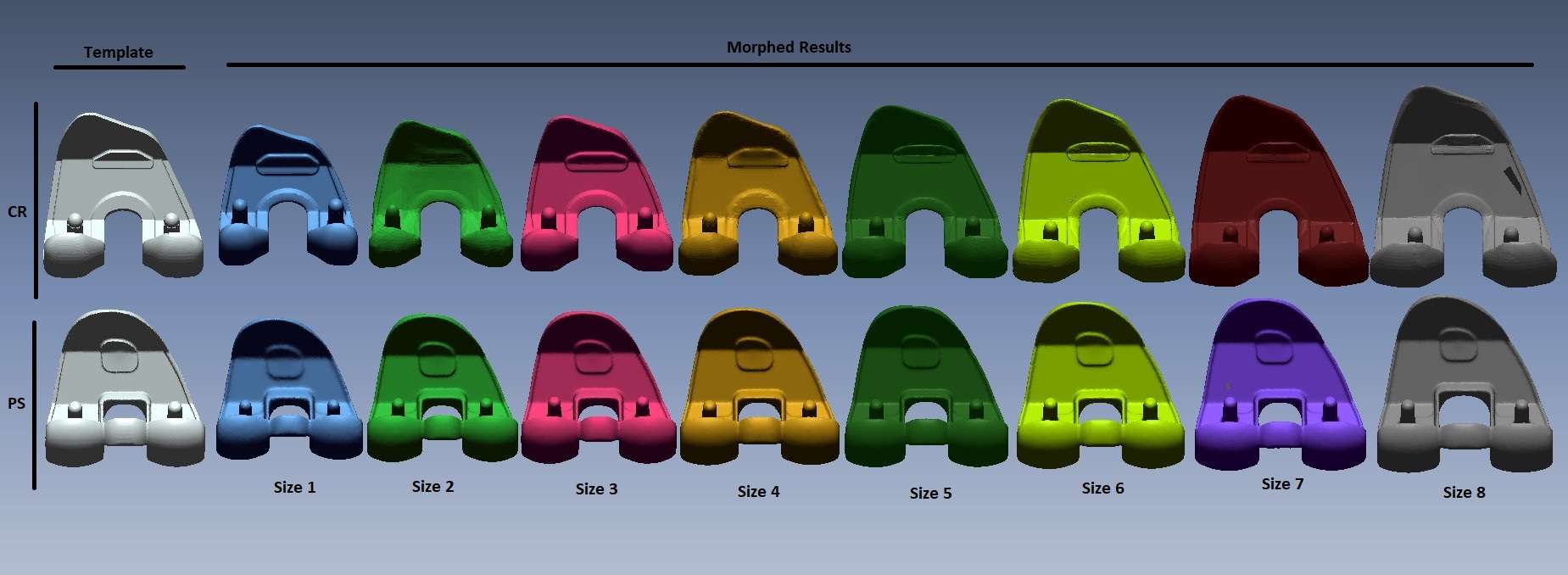
Figure 3#7949
Automatic 3D-to-2D Registration for Total Knee Arthroplasty Fluoroscopy Video by Non-Learning Optimization Method
*Viet-Dung Nguyen - The University of Tennessee at Knoxville - Knoxville, United States of America
Michael LaCour - University of Tennessee - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: vnguye28@vols.utk.edu
Introduction: 3D-to-2D fluoroscopic registration techniques are important steps when analyzing weight-bearing total knee arthroplasty (TKA) kinematics, achieved by overlaying a knee implant model onto multiple fluoroscopy images. Many studies have tried to implement optimization techniques in the past, with varying degrees of success, but the results from these algorithms can be unstable and often require human intervention or confirmation. Thus, 3D-to-2D registration often still requires significant manual work. With advancements in computational technology, many powerful tools have been developed to find more robust solutions to the 3D-to-2D registration problem. While machine learning is a useful tool to solve this problem, it relies on a large dataset and is not always available. Thus, this study compares multiple different non-learning optimization methods and then shows an approach to registering a knee implant onto multiple fluoroscopy images with a high accuracy 3D-to-2D registration method.
Methods: Our registration method uses edge-based registration to compare the edge of the knee implant on the fluoroscopy image with the edge of the projection of the knee implant model onto the fluoroscopy plane as shown in Figure 1. The optimization problem is created with the minimizing objective function as the matching energy between those two edges, while the orientation of the model (3 translations and 3 rotations) is the searching variable. We compared the performance of multiple optimization methods, including Powell optimization (PO), interior-point (IP), Quasi-Newton (QN), and sequential quadratic programming (SQP), to find the method with the highest accuracy and fastest running time. This method was then used to predict the pose at full extension. From there, the registered results were rotated 30° about the Medial/Lateral axis (based on previously known flexion changes between images), yielding the initial pose of the next frame, as shown in Figures 2 and 3. This procedure repeats until all fluoroscopy frames have been registered.
Results: By comparing the performance of multiple optimization methods, we found that the PO method converges to the global solution at a faster time than the IP method, while both the QN and SQP methods fail to converge to the global solution. The registered results through edge-based registration using the PO method are shown in Figure 3. While the green bounds of the initial pose are registered incorrectly, the red bounds of the predicted poses by the automatic registration tool show that the Powell method successfully predicts the final pose for all frames.
Conclusion: This study shows a methodology for the automated 3D-to-2D registration of a knee implant model on a fluoroscopy video and its application in TKA evaluation. While a common drawback of non-learning optimization methods is the need for a “good” initial pose, our framework in Figure 1 demonstrates that the predicted pose from a given image can successfully be modified and used at the initial guess for the subsequent frame. Our proposed approach not only reduces the manual workload for TKA analyses but also can be extended to other implanted joints such as the hip and ankle.
Figures
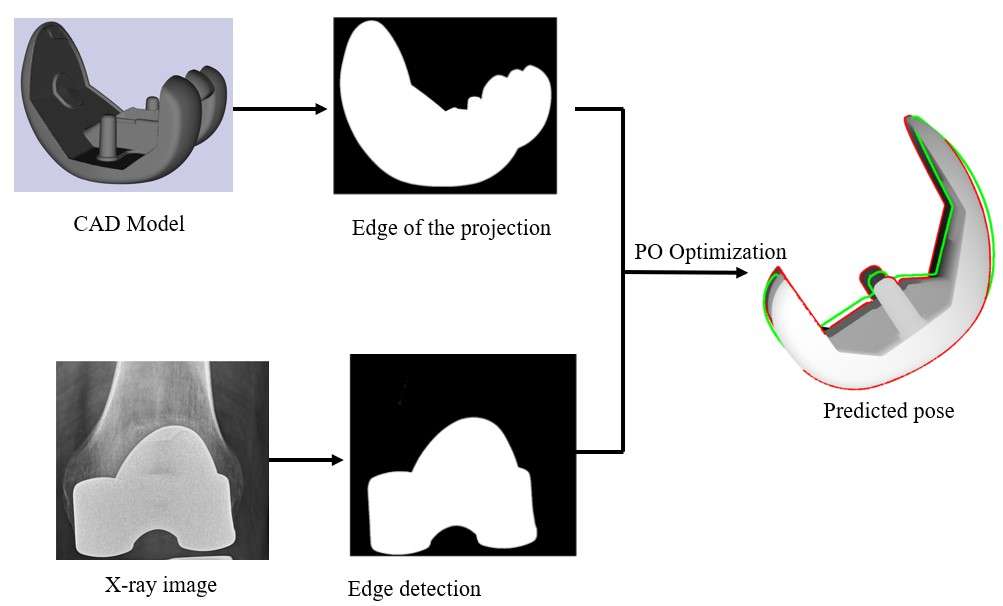
Figure 1
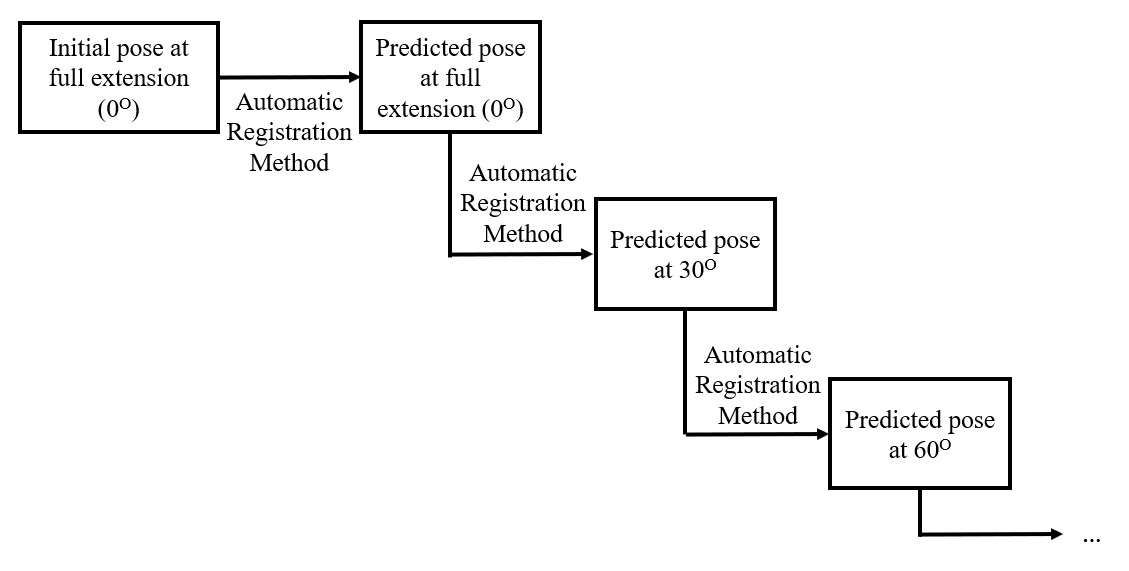
Figure 2
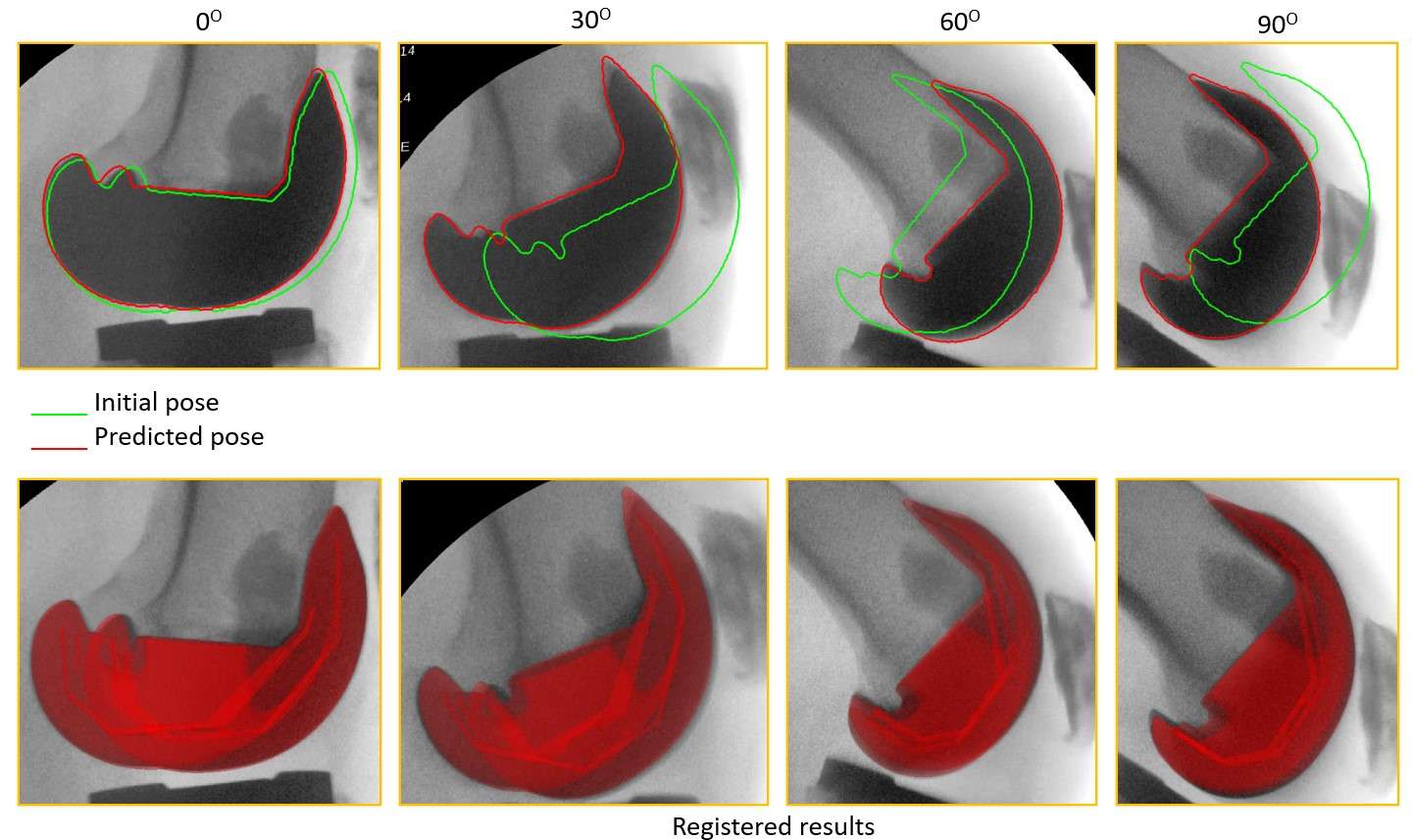
Figure 3#8014
Contact Simulation Model of Knee PSI Guide Fit Accuracy
*Vincent Nierste - DePuy Synthes - Warsaw, USA
*Email: vincent.nierste@gmail.com
Patient specific instruments (PSI) are custom designed guides used by surgeons to execute a total knee replacement procedure. These guides are created using a segmentation of the patient’s anatomy so that when aligned with the bone during surgery, they ideally fit a singular position, allowing for precise placement of pins and cutting tools. One of the issues that can occur with PSI is misalignment of the guide in surgery. If the guide is not accurately fitted onto the femur or tibia, it can affect the final implant position, resulting in misalignment during surgery. Two major sources of misalignment are guide geometry and surgical technique. Evaluating new guide designs or techniques to improve accuracy is traditionally a resource intensive exercise that involves both cadavers and surgeons, creating a situation that is prime for computational analysis. This study sought to utilize a contact simulation model to replicate the results of a cadaver lab which explored multiple surgical techniques.
A contact simulation using finite element analysis was used to determine the expected position of a guide given variations in surgical technique. For this model, there were two main variables: application of force representing surgical technique and bone imperfections created by segmentation errors. The primary variable was surgical technique. A cadaver lab and finite element based contact model were used to compare variations in surgical technique on the final position of the PSI guides. Five techniques were evaluated for femur and tibia guides, emphasizing anterior or distal/proximal pressure, crossed with emphasizing flexion or extension torque. For the cadaver lab (N=4), the XR based guides were designed and a Knee3 CAS system was used to verify final guide position using each surgical technique intraoperatively without resecting the bone. For the computational model, CT was used for segmentation of bones while XR based segmentation was used for guide design, resulting in imperfect fits between guides and bones. This simulated the inaccuracies present between segmented geometry and true bone geometry. The five surgical techniques were recreated in the contact simulation model and evaluated to find the final guide position. The contact parameters and magnitude, distribution, and directionality of loads were adjusted to best match the outcomes recorded in the cadaver lab.
The results of the cadaver lab portion of this study indicated a higher accuracy of the PSI guides in the Flexion/Extension axis when an emphasis was placed on applying an extension torque to femur guides, and when applying a flexion (posterior slope) torque to tibia guides. Emphasis on anterior or distal/proximal pressure did not have a clear effect on the final accuracy of the guides.
The computational model shows similarities to the cadaver lab results in both the Flexion/Extension and Varus/Valgus axes, but is not yet accurate enough to replace the evaluation of guide designs in a cadaver lab setting. The model may however be used to cull a large number of guide designs or surgical techniques down to a select few for cadaver lab evaluation.
Figures
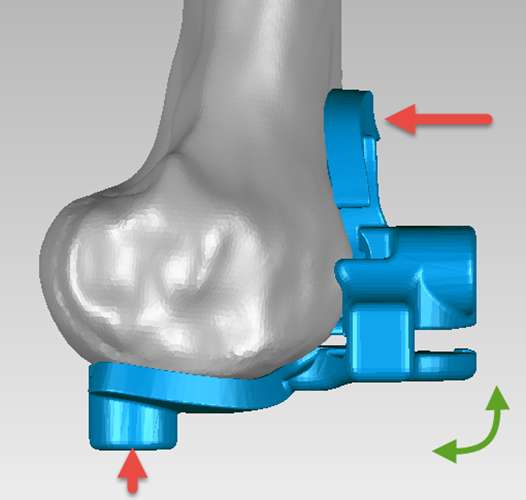
Figure 1
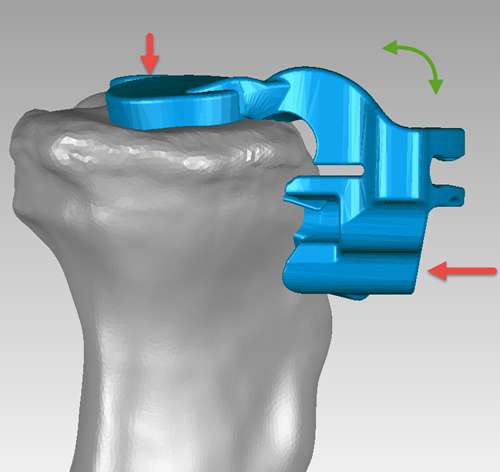
Figure 2#7413
Error in Maximum Total Point Motion of a Tibial Baseplate Is Lower With a Reverse-Engineered Model Versus a CAD Model Using Model-Based Radiosteremetric Analysis
*Abigail Niesen - University of California, Davis - Davis, USA
Anna Garverick - University of California, Davis - Davis, USA
Maury Hull - University of California Davis - Sacramento, USA
*Email: abniesen@ucdavis.edu
INTRODUCTION: Model-based radiostereometric analysis (MBRSA) assesses risk of tibial baseplate loosening after total knee replacement by computing in vivo baseplate migration from biplanar radiographs of patients’ knees. Accuracy of computed migrations depends on accurately registering a 3D model onto the biplanar radiographs; hence, use of a 3D model representative of the baseplate implanted in the patient will minimize registration error. Due to manufacturing tolerances, registration error may differ for computer-aided-design (CAD) models and reverse-engineered (RE) models. Previous research suggests that registration error of a single RE model was less than that of a CAD model in vitro, but no research has quantified differences in registration error among several RE models relative to their CAD model in vivo. The present study determined whether (1) three RE models of the same size baseplate reduce registration error compared to the equivalent size CAD model and (2) RE models of multiple size baseplates reduce registration error compared to CAD models, in vivo.
METHODS: Two pairs of independent biplanar knee radiographs were acquired on the same day from 35 patients enrolled in a study of baseplate migration. A CAD model and at least one RE model were obtained for each size baseplate. For the most common size (size 5), three RE models (termed RE1, RE2, and RE3) were obtained. Radiographs were analyzed using MBRSA. Since the radiographs were acquired on the same day, no true migration occurred and the computed migration, summarized as artifactual maximum total point motion (aMTPM) (i.e. the point on the baseplate that moved the most), represents registration error. For patients with a size 5 baseplate, aMTPM was computed four times by analyzing their radiographs with the CAD, RE1, RE2, and RE3 models (1st objective). Radiographs of the remaining patients were analyzed twice (using the CAD model and single RE model). To obtain 35 paired values, these aMTPM values were pooled with the aMTPM values from the size 5 RE model with the lowest mean error (RE3) (2nd objective). Differences were assessed using Wilcoxon signed-rank tests (p < 0.05 significance).
RESULTS: Mean aMTPM was reduced for all three size 5 RE models compared to the CAD model; however, differences were only significant for one of the RE models (RE3, p = 0.0416, Figure 1). For multiple baseplate sizes, mean aMTPM was reduced by 24% using RE models instead of CAD models, but differences were marginally not significant (0.21 mm ± 0.12(SD) vs. 0.28 mm ± 0.21, p = 0.0658, Figure 2).
CONCLUSION: Because mean aMTPMs for all three size 5 RE models were less than that of the CAD model, and because mean aMTPM was reduced by 24% when using RE models instead of CAD models for multiple baseplate sizes, RE models offer the potential to reduce registration error in MBRSA. Reducing registration error will improve the accuracy with which new baseplate designs are evaluated for risk of loosening. Due to variations in geometry and manufacturing, other baseplate designs should be analyzed using the framework described herein to quantify the improvement.
Figures
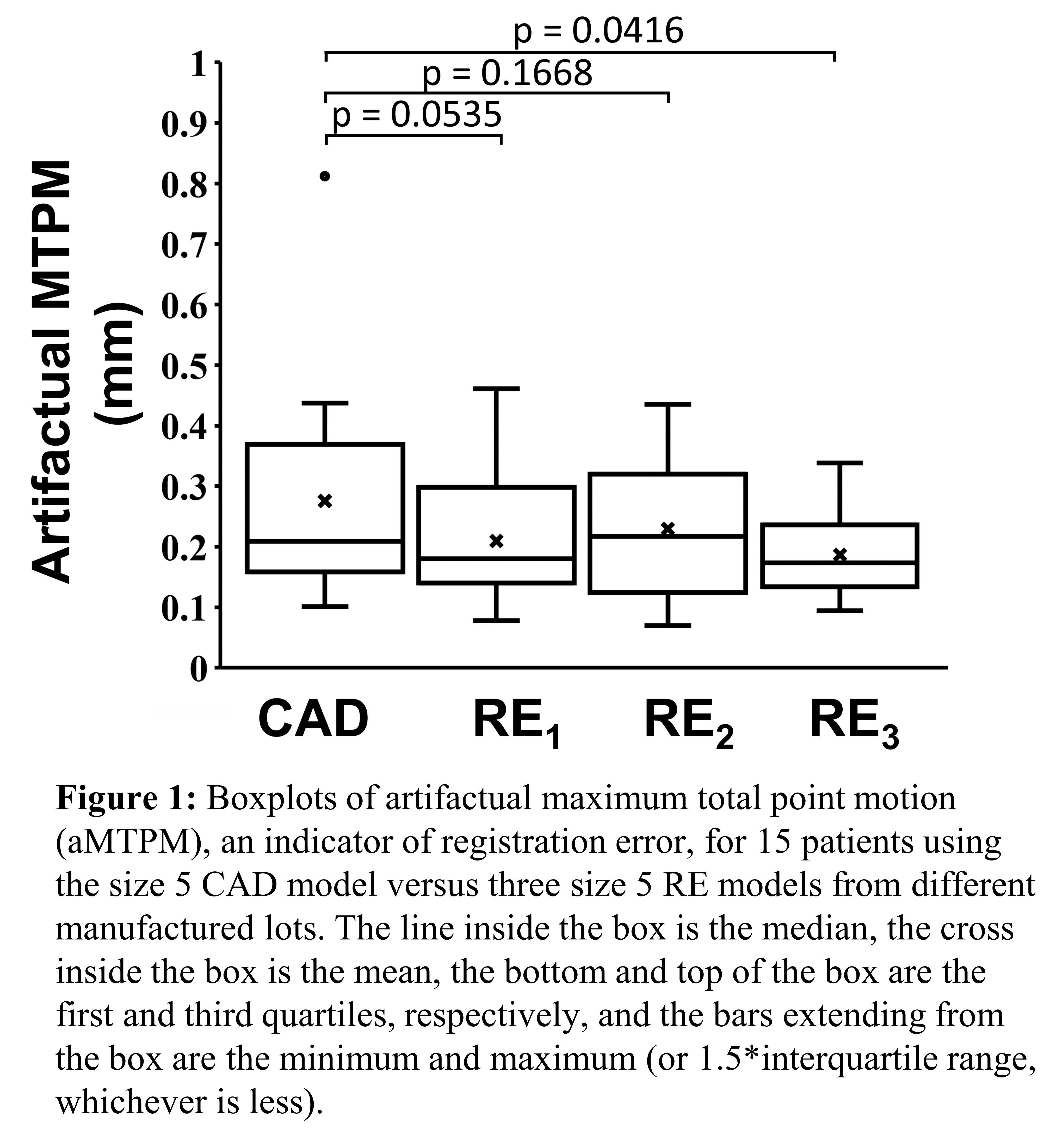
Figure 1
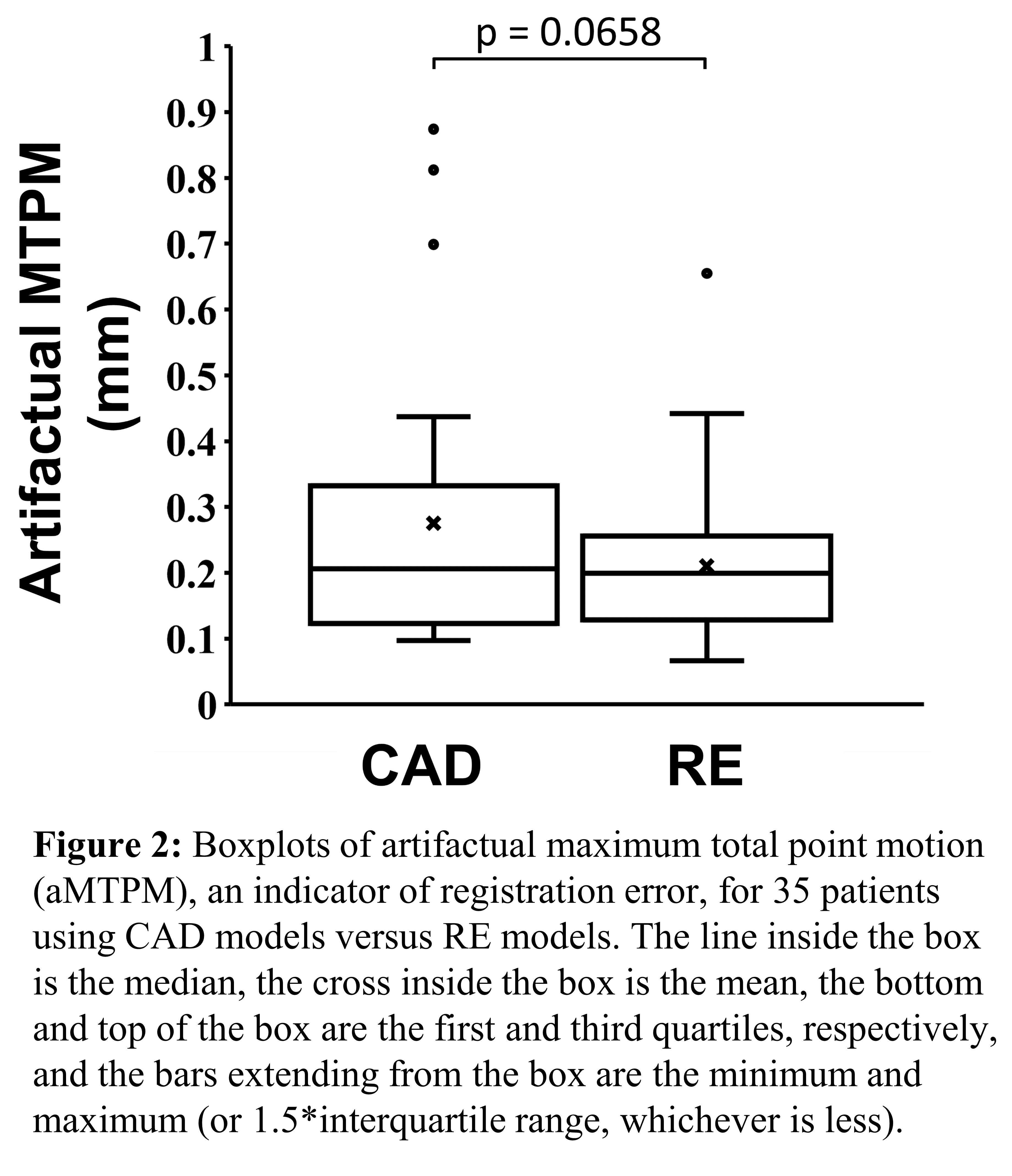
Figure 2#7412
Tibial Baseplate Migration Six Months After Unrestricted Kinematically Aligned Total Knee Arthroplasty Indicates a Low Risk of Baseplate Loosening
*Abigail Niesen - University of California, Davis - Davis, USA
Anna Garverick - University of California, Davis - Davis, USA
Maury Hull - University of California Davis - Sacramento, USA
*Email: abniesen@ucdavis.edu
INTRODUCTION: There are concerns that postoperative varus outlier alignment (i.e. > 3°) of the tibial component might adversely affect long-term tibial baseplate fixation after kinematically aligned (KA) total knee arthroplasty (TKA) particularly when patients are selected without restrictions on the severity of their preoperative varus-valgus deformities. Using radiostererometric analysis (RSA) to quantify baseplate movement over time (i.e. migration), a comprehensive meta-analysis determined that the risk of tibial baseplate loosening is <5% at 10 years when the mean maximum total point motion (MTPM) (i.e. largest displacement of a point on the baseplate) is below 0.5 mm at 6 months. The present study determined whether (1) there was a progressive increase in mean MTPM of the tibial baseplate after unrestricted KA TKA over 6 months, (2) mean MTPM was significantly below the 6-month stability limit of 0.5 mm, and (3) there was a relationship between either proximal medial tibial angle (PMTA), distal lateral femoral angle (DLFA), or hip-knee-ankle (HKA) angle and MTPM at 6 months.
METHODS: Thirty-five patients underwent unrestricted, cemented, caliper-verified KA TKA using a medially constrained insert that retained the posterior cruciate ligament (GMK Sphere, Medacta International, Castel San Pietro, Switzerland). Biplanar radiographs were acquired postoperatively on the day of surgery and at three follow-up time points (6 weeks, 3 months, and 6 months). MTPM was determined at each follow-up time point relative to the day-of-surgery using model-based RSA. A one-way ANOVA determined whether mean MTPMs at 6 weeks, 3 months, and 6 months were different. A one-sided t-test determined whether mean MTPM at 6 months was significantly below 0.5 mm. Simple linear regression models determined whether there was a relationship between either PMTA, DLFA, or HKA and MTPM at 6 months. Significance was p < 0.05 for all tests.
RESULTS: Preoperative age, body mass index, and Oxford Knee Score were 68 ± 7 years, 31 ± 5 kg/m2, and 23 ± 8 (mean ± SD), respectively. There were no differences in mean MTPM at 6 weeks, 3 months, and 6 months (p = 0.8403). Mean MTPMs were 0.31 mm (0.24 mm – 0.37 mm 95% confidence interval) at 6 weeks, 0.31 mm (0.25 mm – 0.37 mm) at 3 months, and 0.30 mm (0.24 mm – 0.35 mm) at 6 months (Fig 1). Mean MTPM was significantly below 0.5 mm (p = 0.0001). There was no relationship between PMTA, DLFA, HKA angle and MTPM at 6 months (|r| ≤ 0.244, p ≥ 0.164) (Fig 2).
CONCLUSION: No differences among mean MTPMs at 6 weeks, 3 months, and 6 months indicate no progression in MTPM over time. Further, since mean MTPM at 6 months was significantly below 0.5 mm, unrestricted KA TKA presents a low-risk of 10-year tibial baseplate loosening. Also, there was no relationship between varus alignment of the baseplate and MTPM at 6 months. These results counter previous studies of mechanical alignment that associated varus alignment of the tibial component with early loosening. To augment these 6-month results, the longitudinal study will be continued over 2 years.
Figures
Figure 1
Figure 2#8002
The Influence of Digital Radiography on Improving Component Placement During Total Hip Arthroplasty
*Evan Nigh - Cedars Sinai Medical Center - Los Angeles, United States of America
Brad Penenberg - Cedars Sinai Medical Center - Los Angeles, USA
Andrew I Spitzer - Los Angeles, USA
Sean Rajaee - Cedars-Sinai Medical Center - Los Angeles, USA
Guy Paiement - Cedars-Sinai Medical Center - Los Angeles, USA
Kevin Rezzadeh - Cedars-Sinai Medical Center - Los Angeles, USA
Caleb Durst - Cedars-Sinai Medical Center - Los Angeles, USA
*Email: evan.nigh@cshs.org
INTRODUCTION:
Optimal implant positioning and sizing during total hip arthroplasty (THA) is associated with improved patient outcomes and implant survival. Intraoperative digital radiography has been shown to improve the accuracy of component placement for patients undergoing posterior approach THA in the lateral decubitus position. Despite being based on a technology that is familiar, reliable, and cost-effective, the use of digital radiography for THA has had slow adoption. There is limited data on the type and frequency of intraoperative changes made as a result of digital radiography, especially among experienced, high-volume surgeons. The purpose of this study was to quantify the value of intraoperative digital radiography to experienced arthroplasty surgeons performing posterior approach THAs at a single institution.
METHODS:
From March 2020 through September 2020, 100 consecutive hips undergoing primary THA by four experienced fellowship trained arthroplasty surgeons were included in the study. Following placement of the acetabular implant and trial femoral components, the surgeon was asked to estimate the adequacy of several parameters: limb length, femoral offset, cup abduction and anteversion angles, and the size and position of the acetabular cup and femoral stem. An intraoperative digital radiograph was then taken, and image analysis software (Radlink™, Inc.) was utilized to measure the parameters of interest. The accuracy of surgeon prediction and frequency of changes made after intraoperative x-ray were recorded and analyzed using McNemar’s test with SPSS software.
RESULTS:
Surgeons accurately predicted cup abduction within ±3 degrees only 45% of the time and cup anteversion within ±3 degrees only 46% of the time. Surgeons were less accurate in predicting appropriate limb length (48%, p=0.014), appropriate femoral stem size (66%, p=0.047), and femoral offset (66%, p=0.089), but had higher accuracy in predicting femoral stem position (varus/valgus) (78%, p=0.27), appropriate acetabular cup size (99%, p=0.999) and cup positioning (medial/lateral positioning) (87%, p=0.123) [Fig 1]. After an intraoperative x-ray was taken, changes to implants were made in 91% of cases, see Figure 2. The most common changes made was to that of limb length (68%), followed by stem size change (51%), cup abduction angle (30%) and cup anteversion angle (19%). Final cup position was more likely to be placed in appropriate abduction/anteversion with fewer outliers after using intraoperative radiograph to guide intra-operative changes [Fig 3].
DISCUSSION and CONCLUSION:
Among experienced, high-volume surgeons, the use of digital radiography led to intraoperative changes in 91% of cases. Surgeons’ estimates of limb length, femoral stem size, and acetabular cup orientation were significantly different than digital radiography measurements and were the parameters most frequently changed intraoperatively. The ability for digital radiography to assess the femoral stem is a distinct advantage of this technique, and this study emphasized its importance finding a high rate of intraoperative changes made to femoral stem size. In conclusion, digital radiography is a valuable and influential navigation tool to ensure reliable implant positioning and restoration of limb length and offset in THA.
Figures
Figure 1
Figure 2
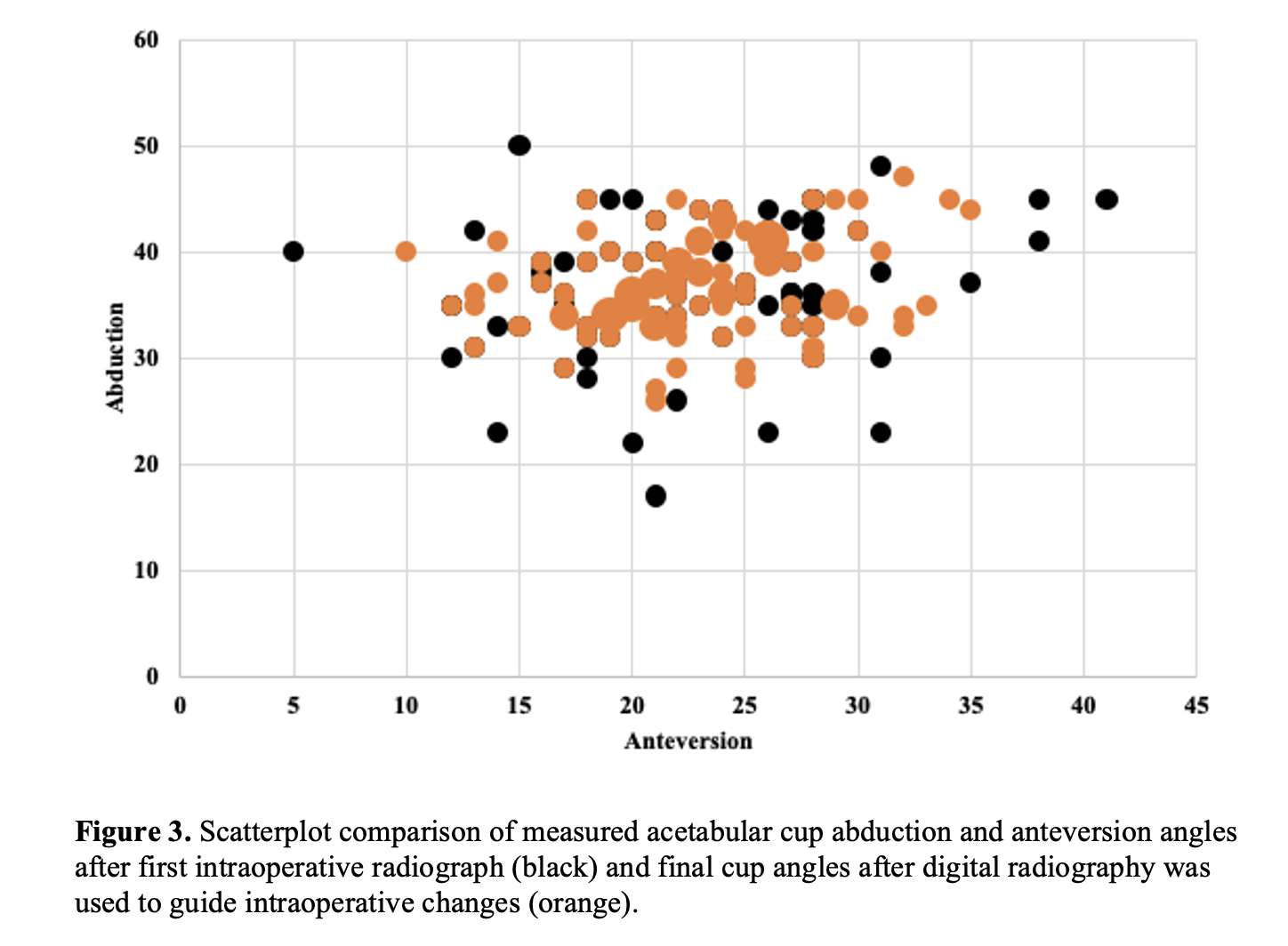
Figure 3#8011
The Influence of Digital Radiography on Improving Component Placement During Total Hip Arthroplasty
*Evan Nigh - Cedars Sinai Medical Center - Los Angeles, United States of America
Caleb Durst - Cedars-Sinai Medical Center - Los Angeles, USA
Sean Rajaee - Cedars-Sinai Medical Center - Los Angeles, USA
Guy Paiement - Cedars-Sinai Medical Center - Los Angeles, USA
Brad Penenberg - Cedars Sinai Medical Center - Los Angeles, USA
Andrew I Spitzer - Los Angeles, USA
Kevin Rezzadeh - Cedars-Sinai Medical Center - Los Angeles, USA
*Email: evan.nigh@cshs.org
INTRODUCTION:
Optimal implant positioning and sizing during total hip arthroplasty (THA) is associated with improved patient outcomes and implant survival. Intraoperative digital radiography has been shown to improve the accuracy of component placement for patients undergoing posterior approach THA in the lateral decubitus position. Despite being based on a technology that is familiar, reliable, and cost-effective, the use of digital radiography for THA has had slow adoption. There is limited data on the type and frequency of intraoperative changes made as a result of digital radiography, especially among experienced, high-volume surgeons. The purpose of this study was to quantify the value of intraoperative digital radiography to experienced arthroplasty surgeons performing posterior approach THAs at a single institution.
METHODS:
From March 2020 through September 2020, 100 consecutive hips undergoing primary THA by four experienced fellowship trained arthroplasty surgeons were included in the study. Following placement of the acetabular implant and trial femoral components, the surgeon was asked to estimate the adequacy of several parameters: limb length, femoral offset, cup abduction and anteversion angles, and the size and position of the acetabular cup and femoral stem. An intraoperative digital radiograph was then taken, and image analysis software (Radlink™, Inc.) was utilized to measure the parameters of interest. The accuracy of surgeon prediction and frequency of changes made after intraoperative x-ray were recorded and analyzed using McNemar’s test with SPSS software.
RESULTS:
Surgeons accurately predicted cup abduction within ±3 degrees only 45% of the time and cup anteversion within ±3 degrees only 46% of the time. Surgeons were less accurate in predicting appropriate limb length (48%, p=0.014), appropriate femoral stem size (66%, p=0.047), and femoral offset (66%, p=0.089), but had higher accuracy in predicting femoral stem position (varus/valgus) (78%, p=0.27), appropriate acetabular cup size (99%, p=0.999) and cup positioning (medial/lateral positioning) (87%, p=0.123) [Fig 1]. After an intraoperative x-ray was taken, changes to implants were made in 91% of cases, see Figure 2. The most common changes made was to that of limb length (68%), followed by stem size change (51%), cup abduction angle (30%) and cup anteversion angle (19%). Final cup position was more likely to be placed in appropriate abduction/anteversion with fewer outliers after using intraoperative radiograph to guide intra-operative changes [Fig 3].
DISCUSSION and CONCLUSION:
Among experienced, high-volume surgeons, the use of digital radiography led to intraoperative changes in 91% of cases. Surgeons’ estimates of limb length, femoral stem size, and acetabular cup orientation were significantly different than digital radiography measurements and were the parameters most frequently changed intraoperatively. The ability for digital radiography to assess the femoral stem is a distinct advantage of this technique, and this study emphasized its importance finding a high rate of intraoperative changes made to femoral stem size. In conclusion, digital radiography is a valuable and influential navigation tool to ensure reliable implant positioning and restoration of limb length and offset in THA.
Introduction:
Optimal size and position of acetabular and femoral components and restoration of limb-length and femoral offset are the key biomechanical factors affecting the outcome of total hip arthroplasty (THA). Failure to achieve proper alignment and sizing of components intra-operatively can be the cause of several complications, all potentially leading to significant patient dissatisfaction and need for revision surgery.
For instance, acetabular and femoral component malposition can lead to dislocation, impingement, and accelerated bearing surface wear (1-6). An oversized acetabular cup can lead to insufficient medialization of the hip center of rotation, resulting in altered hip biomechanics or need for excessive acetabular bone loss. Alternatively, an undersized acetabular cup increases the risk of loosening and instability, particularly by obligating placement of a smaller femoral head. Undersizing the femoral stem is a risk factor for aseptic loosening and early subsidence, while oversizing can lead to intraoperative fracture during insertion or undesired changes in limb length and offset (7-9). Furthermore, varus alignment of the femoral component has been associated with poor outcomes and risk for failure in long-term follow up studies (10-12).
Limb-length discrepancy (LLD) is a common source of patients dissatisfaction as it can lead to limp, functional deficits, instability, pelvic obliquity, and low back pain (13, 14). Furthermore, LLD is the most common causes for litigation after THA, and can be perceived in up to 32% of patients when lengthening exceeds as little as 6 mm, or shortening exceeds 10 mm (14, 15). Achieving appropriate offset in THA plays a critical role in restoring hip abductor biomechanics, improving functional outcomes, increasing implant survivorship, and preventing dislocation (16-18). Inadequate restoration has been found to be associated with increased joint forces, gait disturbances, increased edge loading, pain, impingement, and dislocation (17, 19-21). Excessive femoral offset can increase abductor muscle tension and result in pain, reduced function, and increased polyethylene wear (22, 23).
While the targets of these key parameters during THA are well-recognized by orthopaedic surgeons, consistently achieving them using traditional instrumentation in the operating room can be challenging. This is potentially attributed to the limited accuracy of surgeon’s estimates of component position intraoperatively during conventional THA. For instance, acetabular cup placement within the Lewinnek safe zone (abduction angle 40° ± 10° and anteversion angle 15° ± 10°) has a reported failure rate between 30% and 75% (24-27). Similarly, computer tomography studies measuring femoral stem anteversion postoperatively found between only 45% and 71% of stems were within the expected range predicted by the surgeon (28-30). Although target limb length and offset may be decided upon during preoperative planning, confidently achieving them without radiographic verification can be daunting (13).
We recently described methods to achieve targeted acetabular cup position and limb length and femoral offset targeted measurements with use of intraoperative digital radiography (DR) (31-33). In addition, we have described how DR can reliably control for the effect of pelvic position intraoperatively to facilitate accurate placement of the acetabular component (31-33). There is a paucity of data, however, describing the frequency and type of intraoperative changes made as a result of using digital radiography guidance. Furthermore, no known study has simultaneously evaluated all the key parameters detailed in this study using DR, thus a comprehensive assessment of its utility is lacking.
In the present study, we aim to quantify the value of intraoperative digital radiography as a navigation tool to experienced arthroplasty trained surgeons performing primary THA. We compare surgeons’ estimations of key measurements with those measured after intraoperative DR and recorded any subsequent changes made. We hypothesize that surgeon measurement estimates are less accurate than expected, and the use of DR leads to significant intraoperative changes that augment surgeons’ ability to assure optimal component placement during THA.
Methods:
Study Cohort:
One hundred consecutiveposterior approach primary total hip arthroplasty cases performed in the lateral decubitus position by four fellowship trained arthroplasty surgeons at our institution between March 2020 through September 2020 were included. There were 55 right total hip arthroplasties and 45 left total hip arthroplasties. Revision THA was excluded.
All patients were positioned in the lateral decubitus position and secured using a peg-board with radiolucent pegs. Sixty-eight cases were performed using an IT band sparing superior approach and 42 cases with a mini-postero-lateral approach (34). Traditional techniques were used for cup and screw placement, femoral broaching, and limb-length and offset assessment. The distance from the interteardrop line to the lesser trochanter was used to determine limb length. The actual acetabular cup, not a trial, was positioned using standard alignment guides along with observation of the cup relationship to the anterior and lateral acetabular rim. The decision to place screws or not was made based on the surgeons’ preferred technique. A trial liner was utilized, anticipating the possibility of cup or screw adjustment. Femoral broach placement was completed based on the surgeons’ best guess from preoperative templating and canal fit. Neck and head choices were made based on surgeon estimates of limb length and offset, then trial range of motion was performed. Following placement of the actual cup and trial components and before the first intraoperative radiograph was taken, the surgeon was asked to estimate the following parameters:
- Limb length (appropriate, short, or long)
- Cup abduction and anteversion (degrees)
- Stem position (neutral, varus, or valgus)
- Stem size (appropriate, small, or large)
- Cup size (appropriate, small, or large)
- Cup position (appropriate, medial, or lateral)
- Femoral offset (appropriate, too little, too much)
These estimates were recorded, and then intraoperative digital radiography was performed using a standard portable x-ray unit, a digital flat panel detector, and a portable digital radiography processing system (Radlink™) (Fig. 1). All radiographs were made with the center of the beam directed to the pubic symphysis with both lower extremities in equal neutral alignment. If necessary, adjustments were made to the operating table, x-ray unit, or limb position to obtain neutral pelvic rotation and to match pelvic tilt and limb alignment to preoperative radiographs.
Intraoperative Measurement Techniques
The surgeon remained scrubbed and performed all radiographic measurements on a touchscreen using a Kocher clamp to activate imaging analysis software. Gloves were changed prior to returning to the surgical field. A study member was present throughout the procedure to record pertinent study data. The Surgeon’s Checklist software program was used to measure cup abduction and anteversion angles by matching an ellipse to the rim of the acetabular component. Changes in limb length was measured as the distance from the interteardrop line to the center of the lesser trochanter bilaterally as described in previous studies (35). Femoral offset was measured from the level of the femoral neck cut to the ischium, using an equivalent femoral neck level of the contralateral hip as reference. (Fig. 2) Appropriateness of the size and position of the femoral stem was made based on canal fit and alignment, respectively. Appropriateness of acetabular cup size and position was made based on its fill of the reamed acetabulum and its reference to the ilioischial line, tear drop, and lateral coverage.
After the parameters of interest were measured and recorded, the surgeon returned to complete the procedure, making adjustments as deemed necessary based upon the intraoperative radiograph and surgeon preference. Any changes made in the position or size of components from after the first intraoperative radiograph were communicated by the surgeon and recorded by a study member. Final cup abduction and anteversion of the acetabular components were measured by two independent physicians not involved in the procedure (Fig. 3).
Statistical Analysis
Descriptive statistics were conducted on outcomes, in the form of means and standard deviations for continuous variables and percentages for categorical variables. The frequency of component or cup position changes intraoperatively was calculated. Cup position outliers were identified when cups were placed outside of the Lewinnek safe zones for abduction (30-50 degrees) and anteversion (5-25 degrees) [12]. Accurate surgeon predictions for abduction and anteversion were defined as pre-radiograph intraoperative surgeon estimates within three degrees of radiographically determined angles. McNemar’s test was used to compare the performance of intraoperative surgeon estimation of cup position to radiographic assessment of cup position. Agreement between two independent reviewers in determination of abduction angles and anteversion angles was assessed via a two-way mixed model single measures intraclass correlation coefficient. This correlation coefficient was reported followed by 95% confidence interval (CI). The threshold for statistical significance was 0.05.
Results:
One hundred hips in 95 patients are included in the study who underwent primary total hip arthroplasty; five patients underwent staged bilateral total hip arthroplasty. 35 patients were male and 60 were female. Average (SD) body mass index was 29.67 (± 2.46) and age was 72.1 (±5.36).
Accuracy of Surgeon Prediction
Surgeons accurately estimated cup abduction within ±3 degrees in 45% of cases and cup anteversion within ±3degrees in 46% of cases. Surgeons were less accurate in correctly predicting limb length (48%, p=0.014), femoral stem size (66%, p=0.047), and femoral offset (66%, p=0.089), but demonstrated higher accuracy in predicting femoral stem position (varus/valgus) (78%, p=0.27), appropriate acetabular cup size (99%, p=0.999) and cup positioning (medial or lateral position) (87%, p=0.123) (Table 1).For limb length, the most common error was predicting the length was appropriate when it was too short after IODR. Interestingly, the second most common error for limb length was predicting it was too long when in fact it was too short, suggesting surgeon judgement alone is insufficient (Fig. 4).
After the first intraoperative digital radiograph, 59% of acetabular cups were placed within the Lewinnek safe zone of abduction between 30-50° and anteversion between 5-25° (Fig. 5). Figure 6 demonstrates an example where cup position was changed after the intraoperative x-ray in order to improve the acetabular cup abduction. Overall, surgeons were more accurate in placing cups within this range for abduction (89%) than for anteversion (67%). The intraclass correlation coefficient between the two raters assigning radiographic measures for abduction was 0.907 [95% CI: 0.865-0.937] (p<0.001) and for anteversion was 0.916 [95% CI: 0.877-0.943] (p<0.001).
Changes made after IODR
After the first intraoperative digital radiograph was taken, surgeons made subsequent changes in 91% of cases (Table 2). The most common changes made was to that of limb length (68%), followed by stem size change (51%), cup abduction angle (30%) and cup anteversion angle (19%). An example of a case where intraoperative x-ray led to a larger femoral size can be found in Figure 7. Final cup position was more reliable with less outliers after using intraoperative digital radiography measurements to guide intraoperative changes (Fig. 8).
Discussion
This study shows that intraoperative digital radiography is a valuable navigation tool to improve accuracy of implant positioning and sizing during total hip arthroplasty. Despite advanced fellowship training, surgeon’s estimations of limb length, femoral stem size, and acetabular cup abduction and anteversion angles were significantly different than measurements from intraoperative digital radiography. This led to one or more intraoperative changes of component size or position in 91% of cases to ensure appropriate implant positioning and restoration of limb length and offset.
Before making intraoperative changes, 59% of acetabular cups were placed within the Lewinnek safe zone, which is consistent with reported rates of free-hand technique (25, 36). Our data demonstrates that even experienced surgeons have limited accuracy in predicting cup abduction and anteversion angles, with less that 50% of cups correctly predicted within 3°. If the margin of error increased to within 5°, correct predictions increased to 70% for abduction and 66% for anteversion. These results are markedly similar to a study by Dorr et al, which reported experienced surgeons corrected estimated cup position within 5° at a rate of 70% for abduction and 62% for anteversion (37). After adjusting cup position using DR guidance, final radiographs demonstrated reliable placement of the acetabular cup with fewer outliers.
Surgeons were significantly less accurate in predicting limb length and femoral stem size, resulting in these parameters being the two most common intraoperative changes made after DR. In addition to the low accuracy rates reported for femoral offset, it should not be unexpected that these parameters best assessed radiographically benefitted the most with DR. In comparison, surgeons were more accurate in correctly predicting stem coronal position, acetabular cup size, and cup medial/lateral position. An explanation for this difference may be that deviations outside the norm for these parameters can often be directly visualized or inferred by surgeon expertise and corrected prior to intraoperative DR. Conversely, the parameters of proper cup orientation, limb length, femoral offset, and the canal fit of the femoral stem are less amenable to clinical acumen. Thus, achieving accuracy relied on the use of digital radiography to guide intraoperative changes resulting in decreased incidence of outliers and targeted component placement.
Intraoperative digital radiography with Radlink™ software described in the present study has been routinely used at the authors’ institution for approximately the past 10 years. Detailed technique guides and radiographic results have previously been published with 97.8% of acetabular cups placed within the target range, while 2.2% were placed purposefully outside the range given patient-specific factors (32, 33, 38). Debbi et al. also introduced a method for determining and achieving target limb length and offset using DR (31). The authors reported limb length was within 5mm of targets in 100% of patients and offset was within 5mm of targets in 97.1% with excellent clinical outcomes (31).
Despite these positive results and advancements in digital imaging capabilities, persisting doubts have deterred the adoption of DR during THA. These include increased procedural time, additional room setup, the accuracy of imaging obtained from the lateral decubitus position, and finally, how often imaging results in intraoperative changes being made, especially among experienced, high-volume surgeons (39). These previously voiced concerns have since been overcome in a recent review by Siebenmorgen et al. (39). The present study specifically addresses the last question; even in a group of experienced, high-volume surgeons, DR led to intraoperative changes 91% of the time. There are two known studies that also report frequency of intraoperative changes made after DR. In a retrospective review, Hambright et al. found that after intraoperative DR and Radlink™ analysis, changes were made in 86% of cases with limb length and femoral offset being the most commonly adjusted parameters (40). Ezzet and McCauley reported intraoperative x-ray led to subsequent changes in 50% of cases; however, acetabular anteversion could not be quantified by the imaging software which limit their results (41). The present study is the first to prospectively analyze all the above parameters using intraoperative DR for THA, including the first to assess appropriate femoral stem size using this technique. Taken together, these findings augment the support for DR as a valuable navigational tool during THA and demonstrate it leads to a high frequency of intraoperative changes deemed necessary by the surgeon to assure satisfactory implant placement. As the value of this technique is recognized, several guides are available which describe preoperative planning methods, proper patient positioning, and equipment setup to optimize workflow and ease adoption (32, 33, 38, 39).
Alternative methods to improve surgeon accuracy of component placement have been recently introduced, namely computer-based navigation and robotic systems (42). Meta-analyses of these new technologies concluded that their primary benefit is reducing the number of outliers during acetabular cup positioning (43, 44). Other studies suggest these technologies can accurately reproduce limb length and hip offset; however, there is no clear evidence that it does so better than conventional THA, or if it results in meaningful improvements in clinical outcomes (42, 45, 46). While computer navigation and robotics have recently become popularized across many orthopaedic fields, these systems are not perfected for THA as their success relies on a very reliable understanding of the position of the pelvis intraoperatively. Commonly reported challenges include errors in bony landmark registration and accounting for variations in functional pelvic tilt, raising concerns of their accuracy (47-54). Furthermore, the increased cost, increased perioperative time, and need for preoperative CT scans can be prohibitive to practical use in many settings.
The most significant restriction of robotic and computer navigation systems, however, is their limited assessment of the femoral side. They are incapable of verifying appropriate femoral stem size in order to avoid placement of undersized femoral stems which can lead to loosening, malalignment, and subsidence. In comparison, x-ray remains the current best method for assessing femoral fit to assure appropriately sized implants. Furthermore, intraoperative DR provides a simple, reliable method to account for changes in pelvic tilt to achieve patient-specific cup positioning. Functional spinopelvic motion is assessed preoperatively, and the standing preoperative radiograph is used as reference and matched with the radiograph obtained with the patient in the lateral decubitus position (38). This technique enables the intraoperative radiograph to be standardized even if there is movement of the patient or poor visualization of bony landmarks by manipulating the x-ray beam as necessary to reproduce the reference image. Using this technique, the accuracy of functional cup position is directly in the hands of the surgeon, not at the mercy of computer-based registration.
A unique strength of this study is its comprehensive evaluation of surgeon perceived estimates and DR measurements for all the parameters of interest, particularly the assessment of femoral stem size. Other strengths include prospectively collected data from a single institution, high intraclass correlation between independent raters, and findings consistent with prior literature. The target measurements for each parameter were made at the discretion of the surgeon, not specified by the study protocol, which may be a limitation of the study. This decision was intentional, however, given that parameter targets can often vary between surgeons and patient-specific factors.
In conclusion, DR navigation, based on a familiar technology that is reliable, cost-effective, and user-friendly, significantly contributes to assuring appropriate component size and position during posterior THA. Perhaps one of its strongest advantages is that it provides information on the femoral component’s size and position which current computer navigation systems do not offer. This provides the surgeon the opportunity to intraoperatively correct undersized or varus malpositioned stems which was performed in over half of the cases in this series, emphasizing the importance of this capability. It provides a true, real-time representation of the pelvic anatomy with immediate upload to image analysis software for verification of component positioning. Available software analysis currently includes all the parameters evaluated in this study—acetabular component abduction and anteversion, femoral component alignment and sizing, limb length, and femoral offset. Every one of these parameters represent modifiable factors impacting the success of THA, and IODR navigation empowers the surgeon with the assurance each is optimally achieved.
References:
1. Biedermann R, Tonin A, Krismer M, Rachbauer F, Eibl G, Stockl B. Reducing the risk of dislocation after total hip arthroplasty: the effect of orientation of the acetabular component. J Bone Joint Surg Br. 2005;87(6):762-9. Epub 2005/05/25. doi: 10.1302/0301-620X.87B6.14745. PubMed PMID: 15911655.
2. Gallo J, Havranek V, Zapletalova J. Risk factors for accelerated polyethylene wear and osteolysis in ABG I total hip arthroplasty. International orthopaedics. 2010;34(1):19-26.
3. Kennedy J, Rogers W, Soffe K, Sullivan R, Griffen D, Sheehan L. Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. The Journal of arthroplasty. 1998;13(5):530-4.
4. Kluess D, Martin H, Mittelmeier W, Schmitz K-P, Bader R. Influence of femoral head size on impingement, dislocation and stress distribution in total hip replacement. Medical engineering & physics. 2007;29(4):465-71.
5. Kummer FJ, Shah S, Iyer S, DiCesare PE. The effect of acetabular cup orientations on limiting hip rotation. The Journal of Arthroplasty. 1999;14(4):509-13.
6. Shon WY, Baldini T, Peterson MG, Wright TM, Salvati EA. Impingement in total hip arthroplasty: a study of retrieved acetabular components. The Journal of arthroplasty. 2005;20(4):427-35.
7. Magill P, Hill J, O’Brien S, Stevenson M, Machenaud A, Beverland D. Observed effect of femoral component undersizing and a collarless design in the development of radiolucent lines in cementless total hip arthroplasty. Arthroplasty today. 2020;6(1):99-103.
8. Fottner A, Woiczinski M, Kistler M, Schröder C, Schmidutz TF, Jansson V, et al. Influence of undersized cementless hip stems on primary stability and strain distribution. Archives of orthopaedic and trauma surgery. 2017;137(10):1435-41.
9. Ponzio DY, Shahi A, Park AG, Purtill JJ. Intraoperative proximal femoral fracture in primary cementless total hip arthroplasty. The Journal of arthroplasty. 2015;30(8):1418-22.
10. Devitt A, O'Sullivan T, Quinlan W. 16-to 25-year follow-up study of cemented arthroplasty of the hip in patients aged 50 years or younger. The Journal of arthroplasty. 1997;12(5):479-89.
11. Gill TJ, Sledge JB, Orler R, Ganz R. Lateral insufficiency fractures of the femur caused by osteopenia and varus angulation: a complication of total hip arthroplasty. The Journal of arthroplasty. 1999;14(8):982-7.
12. Khalily C, Lester DK. Results of a tapered cementless femoral stem implanted in varus. The Journal of arthroplasty. 2002;17(4):463-6.
13. Desai AS, Dramis A, Board TN. Leg length discrepancy after total hip arthroplasty: a review of literature. Current reviews in musculoskeletal medicine. 2013;6(4):336-41.
14. Sarangi P, Bannister G. Leg length discrepancy after total hip replacement. Hip International. 1997;7(3):121-4.
15. Hofmann AA, Skrzynski MC. Hip Arthroplasty: Headaches & Migraines: Leg-Length Inequality and Nerve Palsy in Total Hip Arthroplasty: A Lawyer Awaits! : SLACK Incorporated Thorofare, NJ; 2000.
16. Clement ND, S. Patrick-Patel R, MacDonald D, Breusch SJ. Total hip replacement: increasing femoral offset improves functional outcome. Archives of Orthopaedic and Trauma Surgery. 2016;136(9):1317-23. doi: 10.1007/s00402-016-2527-4.
17. Shapira J, Chen SL, Rosinsky PJ, Maldonado DR, Meghpara M, Lall AC, et al. The effect of postoperative femoral offset on outcomes after hip arthroplasty: A systematic review. Journal of Orthopaedics. 2020;22:5-11. doi: https://doi.org/10.1016/j.jor.2020.03.034.
18. Forde B, Engeln K, Bedair H, Bene N, Talmo C, Nandi S. Restoring femoral offset is the most important technical factor in preventing total hip arthroplasty dislocation. Journal of Orthopaedics. 2018;15(1):131-3. doi: https://doi.org/10.1016/j.jor.2018.01.026.
19. Charles MN, Bourne RB, Davey JR, Greenwald AS, Morrey BF, Rorabeck CH. Soft-tissue balancing of the hip: the role of femoral offset restoration. Instructional course lectures. 2005;54:131-41.
20. Malik A, Maheshwari A, Dorr LD. Impingement with total hip replacement. JBJS. 2007;89(8):1832-42.
21. Rüdiger HA, Guillemin M, Latypova A, Terrier A. Effect of changes of femoral offset on abductor and joint reaction forces in total hip arthroplasty. Archives of Orthopaedic and Trauma Surgery. 2017;137(11):1579-85. doi: 10.1007/s00402-017-2788-6.
22. Little NJ, Busch CA, Gallagher JA, Rorabeck CH, Bourne RB. Acetabular polyethylene wear and acetabular inclination and femoral offset. Clinical Orthopaedics and Related Research®. 2009;467(11):2895-900.
23. Liebs T, Nasser L, Herzberg W, Rüther W, Hassenpflug J. The influence of femoral offset on health-related quality of life after total hip replacement. The Bone & Joint Journal. 2014;96(1):36-42.
24. Bosker BH, Verheyen CCPM, Horstmann WG, Tulp NJA. Poor accuracy of freehand cup positioning during total hip arthroplasty. Archives of orthopaedic and trauma surgery. 2007;127(5):375-9. Epub 2007/02/13. doi: 10.1007/s00402-007-0294-y. PubMed PMID: 17297597.
25. Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, et al. The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clinical Orthopaedics and Related Research®. 2011;469(2):319-29.
26. Saxler G, Marx A, Vandevelde D, Langlotz U, Tannast M, Wiese M, et al. The accuracy of free-hand cup positioning-a CT based measurement of cup placement in 105 total hip arthroplasties. International orthopaedics. 2004;28(4):198-201.
27. Epstein NJ, Woolson ST, Giori NJ. Acetabular component positioning using the transverse acetabular ligament: can you find it and does it help? Clinical Orthopaedics and Related Research®. 2011;469(2):412-6.
28. Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. The Journal of arthroplasty. 2006;21(5):696-701.
29. Dorr LD, Wan Z, Malik A, Zhu J, Dastane M, Deshmane P. A comparison of surgeon estimation and computed tomographic measurement of femoral component anteversion in cementless total hip arthroplasty. JBJS. 2009;91(11):2598-604.
30. Belzunce MA, Henckel J, Di Laura A, Hart A. Uncemented femoral stem orientation and position in total hip arthroplasty: A CT study. Journal of Orthopaedic Research®. 2020;38(7):1486-96.
31. Debbi EM, Rajaee SS, Mayeda BF, Penenberg BL. Determining and achieving target limb length and offset in total hip arthroplasty using intraoperative digital radiography. The Journal of arthroplasty. 2020;35(3):779-85.
32. Penenberg BL, Samagh SP, Rajaee SS, Woehnl A, Brien WW. Digital radiography in total hip arthroplasty: technique and radiographic results. JBJS. 2018;100(3):226-35.
33. Penenberg B, editor INTRAOPERATIVE DIGITAL RADIOGRAPHY: ASSURING COMPONENT ALIGNMENT. Orthopaedic Proceedings; 2015: The British Editorial Society of Bone & Joint Surgery.
34. Penenberg BL, Bolling WS, Riley M. Percutaneously assisted total hip arthroplasty (PATH): a preliminary report. JBJS. 2008;90(Supplement_4):209-20.
35. Sculco PK, Cottino U, Abdel MP, Sierra RJ. Avoiding hip instability and limb length discrepancy after total hip arthroplasty. Orthop Clin North Am. 2016;47(2):327-34.
36. Bosker B, Verheyen C, Horstmann W, Tulp N. Poor accuracy of freehand cup positioning during total hip arthroplasty. Archives of orthopaedic and trauma surgery. 2007;127(5):375-9.
37. Dorr LD, Malik A, Wan Z, Long WT, Harris M. Precision and Bias of Imageless Computer Navigation and Surgeon Estimates for Acetabular Component Position. Clinical Orthopaedics and Related Research®. 2007;465:92-9. doi: 10.1097/BLO.0b013e3181560c51. PubMed PMID: 00003086-200712000-00015.
38. Penenberg B, editor INTRA-OPERATIVE DIGITAL RADIOGRAPHY: PARADIGM SHIFT IN STANDARD OF CARE. Orthopaedic Proceedings; 2014: The British Editorial Society of Bone & Joint Surgery.
39. Siebenmorgen JP, Stronach BM, Mears SC, Stambough JB. The Use of Intraoperative Digital Radiography Alignment Software to Assess Implant Placement in Total Hip Arthroplasty. Current Reviews in Musculoskeletal Medicine. 2021:1-9.
40. Hambright D, Hellman M, Barrack R. Intra-operative digital imaging: assuring the alignment of components when undertaking total hip arthroplasty. The bone & joint journal. 2018;100(1_Supple_A):36-43.
41. Ezzet KA, McCauley JC. Use of intraoperative X-rays to optimize component position and leg length during total hip arthroplasty. The Journal of arthroplasty. 2014;29(3):580-5.
42. Wasterlain AS, Buza JAI, Thakkar SC, Schwarzkopf R, Vigdorchik J. Navigation and Robotics in Total Hip Arthroplasty. JBJS Reviews. 2017;5(3):e2. doi: 10.2106/jbjs.Rvw.16.00046. PubMed PMID: 01874474-201703000-00002.
43. Beckmann J, Stengel D, Tingart M, Götz J, Grifka J, Lüring C. Navigated cup implantation in hip arthroplasty: a meta-analysis. Acta orthopaedica. 2009;80(5):538-44.
44. Xu K, Li Y-m, Zhang H-f, Wang C-g, Xu Y-q, Li Z-j. Computer navigation in total hip arthroplasty: a meta-analysis of randomized controlled trials. International Journal of Surgery. 2014;12(5):528-33.
45. Ellapparadja P, Mahajan V, Deakin AH, Deep K. Reproduction of hip offset and leg length in navigated total hip arthroplasty: how accurate are we? The Journal of arthroplasty. 2015;30(6):1002-7.
46. Weber M, Woerner M, Springorum R, Sendtner E, Hapfelmeier A, Grifka J, et al. Fluoroscopy and imageless navigation enable an equivalent reconstruction of leg length and global and femoral offset in THA. Clinical Orthopaedics and Related Research®. 2014;472(10):3150-8.
47. Lembeck B, Mueller O, Reize P, Wuelker N. Pelvic tilt makes acetabular cup navigation inaccurate. Acta orthopaedica. 2005;76(4):517-23.
48. Yamada K, Endo H, Tetsunaga T, Miyake T, Sanki T, Ozaki T. Accuracy of cup positioning with the computed tomography-based two-dimensional to three-dimensional matched navigation system: a prospective, randomized controlled study. The Journal of Arthroplasty. 2018;33(1):136-43.
49. Hayashi S, Hashimoto S, Kuroda Y, Nakano N, Matsumoto T, Ishida K, et al. Accuracy of cup position following robot-assisted total hip arthroplasty may be associated with surgical approach and pelvic tilt. Scientific Reports. 2021;11(1):1-9.
50. Wolf A, DiGioia III AM, Mor AB, Jaramaz B. Cup alignment error model for total hip arthroplasty. Clinical Orthopaedics and Related Research (1976-2007). 2005;437:132-7.
51. Spencer J, Day R, Sloan K, Beaver R. Computer navigation of the acetabular component: a cadaver reliability study. The Journal of Bone and Joint Surgery British volume. 2006;88(7):972-5.
52. Ybinger T, Kumpan W, Hoffart H, Muschalik B, Bullmann W, Zweymüller K. Accuracy of navigation-assisted acetabular component positioning studied by computed tomography measurements: methods and results. The Journal of arthroplasty. 2007;22(6):812-7.
53. Tsukada S, Wakui M. Decreased accuracy of acetabular cup placement for imageless navigation in obese patients. Journal of Orthopaedic Science. 2010;15(6):758-63.
54. Parratte S, Argenson J-NA. Validation and usefulness of a computer-assisted cup-positioning system in total hip arthroplasty: a prospective, randomized, controlled study. JBJS. 2007;89(3):494-9.
Figures
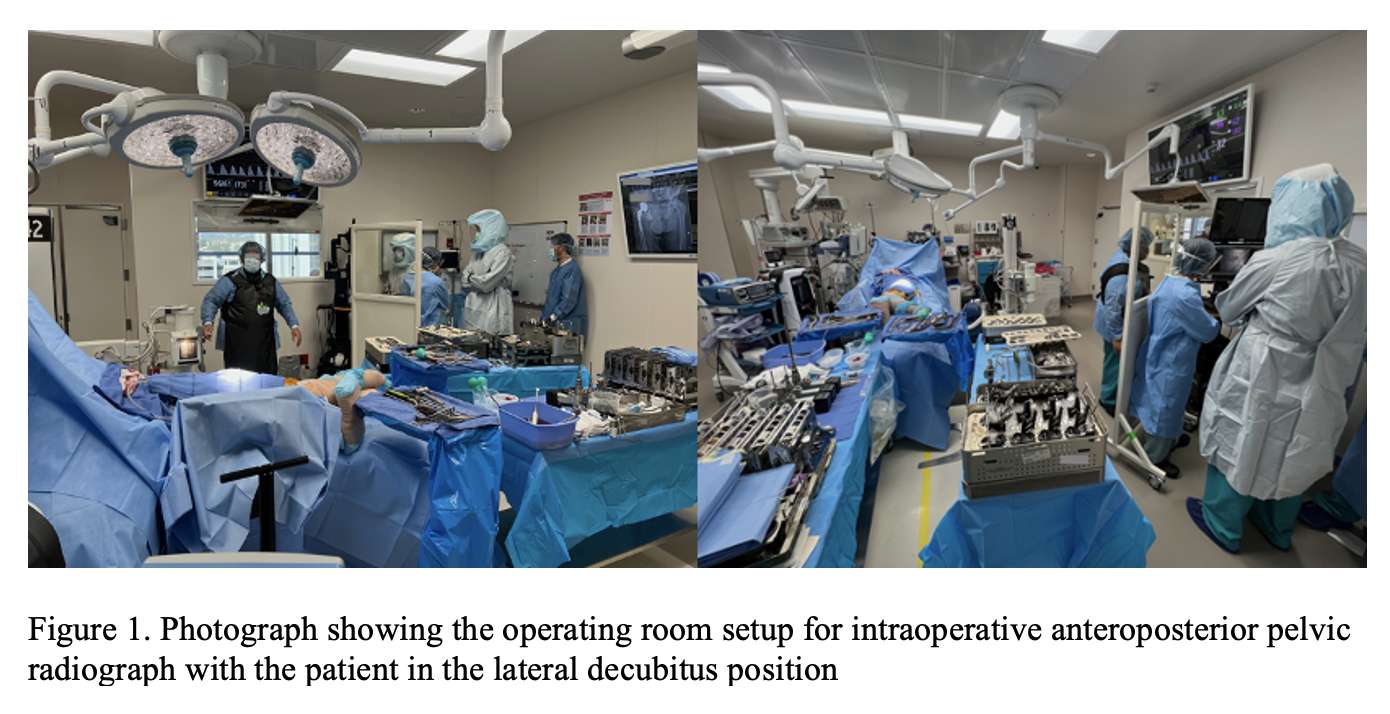
Figure 1
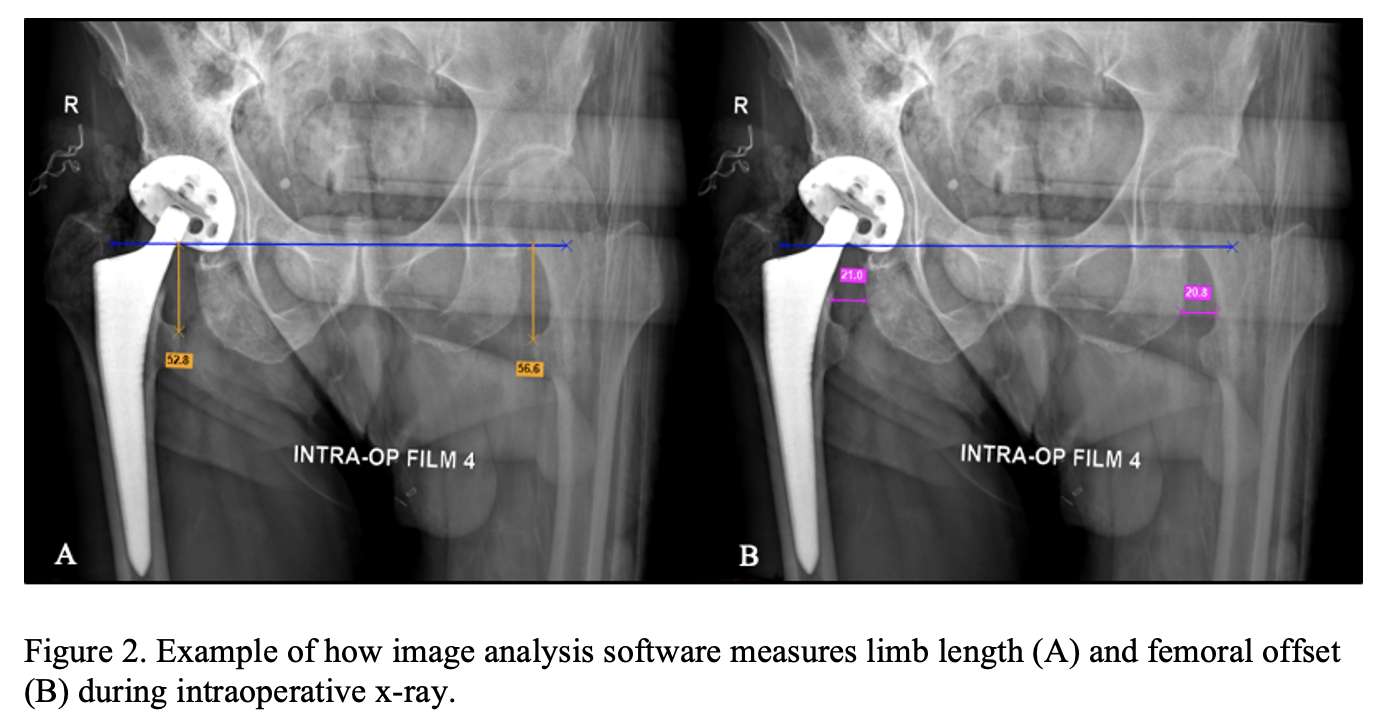
Figure 2
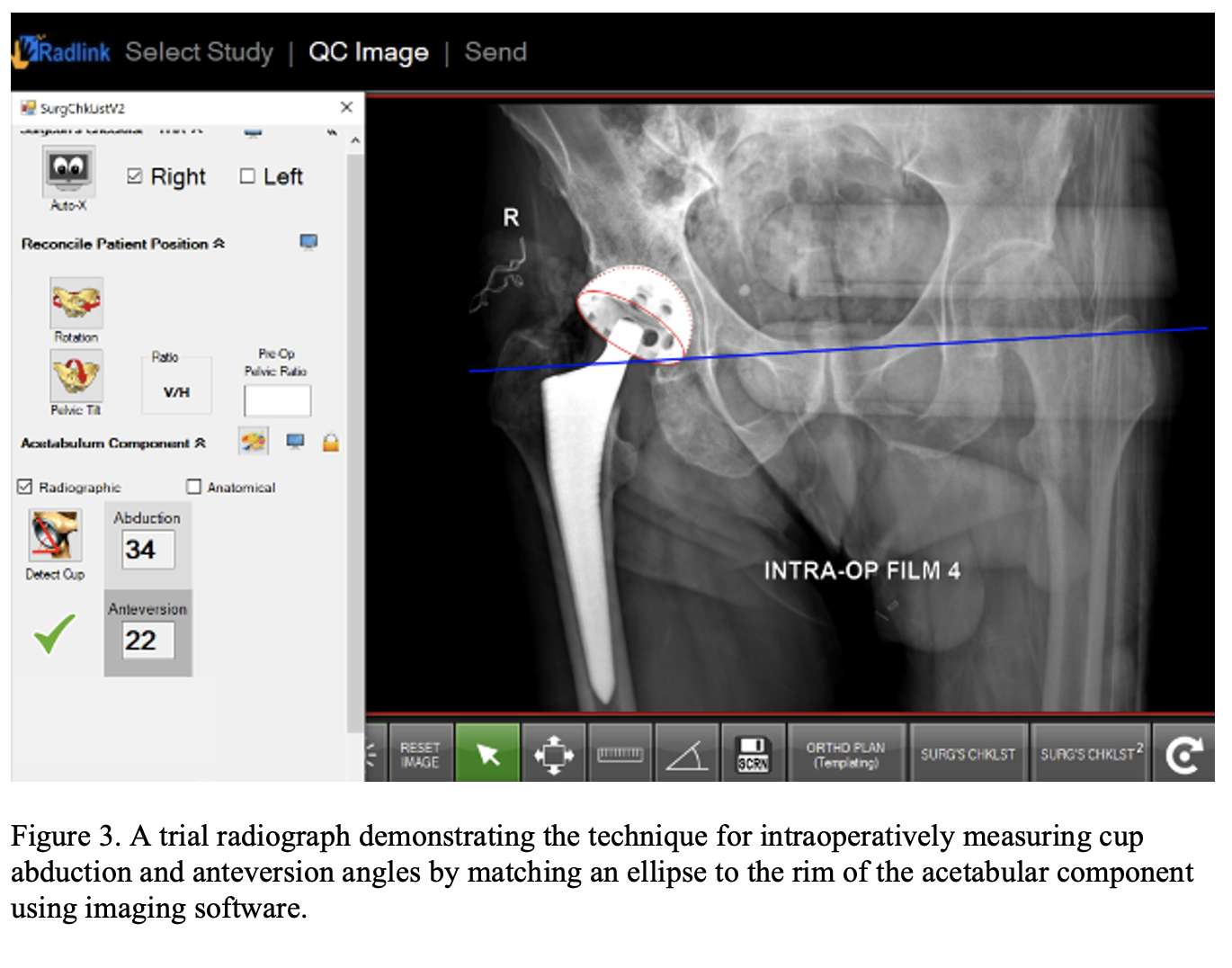
Figure 3
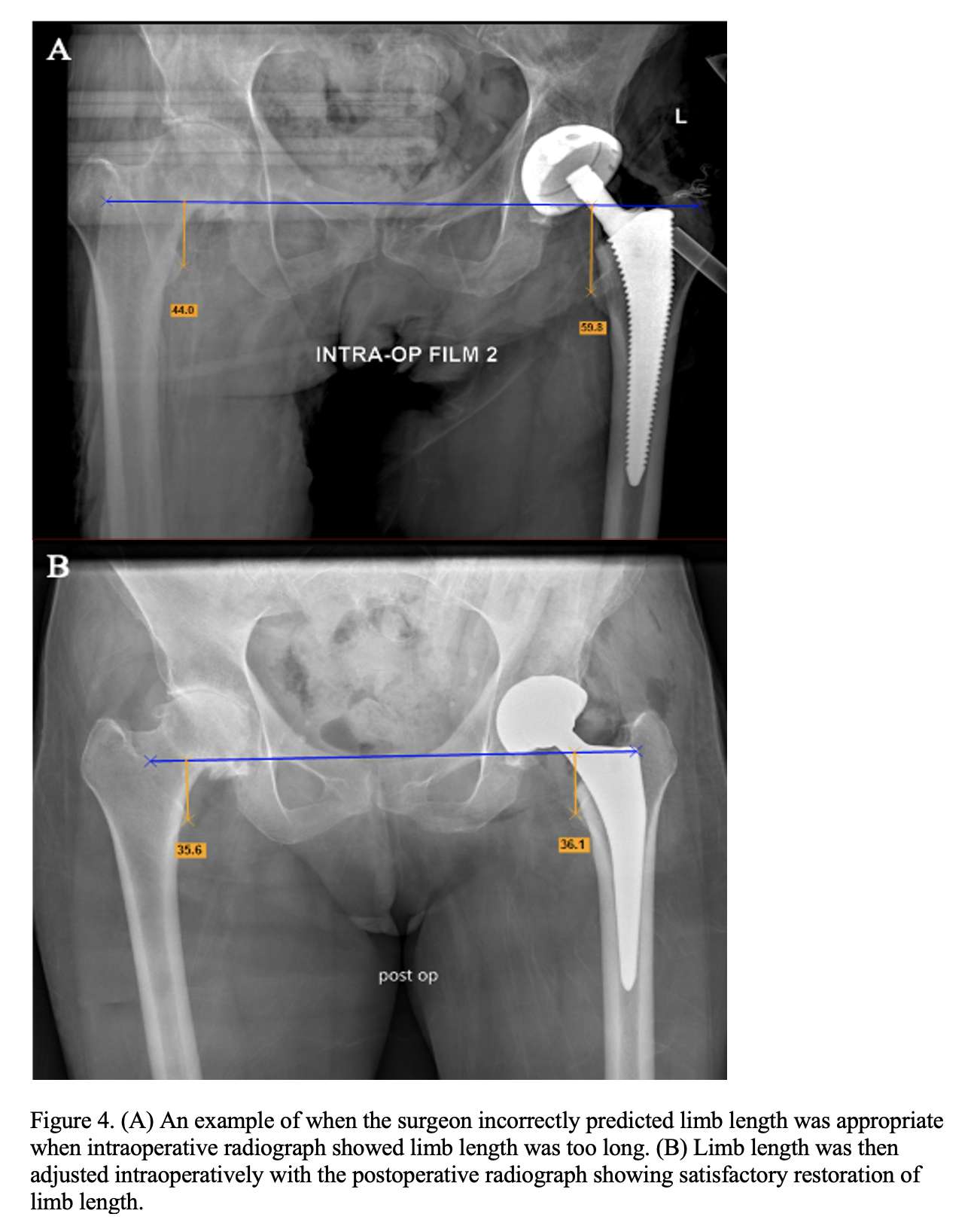
Figure 4
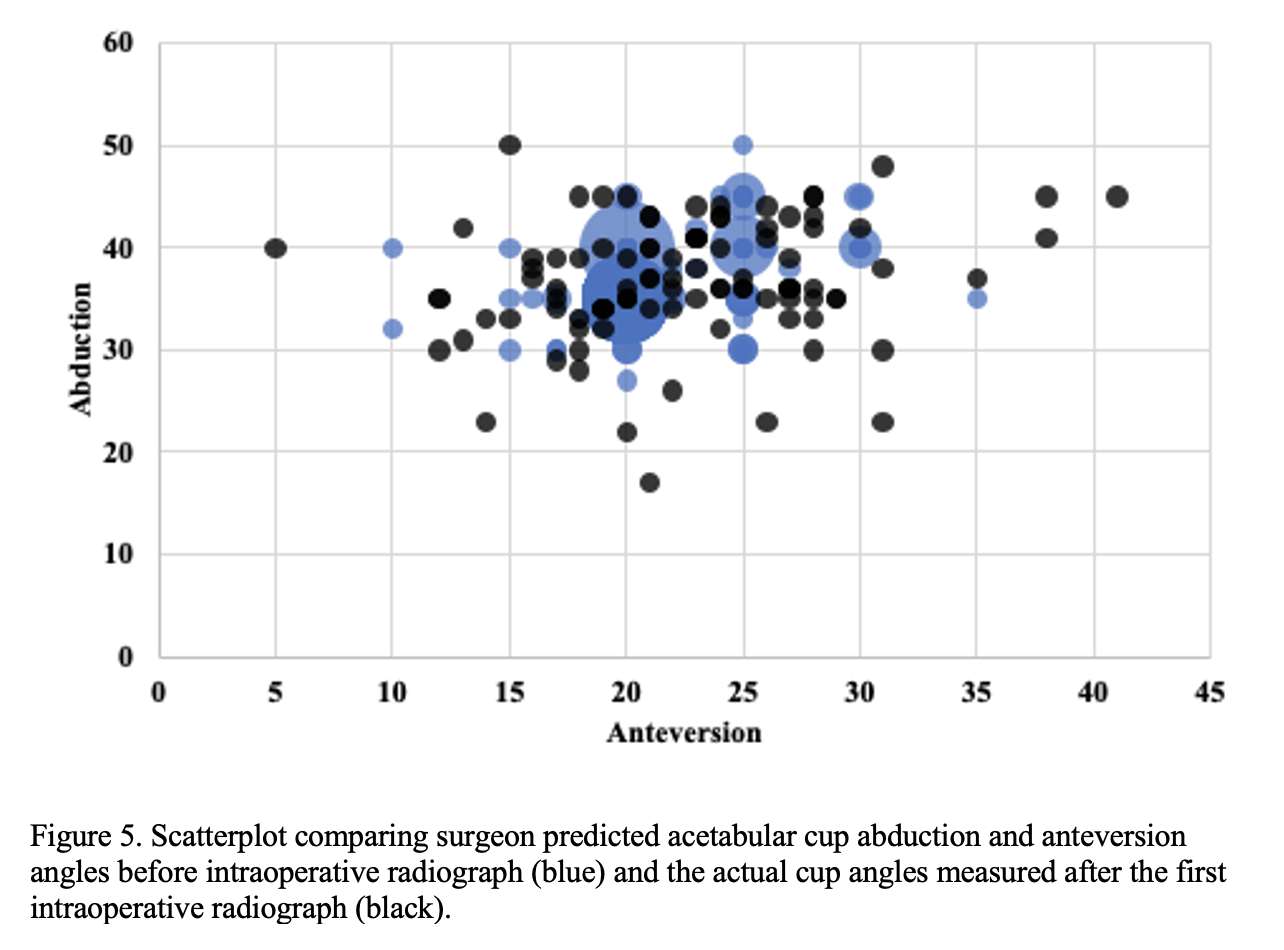
Figure 5
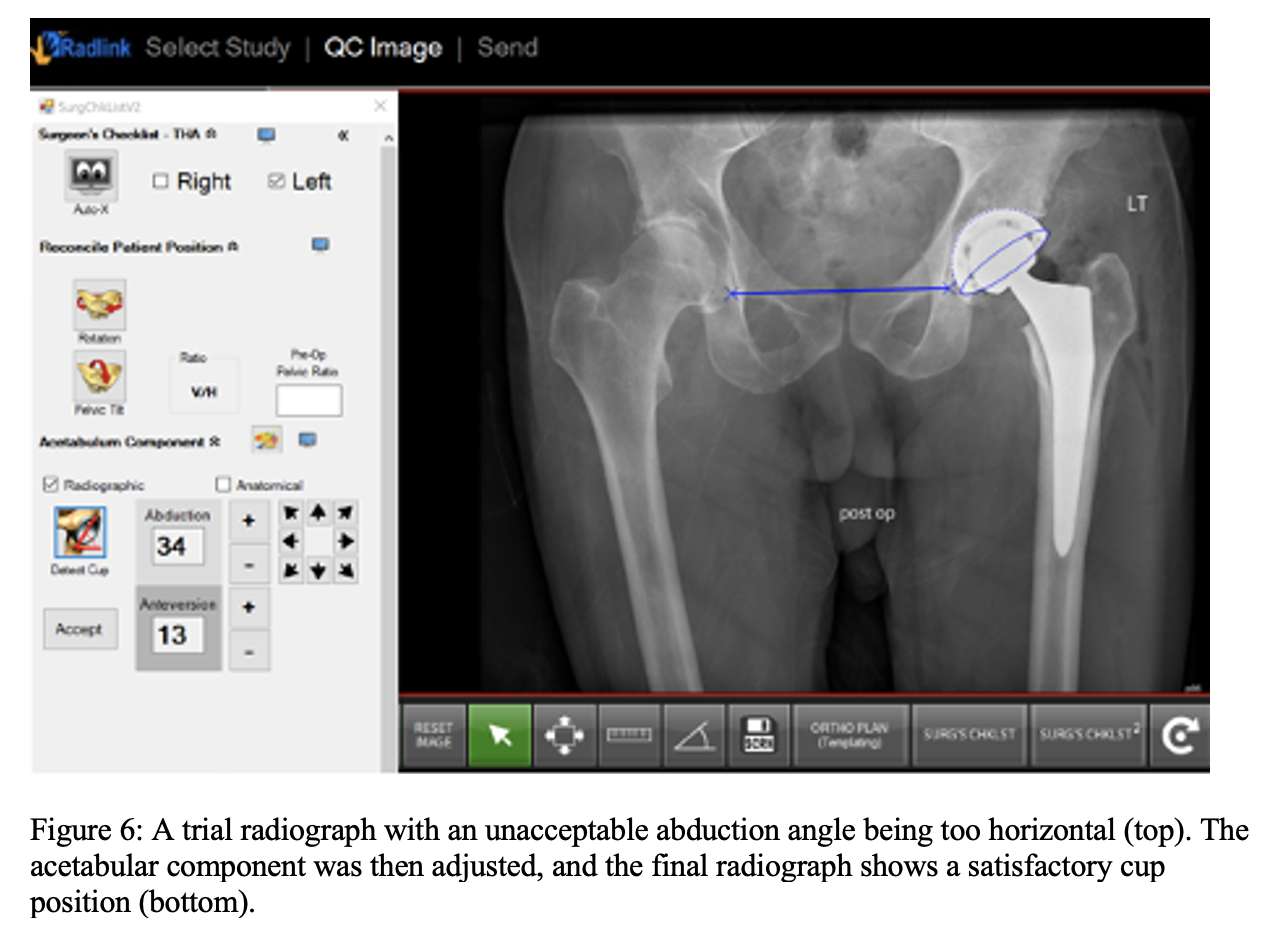
Figure 6

Figure 7
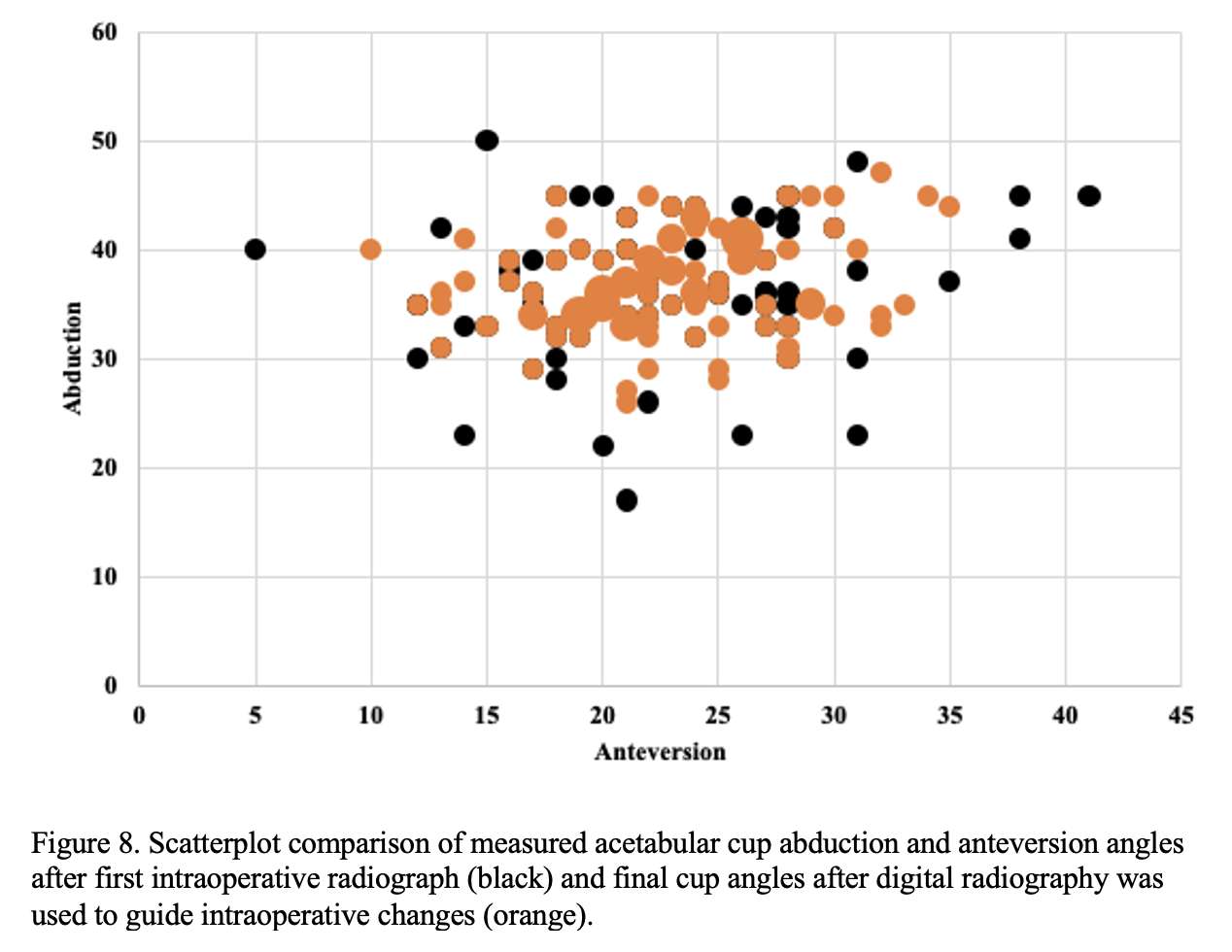
Figure 8
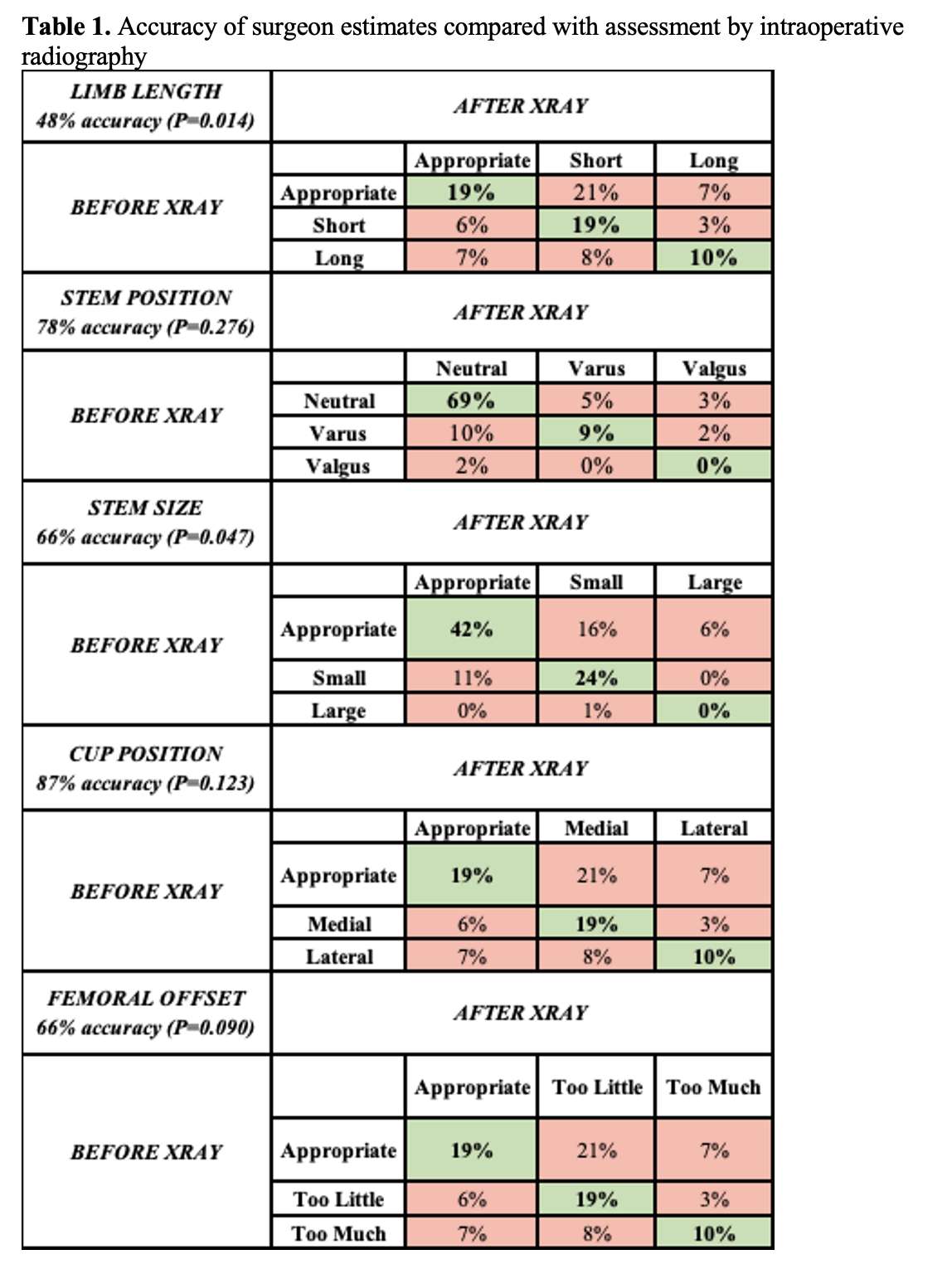
Figure 9
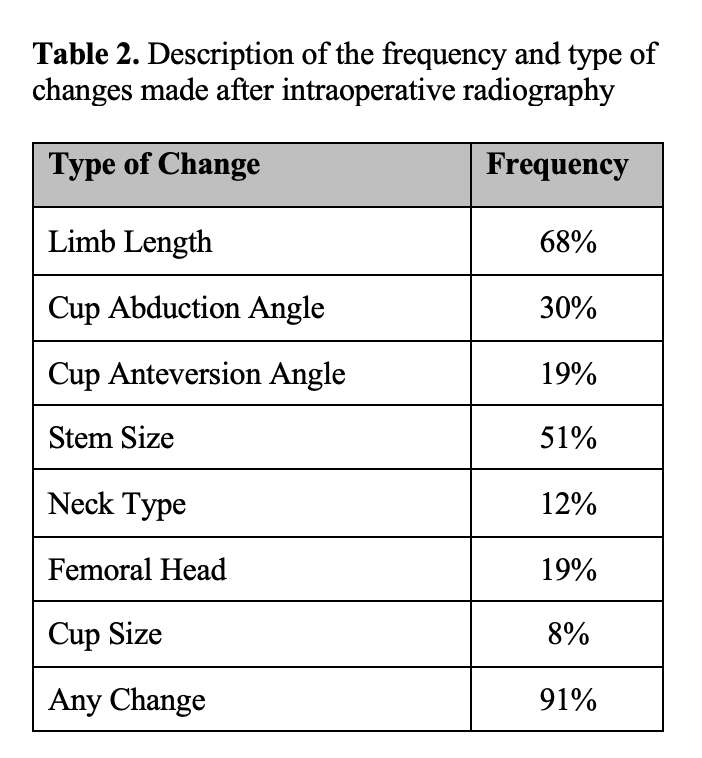
Figure 10#7599
The Efficacy of New Total Knee Arthroplasty Rehabilitation Protocol for Good Range of Motion After Follow-Up of 2 Years
*Masataka Nishikawa - Japan Community Healthcare Organization (JCHO) Osaka Hospital - Osaka City, Japan
Katsuya Nakata - Osaka Hospital, Japan Community Healthcare Organization - Osaka, Japan
*Email: ni4kawama@gmail.com
[Introduction]
Total knee arthroplasty (TKA) has good clinical result and longevity. However, many patients unsatisfied with their range of motion (ROM). We modified our TKA rehabilitation protocol to obtain good post-operative ROM. We evaluated the efficacy of new TKA rehabilitation protocol compared with old one for good ROM after follow-up of 2 years.
[Methods]
Continuous passive motion (CPM) and a standing gait exercise program were started on post-operative (PO) day 2 as standard rehabilitation protocol previously (old rehabilitation). We modified TKA rehabilitation protocol for good ROM (new rehabilitation). First, we discontinued CPM and started self ROM exercise using triangular shaped knee rehabilitation cushion. Second, we did not encourage a standing gait exercise, and recommended the elevation of operated lower leg to avoid swelling. Third, all rehabilitation exercise were started on PO day 1. Forty-seven TKAs with old rehabilitation (old) and forty-six TKAs with new rehabilitation (new) by single surgeon were enrolled in this study. Next, we defined pre-operative ROM as 100% and also evaluated ROM% at post-operative period. We compared with the ROM and ROM% at pre-operation, PO week 1, 2, 3, month 2, 6, 12, 18 and 24 between old and new groups to evaluate the efficacy of new rehabilitation protocol for good ROM. Statistical analysis was performed using Mann-Whitney U test, and p<0.05 was considered to indicate statistical significance.
[Results]
There was no significant difference between 2 groups in pre-operative ROM (old/new; 14-128°/16-124°). However, there were significant differences between 2 groups in PO week 1 (6-99°/4-117°: p<0.001), 2 (4-109°/3-123°: p<0.001), 3 (2-116°/2-126°: p<0.001), month 2 (5-125°/5-132°: p=0.03), 6 (4-127°/3-134°: p=0.02), 12 (3-129°/2-136°: p=0.03), 18 (2-128°/1-137°: p=0.003), and 24 (2-129°/1-138°: p=0.005). Moreover, there were significant differences between 2 groups (ROM%) in PO week 1 (old/new; 84%/106%: p<0.001), 2 (94%/113%: p<0.001), 3 (102%/117%: p<0.001), month 2 (108%/119%: p<0.001), 6 (111%/122%: p<0.001), 12 (114%/126%: p<0.001), 18 (113%/128%: p<0.001), and 24 (114%/129%: p<0.001). All results showed significantly good post-operative ROM in new rehabilitation group compared with old one.
[Conclusion]
The usefulness of CPM after TKA was reported in 1980s. However, many recent studies reported that CPM provided no benefit to patients recovering from TKA. CPM is passive exercise and patients are able to exercise at only setting angle and time. The cost of CPM is also high. The self ROM exercise using triangular shaped knee rehabilitation cushion is active exercise and patients are able to exercise at maximum angle and time as much as possible. This exercise is easy to encourage patients’ motivation for ROM exercise. In addition, all rehabilitation exercise were started on POD 1; one day earlier that previous protocol. This ROM exercise in early post-operative period is able to start before post-operative joint contracture. These modifications of TKA rehabilitation protocol are considered to contribute good ROM after follow-up of 2 years. However, this protocol is not suitable for the unmotivated or upper extremity disability patients such as dementia, post-operative delirium, and rheumatoid arthritis.
#7879
Contributions of Capsular Releases to Femoral Exposure in THA via a Direct Anterior Approach How Much Is Enough?
Zackary Byrd - UTH Texas Medical College - Houston, USA
Shuyang Han - University of Texas Health Science Center at Houston - Houston, USA
Sabir Ismaily - Institute of Orthopedic Research and Education - Houston, USA
Luis Delgadillo - Institute of Orthopedic Research and Education - Bellaire, USA
Adam Freedhand - The University of Texas Health Science Center at Houston - Houston, USA
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
*Email: philipnoble66@gmail.com
INTRODUCTION: The Direct Anterior Approach (DAA) has become popular for performing THA due to faster recovery and reduced risk of dislocation. However, adequate femoral exposure can be difficult due to obstruction of the broach path by the ilium, necessitating multiple soft tissue releases. The number of releases required and the difficulty of each procedure is unpredictable due to morphological and ligamentous differences between patients. This study was performed to answer the following research questions:
1. How much displacement and rotation of the hip are required to provide access to the femur?
2. Which releases are necessary to provide this access?
METHODS: 3D specimen-specific models were reconstructed from CT scans of 7 fresh cadavers (14 hips). Retro-reflective markers were rigidly fixed to the femur and the pelvis. Each cadaver was placed on a Hana Table with the hip at 20°of extension and 20°of adduction. An experienced joint surgeon performed THA via the DAA after dissecting the hip to the capsule and transection of the femoral neck via the iliofemoral ligament (IFL). Then, five releases were performed in the following sequences: (1) Transverse IFL, (2) Descending IFL, (3) Ischiofemoral ligament, (4) Conjoint tendon, and (5) Obturator externus. After each release, a 6 Nm external rotation torque was applied to distal extremity and a 120N retraction force was applied at 45° to the proximal femur. The displacement and rotation of the femur and pelvis were tracked with an 8-camera motion analysis system (Vicon). Next, the experimental procedures were recreated in a virtual environment. The implantation paths of 3D models of a femoral stem and broach handle was reproduced at each step of soft-tissue release for each specimen. The minimum 3D distance between the broach assembly and the pelvis. Once clearance was achieved between the ilium and the broach assembly, the exposure was considered adequate for femoral preparation.
RESULTS: Under the 6 Nm rotational torque, the external rotation of the intact femur averaged 29.9°±14.7°. This rose incrementally with each soft-tissue release (p<0.001), up to 108.8°±16.4° after completion of all releases (Figure 1). Application of the 120N retraction force generated 17.3±6.7mm of displacement of the femur with respect to the acetabular center after resection of the femoral head. This value increased from 20.5±5.8mm after release of the TransIFL (p<0.05) to 21.9±6.1mm (DecIFL), 21.8±7.2mm (IscFL), 22.2±5.5mm (CJtendon), and 24.9±7.0mm (ObtEx) after additional releases (p>0.05). Virtual simulations showed that femoral exposure was adequate in 13/14 specimens after release of the descending limb of the IFL. Additional releases were necessary to avoid contact between the broach handle and soft tissue.
CONCLUSION: Via the DAA, adequate exposure can be gained in most cases after releasing the transverse and descending bands of the ilio-femoral ligament. The findings provide references to achieve minimal and optimal capsular releases in THA performed via DAA, thereby contributing to advance patient care, improve surgery efficiency.
Figures
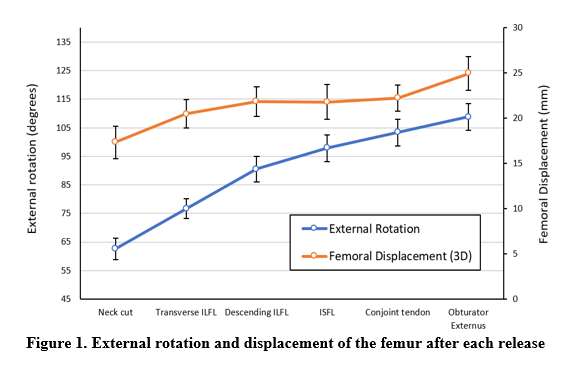
Figure 1
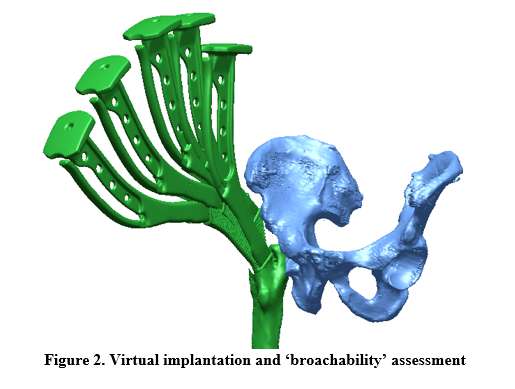
Figure 2#7889
Predictors of Failure of Fixation and Nonunion in Periprosthetic Distal Femur Fractures
*Philip Noble - Institute of Orthopedic Research and Education - Houston, USA
Matthew Hnatow - University of Texas - Houston, USA
Cristian Ybarra - Univesity of Texas Health Science Center - Bellaire, USA
Jerry Wang - University of Texas Health Science Center - Houston, USA
Abhi Rashiwala - University of Texas Health Science Ctr - Houston, USA
Sabir Ismaily - Institute of Orthopedic Research and Education - Houston, USA
Steven Schroder - University of Texas Health Science Ctr - Houston, USA
David Rodriguez - University of Texas - Houston, USA
*Email: philipnoble66@gmail.com
Introduction
Distal femoral periprosthetic (DFPP) fractures are a potential complication following total knee arthroplasty (TKA) and are associated with significant morbidity and mortality. Operative treatments include open reduction and internal fixation (ORIF) or retrograde intramedullary nailing (rIMN). There is no clear consensus which is best. As failure of fixation or nonunion often leads to revision ORIF or a distal femoral replacement, optimization of outcome to reduce risk is imperative. This study is to determine the factors that are associated with early failure of DFPP fractures treated with ORIF or rIMN.
Methods
We performed a retrospective chart review of patients with DFPP fractures treated by fellowship-trained orthopedic trauma surgeons from 2016-2020. Our outcome measures were failure of fixation, nonunion of the fracture or return to the OR to address complications related to the fracture. To examine factors affecting outcome, we collected parameters describing the demographic, clinical and injury status of each patient, including the design of the femoral component (CR or PS), the type of fracture (Rorabeck and Taylor classification) and the presence of anterior and/or medial comminution or bone loss (Figure 2). Post-operative imaging was used to identify the type of fixation construct (intra-medullary nail (IMN), bone plating, or any combination of the two.) The presence and number of any interfragmentary lag screws was also recorded. Post-operative fracture alignment was defined by the distal femoral valgus angle, femoral component flexion or extension, and posterior condylar offset ratio (Figure 3).
Results
There were 83 fractures in 80 patients. The average patient was female, 76 years old (range 55-95) with a BMI of 31.6 kg/m2. The mechanism of injury was a fall from sitting or standing in 95% of cases. Thirty-six fractures were treated with IMN (43%), 42 with ORIF with plate(s) and screws (51%), and 5 with a combination of these modalities (6%). Sixteen patients (19%) were lost to follow-up. Fifteen patients (18%) returned to OR for a total of 21 visits. Eleven fractures (13%) proceeded to nonunion. Failure of fixation was associated with the use of fewer screws in the distal segment (Nonunion group: 4.1 vs. 5.7 in the union group (p=0.001)). Additionally, 78% of the union group had a cruciate retaining femoral component vs. 46% of the nonunion group (p=0.014). Knee alignment following ORIF was highly variable. Post-operatively, the lateral distal femoral angle was 83.9±3.4 degrees, ranging from 74 to 90 degrees, while flexion of the femoral component ranged from -20 to 21 degrees. The average posterior condylar offset ratio was 0.7±0.2 (range: 0.23 to 1.50).
Conclusions
Periprosthetic distal femur fractures have a relatively high nonunion and return to OR rates. Lower number of screws in the distal segment was associated with failure of fixation and nonunion. Additionally, posterior stabilized TKA design is also associated with failure of fixation and nonunion. Improvements in implant design and fracture reduction are needed to reduce patient mortality and morbidity following these serious injuries.
Figures
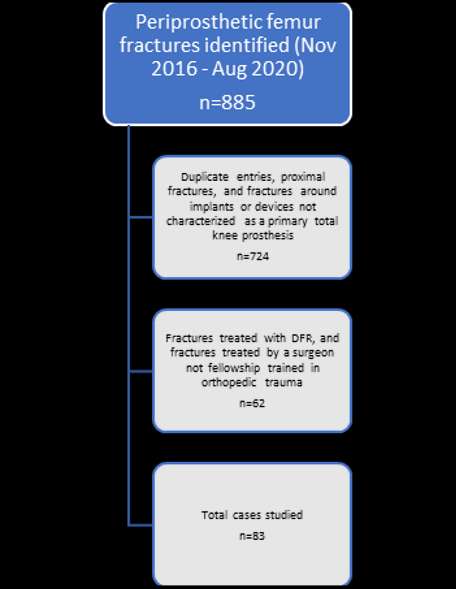
Figure 1

Figure 2
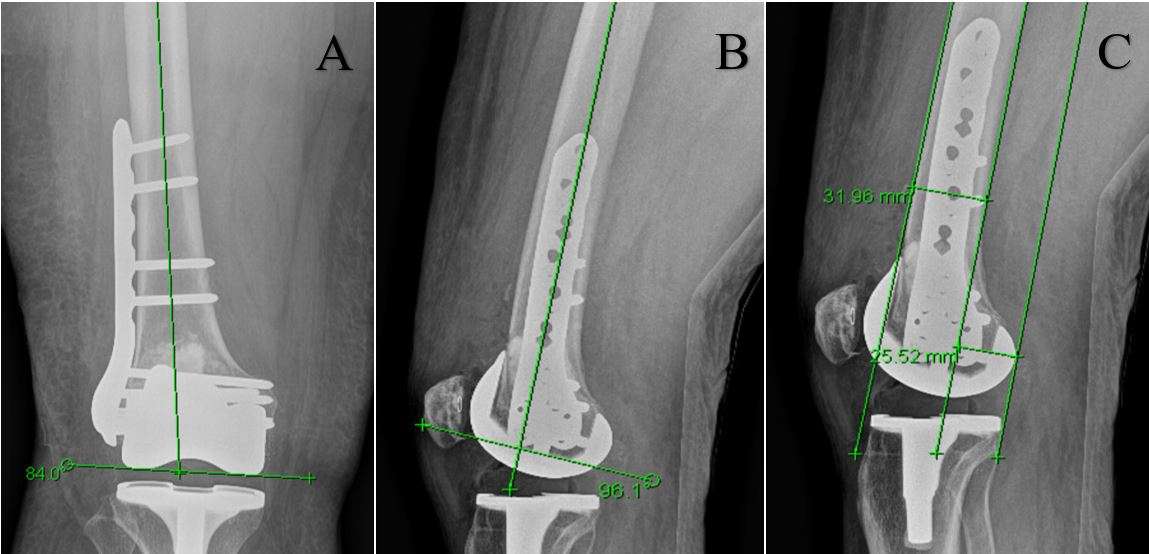
Figure 3#7268
Total Hip Arthroplasty After Seven Decades of a Girdlestone Situation Due to Tuberculous Coxitis in Childhood
*Andrej Nowakowski - Kantonsspital Baselland - Bruderholz, Switzerland
Michal Pelczar - Kantonsspital Baselland / University of Basel - Bruderholz, Switzerland
*Email: andrej.nowakowski@unibas.ch
Introduction: Tuberculous coxitis accounts for about 15 % of all osteoarticular tuberculosis cases and is the second most frequent after spinal tuberculosis. A common surgical treatment option for patients with extensive tuberculous coxitis is excision arthroplasty (Girdlestone). However, this is not regarded as being the final treatment step, total hip arthroplasty should still be kept in mind. There are hip stems on the market that offer good preconditions for bone restoration even in cases with significant bone loss. To the best of our knowledge, no published data exists that examines the assessment and outcome of re-articulation by using a prosthesis more than seven decades after Girdlestone.
Case Presentation: A 76-year-old male patient presented with a painful hip in our department. He had previously been treated with Girdlestone at the age of five years after being diagnosed with tuberculous coxitis. After an intensive and very detailed evaluation of treatment options, the patient agreed upon re-articulating the joint with a total hip implant. On the acetabular side, an acetabular reinforcement ring was inserted and a PE low profile cup was cemented with less inclination, to avoid or reduce hip instability. On the femoral side, a Wagner cone stem was implanted. A fissure around the stem was secured with numerous cerclages. Postoperatively the patient suffered a prolonged delirium, which however had no affect on the healing process of the total hip arthroplasty. At a follow-up appointment 10 months postoperative, the patient was satisfied with the results of the surgery and reported a meaningful improvement in his daily quality of life. His mobility increased significantly, represented by his ability to climb stairs without sensing pain or needing walking aids.
Conclusion: Despite suffering transient complications postoperatively, ten months after surgery the patient is satisfied with the treatment option, has an increased daily quality of life and both the clinical as well as the radiologic outcomes are promising. However, complications associated with this surgery need to be kept in mind. Furthermore, the long-term effects and survival rate of total hip arthroplasty following such a long Girdlestone situation due to tuberculous coxitis, needs to be followed up for a longer time span to develop a concluding statement on this treatment option.
Figures

Figure 1
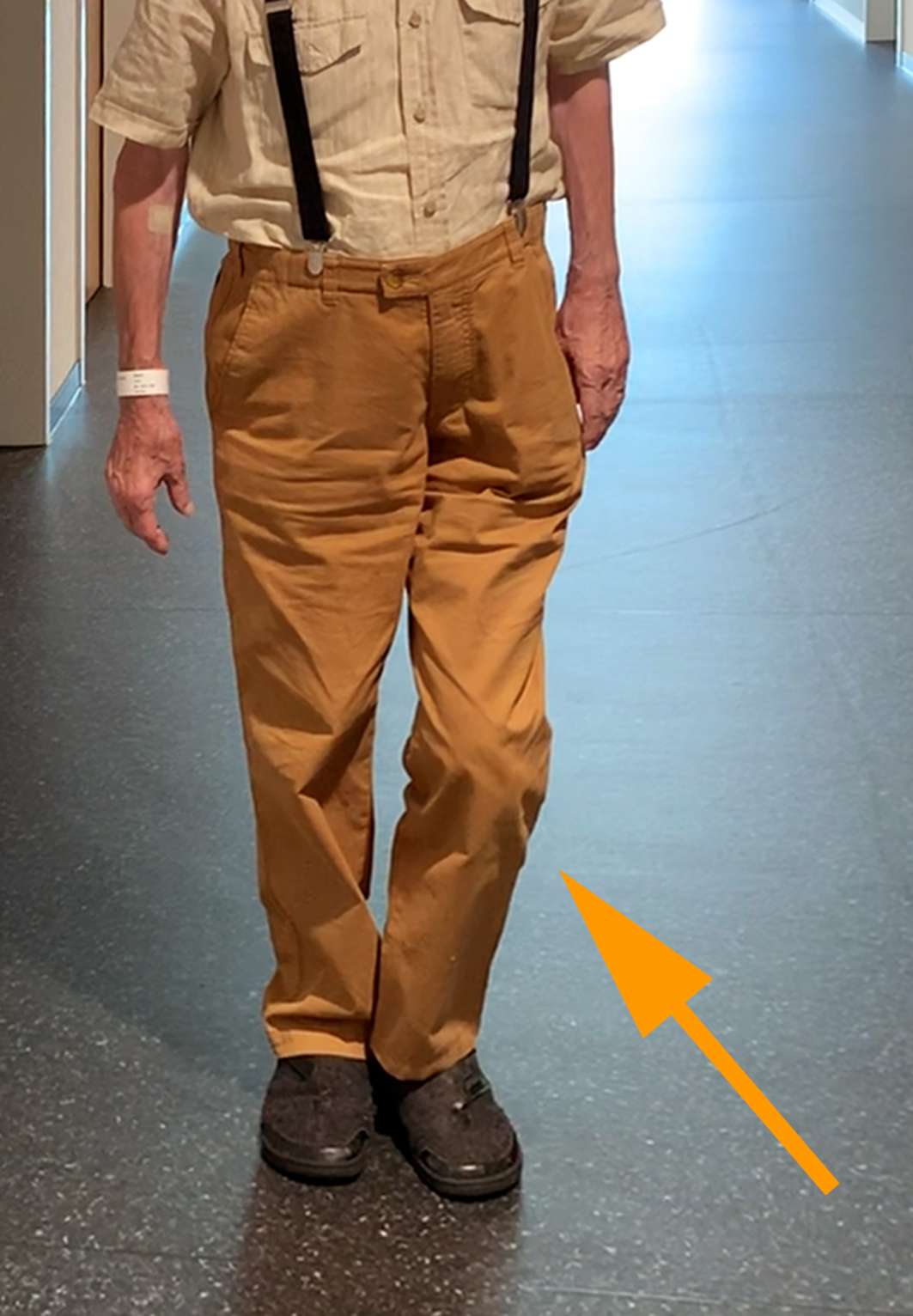
Figure 2
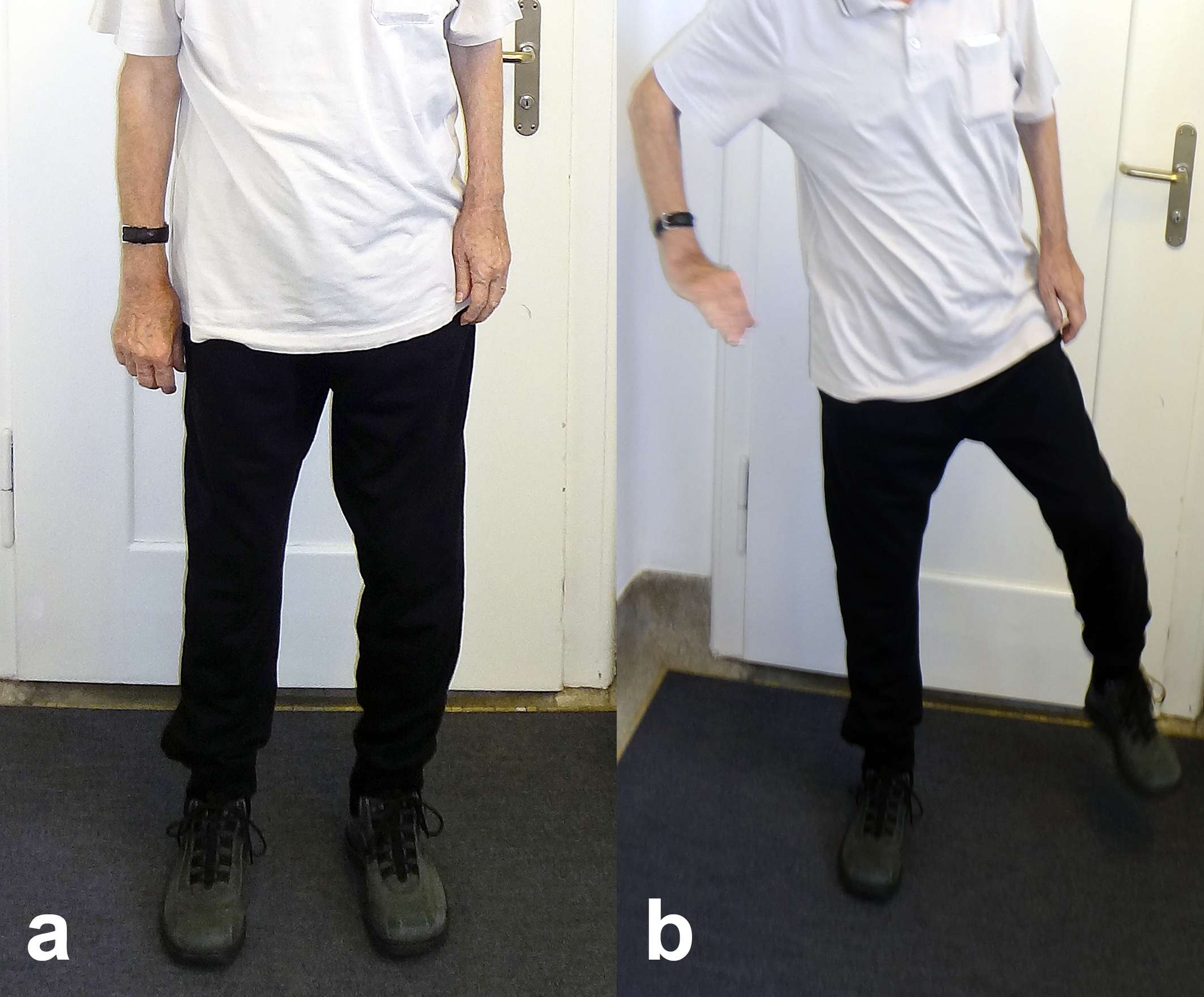
Figure 3#7269
Modified Winged Charnley Retractor for the Use in Total Hip Arthroplasty With Direct Anterior Approach
*Andrej Nowakowski - Kantonsspital Baselland - Bruderholz, Switzerland
Alexander Vacariu-Seelig - Kantonsspital Baselland / University of Basel - Bruderholz, Switzerland
*Email: andrej.nowakowski@unibas.ch
Introduction:
In total hip arthroplasty (THA) with direct anterior approach (DAA) the Charnley Retractor frame is a well-known tool to create a good view of the deep situs. The approach is described as minimal invasive and muscle sparing. Yet there are some described lesions to the musculus tensor fasciae latae (TFL) due to Charnley Retractor use. Our group designed a modification of the lateral hook to improve the muscle sparing.
Material/Methods:
We designed a CAD Modell with successive adjustments. Then an illustration model was worked over several times. The second prototype was established as a custom-made titan hook. This prototype hook was tested intraoperatively for DAA and was considered pleasing. A definitive instrument was built.
Results:
Intraoperatively comparison of the original vs. the modified retractor could be demonstrated easily with photo documentation: the new designed Charnley Retractor showed less impairment of the TFL in the first applications via DAA.
Conclusion:
The Muscle sparing effect of the “winged” Charnley Retractor seems to work very well. With this modified hook we can reduce intraoperative muscle lesions. Especially in the setting of a teaching hospital with residents or young consultants operating via DAA or with low-volume surgeons this modification has probably a positive effect on postoperative outcomes.
#7517
Effectiveness of Drain Insertion and Irrigation in the Treatment of Septic Arthritis of the Knee Under Local Anesthesia
*Byung Hak Oh - Konyang University Hospital - Daejeon, South Korea
*Email: sebslab@hanmail.net
Purpose: Septic arthritis of the knee is an orthopedic emergency that requires early diagnosis and surgical treatment. This study examined the effectiveness of drain insertion and irrigation in the treatment of septic arthritis of the knee under local anesthesia. Materials and Methods: A retrospective study was conducted on nine cases (eight patients) diagnosed with septic arthritis of the knee from September 2017 to February 2020 and treated with drain insertion and irrigation under local anesthesia. After penetrating through the superolateral portal to the superomedial portal and inserting the drain, daily irrigation of approximately 3 L of normal saline was done. The following were investigated: age, sex, underlying disease, cause, degree of osteoarthritis, time from diagnosis to surgery, duration of hospitalization, duration of normalization of C-reactive protein, and smear and culture. Results: The initial white blood cell count of joint fluid was 71,472±51,667/mm3 (32,400–203,904/mm3 ), and polymorphic leukocytes were 91.1%±2.6% (86%–95%). The average time from diagnosis to surgery was 8.3±1.3 hours (6–10 hours), and the irrigation period was 8.2±3.2 days (4–15 days). The average length of hospitalization was 20.8±8.7 days (9–37 days). There was no reoperation or recurrence. Smear and culture tests were not identified. Conclusion: In the treatment of septic arthritis of the knee, the insertion of a drain tube and irrigation under local anesthesia is a relatively fast and simple method to reduce pain by repetitive draining of purulent joint fluid and can be used as an alternative treatment for patients with a risk of general or spinal anesthesia.
#7614
Measuring Three Dimensional Alignment of Lower Limb After High Tibial Osteotomy With EOS System
*Byung Hak Oh - Konyang University Hospital - Daejeon, South Korea
*Email: sebslab@hanmail.net
Introduction: Unintended internal rotation of distal tibia occurs during the procedure of medial open wedge high tibial osteotomy. CT is the standard method for measuring the changes of lower limb alignment throughout the osteotomy procedure. The EOS system is a new biplanar low dose radiographic device that allows 3-dimentional limb modelling with automated measurement of lower limb alignment. The Authors assumed that the changes of lower limb alignment profiles obtained by the EOS system are equivalent to those obtained by CT.
Materials and methods: 51 lower limbs from 46 patients were enrolled to the analysis. Changes of lower limb alignment profiles including femoral and tibial torsion were measured on both CT and EOS images before and after the osteotomy by 2 orthopaedic surgeons. Agreement between CT and EOS values was assessed by inter-observer reliability and inter-modality reliability.
Results: Changers of femoral torsion was 0.2◦by EOS vs. 0.1◦by CT (P = 0.5) and changes of tibial torsion was -2.5◦by EOS vs. -.2.3◦by CT (P = 0.4). Strong associations were found between EOS and CT values for both femoral torsion (P = 0.87) and tibial torsion (P = 0.9).
Discussion: EOS system can be a valid alternative to CT for lower limb torsion measurement in patients underwent OWHTO. EOS imaging shows a comprehensive evaluation in all three planes with less radiation exposure to the patient.
#7615
Comparison of Continuous Lavage by Tube With Arthroscopic Treatment of Acute Septic Arthritis of Native Knee
*Byung Hak Oh - Konyang University Hospital - Daejeon, South Korea
*Email: sebslab@hanmail.net
Objective: The purpose was to compare the treatment efficacy of continuous lavage after tube insertion by local anesthesia and arthroscopic treatment.
Methods:Patients who treated with arthroscopic treatment included in group I and treated with continuous lavage by tube included in group II. We investigated the following variables in all patients: demographics, underlying disorders (hypertension and diabetes), initial serum white blood cell (WBC) count and C-reactive protein (CRP) levels, synovial fluid WBC and polymorphonuclear cells, causative organisms, initial Kellgren-Lawrence grade (K-L grade), lavage number, time to intervention, hospitalization day, and CRP normalization time, clinical outcomes of 3 months postoperatively.
Results:There were statistically significant differences in the lavage number and time to the intervention. Lavage number was significantly larger in group II (7.5 ± 3.0) than in group I (1.1 ± 0.3 and p<0.001). Time to the intervention was significantly delayed in group I (23.6 ± 15.6) than in group II (8.7 ± 9.3, p<0.001).
Conclusion: In terms of efficacy, the continuous lavage by tube had significantly less delay time and more opportunity for intervention. The continuous lavage by tube had no re-aggravations and faster declination at early 2 weeks on CRP, but the difference was not statistically significant. Moreover, continuous lavage by tube had no significant differences in outcomes, including laboratory results and functional outcomes at POD 3 months.
Key points
- Delayed treatment of septic arthritis was associated with poor prognosis.
- Local anesthesia does not require delaying time for preparing operability and it is possible that continuous lavage with no delay.
- Continuous lavage had no significantly different outcomes compared to arthroscopic intervention.
#7923
Usefulness of Intraoperative C-Arm Image Intensifier in Reducing Errors of Acetabular Component During Primary Total Hip Arthroplasty: An Application of Widmers Method
*Seungbae Oh - Department of Orthopaedic Surgery, College of Medicine, The Catholic University of Korea - Seoul, South Korea
Joo-Hyoun Song - St. Vincent;S Hospital, the Catholic University of Korea - Suwon, South Korea
*Email: minerba5@hanmail.net
Background: Acetabular prosthesis positioning in total hip arthroplasty (THA) is crucial in reducing the risk of dislocation. There has been minimal research on the proper way to put the acetabular components into the safe zone intraoperatively. Assessment of version by intraoperative imaging intensifier is very valuable. The value of Widmer’s method, using the intraoperative C-arm available to determine cup anteversion was assessed.
Methods: 101 hips in 91 patients who underwent primary THA were eligible for inclusion. Utilizing intraoperative C-arm images, measurement was performed using the technique described by Widmer. The values obtained using 3D computed tomography postoperatively, which determined the anteversion of the acetabular component, were regarded as the reference standard.
Results: The method of Widmer obtained values similar to those obtained using 3D computed tomography and was considered accurate (n.s.). All 101 hips were positioned in the set target zone. Among the 101 hips, the cup position in nine hips (8.9%) was changed. The dislocation rate in our study was 1.0% with all dislocations occurring in hips placed in the target zone. The mean Harris hip score after THA in one year was 94.2 (82-98).
Conclusions: The method of Widmer was accurate using intraoperative imaging intensifier for the measurement of the anteversion of the acetabular component during THA, with reference to the anteversion obtained from the 3D computed tomography. Also, utilizing intraoperative C-arm imaging was very useful because it allowed for correction of the position of the acetabular cup.
Keywords: X-Rays, Hip, Arthroplasty, Replacement, Acetabulum
#7924
Use of a Constrained Acetabular Liner to Prevent and Treat Recurrent Dislocation After Total Hip Replacement Arthroplasty
*Seungbae Oh - Department of Orthopaedic Surgery, College of Medicine, The Catholic University of Korea - Seoul, South Korea
Joo-Hyoun Song - St. Vincent;S Hospital, the Catholic University of Korea - Suwon, South Korea
Jong-Hun Ji - Daejeon St. Mary's Hospital, The Catholic University of Korea - Daejeon, South Korea
*Email: minerba5@hanmail.net
Background: The aim of the present study was to evaluate the dislocation rate and the risk factors leading to instability after primary and revision total hip replacement arthroplasty (THRA) with constrained acetabular liners (CAL), as well as treatment strategies for prevention of dislocation.
Methods: From 1999 to 2017, drawing on two institutions’ THRA registries, we retrospectively identified 46 THRA cases using a CAL that had been followed up for a minimum of 4 years. The patients comprised 39 women and 7 men, with an average age of 69.1 years (age range, 41–98). Of the 46 patients, CAL were used in 12 patients for prevention of dislocation in primary THRA and in 34 patients for treatment of recurrent dislocation after primary THRA.
Results: Clinical and radiological evaluation were performed. We evaluated the failure rate of CAL as well as the risk factors. The 12 patients who used CAL for prevention of dislocation in primary THRA had no dislocation. However, 12 (35%) of the 34 hips had a dislocation after use of CAL in revision THRA. Patients with an abductor muscle weakness grade of ≤3 had a higher rate of dislocation than those with a grade of ≥4 (grade 1; likelihood ratio = ∞, grade 2; likelihood ratio = 1.83, grade 3; likelihood ratio = 1.05, grade 4; likelihood ratio = 0.46, and grade 5; likelihood ratio = 0). The group of primary THRA with CAL had no dislocations, and this is a proper way for prevention of dislocation in high-risk patients. The group of revision THRA with CAL had a high dislocation rate (35%). Abductor muscle weakness below grade 3 was a risk factor for failure of CAL for hip dislocation.
Conclusions: We recommend treating patients with recurrent dislocations with the presence of abductor muscle weakness below grade 3 with not only THRA using CAL but also applying additional abductor muscle reconstruction to reduce the risk of dislocation.
#7556
The Effect of Total Hip Arthroplasty on Low Back Pain
Masakazu Okamoto - Nara Medical University - Kashihara, Japan
*Yoshinobu Uchihara - Nara Medical University - Kashihara, Japan
Kenichiro Saito - Nara Medical University - Nara, Japan
Yusuke Inagaki - Nara Medical University - Kashihara, Japan
Yasuhito Tanaka - Nara Medical University - Kashihara, Japan
*Email: y-uchihara@naramed-u.ac.jp
【INTRODUCTION】It has been reported that among patients undergoing total hip arthroplasty (THA), the proportion of patients suffering from different degrees of low back pain (LBP) ranged from 21.2% to 60.4%. Some literature reported improvement in LBP after THA. However, whether there was improvement in LBP after THA remains unclear. In this study, we examined whether LBP improves and whether sagittal alignment of pelvis, hip, and spine changes at a relatively early stage at six months after THA.
【METHODS】A total of 29 patients with 31 hips (eight males and 21 females, mean age 65.7 years) who underwent THA for osteoarthritis between January 2020 and March 2021 at our hospital were included in this study. The Japanese Orthopedic Association Hip Disease Evaluation Questionnaire (JHEQ), the Oswestry Disability Index (ODI), and the Visual Analogue Scale (VAS) for LBP were compared preoperatively and six months postoperatively. Sagittal alignment of the pelvis, hip, and spine was analyzed on lateral radiographs taken with the subject standing upright before (baseline) and six months after (follow-up) THA. Sagittal alignment of the pelvis and hip was measured by pelvic incidence (PI), pelvic tilting (PT), sacral slope (SS), pelvic femoral angle (PFA), and femoral inclination (FI), while sagittal alignment and balance of the spine were measured by lumbar lordosis (LL) and T1 spinal–pelvic inclination (T1-SPI).
【RESULTS】The mean JHEQ score improved significantly from 17.5±9.4 preoperatively to 62.9±17.5 at six months postoperatively (P<0.001), ODI improved from 42.3±16.7% to 11.8±11.9% (P<0.001), and the mean VAS of LBP significantly improved from 5.3±2.7 to 1.6±1.7 (P<0.001). There was a significantly larger PFA, but smaller SS and FI at six months after THA when compared to the baseline (P<0.05) in the sagittal alignment parameters.
【DISCUSSION】Preoperative LBP significantly improved, along with JHEQ at six months after THA. The significantly larger PFA, but smaller FI suggested that THA improved the range of motion of the hip extension, and the significantly smaller SS suggested that sagittal alignment of the pelvis and hip was improved. Weng et al. reported that THA was helpful in correcting the abnormal arrangement of spine-pelvis-leg sagittal position and reduced the comorbid LBP. This study also shows that THA is effective in improving the spinal and pelvic parameters and restoring spinal balance, which may be one of the mechanisms of LBP reduction.
【CONCLUSION】LBP, as well as hip pain, significantly improved at a relatively early stage at six months after THA. THA also improves the range of motion of hip extension, which may be effective in restoring spinal balance.
#7488
Surgical Tips of Total Hip Arthroplasty After Failed Trans-Trochanteric Rotational Osteotomy for Osteonecrosis
Masamichi Onaga - Graduate school of medicine, university of the Ryukyus - Nishihara Nakagami-gun, Japan
*Satoshi Nakasone - Graduate School of Medicine, University of the Ryukyus - Nishihara, Japan
Takahiro Igei - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
Fumiyuki Washizaki - Graduate school of medicine, University of the Ryukyus - Nishihara Nakagamigun, Japan
Kotaro Nishida - Graduate school of medicine, University of the Ryukykus - Nishihara Nakagamigun, Japan
*Email: satoshi_nakasone@hotmail.com
【Introduction】Total hip arthroplasty (THA) after failed trans-trochanteric rotational osteotomy (TRO) might have some problems with morphologic change of the proximal femur, muscle atrophy and soft tissue thickening. These may cause malalignment insertion of the femoral component and postoperative dislocation due to cup impingement. The purpose of this study was to evaluate the morphologic change of the proximal femur, muscle atrophy, and soft tissue thickening in THA after failed TRO and their impact on surgery and clinical outcomes.
【Methods】17 patients with 18 hips who underwent THA after failed TRO during the period 1998-2015 were included (TRO group) (Fig. 1). 27 hips in 21 patients who underwent THA for osteonecrosis of the femoral head during the same period were included in the control group. Clinical evaluation included operative time, blood loss, complications, hip function score and hip range of motion between each group. Radiological assessment included cup and stem alignment. In addition, to evaluate the shape of deformity of the proximal femur, the anteroposterior and transverse diameters of the femur on the sliced 5mm proximal from the lesser trochanter were measured on CT images before THA. The thicknesses of the psoas major, iliac muscle, gluteus medius and the anterior capsule of the hip joint (Fig. 2a, b, c) were measured to evaluate muscle atrophy and soft tissue thickening.
【Results】Operative time and blood loss were significantly increased in the TRO group (203 vs 123 min, 717 vs 370 ml, p<0.01). Varus or valgus stem alignment (> 3°) was found in 8 hips (44%) in the TRO group and 1 hip (4%) in the control group (p<0.01). posterior dislocation was observed in 4 hips (22%) in the TRO group (Fig. 3) and 1 hip (4%) in the control group (p=0.07). The ratio of anteroposterior to transverse diameters of the proximal femur was significantly increased in the TRO group (1.01 vs. 0.79, p<0.01). There was no difference in thickness of the psoas major, iliac muscle, and gluteus medius between groups, while thickness of the anterior capsule was significantly increased in the TRO group (10.3 vs 8.1mm, p<0.05).
【Conclusion】Our results showed that THA after failed TRO was considered a technically demanding procedure. After TRO the proximal femur was deformed into square shape, making it difficult to determine the stem insertion point and causing stem malalignment. Anteriorly protruding bone of the proximal femur and thickening of the anterior capsule were thought to cause posterior dislocation due to anterior cup impingement. The tips to performing THA after failed TRO requires preoperative three-dimensional evaluation of the deformity, using image intensifier intra-operatively for optimal stem placement and resection of overhanging anterior bone for prevention of cup impingement.
Figures

Figure 1
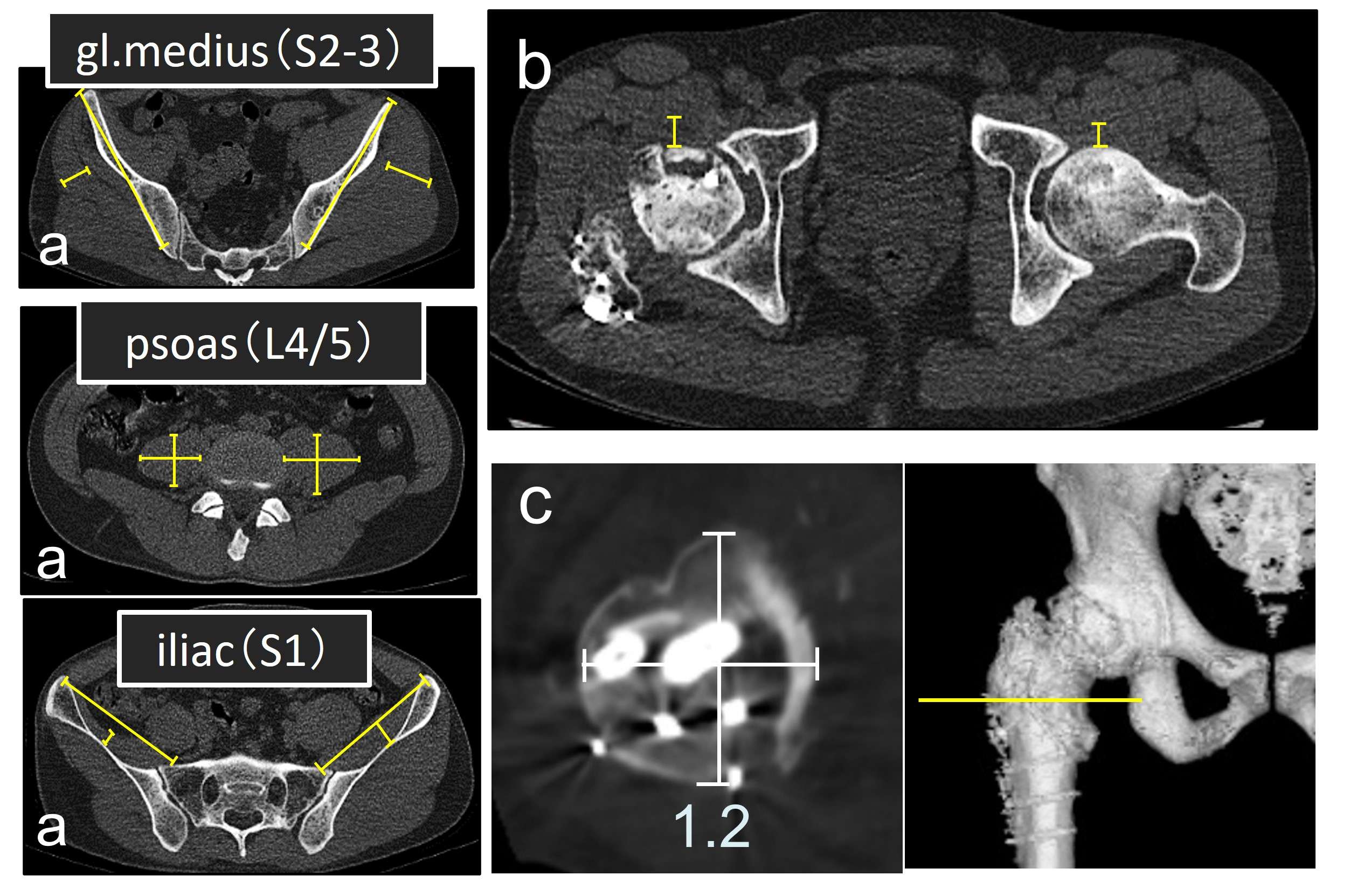
Figure 2

Figure 3#7582
Invited Talk: Antibiotic-Loaded Ultrahigh Molecular Weight Polyethylene (UHMWPE)
Sashank Lekkala - Massachusetts General Hospital - Boston, United States of America
Jaynie Criscione - Massachusetts General Hospital - Boston, USA
Keith Wannomae - Massachusetts General Hospital - Boston, USA
Cecilia M. Nepple - Massachusetts General Hospital - Boston, USA
Amita Sekar - Massachusetts General Hospital - Boston, USA
Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
*Ebru Oral - Massachusetts General Hospital - Boston, USA
*Email: eoral@partners.org
Introduction: Periprosthetic joint infection (PJI) is one of the major causes of revision surgery which requires a two-stage revision with a temporary antibiotic-eluting bone cement spacer. But these spacers often elute less than minimum inhibitory concentration (MIC) of common PJI bacteria after one week.1 We previously showed that vancomycin and rifampicin eluting UHMWPE can eradicate planktonic and biofilm-forming Staphylococci in a lapine model.2 In this study, we investigated the thermal stability of common antibiotics for incorporation into UHMWPE and determined the elution and antibacterial properties of these implants.
Methods: Thirteen antibiotics were characterized by measuring weight loss over time (n=3) with thermogravimetric analysis at molding temperatures of UHMWPE. Thermally stable drugs were blended at 7% and 10% w/w with UHMWPE followed by compression molding. 1H nuclear magnetic resonance (NMR) was used to confirm the molecular stability of the drugs after molding. Energy-dispersive X-ray analysis was used to visualize the drug domain morphology. Antibiotic-loaded UHMWPE strips (n=6, 3×5×20 mm3) were eluted for three weeks and the eluent concentration was measured using UV spectroscopy or o-phthaldialdehyde tagging.3 Intraarticular concentration of the drug was estimated by a single-compartment pharmacokinetic model. The synovial half-life of the antibiotics was assumed to be 6 hours (same as vancomycin4) or 3 hours (worst-case scenario5). To determine antibacterial activity, one 3×5×10 mm3 strip was incubated in 105 CFU/ml Staphylococcus aureus (ATCC12600) at 37°C, 100rpm (n=3). At each time point, viable bacteria concentration was determined by luminescence assay (BacTiter-Glo™, Promega);6 the remaining solution was centrifuged, and the bacteria were resuspended in fresh broth.
Results and discussion: Eight antibiotics lost <2% weight when heated to 200°C and were considered stable for molding with UHMWPE. Concordantly, NMR spectra of these drugs and the eluents matched, confirming thermal stability. The drug domains were eccentric clusters, except for gentamicin and tobramycin which had largely spherical domains, resulting in lower drug release (Figure 1). When 7% w/w antibiotic-loaded strips were incubated with bacteria, the bacteria concentration fell below the detection limit (100 CFU/ml) by the end of day 3 (Figure 2) and no adherent bacteria were detected (vs. control UHMWPE: 2×105 CFU/cm2). However, this semi-static assay may not represent in vivo clearance. To simulate in vivo drug decay kinetics, we used pharmacokinetic modeling which revealed that both 10% w/w and 7% w/w implants with a surface area of 100cm2 (vs. 2cm2 experimental strip) can maintain intraarticular drug concertation higher than the MIC (4µg/ml) of common PJI bacteria for at least 3 weeks (Figure 3).
Conclusion: Local delivery of antibiotics is a more efficient way to treat PJI than systemic administration due to sustained high concentration at the infection site. This work supports the potential use of UHMWPE joint replacement components as delivery devices for antibiotics.
[1] Jill et al. J Bone Jt Surg (2011); [2] Suhardi et al. Nature Biomed Eng (2017); [3] Gubernator et al. Int J Pharm (2006); [4] Bue et al. J Knee Surg (2021); [5] Pezzanite et al. Front Vet Sci (2021); [6] BacTiter-Glo™ #TB337, Promega Corporation.
Figures
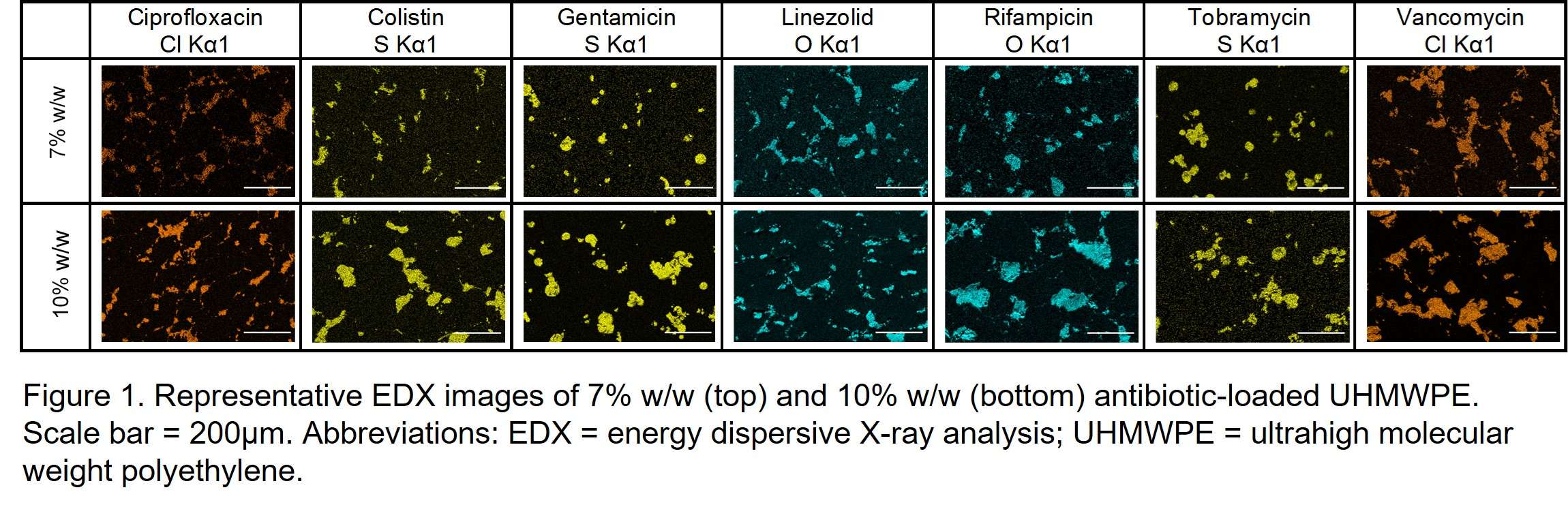
Figure 1

Figure 2
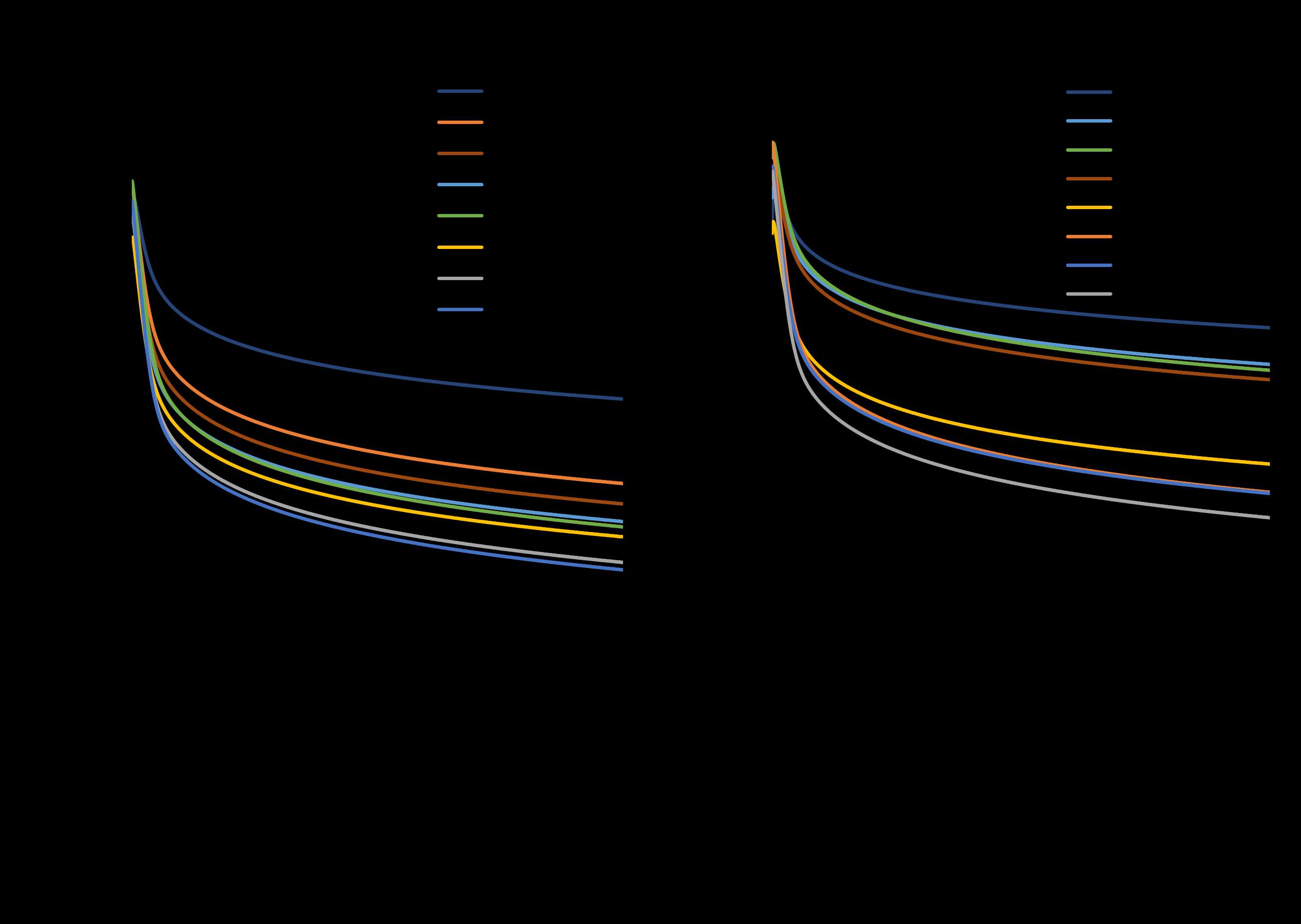
Figure 3#7738
Markerless Motion Tracking via Deep Learning Improves Gait Analysis of Rats in a Periprosthetic Joint Infection Model
Alireza Borjali - Harvard Medical School/ Massachusetts General Hospital - Boston, USA
*Ebru Oral - Massachusetts General Hospital - Boston, USA
Orhun Muratoglu - Massachusetts General Hospital - Boston, USA
*Email: eoral@partners.org
Introduction: Assessing in-vivo animal function is critical for evaluating the outcome of animal studies. Although there is no standard way of assessing animal function, gait analysis has been widely used in the literature. A fundamental deficiency of current gait analysis methods is that to keep the manual/semi-manual data postprocessing manageable, parameters are usually measured at set intervals that might not fully capture the animal recovery trajectory. Furthermore, they require manual handling of the animal, which can cause stress-induced confounds and additional discomfort in the animal. With that being said, the objectives of this study were to 1) develop a fully automatic and hands-free animal gait analysis method, and 2) compare its performance with the state-of-the-art method for analyzing gait in a periprosthetic joint infection (PJI) rat model.
Methods: Gait videos of 21 adult male Sprague–Dawley rats that were included in our previously reported PJI model1 were analyzed. Animals were randomly assigned to the control (n=9) and infected (n=12) groups. All animals underwent surgery to receive a titanium screw in their tibia and a polyethylene pin in their femur. The infected group subsequently was injected with S. aureus, while the control group received saline. Gait videos were recorded 1 day before the surgery and on postoperative days (PODs) 1, 3, 7, 14, 21, and 28. Not all animals walked on the data collection days and a total of 67 gait videos were collected. In the first step, these videos were analyzed with the semi-manual state-of-the-art AGATHA MATLAB script to calculate duty factor, temporal symmetry, spatial symmetry, and phase dispersion. We subsequently implemented the ArtTrack deep learning (DL) markerless tracking model2 and modified it to automatically track multiple points of interest in the rats (Fig. 1) calculating the same gait parameters as the semi-manual analysis. We then built two decision tree (DT) models using semi-manual measurements (DT-1) or DL measurements (DT-2) as inputs categorizing the rats into saline or infected groups and compared the results.
Results: DT-2 outperformed DT-1 in distinguishing between infected vs. saline rats. DT-2 achieved 76.50% overall accuracy, 73.33% precision in identifying infected rats, and 77.42% precision in identifying saline rats. On the other hand, DT-1 achieved 62.50% overall accuracy, 53.33% precision in identifying infected rats, and 67.74% precision in identifying saline rats.
Conclusion: We developed a fully automated markerless motion tracking model to analyze rat gait in a PJI model. We also compared this model’s performance with the state-of-the-art method. We showed that our fully automated method outperformed the state-of-the-art in categorizing rats as saline or infected. This method could be used in future studies to scale up data collection while eliminating the need for any handling of the animal due to its markerless nature.
References:
1. Fan Y, et al. 2020. Longitudinal Model of Periprosthetic Joint Infection in the Rat. J. Orthop. Res. 38(5):1101–1112
2. Insafutdinov, E. et al. ArtTrack: articulated multi-person tracking in the wild. in Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition 1293–1301 (IEEE, Piscataway, NJ, USA, 2017)
Figures
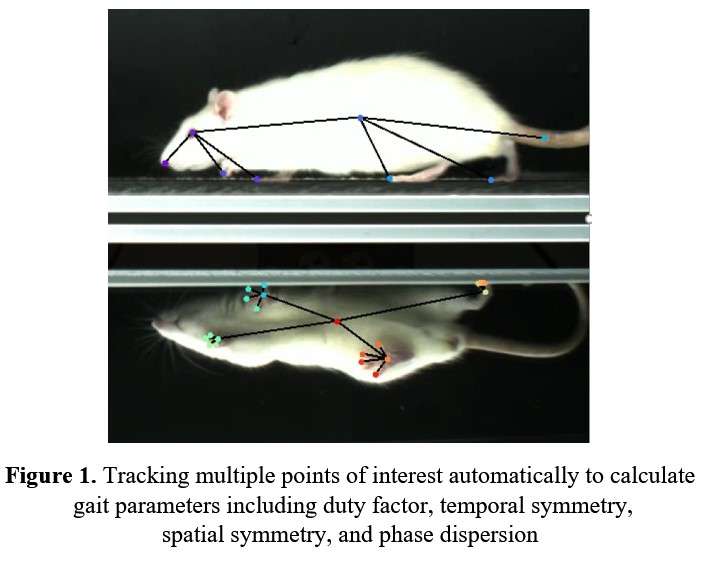
Figure 1#7938
The Effect of Vitamin E in Preventing Arthrofibrosis After Joint Replacement
Yingfang Fan - Massachusetts General Hospital - Boston, USA
Jean Yuh - Massachusetts General Hospital - Boston, USA
Sashank Lekkala - Massachusetts General Hospital - Boston, United States of America
Andrew Thompson - Massachusetts General Hospital - Boston, USA
Madeline McCanne - Massachusetts General Hospital - Boston, USA
Mark A. Randolph - Harvard Medical School - Boston, USA
*Ebru Oral - Massachusetts General Hospital - Boston, USA
Antonia F. Chen - Brigham and Women’s Hospital - Boston, USA
*Email: eoral@partners.org
INTRODUCTION: Arthrofibrosis is a fibrotic joint disorder characterized by excessive scar tissue production within the joint and in surrounding soft tissues. It is a common complication after total knee arthroplasty. Nearly 85,000 cases of arthrofibrosis occur following knee surgery in the United States per year. The development of minimally invasive treatment of arthrofibrosis is highly desirable. Vitamin E is an antioxidant with anti-inflammatory, anticoagulant, and anti-fibroblastic effects. It has been shown to effectively decrease fibrosis in fatty liver disease. The objective of this study was to establish an arthrofibrosis rat model following joint replacement and to assess the effects of vitamin E supplementation on joint fibrosis.
METHODS: The IACUC approved the following procedures under protocol 2020N000081. Eighteen male Sprague-Dawley rats received a simulated knee replacement procedure involving a transcondylar femoral implantation of a 3.0 x 3.0mm cylindrical polyethylene (PE) plug and implantation of a titanium screw in the tibial canal (Figure 1). The surgical leg was immobilized with a suture in a full flexion position to assist in fibrosis formation. Sutures were removed after two weeks. One control group was sacrificed at two weeks at suture removal (C1, n=6), another control group was monitored until 12 weeks (C2, n=6), and the test group was supplemented daily with vitamin E in their drinking water until 12 weeks (0.2 mg/ml; E1, n=6). To investigate the presence and severity of arthrofibrosis and systemic inflammation, we performed the fibrosis tissue histological (H&E, picrosirius red), immunofluorescent staining (IL-6 and TNFa) analysis, and plasma Alpha 2 Macroglobulin (α2M) ELISA. Static weight bearing (TIR) and range of motion were collected for rat wellbeing. All the data were collected on post-operative days (POD) 0, 14, 28, 42, 56, 70, 84.
RESULTS: The α2M of the control group increased, while the Vitamin E group decreased at POD14, suggesting that pretreated vitamin E help avoid the acute early phase inflammation. The histology results in the control group showed a higher presence of fibroblasts and synovium hyperplasia; increased picrosirius staining of collagen fibers in the surgical leg compared to the non-surgical leg of the control group (Figure 2). Immunofluorescent staining showed that the vitamin E group presented an excellent anti-inflammatory effect after 12 weeks from lateral implant sight and posterior capsular. Range of motion and weight-bearing asymmetry within the control and vitamin E groups differed significantly at different time points (Figure 3). The difference between the control and vitamin E groups showed in POD 0 (Figure 3).
CONCLUSION: The time-dependent changes in the range of motion for all animals and the histology results showed that this model is viable for simulating arthrofibrosis after joint replacement. Vitamin E could prevent arthrofibrosis formation and accelerate post-operative recovery. Vitamin E supplementation showed a moderate anti-inflammatory effect on local and systemic inflammation. Although the range of motion level did not get back to the normal range, increasing the dosage of vitamin E or using a more direct and quantifiable route of administration (subcutaneous, intra-articular) may show more significant effects on the formation of fibrosis.
Figures
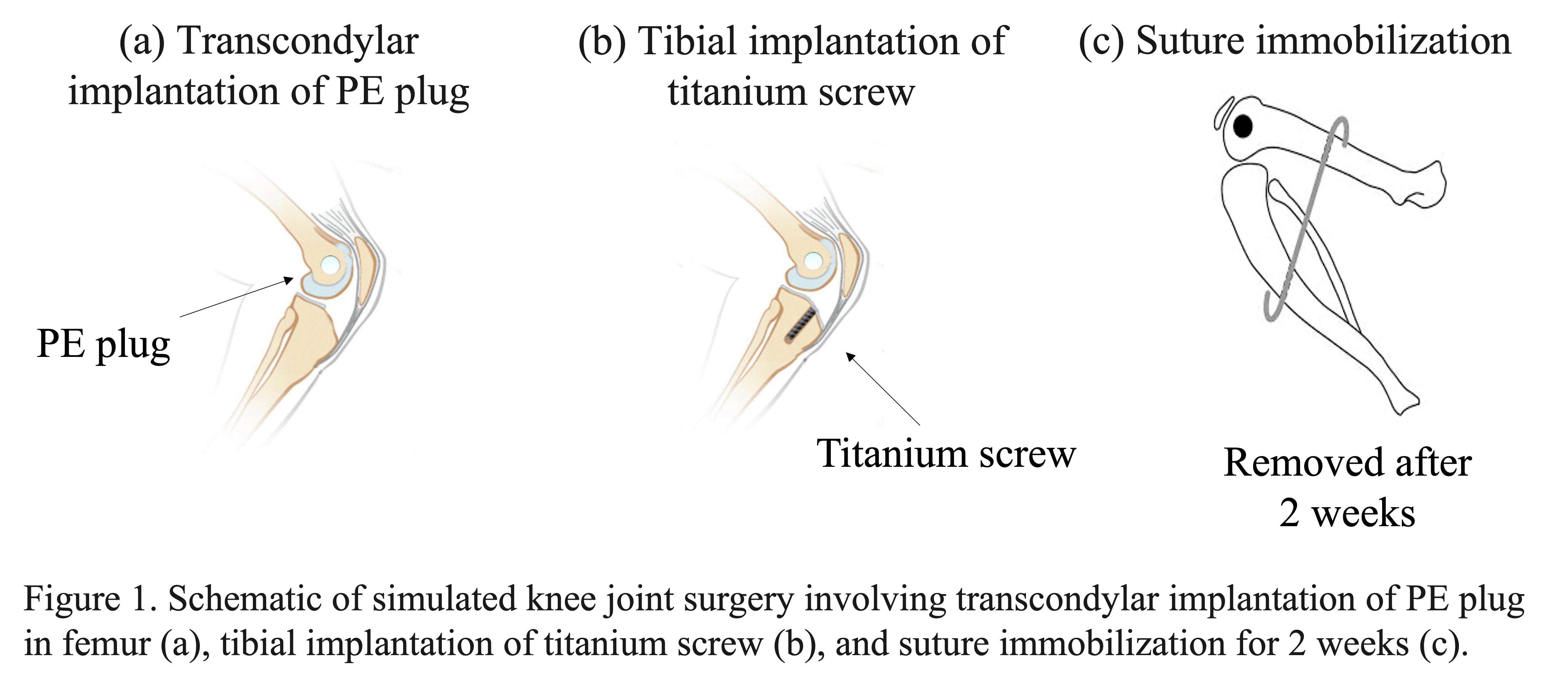
Figure 1
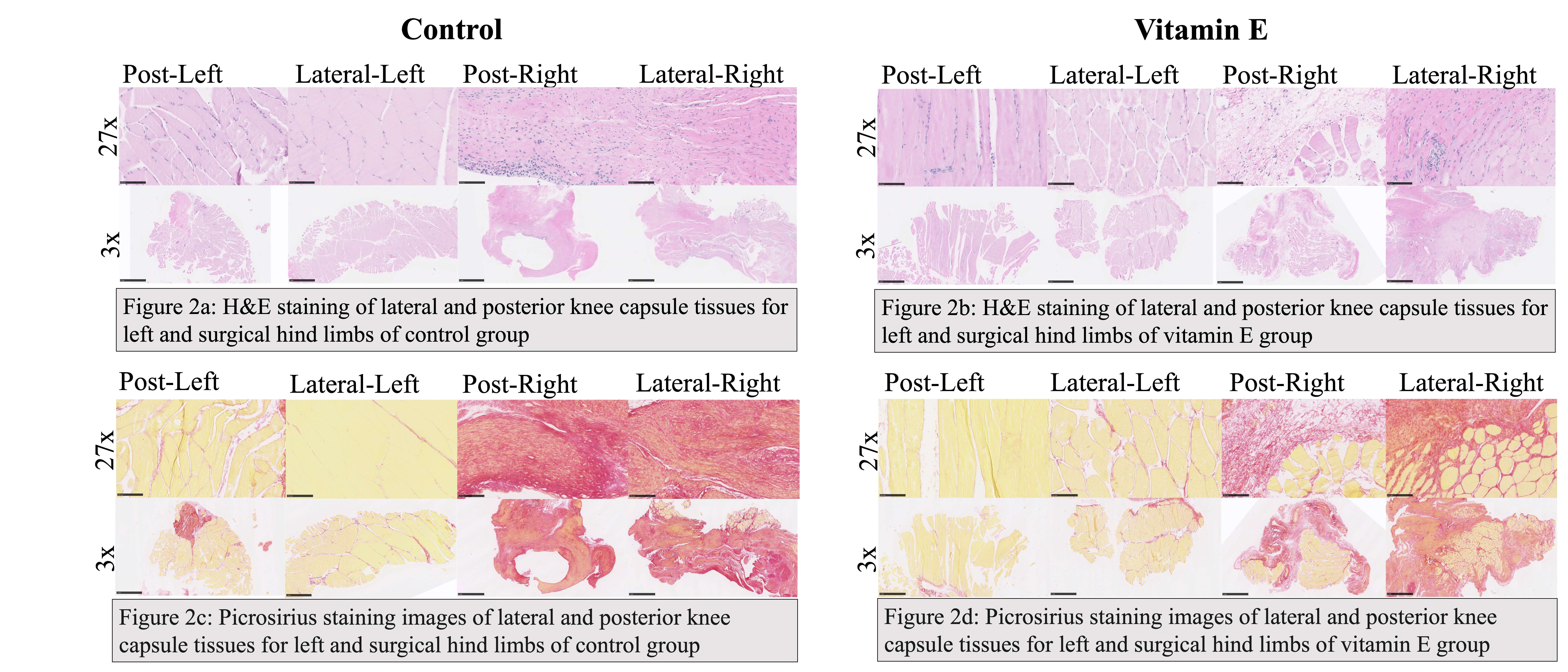
Figure 2
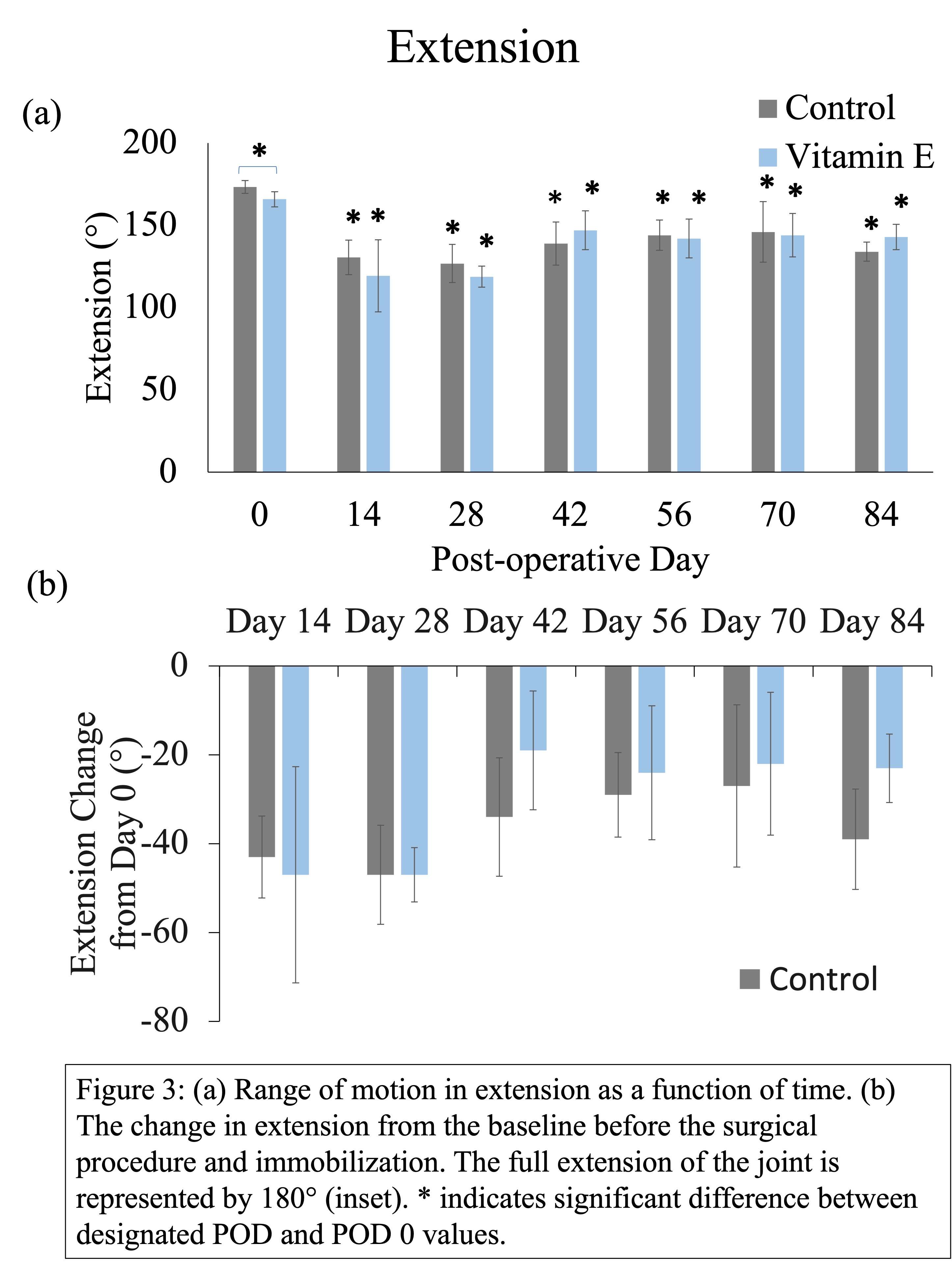
Figure 3#7951
Utilizing Tibial Stems in Primary Total Knee Arthroplasty; Analysis of Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) Data.
*Jess Osan - Perth, Australia
Christopher Jones - Fiona Stanley Hospital Group - East Fremantle, Australia
Benjamin Wall - Orthopaedic Research Foundation Western Australia - Perth, Australia
Piers Yates - University of Western Australia - Perth, Australia
Ian Alexander Harris - UNSW - Sydney, Australia
Yi Peng - South Australia Medical Research Institute - Adelaide, Australia
*Email: jesskosan@gmail.com
Introduction
We aimed to analyse the utilization of tibial stems for primary TKA performed for osteoarthritis in Australia.
Methods
Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were used to compare all cause revision, reason for revision and type of revision between primary TKA using stemmed tibial prostheses to those using non-stemmed prostheses.
Results
There were 131463 primary TKA (88% no stem extension, 22% stem extension) performed during the study period. Osteoarthritis was the most common reason for implantation across the two groups (98% no stem extension, 96% stem extension) yielding 98219 cases considered for analysis [Fig. 1]. Compared to TKA with no stem extension, all cause revision for TKA with stem extension is higher for the first 1.5 years (HR 1.30, 95% CI 1.09, 1.55 p= 0.003); thereafter TKA with stem extension had a lower rate of revision (HR 0.80, 95% CI 0.67, 0.94, p=0.006) [Fig. 2]. Stemmed components were more likely be revised for infection in the first 6 months (HR 1.66; 95% CI 1.23 to 2.25; p < 0.001); thereafter there was no difference. Aseptic loosening was higher in the non-stemmed group beyond 2 years follow-up (HR=2.39; 1.6, 3.58. p<0.001); there was no difference up to 2 years [Fig. 3]. Insert only revision was higher in the stemmed group (HR=1.58; 1.32, 1.91. p=0.001). Isolated tibial component revision was increased in the non-stemmed group (HR=2.4; 1.41, 4.11. p=0.001). Aseptic loosening as the indication for tibial component-only revision was significantly higher in the non-stemmed group (HR=4.32; 1.92, 9.72. p<0.001).
Conclusion
Patients undergoing primary stemmed TKA have lower rates of all cause revision beyond 1.5 years and tibial component only revision, particularly for aseptic loosening. Further investigation is required to identify factors affecting this relationship to pre-operatively select patients who may benefit from augmentation with stems in primary TKA.
Figures
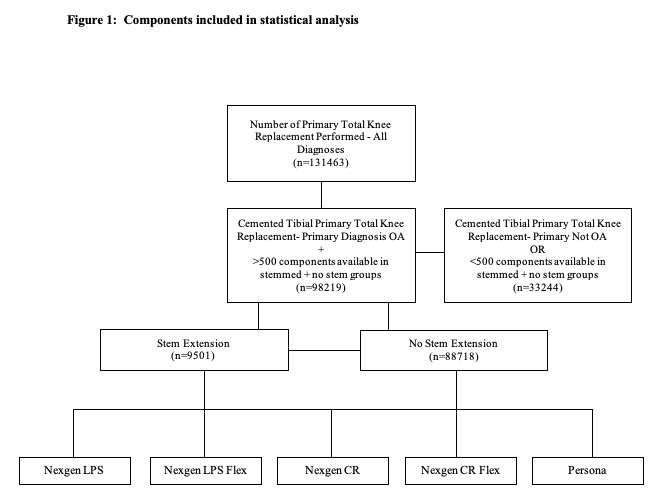
Figure 1
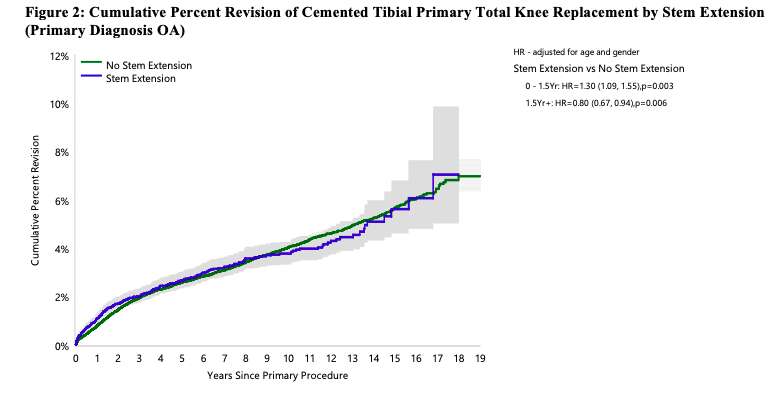
Figure 2
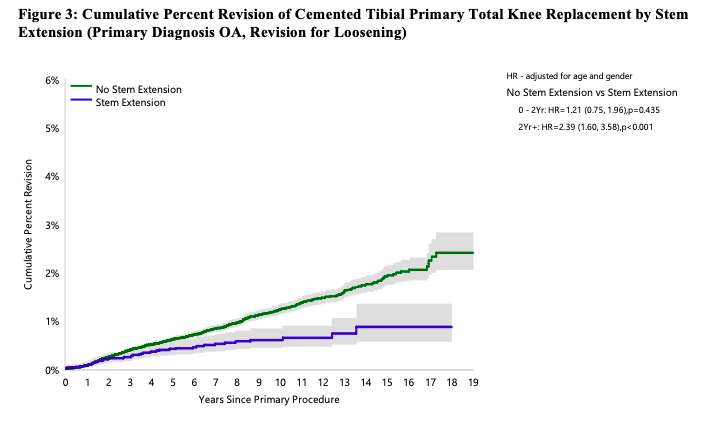
Figure 3#7952
Utilizing Augmented Tibial Fixation for Primary Total Knee Arthroplasty (TKA) in Obese Patients; Analysis of Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) Data.
*Jess Osan - Perth, Australia
Benjamin Wall - Orthopaedic Research Foundation Western Australia - Perth, Australia
Ian Alexander Harris - UNSW - Sydney, Australia
Yi Peng - South Australia Medical Research Institute - Adelaide, Australia
Piers Yates - University of Western Australia - Perth, Australia
Christopher Jones - Fiona Stanley Hospital Group - East Fremantle, Australia
*Email: jesskosan@gmail.com
Introduction
We aimed to determine if the utilization of augmented tibial fixation with stems in primary total knee arthroplasty (TKA) for the obese patient was associated with a difference in the reason for revision or the revision rate over time.
Methods
Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were used to compare the reason for revision, rate and type of revision between primary TKA using stemmed tibial prostheses to those using non-stemmed prostheses, stratified by body mass index (BMI). Cox proportional hazards models were employed, with data presented as cumulative percent revision (CPR) and/or hazard ratios (HR) (adjusted for age and gender) with 95% confidence intervals. All tests were two-tailed at the 5% level of statistical significance (p<0.05). Survival curves were calculated using the Kaplan-Meier method.
Results
32357 prostheses were available for analysis. There was no significant difference in the reason for revision and/or the cumulative percent revision between non-stemmed and stemmed tibial prostheses in any BMI group [Table 1].
Conclusion
Based on AOANJRR data, the addition of a tibial stem during primary TKA for osteoarthritis in patients with increased BMI was not associated with lower rates of revision, including revision for aseptic loosening. Given the increased implant cost with similar results, the use of augmented tibial fixation with stemmed prosthesis for patients with increased BMI may not reduce the risk of revision.
Figures
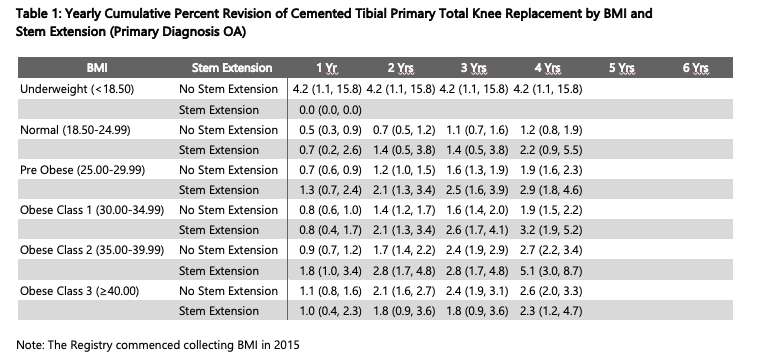
Figure 1#7426
Improvement of Global Body Posture Post Total Knee Arthroplasty as Knee-Hip-Spine Syndrome Is Affected by Contralateral Knee Condition
*Yasushi Oshima - Nippon Medical School - Japan
Nobuyoshi Watanabe - Kyoto Kujo Hospital - Kyoto, Japan
Toru Takeoka - Kyoto Kujo Hospital - Kyoto, Japan
Yoshiteru Kajikawa - Kyoto Kujo Hospital - Kyoto, Japan
Tadahiko Yotsumoto - Kyoto Kujo Hospital - Kyoto, Japan
Norishige Iizawa - Nippon Medical School - Tokyo, Japan
Tokifumi Majima - Nippon Medical School - Tokyo, Japan
*Email: y-oshima@nms.ac.jp
Introduction
In an aging society, prevention and treatment of an abnormal body posture are critical issues, as abnormal posture is associated with a risk of body unbalanced and falls, which can result in fractures, the need for surgical interventions, and nursing conditions for older people (1). Aside from adult spinal deformity and osteoarthritis (OA) of the hip as a hip-spine syndrome (2,3), knee OA is linked with abnormal body posture as a knee-spine syndrome (4), and the posture may be improved with total knee arthroplasty (TKA) as a knee-hip-spine syndrome (5). However, we hypothesized that the contralateral knee condition influenced posture improvement. The purpose of this study was to compare the clinical outcomes of TKA in patients with knee OA and those who had previously had TKA in the contralateral knee.
Methods
Patients with primary knee OA scheduled to undergo primary TKA were enrolled and divided into two groups based on the contralateral knee condition; patients in the unilateral group had not received any surgery, while patients in the bilateral group had already undergone TKA.
The variations in knee range of motion (ROM) and the Knee injury and Osteoarthritis Outcome Score (KOOS) were assessed at 6, 12, and 24 months after TKA. The hip and knee flexion angles as well as the sagittal vertical axis (SVA) as an index of sagittal alignment were measured in standing roentgenography. The repeated measures ANOVA test was used for statistical analysis, and p< 0.05 was considered statistically significant. An institutional review board approved this study, and patients provided informed consent to participate.
Results
Of 24 patients, 12 females were in the bilateral group, and 12 females were in the unilateral group with contralateral knee OA (Kellgren–Lawrence classification: grade II for 3; grade III for 8; and grade IV for 1).
At 24 months, both groups' knee ROM, particularly in extension, and all KOOS items had significantly improved. The hip and knee flexion angles in the unilateral group were improved from 8.5° and 15.6° to 6.9° and 12.2° for 24 months, respectively. Moreover, in the bilateral group, the hip and knee flexion angles were significantly improved from 7.6° and 13.0° to 3.6° and 6.8°, respectively. SVA was significantly improved at 6 months in both groups, and it was maintained until 24 months in the bilateral group. The unilateral group, however, has deteriorated again at 24 months (Fig.).
Conclusion
TKA may improve body balance and reduce the risk of falls because SVA was reduced. However, SVA improvement in the unilateral group has regressed at 24 months. Thus, an additional TKA should be considered before this period for the contralateral knee to preserve sufficient outcomes post unilateral TKA in both knee OAs. The study’s limitations include an all-female patient population and a small number of patients. In conclusion, the improvements in the preoperative abnormal posture after TKA are influenced by the contralateral knee condition.
References
(1) Kim J., 2017. (2) Schwab F., 2012. (3) Offierski CM., 1983. (4) Murata Y., 2003. (5) Oshima Y., 2019.
Figures
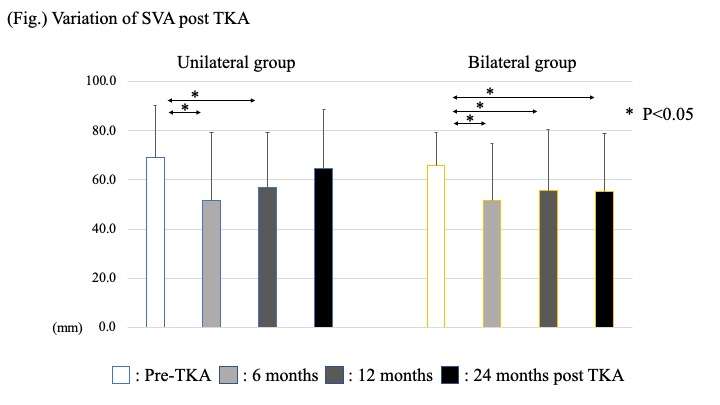
Figure 1#7635
Improved Accuracy in Restoring the Pre-Arthritic Static & Dynamic Alignments, Component Placement in UKA With Semi-Autonomous Handheld Robotic Systems.
*Shantanu Patil - SRM Medical College, SRM Institute of Science and Technology - Kattankulathur, India
Ashok Kumar P. S. - CHENNAI, India
Karthik Jayachandran - SRM Medical College - Trichy, India
Suchitra Gopinath - Asian Joint Reconstruction Institute - Chennai, India
Kalaivanan Kanniyan - Asian Joint Reconstruction Institute AJRI @SIMS Hospitals - Chennai, India
Vijay C Bose - AJRI - chennai, India
Pichai Suryanarayan - India
*Email: shantanup@srmist.edu.in
Introduction: The surgical challenges in restoring the pre arthritic alignment, precise component positioning and a kinematic balance while performing Unicondylar replacements (UKA) is known. Modern instrumentations have addressed some of these. Surgical navigation and robot assisted technologies are being increasingly employed in joint replacement surgeries to advantage. Both the Autonomous (based on preoperative CT scans) and Semi-autonomous (based on landmarks digitized by the surgeon) robot assisted systems have enabled overcome the earlier challenges to planning and execution. We present the early results for UKA done with a semi-automated handheld robotic sculptor from a single tertiary care center in subjects clinically diagnosed with antero-medial osteoarthritis (AMOA).
Aim: To determine the accuracy of Handheld Robot assisted UKA with respect to the planned sagittal and coronal tibial component positioning and evaluate the restored Hip-Knee-Ankle alignment both Static weight bearing and Dynamic nonweight bearing (lying down) with the robot assisted plan.
Methods: 53 consecutive patients with AMOA underwent handheld robot assisted UKA. Intraoperative assessment of the dynamic HKA axis was recorded. Based on the degree of correctability and patient specific morphology, the desired slope, depth and the rotational position of the tibia were set. The planned target in surgery for AMOA was a static weight bearing alignment within 4* of neutral or around 50% correction of the preoperative dynamic deformity. The posterior tibial slope and the coronal placement (varus/valgus) angles of the tibia base plate were measured on the postoperative scanograms. These were compared with the intraoperative planned values.
Results: The mean age of the cohort was 62.2 (±8.4; range 45-76 yrs.) with average BMI of 30.1 (± 4.5; range 21.0-40.1). The gender distribution was M: F: 11: 40. The postoperative stay in hospital was 3.2 (±1.1; range 1-6 days). The mean pre-operative and post-operative Oxford knee scores were 25.5 (±1.2; range 24-29) and 44.3 ± 2.7; range 40-48). The mean intraoperative NWB-HKA axis was 7.1 (± 3.0; range 3-17°) while the planned NWB-HKA was 5.0 (± 2.8; range 1-17°). The pre-operative static/WB-HKA was 8.4 (± 3.6; range 2-17.6°) as compared to the post-operative mean of 4.0 (± 3; range 0.1-15.8°). The mean tibial slope was 8.8 (± 5.0; range 1.8-21.8°) preoperatively. The Intraoperative targeted tibial slope was between 4-6°. The postoperative mean tibial slope measured was 4.3 (± 2.1; range 0.5-9.4°)
Conclusion: In our study, the difference in planned and achieved posterior tibial slope was 0.7° and varus/valgus deviation of the tibial component was 1.2°. The difference in pre- and post-operative HKA static/WB was 0.6°; while the difference for the dynamic/NWB HKA axis target was 1.3°. These results support benefits of the use of semi-autonomous handheld robotic device assisted UKA. This outcome without the need for pre op CT scans, enabled achieving the planned target alignments and implant positions, while overcoming the surgeon associated malpositioning.
#8045
Invited Talk: Anatomy of a Recall
*Douglas E Padgett - Hospital for Special Surgery - New York, USA
*Email: padgettd@hss.edu
Historical factors impacting longevity of total joint replacements have included implant fixation and bearing failure. The introduction of crosslinked polyethylene has dramatically reduced the incidence of wear and osteolysis in hip arthroplasty while direct compression molded polyethylene has performed remarkably well in knee arthroplasty. Over the past 2 decades, the incidence of polyethylene delamination and particle induced synovitis leading to failure has been almost negligible as reported by registries here and abroad.
Beginning in 2017, we observed several severely delaminated and oxidized tibial inserts from a single manufacturer revised at our institution. This prompted an extensive review of retrieved polyethylene bearings in our retrieval archive. This analysis revealed a marked incidence of severely oxidized inserts. Following a thorough analysis of potential factors which may have been associated with our observations, we shared these findings with the manufacturer and a product recall was initiated.
This experience reinforces our contention that implant retrieval analysis remains the best early warning system for the detection of premature implant failure and is a crucial element in the design loop cycle.
#7807
Systematic Review on 3D Bioprinting of Composite Orthoregenerative Tissues
Rachel Pan - University of Central Florida - Orlando, Select Country
Kari Martyniak - University of Central Florida - Orlando, United States of America
David Gelikman - UCF College of Medicine
Makan Karimzadeh - UCF - Orlando, United States of America
Kelly Sutter - University of Central Florida College of Medicine - Orlando, United States of America
Jonathan deVries - UCF - Orlando, United States of America
Rajendra Sawh-Martinez - AdventHealth - Orlando, USA
*Thomas Kean - University of Central Florida - Orlando, United States of America
*Email: thomas.kean@ucf.edu
Introduction: The prevalence of joint injuries is expected to increase as the population ages, leading to greater morbidity and cost. Clinically available restoration options, such as autologous grafting and prostheses, are limited in their longevity and ability to integrate into native tissues. 3D bioprinting (3DBP), the use of computer-aided design and cell-containing ink, has great potential as an alternative to restore joints by recapitulating structure and function of native joint tissues ex vivo, or even in situ. Patient-specific constructs can be generated by combining imaging techniques such as microCT with multi-axis printing devices which allow for a high degree of geometric control. Bioprinted composite osteochondral and vascular bone structures are reaching a level of maturation where clinical translation is a distinct possibility, though developing a fully functional implant remains an elusive goal. This systematic review focuses on the latest developments in 3D bioprinting-based tissue engineering techniques, strategies, and methods for testing composite joint tissues.
Methods: A systematic literature review was performed using PubMed and Web of Science. Primary research articles reporting 3DBP osteochondral and vascular bone structures were considered. Articles published before 2011 or in a journal with impact factor < 2 were excluded. Papers which did not report on a digital design-aided engineering strategy involving cell-containing inks were excluded.
Results: After screening 119 results, ten osteochondral and twelve vascular bone articles underwent full review. All constructs were generated via extrusion-based bioprinting. The most-used materials were gelatin-derived (44% of articles) followed by poly(caprolactone) (31%) and alginate (26%) derivatives. Mesenchymal stromal cells were featured most frequently in both osteochondral and vascular bone implants. All papers sought to determine the effect of the 3DBP process on cell survival. Few groups performed physical characterization of their 3DBP constructs, such as gelation and rheology, and there were no mechanical standards to which constructs should be compared. Other in vitro testing methods assessed markers of extracellular matrix production or cell differentiation into respective lineages. This included molecular methods such as qPCR, histology, or immunohistochemistry. In vivo proof-of-concept studies included full-thickness long bone and patellar defects as well as subcutaneous implantation in rodents followed by histological and uCT analyses to demonstrate implant growth and integration into surrounding native tissues. Notably, researchers encountered pitfalls in scaling up constructs and establishing implants’ continued function and viability in animal models beyond twelve weeks.
Conclusion: Despite its relative infancy, 3DBP is making an impact in joint and bone engineering. Several groups have demonstrated preclinical efficacy of mechanically robust constructs which integrate into articular joint defects in small animals. However, notable obstacles remain. To translate from the laboratory to the clinic, standardized quality control metrics such as construct stiffness and graft integration should be established with consensus among investigators. While there is much work to be done, 3DBP implants have great potential to treat degenerative joint diseases and provide benefit to patients globally.
Acknowledgement: This review was supported by the OrthoRegeneration Network Foundation Innovation Grant.
Figures
Figure 1#7388
Simultaneous Bilateral Total Knee Arthroplasty Itself Does Not Increase the Risk of Short-Term Major Medical Complications Compared With Those of Staged Bilateral Total Knee Arthroplasty: An Analysis
*Jun-gu Park - Korea university - SEOUL, Select Country
Seung-Beom Han - Korea University Medical center - Seoul, South Korea
Woo-Young Jang - Korea University - Seoul, South Korea
Taeyeong Kim - Anam hospital,Korea university - Seoul, Korea (Republic of)
SungJin Ahn - Korea University - Seoul, Korea (Republic of)
Joonsuk Lee - Korea University Anam Hospital - Seoul, Korea (Republic of)
*Email: jgpark11@gmail.com
Introduction
Simultaneous bilateral total knee arthroplasty (TKA) is still controversial compared with staged bilateral TKA (BTKA) in patients requiring BTKA because of concerns about an increased risk of postoperative complications. The optimal interval for staged BTKA has not yet been determined. This study aimed to analyze and compare the postoperative medical and surgical complications after BTKA and determine the optimal intervals in staged BTKA.
Methods
This study included 58,583 patients who underwent BTKA between January 2009 and July 2019 using the Korean National Insurance Database; data on patient characteristics, including demographics, hospital type, and comorbidities, were collected. Major medical complications, such as acute myocardial infarction, pneumonia, intracranial hemorrhage, and ischemic stroke, within 30 days, and surgical complications, including infection and revision, within 90 days of BTKA were assessed. Patients were categorized into six groups according to operative intervals: simultaneous, 1–7 days, 8–14 days, 15–30 days, 31–90 days, and 91–180 days. The 30-day medical and 90-day surgical complication rates were compared among the six groups. The annual trends in the complication rates during the study period were analyzed. The risk factors for postoperative complications were assessed using multivariable logistic regression analysis to adjust for confounding variables.
Results
Of 58,838 patients, 24,379 underwent simultaneous BTKA, while 34,459 underwent staged BTKAs. The number of BTKAs increased from 2,276 in 2009 to 8,703 in 2018. The proportion of patients who underwent simultaneous TKA increased from 9.8% in 2009 to 57.3% in 2018 (See Figure 1). The 30-day medical complication rates of simultaneous and staged BTKA were 2.0% and 2.2%, respectively and were not significantly different (p = 0.069). The medical complication rate in simultaneous BTKA decreased annually from 6.7% in 2009 to 1.7% in 2013 (relative risk [RR] = 0.69, 95% confidence interval [CI] 0.60 to 0.79, p < 0.001). During the same period, simultaneous BTKA showed a higher medical complication risk than staged BTKA (RR = 1.40, p = 0.005, 95% CI 1.10 to 1.78). Conversely, over the last 5 years after 2014, the medical complication rates of simultaneous BTKA were significantly lower (1.9%) than those of staged BTKA (2.2%) (p = 0.023). However, these difference was minimal. After adjusting for confounding factors, simultaneous BTKA and intervals between 8 and 14 days did not significantly increase the risk of postoperative medical complications. Cardiopulmonary comorbidities (angina, ischemic stroke, heart failure, and chronic obstructive pulmonary disease) and age (> 70 years) were associated with postoperative medical complications (See Figure 2).
Conclusion
The complication rate of simultaneous BTKAs has recently decreased and is comparable to that of staged BTKA. Simultaneous BTKA did not increase the incidence of postoperative complications. The interval between 1 and 2 weeks would be suitable for staged bilateral total knee arthroplasty. Cardiopulmonary comorbidities were associated with a higher risk of major medical complications after bilateral total TKAs. Considering the surgeons' preferences and patients' desires, including careful preoperative patient evaluation, simultaneous BTKA could be an appropriate option for patients requiring BTKAs.
Figures
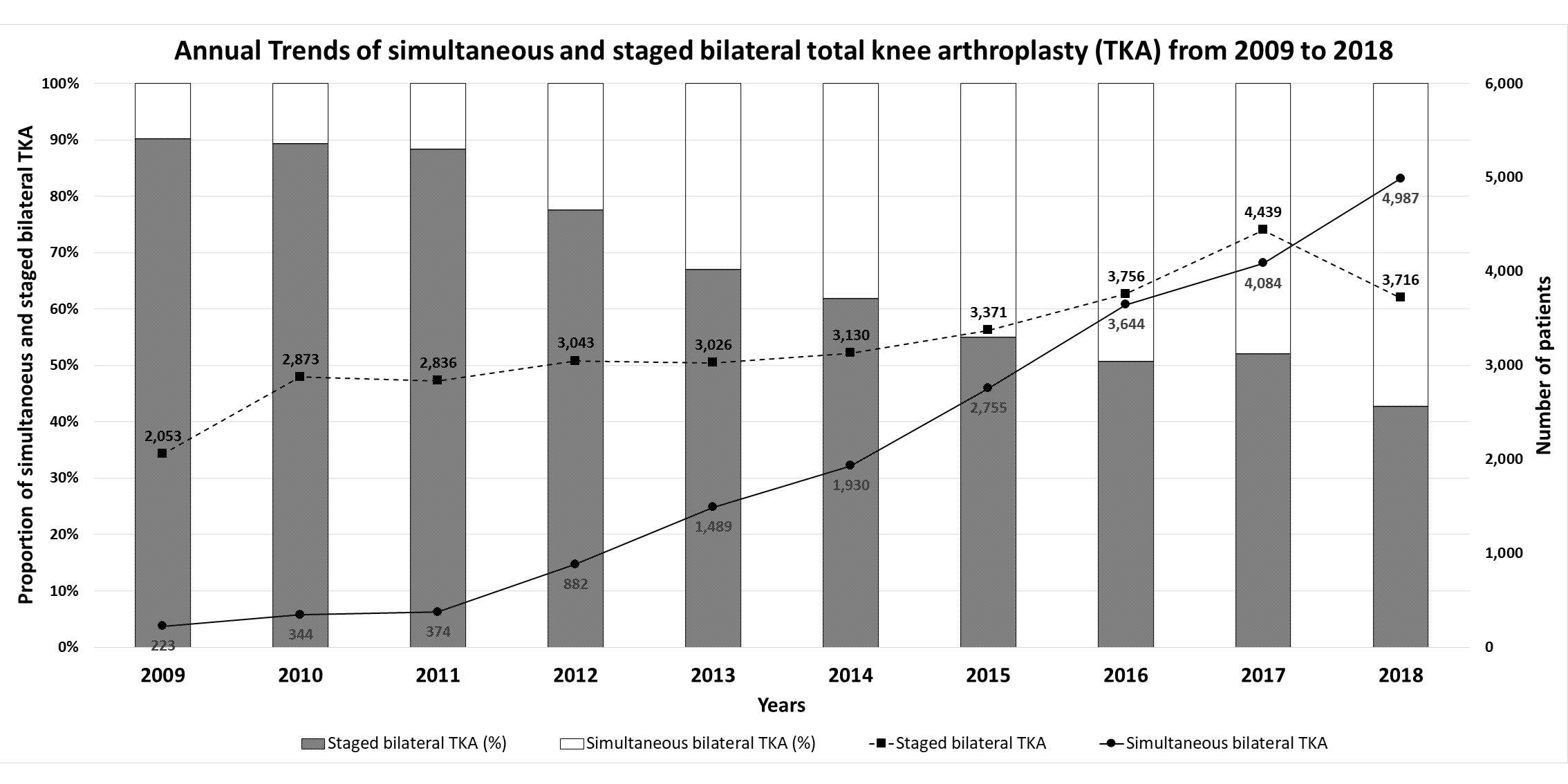
Figure 1
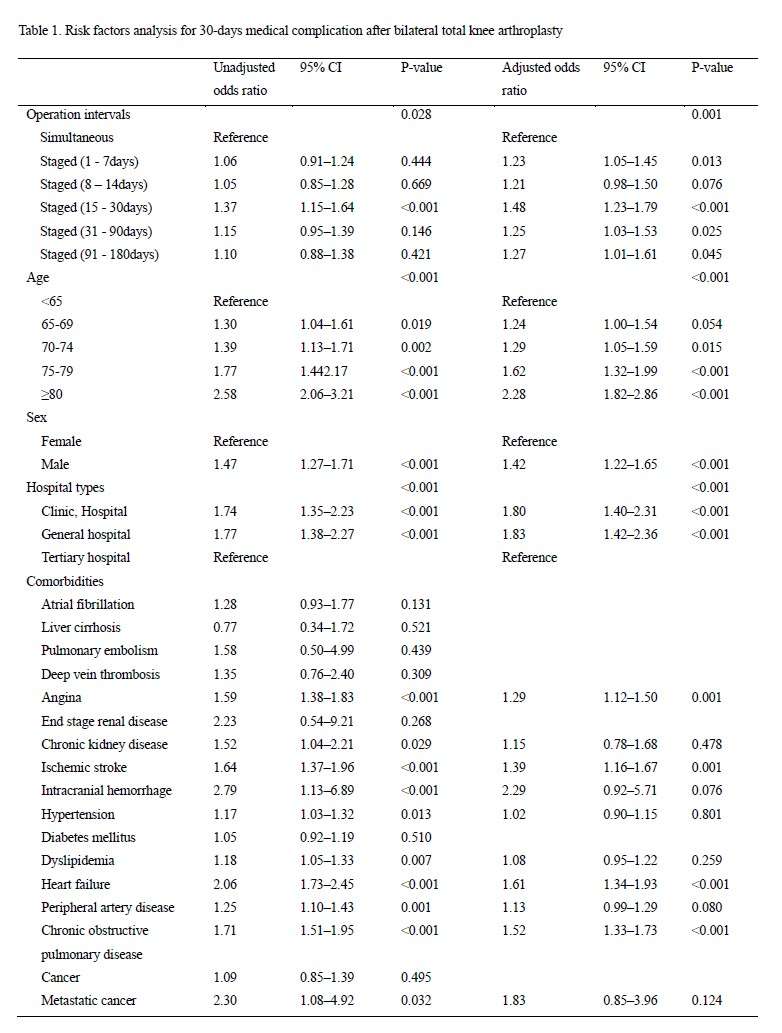
Figure 2#7429
Incidence, Risk Factors, and Treatment Outcomes of Symptomatic Iliopsoas Tendinopathy After Total Hip Arthroplasty
Chan-Woo Park - Samsung Medical Center - Seoul, South Korea
Seung-Jae Lim - Sungkyunkwan University School of Medicine, Samsung Medical Center - Seoul, South Korea
*Youn-Soo Park - Sungkyunkwan University School of Medicine, Samsung Medical Center - South Korea
*Email: ysp3504@skku.edu
Introduction:
Iliopsoas tendinopathy (IPT) can cause persistent groin pain after total hip arthroplasty (THA). The exact etiology and prognosis of this condition is not well understood. This study aimed to report the incidence, risk factors, and treatment outcomes of symptomatic IPT after primary THA.
Methods:
A retrospective case-control study was conducted on patients who underwent primary THA between January 2012 and May 2018. A total of 1602 THAs (1370 patients) performed by a single surgeon with an identical acetabular and femoral implant were included. Patient characteristics, component sizes, cup inclination and anteversion angles, and anteroinferior cup prominence (>8 mm) were compared between the patients with and without IPT. Changes in teardrop to lesser trochanter distance were measured to estimate changes in leg length and offset by THA. A multivariate logistic model was used to identify the risk factors for IPT. Treatment outcomes were compared between patients with arthroscopic iliopsoas tenotomy and those with nonoperative management.
Results:
IPT was identified in 53 hips (3.3%) after THA. Patients with IPT had greater leg lengthening (12.3 mm vs. 9.3 mm; P=0.001) and higher prevalence of anteroinferior cup prominence (5.7% vs. 0.4%; P=0.002). There was no significant difference in inclination, anteversion angle, and offset changes between the patients with and without IPT. In multivariate analysis, female sex, higher body mass index, prominent acetabular cup, and greater leg lengthening were found to be associated with IPT. All patients reported improvement in groin pain after arthroscopic surgery, while 35.7% reported improvement after nonoperative management (P<0.001).
Conclusion:
Symptomatic IPT occurred in 53 (3.3%) of the 1602 primary THAs. Our findings suggest that leg lengthening as well as prominent acetabular cup in THA can be related to the development of IPT. Arthroscopic iliopsoas tenotomy was effective in relieving groin pain caused by IPT.
#7734
Greater Trochanteric Fracture Fixation in Complex Primary and Revision Total Hip Arthroplasty
*Kwan Park - Houston Methodist Hospital - Houston, USA
Patrick Schafer - Houston Methodist Hospital - Houston, USA
Terry Clyburn - Houston Methodist Hospital - Houston, USA
Stephen Incavo - The Methodist Hospital - Houston, USA
Bradley Lambert - Houston Methodist Hospital - Houston, USA
*Email: kwanjunpark@gmail.com
Introduction:
Successful fixation of the greater trochanter (GT) fracture during or after total hip arthroplasty (THA) is a challenging task. A wide range of clinical results have been reported in the literature and multiple factors may influence successful outcome. Our study is the largest study to date to evaluate nonunion and reoperation rate and to determine factors influencing successful fixation of the GT using third-generation cable-plate devices.
Methods:
This retrospective study included 76 patients with a mean age of 67.9 years (29 males, 47 females) who underwent surgery requiring fixation of their GT with third-generation cable-plate device and had at least 1 year radiographic follow-up. Indications for surgery were: periprosthetic fracture (n=25), revision THA requiring an osteotomy (n=30), intraoperative greater trochanter fracture: (n=3), chronic greater trochanter fracture nonunion (n=9), and complex primary THA (n = 3).
Primary outcomes were radiographic union and reoperation rates. Secondary objectives were patient and plate factors influencing radiographic union including plate positioning relative to the patient’s proximal femur anatomy.
Comparison between union and nonunion cases, primary variables, demographic, and surgical data were compared using an independent samples t-test. Chi-Square test was used for comparison of frequency (%) based data between union and nonunion cases.
Results:
At a mean radiographic follow-up of 2.5 years, union rate was 76.3%. Twenty-one patients required plate removal for prominence or pain. Anatomic positioning of the plate (p=0.031) and number of cables used (p=0.0350) were associated with radiographic union. Nonunion was associated with a higher incidence of broken cable(s) (p=0.005).
Conclusion:
Greater trochanteric fracture nonunion remains a problem during or after THA. Successful fixation using third generation cable plate devices may be influenced by anatomic plate positioning and number of cables used, however symptomatic hardware remains to be an issue.
Keywords: complications, greater trochanter fracture, cable-plate system, nonunion, total hip replacement
Figures
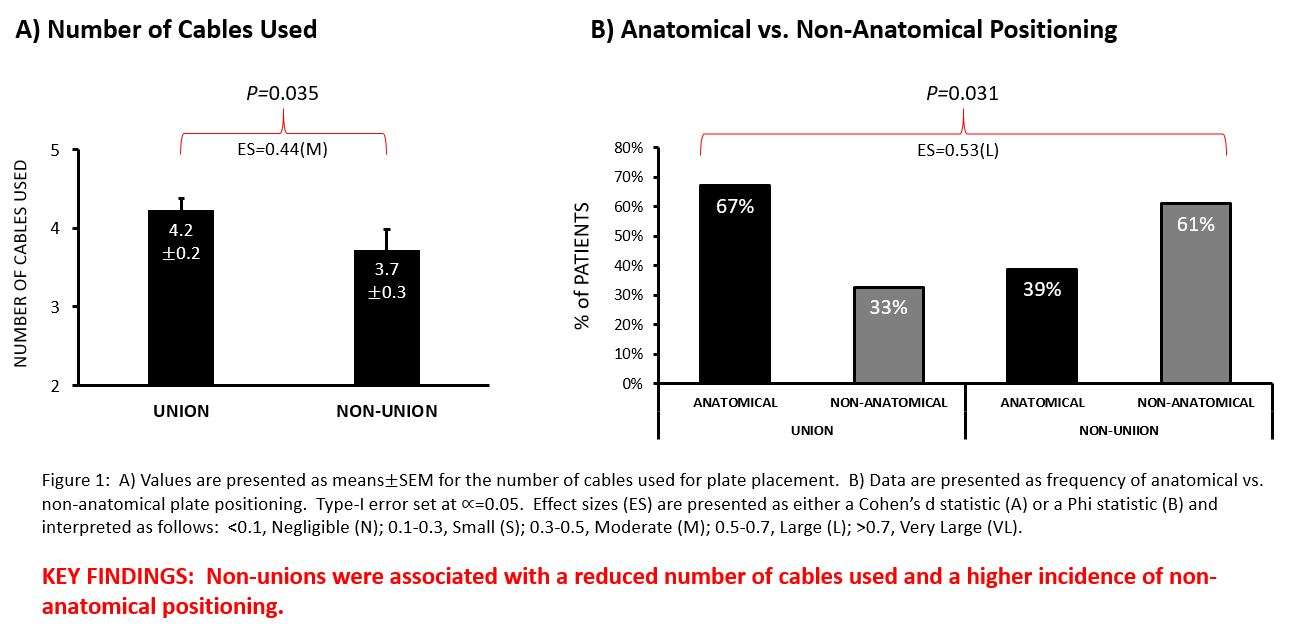
Figure 1
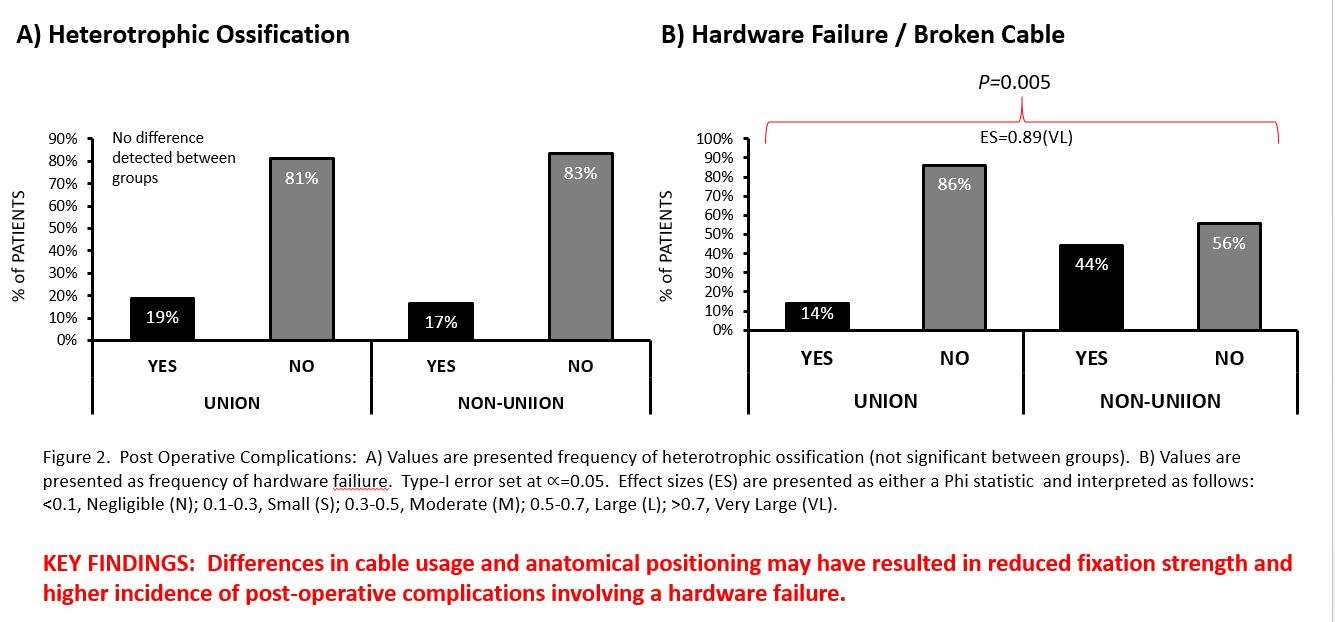
Figure 2#7733
Intraosseous Ketorolac and Morphine Injection Decreases Pain Compared to Intraosseous Morphine Alone in Primary Total Knee Arthroplasty
*Kwan Park - Houston Methodist Hospital - Houston, USA
Jason Laurita - Houston Methodist Hospital - Houston, USA
Stephen Incavo - The Methodist Hospital - Houston, USA
Timothy Brown - Houston Methodist Hospital - Houston, USA
Bradley Lambert - Houston Methodist Hospital - Houston, USA
Terry Clyburn - Houston Methodist Hospital - Houston, USA
*Email: kwanjunpark@gmail.com
Introduction:
Intraosseous (IO) injection of antibiotics and analgesics has been increasingly used to decrease infection rate and to improve pain control after total knee arthroplasty. We investigated an addition of anti-inflammatory agent, ketorolac, to our standard intraosseous mixture of antibiotics and morphine to determine if there is a clinically significant improvement in pain control.
Methods:
IO injection of 10mg morphine (Age > 65) and 30mg ketorolac (Age < 65) was performed on 24 patients (experimental group) undergoing primary total knee arthroplasty at a single institution between October 2021 and July 2022. We compared VAS pain scores and opiate use in this cohort to previously studied morphine-only IO injection cohort at the same institution (control group). Pain, opiate use, and nausea, were assessed up to 14 days postoperatively.
Patients were excluded for weight less than 100 pounds, BMI > 35, past medical history of opioid addiction, established hypersensitivity to morphine, acute or chronic liver disease, chronic kidney disease, narcotics use within 5 days of surgery.
Results:
The experimental group did not have significantly different VAS pain scores in the perioperative period, but did use significantly less opioid analgesia in the first 48 hours after surgery (p=0.031), and this was effective up to two weeks. The experimental group also significantly less IV breakthrough analgesia overall (p=p=0.015).
No adverse outcome such as acute kidney injury or venous thoromboembolitic events was reported in the study group.
Conclusion:
The use of IO ketorolac in conjunction with IO morphine significantly reduced the opiate use in patients undergoing TKA compared to patients who received IO morphine only. This was effective up to two week after the surgery. However, there was no significant difference in VAS pain scores in the perioperative period between the two groups.
Keywords: primary total knee arthroplasty, intraosseous, pain control, multi-modal pain management
Figures
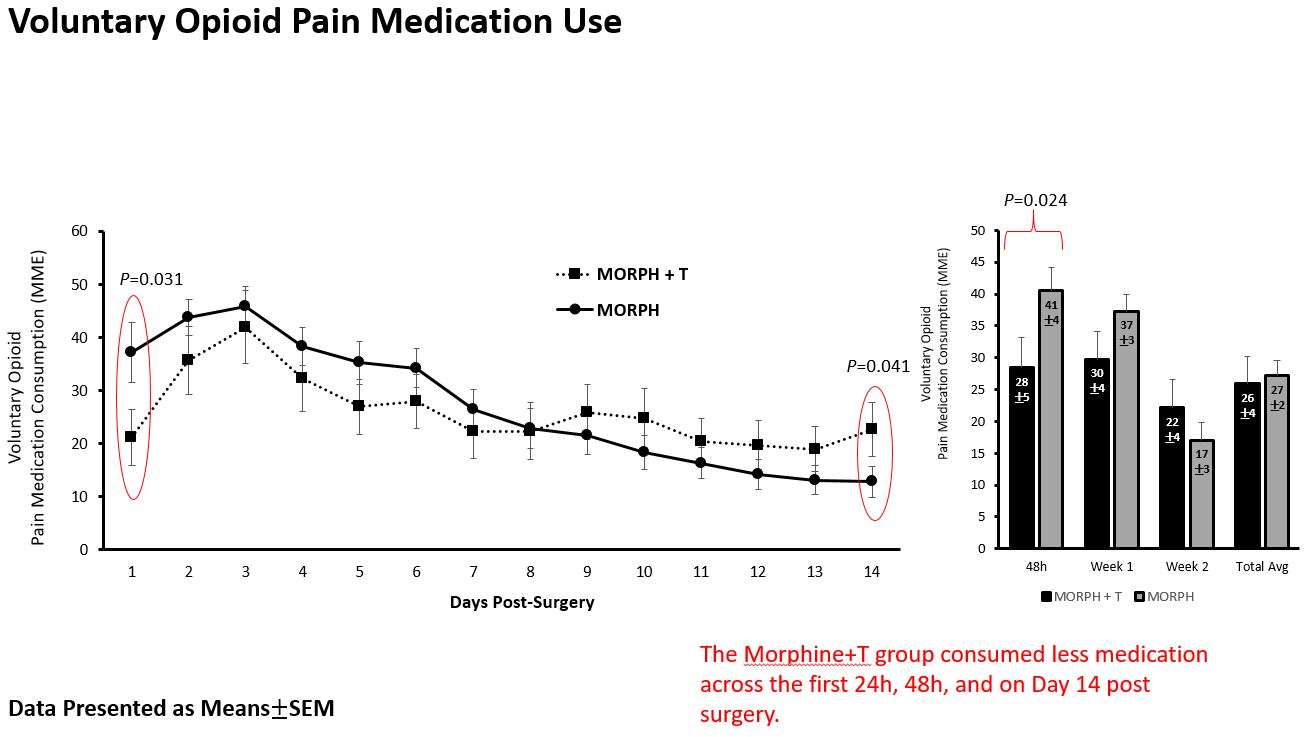
Figure 1
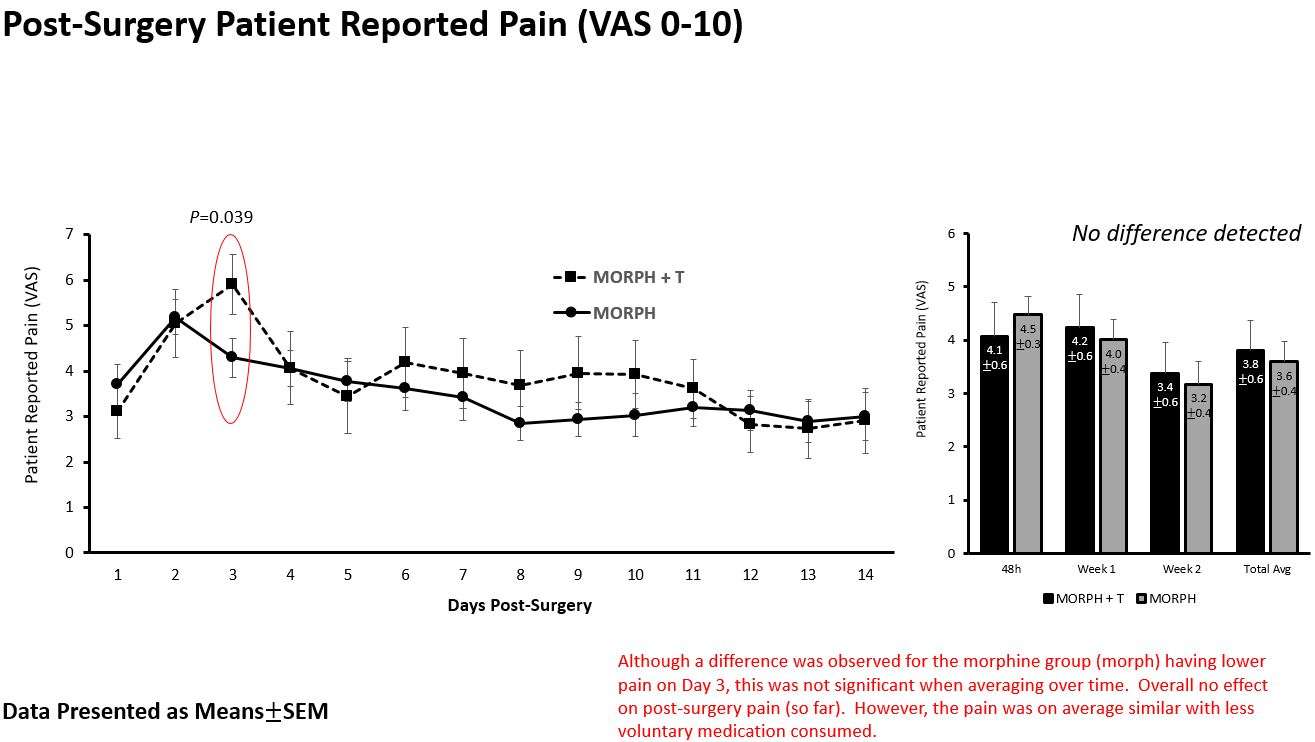
Figure 2#7737
Patient Perceptions of Same Day Discharge Versus Overnight Stay After Total Joint Arthroplasty
Daniel O'Brien - Houston Methodist Hospital - Houston, USA
*Kwan Park - Houston Methodist Hospital - Houston, USA
Bradley Lambert - Houston Methodist Hospital - Houston, USA
Stephen Incavo - The Methodist Hospital - Houston, USA
Timothy Brown - Houston Methodist Hospital - Houston, USA
Terry Clyburn - Houston Methodist Hospital - Houston, USA
*Email: kwanjunpark@gmail.com
Introduction:
During COVID-19 pandemic, there has been increasing interest in same day discharge (SDD) after total joint arthroplasty due to limited resources. The purpose of this study was to investigate patients’ preferences regarding their postoperative care by surveying patients who have completed both an overnight stay and a SDD.
Methods:
We surveyed 67 patients who previously underwent either two previous total hip arthroplasties (THA) or two total knee arthroplasties (TKA), of which one was followed by an overnight stay in the hospital and the other was followed by a SDD. The survey was administered through an email link and responses were recorded through a web-based program.
Results:
Fifty-two patients (78%) responded to the survey. The average age was 65 2 years and 46% were female. Thirty-four patients underwent 2 TKAs and 18 patients underwent 2 THAs. Overall, 63% of patients preferred SDD, 12% had no preference, and 25% preferred their overnight stay. Those who preferred their SDD reported being more comfortable at home. Those who preferred their overnight stay felt their pain and concerns were better addressed in the hospital. There were no differences in patient reported comfort levels, sleep quality, appetite, burden on family, return to function, feelings of being discharged too soon, overall experience, ED visits, or readmissions between patients’ SDD and overnight stays. There was a small statistically significant difference between patient perception of safety between SDD versus overnight stay on a 5-point scale where 5 was “very safe” (4.29 0.25 v. 4.60 0.16, p=0.031)
Conclusion:
These observations suggest that most patients who have experienced both overnight stay and SDD after arthroplasty preferred their SDD experience. Although there was a small difference in patient perception of safety, there were no differences in return to the ED or readmissions after SDD and overnight stay.
Keywords: outpatient surgery, same day discharge, total knee replacement, total hip replacement, rapid-recovery
Figures
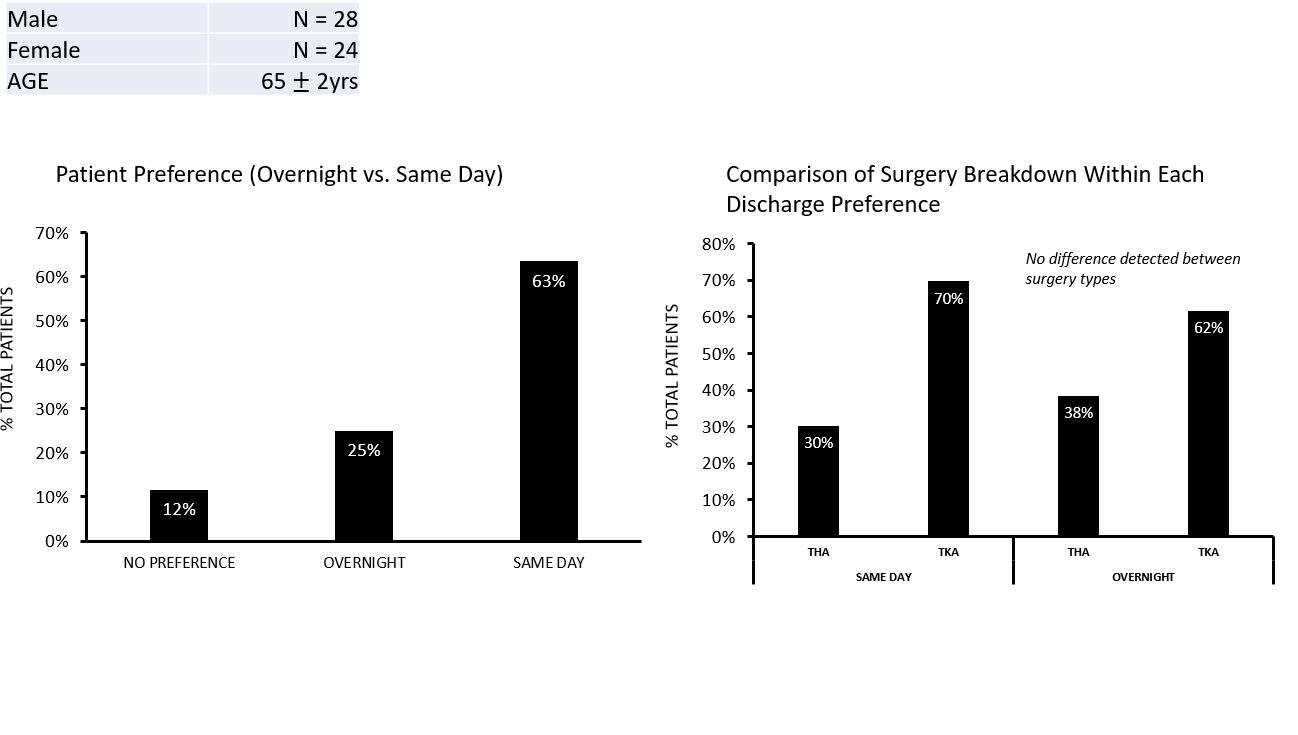
Figure 1
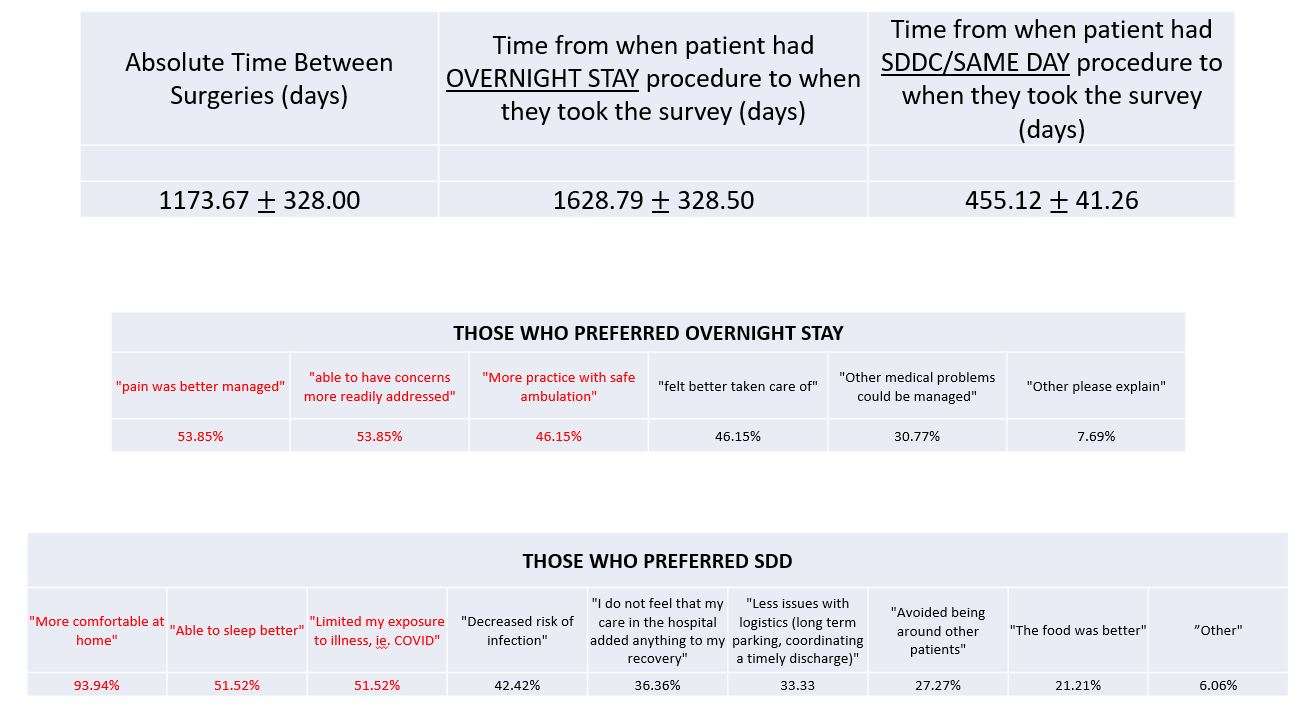
Figure 2
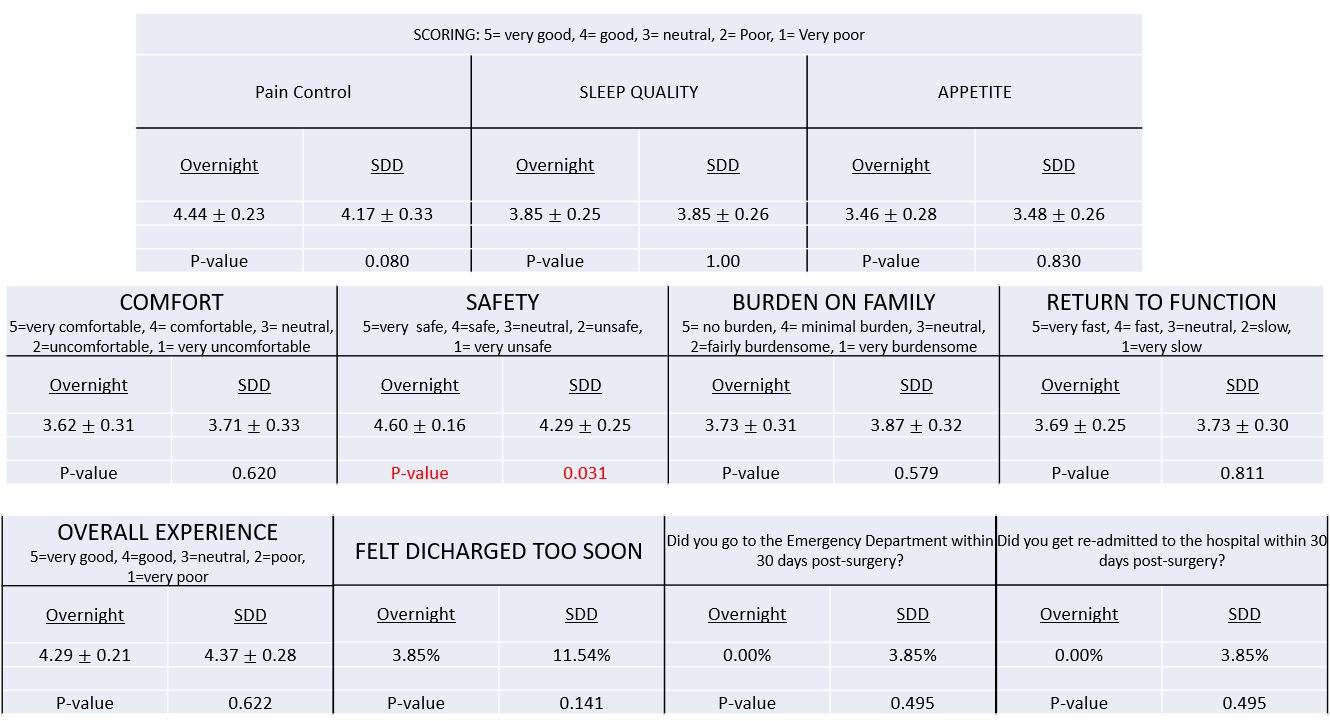
Figure 3#7670
Survival Analysis of Total Hip Arthroplasty for High Hip Dislocation Secondary to Developmental Dysplasia or Septic Arthritis of the Hip
MIN GWANG KIM - CHONNAM NATIONAL UNIVERSITY HOSPITAL - Gwangju, South Korea
Yoon Taek Rim - Chonnam National University - Hwasun-Gun, Korea
*Kyung-Soon Park - Center for Joint Disease,Chonnam National University Hwasun Hospital - Hwasun-gun, South Korea
Joon Kyoo Kang - Chonnam national university - Gwangju, South Korea
Chae Jin Lim - Chonnam national university - Hwa sun, South Korea
*Email: chiasma@hanmail.net
Introduction
This retrospective study was conducted to know clinical and radiographic outcomes, complication rate, and survival of THA in patients with high hip dislocation secondary to developmental dysplasia(DDH) or septic arthritis of the hip(SSH).
Methods
Between March 2005 and September 2014, there were consecutive series of 53 THAs in patients with a highly dislocated hip secondary to DDH or SSH. Of these, 48 hips (DDH 24 and SSH 24) were reviewed at a mean follow-up of 7.9 years(range, 5.0-14.3 years). The mean age at the time of THA was 39.1 years(range, 18.0-59.0 years).
Results
Intraoperative blood loss, total drainage and blood transfusion amounts, and mean time to greater trochanter union were significantly lower in the DDH group than in the SSH group (P = .001, P = .039 and P = .014, and P = .015, respectively). No significant difference in Kaplan-Meier survivorship was observed between groups (log-rank, P = .343). The survival rates with an endpoint of cup aseptic loosening in cases with a cemented cup at 7.9 and 10 years (68.1% and 60.5%, respectively) were significantly lower than those in cementless cup cases (100%) at the same checkpoints (P = .019).
Conclusion
We found similar clinical outcomes between the DDH and SSH groups. However, due to poor bone quality and a lack of containment, cementless acetabular cups could not be performed in more than 50% of patients. Our experience shows that revision cementless fixation cup was possible due to reconstitution of the acetabulum in cases with failed cemented fixation.
Keywords: developmental hip dysplasia; metal-inlay polyethylene liner; septic arthritis; sequelae; total hip arthroplasty.
Keywords: bilateral simultaneous, total hip arthroplasty, drainage, blood loss, pain.
#7672
Long-Term Outcomes of Cementless Femoral Stem Revision With the Wagner Cone Prosthesis
MIN GWANG KIM - CHONNAM NATIONAL UNIVERSITY HOSPITAL - Gwangju, South Korea
Yoon Taek Rim - Chonnam National University - Hwasun-Gun, Korea
Chae Jin Lim - Chonnam national university - Hwa sun, South Korea
Joon Kyoo Kang - Chonnam national university - Gwangju, South Korea
*Kyung-Soon Park - Center for Joint Disease,Chonnam National University Hwasun Hospital - Hwasun-gun, South Korea
*Email: chiasma@hanmail.net
Introduction
The procedure of femoral stem revision is challenging, and bone conservation with less stress shielding is a mandatory effort in these cases. Although there are several reports of stem revision with stems designed for primary total hip arthroplasty (THA), there is no report on stem revision with the Wagner cone prosthesis.
Methods
Between 1996 and 2008, 41 hips of 41 consecutive patients were subjected to femoral revision THA using the Wagner cone prosthesis. The mean age during revision surgery was 56.1 years, and the mean follow-up period was 14.8 years. The clinical results were evaluated, and the femoral component was assessed radiologically.
Results
The results showed that the average period from the first operation to revision THA was 8.0 years. Additionally, the mean Harris hip score improved from 52 points preoperatively to 83 points at the final follow-up. All stems showed bone integration in the radiological evaluation. A subsidence of more than 5 mm was observed in 3 out of 28 (10.7%) femoral stems. Two patients needed an acetabular revision for acetabular cup loosening during the follow-up period. Furthermore, one patient had recurrent dislocation and had to undergo revision surgery for soft tissue augmentation.
Conclusion
We achieved favorable clinical and radiological long-term outcomes in femoral stem revision using the Wagner cone prosthesis. This cementless femoral stem could be an option for femoral stem revision in cases with relatively good bone stock.
Keywords
Cementless femoral stem; Revision total hip arthroplasty; Stress shielding; Wagner cone prosthesis.
#8046
Invited Talk: High incidence of stem loosening in association with periprosthetic femur fracture in previously well-fixed cementless grit-blasted tapered-wedge stem
*Youn-Soo Park - Sungkyunkwan University School of Medicine, Samsung Medical Center - South Korea
*Email: ysp3504@skku.edu
#7562
Impact of Muscle Activity Monitoring in Postoperative Treatment of TKA Regarding the Guidance of Physiotherapy
*Thomas Paszicsnyek - medFit GmbH - Kapfenberg, Austria
Edoardo Bori - BEAMS Department ULB - Bruxelles, Belgium
Bernardo Innocenti - Universite' Libre De Bruxelles - Bruxelles, Belgium
Selina Ovcak - Physiotherapie ortho-unfall - Kapfenberg, Austria
Sandro Pramstaller - Physiotherapie ortho-unfall GmbH - Kapfenberg, Austria
*Email: tp@ortho-unfall.at
Introduction:
The increasing number of joint replacements needs new approaches to improve the patient outcomes. The development of new surgical systems including robotic systems allows to increase the accuracy of the surgical procedure, but, as shown by several studies, this factor alone is not always able improve the patient outcome. Therefore, a new postoperative treatment approach, focusing on the use of muscle activity level as a guide for rehabilitation, was defined to provide a tool able, coupled with the currently available pre and intra-operative technologies, of improving further the final patient outcomes after TKA.
Method:
80 patients were divided in two groups, one implanted with[BI1] a cruciate retaining implant and the other with a posterior stabilized implant (in order to analyze the effect of the approach developed in case of different levels of constraint); each group was then further divided in two subgroups, and for each implant design one group followed the “muscle activity level”-guided physiotherapy while the other underwent traditional approach (control group).
Each group was then tested at defined intervals to check the patient outcomes and thus evaluate the impact of muscle activity on the performances after TKA.
The “muscle activity level”-guided physiotherapy was performed under a standardized testing protocol, using a Noraxon transcutaneous EMG paired with kinematic sensors (fig.1) to generate a virtual personalized musculoskeletal model of the patient[BI2] . During the physiotherapy, the system was used to perform the so called individual coordinative training (ICT) by identifying weaker structures and focusing on training these latter, in order to balance with the more active one.
The performance tests were performed for both control groups and ICT ones preoperatively, postoperatively, after 3 weeks, after 6 months and after 1 year. Load distribution analysis, gait analysis, PROMs and the progress in the postoperative recovery process were recorded and compared.
Results:
In the cohort which received the cruciate retaining implant, muscle activity guided physiotherapy showed [BI3] a faster and more regular improvement, confirming the importance of proper muscle activity, together with the preserved ligaments, to stabilize the knee joint. Function, subjective feeling and objective results showed an increase of 10% in comparison to the control group.
In the posterior stabilized groups, instead, the impact on the joint stability returned to be less remarkable, mainly due to the additional stabilizing factor provided by the prosthesis design. Nevertheless, in comparison with the control group, a faster improvement of the rehabilitation progress was obtained also in this group thanks to the focused muscle training.
Conclusion:
After TKA, not only a correct implant placement and soft tissue balancing are sufficient to guarantee a good satisfaction rate but also the muscle activity covers an important role on the outcomes. The use of a muscle activity-focused physiotherapy approach was thus able to reduce the duration of the rehabilitation process, by improving the quality of the individual training. For these reasons, this kind of procedure has been in use for 5 years in our clinic and great impact on the satisfaction rate of the patients has consequently emerged.
#8003
Mobile Application-Based Pilot Project for Achieving 3D Balancing in Total Hip Arthroplasty Using Digital Inclinometer and Coaxial Stitch Technique, Di-CAST.
*Kalaivanan Kanniyan - Asian Joint Reconstruction Institute AJRI @SIMS Hospitals - Chennai, India
Ashok Kumar P. S. - CHENNAI, India
Pichai Suryanarayan - India
Vijay C Bose - AJRI - chennai, India
Shantanu Patil - SRM Medical College, SRM Institute of Science and Technology - Kattankulathur, India
Sawankumar Pawar - Asian Joint Reconstruction Institute @ SIMS Hospitals - chennai, India
*Email: drkkbriyan@gmail.com
Background: Acetabular Inclination and version are dependent on each other and influential. Effective lower limb version (ELLV) is the appropriate dynamic version of the femoral stem in relation to the long axis of tibia. The coaxial stitch technique used to correct and avoid any sort of Limb length discrepancy (LLD). Achieving appropriate combined version (CV) with no LLD is the key factor while performing 3D balancing of Total Hip Arthroplasty (THA).
Methods: Ongoing prospective study including 30 patients using Mobile application along with coaxial stitch technique, between the study period of February and April 2022. The results primarily to be analyzed clinically and radiologically to ascertain the implications of functional 3D balancing on x-ray parameters, clinical outcome scores (Harris Hip Score), ability to squat, and perception of LLD. Secondary results included complications like infection, dislocation and periprosthetic infection.
Results: The original socket was placed with appropriate inclination angle as of the trial component checked using mobile application. The post operative socket version using ischiolateral view method conformed the same finding. The average socket inclination angle was planned between 31* to 35* and version of 10* to 15*. The combined version was to be placed between 30*to 45* using mobile app. HHS improved with significant statistical significance (P< 0.001). There was significant improvement in terms of VAS preoprative and postoperative with no limb length discrepancy.
Conclusion: This study underlines the fact that even young surgeons with less experience can improve their cup placement in terms of inclination and version. 3D balancing of the hip with no LLD using angle inclinometer mobile application is an easy and cost effective method in developing nations.
#7378
Metallic Versus Non-Metallic Cerclage Cables System in Periprosthetic Hip Fractures: Single-Institution Experience at a Minimum 1-Year Follow-Up
*Stefano Pecchia - University of Rome - Rome, Italy
Attilio Speranza - Sapienza University of Rome/Sant' Andrea Hospital - Rome, Italy
Carlo Massafra - University of Rome La Sapienza - Rome, Italy
Riccardo Di Niccolo - University of Rome La Sapienza - Rome, Italy
Natale Criseo - University of Rome La Sapienza - Rome, Italy
Raffaele Iorio
Andrea Ferretti - roma university
*Email: ste.pecchia@gmail.com
Introduction:
Metallic cerclage cables are reliable and cost-effective internal fixation devices, broadly used in surgical practice for treatment of periprosthetic fractures. Nevertheless, complications connected with their use have been described in literature: third – body generation, failure and consequent migration, fraying, allergies, and injury to the surgical team. The development of new materials offers alternatives to traditional metallic cables: this study compares outcomes between two groups of patients affected with peri prosthetic hip fractures treated with titanium cables or with ultra-high molecular weight polyethylene iso-elastic cables.
Our retrospective study aims to compare clinical and radiological outcomes of titanium cables and UHMWPe isoelastic cables, isolated or associated with dedicated plates, for surgical treatment of periprosthetic fractures with stable implants.
Methods:
Two groups of 30 (group A) and 24 (group B) patients have been surgically treated in our institution for hip periprosthetic fractures between September 2016 and June 2020. Mean age of the patients was 81 years in group A and 80 years in group B; we included in our study fractures classified as B1 or C according to Vancouver postoperative fractures classification; fractures involving the trochanteric are alone (A), with loose implants (B2) and poor bone stock (B3) have been excluded. The procedure was performed by a single experienced surgeon using titanium (group A) or UHMWPe (group B) cerclage cables (Fig. 1) alone or with dedicated titanium hook plates. All patients underwent the rehabilitation protocol at specialized institutions. Patients were evaluated retrospectively at 1 year post operatively regarding: surgery time, blood loss, partial weight-bearing time, radiographical healing time, Harris Hip score and post – operative complications.
Results:
Mean operative time in group A was 87.3 ± 16.2 minutes with a mean hemoglobin loss of 2.6 ± 1.4g/dl, while in group B was 83.6 ± 17.3 minutes with a mean hemoglobin loss of 2.9 ± 1.3 g/dl. Weight bearing concession was given at a mean of 36 days in group A and 28 days in group B. Fractures showed a mean full radiographical and clinical healing time of 12.6 ± 4.3 weeks in group A and 12.8 ± 2.7 days in group B. Among patients treated with titanium cables, we report two cases of cable rupture, two cases of osteolysis, and one case of non-union., all treated with reintervention. In the UHMWPe cables group we report we reported one case of THA posterior dislocation, treated with closed reduction and rehabilitation, one case of superficial wound infection, treated with antibiotics and surgical debridement, and one case of malunion. Mean Harris Hip score at 12 months follow – up was 72.5 ± 10.1 in group A and 72.9 ± 8.4 in group B.
Conclusions:
Comparable outcomes were observed in both groups. Group A showed higher complication rates compared to group B at 1 year. Nonmetallic nylon fiber and UHMWPe cerclage cables could represent a reliable fixation device, ensuring comparable healing and complication rates with traditional titanium cerclage cables. However, high volume studies are needed to assess long-term complications and compare functional outcomes.
Figures

Figure 1
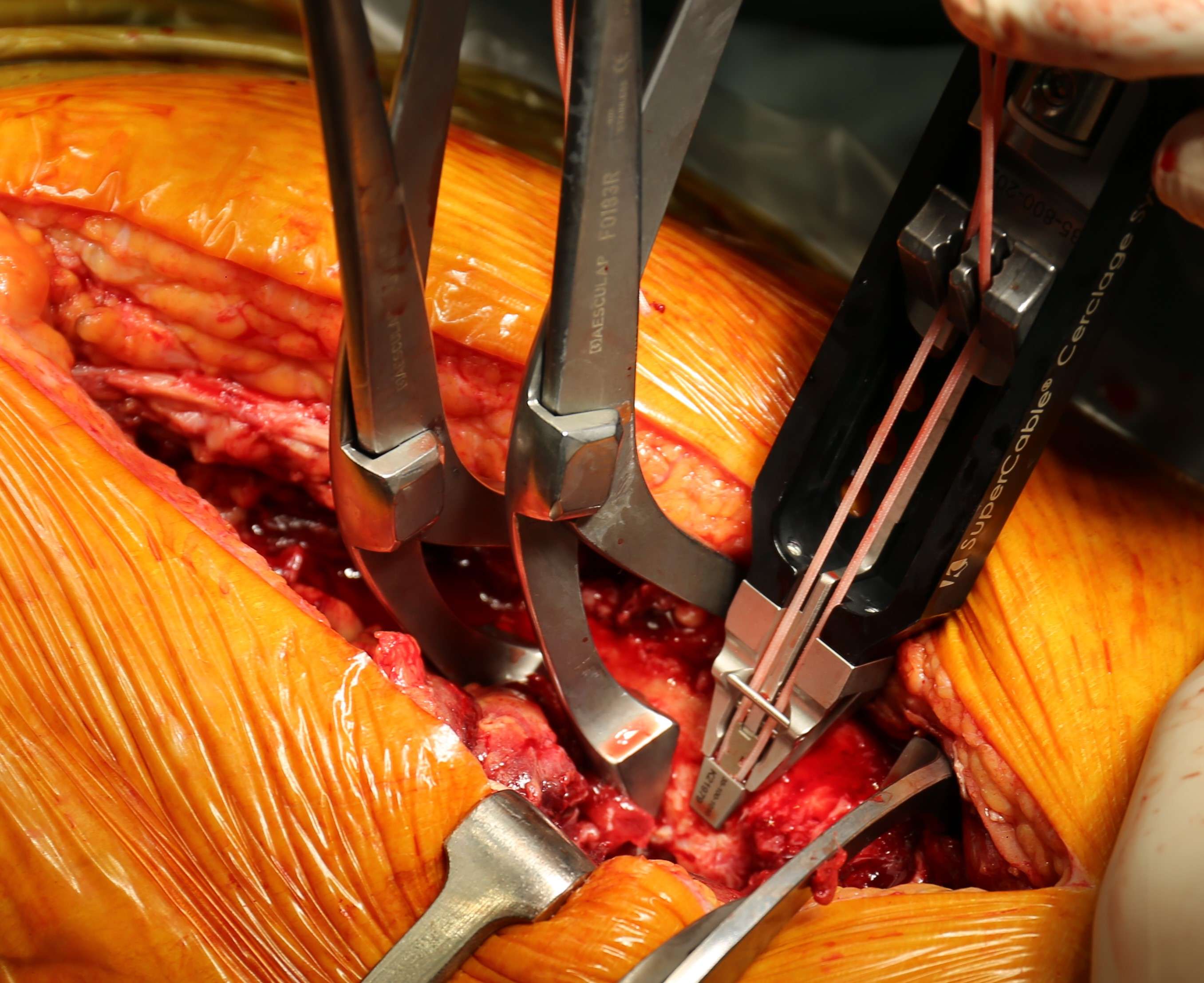
Figure 2
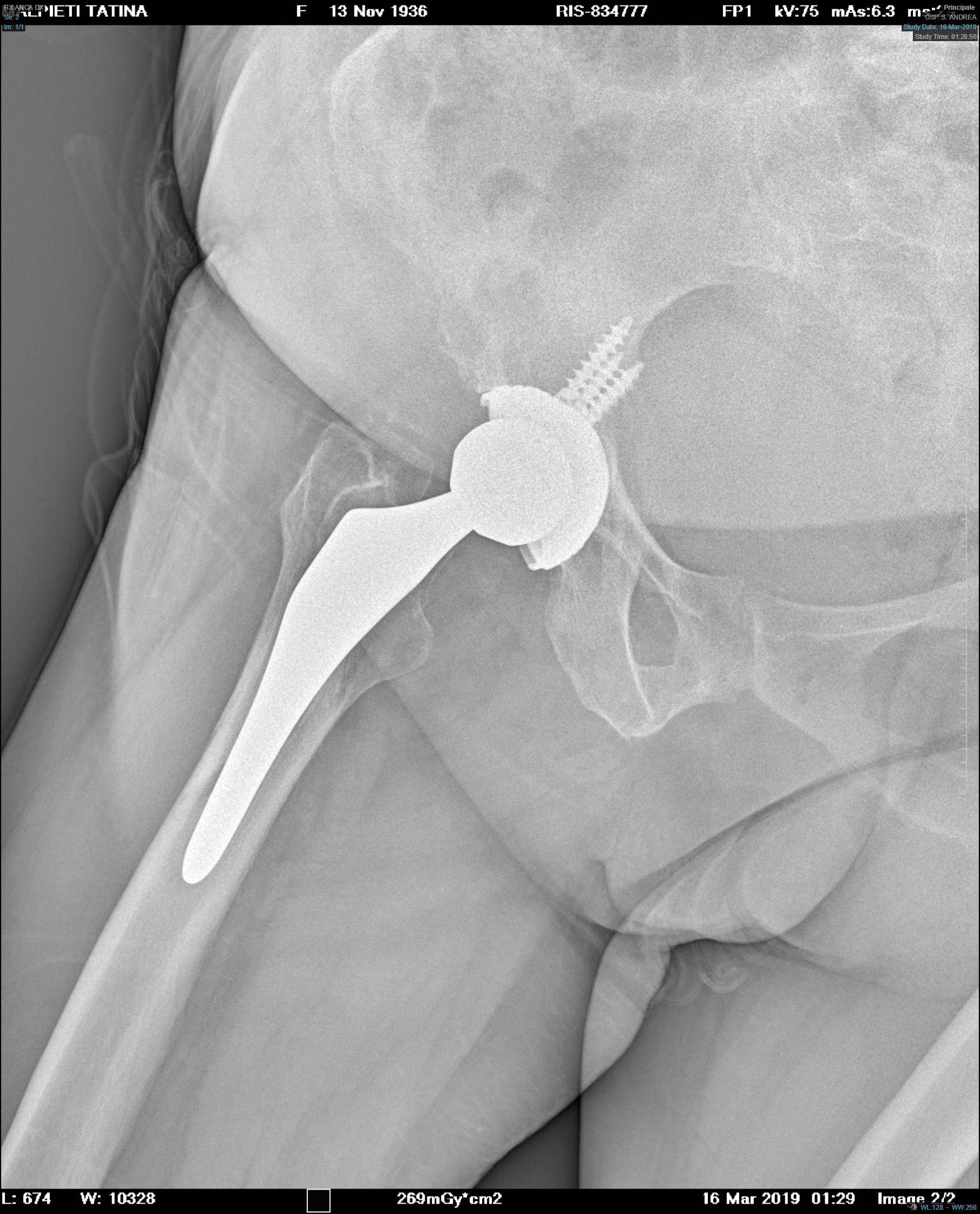
Figure 3
Figure 4#7726
Design Thinking for Arthroplasty Advancement
*David Pienkowski - University of Kentucky - Lexington, USA
*Email: pienkow@uky.edu
Introduction: John Charnley challenged existing paradigms and enabled major advances in arthroplasty. These advances occurred through achievements in new products (implant designs, materials, pharmaceuticals, etc.) and new processes (surgical techniques, rehabilitation methods, etc.). Such advances were attributable to the collective innovativeness of Orthopaedic surgeons, materials engineers, implant designers, and others working collaboratively.
Unfortunately, the pace of all technological advancements eventually declines. This occurs because each technology has an ultimate scientific limit which, as approached, yields less incremental benefit for increasing marginal cost. Advances in arthroplasty are no exception to the “diminishing law of innovation returns” (Fig. 1). Sustainment of arthroplasty advances is important given the growing demand for this technology, but such advances are confounded by healthcare cost containment initiatives imposing a pivotal metric of value created versus costs incurred. Fortunately, a new opportunity exists to facilitate cost-effective advances in arthroplasty technology.
Method
Almost in parallel with Charnley’s contributions, a significant development in problem-solving methodology was disseminated. Nobel Laureate Herbert Simon published “Sciences of the Artificial” in which he advanced the concept of “design-thinking” as a systematic means of creatively solving vexing challenges. Design-thinking is currently defined as a non-linear iterative process that seeks to: better understand user needs, challenge accepted assumptions, redefine problems and create innovative product ideas worthy of evaluation using accompanying new test methods. Five separate activities now comprise the process of design-thinking: empathize with the user(s), define the problem, create new ideas, develop prototypes, test and evaluate.(Fig.2).
History reveals that technology advances require both new products and new processes. New approaches to reasoning can be a source of both, and thus design-thinking merits consideration as a novel means of advancing technology. Formerly the exclusive province of industrial designers, successful adaption of design-thinking as an integral part of technology innovation led to specialized design-thinking practitioners. These professionals are often found within the subspecialty field of product design. Product design professionals are thus increasingly included among technology development teams of leading organizations. Implementation of “design-thinking” methods and inclusion of related product design professionals in the collective technology development effort is a proposed method of cost-effectively advancing arthroplasty.
Results
Design-thinking has been successfully applied to creatively address problems in architecture and engineering. Experience obtained helped refine design-thinking methods, and these methods are currently used by Apple and Google. While design-thinking related activities have occurred in prior arthroplasty development circumstances, systematic incorporation of is not routine. Although design-thinking has an established success record, regular implementation of this approach and related professionals in arthroplasty technology advancement activities may await formal testing and analysis of objective data.
Conclusion
Sustaining a robust pace of technological innovation is difficult and may become cost-inefficient following harvest of the “low-hanging fruit on the tree of technology”. Inclusion of product design professionals as integral team members and allowing challenges and changes to existing technology development paradigms using design-thinking offers an opportunity to creatively enhance the pace of innovation and enable the next generation of efficacious cost-effective advances in arthroplasty.
Figures
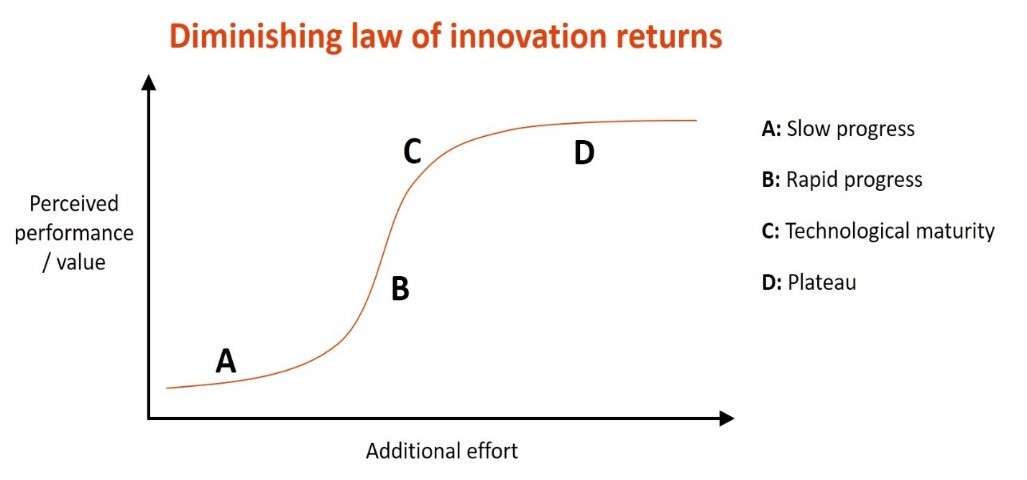
Figure 1
Figure 2#7836
Obtaining an Accurate Intraoperative Leg Length and Offset Measurement During THA Using 3-D Imaging and a Novel Computer Software Program
*Justin Than - Cedars Sinai Medical Center - Los Angeles, United States of America
Wenchao Tao - University of California, Los Angeles - Los Angeles, USA
Landon Polakof - Cedars Sinai Medical Center - Los Angeles, USA
Brad Penenberg - Cedars Sinai Medical Center - Los Angeles, USA
*Email: justinpthan@gmail.com
INTRODUCTION: Achieving accurate and consistent limb length and offset in total hip arthroplasty (THA) measurements using intraoperative radiographs is challenging due to patient positioning and parallax. The goal of this study is to introduce a method of achieving an accurate intraoperative limb length and offset measurement using 3-D imaging combined with a novel computer software program.
METHODS: Patients who underwent THA using intraoperative 3-D imaging with a novel computer software program were evaluated. A 3-D model of the pelvis was acquired from an intraoperative computed tomography (CT) scan in the operating room immediately before patient positioning. Intraoperative limb length and offset measurements were determined using a 3-D overlay technique using trial radiographs with computer assistance during surgery. These measurements were then compared with limb length and offset measurements from postoperative radiographs.
RESULTS: There were 35 patients in the cohort. There was no significant difference (p = 0.52 and 0.87, respectively) between the limb length and offset change measurements from intraoperative 3-D overlay compared to the post-operative measurements. 100% of cases had postoperative limb length measurements within 2mm of intraoperative measurements based on 3-D overlay, and 90% had postoperative offset within 2mm of intraoperative measurements.
CONCLUSION: Using intraoperative 3-D imaging combined with this novel software program may help surgeons obtain accurate intraoperative limb length and offset.
#7651
Machine Learning to Set Expectations and Improve Satisfaction Following Total Knee Arthroplasty
*Jennifer Polus - University of Western Ontario - London, Canada
Tom Appleton - Western University - London, Canada
Edward Vasarhelyi - Western University - London, Canada
Steven MacDonald - London Health Sciences Centre - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Matthew Teeter - Western University - London, Canada
*Email: jpolus@uwo.ca
Introduction
Total knee arthroplasty (TKA) is the only viable treatment for end-stage osteoarthritis, however, 20% of patients consistently report being dissatisfied with the outcome of their procedure. Patient dissatisfaction has been linked to unmet expectations of functional recovery. One way to potentially improve patient satisfaction is to counsel patients on what they can expect of their personal recovery. Our group has developed a tool to predict whether a patient is more likely to meaningfully improve on (responder) or keep (maintainer) their level of preoperative function after undergoing surgery. The purpose of this study is to assess the impact providing patients with a personal functional prediction has on their satisfaction and investigate relationships between patient satisfaction, functional ability, and local knee inflammation with machine learning techniques.
Method
Patients (n=50) undergoing primary TKA for osteoarthritis will be recruited and randomized to either receive the prediction of their functional recovery or to have surgery as normal. Preoperatively, patients perform the timed-up-and-go (TUG) walking test while instrumented with wearable sensors. Using the data collected from the wearable sensors, the machine learning classifier predicts whether each patient is a functional responder or maintainer. Patients repeat the TUG test again at 3-months and 1-year postoperatively to evaluate the prediction accuracy. To determine if dissatisfied patients have experienced truly poor outcomes due to ongoing pain and stiffness, ultrasound imaging is performed to grade the severity of synovitis. Patient reported outcome measures (PROMs) are recorded preoperatively and at follow-up appointments.
Preliminary Results
Recruitment for this study is ongoing. Thus far, 17 patients have consented to participate and 11 have undergone TKA. Patients were randomized to either receive their functional prediction (n=6) or have surgery with no knowledge of their prediction (n=5). Two patients were predicted to be “responders” and the remaining nine were predicted to be “maintainers.” The mean preoperative total TUG times were 17.85 seconds for responders and 14.23 seconds for maintainers (mean difference = 3.62 seconds). So far, six patients have completed their 3-month follow-up. Although all six of these patients were preoperatively predicted to be maintainers, two patients improved on their preoperative TUG times by more than 2.27 seconds, making them responders. Ultrasound synovitis grading of eight patients shows grade 0 to grade 2 synovitis for seven predicted maintainers and grade 0 synovitis for one predicted responder. Further, the mean KOOS pain score for the responder and the maintainer groups were 43 and 51, respectively, where a lower score indicates more pain.
Conclusion
Patient dissatisfaction following TKA is widespread and costly. This ongoing study is the first to evaluate an objective tool for management of preoperative expectations of functional recovery and will contribute to the growing recognition that synovial inflammation may be a significant cause for ongoing pain and stiffness after surgery. So far, the algorithm is performing as expected, with a bias towards setting a lower expectation to ensure satisfaction with functional outcomes. As recruitment is completed, the relationship between functional ability and inflammatory status will be related to other patient outcomes, including satisfaction.
#8007
Immersive Virtual Reality Is Superior to Conventional Training for Novice Scrub Nurses Learning Intramedullary Tibial Nailing: A Randomised Controlled Trial
*Jonathan Edwards - Imperial College - London, GB
Isabelle Poole - Imperial College - London, United Kingdom
Thomas Edwards - Imperial College London - London, United Kingdom
Francesca Kablean-Howard - Imperial College London - London, United Kingdom
Kathryn King - King's College London - London, United Kingdom
Julie Bliss - King's College London - London, United Kingdom
Alexander Liddle - Imperial College - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
Kartik Logishetty - Imperial College - London, United Kingdom
*Email: jonathanwedwards@me.com
Introduction: Superior team performance in surgery leads to fewer technical errors, shorter operation time, reduced mortality and improved patient outcomes. Scrub nurses are a pivotal part of this team, yet they have very little structured training. This lack of training leads to high levels of stress, low confidence and concerns that their poor knowledge may cause patient harm. Immersive virtual reality (iVR) simulation is a low cost, easily accessible technology which allows novice scrub nurses to enter a virtual operating theatre and repetitively practise these skills in a risk-free environment. It has demonstrated excellent efficacy in training surgeons, however there is a paucity of literature investigating its role in training scrub nurses. This randomised study therefore investigates the impact of an iVR curriculum on training prospective scrub nurses to perform their role for intramedullary tibial nailing.
Materials and Methods: 60 undergraduate nursing students were included in this study and randomised in a 1:1 ratio to learning the scrub nurse role for a tibial nail using either conventional training or iVR. Participants were excluded if they had previously scrubbed for >5 intramedullary nailing operations or had prior iVR surgical simulation experience. The conventional training was derived through expert consensus, consisting of a 1-hour seminar including a Q&A session and 2 hours of e-learning where participants were taught the equipment and sequence of steps. The iVR training consisted of 3 separate hour-long sessions where participants performed the key steps of the operation in a virtual operating room. The primary outcome was their performance in a physical world practical assessment with real equipment. Participants were asked a series of questions designed to test the knowledge and skills needed to perform their role in the operation, including operative sequence, equipment identification and assembly. This assessment was developed and validated using a modified Delphi process with a panel of experts consisting of expert scrub nurses, surgeons and industry representatives.
Results: 53 participants successfully completed the study (26 iVR, 27 conventional) with a mean age of 31 ± 9 years. There were no significant differences in baseline characteristics or baseline knowledge test scores between the two groups (p>0.05). The iVR group significantly outperformed the conventionally trained group in the real-world assessment, scoring 65.4 ± 17.7% vs 37.3 ± 15.9%, p<0.0001.
Conclusion: Immersive virtual reality training was superior to conventional training in teaching novice scrub nurses to perform their role for intramedullary tibial nailing. This easily accessible, low cost training modality could be integrated into scrub nursing curricula to address the current shortfall in training.
#7975
Specification and Verification Practices for Synthetic Bone Models Used in Implant Testing
*Amy Posch - Pacific Research Laboratories - Vashon, USA
Rusty Knowler - Pacific Research Laboratories - Vashon, USA
McKee Buxton - Pacific Research Laboratories - Vashon, USA
John James - Pacific Research Laboratories - Vashon, USA
Forrest Miller - Pacific Research Laboratories - Vashon, USA
Hani Haider - UNMC - Omaha, USA
*Email: AMY@PACIFIC-RESEARCH.COM
Introduction
Synthetic bone models intended for testing implants undergo a development process to define materials and shapes that closely match characteristics of bone tissue and anatomy. This work is accompanied with verification using standard test methods for material characterization, 3D morphology measurements with computed analyses, and experimental methods in orthopaedic biomechanics often with expertise from academic institutions. A written standard practice for specification and verification, ISO/CD 22926, is due for publication in 2023. Presented here is an early case of using the standard on a synthetic femur model that has been commercially available for over 15 years.
Methods
Specification and verification were analyzed on a synthetic femur for material, shape and structural characteristics. Material metrics included apparent density, ultimate strength, ultimate strain, elastic modulus, fracture toughness and screw pullout normalized with screw outer diameter and insertion depth. Shape metrics were calculated from an algorithm expressing normal distances between two surface meshes and applying this computation as a three-dimensional (3D) colorized surface map (Cignoni et al. 1998). Shape deviation was expressed as a percentage calculated from the maximum distance (Hausdorff distance) divided by length of the bounding box diagonal where good agreement was specified as 1% or less. Structural metrics were calculated as rigidities measured in bending, torsion and axial compression with a specification that values are within min-max range for cadaver femurs (Heiner 2008).
Results
Materials selected to simulate cortical and cancellous bone tissues were short fiber filled epoxy and rigid polyurethane foam, respectively. Materials were tailored to reflect characteristics obtained from a literature review of healthy adult bone (Figure 1). A cadaver femur was converted into a reference digital model (RDM) containing surfaces that defined cortical, cancellous and intramedullary regions. Synthetic femurs were cast in a manufacturing process based on the RDM. Shape verification was performed on digitized surfaces generated from 3D scans of the synthetic femur cortical and cancellous regions. Computed 3D surface analyses verified synthetic femurs met their specification for good agreement with a maximum deviation in shape for cortical and cancellous surfaces of 0.6% and 0.4%, respectively. Colorized 3D surface maps with scaled histograms explicitly describe shape variations (Figure 2). Structural verification is summarized graphically (Figure 3).
Results indicate synthetic femurs produced met their specified material, shape and structural measurement parameters. Furthermore, to affirm their intended use for testing implants, a high-cycle fatigue study with cemented hip stems was conducted (Chong et al. 2007).
Conclusion
Reporting specification and verification activity acts as a foundation to describe and evaluate synthetic bone models. Adoption of this standard practice supports a global expectation among orthopaedic experts that can be met by users and producers of these specialized synthetic bone models.
References
Morgan, EF et al. (2018). Annu Rev Biomed Eng.
Chong, ACM et al. (2007). Ann Biomed Eng.
Cignoni, P et al. (1998). Computer Graphics Forum.
Heiner, AD. (2008). J Biomech.
Zdero, R et al. (2009) J Biomech Eng.
Zdero, R et al. (2008). Proc Inst Mech Eng H.
Chen, MJ et al. (2020). J Am Acad Orthop Surg.
Figures
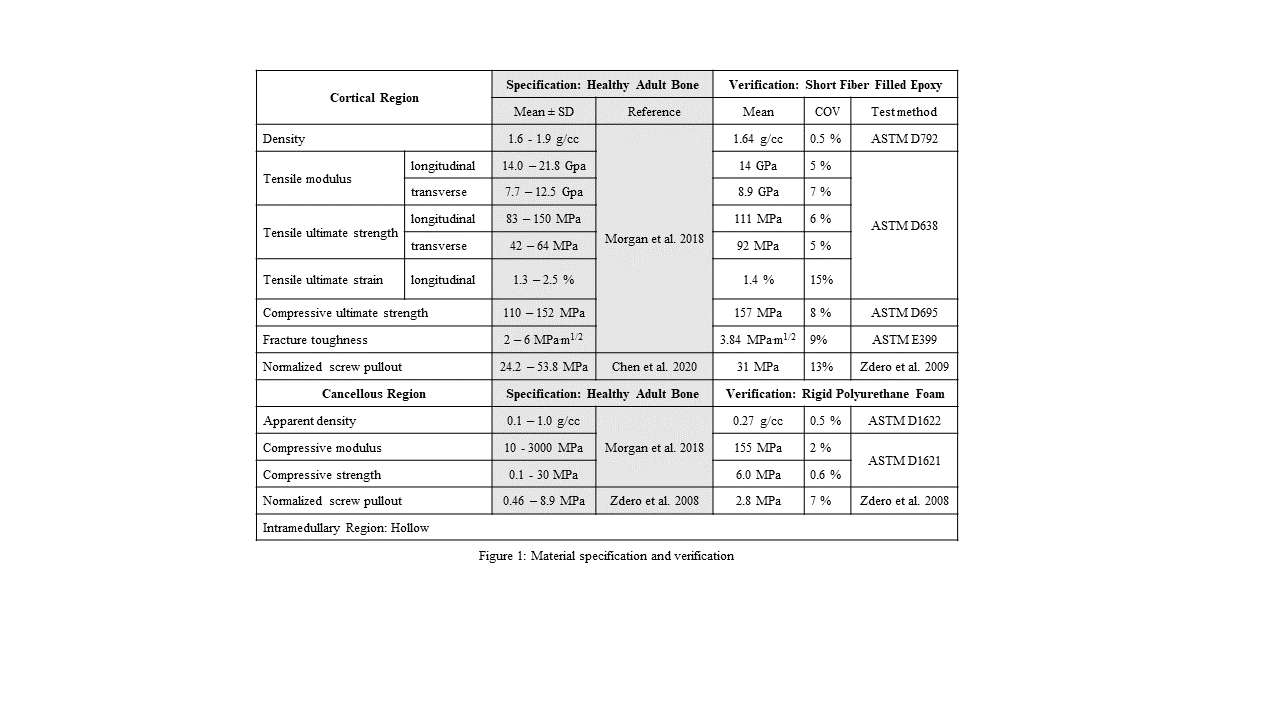
Figure 1
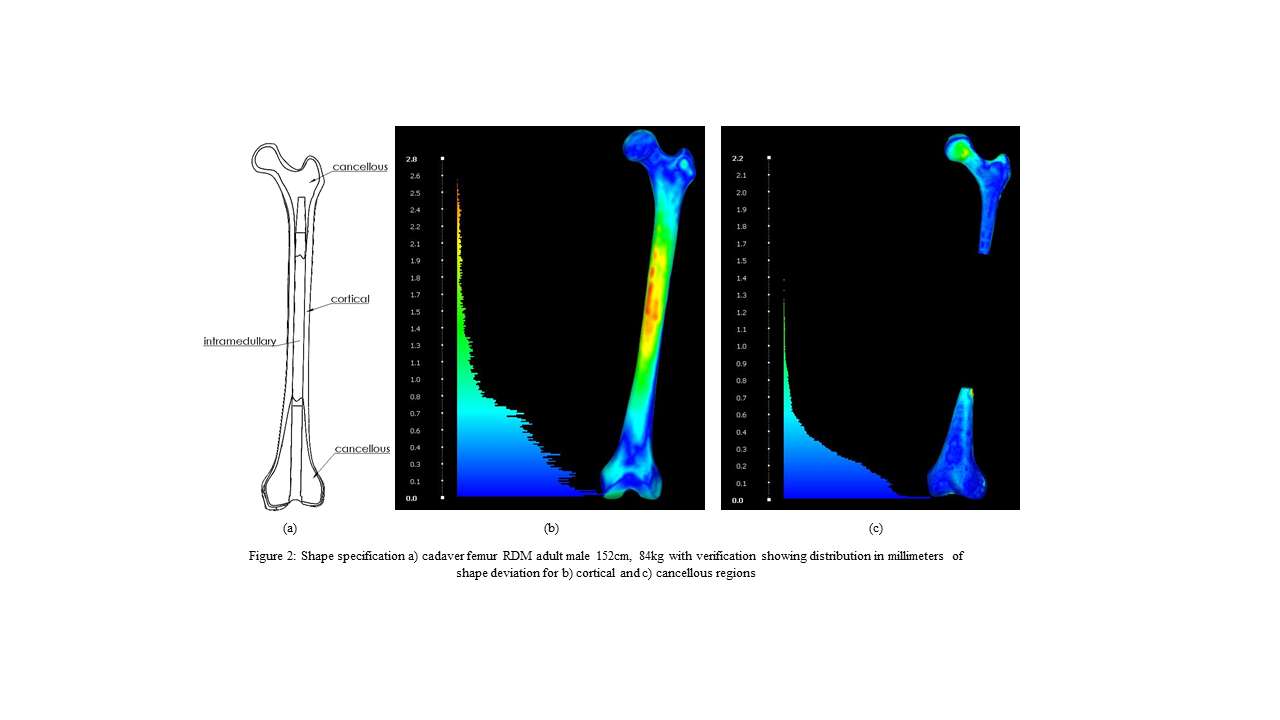
Figure 2
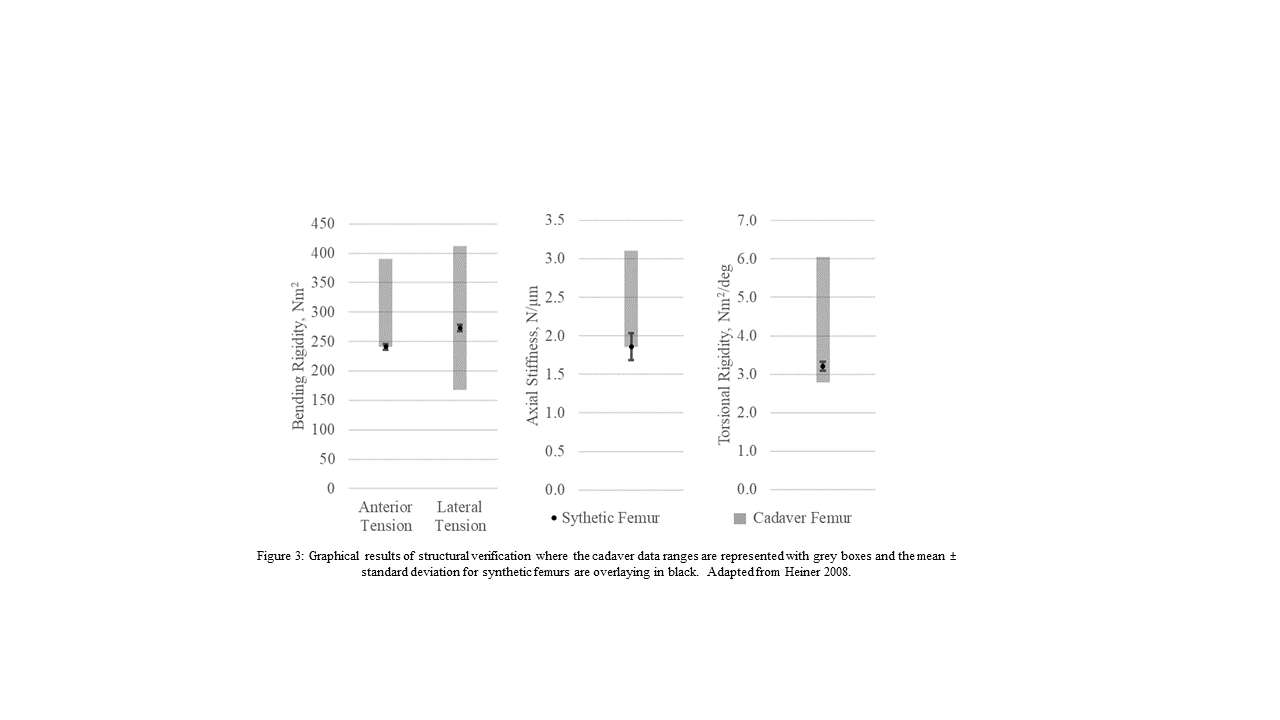
Figure 3#7676
Finite Element Study on the Effect of Interference Fit and Coefficient of Friction on the Primary Fixation of a Cementless PEEK Tibial Component
*Corine Post - Radboud university medical centre - Nijmegen, Netherlands
Thom Bitter - Raboud University Nijmegen Medical Centre - Nijmegen, Netherlands
Adam Briscoe - Invibio Ltd - Lytham St. Annes, United Kingdom
Nico Verdonschot - Radboudumc - Nijmegen, Netherlands
Dennis Janssen - Radboud University Nijmegen Medical Centre - Nijmegen, Netherlands
*Email: Corine.Post@radboudumc.nl
Introduction
Aseptic loosening is one of the most common indications for a revision of the total knee arthroplasty (TKA). The main reason for aseptic loosening is the decrease in bone mineral density which can be caused by stress-shielding of the peri-prosthetic bone. To avoid this, TKA components of a more compliant material such as polyetheretherketone (PEEK-OPTIMATM) could be used. The introduction of a new material for the application in a cementless TKA component requires a thorough investigation of the primary fixation, with the micromotions, the shearing movements on the bone implant interface as important outcome measures. Both the interference fit and coefficient of friction play an important role in the primary fixation and need to be investigated for cementless tibial components of a less stiff material such as PEEK. This finite element (FE) study investigates the effect of variations of interference fit and coefficient of friction on the micromotions of a cementless PEEK tibial component. Additionally, these results are compared with a cementless titanium (Ti) tibial component.
Methods
FE models based on 9 different knees were created of the tibia and tibial component including polyethylene insert (5 left, 4 right tibiae). The forces and moments of a gait and squat activity from the Orthoload database were incrementally applied to the model and linked to the lateral and medial surfaces of the insert [1]. This was simulated four times, resulting in four activity cycles. The tibial component was modelled with a Young’s modulus for PEEK (3.7 GPa) or Ti (109 GPa). Two variations of interference fit (500, 750 µm), defined through the contact algorithm and applied at the bone-implant interface, and two variations of coefficient of friction (0.5, 1.5) were investigated. To quantify the primary fixation, the 95th percentile of the maximum resulting micromotions was analyzed for each FE simulation.
Results
Both the interference fit and coefficient of friction do not have a major impact on the micromotions of the cementless PEEK tibial component (Figure 1). Additionally, the 95th percentile of the maximum resulting micromotions of the cementless PEEK tibial component are similar to the 95th percentile of the maximum resulting micromotions of the cementless Ti tibial component.
Conclusion
This study showed that the primary fixation of a cementless tibial component has minor effects caused by the in this study researched variations of interference fit, coefficient of friction and implant material unlike what has been found for the cementless femoral component. Additionally, the resulting micromotion values generated by the PEEK tibial component were similar to the resulting micromotion values generated by the Ti tibial component. The current FE simulations give insights into the effect of interference fit and coefficient of friction on the micromotions. This may be further assessed in a larger population of models to investigate the influence of patient related parameters on micromotion outliers.
References
[1] Bergmann, G. et al. Standardized Loads Acting in Knee Implants. PLoS ONE 9(1), 1-12 (2014).
Acknowledgements
PEEK-OPTIMATM is a trademark of Invibio Ltd. Implant geometry was supplied by Maxx Orthopaedics Inc.
Figures
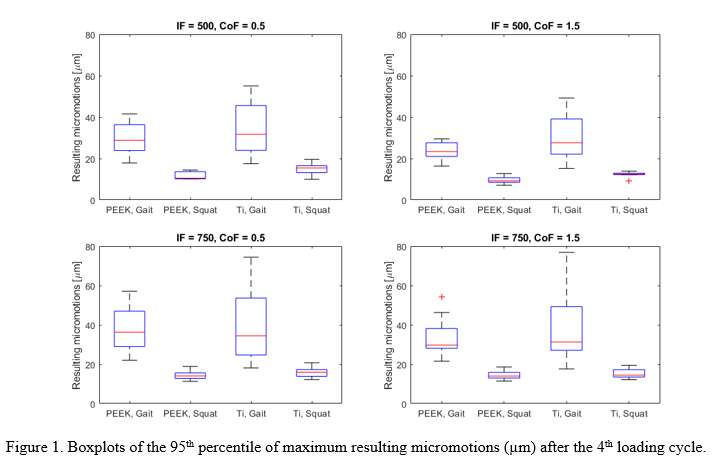
Figure 1#7692
The Role of Design, Microstructure, and Malseating in the Fretting and Corrosion of Dual Mobility Hip Metal Liners
*Deborah Hall - Rush University Medical Center - Chicago, USA
E. Bailey Terhune - Rush University Medical Center - Chicago, USA
Joseph Serino - Rush University Medical Center - Chicago, USA
Denis Nam - Rush University Medical Center - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Craig Della Valle - Rush University - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: deborah_hall@rush.edu
Introduction: As most modular DM bearings have a junction between a CoCrMo liner and titanium shell, the risk of corrosion at this interface and potential subsequent failure due to adverse local tissue reactions remains a concern. The purpose of this study was to determine the occurrence and extent of fretting corrosion on the backside of DM acetabular liners made from CoCrMo alloy by two different manufacturers in context of design features, alloy microstructure, and malseating.
Methods: Twenty-eight surgically retrieved DM acetabular liners with mean time in-situ of 14.3 months (range 1-83) were evaluated. Two manufacturers were included (Type A: n=16, Type B: n=12). Each liner taper was scored with a modified Goldberg scoring system (mGS). Local damage modes were determined by SEM. Quantification of volumetric material loss was conducted with an optical CMM. One cup per manufacturer was sectioned for metallographic analysis and determination of bearing wall thickness. Malseating was evaluated on postoperative radiographs and defined as a visible, distinct divergence between liner and shell.
Results: Six liners had severe mGS damage on the taper surface, 6 had moderate, 11 mild, and 5 none. Liner A and B had different wall thicknesses and alloy microstructures (Figure 1). Liner A exhibited symmetric out-of-roundness (OOR) that appeared to originate from the machining process (Figure 2A). SEM observations were used to ensure surface depressions resulting from OOR were not mistaken as material loss such that total volume loss was determined by summation of local scars loss (Figure 2B). Damage features on all liners of type A were consistent with fretting and fretting corrosion (Figure 3A-B). One case exhibited chemical etching in non-contact areas due to OOR. Five A liners were malseated. While Liner B also showed OOR, it appeared mostly unsymmetrical, possibly the result of the casting process, or deformation during assembly. SEM analysis revealed no fretting or corrosion damage features. Damage features observed by light microscopy initially suggested the occurrence of imprinting on type B liners, but SEM revealed the parallel lines on the surface to be organic residue (Figure 3C-D). None of the B liners were malseated.
Conclusion: Different DM liner designs cannot be directly compared for corrosion behavior due to broad design, surface finish and material differences. Our findings provide important insights to the corrosion performance of each liner type. Type A, a sturdier liner based on design (wall thickness) and material (wrought CoCrMo), does not appear to deform during assembly but exhibits mild initial OOR. The combination of these factors may result in reduced contact area after seating, potentially making micromotion more likely. Further increasing this risk is malseating. Fretting corrosion was observed mostly in contact areas, while one case also exhibited chemically induced corrosion in an area that was likely out of contact. Type B liners exhibited no material loss. The combination of a central nub, less wall thickness and the use of the more ductile cast alloy seem to enable a good seating and bedding-in of the liner into the cup.
Figures
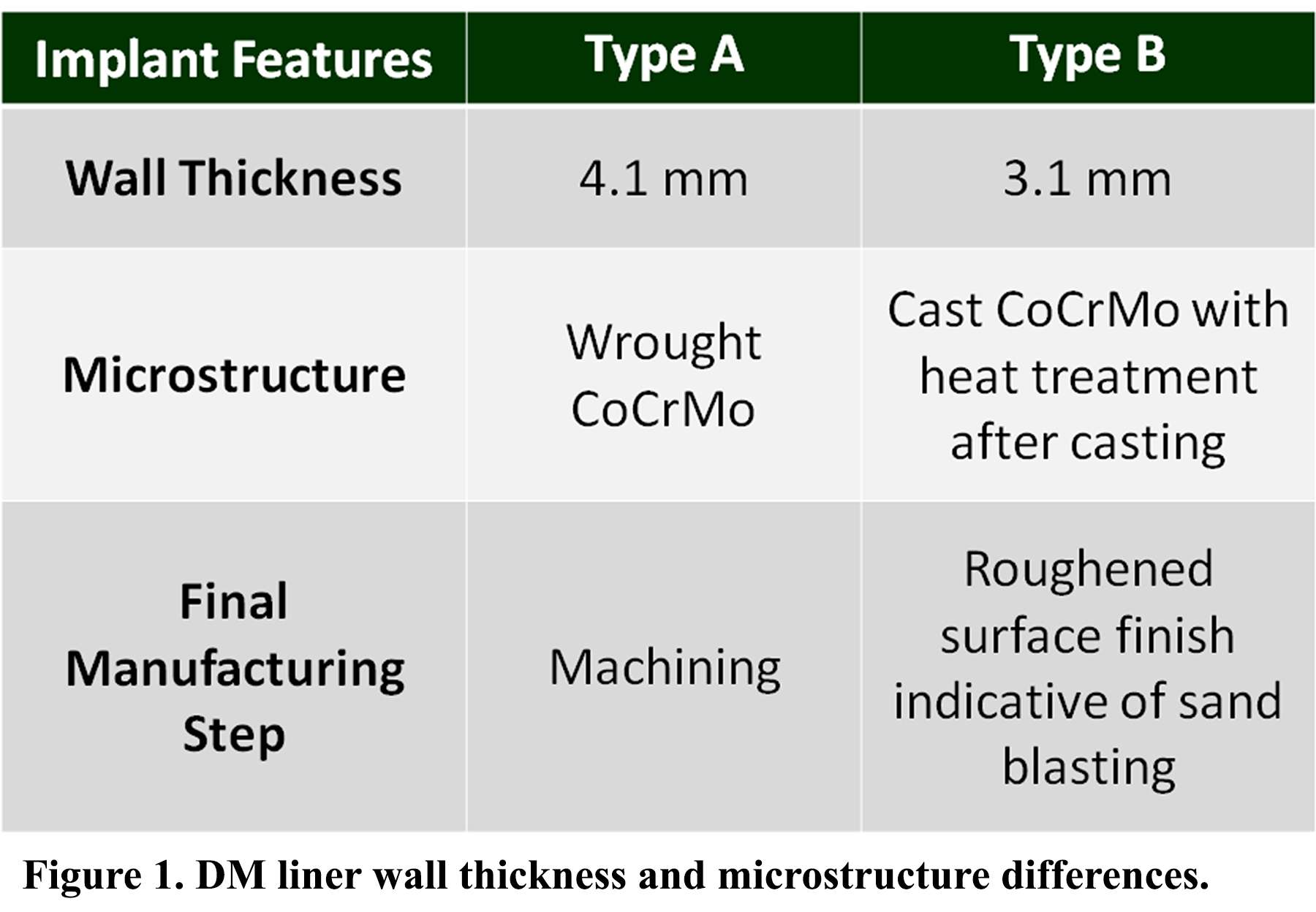
Figure 1
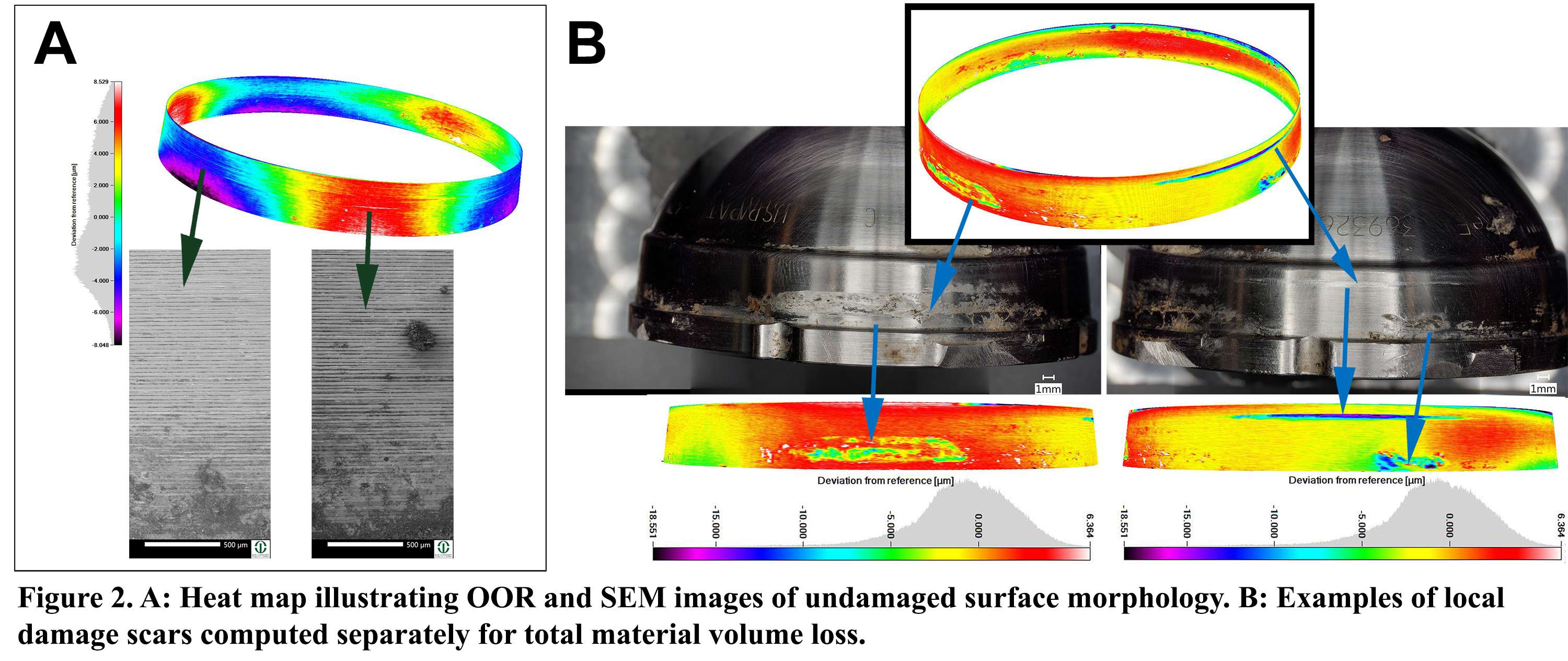
Figure 2
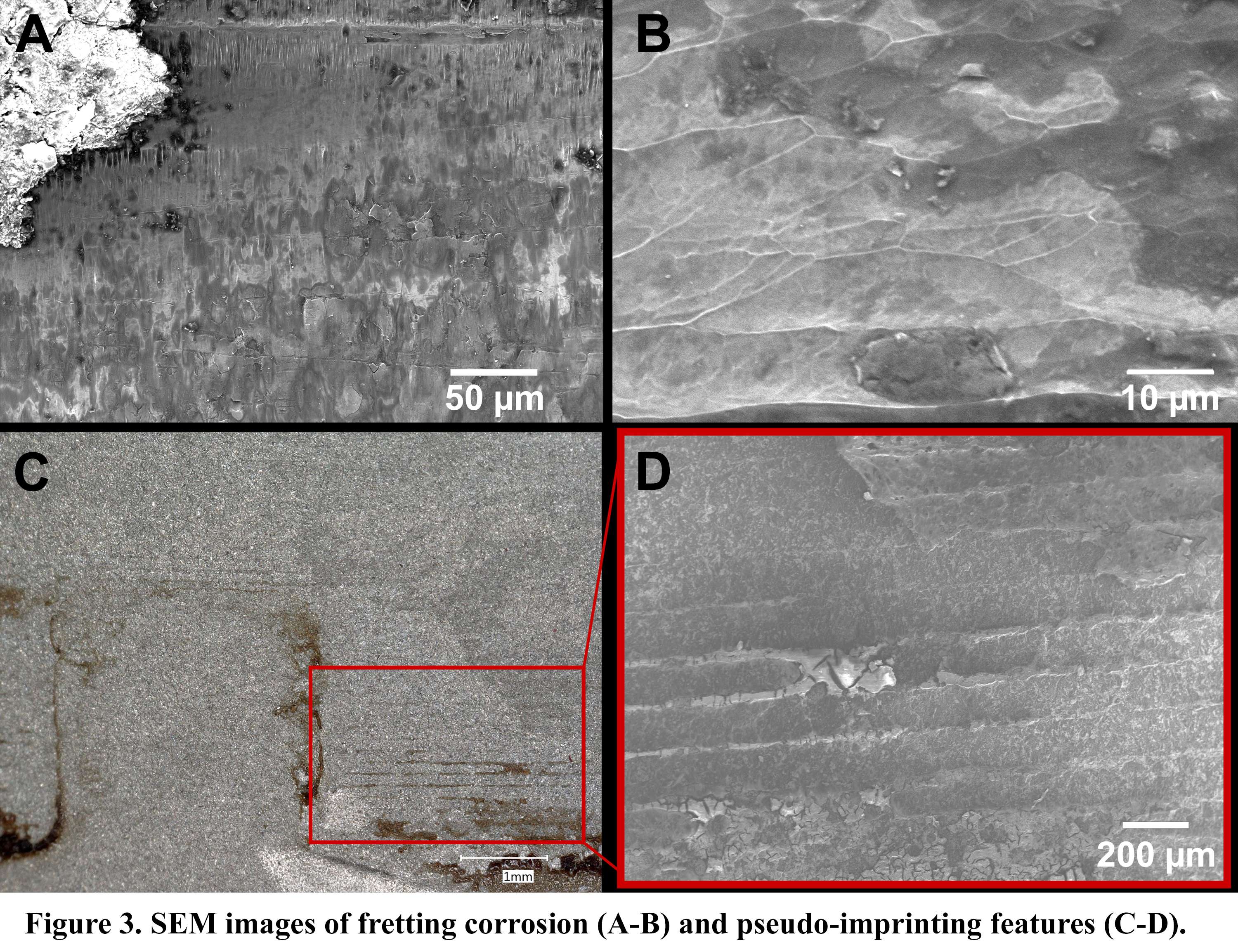
Figure 3#7715
In Vitro and in Vivo Corrosion Behavior of CoCrNiFeMo Alloy in Total Shoulder Arthroplasty
Daehan J. Yi - Rush University Medical Center - Chicago, USA
Alexander Hornung - Rush University Medical Center - Chicago, USA
Mozart Neto - Rush Medical Center - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Bianca Romay - Rush University Medical Center - Chicago, USA
Gregory Nicholson - Rush University Medical Center - Chicago, USA
Grant Garrigues - Rush University Medical Center - Chicago, USA
*Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: robin_pourzal@rush.edu
Introduction: The Aequalis Pressfit from Tornier has been one of the most common and successful implants in total shoulder arthroplasty (TSA). Unlike most of its peers, this device relied on a modular humeral head made from a wrought CoCrNiFeMo alloy instead of the more common wrought or cast CoCrMo alloy. In total hip arthroplasty (THA), CoCrMo alloy has been associated with implant failure due to adverse local tissue reactions in response to corrosion debris from the femoral head/neck junction. In TSA, there has been, so far, only little attention given to corrosion, but recently more reports have emerged. It was the purpose of this study to contrast the in vitro and in vivo corrosion behavior of CoCrNiFeMo alloy and its utility as a humeral head alloy.
Methods: 21 surgically retrieved Aequalis Pressfit humeral heads were studied. Modular taper corrosion was determined by means of an optical coordinate-measuring-machine (Redlux) and scanning electron microscopy (SEM). Three heads where sectioned longitudinally to determine alloy microstructure and to manufacture samples for potentio-dynamic polarization tests in simulated joint fluid (30g/L protein, pH 7.6, 37C). The corrosion potential (Ecorr), corrosion current density (icorr), and pitting potential (Epit) as derived from the potentio-dynamic curves, were determined. Additionally, three cast and wrought CoCrMo heads from contemporary devices were tested as well for reference.
Results: The microstructure of both wrought alloys was comparable and characterized by fine grains and microstructural banding (molybdenum segregations) visible at low magnifications (Figure 1). The cast alloy had a coarse grain size and exhibited large carbides. In vitro corrosion tests revealed that the CoCrNiFeMo alloy exhibited the highest Ecorr and Epit, and the lowest Icorr (Figure 2), thus indicating a superior corrosion behavior compared to both wrought and cast CoCrMo alloy. Retrieval analysis revealed that the taper surface of 13 out of 21 heads had measurable corrosion with an average material loss of 0.007mm3 (95% CI, -0.00067, 0.0147). Seven heads exhibited column damage, a severe form of chemically induced corrosion known from THA (Figure 3).
Discussion: In vitro,the CoCrNiFeMo of the Aequalis Pressfit humeral head exhibited a superior corrosion behavior compared to wrought and cast CoCrMo alloys from contemporary TSA implants. Specifically, the in vitro test revealed a lower corrosion tendency, lower corrosion rate, and better pitting behavior of CoCrNiFeMo. This can be explained by the addition of Ni to the alloy which is known to improve corrosion properties. Interestingly, the retrieval analysis revealed that there were several cases of in vivo corrosion. Furthermore, microstructural banding occurred in this alloy, known from CoCrMo femoral heads in THA, that can be a preferential corrosion site leading to column damage and elevated material loss. Thus, despite theoretical superior corrosion properties, this alloy can corrode in vivo, and even enable the release of Ni, which has been linked to metal hypersensitivity reactions. The results of this study suggest that preclinical corrosion testing methods as well as implant alloy metallurgy need to be improved to reduce the risk of corrosion and potential adverse reactions to metal debris.
Figures
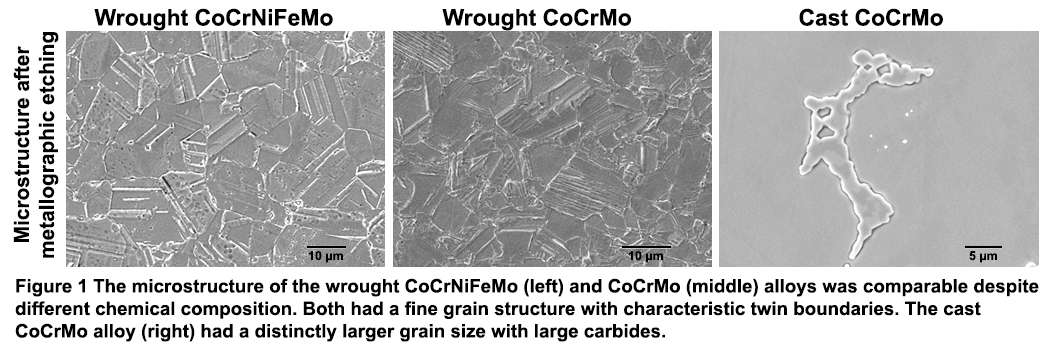
Figure 1
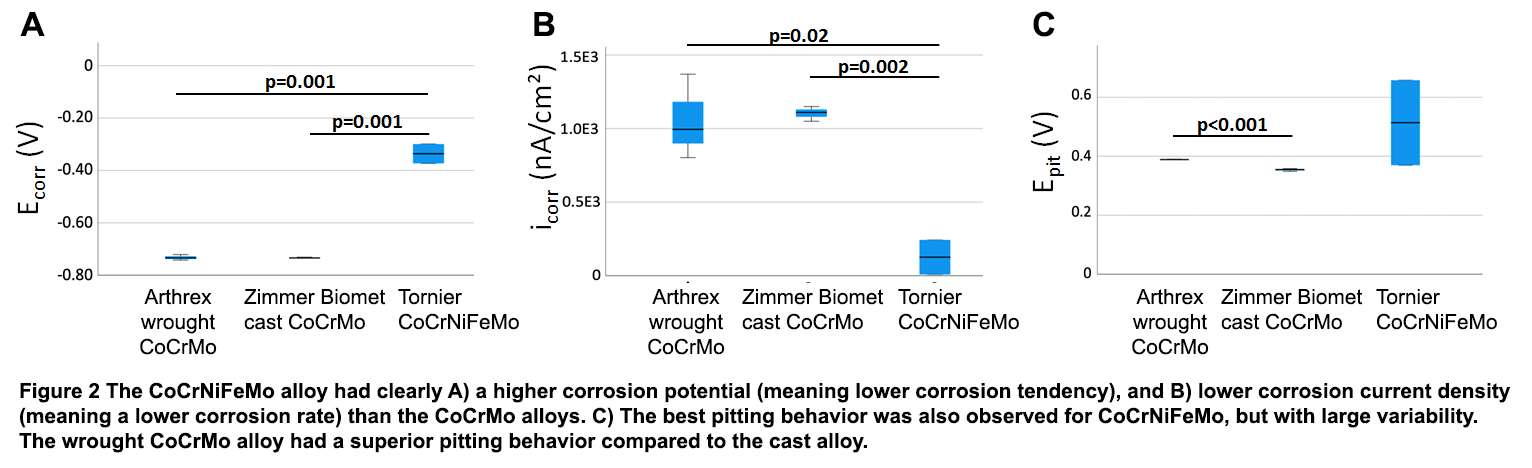
Figure 2
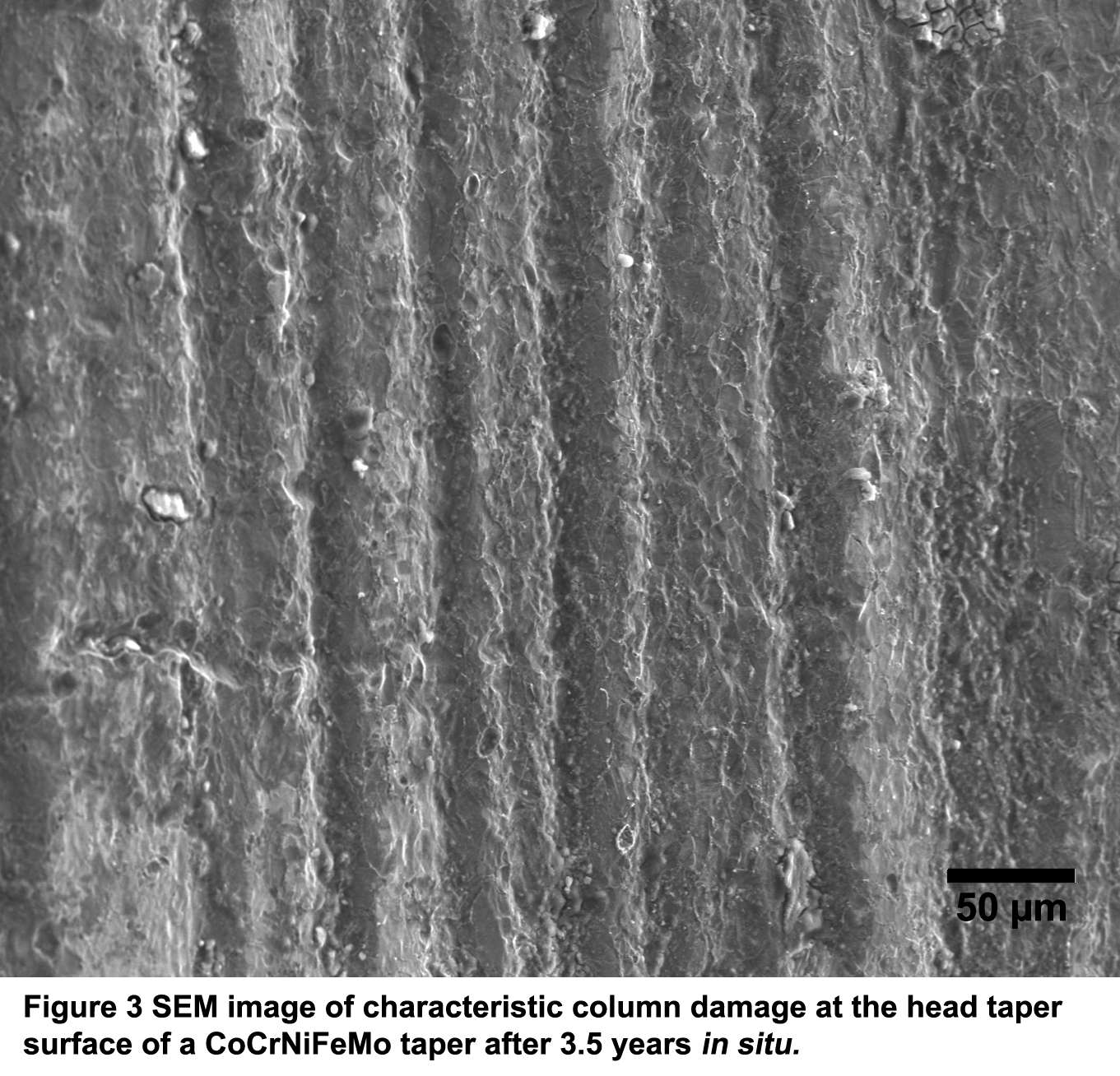
Figure 3#7537
Impingement in the Reverse Shoulder During Activities of Daily Living: The Effect of Humeral Neck-Shaft Angle on Glenosphere Lateralization and Size.
*Andrea Fattori - Lima Corporate - Villanova Di San Daniele del Friuli, Italy
Andreas Kontaxis - Hospital For Special Surgery - New York, USA
amirhossein jahandar - Hospital for Special Surgery - brooklyn, USA
Gabriele Vidoni - LimaCorporate SpA - Villanova di San Daniele del Friuli, Italy
Alessandro Castagna - Istituto Clinico Humanitas - Milano, Italy
Kevin J Setter - Upstate Orthopedics - Syracuse, USA
Michele Pressacco - LimaCorporate Spa - Villanova di San Daniele del Friuli, Italy
*Email: andrea.fattori@limacorporate.com
Introduction. The Reverse Shoulder Arthroplasty (RSA) was popularized by the Grammont design and is an effective treatment for rotator cuff deficient arthritic shoulders, but despite the popularity, there are still concerns about impingement and limited range of motion (ROM). Modern commercial RSA designs deviate from the original Grammont design by lateralizing the humerus either by lateralizing the glenoid center of rotation (COR) or by changing the neck-shaft angle (NSA). Even if there is plethora of literature on how lateralization is affecting ROM in planar motions (e.g. abduction), it is not well understood how the different methods of lateralization affect impingement during Activities of Daily Living (ADLs) and whether one parameter is more effective than others. The primary aim of this study was to evaluate how NSA can affect impingement during ADLs and whether glenosphere size and COR lateralization had the same effect on different NSA configurations.
Methods. Nine shoulder CT-scans subjects with no shoulder OA were used to build 3D-models. A reverse SMR implant (LimaCorporate, IT) was virtually implanted as per surgical technique in two NSA configurations (150° and 140°). The models were imported to an established shoulder computational model (Fig. 1) to investigate impingement during ADLs. The main design parameters considered for both NSA were: i) glenosphere diameter (Ø36mm, Ø40mm, Ø44mm) and ii) COR offset (standard, +5mm). The model calculated the percentage of intra-articular impingement (contact of the cup with scapula neck) and extra-articular impingement (contact of humerus with acromion and coracoid) during 5 ADLs (hand to opposite shoulder, hand to back of head, hand to mouth, drink from mug and place object to head height).
Results. The overall (intra + extra-articular) impingement, for each glenosphere and NSA, are shown in fig. 2. The results showed that the 140° NSA decreased intra-articular and increased extra-articular impingement across all glenosphere sizes. However, the 140° NSA decreased the overall impingement only for the 36mm size (16.8% vs 14.6% for 150° and 140° respectively). The use of a lateralized COR had a significant impact on reducing intra-articular impingement on both 140° and 150° NSA designs (Fig. 3). However, the impact was bigger for the 36mm glenosphere and especially benefited 150° NSA the most (10.1% and 7.0% reduction for 150° and 140° respectively). Lateralization did not affect significantly the extra-articular impingement.
Conclusions. The results suggest that, for the SMR Reverse, the 140° NSA and COR lateralization can decrease the risk of intra-articular impingement during ADLs, but all factors had a bigger impact on the 36mm glenosphere. The COR lateralization was more effective on the 150° NSA. However, the 140° NSA design also significantly increased the risk of extra-articular impingement which can limit ROM and increase risk of acromion fractures. This type of impingement is not very well understood and in this study the results of extra-articular impingement may have been affected by scapula kinematics that are derived from healthy cohort. Increased media-lateral rotation (often observed on RSA patients) may decrease the risk of extra-articular impingement in the 140° NSA designs.
Figures
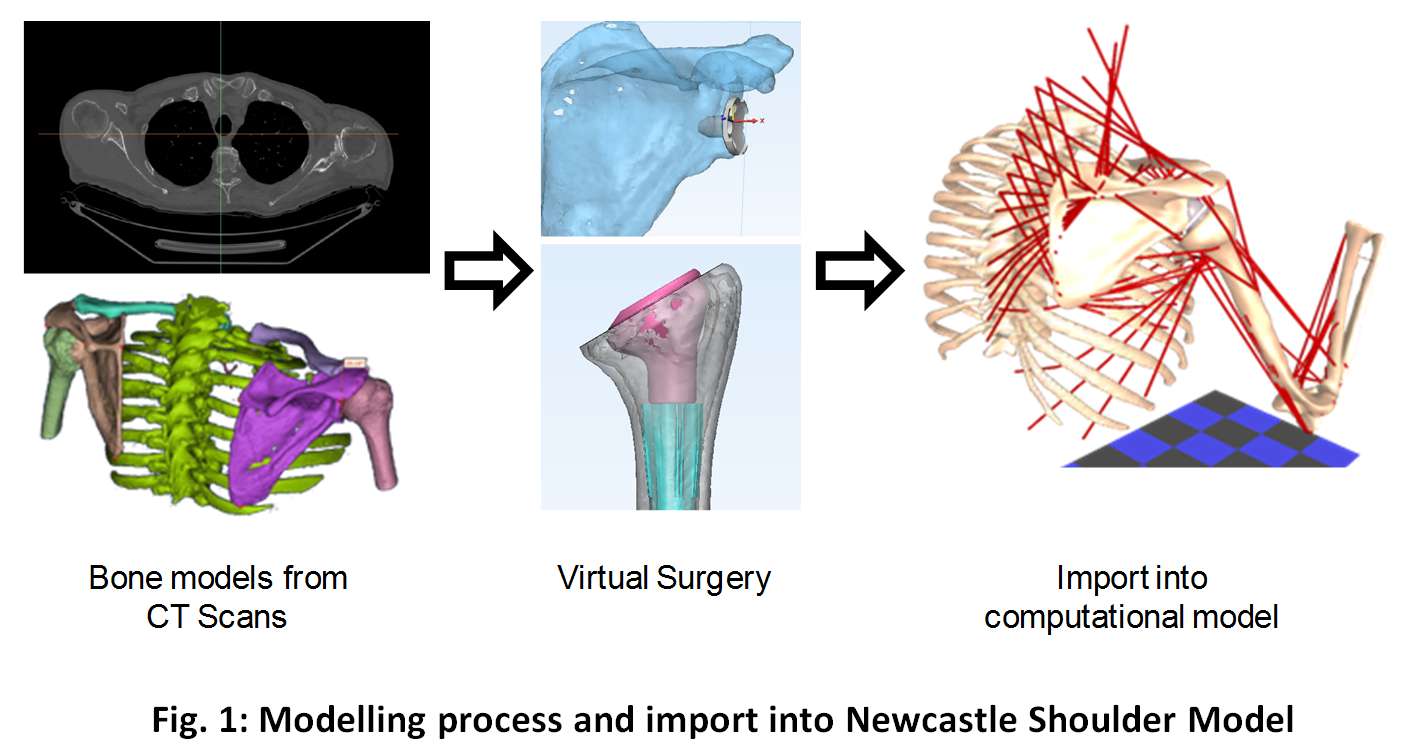
Figure 1
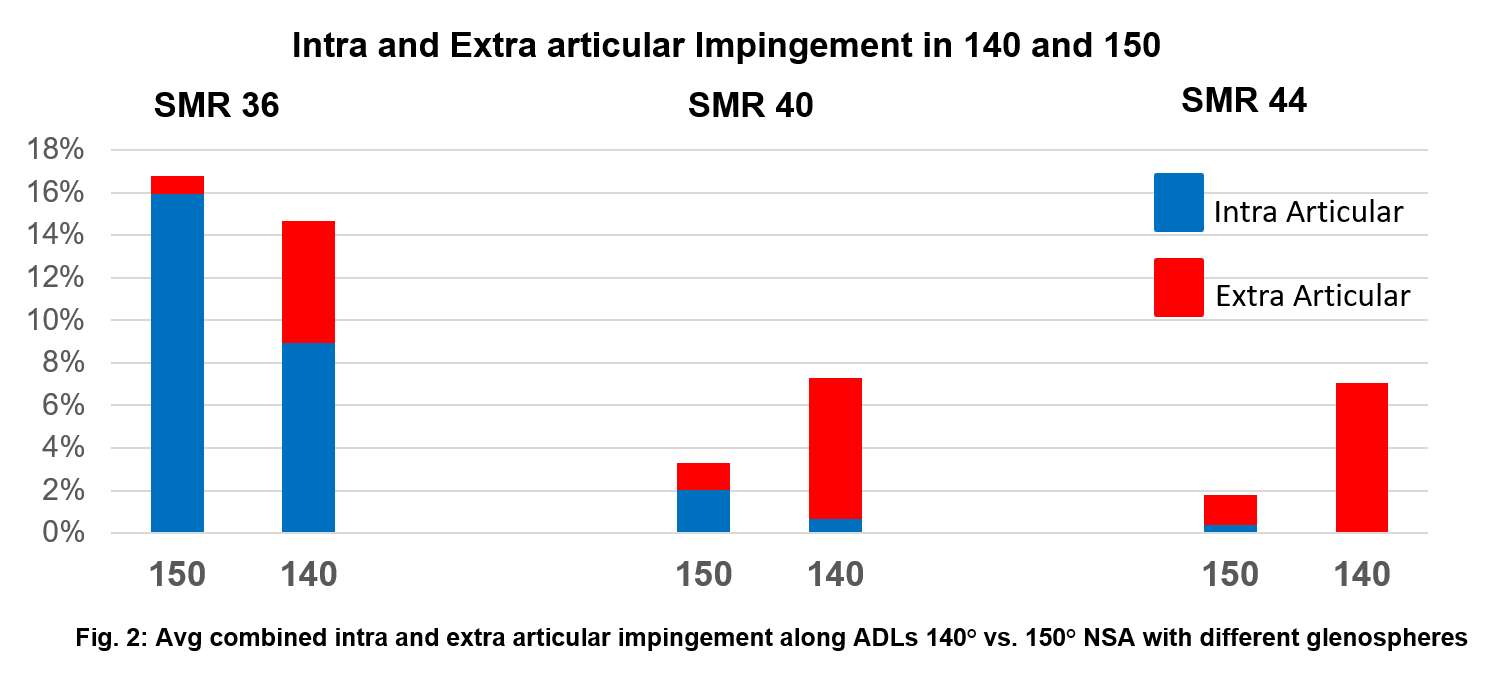
Figure 2
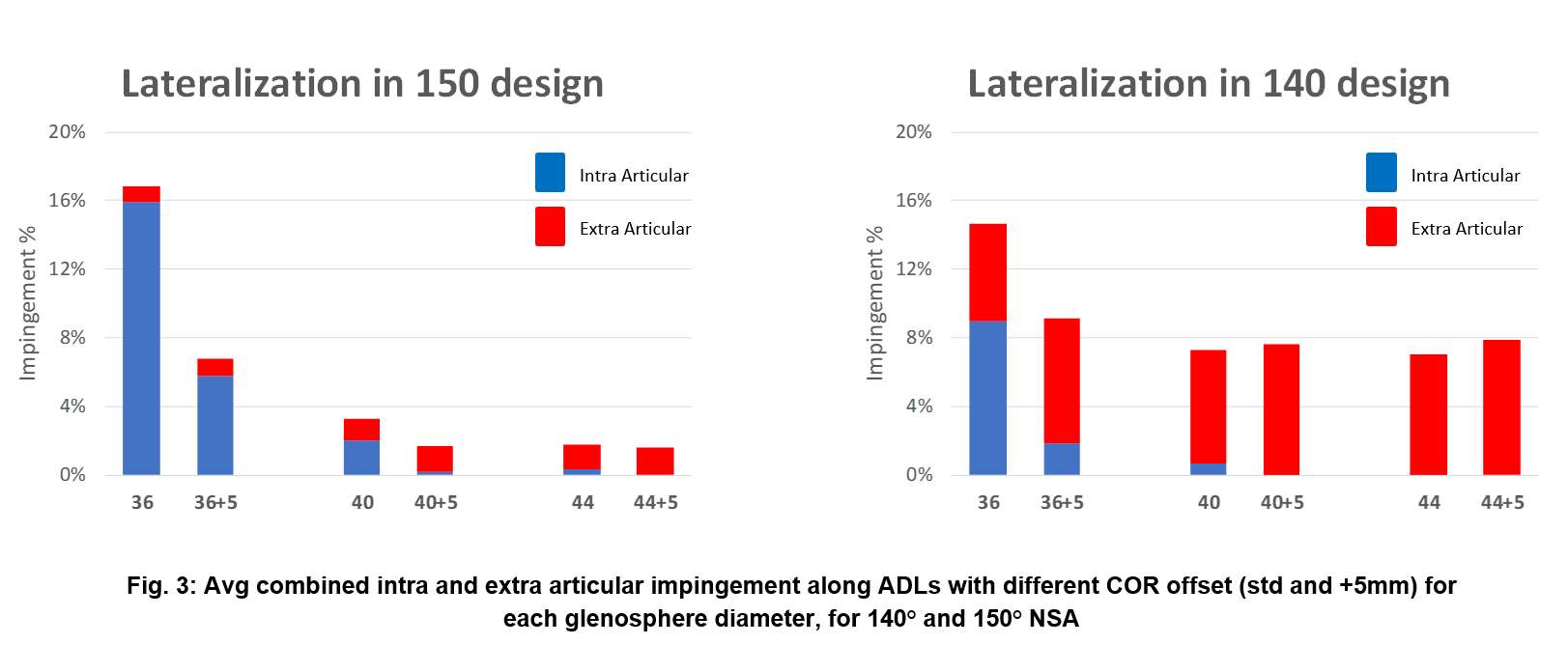
Figure 3#7571
A Computational, Contact-Based Algorithm for Evaluating Possible Positions of a Blade Stem Design
*Nathaniel Pyle - DJO Surgical - Austin, USA
Bryan Kirking - Enovis - Austin, USA
*Email: nathaniel.pyle@enovis.com
Introduction
Press-fit hip stem placement must satisfy anatomical requirements (e.g. leg length and joint tension) and stability requirements (e.g. 3-point contact between the implant and cortical bone). Final positioning is often discussed as an idealized condition, but there may be many acceptable positions. We developed a method to evaluate implant placement over a likely range of positions.
Methods
Three-dimensional cortical bone and implant CAD geometries were algorithmically positioned to recreate possible conventional surgery outcomes. Cortical inner-wall geometries were reconstructed from patient CT scans. The implant geometry was all sizes of a blade-stem style hip implant.
The frontal plane of the implant was aligned with the plane created by the femoral head center and the proximal canal axis. The initial superior-inferior location of the implant was then established by contacting the medial porous region of the implant onto the bone. The set of possible positions was created by perturbating implant position in all 6 degrees of freedom in discrete increments across a predefined range.
For each position of the implant in the bone, the quality of fit was scored. The distances between the medial porous, lateral porous, and distal surface regions and nearest cortical nodes were calculated; creating three distance metrics in each region: penetration, contact, and gap. Each metric was thresholded to eliminate obviously bad positions and weights were manually developed to calculate a position score. See Figure 1 for the region and equation details. Positive scores were labeled “successful implantations” and negative scores were labeled “failed implantations”.
Qualitative validation of the position method was attempted by comparing the simulation positioning to fluoroscopic images taken during implantation in cadavers. Digital 3D geometry of the cadavers was not available, so the cadaver bones were matched to existing scans using the Dorr ratio. The fluro image was then qualitatively compared to the highest scoring simulated position for the matched bone, out of many acceptable positions.
To assess the validity of the scoring algorithm, a commercially available implant was processed through a database of 47 digital patient bones. Based on feedback, the expected outcome was that the device would fit most bones while being challenged by small, champagne-fluted bones.
Results
In the positioning validation, the simulation successfully placed the implant in 9/12 femurs. Figure 2 shows one matched pair with positioning descriptions. In each, the medial curve shows gap at the resection plane and porous contact, the lateral region near the implant shoulder shows gap and the distal stem shows contact, biased laterally.
In the scoring validation, the simulation successfully placed the commercial device in 35/47 CAD bones. Figure 3 shows 7/12 implantation failures in small, champagne-fluted bones. Causes of the remaining 5 simulation implantation failures included distal potting, anterior bow, and neck angle.
Conclusion
We demonstrated a contact-based method sensitive to implant shape for evaluating designs. Qualitative assessment showed the simulation in agreement with cadaveric surgeries. Additionally, the method was sensitive to geometric challenges from small, champagne-fluted bones. Future applications could include patient-specific design, and preoperative positioning assessment.
Figures
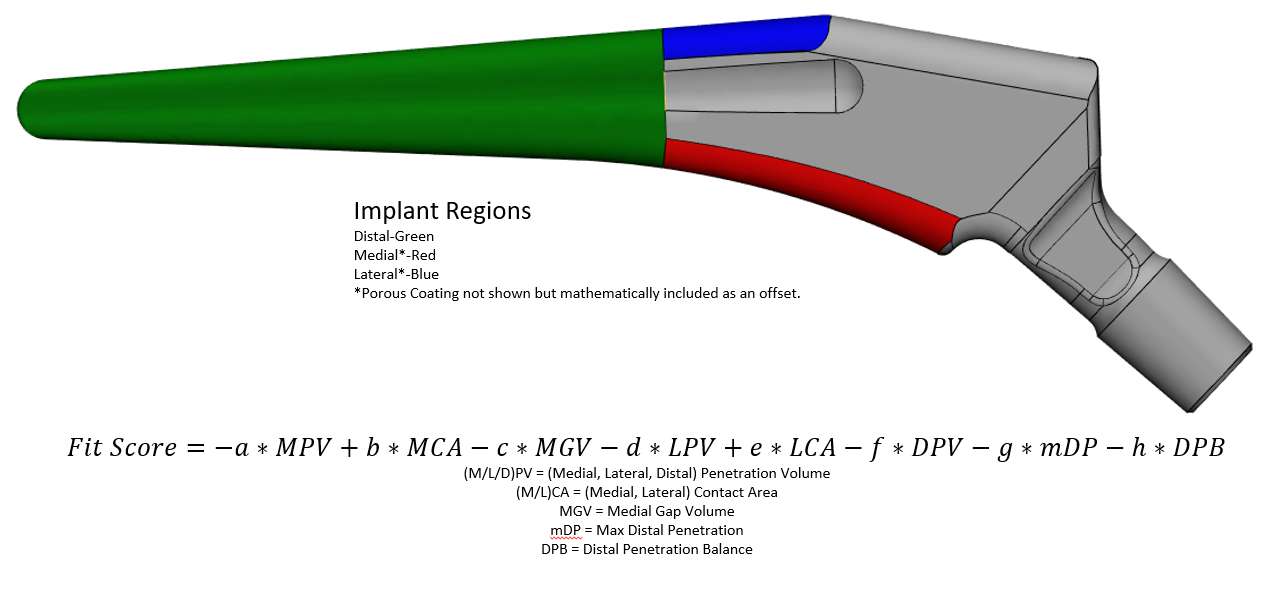
Figure 1
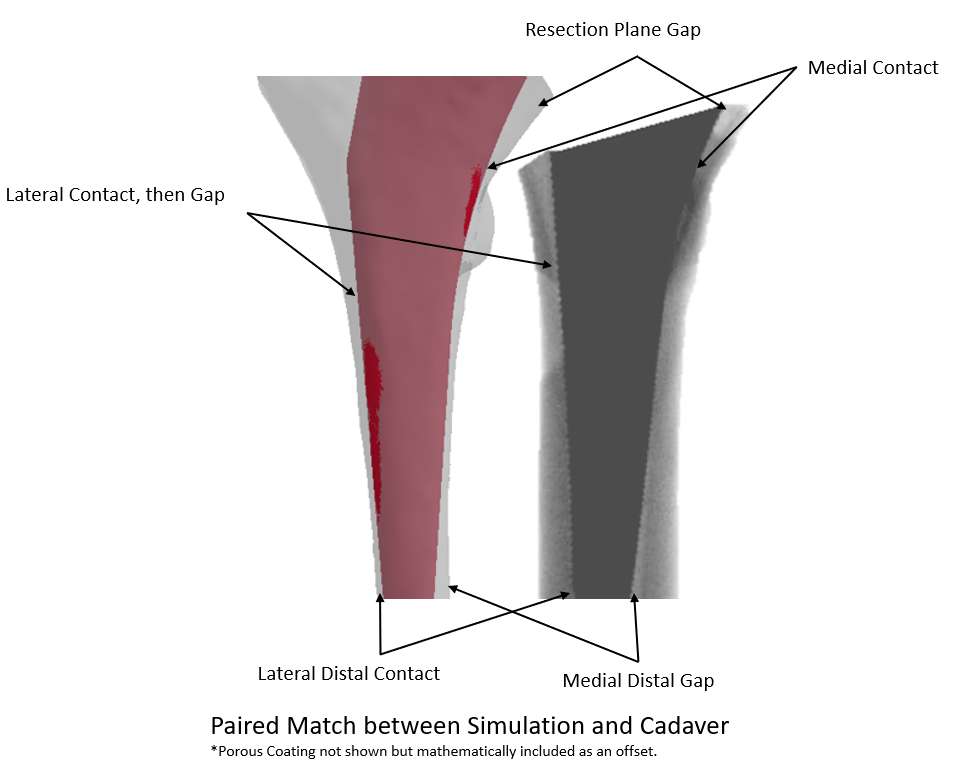
Figure 2
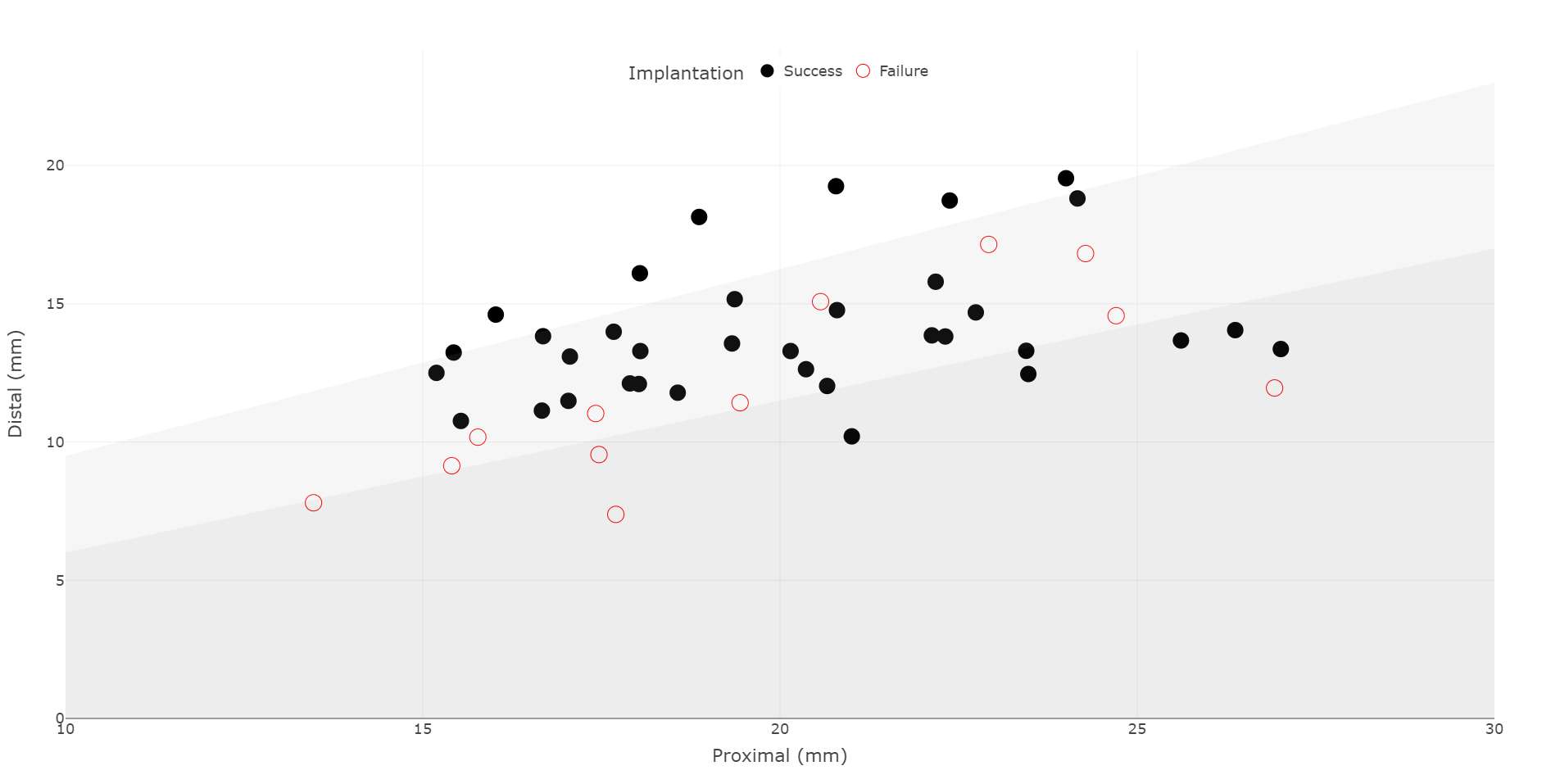
Figure 3#7575
Using a Virtual Surgery Method to Design Stem Boss Position and Offsets for a Revision Knee Implant
*Nathaniel Pyle - DJO Surgical - Austin, USA
Laura Small - DJO Surgical - Austin, USA
*Email: nathaniel.pyle@enovis.com
Introduction
The location of the femoral stem boss is critical to long-term fixation of press-fit revision knee femoral implants. The implant stem would ideally be collinear with the diaphyseal canal axis. For cemented stems, axial alignment is preferred but not necessary for the long-term success of the operation. The objective of this study was to check the current mediolateral (ML) and anterioposterior (AP) location of the stem boss on the femoral implant from the EMPOWR Revision™ Knee and identify the distribution of radial offsets required to achieve coincident axes.
Methods
This investigation was undertaken through virtual surgeries of patients’ femurs, without the tibia present. Utilizing digitized bones generated from a femoral statistical shape model (SSM), a surgical technique was scripted using Materialise 3-matic 14.0 to position femoral implants. Scans from 70 European patients (32 Female, 38 Male, 67.5±14.3 years old) were used to create the SSM. Femur size was identified using an algorithmic version of the femoral sizer instrument. Finally, a plane was created at the top of the femoral implant stem boss. The intersection of the intramedullary (IM) axis with this plane was located and the ML and AP distances between the stem boss center and the IM axis intersection point were calculated.
Results
The ML and AP offset data for each virtual surgery was plotted on the stem boss plane with the stem boss center as the origin. This common datum allows for the data to be considered as a distribution of offset distances. The data was plotted to scale overlaid on a size 8 femoral implant in Figure 1 to provide context for the scatter and location of the data points. Figure 2 shows the distributions of the AP and ML offsets, with the median of the distributions located 0.7mm posterior and 1mm medial from the center of the boss.
Looking at required stem offsets from the centered position, the radial offset of each datapoint was calculated to provide data for the cumulative histogram in Figure 3. The two horizontal lines are at the 50th percentile (2.3mm) and 95th percentile (4.5mm) occurrence points. Two radial offsets of 2.5mm and 5mm would encircle 57% and 97% of the 70 patients in this analysis, respectively.
Conclusion
The current position of the stem boss on the implant is 0.7mm posterior and 1mm medial from the median IM axis. Ideally, this distribution would be centered on the stem boss neutral position and the design was adjusted accordingly. Axial alignment of the stem boss to the intramedullary canal is optimal for appropriate distal femoral component positioning, alignment, and fixation in a revision knee system that is reliant on press-fit (splined) stems. However, when there are larger differences in these two points/axes, the ability for a system to incorporate offsets is necessary. The distribution of points around the stem boss center indicates that a mix of stem offsets between 1mm and 5mm would allow for axial coincidence for up to 97% of the 70 patients analyzed here.
Figures

Figure 1
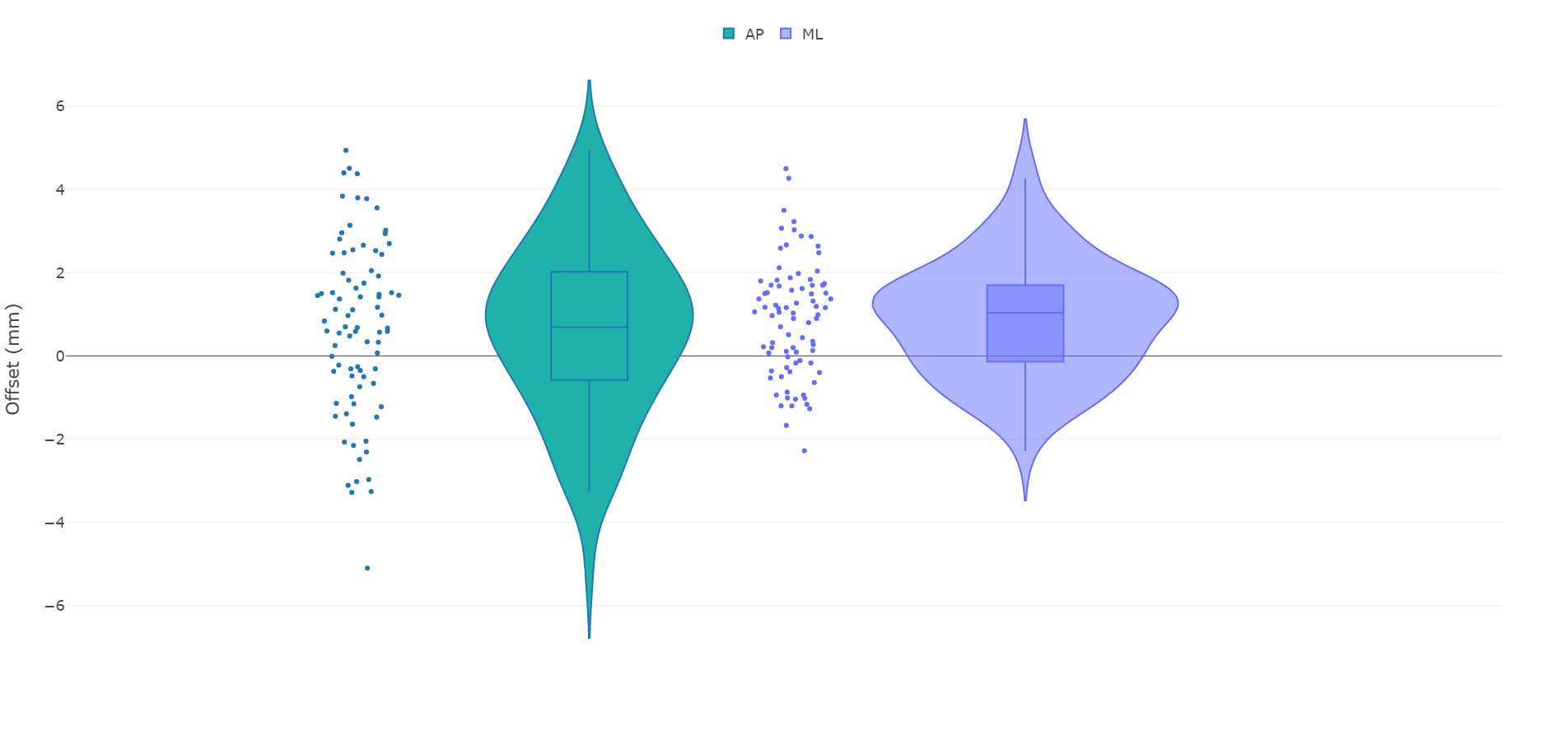
Figure 2
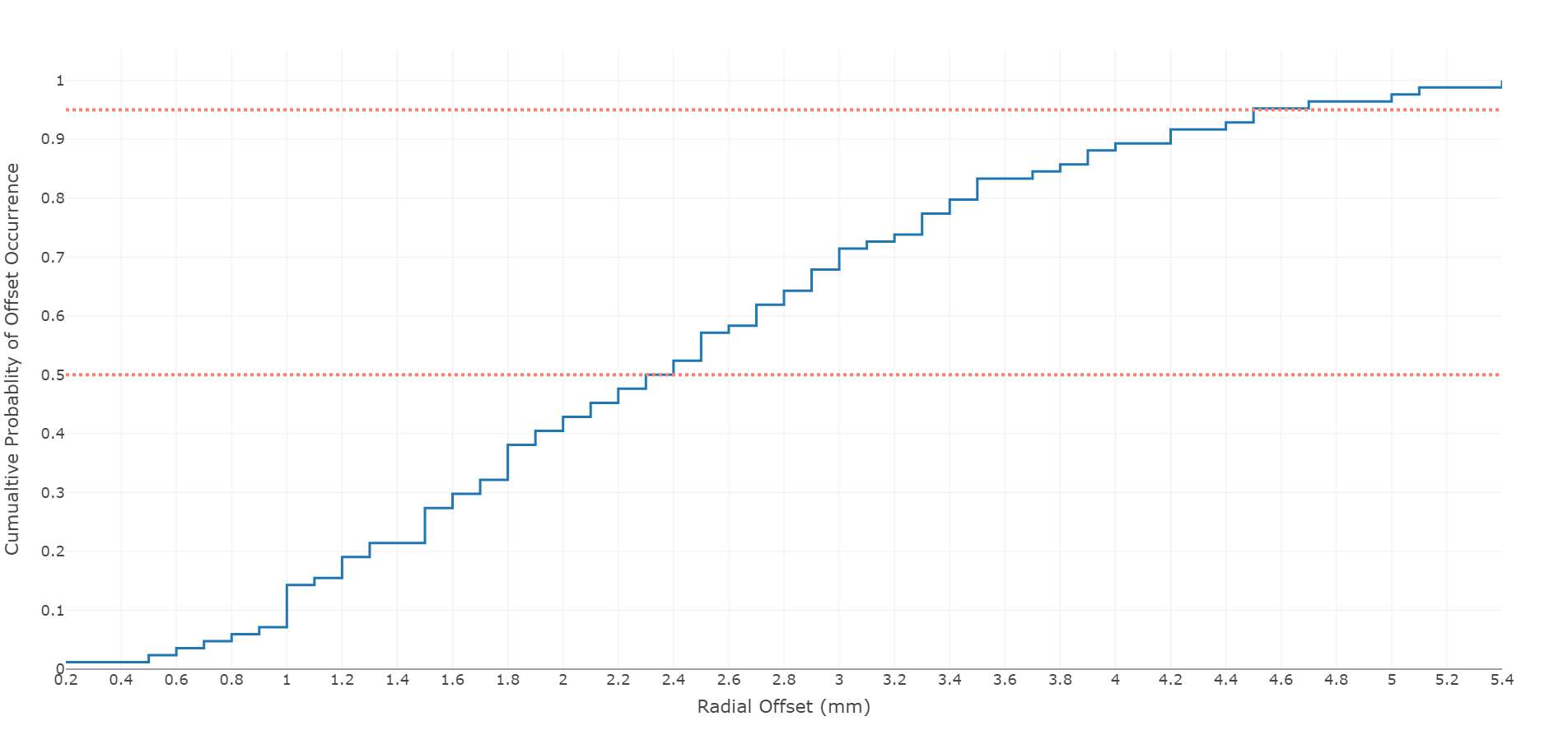
Figure 3#7647
Anterior Fixation Features Help Decrease Bone-Implant Micromotion in Cementless Tibial Baseplates for Total Knee Arthroplasty
*Fernando Quevedo Gonzalez - Hospital for Special Surgery - New York, USA
Joseph Lipman - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
Thomas Sculco - Hospital for Special Services - New York, USA
Ivan De Martino - Hospital for Special Surgery, New York, NY, USA - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
*Email: quevedogonzalezf@hss.edu
Introduction: Cementless fixation by bone ingrowth is increasingly popular in total knee arthroplasty (TKA), especially for younger and more active patients [1]. The design of the fixation features of cementless implants is crucial to ensure the low relative motion (micromotion) between the implant and the bone required for bone ingrowth [2]. We previously determined that the largest micromotion for cementless implants with a two-peg fixation design occurred at the anterior-lateral edge of the implant [3]. Therefore, we asked the question: can an anterior fixation feature help reduce the bone-implant micromotion of cementless implants compared to two pegs alone?
Methods: We performed computational finite element (FE) analyses using data from 13 female patients indicated for TKA due to end-stage osteoarthritis (age: 58-80 years, weight: 53-83 kg; height: 150-167 cm). From the preoperative CT-scans, we extracted the geometry and Hounsfield Units of the proximal tibia. We resected the tibiae 8mm from the lowest point of the lateral plateau, with 3 degrees of posterior slope. Each bone was implanted with the largest tibial baseplate possible, avoiding overhang. Two theoretical fixation designs were considered: 1) two pegs located posteriorly to the midline of the implant, and 2) two posterior pegs supplemented with an anterior spike. We considered materials to be linear, elastic, and isotropic. The bone was modeled as non-homogeneous, with an elastic modulus (E) derived from the Hounsfield Units using empirical relationships specific to the proximal tibia [4], and a constant Poisson’s ratio (v) of 0.3. The insert, baseplate, and fixation features were modeled as homogeneous ultrahigh molecular weight polyethylene (E=846 MPa, v=0.4), Ti6Al4V alloy (E=114.3 GPa, v=0.33), and Trabecular Titanium® (E=1.1 GPa, v=0.3), respectively. We assumed line-to-line contact between implant and bone, with a friction coefficient of 1.1. We considered the most critical loads for bone-implant micromotion from the demanding activity of stair ascent [3]. We calculated the peak micromotion and the amount of baseplate-bone interfacial area that fell below a restrictive threshold for bone ingrowth of 20 µm [2].
Results: For both fixation designs, the peak bone-implant micromotion occurred at the anterior-lateral edge of the implant (Fig.1). For the two-peg design, the peak micromotion ranged from 25 µm to 89 µm (Fig.2). With an anterior spike, the peak micromotion ranged from 24 µm to 78 µm, an average decrease of 8.5% (range: 0.9%-15.4%). For the two-peg design, 62%-98% of the baseplate had micromotions ≤20 µm (Fig.3). With an anterior spike, the baseplate surface area below the 20 µm threshold range was 70%-99% of the baseplate surface area, an average increase of 6% (range: 0.6%-13.7%).
Conclusion: Because the peak bone-implant micromotion during the most critical instant of stair ascent occurs anterior-laterally, an anteriorly placed fixation feature reduces the bone-implant micromotion and increase the interfacial area suitable for bone ingrowth for cementless TKA tibial components.
References: [1] AJRR 2020 Annual Report; [2] Jasty et al., 1997; [3] Quevedo González et al., J Orthop Res, 2018; [4] Morgan et al., J Biomech 2004
Figures
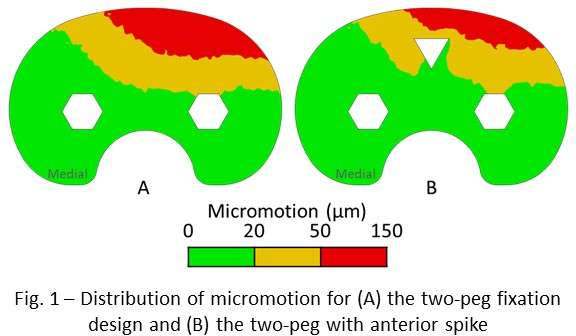
Figure 1
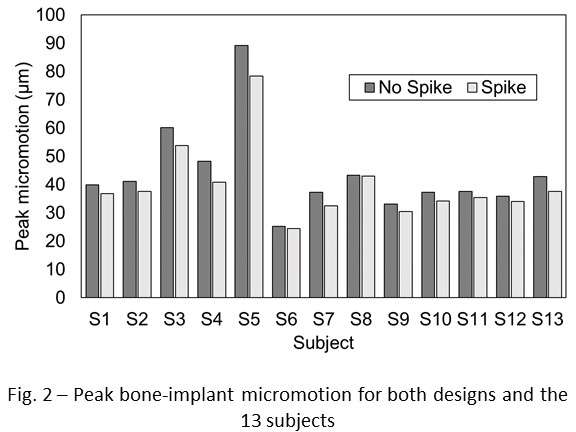
Figure 2
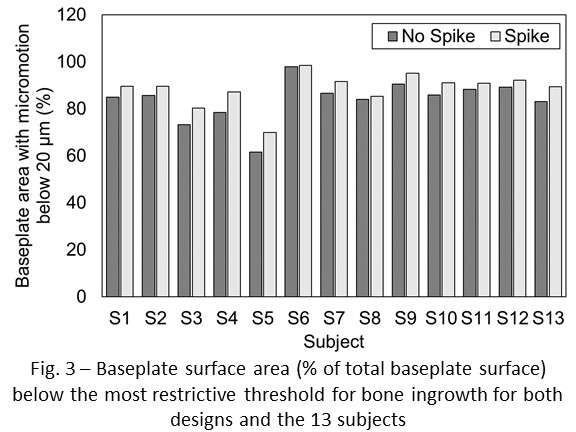
Figure 3#7928
Bone Quality and Cortical Thickness Impact the Risk of Periprosthetic Fracture Between Adjacent Stem Tips
*Fernando Quevedo Gonzalez - Hospital for Special Surgery - New York, USA
ELIZABETH DAVIS - Hospital for Special Surgery - NEW YORK, USA
Joseph Lipman - Hospital for Special Surgery - New York, USA
Timothy Wright - Hospital for Special Surgery - New York, USA
Mark P. Figgie - Hospital for Special Surgery - New York, USA
*Email: quevedogonzalezf@hss.edu
Introduction: In the case of concurrent ipsilateral total hip arthroplasty (THA) and total knee arthroplasty (TKA), the distance between adjacent stem tips is regarded as one of the most critical variables affecting the risk of periprosthetic fracture. However, little is known about the role of bone quality and cortical thickness on the risk of periprosthetic fracture between adjacent TKA and THA stems. Our goal was to quantify the effect of bone density and cortical thickness on the risk of periprosthetic fracture when THA and TKA stems are simultaneously present.
Methods: We developed two finite element (FE) models from the CT-scans of a 23-year-old male and an 80-year-old female, representative of the extreme cases of bone density and cortical thickness. The bones were virtually implanted with a 150 mm cementless fluted straight THA stem (Restoration Modular, Stryker, Mahwah, NJ) and a cemented revision TKA component (Triathlon TS, Stryker, Mahwah, NJ). The length of the stem for the TKA component was chosen to achieve an extreme distance between the tips of 20 mm (Fig. 1). The cement mantle for the TKA component filled the canal from 10 mm distal to the tip of the THA stem. All materials were considered linear, elastic, and isotropic. The implants and the cement were assigned elastic modulus (E) and Poisson’s ratio (v) of Ti6Al4V alloy (E=110 GPa, v=0.33) and polymethylmethacrylate (E=2.2 GPa, v=0.4), respectively. For the bone, E was derived from the CT Hounsfield Units, with empirical relationships specific to the femur [1], and we assumed v=0.3. We modeled line-to-line contact between the THA stem and the bone with a friction coefficient of 0.3 for the fluted region and 0.6 for the proximal ingrowth surface. We assumed perfect interdigitation between cement and bone (i.e., no relative displacement), and we considered cohesive contact between the TKA components and the cement [2]. We simulated the instant with the largest measured hip joint force during stair ascent, and we included the corresponding muscle forces for the abductor, ilio-tibial tract, fascia latae, and vastus lateralis and medialis [3]. The loads were adapted to each patient’s body weight. We evaluated the risk of bone failure by comparing the strains in the cortical bone between the tips of the two stems against the bone yield strain (0.65% in tension and 0.73% in compression) [4].
Results: The 24-year-old male had thicker cortices and stiffer bone than the 80-year-old female (Fig. 2). For both specimens, all cortical bone had strains below yield (Fig. 3). For the female specimen, 11% of the cortical bone between the stem tips had strains greater than 50% of the yield strain of bone. Conversely, the male specimen had only 1% of the inter-tip cortical bone with strains greater than 50% of yield.
Conclusion: Thinner and less dense cortex increase the risk of periprosthetic fracture between stem tips.
References: [1] Morgan et al., J Biomech 2003; [2] de Ruiter et al., J Exp Orthop, 2017 ; [3] Heller et al., J Biomech 2005; [4] Morgan et al., 2001
Figures
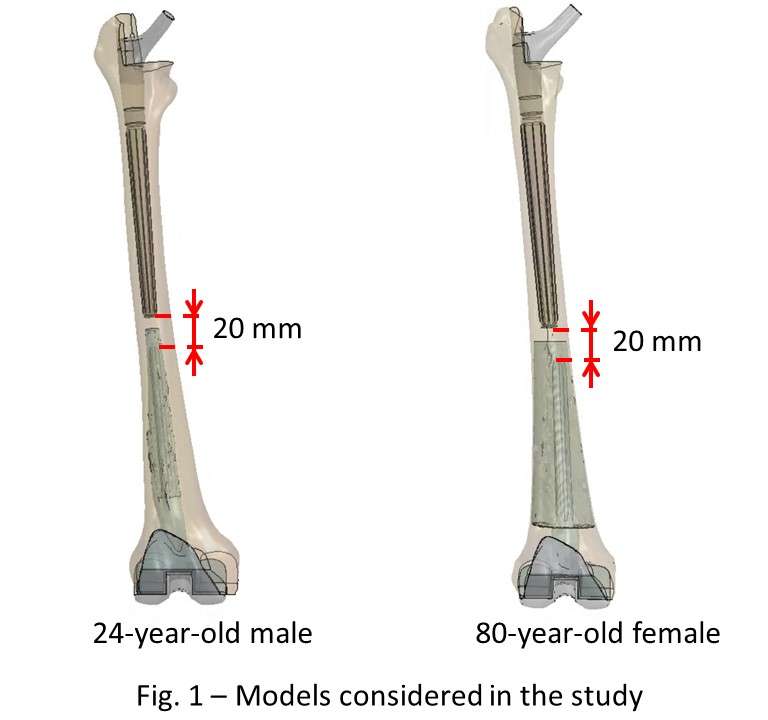
Figure 1
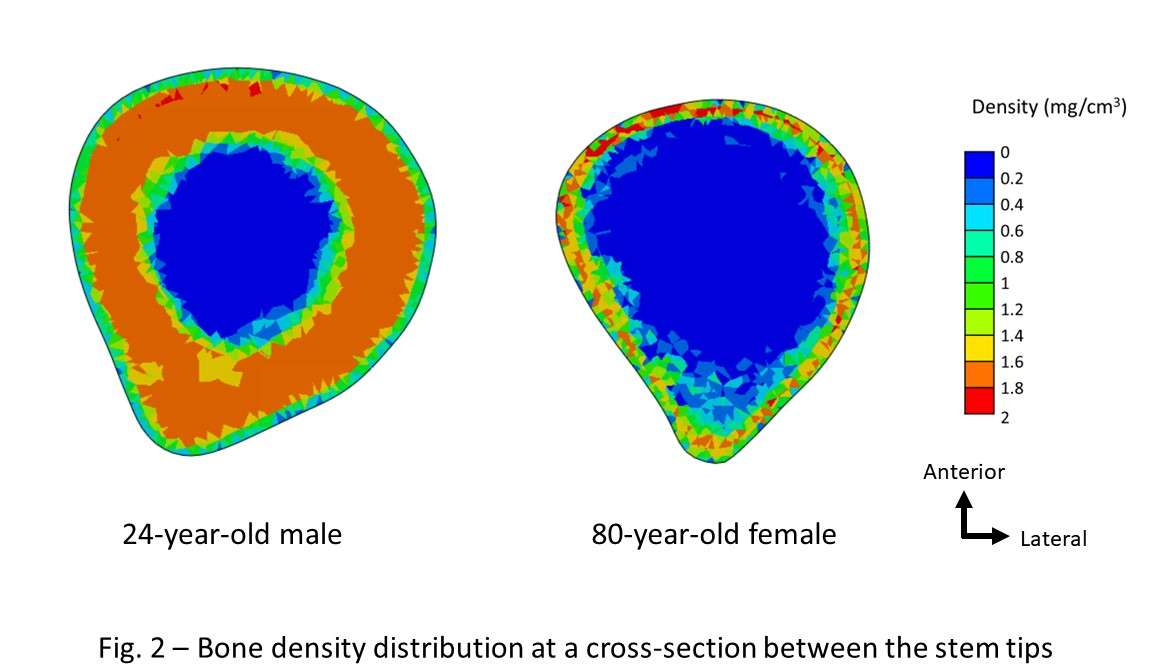
Figure 2
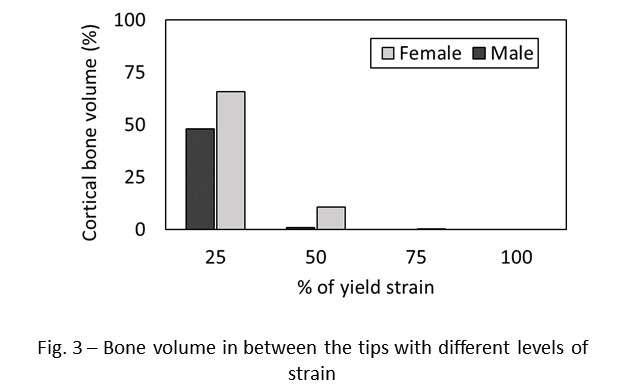
Figure 3#7290
Nonischemic Cardiomyopathy Associated With Elevated Serum Cobalt and Accelerated Wear of a Metal-on-Metal Hip Resurfacing
*Tahsin Rahman - Henry Ford Health System - Detroit, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Brian Darrith - Henry Ford Hospital - Detroit, USA
Songyun Liu - University of Illinois at Chicago - Chicago, USA
Joshua Jacobs - Rush University Medical Center - USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
Craig Silverton - Henry Ford Hospital - Detroit, USA
*Email: trahman1@hfhs.org
Introduction & Case: A 39-year-old male developed non-ischemic cardiomyopathy due to systemic cobalt toxicity associated with accelerated bearing surface wear from metal-on-metal hip resurfacing implanted 6 years prior. The patient initially presented with shortness and breath and went without a discrete diagnosis for his cardiac dysfunction for at least a year until serum cobalt levels were drawn and shown to be >140 ng/mL. At that time, the patient’s left ventricular ejection fraction was 30% and he required intravenous inotropes. Pre-operative radiographs and CT scan demonstrated acetabular component mal-positioning with 51 degrees of inclination and 48 degrees of anteversion. The patient was initially treated with acetylcysteine chelation therapy prior to orthopaedic surgical intervention. Intraoperatively, the patient was found to have significant metal debris with pseudocapsular reaction (Figure 1). Following revision arthroplasty to ceramic-on-ceramic total hip components, the patient regained baseline cardiac function and his serum cobalt levels normalized. The patient subsequently improved clinically and was able to return to most recreational activities while taking chronic oral inotropes at a year post-revision.
Methods: Both head and liner were measured with an optical coordinate-measuring machine (OrthoLux, RedLux) for 3D-reconstruction of the original bearing surface and computation of volumetric wear. Tissue analysis was performed on joint pseudocapsule and heart biopsy tissues. Tissue samples were assessed via light microscopy for histopathological analysis of H&E-stained sections, SEM analysis (JEOL, IT500HR-LV) with energy dispersive x-ray spectroscopy (EDS, Oxford Instruments) for localization of wear debris within tissue and chemical mapping and quantification of implant metals, and Fourier Transform Infrared spectroscopy (FTIR) for chemical analysis of periprosthetic and cardiac tissue.
Results: Wear features on head and liner were consistent with edge-loading (Figure 2). SEM analysis revealed multiple grooves and scratches, indicating the acting wear mechanism was abrasion. The total wear volume was 168.5 mm3 (head: 46.3 mm3, cup: 122.2 mm3) resulting in a wear rate of 24.4 mm3/year (head: 6.7 mm3/year, cup: 17.7 mm3/year).
The joint pseudocapsule tissue was dominated by a marked macrophage response, with only mild to moderate perivascular infiltrate of lymphocytes and plasma cells. The SEM/EDS analysis of the pseudocapsule revealed large, mostly extracellular CoCrMo particles ranging in size from 1 to 7 µm. Intra-cellularly, mostly chromium phosphate was observed. FTIR univariate imaging of cardiac tissue demonstrated interstitial fibrosis and glycogen deposition , which are hallmarks of cardiomyopathy pathology. Surprisingly, CoCrMo particles ranging in size from 0.16 - 15.9 micrometers were found within the heart tissue (Figure 3). 18 particles were found within 2 sections of the same biopsy sample.
Conclusion: Cobalt-induced cardiomyopathy is a grave condition that deserves early consideration due to potentially irreversible morbidity. Patients with mal-positioned and edge-loaded metal-on-metal components are likely at increased risk for developing this complication. The current study suggests the problem may be further exacerbated by the hematogenous spread of large metallic debris to the heart with subsequent local cobalt ion leeching. We present this case to increase awareness, facilitate early detection and emphasize the need for research into the diagnosis and management of at-risk patients.
Figures
Figure 1
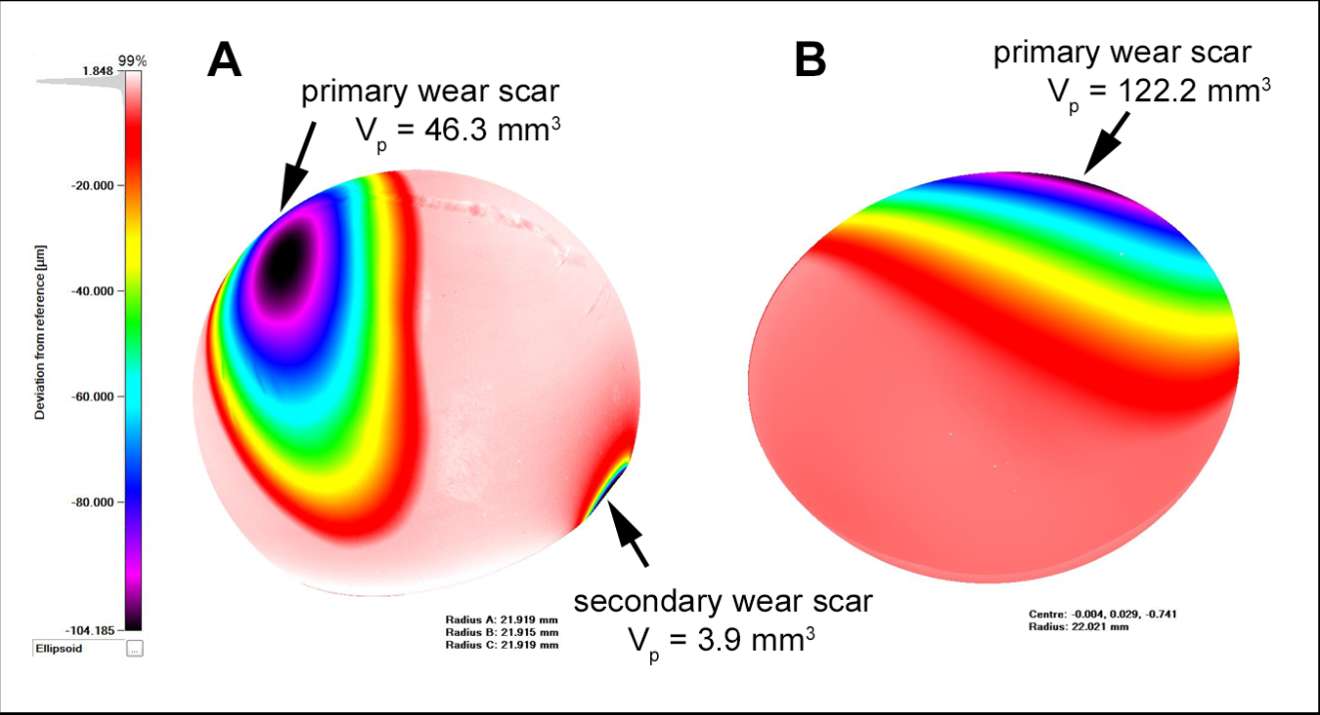
Figure 2
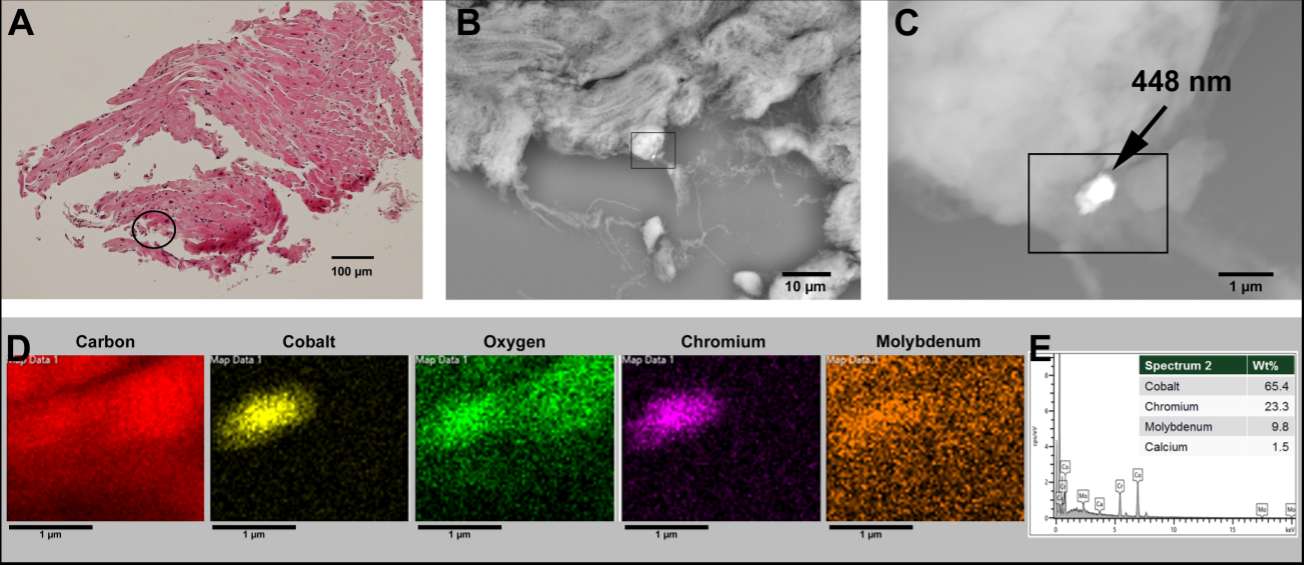
Figure 3#7396
Predictive Factors in Sub-Acutely Achieving KOOS, JR MCID in Patients Undergoing Total Knee Arthroplasty: A Retrospective, Database Study
*Tahsin Rahman - Henry Ford Health System - Detroit, USA
Logan Hansen - Henry Ford Health - Detroit, USA
Mary Hennekes - Henry Ford Health - Detroit, USA
Kevin Lindsay-Rivera - Henry Ford Health - Detroit, USA
Erickson Andrews - Henry Ford Health system - Detroit, USA
Craig Silverton - Henry Ford Hospital - Detroit, USA
*Email: trahman1@hfhs.org
Introduction: The purpose of this study was to identify predictive variables for patients achieving a minimal clinically important difference (MCID) in KOOS-JR scoring after TKA.
Methods: A retrospective cohort study was conducted on 2,905 TKA cases between 2014-2020 at a single multi-center hospital system that had KOOS, JR scores collected pre- and between 1-2 months post-operatively. Patient data was collected by means of inquiry to the Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI). Data points requested include demographics, length of stay, same day discharge, disposition status, medical history, social history, types of perioperative anesthesia, postoperative opioids prescribed in morphine milligram equivalents, and KOOS-JR scores pre- and post-operatively. Based on recent literature, a threshold of 14 was used to define KOOS-JR MCID.
Results: Univariate analysis was initially used to determine potentially significant predictors for achieving KOOS, JR MCID. Significant predictive variables (p < 0.05) included ASA Score (I: 55%, II: 60%, III: 67.2%, IV: 71.8%), history of DVT (No: 65.3%, Yes: 56.8%), spinal anesthesia (No: 66.2%, Yes: 61.8%), regional block (no: 50.7%, yes: 65.4%), local anesthesia (no: 69.7%, yes: 62.1%), postoperative MME prescribed (362.3 ± 202.7 +MCID, 385.6 ± 188.5 -MCID), and preoperative KOOS, JR score (42.48 ± 11.89 +MCID, 53.51 ± 11.11 -MCID). Upon multivariate regression controlling for age, BMI, and surgeon, only preoperative KOOS, JR was found to be significant with a negative, linear relationship (p < 0.001).
Conclusions: Patients with greater impairment from knee osteoarthritis as determined by preoperative KOOS, JR are more likely to sub-acutely, clinically improve following TKA. Regional and local anesthesia may improve patient reported outcomes while spinal anesthesia may limit clinical improvement. Greater comorbid burden may also significantly increase rates of clinical improvement following TKA.
#7397
The Impact of Preoperative Joints Education Classes on Outcomes and Complications Following Total Knee Arthroplasty: A Retrospective, Database Study
*Tahsin Rahman - Henry Ford Health System - Detroit, USA
Madison Mervis - Wayne State University School of Medicine - Detroit, USA
Logan Hansen - Henry Ford Health - Detroit, USA
Brian Darrith - Henry Ford Hospital - Detroit, USA
Jonathan Shaw - Henry Ford Health System - Detroit, USA
Kevin Lindsay-Rivera - Henry Ford Health - Detroit, USA
Erickson Andrews - Henry Ford Health system - Detroit, USA
Craig Silverton - Henry Ford Hospital - Detroit, USA
*Email: trahman1@hfhs.org
Introduction: The purpose of this study was to investigate the impact of preoperative joints education classes on outcomes and complications following total knee arthroplasty (TKA).
Methods: A retrospective cohort study was conducted on 9,630 consecutive TKA cases between 2014-2021 at a single multi-center hospital system. Patient data abstraction was done by means of inquiry to the Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI). Data points requested include attendance of a joint’s education class, demographics, perioperative course and KOOS, JR scores, and incidence of complications (death, DVT, PE, dislocation, fracture, hardware failure, prosthetic joint infection (PJI), any purpose ED visit, and hospital readmission) within 3 months of surgery. Univariate and subsequent multivariate analyses was conducted between patient groups.
Results: Univariate analyses showed that patients with preoperative joints education had lower incidence of same day discharge (24.8% vs 40.0%), lower incidence of pulmonary incidence (0.4% vs 0.8%), shorter average length of stay (1.94 ± 1.44 days vs 2.04 ± 1.65 days), lower postoperative KOOS, JR change (20.80 ± 17.86 vs 23.40 ± 17.62), and greater postoperative prescribed morphine milligram equivalents (MME) (396.26 ± 221.12 vs 336.69 ± 204.50). Upon subsequent multivariate analysis, patients with joints education were significantly correlated to lower incidence same day discharge and pulmonary embolism, shorter postoperative length of stay, lower postoperative KOOS, JR change, and greater postoperative prescribed MME. Joints education did not significantly impact other complications, including rate of dislocation, fracture, and PJI.
Conclusions: Despite significant statistical findings, preoperative joints education has questionable clinically relevant impact on outcomes and particularly does not significantly impact rates of subacute dislocation, fracture, and PJI.
#7417
A Dose Dependent Relationship Between Intraoperatively Administered Opioids and Postoperative Opioid Refill Requests After Total Joint Arthroplasty
*Tahsin Rahman - Henry Ford Health System - Detroit, USA
Logan Hansen - Henry Ford Health - Detroit, USA
Nicholas Blackmond - Henry Ford Health System - Detroit, USA
Mary Hennekes - Henry Ford Health - Detroit, USA
Craig Silverton - Henry Ford Hospital - Detroit, USA
*Email: trahman1@hfhs.org
Introduction: The purpose of the study is to determine the impact of perioperative opioid administration on postoperative opioid prescription.
Methods: A retrospective review was conducted on 547 total hip (THA) and 453 total knee (TKA) cases conducted between January 2000 and December 2021 at a single, multi-center hospital system. Data was abstracted via review of patient electronic medical records. Demographics, medical history, operative details, opioid use history, intraoperative and recovery opioid administration, and postoperative opioid prescription data was collected. Opioid refill information was corroborated using the statewide opioid tracking system. Opioid dosages were converted to total morphine milligram equivalents (MME) intraoperatively, postoperatively in recovery/hospital, and at discharge.
Results: Student’s t-tests and chi-square analyses were used to compare patients who did and did not request an opioid refill. Intraoperative, recovery/in hospital, and discharge MMEs were not significantly different between binary refill groups (p > 0.05). Incidence of preoperative opioid use and TKA (versus THA) was greater in the opioid refill group.
ANOVA analysis was then used to compare discrete refill count groups (i.e., 1 refill, 2 refills, 3 refills…27 refills) and showed a significant difference in intraoperative and recovery/in hospital MMEs between groups (p < 0.002). Subsequent multivariate linear regression of the various phase of care MMEs while controlling for operative joint (hip or knee) and history of preoperative opioid use showed a significantly positive correlation with TKA, preoperative opioid use, and intraoperative opioid MME (p < 0.001).
Conclusions: While greater intraoperative opioid administration did not differ between patients with and without opioid refill requests, there may be a dose dependent relationship between intraoperative opioids and postoperative opioid refill counts that necessitates greater awareness by the surgical team.
#7774
Validation of a Novel Host Response Assay, SynvIchor, for Discriminating Infectious and Non-Infectious Joint Pain
*Antony Rapisarda - OrthoDx - Sydney, Australia
Robert Johnston - OrthoDx - Sydney, Australia
Kevin Tetsworth - Royal Brisbane and Women's Hospital - Herston, Australia
Andrew Kurmis - Modbury Hospital - Modbury, Australia
Jeffrey Lipman - Royal Brisbane and Womens Hospital and The University of Queenslan - Herston, Australia
William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
Matthew Hartley - Hartley Hip and Knee - Mudgeeraba, Australia
*Email: antony.rapisarda@orthodx.com.au
Background: Acutely swollen or painful joints are common with Australian data suggesting over 300,000 such presentations to Emergency Departments (EDs) and general practices each year. Septic arthritis can be a challenging but crucial diagnosis – inaccuracies are often associated with lengthy/costly delays to definitive treatment as well as substantial potentially-avoidable patient morbidity. Despite international ‘guidelines’, there exists no current gold standard test for septic arthritis. While useful in the contemporary context, microscopy and culture from invasive joint aspirates are both slow (often taking days for the ‘final’ result) and have a high level of diagnostic uncertainty. Poor inherent pretest probability also makes such testing prone to high false negative rates – patients often languish in EDs or are unnecessarily admitted to wards awaiting such results. Both pathways are cost/resource intensive. A patient-specific genomic diagnostic assay to distinguish between infectious and non-infectious joint pain with high sensitivity and specificity would have tremendous clinical utility, while aiding patient-flow through busy EDs by returning a prompt, actionable, result.
Objectives: To evaluate the diagnostic performance of a molecular host response assay, designed to distinguish between infectious and non-infectious causes of joint pain in both native and prosthetic joints.
Methods: The study employed a retrospective, observational, noninterventional design, and recruited a heterogeneous cohort of adult patients in various clinical settings from seven sites across Australia (n =84). The performance of the molecular host response assay was compared with retrospective physician diagnosis by a panel of three experts and culture results where available.
Results: In receiver operating characteristic curve (ROC) analysis, the molecular host response assay had an estimated area under the curve of 0.94 for discriminating joint infection from sterile arthropathy. The relative likelihood of non-infectious joint inflammation vs infectious joint inflammation was optimised for high Negative Predictive Value (NPV). Our results indicate an NPV of greater than 95% when targeting non-infectious joint inflammation.
Conclusions: This novel molecular host response assay appears to be a promising diagnostic tool for patients presenting with joint pain or swelling - complementing clinical acumen and existing methods – increasing the possibility of safe patient discharge from the ED with non-infectious joint inflammation.
#7831
Innovative Single Use Instrumentation for Performing Balanced Gap Resection in Total Knee Arthroplasty
*Gary Rasmussen - The Orthopedic Specialty Clinic - Murray, USA
*Email: glrasmussen@msn.com
Total Knee Arthroplasty (TKA) has become a very successful joint reconstructive procedure. However, a significant percentage of patients are not satisfied with their replaced knee. Of those unsatisfied patients, most of them complain of instability and lack of confidence in their knee with high demand activities. Many of these patients who are healthy and active are having their TKAs performed in an Ambulatory Surgical Center which adds an additional challenge to achieve the best patient outcome in the most efficient way. To address these problems, the author has invented and developed innovative novel unique single use instruments for performing balanced gap resection in TKA. These instruments are embodiments within the Intellectual Property of over 40 United States and International Patents and/or Patents Pending. The procedure and instruments consist of: 1- Making a proximal tibial resection. 2- Placing a Tibial Baseplate. 3- Placing a central tensioning device with the knee in flexion. 4- Shimming the medial and lateral joint with asymmetric shim spacer blocks. 4- Attaching a gap resection block to guide the posterior femoral condyle resections. 5- Extending the knee and re-shimming the joint. 6- Attaching the same gap resection block to guide the distal femoral condyle resections and ensure the gaps are equal when the ligaments are balanced. The instrumentation and technique is open platform at this point in the procedure. The procedure becomes implant specific when the femoral chamfer cuts are made. The author has presented patient outcome results at previuos ISTA Meetings as the instrumentation and technique has evolved. In the most recent study was titled: The Effect of Greater External Rotation of the Femoral Component as a Result of Gap Ligament Balancing on Patellar Tracking, Flexion Stability and Function of Different TKA Implant Designs. The results, discussion and conclusions were: -External rotation values are higher on average, when ligament tensioning/balancing is employed with this novel Gap Balancing Instrumentation System. -In this study this resulted in consistent matching of the Flexion Gap to the Extension Gap and better Patellar Alignment. -In a comparison outcome study using this same Gap Balancing Instrumentation to implant different knee designs, a “Single Radius” femur design with medial constraint had a higher arthrofibrosis/Manipulation Under Anesthesia (MUA) rate (6% vs 1%) than a “Single Radius” femur design with less medial constraint. -Also, preliminary results with knees that have a changing radius, “J-Curve” or “Hybrid Curve”, femur show that better balance may be achieved if the Flexion Gap is cut 1mm greater than the Extension Gap. -These findings suggest that limiting the surgeon to discrete rotation values may be at odds with where the femur “desires” to be, given soft tissue considerations for each individual patient. These instruments and the technique for using them meet the goals of better patient outcomes, simplicity in use, and reproducibility while eliminating the inefficiency costs and time associated with reprocessing.
Figures
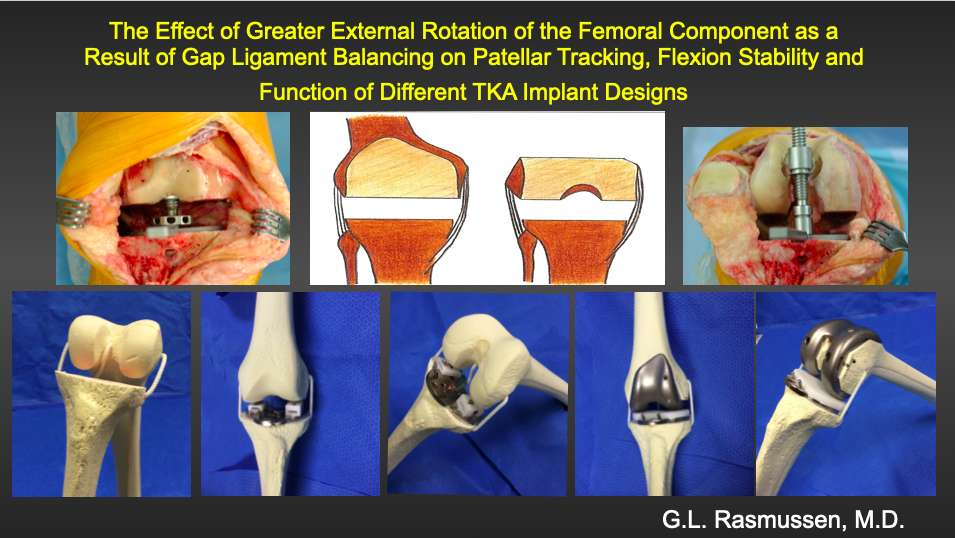
Figure 1

Figure 2
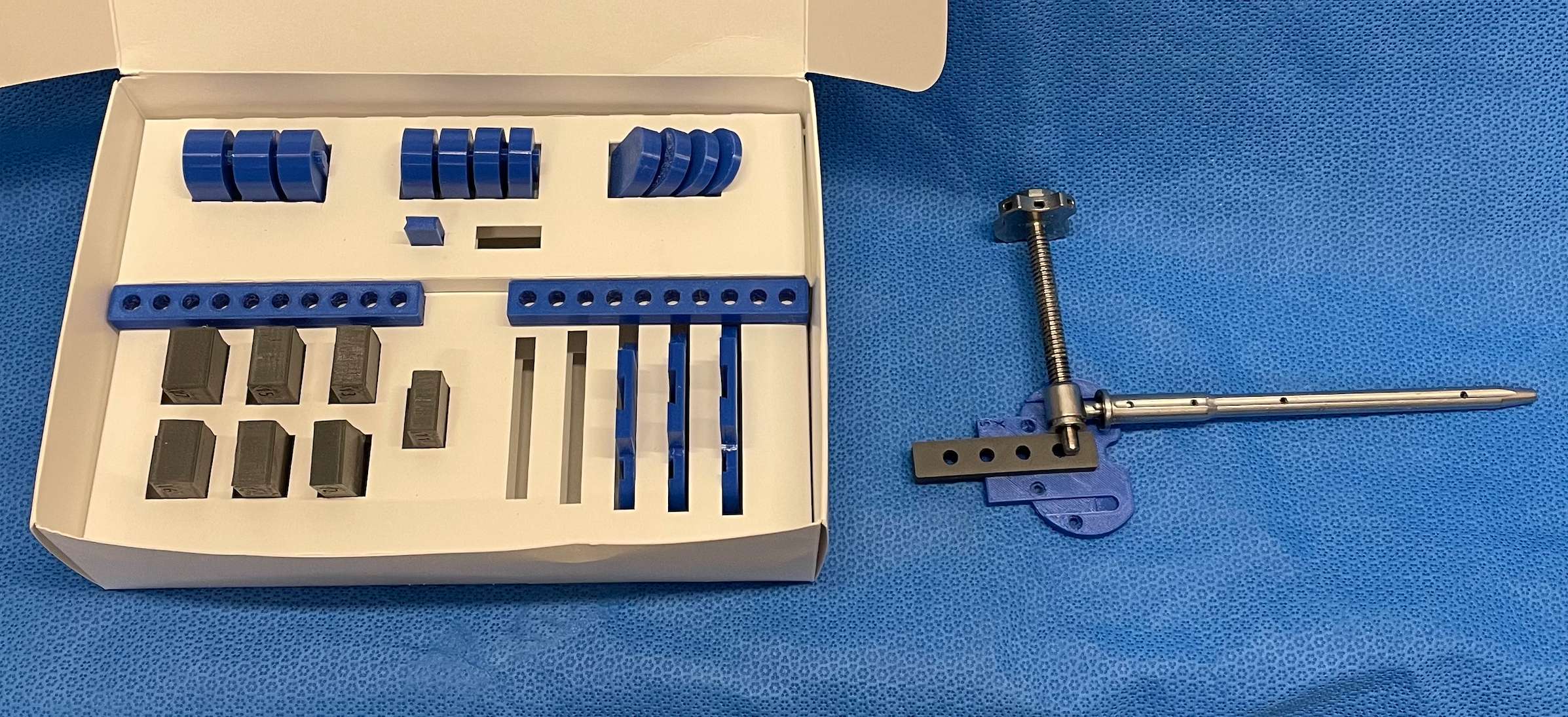
Figure 3#7306
Novel Use of an Accelerometer to Measure Load Asymmetry in Hip Arthroplasty Patients
*Jonathan Spaan - Hospital for Special Surgery - New York, United States of America
Edwin Su - Hospital for Special Surgery - New York, USA
Alexander Shafiro - Hospital for Special Surgery - New York, USA
Renee Ren - USA
*Email: spaanj@hss.edu
INTRODUCTION:
One of the benefits of hip resurfacing arthroplasty is the potential of returning to high levels of activity post-operation. Previously, different technologies such as an accelerometer have been used to measure and track various athletic movements; however, to date, an accelerometer has not been utilized to follow hip resurfacing patients post-operation. Therefore, this study aimed to evaluate the use of an accelerometer as a beneficial resource in the recovery of hip resurfacing arthroplasty.
METHODS:
An analysis on 22 primary hip re-surfacing arthroplasties performed by a single surgeon was conducted. Subjects were examined pre-operation, as well as at 3 and 6 months post-operation. Subjects were put through a series of physical exercises including broad jump, double leg vertical jump, hop test, lateral single leg jump, and a single leg vertical jump. Measurements of impact load per minute, average intensity, bone stimulus, and overall asymmetry were collected using an IMeasureU accelerometer.
Non-operated vs. operated legs were compared for the measurements of impact load per minute, average intensity, and bone stimulus at each time point using a Paired T-Test. Overall asymmetry between non-operated and operated legs was analyzed using a One Sample T-Test. All statistical tests were two sided with a significance level of 0.05.
RESULTS:
Mean age at the time of surgery was 53.62 (±10.86) years old and the mean BMI was 28.67 (±3.78) kg/m². Pre-operation the symmetry between non-operated and operated leg differed both in the double leg vertical jump and lateral single leg jump (p=0.0201 and p=0.0447, respectively). Here, asymmetry refers to the amount of impact load as calculated by the sensors, with the operated leg showing less impact load. At 3 months post-operation there was significant asymmetry between the operated and non-operated legs in both the broad jump and lateral single leg jump exercises (p=0.0359 and p=0.0058, respectively). There were no statically significant asymmetries for any of the five exercises at 6 months post-operation (Table 1).
Overall asymmetry between the non-operated and operated legs for all five exercises performed was 13.87% pre-operation, 13.35% at 3 months post-operation, and 2.69% 6 months post-operation, with the non-operated leg producing a higher impact load at each time point.
CONCLUSION:
In our cohort we found significant asymmetries between the operated and non-operated leg in multiple exercises both pre-operation, and at 3 months post-operation. However no significant difference in performance was discovered at 6 months post-operation. Additionally, subjects were within 3 percent symmetry at 6 months post-operation. Our findings indicate that an accelerometer can be a beneficial resource moving forward to track patient recovery from hip resurfacing arthroplasty, and shows promise for future research using this technology in arthroplasty patients.
Figures
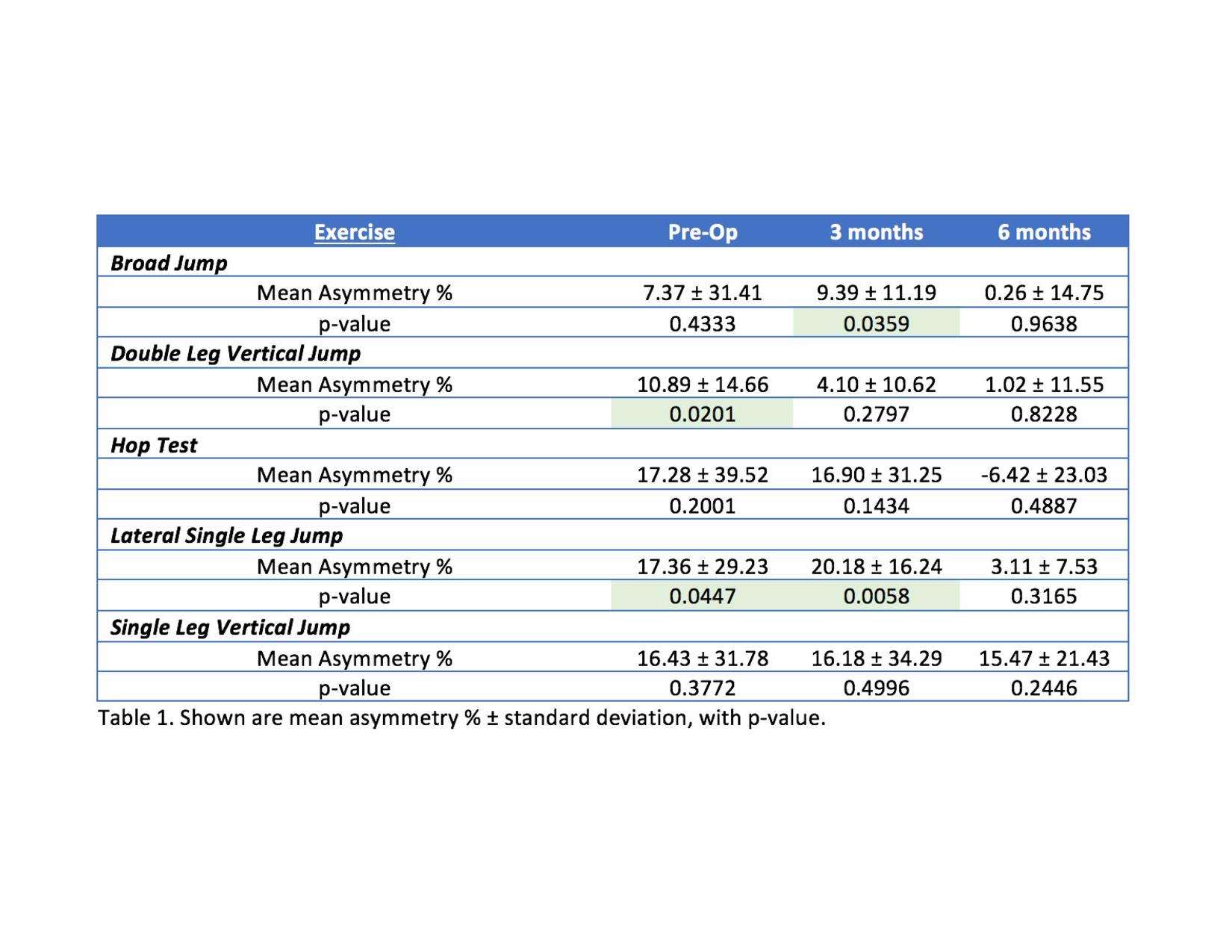
Figure 1#7638
Motion Tracking Study of Surgical Impaction During THA
*Adam Reynolds - Imperial College - London, GB
Ruben Doyle - Imperial College London - London, United Kingdom
Oliver Boughton - Dr - London, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
Jonathan Jeffers - Imperial College London - London, United Kingdom
Sarah K Muirhead-Allwood - Royal National Orthopaedic Hospital, Stanmore - Stanmore, United Kingdom
*Email: asr21@ic.ac.uk
Introduction:
Previous studies have investigated the forces and energies involved in acetabular cup impaction during THA. There is, however, yet to be a study that investigates the accuracy and precision of the motion of the strike during cementless cup impaction. As a motion employing multiple muscle groups and several joints, there is bound to be variability, but this has yet to be defined. This study aims to analyse the kinematics of the strike and quantify the alignment precision and accuracy, relative to the introducer at the point of impact.
Methods:
3 cadavers (6 hips) were prepped for a posterior approach THA. An expert orthopaedic consultant surgeon used a traditional method to impact acetabular cups. The 700g surgical hammer and introducer were instrumented with a 100kN impact load cell (PCB 200C20) and retroreflective passive marker spheres. The surgeon was asked to impact the cup using three levels of effort: low, medium, and high. A total of 110 strikes were recorded. Force data for each strike were acquired at a rate of 51.2kHz and the position and rotation of each instrument were recorded using a stereo camera motion tracker (fusionTrack 500) at a rate of 355Hz. A custom Matlab script was used to analyse the alignment and accuracy of the hammer relative to the introducer.
Results:
The average misalignment of the hammer face, relative to the introducer strike face, was 15.2 degrees (1.6 - 61.6, SD 7.7). The misalignment of the strike vector, relative to the axis of the introducer, was 18.1 degrees (0.9 – 46.4, SD 9.8) (Figure 1) which results in an average minimum wasted energy (discounting heat and sound) of 6.1% (0.0 – 21.1, SD 6.3). Finally, the centre point of the strike was offset, relative to the introducer axis, by an average of 19.9mm (1.4 – 48.0, SD 8.7). This is shown in figure 2. There was no significant correlation between perceived strike effort and strike motion inaccuracies, with strike inaccuracy and inconsistency being present for all efforts.
Conclusions:
An ideal hammer strike would hit the introducer in the centre of the strike face and be colinear to the introducer at the point of impact. However, deviation from this ideal strike was seen in all cases with little consistency in the inaccuracies. The clinical implication of this is that the surgeon is hindered from translating their intuition and experience of ‘how hard to hit’ to the implant. Furthermore, wasted energy is shown to impart torque on the introducer and cause angular displacement of the cup during impact. Wasted energy may also lead to increased fatigue in the surgeon.
Figures
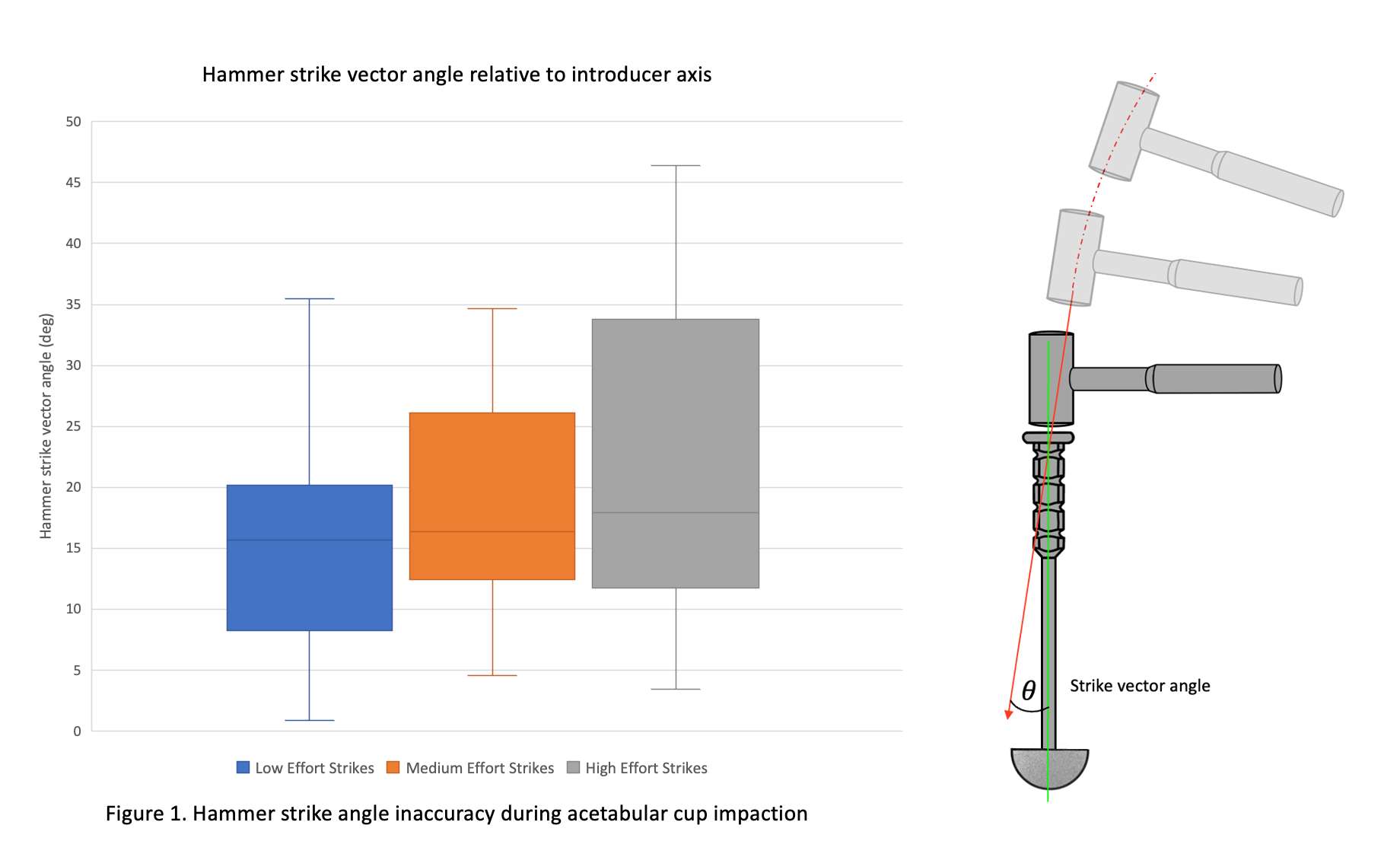
Figure 1
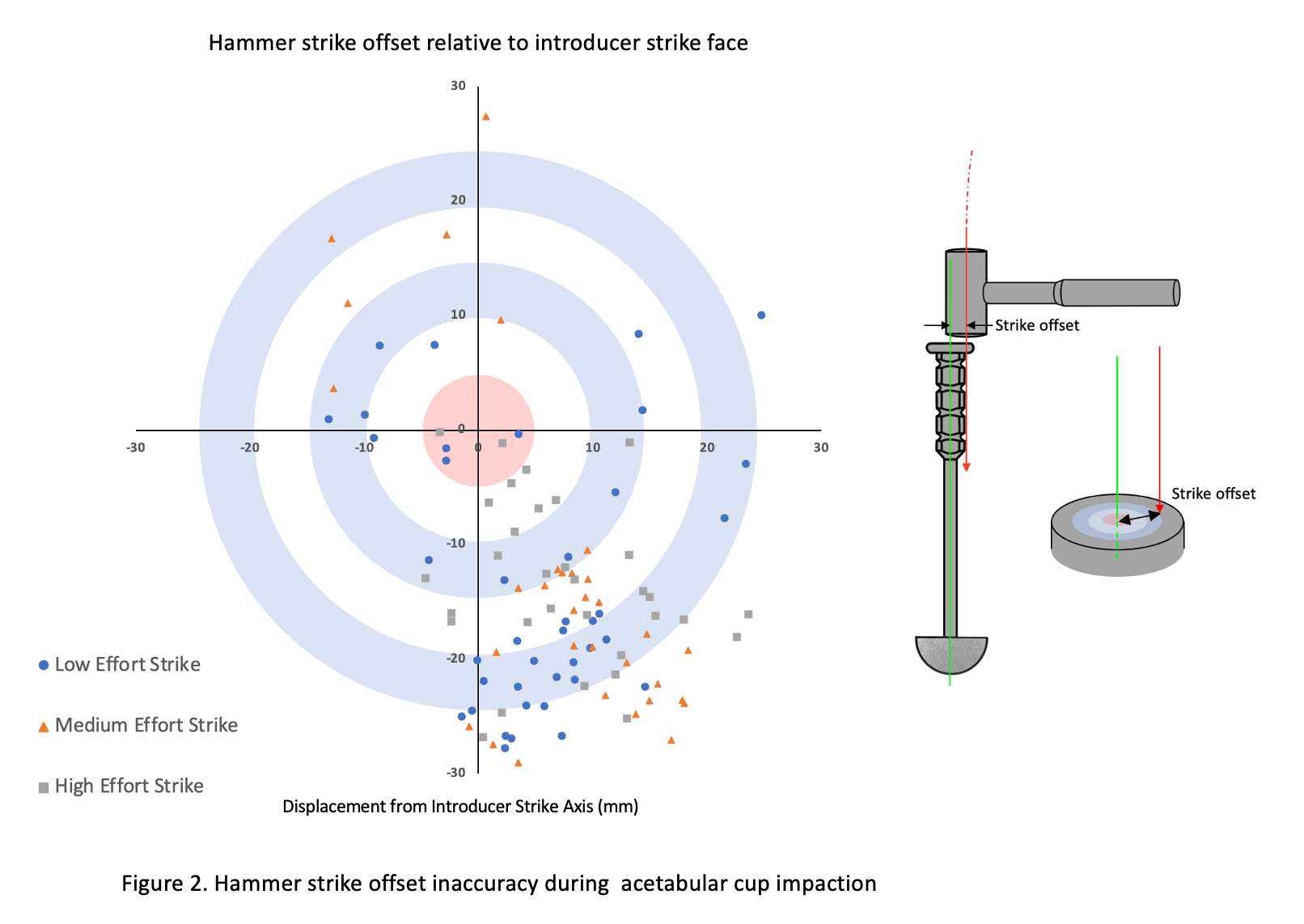
Figure 2#7845
Coronal Plane Femoral Bowing in Far East Asians: Implications for the Strategy of Distal Femoral Resection in Total Knee Arthroplasty
*SeungJoon Rhee - Pusan National University Hospital - Busan, Korea (Republic of)
*Email: rheefury@naver.com
Abstract
Background: The accuracy of distal femoral resection in intramedullary (IM) guided total knee arthroplasty (TKA) depends on femoral morphology and thus varies according to individual anatomy. However, a good guideline to determine optimal surgical approach to achieve an accurate distal femoral resection in Far East Asians is still lacking. This study aimed to characterise coronal plane femoral bowing in Far East Asians according to age, sex, and severity of coronal plane deformity to identify optimal strategies for distal femoral resection in TKA.
Hypothesis: (1) Coronal plane femoral bowing in different demographic groups in Far East Asians will differ significantly. (2) Grossly laterally bowed femur will be revealed as a dominant bowing pattern in Far East Asian femora. (3) Coronal plane bowing of the distal femur will affect the feasibility of IM-guided distal femoral resection in TKA.
Patients and Methods: Femoral anatomical parameters in 656 patients (232 male and 424 female) were assessed using standing long-leg anteroposterior radiography which was fulfilling strict standard. The femur was divided into three longitudinal segments to measure the segmental anatomical axial deviation from the mechanical axis and intersegmental bowing. Coronal plane femoral bowing pattern was categorised based on combined gross bowing and distal bowing.
Results: The mean hip–knee–ankle angle; neck-shaft angle; proximal, middle, and distal segmental axial differences; mechanical lateral distal femoral angle; and femur length were 6.7±6.8°, 125.0±5.5°, 5.9±1.7°, 6.1±1.1°, 5.3±1.6°, 88.4±2.6°, and 432.3±23.9 mm in male and 8.4±5.5°, 126.4±5.6°, 5.4±1.5°, 6.6±0.9°, 5.6±1.6°, 89.3±2.6°, and 410.6±23.3 mm in female, respectively. The mean proximal, distal, and gross femoral bowing was 0.3±1.8°, −0.8±1.8°, and −0.5±2.9° in male and 1.2±1.6°, −1.0±1.6°, and 0.2±2.7° in female, respectively.
Discussion: Grossly straight femur with a straight distal part were the most common femoral bowing pattern in Far East Asians. Distal bowing was proved to be a key factor to choose a method for distal femoral resection in TKA. We conclude it is feasible using IM guide to achieve accurate distal femoral resection in the femora with distal segmental axial deviation between 4-8° and distal bowing less than ±1°.
Keywords: distal femoral resection; femoral bowing
#7846
A Comparison of Long-Term Outcomes of Computer-Navigated and Conventional Total Knee Arthroplasty a Meta-Analysis of Randomized Controlled Trials
*SeungJoon Rhee - Pusan National University Hospital - Busan, Korea (Republic of)
*Email: rheefury@naver.com
Background: It is not clear whether long-term outcomes differ between computer-navigated and conventional total knee arthroplasty.
The purpose of this study was to perform a meta-analysis comparing the radiographic outcomes, the long-term functional
outcomes, and survivorship between computer-navigated total knee arthroplasty and conventional total knee arthroplasty.
Methods: We searched MEDLINE, Embase, and the Cochrane Library to identify studies comparing long-term outcomes
between computer-navigated total knee arthroplasty and conventional total knee arthroplasty. Randomized controlled trials with
mean follow-up durations of >8 years were included. The meta-analysis compared radiographic outcomes (postoperative
alignment), functional outcomes (range of motion and patient-reported outcomes), and survivorship of the 2 techniques.
Results: Nine studies were included. A meta-analysis of accuracy revealed better outcomes in computer-navigated total
knee arthroplasty when compared with conventional total knee arthroplasty in terms of the sagittal alignment of the
femoral component (risk ratio [RR], 0.69; [95% confidence interval (CI), 0.51 to 0.93]; p = 0.02) and the coronal alignment
of the tibial component (RR, 0.75 [95% CI, 0.60 to 0.95]; p = 0.02). The mechanical axis of the lower extremity, the
coronal alignment of the femoral component, and the sagittal alignment of the tibial component did not differ significantly
between the 2 groups. The functional outcomes did not differ significantly between the 2 techniques. Both in terms of the
revision rate and the incidence of aseptic loosening, there were no differences between the 2 techniques.
Conclusions: Although computer-navigated total knee arthroplasty resulted in better outcomes in postoperative component
alignment than conventional total knee arthroplasty, there were no significant differences in long-term functional
outcomes and survivorship between the 2 techniques. To fully evaluate the utility of computer navigation in total knee
arthroplasty, additional randomized controlled studies including diverse ethnic groups and countries, as well as studies
evaluating the correlation between postoperative alignment and long-term survivorship, are necessary.
#7313
Comparison of Patient Demographics, Utilization Trends, and Costs of Total Ankle Arthroplasty and Ankle Fusion for Tibiotalar Osteoarthritis From 2010-2019
*Aaron Lam - Maimonides Medical Center - Brooklyn, USA
Adam Gordon - maimonides Medical Center - Brooklyn, USA
Mitchell Ng - Maimonides Medical Center - Brooklyn, United States of America
Andrew Horn - Maimonides Medical Center - Brooklyn, USA
Ariel Rodriguez - Maimonides Medical Center - Brooklyn, United States of America
Amr Abdelgawad - Maimonides Medical Center - Brooklyn, USA
*Email: aarlam@maimonidesmed.org
Introduction: Tibiotalar osteoarthritis is a disabling condition that results in mobility impairment, functional loss, and decreased quality of life. While the gold standard for the treatment of tibiotalar osteoarthritis is an ankle fusion (AF), improved techniques and designs have made total ankle arthroplasty (TAA) a viable alternative option. Contemporary studies evaluating utilization and trends of total ankle arthroplasty (TAA) and ankle fusion (AF) for tibiotalar osteoarthritis are sparse. Therefore, the purpose of this study was to utilize a nationwide administrative claims database from 2010 to 2019 to compare: 1) baseline demographics; 2) utilization, (2) in-hospital length of stay (LOS) (3) costs of care.
Methods: Using the Pearldiver supercomputer, a retrospective query from January 1st, 2010 to December 31st, 2019 was performed for all patients who underwent TAA and AF for tibiotalar osteoarthritis. Baseline demographics, comorbidities, and geographic utilization were compared using Pearson Chi-Square analyses. Linear regression was used to compare differences in procedure utilization and in-hospital LOS during the study interval. Reimbursements between the two cohorts during the study interval were compared. A p-value less than 0.05 was statistically significant.
Results: In total,14,248 patients underwent primary TAA (n = 5,544) or AF (n = 8,704).Patients undergoing AF were generally younger (<60) with greater comorbidity burden driven by hypertension, diabetes mellitus, obesity, and tobacco use compared to TAA patients (p<0.0001). Over the study interval, TAA utilization remained constant (912 vs 909 procedures; p=0.807), whereas AF utilization decreased by 42.5% (1,737 vs 998 procedures; p=0.0001). Mean in-hospital LOS for patients undergoing TAA decreased (2.5 days vs. 2.0 days, p=0.0004), while AF LOS increased (2.6 days vs. 3.5 days, p=0.0003). Reimbursements for both procedures significantly declined over the study interval (TAA: $4559 to $2156, AF: $4729 to $1721; p<0.013).
Conclusion: TAA utilization remained constant while AF utilization declined by 42.5% from 2010-2019. There was divergence in the LOS for TAA versus AF patients. Both procedures significantly declined by over 50% in reimbursements over the study interval.
Keywords: ankle arthroplasty; ankle fusion; tibiotalar; costs; length of stay; utilization; trends
Figures
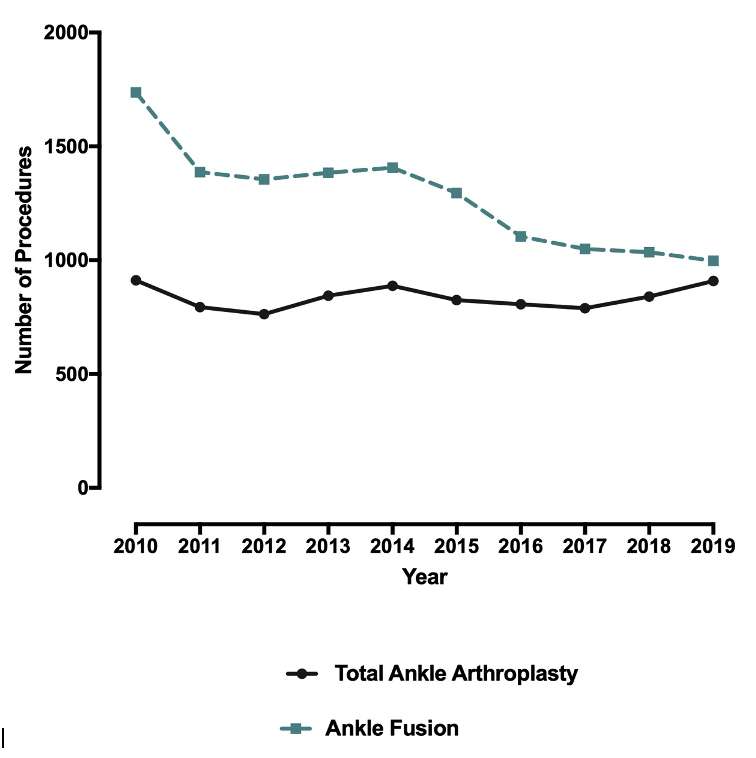
Figure 1
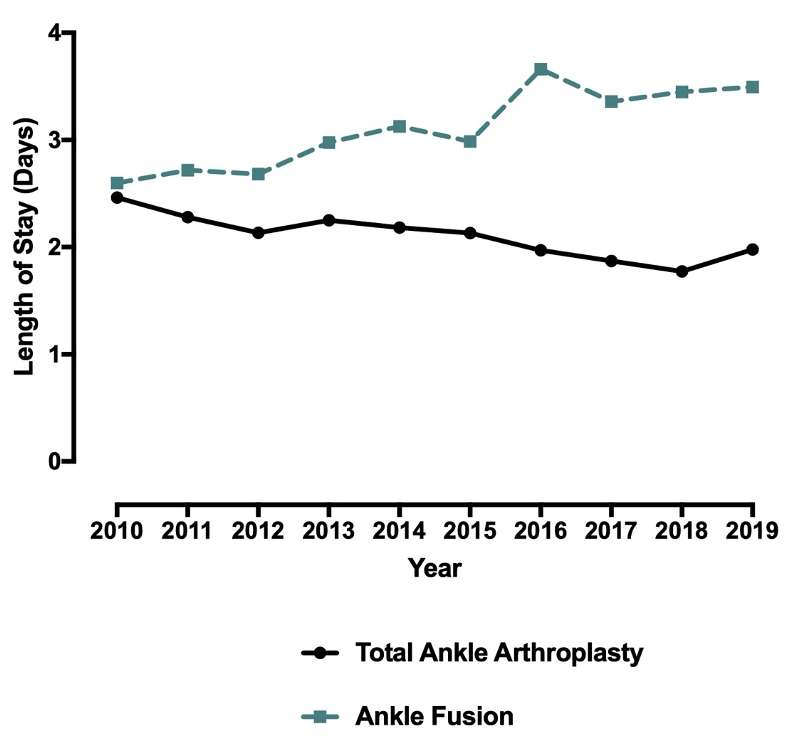
Figure 2
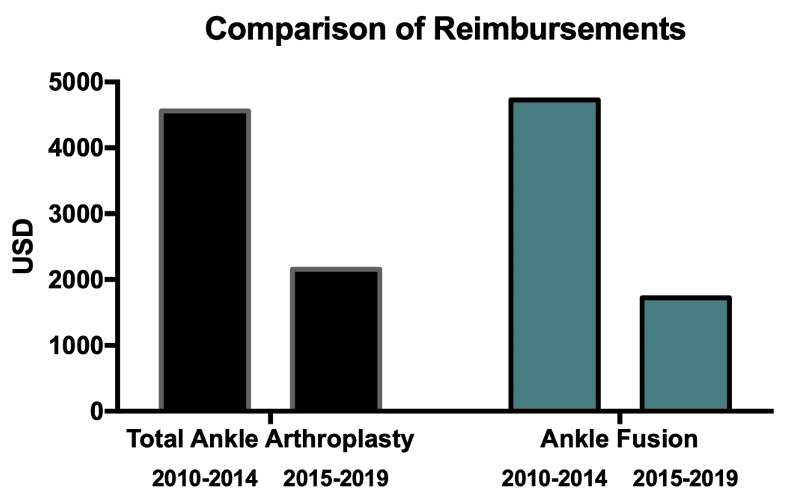
Figure 3#7276
Causes, Costs and Risk-Factors for Emergency Department Visits Following Primary Total Hip Arthroplasty
*Mitchell Ng - Maimonides Medical Center - Brooklyn, United States of America
Aaron Lam - Maimonides Medical Center - Brooklyn, USA
Keith Diamond - Maimonides Medical Center - Brooklyn, USA
Andriy Kobryn - SUNY Downstate College of Medicine - Brooklyn, USA
Nikhil Vasireddi - Case Western Reserve University School of Medicine - Cleveland, USA
Nicolas Piuzzi - Cleveland Clinic - Cleveland, USA
Martin Roche - Holy Cross Hospital - Fort Lauderdale, USA
Orry Erez - Maimonides Medical Center - Brooklyn, USA
Che Hang Jason Wong - Maimonides Medical Center - Brooklyn, USA
Ariel Rodriguez - Maimonides Medical Center - Brooklyn, United States of America
Michael Mont - Sinai Hospital of Baltimore - Baltimore, USA
*Email: mitchng77@gmail.com
INTRODUCTION: A wide range of studies have examined 90-day re-admissions following primary total hip arthroplasty. However, well-powered studies analyzing the relationship of emergency department (ED) visits following primary total hip arthroplasties (THAs) have been limited to single-center studies, which have estimated ~9% incidence of ED visits within 90 days post-operatively. The aim of this study was to: 1) compare baseline demographics of patients who did/did not have an ED visit; 2) determine leading causes of ED visits; 3) identify patient-related risk factors; and 4) quantify associated healthcare costs for these different ED visits.
METHODS: Patients undergoing primary THA who had an ED visit within 90-days following the index procedure were identified using International Classification of Disease (ICD-9,10) and Current Procedural Terminology (CPT) codes from the Mariner insurance claims of the Pearldiver database dataset. The query yielded 682,950 patients who did (n = 21,836) and did not have (n = 661,114) an ED visit within 90-days following their index procedure between January 1, 2010 and March 31, 2018. Baseline demographics/co-morbidities between control and study cohorts, ED visit causes, associated patient-related risk-factors, and subsequent costs of care were collected and compared.
RESULTS: Musculoskeletal etiologies/complaints were the most common cause of ED visits following primary THA. Risk factors associated with increased ED visits were alcohol abuse (Odds Ratio (OR): 1.90, p=0.0003), depressive disorders (OR: 1.10, p<0.0001), congestive heart failure (CHF) (OR: 1.12, p<0.0001), coagulopathy (OR: 1.11, p<0.0001), and electrolyte and fluid derangements (OR: 1.33, p<0.0001), as the greatest risk factors for post-operative ED visits. Additionally, the study found pulmonary ($28,928.01) and cardiac ($28,574.69) associated ED visits attributed to highest costs of care within the study.
CONCLUSION: Musculoskeletal complaints were the leading driver for ED visits following primary THA, followed by cardiac and gastrointestinal complaints. A plethora of risk factors were associated with increasing odds of ED visits with the top 5 being alcohol abuse, electrolyte/fluid derangements, CHF, coagulopathy, and depression (p<0.0001). By identifying demographic patterns of patients, causes, risk factors, and associated costs, this study highlights potential areas of pre-operative medical optimization to reduce 90-day ED visits following primary THA.
Figures
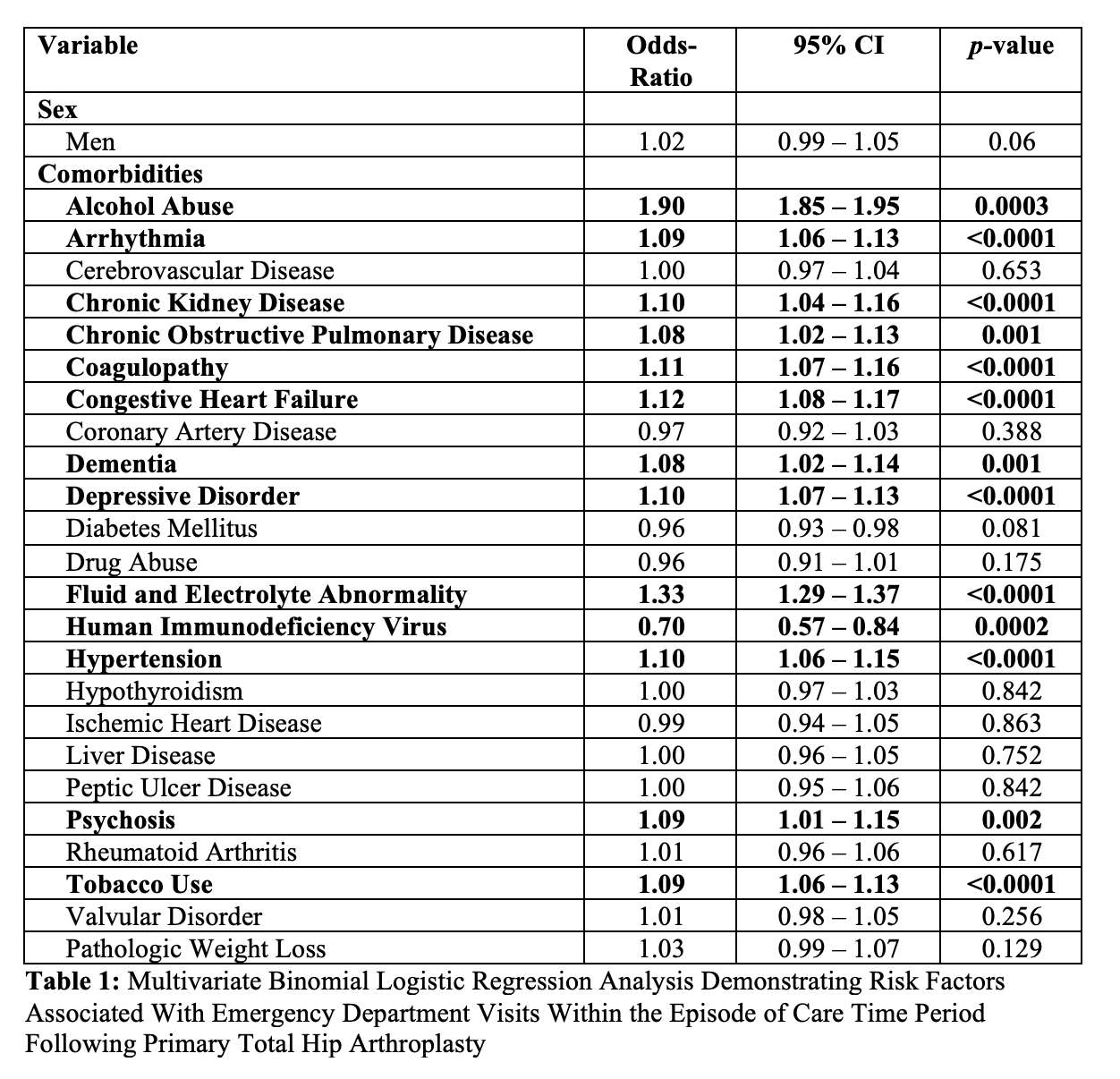
Figure 1#7272
Multi-Level Posterior Cervical Foraminotomy Associated With Increased Peri-Operative Infection Rates Relative to Anterior Cervical Discectomy With Fusion and Cervical Disc Arthroplasty
*Mitchell Ng - Maimonides Medical Center - Brooklyn, United States of America
Ahmed Emara - Cleveland Clinic - Cleveland, USA
Aaron Lam - Maimonides Medical Center - Brooklyn, USA
Bhavya Seth - Florida International university - Miami, USA
Lasya Manne - University of Texas at Dallas - Dallas, USA
Vinati Pillutla - Maimonides Medical Center - Brooklyn, USA
Andriy Kobryn - SUNY Downstate College of Medicine - Brooklyn, USA
John Houten - Maimonides Medical Center - Brooklyn, USA
Ahmed Saleh - Maimonides Medical Center - Brooklyn, USA
Ariel Rodriguez - Maimonides Medical Center - Brooklyn, United States of America
Afshin Razi - Maimonides Medical Center - Brooklyn, USA
*Email: mitchng77@gmail.com
Introduction: Anterior cervical discectomy with fusion (ACDF) is considered the gold standard for treating cervical radiculopathy, however cervical disc arthroplasty (CDA) or posterior cervical foraminotomy (PCF) are also reasonable surgical options. The advantages and disadvantages of these three procedures remain incompletely understood. The purpose of this study was to determine if there are differences in peri-operative outcomes of patients undergoing ACDF, CDA, or PCF.
Methods: Cervical radiculopathy patients who underwent multi-level ACDF, CDA, or PCF between 2012 and 2019 were identified from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. Patients were subsequently stratified into those who underwent ACDF, CDA, or PCF groups. Differences in baseline patient demographics, steroid use, functional status and ASA classification were resolved using propensity score-matching. Analysis of variance (ANOVA) was conducted to identify differences in peri-operative outcomes in terms of operative time, medical/surgical complications, and healthcare utilization metrics (reoperations, readmissions, lengths-of-stay).
Results: A total of 31,344 cervical radiculopathy patients undergoing surgery were identified (ACDF: n=28089, CDA: n=1748, PCF: n= 1507). After 1:1 propensity score matching (n=684 each), there were no differences in patient characteristics of ACDF, CDA, or PCF groups (p>0.05). PCF patients had statistically higher rates of reoperation (2.0%) than ACDF (1.%), CDA (0.4%) patients (p=0.020). PCF patients also experienced higher rates of superficial infection (PCF:1.3%, ACDF: 0.3%, CDA: 0.1%, p=0.008) and deep infection (PCF:1.2%, ACDF:0%, CDA:0%, p<0.001) relative to ACDF and CDA patients. There were no other significant differences in medical/surgical complications between the ACDF, CDA, or PCF patients.
Conclusions: Cervical radiculopathy patients undergoing multi-level PCF are associated with higher rates of peri-operative infection (superficial skin infection, deep infection, and overall reoperation) than multi-level ACDF or CDA. Our findings are consistent with current literature that have associated posterior exposures with higher infection rates relative to anterior approach. Surgeons should aware of this increased relative risk when considering the risks and benefits of potential surgical options for patients. Further research is required to elucidate the mechanism behind this association, and determine if these have an effect on long-term outcome differences.
Figures
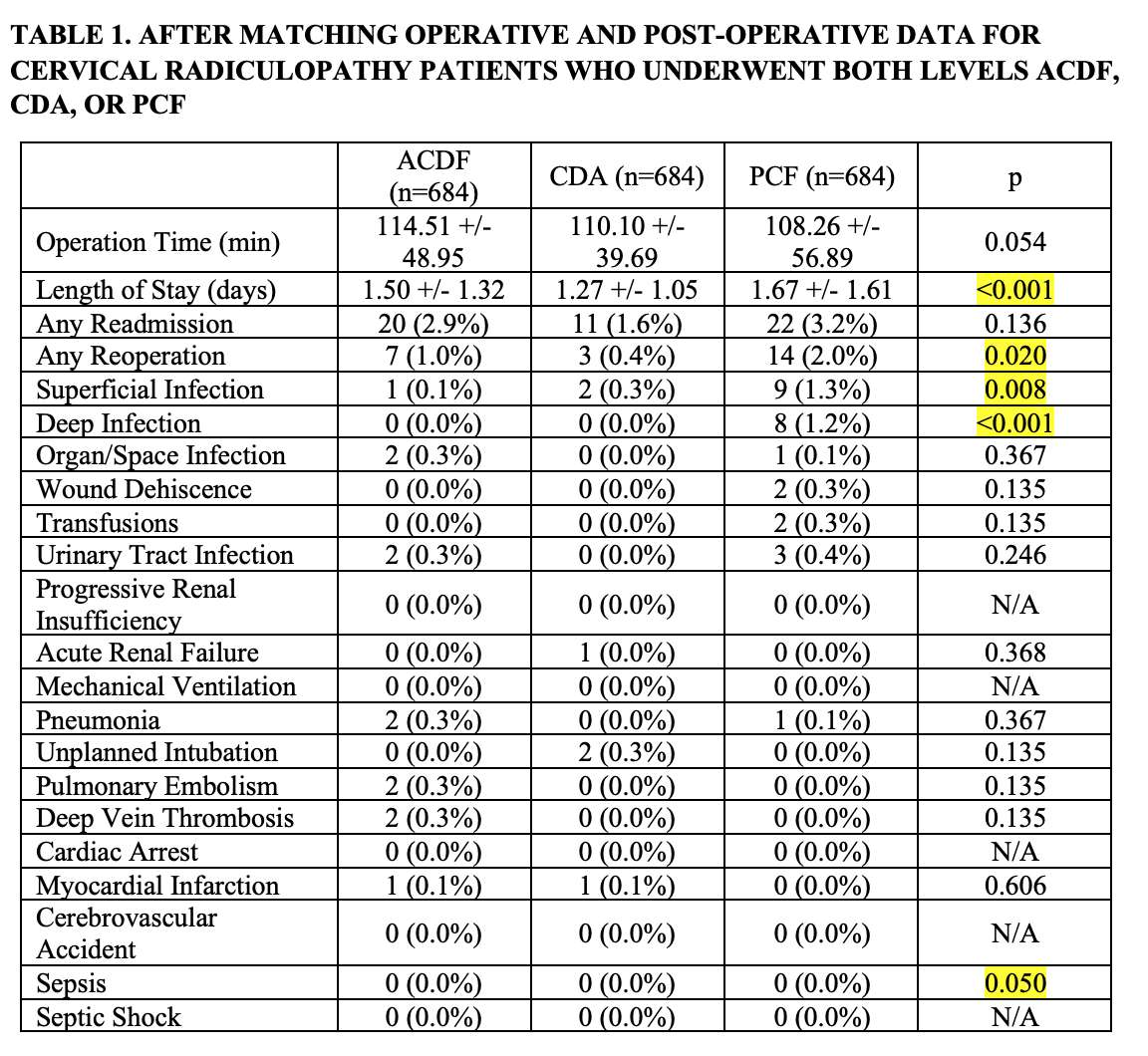
Figure 1#7312
The Association of Benign Prostatic Hyperplasia on Postoperative Complications and Periprosthetic Joint Infections Following Total Shoulder Arthroplasty
*Aaron Lam - Maimonides Medical Center - Brooklyn, USA
Adam Gordon - maimonides Medical Center - Brooklyn, USA
Andrew Horn - Maimonides Medical Center - Brooklyn, USA
Mitchell Ng - Maimonides Medical Center - Brooklyn, United States of America
Ramin Sadeghpour - Maimonides Medical Center - Brooklyn, USA
Ariel Rodriguez - Maimonides Medical Center - Brooklyn, United States of America
Jack Choeuka - Maimonides Medical Center - Brooklyn, USA
*Email: aarlam@maimonidesmed.org
Background: Periprosthetic joint infection following total shoulder arthroplasty is a dreaded complication associated with significant morbidity and healthcare cost. A recently proposed risk factor for periprosthetic joint infections (PJI) in men is benign prostatic hyperplasia (BPH), a common health problem with a lifetime prevalence estimated to be about 26%. Despite the high prevalence among men, limited studies have evaluated the association of BPH on outcomes following total shoulder arthroplasty. The objective was to explore the association of BPH on 1) 90-day complications, 2) length of stay (LOS), 3) readmission rates, and 4) healthcare expenditures following total shoulder arthroplasty (TSA).
Methods: Using the Pearldiver supercomputer, a retrospective query was performed from January 2005 to March 2014 for male patients with and without BPH who underwent primary TSA. Baseline demographics and comorbidities were compared using Pearson Chi-Square analyses. Welch’s t-tests were used to assess for significance for length of stay (LOS), healthcare expenditures and mean ECI scores between the two cohorts. Logistic regression determined the association of BPH on medical complications and readmissions. A p value less than 0.001 was statistically significant.
Results: In total,5,067 patients with BPH underwent primary TSA while 50,720 patients served as the comparison cohort. Patients with BPH had higher incidence and odds (36.8 vs. 6.2%; OR: 2.73, p<0.0001) of all ninety-day medical complications including PJIs (0.49 vs. 0.32%; OR: 1.54, p<0.001). BPH patients had longer in-hospital LOS (3- vs. 2-days, p<0.0001). Study group patients had higher 90-day episode of care reimbursements ($13,653 vs. $12,688), p<0.0001).
Conclusions: BPH is associated with increased complications and healthcare expenditures following total shoulder arthroplasty. The investigation can be used to educate BPH patients of the possible adverse events which may occur within ninety-days following primary TSA for the treatment of glenohumeral osteoarthritis.
Keywords: benign prostatic hyperplasia; total shoulder arthroplasty; periprosthetic joint infection; postoperative outcomes; costs
Figures
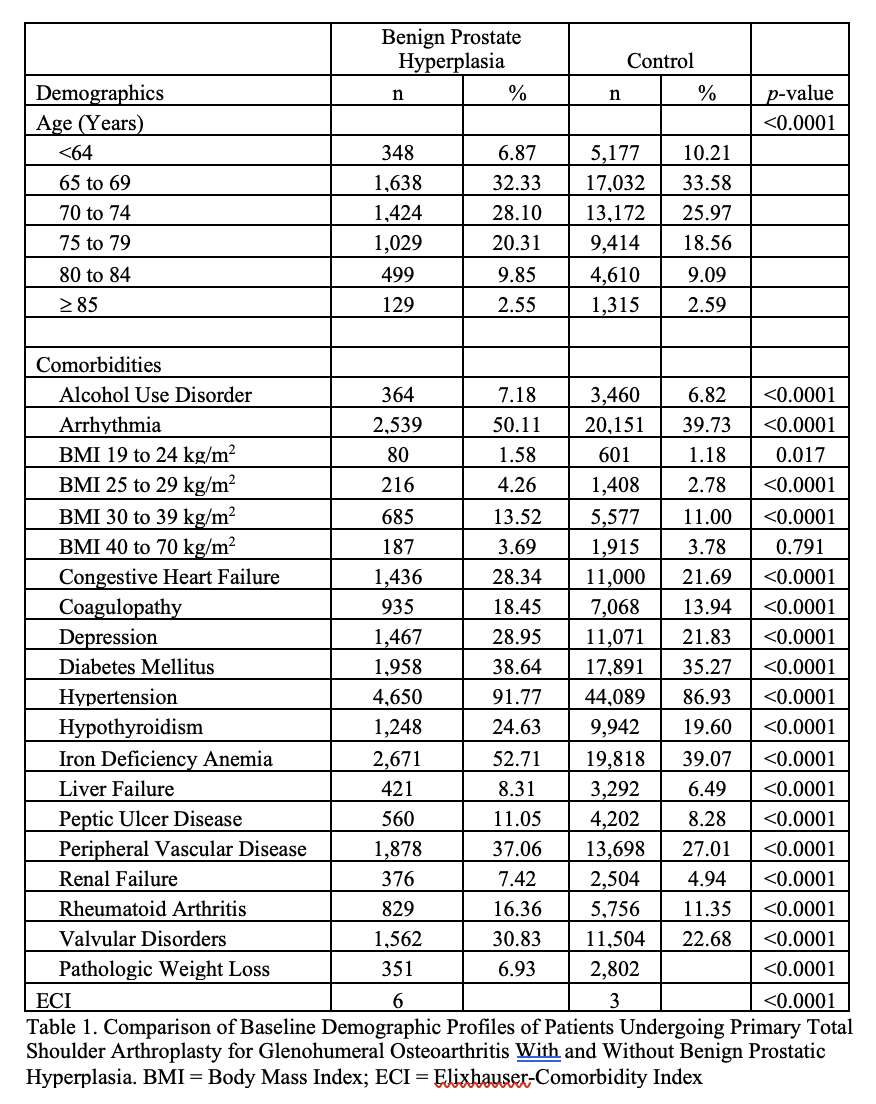
Figure 1
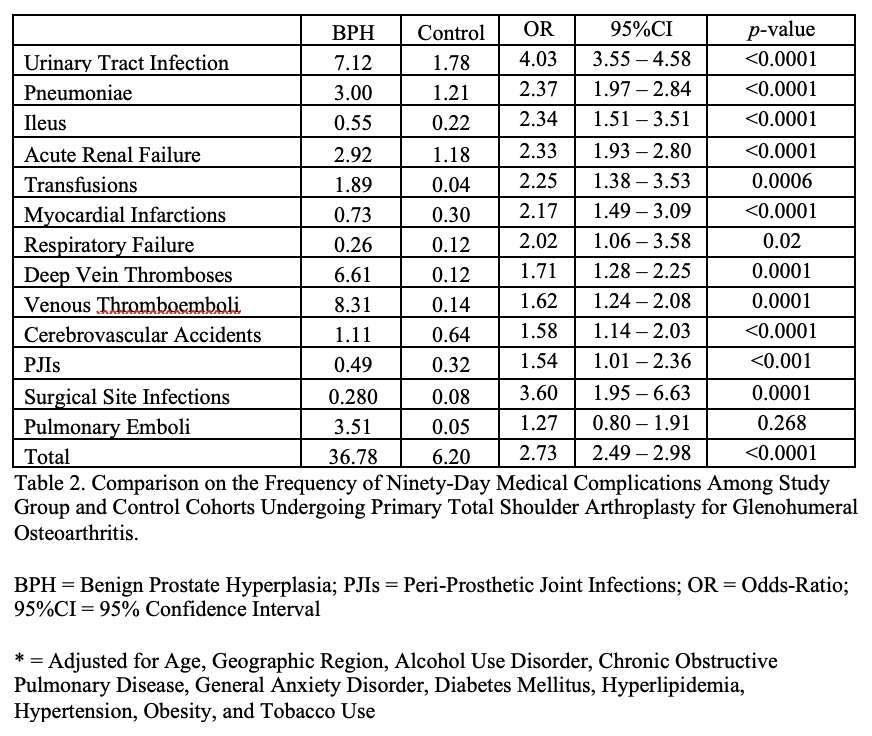
Figure 2#7275
Decreasing Trend in Mortality Rates of Aseptic Versus Septic Revision Total Hip Arthroplasty: An Analysis of 681,034 Cases
*Mitchell Ng - Maimonides Medical Center - Brooklyn, United States of America
Andriy Kobryn - SUNY Downstate College of Medicine - Brooklyn, USA
Ahmed Emara - Cleveland Clinic - Cleveland, USA
Matthew Magruder - Maimonides Medical Center - Brooklyn, USA
Nikhil Vasireddi - Case Western Reserve University School of Medicine - Cleveland, USA
Afshin Razi - Maimonides Medical Center - Brooklyn, USA
Che Hang Jason Wong - Maimonides Medical Center - Brooklyn, USA
Viktor Krebs - Cleveland Clinic - Cleveland, USA
Michael Mont - Sinai Hospital of Baltimore - Baltimore, USA
Ariel Rodriguez - Maimonides Medical Center - Brooklyn, United States of America
Nicolas Piuzzi - Cleveland Clinic - Cleveland, USA
*Email: mitchng77@gmail.com
Objective: While the majority of revision total hip arthroplasty (rTHA) are for aseptic loosening or instability, infection accounts for ~16% of rTHAs. The purpose of our study was to: 1) quantify mortality rates of aseptic versus septic rTHA; 2) determine if mortality rates have changed over the past 20 years; and 3) identify associated preoperative risk factors, focusing on the utility/validity of the Elixhauser Comorbidity index (ECI).
Methods: ICD-9/ICD-10 codes were used to identify patients undergoing rTHA in the National Inpatient Sample database between 1998 and 2018. For each patient, demographic variables including age, gender, race, insurance type, ECI variables, and in-hospital mortality were gathered. Based on these demographics, a logarithmic regression model was constructed to assess risk of in-hospital mortality for septic rTHA compared to aseptic rTHA.
Results: A total of 681,034 cases (576,143 aseptic THA and 104,891 septic THA) were identified. 4,025 deaths (0.70%) and 2,149 deaths (2.05%) were observed in aseptic and septic cohorts. From 1998 to 2018, mortality rates of aseptic and septic rTHA decreased from 0.83% to 0.45%, and from 2.58% to 1.24% respectively. Septic rTHA was independently associated with higher odds of mortality relative to aseptic (Odds ratio (OR): 2.305, 95% confidence interval (CI): (2.014, 2.638), p<0.0001). Increased ECI was associated with higher odds of mortality at both medium (OR: 5.147, 95% CI: (4.433,5.977), p<0.0001) and high index scores (OR: 13.714, 95% CI: (11.519,16.326), p<0.0001).
Conclusion: Mortality rates for both aseptic and septic rTHA have been declining over the past 20 years. This is potentially due to more thorough guidelines regarding patient selection and advances in medical management, as this mortality decline correlates with an overall mortality decline of primary THA. Our study affirmed the utility/validity of the ECI, wherein medium/high ECIs are independently associated with increased mortality relative to a low baseline index.
Figures
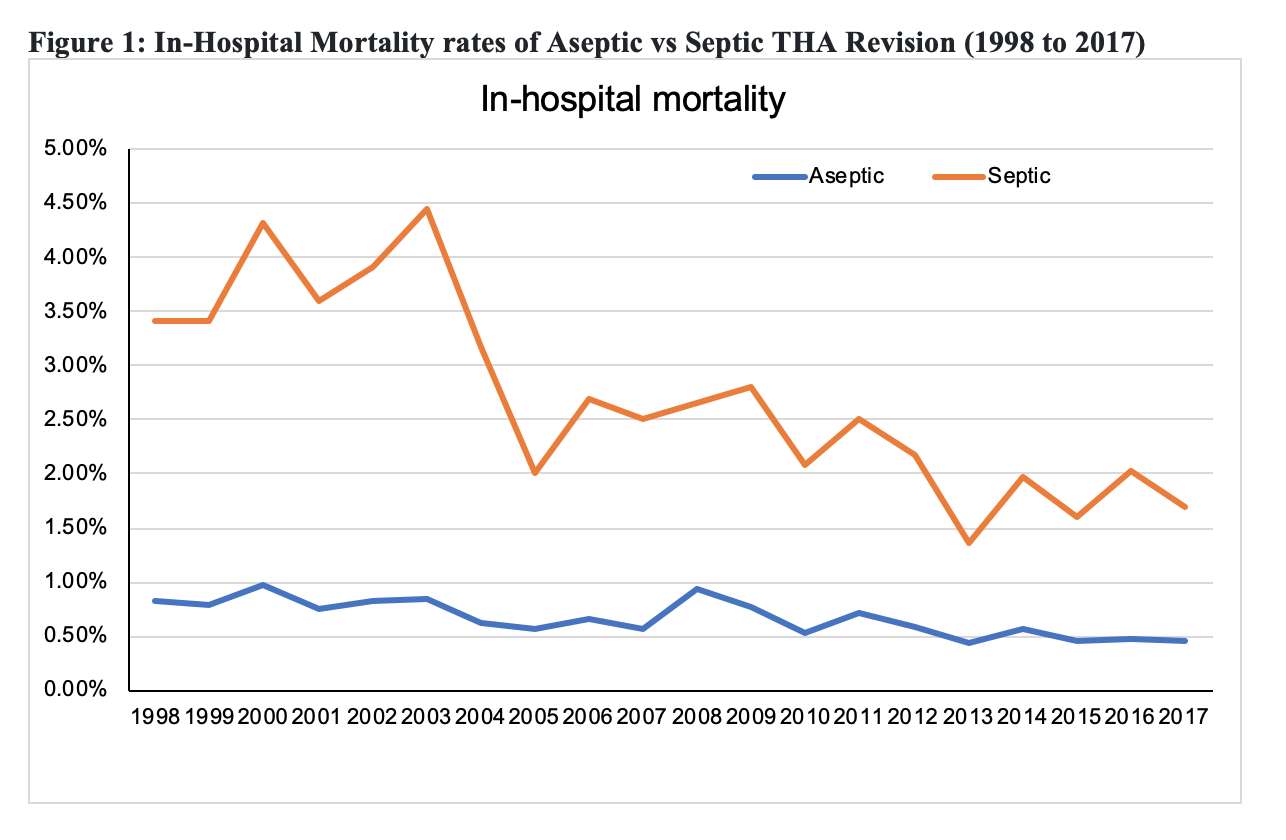
Figure 1#7346
The Effect of Leg Length Discrepancy and Metal Ion Release Following Ceramic-on-Metal Total Hip Arthroplasty
Young-Ho Roh - Jeju National University Hospital - Jeju, Korea (Republic of)
Taehan Kang - Jeju National University Hospital - Jeju, South Korea
Yong Hwan Choi - Jeju National University Hospital - Jeju, South Korea
Chaemoon Lim - Jeju National University Hospital - Jeju, South Korea
*Kwang Woo Nam - Uijeongbu Eulji University Hospital - Uijeongbu, South Korea
*Email: shdudgh@daum.net
Introduction: The ceramic-on-metal (CoM) bearing has the theoretical advantages over ceramic-on-ceramic (CoC) and metal-on-metal (MoM) bearings. The objective of this study was to analyze factors that affect the metal ion release of the CoM bearing and to compare clinical performance with CoC bearings.
Methods: The 147 patients enrolled in our study were divided into 96 patients in Group 1 (CoM group) and 51 patients in Group 2 (CoC group). In addition, within the group 1, 48 patients and 30 patients were sub-categorized into group 1-A with leg length discrepancy (LLD) less than 1 cm and into group 1-B with LLD greater than 1 cm. The level of serum metal ions was measured before operation and postoperative 3 months, 6 months, 1 year and annually thereafter. Functional scores and plain radiographs were obtained for the analysis.
Results: The level of cobalt (Co) 2 years after surgery and the level of chromium (Cr) 1 year after surgery showed significantly higher in the group 1 than the group 2. LLD indicated statistically significant positive correlation between serum metal ion levels among CoM bearing THAs. In comparison of the average metal ions level changes, group 1-B showed higher level of Co and Cr ion than group 1-A. In this study, there were 2 patients in group 1 who suffered from metal liner wear along with outlier serum metal levels, and both patients received revision arthroplasty with CoC bearings [Fig. 1].
Conclusion: Patients who underwent with CoM bearing THAs with large LLD are at higher risks of complications associated with metal ions. In addition, it is critical to maintain the LLD less than 1 cm especially in using CoM bearing.
Keywords: Ceramic-on-metal bearing; Total hip arthroplasty; Leg length discrepancy; Metal ion release; Cobalt; Chromium
Figures
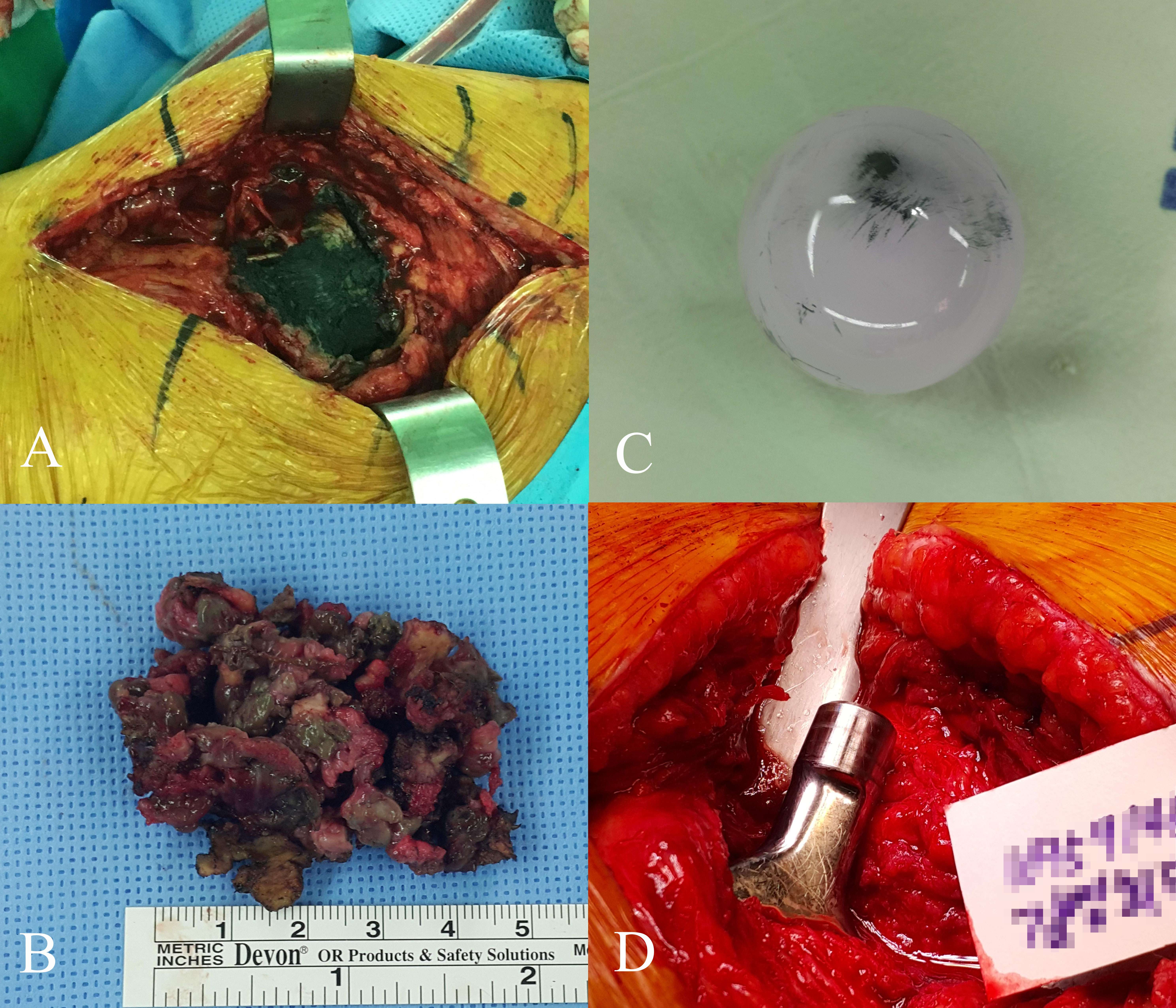
Figure 1#7389
Radiographic Differentiation Between Nutrient Artery Canal and Periprosthetic Femoral Fracture Following Hip Arthroplasty
Young-Ho Roh - Jeju National University Hospital - Jeju, Korea (Republic of)
Seung Jin Yoo - Jeju National University - Jeju, South Korea
Choi Tea Hyun - Jeju National University Hospital - jeju, South Korea
*Kwang Woo Nam - Uijeongbu Eulji University Hospital - Uijeongbu, South Korea
*Email: shdudgh@daum.net
Abstract
Introduction: Accurate diagnosis of undisplaced periprosthetic femoral fracture (PFF) after hip arthroplasty is crucial, as overlooked PFF may affect its treatment and prognosis. The undisplaced PFF is often difficult to distinguish from radiolucent lines of nutrient artery canal (NAC) of the femur present on postoperative radiographs. We aimed to identify the radiographic features of NAC to distinguish them from PFFs.
Methods: In this retrospective radiological study, a total of 242 cases in 215 patients with hip arthroplasty were analyzed using preoperative and postoperative anteroposterior (AP) and translateral (TL) radiographs.
Results: The NACs were found preoperatively in 94 (39.8%) cases on AP views and in 122 cases (50.4%) on TL views. The radiolucent lines were observed postoperatively in 42 (17.4%) on AP views and 122 (50.4%) on the TL views. three cases (1.2%) had a fracture around the stem that were detected on radiographs. One case with PFF presented simultaneously with NAC on the immediate postoperative radiographs. All patients were treated by conservative measures, and the radiolucent lines did not appear on follow-up radiographs.
Conclusion: It is not easy to differentiate undisplaced PFFs that can occur after hip arthroplasty operation from NACs. However, accurate diagnosis is possible through careful observation and comparison of preoperative and postoperative radiologic images.
Keywords: hip arthroplasty; nutrient artery canal; periprosthetic femoral fracture; cementless stem; radiographic study
#7390
Extensive Deep Vein Thrombosis Complicating Total Hip Arthroplasties Caused by Undiagnosed May-Thurner Syndrome
Young-Ho Roh - Jeju National University Hospital - Jeju, Korea (Republic of)
Taehan Kang - Jeju National University Hospital - Jeju, South Korea
Chaemoon Lim - Jeju National University Hospital - Jeju, South Korea
Choi Tea Hyun - Jeju National University Hospital - jeju, South Korea
Seung Jin Yoo - Jeju National University - Jeju, South Korea
*Kwang Woo Nam - Uijeongbu Eulji University Hospital - Uijeongbu, South Korea
*Email: shdudgh@daum.net
Introduction: Deep vein thrombosis (DVT) is a serious and potentially life-threatening complication after total hip arthroplasty(THA). May-Thurner syndrome (MTS) is an iliac vein compression syndrome associated with DVT resulting from chronic compression of the left iliac vein by lumbar vertebrae and overlying right common iliac artery. We investigated the patients presenting with the painful swelling of the lower extremity related to extensive DVT caused by MTS following THA.
Methods: We reviewed the patients underwent THA and had screened for DVT from March 2009 to March 2014 at our institution. We evaluated the clinical and radiological characteristics of DVT using Doppler sonography, venography or CTangiography(CTA). MTS was diagnosed when a common left iliac vein stenosis was found due to compression by lumbar vertebral body and right common iliac artery.
Results: A total of 195 patients were enrolled, 40(21%) patients were diagnosed with DVT. 4(2%) patients had severe and extensive DVT were diagnosed with MTS. All patients diagnosed with MTS were females with a mean age of 63 years and mean BMI of 25.9kg/m2. Painful extensive swelling and erythema to the left lower extremity lasting for a mean of 13days. Radiologic analyses revealed long and extensive thrombi from left common iliac vein to left popliteal vein in the all MTS patients. Pulmonary embolism occurred in 1(0.5%) patient. Systemic anticoagulation was immediately started and interventional procedures was performed combined and selectively [Fig. 1]. In all treated patients, the symptoms improved and subsequent full weight bearing was possible.
Conclusion: MTS is not a rare disease and is reported to occur 22% and 66% of the population. Untreated MTS can cause extensive ilio-femoro-popliteal thrombosis, in orthopedic procedures and can be life-threatening. Increased awareness of orthopedic community is required for early diagnosis and prompt treatment in MTS cases who present with swelling in the left lower extremity after THA surgery.
Figures
Figure 1#7825
Error Analysis of a Shear Wave Tensiometer to Measure Ligament Mechanics: The Next Step Towards Translation to Enhance Knee Arthroplasty
Lesley Arant - University of Wisconsin-Madison - Madison, USA
Mary Laudon - University of Wisconsin-Madison - Madison, USA
Matthew Blomquist - University of Wisconsin-Madison - Madison, USA
*Joshua Roth - University of Wisconsin-Madison - Madison, USA
*Email: roth@ortho.wisc.edu
Introduction
Soft tissue balancing to achieve a desired ligament tension and engagement is a key step during total knee arthroplasty (TKA) [Babazadeh 2009]. Despite its importance, there are no techniques to directly and noninvasively measure the tension and engagement of ligaments. Shear wave tensiometers [Martin 2018] are an emerging technology to directly measure the tension in ligaments [Blank 2020, Arant 2021]. Coupled with a technology to measure joint kinematics (e.g., optical motion capture), shear wave tensiometers might also be able to determine other key metrics of ligament mechanics (e.g., engagement length). However, the accuracy of these measurements has yet to be determined.
Accordingly, the objective of the present study was to determine the errors in ligament mechanics measured in situ using a handheld shear wave tensiometer.
Methods
We performed this study using a mechanical knee model that enables direct tension measurements in a ligament phantom [Arant 2021] (Figure 1). To mimic a patient cohort, we created nine model configurations by varying both the slack length of the phantom and the initial tension in a secondary restraint (Figure 1) at three levels each. For three trials of each knee configuration, we applied a varus-valgus moment up to 20 Nm to the knee model. We simultaneously tracked phantom length using motion capture and phantom tension using a single-axis load cell (Figure 1). We measured shear wave speed using a handheld shear wave tensiometer. We calibrated the shear wave speed – Δtension relationship using estimated Δtensions computed from the applied moment, the functional moment arm of the phantom (Figure 1), and the percentage of the applied moment resisted by the phantom [Grood 1981] (Figure 2).
We used the calibrated relationships to predict Δtension from shear wave speeds measured in each trial. We determined the absolute predicted tension using Δtension and an approximation of the resting tension (i.e., tension at zero applied load) (Figure 2). From piecewise model fits [Tanaka 2011] between calibration-predicted or gold-standard measured tensions (dependent variables) and the phantom length (independent variable), we extracted the phantom slack length, engagement point, and stiffness. We assessed the calibration by computing the errors in tensions, lengths, and stiffnesses between the calibration-predicted and gold-standard values for each trial. We then computed the bias and precision errors pooled across all knee configurations.
Results
The average percent restraint of the phantom was 76% (range: 30% to 97% across configurations). We found errors in predicted tension to be -19.0 ± 47.5 N and errors in engagement length to be -0.02 ± 0.45 mm (Figure 3).
Conclusion
Our results indicate that calibrating a shear wave tensiometer by approximating the percent restraint and the resting tension results in relatively high errors in predicted tension. Our ongoing work is focused on refining these calibration methods to reduce errors in predicted tension. Nonetheless, when coupled with existing surgical technologies to track bone motion, our tensiometer can accurately predict engagement length, which is an important metric of ligament mechanics. These findings push shear wave tensiometers one step closer to translation into the clinic.
Figures
Figure 1
Figure 2
Figure 3#7840
Effect of in Situ Calibration Algorithm on Measurement Errors of Ligament Tension Using a Shear Wave Tensiometer: A Probabilistic Modeling Study
Matthew Blomquist - University of Wisconsin-Madison - Madison, USA
Lesley Arant - University of Wisconsin-Madison - Madison, USA
*Joshua Roth - University of Wisconsin-Madison - Madison, USA
*Email: roth@ortho.wisc.edu
Introduction
Shear wave tensiometry is a novel approach to directly and non-invasively measure ligament tension [Blank 2020, Blomquist 2022]. These direct measurements promise to enhance the surgeon’s ability to properly tension the ligaments during total knee arthroplasty. As with any transducer, shear wave tensiometers need to be calibrated; however, to do so, the tension in the ligament needs to be estimated in a single pose, which can be accomplished by estimating the percentage of an applied joint load restrained by that ligament (%R) at that particular pose. Accordingly, our objectives were to (1) develop calibration algorithms to reduce uncertainty in %R of the collateral ligaments, and (2) determine measurement errors of ligament tension changes using a shear wave tensiometer calibrated with these algorithms.
Methods
To account for patient-to-patient variability in knee mechanics, we generated a virtual cohort of 1000 patients using a probabilistic framework [Smith 2016] and a 12-degree-of-freedom, musculoskeletal model of the knee [Lenhart 2015] (Figure 1). For each model, we performed forward dynamic simulations in OpenSim-JAM of varus-valgus (V-V) and internal-external (I-E) laxity assessments at 0°, 25°, and 45° flexion. We separated the cohort into 500 training models and 500 validation models.
Data from the training models were used to predict %R of the medial and lateral collateral ligaments (MCL and LCL) at 25° flexion under applied V-V moments. We evaluated 5 different cases of predicted %R. For Cases A-C, we fit multivariate regression models to predict the %R as a function of applied moment using three sets of inputs (Figure 2): A) V-V laxities and ligament engagement lengths, B) Case A+I-E laxities, C) Case B+coupled excursions in secondary degrees of freedom. In Case D, we averaged %R of the training models over all applied moments. In Case E, we used the actual %R for each model.
To simulate the application of these calibration algorithms, we computed simulated shear wave speeds (SWS) for the validation models [Blank 2020]. Next, we predicted the tension changes in the MCL and LCL using the %R determined using the 5 cases above. We then virtually calibrated the SWS-estimated tension change relationship at 25° flexion for each of the 5 cases. Finally, we predicted MCL and LCL tension changes using these calibrations at 25° and 45° flexion for each validation model and case. We computed the errors in ligament tension changes between predictions and simulation values.
Results
The predicted error in %R was reduced as more input data was included (Figure 3). Specifically, at 25° flexion, the RMSE of predicted tension changes decreased up to 64% and 61% for the MCL and LCL, respectively. At 45° flexion, RMSE decreased up to 52% and 42% for the MCL and LCL, respectively.
Conclusion
The key findings of this study are (1) considering additional measures of knee biomechanics can reduce the uncertainty in the %R of a particular ligament, and (2) the relationships determined at 25° flexion gave reasonable estimates of tension changes at 45° flexion. Moving forward, we will evaluate these approaches in cadaveric knees.
Figures
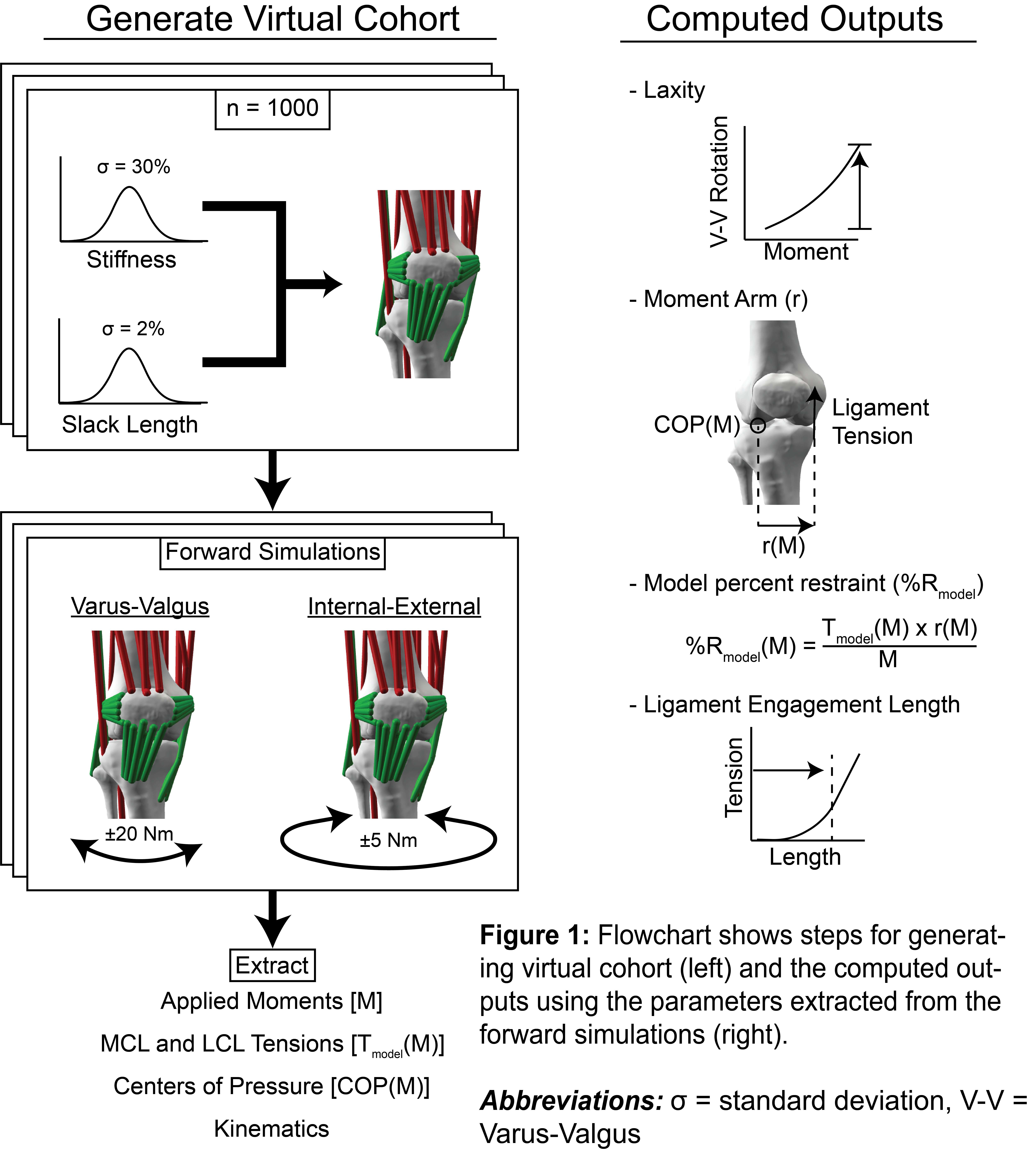
Figure 1

Figure 2
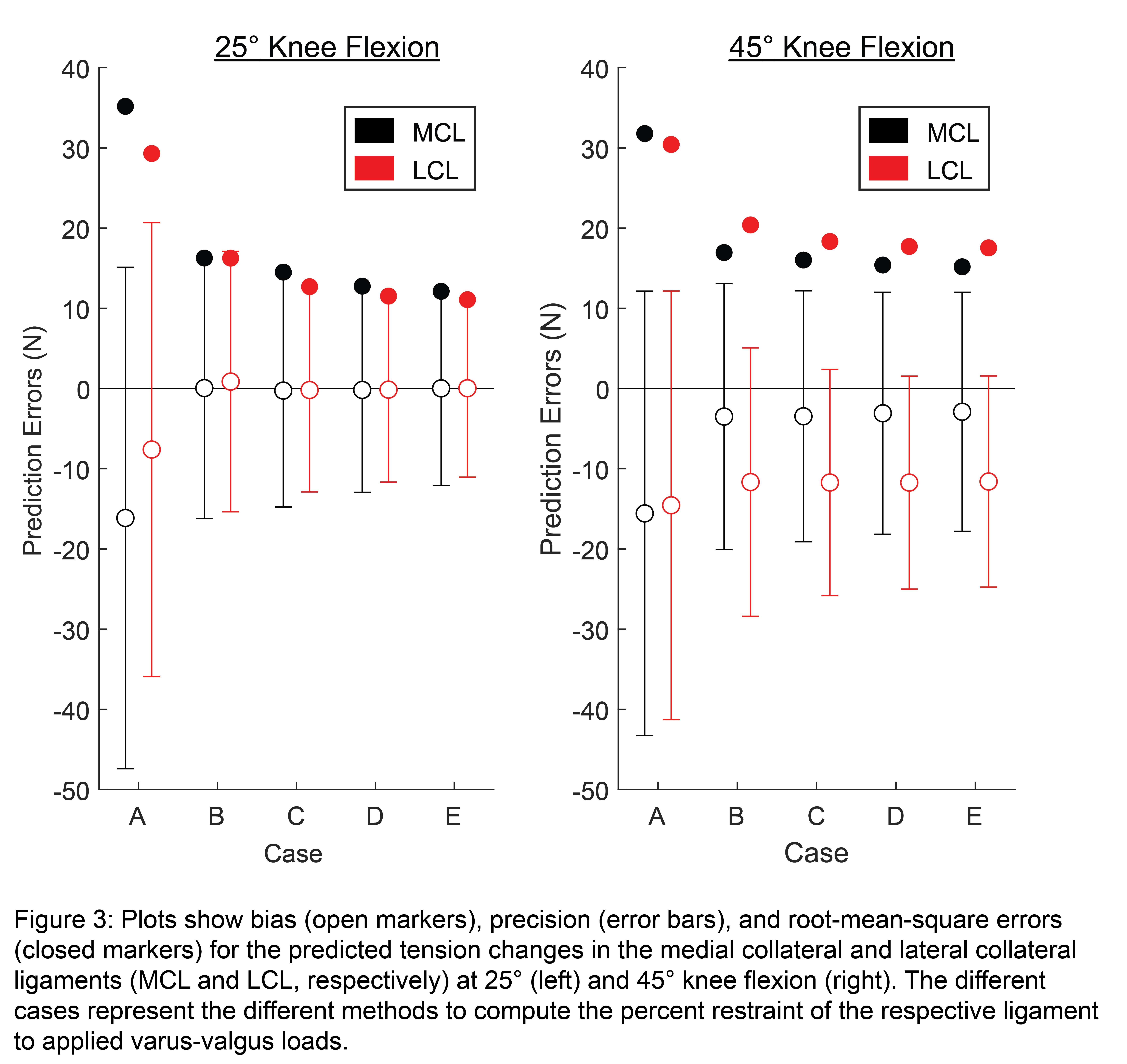
Figure 3#7551
Impaction Method for Implantation Influences the Primary Stability of Press-Fit Hip Cups
*Miriam Ruhr - TUHH Hamburg University of Technology - Hamburg, Germany
Fenna Neumann - Hamburg University of Technology - Hamburg, Germany
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: miriam.ruhr@tuhh.de
Introduction: Bony fixation of acetabular press-fit cups is a prerequisite to prevent early revision due to cup loosening [1,2]. Primary cup stability depends on the press-fit and friction between bone and cup. It is gradually increased during implantation, while it is decreased afterwards due to relaxation of the viscoelastic bone. Differences in the used impaction protocol might affect the stability of the cup in the acetabulum. The aim of the study was to improve the surgical impaction technique by identifying impaction protocols which improve the primary stability.
Materials and Methods: Three impaction protocols were used to implant press-fit cups into porcine pelvises with a powered impactor (3.5 J, Kincise, Fig.1) until no further cup seating was observed (< 0.1 mm, DIC system). In the first group, the impactor was used with an impaction frequency of 1 Hz (n = 5), in the second group a subsequent single blow was applied 20 s after a 1 Hz impaction (n = 5 each). In the third group the cups were impacted with 6 Hz (n = 6). Impaction forces were measured with a load cell at the lower end of the impactor. Impulse and impulse duration were calculated. Strain gauges on the inner cup surface were used to determine cup deflection – caused by the radial forces between bone and cup – during implantation. The actual press-fit was determined based on laser scans before and after implantation. Primary stability was accessed by lever-out testing. Fractures and cracks of the acetabula were identified visually after removal of the cup.
Results: Cups impacted at 6 Hz showed higher lever out moments (p < 0.001, Fig.2A) than cups implanted at 1 Hz and 1 Hz + blow, which showed similarlever out moments (p = 0.841). All three protocols did not differ in terms of deformation (p = 0.585), number of blows (p = 0.098) and press-fit (p = 0.139). Strain relaxation between the blows was higher for the 6 Hz impaction protocol (p=0.039). A tendency towards higher impulses (p = 0.059) and smaller impulse durations was observed for the 6 Hz impactions (p = 0.059). Bone damage was found for all acetabula in the 1 Hz + blow group and for 3 acetabula in the 1 Hz group, but only 2 damages were visible in the 6 Hz group (Fig.2B). The lever out moment for the fractured acetabula independent of groups was reduced by approximately 40 % compared to the intact bones (p = 0.115).
Conclusion: High impaction frequencies were found to be superior in terms of primary stability and bone damage achieving similar cup deformation. Despite the smaller relaxation period between the blows, higher relaxations at high impaction frequencies were found. This indicates together with the smaller pulse durations an increased system stiffness. An additional blow after 20 s showed no benefit. The implantation of press-fit cups might benefit by the use of powered impaction tools, which enable a controlled energy input and the use of higher frequencies.
Acknowledgements: The study has been financially supported by DePuy Synthes.
References:
[1] Jasty et al., J Bone Jt Surg 1997
[2] Pilliar et al., Clin Orthop Relat Res 1986
Figures
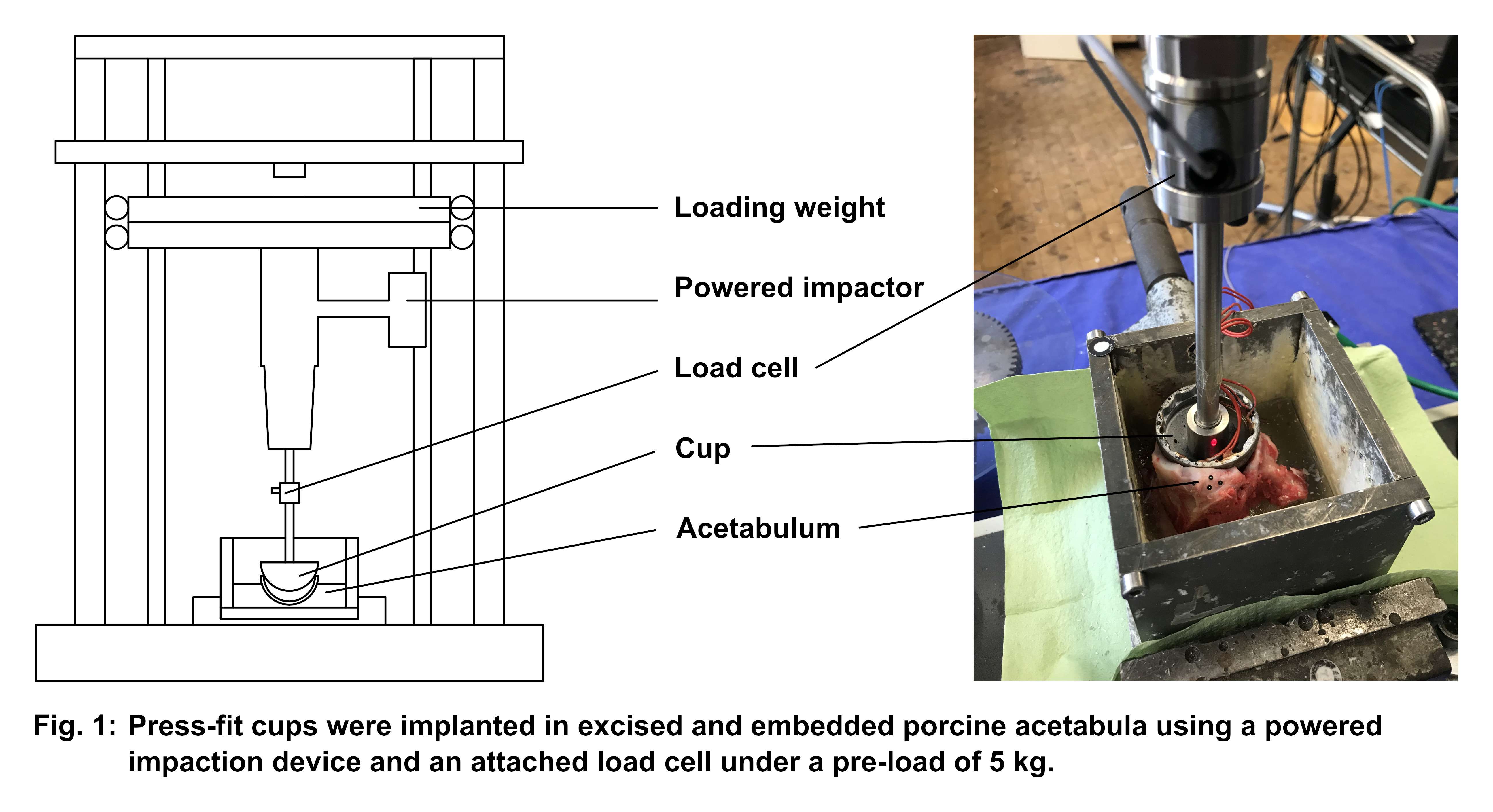
Figure 1
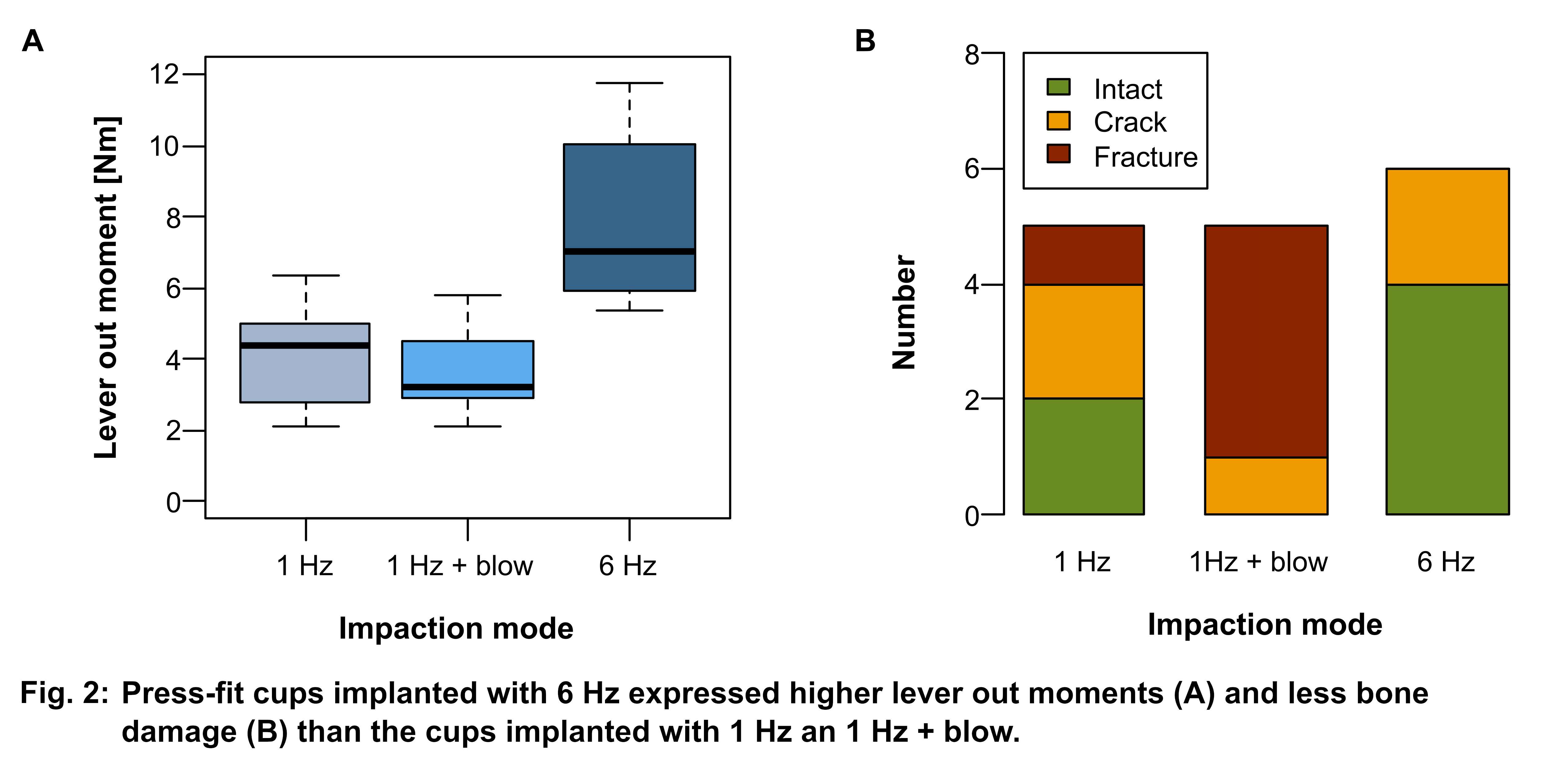
Figure 2#7411
Drivers of Initial Stability in Cementless TKA: Isolating Effects of Tibiofemoral Articulation and Fixation Features From Current Implants
*Paul J. Rullkoetter - University of Denver - Denver, USA
Chadd Clary - University of Denver - Denver, USA
Yashar Behnam - University of Denver - Denver, USA
Huizhou Yang - University of Denver - Denver, USA
*Email: prullkoe@du.edu
Introduction
Initial fixation of cementless tibial trays after total knee arthroplasty (TKA) is crucial to ensure bony ingrowth and long-term fixation. Various implant designs that utilize different features to facilitate this initial stability are currently available. This study aimed to assess the isolated impact of articular conformity and tray features on micromotion during a series of simulated activities, including both cadaveric testing and corresponding computational models.
Methods
Two current fixed-bearing cementless TKA systems were evaluated, including a knee system (Design I) with a semi-constrained tibiofemoral articulation, an intermediate-length cruciform stem, and four peripheral cylindrical pegs. Design-II has lower articular conformity, and the tibial tray includes a large central keel and four bullet cruciform pegs (Fig.1). Note that Design-II is commercially available and clinically successful. Six cadaveric lower limb specimens were implanted with a Design-I TKA on one side and an equivalent size Design-II TKA on the contralateral side, potted into fixtures, and mounted into the AMTI VIVOTM to simulate gait, deep knee bending, and stair descent. Experimental boundary conditions were derived from telemetric implant data and ASTM standards (displacement-control for flexion-extension rotation; force-control for the other degrees of freedom). Relative displacements between the anterior tray-bone interface were recorded using a digital image correlation system (Fig.1).
Two previously-validated cadaveric tibial finite element models were implanted with equivalent sizes of the two designs and evaluated using the same experimental loading conditions (Fig.1). The anterior tray-bone displacements were predicted and compared with the experimental measurements. After validation, the full-field tray-bone interface micromotion and the porous coating area favorable for bone ingrowth (surface area<50µm) were investigated. To study the isolated effect of femoral-insert conformity and fixation features on micromotion, the fixation features of the Design-I and II tibial trays were virtually exchanged, where the respective insert, locking mechanism, and tibial base shape maintained unchanged (Fig.2). The models with swapped fixation features were re-tested. The predicted tray-bone interface micromotions were then compared with the initial models, isolating the impact of the articulation or specific tray features.
Results
The peak interface micromotions predicted for the Design-II knee system was on average 50.2±4.5, 95.0±0.2, and 19.4±0.2µm (GT, SD, DKB), which was at least 42% larger than those predictions for Design-I (Fig.3). This was a combined result of different femoral-insert conformity (contributed 81% of the micromotion difference) and fixation design features (19%). The maximum difference in peak micromotions by only optimizing the specific fixation features used here was up to 55.8µm (30%). The predicted surface area<50µm for Design-I was on average 9.5cm2 (40%) larger than Design-II (Fig.3).
Conclusion
During force-controlled simulation, implant conformity was the key driver of tray-bone interface micromotion, with a more posterior femoral-insert contact due to lower conformity significantly increasing the micromotion and reducing the surface area ideal for bone ingrowth. The impact of different tray features was relatively smaller but still considerable, indicating the potential to improve implant stability by further optimizing the fixation features.
Figures
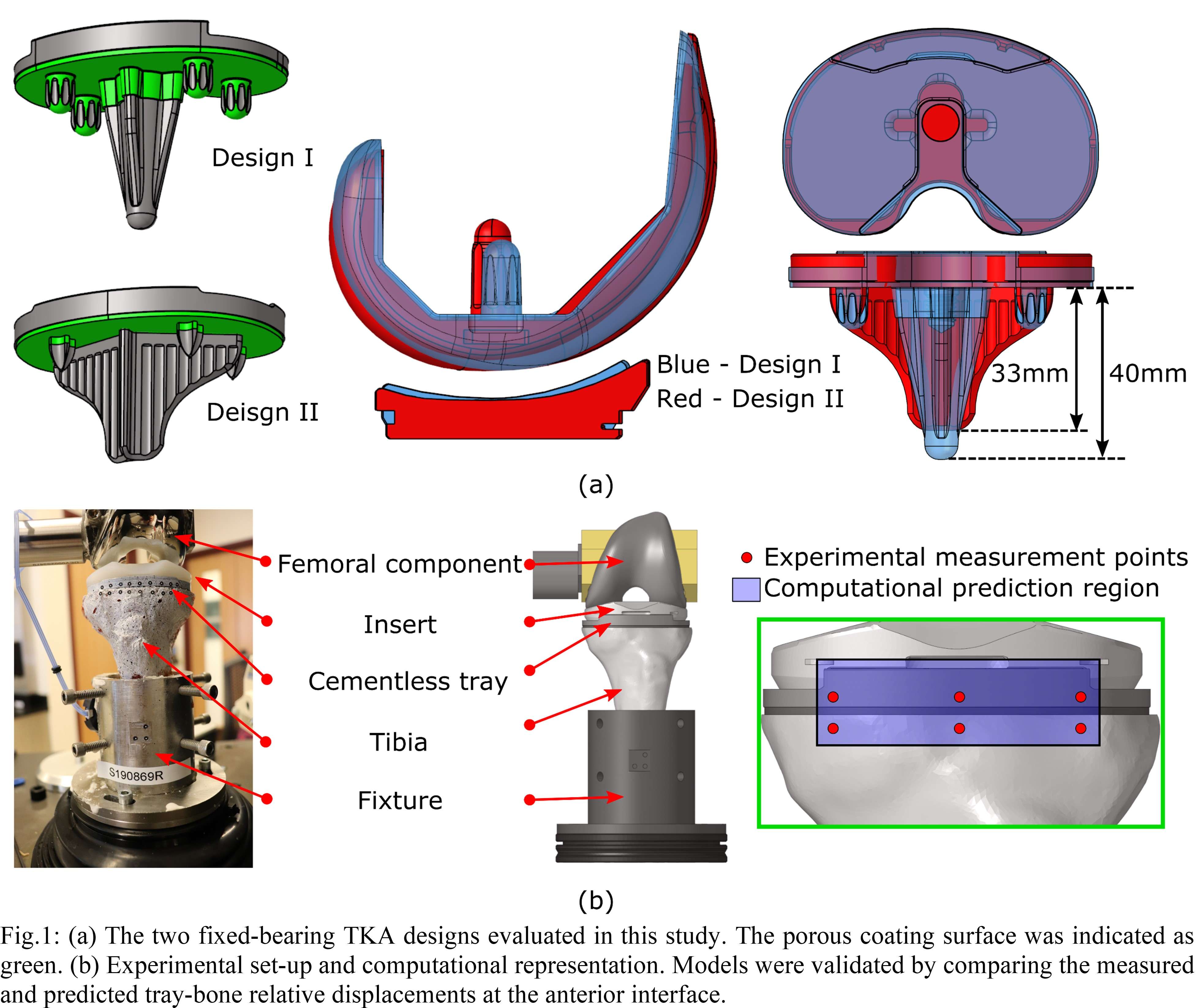
Figure 1
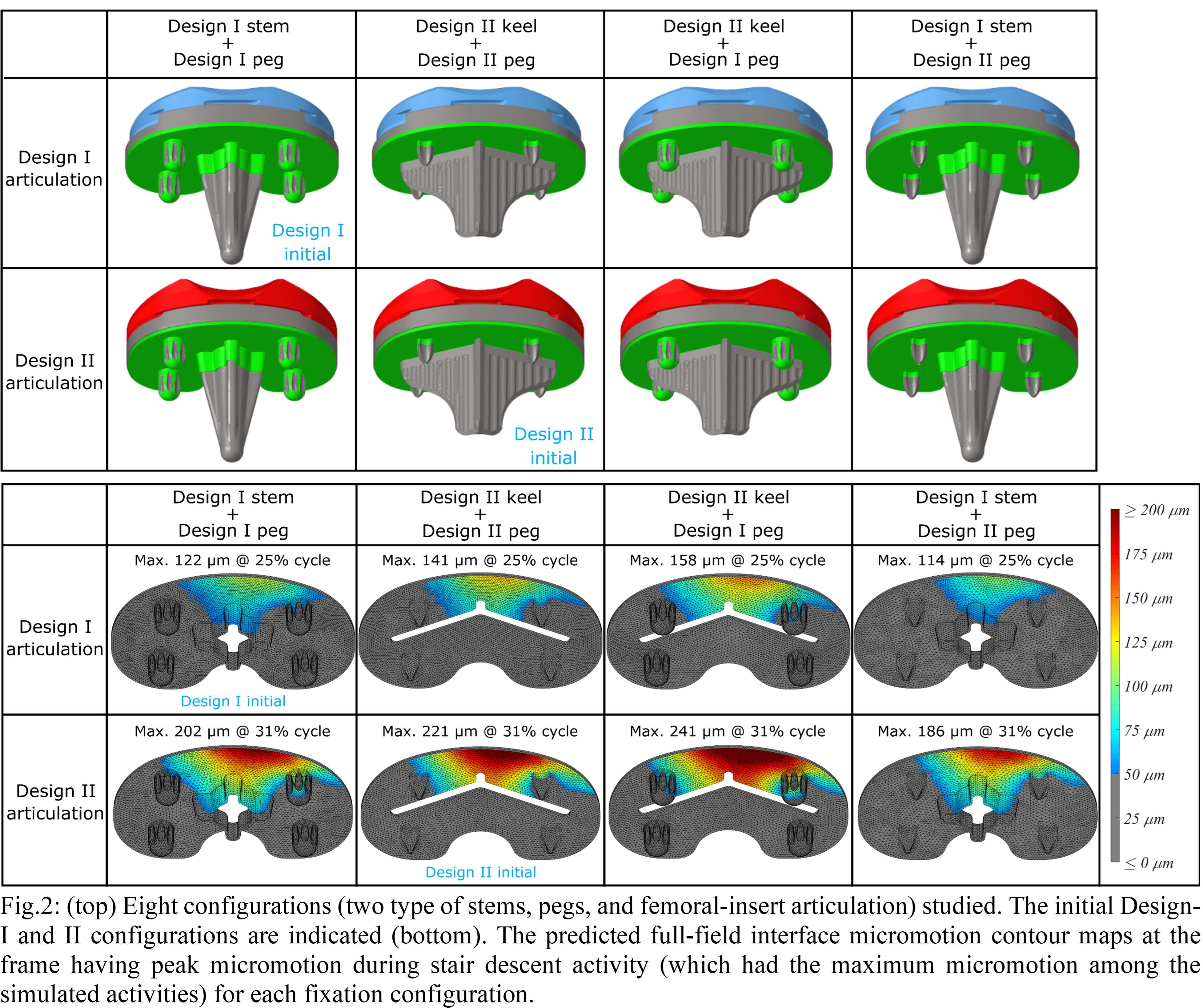
Figure 2
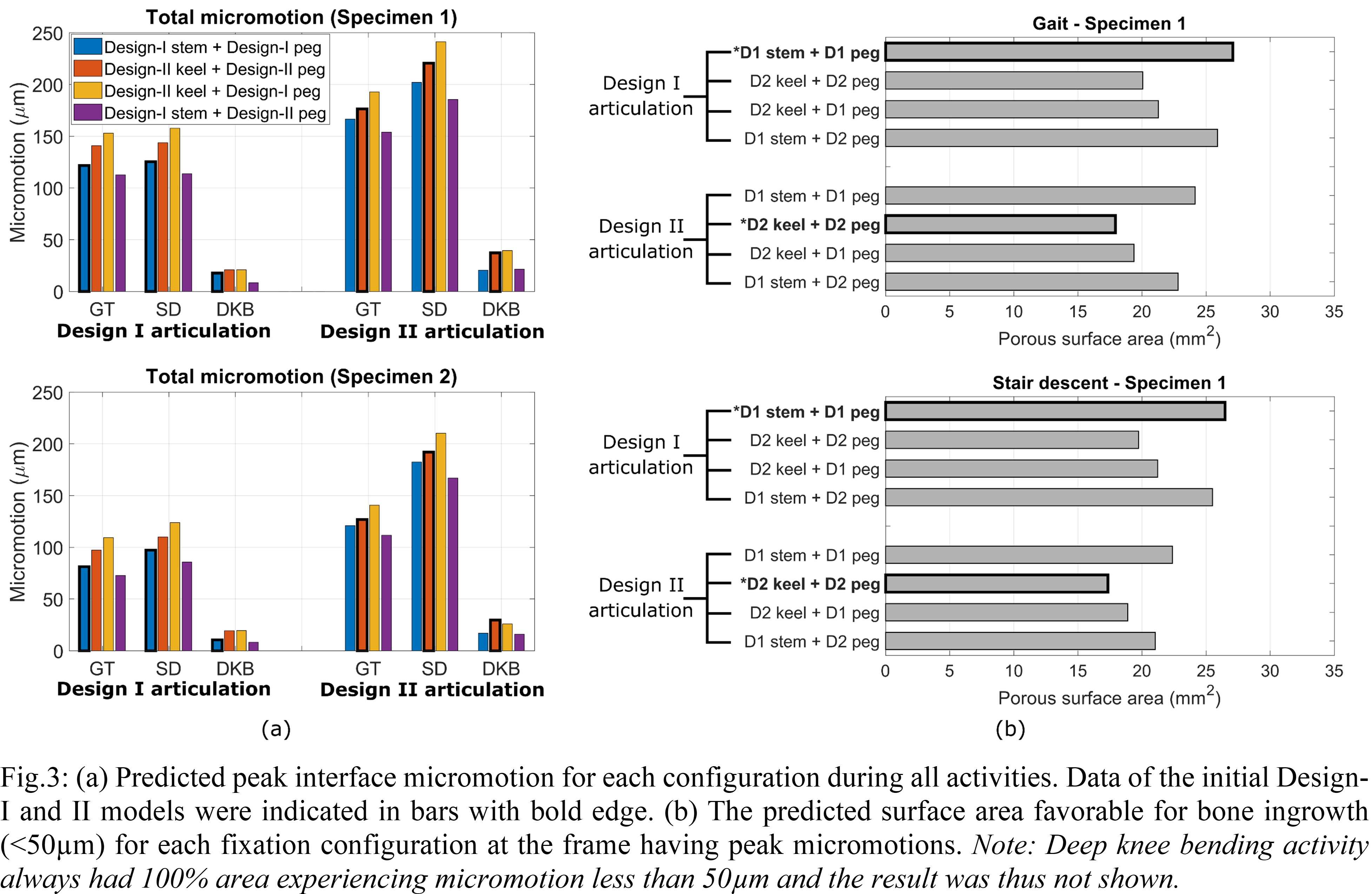
Figure 3#7644
No Difference in Antero-Posterior Position Between Bi-Crusiate Substituting Total Knee Arthroplasty and Healthy Knee
*Keinosuke Ryu - Surugadai Nihon University Hospital - Chiyodaku, Japan
Takanori Iriuchishima - Kamimoku Hot Springs Hospital - Gunma, Japan
Takashi Suzuki - Nihon University School of Medicine - Itabashiku, Japan
Hyunho Lee - Nihon University - Tokyo, Japan
Kazuyoshi Nakanishi - Nihon University - Tokyo, Japan
*Email: kei0202@nifty.com
Introduction
The JOURNEY II Bi-Cruciate substituting (BCS) Knee System is a recently developed system with a cam-post structure designed to possess the functions of both the ACL and the PCL, reproducing the kinematics, function, and stability of a healthy knee. Several studies have reported that it shows similar knee kinematics in BCS-TKA as in normal knee function and favorable clinical results. However, no study has yet addressed the question of anteroposterior tibiofemoral positioning. In this study, the posterior offset ratio (POR) was used to evaluate the anteroposterior positioning of the femur with respect to the tibia in TKA using the Journey II BCS, and its associations with posterior tibial slope and lateral femorotibial angle (FTA) were investigated.
Materials
The study evaluated 124 knees of 82 patients who underwent surgery using the BCS-TKA procedure. They comprised 12 knees of 9 men and 112 knees of 73 women, with a mean age 74.8 years (58–96 years) and mean preoperative FTA of 183.9° (177°–200°), with all knees showing varus knee deformity. The preoperative diagnosis of all patients was osteoarthritis.
Methods
The POR was calculated from postoperative lateral radiographs in the fully extended position, using the method described by Onodera et al. The posterior tibial slope was measured on lateral radiographs and the lateral femorotibial angle (lateral FTA) was also measured. We investigated the relationship between POR and posterior tibial slope, POR, and lateral FTA.
Results
The mean POR in BCS knees was 6.7%±3.6% (−2.6% to 13.6%) (Figure1). The posterior tibial slope was significantly correlated with the POR (r=0.21, P<0.05), and the lateral femorotibial angle was significantly correlated with the POR (P=-0.18, P<0.05) (Figure2, 3).
Discussion
According to previous study, the mean POR is 5.6% in healthy adults, 14.1% after cruciate-retaining TKA, 19.2% after posterior-cruciate-substituting TKA, and 24.3% after mobile-bearing TKA. In the present study, the POR after BCS-TKA was 6.7% lower than for any of the other types and closer to that of healthy adults. BCS-TKA, which incorporates reproduction of ACL function into its design, thus positions the femur further forward with respect to the tibia than does any other type of device, more closely reproducing the anteroposterior tibiofemoral positioning seen in healthy adults. This suggests that using the BCS-TKA may help increase patient satisfaction by providing kinematics that are closer to normal and better knee function. In the present study, the POR after BCS-TKA was positively correlated with the posterior slope and negatively correlated with the lateral FTA. This suggested that too steep a posterior slope or postoperative flexion contracture may increase the POR in BCS-TKA, impeding the BCS design concept.
Conclusions
The POR was used to evaluate anteroposterior femorotibial positioning in 145 knees of 82 patients who underwent BCS-TKA. The value of the POR was lower for the BCS than for other types of devices and closer to that of healthy knees.
Figures
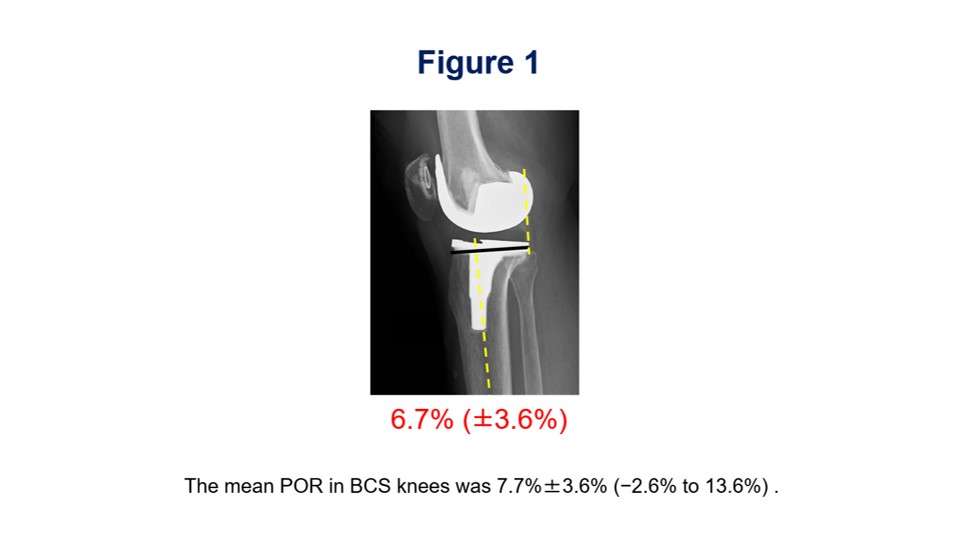
Figure 1
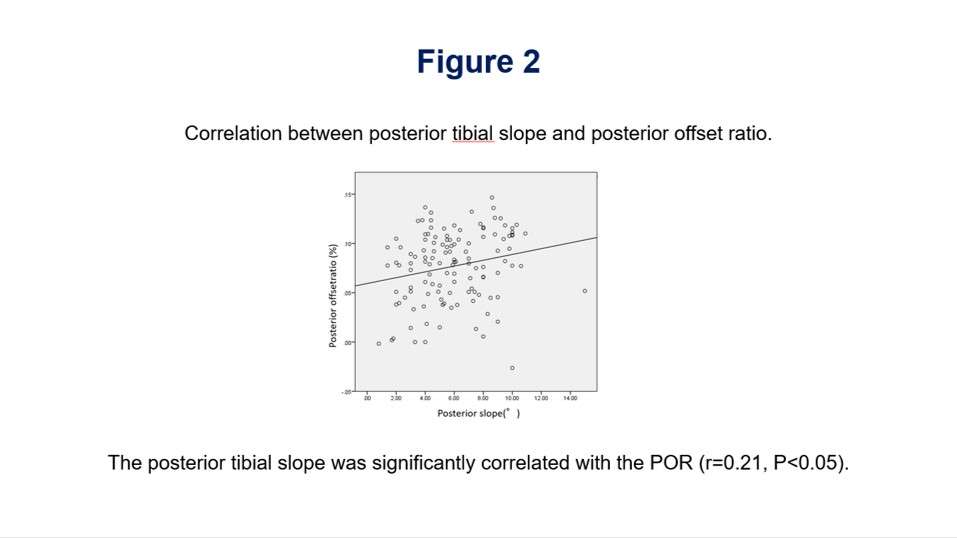
Figure 2
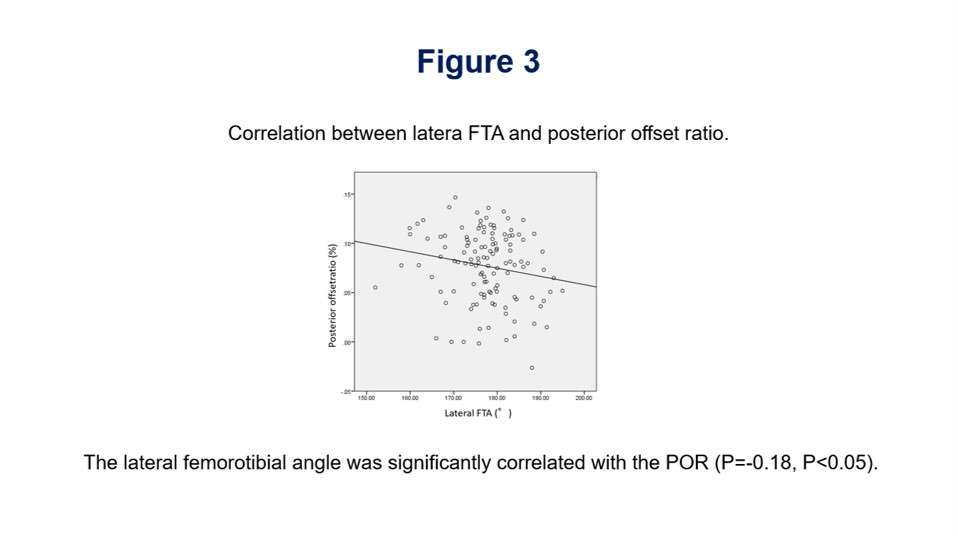
Figure 3#7343
The Usefulness of an Extensible Trial Neck in Total Hip Arthroplasty
*Takashi Suzuki - Nihon University School of Medicine - Itabashiku, Japan
Keinosuke Ryu - Surugadai Nihon University Hospital - Chiyodaku, Japan
Kei Kojima - Surugadai Nihon University Hospital - Tokyo, Japan
Takanori Iriuchishima - Kamimoku Hot Springs Hospital - Gunma, Japan
Tatsuya Kubomura - Eisei Hospital - Hachiojishi, Japan
*Email: rastavibration2328@yahoo.co.jp
Introduction: Dislocation is one of the most common complications after total hip arthroplasty (THA). It is very important to attain adequate soft tissue tension to prevent dislocations. Surgeons control this tension with the neck length after placing implants. However, experimenting with different necks can be troublesome for surgeons, since a hip dislocation is needed each time. We have developed a new trial neck device named Multi-trial neck that can easily change the neck length in the surgical field(Fig 1,2). This device can help surgeons avoid the need to dislocate the hip over and over to find the right neck size. The objective of this research was to investigate whether this device could help shorten the operation time and decrease surgical invasion of the patient.
Method: A total of 36 hips of 32 subjects (7 men and 29 women) with a mean age of 71.8 years were investigated. The mean BMI of the subjects was 23.7. Total hip arthroplasty was performed on all hips at our institute; 32 of them had osteoarthritis; 3 femoral head necrosis; 1 Rapidly Progressive Coxopathy. All THA procedures were performed with antero-lateral supine approach using Kinectiv stem (ZimmerBiomet) by a single surgeon. Leg discrepancy and femoral offset were considered using fluoroscopy and trial reduction was performed on all subjects after stem and cup were placed. Subjects were randomly divided into two groups. The first group used the Multi-trial neck (ZimmerBiomet Japan, Tokyo) during trial reduction (group M) and the other group used a conventional trial neck (group C).Student’s t-test was performed to compare both operative time and blood loss, and Mann-Whitney’s U test was performed to compare the number of times an additional dislocation was needed during operation between group C and group M. P<0.05 was adopted as the level of statistical significance.
Result: The mean elongation of Multi-trial neck in group M was 3.3±1.3 times. Mean operative time for group M was 100±9 min and 117±17 min for group C. Operative time in group M was significantly shorter compared with group C (p<0.05). Mean blood loss during operation for group M was 600±232 ml and 529±192 ml for group C. No significant difference in blood loss was observed between the two groups. Additional dislocation during operation for group M was 0.8±0.9 times and 3.3±1.3 times for group C. The results show that the number of dislocations needed in choosing the final neck size was significantly less for group M (p<0.05).
Conclusion: The newly developed Multi-trial neck was revealed to be useful in selecting an appropriate neck size easily and speedily. It was able to reduce the number of dislocations needed to determine the appropriate length of the trial neck, resulting in a shorter operative time. Moreover, the device helped make THA surgery less invasive, and stress on both the patient and surgeon was greatly reduced.
Figures
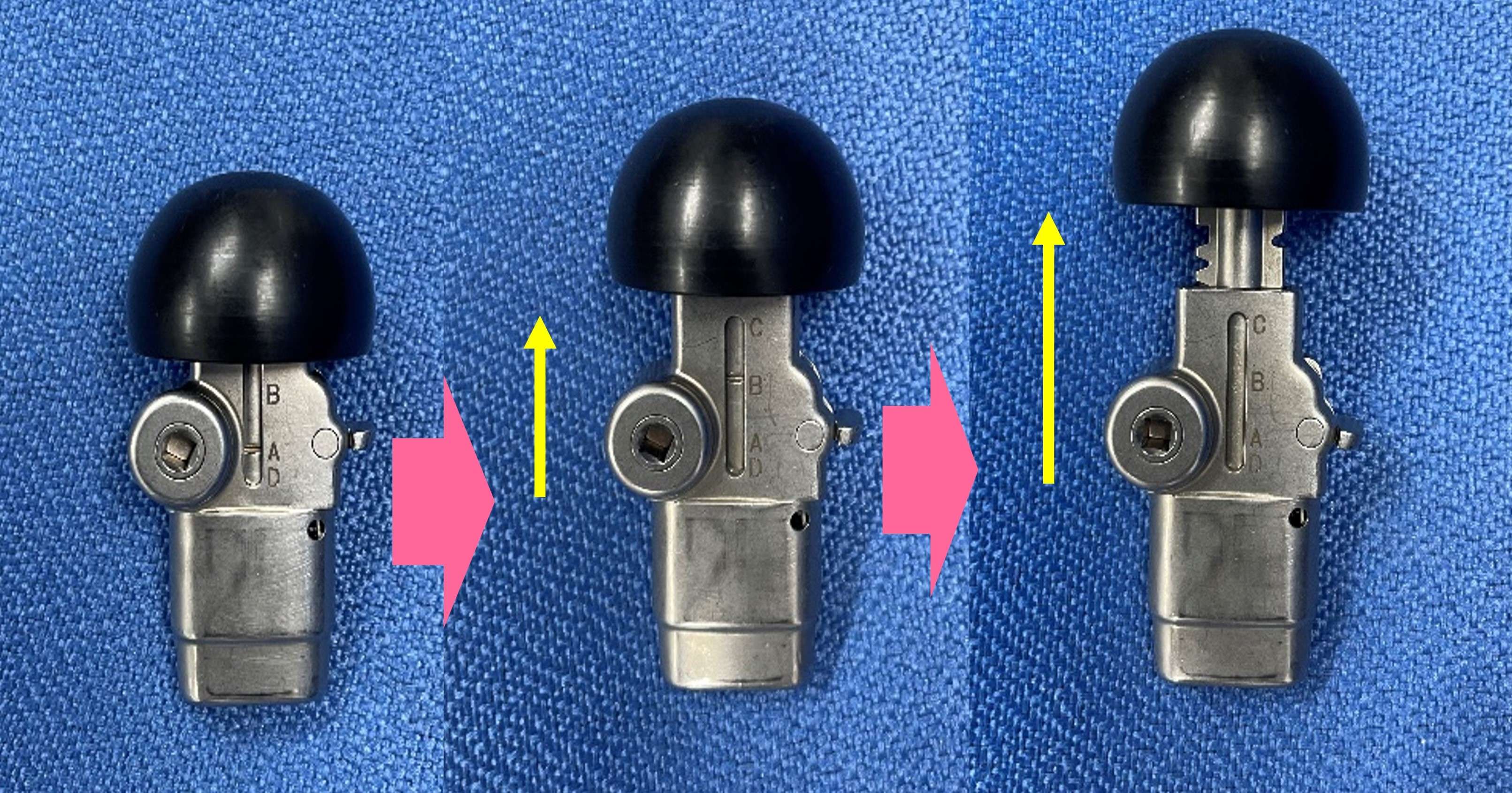
Figure 1
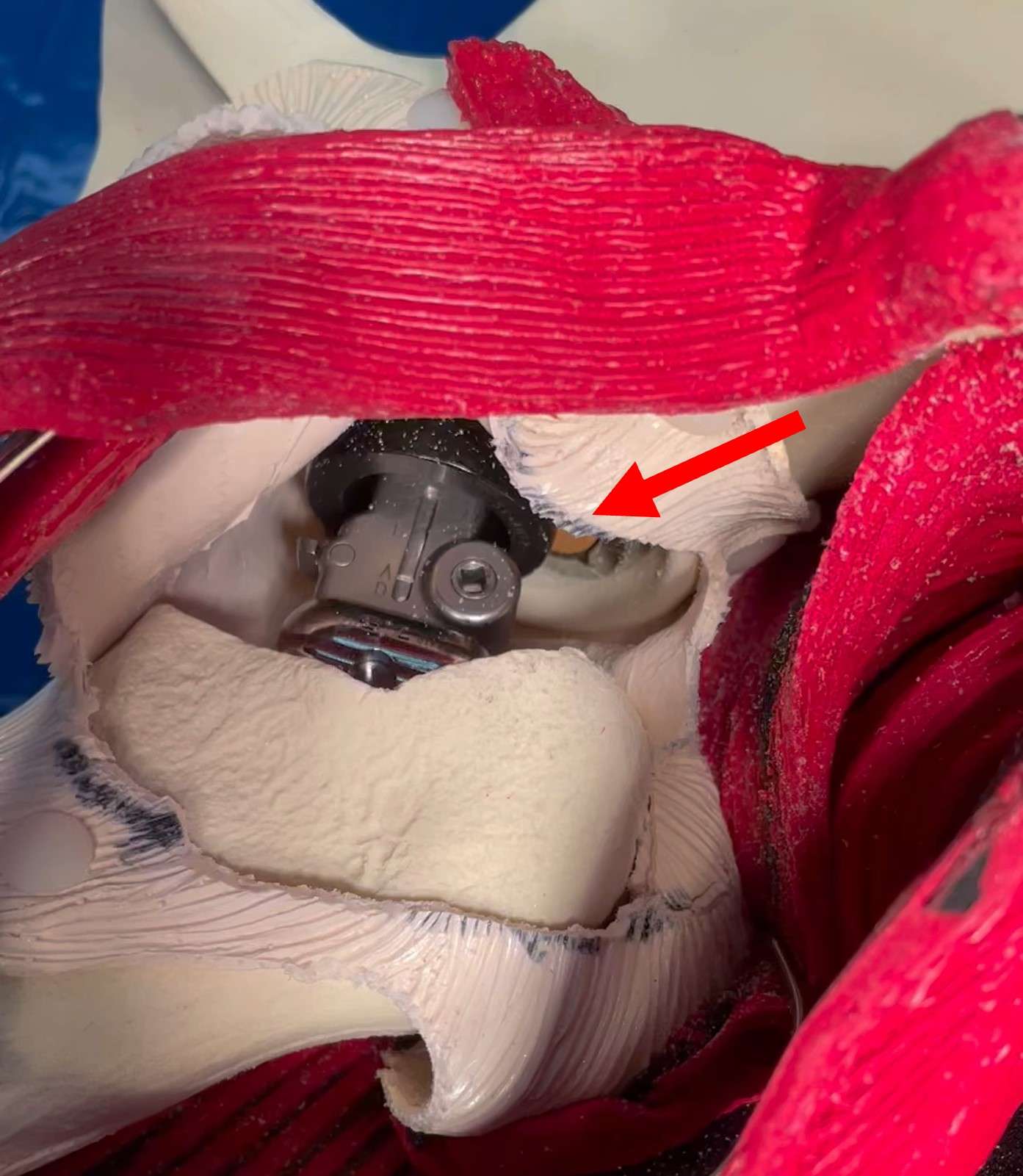
Figure 2#7843
The Natural Trends of C-Reactive Protein After Hip Arthroplasty for Femoral Neck Fracture Without Infection
*Suk Kyoon Song - Daegu Catholic University Medical Center - Daegu, South Korea
Cheol-Hwan Ryu - Daegu Catholic University Medical Center - Daegu, South Korea
Hee-Chan Kim - Daegu Catholic University Medical Center - Daegu, South Korea
*Email: ryansong10@naver.com
The aim of this study was to estimate the degree of normalization of C-reactive protein (CRP) at 2-weeks and 4-weeks after hip arthroplasty after femoral neck fracture. We also wished to determine whether the degree of CRP normalization differs after total hip arthroplasty (THA) compared to bipolar hemiarthroplasty (BH). We also wanted to analyze the patient factors that may influence CRP normalization. We conducted a retrospective study of 135 patients who had undergone THA (32 cases) or BH (103 cases) for femoral neck fracture by single surgeon from January 2015 to December 2019. We analyzed CRP levels during the preoperative period, the early postoperative period, the 2-week postoperative period, and the 4-week postoperative period. In THA, CRP was normalized in 4 patients (12.5%) and in 15 patients (46.9%) within 2-weeks and 4-weeks after surgery, respectively. In BH, CRP was normalized in 16 patients (15.5%) and in 52 patients (50.5%) within 2-weeks and 4-weeks after surgery, respectively. There were no statistical differences between THA and BH. Compared to women, men were 3.78 (95% confidence interval, 1.05–13.63) times less likely to have normalized CRP at 2-weeks after surgery (P=.042). Compared to women, men were 3.01 (95% confidence interval, 1.44–6.27) times less likely to have normalized CRP at 4-weeks after surgery (P=.003). Only 50% of patient’s CRP level was normalized during 4-week postoperative period. In men, CRP levels were significantly higher than women in whole period. In the case of THA, the CRP level was higher only in early postoperative period compared to BH, and there was no difference since then.
#7327
Outcome of the Hip Arthroplasty Performed by Low-Volume Operators
*Suenghwan Jo - Chosun University Hospital - Gwangju, Korea (Republic of)
Hyeon Joon Lee - Chosun University Hospital - Gwagnju, South Korea
Hyo Jun Lee - Chosun University Hospital - Gwangju, South Korea
Jae Hong Ryu - Chosun University Hospital - Gwangju, South Korea
*Email: sueng78@gmail.com
Introduction : Hip arthroplasty (HA) is recognized as the most successful orthopaedic intervention to the debilitating hip. However, while the operation often result in excellent outcome, the literature recommends minimum of 20 to 50 operations per year in order to achieve consistent results. In the current study, we aim to report the outcome of the HA that were performed by the low volume surgeons.
Materials and methods : The inclusion criteria for the current study is HA operated by the surgeons who had performed less than 20 HA per year between January 2011 and September 2020. Total of 689 hips (631 patients) were included in the current study which consist of 15 surgeons from 8 institutions. The mean number of operations per surgeon was 9.0 per year ranging 2 to 19 operations. The general demographic data were retrieved from the hospital records while initial diagnosis, adequacy of operation were assessed and evaluated by preoperative and postoperative radiographs. Additionally, postoperative complications were recorded.
Results : The mean age of the patients was 64.7 years (range, 36 to 102 years) and included 174 males and 457 females. Overall, 61 total hip arthroplasties and 628 hemiarthroplasties were performed. The preoperative diagnosis was femoral neck fracture in 524, intertrochanteric fracture in 47, osteonecrosis in 59, primary or secondary osteoarthritis in 24 and any other reasons in 35. Of the hips that underwent total hip arthroplasty, cup position were noticed to be outside the safe zone in 18%. Overall, stem malalignment was observed in 9.25% of the operations. Postoperatively, dislocation was developed in 16 hips (2.3%), infection in 29 (4.2%) and periprosthetic fracture in 17 (2.5%).
Conclusion : The result of the current study shows that the fracture around the hip is the main indication for performing HA in low volume surgeons. While the incidence of postoperative complications were comparable to that of the previous reports from the high volume institutions, high incidence of malpositioned cup and stem remains a problem.
#7681
The Use of Preoperative Planning to Decrease Costs and Increase Efficiency in the OR
Alessia Lavin - Palm Beach Shoulder Service Atlantis Orthopaedics - Lake Worth, United States of America
*Vani Sabesan - Cleveland Clinic Florida - Weston, USA
Bhavya Sheth - Florida International University - Miami, USA
Christian Martinez - Ponce University - Puerto Rico, USA
*Email: sabes001@gmail.com
Background: Shoulder arthroplasty (SA) has been shown to incur up to $1.8B per year in societal costs. With the increasing demand for SA and the steady decrease of annual reimbursements for orthopedic procedures, it has become crucial to control costs. In SA there has been interest in using preoperative planning software to improve accuracy in positioning and implant selection, ultimately to optimize outcomes. However the use of preoperative planning to increase efficiency has not been studied. The purpose of this study was to determine if preoperative planning could increase efficiency and decrease costs in the operating room.
Methods: This retrospective review included 94 who underwent shoulder arthroplasty and had a CT scan with a preoperative plan by a single orthopedic surgeon between 2017-2020. The patients were divided into two groups based on the use of the preoperative plan during surgery. Group 1 included 28 patients who underwent SA without a preoperative plan utilized during surgery and group 2 included 66 patients with a preoperative plan used during surgery. Procedure time in minutes, average number of trays sterilized, and postoperative outcomes were analyzed between the two groups. Sub-analysis was done to find a statistical difference in the cost of sterilization for both groups. Statistical analyses included the T-test and Pearson’s correlation.
Results: The cohort had 55% males with an average age of 71 years and average BMI of 29.9. There were no significant differences between the groups for age, BMI, nor ASA class. There was no significant difference between groups in average operative time (119.7 minutes for group 1 and 111.8 minutes for group 2 (p = 0.87)) or average time in the OR (173.2 minutes for group 1 and 183.6 minutes for group 2 (p = 0.87)). However, there was a significant difference in average trays prepared and sterilized between the groups with 5.6 trays for group 1 and 4.8 trays for group 2 (p < 0.0005). This yielded a significant difference in cost of sterilization between the groups with group 1 costing on average an additional 17% (p < 0.0005). There were no significant differences in postoperative outcomes between the groups.
Conclusion: While preoperative planning did not reduce time in the OR for shoulder arthroplasty, it was correlated to a significant reduction in the number and cost of sterilized trays with comparable postoperative outcomes. Better cost data and transparency for future studies will further elucidate the cost impact of preoperative planning in the OR. With decreasing reimbursement for orthopedic surgery, administrators and physicians must find more tools to control operating costs.
#7682
Invited Talk: Patients Perceptions and Utilization of Physical Therapy After Shoulder Surgery
Alessia Lavin - Palm Beach Shoulder Service Atlantis Orthopaedics - Lake Worth, United States of America
Brett Stephens - Nova Southeastern Univeristy College of Osteopathic Medicine - Davie, USA
*Vani Sabesan - Cleveland Clinic Florida - Weston, USA
*Email: sabes001@gmail.com
Background: Formal Physical Therapy (PT) traditionally has been a critical part of postoperative recovery but recently due to cost containment, coverage of PT has become limited. Alternatives to formal PT have been proposed, including telerehabilitation, internet-based PT (IBPT), and home-based physician-guided PT. The purpose of this study was to understand patient perceptions of PT, the benefits, perception of improvements, access to PT and alternative forms of PT after shoulder surgery.
Methods: Eighty orthopedic surgery shoulder patients were anonymously surveyed at one institution. Demographics, PT access, number of PT sessions, insurance, copayment, patients’ perceptions of improvement, and their opinion about IBPT was collected. Answers were designed using Likert-scale or open-ended questions. Descriptive statistics were used to report survey data. Analyses were performed based on demographic variables using independent t-test, chi-square tests, and analysis of variance (ANOVA).
Results: Patients attended an average of 16.3 ± 13.8 PT sessions, with 65% ± 32.2 attributing average improvement to their sessions. Average copay was $18 ± 20.8 per session, which 56.1% agreed was reasonable. Almost all patients (94.8%) agreed their therapist took time to educate them. Half (52.5%) disagreed that successful PT could be achieved by IBPT and 68.6% of patients responded they would not consider using IBPT even after a few in-person sessions.
Conclusion: Orthopaedic surgeons need to be aware that patients have a positive perception of their therapy, cost, number of sessions, and utility of PT to impact their improvement following orthopedic shoulder surgery. For IBPT to be a viable alternative, it should involve close engagement of a physical therapist given patient’s perception of PT. Orthopaedic surgeons can reinforce the notion to patients that the referral to physical therapy is a critical part of recovery and has a direct impact on their outcome.
#7684
Acromiohumeral Distance: Can Radiographic Factors Impact Outcomes After Reverse Shoulder Arthroplasty?
Alessia Lavin - Palm Beach Shoulder Service Atlantis Orthopaedics - Lake Worth, United States of America
Feyikemi Ogunfuwa - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Ajay Desai - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Howard Routman - Atlantis Orthopedics - Atlantis, USA
*Vani Sabesan - Cleveland Clinic Florida - Weston, USA
*Email: sabes001@gmail.com
Introduction: Reverse shoulder arthroplasty (RSA) has demonstrated to be highly effective in restoring clinical function and reducing pain however, complications following RSA persist and various outcome predictor tools have been investigated to give providers and patients realistic expectations. Radiographic shoulder measurements have emerged as a possible tool useful to predict clinical outcomes following shoulder surgery and potentially identify complications. The purpose of this study was to investigate the association between preoperative and postoperative radiograph measurements and clinical outcomes in patients following (RSA).
Methods: A retrospective review of 139 patients who underwent RSA performed by a single surgeon in a single institution from April 2018 to July 2020 was performed. The pre- and postoperative radiographic measurements included acromiohumeral distance (AHD) and β-angle. Measurements were correlated to clinical, functional, and patient satisfaction outcome scores using Pearson’s correlation coefficient tests. Functional outcomes included forward flexion, abduction, internal rotation, and external rotation. Clinical outcomes included the Simple Shoulder Test (SST), Constant score, American Shoulder and Elbow Surgeons (ASES), University of California at Los Angeles (UCLA) Shoulder Score, Shoulder Pain and Disability Index (SPADI), and Shoulder Arthroplasty Smart Score (SAS). Functional, clinical outcomes, and patient satisfaction scores were obtained at a minimum 1-year follow up.
Results: The mean age of the cohort was 72 years and with and average BMI of 30 at the time of surgery. Majority of the cohort was Caucasian (91.4%) and female (63.7%). The mean postoperative AHD was 35mm which was significantly higher than preoperative AHD at 8.4 mm (p < 0.01). Preoperative AHD was significantly correlated to patient satisfaction scores (p=0.027, r=0.21). Postoperative β-angle was found to be significantly correlated to passive external rotation (p=0.018, r=0.21). All other correlations were not statistically significant.
Conclusion: The results of our study showed AHD significantly changed postoperatively after RSA, however this change was not correlated with outcomes scores or function except for external rotation. Subsequently, there remains a debate regarding the ideal placement of the components during RSA and the value of these measurements to predict optimal active ROM and patient reported outcomes while minimizing complications.
#7685
Optimal Treatment for Glenoid Bone Loss: Augmented Versus Standard Reverse Shoulder Arthroplasty?
Alessia Lavin - Palm Beach Shoulder Service Atlantis Orthopaedics - Lake Worth, United States of America
Sarah Girshfeld - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Christian Martinez - Ponce University - Puerto Rico, USA
Howard Routman - Atlantis Orthopedics - Atlantis, USA
*Vani Sabesan - Cleveland Clinic Florida - Weston, USA
*Email: sabes001@gmail.com
Introduction: As many as 15-30% of patients with glenohumeral arthritis have glenoid bone loss that presents a challenge for orthopedic surgeons. With higher failure rates and diminished outcomes in the setting of glenoid bone loss with glenohumeral arthritis, augmented glenoid implants have shown encouraging results as an improved treatment option. With a lack of follow up studies comparing the use of augmented glenoid components in reverse shoulder arthroplasty (aRSA), the decision is not always clear when and if to you use them. The objective of this study is to compare the postoperative outcomes between augmented and standard RSA.
Methods: A retrospective review was performed on an IRB-approved database of 629 patients treated with primary RSA by a single fellowship-trained orthopedic surgeon between 2017-2020. Cohort was divided based on the type of RSA procedure: 169 patients in the aRSA group and 279 patients in the sRSA group. Demographic variables, glenoid version, baseplate type, and preoperative diagnosis were collected. Patient reported outcomes, functional outcomes, and pain scores were recorded from the preoperative and latest follow-up visits.
Results: Majority of the cohort was male (62%) of an average age of 73.2 years and 26.0 month mean follow-up. Baseline demographics were comparable except aRSA group had a higher BMI (p=0.007) and fewer males (p=0.005). Preoperatively, the aRSA group had a significantly higher mean glenoid version (–13.53° v. –6.2°; p <0.005) and less external rotation (16.9° vs 20.2°, p=0.01) compared to the sRSA group. Preoperative patient reported outcomes, pain scores, shoulder function were comparable between the two groups. Postoperatively, the aRSA group had significantly higher abduction (133.5° vs.124.7°; p=0.010), lower pain scores (2.95 vs 4.02; p=0.010), better shoulder function (8.13 vs 7.45, p<0.05) and greater satisfaction (p=0.005). No significant difference was seen in postoperative complications or revisions rates (p>0.05).
Conclusion: Augmented baseplates performed better than the standard baseplates in RSA with no significant difference complication or revision rates. The results of this study provide surgeons with reassurance that augmented baseplates are a safe and effective option for managing glenoid bone loss and may improve biomechanics leading to better outcomes in glenohumeral arthritis. Further research is needed to help guide surgeons on when to select the augmented baseplate and who the optimal patients are for these innovative implant option in RSA.
#7568
What Factors Contribute to Reduced Amplitude in Intraoperative Motor Evoked Potential Monitoring in Patients Undergoing Primary Total Hip Arthroplasty?
Kenichiro Saito - Nara Medical University - Nara, Japan
*Yoshinobu Uchihara - Nara Medical University - Kashihara, Japan
Masakazu Okamoto - Nara Medical University - Kashihara, Japan
Yusuke Inagaki - Nara Medical University - Kashihara, Japan
Yasuhito Tanaka - Nara Medical University - Kashihara, Japan
*Email: y-uchihara@naramed-u.ac.jp
Introduction
Postsurgical nerve palsy is a rare complication of total hip arthroplasty (THA). Motor evoked potential(MEP) monitoring is reportedly useful for nerve monitoring in spine and spinal cord surgery. MEP monitoring in THA is expected to be useful in preventing nerve injuries. We believe it might be possible to identify the etiology of this disorder. In this study, we examined the factors that can cause a decrease in the amplitude of potentials in MEP monitoring of THA.
Methods
The participants were 35 patients who underwent primary THA with intraoperative MEP monitoring between July 2020 and January 2022. There were 6 males and 29 females, with a mean age at surgery of 66 (48–84) years. There were 27 cases classified as Crowe 1, 7 as Crowe 2, and 1 each as Crowe 3. All cases underwent THA with anterolateral approach in the lateral decubitus position. The tibialis anterior, gastrocnemius, and quadriceps muscles were monitored, and a decrease of more than 50% in the amplitude of the potential was defined as abnormal. Factors contributing to the decrease in amplitude, such as sex, age, body mass index, approach, operative time, blood loss, lower extremity extension, and offset change, were compared between the decrease and no-decrease groups. All analyses were performed using multivariate analysis.
Results
Intraoperative amplitude reduction of 50% or more was observed in seven of 35 patients. None of cases had postsurgical nerve palsy. Moreover, there was no significant difference in any of the factors between the decrease and no-decrease groups (p>0.05). Intraoperative amplitude reduction was observed during femoral rasping in three cases, insertion of the anterior acetabular retractor in two cases, trial reduction in one case, and dislocation before neck osteotomy in one case. The site of reduction was the tibialis anterior in three cases, gastrocnemius in one case, and quadriceps femoris in one case. Adverse events included postoperative numbness on the radial side of the right thumb in one case.
Conclusion
There were no significant differences among the factors contributing to the amplitude reduction in this study. However, it was found that intraoperative actions were responsible for the decrease amplitude in MEP. Specifically, we predict that femoral limb and retractor positions are related to amplitude reduction. Further studies with a greater number of cases and a focus on the intraoperative limb and retractor positions are required in future.
#7668
Preliminary Comparison Between Trabecular Titanium Porous Structure Manufactured via EBM and SLM Technologies: Friction and Primary Stability Performances
*Elisa Salatin - Limacorporate - San Daniele Del Friuli, Italy
Giulio Cattano - Limacorporate S.p.A. - Villanova di San Daniele del Friuli, Italy
Riccardo Toninato - Limacorporate - San Daniele Del Friuli, Italy
Michele Pressacco - LimaCorporate Spa - Villanova di San Daniele del Friuli, Italy
*Email: elisa.salatin@limacorporate.com
Introduction: Additive Manufacturing (AM) is successfully used to produce orthopaedic implants. Since 2007, LimaCorporate provides products manufactured via Electron Beam Melting (EBM) with good long-term clinical outcomes. EBM and Selective Laser Melting (SLM) are the main AM technologies used to manufacture porous structures, whose macro- and micro-characteristics are strongly correlated to friction force at the interface between implant and bone (Marin et al., 2010; Regis et al., 2014). Friction properties combined with the appropriate press fit are essential to provide primary stability of implants. Morphology and porosity of the lattice are instead important parameters for bone ingrowth and long-term fixation of the implants (Benazzo et al., 2014; Sollazzo et al., 2011; Gastaldi et al., 2010). In this study, we compare friction and initial stability performances of Trabecular Titanium (TT) manufactured with SLM and EBM technologies.
Methods: Standard parameters were adopted for producing EBM samples; SLM samples required preliminary parameters optimization. The friction coefficient (COF) was measured as a function of the applied normal load against different tribological counter-surfaces (Marin et al., 2012) simulating trabecular and cortical bone (foam blocks from Sawbones®, 10 PCF and 30 PCF, corresponding to 0.16 g/cm3 and 0.48 g/cm3 respectively). Friction samples were parallelepiped shaped (30x10x10mm). For each load and block density test was repeated 3 times.
Initial stability test was performed to simulate primary stability behavior of an acetabular cup inserted in a solid foam block (Sawbones®,15 PCF, corresponding to 0.24 g/cm3, simulating average properties of trabecular bone) replicating surgical conditions (Small et al., 2013). Insertion energy was calculated as the area under the force-displacement curve during implantation up to full seating, while lever out peak force as the maximum load to be applied until gross cup displacement is observed. Lever out peak energy is the corresponding area under the force-displacement curve. For each technology, 8 Delta TT cups with 57 mm outer-diameter were used. 1 mm nominal press fit was imposed and test was repeated 3 times.
Results: When tested against simulated trabecular bone (fig. 1), COF shows a nearly linear behavior ranging between 0.94 and 1.24 for EBM and between 0.86 and 1.19 for SLM, due to porous structure penetration inside the synthetic bone. When tested against simulated cortical bone (not showed), the COF exhibits a smoother variation ranging across 0.7 ± 0.06 for both technologies. Initial stability test results show that for trabecular bone (fig. 2) insertion energy and seating force are around 8100 mJ and 4300 N for both technologies. The lever out peak energy (fig. 3) is around 3030 mJ for EBM and 3570 mJ for SLM while the peak force is 3330 N and 3630 N for EBM and SLM technologies, respectively.
Discussion: The results of our study demonstrate that both technologies provide comparable results as concerns the COF and initial stability within the interval of confidence. When same micro- and macro-porous characteristics are achieved, the manufacturing technology is not relevant for the end result. Overall, process parameter optimization for porous structure manufacturing is crucial to achieve these results.
Figures
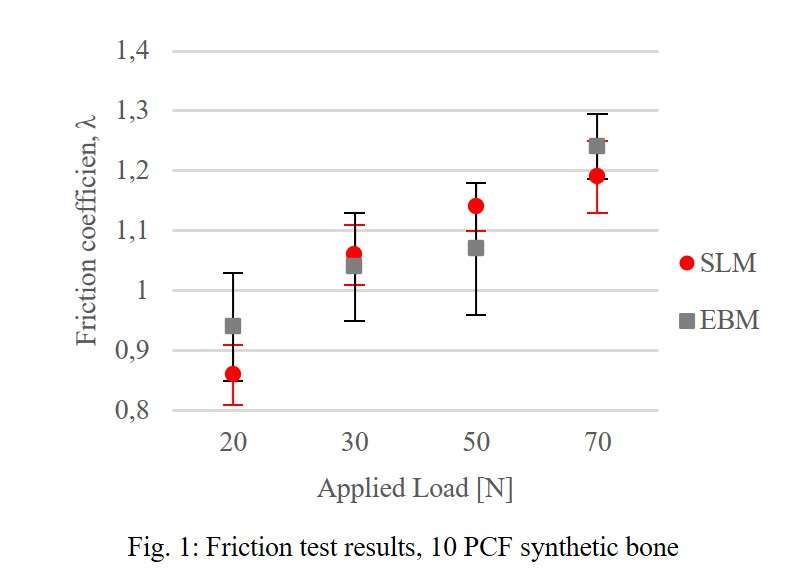
Figure 1
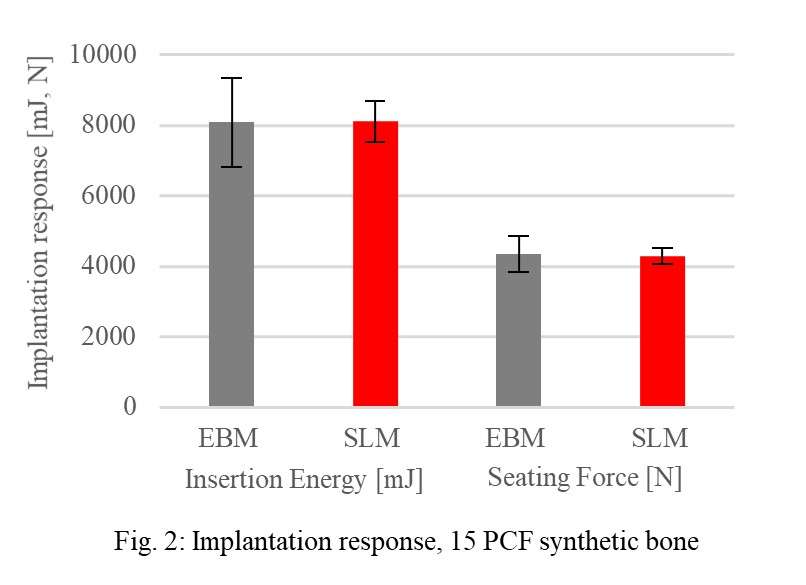
Figure 2
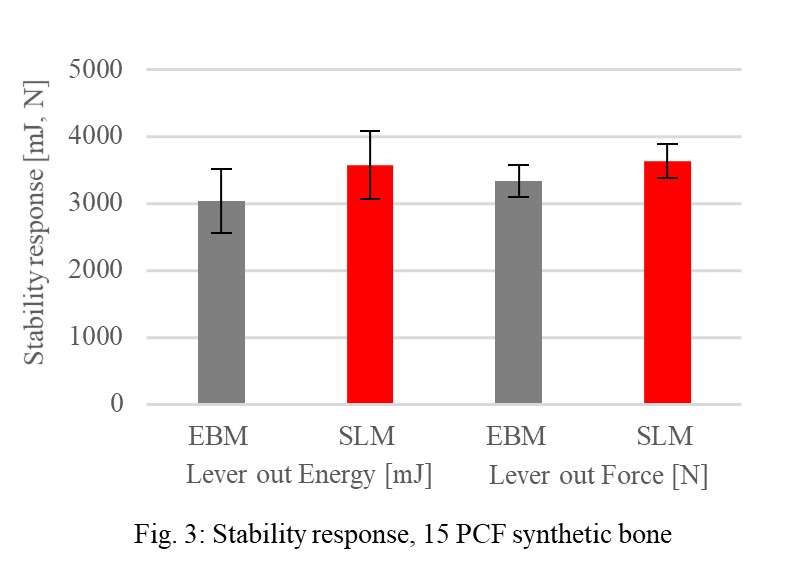
Figure 3#7755
Evaluation of the Course of Asymptomatic Pulmonary Thromboembolism After Total Knee Arthroplasty
*Atsushi Sato - Showa University Koto Toyosu Hospital - Tokyo, Japan
Takayuki Koya - Showa University Koto Toyosu Hospital - Tokyo, Japan
Masataka Ota - Showa University Koto Toyosu Hospital - Tokyo, Japan
Jun Oike - Showa Univercity Koto Toyosu Hospital - Tokyo, Japan
Kanako Iizukashi - Showa University Fujigaoka Hospital - Yokohama, Japan
Takayuki Okumo - Showa University Fujigaoka Hospital - Yokohama, Japan
Saki Yagura - Showa University Fujigaoka Hospital - Yokohama, Japan
Naoki Okuma - Showa University Fujigaoka Hospital - Yokohama, Japan
Fumiyoshi Kawashima - Showa Uniersity Fujigaoka Hospital - Yokohama, Japan
Koji Kanzaki - Showa University Fujigaoka Hospital - Yokohama, Japan
*Email: atsushi@med.showa-u.ac.jp
(Introduction) Total knee arthroplasty (TKA) is one of the most successful surgeries to relieve pain and dysfunction caused by severe arthritis. However, it is a still big problem that there is a possibility of death in pulmonary embolism (PE) after TKA. We previously reported that there was more incidence of asymptomatic PE than estimated in general by detail examinations. There are few reports of asymptomatic pulmonary embolism, therefore, we investigated the course of asymptomatic PE after primary TKA.
(Methods) Consecutive 185 patients who underwent primary TKA from January 2015 to March 2020 were applied. There were 142 females and 43 males included, and the mean age was 74.3 years old. There were 66 cases of one-stage bilateral TKA and 119 cases of unilateral TKA.
A single knee surgery team performed all operations with cemented-type prostheses and air tourniquet during operation. Detail examinations with contrast-enhanced CT (CE-CT) and venous ultrasonography (US) were performed on the 3rd day after surgery. Next, we applied ultrasound cardiogram (UCG) to the patients diagnosed as PE by CE-CT, we checked right ventricular overload (RVO) to treat PE. These images were read by a single senior radiologist team.
(Results) The incidence of deep vein thrombosis (DVT) was 121 patients (65.4%) , and all of these was distal type DVT. PE was 34 patients (18.4%), and each of patients had no symptoms. RVO was detected in 9 patients (4.9%), and three of them (1.6%) had SpO2 decrease to require oxygen administration in early perioperative period. Contrast-enhanced CT was performed for follow-up of PE after discharge in 22 cases (64.7%), and disappearance of PE was confirmed in all cases. The average postoperative days until the disappearance of PE was confirmed was 42.8 days. All patients did not change rehabilitation protocol and progress was good until discharge.
(Conclusion) We recognize that the incidence of asymptomatic PE after TKA is high, and we think that PE examination by contrast-enhanced CT is necessary at least in cases with low SpO2 even if there are no symptoms. PE disappeared on average 6 weeks after surgery, suggesting that it may be an important indicator of anticoagulant administration period and perioperative management. However, all PE cases have not been tested for follow-up, and the number of cases should be increased and careful examination is required in the future.
#7657
The Sensor Enabled TKA - a Novel Approach to Gait Analysis
*Kaitlin Carroll - United States of America
Kevin Gemmell - Canary Medical - Carlsbad, USA
Patrick Aubin - Canary Medical - Carlsbad, USA
Hsiang-Ling Teng - California State Long Beach - Long Beach, USA
Peter Schiller - Canary Medical - Carlsbad, USA
Jeffrey Gross - Canary Medical - Carlsbad, USA
William Hunter - Canary Medical - Carlsbad, USA
Fred Cushner - Hospital for Special Surgery - New York, USA
*Email: kaitlincarroll@gmail.com
Introduction: Gait analysis is a well-described method of not only analyzing post-operative recovery but also as a diagnostic tool to evaluate a painful total knee arthroplasty (TKA). While the use of gait labs provides extensive post-operative kinematic information, they are costly, and not easily accessible. A sensor enabled TKA device would obviate these constraints, and since each patient would act as their own control, the generation of longitudinal data could provide a powerful tool in discriminating small changes for clinicians’ functional assessment of TKA performance. The ability capture data during daily activities makes this type of technologic advancement even more salient as a tool for remote patient monitoring (RPM). The objective of this study was to evaluate the use of the novel smart stem extension for TKA with embedded sensors, the canturio™te,implant to capture gait parameters in comparison to a gold standard camera-based motion capture system.
Materials and Method: Fifteen participants (7 Male, 8 Female, Height 171.4 cm  9.0cm) wore an externally mounted canturio™te implant in a custom harness with motion capture system fiducials (Figure 1). The canturio™te was affixed medially on the proximal aspect of the tibia to minimize relative motion of the canturio™te to the participant’s tibia during activity. Motion capture clothes with additional fiducial markers were placed on the participant to track movement. Participants performed multiple walking trials on a treadmill at different walking speeds while simultaneously collecting canturio™te and motion capture system kinematic data. Sensitivity and Bland-Altman analyses were performed to analyze comparisons. We reviewed the following calculated gait parameters (CGP) – Average Walking Speed, Cadence, Stride Length, Functional Knee Range of Motion (ROM), and Tibial ROM. Data are reported as mean error (95% CI LB, UB).
Results: Analysis of the Average Walking Speed demonstrated the canturio™te underestimated this CGP parameter (Table 1; mean error being negative indicated underestimation). However, based on an Average Walking Speed clinical equivalence margin of 0.32 m/sec, the two one-sided t-tests (TOST) demonstrated equivalence between the canturio™te measure of walking speed and the motion capture system at P-values less than 0.001 for all speeds (Table 1). In additional sensitivity analyses, accounting for within-subject correlation by use of a linear repeated measures model, the mean error for walking speed was -0.0709 m/s with 95% confidence limits of -0.092, -0.050, again supporting the conclusion of equivalent walking speed. A statistical equivalence agreement was demonstrated between canturio™te and the motion capture-based gait lab testing.
The mean error for the 0.5 m/s, 0.9 m/s, and 1.4 m/s walking speed conditions for the remaining CGP were consistent with the equivalence conclusion: Cadence [-0.244, -0.463, -0.220] step/min, Stride length [-0.116, -0.124, -0.130] m, Functional knee range of motion [1.84, -5.29, -3.15] deg, Tibia range of motion [-4.82 -6.41, -6.94] deg.
Conclusion: The canturio™te provides accurate and more easily accessible gait analytics. Further studies are needed to determine if internal canturio™te placement will provide gait analytics but will also serve as a future diagnostic tool for TKA patients and a novel approach to RPM in TKA.
Figures

Figure 1#7489
Numerical Evaluation of the Implanted Stem Size - an Interaction of Implant Size, Position and Bone Morphology
*Peter Schlieker - TUHH Hamburg University of Technology - Hamburg, Germany
Michael Morlock - TUHH Hamburg University of Technology - Hamburg, Germany
Tobias Konow - TUHH Hamburg University of Technology - Hamburg, Germany
*Email: peter.schlieker@tuhh.de
INTRODUCTION:
Periprosthetic fractures (PPF) are one of the main reasons for revision surgery [1]. It is assumed that the implanted stem size effects the PPF risk. Since surgeons follow different philosophies regarding size selection and positioning [2], a reference stem size is difficult to define. Current methods to evaluate the implanted stem size in relation to the geometry of the proximal femur, like the canal-fill-ratio (CFR) [3], use manually determined distances at defined locations from X-ray images. The aim of this study was to develop an objective method to determine the relative implant size using pre- and postoperative CT scans of the femur.
METHODS:
Three experienced surgeons implanted uncemented hip stems (Corail, DePuy Synthes, UK) in 20 human femur pairs [2]. Micromotion between stem and bone was measured (ARAMIS 3D Camera, GOM, GER) during dynamic physiological loading (1600 N, 2400 cycles, 1 Hz) followed by load to failure tests. Pre- and postoperative qCT-scans (Incisive CT 128, Philips, NL) were aligned by superimposing the cortices based on BMD. The implant-to-cortex gap (ICG) was analyzed in every transverse slice with directional vectors (5°-steps over 360°, Fig. 1a) for each point on the stem surface. The smallest distance between each point of the stem and the cortex was averaged for the whole stem length up to the lesser trochanter (Fig. 1b). The new ICG approach was compared with a modified CFR adapted to CT scans by using cross-sectional areas (Fig. 1c) instead of distances. The mean CFR was calculated over the same femoral region as for the ICG.
RESULTS:
A higher ICG was associated with a lower CFR (Fig. 2, R2 = 0.847, p < 0.001). An increased ICG resulted in higher micromotions and decreased load to failure (Fig. 2, R2 = 0.672, p < 0.001; R2 = 0.210, p = 0.056). ICG varied greatly between the surgeons with surgeon C using the largest stems (lowest ICG, Fig. 3, surgeon A vs. B: p = 0.057, A vs. C: p < 0.001, B vs. C: p = 0.005).
CONCLUSION:
The ICG can be used postoperatively to evaluate the implanted stem size or preoperatively in CT-based templating. ICG and CFR showed opposite but similar trends for the Corail stem, which might not be the case for other stem designs. The CFR might imply undersizing for plate type stems due to their small CFR, whereas the ICG should represent more reliably the relative implant size. The ICG does account for a transversal offset position of the stem while the CFR is independent of the stem position. This is relevant in cases of severe femoral curvature, when the stem size is approaching a three-point cortical contact. The differences in ICG observed between surgeons nicely show the different philosophies regarding the proximity of the implant to the cortex. Whether and how these philosophies reflect on migration behavior or PPF risk needs to be investigated.
ACKNOWLEDGEMENT:
The authors appreciate the financial support of DePuy Synthes for the CT scans.
REFERENCES:
[1] Grimberg et al., EPRD 2021
[2] Konow et al., ARTD 2022
[3] Parsley et al., J ARTHROPLASTY 2003
Figures
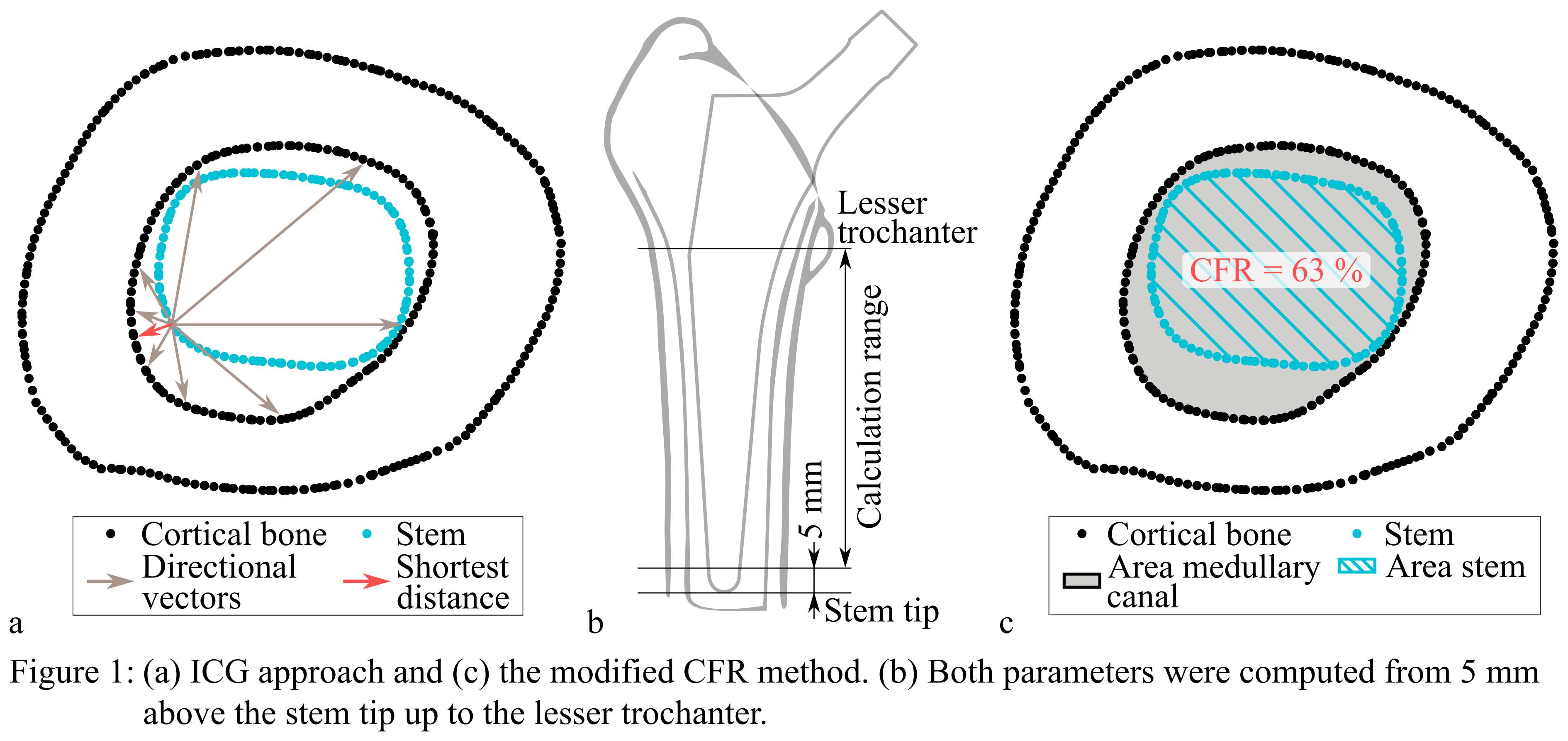
Figure 1
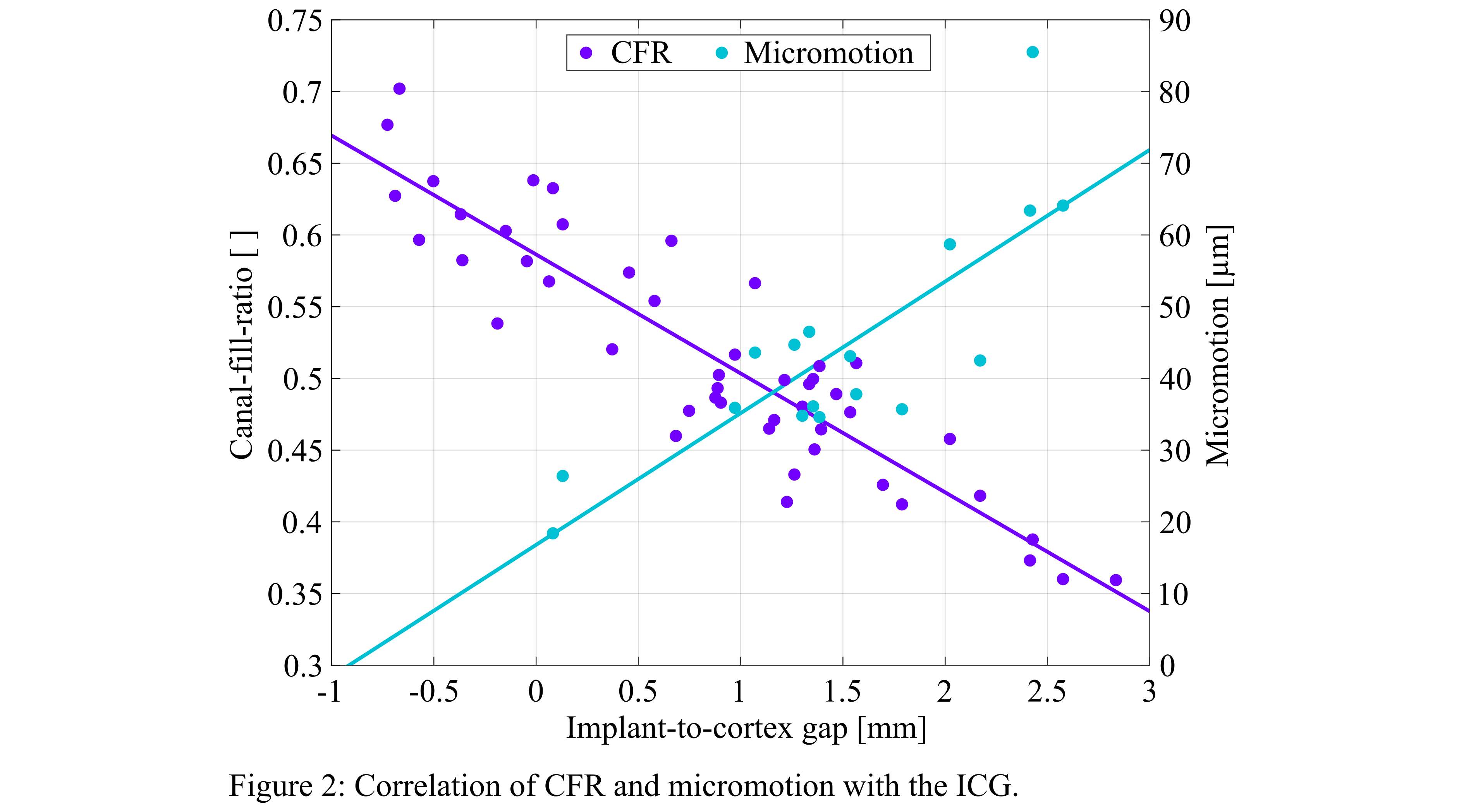
Figure 2
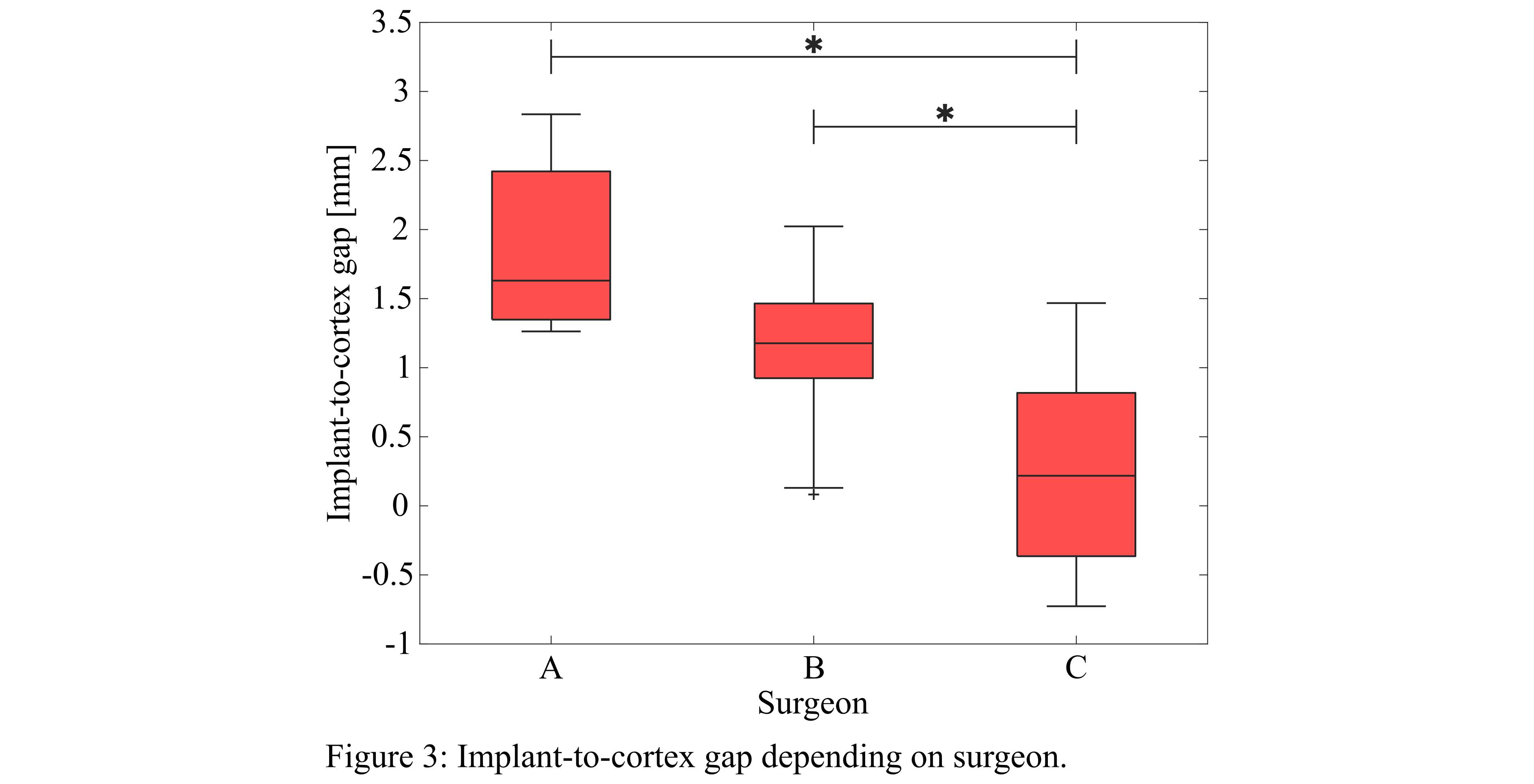
Figure 3#8054
Invited Talk: Bill Harris� Unrecognized Contribution to Knee Arthroplasty
*Thomas Schmalzried
*Email: tpschmalzried@gmail.com
In the early 1990’s, a PhD student in the Harris lab made a novel observation, interfacial porosity: extensive porosity located at the cement-metal interface of femoral total hip components (1). These small pores decrease the strength of the cement-prosthesis interface and jeopardize the mechanical integrity of the cement mantle. The presence of these pores was explained by the rheological characteristics of the cement. On this basis, “wet” cement makes a better bond to metal than “dry” cement. Roughly a decade later, failure of cemented total knees due to de-bonding of the tibial component was reported (2). Tibial de-bonding has subsequently been reported with several different knee systems from different manufacturers. A common denominator is dry (high viscosity) cement. In a laboratory study, “wet” cement increased the mean strength of the tibial component-cement interface 72% while “dry” cement reduced the strength by 73%. To maximize the strength of the cement-metal interface, cement should be applied to the component soon after mixing (3). Thus, the discovery of interfacial porosity is Bill Harris’ (previously) unrecognized contribution to knee arthroplasty.
- James, S.; Schmalzried, T.P.; McGarry, F.J., and Harris, W.H.: Extensive porosity at the cement-femoral prosthesis interface: A preliminary study. Biomed. Biomat. Res. 27:71-78, 1993.
- Mikulak, S.A.; Mahoney, O.M.; Dela Rosa, M.; Schmalzried, T.P.: Loosening and osteolysis with the Press-Fit Condylar posterior-cruciate-substituting total knee replacement. Bone Joint Surg. 83-A:398-403, 2001.
- Billi F, Kavanaugh A, Schmalzried H, Schmalzried TP. Techniques for improving the initial strength of the tibial tray-cement interface bond. Bone Joint J. 2019 Jan;101-B (1 Supple A):53-58.
#7416
Gait Analysis in Total Knee Arthroplasty
Neeraj Vij - University of Arizona College of Medicine - Phoenix - Phoenix, United States of America
*Kenneth Schmidt - Banner University College of Medicine - Phoenix - Phoenix, USA
Christian Leber - University of Arizona College of Medicine Phoenix - Phoenix, USA
*Email: kschmidt@orthoarizona.org
Introduction: Total knee arthroplasty is a common procedure with an expected increase of nearly two-fold by 2050. Though the outcomes are good, it is well known that the biomechanics of the knee do not fully return to their normal state. The purpose of this scoping review is to summarize the current use of gait analysis in total knee arthroplasty and to identify the preoperative motion analysis parameters for which a systematic review aimed at determining the reliability and validity may be warranted.
Methods: This IRB-exempt scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist strictly. Five search engines were searched for a total of 279 articles. Articles underwent a title and abstract screening process followed by full-text screening. Included articles were placed in the following sections: the role of gait analysis as a research tool for operative decisions, other research applications for motion analysis in total knee arthroplasty, gait analysis as a tool in predicting radiologic outcomes, gait analysis as a tool in predicting clinical outcomes.
Results: Eleven articles studied gait analysis as a research tool in studying operative decisions. Motion analysis is currently used to study surgical approaches, surgical techniques, and implant choice. Five articles studied other research applications for motion analysis in total knee arthroplasty. Other research applications for motion analysis currently include studying the role of the unicompartmental knee arthroplasty and novel physical therapy protocols aimed at optimizing post-operative care. Two articles studied motion analysis as a tool for predicting radiographic outcomes. Preoperative gait analysis has identified parameters than can predict postoperative tibial component migration. 15 articles studied motion analysis in conjunction with clinical scores.
Conclusion: The current literature is limited by vague definitions of ‘gait analysis’ or ‘motion analysis’ and a limited number of articles with preoperative and postoperative functional and clinical measures. Knee adduction moment, knee adduction impulse, total knee range of motion, varus angle, cadence, stride length, and velocity have the potential for integration into composite clinical scores.
Keywords: motion analysis, knee replacement, patient-reported outcomes, patient-specific implantation, knee surgery
#7476
Determination of Tibial Implant Stability in Reference to Complete Implant Loosening
*Sebastian Jaeger - Heidelberg University Hospital - Heidelberg, Germany
Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Andre Lunz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: sebastian.jaeger@med.uni-heidelberg.de
Introduction:
Implantation of a cemented total knee endoprosthesis is a well-established orthopaedic procedure. Publications and registry data document very good long-term results in this regard. Aseptic prosthesis loosening is still considered the most common reason for revision surgery. The aim of this experimental in vitro study on human specimens was to compare the migration behavior and relative motion of a cemented tibial component of a bicondylar knee replacement under "best case" (ideal fixation) and "worst case" (complete loosening) conditions. In this manner, the increase in implant migration and relative motion due to a failure at the metal-cement interface can be evaluated.
Methods:
A cemented tibial component without cement pockets (Attune, DePuy) was implanted in 13 "fresh frozen" human legs under standardized conditions (best case group). The worst case group was obtained after the test sequence of the best case group by a debonding between the metal-cement interface caused by a pull out test. For the worst case group, the identical prosthesis was placed in the existing cement mantle without any adhesive bonding and the test procedure was repeated. The specimens were integrated into a hydraulic testing machine and dynamically loaded. Stair climbing was simulated with an extension-flexion angle of 20°-50°. Axial loading was performed at 4 load levels (1200 N, 1500 N, 1800 N, 2100 N) for 1000 cycles each. Implant migration and relative motion between implant and bone were measured during the loading simulation using a 3D optical measurement system.
Results:
Overall, there were considerable differences in implant migration and relative motion between ideal cementation (best case) and the implant after debonding (worst case). However, at a flexion angle of 50° the worst case group showed only an increase in relative motion depending on the load level between 13% and 28%. At a flexion angle of 20°, the increase ranged from 56% to 73% which corresponds to an increase between 11 µm and 34 µm (Figure1).
Conclusion:
Comparison between an ideally cemented tibial component of a bicondylar knee replacement and a fully loosened component showed an increase in relative motion in vitro. It could be possible that the tapered tibial stem design of the prosthesis counteracts a more pronounced effect of relative motion, which remains the subject of further investigation.
Figures
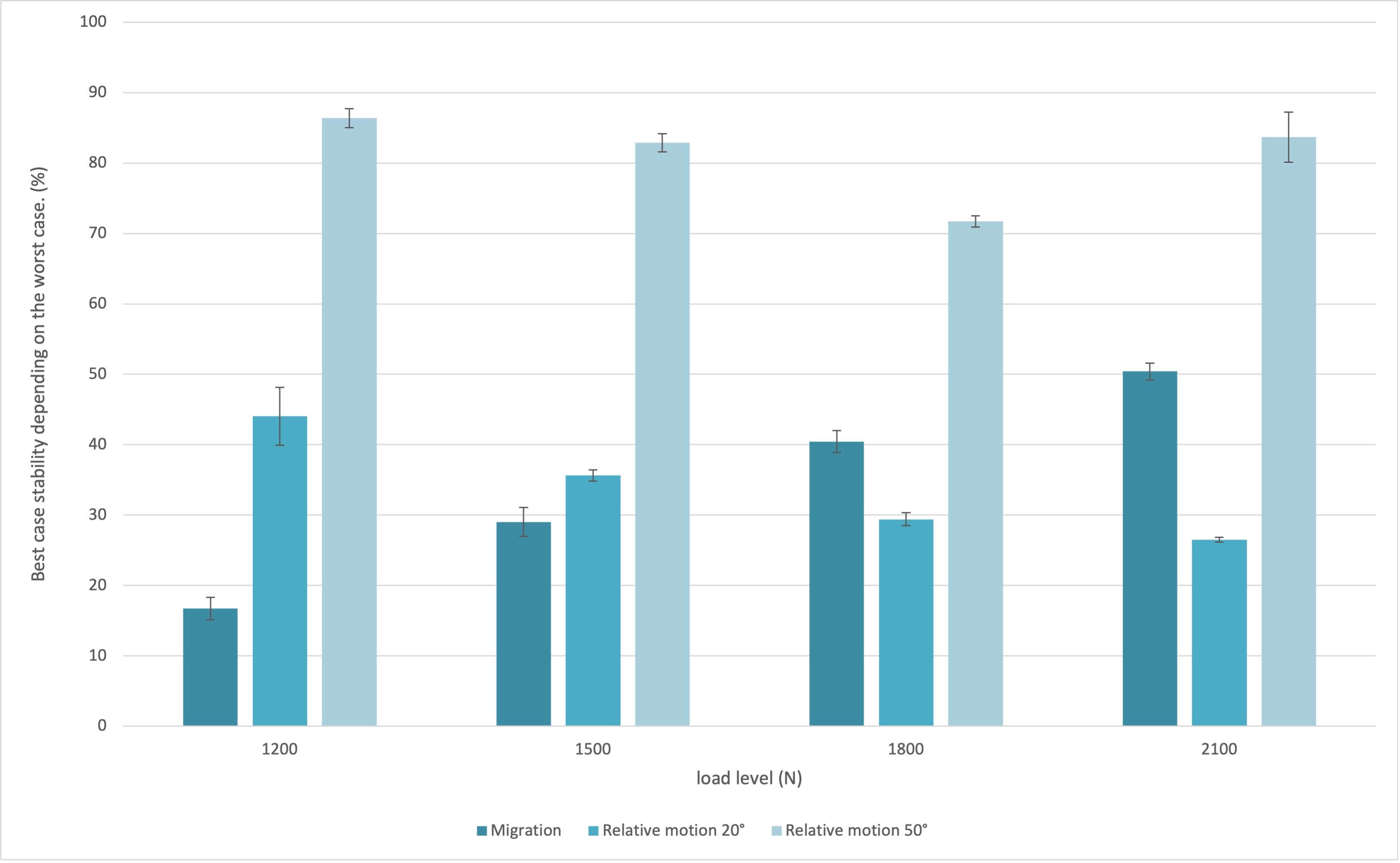
Figure 1#7486
Femoral Cementation in Total Knee Arthroplasty - an in-Vitro Study Comparing the Cement Penetration of Two Cementing Techniques
*Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Martin Schwarze - University of Heidelberg - Heidelberg, Germany
Andre Lunz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
Kevin Knappe - Heidelberg University Hospital - Heidelberg, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
J. Philippe Kretzer - University of Heidelberg - Heidelberg, Germany
Sebastian Jaeger - Heidelberg University Hospital - Heidelberg, Germany
*Email: mareike.schonhoff@med.uni-heidelberg.de
Introduction:
While implanting total knee prosthesis is an established procedure, aseptic loosening is the most common cause of revisions. The femoral component is predominantly anchored with bone cement but the geometry of the femoral component makes the application of the bone cement more difficult. Especially the posterior and anterior areas are critical. An insufficient thickness of the bone cement layer can lead to aseptic loosening. In this experimental in-vitro study, cement penetration was compared between two different cementation techniques. The influence of a pressurizer for pressure application during femoral cementation was to be investigated.
Methods:
We used 6 paired fresh-frozen human cadaver legs for the implantation of the femoral component. Two different cementing techniques were applied. Technique A is a manual technique and technique B is an application with a pressurizer for the cement gun. Defined saw cuts were then made centrally through the posterior and anterior condyle. Standardized digitization of the cut surfaces, the cement mantle could be analyzed and a zone classification according to the Knee Society Score (KSS) could take place. Thus, the anterior (zones 1 and 2) and posterior (zones 3 and 4) areas could be differentiated. The average cement depth was calculated.
Results:
The evaluation showed that in all zones there was no significant difference between technique A and technique B (zone 1: p = 0.514; zone 2: p = 0.380; zone 3: p = 0.45; zone 4: p = 0.877; zone 5/7: p = 0.074) (See Figure 1).
Conclusion:
The in-vitro investigations have shown that the pressurizer technique does not significantly improve the cement penetration into the critical area compared to the manual technique.
Figures
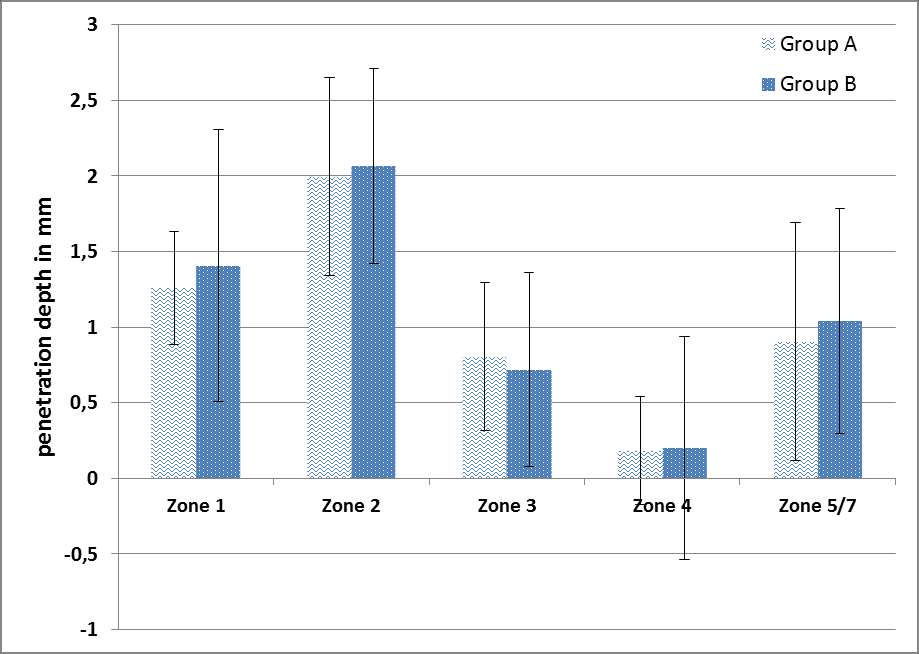
Figure 1#7540
Increasing the Fatigue Strength of 3D-Printed Hip Stems Using Suitable Post-Treatment Procedures
Stefan Schroeder - Heidelberg University Hospital - Heidelberg, Germany
Jens Gibmeier - Karlsruhe Institute of Technology - Karlsruhe, Germany
Phuong Thao Mai - Karlsruhe Institute of Technology - Karlsruhe, Germany
Moritz M. Innmann - Heidelberg University Hospital - Heidelberg, Germany
Tobias Renkawitz - Department of Orthopaedic Surgery | Heidelberg University Hospital - Heidelberg, Germany
*Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: kretzer@arthroplasty-research.com
Additive manufacturing like Laser Powder Bed Fusion (LPBF) of titanium-aluminium-vanadium (Ti6Al4V-) powder is already used in different endoprosthetic applications. LPBF would also offer the possibility of 3D-printing patient-specific hip stems. However, a critical point of these 3D-printed implants is their porosity and the associated low fatigue strength. Due to the high bending stresses hip joints are subjected to in the application, sufficient fatigue resistance of the artificial joint is crucial to ensure patient health. Therefore, the aim of this study was to investigate whether the fatigue strength of 3D-printed hip stems processed via LPBF can be optimized by suitable thermal and mechanical post-treatment procedures.
In a simplified dynamic 4-point bending experiment, the fatigue strength of 3D-printed cylinder specimens was determined and compared to the fatigue strength of a standard forged titanium base alloy using a Locati test (Figure 1). By this means, the influence of different post-treatment processes to optimize the fatigue strength was investigated. The influence of hot isostatic pressing (HIP), of various mechanical surface treatments as well as the combination of both on the fatigue strength was analyzed. A machining process (turning), deep rolling using two rolling pressure variants (Rolling_M1 and Rolling_M2), laser shock peening with two different intensities (LSP_M1 and LSP_M2) as well as shot peening also using two process parameter sets (SP_M1 and SP_M2) were selected as mechanical surface treatments that results in different surface topographies in combination with characteristic residual stress depth distributions and depth distributions in the process induced work hardening in the near surface region. The cylindrical specimens were cyclically loaded at a frequency of 12Hz. As shown in Figure 1 on the right, the specimen was initially loaded sinusoidally with a force Fz between 100 N and 2000 N for 106 cycles. If no fracture of the specimen occurred, the maximum force was increased by 500 N and the specimen was loaded for additional 106 cycles. The increase in force was carried out until failure.
The maximum force levels until specimen failure are listed in Figure 2. The results of the bending tests showed that a HIP process alone, as well as a finishing by conventional machining (turning) alone, is not sufficient to obtain fatigue strengths that are in the range of the standard alloy (forged part). Only by combining the HIP process with a subsequent mechanical surface treatment, sufficient fatigue strengths can be achieved. However, laser shock peening with its chosen process parameters was not convincing in this series of tests. In contrast, excellent fatigue strengths were achieved with both, shot peening and deep rolling.
Of these, the greater application potential in the targeted application on 3D-printed parts can be assigned to shot peening, since this process can be adapted very easily to complex shaped parts, hence it can be excellently applied for mechanical post-treatment of patient-specific 3D-printed hip stems.
Figures
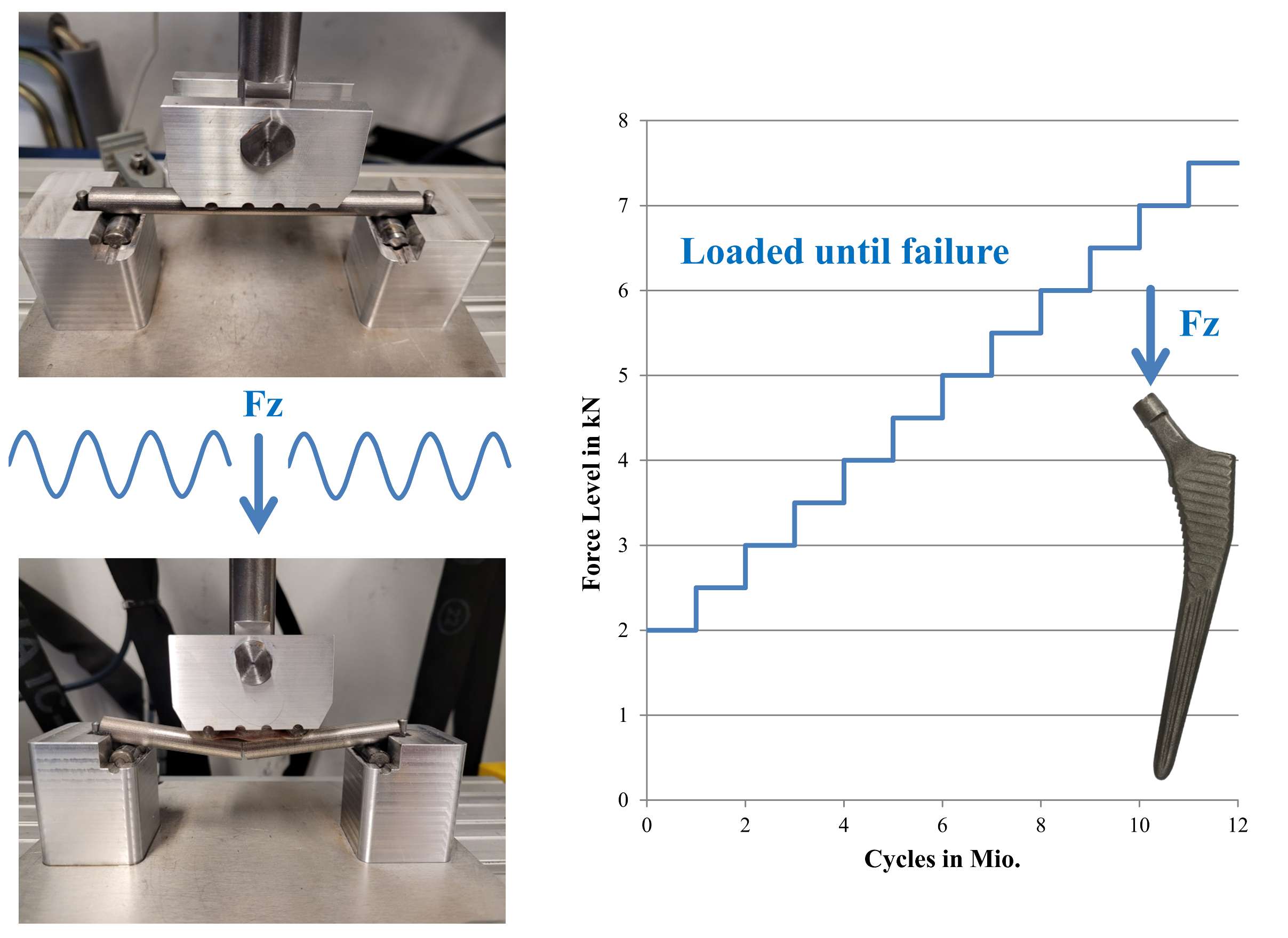
Figure 1
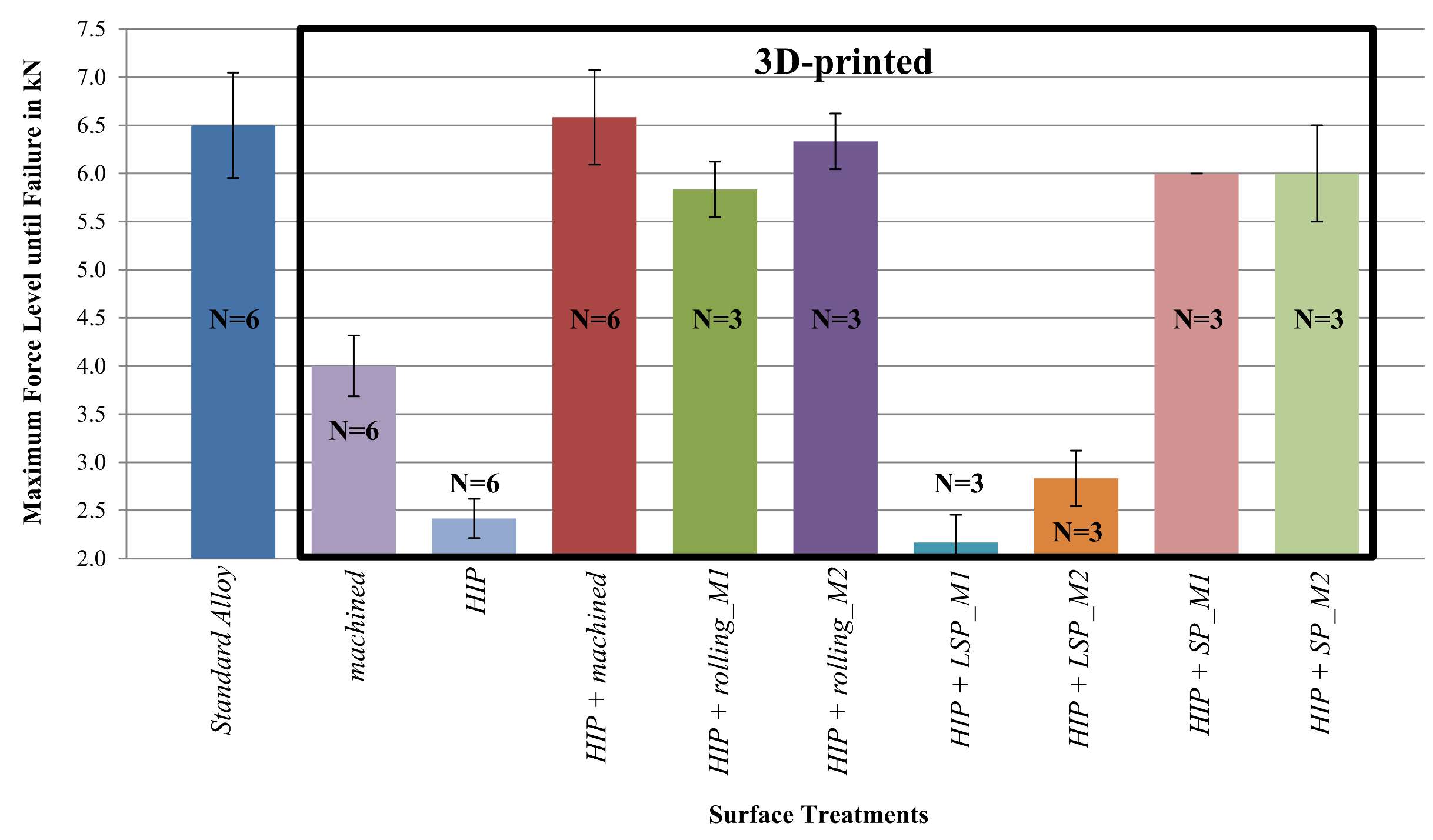
Figure 2#7442
Kinematic Alignment in Total Knee Arthroplasty: A Wear Simulation Study
Stefan Schroeder - Heidelberg University Hospital - Heidelberg, Germany
Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Maximilian Uhler - Laboratory of Biomechnics and Implant Research - Heidelberg, Germany
Steffen Braun - University of Heidelberg - Heidelberg, Germany
Sebastian Jaeger - Heidelberg University Hospital - Heidelberg, Germany
*Philippe Kretzer - Laboratory of Biomechanics and Implant Research, University of Heidelberg - Heidelberg, Germany
*Email: kretzer@arthroplasty-research.com
Kinematic alignment is an alternative approach to mechanical alignment with the goal of restoring the prearthrotic joint line. A ligament release is typical not necessary using kinematic alignment and studies already reported good mid-term functional and clinical results. However, due to the non-perpendicular orientation of the joint axis and tilted implant components concerns rose of the kinematic alignment technique. Similar to malaligned knee implants, these tilted components change the pressure distribution between medial and lateral side of the polyethylene inserts, which may lead to higher wear and thus connected implant loosening in the long-term. Therefore, an in vitro wear simulation study was performed to compare the wear behavior of mechanical, kinematic and malaligned knee implants.
A force-controlled AMTI knee simulator was used for the comparison. For simulating the optimum mechanical alignment condition the machine axes of the simulator were in line with the joints flexion-extension (Flex/Ex-) axis and the axis for the internal-external (I/E-) rotation, which was in line with the force axis (Figure 1). To simulate the malaligned condition, the joint axis was tilted by 4°, but the Flex/Ex-axis and the axis for I/E-rotation were not tilted. For simulating the kinematic alignment condition, a tilted joint axis of 4° was chosen, and the machine axes were tilted by 4° as well. To bring the machine axes in line with the tilted Flex/Ex-axis and the axis for I/E-rotation, mechanical adjustments of the simulator were necessary for the kinematic alignment condition (Figure 2). For each alignment 3.0x106 cycles of wear simulation according to ISO 14243-1 were performed and wear was measured gravimetrically after every 0.5x106 cycles. The tests were performed with two different types of cruciate retaining knee implants from Depuy Synthes (PFC Sigma and Attune).
For the PFC Sigma the wear rates of the malaligned group was lowest, but ANOVA revealed no significant difference between the three alignments (p = 0.061) regarding the wear rates (Figure 3). For the Attune implant a significant difference of the wear rates was found between the mechanical and malalignment groups (p = 0.013) as well as between the kinematic and malalignment group (p = 0.005), but no difference was found between the mechanical and kinematic alignment group (p > 0.99). The worn areas on the polyethylene inserts after 3.0x106 cycles were lowest for the malaligned condition for both implant types.
The similar wear behavior of the mechanical and kinematic alignment group may give the surgeon a certain safety to perform the kinematic alignment technique with tilted components up to 4° without worrying about possible wear related consequences. The malaligned group showed the lowest wear rate. However, due to the small worn area it is assumed, that only the rim of the femoral condyle was in contact with the insert. This may lead to a low wear behavior in the first place, but due to the small contact area high pressures can occur, which may lead to delamination of malaligned components in the long-term.
Figures
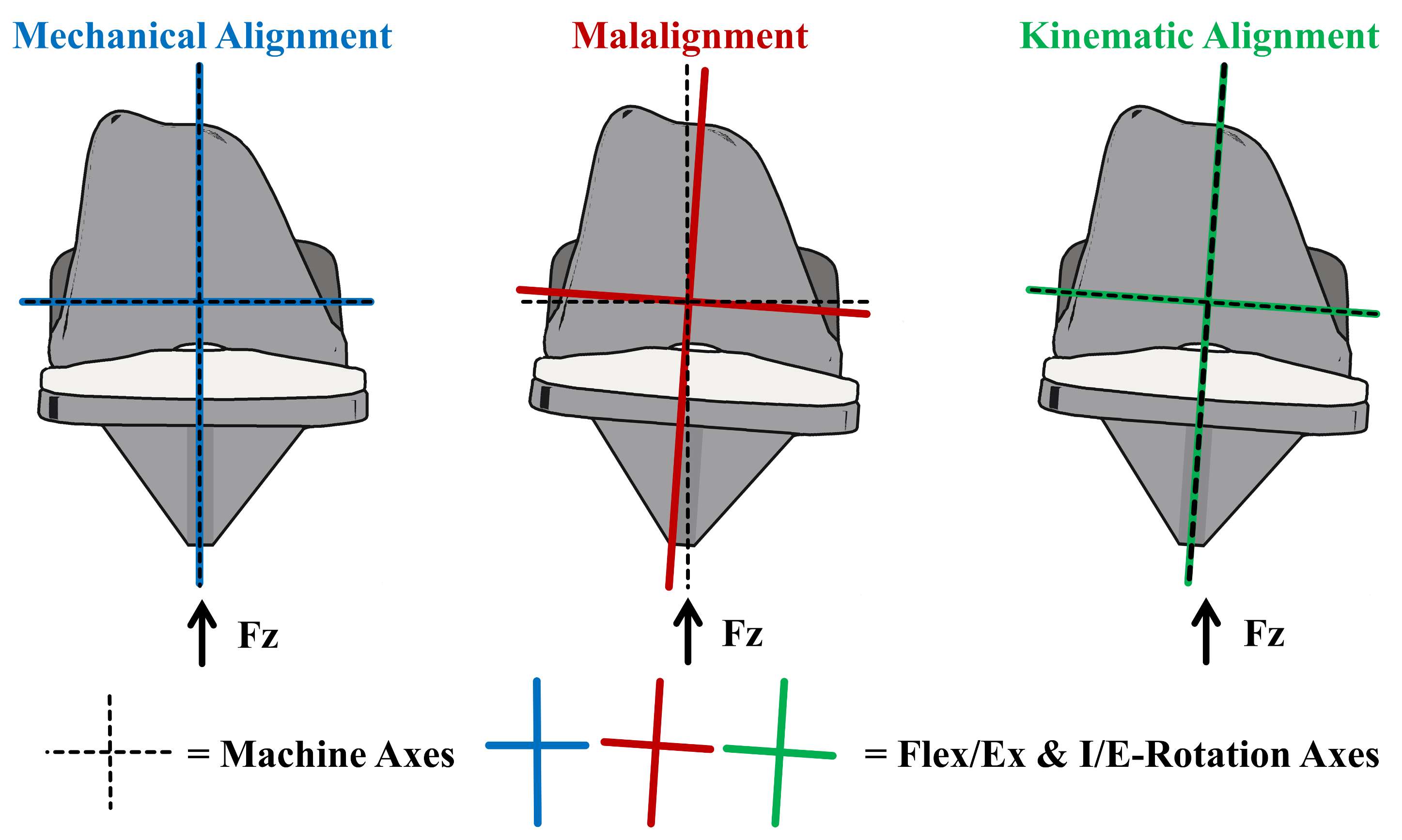
Figure 1
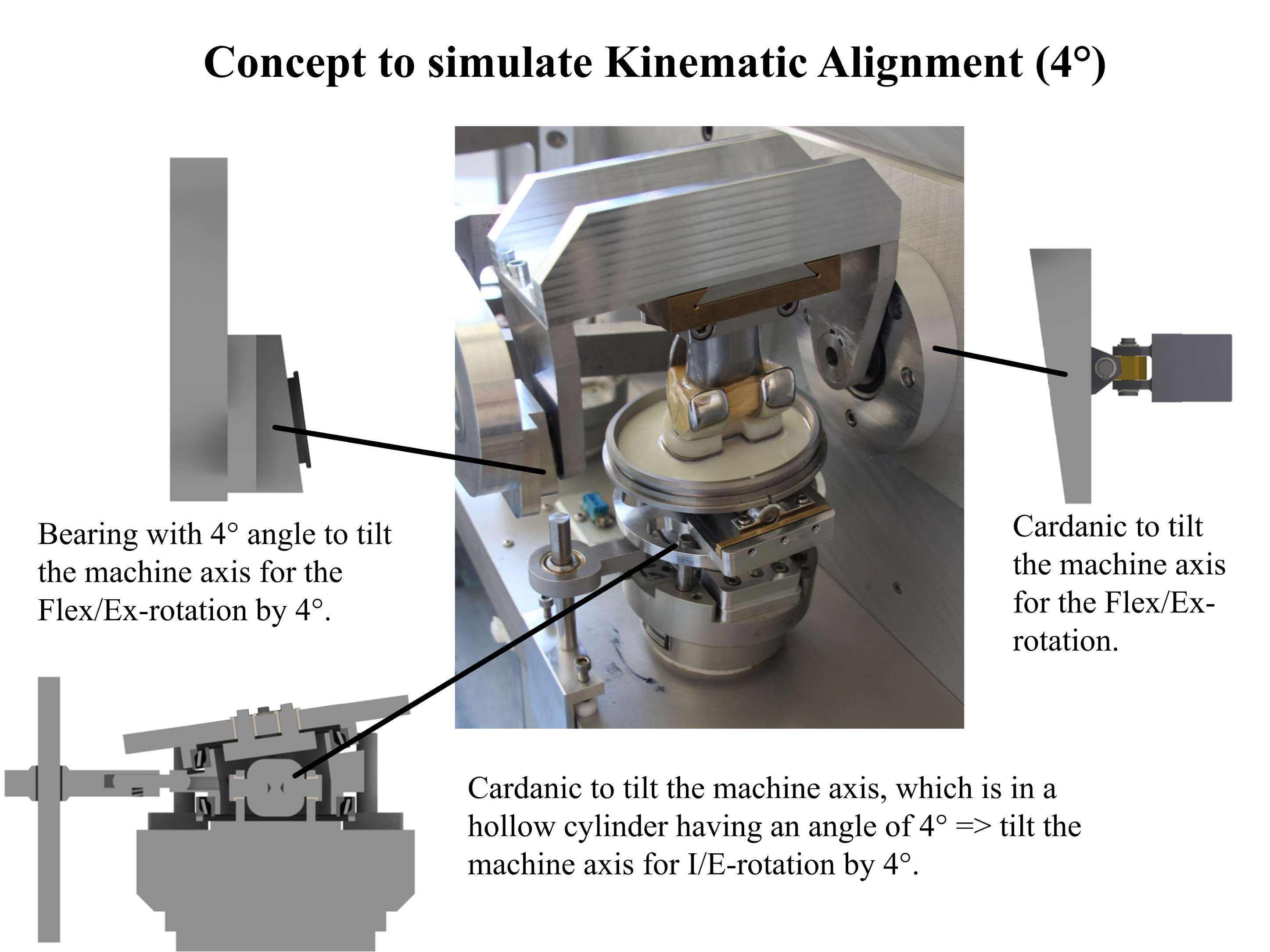
Figure 2
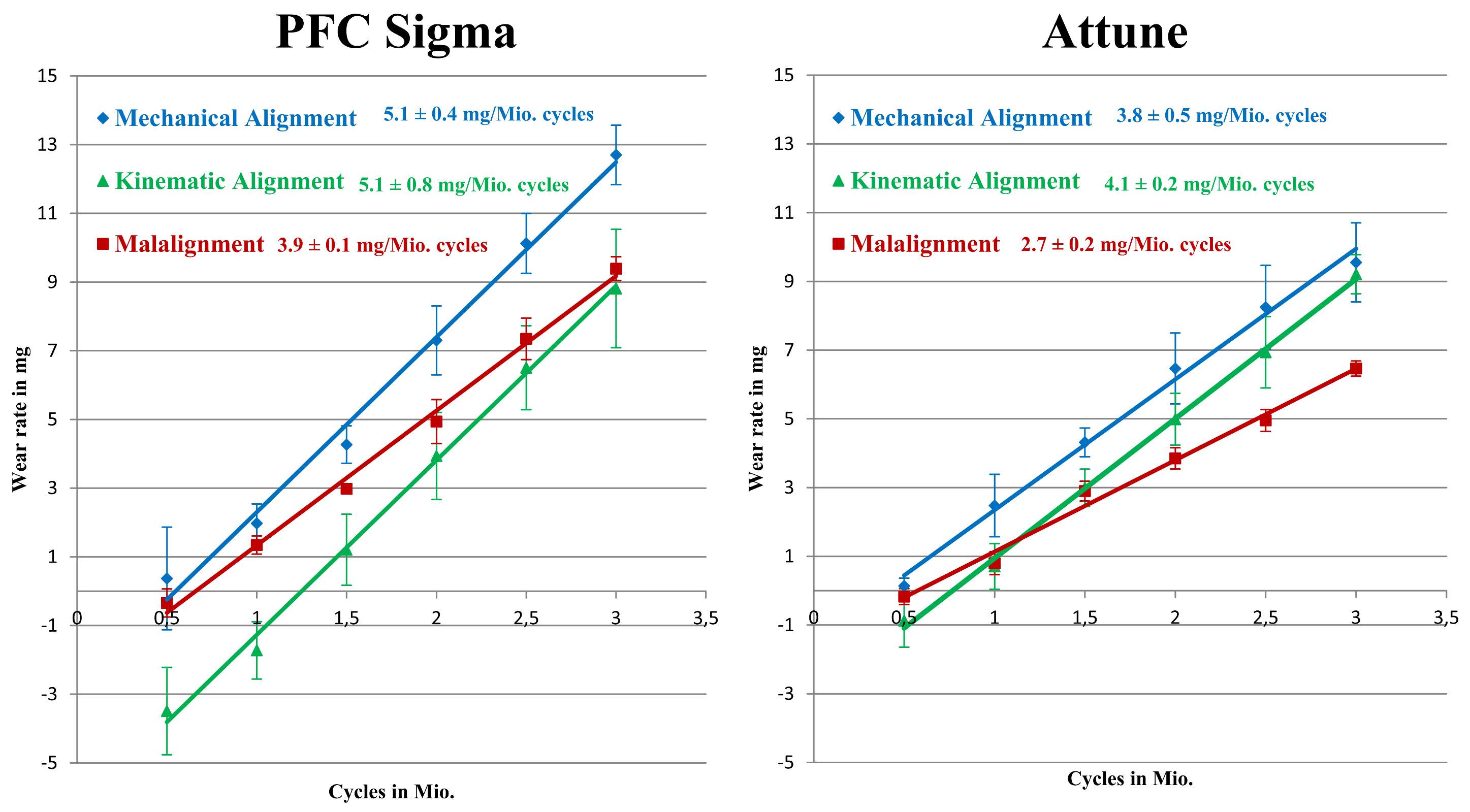
Figure 3#7679
Do Steroid Injections Affect Outcomes of Shoulder Arthroplasty? Why Risk It?
Alessia Lavin - Palm Beach Shoulder Service Atlantis Orthopaedics - Lake Worth, United States of America
*Vani Sabesan - Cleveland Clinic Florida - Weston, USA
Gabriel Lama - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Sarah Girshfeld - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Brandon Macknofsky - Florida Atlantic University Charles E Schmidt College of Medicine - Boca Raton, USA
Howard Routman - Atlantis Orthopedics - Atlantis, USA
Madison Schwerzler - Atlantis Orthopedics - West Palm Beach, United States of America
*Email: sabes001@gmail.com
Introduction: Steroid injections are well-known short-term treatments for glenohumeral osteoarthritis; however, many patients eventually require more definitive management with surgical treatment. Recent literature has called into question the utility and safety of steroid injections prior to shoulder surgery regarding their effect on infections and revision rates. Conclusive data regarding the relationship of preoperative injection and postoperative outcomes is lacking. The purpose of this study is to determine the effect of ipsilateral preoperative injections on clinical outcomes following shoulder arthroplasty (SA).
Methods: A retrospective study was performed on 563 patients who underwent SA by a single fellowship-trained orthopedic surgeon from 2017-2020. Patients were divided into two groups: 240 who received a preoperative injection (IG) and 323 were the control group (CG). Patient reported pain and satisfaction, simple shoulder test (SST), shoulder pain and disability index (SPADI), complications, reoperations, and range of motion (ROM) were compared between groups. Change (delta) in clinical and functional outcomes were calculated from the pre- to postoperative period and compared. Statistical analysis included t-test and chi-squared test with significance defined as p <0.05.
Results: The cohort was comprised of 55% females with an average age of 71.1, BMI of 29.6, and mean follow-up of 21.5 months. The IG group had a significantly greater proportion of females (64%; p<0.01) and older age of 72.9 (p<0.01). The number of comorbidities between groups was comparable. No significant difference in delta in any range of motion or pain was found between groups. Patients in the IG group had significantly greater delta in reported outcomes on both the SST (+6.25 vs. +5.37, p = 0.005) and SPADI (-56.95 vs. -50.56, p = 0.02). Patient satisfaction, complication rates (p=0.98) and reoperation rates (p=0.98) were comparable between groups.
Conclusions: Ipsilateral shoulder injections lead to similar postoperative functional outcomes with superior patient report outcomes and no concurrent increase in complications. Surgeons can maintain injections as a viable first line management option for patients with Rotator Cuff deficiency without concern for inferior postoperative outcomes. Further randomized controlled prospective trials should be undertaken to understand the relationship between ipsilateral corticosteroid injection and subsequent shoulder arthroplasty.
#7334
Impact of Anisotropy on Predicting Mechanical Properties of Trabecular Bone From CT Imaging
*James Scott - Imperial College London - London, United Kingdom
Jonathan Jeffers - Imperial College London - London, United Kingdom
*Email: j.scott19@imperial.ac.uk
Introduction
Trabecular bone exhibits a degree of structural and mechanical anisotropy, with the principal trabecular direction influenced by stress trajectories acting through the bone that relate to the direction and magnitude of joint loading.
Clinical CT derived bone density is a common predicting factor for estimating mechanical properties of trabecular bone. However, whether the relationship between density and mechanical properties holds true for different degrees of bone anisotropy remains to be seen. This is particularly important for the distal femur were the bone properties range from highly anisotropic (generally in the condyles) to less anisotropic (generally in the trochlea). The aim of this study is to investigate the relationship between CT bone density and mechanical properties in these regions.
Methods
66 trabecular cores from 9 distal femur cadavers were imaged through micro-CT. Apparent density was calculated and the scans analysed to identify each cores structural ‘fabric’ components (Figure 1). The axis of all specimens was aligned with the principal trabecular direction. Specimens were taken from a total of 10 locations that covered the trochlear and condyle regions. Once removed, the extracted cores underwent quasi-static compression testing to identify the Young’s modulus and yield strength at each site.
Results
70% of core locations tested had a high degree of anisotropy, the remaining 30% had a low degree of anisotropy. For the high anisotropic regions there was a good relationship between apparent bone density and modulus (R2 = 0.69) and yield strength (R2 = 0.65). For the low anisotropic regions there was a poor relationship between the apparent bone density and both modulus and yield strength (R2 <0.2 for both). This means that in regions with a low degree of anisotropy, there is a risk of overestimating mechanical properties from apparent density. This could lead to an over-estimation of 117% and 53% for modulus and yield strength respectively in low anisotropic regions of the distal femur (Figure 2).
Conclusions
Estimating mechanical properties in regions that have a low degree of anisotropy from bone density should be done with caution.
The results of this study will help to generate better computational models, understand the mechanical environment for novel chondral repair materials and inform the mechanical properties of additively manufactured implants that maintain natural bone strains.
Figures
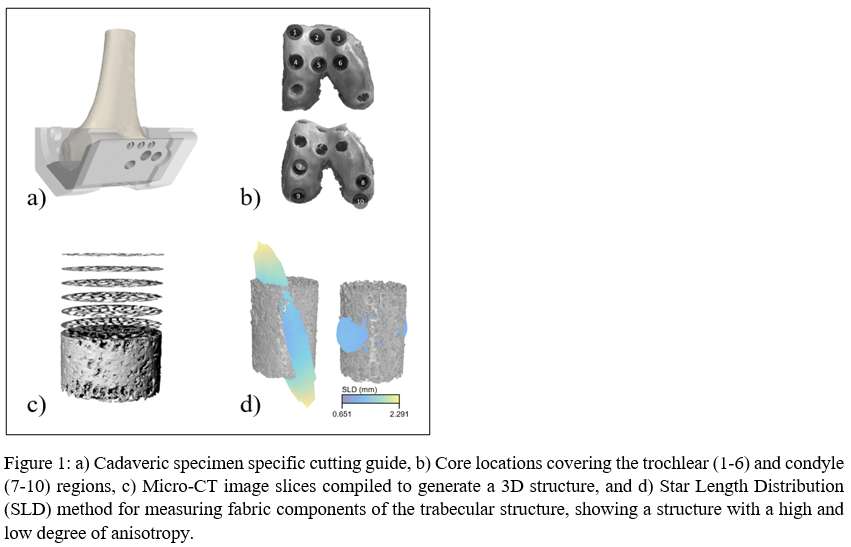
Figure 1
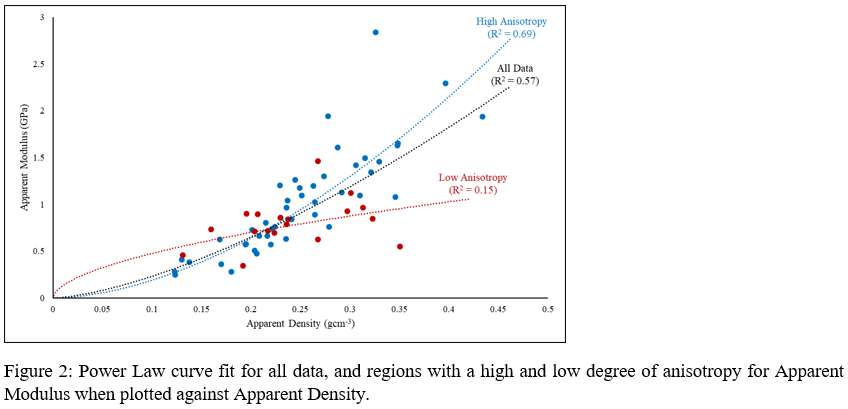
Figure 2#7355
Variation in Mechanical Properties of Trabecular Bone in the Distal Femur
*James Scott - Imperial College London - London, United Kingdom
Jonathan Jeffers - Imperial College London - London, United Kingdom
*Email: j.scott19@imperial.ac.uk
Introduction
Asymmetric joint loading during knee flexion influences the mechanical properties of trabecular bone in the distal femur. Trabecular bone responds to the variation in direction and magnitude of loading across the articulating surface by exhibiting differing Young’s modulus that is suited to each region’s mechanical environment.
The extent of the variation in mechanical properties across the articulating surface is not fully understood. The trochlear and condyle articulating regions of the distal femur experience different loading patterns. Mapping the change in mechanical properties across the distal femur will help understand how trabecular bone varies to the different loading environments noticed especially during knee flexion.
Methods
116 trabecular cores from 16 distal femur cadavers were extracted from 10 locations that covered the trochlear and condyle regions of the distal femur (Figure 1). Each cadaver was imaged using a clinical CT scanner and imported into a visual programming design application to optimally position core locations within the articulating regions. A specimen specific cutting guide based on the femur was additively manufactured to ensure the extracted cores were aligned with the principal trabecular direction. Quasi-static compression testing for each core identified the apparent modulus and yield strength. A load cycle with a hysteresis loop between 40% and 20% of estimated yield was used to estimate apparent modulus.
Results
Trabecular bone apparent modulus and yield strength differs significantly (p <0.0005) when comparing the trochlear (n=61) and condyle (n=58) regions, with median values of 0.62 GPa and 1.09 GPa respectively for apparent modulus and 6.64 MPa and 11.86 MPa respectively for yield strength. A box plot showing the variation in apparent modulus for the trochlear and condyle regions is shown in Figure 2.
In the condyle region the medial condyle (n=28) has a significantly higher apparent modulus and yield strength compared to the lateral condyle (n=30) (p <0.0005), while there was no significant variation in apparent modulus within the trochlear region (p=0.063). Yield strength did however display some significant variation within the trochlear region. Pairwise comparisons found the most significant (p <0.005) difference seen between proximal medial region and the distal lateral region of the trochlea with median values of 5.06 MPa and 9.21 MPa respectively. A box plot showing the variation across all core locations are shown in Figure 3.
Conclusions
There are clear regional differences in mechanical properties when comparing the two articulating regions of the distal femur. A variation in trabecular structure, surface contact patten and joint loading contribute to variation in mechanical properties. Asymmetric joint loading during flexion is mirrored in measured mechanical properties within the articulating regions.
The results of this study will help in the development of regional joint arthroplasty, where implant materials or the surgical approach may vary depending on the mechanical properties and structure of the trabecular bone underneath the articulating surface.
Figures
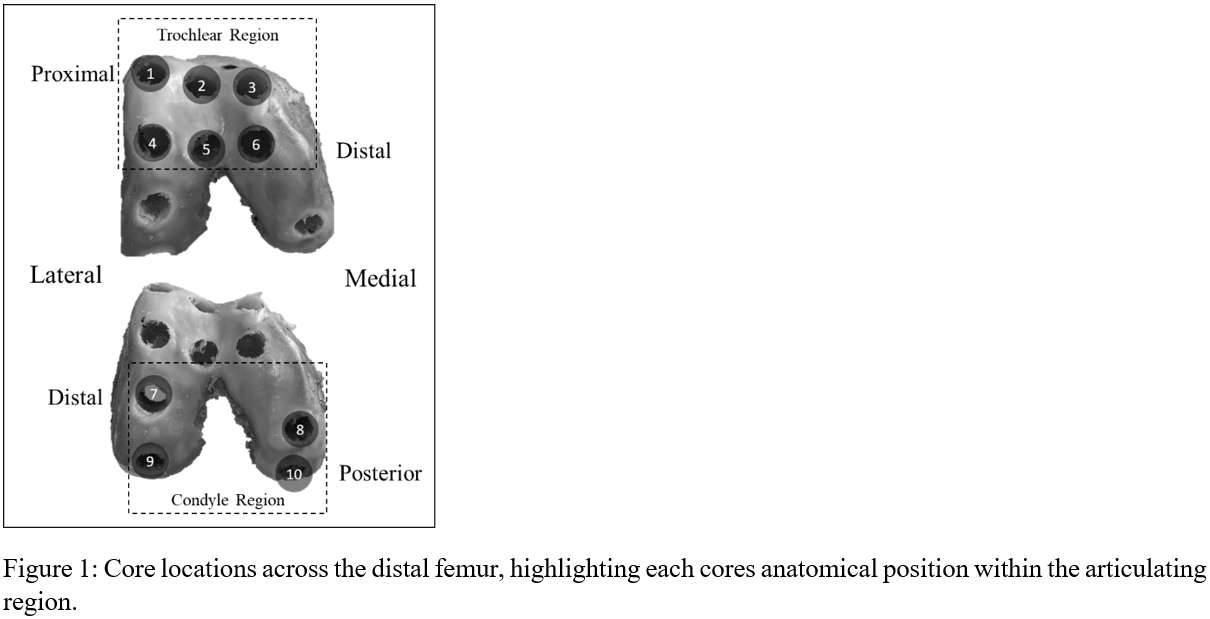
Figure 1
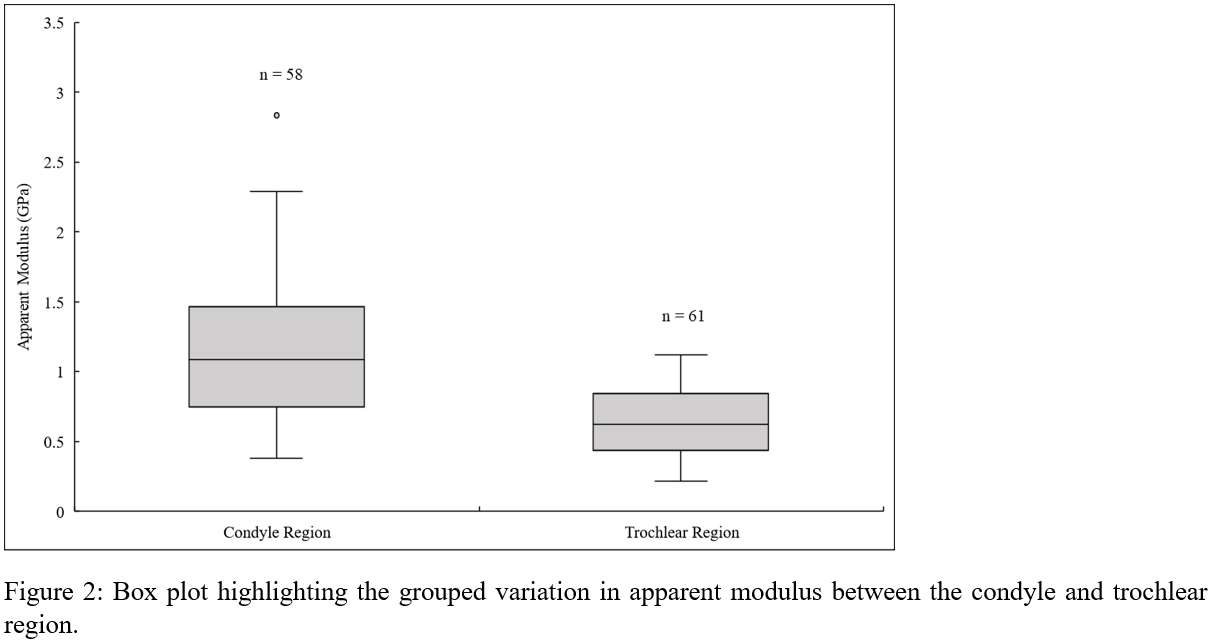
Figure 2
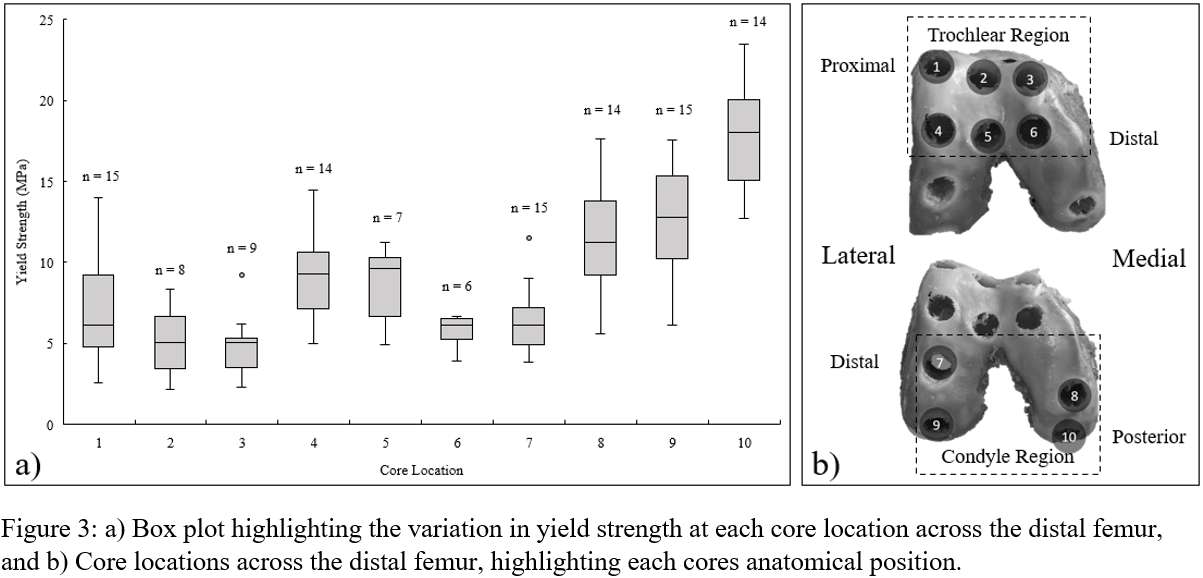
Figure 3#7778
How Do Surface Finish and Taper Design Influence Corrosion Modes and Mechanically Assisted Crevice Corrosion Behavior in Modular Dual Mobility Acetabular Tapers? A
Aarti Shenoy - Hospital for Special Surgery - New York, USA
John Steele - Hospital for Special Surgery - New York, USA
Douglas E Padgett - Hospital for Special Surgery - New York, USA
*Timothy Wright - Hospital for Special Surgery - New York, USA
*Email: wrightt@hss.edu
INTRODUCTION: With expanding use of modular dual mobility (MDM) acetabular components to combat instability in total hip arthroplasty, and reports of mechanically-assisted crevice corrosion (MACC) and associated adverse local tissue reactions in MDM devices, understanding MDM performance metrics is important to the arthroplasty community. We propose investigating three MDM designs in clinical use in the United States. Our goal is to investigate the effect of surface finish and design on taper corrosion among these MDM shell-liner couples using an in vitro corrosion chamber test method.
METHODS: Pairs of pristine commercial Ti6Al4V shells and CoCrMo liners from two of the three groups (MDM® X3® Dual Mobility System (Stryker, Mahwah NJ), and G7® Acetabular Dual Mobility System (Zimmer Biomet, Warsaw IN) were included (n=3 per group). Pinnacle® Dual Mobility System (Depuy Synthes, Warsaw IN) components remain to be tested. Shell-liner couples were assembled with an impaction load of 2000N using a previously established protocol [1].
Each assembled device was placed into an electrochemical chamber with a three-electrode assembly and phosphate buffered saline as electrolyte. Physiological cyclic loading (100N to 1000N in 100N increments; 1000N to 4000N in 200N increments) was simulated while measuring currents generated at the shell-liner taper. Onset load for fretting corrosion and average fretting currents at each load were calculated. Both metrics will be compared across groups using one-way ANOVA with Tukey’s post-hoc analysis, with p=0.05 set as level of significance.
RESULTS: The G7 liner has a sandblasted surface treatment, creating a rougher topography compared to the machined smoother finish of the other two designs. Preliminary results from a Stryker MDM (Fig. 1) and a Biomet G7 (Fig. 2) sample each show a difference in instantaneous spikes in current at the start of the loading cycle. The Stryker sample had spikes rising to an order of magnitude higher than that for the Biomet G7. The fretting current immediately subsides to a steady state between 0-6 µA for both designs (Fig. 3). Fretting onset occurred at 1600N loading cycle for the Stryker sample, and at 2600N for the G7 sample. Average fretting current at 3800N recorded for the Stryker MDM sample was 0.08 µA, and 4.25 µA for G7. Data analysis for other samples and statistical analysis are in progress.
CONCLUSION: From preliminary data, the Stryker MDM design exhibits a higher initial spike at start of loading than the G7 sample, indicating a difference in taper mechanics between the two designs. The rougher surface of the G7 might also contribute to a crevice-like environment, in turn leading to lower average fretting current in the Stryker design than in the G7. Average fretting currents in both designs remain low, especially in comparison with head-neck tapers, where average currents ranging from 14 µA to 40 µA have been reported [2].
References:
[1] Romero J et al., Malseating of modular dual mobility liners. Bone Joint J. 2020 Jul;102-B, p20-26
[2] Mali S.A. et al., “Correlating Fretting Corrosion and Micromotions in Modular Tapers: Test Method Development and Assessment,”, ASTM STP1591 2015, pp. 259–282
Figures
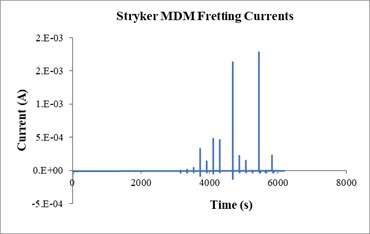
Figure 1
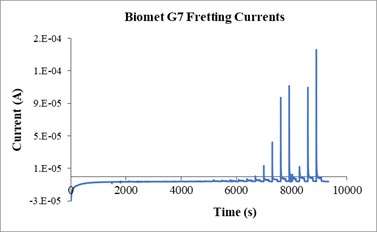
Figure 2
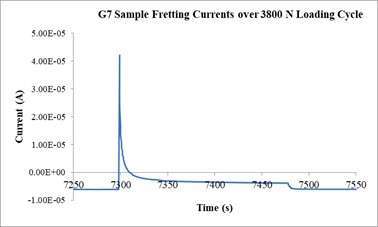
Figure 3#7826
Post Fractures in Total Knee Arthroplasty: Differences in Fracture Progression Between UHMWPE and HCLPE Posts
Aarti Shenoy - Hospital for Special Surgery - New York, USA
Cynthia Kahlenberg - Hospital for Special Surgery - New York City, USA
Elexis Baral - Hospital for Special Surgery - New York, USA
Ashley Pekmezian - Hospital for Special Surgery - New York, USA
Alberto Carli - Hospital for Special Surgery - New York City, USA
Michael Ast - Hospital for Special Surgery - New York, USA
Peter Sculco - Hospital for Special Surgery - New York, USA
Geoffrey H Westrich - Hospital for Special Surgery - New York, USA
*Timothy Wright - Hospital for Special Surgery - New York, USA
*Email: wrightt@hss.edu
INTRODUCTION: Posterior Stabilized Total Knee Arthroplasty (PS-TKA) tibial inserts were revised for post fracture. These inserts were made of ultra-high molecular weight polyethylene (UHMWPE) or highly cross-linked polyethylene (HCLPE). Neither material is known to be more susceptible to post fracture. We sought to characterize the fracture mechanism of contemporary PS-TKA posts to determine if material, design, or patient factors influence fracture patterns and to describe differences in fracture progression between the two materials.
METHODS: 1,363 PS-TKA implants were retrieved between January 2015 and October 2021. 33 implants (2.42%) from five manufacturers had fractured posts that had been confirmed intraoperatively (21 UHMWPE, 11 HCLPE). The articular surfaces were sputter-coated with palladium for enhanced visualization of damage features and subjective Hood scoring for damage to the post surfaces and for scanning electron microscopy (SEM) imaging of the fracture surfaces of13 representative implants. Patient demographics were collected for all patients. T-test was used to compare mean damage scores between the UHMWPE and HCLPE inserts across damage modes.
RESULTS: Fracture initiation generally occurred on the posterior side of the post, and progressed towards the anterior side, often with shifts in the horizontal plane (Fig. 1). Mean length of implantation was 10.3±4.4 years, average age at implantation was 54±1.5 years, BMI was 30±4.4, and 82% (27/33) of patients were males. Eleven patients reported normal activities at the time of post fracture, six reported high impact activities, and four reported being in deep flexion. For four patients, no reported cause of fracture was included in the medical record. No instances were found of sagittal femoral or tibial component malpositioning, defined as >10° flexion or >5° extension. In addition to the common damage modes observed like pitting, burnishing and scratching, more than 75% of the cohort had evidence of abrasion and surface deformation. SEM showed distinct clamshell markings in all 13 imaged implants. Overall damage scores were statistically higher for the UHMWPE inserts than in the HCLPE cohort. The fracture surface of UHMWPE posts had a more tufted, irregularly distributed clamshell progression whereas those on the HCLPE had more precise clamshell marks (Fig. 2), as well as diamond patterns on the acute, final fracture portion of the surface, usually on the anterior side of the post (Fig. 3).
CONCLUSION: Most of the patients who experienced the post fracture were predominantly male and reported a high level of activity, which could have increased risk of crack initiation and fracture progression due to modified or improper femoral cam contact on the posterior surface of the post. Crack initiation usually occurred on the posterior side and likely initiated secondary to damage caused by the femoral cam contacting the post. Fatigue fracture progression patterns differed between HCLPE and UHMWPE inserts and is likely related to the decreased caused by higher degree of crystallinity. The diamond markings on the anterior side of the post fracture surface indicates acute final failure. Neither material appeared to be superior in terms of fatigue resistance.
Figures
Figure 1
Figure 2
Figure 3#7552
Comparison of Taric and Hintegra Prostheses in Total Ankle Arthroplasty; Short-Term Results
*Dong Woo Shim - Catholic Kwandong University International St.Mary's Hospital - Incheon, Korea (Republic of)
Hyunjoo Hong - Severance Health Check-up - Seoul, South Korea
*Email: dcastle@hanmail.net
Introduction
Total ankle arthroplasty (TAA) has become the backbone of treatment for end-stage ankle osteoarthritis with improving clinical outcomes in the past few decades. Several prostheses for TAA have been developed to date. We compared short-term clinical and radiological outcomes between Taric® and Hintegra® prostheses for TAA.
Methods
Total 60 consecutive ankles with TAA were investigated. We included 12 ankles (12 patients, Group 1) who underwent Taric® TAA and 35 ankles (31 patients, Group 2) who underwent Hintegra® TAA in a retrospective design. Age, gender, body mass index (BMI), etiology of osteoarthritis were compared between two groups. Clinical outcomes were evaluated with visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) score, Ankle Osteoarthritis Scale (AOS) pain and disability score, and ankle range of motion (ROM) in dorsiflexion/plantarflexion. Radiological outcomes included tibial angle and tibial slope on weight-bearing radiographs. Revision surgeries for any reason were investigated either.
Results
Mean age at the time of surgery was 62.4 (range, 51 – 88) years and mean follow-up duration was 20.2 (range, 12 – 40) months. There were no demographic data differences between two groups. All patients showed significant improvement at VAS, AOFAS score, AOS score, and ROM (P < 0.001, P < 0.001, P < 0.001, P = 0.028) post-operatively. There were no significant differences in VAS and AOS score (P = 0.128, P = 0. 223) except AOFAS score (P = 0.038) between two groups. In addition, ROM and radiological parameters did not show significant differences (P = 0.532, P = 0.681). Three ankles in Group 1 underwent revision surgery (25%) while one ankle in Group 2 underwent revision surgery (2.9%) during the follow-up period (P = 0.046).
Conclusion
There were no significant clinical and radiological differences between Taric® and Hintegra® prostheses for TAA except in AOFAS score during short-term follow-up. However revision surgery rate was significantly higher in Taric® prosthesis group.
#7280
Risk of Periprosthetic Joint Infection in Patients With Total Knee Arthroplasty Undergoing Colonoscopy: A Nationwide Propensity-Score-Matched Study
Kyun-Ho Shin - Nanoori Hospital Incheon - Incheon, South Korea
*Seung-Beom Han - Korea University Anam Hospital - Seoul, South Korea
*Email: s1113k1209@daum.net
Background
The post-colonoscopy periprosthetic joint infection (PJI) risk in patients with total prosthetic knee joints has limited research. The present study investigated the PJI risk and determined the risk factors for post-colonoscopy PJI in total knee arthroplasty (TKA) recipients. The hypothesis was that colonoscopy is associated with an increased PJI risk in patients with total prosthetic knee joints. This study can potentially help guide the decision making for prophylactic antibiotic use for colonoscopy.
Methods
This nationwide matched cohort study used claims data from the Health Insurance Review and Assessment Service database and enrolled patients who underwent unilateral TKA between 2008 and 2016. The history of diagnostic colonoscopy was investigated at least one year postoperatively. The propensity score was matched between colonoscopy and non-colonoscopy cohorts, and the post-colonoscopy PJI risk was compared. In addition, the PJI risk following invasive colonoscopic procedures, including biopsy, polypectomy, and mucosal or submucosal resection, was further investigated, and the risk factors for post-colonoscopy PJI were determined.
Results
45,612 and 211,841 patients were matched in the colonoscopy and control cohorts, respectively (Figure 1). After propensity score matching, there was a balance between both groups in terms of baseline covariates, except age (Figure 2). The colonoscopy cohort had greater 9-month and 1-year PJI risks from the index colonoscopy date than the matched controls (9-month: hazard ratio [HR], 1.836; p=0.006; 1-year: HR, 1.822; p=0.031). The cumulative incidence rate of PJIs was 0.038% in non-recipients of colonoscopy within 1 year from the index date, whereas the rate was 0.070% in colonoscopy recipients (p=0.005, Figure 3). Invasive colonoscopic procedures did not increase the PJI risk at any time point post-colonoscopy. The only significant risk factor for PJI was post-traumatic arthritis (adjusted HR, 4.034; p=0.023).
Conclusions
Colonoscopy was associated with an increased PJI risk in TKA recipients, regardless of concomitant invasive colonoscopic procedures.
Figures
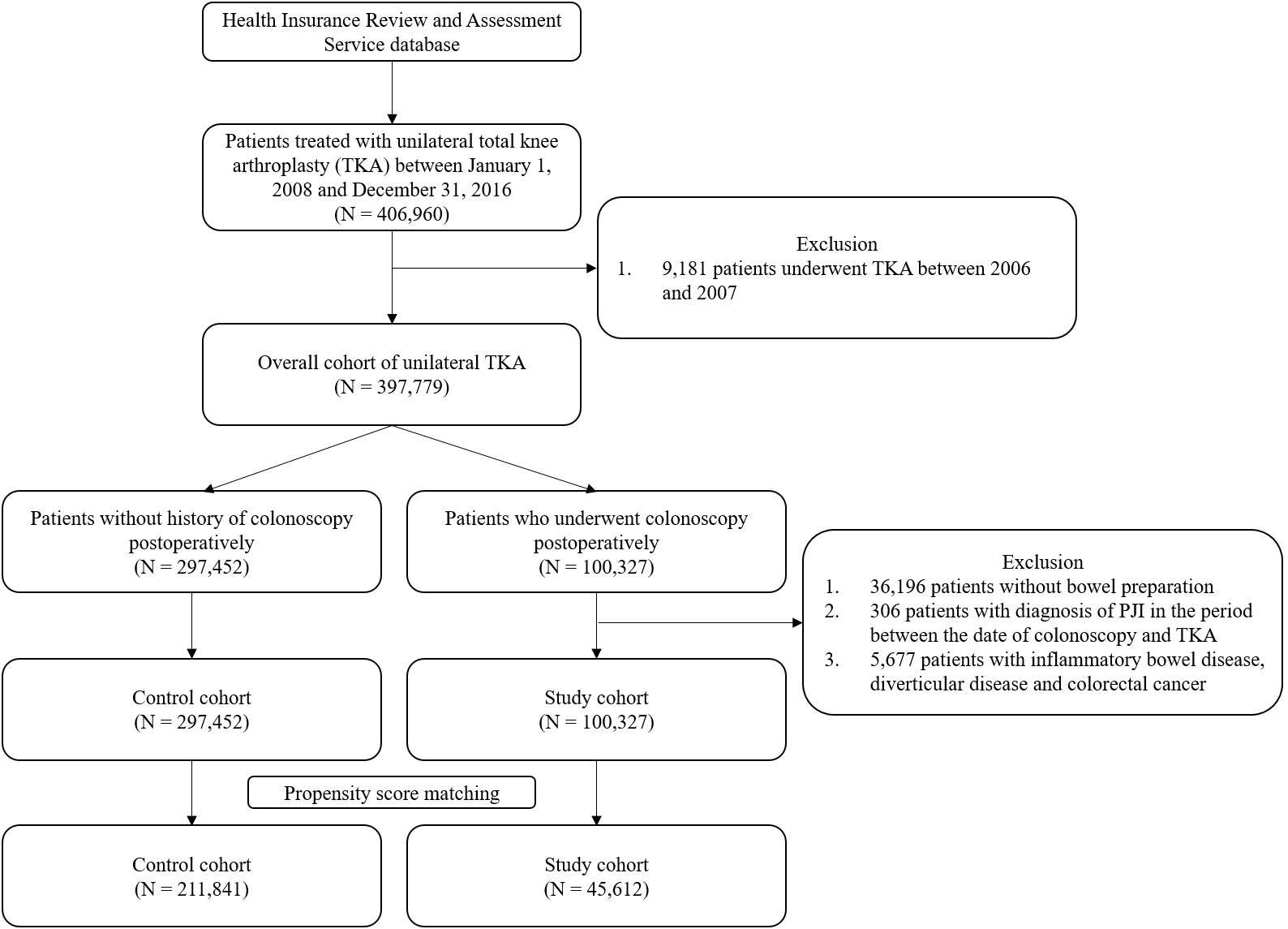
Figure 1
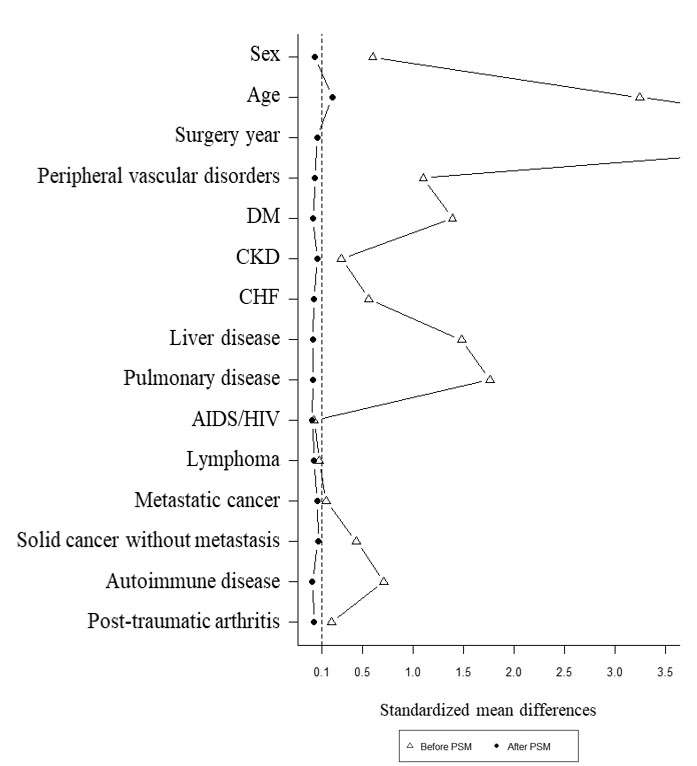
Figure 2
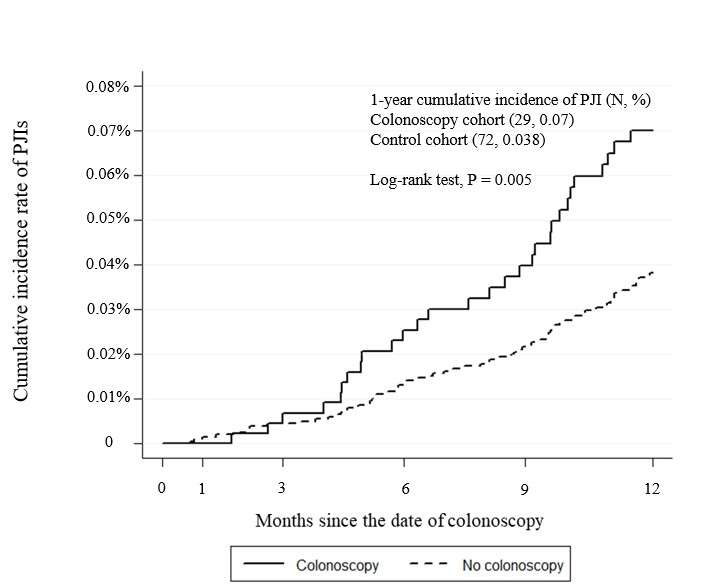
Figure 3#7990
Patient Reported Outcomes and Engagement Following Shoulder Surgery: The Effect of Using a Digital Remote Patient Monitoring Application
*Yousef Shishani - Cleveland Shoulder Institute - Beachwood, USA
Reuben Gobezie - Cleveland Shoulder Institute - Mayfield Heights, USA
Cory Ohradzansky - Ohio University - Athens County, USA
Stacy Jones - Cleveland Shoulder Institure - Beachwood, USA
*Email: yousef@clevelandshoulder.com
Introduction: Traditionally, physical therapy following shoulder surgery has occurred via in-office supervised visits. With the increased use of digital health applications and the impact of COVID-19 on the healthcare system, the development of human motion technology has emerged as a tool for remote patient monitoring (RPM) and peri-operative patient engagement. AI-powered apps can measure range of motion, provide exercise corrections, and help the patient recover remotely. The purpose of this study was to report patient outcomes following shoulder surgery by using a smartphone rehab app (PT Genie, Fl) compared to patients who just did in-office physical therapy. We also wanted to report on the age distribution and engagement of the patients using the digital rehab app.
Methods: In a single orthopedic practice between April 2020 and May 2021, patients who underwent a shoulder procedure were identified and grouped into two categories a) Shoulder arthroplasty and b) Shoulder arthroscopy. Within these two groups, we also identified patients who used the PT Genie (PTG) digital platform to perform their home-based therapy and age-matched a cohort from our research registry (Surgical Outcomes System (SOS), Arthrex, Naples) with patients who just completed in-person rehab sessions at the same practice. Outcome scores included, pre and 1-year post-op visual analog scale pain score (VAS), American Shoulder Elbow Surgeons Score (ASES), and Single Assessment Numeric Evaluation (SANE). All patients in both groups reported the outcome scores in our SOS database. Finally, the age distribution for the digital app users was divided into 6 groups (≤40, 41-50, 51-60, 61-70, 71-80, and 81+). Statistical analysis using the student t-test to compare means was performed using version 17 of SPSS (IBM).
Results: A total of 862 patients were identified. There were 396 patients in the arthroscopy group (198 PTG and 198 non-PTG). In the arthroplasty group, there was a total of 466 patients (233 patients in each of the subgroups). In the PTG arthroscopy group, there were 118 females, and the average age was 52.4 ±14.2 (15-90). In the non-PTG arthroscopy cohort, there were 112 females, and the average age was 52.8 ±15.0 (16-85) (p=0.732). There were 148 females in the PTG arthroplasty group with an overall average age of 67.1 ±8.5 (41-93). For the non-PTG group, there were 130 females, and the average group age was 68.5 ±11.1 (28-90) (p=0.120). Interestingly, the highest engagement in performing home-based rehab on the digital platform was observed in the arthroplasty age groups of 51-60 (72 completed sessions) and 61-70 (81 completed sessions) (Figure 1). Table (1) and table (2) outline the differences in the outcome scores between the two groups.
Conclusion: Digital rehab apps are a viable option for remote patient monitoring following shoulder surgery. Our results showed no significant differences in the outcomes measures reported by the users in the two groups. A larger cohort with multiple joints tracked over a longer period of time will need to be studied in the future.
Figures
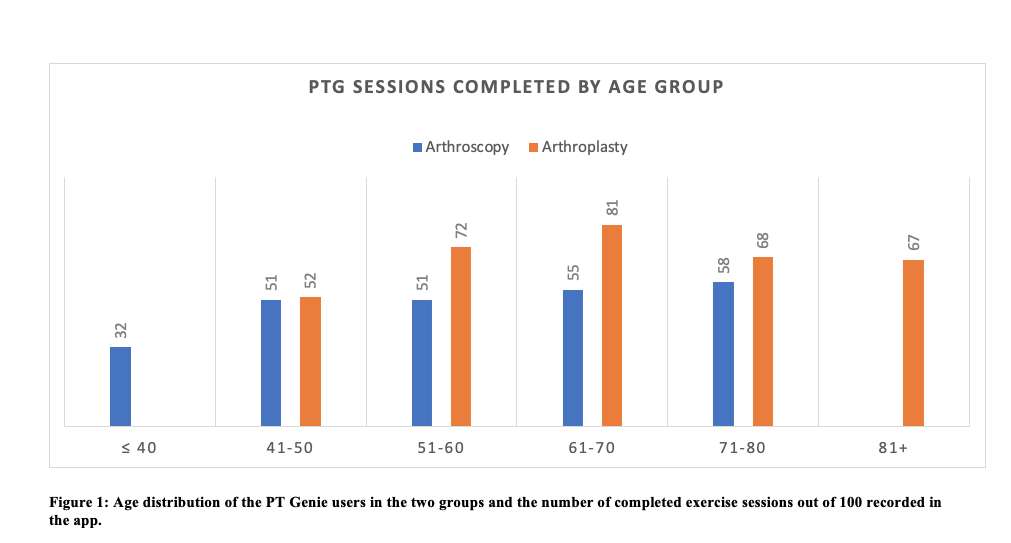
Figure 1
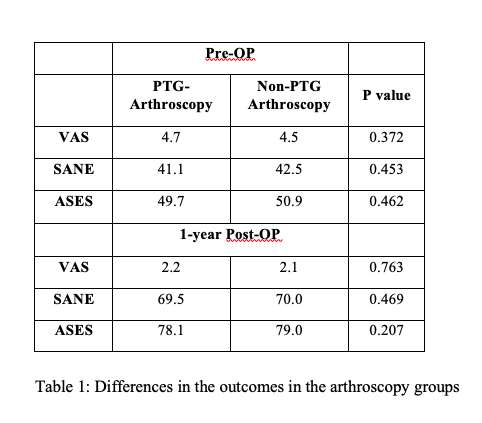
Figure 2
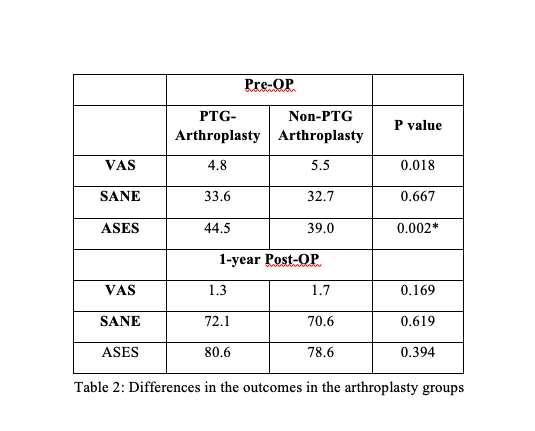
Figure 3#7993
Measuring Shoulder Forward Flexion ROM Using a Digital Rehab Application Versus a Laser Powered Hand-Held Digital Goniometer: A Comparative Study
*Yousef Shishani - Cleveland Shoulder Institute - Beachwood, USA
Reuben Gobezie - Cleveland Shoulder Institute - Mayfield Heights, USA
*Email: yousef@clevelandshoulder.com
Introduction: Shoulder range of motion (ROM) is an important criterion in diagnosing and evaluating the shoulder joint. It is equally important to establish an accurate ROM measurement pre-operatively and to track the progress at specific intervals following shoulder surgery. With the recent advances in human pose estimation algorithms, it has become possible to estimate human joint positions in real-time and to automatically measure the ROM for most of the human joints. The purpose of this study was to compare and evaluate if the results of measuring the shoulder ROM in the Forward Flexion (FF) plane using an AI-powered application (PT Genie, Orlando, Fl) (Figure 1) were as reliable as measurements using a hand-held laser-powered digital goniometer (Halo Medical Devices, Australia) (Figure 2)
Methods: In a busy orthopedic practice, we randomly asked adults to participate in this experiment. Participants were asked to perform 3 consecutive shoulder FF movements measured first by the digital goniometer and then followed by 3 consecutive shoulder FF movements in front of the PT Genie app. All measurements using the digital goniometer were conducted by the same medical professional. All the measurements using the PT Genie app were done using the same iPhone 11 running iOS 15.4.1, and the PT Genie app version 2.2.5. The iPhone was always placed at the same height and distance from the user in the exam rooms (Figure 3). To avoid any aggravation to any existing shoulder injury, all participants had the freedom to choose the side they wanted to move, regardless of dominance (Figure 4). The mean from the 3 measurements was calculated and the mean differences between the two measurement options were then compared.
Results: Thirty-two subjects agreed to evaluate their shoulder ROM. There were 16 males (50%) and 16 females (50%). The average age of the cohort was 58.5 ± 17.4 years (range 24-80). There were 21 right shoulders and 11 left shoulders. There were 7 females with left shoulders and 9 with right shoulders. In the male population, there were 4 with left shoulders and 12 with right shoulders. The mean ROM from each of the three consecutive measurements using the goniometer were as follows: 119.8°±24.4°, 119.9° ±24.7°, and 120.7° ±25.3°. For the ROM using PT Genie, the averages for the 3 measurements were: 123.3° ±25.7°, 123.4° ±26.6°, and 123.8° ±26.4°. The overall difference in measuring the shoulder FF ROM was 3.4° more on the PT Genie application compared to the digital goniometer. Comparing the overall ROM means for the two groups, the digital goniometer was 120.1° ± 24.7° (range 71.7° - 164.7°), and the PT Genie application was 123.5° ± 26.0° (range 74.7° – 173.0°) (p<0.001).
Conclusions: The results from this experiment indicate that the digital PT Genie application is a reliable tool to measure the shoulder joint ROM. The AI-powered algorithms are accurate to within 3° from a digital laser goniometer. Further statistical analysis, such as using the intra-class correlation coefficient and Pearson correlation coefficient can be performed on a larger cohort in the future.
Figures
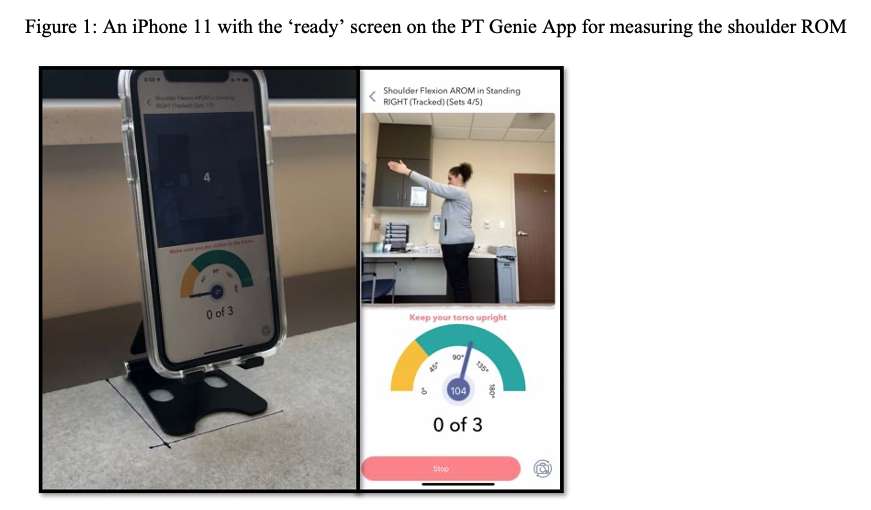
Figure 1
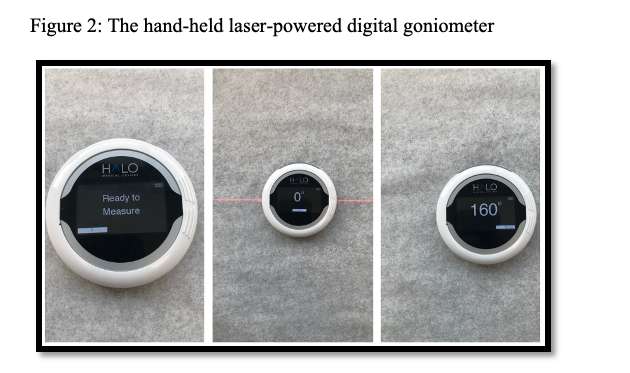
Figure 2
Figure 3#7609
Amorphous Diamond-Like Carbon (ADLC) for Total Joint Arthroplasty
*Ryan Siskey - Exponent - Philadelphia, USA
Alex Avendano - Exponent - Philadelphia, USA
Kapil Raghuraman - Enovis - Ausitn, USA
John Vinciguerra - DJO Surgical - Austin, USA
*Email: RSISKEY@EXPONENT.com
Introduction
Diamond-like carbon (DLC) coatings are a specific class of advanced coating that have been utilized in high wear and performance applications such as in aerospace and motorsports technologies. Compared to previously used DLC coatings, modern amorphous diamond-like carbon (ADLC) coatings incorporate more robust mechanisms of application and better substrate-coating interfaces to address historical surface-finish and delamination concerns. These advancements in ADLC coatings, and their ability to be applied to a variety of substrate materials, make them an attractive solution for providing wear resistance in orthopedic total joint applications. The aim of this study was to evaluate the tribological performance of a titanium femoral component coated with a modern ADLC coating in both clean and abrasive pre-clinical conditions.
Materials and Methods
A total knee replacement system with crosslinked and vitamin E stabilized UHMWPE was tested under clean conditions against an ADLC-coated titanium femoral component. The methods prescribed in ISO 14243-1 were used to guide the input parameters for the test. The test was stopped at least once every 0.5 MC up to 10.0 MC to inspect and characterize the parts. The tibial components were cleaned and dried, photodocumented, and weighed for mass loss throughout the test. At 5.0 MC, the femoral components were intentionally damaged using a particle slurry and the test continued to 8.0 MC. At 8.0 MC the femoral components were replaced with new femoral components and the test continued to 10 MC. Samples were also characterized using SEM, interferometry, and microCT to document the damage modes and effect of abrasive damage.
Results
The UHMWPE tibial inserts demonstrated evidence of microabrasive damage modes typical of UHMWPE-on-hard bearings. The ADLC coating demonstrated multidirectional scratching and polishing in the area of contact but no evidence of coating breakdown or wear-through. Intentional damage of the femoral component showed limited titanium substrate exposure in the region of contact. The mass wear rates across the three phases of testing have been presented in Table 1.
Discussion
Overall, the results suggest the ADLC remains intact through 5 MC of clean wear testing and demonstrate wear mechanisms and wear rates consistent with traditional vitamin-E inclusive cross-linked UHWMPE-on-hard bearing couples. While intentional abrasive damage increased the wear rate of the tibial inserts, it did not result in runaway wear and when removed, the wear rates recovered to rates comparable to conventional TKA. The results suggest that a modern amorphous diamond-like carbon coating could augment the tribological profile of a total joint bearing couple with minimal increase in the risk profile for implant design.
Figures
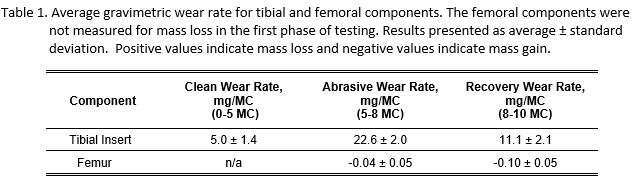
Figure 1#7574
Does It Matter Which PRO You Collect to Measure Health-Related Quality of Life (HRQoL) in THA?
Raj Karia - NYU Hospital for Joint Diseases - New York, USA
*Jerry Arraut - NYU Langone Health - New York, Select Country
Thomas Christensen - NYU Langone Health - New York, USA
Christian Oakley - NYU Langone Health - New York, USA
Thomas Bieganowski - NYU Langone Health - New York, USA
James Slover - New York University-Hospital for Joint Diseases - New York, USA
*Email: jerryarraut1@gmail.com
Introduction:
Health-related quality of life (HRQoL) measures have become the common method of assessing the benefit of healthcare interventions. The Comprehensive Care for Joint Replacement (CJR) includes a measurement of HRQoL in their performance metrics within their patient-reported outcomes (PRO) component of the program. Hospitals submitting PRO data have the option to submit either the Veterans RAND 12 Item Health Survey (VR-12) or the Patient-Reported Outcomes Measurement Information System (PROMIS) ® Global-10 survey. In this study, we evaluated the relationship between these two HRQoL measures to determine if there is a high level of concordance between the measurements in a THA population.
Methods:
A retrospective analysis was performed on primary THA patients from October 2018 to April 2019. Patients completed pre-operative HRQoL measures within a 3-month window prior to their procedure. The VR-12 was completed once a patient was scheduled for the procedure and the PROMIS® Global-10 (v1.2) was completed via tablet or patient portal during a prior outpatient clinic visit. HRQoL questionnaires were scored and reported into their component mental composite score (MCS) and physical composite score (PCS). Pearson correlations were performed to assess the relationship between the two HRQoL instruments.
Results:
A total of 130 primary total hip arthroplasty patients completed both the PROMIS® Global-10 and VR-12 questionnaires. There was only a moderate correlation between VR-12 MCS and PROMIS-10 MCS (r=.549, p<0.01). There was also only a moderate correlation between VR-12 PCS and PROMIS-10 PCS (r=.479, p<0.01).
Conclusion:
The collection of health-related quality of life measures is becoming more prevalent in orthopedics and is an important part of new payment models such as CJR. This study showed only a moderate correlation between two widely used HRQoL measures. Future studies should further investigate the differences between these measures within the total hip replacement population before widely using this data for health economic evaluation.
#7707
Routine Collection of Patient Reported Outcome Scores in Hip/Knee Replacement Patients Using an EMR Integrated App for a Contactless Experience
*Raj Karia - NYU Langone Health - New York, United States of America
James Slover - New York University-Hospital for Joint Diseases - New York, USA
*Email: raj.karia@nyulangone.org
Introduction
Patient-reported outcomes (PROs) are being increasing used in TJA as a measure of care and quality. Providers are increasingly attempting to use PRO data to measure a patient’s status and the impact of various treatment interventions. Furthermore, government programs and private insurers have increasingly asked sites to submit PRO data for a variety of functions. However, challenges to collecting this data routinely in the office setting have been reported. Our objective was to determine the feasibility of implementing PRO collection and clinical use through native tools within our electronic medical record (EMR) system and its associated patient smartphone APP.
Methods
Patients were asked to complete the PROMIS Global-10, PROMIS Physical Function Computer Adaptive Test (CAT), PROMIS Pain Interference CAT, PROMIS Pain Intensity and KOOS/HOOS JR questionnaires at home prior to their visit using a patient portal, which can be accessed via a smartphone APP integrated directly into the EMR. If a patient does not complete prior to the visit, the front desk staff directed them to complete via a tablet or using the smartphone app on their phone in the waiting room prior to their appointment. Scores are available in real-time for provider to view in graphical form in multiple areas of the EMR and can be automatically incorporated into visit notes.
Results
Between February 1, 2021 and March 31st 2022, PRO scores were completed for 9,744 total joint arthroplasty patient-encounters, representing 85% overall completion for visits to the practice. 4,092 were seen for a hip-related complaint and 5,952 were seen for knee-related complaints among 9 orthopedic surgeon practices. 32% were completed at home via smartphone app and 68% were completed in the office on the day of the visit. Median time for completion was 6 minutes.
Conclusion
PRO Collection via an EMR native platform without use of an outside vendor can result in robust collection rates. Advantages of using an EMR native platform include integration with the existing administrative and clinical workflow and ability to complete using a smartphone APP with real time availability of responses for providers caring for patients. Future efforts in PRO collection should leverage this technology and continue to investigate other solutions that increase patient and provider engagement with the collection and use of scores and decrease the burden of collection.
#7712
Implementation of an EMR Based Interactive Virtual Care Management Platform for Perioperative Care After Total Joint Arthroplasty
*Raj Karia - NYU Langone Health - New York, United States of America
James Slover - New York University-Hospital for Joint Diseases - New York, USA
*Email: raj.karia@nyulangone.org
Patients are spending substantially less time in the acute care setting after TJA(total joint arthroplasty), a factor enhanced by the recent removal of TKA from the Center for Medicare and Medicaid Services’ (CMS) Inpatient Only List. As a result, increased communication, coordination and patient engagement in their care plan is needed given the decreased direct contact with the care team after surgery. Patients’ desire to have an elective TJA has been cited as a potential teachable moment to activate patients to optimize their health to reduce the risks of surgery, but little work has been done to determine the potential for increasing patient engagement perioperatively, or the optimal tools or protocols to use. This study describes the implementation of an interactive virtual care management platform using a smartphone app to deliver perioperative education, evaluation and care in a TJA population.
Methods
The implementation took place in a large urban academic medical center with adult patients after joint replacement for hip and knee who were able to use in interactive care plan via mobile app. The interactive virtual care manage platform is highly individualized plan of care delivered to patients directly via an EMR based patient mobile app. The care plan begins 30 days pre-op and continues for the 90 day postop period. Patients receive education that is delivered through formatted text, videos and audio. Also included are general tasks for medications, dressing change and scheduling follow-up appointments. Questionnaires for pain and symptom monitoring are administered at defined time points. Bi-directional communication between the surgeon and their team and patients is part of the system and escalation of responses that require clinical attention are automated through the APP and EMR.
Results
Since its launch, 3,127 patients have been assigned the interactive virtual care plan. In this cohort, there were 34,434 total possible tasks included in the virtual care plans. Of these total possible tasks, 14,654 (43%) were viewed or completed. Providers sent 243 messages to patients that required clinical attention and were identified through the system's escalation reports.
Conclusion
Perioperative care using an interactive virtual care platform is feasible and can increase patient engagement and care coordination needed among providers in a more real time less resource intensive fashion. Additional benefits include reducing the economic and time burden for patients and their home supporters related to traditional perioperative care often requiring many trips to and from various settings with many hours away from work and family. Future studies will be needed to determine its precise role in the perioperative period and impact on TJA outcomes.
#7698
In Vivo Knee Kinematics: Are Bi-Cruciate Substituting TKAs More Likely to Achieve Optimal Kinematics?
*Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: lsmit186@vols.utk.edu
Introduction:
The bi-cruciate stabilized (BCS) TKA features a dual cam-post mechanism to substitute for the ACL and the PCL, while the posterior stabilized (PS) TKA provides a singular cam-post mechanism to replicate the functionality of the PCL alone. Will adequate substitution of both cruciate ligaments result in more normal-like kinematics than seen in traditional PS TKAs? This research study assesses the importance of replicating the function of the ACL in BCS TKAs compared to its PS counterpart and the normal knee.
Methods:
The in vivo 3D kinematics were determined for 28 subjects having a PS TKA (14 Type # 1, 14 Type #2), 14 subjects having a BCS TKA and 10 having a normal knee. Kinematics were obtained using validated fluoroscopic and 3D-to-2D registration techniques. All subjects were asked to perform a weight-bearing deep knee bend (DKB) maneuver intended to flex the knee from full extension to maximum flexion. The kinematic parameters assessed for each subject were lateral and medial anterior/posterior (LAP, MAP) condylar position and axial orientation (Figure 1).
Results:
During DKB, the average lateral rollback for the PS #1 cohort was -4.0mm while the average medial rollback was -1.6mm. The PS #2 cohort also exhibited an average axial rotation of 3.1° of external rotation. The PS #2 average lateral rollback was -5.2mm, the average medial rollback was -3.3mm, and the average axial rotation was 2.8° external. The BCS average lateral rollback was -14.1mm, the average medial rollback was -8.1mm, and the average axial rotation was 7.5° external. Lastly, the normal knee cohort had an average lateral rollback of -17.8mm, an average medial rollback of -9.1mm, and 23.7° of external axial rotation. Detailed kinematics can be found in Table 1, while a visual representation of these motion patterns can be seen in Figure 3.
Discussion:
Because the BCS TKA design has two cam/post mechanisms to mirror the functionality of not only the PCL but the ACL, it can be discerned from this data that it replicates more normal-like kinematics in comparison to the analyzed PS TKAs. Because of the dual cam/post interaction with this design, the BCS cohort displayed a more anteriorized position at full extension, much like the normal knee. In early flexion (0-30°), the BCS TKA displays much higher amounts of posterior femoral rollback of both medial and lateral condyles, as one would expect to see in the normal knee; this can be strongly attributed to the design accounting for the ACL. Once in deeper flexion (90°+), and the PCL becomes dominant, all designs begin to translate posteriorly, as they all share commonality in their design to mimic the PCL. Although all three designs fall short on weight-bearing flexion compared to the normal knee, the BCS design achieves the highest flexion of the three implanted cohorts. Although both PS designs appear to have more rollback during mid-flexion (30-60°), the absence of the ACL seems to affect the performance of these implants during the crucial part of early flexion.
Keywords: PS, BCS, Normal, Knee, Fluoroscopy, Kinematics
Figures
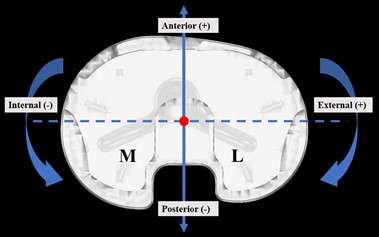
Figure 1
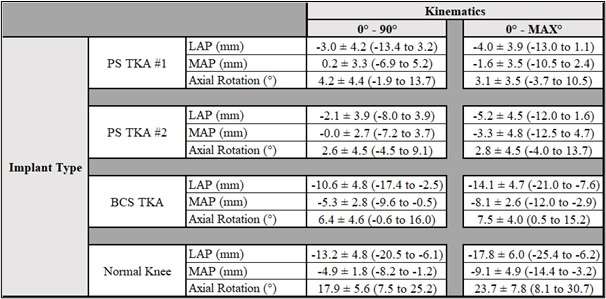
Figure 2
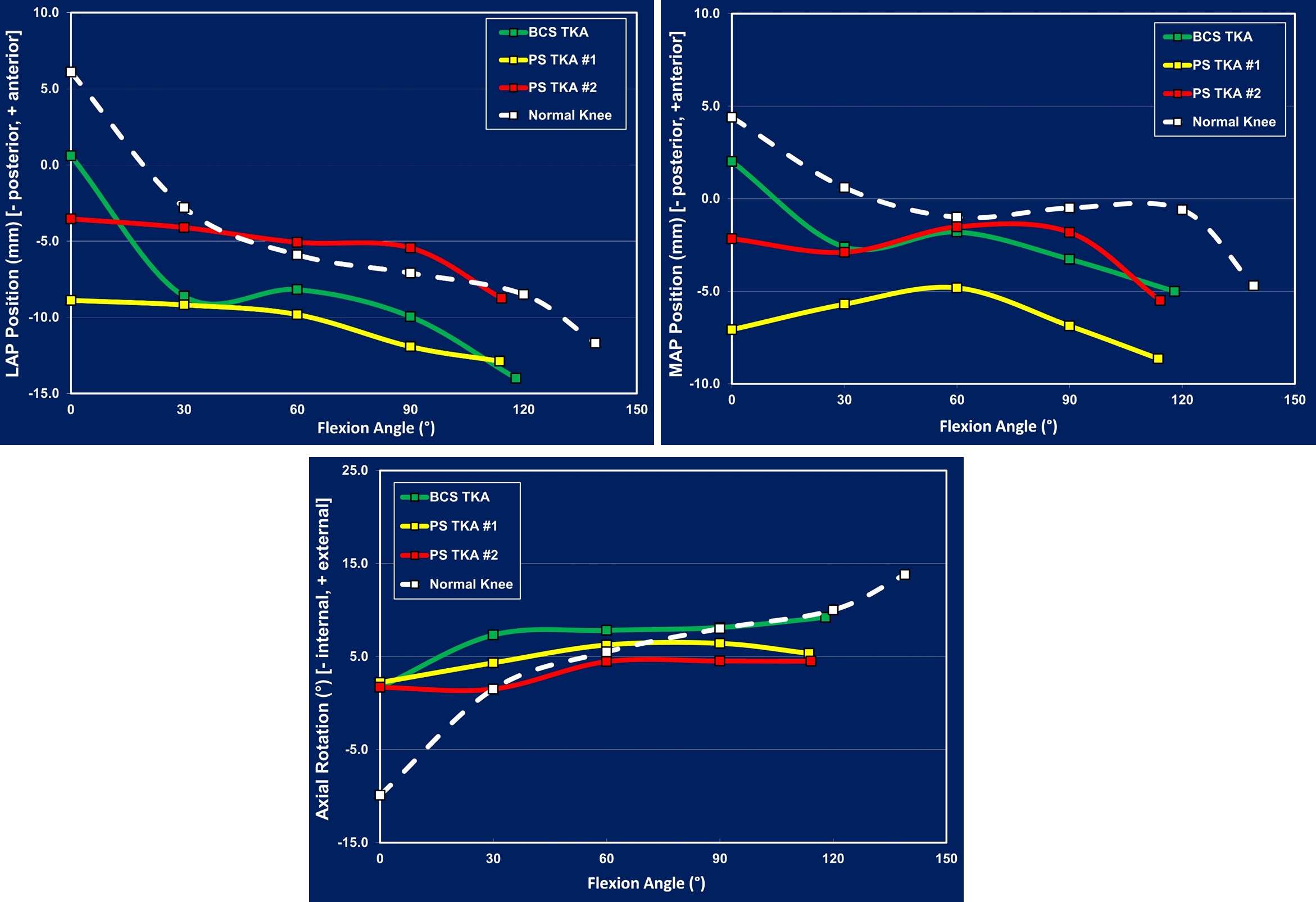
Figure 3#7699
Kinematic Outcomes of a Single Surgeon Implanting Multiple Posterior Cruciate Retaining (PCR) TKA Designs: Does the Implant Really Matter?
*Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: lsmit186@vols.utk.edu
Introduction:
Fluoroscopic studies have historically focused on determination of kinematics of diverse populations but haven’t isolated differentiators that affect motion patterns, such as single surgeon implantation of three different total knee arthroplasty (TKA) systems. While ACL resection hinders the ability to fully replicate motion of normal knee, implant systems strive to alter designs to combat this. While surgical technique has been shown to alter TKA kinematics, do different implant systems make an even greater difference? This research study strives to control for surgeon variability by comparing kinematic results of PCR TKA systems from 3 different manufacturers, all implanted by a single surgeon.
Methods:
The in vivo 3D kinematics were determined for 85 subjects having a PCR TKA (31 Type # 1, 29 Type #2, 25 Type #3) and 10 having a normal knee. All knees were deemed well-functioning, and subjects were recruited using guidelines to maintain similar demographics as defined in the approved IRB. Kinematics were obtained using validated fluoroscopic and 3D-to-2D registration techniques. All subjects performed a weight-bearing deep knee bend (DKB) intended to flex the knee from full extension to maximum flexion. The kinematic parameters assessed were lateral and medial anterior/posterior (LAP, MAP) condylar position and axial orientation (Figure 1).
Results:
During DKB, the average lateral motion for the PCR #1 cohort was +0.7mm while the average medial motion was +4.2mm and the average axial rotation was 4.3° external. The PCR #2 average lateral motion was +0.6mm, the average medial rollback was -0.5mm, and the average axial rotation was 1.5° internal. The PCR #3 average lateral rollback was -4.7mm, the average medial rollback was -0.2mm, and the average axial rotation was 5.6° external. Lastly, the normal knee cohort had an average lateral rollback of -17.8mm, average medial rollback of -9.1mm, and 23.7° of external axial rotation. Detailed kinematics are found in Table 1, with a visual representation of these motion patterns in Figure 3.
Discussion:
Due to the absence of the ACL, all TKA types remain posteriorized throughout flexion, causing varying cases of paradoxical motion. While PCR TKA #3 exhibits the largest amounts of lateral condyle rollback compared to its counterparts in early (0-30°) and late flexion (90°+) leading to positive, external axial rotation, paradoxical motion can be observed in mid-flexion. On the contrary, while PCR TKA #2 shows the most stability in mid-flexion, it does not account for rollback that we expect to see in the normal knee, leading to inverse rotation. These divergent results pose the question, “Are implant systems the real difference maker here?” Overall, this study helps to promote discussion on differing surgical outcomes of single surgeon implantation of the same TKA type. Even when controlling parameters such as successful outcome score, demographics, etc., the kinematic results shown here still show great variety. These results are evidence that under the same surgeon, the implant system does indeed make a difference, and you can expect to get various maximum flexion averages and diverse kinematic profiles that are either more or less like the normal knee.
Figures
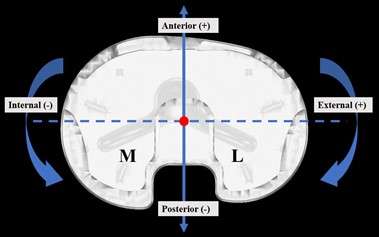
Figure 1
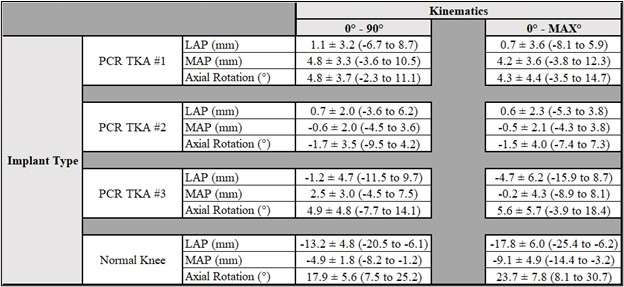
Figure 2
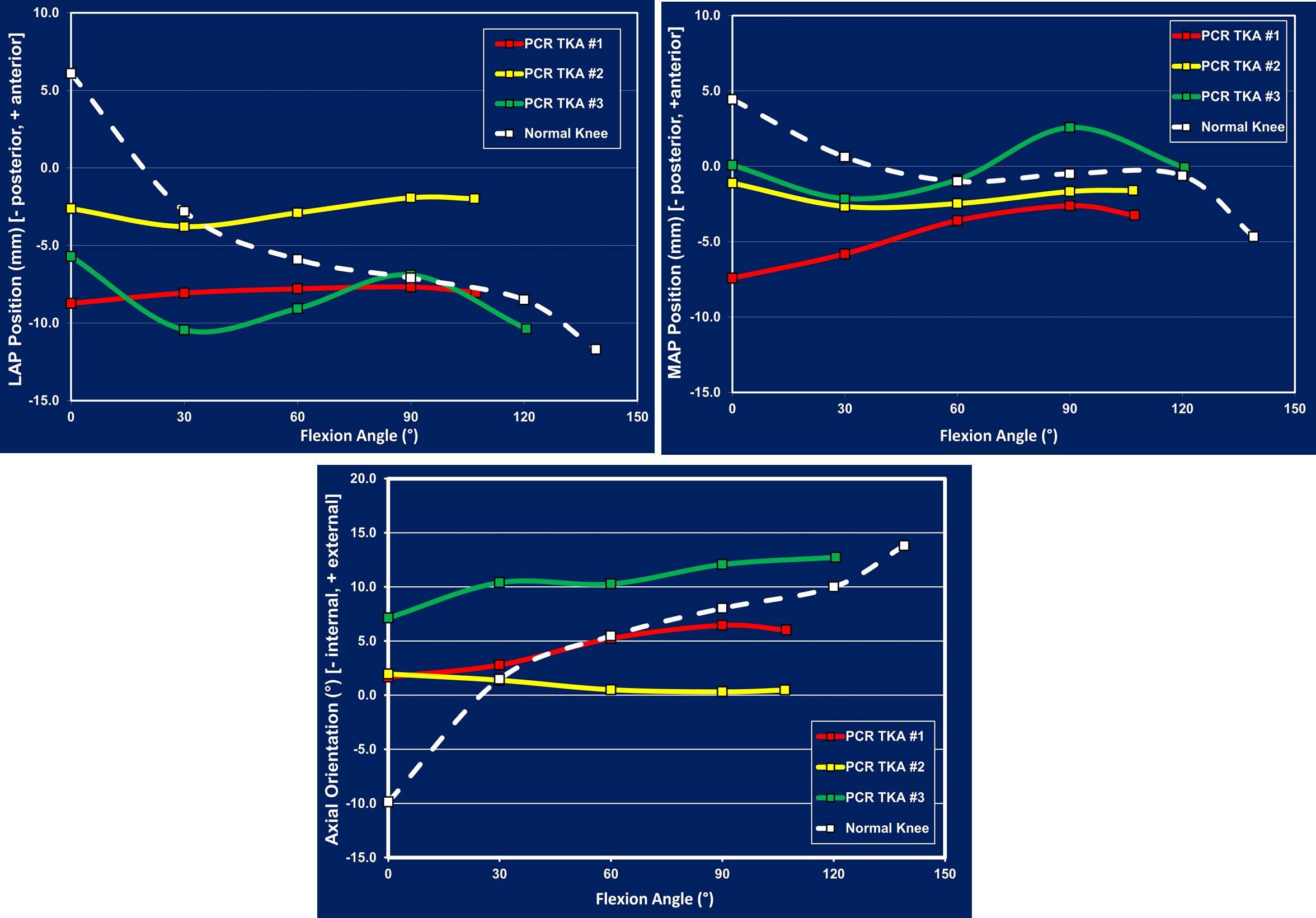
Figure 3#7700
In Vivo Knee Kinematics: How Important Is ACL Retention in Restoring Native Knee Kinematics?
*Lauren Smith - University of Tennessee, Knoxville - Knoxville, USA
Michael LaCour - University of Tennessee - Knoxville, USA
Garett Dessinger - Center for Musculoskeletal Research - Knoxville, USA
Richard Komistek - The University of Tennessee - Knoxville, USA
*Email: lsmit186@vols.utk.edu
Introduction:
Throughout the history of total knee arthroplasty (TKA), it has often been discussed which cruciate ligaments of the knee joint should be retained, substituted, or resected entirely. Discussions analyzing kinematics post-operatively have also been entertained when comparing these outcomes to those of the normal knee. Various fluoroscopic studies have focused on determination of kinematics but haven’t defined differentiators that affect motion patterns, such as retention of the cruciate ligaments. It has been shown in previously published studies that retention of the anterior cruciate ligament (ACL) can promote more normal-like kinematics, such as posterior femoral rollback in early flexion as well as anteriorization of both condyles throughout flexion. This research study assesses the importance of retaining the ACL for Bi-Cruciate Retaining (BCR) TKAs, compared to the normal knee and promotes the discussion of the significant role(s) that ACL retention can play in achieving optimal kinematics.
Methods:
The in vivo 3D kinematics were determined for 30 subjects having a BCR TKA (10 Type # 1, 20 Type #2) and 10 having a normal knee. All knees were deemed well-functioning, and subjects were recruited using guidelines to maintain similar demographics as defined in the approved IRB. Kinematics were obtained using validated fluoroscopic and 3D-to-2D registration techniques. All subjects were asked to perform a weight-bearing deep knee bend (DKB) maneuver intended to flex the knee from full extension to maximum flexion. The kinematic parameters assessed for each subject were lateral and medial anterior/posterior (LAP, MAP) condylar position and axial orientation (Figure 1).
Results:
During DKB, the average lateral rollback for the BCR #1 cohort was -13.6mm while the average medial rollback was -6.1mm. The BCR #1 cohort also exhibited an average axial rotation of 8.1° of external rotation. The BCR #2 average lateral rollback was -6.3mm, the average medial rollback was -1.4mm, and the average axial rotation was 6.5° external. Lastly, the normal knee cohort had an average lateral rollback of -17.8mm, an average medial rollback of 9.1mm, and 23.7° of external axial rotation. Detailed kinematics can be found in Table 1, while a visual representation of these motion patterns can be seen in Figure 3.
Discussion:
The results demonstrate that in early flexion (0-30°), both TKAs display very similar kinematic patterns like the normal knee, however lesser in magnitude. Because early flexion is where the ACL is dominant, one can infer that retention of this cruciate ligament in TKA can lead to more normal like kinematics, especially in early flexion. Both BCR TKAs also appear to display a similar trend throughout flexion, indicating that retention of both cruciate ligaments helps guide posterior movement on the lateral side with less on the medial, leading to axial rotation patterns like the normal knee. Whereas in other studies, it is regularly shown that non-ACL retaining TKAs exhibit generally posteriorized positions of both condyles, both BCR TKAs in this study have more of an anteriorized orientation, as one would see in the normal knee. This study poses the question, “Is ACL retention the real difference maker?”.
Figures
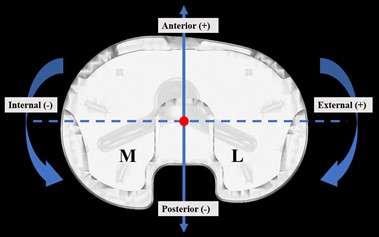
Figure 1
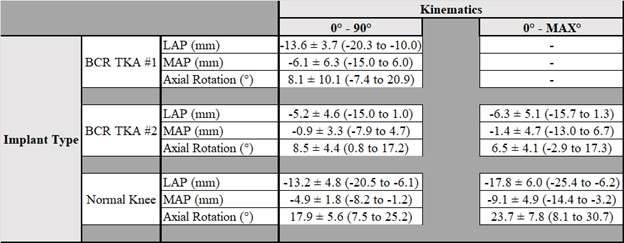
Figure 2
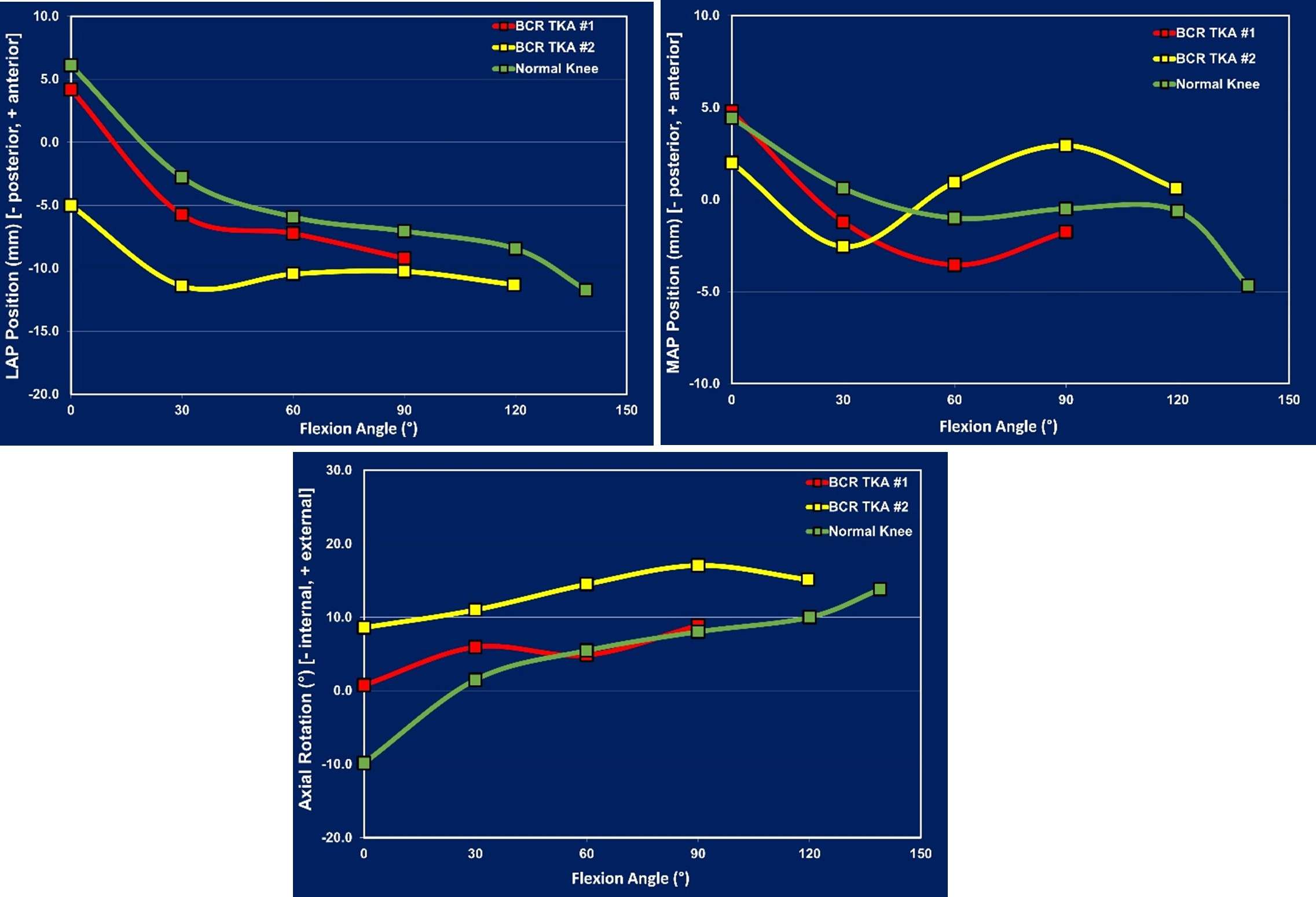
Figure 3#7588
The Effect of Press-Fit on Initial Stability in Stemless Shoulder Arthroplasty
*Kyle Snethen - Zimmer Biomet - Warsaw, USA
Yang Son - Zimmer Biomet - Warsaw, USA
Christine Mueri - Zimmer Biomet - Winterthur, Switzerland
Jeffrey Bischoff - Zimmer, Inc. - Warsaw, USA
*Email: kyle.snethen@zimmerbiomet.com
Introduction: Stemless humeral implants provide a more conservative and efficient approach to shoulder arthroplasty than stemmed prostheses and rely on a press-fit between implant surfaces and proximal humeral bone for initial fixation. Thus, determining the appropriate press-fit for a stemless implant design is imperative to achieve adequate stability. Traditionally, forces required to push-in and pull-out the implant have been used to determine the optimal press-fit and to characterize initial stability. The objective of this study was to determine the effect of press-fit on initial stability of a stemless humeral implant through a combination of push-in/pull-out testing and micromotion analysis.
Methods: 15PCF solid rigid polyurethane foam (Sawbones®) was pre-machined to create different nominal press-fit conditions between 0.375mm to 1mm per surface of a 6-fin, porous-coated stemless humeral implant. The stemless implant was axially pushed-in and pulled-out of the foam at a rate of 0.5mm/sec and the maximum push-in and pull-out forces were recorded for each press-fit a minimum of four times. Subsequently, micromotion of the stemless implant was measured under cyclic loading for the range of press-fit conditions that generated maximum pull-out force. With the implant inserted flush with the surface of the foam block, a 300N cyclic load (R=0.1 @ 1Hz) was applied for 100 cycles at a 30mm distance and 45o angle with respect to the same surface (Figure 1). Maximum relative motion between the implant and foam at the 100th load cycle was measured using digital image correlation. One-way ANOVA and Tukey’s post-hoc pairwise comparison were performed to determine if pull-out force and micromotion were significantly (α=0.05) different between press-fits.
Results: While push-in forces increased with higher press-fit conditions, the pull-out forces only increased at smaller press-fits before peaking at 0.75mm press-fit (901±60N) (Figure 2). No further increase in pull-out force was observed with a higher press-fit. Micromotion testing was performed on press-fits of 0.625, 0.75 and 1.0mm. Similarly, additional press-fit did not increase stability as averaged micromotion ranged between 29-53um and were not significantly (α=0.05) different over that press-fit range (Figure 3).
Discussion: This study demonstrated that increasing the press-fit of a stemless humeral implant does not lead to increased initial fixation, and that there exists a threshold press-fit beyond which the design requires higher insertion forces, thus increasing the risk of bone fracture, without benefiting implant stability. The threshold press-fit was 0.75mm in this analysis, however, it is expected to be unique to each implant design and bone analog material. Traditionally, the optimal press-fit of a non-cemented implant is determined solely from push-in/pull-out testing. The presented method also measured micromotion under cyclic loading which is more representative of implant stability than a static tensile force. The micromotion results suggest that press-fit does not have a significant effect on stability once the pull-out force has been maximized.
Conclusion: There exists a press-fit for stemless humeral implants beyond which initial fixation is not improved. It is important to determine this press-fit for each design to minimize the amount of force required for implant insertion.
Figures
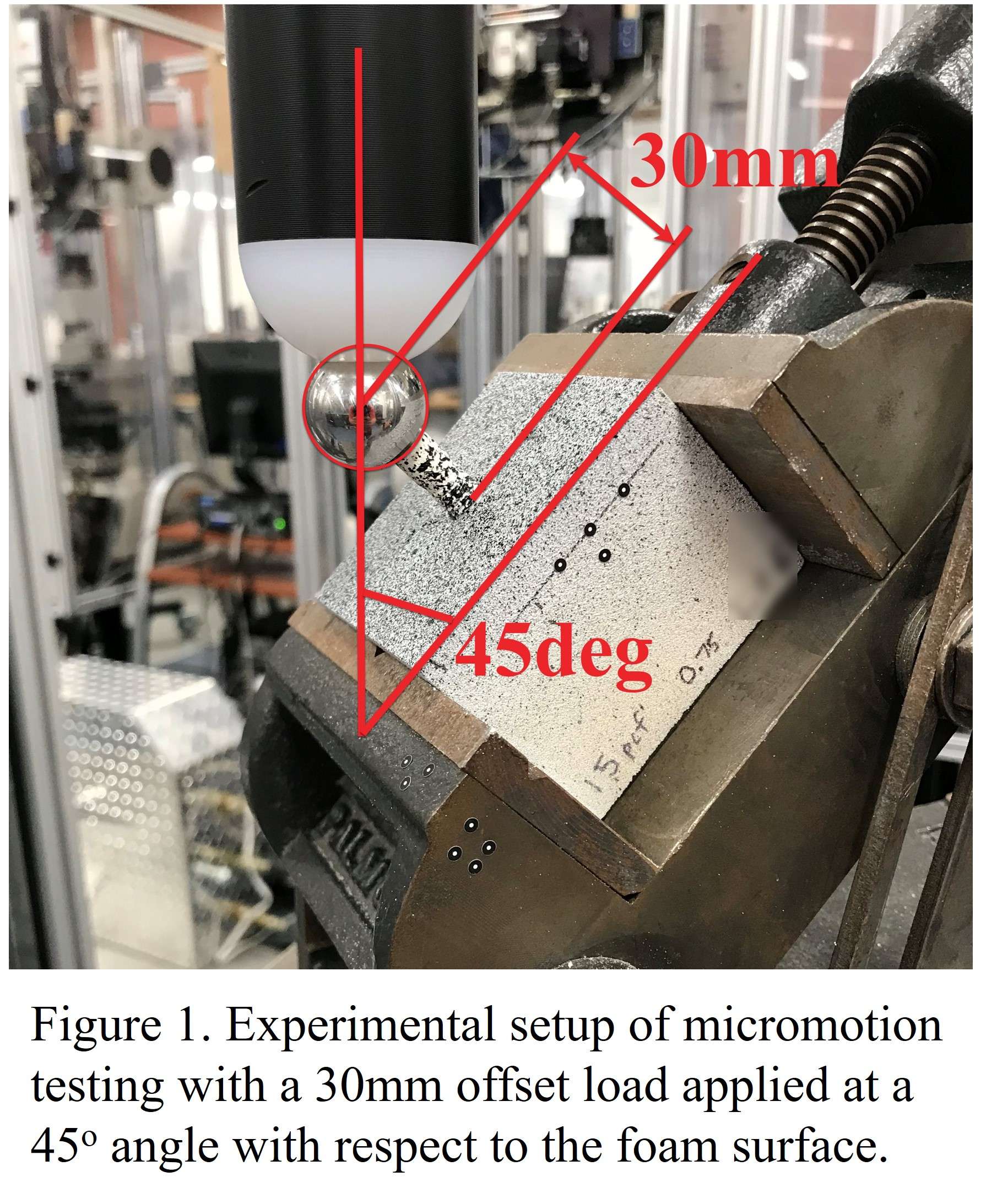
Figure 1
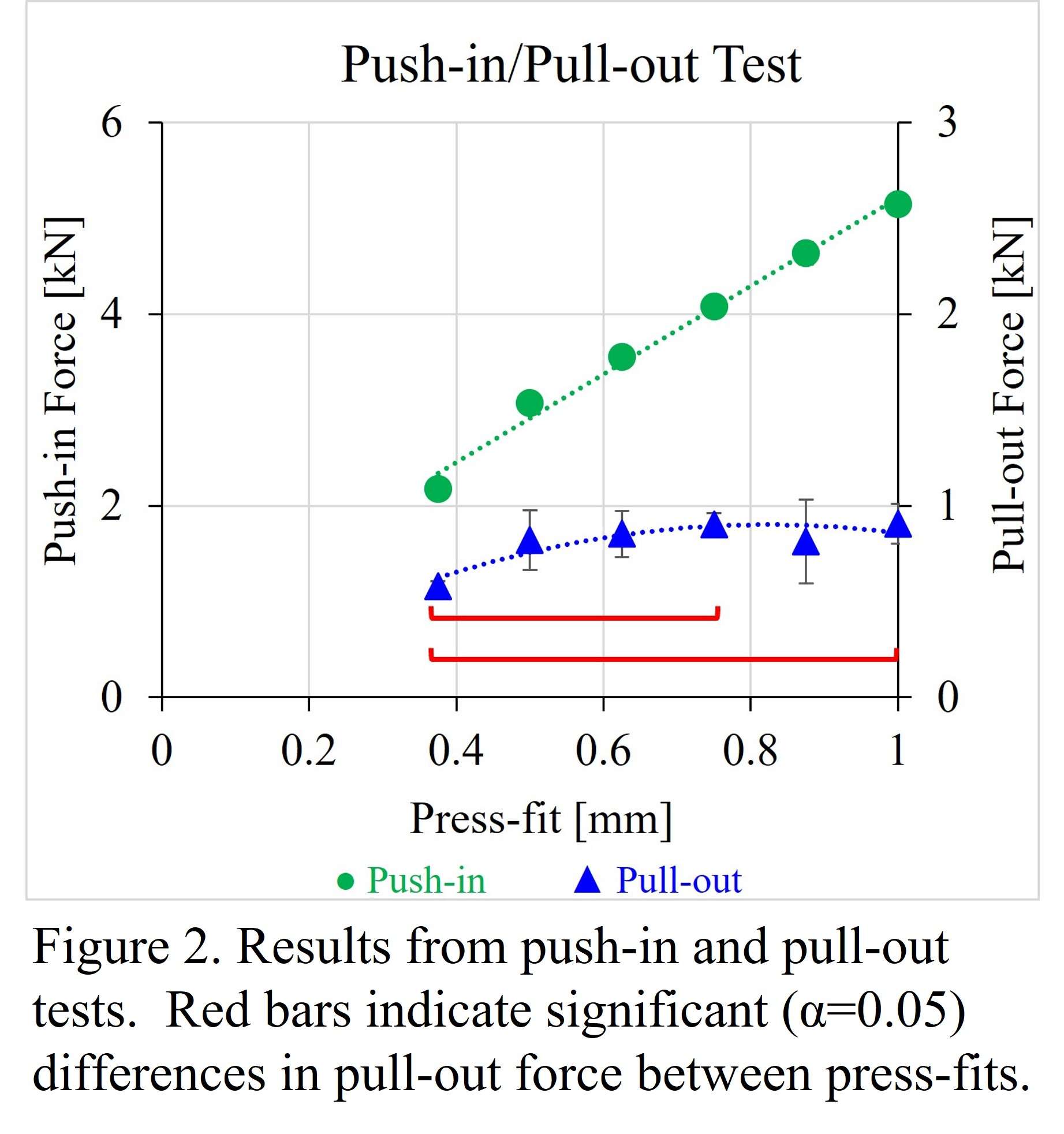
Figure 2
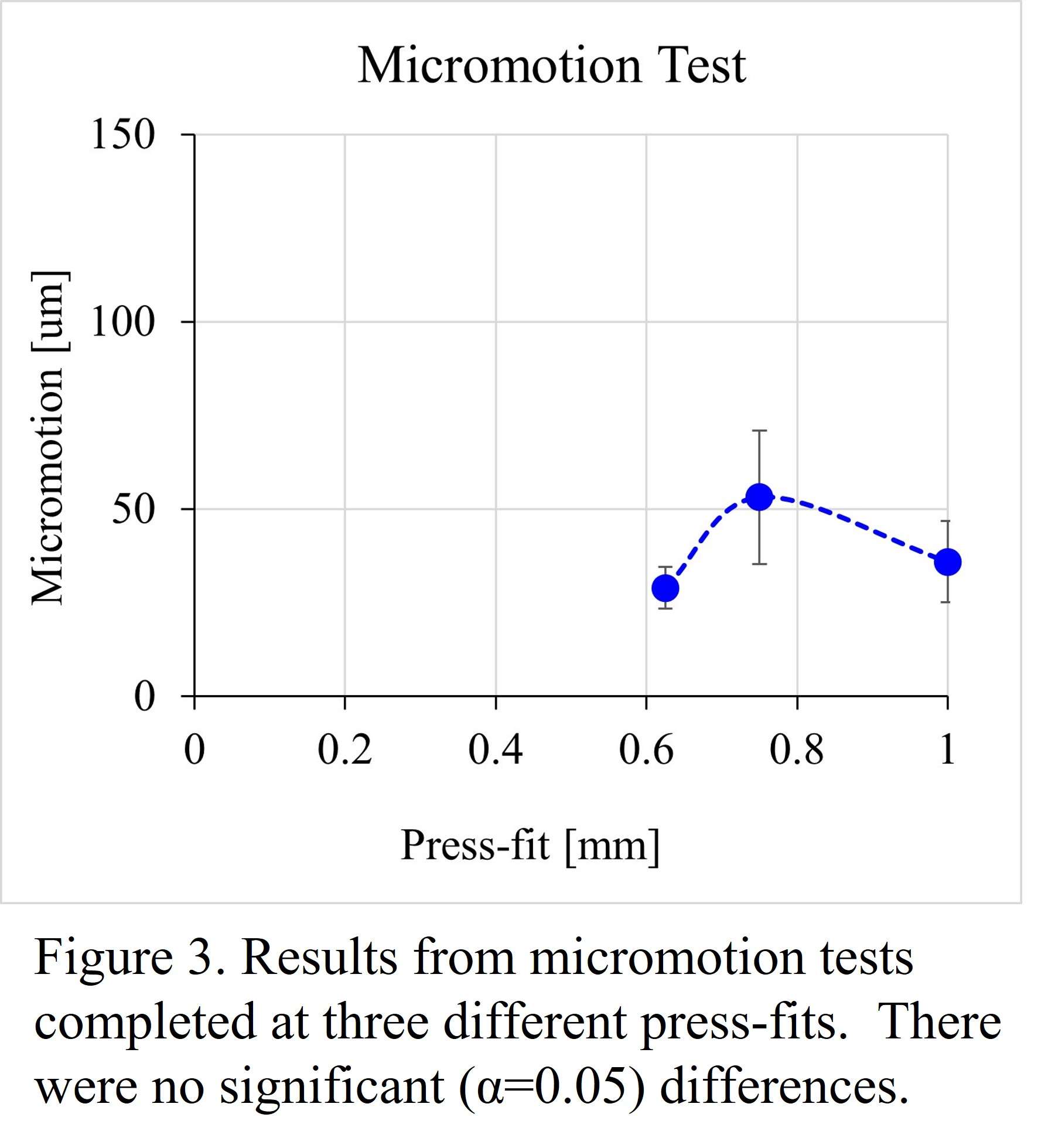
Figure 3#7589
Development of a Robotic Test Method to Assess Key Clinical Measures in Shoulder Arthroplasty
*Kyle Snethen - Zimmer Biomet - Warsaw, USA
Charlie Parduhn - Zimmer Biomet - Warsaw, USA
Vani Sabesan - Cleveland Clinic Florida - Weston, USA
Jonathan Braman - University of Minnesota - Minneapolis, USA
Marc Bandi - Zimmer GmbH - Winterthur, Switzerland
Jeffrey Bischoff - Zimmer, Inc. - Warsaw, USA
*Email: kyle.snethen@zimmerbiomet.com
Introduction: Shoulder arthroplasty aims to restore joint function by locating and orienting implants such that range of motion (ROM) and joint stability is optimized. Surgical planning platforms are being developed to help predict these optimal implant positions complemented by computer navigation and robotic-assisted technologies to execute these plans. It is important that experimental method development parallels these advancements in technology in order to facilitate validation efforts and further innovation. A robotic-based test method for assessing shoulder joint laxity and ROM was developed and previously presented for application in the natural shoulder. The current study focuses on the continued development of this method for application in anatomic and reverse shoulder arthroplasty, with the purpose of informing technologies utilized during pre-operative planning and intra-operative execution of shoulder arthroplasty.
Methods: An in vitro test method assessed shoulder ROM and joint laxity using a robotic arm instrumented with a six degree-of-freedom load cell (Fig. 1). From sixteen fresh-frozen cadaver shoulders, orthopaedic surgeons performed anatomic (TSA) and reverse (RSA) total shoulder arthroplasty on eight specimens each. The ROM simulation abducted the glenohumeral joint from 0o until 90o or 5Nm torque. Subsequently, separate laxity tests applied a ±2Nm internal-external (IE) torque, ±20N anterior-posterior (AP) force, ±20N superior-inferior (SI) force and a 44N medial-lateral (ML) distraction force at six glenohumeral abduction levels. For both the TSA and RSA groups, test method repeatability was characterized by performing four sequential ROM simulations and three sequential laxity tests and calculating the standard deviation of the combined runs.
Results: Simulated ROM averaged maximum abduction of 83o (±10o) and 74o (±10o) for the TSA and RSA groups, respectively. The RSA group also achieved slightly less adduction. While IE and ML laxities were similar between the two groups, translational laxities were significantly (α=0.05) less for the RSA group at all abduction levels (Fig. 2). Repeatability of kinematics during the ROM simulation typically averaged standard deviations within 1o rotations and 0.5mm translations for both groups. Laxity repeatability was evaluated at 15o, 30o and 60o abduction and determined maximum average standard deviations of 4.0o rotational laxity for both groups (Fig. 3) and 3.6mm and 1.5mm translational laxity for TSA and RSA, respectively.
Discussion: Overall, the ROM and laxity measures agreed with the clinical consensus for anatomic and reverse arthroplasty techniques. The RSA condition experienced limited ROM due to scapular notching and bony impingement, and less translational laxity given the higher constraint of reverse shoulder designs. ROM measures and trends in joint laxities were also consistent with in vivo and in vitro methods performed in the literature. Furthermore, the test method was repeatable within clinically relevant detectability thus demonstrating the necessary precision to inform utilization and development of emerging technologies in shoulder arthroplasty.
Conclusion: The developed robotic test method demonstrated the ability to accurately and repeatably assess shoulder ROM and laxity for anatomic or reverse shoulder arthroplasty applications. Exercising this test method will provide value to technologies aiming to optimize ROM and joint stability through implant design, planning, and surgical delivery.
Figures
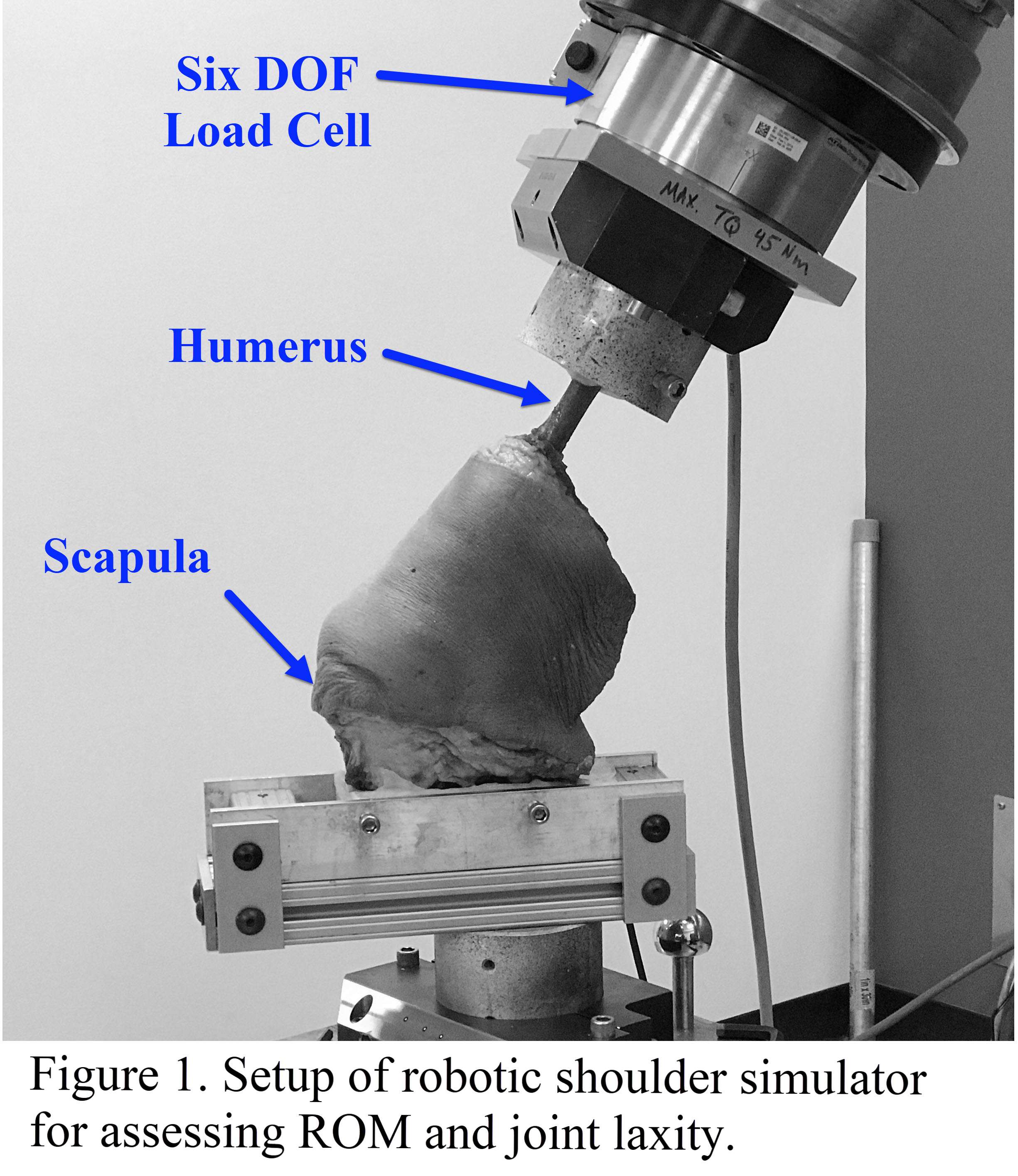
Figure 1
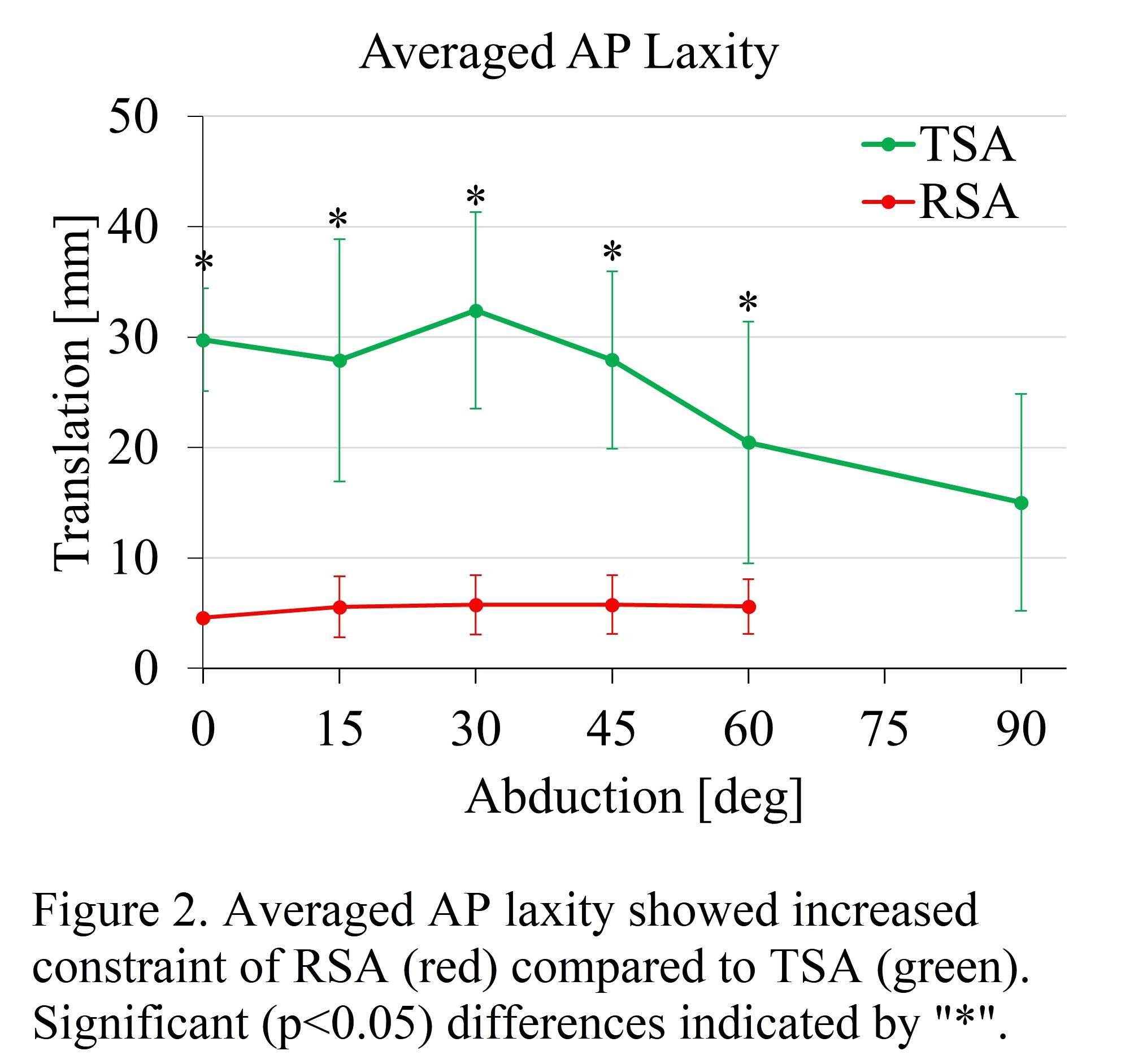
Figure 2
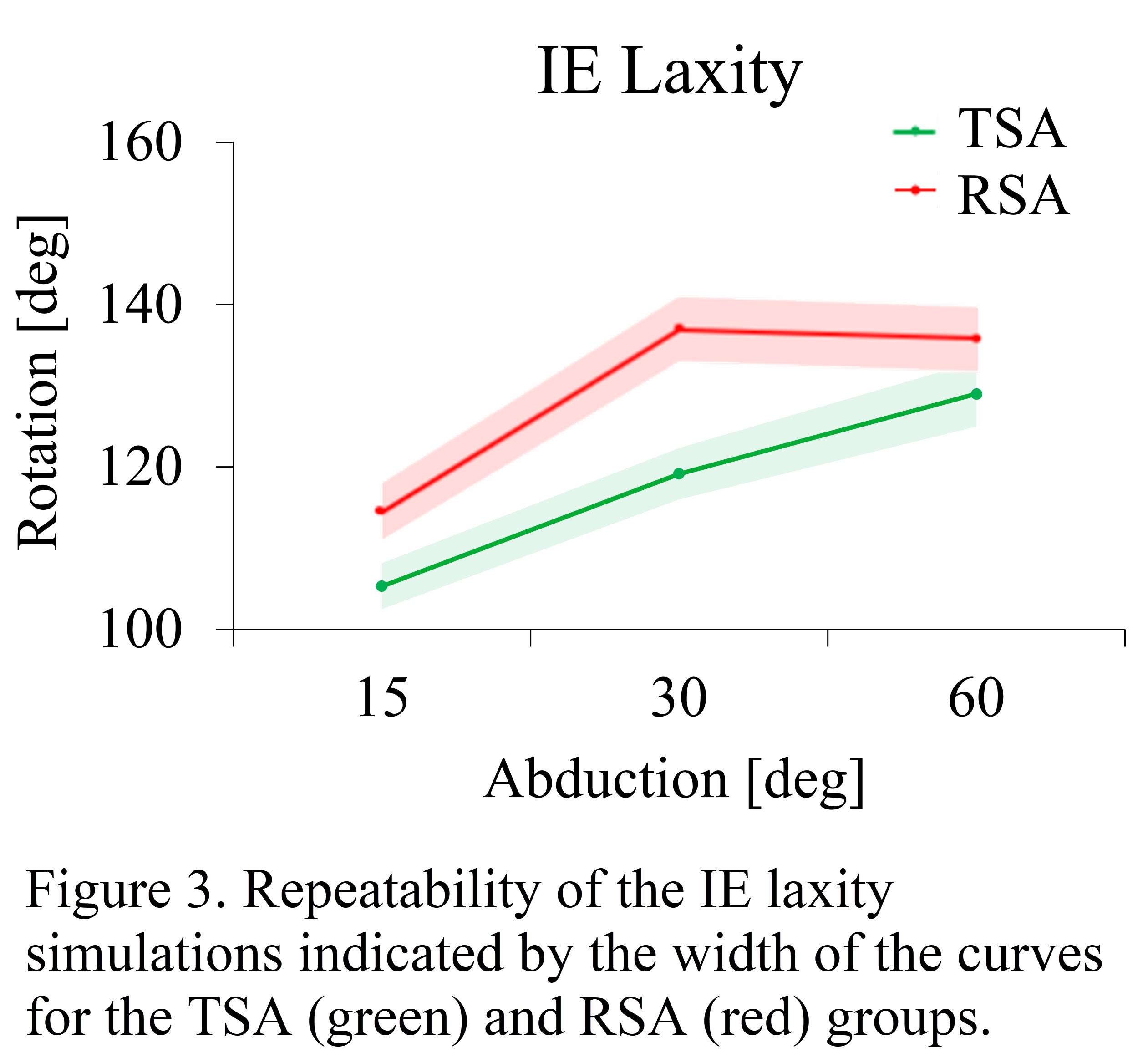
Figure 3#7805
Method and Device for Continuous Monitoring of Anatomic Glenoid Loosening Tests
*Peder Solberg - Dartmouth College - Hanover, United States of America
John-Erik Bell - Dartmouth Hitchcock Medical Center - Lebanon, USA
Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: peder.solberg.th@dartmouth.edu
Introduction:
ASTM F2028 describes a method for measuring prosthetic glenoid component loosening following dynamic, loaded rocking tests. Our shoulder simulator design sought to address two challenges faced in these tests: (1) relieving design challenges associated with linearly displacing a submerged glenoid testing assembly under the high loads (750N) and lubrication conditions (submersion in water) required by the ASTM standard, and (2) enabling continuous video-based monitoring so glenoid loosening characteristics can be ascertained with greater resolution.
Methods: To address the first challenge, the traditional linear-displacement system for the glenoid assembly was replaced by a long pivoting arm (Figure 1). A pneumatic cylinder is used to apply a horizontal load to the rigid arm above water height (Figure 1). This design achieves near-linear displacement of the glenoid without the corrosion or friction challenges associated with submerging linear bearings or subjecting them to offset loads. With a 470mm pivoting arm and a typical large glenoid height of 26mm, top and bottom x-displacement and force are different by less than 6%. This is deemed acceptable given the magnitude of differences in consideration for other variables. A gearmotor-driven linkage displaces a humeral head at 1.5Hz to a translation distance of interest (i.e. subluxation translation distance).
A video-based system was developed to track glenoid loosening at regular intervals. A transparent viewing window allows a view of the submerged glenoid assembly with fiducial marks on the glenoid, bone substitute, and mounting box. A custom Matlab code commands a video software (Debut) to automatically gather five-second videos of the glenoid at user-specified intervals, e.g. every 1000 cycles. Then, a spatially calibrated video analysis software (Tracker) is used to determine glenoid loosening in multiple dimensions by tracking motion of the marks on the top and bottom of the glenoid relative to the bone substitute (Figure 2).
To confirm the functionality of the system, tests were run on an all-polyethylene glenoid component with a 5-peg design cemented in CNC-milled bone substitute. Positions of fiducial marks were tracked over 500,000 cycles of ±5mm SI displacement.
Results:
Average y-direction amplitudes of displacement were used as a comparative loosening metric. Cycle-dependent loosening characteristics of the glenoid being tested can then be determined from the resulting plots (Figure 3). Change in micromotion at the ASTM-recommended 100,000 cycles was very small in each of the glenoids (50-75 um) but detectable by the video-based system. Throughout the tests, the two samples had similar micromotion results; however, some expected sample-to-sample variation was observed. Neither test resulted in gross disassociation at 0.5 M cycles.
Conclusions:
A video-based method for tracking glenoid loosening provides a high-resolution means by which the glenoid loosening can be tracked continuously without the need to stop the test to measure displacement with an LVDT. In addition, a long pivoting-arm design successfully averts the challenges associated with linear displacement of a submerged glenoid assembly while minimizing error associated with the linear displacement approximation.
Acknowledgements: We thank Medacta for their generous donation of glenoids and OREF Grant #19-004 for student support.
Keywords: Shoulder, ASTM, Loosening, Glenoid
Figures
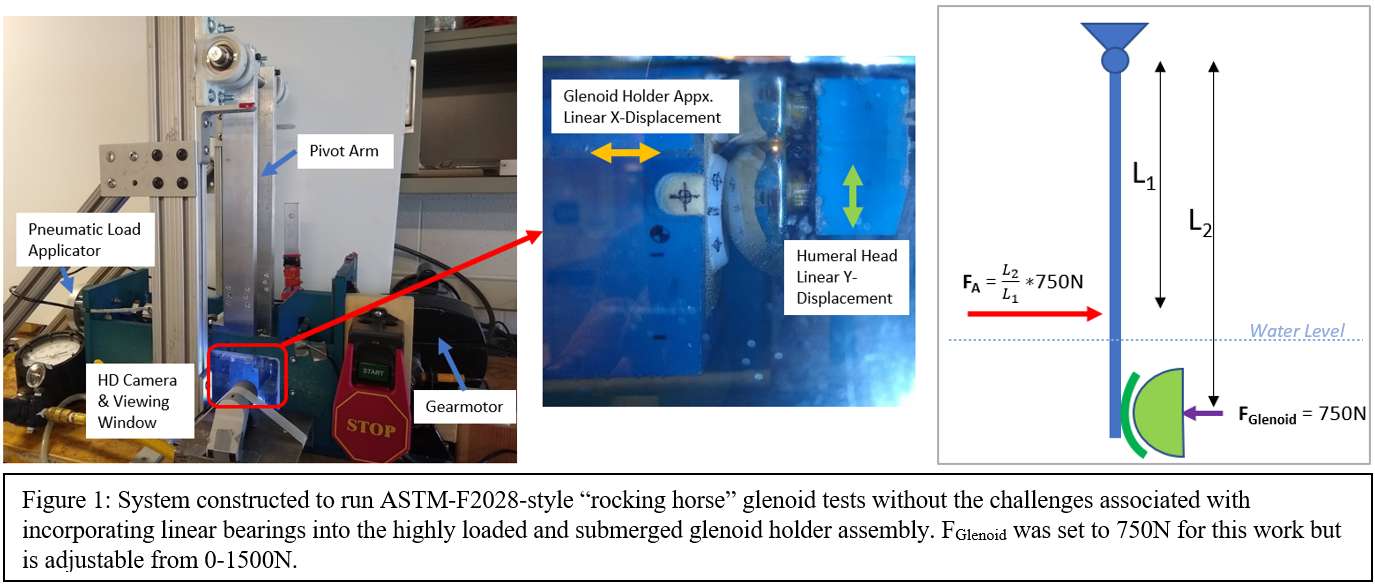
Figure 1
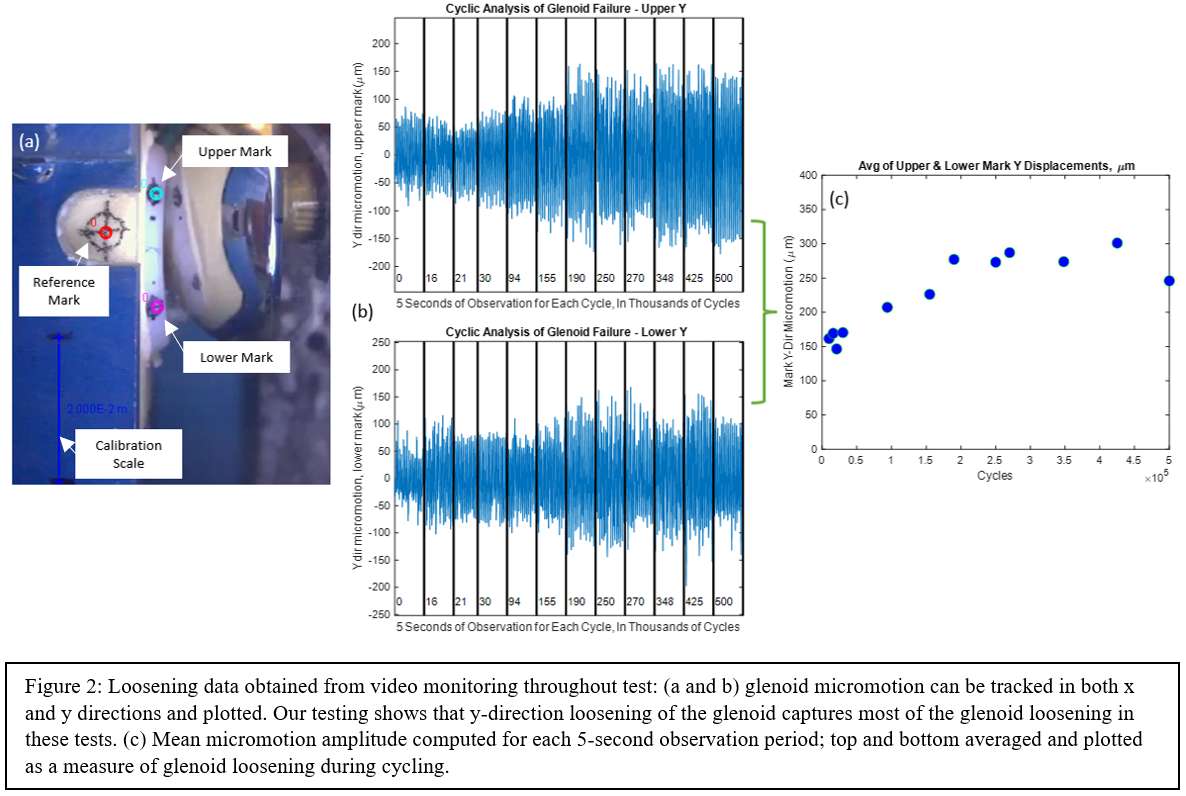
Figure 2
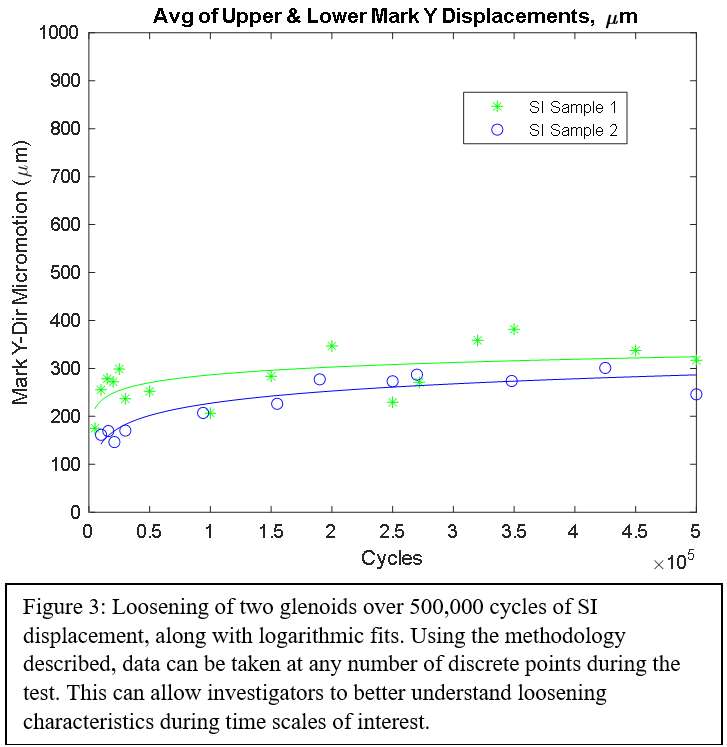
Figure 3#7797
Toughness of a Conductive UHMWPE-Carbon Composite: Materials Progress Toward Smarter Orthopedic Bearings
*Peder Solberg - Dartmouth College - Hanover, United States of America
Hannah Favreau - Dartmouth College - Hanover, USA
Rebecca Thomson - Dartmouth College - Hanover, United States of America
Abigail Chase - Dartmouth College - Hanover, USA
Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: peder.solberg.th@dartmouth.edu
Introduction:
Carbon-UHWMPE composites for use in orthopedic bearings have been investigated since the 1970s. Initial attempts failed, partly due to decreased resistance to fatigue crack propagation of carbon fiber-reinforced UHMWPE [1]. Conferring conductivity to orthopedic bearings without significantly compromising mechanical properties may enable strain sensing devices or biofilm-disrupting “electricidal” treatments of the polyethylene insert [2,3]. To understand the mechanical integrity of a conductive material in a high-stress environment, such as a joint, its toughness must be assessed according to fatigue, impact, and high-stress conditions.
Methods:
Materials were subjected to: (1) fatigue testing to assess resistance to crack propagation, (2) impact testing to assess resistance to fracture under sudden load, and (3) tensile testing to determine work-to-failure at low strain rates using a modified ASTM Type V test. Testing was performed following previously established protocols and conductivity testing was performed on neat and composite materials [4-6]. A 2.5 wt% conductive carbon black (CCB) composite and neat control were compression molded. Commercially available 75 kGy, remelted bar stock (Quadrant) served as a clinically relevant reference. All materials used GUR 1020.
Results:
The 2.5 wt% CCB composite possessed 91.6% and 80.3% of the impact and tensile toughness, respectively, of the neat material while the 75 kGy remelted material had 42.8% and 69.1%, respectively (Figure 1). Fatigue testing, Figures 2-3, revealed little to no difference between the composite and neat materials. The 75 kGy remelted material showed lower resistance to fatigue crack growth, as expected. Under an applied voltage of 5 V the electrical current in the neat material measured ~100 pA, the detection limit of the measuring device, and therefore the conductivity was negligible. The 2.5 wt% CCB sample possessed a conductivity of 2.90±0.16 S/m (n=20).
Conclusion:
The addition of conductive carbon black to UHWMPE imbues it with conductive properties that could enable new possibilities for orthopedic bearings. The carbon composite demonstrated decreased tensile and impact toughness as a trade-off for conductivity (though the latter was not statistically significant). From this work, tensile, and perhaps impact toughness, can be related in composite materials as has been seen in irradiated materials [5]. However, fatigue properties do not coincide with other mechanical property losses in this composite material, suggesting that the incorporation of carbon may affect fatigue crack propagation via microstructural inhibition of crack growth. These results help to demonstrate that UHMWPE-CCB composites are promising biomaterials that may mitigate fatigue cracking, allow for strain sensing in high-load “smart material” applications, or aid in biofilm mitigation.
References:
[1] Connelly, G. et al. J. Ortho Research, 1984,2(2),119–125.
[2] Gupta, T.K. et al. J. Mater. Sci. 2018,53,7939.
[3] Clark, A.C. et al. Tribol. Int. 2006,39,1327.
[4] Atwood, S.A. et al. J. Mech. Behav. Biomed. Mater. 2011,4,1033–1045.
[5] Huot, J.C. et al. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011,97B,327–333.
[6] Favreau, H.J. et al. J. Appl. Polym. Sci. 2022,139,20.
Acknowledgements:
The NH EPSCoR BioMade Project is supported by NSF’s Research Infrastructure Improvement Award #1757371.
Keywords:
UHMWPE, Composites, Impact, Tensile, Fatigue, Toughness, Smart Materials, Bearings, Biofilm, Infection
Figures
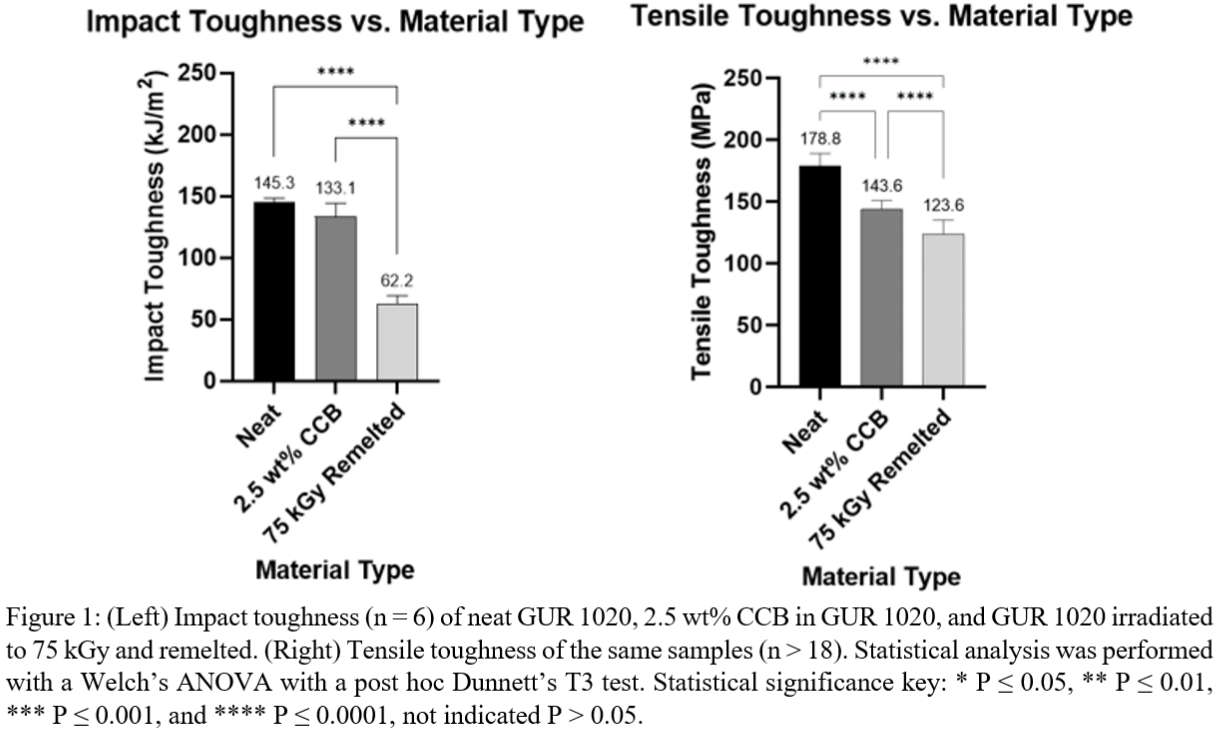
Figure 1
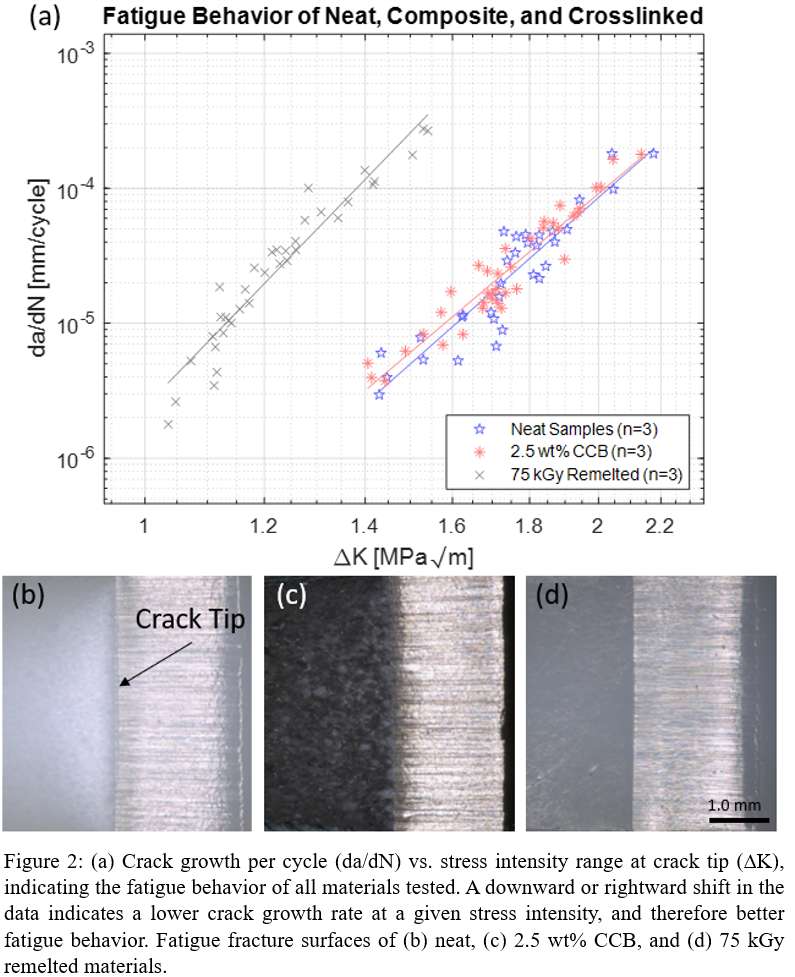
Figure 2
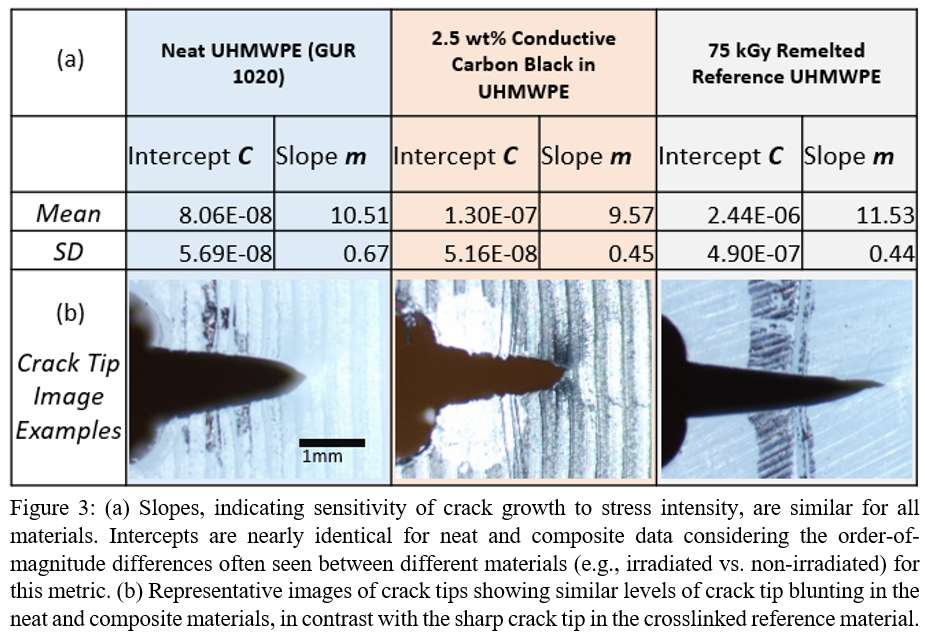
Figure 3#7278
Risk Factors Responsible for Mortality in Total Hip Arthroplasty for Femoral Neck Fracture in Elderly Patients
*Hyung Gon Ryu - Seoul Medical Center - Seoul, South Korea
Se Yong Song - Seoul medical center - SEOUL, South Korea
*Email: hg400@hanmail.net
Purpose : Total hip arthroplasty (THA) using dual mobility component (DMC) is a reasonable surgical option for displaced femoral neck fracture in elderly patients, for lower dislocation rate and instability. The purpose of this study was to investigate the clinical outcomes and risk factors responsible for mortality in elderly patients who diagnosed with displaced femoral neck fracture and undergone DMC-THA
Materials and Methods : Among 147 cases of THA from December 2018 to June 2020, a total of 79 cases were enrolled in this study, with (1) Garden stage III or IV, (2) over 75 years of age, and (3) over 1 year of follow up period. All the patients received DMC-THA surgery using anterolateral approach(See Fig. 1).
Results : The mean follow-up period was 15.0±8.43 months and a total of one dislocation case was observed(See Fig. 2). Mortality rate was 17.7% (14/79), and mortality rate was especially higher when the patient had past medical history of malignancy(OR=7.18, p=0.03) or cognitive disorder such as dementia(OR=5.48, p=0.03). Preoperative initial hemoglobin levels(OR=0.65, p=0.04) and low UCLA score(OR=0.47, p=0.02) were also associated with mortality(See Fig. 3).
Conclusion : When considering THA as treatment method in elderly patients with displaced femoral neck fracture, High mortality rate is expected in patients with low preoperative hemoglobin levels or history of malignancy or cognitive disorder. So, thorough monitoring and management should be taken before and after surgery.
Key Words : Femur, Femur neck fracture, Total hip arthroplasty, Mortality
Figures
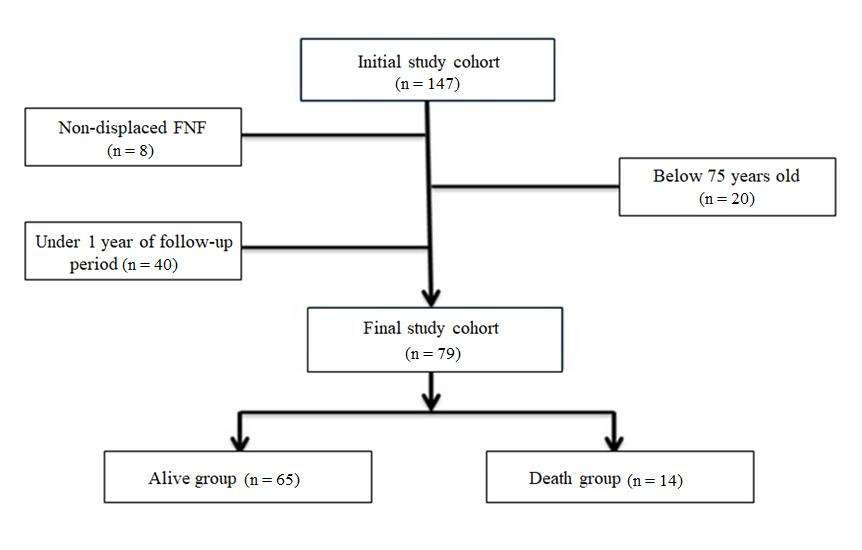
Figure 1
Figure 2
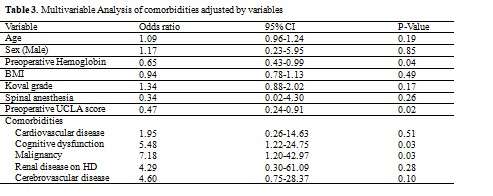
Figure 3#7671
Is Fretting Corrosion Damage a Concern for Titanium-Backed Acetabular Liners in Ceramic-on-Ceramic Total Hip Arthroplasty?
*Hannah Spece - Drexel Implant Research Center - Philadelphia, USA
Eric Ouellette - Exponent - Philadelphia, USA
Greg Klein - Hartzband Center for Hip and Knee Replacement - Hackensack, USA
Michael Mont - Northwell Hospital - New York, USA
Steven Kurtz - Drexel University - Philadelphia, USA
*Email: hannahspece@gmail.com
Introduction
Ceramic-on-ceramic (COC) articulations are commonly used in total hip arthroplasty (THA) due to their tribological properties and biocompatibility. In one COC design, the ceramic acetabular liner has a titanium alloy backing that interfaces with a shell of the same material. Although metal taper interfaces such as this have been investigated extensively across arthroplasty devices, the risk of fretting corrosion for the titanium liner in COC THA devices remains poorly understood. In this study, we aimed to determine the extent to which titanium liner-shell taper interfaces in ceramic-on-ceramic THA devices undergo fretting corrosion and potential material loss in vivo.
Methods
Components from 44 cases (n = 22 shell-liner pairs, n = 22 liners without shells) were retrieved during revision surgery as part of a multi-institutional implant retrieval program. The acetabular components were of a single design and were implanted for an average of 5.5 ± 4.2y (range: 0.0 – 13.0y). The shell-liner taper interface surfaces were analyzed using the Higgs-Goldberg scoring method in which scores of 1 through 4 indicate minimal, mild, moderate, and severe fretting corrosion. Five components with the most distinct areas of fretting corrosion also underwent analysis with a coordinate measuring machine (CMM). The point clouds were analyzed with a custom, validated MATLAB script that uses a least squares cone fitting method to calculate volumetric material loss and maximum wear depth, in accordance with ASTM F3129. Material adhered in the direction opposite wear was excluded. Areas of acute corrosive attack were also imaged using scanning electron microscopy (SEM) and energy dispersive X-ray spectroscopy (EDS).
Results
The retrievals were most commonly revised for loosening (n = 14/44) and infection (n = 8/44). Metallosis was reported in 3 cases: 2 with impingement between the femoral neck and liner, and 1 with a loose shell. Squeaking was also reported in 6 cases. Fretting corrosion at the taper interfaces was minimal to mild for 95% of liners, and 100% of shells. For liners, 43% (n = 19/44) of the components received a Goldberg-Higgs score of 1, 52% (n = 23/44) received a score of 2, and 5% (n = 2/44) received a score of 3. For shells, 41% (n = 9/22) received a score of 1 and 59% (n = 13/22) received a score of 2. There were no cases of severe corrosion for any component, though small areas of corrosive attack were periodically observed. Material loss was minimal for components that underwent CMM measurement. Estimated material loss ranged from 0.2 to 1.3 mm3 for liners and 0.5 to 1.1 mm3 for shells. Maximum wear depth for all 5 components was 0.03 mm or less.
Conclusions
In this study, we elucidated the presence and severity of fretting corrosion for the titanium shell-liner taper interface for retrieved ceramic-on-ceramic THA devices. We found that fretting corrosion was minimal to mild for both the liners and shells. The results of this study provide in vivo evidence supportive of modular Ti alloy taper junctions in acetabular components for total hip arthroplasty.
Figures
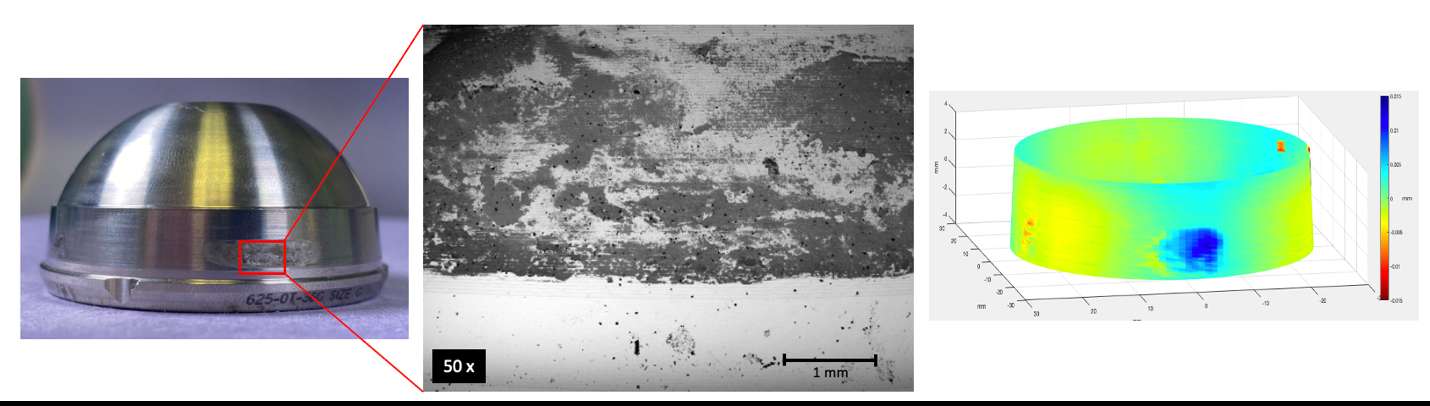
Figure 1#7811
In Vivo Performance of Vitamin E-Doped Polyethylene Implants: A Systematic Review
*Hannah Spece - Drexel Implant Research Center - Philadelphia, USA
Ron Yarbrough - 3Spine - Chattanooga, USA
Steven Kurtz - Drexel University - Philadelphia, USA
*Email: hannahspece@gmail.com
Introduction
Vitamin E stabilization was introduced to improve the oxidative stability, wear resistance, and mechanical properties of highly crosslinked polyethylene (HXLPE) used in total joint arthroplasty (TJA). Existing reviews for vitamin E-stabilized polyethylene (VEPE) report that VEPE demonstrates wear resistance superior to conventional ultrahigh molecular weight polyethylene (UHMWPE) and may lead to decreased risk for osteolysis and implant loosening. Given the limited scope of some previous reviews and the recent increase in VEPE-related studies, an updated review of the literature is warranted.
The aim of this systematic review is to provide an overview of in vivo performance for vitamin E UHMWPE and comparison with non-stabilized UHMWPE. We also aimed to determine whether the use of VEPE has expanded beyond lower extremity arthroplasty devices and if there are reports of VEPE in spinal or upper extremity implants.
Methods
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were used. A systematic review of the literature was performed using PubMed and Embase on March 18, 2022, using search terms: (UHMWPE OR polyethylene OR HXLPE) AND (vitamin E OR "alpha-tocopherol" OR "α-tocopherol") AND (implant* OR Arthroplasty OR "Joint replacement" OR prosthesis OR orthopaedic OR orthopedic OR spinal OR spine OR "upper extremity" OR shoulder OR elbow OR histolog*). Database searches resulted in 250 studies from PubMed, 381 from Embase, and 1 from source bibliographies, totaling 367 unique papers. Following title/abstract screening and assessment of full texts according to inclusion/exclusion criteria, 45 studies were included for review.
Results
We reviewed 36 cohort studies, 5 case studies, and 4 retrieval analyses. For the cohort and retrieval studies, most (n = 26/40) compared VEPE with controls of conventional UHMWPE or HXLPE. The number of implants in the cohort studies ranged from 34 to 53842 (range 17 to 5069 for VEPE alone) with follow-up ranging from 2 to 11 years. Average wear rate ranged from -0.01 to 0.13 mm/year for the VEPE groups and 0.00 to 0.27 mm/year for the controls. Steady-state wear rate, with early creep-dominated penetration excluded, tended to be much lower. For all studies that compared VE-stabilized and non-stabilized polyethylene, outcomes for VEPE were as good or better than the control group, and most VEPE wear rates were <0.1 mm/year, the threshold below which osteolysis is not expected to occur. Reports of polyethylene-related complications were infrequent but included component wear and fracture, most of which were reported as single instances. No cases of osteolysis or adverse outcomes related to VEPE were reported.
Across the literature, we found no studies regarding the use of VEPE in spinal applications. For upper extremities there were reported uses in shoulder arthroplasty, but no studies explored in vivo performance given the relative newness of VEPE for shoulders.
Conclusion
Overall, the literature for vitamin E-stabilized HXLPE indicated positive clinical results and supports its safety and efficacy for use in TJA, with much of the research reporting lower wear rates than for conventional UHMWPE. Adoption of VEPE for spinal and small joint applications is still limited.
Figures
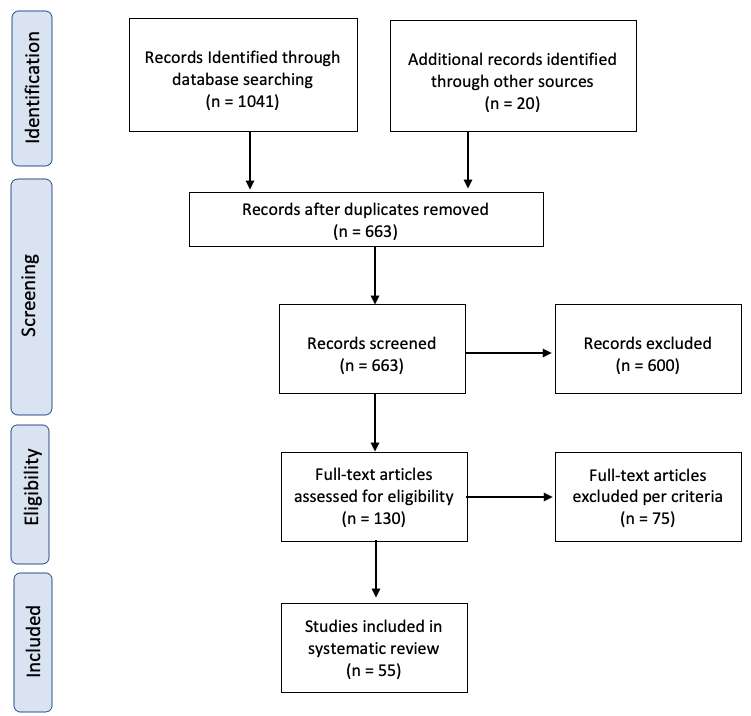
Figure 1#7721
Retrospective Analysis of a Novel Augmented-Reality Templating Solution for Total Knee Arthroplasty
Parth Desai - Ochsner Clinic Foundation - New Orleans, USA
Hunter Starring - Ochsner Medical Center - New Orleans, USA
*Michael Stallard - Ochsner Medical Center - New Orleans, USA
Connor Soles - University of Queensland- Ochsner Clinic Foundation - New Orleans, USA
George Chimento - Ochsner Health System - New Orleans, USA
*Email: michael.stallard@ochsner.org
Introduction: Templating is an important component of pre-operative planning for total knee arthroplasty. Acetate and digital templating are the most widely accepted modalities for templating used worldwide. These modalities are typically accurate within one implant size, however do have limitations. The advent of augmented reality (AR) has allowed for the development of mobile smart phone or tablet solutions for pre-operative templating. The purpose of this study is to evaluate the accuracy of a novel AR-based templating application at predicting implant size for primary total knee arthroplasty (TKA).
Methods: Templating analysis using the AR-based templating application was conducted retrospectively on 20 randomized pre-operative radiographs of primary TKA patients completed by one orthopaedic surgeon over a seven-month period. The femoral and tibial component sizes predicted by the trained user of the templating application were compared to the actual implant sizes utilized. Approval was obtained from the Institutional Review Board for this retrospective study.
Results: The exact femoral component size was predicted using the AR-based templating application in 60% of cases (12/20) while 90% (18/20) of cases were predicted within one size of the eventual implant used. The exact tibial component size was predicted in 45% (9/20) of cases while 100% (20/20) of cases were predicted within one size. For both femoral and tibial components together, 100% of cases were predicted within two sizes.
Discussion: Based on the limited results of this study, AR-based templating is effective at predicting within one implant size for primary TKA. These results indicate the need for future, high-powered prospective studies to validate the accuracy of AR-based templating, in comparison to the currently accepted templating modalities. Over the last few years, AR-technology has become more available and inexpensive on modern mobile phones and tablets. AR-technology may allow for faster and more efficient templating and this study demonstrates that it may be just as accurate as standard modalities.
Figures
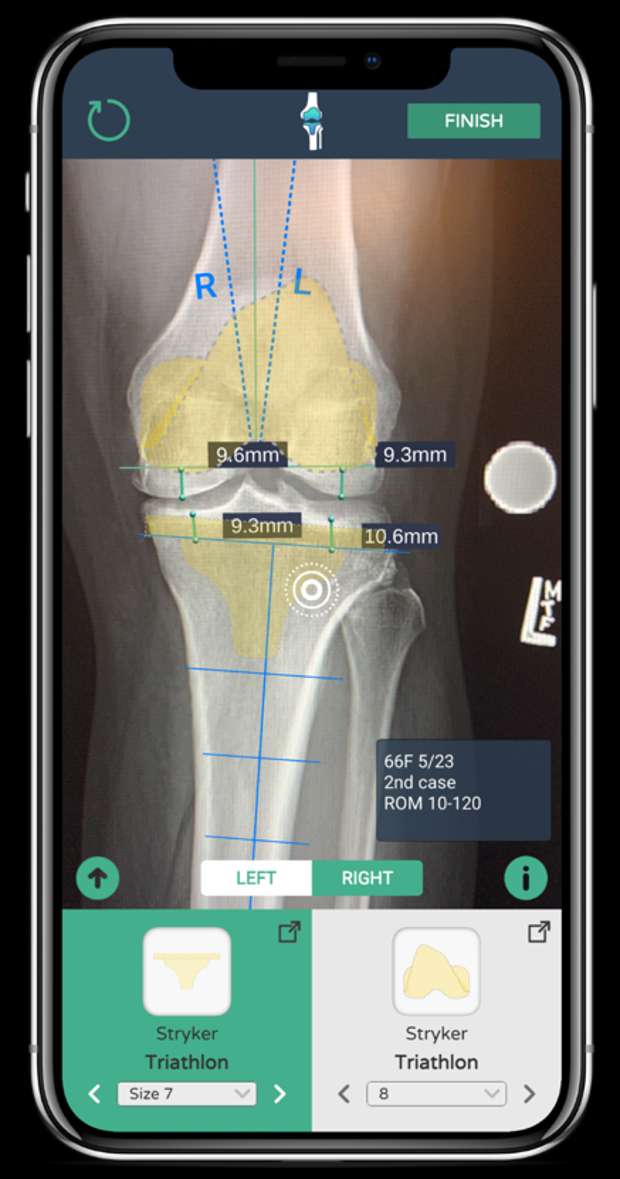
Figure 1

Figure 2
Figure 3#7661
Changes in Load Transfer in Bone Following Combined Partial Knee Arthroplasty
Jennifer Stoddart - Imperial College London - London, United Kingdom
Amy Garner - Imperial College London - London, United Kingdom
Mahmut Tuncer - Meshworks, Alloyed Ltd. - Oxford, United Kingdom
Justin Cobb - Imperial College - London, United Kingdom
*Richard van Arkel - Imperial College London - London, United Kingdom
*Email: r.vanarkel@imperial.ac.uk
Introduction: Metal implants alter the natural load transfer in bone, and in extreme cases this can lead to gross bone loss and complex revision surgery. Combined partial knee arthroplasty (CPKA) has recently emerged as a topic of interest in the field, however it is unknown how combining multiple implants will affect load transfer in the proximal tibia and distal femur, and how this might affect bone remodelling.
Methods: Previously experimentally validated finite element models of a female proximal tibia and distal femur were analysed native, and then: medial (UKA-M) and lateral (UKA-L) unicondylar arthroplasty, patellofemoral arthroplasty (PFA), bi-unicondylar arthroplasty (Bi-UKA), medial (BCA-M) and lateral (BCA-L) bicompartmental arthroplasty, tricompartmental arthroplasty (TCA) and posterior-stabilised total knee arthroplasty (TKA). The implants were sized and positioned by a surgeon familiar with these procedures. Muscle, ligament and joint contact loads representing toe-off in gait were applied to each of the models. The difference in the equivalent strain predicted between the native knee and each of the implanted states was investigated by examining cross-sections in the femoral condyles, and 15 and 30 mm distal to the tibial plateau. The overall effect on load transfer was also quantified by sampling at 5 mm intervals throughout the proximal tibia or distal femur and calculating the percentage of bone which was strain shielded or overstrained by more than 50%.
Results: Tibial load transfer was largely maintained with UKA-M, UKA-L and Bi-UKA, though overstraining was observed immediately under the implant keels and anteriorly near the ACL attachment. Conversely, the tibia was proximally strain shielded following TKA, with a more than 50% reduction compared to native strain predicted close to the stem of the implant. The bone near the tip of the TKA stem was predicted to be highly overstrained compared to native. For procedures that resurfaced the medial condyle (UKA-M, BCA-M, Bi-UKA and TCA) strain shielding was predicted around the length of the fixation pegs [Fig. 1] and overstraining predicted at the peg tips and the anterior notch [Fig. 2]. Conversely, for TKA nearly the entire cross-section was strain shielded. Similar effects were observed in the lateral condyle. For both the tibia and femur, the percentage of bone that was strain shielded by more than 50% increased with increasing amount of metal implanted into the joint: isolated PKA < combined PKA < TKA [Fig. 3]. The same was not true for regions of bone overstrained by more than 50%: in the femur partial knee arthroplasty was associated with more regions of bone overstrained than TKA, which may be a result of the bone surface preparation. There was only limited interaction between the combined partial implants.
Conclusion: Knee arthroplasty disrupts load transfer in the femur and tibia during gait. A compartmental approach to knee arthroplasty inherently preserves more bone stock at the time of the operation and may also lead to less longer-term bone loss as less bone is strain shielded compared to TKA. Further work will consider other ADLs at a range of flexion angles.
Figures
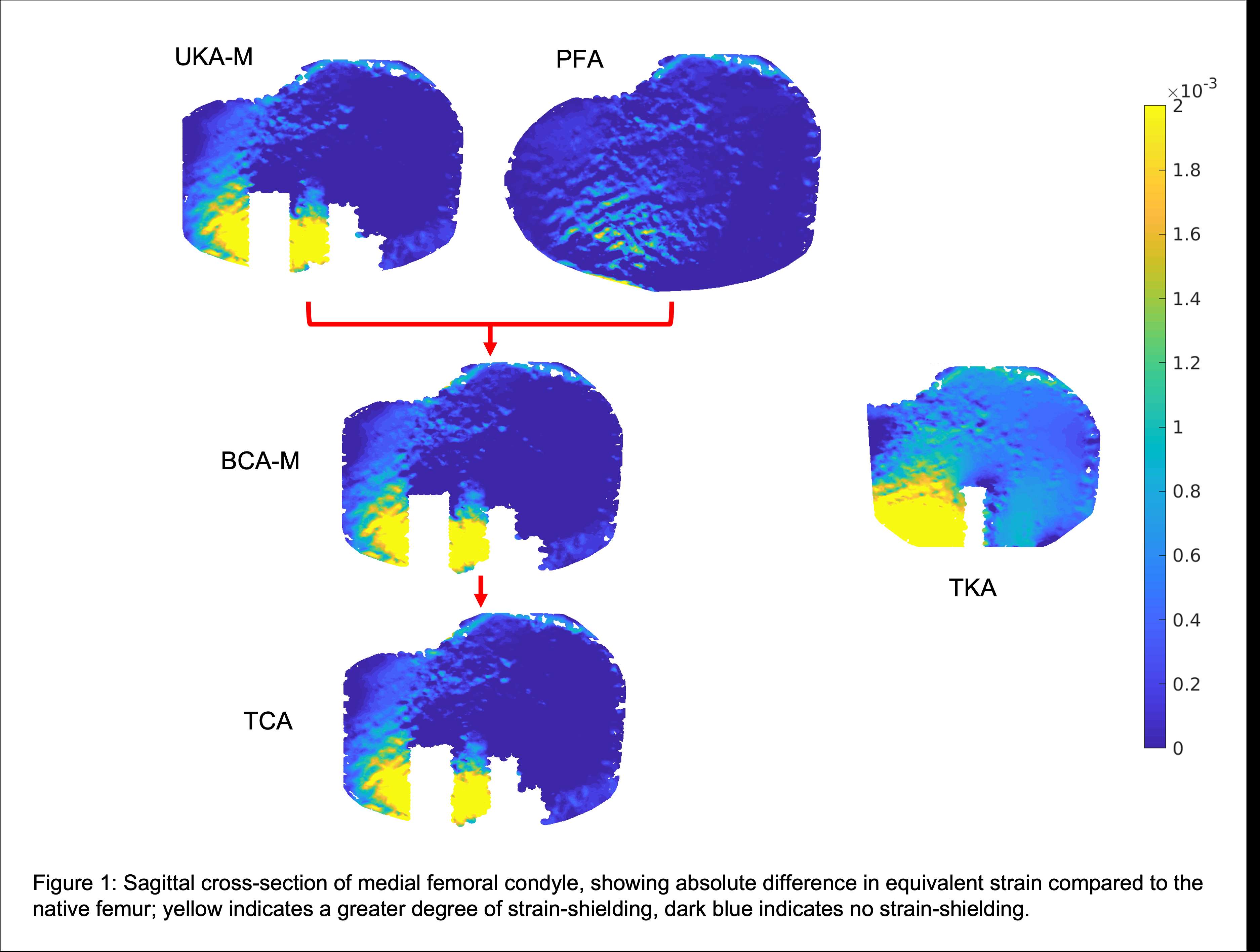
Figure 1
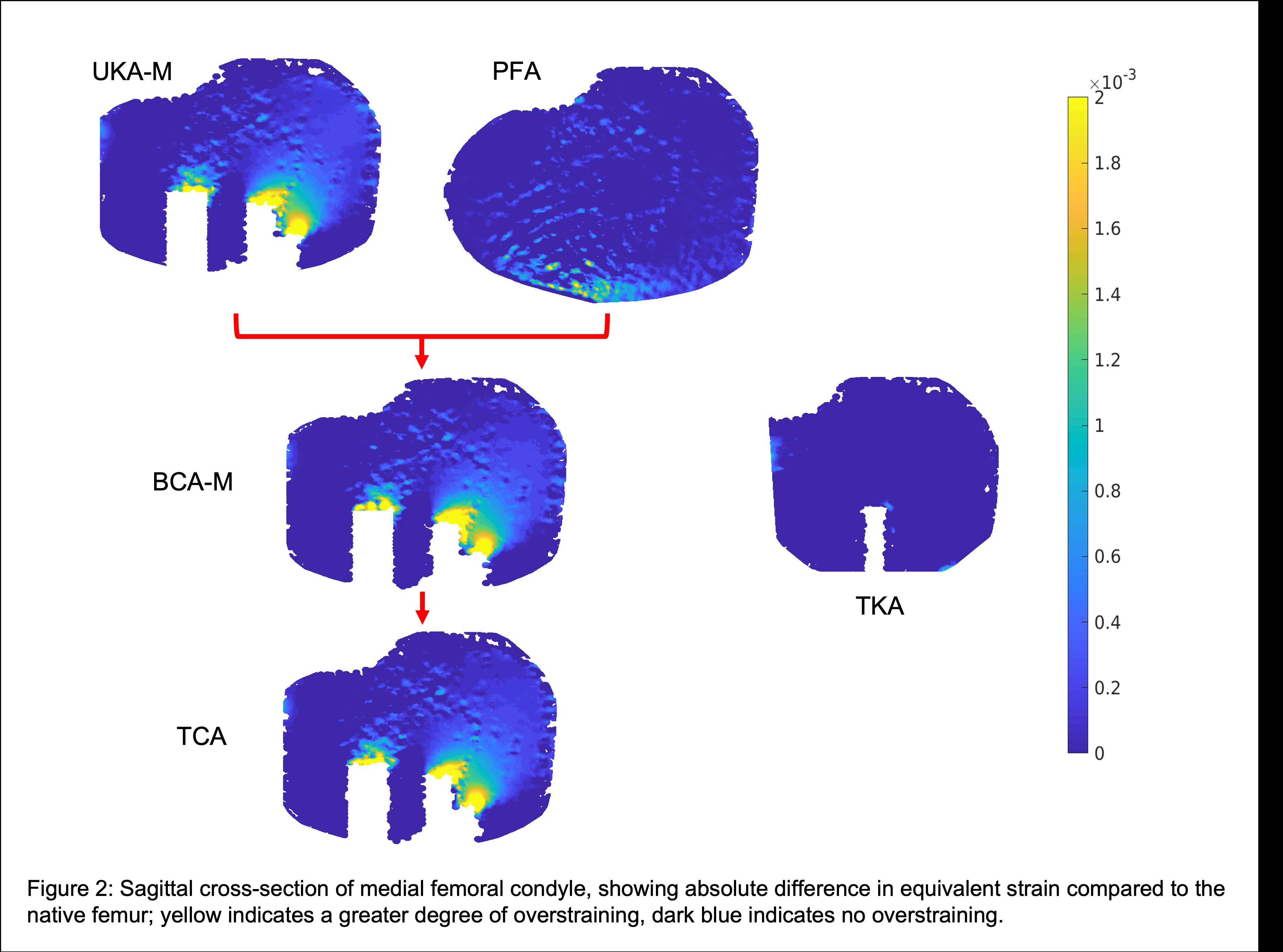
Figure 2
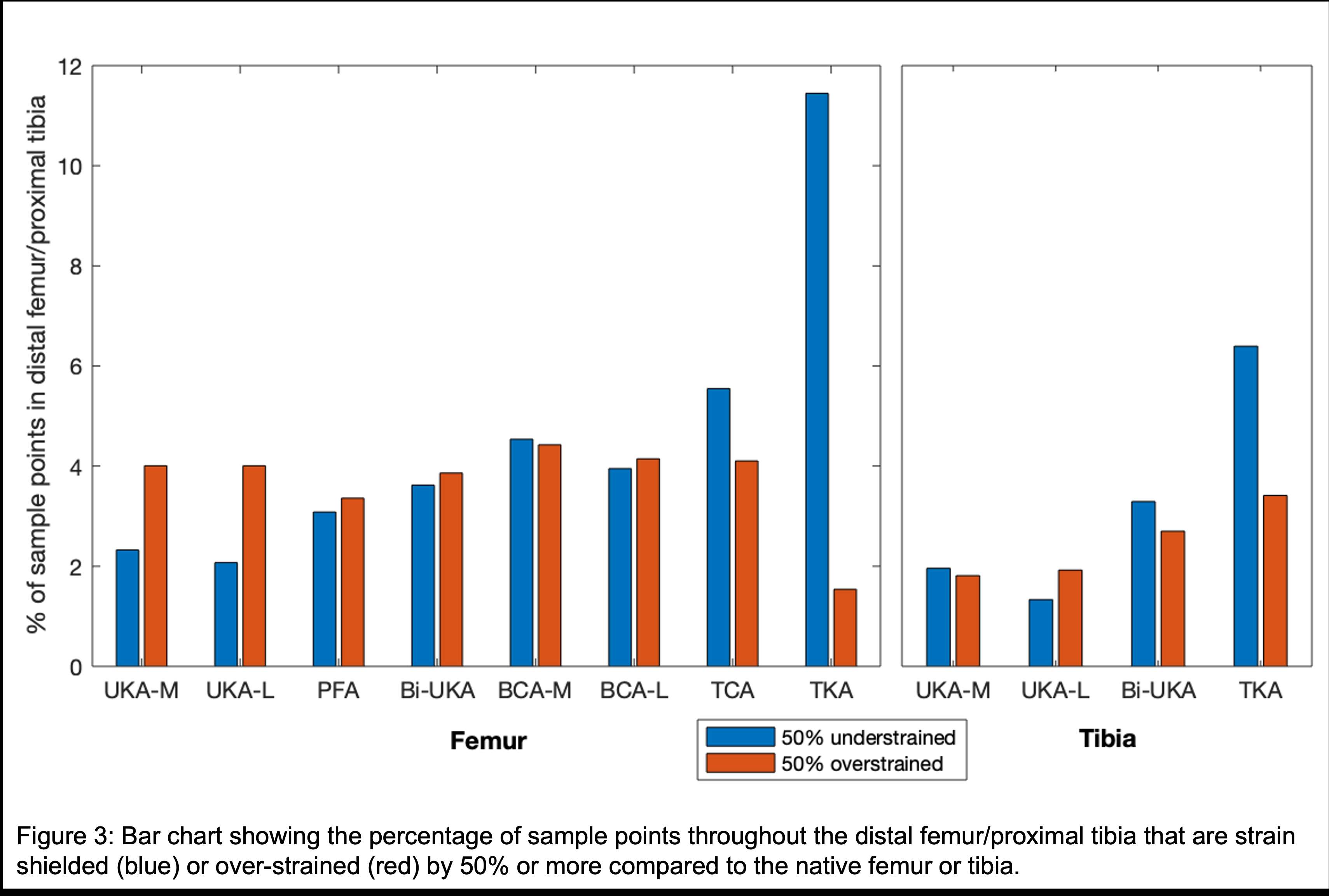
Figure 3#7764
Femoral Closure Fatigue of IBED TiN Coated Wrought Titanium Femurs Compared to CoCrMo Femurs
*Anna Sullivan - Total Joint Orthopedics - Salt Lake City, USA
Chris Weaber - TJO Inc. - Salt Lake City, USA
Dermott McHugh - Total Joint Orthopedics - Salt Lake City, USA
*Email: asullivan@tjoinc.com
Introduction: Although most femoral knee implants are manufactured from cast CoCrMo1, there is an increasing need for alternative femoral implant materials2. Ti6Al4V is a commonly used implant material, but there is a potential concern of fatigue fracture under gait loading when applied to a femoral implant geometry. A novel ion beam enhanced deposition (IBED) TiN coating process has been developed for titanium femoral components3. This study aims to compare the fatigue strength of cast CoCrMo femurs and IBED TiN coated femurs manufactured from wrought Ti6Al4V.
Methods: Finite Element Analysis per ASTM F3161 was conducted utilizing Solidworks on all sizes of the subject modern, universal knee femur components. The highest stresses were found with the size 7 modern, universal component. The subject femur geometry is symmetric, therefore medial/ lateral condyle load application is not a factor.
Size 7 femur implants were manufactured to the same geometry and specifications in the following material conditions: cast CoCrMo per ASTM F75 and wrought Ti6Al4V per ASTM F136. The articular surface of the titanium femurs was coated with a 5µm thick, IBED TiN coating3. A fatigue life curve (n=6) was developed for the two material conditions to determine which is worst-case for fatigue.
Femurs were potted in PMMA with the potting level at least 5mm below the intercondylar notch. A sinusoidal load (R=10) was applied through a thrust bearing and lubricated load applicator to the posterior condyle at 90° of tibiofemoral flexion at a frequency of 15Hz [Figure 1]. Frequency was reduced to a minimum of 5hz on higher load specimens. Testing was performed by Element Materials Technology.
Results: A power fit fatigue life curve for cast CoCrMo and IBED TiN coated wrought Ti6Al4V gave a runout load to 10MC of 2,702N (R2=0.8817) and 2,676N (R2=0.5976) respectively. The highest cyclic load that reached 10MC was 3,000N for both material conditions. Runout testing (n=5) was performed for the worst-case group (IBED TiN coated wrought Ti6Al4V) and all samples ran out to 10MC at a load of 2,676N [Figure 2 and 3].
Conclusion: Cast CoCrMo and IBED TiN coated wrought Ti6Al4V were found to be very similar in strength, but CoCrMo may be slightly stronger due to the runout load calculated by the fatigue life curve. Both material conditions are sufficiently strong for the application of knee replacement based on data from in-vivo knee loading which was measured by Bergmann et al4. This study found that the highest load of the Aver75 dataset above 30 degrees of knee flexion for a high cycle activity (walking) was 907N. The runout loads for both material conditions are significantly higher than this representative in-vivo knee loading, even in a worst-case fixation and loading scenario. This testing suggests that IBED TiN coated wrought Ti6Al4V femurs have sufficient fatigue strength and perform similarly well to CoCrMo femurs under worst case physiological loading conditions.
References:
1AAHKSPatientandPublicRelationsCommittee,AAHKSEvidenceBasedMedicineCommittee.“WhatAreHipandKneeReplacementsMadeOf?”AmericanAssociationofHipandKneeSurgeons,https://hipknee.aahks.org/what-are-hip-and-knee-replacement-implants-made-of/.
2Hallab,NadimPhD;Merritt,KatharinePhD;Jacobs,JoshuaJ.MDMetalSensitivityinPatientswithOrthopaedicImplants,TheJournalofBone&JointSurgery:March2001-Volume83-Issue3-p428
3Deutchman,ArnoldPhD.“IntroductiontoIonBeam-BasedCoatingTechnology.BeamAlloyTechnologies, https://beamalloy.net/ibed-technology/
4Bergmann G, Bender A, Graichen F, Dymke J, Rohlmann A, et al. (2014) Standardized Loads Acting in Knee Implants. PLoS ONE 9(1): e86035. doi:10.1371/journal.pone.0086035
Figures
Figure 1
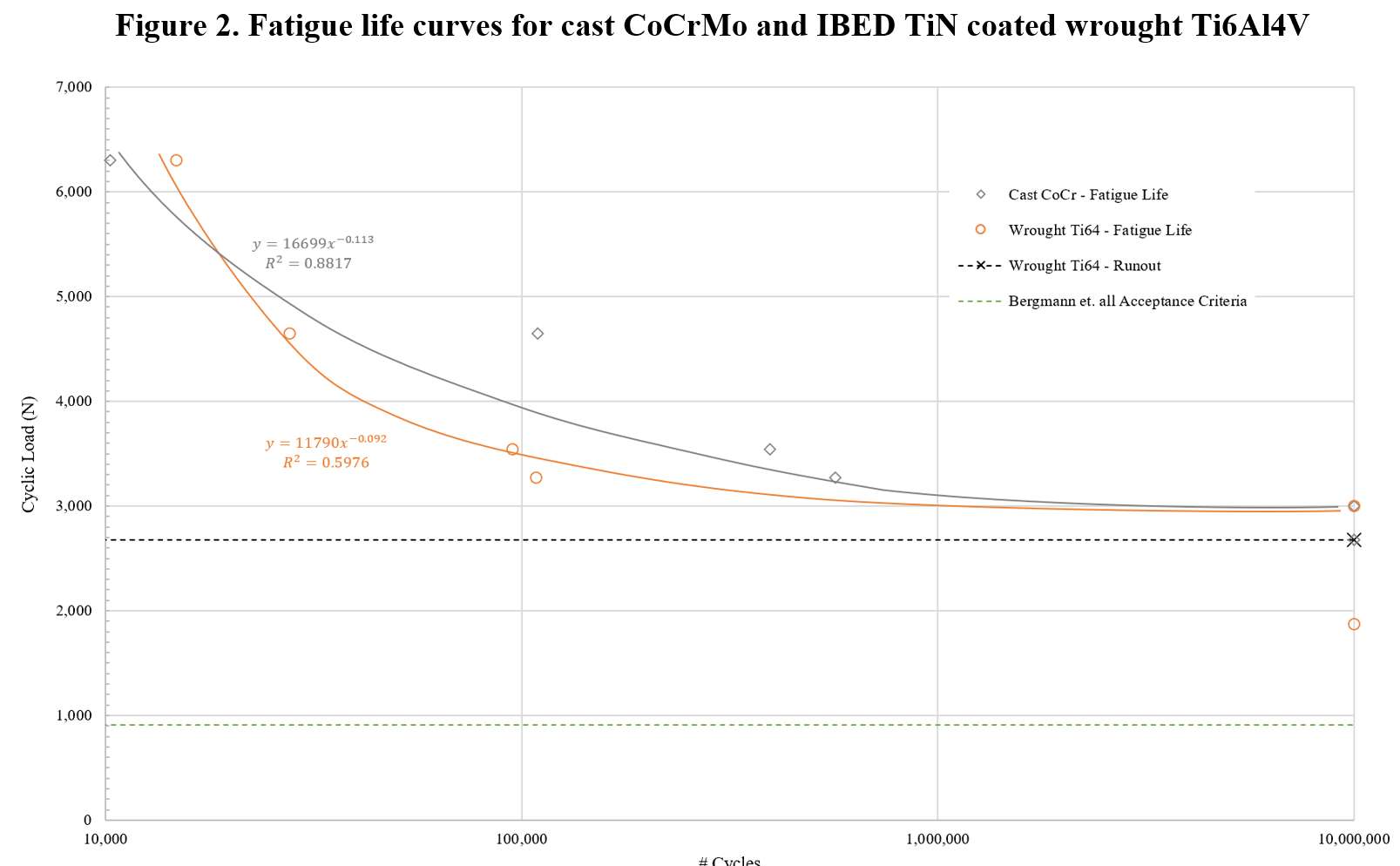
Figure 2
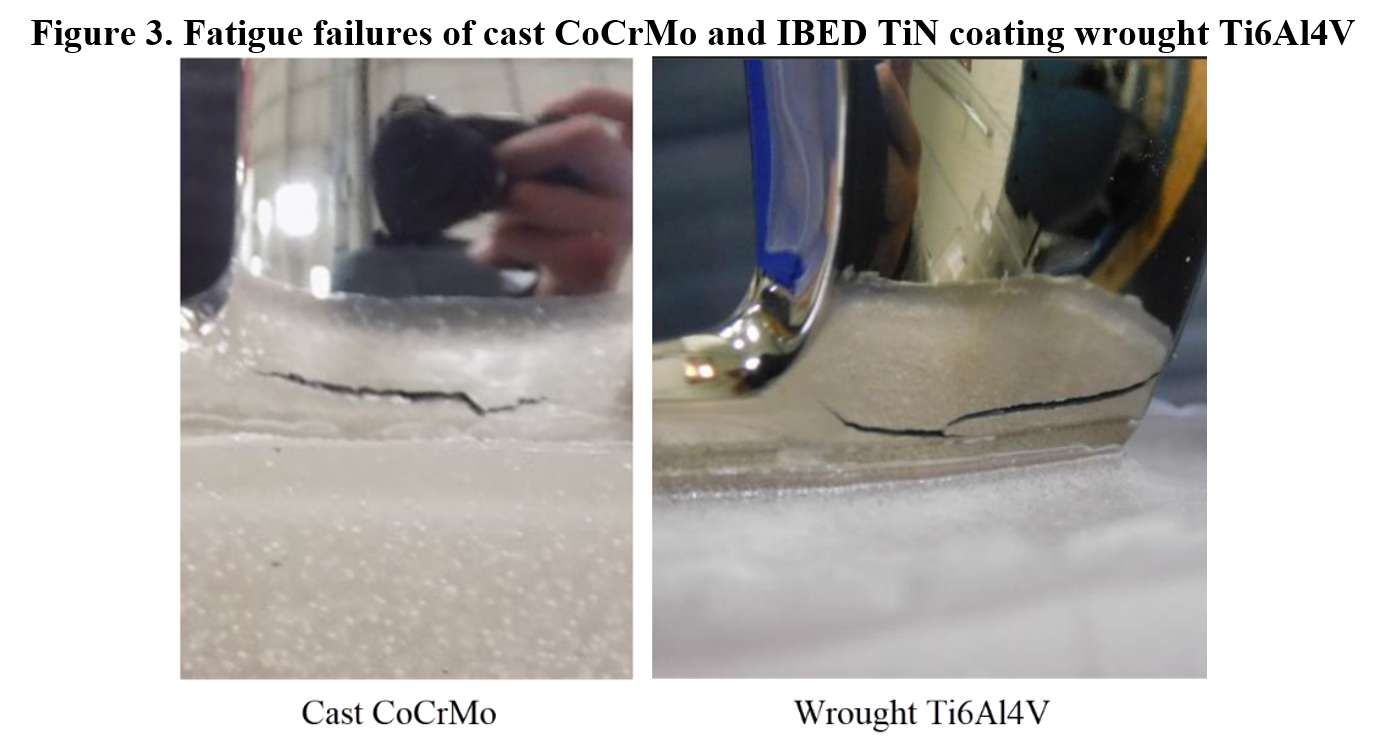
Figure 3#7756
Scratch Hardness of CoCrMo Compared to an IBED TiN Coated Ti6Al4V Substrate
*Anna Sullivan - Total Joint Orthopedics - Salt Lake City, USA
Chris Weaber - TJO Inc. - Salt Lake City, USA
Dermott McHugh - Total Joint Orthopedics - Salt Lake City, USA
*Email: asullivan@tjoinc.com
Introduction: Most femoral knee implants are manufactured from CoCrMo1, but there is an increasing desire to find alternative femoral implant materials2. Ti6Al4V is a commonly used implant material but requires a hard ceramicised coating to provide adequate wear properties3. Aurum® modern, universal femoral components utilize a novel Ion Beam Enhanced Deposition (IBED) titanium nitride (TiN) coating applied to a Ti6Al4V substrate4. Aurum® femoral components could provide an improved articulating surface that matches the durability of CoCrMo. The objective of this study is to compare the scratch hardness of CoCrMo and Aurum® femoral components.
Methods: Modern, universal femoral knee implants were manufactured to the same geometry and specifications in two material conditions: cast CoCrMo per ASTM F75 and Aurum®. The distal condyles of three CoCrMo and five Aurum® femurs underwent scratch hardness testing at MechAction in accordance with ASTM G171 using an Anton Paar Revetest scratch system. Loads of 10N and 80N were applied at 0.5mm/s with a 200µm radius diamond tip to create a 5mm scratch. These loads were chosen to be above and below the cohesive failure of the Aurum® coating. Two to three scratches were applied to each sample at each load. The scratch width was measured at two to three locations along each scratch track and was then used to calculate hardness.
Mode III wear testing was performed with five femorals of each material condition that were scratched with 400 grit sandpaper and run to 3.5MC according to the test parameters at Harris Orthopedic Laboratory [Figure 1].
Results: For the 10N load, the average scratch hardness and scratch width of the CoCrMo and Aurum® femurs were 4.33±0.09GPa/76.73±0.84µm and 4.52±0.08GPa/75.09±0.68µm, respectively (p=<.01). For the 80N load, the average scratch hardness and scratch width of the CoCrMo and Aurum® femurs were 5.17±0.68GPa/199.73±13.69µm and 4.93±0.09GPa/203.38±1.96µm, respectively (p=.19/p=.33) [Figure 2]. CoCrMo had a maximum scratch track pile up of 14µm at the 80N load while Aurum’s® maximum was 6µm [Figure 3].
The average Mode III wear rate of the CoCrMo and Aurum® femurs was 71.6±0.9mg/MC and 43.1±2.7mg/MC, respectively (p=<.01) [Figure 2].
Conclusion: At the 10N load, the scratches were small enough to only test the hardness of the coating of the Aurum® femurs, which had a hardness measurement that was significantly higher than that of CoCrMo. At the 80N load, the Aurum® femurs had equivalent hardness to CoCrMo. The increased scratch hardness of Aurum® at lower loads resulted in significantly lower Mode III wear rates due to the lack of scratches present after applying 400grit sandpaper.
CoCrMo femurs have excellent survivorship and clinical track records. However, 98% of long term CoCrMo retrievals (in vivo>15years) exhibit abrasive wear/scratching5. Aurum® demonstrated improved scratch hardness at lower loads, equivalent scratch hardness at higher loads, significantly improved Mode III wear rates, and decreased scratch track pile up. This data suggests that this novel coating is at least as durable as CoCrMo and has the potential to improve long term TKA outcomes.
References:
1AAHKSPatientandPublicRelationsCommittee,AAHKSEvidenceBasedMedicineCommittee.“WhatAreHipandKneeReplacementsMadeOf?”AmericanAssociationofHipandKneeSurgeons,https://hipknee.aahks.org/what-are-hip-and-knee-replacement-implants-made-of/.
2Hallab,NadimPhD;Merritt,KatharinePhD;Jacobs,JoshuaJ.MDMetalSensitivityinPatientswithOrthopaedicImplants,TheJournalofBone&JointSurgery:March2001-Volume83-Issue3-p428
3“KneeJointPatellofemorotibialandFemorotibialMetal/PolymerPorous-CoatedUncementedProstheses–Class IISpecialControlsGuidanceDocumentforIndustryandFDA.”USFoodandDrugAdministration,https://www.fda.gov/medical-devices/guidance-documents-medical-devices-and-radiation-emitting-products/knee-joint-patellofemorotibial-and-femorotibial-metalpolymer-porous-coated-uncemented-prostheses#_Toc32397782
4Deutchman,ArnoldPhD.“IntroductiontoIonBeam-BasedCoatingTechnology.BeamAlloyTechnologies,https://beamalloy.net/ibed-technology/
5ArnholtCM,MacDonaldDW,MalkaniAL,KleinGR,RimnacCM,KurtzSM;ImplantResearchCenterWritingCommittee,KocagozSB,GilbertJL.CorrosionDamageandWearMechanismsinLong-TermRetrievedCoCrFemoralComponentsforTotalKneeArthroplasty.JArthroplasty.2016Dec;31(12):2900-2906.doi:10.1016/j.arth.2016.05.006.Epub2016May12.PMID:27426028;PMCID:PMC5107165.
Figures
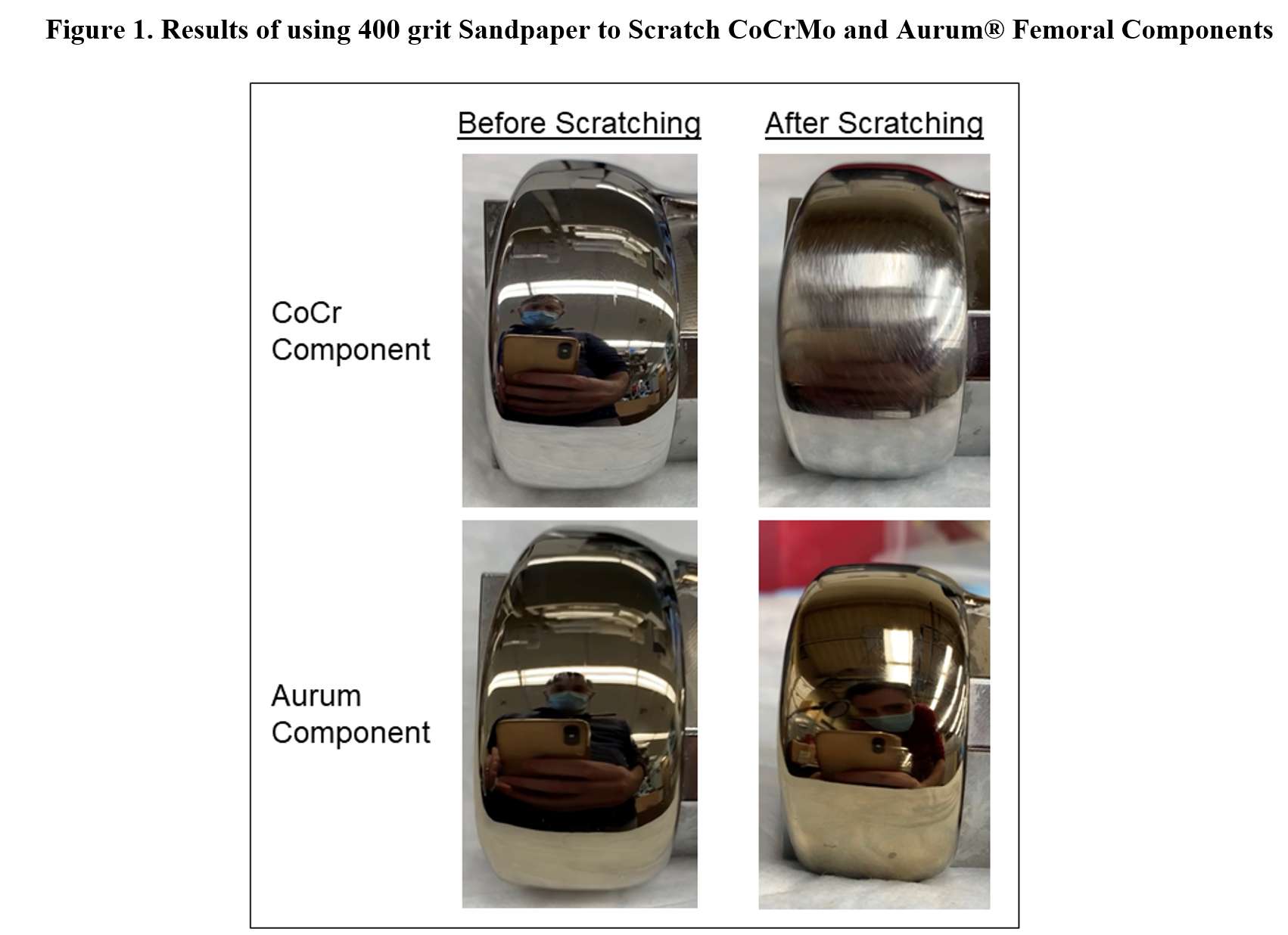
Figure 1
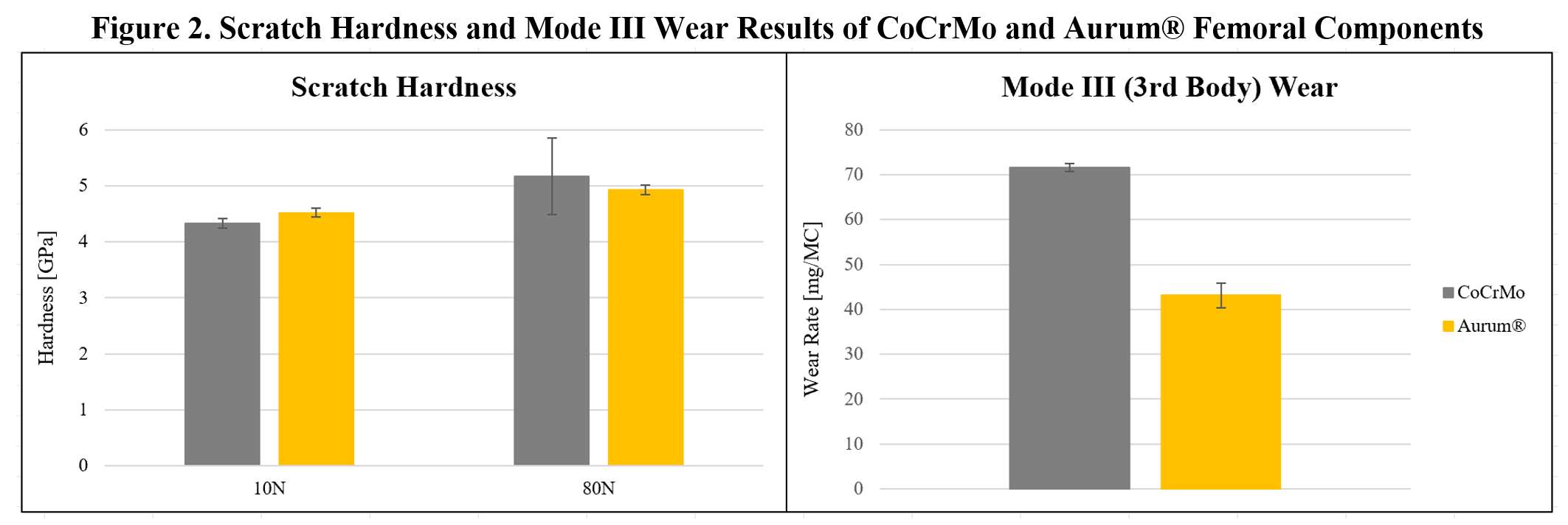
Figure 2
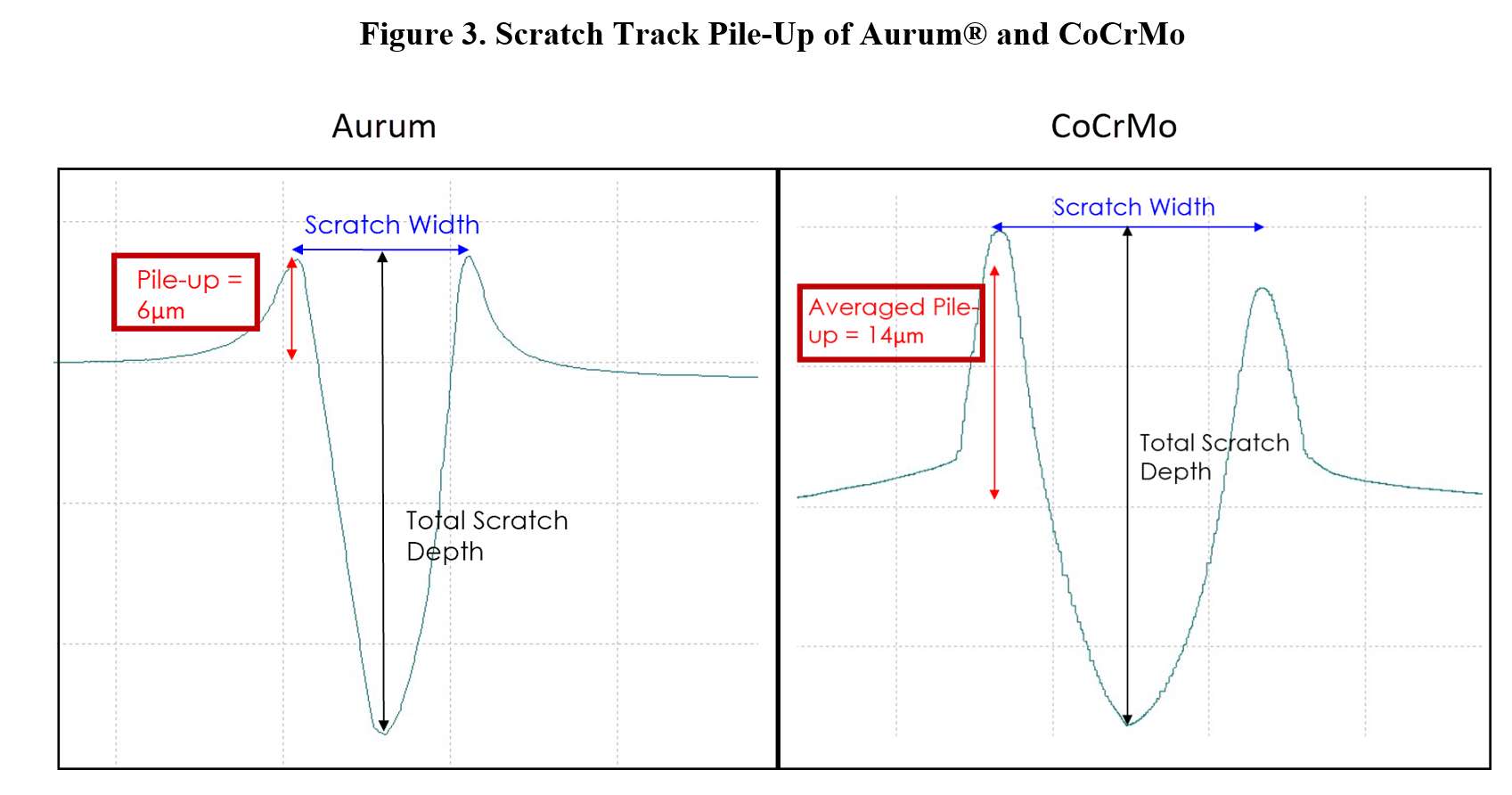
Figure 3#8047
Invited Talk: Does Posterior Cruciate Ligament Resection increase the tibiofemoral joint gap under the preservation of medial soft tissues?
*Shinro Takai - Nippon Medical School - Tokyo, Japan
Yasushi Oshima - Nippon Medical School - Japan
Tokifumi Majima - Nippon Medical School - Tokyo, Japan
*Email: takai@kta.att.ne.jp
Introduction
In performing posterior stabilized (PS) -total knee arthroplasty (TKA), posterior cruciate ligament (PCL) resection has been considered to cause a substantial increase in the tibiofemoral flexion gap than in the extension gap. However, previous evaluations had been performed after bone resections and soft tissue release, which is considered to be an abnormal knee condition and does not represent physiological knee kinematics.
Recently, we performed TKA with less soft tissue release in order to preserve natural knee kinematics. In this procedure, we hypothesized that PCL resection does not affect the extension and flexion gaps. Thus, we evaluated the effect of PCL resection, without any bone resection or soft tissue release during PS-TKA.
Patients and methods
Primary TKA patients with PS implants due to varus knee osteoarthritis (OA) were enrolled in this investigation. After knee arthrotomy, the medial joint capsule was subperiosteally separated 10 mm caudally from the tibial joint line reaching the anterior edge of the deep medial collateral ligament (dMCL); however, the dMCL itself was left intact. The anterior horn of the medial meniscus and the anterior segment of the lateral meniscus were excised to make space for insertion of a force-controlled ligament tensioner. At this stage, osteophytes of the femur and tibia, the dMCL, the superficial medial collateral ligament, the anterior cruciate ligament (ACL), and the PCL were not treated. The medial and lateral joint gaps were measured with the ligament tensioner in full extension and at 90° in flexion at a distracting force of 120 N. Throughout the study, to maintain the tibia's anteroposterior position relative to the femur when measuring the tibiofemoral joint gaps, after knee arthrotomy, the medial edges of the femur and tibia were marked with a surgical marking pen when extended as much as possible and at 90° flexion. The ACL and PCL were resected, and the tibiofemoral joint gaps were measured again.
Results
Analysis of the physiological gaps just after knee arthrotomy showed that the flexion gap was significantly larger than the extension gap in both medial and lateral compartments and was trapezoidal in shape, with the lateral compartment wider than the medial compartment in both extension and flexion. However, the results showed no clinically significant change of either the extension or the flexion gap by ACL and PCL resections.
Discussion
Although PCL resection is believed to increase the flexion gap more than the extension gap, it did not affect the extension or flexion gap in our study. This contradiction is probably due to the existence of medial soft tissues. Therefore, TKA surgeons should carefully consider the distinct effects of PCL resection with and without medial soft tissue release in TKA.
Conclusions
PCL resection does not affect the tibiofemoral gap in varus knees when medial soft tissue conditions are similar to preoperative knee OA kinematics.
#7748
Quantitative Susceptibility Mapping of Brain Regions to Evaluate Metal Deposition in the Brain Following Long-Term Total Hip Arthroplasty and Hip Resurfacing Arthroplasty
*Shahnaz Taleb - Western University - London, Canada
Gabriel Varela-Mattatall - Western University - London, Canada
Abbigail Allen - London Health Sciences Center - London, Canada
Chaithanya Nair - Western University - London, Canada
Roy Haast - Western University - London, Canada
Ali Khan - Western University - London, Canada
Vishal Kalia - St. Joseph’s Health Care London - London, Canada
Steven MacDonald - London Health Sciences Centre - London, Canada
Ravi Menon - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Matthew Teeter - Western University - London, Canada
*Email: staleb3@uwo.ca
Introduction: Wear and corrosion of implants used in total hip arthroplasty (THA) and hip resurfacing arthroplasty (HRA) release metal ions which can cause adverse local and distant tissue reactions. Cobalt and chromium can even cross the blood-brain barrier to deposit in the brain. Imaging evidence has described changes in brain anatomy and metabolism after exposure to heightened levels of cobalt from metal-on-metal and metal-on-polyethylene hip implants. Quantitative susceptibility mapping (QSM) is an emerging MRI technique used to measure the magnetic susceptibility of tissues; therefore, it can be used to study the presence of cobalt and chromium in the brain. The objective of this study is to use QSM to evaluate the association between susceptibility in brain structures and blood metal ion levels in subjects with THA and HRA implants at long-term follow-up, and in comparison, to age- and sex-matched controls.
Methods: Ethics approval from the institutional review board and informed consent from participants were obtained. Subjects included have had a THA or HRA implant for a minimum of eight years or have been referred to undergo a hip replacement but have not yet received an implant. Four cortical and five deep brain structures were identified from case reports describing anatomical changes in patients with implant wear-related cobaltism [Fig. 1]. Subjects were examined using 3T MRI (Siemens Prisma Fit). A T1-weighted MPRAGE sequence was used to segment brain regions using FreeSurfer (v7.1). A multi-echo GRE sequence was used to create susceptibility maps. Blood cobalt and chromium levels were measured at the time of imaging in subjects with implants. The Montreal Cognitive Assessment (MoCA) test was performed. A Friedman test, Spearman correlation, and two-way ANOVA were computed.
Results: 39 subjects have been recruited at present. Implant types consisted of metal-on-metal THA (n = 19), dual-modular neck metal-on-polyethylene THA (n = 6), metal-on-metal HRA (n = 2), and ceramic-on-metal (n = 1). Partial recruitment (n = 11) of matched controls was completed. The mean age was 67 years (56-79) and 64 years (58-75) for implanted and control subjects, respectively. Mean device implantation was 13 years (8-20 years). Mean Co was 6.5 μg/L (0.2-40.0 μg/L), and mean Cr was 2.2 μg/L (0.3-7.4 μg/L). Only 4/28 implanted subjects had blood cobalt levels above the toxic risk threshold and most subjects have well-functioning implants. Mean MoCA scores were 26 in both groups. Most implanted subjects displayed normal anatomical features for their age; however, three subjects displayed chronic ischemic changes, one showing concern for pituitary lesions. Susceptibility varied between brain regions, with susceptibility being the greatest in deep brain regions (p < 0.0001) [Fig. 2]. No correlation was found between susceptibility and blood ion levels of cobalt or chromium for any regions.
Conclusions: Susceptibility levels in both groups were comparable; however, full recruitment of matched controls is needed before conclusions can be determined with respect to metal ion deposition in the brain. Susceptibility was found to vary similarly between different anatomical regions of the brain in both implanted subjects and controls, consistent with aging patterns.
Figures
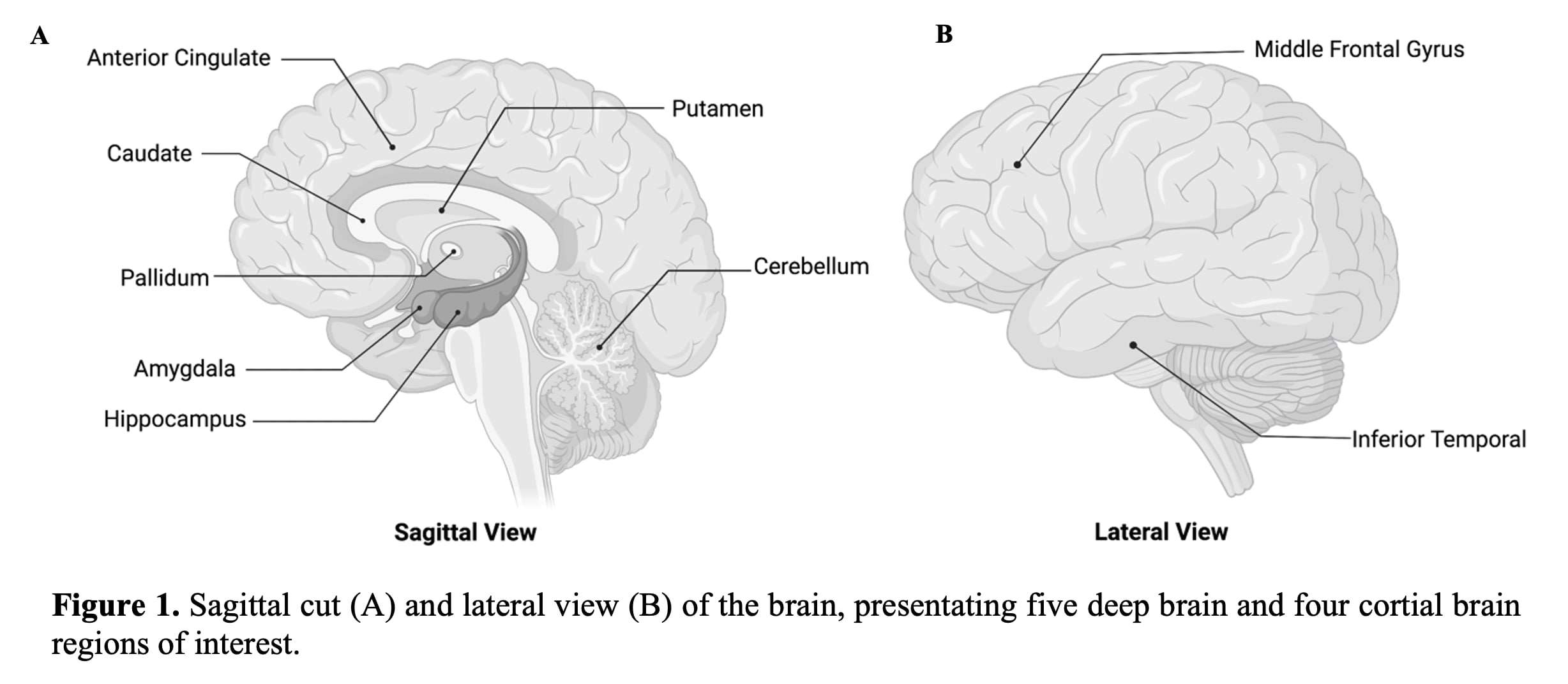
Figure 1
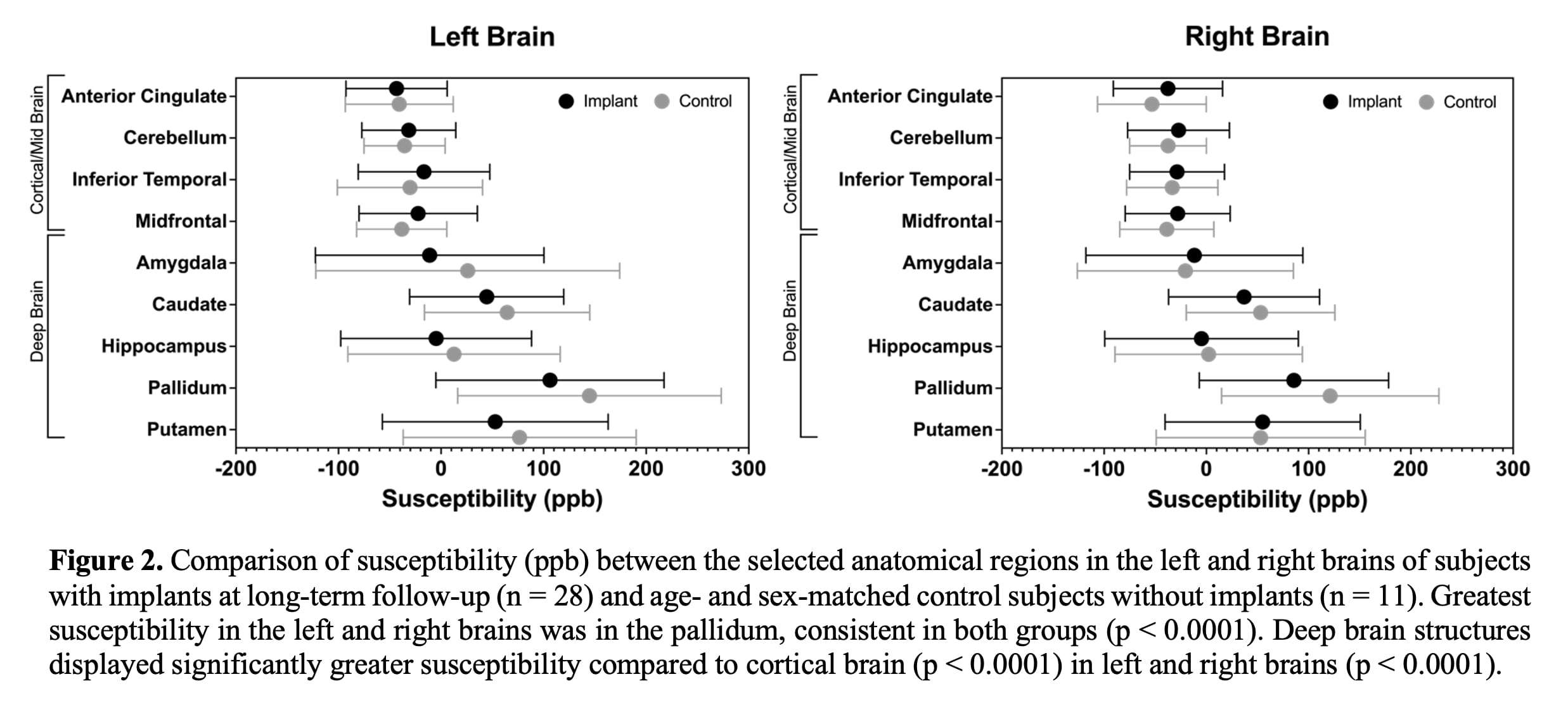
Figure 2#7384
A Novel Algorithm to Balance Varus Knee Without Releasing Superficial MCL Based on the Pathological Changes in Varus Knee.
*Samih Tarabichi - Dubai, UAE
Mohamed Elfekky - Dubai Health Authority - Dubai, United Arab Emirates
*Email: samtarabichi@yahoo.com
Introduction:
John Insall described medial release to balance the varus knee, the release he described included releasing the superficial MCL in severe varus cases. however, this release can create instability in the knee furthermore this conventional wisdom does not correct the actual pathology which is normally exist at the joint line, and instead it focuses on the distal end of the ligament where there is no pathology.
We have established a new protocol consisting of 5 steps to balance the varus knee without releasing the superficial MCL and we tried this algorithm on a series of 115 patients with varus deformity and compared to the outcome with a similar group that we have performed earlier using the traditional Insall technique.
Material and method:
115 TKR were performed by the same surgeon using Zimmer Persona implant in varus arthritic knees. The deformities ranged from 15 to 35 degrees. First, the bony resection was made using persona instrumentation as recommended by the manufacturer. The sequential balancing was divided into 5 steps (we will show short video demonstrating the surgical techniques for each step) as follow;
|
Step 1
|
:
|
Releasing of deep MCL
|
|
Step 2
|
:
|
Excising of osteophyte
|
|
Step 3
|
:
|
Excising of scarred tissue in the posteromedial corner soft phytes
|
|
Step 4
|
:
|
Excision of the posteromedial capsule in case of flexion contracture
|
|
Step 5
|
:
|
Releasing the semi-membranous (in gross deformity)
|
We used soft tissue tensioner to balance the medial and lateral gaps. When the gaps are balanced at early step there was no need to carry on the other steps. we used only primary implant and we did not have to use any constrained implant. We have compared this group with a similar group matched for deformity from previous 2 years where the conventional medial release as described by Insall.
Results:
We could balance all knee without releasing the superficial MCL ligament as follows:
In 31 cases we were able to balance the knees performing step 1 and step 2 only
In 35 cases, we had to do step thee on addition to 1and 2 to achieve balance of cases we had to
In 25 cases, we performed step 4: those cases had pre-operative flexion contracture
We had to proceed to step 5 only in 14 cases. These patients had the worst deformity in the group
we have used primary TKR in all cases; in 83 cases, we used a CR implant and in the rest, we used PS implant. Comparing this to the earlier conventional release we had to use 11 CCK implant on severe cases.
Patient satisfaction was better with the new algorithm group when compared with the traditional release
Preserving the superficial MCL allowed us to maintain stability post-operatively and allowed us to use minimum constraint such as CR in severe deformity.
Discussion:
Many literatures have confirmed that cutting superficial MCL causes major medial instability after TKA. Releasing or pie crusting the superficial MCL can cause MCL insufficiency. Our protocol enable the surgeon to tackle the pathology rather than take a short-cut and releasing the superficial MCL. reserving the superficial MCL allowed us to use minimal constraint even in severe deformity of 40 degrees of varus deformity. The conventional release has resulted in some cases instability, forcing us to use higher constraint such as CCK.
Conclusion:
Although releasing the superficial MCL has been described in different ways in multiple literature, little attention has been paid to the pathology of the posteromedial corner. This paper clearly shows that the complex anatomy of the posteromedial corner require us to pay better attention and this paper present better algorithm reserving the superficial MCL and enabling us to correct the deformity and balancing the soft tissue without instability. We strongly recommend surgeons not to release the superficial MCL because this will create instability in some cases.
#7483
Posterior Stabilized Total Knee Arthroplasty Increases the Risk of Postoperative Periprosthetic Fractures
*Samih Tarabichi - Dubai, UAE
Mohamed Elfekky - Dubai Health Authority - Dubai, United Arab Emirates
*Email: samtarabichi@yahoo.com
Background: The Insall-Burstein posterior-stabilized knee design was first developed in 1978 by adding a central cam mechanism to the articular surface geometry of the total condylar prosthesis to correct its problems being not “rolling back”. Since then, the use of posterior-stabilized (PS) implants in total knee arthroplasty (TKA) is becoming increasingly popular. However, one of the main disadvantages of PS designs is related to the amount of bone removed during femoral box osteotomy to create the housing of the PS mechanism, the clinical value of removing more or less bone during primary TKA remains to be fully established. The objective of this study was to compare the incidence of early postoperative peri- prosthetic fractures in the cruciate retaining (CR) and posterior stabilized (PS) knee prosthesis. Methods: An institutional high volume arthroplasty unit database was reviewed to identify all patients who sustained a postoperative periprosthetic fracture following primary TKA between January 2014 and May 2018. A retrospective chart review was performed to col- lect clinical, radiographic, and operative report data. A total of 352 patients with 600 primary TKAs were identified. (300 cases of cruciate retaining TKAs from 178 patients and 300 cases of posterior stabilized TKAs from 174 patients) were retrospectively reviewed. Results: Eleven patients (1.83%) sustained periprosthetic fractures in the postoperative setting following primary TKA. All of the fractures were located on the femur and were treated surgically. Only one knee (one patient) from the CR group sustained a periprosthetic fracture, while 10 knees (from 10 patients) from the PS group sus- tained a fracture. The relative risk of sustaining a fracture in the CR group was 0.10 times relative to the PS group (RR = 0.10, 95% CI 0.0129 – 0.776). Conclusion: Posterior stabilized total knee arthroplasties (TKAs) significantly increase the risk of periprosthetic fractures in obese Asian patients compared to cruciate retaining TKAs.
#7485
Comparing Two Techniques for Establishing Intraoperative Tibial Component Rotation in Total Knee Arthroplasties: In Vivo Study
*Samih Tarabichi - Dubai, UAE
Mohamed Elkabbani - Mansoura University - Mansoura, Egypt
*Email: samtarabichi@yahoo.com
Introduction
•Although, tibial component rotation plays a big role in total knee arthroplasty (TKA) success, there is no consensus on ideal tibial component rotation.
•Several techniques have been mentioned for tibial component placement intraoperatively, including anterior cortex referencing, medial third of tibial tubercle referencing, and allowing the tibial component to float during passive range of motion with cruciate retaining implants or box method with posterior stabilized implants.
•In this study, we compared two commonly used techniques for tibial component rotational adjustment while performing TKA, 1) curve on curve, and 2) box techniques.
• Our hypothesis is that the curve-on-curve technique allows for more externally rotated tibial components when compared to the box technique.
MEtodes In 18 consecutive patients with advanced varus osteoarthritis scheduled for cemented posterior stabilized total knee replacement using symmetrical tibial components in a high-volume arthroplasty institution between January 2019 and April 2019, the location of the trial tibial component center being placed through free floating tibia technique was compared intraoperatively to its location after being placed through curve on curve technique after performing all the femoral and tibial bone cuts, appropriate sizing, and finalizing soft tissue balance and required releases. The distance in between was measured regardless of its relation to the tibial tubercle.
Results;
•The mean distance between the centers of the trial tibial components being placed through curve-on-curve technique and the centers of the trial tibial components being placed through free floating tibia technique on the anterior tibial border was 10.56 ± 5.75 mm (range:3-19 mm) (95% confidence interval of the difference was 7.7-13.42 mm).
• In all the cases, the centers of the trial tibial components being placed through curve-on-curve technique were located more laterally on the anterior tibial border rather than the centers of the trial tibial components being placed through free floating tibia technique.
• All the tibial components inserted with the curve-on-curve technique are more externally rotated than those inserted with free floating tibia technique, i.e., the curve-on-curve method achieved more external rotation in all cases with a statistically significant difference (p-value<0.001).
Conclusion
ØThe curve-on-curve technique is more reliable among training surgeons during their learning curve rather than free floating tibia technique, for establishing tibial component rotation while performing posterior stabilized total knee arthroplasty using symmetrical tibial components.
#7487
Evaluation of Tibial Component Rotation in Painful Total Knee Arthroplasties by Mri Enhanced With Metal Artifact Reduction Technique
*Samih Tarabichi - Dubai, UAE
Mohamed Elfekky - Dubai Health Authority - Dubai, United Arab Emirates
*Email: samtarabichi@yahoo.com
ABSTRACT
Background: Tibial component malrotation is one of the commonest causes of pain and stiffness following total knee arthroplasties, however, the assessment of tibial component malrotation on im- aging is not clear-cut. The objective of this study was to assess tibial component rotation in cases with pain following total knee replacement using MRI with metal artifact reduction technique.
Methods: In 15 consecutive patients presented in our clinic | a high-volume arthroplasty institution | between January 2017 and June 2017 with persistent unexplained moderate to severe pain for at least 6 months following total knee arthroplasties, which were ALL done outside our institution, after exclusion of infection and loosening (tibial or femoral), MRI evaluation of tibial component rotation using metal artifact reduction for orthopedic implants (O-MAR) technique | to improve visualization of soft tissue and bone by reducing artifacts caused by metal implants | was done according to the technique of Berger et al. [Malrotation causing patellofemoral complications
after total knee arthroplasty. Clin Orthop Relat Res 144–153, 1998].
Results: Eleven cases showed an internal rotation of tibial components (73.3%), four cases showed a neutral or external rotation of tibial components (26.6%), however, with the presence of abnormal intraarticular fibrous bands in two of them.
Conclusions: Two main conclusions are obtained from this study: Firstly, internal rotation of tibial component must be excluded in all cases of persistent pain following total knee replacement. Secondly, magnetic resonance imaging with the newly developed metal artifact reduction techniques is a very useful tool in evaluating cases of unexplained pain following total knee replacement.
#7795
An in-Vitro Study of Glenoid Implant Peripheral Peg-Cement-Bone Interface Mechanics Under Simulated Glenoid Lift-Off Loading
Jakub Targosinski - University of Western Ontario - London, Canada
Jonathan Kusins - The University of Western Ontario - London, Canada
*Louis Ferreira - University of Western Ontario - London, Canada
Andrew Nelson - The University of Western Ontario - London, Canada
Travis Puhr - University of Western Ontario - London, Canada
*Email: louis.ferreira@sjhc.london.on.ca
Introduction
Aseptic loosening of the glenoid implant remains the largest single mode of failure in total shoulder arthroplasty. The mechanical basis for the glenoid implant loosening is thought to be caused by the rocking horse mechanism, whereby cyclic eccentric loading of the glenoid implant rim causes progressive damage to the cement-bone interface of the implant. A common design of glenoid implants incorporates a large central peg flanked by smaller peripheral pegs designed to accommodate the large superior-inferior loads generated in-vivo through the rocking-horse mechanism. Digital volume correlation used in concert with micro-computed tomography can provide more localized information about the role of failure of specific locations of interest in the glenoid implant such as the interface between glenoid implant peripheral pegs, the bone cement mantle, and the trabecular bone of the glenoid. This study used a DVC+micro-CT approach to measure the bone and interfacial strains in a osteoarthritic patient specific tissue model of the glenoid peripheral peg-cement-bone interface.
Methods
10 (n=5 for both tensile and compressive loading) bone cores were recovered from humeral osteotomies post-total shoulder arthroplasty. The bone cores were implanted with a modelled glenoid peripheral peg and the resulting constructed specimens were loaded using a radiolucent hexapod robot inside of a cone beam micro-CT scanner. Stepwise compressive and tensile displacements that emulate glenoid lift-off were applied to the peg constructs, and micro-CT images were captured of the peg-cement-bone interfaces in both an unloaded and loaded state (Fig. 1). DVC-derived maximum and minimum principal strains were calculated at multiple locations of interest inside the peg-cement-bone interface and were examined for any site-specific significant relationships (Fig. 2).
Results
There was a significant relationship between location along the axial length of the peg and magnitude of maximum and minimum principal strains within the interface in the tensile loading of the peg constructs (F(3)=7.642, p<.001). There was also a significant relationship between lateral distance from the pegs and the magnitude of maximum and minimum principal strains within the interface (F(1)=75.281, p<.001). In the compressive loading, there was a significant effect of lateral distance from the peg (F(1)=63.227, p<.001), but not of axial distance along the peripheral peg. Maximum and minimum principal strains in the interface were highest closest to the root of the peg with a mean magnitude of 1.7*105µε and 1.8*105 µε at maximum displacement in the tensile loading, respectively (Fig. 3).
Conclusion
The rocking-horse mechanism provides a sound mechanical explanation for the apparent-level dynamics of glenoid implant loosening, but not the specific location of the initiation of failure in the glenoid implant-cement-bone interface. This in-vitro study used patient-specific osteoarthritic tissue to model glenoid implant peripheral pegs designed to support areas of high stress in-vivo. It found that locations near the root of the peg experience the highest principal strains, of which the mean magnitude was higher than reported yield failure strains for trabecular bone tissue in both tension and compression. This location is a likely candidate for the initiation of failure of the glenoid implant-cement-bone interface following total shoulder arthroplasty.
Figures
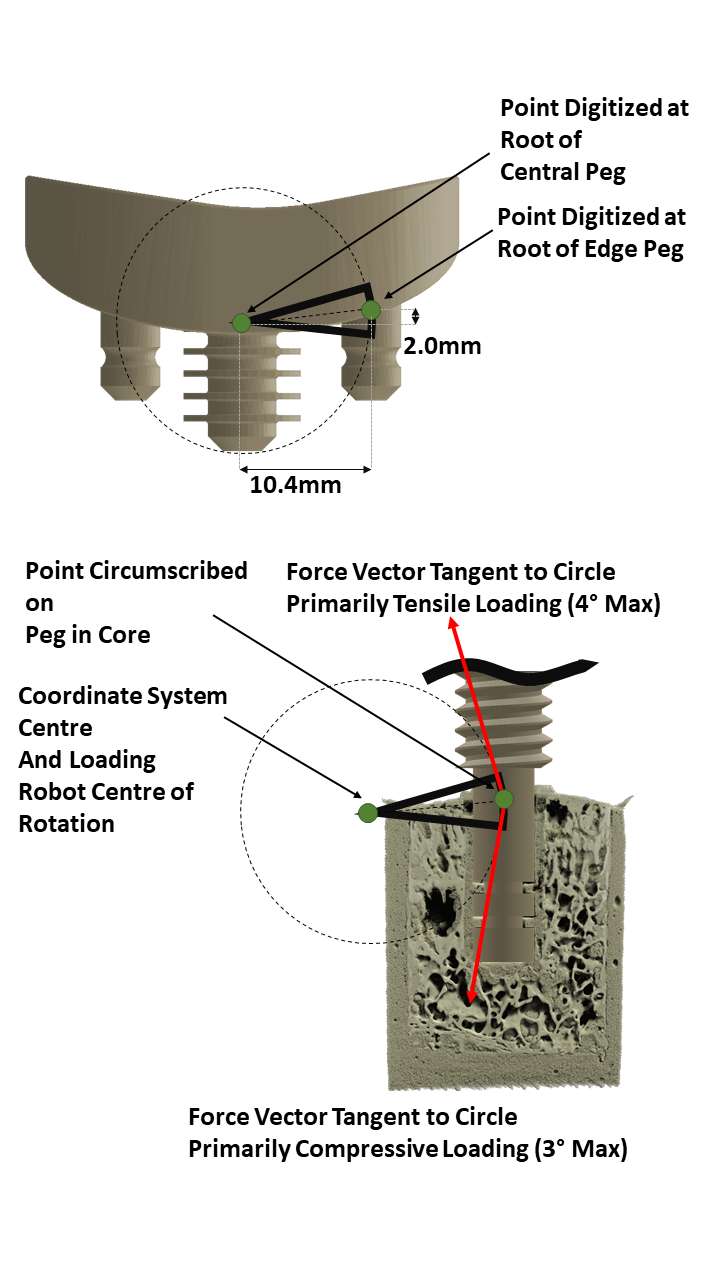
Figure 1
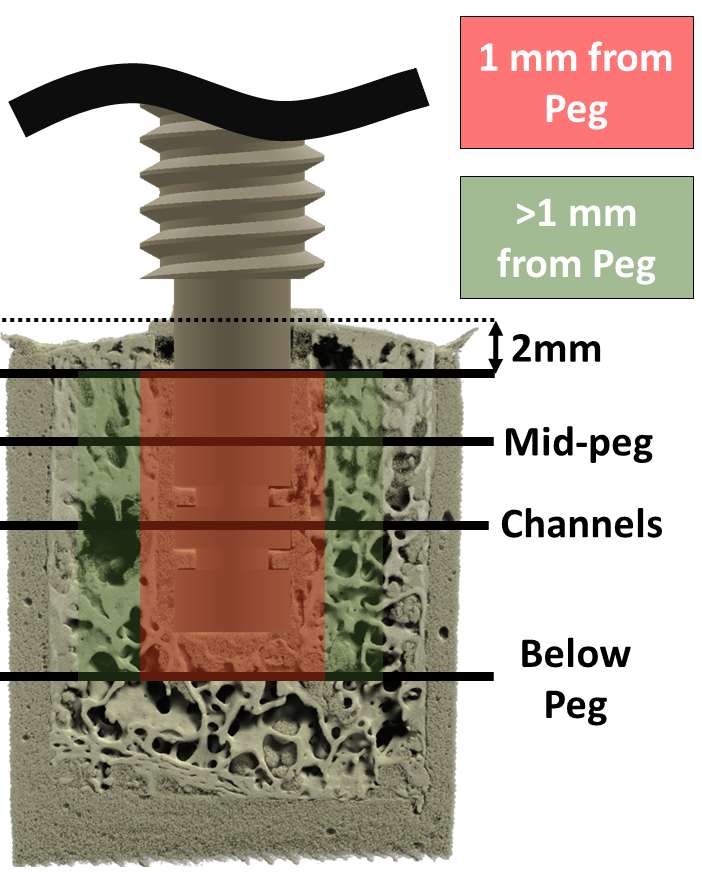
Figure 2
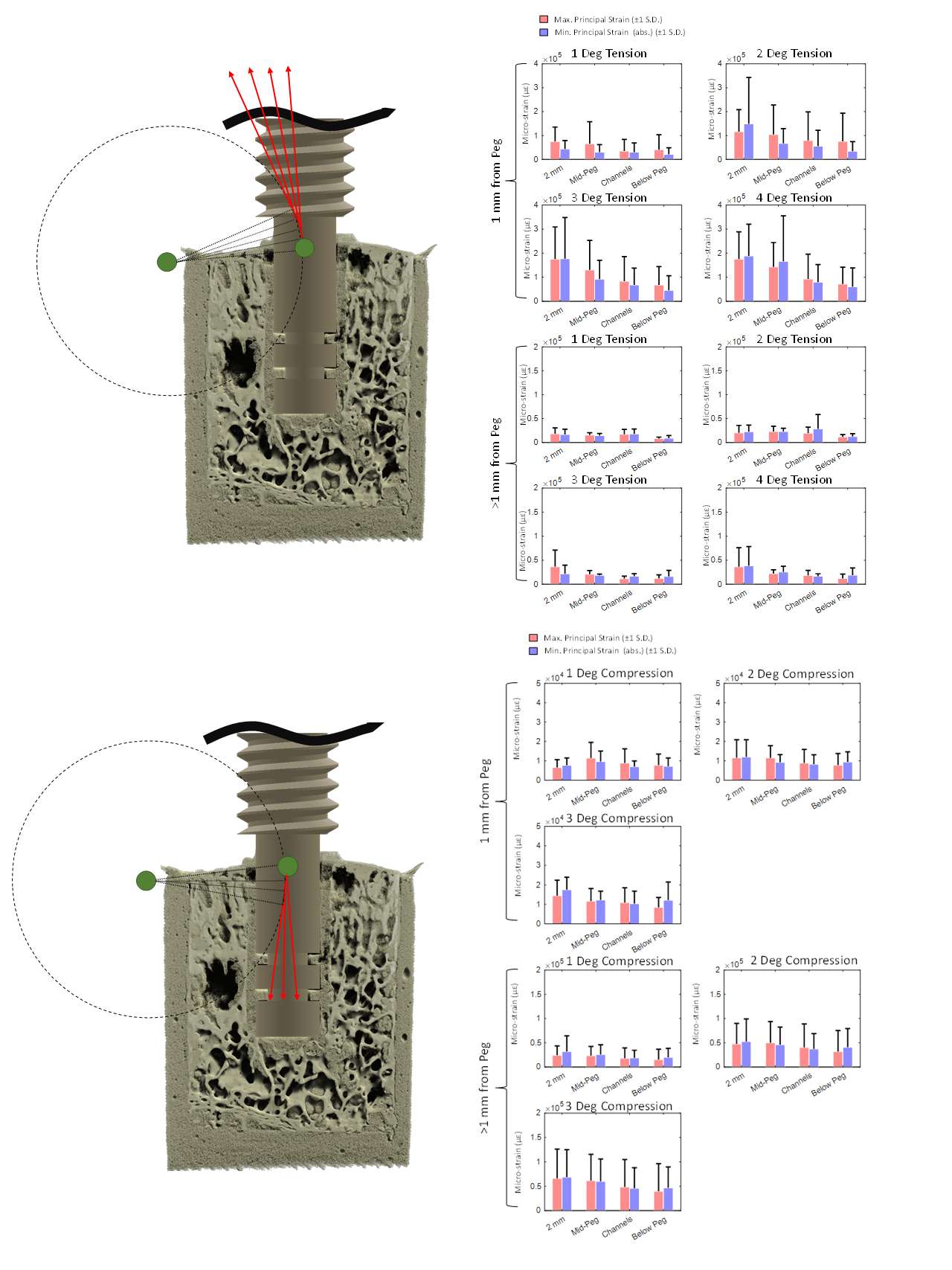
Figure 3#7812
3D Strain Analysis of Osteoarthritic Trabecular Bone Within the Humeral Head Subjected to Stepwise Compressive Loads
Jakub Targosinski - University of Western Ontario - London, Canada
Jonathan Kusins - The University of Western Ontario - London, Canada
Nikolas Knowles - University of Waterloo - Waterloo, Canada
*Louis Ferreira - University of Western Ontario - London, Canada
Melanie Columbus - The University of Western Ontario - London, Canada
George Athwal - University of Western Ontario - London, Canada
*Email: Lferreir@uwo.ca
Introduction:
To improve clinical outcomes of total shoulder arthroplasty, recent interest has grown in the design of stemless humeral head components that require less bone removal. Recent work has focused on quantifying the apparent mechanical properties of trabecular bone from patients with end-stage osteoarthritis (OA) in the humeral head [1,2]. However, local load carrying characteristics of trabecular bone within OA humeral heads is still poorly understood. Recent developments in experimental methods and high-resolution volumetric imaging combined with digital volume correlation (DVC) have been used to quantify in-situ the magnitude of full-field 3D strain that vertebral bone can withstand prior to macroscopic failure [3] but has yet to be conducted to investigate the local failure properties of trabecular bone within the normal or osteoarthritic humeral head. This study aimed to quantify the local load carrying characteristics of OA humeral head trabecular bone.
Methods:
Six osteoarthritic humeral osteotomies were harvested from patients that had undergone TSA. Stepwise mechanical testing was performed within a microCT scanner (Nikon XT H 225ST). A seven-pegged acrylic indenter applied mechanical loads to the resection surface of the osteotomies. Stepwise compressive loads at 250N increments were applied with scans acquired at every increment until macroscopic failure was visualized. DVC was used to quantify full-field strains immediately prior to macroscopic fracture (Fig. 1).
Seven regions of interest were defined underneath each of the indenter pegs. Morphometric parameters (bone volume fraction (BV/TV), trabecular thickness (Tb.Th), trabecular separation (Tb.Sp), trabecular number (Tb.N), and degree of anisotropy (DA)) were calculated for each ROI. Each ROI was classified as either a fracture or non-fracture ROI. Third principal strains between the groups (fracture vs. non-fracture) were compared using a Mann-Whitney U test. To determine if bone morphometric parameters influenced an ROI eventually fracturing, a binomial logistic regression was performed.
Results:
Third principal strains were significantly higher (p < 0.001) in ROIs that fractured (third principal strain: median = -6,511 µstrain, 95th percentile = -12,558 µstrain) compared to ROIs that did not fracture (third principal strain: median = -2,944 µstrain, 95th percentile = -7,806 µstrain) (Fig. 2). Of the five predictor morphometric parameters tested, BV/TV, Tb.Sp and Tb.N were significant (p ≤ 0.037) at predicting fracture (Fig. 3). BV/TV best predicted fracture or non-fracture (p = 0.001) with an accuracy classification rate of 81%.
Conclusion:
This study quantified in-situ 3D mechanical strain distributions throughout the trabecular structure within end-stage OA humeral heads. We measured magnitudes of third principal strain up to -22,000 µstrain with a 95th percentile strain of -12,558 µstrain for trabecular bone ROIs that eventually fractured. We found that when considering if the trabecular bone morphometric parameters were predictive of trabecular fracture or non-fracture, BV/TV was statistically significant (p = 0.019) with a critical threshold of 20.01 and a correct prediction rate of 81%. Therefore, to maximize longevity of the implant interface, trabecular regions with low BV/TV should be avoided.
References: [1] Zdravkovic et al. J. Orthop. Res. 2020. [2] Knowles et al. J. Orthop. Res 2020. [3] Tozzi et al. Strain 2016.
Figures
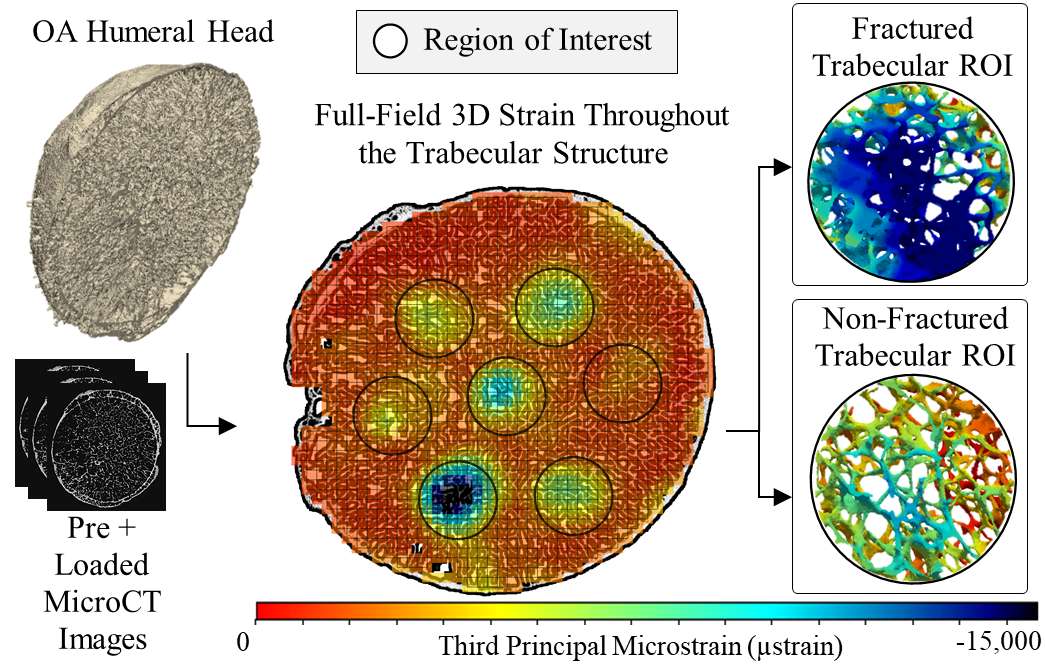
Figure 1
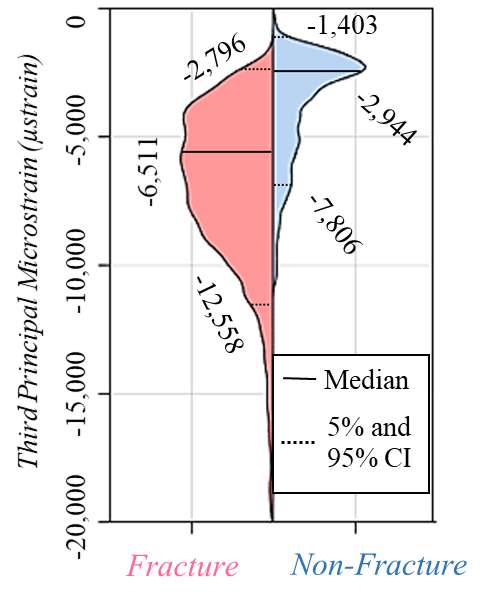
Figure 2
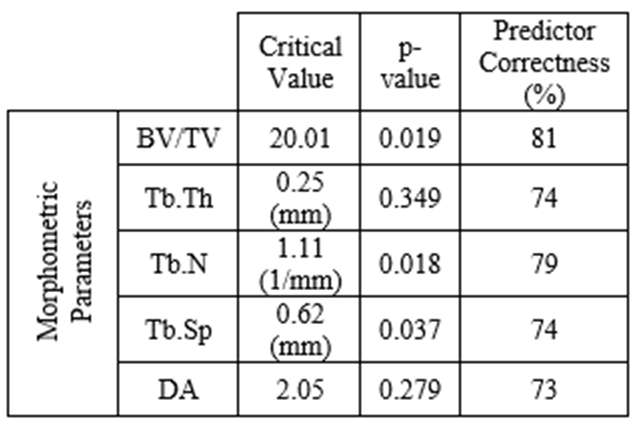
Figure 3#7821
Effect of Metal and Ceramic Artifacts on Digital Volume Correlation Strain Measurements in Cadaveric Shoulder Hemiarthroplasty Models
Jakub Targosinski - University of Western Ontario - London, Canada
Jonathan Kusins - The University of Western Ontario - London, Canada
*Louis Ferreira - University of Western Ontario - London, Canada
Andrew Nelson - The University of Western Ontario - London, Canada
*Email: Lferreir@uwo.ca
Introduction
Glenoid erosion following shoulder hemiarthroplasty remains a large concern in young and active patients not suitable for total shoulder arthroplasty. The mechanism which is thought to drive the accelerated erosion of the glenoid in shoulder hemiarthroplasty is thought to be at least in part a function of the differential mechanical stiffness between natural bone and the material of the humeral head implant. A combination of digital volume correlation (DVC) and high resolution micro-computed tomography imagery can potentially be used to analyse this mechanism and the advantages of new advances in humeral head materials which aim to alleviate glenoid erosion. However, common humeral head implant materials cause significant imaging artifacts which can affect the measurement error associated with DVC in this application; this measurement error must first be quantified before study of various humeral implant materials and their role in glenoid erosion following shoulder hemiarthroplasty. This study aims to quantify the measurement error of DVC applied to micro-CT imagery of cadaveric scapulae interfacing with a ceramic and CoCrMo humeral head.
Methods
A single denuded cadaveric scapula was placed inside a cone-beam micro-CT scanner and was imaged in contact with a ceramic humeral head and a CoCrMo humeral head (Fig. 1.). A reference image of the scapula was also captured without either humeral head implant. A zero-strain DVC uncertainty analysis was performed on the scans captured, and the strain measurement error was quantified as a function of the spatial resolution of the measurement. The relationship between the strain measurement error and the measurement distance from the humeral head implant was also quantified.
Results
Strain mean absolute error (MAE) and standard deviation of error (SDE) began to significantly increase (p<0.001) at a mean distance of 0.69mm and 0.86mm from the CoCrMo humeral head implant and the ceramic humeral head implant, respectively (Fig. 2). DVC correlation values first began to significantly (p<0.001) decline at a mean distance of 1.25mm and 0.86mm from the CoCrMo humeral head implant and the ceramic humeral head implant, respectively (Fig. 3). At a DVC strain measurement spatial resolution of 1.072mm, the MAE and SDE were (MAE=811.6µε, SDE=2574µε) in the CoCrMo humeral head and (MAE=541.8µε, SDE=534.1µε) in the ceramic humeral head.
Conclusion
There was a significant relationship between distance from implant humeral head and measurement MAE and SDE. This relationship also existed in DVC correlation values. This indicates that there is an important effect of image artifacts on DVC strain measurements that must be considered before using DVC in a shoulder hemiarthroplasty glenoid application. However, this effect became only significantly pronounced at distances of ~1mm from each implant humeral head, indicating that only bone structures very close to the implant humeral head are strongly effected by the image artifacts, and DVC strain measurements made elsewhere are still sound. Moreover, the magnitude of measurement error is low enough that the DVC+micro-CT strain measurement technique is feasible to study physiologically relevant strains that may have a significant impact on the differential erosion of glenoids in varied humeral head implant materials.
Figures
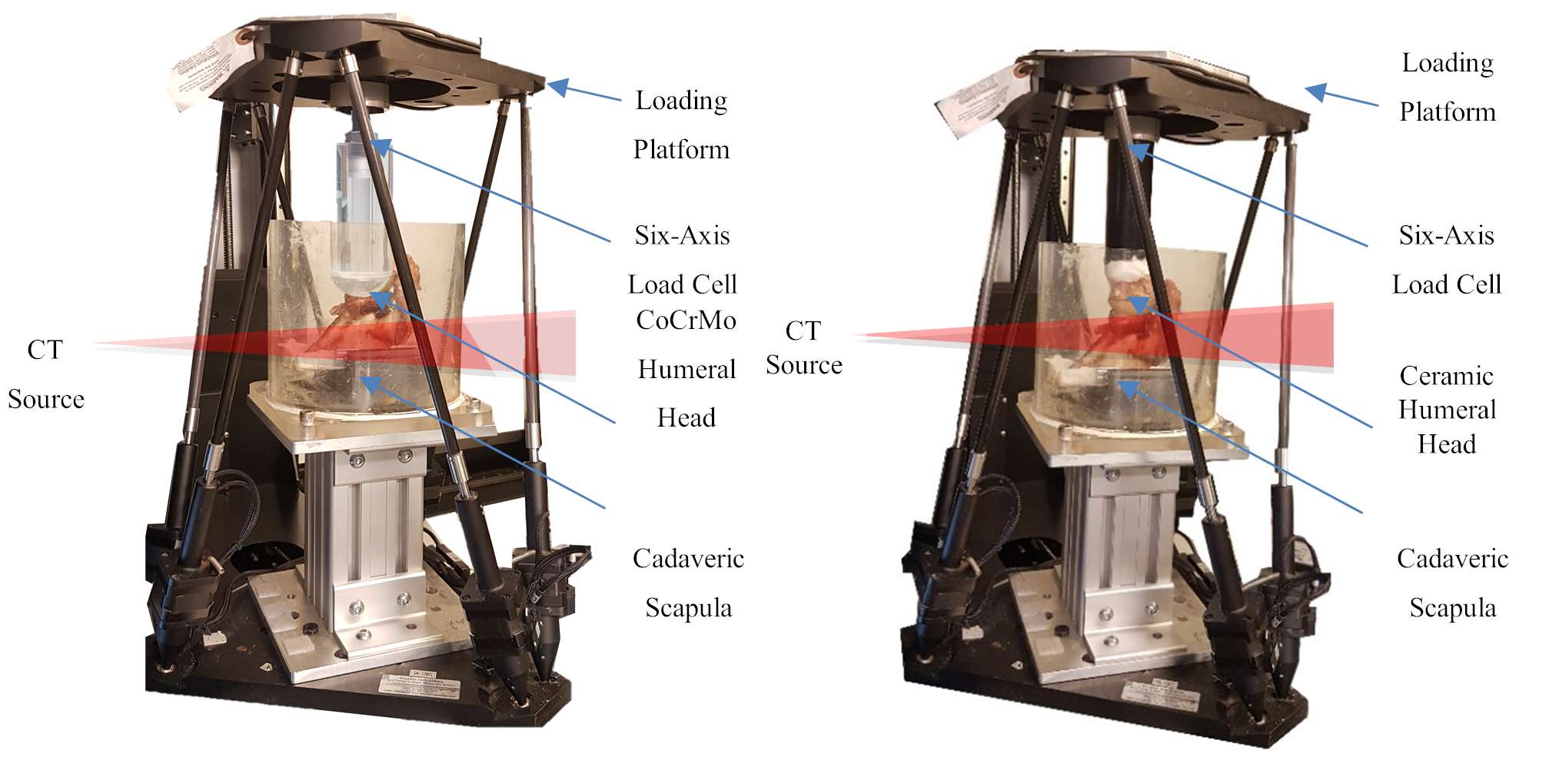
Figure 1
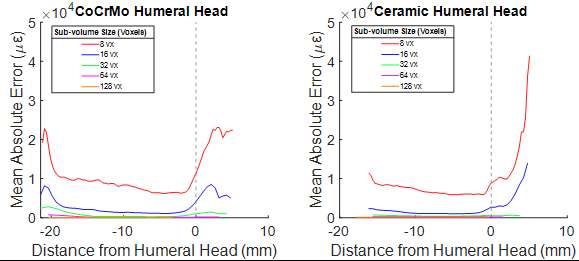
Figure 2
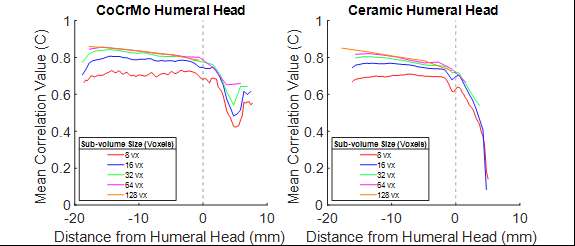
Figure 3#7318
Evaluation of a Proof-of-Concept Platform for Markerless Robot-Assisted Orthopaedic Surgery
*Fabio Tatti - Imperial College London - London, GB
Xue Hu - Imperial College London - London, United Kingdom
Matteo Bermond - Imperial College London - London, United Kingdom
Ferdinando Rodriguez-Y-Baena - Imperial College London - London, United Kingdom
*Email: f.tatti@imperial.ac.uk
Introduction: Robot-Assisted Orthopaedic surgery is gaining popularity as a tool that promises to increase the accuracy and repeatability of implant placement and provide quantitative real-time intraoperative metrics. Patient registration is a crucial step that currently requires substantial manual intervention. Furthermore, most current systems rely on reflective markers that need to be rigidly drilled into the patient’s bone, increasing the risk of infection or fracture. Markerless registration and tracking using 3D RGBD cameras could substantially reduce the amount of manual intervention and eliminate the need for rigidly attached markers. This work presents and evaluates a proof-of-concept demonstration where markerless tracking is used to guide a robotic system towards target poses on a phantom knee model.
Methods: The experimental setup is shown in Fig.1. A Microsoft Kinect Azure DK camera was mounted on a custom 3D printed tool attached to a robotic arm. Deep learning-based algorithms were used to identify the distal femur from real-time RGBD frames (Fig.2a). A preoperative patient-specific model was then registered to the detected points using ICP, and the current femur pose was displayed to the user in a virtual environment (Fig. 2b). A target position and orientation on the femur surface were selected preoperatively and a virtual visuohaptic guide was placed on the model (Fig. 2b). Movements of the tool were controlled by the user through a haptic interface, which also provided active force feedback when the tool touched the virtual guide, helping the user reach the desired pose. An Atracsys fusionTrack 500 optical tracker was used to obtain gold standard reference poses of the phantom limb and custom tool and evaluate the accuracy of the system.
Results: The accuracy of the system was evaluated at 6 different target poses. For each pose, the user guided the robot to the desired target and manually indicated completion. The pose of the surgical tool relative to the phantom limb was then recorded and compared to the surgical plan, to evaluate accuracy. The overall results are shown in Fig. 3. The Root Mean Squared (RMS) translational error was 12.1 mm in the mediolateral direction, 20.2 mm in the anterior-posterior direction, and 2.9 mm in the superior-inferior direction. The RMS orientation error was 5.3°.
Conclusion: This study successfully demonstrates the use of markerless patient tracking and registration for robot guidance, in a controlled laboratory setting. While the level of accuracy in this preliminary study is not yet sufficient for surgical applications, several steps can be taken to improve the system. Firstly, good visibility of the distal femur is crucial, and decoupling the camera from the surgical tool would allow to move the camera independently and optimise its point of view in real time. Secondly, previous studies have shown that bounded-ICP can improve the accuracy of registration, compared to standard ICP [1]. Finally, the accuracy of the robotic platform itself affects the results and could be improved by reducing its workspace and recalibrating the robot in the region of interest.
References:
[1] Hu et al., IEEE Tran Inst Meas, vol. 71, 2021
Figures
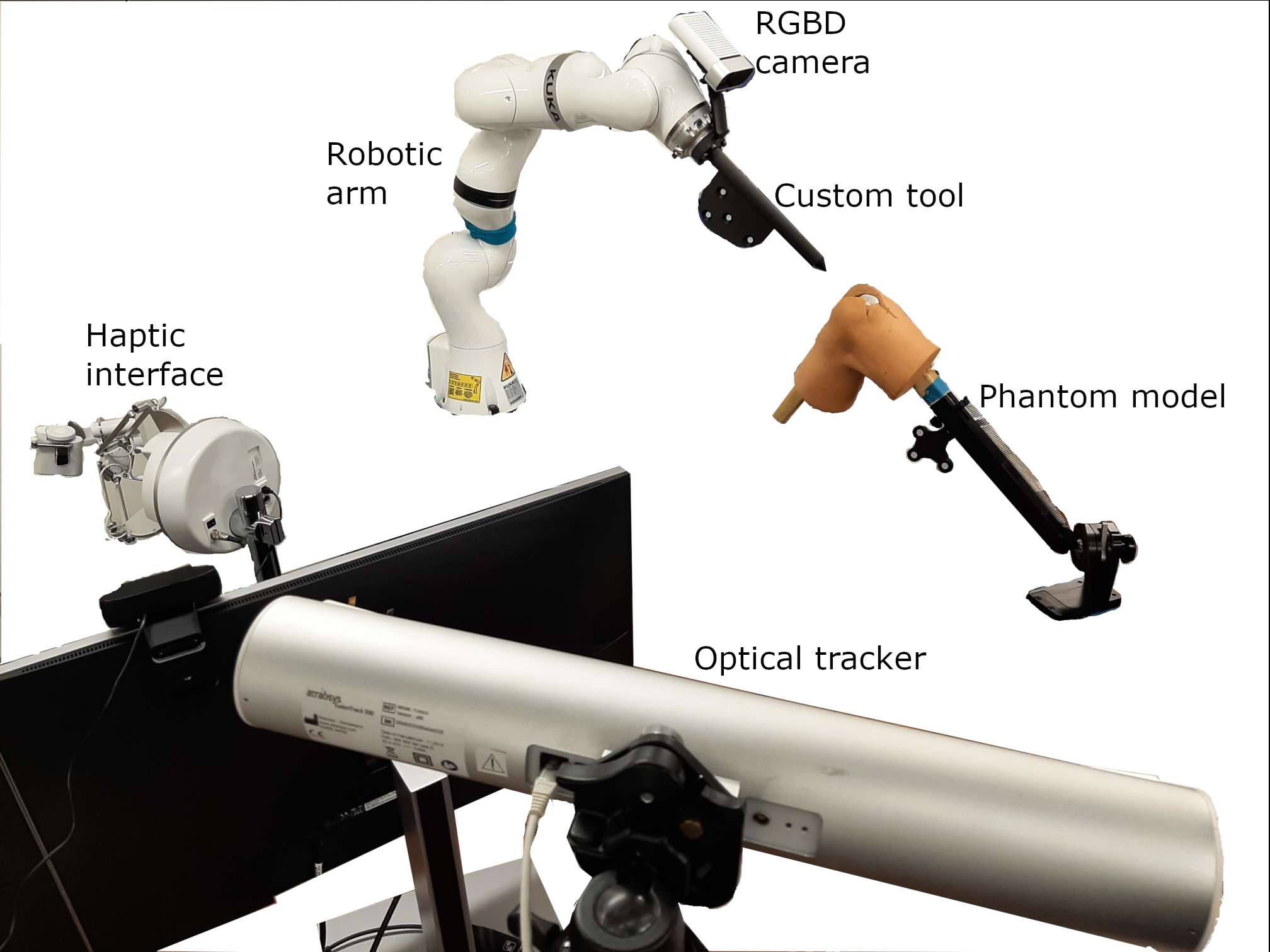
Figure 1
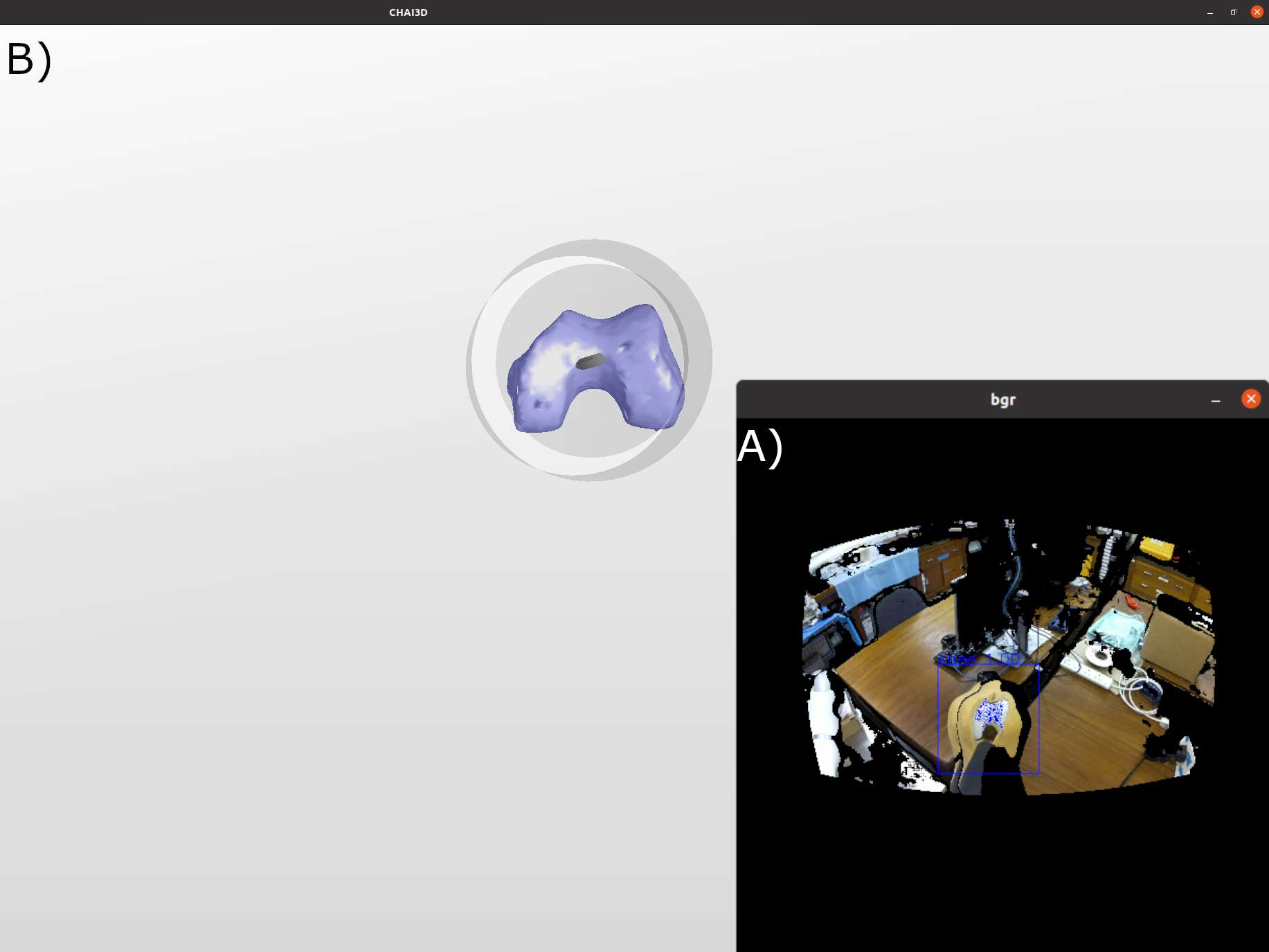
Figure 2
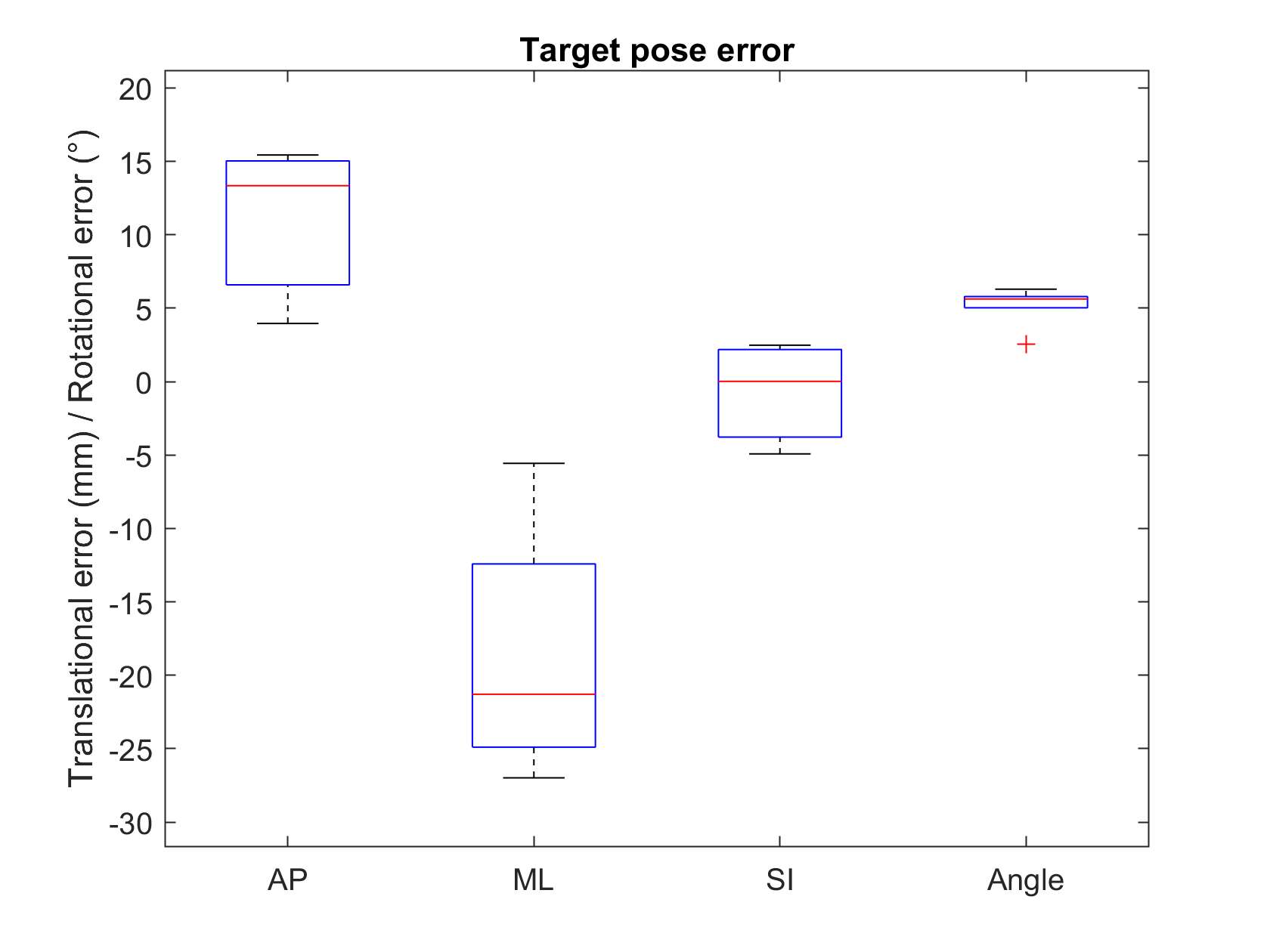
Figure 3#7944
What Patient and Implant Factors Affect Trunnionosis Severity? an Implant Retrieval Analysis of 664 Femoral Stems
*Mathew G Teeter - Schulich School of Medicine and Dentistry, Western University and London Health Sciences Centre - London, Canada
Anastasia Codirenzi - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
*Email: matthew.teeter@lhsc.on.ca
What patient and implant factors affect trunnionosis severity?
An implant retrieval analysis of 664 femoral stems
Anastasia M. Codirenzi1, Brent A. Lanting1, Matthew G. Teeter1
- School of Biomedical Engineering, Western University, London, Ontario, Canada
- Division of Orthopaedic Surgery, Department of Surgery, Schulich School of Medicine & Dentistry, Western University, London, Ontario, Canada
- Department of Medical Biophysics, Schulich School of Medicine & Dentistry, Western University, London, Ontario, Canada
Corresponding author:
Matthew G. Teeter, PhD
Western University
1151 Richmond Street
London, ON N6A 3K7
matthew.teeter@uwo.ca
Abstract
Background: Corrosion at the modular head-neck taper interface of total and hemiarthroplasty hip implants (trunnionosis) is a cause of implant failure and thus a clinical concern. Patient and device factors contributing to the occurrence of trunnionosis have been investigated in prior implant retrieval studies, but generally with limited sample sizes and a narrow range of models. The purpose of the present investigation was to determine which patient and device factors were associated with corrosion damage on the femoral stem taper across a large collection of different implant models retrieved following revision hip arthroplasty.
Methods: A retrieval study of 664 hip arthroplasty modular stem components was performed. Patient and device information was collected. Trunnions were imaged under digital microscopy and scored for corrosion damage using the Goldberg scale. Damage was related to patient and device factors using regression analysis.
Results: Greater duration of implantation (p = 0.005) and larger head size (p < 0.001) were associated with an elevated corrosion class. Older age at index surgery (p = 0.035), stainless steel stem material (p = 0.022), indication for revision as bone or periprosthetic fracture (p = 0.017) and infection (p = 0.018), and certain larger taper geometries were associated with a decreased corrosion class.
Conclusions: Factors identified as contributing to a higher or lower risk of more severe corrosion are consistent with most prior smaller retrieval studies. Surgeons should be aware of these risk factors when selecting implants for their patients, and when diagnosing trunnionosis in symptomatic hip replacement patients.
Introduction
Modularity in modern hip arthroplasty implant designs enable surgeons to closely match the original anatomy of the patient [1]. Most devices provide modularity at the head-neck interface using a Morse taper, where the head and trunnion are attached using an interface fit [2]. The disadvantage of modularity is the potential for fretting and corrosion to occur due to the biomechanical forces acting at the head-neck taper junction [3]. This can produce debris in the form of metal ions, particles, and other corrosion products [4]. The presence of this debris can cause adverse local tissue reactions [5]. The corrosion process, termed trunnionosis, has been identified as a cause of hip arthroplasty failure and thus a clinical concern [6–8]. Corrosion-related soft-tissue reactions may potentially be overlooked and misdiagnosed as recurrent instability or infection [9]. Therefore, understanding potential risk factors for the development of trunnionosis can assist surgeons in making a proper diagnosis.
Implant retrieval studies have had an important role in identifying a variety of implant and patient factors that contribute to trunnionosis, including head material, taper design, implantation time, femoral offset, body mass index (BMI), and taper rigidity [10–16]. However, such studies have made these observations from a limited number of devices sampled from select manufacturers. At most, these studies have included 252 femoral heads with 148 femoral tapers, with some studies including as few as 46 implants [13,16]. In contrast, large-scale implant retrieval studies examining other device failure modes such as polyethylene wear have provided a more rigorous assessment of the variables contributing to implant damage [17].
The purpose of the present investigation was to determine which patient and device factors were associated with corrosion damage on the femoral stem taper across different implant models retrieved following revision hip arthroplasty.
Methods
Study population
Institutional research ethics board approval was obtained for review of patient charts and implant retrieval analysis. All hip implants in our institutional implant retrieval laboratory were reviewed for inclusion (Figure 1). Implants included for analysis were designs with a modular head-neck taper where the femoral head and stem were retrieved at the time of revision surgery. Excluded were implants that were non-modular, cases where the femoral stem was not retrieved or had gross taper failure, and when there was fewer than five instances of a particular femoral stem model. Patient information including sex, age at implantation, hip joint laterality (left or right), reason for revision, and length of stem implantation were obtained from chart review. Implant information including taper design, stem material, head material, head size, stem model, and manufacturer was collected from the institutional implant retrieval laboratory catalogue and analysis of the device.
Visual scoring
Each stem was imaged using a digital microscope at 20x magnification (DSX1000, Olympus Corporation, Tokyo, Japan). The surface was divided into four areas each represented by one image. The images (Figure 2) were then examined and assigned a corrosion score using the method of Goldberg et al. [18], described in Table 1. A single score was assigned to each image and recorded; the maximum score observed on the implant from the four sides of the taper was used as the score for statistical analysis.
Statistical analysis
Ordinal logistic regression was used to compare the maximum observed trunnion corrosion score with the gathered device and patient factors. Odds ratios (OR) were calculated to by exponentiating the parameter estimates of the final ordinal logistic regression model.
Possible interactions between patient and device factors identified in the ordinal logistic regression were further investigated. A Shapiro-Wilk test was used to determine normality. Accordingly, the Kruskal-Wallis one-way ANOVA was used to delineate differences in the factors with an alpha-value of 0.05. Data analysis was performed using IBM SPSS for Windows OS, version 28.0.1.1 and Prism 9 for Windows, version 9.3.1.
Results
In total, 664 implants were included in the analysis. Mean patient age at original implantation was 66 years (range, 23 to 97 years). Most patients were female (51.3%, n = 339) and most were right hips (57%, n = 376). The mean length of implantation was 5 years (range, <1 to 24 years). Reasons for revision included bone and periprosthetic fracture (19.3%, n = 127), implant fracture (2.0%, n = 13), infection (37.9%, n = 249), instability (3.7%, n = 24), metal debris reaction (3.0%, n = 20), polyethylene wear, osteolysis and aseptic loosening (32.4%, n = 213), and undifferentiated pain (1.7%, n = 11). Details on the implants included in the analysis are shown in Table 2.
The ordinal logistic regression revealed length of implantation, age at implantation, reason for revision, head size, stem material, and taper design to be significant factors associated with the severity of corrosion class, as shown in Table 3.
For patient factors, increasing length of implantation was associated with a greater probability of elevated corrosion class (OR 1.049, p = 0.005), while increasing patient age at implantation was associated with a lower probability of elevated corrosion class (OR 0.985, p = 0.035). Two reasons for revision were associated with a lower probability of elevated corrosion class: bone or periprosthetic fracture (OR 0.230, p = 0.017) and infection (OR = 0.238, p = 0.018).
For device factors, increasing head size was associated with a greater probability of elevated corrosion class (OR = 1.096, p < 0.001). Stainless steel stem material was associated with a lower probability of elevated corrosion class (OR = 0.362, p = 0.022). Five taper geometries were associated with a lower probability of elevated corrosion class: D12/14 (OR = 0.120, p = 0.001), D14/16 (OR = 0.061, p = 0.003), PCA (OR = 0.043, p < 0.001), S12/14 (OR = 0.254, p = 0.030), and Z12/14 (OR = 0.273, p = 0.045).
There were two interactions between patient and device factors. Length of implantation varied between reasons for revision (p < 0.001) with median implantation times of 1.1 years for infection, 1.1 years for instability, 3.2 years for bone and periprosthetic fracture, 5.2 years for undifferentiated pain, 5.3 years for metal debris reactions, 6.1 years for implant fracture, and 7.1 years for wear/osteolysis/loosening. Head size varied between stem material (p < 0.001) with median head size of 28 mm for the cobalt-chromium and stainless-steel stems, and 32 mm for the titanium stems.
Discussion
Trunnionosis and the potential for adverse local tissue reactions remains an area of concern for modular hip arthroplasty devices. Although prior implant retrieval studies have identified multiple risk factors associated with trunnionosis (Table 4), these studies have generally examined only specific models of devices with low population numbers (typically below 150 implants). The purpose of this study was to determine which patient and device factors were associated with corrosion damage on the femoral stem taper across different implant models retrieved following revision hip arthroplasty. With 664 femoral stems examined for corrosion severity, this is the largest implant retrieval study of its kind.
Longer implantation duration (time in vivo) was associated with higher corrosion scores. This finding is consistent with prior literature [11,13–16,27]. With increased time implanted, there is more time for corrosion to occur. This is furthered by shear stresses and mechanically assisted wear, such as crevice corrosion, that has been associated with repeated load cycling [28].
Greater age at the time of implantation was associated with lower corrosion scores. This finding is inconsistent with a prior study by Tan et al., who found no difference, but consistent with a study by Siljander et al., who also found that older patients had lower corrosion [11,21]. Younger patients would potentially have had an implant for a longer time before revision and may be more active than older patients, increasing stress on the modular head-neck taper junction. Younger patients would also be more likely to receive a cementless cobalt-chromium or titanium femoral stem than a cemented stainless-steel stem, where stainless steel material was also associated with lower corrosion scores in the present study.
Infection and bone and periprosthetic fracture as the reason for revision were associated with lower corrosion scores. Prior studies have not reported on reason for revision as being associated with corrosion. Stems within the infection and bone and periprosthetic fracture groups had some of the lowest durations of implantation in the study, and length of implantation was associated with corrosion severity. However, instability also had a low implantation time, but was not significantly associated with lower corrosion scores, albeit with a p value approaching significance (p = 0.070). Instability may affect the stresses at the head-neck taper junction causing increased mechanical wear and contributing to a higher corrosion score even with less time implanted. Conversely, corrosion and local debris could cause the soft tissue damage and subsequent dislocation.
Larger head sizes were associated with higher corrosion scores. This finding is consistent with prior literature [12]. This has previously been attributed to larger heads having a greater torque acting along the taper junction during daily activity, leading to more micromotion and increased deterioration of the passive oxide film.
Certain taper designs were associated with lower corrosion scores. Prior studies have found a difference in corrosion severity between taper designs, with smaller tapers having greater corrosion than larger tapers (e.g. 11/13 versus 12/14 tapers, where the numbers refer to the proximal and distal diameter of the trunnion, respectively) but this finding has been inconsistent, with Brock et al. claiming the opposite on a single-manufacture study [10,23,25,27,29]. In the current study, 12/14 tapers from several manufacturers were associated with lower corrosion scores. Although all are labelled as 12/14 tapers, it is important to note that the cone angle and trunnion length differ between them. Two additional taper deigns, both larger than the 12/14 tapers, were also associated with lower corrosion scores. Having a smaller taper geometry with a smaller contact surface may increase the stress concentrations within the head-neck taper junction.
Previous studies have identified head material as a significant contributing factor to corrosion, but that factor was not found to be significant in this study [11,19,26]. Since 93% of heads in this study were cobalt-chromium, this likely affected the model as there was little representation of other head materials. Weight has previously been reported as a significant factor in increased corrosion by Higgs et al., but Tan et al. has reported that BMI is not [11,13]. As height, weight, and BMI data was missing for a large portion of the retrieved stems, these variables were not examined in the present study.
A limitation of this study is that we were unable to include head offset due to lack of information in implant database systems and inconsistent presence of offset printed on the physical components. This factor has been identified as contributing to greater corrosion scores [13]. Similarly, we did not examine flexural rigidity [30]. We scored only corrosion and not fretting, but the two scores are related. Although with 664 femoral stems examined this is a large study including many different implant models and manufacturers, it reflects a single institution and does not include every device available on the market. A subset of the implants examined were also included in previously published retrieval studies by our group, although we have included a discussion of literature from multiple institutions. We assessed damage visually with the common Goldberg score and did not directly measure volumetric changes to the stem tapers, which might yield different results [31]. This study should be considered as confirmation of the findings of prior retrieval studies using visual damage scoring, which are only one important piece of the puzzle alongside quantitative retrieval studies and in vitro investigations of corrosive behavior. Finally, all implant retrieval studies examine failed implants and may not be entirely representative of well-performing devices that have not been revised.
In this large-scale study, the first of its size for retrieved hip arthroplasty devices, length of implantation time, age at implantation, reason for revision, head size, and taper design were found to have a significant effect on corrosion score. These findings are generally supportive of prior implant retrieval studies that examined fewer implants. Surgeons should be aware of these risk factors when choosing femoral stems and heads for their patients, and in diagnosing trunnionosis in patients presenting with complaints after surgery.
Acknowledgements
The authors would like to thank Dr James Howard, Dr Robert Bourne, Dr Steven MacDonald, Dr Richard McCalden, Dr Douglas Naudie, Dr Cecil Rorabeck, and Dr Edward Vasarhelyi for their contribution. Anastasia M. Codirenzi is supported by a Transdisciplinary Bone and Joint Training Award. This study was supported in part by a Discovery Grant from the Natural Sciences and Engineering Research Council of Canada.
References
[1] Vierra BM, Blumenthal SR, Amanatullah DF. Modularity in total hip arthroplasty: Benefits, risks, mechanisms, diagnosis, and management. Orthopedics 2017;40:355–66. https://doi.org/10.3928/01477447-20170606-01.
[2] Hernigou P, Queinnec S, Flouzat Lachaniette CH. One hundred and fifty years of history of the Morse taper: from Stephen A. Morse in 1864 to complications related to modularity in hip arthroplasty. International Orthopaedics 2013;37:2081. https://doi.org/10.1007/S00264-013-1927-0.
[3] Lavernia CJ, Iacobelli DA, Villa JM, Jones K, Gonzalez JL, Jones WK. Trunnion–Head Stresses in THA: Are Big Heads Trouble? The Journal of Arthroplasty 2015;30:1085–8. https://doi.org/10.1016/J.ARTH.2015.01.021.
[4] Shulman RM, Zywiel MG, Gandhi R, Davey JR, Salonen DC. Trunnionosis: the latest culprit in adverse reactions to metal debris following hip arthroplasty. Skeletal Radiology 2015;44:433–40. https://doi.org/10.1007/S00256-014-1978-3/FIGURES/10.
[5] Cooper HJ, della Valle CJ, Berger RA, Tetreault M, Paprosky WG, Sporer SM, et al. Corrosion at the Head-Neck Taper as a Cause for Adverse Local Tissue Reactions After Total Hip Arthroplasty. The Journal of Bone and Joint Surgery American Volume 2012;94:1655. https://doi.org/10.2106/JBJS.K.01352.
[6] Berstock JR, Whitehouse MR, Duncan CP. Trunnion corrosion: What surgeons need to know in 2018. Bone and Joint Journal 2018;100B:44–9. https://doi.org/10.1302/0301-620X.100B1.BJJ-2017-0569.R1/ASSET/IMAGES/LARGE/BJJ-2017-0569.R1-GALLEYFIG1.JPEG.
[7] Banerjee S, Cherian JJ, Bono J v., Kurtz SM, Geesink R, Meneghini RM, et al. Gross Trunnion Failure After Primary Total Hip Arthroplasty. The Journal of Arthroplasty 2015;30:641–8. https://doi.org/10.1016/J.ARTH.2014.11.023.
[8] Hussenbocus S, Kosuge D, Solomon LB, Howie DW, Oskouei RH. Head-Neck Taper Corrosion in Hip Arthroplasty. BioMed Research International 2015;2015. https://doi.org/10.1155/2015/758123.
[9] Bijukumar DR, Segu A, Souza JCM, Li XJ, Barba M, Mercuri LG, et al. Systemic and local toxicity of metal debris released from hip prostheses: A review of experimental approaches. Nanomedicine 2018;14:951–63. https://doi.org/10.1016/J.NANO.2018.01.001.
[10] Tan SC, Teeter MG, del Balso C, Howard JL, Lanting BA. Effect of Taper Design on Trunnionosis in Metal on Polyethylene Total Hip Arthroplasty. The Journal of Arthroplasty 2015;30:1269–72. https://doi.org/10.1016/J.ARTH.2015.02.031.
[11] Tan SC, Lau ACK, del Balso C, Howard JL, Lanting BA, Teeter MG. Tribocorrosion: Ceramic and Oxidized Zirconium vs Cobalt-Chromium Heads in Total Hip Arthroplasty. The Journal of Arthroplasty 2016;31:2064–71. https://doi.org/10.1016/J.ARTH.2016.02.027.
[12] Dyrkacz RMR, Brandt JM, Ojo OA, Turgeon TR, Wyss UP. The influence of head size on corrosion and fretting behaviour at the head-neck interface of artificial hip joints. J Arthroplasty 2013;28:1036–40. https://doi.org/10.1016/J.ARTH.2012.10.017.
[13] Higgs GB, Macdonald DW, Gilbert JL, Rimnac CM, Kurtz SM. Basic Science Does Taper Size Have an Effect on Taper Damage in Retrieved Metal-on-Polyethylene Total Hip Devices? The Journal of Arthroplasty 2016;31:277–81. https://doi.org/10.1016/j.arth.2016.06.053.
[14] Hothi HS, Eskelinen AP, Berber R, Lainiala OS, Moilanen TPS, Skinner JA, et al. Factors Associated With Trunnionosis in the Metal-on-Metal Pinnacle Hip. J Arthroplasty 2017;32:286–90. https://doi.org/10.1016/J.ARTH.2016.06.038.
[15] del Balso C, Teeter MG, Tan SC, Lanting BA, Howard JL. Does the Additional Articulation in Retrieved Bipolar Hemiarthroplasty Implants Decrease Trunnionosis Compared to Total Hip Arthroplasty? The Journal of Arthroplasty 2018;33:268–72. https://doi.org/10.1016/J.ARTH.2017.08.027.
[16] del Balso C, Teeter MG, Tan SC, Howard JL, Lanting BA. Trunnionosis: Does Head Size Affect Fretting and Corrosion in Total Hip Arthroplasty? The Journal of Arthroplasty 2016;31:2332–6. https://doi.org/10.1016/J.ARTH.2016.03.009.
[17] Currier JH, Currier BH, Abdel MP, Berry DJ, Titus AJ, van Citters DW. What factors drive polyethylene wear in total knee arthroplasty? Https://DoiOrg/101302/0301-620X103B11BJJ-2020-2334R1 2021;103-B:1695–701. https://doi.org/10.1302/0301-620X.103B11.BJJ-2020-2334.R1.
[18] Goldberg JR, Gilbert JL, Jacobs JJ, Bauer TW, Paprosky W, Leurgans S. A multicenter retrieval study of the taper interfaces of modular hip prostheses. Clinical Orthopaedics and Related Research 2002;401:149–61. https://doi.org/10.1097/00003086-200208000-00018.
[19] El-Zein ZS, Gehrke CK, Croley JS, Siljander MP, Mallow MA, Flierl MA, et al. Assessing Taper Geometry, Head Size, Head Material, and Their Interactions in Taper Fretting Corrosion of Retrieved Total Hip Arthroplasty Implants. The Journal of Arthroplasty 2021;36:S386-S394.e4. https://doi.org/10.1016/J.ARTH.2021.02.041.
[20] Hampton C, Weitzler L, Baral E, Wright TM, Bostrom MPG. Do oxidized zirconium heads decrease tribocorrosion in total hip arthroplasty? Https://DoiOrg/101302/0301-620X101B4BJJ-2018-1316R1 2019;101 B:386–9. https://doi.org/10.1302/0301-620X.101B4.BJJ-2018-1316.R1.
[21] Siljander MP, Baker EA, Baker KC, Salisbury MR, Thor CC, Verner JJ. Fretting and Corrosion Damage in Retrieved Metal-on-Polyethylene Modular Total Hip Arthroplasty Systems: What Is the Importance of Femoral Head Size? The Journal of Arthroplasty 2018;33:931–8. https://doi.org/10.1016/J.ARTH.2017.10.010.
[22] Lange J, Wach A, Koch CN, Hopper RH, Ho H, Engh CA, et al. Do Well-functioning THAs Retrieved at Autopsy Exhibit Evidence of Fretting and Corrosion? Clinical Orthopaedics and Related Research 2018;476:2017. https://doi.org/10.1097/CORR.0000000000000369.
[23] Triantafyllopoulos GK, Elpers ME, Burket JC, Esposito CI, Padgett DE, Wright TM. Otto Aufranc Award: Large Heads Do Not Increase Damage at the Head-neck Taper of Metal-on-polyethylene Total Hip Arthroplasties. Clinical Orthopaedics and Related Research 2016;474:330. https://doi.org/10.1007/S11999-015-4468-6.
[24] Higgs GB, MacDonald DW, Gilbert JL, Rimnac CM, Kurtz SM, Chen AF, et al. Does Taper Size Have an Effect on Taper Damage in Retrieved Metal-on-Polyethylene Total Hip Devices? The Journal of Arthroplasty 2016;31:277–81. https://doi.org/10.1016/J.ARTH.2016.06.053.
[25] Brock TM, Sidaginamale R, Rushton S, Nargol AVF, Bowsher JG, Savisaar C, et al. Shorter, rough trunnion surfaces are associated with higher taper wear rates than longer, smooth trunnion surfaces in a contemporary large head metal-on-metal total hip arthroplasty system. Journal of Orthopaedic Research 2015;33:1868–74. https://doi.org/10.1002/JOR.22970.
[26] Kurtz SM, Kocagöz SB, Hanzlik JA, Underwood RJ, Gilbert JL, MacDonald DW, et al. Do Ceramic Femoral Heads Reduce Taper Fretting Corrosion in Hip Arthroplasty? A Retrieval Study. Clinical Orthopaedics and Related Research 2013;471:3270. https://doi.org/10.1007/S11999-013-3096-2.
[27] Tan SC, Teeter MG, del Balso C, Howard JL, Lanting BA. Effect of Taper Design on Trunnionosis in Metal on Polyethylene Total Hip Arthroplasty. The Journal of Arthroplasty 2015;30:1269–72. https://doi.org/10.1016/J.ARTH.2015.02.031.
[28] Panagiotidou A, Meswania J, Hua J, Muirhead-Allwood S, Hart A, Blunn G. Enhanced Wear and Corrosion in Modular Tapers in Total Hip Replacement Is Associated With the Contact Area and Surface Topography 2103. https://doi.org/10.1002/jor.22461.
[29] Kao YYJ, Koch CN, Wright TM, Padgett DE. Flexural Rigidity, Taper Angle, and Contact Length Affect Fretting of the Femoral Stem Trunnion in Total Hip Arthroplasty. The Journal of Arthroplasty 2016;31:254–8. https://doi.org/10.1016/J.ARTH.2016.02.079.
[30] McCarthy SM, Hall DJ, Mathew MT, Jacobs JJ, Lundberg HJ, Pourzal R. Are Damage Modes Related to Microstructure and Material Loss in Severely Damaged CoCrMo Femoral Heads? Clin Orthop Relat Res 2021;479:2083–96. https://doi.org/10.1097/CORR.0000000000001819.
Figures
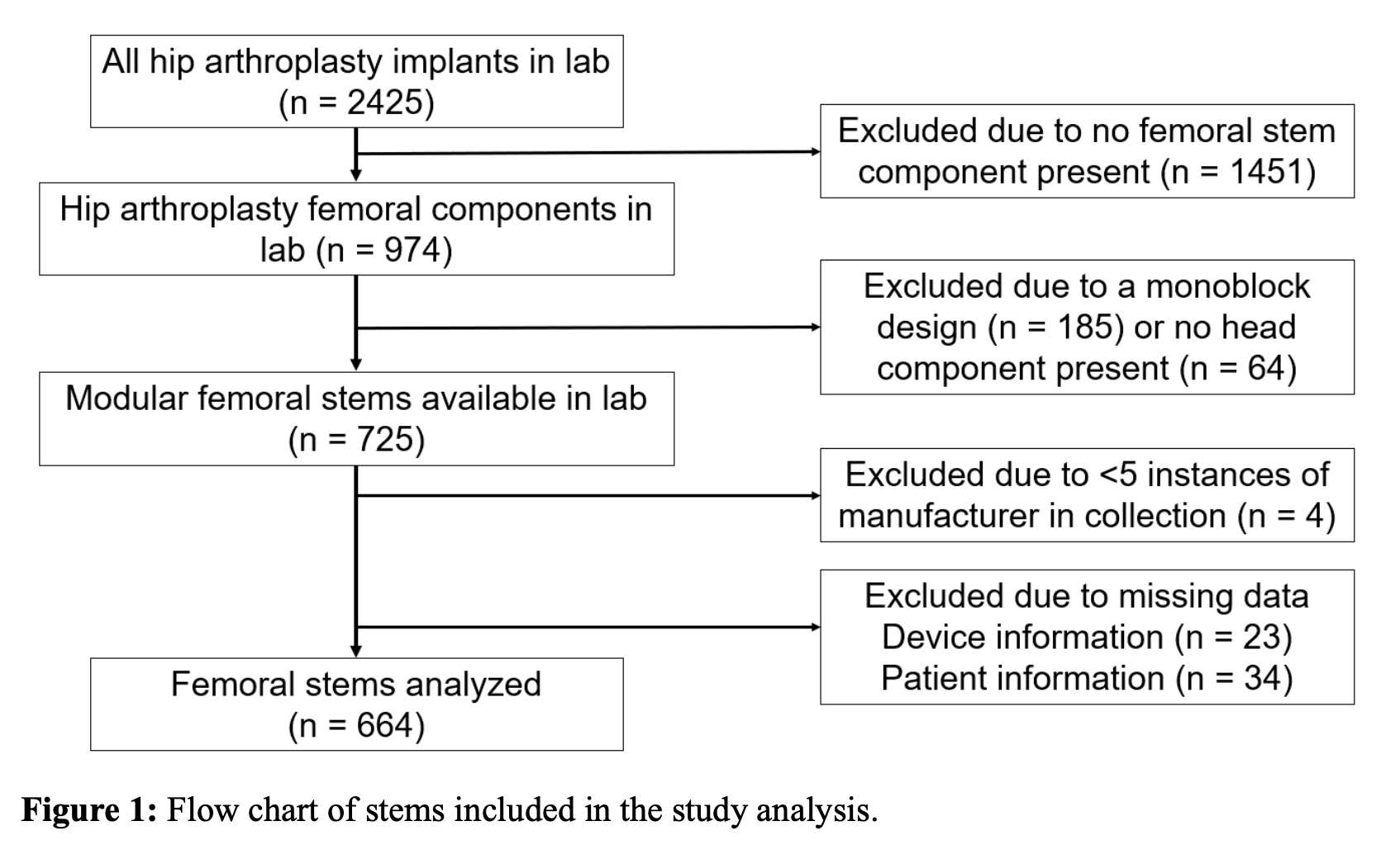
Figure 1
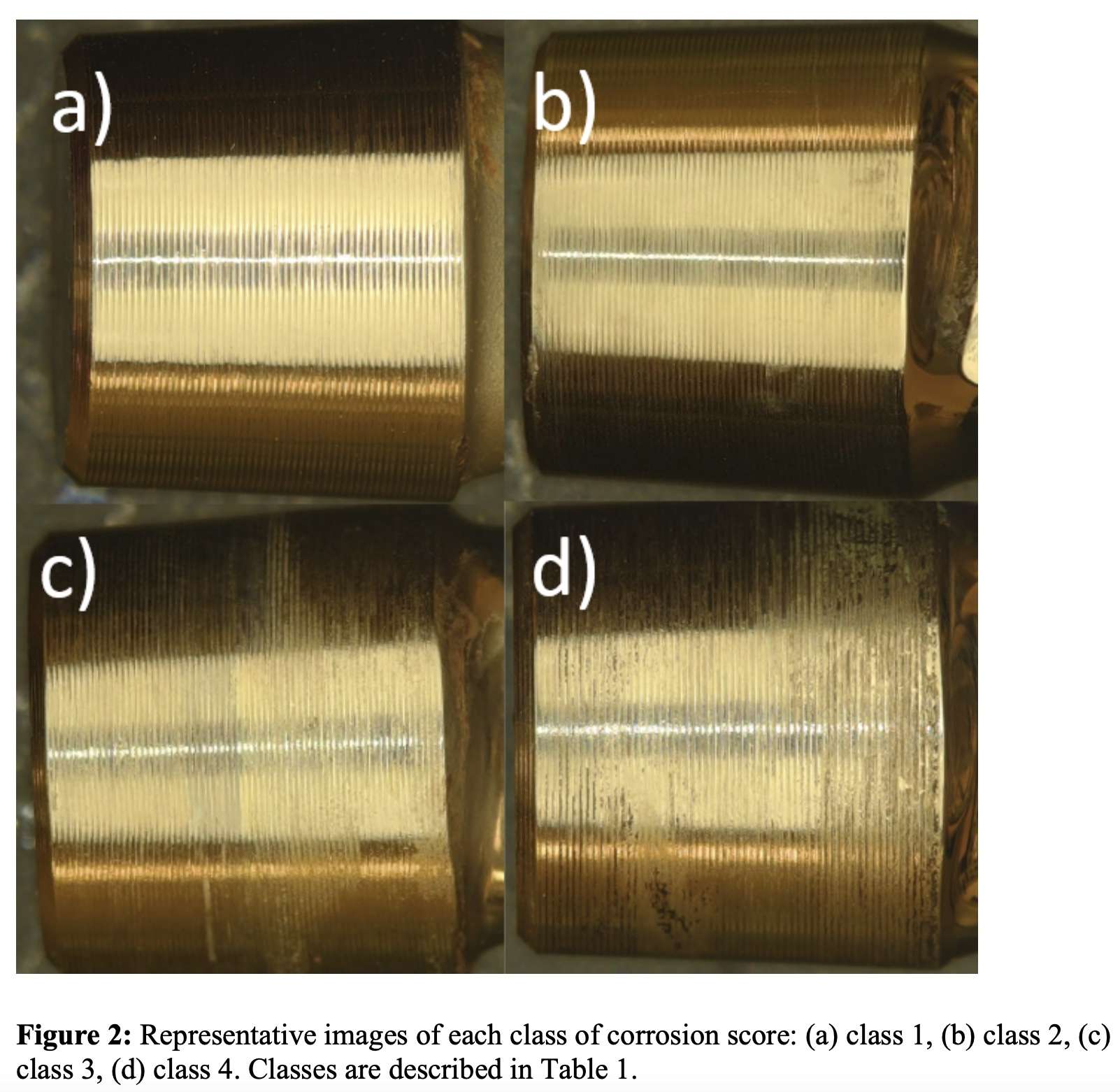
Figure 2
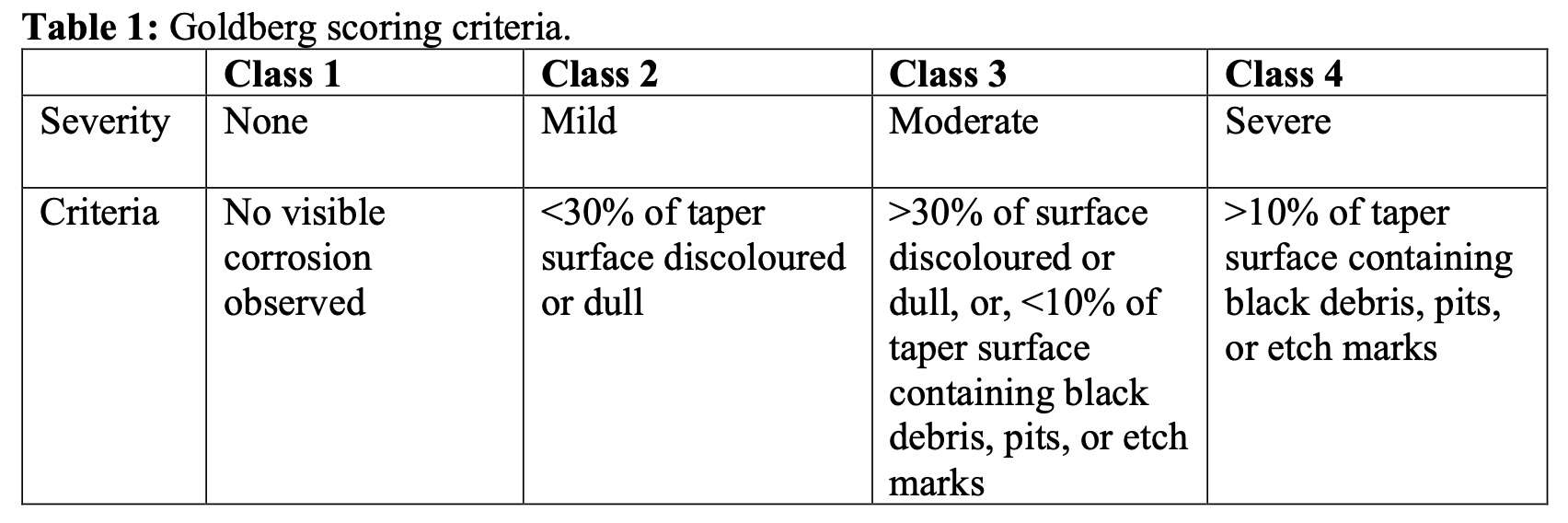
Figure 3
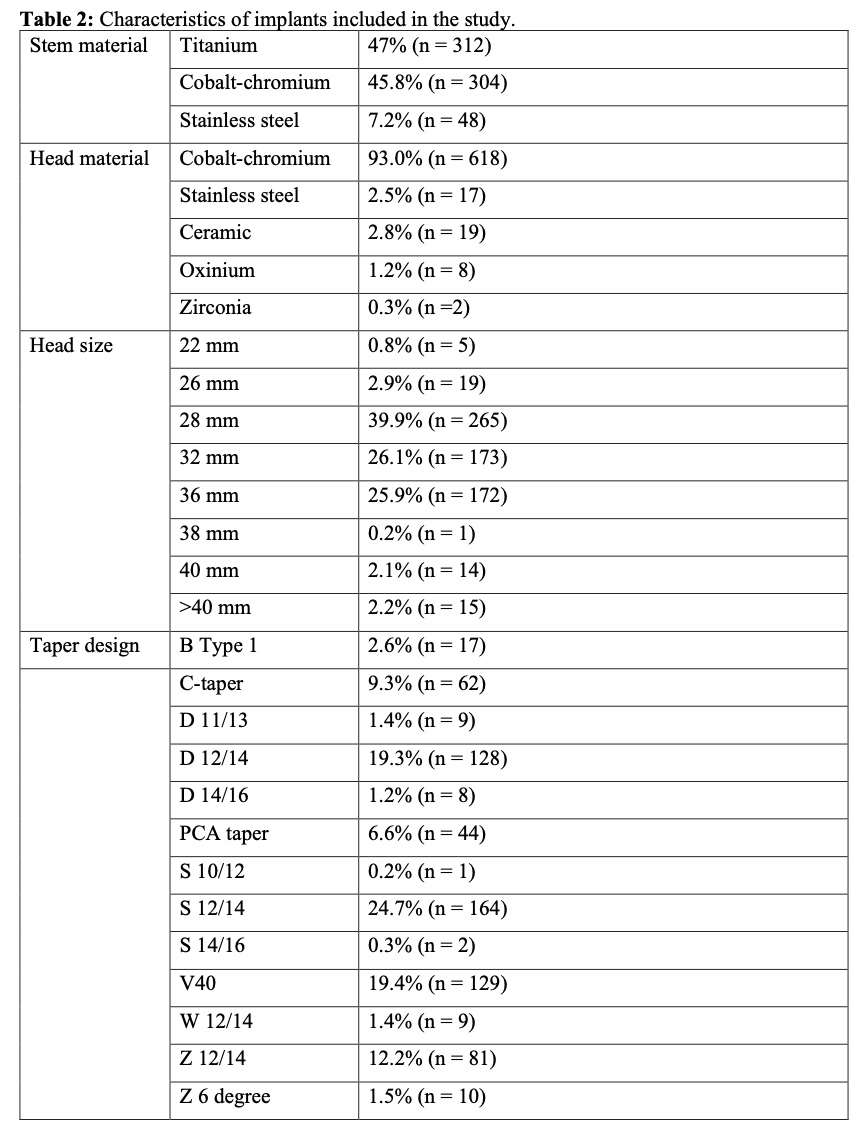
Figure 4
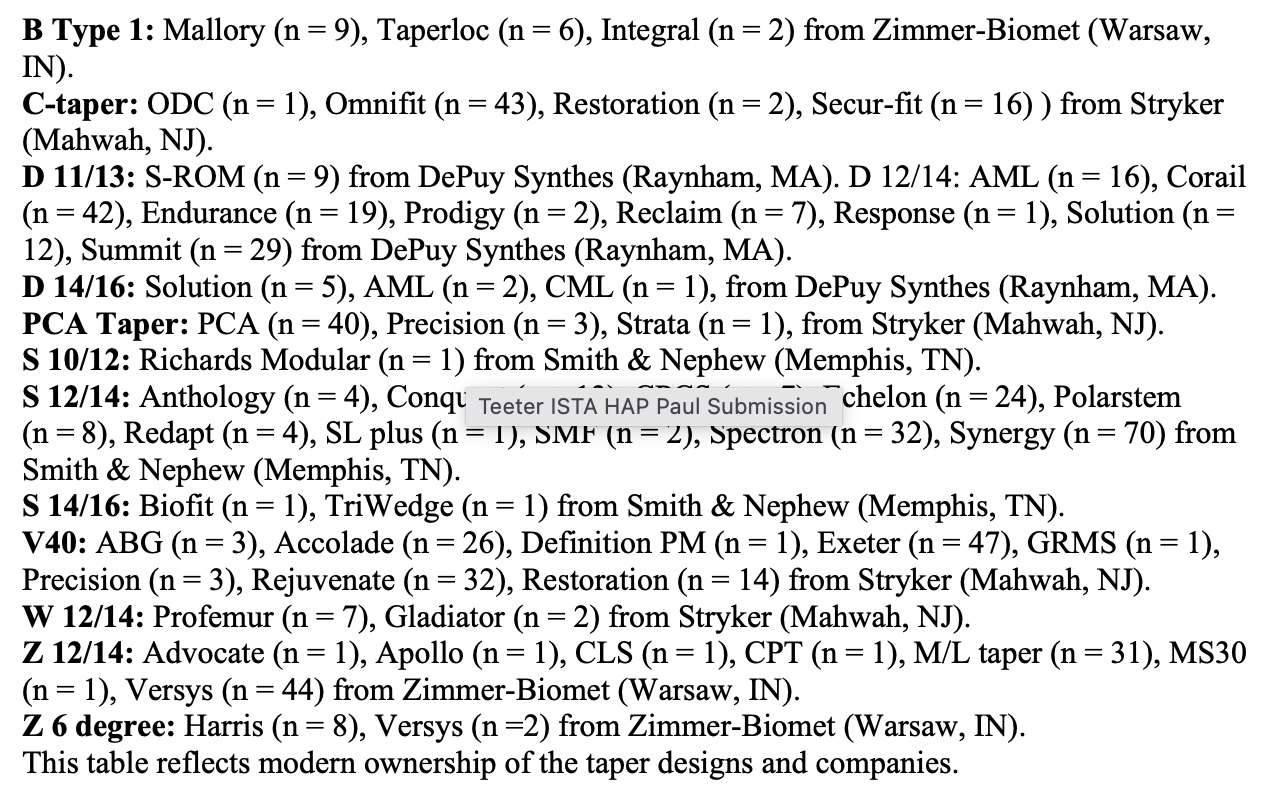
Figure 5
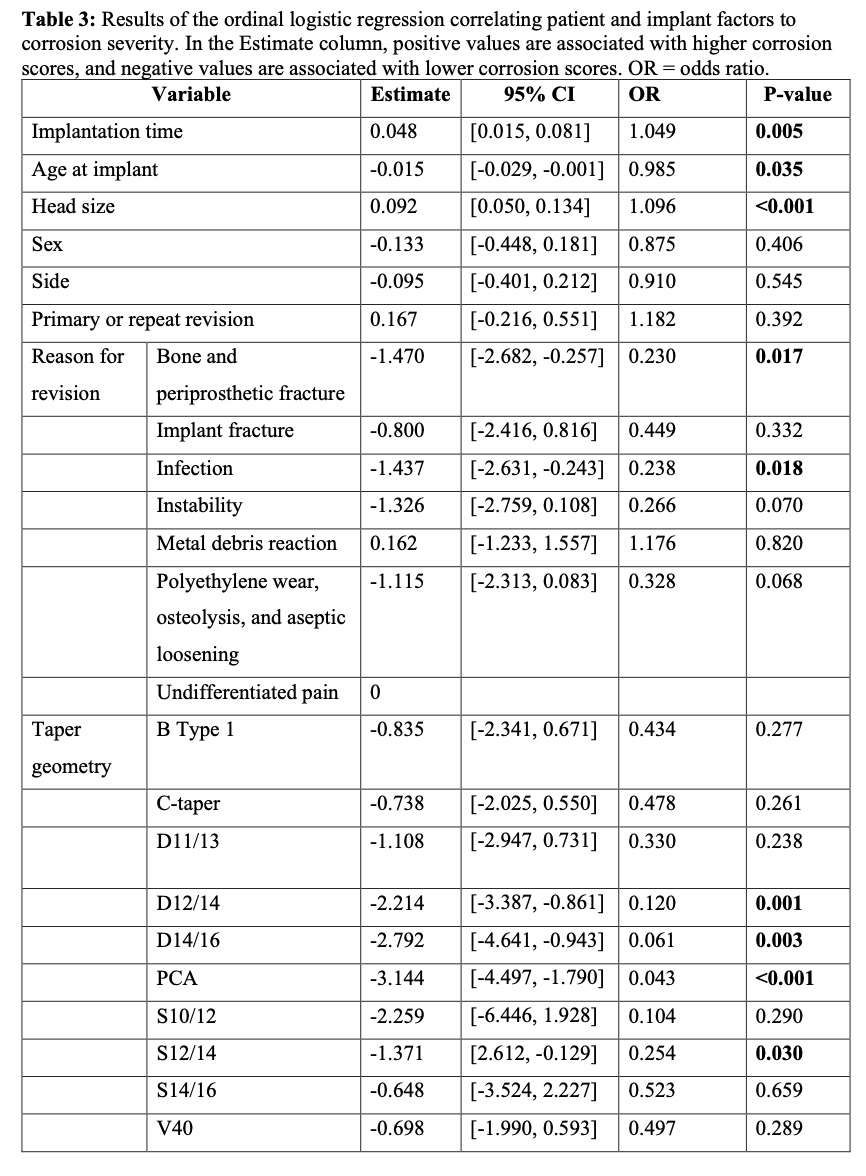
Figure 6
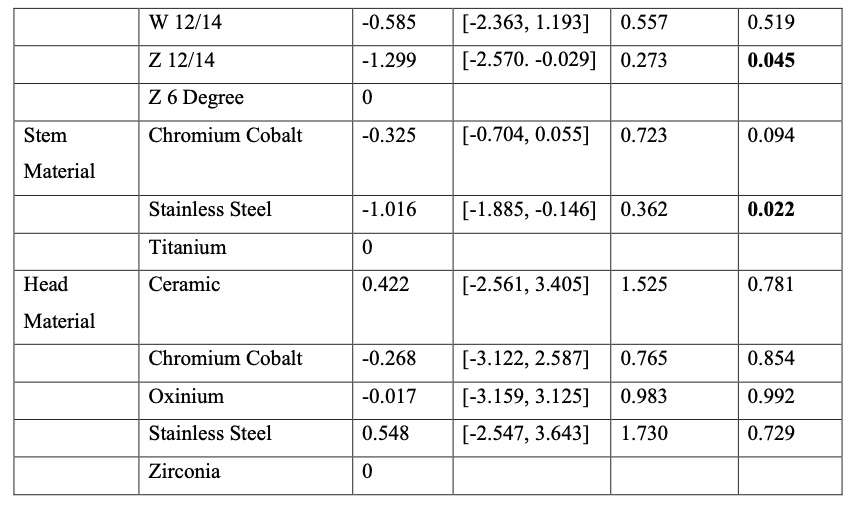
Figure 7
Figure 8
Figure 9#7729
Sheared Carbon-UHMWPE Composites: A Continued Movement Towards Smart Materials
*Rebecca Thomson - Dartmouth College - Hanover, United States of America
Hannah Favreau - Dartmouth College - Hanover, USA
Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: rebecca.j.thomson.th@dartmouth.edu
Introduction:
Recent interest in “smart” materials in orthopedic bearings has led to a return of research into carbon-containing polymers. Older formulations highlighting carbon fiber reinforcement were plagued with significant failure modalities in part driven by the poor adhesion of the carbon fibers to the UHMPWE matrix exacerbated by gamma-induced oxidation [1,2] (Figure 1). Previous studies of additional carbon additives show decreased mechanical properties due to poor consolidation, agglomerations serving as stress concentrators, and interruption of the polymer continuum [3]. The introduction of smaller spherical carbon particulates, such as conductive carbon black (CCB), combined with modern processing may overcome these historical challenges. Equal channel angular processing (ECAP) has previously been shown to increase the toughness of a nano-graphite carbon composites through addressing each of the aforementioned drawbacks [4]. Herein we apply ECAP to a high conductivity carbon allotrope in UHMWPE to identify the toughness/conductivity relationship.
Methods:
Neat and composite GUR 1050 UHWMPE powder blends containing CCB (1%, 1.5%, 2.5%, 5% by weight) were either compression molded (CM) or sheared through ECAP. Conductivity was measured through a previously reported method [4] and tensile toughness was measured via a modified ASTM Type V tensile test. Microstructure was assessed using optical and electron microscopy.
Results:
CCB composites show superior toughness and conductivity in comparison to trends previously reported for NG composites of the same weight percentage [4] (Figure 2). The choice of carbon allotrope shows reduced cracks and agglomerations. ECAP increased CCB tensile toughness while decreasing conductivity for most samples (Figure 3). The conductivity of CCB composites can be significantly increased with minimal differences in mechanical properties from 1.0 wt% to 5 wt%. While microscopy shows conductive particles impede consolidation of adjacent UHMWPE particles, increasing from 1 wt% to 5 wt% decreased the toughness by only 11% (CM) and 5% (ECAP).
Conclusion:
The interaction between the polymer matrix and carbon particulate must be carefully considered when fabricating conductive UHMPWE. ECAP consistently increased the tensile toughness of CCB composites, as occurred in NG composite materials, due to a better interaction between the polymer matrix and CCB particulates, along with better bridging of grain boundaries by polymer chains during consolidation. CCB has shown to be a promising material demonstrating acceptable toughness values of composites while providing UHMWPE with considerable conductivity. These results help to establish a pathway for producing “smart” orthopedic bearings which could be utilized as in vivo strain sensors or as bactericidal constructs [5,6].
References:
[1] S. Suñer, et al. Wear 2014, 317, 163.
[2] F. Medel, et al. Long. Term. Eff. Med. Implants 2008, 18, 151.
[3] Kaur, G., et al. RSC Adv. 2015, 5, 37553–37567.
[4] Favreau, H. J, et al. J. Appl. Polym. Sci. 2022, 139, 20.
[5] A. C. Clark, et al. Tribol. Int. 2006, 39, 1327.
[6] Mahat, M. M., et al. Emergent Mater. 2021, 4, 279–292.
Acknowledgements: Support for the NH EPSCoR BioMade Project is provided by the National Science Foundation's Research Infrastructure Improvement Award # 1757371.
Keywords: UHMWPE, carbon black, orthopedics, smart materials, composites
Figures
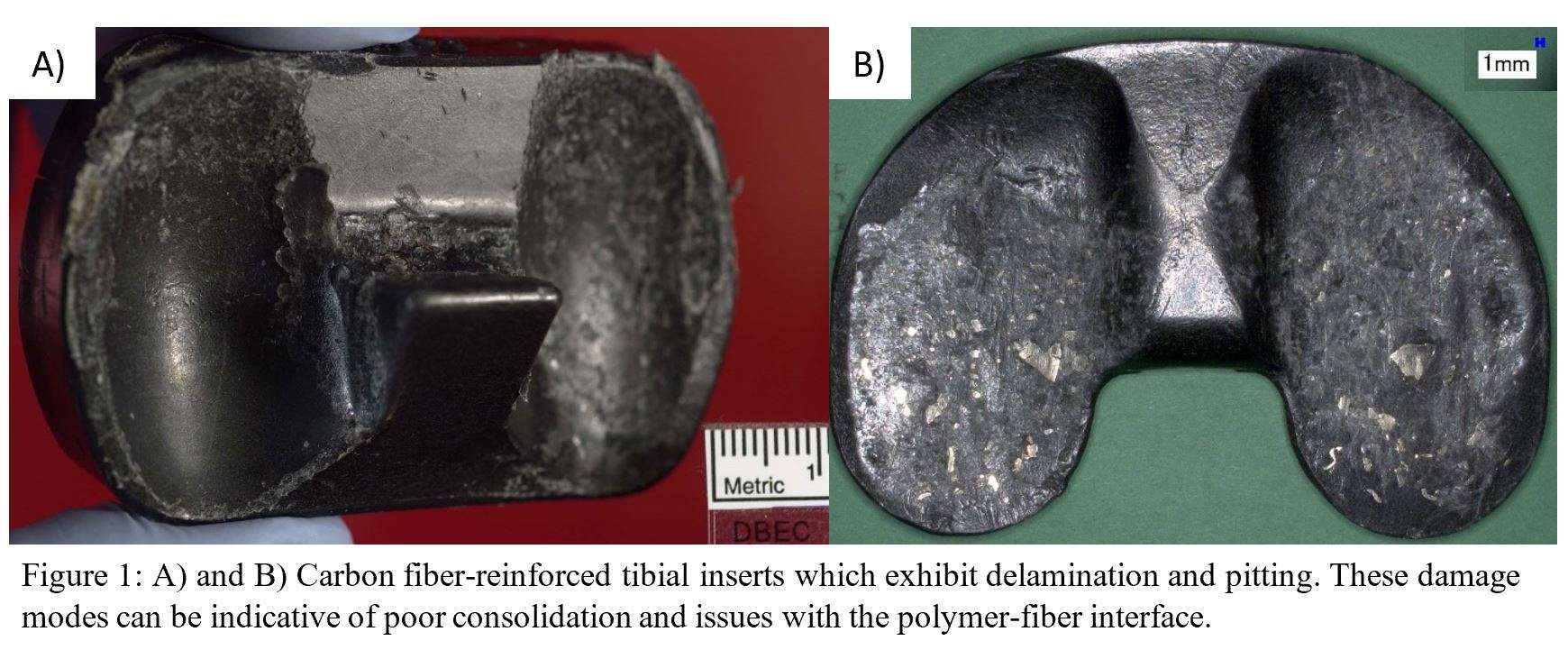
Figure 1
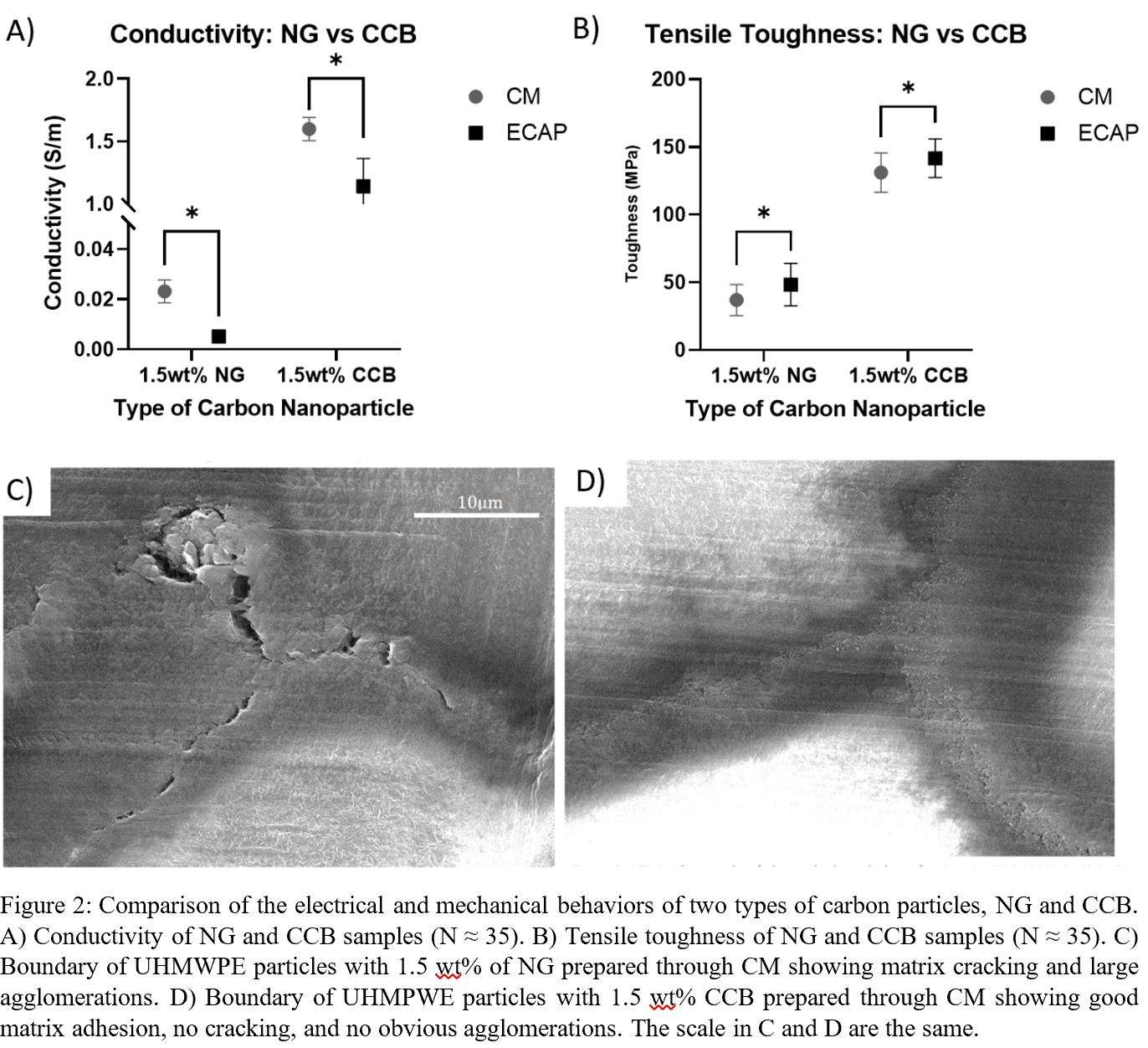
Figure 2
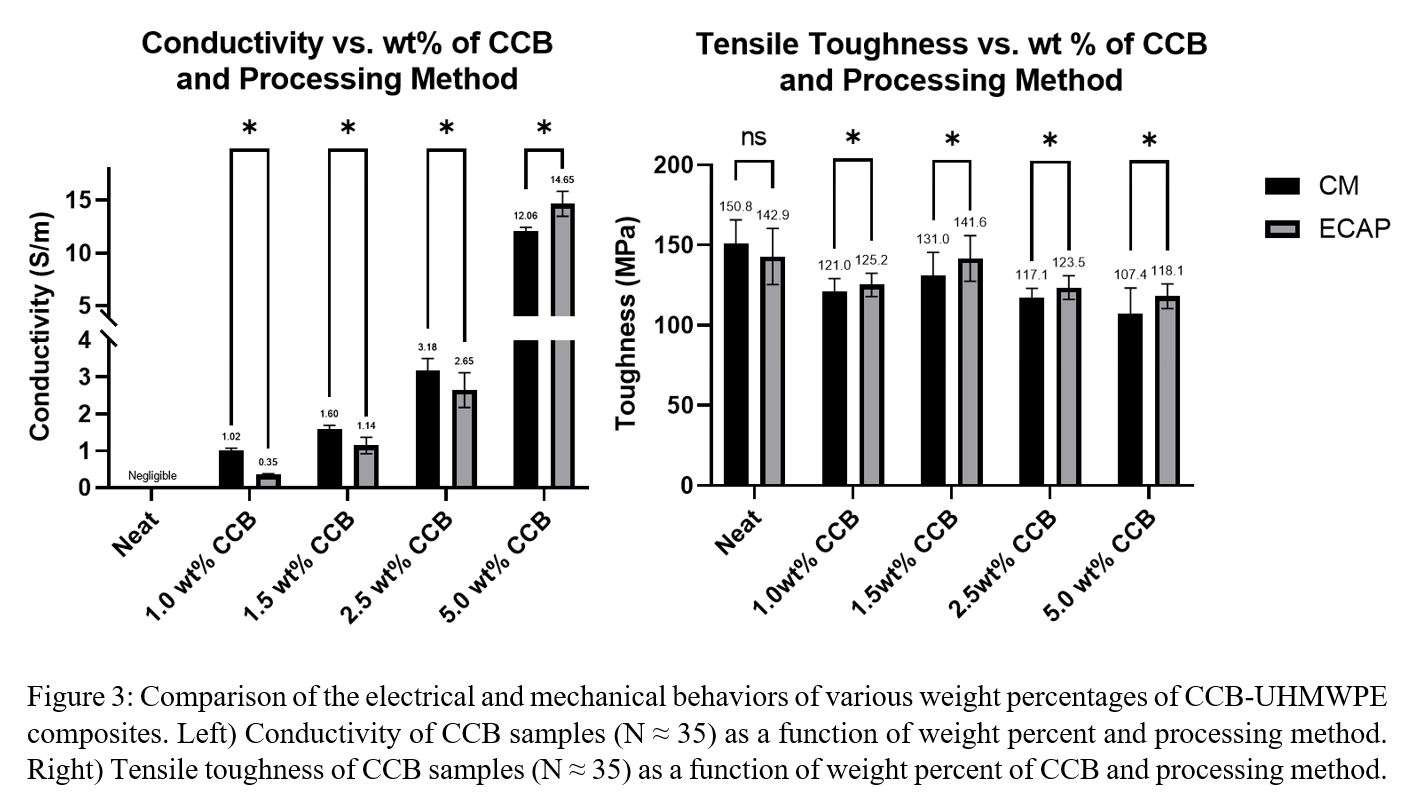
Figure 3#7896
The Charlson Comorbidity Index May Underestimate Health Status for Minorities
*Tyler Thorne - University of Hawaiʻi at Mānoa - Mānoa, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: tthorne@hawaii.edu
Introduction: The Charlson Comorbidity Index (CCI) is a useful tool in predicting post-
operative complications. However, ethnicity may impact CCI’s utility in risk assessment
following arthroplasty if comorbidity profiles are different among minority groups. The
current study aimed to identify the most prevalent comorbidities, as identified by the CCI
score, in an ethnically diverse arthroplasty patient population.
Methods: Data were retrospectively reviewed from 930 hip or knee arthroplasty
patients, with a primary analysis of 537 (57.7%) Asians, 302 (32.5%) Caucasian and
91(9.8%) Native Hawaiian/Pacific Islander (NHPI). The overall CCI score and number of
total comorbidities were determined for each patient through electronic medical record
review. Analyses of variance (with pairwise post-hoc analysis) and Chi-squared tests
were performed to evaluate continuous and categorical variables between ethnicities.
Results: Overall, NHPI were younger (Asian (69.6 years), Caucasian (69.1 years),
NHPI (64.4 years)), predominantly males (Asian (42.3%), Caucasian (48.7%), NHPI
(61.5%)) and had a higher body mass index (Asian (28.0kg/m 2), Caucasian
(28.6kg/m 2), NHPI (32.8kg/m 2)). While no difference in CCI score was noted between
ethnicities, Caucasian patients had a lower number of comorbidities (1.52±1.3)
compared to Asians (1.75±1.2) and NHPI (1.89±1.4). Caucasians had lower rates of
hypertension (56.6% vs Asian (76.0%), NHPI (78.0%)), lower rates of diabetes (8.3% vs
Asian (18.4%), NHPI (18.7%)) but had more cases of depression (15.6% vs Asian
Discussion: Although no difference in CCI score was present across ethnicities, Asian
and NHPI averaged a greater number of comorbidities compared to Caucasians,
suggesting a different postoperative complication risk category. The
differences in patient demographics, specifically in the NHPI group, could predispose
patients to different and/or additional comorbidities that may not be fully appreciated by
the CCI score. While further research is required, the CCI score may fail to provide an
operative risk assessment in an ethnically diverse population.
#7631
Evaluation of Changes Over Time the Bone Formation Around the Fully Hydroxyapatite-Coated Stem Using Digital Tomosynthesis
*Sho Totsuka - University of Tsukuba, - Tsukuba, Japan
Tomofumi Nishino - University of Tsukuba - Tsukuba, Japan
Ryunosuke Watanabe - university of tsukuba - Tsukuba, Japan
Masashi Yamazaki - University of Tsukuba - Tsukuba, Japan
Hajime Mishima - University of Tsukuba - Tsukuba, Japan
*Email: s.totsuka0705@gmail.com
[Introduction]
Digital tomosynthesis (DTS) is an imaging technology derived from radiography that has metal artifact reduction technology and enables observation of prosthetic joints.We performed DTS observation of a THA using a fully HA coated stem. Bone formation around the stem from proximal to distal was clearly observed, which could not be reproduced by plain radiograph, and this response showed temporal changes. In this study, we evaluate the bone reaction around the fully HA coated stem used DTS.
[Method]
Patients who underwent primary THA with fully HA coated stem were included in this study. There were twenty joints in the 1 y postoperative group (all patients had a postoperative observation period of 12 mo) and twenty joints in the 3 y postoperative group (mean postoperative observation period was 41.7 (range: 36 – 49) mo). Plain radiography was used to evaluate RL, cancellous condensation, cortical hypertrophy (CH), and stress shielding (SS). DTS was used to evaluate RL, the presence of periprosthetic bone formation, and the thickness of the layer of bone formation.
[Result]
By plain radiograph, no cases of an RL with osteopetrosis of 2 mm or more in either group were noted. Furthermore, CH was not observed in either group. First- and second-degree SS was observed in sixteen and four cases in the 1 y group and two and eighteen cases in the 3 y group, respectively. No cases of third-degree or higher SS in either group were noted. Cancellous condensation was observed in two (10%) and fourteen (70%) patients in the 1 y group and 3 y group, respectively.
By DTS, in all cases, bone formation was observed uniformly around the stem from proximal to distal. In the AP view, the thicknesses of the osteogenic layer were 0.54 ± 0.19 and 0.91 ± 0.31 mm in the 1 y group and 3 y group (p < 0.001), respectively, and there was a significant difference. In the lateral view, the thicknesses of the osteogenic layer were 0.69 ± 0.20 and 1.16 ± 0.27 mm in the 1 y group and 3 y group (p < 0.001), respectively, and this was also significantly different. No RLs with osteopetrosis in either group were noted.
[Conclusion]
In this study, we confirmed the osteogenic response around the stem using DTS. This is a layer of bone formation that occurs uniformly from proximal to distal on the surface of the HA-coated stem, and this reaction was defined as the surrounding bone formation (SBF). In some cases, the SBF could not be seen on plain radiography, and in other cases, cancellous condensation was seen around the stem as a permeable line, which at first glance appeared as an RL. By contrast, on DTS, no radiolucent image was observed at the stem–bone interface in all cases. The results of this study confirmed the usefulness of the detailed evaluation by DTS, especially in cases where an RL is suspected in fully HA-coated stems.
#7622
Post-Operative External Rotational Laxity Was Significantly Decreased Compared to the Preoperative Level Throughout Flexion in CR-TKA.
*Takashi Tsuda - Ehime University Graduate School of Medicine - Toon, Japan
Kazunori Hino - Ehime University - Toon, Japan
Tatsuhiko Kutsuna - Ehime University Graduate School of Medicine - Toon-city, Japan
Kunihiko Watamori - Ehime University Graduate School of Medicine - Toon-city, Japan
Tomofumi Kinoshita - Ehime University - Toon City, Japan
Hiromasa Miura - Kyushu Rosai Hospital - Kitakyushu, Japan
Masaki Takao - Ehime University - Toon City, Japan
*Email: maxlevel255@hotmail.co.jp
Introduction: Optimal soft tissue balance is crucial for successful clinical results in total knee arthroplasty (TKA). Despite midflexion stability is considered as a key factor for improving the outcome of TKA, there have been few reports on the rotational laxity.The aim of this study is to evaluate the changes of midflexion rotational laxity between pre and postoperative cruciate-retaining(CR)-TKA. Moreover, we compared the rotational laxity between two different design concept models of CR-TKA: symmetric (group S) and asymmetric-designed (group A).
Methods: 63 knees which underwent CR-TKA were evaluated. In accordance with procedures outlined in a previous study, manual maximum passive rotational stress was applied to the knees, and the internal–external rotational angle was measured automatically by a navigation system at 30°, 45°, 60°, and 90° of knee flexion [1]. Non-parametric Wilcoxon’s signed-rank tests were performed for comparisons between two groups, and Dunnett’s tests for multiple groups, respectively. The statistical analyses were conducted by software JMP version 16.0 (SAS Institute, Tokyo, Japan). In all studies probability level of 95% (p < 0.05) were considered statistically significant.
Results: The post-operative external rotational laxity were significantly decreased compared to the preoperative level at 30°, 45°, 60°, and 90° of knee flexion. On the other hand, although no significant difference was observed, the postoperative internal laxity tends to be higher than those at the preoperative level throughout flexion. As a results the post-operative internal-external laxity was statistically significantly decreased compared to the preoperative level only at 30° of knee flexion. Moreover, The post-operative internal-external laxity of group A were significantly lower than those of group S level at 30°, 45°, 60° of knee flexion, whereas no significant difference was found at 90° of knee flexion.
Conclusion: Post-operative external rotational laxity was significantly decreased compared to the preoperative level throughout flexion. Difference of design concepts of the implants affect to the rotational stability at mid-flexion range in CR-TKA.
References:
1.Hino K, et al. Assessment of the midflexion rotational laxity in posterior-stabilized total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2017; 25(11): 3495–3500
Keywords: Total knee arthroplasty; design of implants; Rotational laxity; Cruciate-retaining
#7367
Validation of a Patient Outcome Prediction Tool Relative to Surgeon Predictions of Patient Outcome in Total Knee Arthroplasty
*Ishaan Jagota - 360 Med Care - Sydney, Australia
Justin Roe - North Sydney Orthopaedic and Sports Medicine Centre - Sydney, Australia
David Parker - Sydney Orthopaedic Research Institute - Chatswood, Australia
Brett Fritsch - SORI - Sydney, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
David Liu - Gold Coast Centre for Bone and Joint Surgery - Tugun, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Max Hardwick-Morris - 360 Med Care - Sydney, Australia
*Email: ishaan.jagota@360med.care
Introduction & aims
The current decision-making process when evaluating whether a patient is suitable for a Total Knee Arthroplasty (TKA) involves a combination of patient reported symptoms, clinical examination findings and radiological criteria. Both the patient’s expected outcome from the surgery (as assessed by the surgeon) as well as diagnostic need for the surgery must be considered. This study aims to investigate ability of the Patient Expectation Management (PEM) tool, an artificially intelligent predictive tool, relative to surgeon predictions of patient outcome.
Method
A prospective study was performed involving 89 patients totalling 100 operated knees (11 bilateral) recruited from 4 experienced TKA surgeons between May 2018 and September 2019. Pre-operative KOOS and 12-month post-operative KOOS were obtained for all patients. All patients were surveyed using the PEM tool prior to surgeon consultation. The tool assessed the patient’s current pain state and provided a prediction for the patient’s post-operative pain outcome on a 100-point scale. After the surgeon consultation but prior to seeing the PEM results, the surgeon noted their understanding of the patient’s current pain levels and also predicted the patient’s post-operative pain level on the same 100-point scale.
Results
Average age of patients was 70.22 ± 6.65 years and 56% (56) of the joints were of a female patient. The reported change in patient pain outcome for patients predicted to experience a significant improvement (change in KOOS Pain score ≥ 40) according to the PEM tool was 40.9 ± 13.0, compared to 21.9 ± 22.7 for patients predicted to experience an insignificant improvement (p < 0.001). The reported change in patient pain outcome for patients predicted to experience a significant improvement according to surgeons was 51.2 ± 23.2, compared to 50.0 ± 15.6 for patients predicted to experience an insignificant improvement (not statistically significant) [Fig. 1]. Overall, the predicted change in pain outcome by the PEM tool and surgeon group were 31.4 ± 20.7 and 50.6 ± 19.7, respectively (p = 0.003) [Fig. 2].
Conclusions
The PEM tool was able to predict significant improvements in patient pain outcomes more accurately than surgeons. This may in part be due to the more conservative predictions by the tool relative to surgeons creating a ‘ceiling effect’ on the surgeons’ predictions. This tool can be clinically implemented to assist surgeons during their evaluation of patient suitability, in attempt to improve patient pain and satisfaction outcomes post-operatively.
Figures
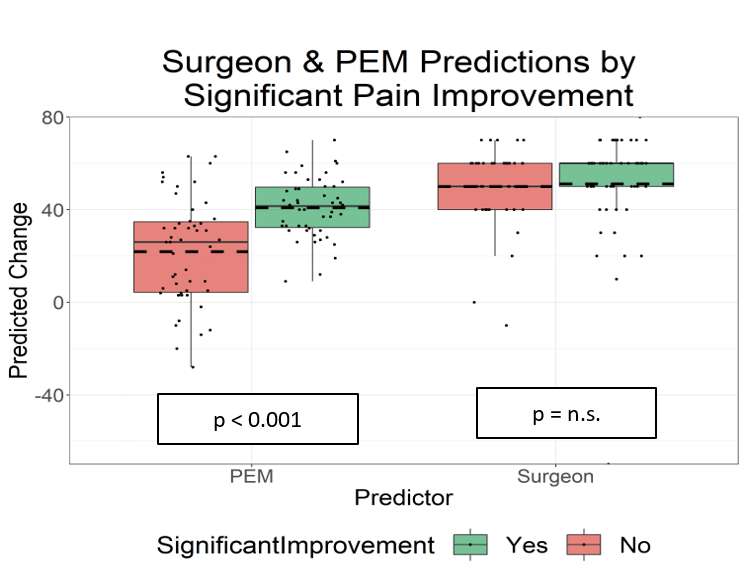
Figure 1
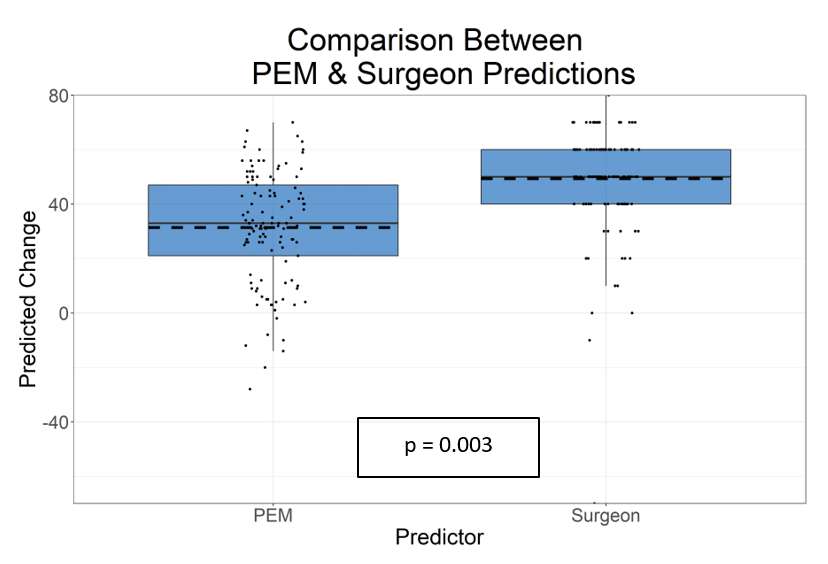
Figure 2#7368
Population Level Validation of a Novel Joint Distraction Radiology Protocol in Total Knee Arthroplasty Planning
*Ishaan Jagota - 360 Med Care - Sydney, Australia
David Liu - Gold Coast Centre for Bone and Joint Surgery - Tugun, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Max Hardwick-Morris - 360 Med Care - Sydney, Australia
*Email: ishaan.jagota@360med.care
INTRODUCTION: TKA alignment strategies aim to achieve joint balance. Historically this has been achieved by restoring the joint to a neutral mechanical alignment and releasing ligaments, but non-mechanical alternatives are now often practiced. This study aims to compare the alignments achieved by pre-operatively planning to a novel distracted joint gap protocol to anatomically referenced Kinematic and Mechanical Alignment (KA & MA) and the alignment of a healthy non-arthritic population as described by Bellemans et al (2012).
METHODS: A retrospective study comprised of 138 patients totaling 145 operated knees (7 bilateral) was performed. All patients were recruited from a single experienced orthopaedic surgeon between March 2020 and March 2021. A long-leg supine CT scan, weightbearing AP knee X-ray and two distracted knee X-rays (one each in extension and flexion, making use of an ankle weight to open the joint) were taken pre-operatively. Segmentation and landmarking of the CT scans were performed. The output bone models were then registered onto the 3 different X-rays via 3D-to-2D registration, and the medial and lateral joint gaps were determined in extension and flexion. An algorithm corrected for geometrically determined osteophyte tenting of ligaments and a surgical plan to fill the expected gaps was formed.
RESULTS: The mean patient age was 70.9 ± 8.5 years with 52% (75) female joints. The mean distracted medial and lateral joint gaps were 3.0mm ± 2.2mm and 5.9mm ± 2.0mm in extension and 2.7mm ± 2.1mm and 6.2mm ± 2.2mm in flexion, respectively. After accounting for osteophyte tenting, these medial and lateral joint gaps increased by 0.8mm ± 0.9mm and 0.4mm ± 0.6mm in extension and 1.3mm ± 1.2mm and 0. 7mm ± 1.0mm in flexion, respectively. The mean weightbearing Hip-Knee-Ankle angle (HKA), KA planned HKA and distracted joint planned HKA were 4.7° (±5.9°) varus, 0.3° (±3.2°) varus, and 2.2° (±3.5°) varus. This compares to a healthy adult HKA of 1.3° (±2.3°) varus[Fig.1]. A patient level analysis between the planned KA and distracted joint HKA angles found that the coronal angles of the two alignments are within 3° of each other for 64% patients, within 3-5° for 26% of patients and greater than 5° for the remaining 10% of patients[Fig.2].
DISCUSSION: The change in joint gaps observed when pre-operatively accounting for osteophyte tenting is comparable to the interoperative observations of Sriphirom et al (2018). A population level analysis displayed that out of the HKA angles analysed, the planned distracted HKA was the closest to the constitutional varus HKA angle of a healthy population.
Most current surgical plans aim to either restore the joint to a neutral mechanical alignment or an alignment based on the arthritic state of the joint, both of which often fail to consider information about the soft tissue within the joint, particularly regarding ligament laxity. The alignment resulting from the stress radiology protocol discussed in this study accounts for the bony and soft-tissue anatomy and could perhaps act as a proxy for a patient’s pre-osteoarthritic alignment and thus provide a better foundation for patient-specific pre-operative surgical planning.
Figures
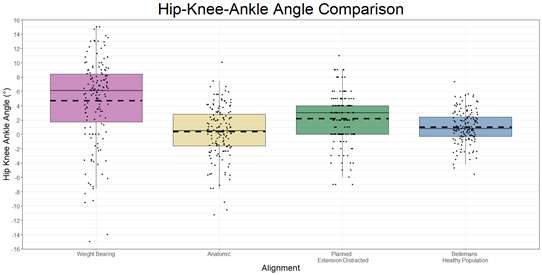
Figure 1
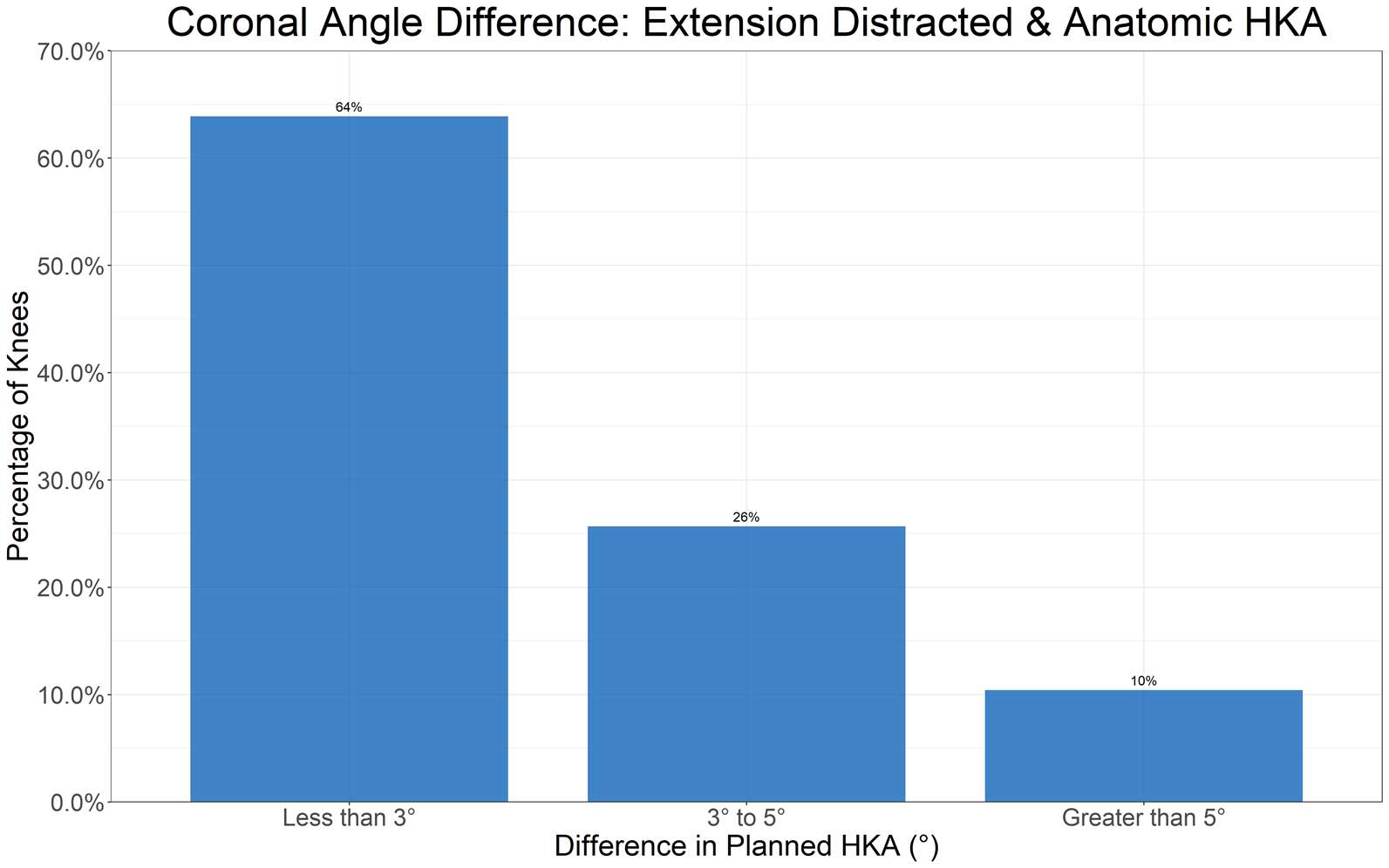
Figure 2#7467
Prediction of Postoperative Impairment With Simulation: Validation of a Patient Specific Planning Tool
*Joshua Twiggs - University of Sydney - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Andrew Shimmin - Melbourne Orthopaedic Group - Melbourne, Australia
Justin Roe - North Sydney Orthopaedic and Sports Medicine Centre - Sydney, Australia
David Liu - Gold Coast Centre for Bone and Joint Surgery - Tugun, Australia
David Parker - Sydney Orthopaedic Research Institute - Chatswood, Australia
Brett Fritsch - SORI - Sydney, Australia
*Email: joshua_twigg@msn.com
Introduction
Joint dynamics following TKA drive tibio-femoral balance and in doing so might influence patient outcome. Computational simulations allow preoperative modelling of joint dynamics outcomes. The Dynamic Knee Score (DKS) is a machine learning predictive algorithm derived from a patient specific multibody computational simulation. The DKS is designed to be used pre-operatively to select a predicted optimal surgical plan. This study aims to validate the DKS as a predictive model of surgical alignment and component orientation decisions that are likely to reduce instances of post-operative patient functional impairment.
Method
A series of 1074 TKAs using the DKS as a predictive tool were performed between Jan-2014 and Aug-2020. Pre- and post-operative CT scans and 12-month Knee Injury and Osteoarthritis Outcomes Score (KOOS) were collected. Implants used were Corin (Cirencester, UK), APEX, Depuy (Raynham, USA) Attune and MatOrtho (Surrey, UK) Saiph CR & PS designs. Landmark localisation and 3D registration of implants were performed on the post-operative CT scans and the achieved implanted position. In addition, a series of simulations covering variant tibial slopes (0°, 3°, 6°, 9° and 12°), variant posterior resections of the femur (+3mm to -3mm, 1mm increments) and variant rotations of the femur (snapping to the Trans-epicondylar and Posterior Condylar axes) was performed. These simulated knees & variant DKS plans were matched with postoperative KOOS questions covering various dimensions of patient impairment. The level of impairment within those patients for whom the best DKS plan was surgically achieved and those in whom it was not was determined and compared
Results
Of the 1074 identified TKA patients, 54.6% (586) were female and the average age was 69.6 ± 9.4 years old at the time of surgery. Patient reported impairment with the knee catching and squatting was shown to be 30% lower (p=0.008) and 22% lower (p=0.038) respectively in patients where the best possible DKS plan was surgically achieved in femoral rotation. Similar findings were found with tibial slope and posterior femoral resection DKS plans and difficulty straightening the knee (p=0.005) and descending stairs (p=0.011). When the best possible DKS result was achieved for tibial slope and posterior resection, 3% of patients reported postoperative difficulty straightening their knee – 17% did when only one of these parameters was optimal to the plan and 18% when neither was optimal, and this finding was also statistically significant (p=0.039).
Conclusions
When the DKS’s predicted optimal plan is surgically achieved, there has been shown to be a reduction in instances of difficulty squatting, straightening and poor patello-femoral function post-TKA. This algorithm can be applied in a pre-operative planning setting to optimise surgical planning. Outcome optimisation may be possible with patient specific selection of alignment strategy and simulations may be a technological enabler of this trend into the future.
Figures
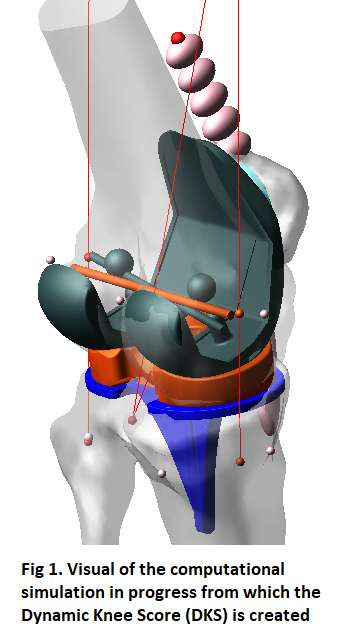
Figure 1
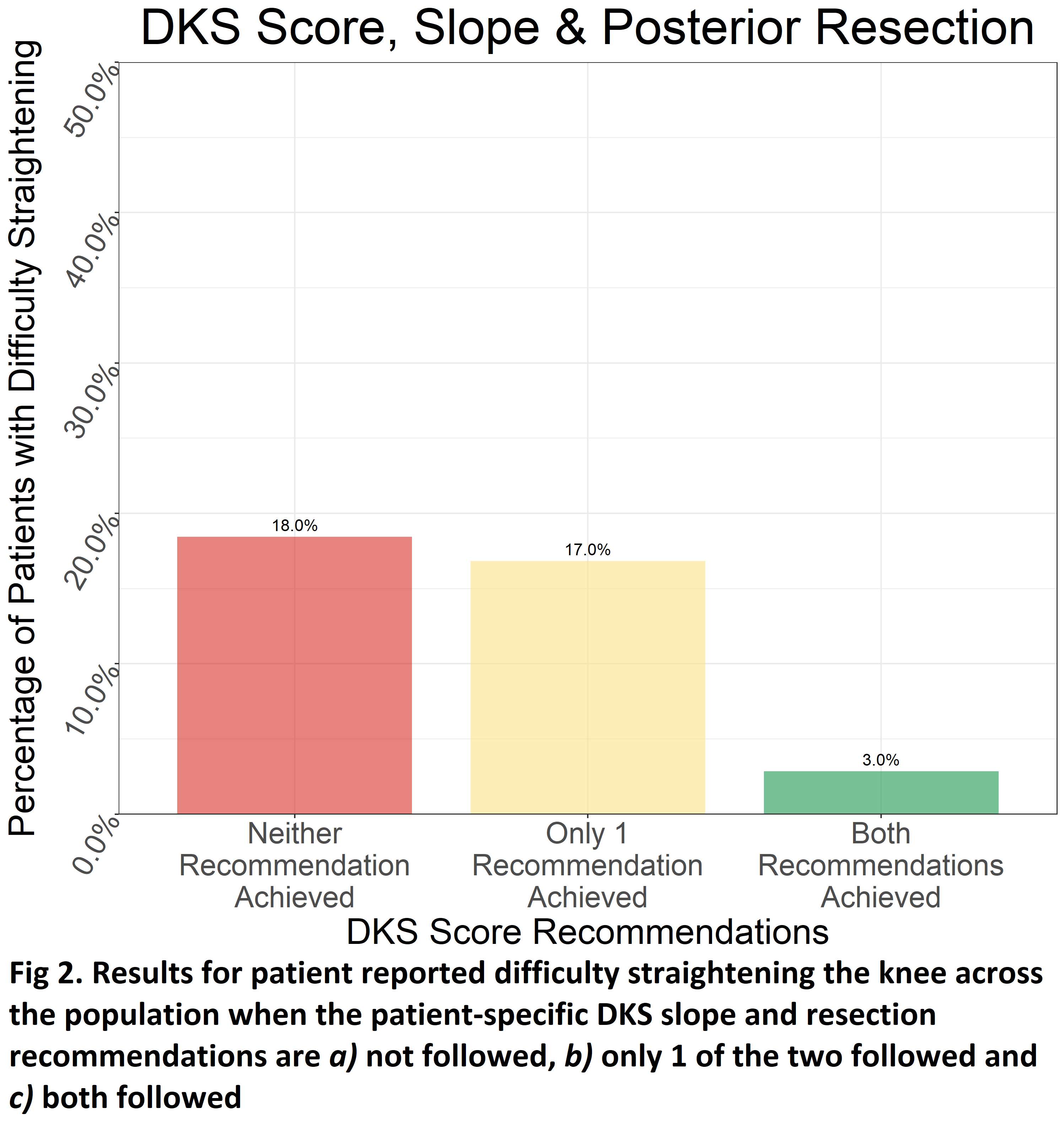
Figure 2#7570
Optimization of Implant Positioning Towards Reconstructing the Premorbid State in Robotic-Arm Assisted Total Knee Arthroplasty
*Periklis Tzanetis - University of Twente - Enschede, Netherlands
Kevin de Souza - Stryker - Manchester, United Kingdom
Rene Fluit - University of Twente - Enschede, Netherlands
Seonaid Robertson - Stryker - Manchester, United Kingdom
Bart Koopman - University of Twente - Enschede, Netherlands
Nico Verdonschot - Twente - Nijmegen, Netherlands
*Email: p.tzanetis@utwente.nl
Introduction
Implant positioning in total knee arthroplasty (TKA) is critical in restoring the function of the arthritic knee. Robotic-arm assisted surgery is highly precise in preoperatively planned bone resections and positioning of components [1]. However, what is yet unclear is the optimal position of the implant in order to achieve restoration of the premorbid joint state. The aim of this study was first to investigate differences in tibiofemoral kinematics and ligament strains between premorbid and their corresponding implanted knees, and second, to optimize the positioning of the femoral component, thereby emulating the premorbid kinematics after a cruciate-retaining (CR) TKA.
Methods
A cadaver-specific musculoskeletal knee model was developed using a previously established methodology [2]. To scale the model to a patient-specific morphology, the preoperative computed tomography (CT) image of a single patient with severe knee osteoarthritis was segmented using a statistical shape and appearance model that identified the arthritic and premorbid femoral and tibial bone surfaces [3]; and a magnetic resonance imaging-based statistical shape model trained to estimate cartilage thickness from the segmented bones. A Triathlon CR-TKA system (Stryker Orthopaedics, Mahwah, NJ, USA) was mechanically aligned to the reconstructed knee (Figure 1). The femoral component’s position was varied from −6 to 6 mm for medial-lateral, anterior-posterior, and proximal-distal translations, −3° to 3° for flexion-extension, and −6° to 6° for varus-valgus and internal-external rotations. The covariance matrix adaptation evolution strategy was used to find the implant position that minimizes the root-mean-square deviation (RMSD) between the premorbid and post-TKA tibiofemoral kinematics within the specified ranges.
Results
Compared to the premorbid state, the mechanically aligned TKA model predicted tibiofemoral kinematics with an average RMSD of 2.53±1.24 mm and 2.45±0.98°. Strain profiles exhibited deviations up to 3% and 5% for the medial and lateral collateral ligamentous structures, respectively. The positioning parameters of the femoral component corresponded to 0.67 mm medial translation, 2.33 mm anterior translation, 4.29 mm proximal translation, 1.97° extension, 0.30° valgus, and 4.07° external rotation, with respect to mechanical alignment in order to optimally resemble premorbid kinematics (Figure 2). We found an average RMSD of 0.95±0.31 mm for translations and 1.35±0.01° for rotations between the premorbid and optimally aligned TKA model; and ligament strain deviations of less than 1%, except for deep medial collateral ligament (Figure 3).
Conclusion
Mechanically implanted knee substantially altered the kinematic predictions, hence the ligament strains, relative to the premorbid state. The reported kinematic differences are larger than the accuracy attained in robotic-arm assisted surgery [4]. We demonstrated that premorbid kinematics could be reproduced more closely in TKA by optimizing the positioning parameters of the femoral component from mechanical alignment. Different goals for robotic surgery can be further discussed, such as maximum joint stability during mid-flexion, achieving balanced collateral ligaments, or reproducing premorbid ligament strains.
References
- Hampp et al, J Knee Surg, 32:239-250, 2019.
- Marra et al, J Biomech Eng, 137:020904, 2015.
- Bowes et al, Ann Rheum Dis, 80:502-508, 2021.
- Sires et al, J Knee Surg, 34:745-748, 2021.
Figures
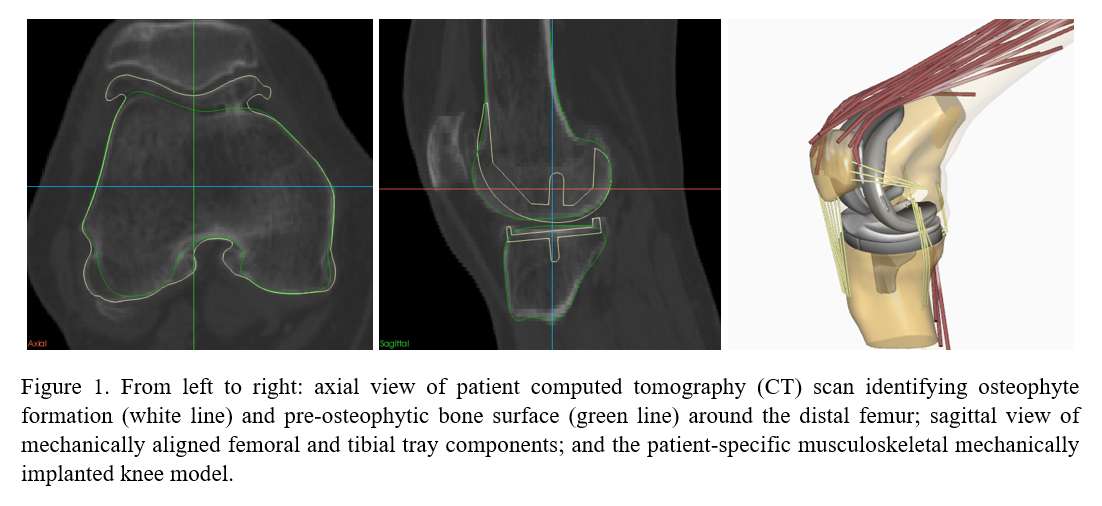
Figure 1
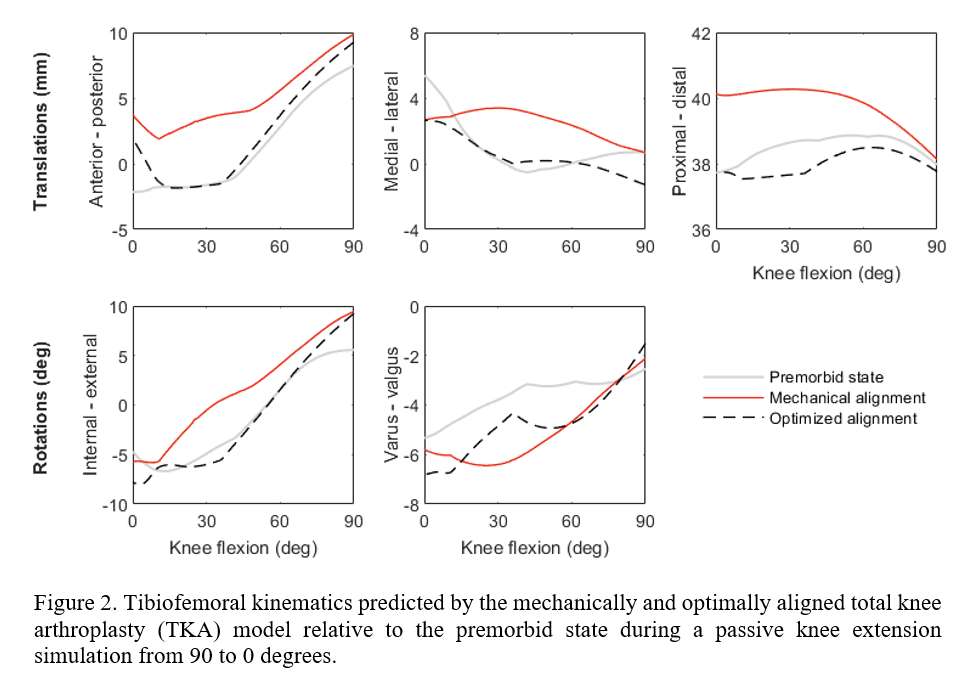
Figure 2
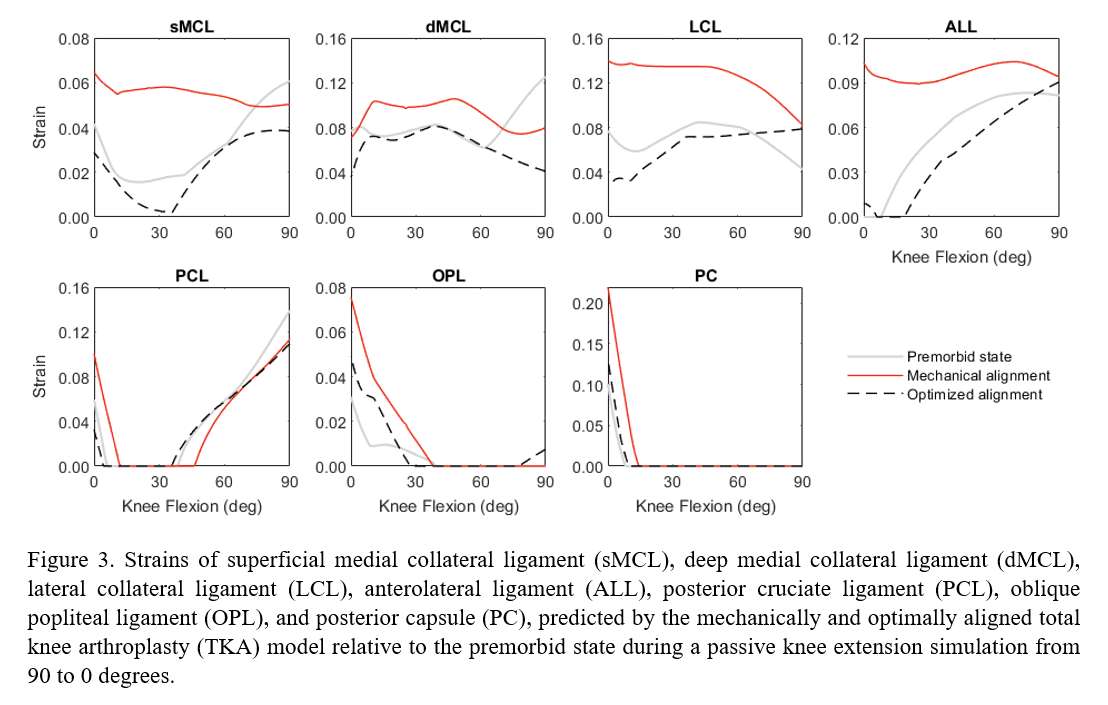
Figure 3#7634
Validation of Naviswiss Imageless Portable Navigation System for Accurate Acetabular Cup Positioning During Total Hip Arthroplasty in the Lateral Decubitus Position: A Retrospective Analysis
*Yoshinobu Uchihara - Nara Medical University - Kashihara, Japan
Kenichiro Saito - Nara Medical University - Nara, Japan
Masakazu Okamoto - Nara Medical University - Kashihara, Japan
Yusuke Inagaki - Nara Medical University - Kashihara, Japan
Yasuhito Tanaka - Nara Medical University - Kashihara, Japan
*Email: y-uchihara@naramed-u.ac.jp
Introduction
Accurate acetabular cup positioning is necessary during total hip arthroplasty to avoid complications due to acetabular cup malposition such as dislocation, polyethylene wear, and iliopsoas impingement. Naviswiss is an imageless portable navigation system that can register the functional pelvic plane (FPP) in the supine position as a baseline position before the patient is repositioned into the lateral decubitus position for surgery. This is different from the existing portable navigation systems that can register only the placement of a patient in the longitudinal axis as a baseline, with less certainty. We report the validation of the Naviswiss imageless navigation system for accurate acetabular cup positioning during total hip arthroplasty (THA) in the lateral decubitus position.
Methods
We retrospectively analyzed the data of 85 patients (16 men and 69 women) who underwent THA using Naviswiss in the lateral decubitus position between November 2020 and March 2022. The mean age of the participants was 69 (range 40–92) years, and their mean body mass index (BMI) was 24.0 (range 14.2–38.4) kg/m2. The anterolateral approach in the lateral decubitus position was used with the FPP preoperatively registered in the supine position as the baseline in all cases. The absolute navigation error values were calculated as the absolute difference between the intraoperative cup angles measured using Naviswiss and postoperative angles measured using computed tomography. The number of outliers of the absolute error (>10°) was evaluated.
Results
The mean absolute navigation error values were 2.8° ±2.1° in inclination and 3.9° ±2.8° in anteversion. Only one (1.2%) case had an outlier of >10°. In one case of anteversion extending beyond 15° than that measured by the navigation, the BMI was high (30.8 kg/m2). However there were no significant differences in the BMI between the groups having navigation error >5° or ≤5°.
Conclusion
The proprietary imageless portable navigation system provides good accuracy of cup positioning during THA in the lateral decubitus position with the FPP preoperatively registered in the supine position as the baseline surgical position.
#7510
Investigation of the Friction Behavior of Different Head Materials in Shoulder Arthroplasty
Maximilian Uhler - Laboratory of Biomechnics and Implant Research - Heidelberg, Germany
Stefan Schroeder - Heidelberg University Hospital - Heidelberg, Germany
Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
*J. Philippe Kretzer - University of Heidelberg - Heidelberg, Germany
*Email: philippe.kretzer@med.uni-heidelberg.de
Introduction:
The Australian Orthopaedic Association National Joint Replacement Registry showed 12.3% revisions in total shoulder replacements after a ten-year follow-up. One of the most common reasons for this is aseptic loosening, which can be minimized through technical progress. The use of ultra-high-molecular-weight polyethylene (UHMWPE) as glenoid material is known to be the gold standard. In addition to the different head material, the influence of the conformity between the sliding partners has already been described as an influencing factor. The present study investigated whether these two influencing factors had a significant effect on the friction behavior of the implant system.
Methods:
To determine the frictional torque between the glenoid and humeral head of the implant systems, they were placed in a physical pendulum. The moments resulting after a defined deflection were recorded and evaluated with a measurement repetition of n=10 using a 6-component load cell. To compare the groups, an ANOVA with a Bonferroni correction was used. The level for statistical significance was set at p < 0.05. The investigated implant systems with the corresponding head material and radial mismatches are shown in Table 1.
Results:
The comparison of the frictional torques shows that the torque of the DJO implant system is reduced when a ceramic head is used. The Mathys implant system tends to show an inverted behavior. In addition, an increase in friction with an increase in conformity is seen here (Figure1). The statistical evaluation of the groups within the material compositions is shown in Table 2. When considering the combination of materials, it is noticeable that when metallic humeral heads are used, that there is a significant difference in terms of measured friction for different manufacturers but the same radial mismatch (1a vs. 2a-L). When looking at the influence of conformity within a company, a smaller difference in radial mismatches did not produce a significant difference in metallic heads (2a-L vs. 2a-M & 2a-M vs 2a-S), but a large difference did (2a-L vs. 2aS). However, when ceramic head material is used, the comparison between the manufacturers does not show any significant difference (1b vs. 2b-L). In addition, conformity plays a more crucial role in ceramic head material.
A direct comparison of the head materials within the manufacturers shows a significant difference between the combinations in the DJO Surgical implant systems (p<0.001). In the case of the Mathys AG systems, a direct comparison of the metallic and ceramic heads with the same radial mismatch shows no significant difference (p>0.657).
Conclusion:
In summary, both the head material used and a different conformity of the systems have an influence on the friction behavior. Another important aspect not considered in this study is the PE of the glenoid used. These differ between the manufacturers with regard to their post-processing, which can also have an effect on the friction behavior. Nevertheless, it can be shown that the friction behavior of a shoulder arthroplasty can be influenced by varying the head materials and the conformity between the components.
Figures
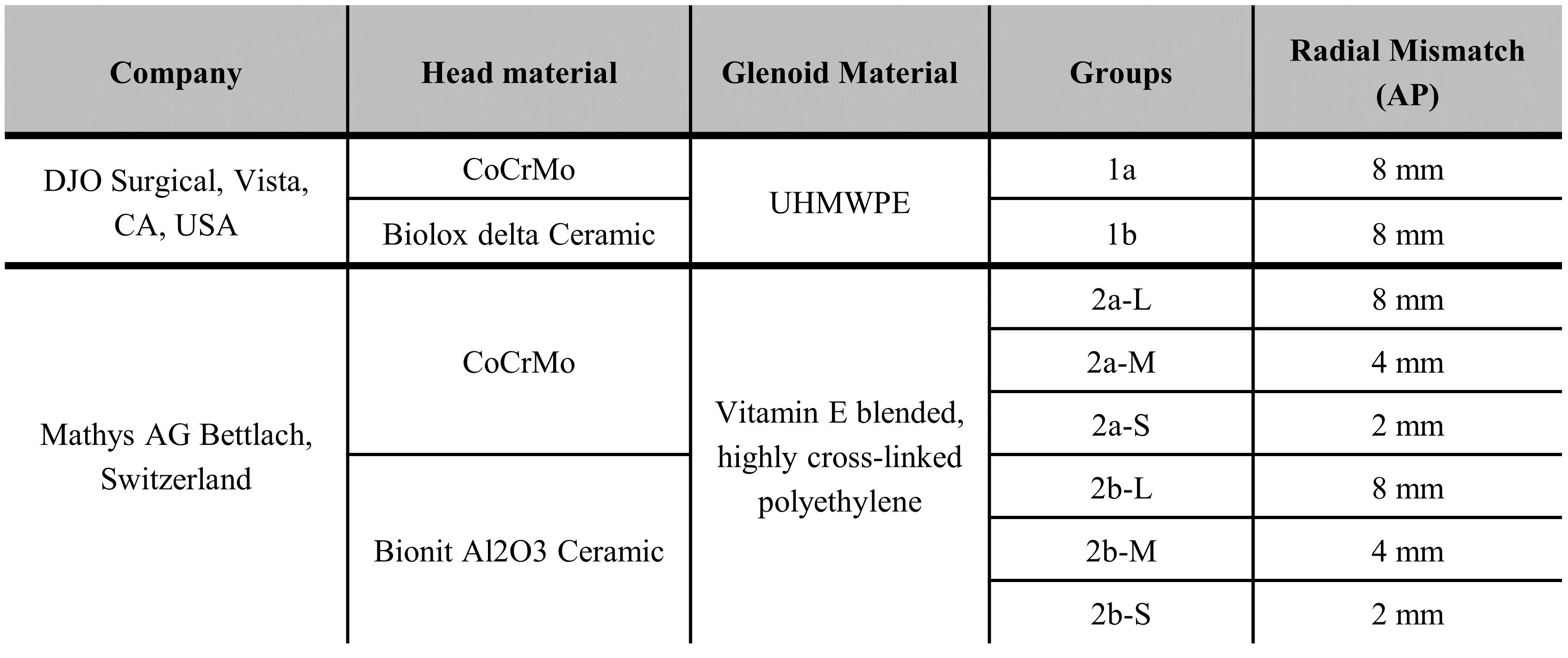
Figure 1
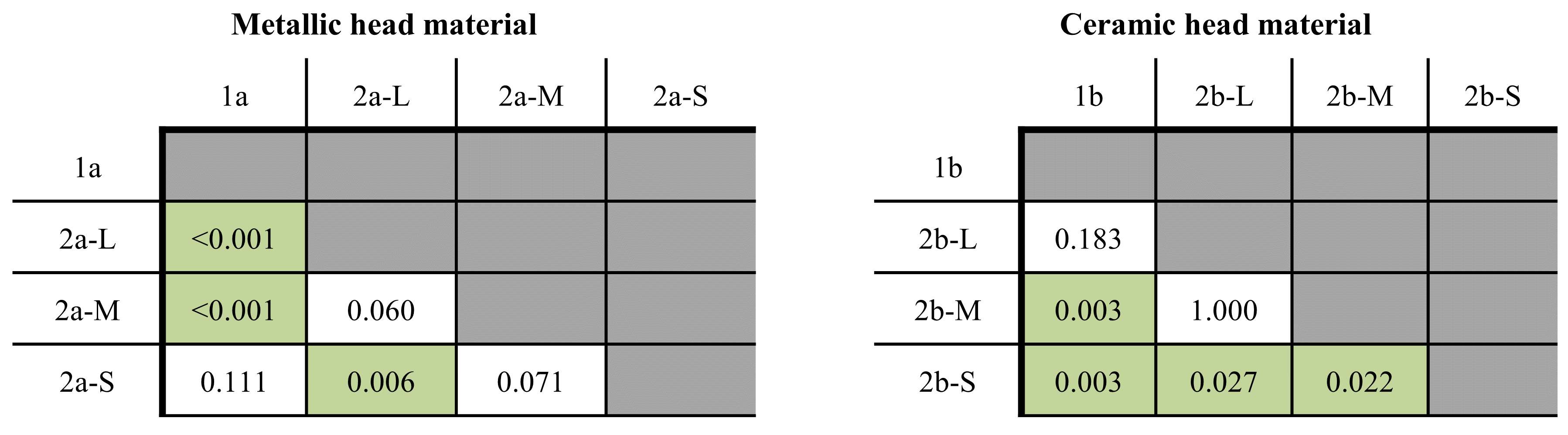
Figure 2
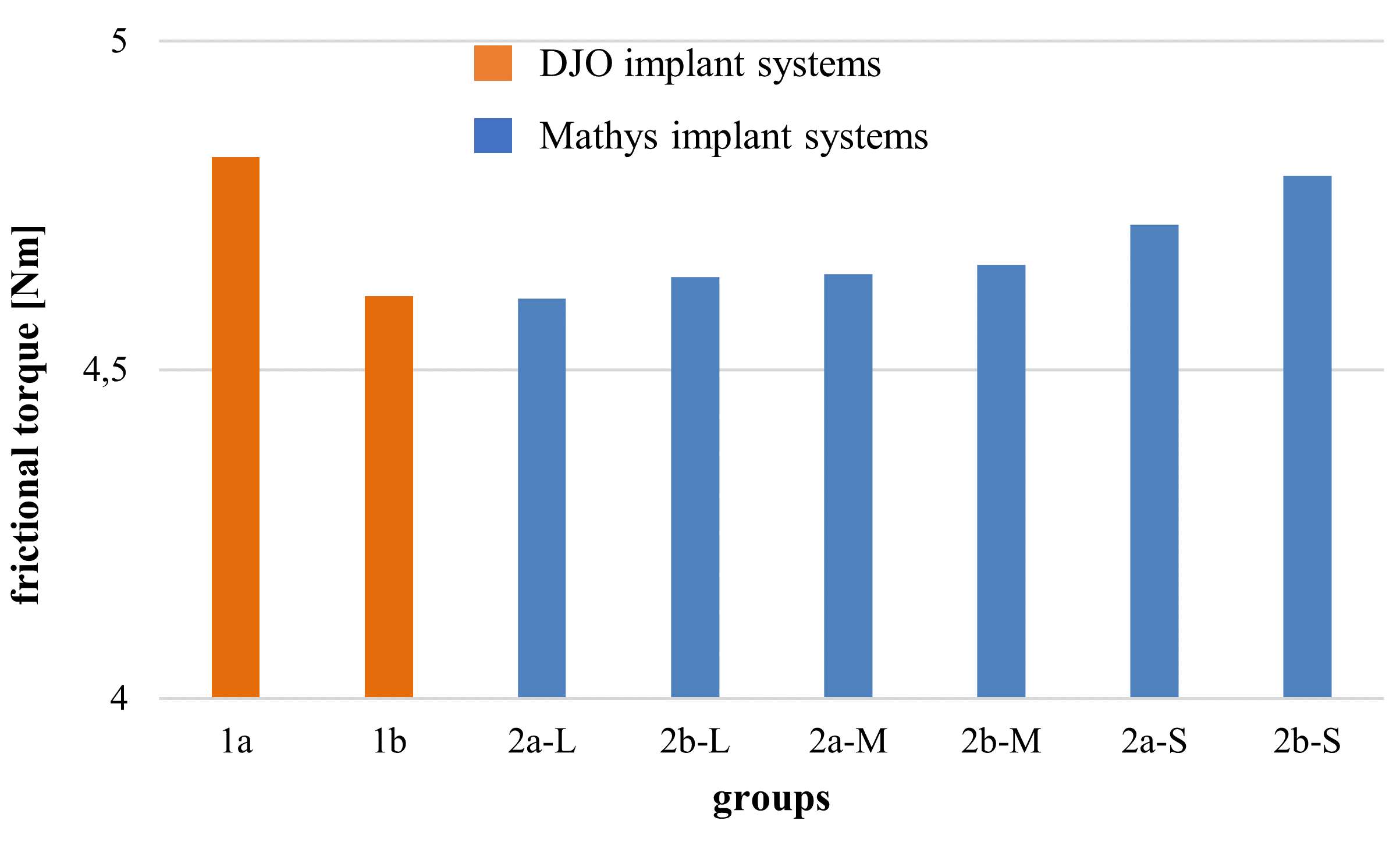
Figure 3#7511
Rheological Behavior of Different Calf Sera Before, During and After Wear Simulation
Maximilian Uhler - Laboratory of Biomechnics and Implant Research - Heidelberg, Germany
Mareike Schonhoff - Laboratory of Biomechanics and Implant Research - Heidelberg, Germany
Timo Nees - Heidelberg University Hospital - Heidelberg, Germany
Tanja Wonerow - Helmut-Schmidt-University - Hamburg, Germany
Jens Nuppnau - Helmut-Schmidt-University - Hamburg, Germany
*J. Philippe Kretzer - University of Heidelberg - Heidelberg, Germany
Stefan Schroeder - Heidelberg University Hospital - Heidelberg, Germany
*Email: philippe.kretzer@med.uni-heidelberg.de
Wear-induced aseptic loosening is still one of the most common reasons for revision in arthroplasty. To guarantee the patient’s safety of implants, well established tribological wear examinations of implants as defined in standards (ISO14242, ISO14243) are essential. Due to the different rheological behavior of human synovial fluid and the test mediums for in-vitro examinations, the wear tests cannot replicate the in-vivo situation completely. The standards for wear testing indicate calf serum as in-vitro test medium. However, these standards do not contain precise information on the main constituent components and the rheological properties. The aim of this study was to characterize the rheological properties of two possible test mediums to detect differences before and during the tribological simulation.
The rheological properties of Newborn-Calf-Serum (NCS) and Bovine-Calf-Serum (BCS) with a protein concentration of 20g/l (ISO14243) were compared by performing a tribological test using a servo-hydraulic-knee-simulator according to ISO 14243-1. Four Attune implants (DePuy-Orthopaedics) were used as test components. For both tests the procedure was divided into 5 intervals (Table1), between which the tested serum was exchanged. The rheologic behavior of the collected fluids at the different cycle numbers was determined using a Physica-MCR-702-rheometer (Anton Paar GmbH). The dynamic viscosity was measured as a function of the shear rate ranging from 10-1000s-1 with n=10 measurement repetitions.
Direct comparison of the dynamic viscosity of the two test sera before testing showed a significant difference regarding the rheological properties (p=0.041). Both fluids showed a shear-thinning behavior merging into nearly Newtonian behavior at high shear rates. From 0.1Mio cycles, there is no significant difference between the two fluids anymore (Figure1) (Table1). The dynamic viscosity at different test intervals for BCS and NCS showed obvious differences (Figure2). For BCS, an increase in dynamic viscosity can initially be identified after 100 cycles. In the interval range from 100 to 0.1Mio cycles a tendency of decreasing viscosity with increasing testing cycles can be seen. For the testing intervals 0.5 and 1.0Mio cycles this tendency is inverted. For NCS a change could also be seen after the start of the test and in the interval range from 100 to 1.0Mio cycles the same tendencies as at BCS can be obtained for lower shear rates. For shear rates , no clear trend in dynamic viscosity can be determined.
In summary, the two test fluids differ in their rheological properties before and during the test and can therefore lead to deviating results in tribological testing, although both are approved according to ISO 14243-1:2009. Thus, the choice of medium already impacts tribological test results which should be considered for the interpretation of tribological studies. Furthermore, both test media changes considerably over test duration. At a test duration of 0.5Mio cycles, both fluids have changed so that there is no longer any difference between them in terms of rheological properties. These changes could be attributed to denaturation and continuous protein shattering. Whether and at what time the test fluids reflect the in-vivo situation needs to be investigated in the further studies.
Figures
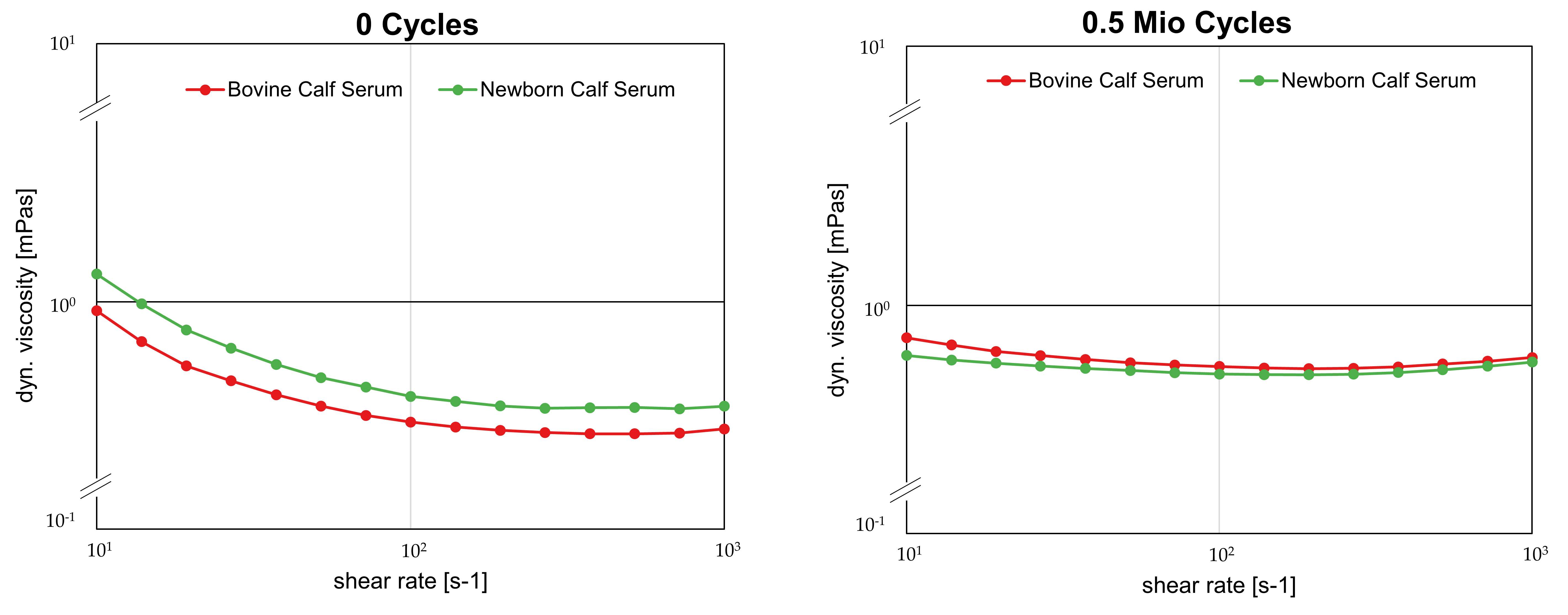
Figure 1
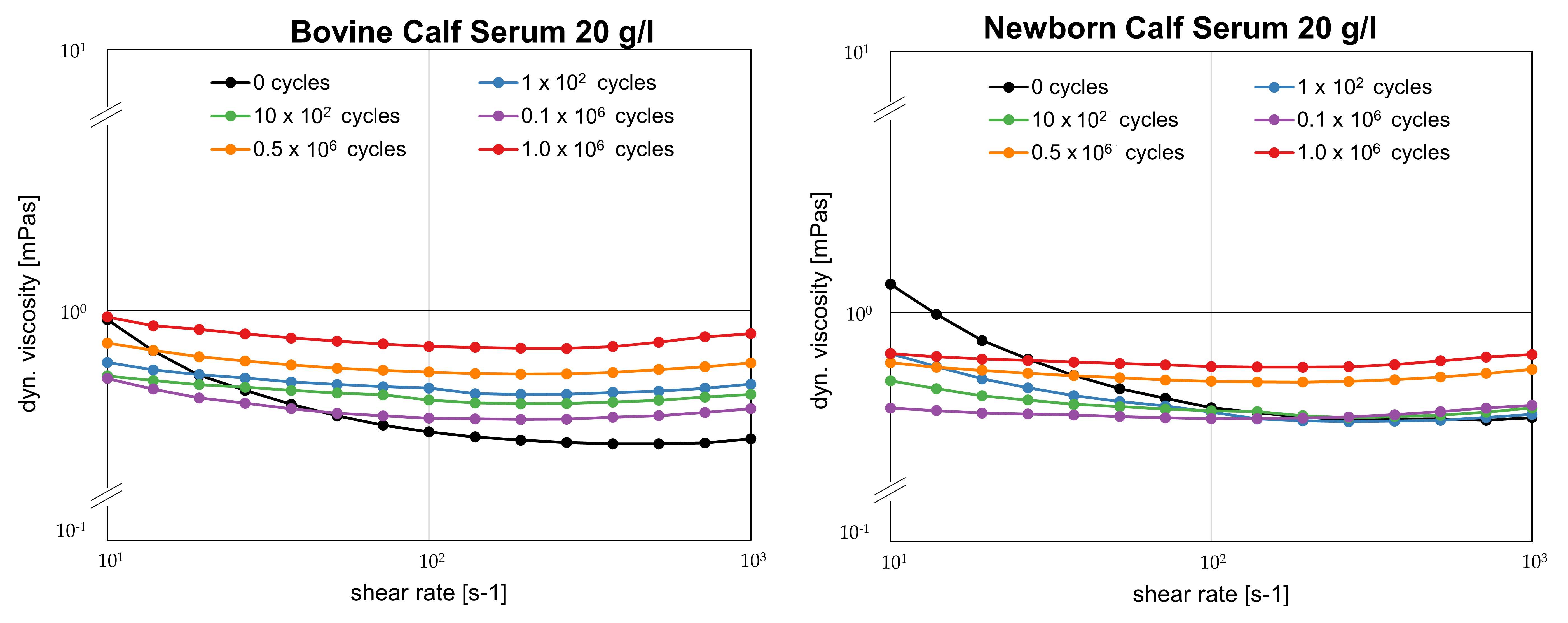
Figure 2
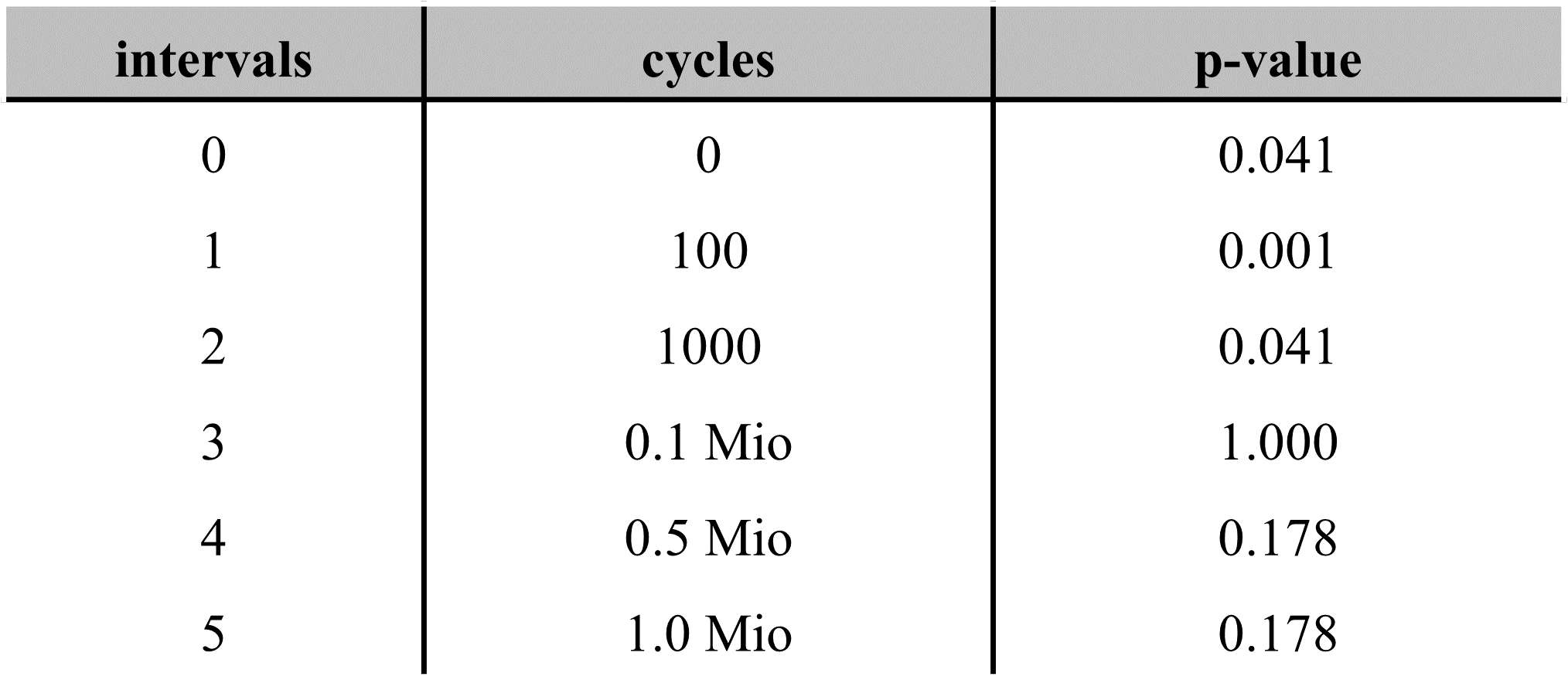
Figure 3#7680
Machine Learning Model Based on Historical Free-Living Activity Data to Improve Identification of Gait Exceptions Following Arthroplasty
*Karl Surmacz - Zimmer Biomet - Swindon, United Kingdom
Alex Ribeiro-Castro - Zimmer Biomet - Swindon, United Kingdom
Mark Brincat - Zimmer Biomet - Swindon, United Kingdom
Roberta Redfern - Zimmer Biomet - Pemberville, USA
Dave Van Andel - Zimmer Biomet - Grand Rapids, USA
*Email: karl.surmacz@zimmerbiomet.com
The current model of care after joint arthroplasty is considered reactive, in which clinicians are unable to closely follow each patient’s recovery postoperatively, addressing only immediate issues as they arise in their patient populations. The advent of digital and mobile health innovations, particularly those that incorporate the use of wearables for passive data collection, allow for remote monitoring in an extremely granular fashion. In order for this abundance of information to be useful, the need for machine learning to process data and provide meaningful, predictive insights is apparent. This study details the creation of a machine learning model and its use in determining exceptions to the early recovery period following total joint replacement.
A commercial database of patients using a smartphone-based care management platform (sbCMP), mymobility®, was used to inform the machine learning models for exceptions following joint replacement. The sbCMP collects information pre- and postoperatively including passive collection of mobility metrics such as step counts, gait speed, gait asymmetry, and other Healthkit data as previously described. Individual patient data is made available via a provider-facing platform for remote monitoring. Previously, gait exceptions based on normative data were employed to notify clinicians in cases where a patient’s gait speed dropped below defined thresholds. The machine learning model, WalkAI®, was trained and validated based on historically collected data from the sbCMP to more accurately identify gait speed recovery curves and anticipate future walking behavior based on real-world preoperative gait behavior. Predictions of 90-day gait speed are calculated at each day postoperatively from days 15 through 40, and exceptions are generated based on a comparison of a patient’s predicted outcome to patients in a similar sub-group. Cross validation was performed using the training set, with 30% being reserved as a test set for final validation. The model was tuned to prioritize precision and reduce the number of false positives resulting in notification. Performance of the model, including sensitivity, specificity, precision, and accuracy were determined; ROC analysis was used to compare false positive and true positive rates. Mean absolute error was calculated and compared to baseline heuristic model results for quantification of improvement of the model.
Including the iterative model training and validation based on real-world mobility data from the historic sbCMP, the performance of the predictive model was significantly improved compared to the historic gait exceptions model, where mean absolute error in 90-day gait speed prediction was reduced from 0.075 m/s to 0.049 m/s in the test set (Figure 1). The model currently provides 60% precision, 89% accuracy, 38% sensitivity and 96% specificity, as this model was trained to reduce false positive results. The ROC analysis (Figure 2) suggests good clinical performance of the current model.
Utilization of machine learning to determine exceptions in gait recovery following total joint replacement is feasible and provides results with exceptional specificity. This model will allow for additional patient data to be included for retraining to adapt to changing patient populations. In addition, clinician feedback regarding notifications, including resulting actions and outcomes, can be used to further inform the model and improve its clinical utility.
Figures
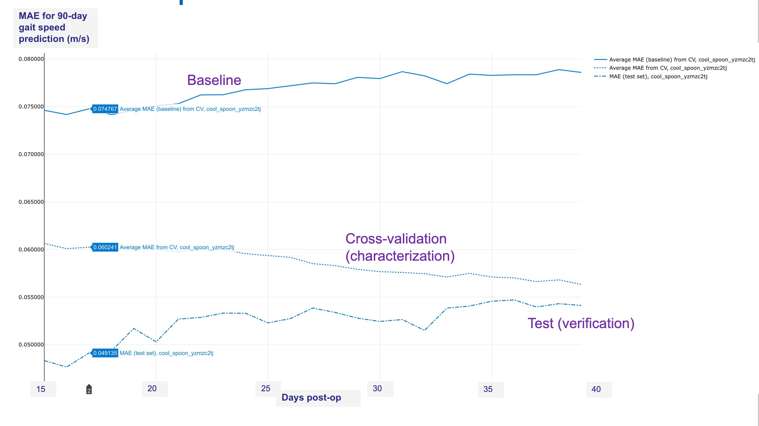
Figure 1
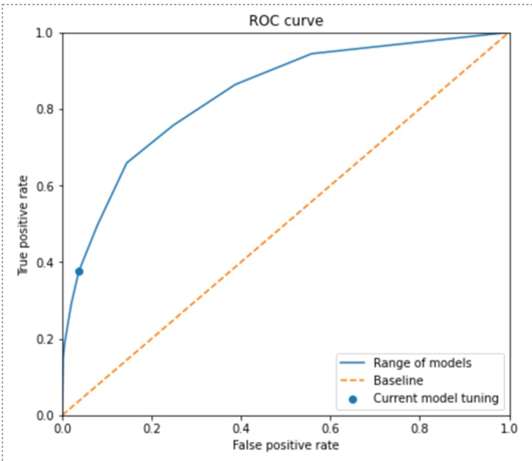
Figure 2#7662
Comparison of Stair Count and Speed Recovery in Patients Following Partial or Total Knee Arthroplasty
Mike Berend - Ortho - Mooresville, USA
Roberta Redfern - Zimmer Biomet - Pemberville, USA
Dave Van Andel - Zimmer Biomet - Grand Rapids, USA
Mike Anderson - Zimmer Biomet - Lehi, USA
Anna N Ren - Zimmer Biomet - Gibsonia, USA
Robert E Neher - Zimmer Biomet - Roanoke, USA
*Jared Foran - Panorama Orthopaedics and Spine Center - Golden, USA
*Email: jaredforan@yahoo.com
Partial knee arthroplasty (PKA) is often employed in the treatment of unicompartmental osteoarthritis and has been reported to provide superior range of motion (ROM), more rapid recovery, and improved gait metrics over total knee arthroplasty (TKA). However, studies have suggested up to 32% fail within seven years and are converted to TKA. The goal of this study was to investigate functional recovery of PKA and TKA cohorts utilizing a smartphone-based care management platform (sbCMP).
Analysis of data from a post-market prospective, multicenter longitudinal study of patients undergoing total joint arthroplasty and prescribed the use of a sbCMP paired with Apple Watch. Only subjects who underwent PKA or TKA and reported living in a multilevel home environment were included. Subjects completed the KOOS JR preoperatively and at 30, 90, 180 and 365 days postoperatively. ROM data was collected at 30 and 90 days postoperatively and investigated as a function of reaching 90° and 110° flexion at 30 and 90 days, respectively. Stair counts, as well as ascending and descending speeds, were collected passively by the sbCMP for 365 days after surgical intervention. Decision to perform manipulation under anesthesia (MUA) due to ROM concerns was based on individual surgeon’s discretion. Average stair counts and KOOS JR scores were compared by t test; changes were compared by paired t test or Wilcoxon rank sum test, where appropriate. Multivariate models were created to investigate the association of baseline characteristics on stair count recovery.
In total, 1,121 patients were eligible for inclusion in this analysis. The average age was 62.5 ±8.8 years; 59.7% of subjects were female. PKA patients reported higher overall KOOS JR scores than the TKA cohort, however the improvement in scores was higher in the TKA patients at 1 year postoperatively. Significantly fewer subjects in the TKA cohort attained 90° flexion at 30 days compared to PKA (86.9% vs 92.9%, p =0.02); similar trends were observed comparing 110° at 90 days (86.2% vs 96.9%, p<0.001). MUA was performed in 3.6% of the cohort. Stair counts were higher in PKA patients preoperatively and through 6 months, however the difference was not significant at one year, at which point both groups exceeded preoperative stair counts (7.4 ±7 vs 6.8 ±15.1). Stair count recovery appeared to be reached between 10-14 weeks postoperatively. Ascending and descending speeds varied between TKA and PKA subjects only at 30 days and did not differ based on ROM goals at 30 and 90 days. Multivariate analysis suggests that stair counts are associated with age, gender, preoperative pain, procedure, time, and flexion at 30 days. Ascending stair speeds were associated with age, procedure, and time whereas descending speeds were associated only with age and time since procedure.
At one year postoperatively, subjects who underwent TKA and PKA had demonstrated similar function as evidenced by KOOS JR scores, stair counts, and stair speeds. Significantly fewer TKA patients met ROM goals, which did not appear to affect patient reported or objective measures of function in this cohort.
#7664
Effects of Increased Use of Self-Directed Therapy on Rehabilitation During the COVID-19 Pandemic Following Knee and Hip Arthroplasty
*Todd Miner - Colorado Limb Replacement - Denver, USA
Mike Anderson - Zimmer Biomet - Lehi, USA
Dave Van Andel - Zimmer Biomet - Grand Rapids, USA
Robert E Neher - Zimmer Biomet - Roanoke, USA
Roberta Redfern - Zimmer Biomet - Pemberville, USA
Paul Duwelius - Orthopedic and Fracture Specialists - Portland, USA
*Email: ToddMiner@Centura.Org
Postoperative physical therapy (PT) has remained the standard of care after many orthopaedic procedures. Smartphone-based care management platforms (sbCMP) have been increasing in popularity and the COVID-19 pandemic has triggered additional adoption of new technologies in order to eliminate the need for in-person PT. The purpose of this study was to evaluate the impact of the COVID-19 pandemic on the PT utilization and outcomes of patients enrolled in a cohort study of patients prescribed a sbCMP for self-directed rehabilitation (SDR).
This study is a secondary data analysis of patients enrolled in a multicenter, industry sponsored, prospective cohort trial. Only patients who met criteria and used the mymobility sbCMP for at least 2 weeks prior to undergoing partial knee arthroplasty (PKA), total knee arthroplasty (TKA) or total hip arthroplasty (THA) and had a minimum three months of postoperative follow-up data were included. Step counts were passively recorded by the sbCMP; patients reported the use of adjunct PT at three months as well as KOOS JR and HOOS JR scores. Cases were separated in two groups as a function of the date of surgery with respect to occurrence in the COVID-19 pandemic and incidence of COVID-19 cases per period (lower cases and higher cases). Step counts, adjunct PT use, and outcomes were compared by parametric and non-parametric tests as appropriate; p<0.05 were considered statistically significant.
Evaluable data was available for 766 (46.0%) TKA, 193 (11.6%) PKA, and 706 (42.4%) THA patients. Baseline patient characteristics (age, gender, and BMI) were similar between the two groups across procedure types, as were preoperative step counts (all, p>0.05). Postoperative step counts improved at three months compared to preoperative levels in all procedure types. The use of SDR alone was significantly higher in the early period when COVID-19 case counts were considered low in patients undergoing TKA (35.3% vs 27.6%, p=0.03) and THA (72.5% vs 59.3%, p<0.001), though this did not reach significance in the PKA cohort (58.9% vs 53.3%, p=0.53). Postoperative step counts exceeded preoperative activity across procedure types and did not vary significantly by COVID-19 period. The change in KOOS JR and HOOS JR scores from preoperative to postoperative levels were similar by pandemic period in all cohorts: TKA (17.7 vs 18.4, p=0.54), PKA (16.0 vs 16.5, p=0.80), and THA (28.6 vs 29.0, p=0.75).
The COVID-19 pandemic affected access to healthcare in all disciplines of medicine, including orthopaedics. The use of SDR increased early during the COVID-19 pandemic, when cases counts were considered low and were associated with local and national lockdowns. Decreases in the use of in-person PT in this study were observed while patient outcomes did not appear to be negatively impacted. SDR as facilitated via a sbCMP may be beneficial for patients who may be unable or unwilling to participate in in-person PT visits.
#7917
Numeric Pain Rating Correlates With Patient Reported Outcome Measures and Passively Collected Mobility Metrics Following Total Hip and Knee Arthroplasty
Karl Surmacz - Zimmer Biomet - Swindon, United Kingdom
Alex Ribeiro-Castro - Zimmer Biomet - Swindon, United Kingdom
Mike Anderson - Zimmer Biomet - Lehi, USA
Dave Van Andel - Zimmer Biomet - Grand Rapids, USA
Roberta Redfern - Zimmer Biomet - Pemberville, USA
*Paul Duwelius - Orthopedic and Fracture Specialists - Portland, USA
*Email: pduwelius@gmail.com
Patients undergo total joint arthroplasty to return function and resolve pain. Patient reported outcome measures (PROMs) are often sought to determine surgical success but are time-consuming and patient response rates are often low. This study sought to determine whether pain numeric rating scores (NRS) were associated with PROMs and objective mobility outcomes.
This is a retrospective review of data in patients who utilized a smartphone-based care management application prior to and following total joint arthroplasty. NRS, PROMs (HOOS JR and KOOS JR), were collected up to 30 days preoperatively; objective mobility data (step counts, gait speed, and gait asymmetry) were collected on a continuous passive basis. Analyses of correlations to PROMs and mobility metrics were limited to those with available data during the preoperative period (-30 to -1 days), 30-day postoperative period (25 to 35 days) to 90-day postoperative (85 to 95 days) timeframe. Correlations were evaluated by univariate quantile regression, comparing NRS pain scores with the corresponding timeframe’s PROMs or mobility metrics, where both NRS and PROMs are normalized on a 0 – 1 scale. Univariate quantile regressions were also performed to investigate the relationship between pain and change in gait speed, where median gait speed over the time window of interest (30±5 or 90±5 days) was used to determine the change from the median preoperative gait speed.
TKA patients reported consistently higher NRS than THA postoperatively. NRS was significantly correlated with step counts, gait speed, and gait asymmetry preoperatively and at 30 and 90 days postoperatively on quantile regression. Regression results suggested significant correlations between NRS and PROMs scores, with stronger relationships observed between NRS and HOOS JR, -0.55 (95% CI -0.67 – -0.43, p<0.001) than with KOOS JR, -0.24 (95% CI -0.10 – -0.43, p = 0.003). The preoperative NRS showed borderline association with gait speed (-0.07, 95% CI -0.14 – 0, p=0.05), but not the preoperative step count or gait asymmetry. Pain score did show significant associations with all remaining mobility measures at both 30 days and 90 days postoperatively, where step counts and gait speed returned negative coefficients, demonstrating higher pain reports were associated with fewer steps and slower walking speeds. The regression analyses of gait asymmetry suggest that patient reported NRS is a significant predictor at 30 days, where higher pain levels are correlated with higher percentages of gait asymmetry. Change in walking speed from preoperative levels to 30 postoperatively demonstrates that 30-day NRS is significantly associated with the median change in speed at 30 days, however the 90-day NRS is not significantly correlated with change in gait speed from preoperative levels at 90 days.
NRS is correlated with both objective and subjective measures of function in patients undergoing arthroplasty. Simple pain ratings and may be a valid measurement to help predict functional outcomes when repeated collection of traditional PROMs is not feasible. NRS scores can be administered using mobile devices for remote monitoring of patient recovery, potentially allowing earlier intervention where necessary.
Figures
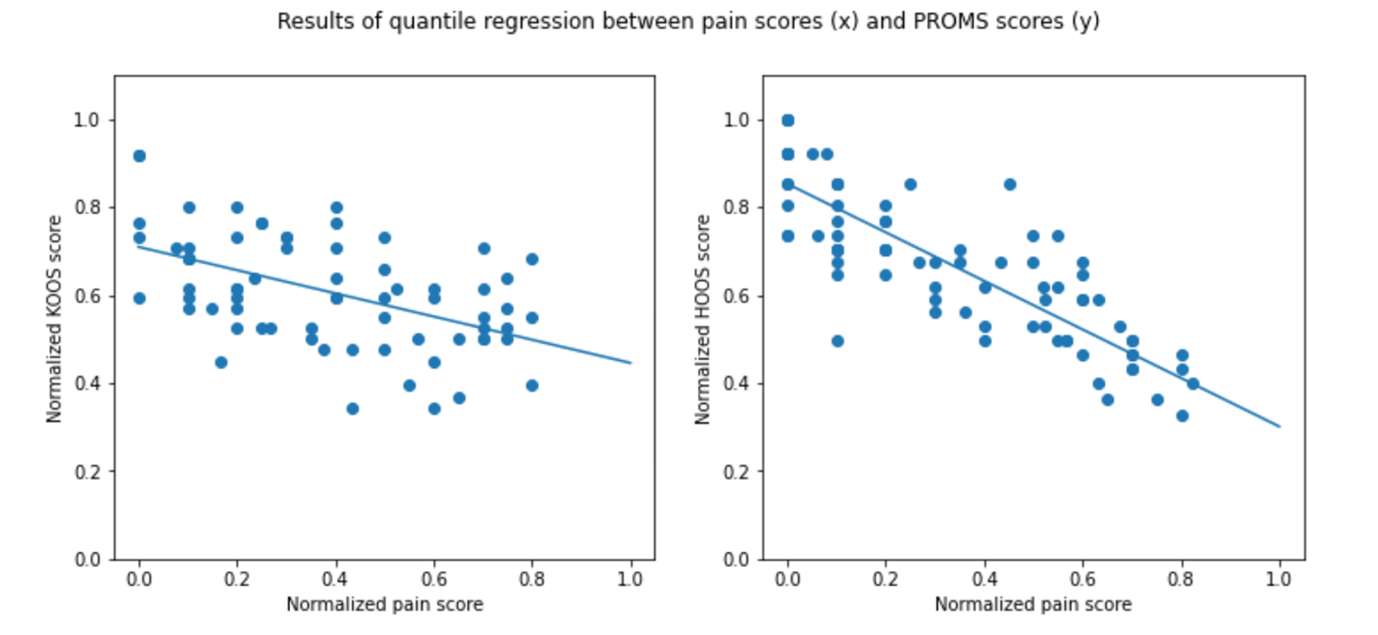
Figure 1#7957
Early Postoperative Walking Bouts Are Associated With Improved Gait Speed and Symmetry at 90 Days
Karl Surmacz - Zimmer Biomet - Swindon, United Kingdom
Mara Catalina AguileraCanon - Zimmer Biomet - Swindon, United Kingdom
Alex Ribeiro-Castro - Zimmer Biomet - Swindon, United Kingdom
Dave Van Andel - Zimmer Biomet - Grand Rapids, USA
Mike Anderson - Zimmer Biomet - Lehi, USA
Roberta Redfern - Zimmer Biomet - Pemberville, USA
*Chad E Cook - Duke University - Durham, USA
*Email: chad.cook@duke.edu
Walking is recommended as the best method to expedite recovery after lower limb arthroplasty; however, little is known about the optimal daily walking patterns postoperatively to achieve recovery of step counts, gait speed, and gait symmetry. This study aims to investigate whether the distribution of walking bouts early in the postoperative period is associated with these gait metrics at 90 days postoperatively.
Mobility data was passively collected using a smartphone-based care management platform in patients undergoing joint replacement procedures. Bout data were investigated as a function of the longest walking session of the day and were used to create a ratio to the total daily active time, representing the fraction of walking done during a single session per day (aggregation score). Quantile regression was performed to evaluate the association between the longest walking session or aggregation score at 30 days postoperatively and HealthKit mobility metrics at 90 days.
In total, 2317 patients provided evaluable data. At 30 days postoperatively, less than 20% of time was spent logging steps and the majority of steps were logged around the midday hours. Preoperative walking session length appeared to reach preoperative levels sooner in patients undergoing total hip arthroplasty compared to total knee arthroplasty and exceeded preoperative session lengths. Similar trends were observed in comparing aggregation scores, where high scores were observed immediately following surgery and improved to preoperative levels more quickly in the total hip arthroplasty (THA) and partial knee arthroplasty (PKA) populations compared to total knee arthroplasty (TKA). The longest walking session at 30 days was positively associated with 90-day gait speed across in THA (0.17, p<0.001) and TKA (0.15, p<0.001). Aggregation score, on the other hand, was negatively associated with gait speed at 90 days across procedure types, with coefficients ranging from -0.18 to -0.12. High aggregation scores early in the postoperative period were associated with increased asymmetry later in the TKA cohort (0.03, p=0.001) and THA cohorts (0.02, p=0.05).
The duration and frequency of walking bouts appears to be associated with recovery of gait speed following lower limb arthroplasty. Higher aggregation scores were associated with slower gait speeds at 90 days postoperatively, while logging longer walking sessions was associated with faster gait speeds later in recovery. These data provide evidence that supports the role of more frequent walking sessions to facilitate recovery following joint replacement.
#7788
Quantitative Determination of Wear Rate and Wear Location in Retrieved Polyethylene Glenoid Components
Peder Solberg - Dartmouth College - Hanover, United States of America
John-Erik Bell - Dartmouth Hitchcock Medical Center - Lebanon, USA
Peter Shaughnessy - Dartmouth Hitchcock Medical Center - Lebanon, USA
Jacob Torrey - Dartmouth College - Hanover, USA
*Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: dvancitters@Dartmouth.edu
Introduction:
Glenoid loosening is the most common cause of total shoulder arthroplasty failure1,2, and osteolysis is a common intraoperative and radiographic finding associated with these failed arthroplasties2. While preclinical testing can estimate failure mode and wear rates in the laboratory, there is limited in vivo data measuring polyethylene wear rate and location. As polyethylene wear in anatomic total shoulder arthroplasty is responsible for osteolysis we hypothesize that higher polyethylene wear in total shoulder arthroplasty leads to shorter time to revision surgery. In addition, we hypothesize that the principal wear location of the humeral head on glenoids is not in the anteroposterior or superoinferior direction, but rather is along an intermediate axis.
Methods:
Using an IRB-approved total joint arthroplasty retrieval collection, 45 gamma-barrier and gamma-air polyethylene glenoid components from ten different manufacturers were analyzed for in vivo dimensional change. Polyethylene thickness measurements were obtained at the anterior, posterior, superior, and inferior aspects of the implant, being careful to avoid regions of obvious delamination or osteophyte-related wear. As there was radial symmetry in all the as-manufactured devices, the differential measurement between each of the anteroposterior values and superoinferior values was calculated to provide a conservative estimate of dimensional change along that axis. The maximum value of the two differential measurements is reported as a conservative estimate of wear rate in vivo, recognizing that the dimensional change may also include creep of the bearing. A physiologic wear vector was determined for each retrieved device by taking the arctangent of the SI and AP measurements, giving a mean wear angle relative to the AP axis.
Results:
The median material loss rate for all samples was 0.14 mm/year. 17 specimens (38%) had wear rates ≤0.1mm/year and 16 specimens (36%) had wear rates ≥0.2mm/year. Specimens with >0.2mm/year of polyethylene wear had an average time to revision of 51.3 months, compared to an average of 146 months in those with <0.1mm/year wear (p<0.002) [Fig. 2]. The superoinferior material loss was greater than the anteroposterior loss in 24/45 specimens (53%). The mean wear vector was 48 degrees above horizontal with a distribution skewed to higher values [Fig. 3].
Conclusion:
The median linear wear rate demonstrated here has been shown previously to be associated with osteolysis in total hip arthroplasty3, and these data suggest that increased polyethylene wear rates in total shoulder arthroplasty lead to earlier revision surgery, likely from osteolysis. The mean wear locus in retrieved glenoids was found to be at an intermediate angle rather than the SI axis most often used to test loosening in ASTM F2028 benchtop tests. These results suggest that glenoids should be designed and tested to minimize loosening resulting from loading along these clinically-relevant wear paths.
References:
1. Matsen FA et al. JBJS Am. 2008;90:885-896. doi:10.2106/JBJS.G.01263
2. Papadonikolakis A et al. JBJS Am. 2013;95(24):2205-2212. doi:10.2106/JBJS.L.00552
3. Wilkinson JM et al. J Orthop Res. 2005;23(3):520-525. doi:10.1016/j.orthres.2004.11.005
Acknowledgements: OREF Grant #19-004 provided funding for this study.
Keywords: Arthroplasty, Shoulder, Retrieval, Glenoid, Polyethylene
Figures
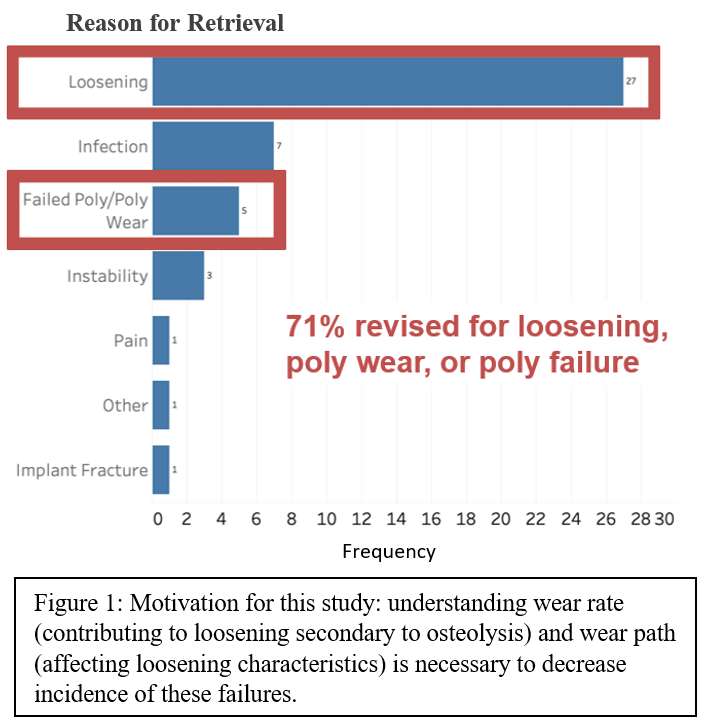
Figure 1
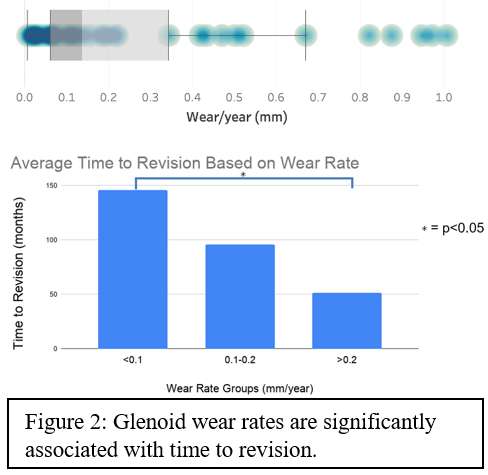
Figure 2
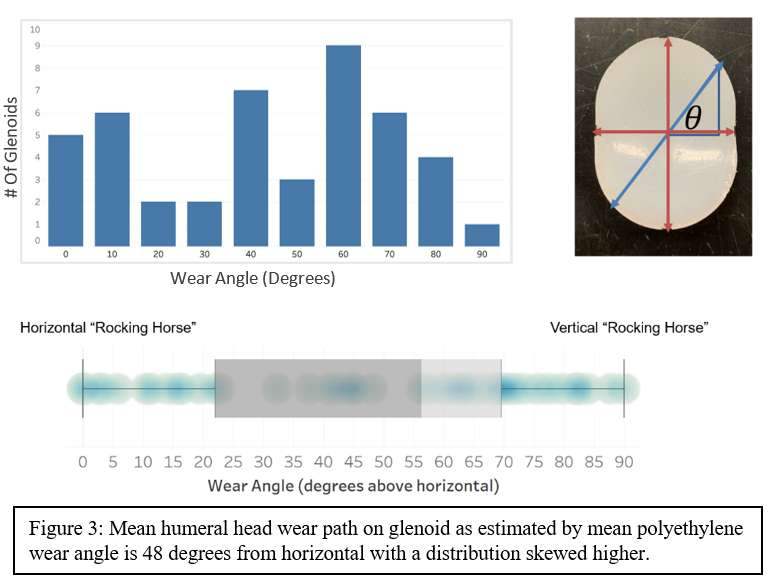
Figure 3#7645
Attune AOX Retrievals: How Do Wear and Oxidation Compare to Highly Cross-Linked UHMWPE?
Barbara Currier - Dartmouth College - Hanover, USA
Kori Jevsevar - Dartmouth College - Hanover, USA
*Douglas Van Citters - Dartmouth College - Hanover, USA
*Email: dvancitters@Dartmouth.edu
Introduction
UHMWPE bearing surfaces are subject to wear, and in vivo oxidation that can lead to bearing fatigue or fracture. To provide TKA bearing materials that balanced resistance to wear, mechanical failure, and oxidation, manufacturers introduced antioxidant polyethylene. This study reports dimensional change (representing wear and deformation) and oxidation performance of an expanded series of hindered phenol (PBHP) antioxidant retrievals, asking: 1) How do dimensional change and oxidation of a series of fixed-bearing antioxidant devices compare to currently-marketed highly cross-linked (HXL) UHMWPE inserts? and 2) Does dimensional performance vary between antioxidant fixed-bearing and rotating-platforms?
Methods
A series of 165 consecutive Attune™ AOX knee inserts (DePuy Synthes, Warsaw, IN), including both fixed-bearing (FB, n=111) and rotating-platform (RP, n=54) designs, were received at revision by an IRB approved retrieval laboratory between September 2014 and January 2022, with in vivo duration of 0-7 years. AOX fixed-bearing (AOX-FB) results were compared to a series of annealed (n=188) and remelted (n=254) HXL tibial inserts with similar in vivo duration. Thickness change of each insert was estimated using a previously published method, calculated by subtracting measured thickness dimension from the as-manufactured dimension, estimated from retrievals in vivo < 16 months (n = 206). Oxidation was measured by FTIR and reported as maximum ketone oxidation index (KOI) measured in the cross-section of each medial condyle. Statistical analyses used SPSS, with a p-value <0.05 considered statistically significant.
Results
Never-implanted AOX knee inserts (n=13) provided a base-line median KOI=0.08. Patient variables and time in vivo were similar among AOX-FB, annealed HXL, and remelted HXL retrieved inserts (Figure 1-Table1). Thickness-change rate (Figure 2) for AOX-FB was higher than for the annealed inserts (Figure 1-Table2), but the difference when compared to remelted insert thickness-change rate was not significant (Figure 1-Table2). The range of measured KOI for AOX-FB inserts was smaller and lower than either annealed or remelted HXL inserts (Figure 3, Figure 1-Table2). Comparing AOX-FB (n=54) and AOX-RP (n=26) inserts in vivo ³16 months, showed that AOX-RP inserts had significantly lower thickness-change rate (RP=0.0114 mm/year, FB=0.0256 mm/year, p=0.012) than AOX-FB.
Discussion
Using thickness change to assess insert wear had the potential for creep to be included in estimates of material loss, potentially overstating wear for less creep-resistant materials. However, this study demonstrated that the thickness-change rate of fixed-bearing, moderately cross-linked AOX-FBinserts was similar to currently-marketed HXL tibial inserts, previously shown to reduce wear rate and nearly eliminate osteolysis compared to conventional UHMWPE. The lower thickness-change rate of AOX-RP inserts compared to AOX-FB was consistent with earlier published studies and might be attributed to lower contact stress, patient variables, or reduced crossing motion at the articulations.
PBHP antioxidant contains ketone functional groups, seen as median KOI=0.08 in never-implanted AOX inserts. AOX KOI did not increase appreciably above this value over time in vivo, demonstrating the effectiveness of PBHP in preventing UHMWPE oxidation. Both annealed and remelted insert KOI increased over time in vivo, approaching critical oxidation, resulting in loss of mechanical properties sufficient to lead to fatigue damage observed in 4 devices.
Acknowledgement
Tibial dimensional change measured by John Currier.
Figures
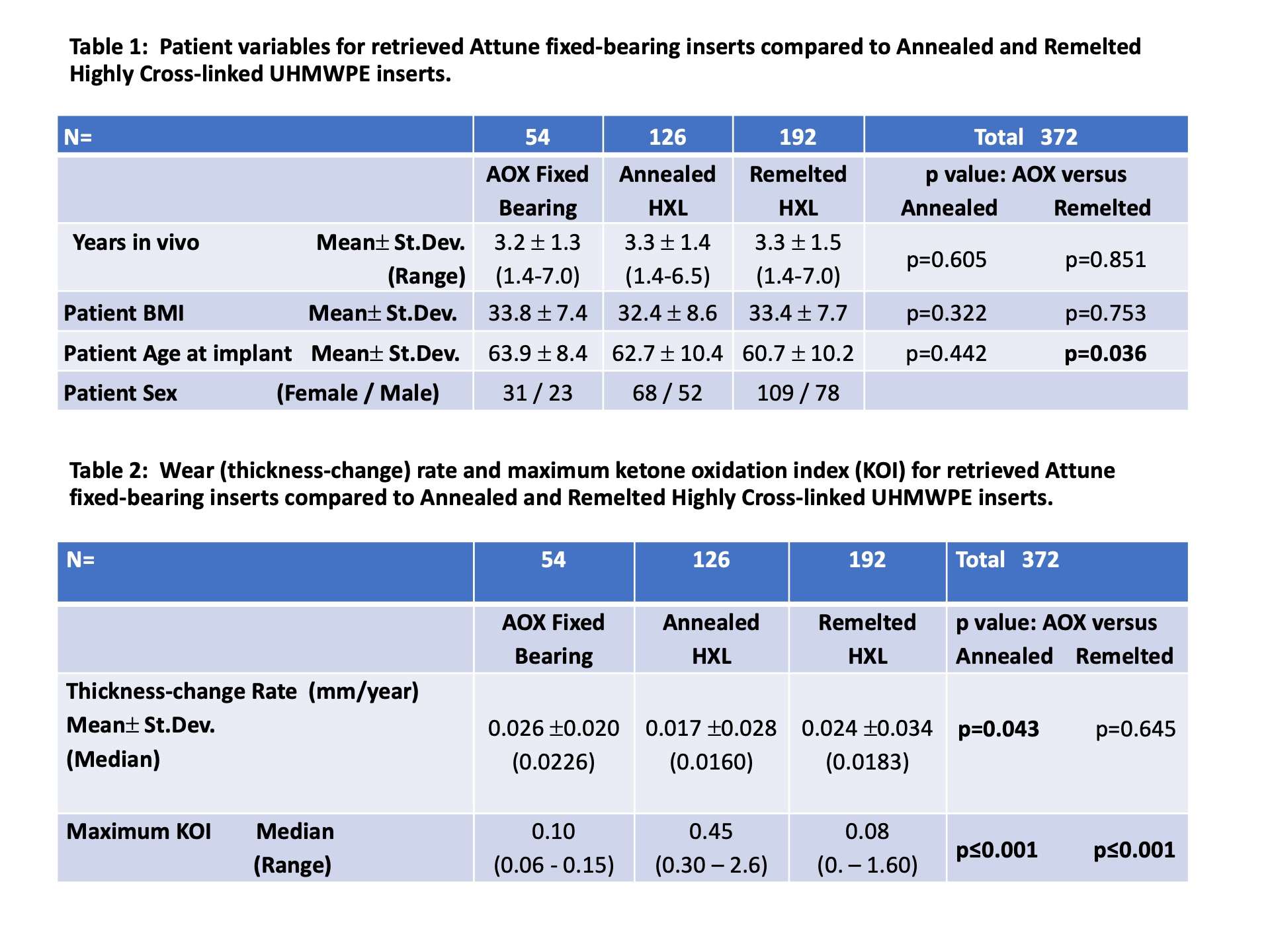
Figure 1
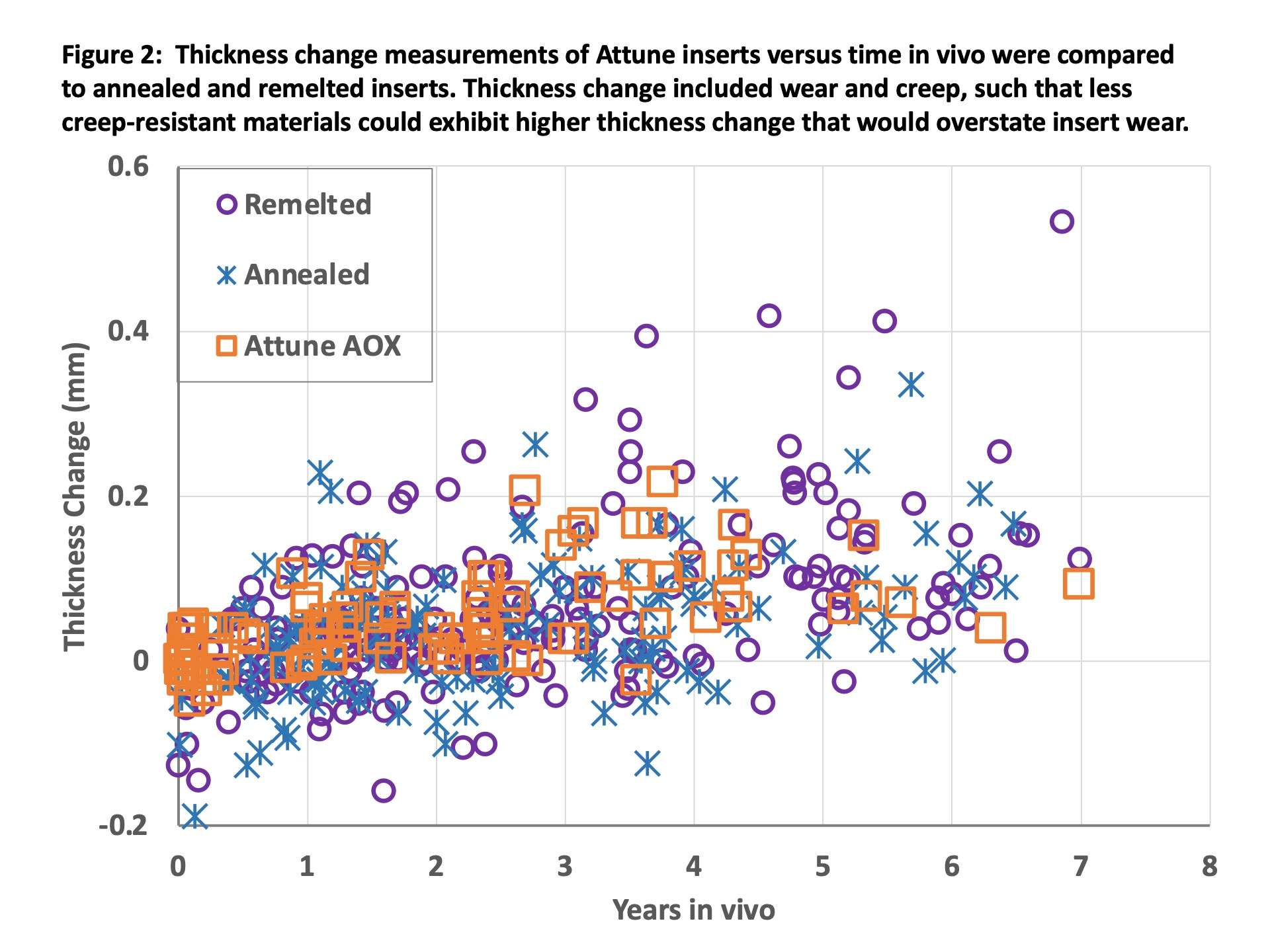
Figure 2
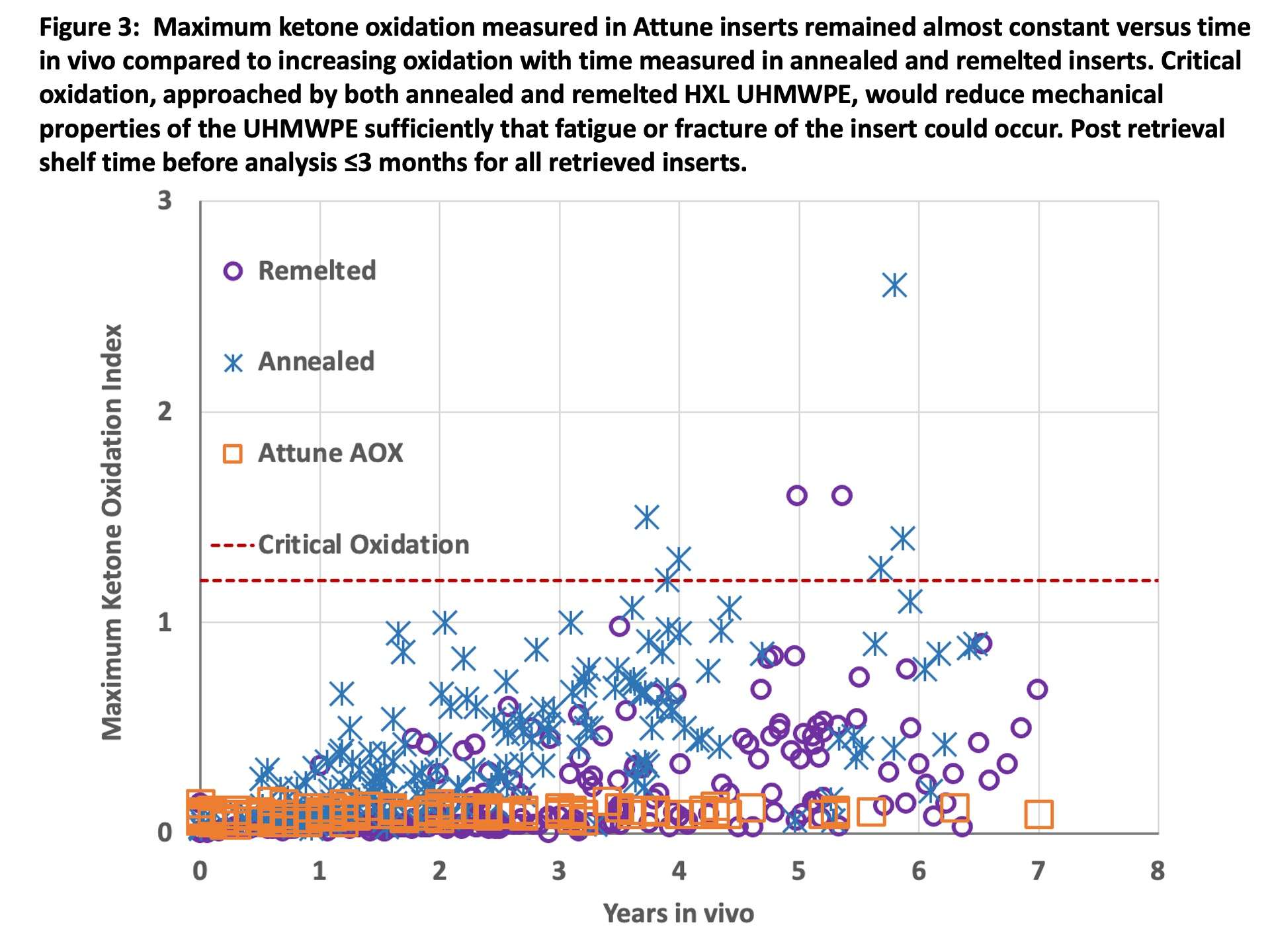
Figure 3#8053
Invited Talk: Surprising Results From a National Randomized Controlled Trial Comparing Standard Physical Therapy With a Rehabilitation App After THA and TKA in Belgium
*Catherine Van Der Straeten - Ghent University Hospital - Ghent, Belgium
*Email: cathvds@telenet.be
Introduction
In 2020, mobile applications are included in a Belgian national treatment plan for patients who receive a total hip or knee prosthesis. In a first phase, the National Institute for Health and Disability Insurance (NIHDI) finances its use in a randomized controlled clinical trial comparing classic rehabilitation with a physical therapist with a program of personalized rehabilitation at home through daily remote follow-up supported by a CE-marked app in patients undergoing primary knee or hip arthroplasty. In addition to the investigation of the effectiveness of mobile applications on rehabilitation outcomes (PROMS) and quality of life, policymakers, healthcare providers and app developers want to collect information on cost-effectiveness of rehabilitation supported by an app, to decide on its definitive reimbursement. Ghent University Hospital coordinates the study, under the supervision of the Belgian Federal Knowledge Center.
Patients and Methods
The study is a national, multi-center, open-label, randomized controlled, three-arm, parallel-group, non-inferiority trial in patients who receive a primary total hip or knee arthroplasty and compares 1) postoperative rehabilitation with a physical therapist to 2) a personalized program of rehabilitation with a mobile app combining patient feedback with standardized recovery protocols to generate daily personalized care plans and information support including exercise videos and remote physiotherapy advice and 3) a mixed model of physical therapy and remote support with the app. Primary endpoint is to evaluate whether equivalent clinical results were obtained at 6 months postop. To this end data on complications and PROMs are collected (HOOS/KOOS). The secondary endpoint is to assess and compare generic quality of life using EQ5D-5L questionnaires at 6 months postop. The necessary sample size to achieve over 80% power to conclude on non-inferiority of the app is 1011 (615 knee- and 396 hip) arthroplasty patients. Prior to the inclusion in the study, patients were asked to complete a questionnaire online to check their ability to use the app and fill out the PROMs online.
Preliminary results
The study started in January 2021 and is now running in 11 sites in Belgium. Recruitment is substantially delayed by the Sars-Cov-2 pandemic leading to a temporary block of elective surgery at many hospitals and many patients postponing their surgery out of fear.
At 17 months, only 368 patients have been randomized in the study, 174 knee and 194 hip arthroplasty patients. Mean and median age is 62 years in both in knee and hip groups.
However, despite the COVID situation, 1130 patients have been screened for participation in the study, but 762 of these patients (67.4%) were not eligible or preferred not to participate. The most important reasons for not participating are 1) preference to exercise with their own physiotherapist (32%) and 2) insufficient digital literacy and/or no access to internet (18%). The latter is probably an underestimation as another 16% of patients did not want to give up a reason for not participating. Less than 1% refused to participate because they absolutely wanted to use the app.
Discussion and Conclusion
The theoretical advantage of personalized rehabilitation with a mobile app and the possible savings for the healthcare payer, greatly depends on the adoption of mobile rehabilitation (mRehab) technology and apps in practice. Besides patients still preferring the direct human interaction with a physiotherapist (probably even more after Covid social restrictions), patients being unable to learn or correctly use the app has been identified in this trial and in other broad surveys, to be the most common barrier to the adoption of mRehab. Especially older people, who are the most common type of patients needing an arthroplasty, often lack the necessary digital literacy. Additionally, patients with limited or no access to internet will remain excluded from this technology. These problems will need to be addressed for mRehab to become a successful large scale treatment option.
#8048
Invited Talk: Defining the Target of Alignment In Total Knee Arthroplasty
*Nico Verdonschot - Twente - Nijmegen, Netherlands
*Email: n.verdonschot@orthop.umcn.nl
There are different technologies to make total knee surgery more precise. Surgical navigation has been introduced a few decades ago; personalized cutting guides have the potential to lead to a predictable implantation of the components and surgical robotics have been introduced to enhance precision and reduce human error. These technologies have clearly reduced the number of outliers of mal-placements.
However, from a clinical perspective, it remains difficult to demonstrate that these (rather expensive) technologies have led to clear benefits for the patient and thereby lead to a cost-effect solution for the society as a whole.
One important aspect in this matter is the difficulty of specifying what exactly the target of these precision instruments should be. Kinematic or anatomical alignment have become more popular and it seems logical that the anatomy is better respected than in a more traditional approach of mechanical alignment. If the target is to reconstruct the original anatomy, we should ask ourselves whether the pre-operative imaging data provides us with the original anatomy or whether this is obscured by the osteoarthritic process.
Recent developments in artificial intelligence, fed with large data sets, have shown that it becomes possible to reconstruct the pre-operative imaging data to that of the pre-diseased state. Hence, we can reconstruct the bony anatomy of the pre-diseased state for an individual patient, which could serve as a target for the precision instruments.
Musculoskeletal models can aid an important parameter in the definition of the target: once the pre-diseased state is reconstructed, we can simulate the kinematics of the knee joint and subsequently, we can optimize the placement of the components such that the kinematics of the TKA joint is as much alike with the pre-diseased knee as possible.
However, new questions come up: is it enough to focus on minimizing the kinematic difference between pre-diseased bone and TKA joint, or should we take the soft tissue strains around the joint into account in our optimization algorithms?
Furthermore, optimization of placement of the components in a personalized manner will result in variations in alignment. The question becomes whether current knee designs are capable of adopting these variations in a safe manner. For example, personalized alignment may lead to challenges in term of fixation and adverse longer-term bone remodeling. In this respect finite element models can provide insights in the robustness of these components using variable loading conditions, simulating various alignment approaches in different populations (population based modeling).
In conclusion the computational simulation community could generate a large impact to enhance the clinical benefits of precision surgical technologies by identifying the surgical targets and enhance the robustness of TKA implants.
#7801
Grit and Preoperative Pain Ratings in Rotator Cuff Repair
*Arjun Verma - Ochsner Sports Medicine Institute - New Orleans, USA
Misty Suri - Ochsner Sports Medicine Institute - New Orleans, USA
Sarena Matriano Lim - Ochsner Sports Medicine Institute - New Orleans, USA
Collyn O'quin - Ochsner Sports Medicine Institute - New Orleans, USA
*Email: arjun.verma248@gmail.com
Introduction:
Grit is a statistically validated psychological concept introduced by Angela Duckworth in 2007. Duckworth defined Grit as a passion and perseverance for long-term goals, and she developed a short questionnaire to assess Grit. Grit scores range from 1 to 5, with 1 being not at all gritty, and 5 being extremely gritty. Higher Grit scores have been shown to be associated with increased pain tolerance in the context of high-level sport (Pettersen). Buckingham showed that Grit is strongly positively correlated to time to pain threshold and tolerance. With this context, this study was conducted to examine if there is a statistically significant relationship between patients’ Grit scores and their assessment of preoperative VAS pain in rotator cuff injury.
Methods:
This study was an IRB-approved prospective study in which VAS pain ratings and Grit scores were collected for 97 patients undergoing arthroscopic rotator cuff repair. Grit scores were assessed using the Short Grit Scale. SPSS statistical software (IBM) was used to conduct multivariate regression analysis of the relationships between Grit score, preoperative VAS pain, BMI, and age.
Results:
Multivariate regression analysis illustrated that Grit score had the greatest Pearson correlation coefficient with preoperative VAS pain rating (r=0.095). However, Grit score, BMI, and age were not significantly correlated with preoperative VAS pain rating.
Conclusion:
This study illustrates that although the topical literature suggests Grit is a powerful measure in determining pain tolerance and pain rating, the Grit score is not significantly correlated with preoperative VAS pain rating in patients requiring rotator cuff repair. This study suggests that there is a definitive delineation between the psychological and physical aspects of pain interpretation. This finding also warrants further research into distinguishing the role of grit in healthy patients from that in physically injured patients.
#7802
The Effects of Obesity on Hip Arthroscopy Outcomes
*Arjun Verma - Ochsner Sports Medicine Institute - New Orleans, USA
Misty Suri - Ochsner Sports Medicine Institute - New Orleans, USA
Brian Godshaw - Ochsner Medical Center - New Orleans, USA
Mohammed Asad Khalid - Ochsner Sports Medicine Institute - New Orleans, USA
*Email: arjun.verma248@gmail.com
Introduction:
Hip arthroscopy is a commonly employed technique for the treatment of various hip pathologies, including labral tears, femoral-acetabular impingement, and osteonecrosis. Many patient-specific variables, such as tobacco use, have been examined to identify their effects on arthroscopic outcomes. This investigation examined the role of body-mass-index (BMI) in impacting postoperative outcomes in patients undergoing arthroscopic hip repair.
Methods:
This investigation was a single-center, single-surgeon, Institutional Review Board approved retrospective review of 484 consecutive patients undergoing hip arthroscopy from 2008 – 2016. Patients were identified via CPT-code search and stratified into 4 cohorts: underweight with BMI < 18.5 (n=16), normal with BMI 18.6 – 24.9 (n=217), overweight with BMI 25 – 29.9 (n=147), and obese with BMI > 35 (n=83). Harris Hip Score (HHS) and Short Form 12 (SF-12) scores were used to measure outcomes. Scores were collected at 7 intervals: pre-operatively and post-operatively at 6 weeks, 3 months, 6 months, 1 year, 2 years, and 3 years. Statistical analyses were performed using multivariable analysis of variance Wilkes Lambda test with p < 0.05 being significant.
Results:
All groups exhibited statistically significant improvements in HHS and SF-12 scores at 3 years follow-up compared to preoperative scores. Intra-cohort analysis illustrated that the obese cohort achieved the greatest magnitude of improvement in both the HHS and SF-12. The underweight cohort had the smallest improvement in HHS and SF-12 scores. However, these inter-cohort differences were not statistically significant, thereby obscuring the role of BMI in functional recovery following hip arthroscopy.
Conclusion:
This investigation of 484 patients is the first to suggest that BMI does not have a statistically significant impact on patient reported outcomes following hip arthroscopy. All patients showed significant improvement in their outcome scores; however, inter-cohort differences were not statistically significant.
#7803
Sexual Dysfunction Following Hip Arthroscopy: Identifying the Variables That Matter
*Arjun Verma - Ochsner Sports Medicine Institute - New Orleans, USA
Misty Suri - Ochsner Sports Medicine Institute - New Orleans, USA
Sarena Matriano Lim - Ochsner Sports Medicine Institute - New Orleans, USA
Collyn O'quin - Ochsner Sports Medicine Institute - New Orleans, USA
*Email: arjun.verma248@gmail.com
Introduction:
Hip arthroscopy is a widely utilized technique for surgical intervention for hip pathology. Multiple studies have illustrated that patients with hip pathology report sexual limitations and growing disinterest in sexual activity, primarily due to hip pain. The investigation was conducted to determine the relationship between patient-reported sexual dysfunction and hip arthroscopy.
Methods:
This investigation was an Institutional Review Board approved, single-center, single-surgeon retrospective review of 327 patients who underwent arthroscopic hip surgery. Patients were filtered to include only those who scored ≤ 40% on question nine of the International Hip Outcomes Tool (iHOT-12), which specifies trouble with sexual activity due to hip issues. Multivariate analyses were then conducted to elucidate the associations between postoperative sexual dysfunction and multiple patient variables, including patient demographics, Modified Harris Hip Score (mHHS), Short Form 12 (SF-12), and intra-operative findings. Statistical significance was defined as p<0.05.
Results:
In this investigation of 327 patients, statistically significant associations between sexual dysfunction and the following variables were identified: age at time of surgery(p=0.03), chondromalacia size (p=0.0003), female sex (p=0.02), trochanteric bursectomy (p=0.01), and psoas tenotomy (p=0.0005). Interestingly, mHHS and SF-12 scores did not yield statistically significant relationships with sexual dysfunction.
Conclusion:
This investigation illustrates that sexual dysfunction following hip arthroscopy is influenced by age at time of surgery, chondromalacia size, female sex, trochanteric bursectomy, and psoas tenotomy. These findings are clinically important for orthopedic surgeons, as they may aid in identifying patients who may be at higher risk for sexual dysfunction after hip arthroscopy.
#7581
A Non-Contact Method for Measuring Separation During Subluxation Events in Total Hip Replacements
*Oliver Vickers - University of Leeds - LEEDS, GB
Matthew Shuttleworth - University of Leeds - Leeds, Select Country
Graham Isaac - University of Leeds - Leeds, United Kingdom
Peter Culmer - University of Leeds - Leeds, United Kingdom
Tim Board - Wrightington, Wigan & Leigh NHS Foundation Trust - Wigan, United Kingdom
Robert Kay - University of Leeds - Leeds, GB
Sophie Williams - University of Leeds - Leeds, United Kingdom
*Email: o.g.vickers@gmail.com
Introduction: Subluxation in total hip replacements (THRs) can lead to liner damage, cause patient discomfort and be a precursor to dislocation. Therefore, there is a need to further investigate the mechanism of subluxation, yet current in-vitro methods do not allow for a line-of-sight view and are often not feedback driven making studying this phenomenon challenging. Previous work has shown that magnetic sensing technology can track the position of a joystick and the angle and position of a THR femoral head within an acetabular liner. The aim of this work is to see if the same approaches can measure displacement of the femoral head during a re-creation of subluxation.
Methods: A tri-axis magnetometer (mlx90393, Melexis) and a magnet (N42 Neodymium, Magnet Experts Ltd) were integrated into clinically available components. The metal femoral head was positioned onto a 3D printed polymer stem and whilst the femoral head was located in an acetabular shell and liner, a robot arm (UR3, Universal Robots) was used to rotate the stem. The stem was rotated to the maximum inclination angle of 66° (impingement occurrence only) and then three angles beyond the working range of the THR components (70°, 72° & 74°) in turn and thus levering the femoral head out of the cup. The stem was returned to an inclination of 45° between each angle and the motion profile was repeated (n=3). To validate the magnetic tracking system (MTS) a camera (Lumix GF6, Panasonic) and Computer Vision Toolbox (MATLAB, MathWorks) acted as a camera tracking system (CTS) and was used to track the position and orientation of the femoral head.
Results: When comparing inclination angle measured by the robot with that of the CTS and MTS (Figure 1), error when the stem had not impinged (i.e. robot arm angle at 66° and 45°) was 0.86°±0.30° (mean±SD) and 1.47°±0.27° for the CTS and MTS respectively. This underestimation of stem angle meant that the MTS did not detect the occurrence of the initial impingement contact as impingement was inferred as whenever the stem angle was >66°. Closer agreement was seen when comparing angle measured by the CTS and MTS over the entire dataset with error of 0.61°±0.92°. This was expected as the 3D printed stem appeared to flex during subluxation. The estimated femoral head position in the z axis showed good agreement to that of the CTS with error of -0.06mm±0.18mm. A plot of impingement occurrence measured by the robot and MTS, and subluxation distance in the z axis measured by the CTS and MTS is shown in Figure 2.
Conclusion: This preliminary work has shown that magnetic sensing technology can track the position and orientation of a femoral head within an acetabular cup during complex adverse motions. Future, work will further develop the method to improve accuracy of impingement occurrence detection. Additionally, a more representative re-creation of a subluxation event is needed in which anatomical loads are included.
Acknowledgements: Oliver Vickers’ studentship is funded by the EPSRC CDT in Tissue Engineering and Regenerative Medicine (Grant number EP/L014823/1)
Figures
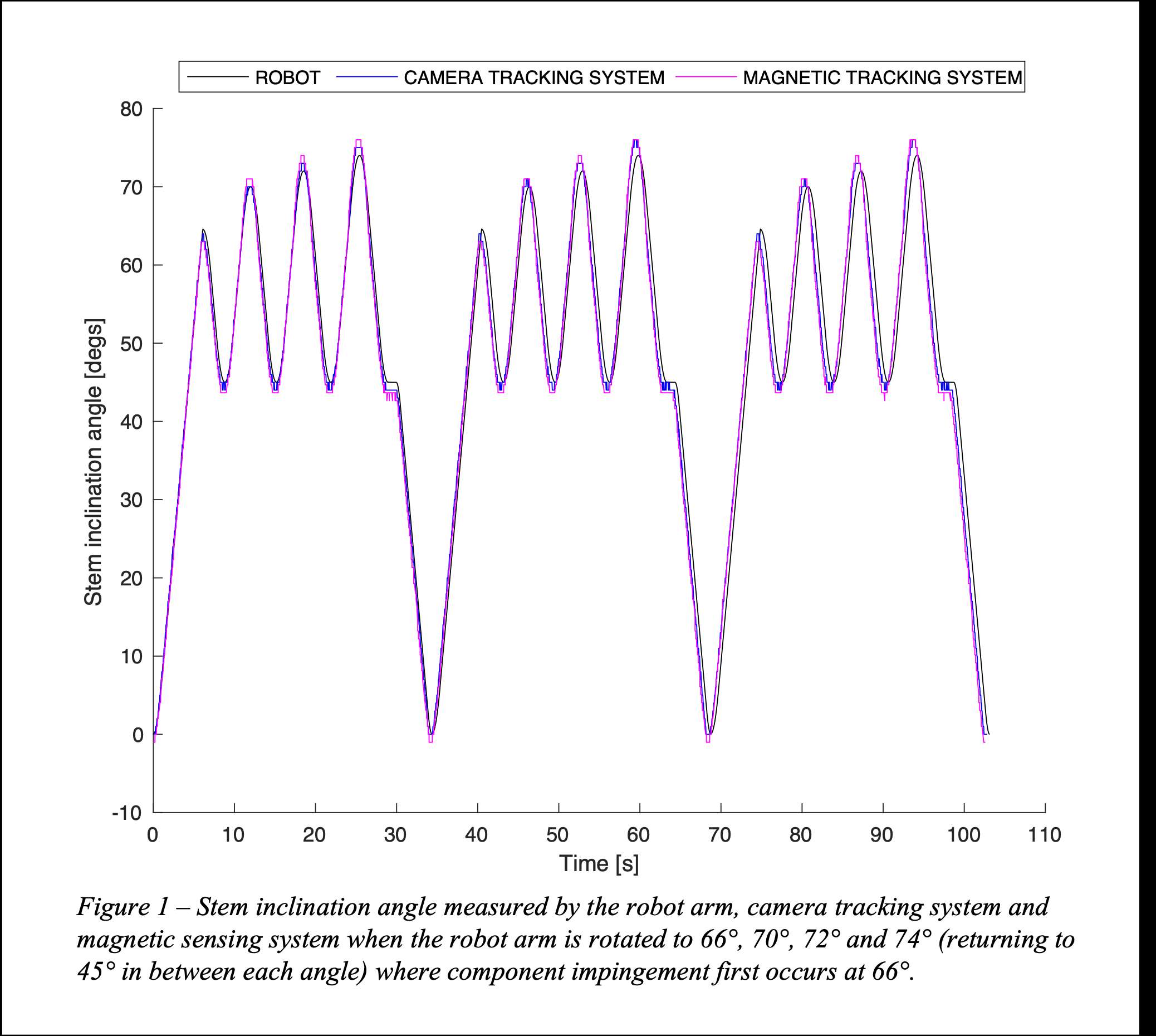
Figure 1
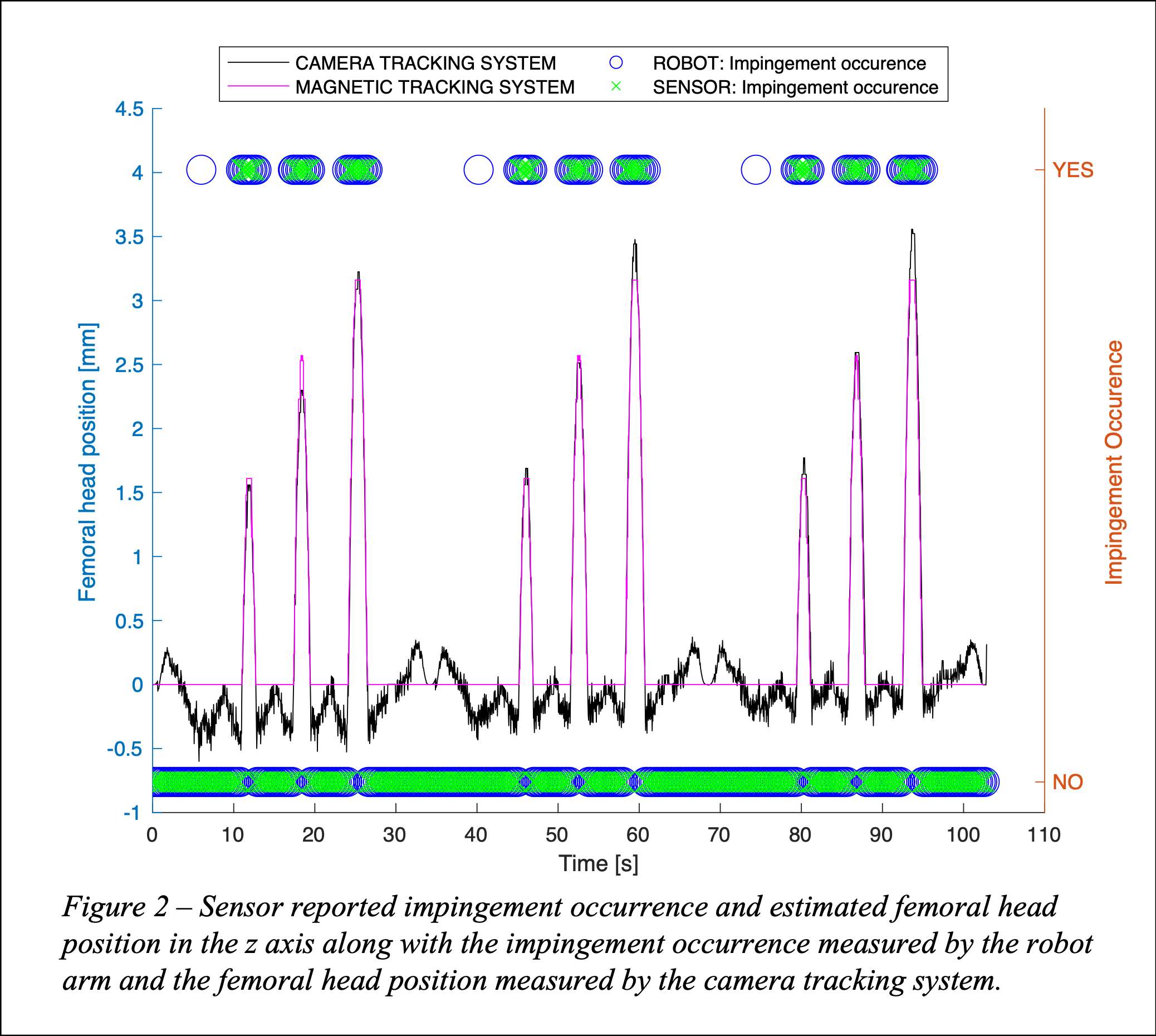
Figure 2#7605
3D-Printed Biomimetic Cervical Vertebral Body for Spinal Arthroplasty Testing
Jenna Wahbeh - University of California, Los Angeles - Los Angeles, United States of America
Stephanie Kehoe - University of Southern California - Los Angeles, USA
John Lama - University of California, Los Angeles - LOS ANGELES, USA
Sang-Hyun Park - Orthopaedic Institute for Children /UCLA - Los Angeles, USA
Edward Ebramzadeh - Orthopaedic Institute for Children/UCLA - Los Angeles, USA
*Sophia Sangorgio - Orthopaedic Institute for Children/UCLA - Los Angeles, USA
*Email: ssangiorgio@mednet.ucla.edu
Introduction: Cervical disc arthroplasty is a promising, motion-sparing, alternative to anterior cervical discectomy and fusion. Few biomechanical studies have been conducted to promote the use and success of these implants. The paucity of cervical spine biomechanical testing may be due to the lack of biofidelic, reproducible cervical vertebral body models. Biomechanical assessments in weight-bearing implants tend to utilize fine-tuned, commercially available composite models for highly reproducible and time-independent testing. Unfortunately, composite vertebrae for the testing of novel cervical devices are currently not available and prove difficult to replicate due to the varying strengths of the vertebral body, anisotropic ultrastructure, and high porosity of cancellous bone in the spine. The goal of this study was to validate different 3D printing techniques for use in the design of a biomimetic vertebral body model for biomechanical testing of cervical devices.
Methods: Using the Ultimaker Cura software, rectangular prints of known dimensions were performed using varying in-fill densities and print patterns for compressive stiffness testing. The chosen in-fill densities in the present study ranged from a 5% to 25% in-fill density, increasing by 5% for a total of 5 different in-fills. Three print patterns were tested: triangle, zig-zag, and gyroid with all in-fill densities (Figure 1). Following successful prints, each specimen was tested for axial compressive strength using a custom pure compression apparatus on a servo-hydraulic load frame (Figure 2).
Results: From a thorough literature review, compressive strength of vertebral cancellous bone ranges from 2 to 20 MPa in the coronal plane, with most models having a compressive strength of 6 MPa (Figure 3). Of most promise for maintaining cancellous properties is the gyroid print patterns which had a compressive strength of 5.7 MPa at 25% in-fill. Triangle and zig-zag specimens buckled at failure while gyroid specimens were crushed, similar to the failure pattern observed in cancellous bone. Gyroid patterns with a 5% in-fill pattern could not be tested as the in-fill density was too low for the chosen print pattern and the print did not yield testable specimens.
Conclusions: This study shows the successful use of 3D printed techniques and materials to recreate mechanical properties of cancellous bone in the vertebral body. As the cervical spine has varying compressive strengths from the lateral edges to the central portions, these iterations are necessary to match combinations of in-fill density and print pattern to the respective strengths in the cervical vertebra for a complete model. The results from this study will be used to create a biomimetic cervical vertebral body model with higher strengths around the lateral edges, using a stronger combination of pattern and in-fill density, and a weaker combination centrally. The final vertebral model will allow for highly reproducible, time-independent, and cost effective biomechanical evaluation of cervical devices. Continuing studies include a finite-element model to assess the different combinations in a single vertebral body and subsequent biomechanical studies comparing cadaveric specimens to the final 3D-printed model.
Figures
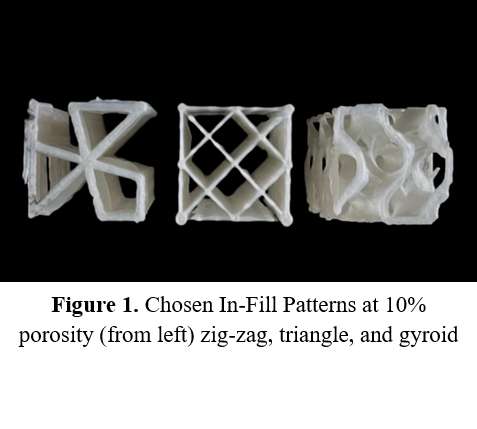
Figure 1

Figure 2
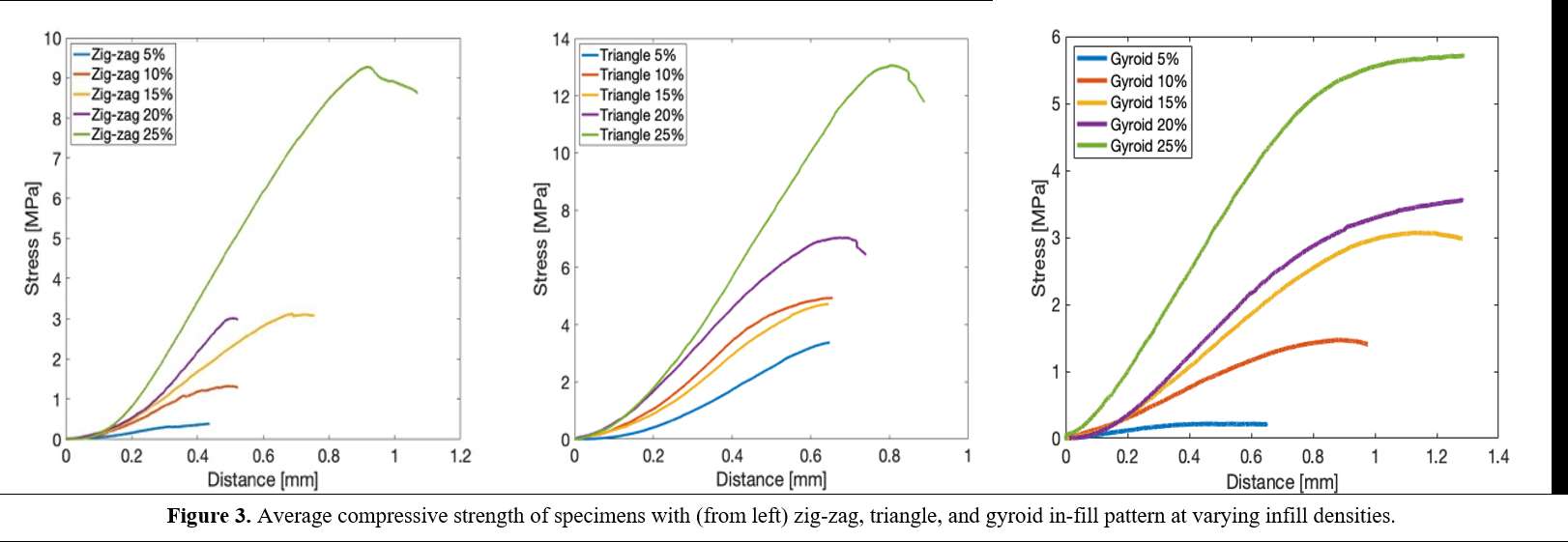
Figure 3#7607
Is Bone Ongrowth in Total Disc Replacements Necessary for Clinical Fixation
Jenna Wahbeh - University of California, Los Angeles - Los Angeles, United States of America
Sang-Hyun Park - Orthopaedic Institute for Children /UCLA - Los Angeles, USA
Edward Ebramzadeh - Orthopaedic Institute for Children/UCLA - Los Angeles, USA
*Sophia Sangorgio - Orthopaedic Institute for Children/UCLA - Los Angeles, USA
*Email: ssangiorgio@mednet.ucla.edu
Introduction: Explant analyses are crucial to understand the in vivo performance of new implants. Historically, total disc replacements have relied on both successful surgical preparation and strong bony growth for successful clinical outcomes. Current spinal arthroplasty designs utilize textured coatings, such as titanium plasma-spray, intended to increase the surface area and maximize bony ongrowth. However, the contribution of direct bony attachment to overall fixation has not been established. The goal of the present retrieval analysis was to document the extent of bony attachment to the fixation surfaces of two clinically functional total disc replacements that were not loose at the time of revision.
Methods: Two metal and polymeric disc replacements were evaluated for bony ongrowth. Non-destructive visual inspection was performed to determine possible failure mechanisms and grossly assess fixation. Devices were then embedded in polymethyl methacrylate (PMMA) and sliced using a diamond band saw into 5 coronal cuts for the lumbar specimen and 3 coronal cuts for the cervical specimen. High resolution photographs and contact micro-radiographs were taken to precisely assess bony ongrowth to the textured plasma-sprayed coating on the endplates.
Results: The lumbar device was removed due to radiographic evidence of osteolysis after 28 months in vivo with no evidence of polymeric wear debris or mechanical failure. The cervical device was removed due to suspected immunological reaction after 8 months in vivo. Initial inspection of both the lumbar and cervical devices, including the observation of large bone masses on the endplates, surgical extraction damage, and lack of radiographic migration suggested that both had been well-fixed at the time of removal (Figure 1). After sectioning, micro-radiographs revealed radiolucent gaps between the endplates and bone mass on the lumbar device (Figure 2). Specifically, little direct bone contact between the bone and endplate surface was identified and the original surgical cuts were still visible. In contrast, direct bony attachment was visible on the cervical endplate.
Conclusions: Both devices were clinically well-fixed at the time of removal and neither had complications associated with loosening; however, after closer inspection, fixation of the lumbar implant was not due to bony ongrowth. Both devices in the present study have a titanium plasma-spray which has been shown to significantly enhance bony ongrowth and have successful integration of new bone onto coated weight-bearing implants after as little as 6 months. However, the micro-radiographs of the lumbar endplate in the present analysis showed the precise straight-edged cuts formed by milling of the bone in surgical preparation and subsequent radiolucent gaps. Regardless, the lumbar implant appeared to have adequate clinical fixation, despite the lack of ongrowth, potentially due to successful surgical preparation. This could indicate that the surgical preparation may have been sufficient to rigidly fix the device and avoid common complications associated with lack of bony ongrowth such as migration, subsidence, and loosening. Future explant analyses for total disc replacements with more clinical information and longer durations of time in situ are necessary for assessing the impact surface coatings may have on successful clinical fixation.
Figures
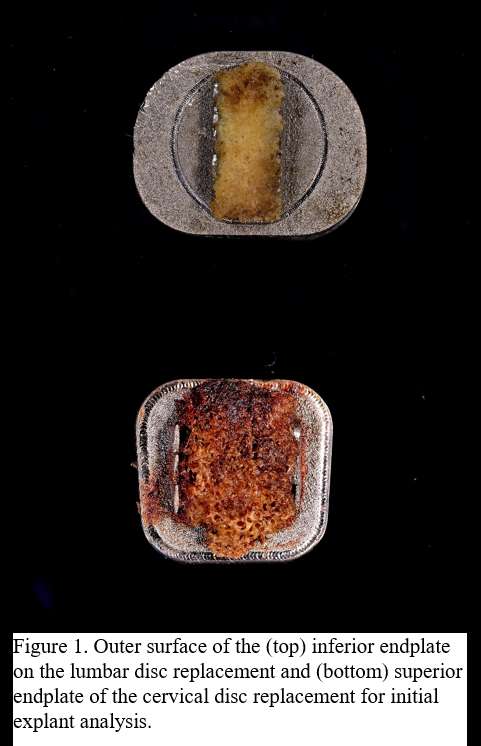
Figure 1
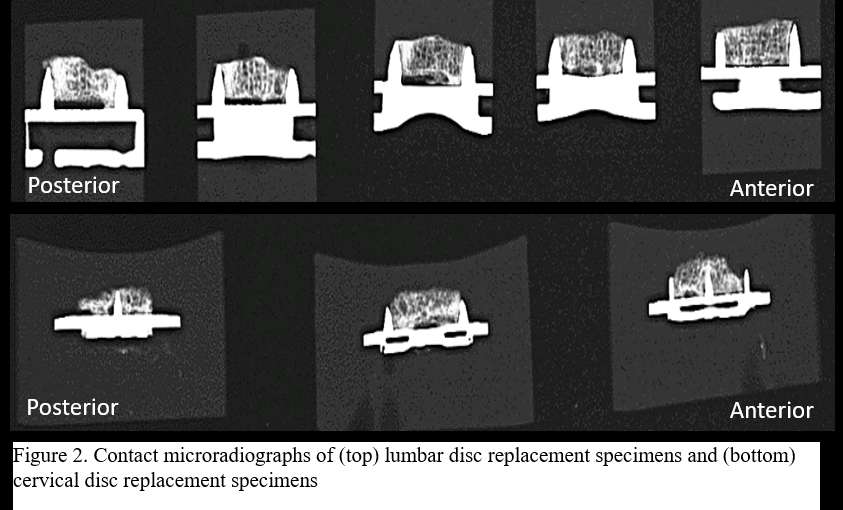
Figure 2#7393
New Minimally Invasive Hip Technique
*peter walker - Concord Hospital - Bellevue Hill, Australia
*Email: pw@hipandknees.com
Described is a new less invasive technique to perform a total hip replacement. There are numerous approaches to perform THR each of which has their own advantages and disadvantages. All of them require some form of dislocation of hip or moving of the femur away from the acetabulum so that it can be reamed. The further it is moved away the more soft tissue is either cut or torn.
This new approach aims to perform a total hip replacement and minimise this trauma by reaming through a small hole in the lateral femur.Fig 1. The potential advantages include less soft tissue dissection ,quicker recovery and less chance of dislocation since all stabilising structures are left intact.
The initial approach is similar to the superior approach which utilises the plane between the gluteal tendons and external rotators with the hip located. This leaves a soft tissue envelope to insert the reamers.
In this approach the acetabulum is prepared with the femur lying flat on a pillow in a flexed position correlating with the desired acetabular angle position.The broaching is performed prior to a femoral neck osteotomy. Once the osteotomy is performed a 5.5 mm hole is then drilled though the lateral femoral cortex using a special jig that attatches to the broach handle.Fig 1 The broach has a 5.5 mm hole lateral to medial at the same angle as the neck of the implant.
A 5.5 mm reamer shaft is then passed through the hole in the lateral femoral cortex and the hole in the broach. Fig 1.The reamer shaft is then attatched to the acetabular reamer which is passed into the joint superiorly and then a specialised C arm is used to apply the pushing force to ream the acetabulum.Fig 2
The reamer shaft is simply rotating and is protected by the broach such that it cannot cause a fracture of the bone. This hole has been shown to have minimal effect on the strength of the bone and is bypassed by the final implant. The pushing force is expended by the C arm which has a flat end to push on the acetabular reamer.Fig 2. No retraction from an assistant is required whilst reaming. To remove and insert another reamer the Carm is simply pulled away from the acetabulum which pulls on the top of the femoral broach allowing access to the joint.
The main advantage of this approach are its simplicity ,minimal invasiveness and minimal assistance required. The acetabular position is directed by the position of the femur and directly related to the angle of the hole in the broach. The procedure can easily be adapted to a mechanical holding device or robotic arm.
Currently this technique is being adapted to a universal robot Fig 3 and cadaver surgeries have been performed to refine the technique and instrumentation. The future possibilities enable more simplified instrumentation and more minimally invasive surgery including incorporating a simple to use EM navigation system which is being worked on.
Figures
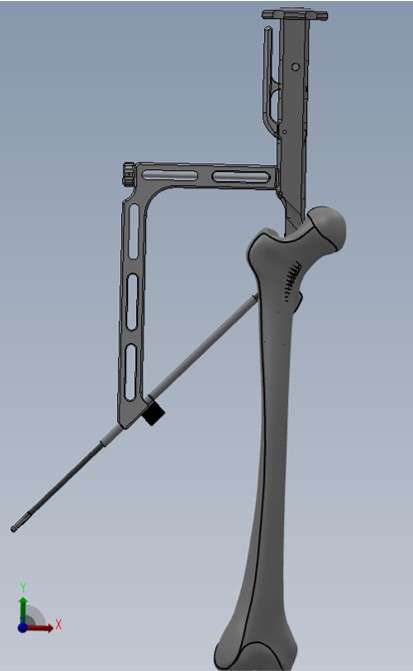
Figure 1

Figure 2
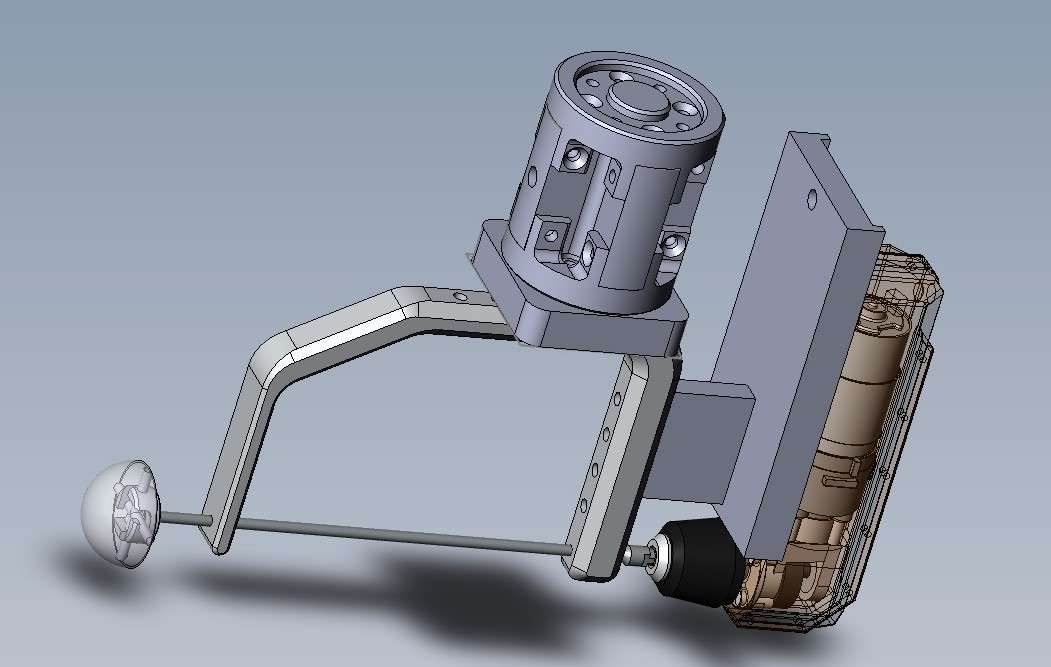
Figure 3#8049
Invited Talk: Is there an ideal total knee design and surgical technique for optimal function?
*Peter Walker - New York University Langone Orthopedic Hospital - New York City, USA
*Email: ptrswlkr@aol.com
Since the first total knees were introduced in the late 1960’s, designers have sought to include design features and techniques which will produce a satisfactory functional result. As the designs have become more anatomic in shape, and the techniques more precise, the expectations for yet further improvements in function have become more intense. The most commonly used functional evaluation schemes are PROMS, because of the ease of obtaining the information, and the inclusion of both objective and subjective factors. However the results are not easy to interpret due to the wide variety in abilities between each individual, and the effect of co-morbidities which impair the function. Typically, in many clinical studies which compare one type of total knee design or technique, with another, no statistically significant differences can be demonstrated. In many of the studies, the total knee designs had completely different geometries, or the techniques used different landmarks for alignment strategies or performing soft tissue balancing.
As an alternative to PROMS, many ‘mechanical’ evaluations schemes have been used. Gait analysis has been used since early times, where selected parameters of the gait variables are compared between cohorts. More recently the simpler Timed-up-and-Go (TUG) test has been used effective. Force plate studies comparing opposite limbs have been used, and well as sensors on the shoe soles or attached to the limb segments of the patients. Measuring muscle strengths has shown the importance of muscle condition on function. In recent years, sophisticated fluoroscopic evaluations have been devised where the fluoro unit follows the patient’s knee during the activity. However, as with the PROM evaluations, for these different mechanical methods, variations between individuals, and co-morbidities, have been problematic. Nonetheless, charting the progress of a particular patient over time, is a useful way of using the evaluation schemes.
One approach to obtaining objective data, where reproducible comparisons between designs or techniques can be obtained, is to use computer or experimental modelling. The overall premise is similar in both methods. A model of the joint is defined, input forces and motions are applied, and the outputs measured. The forces and moments can be those which simulate activities of everyday living, or simpler inputs such as applying combinations of forces in sequence. Likewise the outputs can be displacements, or contact stresses or soft tissue forces. While these methods can demonstrate comparisons, the challenge is to define the target output. As an example, in the balancing of knees at surgery, surgeons will ask what are the target values which will produce the best results to the patient? The question might be reframed as to which values are the best for this particular patient.
In summary, all evaluation schemes for total knee designs or surgical techniques have limitations. However, identifying the factors which produce either a positive or negative effect on the result will be useful in interpreting the results of present methods. Is the anterior-posterior displacement of either the lateral or medial side during functions, the major influence in the feeling of instability or stability to the patient? Do excessively loose or tight soft tissues during an activity cycle, result in feelings of either pain or instability? Is muscle strength and coordination the over-riding factor in a high level of function, over all other factors? It is likely that over time, the best design features and surgical techniques will become evident, and practice will shift in those directions.
#7528
Evaluating Alternative Registration Methods and Reference Planes for Imageless, Computer-Assisted Navigation During Supine Total Hip Arthroplasty
John Farey - The Kolling Institute - Sydney, Australia
*Yuan Chai - University of Sydney - Sydney, Australia
Joshua Xu - Royal North Shore Hospital - St Leonards, Australia
Ameneh Sadeghpour - Navbit Pty Ltd - Sydney, Australia
Neri Baker - Navbit - St. Leonards, Australia
William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
*Email: yuan.chai@sydney.edu.au
Introduction
Computer navigation improves acetabular cup position in total hip arthroplasty (THA), thereby reducing the risk of revision surgery for all causes as well as dislocation. Navigation during supine THA via the direct anterior approach (DAA) is usually image-based via intra-operative fluoroscopy. Imageless computer navigation systems have the potential to improve the uptake of navigation by addressing the disadvantages of image-based systems. We aimed to evaluate the accuracy of 3 combinations of registration methods and reference planes in the supine surgical position generated using imageless navigation for patients undergoing THA via the direct anterior approach (DAA).
Method
A prospective, observational study was conducted with 51 participants undergoing a primary THA for osteoarthritis in the supine position using both an imageless optical navigation system (Stryker OrthoMap, Kalamazoo, MI) and an imageless inertial sensor system (Navbit, St Leonards, Australia). Radiographic inclination and anteversion were obtained by three measurement methods, which were three combinations of a registration method and a reference plane: the ASIS anatomic method (landmarking registration method and anatomic pelvic reference plane), the TT functional method (table tilt registration method and functional pelvic reference plane), and the ASIS functional method (landmarking registration method and functional pelvic reference plane. See Figure 1). Post-operative acetabular cup position was assessed using CT scans and converted to Murray’s definitions of radiographic inclination and anteversion. Two repeated measures analysis of variance (ANOVA) were used to compare mean absolute errors. Post-hoc paired comparisons were conducted for significant ANOVA findings. Bland-Altman plots were used to assess agreement between the 3 measurement methods and the final cup position according to the CT scan. Clinically relevant limits of accuracy were defined as ± 10° a priori.
Results
For inclination, the mean absolute error was significantly lower for the ASIS functional method (2.8°±1.7°) than for the ASIS anatomic method (3.7°±2.1), p < 0.001. The mean absolute error was significantly lower using the TT functional method (2.4°±1.7°) than the ASIS anatomic method (3.7°±2.1°), p < 0.001. For anteversion, the mean absolute error was significantly lower for the ASIS functional method (3.9°±3.2°) than for the ASIS anatomic method (9.1°±6.2°), p < .001. The mean absolute error was significantly lower for the TT functional method (2.4°±1.8°) than for both the ASIS functional method (3.9°±3.2°, see Figures 2 and 3), p = .005 and the ASIS anatomic method, p < 0.001. All measurements of inclination and anteversion were within ± 10° for the TT functional method, but not the ASIS functional or ASIS anatomic methods.
Conclusion
The use of an anatomic reference plane leads to an increase in measurement error that is likely to be clinically significant, with nearly one-third of anteversion results outside of a ± 10° target window. Therefore, the use of a functional registration plane is preferable to an anatomic reference plane, to accurately measure intra-operative acetabular cup inclination and anteversion. Accuracy may be further improved by registering patient location using their position on the operating table rather than anatomic landmarks, particularly if a tighter target window of ± 5° is desired.
Figures
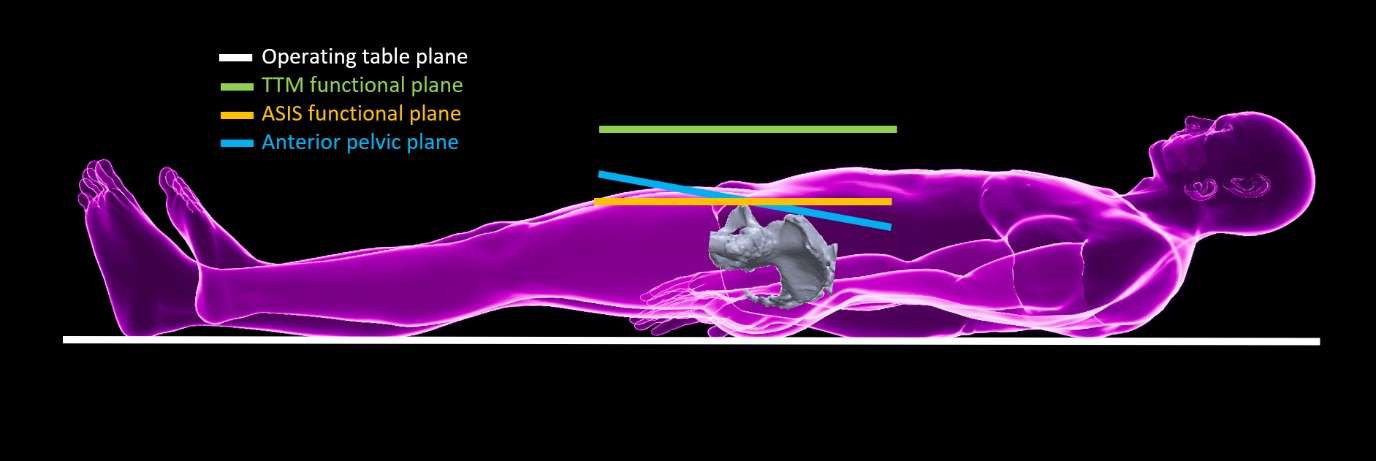
Figure 1
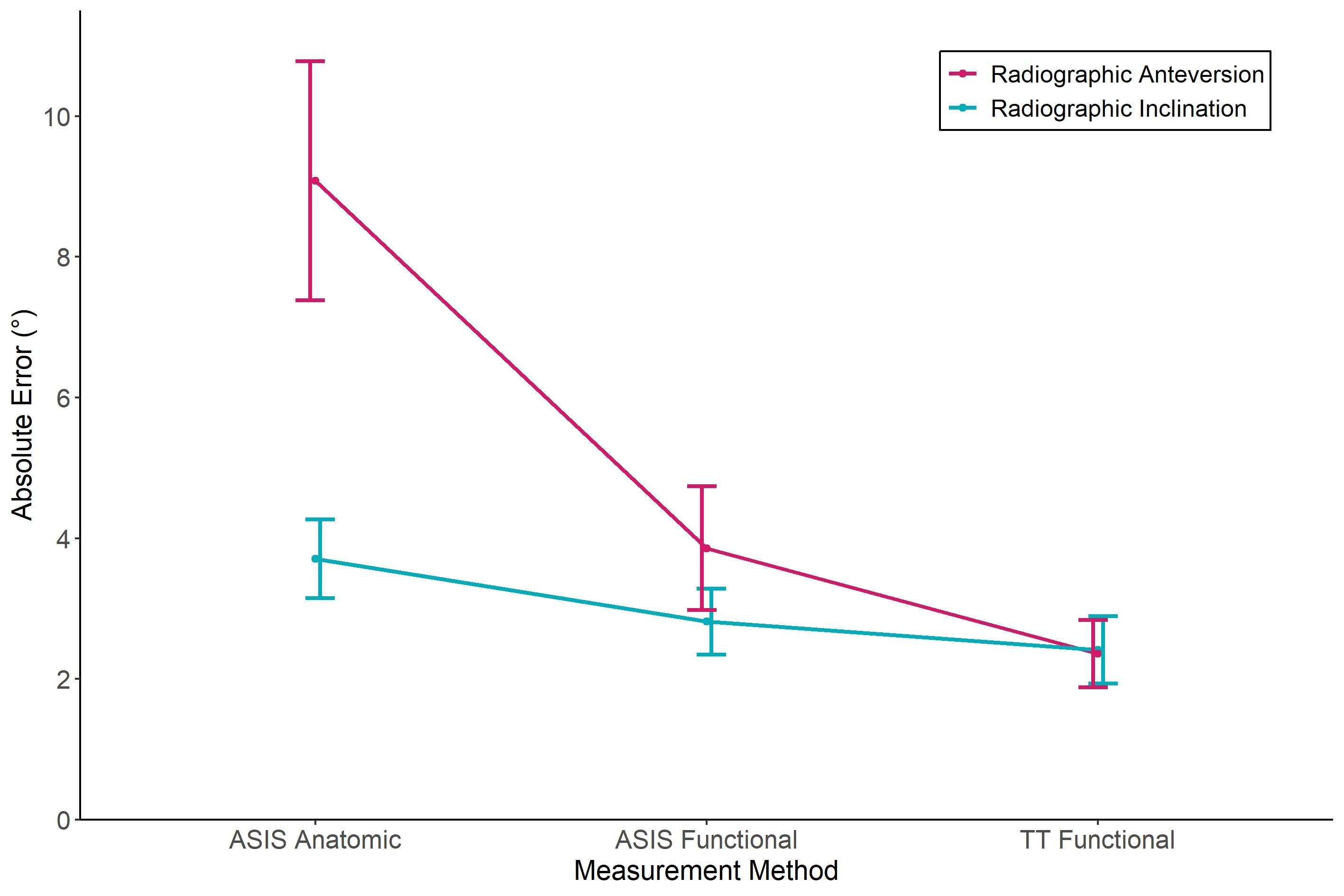
Figure 2
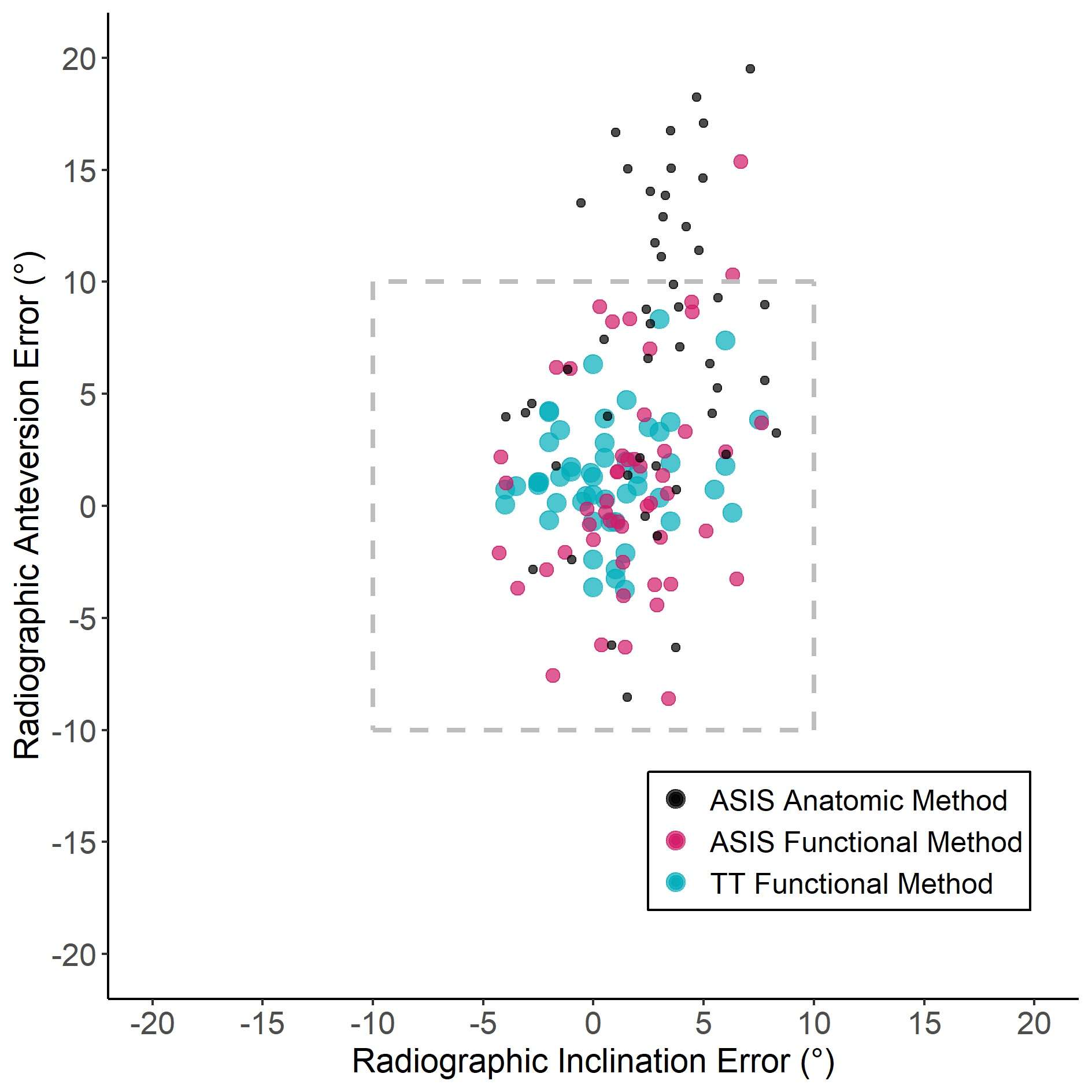
Figure 3#7531
Novel Methodology for Measuring the Medial Proximal Tibial Angle in Total Knee Arthroplasties
William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
*Ishaan Jagota - 360 Med Care - Sydney, Australia
Matthew Lim - 360 Med Care - PYMBLE, Australia
Joshua Twiggs - University of Sydney - Sydney, Australia
Brad Miles - 360 Knee Systems - Pymble, Australia
Max Hardwick-Morris - 360 Med Care - Sydney, Australia
*Email: ishaan.jagota@360med.care
INTRODUCTION:
The Medial Proximal Tibial Angle (MPTA) is a key input for coronal alignment classification systems of the knee and alignment strategies for total knee arthroplasties (TKA). The MPTA is most frequently measured using 2D AP radiographs, but technological advancements have allowed for the development of 3D analysis techniques. This study investigates different 3D analysis methods which can be used to measure the MPTA.
METHODS:
A retrospective series of 209 knees from 158 patients (51 bilateral) was analysed. All patients were recruited from a single experienced orthopaedic surgeon between April 2018 and August 2021 and received a pre-operative long-leg supine CT scan. Segmentation and landmarking were performed to output 3D bone models. The MPTA was calculated using two distinct methodologies, 3D landmarks and 3D geometric analysis, both of which measured the coronal tibial angle with respect to the tibial mechanical axis (centre of proximal tibia to ankle centre). The landmarks technique involved creating a line joining the medial and lateral tibial wells[Fig 1.A.]. The 3D geometric analysis consisted of a selection of 20 points spaced evenly across the anterior (A), centre (C), posterior (P) portions of the proximal tibial surface. Regression lines were created for each set of points and for the combination of the anterior and centre points (AC) and anterior, centre and posterior points (ACP)[Fig. 1.B-F]. The algorithm was created and operated using R Studio v1.3.1903. The MPTA measurements were also categorised as being either ‘less than 87’, ’87 to 90’ or ‘greater than 90’ degrees for additional comparative analysis.
RESULTS:
The mean patient age was 69.7 ± 8.8 years with 56% (116) female joints and 56% (116) right joints. The mean MPTA for the landmark technique and the five 3D geometric analyses (A, C, P, AC and ACP) were 86.0°±2.5°, 89.1°±2.5°, 87.3°±2.4°, 86.7°±2.7°, 88.1°±2.3° and 87.4°±2.3°, respectively[Fig. 2]. The MPTA measurement using the landmark technique was relatively more varus than and statistically significantly different to all the 3D geometric measurements.
The categorisation of the MPTA measurements further highlights this trend, with over 60% of these measurements being greater than 3 varus and fewer than 10% having a valgus MPTA[Fig. 3]. Comparison of the measurements for the A, C and P 3D geometric analyses in Figure 3 also suggests that a relatively more varus alignment is observed further posterior along the proximal tibial surface.
DISCUSSION:
Through consideration of the 3D tibial geometry, determining MPTA using landmarks on 3D bone models allows for greater accuracy than measuring the MPTA directly from AP radiographs. Nonetheless, both methodologies involve using two landmarks to describe the coronal alignment of the proximal tibia. The accuracy of these methods is questionable, which has clinical implications as MPTA measurements are utilised by engineers and clinicians for surgical planning and execution. The novel 3D geometric analyses methodologies described in this study consider numerous points on the proximal tibial surface and were observed to be significantly different to the landmark technique. It is also important to consider the region of the proximal tibial surface being measured.
Figures
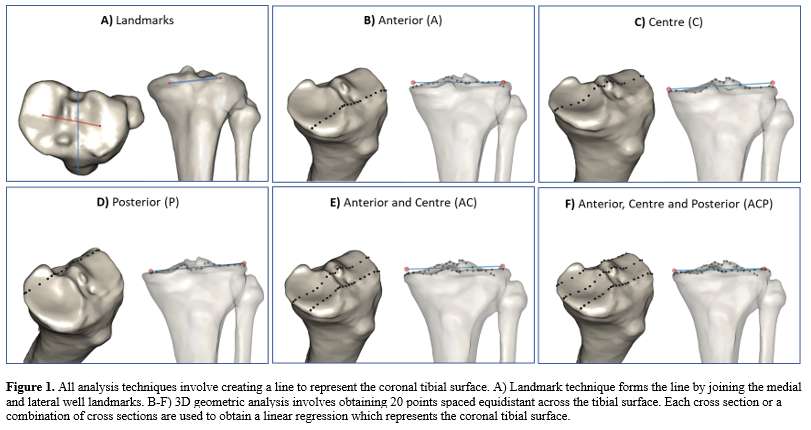
Figure 1
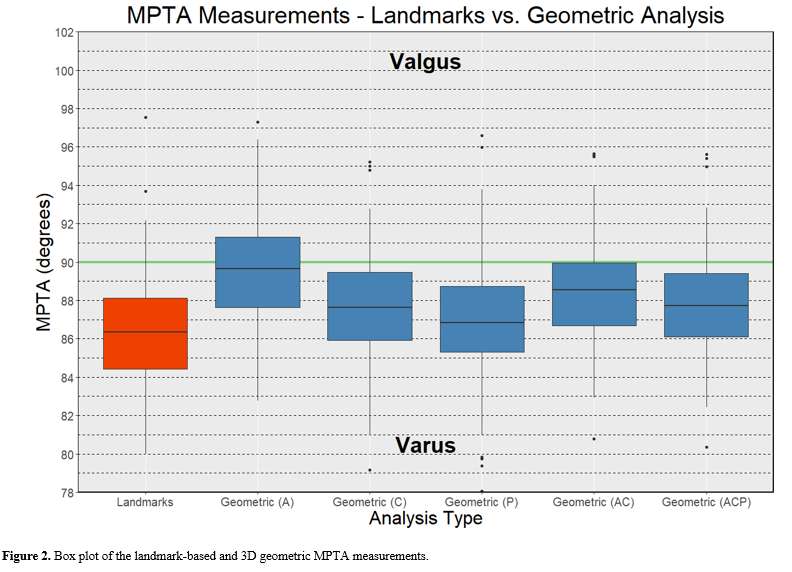
Figure 2
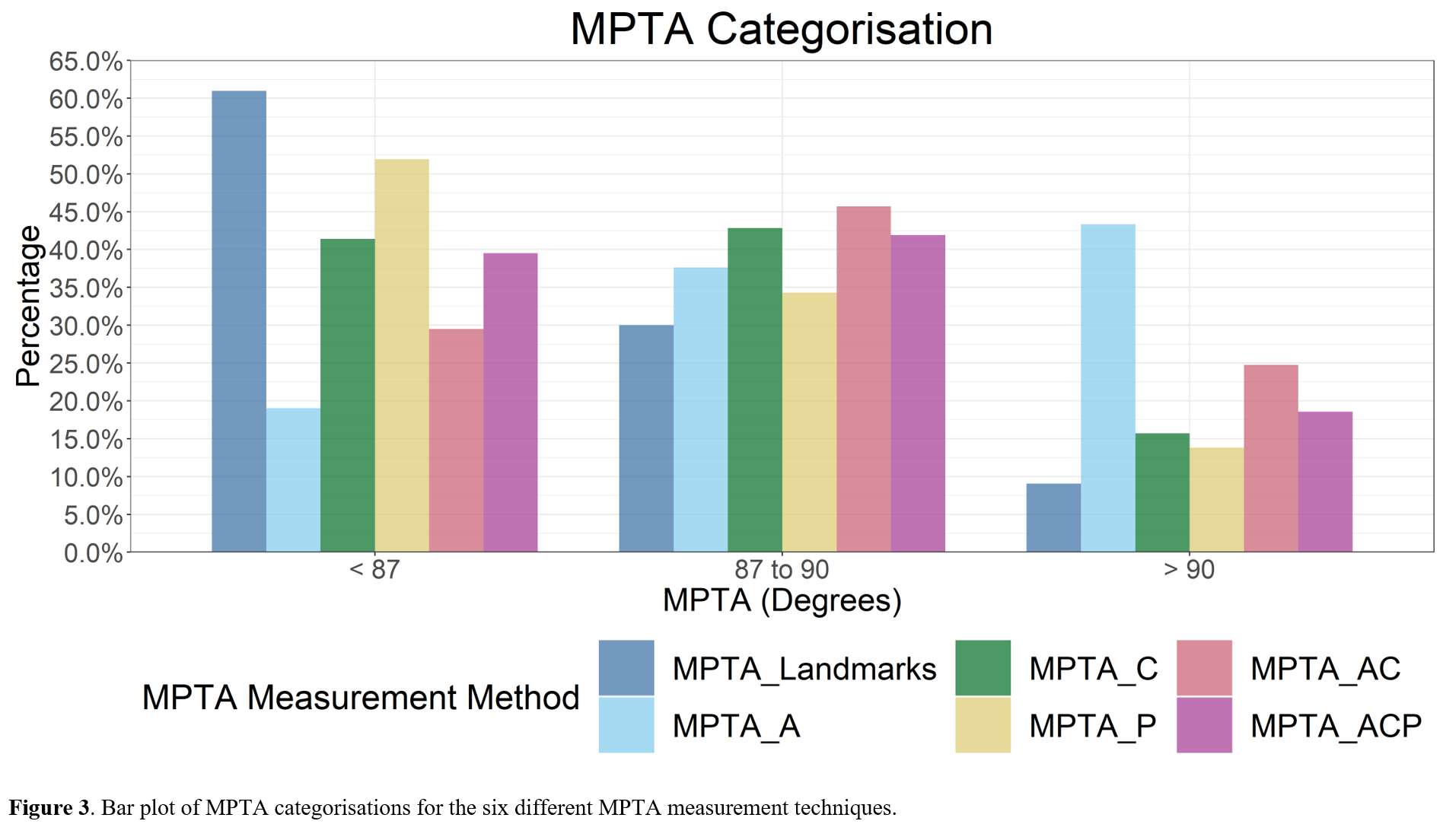
Figure 3#8050
Invited Talk: Inertial-based navigation tools for cup placement
*William Walter - Specialist Orthopaedic Group - Wollstonecraft, Australia
*Email: bill.walter@hipknee.com.au
#7376
Advanced Wear Testing of a Novel Shoulder Prostheses System
*Dong Wang - University of Exeter - Exeter, GB
Andrew Amis - Imperial College of London - London, UK
Hamidreza Alidousti - Imperial College - London, United Kingdom
*Email: d.wang2@exeter.ac.uk
Introduction
Medical advances and an ageing population mean that more people than ever rely on artificial joints. In the past years, shoulder joint replacement has developed rapidly, and the numbers of shoulder prostheses implanted increased dramatically. Despite being used since 1980s, anatomical total shoulder replacement (TSR) yields poor outcome in comparison to knee and hip counterparts. The main reasons for failure of TSR are lack of glenoid component fixation, joint instability and excessive wear of the polyethylene. A new minimally invasive TSR system with superior fixation to the bone and ability to preserve soft tissue around the joint has been designed. The current study aims to assess the wear performance of the newly designed shoulder prostheses system using a state-of–the-art multi-station shoulder simulator which has been specifically designed (but not limited to) for testing the implants under realistic physiological loading conditions. Investigation of wear characteristics through a comprehensive range of motion using the sophisticated shoulder simulator revealed the durability of the implant material, the performance of the implant design and its safety in the laboratory.
Methods
A novel glenoid component with a plurality of fixation elements was designed for securely press fitting in position on a patient’s scapula. And a ceramic humeral head has been developed featuring stemless designs. To facilitate the wear tests of the newly designed prostheses, a six-station shoulder simulator has been developed. It was built to accurately simulate physiological gleno-humeral forces and displacements during activities of daily living. A wear testing study was conducted using the simulator when shoulder implants were subject to rotational and translational motions and loading to replicate the ‘combing’ activity of daily living.
Results
The shoulder prostheses were wear tested for 2 million 'combing' cycles at a waveform frequency of 1 Hz. The results from kinematic and kinetic inputs and outputs were obtained from the study. The volumetric wear results for the glenoid components were calculated from weight losses with comparisons of commercial counterparts. A scanning electron microscope (SEM) was also used to evaluate the wear surface morphology on the glenoid components.
Conclusion
Our data shows the new TSR wear generation is equal to the best commercially available implants on the market.
#7512
Validating Accuracy of an Imageless Computer-Assisted Navigation System for Total Knee Arthroplasty
*Sheila Wang - Intellijoint Surgical, Inc. - Kitchener, Canada
James Howard - London Health Sciences Centre - London, Canada
*Email: s.wang@intellijointsurgical.com
Introduction
A primary reason for total knee arthroplasty (TKA) failure is the suboptimal alignment of implants, which can lead to complications including aseptic loosening, abnormal wear, impairment of functional ability, and the need for revision. Computer-assisted navigation systems (CAS) have been shown to improve accuracy and consistency in implant position and orientation and therefore provide a viable and trusted method for improving alignment and addressing these potential complications. CAS navigation systems are classified based on referencing methods: CT-based, fluoroscopy based, and imageless systems. Imageless CAS uses anatomical reference points that are registered at the start of the procedure and offer advantages over image-based CAS in that they limit exposure to radiation. In order to be a useful adjunct to TKA, CAS systems need to cause minimal disruptions in the surgical workflow while providing accurate information in a safe manner. The purpose of this study was to evaluate the accuracy of a novel, imageless, optical computer assisted navigation system for TKA.
Methods
Forty-two consecutive patients who underwent primary TKA between September 2020 – March 2021 with the assistance of a novel CAS (Intellijoint KNEETM, Intellijoint Surgical, Kitchener, ON) were retrospectively reviewed. Patient demographics including age, sex, BMI, as well as 90-day postoperative complications were collected. Post-operative antero-posterior (AP) radiographs were obtained, from which mechanical lateral distal femoral angles (mLDFA) and mechanical medial proximal tibial angles (mMPTA) were measured. AP femur and tibia cut values were extracted from the navigation device. The primary outcome was the mean absolute difference of femoral and tibial varus/valgus angles between radiograph and intra-operative device measurements. Level of agreement between the two methods were compared using the Bland-Altman technique. Outcomes are reported as means ± standard deviation.
Results
Of the 42 patients, 40.5% (17/42) were female. Mean age and BMI of the cohort was 66.7 ± 7.7 years and 36.56 ± 8.81, respectively. The mean absolute difference between measurements from the navigation device and post-operative radiographs was 1.16⁰ ± 0.95⁰ for femoral coronal alignment, and 1.87⁰ ± 1.43⁰ for tibial coronal alignment. The Bland-Altman analysis demonstrated that for both femur (Figure 1A) and tibia (Figure 1B) cuts, 92.7% (38/41) of paired varus/valgus measurements were within the statistical limit for agreement. Mean operative time was 62.9 ± 11.2 minutes. There were no complications or adverse events associated with the use of the navigation system.
Conclusion
This study demonstrated that a novel imageless navigation system was able to measure coronal femoral and tibial cuts to within 2.0⁰ of post-operative imaging. The Bland-Altman analysis showed strong level of agreement between the two methods. The present study further validates the device’s ability to reliably display accurate intra-operative values, thereby assisting surgeons in achieving their desired cuts and optimal component placement.
Figures
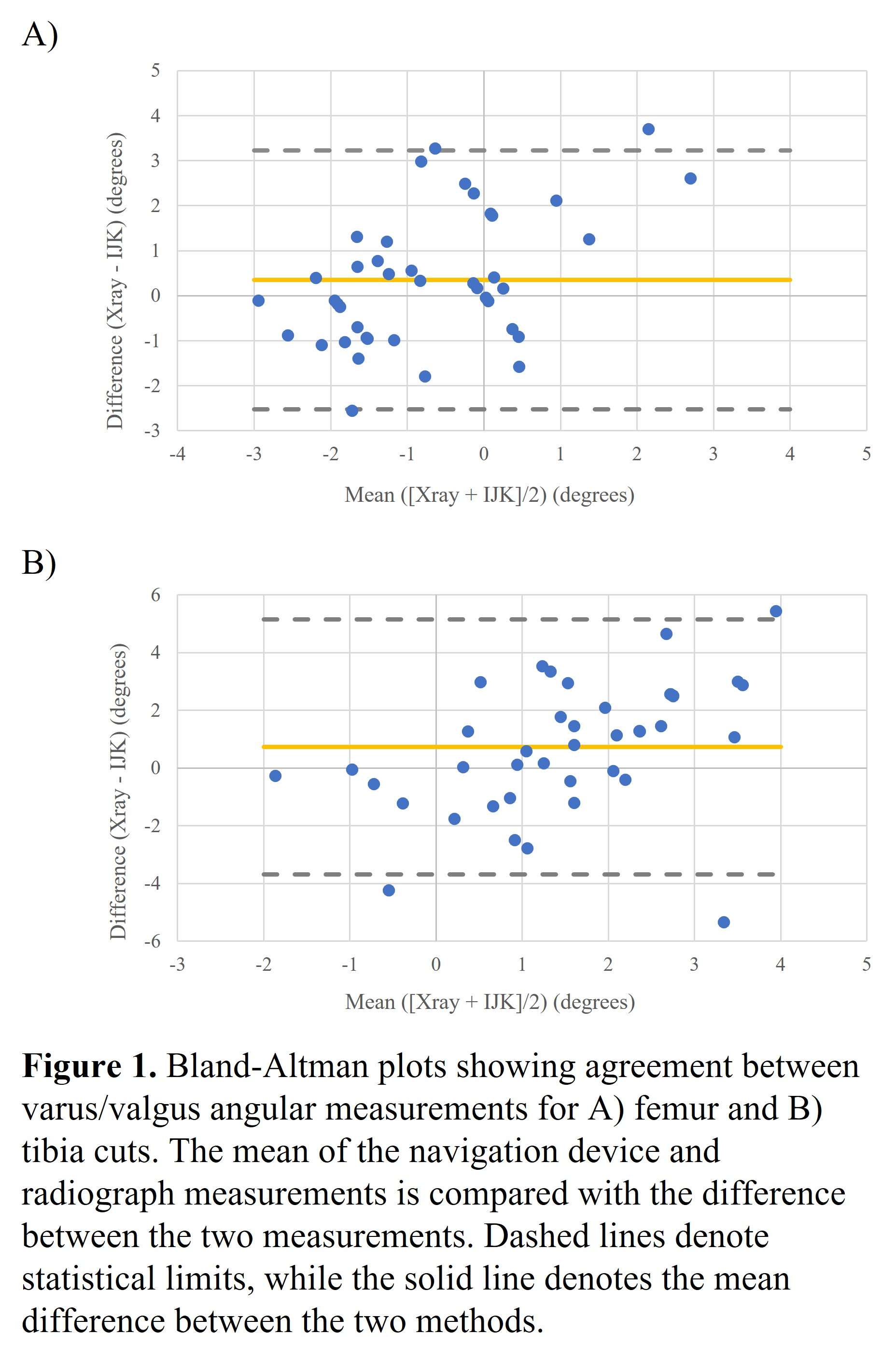
Figure 1#7566
Femoral Abduction/adduction Changes Do Not Significantly Affect Leg Length Measurements on Anteroposterior Pelvic Radiographs
Jeff Muir - Intellijoint Surgical - Waterloo, Canada
Wayne Paprosky
Justin Wagler - University of Waterloo - Waterloo, Canada
*Kelly Foley - Intellijoint Surgical Inc. - Kitchener, Canada
Sheila Wang - Intellijoint Surgical, Inc. - Kitchener, Canada
*Email: k.foley@intellijointsurgical.com
Introduction
Assessment of leg length (LL) discrepancy and pre-to-post-operative leg length change (LLC) are essential components of total hip arthroplasty (THA). The use of plain film radiographs, while common in THA, is associated with known limitations, due to the distortion and patient positioning errors that occur commonly. We previously investigated the role of pelvic tilt in leg length measurement during THA by measuring the pre-to-post-operative change in the non-operative leg of patients undergoing primary THA and noted that there was a predictable relationship between the direction and magnitude of pelvic tilt and the subsequent distortion of leg length measurements. In the current study, we focused on the role of changes in abduction/adduction of the femur on leg length measurements in the non-operative leg of THA patients.
Methods
We retrospectively reviewed anteroposterior (AP) pelvic radiographs of patients undergoing primary THA between February 2016 and November 2017. The pre-to-post-operative LLC in the non-operative leg was measured for each patient, as was the degree of abduction/adduction of the femur, defined as the angle between the trans-ischial line and the anatomical axis of the femur. LL was measured as the vertical distance between the trans-ischial line and the midpoint of the lesser trochanter. The change in abduction/adduction was calculated as the difference between the pre- and post-operative measurements and was correlated with LLC for each image. All measurements were completed in triplicate, by two independent reviewers, using Intellijoint VIEWTM (Intellijoint Surgical, Kitchener, ON).
Results
Radiographs from 75 procedures (150 images) were reviewed. The non-operative leg was the left leg in 53% (40/75) of cases; females comprised 51% (38/75) of the study cohort. The mean change in abduction/adduction angle between pre- and post-operative imaging was 2.9°±2.1°. Only 8 cases (11%) showed no change in abduction/adduction angle between pre- and post-operative imaging. Of the cases with a discrepancy in abduction/adduction angle, the mean change was 3.3°±1.9°, which was evenly distributed amongst cases between the femur appearing more abducted (44%, 33/75) or more adducted (44%, 33/75) on the post-operative image. The relationship between change in abduction/adduction and change in leg length was defined by the equation: y=-0.28x + 0.03, although the magnitude of abduction/adduction change did not correlate well with the observed LLC (r=-0.23, p=0.04) (Figure 1). A subgroup analysis indicated that neither adductors (r=-0.26, p=0.14) nor abductors (r=0.14, p=0.45) saw a strong correlation between change in abduction/adduction angle and LLC.
Conclusion
Inconsistencies in abduction/adduction of the femur are anecdotally thought to contribute to inaccuracies in LL measurement in THA. We examined this change in the non-operative leg of THA patients (where no change in LL is expected) and noted that while a pre-to-post-operative discrepancy in abduction/adduction was common (88%), this discrepancy was small in magnitude and did not correlate well with observed changes in LL between the pre- and post-operative images. This data suggests that while discrepancies in pre- and post-operative abduction/adduction of the femur play a role in leg length measurement accuracy, this role may not be as significant as generally thought.
Figures
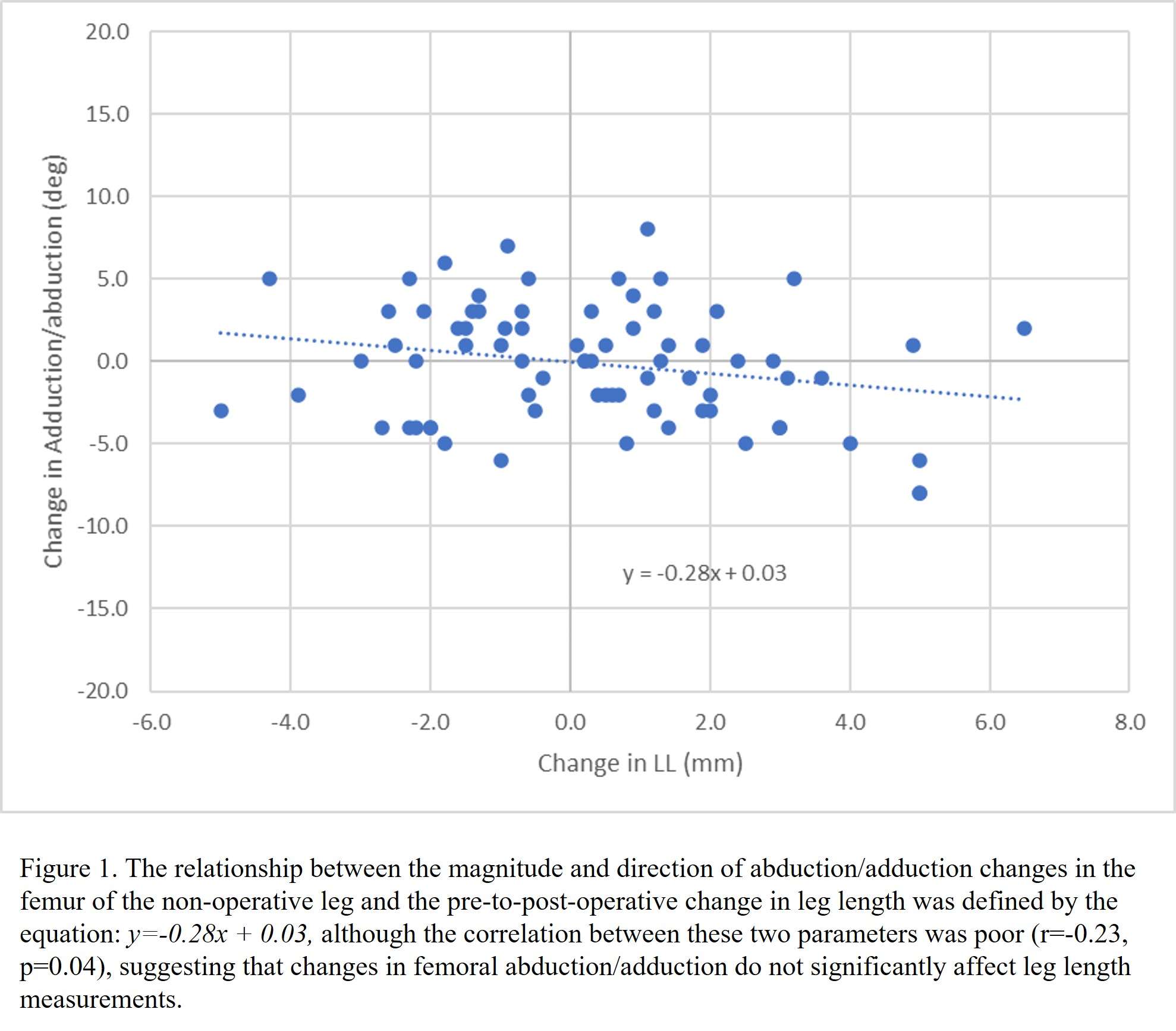
Figure 1#7865
Primary Stability of Collared and Collarless Cementless Femoral Stems - a Finite Element Analysis Study
*Ryunosuke Watanabe - University of Tsukuba - Tsukuba, Japan
Hajime Mishima - University of Tsukuba - Tsukuba, Japan
Sho Totsuka - University of Tsukuba, - Tsukuba, Japan
Tomofumi Nishino - University of Tsukuba - Tsukuba, Japan
Masashi Yamazaki - University of Tsukuba - Tsukuba, Japan
*Email: ryuwatanabe_tuk@yahoo.co.jp
Introduction
The primary stability of cementless femoral stem is important for long-term results in total hip arthroplasty. This study aimed to investigate the difference in stability between collared and collarless cementless femoral stems using finite element analysis (FEA).
Methods
A finite element model was constructed and analyzed using the Mechanical Finder ver. 11.0 (Research Center of Computational Mechanics, Japan). DICOM data of a synthetic femur (Composite femur🄬 #3403, Pacific Research Laboratories, USA) was used for the femur. CAD data of collared and collarless stem of UNIVERSIA stem (Teijin Nakashima Medical, Japan), a fully hydroxyapatite-coated stem, was used for the stem. The stem was positioned to reproduce the center of the femoral head. Three finite element models were constructed. The “contact model” was in contact with the cut surface of the medial calcar and collar. In the “non-contact model,” the cut surface of the calcar was moved 1 mm distally without changing the position of the “contact model” stem while the collar was made non-contact. The “collarless model” replaced the stem of the “contact model” with the collarless stem. Joint contact and muscle forces simulated peak forces in level gait and stair climbing. The femoral condyle was fully fixed and a coefficient of friction of 0.6 was set for the contact surface between the stem and bone. The relative displacement between the nodes of the stem and bone contact surface was defined as micromotion (MM), which was compared among the three models in two loading conditions. Gruen zones 1 and 7 were set as proximal stem, 2 and 6 as central, and 3 and 5 as distal. MM for each of the three zones was also compared among the three models.
Results
The median MM under level gait conditions was 56 μm for the contact model, 67 μm for the non-contact model, and 66 μm for the collarless model. The median MM under stair climbing conditions was 79 μm for the contact model, 99 μm for the non-contact model, and 98 μm for the collarless model. Statistical analysis showed significant differences between the contact and non-contact models and the contact and collarless models under both conditions (Dunn test, p < 0.05). The collar contact was highly effective in suppressing MM proximal of the stem in both conditions.
Conclusion
The collared stem provides greater stability than the collarless stem due to the contact of the collar with the cut surface of the medial calcar.
#7961
The Learning Curve Associated With Computed Tomography-Based Navigation in Total Hip Arthroplasty
*Hiroshi Watanabe - Nippon Medical School - Tokyo, Japan
Tokifumi Majima - Nippon Medical School - Tokyo, Japan
Kohei Murase - Nagoya University - Nagoya, Japan
*Email: watanabehiroshi@nms.ac.jp
Objective: Computer-assisted navigation systems (CAS) are increasingly used in total hip arthroplasty (THA), meanwhile its proficiency might require more cases than expected, considering the quitters. The objectives of this study are to investigate the accuracy of cup orientation and evaluate the registration error of computed tomography (CT)-based navigation in THA with its learning curve.
Methods: This study retrospectively investigated 75 patients who underwent CT-based navigation THA between April 2018 and March 2022. Consecutive cases using CAS by a single surgeon were included in the study. We compared the intraoperative acetabular cup alignment using navigation records with the postoperative cup alignment using postoperative CT data. All patients were categorized into the following three groups according to the course of three sequential operative time periods: 1–25 (initial group, A), 26–50 (intermediate group, B), and 51–75 (recent group, C).
Results: The mean absolute errors of cup angle were 5.4 ± 4.2 mm, 2.7 ± 2.7 mm, and 2.5 ± 2.0 mm for radiographic inclination (RI), and 4.1 ± 5.2 mm, 3.4 ± 2.4 mm, and 3.1 ± 2.4 mm for radiographic anteversion (RA) on group A, B, and C, respectively. In initial 10 patients, the mean absolute errors of cup angle were 7.0 ± 4.6 mm for RI, and 5.4 ± 7.4 mm for RA.
Conclusions: CT-based navigation offers excellent accuracy of cup orientation than expected, and therefore the proficiency would be acquired at no less than 25 cases. The initial 10 cases would be the minimum number for the learning curve.
#7673
The Non-Uniformity of Regional Strain in the Patellar Tendon Significantly Increases the Shear Strain Distribution at the Proximal Tibial Epiphyseal Plate: Three-Dimensional Finite Element Analysis
*Hiroshi Watanabe - Nippon Medical School - Tokyo, Japan
Kohei Murase - Nagoya University - Nagoya, Japan
Tokifumi Majima - Nippon Medical School - Tokyo, Japan
*Email: watanabehiroshi@nms.ac.jp
Objective:
Recently, we have reported the association between the increased PTSA and PTE injury during adolescent athletes. Meanwhile, the mechanism of the increasing stress at the proximal tibial epiphysis (PTE) remain unknown in Osgood-Schlatter disease (OSD). In the recent studies, the non-uniformity of regional strain in the patellar tendon has been reported, and we have proposed the mechanism of the increasing stress at PTE in OSD (Figure 1). To elucidate the effects of non-uniformity of regional strain in the patellar tendon on PTE, we simulated the different PTSA and patellar height model in the knee of OSD adolescent and studied the mechanical stress distribution in PTE using three-dimensional finite element (FE) analysis.
Methods:
FE models of the proximal tibia were reconstructed from computed tomography images and consist of cancellous bone, cortical bone, and epiphysis. The variations of PTSA and patellar height were prepared. The strain distribution in PTE with different PTSA and patellar height was examined by FE analysis using CalculiX software (Convergent Mechanical, United States).
Results:
On the increased PTSA and patellar height model, the increased strain in PTE was found and the maximum stress was confirmed in the edge of PTE. On partially open PTE models, the maximum shear strain distribution in anterior lesion of PTE was significantly different compared to normal PTSA and patellar height model.
Conclusions:
The increased PTSA and patellar height are associated with the increasing stress on PTE in OSD, due to the non-uniformity of regional strain in the patellar tendon.
Figures
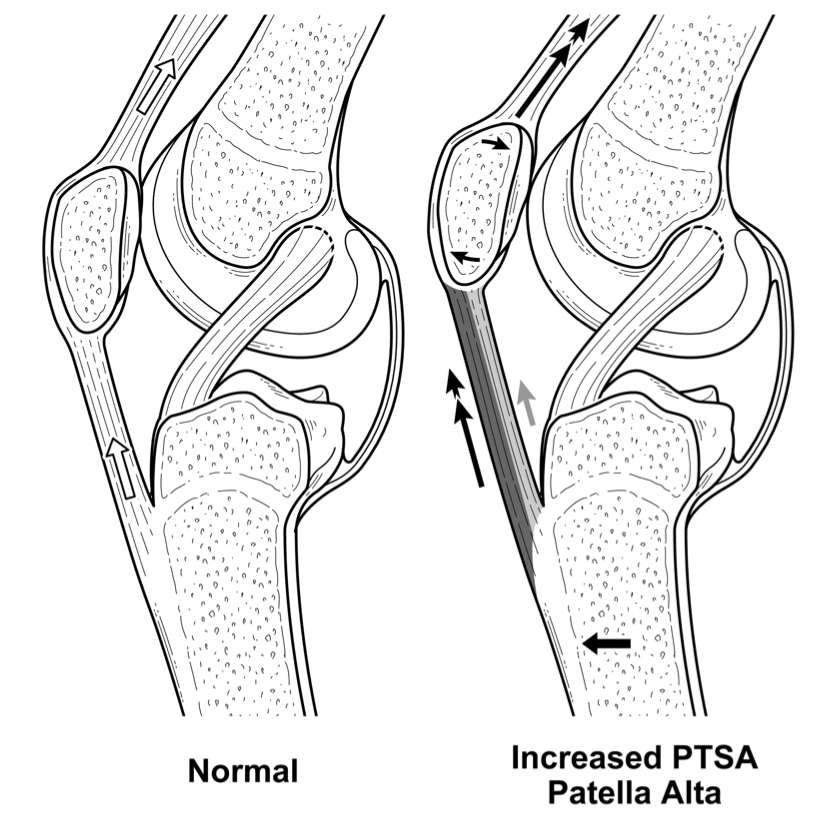
Figure 1#7351
Biologic Response to Metals: the FDA Experience
*Stephen Weber - Sacramento Knee & Sports Medicine - Sacramento, USA
*Email: webersc@earthlink.net
Although disregarded for decades, adverse biologic response to metal implants has recently come to the forefront with the early failures noted with metal on metal (MOM) total hip replacements. These failures have inspired significant new clinical data regarding the biologic responses to metals in general. In 2019 the FDA presented a major panel discussion regarding biologic response to metals to address the recent issues associated with a variety of metal devices of which the presenter was a co-author. While true metal allergy exists, it is an uncommon mechanism for device failure. While complex, the failure mode for MOM (metal-on-metal0 hips and other orthopedic implants is more likely to be local toxicity combined with a type IV delayed sensitivity reaction. These reactions occur not only in MOM devices but also with trunnion corrosion, dual mobility hips and mixed metal devices. Mechanisms for this reaction, diagnosis, and treatment remain challenging. This presentation will review the latest information available regarding this rapidly changing area, focusing on the regulatory issues involved with metal implants and up to date responses for diagnosis and treatment in this challenging area.
#7354
Reverse Shoulder Arthroplasty: Trends in the Incidence, Indications and Complications as Reported by ABOS Part II Oral Examination Candidates From 2005 Through 2017
*Stephen Weber - Sacramento Knee & Sports Medicine - Sacramento, USA
Edward McFarland - Johns Hopkins School of Medicine - Baltimore, USA
Jorge Rojas Lievano - Johns Hopkins School of Medicine - Baltimore, USA
Prashant Meshram - Johns Hopkins - Baltimore, USA
Uma Srikumaran - Johns Hopkins - Baltimore, USA
*Email: webersc@earthlink.net
Background: The experience of early-career orthopedic surgeons performing reverse shoulder arthroplasty (RSA) has not been previously reported. The aim of this study was to evaluate the temporal trends in the incidence of and indications for RSA procedures and reported complications performed among board-eligible orthopaedic surgeons in first 6 months of their career.
Methods: A query of the American Board of Orthopaedic Surgery (ABOS) Part II Oral Examination database for all cases of RSA from 2003 through 2017 was performed. The data over this time period was analyzed for incidence, indications, and complications. Risk factors for complication including patient demographics and shoulder fellowship-training were evaluated.
Results: A total of 2,633 RSA procedures were reported. There was an increased incidence of RSA (23-fold) and increased proportion of candidates performing RSA (19-fold) (P-trend < 0.001) (Figure 1). While there was an increasing trend seen in the primary (P-trend = 0.009) and trauma cases (P-trend < 0.001), declining was seen in the revision cases (P-trend < 0.001). Shoulder fellowship-training was reported by 27% of the candidates, and these candidates performed 42% of all RSA procedures. The complication rate over this time period was 34% and increased over the study period (P-trend < 0.001) (Figure 2). The incidence of medical, surgical and anesthesia complications was 18%, 15%, and 1.2%, respectively. Mortality, reoperation, and readmission rates were 0.6%, 3.2%, and 6.4%, respectively. Risk factors for medical complications were age and trauma cases, whereas revision RSA was a risk factor for surgical complications. Shoulder fellowship-training was not associated with a decrease in any of the complications.
Conclusions: There was a dramatic increase in the use of RSA among board eligible orthopedic surgeons in the United States. The early complication rates for ABOS candidates performing RSA are above others reported in the literature and showed an increasing trend over the study period.
#7854
Mismatched Tibial and Femoral Components: Is It a Viable Option in Total Knee Replacement?
Joel Weisenburger - The University of Nebraska Medical Center - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
*Hani Haider - UNMC - Omaha, USA
*Email: hhaider@unmc.edu
Ultra-high molecular weight polyethylene (UHMWPE) bearings in Total Knee Replacements (TKR) have shown significantly reduced wear when highly cross-linked (HXL) and stabilized with vitamin E to preserve material properties. In patients presenting with a varus or valgus deformity or needing more or less laxity on a given condyle, the use of an intentionally mismatched tibial bearing (i.e. a RIGHT bearing design on a LEFT knee) may assist in balancing the ligament tension around the joint, making the TKR feel more stable and natural to the patient. However, such a mismatch could result in unexpected increases in stress, contact area, and ultimately UHMWPE wear. This study investigated whether intentionally mismatched tibial bearings and femoral components would show wear rates that were significantly different than properly matched TKR components in an in vitro wear test.
Eight cruciate retaining (CR) tibial bearings made from compression-molded GUR 1020-E UHMWPE (0.1% vitamin E) irradiated with 100±10 kGy to achieve crosslinking were tested. The bearings were large size (81mm wide, 9mm thick) to maximize contact area. LEFT and RIGHT tibial bearings were paired with large highly polished CoCr LEFT femoral components, creating the properly matched group and an intentionally mismatched group (Fig.1), respectively (N=4 in each). The bearings were locked into titanium alloy tibial trays designed to work on either knee.
Testing was conducted on a significantly upgraded (in house) 4-station Instron-Stanmore force-controlled knee simulator. The machine simulated flexion with anatomically realistic joint reaction forces and torques between tibia and femur and included a spring-based system to simulate soft-tissue restraining forces and torques of a CR knee. The force-control waveforms of the walking cycle specified in ISO-14243-1 were applied for 5 million cycles (Mc) at 1Hz, with bovine serum lubrication with 20g/L protein concentration at 37°C. The tibial bearings were weighed at standardized intervals, and active soak control bearings were used to compensate for fluid absorption.
Over the 5Mc test, the properly matched group wore at an average rate of 15.2±2.01mg/Mc while the mismatched group wore at a nearly identical rate of 15.0±2.36 mg/Mc (p=0.880, not significantly different, Fig.2). The tibial bearing anterior-posterior movement during a walking cycle for both groups was similar, while the internal-external (IE) rotation of the properly matched group was slightly more than that of the mismatched group. The wear patches on the UHMWPE bearing surface of the properly matched group also appeared larger (Fig.3), perhaps partially due to the marginally increased IE rotation, but more likely due to the better-matching femoral-tibial bearing surface conformity. However, because the wear rates of both groups were nearly identical, any difference in IE rotation or wear patch size is likely of little consequence.
For this CR design, the study showed that mismatching the tibial bearing did not result in additional wear, and the knee kinematics during testing differed very little from that of the properly matched TKR. Perhaps mismatching the tibial bearing in certain surgical cases is an option that surgeons may consider for some specific TKR system designs.
Figures
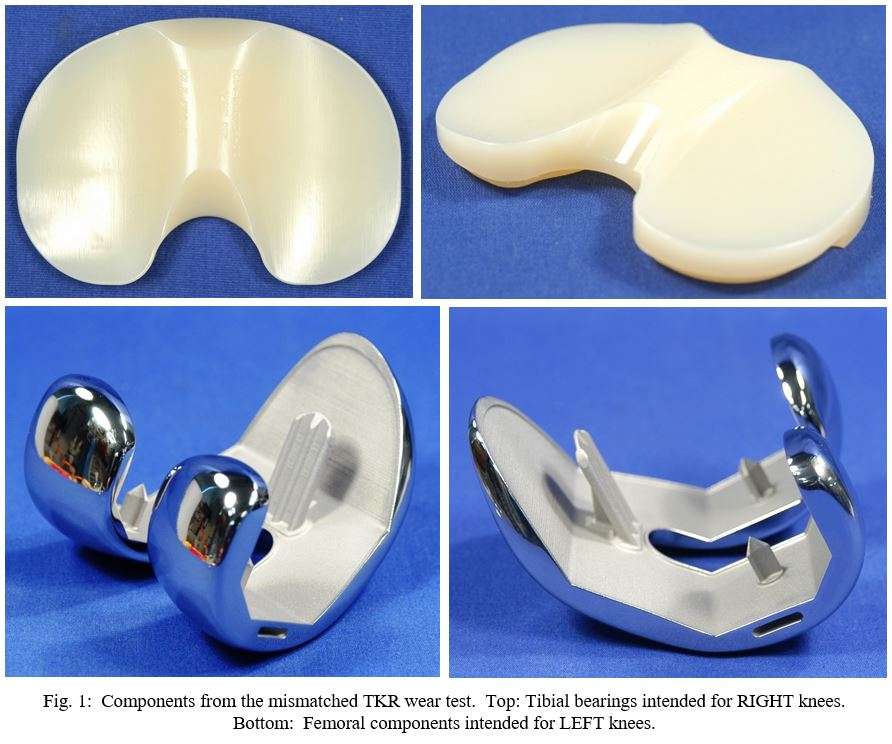
Figure 1
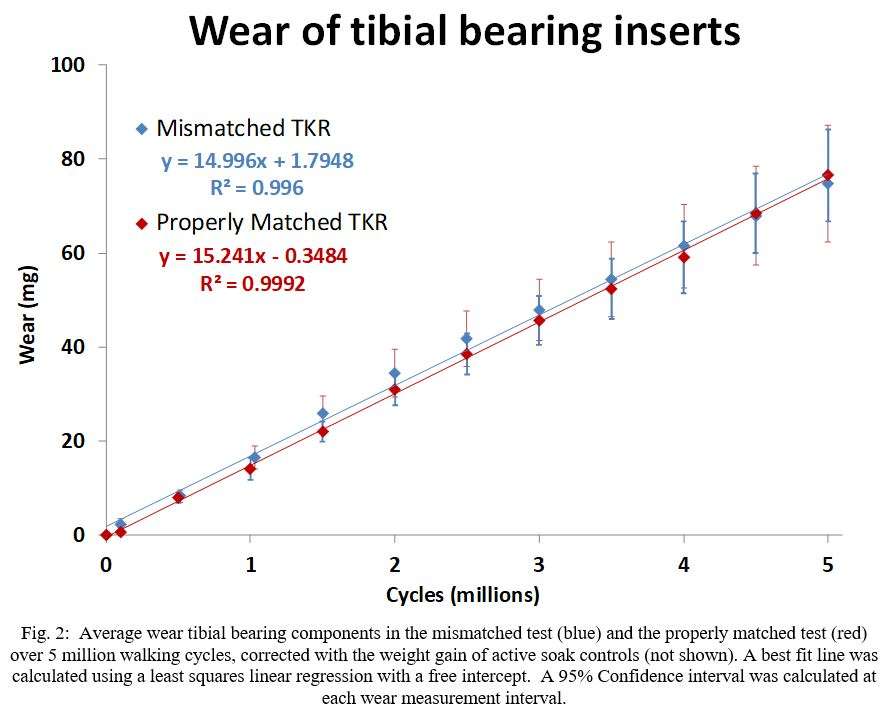
Figure 2
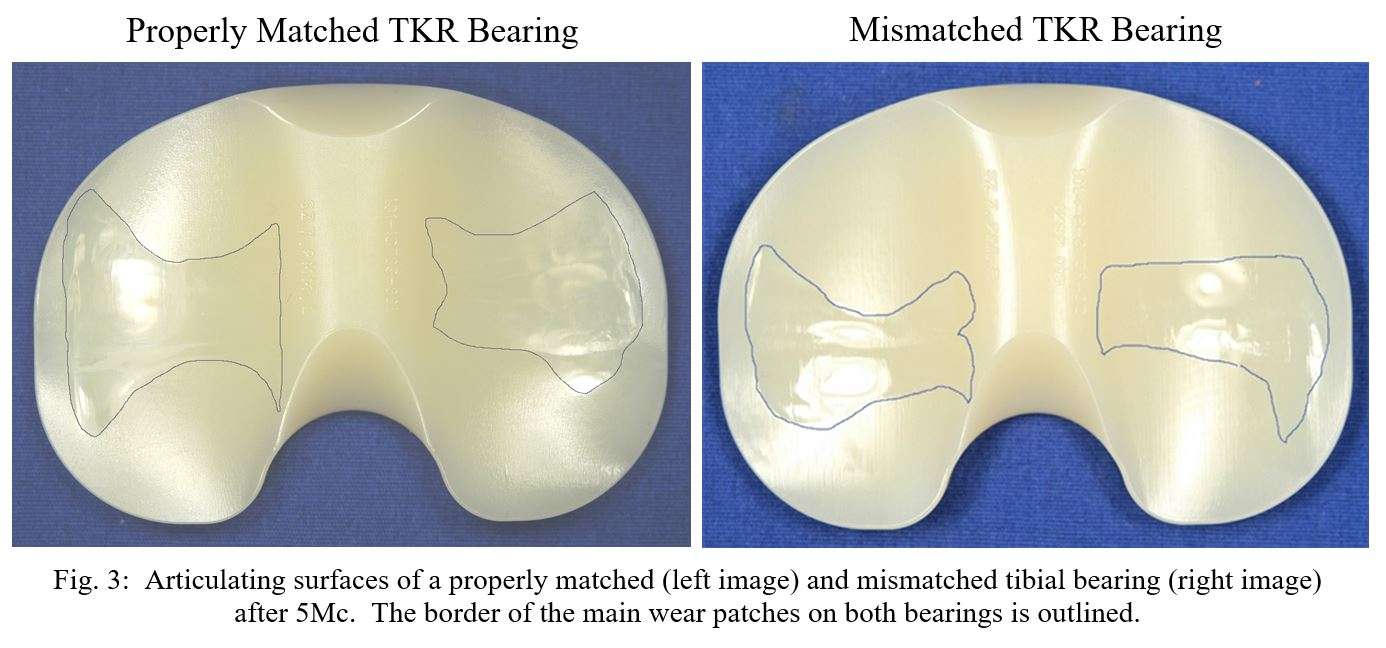
Figure 3#7969
Friction and Joint Reaction Torque in Dual Mobility Hips
Joel Weisenburger - The University of Nebraska Medical Center - Omaha, USA
Curtis Hartman - UNMC - Omaha, USA
Beau Kildow - UNMC - Omaha, USA
Beau Konigsburg - UNMC - Omaha, USA
Kevin Garvin - Univ of Nebraska Med Ctr - Ortho Dept. - Omaha, USA
Ryan Siskey - Exponent - Philadelphia, USA
*Hani Haider - UNMC - Omaha, USA
*Email: hhaider@unmc.edu
Dual Mobility (DM) Total Hip Replacements (THR) have emerged as a viable option in primaries and when revision surgery is necessary for improved range of motion with less dislocation risk. The tribology of DM THRs and their multiple articulating bearing surfaces is complex and poorly understood. This in-vitro hip simulator study investigated and compared the joint reaction torques and friction of DM and fixed-bearing (FB) THRs using novel measurement techniques.
12 hips were tested, in four different groups (n=3 each), 1 FB and 3 DM groups. The DM groups were as follows: fully dual mobility articulations, outer articulation surfaces allowed only, and inner articulation only. All DM groups had inner 28mm CoCr femoral heads, while the FB had 44mm dia. heads. The ultra-high molecular weight polyethylene (UHMWPE) components in all groups were GUR1020-E 150KGy UHMWPE. The DM and outer articulation UHMWPE bearings had identical 58mm outer dia.
Friction was measured based on equilibrium of forces and moments measured by a 6-DOF load cell on each station of an AMTI hip simulator. The force and moment data from the load cells were utilized to calculate the frictional torque about each of three rotational axes (flexion/extension, abduction/adduction and internal/external rotation). The frictional torques were transformed to account for the offset in load cell position from the hip center and were then vector summed to yield an overall frictional torque about the femoral head. The friction factor was then computed by dividing the overall frictional torque by the compressive load and femoral head radius. The ISO-14242-1 waveforms were used at 1Hz up to 10million cycles (Mc). Diluted bovine serum at 37ºC with 30 g/L protein concentration lubricated the specimens.
The isolated outer articulation group had the highest initial net frictional torque of 4.70±1.05Nm during peak stance-phase loading (Fig.1) and an average friction factor of 0.169±0.006 which decreased to 0.137±0.031 by the end of 7.5Mc (Fig.2). The 44mm FB group showed the next highest initial torque (2.35±0.784Nm) and a friction factor (0.117±0.007) decreasing to 0.072±0.008 after 10Mc. The isolated inner group showed a lower initial torque (1.42±0.210Nm) and a friction factor of 0.110±0.007 which decreased to 0.090±0.013. The full DM group displayed the lowest initial torque of all groups (0.925±0.272Nm) and the lowest initial and final friction factors (0.086±0.012 and 0.055±0.013, respectively). The average friction factors differed significantly between all groups (p<0.05).
All groups showed joint reaction torques and friction that decreased over testing after initial bedding-in wear/deformation occurred. The outer articulating surface of a full DM does not contribute to the overall friction/torque, with most of the articulation occurring between the femoral head and UHMWPE bearing. This becomes clear when comparing the DM torque/friction with that of the isolated outer articulation group. Additionally, the UHMWPE DM bearing decoupled some of the rotations which reduced joint reaction torque. Therefore, the DM torque and friction values were lower than even the isolated inner articulation group which could decouple rotations. These results indicate that high friction/torque in full DM THRs is not a concern.
Figures
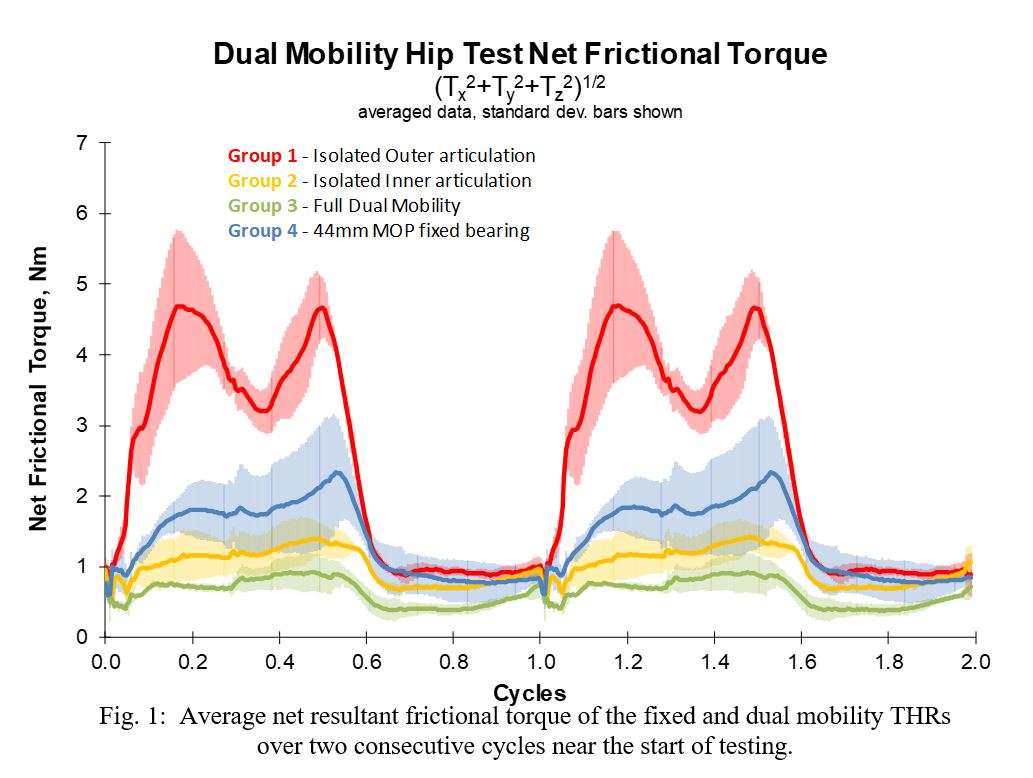
Figure 1
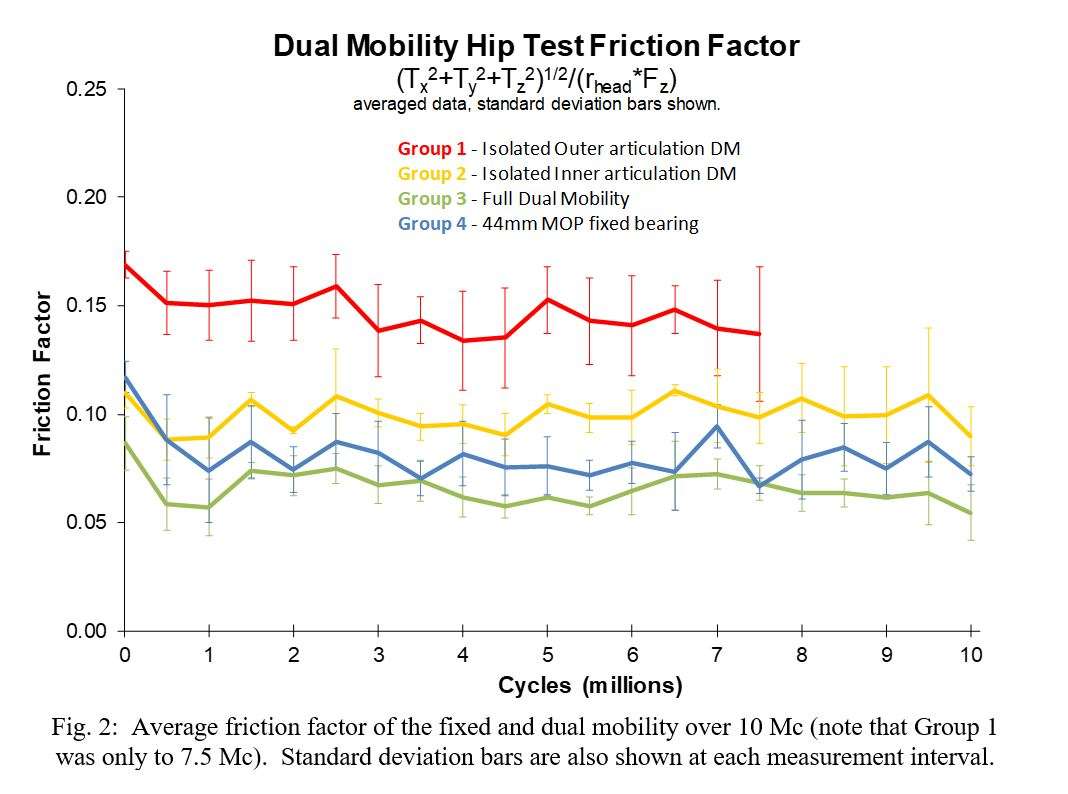
Figure 2#7919
Extended Offset Femoral Stem Use in Anterior Approach Total Hip Arthroplasty
*Edward Weldon - John A. Burns School of Medicine - - Honolulu, HI - Honolulu, USA
Keinan Agonias - John A. Burns school of medicine - Honolulu, United States of America
James DeJesus IV - University of Hawaii - Honolulu, United States of America
Dylan Lawton - Straub Medical Center - Honolulu, USA
Samantha Andrews - Straub Medical Center - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: ejweldon@hawaii.edu
Extended Offset Femoral Stem Use in Anterior Approach Total Hip Arthroplasty
Introduction: Dislocation remains a feared complication of total hip arthroplasty (THA). To decrease the risk of dislocation, extended offset (EO) femoral stems are used to increase muscle tension around the implant following posterior THA. The anterior approach is suggested to reduce dislocation risk and thus reduce the need for EO stems. The purpose of this study was to report on the overall usage rates of EO stems and compare radiographic outcomes and complications between EO stems and a matched standard offset cohort following anterior approach THA.
Methods:A retrospective review was performed on 1515 consecutive anterior approach THA to determine rates of EO use. The most recent 100 EO were included in the radiographic and complication analysis and were matched to 100 standard offset stems based on stem size, procedure (unilateral/bilateral), sex, body mass index and age. Data collection included patient demographics, pre- and post-operative radiographic outcomes, and complications within one year. Independent t-tests and Chi-squared analyses were performed to compare extended offset and standard offset groups.
Results: EO was used in 8% of all THA. Rates for extended offset use in Asian, Caucasian, and NH/PI patients were 1.6%, 13.1%, and 7.1%, respectively. Despite rigorous matching procedures, the distribution of ethnicity was different between extended and standard offset groups: Caucasian (75% vs. 43%), Asian (12% vs. 35%), NH/PI (9% vs. 13%), and other (4% vs. 9%) (p<0.001). No fractures, dislocations, or revisions occurred within one-year after surgery, and one deep infection was noted in the standard offset group. Hip offset difference was greater than 6mm in 24% and 18% of extended and standard offsets (p-0.193), respectively. Leg length difference was greater than 6mm in 19% and 15% of extended and standard offsets (p=0.223), respectively. EO was utilized much less frequently in this single surgeon, anterior approach THA cohort compared to previously reported rates for posterior approach THA (8% versus 49%, respectively).
Conclusion: The lack of dislocations and the ability to achieve limb symmetry suggests the use of EO is required to restore hip symmetry and not to achieve stability with anterior approach THA. The difference in the proportion of extended offset use between ethnicities was likely due to racial differences in hip anatomy.
Keywords: Total Hip Arthroplasty; Anterior Approach; Hip Dislocation; Extended Femoral Offset
#7493
Experimental Methodology to Evaluate Degradation on Human Cadaveric Hip Joints Subjected to Normal Loading Conditions on an Anatomical Hip Simulator.
*David Jimenez-Cruz - University of Leeds - Leeds, GB
Mudit Dubey - University of Leeds - Leeds, United Kingdom
Tim Board - Wrightington, Wigan & Leigh NHS Foundation Trust - Wigan, United Kingdom
Sophie Williams - University of Leeds - Leeds, United Kingdom
*Email: d.jimenez-cruz@leeds.ac.uk
Introduction
The mechanical environment of the natural hip joint is altered when conditions such as femoroacetabular impingement, developmental dysplasia or slipped capital femoral epiphysis occur. The geometric abnormalities of the femoral head and/or acetabulum alter the normal biomechanics and affect the tribology, range of motion and the stress distribution on the articular surfaces of the hip joint leading to mechanical failure and degradation of the tissue. Experimental hip simulators have been used to study effects of different mechanical environments on total hip replacements; however, their use investigating the effects of altered mechanical environments on the natural hip joint has been limited. The aim of this study was to assess changes to the articular surfaces of cadaveric hip joints after extended testing using an anatomical hip simulator that provides clinically relevant loading and motion.
Methods
Four cadaveric right hips were dissected (mean age = 62 years, male; United Tissue USA). The capsule was removed and joints were disarticulated. Custom designed cementing rigs and holders were used to position the sample into the anatomical hip simulator (AHS). The femur and acetabulum were secured into these fixtures using PMMA bone cement and mounted in the AHS so the centre of rotation of the hip and simulator were coincident [Fig 1]. Hydration of cartilage surfaces was maintained throughout tissue preparation.
Simulations consisted of applying a simplified twin peak gait cycle (peak load of 3kN; 25° to -18° flexion-extension, -10° to 2°, internal–external rotation and 7° to -4° abduction-adduction) at 1 Hz for 32 hours with the joints submerged in Ringers solution (0.04% sodium azide) . Photogrammetry was used to characterise the articular surface and labrum at 2hr intervals (initial 8hrs of testing) and at 4hr intervals (following 24hrs of testing). The appearance of the surfaces in terms of degradation and damage was recorded.
Results
All four hips were successfully tested for 32 hrs. Prior to simulation, some samples (n=2) exhibited signs of osteoarthritis and ossification on the articular surface, additionally, one sample suffered a minor surface laceration to the labrum during preparation. This sample also showed a small area of cartilage delamination. This damage progressed slightly during testing. For all the samples, the labrum appeared lax, which progressively increased within the first 16 hrs, but no new areas of damage were detected. The joints remained stable and the sealing effect of the labrum remained evident in the two samples with no signs of osteoarthritis after 32 hrs of simulation, these joints were difficult to disarticulate and the characteristic suction sound indicated that the labrum continued to act as an effective seal [Fig 2].
Conclusion
This study has demonstrated an effective experimental simulation methodology for evaluating damage and degradation in hip joints in a mechanical environment mimicking in vivo conditions. Future studies will assess degradation of the joint in altered mechanical environments and assess surgical repair strategies.
Figures

Figure 1
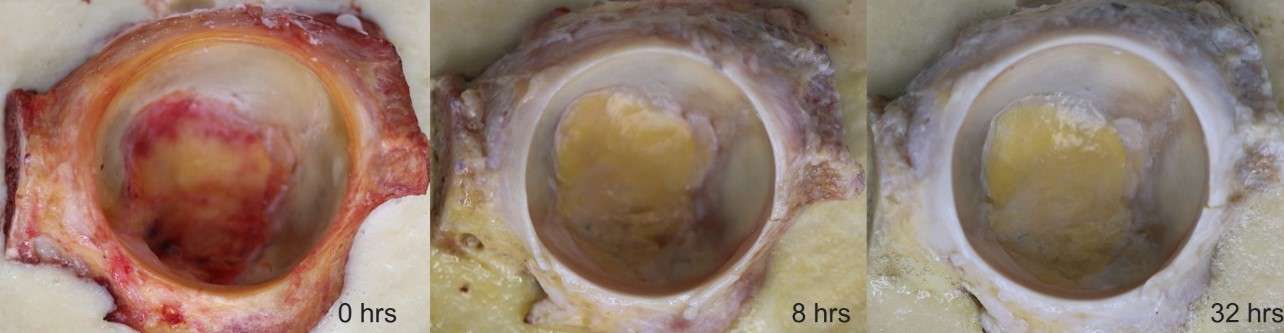
Figure 2#7717
Quantification of Trunnion Damage in a Series of Intact Total Hip Arthroplasty Femoral Stems Previously Identified to Be at Risk of Catastrophic Failure
*Olawale Sogbein - London Health Sciences Centre/Western University - London, Canada
Mathew G Teeter - Schulich School of Medicine and Dentistry, Western University and London Health Sciences Centre - London, Canada
Steven MacDonald - London Health Sciences Centre - London, Canada
Tea-Lyn Kok - London Health Sciences Centre - London, Canada
Ryan Willing - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
*Email: olsogbein@nosm.ca
Introduction: Corrosion at the head-neck junction of femoral stems is a rare complication of total hip arthroplasty (THA) with manifestations ranging from subclinical wear to catastrophic failure. Prior studies have identified a single femoral component design with an increased propensity for catastrophic trunnion failure. The purpose of the present study was to quantify trunnion damage of this femoral component retrieved from patients undergoing revision THA for non-trunnionosis indications.
Methods: Twenty-four femoral components from a single manufacturer were identified for study inclusion. Indications for revision included periprosthetic fracture (n=9), aseptic loosening (n=8), and infection (n=7). Revisions occurred at a mean 4 years after index THA. Each prosthesis underwent stereomicroscopic inspection. Corrosion and fretting scores were assigned per the Goldberg criteria to each quadrant zone of the trunnion. Material loss was calculated based on cone angles across trunnion quadrants. This was carried out using a coordinate measuring machine that digitized each trunnion surface. Stems were compared to a series of femoral stems with the same trunnion design with excellent clinical outcomes and longevity.
Results: Twenty of the 24 (83%) trunnions demonstrated corrosion, while all 24 trunnions demonstrated fretting. Corrosion scores did not statistically differ with respect to trunnion zone (p=0.53), while fretting scores were higher in the inferior zones compared to the superior zones (p<0.001). There was no statistically significant difference in cone angles assessing material loss between stems (p=0.25).
Conclusions: Evidence of trunnion damage was observed in each stem retrieved for non-trunnionosis revision THA. Specifically, fretting occurred more frequently about the inferior quadrants of the trunnion. However, digitized trunnion shapes were similar between implants with the control group of stems exhibiting no material loss. This calls into questions whether material loss occurred at all. Therefore, it is possible that previous reports of trunnion failures for this implant are not a systemic issue, and that further investigation is required.
Keywords: trunnionosis, corrosion, fretting, mechanically assisted crevice corrosion, revision total hip arthroplasty
#7735
Cementless Tibial Baseplates: A Biomechanical Study of Fixation Patterns
*Olawale Sogbein - London Health Sciences Centre/Western University - London, Canada
Ryan Willing - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Brett MacDonald - Western University - London, Canada
*Email: olsogbein@nosm.ca
Introduction: As understanding of early cementless TKA failure mechanisms improved with additional advancements in biomaterials, there has been improved survivorship of modern cementless TKA implants, especially in younger, obese, and active patients. Failure secondary to aseptic loosening, however, is still reported in this patient population. Migration of tibial components secondary to micromotion has been a common mode of failure with previous studies demonstrating that motion >150 µm inhibits bone ingrowth. Furthermore, studies have analyzed potential micromotion in tibial component designs with compressive, shear, and torsional loads applied through an articulating femoral component. A modular design featuring a keel with four adjuvant cruciform pegs was found to have less micromotion and therefore better initial stability than a monoblock porous tantalum baseplate with two hexagonal pegs. The objective of our study was to evaluate the stability of two cementless baseplate designs with different fixation patterns under simulated physiological loading conditions.
Methods: Two cementless tibial baseplate designs were implanted into ten sawbones. Five were a titanium modular design consisting of a keel with four surrounding cruciform pegs. The remaining five received a modular design with four peripheral porous coated pegs around a proximally coated central cone. All ten constructs were subjected to a previously validated physiological loading protocol simulating 6-8 weeks of stair descent activity, using a 6 degrees of freedom joint motion simulator. Compressive and shear implant-bone micromotion was measured continuously using 4 vertically oriented and 4 horizontally oriented LVDT’s.
Results: The central cone baseplate experienced significantly more vertical micromotion during the cyclic loading cycle. Specifically, micromotion was significantly larger anteriorly (p=0.03) and posteriorly (p<0.001) for this baseplate design.
Conclusions: The peripheral coated pegs with a central cone baseplate demonstrated significantly greater subsidence and liftoff compared to the baseplate with a keel and surrounding cruciform pegs. This may indicate lower initial mechanical stability with possible inhibition in biological fixation. Based on our results, additional studies investigating motion in these fixation designs with clinical correlation is warranted.
#7785
Development of Multi-Bundle Virtual Ligaments to Simulate Knee Mechanics After Total Knee Arthroplasty
*Samira Vakili - Western University - London, Canada
Brent Lanting - London Health Sciences Centre - London, Canada
Alan Getgood - Fowler Kennedy spirt medicine Clinic - London, Canada
Ryan Willing - Western University - London, Canada
*Email: svakili4@uwo.ca
Purpose: Total knee arthroplasty (TKA) aims to improve joint kinematics and hence restore joint stability. Preclinical testing of TKA implants is essential to understanding their mechanical performance and for developing strategies to improve joint stability. Ideally, such preclinical tests should reproduce the physiological behavior of the knee joint, which is guided by the articular geometries of the implants in conjunction with the capsule and ligaments. The purpose of our study was to design subject-specific virtual ligaments based on native ligaments and to determine if subject-specific virtual ligaments accurately reproduce the same mechanical behavior as real ligaments surrounding TKA implants on a joint motion simulator.
Method: Five cadaveric knee specimens with TKA implants were mounted onto the 6 degrees of freedom AMTI VIVO joint motion simulator (Advanced Mechanical Technology, Inc, Watertown, MA). Each knee was subjected to loads that simulated neutral flexion-extension (FE) and knee laxity tests. FE kinematics were determined by flexing and extending the knee between 0° and 90° while applying a 200N constant compression force. Knee laxity tests also were simulated by applying constant anterior-posterior (AP) forces, varus-valgus (VV), or internal-external (IE) torques to the tibia while maintaining 200 N of compression, across the full range of flexion and extension. Tibiofemoral kinematics were recorded during each motion. The forces transmitted through major ligaments (medial, lateral, and the posterior cruciate ligament) were measured using a sequential resection and superposition technique whereby each ligament was individually dissected, the kinematics were repeated, and the changes in joint reaction force were measured. Ligament lengths were calculated based on the point-to-point distances between the femoral and tibial insertions. Ligament properties (stiffness, slack length, ligament insertion points, and the number of bundles) were calibrated by tuning the measured ligament force to an established nonlinear force-length relationship. Based on this, virtual ligaments were developed for each specimen and were used to simulate the soft tissue envelop around isolated TKA implants mounted on the motion simulator. The same motions were then repeated allowing the comparison of joint kinematics resulting from native versus virtual ligaments.
Results: The mean difference between virtual and native ligament knee kinematics during FE was less than 3 mm in terms of AP displacement, 2° for IE rotation, and 2° for VV. The average RMSE between virtual and native ligament knee laxities was less than 3.6 mm for AP, 7.6° for IE, and 1.7° for VV. There were similar errors recorded in the present study as in previous studies, such as an average RMSE of less than 2 deg during VV rotations, less than 6 deg during IE rotations, and less than 3 mm of translation during AP displacements (Harris et al. 2016).
Conclusion: In this study, virtual ligament properties were calibrated to best match native ligament behaviors. When used to stabilize isolated implants, the resulting behaviors were comparable to those of the real ligaments. These results suggest that databases of subject-specific knee ligaments could be developed and employed on joint motion simulators to simulate prosthesis behaviors in a large population of knees.
#7817
Comparing Simulation Approaches Used in Finite Element Modelling of Medial Opening Wedge High Tibial Osteotomy
Victor Carranza - Western University - London, Canada
Ryan Willing - Western University - London, Canada
Alan Getgood - Fowler Kennedy spirt medicine Clinic - London, Canada
*Timothy Burkhart - University of Toronto - Toronto, Canada
*Email: timothy.burkhart@utoronto.ca
Purpose: Finite element (FE) modelling has been widely used in research related to medial opening wedge high tibial osteotomy (HTO) of the knee to investigate the stress and strain patterns in the tibial bone, plate, and screws. There are, however, elementary aspects of modelling HTO in a FE modelling study that must be addressed. In previous studies, the osteotomy cut has been performed in one of two ways: i) the clinically relevant method (CRM) - open the tibial wedge through simulation of the intra-operative procedure1; or ii) the simplified method (SM) - cut out the tibial wedge to the desired correction angle without performing the opening2 (Figure 1). The purpose of this study is to determine whether the simplified method is an acceptable assumption for a HTO FE modelling study when analyzing the stresses and strains in the plate, screw, and throughout the proximal tibia.
Methods: Seven tibia models were reconstructed from computed tomography (CT) scans of seven cadaveric specimen. Two sets of models were created from the same set of specimens to create the CRM and SM dataset. The osteotomy in the CRM was simulated by virtually creating an osteotomy whose orientation and thickness correspond to the angle and kerf of the osteotomy saw blade and virtually opening the wedge to 10mm. In the SM, the osteotomy was simulated by simply removing a wedge from the proximal tibia the size of which would match the void normally created by a 10mm opening height, without changing the tibial geometry. To test the differences between both methods, a simplified Tomofix fixation plate and screw system was modelled and fixed to the tibia to maintain the position of the wedge and loaded evenly across the tibial plateau.
Results: A statistically significant difference in the mean plate stresses were found, with the SM experiencing 36% greater stresses through the plate construct. A statistically significant difference in mean screw stresses was found between the CRM and SM with the SM experiencing up to 43% more stress. Finally, the SM model experienced 24% greater stresses around the apex of the osteotomy hinge when compared to the CRM.
Discussion: Selecting the appropriate modelling method that best represents the clinical scenario is a crucial step in creating a representative FE model. With the CRM, the proximal wedge is moved from its original position, virtually shifting the loading axis. Alternatively, the SM does not account for the geometric changes in the tibia which may cause the differences in the outcome measures. Secondly, the positioning of the plate in the SM is more proximal on the tibia due to the lack of bone stock (i.e., the wedge was cut out of the tibia). This creates an unrealistic plate and screw position on the SM which cause the increase in stresses experienced. To account for the mechanical change in a MOWHTO, it is recommended to perform the opening (CRM) of a HTO FE modelling study when analysing the stresses and strains in the plate or screws.
Figures
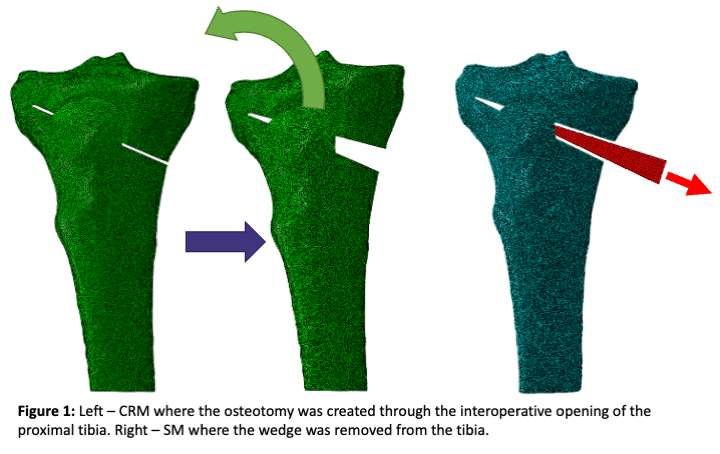
Figure 1

Figure 2#7421
The Effect of Stem Size on Late Revision of the Exeter Femoral Hip Stem
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
Jonah Poo - Flinders University - Adelaide, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
Stephen Graves
*Email: chriswilson42@hotmail.com
Introduction
Since 1970, the Exeter cemented femoral stem has demonstrated excellent clinical and radiographic outcomes as well as long-term survivorship for primary total hip arthroplasty. However, recent studies have shown a potential trend of increased late revisions for larger stem sizes (size 4-6) for loosening and for peri-prosthetic fractures. This study aims to compare the cumulative percentage revision of large Exeter stems (sizes 4-6) to other smaller Exeter stem (sizes 0-3) to evaluate whether there exists a statistically significant increased risk in late revision for larger sizes for loosening and peri-prosthetic fracture.
Methods
Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were analysed for all primary total conventional hip procedures undertaken for osteoarthritis using the Exeter stem for the period September 1999 to December 2019. The primary outcome measure was the cumulative percent revision (CPR) for all causes and the CPR for fracture. Results were adjusted for age and gender. A sub-analysis was performed comparing the Exeter stems by offset sizes 37.5mm, 44mm, 50mm and 56mm.
Results
There were 84,037 primary THA procedures undertaken for OA. Of these, 81,976 were size 0-3 and 2,061 were size 4-6. The CPR at 17 years was 7.8% (95% CI 7.3, 8.4) for the size 0-3 group and 10.7% (95% CI 7.9, 14.4) for the size 4-6 group. There was no difference in the risk of revision when the two stem size groups were compared (entire period HR=1.17 (95% CI 0.94, 1.45), p=0.169). There was a higher CPR for fracture for size 4-6 stems compared to size 0-3 from 3.5 years onwards (HR=2.23 (95% CI 1.41, 3.53), p<0.001), with no difference between the two groups prior to this time. Large offset size was a risk factor for revision, with size 56mm having a higher rate of revision when compared to offset size 37.5mm (entire period HR=1.68 (95% CI 1.00, 2.81), p=0.050). There were no other differences between the remaining offset sizes.
Conclusion
The data obtained confirms our initial hypothesis that a statistically significant increased risk of late revision for fracture exists for larger stem sizes (Size 4-6) as compared to smaller sizes (Size 0-3). Fracture was also identified as the commonest cause for late-stage revision in larger sizes, specifically starting from 10 years post-primary procedure.
#7424
Design, Construction, and Early Results of a Formal Local Revision Hip Arthroplasty Registry
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
Ben Piotrowski - Flinders University - Adelaide, Australia
*Email: chriswilson42@hotmail.com
Introduction:
National Registries for arthroplasty surgery have been successful in improving outcomes and quality control by large scale data collection and analysis. Data from the national registry has suggested room for improvement in our local revision hip arthroplasty outcomes. Using this data we have a standardised diagnostic and management pathway for revision hip arthroplasty combined with a local revision hip arthroplasty registry provides granular data applicable to our local hospitals. The aim is to evaluate the performance of our local hospitals against the national standard to improve patient outcomes and care. This is achieved through comparing data of revision types, revision diagnosis and incidence of revisions performed.
Methods:
In our centre in 2014 we introduced a standardised diagnostic algorithm for hip revision arthroplasties. From December 2014 to December 2020, our centre applied the algorithm to all cases of revision hip arthroplasty and investigated their indication. This data was then compared with the results procured from the with Australian Orthopaedic Association National Joint Replacement Registry.
The primary outcome of our research was used to compare hip revision arthroplasty at our centre pre and post the algorithm intervention whilst simultaneously comparing against national standards. The secondary outcome was to analyse the re-revision rates of hip arthroplasty’s pre and post intervention and locally vs nationally. Re-revision rates was used as a proxy of the success of our initial revision surgeries. Finally, our third outcome was to analyse the propensity of our centre to perform more minimally invasive hip arthroplasty procedures.
Results:
When comparing with historical local data, the diagnosis of “Loosening” decreased (25.0% vs. 14.1%), “Infection” had increased (23.2% to 29.6%) and “Fracture” had increased (12.5% to 18.5%). Additionally, Our Centre improved our proportion of “minimally invasive” revision types from 25.7% to 40.7%. When comparing our historical data to national standard at 8+ years since the primary procedure, our centre was 28% more likely to perform hip revision arthroplasty (HR = 0.72).
Our historical data showed a higher rate of re-revision hip surgery compared to the national average. After implementation of our diagnostic pathway the re-revision rate fell to below national average and the reduction was significant. (p=0.047)
Conclusion:
Our research shows that the use of a standardised diagnostic algorithm was instrumental in improving our surgical outcomes for hip revision arthroplasty. We have increased our use of more conservative revision surgery and our rates of re-revision surgery have significantly reduced.
#7427
Long Leg Radiographs vs CT Perth Protocol: Mechanical Alignment Analysis
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
Matthew Cehic - Flinders Medical Centre - Adelaide, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
*Email: chriswilson42@hotmail.com
Background
Long leg radiographs are commonly used to measure alignment in Total Knee Arthroplasty surgery. However, they are time consuming to perform and provide no information regarding implant rotation. The aim of this study was to compare the accuracy of measuring mechanical alignment in the coronal plane between long leg radiographs and CT Perth protocol.
Methods
Patients were recruited from our waiting list for routine TKA surgery. Pre-operative and post-operative Long Leg Radiographs and Perth protocol CT scans were performed. LLR’s were reported by 2 blinded orthopaedic surgeons and the CT scans by a blinded consultant radiologist. Intra-class correlation coefficient was compared between the scan results.
Results
Pre-operatively 132 (73 female and 59 male), meet the inclusion criteria with 120 patients completing the post op scans due to loss to follow up. The agreement between the pre-op LLD’s and CT scans was excellent with and average difference of 1.8 degrees and an ICC of 0.82. Post-op the agreement was good with an average difference in measurements of 1.58 degrees and an ICC of 0.69.
Conclusions
This study show that CT Perth Protocol achieves similar, reproducible results in determining mechanical alignment in the coronal plane when compared to LLRs. CT scans provide more information and integrate with modern robotic surgical techniques. We propose that all patients undergoing elective TKA should have a pre-operative CT for planning purposes.
#7432
An Australian Algorithm to Guide the Surgical Management of Chronic Prosthetic Joint Infection: A Multi-Disciplinary Team Approach
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
Melinda Jiang - Flinders Medical Centre - Adelaide, Australia
James Sires - Flinders - Adelaide, Australia
Santhosh Daniel - Flinders Medical Centre - Adelaide, Australia
Matthew B Roberts - Flinders Medical Centre - Adelaide, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
*Email: chriswilson42@hotmail.com
Introduction:
Chronic prosthetic joint infection (PJI) is a leading cause of failure for total joint arthroplasty. Historically, two-stage revision arthroplasty has been considered the gold standard approach to chronic PJI, however emerging evidence suggests one-stage revision arthroplasty may be underutilised. To our knowledge, there have been no previously published guidelines for the surgical management of chronic PJI in Australia, resulting in significant heterogeneity in management within and across centres.
We aim to review contemporary concepts in the surgical management of PJI and develop an evidence-based algorithm to optimise the management of chronic hip and knee PJI, incorporating a multidisciplinary team (MDT) approach.
Methods:
A review was conducted to identify existing articles discussing surgical management of chronic PJI, specifically contraindications to one-stage revision arthroplasty. Absolute contraindications for one-stage revision include difficult to treat organisms, significant soft tissue compromise and concurrent sepsis. Relative contraindications include lack of pre-operative identification of organism, presence of a sinus tract, fungal infections, significant bone loss, and immunocompromise. In determining management for patients with a relative contraindication, MDT discussion with consideration of the patient’s overall local, host and microbiological profile is necessary.
Results:
Using gathered evidence, absolute and relative contraindications for one-stage revision arthroplasty were developed into an algorithm. The algorithm is designed to assist our PJI MDT in making optimised decisions when choosing between a one-stage versus two-stage approach. Ongoing follow-up is underway to determine the effect of implementing this algorithm on patient outcomes, eradication rates and revision rates within our centre.
#7433
A Multi-Disciplinary Approach for the Management of Prosthetic Joint Infections: an Australian Perspective
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
James Sires - Flinders - Adelaide, Australia
Santhosh Daniel - Flinders Medical Centre - Adelaide, Australia
*Email: chriswilson42@hotmail.com
Background:
Prosthetic joint infections (PJI) are a major complication of hip and knee arthroplasty, imposing significant morbidity and mortality. Orthopaedic oncology units have utilised a multi-disciplinary team (MDT) approach for some time. PJI is not only an equally life-threatening condition, it also requires input from multiple healthcare personnel and treatment can vary significantly between individuals given the diversity in microbiological, surgical and host factors. Our arthroplasty service established an MDT meeting to manage this complex patient group. This study describes the philosophy and implementation of an MDT approach to the management of PJIs at a tertiary hospital in Australia.
Methods:
A retrospective review of all patients that presented to the MDT PJI meeting from October 2017 to April 2020 was performed. Patient characteristics, microbiological profile and management were reviewed.
Results:
101 patients were reviewed over a 2.5-year period with a mean age of 69.2 years (SD 11.9). Patients presenting predominantly had a primary TKR (32%) or primary THR (22%). Results of Microbiology cultures varied, with 42% Gram-positive organisms, 13% Gram-negative organisms, 2% fungus and 1% yeast origin. Management mainly consisted of two-stage revision (28%), debridement-antibiotics-and-implant retention (22%) and antibiotic suppression (14%). 91.5% of patients who underwent surgical management were considered cured at one year.
Conclusion:
PJIs are complex and require coordinated care by a number of healthcare personnel. The MDT process has allowed collaboration between Orthopaedic, Infectious Disease and Microbiology departments and aims to improve quality of care provided to patients, potentially reducing morbidity and mortality of patients with PJI.
#7428
The Pericapsular Nerve Group (PENG) Block Combined With Local Infiltration Analgesia (LIA) Provides Superior Short-Term Analgesia Compared to Non-Invasive Sham and LIA in Hip Arthroplasty Surgery:
Emma Jackman - Flinders Medical Centre - Bedford Park, Australia
*Chris Wilson - Repatriation General Hospital - Adelaide, Australia
Matthew Cehic - Flinders Medical Centre - Adelaide, Australia
D-Yin Lin - Flinders Medical Centre - Adelaide, Australia
Craig Morrison - Flinders Medical Centre - Bedford Park, Australia
Ruurd Jaarsma - Flinders Medical Centre - Bedford Park, Australia
Brigid Brown - Flinders Medical Centre - Adelaide, Australia
*Email: chriswilson42@hotmail.com
The Pericapsular Nerve Group (PENG) Block Combined with Local Infiltration Analgesia (LIA) Provides Superior Short-Term Analgesia Compared to Non-Invasive Sham and LIA in Hip Arthroplasty Surgery: A Multi-Centre Double-Blinded Randomized Controlled Trial.
Background:
The Pericapsular Nerve Group (PENG) block is a novel regional analgesia technique that has shown to provide superior analgesia in patients undergoing hip fracture surgery while preserving motor function. In this study the use of the PENG block was investigated in elective total hip arthroplasty (THA).
Methods:
In this multi-centre double-blinded randomized-controlled trial, THA patients were randomized to receive either a PENG or a sham block. The primary outcome was pain score (numeric rating scale 0-10) 4 hours post-operatively (Day 0). Secondary outcomes were postoperative quadriceps muscle strength, postoperative day one pain scores, opiate use, complications, length of hospital stay, and patient-reported outcome measures.
Results:
Sixty THA patients were randomized and equally allocated between groups. Baseline demographics were similar. Postoperative Day 0, the PENG group experienced less pain compared to the sham group (PENG group 14 (47%) patients no pain, 14 (47%) mild pain, 2 (6%) moderate/severe pain versus sham 6 (20%) patients no pain, 14 (47%) mild pain, 10 (33%) moderate/severe pain; p=0.03). There was no difference in quadriceps muscle strength between groups on Day 0 (23 (77%) intact PENG group versus 24 (80%) sham group; p=0.24) and no differences in other outcomes.
Conclusions:
Patients receiving a PENG block for analgesia in elective THA experience less postoperative pain on Day 0 with preservation of quadriceps muscle strength. There was no impairment of mobilisation or loss of quadriceps muscle strength.
#7439
Why Surface Topography of Hip Trunnions Matters Under Fretting Corrosion
*Markus Wimmer - Rush University - Chicago, USA
Alfons Fischer - University of Duisburg-Essen - Duisburg, Germany
Philippe Telouk - Universite de Lyon - Lyon, France
*Email: markus_a_wimmer@rush.edu
Introduction: Fretting corrosion of biomedical taper junctions has raised concerns about adverse local tissue reactions. Particularly some CoCr29Mo6/TiAl6V4 couplings produced excessive cobalt and chromium ion release; however, the exact mechanism is still not fully understood. A lower release of wear products into the body is always desired. This is typically achieved by lowering the local contact pressures within the real contact area making the topography one of the optimization parameters. Still, a taper topography of circumferential machining marks with high ridges and low valleys (leading to high local contact pressures) appears to enable a reduction of the release of corrosion wear products. The purpose of this study is to clarify this obvious contradiction to classical wear models and identify the mechanisms and submechanisms of CoCr/Ti taper couplings under gross-slip fretting conditions.
Methods: Gross slip fretting tests (as previously described) were carried out in bovine calf serum (BCS) at 37degC with polished low-carbon CoCr29Mo6 alloy pins (Ra»0.006 µm) against fluted TiAl6V4 cylinders (Ra»2.4 µm). The circumferential machining provided ridges with a distance of about 190 µm and valleys of 10 µm depth. Wear mechanisms and submechanisms were analyzed by SEM after 40,000 fretting cycles. ICP-MS was used to measure metal content (ions and particles) within the lubricant (representing the wear loss). These were compared with former results of polished CoCr29Mo6 pins against fine machined (Ra»0.245 µm) TiAl6V4 cylinders.
Results: Fine machined surfaces of CoCr29Mo6 showed microploughing, tribooxidation, and tribocorrosion, while the TiAl6V4 counterbody showed mechanical mixing and microploughing. The nanostructured tribomaterial consisted of oxidic wear particles predominantly from the Ti-side as well as denatured/cleaved proteins. With increasing numbers of cycles, it is squeezed out of the contact area to both sides of the wear groove, remaining on the surfaces without contributing to wear loss. The steady state wear rates by metal ion release into BCS were 1.25 ng/m wear path for CoCr29Mo6 and 0.09 ng/m for TiAl6V4. Tribocorrosion dominated the wear loss, while the other submechanisms mainly generated tribomaterial.
With the rougher fluted topography the acting submechanisms altered into microploughing triggering tribooxidation and tribocorrosion on both bodies. In contrast to above, the oxidic wear particles escaped into the valleys of the topography. Here, they remained with residues of the denatured/cleaved proteins, while the latter also covered the ridges acting as boundary lubricant. The steady state wear rate decreased to 0.6 ng/m for CoCr29Mo6, while it increased for TiAl6V4 to 0.18 ng/m.
Conclusion: A fluted topography allows for a shorter dwell time of oxidic wear particles within the contact, as well as for a quicker escape from the real contact area. Thus, tribocorrosion as results of the removal of the passive films by microploughing is reduced on the CoCrMo-side of the contact, while the same submechanism increases the wear loss on the Ti-side. Still, the total wear of the fluted system was half of the fine machined system, despite the higher local contact pressure, while the soft constituents still acted as boundary lubricants.
#8051
Invited Talk: Hip trunnion fretting & corrosion
*Markus Wimmer - Rush University Med Ctr - Chicago, USA
*Email: markus_a_wimmer@icloud.com
#7649
Functional Gait After Inverse Kinematic Aligned (IKA) Total Knee Arthroplasty Resembles Healthy Controls - a Comparative, Blinded, Gait Analysis of 45 Subjects at 2 Years Postop
*Philip Winnock De Grave - AZ Delta - Roeselare, Belgium
Tamaya Van Criekinge - KU Leuven - Brugge, Belgium
Thomas Luyckx
Kurt Claeys - KU Leuven - Brugge, Belgium
*Email: philip.winnockdegrave@azdelta.be
Introduction
Reports on patient specific alignment in total knee arthroplasty (TKA) show prosperous patient reported outcome measures (PROMs), however, the clinical effect of restoring native joint line obliquity (JLO) and native knee anatomy is still debated. The purpose of this study was to compare the gait of a mechanical aligned TKA cohort (adjusted mechanical alignment; aMA) with a patient specific alignment TKA cohort (inverse kinematic alignment; iKA).
Methods
At 2 years postoperative, 15 aMA and 15 iKA patients were analyzed. All patients were operated with robotically assistance (Mako) using an identical perioperative protocol. Patients’ demographics were identical. As a control group, 15 healthy subjects were used, matched for age and sex. (Figure 1) Gait analysis was done using a 3D motion capture system (VICON). Data collection was done by a blinded investigator. Primary outcomes were sagittal knee kinematics, knee adduction moment and spatiotemporal parameters (STPs). Secondary outcomes were Oxford Knee Score (OKS-12) and Forgotten Joint Score (FJS-12).
Results
Concerning sagittal knee kinematics during gait, no significant differences were observed regarding functional knee flexion between iKA and healthy controls, while aMA differs significantly with iKA and healthy controls (p<0.001; aMA 41,8°; iKA: 50,4°; controls 52,0°). (Figure 2) Knee adduction moments during stance with iKA are lower (225 Nmm/kg) compared to aMA (276 Nmm/kg) and healthy controls (280Nmm/kg), though none were significant. (Figure 3) Regarding STPs, no significant differences are seen between iKA and healthy controls. Six out of 7 STPs differ significantly between aMA and healthy controls. OKS-12 of iKA is significantly better compared to aMA: 45.4 vs. 40.9; p=0.05. FJS-12 is significantly better with iKA compared to aMA: 84.8 vs. 55.5; p= 0.002.
Conclusion
At 2 years postoperative, functional knee flexion and quality of the gait is better with iKA, compared to aMA. The restoration of joint line obliquity and native anatomy enhances clinical and patient reported outcomes.
Figures
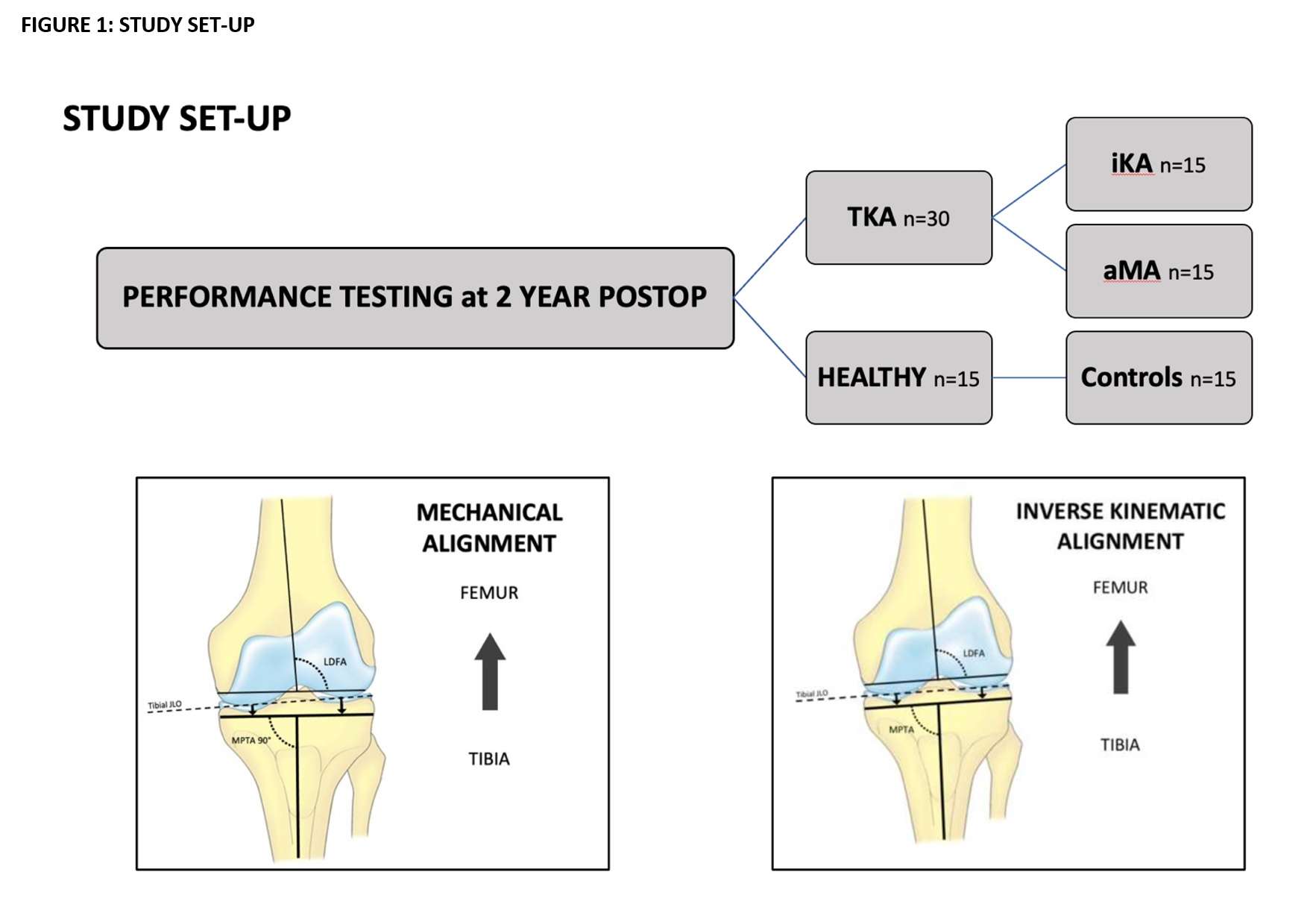
Figure 1
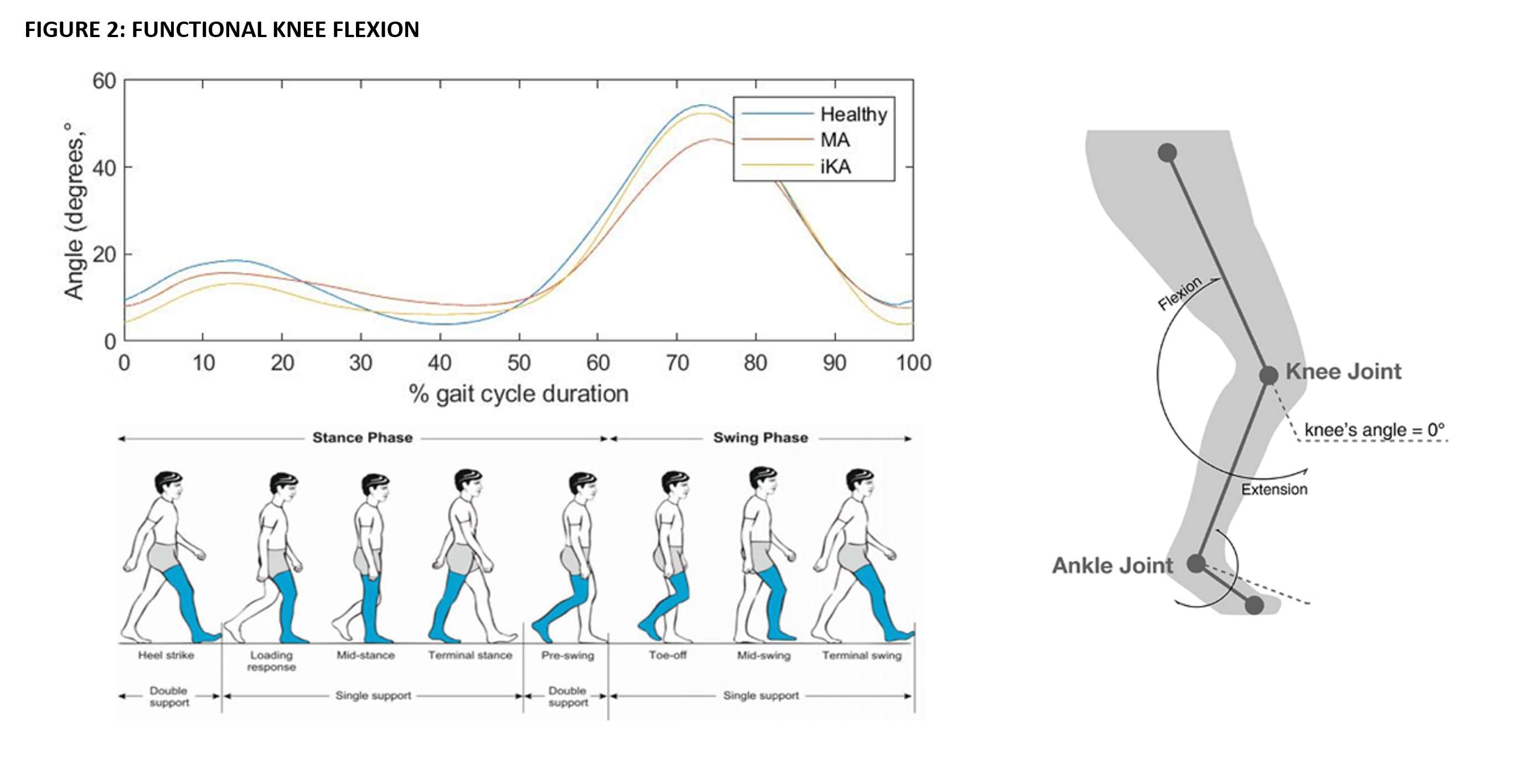
Figure 2
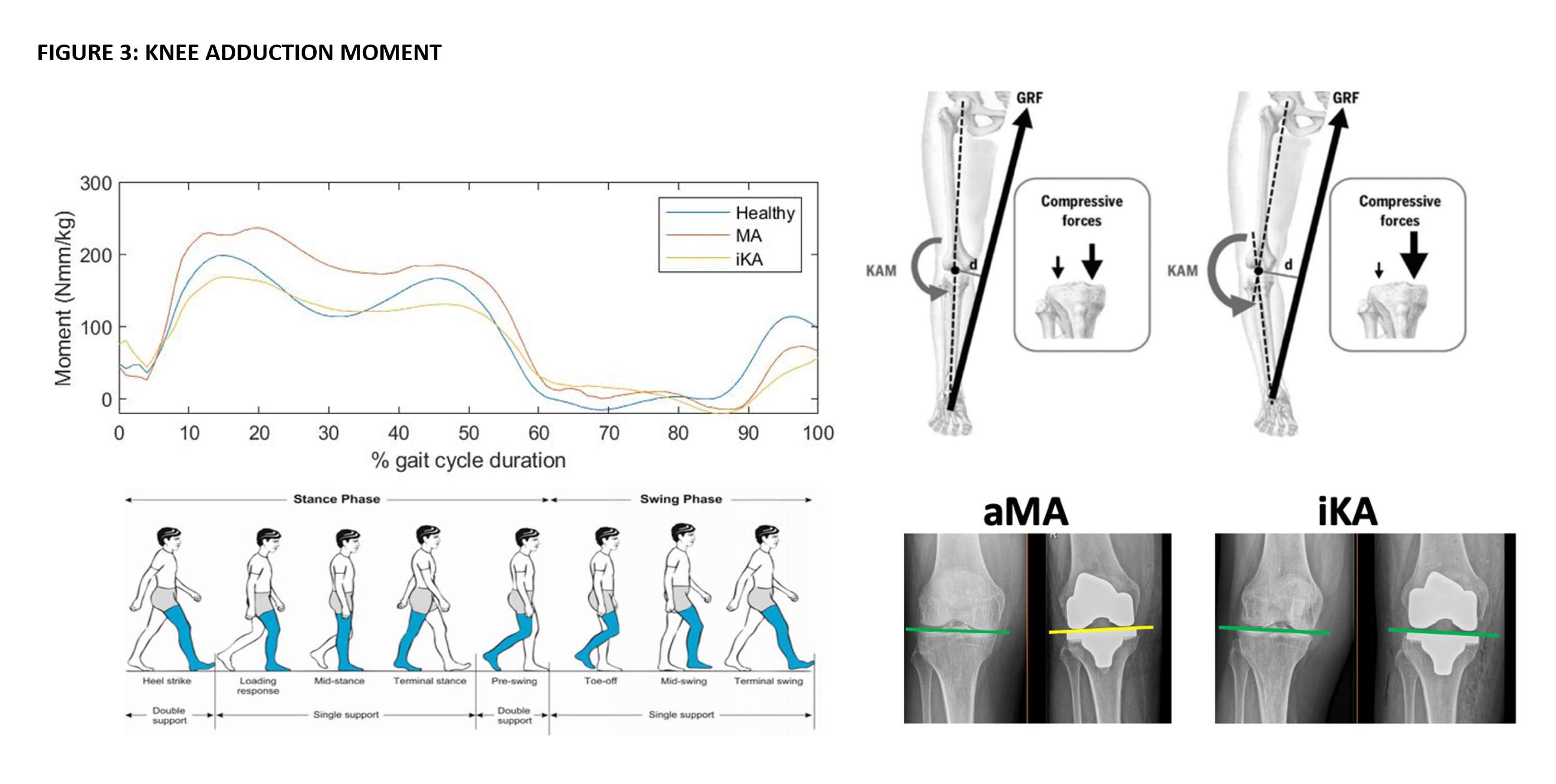
Figure 3#7653
Effect of Hybrid Alignment Techniques on Native Coronal Alignment and Soft Tissue Balance in Total Knee Arthroplasty
*Philip Winnock De Grave - AZ Delta - Roeselare, Belgium
Cobus Muller - Resurg - Madrid, Spain
Kurt Claeys - KU Leuven - Brugge, Belgium
*Email: philip.winnockdegrave@azdelta.be
Introduction: Hybrid alignment techniques in TKA, such as adjusted mechanical alignment (aMA), restricted kinematic alignment (rKA) and inverse kinematic alignment (iKA), allow restoration of prearthritic knee alignment, but within defined limits or target zones. The purpose of this study was, first, to determine the proportion of native non-arthritic knees that fit within the target zones of aMA, rKA, and iKA. Second, to estimate required adjustments in native coronal alignment and soft tissue balance to bring outlier knees within the respective target zones.
Methods: The study used measurements obtained from a computed tomography (CT) scan database of 1005 healthy knees. HKA, MPTA and LDFA were used to estimate the proportions of knees within the hybrid alignment target zones; and to estimate adjustments of MPTA, LDFA and soft tissue balance to bring outlier knees within target zones.
Results: Of the 1005 knees, 81 (8.1%) were in the aMA target zone, 544 (54.1%) were in the rKA target zone, and 748 (74.4%) were in the iKA target zone. To bring knees within the target zones, estimated proportion of coronal alignment adjustments are, for aMA (MPTA, 90%; LDFA 91%), for rKA (MPTA, 45%; LDFA 28%), and for iKA (MPTA, 25%; LDFA 22%). Soft tissue balance adjustment would be required in 29% for aMA, 26% for rKA, and 7% for iKA.
Conclusion: There is considerable variability in native knee alignment that correspond to hybrid alignment techniques: iKA represents the greatest proportion of knees (74.4%), followed by rKA (54.1%), whereas aMA only represents a small proportion (8.9%). Less soft tissue releases are necessary with iKA, due to its target zones which better represent the variability in native knee alignment.
Figures
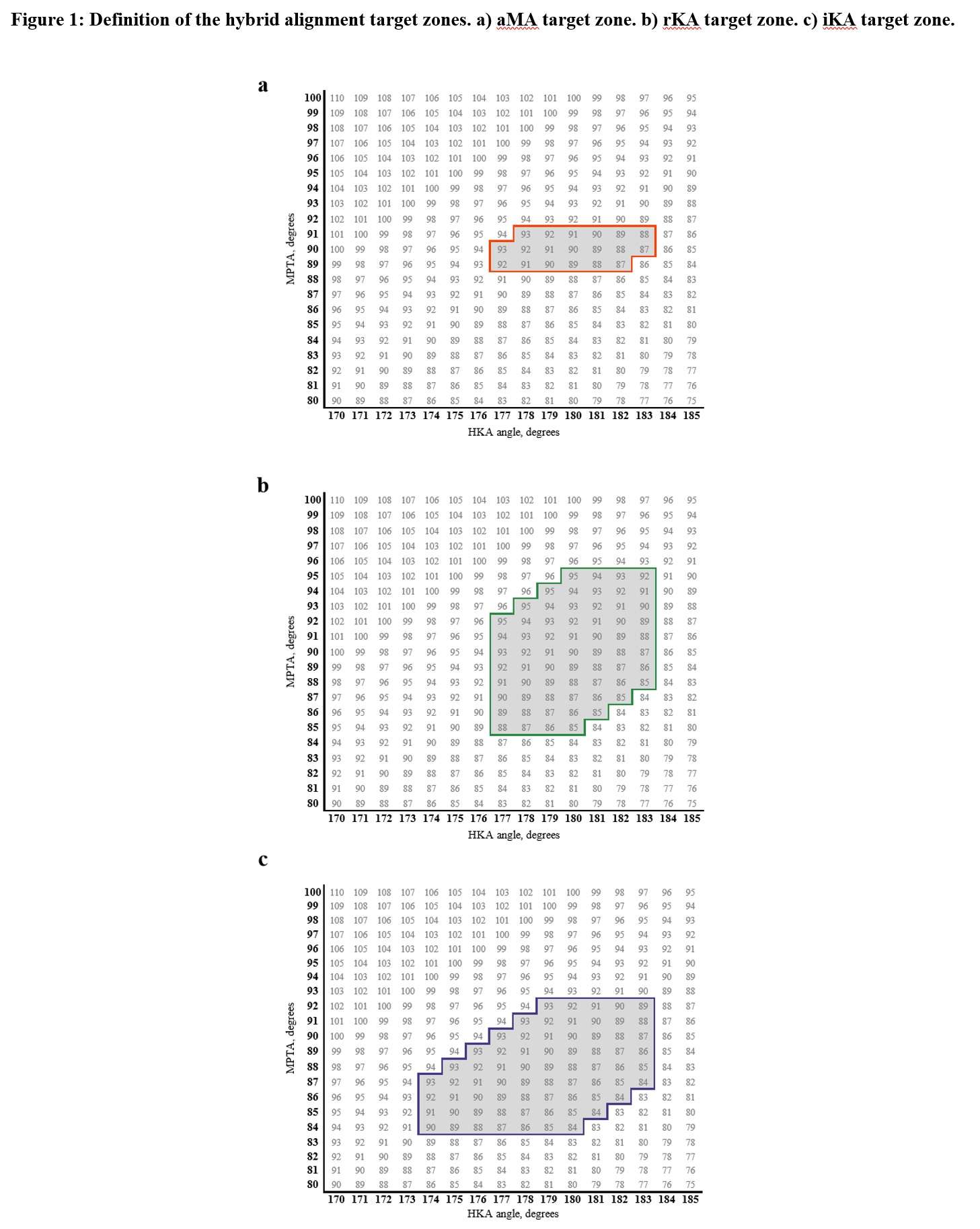
Figure 1
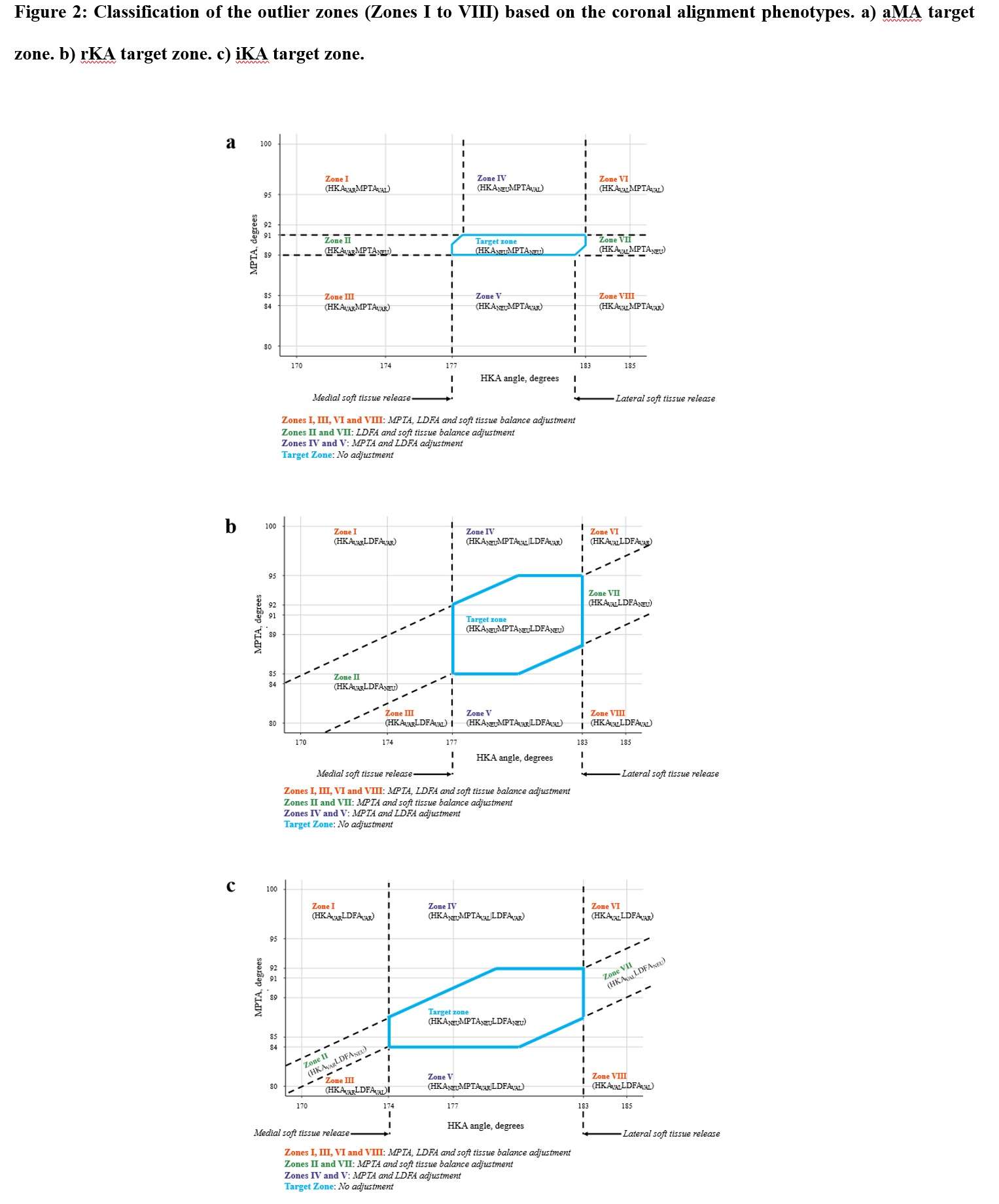
Figure 2
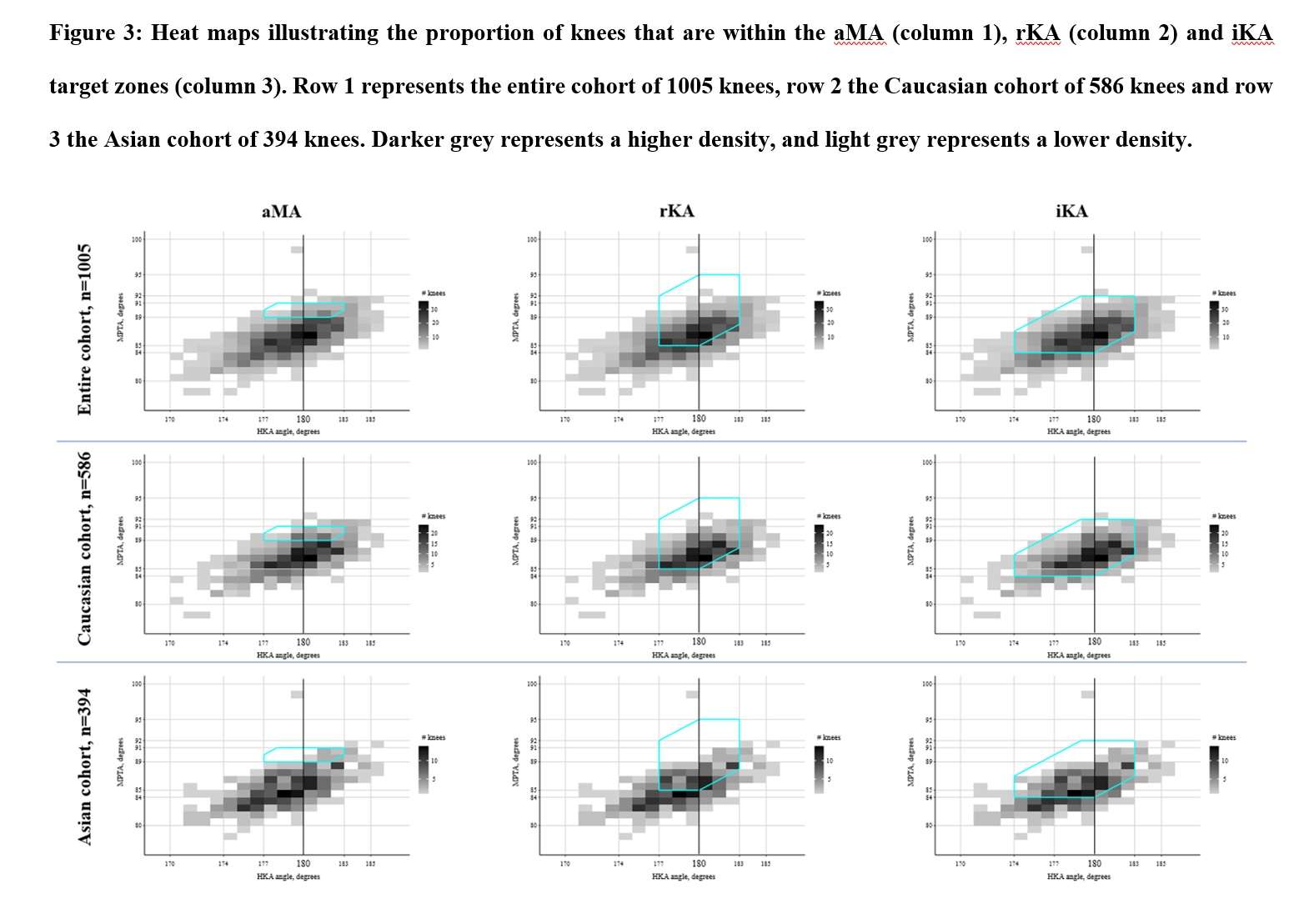
Figure 3#7365
The Morphology of a Kinematically Aligned Distal Femoral Osteotomy Is Different From That Obtained With Mechanical Alignment and Could Have Implications for the Design of Total Knee Arthroplasty
*Ye Yeon Won - Ajou University Medical Center - Suwon, South Korea
Quan Hu Shen - Ajou - Suwon, South Korea
Seok-Hyung Won - Ajou University Hospital - Suwon, South Korea
*Email: thrtkr@ajou.ac.kr
Introduction: Kinematically aligned total knee arthroplasty (KA-TKA) may lead to a
different pattern of osteotomy from mechanically aligned total knee arthroplasty (MA-TKA). This
paper aims to analyze the effects of KA and MA on the morphology of the distal femoral osteotomy
surface.
Methods: Computed tomography scans of 80 TKA candidates were reconstructed into 3D
models. The measurement of bone morphology was performed after the distal femur cut according to
two different alignment techniques. The aspect ratio, trapezoidicity ratio, and asymmetry ratio of the
distal femur were assessed. (Figure1,2,3)
Results: The aspect ratio and the asymmetry ratio in the KA group was significantly lower than that in the MA group in the general population (p < 0.001). The trapezoidicity ratio in the KA group was significantly higher than that in the MA group in the general population (p < 0.001).
Conclusions: It was found that KA-TKA and MA-TKA presented different morphologies
of the distal femoral osteotomy surface, and this difference was also influenced by gender. The
surgery pattern of KA-TKA and MA-TKA and gender should be considered when surgeons choose
femoral prostheses.
Figures
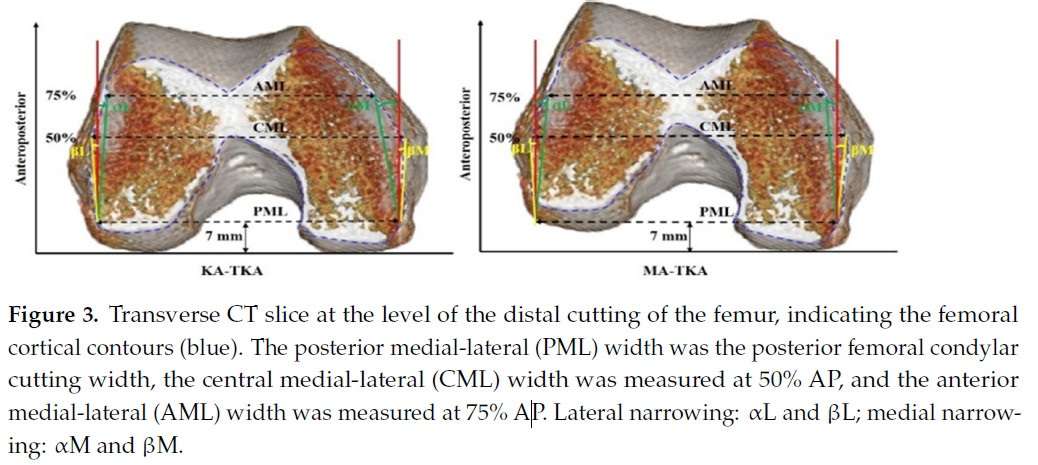
Figure 1
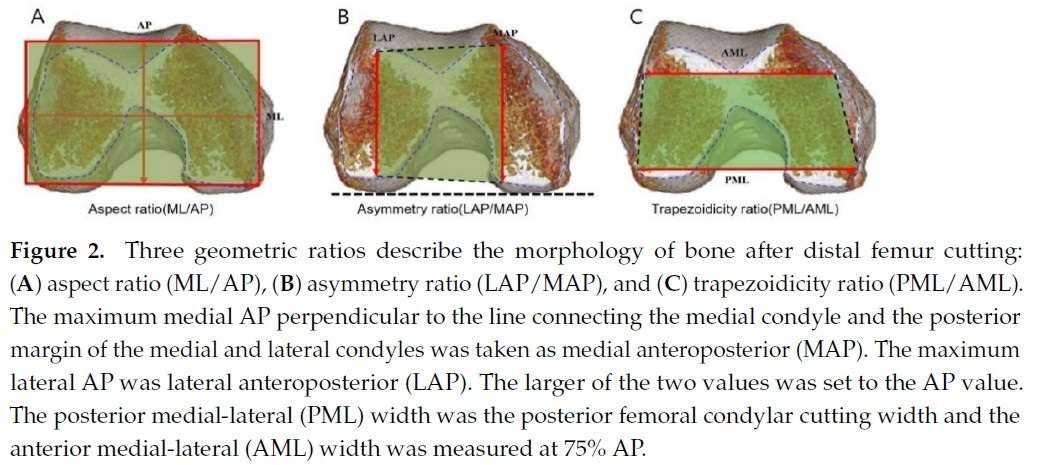
Figure 2
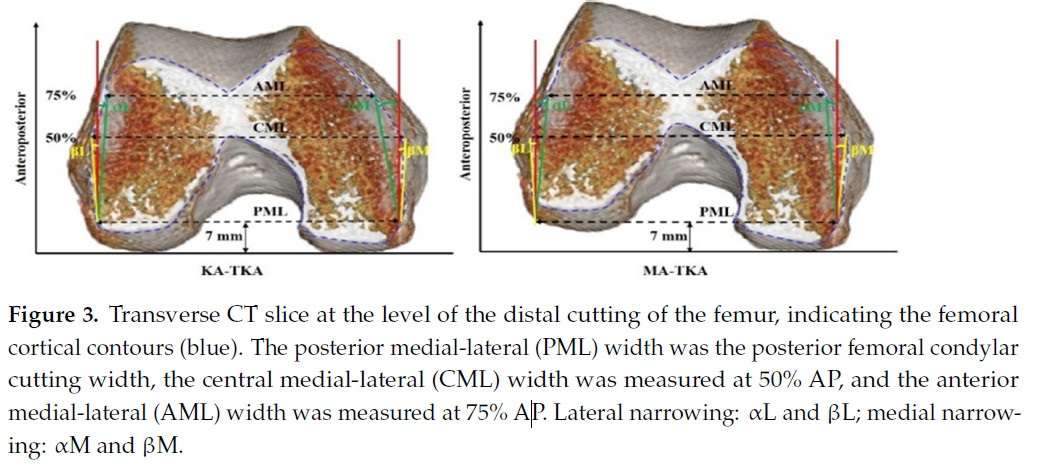
Figure 3#7870
OARA Score, ASA and CCI Are Poor at Predicting Failure in Outpatient Total Joint Arthroplasty
*Krystin Wong - Straub Medical Center - Honolulu, USA
Scott Nishioka - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Dylan Lawton - Straub Medical Center - Honolulu, USA
Tyler Thorne - University of Hawaiʻi at Mānoa - Mānoa, USA
Samantha Andrews - University of Hawaii John A. Burns School of Medicine - Honolulu, USA
Cass Nakasone - Straub Medical Center/Hawaii Pacific Health/University of Hawaii - Honolulu, USA
*Email: krystinw@hawaii.edu
INTRODUCTION: The Outpatient Arthroplasty Risk Assessment (OARA) score was designed to identify suitable patients for outpatient total joint arthroplasty (TJA). However, there is limited research on its validity or applicability to minority racial groups. The American Society of Anesthesiologist (ASA), and the Charlson Comorbidity Index (CCI) are tools that have previously been studied for predicting safety in outpatient discharge, however these scores lack guidelines specific to arthroplasty outcomes. Therefore, the purpose of this study was to compare the predictive values of the OARA score, ASA, and CCI in predicting outpatient discharge, and further determine whether these scoring systems differ amongst racial groups.
METHODS: This retrospective review included 288 consecutive total knee and hip arthroplasty patients (368 joints) for which OARA scores, ASA, and CCI were calculated. Ethnicity was self-reported as Caucasian, Asian, or Native Hawaiian/Pacific Islander (NHPI). Positive (PPV) and negative predictive values (NPV) were calculated for outpatient discharge for all three indices.
RESULTS: Compared to Caucasians and Asians, NHPI had the highest body mass index yet the youngest age. There were no significant differences for OARA scores (51.4-67.1), ASA ≥ 3 (58.1-72.0%) or CCI (2.0-2.6) amongst all three racial groups. There were no significant differences in the PPV for all three scoring systems amongst the racial groups for either unilateral (91.9-95.4%) or bilateral (65.3-73.7%) procedures. The NPV for all three indices were equally poor amongst all racial groups for both unilateral (7.8-12.3%) and bilateral (34.9-40.0%) cases.
CONCLUSION: While the OARA score, ASA, and CCI did not show any significant differences amongst the three racial groups, all three scoring systems were equally poor in predicting which patients would fail to achieve outpatient discharge following TJA. Furthermore, all three scoring systems showed acceptable and equivalent PPV for unilateral TJA only. There is clearly a need for better assessment tools to accurately predict which patients are poor candidates to attempt outpatient TJA.
#7546
Accuracy of Acetabular Component Alignment With Surgical Guidance Systems During Hip Arthroplasty
*Joshua Xu - Royal North Shore Hospital - St Leonards, Australia
Wout Veltman - Royal North Shore Hospital - St Leonards, Australia
Yuan Chai - University of Sydney - Sydney, Australia
William Walter - Specialist Orthopaedic Group - North Sydney, Australia
*Email: joshua.xu@msn.com
Background:
Accurate acetabular component alignment during hip arthroplasty is critical to ensure satisfactory post-operative outcomes and to minimise complications. Optical navigation systems (ONS) have been widely demonstrated to improve implant positioning but have limitations including the need for bulky equipment and variable reproducibility in registering landmarks. Subsequently there has been increasing interest in inertial navigation systems (INS) as they are more compact and do not rely as heavily on landmark acquisition. Thus, the aim of this study was to assess the accuracy of an INS and ONS by comparing intra-operative measurements of acetabular component inclination and anteversion with a post-operative CT scan.
Methods:
We prospectively collected intra-operative navigation data from 102 hips receiving conventional total hip arthroplasty or hip resurfacing arthroplasty through either a direct anterior or posterior approach. Two guidance systems were used simultaneously: an inertial navigation system (INS) and optical navigation system (ONS). Acetabular component anteversion and inclination was measured on a post-operative pelvis CT scan.
Results:
The mean age of the patients was 64 years (range: 24-92) and average BMI was 27 kg/m2 (range 19-38). There were approximately equal patients having hip surgery through an anterior approach versus a posterior approach (52% vs 48% respectively). From the navigation output, 98% of the INS measurements (Figure 1) and 88% of the ONS measurements (Figure 2) were within 10° of the CT measurements. The mean (and standard deviation) of the absolute difference between the post-operative CT and the intra-operative measurements for inclination and anteversion were 3.0° (2.8) and 4.5° (3.2) respectively for the ONS, along with 2.1° (2.3) and 2.4° (2.1) respectively for the INS. There was a significantly lower mean absolute difference to CT for the INS when compared to ONS in both anteversion (p<0.001) and inclination (p=0.02).
Conclusions:
The INS demonstrated greater accuracy compared to the ONS in the measurement of acetabular inclination and anteversion. However, both navigation systems provided reliable intra-operative feedback to allow nearly all acetabular components to be placed within an acceptable range.
Figures
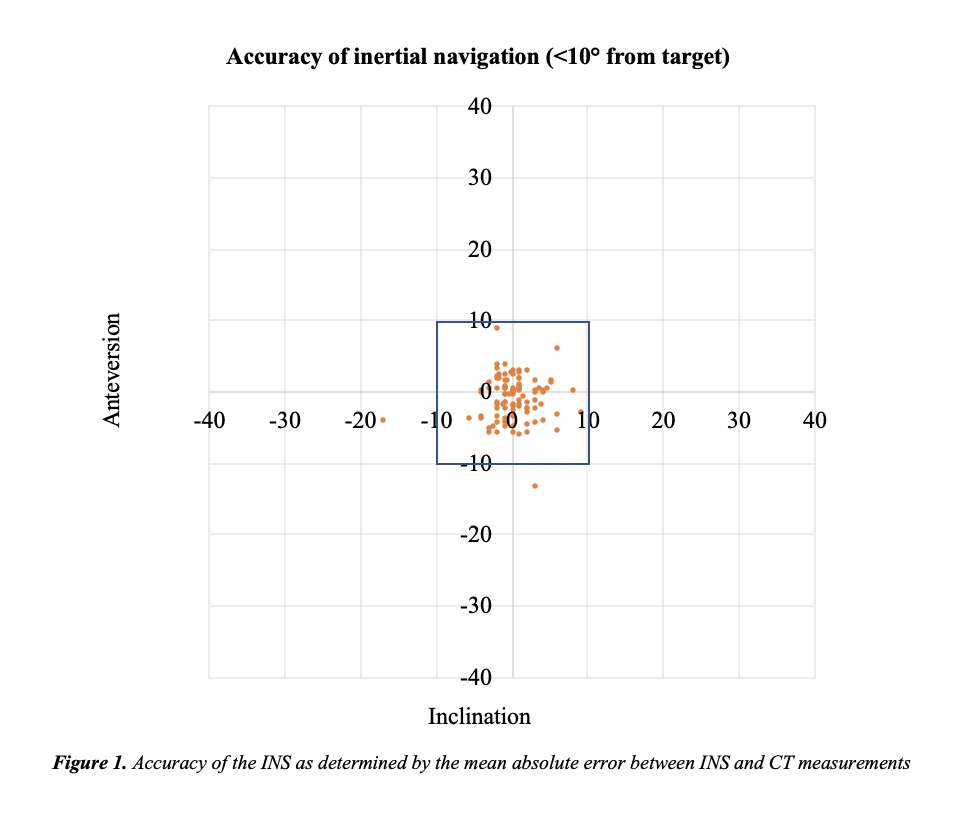
Figure 1
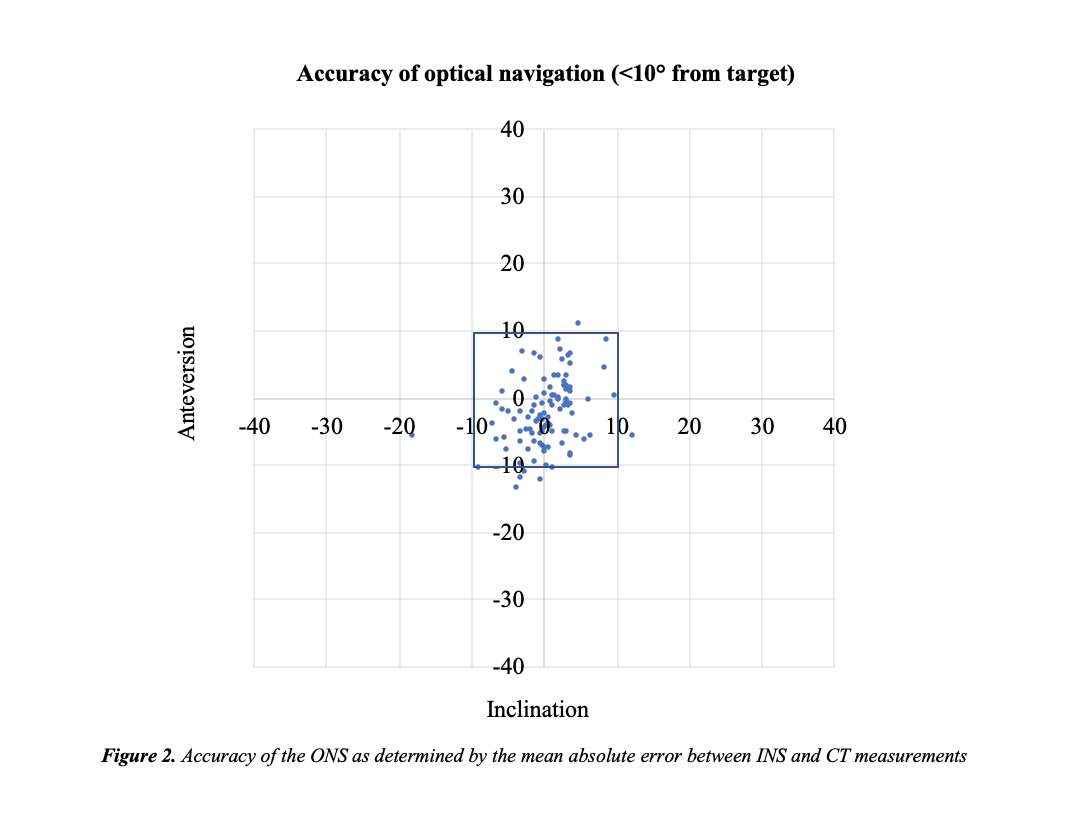
Figure 2#7386
Comparative Study Between Glenoid Versus Humerus Lateralization Design in the Reverse Total Shoulder Arthroplasty : Which Lateralization Design Is Better?
Jun Seo Yang - Daejeon St. Mary's Hospital, Catholic University of Korea - Daejeon, Korea (Republic of)
*Jong-Hun Ji - Catholic University - Daejeon, South Korea
*Email: jijh87@gmail.com
Introduction: The reverse total shoulder arthroplasty (RSA) leads to medialization of shoulder joint and often causes complications such as increased scapular notching and decreased external rotation. With glenoid and humeral lateralization, such problems can be addressed, however, the lateralization is known to cause tension in soft tissue, difficult prosthesis reduction during the procedure. Its more so in rather small statured patients, such as in Asian populace. In this study, we report clinical and radiologic outcomes of the two lateralized designs of RSA in Asian patients and compare those results between two different design.
Materials and Methods: From June, 2012 to June, 2020, total 152 shoulders of 147 patients [mean age: 73.8±6.8years (56-88 years)] who received either glenoid or humeral lateralization design RSA with minimum 18 months follow-up were enrolled. We divided these patients into 2 groups: Group I (glenoid lateralization design, BIO-RSA) included 60 shoulders (40 cemented, 20 cementless stem), and Group II (humeral lateralization design, a short curved onlay stem) in 92 shoulders (8 cemented, 84 cementless stem). At the final follow-up, clinical and radiologic outcomes were compared between 2 groups.
Results: Between two groups, there were no significant differences of clinical and radiologic outcomes except glenoid-tuberosity (GT) distance and loosening. Group I had 1 1 acromion fracture, 1 loosening (stem) and 1 infection in which implant removal was performed. Group II had 1 scapular neck fracture and 3 loosening (1 glenoid, 2 stem) were related to the trauma..
Conclusion: Compared to glenoid lateralization (Group I), humeral lateralization (Group II) showed better shoulder contour closer to normal anatomy, due to larger GT distance (more lateralization), while radiologic complications were more frequent; 1 scapular neck fracture and 3 loosening (1 glenoid, 2 stem) among which 1 glenoid and 2 stem loosening were related to the trauma.
Key words: reverse total shoulder arthroplasty, glenoid lateralization, humeral lateralization, complication.
Figures
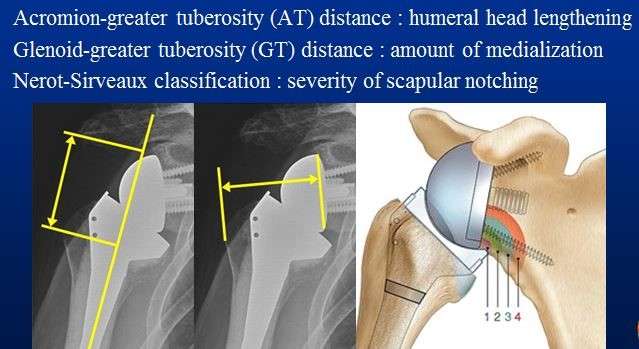
Figure 1#7958
No Difference in Survival Rate Between Posterior Stabilized and Constrained Condylar Articulations in Revision Total Knee Arthroplasty : A Minimum 5-Year Follow-Up Analysis
Hong Yeol Yang - Chonnam national university - Gwangju, South Korea
Dong Min Jung - Chonnam national university hospital - Gwangju, South Korea
Woo Kyoung Kwak - Chonnam national university hospital - Gwangju, Korea (Republic of)
*Jong-Keun Seon - Chonnam National University - Hwasun Gun, South Korea
*Email: seonbell@jnu.ac.kr
Introduction
Revision total knee arthroplasty (RTKA) is a technically demanding procedure for failed primary total knee arthroplasty. Posterior stabilized (PS) and constrained condylar knee (CCK) articulations are commonly used for RTKA. Comparison of these articulations in RTKA is scarce. The aim of this study was to compare survival rates and clinical outcomes between RTKA with a PS articulation and that with a CCK.
Methods
This study conducted a retrospective analysis of 86 RTKAs (PS = 41/CCK = 45) with a mean follow-up of 9.15 ± 2.79 years. Clinical outcomes were evaluated using the Hospital for Special Surgery score(HSS), Knee Society Score(KSS) and The Western Ontario and McMaster Universities Osteoarthritis Index(WOMAC)at final follow up. The survival rate of each group were analyzed by Kaplan-Meier survival analysis and Cox-hazard progression model
Results
The clinical outcomes were improved in both groups without significant difference. 12 patients had orthopedic complications (PS=5/CCK=8). eight of them underwent re-RTKA (PS=3/CCK=5). The articulation design did not influence the complications (p = 0.713) and failure (p = 0.599). The survival rate was 92.7% in the PS group and 88.2% in the CCK group with no significant difference (p = 0.6). Also in septic failure, there was no significant difference in survival rate (92.7% in PS, 92.5% in CCK, p=0.87) Also, the hazard ratio in the PS group was no significant difference (p = 0.6).
Conclusions
PS and CCK articulations in RTKA showed similar clinical outcomes at final follow up. In addition, the survival rate was similar either total failure and septic failure between the groups.
Keywords : revision total knee arthroplasty; survival rate; constrained condylar knee; posterior stabilized
#7940
Preoperative Bone Marrow Edema Negatively Impacts Long-Term Outcomes After Unicompartmental Knee Arthroplasty
*Jong-Keun Seon - South Korea
Hong Yeol Yang - Chonnam national university - Gwangju, South Korea
Sun-Ho Lee - Chonnam National University Hospital - Gwangju, South Korea
Dong-Min Jung - Chonnal national university of hospital - Gwangju, Korea (Republic of)
*Email: seonbell@chonnam.ac.kr
Aims: The aim of this study was to investigate the association between extent of subchondral bone marrow edema (BME) as classified by magnetic resonance imaging (MRI) and long-term outcomes after unicompartmental knee arthroplasty (UKA) for medial compartment osteoarthritis.
Patients and Methods: We enrolled 150 knees (144 patients) that underwent fixed-bearing UKA between April 2003 and December 2014 with a minimum follow-up of 5 years; the mean overall follow-up duration was 9.8 years (5.1 to 17.7 years). We divided the patients into two groups based on the presence or absence of preoperative BME. Patients were also subdivided into four groups according to their BME scores determined by the MRI Osteoarthritis Knee Score (MOAKS) method. Clinical outcomes were assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Forgotten Joint Score. Furthermore, survival rates and relevant risk factors that affect joint survivorship were analyzed.
Results: The groups with BME demonstrated significantly worse postoperative WOMAC pain and Forgotten Joint Scores at the final follow-up than the group without BME. (all p < 0.05). We also found significant differences among the scores of groups with different BME grades (all p < 0.05). Post hoc analysis demonstrated differences between groups 1 and 2, 1 and 3, 1 and 4, and 2 and 4 (all p < 0.05) with a significant correlation between postoperative clinical outcome and the extent of BME (r = 0.430 [WOMAC pain], r = −0.342 [Forgotten Joint Score]; p < 0.05). The survival rate was 95.4% at a mean period of 9.8 years, and survival was not associated with the presence of BME (p = 0.232; log-rank test). According to multivariate regression analysis, higher body mass index (hazard ratio, [HR] = 1.266, p = 0.021) and postoperative malalignment (HR = 5.193, p = 0.019) were related to implant failure.
Conclusion: Preoperative BME negatively impacted the long-term clinical outcomes after UKA, although UKA contributed to excellent survival rates after a mean follow-up of 9.8 years regardless of BME severity.
Figures
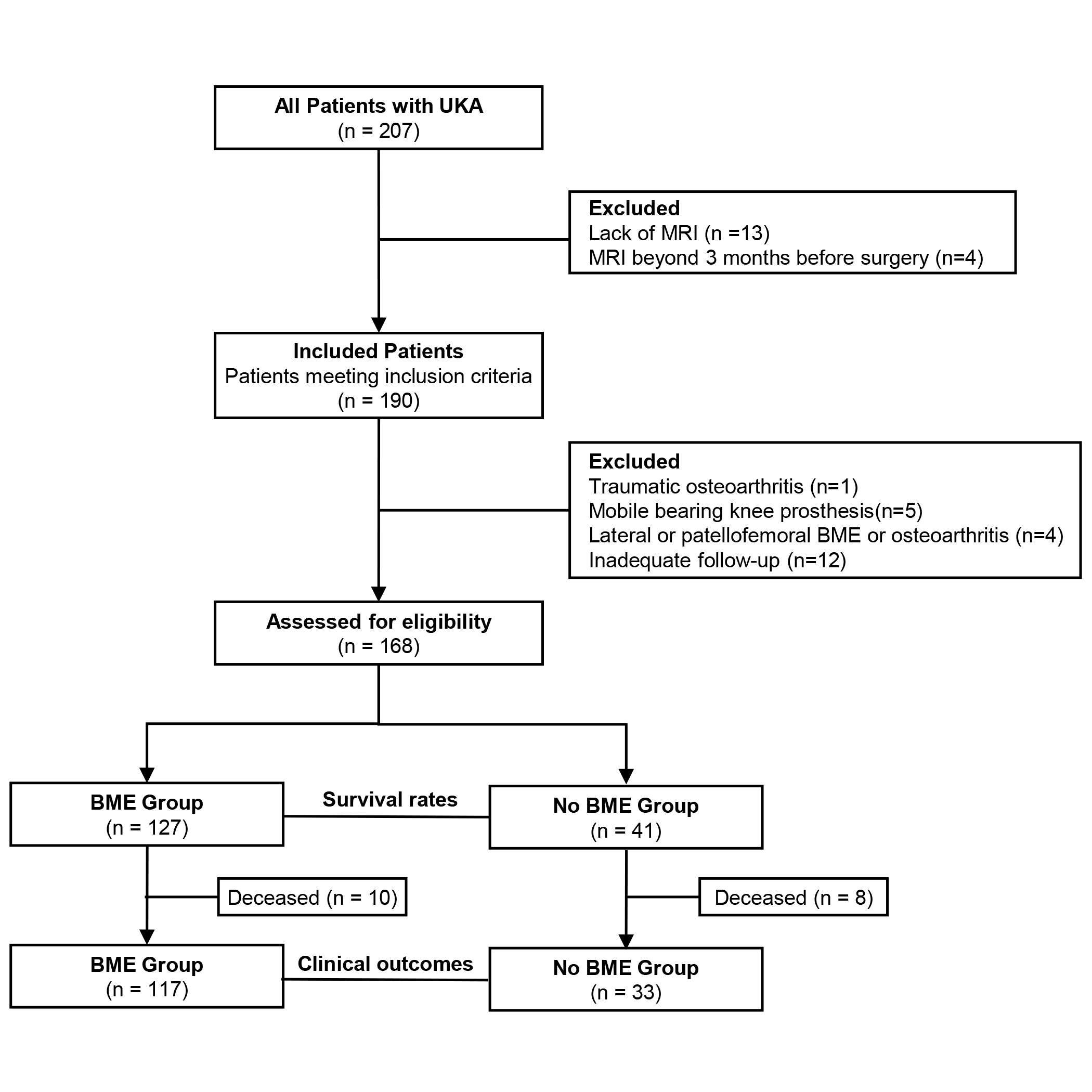
Figure 1
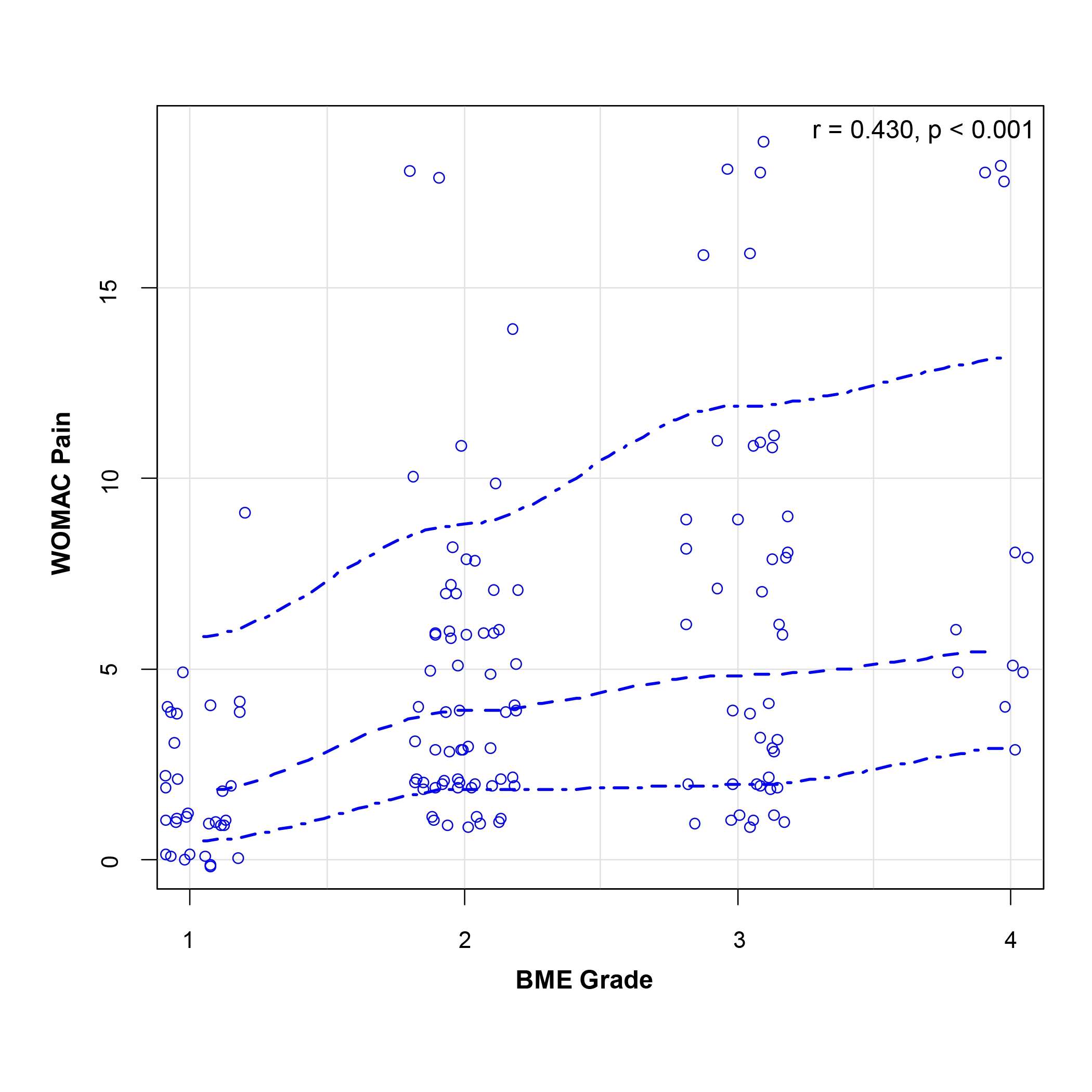
Figure 2
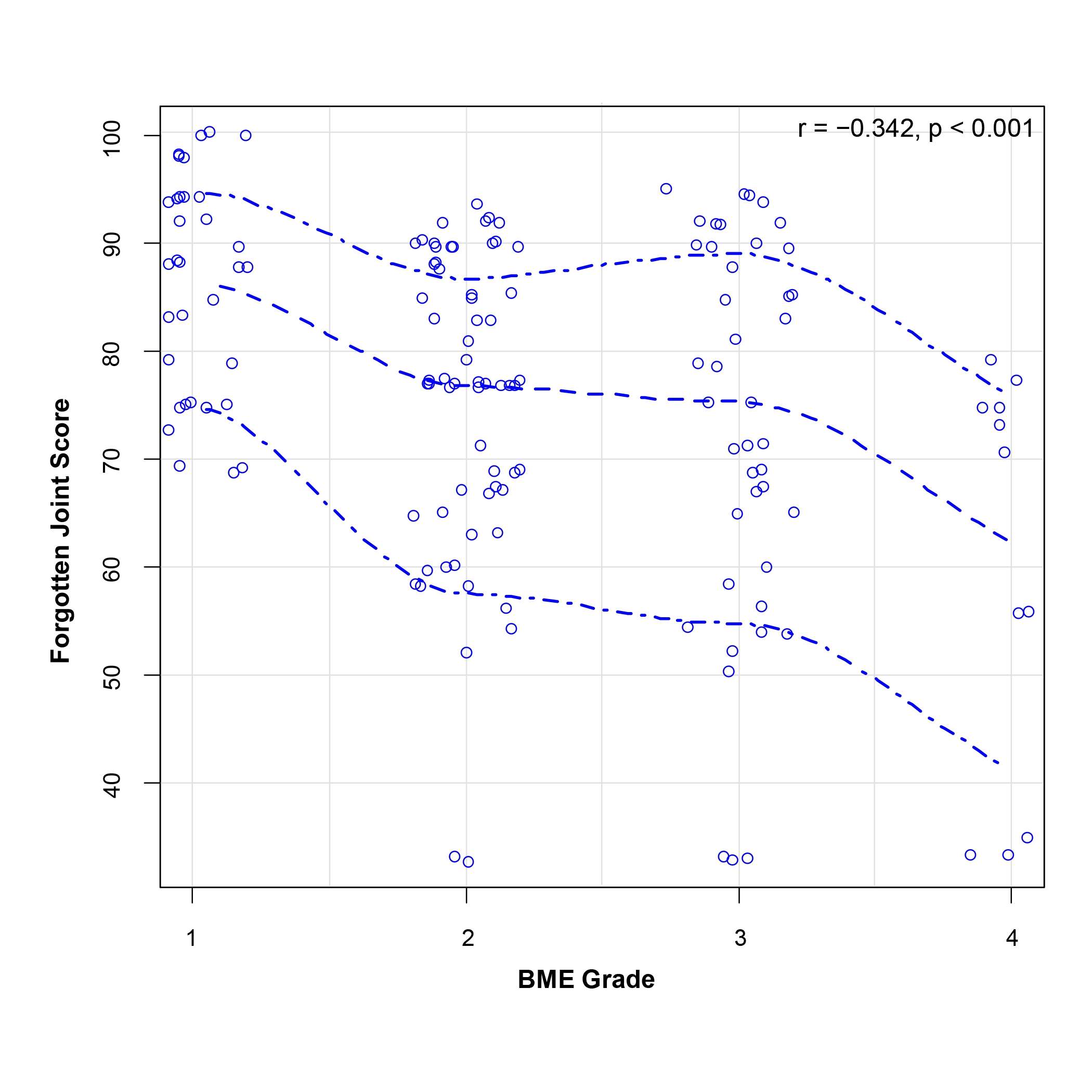
Figure 3
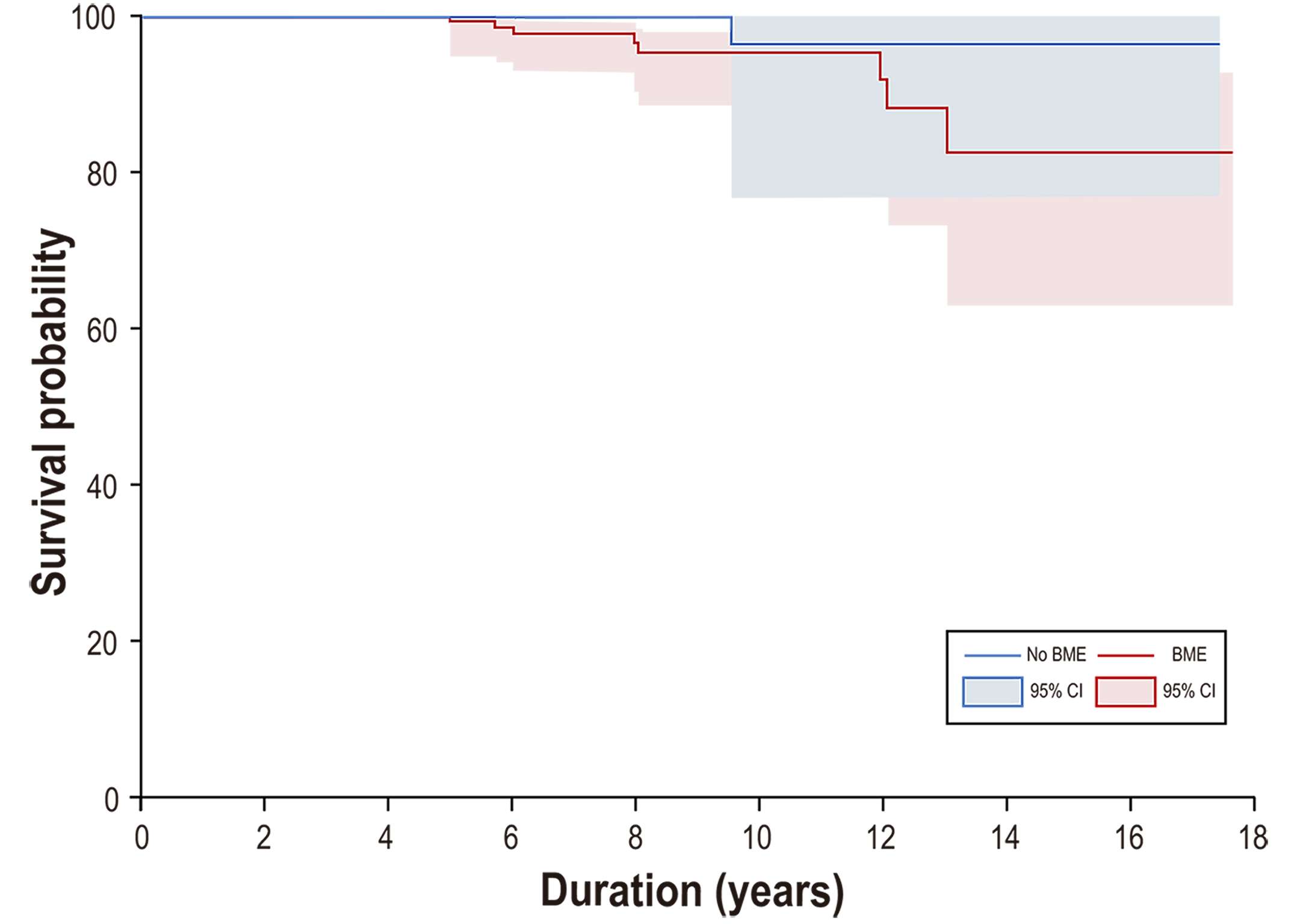
Figure 4#7401
Long-Term Report of Complications After Unicompartmental Knee Arthroplasty (UKA) in Asian Patients
*Dong Whan Suh - SMG-SNU Boramae Medical Center - Seoul, South Korea
KWANGHYUN CHO - Daejeon St. Mary's hospital - Daejeon, Korea (Republic of)
Jun Seo Yang - Daejeon St. Mary's Hospital, Catholic University of Korea - Daejeon, Korea (Republic of)
*Email: eastlight83@gmail.com
long-term report of complications after Unicompartmental knee arthroplasty (UKA) in Asian patients
Purpose
To analyze the causes and types of complications after unicompartmental knee arthroplasty (UKA) after 10 years follow up.
Materials and Methods
A total of 180 mobile bearing UKAs were performed between May 2008 and April 2012 at our institution. Medical records were reviewed for pre and postoperative assessment, retrospectively. The mean age of the patients were 54.7 years old (range 44-59 years) and mean follow up period was 11 years (range 10-13 years). The cause of complications, its solution, clinical score, knee range of motion and radiologic outcomes were assessed.
Results
50 complications (27.7%) occurred after 180 UKAs. Regarding the type of complications, there were 16 cases of dislocation of the mobile bearing, 14 cases of loosening of the femoral prosthesis, 2 cases of loosening of the tibial prosthesis, 7 cases of polyethylene wear, 5 cases of progression of arthritis in the contralateral compartment, 4 cases of infection, 3 cases of loose body formation, 1 case of periprosthetic fracture. The complications were treated with conversion to total knee arthroplasty in 35 cases and simple bearing change in 11 cases, and arthroscopic loose body removal with synovectomy in 4 cases.
Conclusions
The most common complication after UKA was dislocation of the mobile bearing and femoral component loosening. When a complication occurs after UKA, appropriate treatment should be performed after accurate analysis of the cause of complication.
#7391
A Novel Method for Postop Implant Evaluation for Bone Remodeling
*Gokce Yildirim - Vent Creativity Corporation - Weehawken, USA
Andrew Pearle - Hospital for Special Surgery - New York, USA
Tarik Bayoumi - Hospital for Special Surgery - New York, USA
*Email: gyildirim@ventcreativity.com
Introduction: Orthopedic cementless implants require good fixation features, sufficient contact with the bone, and forces that are directed towards the intended directions of the implant to be successful. Cementless implants have been designed based on animal studies showing good bone in-growth over different periods of time, but human in-growth has been difficult to prove outside of retrieval studies.
Methods: A previously validated point clouds method using CT data was used to segment bone models. Patients were scanned both preop and postop with recorded time out of surgery. The patient information was de-identified by the clinicians.
The implant distal surface points were used to generate a plane, and the distance of this plane to the points making up the cut bone surface were measured. Percentage of points that are under 0.5mm were deemed viable for in-growth1. The first goal was to determine the convergence of all patients and their grouping in various time stamps to the final percent contact area once an implant settled. The variance of each time stamp is also important as closely clustered results for a time stamp is hypothesized to indicate a time point where implant is reproducibly generating in-growth. However, contact due to high pressure can have negative effects. Therefore density mapping of tibial sulcus bone centroid compared to a healthy cohort is necessary to determine the success in recreating a healthy bone composition state2.
The surface points from the distal and eminence wall are used to generate two planes. The midpoint of the intersecting line is used to generate a cylinder orthogonal to the distal cut. The common aligned ‘pucks’ are retrieved for the Hounsfield Units that are 25% or higher for the patient’s range in order to normalize data representing cortical bone. The resulting mesh volume centroid is measured from the anterior most edge of the puck, compared to the A/P distance to generate a percent deviation value. This value is compared to previous literature to determine the pre-op to post-op centroid. Coupled with the contact area measurements, the values are plotted to determine how these blinded results correlate with the patient and surgeon reported outcomes.
Results: Each of the 6 matched pairs of scans showed a migration of density centroid from anterior positions to central sulcus position. Additionally, all 19 postop scans evaluated for contact area under 0.5mm showed a convergence to 80% contact at 150 days post op for the specific implant tested for the method in this study. A large variance was observed in all initial readings leading up to 150 days, which supports the hypothesis of a potential well-fixed implant timeline, previously shown in animal studies.
Conclusion: The test method proposed in this study can be a good approach to characterizing implant placement, in-growth, and bone remodeling to prevent revisions, as well as the expected time to good fixation of the implant. This tool can then be used in rehab and patient expectation to address days post op for any implant type to aim for reduced revisions.
Figures
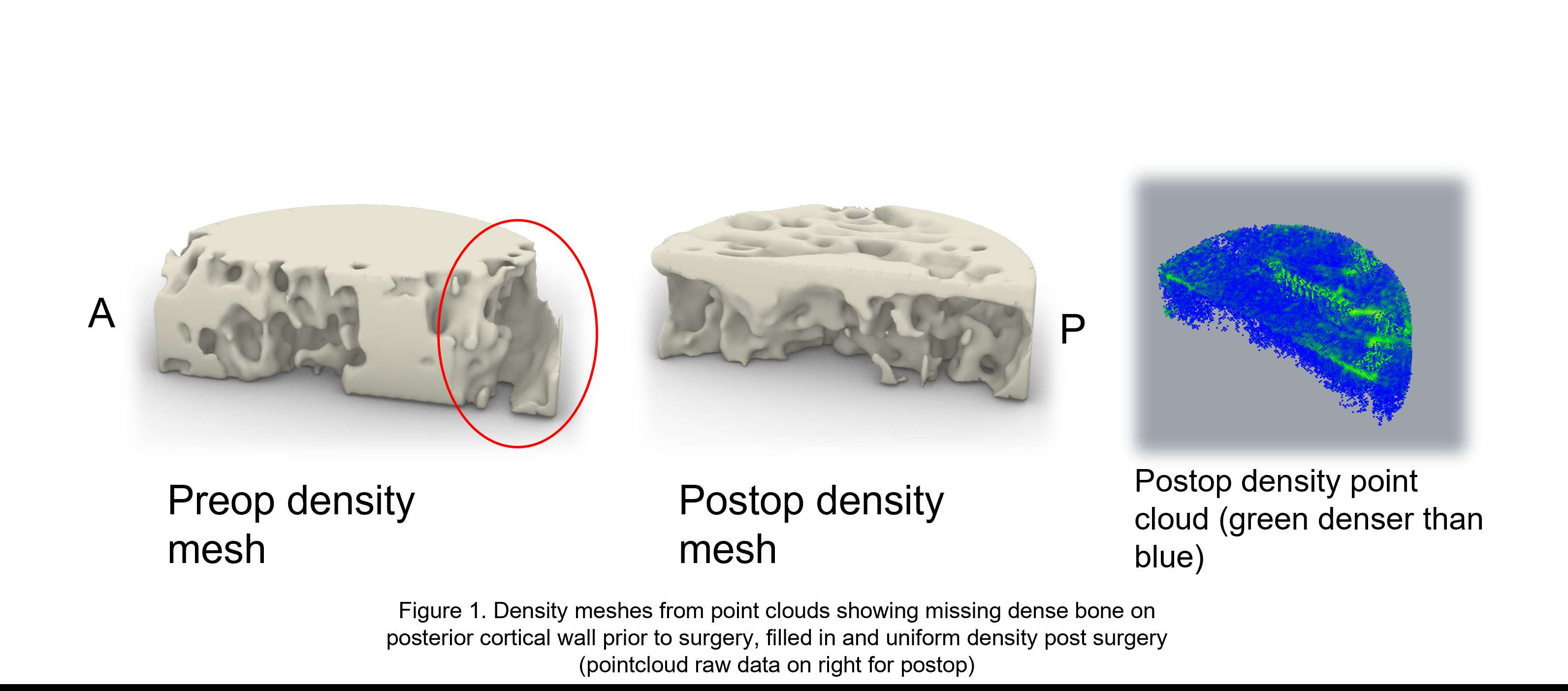
Figure 1
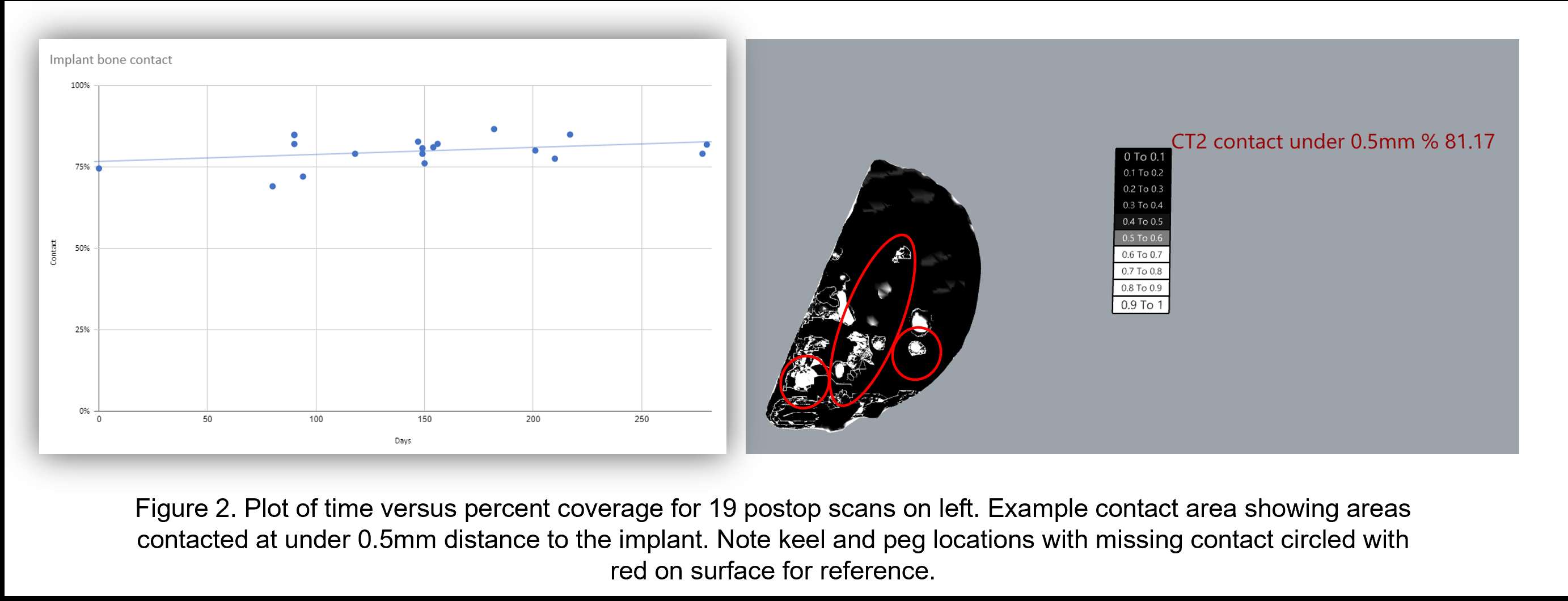
Figure 2
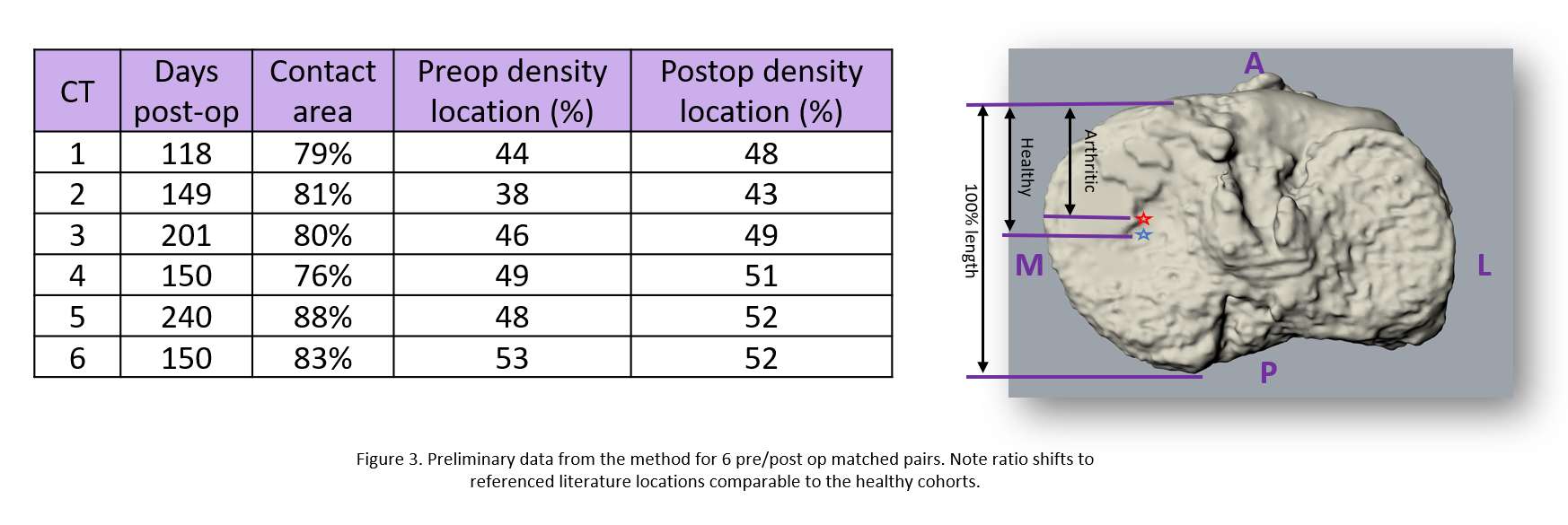
Figure 3#7604
A Novel Autosegmentation Tool for Orthopaedic Surgery Planning
*Gokce Yildirim - Vent Creativity Corporation - Weehawken, USA
Eric Bogner - Hospital for Special Surgery - West Palm Beach, USA
Dimitrios Georgopalis - Vent Creativity - Weehawken, USA
Rachel Alexander - Vent Creativity Corporation - Weehawken, USA
*Email: gyildirim@ventcreativity.com
Introduction: Medical imaging for orthopedic surgical planning relies on manual or semi-automatic techniques that generate 3D models. This process can be costly and time consuming. Most automatic systems rely on edge-detection methods, and can generate error in more arthritic joints depending on the training sets used. The Minerva system collects the point cloud data from the source files and clusters them to generate the final segmentation, preventing the averaging or omission of critical features that may be missed, which is critical to the robotic and PSI procedures.
Methods: CT data, in the form of point clouds, is used and clustering methods at various thresholds allow the new proposed system to generate more accurate and labeled bones. A separation software was created which is used to feed training datasets to the Convolutional Neural Networks algorithms. The weights were adjusted with backwards propagation penalty methods, widely discussed in the literature. Thirty knee joints were used to test the autosegmentation system against the widely used Materialise Mimics 24 and Synopsys Simpleware AS Ortho autosegmentation tools, and manual segmentation by consensus expert review. Images were masked, and the area for each mask was measured, and total volume was calculated using CAD modeling tools. Additionally, the two alternative software outputs were measured against the Minerva bone volumes using Iterative Closest Point analysis to identify point-to-point normal distance deviations between the results. Finally, the expert radiologist was consulted on the masks generated from the source image versus their preferred best in class method to determine the validity of the segmentation tools. For each of the area and volume comparisons, one of the software was considered ground truth and Minerva difference calculated against it, and the manual segmentation was considered best in class versus Minerva.
Results: Surface area of each image for each time the slices were segmented was calculated and the average deviation was 6% for Mimics, 25% for Synopsys, and 4% for manual versus Minerva. For each representative worst case and comparable image, an expert radiologist was consulted on the deviations and the Minerva system was selected as the more accurate outline. Large (>50%) deviations (8/30 cases) were attributed to the missing areas in Minerva compared method outlines according to the radiologist. Volume deviations for femur, generated by the ICP analysis averaged 0.5mm for Mimics, 0.2mm for Synopsys, and 0.2mm for manual models compared to Minerva, and for tibia was 1.3mm for Mimics (std 4.02), and 0.3mm (std 4.02) for Synopsys due to the inclusion of fibula in some scans for Mimics. The radiologist picked Minerva as the more accurate segmentation for these comparisons.
Conclusion: Compared to the manual and automated segmentation tools available to the research and development community in orthopedics, Vent is shown to create masks and 3-D models at a higher accuracy as determined by the expert radiologist. Additionally, density maps of the 3-D contours add value by providing insights on intuitive positioning of the dense locations which can benefit surgical decision making.
Figures
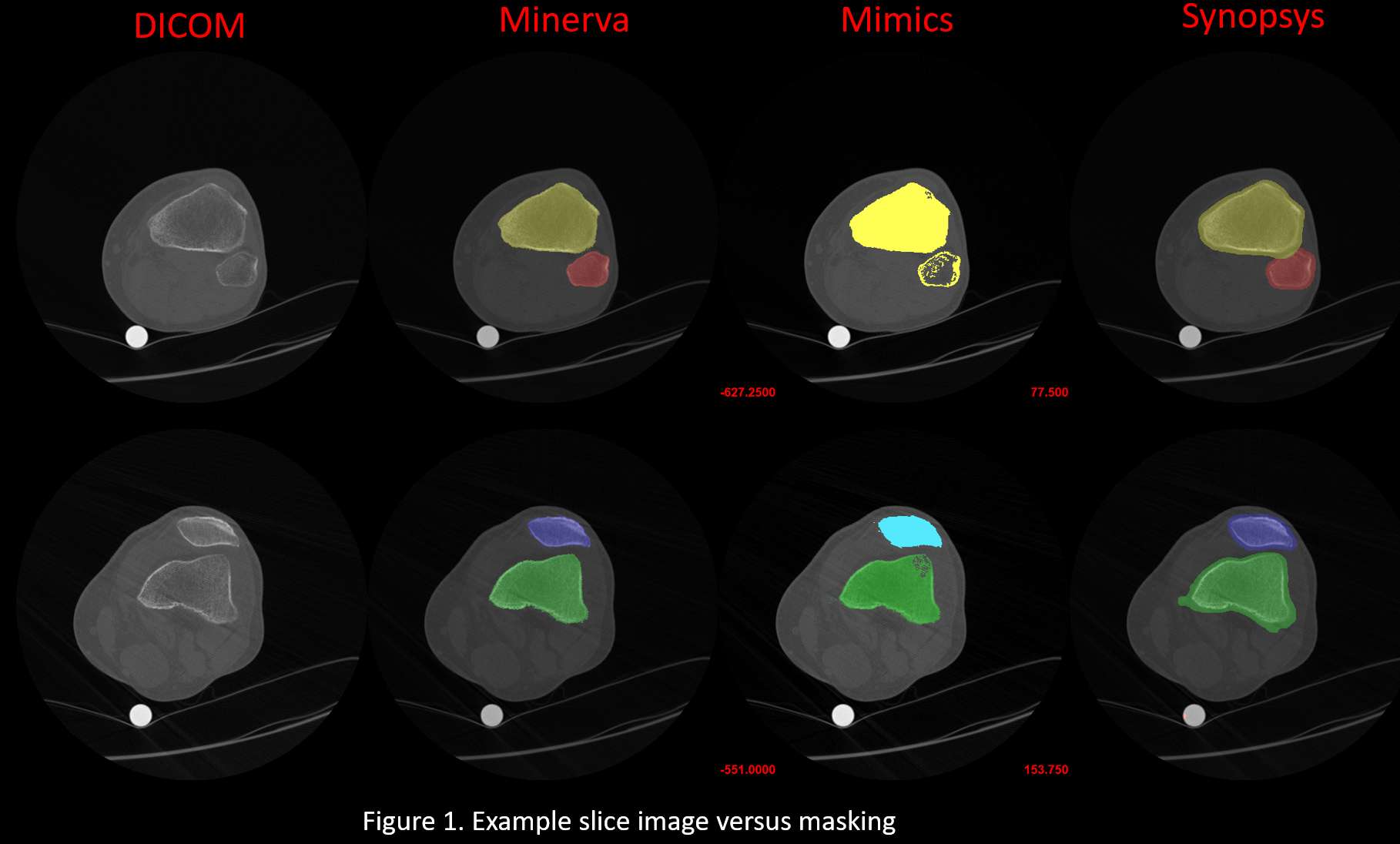
Figure 1
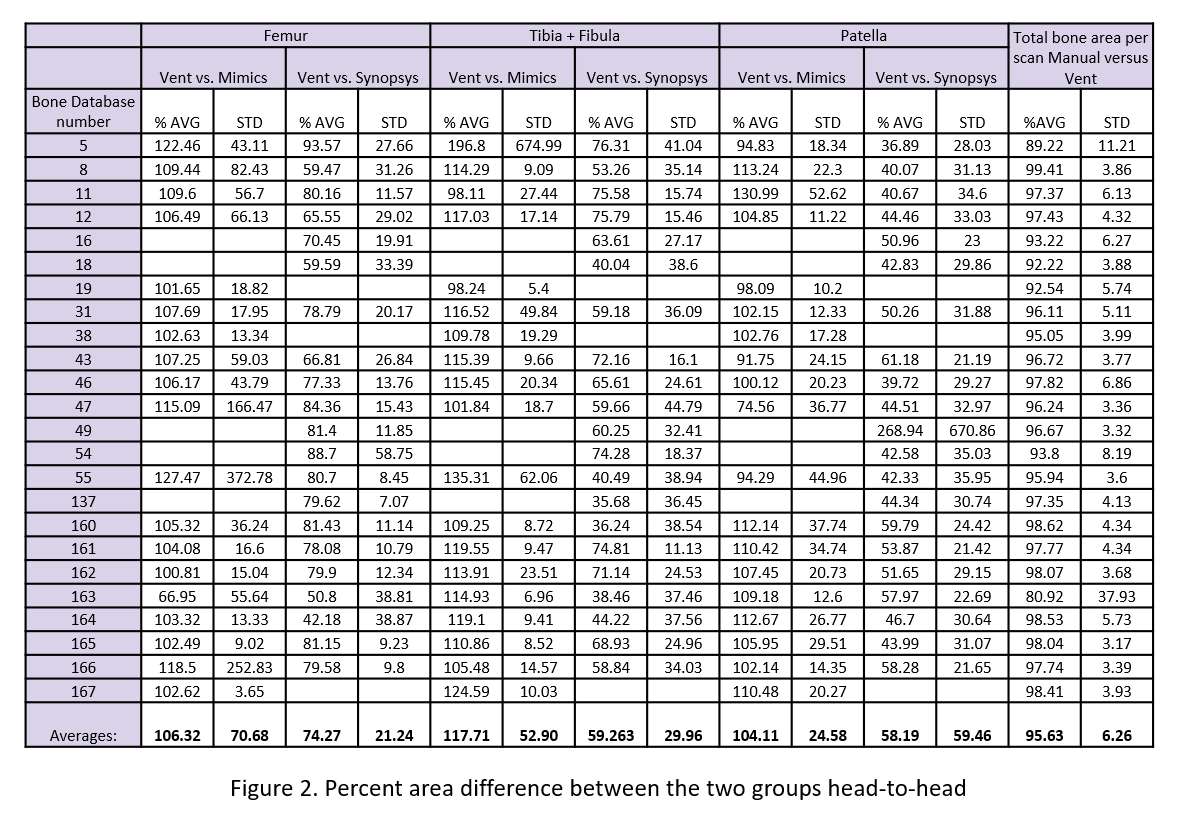
Figure 2
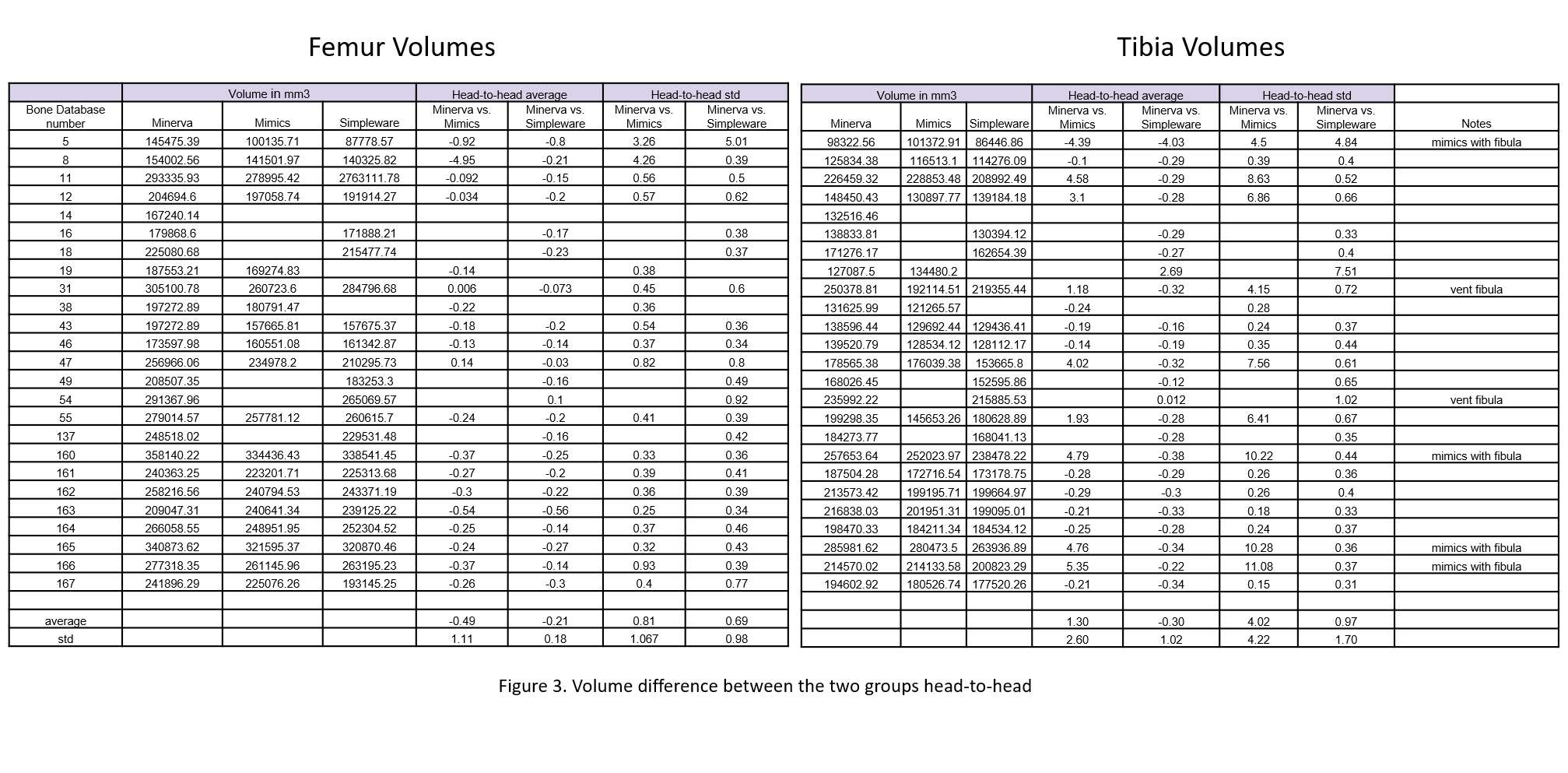
Figure 3#7400
Early Result of a Prospective, Randomized, Controlled Study on Radiologic and Functional Outcomes Between Patient-Specific Instrument and Conventional Total Knee Replacement Arthroplasty Instrument.
*Sung-Wook Choi - Jeju National University - Jeju, South Korea
Seung Jin Yoo - Jeju National University - Jeju, South Korea
Taehyeong Lim - Jeju national university - Jeju, South Korea
*Email: swchoi1115@gmail.com
Introduction: Total knee replacement arthroplasty (TKRA) is a one of the most successful orthopedic procedure to restore a significant degree of lower limb alignment and function in osteoarthritic knees. While TKRA is one of most regularly performed musculoskeletal procedures, postoperative limb alignment and component position has been considered critical influences on longevity, outcomes, and revision rates after TKRA. With technological advancement to improve the likelihood of achieving neutral TKRA alignment, patient-specific instrument (PSI) TKRA has received vast attention to arthroplasty surgeons. PSI utilizes patient specific cutting blocks, generated by an ideal 3 dimensional model of the patients’ lower limb anatomy to create optimal size, position, and alignment. The current study aims to compare radiologic and functional outcomes between PSI and conventional TKRA instruments through a prospective, randomized, controlled study.
Method: We randomized 100 patients, who were due to undergo TKRA, to have the procedure performed either PSI or conventional instrumentation (CI). Radiologic primary endpoint was deviation from the mechanical axis greater than 3 degrees, and radiologic assessment included preoperative and postoperative measures of alpha, beta, gamma, and delta angles of tibial and femoral components in both PSI and CI (Figure 1). Secondary outcome measures included component position, operative time, blood loss, and length of hospital stay. Serial functional assessment included Knee Society Score (KSS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
Result: A total of 100 patients (50 in PSI group and 50 in CI group) had all completed clinical and radiologic data. There were 73 female and 27 male patients with a mean age of 72 years old (range: 65 to 82). The postoperative hip-knee-ankle angle was 178.3 degrees (range: 175.4 to 179.4) in PSI group and 178.9 degrees (range: 176.2 to 180.1) in CI group (p-value: 0.42). There were no significant differences in functional outcomes and radiologic parameters of component position between PSI and CI groups (p-value: 0.85 and 0.67, respectively). Operation time, blood loss, and lengths of hospital stays were similar in both groups. (p-value: 0.12, 0.52, 0.64, respectively).
Conclusion: The use of PSI in primary TKRA did not show significant improvement in postoperative lower limb alignment and component positioning as well as functional outcomes compared to CI.
#7399
A Randomized, Controlled Study on Early Versus Delayed Rehabilitation Protocols After Reverse Total Shoulder Arthroplasty in Massive Rotator Cuff Tears
*Sung-Wook Choi - Jeju National University - Jeju, South Korea
Seung Jin Yoo - Jeju National University - Jeju, South Korea
Taehyeong Lim - Jeju national university - Jeju, South Korea
*Email: swchoi1115@gmail.com
Introduction: Reverse total shoulder arthroplasty (rTSA) has gradually gained its popularity over the past two decades as a treatment option for those who require shoulder replacement surgeries for the treatment of glenohumeral arthritis associated with irrepairable rotator cuff tear, complex proximal humeral fracture or revision of a previously failed conventional total shoulder arthroplasty (TSA). Even though there have a number of previous literature on rehabilitation protocols after TSA in those with intact rotator cuff function, there has been a paucity of high-quality evidence regarding rehabilitation following rTSA. In addition, due to its unique biomechanics and a wider spectrum of shoulder pathology associated with rTSA, its rehabilitation protocol must be considered as a separate entity from TSA. The current randomized, controlled trail aims to compare early versus delayed rehabilitation involving range of motion after rTSA in massive rotator cuff tears.
Method: Eighty patients were randomized to early rehabilitation (ER) group and delayed rehabilitation (DR) group after rTSA in those with massive rotator cuff tears. Range of motion (ROM) and functional outcomes by visual analogue scale (VAS) and University of California, Los Angeles scales (UCLA) score were compared serially at 4 weeks, 8 weeks, 3 months, 6 months, and 12 months postoperatively. All patients began shoulder pendulum exercises immediately after the surgeries, and detailed rehabilitation protocols are outlined in the Table 1.
Result: A total of eighty (40 in ER group and 40 in DR group) all completed surgical treatment and full rehabilitation protocols with a minimum one-year follow-up. There were 58 female and 22 male patients with a mean age of 68 (range: 60 to 79), and preoperative baseline demographics between two groups did not show any statistical difference. Compared to the preoperative status, the both groups showed statistically significant improvement in forward flexion, abduction, external rotation, and internal rotation, and the differences in ROM improvement between the two groups did not show statistical differences at the final follow-up (p-value 0.34). However, the ER group showed early regain of motion. Both groups showed similar improvement in functional outcomes at the final follow-up (p-value 0.12), but ER group showed higher functional outcomes by the postoperative 3rd month. In addition, postoperative complication such as dislocation, implant loosening, periprosthetic fracture did not differ between the two groups (p-value 0.75)
Conclusion: ER group demonstrated a more rapid return of function and pain relief compared to DR group after rTSA. However, there were no differences in final ROM and functional outcomes between the two groups.
#7674
Minimum 15-Year Results of Metasul 28-Mm Metal-on-Metal Total Hip Arthroplasty in Patients Younger Than 50 Years of Age
MIN GWANG KIM - CHONNAM NATIONAL UNIVERSITY HOSPITAL - Gwangju, South Korea
Taek Rim Yoon - Center for Joint Disease, - Hwasun-gun, South Korea
*Kyung-Soon Park - Center for Joint Disease,Chonnam National University Hwasun Hospital - Hwasun-gun, South Korea
Chae Jin Lim - Chonnam national university - Hwa sun, South Korea
Joon Kyoo Kang - Chonnam national university - Gwangju, South Korea
*Email: chiasma@hanmail.net
Introduction
Some propitious mid- and long-term studies had been reported for MoM bearings; however, most studies have addressed specific patient groups rather than younger, active patients, who probably represent the most suitable population for investigations on wear and osteolysis. The purpose of this study to evaluate the long-term results of second-generation metal-on-metal cementless total hip arthroplasty (THA) in patients aged <50 years.
Methods
From December 1997 to January 2004, primary THA using a metal-on-metal bearing cementless implant was performed in 63 patients (72 hips) aged <50 years. The mean follow-up duration was 18.6 (range, 15.9-22.1) years, and the mean age at initial operation was 39 (range, 22-49) years. Clinical results, complications, survivorship, osteolysis, and aseptic loosening were evaluated.
Results
The mean Harris hip score and Western Ontario and McMaster Universities Arthritis Index scores were improved from 57.8 (range, 28-69) points and 73.4 (range, 63-94) points preoperatively to 91.7 (range, 80-100) points and 25.5 points (range, 17-38) points, respectively, at the last follow-up. Osteolysis lesions were found in 12 hips (acetabulum, 6 and femur, 6). The notching occurred on the femoral stem neck occurred in 12 hips. The mean serum cobalt and chromium concentrations were 2.3 (range, 0.2-10.6) μg/L and 1.7 (range, 0.4-8.1) μg/L, respectively, at a mean follow-up of 12.7 years in 32 patients (50.1%). The Kaplan-Meier survivorship curve analysis with revision for any reason as the endpoint revealed that 93.1% survived at 18.6 years' follow-up.
Conclusion
Second-generation metal-on-metal cementless THA was found to produce satisfactory clinical and radiographic results with a low revision rate for osteolysis and aseptic loosening in patients aged less than 50 years.
Keywords: Cementless total hip arthroplasty; Long-term result; Metal-on-metal; Survivorship
#7833
Prediction of Cage Subsidence in Relation to Insertion Position and Angle With Different Cage Sizes Following Oblique Lumbar Interbody Fusion
Jin-Ho Youn - Inje University - Gimhae, Select Country
Sung-Jae Lee - Inje Univ. - Gimhae, South Korea
Jae-Won Lee - GS medical - Cheongju, South Korea
Ji-Eun Jang - GS medical - Cheongju, South Korea
Eghan-Acquah Emmanuel - Griffith University - Gold Coast, Australia
*Jung-Woo Hur - Eunpyeong St.Mary's Hospital - Seoul, South Korea
*Email: neurotique79@gmail.com
Objectives:
Oblique lumbar interbody fusion (OLIF) is a minimally invasive surgical technique for the treatment of degenerative lumbar diseases with favorable clinical results and few complications. Cage subsidence after OLIF surgery is a common problem, causing neurological symptoms by segmental instability and reduction of disc space and formal height. Retroperitoneal pre-psoas approach compels cage to be inserted more obliquely compared to direct lateral transpsoas approach, where cage is inserted more vertically. However, the effect of cage position and insertion angle on postoperative stability and subsidence has not been fully understood yet. In this study, we aimed to predict the risk of subsidence according to the cage position & insertion angle for each cage size during the OLIF procedure using finite element analysis (FEA).
Methods:
Surgical models were constructed from a previously validated 3-dimension intact lumbar finite element model(L1-S1) for this study. An OLIF cage(PEEK, E=3.5GPa, v=0.3, two different anteroposterior width(18mm; 22mm)) [Figure 1] and pedicle screws(titanium, E=110GPa, v=0.3) were inserted at L4-L5. A total of 18 post-op models were constructed according to cage width(narrow, 18mm; wide, 22mm), cage position(anterior, A; middle, M; posterior, P) and insertion angle(0°; 15°; 25°) with respect to the center of the vertebral body(For example, Type A0 denotes a cage with the anterior placement at 0 degree insertion angle) [Figure 2]. The nucleus pulposus of the disc was removed, whereas the annulus fibrosus and ligaments were only removed at the insertion site of the cage. A ‘tie contact’ condition was assigned to the bone-implant interface assuming complete bone union. The lower endplate of S1 was fixed and a compressive follower load of 400N and a pure moment of 10Nm were applied. Peak von Mises Stress(PVMS) generated in the vertebral body for each surgical model was calculated and compared to the yield strength(16.3MPa) of the vertebral body(ABAQUS_2021, Dassault Systems Inc., France) to predict the risk of subsidence.
Results:
The PVMS generated in the vertebral body decreased with increasing cage width(18mm to 22mm). In particular, the risk of subsidence was reduced the most in Type M15(48%). Furthermore, as the cage was positioned posteriorly rather than anteriorly, the risk of subsidence increased more with high insertion angles(15° and 25°), the most prominently in narrow cage Type A15 to P15 (by 136%). The models with 25° cage insertion angle showed higher risk of subsidence as compared to the models with 0° cage insertion angle in middle and posterior positions, notably the most in narrow cage Type P0 to P25(by 95%). Anterior placement of the cage exhibited lower risk of subsidence than the control group, the middle placement with 0 degrees of insertion angle(Type M0). In addition, increased insertion angle does not have a significant effect in cage subsidence [Figure 3].
Conclusion:
The insertion position was found to be a more sensitive factor than the insertion angle that could affect cage subsidence. Our study demonstrated that during OLIF surgery, insertion of wider cage more anteriorly with less insertion angle may provide better stability and lower risk of subsidence.
Figures
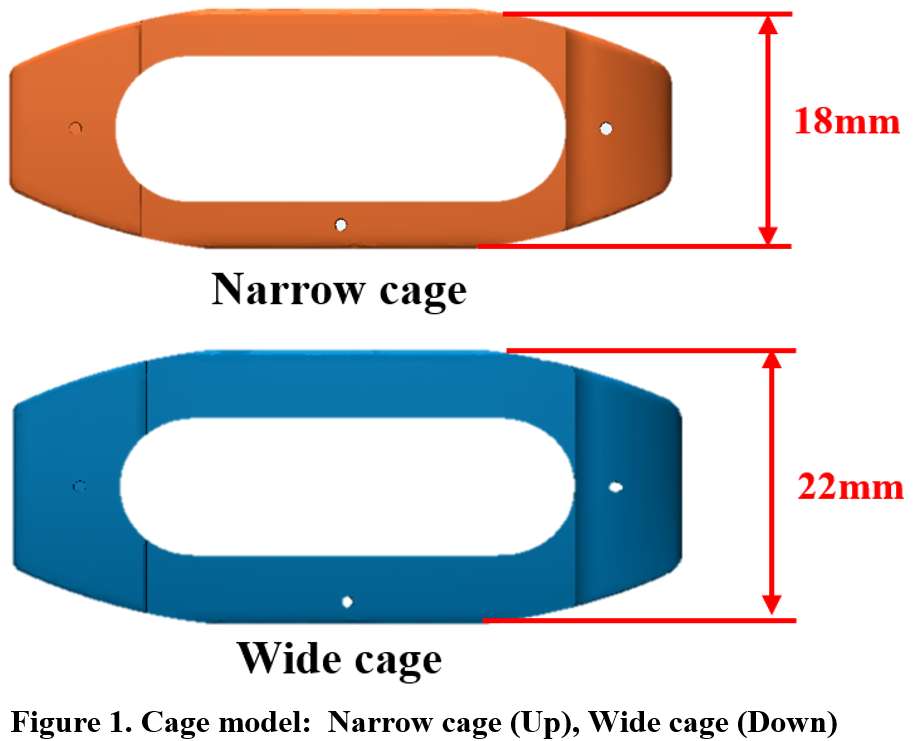
Figure 1
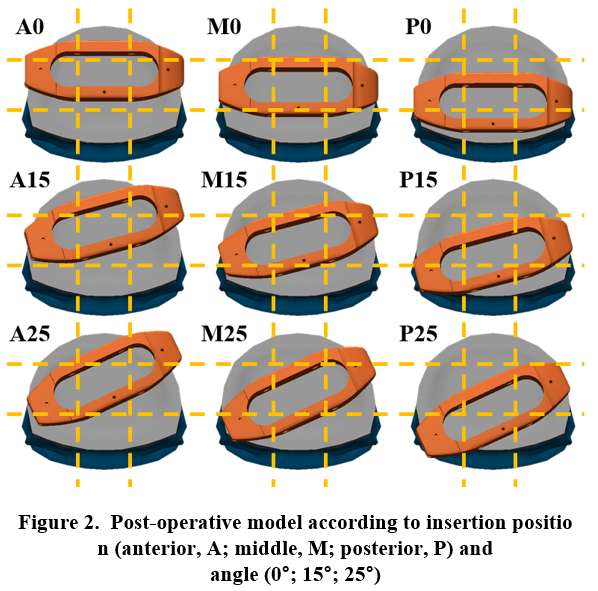
Figure 2
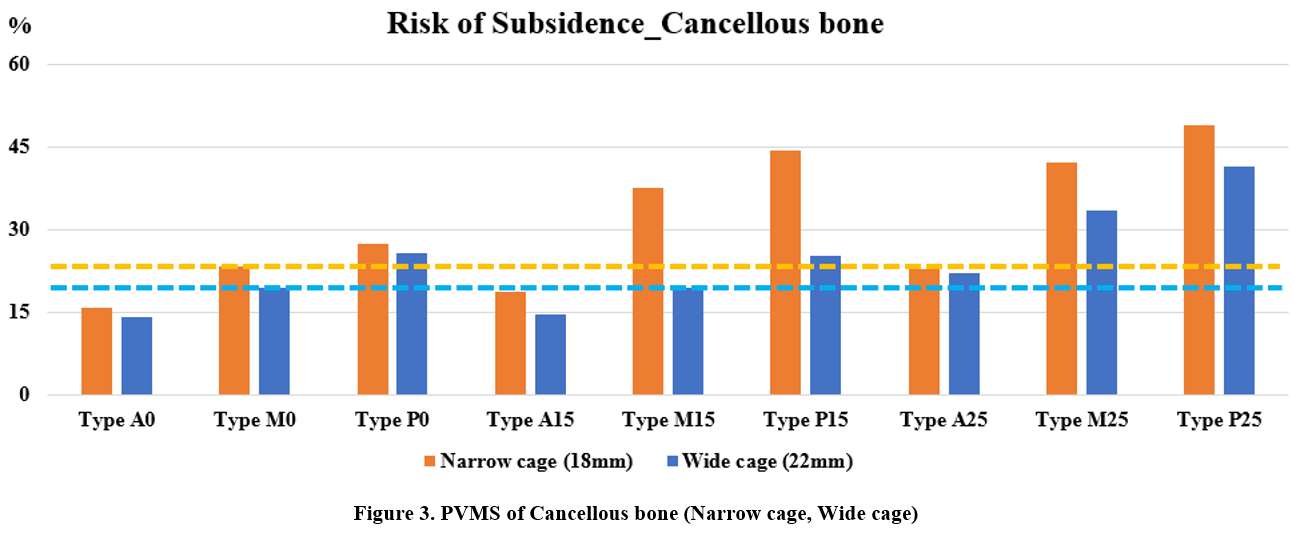
Figure 3#7595
In Vitro Comparison of High and Low Viscosity Cement 'Lack of Bonding' at the Cement-Implant Interface in Total Knee Arthroplasty
*Catherine Yuh - Rush University Medical Center - Chicago, USA
Robert Burnett - Rush University Medical Center - Chicago, USA
Alannah Rodrigues - University of Illinois at Chicago - Chicago, USA
Deborah Hall - Rush University Medical Center - Chicago, USA
Denis Nam - Rush University Medical Center - Chicago, USA
Robin Pourzal - Rush University Med Ctr - Chicago, USA
*Email: catherine_yuh@rush.edu
Introduction: Use of high viscosity cement (HVC) during total knee arthroplasty (TKA) has been reported to decrease the total time of surgery and improve handling characteristics. HVC use has increased from 46% to 61.3% in TKAs between 2012-2017, during which low viscosity cement (LVC) use decreased from 47.9% to 30.9%. However, recent studies have reported cases of premature failure due to a ‘lack of bonding’ between HVC and the tibial component backside. In this study, we assessed the bonding quality of HVCs and LVCs at the cement-implant interface using a mock TKA surgery model. We investigated how variable waiting times following cement mixing and preceding implantation affected bonding quality. The goal of this work is to establish methods that will be applied in a larger scope investigation on implant-cement bonding properties and to identify potential modes of failure related to interface lack of bonding.
Methods: Mock TKA surgeries were performed using six NexGen tibial component retrievals in porous cancellous saw bones. Tibial components were implanted using either HVC (DePuy High Viscosity) or LVC (Stryker Simplex P, Low Viscosity) at various waiting times. All experimental groups are indicated in Figure 1. After all implants were placed in the sawbones, a 10 lb weight was placed on the components to simulate knee extension that would apply pressure to the implant, followed by drying for at least 24 hours after mock surgery under no weight. All implanted bone blocks were sectioned at 3 mm thickness using a Secotom Precision Cutting Machine (Struers). Sections were assessed macroscopically using a light microscope (Keyence) along the cement-implant interface using a 100X objective. Lack of bonding was determined at the interface. Additionally, estimated cement mantle thickness was also calculated as the average between the minimum and maximum thickness.
Results: Macroscopic imaging of the cement-implant interface indicated differences between HVC and LVC lack of bonding, cement mantle thickness and heterogeneity of cement material. The lack of bonding pattern in the HVC groups were observed to span longer lengths along the interface, whereas that of the LVC groups appeared to be more dispersed, with lack of bonding present in smaller lengths along the interface (Figure 2). HVC groups also had noticeably increased cement mantle thicknesses compared to LVC groups (Figure 3). Estimated thickness was observed to be dependent on waiting time, with increasing thickness with longer waiting times for both cements.
Conclusion: This assessment of cement-implant interface bonding demonstrates multiple differences between HVC and LVC in TKA at the cement-implant interface. These findings indicate that lack of bonding may be dependent on the timing of the cementing process, where longer waiting times prior to implantation may lead to lack of bonding. Cement mantle thickness was also observed to be different between HVC and LVC use, which may be related to joint-line elevation that can impact knee kinematics and implant alignment. In future work, additional parameters, such as temperature and load will be assessed. Additionally, quality of bonding at the interface will be further assessed using techniques such as pull-out testing.
Figures
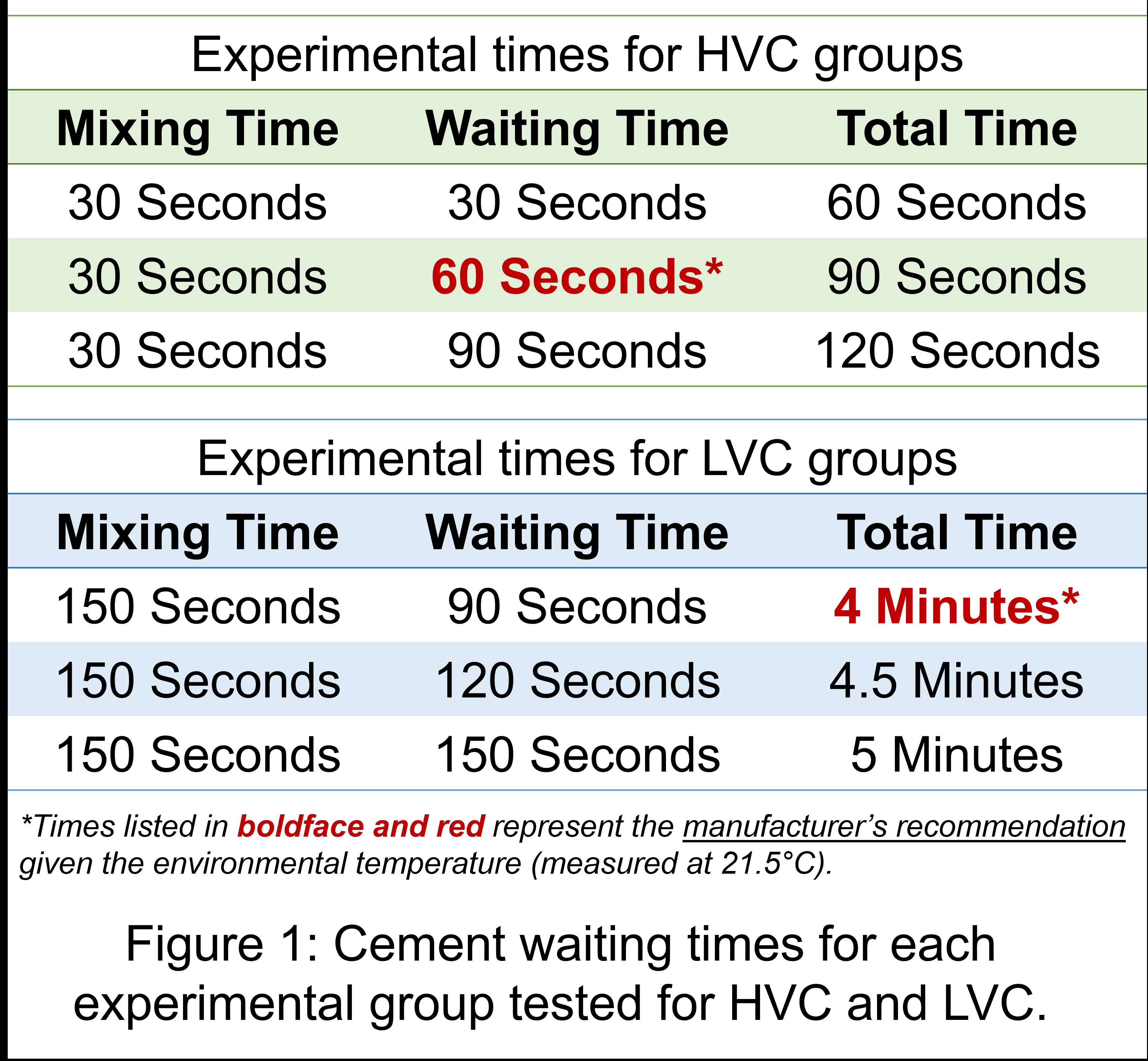
Figure 1
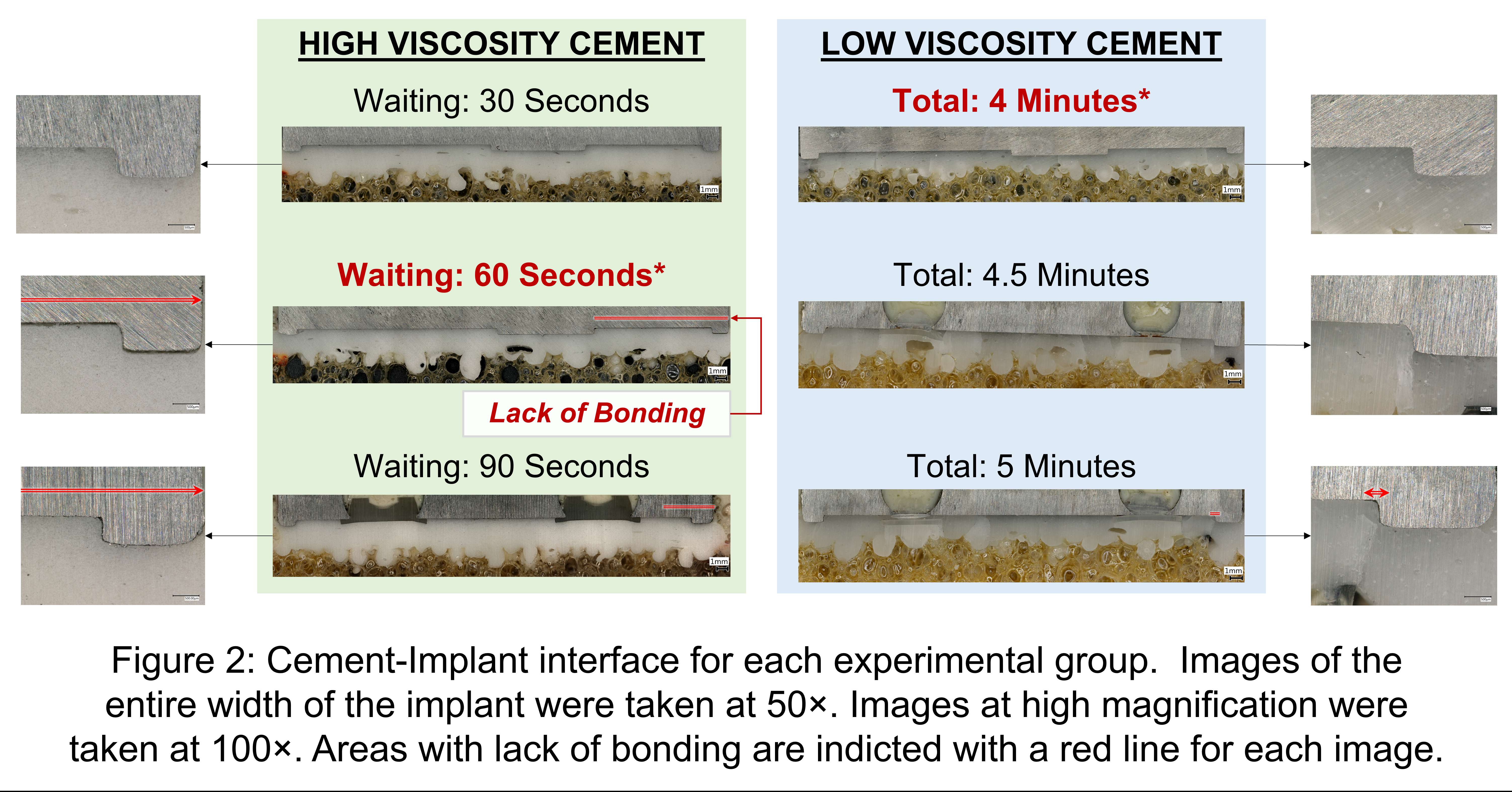
Figure 2
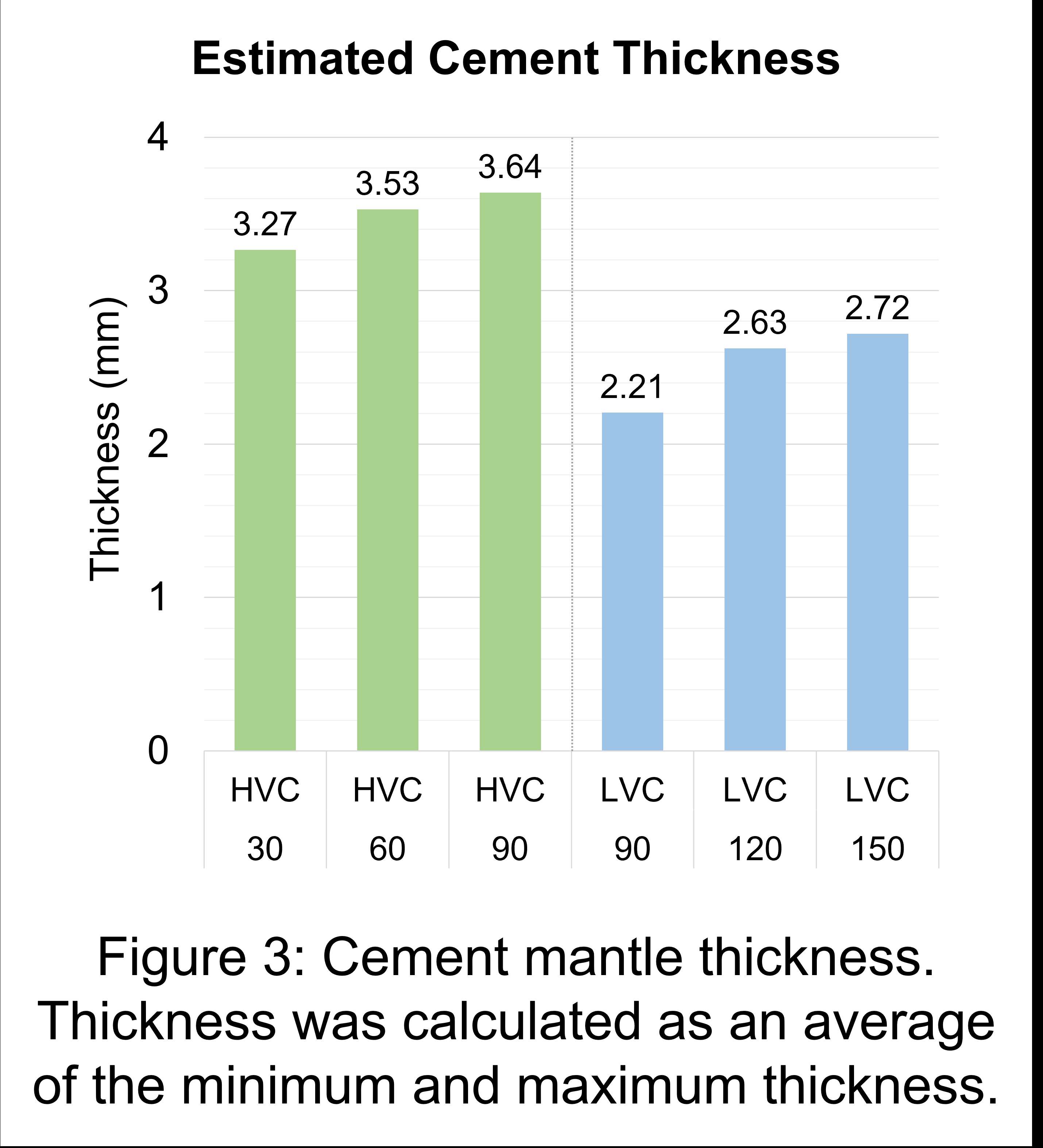
Figure 3#7934
A New Methodology for Extension Gap Planning in Robotic TKA
*Jayson Zadzilka - JZ Biomedical LLC - Brunswick, USA
Bernard Stulberg - Saint Vincent Charity Medical Center - Cleveland, USA
*Email: jzbiomedical@gmail.com
Introduction
Preoperative planning is an integral part of the Total Knee Arthroplasty (TKA) process. CT-based robotic systems for TKA allow the surgeon to preoperatively plan each case three-dimensionally and accurately execute that plan. With these preoperative plans readily accessible, there’s opportunity to review specific steps in the planning process to see how they relate to outcomes.
Tibial and femoral resection depths are planned with several factors in mind including varus/valgus, flexion contracture and compromised bone structure. Improper resection depth can result in postoperative instability or contracture. Kishimura et al showed a slight correlation between postoperative knee extension angle and a measure that subtracts the extension gap from the polyethylene thickness [1]. Patients tended toward full extension as that calculated difference approached zero. Nagai et al showed a slight correlation between the joint center gap and early postoperative flexion being close to preoperative values [2].
In this pilot study, our objective was to identify a predictable measure of planned robotic resection gap to assess relationships of resection depth to early postoperative recovery.
Methods
A CT-based active robotic platform allows for submillimeter resection based on a preoperatively determined surgical plan. We developed a simple methodology to measure gap difference to accommodate the various implant designs available on this open platform system. Known device thickness, which is the combined thickness of the distal femoral component and the tibial construct, was compared to the robotically planned extension gap. The difference between device thickness and planned extension gap was calculated. This number, which we called gap difference, was assessed with the postoperative outcomes to identify associations. In this preliminary study, a single surgeon robotic TKA case series was retrospectively reviewed. Preoperative deformity, planned resection depth, and implant selection (manufacturer and sizes) information was retrieved from the robotic system. Reviewed six-week postoperative clinical measures included obtained ROM, ligamentous stability, and the presence of flexion contracture or extension lag.
Results
The review included 29 robotic TKA cases. Active flexion tended to be better for gap differences close to zero (Figure 1). There was also a trend toward full extension for gap differences close to zero or slightly larger (Figure 2). However, neither of the trends identified for flexion and extension were statistically significant. No associations were identified between gap difference and any other outcome measures assessed.
Conclusion
This study presents a straightforward method to plan resection depths to achieve predictable early ROM, independent of implant design. Preliminary findings suggest that early postoperative range of motion may be affected by cutting the extension gap to match the combined device thickness.
References
[1] Kishimura Y, Matsui Y, Matsuura M, Hidaka N. Changes in postoperative extension angle after total knee arthroplasty: Effect of polyethylene insert thickness. J Orthop Sci 2019;24:674–9. https://doi.org/10.1016/j.jos.2018.12.013.
[2] Nagai K, Muratsu H, Matsumoto T, Maruo A, Miya H, Kuroda R, et al. Influence of intra-operative parameters on postoperative early recovery of active knee flexion in posterior-stabilized total knee arthroplasty. Int Orthop 2013;37:2153–7. https://doi.org/10.1007/s00264-013-2018-y.
Figures
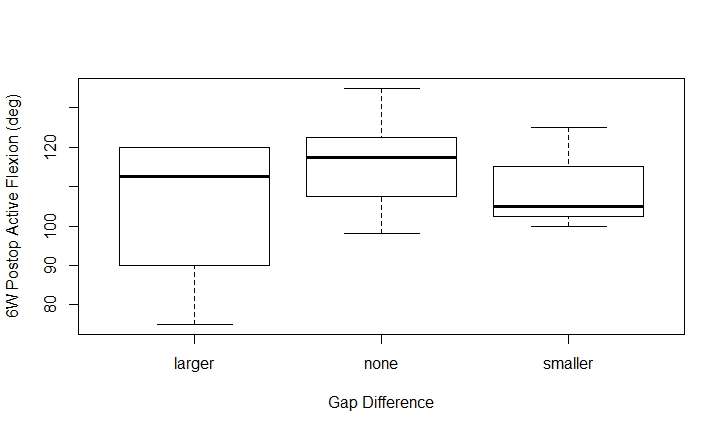
Figure 1
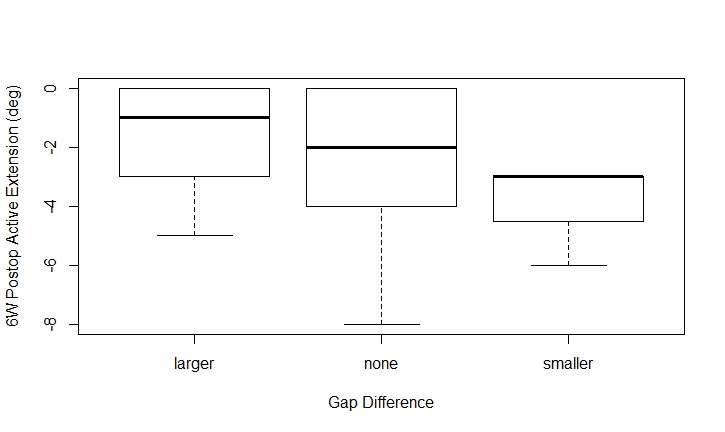
Figure 2POSTERS